The 2020 European Conference on Embolotherapy (ET), run by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), has been postponed until 16–19 December due to the coronavirus pandemic.
In full, the statement from CIRSE president Afshin Gangi (University Hospital Strasbourg, Strasbourg, France), ET chairperson Christoph Binkert (Institute of Radiology and Nuclear Medicine Kantonsspital, Winterthur, Switzerland), and ET deputy chairperson Patrick Haage (HELIOS Universitätsklinikum, Wuppetal, Germany) reads:
“After careful consideration of the conditions surrounding the continuing spread of the COVID-19 epidemic throughout Europe and the uncertainty regarding the severity and duration of restrictions on travel and gatherings in Austria and globally, the CIRSE leadership has had to take the difficult decision of postponing ET 2020 in Vienna, Austria, to December 16-19.
“We are very grateful for the understanding and support we have received from our community in these challenging times and look forward to welcoming you to another engaging ET in December!”
The American Journal of Kidney Diseases (AJKD) has published the National Kidney Foundation’s KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update, a completely revamped set of 26 individual guidelines for clinicians that focuses on dialysis access choices tailored to individual patients’ goals and preferences, as well as clinical outcomes.
It is the third time the Kidney Disease Outcomes Quality Initiative (KDOQI) team has developed a vascular access guideline and the first time the guideline has been updated since 2006. About 500,000 patients in the USA receive dialysis treatment and in 2016 alone, nearly 125,000 people started treatment for end-stage kidney disease (ESKD).
This comprehensive update was developed due to the significant growth in the evidentiary database for vascular access. Haemodialysis access issues are managed by a multidisciplinary team of medical professionals, thus the working group that developed this update includes members representing not only clinical and academic-based adult and pediatric nephrologists, but also interventional nephrologists, radiologists, surgeons, and vascular access nurses.
“It is gratifying to see how much progress has been made in understanding how to place and maintain the various types of vascular access to maximise the effectiveness and reduce complications,” said NKF chief scientific officer Kerry Willis. “One of KDOQI’s most important contributions to improving outcomes for dialysis patients has been the stimulation of new research such as the studies used in creating this groundbreaking update.”
An important new approach introduced in this guideline is an individualised and comprehensive map for dialysis modalities for the lifetime of the patient called the “ESKD Life-Plan,” achieved by creating a “P-L-A-N” for each patient that considers the Patient’s Life-Plan and corresponding Access Needs. For each access, the “Access Needs” part of the P-L-A-N includes designing and documenting the patient’s access creation plan, contingency plan, succession plan and underlying vessel preservation plan. The end-result is a comprehensive vascular access management plan that will best suit the patient throughout his or her time with end stage kidney disease.
The Evidence Review Team from the University of Minnesota reviewed more than 4,600 peer-reviewed publications, of which 286 were included in the evidence tables. These evidence tables were used by the workgroup, chaired by Charmaine Lok from the University of Toronto, to develop this fresh and more patient-focused approach to vascular access care that takes into consideration each patient’s needs and preferences.
“The new guideline will have many benefits for patients on dialysis, including to help preserve vessels needed for successful future access creation and to minimise unnecessary access-related procedures and complications,” said KDOQI chair Michael Rocco.
NKF has produced clinical practice guidelines through KDOQI on all stages of kidney disease and related complications since 1997. Recognised around the world for improving the diagnosis and treatment of kidney disease, the KDOQI guidelines have changed the practices of numerous specialties and disciplines and improved the lives of thousands of kidney patients. All KDOQI guidelines and commentaries are published in AJKD.
“These Guidelines emphasise an integrated, individualised approach to patient care that promotes optimal dialysis access management based on the best available evidence,” said Guideline Chair Charmaine Lok. “It recognises the need for further research, data, and timely revision that incorporates evolving practices, innovation, and new advances in vascular access. We are excited for clinicians to start using these Guidelines to help get the right access in the right patient at the right time for the right reasons.”
The guidelines will appear in the National Kidney Foundation’s AJKD today. AJKD is the leading kidney disease journal. It reaches thousands of healthcare professionals each month. To read more about the authors and to read the commentary, please visit: https://www.ajkd.org/issue/S0272-6386(20)X0004-7.
NOTE: This video is ONLY available to watch in selected countries and geographies
Geert Maleux (Leuven, Belgium), one of the first users of the SeQure® reflux control microcatheter (Guerbet) in Europe, shares his experience with the new device. He tells BLearning IR that the current challenges of embolotherapy include incomplete devascularisation, which can occur in some cases of liver chemoembolisation procedures, as well as non-target embolisation.
Maleux shares that he was drawn to using the SeQure® microcatheter because it is a novel device that is designed to help reduce the risk of non-target embolization. “[.] I have also the impression that we can deliver more microparticles into the targeted areas, for instance in cases of liver chemoembolization, into the tumour,” he adds.
Guerbet sponsored this video and its distribution in association with Interventional News.
A review of data from Veteran Health Administration shows that there was a temporal increase in the use of revascularisations for the management of critical limb-threatening ischaemia (CLTI) between 2005 and 2014. This increase correlated with a reduction in both mortality and major amputation during the same time period. However, contrary to data for non-veteran association patients, the new data did not indicate a shift towards endovascular revascularisation strategies.
Amgad Mentias (University of Iowa Carver College of Medicine, Iowa City, USA) and others write in Circulation: Cardiovascular Interventionsthat prior studies of non-veteran patients have already shown a temporal increase in both the use of revascularisation and the use of statin therapy for the management of critical limb ischaemia, and these trends have been linked to a reduction in mortality. “However, contemporary studies of critical limb ischaemia incidence, clinical management, and outcomes among veterans remain limited,” the authors report. The senior study author Saket Girotra (University of Iowa Carver College of Medicine, Iowa City, USA) told BIBA Briefings via email that there is a general lack of research on peripheral arterial disease among veterans. He noted that “we do not know with any degree of certainty how common peripheral arterial disease is among veterans”. “How does peripheral arterial disease affect veterans’ health status and quality of life both in the short-term and the long-term? And are veterans with this condition being appropriately managed? If not, what are the barriers and how can we improve care?” he adds.
Therefore, the team reviewed data from the Veterans Health Administration to provide further information in critical limb ischemia, which represents an advanced stage of peripheral arterial disease. They identified data for 20,938 patients (mean age 67.8 years; range 40–100 years) who were admitted to a Veterans Affairs (VA) facility with a diagnosis of critical limb ischaemia between 2005 and 2014 (fiscal years). Overall, the incidence of critical limb ischaemia was 0.25 per 1,000 enrolees. The authors report that across the study period, there was a “modest” decrease in the incidence of critical limb ischaemia: 0.3 per 1,000 enrolees to 0.24 per 1,000 enrolees (p<0.01).
The authors note: “There was a significant temporal increase in the overall use of revascularisation at 90 days (41.4% in 2005 vs. 57.9% in 2014; p<0.01 for trend) and this trend was consistent across all modalities [surgery, endovascular, and hybrid] as well as revascularisation during hospital stay.” Furthermore, between 2005 and 2014, risk-adjusted 90-day mortality decreased: 11.8% in 2005 and 9.4% in 2014 (p<0.01). Both revascularisation and statin use (which also increased) were strongly associated with a lower risk of 90-day mortality; revascularisation was also associated with reduced rates of major amputation at 90 days.
The authors found that surgery was the primary method of revascularisation: 25.4% vs. 14.9% for endovascular vs. 9.2% for the hybrid approach. They note that although the ongoing BEST-CLI trial is evaluating the optimal revascularisation approach, “endovascular techniques provide a lower risk option for revascularisation in patients with critical limb ischaemia”. Furthermore, they observe their findings are in “sharp contrast” to non-VA studies that have “demonstrated a general shift in revascularisation towards an endovascular approach”. Girotra comments: “The suitability of treatment depends on several factors such as the extent and complexity of vascular disease, the availability of conduits, potential for wound healing, patient preference as well as availability of appropriate expertise. Our study did not capture these data to inform us about the reasons for this divergent pattern of care. There is currently equipoise between endovascular therapy and surgical revascularisation as treatment options for critical limb ischaemia and, thus, the result of BEST-CLI are eagerly awaited.”
The study also found more than four-fold variation in the use of revascularisation across the sites and differences in patient factors could only account for less than 10% of this variation. The authors comment that they could not determine, with the current analysis, if these differences were because of differences in speciality expertise or in the number of available operators. Therefore, future studies are needed. “Given the strong association of revascularisation with patient outcomes, the findings highlight an urgent need to develop processes for ensuring that patients with critical limb ischaemia receive care from specialists with expertise in critical limb ischaemia management,” they say.
The authors conclude: “Further studies are needed to examine the reason of low use of endovascular revascularisation in VA hospitals compared with surgical revascularisation.”
An ahead-of-print article in the April issue of the American Journal of Roentgenology (AJR) reviewing various techniques and clinical management paradigms to treat severe frostbite injuries—relevant for interventional radiologists, especially—shows promising results using both intra-arterial (IA) and intravenous (IV) tissue plasminogen activator (tPA) to reduce amputation.
“Severe frostbite injuries can lead to devastating outcomes with loss of limbs and digits,” write radiologists Mikhail Higgins and John Lee (both Boston Medical Center, Boston, USA). Speaking specifically to this newspaper, they add: “In an era where the clinical paradigm for management of frostbite injuries has been primarily tissue rewarming, prolonged watchful waiting, and often delayed amputation, it is particularly exciting to have a meta-analysis that supports and validates a promising endovascular therapy performed by interventional radiologists that can significantly mitigate digit loss.”
Elaborating to Interventional News, Higgins and Lee comment: “The management of frostbite injury has been limited to conservative management and supportive care until now, mainly due to lack of studies on additional treatment options. Patients with severe frostbite injuries have often had bad outcomes—including amputations—due to the lack of reliable treatment options in the acute setting. Our meta-analysis shows promising results of intra-arterial and intravenous tPA therapy in the acute management of severe frostbite involving thrombosis of the digital arteries.”
A search of the literature by Lee and Higgins yielded 157 citations. After manually screening for inclusion criteria of case reports, case series, cohort studies, and randomised prospective studies that reported the use of tPA to treat severe frostbite injuries, 16 qualified for review.
Higgins and Lee analysed series included 209 patients with 1,109 digits at risk of amputation treated with IA or IV tPA—116 and 77 patients, respectively. A total 926 at-risk digits were treated with IA tPA and resulted in amputation of 222 digits, for a salvage rate of 76%. Twenty-four of 63 patients underwent amputation after IV tPA, resulting in a 62% salvage rate.
Both digital subtraction angiography (DSA) and triple-phase bone scan were utilised for initial imaging evaluation of patients with severe frostbite injuries.
Additional concurrent treatment included therapeutic heparin at 500U/h, warfarin with target international normalised ratio of 2:3, nonsteroidal anti-inflammatory drugs, pain management, and light dressings with topical antimicrobial agents.
Interventional radiologists are well-placed to be offering this digit-saving treatment, they add. “Not only are we interventional radiologists trained in catheter and guidewire manipulation skills to successfully navigate the arterial anatomy, but we are also clinically facile with managing patients’ unique endovascular needs with tPA therapy, given our deep experience with its use in catheter-directed thrombolytic therapy of other pathologies, such as pulmonary thromboembolism and thrombosed arteriovenous fistulas and grafts. In addition, the skill of diagnostic angiography, particularly of micro-arterial anatomy, that is needed to quickly and accurately diagnose frostbite-related thrombosis of the digital arteries as well as during post treatment evaluation is a long-held point of expertise by the clinically trained interventional radiologist.”
“For many years,” Higgins and Lee concluded, “the axiom ‘frostbite in January, amputate in July’ was an accurate description of the common outcome in frostbite injuries. Through a meta-analysis of thrombolytic therapy in the management of severe frostbite, this article provides a useful guideline for interventional radiologists, including a suggested protocol, inclusion and exclusion criteria, and potential complications.”
The author’s recommendation is based off the multidisciplinary care protocol that they co-implemented at their own institution, Boston Medical Center. Higgins and Lee say this “begins with an objective evaluation of the affected digits, including grading post-rapid rewarming in the emergency department.” This might then include collaborative clinical triaging of severe frostbite injury patients to intravenous or intra-arterial thrombolytic management with conservative management for low grade injuries, with contributions from emergency medicine, trauma surgery, podiatry, orthopaedics, internal medicine, diagnostic and interventional radiology.
“It is important to note,” they add, “that such multidisciplinary efforts reliably and reproducibly support early and accurate diagnosis and triaging of patients with frostbite injuries and are vital in providing appropriate management and oversight of these patients, particularly during thrombolytic therapy.”
When asked how this research will impact clinical practice, Higgins emphasises the importance of promoting these procedures: “Publicity on the use of thrombolytic therapy in treating acute severe frostbite is vital to ensure that frostbite patients are afforded the most efficacious management option to preserve their digits in the unfortunate event of an acute frostbite injury. With global warming as a real though daunting consideration, who knows which city or hospital might experience a rush of frostbite cases amenable to this important digit-salvaging therapy, and when? Knowing how to protect our patients from digit loss should such events occur is now a critical consideration for the forward-thinking, patient-centric interventional radiologists that we all aspire to be. In that vein, I would consider encouraging periodic efforts to inform healthcare providers about thrombolytic management of severe frostbite, especially during each winter season.”
Higgins and Lee hope to see the results of randomised trials in comparing the effectiveness and complications of intra-arterial and intravenous thrombolytic therapy. “With these results,” they determine, “we will be able to provide more effective and safe digit-saving care for patients with acute severe frostbite injuries.”
The Society of Interventional Radiology (SIR) has cancelled its upcoming conference due to the coronavirus outbreak. The conference was to be held in Seattle, USA, from 28 March–2 April.
“Based on these recommendations, US Centers for Disease Control and Prevention (CDC) and World Health Organization (WHO) information, and numerous travel restrictions issued by companies and medical institutions, SIR and SIR Foundation leadership have made the difficult, but necessary and responsible, decision to cancel the SIR 2020 Annual Scientific Meeting in Seattle,” the society said.
SIR plans to refund attendees’ and exhibitors’ registration fees and will cancel any hotel reservations made through its official hotel block, it said. It will not refund individual travel costs. Exhibitors’ space rental fees will be refunded upon written request.
The society plans to explore other meeting options.
“In the coming weeks, we will tap into the innovative and agile spirit of [our] specialty to explore virtual meeting options that deliver world-class education, spotlight interventional radiologists’ ingenuity, and celebrate the many achievements we had planned to recognize in Seattle,” SIR said.
In addition, the European Society of Radiology (ESR) announced last week that is has postponed its annual meeting, the European Congress of Radiology (ECR), originally scheduled for 11–15 March in Vienna, Austria. This will now be held on 15–19 July.
Boris Brkljačić, ESR president, comments on the society’s website: “After careful evaluation of the spreading coronavirus epidemic, and considering the recent statements issued by the World Health Organization (WHO) and the European Centre for Disease Prevention (ECDP), and the related evolving world-wide restrictions and crisis, the ESR was forced to make this decision. Above all, we have analysed the recommendations from the Austrian health authorities for large-scale events and came to the conclusion that we are not in a position to fulfil their requirements and guarantee a safe congress for our participants and industry partners at this time. The safety, health and well-being of our delegates and partners will always be the highest priority for the ESR.”
Okami Medical has announced the successful completion of the first cases with the Lobo vascular occlusion system. The first offering in the company’s product portfolio, Lobo-3, recently received 510(k) clearance from the US Food and Drug Administration (FDA) for the occlusion of peripheral arteries.
The Lobo (Low-profile braided occluder) system is uniquely designed to provide interventional physicians with a single-device, one-and-done solution for the occlusion of various arterial targets without the need for multiple embolic devices. The Lobo system combines a patented design with proprietary Hdbraid technology to create a highly occlusive pore structure that substantially reduces blood flow and accelerates vessel closure. The Lobo-3 occluder is intended for use in 1.5–3mm diameter vessels.
Ripal Gandhi, interventional radiologist, Miami Cardiac and Vascular Institute, performed the first Lobo-3 implant. “We have successfully utilised the Lobo-3 occluder to embolise several small vessels via a microcatheter. The device has resulted in immediate occlusion of the target vessels. The device tracks well and deploys precisely at the desired location. The Lobo-3 occluder is a great addition to the embolic armamentarium for the occlusion of small vessels,” said Gandhi.
“Guided by world-class physician collaborators, Okami is committed to addressing numerous challenging aspects of peripheral vascular occlusion,” said Bob Rosenbluth, president and CEO of Okami Medical. “We are very pleased with the clinical performance of the Lobo-3 occluder in the initial cases. The device is in clinical use at key centres and we look forward to expanding our launch in 2020.”
Medtronic has issued an urgent field safety notice to warn on specific production lots of its Pipeline Flex embolization devices due to the potential for device fracture.
The company initiated verbal communication about the issue last month after identifying the potential for device fracture at the distal section during use, due to a weakened bond in a subset of recently manufactured devices.
Use of the affected product could result in unintended separation, where the distal portion of the device delivery system remains in the patient, which could cause significant patient injury, including a prolonged procedure, ischaemic stroke, intracranial haemorrhage, neurological deficit and/or death.
Medtronic has not received complaints related to the issue within the affected population, but the company is recalling the affected products due to the increased potential for fracture, according to the field safety notice.
If a Pipeline Flex embolization device was already successfully implanted, there is no increased risk to patients due to the issue, and those patients can continue with their normal course of treatment. The affected lots include devices with a “use-before” date on or after 21 October 2022.
The company urged those affected by the issue to cease the use of any affected products and to remove and quarantine all unused devices in their inventory before returning them to Medtronic.
Pipeline Flex is designed for the endovascular treatment of adults with large or giant wide-necked intracranial aneurysms from the petrous to the superior hypophyseal segments. In February 2019, it won expanded US Food and Drug Administration (FDA) indication for patients with small or medium wide-necked brain aneurysms in the territory from the petrous to the terminus of the internal carotid artery.
NOTE: This video is ONLY available to watch in selected countries and geographies
[xyz-ihs snippet=”vid-01″]
Andrew Holden (Auckland, New Zealand), Alexandros Mallios (Paris, France), Robert Lookstein (New York, USA) and Tobias Steinke (Dusseldorf, Germany) talk to BLearning Peripheral about the 12-month results of the IN.PACT AV Access randomised controlled trial (RCT) which compared drug-coated balloon (DCB) angioplasty to plain balloon angioplasty.
Holden, who presented the 12-month primary patency data for the first time at LINC 2020 (Leipzig Interventional Course; 28–31 January, Leipzig, Germany), explains that the data showed a “highly significant difference in patency” in the paclitaxel DCB arm (63.8%) when compared with the plain balloon arm (43.6%). He also highlights other key data including a 35.4% reduction in the number of reinterventions in the DCB group, which he notes “really resonates with clinicians as well as patients”.
Mallios notes that the six-month data was not only sustainable but improved and claims that another important point is that, regarding the risk of mortality, “apparently there is no evidence supporting this risk for arteriovenous access”. He discusses the clinical importance of the data which he believes is “very reassuring” and provides a “better quality of life for the patient”.
Lookstein for his part discusses the Economic Impact Model of the German and American healthcare systems which he says provided “a very telling argument” that the technology should be used in the “broadest population possible”. He goes on to look at how these “impressive” datasets, including both the 12-month data and the Economic Impact Model—which showed a DCB cost benefit—have led him to think “even more about using DCBs in AV access patients”.
Finally, Steinke gives his view on the 12-month IN.PACT AV Access data which he says was “really impressive”, noting that this was the first time that “significant results” were seen over this length of observation.
Reflow Medical has announced that they have received US Food and Drug Administration (FDA) clearance for an expanded indication for the Wingman crossing catheter after completing the Wing-IT clinical trial. The Wingman catheter crosses peripheral chronic total occlusions (CTOs) using an extendable bevelled tip that creates a channel to help penetrate, or cross, the occlusion with a guidewire, enabling further treatment of the lesion with therapeutic devices.
The Wing-IT CTO clinical trial was a prospective, international, multicentre study that treated 85 patients and followed them for 30 days. The Wingman catheter was able to demonstrate a 90% crossing rate when up to two previous guidewires could not cross these challenging lesions, meeting its primary safety and efficacy endpoints. These clinical trial results have garnered positive feedback in the physician community.
“With this expanded indication, physicians gain the ability to cross [CTOs] in peripheral lesions with a simple and very effective device,” according to John R Laird (Adventist Heart and Vascular Institute, St Helena, USA). Laird was the principal investigator for the study.
S Jay Mathews (Bradenton Cardiology Center, Bradenton, USA), who performed initial patient enrolments, said, “Reflow goes the extra mile to provide physicians with real clinical evidence for utilising their technology, including this new indication for the Wingman.”
Company co-founder and CEO Isa Rizk noted, “We are extremely grateful to the physician investigators, patients, research staff and employees who helped us conduct this very important and compelling clinical study that supported this expanded treatment option for crossing peripheral CTOs.”
A world map showing the “huge disparity” between the number of UAEs and the number of uterine surgeries performed annually in Spain, France, Australia, and at one institution in El Salvador
On average in France, 2,000 uterine artery embolizations (UAEs) are performed each year. In contrast, 40,000 patients have hysterectomies annually. This has led French interventional radiologists to protest the high number of “unnecessary” surgeries, and spurred the development of a nation-wide public awareness campaign. However, this is not just a French issue.
James Spies (Georgetown University Hospital, Washington, DC, USA) reports that, “despite some progress in reducing the number of hysterectomies for benign conditions such as fibroids, with about a 10% reduction in the past decade, there are still eight to 10 times the number of hysterectomies as UAEs for fibroids in the USA.”
A 2017 report by the Society of Interventional Radiology (SIR), The Fibroid Fix: What women need to know, provided insights into the lack of awareness. SIR commissioned a Harris Poll in June 2017 that surveyed 1,176 US women ages 18 and over. The poll found 62% of respondents had never heard of UAE and that 20% believed hysterectomy was the only treatment option for fibroids. Even those who were diagnosed with fibroids reported a lack of awareness, with 44% saying they had not heard of UAE. Of those who had, 75% said they did not learn about it from a gynaecologist.
“Our numbers for UAE are ridiculous,” José Urbano (Ramon y Cajal University Hospital, Madrid, Spain) says of Spain. According to the Spanish Society of Vascular and Interventional Radiology (SERVEI), 120–150 UAE are performed each year in the country, which has a population of 44 million. These experiences are echoed in Central America. Speaking at SIR’s annual meeting last year (23–28 March, Austin, USA), the only interventional radiologist in El Salvador, Ethel Rivas Zuleta (Universidad Dr José Matías Delgado, San Salvador, El Salvador), told delegates: “We face the same problems in our region”. Fibroids are the leading indication for hysterectomy in El Salvador. In 2018, 746 hysterectomies were performed in Zuleta’s institution, mostly in women between 30 and 50 years of age. Six women were treated with UAE. Zuleta noted that none of these six patients were referred by an obstetrician or gynaecologist: four were either doctors themselves, or related to one, and two had found out about UAE themselves online.
On the other side of the world, Gerard Goh (The Alfred Hospital, Melbourne, Australia) and colleagues recently analysed Australian Medicare data, and found a “huge disparity” between the number of hysterectomies performed each year compared with the number of UAEs. The data showed that, on average over the last five years, 30,332 uterine surgeries are performed each year. According to Goh, you would expect four to five thousand of these (approximately 30%) to be treatment for fibroids. Fewer than 145 UAEs were performed on average per year. “Based on the suggestion that 20% of hysterectomies in Australia are for fibroid-related disease, this estimates 6,066 fibroid-related surgeries per year,” Goh comments.
He adds that he thinks it is “interesting” that a procedure which has been proven to be efficacious has such a poor take-up globally. A major reason for this, he posits, is the lack of “patient and referrer awareness”. To tackle this issue, he believes interventional radiologists from across the world need to “come together” and work with societies to help educate patients and referrers, because currently “a lot of women are really missing out on uterus-sparing surgery for fibroids”.
Why this discrepancy?
Speaking specifically of the US population, Spies expands on his thoughts for the causes of the discrepancy between hysterectomy patient numbers and UAE patient numbers: “I believe that there are a range of factors, which could include economic considerations, but also persisting scepticism among gynaecologists about UAE. Despite considerable evidence of excellent outcomes after UAE, UAE patients are more likely to need additional interventions than those that have hysterectomy and many gynaecologists seem convinced that a definitive treatment like hysterectomy is best. [However, we must take into account] women’s desire to avoid hysterectomy.
“In the USA, we have made efforts for years to raise the profile of UAE, with some success. Still, it is an effort of decades that will cause change. Currently, SIR is engaged in a multi-disciplinary creation of practice guidelines for the procedure.”
These guidelines, which are expected to be published in early 2021, are being developed by physicians from the specialties of gynaecology, body imaging, and IR. “The guidelines will amplify SIR’s past awareness and education efforts by providing physicians and patients with evidence-based recommendations for the optimum care of patients with symptomatic fibroids,” SIR president Laura Findeiss (Grady Memorial Hospital, Emory University School of Medicine, Atlanta, USA) comments.
In addition to SIR, the participating societies are Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Fédération Internationale de Gynécologie et d’Obstétrique (FIGO), the American Association of Gynaecologic Laparoscopists (AAGL), the American Society for Reproductive Medicine (ASRM), and the Society for Advanced Body Imaging (SABI).
To attract a Medicare rebate for UAE in Australia, the patient must be referred by an obstetrician/gynaecologist, which Goh says “brings up potential referral bias”. However, he notes that the low UAE rate in Australia is “likely multifactorial”, and that IR can only fulfil its potential in terms of treating the appropriate number of eligible patients when interventional radiologists “take greater clinical ownership of their patients”. To Goh, this looks like preprocedural consultations with patients, postprocedural care, and having an inpatient bed card. He also stresses that gynaecologists and interventional radiologists alike should have an understanding of the pros and cons of both embolization and surgical options, to allow patients to make an informed decision about their fibroid treatment.
Urbano concurs with Goh’s assessment that there are numerous reasons for the underutilisation of UAE globally, and particularly in Spain. “Of course, like in France, gynaecologists actively block this treatment because they fear losing patients,” he says. “Furthermore, when obtaining informed consent for hysterectomy, it is mandatory to notify the patient that UAE is offered as an alternative, but it is often not even mentioned. Gynaecology tends to be a speciality that does not participate in multidisciplinary work. They have countless patients, they do their own diagnostic tests, and their patient management is routine.
“Interventional radiologists have too much work in Spanish public hospitals, so UAE is not an important focus for them. In addition, while they are experts at doing the procedure, they are not always involved in the diagnosis, pain management, and patient follow-up. Interventional radiologists are only fully involved in the UAE process in private practice and some public hospitals. Less than 50% of IR services in Spain have a clinic and beds. In my experience, this is crucial for us to do all those type of procedures in which IR competes with other specialties.”
Zuleta argues the same in El Salvador. She says the underutilisation of UAE is due to “a lack of knowledge by other specialties, the usage of old protocols and guidelines, and highly unequal access to healthcare for women. We do have access to technology: we have angiosuites, CTs, ultrasounds, MRI, but what we lack is education. We at SIDI [Sociedad Iberoamericana De Intervencionismo] believe that supporting education in our countries is the best way to improve the management of patients, especially in IR.”
Public awareness initiatives
In the USA, SIR is running its own campaign—the Vision to Heal, Together, launched in September 2019—to bring IR procedures to the forefront of the public consciousness. According to an SIR press release, this aims to “build stronger partnerships with referring physicians and to empower patients to ask about IR as a treatment option.” The campaign is not specific to UAE, it is focused more broadly on vascular disease, cancer, and men’s health conditions, which includes uterine fibroids. SIR is using a combination of radio, digital, and social media advertising in four pilot US markets (Washington, DC; Rochester; Little Rock; Portland) to spread its messaging.
The campaign was inspired in part by SIR’s 2017 report finding the lack of awareness among patients and the lack of information from referring physicians. “By educating both groups, we hope to not just reduce the knowledge gap, but to build trust among the specialties so that patients are presented with all of their treatment options up front,” says Findeiss.
The Vision to Heal, Together campaign ran through to the end of March 2020. SIR reports positive engagement and social media posts. “We have seen friends sharing information with friends in need and others simply commenting to vouch for the life-saving and quality-of-life improving power of interventional radiology,” Findeiss comments. “There is a real desire and need for more information about minimally invasive treatments across the board.”
In Australia, the wording of the Medicare item for UAE is under review, which Goh hopes will change to improve patient access to the procedure. The Interventional Radiology Society of Australasia (IRSA), of which Goh is president, is “working on the UAE issue.” Goh says: “We are working with some other stakeholders to increase public awareness online, and via print and social media.” IRSA is updating its website to list practitioners who can perform UAE, and is leading a global position statement to help further increase awareness.
In Spain, Urbano stresses that the key lesson from the French action is that it is patient-focused. “SERVEI’s position is not to start turf battles,” he says. “We have lost too much time and energy in the past with no-way fights. Our policy is to show what IR work is, and to demonstrate he advantages of our treatments to patients.”
French interventional radiologists are protesting the high number of “unnecessary” surgeries taking place nationwide, stressing that there are minimally invasive alternatives with fewer complications available. The Federation de Radiologie Interventionnelle (FRI), has launched a public awareness campaign to educate potential patients about interventional radiology (IR) procedures, with a specific emphasis on uterine artery embolization (UAE), which it claims is an underutilised, safe, and effective option for patients who do not want a hysterectomy. To read about this issue on an international stage, read the full coverage here.
“I think gynaecologists have a real scepticism of the effectiveness of UAE,” FRI president Hélène Vernhet-Kovacsik (Arnaud de Villeneuve Hospital and Montpellier University, Montpellier, France) tells Interventional News. “They do not trust this technique, which they do not practice.”
The French guidelines for the therapeutic management of uterine fibroid tumours, published in the European Journal of Obstetrics and Gynecology and Reproductive Biology and last updated in 2012, state that “Because UAE is an effective treatment with low long-term morbidity, it is an option for symptomatic fibroids in women who do not want to become pregnant, and a validated alternative to myomectomy and hysterectomy that must be offered to patients.” However, Vernhet-Kovacsik says that though UAE is in the guidelines, and “should be offered as an alternative to hysterectomy for all patients”, it is not. On average 2,000 UAEs are performed a year in France. In contrast, 40,000 patients have hysterectomies annually.
Raising awareness
When first elected president of the FRI, Vernhet-Kovacsik set up specific working groups within the society. The communications working group, headed by Vincent Vidal (Hôpital de la Timone, Marseille, France), have launched a public awareness campaign in an effort to educate the public about UAE and other minimally-invasive options. With a focus on pelvic interventional radiology (IR) in 2020, the society’s edifying efforts are dedicated to UAE, haemorrhoids, and prostate artery embolization (PAE). As a world-leading advocate of the “emborrhoid” technique—the embolization of the superior rectal arteries—and the lead author of the 2015 study demonstrating the procedure’s efficacy, Vidal is a global specialist on haemorrhoids. PAE is the principle purview of Marc Sapoval (Georges Pompidou European Hospital, Paris, France, and founder of the GEST Symposium), who is a prominent member of FRI. UAE was chosen for more political reasons: in Vernhet-Kovacsik’s words, the lack of referrals and general awareness “seemed to us very stigmatising and unfair. How is it that a technique recognised as effective and less morbid than hysterectomy, cited in the gynaecology guidelines [and] with long established scientific evidence, remains as little used?”
The communications working group organised a press conference with French media on 23 January at the Georges Pompidou European Hospital in Paris. This resulted in a double page spread appearing in the non-specialist daily newspaper Le Parisien, featuring patient testimonials in favour of UAE, and interviews with Vernhet-Kovacsik, Sapoval, and other French interventional radiologists with private practices explaining technical details of the procedure, as well as describing how and why it is underutilised. The article cited a lack of information provided to the patient from interventional radiologists’ medical colleagues leading to a low referral rate.
Following this, Vernhet-Kovacsik recounts how Sapoval appeared on French radio to discuss embolization. “[He] brilliantly exposed the clinical and economic effectiveness of all the IR treatments, and presented emerging techniques,” she enthuses. Following the success of these media engagements, FRI produced a press kit summarising current scientific data on pelvic IR, which can be used to inform future media opportunities, in France or abroad.
“We also wanted to communicate [the impact on] quality of life,” Vernhet-Kovacsik says of the FRI media strategy, “because it has become a major concern for patients, and is an advantage of IR procedures, which have very low morbidity and require very short hospitalisations in comparison with alternative surgical techniques. This also made it possible for us to directly address patients by proposing solutions to symptoms that are not always recognised as pathological, but [are] handicapping in everyday life, such as pelvic pain or urinary discomfort.”
FRI has taken a multimodal approach to disseminating their message. The society made a short animated film about pelvic IR, which is freely available on their YouTube channel. This also hosts video coverage of radiology congresses and the preprocedural film shown to patients in waiting rooms. Additionally, Sapoval is working on a patient-facing website, to launch 13 June this year. “We are testing and finalising it now,” Sapoval tells Interventional News, “then we will be launching it nationwide. The website will inform patients of treatments for fibroids other than hysterectomy, so they can be aware that they may not need one.” FRI also plans to use Facebook to engage the online community through question and answer sessions, mediated by specialised health publications, designed to offer patients a chance to speak directly with an interventional radiologist.
This direct engagement is part of a trend Vernhet-Kovacsik has identified. “The patient-doctor relationship is changing—it is no longer directive, but participative. The dissemination of information on the web via social media and the creation of user groups should be [a step] in the right direction.” Following the increased interest in UAE that succeeded the Le Parisien article, FRI set up an online directory of pelvic IR centres in France, allowing patients to find these services more easily.
Sapoval believes this increasingly participative relationship is important because patients will have to lead the charge in advocating for UAE. “We have a very unethical situation in France where women get hysterectomies instead of embolizations because the obstetricians/ gynaecologists are operating on patients instead of referring them to interventional radiologists. This is one of the interventions where we have strong, level one evidence, and despite a lot of effort, we have not seen a lot of movement in the last few years. This is the case in many other countries as well, so we wanted to take the lead and raise the flag for UAE.”
“Some resistence” to uterine artery embolization from referrers
When questioned about why he thinks the discrepancy between hysterectomy and UAE numbers exists, Sapoval is categorical: “There is some resistance. Some [obstetricians/ gynaecologists] do not know about UAE, and some do know, but do not want to refer patients because they are paid to perform hysterectomies.”
Vernhet-Kovacsik proposes another reason for the low referral rate: “In my opinion, this goes beyond simple corporatist considerations. Women have a doctor who has looked after them for years, has helped them give birth to their children, knows their intimate problems. A recognition has been created and it is difficult for patients to dare to express desire for a treatment different to the one proposed by the gynaecologist! However, it is shocking to offer a firstline technique (hysterectomy) which has twice as many serious complications as embolization, sometimes requires transfusions, and always prolongs work stoppage. Gynaecologists’ main argument is the increased risk of embolization versus myomectomy regarding fertility, but the vast majority of patients are over 43 years old, are not keen on pregnancy, and are treated by hysterectomy and not myomectomy: so why not perform an embolization? I think our target must be this population precisely!”
UAE preserves sexual function and bodily integrity
The EFUZEN study, conducted in 2017 by Vernhet-Kovacsik, Sapoval, and others from the French Society of Interventional and Cardiovascular Imaging (SFICV) research group, evaluated sexual function before and one year after UAE. The authors concluded that at one-year post-embolization, UAE significantly improves all aspects of sexual function and quality of life. Vernhet-Kovacsik stresses the pertinence of this finding: patient’s quality of life and sexual function “are rarely addressed by gynaecologists”, she says, adding that “there is a close link between fibroids and their treatment, and these aspects of life.
“The uterus is not only used for reproduction; preserving bodily integrity is also a current demand,” she comments. “I think we should all take advantage of the ‘me too’ phenomenon and, as interventional radiologists, speak out and encourage women to dare to ask for fair treatment when it comes to preserving their femininity and their quality of life. We could certainly work together: interventional radiologists, gynaecologists, and patients. I am less concerned about the future of PAE, however technically more difficult, because the importance of preserving sexual function in men will never be questioned!”
The US Food and Drug Administration (FDA) is hosting a public workshop entitled “Medical Extended Reality: Toward Best Evaluation Practices for Virtual and Augmented Reality in Medicine”. According to the agency’s website, the purpose of the public workshop is “to discuss evaluation techniques for hardware, standards development, and assessment challenges for applications of Extended Reality (XR) in medicine. The goal is to identify critical gaps that may impede medical XR device development, innovation, and to advance the evaluation of medical XR devices and applications, thus accelerating the development of safe and effective medical XR devices benefiting patients and healthcare.” Follow for live updates from Interventional News here.
13:41 GMT
Edward Margerrison (director, Office of Science and Engineering Labs, Center for Devices and Radiological Health, FDA) welcomes attendees. “I want to set the scene a bit, and explain why the FDA is involved,” he says. “We have representatives here from industry, from academia, we have healthcare professionals, and we have members of government as well. So we really have the whole community here.
“Much of the technology has been developed outside of healthcare, outside of medical devices, and is beginning to come into FDA to be regulated. It is a very interesting area for us, because companies are developing products that haven’t previously been in a regulated environment. Now is the time to get everyone on the same page, to have real discussions about how we are going to develop these technologies, and stimulate innovation.
“We are looking in a pre-competitive space. […] The technologies and products of the future should compete on how good they are for the customer. […] Being the FDA, a lot of people look to us as leaders. I anticipate a lot of people asking today, is this the end of the beginning, or the beginning of the end? We think it really is the end of the beginning. Particularly the AR/ VR space (augmented reality/ virtual reality), we know it is coming, but what are the things that we do not know yet? We want you to explain so we do not become a barrier.”
13:49 GMT
Technical session begins.
“At the end of the day, at around 4pm [ET], we will need to come up with ideas for how to move forward, and we want those ideas to come from you,” Aldo Badano (deputy director, DIDSR, OSEL, CDRH, FDA) says, encouraging attendees to “be bold” and come up to the microphone to ask questions and air opinions.
“With the exception of our keynote speaker, we do not want to focus on the hype or what would be possible if we had infinite amount of time and resources, but rather what are the current challenges that are impeding the application of these technologies in the medical field.”
13:55 GMT
General trauma surgeon Rafael Grossmann (Maine, USA), the first surgeon to use Google Glass, starts his keynote lecture.
Talking of VR, Grossmann enthuses: “It blows my mind, what the technologies allows you [to do] today. What you can see through s VR headset is incredible, and this is just the beginning. The future of this technology is to become more ergonomic, more economically viable, and, ultimately, much more common.
“We are going to see a paradigm cost in the cost, weight, size of these devices that will transform the way we do health care.”
He shares BrainLab, a company he claims is “revolutionising how we educate patients and providers in regards to surgery and planning”. A representative from BrainLab will speak later. Grossman stresses the importance of haptic feedback when using VR or AR in surgery, and says that BrainLab is a “pioneer” in this field.
Grossman is currently not using VR headsets clinically, but for teaching purposes. “This is not a matter of sterility, there is no infectious concern, but we have not found the right combination of this technology and procedure in the operating room. We are still waiting on regulations.”
14:23 GMT
Bernard Kress, an optical engineer at Microsoft, takes to the podium to present on advances in mixed reality devices and new evaluation challenges.
He says HoloLens is not advertised for general consumers, but is specifically for healthcare providers. The legal team at Microsoft requested Kress read the following disclaimer ahead of his talk: “HoloLens is not intended to be a medical or surgical device, but our clients say it can be effectively used in medical imaging and image assistant surgical planning.”
Several companies, including Philips, are already using HoloLens in the medical space, Kress comments. Atul Gupta will speak on behalf of Philips later in the programme.
“Everything that we do is centred on the human,” Kress explains. “The first pillar of mixed reality is immersion. Immersion has to be matched with what the human can actually sense. This is very difficult. You do not want to over-design your system; it has to fit what the actual human can see. You have to match the optical resolution and the field of view with that of the human eye.”
The second “pillar” is comfort. “This is especially important if the surgeon has to wear the headset for multiple hours”. There are four types of comfort Microsoft take into account: wearable comfort (taking into account size, weight, temperature, centre of gravity), vestibular comfort (the device has to be physically untethered, and a large, transparent, unobtrusive peripheral see-through is required so wearers are aware of their surroundings), visual comfort (having non-conflicting 3D cues and the shortest “motion to photon” latency possible), and social comfort (need to be able to make eye contact with nurses and technicians in the room, and not put off the patient).
“So where are we today with MR hardware?” Kress asks. “There is still a long way to go to provide full comfort to surgeons and medical professionals to allow for a revolutionary imaging and augmentation tool which will change forever the medical imaging field. This is just the tip of the ice berg.”
When asked by an audience member when the cost of MR headsets will go down (“Like VR headsets, which can be very cheap”), Kress says “It will take a long time. There is no AR market today for consumers, so we are not even looking at a consumer price point. For industry, right now, I think the device is around US$3,500. This will go down, but we are not constrained by consumer requirements.
“However, this ecosystem of companies that are trying to reduce the cost of these very complicated optics are emerging, so in five to ten years I think you will see a price decline of a degree of magnitude.”
14:52 GMT
Hiroshi Mukawa, of Sony, speaks on “Emerging technologies for addressing performance limitations in extended reality devices, such as motion-to-photon latency compensation, and retinal scan displays”.
15:09 GMT
Vinay Narayan, from HTC, delivers his talk, “Advances in virtual reality devices and characterization methods”.
“We started off in VR,” he says, “but the ability to build products that can scale in a meaningful time frame really made us switch our priorities to the VR space.” Echoing Kress, Narayan stresses that one of the key differences between AR and VR when thinking about commercialisation is that VR products are available for general consumers.
17:05 GMT
John Penczek, from NIST, takes to the podium to discuss progress in standards for extended reality devices. Providing a review of the International Organization for Standardization (ISO), he outlines how the standard-setting body has robust, specific guidance for consumer requirements for finding eye point, but that there is still more work to be done, in particular in the realm of eye tracking and direct retinal tracking.
18:45 GMT
Atul Gupta, from Philips, outlines the opportunities and challenges for extended reality devices in medicine.
Andrea Kahlberg (Milan, Italy) talks to BLearning Peripheral at LINC 2020 (Leipzig Interventional Course; 28–31 January 2020, Leipzig, Germany) about a novel sirolimus-eluting self-expanding nitinol stent that Kahlberg claims “has the ability to improve the long-term results” of superficial femoral artery (SFA) endovascular treatment.
Kahlberg outlines some of the main features and unique properties of the stent. He notes that one of the “unmet needs” of SFA stenting is durability over time, explaining that the Sirolimus is combined with fatty acids helps to improve the dispersion of the drug inside the arterial wall which helps improve durability.
He finally goes on to discuss the first in-human trial with the device, which enrolled 100 patients across Europe, and notes that the two year results were “very satisfactory” compared to other major trials that involved drug-eluting stents.
The first prospective study on the combination of peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTATATE and Holmium-166 (166Ho) radioembolization has shown that significant tumour reduction can be achieved in patients with bulky liver disease, a significant advancement considering the liver is the most commonly affected organ in metastatic disease and is the most incriminating factor for patient survival. Just published in Lancet Oncology, Arthur Braat (University Medical Center Utrecht, The Netherlands) et al conclude that the additional radiation boost provided by 166Ho-radioembolization following PRRT leads to a high objective response rate with acceptable side effects and only temporary changes in quality of life.
The HEPAR PLuS study (Holmium Embolization Particles for Arterial Radiotherapy Plus 177Lu-DOTATATE in Salvage NET [neuroendocrine tumour] patients) was a phase 2, single centre, non-randomised, noncomparative, open label study. Patients received additional 166Ho-radioembolization within 20 weeks after the fourth cycle of 177Lu-DOTATATE. Senior author Marnix Lam speaks about the study’s implications, highlighting the investigators’ use of Quiremspheres (Quirem/ Terumo Europe), and how these particles are helping to usher in a new era of more individualised treatment planning when it comes to selective internal radiation therapy (SIRT):
How is this data breaking new ground?
In my opinion, the phase 3 NETTER-1 trial in patients with grade 1 and 2 gastrointestinal neuroendocrine neoplasms was a landmark study, showing that PRRT has a huge benefit for patients in terms of progression-free survival [PFS] and overall survival [OS]. However, objective response rate after PRRT was limited to only 18%. In addition, a subanalysis showed that 68% of patients in the NETTER-1 study had bulky disease, and of those patients, 70% had bulky disease in the liver. The outcomes in terms of progression-free survival are much worse: most patients with bulky disease did not reach the median PFS of >40 weeks of the NETTER-1 trial. In other words, for patients with bulky liver disease, there is definitely room for improvement.
I was discussing this with Dik Kwekkeboom (Rotterdam, The Netherlands), one of the founders of PRRT, and a friend and colleague of mine who sadly passed away in 2017. He told me he had a fantastic new treatment for neuroendocrine tumours, but that improvements were needed for patients with bulky liver disease. At the time, we were developing 166Ho-radioembolization for liver disease, so we joined forces and came up with the design of the HEPAR PLuS study, which combines the treatments: four cycles of PRRT followed by additional 166Ho-radioembolization, which provides a radiation boost. While PRRT is a systemic treatment, 166Ho-radioembolization is a local treatment, targeting the liver metastases.
With this method, we were able to improve that 18% response rate. Total hepatic objective response rate at six months was 47% in HEPAR PLuS—a huge increase. Of course, we always have to keep in mind that response rates do not necessarily translate into improved PFS or OS, and that is definitely the next step that we want to take: conduct a randomised controlled trial to evaluate whether the increased response rate translates into a better outcome for patients with bulky liver disease.
The timing of this publication is significant. PRRT is now the standard of care, as a lot of hospitals around the world have been performing this therapy for six to 12 months. They have gained experience with PRRT, which is great, but have also found that the response rate for patients with bulky liver disease is limited.
What do you think is the future of SIRT?
I think the future of SIRT is individualised treatment planning. The HEPAR PLuS study shows that it is safe to combine PRRT and 166Ho-radioembolization. However, when combining two treatment modalities that involve radiation doses, dosimetry is essential. You have to calculate the absorbed dose coming from PRRT and from radioembolization, so combining these modalities is a call for improved treatment planning.
This is where the benefit of the 166Ho-microspheres comes in: we can use the exact same particles (QuieremScout) in the test procedure as in the treatment (QuieremSpheres). During the test, we only administer a small fraction of the microspheres to the patients for diagnostic purposes—a scout dose. We evaluate the biodistribution of the microspheres, and then draw an individualised treatment plan. This is possible because, even at low activities, 166Ho-microspheres are fit for imaging, unlike Yttrium-90 (90Y)-microspheres, which can only be properly imaged at high activities. Therefore, when using 90Y-microspheres, you have to use a surrogate for the pre-treatment testing, and this is not always predictive enough for the final outcome.
Having an individual treatment plan in place is crucial when combining treatments. This is not only true for PRRT, but also if we start combining immunotherapy or chemotherapy with radioembolization. This is really where the benefit of 166Ho-microspheres lies in comparison to the 90Y-microspheres.
How can other centres benefit from this combined treatment approach?
As with all innovation, study results need to be translated into clinical guidelines for reimbursement. In Germany and Belgium, 166Ho-radioembolization is already reimbursed specifically in the treatment of neuroendocrine tumours and liver metastases.
In the most recent US guidelines for neuroendocrine neoplasm patients with liver disease, PRRT is the standard of care. Radioembolization is listed as an option following the failure of systemic treatment such as PRRT, but is also considered investigational. We want to change that. This is the first step: we have shown that the combination is safe and effective in a prospective study; now we have to conduct a randomised controlled trial. If the outcomes of this concord with those of our present study, then I am convinced we will be able to change the guidelines and offer this combined treatment approach to patients with bulky liver disease.
Preliminary experience with 166Ho-radioembolization
Irene Bargellini (University of Pisa, Pisa, Italy) shares her early experience using 166Ho-microspheres (Quirem/ Terumo): “The initial cases we have performed have confirmed that there is something really interesting going on here that deserves more attention.
What drew you to 166Ho-microspheres?
Several interesting features attracted us to 166Ho-microspheres. Our physicists and nuclear medicine physicians in particular were very interested in the dosimetry—the idea of the scout dose (QuiremScout) was intriguing to them. The concept of being able to evaluate the distribution of the microspheres with MRI was also interesting to us.
How was incorporating 166Horadioembolization into your practice?
Initially, we had to set up a specific acquisition protocol for MRI and SPECT [Single photon emission computed tomography].
What therapeutic feedback have you got from using 166Homicrospheres?
We have treated 15 patients so far. In our limited experience, we have seen the majority of our patients responding much quicker than what we are used to seeing with 90Y microspheres. The lesions were already shrinking just 45 days post-procedure. In fact, two of our patients originally deemed to be non-surgical candidates had a resection and a transplant, respectively, after radioembolization with QuiremSpheres. The response might be so quick because 166Ho has a shorter half-life than 90Y, so the dose is deposited much quicker. This is the reason why we are currently using 166Ho-microspheres for patients that could be resected or transplanted after an adequate and fast tumour downstaging. In five patients, the Holmium scout dose (QuiremScout) was performed after an initial 99mTc-MAA diagnostic work-up, whose findings would have excluded the patients from treatment, due to high lung shunting in one patient and to heterogeneous 99mTc-MAA distribution within the tumours in the remaining four cases. In all 99mTccases, the scout dose provided different information that allowed us to safely and effectively perform Holmium radioembolization. We also try to use 166Ho-microspheres in patients with colorectal metastases, because so far we have not had very good results with 90Y in this cohort.
Mohamad Hamady (L), Oliver Llewellyn, and Neeral Patel
“Current evidence shows uterine artery embolization (UAE) is a safe and effective option to treat giant fibroids,” Oliver Llewellyn (Royal Infirmary of Edinburgh, Edinburgh, UK), Neeral Patel, and Mohamad Hamady (Imperial College NHS Trust, London, UK) et al conclude in Cardiovascular and Interventional Radiology (CVIR). They recommend that “patients should be selected, counselled, and managed accordingly” in order to benefit from this minimally invasive therapy and limit the “relatively higher risk of complications and reinterventions when compared with non-giant fibroids.”
Evidence supporting UAE for giant fibroids—defined as having a diameter of at least 10cm, and/ or with a uterine volume equal to or greater than 700cc—is sparse, according to Llewellyn and co-authors. They therefore performed a systemic review and meta-analysis of UAE outcomes for symptomatic giant versus non-giant fibroids to try and consolidate existing knowledge.
“This systematic review and meta-analysis of the current available data on the treatment of giant fibroids with UAE indicates there are several key factors required for the successful management of this unique cohort of patients,” Llewellyn tells Interventional News. “This includes close collaboration between gynaecology and interventional radiology colleagues, as well as careful follow-up in the post-procedure period.”
Primary outcome measures of the study were fibroid size, uterine volume reduction, procedure time, length of hospital stay, patent symptom improvement, reintervention rate, and complication rate. Following a systematic literature review, the authors extracted data from four relevant retrospective cohort studies, including a sum of 843 patients in their analysis. Of these, 163 (19.34%) had giant fibroids, and 676 (80.19%) had non-giant fibroids.
The main findings were:
UAE resulted in uterine volume reduction in both groups: patients with giant fibroids, 38.6%±16.2; non-giant fibroids, 37.5%±18.7. The difference between the groups was not significant.
Two studies indicated a statistically significant, but not clinically significant longer operative time for giant fibroids than non-giant fibroids (49±13.3 minutes versus 44.9±12.7 minutes, respectively, in one study, and 55.3±15.8 minutes versus 46.6±14.3 minutes; MD: 5.58 minutes; CI: 2.58–8.57; p=0.0003).
There was a statistically significant but not clinically significant longer hospital stay for the giant fibroid group, as reported in two studies (p=0.01).
Individually, included studies showed good overall patient satisfaction with the procedure, as well as effective postoperative symptom improvement, but meta-analysis was not possible.
All studies reported a higher reintervention rate when embolizing giant fibroids (odds ratio [OR]: 3.57; 95% CI: 1.7–7.49; p=0.0008).
Pooling analysis of all four studies found no significant difference in total postoperative complication rate associated with embolization of giant versus non-giant fibroids (OR: 1.45; 95% CI: 0.94–2.24; p=0.09).
The rate of major complications was relatively higher in the giant fibroid cohort (OR: 4.71; 95% CI:1.51–14.64; p=0.007).
Commenting on the reported major complication rate following embolization of giant fibroids, Llewellyn et al write: “Broadly, of the seven major complications within the giant fibroid group, three related to fibroid expulsion requiring reintervention/ endocavitatory transformation, three related to uterine infection, and one patient suffered sexual dysfunction post-UAE.” Complications can be minimised with meticulous post-procedure follow-up for women undergoing UAE for giant fibroids and dedicated management pathways for patients who present with uterine infection may expedite treatment in this patient group, subsequently reducing the requirement for emergency surgery.
Elaborating on the clinical implications of this research, Llewellyn says to this newspaper: “The results from this meta-analysis will allow interventional radiology clinicians to fully discuss the risk profile with patients in the clinic setting, allowing a fully informed decision to be made. Further work in this patient population includes a comparison with current surgical techniques such as myomectomy and hysterectomy, as well as standardising patient outcome measures for UAE, which will allow patient centred data to be pooled and compared, as has been achieved with the International Prostate Symptom Score (IPSS) for prostate artery embolization.”
While the study investigators conclude that UAE is safe and effective in the treatment of uterine fibroids of various sizes, they highlight “the heterogeneous methods used by included studies in assessing symptom severity and quality of life pre- and post-UAE”. None of the included papers used a validated measure such as the uterine fibroid symptom and health-related quality of life (UFS-QoL) questionnaire. Instead, each publication utilised their own local questionnaires, which Llewellyn and co-authors say “prevented direct comparison between studies”, missing a valuable opportunity to pool patient related outcome measures for UAE.
Cerus Endovascular receives FDA approval for its first microcatheter. The 021 microcatheter will be offered with three different distal configurations, and commercial sales are expected to begin during the second quarter of 2020.
According to a press release, the company will be developing additional microcatheters of various dimensions to offer a comprehensive selection of instrumentation for the needs of interventional neuroradiologists.
Moreover, the company announced it has successfully completed its Series B financing that has raised a total of US$19 million from current and new institutional investors since the commencement of the round in July 2018.
Completion of the Series B financing will allow the company to execute on its go-to-market strategy and to complete the planned expansion of its product portfolio, including a smaller delivery platform for its recently CE marked Contour Neurovascular System, for the treatment of intracranial aneurysms.
The company’s second implant device, the Neqstent aneurysm bridging device, is advancing through the regulatory process, with a clinical trial currently enrolling, aimed at providing additional safety and efficacy data. The Neqstent is designed to be used in conjunction with conventional embolic coils for endovascular embolisation of bifurcated saccular intracranial aneurysms.
February 2020 brings another paclitaxel device meta-analysis of randomised controlled trials in chronic limb-threatening ischaemia (CLTI) patients. Krystal Dinh (Westmead Hospital, Sydney, Australia) et al report online ahead of print the risk of all-cause mortality after treatment with paclitaxel-coated devices vs. uncoated controls in patients with CLTI in the Journal of Vascular and Endovascular Therapy (JEVT) very differently than did Katsanos and colleagues earlier this year.
Dinh and colleagues, including Ramon Varcoe (Prince of Wales Hospital, Sydney, Australia), Andrew Holden (Auckland Hospita, Auckland, New Zealand) and Peter Schneider (University of California San Francisco, San Francisco, USA) performed a systematic review on 5 November 2019 to identify randomised controlled trials using intention-to-treat analysis to compare a paclitaxel-coated device to an uncoated device in peripheral arterial disease patients having clinical follow-up of at least six months. Half of the study population had to have CLTI, or extractable data on the CLTI subgroup, if this constituted less than 50%, write the authors.
The search revealed 11 trials with 1,450 patients who were randomised to treatment with a paclitaxel-coated device (n=866) or an uncoated control (n=584). The group included 94.3% (1,367) patients with CLTI. The single endpoint was all-cause mortality, which was analysed by pooling the mortality data in a random effects model. Summary statistics are expressed as relative risk ratios (RR) with a 95% confidence interval (CI).
Ramon Varcoe
Importantly, Varcoe clarified that this meta-analysis included the five-year IN.PACT DEEP results that were overlooked by Katsanos and colleagues. Further, they included only studies that were published, or those that authors were able to confirm had been accepted for publication and were in press.
As described in JEVT, the mean follow-up was 25.6 months (range 6–60) and 10 of 11 studies reported a minimum 12-month follow-up. There were 18.6% (161) deaths in the 866 patients in the paclitaxel device group and 19.9% (116) deaths in 584 patients who received treatment with a non-coated devices (RR 0.93, 95% CI 0.78 to 1.12, p=0.45).
This led the investigators to conclude that “there was no observed difference in short- to mid-term mortality among a pooled patient population of predominately CLTI patients treated with paclitaxel-coated balloons or stents compared with uncoated controls”.
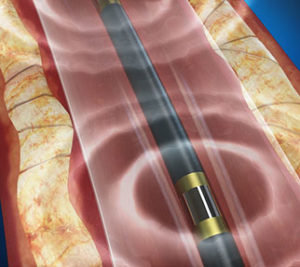
Ablative Solutions has announced that positive six-month results from the Peregrine post-market study demonstrating the safety and efficacy of the company’s CE-marked Peregrine System infusion catheter were published in the Journal of the American College of Cardiology: Cardiovascular Interventions.
The Peregrine post-market Study is a European multicentre open-label trial that evaluated additional safety and performance of the Peregrine System infusion catheter using a neurolytic agent (dehydrated alcohol) delivered into the space outside of the renal (kidney) arteries in 45 patients with systemic hypertension. Patients included in the study were taking at least three anti-hypertensive medications.
At six months, mean 24-hour ambulatory SBP was reduced by 11mm Hg, and diastolic blood pressure was reduced by 7mm Hg. Medication adherence was monitored and remained stable throughout the study. The primary safety endpoint, defined as absence of periprocedural major vascular complications, major bleeding, acute kidney injury, or death within one month, was met in 96% of patients (95% CI: 85–99%).
“Publication of the Peregrine post-market study results in a respected peer-reviewed journal is a significant milestone for Ablative Solutions and shows the potential of the Peregrine System to become an important adjunctive therapy for managing uncontrolled blood pressure in this large patient population,” said Kate Rumrill, president and chief executive officer at Ablative Solutions. “We are committed to robust clinical research through our ongoing Target BP clinical trials program to further substantiate the procedural, clinical, and health-economic benefits of the Peregrine catheter for the treatment of hypertension.”
In an accompanying editorial, Deepak L Bhatt and Arjun Majithia (Harvard Medical School, Boston, USA) noted that “although the Peregrine system will clearly need to be tested in a randomised, blinded, sham-controlled clinical trial environment, the study investigators should be complimented for using rigorous, contemporary methods including objective adherence measurements (urine toxicology analysis) and appropriate, clinically relevant endpoints (ambulatory blood pressure).”
Twelve-month results from the study presented last fall at the 2019 European Society of Cardiology (ESC) Congress (31 August–4 September, Paris, France) showed that the statistically significant reduction of 24-hour mean systolic ambulatory blood pressure measurement (ABPM) at six months was sustained at 12 months, providing evidence of consistent blood pressure-lowering effect. Twelve-month results also showed a reduction of mean systolic 24-hour ambulatory blood pressure of 10mmHg (±17mmHg, p=0.001) and a reduction in systolic office blood pressure of 20mmHg (±23 mmHg, p=0.001). No patients had major adverse events.
“Results from this trial show that the renal denervation procedure using the Peregrine Catheter and alcohol as a neurolytic agent may be safe and effective for lowering blood pressure in patients with poorly controlled hypertension on medications,” said Prof. Felix Mahfoud, Saarland University Hospital, Homburg, Germany. “The publication of these data further proves the potential value of the system for both physicians and patients. We look forward to further studying the investigational product in the randomised, sham-controlled TARGET BP clinical programme.”
Worldwide, hypertension affects more than one billion people. Management of hypertension often requires multiple medications. More than half of those treated with antihypertensive medications do not achieve their target blood pressure. High blood pressure can eventually lead to serious health problems such as heart attack, stroke and loss of vision. Approximately half of people with uncontrolled hypertension die of heart disease related to poor blood flow, and another third die of stroke.
The investigational Peregrine Kit, which includes the Peregrine System Infusion Catheter (Peregrine Catheter) and Ablative Solutions dehydrated alcohol, is currently being investigated in the TARGET BP clinical program which comprises two clinical trials. Data from the TARGET BP I and TARGET BP OFF-MED trials will be used to continue to advance the understanding of renal denervation.
At CRT 2019, (2–5 March (Washington, DC, USA) Horst Sievert (Sankt Katharinen Hospital, Frankfurt, Germany) shared early results of alcohol-mediated renal denervation, which were presented as a late-breaking abstract at the conference. Watch the video here.
Peter Schneider (San Francisco, USA) talks to BLearning Peripheral at LINC 2020 (Leipzig Interventional Course; 28–31 January 2020, Leipzig, Germany) about the relevance of dose relationship and geographical data when discussing the controversy surrounding the use of paclitaxel devices in peripheral arterial disease patients.
Schneider says that the key thing is to understand whether the relationship between paclitaxel and mortality is just an association” or “an actual causal relationship”. He notes that “if we have a dangerous agent on our hands”, it should be consistent in terms of being equally dangerous no matter where it is employed. However, Schneider highlights that looking at the data of paclitaxel-coated balloons in various countries has shown that there is “no signal” in Japan, “little or no signal” identified in the EU” and that the only signal seems to be related to the US, which Schneider describes as a “geographical inconsistency”.
Schneider believes that the importance of understanding these issues is of paramount importance and that as a physician he takes any signal on mortality “extremely seriously” but also does not want to leave “our most efficacious tool on the shelf gathering dust” if the risk is not significant.
The UK Royal College of Radiologists (RCR) has unveiled its new curricula for clinical radiology and interventional radiology. These are “based around a small number of high-level learning outcomes that describe the holistic capabilities needed for day-one consultant practice”, according to a press release.
The reshaped curricula reflect the General Medical Council’s Excellence by Design standards for postgraduate curricula. They replace the old extensive and granular lists of knowledge, skills and behaviours with concise outcomes and tables showing the presentations, conditions, and procedures that clinical and interventional radiologists in the UK need to be proficient in.
The curricula include a requirement to maintain general radiology skills alongside special interest or subspecialty practice, ensuring that all radiologists can meet changing patient and service needs. They also include a requirement for trainees to embrace and evaluate emerging techniques and technologies, such as AI and hybrid imaging.
All trainees will transfer to the new curricula by August 2020, except those due to achieve their Certificate of Completion of Training before September 2021.
Stephen Harden, Medical Director for Education and Training in Clinical Radiology at the RCR, says: “Under the new curricula, training activities on the hospital ‘shop floor’ will not be affected—what is changing is how trainee progress is monitored and how and when training requirements are deemed to be met fully.
“The expectation is that trainees will be able to deliver a broad range of care, as part of maintaining a generalist skill set.”
Under the current 2016 curricula, trainees are assessed against long lists of competencies. Under the new 2020 curricula, they will instead be judged against 12 high level capabilities in practice. Six of these describe generic capabilities that apply to all doctors, including areas such as ongoing professional and reflective practice, commitment to quality improvement, leadership and teaching and supervision abilities.
There are six radiology-specific capabilities in practice that describe the unique role of a radiologist, plus two additional capabilities for interventional radiology subspecialty trainees, which focus on the ability to provide high-standard interventional care to emergency and elective patients, and the ability to clinically manage all stages of a patient’s admission and treatment.
Assessment of the capabilities is based on intuitive entrustment scales that will support professional judgement and, along with progression grids, provides clear expectations for trainee progress.
Harden continues: “The idea behind the collated capabilities is that these rounded skills are what are expected of a new clinical or interventional radiologist on day-one of consultant practice.
“The new curriculum states much more clearly what is expected of—and to be demonstrated by—trainees, and makes clear to the public and the medical community just how broad the role of hospital radiologist is, around and beyond our core function of image interpretation.
“The inclusion of emerging technology and techniques future-proofs the curriculum and ensures that trainees are able to embrace new advances.”
The curricula and a package of key documents, implementation tools and supporting information are hosted on a dedicated section of the RCR website.
Robert Shahverdyan, head of the Vascular Access Center at Asklepios Klinik Barmbek, Hamburg, Germany, has recently published a retrospective analysis of his first 32 consecutive radiocephalic (forearm) VasQ External Support procedures in the Journal of Vascular Access. The paper demonstrated that using VasQ as standard of care for radiocephalic fistulas resulted in a significant improvement in his centre’s primary fistula failure and longer-term secondary patency rates with less repeat interventions when compared to historical controls.
Radiocephalic fistulas are the preferred vascular access to facilitate dialysis treatment as compared to other modalities despite the reported high rates of primary failure and need for frequent interventions. Historically, the primary fistula failure rate for radiocephalic fistulas at Shahverdyan’s centre before the use of VasQ was 29%, which compares well to the typically higher rates reported in the clinical literature for this type of fistula. That primary failure rate has dropped to 6% since he began using VasQ as the standard of care for his radiocephalic patients.
Additionally, his rate of repeat procedures required to make the fistulas usable dropped from 0.62 per pt-yr to 0.26 per pt-yr with VasQ. For context, typically reported rates for repeat procedure are between one and two interventions per pt-yr in Europe with rates in the USA reported at over three per pt-yr. His data aligns well with previously reported clinical studies for VasQ for upper arm fistulas and shows that the adoption of VasQ as the standard of care improved patient outcomes of an already high performing centre.
Shahverdyan commented: “Haemodialysis patients are a particularly challenging patient population with historically poor outcomes related to vascular procedures. As surgeons we must be skeptically optimistic about any new technology that promises better outcomes for our patients until we see it perform in a real-world setting. After careful review of my results over the last few years, I was excited to learn of the beneficial impact VasQ has had on my haemodialysis patient outcomes and am happy that I can offer them a better option with VasQ as my new standard of care for their vascular access.”
“The results from Shahverdyan’s practice is a significant step forward for Laminate to meet our goal of providing surgeons tools to create more usable fistulas,” said Laminate CEO Tammy Gilon. “We are excited to continue to partner with physicians like Shahverdyan as they work to create functioning fistulas for each of their patients.”
Left to Right: Julius Chapiro, Leigh Casadaban and Luigi Solbiati during the Hackathon Winner Announcement Ceremony at the SIO Annual Meeting 2020 in New Orleans, USA.
The Society of Interventional Oncology (SIO) hosted its first artificial intelligence (AI) hackathon at this year’s annual meeting (31 January–3 February, New Orleans, USA). Out of 11 international contestants, Leigh Casadaban (Brigham and Women’s Hospital, Boston, USA) won the competition for her project entitled “Feasibility study of deep learning convolutional neural networks to predict clinical benefit of transarterial radioembolization using pretreatment CT and SPECT imaging”.
“Our study plans to look for imaging or patient/treatment factors that predict outcome after transarterial radioembolization (TARE) with Yttrium-90 (Y-90) microspheres,” Casadaban explains. “Our hypothesis is that the deep learning system using 3D treatment planning data will outperform standard dosimetry estimates in predicting progression-free survival.”
Julius Chapiro (Yale School of Medicine, New Haven, USA) from the SIO Research Committee hosted and moderated the AI hackathon, which was funded with unrestricted grants from Guerbet and Visage Imaging. This novel type of session gave the opportunity to 11 international teams to pitch their pre-selected proposals to a jury panel, composed of international interventional oncology (IO) experts and industry representatives. The jury evaluated the proposals on the criteria of healthcare impact, innovation, translatability to product, and presentation. Each five-minute pitch presented “AI-driven research project proposals with high translational value”. The proposed projects all offered AI-based solutions to a specific clinical problem in IO, and presentations were followed by one minute of questioning from the judging panel.
Speaking to Interventional News about her win, Casadaban says: “I am happy to have won the hackathon because it validates our project idea. The prize money also helps us to afford software and hardware for data processing, and for our data scientists and software engineer collaborators.”
Some of the US$7,000 prize money will go towards a new computer with imaging software to process images, Casadaban shares, as well as statistical software for data crunching. The rest will go towards the Brigham and Women’s Hospital and Massachusetts General Hospital Center for Clinical Data Sciences, which hosts data scientists, software engineers, and clinicians working to solve healthcare problems.
AI hackathon “incredibly powerful” format in a quickly evolving field
“The hackathon was a fun format,” Casadaban says, as it is “different from other formal talks, in that presenters stood directly in front of the judges, not behind a podium”. She continues: “We had five minutes to ‘pitch’ our idea before the buzzer went off. I think the format made the session fun and exciting.
“AI already influences many things around us, and is incredibly powerful. The field is evolving quickly, and an event like this raises awareness of new developments and tools, encourages brain storming, and also enables IO projects to get their feet off the ground. We have just started to scratch the surface of how AI can improve our clinical practice. The opportunities are boundless.”
“We did not expect to collect so many excellent proposals as the AI hackathon was announced on very short notice”, says Chapiro. “The number of excellent and mature proposals and the great variety of different scientific questions raised during our session clearly illustrates the untapped potential of our community and the need for funding of structured machine learning-driven research. With this format, we can mobilise the IO community to enter the era of data science”. The SIO confirmed plans to make the AI hackathon a recurring session for upcoming meetings, including during the next SIO annual meeting, which will take place in San Francisco, USA, in January 2021.
Sirtex Medical has announced a collaboration with MIM Software. Under the terms of the agreement, Sirtex’s sales teams in the USA, Europe, and other key global markets will offer MIM SurePlan LiverY90 software alongside the company’s SIR-Spheres Y-90 resin microspheres to improve treatment precision for patients with hepatic tumours.
According to a company press release, MIM SurePlan LiverY90 provides timesaving tools and post-treatment dosimetry for interventional radiologists and nuclear medicine physicians treating hepatic tumours with SIR-Spheres. The software allows physicians to calculate the dose delivered by the microspheres to improve treatment decisions and patient care. The technology also incorporates CT, PET, SPECT and MRI scans simultaneously to deliver results on spheres deposition, coverage, and absorbed dose.
“Given the overlap of their technology and our SIR-Spheres product, Sirtex and MIM have a long history of working alongside clinical care teams,” comments Kevin Smith, Chief Executive Officer of Sirtex. “Now as partners, we will be able to combine our expertise and resources to provide an even higher level of support to treat liver tumours. We are excited to see how this collaboration will benefit physicians and ultimately improve treatment outcomes for patients.”
“We are proud and excited to partner with Sirtex, mainly because it will provide access to personalised dosimetry for a large number of patients across the globe,” says Andrew Nelson, Chief Executive Officer of MIM Software. “The treatment of liver tumours requires a multi-disciplinary approach, so it is a natural evolution for companies like ours to partner to provide an even faster, higher level of support and resources to treatment teams.”
In the USA, SIR-Spheres Y-90 resin microspheres received Premarket Approval (PMA) from the US Food and Drug Administration (FDA) and are indicated for the treatment of non-resectable metastatic liver tumours from primary colorectal cancer in combination with intrahepatic artery chemotherapy using floxuridine. SIR-Spheres Y-90 resin microspheres are approved for the treatment of inoperable liver tumours in Australia, the European Union, Argentina, Brazil, Canada, and several countries in Asia, such as India and Singapore.
Sean Lyden (Cleveland, USA) talks to VEITHtv at the VEITHsymposium 2019 (19–23 November, New York, USA) about the “tumultuous” year for the industry following the publication of the 2018 Katsanos meta-analysis which showed an increased mortality risk with the use of paclitaxel-coated balloons at five-years in intermittent claudication patients.
Despite FDA analysis which indicated that there “was something to this signal”, Lyden explains that that the Katsanos meta-analysis “did not have patient-level data” and says VIVA Physicians’ findings saw the FDA’s 58% mortality signal fall to 27% through five-years. Lyden goes on to discusses his views on the inconsistent data and how it might affect practitioners, outlining the need for “informed consent” from patients.
“We have seen a huge downturn in the use of paclitaxel” says Lyden, adding however that there is now “a light at the end of the tunnel” with the FDA, regulators, physicians and industry all partnering to decide on the next steps including looking at “improving trial design”.
Dierk Scheinert (Leipzig, Germany) moderates a panel with Eva Freisinger (Münster, Germany) and Thomas Zeller (Bad Krozingen, Germany) to discuss the developments over the past 12 months surrounding the safety of paclitaxel.
Zeller notes that further analyses of the randomised controlled data of drug-coated device use in claudicants has indicated a lower risk of mortality. Importantly, he states that the addition of patient-specific data information, as requested by the US FDA, has highlighted a “significant reduction” in the overall risk. Zeller adds that with the inclusion of large real-world data analysis with appropriate sample size, the mortality risk totally disappears. He goes on to highlight his own centre’s findings of more than 1,500 patients suffering claudication or rest pain, split between a control group and those treated with a drug-coated balloon (DCB). The “major finding” of this comparison was a mortality benefit favouring the DCB approach, which Zeller notes contradicts the Katsanos et al findings in a real-world setting.
Freisinger discusses her team’s analysis of a real-world dataset which included insurants from German company BARMER Health Insurance. The findings showed “no evidence of a long-term mortality signal” at 7.6 years and a “slight beneficial signal” favouring DCB use. She outlines some of the study’s strengths, but cautions that there is “no study without limitations”.
Zeller maintains that it is important to complete the long-term follow-up of current trials, which he believes “will tell us that there is no real mortality issue”. He finally addresses Katsanos et al’s most recent meta-analysis (January 2020, Journal of Vascular and Interventional Radiology) – which he claims has “many limitations” – of DCB versus plain balloon angioplasty in below-the-knee lesions, which suggests a higher mortality in the short-term. This, according to Zeller, goes against the grain of the original findings which only showed a signal in the long-term.
Both Zeller and Freisinger conclude by agreeing that they will continue to use paclitaxel-coated devices, and Scheinert, for his part, says this new real-world safety data is “reassuring”.
Bluegrass Vascular Technologies (Bluegrass Vascular) announced today that the US Food and Drug Administration (FDA) has granted a de novo classification order for its Surfacer Inside-Out access catheter system. The Surfacer system is intended to obtain central venous access to facilitate catheter insertion into the central venous system for patients with upper body venous occlusions or other conditions that preclude central venous access by conventional methods. The Surfacer system employs a novel Inside-Out approach.
“The Surfacer system offers a safe and effective approach to reliably preserve and restore critical upper body vascular access sites,” stated Mahmood Razavi, interventional radiologist at St. Joseph Hospital in Orange, USA and lead principal investigator of the SAVE-US (Surfacer system to facilitate access in venous Occlusions—United States) IDE study. “This is an unmet clinical need for patients who require life-saving therapies, such as dialysis, and who have limited options due to venous obstructions.”
The Surfacer system is the first FDA cleared medical device to facilitate upper body central venous access in patients with venous obstructions or other conditions that preclude access by conventional methods. Approval is based on the results of the SAVE-US trial. Of the thirty enrolled patients, 90% met both the primary and secondary efficacy endpoints despite a complex patient population comprised largely of Type 3 and 4 obstructions (3 or more obstructed vessels). No device related adverse events were reported, confirming the safety and performance of the Surfacer system.
“Thoracic central venous obstruction (TCVO) is a costly problem associated with increased patient morbidity and reduced quality of life,” stated Bart Dolmatch, interventional radiologist at The Palo Alto Medical Foundation (Palo Alto, USA). “We have recently published reporting standards that create a common language for understanding and describing signs, symptoms, functional impairment, and anatomy of TCVO. BVT incorporated elements of these reporting standards into the SAVE-US trial, demonstrating the clinical impact of the Surfacer system. Now that it has been FDA cleared, the Surfacer will be part of the treatment algorithm for my patients with TCVO.”
Thoracic central venous obstruction occurs in roughly 40% of patients where haemodialysis is performed via a central venous catheter. While permanent arteriovenous fistulas are the preferred form of vascular access for haemodialysis patients, central venous catheters continue to serve as an important bridge to securing long-term access for life-saving haemodialysis treatment. The current approach for most patients with central venous obstructions is to use an alternative vein, which reduces the ability to place and mature a functioning fistula, resulting in increased catheter days and costs.
Rist Neurovascular recently announced that it has received US Food and Drug Administration (FDA) 510(k) clearance to market the Rist Cath Radial Access Long Sheath (Rist Cath) for the introduction of interventional devices into the peripheral, coronary, and neurovascular system.
Rist Cath is the first device specifically designed for the unique demands of accessing the neurovasculature through the radial artery in the wrist, enabling the full gamut of neurovascular procedures to be performed transradially.
“Although transradial techniques have become the standard of care in the cardiac interventional communities, neurointerventionalists have not previously had the appropriate tools to allow these advantages for patients undergoing neurovascular procedures,” said Pascal M Jabbour, professor of neurological surgery and chief of the Division of Neurovascular and Endovascular Neurosurgery in the Department of Neurological Surgery at the Sidney Kimmel Medical College at Thomas Jefferson University (Philadelphia, USA).
He continued: “Clearance of the Rist Cath provides neuroendovascular specialists a safe and durable tool to perform neuroendovascular interventions via a transradial approach, and allows us to offer improved care for patients while pushing the envelope of what our field has to offer.”
“The Rist Cath was developed to meet a well-documented need expressed among physicians conducting neurovascular surgeries,” said Martin Dieck, director, Rist Neurovascular. “This FDA clearance will allow us to make the Rist Cath broadly available to these surgeons, improving care for the millions of patients undergoing procedures to treat conditions such as stroke, brain aneurysms and other neurovascular conditions.”
While the American Heart Association has recommended a radial-first strategy for acute coronary syndrome since 2018, there has never before been a FDA cleared device that enabled the use of this strategy specifically for neurointerventional procedures.
Cardiology studies have demonstrated a significant reduction in access site complications as well as mortality with radial access. Furthermore, radial access procedures offer several additional advantages, including strong patient preference, immediate ambulation, and reduced costs.
At the International Stroke Conference 2020 (18–21 February), being held in Los Angeles, USA, there will be several presentations exploring the benefits of radial access for neurointerventional Surgery.
XableCath has announced that its XableCath Crossing catheters have received CE mark for peripheral use. Its crossing devices will be available for sale in Europe in two versions, a blunt tip and an abrasion tip, in a variety of diameters and lengths. XableCath received US Food and Drug Administration (FDA) clearance for its crossing devices last year.
Physicians in the USA have had remarkable success using the XableCath Crossing devices to cross challenging lesions in the peripheral vasculature. The product has been used to successfully cross recalcitrant chronic venous obstructions, including what is considered by many clinicians to be the most challenging venous procedures—crossing in-stent restenosis.
“I am pleased XableCath intravascular products continue to demonstrate a high degree of safety and effectiveness crossing a variety of challenging lesions successfully in both venous and arterial disease. Our devices have helped many patients and physicians in the U.S. Now that we have achieved CE mark, we will be able to offer our crossing solution to help patients and healthcare providers in Europe.
In a time where the vast majority of new products are more costly and complex than the technologies they propose to displace, it is especially fulfilling to our team to bring a new product to market that is easy to use, effectively crosses occlusions, and more favorably priced than the existing crossing devices. Economic pressures on our global healthcare system are tremendous and XableCath Crossing devices were conceived to improve patient care at a lower overall procedural cost, which I believe we have achieved,” said XableCath president and chief executive officer, Lisa Dunlea.
“With a CE mark, we look forward to bringing this wonderful, easy to use, and highly applicable interventional device into our Neu-Bethlehemcath-lab in Germany. Our centre conducted the first-in-man studies using the device to recanalise very challenging lesions in patients with no other interventional options and critical limb ischaemia. I am excited to bring it back more fully into my lab to help me and my patients,” said Johannes Dahm, professor of Medicine-Cardiology-Angiology in Göttingen, Germany.
Laminate Medical Technologies has announced the completion of enrolment into the VasQ external support US pivotal study. The study was conducted at 17 sites across the USA and prospectively enrolled 144 male and female patients in need of an arteriovenous fistula (AVF) for haemodialysis. Both brachiocephalic and radiocephalic AVF patients were included in the study. The patients will be followed for two years with the primary endpoint of primary patency analysed at six months.
AVFs are the preferred vascular access to deliver haemodialysis treatment due to the low rates of infection and mortality relative to alternative options for patients. However, the natural biologic responses to the changes in haemodynamics and mechanical stress at the vein wall from the arterial flow tends to induce in inward tissue growth and ultimately AVF failure. Reported failure rates for AVFs are as high as 60% and require costly additional procedures to correct or a new AVF creation altogether.
VasQ is designed to address both the haemodynamic and mechanical factors associated with AVF failure. The device is a nitinol external support placed around the artery and vein at the creation site that optimises the transition of arterial flow to the vein while reinforcing the vessel wall against the increase in mechanical stress. VasQ patients in Europe have demonstrated increased rates of receiving a usable AVF with fewer early failures and additional procedures in multiple prospective and retrospective studies. The clinical benefits of VasQ experienced in Europe are expected to be validated in the US dialysis patient population within this fully enrolled pivotal study.
Ellen Dillavou of Duke University (Durham, USA) stated: “VasQ promises to be a new standard of care for fistula creation to give my haemodialysis patients the greatest probability of success. The device has performed as expected in my study patients so far, and I look forward to continue to utilise it once commercially available in the USA.”
“We are grateful to our principle investigators for their commitment to this study,” said Laminate CEO Tammy Gilon. “The results will be an important addition to the mounting evidence supporting the benefits of VasQ to promote the usability of both forearm and upper arm fistulas.”
The first head-to-head randomised controlled trial to directly compare two different drug-coated balloons—the lower-dose density (2μg/mm2) Ranger and higher-dose density (3.5μg/mm2) IN.PACT—showed similar results with regard to effectiveness and safety through 12 months for femoropopliteal interventions, Dierk Scheinert (Leipzig, Germany) tells BLearning at LINC 2020.
A proof-of-concept study has demonstrated the feasibility of using computed tomography (CT) with a novel composition of radiopaque microspheres in Yttrium-90 (Y-90) radioembolization to determine tumour radiation dose exposure. Presenting these early results at Spectrum (18–21 January, Miami, USA), Robert Abraham (Dalhousie University QEII Health Sciences, Halifax, Canada), told delegates that this technique “may provide increased confidence in the true spatial distribution of the microspheres, and hence the distribution of Y-90 activity in tumour”.
Outlining his hopes for Y-90 based CT radiopacity, Abraham said he thinks it “may improve characterisation of the absorbed dose heterogeneity in radioembolization”, and “may improve our understanding of the relationship between absorbed dose and tumour response, which could ultimately translate into improved patient outcomes.”
Using a proprietary blend of non-irradiated radiopaque Y-89 glass microspheres (30µm in diameter), Abraham described how the investigators injected 480mg through a 0.021” Cook Cantata microcatheter into the segmental arteries in the left kidney of a hybrid farm pig. Following sacrifice, the kidney was explanted and imaged by conventional CT scan. Three-dimensional convolution of the activity distribution with a validated Y-90 dose point kernel was implemented to produce a high-resolution dose distribution.
“The dose distribution images in the axial plane using MATLAB software simulates the effect of increasing microsphere deposition,” Abraham stated, showing the Spectrum audience five axial CT images of the left kidney with increasing amounts of deposited microspheres. “As you can see, from left to right, as you increase the quantity of microspheres that are deposited in the tissue, the radiopacity increases accordingly”, he shared. Indeed, there is a linear relationship between CT Hounsfield Units (HU) and microsphere concentration per CT voxel, according to previously published work by ABK Biomedical.
Explaining the implications of this relationship between increased deposition and increased radiopacity, he continued: “Using the specific activity at the time of administration, we could potentially convert radiopacity threshold maps to dose threshold maps.” As increased deposition of microspheres correlates with an increased dose, Abraham described how it is possible to build a colour map depicting specific thresholds. “For example, here we used a threshold of 210Gy which some studies have suggested is a minimum target threshold in order to obtain tumour kill with glass Y-90. Based on radiopacity mapping and conversion to dose we may be able to confirm a minimum of 210Gy in the target tissue” he said, again showing a CT scan of the left kidney coloured according to dose.
Turning to future work, Abraham said: “We are doing ongoing studies on different compositions that have been developed. We will evaluate the potential of CT dosimetry with both cone beam CT, to allow intraprocedural dosimetry, as well as post-procedural conventional CT. We will also be commencing a hypervascular tumour model trial with activated Y-90 product. This will compare CT radiopacity-based dosimetry with time of flight PET [positron emission tomography] dosimetry.”
ABK Biomedical products are not approved for clinical use; the radiopaque microspheres are strictly investigational.
Abraham is a co-founder and shareholder of ABK Biomedical Inc., co-inventor of ABK’s proprietary investigational products, and serves as ABK’s Chief Medical Officer.
Kenneth Ouriel (New York, USA) talks to BLearning Peripheral at LINC 2020 (Leipzig Interventional Course; 28–31 January 2020, Leipzig, Germany) about a recent independent analysis to assess safety outcomes of femoropopliteal drug-coated balloon (DCB) angioplasty using patient-level data from the Lutonix clinical programme—and further studies looking at data with the IN.PACT DCB and Stellarex DCB.
This particular independent analysis, explains Ouriel, included an oncologist on the review committee to re-examine the adverse events and deaths in order to determine if these were related to paclitaxel. The findings of this review committee found that the deaths “appeared not to be related to the paclitaxel” but rather other patient issues like heart disease or lung cancer caused by smoking for example.
Ouriel concludes that he believes it was the trial design and a “failure to follow patients through five years” rather than a problem with the drug which led to the mortality signal described by Katsanos et al in the 2018 meta-analysis. He adds that he is “95% sure that what we see is not related to a few milligrams of a drug that the oncologists have been using for a long time”.
Medtronic has announced that it will begin enrolment in a pilot study evaluating the safety and efficacy of the Symplicity Spyral renal denervation (RDN) system using a targeted procedural approach with a reduced number of radio frequency (RF) ablations. Set to enroll 50 patients at up to 15 sites in the USA and Europe, the single-arm study is designed to focus on ablating the distal main renal artery and primary branches to lower blood pressure utilising a simplified procedural approach.
“In depth anatomical study indicates the renal nerves are closer to the renal artery in the distal renal artery and branches. Focusing the procedure on these targeted locations may help us understand if we can achieve meaningful blood pressure reductions more efficiently,” said Andrew Sharp, interventional cardiologist at the University Hospital of Wales, in Cardiff, UK, and co-principal investigator of the SPYRAL DYSTAL study. “Early evidence using this modified approach has been encouraging and we intend to build on that data with the DYSTAL study.”
Renal denervation is a minimally invasive procedure intended to regulate overactivity of nerves that lead to and from the kidney, which play an important role in controlling blood pressure.
“As we strive to build upon the rigorous renal denervation studies within the SPYRAL HTN clinical programme, the DYSTAL study will help inform how we can fine-tune the procedure and continue to address the unmet need in hypertension management,” said Dave Moeller, vice president and general manager of the Coronary and Renal Denervation business, which is part of the Cardiac and Vascular Group at Medtronic.
Spyral HTN-OFF MED pivotal trial data at ACC.20
Results from the SPYRAL HTN OFF MED pivotal trial will be presented as a late-breaking clinical trial at the American College of Cardiology 69th Annual Scientific Sessions on 29 March, 2020, in Chicago, USA. The prospective, international, randomised, sham-controlled study is investigating the blood pressure lowering effect and safety of renal denervation with the Symplicity Spyral system in the absence of medication.
“Medtronic is committed to realising the full potential of renal denervation, and we look forward to the highly anticipated results of the SPYRAL HTN-OFF MED Pivotal Trial to be unveiled at ACC in March,” said Moeller.
In addition to the SPYRAL DYSTAL Study, the Medtronic SPYRAL HTN Global Clinical Program includes the SPYRAL HTN-OFF MED Pivotal and SPYRAL HTN-ON MED trials, both prospectively powered, randomised, sham-controlled studies evaluating patients with uncontrolled blood pressure in the absence and presence of prescribed anti-hypertensive medications, respectively. The program also includes the real-world GLOBAL SYMPLICITY REGISTRY that has enrolled over 2,700 patients with the Medtronic Symplicity RDN system, including 600 patients with the Symplicity Spyral catheter.
Approved for commercial use in more than 50 countries around the world, the Symplicity Spyral system is limited to investigational use in the USA, Japan, and Canada.
IR practice has changed significantly from diagnostic radiology, and interventional radiologists are in practical terms image-guided surgeons. Within the Royal College of Radiologists (RCR), IR is almost identical to Clinical Oncology in terms of its pattern of practice: it is a predominantly procedural specialty, the main purpose of which is to offer treatment. Although imaging remains at the heart of IR, images are primarily for guidance rather than diagnosis. Interventional radiologists must have the confidence and ability to see patients before treatment in order to consent them appropriately and discuss all options with them; in order to do that well, they need to have sufficient clinical knowledge, including a good understanding of what other specialties have to offer for the same condition.
Interventional radiologists need to have the confidence and ability to take primary responsibility for the patient during the treatment episodes, and interventional radiologists need to follow up their own patients; if they do not things will go wrong. In order to do this, interventional radiologists require better training in clinical practice and procedures than is possible under the current system. As with surgery, interventional radiologists need training in clinical and interventional techniques. Currently, however, the training of interventional radiologists is patchy, and results in huge knowledge gaps that potentially compromise patient safety. We of course have stringent requirements about knowledge in imaging, but no formally defined comprehensive requirements for IR procedures. The focus of training and examinations for future interventional radiologists therefore still involves having to know the detailed characteristics of imaging for cases they will likely never see once they leave FRCR [Fellow of the Royal College of Radiologists], such as certain rare bone tumours, but does not necessitate having an intimate knowledge of clinical management, techniques, procedures, and equipment, such as microwave or radiofrequency equipment that the interventionalist may use several times per week.
Many trainees who might be considering a career in IR are put off applying as they still see radiology as predominantly an imaging specialty, particularly those with a surgical interest. Trainees spend much of their time in the first three years doing few or, in many cases, no IR cases at all.
An IR specialty would result in a better-defined training, assessment, and career path for interventional radiologists, and the College would be in a better position to define the numbers of interventional radiologists required in hospitals and regions. The benefit and success of an IR specialty has been shown in the USA, where it is the country’s most sought after specialty.
Specialty of course would not only improve individual training; it would also help workforce planning, and ultimately allow provision of a national 24/7 service. There are currently no defined IR numbers, so it is impossible to undertake workforce planning, with huge implications for providing 24/7 IR care. Approximately, only one in seven units is currently able to provide a comprehensive lifesaving out-of-hours service in the UK. Without a specialty, workforce planning is not possible, because there is no generally accepted definition of who is and who is not an interventional radiologist. This does not mean that radiologists who do not belong to the IR specialty would be precluded from performing certain procedures, in the same way that radiologists can do endoscopy without being gastroenterologists. Nobody would be disenfranchised, as long as they have the required skills. In fact, it is vital that interventional radiologists are available in all hospitals and settings. Drainages and biopsies will remain a core radiology procedure, with interventional radiologists also having additional training to undertake more complex and varied interventions.
The RCR is the natural home of IR, with key shared competencies and interests in patient care. With the overwhelming vote endorsing the proposal to set up an IR specialty at the annual scientific meeting of the British Society of Interventional Radiology (BSIR) in November 2019 (see above), we now have a mandate from members to approach the RCR in taking the next steps in the creation of a new specialty. The process for the creation of a new specialty is not going to be quick, easy, or straightforward. It will be necessary not only to get the full backing of the RCR, but to obtain four-nation support from various relevant bodies—for example: NHS Improvement, NHS Employers, Scottish Association of Medical Directors, Health Education England, NHS Education for Scotland, Health Education and Improvement Wales, Northern Ireland Medical and Dental Training Agency. With this support, we should then be able to get endorsement from the UK Medical Education Reference Group (UKMERG), and then submit an application with UKMERG endorsement to the Department of Health. The decision of course will ultimately be made by the privy council. There have already been some informal discussions with the General Medical Council (GMC) last summer, and more formal discussions are planned for early in 2020. To achieve specialty status, we will need strong support from many quarters, but ultimately a lot of time and hard work will be essential from many colleagues to succeed in completing this process and achieve specialty status.
Raman Uberoi is a consultant interventional radiologist and Honorary Senior Lecturer at the John Radcliffe Hospital, Oxford, UK. He is a past president of the British Society of Interventional Radiology, and is running for vice president of the Royal College of Radiologists in the UK.
With an increasing number of interventional radiologists turning their technical and clinical expertise to musculoskeletal embolization, Sandeep Bagla and Abin Sajan believe it is important to have a thorough understanding of the anatomy specific to these procedures. Here, they detail the genicular artery anatomy, in the hope that increased physician familiarity translates into an increased ability to treat patients with challenging vasculature.
In an era of cutting-edge interventional procedures, genicular artery embolization (GAE) is a minimally invasive solution for patients with mild to moderate osteoarthritic (OA) knee pain. The primary goal of GAE is to disrupt the inflammatory process by embolizing the hypervascular synovium causing the pain and disability. Successful preliminary results in pilot clinical studies have fostered a randomised control trial (RCT) at the Vascular Institute of Virginia and UNC Chapel Hill, which has finished recruitment and we hope to present our findings at the annual meeting of the Society of Interventional Radiology (SIR) next year (28 March–2 April, Seattle, USA).
As the popularity of GAE increases, it is important to have a thorough understanding of the genicular arterial anatomy. The success of GAE, as well as the prevention of non-target embolization, is associated with recognising patterns on the initial angiogram and anticipating potential obstacles during the procedure. Possible anatomic challenges include variable presence of vessels, small sized vessels, acutely angled vessel origin, presence of atherosclerosis, and collateral supply. Familiarity with typical patterns and an understanding of angiographic relationships provide a dynamic foundation when presented with challenging anatomy.
Figure 1 (left) and Figure 2 (right): Angiography at the level of the upper and lower knee. Descending Genicular Artery (A) divides classically in to Saphenous Branch (G) and Articular Branch (H). The Superior Medial Genicular Artery (B) and Superior Lateral Genicular Artery (D) typically have a reversed curve origin from the popliteal artery. The Inferior Medial Genicular Artery (C) demonstrates its classic J shaped pattern and the Inferior Lateral (E) may arise at, or in this case, slightly below the joint. The Anterior Tibial Recurrent (F) originates from the proximal Anterior tibial artery as displayed.
We reviewed the angiographic patterns from our first two clinical trials to identify the basic arterial anatomy and review technical pearls for the procedure. We identified six main arteries: descending genicular artery (DGA), medial superior genicular artery (MSGA), medial inferior genicular artery (MIGA), lateral superior genicular artery (LSGA), lateral inferior genicular artery (LIGA), and anterior tibial recurrent artery (ATR). Since osteoarthritic knee pain can be lateralised to either the medial or lateral aspect of the knee, we present the anatomy using the same approach (Figure 1). Of note, other vessels, including the median genicular artery, contribute to the knee joint but were not included in our study.
The medial compartment of the knee is mainly perfused by the DGA, MSGA, and MIGA. The DGA originates from the distal superficial femoral artery and has a classic inverted “Y” appearance. It divides into a straight medial saphenous branch which courses superficially, and a more torturous lateral musculoarticular branch which courses deeper in the knee.
The MSGA arises from the proximal-mid popliteal artery just above the medial femoral condyle and classically courses superiorly before travelling down to the medial knee joint. Although the MSGA is often difficult to visualise given its smaller calibre, we have noted that the luminal size of the MSGA is inversely related to the size of the DGA. The MIGA originates from the popliteal artery near the joint space and descends along the upper margin of the popliteus, before coursing anteriorly and superiorly, creating an angiographic “V” around the medial tibial condyle. The MIGA arises adjacent to the sural arteries, which are distinguished by their steeper trajectory towards the gastrocnemius musculature.
The lateral compartment of the knee is mainly perfused by the LSGA, LIGA, and ATR. The LSGA arises from the mid-popliteal artery at the level of the lateral femoral condyle. Like the MSGA, it initially courses superolateral before travelling down to the lateral knee joint. The LIGA originates around the joint space and courses laterally above the fibular head before wrapping around the lateral tibial condyle, creating a “J” appearance. In addition, this reversecurved vessel may share a common trunk with the SMGA, making catheterisation more challenging. The ATR is the most inferior branch supplying the knee and originates from the very anterior tibial artery just beyond its origin.
Although the six arteries are typically present in all patients, absence of one or more arteries might suggest that another artery is more dominant in the affected compartment. Additionally, collateral supply can cross the joint space and embolizing in such cases can lead to non-target embolization of the asymptomatic side. Cutaneous branches often appear perpendicular to the main genicular artery and terminate at the skin surface. Skin purpura from embolizing these vessels is the most common side effect of GAE, and an attempt should be made to deliver particles distal to cutaneous branches, however this may be challenging given their ubiquitous presence. Ice-packs placed on the skin may minimise the risk of non-target related cutaneous changes.
The most technically challenging aspect of GAE is catheterising the acutely angled vessel origins (Figure 2). Wire placement can be challenging in the first 3cm, and wires with a floppy tip may not allow ample support during catheterisation. In our experience, a 2.4F microcatheter was adequate in catheterising these arteries. However, there is a role for pre-shaped microcatheters, especially in acutely angled vessel origins, most notably the SMGA and the SLGA.
GAE is an exciting procedure that is leading the way for musculoskeletal embolization. We believe that a thorough understanding of the angiographic anatomy and knowledge of commonly encountered challenges will increase interest in GAE and promote future cutting-edge interventional procedures.
Sandeep Bagla is the chair of Interventional Radiology at the Vascular Institute at Virginia, Woodbridge, USA. For his GAE clinical studies, Rachel Piechowiak and Ari Isaacson are coinvestigators.
Abin Sajan is a medical student at the State University of New York (SUNY) Downstate College of Medicine, New York, USA. He was awarded the SIR Dr and Mrs WC Culp Student Research Grant for his work on the “Cadaveric Classification of the Geniculate Artery Anatomy”. He is working with Maziar Sighary on the cadaveric studies.
For some patients, kidney cancer can be effectively treated without surgery, according to the Society of Interventional Radiology’s first-ever position statement on the role of percutaneous ablation in the treatment of renal cell carcinoma (RCC). The position statement was published with an accompanying quality improvement document, which establishes performance thresholds for patient safety for interventional radiology (IR) groups who wish to develop a renal ablation practice.
The position statement and quality improvement document, published in the February issue of SIR’s flagship Journal of Vascular and Interventional Radiology (JVIR), were written by a multidisciplinary group of experts, including interventional radiologists and urologists. They were endorsed by the Canadian Association for Interventional Radiology (CAIR) and the Society of Interventional Oncology (SIO).
The authors recommend thermal percutaneous ablation for kidney cancer patients with small renal tumors, calling it “a safe and effective treatment with less [sic] complications than nephrectomy [surgery] and acceptable long-term oncological and survival outcomes.” Unlike current existing guidelines, the position statement offers recommendations on the consideration of treatment over active surveillance and discusses the incorporation of ablation for appropriate patients with T1b disease.
“Interventional radiologists are critical members of the multidisciplinary team caring for patients with kidney cancer. They have an important role, not only in the diagnosis of cancer but in its definitive treatment,” says SIR president Laura Findeiss, (Grady Hospital and Emory University School of Medicine, Atlanta, USA). “An image-guided biopsy by an interventional radiologist can confirm a diagnosis of cancer, and the interventional radiologist can be a game-changer as a partner physician on the cancer care team, expanding access to the complete range of therapeutic options, tailored to the individual patient.”
Lead author of the quality improvement document Andrew Gunn (University of Alabama, Birmingham, USA) elaborates: “These documents should expand the interventional radiologist’s approach in recommending image-guided ablation for renal cancer. First, there is sufficient evidence to suggest that image-guided ablation has nearly equivalent oncologic outcomes to traditional surgery for tumours up to 4cm in size. Additionally, ablation has fewer complications and is less detrimental to renal function than surgery. Second, there is increasing evidence that ablation can be performed for curative intent in tumours up to 7cm. While surgery is still the preferred approach for tumours this size, many patients cannot or will not undergo traditional surgery. Therefore, interventional radiologists can now recommend ablation in this patient population with more confidence.”
The position statement’s authors deemed radiofrequency ablation, cryoablation, and microwave ablation “appropriate modalities”, noting that the “method of ablation should be left to the discretion of the operating physician.”
According to the statement, thermal percutaneous ablation may have a potential beneficial role to play in the treatment of high-risk patients with more advanced disease who are not candidates for surgery, but further research is necessary. Read the full position statement and quality improvement guidelines here.
Speaking to Interventional News, Gunn comments on the timeliness of these publications: “Image-guided renal ablation is a safe and efficacious procedure for many patients with renal cancer. Despite this, there is heterogeneity among medical organisations about who might be eligible for this procedure. For example, some organisations only recommend ablation for tumours <3cm in size, while others allow ablation as a viable option for tumors up to 4cm. Furthermore, there are increasing reports of safe and effective image-guided ablations for tumours up to 7cm, but this has yet to be addressed from a societal standpoint. Thus, it was an opportune time for the SIR to release an updated position statement and quality improvement guidelines.”
RCC is the most common type of kidney cancer and an estimated 73,820 new cases of kidney cancer will be diagnosed in the USA in 2019, resulting in 14,770 new deaths.
Merit Medical announces that both its EmboCube (syringe-loaded embolization gelatin foam) and Torpedo (uniform, pre-shaped gelatin foam loaded into a cartridge with optional blunt stylet) devices are now US Food and Drug Administration (FDA)-indicated for the embolization of blood vessels to occlude blood flow, which helps control bleeding and haemorrhaging in the peripheral vasculature.
EmboCube is the only gelatin foam that is delivered pre-cut and pre-loaded into a syringe for efficiency and ease of use. Torpedo provides physicians a uniformly pre-shaped gelatin foam loaded into a cartridge with an optional blunt stylet, removing the need for manual foam shaping, providing fast and easy attachment to the catheter for delivery, a Merit press release states. EmboCube and Torpedo are made of porcine gelatin and have no ferrous composition, making it safe for use in patients undergoing magnetic resonance imaging (MRI).
Frank Arko (Charlotte, USA) talks to VEITHtv at the VEITHsymposium 2019 (19–23 November, New York, USA), about the benefits of using Shockwave Intravascular Lithotripsy (IVL) when performing EVAR and TEVAR through calcified iliac arteries.
Arko, who shares some of the downsides of traditional procedures to deliver endografts in the presence of heavy calcification, underlines that Shockwave IVL technology has been a “game-changer”. The use of IVL, he points out, can help to avoid other costly, complicated or risky adjunctive procedures, keeping EVAR and TEVAR minimally invasive just as if a patient had non-calcified anatomy—and it enjoys “fantastic” results, he notes.
MedAlliance has announced the award of its first CE mark approval: for SELUTION SLR, a novel sirolimus drug-eluting balloon (DEB), for the treatment of peripheral arterial disease. This approval applies to sizes from 2x20mm to 7x150mm.
This award was supported by two-year results from the SELUTION SLR first-in-human study, involving 50 patients enrolled across four German centres. SELUTION SLR is the first and only sirolimus drug-eluting balloon to have six months’ clinical follow-up demonstrating a 2.3% target lesion revascularisation (TLR) and a 0.19 late lumen loss (LLL). Two-year clinical results confirmed no deaths or amputations. Patients demonstrated clinical improvement as measured by Rutherford classification, ABI and walking distance at six months and one year, which was maintained out to two years. This evidence demonstrates that a sustained limus release drug-eluting balloon is both safe and effective for the treatment of femoropopliteal lesions over a prolonged period.
The study involved 50 patients enrolled across four German centres and achieved excellent freedom from TLR through to two years in 87.5% of subjects, with no primary TLR event observed after month 11. These figures are low compared to reported historical first-in-human studies. There were no incidences of death or the need for minor and/or major amputations over this period. These Patients demonstrated clinical improvement as measured by Rutherford classification, ABI and walking distance at six months and one year, which was maintained out to two years.
“We are very excited to have been awarded our first CE mark, which is testament to the documented efficacy and safety of our novel sustained limus release eluting balloon”, said MedAlliance Chairman and CEO Jeffrey B Jump. “We now anticipate that patients in all markets where the CE mark is recognised will be able to benefit from this breakthrough in drug-eluting technology.”
MedAlliance has recently announced completion of its below-the-knee (BTK) first-in-human study in Singapore. Studies in arterial venous fistula (AVF) and pedal arch are to start enrolling soon. A 500 patient post marketing clinical study will follow shortly.
Philips today announced four-year results from the randomised controlled ILLUMENATE pivotal trial in the USA. The data show similar mortality rates through four years for patients treated with Stellarex compared to those treated with percutaneous transluminal angioplasty (PTA). The results were presented at the Leipzig Interventional Course (LINC; 28–31 January, Leipzig, Germany) by Sean Lyden (Cleveland Clinic Ohio, USA), the co-primary investigator for the ILLUMENATE trial.
The four-year ILLUMENATE pivotal trial data are the latest data from a series of trials evaluating the safety and efficacy of the Philips Stellarex 0.035″ low-dose drug-coated balloon (DCB) in restoring and maintaining blood flow in the superficial femoral artery and popliteal arteries of patients with peripheral arterial disease (PAD). The results were evaluated compared to PTA treatment with uncoated balloons, the current standard of care.
“The four-year data from the ILLUMENATE pivotal trial further substantiates the three-year results that were presented at LINC 2019 and published in Circulation in 2019,” said Sean Lyden. “The high compliance follow-up rate further affirms the findings of these data in a complex patient population.”
The study’s patient population is complex with a high proportion suffering from severely calcified lesions. The mortality rate at four years was virtually identical between the two patient groups, at 15.6% for the Stellarex patient group and 15.2% for the control group. Secondary safety outcomes were also similar across the two groups. The four-year data also show a clinically relevant lower rate of clinically-driven target lesion revascularisation (CD-TLR) in the Stellarex DCB patient group of 28.2%, vs. 34.1% in the control group. CD-TLR is a commonly used indicator of treatment efficacy durability.
“The ILLUMENATE pivotal four-year data builds on the robust, consistent long-term data of the Stellarex clinical evaluation program,” said Chris Landon, general manager, Image Guided Therapy Devices at Philips. “We continue to make relevant data available to healthcare providers in order to help them make an informed decision on the optimal treatment for often complex disease patients with peripheral arterial disease.”
Today at the 2020 Leipzig Interventional Course (LINC; 28–31 January, Leipzig, Germany), BD announced that interim findings from the Lutonix below-the-knee (BTK) investigational device exemption (IDE) trial show positive safety results at three years for freedom from mortality, freedom from major amputation and amputation-free survival.
The clinical study is a prospective, global, multicentre, single-blind, randomised (2:1 randomisation), controlled trial comparing the Lutonix 014 drug-coated balloon (DCB) to percutaneous transluminal angioplasty (PTA) for the treatment of narrowed or obstructed arteries below the knee. The safety endpoints were assessed using a Kaplan-Meier analysis through 36 months for the intent-to-treat population, with 70% of patients having completed three-year follow up at the time of analysis. At 1,095 days, there is no significant difference in freedom from mortality (DCB: 81% and PTA: 81%, p=0.946), freedom from major amputation (DCB: 95.5% and PTA: 93.8%, p=0.268) or amputation-free survival (DCB: 77.8% and PTA: 77.8%, p=0.495).
The Lutonix 014 DCB demonstrated statistically improved primary efficacy at six months when compared to PTA (K-M analysis), with K-M curves merging at one year. There were no statistical differences in safety or efficacy beyond six months in this interim analysis. These results show that the Lutonix 014 DCB versus PTA provided statistically significant efficacy outcomes at six months with no observed safety issues out to three years.
“Critical limb ischemia (CLI) is an aggressive disease affecting approximately 3.4 million patients in the USA,” said JD Meler, vice president, Medical and Clinical Affairs at BD. “The interim long-term Lutonix BTK IDE safety and efficacy data presented at LINC is a step toward advancing CLI research and finding new treatment options for this difficult-to-treat disease.”
The Lutonix 014 DCB has been commercially available in Europe, Canada and Australia for treatment of the below-the-knee arteries in patients with CLI since 2013. The product is an investigational device in the USA.
At the 2020 Leipzig Interventional Course (28–31 January, Leipzig, Germany), Sabine Steiner (University of Leipzig, Leipzig, Germany) presented one-year results of the COMPARE-RTC of low-dose versus high-dose paclitaxel balloons. Both types of balloons exhibited comparable results with excellent effectiveness and safety through 12 months for femoropopliteal interventions including a wide range of lesion lengths. The results were also published online ahead of print in the European Heart Journal.
The authors of the study, Steiner and colleagues, note that drug-coated balloons (DCBs) for femoropopliteal interventions have not been tested against each other. They aimed, therefore, to directly compare the efficacy and safety of a high-dose (IN.PACT) versus a low-dose (Ranger) DCB, with nominal paclitaxel densities of 3.5 vs. 2μg/mm2, respectively.
This prospective, multicentre, non-inferiority clinical trial included 414 patients with symptomatic femoropopliteal lesions (Rutherford classification 2–4). Patients were randomised 1:1 to endovascular treatment with either high- or low-dose DCB after stratification for lesion length. Primary efficacy and safety endpoints comprised primary patency and freedom from major adverse events. The investigators set a non-inferiority margin of -10% at 12 months.
Total occlusions were observed frequently (>40%) and provisional stenting was performed in every fourth intervention, and non-inferiority was determined for both primary efficacy and safety endpoints at 12 months.
Primary patency was 81.5% in the high-dose and 83% in the low-dose DCB group. Freedom from major adverse events was determined in 92.6% in the high-dose and in 91% in the low-dose DCB group. The overall death rate was low (2%) and no major amputation occurred.
Profusa has announced research findings that suggest the company’s Lumee oxygen platform may help improve the clinical management of patients with critical limb ischemia (CLI) who are undergoing endovascular revascularisation treatment (EVT). The data, from a recent post-market clinical study called OMNIA (Oxygen monitoring near ischaemic areas), were detailed in a series of presentations at the 2020 Leipzig Interventional Course (LINC; 28–31 January, Leipzig, Germany).
The Lumee oxygen platform is a tiny, injectable tissue-integrated biosensor with an intelligent data platform intended for continuous, real-time monitoring of tissue oxygen levels.
“Performing revascularisation in patients with critical limb ischemia is standard practice, but the tools surgeons and interventionalists typically use to gauge effectiveness of the procedure are not ideal,” said Marianne Brodmann, interim head of the Clinical Division of Angiology, Department of Internal Medicine, at Medical University in Graz, Austria. “These research findings from OMNIA suggest that continuously measuring tissue oxygen may result in better outcomes for these patients.”
OMNIA, a multicentre trial of the Lumee oxygen platform, monitored tissue oxygen levels in the affected limbs of 35 CLI patients who underwent EVT procedures, which are designed to clear obstructed arteries. Study participants were injected with four Lumee biosensors, three in the foot and one as a reference sensor in the arm. OMNIA collected measurements of oxygen throughout the revascularisation process (with measurements performed before, during, and one, three, six, and twelve months post-procedure). OMNIA also recorded traditional haemodynamic metrics, including ankle-brachial index and toe-brachial index, and clinical assessments of wound healing at each follow-up visit.
The OMNIA data presented by Brodmann showed that increases in tissue oxygen during EVT were significantly higher in patients who experienced wound healing than in those who did not (p<0.01). In addition, tissue oxygen levels during revascularisation were a better predictor of wound healing than traditional clinical measures, such as ankle-brachial index or toe-brachial index (p=0.59 and p=0.14, respectively).
“These findings show the importance of further investigating how continuous tissue oxygen measurements may satisfy an unmet clinical need to objectively evaluate how the increases in blood flow offered by EVT actually translate into nutritive oxygen delivery to the injured tissue,” added Brodmann.
Martin Werner, an angiologist at Hanusch Hospital in Vienna, noted that traditional angiography during EVT does not sufficiently measure microvascular blood flow, a special concern for people with diabetes who may have microvascular impairment. He presented results of a retrospective classification analysis from OMNIA in which continuous oxygen traces measured by the Lumee oxygen platform were analysed throughout EVT. Findings showed that oxygen changes between discrete time points, specifically start and end of EVT, may not be predictive of wound healing, but dynamic changes continually assessed throughout the procedure were.
“These results indicate that continuous measurements of blood flow in the foot during EVT may reveal factors that provide clues to treatment outcome that would have been missed if only measured at the start and end of the procedure,” said Werner.
Stephen Kanick, data science lead for Profusa, presented data from OMNIA that evaluated how Lumee biosensors assess long-term tissue viability following EVT treatments in patients with CLI. Results showed that patients who improved showed larger oxygen increases after EVT and maintained larger oxygen values at a three-month follow-up compared to patients who did not improve.
Miguel Montero-Baker, vascular surgeon and associate professor in the Division of Vascular Surgery and Endovascular Therapy at Baylor College of Medicine in Houston, USA, discussed how tissue oxygen measured before, during and after EVT can be combined to provide a more accurate predictor of patient healing. According to Montero-Baker, “The Lumee oxygen platform gives us insights we have not had before about how CLI patients are responding to treatment.”
“These findings from OMNIA affirm the emerging role of injectable biosensors in informing the treatment of patients with limb-threatening ischemia,” said Ben Hwang, chairman and CEO of Profusa. “Being able to monitor biochemical data such as tissue oxygen on a real-time basis may mean the difference between effective interventions and a catastrophic worsening of the condition.”
New arteriovenous (AV) access results were presented at the 2020 Leipzig Interventional Course (LINC; 28–31 January, Leipzig, Germany), including data on percutaneous AV fistula creation and also the use of drug-coated balloons (DCBs) in AV access interventions. While Robert Jones (University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK) opened the session by revealing a high functional patency for endoAVF at six months, Andrew Holden (Auckland University School of Medicine, Auckland, New Zealand) revealed a sustained patency advantage for a DCB compared to percutaneous transluminal angioplasty (PTA).
EndoAVF shows high functional patency at six months
WavelinQ (BD)
Jones opened the session by presenting initial multicentre experience results of the WavelinQ catheter. Concluding that “AV is now endovascular,” results of and EU and Canada post-market study showed 95% functional patency at six months as well as a limited need for secondary procedures.
“This is the first time that this additional data on the multicentre WavelinQ study has been seen,” Jones began. Endovascular AV fistula (endoAVF) devices—created with the intention of improving fistula outcomes—have performed well in clinical studies. “There are high rates of technical success in terms of creation, higher rates of maturation and patency and low rates of complications. But we have got to bear in mind that these closely monitored clinical trials are not the real world,” Jones commented.
At the University Hospitals Birmingham NHS Foundation Trust Jones and colleagues carried out a matched comparison of WavelinQ fistulas with surgical fistulas. They had 30 in the WavelinQ arm and 40 in the surgical arm. Patency results showed that WavelinQ fistulas outperformed those created surgically.
In terms of the post-market study, this was intended to collect data on WavelinQ cathether performance and outcomes in a prospective, multicentre, international study, which recruited 100 patients across 13 sites in the EU and Canada. Jones remarked: “The post-market study forms part of a wider programme of clinical trials looking at the WavelinQ device, most of which have already either completed or been published”.
Looking to the future, Jones informed the LINC audience that there are two other studies that are being lined up—a prospective, multicentre study in the USA, which aims to recruit 250 patients and a global study looking at another 100 patients. “Hopefully both of these will be rolled out in 2020,” Jones added.
Jones concluded: “In summary, this is the first time that this post-market data is being seen. We have got 95% functional patency at six months with a limited need for secondary reinterventions.”
DCB shows sustained patency advantage over PTA
IN.PACT Admiral DCB (Medtronic)
Subsequently, Holden presented 12-month outcomes of the IN.PACT AV access study, showing a 63.8% target lesion primary patency in the DCB arm compared to 43.6% in the PTA arm, with no difference in mortality.
The AV access investigational device exemption (IDE) trial was designed to evaluate safety and effectiveness of the IN.PACT AV DCB compared to PTA for de novo or restenotic obstructive lesions of native AV fistulae in the upper limbs. This was performed in the USA, in Japan and in New Zealand.
A total of 330 patients were randomised 1:1. The primary safety endpoint was serious adverse event rate within 30 days and primary effectiveness endpoint was target lesion primary patency through six months, which is defined as freedom from clinically-driven target lesion revascularisation (CD-TLR) or access circuit thrombosis measured to six months post-procedure.
It was revealed last year that IN.PACT AV access was the first DCB versus angioplasty trial to meet its primary effectiveness endpoint—a “highly impressive” primary patency of 82.2% at six months compared to 59.5% with PTA with high statistical significance and also a significant advantage in terms of freedom from CD-TLR.
“I am delighted to share for the first time the 12-month primary effectiveness endpoint. Again, a highly significant difference in target lesion primary patency—63.8% in the DCB arm compared to 43.6% for the PTA arm,” Holden revealed, adding that “there was also a highly significant difference in CD-TLR, at 35% for the DCB arm and 54.3% in the PTA arm”.
Holden added that there was less than half the rate of access circuit thrombosis in the DCB arm. “This is such a severe and catastrophic complication that, even though it did not reach clinical significance, I think is worth mentioning”.
In terms of safety at 12 months, the serious adverse event rate for the DCB arm was 46.9% compared to 69.2% for the PTA group. In the DCB arm, 40.1% had lesion revascularisations compared to 62.4% in PTA arm. Holden added that there is “absolutely no mortality signal between the two groups at 12 months,” detailing that freedom from all-cause mortality in DCB arm was 90.6% and in PTA arm was 90.4%.
Holden summarised: “For the first time we have seen sustained patency advantage for a DCB over PTA using a combination of vessel preparation with a high-pressure balloon and DCB angioplasty with a target lesion primary patency of 63.8% for the DCB compared to 43.6% for PTA arm. Fewer interventions were required to maintain target lesion primary patency in the DCB arm compared to the PTA arm, and we also saw the incidence of access circuit thrombosis more than half—something I think is very important given the severity of that complication—and no difference in mortality out to 12 months.”
The US Food and Drug Administration (FDA) have granted Intact Vascular pre-market approval application for an additional size of its Tack Endovascular System, a dissection repair device used to treat peripheral arterial dissections after balloon angioplasties.
A larger version of the device has now been cleared for superficial femoral and proximal popliteal arteries ranging from 4–8mm in diameter.
The device features adaptive sizing, which allows the implant to adapt to tapering vessels while maintaining a relatively steady radial force.
The Flex vessel preparation system (VentureMed group) is safe and effective, and appears to limit the potential risks of dissection and perforation of chronic total occlusions. This is the conclusion given by Constantino Peña (Miami Cardiac and Vascular Institute, Miami, USA) at the 2020 International Symposium on Endovascular Therapy (ISET; 22–25 January, Hollywood, USA) in his featured abstract presentation. Peña is a member of the scientific advisory board for Venture Medical.
“The Flex vessel preparation system effectively modified real-world plaque, including chronic total occlusions in the superficial femoral and popliteal arteries,” he said. “Furthermore, post-Flex subnominal inflation pressures demonstrate improved vessel compliance.” However, he added that “Further studies are warranted to confirm reduction in long-term re-intervention rates.”
In an initial, multicentre, retrospective review, investigators used the Flex vessel preparation system in 185 real-world cases: all lesions were long (over 20cm in length), and 69% had moderate to severe calcification. In 100% of lesions, there was some type of chronic total occlusion. Lesions were prepped just with the Flex system prior to either plain balloon angioplasty or treatment with drug-coated balloons (DCBs). The researchers collected angiograms at baseline, post-Flex, and post-procedurally.
Crucially, Peña said, there was a 34% mean luminal gain prior to treatment after the Flex vessel preparation system was used. Peña also reported sub-nominal inflation pressures averaged 4atm, and that there was a low rate (4%0 and grade (A or B) of dissections. He added that there were no flow-limiting dissections, perforations, or embolizations, and that provisional stenting “only occurred” in 28% of cases.
Illustrating these findings with some case examples, he talked the audience through the use of the Flex vessel preparation system in a 71-year-old man with Rutherford class 5 peripheral arterial disease (PAD). The pre-procedural stenosis rate of the target lesion was 100%. Following treatment with the Flex vessel preparation system, this dropped to 30%. There was also a 70% luminal gain post-Flex. After angioplasty, stenosis was 0%.
In the second case Peña recounted, vessel preparation with the Flex system prior to angioplasty reduced the stenosis rate from 100% to 50% in a 72-year-old woman with Rutherford class 3 PAD. There was a 50% luminal gain following use of the Flex system. Following angioplasty, the stenosis rate was 10%. These results are reported for a 41cm long lesion.
Vessel preparation aims to improve outcomes
Before discussing its importance, Peña first defined vessel preparation for the ISET attendees: “Its goal is the safe dilation of vessels to improve outcomes. This can be achieved through the modulation of a vessel in order to allow dilatation to its final diameter for definitive therapy or by modifying plaque to improve vessel compliance and reduce dissections. Vessel preparation can potentially improve diffusion of drug-coated balloon [DCB] therapy.”
Specifically referring to the Flex vessel preparation system, Peña described how it is able to “optimise the revascularisation of long, complex lesions with micro-incisions.” He highlighted multiple characteristics of the system that facilitate this.
“Firstly it is safe,” he said. “The Flex vessel preparation system creates predictable, depth-controlled micro-incisions that minimise the risk of dissection, perforation, and other complications.” Next, Peña informed delegates that the system is easy to use: “It has a simple design for treating long, complex lesions. It has a retrograde pull-back with minimal user variation, and no vessel sizing is needed.”
The Flex vessel preparation system is also cost-efficient, according to Peña. No capital equipment is required, as only one or two catheters are necessary to use Flex, which has a “quick, over-the-wire set-up”. The system has two working lengths–40cm and 120cm (in US and outside US markets, respectively). It has a reinforced braided shaft “for enhanced deliverability and torque performance”, and an atraumatic tip for “improved trackability and crossing profile”.
The Flex vessel preparation system is for use in the femoral and popliteal arteries, as well as for arteriovenous fistulas and grafts.
Stratus Medical, a new company created to focus on advancing radiofrequency (RF) ablation treatment for chronic pain, has announced that it completed a private placement to acquire the assets of NimbusRF from Biomerics and provide growth capital funding to support the continued global expansion of the Nimbus RF Multitined Expandable Electrode for chronic pain. The investment was led by Med Venture Holdings.
Nimbus was developed to address the unmet need for an easy to use, efficient, cost-effective RF device that provides a large volume and optimally shaped lesion, which interventional pain specialists, orthopaedic surgeons and neurosurgeons can use to treat pain. Nimbus has been shown to reduce procedural time and increase efficiency for hospitals and surgery centres where Nimbus is utilised. The Nimbus device is US Food and Drug Administration (FDA) cleared and CE marked. Nimbus has been utilised in over 100,000 patient treatments in Australia, Brazil, Canada, USA, UK and other countries.
Bret Boudousquie, Stratus Medical CEO offered, “The rapidly growing global radiofrequency (RF) ablation for chronic pain market has been asking for innovation and Nimbus is well positioned to become the market leader in this space to treat chronic pain. Nimbus offers a highly differentiated and patented technology to meet the needs of patients and physicians alike. With the financial support and expertise from our lead investor, Med Venture Holdings, we will accelerate the global sales and marketing efforts of Nimbus and fund development of our new product pipeline.”
Travis Sessions, Med Venture Holdings Managing Partner commented, “We see great value in the interventional pain medicine space as so much emphasis is being placed on reducing the use of narcotics and improving interventional therapies to address chronic pain and improve quality of life. We have been involved with the Nimbus product line for some time and have seen an excellent response from physician users, hospitals and ASC customers. Under Bret’s proven leadership, we expect Nimbus to increase its global presence and Stratus Medical to bring innovation to the interventional pain space.”
NOTE: This video is ONLY available to watch in selected countries and geographies
The one-year IN.PACT AV trial results, first presented at LINC 2020 (28–31 January, Leipzig, Germany), reveal that the target lesion primary patency in the patient group treated with the IN.PACT drug-coated balloon (DCB; Medtronic) was 63.8% compared to 43.6% in the group treated with plain balloon angioplasty (p<0.001) for the treatment of arteriovenous (AV) access site lesions. The trial also showed a 35% reduction in reintervention rates when a drug-coated balloon was used instead of a plain balloon and “nearly identical” safety data in the two groups with respect to mortality.
Panel discussion
Tobias Steinke (Düsseldorf, Germany; pictured in the centre) discusses this trial’s distinctive results with principal investigators Andrew Holden (Auckland, New Zealand; pictured on the right) and Robert Lookstein (New York, USA) and establishes the importance of considered vessel preparation using a high-pressure balloon. The panel also reflects on the data from a budget impact, economic model based on the German and US healthcare systems that shows substantial cost savings when the IN.PACT DCB is used. The physicians also emphasise the enthusiasm displayed by the audience to use DCBs in this patient population, when these striking results were presented.
The IN.PACT AV access trial was the first trial to meet its primary endpoint.
Margin assessment using white light (left) versus intraoperative molecular imaging with OTL38 (right)
A ground-breaking tumour-highlighting technology—OTL38—enhances the visualisation of lung cancer tissue, providing surgeons with a significantly better chance of finding and removing more cancer than previously possible, according to a scientific presentation at the 56th Annual Meeting of the Society of Thoracic Surgeons (STS 2020; 26–29 January, New Orleans, USA).
“Lung cancer is the most common and lethal cancer worldwide,” comments Inderpal (Netu) S Sarkaria, of the University of Pittsburgh Medical Center, Pittsburgh, USA. “Technologies to improve the care of these patients are needed. Near-infrared imaging with OTL38 during surgery for lung cancer is one such promising technology with the potential to significantly improve the completeness and quality of the operation, therefore improving patient outcomes.”
Sarkaria and colleagues at six institutions (University of Pittsburgh, University of Pennsylvania, Harvard University, Cleveland Clinic, Leiden University, and MD Anderson) participated in a phase 2 clinical trial, identifying 92 patients who had lung lesions and were to undergo pulmonary resection for non-small cell lung cancer (NSCLC). Before their operations, each patient received a measured intravenous dose of OTL38, composed of near-infrared dye and a targeting molecule. The molecule attaches to folic-acid-based receptors on cancer cells and can be illuminated during surgery using a special surgical endoscope. This helps identify small, hard-to-detect cancer lesions that might otherwise have been missed and should be surgically removed.
The researchers made assessments in three phases: “lung inspection,” “tumour resection,” and “specimen check.” During the inspection phase, the molecular imaging identified 10 additional cancers—all missed when using visual examination and manual touch—in seven patients (8%). In the resection phase, researchers determined that OTL38 enabled localisation of lesions that were not found in 11 patients (12%). After surgeons found that all margins were visually adequate or clear in the specimen check, the resected specimens were further assessed using the molecular imaging. Inadequate margins (microscopic residual tumour left at the edges) were uncovered in eight patients (9%). Overall, researchers determined that the OTL38 molecular imaging helped improve outcomes for one in four patients (26%).
“OTL38 is the first technique that is specific to imaging adenocarcinomas of the lung, which is one of the most common types of invasive lung cancer, making it unique and clinically useful in this respect,” says Sarkaria. “Localisation of tumours, identification of occult tumours, and immediate tumour margin assessment during surgery for adenocarcinomas of the lung were significantly improved with the use of this technology.”
Surgery remains the best potentially curative treatment for early stage NSCLC. However, research has shown that 30–55% of patients with NSCLC develop recurrence, which often is caused by microscopic clusters of cancer cells that were undetected by standard staging methods. This suggests that complete removal needs to be ensured both macroscopically and microscopically during surgery.
“Near-infrared imaging with OTL38 may be a powerful tool to help surgeons significantly improve the quality of lung cancer surgery by more clearly identifying tumours and allowing the surgeon to better see and completely remove them—one of the most vital components in the overall care of patients with this disease,” Sarkaria posits.
Surgeons traditionally use X-rays, magnetic resonance imaging, computed tomography (CT) scans, positron emission tomography, and/or ultrasound to determine the size and location of tumours before surgery. However, these imaging modalities are rarely, if ever, used during surgery.
OTL38 is believed to be the first targeted fluorescent marker to provide this type of benefit for lung cancer. The OTL38 technology is different in its ability to detect cancerous tissue not previously identified on preoperative scans and do so in real-time, while the surgeon is operating. This is crucial in ensuring that surgeons adequately detect and remove cancer cells that may not be visible to the naked eye or located through touch. The complete removal of diseased tissue during surgery helps to avoid additional surgeries and cancer relapse, as well as increase patients’ overall chances of survival.
“Use of advanced near-infrared imaging techniques such as OTL38 may provide surgeons with powerful tools to improve the quality of lung cancer operations by better identifying small, hard-to-find tumours, finding previously undetected cancers at the time of surgery, and better assessing if the entire tumour has been removed,” says Sarkaria.
In addition, with the implementation of lung screening and the increased use of CT scans in general, cardiothoracic surgeons are seeing more patients with small or undefined nodules, so the timing of the availability of technology such as OTL38 is just right, according to Linda W Martin, of the University of Virginia in Charlottesville, USA, who was not directly involved with this research.
“In many circumstances, a preoperative biopsy is not practical or feasible, and we are faced with the need for intraoperative identification of these nodules,” she says. “This research describes an exciting new approach to localise nodules that are difficult to find without a separate procedure. More importantly, the study showed that because of this technology, additional nodules that were in fact separate cancers were found, and useful information about margin status also resulted.”
Martin describes another significant advantage that the OTL38 technology offers—the ability to better identify small nodules. This may allow surgeons to more often utilise minimally invasive operative approaches in some patients who otherwise would have been required to undergo a thoracotomy in order to find these nodules. The completion of the OTL38 Phase 2 trial in lung cancer is a major milestone, advancing the technology closer to US Food and Drug Administration (FDA) approval and commercialisation. Phase 3 trials are currently under way.
Merit Medical has announced the official market launch of its Arcadia steerable and straight balloons for vertebral augmentation. These balloons are designed to help physicians achieve controlled, precise cavity creation during unipedicular or bipedicular vertebral augmentation procedures, the company state.
The Arcadia steerable balloon provides a bipedicular footprint through a unipedicular approach for increased control of balloon placement and cement delivery when treating vertebral compression fractures. The Arcadia steerable balloon’s design has the potential to reduce procedural and fluoroscopy times and lower costs associated with additional incisions, according to a Merit press release. The Arcadia straight balloon is designed for simplified cavity creation when treating vertebral compression fractures via a standard bipedicular approach.
“The Arcadia steerable balloon offers highly accurate balloon placement through a unilateral approach, as well as a balloon with enough size and durability to reduce prominent fractures and optimise cement fill,” explains Douglas P Beall, (Clinical Radiology of Oklahoma, USA). “This system has the capability to offer bilateral results with a unilateral approach.” Beall consulted with Merit Medical as part of its development and early evaluation teams for the Arcadia steerable balloon.
Pitching the positive design features of the device, Merit Medical claim that the pre-inflation length of both product offerings—five sizes ranging from 10mm to 30mm—accommodates diverse anatomies while providing reduced compliancy and increased balloon volumes. The company also state that the size range combined with steerability enables the ability to straddle the centre midline of the vertebral body, providing a balanced inflation footprint between endplates. A high-pressure rating of 700psi helps to form even cavity creation in varying vertebral body anatomies.
Imricor Medical received CE mark certification for its Vision-MR ablation catheter, a device guided by real-time magnetic resonance imaging (MRI).
The device, which is constructed to feel like a traditional ablation catheter, uses a fibre optic tip to provide temperature sensing and comes with active MR tracking features.
The ablation catheter is designed “with the intent of enabling higher success rates along with a faster and safer treatment compared to conventional procedures using X-ray guided catheters,” the company said.
Introduced as “a pioneer in the vascular arena”, Michael Dake, senior vice president of the University of Arizona Health Sciences, Tucson, USA, addressed the audience at the 2019 meeting of Vascular and Interventional Advances (VIVA; 2–5 November, Las Vegas, USA) in a keynote lecture entitled “The future of medicine and medical education: How do we prepare the next generation?” Responsible for the integration of undergraduate and graduate education at his institution, Dake enumerated the lessons he had learned from personal experience concerning physician training.
“Big biology and big medicine is meeting big data,” he began, elaborating: “Some have called it the fourth industrial revolution, where we have an accelerated, exponential convergence of data science, physical science, and life sciences. These are creating enormous opportunities, but also challenges, for all of us. Our main task as educators is to figure out how to integrate large scale, multidisciplinary datasets into our education.”
He is enthusiastic about the prospect, fervently anticipative of the future he is advocating: “We are in a period of great innovation. There are tremendous opportunities, and these will continue to grow with technological advances that promise to impact clinical practice and transform medicine and medical education. The pace of change is rapid; thinking outside the box is essential. The potential impact on medical education and medical care is enormous.”
The convergence of precision medicine and digital medicine
“How do we drive precision medicine and data-driven healthcare into routine clinical practice?” Dake asked. He believes the answer lies with artificial intelligence (AI). “Where AI can really help in the future of healthcare,” he said, “is with merging these two dominant trends: precision medicine and digital medicine.”
Dake detailed how new technology platforms that use profiling, automation, and computing to provide deep phenotyping and risk profiling will interact with the “expanded care space”—wearables, sensors, telemedicine, social media and lifestyle metrics, data on consumer patient engagement—to enable remote monitoring of patient health status. This interaction will be mediated by machine learning algorithms. The “potential power” of AI in this context, Dake explained, is to provide analytics for improved decisions and clinical outcomes at lower cost.
Indeed, the cost of big data has decreased dramatically over the last decade. Showing a graph plotting the cost of data relative to speed versus data consumption, Dake demonstrated that the cost of data per second has dropped from nearly $3 per Mbps in 2004 to less than $0.1 per Mbps by 2013, while data consumption per subscriber per month rose from less than 10MB a month in 2006 to 225MB a month in 2013. “We can feel confident that at least computation comes cheaply. All this big data certainly is not as expensive to process as it was years ago,” he said. “That is good for us.”
Exemplifying the uses of big data, he continued: “Everyone in any healthcare centre or academic community is aware of the buzzwords around precision medicine. There is a lot of emphasis on deep phenotyping: taking large-scale datasets, predicting complex traits and disease risk, whether it is by a variety of ‘omics’ that take large cohorts of individuals and stringently control for clinically phenotyped outcomes, or by mapping genetic overlap between different diseases involving shared pathogenic elements and co-morbidity risks.”
Illustrating the idea of genetic phenotype mapping with an example, he cited a study published in Nature Genetics in 2018 by Rainer Malik (Institute for Stroke and Dementia Research, University Hospital, LMU Munich, Munich, Germany) et al that identified a genetic overlap between stroke and related vascular traits at 32 genome loci in 521,612 people. Twenty-two of these loci were new to the designation “stroke risk”. This is one example of the “tremendous opportunities” afforded to researchers with access to large datasets, Dake opined.
However, he did enumerate several challenges presented by the emergence of big data. “The problem with real world data,” he said, “is that it is, indeed, real world.” Elaborating, he explained how people analytics and large scale databanks had blurred the boundaries between medical research, clinical care, and daily life, rendering every monitored event as a potential data point, every individual as a data node and research asset. Social spaces are also becoming quantifiable, and with sufficient data, investigators could reveal increasingly predictable behaviour and individual risk patterns. “This blurring of private and public spaces could lead to complex ethical and legal issues,” Dake commented, noting that consent, privacy, security and surveillance were factors society was “only beginning to address”, and that they would be “increasingly important as areas of focus”.
One of the key benefits of AI, though, is the fact that it can overcome the “bandwidth” limits of humans, Dake enthused. “There is currently a data deluge,” he said. “Our cognitive bandwidth is certainly challenged and overwhelmed, but I think there is great promise in decision support, and ways that we really can impact the future of medical education for the better.”
He informed the VIVA audience that society was at the cusp of the “era of cognitive computing and decision-support systems”. Using AI algorithms can help draw patterns and sense from such large datasets. “Clearly we have limits to individual expertise,” Dake said. “We have limits to our individual abilities to multi-dimensionally evaluate data, we have limits to our sensory systems, cognitive experiences and perceptions, and limits to our objective decision-making. This is where AI, deep learning, and machine learning can come to help us.”
Envisioning the future of medicine as made possible by AI and big data, Dake predicted: “As we evolve from qualitative, descriptive information of variable quality and provenance to quantitative data of known provenance and validated quality, [we will] change from a complex ecosystem of largely unconnected data sources to an evolving, interconnected network of data sources for robust decisions and improved care.”
Digital Darwinism: A looming data divide in medical education
“If you are teaching today what you were five years ago, either the field is dead, or you are,” Noam Chomsky (University of Arizona, Tucson, USA) said. Sharing this quote, Dake added: “Noam Chomsky is 95 years of age, and he is aware of this—so should we be”.
Dake highlighted a shift in medical education, from being science-centric in the 20th century, to becoming more data-centric between 2000 and the present day. Extrapolating this trend, he said that education will next become network-centric, stressing the importance of students gaining mastery of escalating complexity and massive data.
“There is a digital Darwinism looming,” Dake warned. “Understanding data structure and application to improve decisions and outcomes will become a critical institutional competency. With major skill gaps and predicted personnel shortages, we are going to have to train a new cadre of data scientists, both medical and non-medical, and institutions that lack adequate computation infrastructure and are not committed to this training are going to suffer ‘cognitive starvation’ and relegation to competitive irrelevance.”
So how will medical education adapt to this demand? Dake outlined his thoughts on curricular emphasis in the 21st century, believing that knowledge capture and creation, not information retention, should be the priority, and that students should be taught to distinguish between information and knowledge. He said that he would like to see future physicians have a deep understanding of probabilistic reasoning, as well as collaboration with and management of AI applications. Lastly, he underlined the importance of cultivating empathy and compassion in the next generation of doctors, emphasising the “very real” issue of physician burnout, and advocating for a more holistic curriculum prioritising students’ mental health.
The University of Arizona has implemented a programme to “future-proof” its graduates, Dake recounted, taking all of these factors into account. The institution is following a health sciences strategic plan, comprised of 26 initiatives, which cover a range of topics, from reducing student debt, to increasing the number of nurses and primary care physicians, to creating more flexible learning pathways. While every institution will need to explore ways of tackling its own specific challenges, Dake said, his keynote lecture serves as a blueprint for building a comprehensive medical curriculum capable of reimagining the physicians of the future.
“Institutions should make every effort to take advantage of the strategic synergies that can arise by creating a virtuous cycle connecting education with research and patient care in a continuous feedback loop,” he concluded. “The ultimate goal is the creation of a real-time learning health system, in which the practice and teaching environments learn from each other and are informed by research.”
Stereotactic body radiation therapy (SBRT) in previously irradiated patients “appears clinically feasible”, and provides good disease control out to five years for men with locally recurrent prostate cancer. This is the conclusion of a recent prospective study from Donald Fuller (Genesis Health Care Partners, San Diego, USA), published in the International Journal of Radiation Oncology Biology Physics.
The investigators set out to evaluate the use of SBRT retreatment for biopsy-proven local persistence in prostate postradiation therapy, evaluating efficacy and toxicity. For this patient cohort, the authors explain how a number of local salvage methods have been described, but say that none have been widely used, “primarily owing to elevated toxicity concerns”.
Analysing outcomes in the 50 patients enrolled in the study from February 2009 to March 2018 from two community-based radiation oncology centres, Fuller et al assessed toxicities before and after SBRT salvage using CTCAE v.3 criteria and International Prostate Symptom Score (I-IPSS). SBRT was performed with the CyberKnife system from Accuray.
The authors report that 69% of the patients required no androgen deprivation therapy (ADT) treatment within the first five years following CyberKnife prostate SBRT. There were also low overall rates of toxicity among the patients, all of whom had undergone radiation therapy treatment prior to SBRT.
“Most men, if treated, receive only ADT, which has the potential for long-lasting whole-body side effects while rarely eradicating the tumour completely,” Fuller comments. “Without effective local retreatment, it is likely that most, if not all of them [the patients treated in this study], would have needed ADT treatment at a far earlier point in their history. Because ADT has many long-lasting detrimental ‘whole body’ symptoms, effective SBRT local salvage thus preserves better quality of life, greatly delaying or avoiding ADT systemic effects for most patients.”
Furthermore, at five years, the disease-free survival rate was 60%, indicating patients experienced no signs or symptoms of their cancer during that time. The authors write: “In spite of the relatively high-risk patient population described herein, the five-year biochemical relapse-free survival rate of 60% confirms extended disease-free survival in the majority of SBRT salvage cases.”
Comparing SBRT favourably to radical prostatectomy, Fuller and colleagues say: “We also report a biochemical relapse-free efficacy rate that appears at least comparable to that reported with salvage radical prostatectomy; 60% five-year biochemical relapse-free survival in the present series versus 57% three-year biochemical relapse-free survival in a contemporary salvage radical prostatectomy series of similar size and similar median follow-up. This suggests a definite role for salvage SBRT, particularly well-suited for those who either do not desire to or are not physically able to withstand the rigors and potential complications of a salvage radical prostatectomy procedure.”
The median prostate-specific antigen decreased to 0.16ng/mL at five years, similar to initial treatment with brachytherapy and lower than typical conventional fractionation, based on results from other studies.
No grade two or higher gastrointestinal events were reported. Genitourinary toxicity also was lower than reported rates for salvage radical prostatectomy and seems less frequent after prior standard external radiation treatment.
“Our results suggest that efficacious salvage of locally recurrent prostate cancer with SBRT is possible, with an acceptable toxicity risk, in appropriately selected patients,” Fuller et al conclude.
David Hayes, former physician administrator at Mayo Clinic, Rochester, USA, has been appointed chief medical officer of Biotronik, a company press release reports.
“Our focus has always been on the patient. To help patients live their best lives, we remain in constant collaboration with physicians so we can intimately understand the challenges they face every day. Hayes’ clinical, teaching, and publishing accomplishments bring a new level of experience and expertise to the company,” comments Ryan Walters, Biotronik president. “His commitment to understanding the dynamics of patient care, the challenges health systems face, and the impact of technology aligns perfectly with our focus on expanding partnerships with physicians and institutions throughout the USA. With Hayes on our team, we are positioned to set a new standard in delivering cardiovascular care.”
Hayes joins Biotronik following a more than 40-year career with Mayo Clinic in Rochester, USA, where he held various roles including professor of Cardiovascular Medicine and physician administrator. He most recently served as medical director, Mayo Clinic Care Network. His career has been dedicated to treating patients and helping advance electrophysiology and cardiology through teaching.
“This is an opportunity for me to drive change and create positive patient impact from a very different perspective,” states Hayes. “As the chief medical officer of Biotronik, I have assumed a role rooted in collaboration, understanding, and action. We are ready to challenge norms and shake things up. Cardiology is an area of healthcare that should always be evolving and advancing. We are making sure that happens. I am personally committed to ensuring physicians know they have a trusted partner in Biotronik.”
Juan Granada (New York, USA) chats to Sahil Parikh (New York, USA) for VEITHtv about below-the-knee (BTK) intervention and innovation and how the paclitaxel controversy has influenced the treatment of BTK disease.
Parikh says: “Frankly there is a lot of dampened enthusiasm” about the use of paclitaxel for drug delivery below the knee and that “if there is any good that came from this controversy is that it has stimulated innovation”. Granada agrees, noting that the field is “wide open” for the development of alternative therapeutic solutions.
The duo also discuss the benefits of stents/scaffolds compared with balloons with Granada noting that recent data suggests stents/scaffolds may have the edge. Scaffolds are “intrinsically and intuitively attractive” says Parikh, adding however that many physicians, including himself, are reluctant are to stent below the mid-level of the calf.
Argon Medical Devices has announced the commercial launch of its Single-loop and Triple-loop retrieval kits for sale in the USA. The Single-loop and Triple-loop Retrieval Kits are intended for percutaneous removal of retrievable inferior vena cava (IVC) filters that are no longer medically required, via a jugular approach.
“We are excited to improve the IVC filter retrieval options available to our customers with the introduction of these new products,” said George A Leondis, president and CEO of Argon Medical.
According to a statement, Argon Medical’s Single-loop and Triple-loop retrieval kits were designed with the rigour of IVC filter retrieval in mind, offering the following key features:
A coil-reinforced outer sheath with the strength needed to detach filter legs from the IVC wall
Radiopaque bands on the distal end of the inner sheath, outer sheath and the snare catheter for enhanced visualisation
A 15-degree curve at the distal tip of the snare catheter for directional control
“IVC filters are a safe and effective treatment for the prevention of pulmonary embolism, however they should be removed when the need for the filter subsides,” said David Trost (Weill Cornell Medical Center, New York, USA). “I like that Argon’s new retrieval kits can be used on all retrievable IVC filters, regardless of brand, from the jugular vein, providing unique versatility,” he added.
Terumo has announced the launch of a new randomised clinical trial: the DIStal vs. COnventional RADIAL access trial (DISCO RADIAL). The trial compares the novel distal radial access with conventional radial access approach, in terms of radial occlusion rates at discharge. The first patient has been enrolled.
Transradial approach is the preferred vascular access for coronary angiography and interventions, a Terumo press release asserts. Recently, the distal radial artery from the anatomical snuffbox on the dorsal side of the hand (“distal TRA” or “snuffbox access”) has emerged as an alternative access to the conventional forearm radial artery for coronary angiography and interventions.
DISCO RADIAL is the first large international randomised study designed to investigate the benefits of distal radial access over conventional radial access approach. The study plans to enrol 1,300 patients, in approximately 13 centres in Europe and Japan. The patients will be randomly assigned to one of the two access groups.
DISCO RADIAL aims to generate clinical evidence on the potential benefits of this novel distal access approach over the conventional radial approach, and to support the use of the distal radial approach as an alternative to the conventional radial approach.
Principal investigator Shigeru Saito, interventional cardiologist from Shonan Kamakura General Hospital, Kamakura, Japan, comments: “The radial approach is a small world and just one of the access methods. However, its impact on the clinical field has been proven potent and significant. Everybody was thinking we will never have anything novel in this small world. However, unexpectedly it was not true. The distal radial approach is truly novel, and nobody has evidence yet proving its advantage over the conventional radial approach. As the group of physicians working in this field, we have the responsibility to show its efficacy. That is the reason to initiate the trial.”
Principal investigator Adel Aminian, an interventional cardiologist from the Centre Hospitalier Universitaire de Charleroi, Charleroi, Belgium, says: “This novel access has raised great enthusiasm among the radial community, despite the paucity of clinical evidence supporting its use. Beyond potential advantages related to improved operator/patient comfort, easier and shorter haemostasis, an important feature of this technique is a puncture distal to the superficial palmar arch. Distal transradial access has the potential to maintain antegrade flow in the forearm radial artery during haemostatic compression, reducing thereby the risk of retrograde thrombus formation in the forearm radial artery and therefore the risk of radial occlusion. The current available data on distal transradial access is limited to relatively small prospective and retrospective case series looking primarily at the feasibility and success rates with this approach. By assessing the potential benefit and limitations of this alternative access, DISCO RADIAL will have an important clinical impact for radial operators.”
Christophe Giot, chief medical officer, Terumo Europe, says that this study will generate clinical evidence for this novel distal access approach, and reflects Terumo’s commitment to evidence based clinical practice and to the improvement of patients’ healthcare.
Enrolment is expected to be completed within one year, and results are expected to be available in 2021. Terumo is sponsoring this new study.
Speaking at the 32nd Annual International Symposium on Endovascular Therapy (ISET; 22–25 January, Hollywood, USA), Lindsay Machan (University of British Columbia, Vancouver, Canada) said that there had been “significant advancements” in the development of radiation protection options, though added that it was “important to remember that all devices are tested in optimised, non-real world conditions”.
“We are all aware of some very inconvenient truths about radiation,” he began, highlighting how, in 2017, “It was pointed out that in all these procedures we are performing, not only do they cause evidence of radiation-induced DNA damage, but we are individually predisposed, and actually the less radiation we get exposed [to], the less DNA damage we get from doing those procedures.”
Of the multitude of new procedures for radiation protection that have emerged in the last few years, Machan said he believes they could be categorised into three general brackets. These are: protective shielding, reducing the radiation output, and reducing the biological effect.
Protective shielding
“I think most of us are used to the idea of using shielding,” Machan said. “If you use the new three metal shielding [triple layer non-lead skirts], it actually works profoundly well.” He showed the ISET audience a video of physicians performing an endovascular aneurysm repair (EVAR), commenting that his own data show that if, in addition to the “typical shielding and the bedside shielding”, a triple layer non-lead skirt was added to the theatre set-up, “you can actually reduce radiation to the operator by 91% compared to what we call ‘commando’, or just wearing a lead [apron]”.
Adding more additional shielding resulted in a further 80% reduction in radiation exposure to the operator and staff, Machan shared. He showed the ISET audience “some pretty innovative lead gowns”, again with the tripe metal layering. The gowns are made from tungsten, antimony, and bismuth, the “secret sauce”, in Machan’s words. Speaking of this metal triplet, he said he “highly encouraged” his listeners to look into acquiring such a combination gown for their own practice.
“It is actually very light,” he said of the gown. “Compared to standard non-lead, so called ‘light’ lead, this is profoundly better in terms of radiation protection,” he emphasised. For a 0.25mm thick gown, the wearer would get 3.7% transmission from a 70kV beam, Machan said. In contrast, this drops to 1.7% transmission with a 0.35mm thick gown, and reduces further to 0.6% transmission with the triple metal gown, which is 0.5mm thick.
However, he also offered a word of caution. When investigating the radiation protection conferred by lead glasses, Machan reported that they were not particularly effective. Describing their experimentation, Machan said: “The magic innovation was eyelash glue that allowed us to put dosimeters on the face—the eyelids and the cheeks. We then put lead glasses over the top, and it was a little bit disturbing to find that in real-world circulations, lead glasses only reduce the radiation dose to the eye by 9.5%. If you look at the right eye, it is 14.2%, so in other words, our nose actually provides 15% of radiation protection. These things are tested in non-real-world circumstances; this needs our attention.”
Reducing the radiation output
In terms of reducing the radiation output, Machan said he was “conflicted”.
“There are many different ways of doing this, he stated. One way utilises artificial intelligence (AI) to limit the radiation exposure when using fluoroscopy to navigate intraprocedurally. “When we are doing procedures,” Machan explained, “we are usually focusing on a relatively small area of the image [generated by fluoroscopy]. We have used AI, and we have taught it to recognise catheters, guidewires, and contrast, and then we use that to guide sub-second coning to our areas of interest. Once per second, we open up the full field, so you get context.
“You step on the fluoro-pedal, and where the white box is [a white box is visible over a subsection of the fluoroscopy image], that is the AI actually changing the cones actively. It just looks like normal fluoroscopy.”
The first application of AI-enabled fluoroscopy demonstrated that it facilitated a median 61.8% radiation dose reduction to the patient, and a 59.4% reduction to everybody else in the operating theatre.
Reducing the biological effect
“This is interesting work reducing the biological effect of radiation,” Machan said, introducing work by Kieran Murphy (University Health Network Toronto Western Hospital, Toronto, Canada).
Explaining this research, Machan recounted: “All of us sitting here, we have this balance of excess free radicals and anti-oxidants to prevent DNA damage and oxidative stress. Radiation creates free radicals, which damage DNA, and results in all those noxious things that we talk about: stroke, heart attack, cancer, cataracts, and accelerated aging. Kieran [Murphy]’s thought is that if you take an anti-oxidant mixture dissolved in any drink, even ones we do not think of as being healthy, and if you do this every day before you go in and do a procedure, then actually the idea is that you prevent those free radicals from damaging your DNA.”
In a clinical study of 10 patients published in the Journal of Vascular and interventional Radiology (JVIR) in 2017 by Murphy et al, the investigators found that premedication with an oral antioxidant cocktail before medical imaging exams could significantly reduce DNA injury from the ionising radiation dose. Murphy claimed at ISET that this was “pretty impressive early phase work”, and teased that Murphy’s group were preparing to do the same kind of study on people before they do endovascular procedures.
However, whilst Machan is enthusiastic about these various options for radiation protection, eh concludes by saying that “There is no safe dose”.
Addressing the audience at the Spectrum meeting (18–21 January, Miami, USA), Theresa Caridi (MedStar Georgetown University Hospital, Washington, DC, USA) expands on the pros and cons of uterine artery embolization (UAE), and shares what factors she believes are necessary to discuss with the patient prior to the procedure.
Firstly, Caridi discussed the issue of fertility. In a 2008 study published in the Journal of Cardiovascular and Interventional Radiology (CVIR) by Michal Mara (General Faculty Hospital and First Medical Faculty of Charles University, Prague, Czech Republic) and colleagues, the authors concluded that, while UAE is less invasive and as symptomatically effective and safe as myomectomy, but has inferior reproductive outcomes in the first two years after treatment. One-hundred-and-twenty-one women with reproductive plans who presented with an intramural fibroid(s) larger than 4cm were randomly selected for either UAE or myomectomy; 58 embolizations and 63 myomectomies (42 laparoscopic, 21 open) were performed. Mara et al reported significantly more pregnancies and labours (33 and 19, respectively) and fewer abortions (six) following surgery than after embolization (17 pregnancies, five labours, nine abortions; p<0.05).
Listing her first positive for UAE, Caridi told the Spectrum audience how the procedure is uterine-sparing. Citing a study by Shannon Laughlin-Tommaso (Mayo Clinic, Rochester, USA) published in Menopause in 2018, Caridi demonstrated that ovarian-sparing hysterectomy, which had been touted as a potential way of avoiding some of the detrimental effects of hysterectomy, did not fully eliminate the risks. The Menopause study looked at approximately 2,000 women who had an ovarian-sparing hysterectomy and compared them to age-matched controls. Laughlin-Tommaso and colleagues found that even with ovarian conservation, there is an elevated long-term risk of cardiovascular disease and metabolic conditions, especially in women who undergo hysterectomy when 35 or younger. The authors concluded: “If these associations are causal, alternatives to hysterectomy should be considered to treat benign gynaecologic conditions.”
“Women are talking about this on social media,” Caridi commented. “They are asking ‘What are the risks if I have a hysterectomy, even if I leave the ovaries behind?’ I think it is important to know about this.”
However, while UAE offers a uterine-sparing alternative to hysterectomy, Caridi said that the presence of the uterus “means that we can get fibroid recurrence”. Sharing the five-year results of the prospective, randomised controlled REST trial, which directly compared UAE to surgical treatments—both myomectomy and hysterectomy—in patients with symptomatic uterine fibroids, Caridi reported how the authors, Jon Moss (Gartnavel General Hospital, Glasgow, UK) et al, found that adverse event rates were no different between the UAE and surgical arms, but that the reintervention rate was much higher with UAE. Moss and colleagues’ conclusion in 2011 was that “UAE is a satisfactory alternative to surgery for fibroids”, but that “the less invasive nature of UAE needs to be balanced against the need for re-intervention in almost a third of patients”. They recommended that the choice should lie with the informed patient.
In defence of UAE, Caridi added: “That being said, some of those people who got surgery actually got a hysterectomy, so of course they are not going to need a reintervention more than likely, whereas people who get a myomectomy may, so there is a little bit of bias. But several studies, some out to ten years, do show that the reintervention rate with UAE is about 30%.”
Moving on to her next pro of UAE, Caridi said: “UAE is very efficacious. In fact, it is one of the most efficacious procedures we do in interventional radiology (IR).” The clinical practice guidelines from the Society of Interventional Radiology (SIR) summarise the data in the literature, and show that, on average, “rates of success are really good”: leiomyoma size reduction, 50–60%; uterine size reduction, 40–50%; reduction of bulk symptoms, 88–92%; elimination of abnormal uterine bleeding, >90%; successful elimination of symptoms, 75%; patient satisfaction (would recommend UAE to a friend), 80–90%.
However, another con of UAE is the possibility of fibroid passage. “We treat fibroids really well, but sometimes they detach and pass,” Caridi explained. “We have to worry about that, particularly in submucosal fibroids.”
A meta-analysis from Sundeep Toor (The Ottawa Hospital and University of Ottawa, Ottawa, Canada) et al published in the American Journal of Roentgenology in 2012 reported an incidence of leiomyoma tissue passage of 4.7% (with a range of 3.9–5.7% in 8,159 patients). “That is much higher in a risky site like the submucosal location,” Caridi commented. “It is something we have to worry about. What is the consequence of this [fibroid passage]? Patients can get endometritis and infection and require a secondary intervention. Maybe it is a myomectomy, maybe it is a hysterectomy, if you cannot get the infection under control. Or, they can just get a chronic vaginal discharge that lasts upwards of six months or even a year, and some would like to have a hysterectomy for that reason.”
Returning to her pros of UAE list, Caridi said that “probably one of the key reasons why women seek” UAE is that the recovery time is shorter than for surgical intervention. In the CVIR study by Mara and colleagues that demonstrated the inferior reproductive outcomes of UAE when compared with myomectomy, the authors also reported that the minimally-invasive option fared much better than myomectomy, with significance, for average length of hospital stay, recovery period, and disability greater than two weeks. “It is a quicker recovery, no doubt,” Caridi stated.
She continued, “Though there is a lot of pain associated with UAE”. She elaborated: “Despite our best efforts to look into this in many ways, and all the research that has been done—we have this arsenal of anti-inflammatory and PCA [patient-controlled analgesia] medications, [but] more than 90% of women still report post-procedural pain, and about 35% of women experience pain that is equal to or greater than [that experienced in] labour. So this is a real issue.
“In terms of how to mitigate this, we have some adjunctive techniques, but some of them require a second procedure or have their own risks. We could use superior hypogastric nerve block, intra-arterial lidocaine after embolization—this is pretty widely used as its low-risk profile has been shown in a prospective randomised controlled trial—and then you could go as far as to perform an epidural if you cannot get the pain under control.”
Informed consent is key
Concluding, Caridi commented: “All that being said, I think the summary of this lecture is that there are a lot of pros and a lot of cons to doing a UAE, but the most important factor is to discuss these in a clinic visit.”
Caridi showed the Spectrum audience a consent form that she uses in her own institution, Georgetown University Hospital, that she said she would be happy to share with any interested parties. “We go over all these things with the patient,” she explained. “It helps me stay on track. I sign it, they sign it, I give them a copy.”
The form covers a description of the procedure and the anticipated outcomes: “I tell them [the patient] this is a global treatment, it is uterine-sparing, it is about 90% efficacious, the recovery time is limited. I tell them to take a week off work, although they oftentimes do not need it, but at least they have planned ahead.
“We talk about the alternatives. We talk about the risks, some of which—but this is not an inclusive list—are fibroid recurrence, passage, and pain. Then we talk about future fertility, this actually has its own category. There is no guarantee for future fertility, and if someone desires that, we certainly talk about whether they are a myomectomy candidate.”
Rabih Chaer (left) and Efthymios Avgerinos (right)
Rabih Chaer (left) and Efthymios Avgerinos (right)
The “Standard versus ultrasound-assisted catheter thrombolysis for submassive pulmonary embolism” (SUNSET sPE) trial, a randomised, single-blinded clinical trial comparing ultrasound-assisted thrombolysis (USAT) to standard catheter-directed thrombolysis (SCDT), has completed enrolment, as announced on Friday 17 January by principal investigators Efthymios Avgerinos and Rabih Chaer (University of Pittsburgh Medical Center, Pittsburgh, USA).
The SUNSET sPE trial was designed to address the controversy of the role of ultrasound in improving clot reduction during catheter-directed thrombolysis for acute submassive pulmonary embolism. The study was launched as an institutional trial at the University of Pittsburgh Medical Center in 2016, and more recently two more institutions joined as collaborators; the Department of Cardiology, Emory University, and the Piedmont Heart Institute, both in Atlanta.
As reported in Venous News, participants were randomised 1:1 to a USAT catheter (EKOS System) or a SCDT catheter (Unifuse, Cragg-McNamara). Technical details of the procedure were left to the discretion of the treating physician, with a general guidance for short periods (less than 12 hours) of thrombolysis to match the favourable outcomes demonstrated by the “Optimum duration of acoustic pulse thrombolysis procedure in acute pulmonary embolism” (OPTALYSE) study.
In order to simulate real-life practice, termination was recommended when there was an objective improvement of vital or echocardiographic signs (pragmatic trial). The primary outcome was clearance of pulmonary thrombus burden, assessed by post-procedure computed tomography angiography using a modified Miller score.
According to the investigators, this was partly chosen due to thrombus clearance being the distinct assumed advantage of ultrasound-assisted catheter-directed thrombolysis, but most importantly because it is the only outcome that could power this randomised clinical trial, since the use of clinical outcomes would require a prohibitive sample size.
The study was powered for 80 patients to detect a 50% improvement in pulmonary artery thrombus clearance. Secondary outcomes include resolution of right ventricular strain by echocardiography; improvement in pulmonary artery pressures; and a three- and 12-month improvement in echocardiographic, functional capacity, and quality of life measures.
Efthymios Avgerinos (University of Pittsburgh Medical Center, Pittsburgh, USA) presented interim results of the overall outcomes at the Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM; 12–15 June, National Harbor, USA).
It was shown that catheter thrombolytic techniques can achieve a significant and quick thrombus and RV/LV ratio reduction, and are safe and effective. With enrolment complete, follow-up data and analyses are pending, and comparative results will be announced within the forthcoming months.
George Adams (Raleigh, USA) talks to VEITHtv at the VEITHsymposium 2019 (19–23 November, New York, USA) about the benefits of using easy-to-use Shockwave IVL (Intravascular Lithotripsy) in calcified below-the-knee vessels, which he says, results in “great outcomes”.
Adams explains that calcific plaque, particularly medial calcification in smaller below-the-knee vessels can contribute to adverse events and poor acute outcomes, such as vessel recoil and dissections. However, Adams explains that the use of Shockwave IVL, in which pulsatile sonic pressure waves fracture intimal and medial calcium, can help avoid these events and maximize luminal gain in order to get much-needed blood supply to non-healing wounds in critical limb ischaemia patients.
Investigators report a 100% technical success rate in creating their planned ablation volume and no major device-related complications in the first-in-human clinical cases using histotripsy, a novel ablation modality. Presented at Spectrum (18–22 January, Miami, USA) by Emily Knott, a research intern at the Department of Radiology, University of Wisconsin, Madison, USA, and currently applying to medical school, these early positive results offer “real potential” for the future of this therapy.
Histotripsy is a non-invasive, non-thermal ablation modality that uses focused ultrasound to create a cavitation bubble cloud which destroys the target tissue. This cavitation bubble cloud is precise at the histologic level: the resultant ablation zones are within millimetres of the prescribed location. “Coupled with a robotic arm, you can virtually prescribe any size and shape of ablation zone,” Knott described. The tissue within the ablation zone is completely necrotic.
“An interesting characteristic,” Knott observed, “is that because of these mechanical tissue destruction effects, there is architecture preservation within the ablation zone, including bile ducts and large vessels.
“The most interesting part of this technology, though,” she continued, “is the potential for an immune response.” Sharing early histotripsy studies conducted in mice at the University of Michigan, she described how investigators witnessed an abscopal response that is greater than radiation therapy and thermal ablation, as well as finding decreased metastases in the pulmonary area.
Describing the first ever human clinical cases, Knott told the Spectrum audience of the 100% technical success rate in creating the planned ablation volume, and of the lack of device-related complications.
Two patients demonstrated a potential abscopal response to therapy. Showing the MRI scans of one of these patients on her slides, Knott said: “The really exciting thing with this patient is that when we treated one tumour, a small percentage of this patient’s disease, the AFP [alpha-fetoprotein, a tumour marker] dropped disproportionately over eight weeks.”
In a second patient, with metastatic colorectal cancer, Knott recounts how the team treated a single tumour in the left lobe of the liver. One day post-treatment, imaging showed the tumour swelling slightly “with some inflammation”, but over time, it decreased in size to smaller than before ablation. “CEA [carcinoembryonic antigen, used as a diagnostic and prognostic tumour marker] also dropped disproportionately to the one tumour that we treated in the liver,” Knott said.
She concluded: “Histotripsy is a non-thermal and non-invasive ablation modality. It can safely create a planned ablation volume, and there is a potential immune stimulation in early pre-clinical results in mouse models, and in two of eight patients in an early clinical trial. This clinical trial will be more finalised and [eventually] published, and will also be presented at SIO [the annual meeting of the Society of Interventional Oncology; 31 January–3 February, New Orleans, USA].”
Shimadzu Medical Systems USA, a subsidiary of Shimadzu, along with NZ Technologies of Vancouver, Canada, and developers of TIPSO technology, have announced that they have signed a one-year renewable agreement that allows Shimadzu to market and sell the innovative TIPSO AirPad in the US healthcare market.
TIPSO is a specialised medical technology that has evolved from the technical expertise and industrial experience of its engineering team through contributions from physicians as co-inventors who practice in the field of interventional radiology.
Proprietary technology enables various modes of image navigation over the TIPSO AirPad surface (functioning as mouse and keyboard at bedside) while a real-time representation of the hand and menu is shown on the system monitor display. A simple USB dongle connects the AirPad to any workstation wirelessly without having a connection to the hospital network or any type of transfer/storage of patient data to keep within HIPAA (Health Insurance Portability and Accountability Act) compliance.
AngioDynamics has announced the launch of the PATHFINDER I: Post-Market Registry (PATHFINDER I-Registry, EX-PAD-05), a pilot study to evaluate the safety and efficacy of the company’s AURYON atherectomy system in the treatment of de novo, re-stenotic, and in-stent restenosis (ISR) lesions in infrainguinal arteries of patients with peripheral arterial diseases (PAD).
The AURYON atherectomy system, previously known as the Eximo B-Laser, is a proprietary 355nm wavelength laser-technology platform that was acquired by AngioDynamics in October 2019.
“The PATHFINDER I study will provide valuable, scientifically-backed data to further differentiate the AURYON system from competitive products in this space and build upon the excellent long-term results that patients experienced during the IDE,” says Juan Carlos Serna, AngioDynamics Vice president for Clinical Affairs and Healthcare Economics.
AngioDynamics’ PATHFINDER I registry is a prospective, non-randomised, single arm, multicentre observational study that will evaluate the performance of the AURYON atherectomy system during procedures and measure clinical outcomes, both intermediate and long-term. A total of 100 eligible PAD patients treated with the AURYON atherectomy system in a post-market setting will be enrolled and tracked for a 36-month period after the initial procedure.
Initial findings from the pilot registry study will contribute to a subsequent large pivotal phase registry that is expected to include approximately 1,000 patients.
The commercial release of the AURYON atherectomy system in the USA will occur in the second half of the fiscal year.
The TriForce peripheral crossing set, from Cook Medical, is now commercially available in the USA. As of January 2020, these products are available to physicians in the USA to support procedures to treat patients with vascular obstructions.
According to the company, the TriForce peripheral crossing set is designed to be percutaneously introduced into blood vessels and support a guidewire while performing a peripheral intervention. The device is also intended for injection of radiopaque contrast media for angiography.
It is offered in two lengths and four configurations, providing several product options to treat blocked or restricted vessels in a variety of locations in the body, Cook Medical state.
With provision of interventional radiology (IR) services varying across the UK, the Getting It Right First Time (GIRFT) programme aims to identify and reduce unwarranted variation in English trusts to help bring about improvements. GIRFT is publishing a report later this year outlining the issues that have led to this discrepancy, and providing recommendations for solutions at the local and national level. Katharine Halliday anticipates this report here, elaborating on her keynote lecture at the British Society of Interventional Radiology annual meeting (13–15 November, Manchester, UK).
Introduction to GIRFT
GIRFT is a national programme aimed at reducing unwarranted variation in the National Health Service (NHS). It began as a pilot in orthopaedic surgery, led by Professor Tim Briggs, who visited orthopaedic units across the country and led peer-to-peer discussions about the local service. The pilot was very successful, improving the standard of care for orthopaedic patients and reducing costs. The model has subsequently been rolled out to 40-plus clinical specialties, including radiology.
For each trust, a pack of comparative data is produced from national sources—this forms the basis of a discussion with clinical staff and mangers, facilitated by the clinical lead. The visit provides an opportunity for departments to showcase their good work to their executive team and for the senior managers to fully understand the vital role played by radiology in most patient pathways. The clinical lead identifies areas of good practice which can then be shared with other departments. Areas the department would like to work on are also discussed and documented.
The GIRFT radiology team has now visited almost every trust in England. The process has been a hugely educational one and we have been very impressed by the enthusiasm with which the radiology community has embraced the opportunity to review services, identify possible areas for improvement, and learn from others
Regarding interventional radiology, some strong themes have emerged:
Workforce
In 2018, the Royal College of Radiologists (RCR) identified that only one in five trusts had six interventional radiologists, considered to be the minimum number necessary to cover a comprehensive on-call service. There is no evidence that this situation is improving.
In many trusts the shortfall in the elective interventional service is mitigated by extending the role of radiographers and nurses, who now undertake many and varied interventional procedures. But radiographers and nurses are also in short supply, and some trusts are not capitalising on their training investment because staff cannot be released from image acquisition or other duties. Innovative departments have maximised the contribution of healthcare assistants to release higher banded staff for advanced practice, but over recruitment is essential for role extension to be effective.
The stimulating and varied nature of radiology nursing is not always recognised, and, on the background of a national nursing shortage, recruitment issues are keenly felt. In some cases, working with theatres has enabled a more sustainable workforce. Close liaison with other nurses from across the hospital, including students, is helpful when attracting staff. Several interventional radiology (IR) nurses have mentioned that there are few nationally-run training courses. There is an opportunity here to strengthen the nursing division of the British Society of Interventional Radiology (BSIR).
Some departments are more successful than others at recruiting and retaining their staff. A focus on training and continuing professional development proves very popular with all grades. Ideally more staff would be able to progress from the lower bands to Bands 5 and 6, but this is still challenging. GIRFT is working with national bodies to identify and reduce barriers.
Environment
We have seen wide variation in the environments for patients and staff. Those departments that operate most efficiently can admit and discharge patients from radiology, ideally with a small day case unit dedicated to imaging, overseen by nursing staff. These units are often shared with cardiology and provide a safe environment for patients and avoid expensive and frustrating delays waiting for inpatient beds. We have seen excellent radiology day case units in hospitals where there are no vascular beds which allow patients to be treated much closer to home.
Paediatrics
Paediatric intervention is particularly challenging. Although facilities and expertise in children’s hospitals are excellent, most children are seen and treated in general hospitals. Even in very small departments where most patients are adults, liaison with play therapists and the identification of a lead radiographer for paediatrics can vastly improve the experience for paediatric patients and their families. Volumes of paediatric intervention are too low to have a dedicated paediatric IR team in any but the largest specialist centres, and it is necessary for adult IR teams to develop and maintain some skills in this area.
Data
Although large quantities of radiology data are collected, the quality is often poor because there is huge local variation in the way individual procedures are coded and counted. There is also no unifying code for interventional procedures so collecting outcome data for appraisal and audit is difficult locally and impossible at a national level. GIRFT is working with a team of data experts to address these issues.
Networking
The challenges identified above result in very variable access to interventional procedures, particularly for patients presenting out of hours. The vascular surgical networks supported by the vascular surgery GIRFT work stream are maturing and continue to improve pathways for vascular patients, while many radiology departments are working together to form IR networks. The model varies depending on local circumstances and expertise but in the best departments individual pathways are identified for specific conditions and these are clearly conveyed to clinical teams. The document recently published by NHSI/E—Transforming Imaging services in England: A national Strategy for imaging networks—sets out a vision for networking in radiology which will be helpful for developing robust IR services. Strong leadership from interventional radiologists and close liaison with clinical colleagues is essential if these are to be successful.
Next steps
At the end of each GIRFT presentation the local team are asked to identify issues they would like to work on, together with good practice. These are summarised in a short report which is sent back to each trust within a couple of weeks. Local support is offered to the trust by the GIRFT implementation team who help to develop the themes and put together an action plan. Many trusts have also appointed their own GIRFT lead who will assist with local improvements. It is often possible to put departments in contact with other people who have overcome similar challenges and for good practice to be shared between institutions.
Each GIRFT work stream publishes a national report and in many of those, the essential role of radiology has been highlighted. The radiology GIRFT national report will be published in 2020. In several areas the team are already working with national bodies, but the report will highlight the issues identified across imaging departments and will make national recommendations.
Katharine Halliday isthe clinical lead radiologist for the GIRFT programme and is a consultant paediatric radiologist at Nottingham University Hospitals NHS Trust, Nottingham, UK. She is past chair of the British Society of Paediatric Radiology from 2010 to 2016.
A new meta-analysis, just published in the Journal of Vascular and Interventional Radiology (JVIR), suggests significantly worse amputation-free survival at one year with the use of paclitaxel-coated balloons in arteries below the knee in the treatment of chronic limb-threatening ischaemia (CLTI). However, some experts advise cautious interpretation of results and question whether these data will impact practice. The new systematic review and study-level meta-analysis of eight randomised controlled trials was conducted by Konstantinos Katsanos (School of Medicine, University of Patras, Patras, Greece) and colleagues.
Several physician thought-leaders believe that the conclusions are not yet definitive, with multiple vascular interventionalists and surgeons cautioning how these data should be interpreted. Most emphasised the challenge of teasing out scientifically meaningful information from a patient cohort that suffered from CLTI, which is associated with “mortality, amputation, and impaired quality of life”. They also point to the inclusion of unpublished data (which has therefore not gone through the peer-reviewed process); the inclusion of summary-level data; the inclusion of the IN.PACT DEEP data (which used a device that has long since been withdrawn from the market); and the study’s short-term follow-up period.
As reported in JVIR, the eight randomised controlled trials included in this most recent summary-level analysis included 1,420 patients, of which 1,380 (97.1%) had CLTI. The primary safety and efficacy endpoint was amputation-free survival, defined as freedom from all-cause death and major amputation (above the ankle). At one year, there was a 13.7% crude risk of death or limb loss among the 835 patients who had received treatment with paclitaxel-coated balloon—74 deaths and 40 major amputations. In comparison, the crude risk of death or limb loss in the cohort treated with an uncoated balloon was 9.4%—39 deaths and 17 major amputations. For the primary amputation-free survival endpoint, the number needed to harm was estimated to be 22 patients (95% confidence interval [CI] 11–94). The authors claim there was consistent evidence from the randomised studies that freedom from major amputation or death was significantly lower in cases with paclitaxel-coated balloons with a pooled hazard ratio (HR) of 1.52 (95% CI 1.12–2.07; p=0.008).
However, Katsanos et al also report consistent evidence that paclitaxel reduces the need for target lesion revascularisation in below-the-knee arteries by approximately 40%. Target lesion revascularisation constituted the secondary efficacy endpoint. The crude risk of target lesion revascularisation was 11.8% (103 revascularisation events among 875 cases) versus 25.6% (159 events among 620 control patients) for patients treated with a paclitaxel-coated balloon and an uncoated balloon, respectively. The calculated pooled risk ratio was 0.53 (95% CI 0.35–0.81; p=0.004), with a corresponding number needed to treat of eight patients (95% CI 4–25).
The study authors claim there is a dose–response relationship between paclitaxel and amputation-free survival. They compared outcomes with low and high doses of paclitaxel, and found significantly more deaths or amputations (lower amputation-free survival) in cases with high-dose devices, defined as 3–3.5µg/mm2 (HR 1.62; 95% CI 1.16–2.27; p=0.005). In comparison, amputation-free survival was higher (fewer deaths or fewer major amputations) when a low-dose device (2µg/mm2) was used (HR 1.06; 95% CI 0.48–2.34). This low-dose was found to be safe and effective, the authors report.
The authors of the present study say they performed a “comprehensive literature review” due to the “major concerns about systemic safety of paclitaxel” prolific in the endovascular community today as a result of their earlier meta-analysis published in the Journal of the American Heart Association (JAHA) in 2018. This concluded that there was an increased association of mortality beyond two years through five years of follow-up when paclitaxel-coated balloons and paclitaxel-eluting stents were used in the femoropopliteal arteries.
Concerns of the medical community: The interventional radiologist perspective
Laura Findeiss, president of the Society of Interventional Radiology (SIR); Emory University School of Medicine, Atlanta, USA
Laura Findeiss
“The paper published today by Konstantinos Katsanos and colleagues raises important questions about the treatment of patients with CLTI, and is an important contribution to the medical literature. As with any meta-analysis, validation of the findings will require further dedicated investigation. In particular, the lack of patient-level data and the inclusion of unpublished data sets in this analysis may weaken the strength of the conclusions.
“Patients with CLTI are vulnerable and have few care options. It is important to know what treatments will best enhance their life expectancy and quality of life. The Society of Interventional Radiology will continue to work with the [US] Food and Drug Administration to support its work in developing practice guidance on the use of paclitaxel-coated balloons in the infrapopliteal arteries for CLTI treatment as we look to build rigorous scientific evidence for available treatments.”
Robert Morgan, past president of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE); St George’s Hospital, London, UK
Robert Morgan
“It is an interesting publication that unfortunately adds little to the overall lack of conclusive evidence supporting the use of paclitaxel-coated devices in the infrapopliteal circulation in patients with CLTI.
“I am concerned that flaws in systematic reviews highlighted in universal comments on the authors’ previous meta-analysis in JAHA may also have contributed to the negative results for paclitaxel-coated balloons in this systematic review. No doubt this paper will excite many comments and publications on this topic in the next 12 months.
“The topic is a very important one considering the ongoing controversy of paclitaxel-coated devices in the femoropopliteal circulation. The subject is muddied by the potential adverse effects of different excipients and the lack of individual patient safety data. I do not think that this contributes significantly to the ongoing controversy regarding any potential link between paclitaxel-coated balloons and mortality. However, the authors’ conclusion that distal embolization of paclitaxel and/or excipient may adversely affect amputation-free survival is reasonable. Finally, the inclusion of the IN.PACT DEEP data (using a withdrawn device) involving almost a third of the patients in this review, with its known negative influence on mortality and amputation-free survival, is likely to have adversely contributed to the overall negative results on amputation-free survival in this publication.
“In common with most vascular practitioners in the UK, I do not use paclitaxel-eluting devices below the knee in patients with CLTI. This is partly due to the Medicines and Healthcare products Regulatory Agency (MHRA) statement on paclitaxel devices in 2019, and partly due to a perception of lack of efficacy of these devices in CLTI. In view of the above, these data will not impact my current vascular practice.”
Michael Dake, president-elect of the Society of Interventional Radiology (SIR); University of Arizona Health Sciences, Tucson, USA
Michael Dake
“Aside from The Godfather Part II, sequels are rarely as compelling as the original version, often with an impact that is a mere ripple of the force produced by the initial statement. Predictably, I suspect this will be the case for the current report, although its contribution to the medical literature will be of interest to many stakeholders in the field of vascular disease.
“The results of this meta-analysis of randomised controlled trials focused on patients with CLTI are more difficult to interpret than the earlier femoropopliteal publication. The medical complexity of the underlying disease and the vulnerability of CLTI patients contribute to a greater heterogeneity in the population studied. Consequently, added caution must be exercised when attempting to make conclusions from this meta-analysis.
“In terms of the methodology used, the current study shares some of the frequently noted limitations of the original femoropopliteal meta-analysis. The lack of patient-level data available to the authors from the randomised studies included in the meta-analysis restricts evaluation of the total dose of paclitaxel used in individual patients and any correlation with mortality. In addition, the relatively small number of patients analysed and [the] short follow-up (46% of the patients had only six-month follow-up) make any conclusions problematic. Unlike the first meta-analysis, however, an additional limitation is noted. The current report of pooled trials includes unpublished data. Results from three of the eight trials used in the analysis have not been published. This represents one-quarter of the patients included.
“Nevertheless, the paper raises interesting points about the effect of drug-coated balloon treatment for patients with CLTI, and questions the possible association of downstream drug embolization and amputation in patients with compromised distal arterial circulation. In addition, it echoes the call after the earlier femoropopliteal publication for more data and an urgent need for adequately-powered multicentre studies with longer follow-up. Its effect on clinical practice for management of CLTI patients with limited treatment options is questionable. Most likely, future substantiation using larger, well-controlled trials will be required before changing strategies for the application of drug-coated balloons in treating CLTI.”
John Kaufman, Oregon Health & Science University, Portland, USA
John Kaufman
“Concerns about drug-eluting balloons in the tibial arteries have been around since the DEBATE-BTK and IN.PACT DEEP trials, so while not as disruptive as the prior study from this group, this new meta-analysis certainly adds more grist to the paclitaxel mill. Some of the same limitations of the previous study apply here: the absence of patient-level data, and differences in the technologies between trials. Most patients in this meta-analysis had CLTI, a more challenging population than the patients with claudication due to the femoropopliteal artery that dominated the previous study. Other differences are that only balloon-based devices were studied, there are a paucity of data on inflow and target lesion revascularisation procedures, and the number of patients analysed is smaller. Of note, data from several of the included trials are only available as conference presentations online, rather than peer-reviewed publications. However, most important is that the follow-up is far shorter than in the previous meta-analysis—between six months and 12 months. Is it possible that over time we will see these amputation and mortality rates stabilise or even equalise? Will extended follow-up of patients treated with new devices bend the curves in the right direction? With this new analysis we are left in the same place as before; paclitaxel devices have better lesion-based outcomes, but there may be trade-offs. We need to be really thoughtful as we learn how and when to best use them, especially in the tibial arteries.”
Jim Reekers, CVIR Endovascular editor-in-chief; Academic Medical Center, Amsterdam, The Netherlands
Jim Reekers
“Reading the methodologically-excellent paper by Katsanos et al, their conclusions do not come as a surprise. The so called “low flow” phenomenon after drug-coated balloon use was recognised in coronary arteries four years ago. Also, the observation of “slow flow” directly after peripheral drug-coated balloon [use] has been discussed by others in the corridors of several meetings. In our department, drug-coated balloons are used very scarcely (four a year for recurrent early superficial femoral artery restenosis only), but we have already seen two patients with instant reduction of foot perfusion after drug-coated balloon use in the superficial femoral arteries. This acute reduction in flow was documented with perfusion angiography. These were both patients with intermittent claudication where no clinical consequences were seen, probably due to the sufficient reserve capacity of the microcirculation perfusion. However, in serious CLTI, this embolization could have devastating consequences for the outcome. This also proves that, at least partly, micro-particles loaded with paclitaxel are trapped in the microcirculation. A simple prospective trial using perfusion angiography after drug-coated balloon implantation would be enough to prove this micro-particle embolization as cause for a reduction in amputation-free survival.
“In Katsanos et al’s paper, the hazard ratios are calculated for amputation-free survival as a primary clinical endpoint, and target lesions revascularisation is a secondary non-clinical endpoint. A secondary endpoint can sometimes be used for clinical decision-making if the primary endpoint of a study is borderline statistically not significant or equivalent. Mostly, a secondary endpoint is used to calculate the cost-efficacy of a treatment. The fact that the target lesion revascularisation is 50% better after drug-coated balloon use is, however, irrelevant if the primary clinical endpoint (amputation-free survival) shows that the hazard ratio for a lower amputation-free survival is 1.52 after the use of a drug-coated balloon. This strong primary clinical endpoint makes any drug-coated balloon treatment questionable.
“Combining the previously-documented data of a mortality increase with paclitaxel-coated devices after two and five years with this new findings of a lower amputation-free survival after drug-coated balloon use in CLTI patients should make us seriously re-think the concept of drug-coated balloons in CLTI as a (failed) treatment concept.”
Gunnar Tepe, Klinikum Rosenheim, Rosenheim, Germany
Gunnar Tepe
“I have two immediate remarks:
“It is very important to look into safety issues of devices in general. Therefore, all data have to be taken seriously.
“Compared to the first publication from Katsanos et al, the statistical part is much more solid.
“Nevertheless, there are several major limitations of the recent publication:
“In order to achieve a certain number of patients, the follow-up time was mixed—some studies follow the patients for six months, some trials have a 12-month follow-up.
“Katsanos et al state that they did a meta-analysis based on eight studies. In fact, the meta-analysis is driven by two high-volume studies only. This is the Lutonix BTK study with a six month endpoint, and the IN.PACT DEEP study with a 12 month endpoint. The finding that amputation-free survival is decreased in patients who received paclitaxel-coated balloon angioplasty below-the-knee is driven by the IN.PACT DEEP study, which has high patient numbers. This is nothing new and has been published. Nevertheless, even the data available to Katsanos et al do not discuss that. For the IN.PACT DEEP study, we know from data presented at conferences that at five years, patients who received drug-coated balloons had a better amputation-free survival.
“Dose issue: Katsanos et al state that a higher dose is followed by more amputations. This is a wrong statement. All below-the-knee drug-coated balloons are low-dose applications compared to what is given in the superficial femoral arteries. We know from several studies that patients with CLTI and drug-coated balloon treatment in the superficial femoral arteries do fine. There were fewer target lesion revascularisations, but no increase of amputations or deaths. It is totally misleading the Katsanos et al ignore this fact.
“Another mistake is that Katsanos et al do not take into account that most likely almost all patients have received paclitaxel-coated balloons in their history—either in the same leg, in another location, or for target lesion revascularisation. It is not OK that he just states in the discussion that this is unknown.
“In summary: Katsanos et al unfortunately increase the uncertainty in the safety of drug-eluting technology. What does it end with? Fewer patients will get drug-coated balloons and more target lesion revascularisations and [consequently] more amputations may occur. Does it affect my clinical practice? No, for two reasons:
“I think (also [in accordance with] what has been published within the last year) that paclitaxel-coated balloons are safe
“In CLTI patients with below-the-knee treatment, the long-term patency is not as important as in claudicants patients. It is also feasible to proceed with plain balloon angioplasty. In the superficial femoral artery, my primary choice is drug-coated balloon treatment; in below-the-knee arteries it is plain balloon angioplasty.
Concerns of the medical community: The vascular surgeon perspective
Kim Hodgson, president of the Society for Vascular Surgery (SVS); Southern Illinois University School of Medicine, Springfield, USA
Kim Hodgson
“While this analysis of the efficacy and mortality of paclitaxel use in the infrapopliteal CLTI population has similar methodological limitations to the first Katsanos publication of paclitaxel used to treat claudication, it also reaches the similar concerning conclusion that paclitaxel use in peripheral vascular disease is associated with increased mortality. But this time the authors use the most relevant of clinical endpoints for this population, amputation-free-survival, to evaluate for the ultimate goal of an intact living patient. While it took use of this composite endpoint to achieve statistical significance, it is alarming that both mortality and amputation came very close to independently reaching statistical significance (p=0.1; p=0.09, respectively), and I suspect that with a larger sample size one or both may have. If further evidence confirms either that paclitaxel does not decrease the rate of amputation but does increase the mortality, then the prospects for its continued use appear bleak. The possible ray of sunshine in this cloud is the observation that the lowest dose paclitaxel device analysed (Lutonix, BD) appeared to be free of increased mortality yet still effective, perhaps indicating that the dosing sweet-spot has yet to be found while acknowledging that we have no accurate way of measuring actual paclitaxel tissue delivery or systemic release. The complicated nature of paclitaxel delivery and its pharmacology, however, portend that this will remain a complicated mystery to unravel.
“There has been a significant shift towards the use of paclitaxel delivering devices in treating peripheral vascular disease since their introduction several years back. Given this and the ever-growing population of peripheral vascular disease patients being treated, it is critical that physicians know the full risk:benefit profile of the therapies they employ and always put the patient’s outcome first. The methodological limitations of this pooled analysis are divulged by Katsanos et al and are similar to those of the group’s previous publication on the use of paclitaxel in the claudication population. Nonetheless, his prior report called attention to a signal that was, in fact, subsequently confirmed, though still not understood, so the findings of this analysis are highly relevant and need further analysis.
“When considering a risk like mortality, erring on the side of caution only makes sense, especially considering the multitude of other revascularisation options available to most patients, the irreversibility of death, and the risk of litigation. This is especially true when the effectiveness of the therapy itself is in question, as this analysis has suggested. Until we have greater clarity on the safety and efficacy of paclitaxel devices, I believe that most will opt to use them very selectively in the small subset of patients at high risk for restenosis and no other reasonable revascularisation options.”
Ramon Varcoe, Prince of Wales Hospital and University of New South Wales, Sydney, Australia
Ramon Varcoe
“My first reaction was that it was good to see a group looking to define the risks of paclitaxel devices in the CLTI population. The CLTI group is very different to the claudicants evaluated in the previous meta-analysis and warrants specific attention.
“My reaction to the results was mixed. The authors showed no difference in all-cause mortality or major amputation rates but when they combined the two as the endpoint amputation-free survival, they appeared to find a difference between drug-coated balloons and percutaneous transluminal angioplasty, with better amputation-free survival in the control group. The other positive finding was that they showed a 47% reduction in reinterventions, underlining the well-established effectiveness of these devices.
“It must be said from the outset that—with limited numbers and such short-term follow-up—care must be taken not to overreach in our conclusions. Moreover, taking a deeper dive into the meta-analysis revealed several methodological questions and important validity concerns.
“For example, why were only drug-coated balloons evaluated and not drug-eluting stents? This differed from the methodology of the previous meta-analysis and meant excluding the PADI trial, which has published five-year follow-up. This is the very group identified in the previous meta-analysis as having the most pronounced safety signal. Second, why was amputation-free survival determined to be the primary endpoint, when all-cause mortality was used in the previous meta-analysis? Why was no protocol published on the PROSPERO database to assure the reader that the endpoint was determined a priori, not after the analysis? Third, why were only below-the-knee studies included when the authors speculate it is the particulate embolisation of the drug that provides an explanation for the safety signal? Particulate embolisation is known to occur when CLTI patients are treated for above- and below-the-knee disease. However, ultimately these are questions for the authors, which may have a reasonable explanation.
“My major concern is the inclusion of unpublished data. This was the case in three of the eight studies pooled. We must take great care in including data that has not been peer reviewed. It is common that event rates change between presentation and final publication, which may alter the findings of a meta-analysis and its conclusions. This is particularly true for low-frequency endpoints such as amputation-free survival at six to 12 months. It is also very difficult for the reviewers to grade the quality of evidence from a short congress presentation, as opposed to a peer-reviewed manuscript. However, including unpublished data is not unheard of, particularly when there are few published studies in the literature. What concerns me most is the glaring omission of the most significant study of drug-coated balloon use in below-the-knee arteries of CLTI patients. The five-year results of the IN.PACT DEEP study were presented by Thomas Zeller at the AMP symposium last year (14–17 August, Chicago, USA). Like the other three studies, it was unpublished in September 2019 when the systematic review was conducted. However, if you include some unpublished data you must include all.
“IN.PACT DEEP was a rigorously conducted trial which fulfilled all of the inclusion criteria for the meta-analysis, as evidenced by inclusion of its earlier 12-month results. In that study, amputation-free survival was numerically better in the drug-coated balloon group (drug-coated balloon 135/239 [56.5%] vs percutaneous transluminal angioplasty 65/119 [54.6%]). The inclusion of such a study is important for two reasons. It provides long-term follow-up, which was linked to mortality in the original meta-analysis in claudicants and it had a high number of events (death and amputation). Statistically, meta-analysis gives additional weight to large studies with high event rates because observed differences are less likely to be due to chance. It is my view that if those contemporary results had been included in this meta-analysis, the conclusions regarding amputation-free survival and safety would have been very different. Given the reintervention reducing benefit of drug-coated balloons, the authors have demonstrated we must get this right. A serious omission such as this must be corrected if we are to determine the truth—our very patients’ lives depend on it.
“These results are under a cloud due to methodological questions and the omission of the most important study. This should not impact anyone’s practice until those issues have been addressed.”
Michael Conte, Heart and Vascular Center, University of California, San Francisco, San Francisco, USA
Michael Conte
“I do not think this is really a big surprise, as the results from IN.PACT DEEP regarding a higher observed rate of major amputation in the paclitaxel-coated balloon arm have been known, and the only other reasonably large study (Lutonix-BTK) has yet to report one-year data. The other six trials are modest in size and the number of events is small. So the pooled data is dominated by the two larger trials, only one of which has reported one-year data with these effects known. There are and have been concerns about the adverse effects of paclitaxel embolisation in CLTI patients and this publication keeps the issue on the front-burner but does not resolve it much further.
“CLTI is a major global health problem and current treatments have significant limitations, contributing to high morbidity and mortality rates in these patients. Interventions for infrapopliteal arteries, in particular, have high rates of failure and thus there is considerable unmet need for more effective approaches. Thus the interest in various methods to improve the results of angioplasty, such as drug-elution, remains high.
“The limitations of this study relate to both the analysis itself and, more importantly, the state of the field it reflects. The meta-analysis involves pooled data and is not patient-level. Thus it is not possible to evaluate confounders (e.g. unbalanced comorbidities or clinical severity) that may be driving the outcomes. The actual event rates in these trials are lower than expected across the board, e.g. overall major amputation rate of 4% suggesting that the degree of limb threat at presentation may have been modest. The two larger trials employed a 2:1 randomisation ratio, leading to a significantly larger population with PCB exposure than controls. As stated above, the results are dominated by the two larger studies, and these studies have only reported short to mid-term outcomes. This is particularly relevant for the death outcome. CLTI itself has a broad clinical spectrum and the need for improved staging systems (for example, the Society for Vascular Surgery Wifi classification system) is evident to allow for better trial designs and balanced randomisation by limb severity. Finally, one has to ask—where are the five-year data from IN.PACT DEEP and where are the one-year data from Lutonix BTK? The vascular community deserves timely, complete, and honest reporting from the trials.
“The conclusions are cautiously stated by the authors and reflect the current data available. But the quality and quantity of data available in this space remains seriously lacking.
“No [I do not think the paper will change practice] because in the USA there are no currently approved paclitaxel-coated balloons for the infrapopliteal arteries at this time. It will be interesting to see if the final results of Lutonix BTK are reported and whether they allow for regulatory approval by the FDA. Until then I believe it is reasonable to continue to conduct appropriately monitored, well-designed RCTs to evaluate the safety and efficacy of drug-eluting devices for CLTI given the significant unmet need.”
Concerns of the medical community: The interventional cardiologist perspective
Gary Ansel, OhioHealth Heart and Vascular Physicians, Columbus, USA
Gary Ansel
“In my view, this manuscript may very well misinform the medical community and the patients we serve. It is important to note that the scientific community has been utilising higher level scientific analyses (i.e. patient-level data) to evaluate the role of paclitaxel in peripheral vascular procedures. The original question of whether paclitaxel has adverse outcomes in these procedures was a good one. However, there is a need to react scientifically to any potential investigator bias and ascertainment bias in the original data sets as well as the patient level data from the randomised trials and very large real-world data.
“First, patient care including safety and outcomes are foremost in my thoughts. However, this manuscript included data from non-peer reviewed studies presented at medical symposia as well as single-centre datasets and data published in lower-tiered journals. Both of these types of data, especially with the low total number of patients may be interesting, but do not have the level of accuracy to apply to a meta-analysis trying to make definitive patient safety claims. One of the cardinal sins for meta-analyses is to try and prove a point or to go in with an agenda.
“It is interesting that the authors chose to utilise certain data sets from the public sector, while at the same time leaving out others such as the many presentations of the longer-term follow-up of the INPACT DEEP study where the risk of amputation and survival actually reverse with uncoated balloon angioplasty demonstrating more risk. There have also been numerous presentations in the femoropopliteal bed with DCB (with an actual patient-level data meta-analysis) demonstrating a continuously decreasing relative risk as more complete follow-up data is obtained. These data have been submitted for publication and are under evaluation.
“The relevance of CLTI is important as typically there has been a “mantra” from the current authors that much larger public data sets that have been published without any safety signal has been due to the dilution by the increased risk of the critical limb population. The authors do not even address the fact that their first data sets evaluating the potential mortality signal appeared at a delayed time point of over a year, and here they seemingly find it at 6–12 months? This publication serves no useful purpose, in my opinion.”
Thomas Zeller, Universitäts-Herzzentrum Freiburg, Bad Krozingen, Germany
Thomas Zeller
“I was surprised about the inclusion of short-term outcomes in this study—the follow-up period ranges from six to 12 months. In a previous meta-analysis of the same study group regarding safety of paclitaxel-coated balloon use in femoropopliteal artery disease, absolutely no safety concern was evident at one-year follow-up. Now, in the present study, the authors raise a safety concern already within a couple of months after paclitaxel exposure that does not fit together with their assumption of an increased mortality risk as the consequence of a chronic paclitaxel toxicity due to disseminated multi-organ embolisation.
“The study data must be interpreted with caution due to several reasons. The limitations of the present meta-analysis are even more relevant as compared to the previous one related to femoropopliteal disease treatment. The overall study size of 1,420 patients is meaningful but still underpowered regarding the primary endpoint amputation-free survival considering the wide variation of the numbers found in the literature for the both individual endpoints: all-cause death and major amputation rate. In five of the eight studies, data from congress reports are included in the meta-analysis. The primary endpoint of the study is amputation-free survival. Secondary endpoints are all-cause death, major amputation, and target lesion revascularisation rates. Amputation-free survival was significantly worse for the drug-coated balloon group (HR 1.52, 95% CI 1.12–2.07, p=0.008), whereas all-cause mortality and amputation rates were not statistically significant different. The target lesion revascularisation rate was significantly lower after drug-coated balloon treatment (HR 0.53, 95% CI 0.35–0.81, p=0.004). Again, same as for drug-coated balloon application in femoropopliteal arteries, the authors postulate a dose-dependent increase of risk of mortality and amputation rate with “high-dose” drug-coated balloon devices.
“Katsanos et al conclude: “There appears to be an increased risk of death or major limb loss during the first year when paclitaxel-coated balloons are applied in the infrapopliteal arteries for CLTI treatment. Actual causes for this detrimental clinical outcome remain largely unknown, but downstream and systemic paclitaxel embolization is a plausible mechanism.
“First of all, the conclusion is wrong. The study does not show an increased risk of “death or major limb loss”: all-cause death rate does not significantly differ between the study groups (HR 1.39, 95% CI 0.94–2.07) nor does major amputation rate (HR 1.63, 95% CI 0.92–2.90). It is the combination of both endpoints—amputation-free survival—that is favouring the percutaneous transluminal angioplasty strategy.
“Are the findings real? The review includes study data derived from study-level data published or presented on recent congresses. Three out of eight studies are single-centre studies without independent clinical events committee adjudication of the safety events, three out of eight studies analysed are not yet published congress reports and the data may be subject of change during the publication process.
“The “trend to an increased all-cause mortality risk” following drug-coated balloon exposure in this study is not in line with the finding of the same study group for the treatment of femoropopliteal disease with drug-coated balloon. In the former study, the all-cause mortality rate was identical at one-year follow-up, whereas in the present study mortality rate was already higher after a short-time follow-up of six to 12 months only. If paclitaxel exposure during drug-coated balloon treatment should result in a chronic systemic toxic effect, as claimed by Katsanos et al, it should result in a uniform time to harm from exposure in particular considering that the paclitaxel doses applied during treatment of femoropopliteal disease is much higher as compared to below-the-knee disease. In addition, assuming a toxic drug effect, a dose–dependency of the mortality endpoint is crucial. The study found a lower mortality rate for “low-dose” drug-coated balloon, defined as 2μg/mm2, compared to “high-dose” drug-coated balloon (3–3.5μg/mm2). However, only one out of eight studies used a “low-dose” device and for this particular study only six-month follow-up data are published.
“The trend towards a non-significant higher major amputation rate following drug-coated balloon treatment in short-time follow-up must be interpreted with caution. Only one study (SINGA-PACLI) reported a significantly increased one-year amputation rate at one year. Major amputation rate is a study endpoint with high potential for bias due to the lack of uniform post-procedure wound care guidelines. In addition, study cohorts included in the meta-analysis are hard to be comparable regarding disease severity, in particular regarding the presence of wounds or ulcers ranging from 56.1% in Lutonix BTK—the only “low-dose” drug-coated balloon study—to 96.5% in DEBATE-BTK and SINGA-PACLI. In addition, patients included DEBATE-BTK were in 100% diabetics. The combination of diabetes and wounds characterises a high-risk patient population for amputation. Nevertheless, DEBATE-BTK resulted in the lowest odds ratio for major amputation despite the use of a “high-dose” DCB (3.5μg/mm2) that disproves the suggestion of the authors of dose-dependent local tissue toxicity.
“In summary, the current meta-analysis raises concerns regarding the short-term safety of paclitaxel-coated balloon treatment of below-the-knee disease in a CLTI study population resulting in a significantly reduced amputation-free survival rate after a follow-up of six to 12 months. Not going into statistical details, the study is characterised by major limitations but the safety signal deserves a higher quality data work-up including patient level data analysis and a longer-term follow-up of at least three years considering the high general mortality rate of a CLTI study population.
“These data will not impact practice because, as a result of the JAHA publication in 2018, drug-coated balloons are, in general, already used with caution. In addition, until the recent congress presentations of ACOART II (Guo et al, LINC 2019, Leipzig, Germany) and ACOART BTK (Liistro, VEITH 2019, New York, USA) no clear evidence existed regarding the technical efficacy of drug-coated balloons in below-the-knee lesions. Both afore mentioned studies for the first time demonstrated a patency benefit of a drug-coated balloon over percutaneous transluminal angioplasty. Therefore, so far the use of drug-coated balloon in below-the-knee disease in daily practice was experimental and limited to “drug-coated balloon believers” that will not be changed by the present publication. In my daily practice I will still use the drug-coated balloon brand investigated in the two ACOART studies in long below-the-knee total occlusions. Interestingly, in IN.PACT DEEP, the to date only study with a published five-year follow-up using a “high-dose” drug-coated balloon, the composite endpoint consisting of all-cause death, major amputation, and clinically-driven target lesion revascularisation was identical for both study cohorts (drug-coated balloon 59.8% vs. percutaneous transluminal angioplasty 57.5%, p=0.309) as well as the all-cause mortality rate (drug-coated balloon 39.4% vs. percutaneous transluminal angioplasty 44.9%, p=0.727).”
A range of interventional radiologists experts including Michael Dake (Tucson, USA), John Kaufman (Portland, USA), Jim Reekers (Amsterdam, The Netherlands) and Gunnar Tepe (Rosenheim, Germany) give their thoughts on the recently released meta-analysis in JVIR, which has suggested an increased risk of death or amputation at 12 months when paclitaxel-coated balloons are used in the infrapopliteal arteries for the treatment of critical-limb threatening ischaemia (CLTI).
Vascular and interventional cardiology experts including Kim Hodgson (Springfield, USA), Ramon Varcoe (Sydney, Australia) and Gary Ansel (Columbus, USA) give their thoughts on the recently released meta-analysis in JVIR, which has suggested an increased risk of death or amputation at 12 months when paclitaxel-coated balloons are used in the infrapopliteal arteries for the treatment of critical-limb threatening ischaemia (CLTI).
MedAlliance, the first drug-eluting balloon (DEB) company in the world to receive US Food and Drug Administration (FDA) breakthrough device designation status for a sirolimus DEB, has now been awarded breakthrough status for SELUTION SLR, its sustained limus release DEB catheter, in the treatment of AV fistula indications. This is the third breakthrough designation awarded to MedAlliance for its sirolimus DEB, following coronary in-stent restenosis and peripheral below-the-knee indications.
According to a press release, SELUTION’s technology involves unique micro-reservoirs made from biodegradable polymer intermixed with the antirestenotic drug sirolimus. These micro-reservoirs provide controlled and sustained release of the drug. Extended release of sirolimus from stents has been demonstrated highly efficacious in both coronary and peripheral vasculatures. MedAlliance’s proprietary CAT (cell adherent technology) enables the micro-reservoirs to be coated onto balloons and adhered to the vessel lumen when delivered via an angioplasty balloon.
“MedAlliance is honored to have our sirolimus DEB selected for the FDA’s breakthrough device programme for a third time. This may provide US patients faster access to a new technology with the potential to provide safer and more effective treatment,” said Jeffrey B Jump, chairman and CEO of MedAlliance.
The FDA breakthrough device programme is intended to help patients receive more timely access to breakthrough technologies that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions. Under the programme, the FDA will provide MedAlliance with priority review and interactive communication regarding device development and clinical trial protocols, through to commercialisation decisions.
The goal of the breakthrough devices programme is to provide patients and healthcare providers with timely access to these medical devices by speeding up their development, assessment, and review, while preserving the statutory standards for premarket approval, 510(k) clearance, and de novo marketing authorisation, consistent with the agency’s mission to protect and promote public health.
Two-year clinical follow-up data on the company’s SFA (superficial femoral artery) sirolimus DEB and six-months follow up data on the coronary de novo and in-stent restenosis DEB were presented at TCT and VIVA last year.
Reflow Medical has announced that its Temporary Spur stent system for treating below-the-knee peripheral arterial disease (PAD) won US Food and Drug Administration (FDA) breakthrough device designation.
The Temporary Spur stent system includes radially expandable spikes designed to create multiple pathways for delivering antiproliferative drugs for increased uptake into the vessel wall for facilitating acute luminal gain without leaving anything behind, a company press release explains.
Reflow Medical developed the device in response to unmet clinical needs that resulted in high rates of restenosis and treatment challenges for patients with below-the-knee PAD, according to a news release.
The San Clemente, US-based company said it plans to build on clinical evidence supporting the Temporary Spur stent system and continue development in other clinical areas based around the Spur platform.
“We are extremely grateful to the FDA for their expedited designation of the Temporary Spur stent system as a breakthrough device,” Reflow Medical CEO Isa Rizk says. “We plan to take full advantage of the programme’s benefits, accelerating our efforts towards meeting the requirements of the review process as we advance this novel technology, with the goal of improving the lives of patients.”
There is no sign of increased all-cause mortality following the use of paclitaxel-coated devices for the treatment of symptomatic peripheral arterial occlusive disease, a new study based on German claims data attests in the European Journal of Vascular and Endovascular Surgery.
The study investigators set out to determine the survival of patients after use of paclitaxel-coated devices using a propensity score matched retrospective analysis of German health insurance claims. BARMER is the second largest insurance fund in Germany, and lead author Christian-Alexander Behrendt (University Medical Centre Hamburg-Eppendorf, Hamburg, Germany) and colleagues used this dataset to identify index femoropopliteal arterial interventions between 1 January 2010 and 31 December 2018. To ensure first paclitaxel exposure, patients with prior deployment of paclitaxel were excluded.
The study cohort—37,914 patients; mean age 73.3 years; 48.8% female—was stratified into patients with chronic limb threatening ischaemia (CLTI) and intermittent claudication, then into balloon versus stent cohorts. Within each stratum, paclitaxel was compared with uncoated devices.
Contextualising this research by highlighting how multiple US and European guidelines have recommended drug-eluting devices as “first-line treatments in the femoropopliteal segment”, Behrendt et al cite a 2018 meta-analysis published in the Journal of the American Heart Association (JAHA) as the cause for heightened scrutiny on these devices in recent months. The JAHA meta-analysis, authored by Konstantinos Katsanos (School of Medicine, University of Patras, Patras, Greece) and colleagues, evaluated data from 28 randomised controlled trials, and reported a higher risk of death at two and five years following the use of paclitaxel-coated balloons and paclitaxel-eluting stents in the femoropopliteal arteries.
However, this finding was not repeated in analyses involving “real-world data”. As reported in this newspaper, Eva Freisinger (University Hospital Münster, Münster, Germany) also used the BARMER dataset to conduct a real-world safety analysis of paclitaxel-based devices in peripheral arteries, concluding in the European Heart Journal that the use of drug-eluting devices is “safe for endovascular therapy of the lower limbs”. Indeed, Freisinger et al explicitly stated: “Particularly with regard to long-term mortality, neither drug-coated balloons nor drug-eluting stents was associated with increased risk compared to non-drug-eluting devices”.
The present study is differentiated from that of Freisinger et al by restricting the included patients to ensure a more homogenous study population. Behrendt and his co-investigators write: “Aiming to add to the existing evidence, the current approach rested on a rigorous study design involving a more homogeneous study population (only femoropopliteal segment, no prior major amputation), with a lookback period of up to five years and follow-up periods (left and right censoring) of five years.”
In this most recent analysis of the BARMER insurance claims dataset, Behrendt and co-authors also have opposing conclusions to the Katsanos et al JAHA meta-analysis. They report that paclitaxel-coated balloons and stents were associated with improved overall survival (hazard ratio [HR] 0.83, 95% confidence interval [CI] 0.77–0.90), amputation-free survival (HR 0.85, 95% CI 0.78–0.91), and freedom from major cardiovascular events (HR 0.82, 95% CI 0.77–0.89) versus uncoated devices at five years for CLTI. In the intermittent claudication cohort, mortality was significantly lower after using drug-coated balloons (HR 0.87, 95% CI 0.76–0.99) or combined drug-coated balloons and drug-eluting stents (HR 0.88, 95% CI 0.80–0.98).
Additionally, Behrendt et al note that the annual proportion of paclitaxel use increased from 3% to 39% during the study period for CLTI, and from 4% to 48% for intermittent claudicants (both p<0.001).
“In this propensity score matched retrospective analysis of health insurance claims,” the authors summarise, “comprising a rapidly increasing proportion of paclitaxel-coated devices in the treatment of peripheral arterial occlusive disease, higher long-term survival, amputation-free survival, and adverse cardiovascular event-free survival after the treatment of CLTI with paclitaxel-coated devices (both balloon and stent) was found, when compared with the uncoated control group. In patients with intermittent claudication, paclitaxel-coated devices were associated with higher long-term survival only, visible in the group where balloons and stents were combined and for balloons but not for stents. Unlike any other prior analysis, a persistent, robust, and positive association of paclitaxel exposure and survival is documented for a wide range of subgroups.”
The US Food and Drug Administration (FDA) has released draft guidance detailing the information device-makers should include in 510(k) submissions of catheter-based devices intended to treat peripheral vasculature lesions.
The guidelines, which cover class II peripheral percutaneous transluminal angioplasty (PTA) balloons and specialty catheters—including infusion catheters, PTA balloon catheters for in-stent restenosis and scoring/cutting balloons—include suggestions on labelling, performance testing, biocompatibility, and other issues.
Labelling should include information on indications, contraindications, warnings, product information, directions for use and a summary of clinical trial data, if applicable, the agency said.
TriNav infusion system powered by PEDD with SmartValve improves delivery and penetration of therapy into tumours.
TriSalus Life Sciences (“TriSalus”, formerly Surefire Medical) today announced the launch of its TriNav infusion system (“TriNav”). Powered by its proprietary pressure-enabled drug delivery (PEDD) approach with SmartValve technology, TriNav is designed to help overcome the infusion barriers that limit therapeutic uptake in solid tumours, including hepatocellular carcinoma (HCC) and liver metastases.
The TriNav system can provide interventional radiologists intravascular tumour access with improved trackability, compatibility with standard angiographic catheters, and workflow comparable to standard interventions, a TriSalus press release states.
The tumour microenvironment creates pressure barriers that limit flow into solid tumors. PEDD with SmartValve creates a high-pressure gradient that improves delivery and penetration of therapy into tumours. The porous expandable SmartValve is designed to allow antegrade flow, and leverages blood flow to carry the dose deep into the solid tumour. SmartValve enables therapy delivery to the intended target while minimising non-target delivery that has been shown to damage healthy tissue.
In a clinical study, PEDD with SmartValve demonstrated the ability to overcome tumour infusion barriers and significantly improve response rates in HCC. Outcomes from a retrospective, single-centre study of patients with solitary HCC tumors who underwent treatment utilising either PEDD or standard end-hole microcatheters, showed 100% objective response (OR) with PEDD versus 76.5% with standard end-hole microcatheters (p=0.019). Additionally, after first treatment, Pathological response (PR) as shown by tumour necrosis percentage was significantly greater with PEDD (88.8%) versus standard end-hole microcatheters (33.8%; p=0.026). Improving response rates could potentially help more patients meet transplant criteria, lead to successful down-staging, bridging, and post-transplant survival.
“Tumour-directed delivery of therapeutics is an exciting opportunity to help improve outcomes across a wider range of procedures by overcoming intratumoral pressure that can prevent drugs from adequately penetrating the tumour,” says Mary Szela, president and CEO of TriSalus. “The new TriNav infusion system utilises SmartValve, a first-in-kind, proprietary technology that has been shown to modulate pressure and flow with the goal for improved therapeutic delivery and deeper penetration into the tumour while helping to protect healthy tissue.”
Proprietary PEDD approach with SmartValve technology enables deep penetration of therapeutics.
Acknowledging its technology for therapeutic delivery, the Centers for Medicare and Medicaid Services (CMS) granted TriNav transitional pass-through payment as part of the 2020 Medicare Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System (CMS-1717-FC), effective 1 January, 2020.
This supplemental payment is intended to “facilitate access for [Medicare] beneficiaries to the advantages of new and innovative devices”. The TriNav infusion system met the required criteria to receive transitional pass-through status, including the demonstration of substantial clinical improvement, with the CMS saying it believes there is no existing pass-through payment category for this device because its SmartValve technology offers a unique mechanism for therapy delivery to selected sites in the peripheral vascular system, including solid tumours in the liver.
Patient enrolment in the PRESTIGE below-the-knee (BTK) clinical trial has been completed. The objective of this clinical investigation is to evaluate the six-month safety and performance outcomes of SELUTION SLR, MedAlliance’s novel sirolimus-eluting balloon, for the treatment of long tibial occlusive lesions (TASC C and D) in patients with critical limb ischaemia (CLI).
PRESTIGE is a prospective, single-centre, physician-initiated clinical study, being run at Singapore General Hospital, Singapore, by Chong Tze Tec and Tang Tjun Yip. Twenty-two patients have now been enrolled. Clinical follow-up will be at one, three, six and 12 months.
“The initial performance of SELUTION SLR has been very encouraging”, Tec says. “We have observed good blood flow in the amputation segment and some cases of fast wound healing. The device is also easy to track and deliver. We are eagerly awaiting the study’s follow-up data”.
Singapore has a high percentage of diabetics in its population, and CLI therefore constitutes a major challenge among patients seen with peripheral arterial disease (PAD). Singapore General Hospital (SGH) performs over 1,000 interventional procedures a year on patients suffering from CLI.
The PRESTIGE study, utilising a sirolimus-eluting balloon, is particularly significant in the wake of current controversy surrounding paclitaxel-coated balloons, a MedAlliance press release states.
Historically, paclitaxel has been the drug of choice for use in drug-coated balloons (DCBs). SELUTION SLR is the first sirolimus drug-eluting balloon specifically designed to treat PAD. This device combines the safety and efficacy of sirolimus with advanced MicroReservoir and cell adherent technology to offer a sustained therapeutic effect for over 60 days, achieving long-term clinical benefits.
The MicroReservoir combines sirolimus with a biodegradable polymer. Millions of these MicroReservoirs act as miniature drug delivery systems, achieving sustained sirolimus release.
The cell adherent technology achieves an unmatched drug bioavailability and minimal systemic loss, allowing for a lower drug dose concentration on the balloon surface (1μg/mm²). Proprietary amphipathic lipid technology binds micro-reservoirs to the balloon surface to protect during insertion and navigation of the balloon. Once the balloon is inflated, the cell adherent technology ensures transfer of micro-reservoirs to the tissue and cellular uptake of the sirolimus drug.
“We are excited at the prospect of demonstrating that our breakthrough technology is effective in below-the-knee lesions, so bringing much-needed relief to a substantial group of patients who might otherwise not be effectively treated”, adds MedAlliance chair and CEO Jeffrey B Jump.
MedAlliance was granted breakthrough designation by the FDA on 20 September 2019.
Alucent Biomedical has received US Food and Drug Administration (FDA) approval to proceed with a phase 1 clinical trial to evaluate the safety and efficacy of its Natural Vascular Scaffolding (NVS) technology. The therapy is designed to treat peripheral arterial disease (PAD) of the lower extremities, a condition that affects over 200 million people worldwide.
According to a press release, the Alucent NVS vessel restoration system with photoactivated linking combines standard angioplasty with linking of the structural proteins in the wall of a blood vessel. The intervention is designed to deliver immediate restoration of the vessel’s lumen and sustained improvement of blood flow, without the introduction of a foreign implant, such as a metallic stent, into the patient’s body. Because there is no rigid foreign material, the arterial wall has the potential to retain its natural functionality and flexibility, and avoid the complications of permanent stents. Alucent NVS photoactivated linking is also designed to mitigate the adverse effects of angioplasty, such as vessel recoil. Sustained, improved blood flow is expected to result in pain relief, limb preservation, and an improved quality of life for patients.
“FDA approval to commence human clinical testing allows us to move this revolutionary therapy into PAD patients, many of whom are in acute need of a better and more durable alternative to currently available treatments,” comments Myles Greenberg, CEO of Alucent.
Preclinical testing of NVS in animal studies has shown acute and long-term safety and patency without the pro-inflammatory and mechanical risks of placing a rigid foreign implant into the blood vessel.
“Alucent NVS is a novel and disruptive medical therapy that may promote better clinical outcomes in patients with symptomatic femoropopliteal atherosclerosis without the use of a metallic implant. Moreover, given the novel nature of this therapy, which in animal models was able to restore vessel wall architecture, it has the potential to dramatically improve quality of life in patients with peripheral arterial disease”, says Krishna Rocha-Singh, chief scientific officer at HSHS St John’s Prairie Heart Institute in Springfield, USA, and chief medical advisor of Alucent Biomedical.
Enrollment for the phase 1 clinical trial is expected to begin in Q1 2020. Up to 15 patients will be enrolled across five research sites, including the Cardiovascular Institute of the South in Houma, USA, and the Wellmont Hollston Valley Medical Center in Kingsport, USA.
An artificial intelligence (AI) programme has been developed that is better at spotting breast cancer in mammograms than expert radiologists, an article published in Nature reports.
“Screening mammography aims to identify breast cancer at earlier stages of the disease, when treatment can be more successful,” lead author Scott Mayer McKinney (Google Health, Palo Alto, USA) et al write. “Despite the existence of screening programmes worldwide, the interpretation of mammograms is affected by high rates of false positives and false negatives.”
To assess the performance of their AI system in the clinical setting, the investigators curated a large, representative dataset of mammograms for 25,856 patients in the UK, and a large, enriched dataset of 3,097 patients from the USA. These datasets were used to train the AI system, before it was used to identify the presence of breast cancer in mammograms of women who were known to have had either biopsy-proven breast cancer or normal follow-up imaging results at least one year later.
In an independent study of six radiologists, the AI system outperformed all of the human readers: the area under the receiver operating characteristic curve (AUC-ROC) for the AI system was greater than that AUC-ROC for the average radiologist by an absolute margin of 11.5%. Mayer McKinney and colleagues further demonstrate an absolute reduction in false positives of 5.7% in the USA and 1.2% in the UK, and an absolute reduction in false negatives of 9.4% in the USA and 2.7% in the UK.
“This robust assessment of the AI system paves the way for clinical trials to improve the accuracy and efficiency of breast cancer screening,” Mayer McKinney et al conclude.
If the programme proves its worth in clinical trials, the software, developed by Google Health, could make breast screening more effective and ease the burden on health services such as the UK’s National Health Service (NHS), where radiologists are in short supply.
Writing in an accompanying editorial in Nature, Etta Pisano (American College of Radiology, Philadelphia, USA, and Beth Israel Lahey Medical Center, Harvard Medical School, Boston, USA) says “Screening is used to detect breast cancer early in women who have no obvious signs of the disease. This image-analysis task is challenging because cancer is often hidden or masked in mammograms by overlapping ‘dense’ breast tissue. The problem has stimulated efforts to develop computer-based AI systems to improve diagnostic performance. […] Despite some limitations, McKinney and colleagues’ study is impressive. Its strengths include the large scale of the data sets used for training and subsequently validating the AI algorithm.
“McKinney and colleagues’ results suggest that AI might someday have a role in aiding the early detection of breast cancer, but the authors rightly note that clinical trials will be needed to further assess the utility of this tool in medical practice.”
Several reports emerged last year concerning issues with MRI safety.
In October 2019, officials at Sunderby Hospital in Luleå confirmed that a hospital staff member and two security guards were injured in an accident at a mobile MRI unit outside the hospital. According to the Swedish press at the time, a specialist nurse got stuck outside the gantry. When his screams and the appearance of a hand inside the scanner alerted the patient that something was wrong, the patient reportedly got out of the machine and tried to help the nurse. With the help of a security officer, the nurse was pulled out of the mobile unit, although he was unconscious at this stage.
At a press conference on 24 October, Aleris, the company that owns the equipment, the MR trailer, and employs the injured person) reported that the nurse had been moved from the intensive care unit to a regular ward. His condition has improved, and he said he was feeling OK under the circumstances, Emma Bergström Wuolo, press officer of the Norrbotten region, noted.
In early November 2019, reports appeared in the Swedish press about a second MRI accident that occurred in Varberg, Sweden, in April. A staff member at the Halland hospital in Varberg, who was accompanying an anxious patient into the MRI scanner room, was wearing a metallic ankle band with steel balls, and their leg got stuck to the scanner, according to a report in Aftonbladet, a Stockholm-based tabloid newspaper.
There were no injuries, but the machine had to be shut down for more than two weeks. The total cost to the hospital was around 1,000,000 Swedish krona (£82,800), Magnus Warfvinge, deputy head of X-ray operations in Halland, told Aftonbladet.
Meanwhile, a court case continues following the death of a man in India in January 2018 following an MRI accident. The man was accompanying his mother-in-law into an MRI suite, and was killed when he was sucked into the magnet bore while carrying an oxygen tank.
An analysis of data from the ATTRACT trial, published in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (JVSVL), has revealed that quality of life (QoL) measures improve after pharmacomechanical catheter-directed thrombolysis (PCDT). According to the findings of the analysis, this is particularly true early on and for iliofemoral deep venous thrombosis (DVT).
It is said that, despite treatment with anticoagulation and compression stockings, up to 50% of patients with proximal DVT develop post-thrombotic syndrome (PTS), which causes patients to experience severe pain and swelling of the limb, as well as increasing the risk of pulmonary embolism (PE).
As Venous News has previously reported, the results of the ATTRACT trial showed that PCDT does not reduce the occurrence of PTS at two years but does lessen its severity, as well as treating acute symptoms faster.
In this analysis, lead investigator Susan Kahn (Jewish General Hospital, Montreal, Canada) and colleagues aimed to assess the effect of PCDT on both short-term and long-term QoL in all of the patients enrolled in the ATTRACT trial—as well as predefined subgroups with (iliofemoral DVT) or without (femoral-popliteal DVT) involvement of the iliac or common femoral vein—before examining whether this effect differed over time.
As part of the investigation, QoL was evaluated in a total of 692 patients between 2009 and 2014, with follow-up taking place at one, six, 12, 18 and 24 months. Randomisation resulted in 337 being allocated to PCDT, and 355 to no PCDT; upon analysis, it was found that VEINES-QOL change scores were greater (and therefore better) in the PCDT cohort vs. no PCDT from baseline to one month (difference, 5.7, p=0.0006), and from baseline to six months (5.1; p=0.0029). For all other intervals, there was no difference.
According to the 36-Item Short Form Health Survey (SF-36) physical component summary (PCS), scores were greater in PCDT vs. no PCDT from baseline to one month (difference, 2.4; p=0.01), but not for other intervals.
However, among iliofemoral DVT patients, VEINES-QOL change scores from baseline to all assessments were greater in the PCDT vs. no PCDT group, and this was statistically significant in the intention-to-treat analysis at 1 month (difference, 10.0; p<0.0001) and 6 months (8.8; p<0.0001). SF-36 PCS change scores were greater in PCDT vs. no PCDT from baseline to 1 month (difference, 3.2; p=0.0010), but not for other intervals. In contrast, in femoral-popliteal DVT patients, change scores from baseline to all assessments were similar in both cohorts.
Commenting on these findings, Kahn said: “First, most of the improvement in QoL was in the first six months, and the trial did find that PCDT reduced clot burden and early leg pain and swelling over no PCDT, and was associated with a reduced point prevalence of PTS at six months, but not thereafter. Though PCDT did not prevent PTS, it did reduce its severity.”
Furthermore, a statement from the Society for Vascular Surgery (SVS) noted that the decision to proceed with lytic therapy for patients with iliofemoral DVT can be complicated. “This data supports offering this therapy to selected patients with severe symptoms, low bleeding risk and a willingness to undergo a catheter-based procedure,” it read.
The Society of Interventional Oncology (SIO) has announced that Jena Eberly Stack will assume the role of executive director effective 1 January, 2020. As a certified project management professional through the PMI Institute, Stack brings expertise in strategic development, change management, and association governance, a society press release states.
“I am thrilled to be joining SIO as the new executive director,” Stack comments. “This is such an exciting time for the society and for the field of interventional oncology. I have had the pleasure of getting to know SIO’s board of directors in recent weeks and I know we will continue to accomplish great things for SIO’s members and the industry.”
Stack has worked in association management for the past six years, previously having worked in other non-profit management and education settings. Her association management experience has been focused in healthcare organisations, having served a variety of clinical societies. She is excited to join SIO in this capacity and help further advance the field of interventional oncology.
Cameron Curtis, the current executive director, is leaving SIO to pursue another opportunity. “On behalf of the SIO board of directors, I would like to thank Cameron for her strong leadership,” said board president William Rilling. “We have accomplished a great deal with her energy and guidance and look forward to building on our momentum as Jena assumes executive leadership of SIO.”
“Cameron has served as an exceptional leader and partner of the board, playing an integral role in the evolution and success of the society,” continued Rilling. “Under her leadership, SIO has achieved tremendous success, and we cannot thank her enough for her commitment and service to SIO. Although she will be greatly missed, we wish her all the best in her future endeavours.”
PQ Bypass announced today that it has received approval for coverage from the Centers for Medicare and Medicaid Services (CMS) for the Investigational Device Exemption (IDE) study titled TORUS 2. This approval will affect coverage across all Medicare administrative regions.
TORUS 2 (The PQ Bypass pivotal IDE intra-arterial stent graft study for occlusive and restenotic fem-pop revascularisation) will evaluate the safety and effectiveness of the TORUS stent graft system in the treatment of obstructive atherosclerotic lesions of the superficial femoral and/or proximal popliteal arteries. Led by national coprincipal investigators Peter Schneider (Division of Vascular and Endovascular Surgery, University of California San Francisco, San Francisco, USA) and Ehrin Armstrong (Director of Interventional Cardiology, Rocky Mountain Regional VA Hospital; University of Colorado School of Medicine, Aurora, USA), this prospective, single arm study will enrol up to 188 patients at up to 40 sites.
“The TORUS Stent Graft System represents the first major stent graft advancement in more than a decade for patients with SFA lesions and is the vanguard for the next generation of medical devices,” says Heather Simonsen, General Manager of PQ Bypass. “Currently, patients and physicians have only one stent graft option, which gained approval for the SFA in 2005, on the market in the USA.”
Previously studied in the DETOUR 1 and TORUS 1 studies in Europe, and currently under investigation in the DETOUR 2 IDE trial, the TORUS stent graft was granted CE mark as a part of the DETOUR procedure in 2017.
The TORUS stent graft is limited by federal law to investigational use only and is not available for sale in the USA. For more information, please visit www.pqbypass.com
The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust, Bournemouth, UK, has become the first in the country to offer patients audio-visual goggles to distract and comfort them when undergoing an IR procedure without general anaesthesia or with only local anaesthetic. With a 100% patient satisfaction, the iTV FPView 3D HD goggles have been used in a variety of interventional radiology procedures where the patient lies supine for longer than 20 minutes, including prostate artery embolization, transarterial chemoembolization, superior rectal artery embolization, complex vascular recanalisation, and for GI bleeds. Here, project leader Clare Bent discusses the lessons learned from the patient experience, and how her Trust could serve as a model both nationally and internationally.
Audio-visual (AV) technology may be the next global initiative within interventional radiology (IR) to improve the patient experience during invasive medical care.
I have been leading the IR team at the Royal Bournemouth and Christchurch Hospitals (RBCH; Bournemouth, UK) in a quality improvement project to assess the benefits of AV goggles in the IR setting. These video goggles stream personal entertainment directly to the patient during IR procedures (HD and 3D videos, daytime television, box sets or real-time procedural imaging), aiming to distract and reduce anxiety and awareness. Published data suggests that AV distraction is a promising analgesic technique that is safe, reduces intravenous sedation and general anaesthetic requirements, and consequently allows for earlier ambulation and discharge following medical treatment.
Why were the goggles introduced?
With IR at the front-line of medical innovation, newer complex procedures frequently result in an increase in procedural duration. Further research into non-pharmacological methods to optimise patient experience and complement these technical advancements is warranted.
For longer procedures, a static position, lying on a relatively hard IR table, can be poorly tolerated by patients. With pain perception known to have a large psychological component, distraction techniques such as AV use a) allows time to pass expeditiously and b) deflects the patient’s attention from noxious stimuli with a consequential reduction in perceived pain.
Patient experience and pain measures—using visual analogue score (VAS), sedation requirements, length of postprocedural hospital stay, and a cost-benefit analysis—are examined. The RBCH IR team is hopeful that the AV goggles will benefit the patient and improve hospital throughput.
What was the patient experience like?
To date, 30 patients have trailed the AV goggles with 100% positive feedback.
Patients have commented that the focus of attention to streamed media has meant they have not noticed the invasive treatment being undertaken.
One patient undergoing resuscitation and embolization for a gastrointestinal bleed requested to watch Formula One during the procedure to distract him from the resuscitation team’s clinical management, and fed back positively that the distraction had improved his otherwise traumatic experience.
Clare Bent with patient
What are the key lessons from the quality improvement project?
Not all patients want to be distracted during invasive procedures.
A small proportion of patients experience simulator sickness.
Infection control requires early involvement to ensure the device adheres to Trust guidance:
Use of eye guards to prevent skin contamination
Use of disposable earphones
Ensure AV equipment chosen is robust enough to undergo thorough cleaning with Universal wipes between patients.
Confirm with BBC [British Broadcasting Corporation] Licensing that your hospital trusts current TV Licence covers streaming and goggle use in this way. Notify the Trusts IT department to ensure WiFi capacity supports use of streaming.
Consider a smaller monitor to video loop streamed media to enable the operating team to trouble shoot viewing issues to assist the patient.
Consider which streaming tool to use—RBCH use a Now TV USB stick which has a remote control and also voice recognition to facilitate patient use.
Counsel patients on the need for compliance with instructions and that excessive fidgeting from funny or scary imagery may require a change of channel!
How could this be rolled out nationally and internationally?
The quality improvement project will run initially for a six-month period to enable data collection. Following completion, the RBCH IR team aim to present and publish their findings to Trust management and to a wider audience within IR.
Internally, endoscopy, day theatres, and cardiac intervention have already requested a roll out of AV goggle use to facilitate improved patient experience in their own departments drawing on data and learning from this quality improvement project. Additionally, RBCH have received positive enquiries from national hospitals and industry, with the latter considering inclusion as part of IR suite specifications for future projects.
This quality improvement project hopes to recommend the use of AV goggles as a simple, non-invasive, low cost, and non-pharmacological method to improve patient experience and hospital throughput, which will in turn complement recent and future advances in IR.
Clare Bent is an interventional radiologist at the Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust, Bournemouth, UK.
Lead authors João Pisco (L) and co-author Tiago Bilhim
The improvements in quality of life measurements and International Prostate Symptom Score (IPSS) in patients following prostatic artery embolization (PAE) are “far superior” to those due to the placebo effect, a new study just published in European Urology, the official journal of the European Association of Urology (EAU), concludes. Publishing a paper positively describing PAE in a urology journal has historically been difficult for interventional radiologists, and co-author Tiago Bilhim (Hôpital Saint-Louis, Lisbon, Portugal) tells Interventional News that this publication “might help our way into the urology guidelines with PAE”.
The most recent EAU guidelines for the diagnosis and treatment of men with lower urinary tract symptoms (LUTS)/ benign prostatic hyperplasia (BPH), published in 2017, are cautious when describing the potential clinical role of PAE, saying that the selection of LUTS patients who will benefit from the procedure still needs to be defined, and highlighting that PAE is technically demanding. The European guidelines state: “A multidisciplinary team approach of urologists and radiologists is mandatory as the basis for future RCTs [randomised controlled trials] of good quality with long-term follow-up in order to integrate this treatment option into the spectrum of efficient, minimally invasive treatment options.”
Bilhim says that the present study is the “kind of research” called for by the European urology community in order to accept PAE into their guidelines for the treatment of LUTS due to BPH. He therefore hopes that this research, which he says demonstrates that PAE is not a placebo procedure, “will be a fundamental study to raise the level of evidence of PAE to treat LUTS due to BPH, and to help get PAE in the [European] urology guidelines.”
In the USA, the American Urological Association (AUA) also mention PAE in their guidelines, published in The Journal of Urology—but only to explicitly not recommend the procedure outside the context of a clinical trial. Interventional radiologists have been advocating for the procedure’s acceptance by urologists, with several prominent figures in this community calling for more widespread awareness of the safety and efficacy of this minimally invasive treatment option for select LUTS/ BPH patients.
The authors of this recent publication therefore underline the importance of sharing their data with the urology community, writing: “PAE is considered experimental in the urology guidelines. For a novel technique such as PAE to be considered as a first-line option, sham-controlled trials are very helpful, and hence the present study.”
In light of the positive outcomes observed in the PAE group, they believe “The results of this clinical trial will be a reference for future research consensus panels and guidelines on the management of LUTS/BPH.”
Speaking to this newspaper in May 2019, Ari Isaacson (Department of Radiology, University of North Carolina, Chapel Hill, USA) highlighted the importance of interventional radiologists publishing their work in urology specific journals, as a way of communicating their views directly to this community. However, he reported that this is challenging: “We have attempted to [publish in a urology journal] several times; it is very difficult to get a PAE paper in a urology journal”. Riad Salem (Northwestern University, Chicago, USA), who is one of few US interventional radiologists that has published a PAE paper in a urology journal, supports this assertion, commenting earlier this year: “In my 20 years of publishing over 330 papers, getting accepted into a urology journal was the most difficult, challenging, controversial process I have ever been through. The reviews were replete with opinions that seemed to have been made before even reading the study. We tried several times, and finally got accepted into the fourth urology journal. This was a prospective, phase II, FDA [US Food and Drug Administration]-approved study, so it met all the high level criteria, but it was still dismissed by many urology journals.”
However, the European urology community has been more welcoming, as Bilhim describes. “The overall experience was very positive,” he says. “We received very constructive reviews from urology experts in the field of BPH that helped make the manuscript better. We wanted to target the urology community because the major goal of this manuscript was to prove to the urology community that PAE is not a sham procedure, and is in fact safe and effective for the treatment of LUTS, without compromising sexual function.
“The major goal of this study was to raise the level of evidence for PAE as a safe technique to treat LUTS due to BPH, so that PAE can be considered as [an] effective alternative in the urological guidelines for patient management. The submission process in the urology journal was similar to standard scientific journals and it took around four to six months from submission to final acceptance.”
Trial findings: PAE superior to sham procedure
Lead author João Pisco (Hôpital Saint-Louis, Lisbon, Portugal), who died in March 2019 after completion of the trial, and co-authors set out to assess the safety and efficacy of PAE “above and beyond the placebo effect” compared to with a sham procedure for the treatment of LUTS/BPH. They conducted a parallel-group, single-blind, sham-controlled superiority randomised clinical trial in 80 men, aged 45 or above, with severe LUTS/BPH non-responsive to medical treatment between 2 September 2014 and 3 March 2018 at Hôpital Saint-Louis, Lisbon, Portugal, with an efficacy assessment at six months after randomisation. This was followed by an open extension phase, where all 38 patients of the sham trial arm who completed the single-blind period crossed over to the PAE arm (underwent the procedure). A final evaluation was conducted at 12 months after randomisation. One patient in the PAE group and three in the sham group did not complete the study.
Patients were randomised 1:1 upon successful catheterisation of a prostatic artery to either PAE or a sham PAE procedure without embolisation. Pisco and colleagues describe the procedure: “In the PAE group, Bead Block (BTG plc, London, UK) 300–500mm was used; in the sham group, after catheterisation of one prostatic artery, the catheter was removed and no particles were injected, but there was a wait of some minutes before the removal of the catheter in order to avoid revealing the treatment arm to patients of the sham group.” All procedures were performed by five interventional radiologists with between three and 10 years of experience in PAE.
The investigators performed an intention-to-treat analysis of all randomised patients. The co-primary outcomes were the change from baseline to six months in the IPSS and the quality of life score at six months, analysed with analysis of covariance and t test, respectively.
At six months, patients in the PAE arm had a greater improvement in IPSS than patients in the sham arm. For those that underwent PAE, the decrease from baseline to month six in IPSS was 17.1±7.25. In comparison, the decrease in IPSS from baseline to six months for patients who underwent the sham procedure was only 5.03±8.13 (difference between groups in changes from baseline: 13.2, 95% confidence interval [CI]: 10.2–16.2, p<0.0001). After six months, the mean IPSS in the PAE group was 8.75±5.73, and 21.9±7.34 in the sham arm.
This pattern was also true of improvements in quality of life: for patients treated with PAE, mean quality of life score at six months was 3.48±1.38, while for patients treated with the sham procedure, mean quality of life score at six months was 1.35±1.12 (difference in the means of quality of life scores between groups at month six: 2.13, 95% CI: 1.57–2.68, p<0.0001).
The occurrence of adverse events was similar between the two groups: 16 events in 14 patients (35%) after PAE, and 17 events in 13 patients (32.5%) following the sham procedure. One serious adverse event took place in the sham group during the open period.
“The results of this randomised clinical trial provide clear evidence that the improvement experienced by patients after PAE is due to a real treatment effect that is much larger than the placebo effect associated with the procedure,” Pisco et al summarise. “The marked and sustained amelioration in all primary and secondary outcomes, with no negative influence on erectile function, offers strong evidence that PAE, through the reduction it imposes on prostate size and possibly because of several other mechanisms, actually modifies the course of LUTS/BPH, and this explains the high clinical success rates reported so far with this treatment.”
PAE “still in the investigational phase” but this study “fills the gap in the evidence base”
Setting out the case for PAE, Pisco et al write: “PAE is a minimally invasive treatment that has been shown in many observational studies and meta-analyses to be safe and effective, reducing LUTS/BPH. In addition, many phase II trials without controls already exist, showing the safety and efficacy of PAE for BPH.
“However,” they add, “LUTS/BPH is known to be very susceptible to placebo treatments, and conclusive demonstration of efficacy will require randomised controlled trials, but until now only three randomised clinical trials of PAE have been published, all comparative to TURP [transurethral resection of the prostate], and none has conclusively demonstrated the efficacy of PAE in LUTS/BPH.” They therefore conclude that, prior to their present study, PAE was “still in the investigational phase”, as “as evidence of efficacy compared with standard treatment has not yet been clearly demonstrated and randomised placebo-controlled clinical trials have not previously been conducted.”
The authors conclude that “The single-blind period of this randomised clinical trial fills the gap in the evidence base on the treatment effect of PAE by demonstrating both clinically and statistically significant differences in patients treated with PAE as compared with patients submitted to a sham procedure. In addition, the trial open extension period offers evidence of sustainability of effects up to 12 months.”
Nonetheless, they concede that “major questions still remain”, especially regarding the durability of the treatment effect. Pisco et al call for non-inferiority clinical trials providing data on long-term outcomes after PAE in large patient cohorts, and say that future research should focus on providing comparative studies of PAE with surgery or medical care with appropriate cohort sizes and long-term follow-up.
Thrombolex has announced that the company has received US Food and Drug Administration (FDA) clearance for the Bashir Endovascular Catheter – Short Basket (BEC S-B). The indication for use of the BEC S-B is for the controlled and selective infusion of physicianspecified fluids, including thrombolytics, into the peripheral vasculature.
Thrombolex provides an innovative line of endovascular catheters, which feature a unique combination of mechanical-pharmaco, expandable infusion basket for effective treatment of venous thromboembolic (VTE) conditions.
According to Thrombolex, the BEC S-B represents the third FDA 510k premarket pathway clearance achieved this year by the Company. This new medical device is part of the Company’s platform technology.
The Bashir line of interventional catheters are the first interventional catheters to rapidly create multiple cross-sectional channels to allow the patient’s own endogenous lytics to immediately begin to flow into the culprit thrombus. The treatment is then enhanced by infusing small amounts of exogenous thrombolytics directly into the culprit thrombus, the combination of which accelerates the dissolution of the clot burden.
The Bashir Endovascular Catheter (BEC) and the Bashir N-X Endovascular Catheter (BEC N-X) previously received FDA 510k premarket pathway clearance earlier this year. The BEC is cleared for the controlled and selective infusion of physicianspecified fluids, including thrombolytics, into the peripheral vasculature. The BEC N-X is a device intended for the localised infusion of physician specified fluids, into the peripheral vasculature, including the pulmonary arteries.
The company has advised that the BEC S-B will be introduced into the USA through a controlled roll-out at hospitals with established VTE treatment protocols.
Cardiovascular Systems announced today that the first patient in Europe has been treated with its Stealth 360 peripheral orbital atherectomy system (OAS) 1.25mm Micro Crown with GlideAssist (1.25 Micro Crown).
According to a press release, the 1.25 Micro Crown is designed with flexibility for tortuous vessels and tight bends below the knee. The GlideAssist feature enables the crown to spin at a slow speed of 5K rpm, facilitating tracking and smoother movement to access diffuse, calcified lesions below the knee.
Michael Lichtenberg, chief physician, Clinic for Angiology, Hochsauerland Hospital, Arnsberg, Germany, successfully treated the first peripheral patient with the 1.25 Micro Crown.
Lichtenberg said, “CSI’s new Stealth OAS 1.25 Micro Crown with GlideAssist is a welcome addition to my toolbox for treating challenging critical limb ischemia, or CLI, cases. In particular, the device’s dual mechanism of action of differential sanding and pulsatile forces will be instrumental in the treatment of the challenging calcified lesions I often see in lesions below the knee.”
Scott Ward, chairman, president and chief executive officer of CSI, said, “With our distribution partner, OrbusNeich, we are excited to introduce the 1.25 Micro Crown in Germany. One million German patients suffer from CLI, a severe condition that can result in severe pain, tissue damage and loss of limbs. The 1.25 Micro Crown provides physicians with a minimally invasive therapy to access and effectively treat this condition by modifying calcified lesions below the knee and restoring blood flow to the foot.”
The product has clearance from the US Food and Drug Administration (FDA) and has CE mark in the EU for use in diagnostic cardiac catheterisation procedures and percutaneous coronary interventions (PCIs).
Merit’s PreludeSYNC EVO is a sterile, single-use, disposable device used to assist in gaining haemostasis of the arterial percutaneous access site following catheterisation procedures.
“PreludeSYNC EVO adds to our extensive line of radial compression devices that support PCI from start to finish. It was developed to meet the evolving clinical and health economic needs of physicians, administrators and catheter lab teams around the globe. Our intent with PreludeSYNC EVO, the latest innovation in our premium cardiology product portfolio, is to provide physicians with even more procedural clarity and uniformity and their patients with safety and comfort,” says Fred P Lampropoulos, Merit Medical’s founder, chair, and Chief Executive Officer.
The device has a large, clear window area, which provides unobstructed site visibility. It is also optimised for diffuse and uniform balloon pressure. The safety features include a specialised connection and Slip-n-Lock cap that secures the syringe during inflation and deflation. A soft, comfortable band, which is easy to secure, adjust and clean, is available in 24 and 29cm sizes.
The PreludeSYNC EVO is immediately available in the EU, with registration coming in Middle East and Africa.
Imperative Care has completed the initial closing of a Series C financing of US$85 million to support the commercial launch of the company’s portfolio, which is composed of the latest advances in neurovascular devices treating ischaemic and haemorrhagic strokes.
The round was co-led by new investors Ally Bridge Group and Bain Capital Life Sciences. Existing Imperative Care investors Ascension Ventures, Delos Capital, Rock Springs Capital, 3H Health Investment, and Incept LLC also strongly participated in the round. Frank Yu, Ally Bridge’s founder, and Andrew Hack, managing director of Bain Capital, will join Imperative Care’s board of directors.
“We are thrilled to have Ally Bridge and Bain Capital leading this round of financing at this important stage in our company’s growth. We look forward to Frank and Andrew’s support and guidance as we continue to propel forward Imperative Care’s unique mission,” said Fred Khosravi, Chairman and CEO of Imperative Care. “This is an exciting time for our company. We are poised to launch the industry’s first Large Distal Platform (LDP) access technology and our unparalleled ZOOM Aspiration System. In addition, we continue to develop a pipeline of innovations in the continuum of stroke-care, with significant investment and emphasis on clinical evidence.”
Imperative Care has received 510(k) clearance from the US Food and Drug Administration (FDA) for its family of access catheters designed to facilitate smooth, consistent navigation into blood vessels of the brain. The company has also received FDA clearance for its ZOOM Aspiration System, a family of products designed to facilitate clot removal during ischaemic stroke.
Canon Medical has concluded a contract to acquire all shares of Skope Magnetic Resonance Technologies AG. Skope specialises in the development and sales of magnetic field monitoring systems and image reconstruction software for MRI. The acquisition was completed according to the required approval procedures.
A press release details how Skope is equipping leading MRI research sites with its high-precision magnetic field monitoring systems and sophisticated image reconstruction software to facilitate next-generation MR imaging and diagnostics.
Canon Medical Systems developed and introduced the first Japanese MRI in 1983, and today is dedicated to the research and development of innovative MRI technologies, such as Pianissimo, the company’s unique acoustic noise reduction technology.
Narayan Karunanithy outlines the benefits of intravascular ultrasound (IVUS) during haemodialysis access intervention.
Thoracic central veins include intra-thoracic segments of the internal jugular, subclavian, brachiocephalic veins and superior vena cava. These veins are located central to the superior thoracic aperture (C7–T1 intervertebral disc level), central to the lateral margin of the first rib and superior to the diaphragmatic caval opening.1 Patients with haemodialysis access are prone to developing Thoracic Central Vein Obstruction (TCVO) due to their underlying renal failure, altered haemodynamics of the arteriovenous circuit and previous central vein catheter, pacemaker or defibrillator placement. The incidence of TCVO in this patient cohort is thought to be rising and currently estimated to be 20–40%.2 TCVO may be partial (i.e. stenosis) or complete (i.e. occlusion).
Patients with TCVO can present with arm/neck/face/breast swelling, pain, access dysfunction and respiratory distress. Visible chest wall collaterals may also be unsightly for the patient.
Most of the haemodialysis circuit can be imaged readily with standard ultrasound, as the circuit is very superficial. However, TCVO can be virtually impossible to image with ultrasound. CT or MR venography can provide excellent depiction of central venous anatomy. However, CTV carries an additional radiation burden and MRV usually requires administration of gadolinium, which may be complex in this cohort of patients with end stage renal failure or approaching it. Hence the mainstay of CVS assessment currently is digital subtraction angiography (DSA).
IVUS is an invasive modality that provides cross-sectional imaging of the veins but without the need for ionizing radiation or contrast administration. In addition to being a diagnostic tool that is easy and repeatable, it aids treatment decision-making.
The VIDIO trial has demonstrated that DSA can underestimate the degree and morphology of iliofemoral vein stenosis when compared to IVUS. There is paucity of published literature evaluating IVUS for TCVO assessment in haemodialysis patients.3 de Graaf et al performed DSA and IVUS on 12 patients with suspected TCVO. IVUS showed significant stenosis in 12/12 versus 8/12 with DSA. After angioplasty, significant residual stenosis was demonstrated in 10/12 versus 3/12 with DSA. The authors concluded that IVUS was more sensitive in diagnosing significant TCVO and aided the decision-making process in deciding treatment strategy.4 This is in line with what we have learned from the iliofemoral venous treatment literature that IVUS aids precise device dimension selection (diameter and length of stenosis), appropriate landing zones and adequacy of treatment (for e.g. wall apposition of stent). These are fundamentally important steps that contribute to optimised outcomes.5 Clearly high quality large data studies are required to demonstrate the benefit of IVUS in haemodialysis access.
Currently no consensus exists on the optimum treatment of TCVO. The mainstay of treatment is high-pressure balloon angioplasty but the outcomes are generally poor with reported patency at six and 12 months 29–60% and 25% respectively. The use of bare metal stents has similarly poor outcomes with one-year patency 33–56%. The reported outcomes even with stent grafts are as low as 40% patency at 12 months. The patency rates with drug coated balloon angioplasty are better.6 Reliance on DSA alone to determine adequate treatment may have contributed to these relatively poor outcomes.
In conclusion, reliance on DSA alone for TCVO can under-estimate the extent and severity of these lesions. This can be overcome with use of IVUS. IVUS use during treatment aids appropriate device selection and adequacy of treatment.
References
Dolmatch BL, Gurley JC, Baskin KM et al. Central Vein Work Group and the Technology Assessment Committee. Society of Interventional Radiology Reporting Standards for Thoracic Central Vein Obstruction: J Vasc Access. 2019 Mar; 20(2): 114–122
McFall RG, Lu T. Application of Intravascular Ultrasound in End-Stage Renal Patients with Central Venous Occlusive Disease. Methodist Debakey Cardiovasc J. 2018 Jul-Sep; 14(3): 196–1993.
Gagne PJ, Tahara RW, Fastabend CP et al. Venography versus intravascular ultrasound for diagnosing and treating iliofemoral vein obstruction. J Vasc Surg Venous Lymphat Disord. 2017 Sep; 5(5): 678–6874.
de Graaf R, van Laanen J, Peppelenbosch N et al. The value of intravascular ultrasound in the treatment of central venous obstructions in hemodialysis patients. J Vasc Access. 2016 Mar;17 Suppl 1:S12–5
Murphy E. Use of IVUS to optimise outcomes in venous stenting. Venous News 6th April 2018
Kitrou PM, Papadimatos P, Spiliopoulos S et al. Paclitaxel-Coated Balloons for the Treatment of Symptomatic Central Venous Stenosis in Dialysis Access: Results from a Randomized Controlled Trial. J Vasc Interv Radiol. 2017 Jun;28(6):811–817.
Narayan Karunanithy is a consultant interventional radiologist at Guy’s and St Thomas’s Hospital (London, UK) and honorary senior lecturer at the School of Biomedical Engineering and Imaging Sciences at King’s College London (London, UK).
Merit Medical has announced the commercial launch of the Resolve mini locking drainage catheter, the most recent addition to the company’s line of innovative Resolve locking drainage catheters. The Resolve mini is intended for the percutaneous drainage of fluid from body cavities, and its mini pigtail design—which is up to 42% smaller than the standard Resolve locking drainage catheter pigtail—allows the catheter to be placed into small fluid pockets.
The Resolve mini features a tapered tip and hydrophilic coating for smooth introduction, designed to reduce patient discomfort, a Merit Medical press release reports. Depth markers located on the catheter shaft aid accurate placement and act as a reference for correct positioning, and a radiopaque marker band denotes where the pigtail is to ensure all the holes are in the fluid pocket. The device features multiple large holes to help maximise drainage.
Additionally, the Resolve mini includes a secure locking mechanism that makes it difficult for patients to unlock the catheter, a pigtail straightener to help insert the cannulas into the catheter easier, and a catheter tip positioned within the pigtail curve, designed to reduce tissue irritation. Flexible polyurethane material prevents kinking and ensures catheter rebound, and an included repositioning tool helps unlock and reposition the catheter at any time.
“For years, Merit has been deeply committed to the drainage space, developing novel and innovative catheters and drainage devices that improve the standard of care,” comments Fred Lampropoulos, chair and CEO of Merit Medical. “The commercial launch of the Resolve mini furthers that legacy by offering customers a device designed to provide safety, usability, and patient comfort.”
Last month (November), the FDA approved Medtronic’s paclitaxel-coated balloon IN.PACT AV for the management of failing arteriovenous fistulae (AVF). Approval for the device was based on data from the IN.PACT AV Access trial, which showed the device to significantly increase primary patency compared with standard percutaneous transluminal angioplasty. Andrew Holden (Department of Interventional Radiology, Auckland, New Zealand), the principal investigator of IN.PACT AV Access, says having a treatment that improves access circuit patency is a “huge gain”.
According to Holden, ensuring the patency of arteriovenous fistulae is an ongoing concern. He notes that while haemodialysis is the most common method of renal replacement therapy, “dialysis access circuits are prone to high rates of dysfunction” and this is primarily because of access circuit stenotic lesions. Furthermore, he says, these lesions are “often refractory” to standard percutaneous transluminal angioplasty and “require high pressure or specialty balloons to adequately dilate”. “Of more concern is the extremely high rate of restenosis, with many studies reporting a primary patency rate below 50% at six months,” Holden observes.
Therefore, given outcomes seen with drug-coated balloons for treating femoropopliteal lesions, interest in the use of these devices to treat failing arteriovenous fistulae has been considerable. However, until recently, the efficacy of drug-coated balloons in this context had not been definitively demonstrated. Holden explains: “Although many studies reported a trend towards better patency with drug-coated balloons compared with plain balloon angioplasty, the confidence intervals were wide and some studies failed to showed a benefit. Not surprisingly, there was considerable heterogeneity in technique in the papers, particularly the requirement and quality of vessel preparation prior to drug-coated balloon deployment.” He adds these studies reinforced the need for larger, multicentre, randomised trials.
Efficacy data
IN.PACt AV
The Lutonix AV Access investigational device exemption (IDE) trial was the first such randomised trial, and it evaluated the drug-coated balloon Lutonix 035 (BD). Scott Trerotola (Department of Radiology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA) and others recently reported the two-year results of this study (285 patients with dysfunctional arteriovenous fistulae) in the Journal of Vascular and Interventional Radiology. They note that the study did not meet its primary endpoint—superior target lesion primary patency (TLPP) at six months compared with control therapy (standard percutaneous transluminal angioplasty)—but did show statistically significant TLPP at nine months (58%±4 vs. 46%±4 for control therapy; p=0.02). Lutonix AV was not associated with better TLPP at any other time point (12 months, 18 months, and 24 months). Trerotola et al conclude that the data represent “an important step forward in the development of novel therapies that improve the quality of life of patients undergoing haemodialysis”. “We hope the further introduction of other such therapies, as well as the analysis of more patients treated with drug-coated balloons, will result in a future precision-based approach to arteriovenous fistulae stenosis,” they add.
Unlike the Lutonix AV Access IDE trial, Holden reports, IN.PACT AV Access trial (330 patients) “well and truly met its primary efficacy endpoint”. At 210 days, per Kaplan-Meier estimates, the primary patency of the target lesion was 81.4% in the IN.PACT AV arm vs. 59% in the control arm (p<0.01). Additionally, patients in the IN.PACT AV arm required 56% fewer reinterventions to maintain target lesion patency through 210 days compared with those in the control arm. Holden observes: “It is highly likely that this reduced reintervention rate will make a primary drug-coated balloon angioplasty approach to arteriovenous access circuit stenoses a very cost-effective treatment.” He adds that a detailed cost-effectiveness analysis of the IN.PACT AV Access Study will be presented early 2020.
The six-month data were reported at the 2019 Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 7–11 September, Barcelona, Spain) and subsequent data were presented at the recent VIVA meeting (2–7 November, Las Vegas, USA). Holden comments that these data show “a significant patency advantage for the drug-coated balloon in de novo and restenotic lesions and all anatomic locations, particularly for the arteriovenous anastomosis and cephalic arch”.
Safety data
As Holden puts it, the possible relationship between paclitaxel exposure and all-cause mortality in claudicants (for the management of femoropopliteal lesions) “is a hotly debated issue” at present. However, he says that there “should be great caution” about extrapolating these data to the use of paclitaxel devices for “other arterial devices and for different clinical indications.” “The life-expectancy of haemodialysis patients may be very different to a claudicant population and the benefits of a patent vessel even more profound. In the USA, it is estimated the two-year mortality for haemodialysis patients is 33.2%, more than twice that of a claudicant population,” Holden observes.
Additionally, none of the studies evaluating drug-coated balloons for haemodialysis patients have identified any safety concerns (so far). For example, there were no significant differences in mortality between the IN.PACT AV group and the control group at 12 months—90.6% vs. 90.4%, respectively—in the IN.PACT AV Access trial. Also, Holden notes: “A recently published meta-analysis of mortality after paclitaxel-coated devices in arteriovenous access showed no difference in short to mid-term mortality for drug-coated balloon compared to plain balloon angioplasty”.
Future devices
Merit Medical is hoping to following Medtronic in having a FDA-approved device for the management of failing arteriovenous fistulae. On the same day that Medtronic announced that it had received FDA approval for the IN.PACT AV (21 November 2019), Merit announced that it had received FDA Breakthrough Device Designation for its Wrapsody endovascular graft system. According to a press release, the system is a flexible, self-expanding endoprothesis for use in haemodialysis patients for the treatment of stenosis within the central veins of the outflow circuit of arteriovenous fistula (up to the superior vena cava).
Concept Medical also has FDA Breakthrough Device Designation (as of August 2019) for a device for treating dysfunctional arteriovenous fistulae—the MagicTouch AVF sirolimus-coated catheter. A press release reports that the proposed indications for the catheter are “for use in percutaneous transluminal angioplasty, after appropriate vessel preparation, for the treatment of stenosis lesions of dysfunctional native arteriovenous dialysis fistula or graft”.
Whether or not Merit Medical and Concept Medical get a device onto the US market, Holden believes, just having IN.PACT on the market is good news for all concerned. He says: “It is well recognised by clinicians, funders and—most importantly—patients that a technology that significantly improves access circuit patency and reduces reinterventions is a huge gain. Haemodialysis patients have a challenging quality of life and will be delighted at a more effective treatment with reduced reintervention.”
Of note, in Europe, the MagicTouch AVF received CE mark approval in November this year and the IN.PACT Admiral was CE-marked approved for treating arteriovenous fistulae in 2016. Furthermore, the Lutonix 035 received FDA approval for this indication in 2017.
This article is part of a series of BIBA Briefings columns published in Interventional News. For previous columns, click here.
BIBA Briefings Insights reports give in-depth analysis of market intelligence from BIBA MedTech Insights. They also review that the latest technology news and pipeline developments.
For editorial enquiries, please contact Dawn Powell: [email protected]
Internal BIBA MedTech data show that perceptions on paclitaxel devices have shifted considerably in the twelve months that have elapsed since Konstantinos Katsanos (Patras, Greece) et al published their meta-analysis in the Journal of the American Heart Association (JAHA) alleging an increased death rate in patients treated with paclitaxel-coated balloons or paclitaxel-eluting stents in the femoropopliteal arteries. A recent survey reports that for 43% of physicians, the leading cause for this increased concern is due to published statements from regulatory bodies and international societies. Exactly one year on from the initial JAHA publication, Interventional News collates these position statements.
Society for Cardiovascular Angiography and Interventions (SCAI):
After reviewing the Katsanos et al meta-analysis, experts from the Society for Cardiovascular Angiography and Interventions (SCAI) concluded in a statement published on 25 January 2019 that the methods used by Katsanos et al were appropriate and within constraints of trial-level meta-analysis. However, the society statement said: “It is important to note that SCAI believes the associations are hypothesis-generating and require further investigation with patient-level data.”
Cardiovascular and Interventional Radiological Society of Europe (CIRSE):
On 29 March 2019, CIRSE made the following recommendations:
In the majority of patients undergoing lower limb recanalisation therapies, alternatives to drug-eluting devices should be used.
For some individual patients at particularly high risk for restenosis, clinicians may decide that the benefits of using a paclitaxel-coated device may outweigh the risks.
Drug-eluting devices should only be used after a full informed consent process that has discussed the mortality implications from the Katsanos meta-analysis.
All patients who have already received paclitaxel-eluting devices should be followed up to assess for a potential effect on mortality.
Medicines and Healthcare products Regulatory Agency (MHRA):
The MHRA issued a medical device alert (MDA) on 4 June 2019 warning physicians not to use paclitaxel-coated balloons or paclitaxel-eluting stents in the routine treatment of patients with intermittent claudication until further notice, “as the potential mortality risk generally outweighs the benefits”. However, the agency accedes that use of these devices may still be considered in patients with critical limb ischaemia, taking National Institute of Care Excellence (NICE) guidance into consideration, in view of their increased risk of stenosis and reduced life expectancy. This MDA was published one day after an independent expert advisory group (EAG), consisting of leading UK clinicians from multiple specialties (including interventional radiology, vascular surgery, toxicology and statistics) advised the MHRA to limit the use of paclitaxel devices to patients with CLI. The EAG was established following the publication of the Katsanos et al meta-analysis.
Society for Vascular Surgery (SVS):
The SVS Vascular Quality Initiative (VQI) used large, multicentre registries as datasets for the analysis of vascular patient care in the USA. At the SVS annual meeting (12–15 June, National Harbour, USA), Daniel Bertges (Burlington, USA) demonstrated how the VQI could potentially be used for surveillance of the safety of new peripheral arterial devices. “In this large, real-world sample,” he shared, “there is no difference in mortality at a mean of 12.4 months. The results are similar for patients treated with paclitaxel-coated balloons or paclitaxel-eluting stents. Certainly, a longer registry follow-up is required and ongoing, and we hope that the VQI Peripheral Vascular Interventions Registry will be part of that cumulative body of evidence on this important topic.”
In Spring 2019, the SVS formed a Paclitaxel Safety Task Force, with the mission of facilitating the performance and interpretation of an Individual Patient Data meta-analysis using patient-level randomised controlled trial data from industry partners.
US Food and Drug Administration (FDA):
The FDA admitted in an update from 7 August 2019 that treatment of peripheral arterial disease (PAD) with paclitaxel-coated balloons and paclitaxel-eluting stents is potentially associated with increased mortality. While the regulatory body reported the presence of the mortality signal in its own analysis, it said that the magnitude of the signal should be interpreted with caution due to several limitations in the available data. The FDA advises diligent patient monitoring, that the Katsanos et al meta-analysis be included in the patient consent process, that the device risks and benefits are discussed prior to treatment, and that physicians report any adverse events experienced with the use of paclitaxel-coated balloons and/or paclitaxel-eluting stents. These recommendations are based on the agency’s analysis of long-term follow-up data from premarket trials. The FDA is working with manufacturers and investigators to update device labels and to garner additional clinical evidence for assessment of the long-term safety of these devices.
Women of reproductive age with symptomatic fibroids experience significantly improved quality of life and significantly reduced symptoms following treatment with uterine fibroid embolization (UFE), a recent study reports. Published in Cardiovascular and Interventional Radiology (CVIR) Endovascular, the authors also conclude that functional uterine contractility seems to have a positive impact on quality of life and sexual function in this population.
While changes in uterine contractility pattern after UFE have already been assigned by cine magnetic resonance imaging (MRI), the impact of these changes had not been evaluated previous to this study. Lead author Vinicius Adami Vayego Fornazari (Universidade Federal de São Paulo, São Paulo, Brazil) and colleagues therefore set out to investigate the impact of uterine contractility on the quality of life of women undergoing UFE, measured by the Uterine Fibroid Symptom and Quality of Life questionnaire. The questionnaire, they say, is “a validated tool for measuring patient-reported symptoms and documenting clinical outcomes from surgical and interventional procedures.”
Whilst UFE is recognised as a Level A treatment option for managing leiomyomas in carefully selected patients, Fornazari et al claim that the procedure’s use for women of reproductive age “is still controversial”, and that the impact of fibroids on infertility is “not yet clear”. The majority of patients who wish to become pregnant therefore opt for a myomectomy, though there have been some studies that demonstrate successful pregnancies post-UFE. “One of the hypotheses for the association between fibroids and infertility,” the study authors write, “is alteration of uterine contractility.”
Uterine contractions act to eliminate peeling endometrium during the menstrual period, and also have various functionalities relating to pregnancy maintenance and fertility. However, these contractions are also implicated in dysmenorrhea (menstrual cramps). It has been hypothesised that fibroids could alter uterine contractility and functionality, Fornazari and colleagues write.
The present study supports this theory: half of the 26 patients prospectively included in the study experienced positive changes in their uterine contractility pattern following UFE. These patients were classified as group A during analysis. However, in a significant minority (38%) of patients, the uterine contractility pattern was unchanged after the procedure. These patients made up group B. Three patients (11%) lost uterine contractility after the procedure, and were categorised as group C.
The study investigators gave each of the 26 patients a questionnaire at their first MRI scan, which varied from 30 to seven days prior to undergoing UFE. All patients were then given the questionnaire again at their one-year follow-up consultation. Fornazari et al then analysed the survey results according to change in contractility from baseline after UFE (whether the patients were group A, B, or C).
All UFE patients presented a statistically significant reduction in mean symptom score, as well as a statistically significant increase in mean quality of life scores. Quality of life scores included worry, activity, energy, self-control, self-confidence, and sexual function.
Breaking this down by group: in those patients with an unchanged uterine contractility pattern (group A), the authors report a statistically significant reduction in mean symptom score, and an increase in the mean score of all quality of life scores, with the exception of the sexual function subscale (p=0.3232). For the 50% of patients with a favourably modified uterine contractility pattern (group B), there was a statistically significant reduction in mean symptom score, and an increase in mean quality of life score. As there were only three patients with loss of uterine contractility after UFE (in group C), no analysis could be performed.
Form these results, Fornazari et al surmise that “The significant improvement of uterine contractility and simultaneous improvement of quality of life these patients experienced after UFE suggests that uterine contractility may have a positive impact on quality of life.”
A comparative analysis between groups A and B found that, before UFE, group A had a higher sexual function score. As sexual function is a quality of life metric, the higher the score, the better. In patients with no change in uterine contractility pattern after UFE, there was also no significant change in sexual function. For patients who did experience a beneficial change in uterine contractility pattern (group B), however, there was a statistically significant increase in sexual function score. Fornazari and colleagues say that, in their previously published work, they “did not identify statistically significant variables that could be correlated to this data. In this study, the only potentially relevant variable that could be associated with a low interference in sexual function, both before and after UFE, is the fact that this group experienced no change in uterine peristalsis.”
However, Fornazari et al do note that their sample size was small, and say that additional studies are required to confirm or denounce their finding that functional uterine contractility has a positive impact on fertility and quality of life.
The first UK clinical trial site for the treatment of diabetic patients with chronic limb-threatening ischemia (CLI) using a novel patient-specific regenerative therapy has opened for patient recruitment at the University Hospital of Wales in Cardiff, UK. The site will be evaluating Rexgenero’s REX-001 in two Phase III trials, codenamed the SALAMANDER trials. The trials are being led by Ian Williams, a consultant vascular surgeon and the principal investigator at the site. recruiting
The University Hospital of Wales is participating in the trials through a consortium, the Midlands-Wales Advanced Therapy Treatment Centre (MW-ATTC), part of the Advanced Therapy Treatment Centre Network (ATTC) which aims to bring pioneering advanced therapy medicinal products (ATMPs) to patients. THE MW-ATTC has been working in collaboration with the Cardiff and Vale University Health Board to progress the initiation of the two SALAMANDER trials and is planning to activate new clinical trial sites in the Midlands in England shortly.
REX-001 represents a new class of regenerative medicines. It is an autologous cell therapy manufactured using the patient’s own bone marrow and consists of immune cells (lymphocytes, monocytes, and granulocytes) and progenitor cells involved in immune modulation and tissue regeneration. It is administered as a single dose within four days after collection of bone marrow cells.
Williams comments: “Chronic limb-threatening ischaemia is a serious disease with severe consequences and limited treatment options. There is a high unmet need for novel and innovative therapies—such as REX-001—that have the potential to be a highly effective treatment and to reduce amputation and mortality rates amongst the patient population.”
Rexgenero, the company pioneering the development of REX-001, says that the experimental product has already demonstrated efficacy in Phase I/II studies. In the Phase II clinical trial, 82% of patients with non-healing ischaemic ulcers were healed within the first 12 months after a single administration dose of REX-001.
Joe Dupere, CEO of Rexgenero, adds: “Treating our first patient with REX-001 in the UK represents an important milestone for our Phase III programme in diabetic patients with chronic-limb threatening ischaemia, a severe condition with high unmet need. With clinical trial sites and manufacturing bases now open across multiple countries in Europe, we are one step closer to completion of the Phase III studies and potential regulatory and market approval for an innovative and much-needed product.”
Rexgenero is planning to treat a total of 60 patients with CLI and rest pain and 78 patients with CLI and non-healing ischaemic ulcers in two independent Phase III SALAMANDER trials in approximately 25 hospitals across Europe. In addition to the trial sites in the UK, Rexgenero is also recruiting patients for both trials at sites in Spain, Austria, Portugal, Poland, Hungary, The Netherlands and the Czech Republic.
Akhilesh Sista (New York, USA) talks to Interventional News at VIVA 2019 (Vascular InterVentional Advances; 4–7 November, Las Vegas, USA) about the results of the EXTRACT-PE study, that were presented in a late-breaking clinical trial session at the meeting.
EXTRACT-PE successfully met the primary endpoints, demonstrating the safety and efficacy of the Indigo Aspiration System (Penumbra) for aspiration mechanical thrombectomy in patients with acute pulmonary embolism (PE).
Sista says that “up to this point, there had been no prospectively collected data on this new but promising device”. Catheter-directed thrombolysis and systemic thrombolysis both carry the risk of bleeding and the inconvenience of having to drip the patient with tissue plasminogen activator (tPA) over the course of time. That is why, Sista says, the purpose of the EXTRACT-PE study, was to evaluate the efficacy and safety of aspiration thrombectomy with the Indigo Aspiration System.
While Sista says that the data indicates “this is another tool in our toolbox to remove thrombus quickly in patients who need thrombus removal”, he also believes that the “scientific pulmonary embolism (PE) community” has to go beyond the RV to LV ratio and needs to look at clinical outcomes and randomise patients, both for this device and in general, to try to evaluate whether clot removal in submassive PE “is the right thing to do, and if so, in whom”.
A real-world study investigating the luminor drug-coated balloon (DCB; iVascular) in Brazil has started, following approval for commercialisation of the device by ANVISA, the Brazilian regulatory authority. LUMBRA (LUMinor balloon in a BRAzilian registry for real world lesions) aims to corroborate the efficacy and safety results of luminor in Europe demonstrated by the EFFPAC and TINTIN trials.
The LUMBRA trial has the objective of evaluating the long-term outcomes of treatment with the luminor DCB, followed by potential bail-out stenting with the iVolution stent (iVascular) in symptomatic femoropopliteal arterial stenotic or occlusive lesions in 200 patients from Brazil. The first patient to be enrolled was included on 30 November 2019.
The primary endpoint of the registry is primary patency at 12 months. The secondary endpoints include: technical success, procedural success, primary patency rate freedom from target lesion revascularisation, changes in ankle-brachial index measurements, and serious adverse events, as defined per ISO 14155:2011.
Pierre Galvagni (Federal University of Santa Catarina, Florianopolis, Brazil), principal investigator of the trial states: “We were expecting to have luminor in Brazil; this trial will allow us to corroborate in [a] real-world Brazilian population the great outcomes of luminor DCB”.
During the November SIR and SIR Foundation Nominating Committee meetings, the Society of Interventional Radiology (SIR) elected a new Executive Council for 2019–2020. Following the Annual Members’ Business Meeting in spring this year (28 March–2 April, Seattle, USA), Katharine Krol (Lafayette, USA) will become chair of the SIR Foundation Board of Directors.
Theresa Caridi (Washington, DC, USA), currently serving as development division chair, has been elected vice chair of the society. She will hold this position for a two-year term, before succeeding to chair in 2022.
Parag Patel (Milwaukee, USA) has been elected SIR secretary, and will succeed to president-elect in 2021 following his one-year term as secretary.
Akhilesh Sista (New York, USA) has been elected as councillor-at-large, for a four-year term.
Alda Tam (Houston, USA) has been reappointed standards division councillor, and will serve a three-year term.
Clifford Weiss (Baltimore, USA) has been appointed grants and education division chair, a position he will hold for a three-year term.
Philips has announced a major clinical trial to assess the impact of a direct-to-angiosuite workflow on stroke patient outcomes. The study will assess whether with Philips’ advanced image-guided therapy platform it is possible to diagnose, plan and treat stroke patients in the interventional suite without requiring an initial CT or MRI exam. The multicentre, prospective, randomised, controlled, open-label, blinded-endpoint trial will be run across eight sites and over 460 patients globally. It will begin in the first half of next year and is expected to be completed in 2022.
Outcomes for stroke patients are closely tied to how quickly they receive treatment: every 30 minutes’ delay before treatment reduces the chance of a good outcome by 14%1, and every hour of delay ages the brain by 3.6 years compared to a normally aging brain2.
Currently, when a possible stroke patient arrives at the emergency department, they typically first undergo a CT or MRI exam and, in the case of an ischaemic stroke, are then treated in an interventional suite. Several studies have indicated that a direct-to-angiosuite workflow can reduce the time to treatment and improve patient outcomes. Philips is developing new technology to further improve the CT-like images of the brain created with the X-ray system in the suite. The WE-TRUST (Workflow optimisation to reduce time to endovascular reperfusion in stroke treatment) trial will provide the most comprehensive assessment to-date of the impact of this technology and workflow innovation on time to treatment and patients’ neurological outcomes.
“Significant advances in technology mean that we are now able to identify, plan and treat ischaemic stroke patients in the angiography suite, without the need for a separate CT or MR scan” said Raul G Nogueira, director, Neuroendovascular Service Marcus Stroke & Neuroscience Center at Grady Memorial Hospital in Atlanta, USA, and principal investigator for the WE-TRUST trial. “Now is the right moment to perform a randomized controlled trial to objectively assess the benefits of a streamlined Direct to Angio Suite workflow on patient outcomes.”
“With extensive clinical research demonstrating the benefit of a treatment approach that combines thrombectomy and clot-busting drugs, stroke patient triage and treatment has changed dramatically in recent years,” said Ronald Tabaksblat, General Manager Image Guided Therapy Systems at Philips. “For stroke patients, ‘time is brain’. The WE-TRUST trial will assess the impact of a streamlined direct-to-angiosuite workflow on patient outcomes and has the potential to make a significant impact in this rapidly advancing field.”
The trial will primarily be carried out on Philips Azurion, the company’s platform for interventional procedures, at eight leading stroke sites in Europe and the USA. The primary endpoint of the WE-TRUST trial is patients’ cognitive function at three months after the procedure.
Additional ultrasound-accelerated catheter-directed thrombolysis does not lower the risk of post-thrombotic syndrome in patients with acute iliofemoral deep-vein thrombosis (DVT), according to findings of the CAVA trial presented at the International Union of Phlebology chapter meeting (UIP 2019; 25–27 August, Krakow, Poland). Preliminary results of a post-hoc subgroup analysis suggest that if recanalisation is successful, post-thrombotic syndrome is less severe and quality of life scores are higher one year after an acute DVT.
Examined in presentations by both Pascale Notten (Maastricht, the Netherlands) and Cees Wittens (Maastricht, the Netherlands)—winners of the best abstract session at UIP— and published in The Lancet Haematology, results of the CAVA trial also showed a high rate of thrombotic events, mostly due to in-stent thrombosis.
Post-thrombotic syndrome is a common long-term complication of deep-vein thrombosis , particularly in cases where the localisation of the thrombus is iliofemoral or more cranial. The ‘open vein hypothesis’ suggests early removal of the thrombus as a means of preserving venous function and restoring venous outflow, thereby preventing the development of post-thrombotic syndrome; ultrasound-accelerated catheter-directed thrombolysis was considered a promising option for this removal.
As part of the multicentre, randomised controlled CAVA trial, which aimed to determine whether additional ultrasound-accelerated catheter-directed thrombolysis can decrease the risk of post-thrombotic syndrome, 184 patients with a first-time acute iliofemoral deep-vein thrombosis were randomly assigned to one of two treatment groups; either standard post-thrombotic treatment with additional ultrasound-accelerated catheter-directed thrombolysis or standard treatment (including early anticoagulant therapy, compression therapy, and mobilisation) alone.
Results of the trial showed that post-thrombotic syndrome occurred in 22 of the 77 patients (29%) randomised to the additional thrombolysis group, compared to 26 out of 75 patients (35%) in the standard treatment cohort (odds ratio 0.75, 95%CI, 0.38-1.50, p=0.42). Major bleeding occurred in four patients (5%) from the intervention group, compared to none in the control group, (p=0.06). Furthermore, a total of 24 thrombotic events occurred in 20 patients: 14 patients (18%) from the intervention group developed 17 events versus seven events in six patients (8%) from the control group (P=0.06). Of the 17 thrombotic events in the intervention group, more than 70% (12 out of 17) were due to in-stent thrombosis.
Speaking to Venous News about the results, presenter Notten said: “When comparing our results to the two previous large trials (CaVenT and ATTRACT), our outcomes regarding the development of post-thrombotic syndrome are similar to those found in the ATTRACT trial and show no statistically significant difference between treatment groups as opposed to the CaVenT trial.
“With the CAVA trial being inconclusive, the discussion regarding the role of additional catheter-directed thrombolysis in the treatment of acute iliofemoral deep-vein thrombosis persists. Further research including optimising patient selection, interventional techniques, and peri-interventional treatment regimens is essential.”
Can successful thrombolysis prevent post-thrombotic syndrome?
Presented by Wittens at UIP, a sub-group analysis of the results aimed to assess the success rate of additional ultrasound-accelerated catheter-directed thrombolysis in restoring patency (to 90% or more) and its relation to development of post-thrombotic syndrome at one year. As the degree of residual vein occlusion correlates with the risk of post-thrombotic syndrome, it has been said that the preventative impact of ultrasound-accelerated catheter-directed thrombolysis might depend on its ability to achieve successful recanalisation.
According to the preliminary analysis, recanalisation was considered successful in 41 out of the 77 patients (53%) who received additional ultrasound-accelerated catheter-directed thrombolysis, while a total of 75 patients in the CAVA trial received standard treatment only. Overall, post-thrombotic syndrome developed in nine patients (22%) from the successful thrombolysis subgroup and 26 (35%) of the control patients (P=0.15).
Comparing the successful thrombolysis sub-group to those who underwent unsuccessful thrombolysis—post-thrombotic syndrome developed in 13 out of 36 patients (37%) —no significant difference in proportion of post-thrombotic syndrome was seen (p=0.17). However, the severity was significantly lower in those successfully treated. Generic and disease-specific quality of life questionnaires also differed significantly between groups, once again favouring those who had been successfully treated.
Based on the findings of the sub-group analysis, successful thrombolysis does result in benefits such as less severe symptoms and improved quality of life when considering multiple aspects. Commenting on these results, Cees Wittens said to Venous News: “The subgroup analysis shows that proper quality control of an intervention is essential to evaluate an intended treatment. Unfortunately, this trial shows that only 53% of the patients who received the intervention had a successful intervention.
“Since the preliminary subgroup analysis showed a significant improvement in clinical scores and quality of life in those successfully recanalised, the overall conclusion of the various trials should not be that early thrombus removal is not effective in achieving better clinical outcomes and that this treatment should be abandoned; it tells us that early thrombus removal actually has the capacity to limit long-term post-thrombotic morbidity, if only we are able to improve the process of patient selection and develop better interventional treatments.”
Ultrasound-only guidance is technically feasible for a substantial proportion of cryoablation procedures, Alex Barnacle (Great Ormond Street Hospital, London, UK) reported at the 2019 annual meeting of the British Society of Interventional Radiology (BSIR; 13–15 November, Manchester, UK). Using ultrasound instead of computed tomography (CT) for intraprocedural imaging eliminates the radiation burden, which Barnacle said “is of primary importance”, especially when treating children.
“Wherever possible, ultrasound is the preferred imaging modality in paediatric interventional radiology, to avoid or minimise radiation dose in childhood,” she stated. Therefore, Barnacle and colleagues set out to investigate if ultrasound-only guidance was viable for intraprocedural navigation, and an assessment of their initial experience proves that it is.
The team reviewed all cryoablation procedures performed at their institution, and selected those for which only ultrasound was used. They collected their data prospectively, and had institutional review board approval for the study.
Over 29 months, interventionalists at Great Ormond Street Hospital performed 25 cryoablation procedures using only ultrasound as image guidance. Twenty-one lesions were treated in 20 children; most of these were soft tissue lesions in the extremities. “The age range and therefore the weight range was really diverse in this paediatric group”, Barnacle said. The median age was 11.4 years (ranging from five months to 16.5 years), and the median weight was 37.9kg (ranging from 7.5kg to 94.2kg). Whilst cone beam CT was available as back up for all cases, no procedure required the investigators to convert to CT guidance.
Since starting a new ablation service, interventional radiologists at the London-based paediatric hospital have been referred increasingly complex cases. “As often happens when you start a new service, you get sent quite a hodgepodge of cases,” Barnacle explained. “We were often sent patients as a last resort, where people had tried every other therapy first, so our initial experience was with a whole bunch of different conditions, from venous malformations to fibro-adipose vascular anomaly (FAVA), which is one of the primary diseases that we use cryoablation for in our centre.” Incidentally, this latter pathology was the first condition in children for which treatment with cryoablation was fully described. “Increasingly,” Barnacle continued, “we are being referred more aggressive diseases, and some oncological diseases as well.”
Detailing some examples of these more complex cases, Barnacle went on to describe a patient with a fast flow vascular anomaly in their forearm. Surgical debulking had been attempted twice previously, but had been followed by rapid regrowth. There was a large vessel in the centre of the lesion, and the arm was “very hot”, Barnacle recounted. “We wanted to cryoablate this,” she said, “but we were not sure what to do about the temperature.” The interventionalists performed an angiogram and embolized the central vessels, before going on to cryoablation. This had “really good results”, according to Barnacle, who enthused: “We are trying to push the boundaries with what we are doing in these patients.”
This involves being more aggressive in their treatment. Whilst Barnacle and colleagues used a range of one to five probes per procedure for the 20 patients in this study, they now sometimes use significantly more than five in some circumstances. The team use a standard freeze-thaw cycle twice, and lots of hydrodissection. Commenting on this, Barnacle opined: “I think this just reflects the fact that many of these lesions are very superficial, especially in children, who by their very nature do not have much subcutaneous fat.”
Speaking from the floor, Society of Interventional Oncology (SIO) president-elect Matthew Callstrom (Mayo Clinic, Rochester, USA) asked about the natural history of these vascular malformations in children, and how aggressive Barnacle felt the interventionalists need to be to have an impact on tumour growth over time. “Do you treat the entire mass, or do you try and treat 80%—what is your goal?”, he asked.
“We are getting more aggressive now,” Barnacle replied. “The nice thing is you are not having to get margins, so you have some leeway. […] Increasingly, we are trying to get the whole thing in one go.” However, she cautioned against using very aggressive cryoablation with large ice balls in very small children, describing a one-and-a-half-year-old patient who did not respond well to this type of intervention. “She was pretty unwell for a few days [after cryoablation]”, Barnacle reported. “She clearly had some kind of immune response and a cytokine storm afterwards. She tolerated the second procedure much better, when we used a decreasing dose of steroids over a week and gave her antibiotics and other support, but that initial experience made us wary.”
Many regulatory jurisdictions are establishing different approaches for medical devices, Misti Malone, assistant director in the Office of Cardiovascular Devices at the US Food and Drug Administration (FDA) said recently at the 2019 Vascular and InterVentional Advances meeting (VIVA; 4–7 November, Las Vegas, USA). She talked the audience through recent regulatory changes across the world, and outlined her vision for a global regulatory consensus.
Speaking in the “Most controversial clinical challenges of 2019” session at VIVA, Malone joked, “I hope you do not consider the FDA the most challenging and controversial aspect of clinical care” as she took to the podium to deliver her talk “Shifting worldwide regulatory priorities: How will changes in the 510(k) and CE mark process affect device availability for patients?”
“We [the FDA] are here to interact and collaborate with you,” she told the physicians, “and we appreciate the hard work you are doing. […] Regulatory pathways are evolving across the world. While I was asked to comment on whether this may affect device availability, our primary mission is to promote and protect public health, and our goal is to bring safe and effect devices to patients. We try to do this as quickly as possible, so we hope that our pathways are not changing how devices are available, other than potentially making devices available more quickly, and as needed by some of our new pathways.”
While she detailed how many regulatory jurisdictions are establishing different regulatory approaches for medical devices, exploring the changes to the FDA pathways in the US, she urged the VIVA audience to consider global strategies when appropriate. “We [the FDA] highly recommend discussing these proposals with multiple regulatory agencies early in the process,” she counselled, “so they can be efficient and predictable”.
The FDA 510(k) pathway
The FDA’s 510(k) pathway is required for most medium-risk devices, classified as Class II by the agency. These include guidewires, introducers, balloon catheters, and peripheral atherectomy devices. Approval via this pathway requires the demonstration of “substantial equivalence to a legally marketed, predicate device”, meaning that the new device design, performance, and intended use must be similar enough to an existing device.
On 20 September 2019, the FDA released a guidance document outlining a new “safety and performance-based pathway”, representing an alternative to the 510(k) process. According to Malone, the clearance was based on the intended use being equivalent to the predicate, and performance testing following FDA-specified methods and criteria, which may be based on recognised standards and the historical performance of comparable products, rather than testing intended to demonstrate substantially equivalent performance to a specific marketed device via methods selected by the manufacturer.
However, Malone acknowledged that this new 510(k) pathway may not be suitable for all devices: “Due to the lack of comprehensive standards and guidances available, particularly for cardiovascular devices […], identifying performance criteria and placing devices in a box may be challenging. Our goal is not to reduce innovation—it is to support innovation by allowing the process to move as efficiently as possible.”
One of the goals of this new pathway, Malone shared, is to make the approval process in the USA “more similar to regulatory paradigms in other countries”, such as the third party certification in Japan, which relies on performance criteria set by the Japanese government. As this only includes a limited number of cardiovascular devices, Malone anticipated that “This [system in Japan] may be pathway that will be valuable for some of our simpler devices for which we can set our performance criteria, but not for all devices.” She was enthusiastic, though, about the potential for global regulatory synergy, commenting: “It may facilitate convergence for global regulatory decision-making.”
EU MDR changes will take effect from May 2020
The European Union is moving to replace its Medical Device Directive (MDD) with the Medical Devices Regulation (MDR), a more extensive regulatory document, introducing significant revisions to quality and safety standards, and the range of regulated devices. The MDR was initiated in May 2017, and a three-year transition period applies. The changes outlined in the MDR legislation are currently due to take effect from May 2020, though, as Malone pointed out, “There is continual discussion on the topic at these forums [referring to meetings like VIVA] and from the EU”.
The goals are to reinforce provisions for clinical evidence. Clinical evaluation will be required pre-market for some devices and modifications, and it will continue into post-market with regular updates, surveillance, and analyses. Another goal is to encourage transparency, using unique device identification (UDI) traceability and data availability for both clinicians and patients. “We hope that this will provide more information, or at least that the EU will provide more information to support clinical decision-making and patient decision-making,” Malone stated.
One worry she shared with the VIVA audience was that clinical data may be required, and that this may affect device availability. Devices that are most likely to require clinical investigation are those that are implants and high-risk devices, those assigned to Class II, low-risk devices where the technology has little or no experience, or devices that extend the intended purpose of an existing technology, Malone informed delegates. For devices classified as Class III and implantable devices, a post-market clinical follow-up report may be required to update a summary of safety report, and clinical performance needs to be updated at least annually with these data.
“How this will affect device availability I think is more of a question for industry,” Malone opined. “I think it may be based on their cost-analysis. However, we look to clinicians to help us understand the ramifications of some of the regulatory decisions, and also to develop a global consensus, so the process can be efficient.”
Harmonising global regulatory requirements
“We have global groups, such as the International Medical Device Regulators Forum, in which we cooperate with numerous countries across the globe,” Malone said. This is a voluntary effort among medical device regulators to, in Malone’s words, “harmonise various regulatory requirements across their jurisdictions. The goal”, she elaborates, is “to be transparent and predictable, and create a reliable pathway, that is efficient for industry, clinicians, and regulators. It is currently high-level, but it is driving cooperation at the device level.”
The FDA and the Center for Devices and Radiological Health (CDRH)—the branch of the FDA responsible for the premarket approval of all medical devices—consider it a strategic priority to use opportunities and collaborations like IMDRF to put in place building blocks for creating a medical device single review programme with the potential goal that, once established, market authorisation and decision in one place may be supported in another country.
The clause in the 2018–2020 CDRH strategic priorities document, published January 2018, outlining how this may work reads: “We also will explore international convergence of some of these pathways—but not change our regulatory standard for market authorisation nor our reliance on valid scientific evidence—as we continue to work under the auspices of the International Medical Device Regulators Forum to put in place the building blocks for creating a Medical Device Single Review Program. Under such a programme, should it be established, the market authorisation decision made by or on behalf of one participating jurisdiction would be relied on wholly or in part to support marketing authorisation by other participating jurisdictions.”
Malone drew the audience’s attention to Japan as a case study of international collaboration. She described a successful harmonisation between the USA and Japan: “The USA collaborates closely with Japan due to the similar regulatory environments and patients. They [Japan] have made some recent policy developments, including [the] Sakigake (pioneer) device scheme, shifts in pre- and post-market balance, similar to the FDA, the use of non-domestic data, establishment of registries and use of real-world evidence, and pathways for early feasibility studies. We have continuing US and Japanese collaboration via HBD [harmonisation by doing].”
HBD facilitates the cooperation of industry, government, and academia in Japan and the USA to align medical device regulations in both countries through clinical trials and the approval review process.
Endovascular arteriovenous fistulas (endoAVF) platforms add additional fistula options for patients and physicians, argues Dheeraj Rajan (University Health Network, University of Toronto, Toronto, Canada, and a paid consultant for BD) at the 2019 Vascular and InterVentional Advances meeting (VIVA; 4–7 November, Las Vegas, USA). He argues that, due to higher patient satisfaction, good technical success, and low complication rates, as well as the attendant cost savings, endovascular AVF creation will soon be “essential” for any dialysis programme.
The first AV fistula, described in 1966 by Michael Brescia, James Cimino, Kenneth Appel, and Baruch Hurwich (all Veterans Administration Hospital, New York, USA), involved the side to side surgical anastomosis of the patient’s cephalic vein and radial artery near the wrist.
“It is important to note,” Rajan said to the VIVA audience, “that over 50 years [since the first AV fistula], we are still talking about the surgical creation of AV fistulas; not a lot has changed in that time. If you think about what kind of innovation has happened in different areas of medicine over those 50 years, and compare it to that in dialysis access, then you can see that we have not really had a lot of innovation in this space.”
He thinks this is changing, however, predicting the mainstream adoption of endovascular AVF creation.
Rajan highlighted the 20–60% failure rate of surgical AVFs to mature, as reported in “meta-analyses and multiple, large studies”—though he did also note that, anecdotally, AVFs may have a higher maturation rate, with several conference attendees reporting a 90% success rate in their own experience. In addition, he told delegates that 80% of patients start dialysis with a central venous catheter (CVC) in place, which he said “is not good for the patient”. Added to these downsides of surgical AVF creation, he commented, “In the world of patient-centred care, it is important to note that 30% of patients do not want to get surgery. It is something we rarely talk about.”
There are two devices currently commercially available for endovascular AVF creation: the 4Fr or 6Fr WavelinQ endoAVF platform, from BD, and the 6Fr Ellipsys vascular access system, from Avenu Medical. These were both approved by the US Food and Drug Administration (FDA) in 2018, following CE mark approval for Ellipsys in 2016, and WavelinQ in 2017. The WavelinQ system is a dual catheter system, which uses radiofrequency (RF) energy to vaporise tissue between the artery and the vein, thereby creating an anastomosis between the two vessels.
Describing the commonalities between surgical and endovascular AVF creation, Rajan says screening is “relatively similar”, with both requiring ≥2mm vessels and a perforator. The interventionalist arterialises the deep venous system to the superficial system.
However, he then went on to detail the differences in outcomes between the two methods. The prospective, multicentre NEAT (novel endovascular access) trial, published in the American Journal of Kidney Diseases in 2017 by Charmaine Lok (University Health Network, University of Toronto, Toronto, Canada) et al, concluded than “An endoAVF can be reliably created using a radiofrequency magnetic catheter-based system, without open surgery and with minimal complications. The endoAVF can be successfully used for haemodialysis and demonstrated high 12-month cumulative patencies. It may be a viable alternative option for achieving AVFs for haemodialysis patients in need of vascular access.”
Indeed, primary and secondary patency were better for endovascular AVF creation than outcomes from surgical creation. Primary patency was time from successful AVF creation to the first intervention designed to address thrombosis or stenosis, assist in maturation, or cannulation of AVF abandonment. Secondary patency was time from creation to the abandonment of AVF.
“Maturation rate, with both devices [WavelinQ and Ellipsys], was better than what we see typically with surgery,” Rajan said. Presenting data on WavelinQ from Lok et al’s NEAT trial, he said that the maturation rate in this study for endovascular AVF creation was 91%. In comparison, Rajan showed data from Michelle Robbin (University of Alabama, Birmingham, USA) et al, published in Radiology, that reported a maturation rate of 76% in the upper-arm and 53% in the forearm when using surgical AVF creation.
Patient satisfaction is also superior with endovascular haemodialysis AVF creation, Rajan reported. Indeed, Lok et al found that 96% of patients said they were “satisfied” with endovascular AVF creation. Illustrating this statistic with an anecdote, Rajan recounted: “I will never forget a conversation I had with a vascular surgeon where he grabbed me, physically grabbed me by my lapel, and said ‘I want in’. I asked him what he meant, and he said ‘You are working on this endovascular fistula thing, I want to invest’. I said ‘We do not know if it really works or not yet or how good our numbers are going to be’, and he said ‘It does not matter, every patient is going to want this first before they want surgery’.”
Another advantage of the endovascular approach listed by Rajan is the reintervention rate. He continued: “In terms of post-creation procedures,” Rajan continued, “the total number of interventions with endovascular access, using WavelinQ specifically, is 0.6 per patient year, compared to surgical, where it is 3.4 per patient year. So looking at our intervention rate, that is six times’ lower than with the surgical approach.” In addition, time to first intervention is longer when the endovascular approach is used.
Rajan also outlined how these factors translate into cost savings: a study by Shuo Yang (Quorum Consulting, San Francisco, USA) and colleagues, published in Journal of Vascular Access in 2017, found that US$11,240 was saved per patient-year following endovascular haemodialysis AVF creation compared with surgically created AVFs, due to the reduced number of reinterventions. “We have follow-up data that shows the cost-savings are even better than that,” Rajan added.
“One of the things to note is, with both devices [WavelinQ and Ellipsys], you are actually not getting rid of traditional surgical options. This actually adds more options for the patient, so you are not eradicating surgical choices. Working distal to proximal, you are adding more sites to create accesses, and these are autogenous fistulas: you are not leaving prosthetic material behind, you are not leaving a stent graft, you are not leaving a stent, there is no suture material here, and that all translates into better outcomes.”
To demonstrate this, Rajan collated the outcomes of major studies published recently, where the technical success rate with endovascular access was consistently above 80%. These studies included the Flex study (2015), the NEAT study (2017), and the EASE study (2019), which all used WavelinQ, as well as the two Hull studies (2017 and 2018), and the Mallios study (2018), which utilised the Ellipsys device. Mean maturation time ranged from 42 days to 118 days, and functional patency was “very high” for both devices, ranging from 87% to 100%.
Adverse events are also rare in endovascular AVF creation, Rajan commented. The number of serious adverse events recorded in these major studies ranged from 0% to 8%, though Rajan noted that events may not always be due to AVF creation. “Depending on the study and how you record adverse events,” he said, “keeping in mind that in studies, when you talk about serious adverse events, this includes strokes, cardiac attacks, car accidents and so on, so there are different adverse events that can be attributed to devices.”
He summarised: “I think this will accelerate and improve patient care. We are talking about not needing pre-operation visits. You could potentially screen patients with ultrasound the day they get a dialysis catheter; you do not need anaesthesia, these are outpatient procedures that can be done with conscious sedation, and this all potentially gets you to getting a fistula on a patient sooner, but also potentially cannulating sooner as well.
“This is coming. I think this adds a different platform for patients, the data suggests technical success and the complication rates are acceptable, there is high cannulation success, high patency with low interventions, and, most importantly, high patient satisfaction. I do think this will be a key part of any dialysis programme going forward, and there have probably been around 2,000 cases performed between both devices globally. I think patients will demand this, and they will actually drive a large part of the adoption.”
Writing to members of the American Venous Forum (AVF), president Brajesh K Lal (Baltimore, USA), has revealed that the AVF has established a partnership with the C-TRACT study, a randomised controlled trial funded by the National Institutes of Health. As part of the collaboration, AVF will contribute its expertise, perspective, and work effort to advance the trial’s success.
In his letter, Lal described the C-TRACT trial as a large study of endovascular therapy for post-thrombotic syndrome (PTS). Furthermore, the aim of the study is to understand whether image-guided procedures reduce the severity of PTS and improve patients’ quality of life. While long-term safety and costs of endovascular procedures are also being evaluated, the findings of the trial will provide new information on optimal ways to care for patients with PTS. Twenty-three clinical centres are currently participating in C-TRACT, with availability for more to join.
The partnership expands AVF’s tradition of leadership in promoting evidence-based practice in venous and lymphatic disease. As part of agreement with C-TRACT, which is led by Suresh Vedantham (St Louis, USA), AVF will leverage its knowledge and resources to increase awareness of the study, as well as helping to identify investigators and sites to participate in the study, encourage enrolment in the trial, and promote best practices for study conduct.
Discussions of C-TRACT will be presented at AVF meetings, including the 32nd annual meeting of AVF (March 3–6 2020, Amelia Island, Florida) and the Fall and Spring AVF Fellows’ courses. It will also be discussed during AVF sessions at other society meetings and in AVF’s scientific journal, Journal of Vascular Surgery: Venous and Lymphatic Disorders.
Speaking to Interventional News, chief investigator of the C-TRACT trial Vedantham said: “We are grateful to the AVF for its strong support of the C-TRACT Trial. The AVF has a distinguished history of advancing venous research, so this is a perfect fit. This partnership will promote the study’s success and provide insights into a new community partnership model that can be applied to benefit future studies.
“The investment of $12 million in this study by the NIH demonstrates its awareness of the potential for endovascular stent therapy to reduce disability in patients with post-thrombotic syndrome. As such, the C-TRACT Investigators and the AVF have a golden opportunity to develop high-quality evidence that secures access to innovative therapy for patients suffering with this condition.”
The Society of Interventional Radiology (SIR) Foundation is already partnering with C-TRACT investigators. Since January 2019, SIR Foundation has worked with Vedantham to raise awareness of the trial within the IR community, support site and patient enrolment, and encourage patient follow-up activities.
“Studies such as C-TRACT exemplify SIR Foundation’s mission to further interventional radiology through high-quality research that impacts our patients,” comments SIR Foundation chair Jeremy C Durack (Memorial Sloan Kettering Cancer Center, New York, USA). “We are proud to support this effort and continue to raise awareness among SIR members and the IR community about the value of this ground-breaking trial.”
Medtronic today announced US Food and Drug Administration (FDA) approval of the IN.PACT AV drug-coated balloon (DCB), a paclitaxel-coated balloon indicated for the treatment of failing arteriovenous (AV) access in patients with end-stage renal disease (ESRD) undergoing dialysis.
AV fistulae are created and used to enable haemodialysis for patients with ESRD. Over time, vessel restenosis limits the ability to use AV fistulae effectively. In order to restore function, patients often undergo one to three maintenance procedures per year,1 which can result in significant disruptions to critical haemodialysis care and increased costs to the healthcare system. Pivotal randomised trial results from the IN.PACT AV Access trial have shown IN.PACT AV DCB can extend the time between reinterventions by maintaining AV access site patency, therefore maximising a patient’s uninterrupted access to lifesaving dialysis care.
“In many cases, AV fistula are considered lifelines for patients with ESRD as they are the primary access point for life-saving dialysis treatment. When these access sites fail, patients experience delays in their dialysis treatment and require multiple reinterventions to keep the site functioning,” said Vincent Gallo, interventional radiologist at Holy Name Medical Center in Teaneck, USA, and an investigator for the IN.PACT AV Access trial. “With this approval physicians now have access to a safe and extremely effective therapy to slow the progression of restenosis, which results in fewer reinterventions and disruptions in care for these patients.”
The FDA approval is based on data from a prospective, global, multicentre, blinded, randomised (1:1), investigational device exemption (IDE) study, which enrolled 330 subjects, and evaluated the safety and effectiveness of the IN.PACT AV DCB at 29 sites in the USA, Japan, and New Zealand. Early data presented at the Cardiovascular Interventional Radiological Society of Europe (CIRSE) met the primary endpoints in demonstrating the comparable safety and the superior effectiveness of IN.PACT AV DCB compared to percutaneous transluminal angioplasty (PTA). Patients treated with IN.PACT AV DCB maintained patency longer and required 56% fewer reinterventions compared to those treated with standard PTA through six months. Through 12 months the data also showed no difference in mortality rates between the IN.PACT AV DCB group and the PTA control group. Finally, data presented at VIVA 2019 demonstrated superior patency was achieved with IN.PACT AV DCB versus PTA in both de novo and restenotic lesions, and all studied types of AV access.
“Until now, there were virtually no therapies available to treat AV fistulae lesions that had demonstrated an ability to maintain primary patency and reduce reinterventions over time,” said Robert Lookstein, national principal investigator in the USA and professor of radiology and surgery, vice-chair of interventional services, and medical director of clinical supply chain at Mt. Sinai Healthcare System in New York, USA. “In the largest AV DCB pivotal study to-date, IN.PACT AV DCB demonstrated the highest primary patency rate through six months and significantly lowered the rate of reinterventions required to maintain patency. With this evidence and approval in hand, we now have a technology that provides a significant clinical benefit of a 56% reduction in repeat interventions, which I believe is a huge win for the haemodialysis community and the patients we treat.”
IN.PACT AV DCB, leveraging technology from Medtronic’s IN.PACTTM AdmiralTM platform, increases blood flow and reduces thickening of the vessel wall by delivering the proven anti-proliferative drug paclitaxel. This drug penetrates deep into the vessel wall to prevent restenosis and has the potential to extend time between reinterventions. In 2016, the CE Mark indication for IN.PACT Admiral DCB was expanded for the treatment of failing arteriovenous (AV) access in patients with end-stage renal disease undergoing dialysis.
“The FDA approval of IN.PACT AV DCB marks a significant step forward for paclitaxel-coated devices. Importantly, it allows us to expand our proven IN.PACT DCB platform beyond the superficial femoral artery,” said Mark Pacyna, vice president and general manager of the Peripheral Vascular business in the Medtronic Cardiac & Vascular Group. “We are excited to bring this technology to physicians in the U.S. and to help improve the lives of patients living with ESRD.”
In collaboration with leading clinicians, researchers, and scientists worldwide, Medtronic offers the broadest range of innovative medical technology for the interventional and surgical treatment of cardiovascular and end-stage renal disease. The company strives to offer products and services that deliver clinical and economic value to healthcare consumers and providers around the world.
References
THE USRDS Special Study Center. Transition of care in CKD. Prelude to Dialysis: Trends and Timely Transitions. Kalantar-Zadeh K et al. 2016
Merit Medical Systems has announced that it has been granted breakthrough device designation by the US Food and Drug Administration (FDA) for the Merit Wrapsody endovascular stent graft system. The Wrapsody system is a flexible, self-expanding endoprosthesis for which Merit intends to seek indication for use in haemodialysis patients for the treatment of stenosis within the central veins of the outflow circuit of an arteriovenous fistula (AVF) up to the superior vena cava.
The FDA breakthrough devices programme is intended to help patients receive more timely access to breakthrough technologies that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions. Under the programme, the FDA provides priority review and interactive communication regarding device development and clinical trial protocols, through to commercialisation decisions. The Wrapsody system is nearing completion of its “first-in-man” studies, and is not currently available for sale.
“We are pleased with the recognition by the FDA of this worthwhile technology as well as the efforts of many members of our research and development team to bring the project to this point,” says Fred P Lampropoulos, Merit Medical’s chair and CEO. “Most importantly, we believe this system will provide substantial benefits to patients who may be treated with it in the future.”
Siemens Healthineers presents its new Somatom X.cite single-source CT scanner, together with the new myExam companion user guiding system, based on artificial intelligence (AI).
The intelligent user guidance system guides the user through the workflow using specific questions. The user interface works with the latest scanner hardware “to open up new possibilities,” a company press release states. myExam companion makes use of available patient data, such as sex, height, and age, and combines these with additional patient-specific information gathered by asking the user specific questions; for example, about the presence of metal implants, or the ability of patient to hold their breath. The scanner then optimises the scan parameters accordingly to ensure the best possible result. Siemens say that, in combination, these innovations help structure workflow more efficiently, smooth out differences in experience between the users, and achieve extremely high-quality results even in difficult diagnostic situations.
The first CT scanner with myExam companion is the new Somatom X.cite, featuring the Vectron X-ray tube that has previously only been used in the Somatom Force dual-source CT scanner.
“We have been testing Somatom X.cite with the new software platform for the past two months with successful results. We were impressed by both the excellent images and the way the new user guidance system made the workflows faster. The large gantry [82cm] facilitates the examination of seriously ill patients”, comments Christoph Stippich, chair and director, University Hospital Zurich, Zurich, Switzerland.
“We are driving the digital transformation of radiology through constant innovation of our devices. At the same time, we offer—for example, through remote solutions—more and more ways for our partners to create high-quality diagnostics. Somatom X.cite and myExam companion are a big step for our imaging portfolio along this plan into the world of intelligent user support and for Siemens Healthineers on our way to becoming a leader in clinical decision support “, says André Hartung, president Diagnostic Imaging at Siemens Healthineers.
myExam companion
The new intelligent user guidance system lets users utilise the full potential of the new Somatom X.cite, as well as the Somatom go scanner platform, which is already used on the market. It is now also possible to share established examination protocols between scanners quickly and without complications. Using AI, Siemens Healthineers has analysed thousands of scanning processes and identified key questions about the general conditions for achieving optimized scanning results. This led to the development of decision trees that ask the users relevant questions at each stage, thus guiding them through the scan preparations without complications. Workflows and their results are also more standardised, since this makes it possible to reduce deviations at a patient and user level.
“The decision trees found in almost every hospital, which have often previously been sketched on paper at an individual department level and define particular scanning parameters for different cases, are now directly integrated in the scanner software—in other words, exactly where they are needed,” comments Hatem Alkadhi, consultant radiologist at University Hospital Zurich (Zurich, Switzerland).
TriSalus Life Sciences (formerly Surefire Medical) has announced that the Centers for Medicare and Medicaid Services (CMS) granted approval for transitional pass-through (TPT) payment for its Surefire Spark Infusion System. Effective 1 January 2020, Surefire Spark Infusion System (to be known as TriNav) was granted transitional pass-through payment status as part of the 2020 Medicare Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System (CMS-1717-FC) final rule posted on 1 November 1 2019.
TriNav is designed to improve therapeutic distribution and penetration into solid tumors. This system, using pressure-enabled drug delivery technology, has demonstrated the ability to overcome intratumoral pressure in solid tumors and potentially improve distribution and penetration of therapy during transcatheter arterial chemoembolization (TACE) and transcatheter arterial radioembolization (TARE) procedures.
This additional payment is intended to “facilitate access for [Medicare] beneficiaries to the advantages of new and truly innovative devices”. The Surefire Spark Infusion System met the required criteria to receive transitional pass-through status, with the CMS saying it believes there is no existing pass-through payment category for this device because of its pressure-enabled drug delivery (PEDD) valve, which offers a unique mechanism for therapy delivery to selected sites in the peripheral vascular system, including solid tumors in the liver and pancreas.
“We thank CMS for its efforts to expand access to devices such as our Surefire Spark Infusion System that provide improved benefits to patients,” says Mary Szela, president and CEO of TriSalus. “As we transform TriSalus into an oncology therapeutics focused company dedicated to improving outcomes in solid tumors, this highly favourable reimbursement status validates our innovative delivery system and confirms its role in our unique, multi-pronged approach to treat liver metastases and pancreatic cancer.”
With widespread urological acceptance of prostate artery embolization (PAE) impending, Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) calls for caution when selecting patients for the minimally invasive treatment of benign prostatic hyperplasia (BPH). In a recent commentary published in the Journal of Vascular and Interventional Radiology (JVIR; doi: 10.1016/j.jvir.2019.08.003), Bilhim says “It is important to better select patients before PAE to avoid clinical failures”, emphatically concluding: “Avoid pedunculated intravesical prostatic protrusions!”
The commentary was written following another article published in JVIR (doi: 10.1016/j.jvir.2019.07.035) in November 2019 by Simon Yu (Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, China) and collaborators, who reported that the thickness-to-height ratio of intravesical prostatic protrusions (IPPs) predicts the clinical outcome and morbidity of PAE for BPH.
Both the prospective, single centre study conducted by Yu et al and the subsequent commentary from Bilhim were carried out within the context of a dearth of information regarding the implications of the median lobe for patients with BPH. Defining the median lobe, Bilhim writes: “There are many different types of IPPs (intravesical prostatic protrusions) that may be due to median lobe overgrowth, but also from the central or transitional zone of the prostate, or even the anterior fibromuscular stroma. Usually, the terminology of ‘median lobe’ refers to the continued growth of the periurethral glands, leading to a well-demarcated expanding midline retrourethral tissue; thus, IPP connotes a broader reach, encompassing both the median lobes, as well as all IPP from other glandular zones of the prostate.”
According to Bilhim, a frequent question posed by physicians and patients alike is whether the median lobe is a contraindication for PAE. In praise of the study from Yu and colleagues in Hong Kong, Bilhim writes that “the present study sheds some light on this specific topic”. Indeed, the answer provided by Yu and his team is that not all median lobes are the same.
Yu and collaborators found that pedunculated IPPs, which are taller than they are wide, are indicative of poor outcomes after PAE. They postulate that this is due to a bladder outlet obstruction that “becomes more prominent after embolization, as the prostatic tissue gets softer and more mobile with ischaemia”. In their study, they evaluated 82 patients with an International Prostate Symptom Score (IPSS) ≥15 and a quality of life score ≥3, treated between June 2015 and December 2018 at their institution. IPPs were present in 57 of 82 patients (69.5%). They reported the presence of IPPs correlated with the occurrence of post-procedure complications (p=0.009), but not with suboptimal IPSS at 12 months (p=0.758). However, IPPs with a thickness-to-height ratio ≤1.3 did correlate with suboptimal IPSS at 12 months (p=0.025) and suboptimal quality of life at six months (p=0.025) and 12 months (p=0.008), as well as with the occurrence of post-procedure complications (p=0.009). They therefore concluded that while IPPs with a thickness-to-height ratio ≤1.3 predicted the occurrence of post-procedure complications with urinary obstruction up to 12 months after PAE, merely the presence of IPPs alone did not predict the clinical outcome.
This raises several questions about the median lobe, Bilhim argues: “What type of imaging classification can we use to assess it? What is the impact of the median lobe on the natural progression of disease in patients with BPH? Does the median lobe also limit the efficacy of other minimally invasive surgical techniques such as prostatic urethral lift (PUL) or water vapour thermal therapy? What do we know already about the effect of PAE for the median lobe? Can we target the median lobe during PAE? Is PAE effective when treating patients with BPH and a median lobe?”
Whilst seeking answers to these questions, Bilhim acknowledges that what Yu et al’s study does elucidate is that PAE can target the IPP, but it highlights that there are different clinical outcomes depending on the subtypes of IPP present. “Clearly,” Bilhim writes, “pedunculated IPPs with taller than wide protrusions into the bladder neck are poor candidates for PAE, with 34% of patients presenting worsening of bladder outlet obstruction symptoms, acute urinary retention, or failure to remove the bladder catheter, and 11% requiring bailout surgery after embolization. One would not want to end up as Stealers Wheel: ‘Here I am stuck in the middle with you’.”
However, he ends on a positive: “The good news is that these types of pedunculated IPPs have an overall reported prevalence of 10%, even though they were documented in 43% of patients from the study of Yu et al, which may be due to selection bias. The vast majority of IPPs are broad-based and respond well to PAE.”
Members of the British Society of Interventional Radiology (BSIR) have voted overwhelmingly in favour of interventional radiology (IR) becoming a specialty in the UK. Of 350 votes cast, 80% (279) were in favour, and 20% (71) were against.
BSIR members had 24 hours to vote on the motion “Should interventional radiology become a specialty?” during the society’s 2019 annual scientific meeting (13–15 November, Manchester, UK). The society’s annual general meeting (AGM) took place during this voting window, and allowed participants to discuss the ramifications of voting for or against granting IR specialty status.
Whether or not interventional radiology will become a specialty is still under the auspices of the Royal College of Radiologists (RCR), explained BSIR vice president Philip Haslam (Freeman Hospital, Newcastle-Upon-Tyne, UK), but he said that the results of this vote “give us [BSIR] a mandate now, from our members, to take this forward with the college of radiologists, with the General Medical Council (GMC), and hopefully achieve our aims”.
IR became a specialty in the USA in 2014 and, by 2018, was the most sought after specialty amongst medical students. While the healthcare system differs between the USA and UK, proponents of IR becoming a specialty in the UK argued that “there is much to learn” from this US success. The Royal Australian and New Zealand College of Radiologists (RANZCR) have recently published a white paper looking to develop an IR specialty in Australasia. In continental Europe, the German Society of Interventional Radiology and Minimally Invasive Treatment (DeGIR) have their own exam, which implements a modular system for training. France and The Netherlands are currently exploring options for IR to become a specialty.
What happens next?
“This is the start of a long and slightly painful process,” Raman Uberoi (Oxford University Hospitals NHS Foundation Trust, Oxford, UK) told BSIR delegates, “because it is tricky to become a specialty”.
BSIR will begin talks with the RCR, and then jointly with national training bodies, including the GMC, the clinical oversight group (COG), and the UK Medical Education Reference Group (UKMERG), to make the case for IR becoming a specialty. This decision will ultimately come from the Privy Council, but Uberoi emphasised that “the message needs to come from the bodies to say that it is vitally important that IR becomes a specialty”.
The Privy Council is a formal body of advisers to the Sovereign of the UK, and is responsible for some of the affairs of the GMC. Following an initial, positive reaction from the GMC, Uberoi reported that the Privy Council were not supportive of IR becoming a specialty (“Their knee-jerk response is ‘no’ to any new specialty,” he said). However, he added that the case had never been made directly to the Privy Council, and that BSIR needed to work with the RCR and GMC “to make the arguments cogent” before making the final submission to the body.
This process may take “many years”, he said. Specifically addressing the BSIR members, he urged: “A lot of us will need to go into the college, a lot of us will need to be involved in the creation of the specialty and actually delivering for the future.
“Ultimately, this is about quality and patient safety, and improving outcomes,” he continued. “That means, we have to have better training, we need better access to clinics, and to occupy those clinics, and then to get better workforce planning for the future. But this needs buy in from all interventional radiologists, because this is not something that Council or a small group of people can take forward. We all need to push for this and we all need to believe in this project, because it will take some time. It will not impact on any consultants working today. This is the future; this is next generation of interventional radiologists that we are looking to. So we are looking at something that is going to take eight or nine years before we see the full benefits. We need to be doing other things besides, but I think this is vital for the future survival of IR, and more importantly, it is going to give us high-quality, focused care.”
Graham Plant Lecture advocates for IR to become a specialty
In his Graham Plant Lecture at the annual meeting, entitled “Interventional Radiology: A 21st century specialty”, Uberoi took the opportunity ahead of the vote to make the case in favour of IR gaining specialty status. “We have become integral to the management of not all, but a large number of patients in virtually every specialty in the hospital setting,” he said. “We play a key role in their treatment in nearly every sense that I can think of.”
However, he continued: “I think there is a problem. […] This issue that Charles Dotter [founder of interventional radiology] himself identified, and others after him identified, is the role of clinician versus technician. It is really about who is clinically responsible for the patient? Who is clinically responsible for the patient has huge connotations: the hospital management team, NHS England, the Trust, really focus on those individuals, supporting them with infrastructure and resources. They are seen as the primary clinician managing that patient. I argue that many of us are still behaving very much as technicians; the responsibility lies with surgeons or physicians. They are seen as the specialist clinician and, not unreasonably, a lot of organisations will focus their attention and their resources on those areas.”
Speaking in advance of the BSIR membership vote on the matter, Uberoi said, “I think it is vitally important that we consider becoming a specialty. I am not one for doing things just for the sake of it; I really believe this is crucial for our future development and survival. We can carry on sculling, keep doing the same things that we have been doing for the last 20 years, but I can tell you that, yes, it has given us some benefit, but I do not think that we can do much more.” Listing what he saw as the potential benefits, he enumerated:
Improved provision of 24/7 IR services, quality of IR training and patient safety throughout the UK
Improved IR workforce planning by matching training to need
More defined career path for IR
Widen the pool of doctors considering a career in IR
Strengthen the voice of the RCR nationally by creating a three-specialty college—both therapeutics and diagnostics
Uberoi did mention concerns his IR colleagues had raised with him over the last few months about becoming a specialty, though, which he hoped to alleviate in his Graham Plant Lecture. Firstly, he said, some people worried that becoming a specialty may adversely impact the number of doctors joining IR. Addressing this concern, he said: “I think we are in a poor place [with recruitment]; I think we can only get better.”
Furthermore, he said there is “a lot of confusion” about what happens with diagnostic radiologists who currently do IR. “This does not stop anybody from doing IR. On the contrary, it gives greater guidance and support for their practice in their roles from the specialty, which will ensure the quality standards that we need to adhere to,” he explained. “Similarly, those who do diagnostic radiology (DR) and IR will be able to continue doing so. DR is key to what we do, it is what distinguishes us from other surgeons. We need imaging, and we can and should continue to do DR, as long as we adhere to the RCR quality standards and look to our patient’s needs. We will continue to be trained in imaging, and we will continue to do imaging.”
This concern was discussed further by BSIR members after the Graham Plant Lecture, before voting closed. In particular, congress attendees asked about the RCR’s attitude towards IR becoming its own specialty, with one audience member flagging that the college may view this as taking numbers away from DR. “I do not think they are overjoyed,” Uberoi conceded, “because I think this is an unnecessary, from their perspective, headache, and it is a real problem for them.” However, he went on to counter: “Yes, we will be taking numbers from DR initially, but of course, these would reflect for trainees who are currently going into IR. Over time, I think we will increase IR numbers not at the expense of DR.”
Uberoi described the RCR’s stance towards designating IR specialty status as “lukewarm”, in his opinion, and announced his intention to run for vice president of the college once nominations open, as he believes it is important for the IR voice to be represented. “My intention is to do this from within the college. I think we can only do this with full college support. I think we need to make people understand why we want to do this: it is not a backlash against DR, it is about our future, the future survival of our specialty.”
Following dialogue with RCR, BSIR president Ian McCafferty (Queen Elizabeth Hospital Birmingham, Birmingham, UK) was positive about the college’s response: “They [RCR] also understand that we cannot stay where we are. They know we have to evolve in some shape, way, or form.”
Professor Anna Maria Belli Travelling Grant launch event at BSIR 2019. Professor Belli in centre.
The BSIR women and diversity committee formally launched the Professor Anna Maria Belli Travelling Grant on 14 November, at the 2019 annual scientific meeting of the British Society of Interventional Radiology (BSIR; 13–15 November, Manchester, UK). The launch took place during the first ever women and diversity networking luncheon to be hosted at the annual congress.
Speaking to Interventional News at the launch, the grant’s namesake, Anna Maria Belli (recently retired from St George’s University Hospitals NHS Foundation Trust, London, UK), commented: “More than half of medical graduates are female, yet we still do not have them entering interventional radiology (IR), because they perceive it as a very male-dominated specialty. Women make fantastic interventional radiologists. They bring a different perspective and have a healthy team approach, and we really need to attract them for our specialty to thrive.”
BSIR women and diversity committee co-chair Fiona Miller (King’s College Hospital NHS Foundation Trust, London, UK) shared Belli’s enthusiasm, saying: “I am delighted that the BSIR committee decided to support this grant to promote interventional radiology, while carrying the message that everyone is welcome to join our team.”
Tze Wah (The Leeds Teaching Hospitals NHS Trust, Leeds, UK), also BSIR women and diversity committee co-chair, added: “It has been a real privilege to celebrate this amazing milestone with professor Anna Maria Belli. We would like to spread this magical ripple forward, and I believe we can change the landscape for women in interventional radiology, and increase the colour in our IR community. All good standing BSIR members can apply for it [the grant], so they can go out and promote diversity in IR.”
Funds from the Professor Anna Maria Belli Travelling Grant will be used to cover second class travel expenses for individual lecturers to deliver talks to medical students, junior doctors, and consultants regarding women in IR, diversity and recruitment. One night’s accommodation, if necessary and at “reasonable costs”, may also be included.
According to BSIR, the purpose of the travelling grant “is to showcase IR, facilitate access to female and other role models, allowing trainees the opportunity to discuss as well as ask sensitive questions relating to a career in IR. The hope would be that these visits would in addition result in informal/ formal point of contact that would blend with our vision to commence a mentoring programme.”
Applicants must be UK-based IR consultants, a current member of BSIR, have a track record of teaching and education, and submit a statement explaining what the lecture would be based on. The women and diversity committee will then review applications and select the grant recipients.
Raman Uberoi (Oxford University Hospitals NHS Foundation Trust, Oxford, UK), another member of the BSIR women and diversity committee, explained the importance of the grant to this newspaper: “What we need are role models; we need mentors who are going to inspire people, give them the opportunity to see interventional radiologists as being an embracing community of like-minded doctors who are using image-guiding treatments. Having this diversity group [the women and diversity committee] means we are inclusive, we are trying to bring everybody into IR who is interested in treating patients using minimally invasive techniques, regardless of their gender, ethnicity, or orientation—that should not be the issue. The only issue is that they are keen on patient care, on improving outcomes, on quality and safety, and really, getting the best results for our patients. Having people who are going out from the BSIR demonstrating that we are very open and receptive to any ethnicity, any gender, is important. We want them to become skilled in interventional radiology, ultimately to provide the best possible care for our patients.”
Professor Anna Maria Belli at the podium
During the official launch of the travelling grant, incoming BSIR women and diversity committee chair Rosemina Ahmad (University Hospitals of Leicester NHS Trust, Leicester, UK) spoke on unconscious bias in interventional radiology. In her presentation, she highlighted how innate human unconscious bias was seeping into machine learning algorithms, warning: “Early evidence shows that unconscious bias is magnified by artificial intelligence. We need to be aware of this, because this is shaping the future.”
The BSIR women and diversity committee, and the new Professor Anna Maria Belli Travelling Grant, hope to address both unconscious and conscious biases facing women and marginalised groups interested in a career in interventional radiology. The ultimate goal, Elika Kashef (Imperial College Healthcare NHS Trust, London, UK) explained, is to further the conversation around diversity so that it goes beyond “simply celebrating being a woman, for example, and an interventional radiologist”, but matures to the point when the discipline is so inclusive for its diversity to be unremarkable.
Figure 1. As presented at FDA Panel in June 2019. BSC Data on File. As-treated ELUVIA patients. Abbreviations: CTO, chronic total occlusion; RCT, randomised controlled trial.
This advertorial is sponsored by Boston Scientific.
Boston Scientific leads the largest clinical programme investigating drug-eluting therapy for the treatment of peripheral arterial disease (PAD), in an effort to capture safety and efficacy data, and to help physicians make informed decisions. PAD affects an estimated 27 million adults in Europe and North America, and is associated with significant morbidity and mortality, as well as impaired quality of life and lower-extremity functioning over time. Boston Scientific’s ELUVIA® drug-eluting stent is a safe, effective option for these patients, writes Yann Gouëffic, MD, PhD (Paris, France).
Endovascular intervention for the treatment of femoropopliteal lesions is established as a first-line strategy. In the 2000s, self-expandable stents showed superiority over percutaneous transluminal angioplasty (PTA), but in-stent restenosis rates were still high (19–37%). Paclitaxel-coated balloons have been shown to successfully prevent intimal hyperplasia, but the use of scaffolding appears to be a more effective option to reduce restenosis.
In 2011, Michael Dake (Tucson, USA) et al evaluated a polymer-free, paclitaxel-eluting stent (ZILVER® PTX®, Cook Medical), and showed that it was superior to balloon angioplasty in terms of patency and reintervention, with provisional stenting. However, there was still room for improvement, notably in terms of controlled drug release: ZILVER® PTX® does not utilise a polymer to release paclitaxel, and delivers approximately 95% of the total drug load within 24 hours of deployment. Paclitaxel levels are sustained in the artery wall for 56 days. However, in-stent restenosis predominantly occurs a year after nitinol stenting in the femoropopliteal segment, so the kinetics of paclitaxel release by ZILVER® PTX® do not match the kinetics of restenosis at the femoropopliteal level.
ELUVIA® is characterised by its nitinol platform (INNOVA®), low paclitaxel loading (0.167μg/mm2 dose density), and use of polymer to control drugelution. The amount of paclitaxel is much lower for ELUVIA® compared with other drug-eluting devices. The polymer is similar to the polymer used in coronary paclitaxel-eluting stents, and, as a result, its safety and biocompatibility have been well studied.
The polymer is composed of a dual layer. The primer layer (poly n-butyl methacrylate) promotes adhesion of the active layer (poly[vinylidiene fluoridehexafluoropropylene]) to the stent, while the active layer controls the release of paclitaxel.
After promising preclinical studies, ELUVIA® was first evaluated in humans in the MAJESTIC registry. In MAJESTIC, 57 patients were treated for femoropopliteal lesions with an average length of 70.8mm±28.1. The primary patency at one year reached 96.4% (Kaplan-Meier [KM] estimate). Subsequently, a randomised (2:1) controlled trial was launched comparing ELUVIA® to ZILVER® PTX® for femoropopliteal lesions: IMPERIAL.
The IMPERIAL trial
The IMPERIAL trial was designed as a non-inferiority study, including patients with Rutherford category 2–4, with lesions that range from 30–140mm in length. Sixty-five centres were included to enrol 465 patients. The primary efficacy endpoint was primary vessel patency at 12 months, defined as a binary endpoint based on a duplex ultrasound peak systolic velocity ratio of 2.4 or lower at the 12-month follow-up visit in the absence of clinically-driven target lesion revascularisation or bypass of the target lesion.
The primary safety endpoint was the occurrence of major adverse events, defined as all causes of death through one month, major amputation of the target limb through 12 months, or target lesion revascularisation (TLR) through 12 months. Additionally, a prespecified post-hoc superiority analysis for the primary efficacy endpoint was included within the statistical analysis plan. A duplex ultrasound core laboratory and a clinical events committee were involved to assess the primary endpoints.
Between December 2015 and February 2017, 309 patients were included in the ELUVIA® group and 156 in the ZILVER® PTX® group. The mean age of participants was 68.5 and 67.8 years old, respectively, and 42–44% of the patients were diabetic. The mean length of the treated lesions ranged from 81.8–86.5mm. Non-inferiority was shown for both efficacy and safety endpoints at 12 months. Primary patency was observed for 231 (87%) of 266 patients in the ELUVIA® group, and for 106 (82%) of 130 patients in the ZILVER® PTX® stent group (difference 5.3% [one-sided lower bound of 95% CI –0.66]; p<0·0001).
Moreover, statistical superiority was met in the post-hoc analysis of 12-month primary patency in the full cohort analysis. Among the secondary endpoints, the rates of thrombosis in the ELUVIA® and ZILVER® PTX® groups were 1.7% and 4%, respectively (p=0.20). One year TLR rates were 4.6% for ELUVIA® and 8.1% for ZILVER® PTX® (p=0.0142). This statistically significant difference is maintained out to two years, with TLR rates of 12.9% and 20.5% for ELUVIA® and ZILVER® PTX®, respectively (p=0.0472).
Prespecified subgroups at high risk of restenosis and reintervention, namely chronic total occlusion (CTO), high calcium lesion, diabetes, and long lesions, were analysed in the IMPERIAL dataset. Lesions at high risk of restenosis demonstrated a consistent two year TLR rate (Figure 1).
In the ELUVIA® group, non-CTO lesions had a higher average one-year primary patency (90.6% vs. 83.9%). Of the 193 lesions considered to have moderate or severe calcifications, a primary patency rate of 89.2% was recorded at one-year compared to lesions with no or mild calcification, which had a patency of 87%. In diabetic patients, ELUVIA® showed primary patency results of 87.4%, consistent with the overall cohort, and in comparison to 80.2% with ZILVER® PTX® at one-year.
Lastly, the 50 long femoropopliteal lesions in IMPERIAL (mean length 162.8mm) had an 87.9% primary patency rate at one year (KM estimate). These data are in line with a previous long femoropopliteal lesion ELUVIA® registry. At one-year, the primary patency rate was 87% (KM estimate). There is remarkable consistency in efficacy across all lesions at high risk of restenosis for this device.
Paclitaxel-coated devices under scrutiny, but benefits outweigh risks
In December 2018, a meta-analysis showed a late mortality signal with certain paclitaxel-coated devices compared to non-coated devices. Notably, the ELUVIA® stent was not included in this. Recently, a new meta-analysis was presented at the FDA Panel in June 2019, though, again, ELUVIA® was not part of these contributing datasets.
However, during this June meeting, additional data were released regarding the comparison between ELUVIA® and coronary drug-eluting stent designs. Interestingly, the polymer release design principles are similar between both, but paclitaxel concentration is higher in coronary paclitaxel-eluting stents. Over 4,000 patients have been included in randomised clinical trials comparing paclitaxel-eluting coronary stents versus bare metal stents, and no all-cause mortality signal has been observed in a meta-analysis, negating the hypothesis of a systemic effect of paclitaxel delivered by this method. The FDA highlighted “that for individual patients judged to be at particularly high risk for restenosis and repeat femoropopliteal interventions, clinicians may determine that the benefits of using a paclitaxel-coated device outweigh the risk of late mortality”.
Boston Scientific has developed the largest clinical programme regarding drug-eluting therapy for PAD. The EMINENT RCT is recruiting 750 patients to compare ELUVIA® to bare-metal stents. To ensure long-term data capture both IMPERIAL and EMINENT, follow-up has been extended to five years. SPORTS, an investigator-sponsored study, is an RCT with three arms (total 222 patients) to compare a bare metal stent, a paclitaxel-eluting stent, and a paclitaxel-coated balloon (SeQuent Please®, from B Braun) for long femoropopliteal lesions.
Data from this clinical programme, as well as from other ongoing drug-eluting device trials and analyses, should provide further information to help physicians with patient-centric decision-making in the endovascular treatment of femoropopliteal disease, and in particular the treatment of lesions at high risk of restenosis.
Yann Gouëffic, MD, PhD, is affiliated with the department of vascular and endovascular surgery, Hôpital Paris St Joseph, Paris, France.
Establishing the first Interventional Radiology department in Argentina, Ricardo García-Mónaco is a pioneer of minimally invasive, image-guided therapies in South America. Looking back on a career that spans more than three decades, he discusses how establishing interventional radiology (IR) as a clinical discipline rather than a technical one is crucial for the field’s survival and success, and recalls a particularly memorable case where IR intervention in a two-day-old baby saved the patient from amputation and enabled her to go on to become the healthy, active teenager she is today.
What initially attracted you to interventional radiology (IR)?
When I was in my second year of residency in radiology, in 1985, my hospital incorporated digital subtraction angiography equipment, the first of its kind in my country. Before that the Radiology departments in Argentina did not have vascular suites. I was selected by the chair of Radiology to join the new Angiography Unit (at the time the unit only performed diagnostic examinations), in addition to the regular residency curricula. I was very happy with the patient commitment I could get in radiology through this subspecialty, and started reading about the subject in the radiology journals that we had at the time in Argentina: American Journal of Roentgenology (AJR) and Radiology. I was rapidly fascinated by the possibilities of therapeutic angiography, as it was then called. I foresaw the tremendous future of the endovascular approach as a proper tool to treat different diseases, especially through embolization procedures that were not recognised or regularly performed at that time in my country. Except for cardiologists performing angioplasty procedures, there were not many physicians interested in vascular procedures, and I realised it was a great opportunity to develop my career in what was a rather “unknown” area in Argentina at the time.
Who have been important mentors for you throughout your career?
I was very lucky to have important mentors in my career, who positively marked my professional and personal pathways. First of all, during my residency, Eduardo De Santibanes, an outstanding young liver surgeon at the time, introduced me to the importance of clinical commitment and patient follow-up—not very common amongst radiologists. He always encouraged me to be in the operating room while surgery was being conducted on any of my angiography patients, and then to go to the pathology department to observe the specimen resected. He was very keen to explain every detail of the surgery to me, and to elucidate the correlation with the imaging studies I had performed preoperatively. Years later, when I went to France to train in vascular and interventional radiology, I was lucky enough to meet two outstanding mentors: Pierre Lasjaunias and Alain Roche. Knowing them and incorporating their ways of practicing IR was a breakthrough in my career. They were top IR physicians ahead of their time, and they developed the foundations of many of the clinical and technical interventions still performed to this day worldwide. Indeed, both of them were mentors for a whole generation of interventional radiologists, and many that trained with them are now successful professionals at different international facilities.
Which innovations have most influenced your career, and how?
As I have been in IR for 30 years, I have seen many innovations, including technical developments, material refinements, new devices, new interventions, new indications of IR treatments, and improvements in equipment and software. But what has most influenced my career has been the conceptual shift from IR being a technical speciality to becoming a clinical, patient-centred one. Indeed, this “innovation” is increasing IR recognition among other clinical and surgical specialties, allowing interdisciplinary interactions to offer IR as a solution to the patient as it occurs with medical or surgical therapies. A nice example of innovation in this setting is the recent development of interventional oncology, now regarded as the forth pillar of cancer care, joining medical, surgical, and radiation oncology.
What were the biggest challenges and rewards in establishing Argentina’s first interventional radiology department?
Argentina being a rather conservative country, one of the biggest challenges was overcoming the disbelief that a radiologist could have a therapeutic role and run an interventional department. As radiologists are commonly regarded as physicians who only work with images and who do not interact with patients, both patients and doctors were unaware of the possibilities of IR. I remember in my early days back from France, every indication and every procedure I performed were like tests, because my results were under constant scrutiny from other physicians. Demonstrating that IR training differs a lot from that of diagnostic radiology and that we are specifically trained to treat certain diseases, along with our positive results, minimised this reluctance. Another big challenge was to organise all the staff, including nurses and technicians, as the path to success is dependent on paramedical staff as well as IR. Doing so many procedures requiring specific materials for the very first time in my country (such as transarterial chemoembolization (TACE), radiofrequency ablation (RFA), transjugular intrahepatic portosystemic shunt (TIPS), and venous stenting), I had to explain the advantages of IR to the hospital administrators and payers, as these were initially regarded just as additional costs. Indeed, this challenge still continues today with procedures recently introduced to my country, such as radioembolization, cryoablation, and venous deprivation. On the other hand, establishing an Endovascular Therapy and Interventional Radiology department was very rewarding. Developing a single department performing all types of image-guided therapies regardless of the organ (except for the heart) prevented other specialties from developing these types of procedures in their own domain. This was different to other hospitals, where neurointerventions, peripheral angioplasty, aortic aneurysm grafts, vertebroplasty, and many other procedures were being performed by other specialities. A single, broad department allowed not only important clinical activity, but also enabled educational endeavours, evidenced by the number of young Latin American interventional radiologists trained at our facility. Being recognised as one of the best teaching centres in Latin America and the high quality standards advocated by the Joint Commission is one of the biggest rewards for me.
As a founding member of the Argentine College of Vascular and Interventional Radiology (CARVI), what are your ambitions for the society?
I was the first president of this recently created society. The main goals are to foster education in IR and to work with the national government to recognise IR as a true speciality. Additionally, it is a facilitator for physicians interested in the subject and wanting to pursue an IR career. It is also a professional and juridical way to interact with other medical specialities and the minister of health from an official position.
What is the most exciting research coming from South America in IR right now, in your opinion?
The expenditure on research in South America is very low compared to other regions. However, some exciting research has originated from South America, such as the introduction of stent grafts to treat aortic aneurysms (albeit developed by a vascular surgeon), or the first prostate arterial embolization (together with Portugal). The latter, developed by Francisco Carnevale in Brazil, is probably the most relevant research to come out of South America in recent years. The same group is still performing additional work on the matter, and we have studied the macro- and microvascular anatomy of the prostate and its implications for embolization. The field of interventional oncology is very exciting, and we are part of some international randomised controlled trials, including RETNET, the first study to compare bland embolization versus conventional TACE versus DEBTACE in neuroendocrine liver tumours.
Would you describe a particularly memorable case?
I have many memorable cases—some due to amazing, positive results, and others that have saved patients’ lives or much improved their quality of life. Among these, maybe the most memorable was a newborn with a life-threatening condition due to multi-organ haemorrhages and congestive heart failure, secondary to a giant right lower limb tumour (Kaposiform Hemangioendothelioma). The patient was so critically ill, despite medication, that amputation of her right leg was considered to stop the irreversible coagulopathy caused by the tumour. Instead, we intervened to embolize the tumour early on the second day of life—a challenging intervention in this 3kg, decompensated newborn—which lead to a dramatic and total recovery. Most memorably, I met the patient recently, now a teenager with a normal life, practicing several sports, including volleyball and dancing. This made me very happy, especially considering she risked amputation as a newborn, and this was not done thanks to our IR decision.
What do you think the future of IR will look like?
IR has a bright future, because innovations and improvements in imaging capabilities are constant. However, IR needs to become a true clinical specialty, just like surgery or paediatrics. IR has not yet found the correct pathway to succeed and survive. Should it be a subspecialty of radiology, or should it run separate and by itself? Should the medical community or payers accept IR as a self-specialty, or as a therapeutic technique inside a broad specialty (as is the case with “interventional neurosurgery”, performed by neurosurgeons, and “endovascular surgery”, performed by vascular surgeons)? Of course I do not have the answer, but new generations of interventional radiologists should consider that clinical competence is as important as technical skill. IR procedures will continue to grow, because in my view the number of open surgeries being performed will continue to fall, and ultimately these will be replaced by minimally invasive or medical options, except for in a few indications.
What is the biggest challenge in IR today?
Atomisation of the specialty by other disciplines could jeopardise the future of IR. The most notorious examples are neurointerventional procedures that in many countries are performed by neurosurgeons, or endovascular interventions performed by vascular surgeons. Interestingly, in some countries there is a trend for surgical departments to establish a “percutaneous surgery unit” that performs drainage of fluid collections, gastrostomy, bile duct interventions, and even tumour ablations. I think this is one of the biggest challenges in IR at the moment; strategies must be built accordingly. Fortunately, SIR, CIRSE, and many other IR societies are aware of this and are currently facing this problem.
Ricardo García-Mónaco
What are your hobbies and interests outside of medicine?
I am a family man, so enjoy spending time with my family, watching soccer games with my son or daughter in stadiums, and seeing my son play in the Argentinian Rugby Union tournament. I love sports, and played rugby in the first division during my youth. More recently, I have been coaching young rugby teams for several years. I used to ski with the family every winter and like to fly cast in Patagonia lakes and rivers in the summer. I also like to cook a typical Argentine meal called “asado” on Sundays, a kind of firewood grilled beef, and to watch movies or TV series at night, or dine with friends and family.
Fact file
Current positions
1992–Present: Head of Interventional Radiology and Endovascular Therapy, Hospital Italiano, University of Buenos Aires, Buenos Aires, Argentina
2005–Present: Head of Vascular and Interventional Radiology, Hospital Italiano, University of Buenos Aires, Buenos Aires, Argentina
Previous positions
2005–2018: Chair of Department of Radiology, Hospital Italiano, University of Buenos Aires, Buenos Aires, Argentina
1991–1992: Medecin Consultant, Radiologe Interventionelle, IGR, Villejuif, France
1991: Medecin Assistant a Titre Etranger, Bicêtre Hospital, University of Paris, Paris, France
1990: Visiting Fellowship, Toronto Western Hospital, Toronto, Canada
1990: Visiting Fellowship, New York University, New York, USA
1988–1992: Training in Angiography and Interventional Radiology, Bicêtre Hospital, University of Paris
1987–1988: Senior Chief Resident, Hospital Italiano, University of Buenos Aires, Buenos Aires, Argentina
1983–1987: Residency in Radiology, Hospital Italiano, University of Buenos Aires, Buenos Aires, Argentina
Society positions
2016–2018: President of the International Society of Radiology (ISR)
2014–2018: President and founding member of the Argentine College of Vascular and Interventional Radiology
2006–2008: President of Inter-American College of Radiology (CIR)
2000–2006: President of the Argentine Society of Radiology (SAR)
Konstantinos Donas (Münster, Germany) reported five-year data from a single-centre, retrospective study with 238 patients in the first CIRSE session. The long-term, real-world dataset showed no increased mortality for the matched patients who underwent paclitaxel-coated balloon treatment vs. those treated with plain balloon angioplasty.
“In addition, there was no correlation between mortality and the dose of paclitaxel used,” the researchers write in the study that was published in CVIR.
These data, which refute the findings from the Katsanos et al meta-analysis, are important as they shed light on whether the meta-analysis can be replicated in a real-world setting, says Donas. He also notes that the researchers designed this study to avoid the limitations of the randomised data included in the meta-analysis.
This investigator-initiated study set out to assess the long-term mortality of patients treated by the IN.PACT Admiral (Medtronic) compared with standard plain balloon angioplasty.
Since founding the Ghana Society of Interventional Radiologists in November 2015, Benjamin Dabo Sarkodie has been working to establish the offering of minimally invasive, image-guided procedures in the west African nation. He describes his recent successes performing the first cerebral aneurysm coiling in West Africa, and discusses how, through collaboration with interventionalists from Hungary, he is setting his sights on hyper-acute stroke management as the next frontier in Ghanaian interventional radiology.
Ghana is a developing country located in West Africa, bordered by Ivory Coast, Togo, Burkina Faso, and the Atlantic Ocean, with a growing population of 30 million people. Although endovascular neurointerventional practices are well-established in many developed countries, they are non-existent in many low- and middle-income countries, due to a shortage of doctors with the required training, and to limited infrastructure. This is despite the huge demand. Until recently, there were minimal treatment options in Ghana for neurovascular conditions such as arteriovenous malformation (AVM) or cerebral aneurysms. Many patients travel thousands of miles to access treatment, an expensive venture that some patients are not fit for. Indeed, several developed complications like deep vein thrombosis during these long haul, transatlantic flights.
The infrastructure needed for this specialty is not readily available in Ghana. The establishment of a neurointerventional service is also hindered by the lack of good quality angiographic machines and trained angiographic laboratory personnel. However, adequate resources are emerging.
In March 2019, supported by interventional radiologist Istvan Lazar (Borsod County University Teaching Hospital, Miskolc, Hungary), we successfully completed the first case—to our knowledge—of cerebral aneurysm coiling in West Africa. This was after the acquisition of a digital subtraction angiogram (DSA) and road mapping software at the Euracare Advanced Diagnostics and Heart Center in the Ghanaian capital, Accra. We continue to collaborate with Lazar for assistance with difficult cases. Our team is comprised of doctors, nurses, and radiographers who have been adequately trained to assist with these endovascular neurointerventions.
Since this first case, we have successfully completed six cases of coiling and one case of flow diverter stent insertion. We have also undertaken 22 cases of diagnostic cerebral angiograms, two cases of tumour embolization, and three cases of AVM embolization.
(L to R): Head nurse Hagar Bandoh, Dr Benjamin D Sarkodie, Dr Itsvan Lazar, Dr Owusu Darkwa
With the good outcomes from these initial procedures, coupled with awareness creation, we are set to embark on even more endovascular neurointerventions.
It is an exciting time for healthcare in Ghana, as we are now equipped to cater for both ruptured and unruptured cerebral aneurysms, as well as other neurovascular conditions.
With the launch of a stroke centre at Euracare, hyper-acute stroke management is our next major focus. We have acquired various devices to aid us in offering mechanical thrombectomy to people with large vessel ischaemic infarcts.
As all patients are evaluated by a neurologist prior to intervention, a strong partnership with other specialties, such as neurology, neurosurgery, and anaesthesia, is needed as the basis for these procedures.
As we forge ahead with our endovascular offering, we hope that the surgical options for treating some of these conditions will also become more readily available. These will serve as an alternative modality, in addition to treating those conditions unsuitable for endovascular management.
We are also embarking on conferences and workshops, backed by the Ghana Society of Interventional Radiologists, to aid physicians in identifying common conditions like subarachnoid haemorrhage. There is a low level of awareness among general practitioners, who serve as the first point of call.
To provide an example of this: a client of mine had been on admission for a week in a small facility receiving treatment for malaria. She had been suffering from severe headaches and suddenly collapsed whilst singing at church. Fortunately for her, the pastor presiding over the assembly thought it prudent to request a transfer to a tertiary facility, as her condition was not improving. A head CT scan was requested on admission to the facility: the diagnosis, an acute subarachnoid haemorrhage.
Many patients are not able to afford these interventions, as treatment is on a “cash and carry” basis. Local insurance companies, as well as the National Health Insurance Scheme, do not offer cover for these procedures. However, an altruistic cerebral aneurysm survivor has founded the Ghana Brain Aneurysm Foundation, which aims to fund and make accessible treatments to those who are not as fortune as he was to receive management abroad.
Benjamin Dabo Sarkodie is aconsultant endovascular and interventional radiologist in the department of Radiology at the School of Medicine and Dentistry, University of Ghana, Legon, Accra, Ghana.
Harel Gadot: founder, executive chair, and president, XACT Robotics
XACT Robotics has announced the successful completion of its latest financing round, totalling US$36 million.
The company intends to use the proceeds to support the commercialisation and continued development activities in support of the recently US market cleared XACT Robotic System, which also has CE mark. The XACT Robotic System is the first hands-free robotic system combining image-based planning and navigation with insertion and steering of various instruments to a desired target across an array of clinical applications and indications.
“As we continue to build momentum for our robotic system, we will use the recent funding to launch the system to select US radiology Centers of Excellence partners,” says Chen Levin, CEO, XACT Robotics. “In addition, we will invest to continue expanding the utilisation of the system and support our future launch cycle, including compatibility of the XACT Robotic System with additional imaging modalities and clinical applications to address a broad range of patient care needs.”
The current financing round included leading investors in the surgical robotics space, such as Chasing Value Asset Management who previously held positions in MAKO Surgical (acquired by Stryker in 2013), Mazor Robotics (acquired by Medtronic in 2018), and most recently Corindus Vascular Robotics (acquired by Siemens in 2019). They join the current shareholders of the company, including Shizim Group and MEDX Ventures Group.
XACT Robotics was founded by entrepreneur Harel Gadot. The technology is based on research originally conducted at the Technion—Israel Institute of Technology, by Moshe Shoham, founder of Mazor Robotics (acquired by Medtronic in 2018).
Nick Hopkins (Buffalo, USA) talks to BLearning Neuro at VEITH Symposium 2018 (13–17 November 2018, New York, USA) about the DAWN trial, which showed that in carefully selected acute ischaemic stroke patients that “intervention out to 24 hours is viable”.
“Stroke intervention is the next horizon in medicine,” says Hopkins, who also discusses the shortage of trained neurointerventionists who can perform stroke thrombectomy. “The only way we are going to solve this problem”, adds Hopkins, “is by training interventional cardiologists, interventional radiologists and vascular surgeons interventionists in outlying areas who can perform endovascular treatment for stroke ‘on the spot.’”
Thomas Zeller presents SELUTION trial results at VIVA 2019
The SELUTION SFA trial met its primary endpoint and demonstrated an late lumen loss of 0.19mm. Furthermore, excellent freedom from clinically driven TLR was achieved through 24 months in 87.5%, with no primary TLR event observed after month 11. Thomas Zeller (Bad Krozingen, Germany) presented these results at the 2019 Vascular Interventional Advances conference (VIVA) in Las Vegas, USA (4–7 November).
SELUTION SFA is a prospective, controlled, multicentre, open-label, single-arm clinical trial treating superficial femoral artery (SFA) lesions (lesion length, 51.3±40.3 mm; 34% moderate to severe calcification). The trial enrolled 50 patients in four German centres between November 2016 and May 2017. Patients enrolled were symptomatic with de novo or restenotic lesions with ≥70% diameter stenosis or occlusion.
Clinical improvements were seen in Rutherford classification, ABI, and walking impairment at six months and were further improved to 12 months and maintained to 24 months. This initial first-in-human trial demonstrates that SELUTION SLR is a viable option to treat lesions in the SFA. It is the first demonstration of a sirolimus safety and efficacy in peripheral intervention.
The SELUTION SLR (MedAlliance) is based on microreservoir balloon coating technology, which provides controlled and sustained sirolimus release with a therapeutic effect for over 60 days. The cell adherent technology is a proprietary amphiphatic lipid technology that binds microreservoirs to the balloon surface, and it contains and protects microreservoirs during insertion and inflation. Also, it facilitates higher drug transfer efficiency, allowing for low drug dose (1 µg/mm2) on the balloon surface, and maximises the drug bioavailability.
Medtronic today announced four-year data from the IN.PACT Global study, which reinforce the long-term durability and safety of the IN.PACT Admiral drug-coated balloon (DCB) in patients with peripheral artery disease (PAD) in the superficial femoral (SFA) and popliteal arteries. The data were presented this morning in the late-breaking clinical trial session at the Vascular Interventional Advances (VIVA) 2019 conference in Las Vegas, USA (4–7 November).
Thomas Zeller, director of the Department of Angiology at Universitaets-Herzzentrum, Freiburg-Bad Krozingen, Germany, presented the new, four-year results from the full clinical cohort of the IN.PACT Global Study. The results are the first four-year, real-world, fully adjudicated DCB data to be presented in a scientific congress. IN.PACT Admiral DCB demonstrated durable effectiveness and a strong safety profile in a real-world population.
“The IN.PACT Global study is the largest independently adjudicated real-world evaluation of any peripheral intervention undertaken and includes patients with the most complex lesions observed in any existing DCB clinical study, many of whom have commonly known risk factors for progressive PAD,” said Zeller. “Even in this real-world patient population, including those with critical limb ischemia, we continue to see durable treatment effect through four years. These data further demonstrate the clinical benefit of IN.PACT Admiral DCB and its ability to be a first-line therapy for patients with challenging lesions.”
Kaplan-Meier estimates demonstrated a freedom from clinically-driven target lesion revascularization (CD-TLR) rate of 73.4% (n=1,406) in a large, real-world patient population through 4-years. Of the subjects enrolled, the mean lesion length was 12.09 ± 9.54 cm, 18.0% had in-stent restenosis, 35.5% had occluded lesions, 39.9% had diabetes, and 68.7% had calcified lesions. Overall, the average time to first CD-TLRs in this complex patient population was approximately 570 days.
Based on Kaplan-Meier estimate, IN.PACT Admiral demonstrated a solid safety profile through four years with a low major target limb amputation cumulative incidence of 1.1% through four years. The freedom from all-cause death through four years was 83.5%, which is comparable to what would be expected in this patient population.1 This rate is based on data from all subjects enrolled in the IN.PACT Global study, among which 98% had known vital status.
Furthermore, an additional analysis was conducted to evaluate the performance of IN.PACT Admiral through four years in patients with intermittent claudication and critical limb ischemia (CLI) based on Rutherford Classification (RCC). The Kaplan-Meier estimated freedom from CD-TLR was 74.5% (n=1,246) in the intermittent claudication (RCC 2/3) patient cohort and 64.8% (n=156) in the CLI (RCC 4/5) patient cohort respectively.
“The body of evidence on paclitaxel-coated devices continues to mature with recent significant publications and presentations, including the IN.PACT Global four year data, adding to the totality of evidence generated,” said Mark Pacyna, vice president and general manager of the Peripheral Vascular business, which is part of the Cardiac and Vascular Group at Medtronic. “Outcomes from the IN.PACT Global study specifically show that IN.PACT Admiral DCB, which has now been used to treat approximately 500,000 patients worldwide, can prolong the time between reinterventions in a very challenging patient population by over a year and a half. Long-term and real-world data continue to demonstrate both the safety of these devices and the overall treatment benefit to the patient.”
In collaboration with leading clinicians, researchers and scientists worldwide, Medtronic offers the broadest range of innovative medical technology for the interventional and surgical treatment of cardiovascular disease and cardiac arrhythmias. The company strives to offer products and services that deliver clinical and economic value to healthcare consumers and providers around the world.
Boston Scientific today announced positive data for two devices within the peripheral drug-eluting product portfolio during separate late-breaking clinical trial presentations at the 2019 Vascular Interventional Advances conference (VIVA) in Las Vegas, USA (4–7 November).
Data presented included a 12-month interim analysis from the RANGER II SFA trial of the Ranger drug-coated balloon (DCB) as well as 24-month results from the IMPERIAL trial of the Eluvia drug-eluting vascular stent (DES), which exhibited the highest 24-month primary patency reported to date for the treatment of femoropopliteal disease in a US pivotal trial with a DCB or DES.1
The RANGER II SFA study evaluated the safety and effectiveness of the Ranger DCB, which has a low drug dose density of paclitaxel, versus standard percutaneous transluminal angioplasty (PTA) for the treatment of patients with peripheral artery disease (PAD) in the superficial femoral artery (SFA) and proximal popliteal artery (PPA).
In the trial, the Ranger DCB exhibited a primary patency rate—a measure of the target vessel remaining unobstructed at 12 months—of 89.2% compared to 72.9% percent in patients treated with standard PTA (p=0.0022), by Kaplan Meier estimate. Additional key findings from the trial include:
Patients treated with the Ranger DCB had a significantly lower target lesion revascularization (TLR) rate of 6%, in contrast to 17.9% observed with standard PTA (p=0.0018), substantially reducing the patient’s need for repeat procedures at 12 months;
No difference in all-cause mortality at 12 months with a 2.3% rate for the patients treated with Ranger DCB vs. 2.5% in patients treated with standard PTA (p>.99);
Data from the Pharmacokinetics (PK) sub-study showed that 11 of 12 patients with an average lesion length of 154.2mm had unmeasurable paclitaxel levels in venous plasma approximately one hour after DCB deployment and removal.
“These excellent clinical data coupled with the ease of deliverability of the Ranger DCB are reassuring for physicians as we evaluate the most appropriate therapies based on individual patient needs,” said Ravish Sachar, University of North Carolina Rex Hospital physician-in-chief for Heart and Vascular services and principal investigator of the RANGER II SFA trial. “The high primary patency rate as well as the significantly lower TLR rate, which reduces the need for repeat procedures, are very encouraging.”
Also presented at the meeting was a 24-month analysis of data from the IMPERIAL trial, which evaluated the Eluvia stent versus the Zilver PTX drug-eluting peripheral stent for the treatment of patients with symptomatic PAD that had SFA and PPA lesions up to 140mm in length. The Eluvia stent utilises a drug-polymer combination and offers controlled delivery and sustained release of the lowest dose of paclitaxel of any peripheral drug-eluting device. In the study, the Eluvia stent exhibited a primary patency rate of 83.0% versus 77.1% with Zilver PTX, by Kaplan Meier estimate, the highest 24-month primary patency reported to date for the treatment of femoropopliteal disease in a US pivotal trial with a DCB or DES.1 The analysis also confirmed:
Statistically significant lower clinically-driven TLR rate of 12.7% for patients treated with the Eluvia stent, in contrast to 20.1% observed within the Zilver PTX cohort (p=0.0495), thus reducing the need for repeat procedures at 24 months;
A low all-cause mortality rate of 7.1% for the Eluvia stent and 8.3% for those treated with the Zilver PTX (p=0.6649), which is within range expected for symptomatic peripheral arterial disease.2
“We are very pleased with the safety and efficacy demonstrated by the Ranger DCB and the Eluvia stent, both of which showed exceptional durability while preventing repeat TLRs in 66% and 40% of treated patients, respectively,” said Ian Meredith, executive vice president and global chief medical officer, Boston Scientific. “The excellent outcomes presented today underscore our commitment to physicians and their patients with PAD. We continue to drive innovation in the drug-eluting vascular space and these results add to the growing body of evidence supporting our therapy options for the treatment of this challenging disease.”
The RANGER DCB gained CE Mark in 2014 and the company submitted for US Food and Drug Administration approval of the device earlier this year. The combination of the RANGER DCB as well as the Eluvia stent positions Boston Scientific as the only company to have both a DES and a DCB for the treatment of PAD in their portfolio.
In the USA, the Ranger DCB is an investigational device and is not available for sale.
References
Highest-two year primary patency based on 24-month Kaplan-Meier estimates reported for IMPERIAL, IN.PACT SFA, ILLUMENATE, LEVANT II and Primary Randomization for Zilver PTX RCT.
Feringa HH, Bax JJ, Hoeks S, et al. A prognostic risk index for long-term mortality in patients with peripheral arterial disease. Arch Intern Med. 2007;167:2482-2489.
Revolution rotational atherectomy system (Rex Medical)
Revolution rotational atherectomy system (Rex Medical)
Findings from the REVEAL study confirm a favourable safety and effectiveness profile through six months for the Revolution peripheral atherectomy system from Rex Medical. The results were presented today at the 2019 Vascular Interventional Advances conference (VIVA) in Las Vegas (4–7 November).
The Revolution rotational atherectomy system incorporates continuous aspiration and has a dual indication for atherectomy and thrombectomy. The device is intended for atherectomy of the peripheral vasculature in patients with obstructive atherosclerotic disease both above and below the knee. No capital equipment is required. The spheroid-shaped burr rotates at 140,000 rpm to ablate plaque, which is aspirated into the catheter.
The primary objective of the REVEAL trial was to evaluate the safety and effectiveness of the Revolution peripheral atherectomy system in patients with symptomatic infrainguinal lower extremity arterial obstructive disease. One hundred twenty-one patients were enrolled at 17 US sites. Patients with Rutherford category 2 to 5 disease and lesions with ≥70% stenosis were eligible.
The primary safety endpoint was a composite of 30-day major adverse events, including all-cause mortality, clinically driven target lesion revascularisation, amputation, vessel perforation, and embolisation. The primary effectiveness endpoint was technical success, defined by core laboratory–assessed ≤ 50% diameter stenosis after treatment prior to adjunctive therapy.
The 30-day primary safety and effectiveness endpoints were met, with freedom from 30-day major adverse events in 110 of 113 (97.3%) intention-to-treat patients at 30 days (both distal embolisations were clinical events committee–adjudicated as nondevice-related) and technical success in 111 of 123 (90.2%) target lesions.
Excluding lesions that were treated with a burr not appropriately sized for the vessel diameter from the data set in which the postatherectomy stenosis was > 50%, the technical success rate was 95.7% (111 of 116 patients) (nonimputed). The procedural success rate was 93.7% (119 of 127 patients). The 6-month outcomes were also favourable.
One-year results of the MIMICS-3D study were announced today at the 2019 Vascular Interventional Advances conference (VIVA; 4–7 November, Las Vegas, USA). Freedom from clinically-driven target lesion revascularisation (CD-TLR) was 89%, which aligns with results from the MIMICS RCT and MIMICS-2 studies, despite treatment of more complex disease.
In addition, the percentage of patients with improvement of ≥1 Rutherford category at one year compared to baseline was 87% (322/370), and for patients treated with or without a drug-coated balloon and BioMimics 3D, there was no difference in CD-TLR (89.5% and 88.5%, respectively; P>0.88).
BioMimics 3D (Veryan Medical) is a nitinol stent designed to provide optimal radial support, flexibility, durability, visualisation, and delivery accuracy for femoropopliteal intervention. The addition of a unique three-dimensional (3D) helical centreline provides the advantages of biomechanical stability and swirling blood flow.
BioMimics 3D was evaluated in the MIMICS randomised controlled trial (RCT) in which patients received either a BioMimics 3D helical stent or a straight stent control. The Kaplan-Meier estimate of freedom from clinically driven target lesion revascularisation (CD-TLR) at 1 year for those treated with BioMimics 3D was 91%. A second study, MIMICS-2, conducted in the USA, Japan, and Europe, met 30-day safety and 12-month primary patency endpoints, and the 1-year Kaplan-Meier estimate of freedom from CD-TLR was 88%.
The MIMICS-3D European registry is now investigating outcomes in patients with longer, more complex lesions; complementary use with drug-coated balloons occurred in 50% of procedures. MIMICS-3D enrolled 507 patients at 23 sites. The primary safety endpoint is a composite of major adverse events (MAEs) or CD-TLR through 30 days. The primary outcome measure for effectiveness is freedom from CD-TLR through 12 months. An independent clinical events committee adjudicated MAEs.
Thomas Zeller gives an update on the DEEPER-OUS trial at VIVA 2019
Thomas Zeller gives an update on the DEEPER-OUS trial at VIVA 2019
Today at the 2019 Vascular Interventional Advances conference (VIVA; 4–7 November, Las Vegas, USA), Thomas Zeller (Bad Krozingen, Germany) gave an update on the DEEPER OUS trial. He concluded that the Temporary Spur stent system (Reflow Medical) appears to be a feasible and safe method for the treatment of disease in the infrapopliteal arteries.
This trial is a prospective, multicentere nonrandomised, single-arm study. Trial enrolment began in July 2019 and is presently ongoing, with anticipated completion in 2020. The study will consist of 100 patients in New Zealand, Germany, and Switzerland.
The purpose of the DEEPER OUS study is to evaluate the safety and efficacy of a novel device, the Temporary Spur stent system in conjunction with a commercially available drug-coated balloon. An angiographic substudy examining recoil will be conducted on the first 10 patients from each site.
Examination of patency rates and long-term safety data is ongoing in the DEEPER OUS trial.
George Adams presents six-month TOBA II BTK results at VIVA 2019
It was announced today at the 2019 Vascular Interventional Advances conference (VIVA) (4–7 November, Las Vegas, USA) that, through six months, TOBA II BTK met all endpoints in a 100% dissected vessel population.
This prospective, multicentre, single-arm global pivotal study was designed to investigate the safety and effectiveness of the Tack endovascular system (Intact Vascular) to repair dissections in below-the-knee (BTK) arteries. Primary safety and efficacy endpoints were analysed at six months and compared with performance goals derived from the critical limb ischemia (CLI) literature.
It was concluded that high rates of dissection resolution, wound improvement, and freedom from clinically-driven target lesion revascularisation (CD-TLR) support the Tack system as an ideal adjunct to PTA and potentially as the first permanent vascular implant to improve results of infrapopliteal angioplasty.
In more detail, TOBA II BTK met both primary endpoints (p<0.0001) of safety (30-day major adverse limb event or perioperative death) and efficacy (six-month major adverse limb event or 30-day perioperative death). All (100%) dissections were resolved following Tack implantation, with 92.0% 6-month Kaplan-Meier freedom from CD-TLR, 87.3% 6-month Kaplan-Meier target lesion patency, and 95.7% 6-month Kaplan-Meier amputation-free survival. Wounds were healed or improved in 73.8% and Rutherford category was ≤3 at six months in 74% of CLI patients.
TOBA II BTK is the first investigational device exemption clinical trial approved to investigate safety and effectiveness of a permanent implant to repair dissections in BTK arteries. The study evaluated the Tack system 233 patients who had ≥1 dissection requiring repair after PTA in the mid/distal popliteal, tibial, and/peroneal arteries. There were 918 Tacks implanted from the mid popliteal to 1 cm above the tibiotalar joint, with 122 placed in the distal third of the vessels.
The Tack system has four preloaded self-expanding nitinol implants on a single catheter. Each implant is 6mm long and self sizes to vessels ranging from 1.5 to 4.5mm in diameter, using sufficient radial force to appose dissected tissue against the vessel wall.
Ramon Varcoe presents five-year results of the ABSORB BTK trial
Ramon Varcoe presents five-year results of the ABSORB BTK trial
Ramon Varcoe today announced positive five-year results of the ABSORB BTK trial at the 2019 Vascular Interventional Advances conference (VIVA) in Las Vegas, USA (4–7 November). Primary patency of the Absorb bioresorbable vascular scaffold (BVS) from Abbott achieved a 72.9% primary patency rate and 90.7% freedom from clinically-driven target lesion revascularisation (CD-TLR).
The ABSORB BTK trial is a prospective, nonrandomised, single-centre study designed to evaluate the novel bioresorbable, drug-eluting Absorb scaffold used for the treatment of peripheral artery disease below the knee. There were 71 scaffolds utilised in 55 limbs of 48 patients who fulfilled the inclusion criteria (72.7% with critical limb ischemia). Most scaffolds were implanted in arteries of the proximal half of the calf, and the mean lesion length was 20.1 mm (range, 5–50 mm). There was 100% procedural and technical success.
Over the 5-year follow-up period, 38% of patients had died, all from causes unrelated to the procedure or study device; 95% of patients had sustained clinical improvement. Complete wound healing occurred in 90% of those treated for tissue loss, with no major amputations and a limb salvage rate of 100%. No late or very late scaffold thromboses were observed.
This novel bioresorbable, drug-eluting scaffold has several inherent advantages over stents, related to its biological resorption. These results represent best-in-class durability for a stent-like device in this challenging vascular territory.
LimFlow SA today announced the presentation of positive six-month data from the full patient cohort in its PROMISE I early feasibility study of the LimFlow percutaneous deep vein arterialisation system. Results were presented on the podium at the 2019 Vascular InterVentional Advances conference (VIVA; 4–7 November, Las Vegas, USA) by Daniel Clair, PROMISE II principal investigator and chair of the department of surgery at the University of South Carolina (USC) and Palmetto Health-USC Medical Group.
“Findings from this early feasibility trial are very promising,” said Clair. “They show that the LimFlow system is a novel, safe and reproducible approach for improving wound healing and reducing amputation rates in a patient population for whom amputation would otherwise be considered inevitable. It is very encouraging to be able to offer hope to patients that cannot be treated with any current technology today.”
PROMISE I is a multicentre, prospective, single-arm study conducted at seven US centres encompassing 32 end-stage—or “no option”—CLTI patients, 100% of whom had non-healing wounds on the target foot, 69% of whom had diabetes, and 34% of whom had renal insufficiency.
At six months, the LimFlow system achieved an amputation-free survival rate of 74%. A strong trend of successful wound healing was also demonstrated, with 67% of wounds classified as healed or healing at six months and 100 percent healed or healing at nine months. Technical success was 97%.
When all other therapeutic options have been exhausted and a CLTI patient is facing major amputation, the minimally-invasive LimFlow system is designed to bypass blocked arteries in the leg and deliver oxygenated blood back into the foot via the veins. For many patients, restoring perfusion in the lower limbs resolves chronic pain, improves quality of life, enables wound healing and prevents major amputation.
“We are enthusiastic about the exceptional results for the LimFlow System,” said LimFlow CEO Dan Rose. “Our goal with the technology is to fully heal previously non-healing wounds and save more patients from amputation, improving their quality of life and preventing the downward spiral that comes from losing a limb. With the recent FDA approval of our pivotal trial, we look forward to shortly commencing enrolment in the USA and continuing to build evidence for the therapy.”
CLTI is the most severe form of PAD and often occurs in patients suffering from coronary artery disease, diabetes, obesity, high cholesterol and high blood pressure. Patients with CLTI often experience profound, chronic pain and develop festering wounds or infections that lead to major limb amputation, an event closely associated with increased mortality and reduced quality of life. To relieve the symptoms of CLTI, patients today are treated primarily with angioplasty or open bypass surgery. In many late-stage patients, however, neither option is feasible due to extensive disease in the target arteries or other anatomical constraints.
Ehrin Armstrong presents initial 12-month outcomes from the TANGO trial at VIVA 2019
It was announced today that results of the TANGO low-dose cohort compared to controls are positive, both for primary and secondary endpoints. These latest findings were presented by Ehrin Armstrong at the 2019 Vascular Interventional Advances conference (VIVA) in Las Vegas, USA (4–7 November). According to Armstrong, perivascular temsirolimus is being developed as a “viable alternative” to prevent restenosis after below-the-knee (BTK) peripheral artery interventions, and TANGO high-dose data is “forthcoming”.
The TANGO trial is a phase II, dose escalation, double-blinded trial comparing the delivery of temsirolimus to saline control in patients with severe claudication or critical limb ischaemia. This is the first US trial to investigate a sirolimus analogue to improve the durability of peripheral revascularisation procedures. Armstrong commented that the present results warrant a move to Phase III trials.
The purpose of the trial is to limit neointimal hyperplastic tissue growth into the artery after endovascular BTK revascularisation procedures, where paclitaxel-coated balloons have had limited success.
Results are now available comparing Bullfrog micro-infusion device (Mercator MedSystems) delivery of either low-dose temsirolimus treatment (0.1mg/mL; n=20) or saline control (n=20) into the perivascular tissue around lesions subsequent to revascularisation. Patients (Rutherford category 3–5) with up to 30cm-long BTK lesions were enrolled in the study.
The primary safety endpoint was 30-day freedom from major adverse limb event or postoperative death, and no events were observed. The primary efficacy endpoint was improvement in 6-month transverse view vessel area loss, an angiographic measure that uses the opacified area of the lesion to approximate the neointimal volume.
At six months, excluding subjects with unstented severe dissections in their target lesion, transverse view vessel area loss improved to 19% in treatment subjects compared to 38% in controls. With respect to secondary endpoints, six-month freedom from target lesion failure was reported in 58% (11/19) of treatment subjects compared to 42% (8/19) of controls, favouring treatment by a relative 38%. In patients with total occlusions at baseline, 78% (7/9) of treatment subjects and 25% (2/8) of control subjects were free from reocclusion at 6 months.
In treatment subjects with wounds upon enrolment or who developed wounds on their target limb during the study, 71% (5/7) of treatment subjects had full healing of wounds by 12 months without the need for clinically driven target lesion revascularisation, whereas 44% (4/9) of control subjects had wound healing without prior clinically driven target lesion revascularisation.
Costantino Del Giudice concludes his VIVA19 late-breaking trial presentation on the ULYSEE registry
Low-frequency, high-intensity ultrasound energy delivery followed by percutaneous transluminal angioplasty (PTA) may improve clinical outcomes in below-the-knee (BTK) lesions without the need for a drug-eluting device, but a larger randomised study is needed to confirm these results. This was the main conclusion presented by Costantino Del Giudice during the ULYSSE registry late-breaking trial presentation at the 2019 Vascular Interventional Advances conference (VIVA) in Las Vegas (4–7 November).
The ULYSSE registry is a retrospective, nonrandomised, single-centre study evaluating the safety and the efficacy of ultrasoundplasty before angioplasty to treat below-the-knee (BTK) lesions in 22 critical limb ischemia (CLI) patients (35 BTK lesions). All patients were Rutherford category 4 to 6 and had moderate-severe calcification. Ultrasoundplasty was performed using the Kapani catheter (Apani Corporation), which delivers a local, low-frequency, high-intensity ultrasound energy to the lesion.
The objective of the study was to demonstrate that locally delivered ultrasound energy may modify plaque structure using microcavitational effects and change plaque compliance without risk of vessel dissection and rupture. Modifications of plaque structure may potentially improve the outcome of a simple balloon angioplasty.
The primary safety outcomes were the major adverse events at 30 days, recurrence of CLI, and surgical or endovascular revascularization at 6 months. The primary efficacy endpoint was angiographic restenosis and target lesion revascularisation at six months. Immediate outcomes showed good results, with 100% technical success and no major adverse events. At six-month angiographic control, primary patency was 97.1%, with 100% ulcer healing and no target lesion revascularisation and no CLI recurrence. At 24 months, freedom from restenosis was 91.4% as evaluated by Doppler ultrasound control, with no target lesion revascularisation and no CLI recurrence. No major adverse events were reported.
Penumbra today announced that the EXTRACT-PE trial successfully met the primary endpoints, demonstrating the safety and efficacy of the Indigo Aspiration system for aspiration mechanical thrombectomy in patients with acute pulmonary embolism (PE). The data were presented in a late-breaking clinical trial session today at the 2019 Vascular Interventional Advances conference (VIVA) in Las Vegas, USA (4–7 November).
“The positive results of the EXTRACT-PE trial, the first prospective safety and efficacy study of the Indigo Aspiration System, are a step forward in building needed clinical evidence around catheter-based embolectomy in patients with acute pulmonary embolism,” said Akhilesh Sista, EXTRACT-PE national principal investigator, chief of Vascular and Interventional Radiology at NYU-Langone School of Medicine, and vice chair of the recently published Interventional Therapies for Acute Pulmonary Embolism guidelines from the American Heart Association. “New AHA guidelines state that catheter-based embolectomy may have an important role in severe PE, but that more study is needed. EXTRACT-PE is an important first step in determining how and when we should employ promising and innovative catheter-based technologies such as the Indigo aspiration device.”
EXTRACT-PE was a prospective, single-arm, multicentre trial conducted under an Investigational Device Exemption (IDE) from the US Food and Drug Administration (FDA) that evaluated the safety and efficacy of the Indigo Aspiration System in the treatment of acute pulmonary embolism (ClinicalTrials.gov Identifier NCT03218566). The study enrolled 119 participants across 22 US study centres. The primary efficacy endpoint was met with a significant mean reduction in right ventricular (RV)/left ventricular (LV) ratio of 0.43, corresponding to a 27.3% reduction, at 48 hours after intervention. The primary safety endpoint was reached with a low major adverse event composite rate of 1.7% within 48 hours. The major adverse event composite included device-related death, major bleeding, and device-related serious adverse events as measured by the clinical events committee. Additional data reported included median time of Indigo System usage (37 minutes) and median ICU stay (one day). No thrombolytic drugs were used in 98.3% of patients.
“From a pulmonologist’s perspective, the results of the EXTRACT-PE trial are another important dataset that help broaden the mechanical treatment options for patients with pulmonary embolism,” said Victor F Tapson, pulmonary critical care specialist at Cedars-Sinai Medical Center in Los Angeles and EXTRACT-PE steering committee member. “The safety profile of the Indigo System and the low rate of bleeding events, combined with the significant reduction in RV/LV ratio seen in the EXTRACT-PE trial, can positively impact the emerging field of acute pulmonary embolism intervention.”
“The Indigo Aspiration System has demonstrated tremendous potential to address patients with clot in other parts of the body, and today’s data show its specific potential in the pulmonary arteries,” said Adam Elsesser, chairman and chief executive officer of Penumbra. “Pulmonary embolism is a deadly disease where we see an unmet clinical need and patient opportunity, and we commend the dedication of physicians who are focused on addressing this area. We are excited about the excellent results of this trial and look forward to working together with physicians in the field to bring better treatment options to patients.”
At this year’s Vascular Interventional Advances (VIVA) conference (4–7 November, Las Vegas, USA), Michael D Dake presented data on Zilver PTX that supports the device’s benefits across different patient groups.
Dake presented the latest data regarding Zilver PTX, Cook Medical’s paclitaxel-coated stent that is used to treat peripheral arterial disease (PAD). His presentation focused on findings that Zilver PTX shows benefits for a variety of patients.
“Our ultimate goal is to help patients suffering from PAD. That is why these data are so important—behind each one of these data points is a real person. As we continue this discussion on paclitaxel-coated devices, we will keep providing as much information on Zilver PTX as we can so that patients and physicians can make the best decisions,” said Mark Breedlove, vice president of Cook Medical’s Vascular division.
In Cook Medical’s ongoing review of data relating to the Zilver PTX peripheral arterial stent, patient-level data for Zilver PTX were evaluated to determine if there was an increased mortality risk due to paclitaxel and the impact of risk factors on outcomes. Data presented at VIVA was collected from a five-year randomised controlled trial. In the trial, patients with PAD were initially randomised to be treated with either Zilver PTX or angioplasty. When the data were analysed, it was discovered that patients assigned to the Zilver PTX group had more risk factors than the control group, despite the trial’s randomisation of patient assignment.
The trial had a study design that allowed for patient crossover to treatment with Zilver PTX within the first year. Taking actual treatment into account, analyses of the complete 5-year data for Zilver PTX show no increase in long-term mortality for the paclitaxel-eluting stent. When evaluating potential risk factors for freedom from target lesion revascularisation (TLR), data continue to support the benefit of Zilver PTX across a variety of patient risk factor groups.
When considering treatment options for PAD, the FDA recommends that physicians discuss both risk and benefit possibilities with their patients.
The first patient has been enrolled in the TORUS 2 multicentre, clinical trial, evaluating the use of the self-expanding Torus stent graft system (PQ Bypass), a novel technology designed for the treatment of peripheral arterial disease (PAD) in the superficial femoral artery. This inaugural enrollment comes less than a month after the study received unconditional approval from the US Food and Drug Administration (FDA) for the TORUS 2 original investigative device exemption (IDE).
The TORUS 2 study (The PQ Bypass pivOtal IDE intra-aRterial stent graft study for occlUsive and re-Stenotic fem-pop revascularization) is a prospective, single-arm trial of 188 patients at up to 40 sites. The study is led by national co-principal investigators Peter Schneider (Division of Vascular and Endovascular Surgery, University of California San Francisco, USA) and Ehrin Armstrong (director of Interventional Cardiology, Rocky Mountain Regional VA Hospital; University of Colorado School of Medicine, Aurora, USA).
The objective of the trial is to evaluate the safety and effectiveness of the Torus stent graft system in the treatment of obstructive atherosclerotic lesions of the superficial femoral and/or proximal popliteal arteries. The Torus stent graft system received CE mark in 2017 for use in the DETOUR percutaneous femoropopliteal bypass procedure, based on the DETOUR 1 global study. The technology has also been evaluated in the TORUS 1 study in Europe and is currently under evaluation in the DETOUR 2 IDE for percutaneous femoropopliteal bypass in the USA and Europe.
“There is an unmet need in our care of PAD patients for an updated, optimised, and specifically designed stent graft for SFA-popliteal use,” Schneider says. “I believe this technology could become an important part of our endovascular armamentarium.”
Armstrong adds, “This study is intended to further the growing body of evidence for the TORUS stent graft. I am pleased to be involved in such an important step forward in the percutaneous treatment of PAD.”
Vaqar Ali, vice president and catheter lab director at First Coast Cardiovascular Institute in Jacksonville, USA, enrolled and treated the trial’s first patient.
“Our patient had a challenging SFA lesion that was treated thanks to the radial strength and flexibility afforded by the robust design of the TORUS stent graft,” Ali says. “We are thrilled to be the first site to enrol in this important trial and to be part of bringing this technology forward as a potential option for our patients.”
PQ Bypass general manager Heather Simonsen called the enrollment of the first patient “a significant milestone for PQ Bypass as we initiate our second pivotal IDE evaluating our unique technology in two different applications for patients with PAD. We are thrilled to commence TORUS 2, continue enrollment in DETOUR 2, and look forward to working with our investigators to execute two efficient and rigorous pivotal trials.”
The first preclinical study of a novel embolization agent, GPX, reports its successful performance in a rabbit aneurysm model. High rates of complete angiographic occlusion were achieved and maintained, said Ruben Mühl-Benninghaus (Saarland University Hospital, Homburg, Germany), presenting these “promising” results at the 2019 annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (7–11 September, Barcelona, Spain).
In recent years, liquid embolic agents have emerged for endovascular treatment of cerebral aneurysm. “There are multiple liquid embolics available right now”, Mühl-Benninghaus said, before describing the properties of the ideal embolic agent: “It should have good control and precision during embolic injection, it should not adhere to any adhesion or clumping within the catheter, and the penetration of the liquid embolic agent should always target the distal vessel, which is the aim of the occlusion. Ease of use is also very important, [to] minimise the preparation steps and minimise complications during preparation. Of course, no fragmentation and no reflux should be achieved in the optimal liquid agent.”
Introducing the CIRSE audience to GPX, he described it as a polymer in a hypersaline solution, which solidifies upon injection into the blood vessel in response to a decreased sodium chloride concentration. The agent is prepackaged in a single, standard syringe and comes with an empty syringe. The interventionalist connects the two syringes and needs to mix them 25 times before the agent is ready to use. “Due to its waterborne composition, no specialised catheters are needed and no DMSO [dimethyl sulfoxide] and no vortexing prior to the procedure is required”, Mühl-Benninghaus explained.
In the present, pre-clinical study, the investigators set out to assess the in vivo performance of the GPX in a rabbit model.
To this end, elastase-induced aneurysms were created in 10 New Zealand white rabbits. Each aneurysm was embolized with low viscosity GPX using an Echelon 10 microcatheter (Medtronic) with balloon assistance. The mean aneurysm neck diameter, width, and height were 3.6±1mm, 3±0.8mm, and 7.4±1.4mm, respectively. The mean dome-to-neck ratio was 0.9±0.2.
Ninety per cent of aneurysms (nine of 10) showed complete stagnation of intra-aneurysmal flow within 30 minutes of device deployment. One aneurysm showed moderately diminished intra-aneurysmal flow within 30 minutes due to distal migration of GPX that still was connected to intra-aneurysmal embolic. This was assessed via digital subtraction angiography (DSA), performed predeployment, as well as five, 10, and 30 minutes post-deployment.
DSA was also performed one month after the procedure in the eight surviving rabbits (two of the study animals did not survive to one-month post-procedure). All eight aneurysms were completely occluded.
“We did not see microscopically any fragmentation of GPX, and we did not see any adhesion to the catheter or the balloon”, Mühl-Benninghaus noted. “We did observe some resistance during injection from the new embolic agent through the Echelon 10 microcatheter. Our impression was that there was a little varying visibility of GPX.”
“Upon gross examination at 28-days, tissue appeared normal”, he reported. Histological examination of the vessel wall, however, did reveal “evidence of some inflammation reaction”, but Mühl-Benninghaus said that he did “not have the final results”.
Compared to stent-assisted coil embolization in the same model, Mühl-Benninghaus said that the occlusion rates achieved with GPX were similar. “We have also performed previously in the same model the same thing with onyx, and we did see less fragmentation with GPX. We did not use any remodelling balloon due to the cost of balloons. The remodelling balloons could provide better stability of the microcatheter. For further investigations, this might be an option.”
When concluding, he outlined some limitations of the present study. Namely, the small study population, and the outstanding final histological results. He summarised that while GPX was easy to use and did not require DMSO, the agent’s viscosity needs improving, and although it has the potential to achieve durable occlusion of cerebral aneurysms, its clinical relevance will have to be assessed in larger and longer-term studies.
“It looks to us to be a promising embolic agent for neuro-intervention therapy,” he stated. embolization embolization
The first-in-human robotic-assisted neurovascular intervention has been performed at the Toronto Western Hospital (Toronto, Canada), by a team led by Vitor Mendes Pereira. A press release states that this “landmark” robotic-assisted stent-assisted aneurysm coiling case marks a “significant milestone” in interventional medicine as the first step in building a new treatment paradigm for patients suffering from neurovascular disease. The technology used for the procedure, the CorPath GRX system, has been developed by Corindus, which has recently been acquired by Siemens Healthineers.
CorPath GRX (Corindus)
Before the procedure commenced on 1 November this month, Pereira performed a rehearsal procedure on a Biomodex three-dimensional (3D)–printed flow model of the specific anatomy of the patient, a 64-year-old female Canadian resident. According to the press release, using the 3D model allowed Pereira to develop a plan for the novel robotic procedure and ensure an optimal treatment approach.
During the procedure itself, Timo Krings and Patrick Nicholson, neuroradiologists, provided bedside physician support while Nicole Cancelliere, medical radiation technologist, acted as the bedside robotic technician.
“Precision is a key element of neurovascular interventions, and it is evident to me that augmenting these delicate procedures with robotic assistance can positively impact how we treat patients,” Pereira commented in the company’s announcement. “I felt honoured to perform this procedure and look forward to continuing to support the development of robotic technology to help address access issues of stroke patients in the community.”
Mark Toland, CEO of Corindus, added: “The field of neurovascular intervention is changing rapidly, but there remains a significant need to expand access to care and reduce treatment times.” He further put forward that implementing robotic capability for neurovascular intervention is the first step toward the company’s vision of providing patients access to the world’s best specialists, regardless of their geographic location. “Building a body of clinical research on neurovascular robotics while training physicians to be robotics experts today will allow us to maximise physician impact and reach with remote telerobotics tomorrow,” said Toland.
Kyaw Zay Ya caught up with Interventional News at the 2019 meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 7–11 September, Barcelona, Spain) to discuss the opportunities and challenges Myanmar faces in developing its interventional radiology (IR) offering.
What is the status of IR in Myanmar?
My country is still developing, so IR in Myanmar is in the very initial phase. For me, I wanted to become an interventional radiologist after my radiology residency. In 2002, I had the chance to apply for fellowship training in Singapore General Hospital (SGH) with Bien Tan Soo—he is my mentor. He helped me a lot, not only to get the training, but also to get continuing interventional activities in Myanmar.
We interventional radiologists need to use so many advanced technologies and equipment, especially consumables—catheters, wires—that were very difficult to get at that time [early 2000s]. Anyhow, I requested that my colleagues at SGH get me some of the instruments and materials, and I tried to develop the interventional procedures in my country. At the same time, I tried to get the younger generation to get similar training like me in Singapore. I try to go to every conference in Singapore and took some of the consumables from SGH. From 2008, I got a chance to get the younger generation, my junior colleagues, training at SGH. One or two radiologists get that chance at SGH each year. Today, I have around 15 to 20 junior colleagues who perform interventional procedures in Myanmar.
Why is Singapore General Hospital a good collaborator?
SGH is very suitable for us. The case load and the instruments available make it the perfect place to train. When I first went in 2002, there were five interventional suites; nowadays, there are about 10 interventional suites in the department, and each and every day, there are at least 15 to 30 cases—on some days, there are 40 cases. Over a training period of one year, therefore, my colleagues can gain a lot of experience.
Primarily, we assist the interventional radiologists at SGH with their procedures. Later, when we [the trainees from Myanmar] are reliable, they give us the chance to do the procedures ourselves, under supervision. If there is a complication, they would come in and help, so it is very good training.
At the same time, Tan Soo and some of the other consultants at SGH not only help us with training and materials, but they also give us the chance to attend international conferences like CIRSE.
In 2010, Myanmar became a member of the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR). Why is this important?
Due to being a member country, we have gained more international exposure. Every year, in January, we have an IR workshop in our country. It is an APSCVIR outreach programme, in collaboration with the Myanmar Radiology Society, in which there is a vascular and interventional radiology section. I am president of this section.
Due to these workshops, the interests of our clinicians and radiologists in IR has become bigger and has spread across the country. Next year, CIRSE president Afshin Gangi and Society of Interventional Radiology (SIR) president Laura Findeiss will come and teach, and help us to improve the status of IR.
This collaboration has led to my attendance at CIRSE this year. This is a great opportunity for me to meet with industry and to discuss access to consumables in Myanmar. My aim at these conferences is to get international contacts, and for my junior colleagues to receive training.
What message would you like to give to your IR colleagues in developed nations?
Our country is now open—politically, socially, and economically. IR is very quickly developing and, to ensure quality of care for our patients, we need international support. Because of the population of our country [54 million people], there is a lot of potential to develop a great IR specialty, but we still need some human resources and consumables.
I would like to invite interventional radiologists across the world to come to my country and help us in any way, through training or instrument support. I hope I can improve the status of IR in Myanmar; within the next five years, it will become an international standard [of IR care]. We must dedicate our time and efforts to improving this valuable specialty.
Collaboration, academic support, and hands-on training provided by the Singapore General Hospital, Singapore, have driven the small interventional radiology (IR) community of Myanmar to the international stage. As one of the organising members of the Asia-Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR), the group of interventional radiologists in Myanmar have been working more closely with members of the Society of Interventional Radiology (SIR) and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) to promote the specialty locally. Despite huge strides over the last decade in the number and complexity of IR cases being undertaken in the country, Myanmar faces several challenges, which Kyaw Zay Ya (an interventional radiologist based in Nyaung, Myanmar; full interview from CIRSE 2019 here) summarised as the “three Ms: man, money, and materials”.
Due to a cancelled flight, Bien Soo Tan (Singapore General Hospital, Singapore) addressed delegates on behalf of Ya, speaking at the 2019 annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 7–11 September, Barcelona, Spain).
Myanmar is a large country in South East Asia with a population of 54 million, and a land area of 676,575km2. In the late 1970s and early 1980s, a conventional angiography system with serial changer was installed for diagnostic purposes in Yangon General Hospital (Yangon, Myanmar). By the end of the 1980s, digital subtraction angiography (DSA) was possible in the country, and some vascular and non-vascular interventional radiology (IR) procedures were performed in the early 1990s, though there was no proper training for interventionalists.
“At that time,” Tan said, “there were several very senior radiologists in Myanmar who were trained in Europe, in particular the UK, and when they went back [to Myanmar], they did introduce some of these procedures, […] primarily angiography and even chemoembolization.”
Following this informal introduction of IR to the country, Tan’s own institution, the Singapore General Hospital, provided IR training to radiologists in Myanmar. This paved the way for the first two Myanmarese interventional radiologists to gradually start working in their home country in the early 2000s, with “very limited consumables available to them”.
Since then, IR has grown steadily in Myanmar. From 2008, interventional radiologists at Singapore General Hospital have trained one or two candidates, and have provided some of the required consumables. These are often consumables in Singapore which are close to expiry, as Tan explained: “They are not freely available; the distributors are not really bringing in these consumables, because there is not much volume in Myanmar itself.”
Today, Myanmar is one of the organising members of APSCVIR, and Tan told delegates that, increasingly, Myanmar is in contact with SIR, based in the USA, and CIRSE, in Europe. Indeed, earlier in the session, APSCVIR president Andrew Holden (Auckland, New Zealand) had praised the “very active outreach programme” in Myanmar; when CIRSE president, Robert Morgan (London, UK) visited the country in January 2019 to take part in said programme. Of this experience, he said: “I was struck firstly by how large Myanmar is as a country, and secondly by how beautiful it is as a country. The people are all very friendly, so I would certainly recommend anyone who wishes to go and visit to do so. I was impressed by the set-up in the hospitals there. I may have had pre-conceived ideas that things would be relatively primitive, but they were not, in fact; there were pretty good facilities in each of the hospitals I went to in Yangon and Mandalay. […] I think it was a very good venture for CIRSE to be involved in, and I am pleased that Afshin Gangi [CIRSE president since September 2019] will continue this in January next year.”
Speaking about convincing hospitals and governments to support the establishment and progression of IR, Tan commented: “For us [in Singapore], I think some of these arguments have been ongoing within our own institutions and national systems, but you can imagine that in Myanmar, the conversations are [at a] much earlier [stage], [as they] try to argue why IR should be supported.” On his presentation slide, Ya had outlined shorter hospital stays, money saving, reduction in transfusion requirements, better quality of life for patients, faster recovery times, and high intensity local treatments as convincing arguments supporting the development of an IR department.
“These advantages are all very clear to us”, Tan acknowledged to the CIRSE audience, while in Myanmar, he explained how the country’s interventional radiologists “have to start the conversation and lobby the hospital administrators, the ministry, to get more training, more equipment.”
Regaling the CIRSE audience with a personal anecdote, Tan shared: “I think one very telling story I have—I have visited Myanmar quite regularly for ten years now—when I went in 2009, they had an angiography unit installed in Yangon General Hospital that was quite new, I think it was two to three years old, but the tube had blown. So in 2009, there was no angiography available in Yangon General Hospital, which is the largest public hospital in the whole of Myanmar. When I went back over the next three to four years, they still had not got the money to buy the tube. Only about six or seven years later did they decide to junk the machine, and they got a new machine in. So these are the challenges that they are facing.”
Despite the difficulties with procurement, a “whole spectrum” of IR procedures are currently being conducted in Myanmar, tailored to the disease distribution seen in the country. There are six public centres and six private centres offering IR services. Between 2015 and 2019, in public centres across Myanmar, there have been, each year, on average: 612 transarterial chemoembolization (TACE) procedures (“one of the main treatments for inoperable HCC”, Tan told the audience, “they do not have the other modalities available, like Y90”), 721 guided biopsies, 67 percutaneous transhepatic biliary drainages (PTBD), 44 angioplasties, 21 intracranial arteriovenous malformations (AVM) treated, and three abdominal aortic aneurysms (AAA) stented. In the private sector, there is on average 352 TACE procedures, 35 guided biopsies, 23 PTBDs, and 18 angioplasties performed each year.
Remarking on the 21 intracranial AVMs treated in the public centre, Tan observed: “Very little neurointervention for such a huge population”.
These procedures have all been conducted by the small group of interventional radiologists working in the country. Modern-day Myanmar has 15 practicing interventional radiologists, trained at several institutions across Asia, including Singapore, Thailand, the Republic of Korea, Japan, and India. There are two senior radiologists in the country with interventional training who have retired from public practice, but still work in the private sector. Twenty Myanmarese trainees have received local training, and are preparing to move abroad to “gain more intense exposure”, in Tan’s words, to the discipline.
In addition to procurement difficulties and the low number of interventional radiologists, Myanmar faces other challenges in being able to offer IR services to its 54 million inhabitants. Access to adequate training stymies the discipline’s development. Furthermore, awareness of IR among interventionalists’ clinical colleagues is low, according to Tan, “and therefore the referral system is not robust.”
However, he then said that the healthcare system is starting to invest in IR. “They [the Myanmarese healthcare system] are now starting to be vendors and distributors, gaining interest, but unfortunately, a lot of the interest is focused on cardiology, because that is where the money comes in, and less on IR.”
Ambitions for a more developed IR programme in Myanmar
Enumerating Ya’s aspirations for the development of IR in Myanmar, Tan listed the following:
To have vascular interventional radiology (VIR) services in all tertiary hospitals
To train more interventional radiologists
To establish a 24-hour VIR service, especially for emergency cases
To build up VIR clinics in all tertiary hospitals
To train neuro-interventionalists
To establish VIR sub-units in the radiology department of every teaching hospital
To conduct up-to-date research within the specialty
Harel Gadot: founder, executive chair, and president, XACT Robotics
XACT Robotics has just received clearance from the US Food and Drug Administration (FDA) to sell its first robotic system in the USA for use during computed tomography (CT)-guided percutaneous interventional procedures. XACT’s technology is the first hands-free robotic system combining image-based planning and navigation with insertion and steering of various instruments to a desired target across an array of clinical applications and indications.
“We are committed to redefining the way the entire medical community utilises robotics, beginning with interventional radiologists,” says Harel Gadot, founder, executive chair, and president of XACT Robotics. “Being the first to introduce a hands-free robotic system, we have the potential to provide significant clinical, technical and economic value while democratising interventional procedures. Our system’s small footprint and high mobility design will enable care providers to treat a broad range of patient care needs in various clinical sites of service.”
“The XACT Robotic system provides a unique platform to the interventional radiology community which can help improve the delivery and quality of care for the patients we serve,” comments Nahum S Goldberg, the principal investigator in a multi-site study using the system, which is still an investigational device in Israel, where XACT Robotics is based. Goldberg is the head of the Interventional Oncology Unit and director of the Applied Radiology Research Lab at Hadassah Hebrew University Medical Center, Jerusalem, Israel. “Based on our experience with this unique robotic technology, we can reach very small targets with unprecedented accuracy. Furthermore, this system holds much promise for enabling more efficient use of time and hospital resources.”
The XACT Robotic system is based on research originally conducted at the Technion—Israel Institute of Technology, by Moshe Shoham, founder of Mazor Robotics (acquired by Medtronic in 2018). The company plans to launch the system to select US radiology centres of excellence partners, and will debut its technology at the 2019 Radiological Society of North America conference (RSNA; 1–6 December, Chicago, USA).
A Philadelphia jury has awarded more than US$33 million to a woman who was injured as a result of a defectively designed inferior vena cava (IVC) filter. The trial was overseen by Philadelphia Judge Michael Erdos.
The litigation focused on allegations that the defendant, the company Rex Medical, failed to properly warn about the dangers of the filter devices, which were designed to prevent blood clots, but can allegedly migrate or fracture in patients’ bodies, causing perforations. The injuries, according to the accusers, put patients at risk for a host of medical problems, including gastrointestinal difficulties, kidney failure and death.
The trial result prompted Cook Medical to release a statement defending their IVC filter devices. Penned by Cynthia Kretz, vice president and general counsel for the company, this reads in full:
“Earlier today, a decision was made in Philadelphia against Rex Argon, an IVC filter device manufacturer.
“Cook Medical’s IVC filters are quality products that have saved thousands of lives and are critical to patient well-being. Our design and materials are different from the Rex Argon Option filter.
“To date, Cook Medical has had over 1,000 cases dismissed by the courts and we will continue to defend all of our IVC filters.
“IVC filters are an important option for physicians working to prevent the estimated 100,000 deaths associated with pulmonary embolism each year in the United States. Physicians and companies like Cook worked together to develop IVC filters to help patients and reduce the risk of these deadly pulmonary embolisms.
“Physicians choose to use IVC filters based on each patient’s medical needs. Every patient’s situation is different, and individual patient factors and risks must be considered when evaluating treatment options.
“We are dedicated to providing life-saving treatment options for patients.”
As of 16 September 2019, federal records showed more than 7,000 cases were pending against Cook Medical in Indiana federal court, and more than 8,600 were pending against Bard in Arizona federal court.
Cook won the first IVC filter trial in 2017, but it lost a US$1.2 million verdict in Texas state court in May 2018. Cook was also lost a US$3 million verdict in February. In March 2018, plaintiffs won a US$3.6 million verdict against Bard. That verdict included a US$2 million punitive damages award against Bard. The company, however, followed up in June 2018 with a defence win.
The first patient in the United Arab Emirates has been treated with the Stealth 360 peripheral orbital atherectomy system (Cardiovascular Systems), intended for the treatment of patients with peripheral and coronary artery disease.
The first peripheral patient in the Middle East was treated by Faisal Hasan at the Cleveland Clinic Abu Dhabi, UAE.
Hasan comments: “Cardiovascular System’s orbital atherectomy simultaneously removes calcified plaque within the vessel and modifies medial calcium. This dual mode of action helped restore blood flow and vessel motility in a very challenging peripheral patient. The ability of orbital atherectomy to safely treat calcified peripheral lesions, both above and below the knee, will allow me to serve an unmet need in the United Arab Emirates.”
Scott Ward, chair, president and chief executive officer of Cardiovascular Systems, says, “In the last year, we have successfully introduced our orbital atherectomy system technology in Asia, Europe and the Middle East. As our distribution partner, OrbusNeich, identifies new markets, we are providing best-in-class training to physicians committed to improving patient outcomes within this underserved patient population.”
Omega Medical Imaging, manufactures of Artificial Intelligence Fluoroscopy/Cine (AIF/C) Imaging systems, has announced US Food and Drug Administration (FDA) 510(k) clearance of FluoroShield with their 2020 cardiac flat panel detector.
The FluoroShield system allows for auto-collimation during interventional fluoroscopy or cine cases, while maintaining a perspective of the surrounding anatomy. The blended image incorporates a lower frequency refresh of the peripheral image area, a press release explains. This combined image (live fluoroscopy or cine and background refreshed at a rate of once or twice per second) increases the quality of information presented during interventional procedures.
Brian Fleming, president of Omega Medical Imaging, states, “Until now, products on the market have only been able to manage radiation to patients and staff. FluoroShield is the only system in the world that provides an actual reduction in dose. The impact of this ground-breaking solution for patients and healthcare providers is substantial. I am very grateful to be a part of a team that pushes the envelope in the development of safer healthcare solutions.”
A recent study comparing holmium-166 (QuiremSpheres, from Terumo) to technetium-99m-macroaggregated albumin (99mTc-MAA) as a work up for selective internal radiation therapy (SIRT) has found QuieremSpheres to be superior in terms of predicting which patients with liver cancer will benefit from SIRT treatment.Theresults were published in the European Journal of Nuclear Medicine Molecular Imaging.
The aim of the study was to analyse whether the intrahepatic distribution of QuiremScout has a better agreement with the QuiremSpheres distribution when compared with 99mTc-MAA. Several scientific papers have indicated that the widely used 99mTc-MAA has limited predictive value, a Terumo press release claims.
The present study included 53 patients that had been included in either phase 1 or phase 2 Holmium Embolization Particles for Arterial Radiotherapy (HEPAR) studies, and showed QuiremScout has superior predictive value for intrahepatic distribution in comparison to 99mTc-MAA.
“Previous studies already demonstrated that QuiremScout is safe in this population, and, moreover, a better predictor for lung shunting than 99mTc-MAA,” first author Maarten Smits comments. “As a result, QuiremScout allows for more accurate SIRT patient selection. Now, our study shows the potential of QuiremScout to also improve the efficacy of SIRT, by allowing a more accurate and truly personalised pre-treatment activity planning.”
“This is an important next step towards unlocking the full potential of Quirem Scout,” says Rijk de Jong, medical director of Quirem Medical. “Smits et al publication further strengthens the evidence base of QuiremScout, demonstrating superiority over 99mTc-MAA in the evaluation of the subsequent treatment. We believe this will translate into enhanced efficacy and safety for the benefit of patients undergoing SIRT procedures.”
“This is a very exciting milestone for QuiremScout and the next step in building the future for SIRT,” adds Peter Coenen, president of Interventional systems, Terumo. “This publication further validates the advantages of QuiremScout over 99mTc-MAA during the SIRT work up, which we at Terumo believe is a vital step in advancing patient selection and optimising dosimetry for better patient outcomes.”
QuiremScout is the first SIRT work up product that utilises the same technology as the therapeutic microspheres, which aims to optimise patient selection and advance treatment planning when compared to using 99mTc-MAA.
Live guidance of a thrombectomy procedure performed with Philips Azurion
Interventional News speaks with Atul Gupta about the future of interventional radiology (IR). As a chief medical officer for Image-Guided Therapy, Philips, he enthuses about the possibilities of radiation-free interventional procedures, and a medical world advanced by augmented reality and artificial intelligence solutions.
How was IR changed over the course of your career?
I have been practicing for about 20 years, so when I first started my career, it was simple: just X-ray and a device. Procedures are becoming increasingly complex. When I do an intervention today, it is no longer just X-ray and device—I have to analyse data from a whole bunch of sources: haemodynamic data, electronic health records, 2D and 3D live imaging, intravascular ultrasound (IVUS) and ablation data.
I have also seen a change in the types of procedure that we do. My entryway to the human body used to be the femoral artery, but now, as we do things like uterine fibroid embolization (UFE), prostate artery embolization (PAE), transarterial chemoembolization (TACE), peripheral vascular disease (PVD) work, and even biliary procedures, we have several different access points: radial, pedal, femoral, jugular, transabdominal. I want to be able to rapidly image wrist to wrist, from head to toe, and I need to be able to do it very quickly and with great image quality. That is the biggest change I have seen in the last 20 years, the increased complexity of these procedures. Fortunately, technology now exists to help us make these procedures a lot more efficient.
What are the challenges for today’s interventional radiologists, and how can these be overcome?
At CIRSE 2019 [the annual meeting of the Cardiovascular and Interventional Radiological Society of Europe; 7–11 September, Barcelona, Spain], we heard a lot about how we as a specialty have an identity crisis. Not just with patients, but also with other physicians. It is well understood that cardiologists treat the heart, neurologists treat the brain—but what do interventional radiologists treat? Put simply, everything, everywhere. What other field can treat a liver blockage, a stroke patient, a trauma patient, a prostate patient, kill a kidney tumour, and drain from the lungs, all in one day? We do it all, and that is a challenge. But there are three ways I think you can overcome this identity issue.
Firstly, education in the impressionable years. Any individual specialist knows us for our procedures specific to them: gynaecologists know us as the UFE expert, trauma doctors know us for doing splenic embolization, and geriatricians know us as the people who perform kyphoplasties. They are amazed to hear of all the things that we do outside of their specialty. At CIRSE, the European Trainee Forum bought 300 medical students to the congress. Not all of those 300 are going to go into IR, but they will be IR ambassadors for us, as they learn about all the things that we do.
Secondly, interdisciplinary congresses such as VIVA, ISET, CX and CIRSE, where all these specialists from across disciplines gather, are important.
Finally, social media, which gives us interventional radiologists the opportunity to get the word out is increasingly playing a role.
The Microsoft Hololens 2 AR headset
What technological developments do you think will be the most disruptive in IR?
Lots of things! That is the cool part of the job, I get a glimpse of the future and help define what the next five to ten years of innovation are going to be, and the world that I and my colleagues are going to work in. Philips is an innovation company, so we are very much about creating technology, but it is very important to remember that it is not just about the technology. We are not here to push technology for technology’s sake—technology is the enabler to help physicians do a procedure better.
I think we are going to be working increasingly in a radiation-less, or maybe even radiation-free, world. We are going to be using ultrasound instead of X-ray. We [at Philips] have technology called TrueView, where I can photo-realistically render 3D ultrasound on the fly, so I can guide a device using ultrasound and see it in 3D, maybe even see it in a hologram in the world of augmented reality (AR). In addition to sound, we are going to be using light to navigate our devices instead of X-ray. Philips is developing devices using technology called Fibre-Optic RealShape (FORS), which lets me visualise wires and catheters in 3D using light, instead of X-ray; this was presented to the world through first-in-human cases shown at the 2019 Leipzig Interventional Course (LINC; 22–25 January, Leipzig, Germany), the International Symposium on Endovascular Therapy (ISET; 27–30 January, Hollywood, USA), and the Charing Cross Symposium (CX; 15–18 April, London, UK). Philips acquired EPD Solutions last year, and we now have a new technology called dielectric imaging, which lets you visualise not just the device, but the anatomy, in high definition and 3D, without X-ray. If we can do all this imaging without X-ray, and support it with artificial intelligence (AI), this is, I think, going to be massively disruptive, not just for IR, but for all interventionalists.
What can other medical disciplines learn from IR?
I think that collaboration is the most important thing that interventional radiologists bring to the table. We know that no two patients are the same, and so we are often asked by other specialities to solve very unique problems, and that lets me as an interventional radiologist be creative. Interventional radiologists are the innovators; we are always inventing new ways of treating patients. That is a hot topic every year, from the annual meeting of the Society of Interventional Radiology (SIR) to CIRSE. By collaborating with industry and with other physicians, the procedures that we develop disseminate into other fields. I think that other medical disciplines love interventional radiologists’ passion for innovation and creativity, but most importantly for collaboration. If I fast forward 10 or 15 years, I would not be surprised to see a blurring of lines between specialties, because a lot of the procedures that we do are increasingly overlapping. What specialist today is the expert in critical limb ischaemia (CLI), or AAA, or venous disease? Many people: cardiologists, surgeons, and interventional radiologists. I think that we are starting to see physicians meet across specialties. I saw vascular surgeons, cardiologists, and radiologists joining CIRSE. At conferences like ISET and Vascular InterVentional Advances (VIVA), we also see multiple specialties coming together. None of us work in a vacuum, and so crossing over to approach patient care is extraordinarily important, not just for physicians, but also for industry. Collaboration leads to the very best in innovation.
How are you working to shape the future of IR?
This is the part of my job that I like the best, the innovation piece. The process of how we innovate and co-create with physicians is both extraordinary and fascinating, because you never want to just push technology out, everything has to start with the end-user and patient. Recently, we brought teenagers into our innovation centre, and allowed them to sit in an interventional suite and start playing with it. These adolescents were born after the iPhone was introduced in 2007, and they are going to be the physicians of the future. Their insights are tremendous. So the process starts early on, but we also work with the world’s leading interventionalists to help us improve our devices, imaging, and software.
Atul Gupta is chief medical officer for Image-Guided Therapy, Philips. He is also a practicing interventional radiologist in Philadelphia, USA.
The 11th Symposium on Clinical Interventional Oncology (CIO; 11–13 October, Miami, USA) hosted a virtual reality (VR) case presentation, where delegates placed their smartphones into a provided cardboard headset and watched Auh Whan Park (UVA Health, Charlottesville, USA) perform a pre-recorded thyroid ablation as though they were in the operating room. This case presentation followed a series of talks discussing state of the art thyroid intervention, versing the audience in the current mainstay of thyroid cancer treatment.
Speaking in his capacity of panel moderator, Ziv Haskal (UVA Health, Charlottesville, USA) introduced the live case: “I have had the great fortune and pleasure of being involved in this meeting for ten years, and they have tolerated a lot of the things I have done. There is a certain atmosphere here—maybe it is the Miami meeting or the southern Florida meeting that just makes it a cool and hip way to learn things—and I think, at least for me, things just stick better when you can meet faculty and talk to them and see things that might be defining. I will never forget the first time I saw a live EVAR [endovascular aortic repair] case at ISET [International Symposium on Endovascular Therapy] a few decades ago. No matter how many papers you had read beforehand, seeing that live was transforming. It was several years before I did my first case, so there is sort of an inertia, but [witnessing that live case is nevertheless] a marked event.
“What we are going to do here is try to give you a little bit of that cool by putting you in that intimate, close-up seat, in the room, where you can watch Dr Park do a thyroid ablation. The purpose is to take something that probably none of you have done, and show you that […] you can actually do this: this is something you can learn and put into your practices. The opportunity is enormous. This will happen in the USA; whether it is going to be interventional radiologists (we all have experience with ablation, after all), or endocrine surgeons [is to be decided]—it is going to be performed by whoever is going to bring it [to institutions], and whoever is going to do it well.”
Prior to the session, attendees downloaded a free application to their smartphones, and then used this to stream the case. By placing a smartphone into the cardboard headsets provided, attendees were transported to Park’s operating room, where they watched a 15-minute thyroid ablation case. Haskal provided commentary throughout, describing operator decisions and drawing the audience’s attention to certain technical aspects of the case. Turning around whilst wearing the VR headset, session participants could see a presentation slide outlining the procedural steps.
Ziv Haskal at CIO 2019
The case
The patient was a woman with two benign nodules in the right thyroid lobe, which had been growing for two years prior to the procedure. Her pre-procedural thyroid function tests were normal. The patient had opted for radiofrequency ablation (RFA) over a thyroidectomy to preserve her singing voice.
The procedure was a success, with Park reporting: “She [the patient] is now really happy. She sent me a thank you letter to say that she had an invitation to perform at a concert, she is a jazz singer, so she is really happy and grateful.”
Prostate artery embolization (PAE) may become the standard of care procedure for the management of symptomatic benign prostatic hyperplasia (BPH), proposed Tiago Bilhim (CHULC, Saint Louis Hospital, Lisbon, Portugal), due to “good clinical results” presented at the 2019 annual meeting of the Cardiovascular and Radiological Society of Europe (CIRSE; 7–11 September, Barcelona, Spain).
The investigators set out to evaluate the outcome of PAE for symptomatic BPH patients with moderate to severe lower urinary tract symptoms (LUTS). The single-centre, retrospective study examined data on 1,550 patients, prospectively-collected between March 2009 and February 2019.
“Subjective and objective parameters were assessed”, Bilhim said. The International Prostate Symptom Score (IPSS), quality of life (QoL) score, and international index of erectile function (IIEF-5) were categorised as subjective measures, whilst the investigators also calculated changes in prostate volume (PV) using trans-rectal ultrasound, peak urinary flowrate (Qmax), post-void urinary residual (PVR), and prostate specific antigen (PSA) concentration. All of these were assessed before PAE, and one, six, and 12 months after PAE, then yearly for up to 10 years.
Clinical outcomes
There was a statistically significant change from baseline in the evaluated parameters (p<0.001) across all time scales. In the short-term, defined as one to 12 months after PAE, the mean cumulative clinical success rate was 88.1% (range: 77.6–92.4%). In the medium-term, two to five years after the procedure, this was 85.1% (range: 71.3–93.1%), and over the long-term, from six to ten years post-PAE, the mean cumulative clinical success rate was 76.8% (range: 69.1–84.6%). Bilhim described the change in cumulative clinical success rate from short- to longterm—88.1% to 76.8%—as “not that much of a drop” over ten years.
Mean IPSS reduction was 13.5±6.9 in the short-term, 14.1±7.3 in the medium-term, and 13.9±8.7 in the long-term. Mean quality of life improvement was also consistent out to ten years: 1.8±1.2 in the short-term, 2.1±1.3 in the medium-term, and 1.7±1.5 in the long-term. Prostate volume reduction was also observed out to ten years, with the mean long-term reduction being 16.9±26.6cm3, and a short-term reduction of 18.3±27.9cm3.
From the 156 patients in acute urinary retention (AUR), 140 (89.7%) had the bladder catheter removed between two days and three months; 10 had repeated successful PAEs, and six had surgery. For the 312 patients with prostates larger than 100mL, there was a high rate of clinical success: in 80.7% of patients (252 individuals) over the short-term; 77.6% of patients (242 individuals) over the medium-term; 75.3% of patients (235 individuals) in the long term. Bilhim reported three major complications: a bladder wall ischaemia, a perineal pain for three months without sequela, and a patient had expelled prostate fragments and AUR treated by trans-urethral resection of the prostate (TURP) without sequela.
Describing the technical outcomes, Bilhim reported that in 90% of patients (1,324 people), the interventionalist gained access to the vasculature through the femoral artery. Since 2016, interventional radiologists at Saint Louis Hospital in Lisbon, Portugal, have been using left radial access, so 10% of the cohort (148 patients) experienced this. “This is our first-line approach”, he said of the technique, adding that now they are using it “more and more”.
Patient characteristics
Enrolled patients were 40 or older (with no upper limit on age; mean age was 65.1 years), and “severely symptomatic”, with an IPSS greater than 18 (mean IPSS: 21.8), a prostate volume greater than 30mL, and a peak urinary flowrate less than 15mL per second. The prostate was larger than 100cm3 in 312 patients, and 156 patients were in acute urinary retention (AUR). In the initial phase of the trial, only patients failing medical therapy were accepted, meaning that 65% of the cohort were given medical therapy prior to PAE. However, Bilhim said that “a significant proportion” (35%) of patients had no medical therapy pre-PAE, as “they do not want the adverse events” attributed with the alpha-blockers and 5-alpha-reductae inhibitors, such as retrograde ejaculation.
MagicTouch—ED (sirolimus-coated balloon catheter) for erectile dysfunction
MagicTouch—AVF (sirolimus coated PTA balloon catheter) for arterio-venous fistula and graft
MagicTouch—PTA is the only commercially available and CE certified sirolimus-coated balloon catheter for peripheral arterial diseases.
Several studies have demonstrated that erectile dysfunction is increasingly prevalent with age. Approximately 40% of men are affected by the age of 40, and nearly 70% of men are affected by the age of 70. MagicTouch ED is the only CE certified, commercially available sirolimus-coated balloon catheter in the world for the therapeutic management of erectile dysfunction.
Concept Medical state in a press release that the company will now intensify its efforts to market and promote its products in all of Europe and other relevant markets that accept the CE certification for marketing authorisation.
Scientists of Jena University Hospital, Germany, conducted a meta-analysis sought to evaluate benefit and risk of paclitaxel-coated balloon angioplasty compared to plain old balloon angioplasty as therapy of intermittent claudication. The study confirms an increased all-cause mortality, which has formerly been stated, and found a broad heterogeneity in the effectivity of the procedure depending on pre-dilation strategy, lesion complexity, and the paclitaxel density. The authors raise doubts about a class effect of drug-coated balloons and suggest a highly individualised therapeutic decision. This meta-analysis has recently been published by The Lancet in EClinicalMedicine.
For intermittent claudication, drug-coated balloon angioplasty is the therapy of choice to reduce the risk of target lesion restenosis, and consequently, the necessity of reintervention. However, numerous types of those balloons are distinguished by drug density and coating. Clinical efficacy is not proven for all that types. Moreover, conflicting evidence exists about the risk of mortality that arose from the meta-analysis of Katsanos et al. one year ago. Scientists of Jena University Hospital, Germany, now conducted a meta-analysis sought to evaluate benefit and risk of drug-coated balloon angioplasty compared to non-coated balloon angioplasty assessing the main outcomes of freedom from target lesion revascularisation and all-cause mortality. Their results are published by The Lancet in EClinicalMedicine.
The authors working in the department of radiology and the centre for clinical studies took a closer look on 14 randomised trials comparing both procedures for the treatment of femoropopliteal artery disease. Including a total of 2504 patients, the trials were conducted between 2005 and 2019. Actually, the risk of all-cause mortality at two years was indeed increased significantly with a trend to a paclitaxel dose-response relationship, but without evidence of causation. Drug-coated balloon angioplasty significantly increased the risk of target lesion restenosis.
However, results showed substantial heterogeneity due to substantial inter-study design differences, inter-study lesion complexity differences and inter-study device differences. There is a risk of overestimation of the benefit due to high risk of bias within studies, mainly driven by missing blinding of study personal. Head-to-head comparisons of different coated balloons under the same conditions will be needed to evaluate different product efficacy. Additional pharmacological studies are needed to generate robust and meaningful evidence on safety or risk of intra-vessel paclitaxel application. Professor Ulf Teichgräber, the corresponding author of this meta-analysis, states: “There are first trials that are already beginning to examine if sirolimus-coated balloons could be an alternative to paclitaxel-coated ones. Also newer coating technologies of paclitaxel-balloons seem to have less drug loss during the procedure and better drug release to the target lesion. Innovation in this field clearly is leading towards better efficacy and safety.”
The National Institute for Health and Care Excellence (NICE) has published the final appraisal determination (FAD) recommending the use of Xarelto (rivaroxaban) by the National Health Service (NHS) in England at a dose of 2.5mg twice daily combined with aspirin (75–100mg) once daily as an option for preventing atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral artery disease (PAD) who are at high risk of ischaemic events.1
Publication of the NICE FAD for Xarelto (rivaroxaban) is based on evidence from the COMPASS study, the largest Phase III study with rivaroxaban (27,395 patients). This study showed that rivaroxaban vascular dose—2.5mg twice daily combined with aspirin 100mg once daily—statistically significantly reduced the risk of the composite of cardiovascular (CV) death, stroke or myocardial infarction (MI) (major adverse cardiovascular events; MACE) by 24% (relative risk reduction, ARR: 1.3%) compared with aspirin 100mg once daily alone amongst patients with stable atherosclerotic vascular disease (379 patients [4.1%] vs. 496 patients [5.4%]; hazard ratio [HR], 0.76; 95% confidence interval [CI], 0.66 to 0.86; P<0.001).2
In the COMPASS trial, for patients with stable CAD, addition of rivaroxaban 2.5mg twice daily with aspirin 100mg once daily lowered major adverse cardiovascular events compared with aspirin once daily (347 [4%] of 8,313 vs. 460 [6%] of 8,261; HR 0.74, 95% CI 0.65–0.86, p<0.0001)3. Moreover, patients with PAD who received rivaroxaban 2.5mg twice daily combined with aspirin 100mg once daily also had fewer major cardiovascular events compared with the aspirin 100mg once daily alone group (126 [5%] of 2,492 vs. 174 [7%] of 2,504; HR 0.72, 95% CI 0.57–0.90, p=0.0047).4
Rivaroxaban is an anticoagulant that targets Factor Xa, an enzyme which acts at a key point in the blood clotting process, inhibiting its ability to generate thrombin.5 NICE is recommending use of rivaroxaban as part of a dual pathway approach (in combination with aspirin) to prevent atherothrombotic events in patients who are at high risk of such events. CAD patients who are at high risk of ischaemic events are defined by NICE as those aged 65 or over, patients with atherosclerosis in at least two vascular territories, or those presenting risk factors such as smoking, diabetes, kidney dysfunction, heart failure or a history of stroke.1
Derek Connolly, COMPASS trialist, consultant interventional cardiologist and honorary senior clinical lecturer at Birmingham city hospital, Birmingham, UK, said: “Cardiovascular disease remains the biggest cause of years of life lost in the UK. There have been few recent major new advances in the medical management of patients with CAD and PAD to protect them against strokes or heart attacks.”
“The COMPASS trial showed that adding rivaroxaban vascular dose (2.5mg) to low-dose aspirin significantly reduced vascular events. The large reduction in events [such as strokes], outweighed the increase in major bleeding events seen. Conducted in more than 30 countries, including the UK, COMPASS was one of the largest ever trials of oral anti-thrombotic therapy providing robust results, overall, and particularly for key patient subgroups at high-risk of recurrent events such as those with renal dysfunction or stable ‘mild’ heart failure.
“Rivaroxaban vascular dose in combination with aspirin is the first treatment of its kind for this patient population and this recommendation from NICE provides clinicians with an important additional option for treating patients at risk of major adverse cardiac events such as CV death, stroke or MI.”
Matthew Fay, General Practioner (GP) in Queensbury, Bradford, UK, with a special interest in cardiology and Trustee of AF Association and Thrombosis UK said: “We are only too aware that cardiovascular diseases carry an unacceptable burden, accounting for a quarter of all deaths in the UK. As GPs, we are always looking for new options for protecting our patients living with cardiovascular diseases, especially as the risk of atherothrombotic events remains high despite current treatment options.
“The COMPASS study showed that the rivaroxaban vascular dose (2.5mg) is an effective option for patients with coronary and peripheral artery disease and holds promise for helping patients with these conditions. I am sure that GPs across England will join me in welcoming this decision by NICE.”
Speaking on 17 October, when NICE made the recommendation, Jo Jerrome, CEO of Thrombosis UK, said: “Cardiovascular disease is one of the leading causes of deaths across the UK, accounting for more than 460 deaths per day. Today’s recommendation from NICE is great news for thousands of patients at risk across the nation.”
More than seven million people are living with cardiovascular disease in the UK. It is estimated that CVD, including CAD and PAD, is responsible for 170,000 deaths in the UK each year, representing a quarter of all annual deaths.6
Lars Bruening, CEO Bayer UK and Ireland, said: “Bayer has a long and successful heritage in cardiology. The NICE recommendation provides those with high risk CAD and symptomatic PAD with an effective treatment option that will provide additional tailored protection from atherothrombosis. Ten years on from the introduction of rivaroxaban into the UK we are continuing to see the enduring impact that it has on patients treated across its licensed indications—and now this new patient population with previous unmet needs can be considered.”
Publication of the NICE FAD for Xarelto (rivaroxaban) follows approval by the European Commission (EC) in August 20187 for the regimen of rivaroxaban 2.5mg twice daily plus aspirin 75–100mg once daily for the prevention of atherothrombotic events in adult patients with CAD or symptomatic PAD at high risk of ischaemic events. Rivaroxaban is the most broadly indicated NOAC worldwide. It is approved in the UK for:8,9,10
The prevention of stroke and systemic embolism in adult patients with non-valvular AF with one or more risk factors
The treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and prevention of recurrent DVT and PE in adults
The prevention of venous thromboembolism in adult patients undergoing elective hip or knee replacement surgery
The prevention of atherothrombotic events in adult patients after an acute coronary syndrome (ACS) with elevated cardiac biomarkers, co-administered with aspirin alone or with aspirin plus clopidogrel or ticlopidine
The prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral artery disease (PAD) at high risk of ischaemic events
It is recommended that physicians assess a person’s risk of bleeding before considering rivaroxaban. Treatment to be commenced once an informed discussion has taken place, weighing up the risk of atherothrombotic events against the risk of bleeding.1
References 1 NICE. Rivaroxaban for preventing atherothrombotic events in people with coronary or peripheral artery disease. Available at: https://www.nice.org.uk/guidance/ta607 [Last accessed October 2019] 2 Eikelboom, JW., et al. N Engl J Med 2017; 377:1319–30. 3 Connolly S. J., et al. Rivaroxaban with or without aspirin in stable coronary artery disease an international, randomised, double blind, placebo-controlled trial. The Lancet 2017: DOI 10.1016/s0140-6736(17)32458-3 4 Anand, SS et al. TheLancet 2018,391:219-229. 5 Turpie AG. Arterioscler Thromb Vasc Biol. 2007; 27(6):1238-1247 6 BHF factsheet UK: bhf-cvd-statistics-uk-factsheet. Available at: https://www.bhf.org.uk/-/media/files/…statistics/bhf-cvd-statistics—uk-factsheet.pdf [Last accessed July 2019] 7 eMC. 2018. Xarelto. Available at: https://www.ema.europa.eu/en/medicines/human/summaries-opinion/xarelto [Last accessed July 2019] 8 eMC. 2018. Xarelto SPC 2.5 mg. Available at: https://www.medicines.org.uk/emc/product/3410/smpc [Last accessed July 2019] 9 eMC. 2018. Xarelto SPC 10 mg Available at: https://www.medicines.org.uk/emc/product/6402/smpc [Last accessed July 2019] 10 eMC. 2018. Xarelto SPC 20 mg. Available at: https://www.medicines.org.uk/emc/product/2793/smpc [Last accessed July 2019] 11 Lloyd-Jones, D., et al. Lifetime risk of developing coronary artery heart disease. The Lancet. 1999;353(9147):89–92. 12 Bosch J, et al. Can J Cardiol. 2017;33(8):1027-1035 13] emc. 2019. Xarelto. Available at: https://www.medicines.org.uk/emc/product/3410/rmms [Last accessed July 2019]
Boston Scientific recently announced that vascular medicine specialist Michael R Jaff (Newton-Wellesley Hospital, Newton, USA) will be joining the company as vice president, clinical affairs, innovation and technology, peripheral interventions. His role will involve, according to Boston Scientific, leading clinical and medical affairs strategies to support the development and commercialisation of the company’s peripheral vascular medical device portfolio. In this interview with Interventional News, Jaff discusses his new position and says that “collaboration and innovation” is at its core.
Why did you decide to make the switch from medical practice to industry?
I have had an amazing career and I have been able to have a positive effect on the lives of many incredible patients. Also, I have had the privilege of participating in some of the most impactful clinical trials that have shaped and evolved our field. Most recently, I had the honour of leading a remarkable group of healthcare professionals at Newton-Wellesley Hospital. This opportunity to join an extraordinary medical technology company [Boston Scientific] is the crown jewel in my career.
Why Boston Scientific?
I have had multiple opportunities to collaborate on clinical trials with Boston Scientific, and I have been impressed with their innovative spirit, integrity and ethical standards. Their business approach has always been of interest to me and I feel honoured to have the opportunity to partner with them to improve the health of patients around the world.
How do you think your experience as a physician will help you in your new role?
Being a physician is key to this role—there is nothing more important that I can bring to the table than the perspective of what matters most to patients. My hope and my goal is that these insights will lead Boston Scientific to innovations and discoveries that will change the outcomes for patients and increase longevity.
What will your new role involve?
At the core of this new role is collaboration and innovation; we want to develop medical solutions that will transform lives. I will collaborate with colleagues at Boston Scientific to develop novel clinical trials, source new technologies and advance innovation.
In your new role, you will be looking at innovation. What do you think will be the biggest innovation in peripheral technologies over the next few years?
I am enthusiastic about advancing revascularisation strategies in peripheral artery disease, particularly given the recent confusion surrounding paclitaxel. I want to help solve the management conundrums of venous thromboembolic disease, advance interventional treatment of various malignancies, and progress artificial intelligence associated with implantable devices.
Are you able to say what Boston Scientific has in the pipeline in terms of peripheral technologies?
This is an exciting time to be joining the Boston Scientific Peripheral Interventions business, especially with the recent merger with BTG. The new portfolio of products will advance care for patients in ways that could not be realised by either company alone. My focus will be on driving innovation and clinical evidence of minimally-invasive treatments. I am excited about the totality of products in the Boston Scientific peripheral portfolio and what they offer physicians and patients.
Michael R Jaff is to be vice president, clinical affairs, innovation and technology, peripheral interventions of Boston Scientific by January 2020. In this role, a press release reports, Jaff will lead clinical and medical affairs strategies to support the development and commercialisation of the company’s peripheral vascular medical device portfolio, and drive engagement with external stakeholders to advance technologies that deliver strong clinical value and enable patient care.
The press release adds that Jaff is currently president of Newton-Wellesley Hospital (part of the Partners Healthcare system in Massachusetts), “where he has been instrumental in the hospital’s growth since 2016”. Previously, he was responsible for process improvement efforts to redesign healthcare delivery at Massachusetts General Hospital and led its Fireman Vascular Center.
With more than 25 years of experience as a vascular clinician, his research has been published in more than 300 peer reviewed medical journals. Jaff is also the founder of VasCore, which is the world’s largest core laboratory for non-invasive vascular imaging and clinical trials. Furthermore, he is currently professor of medicine at Harvard Medical School and has served on multiple professional society and hospital boards of directors.
Jaff says: “I have had the privilege of collaborating with Boston Scientific over the course of my career and have participated in numerous clinical trials investigating the company’s devices. The Boston Scientific culture of innovation, dedication to the highest ethical approach to interventional therapies and commitment to bringing forward solutions that improve the care of patients made this the best decision for the next phase of my career.”
Jeff Mirviss, senior vice president and president, peripheral interventions, Boston Scientific, comments: “Michael’s experience as a clinician, researcher and hospital administrator will bring a unique perspective in our efforts to help solve complex healthcare challenges and support our customers in advancing the care of patients suffering from debilitating vascular diseases and conditions. We are looking forward to Michael joining our Boston Scientific team.”
Philips has received US Food and Drug Administration (FDA) approval for two Stellarex 0.035” low-dose (200mm and 150mm) drug-coated balloons for the treatment of de novo and restenotic lesions in native superficial femoral or popliteal arteries.
According to a press release, the new balloons broaden physicians’ treatment options for peripheral artery disease (PAD) patients with a high risk of restenosis and expand the Stellarex portfolio, which has a proven significant treatment effect and high safety profile. The 200mm and 150mm Stellarex 0.035” low-dose DCBs are now available in the USA and will be rolled out to other markets in due course.
“With its unique coating, Stellarex is unlike any other DCB in the industry for the treatment of PAD,” said Chris Landon, general manager, Image Guided Therapy Devices at Philips. “Stellarex is the only low-dose drug-coated balloon with a proven treatment effect at three years compared to the existing standard of care in the USA and Europe. By expanding our range of Stellarex balloons, we are adding to the treatment options that physicians can use to provide optimal care for each patient with peripheral arterial disease.”
All Philips’ Stellarex DCBs feature EnduraCoat technology, a coating consisting of a polyethylene glycol excipient with amorphous and crystalline paclitaxel particles dispersed in it. The coating provides drug transfer and effective drug residency coupled with high coating durability and minimal particulate loss, thereby enabling a low therapeutic drug dose. The Stellarex balloon is now available in 40, 60, 80, 100, 120, 150, and 200mm lengths for the treatment of lesions in the superficial femoral and popliteal arteries with vessel diameters of 4–6mm.
The results of third-party analyses of patient-level data from worldwide clinical trials of the Philips Stellarex 0.035″ low-dose DCB in lengths under 150mm were recently published in Circulation. Primary safety analysis of Philips Stellarex DCB three-year data, comprising a large published, pooled set of randomised controlled trial (RCT) data for a single paclitaxel-based device, showed no difference in mortality between patients treated with the Philips Stellarex DCB and those treated with percutaneous angioplasty, the current standard of care. The analyses represent one of industry’s most extensive and rigorous safety assessments of a paclitaxel-based device.
During a session on radiation protection technologies at the 2019 Transcatheter Cardiovascular Therapeutics (TCT) meeting (25–29 September, San Francisco, USA), Lloyd W Klein (Rush Medical College, Chicago, USA) said that Henry V led the heavily outnumbered English army to victory at the Battle of Agincourt (1415) because he “figured out how to use an old weapon in a new way”. He added that physicians needed to take a similar innovative approach to developing technologies for reducing radiation exposure.
He explained that, at the Battle of Agincourt: “The French had the best weapons, the best armour; they had the best everything. They [the English] were outnumbered seven to one. And yet, 7,000 French troops died during the battle vs. a few hundred English. How did Henry V do this?” According to Klein, the answer is not the “great motivational speech” that Shakespeare gave him (“probably the best speech ever written in the English language”) but Henry V’s innovative military tactics. “Henry figured out that the French’s armour could be used against them. So, he made them charge through a muddy field. And then to take further advantage, he figured out how to use an old weapon in a new way—the longbow [more than 80% of the English army had longbows]. The longbow made the heavy armour obsolete,” Klein said. He added that physicians were “now looking for our longbow” in terms of innovation to reduce radiation exposure.
Klein made clear that there is a need to reduce radiation exposure, outlining the damaging side effects of exposure to patients, operators and staff. He stated that the side effects could be related to the radiation itself (deterministic injuries and stochastic injuries) and/or to having to wear lead-lined aprons to protect against exposure (musculoskeletal injuries). Therefore, Klein said, it was “time for a safer environment”.
Lloiyd W Klein
While he did acknowledge that technologies for reducing radiation exposure were already available, he said that they had limitations. The Zero-Gravity radiation protection system (Biotronik), for example, was “cumbersome” and the CorPath robotic angioplasty system (Corindus Vascular Robotics) gave “less procedural control than we would like”. Concluding, Klein said: “If the same level of commitment to innovation that has been applied to other fields of interventional medicine was transferred to workplace safety, then the career of the interventionalist and their staff would undoubtedly be more comfortable”.
Jennifer A Tremmel’s (Division of Cardiovascular Medicine, Department of Medicine, Stanford University School of Medicine, Stanford, USA), who was speaking at the same radiation protection technologies session as Klein, agreed that there was a need to reduce radiation exposure and that current technologies have limitations. “The downside to many radiation reduction techniques is that they take effort. You have to push a button, move yourself or a device, or learn a new technique. Ideally, a system would reduce radiation for us and our patients automatically without interrupting our workflow.” She then proposed that ControlRad was such a system.
Tremmel explained that ControlRad worked on the principle that peripheral vision was not as important as central vision. “Peripheral vision has value but there is no need to have the same image quality, [and thus] the same amount of radiation, over the entire field of view. Instead, it would be better to limit the radiation only to the area we are focusing on (which is 5% of our visual field), but keeping the periphery visible.”
According to Tremmel, ControlRad focuses on the operator’s area of interest while maintaining the peripheral view. It attenuates radiation (and image quality) for the peripheral view by using dynamic semi-transparent filters. The system can be integrated into existing fixed and mobile C-arm units, and the operator identifies the area of interest via a tablet (ControlRad Trace) or via eye-tracking (ControlRad View). Tremmel reported, based on the results of a 2016 study, that this leads to a “75% or greater radiation reduction from whatever dose you would have been getting”.
“Radiation risk is a real concern for operators, staff, and patients. It is our responsibility to minimise that risk. This includes getting our administrators to pay for equipment that keeps everyone safe. Technology is increasingly offering us solutions—those that require minimal learning and do not affect our workflow will be easier to adopt,” she concluded.
Following Tremmel, Jean-Michel Paradis (Quebec Heart and Lung Institute, Québec, Canada) spoke about the Newton system. He explained that it was a “double suspension system” that was designed to support the weight of the leaded aprons of two operators, adding that the system could be used “with your personal radiation protection apron, with virtually no motion restriction”. Furthermore, Paradis commented, the Newton system could potentially allow you to choose “a thicker/heavier garment” to improve your radiation protection because you did not have to support the weight of your apron.
In contrast to Paradis, both James A Goldstein (Department of Cardiovascular Medicine, Beaumont Health System, Royal Oak, USA) and Amir Belson (Neoguide Systems) spoke about technologies that were designed to eliminate the need for radiation protection. Goldstein reviewed the Protego system, describing it as a shield that provided “comprehensive total body exposure protection” but one that did not “interfere with procedural performance”. In his talk about a “innovative robotic shield device” (Radiaction), Belson commented: “It is deployed to encapsulate the imaging beam. The system blocks scattered radiation at its source—the patient and the table, and it provides 360-degree, full-body protection”.
During the discussion following the talks on the new technologies, Klein called for action to better protect operators against the dangers of radiation exposure. He said: “Our [interventional] societies should come together to demand technologies that reduce radiation exposure. We need to be clear that this [the current situation] is something we are no longer OK with; change is something we should insist on. It is time for us to say that this is no longer acceptable. We do not want to have to live our lives like this.”
This article is part of a series of BIBA Briefings columns published in Interventional News. For previous columns, click here.
BIBA Briefings Insights reports give in-depth analysis of the latest market intelligence from BIBA MedTech Insights. They also review that the latest technology news and pipeline developments.
For editorial enquiries, please contact Dawn Powell: [email protected]
Gerard Goh (Melbourne, Australia) talks to BLearning IR at CIRSE 2019 (Cardiovascular and Interventional Radiological Society of Europe; 7–11 September; Barcelona, Spain) about Australian public Medicare data which has shown a “huge disparity” between the number of hysterectomies performed each year compared with the number of uterine artery embolisations procedures performed.
The data showed that of the 22,500 hysterectomies each year, of which you would expect to see four to five thousand performed for fibroids, fewer than 150 uterine artery embolisations were actually performed.
Goh says that it is “interesting” that a procedure which has been proven to be efficacious has such a poor take-up globally. A major reason for this, Goh states, comes down to a lack of “patient awareness and referrer awareness”. To tackle this issue, he believes interventional radiologists from across the world need to “come together” and work with societies to help educate women and referrers because currently “a lot of women are really missing out on uterus-sparing surgery for fibroids”.
VEITHsymposium and BLearning, the digital education division of BIBA Medical, are pleased to announce a collaboration on the creation and dissemination of digital education video content, which will be filmed at the 46th Annual VEITHsymposium in New York, USA (19–23 November 2019, New York City).
VEITHsymposium is a leading global conference covering all aspects of vascular medicine, vascular surgery and endovascular intervention. BIBA Medical’s mission is to provide education, news, and insights to connect the global community of physicians, healthcare providers, and medical manufacturing industry. BLearning is the company’s video production capability that seeks to develop and deliver high-quality digital education content.
As part of this specific co-operation project, the VEITHsymposium leadership will work closely with BLearning to create and realise the filming, production and release of digital education videos that will be filmed in a dedicated studio during this year’s conference. The videos will be released on the VEITHsymposium website and its social media as well as BIBA Medical’s flagship newspaper sites, Vascular News and Interventional News, and their associated social media channels.
“VEITHTV is a new initiative from VEITHsymposium that is designed to extend the meeting’s global digital presence and impact throughout the year, after the five days of symposium in New York. Interesting video highlights and late-breaking information will be filmed by our expert faculty during the meeting, edited professionally and released in a timely fashion to provide vital educational material to keep the vascular community clinically up-to-date. This material may also include exciting new developments from our industry partners,” said Frank J Veith, chairman of VEITHsymposium.
“It is a privilege for BLearning to collaborate with VEITHsymposium. The creation of a dedicated studio will ensure that many of the key highlights of the outstanding education presented at VEITHsymposium can be shared with the global vascular community in a new, watchable format,” said Stephen Greenhalgh, business development director, BIBA Medical.
Jos van den Berg (Lugano, Switzerland) tells Interventional Newsat CIRSE 2019 that the results of the APERTO AVF China trial provide strong evidence of the benefits of using the APERTO drug-coated balloon (DCB; Cardionovum) in haemodialysis patients who had stenosis of, mainly, de novo arteriovenous fistulas. The APERTO paclitaxel-releasing haemodialysis shunt balloon was tested against high-pressure balloons in a randomised fashion. Significantly more patients treated with APERTO were free of restenosis at six months and from clinically driven target lesion revascularisation at 12 months, compared to those treated with the high pressure balloon, says van den Berg, who also pointed to the fact that there was no cause for concern in terms of safety of the paclitaxel-coated device at one year.
There is now an “increase in the body of evidence” that supports a primary treatment strategy using DCB for arteriovenous fistula stenosis—and the landscape of treatment for vascular access stenosis “is going to change”, van den Berg, says.
A real-world safety analysis of paclitaxel-based devices in peripheral arteries, recently published in the European Heart Journal, showed no evidence for increased mortality over a period of 11 years. “In summary,” the authors remark, “our analysis found the use of drug-eluting devices to be safe for endovascular therapy of the lower limbs”.
Elaborating on the findings, they comment that “Particularly with regard to long-term mortality, neither drug-coated balloons nor drug-eluting stents was associated with increased risk compared to non-drug-eluting devices”. Furthermore, they say the analysis “exemplarily demonstrates the significance of health claims data for assessing urgent safety concerns without undue delay”.
In 9.2 million insurants of the German BARMER Health Insurance, Eva Freisinger (University Hospital Münster, Germany) and colleagues retrieved data on the application of paclitaxel-based drug-eluting stents (DES) and drug-coated balloons (DCB) from their introduction on the market in 2007 until the present.
They then indexed all patients with first endovascular revascularisation between 2007 and 2015 and followed them until 31 December 2017. Freisinger and colleagues included each subsequently applied DES, DCB, bare-metal stent, and uncoated balloon in further analysis.
Multivariable Cox regression analysis considered potential non-linear time-dependent hazard ratios of DES and DCB over 11 years. The authors identified 64,771 patients who underwent 107,112 endovascular revascularisation procedures using 23,137 drug-eluting devices (DED).
The investigators report that this analysis showed paclitaxel-based DES not to be associated with increased long-term mortality for over 11 years past application (all p>0.057). DCB was associated with decreased long-term mortality for the first year past application (HR 0.92; p<0.001), and indifferent correlation in the years thereafter (all p>0.202).
Addressing the significance of the study, the authors remark: “Our study debilitates current safety concerns resulting from previous findings,” referring to recent data which has indicated a two-fold increase in long-term mortality among patients treated with paclitaxel-based DED.
While DED represent a well-established therapy being widely used for endovascular revascularisation for peripheral vessels, the authors note, these safety concerns affected international regulatory authorities to call for several alerts for further application of DED.
“Compared to the meta-analysis by Katsanos et al that resulted from small-sized selected cohorts of the underlying RCTs,” Freisinger and colleagues continue, “our data reflect the unselected real-world patient collective to which the devices actually apply to.”
Commenting on the patient cohort, they say it is “representative compared to other large epidemiological studies in terms of age, sex, cardiovascular risk burden, and LEAD [lower extremity artery disease] severity,” referring directly to studies by Olinic et al and Fowkes et al.
While the authors stress that the present analysis covers a “large and comprehensive” database of unselected real-world patients, they admit that it is limited by the “general constraints” in the use of secondary healthcare data. Specifically, they note, real-world administrative data do not provide information on the underlying reason for DED treatment, representing a potential selection bias.
Medtronic today announced it has received breakthrough device designation from the US Food and Drug Administration (FDA) for its Valiant TAAA stent graft system for minimally invasive repair of thoracoabdominal aortic aneurysm (TAAA).
The FDA breakthrough device programme is intended to help patients receive more timely access to breakthrough technologies that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions. Under the programme, the FDA will provide Medtronic with priority review and interactive communication regarding device development and clinical trial protocols, through to commercialisation decisions.
The Valiant TAAA is currently being evaluated in the USA within five physician-sponsored investigational device exemption (PS-IDE) trials for treatment of TAAA. The system under evaluation in these trials was developed in collaboration with Patrick Kelly, a vascular surgeon and inventor specialising in complex vascular disease who leads Sanford Health Commercialization. The Valiant TAAA is intended to offer an off-the-shelf endovascular solution with a size matrix to enable broad patient applicability for one of vascular surgery’s most difficult pathologies.
“Breakthrough designation from the FDA means that we will be able to deliver this much needed treatment to patients sooner than expected. With an open surgery mortality rate of 25%, it is critical that we deliver for this unmet patient need,” said Murray Shames, professor and chief division of Vascular Surgery at the University of South Florida Morsani School of Medicine (Tampa, USA) and an investigator for the Valiant TAAA. “Physicians and industry must continue to innovate and provide hope for those with challenging disease states.”
“In addition to a high mortality rate for open surgical repair, physicians do not have good options when it comes to treatment for failed endografts,” said John Farquhar, vice president and general manager of the Aortic business, which is part of the Cardiac and Vascular Group at Medtronic. “The FDA’s breakthrough designation for Valiant TAAA and our collaboration with leading physicians is an example of our willingness to take a courageous approach and challenge the limitations of current treatment options. This is about going further, together to improve patient outcomes.”
Continuing expansion into breakthrough technologies with Valiant Navion LSA
The Valiant Navion LSA branch thoracic stent graft system received breakthrough designation from the FDA in May 2019 to allow for more timely delivery of treatment options for patients in need of left subclavian artery (LSA) coverage during thoracic endovascular aortic repair (TEVAR).
Valiant Navion LSA is based on Valiant Mona LSA investigational device and the FDA-approved Medtronic Valiant Navion stent graft system. Like Valiant Navion, the off-the-shelf, single branch device leverages a low-profile design, which may further enable patient applicability and access. The branch cuff is intended to replicate the natural anatomy of the LSA to maximise seal and patency.
“About 40% of thoracic aortic aneurysms in branch vessels involve coverage of the LSA. With no currently available off-the-shelf solutions, surgical bypass remains the standard of care for these patients,” added Farquhar. “By leveraging our low-profile, Valiant Navion platform, we hope Valiant Navion LSA will expand endovascular treatment options to those in need. It is a matter of putting patients first and delivering innovation where it matters most.”
Luminor 18 and Luminor 35 drug-coated balloons (DCB; iVascular) are now listed on the French LPPR list for de novo lesions of the femoropopliteal arteries.
Luminor is a paclitaxel-coated balloon specifically designed for dilatation of stenosis located in the iliac, femoral, iliofemoral, popliteal, infrapopliteal and renal arteries, as well as for the treatment of obstructive lesions of arteriovenous fistulas, whether original or artificial.
Eric Ducasse (CHU Bordeaux, Vascular Surgery Unit, France) has been one of the first Luminor users in France. He comments: “Luminor is the first paclitaxel DCB reimbursed in France since the Katsanos et al publication. It underlines that French authorities do trust its last generation coating technology, which is unique and has demonstrated efficacy, and, above all, safety. I am confident that French use and data analysis will confirm it shortly.”
The latest EFFPAC trial two-year outcomes with Luminor have shown positive results in terms of primary patency (90.2%) and freedom from target lesion revascularisation (97.2%) in the superficial femoral artery and popliteal artery for TASC A and B lesions. The trial also demonstrated no increased risk of death detected at two-years (one death in the DCB group versus two deaths in the percutaneous transluminal angioplasty group), evidencing a relative risk of 0.48.
The Luminor DCB has a proprietary nanotechnology coating, TransferTech. This uses paclitaxel in a microcrystalline molecular structure that is spread on the balloon, together with the excipient, by ultrasound spray pulse. The balloon surface is covered with multiple and independent nanodrop layers, providing a flexible coating that adapts to the balloon movement and ensures paclitaxel is released in the target lesion without particle loss in the blood flow.
The Society of Interventional Radiology (SIR) Women in IR section has launched the Women in IR Champion Award to recognise an individual who has consistently made a significant contribution to the advancement of women in interventional radiology (IR). The award will be presented each year at the society’s annual meeting, with the first honouree receiving the award at the 2020 Annual Scientific Meeting (28 March–2 April, Seattle, USA).
According to the SIR website, the significant contribution towards women in IR can be in “sponsorship, mentorship, teaching, promotion, advocacy, and recruitment”. The nominee must be a member of SIR for at least 10 years after completing their training, and must be an actively practicing interventional radiologist.
Calls for nominees opened on 9 September 2019, and will be conducted through to 31 October 2019. Individuals can self-nominate or be nominated by a peer. The SIR website details that all nominations must be accompanied by two letters of support (three if it is a self-nomination) outlining how the nominee has contributed to the advancement of women in IR and a copy of the nominee’s CV.
Aneesa Majid, an interventional radiologist based in Chicago, USA, and founder and president of No Limits Radiology, expands on why she believes this award is so important: “Currently, approximately 8% of interventional radiologists are women. While we have had amazing women interventional radiologists achieve great things and lead the society, we are still a minority. Advancement requires advocacy, and recognising those who promote women in IR is important in helping to grow the community of IR to be more inclusive of women interventionalists.”
Majid also tells this newspaper why this award is timely: “Gender equality in the workplace is the topic now, and the focus of gender equality in medicine is front and centre in the discussion. There is not a day that goes by on social media and #medtwitter where this topic is not discussed. It is important for us to join that conversation and highlight those who are active in working to achieve that equality within our field.”
The future of interventional radiology will be more gender inclusive, Majid enthuses. “We are already seeing female medical students and residents learning about IR early in their training, showing interest and pursuing it as their field of choice”, she says. “Data has shown that being gender inclusive results in better performance than single gender teams, provides a wider talent pool, offers different perspectives, which sparks greater creativity and innovation, enhances collaboration, improves staff retention, is a better reflection of the patient population we serve, improves recruitment and reputation, and [leads to] greater profitability. Thus, I look forward to seeing many more amazing innovations from female interventional radiologists, particularly in the areas of women health and women health services that are also consistently ignored. I also look forward to seeing strong interventional departments that break the myth that IR is not a profitable field.”
Andrew Holden (Auckland, New Zealand) provides perspective on the first results from the Disrupt PAD III observational registry that were presented at the Charing Cross International Symposium 2019. This large registry is designed to evaluate the use of Intravascular Lithotripsy (IVL; Shockwave) in the treatment of calcified arteries beyond the femoropopliteal segment, in anatomies such as below the knee and the iliac arteries.
As the clinical experience and evidence base for this technology grows, Holden, one of the earliest users in the world of IVL, shares his views on the broadening applications for IVL in larger vessel beds, such as the common femoral artery and facilitating transfemoral access for large bore devices.
BD has announced the publication of a company-initiated, independent analysis of the Lutonix 035 drug-coated balloon (DCB) femoropopliteal clinical programme in the Journal of the American College of Cardiology (JACC): Cardiovascular Interventions. These data were simultaneously presented in a late-breaking session at Transcatheter Cardiovascular Therapeutics (TCT; 24–29 September, San Francisco, USA), the annual scientific symposium of the Cardiovascular Research Foundation.
This independent analysis evaluated Lutonix 035 DCB (n=1,093) and standard percutaneous transluminal angioplasty (PTA; n=250) safety outcomes using patient-level data and propensity-matching from three Lutonix DCB randomised controlled trials: LEVANT 1, LEVANT 2, and LEVANT Japan, as well as the Continued Access cohort of the LEVANT 2 trial, and confirmed that there was no statistically significant increase in mortality with the use of LUTONIX 035 DCB.
“While the FDA and Advisory Committee of Circulatory System Devices Panel in June identified a late mortality signal after treatment with paclitaxel-coated devices using a meta-analysis of randomised controlled trials at five years from multiple companies, they recognised the benefits of these devices, including fewer reinterventions. They agreed that the magnitude of the signal should be interpreted with caution due to multiple limitations in the available data,” said Kenneth Ouriel, president and CEO, Syntactx, the clinical research firm that conducted the independent analysis, and former chairman of Surgery at the Cleveland Clinic.
He continued: “This large patient-level analysis found no statistically significant increase in mortality associated with LUTONIX DCB treatment. LUTONIX DCB remains a viable medical therapy for patients with peripheral arterial disease who demonstrate a high risk for restenosis and repeat femoropopliteal interventions.”
Further, a medical advisory committee comprised of an interventionalist and oncologist re-evaluated the cause of death in the LEVANT 1 and LEVANT 2 trials, including the LEVANT 2 Continued Access cohort. This independent review confirmed through adjudication that zero deaths were determined to be related to paclitaxel. Moreover, no clustering or pattern of death in any cardiovascular or non-cardiovascular categories was observed, which would have indicated a causal relationship between paclitaxel and death.
“The published patient-level analysis from Syntactx provides important information that health care providers can use to make an informed decision on the use of paclitaxel devices until additional long-term data are available,” said JD Meler, vice president of Medical and Clinical Affairs for BD’s Peripheral Intervention business. “Patient safety is our top priority, and BD remains committed to improving the quality of life of patients with PAD.”
Lorenzo Patrone (London, UK) shares with Blearning at CIRSE 2019 (7–11 September, Barcelona, Spain) the benefits of using the OUTBACK™ Elite Re-entry Catheter (Cordis, a Cardinal Health Company) in chronic total occlusions—in any arterial segment from the iliacs to the toes.
Patrone speaks about the use of the re-entry device used via the standard antegrade access or via a distal superficial femoral artery/below-the-knee retrograde approach to be able to re-enter in the proximal superficial or common femoral artery in patients with history of previous bypass, where the need and the difficulty in achieving an accurate re-entry are maximum.
He emphasises the importance of operator expertise and recommends for the device to be used earlier, rather than later in the treatment plan [to avoid dissection of the subintimal space], in order to achieve effective outcomes. Regarding costs, his opinion is that the cost of the device itself is nothing in compared to [savings] in “time, contrast, and radiation to the patient”.
“In my experience, to cross the lesion is the most challenging part [of the procedure],” says Patrone, “once you cross the lesion, you can angioplasty, you can stent, and the patient will have a new vessel, new vessel means new blood to the limb, and new blood to the limb means new life to the patient”.
This video is sponsored by Cordis, a Cardinal Health Company.
Marianne Brodmann presenting TOBA III data at TCT 2019
Intact Vascular has announced the positive one-year results of its Tack Optimised Balloon Angioplasty (TOBA) III clinical trial, successfully achieving both primary and secondary endpoints. Marianne Brodmann, head of the Clinical Division of Angiology, Medical University of Graz, Austria and principal investigator of the TOBA III trial, presented the data during the high impact clinical research session of the 31st Transcatheter Cardiovascular Therapeutics (TCT) meeting (25–29 September, San Francisco, USA), the annual scientific symposium of the Cardiovascular Research Foundation.
This multi-centre, single-arm, prospective study was conducted in Europe and investigated the combination of the Tack endovascular system with Medtronic’s IN.PACT Admiral drug-coated balloon as a treatment in the superficial femoral (SFA) and/or proximal popliteal (PPA) arteries. The study enrolled 201 patients, including 169 patients with arterial lesions ≤150mm in length and a subset of 32 patients with long arterial lesions (>150 and ≤250mm). All patients suffered from peripheral arterial disease (PAD) and underwent balloon angioplasty, consequently experiencing at least one dissection requiring repair.
Results from the 169 patient standard lesion cohort (≤150mm) impressively demonstrated 97.7% complete dissection resolution, 95% K-M vessel patency and 97.5% K-M freedom from clinically-driven reintervention at 12-months. This was accomplished with a 0.6% bailout stent rate. These results add to the body of clinical evidence supporting the use of the Tack system for post-PTA dissection repair and further demonstrate the long-term effectiveness of the technology, an Intact Vascular press release states.
“I am extremely pleased with the clinically compelling results of the TOBA III study,” comments Marianne Brodmann. “The Tack system provides a safe and effective solution for treating post-angioplasty dissections. I believe this new therapeutic paradigm will change the standard of care for above-the-knee interventions.”
The observational data from the long lesion subset (>150 and ≤250mm) was analysed separately. Results from these 32 patients notably demonstrated 98.8% complete dissection resolution and 89.3% K-M vessel patency, with 96.8% K-M freedom from clinically-driven reintervention at 12-months and a 0% bailout stent rate.
“The data presented at TCT further validates the use of Tack implants to improve balloon angioplasty results,” says Peter Schneider, co-founder and chief medical officer of Intact Vascular. “The data suggest that we have been implanting too much metal for far too long with traditional stents. We are thrilled to offer a minimal metal therapeutic solution that enhances patient outcomes and preserves future treatment options.”
“We would like to thank the excellent team of physicians and coordinators who contributed to the success of the TOBA III study,” states Bruce Shook, Intact Vascular’s president and CEO. “The results presented are the most impressive reported to date for balloon angioplasty in above-the-knee arterial disease. We look forward to offering this technology to more patients as we continue the rapid expansion of our commercial efforts.”
Terumo Medical have announced that it has introduced the Radial to Peripheral (R2P) MISAGO RX self-expanding peripheral stent at the 31st Transcatheter Cardiovascular Therapeutics (TCT) conference (25–29 September, San Francisco, USA). The introduction of R2P MISAGO helps physicians bring the benefits associated with a radial access approach to patients with peripheral arterial disease (PAD).
According to the US Centers for Disease Control and Prevention (CDC), PAD affects approximately 8.5 million people in the USA, and is characterised by a narrowing or blockage of arteries limiting blood flow to the lower extremities; an endovascular approach is often used for treatment.
R2P MISAGO is a device within the R2P portfolio, the first and only portfolio of longer-length radial devices specifically designed for peripheral procedures. R2P MISAGO is the longest stent platform specifically designed for above-the-knee PAD interventions via radial access, incorporating Rapid Exchange (RX) technology and innovative bare metal stent design.
The launch of R2P MISAGO is complemented by the introduction of R2P CROSSTELLA RX PTA balloon dilatation catheter, the longest 0.018″ balloon designed for use in radial to peripheral procedures. Both R2P MISAGO and R2P CROSSTELLA have a 200 cm working length, enabling physicians to perform more peripheral procedures for more patients.
“As the industry leader in radial access, Terumo is very proud of the work we have done in partnership with the medical community to drive utilisation of radial procedures,” says Chris Pearson, Executive Vice President, Commercial Operations, Terumo Interventional Systems. “The launch of these additional devices enhances our existing R2P portfolio, and underscores Terumo’s commitment to developing new, innovative technology to advance peripheral vascular care.”
“Using radial artery access is associated with quicker ambulation, improved patient comfort, and satisfaction. Terumo’s introduction of R2P MISAGO and R2P CROSSTELLA as part of the R2P portfolio provides physicians with additional options to treat PAD patients from the wrist,” comments John Coppola (NYU Langone Medical Center, New York, USA).
R2P MISAGO is currently in a limited market release within the USA, and will have full commercial availability in October 2019. R2P CROSSTELLA is currently commercially available as part of the R2P portfolio of radial length devices.
Bart Dolmatch gives an overview of the history of haemodialysis access in the USA, and balances the pros and cons of current access options. He outlines his hopes for the increasing role he believes interventional radiologists should play in the management of end-stage renal disease patients, and how innovation is helping physicians achieve better clinical results.
While the incidence of end-stage renal disease (ESRD) in the USA has reached a plateau over the past few years, prevalence continues to climb due to lower mortality rates.1 ESRD is treated with renal replacement, but it is costly and places a growing financial burden upon Medicare participants. Medicare-paid claims for ESRD, including renal replacement, represented over 7% of all Medicare payments and exceeded US$35 billion in 2015–2016.2
Renal replacement can be performed with a kidney transplantation, peritoneal dialysis, or haemodialysis. For many people, transplantation may be the best option, but due to the ongoing shortage of donor organs, fewer than 3% of people with ESRD received a pre-emptive transplant. Peritoneal dialysis, conveniently performed at home by most people, accounted for only 9.7% of all renal replacement. Haemodialysis accounted for renal replacement for nearly 90% of the ESRD population in the USA.1
Haemodialysis is simply the process of cycling a person’s blood through a filtration system, removing toxins while balancing fluids and electrolytes, and returning the blood back to the patient’s circulatory system. Efficient cycling of blood requires a way to both remove and replace blood, typically through one of three methods: a dual lumen catheter; an arteriovenous graft (AVG); or an arteriovenous fistula (AVF). An AVG is a surgically inter-posed conduit between an artery and vein that is accessed for haemodialysis. An AVF is the direct connection of an artery to vein, where the venous side of the circuit serves as the access site. Both an AVG and AVF are accessed for haemodialysis using two-needle cannulation—one for cycling blood to the dialyser, the other to return blood to the patient.
All three types of vascular access have pros and cons. Catheters are convenient but have the highest morbidity rates compared to AVGs and AVFs.3,4 AVGs had a high rate of usability, but up to 75% failed in their first year.5 Once an AVF is ready for repeated successful haemodialysis, it is often an excellent long-term vascular access solution with better durability than an AVG. However up to 60% of AVFs were not ready for use within four to five months after surgery, and many were abandoned before any attempt to salvage.6
While there are problems with all forms of haemodialysis access, the AVF remains the preferred modality and accounts for about two-thirds of haemodialysis access in the USA.5 For more than 50 years, creation of an AVF was the purview of surgeons. However, in 2018, two catheter-based systems were cleared for percutaneous AVF creation by the US Food and Drug Administration (FDA)—BD’s WavelinQ and Avenu Medical’s Ellipsys. The hope is that percutaneous AVFs, created without pre-operative delay, will have high rates of early unassisted usability and remain functional. So far, data are encouraging.6,7
AVGs and AVFs often develop stenoses that reduce dialysis efficiency and can lead to thrombosis. Percutaneous transluminal angioplasty (PTA) has been used for decades, though with varying durability. We have learned that bare metal stents do not improve durability over successful PTA.8,9,10 However, covered stents from BD such as the Flair, Fluency and Covera, as well as Gore and Associate’s Viabahn, reduce restenosis rates. These covered stents have demonstrated superior outcomes in prospective clinical trials when compared to PTA.11,12,13,14,15 In addition, BD’s Lutonix drug-coated balloon also confers improved outcomes compared to PTA.16
The past few years have seen great strides in creating and maintaining haemodialysis access. We now have new ways to achieve better results, with the hope that through ongoing innovation and comparative prospective clinical research, we can improve the lives of patients with ESRD.
Bart Dolmatch is an interventional radiologist at The Palo Alto Medical Foundation and El Camino Hospital, Palo Alto, USA.
References
2018, United States Renal Data System Annual Report, End-Stage Renal Disease, Chapter 1, https://www.usrds.org/2018/view/v2_01.aspx, accessed 8/15/2019
2018, United States Renal Data System Annual Report, End-Stage Renal Disease, Chapter 9: Healthcare Expenditures for Persons with ESRD, https://www.usrds.org/2018/view/v2_09.aspx Accessed August 15, 2019.
Charmaine E Lok and Robert Foley, Vascular Access Morbidity and Mortality: Trends of the Last Decade, CJASN 2013; 8 (7):1213–1219.
Gürbey Ocak, et al, Haemodialysis catheters increase mortality as compared to arteriovenous accesses especially in elderly patients Nephrology Dialysis Transplantation, 2011; 26(8):2,611–2,617.
2018 United States Renal Data System Annual Report, End-Stage Renal Disease, Chapter 3: Vascular Access. https://www.usrds.org/2018/view/v2_03.aspx, Accessed August 15, 2019.
Charmaine Lok et al, Endovascular Proximal Forearm Arteriovenous Fistula for Hemodialysis Access: Results of the Prospective, Multicenter Novel Endovascular Access Trial (NEAT). American Journal of Kidney Disease, 2017; 70(4):486–497
Jeffrey E. Hull, William C. Jennings, Randy I. Cooper, et al. The Pivotal Multicenter Trial of Ultrasound-Guided Percutaneous Arteriovenous Fistula Creation for Hemodialysis Access. J Vasc Interv Radiol. 2018; 29(2):149–158.
Quinn S F, Schuman E S, Demlow T A. et al. Percutaneous transluminal angioplasty versus endovascular stent placement in the treatment of venous stenoses in patients undergoing hemodialysis: intermediate results. J Vasc Interv Radiol. 1995;6(6):851–855.
Beathard G A. Gianturco self-expanding stent in the treatment of stenosis in dialysis access grafts. Kidney Int. 1993;43(4):872–877.
Hoffer E K, Sultan S, Herskowitz M M, Daniels I D, Sclafani S JA. Prospective randomized trial of a metallic intravascular stent in hemodialysis graft maintenance. J Vasc Interv Radiol. 1997;8(6):965–973.
Haskal ZJ, Trerotola S, Dolmatch B, Schuman E, et al. Stent Graft versus Balloon Angioplasty for Failing Dialysis-Access Grafts. 2010. N Engl J Med 2010;362:494-503.
Haskal ZJ, Saad TF, Hoggard JG, Cooper RI, et al. Prospective, Randomized, Concurrently-Controlled Study of a Stent Graft versus Balloon Angioplasty for Treatment of Arteriovenous Access Graft Stenosis: 2-Year Results of the RENOVA Study. J Vasc Interv Radiol. 2016 Aug;27(8):1105-1114.
Falk A, Maya ID, Yevzlin AS, and RESCUE Investigators. A Prospective, Randomized Study of an Expanded Polytetrafluoroethylene Stent Graft versus Balloon Angioplasty for In-Stent Restenosis in Arteriovenous Grafts and Fistulae: Two-Year Results of the RESCUE Study. J Vasc Interv Radiol. 2016; 27(10):1465-1476.
Vesely T, DaVanzo W, Behrend T, Dwyer A, Aruny J. Balloon angioplasty versus Viabahn stent graft for treatment of failing or thrombosed prosthetic hemodialysis grafts. J Vasc Surg. 2016 Nov;64(5):1400-1410.
Covera Vascular Covered Stent Instructions for Use. Bard Peripheral Vascular. B05872 Rev.3/05-18. https://www.accessdata.fda.gov/cdrh_docs/pdf17/P170042D.pdf Accessed August 15, 2019.
Scott O. Trerotola, Jeffrey Lawson, Prabir Roy-Chaudhury and Theodore F. Saad; for the Lutonix AV Clinical Trial Investigators. Drug Coated Balloon Angioplasty in Failing AV Fistulas: A Randomized Controlled Trial, CJASN 2018; 13(8):1215-1224.
The late mortality risk associated with paclitaxel-coated balloons and stents when used in the femoropopliteal arteries for the treatment of peripheral arterial disease (PAD) is lower than initially reported, as investigators incorporate more patient-level data into the analysis, but the signal persists nonetheless. This is the finding of a new meta-analysis presented by independent researchers from VIVA/NAMSA at the Transcatheter Cardiovascular Therapeutics (TCT) annual meeting (25–29 September, San Francisco, USA).
The latest data from the independent, patient-level analysis showed a mortality risk (HR 1.27, 95% CI 1.03–1.58) “incrementally” lower than the last update from the US Food and Drug Administration (FDA) device panel convened in June this year (HR 1.38, 95% CI 1.06–1.80), Krishna Rocha-Singh (Prairie Heart Institute, HSHS St John’s Hospital, Springfield, USA) told the TCT audience.
“This updated meta-analysis, which represents the most comprehensive analysis of available individual patient data to date, demonstrated a modest and consistent mortality signal in patients exposed to paclitaxel. However, it did not identify any explanation,” he said.
On 6 December 2018, Konstantinos Katsanos (Patras, Greece) and colleagues published a meta-analysis in the Journal of the American Heart Association (JAHA) reporting an increased association of mortality when paclitaxel devices were used in the leg to treat PAD patients. The mortality signal they found was HR 1.93. Amongst the ongoing international conversation spawned by the publication of these data were criticisms of the lack of patient-level data in the original JAHA meta-analysis. Industry stakeholders and the FDA started working to gather individual-level data.
Today, the paclitaxel device issue is “by no means a done deal” and has “taken over the majority of our work load,” Eleni Whatley, of the FDA, reportedly said at TCT. She informed the audience that any new application for a device containing paclitaxel has to apply at least five years of data and have minimal loss to follow-up.
In June this year, the FDA panel concluded that devices already on the market should remain available given their risk-benefit ratio, but agency advisors also called for a change in labelling. Whatley said at TCT that this was imminent, to be expected in the next few weeks.
No mechanism for increased mortality has been shown.
Rocha-Singh summed up: “The updated met-analyses [sic], which represents the
most comprehensive analysis of available IP [individual patient] data to date, demonstrated a modest and consistent mortality signal in patients exposed to paclitaxel, however, it did not identify an explanation. Consideration of ‘real world evidence’, although hindered by issues of reliability, lack of follow-up, selection bias and internal controls, may offer insights [into] paclitaxel device use and mortality.”
The prospective, randomised SINGA-PACLI trial sought to compare the results of drug-coated balloon (DCB) treatment to plain balloon angioplasty (POBA) for the treatment of infragenicular lesions in patients with critical limb ischaemia.
Tan Bien Soo (Singapore), principal investigator of the trial, reported 12-month results at CIRSE 2019 (Cardiovascular and Interventional Radiological Society of Europe; 7–11 September; Barcelona, Spain). He tells Interventional News that while six-month patency rates (around 42% for DCB group vs. 38% for POBA group) and limb salvage rates (75% for DCB group vs. 85% for the POBA group) were similar between patients treated in both arms of the trial, the results of amputation-free survival was significantly different in both groups. Patients in the group treated with DCB experienced significantly worse amputation-free survival (62% vs. 77% for the POBA group) leading the investigators to comment that there was “no strong evidence to recommend the routine use” of drug-coated balloons in critical limb ischaemia patients below the knee, unless there were “compelling” reasons to do so.
The six-month results of TINTIN (Treatment with the lumINor DCB and The IVolutioN self-expanding stent) trial have been revealed at the annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE 2019; 7–11 September, Barcelona, Spain) by Koen Deloose.
TINTIN is a physician-initiated trial investigating the safety and efficacy of the treatment with the Luminor DCB and iVolution self-expanding stent (both iVascular), in TASC C and D femoropopliteal lesions.
Both iVolution and Luminor present excellent outcomes in TASC A & B lesions, but it is clear, out of the literature, that neither BMS nor DCB alone are winners in long, complex lesions and on the longer run. The combination of both is the key to success in these situations.
TINTIN trial outcomes:
Primary patency of 96.5%
Freedom from TLR of 98.9%
At the end of the presentation Deloose concluded that “The Belgian TINTIN trial shows impressive 6 months results in lesions of 24 cm”.
NOTE: ONLY intended for healthcare professionals outside of the USA and France.
Zoom in on a tête-à-tete between Marianne Brodmann (Graz, Austria) and Giovanni Torsello (Munster, Germany) who talk through the latest clinical evidence that directly compares drug-eluting stents in a head-to-head fashion.
Brodmann and Torsello talk through thorny issues such as which patients qualify as “high-risk” patients who would benefit most from the use of paclitaxel-coated devices in light of the most recent US FDA guidance on the topic. They also outline the poor outcomes obtained before the era of drug-elution with bare metal technologies.
Torsello highlights the latest results from drug-eluting stent trials, particularly the IMPERIAL trial that compares the Eluvia drug-eluting stent platform (Boston Scientific) with the Zilver PTX drug-eluting stent platform (Cook Medical), emphasising the importance of polymer-mediated, low dose, sustained local drug release over time.
Both look to the near future and the upcoming EMINENT trial that will compare Eluvia with best practice US FDA approved bare metal stents, and comment on the importance of long-term data from the Muenster Eluvia registry which is testing this drug-eluting stent system in a complex patient cohort with lesions at high risk of restenosis to provide evidence of its clinical benefits in this patient population.
NOTE: ONLY intended for healthcare professionals outside of the USA.
Ulf Teichgräber (Jena, Germany) and Koen Deloose (Dendermonde, Belgium) discuss the 24-month results of the EFFPAC trial and the six-month outcomes of the TINTIN trial. Both trials used the luminor drug-coated balloon (DCB; iVascular) with TINTIN testing it in combination with the iVolution self-expanding stent (also iVascular). The latest trial results were presented at CIRSE 2019 (Cardiovascular and Interventional Radiological Society of Europe; 7–11 September; Barcelona, Spain).
Teichgräber, analysing the latest EFFPAC data, points out that luminor is a third-generation DCB with a “very innovative nanotechnology” that is designed to release paclitaxel just at the target lesion.
EFFPAC has shown “outstanding” results in terms of patency (90.2%) and freedom from TLR (97.2%) in the superficial femoral artery and popliteal artery for TASC A and B lesions, and at 24 months, no risk of increased death in the paclitaxel group, says Teichgräber.
The TINTIN trial is a physician-initiated trial evaluating the use of combined treatment with two products that have already “proven their efficacy”, says Deloose—the luminor DCB and the iVolution self-expanding stent—in complex and long lesions (mean lesion length of 24cm), such as those seen in real-world practice. At six months, TINTIN data “showed a clear and good signal” with a 96% primary patency and 98% freedom from target lesion revascularisation in patients with difficult disease, says Deloose.
LimFlow has announced that the US Food and Drug Administration (FDA) has approved its investigational device exemption (IDE) for the PROMISE II pivotal study of the LimFlow Percutaneous Deep Vein Arterialisation (pDVA) System.
PROMISE II is a multicentre, prospective, single-arm study to be conducted in the USA and Japan. Using an adaptive statistical design, the study plans to enrol 60 to 120 “no option” chronic limb-threatening ischaemia (CLTI) patients. Endpoints include amputation-free survival at six months, limb salvage and wound healing, and subjects will be followed out to three years. The “no option” patients who are candidates for the PROMISE II study are no longer eligible for conventional endovascular or surgical therapy for CLTI, as determined by an independent physician committee.
The approval to initiate the pivotal trial follows completion of six-month follow-up of the US early feasibility study—PROMISE I—that successfully enrolled 32 patients at seven centres. Interim outcomes from the first 10 patients treated in the PROMISE I study showed nine patients surviving and amputation-free at one year, with seven of these patients experiencing complete wound healing. These results were presented in May at the New Cardiovascular Horizons Conference by Steve Henao, of the New Mexico Heart Institute. The complete results of PROMISE I will be presented during the Late Breaking Trials Session at the VIVA conference in Las Vegas in November.
“For these late-stage CLTI patients, success can be defined in two ways: wound healing and amputation-free survival. This exciting new therapy has the potential to restore blood flow to the ischaemic foot, which may help patients heal their wounds and keep their feet. I am very encouraged by the early experiences in the USA, and outcomes from this pivotal trial may offer hope to the many Americans who might otherwise face major amputations,” said Daniel Clair, PROMISE II principal investigator and chair of the department of surgery at the University of South Carolina (USC) and Palmetto Health-USC Medical Group.
“Major amputations have a devastating effect on the lives of patients and their families, and each one is a personal tragedy. Chronic Limb-Threatening Ischemia is a public health crisis and far too many limb amputations are performed in the world today, costing the healthcare system many billions of dollars,” said LimFlow CEO Dan Rose. “As part of the FDA Breakthrough Devices program, LimFlow is excited to commence its US pivotal trial on the heels of the successful experience from the US feasibility study. This is a tremendous milestone that furthers our mission of empowering vascular specialists to offer new hope to their CLTI patients who may be only days away from losing a limb.”
CLTI is the most severe form of PAD and often occurs in patients suffering from coronary artery disease, diabetes, obesity, high cholesterol and high blood pressure, many of which are growing health problems. Patients with CLTI often experience profound, chronic pain and develop festering wounds or infections that lead to major limb amputation, an event closely associated with increased mortality and reduced quality of life. To relieve the symptoms of CLTI, patients today are treated primarily with angioplasty or open bypass surgery. In many late-stage patients, however, neither option is feasible due to extensive disease in the target arteries or other anatomical constraints.
The results of AVeNEW, the first level one clinical study dedicated solely to the use of a covered stent designed to treat stenosis in the arteriovenous (AV) fistula access circuit, show that the Covera vascular covered stent (Bard) demonstrates “significantly better” target lesion primary patency compared to percutaneous transluminal angioplasty (PTA) at six months, with the difference sustained in the 12-month data, and better access circuit patency was maintained at 12 months.
Lead investigator Bart Dolmatch, (The Palo Alto Medical Foundation, Mountain View, USA) recently presented this “first look” at the 12-month results of the AVeNEW study at the annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE 2019; 7–11 September, Barcelona, Spain).
Dolmatch and colleagues describe AVeNEW as a prospective, international, multicentre randomised controlled clinical trial, designed to assess the Covera vascular covered stent compared to angioplasty for the treatment of stenotic lesions in the venous outflow of upper extremity AV access circuits in patients dialysing with an autogenous fistula.
The Covera stent, which received US Food and Drug Administration (FDA) approval in July 2018, is described on the FDA website as “an expandable, flexible, metal [nitinol] tube covered with a material called expanded polytetrafluoroethylene [ePTFE].”
Dolmatch and colleagues comment that AVeNEW is “the first level-one clinical trial dedicated solely to the use of a covered stent graft designed to treat stenosis in the AV fistula access circuit,” and they conclude that the covered stent group demonstrated “significantly better” target lesion primary patency compared to the PTA group at six months, with the difference sustained at the 12-month data. Access circuit primary patency was numerically different at six months, and “statistically better” for the stent graft group at 12 months.
The investigators enrolled 280 patients with stenosis ≥50 per cent in the venous outflow of the AV access circuit, and with clinical or haemodynamic evidence of fistula dysfunction, at 20 centres across the USA, Europe, Australia, and New Zealand.
They detail that patients received either PTA alone or PTA followed by covered stent placement. The primary endpoints were six-month target lesion primary patency and 30-day safety. Secondary outcomes included target lesion primary patency at 12 months, and access circuit primary patency at six and 12 months.
The majority of patients included in the study were Caucasian (68.6%) with a mean age of 63±12.4 years, and most patients were male (61.8%). Patients included in the study had multiple risk factors for renal dysfunction, including diabetes mellitus (69.6%) and hypertension (97.1%). Lesions were restenotic in 73.2% of cases, were on average 29.3±17.2mm long (diameter stenosis: 72.5±12.5%), and 53% were in the cephalic vein arch.
The proportion of patients free from a primary safety event with the covered stent (95%) was non-inferior to PTA (96.4%) at 30 days (p=0.002, significant for non-inferiority). Target lesion primary patency was significantly better for the covered stent group (78.7%) versus the PTA group (47.9%) at six months (Kaplan-Meier analysis) and remained statistically significant at 12 months (57.5% vs. 21.2%, respectively; p<0.001). Access circuit primary patency at six months numerically favoured the covered stent (50.7%) group compared to the PTA group (43.8%) while at 12 months the difference was statistically significant (28.9% vs. 17.7%, respectively; p=0.016).
The investigators summarise that the results of the AVeNEW study have shown that the covered stent conferred more than a 30% improvement in patency at the target lesion compared to PTA at both six and 12 months. Furthermore, the covered stent group had statistically superior access circuit patency at 12 months. “Clinical follow-up is ongoing,” they comment, “and will continue out to three years”.
Orchestra BioMed, in partnership with Terumo Corporation, today announced that the company has secured breakthrough device designation by the US Food and Drug Administration (FDA) for its Virtue sirolimus-eluting balloon (SEB) in the treatment of below-the-knee (BTK) peripheral arterial disease.
According to a press release, Virtue SEB is a novel, first-in-class drug/device combination product that delivers a sustained-release sirolimus formulation directly to the artery during balloon angioplasty without the need for a coating.
“Virtue SEB’s unique design enables delivery of sustained-release sirolimus during angioplasty without the need for coating or permanent implant. This highly differentiated design makes this product the ideal candidate for Breakthrough Device Designation in BTK peripheral artery disease,” says James P Zidar, clinical professor of medicine, UNC Health Systems, physician-in-chief, Heart & Vascular Corporate.
He continues: “Currently, there is a significant unmet need in the BTK stenosis treatment landscape. The presence of underlying comorbidities renders many patients unsuitable for bypass surgery. Angioplasty with plain balloons, which has been the default endovascular therapy for years, has a low success rate. Adding a proven anti-restenotic agent like sirolimus has the potential to enhance this treatment approach and drive better patient outcomes.”
“Our team is grateful that the FDA has recognised the potential value Virtue SEB can provide patients and physicians by granting this second Breakthrough Device Designation for an important arterial therapeutic indication,” said Darren R Sherman, president, chief operating officer and co-founder of Orchestra BioMed. “This designation will be critical as we continue to work with Terumo to accelerate Virtue SEB’s global clinical and regulatory program in both coronary and peripheral indications. In BTK disease, treatment with Virtue SEB has the potential to improve long-term outcomes and reduce periprocedural complications which can extend hospital stay and increase cost of treatment.”
Artis icono angiography system (Siemens Healthineers)
Artis icono angiography system (Siemens Healthineers)
The US Food and Drug Administration (FDA) has cleared the Artis icono, a family of angiography systems from Siemens Healthineers that permit a range of minimally invasive procedures to be performed in a single interventional suite.
The Artis icono biplane system is engineered for optimal utilisation in neuroradiology and abdominal imaging, while the Artis icono floor is a floor-mounted, single-plane system for vascular, interventional cardiology, surgical, and oncology procedures. Both systems in the Artis icono family expand the reach of precision medicine.
At its core, the Artis icono platform delivers the new OPTIQ image chain, which fundamentally redesigns image processing for 2D imaging. OPTIQ increases image quality across a wide range of C-arm angles and patient weights, regulating acquisition parameters to automatically achieve optimal image contrast at patient radiation doses that conform to the As Low As Reasonably Achievable (ALARA) guiding principal for radiation safety. The platform also improves the Siemens Healthineers roadmap function, which creates subtracted angiography images for easier navigation of the patient’s vascular system during subsequent fluoroscopy, allowing dose reduction during the fluoro mode.
Additionally, the Artis icono platform significantly enhances ease of use through Case Flows, which provide personalised workflow plans to optimise imaging parameters and system positions, in addition to displaying layouts for the entire procedure. Case Flows adapt to user needs, providing flexibility when executing certain sequences. Users can therefore standardise procedures across multiple Artis icono labs for improved outcomes and more consistent documentation.
Scott McLafferty and Hammed Ninalowo performing the first PAE in Nigeria
Hammed Ninalowo (Lagos, Nigeria) and Scott McLafferty (Columbus Radiology Corporation, Cincinnati, USA) performed the first prostate artery embolization (PAE) in Nigeria on 29 August 2019.
The patient was a 77-year-old man with a long history of benign prostatic hyperplasia (BPH) with lower urinary tract symptoms (LUTS), according to Ninalowo and McLafferty, and was initially seen for a consultation in July 2019. Describing the patient’s condition prior to treatment, the interventionalists tell Interventional News that, “A few months prior, he had developed acute urinary retention, necessitating placement of a suprapubic catheter. Since that time, he had a significant worsening in his quality of life due to catheter dependence. The presence of the catheter caused him both significant physical and emotional distress, with the patient regressing into a state of depression, and refusing to have guests around his home. Due to a complex medical history including a prior coronary artery bypass surgery, prostate surgery was not an option.”
Ninalowo and McLafferty say they are “proud” to have performed the first PAE in Nigeria, and to help this patient. “At the time he was seen in clinic”, they recount, “it was clear he was desperate for a solution and prepared to leave Nigeria to find one. However, with [the] continued awareness of local physicians and the possibilities of interventional radiology, he was sent to us for consideration of minimally invasive PAE.”
PAE is a minimally invasive treatment for LUTS secondary to BPH, and is frequently used to treat men who have failed traditional medical management. Ninalowo and McLafferty explain that this is the story for a large number of older men in Nigeria, saying “many are desperate for a solution to improve their symptoms or be free of their catheter dependence”. However, they also state that local options have been limited, especially in high-risk non-surgical candidates.
“Myriad Nigerian men suffered and did not have the means to seek PAE as a therapy locally”, they comment. “This is no longer the case. By offering this in Lagos, we create the first step towards improving access to care for these men.”
Scott McLafferty and Hammed Ninalowo
Nigeria is a country with a long history of its citizens traveling internationally for medical care. Five practising interventional radiologists today serve a country with a population of 200 million people. Ninalowo is helping to lead the effort to establish greater access to interventional radiology for all Nigerians. Following his own medical training in the USA, he founded the organisation IRDOCNIGERIA, which aims to train an additional 100 interventional radiologists in his home country over the next decade. The first interventional radiology training programme in Nigeria also launches this month, with Ninalowo at its helm.
McLafferty expands on the importance of this work: “I think this model of a local physician trained in America repatriating his skills to his own people is the key to achieving a sustainable interventional radiology practice in a virgin country. His [Ninalowo’s] practice, IRDOCNIGERIA, currently offers high-level interventional radiology procedures in Lagos, Nigeria.
“In addition, Ninalowo and I are managers with RAD-AID International’s IR4Nigeria effort to establish a sustainable IR training programme in Nigeria. With this, we have established a primary collaboration with the Nigerian Society of Interventional Radiology (NiSir), and also established a primary training site at the University College Hospital in Ibadan, Nigeria. The enthusiasm of local radiologists to learn interventional radiology has been tremendous and we plan to continue to provide immediate access to simple and complex interventional radiology procedures and help build long-term sustainability.”
According to a press release, Proximo Medical has been announced as the commercial partner for Biotronik’s peripheral vascular intervention (PVI) platform in select US markets.
Proximo Medical is a fractional commercial organisation for start-up medical device technologies and established medical device companies looking to expand adoption on select products in the US market.
Biotronik’s PVI portfolio is designed for the treatment of peripheral artery disease and includes the Pulsar stent, which is the only 4-French (4F) self-expanding stent approved in the USA. Additional products include the Astron stent system, Passeo PTA balloon catheters and Fortress introducer sheaths.
“By partnering Biotronik’s solutions and innovations with Proximo, we accelerate our ability to help physicians deliver improved outcomes to patients,” states Ryan Walters, president, Biotronik. “At Biotronik, our focus is always on innovation that improves patient lives. We know millions of American’s suffer from peripheral artery disease and this partnership will help ensure this patient population has access to safe and effective treatment options.”
“I was an investigator in the trial of the Biotronik Pulsar stent,” states Craig Walker, president and medical director, Cardiovascular Institute of the South; clinical professor of Medicine, Tulane University and Louisiana State University Medical Schools; and chairman, New Cardiovascular Horizons. “I was impressed that this stent, which has a 4F delivery system, was easy to deploy accurately and had good clinical patency. I think this will be very helpful particularly in cases where standard 5F or 6F sheaths may be occlusive.”
The American Urological Association (AUA) have published guideline amendments in the September issue of The Journal of Urology, but have not changed their stance on prostate artery embolization (PAE). The AUA does not recommend PAE for the treatment of lower urinary tract symptoms/benign prostatic hyperplasia (LUTS/BPH) outside the context of a clinical trial, a recommendation attributed to the expert opinion of a panel of urologists. This news is unwelcome to the interventional radiology (IR) community, which has been advocating for the procedure’s acceptance by the wider medical world. US interventional radiologists were awaiting these guideline amendments hopeful that new recommendations would better reflect the conclusion of multiple IR societies that PAE is a safe, effective, minimally invasive treatment option in select BPH patients.
The guidelines, authored by Harris Foster (American Urological Association Education and Research, Linthicum, USA) and colleagues, cite the following as their rationale:
“High level evidence remains sparse, and the overall quality of the studies is uniformly low.
Three randomised controlled trials (n=247) with heterogeneous methods and results.
Concerns regarding radiation exposure, post-embolization syndrome, vascular access, technical feasibility, and quality control at lower volume centres.
PAE should only be performed in the context of a clinical trial, comparing to sham will account for placebo effect.”
SIR urges AUA to reconsider their “unnecessarily restrictive” recommendation, and to expand access to available treatment options for men
This has sparked a response from US interventional radiologists. In May this year, the Society of Interventional Radiology (SIR), the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Société Française de Radiologie (SFR), and the British Society of Interventional Radiology (BSIR) published a position statement in the Journal of Vascular and Interventional Radiology (JVIR) concluding that current evidence supports the use of PAE for the treatment of LUTS for the symptoms of BPH in appropriately selected patients. The AUA has not accommodated this viewpoint in their latest guidelines amendments.
Speaking in her capacity as president of the SIR, Laura Findeiss (Emory University School of Medicine, Atlanta, USA) provides this newspaper with the following statement:
“The AUA’s recent guideline amendment to explicitly not recommend the use of PAE for the treatment of BPH outside of the context of a clinical trial fails to acknowledge the medical evidence supporting the safety and efficacy of this minimally invasive treatment option. It also fails to recognise the US Food and Drug Administration (FDA) approval of embolization devices for this use.
“SIR’s 2019 multi-society position statement on the application of PAE cites multiple randomised controlled trials and comparative studies of PAE versus the gold standard urologic treatment of lower urinary tract symptoms (LUTS) caused by BPH—TURP, or transurethral resection of the prostate. These studies show that symptomatic improvement following PAE approaches are seen after TURP, while maintaining a superior safety profile. The multisociety statement’s authors cite dozens of other prospective and retrospective cohort studies and meta-analyses that also support the safety and efficacy of PAE as a treatment option for LUTS caused by BPH.
“Due to the strong nature of the evidence supporting PAE, the societies endorsed PAE as ‘a definitive treatment option for multiple underserved patient groups, who may not have satisfactory urologic treatment options’. These patient groups include older patients with multiple medical conditions, patients with very large prostates, patients with bleeding from the prostate, patients with long-term bladder catheters, patients who cannot stop anticoagulation therapies and patients who desire to preserve sexual function.
“Furthermore, the National Health Service (NHS) in the United Kingdom has also acknowledged the strength of the evidence and supports the use of PAE to treat BPH symptoms in appropriately selected patients.
“AUA, however, has ignored the peer-reviewed data supporting PAE as appropriate for the sizeable population of men who are poor candidates for surgery and those who seek a nonsurgical, prostate-sparing option to treat their BPH symptoms. While AUA reasonably calls for increasing the level of evidence for the standard patient, the abundance of positive data moves PAE significantly beyond experimental. What is yet to be determined is where this therapy fits in the treatment algorithm. It is our hope that the urology community will partner with IR on behalf of patients in completing such recommended studies. Despite the AUA position, PAE is supportable as an evidence-based treatment modality that will remain available to men with LUTS secondary to BPH who seek this therapy.
“We urge the AUA to reconsider this recommendation, which is unnecessarily restrictive and is not founded in evidence. The SIR and the IR community stand ready to partner with urologists to ensure provision of the treatment that is most appropriate for each patient based on his clinical situation, risk tolerance and priorities.”
While AUA calls for more Level 1 evidence, some interventional radiologists claim this is “an impossibility”
In April this year, an SIR Foundation-sponsored research consensus panel for PAE was convened with urologists from the AUA with the aim of positively establishing the procedure in the urology society’s guidelines. The meeting was chaired by Clifford Davis (University of South Florida, Tampa, USA) and Jafar Golzarian (University of Minnesota, Minneapolis, USA). Davis informs Interventional News that since their conversation in the spring, where the AUA made it clear that it wanted additional Level 1 evidence, nothing has changed. He is therefore “unsurprised” by the consistent recommendation of the AUA to not recommend PAE outside of the context of clinical trials, and is planning funding applications for a randomised controlled trial aimed at producing Level 1 data.
There are multiple barriers to an RCT involving PAE, however. Firstly, the research consensus panellists need to decide on a study design: PAE versus a sham, or PAE versus surgery. There are concerns with conducting a trial of PAE against a sham due to crossover issues. Current guidelines from the AUA are based on RCTs with at least 12 months of data, and many had up to five years of follow-up. Patients randomised to a sham procedure or to PAE may move across to the opposite cohort before the 24-month mark, and could therefore cofound the data, but this would be still be considered as low Level 1 evidence.
Furthermore, as RCTs are so expensive, Davis explains that “industry or our national associations [in the USA] cannot afford to fund them”. Instead, interventional radiologists are looking to the National Institutes of Health (NIH) for funding. Four years ago, following an earlier SIR-sponsored research consensus panel meeting, a decision was made to apply for NIH funding for a PAE versus sham study, but this was rejected. With this precedent in mind, Davis favours “building a large, multicentre RCT comparing PAE to a surgical procedure”. A follow-up meeting to the April research consensus panel is to take place later this year to decide on which surgical procedure this may be.
“This sounds very simple”, Davis says, “but it is complicated because the patients that do best with PAE may have comorbidities for surgery. We feel that the patients who do best with PAE have bigger prostates in general, over 80g, which is not the typical patient seeking surgery. We have to compare PAE to a surgical technique that is generally accepted for a similar population. In my opinion, I think we should do an RCT [on either PAE] versus simple prostatectomy, or versus Holmium laser.” This latter option is a transurethral procedure that enucleates the prostate through the urethra, and is usually performed on men with larger prostates.
“I also think”, Davis elaborates, “an RCT trial with PAE should focus on patient satisfaction, including symptoms, quality of life, pain, and morbidity, and should not solely focus on flow rates and post-void residual (PVR) urine volumes, which are considered to be quantitative measures of surgical success. If PAE is found to be durable but less efficacious (regarding flow rates and PVR) but with fewer complications, lowers costs and reduced hospital time compared to surgical options, then I would hope the AUA would reconsider it in its guidelines for certain populations.
“In all other RCTs of surgery versus a control group, there was noted a significant drop in International Prostate Symptom Score (IPSS) even without therapy. This is a major argument of the urology community against our current data with small samples sizes and lack of long term follow-up.” In terms of data regarding the safety of radiation dose during PAE, Davis says that he and his team are currently working on publishing data from their centre in response to this concern raised by the PAE Research Consensus Panel.
Commenting on the status of the development of an RCT involving PAE, Ari Isaacson (Department of Radiology, University of North Carolina, Chapel Hill, USA), a co-author of the multisociety consensus document published in May, says: “The initial design and protocol and attempt to get funding [from the NIH] is underway, but it is a slow process. In the meantime,” he explains, “I think that a lot of urologists are going to feel handcuffed, because they do not feel that they can go against their society’s guidelines, and therefore there are going to be a lot of patients who either are not told about PAE or who are going to be dissuaded from pursuing it due to these guidelines.”
Even with funding, an RCT may not be feasible due to patient-driven issues with enrolment. Riad Salem (Northwestern University, Chicago, USA), another co-author of the multisociety position statement and an outspoken advocate of PAE, explains to this newspaper why this is the case: “An RCT has been tried, and it has been rejected, not by the medical community, but by the patients that would enroll. The BEST trial, while initiated as an RCT, was subsequently revised to a prospective comparison to TURP, because patients are not willing to be randomised to TURP. Patients are looking for minimally invasive treatments—so an RCT randomising TURP versus PAE is effectively an impossibility. It is not feasible and not constructive to wait for this clinical trial that will never happen.”
Nabeel Hamoui, one of three physicians dual-trained in urology and interventional radiology in the USA (Brooksville, USA) agrees with Salem. Hamoui expands, “I have seen this in my own experience at Northwestern. If you sit a patient down and say ‘we can do this therapy called PAE, which has fewer side effects, where you most likely do not need a catheter for more than a day, if that, and your recovery time is essentially zero, and if it fails, you can always have the other treatment option’, it is going to be very difficult to enroll enough patients into the TURP or surgery arm of an RCT. How do you accumulate Level 1 data if the patient becomes the rate-limiting factor?”
However, Isaacson tells Interventional News that the AUA was unmoved by discussions with interventional radiologists concerning past attempts to get US RCT data on PAE. “We tried to suggest alternatives as far as what types of data we could get”, he explains, “but despite our, I think solid, arguments, the reply was that unless there is RCT data, the AUA will not consider PAE as part of their guidelines. I think this methodology is flawed—their unwillingness to look at studies of other types excludes most of the evidence available that shows PAE is safe, so I think their evaluation of the procedure is limited, and they cannot gain a full, accurate picture of the safety and effectiveness of PAE. In my view, this is narrow-minded.” He adds that he is “disappointed” by the lack of change to the AUA guidelines for the surgical management of BPH.
This difficulty with accumulating Level 1 data on PAE, and the insistence of the AUA that interventional radiologists provide evidence from a US RCT investigating the procedure, has led to a “stalemate”, in Salem’s words.
Multidisciplinary cooperation called for to break the stalemate
As the US healthcare system operates on a fee-for-service model, one criticism levelled against either side in a dispute about procedural choice is that, instead of fighting for the best patient outcomes, individuals are fighting to protect their pay checks. Hamoui explains, “This is the reality of the US healthcare system. Unlike the NHS [in the UK], our system is based on the intensivity of care, not outcomes per se. As a urologist, if my practice is largely BPH-based, and I get paid to do surgery and treat them, then I am not going to want to give that up because that will affect my bottom-line. The opposite is also true: if an interventional radiologist aggressively markets PAE as the ultimate procedure, and recommend it over TURP and prostatectomy in a vast majority of cases, then they are doing so because they want money.”
However, Timothy McClure (Department of Urology, Weill Cornell Medicine, Lefrak Center for Robotic Surgery, New York, USA), a second dual-trained urologist/interventional radiologist in the USA and another co-author of the multisociety consensus position statement, says that urologists are acting solely on behalf of the patient: “I think the AUA is just being overly cautious, in part because of a lack of understanding of PAE. PAE is technically challenging, and they do not want problems arising in their patients. The guidelines are established to protect patients, so the bottom line is that they are trying to protect patients from having a procedure done that either will not make a difference or will potentially harm people. In fact, most urologists I have spoken with think PAE is a good option for certain patient populations. I think their concerns stem from a lack of understanding of what PAE is and what interventional radiologists can do. They view this as a technically challenging procedure that requires a certain level of skill which may not be applicable to the entire IR community. PAE is a complex case but skilled interventional radiologists do complex cases on a daily basis. Their concerns over radiation, complications, and side effects suggests a lack of understanding of PAE. These concerns could have been addressed by having an interventional radiologist participate with the guidelines. It is unfortunate that the AUA did not include a representative from IR.”
Davis likewise sympathises with the AUA guidelines committee, saying: “Some have negative feelings against the AUA; I feel differently. They hold their standards for their recommendations based on Level 1 data. They have held every other surgical procedure to that same level. It is just more difficult to compare a procedure across specialties. There is distrust in the USA, because in an RCT design by definition one specialty will lose patients to the other, which could introduce subspecialty bias during patient selection into the trial.”
The AUA guidelines are not all based on Level 1 evidence, though. For example, they state that “Water vapour thermal therapy may be offered to eligible patients who desire preservation of erectile and ejaculatory function”. This is a conditional recommendation, based on Grade C evidence. Grade C means “Low quality evidence: observational studies that provide conflicting information or design problems (such as very small sample size).” However, Davis notes that, although the evidence is marked as Grace C for this recommendation, it is based on an RCT of a sham versus therapy with three months crossover, and that this trial now has follow-up to two years.
“PAE is not alone in having heterogeneous outcomes”, Salem says. “If you look at a lot of data in urology, that too is heterogeneous. Heterogeneity is unfortunately a reality in medicine. Per the AUA guidelines, urologists should only offer robotic prostatectomy if they possess the necessary skillset. Why could that recommendation also not be made for PAE?”
Hamoui points to the urology procedure transurethral nuclear ablation, TUNA, highlighting its obsolescence. “We ourselves have done procedures that are now in the dustbin of urology”, he comments. “Many of those procedures that people thought were cure-all, and that were advocated for by some of the more prominent names in urology and pushed by industry, were largely financially driven, had poor evidence, and in five to seven years completely failed. The nuclear ablation machine in the practice where I work is now collecting dust in the corner. We no longer use it due to bad outcomes, but when it was recommended, I do not think that was based on Level 1 evidence.”
Salem urges urologists to understand that PAE is not in competition with TURP or prostatectomy. “All interventional radiologists are saying”, he says, “is that PAE should be part of the discussion, and one of the treatment options. Nobody is saying that anything should be replaced. Let the patient participate in the decision-making process. By urologist’s own admission, many of their treatments do not really work in glands over 80g. Most of their trials exclude glands larger than that volume. Glands this size or larger are the ideal candidate for PAE. So we are filling a niche, a treatment gap, that exists. To me, it is short-sighted to acknowledge there is a difficulty in treating larger glands, exclude them from urology studies, and then dismiss PAE.”
That interventional radiologists wish PAE to exist within the current treatment algorithm as one option for patients is something many are eager to highlight. “The key thing that I want to get across is that PAE provides a great addition to the BPH treatment algorithm”, Isaacson articulates. It does not replace the current surgical therapies, but it does provide a nice alternative to certain patients: those with very large prostates, those on anticoagulation medication, or patients with surgical comorbidities.”
“PAE is radically different from any of the urologic treatment modalities”, Hamoui says. However, he explains that this can be a hindrance as well as a positive. “In vascular surgery and IR, there is a huge overlap, so if vascular surgeons were to come up with new guidelines, they would have a lot of legitimacy because they understand IR procedures. For me, having the dual perspective [of urology and IR], I can understand that the treatment options sit alongside each other. I do not think that urologists fully understand the benefits of the procedure.”
Hamoui believes urologist education about PAE is critical. He, alongside McClure, advocates for the involvement of interventional radiologists on the AUA guidelines committee when discussing treatment options for BPH. Speaking at urology conferences is another method used by interventional radiologists to reach out across specialty borders. Salem gave a talk at a recent meeting of the Chicago Urologic Society, which reportedly helped diminish their scepticism of PAE, and aided the attending urologists’ understanding of which patients would and would not benefit from the procedure.
Publishing in urology specific journals would also be an effective communication tool for interventional radiologists to communicate to urologists, suggests Isaacson. However, he reports that this is challenging: “We have attempted to [publish in a urology journal] several times; it is very difficult to get a PAE paper in a urology journal”. Salem, who is one of few US interventional radiologists that has published a PAE paper in a urology journal, supports this assertion, commenting, “In my 20 years of publishing over 330 papers, getting published in a urology journal was the most difficult, challenging, controversial process I have ever been through. The captious reviews were rude, insulting, and, worst of all, replete with emotional bias. We tried several times, and finally got accepted into the fourth urology journal. This was a prospective, phase two, FDA-approved study, so it met all the high level criteria, but it was still dismissed by many urology journals.”
As well as operating on the community level, many interventional radiologists have also expressed the need to start locally. “Where I work”, McClure says, “we have great collaboration with the BPH experts, and we have a good, collaborative, multidisciplinary approach to [treating] men with LUTS. Not every patient is a good candidate for PAE, and not every patient is a good candidate for TURP, so ultimately patients benefit when you have this cross-over between disciplines.”
McClure believes that urologists need to understand that interventional radiologists are clinicians and not just technicians, and that for this there needs to be a “friendly, collegial” relationship between these two specialist groups. Hamoui, who mainly works as a urologist, thinks this is easier for him due to his dual training: “I am able to appreciate what interventional radiologists bring to the table”, he says, “so I can foster that by being friendly and receptive from the get-go, rather than being hostile and looking at them as competition. I think it is unfortunate to have PAE under such hostile attack. My own father, himself also a urologist, declined a TURP and opted for PAE, [performed] by Dr Salem, and was happy with the results.”
Salem is unequivocal in how he believes the debate should move forward: “The only way to break this stalemate is to engage individuals from both sides that can take a reasonable, tempered, non-emotional approach to this therapy. Get patients and get neutral physicians involved. Create a guideline that is tempered, recognises the limitations of the data we have, and incorporates PAE as one of the many treatment options for BPH. Until the loudest, most cynical voices are excluded from the discussion, this sensationalised and vitriolic debate will never end.”
Merit Medical has announced the commercial launch of Torpedo, a proprietary gelatin foam indicated for use in the embolization of hypervascular tumours. The Torpedo provides physicians a pre-shaped gelatin foam loaded into a cartridge with an optional blunt stylet, removing the need for manual foam shaping and providing fast and easy attachment to the catheter for delivery, a press release describes.
The Merit Torpedo is easy to prepare and use, requiring only hydration with a 50:50 saline-to-contrast mixture. The product is available in two diameters (2.5mm and 5mm) and two lengths (10mm and 20mm), and is designed for use with a catheter with an inner diameter large enough to allow delivery of the Torpedo to the target vasculature via syringe injection. The gelatin foam in the Torpedo is biocompatible, hydrophilic, and resorbable.
“In the operating room, time and consistency are crucial,” comments Fred Lampropoulos, chair and CEO of Merit Medical. “The Torpedo device, which includes embolizing gelatin compressed into a cylindrical shape and pre-loaded into a cartridge, will save physicians valuable time and improve material delivery with precision and predictability by eliminating manual cutting and shaping. The Torpedo’s launch exemplifies Merit’s commitment to ongoing innovation in the field of embolotherapy, and we look forward to bringing physicians even more ground-breaking technologies soon.”
The Torpedo’s commercial launch follows the recent 510(k) clearance of Merit’s EmboCube. The EmboCube offers uniformly cut cubes of gelatin foam preloaded into a syringe, specifically designed to save time and avoid inconsistent particle sizes associated with manual preparation of gelatin foam sheets. Torpedo and EmboCube, the newest additions to Merit’s suite of microcatheters and embolic products, together address an important market need: reducing surgical time without compromising quality of care.
Theresa Caridi is an interventional radiology advocate, and believes passionately in spreading awareness of minimally invasive, image-guided procedures to both potential patients and referrers. In July 2019, Caridi appeared on ABC 7 News WJLA, an ABC affiliate covering national and local news in Washington, DC, USA, where she talked about uterine fibroid embolization for Fibroid Awareness Month. Here, she describes why it is important for interventional radiologists to market themselves, and how individuals, as well as organisations like the Society of Interventional Radiology (SIR), can best spread their message about what interventional radiology has to offer. outreach
Understanding interventional radiology (IR) as a specialty and descriptor has been a topic of much discussion over the last two decades, if not for even longer.1–5 The name itself has been questioned for its reductive nature, in that the term “interventional radiology” fails to explain the complexity and value of what we do.1 We interventional radiologists cannot always describe the type of doctor we are, so it is easy to see how our patients and referrers have a gap in understanding in what IR is and how we can help. It has even been speculated that IR cannot be easily understood because both the specialty and term are in the forefront of true interdisciplinary medicine—specifically the blending of image, body, and physician.1 Public outreach in the form of speaking/lectures, radio, media, or print marketing may help to provide clarity to both patients and referring physicians on treatment options provided by IR.
Additional factors play an important role in the lack of awareness of IR. As interventional radiologists, we may become involved in a patient’s treatment plan later than a primary specialty. Once the traditional specialties have offered what they can and failed, or are ruled out as an option due to a patient’s advanced disease, a referrer may think to involve an interventional radiologist, or a patient may ask for other options. Due to the diverse nature of our specialty, we lack the longstanding relationship that begins early in a patient’s life, such as that seen with a primary care physician or obstetrician/gynaecologist. Furthermore, interventional radiologists have knowledge of and treatments for the entire body, and are sometimes lost in the treatment algorithm because we are not the first specialty that comes to mind for a specific organ system. Lastly, there are many different types of IR practices, and the patient or referring physician may only be familiar with one—and this practice model may not be the one they are looking for.
A good marketing tool is one that derives traction from both patients and colleagues. One of the most effective ways that I have found to reach patients and referrers is through educational videos that demonstrate a physician’s knowledge, but perhaps more importantly also their character and disposition. When a patient comes in for consultation after having watched one of my educational videos, I get a sense that it has accelerated their comfort level and also their ability to speak about sensitive issues—this tends to be pretty valuable in a women’s health focused practice where a woman has spent her lifetime building a relationship with her gynaecologist, but has never met her interventional radiologist. This is one of the many challenges that we face.
Podcasts, particularly with video, can have a similar beneficial effect. Any type of video allows viewers to see the physician’s human side and allows for nuances that cannot be demonstrated in a social media snippet. It also seems a bit more credible than the average social media post. This is not to diminish the effect of social media, which has been shown to improve the transparency and accessibility of medicine.6Social media can be very useful in promoting speaking engagements, radio, traditional media, or print marketing. But social medial must be used appropriately. Information that could identify a patient must be removed, including age and specifics about disease. Further, one must be careful not to give medical advice outside of suggesting a person get evaluated by a physician.7
I think most would agree that promoting IR in this manner is necessary, but it is time consuming. It takes institutional infrastructure and often an eager physician to get follow through. Fortunately, the Society of Interventional Radiology (SIR) is launching a national awareness and education campaign this fall—the Vision to Heal, Together—which takes a multipronged approach, with aspects that promote IR to patients and elements that market the discipline to referrers. Stay tuned and, in the meantime, do not be afraid to ask for help from your institution’s marketing team or to learn from an IR colleague who already has a successful marketing plan in place.
Theresa Caridi is an interventional radiologist at MedStar Georgetown University Hospital, Washington, DC, USA.
References:
Iwai YA, Erinjeri JP, What’s in a Name: Is “Interventional Radiology” too Reductive? Journal of Vascular and Interventional Radiology (JVIR), JID—9203369.
Becker G.J: Interventional radiology 2000 and beyond: back from the brink. JVIR 1999; 10: pp.681–687.
Baerlocher MO, Asch MR, Puri G, Vellahottam A, Myers A, and Andrews A: Awareness of interventional radiology among patients referred to the interventional radiology department: A survey of patients in a large Canadian community hospital. JVIR 2007; 18: pp.633–637.
Baum RA, and Baum SB: Interventional radiology: A half century of innovation. Radiology 2014; 273: pp.S75–S91.
Baerlocher MO, and Asch MR: The future interventional radiologist: Clinician or hired gun? JVIR 2004; 15: pp.1,385–1,390.
Pershad Y, Hangge PT, Albadawi H, Oklu RA, Social Medicine: Twitter in Healthcare. LID—E121 pii [LID—10.3390/jcm7060121 doi]. Journal of clinical medicine JID—101606588 PMC—PMC6025547 OTO—NOTNLM.
Ahmed O, Jilani S, Ginsburg M, Hadied O, Tasse J, Loanzon R, et al. You Are What You Tweet: Navigating Legal Issues in Social Media for Interventional Radiologists. JVIR JID—9203369.
Two-year results of EffPac—a randomised controlled trial to assess the safety and efficacy of a novel drug-coated balloon (DCB) with a nanotechnology coating—have been announced. The investigators, Ulf Teichgräber (University Hospital Jena, Germany) and colleagues, report that use of the DCB in question, iVascular’s Luminor, resulted in a significantly lower incidence of binary restenosis compared to plain old balloon angioplasty (POBA).
The new data, presented for the first time at the Annual Scientific Meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE 2019; 7–11 September, Barcelona, Spain), also showed a significant clinical and haemodynamic improvement from baseline, similar to the level of improvement achieved with POBA, but with considerably fewer repeat revascularisations. The investigators found no difference to POBA regarding safety.
The EffPac (Effectiveness of paclitaxel-coated Luminor balloon catheter versus uncoated balloon catheter in the arteria femoralis superficialis) trial was designed to assess the safety and efficacy of the Luminor paclitaxel drug-eluting balloon in inhibiting restenosis and in ensuring long-term patency. The investigators compared the DCB catheter to non-coated POBA in stenotic or occlusive lesions of the femoropopoliteal artery.
Between September 2015 and December 2016, the investigators enrolled 171 subjects across 11 German study centres. Eighty-five of these patients were randomised to DCB angioplasty, with the remaining 86 being assigned to the POBA group. They note that before the 24-month mark, analysis was discontinued for 25 patients in the DCB group and 30 patients in the POBA cohort.
The primary endpoint of the study was defined as late lumen loss at six months. The secondary endpoints at six, 12, and 24 months included primary patency, target lesion (TLR) and vessel (TVR) revascularisation, quality of life—assessed by the EQ-5D—change of Rutherford-Becker classification (RBC), ankle-brachial index (ABI), and major and minor amputation rates, among others.
The authors comment that 12 months in to the study, the investigational DCB catheter proved “highly effective and safe in inhibiting restenosis,” and demonstrated a walking improvement in change of RBC compared to POBA.
Twelve-month results of the safety and efficacy of the Luminor device had been released prior to the CIRSE 2019 presentation. The authors detail that at six months, the late lumen loss was on average 0.92mm lower in the DCB group than in the POBA group (95% confidence interval [CI]: -1.36mm; -0.49mm, p<0.001). Significantly more patients showed a walking improvement after DCB treatment at six months (p=0.021).
Looking now at the 24-month results, Teichgräber and colleagues reveal that primary patency (the rate of freedom from restenosis) was 90.2% (80.4–95.2) in the DCB arm, compared to 94.7% (86.4–98) at 12 months. The corresponding figures for the POBA cohort were 62.7% (50–73) and 71.3% (59.4–80.3).
Freedom from TLR in the DCB group was 97.2% (89.1–99.3) at 24 months, compared to 98.7% (91.1–99.8) at 12 months. In the POBA group, the figures were 78% (66.5–86) and 81.6% (71–88.7), respectively.
The investigators detail that in both groups patients were of similar age. While the DCB cohort was 68±7.5 years old, on average, the POBA group was 68.1±8.8 (p=0.979). There were slightly fewer male patients in the DCB group (60%) than in the POBA group (69.8%; p=0.239), and also slightly fewer diabetic patients in the DCB group (36.5%), compared to 40.4% in the POBA group (p=0.681). There were fewer current smokers in the POBA group than among DCB patients (40.5% vs. 43%; p=0.856). There were just over double the number of patients with critical limb ischaemia in the DCB group (3.6%) than there were in the POBA group (1.2%; p=0.929).
Why were you initially drawn to interventional radiology?
I was just about to finish my undergraduate studies at the Patras School of Medicine in 2001 when I was exposed to a peripheral Angiojet thrombectomy case that was the first one to be performed in Europe, by professor Dimitris Siablis. I still remember my fascination with the specific medical device fragmenting and aspirating the thrombus through remote pinhole access in the groin—being a medical student at the time, the sheer potential of catheter-based technologies was mind boggling to say the least. Over the next couple of years, I slowly became addicted to the field of interventional radiology (IR) and image-guided therapies in general through attending national and international symposia (including CIRSE [the annual meeting of the Cardiovascular and Interventional Radiology Society of Europe]) that confirmed in my eyes the transformational and cutting-edge character of IR.
Today, what is it you enjoy most about interventional radiology?
Nowadays, I most enjoy combining general clinical skills with image interpretation and image guidance to deliver highly accurate therapies with the use of sophisticated catheters and dedicated miniaturised medical instruments. Transcatheter atherectomy for plaque excision/removal, the use of drug-coated balloons and stents for the inhibition of vascular restenosis, utilising radioactive beads for targeted internal organ radiation therapy, balloon kyphoplasty and new-generation vertebral augmentation techniques are some of my favourite procedures—all of which demonstrate the unique, minimally invasive, and highly effective nature of IR treatments.
Have you had important mentors throughout your career? What have they taught you?
Professor Dimitris Siablis has been my IR teacher and mentor from the very beginning. He had the courage to believe in me whilst I was still an undergraduate student, invested his time in teaching me most catheter and guidewire skills, and had the kindness to mentor me through my early academic endeavours. He has actually been more of a coach and mentor then a professor of medicine. His ‘inheritor’ and my current director, professor Dimitris Karnabatidis, has continued the tradition by delivering unlimited, unselfish and considerate education and guidance not only to myself, but to a whole team of more than a handful aspiring junior IR fellows. Finally, Professor Andreas (Andy) Adam, who was my director for nearly five years at St Thomas’ Hospital in London, UK, has been a unique role model by exhibiting exemplary leadership and sharing unparalleled insights into the future of the IR profession.
Having worked in both Greece and the UK, what are the similarities and differences between these two healthcare systems for interventional radiologists?
I have been very fortunate to work in two completely different healthcare systems both as a trainee/fellow and as a consultant/professor. Greece has been the stepping stone in my early training days in IR and the UK has been the landing site for my junior consultant job. I was lucky to enjoy the benefits of the more liberal, more forgiving Greek healthcare system early on followed by the more mature and conservative UK National Health Service later as I was transitioning to a consultant level job with different priorities and responsibilities. I think that in a combined way they both contributed to my education by amalgamating current standards of clinical practice, academic research and medical ethics.
Late last year, you published a paper in the Journal of the American Heart Association (JAHA) that reported an increased mortality with paclitaxel devices in the femoropopliteal arteries. How do you see these findings changing practice in the future?
By employing good research and statistical practice, we showed that there is increased risk of all-cause patient death with the use of paclitaxel-coated balloons and stents in the femoropopliteal artery in the lower limbs for treatment of intermittent claudication. Interestingly, since our contentious publication in JAHA, two companies have produced errata of mortality counts in industry-sponsored studies. Meanwhile, new evidence has also come to light, mostly in the form of so-called individual patient data (IPD). Both the IPD analysis performed by the US Food and Drug Administration (FDA) and the one performed by the non-profit VIVA consortium have confirmed a significant mortality risk with the use of paclitaxel (when analysing the data from the pivotal randomised controlled clinical trials). I personally maintain the view that the future of endovascular peripheral arterial disease (PAD) treatments is going to be drug-coated or drug-eluting, but in a different way. As I have stated before, endovascular treatment is not going back to the Stone Age of plain balloons and metal any time soon. I personally think that had there been an alternative means (other than paclitaxel) to treat restenosis, we would not have had the kind of intense reaction we experienced.
How has your life changed as a result of publishing research that is not positive, and how have your coped with the reaction from the medical community to the JAHA paper specifically?
Our findings have initially been received with anger and denial—often regrettably so by our own peers. However, we are scientists and we need to read the numbers, apply good statistical practice and acknowledge and act on the results regardless of personal, commercial, emotional or other conflicts of interest. The fact that paclitaxel is the only difference in the treatment between active and control arms across all randomised controlled studies makes it very likely that paclitaxel is also the cause of the problem—in a direct or indirect way. This is not to say that we definitively know that paclitaxel causes the problem. Ultimately, we have the responsibility to report both positive and negative findings to be able to advance science for the sake of patient safety and public health. To quote Sir Bradford Hill in his 1965’s presidential address: “All scientific work is incomplete—whether it be observational or experimental. All scientific work is liable to be upset or modified by advancing knowledge. That does not confer upon us a freedom to ignore the knowledge we already have, or to postpone the action that it appears to demand at a given time.” Being in the spotlight should not disrupt or affect in any way solid, credible scientific research.
How do you feel the regulatory bodies across the world have responded to the mortality signal reported in your publication?
I think that regulatory bodies across the world (the FDA, the Medicines and Healthcare products Regulatory Agency [MHRA], etc.) have responded swiftly, responsibly and above all professionally in validating our findings and interacting with the industry to guide next steps. On their mandate, industry stakeholders have quickly collected and delivered a wealth of new data in order to better understand this alarming situation. Unfortunately, however, in my personal opinion it is a real shame that the average researcher or scientist is not allowed access to all that individual patient data for more in-depth analyses and explorations of alternative hypotheses.
You hosted the first ever EndoVascular Access (EVA) meeting this year with Panagiotis Kitrou and Dimitrios Karnabatidis. What are your ambitions for this meeting, and how do you hope to see this field develop?
Our aim has been to create a meeting fully dedicated to the emerging role of endovascular management of dialysis access. EVA encompasses topics from access creation (surgical or endovascular) to percutaneous maintenance and declotting by treatment of stenoses and thromboses. EVA will strive to disseminate the highest quality of relevant medical research and increase awareness among healthcare professionals on the important service they can provide to their dialysis patients by increase access longevity and improving quality of life. This is extremely important as we strongly believe that the future of dialysis access is endovascular. We envision that EVA will soon become the go-to meeting of reference in the field of endovascular access interventions.
In your opinion, what are the most exciting new developments in interventional radiology that we can expect in the next five to 10 years?
I am currently predicting/dreaming of augmented reality in the IR suite for improved perception and manual skills, routine use of perfusion monitors for diagnosis and aftercare of critical limb ischaemia, multi-drug-coated balloons for angioplasty and multichemo-laden microparticles for cancer embolization, integration of optics and photonics for the design of next-generation needles and catheters, and most likely the gradual emergence of completely needleless procedures, for example high-intensity focused ultrasound ablation of a tumour or magnetically guided microparticles to concentrate into particular tissue sites or intravascular micro-robots harnessing energy from the host to propel themselves and clear the arteries and/or deliver medications on demand.
Konstantinos Katsanos
What are your hobbies and interests outside of medicine?
My hobbies outside of medicine are: movies, computers and tech, occasionally running and cycling. Personal interests beyond academia include European and global geopolitics, space exploration and an ongoing fascination with numbers and maths.
Philips and B Braun have announced the launch of Onvision, a breakthrough ultrasound guidance solution for real-time needle tip tracking in regional anaesthesia. Available on the latest version of the B Braun and Philips Xperius ultrasound system, Onvision gives anaesthesiologists the confidence to accurately position the needle tip inside the body. The introduction is part of a multi-year strategic alliance between Philips and B Braun to innovate in ultrasound-guided regional anaesthesia, a rapidly growing alternative to general anaesthesia. Onvision is being launched at the 38th Annual Conference of the European Society of Regional Anaesthesia and Pain Therapy (ESRA) in Bilbao, Spain (11–14 September).
Accurate needle placement is critical to the success of regional anaesthesia procedures, such as peripheral nerve blocks, both in terms of effective pain relief and the avoidance of unintended nerve and vessel punctures or collateral damage to surrounding tissue. While real-time ultrasound imaging has proved to be a valuable tool for needle guidance, failure to optimally visualise the needle tip remains a challenge for both novice and experienced anaesthetists. Currently, 10–20% of all peripheral nerve blocks are ineffective on the first attempt. By simplifying alignment between the needle and ultrasound probe, Onvision reduces the effort needed to interpret the ultrasound image. This allows the anaesthesiologist to more confidently guide the tip of the needle to its target.
“Regional anaesthesia is a rapidly growing alternative to general anaesthesia and has the potential to improve patient outcomes as well as increase workflow efficiency in the hospital,” says Bert van Meurs, chief business leader, Image Guided Therapy at Philips. “By combining B Braun’s expertise in needle design with Philips’ capabilities in real-time image guidance, we have created a solution to one of the biggest challenges in regional anaesthesia—accurate positioning of the needle tip in the body. Our alliance with B Braun is a strong example of our commitment to partner with industry leaders to grow our footprint in the therapy market.”
“Our customers want intuitive solutions that allow them to focus on the patient rather than the technology, so they can achieve the best outcomes. As demand for regional anaesthesia grows, improved efficiency can also help reduce the pressure of an increasing workload,” comments Meinrad Lugan, member of the board for the Hospital Care Division at B Braun. “Onvision is a perfect example of what can be achieved through shared expertise to meet the evolving needs of our customers, bringing regional anaesthesia to more patients in more hospitals worldwide.”
Together, B Braun’s Stimuplex Onvision needles and Philips’ Onvision needle tip tracking technology indicate the position of the needle tip in relation to the ultrasound viewing plane to an accuracy of better than 3mm, a press release reports. A sensitive micro-sensor placed on the needle, combined with advanced signal processing and visualisation techniques on the Xperius system, indicate the real-time location of the needle tip in relation to the 2D ultrasound viewing plane. The solution provides greater flexibility in needle trajectory and can reduce procedure times. The increased confidence and predictability offered by Xperius and Onvision will empower more anaesthesiologists to embrace regional anaesthesia as a viable and effective alternative to general anaesthesia.
Regional anaesthesia or analgesia involves the injection of an aesthetic in the proximity of a nerve, targeting areas of a patient’s body that are subject to surgical intervention. Regional anaesthesia can have significant advantages over general anaesthesia for both patients and hospitals. Patients undergoing regional anaesthesia typically benefit from reduced opioid consumption and fewer side-effects, such as nausea. Moreover, regional anaesthesia may lead to faster post-surgical recovery, allowing patients to ambulate or leave the hospital sooner, which benefits both patients and hospitals.
Together, Xperius and Onvision form an integrated point-of-care solution for supporting current and future needs in regional anaesthesia. They are co-branded and sold via B Braun’s global sales network, with Philips providing installation and service. Xperius is part of Philips’ complete portfolio of point-of-care ultrasound solutions, which offers clinicians the ability to confidently diagnose and care for their patients in any work environment.
CIRSE 2019 Gold Medal awardee, Thierry de Baère (Villejuif, France), tells Interventional News at the society’s annual meeting (7-11 September, Barcelona, Spain) that this award is a reflection of CIRSE’s interest and engagement with interventional oncology (IO).
On the IO education front, the natural next step after the creation of the curriculum, which acts as a foundation for interventional radiologists, will be to have teaching materials as well, he states.
He also addresses the current thinking on drug delivery to tumour, which “does not always need [to be achieved alongside] embolization”, he says, emphasising that interventional radiologists are well placed to deliver drugs directly to the tumour with the view to eliciting an immuno-oncologic response. Such intratumoural delivery enables high local dosage to destroy the tumour, without the toxicity of systemic delivery.
Twelve-month results of the BIOFLEX COF trial have demonstrated that the implantation of stents with low chronic outward force (COF) was associated with less neointimal hyperplasia, consequently resulting in less restenosis. Patients treated with Biotronik’s low COF Pulsar stent showed significantly lower restenosis rates than patients treated with the high COF LifeStent implant. Martin Funovics, Medical University of Vienna, Austria, presented the full cohort primary endpoint data at the annual scientific meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 7–11 September, Barcelona, Spain).
BIOFLEX-COF is the first randomised controlled trial (RCT) to investigate differences in clinical outcomes of nitinol stents with high versus low COF in de novo superficial femoral artery occlusive arterial lesions. The low-COF Pulsar stent had a mean restenosis rate of 26%, while the high-COF LifeStent implant showed 35%, as measured on CT angiography at one year (p<0.001, t-test and Mann-Whitney U test).
“We initiated the BIOFLEX COF trial to close the gap on how COF impacts the human neointima,” explains principal investigator Funovics. “These RCT data support our hypothesis that high COF leads to increased neointimal hyperplasia, which causes restenosis and increases the risk of repeat interventions for the patient. Our results suggest that COF impacts clinical outcomes and should therefore be an important factor in the choice of the stent.”
Self-expanding nitinol stents must be oversized by at least a minimal amount to ensure contact with the vessel wall and prevent migration. Once the stent is deployed, it exerts a continuous force upon the vascular wall, termed COF. While an animal study has found increased neointimal hyperplasia, inflammation and injury scores in vessels treated with high COF stents, human data were not available until now.
The investigator-initiated BIOFLEX-COF RCT enrolled 83 patients with symptomatic peripheral arterial lesions eligible for endovascular stent implantation. The patients were randomised 1:1 to either a high COF group or a low COF group. The trial’s primary endpoint is the amount of in-stent restenosis at one and two years as assessed by contrast-enhanced CTA.
“At BIOTRONIK, we develop our technologies to continuously improve patient outcomes,” comments Alexander Uhl, senior vice president of Corporate Marketing at BIOTRONIK. “With its unique design, Pulsar stent offers the benefits of a low COF stent and thin struts while resisting crush force: the optimal balance of radial forces keeps the vessel open, increase blood flow and reduce stress to the vessel wall. This helps to decrease patients’ risk of restenosis and need for re-interventions.” chronic
Cook Regentec has announced enrolment of the first patient in an international clinical trial evaluating the HemaTrate Blood Filtration System to treat patients with critical limb ischemia (CLI) due to peripheral arterial disease (PAD). To treat CLI, the HemaTrate system produces an autologous, peripheral blood-derived total nucleated cell (TNC) concentrate for intramuscular injection into the ischemic limb.
“Critical limb ischemia is the final stage of peripheral arterial disease and is associated with major morbidity and mortality despite current medical and surgical treatment,” noted Bijan Modarai, the study’s principal investigator, who treated the first enrolled patient at Guy’s and St. Thomas’ Hospital in London, UK. “Circulating nucleated cells are thought to stimulate vascular repair and regeneration and are of growing interest as a potential therapeutic option for these patients.”
The HemaTrate CLI (HT-CLI) trial is an international, multicentre, randomised controlled study that will enrol up to 350 patients. Subjects with Rutherford class 4 or 5 CLI will be randomised to receive a series of three intramuscular injection treatments of TNCs or saline, six weeks apart. The primary endpoint is clinical benefit through 12-month follow-up, defined as freedom from reintervention, major amputation or death. Following the 12-month study period, all patients will be offered TNC treatment for both study and non-study limbs. Patients will be followed for a total of 24 months.
“Patients with PAD-associated CLI who are poor candidates for surgical or endovascular procedures require alternative treatment options that deliver improved long-term outcomes,” said Brad Shirley, business leader at Cook Regentec. “We are excited that patients enrolled in our global CLI trial will begin to receive HemaTrate as treatment for this often-devastating condition.”
Bijan Modarai is a principal investigator of the HemaTrate CLI trial and is a paid consultant of Cook Regentec.
New data on the use of Zilver PTX, Cook Medical’s paclitaxel-coated stent for peripheral arterial disease (PAD), confirms the safety of the device. These data were presented at the Annual Scientific Meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE 2019; 7–11 September, Barcelona, Spain).
Michael Dake, senior vice president of health sciences at the University of Arizona, Tucson, president-elect of the Society of Interventional Radiology Executive Council, and global principal investigator, presented new 5-year data on Zilver PTX that Cook Medical gathered from the randomised controlled trial (RCT) performed to obtain US Food and Drug Administration (FDA) approval.
Cook Medical is the only organisation that has publicly provided long-term, patient-level data on the use of paclitaxel-coated devices for PAD. In addition to previously released information, the presentation included new data that had not been previously published.
These new data include information from patients who had not previously completed the study, such as those who had been lost to follow up, giving a more complete view of how paclitaxel-coated devices affect patients.
The data confirm no significant difference in all-cause mortality for the Zilver PTX drug-eluting stent compared to traditional angioplasty or a bare metal stent (BMS). The findings further show that treatment with Zilver PTX and paclitaxel dose were not predictors of mortality. However, age and other serious conditions common in PAD patients were associated with mortality.
The findings that Dake presented have been published online in CardioVascularand Interventional Radiology (CVIR), a peer-reviewed journal, which can be found here.
“Our clinical program evaluates the Zilver PTX technology across a broad, real-world patient population—including patients at high risk for restenosis and reintervention. Zilver PTX offers proven long-term benefits that help patients get back to living,” said Mark Breedlove, vice president of Cook Medical’s Vascular division.
Geniculate artery embolization (GAE) is responsible for statistically significant improvements in pain scores from baseline out to three months, the preliminary results of the first European prospective study on the procedure show. Mark Little (University of Reading and Royal Berkshire NHS Foundation Trust, Reading, UK) presented these early results of the GENESIS study (Geniculate artEry embolisatioN in patiEnts with oSteoarthritis of the knee) today at the Annual Scientific Meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 7–11 September, Barcelona, Spain).
While cautious about overinterpreting what he stresses are early data, Little is nonetheless optimistic about these positive results, telling delegates at CIRSE: “Musculoskeletal (MSK) embolisation is the next frontier in embolotherapy”.
The GENESIS investigators report “excellent recruitment”, with 34 patients enrolled since the trial started recruiting. Little believes this reflects the fact that GAE is serving an unmet clinical need. Osteoarthritis is a common condition with a growing prevalence due to an increasingly obese and elderly European population. For those patients older than 45 years of age who have mild to moderate osteoarthritis that is resistant to conservative treatment, yet is not severe enough to warrant joint replacement, GAE is being hailed as a potential solution.
Detailing the scientific rationale for GAE, Little explained to the CIRSE audience that inflammation of the knee joint drives synovial angiogenesis through macrophage activation. “It is hypothesised that angiogenesis contributes to structural damage and pain in osteoarthritis”, he explained, “and GAE can be used to treat this pain”.
The single centre, prospective GENESIS study (funded by Merit Medical and the National Institute for Health Research, NIHR) uses changes in pain measurements from baseline to post-procedural follow-up to assess the efficacy of GAE. Consultant interventional radiologists performed the procedure using 100–300micron Embosphere particles (Merit Medical) diluted in 20ml contrast.
Pain is a complex multifactorial process and the GENESIS study protocol is using a number of novel tools to assess patient’s pain. Little’s research group at University of Reading, UK, is using neuropsychological assessments employing functional magnetic resonance imaging (fMRI) of the brain to map pain, in addition to measuring Visual Analog Scores (VAS) pain scores, and using the Knee Injury Osteoarthritis Outcome Score (KOOS), a validated questionnaire used throughout the orthopaedic literature on knee osteoarthritis.
Overall Visual Analogue Scale (VAS) decreased from baseline at both six weeks and three months follow-up: mean VAS was almost 70 pre-GAE, and just below 30 six weeks post-procedure. VAS score was 33 at three months (p<0.005). Meanwhile, Knee Injury and Osteoarthritis Outcome Score (KOOS) increased from baseline to one-year follow-up, representing a reduction in pain and symptoms. Mean KOOS was 39 at baseline, 62 (p<0.005) and 85 one-year post-procedure.
There were two minor complications, observed in the 22 patients treated with GAE for this interim analysis—two cases of transient skin discoloration early on.
Explaining the significance of these results, Little tells Interventional News, “I really want to stress how important it is to precisely measure patient’s pain. We need to up our game in terms of accurate outcome measures in MSK embolization. We are very fortunate to have the Center for Integrative Neuroscience and Neurodynamics (CINN) at the University of Reading to carry out the pain assessments as part of the GENESIS study.”
Little reported that preliminary neuropsychology data reveal signals that may predict treatment failure. “We are continuing to model the neuropsychological pain experiments with the ultimate aim of aiding patient selection”, he said. The triallists are instituting neuromodulation prior to the procedure to improve clinical outcomes.
Omar Ishrak, Medtronic’s chairman and CEO is to retire on 26 April 2020, following the end of the company’s current fiscal year. Also, the Medtronic Board of Directors has announced key leadership appointments as part of its multi-year, leadership succession planning process. A press release reports that these announcements will ensure a smooth and successful transition in leadership across the company.
The Board of Directors has unanimously appointed Geoff Martha, currently executive vice president (EVP) of the company’s Restorative Therapies Group (RTG), to assume the newly created role of Medtronic president and become a member of the Medtronic Board of Directors, effective 1 November 2019. He will also succeed Ishrak as Medtronic CEO, effective 27 April 2020. As president, according to the press release, Martha will lead Medtronic’s operating groups and regions. Brett Wall, president of Medtronic’s Brain Therapies division, was appointed EVP and group president of RTG, succeeding Martha, effective 1 November 2019.
At the start of Medtronic’s next fiscal year, on 27 April 2020, Ishrak will assume a new position of executive chairman. He will provide counsel and guidance to Medtronic’s leadership, oversee CEO succession, and drive the ongoing successful execution of Medtronic’s long-term strategic plan. These changes are designed to ensure a smooth transition, continuity of leadership and a continued focus on delivering Medtronic’s innovation strategy and financial performance.
Ishrak comments: “We have announced leadership changes that meet both the Board’s objective of executing a thoughtful leadership transition as well as my personal desire to begin transitioning my duties as CEO to a new leader coinciding with the start of our next fiscal year. This plan and its timing enable Geoff and I to partner on achieving Medtronic’s key financial performance goals as well as delivering on our critical pipeline milestones, including several important product launches. Leading Medtronic as CEO is an honour and a privilege, and I know that Geoff is the right leader to take Medtronic to the next level of its growth and evolution. Geoff is a results-oriented, dynamic, and innovative business leader who is passionately committed to our mission, the advancement of our growth strategy and the development and diversity of our people. I am confident he has the right track record, commitment, vision and judgment to lead our company.”
Scott Donnelly, Medtronic’s lead director, and chairman, president and CEO of Textron, says: “As Omar approaches the company’s mandatory executive officer retirement of 65 years of age next year, we have ensured Medtronic has the right leadership at the right time to advance its mission and deliver shareholder return through a seamless transition. The Board is extremely grateful to Omar for his outstanding leadership—as the company’s annual revenues have doubled and its market capitalisation has increased by more than US$100 billion during his tenure. We are confident Omar’s contributions to Medtronic will continue as executive chairman. The Board’s succession planning process prioritises developing leaders from within the company, and we are pleased that we could advance Geoff and Brett for these roles. During his time at Medtronic, Geoff has demonstrated his unique ability to lead, innovate and drive results, and the Board has full confidence in him and his ability to take Medtronic into its next chapter of growth.”
Michael Dake (Tucson, Arizona) presented the two-year data from the VERNACULAR trial at CIRSE 2019 on 8 September in Barcelona, Spain.
Dake said: “The 24-month results from the VERNACULAR trial using the BD Venovo stent show absolutely sustained benefit in terms of patency [and] quality of life from one year to two years. We saw a very high follow-up of 83% of patients coming back for a follow-up at two years. We had an overall 83% primary patency of two groups, the non-thrombotic iliac vein lesions and the post-thrombotic syndrome lesions. And again, we can see that the target lesion revascularisation and target vessel revascularisation was less than 11%. These are fantastic results and we coupled that with the fact that radiographic evaluation, a very high percentage of patients, showed zero fractures not only at one year, but at two years.”
This video was filmed by BD and is being sponsored for distribution in association with Venous News, Vascular News and Interventional News.
Speaking at the 2019 annual meeting of the Cardiovascular and Interventional Radiology Society of Europe (CIRSE; 7–10 September, Barcelona, Spain), Vincent Vidal (Marseille, France) describes the Fair-Embo technique, detailing how to obtain the inexpensive embolic agents, the technical efficacy of the procedure, and his ambitions for the project’s future.
An initial preclinical study in a porcine model tested the feasibility and safety of arterial embolization with absorbable and nonabsorbable suture fragments. The investigators reported a technical success, demonstrating the proof of concept of the feasibility and safety of the so-called “FAIREmbo” procedure. Demonstrating the in vivo feasibility of the procedure led Vidal and colleagues to propose what they termed the “FAIR-Embo technique”. Writing in Cardiovascular and Interventional Radiology (CVIR) earlier this year, they concluded: “Embolization by absorbable and non-absorbable suture is a feasible and effective treatment, which opens up the possibility of global use of this inexpensive and widely available embolization agent”.
At present, Vidal is working with the French Society of Radiology (FSR) to send out a survey to countries with emerging economies—“potential Fair-Embo recipients”, in his words—to map interventional radiology services around the world. The survey will be sent to more than 3,000 email addresses across Africa, South America, Asia, the Middle East and eastern Europe. The survey asks basic questions about access to interventional radiology services, such as:
Do you have access to interventional radiology in your hospital/ town/ state/ country?
If yes, which kind of procedures are regularly performed: angioplasty? Embolization? Drainage?
How many interventional radiologists are working in your hospital/ town/ state/country?
Do you have a contact with a local or national interventional radiology organisation or scientific society?
Do you have any difficulty with obtaining implantable medical devices?
Although the survey results are yet to be received, Vidal speaks to Interventional News about his expectations. He tells this paper that he anticipates the results “mapping the places where interventional radiology is possible”, as the answers will delineate where in the world trained physicians are working, the availability of imaging hardware such as X-ray machines, and where access to implantable medical devices is an issue. “The final goal”, he says, “is to target the places where FAIR-Embo will be helpful, and also where the existence of an educational programme will be useful as a first point of action”.
With this in mind, the future steps of the Fair-Embo project that Vidal envisions centre around creating a global community of interventional radiologists. Initially, he plans to create a foundation with the capacity to fund a FAIR-Embo clinical programme in developing nations. Outlining this idea to Interventional News, Vidal enumerates the features of this potential future foundation: “We will get help from a proctor if necessary to set it up. I foresee the foundation as one which can offer tips and tricks to interventional radiologists working in low resource settings, which will help provide any necessary materials, and which can help elaborate an existing clinical research programme.”
Further to the development of a FAIR-Embo foundation, Vidal would like to link this with “all the interventional radiology organisations around the world”. Ambitious in his aims for the project, Vidal says that he would like to collect data from the FAIR-Embo community (such as the number and outcomes of embolizations performed) “in order to give feedback to international healthcare organisations such as the International Atomic Energy Agency (IAEA) and the World Health Organisation (WHO)”.
By taking these steps, Vidal hopes to create “a virtuous cycle”. He imagines it working thus: FAIR-Embo will help to develop embolization practices in low resource settings; data collected from these procedures will help to obtain funding from international organisations; this funding will help interventional radiology research in the form of the development of clinical programmes in emerging countries.
Figure 2: (L) Left kidney before; (Middle) Selective embolization; (R) Control post embolization
At CIRSE, Vidal presented a new study demonstrating how to obtain non-spherical particles with suture material. Using scissors, he advises interventional radiologists to cut sutures into small fragments between 700 and 1,100 microns long. So called “FAIR particles” (Figure 1) are then injected via a catheter to the target site, and their technical success is demonstrated through post-embolization imaging (Figure 2).
Afshin Gangi (Strasbourg, France), CIRSE vice-president, is enthusiastic about FAIR-Embo, commenting: “Even if this concept is not adapted for all cases, if this material becomes clinically available [as an embolic agent], it will be a game changer for developing and even for industrial countries.”
Detailing why he thinks this, Gangi says to Interventional News: “Traumatic, post-partum or post-surgical bleeding is a major cause of mortality. Until the late 1970s, operative management was considered the only legitimate course for blunt and penetrating abdominal and extremity vascular injuries. Interventional techniques first popularised in the early 1970s now offer a wide range of solutions, principally using transcatheter arterial embolization. Various embolic agents (for example, coils or gelfoam) and particles may be used to stop or control bleeding. All these agents used individually or in combination can save lives by stopping life-threatening bleeding.
“An embolization performed by a well-trained interventional radiologist is essential in all centres dealing with bleeding—trauma centres, maternity wards, surgical units where high blood loss is common, to name a few. In developing countries, training interventional radiologists to safely perform embolization is key. However, regardless of IR training or the presence of an angiosuite with high resolution C-arm fluoroscopy capabilities, availability of the embolic agent is an issue. The idea of having an efficient embolic agent which is available anywhere and is cost-effective is very attractive.
“The idea underpinning ‘the FAIR-Embo concept’, which demonstrates the feasibility and efficacy of using non-absorbable and absorbable sutures, is about making a cheap embolic agent available everywhere. In addition to this availability, the benefits of this material are that it is inexpensive, can be temporary or permanent, that it leads to mechanical obstruction, and that suture fragments are easy to work with.”
Medtronic has announced the first-ever results from the IN.PACT AV access clinical study comparing the investigational IN.PACT AV drug-coated balloon (DCB) to percutaneous transluminal angioplasty (PTA) in patients with de novo or non-stented restenotic arteriovenous (AV) fistulae lesions. The study met primary safety and effectiveness endpoints and data were presented today at the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) annual meeting (7–11 September, Barcelona, Spain).
“Maintaining patency and limiting the frequency of reinterventions needed to keep AV access sites functioning properly remain significant treatment challenges for physicians treating AV fistulae lesions,” says Andrew Holden, director of interventional radiology at Auckland Hospital and associate professor of radiology at Auckland University (Auckland, New Zealand). “These results demonstrate the promise of IN.PACT AV DCB to not only address these critical issues, but to potentially improve the quality of life of patients undergoing dialysis.”
AV fistulae, otherwise known as AV access sites, are created and used to deliver haemodialysis to patients with end-stage renal disease (ESRD). Over time, vessel restenosis limits the ability to use AV fistulae effectively. In order to restore function, patients often undergo one to three AV fistula maintenance procedures per year. The need for frequent reinterventions can result in significant disruptions to critical haemodialysis care and increased costs to the healthcare system. Drug-coated balloons have the potential to extend the time between reinterventions by maintaining AV access site patency, therefore maximising a patient’s uninterrupted access to lifesaving dialysis care.
The IN.PACT AV Access study is a randomised controlled trial (RCT), which has enrolled 330 subjects at 29 sites in the USA, Japan, and New Zealand. The primary effectiveness endpoint was defined as freedom from clinically-driven target lesion revascularisation (CD-TLR) or access circuit thrombosis measured through six months post-procedure and the primary safety endpoint was defined as the serious adverse event rate involving the AV access circuit through 30 days post-procedure. Additional endpoints include but are not limited to: access circuit primary patency, cumulative target lesion revascularisations, and number of interventions required to maintain target lesion patency.
The study enrolled a challenging patient population who had been undergoing dialysis for an average of 4.3 years. Overall, the IN.PACT AV DCB group demonstrated clinical benefit compared to the PTA control group. Key data highlights include:
Per Kaplan-Meier estimates, the primary patency rate of the target lesion at 180 days was 86.1% in the IN.PACT AV DCB group compared to 68.9% in the PTA control group (p<0.001).
Per Kaplan-Meier estimates, the primary patency rate of the target lesion at 210 days was 81.4% in the IN.PACT AV DCB group compared to 59.0% in the PTA control group (p<0.001).
Patients in the IN.PACT AV DCB group required 56% fewer reinterventions to maintain target lesion patency through 210 days compared to those in the PTA control group
A low rate of access circuit-related serious adverse events, with 4.2% in the IN.PACT AV DCB study group compared to 4.4% in the PTA control group through 30 days.
“The data presented today at CIRSE demonstrate the potential of IN.PACT AV DCB to address restenosis in high-risk patients who currently have few long-term treatment options available to them,” comments Mark Pacyna, vice president and general manager of the Peripheral Vascular business, which is part of the Aortic, Peripheral, and Venous division at Medtronic. “As part of our commitment to improving outcomes, we look forward to generating further clinical evidence in support of this therapy.”
In the USA, IN.PACT AV DCB is an investigational device and not yet approved for commercial use. In January 2016, the CE (Conformité Européene) indication for the IN.PACT Admiral DCB was expanded for the treatment of failing arteriovenous access in patients with end-stage renal disease undergoing dialysis.
In collaboration with leading clinicians, researchers, and scientists worldwide, Medtronic offers the broadest range of innovative medical technology for the interventional and surgical treatment of cardiovascular disease and cardiac arrhythmias. The company strives to offer products and services that deliver clinical and economic value to healthcare consumers and providers around the world.
A meta-analysis, recently published in Osteoporosis International, has found that the application of percutaneous vertebroplasty (PVP) is safe and effective only in patients with acute osteoporotic vertebral compression fractures (OVCFs) having persistent and severe pain. The investigators recorded no benefits among patients with older fractures or those bearing non-severe symptoms.
According to the authors, S Lou (The First Affiliated Hospital of Harbin Medical University, Heilongjiang, China) and colleagues, OVCFs are common in the elderly population and are often treated using PVP. However, the effectiveness of PVP reported by various randomised controlled trials (RCTs) is inconclusive. This study therefore aimed to analyse, from published literature, the efficacy and safety of PVP for OCVFs.
Lou and colleagues conducted searches in Medline, EMBASE, and Cochrane Libraries since their respective inceptions on 1 January 2019 for RCTs of OVCFs treated with PVP compared with non-operative treatment. The primary outcomes were pain relief at one to two weeks, one to three months, and six to 12 months. The secondary outcome was the rate of occurrence of new vertebral fractures, and the meta-analysis was performed using a random effect model.
The investigators included a total of 12 RCTs, comprising 1,624 patients, in the analysis. For the blinded studies, they found statistical differences between PVP and the sham injection group for the three primary outcomes in the subgroup of the Vertebroplasty for acute painful osteoporotic fractures (VAPOUR) trial. Although pain scores were similar between the PVP group and the sham injection group for the VAPOUR trial at each period, the effect size of PVP increased over time.
They found that in the open label studies, PVP significantly reduced pain at all the time points, and that the risk of the new vertebral fractures was similar between the PVP groups and control groups.
Due to certain limitations of the meta-analysis, Lou and colleagues warn that the results should be “interpreted cautiously”. They note, for example, methodological limitations in the quality of the original studies, such as the unclear random method, the unclear concealment of the treatment allocation, and the inadequate blinding.
In addition, the possibility of publication bias might exist because of the ongoing and unpublished trials, although no statistical evidence for this was detected.
They also note that while the baseline of pain scores and duration of fracture might be key factors affecting the PVP, there might be other clinically relevant but unreported confounding factors, such as the types of patients, the degree of bone mineral density, and the types of PVP techniques. Moreover, owing to the limited studies, whether the baseline of pain scores and duration of fracture truly affect the PVP “still needs to be determined by further trials”.
Considering the direction of future research, the investigators suggest that it should “focus more on [patients with acute OVCFs and experiencing severe pain] and use more consistent inclusion criteria”. They suggest, for example, that each study should add the confirmation of OVCFs with magnetic resonance imaging (MRI) to the inclusion criteria and use the same threshold of the baseline scores for patient eligibility.
Lou and colleagues also suggest that, since they determined that the baseline information could affect the effect of PVP, further studies “should clearly report the baseline information, such as the duration of back pain, the baseline pain scores, the methods of non-operative therapy, the PMAA volume, and the baseline T-scores, and other clinically relevant factors, to find the association between these factors and PVP.”
Finally, they indicate that a longer follow-up—more than 12 months—with a large enough sample size is “necessary for further studies to determine the long-term therapeutic effects of PVP”.
Thousands of eligible patients are not receiving endovascular thrombectomies after suffering a stroke due to a shortage of neurointerventionalists worldwide. In an effort to combat this, the Society of Interventional Radiology (SIR),the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), and the Interventional Radiology Society of Australasia (IRSA) believe interventional radiologists must treat acute ischaemic stroke patients. SIR has today published an update of its stroke guidelines, outlining the pathways to ensure adequate training for those performing the procedure. David Sacks, lead author of these guidelines and a physician who has been involved in stroke intervention since the original publication of the PROACT trial in 1999, here describes why involving interventional radiologists in stroke care is critical.
How many patients with acute ischaemic strokes could be treated with emergency endovascular thrombectomy (EVT) but are not? Why is this happening? What can be done to help?
In the USA in 2015–2016, only 2.6% of stroke patients received EVT.1 A European survey on stroke care authored by Aguiar de Sousa et al on behalf of the European Stroke Organisation (ESO), the European Society of Minimally Invasive Neurological Therapy (ESMINT), the European Academy of Neurology (EAN), and the Stroke Alliance for Europe (SAFE) found that EVT was offered in 40 of 44 European countries. On average across the continent, the procedure was offered for 1.9% of all strokes.2 The highest country rate was 5.6% of all strokes. Assuming that 5% is a reasonable goal, this means that 67,000 patients were clinically eligible for EVT but not treated.
Notably, the European survey considered 5% to be a conservative estimate. There is strong evidence from the DAWN and DEFUSE 3 trials3 to treat selected patients up to 24 hours after stroke onset. Furthermore, patients over 80 years of age have a similar odds ratio of benefit compared to younger patients.4 Randomised trials are underway to evaluate the benefit of EVT for mild strokes, large core infarcts, and patients with moderate baseline disability. In one published national registry of current practice, 11% of treated patients had mild strokes, not currently included in treatment guidelines.5 Patients with large core infarcts are also likely to benefit.6 In the UK, it is estimated that about 10% of stroke admissions would be eligible for EVT, an estimate which does not include patients with mild strokes, large cores, baseline disability, or time from stroke onset >12 hours.7 It is estimated that 30–46% of acute ischaemic strokes involve large vessel occlusions,8–11 and a recent commentary suggests that every stroke patient with an acute large vessel occlusion “should undergo thrombectomy unless the weight of evidence is strongly against treatment”.12
Why are more eligible patients not being treated? In the European survey, the most common reasons were lack of specifically trained personnel, lack of facilities, and costs. Multiple studies have demonstrated that EVT is a highly cost-effective intervention, but stroke interventions involve complex care, from ambulance staff to emergency department and radiology evaluation, patient transport, endovascular treatment, critical care management, stroke unit care, and rehabilitation. The resources to provide this care have not yet caught up with the recent proof of effectiveness of EVT.
One way to provide additional personnel is to train vascular interventional physicians to provide EVT. In theory, this would allow EVT to be provided in locations where neurointerventional physicians are not able to provide 24/7 care, or not available at all. Hospitals that may not have sufficient volumes of cerebral aneurysms or vascular malformations to support multiple neurointerventional physicians may be able to provide EVT by sharing the EVT work with other endovascular colleagues. This raises a series of questions: can other interventional physicians be trained sufficiently to provide EVT such that outcomes meet international benchmarks? Might the learning curve for training be such that patients would be better off not being treated at all, or being transferred to another hospital with delayed treatment? If a hospital cannot provide 24/7 coverage by physicians specifically trained for neurointerventional procedures, might it also lack the infrastructure to provide all of the rest of the complex care that is necessary to achieve good outcomes? Might the treatment of stroke patients at many local hospitals lead to many low-volume centres with suboptimal outcomes compared to a few high-volume centres? Many of these questions will require trials for answers. In the meantime, patients with acute ischaemic strokes are being vastly undertreated with EVT.
Interventional radiology societies believe that appropriately trained interventional radiologists can help address the manpower needs. Interventional radiologists are currently active providers of EVT. The majority of the interventional physicians in The Netherlands who participated in the MR CLEAN trial and registry were interventional radiologists. The odds ratio for benefit in the MR CLEAN trial was the same as for the neurointerventional trial sites.13 The vast majority of the physicians providing EVT in the Czech Republic are interventional radiologists, and published results from the Czech registry are comparable to neurointerventional outcomes. In the USA, 60% of primary stroke centres perform EVT, and of these, 41% rely on interventional radiology physicians,14 and overall, 34% of EVT cases were performed by physicians who had not trained in dedicated neurointerventional fellowships.15 In a survey conducted by the Society of Interventional Radiology (SIR), approximately 25% of interventional physicians providing EVT at certified comprehensive or thrombectomy-capable stroke centres are interventional radiologists. SIR, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), and the Interventional Radiology Society of Australasia (IRSA) have published a joint statement on the role of interventional radiologists in acute stroke interventions.16 Working with neurologic and neurointerventional sister societies, SIR and CIRSE have published international benchmarks for EVT outcomes.17 A European pathway for training interventional radiologists in stroke interventions has been established.18 SIR has just published an update of its training guidelines written by multispecialty authors from Interventional radiology, neurointerventional, combined interventional radiology and neurointerventional, stroke neurology, and endovascular neurosurgery backgrounds. The SIR training guidelines require a background of endovascular expertise supplemented with stroke specific imaging, cognitive, and technical training.
EVT is a powerful tool to reduce disability from acute ischaemic stroke. There is strong evidence that eligible patients are not receiving EVT due to a shortage of EVT physicians. IR physicians are currently working with our neurointerventional colleagues to provide this care with acceptable outcomes.
David Sacks is an interventional radiologist in the Department of Interventional Radiology at The Reading Hospital and Medical Center, West Reading, USA.
References:
Stein et al, Journal of NeuroInterventional Surgery, doi:10.1136/neurintsurg-2019-015019
Aguiar de Sousa et al, European Stroke Journal 2019; 4:13–28
Nogueira et al, New England Journal of Medicine 2018; 378:11–21
Albers et al, New England Journal of Medicine 2018; 378:708–718
Goyal et al, Lancet 2016; 387:1,723–1,731
Asdaghi et al, Stroke 2019; 50:2,101–2,107
Panni et al, Stroke 2019; 50:1,164–1171
McMeekin et al, European Stroke Journal 2017; 2:319–326
Lakomkin et al, Journal of NeuroInterventional Surgery (JNIS) 2019; 11:241–245
Smith, Stroke 2009; 40:3,834–3840
El Tawil et al, European Stroke Journal 2016; 1:264–271
Nogueira and Ribo, Stroke, 50:2,612–2,618
Flynn et al, European Stroke Journal 2017; 2:308–318
Alberts et al, Interventional Neuroradiology 2017; 23:64–68
Kamel, Journal of the American Medical Association (JAMA) Neurology [Year]; [Issue; Pages]
Sacks et al, J Vasc Interv Radiol 2019; 30:131–133
Sacks et al, J Vasc Interv Radiol 2018; 29:441–453
European Board of Neurointervention. Recommendations for acquiring competence in Acute Ischemic Stroke Intervention (AISI). Available at: https://ams3.digitaloceanspaces.com/ebni-document-storage/68903e8bfc62bb742df0191935e6f112/Standards-of-training-in-AISI-APPROVED.pdf
The Society of Interventional Radiology (SIR) has today published new training guidelines for endovascular stroke treatment in the Journal of Interventional Radiology (JVIR). This is the first update since 2009, when the society released training guidelines for intra-arterial catheter-directed treatment of acute ischaemic stroke.
“Obviously, the world of stroke intervention has changed tremendously since then”, lead author of the guidelines David Sacks (The Reading Hospital and Medical Center, West Reading, USA) tells Interventional News. At the time, catheter-directed thrombolysis was the only such therapy studied in randomised trials. In the intervening decade, mounting positive evidence for endovascular thrombectomy from randomised trials and meta-analyses, and the subsequent growth in the number of these procedures being performed each year, has led the SIR to believe that these new recommendations are timely and necessary.
The guidelines were authored by a diverse group of interventional radiologists, specifically-trained neurointerventionalists, endovascular specialists, and stroke neurologists, as well as academics and community hospital staff; they varied to being freshly out of training themselves, to having over 30 years’ experience of stroke interventions. Sacks explains to this newspaper: “We solicited people from a range of backgrounds so that we could have a diversity of opinion, experience and knowledge. We wanted to make sure that we were meeting the needs of people in many different environments, as well as meeting the needs of patients.”
However, no official representative of the Society of NeuroInterventional Surgery (SNIS) participated in the creation of these guidelines. Despite the SIR inviting various leaders and former leaders of SNIS to participate in the creation of these guidelines, “for various reasons those individuals declined”, Sacks reports. Several of the guidelines authors are members of SNIS, though. Sacks also adds, “We [SIR and the guidelines authors] have maintained lines of communication with the current leaders of SNIS, and we remain open to working with them in whatever ways would advance patient care for stroke interventions”.
“Interventional radiologists are seeking guidance as to how they should train”
Earlier this year, SIR, the Cardiovascular and Interventional Radiology Society of Europe (CIRSE), and the Interventional Radiology Society of Australasia published a joint position statement in the Journal of Vascular and Interventional Radiology (JVIR) outlining the role of interventional radiologists in acute ischaemic stroke interventions. Sacks, who was also the lead author of this joint statement, describes this as “an acknowledgement that interventional radiologists have an important role to play in stroke care”, but adds that “it was also cautionary, stating that interventional radiologists must be adequately trained”. These latest guidelines provide the training pathway alluded to in the earlier joint statement.
Sacks says that the new guidelines “make clearer what training and experience interventional radiologists are expected to have to be performing these [endovascular stroke] procedures”. He continues: “I think there are an increasing number of interventional radiologists already who are involved in stroke interventions, and like any kind of medical care, there will be a range of experiences and capabilities. We are trying to bring more uniformity at a high level of what that training and experience should be. I think there are already many hospitals that are turning to their interventional radiologists to help provide this care, and those interventional radiologists are seeking guidance as to how they should train. They want to do a good job, and they need to know what the recommendations are for them to train to be able to do the good job they are committed to.”
Specific training requirements
The updated guidelines state: “The IR physician is expected to have baseline mastery in accordance with the Accreditation Council for Graduate Medical Education (ACGME) milestones of level 4 or higher of arterial access, selective vascular catheterisation, including microcatheters, and mechanical revascularisation, including thrombectomy and thrombolysis of extracranial vessels. The IR physician is also expected, as part of core training and certification in diagnostic radiology, to have experience with neuroimaging including CT, MRI, and perfusion imaging.”
There is no requirement for full-scope neuroendovascular training through either a formal neurointerventional fellowship or near equivalent. “However”, the authors note, “specific and rigorous training with demonstration of competence is required”. Adequate training, according to Sacks et al, involves the following:
Formal training that imparts the required depth of cognitive knowledge of the brain and its associated pathophysiological vascular processes, clinical syndromes, the full array of ischemic stroke presentations, and pre-, peri-, and post-procedural care.
Procedural skill, including management of complications secondary to endovascular procedures, that is achieved by supervised training by a qualified instructor.
Diagnostic and therapeutic acumen, including the ability to recognise procedural/angiographic complications. This is achieved by studying, performing and correctly assessing an adequate number of diagnostic and interventional/endovascular procedures with proper tutelage.
In addition, the new SIR guidelines stipulate that “a minimum of six months of documented cognitive neuroscience training during or post-residency is necessary to become competent in the interventional care of patients with acute ischaemic stroke”.
Three training pathways are outlined in the document to highlight how this competency could be achieved. Firstly, the new ACGME accredited IR/diagnostic radiology residency programme in the USA will provide trainees with at least two years of dedicated clinical and procedural training, with “motivated residents” able to access up to six months of neuroscience training. Alternatively, practicing interventional radiologists could achieve competency to treat ischaemic stroke through a proctorship. The guidelines authors elaborate: “Ideally, supervised training would include robust, hands-on training, not limited to interventional techniques but also workup prior to and management after thrombectomy”. The final training pathway detailed in the guidelines is for physicians to enrol in an educational stroke course involving procedural simulations and potentially virtual reality to supplement stroke training.
The consensus of the guidelines’ authors is that a minimum of 10 procedures per year for each operator is recommended for maintenance of physician competence. The onus also falls on institutions to provide appropriate infrastructure and support, according to Sacks and colleagues. They conclude: “Institutions performing stroke intervention must establish quality assurance programmes to optimise processes and outcomes, and both technical and clinical outcomes must be entered into a database or registry”.
Endovascular thrombectomy procedures on the rise
“I think the number of stroke interventions will continue to increase”, Sacks predicts. The current number of stroke interventions are vastly fewer than the number of patients generally acknowledged to be eligible. A 2018 survey from the European Stroke Organisation (ESO), the European Society of Minimally Invasive Neurological Therapy (ESMINT), the European Academy of Neurology (EAN) and the Stroke Alliance for Europe (SAFE) investigated the access to and delivery rates of stroke care in 44 European countries—and found that over 65,000 stroke patients eligible for endovascular treatment were not provided with this intervention. On average, 1.9% (95% confidence interval [CI], 1.3–2.5) of all patients with an ischaemic stroke in Europe received endovascular treatment, while a recent UK study estimated that approximately 10% of stroke patients are good candidates.
The most common reason that stroke intervention was not performed on an eligible patient was the lack of adequately trained physicians, leading Sacks to argue that there is a need for well-trained interventional radiologists to perform these procedures. “Having more interventional radiologists who are adequately trained will allow more patients in total to be treated when it is appropriate to treat them”, he says.
In addition to the potential increase in stroke interventions caused by treating a greater majority of eligible patients, Sacks also believes the overall number of eligible patients will rise. “The estimates on which these articles are relying [for estimates of eligible patients] are based on the well-accepted indications: patients within six hours, patients with ICA-M1/M2 occlusions, and patients whose strokes are sufficiently severe but do not have large core [infarcts]”, he says. “There are multiple trials underway looking at whether patients with mild strokes or patients with large core [infarcts] will benefit.
“I think that in the future, we are going to be treating increasing numbers of patients with a broader set of indications. Stroke patients will be treated at an increasing number of centres [in the USA] rather than [just at] the current number of thrombectomy-capable stroke centres. I think there will be more uniformity in the way people are training, and more uniformity in the expectations for outcomes.”
Beacon Tip catheters (Cook Medical) are once again available to physicians in Europe. As of September 2019, the catheters are available in the UK, Ireland, Norway, Sweden, Finland, Denmark, Germany, Poland, the Netherlands, Luxembourg, Belgium, France, Switzerland, Austria, Hungary, Spain, and Italy. Cook is continuing to work on releasing the products to customers in the rest of Europe, the Middle East, and Africa in the near future.
“Patient safety is always a priority for us, and we are proud of the changes we have made. Improved packaging allows for physicians to once again have access to catheters, designed for torqueability, visibility and pushability, to improve procedural outcomes”, said Mike Williams, global director of Cook Medical’s Vascular programmes. Beacon Tip catheters are used for diagnostic angiographic procedures and feature a visible distal tip designed to improve visualisation when using fluoroscopic guidance.
In 2016, Cook Medical issued a voluntary global recall of all Beacon Tip catheters following concerns that the tips were fracturing due to environmental factors. As patient safety is always a priority, engineers at Cook began intensive testing to find a solution. The products now come with specialised foil packaging to help protect the catheters from the environmental effects that contributed to the recall.
Cook invested resources into innovating the product packaging and meeting regulatory standards from multiple governing bodies. The catheters were reintroduced in the USA and Canada in 2018 and are now approved for physician use in many countries in Europe.
Foundation trainees’ perception of interventional radiology (IR) is “generally poor due to a lack of adequate knowledge”, a recent survey from the Radiology department of the Pennine Acute Hospitals NHS Trust, Manchester, UK, reports.
Marawan El Farargy, Khalid Bashaeb, Linda Watkins, and Aws Alfahad, all from said institute, set out to assess perceptions of the specialty amongst foundation trainees, with the simultaneous aim of exploring the means by which these perceptions could be addressed, “with the overall outcome of encouraging junior doctors to consider a career in this advancing sub-speciality.”
El Farargy et al distributed a physical copy of an anonymised survey to a total of 79 students in the first and second year of their foundation course (FYs), all of whom responded. Forty-five per cent (34 of 79) were introduced to interventional radiology within their prescribed training posts, and 38% (29 of 79) were “interested enough to learn more through self-directed reading”, El Farargy and colleagues report. Approximately 28% (22 of 79) had heard of interventional radiology during medical school rotations and a few trainees (six of 79) were exposed to the specialty during elective placements.
“The findings of the present survey are indicative of the poor general knowledge of FYs regarding interventional radiology,” the authors surmise, “and highlights that interventional radiology is not introduced appropriately to undergraduates”. They continue: “The Royal College of Radiologists has already made recommendations regarding the embedding of clinical radiology as a whole in medical education. Interventional radiologists must take a leading role in the education of both undergraduate and junior doctors to address the apparent lack of interest in radiology of newly qualified doctors. In addition, universities and societies should ensure that a basic level of general radiology and IR knowledge is obtained by medical students prior to graduation.”
Three-quarters of foundation year students unwilling to consider a career in IR
“Despite reasonable awareness of the IR sub-speciality, 75% of FYs (59 of 79) stated that they were not willing to consider a career in interventional radiology, and around 11% were unsure about pursuing a career in interventional radiology,” the authors write. “Of those who did not wish to consider IR as an option, 53/59 lacked general interest in radiology and 13/59 felt they did not have enough information about this career option”.
While almost all respondents demonstrated awareness that interventional radiology is both an elective and an emergency specialty, over 45% did not know that attending clinic is part of the consultant role. Citing an American study by Julia Fielding (Department of Radiology, University of North Carolina, Chapel Hill, USA) et al that found that less patient contact discourages medical students from selecting radiology as a speciality, El Farargy and colleagues say, “it is understandable that inadequate knowledge of the typical interventional radiology consultant job plan may dissuade junior trainees from pursing interventional radiology as a future career”.
Survey respondents were asked to rate possible ways of raising awareness about interventional radiology on a scale of one to five, with lower scores being worse. “Surprisingly, 65% (50 of 79) rejected the notion of learning more about interventional radiology at all”, El Farargy et al describe, though the most popular method of awareness-raising was deemed to be elective placements and teaching throughout foundation years, followed by lectures in medical schools. Attending multidisciplinary team meetings was the least preferred option.
Discussing these methods, the authors suggest that “multiple strategies can be employed, including radiology placements, electives, and student-selected modules, encouraging attendance at interventional radiology procedures, provision of student access to interventional radiology conferences, and embedding appropriate multidisciplinary team meetings within the student timetable”. For foundation schools, they advise teaching sessions, adequate access to taster week programmes, and the inclusion of radiology rotations within their foundation posts.
“Again,” they write, “the interventional radiology community need to step up and ensure they are involved in both decision-making and face-to-face teaching levels to capitalise on available opportunities”.
They conclude with a call to action for current interventional radiologists: “It is essential that we, as a radiology community, take responsibility for this crucial issue and work to boost perceptions of interventional radiology amongst the consultants of tomorrow”.
Balloon-occlusion prostatic artery embolization (PAE) is as effective as conventional microcatheter PAE in the treatment of benign prostatic hyperplasia (BPH) with a potential to reduce nontarget embolization, Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) and colleagues report in the Journal of Vascular and Interventional Radiology (JVIR). However, the authors were surprised to note that there was no clear advantage of balloon-occlusion PAE over the conventional technique.
The investigators set out to compare the safety and efficacy of these two types of PAE. In this single-centre, prospective, randomised, single-blind clinical trial, 89 patients with symptomatic BPH were assigned to conventional microcatheter PAE (43 patients) or balloon-occlusion PAE (46 patients), and were treated between November 2017 and November 2018. All patients were embolized with 300–500µm Embosphere microspheres (Merit Medical), and were evaluated one and six months post-procedure.
All efficacy variables improved in both groups with statistical significance, with the exception of International Index of Erectile Function, which remained constant in both groups, and prostate-specific antigen levels, which decreased significantly in the conventional microcatheter PAE group (0.9nb/mL±2.22; p=0.01).
Assessments at six months after PAE showed mean International Prostate Symptom Score (IPSS) reduction from baseline was 7.58±6.88 after conventional microcatheter PAE, and 8.30±8.12 after balloon-occlusion PAE (p=0.65).
Mean prostate volume reduction was 21.9cm3±51.6 (18.2%) after conventional microcatheter PAE and 6.15cm3±14.6 (7.3%) after balloon-occlusion PAE (p=0.05).
Additionally, Bilhim et al report no statistically significant difference in the average maximum pain reported within 24 hours after the procedure (0.74±1.31 and 0.93±1.70 in conventional microcatheter PAE and balloon-occlusion PAE groups, respectively; p=0.056).
Longer term data are needed to determine if the relapse rate is different between the two PAE procedural methods.
Comparing the two PAE procedures, Bilhim and colleagues are surprised by their results, writing: “Balloon-occlusion PAE relies on the potential to prevent reflux and to reverse blood flow in the anastomoses between the prostate and surrounding organs. Thus, it would be reasonable to expect fewer adverse events in balloon-occlusion PAE and less need for protective coil blockage of the prostatic anastomoses. These assumptions were not proven here, as the overall rate of adverse events was not significantly different between the two groups.”
Indeed, no major adverse events occurred in either group, whilst minor adverse events occurred in 23 patients (53.5%) in the conventional microcatheter PAE group, and in 26 patients (56.5%) in the balloon-occlusion PAE cohort. Penile skin lesions and rectal bleeding, which the study authors say can be due to nontarget embolization, only occurred in the conventional microcatheter PAE cohort: three patients (7.1%) had penile skin lesions and two (4.7%) had rectal bleeding.
Interpreting these findings, the investigators say that “these observations are probably clinically relevant, as they represent indirect measures of nontarget embolization”. They continue: “The lower rate of these adverse events [penile skin lesions and rectal bleeding] in the balloon-occlusion microcatheter PAE group (with no reported events) could be due to the protective features of balloon-occlusion. However, the wedged embolization technique used as opposed to a free-flow embolization and a low usage of protective coils (14%) could have led to a higher rate of nontarget embolization in the conventional microcatheter PAE group (n=5; 11.9%).”
Bilhim and colleagues recommend that future trials compare the two types of PAE procedures using radiopaque microspheres or macroaggregates, in an effort to clarify “any potential benefits related to reduced nontarget embolization in particular”.
When enumerating the potential benefits of balloon-occlusion PAE in comparison with conventional microcatheter PAE, Bilhim et al list reduced coil usage (as the placement of coils has been shown to increase procedural times and radiation exposure) and the establishment of an intraprostate negative pressure, which the authors claim “could likely allows the use of a larger amount of embolic volume”. If this latter benefit holds true, Bilhim and colleagues postulate that balloon-occlusion PAE “could lead to greater prostatic destruction, together with higher values of prostate-specific antigen in the 24 hours following embolization, and greater clinical relief”. However, this was not proven in the present study.
Furthermore, the authors note that their work corroborates earlier studies in showing that 5α-reductase inhibitors are not detrimental to the clinical outcomes after PAE. In fact, the present study “uncovered a potential positive interaction with PAE outcomes—that is, the use of 5α-reductase inhibitors before PAE may lead to better clinical outcomes”, according to Bilhim and colleagues.
Concept Medical has been granted breakthrough device designation from the US Food and Drug Administration (FDA) for MagicTouch AVF, its sirolimus drug-coated balloon (DCB) catheter, for the treatment of stenotic lesions of arteriovenous fistulae or arteriovenous graft in haemodialysis treatment of renal failure.
The FDA received a request from Concept Medical to designate MagicTouch AVF as a breakthrough device in July 2019. The proposed indications for the breakthrough device designation for the MagicTouch sirolimus-coated balloon catheter is indicated for use in percutaneous transluminal angioplasty (PTA), after appropriate vessel preparation for treatment of stenotic lesions of dysfunctional native arteriovenous dialysis fistula or graft with 4–12 mm diameter and up to 100mm in length.”
On 28 August, Concept Medical was informed by the FDA that “your combination product and proposed indication for use meet the criteria and have been granted designation as a breakthrough device.”
The world’s first pilot study to investigate the safety and efficacy of Magic Touch percutaneous transluminal angioplasty (PTA) sirolimus balloon in vascular access interventions was started in Singapore in 2018. Led by principal investigator, Tan Chieh Suai, a multi-disciplinary team of doctors consisting of interventional nephrologists, vascular surgeons and interventional radiologists, is conducting the study entitled “Sirolimus coated angioplasty balloon in the salvage of thrombosed arteriovenous graft” in Singapore General Hospital.
In response to the breakthrough designation for Magic Touch AVF, adjunct assistant professor Tan Chieh Suai, senior consultant and director for the Interventional Nephrology Program in the Department of Renal Medicine in Singapore General Hospital and Duke-NUS Medical School, said, “The award of the breakthrough device designation for the use of sirolimus-coated balloons in dialysis access is fantastic news for patients on haemodialysis, as there is an urgent need for effective and durable treatment for narrowing (stenosis) within the dialysis circuit.”
Tjun Yip Tang, associate professor and consultant vascular and endovascular surgeon, Singapore General Hospital, Singapore has highly appreciated the success of Concept Medical and said, “We are still in the early stage in the clinical study of drug-coated balloons for haemodialysis access patients. The paclitaxel-based technology study results have certainly been encouraging, but more research is required to determine if other devices may prove to be more effective or uniquely beneficial for specific anatomical or clinical subtype presentations.”
The breakthrough device designation granted to Magic Touch AVF offers Concept Medical an opportunity to interact with the FDA’s experts. Under the programme, the FDA will provide Concept Medical with priority review and interactive communication regarding device development and clinical trial protocols through to commercialisation decisions.
An updated guideline on the prophylaxis and treatment of venous thromboembolism (VTE) in patients with cancer has been unveiled by the American Society of Clinical Oncology (ASCO) in its Journal of Clinical Oncology. An expert panel convened by ASCO reviewed evidence—including randomised controlled trials (RCTs) and meta-analyses of RCTs—from the period between 1 August 2014 and 4 December 2018, before providing a list of findings and recommendations.
Patients with cancer are at a higher risk of developing VTE, including deep vein thrombosis (DVT) and pulmonary embolism (PE), than those without cancer, and have higher rates of VTE recurrence and bleeding during VTE treatment. Consequently, VTE is an “important cause of morbidity and mortality” among cancer patients.
According to the review, two RCTs of direct oral anticoagulants (DOACs) for the treatment of VTE in cancer patients confirmed the efficacy of edoxaban and rivaroxaban, but found that they could be associated with an increased risk of bleeding compared to low-molecular-weight heparin (LMWH). Furthermore, two additional RCTs underlined the potential benefits and side-effects of DOACs for thromboprophylaxis in ambulatory cancer patients at a higher risk of VTE.
Co-chaired by Nigel S Key (Chapel Hill, North Carolina, USA) and Anna Falanga (Bergamo, Italy), the panel’s systematic review included a total of 35 publications (26 meta-analyses and nine RCTs) on VTE prophylaxis and treatment, and 18 publications on VTE risk assessment (six included multiple types of cancer, while 12 focused on individual cancer types). In addition to Key and Falanga, 15 additional authors worked on the project.
Speaking to Interventional News about the importance of these guidelines, Key comments, “This iteration of the ASCO guidelines on VTE prevention and treatment reflects an evolving evidence-based set of recommendations on a common problem in a challenging patient population. Perhaps the greatest advances are the recommendations to consider certain oral direct factor Xa inhibitors for the treatment of VTE and for VTE prevention in higher risk cancer patients.”
Falanga is in accordance, adding, “The updated ASCO guidelines reflect the new evidence from clinical research showing the efficacy of new anticoagulant drugs for VTE management in oncology. The addition of some DOAC to our armamentarium to prevent and treat cancer-associated VTE expands our choice and allows the possibility to personalise treatment based on patient characteristics and type of cancer.”
The updated guideline addresses six clinical questions:
Should hospitalized patients with cancer receive anticoagulation for VTE prophylaxis?
Should ambulatory patients with cancer receive anticoagulation for VTE prophylaxis during systemic chemotherapy?
Should patients with cancer undergoing surgery receive perioperative VTE prophylaxis?
What is the best method for treatment of patients with cancer with established VTE to prevent recurrence?
Should patients with cancer receive anticoagulants in the absence of established VTE to improve survival?
What is known about risk prediction and awareness of VTE among patients with cancer?
In response to the first clinical question, “Should hospitalized patients with cancer receive anticoagulation for VTE prophylaxis?”, ASCO’s guideline states that hospitalised patients who have active malignancy and acute medical illness, or reduced mobility, should be offered pharmacologic thromboprophylaxis in the absence of bleeding, while patients with active malignancy but no additional risk factors may be offered pharmacologic thromboprophylaxis. However, pharmacologic thromboprophylaxis should not be offered to patients admitted for minor procedures or chemotherapy infusion, nor patients undergoing stem-cell or bone marrow transplantation.
On the subject of whether ambulatory patients with cancer should receive anticoagulation for VTE prophylaxis during systemic chemotherapy, a new addition to the guideline is that high-risk outpatients with cancer may be offered thromboprophylaxis with apixaban, rivaroxaban or LMWH Patients with multiple myeloma receiving thalidomide or lenalidomide with chemotherapy should be offered pharmacologic thromboprophylaxis, according to the guideline.
For cancer patients undergoing surgery, it is recommended that all persons with malignant disease undergoing a major surgical intervention receive perioperative VTE prophylaxis with either unfractionated heparin (UFH) or LMWH, unless they present a high bleeding risk or other contraindications. Prophylaxis should be commenced preoperatively and continue after surgery for at least seven to 10 days, while extended prophylaxis with LMWH, for up to four weeks, is recommended for cancer patients undergoing major open, laparoscopic abdominal or pelvic surgery.
Regarding the best method of treating cancer patients in order to prevent VTE recurrence, a number of recommendations are included in the guideline. Initial anticoagulation may involve LMWH, UFH, fondaparinux, or rivaroxaban, though LMWH is preferred over UFH for the initial five to 10 days of anticoagulation for patients with newly diagnosed VTE. For long-term anticoagulation of six months, it is stated that LMWH, edoxaban, or rivaroxaban are more effective and therefore preferred. Patients with active cancer, including those with metastatic disease or persons receiving chemotherapy, should receive anticoagulation with LMWH, DOACs or vitamin K antagonists (VKAs) beyond six months.
Responding to expert opinion in the absence of randomised trial data, uncertainty towards short-term benefits, and evidence of long-term harm from filters, ASCO has recommended against the insertion of a vena cava filter for patients with established or chronic thrombosis. Additionally, the guideline asserts that filter insertion has no role for primary prevention or prophylaxis of PE or DVT, though a vena cava filter may be offered as an adjunct to anticoagulation in patients with progression of thrombosis. Incidental PE and deep vein thrombosis should be treated in the same manner as symptomatic VTE, according to ASCO.
Answering the question of whether patients with cancer should receive anticoagulants in the absence of established VTE to improve chances of survival, anticoagulant use is not recommended to improve survival in patients with cancer without VTE.
Finally, the guideline addresses what is known about risk prediction and awareness of VTE among patients with cancer, recommending that those persons should be assessed for VTE risk initially and periodically, particularly when starting systemic antineoplastic therapy or at the time of hospitalisation. At the same time, individual risk factors do not reliably identify patients with cancer at high risk of VTE. ASCO argues that oncologists should educate patients regarding VTE, particularly in settings that increase risk such as major surgery and hospitalisation.
Oleksandra Kutsenko, a radiology resident at Upstate Medical University, Syracuse, USA, and Society of Interventional Radiology-Resident Fellow Student (SIR-RFS) advocacy chair, has given a TED talk expressing the possibilities of minimally invasive, image-guided medicine.
Focusing on the “science-fiction” like capabilities of interventional radiology (IR), Kutsenko began her talk by describing three case studies where patients were not treated with IR procedures, but could have potentially received better treatment if they had been. In the first example, she detailed how a woman who had a hysterectomy could have been saved an invasive surgery, a long recovery time, and her fertility if she had been treated with a uterine fibroid embolization. In the next example, she detailed how a young veteran treated for back pain with opioids could have been spared his resultant painkiller addiction through original treatment with nerve ablation and vertebroplasty. Lastly, she spoke of a liver cancer patient who could undergo “potentially curative” microwave ablation or chemoembolization in order to avoid either liver transplant and a lifelong immunosuppression, or a long course of chemotherapy with its attendant side effects: infection, bleeding, hair loss, fatigue, and stomach pains.
Reaching an audience of millions, TED talks are an effective means of communicating with large swathes of the general public. This accords with one of SIR’s key mission statements, to reach “around the world and out to partners across corporate, public, and private sectors to ensure the story of interventional radiology is spread through a range of communication channels”. In addition to public outreach, SIR advocates on behalf of its members and interventional radiology as a whole before Congress, insurance carriers and other key decision-makers.
Improving the public awareness of interventional radiology procedures was central to Kutsenko’s talk. “It seems that interventional radiology has been the best kept secret of medicine”, she told the audience. “So let us change this”.
Speaking to Interventional News, Kutsenko comments, “Interventional Radiology covers a broad spectrum of minimally-invasive procedures that diagnose and treat almost every organ in the body; we work with physicians in nearly every specialty of medicine and provide some of the best healthcare value and outcomes, and yet our specialty is strikingly unknown among other physicians, legislative bodies, and most importantly patients.
“To change this, we need to reach out to large masses of people in the general population and spread the word about the treatment options we have to offer. TED is one of the greatest media platforms that is doing exactly that. Extremely popular TED educational videos can increase awareness about IR far beyond single hospitals, cities, or even countries. As a result, the information on value of minimally invasive image-guided procedures can be delivered to large populations, and through them further influence hospital and national policies. The voice of our patients will be heard, and we all should make sure that their health decisions are based on understanding new technically-advanced, IR-inclusive, better medicine.”
After sharing her TED talk on Twitter, Kutsenko was quickly the recipient of much praise from other interventional radiologists on the platform. Replying on the site, aspiring interventional radiologist Alex Sher (Mount Sinai, New York, USA) wrote: “Great talk and thanks for spreading the word about interventional radiology!”
Adept Medical has launches its Antegrade IR platform, which provides a work surface for antegrade femoral approach during interventional radiology vascular procedures. The device sits within the company’s existing range of access and patient positioning devices designed for interventional radiology, cardiology and vascular procedures.
Designed to provide a stable, radiolucent, height- and length-appropriate work surface for supporting light-weight equipment during the antegrade femoral approach, the Antegrade IR Platform offers clinical benefits to the current practice of laying procedural equipment on the mattress and patient, a press release states.
The narrow portion of the Antegrade IR Platform extends alongside the patient towards the femoral artery, offering a steady platform for the clinician to rest their wrists on during wire manipulation. It can be set up at two different lengths and at various heights according to the patient and procedure, providing flexibility.
“Having the Retrograde IR Platform in market now for a few years gave us deeper insights into the requirements surrounding femoral artery access and that product was the conversation starter for the Antegrade IR Platform”, Adept Medical’s product development manager Matt Lazenby comments. “It became a common request when promoting at congress meetings and we worked closely with director of Medical Imaging, Marcus Mykytowycz of Western Health (Melbourne, Australia), with iterations of prototypes before widening our trial sites. Lower leg interventions for ischaemia is going through a rapid upsurge due to the increase in diabetes cases and we felt that the timing was right to release a specific platform for facilitating antegrade femoral access with all the same benefits as our existing retrograde platform.”
Ideally used in conjunction with the Adept Medical Drape Support and ArmSure, these two products offer drape management, patient comfort and security during interventional radiology procedures.
Crafted from carbon fibre composite and high-performance engineering plastics, the platform is light-weight yet strong and has a high resistance to chemical attack from commonly used cleaning products.
According to a press release, Surmodics has completed enrolment in TRANSCEND, its pivotal clinical trial for the SurVeil drug-coated balloon (DCB).
“TRANSCEND is a rigorous level one, randomised controlled trial that comes at a very important time for the vascular and interventional community,” said Kenneth Rosenfield, a principal investigator of the TRANSCEND study. “By providing a head-to-head comparison with today’s market leading DCB, this trial will provide data regarding the relative performance of the SurVeil DCB, which represents a new generation of DCB. Beyond the device itself, the new trial design will ultimately provide insight into clinically important questions regarding long-term results. There is great promise that this third-generation DCB will further improve upon current outcomes for this technology and provide additional benefit for clinicians and the patients that they treat.”
The TRANSCEND trial enrolled 446 patients at 65 global sites. The randomised study will evaluate the safety and efficacy of the SurVeil DCB compared with a commercially available DCB in treating peripheral artery disease (PAD) in the upper leg. The results of the trial will also include long-term, patient-level data out to five years.
“I am excited about the potential of the SurVeil DCB to improve the treatment of PAD,” said Marianne Brodmann, a TRANSCEND principal investigator and the trial’s leading enroller with 44 randomisations. “Our focus now shifts to follow-up and monitoring of these patients and the collection of high-quality data.”
“Completing enrolment in the TRANSCEND trial marks an important milestone and brings us one step closer to bringing this next-generation treatment to PAD patients,” said Gary Maharaj, Surmodics’ president and chief executive officer. “I would like to thank our principal investigators—Kenneth Rosenfield, Marianne Brodmann, and William Gray—our trial advisor, Peter Schneider, and the entire steering committee for their leadership and guidance, all our investigators, support teams and, importantly, the patients we enrolled. Without their participation, we would not be here today.”
In February 2018, Surmodics entered into an agreement with Abbott that provided Abbott with exclusive worldwide commercialisation rights for the SurVeil DCB. Pursuant to the terms of the agreement, Surmodics received a US$25 million upfront payment and will receive a US$10 million milestone payment in connection with the completion of patient enrolment in the TRANSCEND trial. Approximately US$5 million from this milestone payment will be recognised as revenue in the company’s fiscal fourth quarter. Surmodics may earn an additional US$57 million for other various product development milestones.
Upon the regulatory approval of the device, Surmodics will be responsible for manufacturing clinical and commercial quantities of the product and will realise revenue from product sales to Abbott as well as a share of profits resulting from sales to third parties.
The Society of Interventional Radiology (SIR) invites practising physicians, early career professionals, research scientists, clinical associates, trainees and medical students to submit original research for possible presentation during the society’s Annual Scientific Meeting, 28 March–2 April, 2020, in Seattle, USA. Online abstract submission is open at sirmeeting.org until 5pm ET on 26 September, 2019.
“Interventional radiology is constantly redefining the landscape of minimally invasive, image-guided treatments. You can play a role in this evolution by sharing your ideas, innovations and state-of-the-art technology at the SIR 2020 Annual Scientific Meeting. SIR 2020 is the place to see what is at the forefront of the specialty that will enable us to continue to provide the best patient care,” says SIR 2020 scientific chair Baljendra S Kapoor, an interventional radiologist at the Cleveland Clinic, Cleveland, USA. “The SIR Annual Scientific Meeting highlights collaboration in interventional radiology and addresses bold strides in clinical practice. I invite you to join us in Seattle and share your research and expertise with attendees from around the world.”
SIR details how to get involved: “Submissions may be accepted for oral or poster presentation for scientific abstracts and traditional paper posters for educational exhibits. Please note, single-case reports will not be accepted. Original scientific research abstracts accepted for oral presentation, ePoster or traditional poster presentation will be published in the supplement to SIR’s flagship Journal of Vascular and Interventional Radiology (JVIR), and on jvir.org, and will be a citable reference.
“Selected abstracts will be designated as ‘Distinguished’, ‘Featured’ or ‘Abstract of the Year’. Additionally, national and international consumer and trade media will report on ground-breaking research presented at SIR 2020.”
SIR 2020 is expected to attract more than 5,000 attendees from around the globe to Seattle, a city known for germinating new technologies and bold scientific thinking. Researchers who are accepted will have the opportunity to grow the field of image-guided interventions by sharing their discoveries, device and procedure innovations, clinical outcomes, and breaking research in areas that address many of today’s most challenging medical problems, including cancer, vascular disease, and men’s and women’s health.
According to SIR, in 2020 the meeting will include lecture-based didactic sessions; centrepiece plenaries that will inspire and educate; Angio Clubs, a series of case-based workshops; SIRConnectLive, a unique town-halltype session that promotes interactive learning; self-assessment CME (SACME) sessions, which help fulfil maintenance of certification (MOC) requirements; hands-on workshops and much, much more.
High-level scientific abstract presentations are featured during the meeting’s scientific sessions, where attendees will learn about current clinical trials, technical innovations, and the basic science shaping the foundation of the specialty.
Abstracts presented during the scientific sessions span a wide breadth of categories, including arterial interventions; venous interventions; nonvascular interventions; dialysis interventions; education and training; practice management; health care policy; and quality improvement.
SIR Expo
The SIR 2020 exhibit hall at the Washington State Convention Center is open to all registered attendees and guests with a badge. Attendees should watch for special events and hands-on sessions at select booths. Throughout the meeting, attendees will be encouraged to attend “Compelling Conversations,” a series of informal, popular question and answer sessions on timely topics, held at SIR Central in SIR Expo.
About Seattle
Seattle is a world-class metropolis set within beautiful, natural surroundings, offering the best of an urban lifestyle while embracing the outdoors. Many of Seattle’s top visitor attractions are within a few blocks of the Washington State Convention Center, including the Pike Place Market, Seattle Art Museum, ferries, world-class restaurants, and a historic theatre district. Three national parks lie within a two-hour drive of Seattle and the city is a gateway to the San Juan Islands, Washington Wine Country, and British Columbia.
About the Society of Interventional Radiology
The Society of Interventional Radiology is a non-profit, professional medical society representing more than 8,000 practising interventional radiology physicians, trainees, students, scientists and clinical associates, dedicated to improving patient care through the limitless potential of image-guided therapies. SIR’s members work in a variety of settings and at different professional levels—from medical students and residents to university faculty and private practice physicians.
Data from the University of Pittsburgh Medical Center (Pittsburgh, USA) indicate that the open approach to managing thrombosed haemodialysis grafts with venous anastomotic lesions is not associated with superior primary patency when compared to the hybrid approach. These findings also show that an existing stent in an arteriovenous graft (AVG) is a strong predictor of loss of patency and graft abandonment.
Catherine Go (Division of Vascular Surgery, University of Pittsburgh Medical Center, Pittsburgh, USA) presented the data at the 2019 Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM; 12–15 June, National Harbor, USA). She told delegates that AVG were “plagued by poor patency” and failure of an AVG leads to “increased cost and morbidity”, adding that thrombosis in an AVG most commonly occurred because of a venous anastomosis stenosis.
However, according to Go, the “jury is still out” about how to manage such thromboses. Two meta-analyses—published in 2002 and 2019—have reported the superiority of the open treatment over purely endovascular methods, but few studies have investigated the hybrid technique, which Go reported is commonly used at her centre (University of Pittsburgh Medical Center). She explained that this involves “open thrombectomy followed by endoluminal treatment (balloon angioplasty, cutting balloons, or stents/stent grafts)”.
“Based on historical data, we hypothesised that open revision for AVG venous anastomosis is associated with better patency when compared to hybrid therapies”, Go stated. Therefore, in the retrospective study, Go and colleagues compared patency outcomes for patients who underwent open repair for a first-time AVG thrombosis with those for patients who underwent the hybrid approach. The primary endpoints were primary patency (time from index thrombectomy to first reintervention or thrombosis) and secondary patency (time from index thrombectomy to graft abandonment). The investigators also reviewed technical success and primary-assisted patency (time from index thrombectomy to first rethrombosis).
Overall, 97 patients underwent intervention for occluded AVGs at the University of Pittsburgh Medical Center between 2014 and 2018. Of these, 34 underwent the open approach (73.5% patch angioplasty and 26.5% jump bypass) and 63 (22.2% stent graft, 7.9% cutting balloon, and 1.6% bare metal stent) underwent the hybrid approach. At 30 days, there were no significant differences in rate of the failure of the approach: 29.4% for open vs. 27% for hybrid (p=0.799). A multivariate analysis showed that a higher number of prior fistulograms and African-American race were both predictive of protection against failure. There were also no significant differences between groups in primary patency, primary-assisted patency, or secondary patency at either six months or 12 months.
Go reported that the number of prior fistulograms was again predictive of protection against primary patency failure (at six/12 months). Central occlusion and a hypercoagulable state were predictive of loss of primary-assisted patency. An existing venous anastomosis stent predicted both loss of primary patency and loss of secondary patency.
“AVG patency after thrombectomy is poor. Open versus hybrid treatment of AVG venous anastomosis stenosis are not associated with differences in patency. An existing stent at the venous anastomosis is a strong predictor of loss of patency and abandonment,” Go reported. She added that, given the association between an existing stent and graft abandonment, an operator should “start planning future access options” when using a stent to salvage a thrombosed AVG.
Nicholas (Nick) Inston calls for “more creative solutions” to vascular access challenges, commending interventional radiologists’ innovative reputation as instrumental to increasing the number of treatment approaches available to physicians. Outlining the complexities of end-stage vascular access in an ever-increasing patient population, Inston expresses the need for a multidisciplinary team approach, claiming that the “outlook is improving” due to the fruitful cross-pollination of ideas and skills.
The age of the dialysis population continues to increase, and whilst some of this may be attributed to older patients initiating dialysis, the main component is improved survival in prevalent dialysis patients. As a consequence, the vascular access needs of this population become more challenging. As primary access sites become depleted, more creative solutions must be employed.
In a small but increasing group of patients, standard, multiple, autologous, and synthetic options may have all failed, and these patients may be deemed to have exhausted all vascular access options except for the use of a central venous catheter (CVC). This situation may be termed end-stage vascular access (ESVA).1
If a patient with a limited lifespan expresses a wish to remain on a CVC, this may be a suitable option. However, this group of patients are likely to require multiple interventions to maintain their CVC patency and may require kinase infusions and even emergency CVC exchange to maintain an ability to dialyse.2
In those patients keen to pursue definitive access options, classifying the underlying issues is helpful. This can be done on an anatomical basis such as the radiological classification outlined by the Society of Interventional Radiology,3 or by using a simplified, more basic classification, such as that described by Julien Al-Shakarchi (University Hospital Birmingham, Birmingham, UK).1
A simple classification for endstage vascular access failure is proposed based on a sequential broad categorisation of: stage 1) no upper limb vascular access option; stage 2) no lower limb vascular access options; stage 3) no vascular access options at any site.
Stages of ESVA from Al-Shakarchi et al. The classification has arterial insufficiency (including hypotension) which has been removed from this table as different approaches are required
These can have the underlying anatomical problem added to allow more detailed definition (see Table 1).
An illustrative example may be a patient with tight superior vena cava (SVC) and brachiocephalic stenosis who has a right iliac vein occlusion and a left groin line. This would be classed as ESVA 2a, and possible solutions that could be considered are a left femoral vein transposition or loop thigh arteriovenous (AV) graft, attempts at recanalising the upper body central veins with recanalisation and stenting, or use of a Surfacer device (Bluegrass Vascular) and insertion of a HeRO (Merit Medical).4 Other options may be a non-standard graft configuration—here a right axillo-femoral graft may be possible. Peritoneal dialysis should not be forgotten.
When balancing each of these the risks and benefits should be carefully considered.
Lower leg access is not without complications. Femoral vein transposition, whilst having the advantage of use of the autologous vein and of reducing infection, is associated with lower limb congestion and venous insufficiency. Additionally, amputation has been reported with this method. Lower limb prosthetic grafts are associated with high rates of infection and low patency.5
Recanalisation of upper body central vessels may require expert interventional radiology skills and devices. The Surfacer device has potential, but robust data are not yet available to allow evaluation. Even with recanalised vessels the next step towards definitive access requires either extensive stenting or the use of a HeRO device. In patients with CVC infections (common in groin access), this is contraindicated. In such patients, a staged approach to recanalisation with initial upper body CVC, eradication of infection, and subsequent conversion to a HeRO graft may be a better approach.
Patients with arterial insufficiency can pose a problem and inadequate inflow may not only threaten the access, but also the limb. The resistance within longer grafts and HeRO grafts requires a suitable inflow including a reasonable blood pressure. Hypotension should be carefully evaluated when these options are being considered.
A further consideration is that of transplantation. Younger patients with ESVA may have had a long history of renal replacement and multiple CVCs. In the example above, a groin line in the only patent iliac vein poses a great threat to future kidney transplantation. It may be proposed that such patients are considered higher priority in organ allocation schemes as a working transplant is their optimal option. When considering such patients for lower limb access there is little to support avoidance of lower limb options and many transplants have been performed successfully above patent ipsilateral loop thigh grafts.
For patients where attempts to gain access are unsuccessful—stage 3 ESVA—there are still solutions that can be found.
This group traditionally were treated with a translumbar or transhepatic CVC. For many this was seen as a pre-terminal option, although data support reasonable short and mid-term survival.6 A relatively simple definitive option in these patients is the arterial arterial prosthetic loop (AAPL), which is an interposition graft in the subclavian/axillary artery.7
This unique configuration requires special consideration when cannulated and cannot be used for drug delivery but has been shown to have good patency with low complications.
Smaller series of axillary atrial grafts are published and advocated by some authors, however complications are greater and more significant.6
In deciding treatment options, an access life plan should be defined, as highlighted in the recent Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines from the National Kidney Foundation.8 Where multiple options exist, these should be considered and staged with the simplest and safest option first, whilst retaining the possibility of further interventions later down the line.
The best approach to managing these difficult cases is with a multidisciplinary team, using a treatment utilising their experience and expertise, and chosen based on its applicability to the patient. The availability of surgical and radiological expertise is required not only for the index procedure, but also for many of these patients’ subsequent interventions and salvage procedures, conducted to maintain patency. An identified pathway should be defined with access to suitable facilities to allow this.
ESVA provides a very challenging problem for the vascular access surgeon, and the bad news is the incidence is likely to increase. Fortunately, there are an increasing number of possibilities for treatment with innovative devices and techniques. Historically, the prognosis was bleak for patients with ESVA, but by combining surgery and interventional radiology skills, the outlook is improving. As always in access, the approach used should be the right access, for the right patient, at the right time. This applies especially to ESVA, where the whole team’s input and detailed discussion with the patient are essential.
Nicholas Inston is a consultant transplant and vascular access surgeon at the University Hospital Birmingham NHS Trust, Birmingham, UK.
References
Al Shakarchi J, Nath J, McGrogan D, Khawaja A, Field M, Jones RG, et al. End-stage vascular access failure: can we define and can we classify? Clin Kidney J. 2015;8(5):590-3.
Kumwenda M, Dougherty L, Spooner H, Jackson V, Mitra S, Inston N. Managing dysfunctional central venous access devices: a practical approach to urokinase thrombolysis. Br J Nurs. 2018;27(2):S4-S10.
Dolmatch BL, Gurley JC, Baskin KM, Nikolic B, Lawson JH, Shenoy S, et al. Society of Interventional Radiology Reporting Standards for Thoracic Central Vein Obstruction: Endorsed by the American Society of Diagnostic and Interventional Nephrology (ASDIN), British Society of Interventional Radiology (BSIR), Canadian Interventional Radiology Association (CIRA), Heart Rhythm Society (HRS), Indian Society of Vascular and Interventional Radiology (ISVIR), Vascular Access Society of the Americas (VASA), and Vascular Access Society of Britain and Ireland (VASBI). J Vasc Interv Radiol. 2018;29(4):454-60 e3.
Davis KL, Gurley JC, Davenport DL, Xenos ES. The use of HeRo catheter in catheter-dependent dialysis patients with superior vena cava occlusion. J Vasc Access. 2016;17(2):138-42.
Parekh VB, Niyyar VD, Vachharajani TJ. Lower Extremity Permanent Dialysis Vascular Access. Clin J Am Soc Nephrol. 2016;11(9):1693-702.
Inston N, Khawaja A, Mistry H, Jones R, Valenti D. Options for end stage vascular access: Translumbar catheter, arterial-arterial access or right atrial graft? J Vasc Access. 2019:1129729819841153.
Stephenson MA, Norris JM, Mistry H, Valenti D. Axillary-axillary interarterial chest loop graft for successful early hemodialysis access. J Vasc Access. 2013;14(3):291-4.
KDOQI clinical practice guideline for vascular access: 2018. 2018.
Merit Medical have announced the commercial launch of the PreludeSYNC EVO radial compression device in the USA. The PreludeSYNC EVO is a sterile, single-use, disposable device used to assist in gaining haemostasis of the arterial percutaneous access site following catheterisation procedures.
Merit Medical’s launch of the PreludeSYNC EVO follows nearly two decades of innovation in haemostasis band products, the company asserts. The PreludeSYNC EVO was designed to provide operators improved clarity, safety, and patient comfort. According to a press release, the clear balloon and curved backer plate provide optimal visualisation of the puncture site, facilitating easy placement. The band, which is easily adjustable and fits securely around a patient’s wrist, comes in two sizes (24cm and 29cm). The device also features the new Slip-n-Lock Connection for safe and easy inflation and deflation.
“A core part of Merit Medical’s mission is to continually evolve and improve our product offerings, including in the area of access and hemostasis,” says Fred P Lampropoulos, Merit Medical’s founder, chair, and CEO. “Accordingly, the PreludeSYNC EVO is a needed solution that elevates the radial compression experience for operators and their patients. The Merit leadership team is excited to put the EVO in the hands of specialists across the USA.”
Ashutosh Rao (Atlanta, USA) talks to Interventional News at SIR 2019 about the OnControl device. Before switching to OnControl, Rao explains, “we did not realise how easy bone biopsies could be”.
Rao notes that sometimes bone lesions are not on the proximal side of the bone and that the OnControl device, with its outer cannula, allows those using it to drill through the front cortex and “get to difficult lesions we may not have otherwise been able to get to.”
He also talks about how it has transformed his practice for both bone biopsies and bone marrow biopsies and how the patients do not feel “all the pushing and pulling” you would normally get from manual pressure.
“Interventional radiology is uniquely equipped to shape the next generation of nanotherapeutics,” Sarah White, associate professor of Radiation and Surgical Oncology at the Medical College of Wisconsin (Milwaukee, USA) and adjunct professor of Radiology at Northwestern University (Evanston, USA) informed delegates at the 2019 annual meeting of the Society of Interventional Oncology (SIO; 7–11 June, Boston, USA). She presented research detailing how the local delivery of nanoparticles directly to the tumour site enables enhanced care to cancer patients. nanotechnology
“I think nanotechnology really allows us to troubleshoot some of the problems in interventional oncology, and then to find applications and create solutions”, she said.
Globally, US$10 billion is spent on nanotechnology research, across many different disciplines. Explaining why she believes this technology has so much potential in the medical field specifically, White said, “Nanoparticles are the right size. One nanoparticle is a billionth of a metre. To visualise that: a marble to the size of the Earth. The diameter of a DNA double helix is 2nm, and the smallest bacteria is 200nm long. Nanotechnology is the size between cells and their organelles, such as mitochondria. They are right in that cellular realm, which is why it is so advantageous to use them in this field.”
In cancer research, nanoparticles are usually used in a theranostic setting, meaning that the nanoparticle can be used not only as a drug—as the treatment—but also as an imaging tool. Currently, systemic chemotherapy used to treat cancer patients is non-specific and, due to lymphatic drainage of the chemotherapy agent from the target tissue, needs to be administered in such high doses to be concentrated enough in the tumour to destroy the cancer that side effects are common and severe.
However, when the chemotherapy drugs are formulated into a nanoparticle, these do not leach out of the tumour cells as easily. This is because healthy cells are packed close together in an orderly structure, and have tight junctions with a lymphatic outflow system threaded throughout. In comparison, tumour cells have antigenic factors that mean they grow rapidly, proliferating in a disordered fashion without tight junctions. The larger gaps between tumour cells means the normal lymphatic outflow cannot form to drain the tissue correctly, altering what passes into and out of the cancerous cells. Smaller molecules, such as nanoparticles, can enter the tumour, and due to the lack of lymphatic drainage, remain there. This method of drug delivery is known as passive tumour targeting, and it increases the ability of the interventionist to get the drug into the tumorous tissue. Due to the proper lymphatic drainage of the non-tumour cells in the body, the nanoparticles are filtered out of these more effectively, meaning the concentration of these small molecules is greater in the cancer.
Active targeting of the tumour
Active targeting of the tumour by nanoparticles also improves clinical outcomes. White explained at SIO: “Tumours often overexpress receptors, so we can put things on the nanoparticles to actively target those surplus receptors.”
According to White, this active tumour targeting increases the efficacy of the treatment due to greater internalisation of the chemotherapy agent. Another drug delivery method explained by White at SIO is endothelial cell targeting, where, similarly to the overexpression of surface receptors on the tumour cells, investigators can formulate nanoparticles to specifically target overexpressed receptors on angiogenic endothelial cells. These line the newer blood vessels feeding the tumour, and using nanoparticles to target these cells helps eradicate the source of the blood flow to cancerous or benign growths.
“The last thing we can do [with drug delivery] is triggered drug release”, White described, “and this is one of the most interesting to me. We can stimulate the release of the cargo. The cargo is the imaging agent or the treatment.”
Clinical applications of nanotechnology in interventional oncology
Addressing the SIO audience, White described current and potential clinical applications of nanoparticles. The first example she used was in the delivery of hydrophobic drugs: “We want to deliver hydrophobic drugs. We think sorafenib can help us treat the surge in vascular endothelial growth factor receptor (VEGF) after transarterial chemoembolization (TACE) that we see at 24 hours.”
Sorafenib is currently the only first-line multi-kinase inhibitor approved for use in hepatocellular carcinoma (HCC). It inhibits the activity of several kinases, including VEGF, which are involved in tumour cell signalling, proliferation, angiogenesis and apoptosis. Thus, sorafenib inhibits tumour growth and neoangiogenesis. Several recent studies, including work by Baosheng Ren (The Second People’s Hospital of Changzhou, Changzhou, China), Wansheng Wang (The First Affiliated Hospital of Soochow University, Suzhou, China) et al in the Journal of Cancer, have reported that overall survival is improved in HCC patients when treated with a combination of sorafenib and TACE compared with TACE alone.
“But when sorafenib is administered systemically”, White explained, “which is done in order to get high enough levels of the drug into the tumour, it can cause extreme side effects.”
In an effort to eliminate these side effects, nanoparticles can be used to deliver sorafenib locally, rather than systemically. According to White, it is possible to make a nanoconstruct with sorafenib that will deliver and deposit the drug straight to the tumour. White and collaborators have fabricated poly(lactide-co-glycolide) microspheres for local sorafenib delivery to tumours during liver-directed embolotherapies. These constructs co-encapsulated iron oxide nanoparticles (IONP) so that the investigators could observe microsphere delivery via magnetic resonance imaging (MRI). Following intra-arterial microsphere infusions in a rabbit VX2 liver model, White demonstrated in 2015 that these sorafenib particles normalised VEGF activity and decreased microvessel density. Writing at the time in Biomaterials, she concluded “These methods should avoid systemic toxicities, with MRI permitting follow-up confirmation of microsphere delivery to the targeted liver tumors”.
A second clinical application of nanoparticles in interventional oncology is to expand the ablation zone when treating patients with metastatic colon cancer who are not candidates for resection. The ablation zone is limited by size (4mm being approximately the largest possible size) and location (due to the risk of damage to adjacent structures). Using a rat model of colorectal liver metastases, White and colleagues compared the size of ablation zones in three groups—rats injected with hybrid magnetic gold nanoparticles tagged with monoclonal antibodies, rats injected with hybrid magnetic gold nanoparticles only, and a control group.
After undergoing photothermal ablation with a fibre-coupled near infrared diode laser, haematoxylin-eosin staining revealed a significant difference in tumour necrosis across the three groups. In the antibody and nanoparticles group, tumour necrosis was 38%±29. In contrast, tumour necrosis in the nanoparticles only group was 14%±17, demonstrating a lack of toxicity. The control group, which were only injected with the colorectal liver metastasis cell lines, had a tumour necrosis of 7%±8 (p=0.043). The addition of the monoclonal antibodies to the nanoparticles also resulted in statistically significant higher levels of delivery to the tumour compared to nanoparticles alone. Published in Radiology in 2017, the investigators concluded that targeted monoclonal antibody–conjugated hybrid magnetic gold nanoparticles can serve as a catalyst for photothermal ablation of colorectal liver metastases by increasing ablation zones. nanotechnology
Society of Interventional Oncology (SIO) president William (Bill) Rilling notes that you do not need to be a full time cancer specialist to describe yourself as an interventional oncologist, and that such a prescriptive definition is unhelpful. “Being an interventional oncologist is not about how many cases you do or what percent of your practice is IO, it is a mindset and a dedication to be a part of the cancer care team”, he says.
As interventional radiology (IR) continues to evolve and mature, it seems only natural that the development of subspecialties is a part of that evolution. Currently, IR physicians may focus on a variety of subspecialty practices including peripheral arterial disease (PAD), venous disease, musculoskeletal interventions, women’s health, oncology, and many other new and exciting facets of IR. Encouraging and enabling IR physicians to focus on subspecialties is important to drive innovation and research and subsequently advance practice. From a practical perspective, the diversity and richness of IR practice helps protect us as IR physicians from large losses in patient and procedure volumes as we can often compensate by expanding other areas of our practice. If a drug is developed tomorrow that cures atherosclerosis, many interventional radiologists would lose a significant and important part of their practice, but the vast majority would still have a job.
However, the diversity of IR can also be a weakness. Others who practice in the field of oncology, for example, focus exclusively on caring for cancer patients. Very few medical, surgical, and radiation oncologists spend a significant portion of their time on anything but oncology. This presents a challenge for interventional oncologists, as there are very few IR/ interventional oncology (IO) physicians who practice in IO exclusively. It makes it more difficult for us to be part of “the club.” For example, my practice is about 70% IO, but I also treat vascular malformations, hereditary haemorrhagic telangiectasia (HHT) patients, along with all the other things most of us take care of on a daily basis, and still have to be able to treat aortic catastrophes on call. Having a single-minded focus on oncology is a challenge for most interventional radiologists.
How do we overcome this challenge? In my view, there are several solutions. First and foremost, we must practice multidisciplinary patient care at its highest level with patients as the focus. Cancer care is the ultimate team sport and most cancer patients will have many different oncologic specialists caring for them at various times throughout their cancer journey. This requires the IR/IO physician to participate in multidisciplinary tumour boards, have a meaningful role in treatment decision making, see patients in clinic to discuss options, follow them in clinic to assess response, and understand the evidence basis for IO therapies and the complimentary medical and surgical options. If you are doing these things in your practice, even if IO is not the majority, you are an interventional oncologist. Thus, being an interventional oncologist is not about how many cases you do or what percentage of your practice is IO, it is a mindset and a dedication to be a part of the cancer care team, providing a unique perspective on image guided therapy and hopefully helping to move the field forward.
IR/IO physicians have a significant advantage being part of the cancer team: we have a role in cancer care from diagnosis, through treatment, and continuing to palliation. Therefore, the definition of what are “IO procedures” also warrants additional discussion. Targeted biopsies are becoming increasingly important as personalised cancer therapy expands at an exponential rate. We not only biopsy for initial diagnosis but also to identify new mutations and resistant clones to modify targeted therapy. This is a central and critical role in the cancer patient which will continue to expand. Image guided therapeutic procedures are clearly the realm of IO and we all need to work to expand access to these procedures for our patients. Central to this will be proving the effectiveness of IO treatments by expanding clinical trials and other data collection platforms. IO/IR physicians also play a unique role in palliation and improving quality of life for cancer patients with fluid management techniques, pain palliation, management of malignant bowel obstruction and many other interventions to improve quality of life and decrease narcotic usage in this patient population. This broad spectrum of involvement from diagnosis, to treatment and continuing to palliation is a unique advantage and perspective for IO.
Moving forward, I believe we should continue to encourage and enable subspecialty evolution in IR. This does not weaken IR as a whole but strengthens it. As interventional oncology matures as a subspecialty, we should embrace our inherent and significant advantages as cancer specialists. Currently, as patient reported outcomes, quality of life metrics, and cost effectiveness all become central to cancer therapy, we have a unique opportunity to expand the role of IO and expand patient access to IO therapies. We will need all IO/IR physicians functioning at a high level in their cancer centres to accomplish these goals. The door is open, we simply must walk through it.
William (Bill) Rilling is professor of Radiology and Surgery at the Medical College of Wisconsin, Milwaukee, USA.
Automatic characterisation of Lipiodol (Guerbet) deposition is feasible, workflow efficient, and improves consistency across patients, argued Sophie Stark (Yale School of Medicine, New Haven, USA) at the Society of Interventional Oncology’s annual meeting (SIO; 7–11 June, Boston, USA). Stark presented an automated quantitative and pattern-based method for the characterisation of Lipiodol deposits on CT scans taken 24 hours after cTACE (conventional transarterial chemoembolization).
“This work paves the way for the development of automated algorithms that predict tumour response from preprocedural MRI and 24 hour CT, and may allow earlier and more personalised therapy”, she enthused at the meeting.
“Lipiodol use in cTACE plays a unique multifunctional role”, Stark explained. “It has drug delivery capabilities with transient microembolic effects, and its radiopacity allows drug delivery visualisation on post-procedural CT scans. Previous studies already show that Lipiodol deposition is correlated with tumour response.”
The investigators within the Yale Interventional Oncology Research Lab, led by Julius Chapiro, set out to see if they could further establish Lipiodol as an early imaging biomarker for the therapeutic efficiency of cTACE using this automated system on 24 hour CT scans. Contextualising this research, Stark informed the SIO audience that liver cancer is the fourth leading cause of cancer-related deaths worldwide, and that cTACE is a guideline approved treatment option for patients with intermediate to advanced stage disease.
They conducted a retrospective study of 42 primary and secondary liver cancer patients, with a total of 65 tumours between them, who underwent cTACE between 2012 and 2018 at the Yale School of Medicine. All patients had a baseline contrast-enhanced MRI scan before undergoing cTACE, then a CT scan 24 hours after the procedure, followed by a second MRI scan 30 days post-procedure. Detailing this image analysis workflow, Stark explained how she and her colleagues volumetrically segmented all of the tumours at all imaging time points. This was followed by an automatic, enhancement-based quantification of viable and necrotic tumour tissue on MRI. Next, the investigators performed an enhanced-based volumetric response assessment using qEASL (Quantitative European Association for the Study of the Liver).
Figure 1: CT scan of liver with colour coded Lipiodol density overlay
“On the 24 hour CT, which was our focus, we characterised Lipiodol deposition automatically”, Stark continued. The researchers looked at the tumour coverage with Lipiodol, as well as areas of different Lipiodol densities—categorised as low, medium and high—using intensity thresholds from the Hounsfield units scale. The cut-off values were: low density, 87–145 Hounsfield units (HU); mid density, 155–240 HU; high density, 241+ HU. The automated quantification method was developed by one of Stark’s co-workers, Clinton Wang, who is currently a graduate student at the MIT in Boston, USA, and was previously involved with research at Yale. Based on these density values, the developed algorithm creates a colour coded overlay for the CT image of the liver, where low density areas were shaded green, mid density areas shaded yellow, and high density areas shaded red (see Figure 1).
Stark continued: “Specifically, we looked at homogenous deposition of Lipiodol, sparsity, rim deposition of Lipiodol, and peripheral deposition. The homogenous and sparsity deposition of Lipiodol could be determined through volumetric analyses of the whole tumour, whereas for the rim and peripheral Lipiodol deposition, a more complex approach was required.” Expanding on these complexities, she said: “First, we calculated the volume of the tumour, and then created a sphere with exactly the same volume. Then we used operations such as morphological erosion and dilation to separate the core and the periphery of the tumour.”
Lipiodol coverage in viable areas was significantly higher than that of necrotic areas, the investigators found through comparing contrast-enhanced MRI scans. There was approximately 8.2% more Lipiodol coverage in viable areas than necrotic zones, averaged throughout all tumours. “We also looked at several subgroups, and the analysis was consistent throughout”, Stark said.
Looking at Lipiodol density distribution, the fraction of low density deposition was significantly higher in necrotic areas compared with viable areas, whereas the fraction of high density Lipiodol was significantly higher in viable compared to necrotic areas. There was no significant difference for mid density Lipiodol. Also, this analysis was consistent throughout several subgroups, according to Stark.
The investigators reported a stratification of tumour response by Lipiodol density. Areas that deposited Lipiodol became necrotic at a higher rate, as seen on follow up MRI, than areas without Lipiodol (p=0.0475). Higher concentrations of Lipiodol enhanced this effect with increasing Lipiodol densities, there was an increasing percentage of necrotic tissue.
When deposited peripherally, Lipiodol is associated with an improved tumour Homogenous, non-sparse, and rim deposition were all associated with accelerating the slowing of tumour volume growth. In Stark’s words: “Homogenous deposition, non-sparse deposition, and rim deposition within sparse tumours showed an increased decrease of enhancing tumour volume on follow up MRI”.
This led Stark and colleagues to conclude that the automated characterisation of Lipiodol “can be easily incorporated into a standardised framework for cTACE management”. Stark summarised: “Our approach improves the consistency for patients because it leverages the standardised Hounsfield units scale. We show that tumour enhancement on contrast-enhanced MRI can make predictions not only about the presence, but also about the density, of Lipiodol deposition, which is strongly correlated to tumour response to cTACE. Also patterns, including homogenous, non-sparse, rim and peripheral deposition of Lipiodol were positive predictors of tumour response. We think this work paves the way for the development of fully automated algorithms that can predict tumour response from pre-procedural MRI and 24 hour post-procedural CT, and may allow earlier and more personalised therapy to our liver cancer patients”.
The Society of Interventional Oncology (SIO) is working more closely within cooperative groups and taskforces, as well as amongst the guidelines commentariat, to provide a global voice to interventional radiologists working in cancer care. Within the various groups the society is active amongst, SIO president William (Bill) Rilling (USA) tells Interventional News they have the strongest presence on relevant National Cancer Center Network (NCCN) panels.
SIO is working on developing and submitting evidence-based recommendations to various NCCN panels. Commenting on this growing integration into the formal process of commenting on and reviewing guidelines, Rilling says: “We have been very welcomed into this process, especially by medical oncologists. Everyone can recognise that there is a benefit to the patient to have as broad a view as possible. The vast majority of people involved at the moment [with guideline review] are medical oncologists.”
NCCN kidney cancer guidelines
Earlier this year, updates to the NCCN renal guidelines were submitted by Ronald Arellano (Harvard University, Cambridge, USA), Thomas Atwell (Mayo Clinic, Rochester, USA), and S William Stavropoulos (University of Pennsylvania, Philadelphia, USA) on behalf of SIO. Their letter requests the NCCN kidney cancer guideline panel review six specific changes for inclusion in the management of T1a renal masses.
Speaking to Interventional News, Stavropoulos explains the society’s ambitions for how the guidelines will change: “We hope the NCCN guidelines are updated to accurately reflect the latest research showing the oncologic success and safety of percutaneous ablation for renal cell carcinoma (RCC) relative to surgery and active surveillance.
“It is critical that national guidelines reflect the latest developments in research and clinical practice. Updating the NCCN guidelines will help interventional oncologists at the local and national level. Locally, it could help interventional oncologists during discussions regarding treatment options at individual tumour boards. At the national level, updating the role of ablation in the NCCN guidelines could assist with issues such as funding of clinical trials, procedural reimbursement coverage and industry investment in research and development.”
These specific changes SIO are requesting are:
Move text related to thermal ablation to a position in front of surveillance.
When addressing relative incidence of local recurrence following thermal ablation compared to surgery, qualification is needed to state that both techniques are very effective and the difference in treatment success is very small or absent (5% or less). For small renal tumours, cancer specific survival is also similar amongst treatment strategies.
Benefits of thermal ablation deserve mention in Principles of Surgery.
When considering those patients appropriate for thermal ablation, please include “those patients willing to accept a potential very low increased incidence of local recurrence” and “those patients in whom partial nephrectomy is not possible and nephron preservation is imperative”.
Recommend the term “in selected patients” be removed below Ablative Techniques and Ablative Techniques be moved above Active Surveillance on page KID-1.
Recommend the following change be added to page Kid-B, 2-4, Follow-up after Partial or Radical Nephrectomy: Biopsy or repeat biopsy: New enhancement or enlarging nodularity along the surgical margin following partial nephrectomy or new enhancing mass in the surgical bed following radical nephrectomy.
Atwell outlines his ambitions for the guidelines to Interventional News: “My hope is that we could bring the NCCN guidelines closer to those currently provided by the American Urological Association (AUA) and the American Society of Clinical Oncology (ASCO), both of whom include thermal ablation as a front-line treatment alternative for small renal masses. There are particular attributes of ablation that warrant consideration in the NCCN guidelines, including favourable perioperative outcomes.”
Enthusing about the society’s involvement in these requested guidelines changes, Stavropoulos says: “SIO has been critical in spearheading these type of efforts. For interventional oncology (IO) to take its place as the fourth pillar of cancer care, we need to engage with the major oncology organisations. In this instance, the SIO was instrumental in bringing our RCC working group together and helping us through the specifics of the NCCN submission process. Other areas of SIO advocacy include establishing the first IO Working group within ECOG-ACRIN [a cancer research group formed from a 2012 merger between the Eastern Cooperative Oncology Group and the American College of Radiology Imaging Network], spearheading multiple IO clinical trial concepts in gastrointestinal (GI), genitourinary (GU), and thoracic oncology within the National Cancer Institute (NCI) Cooperative Groups. Establishing a footprint within organised oncology increases the visibility of IO and recognition of what we offer patients among our medical, surgical and radiation oncology colleagues.”
NCCN breast cancer guidelines
SIO also submitted updates to the NCCN breast cancer guidelines this year. Submitted by Amy Deipolyi (Memorial Sloan Kettering Cancer Center, New York, USA), Maureen Kohi (University of California, San Francisco, USA), and Gloria Hwang (Stanford University, Stanford, USA).
Deipolyi explains to Interventional News: “The NCCN publishes guidelines that guide physicians and patients on ‘standards of practice’ for cancer treatment. These guidelines not only drive decision making in tumour boards and in clinic, but are also used by insurance companies to justify witholding reimbursement for procedures and diagnostic exams. The current NCCN guidelines for breast cancer do not mention minimally invasive procedures, despite good evidence that local therapies are effective for palliating pain and liver-directed therapies can confer progression free survival intervals. The NCCN committee for breast cancer does not include a single diagnostic or interventional radiologist. We have petitioned the committee to consider including radiologists, and to consider minimally invasive therapies in the treatment of metastatic breast cancer. Our hope is to improve patient outcomes and to help physicians offer these procedures while minimising the difficulty in obtaining insurance coverage. We appreciate the support and effort of SIO to advocate for interventional oncology physicians and their patients.”
To this end, their letter suggests including a section for locoregional therapies for stage IV metastatic breast cancer and illustrates three clinical examples.
These three clinical examples are: if the patient has painful bone metastases, for oligometastatic disease, and for liver-dominant hepatic metastasis refractory to systemic therapy.
Regarding the first example, the authors write: “Bone metastasis occurs in 65–75% of patients with metastatic breast cancer. Image-guided cryotherapy, heat-based thermal ablation, and cementoplasty have been demonstrated to be effective and fast-acting methods to improve bone pain due to metastasis from a wide range of tumours, including breast cancer.”
Similarly, for oligometastatic disease, Deipolyi, Kohi and Hwang justify their recommendation through this statement: “Local ablative therapies for five or fewer sites of metastasis have been shown to provide longer progression free survival and may prolong overall survival. Hepatic resection and/or thermal ablation of hepatic oligometastatic disease can confer disease free intervals lasting several years and perhaps, more importantly, allow long intervals of disease control without chemotherapy. This is particularly beneficial in patients not tolerating systemic therapy.”
For their final clinical example, they expand: “Liver metastasis commonly occurs in breast cancer patients and is associated with poorer oncologic outcomes. Liver tumours may cause abdominal pain or result in compression of the portal vein or obstruction of bile ducts. In selected patients who are not eligible for resection such as chemoembolization and radioembolization have demonstrated radiologic responses that translate to prolonged patient survival. Combining liver-directed treatments in the management of metastatic breast cancer with liver-only or liver-dominant disease can provide longer disease control while delaying the need to change to another line of systemic therapy. Also, in patients with hormonally responsive breast cancer and new-onset liver metastases, transarterial locoregional therapy can delay the initiation of systemic chemotherapy and benefit the patient’s quality of life.”
NCCN lung cancer guidelines
Additionally, SIO submitted updates to the NCCN non-small cell lung cancer guidelines. The letter was penned by Patrick Eiken (Mayo Clinic, Rochester, USA), Florian Fintelmann (Harvard Medical School, Cambridge, USA) and Robert Suh (David Geffen School of Medicine at UCLA, Los Angeles, USA), and requests updating the role of image-guided thermal ablation in the Clinical Practice Guidelines in Oncology for non-small cell lung cancer.
The letter authors describe image-guided thermal ablation as “inclusive of radiofrequency ablation, microwave ablation and cryoablation” and as “a form of ‘local therapy’ or ‘local ablative therapy’ and, generally, may be considered as a potential alternative to other local therapies, particularly for lung lesions <3cm”.
They argue for the inclusion of a section on the principles of image-guided thermal ablation in the NCCN non-small cell lung cancer guidelines, as well as the addition of a section titled “Image-guided thermal ablation” in the discussion of treatment approaches in the guidelines. Currently, the guidelines include a similar section on the principles of radiation therapy; Eiken, Fintelmann and Suh say that as image-guided thermal ablation is “increasingly being studies and used clinically in the treatment of lung cancer”, including a summary of what it is and of its appropriate applications “would be useful to include”.
The third specific change called for by these interventionists is to give greater attention to ablation for medically inoperable stage IA cancer under the “initial treatment” options. Currently, when deemed medically inoperable, the guidelines suggest stereotactic ablative radiotherapy (SABR), with two footnotes, m and n. SIO is calling for NCCN to delete footnote “n” (which reads “Interventional radiology ablation is an option for selected patients”) and to include image-guided thermal ablation in the algorithm proper, alongside SABR. They state their rationale for this: “A growing volume of literature shows the efficacy of image-guided thermal ablation for local control of primary and secondary malignancies of the lung. While the evidence for surgery or SABR may be more robust, use of image-guided thermal ablation may expand the pool of patients for whom local tumour control is possible. Image-guided thermal ablation may be of particular value in patients with limited pulmonary reserve or for those who have reached the limits of tissue toxicity from radiation therapy.”
A further five changes are specified in the letter:
To swap the positions of “Radiation” and “Ablation”, so that ablation is a higher consideration for patients with multiple lung cancers where definitive local therapy is possible. To change “Ablation” to “Image-guided thermal ablation”. The authors justify this recommendation: “In the setting of multiple lung cancers, preservation of lung parenchyma and feasibility of repeat treatments are paramount considerations, as repeat treatments are expectedly necessary over time. Both lung parenchymal sparing and repeatability are strengths of image-guided thermal ablation relative to radiation.”
Add “Image-guided thermal ablation” as a third option, after surgical resection or SABR, for patients where definitive therapy for local disease is feasible. The rationale for this is described thus: “A growing volume of literature shows the efficacy of image-guided thermal ablation for local control of primary and secondary malignancies of the lung. While the evidence for surgery or SABR may be more robust, use of image-guided thermal ablation may expand the pool of patients for whom local control of the tumour is possible. Image-guided thermal ablation may be of particular value in patients with limited pulmonary reserve or those who have reached the limits of tissue toxicity from radiation therapy.”
To add image-guided thermal ablation into the footnote that defines “Definitive local therapy for metastatic site”. This currently reads: “Typically, RT (including SABR) or surgical resection”.
To add “Image-guided thermal ablation” to the algorithm proper under “External-beam RT or SABR” and delete the footnote (where it currently resides) when recommending therapy for recurrence and metastasis.
On NSCL-19, 20, 22 and 23, change each instance of “Consider definitive local therapy (e.g., SABR or surgery) for limited lesions to “Consider definitive local therapy (e.g., Image-guided thermal ablation, SABR or surgery) for limited lesions.
Thierry de Baère during his keynote lecture at SIO
“It is very important that we, as interventional oncologists, embrace the immuno-oncology field,” Thierry de Baère (Institut Gustave Roussy, Villejuif, France) said in his keynote address on the future of interventional oncology at the Society of Interventional Oncology annual meeting (SIO; 7–11 June, Boston, USA). Drawing from an SIO white paper published recently in Radiology detailing the challenges and opportunities of further integrating these two cancer disciplines and from the literature, de Baère outlines why “Immuno-oncology in cancer care is a fantastic opportunity for interventional oncology”.
In the Radiology white paper, lead author Joseph Erinjeri (Memorial Sloan Kettering Cancer Center, New York, USA) and 17 other leading interventional oncology and immuno-oncology experts define the two IOs, and their potential importance in a more synergistic approach to cancer care: “Interventional oncology is a subspecialty field of interventional radiology that addresses the diagnosis and treatment of cancer and cancer-related problems by using targeted minimally invasive procedures performed with image guidance. Immunooncology is an innovative area of cancer research and practice that seeks to help the patient’s own immune system fight cancer. Both interventional oncology and immuno-oncology can potentially play a pivotal role in cancer management plans when used alongside medical, surgical, and radiation oncology in the care of cancer patients.”
Erinjeri et al, as well as de Baère in his keynote lecture, urge the interventional radiology community that this is possible with an increasingly close collaboration with medical oncology colleagues. From an initial meeting on 23 January 2017 at the Memorial Sloan-Kettering Center in New York, USA, and through multiple subsequent teleconferences, the white paper authors evaluated key areas in immuno-oncology considered integral to the interventional oncologist’s practice.
“We are at the beginning of an exciting revolution in cancer care with the advent of immunotherapy,” Erinjeri et al summarise. “The role that interventional oncology will play in immunotherapy will depend on our collective efforts to address rational questions regarding the fundamental immune effects of local and regional image-guided interventions.”
The SIO white paper makes four recommendations for future work on combining immunotherapy and interventional oncology. These are:
Standardise the lexicon between the two disciplines
Define commonly used immunobiology terms as they pertain to interventional oncology procedures and follow-up.
Establish criteria for identification of antitumour immunity, pro-oncogenic effects, and abscopal effects.
Harmonise the description of technique and procedural details (method of tissue injury, margins, particles, etc.) through standardised reporting
Personalise interventional oncology
Determine the effect of organ, tumour type, and interventional oncology procedure on immune system effects through preclinical, translational, and clinical studies.
Investigate the timing of administration of immunotherapy in combination with interventional oncology therapies through clinical trials.
Create multi-institution registries to allow for large-scale data mining and determination of correlations.
Understand the tumour-stimulating effects of interventional oncology procedures
Recognise patient/tumour characteristics and procedural factors that predict pro-oncogenic effects.
Identify optimal methods for eliminating unwanted protumorigenic effects.
Develop imaging biomarkers for interventional oncology procedures combined with immunotherapy
Require use of immune response criteria in addition to conventional imaging criteria in reporting response to interventional oncology treatments.
Validate new early imaging markers of therapeutic efficacy and response.
Design imaging studies that can assess the tumour microenvironment.
Combining interventional oncology therapies with intratumoral immunotherapy
Speaking to Interventional News, de Baère underlines the importance of the coordination of human intratumoral immunotherapy (HIT-IT) and interventional oncology. This year, the American Association for Cancer Research (AACR) held a specific session on HIT-IT at their annual meeting (29 March–3 April, Atlanta, USA), as do the European Society for Medical Oncology (ESMO; 27 September–1 October, Barcelona, Spain). The 34th Annual Meeting of the Society for Immunotherapy of Cancer (SITC) will also host a full day of discussion and presentations on the topic (6–10 November, Fort Washington, USA).
This increasing international discourse on HIT-IT can be traced to an ESMO-sponsored expert meeting held 8 March 2018 in Paris, France. This comprised 11 experts from academia, 11 from the pharmaceutical industry, and two clinician representatives of ESMO. They met to produce a document that would “help to structure the ongoing and future development of HIT-IT”.
The resultant paper, published in Annals of Oncology by lead author Aurélien Marabelle (Villejuif, France) and colleagues, including de Baère, made six recommendations. These are: 1) To carefully select the paptient population for clinical trials, 2) To conduct translational studies systematically to facilitate better understanding of the mechanism of action of HIT-IT, 3) To organise face-to-face meetings or surgeons and oncologists, 4) To use ultrasound guidance for the injection of superficial tumour lesions, ultrasound guidance or CT-scans to guide the injection of deeper tumour lesions, and to use doppler ultrasound to ensure no big vessels are injected in error, 5) To measure injected and noninjected lesions at each injection time point to better capture the kinetics of tumour growth, and 6) To generate diagrams or photographs at every visit or time point of injection, which should be recorded on specific body-map proformas.
Erinjeri and colleagues state in their white paper that interventional radiologists need to work out how to monitor the effects of immunotherapy. They explain that “because immunotherapy mostly facilitates or modulates the inflammatory response rather than causing tumour cell death through cytotoxic effects, to our knowledge no specific guidelines exist to evaluate changes in tumour imaging appearance after treatment.”
Several response criteria have been developed, but to date none have been validated with intratumoural delivery methods or approaches combining locoregional therapy with systemically delivered immune-reactive agents. The SIO white paper authors claim this will be “essential” before physicians can successfully evaluate treatment response.
The group of 18 leading experts are categorical in their conclusion, stating emphatically: “Regardless of the challenges we face in investigating and incorporating immuno-oncology into an interventional oncology practice, immunotherapy is destined to become an integral part of interventional oncology care, and the integration is therefore essential for the future of IO.”
In accordance with this sentiment, de Baère told the SIO audience: “Immuno-oncology will be a much bigger part of practice and research in the next five to 10 years. The reason for this is that we already know how great immuno-oncology is for cancer treatment.” Showing a graph depicting the number of trials investigating intratumoural immunotherapy opening every year, he demonstrated their exponential growth; from fewer than five opening each year between 1992 and 2004, to 40 opening in 2017. de Baère argues that intratumoural delivery allows for a high enough local dose to efficaciously destroy the tumour, without the toxicity of systemic delivery. “We can help medical oncologists specifically target the tumours,” he said.
“There is a lot of noise about this,” he enthused. Indeed, industry have started taking note, with some companies having their own dedicated compounds. One such example is Lytix Biopharma, which manufactures short, oncolytic peptides that cannot be delivered systemically. “Who can inject it locally?” de Baère asked the SIO delegates, “Interventional radiologists. This is the future of interventional oncology, and it is very important that we are part of it”.
“Arm yourself with the comprehensive but nuanced science behind hepatocellular carcinoma (HCC),” Riad Salem (Northwestern Memorial Hospital, Chicago, USA) instructed the audience at the Global Embolization Oncology Symposium Technologies (GEST; 9–12 May, New York, USA) during his Honorary Lecture, which concluded with the warning: “Do not let yourself be bullied by the tyranny of the randomised controlled trial”.
Arguing that “so-called evidence-based medicine is really not [that] 90% of the time”, Salem challenged the notion that randomised controlled trials with a primary endpoint of overall survival should be the gold standard in interventional radiology. However, he began by conceding that “the randomised design is ideal—it is the best. It directly compares [the control] to the treatment, it minimises the bias and gives you causality where you can say ‘this treatment led to this endpoint’. You can power a randomised control trial with a large enough sample size that you minimise type 1 and type 2 error, and of course it is the most influential data”. However, though he says this is all possible in theory, he goes on to recount how in practice, this is often far from the case.
Speaking generally, Salem opined: “In interventional radiology (IR) and other areas, these are very expensive and complicated studies to do, with sample sizes that are sometimes impractical, if not impossible. They take years to complete and, as a result, what is their relevance [when completed]?”.
There is a precedent for using lower level data to inform procedural decisions
Salem argued that there are precedents for not relying on randomised controlled data to guide procedural choice. In the late 1990s, Salem informed GEST delegates that he used to perform a lot of chemoembolization procedures. However, it was only in 2002 that Josep Llovet (University of Barcelona, Barcelona, Spain) and colleagues published in The Lancet findings from a randomised controlled trial that reported chemoembolization improved survival compared with conservative treatment. Writing at the time, Llovet et al said: “There is no standard treatment for unresectable HCC. Arterial embolization is widely used, but evidence of survival benefits is lacking.” In response to this, Salem continued, “Before 2002, we were all performing chemoembolization based on phase II data”. However, Salem emphasised its limitations: “You have a 112 patient clinical trial with three arms; notice each arm is about 35 to 40 patients, so it is very small. This study here, that we all quote [to support the use of chemoembolization as the standard of care in unresectable HCC patients], basically was a single-centre study. There is a low sample size, there is no active control, so there is relatively limited power—all the things that we currently need in a randomised controlled trial are not necessarily present in this clinical trial.” In fact, the trial was stopped when the ninth sequential inspection showed that chemoembolization had survival benefits compared with conservative treatment.
Examining the evidence presented in the various guidelines that help inform physician’s practice, Salem reported a distinct lack of level 1 data. Of the National Comprehensive Cancer Network (NCCN) guidelines, Salem said: “95% of the recommendations are based on non-level 1 evidence”. Continuing through other frameworks, he stated that in the American Association for the Study of Liver Diseases (AASLD) guidelines, two of the 21 recommendations are based on level 1 data. He stressed that “everything else is lower level evidence”. The European Association for the Study of the Liver (EASL) guidelines tell a similar story: three of their 36 recommendations hinge on level 1 evidence.
Salem summarised: “We have guidelines that tell us what we should and should not do, yet most of them are not based on the very data that we are supposed to be generating, so there is some confusion. […] As interventional radiologists, we have to recognise that many standards of care are not supported by randomised controlled trials, particularly with overall survival as the endpoint.”
He then goes on to enumerate the several procedures performed by interventional radiologists for which level 1 evidence does not exist: bland transarterial chemoembolization (TACE), drug-eluting bead (DEB) TACE, or Yttrium-90 (Y-90) TACE to treat HCCs or neuroendocrine tumours; ablation in colon cancers and HCCs; resection for colon cancer or HCC metastases. “Liver transplantation,” he added, “a goal that many of us seek to achieve for our patients, a gold standard, curative option—what is that based on? A phase II, single-arm study published in 1996 and based on 48 patients. It is the standard of care, I understand that, but we have to make sure that we compare our therapies and their respective levels of evidence with what other standards are based on.”
Not all randomised controlled trials change clinical practice
“What we want are randomised controlled trials that provide clinically meaningful results. I think that is what we believe in interventional radiology,” Salem stated. However, he went on to highlight how several randomised controlled trials were far from practice-changing.
Using the example of a phase III pancreatic cancer study published in the Journal of Clinical Oncology in 2007 by Malcolm Moore (Princess Margaret Hospital, Toronto, Canada) et al, Salem explained how, despite filling all the criteria for a randomised controlled trial, the results may still not be illuminating. Moore and colleagues set out to see if they could improve the chances of survival in patients with unresectable, locally advanced or metastatic liver cancer by adding erlotinib to gemcitabine. Comparing the erlotinib and gemcitabine group with the gemcitabine only cohort, the investigators found there was an overall survival benefit of 9.9 days in the combined group. “More than 500 patients, level 1 evidence—and a survival benefit of 9.9 days,” Salem reiterated. “Is erlotinib and gemcitabine the gold standard? I am not a medical oncologist, I do not know, but this trial satisfies everything the purists really want when it comes to generating level 1 evidence. I do not know if it actually changes standard of care though.” A recent publication in Oncology Reviews by Amrallah Mohammad (Zagazig University, Zagazig, Egypt) concluded that “only [a] small set of patients get small benefit” from the combined use of erlotinib and gemcitabine.
Randomised controlled trials “do not necessarily reflect real-world outcomes”
Randomised controlled trials are often designed by statisticians and physicians to fit what is logistically possible, and therefore do not necessarily reflect real-world outcomes, Salem said. He uses several examples to illustrate this point. Firstly, he explained how he suspects there is “a little bit of doctoring” going on when choosing the sample size for a randomised controlled trial: “Interestingly, if you look at many of these trials that we reported, sample size is 300, 400, 600—it is almost always an even number”. The sample size is the result of back and forth between the principal investigator and the statistician, and is, in theory, calculated from the initial hypothesis and the DELTA (difference elicitation in trials). Salem explains how, in practice, determining the sample size is often a case of calculating how many patients a physician believes they may realistically be able to enrol in a trial, and then “reverse engineering” a hypothesis and DELTA from that number (though he accedes he is “a little bit cynical”).
In addition to this alleged data engineering, Salem pointed to narrow inclusion criteria as slowing recruitment to trials. That so many are excluded slows recruitment, he said, and means that by the time enough patients are enrolled and have been followed-up, and the data have been analysed, the findings are no longer timely. According to Salem, there is “about a 90% non-enrolment rate”; he extrapolated from this that “the findings of a randomised study are [therefore] not applicable to 90% of the patients that you see, so it is a very strict patient population you are making conclusions about”.
Recruitment can also be an issue when enrolling for large, multicentre trials, Salem explained, due to the biases and beliefs individual institutions hold. In the mid-2000s, Salem and colleagues were designing a multicentre trial to compare Y-90 with RFA and TACE RFA. However, what was initially intended as a six-centre clinical trial devolved into a single-centre trial of 45 patients. The investigators could not enrol enough patients in each of the three arms—Y-90, TACE and TACE RFA—because of physician and institutional preference over certain procedures. Nevertheless, Salem used the data derived from the beginnings of this trial to redefine the institutional standard of care at Northwestern Memorial Hospital to Y-90.
Using another example from his own work in liver cancer, Salem explained that the STOP-HCC trial, of which he is the global principal investigator, further demonstrates the difficulties of recruitment in a randomised controlled trial. The initial vision was to have STOP-HCC as an open-label, prospective, multicentre, randomised, phase III trial evaluating Yttrium-90 (Y-90) transarterial chemoembolization (TACE) in the treatment of patients with unresectable HCC. “In 2010, when we started the trial, all we had was sorafenib, and we wanted to see if this would add to the standard of care”, Salem said at GEST. “This started as a 400 patient clinical trial; it is now eight years later, the technique has improved, there are seven other drugs approved, and our sample size is now 600. While I hope it will have an effect on standards of care, I am not sure what the impact of this trial will be, whether it is positive or negative.”
Overall survival “is not a good outcome for randomised trials with effective subsequent therapies”
Advising the listening interventional radiologists as to how he believes they should devise trials to further their field, Salem guards against using overall survival as a primary endpoint when the patient will receive multiple interventions. Quoting statisticians writing in the Journal of Clinical Oncology, Salem said that “survival is not a good outcome for randomised trials with effective subsequent therapies”. He elaborated: “We cannot attribute overall survival to the initial treatment, say TACE or radiofrequency ablation (RFA), if later on the patient had other interventions. After a patient progresses, they may be given regorafenib, lenvatinib, nivolumab, cabozantinib, ramucirumab. This gets very complicated.”
Indeed, the Barcelona Clinic Liver Cancer (BCLC) staging system (stages A/B) is predominantly predicated on level 2 data without data on overall survival. “It is too complicated to do overall survival studies, and there is a prohibitive statistical barrier”, Salem explained. “We must use imaging surrogates for BCLC A/B studies, such as time to progression and progression-free survival. Overall survival is possible in end-stage care, but really for everything else, we have to use imaging.”
He emphasised this point in his concluding remarks, reiterating: “I think in our quest to improve overall survival, we have let the statisticians rule a little too much, and we need to push back a little bit, and get a bit more clinical relevance in our clinical trials. For two therapies that might provide the same overall survival, we need to find surrogates that matter and reject the trope that overall survival is the supreme endpoint”.
Designing trials to push practice in interventional radiology
To combat these shortcomings, Salem made two proposals to the GEST audience for how interventional radiologists should go about designing trials in future.
Firstly, he suggested physicians conduct an initial, exploratory analysis. This would be an 80 patient study in a randomised, phase II trial design. “Forty versus 40, this bead versus that bead, this probe versus that probe”, Salem described. “Whatever it is you are investigating, you can compare it to a different option and make sure there is a difference you are identifying between the two.” If the investigators are aiming to change the standard of care, Salem suggested using this same model, but for 100 versus 100 patients: “If you cannot determine a difference in 100 patients versus 100 patients, there probably is not much there that is clinically relevant in the IR space”, he said. “Then you do not have to get a patient population of 1,000 and have a negative clinical trial.”
The second proposition Salem has for the GEST attendees is that investigators largely stop using overall survival as an endpoint, and use a clinically meaningful alternative. “I personally think response is a very important one”, he suggested. He explicated: “Imagine you have three treatments. One gives you stable disease, one gives you minor response, and one gives you major response. All three of those treatments have the same time to progression and the same progression free survival. But if you are a believer in the lethal tumour model in the liver, then the person with the best response rate is the person furthest away from the lethal tumour load line. So, everything else being the same, the best response becomes a relevant and important concept.”
He concluded: “I think we need to limit the amount of weight we give randomised controlled trials, and be careful not to prematurely and quickly discount other types of rigorously developed evidence. I think physicians rely on randomised controlled trials when supportive of their position, but interestingly ignore them when they do not; that is clear, we see that all the time.
“Do not accept in isolation the fact that we have limited level 1 randomised controlled trial data [in IR]. Take everything in totality—phase II, big data, randomised controlled trials—process, triangulate, and carry this knowledge to tumour board. You are certainly not alone in relying too heavily on phase II data, and please, whatever you are confronted with, do not let yourself be bullied by the tyranny of the randomised controlled trial.”
MRI Interventions said its ClearPoint Neuro navigation system has been used in 3,000 neurosurgical procedures.
The milestone procedure was completed at the University of California, San Francisco, USA, according to the vendor.
“This milestone is a testament to the value surgeons are placing on precision guided therapy, especially in neurosurgery where the stakes are the highest,” comments Joe Burnett, president and CEO of MRI Interventions. “Although the timing is coincidental, we were thrilled to share this success with the team at the University of California, San Francisco, who have partnered with us for the last decade in refining our platform and ensuring the voice of not only the doctor, but also that of the patient, is included in every improvement. It is also important to note that not only did UCSF perform the 3,000th case using ClearPoint, they also performed the 3,001st case that same day. UCSF is among the now ten centres scheduling two cases per day utilising the same MRI scanner, which has been a strategic push for us in the past year.”
Cook Medical recently released the second generation of the 2.6Fr CXI support catheter with platinum-iridium marker bands. The CXI catheter is used in small-vessel anatomy or super-selective anatomy for diagnostic and interventional procedures, including peripheral use.
“We strive to offer physicians the tools they need to provide the best possible outcomes for patients,” comments Mike Williams, director of global vascular programmes. “Physicians frequently asked for the 2.6Fr CXI support catheter to have the same visibility as smaller-sized CXI catheters. Platinum-iridium marker bands were added in response to these needs.”
This second-generation CXI catheter provides clinicians with better visualisation under fluoroscopy because of the platinum-iridium marker bands. The catheter comes with additional tip configurations and a new 135cm length. Its stainless steel braid provides responsive torque and pushability, and the 2.3Fr and 2.6Fr sizes can fit coaxially in the 4.0Fr size to increase the amount of support.
The new design of the 2.6Fr platform is now available in Europe, the USA and Canada.
Siemens Healthineers will acquire all issued and outstanding shares of common stock of Corindus Vascular Robotics, Corindus announced this month.
The cash transaction is US$4.28 per share, resulting in an aggregate purchase price of US$1.1 billion by Siemens Medical Solutions, a subsidiary of Siemens Healthineers, according to Corindus.
“We are pleased to have reached this agreement with Siemens Healthineers,” comments Mark J Toland, president and CEO of Corindus, in the news release. “We believe the transaction will deliver immediate, compelling and certain value to all Corindus stockholders, as well as substantial benefits to our customers. The combination of Siemens Healthineers’ advanced, high-quality imaging, digital and artificial intelligence tools with Corindus’ precision robotics platform has the potential to transform the way healthcare is delivered to those suffering from cardiovascular or peripheral disease. The tremendous technology synergies and shared vision between both companies should allow us to achieve a seamless integration between our businesses.”
“Corindus has established a leading position in vascular robotics with a compelling technology platform for robotic-assisted coronary, peripheral, and neurovascular procedures,” says Michel Therin, president of advanced therapies at Siemens Healthineers. “The acquisition of Corindus, combined with Siemens’ strong advanced therapies portfolio, will help further advance the growth of vascular robotics. The integration of our technologies could lead to reduced variability, improved efficiency, expanded access to care, and ultimately improved patient outcomes. We look forward to welcoming the Corindus team to Siemens Healthineers.”
Corindus Vascular Robotics’ CorPath is the first US Food and Drug Administration-cleared medical device to bring robotic technology to percutaneous coronary and vascular procedures. Siemens Healthineers is a multibillion-dollar health-care technology company.
The merger is expected to close in the fourth quarter of 2019, Corindus said.
According to a BIBA MedTech survey, 52% of neurointerventionalists believe that they are the only specialists who have the relevant skills and experience to perform interventional stroke procedures (e.g. mechanical thrombectomy). However, of those who believe other specialities—with the appropriate training—could potentially perform such procedures, 58% propose interventional radiologists. Previous discussions about other specialists performing interventional stroke procedures have focused on interventional cardiologists.
Mechanical thrombectomy is now an established treatment for patients with emergent large vessel occlusion, but who should perform this procedure is controversial. A 2016 multisociety consensus document—published in the Journal of NeuroInterventional Surgery—states that “physicians providing intra-arterial treatment for acute stroke are required to have appropriate training and experience for the performance of neuroangiography and interventional neuroradiology”. However, some believe that restricting interventional stroke procedures (specifically, mechanical thrombectomy) to neurointerventionalists may limit the number of patients who are able to access the therapy given the lack of relevant operators in some areas. For example, in the 2019 Vascular and Endovascular Challenges Update, cardiologist Jan Kovac writes “collaboration of various interventional specialists is desirable to deliver this therapy to a wider population”.
A previous poll on this issue, conducted at the 2019 Charing Cross Symposium (15–18 April, London, UK), indicated that 57% of respondents were against mechanical thrombectomy being restricted to neurointerventionalists. However, these respondents were predominantly vascular and endovascular surgeons. Therefore, BIBA MedTech sought to understand how practising neurointerventionalists felt about the issue.
Of 54 neurointerventionalists surveyed, 52% agreed that “only neurointerventionalists should perform interventional stroke therapy” vs. 48% who did not agree. Of those who did not agree (26), 58% said “interventional radiologists” in response to the question “who else (with appropriate training) do you feel might be able to perform interventional stroke procedures?”. Of note, only 15% said interventional cardiologists. See Figure 1.
In his chapter in the 2019 Vascular and Endovascular Challenges Update, Kovac proposes interventional cardiologists as suitable alternative specialists to perform interventional stroke procedures. He states that cardiologists are “no strangers to stroke care”, commenting that “cardiologists have traditionally played an important role in stroke prevention by providing both comprehensive medical and interventional management of cardiovascular risk factors [for stroke] including atrial fibrillation”. He adds: “It appears reasonable to complement the existing workforce of neurointerventional radiologists by interventional cardiologists being properly trained in mechanical thrombectomy, joining the interdisciplinary stroke teams led by neurologists”. However, Kovac does stress that there is “absolutely no doubt that a fully trained neurointerventionalist, with audited practice outcomes, and adequate skill maintenance, is the optimal provider of mechanical thrombectomy for stroke patients”.
The 2016 multisociety consensus statement observes: “The technical skills needed to safely deliver devices into the intracranial circulation are significantly more involved than simply placing a catheter for medical infusion. Catheter skills from other circulations do not replace the need for formal training in safe intracranial microcatheter navigation and device placement.”
BIBA Briefings is an online platform that gives in-depth analysis of the latest market intelligence from BIBA MedTech Insights. It also reviews the latest industry news and pipeline developments.
For editorial enquiries, please contact Dawn Powell: [email protected]
Irene Bargellini (Pisa, Italy) tells BLearning IR at the first Embolotherapy conference (ET; 26–29 June, Valencia, Spain) that non-target embolization is a frequently under-diagnosed, sometimes fatal, problem that interventional radiologists encounter every time they work with embolics.
Understanding the vascular anatomy, identifying the non-target vessels, positioning the catheter properly, choosing the right embolic, and checking injection under fluoroscopy are all part of reducing the risk of non-target embolization, Bargellini says.
She also draws attention to new devices, such as an innovative novel microcatheter with side-holes that received CE mark in April. This device is designed to reduce the risk of embolic material reflux and works on the principle that fluids, but not embolic material, exit from the side-holes and create a vortex that acts as a barrier to prevent reflux.
Guerbet sponsored this video and its distribution in association with Interventional News.
The statements by Guerbet’s key opinion leader described here are based on results that were achieved in their unique setting. Since there is no “typical” hospital and many variables exist (e.g. hospital equipment, case mix, patients’ conditions) there can be no guarantee that other physicians will achieve the same results. Availability of Guerbet products may vary by country.
Sanjay Misra (Rochester, USA) talks to Interventional News about his research into whether stem cell therapy can help AVFs (arteriovenous fistulas) mature and also prevent venous stenosis. The pilot study with a small group of haemodialysis AVF patients led to “promising results” according to Misra, who is planning a larger study to validate the findings. He also discusses the optimal point to deliver the therapy, its future direction and finally, addresses some of the safety concerns around stem cell therapy.
Boston Scientific has announced the completion of its acquisition of BTG, pursuant to the previously announced scheme of arrangement. BTG develops and commercialises products used in minimally-invasive procedures targeting cancer and vascular diseases, as well as specialty pharmaceuticals.
BTG has three key businesses, the largest of which is its highly-differentiated interventional medicine portfolio that encompasses interventional oncology therapeutic technologies for patients with liver and kidney cancers, as well as a vascular portfolio for treatment of deep vein thrombosis, pulmonary embolism, deep venous obstruction and superficial venous disease.
“The addition of the BTG interventional medicine portfolio reinforces our category leadership strategy and enables us to offer best-in-class technologies, unparalleled clinical evidence and a strengthened commercial infrastructure to support physicians treating some of the most challenging diseases impacting patient health around the world,” comments Mike Mahoney, chairman and chief executive officer, Boston Scientific. “Leveraging the employee talent and clinical and commercial expertise of these two high-performing organisations will generate continued innovation and access so that we may advance patient care in ways that neither company could do alone.”
In addition to the interventional medicine product lines, the BTG portfolio also includes a specialty pharmaceutical business comprised of acute care antidotes to treat overexposure to certain medications and toxins, and a licensing business that receives royalties related to BTG intellectual property and product license agreements.
Upon the effectiveness of the scheme of arrangement, BTG became a wholly-owned subsidiary of Boston Scientific, and BTG shares no longer trade on the London Stock Exchange. Under the terms of the previously announced transaction, holders of BTG common shares will receive 840 pence in cash per share.
Boston Scientific expects to complete the previously announced sale of its global embolic microspheres portfolio—comprised of Embozene, Embozene TANDEM and ONCOZENE brands—to Varian Medical Systems. in due course, a transaction entered into in connection with obtaining the antitrust clearances required to complete the BTG transaction.
In addition, the company is initiating a process to explore the divestiture of the royalty stream associated with BTG’s Zytiga licensing arrangements and anticipates closing this divestiture by the end of 2019.
The transaction is expected to be immaterial to adjusted earnings per share in 2019 as a result of the BTG transaction closing later than originally anticipated, the divestiture of the Boston Scientific embolic microspheres portfolio, and the treatment of the licensing business as an asset for accounting purposes and its intended divestiture. The transaction is expected to be four to five cents accretive in 2020 on an adjusted basis, and increasingly accretive thereafter. On a GAAP basis, the transaction is expected to be less accretive, or more dilutive as the case may be, due to amortization expense and acquisition-related net charges. acquisition
Following the announcement that the trial is set to continue, the Vascular Society for Great Britain and Ireland have provided an update on the trial’s progress. In a news release, the society state: “Based on the aggregate data we have so far on the 411 patients who had been randomised at the time we paused recruitment in December 2018, our statistical colleagues tell us that, maintaining 90% power and a minimum of two-year follow-up (as per the original protocol), we will probably need just short of 500 patients to answer the original question.
“In addition, in concordance with advice from MHRA [Medicines and Healthcare products Regulatory Agency] (and FDA [the US Food and Drug Administration]), we are discussing with NIHR HTA [National Institute for Health Research Health Technology Assessment], and other stakeholders, the possibility of extending follow-up to a minimum of five years (to look at the late mortality).
The FDA has been in touch “very recently” with the British Society of Interventional Radiology (BSIR) regarding a data sharing agreement. The news release on the Vascular Society for Great Britain and Ireland’s website states, “We will be discussing their approach and proposals at our next TMG [trial management group] meeting in September”. BASIL
International Cardio Corporation (ICC) announced that it has achieved the first human use of its high-intensity focused ultrasound (HIFU) system to designed to treat peripheral vascular disease (PVD).
The Minneapolis-based company said its HIFU Synthesiser system is undergoing a 15-patient safety study in The Netherlands to investigate its feasibility and safety for the treatment of atherosclerotic plaques. The system uses high-intensity ultrasound to noninvasively treat vulnerable and occlusive plaques in peripheral arteries to reduce stroke mortality and improve the quality of life for those suffering from PVD.
“The potential for noninvasively ablating and stabilising vulnerable vascular plaques is a compelling opportunity to both reduce stroke risk and deliver better outcomes with higher patient safety than current treatment options for patients suffering from PVD,” says ICC chief operating officer David Lee in a news release.
The safety study is the first step toward achieving the CE mark and FDA approval HIFU Synthesiser.
On The Netherlands Trial Register website, the investigators summarise their study: “Current treatment of lower extremity peripheral arterial disease consists of risk factor modification, exercise therapy and pharmacological treatment initially, but intervention is frequently needed when patients are significantly disabled. Interventional treatment is invasive, either surgical or endovascular. This study investigates a new non-invasive technique that uses high intensity focused ultrasound to treat atherosclerotic arterial disease.”
The primary endpoint of the study is the 30-day major complication rate, which is a composite endpoint that includes 30-day major adverse limb event rate and 30-day mortality rate. Secondary outcomes assessed include a range of technical, MRI, echo-duplex, clinical, and quality of life parameters.
Concept Medical has been granted breakthrough device designation from the US Food and Drug Administration (FDA) for its MagicTouch percutaneous transluminal angioplasty (PTA) sirolimus drug-coated balloon (DCB) catheter, used in the treatment of peripheral arterial disease (PAD) in infra-popliteal lesions. The first breakthrough device designation received by Concept Medical was on 30 April 2019 for its MagicTouch sirolimus-coated balloon, for the treatment of coronary arterial disease (CAD) in patients with in-stent restenosis.
Concept Medical has pioneered the sirolimus drug delivery platform technology (Nanolute Technology) which has been used in more than 30,000 patients worldwide. The MagicTouch PTA sirolimus-coated balloon is developed using this Nanolute Technology for use in PAD.
In an ongoing clinical study (XTOSI), associate professor Edward Choke, principal investigator of the trial and chief of Vascular Surgery, Sengkang General Hospital, Singapore, said, “XTOSI study is the world’s first pilot study to investigate the safety and efficacy of novel MagicTouch PTA sirolimus drug-coated balloon in the treatment of below the knee arterial lesions in addition to femoropopliteal lesions. The majority of patients enrolled had major comorbidities (diabetes and end stage renal failure) and the indication for angioplasty was for severe critical limb ischaemia (more than 90% had the most severe Rutherford scores of 5 or 6). The extent of peripheral arterial disease treated were also severe, and about 80% of patients did not have any patent below the knee arteries before angioplasty.
“I am very encouraged by the excellent results so far in these challenging cohort of patients. Device and technical success were both 100%. Freedom from device and procedure related mortality was 100%. Limb salvage rate at 30 days was 97%. At six months, freedom from clinically driven target lesion revascularisation (TLR) was 91%; and primary patency, independently and blindly assessed by duplex ultrasound, was 82%. I did not encounter any distal embolization or ‘slow flow phenomenon’ after application of sirolimus-coated balloon in below the knee vessels.”
Sahil Parikh, an interventional cardiologist and associate professor of Medicine and director of Endovascular Services at the Columbia University College of Physicians and Surgeons (New York, USA) says, “The breakthrough designation demonstrates how important it is for us to have new technologies for below the knee intervention. Patients with critical limb ischemia (CLI) represent an enormous burden to our healthcare system and comprehensive care for these patients begins with effective revascularisation. The MagicTouch PTA will hopefully bring us closer to our goals of reducing amputations in the USA and the world.”
According to a press release, this breakthrough device offers Concept Medical an opportunity to interact with the FDA’s experts through several different programme options “to efficiently address topics as they arise during the premarket review phase, which can help manufacturers receive feedback from the FDA and identify areas of agreement in a timely way”. Manufacturers can also expect prioritised review of their submission. Under the programme, the FDA will provide Concept Medical with priority review and interactive communication regarding device development and clinical trial protocols, through to commercialisation decisions.
A private equity firm, Palatine (Manchester, UK), has announced that it has made a “significant investment” into a UK centre—Veincentre—that provides endovenous laser ablation (EVLA) for the management of varicose veins. The investment, according to Palatine, is the fourth to be made from the firm’s £100m “Impact Fund” that “targets companies with a social and/or environmental impact, alongside industry-standard returns”.
A press release reports that, in the UK, the NHS withdrew funding for varicose veins treatment after determining it was “non-essential”. Last year, the NHS released a consultation document on stopping or reducing the routine commissioning of 17 interventions for which “less invasive, safer treatments are available and just as effective”. One of these interventions was surgery for varicose veins, with the document noting that patients with varicose veins should only be referred for treatment when they meet specific criteria (such as having a venous leg ulcer). It states: “For patients whose veins are purely cosmetic and are not associated with any symptoms, do not refer for NHS treatment.”
According to the press release announcing the investment from Palatine, EVLA reduces recovery times associated with traditional forms of treatment (i.e. conventional surgery) and significantly reduces scarring. David West, the clinical director of Veincentre, says: “With the help of the Palatine team, our aim to bring this specialist, yet affordable treatment to as many people as possible seems more achievable than ever. The work we do has become increasingly important following falling NHS funding in the sector, and now with the help of this investment, we will be able to offer a necessary social service where access might otherwise be scarce.”
Veincentre now plans to continue to build on its recent nationwide expansion, opening new clinics in Glasgow and Leeds later this year, before carrying out a plan to open two new centres across Britain annually. Beth Houghton (head of the Impact Fund, Palatine) comments: “We are very excited to work with Veincentre; with the lack of NHS funding for what can for some people be a debilitating condition, it is important that people are able to access treatment at affordable prices, in convenient locations. With the planned roll-out of clinics to Scotland and Yorkshire, Veincentre will be able to offer treatment in almost every major region in the nation, and the management team has ambitions to offer full coverage of the UK. Veincentre is exactly the type of business we want to support, and we look forward to working with the management team in order to help accelerate growth and consolidate the company’s position as a leader in the industry.”
West told BIBA Briefings: “I am delighted that we have teamed up with Palatine who recognise the impact varicose veins and other problems with venous insufficiency have on people’s lives and the lack of comprehensive provision of modern treatment by the NHS. Most of our patients are bothered by both the cosmetic appearance and troublesome symptoms and many tell us that treatment has changed their lives. Although in an ideal world, all UK patients would be able to access NHS treatment it is difficult to justify treating all cases at the inevitable expense of patients with other more pressing health issues. This investment ensures that we can achieve our short-term expansion plans in the UK and put us on a firm footing for international growth in the future. Veincentre also encompasses the specialist medical devices company EVLA Expert, which provides UK manufactured all in one kits for EVLA at a fraction of the price of the major laser manufacturers. We are always on the lookout for ‘hungry’ keen vascular specialists to join our friendly multidisciplinary team of nurses, surgeons and radiologists.”
This article is part of a series of BIBA Briefings columns published in Venous News International. For previous columns, see past issues.
In a new consensus statement, the Joint UK Societies (JUKS)—which includes the British Society of Interventional Radiology—say that the evidence for renal denervation is “insufficient” to recommend its routine use in clinical practice. However, they add that they support ongoing clinical trial programmes of renal denervation and “strongly encourage” clinicians to tell their hypertensive patients about ongoing renal denervation studies.
Melvin D Lobo (William Harvey Research Institute, Queen Mary University London, London, UK) and colleagues write in Heart that a previous JUKS consensus statement on renal denervation—published in 2014—“placed a moratorium” on the use of renal denervation in routine UK clinical practice until further “favourable evidence had emerged”. They explain that the 2014 statement was in response to the results of the SYMPLICITY HTN-3 trial, which found that renal denervation with the Symplicity system (Medtronic) did not significantly reduce blood pressure compared with a sham procedure.
According to Lobo et al, recommendations from this 2014 statement and those from the European Clinical Consensus Conferences “led to new and improved clinical trials of renal denervation utilising input from experts in the field to lead on both the design and execution of studies in collaboration with commercial sponsors”. Therefore, now that several of these studies have been published, JUKS have published a new consensus statement to “consider the new evidence that they provide”.
Melvin Lobo
The authors review data both for Medtronic’s radiofrequency Symplicity Spyral system and for ReCor Medical’s ultrasound Paradise system, noting that both system have been associated with significant reductions in ambulatory blood pressure (albeit in different patient populations). “The SPYRAL and RADIANCE [Paradise] study programmes to date have provided encouraging data to suggest that renal denervation may have a role in the treatment of hypertension,” Lobo et al comment. They add that, together, the studies have shown the “value of collaboration” better different disciplines (including industry) and “rekindled enthusiasm for renal denervation in the clinical community”.
However, Lobo et al do outline the limitations of the studies—such as being of short duration—and that the studies have “reported considerable heterogeneity in the response to renal denervation”. Furthermore, they note: “At present, it is unclear which technology may be best for renal denervation, with radiofrequency and ultrasound systems appearing more or less similar in efficacy and ongoing trials of chemical ablation systems are not published yet.”
Thus, Lobo et al report that the JUKS are not changing their position that there is “insufficient evidence to recommend the routine use of renal denervation and that the use of renal denervation should remain restricted to clinical trials”. They do though provide an “agenda” for important areas for future research. These areas include further studies to determine the role of renal denervation in the treatment of hypertension, establishing the safety/durability of different renal denervation technologies, and identifying which patients will be the best responders.
Although they do not advocate the use of renal denervation in routine clinical practice, Lobo et alsay that the JUKS support ongoing clinical trials programmes from the different device manufacturers across the spectrum of renal denervation technologies. They add that they “strongly encourage clinicians who look after patients with hypertension to inform their patients about these studies which are recruiting participants who are on and off medications in order to inform future practice.”
Lobo told BIBA Briefings that he thinks there will be a definitive answer about the role of renal denervation for managing hypertension in “the next two to three years”.
Expanding the role of renal denervation
The need for further studies to better understand the role of renal denervation to manage hypertension has not, however, prevented studies exploring the use of the procedure to treat other cardiac conditions. Lobo said: “I think these studies make a lot of sense particularly where those conditions are characterised by high sympathetic drive. The design of these studies, however, will need to be very carefully thought out given how complex it has been to evaluate the efficacy of renal denervation for hypertension.”
Speaking at EuroPCR 2019 (21–24 May, Paris, France), Marshall Heradien (Department of Internal Medicine, Stellenbosch University, Tygerberg, South Africa) presented a study that evaluated the use of renal denervation for the management of atrial fibrillation. He said that several previous studies “support the idea that renal denervation may have an antiarrhythmic effect”, adding that he and his fellow investigators sought to test the hypothesis that “upstream renal denervation treatment can reduce atrial fibrillation in patients with hypertensive heart disease”.
In the study, 42 patients were randomised to receive treatment with renal denervation (10 with the first-generation Flex catheter and 32 with the second-generation Spyral catheter) and 38 underwent “sham” renal denervation. The primary endpoint was the first event of subclinical atrial fibrillation atrial fibrillation at least six minutes on an implantable loop recorder (which was scanned at six-month intervals).
After an average of three years of follow-up, 19% of the renal denervation group had an episode of atrial fibrillation compared with 47% of the sham procedure group (0.011). Furthermore, patients in the sham procedure experienced significantly more episodes of fast atrial fibrillation: 12% vs. 2% (p=0.002). Renal denervation was also associated with a significant reduction in cardiovascular death at two years: one patient vs. six patients for the sham procedure (p=0.04). However, there were no significant differences in office systolic blood pressure at six months between groups.
Heradien concluded: “In this single-centre randomised controlled trial of patients with hypertensive heart disease, upstream treatment of renal denervation reduced subclinical and fast atrial fibrillation and cardiovascular death.”
Renal denervation has also been explored for the management of heart failure secondary to Chagas’ disease. In Catheterization and Cardiovascular Interventions, André G Spadaro (Heart Institute, University of São Paulo Medical School, São Paulo, Brazil) and others report that renal denervation was “safe and feasible” for patients with Chagas cardiomyopathy. They add that after nine months of follow-up, the primary endpoint (all-cause mortality, myocardial infarction, stroke, need for renal artery invasive treatment or worsening renal function) occurred in 36.4% of 11 patients randomised to undergo renal denervation compared with 50% of six patients randomised to conservative treatment (p=0.06). Spadaro et al state that these findings warrant “future studies to better evaluate the clinical efficacy of the interventional strategy in improving the prognosis of this high-risk population.”
This article is part of a series of BIBA Briefings columns published in Interventional News. For previous columns, see past issues.
BIBA Briefings Insights reports give in-depth analysis of the latest market intelligence from BIBA MedTech Insights. They also review that the latest technology news and pipeline developments.
For editorial enquiries, please contact Dawn Powell: [email protected]
Medtronic has issued the following statement regarding the US Food and Drug Administration’s (FDA) updated letter to healthcare providers for paclitaxel-devices in patients with peripheral artery disease (PAD) in the superficial femoropopliteal artery (SFA):
“Medtronic would like to thank FDA and the panel members for their thoughtful deliberations and dedication to providing physicians, patients, and administrators with updated recommendations following the Advisory Committee meeting of the Circulatory System Devices Panel in June [19–20 June, Washington, DC, USA). The next steps as outlined by [the] FDA are critical to ensuring that physicians and their patients with PAD retain the option to utilise paclitaxel-coated therapies. The IN.PACT Admiral drug-coated balloons (DCB) have demonstrated a clear positive benefit on clinical outcomes and quality of life across multiple randomised controlled clinical trials.
“Importantly, this guidance will allow:
Physicians and patients to discuss the benefits and risks of all available PAD treatment options in order to support an informed treatment decision.
Patients to have continued access to paclitaxel devices as a first-line treatment option, particularly those at high risk of restenosis.
Trial sponsors to continue enrollment in clinical studies to further evaluate the long-term safety and effectiveness of paclitaxel devices.
FDA and industry to analyse of additional randomised controlled trials (RCTs) and registry datasets to help provide more insights into the mortality signal in question.
“Medtronic is encouraged by this path forward, but our work to evaluate the root cause of this safety signal is not complete. It is important to remember that causality was not able to be established in the FDA or VIVA/NAMSA [Vascular InterVentional Advances/ North American Science Associates] analyses. Therefore, it is critical that Medtronic and our industry partners continue to work together to share safety and effectiveness data to further facilitate the benefit-risk conversation. This work is consistent with the Medtronic Mission, and we look forward to continued collaboration with physician societies, FDA, and our industry partners throughout the next phase of this effort.
“Medtronic remains confident in the safety and effectiveness of IN.PACT Admiral. In the IN.PACT SFA trial, three out of four DCB patients remained intervention-free through five years, and for DCB patients who required a repeat procedure, the time to reintervention was prolonged for more than two years. In line with FDA’s recommendations, we encourage physicians to talk to their patients about the benefits and risks of all available treatment options.”
Clinical studies of paclitaxel-coated balloons and paclitaxel-eluting stents “may continue and should collected long-term safety (including mortality) and effectiveness data”, says the US Food and Drug Administration (FDA) in a letter to healthcare providers on 7 August. This is due to “the demonstrated short-term benefits of the devices, the limitations of the available data, and uncertainty regarding the long-term benefit-risk profile of paclitaxel-coated devices”.
The letter provides an update on the agency’s stance on the use of paclitaxel devices to treat peripheral arterial disease (PAD) in the femoropopliteal arteries. The FDA say clinical studies investigating these devices in the lower leg “require appropriate informed consent and close safety monitoring to protect enrolled patients”, and confirm they are working with study investigators to modify informed consent documents to include information about the late mortality signal.
The FDA state: “Based on the conclusions of our analysis and recommendations of the advisory panel, the FDA is taking additional steps to address this signal, including working with manufacturers on updates to device labelling and clinical trial informed consent documents to incorporate information about the late mortality signal. The FDA is also continuing to actively work with the manufacturers and investigators on additional clinical evidence development for assessment of the long-term safety of paclitaxel-coated devices.”
The recommendations
In full, the FDA recommendations are:
Continue diligent monitoring of patients who have been treated with paclitaxel-coated balloons and paclitaxel-eluting stents.
When making treatment recommendations, and as part of the informed consent process, consider that there may be an increased rate of long-term mortality in patients treated with paclitaxel-coated balloons and paclitaxel-eluting stents.
Discuss the risks and benefits of all available PAD treatment options with your patients. For many patients, alternative treatment options to paclitaxel-coated balloons and paclitaxel-eluting stents provide a more favourable benefit-risk profile based on currently available information.
For individual patients judged to be at particularly high risk for restenosis and repeat femoropopliteal interventions, clinicians may determine that the benefits of using a paclitaxel-coated device outweigh the risk of late mortality.
In discussing treatment options, physicians should explore their patients’ expectations, concerns and treatment preferences.
Ensure patients receive optimal medical therapy for PAD and other cardiovascular risk factors as well as guidance on healthy lifestyles including weight control, smoking cessation, and exercise.
Report any adverse events or suspected adverse events experienced with the use of paclitaxel-coated balloons and paclitaxel-eluting stents. Voluntary reports can be submitted through MedWatch, the FDA Safety Information and Adverse Event Reporting programme. Device manufacturers and user facilities must comply with the applicable Medical Device Reporting (MDR) regulations. Health care personnel employed by facilities that are subject to the FDA’s user facility reporting requirements should follow the reporting procedures established by their facilities. Prompt reporting of adverse events can help the FDA identify and better understand the risks associated with medical devices.
FDA actions
In full, the FDA actions are:
The FDA continues to work with the manufacturers and investigators on additional clinical evidence development to assess the long-term safety of paclitaxel-coated devices. Analyses of additional randomised trials and registry datasets are being planned to provide further insights into the magnitude and potential causes of the late mortality risk.
The FDA is working with manufacturers on labelling updates for paclitaxel-coated devices to include information about the late mortality signal.
For ongoing trials of paclitaxel-coated devices, the FDA is working with study investigators to modify informed consent documents to include information about the late mortality signal.
Summary of earlier FDA statements
In June this year, the agency convened a Circulatory Systems Devices Panel meeting (19–20 June, Washington, DC, USA) on the late mortality safety signal associated with paclitaxel-coated balloons and paclitaxel-eluting stents used to treated PAD in the femoropopliteal arteries.
Following the two-day discussion, which included the presentation of the agency’s own analysis of long-term follow-up data from pivotal premarket randomised trials, an FDA Circulatory System Devices Panel Advisory Committee concluded that there is a “late mortality signal”, as first described in the Journal of the American Heart Association (JAHA) paper authored by Konstantinos Katsanos et al (Patras, Greece) in December 2018.
However, they also concluded that better data collection was necessary going forward, as some data were missing, a small sample size meant there were wide confidence intervals, and there was pooling of studies of different paclitaxel devices that were not intended to be combined. The panel determined that there were not enough data to confirm a class effect, and no consensus was reached on the cause(s) of death.
In their most recent letter to healthcare providers, dated 7 August 2019, the FDA summarise the deductions of the advisory committee back in June: “In the three randomised trials which enrolled a total of 1,090 patients, the crude mortality rate at five years was 19.8% (range 15.9–23.4%) in patients treated with paclitaxel-coated devices compared to 12.7% (range 11.2–14%) in subjects treated with uncoated devices. The relative risk for increased mortality at five years was 1.57 (95% confidence interval 1.16–2.13), which corresponds to a 57% relative increase in mortality in patients treated with paclitaxel-coated devices. A meta-analysis performed by VIVA (Vascular InterVentional Advances) physicians of patient-level data provided by manufacturers reported similar findings with a hazard ratio of 1.38 (95% confidence interval 1.06–1.80). […] The Panel determined, and the FDA concurs, that additional clinical study data are needed to fully evaluate the late mortality signal.”
In the largest cohort study to date, new research from Jefferson (Philadelphia University and Thomas Jefferson University, Philadelphia, USA) demonstrates that transradial surgery, done via the wrist, is safe and effective for a broad range of neuroendovascular procedures, and gives patients faster recovery with less procedural risk. Neurointerventionists most commonly use a transfemoral approach, threading instruments through arteries in the groin.
“Despite improved safety shown in large cardiology trials, transradial brain surgeries via the wrist are much less common”, says senior author of the study and neurosurgeon Pascal Jabbour (Jefferson, Philadelphia, USA). “Neurosurgeons tend to prefer the transfemoral approach on which many of us were trained. But our research demonstrates that all kinds of neurological procedures can be done effectively and even more safely via the wrist.”
Transradial access has been widely adopted by interventional radiologists across a range of procedures, with many advocating for its use due to its positive clinical outcomes and patient satisfaction measures.
Jabbour and his team, including first author Omaditya Khanna, retrospectively examined the medical records of 223 patients who underwent 233 consecutive neuroendovascular interventions via radial artery access at Jefferson. The procedures included diagnostic angiograms, mechanical thrombectomies, arteriovenous malformation (AVM)/ arteriovenous fistulae (AVF) embolizations, coiling, stent-assisted-coiling, Woven EndoBridge (WEB) intracranial aneurysm device placement and flow-diversion treatments of cerebral aneurysms, and carotid stent placement.
A subset of 66 patients who had undergone both transfemoral and transradial surgeries were selected to complete a satisfaction survey to assess their preference. As published in Stroke, the majority of patients—94%—said they preferred surgery through the transradial route.
In addition, patients overall reported shorter recovery times with transradial access. It is easier to ensure a blood vessel in the wrist has clotted, and so patients can go home shortly after surgery, rather than laying horizontally for four to six hours after transfemoral surgery. The mean procedure time was also shorter for diagnostic angiograms performed via transradial versus transfemoral access (18.8±15.8 versus 39.5±31.1 minutes; p=0.025).
“Lying flat after certain kinds of brain surgery should be avoided in cases with high intracranial pressure, and yet it is the best way to prevent groin and internal bleeds,” comments Jabbour. “For these cases surgery via the wrist is by far the safest option.”
One of the most compelling reasons to change practice, says Jabbour, is that it eliminates the risk of rare but potentially dangerous complications of post-surgical bleeds in the groin and retroperitoneal area, which can be difficult to detect. The overall incidence of perioperative and postprocedural complications was investigated, and was found to be low across all procedures performed via transradial access. Periprocedurally, only two patients had symptomatic radial artery spasm, and there were no instances of iatrogenic complications (such as vessel dissection, stroke, and haemorrhage).
In 10 cases (4.3%), the intended procedure could not be completed via a transradial approach, and, thus, femoral artery access had to be pursued instead. Ten patients complained of minor postprocedural complications, although none required therapeutic intervention.
Jabbour and colleagues conclude: “Radial artery catheterisation is a safe and durable alternative to perform a wide range of neuroendovascular procedures, with a low rate of complications. On the whole, patients prefer transradial compared with transfemoral access.”
Transradial access in acute ischaemic stroke intervention
Jabbour was one of the first neurosurgeons to perform brain surgery via the wrist and has continued to teach others this technique.
In 2016, Diogo Haussen (Emory University School of Medicine and Grady Memorial Hospital Marcus Stroke and Neuroscience Center, Atlanta, USA) and colleagues set out to describe the feasibility and safety of transradial access in the interventional management of acute ischaemic stroke. Publishing their findings in the British Medical Journal (BMJ), they concluded that failure of transfemoral access in the endovascular treatment of acute ischaemic stroke is uncommon, “but leads to unacceptable delays in reperfusion and poor outcomes. Standardisation of benchmarks for access switch could serve as a guide for neurointerventionalists. Transradial access is a valid approach for the endovascular treatment of acute ischaemic stroke.” neuroendovascular
The US Food and Drug Administration (FDA) have denied BD premarket approval (PMA) for the company’s Lutonix drug-coated balloon (DCB) in the treatment of peripheral arterial disease (PAD).
Speaking in the company’s third quarter conference call on 6 August, BD CEO Vincent Forlenza told analysts: “Regarding our FDA, PMA submission for Lutonix below the knee [BTK], as you are all aware, we have been working with the FDA in a collaborative review process. Subsequent to the FDA Advisory Committee meeting on paclitaxel, the statutory review time for our BTK PMA submission concluded, and the FDA notified us that our PMA was not approvable in its current form.
“While this determination was based on the clinical evidence provided to-date, we continue to review, collaborate and align with the FDA on the path forward regarding our submission, including the need to potentially provide additional clinical data.
“As a result, the approval process timeline has extended out from our previous expectations and we no longer expect approval this calendar year. We will keep you informed as we work with the FDA and make further progress.”
Paclitaxel devices have come under regulatory scrutiny in the last eight months, following the publication of a meta-analysis in the Journal of the American Heart Association (JAHA) by Konstantinos Katsanos (Patras, Greece) and colleagues reporting an increased association of death when paclitaxel devices are used in the lower leg. The FDA analysed all available clinical randomised controlled trials or single-arm registries conducted with agency-approved devices with at least two year follow-up. The investigation compared drug-eluting or coated devices with non-eluting or coated devices.
At two years, the observed mortality rates for the paclitaxel-coated device group were higher for the Zilver PTX (Cook Medical) trial, Levant 2 (evaluating BD’s Lutonix DCB), and IN.PACT SFA I and II trials (looking at Medtronic’s Admiral DCB) in the FDA’s own analysis.
On the same call, the company reaffirmed its full-year revenue and earnings forecasts, and reported quarterly revenues of US$4.35 billion for the third fiscal quarter (which ended 30 June this year). According to a BD press release, this represents an increase of 1.7% over the prior-year period. The company state that on a comparable, currency-neutral basis, revenues increased 5.7% over the prior-year period.
A nurse examines a patient in the Emergency Department of Cincinnati Children’s, where researchers successfully tested artificial intelligence-based technology to improve patient recruitment for clinical trials.
Clinical trials are a critical tool for getting new treatments to people who need them, but research shows that difficulty finding the right volunteer subjects can undermine the effectiveness of these studies. Researchers at Cincinnati Children’s Hospital Medical Center (Cincinnati, USA) designed and tested a new computerised solution that used artificial intelligence (AI) to effectively identify eligible subjects from Electronic Health Records (EHRs), allowing busy clinical staff to focus their limited time on evaluating the highest quality candidates.
The study is published online in JMIR Medical Informatics. It shows that compared to manually screening EHRs to identify study candidates, the system—called the Automated Clinical Trial Eligibility Screener (ACTES)—reduced patient screening time by 34% and improved patient enrollment by 11.1%. The system also improved the number of patients screened by 14.7% and those approached by 11.1%.
Busy emergency departments often serve as excellent locations for clinical trial coordinators to find people who may be good study candidates. According to the study’s lead investigator, Yizhao Ni, (Division of Biomedical Informatics, Cincinnati Children’s Hospital Medical Center, Cincinnati, USA), ACTES is designed to streamline what often proves to be inefficient clinical trial recruiting process that does not always catch enough qualified candidates.
“Because of the large volume of data documented in EHRs, the recruiting processes used now to find relevant information are very labour intensive within the short time frame needed,” comments Ni. “By leveraging natural language processing and machine learning technologies, ACTES was able to quickly analyse different types of data and automatically determine patients’ suitability for clinical trials.”
How it works
The system has natural language processing, which allows computers to understand and interpret human language as the system analyses large amounts of linguistic data. Machine learning allows computerised systems to automatically learn and evolve from experience without specifically being programmed. This makes it possible for computer programs to process data, extract information, and generate knowledge independently.
The automated system extracts structured information such as patient demographics and clinical assessments from EHRs. It also identifies unstructured information from clinical notes, including the patients’ clinical conditions, symptoms, treatments and so forth. The extracted information is then matched with eligibility requirements to determine a subject’s suitability for a specific clinical trial.
The system’s machine learning component also allows it to learn from historical enrolments to improve its future recommendations, according to the researchers. Much of the analyses are handled by carefully designed AI algorithms, essentially procedures or formulas that computers use to solve problems by performing a set sequence of specified actions.
Advanced to live clinical setting
Previously the system was successfully pilot tested in a retrospective study published in 2015 by the Journal of the American Medical Informatics Association. The current study tested the solution prospectively and in real time in a busy emergency department environment, where clinical research coordinators recruited patients for six different paediatric clinical trials involving different diseases.
Using the technology in a live clinical environment involved significant collaboration between data scientists, application developers, information service technicians and the end users, clinical staff.
“Thanks to the institution’s collaborative environment, we successfully incorporated different groups of experts in designing the integration process of this AI solution.” Ni says.
The researchers listed as limitations the small number of clinical trials used in the study, all from a single clinical department. They also pointed to some lingering issues involving the system’s accuracy at interpreting data. These issues will be resolved in future studies through ongoing enhancements to the technologies and also by testing the system in a wider variety of clinical departments, according to the investigators.
Complications are an inevitable component of an interventional radiologist’s practice, says Eric Keller, especially as a newer specialty with a reputation for pushing medical frontiers. As such, he elaborates on the ethics of procedural complications, and describes how he believes physicians should conceptualise and learn from their mistakes. Keller calls for more research on the ethics of complications in interventional radiology (IR), detailing how the innovation that characterises the specialty could be directed towards reimagining approaches to answering hard-hitting questions.
Some people consider “errors” and “complications” distinct, in that an error implies a mistake was made, while complications occur even when everything is done correctly. This distinction is helpful from a systems perspective, but these events do not feel very different personally or ethically.1 When a procedure does not go as expected and hurts someone, it violates a basic assumption held by patients and clinicians: doctors heal people. It leaves us with questions and uncertainty that can undermine our relationships with patients and colleagues and leave clinicians asking, “What if I had…?”. Complications seem particularly personal for interventionalists. When a patient dies on a medical service, people tend to ask, “What happened?”, but when a patient dies on a surgical service, people ask “What did you do?”.2 Although successes define one’s career, it is often responses to shortcomings that defines one’s character. Complications challenge us to be better and to support those hurt in our efforts to improve. When they occur, we should question what we owe our patients, selves, and colleagues, and to some degree, the answers are similar: reflection, confession, and resolution.
First, we should try to understand why a complication occurred and how to best avoid it in the future. It can be tempting to consider a complication merely as something that happens or attribute the fault to someone or something else, but we should always reflect upon our role in the event. Likewise, it can also be tempting to feel like a failure and let complications paralyse us, but the only interventionists that do not have complications are those that do not perform procedures. Neither extreme is helpful.
One useful approach for reflection is Charles Bosk’s categorisation of operator errors,2 which is summarised in Table 1 (below) with examples for interventional radiology (IR). Errors of technique or clinical judgement happen to everyone and are easier to improve with more training and experience. However, errors of character (normative or quasi-normative errors) are more difficult. In the face of these errors, we should look for deeper causes. Was the interventionalist depressed, burnt out, or overwhelmed by other aspects of life? Is the current practice or career not the right fit? If this is the case, we owe it to our patients, selves, and colleagues to step away and get help.
Table 1: Bosk’s four types of operator errors
Once one has reflected upon the cause of the complication, this understanding should be used to provide an explanation and support to patients, families, and colleagues. For patients and families, complications can undermine trust, which is central to the patient-clinician relationship.3 It is trust that allows people to let us render them unconscious and thread catheters and wires into their bodies. Without this trust, it can be difficult for people to get the care they need, so in the face of complications, we owe it to patients to help rebuild that trust, not just in one clinician, but healthcare in general. Rather than abandoning patients, we should advocate for them by providing information, support, and guidance.4 An apology can also go a long way. Some may worry that an apology will increase the risk of a law suit, but research tends to suggest otherwise. Patients that sue tend to be those who did not receive the information or support they felt they deserved.5
Similarly, we should not leave our colleagues to deal with our complications alone. Rather, we should take responsibility for what occurred and partner with them. In IR, referrals networks are important, and complications can weaken these relationships. Just as with patients, we owe our colleagues an explanation and support to rebuild their trust. Colleagues can also be invaluable for stopping a difficult situation from getting worse, and we should have the humility and insight to ask for help when things go awry.6 We can also provide an opportunity for our colleagues to learn from our complications via morbidity and mortality conferences. Ideally these should be constructive and supportive rather than whipping posts for subordinates. Again, everyone has complications, and we owe it to our patients, selves, and colleagues to learn from them together.
This approach of reflection, confession, and resolution is not specific to IR, so it is also worth considering some unique aspects of IR culture related to complications. As a newer specialty, there tends to be less data to guide clinical decision making. The specialty has a reputation of being the cowboys and cowgirls of medicine, always willing to try something. We even have an entire forum to celebrate “extreme” cases that could easily end up in morbidity and mortality conferences of other specialties. This creates a complex relationship with complications. IR has classification systems to measure and report complications but not a robust forum for discussing the cases that did not save the day and how this relates to our drive for innovation or willingness to push the envelope. Furthermore, discussions of complications tend to be limited to more tangible periprocedural events such as bleeding or infection. There is little work in IR exploring issues of consent, futility, conflicts of interest, or tribalism. Overall, there seems to be a need for a balance; forums to celebrate innovation and to discuss the difficult ethical questions that interventionalists face each day.
In summary, complications and errors are likely to feel similar to interventional radiologists, their patients, and their colleagues. These events contradict expectations and hopes and leave people with uncertainty that can undermine relationships with patients, families, and colleagues. In response, we should reflect upon our complications, try to understand what caused them, and give ourselves permission to be human and learn from them. We can then use this understanding to provide an explanation and support to our patients and colleagues to rebuild trust and rapport with them. On a larger scale, we should also consider developing more research on and forums to discuss ethics in IR. Perhaps IR can develop innovative approaches to the difficult ethical questions we all face as well as the clinical ones.
Eric Keller is an interventional radiology resident at Stanford Medical School, Stanford, USA, and has a Master of Arts in Medical Humanities and Bioethics from Northwestern University, Chicago, USA.
References:
Angelos P. Complications, errors, and surgical ethics. World J Surg. 2009;33(4):609-11.
Bosk CL. Forgive and remember : managing medical failure. 2nd ed. Chicago: University of Chicago Press; 2003. xxv, 276 p. p.
Pellegrino ED. Professionalism, profession and the virtues of the good physician. Mt Sinai J Med. 2002;69(6):378-84.
Meruelo NC. Mediation and medical malpractice: the need to understand why patients sue and a proposal for a specific model of mediation. J Leg Med. 2008;29(3):285-306.
Hickson GB, Clayton EW, Githens PB, Sloan FA. Factors that prompted families to file medical malpractice claims following perinatal injuries. JAMA. 1992;267(10):1359-63.
Keller EJ, Crowley-Matoka M, Collins JD, Chrisman HB, Milad MP, Vogelzang RL. Fostering better policy adoption and inter-disciplinary communication in healthcare: A qualitative analysis of practicing physicians’ common interests. PLoS One. 2017;12(2):e0172865.
Thrombolex has announced the enrolment of the first patient in their Early Feasibility and Safety Study, investigating the Bashir Endovascular Catheter for the treatment of submassive pulmonary embolism (PE). The device was designed to quickly and safely dissolve thrombus and restore blood flow in patients with thrombotic vascular occlusions.
The Bashir catheter includes an expandable infusion basket comprised of six mini-infusion catheters with 48 precision, laser-drilled infusion holes. When expanded, it can promptly restore blood flow to enable endogenous lytics in the blood to help accelerate clot lysis. In this investigational study the device is used to administer thrombolytics through multiple cross-sections of the culprit clot to enhance clot dissolution.
“We are pleased to have been the first site to enrol a patient in the Thrombolex Early Feasibility and Safety Study,” said Parth Rali, assistant professor, Thoracic Medicine and Surgery at Lewis Katz School of Medicine at Temple University in Philadelphia, USA. “The catheter removed a large volume of clot from the pulmonary arteries efficiently, and safely restored blood flow, that resulted in a very rapid improvement in the patient’s overall clinical status.”
In this patient with a critical, large submassive PE that severely compromised blood flow to both lungs, a total of 14mg of r-tPA was administered over eight hours. “There was a dramatic improvement in the patient’s haemodynamic state and oxygenation as well as evidence of a marked reduction in clot burden as compared to what has been seen in other catheter-directed thrombolysis studies using a similar dose of r-tPA,” said Riyaz Bashir, director of Vascular and Endovascular Medicine at Temple University Hospital. “We believe that the Bashir Endovascular Catheter may represent a quantum leap in the treatment of venous thromboembolism patients, not just acutely, but also in terms of their longer-term health status,” said Brian Firth, chief scientific officer at Thrombolex.
“Thrombolex is focused on developing more advanced therapies for treatment of patients suffering with venous thromboembolic (VTE) disorders,” said Mike Cerminaro, president & COO of Thrombolex. “We are passionate about our focus because PE is a common disease, which is the third highest cause of cardiovascular mortality and is responsible for up to 180,000 deaths annually in the USA alone.”
“Currently available infusion catheters used to treat PE and other large clots are not able to rapidly restore blood flow through the thrombus and allow for only limited radial diffusion of exogenously administered thrombolytics like r-tPA into a clot,” said Marv Woodall, chairman & CEO of Thrombolex. The Thrombolex investigational trial is designed to examine if lower doses of thrombolytic via the Bashir Endovascular Catheter can be administered much more effectively over less time and thereby minimise major bleeding complications. This investigational study is a 10-patient prospective, multicentre clinical study to evaluate feasibility and safety of the catheter to treat patients with intermediate-risk PE. It represents the first in a series of planned clinical trials to evaluate this new platform technology that has been developed by Thrombolex.
The interim results of a multicentre, European retrospective analysis investigating the use of drug-coated balloons (DCBs) in symptomatic central venous stenosis (CVS) suggest that these devices could be a valid option for treatment, slowing down the effect of neo-intimal hyperplasia (NIH) leading to restenosis. Though with data mining still underway, the investigators warn against drawing any premature conclusions. Panagiotis Kitrou (Patras University Hospital, Patras, Greece) presented these preliminary results at the annual EndoVascular Access Meeting (EVA; 21–22 June, Patras, Greece) earlier this year.
Against the backdrop of the current paclitaxel controversy (where Konstantinos Katsanos, along with Kitrou and other colleagues, reported in the Journal of the American Heart Association (JAHA) an increased risk of death at two and five years following the use of paclitaxel devices), Kitrou first provided insight into how the publication has affected his own clinical practice. He told delegates: “We [at Patras University Hospital] have not changed our practice with regard to DCB use in dialysis access management. We believe that paclitaxel is an independent predictor of death, but its effect is different in different populations. Thus, a claudicant suffering more comorbidities compared to a claudicant with fewer comorbidities will have a greater number of factors antagonistic for the same event, which is death. Hence the signal and the effect of paclitaxel becomes faint and diluted while the actual benefit from NIH inhibition becomes more apparent.”
For patients with CVS, the gold standard treatment is percutaneous transluminal angioplasty (PTA). “However, Kitrou explained, “the patency rates may be as low as 28.9% at six months. This rate doubles to 60% when you use a high pressure balloon. The main problem [when using balloons] remains elastic recoil. You may also use a stent or a covered stent, is the latter being a much more aggressive treatment”.
Going through today’s evidence on CVS treatment, Kitrou showed EVA attendees the results from a 2015 retrospective analysis by Alexander Massmann et al that compared standard balloon angioplasty with paclitaxel-coated balloon angioplasty for symptomatic central vein restenosis in patients with impaired native haemodialysis fistulas. The study investigators concluded that paclitaxel-coated balloon angioplasty yielded a statistically significant longer freedom from target lesion revascularisation compared to standard balloon angioplasty. Although, Kitrou noted, Massmann and colleagues did include axillary veins, so he thinks these results “are not strictly for central veins”.
He next talked the audience through his own randomised controlled trial from 2017, which included 40 patients with de novo, restenotic and occluded lesions. Twenty patients were treated with the Lutonix DCB (BD), and twenty were treated with a non-coated balloon. In this study, the primary end-point was a clinically-assessed intervention-free period. In this, Kitrou et al found a significant difference in favour of DCBs. Additionally, DCB angioplasty was numerically better in the longitudinal analysis compared to plain balloon angioplasty.
Despite the fact that these studies found a significant difference between treatment arms consistently in favour of paclitaxel-coated balloons, Kitrou highlighted that these results have been observed in fewer than 30 patients. The present, multicentre European retrospective analysis therefore will provide data detailing DCB use in a greater number of patients. The primary outcome measures are a clinically assessed intervention-free period of the treated segment at six months, a dialysis access circuit with no need for clinically driven target lesion repeat intervention for symptom recurrence (verified angiographically), and no procedure-related minor and major complications.
The study included 87 patients from 11 centres across Greece, Germany, France, Italy, Portugal, and the UK. Though still only early data, the interim analysis reveals that at six months, the target lesion primary patency was 52%, and the median target lesion primary patency was 280 days, meaning lesions remained open following intervention for an average of nine months. “The results are already much better compared with our randomised controlled trial”, Kitrou said, referring to his 2017 study.
The investigators also measured primary patency of the access circuit. This was 48% at six months, and the median time to reintervention was 257 days. The access circuit survival was approximately 70% at six months, Kitrou shared.
“There is a lot of work in progress, we are still mining data—we are looking at this huge Excel [document] with a lot of data in there, and we will soon have more to share with you”, Kitrou concluded. interim interim
Jos van den Berg (Lugano, Switzerland), Antonio Micari (Bergamo, Italy) and Marianne Brodmann (Graz, Austria) sit down after a specially convened US FDA panel reviewed paclitaxel device data, with recommendations still to come. The physicians discuss the safety of paclitaxel devices and examine what the evidence says.
Micari presented a patient-level analysis from the IN.PACT randomised controlled trials to state that they have collectively shown there is no drug-related mortality signal and suggests that study design and conduct might be responsible for the “transient” mortality signal. He also looks at the long-term effectiveness of paclitaxel devices to state that the IN.PACT DCB (Medtronic) provides a vast improvement over plain balloon angioplasty, and shows “durable treatment benefit”.
Brodmann, meanwhile, outlines evidence from real world data sources – such as Medicare, OPTUM and VQI – which has indicated that there is “no difference in mid-term or long-term survival between patients treated with drug-coated or non drug-coated devices”.
Summing up, van den Berg states that several methods of investigation have demonstrated the absence of a dose relationship to mortality. “What we need to do now,” he says, is to “perform well-conducted real world comparative studies that are followed up for a sufficient duration”.
This webinar was filmed by SparkBio. Medtronic sponsored its distribution in association with Vascular News and Interventional News.
Medical devices manufacturer Boston Scientific has partnered with Mayo Clinic, a non-profit academic medical centre, to launch an accelerator focused on medical solutions for diseases with unmet clinical needs.
Named Motion Medical, the new 1,800ft² venture will receive funds from partners over three years to develop new medical technology and minimally invasive therapies.
Motion Medical research facilities will be located in the Discovery Square research district’s bioscience centre called One Discovery Square in Rochester, USA.
Boston Scientific and Mayo Clinic have been working together for approximately ten years for the development of medical devices and technologies across interventional cardiology, neuromodulation and urology therapeutic areas, among others.
To date, the companies have submitted eight patent applications and partnered on two first-in-human clinical trials, according to Mayo Clinic.
Boston Scientific develops a variety of medical solutions for endoscopy, rhythm management, interventional cardiology, peripheral interventions, neuromodulation, urology and pelvic health.
In November last year, the company signed an agreement to buy BTG for £3.3bn. BTG has three main businesses and Interventional Medicine is said to be the largest.
The acquisition is expected to help boost Boston Scientific’s capabilities in cancer and pulmonary embolism.
The National Institute for Health and Care Excellence (NICE) in the UK has published a positive draft final appraisal determination recommending the use of rivaroxaban (brand name Xarelto, Bayer) by the National Health Service (NHS) in England. The NICE recommendation sets out a dose of 2.5mg twice daily, combined with 75–100mg aspirin once daily, as an option for preventing atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral arterial disease (PAD) who are at high risk of ischaemic events.
Publication of this NICE draft is based on evidence from the COMPASS study, the largest Phase III study with rivaroxaban (27,395 patients). This study showed that rivaroxaban vascular dose, 2.5mg twice daily combined with aspirin 100mg once daily, statistically significantly reduced the risk of the composite of cardiovascular (CV) death, stroke or myocardial infarction (major adverse cardiovascular events; MACE) by 24% (relative risk reduction, ARR: 1.3%) compared with aspirin 100mg once daily alone amongst patients with stable atherosclerotic vascular disease (379 patients [4.1%] vs. 496 patients [5.4%]; hazard ratio, 0.76; 95% confidence interval [CI], 0.66 to 0.86; p<0.001).
In the COMPASS trial, for patients with stable CAD, addition of rivaroxaban 2.5mg twice daily with aspirin 100mg once daily lowered major adverse cardiovascular events compared with aspirin once daily (347 [4%] of 8313 vs. 460 [6%] of 8261; HR 0·74, 95% CI 0·65–0·86, p<0·0001). Moreover, patients with PAD who received rivaroxaban 2.5mg twice daily combined with aspirin 100mg once daily, also had fewer major cardiovascular events compared with the aspirin 100mg once daily alone group (126 [5%] of 2492 vs. 174 [7%] of 2504; HR 0·72, 95% CI 0·57-0·90, p=0·0047).
Rivaroxaban is an anticoagulant that targets Factor Xa, an enzyme which acts at a key point in the blood clotting process, inhibiting its ability to generate thrombin.NICE are recommending use of rivaroxaban as part of a dual pathway approach (in combination with aspirin) to prevent atherothrombotic events in patients who are at high risk of such events. Coronary artery disease patients who are at high risk of ischaemic events are defined by NICE as those aged 65 or over, patients with atherosclerosis in at least two vascular territories, or those presenting risk factors such as smoking, diabetes, kidney dysfunction, heart failure or a history of stroke.
Derek Connolly, COMPASS trialist, consultant interventional cardiologist and honorary senior clinical lecturer at Birmingham City Hospital (Birmingham, UK) said: “Cardiovascular disease remains the biggest cause of years of life lost in the UK. There have been few recent major new advances in the medical management of patients with CAD and PAD to protect them against strokes or heart attacks.
“The COMPASS trial showed that adding rivaroxaban vascular dose to low-dose aspirin significantly reduced vascular events. The large reduction in events [such as strokes], outweighed the increase in major bleeding events seen. Conducted in more than 30 countries, including the UK, COMPASS was one of the largest ever trials of oral anti-thrombotic therapy providing robust results, overall, and particularly for key patient subgroups at high-risk of recurrent events such as those with renal dysfunction or stable ‘mild’ heart failure.”
“Rivaroxaban vascular dose in combination with aspirin is the first treatment of its kind for this patient population and this recommendation from NICE provides clinicians with an important additional option for treating patients at risk of major adverse cardiac events such as cardiovascular death, stroke or myocardial infarction.”
Lars Bruening, CEO Bayer UK & Ireland, said: “Bayer has a long and successful heritage in cardiology. The NICE recommendation provides those with high risk CAD and symptomatic PAD with an effective treatment option that will provide additional tailored protection from atherothrombosis. Ten years on from the introduction of rivaroxaban into the UK we are continuing to see the enduring impact that it has on patients treated across its licensed indications—and now this new patient population with previous unmet needs can be considered.”
Publication of the NICE draft for rivaroxaban follows approval by the European Commission (EC) in August 2018for the regimen of rivaroxaban 2.5mg twice daily plus aspirin 75–100mg once daily for the prevention of atherothrombotic events in adult patients with CAD or symptomatic PAD at high risk of ischaemic events. Rivaroxaban is the most broadly indicated NOAC worldwide. It is approved in the UK for:
The prevention of stroke and systemic embolism in adult patients with non-valvular AF with one or more risk factors
The treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and prevention of recurrent DVT and PE in adults
The prevention of venous thromboembolism (VTE) in adult patients undergoing elective hip or knee replacement surgery
The prevention of atherothrombotic events in adult patients after an acute coronary syndrome (ACS) with elevated cardiac biomarkers, co-administered with aspirin alone or with aspirin plus clopidogrel or ticlopidine
The prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral artery disease (PAD) at high risk of ischaemic events
In a retrospective, single centre study, the vast majority of patients who underwent uterine artery embolization (UAE) were able to have a successful pregnancy after the procedure. This led Muthusubramanian Rajasekaran (Department of Interventional Radiology, HCG Cancer Centre, Bangalore, India) to conclude that UAE has “satisfactory and acceptable outcomes” concerning fertility and pregnancy amongst patients of reproductive age, as he informed the audience at GEST 2019 (Global Embolization Cancer Symposium Technologies; 9–12 May, New York, USA). pregnant
As a commonly performed interventional radiology procedure, UAE is used to treat a variety of pathologies, including leiomyomas (fibroids), arteriovenous malformations (AVMs) and post-partum haemorrhages. “However”, Rajasekaran told the GEST audience, “the beneficial effects of UAE over the surgical treatment are still up for debate in patients of reproductive age, as the adverse effects of the procedure on fertility and pregnancy are not known”. As such, Rajasekaran and colleagues felt further investigation into the effects of UAE on pregnancy and fertility was warranted.
They conducted a retrospective analysis of their hospital records between January 2012 and January 2018, where they found that 42 patients had undergone UAE for various uterine pathologies. Of these, nine were excluded for being over the age of 35, three were excluded as they did not wish to get pregnant in the future, and two were lost to follow-up. This left 28 patients, with an age range of 22 to 35 years, for the analysis. Fourteen per cent underwent UAE to treat AVMs, 43% had post-partum haemorrhage, and the remaining 43% had fibroids.
Twenty-four (86%) of these 28 patients had at least one successful pregnancy after UAE, and 21% of the patients (six of the 28) had two successful pregnancies following the procedure. The majority of these women—62%, or fifteen of the 28—had normal vaginal delivery, and 38% (nine of the 28) had a caesarean section.
The average time interval for the first pregnancy after UAE was 15 months; the shortest time to pregnancy was six months, and the longest gap between pregnancy and procedure was 30 months. No procedure-related complications were observed in any of these patients.
Of the four (14%) patients who did not get pregnant following UAE, one (4%) did not get pregnant at all, and three (11%) had miscarriages. When asked about whether there were any unifying characteristics of these three patients by moderator Robert Mitchell Ermentrout (Department of Radiology, Emory University School of Medicine, Atlanta, USA) at GEST, Rajasekaran said that when they were evaluating the patients during follow-up, they found nothing that specifically explained why these women in particular were having difficulty with pregnancy.
“The more data we have, the more likely that this will become more standard practice”
An American audience member asked Rajasekaran what the referral rate and process was like in India, and if it is standard practice for gynaecologists to transfer patients across to the interventional radiology department. “We are still finding it hard to convince gynaecologists to refer patients to us”, Rajasekaran said. “The practice in India is for these patients to first go to the gynaecologist, and then it is their role to refer back to us.”
The questioner said that this is similar to the case across most of the USA we well. He elaborated: “There are many patients who hear about UAE from advertisements, and that is actually how we built up a lot of our practice. A lot of gynaecologists have started referring many patients to us, and normally it is because the patient already knows about the procedure and asks about it in their consultation, from what I understand. But there is still a recommendation to have them evaluated for myomectomy if they do desire future fertility, at least in the USA. But I think anecdotally, at least in our experience—so this is unpublished—fertility is certainly a possibility for patients who have had this procedure [UAE], and I think the more data we have, the more likely that this will become more standard practice across the world.” Rajasekaran agreed.
Medtronic and Viz.ai have partnered to accelerate the adoption of Viz.ai’s new technology, which helps synchronise stroke care and decrease time to treatment, potentially improving outcomes for patients.
Viz.ai’s technology uses artificial intelligence (AI) to identify suspected large vessel occlusion (LVO) strokes and automatically notify specialists. The Viz.ai software connects to hospital computed tomography (CT) scanners and alerts stroke specialists within minutes that a suspected LVO stroke has been identified, sending the radiological images directly to their smart phones where they can be viewed. Viz.ai enables a physician to provide the patient with the treatment they need as quickly as possible.
“Medtronic is an innovative company focused on therapies that extend life and restore health,” said Chris Mansi, neurosurgeon, co-founder and CEO of Viz.ai. “As the largest medical device company in the world, Medtronic is an ideal partner to help physicians access Viz.ai’s cutting-edge technology to ensure as many patients get the care they need as quickly as possible.”
Stroke is a serious and time-sensitive medical condition that requires emergency care and can cause lasting brain damage, long-term disability and death. A stroke occurs if the flow of oxygen-rich blood to a portion of the brain is blocked. When this happens two million brain cells die every minute. It is the number-one cause of disability in the USA and the leading cause of death outside of the USA.
“Viz.ai allows clinicians to receive an alert for suspected LVO’s and the corresponding visual data” said Elad Levy, chairman in the Department of Neurosurgery with the University at Buffalo’s Jacobs School of Medicine and Biomedical Sciences and medical director of Neuroendovascular Services at Gates Vascular Institute. “The combination of AI powered alerts, mobile image viewing, and HIPAA compliant communication facilitates synchronisation of stroke care with great potential to impactfully reduce door-to-needle time and help an increased number of patients.”
Every two minutes someone in the USA has an LVO, but only an estimated 15% receive a potentially lifesaving mechanical thrombectomy, a minimally-invasive procedure that removes blood clots. A Viz.ai study in two centres showed that in 95.5% of true positive cases, its technology alerted the stroke specialist earlier than the standard of care, saving an average of 52 minutes.
“We are excited about this partnership because Viz.ai’s technology has the potential to significantly reduce the time it takes for patients suspected of LVO stroke to receive the care they need,” said Stacey Pugh, vice president and general manager of Medtronic’s Neurovascular business, which is part of the Restorative Therapies Group at Medtronic. “Viz.ai’s software coupled with our network is going to increase access to needed therapies.”
Through this agreement, Medtronic will distribute Viz.ai’s existing LVO detection and triage software services, which are currently permitted for marketing in the US. It was the first clinical decision support software designed to analyse CT results that may notify providers of a potential stroke in their patients cleared by the US Food and Drug Administration (FDA). The technology is available in over 200 hospitals, with the goal of making Viz.ai available to every stroke centre in the country.
Preliminary results of a first in man trial demonstrate that robotically-assisted sonic therapy (RAST) can create a planned ablation volume without significant device-related adverse events. Timothy Ziemlewicz (Department of Radiology, University of Wisconsin School of Medicine and Public Health, Madison, USA) informed delegates at the 2019 annual meeting of the Society of Interventional Oncology (SIO; 7–11 June, Boston, USA) that short-term local tumour control with RAST may be similar to that of other ablation modalities.
The study investigators conducted a phase I trial with the aim of evaluating the safety and short-term efficacy of RAST for hepatic ablation in patients with primary or metastatic liver cancer. RAST is the automated treatment of a defined volume of tissue utilising histotripsy, the first non-thermal, non-ionizing, non-invasive ablation modality. Prior to this research, RAST had successfully been applied in pre-clinical porcine liver models.
The study patients were recruited from, and procedures were performed at, two hospitals near Barcelona, Spain: Mutua Terrassa, where the study’s principal investigator Joan Vidal-Jove is located, and Vall D’Hebron Hospital, where Xavier Serres is based. The underlying technology was developed by members of the Department of Biomedical Engineering at the University of Michigan.
When delineating the advantages of RAST, Ziemlewicz emphasised the precision, telling the SIO audience that the cavitation bubble cloud is precise at the histologic level (“so you can literally cut cells in half with it”), and that planned treatment volumes are within nanometres of the resultant ablation.
The phase I, open-label, non-randomised trial had a primary endpoint of technical success, defined as the ability to create an ablation zone per the planned volume, as assessed by MRI one-day post-procedure. There were multiple secondary endpoints, the most important of which, according to Ziemlewicz, was safety, measured as the number and severity of adverse events. Adverse events were graded using the Common Terminology Criteria for Adverse Events (CTCAE v4.0), a descriptive scale from Grade 1 (mild) through to Grade 5 (death related to adverse event). The study investigators also evaluated local tumour progression, liver function, involution of the ablation zone, and analgesic requirements. Follow-up MRI, laboratory draws, and clinical visit were planned at one day, one week, one month, and two months.
Eight patients, five female, three male, have had a tumour treated under this protocol. Most patients (six) had a single tumour, one patient had two tumours, and one patient had three tumours. The mean tumour size was 1.3cm, and the range was 0.5cm to 2.3cm. “We were somewhat limited in size by having to fit treatments within livers with multifocal tumours”, Ziemlewicz said.
The triallists achieved 100% technical success in creating the planned ablation volume using RAST. In the axial plane, the ablation zone was within an average of 0.1cm of the plan, and in the coronal plan the ablation zone was an average of 0.5cm larger than the plan. “We did not control for respiration”, Ziemlewicz commented, “so we knew that these would be elongated in the coronal plane”. In terms of targeting tumours, the investigators report a 90.9% success rate—one of the eleven tumours treated was mistargeted immediately adjacent to the 0.5cm tumour. Ziemlewicz ascribed this mistargeting to poor ultrasound visualisation, and explained that the patient is set to undergo a second procedure for local control.
Concerning safety, there was one Grade 4 adverse event (classified as life-threatening, with urgent intervention indicated), which Ziemlewicz explained was not thought to be device-related. The patient was admitted to hospital and the complication was attributed by the independent treating physicians to their underlying Crohn’s disease. In addition, there was one Grade 2 (designated as a moderate complication) adverse event, which was also not attributed to the device. This patient was admitted to hospital for fever and given supportive treatment. One patient had a complication that was device-related; a Grade 1 (mild) adverse event, they presented with post-ablation syndrome one day after the procedure and had a fever of 39°C. This patient was the only one of the eight to have three ablative treatments; 64mL of total ablation. “They had a fever and some malaise for a couple of days after the procedure, which resolved and they are doing fine [now]”, Ziemlewicz assured the audience.
The deepest tumour treated by the study investigators did experience some local progression. Explaining this, Ziemlewicz said: “The prototype transducer we used is only capable of treating to about 10cm; we were pushing it to the edge of the envelope [with trying to treat this tumour].” Showing the audience some post-procedural images of the patient’s liver, he commented “You can see at one month the ablation zone is nicely absorbed, and then at the three-month follow-up scan you can see the progression. One of the benefits of this technology is that you can see this relatively early.”
In terms of analgesic requirements, another of the study’s secondary endpoints, there were no analgesic requests and no reported pain.
The involution data were of particular interest to the investigators as they were unsure how this would translate from previous laboratory studies. Ziemlewicz tells Interventional News: “We did note this in our original study published in Radiology last year. We survived half of those treated animals which is where we noted this involution. We honestly were not sure how this would hold up in human livers, which were either cirrhotic or patients were treated with chemotherapy previously.”
There was significant involution after two months: an average of 88.1% volume contraction and 51.1% diameter contraction. Ziemlewicz suggested that rapid involution may allow earlier identification of incomplete treatment.
All RAST procedures (VORTX RX system, Histosonics) were performed with the patient under general anaesthesia. Speaking from the floor, John Kachura (Toronto General Hospital, Toronto, Canada) asked about this decision: “No patients reported pain afterwards, and all procedures done under general anaesthetic. Has anyone tried doing it without general anaesthetic, and just with conscious sedation, or is there concern about that?”.
Ziemlewicz replied that initially, the investigators did not know how the patients were going to feel, and decided to use general anaesthetic to stay consistent with their institution’s policy of using it for all ablation patients. He did say, though, that “Anecdotally, none of the patients showed any vital sign changes to suggest they were having pain during the procedure. […] In the future, we will definitely consider doing this with conscious sedation”.
Yuji Okuno (Okuno Clinic, Tokyo, Japan) gave an update on the status of musculoskeletal embolization for pain management and sports related injuries at the GEST Symposium this year (Global Embolization Cancer Symposium Technologies; 9–12 May, New York, USA).
He began by detailing the first report on musculoskeletal embolization, published in the Journal of Vascular and Interventional Radiology (JVIR) in 2013 by himself and colleagues, which demonstrated the feasibility and efficacy of transcatheter arterial embolization (TAE) using imipenem and cilastatin sodium for tendinopathy and enthesopathy refractory to nonsurgical management. Imipenem and cilastatin sodium have been used as a temporary embolic agent in Japan since 1990, and the Japanese investigators selected the material for its established safety record. Local tenderness score, used as a proxy for pain, reduced rapidly following the procedure, and pain disappeared at three months.
Okuno and his colleagues were encouraged by the results of this pilot study, seeing potential in the procedure’s use to alleviate pain. Current understanding is that chronic inflammation leads to an increase in abnormal neovessels, and that embolizing these vessels and reduce pain and consequently the dependence on alternative pain management strategies, such as taking opioids. However, more data are needed to solidify TAE’s position as a pain management treatment, and Okuno said at GEST that comparative studies of TAE versus a placebo and TAE versus another treatment are needed.
Recently, there has been an upswell in interest around musculoskeletal embolization, with multiple studies investigating the technique’s use in the knee, shoulder and elbow. Sandeep Bagla (chair of Interventional Radiology at the Vascular Institute at Virginia, Woodbridge, USA) presented the positive results on an early preclinical study of GAE in 20 patients with mild to moderate knee osteoarthritis in spring this year at the Society of Interventional Radiology’s annual meeting (SIR; 23–28 March, Austin, USA). A randomised controlled trial focusing on GAE in a larger cohort is underway. Meanwhile, Mark Little (Royal Berkshire Hospital, Reading, UK) is the principle investigator for the first clinical trial examining GAE in knee osteoarthritis patients in Europe, the GENESIS trial. A placebo-controlled randomised controlled superiority trial embolization in the knee headed by Steve Landers (Barwon Medical Imaging, Barwon Health, Geelong, Australia) has also recently completed enrolment in Australia.
Musculoskeletal embolization for pain management in athletes
Specifically thinking about sports injuries, Okuno believes musculoskeletal embolization will have a much larger role to play in the future of pain management for athletes. He gives two case examples at GEST.
The first case report is of a 26-year-old male patient with patellar tendinopathy. The patient is a professional goal keeper for a football team in the Japanese top league, and does not wish to undergo surgery due to the slow post-operative recovery. The patient’s chief complaint is knee pain, which is exacerbated by running, jumping, flexing and kneeling, Okuno informed the audience, “all movement crucial to his profession”. The goalkeeper was resistant to conservative treatment, having had one corticosteroid injection and two hyaluronic acid injections prior to trying TAE.
Post-procedural imaging revealed that the abnormal vasculature was no longer visible, and the patient’s pain score as measured by the Numerical Rating Scale (NRS) dropped from eight to two within a month, and was zero three months post TAE. Two days after the procedure, the patient returned to light training, and was back to full training with the rest of the football team two weeks after the embolization was performed. Six weeks’ post-procedure, the patient had their first competitive game. “The patient had rapid progression and quick reduction in symptoms after the embolization”, Okuno described. He opined, “This is particularly advantageous for sportspeople, as they cannot rest for long. At two-years follow-up, this patient’s knee has a normal appearance”.
The second case Okuno presented to the GEST audience was a chronic hamstring injury in a long distance athlete, who competed at the Rio Olympics. The 34-year-old female athlete complained of hip pain, and was resistant to conservative treatment after one year. “It is very difficult to have surgery and then go back to training”, Okuno explained, “so she was reluctant to have that treatment, even though this was recommended surgery by the orthopaedic surgeon”. Instead, Okuno performed embolization twice in two months. She was back training again after three to four months.
Okuno used these success stories to promote the potential of embolization to allow athletes and active patients to continue engaging in their chosen sport pain free. Marc Sapoval, who was chairing the session “Vanguard in embolization” at GEST, said in response to Okuno’s presentation: “I am very optimistic about this being a new area of embolization for the future”.
In 2013, the Dutch national guidelines on heavy menstrual bleeding were updated to include, for the first time, a recommendation that uterine artery embolization (UAE) be part of counselling for patients with symptomatic fibroids. Despite this, no increase in the number of UAEs being performed in The Netherlands was observed between 2012 and 2014, according to a recent report published in Cardiovascular and Interventional Radiology (CVIR) Endovascular by Annefleur de Bruijn (Amsterdam University Medical Center, Amsterdam, The Netherlands) and colleagues.
The study authors aimed to evaluate the implementation of UAE in The Netherlands and investigate influential factors concerning gynaecologists’ preference, counselling differences and knowledge. “The UAE/hysterectomy ratio in 2014 was 6.9”, they report, a calculation the authors deem “unacceptably low for a procedure with solid scientific level 1 evidence”.
Indeed, de Bruijn et al write that some “‘urban embolization myths’ tend to persist”, with 40% of gynaecologists in hospitals that do not perform UAE doubting the effectiveness of the procedure. In hospitals that do perform UAE, nearly half of the gynaecologists overestimate the chance of a surgical intervention after the minimally invasive procedure.
This research is specific to The Netherlands, but the authors say that “Although there is no scientific evidence from other European countries, oral communications at scientific meetings seem to support” their findings.
Approximately 10–30% of fertile women suffer from heavy menstrual bleeding, and in 40% of these women, fibroids are present. Although multiple randomised controlled trials have concluded that UAE is a valid, safe, and effective alternative to hysterectomy for patients with symptomatic uterine fibroids, when de Bruijn et al initiated their study, they believed the procedure was “offered infrequently” and that its implementation seemed “slow”.
The 2013 national guidelines published in The Netherlands recommend informing the patient of the following outcomes five years after the initial treatment (UAE versus hysterectomy):
An improved quality of life comparable to that of patients who underwent hysterectomy
Faster recovery and return to work after UAE compared to hysterectomy
In 75% of patients who underwent successful UAE, no hysterectomy was needed
The study investigators asked all 82 Dutch UAE performing and non-UAE performing hospitals to send their annual reports detailing the number of hysterectomies performed. Information about the number of UAEs performed over the same time period was requested from the interventional radiology departments of each hospital. Of 30 requests sent out to UAE performing hospitals, 29 (91%) returned the desired information; 36 of 52 (69%) non-UAE performing hospitals returned the data. The calculated UAE/hysterectomy ratios were 7%, 7% and 6.9% in 2012, 2013, and 2014, respectively.
Additionally, de Bruijn and colleagues sent out questionnaires to the hospitals’ gynaecologists—they received a response from 43 gynaecologists at UAE performing hospitals and from 43 gynaecologists at non-UAE performing hospitals.
The survey indicates that gynaecologists working at UAE performing hospitals counsel more patients for UAE compared to their colleagues at non-UAE performing hospitals. Those working at hospitals that did conduct UAE estimated they counselled a median of 20 patients a year, as opposed to just 10 patients a year at non-UAE performing centres. Furthermore, where UAE was performed, 64% of the hospitals (18 out of 28) involved interventional radiologists in the counselling process. At the remaining 10 institutions that do not involve the interventional radiologists in patient counselling but which do perform UAE, 57% of the gynaecologists thought it should be standard practice to include them.
Over a third of gynaecologists at non-UAE performing hospitals (37%, or 16 of 43) think interventional radiologists should not be involved with patient counselling. At non-UAE performing hospitals, 26% (11 of 43) of gynaecologists think interventional radiologists should not be involved in the patient counselling process; an additional 28% (12 of 43) think they should be involved only if that is the patient’s preference.
The authors advocate for the involvement of interventional radiologists in the counselling process. Over half (51% in UAE+ hospitals and 52% in UAE- hospitals) the gynaecologists working across all the hospitals surveyed mentioned that the patient declines UAE when counselled. de Bruijn and colleagues blame the lack of interventional radiologists in the counselling process, pointing to the fact that gynaecologists from all hospitals tend to overestimate the risk of reintervention. To illustrate this, they highlight how the gynaecologists indicated the statement “the secondary hysterectomy rate is 50%” to be true. de Bruijn et al respond: “Literature (and also the guidelines) state there is a secondary hysterectomy rate of 28% after five years of follow up and 31% secondary hysterectomies after 10 years. Apparently this has not reached the surveyed gynaecologists”.
They suggest “Good counselling should be based on facts and should be free of personal preferences of the health care professional. In the case of UAE, counselling is mostly performed by the physician that does not execute the actual procedure. This could be a major influence [on patients turning down UAE]”.
To overcome this knowledge gap, and to promote the possibility of UAE as a treatment option for patients with symptomatic fibroids, the study authors propose the development of an option grid or decision making tool “in order to offer independent counselling and encourage shared decision making”. They also recommend a standard multi-disciplinary consultation for patients with fibroids.
The first patient has been randomised in the TARGET BP I trial at the Piedmont Heart Institute in Atlanta, USA, to investigate the use of the Peregrine System Kit (Ablative Solutions) in renal denervation.
Target BP I is a blinded, randomised sham-controlled study that is evaluating the safety and efficacy of the system in the treatment of patients with uncontrolled hypertension who are taking two to five anti-hypertensive medications.
The company announced the trial’s commencement in a press release, which explains that the TARGET BP I trial and the ongoing European TARGET-BP OFF-MED trial are part of the TARGET BP clinical trials programme and are designed to evaluate the safety and efficacy of the Peregrine System Kit when used to treat patients with uncontrolled hypertension. The system is comprised of a patented infusion catheter and dehydrated alcohol.
David Kandzari (Piedmont Heart Institute, Atlanta, USA) co-principal investigator of the TARGET BP I trial, comments in the release: “It is exciting to initiate this important trial to evaluate the Peregrine System Kit for the treatment of patients with uncontrolled hypertension. More than half of those treated with anti-hypertensive medications do not achieve their target blood pressure, so there is a great need for improved therapeutic options.”
Prostate artery embolization (PAE) outcomes do not differ significantly when microspheres of different sizes are used as embolic agents, a recent single centre, randomised controlled clinical trial reports. Writing in the Journal of Vascular and Interventional Radiology (JVIR), the authors report no differences between the clinical success rates using 100µm- to 300µm-sized particles at 18 months, although the incidence of minor self-limiting complications such as dysuria was greater with smaller particles.
“Particle sizes used for PAE range between 50µm and 300µm for non-spherical polyvinyl alcohol (PVA) particles and between 100µm and 500µm for spherical embolic agents. The best size with which to obtain optimal clinical success is not known”, senior author Tiago Bilhim, lead author Daniel Torres (both Hospital Saint Louis, Lisbon, Portugal) and colleagues write.
Therefore, they set out to investigate the safety and efficacy of PAE using trisacryl gelatine microspheres of different sizes for the treatment of benign prostatic hyperplasia (BPH).
The study authors randomised 138 patients who underwent PAE for BPH between July 2015 and December 2016 to one of three groups: A, B and C. Embolization was performed using microspheres of different sizes in each group: in group A, the microspheres used were 100–300µm; for group B, 300–500µm microspheres were used; and in group C, patients were first embolized with 100–300µm microspheres before being embolized with 300–500µm microspheres. All patients were evaluated before the procedure, and one, three, six, 12, and 18 months after PAE.
At baseline, the International Prostate Symptom Score (IPSS), quality of life scores, and prostate volume were comparable across all three groups (p>0.05). In group A, these were 23, 4.14, and 87.9cm3, respectively; for group B: 23, 4.09 and 89cm3; in group C: 24.2, 4.29 and 81cm3.
After PAE, the scores and data were:
Group A: 9.98, 2.49 and 65.1cm3 (p=0.23)
Group B: 8.24, 2.26 and 63.1cm3 (p=0.39)
Group C: 10.1, 2.69 and 53.1cm3 (p=0.24)
Specifically comparing groups A and B—patients embolized with 100–300µm microspheres versus patients embolized with 300–500µm microspheres—the authors report no statistically significant differences in IPSS, quality of life or prostate volume. Detailing their results, Bilhim, Torres et al write: “The patients in whom the smaller particle size was used showed a significant regrowth in prostate size from three to 12 months, and there was an increase in minor adverse events in patients who underwent PAE with smaller microspheres, although this was not statistically significant.”
Indeed, the study investigators conclude that PAE using larger particles may be better, as there is a higher rate of minor adverse events when 100–300µm microspheres are used as embolic agents. When a combination of microsphere sizes is used, as in group C, no benefit was seen compared to either groups A or B, and, compared with the 300–500µm cohort, there was a higher rate of adverse events.
Bilhim, Torres and colleagues postulate that, as the number of minor adverse events was significantly lower in group B, the only study arm not to include 100–300µm microspheres, the smaller sized particles were the culprit. They explain that the smaller sized microspheres “could penetrate more distally, causing more inflammation and necrosis”.
Drawing the reader’s attention to previous studies that have found an advantage to using smaller sized embolic agents (“The use of smaller PVA particle sizes led to greater prostate ischaemia, greater prostate volume reduction, and greater clinical improvement, without a higher rate of adverse events. Retrospective analysis looking at spherical embolic agents has also shown that spherical embolic agents <300µm performed best”), the authors note that this potential benefit has to be counterbalanced by the potentially higher rate of adverse events and ejaculation disorders that they say has been “overlooked” in most PAE studies.
All adverse events were mild and self-limited, with the following rates (p<0.001):
Group A: 86% (37 of 43)
Group B: 41.3% (19 of 46)
Group C: 58.3% (28 of 48)
Dysuria was the most frequent adverse event, occurring in 20.4% (28 of 137) of patients.
Ablation costs are significantly less than those of transarterial chemoembolization (TACE) and Yttrium-90 (Y-90), according to a comparative cost analysis of the three procedures at a tertiary care centre. These results were presented at the 2019 annual meeting of the Society for Interventional Oncology (SIO; 7–11 June, Boston, USA) by Damir Ljuboja (Harvard Medical School, Boston, USA).
Ljuboja and colleagues used a relatively novel granular costing methodology developed by accounting academic Robert Kaplan (Harvard Business School, Boston, USA), called time-driven, activity-based costing, to estimate and compare the costs of TACE, Y-90 and ablation for the treatment of hepatocellular carcinoma (HCC) in their centre in Boston, USA. According to the investigators, “Only 36% of Medicare patients diagnosed with HCC receive cancer-directed therapy. Among them, TACE is utilised 10 times more frequently than ablation for these patients. Creation of an HCC-based bundled payment model may improve overall treatment utilisation, use of potentially curative treatments, and patient outcomes. However, the true costs of locoregional therapies are poorly understood.”
To gain a more accurate understanding of the costs of locoregional therapies for treating HCC, then, three observers prospectively recorded the utilisation time for staff members and equipment used to treat ten HCC patients with TACE, Y-90, and ablation procedures. Previous cost comparative studies in interventional radiology have determined prices from Medicare reimbursement rates, whereas in this present study, the investigators prospectively calculated the costs themselves. This bottom-up approach was intended to identify sources of variability in costs as well as provide a direct comparison between the expense of treatment modalities.
Ljuboja explained to the SIO audience the time-driven, activity-based costing methodology: “You first take a procedure and develop a process map for it, in which you identify each step from admission to discharge individually. Then, you prospectively measure [the duration of] each of those steps for each individual personnel member involved. For that person you can calculate a capacity cost rate using salary data, which allows you to estimate their clinical viability, usually measured in [US] dollars per minute. Multiply that by the number of minutes used, and you have the cost for that resource.” The costs of equipment and consumable supplies used in each procedure, as well as their number, were also recorded. The summation of all resource costs then gave the investigators the total procedure cost.
“We decided to do this prospectively initially. Small numbers of direct measurements are very time intensive and labour intensive, but it is very accurate”, Ljuboja said of their approach. In addition to this prospective data collection, the investigators then retrospectively looked at the electronic medical record (EMR) to get time stamp data for the same procedures to verify if retrospective data can be used in place of prospective data. The difference between the retrospectively obtained data and the prospectively obtained data was not statistically significant for any of the three procedures, demonstrating that this analysis can be conducted retrospectively, saving time for the researchers. “Once we had validated that methodology”, Ljuboja continued, “we then retrospectively looked at all the cases from 2018”.
They found that total ablation costs, from admission to discharge, were US$3,813. This was 75% of the total cost for TACE (US$5,097) and 18% of the total cost of Y-90 (US$20,745). The cost for an ablation increased to US$4,245 for one versus two lesions treated, and increased again to US$4,461 for three lesions treated with two probes. The cost of TACE increased from US$5,097 to US$5,296 for non-selective (lobar) versus selective TACE.
Breaking these results down, Ljuboja noted that the greatest personnel cost was observed in TACE. “A large function of that was use of the medicine attending and medicine resident, primarily because the patient was admitted overnight. Another notable thing”, he continues, “is the technologist cost for Y-90 procedures. This factors in to both the treatment stage and the planning stage.” Fixed equipment costs were relatively low, “because the length of the procedures is short relative to the timeline on which these items are used”, Ljuboja explained. “For example, a CT scanner depreciates over the course of eight to 10 years, and if you atomise the cost of that CT scanner across that time horizon, then this is a relatively small amount of time we are talking about.”
Consumables were the greatest cost contributor across all three procedures and accounted for 63% of ablation, 57% of TACE, and 91% of Y-90 costs. “Of note”, Ljuboja wrote in his presentation abstract, “each procedure has a single consumable that accounted for a substantial portion of the overall procedure cost, namely ethiodized oil for TACE (30%), Y-90 resin microspheres for Y-90 (81%), and the probe for ablation (41%).”
“The point of these studies is to identify cost levers that we can pull to minimise the cost to overall maximise the way we are spending our money when it comes to following these procedures, so I think from out study we have identified that there are two different approaches that can be taken. One involves the use of alternative labour sources when it is clinically appropriate; the other is using collective bundled agreements with manufacturers to drive down the price of consumables and equipment”, Ljuboja concluded.
Acknowledging that one of limitations of this study is that it was conducted entirely at a single centre, Ljuboja told the SIO attendees that replication of these methods at other institutions will enable the investigators to determine the inter-centre variability in costs of these procedures, and additionally may allow for the creation of a representative national or regional bundled payment model to improve utilisation of locoregional therapies for patients with HCC.
“As a specialty, we are a little bit guilty of navel-gazing—we are looking inwards a bit. What might be really interesting is to extend some of your methodology to other cancer treatments. I mean radiation therapy, some chemotherapies, and immune oncology, because I think it might be quite surprising to the world to see what our true costs are versus some of the things that are done in other specialties”, commented Fred Lee (University of Wisconsin School of Medicine and Public Health, Madison, USA).
“One thing I will say to address that is that this methodology has been used in other specialties in the past,” a commenter responded from the floor, “primarily surgical specialties on the scale of singular events. A good example is total knee replacements, so they isolated that entire care cycle and calculated all the costs. It has been used to some extent in oncologic procedures, primarily in radiation oncology and surgical oncology, but I think in IR it is a relatively new concept, and we are one of the first studies to evaluate [our procedures in this way].”
Ljuboja noted that studies looking into costs often use Medicare reimbursement rates as the base data, and this does not allow the investigator to determine how best to bring costs down. The granularity of the data provided by the methodology in the current study—using the Harvard-derived time-driven, activity-based costing method—enables exactly that. “As the payment landscape in the USA is moving toward alternative payment models—there is already an oncology care model—one of the biggest challenges that comes with that is that if you are asking payers to pay a bundled payment over the lifetime of a patient, you have to understand your true costs in order to actually generate a profit or make sure that your financial enterprise is viable. So this is where that work fits in,” he opined.
Clifford Weiss (Division of Interventional Radiology, Johns Hopkins University School of Medicine, Baltimore, USA) called for a prospective randomised controlled trial to investigate potential weight loss after left gastric artery embolization (LGAE) in patients with obesity at the GEST Symposium (Global Embolization Cancer Symposium Technologies; 9–12 May, New York, USA) earlier this year. While he concluded that non-randomised trials report a statistically significant and clinically important post-procedural weight loss after the procedure, he says that, given the “limited data” available to interventional radiologists, better quality data are needed to confirm the efficacy of LGAE as an enabler of weight loss.
Weiss first defined the patient population in which he believes LGAE may be most beneficial. For patients with a body mass index (BMI) over 40, who are classed as “severely obese”, he says gastric surgery is an appropriate choice, whether open or laparoscopic. For patients with a BMI between 25 and 30, “a lot of options are available”, according to Weiss, such as dietary changes and exercise. A treatment gap exists, therefore, for patients with a BMI of 30–40.
Before detailing the current evidence in favour of LGAE as a solution interventional radiologists may provide for these patients with intermediate obesity wanting to lose weight, Weiss insists that no “mechanical solution” will be the ultimate obesity treatment. “Any of these solutions […] may only serve as part of the solution”, he tells the GEST audience. “Nothing is going to replace surgery as the gold standard in the population of patients who have severe obesity. More than anything, [LGAE] will be a tool for motivation, or to decrease hunger, or maybe as a standalone tool for limited weight loss”. He also emphasised the psychological, genetic, environmental, sociocultural and behavioural elements of obesity, and the consequent need for an interdisciplinary approach to treatment.
Theoretically, the goal of LGAE is to remove hormone-producing cells from the blood. “Although this has not been fully proven,” said Weiss, “we believe ghrelin, the hunger stimulating hormone, is critical to this process.” By embolizing the left gastric artery, interventional radiologists hope to alter the balance of hunger and satiation hormones. Preclinical studies in both swine and dog models have demonstrated that the procedure leads to a decrease in ghrelin and either a decrease in weight gain or an increase in weight loss.
Following preclinical studies, there have been multiple retrospective studies looking at LGAE in humans, as well as a few prospective single arm trials. The most recent of these Weiss mentioned to the audience was conducted by Mohamed Zaitoun (Department of Radiodiagnosis, Zagazig University, Zagazig, Egypt) et al, and published in the June issue of Journal of Vascular Interventional Radiology (JVIR). Zaitoun and colleagues found that LGAE is well tolerated and leads to clinically significant decreases in weight and glycated haemoglobin in obese, prediabetic patients. They reported a 9.4kg or 8.9% mean weight loss at six months (p<0.0001) and no complications.
Adding to this evidence, Weiss mentions his own physician sponsored IDE (investigative device exemption) single-arm, prospective clinical trial on 20 patients with severe obesity. All participants had a BMI over 40, and were lighter than 400Ibs. They were embolized with 300–500µm Embospheres (Merit Medical). The primary endpoints were weight loss and 30-day adverse events. Weiss reported no major adverse events in this study population, and a minor adverse event in 27% (eight of 20) of the patients. At 12 months, there was a mean weight loss of 16.8kg, or 6% of initial body weight. The mean excess weight loss was 11% at one year (p<0.01).
Describing a graph showing hunger and weight loss over time, Weiss elaborated: “Interestingly, the hunger dropped very acutely and then started to rise again. The weight loss continued, but then lagged behind [the change in hunger]. The hunger started to reverse [appetite increases] at the 13-week time point and then slowly afterwards the weight loss started to decrease as well. So hunger and weight change go hand in hand. Could this be a motivating procedure [to add to] already existing weight loss protocols?” he asked.
Weiss’ residents conducted a meta-analysis to see if they could detect predictors of weight loss after LGAE. They did a systematic literature search to identify studies that reported post-procedure weight changes and, after excluding studies performed for the primary purpose of treating malignancy, ended up with seven publications to examine. From their analysis, which Weiss shared with the GEST attendees, they determined that the most common adverse events were transient abdominal pain and superficial gastric ulceration. The pooled results of the seven studies revealed a mean body weight loss of 8.73% and a mean absolute weight loss of 10.08% (p<0.001 for both figures).
Younger age, female sex, and higher baseline ghrelin levels appeared to be positive predictors of post-procedure weight loss, according to this meta-analysis.
However, Weiss reiterated that interventional radiologists still have “a lot to learn” about this procedure. “This needs randomised controlled data, this is not ‘good to go,’ and this is not yet ready to be conducted in patients. There are a lot of data that we still need to collect, which must be collected in a unified and thoughtful way so that we can actually move this forward, or not, depending on if it really works,” he insisted. Nevertheless, he ended on an optimistic note: “I believe in data, and I believe that our data so far is promising.” gastric
Countries participating in the skill development initiative (map for illustrative purposes only; not to scale). Photo credit: Sharma and Ganga, JVIR
Countries participating in the skill development initiative (map for illustrative purposes only; not to scale). Photo credit: Sharma and Ganga, JVIR
An organised skill development initiative that started in late 2015 offering interventional radiology (IR) training for eight emerging economies has precipitated the development of a global network of trained personnel who can support IR programmes in challenging locations. The initiative has motivated the formation of national IR societies in Nepal, Sri Lanka, Bangladesh and Nigeria, all of which—in addition to Myanmar—now have dedicated IR programmes in their largest hospitals.
The concept and its success is reported in the Journal of Vascular and Interventional Radiology (JVIR) by Sanjiv Sharma and Kartik Ganga (both Department of Cardiovascular Radiology and Endovascular Interventions, All India Institute of Medical Sciences, Ansari Nagar, Delhi, India).
“Integrating IR into clinical practice remains a big challenge in emerging countries in Asia and Africa”, the authors write. “Although IR has changed clinical medicine worldwide, the benefits of these advances have not percolated to the mainstream practice of medicine in these locations. Emerging countries have much to benefit from IR”. With this concept in mind, Sharma and Ganga report how they organised for a group of interested radiologists to travel to their centre and take part in observerships and short-term training courses, typically lasting three months.
Mongolia, Nepal, Bhutan, Bangladesh, Myanmar, Sri Lanka, Ethiopia and Nigeria were the eight countries that participated in the initiative. Since its inception, 51 specialists from these countries have received observerships in IR procedures. These specialists represent a spectrum of disciplines, including radiologists, technologists and nurses, in order to best help establish a comprehensive IR team in their hospitals, the authors say.
Attendees were provided with logistic and financial support during their training period (up to US$500 per month toward stay and up to US$200 per month for reimbursement of observership), as well as samples of consumables for starting an IR practice and various educational materials. These included textbooks and management protocols published by the Society of Interventional Radiology (SIR) and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE).
A further 15 educational events have also been conducted to international audiences to date, some at the authors’ own institution and some within the participating countries’ borders. “Emphasis was placed on teaching and building standards for the ethical practice of IR”, according to the study authors. There is currently no exit-level examination following training, but Sharma and Ganga state that they intend to introduce one this year. To further objectify the results of the initiative, they are designing a survey to assess the impact of their training scheme on alumni who have returned to their native hospitals and started their own specialty practice.
Trainees establishing their own practice was one of the target outcomes of the initiative. Sharma and Ganga explain that trainees “were encouraged to start an IR practice [on return to their native countries] and were supported in decision making and procedure planning by regular communication via various channels, including telephone, WhatsApp, and e-mail on a regular basis”. CME programmes and workshops in their local institutions reinforced this training, and periodic invitations to conferences held at the All India Institute of Medical Sciences updated this learning.
Another key component of the training initiative was to use web-based platforms as “force multipliers”, allowing for wider participation. Virtual lectures and CME programmes were held for audiences across Asia and Africa, and were in fact transmitted live to up to 56 countries.
Radiology residents at medical colleges in India with poor IR utilisation were offered a short stint at an established IR department to raise awareness of the discipline and to encourage recruitment. This aimed to provide first-hand learning experience to acquire basic IR skills, as well as networking opportunities.
This global network building is key: Sharma and Ganga attribute the success of the programme to the participation of experienced interventional radiologists from India, the USA, China, Germany and the UK. “These individuals act as global ambassadors for IR and play an enormous role in both inspiring and imparting knowledge to the budding specialists as well as act as role models for them”, they say.
Sharma and Ganga have also shared a collaboration with the International Atomic Energy Agency (IAEA) to prepare a document outlining the relevance of IR in clinical medicine and methods of establishing it in emerging countries. An expert group formed under the aegis of the IAEA in 2015 has published a report entitled The Needs of IR in Emerging World Countries. Keeping in mind that IR is variously recognised as a subspecialty of diagnostic radiology or is a distinct clinical specialty, Sharma and Ganga impress upon their readers the importance of establishing IR as its own specialty in Asia and Africa. Their work with the IAEA aims to lay stress on this issue.
Collaborating with national and international centres of excellence and setting up more training centres are among the next objectives, according to Sharma and Ganga. They call for large international IR societies to lend their experience and organisation to help support this cause, concluding: “Problems with availability of IR equipment should be addressed by encouraging and fostering indigenisation and locoregional development of such technologies. Until IR gets incorporated and integrated into regional health care systems and university teaching programmes, the nascent regional IR community needs the support of international IR organisations.
“Our specialty shares natural collegial bonds that should be harnessed to help grow rather than wait for external governmental agencies to leapfrog administrative and financial red tape and sluggishness”.
The possibility of spreading interventional radiology across the globe is also one which excited Vincent Vidal, whose FAIR-Embo concept aims to enable the use of an inexpensive and widely available embolization agent to perform minimally invasive procedures.
Speaking at the Charing Cross Symposium 2019 (CX; 15–18 April, London, UK), Jeffrey Jump (Nyon, Switzerland) outlines the impact of the Medical Device Regulations (MDR), which he believes will be “the most devastating thing to happen to European healthcare in Europe since World War Two”.
Patients “will bear the brunt of this hardship” says Jump, who add that as well as regulating new products, the MDR will mean all existing products will have to go through re-certification which will be a “huge drain” on the notified bodies.
The regulations will have more than half of existing products removed from the shelf, according to Jump, who says that everyone will go to the USA or Asia instead as a result.
Jump outlines that he would like to see the current deadline extended and give more time for existing products to “take a bit of pressure off the system”. He also outlines that he would like to see an innovation “fast-track for innovative products”.
Transarterial chemoembolization using microspheres appears to show “much better outcomes” than those seen with conventional TACE, both in the setting of hepatocellular carcinoma (HCC) treatment and when used to treat colorectal cancer patients, Philippe Pereira (Heilbronn, Germany) tells Interventional News at the first European Conference on Embolotherapy (ET; 26–29 June, Valencia, Spain). However, he clarifies that for HCC, the advantages of microspheres over conventional TACE still needs to be demonstrated in a prospective randomised controlled trial.
Pereira says interventional radiologists are demonstrating curative, not only palliative, treatment using microspheres in selected HCC patients with high rates of complete response at one year. On the other hand, they are also observing even better results than some third line treatments in liver-dominant disease in patients with colorectal cancer. These results should be reflected in the “place for TACE” in the European guidelines, he urges, while outlining the goals of the CIRSE-sponsored European registry, CIREL.
Vascular malformations have perplexed a plethora of physicians from diverse specialties for decades, writes Jocelyn Brookes. The British Society of Interventional Radiology (BSIR) has formed a Vascular Anomalies Special Interest Group (VASIG), which met last year for a study day to discuss treatment approaches and outcome measurements. This year, the group welcomes interested specialists to The Royal Free Hospital, London, on 5 December to continue the conversation.
Vascular anomalies (arteriovenous/vascular malformations [AVM]) and associated syndromes have traditionally formed an esoteric area of endeavour for a small group of interested practitioners whose specialist backgrounds reflect the variety and complexity of the lesions themselves.
These non-neoplastic yet proliferative disorders of vascular tissue differentiation may present at all times of life at unpredictable times of growth, causing pain, bleeding, thrombosis, and local space occupation (such as airway embarrassment), with consequent symptoms varying from trivial to catastrophic and lethal. Most are genetically random, but some are familial and syndromic.
Multiple interested specialist backgrounds
Presenting in all tissues of the body, dermatologists and plastic surgeons have taken an interest in superficial vascular malformations (for example, port wine stains), with vascular surgeons and, latterly, interventional radiologists attending to deeper tissue vascular malformations whilst neurointerventionists and surgeons have treated intracerebral ones.
Depending on local interests and referral patterns, specialist centres have developed and dissipated in each generation, usually with the retirement of the central enthusiast of the group.
Complex classification
Over the past 30 years, the International Society for the Study of Vascular Anomalies (ISSVA) has met biannually to develop an internationally agreed classification of these perplexing lesions based originally on descriptive characteristics, separating malformations from vascular tumours and defining separate lesions by their phenotypic approximation to arteries, veins, capillaries or lymphatics.
Distinction of high and low flow lesions has led to the development of observational treatment classifications guiding specific therapeutic approaches; for example, Houbart (neuro AVM), Yakes (peripheral AVM), and Dubois-Puig (peripheral low flow VM).
Many treatment modalities
Treatment methods range from excision surgery to arterial embolization, sclerotherapy to percutaneous coagulation. For high flow AVM lesions, the search for the elusive, transformative “nidus” absorbs practitioners with an intensity as if on a quest for the Holy Grail.
But things are changing in this challenging field.
Multidisciplinary approach
Long-term (officially incurable) chronic vascular lesions with (traditionally) heroic surgical complication rates need a specialist multidisciplinary approach involving appliances, nurse specialists, psychologists, palliative care, haematology and, more recently, genetics and pharmacology all working together to care for this challenging group of patients.
Exciting new developments
Recent exciting developments in understanding of errors of genetic signalling pathways in endothelial cell proliferation and corresponding pharmacological interventions are revolutionising the approach to VM care. Biomarker technologies and sophisticated imaging modalities are now casting light, logic and sense onto this dark and perplexing area with very real benefits to our patients.
Increasing professional interest
For the past five years, the AVM session at the Charing Cross Symposium (CX; London, UK) has begun to attract larger audiences and, with the growth of image-guided embolosclerotherapy as the most popular modality of treatment, the British Society of Interventional Radiology (BSIR) has drawn together the disparate groups interested in vascular malformations to search for commonalities of approach and measurements of outcome.
Come to VASIG meeting 5 December 2019
The Vascular Anomalies Special Interest Group (VASIG) met last year for a study day at The Royal Free Hospital, London, when over 60 delegates of all specialty backgrounds attended. Delegates brought challenging cases to discuss with colleagues from all over the UK and the Republic of Ireland. Offered gratis, the meeting rewarded its participants with five continuing professional development (CPD) points and was universally applauded as interesting, inspiring and relevant to practice.
The VASIG study day will be held on 5 December this year at The Royal Free Hospital, London. Local accommodation can be arranged. Bring your challenging cases.
Jocelyn Brookes is a consultant endovascular radiologist at The Royal Free NHS Foundation Trust and The London Clinic, London, UK.
The US Food and Drug Administration (FDA) has granted 510(k) clearance to Centerline Biomedical’s Intra-Operative Positioning System (IOPS), a device used in endovascular procedures to provide 3D visualisation.
The non-radiation-based surgical navigation system uses anatomical mapping algorithms and electromagnetic tracking to give surgeons 3D colour visualisation and guidance during procedures.
The holographic system, developed at Cleveland Clinic’s Heart and Vascular Institute (Cleveland, USA), offers an alternative to the current standard of care, X-ray fluoroscopy, which exposes surgeons and operating room staff to potentially dangerous radiation.
“Having worked closely with Centerline for almost five years, I am very pleased to see that IOPS will soon be commercially available,” remarks Matthew Eagleton, chief of Vascular Surgery at Massachusetts General Hospital (Boston, USA) and chair of the company’s scientific advisory board. “We hope to use this game-changing technology to revolutionise our approach to vascular procedures and imaging.”
This milestone, achieved working with regulatory partner JALEX Medical, will allow marketing and commercial use of IOPS for endovascular interventions in the descending aorta, though the underlying platform will be applicable to many other minimally invasive procedures in the future, a press release states. Such future indications may include structural heart interventions, an application the company is currently exploring with funding from an NIH small business grant. The company’s research and development efforts will continue in parallel with Centerline’s upcoming market launch.
Rajesh Dave (Camp Hill, USA) talks to iWounds News about his highlights from the 15th annual C3 conference, which included a special session on the paclitaxel controversy.
Dave talks about the “journey of 15 years” and how the meeting started with “an idea that we create something very special and unique” that “fills the gap between the science being produced and the lack of application of that science into clinical practice”.
Dave also discusses the live case education sessions at C3, which covered a range of specific areas including coronary PCI as well a variety of dedicated endovascular sessions for both interventional radiologists and vascular surgeons. Dave also outlines why the use of live cases are such an important teaching tool.
Hammed Ninalowo after completing the first below-the-knee CTO recanalisation with the SAFARI technique in Africa
There are fewer than five practicing interventional radiologists in Nigeria today, a country of 200 million people. Hammed Ninalowo aims to change that ratio, founding the organisation IRDOCNIGERIA, with the aim of training an additional 100 interventional radiologists in his home country over the next decade. Having trained in the USA, Ninalowo describes the experience of performing the first ever transjugular intrahepatic portosystemic shunt (TIPS) in sub-Saharan Africa, and looks forward to the launch of the first interventional radiology training programme in the country in September this year.
When I told my colleagues in America that I was considering performing a transjugular intrahepatic portosystemic shunt (TIPS or DIPS: direct intrahepatic portosystemic shunt) on a Budd Chiari patient in Nigeria (see image below), most said I was crazy. But I remember thinking, “If I do not do this, who will?”. After extensive planning from myself and my team, we were able to pull the procedure off with an amazing clinical outcome. A 20-year-old woman who had had 33 litres of ascites drained from her body over the last three years at monthly intervals and had lost all muscle mass now has no ascites, has regained muscle mass, and is returning to school.
My story of practising interventional radiology in Nigeria did not start there, however. Pulling off the first TIPS/DIPS in sub-Saharan Africa is just a small fraction of our journey.
I was born and raised in Lagos, Nigeria, and left in 1999 to pursue an education, though I always had a homeward focus. I finished by Bachelors degree in 2003 and graduated medical school in 2010. While in medical school, I continued to look back to Nigeria, and spent the summer of my first year at a teaching hospital in Lagos. My guiding principle all through medical school regarding specialty and career choice remained “What can I bring back to my people?”. I was involved in the care of a patient in the intensive care unit in my third year of medical school; he had undergone two endoscopies due to bleeding varices, yet continued to bleed. An interventional radiologist was called in and, through just a tiny hole in the neck, placed a stent graft and coiled off varices, triggering an immediate change in the patient’s haemodynamics. That was it. My specialty was chosen and my interventional radiology journey started.
Hammed Ninalowo with his 20-year-old Budd Chiari patient after the second IVC stent extension
I trained in diagnostic radiology at the University of Maryland. My mentors always asked me what my future plans were, and it always circled back to what I planned to do in Nigeria. I took multiple trips to Nigeria during training to survey the state of medicine and also visited some of the local pioneers who had made a move back home in fields like interventional cardiology and changed the narrative as to what was possible locally. I went on to finish subspecialty training in interventional radiology at the University of Pennsylvania. I have since worked in a large hospital system in Pennsylvania (Geisinger health system), a tertiary care centre with level one trauma and multiple transplant programmes.
In early 2018, I was ready to make my push into Nigeria and heard of a group in Nigeria called the Nigerian Society of Interventional Radiology (NiSIR). I learned this group was attending the Pan Arab Interventional Radiology (PAIRS) meeting in Dubai. I immediately bought a ticket. I met many bright minds, mostly working in the public sector, who had left the country to obtain training and were back in Nigeria providing amazing care to patients. However, there were significant frustrations, as they had not been able to open all the possibilities offered by interventional radiology in the public sector. One of these gentlemen was Professor Ahmed Ahidjo, now the Chief Medical Officer of the University of Maiduguri, who I still credit as the real pioneer of interventional radiology in Nigeria. I knew I had trained at one of the best IR programmes in the USA and had been lucky enough to work and gain experience in a high volume complex practice. I was ready to make my push.
I initially started by collaborating with the public sector—however, it was immediately apparent that the resources there were significantly limited, and getting things done in the government hospitals was a difficult task. I immediately changed my goals to: 1) Look for a progressive organisation that believed interventional radiology was possible in Nigeria and work hard to show what is possible at a complex level immediately providing care to patients; 2) Continue to collaborate with the public sector to create sustainability in the country. With these objectives, I founded IRDOCNIGERIA, a company providing IR services in Nigeria, and started the IR division of RAD-AID international Nigeria.
Since our first case in September 2018, we have completed many complex procedures, including complex venous recanalisations, TIPS/DIPS, transarterial chemoembolizatons (TACE), varicocele embolizations, uterine fibroid embolizations (UFE), biliary stenting and recanalisation for chronic total occlusions using SAFARI, to name a few. We now offer any procedure in interventional radiology except for radioembolization. In September this year, we are hosting a symposium at the University College Ibadan with several SIR Faculty members, and we will launch the first training programme in Nigeria.
Achieving this has not been easy. The time spent across two continents has been a challenge—though the greatest challenge remains the supply chain for interventional radiology in sub-Saharan Africa and the infrastructure in public institutions. It is no secret that interventional radiology consumables are not cheap, but the cost is a minor factor, as most manufacturers (except currently Medtronic) do not do business in Nigeria or many African countries. There is something interesting going on with a lot of African economies; many markets have emerged in the last few decades, and with this, modern medicine is on the rise. African patients spend an incredible amount of money on medical tourism to places like India and the West. In a very small way, I have stopped a few patients from making these trips. We can keep and treat these patients in Africa and keep the money in Africa for Africa. It will require some sacrifice from the industry, but most of the sacrifice will have to be made by Nigerian physicians in the diaspora who have acquired a significant amount of knowledge and thrive in most of their chosen fields. I say the days of “Tent medicine and medical missions” are dying, as these do not create sustainability. We need to improve the long-term state of healthcare in these countries by focusing on people and services who are committed to full time or long term sustainability driven projects.
Hammed Ninalowo
For me, I have simply been on a mission and I have not looked back. I can say with authority that the future of medicine, on any continent, without interventional radiology is no future at all. My goal in the short term is to transition my practice full time to Nigeria, an ambition well known to those around me. A colleague in Nigeria uses the phrase #TheNigerianPatientsAreWorthIt, and I agree. Our journey has just started, but watch this space, as I am committed not only to Nigeria, but to collaborating across Africa to bring the life saving minimally invasive procedures of interventional radiology to the continent at large.
Hammed Ninalowo is an interventional radiologist in Lagos, Nigeria.
Women and Diversity committee collage courtesy of BSIR
The British Society of Interventional Radiology (BSIR) established a Women and Diversity committee earlier this year, with the aim of overcoming obstacles to women and marginalised groups who are either already interventional radiologists or potentially will be in the future. The committee is discussing ways to encourage women to apply to the specialty, as well as how to make the work place as supportive as possible.
The first meeting of the committee resulted in 12 proposals for action being made, which are currently being prioritised and implemented. These included a plan to develop social media forums (WIIGS@BSIR) led by Elika Kashef (London, UK), and a baseline survey with metrics to monitor the progress of the committee’s work over time led by Ros Ahmed (Leicester, UK). The group also intends to work with potential interventional radiology recruits from school age through to radiology trainees.
In full, the 12 initial proposals are:
Develop Women and Diversity social media forums (for example using WhatsApp and Twitter)
Baseline survey of perceptions with metrics to monitor progress over time
Develop a BSIR area blog / newsletter / online forum
Work with Radiology trainees—encourage IR as an open specialty to all
BSIRT [British Society of Interventional Radiology Trainees] survey to identify barriers to entering interventional radiology
Attend / presence at meetings: Annual Scientific Meeting, Advanced Practice Course and Basics Course to access trainees.
Inspire future trainees early—attend A level fairs and medical student careers fairs
Support existing trainees—mentoring programme to include access / support for mentoring coaching
Provide a roadshow at careers fares / BSIRT meetings. With specific attention to barriers—flexible training and pregnancy
Promote leadership among interventional radiologists
Promote resilience / work–life balance / coaching
Produce a workshop for the Annual Scientific Meeting and IOUK [Interventional Oncology United Kingdom]
Speaking of the importance of this work, committee member Shilpi Pal (Dundee, UK) says, “The presence of visible female role models was felt useful as a means to inspire future recruits. There was felt to be a need to encourage women into leadership roles, and to provide support once these roles have been taken on.” With this in mind the group is in the process of setting up a travelling grant. Speaking about this Tze Wah (Leeds UK) says: “It is a great honour that Professor Anna Maria Belli has agreed to allow us to name the grant after her”.
There is a national shortage of trained diagnostic and interventional radiologists in the UK. While women currently make up 50% of junior doctors, just 10% of qualified interventional radiologists are female. This pattern also holds true across continental Europe and the USA.
The BSIR Women and Diversity committee aims to understand the causes of this discrepancy, and its mission statement is to find ways to “overcome the barriers” to potential female interventional radiologists. At the latest committee meeting, the most obvious barriers were felt to be issues around pregnancy and screening, fertility and screening, and access to flexible or part-time working.
“Definitions of diversity abound”, comments Fiona Miller (London UK). “I see diversity as empowering people by respecting and appreciating what makes them different, in any way, including age, gender, ethnicity, religion, disability, sexual orientation, education, and national origin. The main reward for accommodating diverse colleagues is a wealth of new ideas and approaches to our professional lives. A further benefit of working in a diverse peer group where individuality is respected is [a] better work–life balance for all.”
Elaborating on the decision to create the Women and Diversity committee, Miller explains: “In order to attract the best doctors, interventional radiology needs to be welcoming and inclusive to all. It was with this in mind that [the] BSIR council decided to create the Women and Diversity committee with time and resource[s] to focus on barriers to interventional radiology recruitment and retention. The precise remit will be determined by the elected group in discussion with council. At the first meeting, clear aims and objectives were defined, the primary aim being the promotion of equality for all in interventional radiology. The first project will be to address the challenges facing women in interventional radiology, followed by other issues including sexual orientation and gender identity, ethnicity and disability.”
In addition to Wah and Miller, the committee consists of three other elected members: chair Ros Ahmad (Leicester, UK), Shilpi Pal (Dundee, UK), and Elika Kashef (London, UK); Raman Uberoi (Oxford, UK) also “kindly agreed to be co-opted”, in Miller’s words. Any BSIR members who would like to be involved are encouraged to contact the committee directly.
When new rules capped training hours for medical residents at 80 hours per week in 2003, critics worried that the change would leave physicians-in-training unprepared for the challenges of independent practice. New research, published today in the British Medical Journal (BMJ) and led by scientists in the Department of Health Care Policy in the Blavatnik Institute at Harvard Medical School, shows that these warnings were largely unjustified.
The analysis—believed to be the first national study examining the impact of reduced hours on physician performance—found no evidence that reduced training hours had any impact on the quality of care delivered by new physicians.
This is notable given that recent polling from a survey sent out by the Society of Interventional Radiology (SIR) found that there was a significantly increased risk of experiencing burnout, characterised by depersonalisation and emotional exhaustion, for those interventional radiologists who work more than 80 hours per week.
Following a series of high-profile patient injuries and deaths believed to stem from clinical errors caused by fatigue, medical accreditation agencies initiated a series of sweeping changes to the regulations governing resident hours and other aspects of training. These efforts culminated in 2003 with the US Accreditation Council for Graduate Medical Education capping the training of medical residents at 80 hours per week.
“This is probably the most hotly debated topic in medical education among physicians,” says Anupam Jena, the HMS Ruth L Newhouse associate professor of Health Care Policy in the Blavatnik Institute, a physician in the department of medicine at Massachusetts General Hospital (Boston, USA), and lead author of the study. “Many doctors trained under the old system think that today’s residents do not get enough training under the new system. You hear a lot of senior physicians looking at younger doctors coming out of training and saying, ‘They are not as prepared as we were.’”
The findings of the study should assuage these fears, Jena believes.
The researchers found no significant differences in 30-day mortality, 30-day readmissions, or inpatient spending between physicians who completed their residency before and after the residency hour reforms.
“We found no evidence that the care provided by physicians who trained under the 80-hour-a-week model is suboptimal,” Jena comments.
Given the changes in hospital care over the past decade, the researchers knew that they could not just compare the difference between outcomes of recently trained doctors before and after the cap, since overall outcomes have improved thanks to better diagnoses and treatments, better coordination of care and new digital tools designed to prevent harmful drug interactions and other human errors.
Comparing new physicians trained before reform with those trained after would confound the effect of changes in training with the effect of overall changes in hospital care. To avoid conflating the two, the researchers compared new physicians before and after the reforms with senior physicians who had trained before the reform.
The study analysed 485,685 hospitalisations of Medicare patients before and after the reform. The training hour reforms were not associated with statistically significant differences in patient outcomes after the physicians left training.
For example, 30-day mortality rates among patients cared for by first-year attending internists during 2000–2006 and 2007–2012 were 10.6% (12,567 out of 118,014) and 9.6% (13,521 out of 140,529), respectively. In comparison, the 30-day mortality among patients cared for by tenth-year attending physicians was 11.2% (11,018 of 98,811) and 10.6% (13,602 of 128,331) for the same years.
Further statistical analysis to eliminate the unwanted effects of other variables showed that these differences translated into a less than 0.1%-point gap between the groups. The difference in hospital readmission rates was similarly minuscule: 20.4% for patients cared for by first-year physicians in both 2000–2006 and 2007–2012, compared with 20.1% and 20.5%, respectively, among patients treated by senior physicians.
Taken together, these findings suggest that US residency work hour reforms have not made a difference in the quality of physician training, Jena concludes.
As a way of magnifying any possible gaps in care stemming from a difference in training hours, the researchers looked specifically at outcomes for high-risk patients, in whom even small differences in quality of care would become apparent.
“We looked at patients who were particularly ill. In these cases, one little mistake could mean the difference between life and death,” Jena says. “Even for these sickest patients we found that the reduced training hours had no effect on patient mortality.”
Burnout is prevalent among interventional radiologists, with a recent survey finding that both identifying as female and working more than 80 hours per week are significantly associated with high emotional exhaustion and depersonalisation (p=0.009 and p=0.030, respectively).
The survey results were published in the Journal of Vascular and Interventional Radiology by joint first authors Jacob Bundy (Department of Radiology, University of Michigan Health System, Ann Arbor, USA) and Anthony Hage (Department of Surgery, Thomas Jefferson University Hospital, Philadelphia, USA) et al.
Aiming to assess the prevalence of burnout and to determine demographic and practice-related stressors among interventional radiologists, Bundy, Hage and colleagues posted a 34-question survey to the Society of Interventional Radiology (SIR) Connect Open Forum website, which on the day of posting (7 January 2019) had 7,402 members. From the total membership, there were 339 complete responses. The prevalence of burnout was 71.9% (244 respondents).
This abundance of burnout places interventional radiologists in the upper range of that reported amongst all medical specialties. The prevalence of this condition in medicine as described in the literature varies from 30–75%. In fact, the authors write, “Interventional radiologists report manifestations of burnout at a rate higher than not only the general public (28%) but also diagnostic radiologists (54–61%) and surgeons (40%)”.
Bundy, Hage et al believe that the survey answers “indicate that additional harmful external factors exist and may require attention when combating burnout among interventional radiologists”. Highlighting perceived gender stereotypes, bureaucracy and administrative duties as prominent amongst these external factors, the authors say that these “represent problems that may not be resolved through established physician wellness programmes, but instead may require human system interventions driven by organisational restructuring and redirection toward patient-centred care rather than financial obligations”.
Interventional radiologists at high risk of emotional exhaustion and depersonalisation
The study authors define burnout as “a cluster of symptoms that occur in response to chronic emotional career-related stressors resulting in emotional exhaustion, depersonalisation, and lack of personal accomplishment in relation to one’s professional activity”. It was evaluated using the 22-item Maslach Burnout Inventory-Human Services Survey (MBI) for Medical Personnel (Mind Garden). Additionally, the survey included 10 demographic questions, ascertaining age, gender, current level of practice, time since fellowship training, practice setting, number of interventional radiologists in the practice, daily percentage of time spent performing nonprocedural diagnostic radiology, mean weekly hours worked, presence of interventional radiology (IR) call duties, and mean number of call shifts taken per month. An optional, open-ended, free response question regarding the greatest contributor to burnout in the workplace was also included.
A total of 61.9% of responders were at high risk of emotional exhaustion, according to the MBI subscales. A further 15.3% were at a moderate risk, and the remaining 22.7% were low risk. The mean MBI score for emotional exhaustion was 30±13, which is categorised as high (low ≤18; moderate 19–26; high ≥27). The mean depersonalisation score was also high, at 10.6±6.9 (low ≤5; moderate 6–9; high ≥ 10). Just over half of survey respondents—54.3%—were at high risk of depersonalisation. An additional 17.2% were at a moderate risk, and 28.6% were low risk. One-hundred-and-sixty-two (47.8%) responders were at high risk of both depersonalisation and emotional exhaustion.
“Personal achievement scores were high in only 14.7%” of respondents, the authors write. Personal achievement ranking was not used to determine if a participant had burnout. Most responders (59.3%) reported low personal achievement, and 26% reported a moderate personal achievement rating. However, the mean personal achievement rating was 39.6±6.6, just shy of a “high” designation (low ≥40, moderate 34–39, high ≤ 33).
Explaining the open-ended responses received, which were given by 258 survey participants (76.1%), the authors say: “On review of the responses, several themes emerged, including administrative pressures on productivity and administrative tasks, relationships between interventional radiologists and ancillary staff, workload and work hours, electronic medical record and documentations systems, diagnostic radiology responsibilities, contentious relationships with diagnostic radiologists within the same practice, lack of recognition and respect from other medical and surgical subspecialties, and fielding inappropriate consultations from other medical professionals”.
Bundy, Hage et al express concern at their finding, continuing: “The technical challenges, physical demands, and unpredictable work hours of IR likely impart different stressors [to those experienced by other medical specialties, such as diagnostic radiology], and thus rates of burnout may be related to these factors. Regardless, this is an alarming finding given the negative impact burnout has on job satisfaction, career longevity, mental health, and patient care”.
Female interventional radiologists are more likely to experience burnout than male physicians
Gender was significantly associated with increased rates of burnout, with women having 2.4 times’ higher odds of experiencing burnout than men. (See here for a first hand testimonial of burnout). The study authors say that “Gender judgement and stereotypic perceptions of female physicians have been linked to increased rates of burnout and worsened psychological well-being”. To remedy this, Bundy, Hage and colleagues suggest that increasing the number of women in the male-dominated discipline of interventional radiology “may mitigate the relationship between stereotypic perceptions and burnout among women”.
That women have an increased propensity to work more than 80 hours a week compared with their male counterparts is also potentially a contributing factor to their higher incidence of burnout, according to the study investigators. Interventional radiologists who worked more than 80 hours per week were seven times more likely to report traits indicative of burnout than those who worked fewer than 80 hours in a week.
“Of note”, the authors write, “the form of call taken in the present survey was not assessed; however, IR call shifts would likely contribute differently than diagnostic radiology call shifts toward the total hours worked”. They continue, “Whereas physician expectations for acceptable work hours vary by specialty, a dependent response is likely present between work hours and burnout. Although not an easily applicable intervention, decreasing work hours or other contributors to overall workload may have a substantial impact on lowering the incidence of burnout amongst interventional radiologists”.
The authors also note that, despite the fact that the survey was intended to capture a representative cross section of interventional radiologists in training and practice, respondents were disproportionately early career physicians. They suggest additional analyses of burnout within age-specific subsets of IR physicians and trainees to “further delineate the aetiologies of burnout among these groups”.
Teleflex received positive results for a multi-centre study reaffirming the safety and effectiveness of its minimally invasive UroLift system for the treatment of benign prostatic hyperplasia (BPH) in real-world patient populations. These were published in the Journal of Endourology.
The multi-centre, retrospective study examined the results of 1,413 consecutive patients who received the UroLift system for treatment of lower urinary tract symptoms due to BPH. The trial took place over the course of two years across 14 sites in North America and Australia. The study investigators set out to determine whether clinical outcomes are consistent with those found in controlled studies, and found that they were.
Data published from the study show that patients from multiple subgroups treated with the UroLift system experienced improvements in International Prostate Symptom Score (IPSS) and Quality of Life (QoL) score:
Consistent with the previous LIFT study, symptoms improved significantly from baseline at all follow up time points through two years, and most perioperative adverse events were mild to moderate, resolving by four weeks.
In a cohort-matched comparison to LIFT study patients with moderate–severe symptoms (IPSS≥13), symptom improvement was similar at all time points.
Of the 165 patients in retention at baseline, 83% became catheter-free by one-month post-procedure, and 87% were catheter-free by the end of the study; IPSS scores were similar to non-retention patients.
In the 73 patients with prior prostate cancer treatment, mean IPSS improved at all time points with no significant difference in adverse events of interest compared to other patients.
IPSS improvement was similar regardless of prostate volume (<30cc; 30cc to <80cc; ≥80cc)
“Not only are the real-world results from this large, multi-centre study consistent with the LIFT study, this study also provides data in populations of patients who were not studied in the LIFT study but are seen in a real-world clinic setting,” says Gregg Eure, urologist at Urology of Virginia (Virginia Beach, USA), a lead investigator and co-author of the study. “These findings should give urologists and patients the confidence to adopt the UroLift system within the broader BPH population.”
The randomised LIFT clinical trial demonstrated that treatment with the UroLift system provides patients rapid and durable symptom relief. The procedure demonstrates an excellent safety profile and preserves sexual function.
UroLift is a minimally invasive technology cleared by the US Food and Drug Administration (FDA) for treating lower urinary tract symptoms due to BPH. The UroLift permanent implants, delivered during a minimally invasive transurethral outpatient procedure, relieve prostate obstruction and open the urethra directly without cutting, heating, or removing prostate tissue.
Teleflex acquired NeoTract, the privately-held medical device company that developed and commercialised the UroLift system, in Autumn 2017 in a transaction valued at up to US$1.1 billion.
IntelliCath system with Torben Pätz (L) and Jan Strehlow
A new visualisation method enables more precise catheter navigation through the vascular system. It is being developed at the Fraunhofer Institute for Digital Medicine (MEVIS) in Bremen, Germany, and one of its ambitions is to reduce physician radiation exposure.
The “intelligent catheter navigation”, or Intellicath method, uses a catheter equipped with an optical fibre containing tiny “mirrors”. When light passes through the fibre, the mirrors reflect a portion of the light. Whenever the fibre bends, the reflected light changes colour. Sensors can measure the change in colour.
“The signal from the sensors gives us information about the intensity and direction of the curvature,” Torben Pätz, a mathematician at Fraunhofer MEVIS, explains in a news release. “To some extent, the fibre knows how it is formed.”
Around the world, millions of endovascular procedures are performed per year, using X-ray guidance to place stents or remove blood clots. This results in radiation exposure for patients and physicians alike, and an additional challenge is that X-rays do not provide the most precise images, according to Pätz.
Before the procedure, physicians obtain computed tomography (CT) or magnetic resonance (MR) images of the patient. Based on this image data, IntelliCath software creates a 3D model of the vessel system and displays it on a monitor. During the endovascular procedure, live data from the fibre navigation is fed into the model. The doctor views the monitor to see how the device moves through the vascular labyrinth live and in 3D.
MEVIS experts have already been able to test the method’s feasibility using a prototype, according to Pätz. “We connected several silicone hoses into a curved labyrinth,” he says. “Then, we inserted our device containing an optical fibre into the labyrinth.” On the monitor, they were able to locate the catheter’s position in real-time with precision approaching five millimetres. The researchers have applied for two patents.
Although several medical device companies work on similar projects, “they expend a great deal of technical effort into trying to reconstruct the shape of the entire catheter, which can be up to two meters long,” Pätz comments. “Our algorithm, however, only needs a fraction of the data to localise the catheter in a known vascular system.”
As a result, the MEVIS approach promises cost-effective technology without special fibres and measurement systems and is less sensitive to measurement errors than previous approaches, according to the institute.
Next, the researchers will test the IntelliCath system on both a full-body phantom of the human vascular system and on a pig lung. Toward the end of the current project phase in 2020, a prototype will be ready to serve as a foundation for a clinical trial.
Pätz and his team are also developing acoustic feedback to relieve doctors of the constant need to look at the monitor. The idea is to employ various indication sounds to signal how far the next vessel junction is and in which direction the catheter should be inserted.
“It is similar to a car’s parking assistance system, where you also receive acoustic indications about the distance to the next obstacle,” Pätz explains.
William Rilling (Department of Radiology and Surgery, Medical College of Wisconsin, Milwaukee, USA) has assumed the role of president of the Society of Interventional Oncology (SIO), while Matthew Callstrom (Department of Radiology, Mayo Clinic, Rochester, USA) has been named president-elect. A new team of board officers aim, according to the society, to drive strategy and deliver quality resources to medical professionals in the interventional oncology field.
“I am very excited to take on this opportunity to promote interventional oncology as an emerging field of cancer medicine”, says Rilling. “Using advanced imaging and sophisticated tools, we can help patients with minimal invasiveness in order to definitively treat patients and/or preserve patient quality of life”.
In addition to Rilling and Callstrom, the SIO officers, announced at the society’s annual meeting in Boston, USA last month (8–11 June, Boston, USA) include Riad Salem, as treasurer, and Stephen Solomon, the immediate past president.
The directors-at-large of SIO are:
Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA)
Alexis Kelekis (National and Kapodistrian University of Athens, Athens, Greece)
Kevin Kim (Yale School of Medicine, New Haven, USA)
Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA)
Uei Pua (Tan Tock Seng Hospital, Singapore)
The SIO board of directors is responsible for governing the affairs of the society, in addition to establishing its policies and programmes. Members will work in cooperation with the new officers, other board members, and the society’s staff.
Rilling is professor of Radiology and Surgery at the Medical College of Wisconsin, Milwaukee, USA. He completed his diagnostic radiology residency at the Medical College of Wisconsin and his fellowship in Vascular Interventional Radiology at Northwestern University in Chicago in 1996. He has been practicing at the Medical College of Wisconsin since 1996 and is the vice chair of Clinical Operations in Radiology and the former director of the Division of Vascular and Interventional Radiology for 14 years.
Callstrom is vice chair for the Department of Radiology and director of the Ultrasound Research Center at Mayo Clinic, Rochester, USA. He has been on staff at Mayo Clinic for over 15 years. He is board certified in diagnostic radiology. He is active in the use of image-guided intervention to treat cancer and has led several clinical trials in this area. He earned his BS degree and PhD from the University of Minnesota, Twin Cities, USA. He completed medical school, radiology residency training, and fellowship at Mayo Clinic College of Medicine.
Radiation therapy firm Varian Medical Systems has signed an agreement to acquire Boston Scientific‘s portfolio of drug-loadable microsphere and bland embolic bead products designed to treat arteriovenous malformations and hypervascular tumours.
Varian plans to fund the US$90 million transaction through cash and proceeds from borrowing as it adds to its multidisciplinary integrated cancer care product lines, which include its recent acquisitions of Endocare and Alicon.
Varian will not acquire any of the Boston Scientific operations. Instead, Varian plans to manufacture and distribute the Oncozene/Embozene Tandem microspheres and Embozene bland embolic bead products with Boston Scientific through transition services agreements to avoid any interruption in service to customers.
“This acquisition from Boston Scientific will strengthen Varian’s growing position in the high-value interventional oncology segment and is consistent with our long-term strategy to become a global leader in multidisciplinary, integrated cancer solutions,” says Dow Wilson, Varian’s president and CEO, in a statement.
The Boston Scientific assets generated revenue of US$21.2 million in 2018. Varian expects the transaction will not have a material impact on its fiscal year 2019 financial results. The acquisition could close as soon as August, subject to customary closing conditions and regulatory approvals.
Following a keynote lecture on her personal and professional understanding of physician burnout earlier this year at the annual meeting of the Society of Interventional Radiology (SIR; 23–28 March, Austin, USA), Sasha Shillcutt here details the changes physicians can make to best achieve “work/life integration”, emphasising the importance of not compartmentalising yourself.
I was approaching 24 hours in the hospital and waiting for my partner to come into my operating room so we could do “hand-off”, where I spend 15 minutes going over all of the events of the surgical case and explain my patient’s health history, his current status, my current treatment strategies, the echocardiography findings, and our plan for the rest of the case. As I was awaiting my colleague’s arrival, I received a text from my son, AP.
AP: We need to make lunches, when will you be home? Are you taking us to school?
Me: Please make sure everyone is awake and make lunches.
AP: S2 is still asleep. He’s refusing to wake up.
Me: Can you PLEASE wake him up and make lunches. Also, get the papers on the island ready to hand in—they were there two nights ago.
Two nights ago, the last time I was awake in my house.
In comes my partner, and we chat. I tell him about my last 24 hours and the patient in my care. We review the anaesthesia record and the current surgical state. I say goodbye to the surgeon, the third one I have worked within 24 hours. He thanks me for my help throughout the night and wishes me a good day.
I do a five-minute change and rush home, transitioning into mum mode. I call home on the way and put out sibling fires and rally the sleepy preteen over the phone. When I arrive, AP has delivered: everyone is dressed, breakfasted, and lunches are thrown in backpacks. I kiss everyone hello and tell them I have missed them. I drive them to school and hear about yesterday’s events and today’s plans. They exit the car and I kiss them again. A little pang goes off in my heart; I just said hello, and now I am saying goodbye.
When I finally get home, I try and decide: sleep, shower, or coffee? And in what order? Should I empty the dishwasher, go through the mail, or just ignore it until later? Should I catch up on emails, or crash into a few hours of sleep? Should I run errands? After all, I am awake.
This is a very typical day in my life, and in most physicians’ lives. I recognise this does not just happen to doctors, it happens to many of us who work in areas such as healthcare, emergency service personnel, military, and law enforcement. We feel honoured to care for other’s sisters and dads and brothers and friends, yet we are all of those things to others, and find it a difficult balance.
In the last two years, out of complete necessity, I have studied professional burnout. Five years ago, I experienced clinical burnout myself and nearly quit the practice of medicine. Despite years of training and experience, I did not want to be a cardiac anaesthesiologist anymore. I knew I was in danger.
I needed to get a handle of my work/life integration. I do not use the term “work/life balance” anymore; I recognise that the 10-year quest for “balance” left me empty, defeated and more stressed than ever. So this is what I did: I embraced the suck.
Literally and figuratively. I stopped trying to be a “doctor” at work and a “mother” at home. I am both, all the time, and they are integrated. I stopped worrying that if I talked to my son about his homework over the phone at work and someone heard me they would not think I was serious about my job because I am a woman “mumming” at work. I stopped trying to hide in my bedroom to answer a consult at home. I just embraced that I was both of those things, and people who respected me would have to as well.
Burnout, in any profession, will steal your empathy and your innovation and, well, YOU. You will feel less engaged, less motivated, physically and emotionally exhausted, and start to withdraw. It is a dangerous path and can lead to very costly problems for individuals, institutions, and your family. Over 50% of physicians report burnout, and the suicide rate is 1.5–2.3x higher in male and female physicians than the general population. This is a real problem.
For me, when I started embracing that my work would flow into the home and my home would flow into work, suddenly my work became much more manageable. Now, do I answer questions about homework during an emergency at work? Of course not. Do I answer phone calls from work when my son is about to take a penalty kick? Heck no, I am cheering on the sidelines and it can wait 10 minutes. Do I have best friends who I also work with that I meet and have coffee with and decompress about a case that I am struggling to let go of? Absolutely. Do I invite my mother to hear me speak professionally, so she can understand what I do? Absolutely. Do I write manuscripts on the sidelines of my son’s football practice when I have downtime? Of course.
I am both doctor and mother.
It is important to leave work and be a sister, a friend and a dad. It is important to shut down devices and decompress and connect with your loved ones. I am not promoting a 24/7 work life. I am promoting embracing the fact you are ONE. One person, who is many things. And it is OK to be all of yourself, at all times. My patients and my work colleagues deserve my BEST self; that person is a mum, a wife, and a friend. And what I have found is that I have developed resilience and respect from my colleagues by being fully ME.
When I speak professionally on burnout and overcoming professional failure, I encourage physicians and leaders to make these changes:
Set boundaries. When we are burned out, we must pull back from what we are being asked to do (or over-asked to do) and have frank conversations with leadership and say enough. There are limits to what we can do in a day, and we need leaders who listen to our requests for support; whether it is clerical, administrative, or procedural.
Start with one efficiency fix. Identify the area of your workflow that is most problematic and requires you to do things inefficiency or takes your time and steals your joy. If you can recruit stakeholders to make changes, and fix one problem at a time, you will immediately see improvements.
Stop judging yourself for being burned out. Start allowing yourself space to work on your own wellbeing. This is often hard for us as we care for others, we work incredibly long hours, and we feel guilty saying no to extra work. Here is the thing: the hardest working people burnout the most. Give yourself grace to recognise this, and empower yourself to say yes to your own health. Only you know what you need to be mentally and physically healthy—it is different for each individual.
Plan your wellbeing. Wellbeing must be intentional. Wellness is not doing yoga, it is living within healthy boundaries you set for yourself and finding joy in your personal and professional life. Allow yourself to be a whole person—both at work and at home, and understand that requires saying no, thank you. And it may require change.
Let us stop judging one another in healthcare; rather, let us encourage each other to be our whole selves; not half and half. Whole. It is where freedom lives.
Sasha Shillcutt is a professor and the vice chair of Strategy and Innovation in the Department of Anesthesiology at the University of Nebraska Medical Center (UNMC; Omaha, USA). She leads conferences and retreats for women through her organisation, Brave Enough.
While the standard approach for preparing the future liver remnant prior to liver resection is to use portal vein embolization, a new technique—variously either called double vein embolization, or liver venous deprivation—can enhance the rapidity of the desired response. Christoph Binkert (Winterthur, Switzerland), ET 2019 Programme Committee Chairperson speaks to Interventional News at the first Embolotherapy (ET) conference in Valencia, Spain.
The new technique involves embolizing the hepatic vein after embolizing the portal vein in the same session and the desired growth of the future liver remnant is typically achieved in two weeks, rather than the six weeks needed, after portal vein embolization alone.
Cryoablation may be associated with longer overall survival than heat-based thermal ablation in clinical T1a renal cell carcinoma (RCC), concludes a recent study published in the Journal of Vascular Interventional Radiology. To date, this is the largest study comparing overall survival between two ablative therapies in these patients.
“Further research with the use of randomised controlled trials or retrospective studies, with more details on technologies, local outcomes, and complications, is required to identify patients best suited to treatment with either approach”, the authors recommend.
Jing Wu (Second Xiangya Hospital, Central South University, Changsha, China) et al note that a clinical trial comparing the effectiveness of cryoablation with thermal ablation is “not likely to be developed or completed”, and thus set out to assess the survival outcomes of these two treatment modalities using the US’ National Cancer Database (NCDB). Established in 1989, this is a clinical oncology database of hospital registry data gathered from more than 1,500 Commission on Cancer-accredited facilities and sponsored by the American College of Surgeons and the American Cancer Society. Over 70% of newly diagnosed cancer cases in the USA are captured by NCDB data.
A total of 6,258 patients who received either cryoablation (3,936 patients) or heat-based thermal ablation (2,322 patients) between 2004 and 2014 were included in the study.
The three-, five-, and ten-year survival rates were, respectively, 91%, 82%, and 62% for cryoablation and 89%, 81%, 55% for heat-based thermal ablation. Wu and colleagues report that patients treated with cryoablation had more comorbidities that those treated with thermal ablation. They say that this finding “supports previous studies suggesting heat-based thermal ablation as [sic] less effective in managing larger masses”.
Detailing their results, the authors write: “On univariate Cox regression analysis, compared with cryoablation, the hazard of mortality was increased for patients treated with heat-based thermal ablation (p=0.031). On multivariate Cox regression analyses adjusted for age, facility type, facility location, insurance status, education level, income, residence, Charlson-Deyo score, tumour size, and treatment, cryoablation remained associated with longer overall survival compared with heat-based thermal ablation (p=0.021).”
This observed difference in overall survival was only apparent in tumours larger than 2cm, according to the study investigators. The authors say that “This is in accordance with a previous retrospective study of 445 patients that demonstrated similar outcomes between cryoablation and heat-based thermal ablation when treating masses ≤3cm”.
Centre and experience were not found to have an effect on overall survival. “In fact”, the authors write, “patients who went to facilities reporting ≥100 cases over the past 10 years had shorter survival than those who went to facilities reporting <100 cases”. They posit that this difference in survival is due to the fact that patients were sicker in the more experienced centres, as large academic centres take complex cases where patients are more likely to have increased comorbidities. Another explanation the authors suggest is that “with high-volume centres reporting more heat-based thermal ablations than cryoablations, the shorter survival may be related to the shorter survival associated with the procedure itself”.
The study authors describe ablation as “a nephron-sparing minimally invasive approach that is typically used for patients who are not optimal surgical candidates or who have masses within a solitary functioning kidney or in association with renal dysfunction”. They explain that, although partial nephrectomy “remains the most common treatment for clinical T1a RCC, ablative therapies serve as a less invasive alternative and offer distinct advantages in both complications rate and cost-effectiveness”.
Wu and colleagues acknowledge several limitations of their study. Being retrospective, they say that the potential for selection bias “must be considered”. Secondly, the study only reports on overall survival, and not cancer-specific survival, “which would be expected to have more direct implications on treatment consideration”, the authors write. They also list the inability to distinguish approach and ablation type (radiofrequency ablation or microwave ablation) in the NCDB dataset, the potential for underreporting of cases performed by interventional radiologists, the inability to assess impact on patients’ quality of life, and any potential unknown confounders outside of those accounted for in the study as limitations.
Dan Sze (Palo Alto, USA), chair, 2019 Annual Meeting Program and Nadine Abi-Jaoudeh (Orange, USA), chair, 2019 Scientific Program, discuss the highlights of the 2019 Society of Interventional Radiology (SIR) Annual Scientific Meeting. The programme-makers set out to turn some established ways of doing things on their head, and the “off-the-charts” energy of the meeting truly represented the diversity of interventional radiology, they say.
Constantino Peña was the chair of the 2019 Workshop Program.
There is a huge group of knee osteoarthritis patients in whom conservative therapy fails. Yet, many of these patients are not candidates for joint replacement. If proven to have long-term benefits, geniculate artery embolization—a minimally invasive procedure performed in about an hour, under local anaesthesia—could help fill the gaps in the treatment paradigm and have a profound effect on the quality of life of these patients, Mark Little (Reading, UK) tells Interventional News at the first Embolotherapy (ET) conference in Valencia, Spain.
“Deep in my heart, I knew interventional radiology (IR) had a tremendous future,” Alex Tang tells Interventional News. Looking back at his career, Tang talks of setting up IR services in his native Malaysia, and, as the convenor of the Asia-Pacific Congress of Interventional Oncology (APCIO), details the myriad opportunities and challenges interventional radiologists in the Asia-Pacific region face.
What first drew you to interventional radiology?
I joined as a radiology trainee at the National University of Malaysia in 1991. This was an unexpected opportunity: a nurse happened to drop the application for radiology training on to my desk during the peak of the outpatient rush. The chances of enrolling in radiology training 29 years ago were as slim as winning the lottery. I was mesmerised by my radiology counterparts, who were able to biopsy the liver percutaneously in a trauma case, in one instance saving a patient with a massive post-biopsy bleed—this was done by my senior using the frightening Vim-Silverman needle. I then obtained a place on a postgraduate training course to eventually become a specialist; the places were full, but the phrase “I want to do interventional radiology” during my interview secured me the training post. Back then, I was not yet aware of how wide-reaching and interesting the field of IR was.
Have you had important mentors throughout your career? What have they taught you?
My training in IR started in the Hammersmith Hospital, The Royal Postgraduate School University of London, UK, under the guidance of Ann Hemingway and James Jackson, from 1997 to 1998. During my fellowship training, I was also seconded to the Guy’s Hospital, London, UK, where I worked under Andreas Adam. Ann Hemingway created the fellowship opportunity for me despite working around a very busy schedule. James Jackson taught me a complex, state-of-art techniques in embolization. Andreas Adam completed my training in the various non-vascular interventions. In addition, Richard Edwards and John Moss were very important mentors to me, because they exposed me so much to various endovascular revascularisation techniques in the Gartnavel General Hospital, Glasgow, Scotland. I have obtained strong technical skills from all of these mentors. These hands-on training opportunities shaped me to become an all-rounder within IR by the time I returned to Malaysia to start the IR services in my home country. To those who have shaped me to be who I am today, I sincerely thank and appreciate you from the bottom of my heart.
As the convener of APCIO, why did you feel the need for a meeting in the Asia-Pacific region?
Modern oncology is among the fastest-growing fields in medicine. Interventional Oncology (IO) being the fourth pillar of cancer care, it is one of the most rapidly evolving sub-specialties. The practice of IO in the Asia-Pacific region is extremely variable; we have to take into consideration the varying standards of care, technologies, and availability of services, as well as the diverse geographies, ethnicities, socio-economic backgrounds and skills in each and every country.
With the theme “Interventional Therapy in Modern Oncology: Technological Integration Beyond Boundaries”, APCIO 2019 is multidisciplinary and multinational. The meeting aims to establish a regular platform from which to discuss ways of continually improving medical expertise, while also ensuring the delivery of best ethical practices in oncological patient care. APCIO 2019 enrols almost every country in the Asia-Pacific region, with the primary aim of developing an even greater interest in the next generation of interventional radiologists.
APCIO 2019 also wishes to strengthen intersocietal collaborations, with associations such as the Society of Interventional Radiology (SIR), the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR), the Cardiovascular and Interventional Radiology Society of Europe (CIRSE), the Society of Interventional Oncology (SIO), the Asia Pacific Primary Liver Cancer Expert group (APPLE), the Asian Pacific Association for the Study of the Liver (APASL), the local oncology society and many more.
How has the APCIO changed over the last six meetings?
APCIO was first established in 2010 in Beijing, China, by the Asia Pacific Society of Interventional Oncology (APSIO). It is a biennial meeting of interventional radiologists from the Asia-Pacific countries. The last five meetings were held in Beijing, China, 2010; Hangzhou, China, 2011; Guangzhou, China, 2013; Miyayaki, Japan, 2015; and New Delhi, India, 2017. The sixth meeting will be held in Kuala Lumpur, Malaysia, 2–5 October 2019. With the premise of providing a multidisciplinary approach and fostering intersociety collaborations, APCIO 2019 is establishing a collaborative platform in interventional oncology in the region. We see positive steps in having non-interventional radiologists coming forward to collaborate with and to support the meeting. This is very encouraging and favourable development. With IO being the fourth pillar of modern oncology, it is vital that we work with the other three pillars to offer more holistic and multidisciplinary care in the best interest of cancer patients. Moving forward, future APCIO meetings will see a greater symbiosis with our clinical counterparts in surgical oncology, medical oncology, radiation oncology, immunology, stem cell medicine, modern pathology, palliative care and various support groups in the modern oncology field.
What are the challenges and triumphs of interventional radiology specific to the Asia-Pacific region?
Asia Pacific countries are geographically, ethnically and financially diverse. The standard of care in medicine, especially in the field of interventional radiology, varies throughout the region. The disease spectra, presentations, and incidences also vary regionally and are different from in western countries.
Whilst numerous procedures are performed to the best achievable local standards, they frequently have suboptimal outcomes, especially in the economically under-privileged countries. Procedures are also performed in diverse ways, and optimal endpoints for the best result may not have been reached. One example is conventional transarterial chemoembolization (cTACE) in hepatocellular carcinoma (HCC): the technical approach, patient selection, and outcomes are extremely variable. Skill level, equipment availability, and financial constraints—notably a lack of national healthcare financing—present daily challenges.
There is a huge need for streamlining the standard of care, procedural techniques, and skills, regional availability of necessary equipment for procedures—from the very basic to the most advanced—and the training of young interventional radiologists across the region. This should be our priority. APCIO wishes to do this by gathering everyone under one roof on a regular basis, with the hope of strengthening the regional IO/IR fraternity. To this end, 80 young investigator awards are given out at the meeting. These are strongly supported by the industry, with the hope of bringing delegates from financially restricted countries, as well as providing individual benefit to the recipients. Two US$3,000 training scholarships are also provided.
What is the most exciting research coming from the Asia-Pacific region in interventional oncology, in your opinion?
The paper from the Chinese University of Hong Kong, on the “Ablative chemoembolization for hepatocellular carcinoma: a prospective phase I case-control comparison with conventional chemoembolization”, by Simon Yu et al. It was published in Radiology in April 2018. The management of giant HCC, an endemic disease in the Asia-Pacific region, has been a great challenge to all of us. Treating and completely controling a giant HCC in a non-resectable candidate with cTACE or DEB TACE is frequently futile. The use of transarterial ethanol injection (TEE) in the embolization of liver cancer was first attempted in the 1970s in Japan. This treatment technique was abandoned because of multiple technical failures.
Technical improvisation and improvements in safety have optimised this procedure, and Yu et al published a paper in the Journal of Vascular and Interventional Radiology in March 2009 detailing their positive experience of TEE. Ever since, TEE has been gaining momentum, with more interventional radiologists using this new treatment modality in the management of intermediate-stage HCC.
Yu has attempted to further advance the treatment for HCC by adding an element of chemotherapy (cisplatin) into the formulation of TEE, to develop what he calls ablative chemoembolization (ACE). His study published in Radiology has proved the safety of this new and highly effective treatment. A 100% complete remission rate using the ablative chemoembolization protocol has been reported; a very encouraging development.
In my personal experience, TEE/ACE offer numerous advantages and has fewer side effects. It is highly efficacious in controlling the tumour, especially if it is injected super selectively into the tumour. Ethanol has the property of instigating immediate cellular coagulation; hence, it achieves an immediate tumour necrosis, especially if a concentration of more than 66% is used during the procedure.
As president of the MYSIR, what are your goals for society?
The Malaysian Society of Interventional Radiology (MYSIR) is a young society, established in 2013. Our main goals are: to establish a more streamlined standard of care in IR/IO, to train more young blood, to promote IR services locally, and to enhance our presence in the daily clinical workflow. MYSIR is working collaboratively with multiple disciplines to gain greater clinical acceptance of the newer IR technologies and treatment modalities. We are organising more multidisciplinary team meetings, among them the Multidisciplinary Oncology Symposium Malaysia (MOSM) and APCIO 2019.
MYSIR is an organisational member of the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR), and we are looking forward to having a greater presence both regionally and internationally, and to establishing a more cohesive collaboration with larger societies, such as SIR, CIRSE, Society of Interventional Oncology (SIO), ACTA, APPLE and APASL, to promote IR services and to conduct training workshops for local IRs and trainees.
What is the biggest challenge for IR at the moment?
The public awareness of the availability of IR treatment techniques is still low, especially in some Asia-Pacific countries. Similarly, in the medical fraternity, many doctors are unaware of the availability of the state-of-the-art options IR offers in the management of diseases. Clinical acceptance of the new IR techniques is also a big challenge for us, as many of the clinicians prefer to opt for more conventional means.
Evidence-based medicine and clinical outcomes remain the most important determinants of our daily practice. High-quality research and clinical evidence in IO and IR treatment techniques are still lacking, and they are needed to justify our clinical presence and in offering the best medicine for the best interests of our patients.
Alex Tang
What do you anticipate being the most practice-changing technology in IR over the next 10 years?
Artificial intelligence (AI), especially machine learning (ML), is expected to play a primary role in the future of IR. This is especially true for minimally invasive tumour therapies performed by interventional oncologists. The overwhelming amount of disparate clinical, laboratory and imaging data derived from clinical research is beyond anyone’s ability to digest, and thus cannot be systematically applied in the everyday clinical setting. This results in institutional and individual variabilities in multidisciplinary decision-making involved in daily patient management. The growing need for more patient-centred and individualised care necessitates a more systematic and unbiased approach for determining case stratification, treatment protocols, outcome predictions and, most importantly, avoiding those treatments that are not (or less) effective. AI solutions can use ML algorithms in precise planning and may help make sense of the potentially nonsensical. This will cause a paradigm shift for interventional oncologists, improving clinical outcomes to the extent that it will be the mainstay of IR practice.
Micro Medical Solutions has received Investigational Device Exemption (IDE) approval from the US Food and Drug Administration (FDA). IDE approval allows the company to initiate a US pivotal clinical trial to evaluate MicroStent’s safety and efficacy. A press release reports that MicroStent is a vascular stent specifically designed to achieve and maintain vessel patency and improve blood flow in order to reduce below-the-knee amputations for patients with critical limb ischaemia resulting from peripheral arterial disease.
Last year, Micro Medical Solutions completed a three-centre, 15-patient feasibility study of MicroStent in which MicroStent met all primary endpoints for both safety and efficacy. The study demonstrated in the device-related per protocol population that 90.9% of patients had primary patency at six months’ post-index procedure, which is a composite of 90.9% of patients with freedom from occlusion, while 100% were free from a clinically driven target lesion revascularisation. The study also showed 100% of patients had freedom from the primary safety endpoint at six months’ post-index procedure, which is a composite of 100% of patients with freedom from death and 100% freedom from major adverse limb events in the same population.
The FDA has granted IDE status based on these outcomes. Micro Medical Solutions will immediately initiate the process to begin enrolment in the clinical trial, called the STAND study (A clinical evaluation of the MicroStent peripheral vascular stent in patients with arterial disease below the knee).
Robert E Beasley (Mount Sinai Medical Center, Miami Beach, USA), the lead investigator, comments: “Because critical limb ischaemia represents the most severe clinical manifestation of peripheral arterial disease, we are excited to have a device that offers physicians multiple access points, as well as a trial that allows for reintervention to effectively treat and lessen the impending limb and tissue loss.”
Jihad A Mustapha (Advanced Cardiac & Vascular Centers for Amputation Prevention in Grand Rapids, USA), states: “For patients with peripheral arterial disease, the risk of amputation is high, particularly if they have critical limb ischaemia. Amputees face decreased quality of life, as well as amputation-associated mortality. I look forward to the clinical trial for MicroStent because we need new solutions to help save critical limb ischaemia patients from amputation.”
Jason Levy (Atlanta, USA) and Sandeep Bagla (Virginia, USA) talk to Interventional News about preliminary results from the ongoing OPuS One study. The OPuS One post market study is currently collecting real world data on the effectiveness of the OsteoCool radiofrequency ablation (RFA) system (Medtronic) for palliative treatment of spinal metastasis and benign bone tumours. The study is ongoing and continues to enrol patients globally.
Preliminary results for 34 patients treated with RF ablation with lesions in the thoracolumbar spine (predominately) and the pelvis and/or sacrum treated with OsteoCool have been analysed. The study investigators found in these preliminary data that patients exhibited rapid pain improvement at one week with 74% (25/34) patients experiencing significant change from baseline in worst pain of ≥2 points and sustained long-term relief through three months. Levy goes on to talk about the road being “wide open” for RFA therapy while Bagla outlines why the OPuS One study is so important to the field.
This video is sponsored by Medtronic.
Bagla S, Levy J, Hopkins T, et al. Abstract No. 618 Rapid pain improvement in patients treated for painful bone metastases with the Medtronic Osteocool RF Ablation system: the OPuS One study. J Vasc Intervent Radiol. 2019;30 (3 Supplement):S266-S267. doi:10.1016/j.jvir.2018.12.723.
Both Medtronic and BD have released statements in response to the FDA circulatory system devices panel held last week (19–20 June, Washington, DC, USA). The companies reiterate the safety and efficacy of their own paclitaxel devices and state that patient safety is a priority.
For Medtronic, patient safety is our top priority—and has been since our company’s founding more than 60 years ago. These panel deliberations are critically important as the Food and Drug Administration (FDA), societies, physicians, and industry consider and address the recent questions around the safety of paclitaxel devices in peripheral arterial disease (PAD) above-the-knee. As an industry leader, we take our responsibility to patients and physicians very seriously and look forward to further collaboration on a response to the panel’s recommended next steps.
The Medtronic presentation included the independent, patient-level analysis from our two randomized controlled trials (RCTs)—IN.PACT SFA and IN.PACT Japan. This analysis also accounts for vital status data on 97% of patients from our RCTs, representing the highest rate obtained across all industry clinical data presented at the panel. Results demonstrate:
No drug-related mechanism for observed transient mortality signal
No observed dose relationship with mortality
No pattern of adverse events or cause of death to suggest unifying mechanism
No relatedness between deaths and paclitaxel, as adjudicated by a newly convened independent Clinical Events Committee (CEC) with paclitaxel toxicity expertise
Additionally, Peter A Schneider, MD, professor of Surgery, Division of Vascular & Endovascular Surgery, University of California San Francisco and principal investigator of the IN.PACT SFA trial, presented the clinical benefit of IN.PACT Admiral. In the IN.PACT SFA trial, three out of four DCB patients remained intervention-free through five years, and for DCB patients who required a repeat procedure, the time to reintervention was prolonged for more than two years. Medtronic remains confident that the IN.PACT Admiral benefit-risk profile is positive and supports IN.PACT Admiral DCB as a first-line strategy for the treatment of PAD.
The panel presentations and deliberations addressed a wide range of considerations related to paclitaxel drug-coated balloons (DCB) and drug-eluting stents (DES). Laura Mauri, MD, vice president, Global Clinical Research & Analytics, Medtronic also presented alongside Dan Clair, MD, chair of the Department of Surgery for the University of South Carolina (USC) and the Palmetto Health-USC Medical Group and Eric A Secemsky, MD, MSc, RPVI, FACC, FVSM, Beth Israel Deaconess Medical Center, Harvard Medical as part of an unprecedented pan-industry presentation.
Medtronic remains steadfast in our leadership and commitment to data transparency and continues to encourage collaboration across industry and regulatory stakeholders around the world to further address this issue.
The full statement from BD:
The panel discussed the benefits of paclitaxel-coated devices relative to the potential risks and noted strong evidence of benefit and recommended additional efforts to evaluate long-term safety. Additionally, BD presented its own data confirming that the benefits outweigh the risks for LUTONIX drug-coated balloons (DCBs) in SFA. Over the past several months, BD has been working diligently to obtain all available patient follow up data and collaborating with FDA, professional clinical organisations and industry to investigate the important issue of DCB safety. BD continues to stand behind the safety of its LUTONIX DCBs and is committed to improving the quality of life for patients with PAD. BD will continue to collaborate with FDA, industry and professional organisations to collect and analyse data for the benefit of patients. To ensure patients with PAD continue to receive the best care possible, BD will continue to ensure physicians and patients have access to BD’s broad range of treatment options for this serious disease.
Siemens Healthineers and Mentice AB have announced that they are collaborating to fully integrate Mentice’s VIST virtual patient into the Artis icono angiography system from Siemens Healthineers.
According to a press release, the VIST virtual patient thus becomes a fully integrated simulation solution for the angio-suite. The global partnership between the two companies will allow interventional radiologists, neuroradiologists, and cardiologists to perform vascular and cardiac interventions on a virtual patient inside the angiosuite.
“With an ever-increasing complexity of new interventional procedures, our customers strive to acquire and retain procedural skills while optimising their performance and improving patient safety. The Artis icono angiography system equipped with a VIST virtual patient will make it possible to train new interventional procedures directly in the angio room,” says Michael Scheuering, head of Interventional Radiology at Siemens Healthineers.
“The VIST virtual patient integration into the Artis icono angiography system will open new opportunities for clinical teams to improve their overall performance, drive operational efficiency, and more importantly, help improve patient outcomes. By using the Artis icono system on the VIST virtual patient, clinicians may now explore new interventional procedure methods and experience the use of new medical devices while reducing clinical training on actual patients and eliminating exposure to radiation,” comments Göran Malmberg, CEO at Mentice. “The VIST virtual patient provides an immersive, high-fidelity, simulation-based environment accessible right from the Artis icono system, making this integration one of the most sophisticated options in the field of endovascular skills acquisition.”
Interventionalists may now perform simulated cardiac and vascular procedures by using the Artis icono controls to angulate the C-arm, move the angiography table, use the foot pedals, and review fluoroscopic images on the Artis icono screens while deploying actual medical devices in a radiation-free environment. The integrated solution will allow clinicians to perform procedures either by using Mentice’s extensive library of patient cases or by importing actual MR and CT patient data for case training and rehearsal. Transesophageal echocardiography (TEE), intravascular ultrasound (IVUS), optical coherence tomography (OCT), and fractional flow reserve (FFR) procedures are also available.
The US Food and Drug Administration (FDA) convened today and yesterday for a General Issues Panel Meeting on the late mortality safety signal associated with paclitaxel-coated products (i.e. paclitaxel-coated balloons and paclitaxel-eluting stents) used to treat peripheral arterial disease (PAD) in the femoropopliteal arteries.
Following the two-day discussion, an FDA Circulatory System Devices Panel Advisory Committee concluded that there is a “mortality signal” as first described in the Journal of the American Heart Association (JAHA) paper authored by Konstantinos Katsanos et al (Patras, Greece) in December 2018, but that better data collection was necessary going forward, as some data were missing. The panel determined that there were not enough data to confirm a class effect, and no consensus was reached on the cause(s) of death.
“One of the take-aways from this has been that in this field of lower extremity revascularisation, the quality of these data and the rigour of these clinical trials has been somewhat amiss, that even with the adjustments in follow-up, anywhere from 6% to 26% of the patients’ data are missing at one and five-year follow-up,” surmised Todd Rasmussen, a vascular surgeon in Kansas, USA.
On the second day, themes of the meeting included the risk-benefit consideration for patients, and how best to convey the choice of paclitaxel treatment in the context of short-term benefit and improved quality of life weighed against a signal of late mortality risk. The panel largely agreed that patient choice is central, as clinical benefits are clearly demonstrated and increased quality-of-life may be an acceptable tradeoff for long-term risks for many patients.
Furthermore, consistently noted throughout panel discussion was the importance of collaboration between industry, regulatory bodies and other stakeholders to ensure data gaps are filled and strategically tackled. Recommendations regarding future study designs as well as optimisation of ongoing trials were discussed, with no consensus on the value of registry data as opposed to more time-consuming and expensive randomised controlled trials. However, FDA representative Bram Zuckerman stated in the last hour of the meeting, “Unfortunately, we have a signal here that remains undetermined. One of the reasons why is that the death adjudication uniformly in these FDA trials was poor.” He summarised, “going forward, mortality will be given a higher priority, and we will need to think about how it can be best assessed and adjudicated.”
The panel agreed that in terms of determining efficacy, studies can follow up to one year for these endpoints, while safety should be assessed over a longer-term follow-up of three to five years.
Concluding the meeting, Bram Zuckerberg states that the two-day meeting and presentation has been “extremely helpful” for the FDA, who will now consider the analysis of the panel, and “look forward to continued collaboration in this field.”
See below for highlights from 19-20 June:
As laid out in an Executive Summary document prior to the meeting, the aims of this meeting are several-fold. They are to review the available information and provide feedback on:
The presence and magnitude of a late mortality safety signal;
Whether all paclitaxel-coated vascular products (regardless of device platform or dose) are associated with the signal;
The impact of missing data and covariates on the signal;
Potential mechanism of death (causality) considering drug dose exposure and pre-clinical data;
Reconsideration of the benefit-risk profile related to the use of these products;
The need for the collection of additional data and/or device labelling changes;
The impact of the signal on ongoing femoropopliteal disease clinical trials as well as on paclitaxel-coated products marketed or under clinical evaluation for other indications (e.g. treatment of stenoses in arteriovenous dialysis fistulae, critical limb ischemia).
To date, FDA analyses of available data from FDA-approved devices show an increase in late mortality between two and five years associated with paclitaxel-coated devices intended to treat femoropopliteal disease. However, the FDA note in their Executive Summary report, “causality for the late mortality rate increase could not be determined”. The agency recommends that additional data are needed to further assess the magnitude of the late mortality signal, determine any potential causes, identify patient sub-groups that may be at greater risk, and to update benefit-risk considerations of this device class.
Live updates on the meeting below:
19 June, 13:00 BST
Chairing the panel, Richard Lange opens the meeting, and a statement from Evella Washington of the FDA outlines the selection for the panel members, who have been chosen as financially impartial with no conflicts of interest.
19 June, 13:15 BST
Eleni Whatley gives the first presentation to introduce the background and the purpose of the panel. Day one will focus on the presence and magnitude of the mortality signal described by Katsanos et al, whether a class effect is identified, and potential causal mechanisms. On day two, Whatley states, dose effect will be considered along with the benefit/risk profile of paclitaxel devices and finally a discussion of future regulatory actions, including modifications to clinical trial designs, approved product labelling, and additional studies.
Whatley summarises the recently completed analysis by the FDA and outlines the Executive Summary, which is available here: https://www.fda.gov/media/127698/download
19 June, 13:40 BST
Mathematical statistician Adrijo Chakraborty notes “the FDA statistical team conducted a sensitivity analysis to evaluate potential impact of missing data on mortality analysis.”
The findings of this analysis were summarised by Chakraborty as follows: “The meta-analysis results suggest that there is an increasing risk for mortality in patients treated with paclitaxel-coated devices compared to control devices for the as treated population. Similar chain is observed for the intent-to-treat population. The meta-analysis here are based on a small number of studies, based on four studies and analysis of four year and five year are based on three studies. The FDA conducted a sensitivity analysis to evaluate the impact of missing data. The results suggest that the increases risk of mortality remains for the scenarios completed. It is to be noted that the result is the choice of the data.”
Yu Zhao, a second mathematical statistician, reports the FDA conducted a gender analysis to assess heterogeneity and treatment effect regarding cause to mortality between male and female in a similar fashion as the geography analysis. “For all four pivotal RCTs, no evidence of differential treatment effect between the paclitaxel-coated device group and the uncoated device group was no difference between the gender groups,” Zhao says.
19 June, 13:50 BST
Donna Buckley, Interventional Radiologist, presents the FDA’s cause of death analysis, and says “The mortality rate for each cardiovascular subtype was numerically higher for the paclitaxel group versus the non-paclitaxel device group in all subcategories.” Overall, “there were no qualitative trends identified to suggest a particular cancer type was more frequent in the paclitaxel group”, and other causes of death investigated included adverse events classified into 27 FDA specified categories.
“The results qualitatively suggest a higher percentage of patients treated with paclitaxel-coated device groups had more adverse events in all categories except injury”, Buckley says. “Overall, patients treated with paclitaxel-coated devices had higher rates of all death types versus patients treated with uncoated devices, except for infection related deaths and trauma, which trended higher in the control group. There’s also no clear trend from the data provided that treatment with paclitaxel-coated devices was associated with excess rate of cardiovascular or non-cardiovascular death subtypes.”
In terms of causal mechanisms, Buckley notes: “There was no specific group of adverse events identified that would suggest a mechanism for late term mortality and a baseline characteristics and was not specifically instructive, and more detailed statistical analysis would need to be conducted to identify potential covariates and predictors of mortality.”
Summarising the full FDA analysis, Buckley states: “With regard to subgroup analyses, there was no consistent pattern of differences in gender and geography across the studies to suggest a predictable differential treatment effect between patients treated in the USA and outside the USA in male and female patients. With regard to the adjudication of causes of death and adverse events, there were numerous limitations such that conclusion should be viewed with caution. However, given the data provided, FDA were not able to determine a pattern in cause of death or adverse events that would indicate a clear area of exploration regarding a potential biological mechanism.”
19 June, 14:15 BST
Buckley adds, in discussion with the panel, that “one of the challenges that we have for most of the studies there were some restrictions at least in terms of use of paclitaxel-coated device and ipsilateral land within the first 12 months. Beyond that it became a little bit more challenging to collect that data in a robust way.”
Panel member Frank W LoGerfo questions the follow-up on death in non-US studies, where social security numbers may not be implemented, and whether there may be more missing data in non-US trials.
Panel member Joaquin Siguroa states: “a challenge of potential identification of cause versus confounding variables present in risk factors as they evolve in an underlying disease state which has with it associated high mortality and morbidity, in a disease state in which we know effective therapies for secondary prevention are often not prescribed or not compliant. And so trying to identify where that signal comes from remains a challenge which we’ll continue to explore.”
Considering the significant amount of comorbidities in this patient population, Buckley says the cause of death was often unclear, especially at five year follow-up. “I’m not tremendously confident, I think the industry did their due diligence in trying their best to adjudicate those events, but given the patient population I think it was extremely challenging to end up with a very confident single cause of death in those cases,” she says.
Whatley expands on this point, noting that “these randomised controlled studies were not designed to look at five year mortality.”
19 June, 14:45 BST
Combined industry presentations begin.
Daniel Clair, advisor to Medtornic and Boston Scientific and a consultant for BD, provides a pan-industry talk on the “dramatic” and “critical” role drug-eluting technologies have played in patient care. “We believe this technology is safe, effective, and incredibly valuable for our patients and the healthcare system overall”, he says. “To address the issues or the concern regarding paclitaxel and mortality, industry competitors have become partners in an unparalleled way to provide additional information and analysis regarding each of their studies. Honestly I have not ever witnessed this type of collaborative effort on the part of companies living in a very competitive environment to assess the safety and performance of an entire class of devices. Their interaction and cooperation exemplify for clinicians the commitment to ensure the therapies they are offering enhance the options for patients without putting them at increased risk. I am proud ton stand with them as a partner in this effort.”
“Paclitaxel has a long history of use in the vascular system”, Clair reminds the audience, calling the value of paclitaxel devices “indispensable” in the coronary arteries. He says their use in this space informed the later decision to use the drug in peripheral vessels.
Describing the industry response to the FDA letter of 15 March earlier this year, recommending paclitaxel use being limited to patients at greater risk of restenosis, Clair says: “While the intent of this letter was patient safety, the impact of the communication is significant. For many clinicians, health care systems have unilaterally made the decision to withdraw these devices from their shelves. And for many physicians the fear of potential lawsuits has led to these products being essentially unusable in the current environment. For our patients, this means a dramatically increased risk for intervention failure and risks related to reintervention, potentially limb loss in more severe cases. For some patients, this will mean only surgical options will be offered or no treatment at all. And I would particularly like to emphasise the potential impact for our most vulnerable patients, those with critical limb ischemia. These sickest and most frail patients with PAD may be subjected to increasing numbers of interventions, and they have the highest riskof restenosis along with the potential to be pushing to more extensive therapies, which increases their overall mortality and local risk of the rocedures. These patients need these devices.”
“There is no relationship between paclitaxel dose and mortality”, Clair says. He reiterates: “There is no evidence of paclitaxel-related toxicities in the mortalities.”
19 June, 15:00 BST
Aaron Lottes, lead scientist for Zilver PTX (Cook Medical), promises to provide clinical data confirming no mortality signal seen with paclitaxel across the company’s 25 year history with the drug.
As other paclitaxel devices were not available at the time, Lottes says that the original Zilver PTX RCT and Japan PMS provide the best data available to look at paclitaxel data. These compared the Zilver PTX to a bare metal stent (BMS).
Patients enrolled in the Zilver PTX RCT were randomised to percutaneous transluminal angioplasty (PTA) and Zilver PTX. Any cross-over (patients who moved from the PTA to the Zilver PTX group) were analysed as belonging to the paclitaxel group. Forty per cent of the patients initially randomised to PTA were actually analysed as Zilver PTX patients after crossing over.
Michael Dake now provides updates on the clinical results of this study.
An intent to treat analysis is “generally recognised” as the standard for evaluating effectiveness. However, Dake says, “To address questions of safety, regulatory guidance, literature and expert opinions agree that we must consider how patients were actually treated.” As 40% of patients enrolled in the BMS arm of the Zilver PTX RCT were treated with Zilver PTX, he says an intent to treat analysis “is not an appropriate method for answering the question of paclitaxel mortality.”
He says the Katsanos et al data did not account for this crossover, but when Cook Medical accounted for it in their own analysis,”Mortality rates for Zilver PTX and PTA bare metal stent groups were comparable. FDA’s analysis confirms that there was no mortality signal for Zilver PTX”.
In addition to treatment with paclitaxel, the Cook Medical investigators looked at the dose effect. They report finding no association of dose with mortality.
Concluding, Dake says: “We are here because of statistical debate that has raised questions with patient safety. Paclitaxel devices with proven benefit are being restricted from use and these decisions are negatively impacting patient care. Analysing Zilver PTX patients in the PTA stent group does not make sense. When Zilver PTX patients are analysed base on how they were actually treated, the published results for the overall meta-analysis of paclitaxel related mortality become non-significant. That is, there is no class effect. If Zilver PTX patients are analysed based on how they were actually treated, the results for the entire published meta-analysis of paclitaxel-related mortality become non-significant. An appropriate assess must be based on actual treatment with paclitaxel not on how patients were randomised. When appropriately analysed the data clearly shows no mortality signal with paclitaxel stents.”
19 June, 15:15 BST
JD Meler speaks on behalf of BD. He provides an overview of three randomised controlled trials involving the company’s Lutonix drug-coated balloon.
Vascular surgeon Kenneth Ouriel now speaks on behalf of BD. Outlining the Bradford Hill criteria, designed to tease out a difference between association and causality. Ouriel says there is no evidence for causation between paclitaxel and mortality, echoing Dake’s earlier remarks (see above).
“If causation does exist, there should be one or more specific causes of deaths more prevalent in the DCB arm, causes corresponding uniquely to the mechanism of action”, he says.
He continues: “An independent medical advisory committee made up of intervention lists and oncologists reviewed narratives and source documents for the 173 deaths in the Levant 1 and Levant 2 datasets. No deaths were classified as related to paclitaxel based upon the known side effects of the drug.
“Since this might not capture paclitaxel-relatedness from unknown mechanisms, we reviewed causes of death at categorised by the committee. Mechanistically, if paclitaxel caused deaths, there should be a disproportionate frequency in one category or in a group of related categories, a disproportionality that was not observed. Without clustering of death within a category, causation is not supported.”
Questioning if there was an association between dose of paclitaxel and mortality, further analysis of the Levant 2 dataset demonstrates no dose response, according to Ouriel.
“We also looked at the effect of subsequent interventions with paclitaxel devices which increased drug exposure”, he says. “Some of the analysis that had been reported to date did not account for reinterventions. Almost 20% of subjects in the Levant 2 RCT were treated with a paclitaxel device at some point during their five year follow up. And subjects in both arms, PTA and DCB, who subsequently underwent intervention with a paclitaxel device had a higher five year survival rate than those that did not. This finding was confirmed in our other studies. These findings are counterintuitive if additional paclitaxel exposure is harmful in the long run. It should be noted that the mortality rate in Levant 2 study was lower than the pad population as reported in the Swedish vascular registry at five years.”
Concluding the talk, Meler returns to the stage. He states: “There are no statistically significant increases in hazard ratio for mortality in any Lutonix study. When the Levant studies are pooled the hazard ratio is nearly one. There is no plausible mechanism for mortality or evidence of paclitaxel causation identified. And there is no increase in mortality with additional exposure to paclitaxel in either cohort. Reducing interventions is advantageous to patients, but it also reduces additional visits with health care providers, and associated benefits which may ultimately impact mortality. This creates a plausible explanation for the numerical difference.
“Finally, based on all the analyses to date and a large dataset, Lutonix DCB continues to offer meaningful benefit relative to risk in indicated patients. BD is committed to ensuring patient safety and minimising risk and we will continue to monitor safety data on Lutonix DCB in our ongoing clinical programme and in commercial use. BD plans to incorporate additional analyses into our labeling in coordination with the agency to inform physicians and patients of all available information.
“We have a large dataset that has enabled us to rule out causation. However, analysis of even larger datasets that are appropriately structured to evaluate overall patient health may be required to enable additional investigation on the subject of association.”
19 June, 15:30 BST
Following an introduction by Simona Zannetti, Peter Schneider presents data on the IN.PACT IDE and IN.PACT Japan on behalf of Medtronic.
Stressing the benefits of these devices, Schneider says: “Evidence strongly supports the benefits of DCBs. They are a major improvement from what we had to offer our patients previously, and as a result, DCBs have been integrated as standard of care into clinical practice. IN.PACT DCB has demonstrated durable effectiveness in a population of patients and this is sustained through five years. In my opinion, if we restrict the availability of paclitaxel DCBs, we would be turning back the clock to an era of less effective treatments and will likely result in more repeat interventions over the long-term.”
Laura Mauri provides a safety analysis of the Medtronic data. Pooling data from the IN.PACT Admiral IDE and the IN.PACT Japan study, Mauri says, reveals no statistical difference in the incidence of mortality between the PTA arm and DCB arm.
The pooled analysis from Medtronic also reports no gradient of risk (of mortality) according to paclitaxel dose. “Dose was not significant when examined in multiple ways”, she says.
Mauri concludes that the IN.PACT Admiral DCB is safe and effective, but adds that Medtornic “recognise that even these pooled randomised trials are underpowered to detect a difference in mortality.” She calls for “real world comparative studies followed for a sufficient duration of time” to help to better understand the long term safety of paclitaxel products.
19 June, 15:45 BST
Jonathan Batiller, head of Medical and Clinical Affairs at Philips, introduces the company’s presentations on Stellarex data. “We recognise the importance of the work that was published by JAHA in December of 2018″, Batiller says, adding “we realise there are recent publications that arrive at a different conclusion.”
William Gray explains, “After the publication of the JAHA paper, Philips prepared a prespecified analysis of mortality using the data collected from controlled trials using the Stellarex DCB.” In an integrated analysis of all seven Stellarex studies, Gray says the findings “continues to support a low all-cause mortality through 3 years of 7.9%, and compares favourably to the 9.3% pooled randomised Stellarex DCB mortality rate.”
“There is no mortality signal of it with Stellarex we could not find in all of our analysis,” Gray concludes. “We’ve reliably shown this through sizable randomised analysis through single trials through DCB and these are consistent observations. The lack of mortality signal further reinforced the paclitaxel cross-over accounting. Comparing paclitaxel exposure versus non paclitaxel exposure further supports paclitaxel as not contributing to mortality, and absent a complete accounting of paclitaxel exposure in any analysis, and its potential impact on modified as treated outcomes any large scale assessment will be incomplete. And we continue to believe that the benefits of Stellarex outweighs its risks, and improved patients out comes in the long term.”
19 June, 16:00 BST
Ian Meredith, executive vice president and global chief medical officer at Boston Scientific, says their Eluvia drug-eluting stent is “differentiated from other paclitaxel coated technologies used in peripheral vascular disease: Its stable polymer does not break down as compared to all DCB excipients that do break down and contribute to downstream particulates.”
Meredith presents data on paclitaxel use in the coronaries. “Paclitaxel in the treatment of peripheral vascular disease and coronary vas clear disease is safe and effective”, he states. “The design principles of Eluvia and coronary stents are identical in coronary studies to studies comparing paclitaxel stents with bare metal stents, and any effect of paclitaxel would have been observed in those taxus studies.”
Robert Lookstein presents further data on Eluvia, including an ongoing large randomised controlled trial. With “extremely high clinical follow-up” at two years (n=398) all-cause mortality is 6.5%, which is “not distinguishable from” the mortality rate reported in the FDA panel pack. Lookstein reports “to date, we’ve seen no mortality signal whatsoever for the Eluvia drug-eluting stent.”
“The clinical benefit observed with the Eluvia drug eluting stent is observed in all patients studied to date,” Lookstein states, and points out, “The paclitaxel eluting coronary stents, the taxus extent and drug-eluting stent were not included in the JAHA meta-analysis we’re not included in the long term outcomes for the FDA panel pack and were not included in the subsequent VIVA Summit.”
19 June, 16:15 BST
In a final discussion and Q&A before the lunch break, panel member John Hirshfield says “we are being subjected to a forest of duelling numbers: Body counts, crude mortality and subjects under observation, but also all derived coefficients that are derived from these numbers. The problem is that the numbers presented by industry and the numbers presented by the FDA are not the same.” Hirshfield expresses his hope from the panel, to “get a real common agreement of what the actual numbers are between the sponsors and the agencies so we know exactly what data we’re dealing with.”
Panel member David Kandzari adds to Hirshfield’s point, noting “I’m not sure if it’s just the numbers issue or not, I’m trying to sort out two very disparate groups of presentations this morning”.
Panel member Bram Zuckerman says that while the FDA data has been verified, Zuckerman cautions: “I would be careful about utilising of the most up-to-date data analyses. They have not been checked by the FDA, and I can say in general terms, because of a multitude of problems, the FDA has had a lot of back and forth with each company to verify data.” Nevertheless, Zuckerman acknowledges the industry has “stepped up to the plate” in what he calls a “dynamic process”.
19 June, 17:30 BST
Andrew Holden takes to the podium to detail the results of his latest paper, published earlier this week in the Journal of Endovascular Therapy (JEVT), which report finding no causal link between paclitaxel dose and all-cause mortality.
He says: “Probably the biggest limitation in the [dose] equation is the fact that the authors had to use lesion length because they only had summary level data to assist. But of course, lesion length is a poor representative of dose delivered because we do not know the number of balloons used, the amount of overlap, and even treatment beyond the target lesion.”
19 June, 19:30 BST
Presenting the questions for the FDA, Eleni Whatley first permits the panel to discuss the potential presence and magnitude of a late mortality signal associated with paclitaxel devices.
With the panel in agreement in terms of the presence of a signal, the panellists each expressed their concern. Whilst Katsanos’ data was held in high regard, the effect of missing data was discussed at depth, eliciting a variety of responses from the panellists.
“One of the take-aways from this has been that in this field of lower extremity revascularisation, the quality of these data and the rigor of these clinical trials has been somewhat amiss, that even with the adjustments in follow-up, anywhere from 6% to 26% of the patients’ data are missing at one and five-year follow-up,” surmised Todd Rasmussen.
The second question pertains to class effect. “Discuss the strength of the evidence supporting late mortality risk class effect among all US-approved devices,” inquires Whatley, urging the panel to answer irrespective of platform, dose or formulation. The panel expressed a clear consensus that there are not sufficient data to “definitely rule in or out a class effect.”
Although Bram Zuckerman (FDA) alludes to the idea of a new trial comprising a large number of patients, he questioned the panel on whether they are okay with the poolability of devices to address such needs.
Thirdly, the panel are questioned on the impact of missing data, a notably reoccurring topic of today’s meeting. Again, the panel highlight the impact of incomplete data, which, they say, may make the overall data look better or worse if it were to be reported; in turn affecting efficacy analyses.
Moreover, Zuckerman emphasises that increasing the quality and follow-up will not stop after the current evaluation. “This is a very disappointing experience for all. This problem now has significant ramifications,” he adds, and he stresses the need to improve evaluation moving forward.
The penultimate question put to the panel concerns the added value of subgroup analyses. “No clear trends were observed based on region or gender. In addition, baseline characteristics were compared between patients that died and patients remaining alive at the end of available follow-up period for the pivotal studies. In general, patients who died were older with more comorbidities and had longer lesion lengths compared to surviving subjects. However, no consistent pattern was determined,” summarised Whatley.
Addressing the panel, she asks them to discuss the issue of whether such analyses help identify specific patient subgroups that are at increased (or reduced) risk of late mortality following treatment with paclitaxel-coated devices.
However, the panellists maintain that no particular subgroup signal that identifies who might benefit or, more importantly, who might be at risk from drug devices. The consensus calls for more data, and specifically, more heterogeneity within it.
The conclusive question concerns the cause of death. “Do the cause of death data support the presence of a late mortality signal associated with paclitaxel-coated device treatment and suggest a mechanism for this signal?”
Evoking a variety of responses, the panel ultimately concedes that they do not feel comfortable with these data concerning the correct attribution of death. Thus, the panellists also express a lack of consensus regarding whether the data conveys a clear mechanism for such a signal.
20 June, 12:00 BST
The panellists resume their positions, with chairman Richard Lange opening the second day of the meeting. “For today’s agenda the panel will discuss and make recommendations on recent observations of increased long-term mortality and peripheral arterial disease patients treated with Paclitaxel compared to uncoated comparative devices. The FDA requests panel input regarding the presence and magnitude of the signal and potential causes. The FDA also seeks input regarding appropriate regulatory actions associated with the findings.”
Introducing the FDA’s presentation today, Eleni Whatley (Lead Reviewer) acknowledges that given the new information regarding long-term clinical mortality, the FDA reevaluated the preclinical animal studies that were conducted on the five approved devices. She concludes, “Regardless of low dose and single administration, paclitaxel was resident in local and downstream tissue for 60 days and beyond, and in some cases for as long as 270 days. Through no relationship could be gleaned from paclitaxel concentration and local tissue effects, there is the potential that the drug could be having an effect on various tissue systems during its residence and thus allowing for chronic effects.”
Karen Manhart provides an overview of an analyses of the preclinical safety study data. Summarising the studies on animal safety studies, she says, “[There were] no systemic pathologic changes which appear to be device or drug-related. The reviewed data does not suggest a potential mechanism for increased late mortality observed in human study subjects.” Yet she adds that it is important to understand that chronic time-points for animal study data is still short-term compared to the observed safety signal.
Next, Donna Buckley (Interventional Radiologist) presents the dose analysis conclusions. “ZILVER PTX TCT, IN.PACT SFA I and II displayed no clear relationship between dose and mortality. LEVANT 2 RCT shows a possible trend of increased mortality with increased dose.” However, she points to the fact that no consistent association between dose and mortality was detected across studies.
Weighing up the benefits versus the risks of TLR, Buckley surmised, “Overall the class of devices that includes use of Paclitaxel coating to inhibit restenosis have shown consistent and generally sustained benefit in the reduction of reintervention to treat femoral popliteal disease. It is important to emphasise that a qualitative comparison of these findings should be cautioned given that TLR and mortality events are not comparable given differences in severity. Also these events do not fully characterise the totality of the device benefits and risks.”
In relation to the next steps of PAS and labelling, Buckley posits, “Overall, based on the review of the available data, there appears to be a trend of increased mortality three to five years following treatment with Paclitaxel coated stents or balloons in the femoral popliteal arteries. However, as previously emphasised, there are numerous limitations with the currently available clinical data and the result and analysis. In addition, a biological or non-biological cause responsible for this late mortality signal is not evident.”
She adds: “Regarding a new RCT, a fundamental question for the panel is whether a randomised trial of Paclitaxel coated versus uncoated devices is feasible.”
Considering the specifics of labelling, she notes, “[Given] the FDA’s least burdensome principles approach, it may not be possible at the time of device approval to fully predict long-term safety and effectiveness. Note that FDA required for all Paclitaxel coated devices that the pivotal study subjects be followed up to five years as part of the condition of PMA approval, following the collection of these post approval data—whether related to the post approval studies in place or related to new agreed upon data collection efforts. In addition to updating the clinical data, other appropriate modifications may be made to labelling in order to convey appropriate safety information.”
Finally, Buckley concluded the FDA’s presentations for the day: “The FDA reevaluated previously conducted animal PK and safety studies and did not identify information that may suggest a potential mechanism for late mortality. We investigated the observed Paclitaxel doses in the pivotal trials, and did not identify a relationship between mortality and Paclitaxel dose that was consistent across all trials. We also investigated clinically driven TLR in pivotal studies and for all time points the risk ratio values favoured the Paclitaxel device group at five years. The FDA identified approximately 20% decreased risk of clinically driven TLR with patients treated with Paclitaxel coated devices benefit in this regard. This should be considered when we discuss risk and overall adjustments for the risk profile of these devices.” She urges the panel to provide discussion and input on these topics.
20 June, 14:15 BST
Combined manufacturer presentation begins.
Laura Mauri, vice president of global clinical research and analytics at Medtronic, opens the discussion, introducing her fellow speakers Daniel Clair (University of South Carolina, USA) and Eric Secemsky (Harvard Medical School, USA).
Clair gives an anecdote from the recent National Vascular Meeting, where an informal poll revealed that many attendees no longer used paclitaxel devices, demonstrating how the Katsanos et al paper has had “a significant impact on physicians’ ability or hesitation to use these devices”. Clair says it will be good to get closure and clarity on this topic, therefore.
Looking at the use of paclitaxel devices in specific vascular beds, Clair reports no difference in mortality in patients treated with paclitaxel devices compared to without. This held true in the coronary arteries, in arterio-venous access usage, in renal arteries and in below-the-knee patients, Clair informs the audience.
Laura Mauri takes to the podium. She reiterates that the trials discussed yesterday were focused on a narrow patient population and “do not reflect the full spectrum of patients that clinicians see”. She also makes the point that the RCTs under scrutiny were not powered to analyse mortality.
“Real-world analyses, when done properly, can be helpful, but they are not good at avoiding selective bias. They are much more precise, but it is not more convincing to have more precise but biased estimate”, she says. “The only time we can rely on real-world data is if there are robust methods that we are confident about to adjust for selection bias”.
“The study designs were not designed for long term mortality. Regarding paclitaxel treatment; one important thing to point out that has not been stressed before is that we also do not know the treatments that were received before randomisation in almost all of the studies. Drug treated products were available to patients before they were entered [into randomisation], many patients had prior procedures and were being treated for a second time and that was not recorded whether they had had paclitaxel before randomisation”, Mauri criticises.
She summarises: “The observational studies in this space have to be evaluated very carefully and we have to look at those that have been conducted with a high attention to methods. They increase the precision and, if they are reliable in terms of the methods, can be quite important. It is important to know there are unique strengths for this observational data; one is that the completeness and mortality data may actually be better than the randomised trials, which is shocking but true. […] The take home message is in these conducted studies is there are a large number of patients studied representing non-overlapping groups of patients, and hazard ratios are really all right around one with very tight confidence intervals.”
Secemsky says that having a comorbid disease could “negate or impact the potential harm of drug-coated therapy”. He explains: “One of the strengths of our Medicare analysis is the size – not that we have 150,000 patients, but that when we do look at separate subgroups, we have enough patient population to find a meaningful follow-up. I want to highlight here that 60% of our patients are non-CLI patients. In the PAD world, there are two groups of patients, high risk and low risk. High risk are CLI and the non-risk are claudicants and non-CLI. Here we have 90,000 patients; we have more than 17,000 patients contributing data through 1,250 days, we find that there is no associated risk or evidence of harm with drug coated therapy with an upper limit of our confidence interval at 0.96.”
Laura Mauri summarises the industry response to the FDA panel questions. See image below.
Laura Mauri presents the industry response to the FDA’s questions
“For the ongoing studies, it is important that we educate our sites about the importance of good follow-up, and then think about methods in the consent to provide for complete vital status ascertainment with linkage. We can ensure that there is better recording of additional information post procedure, as well as pre-procedure, and maintain that throughout the follow up, not just at the time of randomisation, as well as the important factors of medical therapy that are now incompletely ascertained”, Mauri recommends.
“We would like to work with the FDA to update our datasets and analyses and reflect that in the labelling, and maintain the current indications,” Mauri says.
Outlining her further recommendations, Mauri says that “It is critical really that we continue to assure patient access to treatment. These are very effective products, and we believe that the totality of evidence is supportive in terms of the benefits and risks of these devices. And right now health care providers are not fully able to do what they think is appropriate for their patients.
“We respectfully request the FDA update the 15 March letter to health care providers, really to convey the totality of evidence that is being discussed now”, Mauri says on behalf of Medtronic and industry more generally.
20 June, 14:50 BST
In the discussion following the industry presentations, temporary member Karla Ballman (Weill Cornell Medical College, New York, USA) says that she is “a bit hesitant”. She expands: “I just want to make the observation that I think we need better clinical trial design. When there is an issue with randomised data, you cannot rescue it with very large observational datasets. We take a huge step back if all of a sudden we say we do not even need to do clinical trials, we just neat the observational datasets – we could extend this [discussion] to that extreme. Why do any clinical trials in the first place? So I think there is a place for observational studies, I think they are good for hypothesis-generating, but they are not good for confirming efficacy or clinical benefit. This is why we have clinical trials. Even if they [observational studies] are done well, you can minimise some biases that are in there, but you cannot eliminate them.”
There are general calls from the floor for more information on intervention-free survival rates, which are not known.
20 June, 15:15 BST
Open public hearing session 2 begins.
Evalina Washington, the designated Federal Officer, reminds speakers to provide disclosures at the start of their talk. The FDA has received 14 requests to speak.
The first speaker is Lindsay Machan, an interventional radiologist from Vancouver, Canada. He is one of three that patented the use of paclitaxel for vascular disease, and starts by saying he believes in the drug’s safety and efficacy in treating these patients. Describing early research on the drug, Machan describes how, contrary to research presented by Whitely yesterday, his team “found that paclitaxel is an exquisitely potent inhibitor of angiogenesis at nanomolar concentrations. In fact”, he continues, “even lower than that it was the strongest angiogenesis inhibitor that we identified. In fact, we found paclitaxel did not have any endothelial cell toxicity until we got to 50 micromole concentrations, at least three orders of magnitude greater than we even could detect smooths muscle cell apoptosis.”
“The other thing we found is that the biological effect is extremely localised,” he says. “I work with a group of scientists who have among us greater than 100 man years of experience investigating the local application of paclitaxel and none of us can conceive of a mechanism for this nonspecific mortality.”
20 June, 15:25 BST
Renu Virmani, cardiovascular pathologist and president of the CVPath Institute, says: “CVpath has performed preclinical studies in drug-coated balloons for Lutonix, Medtronic, Spectranetics and now Boston Scientific; we have the largest registry for coronary stent including arteries and have published more than 200 publications regarding stents. I have examined over 100 autopsies of individuals receiving coronary paclitaxel-eluting stents – the cause of death was in no way related to paclitaxel.”
As was also presented this morning, Virmani tells attendees that preclinical studies in swine do not support toxic effects of paclitaxel with the use of DCBs and DESs for the treatment of PAD. Virmani concludes that the major cause of mortality in PAD patients is underlying CAD. “I suggest unrestricted use of DCBs and DESs, monitor and perform autopsy studies, moving forward to be certain of the cause of death”, she advises.
20 June, 15:32 BST
Erica Mayer, a breast cancer pathologist from Boston, USA, takes to the podium. She reviews data from cancer patients demonstrating the benefits of adjuvant paclitaxel.
In a trial of 6,000 patients randomised to anthracycline-based chemotherapy or paclitaxel, Mayer says that “The addition of paclitaxel reduced the risk of recurrence”, and that this what led to approval in 1999 of the drug. She adds that long term follow up showed “there was a decreased risk of all cause mortality at seven years in patients who received paclitaxel, so receiving paclitaxel helped to save lives here. There was also no increase in cardiovascular toxicity or secondary malignancies in patients who received paclitaxel.”
She also says she uses paclitaxel in pregnant patients: “We have seen no increase in maternal or fetal mortality with exposure to paclitaxel, so we feel comfortable enough with this agent that we can give it to pregnant patients.”
She concludes that paclitaxel is established as a safe and effective chemotherapy drug, and that she knows of no data reporting long-term mortality associated with paclitaxel in the oncologic space.
20 June, 15:39 BST
Ramon Varcoe, a vascular surgeon from New South Wales, Australia, speaks of trial design.
“How can we determine whether the finding of this [Katsanos etal] meta-analysis were due to paclitaxel or due to bias from clinical trial design?” he asked. Speaking of his team, he says “We had this idea to perform an identical meta-analysis of randomised controlled trials in the SFA but to exclude all drug-coated devices, so we took paclitaxel completely out of the equation. Our systematic review identified 22 studies that fulfilled the inclusion criteria. […[ Our risk ratio was highly significant at 12 months, showing the patients in the control arm had around 69% fewer mortality compared to the experimental arm. We thought this was quite compelling.”
He concludes: “What we have demonstrated here is that randomised control trials which compare types of experimental controlled trials of SFA can find additional risk of death at 12 months. We see the same risk at 24 and 30 months although we are underpowered and not significant. What if they were independent of paclitaxel completely? In my mind that casts considerable doubt as to the causal link between paclitaxel and mortality.”
He recommends “a more tenacious follow up protocol of those subjects in the experimental arms combined with higher rates of medical interaction in those RCT arms that have more frequent TLRs”.
20 June, 15:46 BST
Alik Farber (Boston, USA) speaks about the BEST-CLI registry. He comments: “The BEST CLI trial and opinion registry will provide a comprehensive and granular dataset on a sizable cohort of patients with CLI treated with paclitaxel devices. So we will be able to provide the use of paclitaxel and its procedure by calendar year by specific arterial segments throughout the course of the study, including reinterventions. We are going to be able to comment on all cause mortality and specific causes of death.”
20 June, 15:51 BST
Yann Goueffic, PI of the BATTLE trial, provides insights from this dataset. The trial compares the Zilver PTX DES with a bare metal stent with a primary endpoint of freedom from in-stent restenosis at one year. Updating the Katsanos meta-analysis with the two year data from the BATTLE trial, “we have no more signal of death in the DES group at two years”, he says. In the BATTLE trial, “there is a trend to have more deaths in the BMS group rather than the paclitaxel-eluting stent [arm]”, he informs listeners. However, he also notes that the BATTLE trial was not powered to assess safety, and so says that “no conclusions can be drawn from this secondary end point.”
20 June, 15:57 BST
Kim Hodgson, representing the Society for Vascular Surgery (SVS) as its president and chair of its paclitaxel safety taskforce, outlines the society’s vision for a pathway forward. He says: “Based on the Katsanos and other subsequent analyses, we assumed a mortality signal would be confirmed. We also assumed this panel would be hearing a lot about patient safety. Striking the right balance requires weighing the increased risk associated with extra interventions against the presumed increased mortality of paclitaxel.”
He says the SVS recommend a spectrum of actions. One is to limit paclitaxel use in claudicants to the anatomic lesion criteria of their original approvals. The SVS should work with RAPID, a public-private partnership, going forward, he says.
20 June, 16:04 BST
Daniel Burgess presents the SVS-VQI registry data. He says he sees two pathways forward, see below:
20 June, 16:10 BST
Schuyler Jones, a cardiologist, speaks now. He believes “There is the opportunity to do traditional observational analyses with adjustment for patient and procedural characteristics that have been described already.” He says “I think our huge challenge and with that the opportunity, is to do prospective registry-based randomised control studies with not just our registry but multiple registries for all of our patients who are cared for in the vascular space.”
His slide on possible next steps:
20 June, 16:17 BST
Statistician Rose Ann White provides her insights. She warns that “We need to be aware of the assumptions.” She adds: “I think we do change over time due to learning [referring to clinicians], and so does our practice. And we can be most efficient through cooperation.”
20 June, 16:23 BST
Stephanie Fox-Rawlings of the US National Center for Health Research praises the FDA’s continued post-market surveillance: “while there are still many questions, the fact that this [mortality] signal was seen in a solid meta-analysis is important. It is a reminder of the value of long-term studies conducted after products are on the market. It also shows the importance of FDA’s continued role in post-market surveillance and communicating about their findings to physicians and patients. This information is absolutely vital for health care providers and patients to make informed decisions about their care.”
20 June, 16:25 BST
“What is unique about my opinion today”, says John Winscott, a cardiologist from Jackson, Mississippi, “is my volume. If you look at the number of patients I have treated with drug-coated balloons in the last four years, I have treated almost 2,400 patients with drug-coated balloons, which is more patients than the [Katsanos et al] meta-analysis and randomised trials all combined.” He gives examples of positive patient stories, playing recording of patient’s testimonies to the beneficial impact paclitaxel therapy has has on their quality of life.
“I would say I have an extremely busy practice and I fight for limb salvage every day. The most powerful tools I have been able to put in my toolbox over the years has been drug-coated balloons, and the biggest change in my practice I have seen in 11 years has been drug-eluting technology. With over 2,000 patients treated and with lesion lengths around 25 centimetres, I personally do not have any concerns for safety or increased mortality. I can tell you honestly that if my mother needed a procedure tomorrow in her femoralpopliteal segment, I would not only request, I would demand she be treated with this technology”, he states.
20 June, 16:31 BST
Robert Yeh of the Beth Israel Deaconess Medical Center (Boston, USA) speaks. Detailing a study of 20,536 patients treated for PAD in the femoropopliteal arteries, he reports no statistically difference in all-cause mortality between patients treated with and without paclitaxel devices. He concludes: “In our interpretation in this large national cohort of PAD procedures, drug-coated devices were not associated with a difference in mortality. These real-world cohorts are more representative of patients undergoing treatment in routine practice, and these conclusions of device safety are more relevant to public health than those seen in the trials.”
Clarifying this statement in later questioning, Yeh says: “I think my main point is that the patients that we see in these observational datasets are actually the ones that are representative of the patients that we are treating in practice. And the one that have public health problems.” He does not believe real-world datasets should replace RCTs.
20 June, 17:40 BST
Eleni Whatley responds to questions in the final FDA Q&A session with industry.
Ian Meredith picks up some unanswered questions regarding the Boston Scientific data, clarifying dose and mortality at 5 years, saying “There is no all-cause mortality difference between bare metal stents and the paclitaxel drug-eluting stent in double blind trials. These are double blind trials with up to 100% follow-up, and the main trial driving this has a 95% follow-up.”
Laura Mauri, representing Medtronic, tells the FDA panel in response to prior questions: “In our trial we had 85% relative risk reduction, so as you expect you see a hazard ratio of 0.13, for the use of the DCB versus PTA which is highly significant; p-value less than 0.001, so that’s the first thing: the treatment is effective. And that’s true after adjusting for the one factor that was an additional independent predictor, prior peripheral revascularization, which is an independent predictor of TLR as we would expect clinically.”
Richard Lange, points out the FDA panel is tasked with “doing a couple things”: one is the address the issue of ascertainment bias, and secondly to pursue comparative analysis of US- versus non-US populations. In response, JD Mueller representing BD, says: “We were able to pull data from our resilient trial and we thought it was relevant because it compares a bare metal stent to PTA and femoral popliteal, and you can see not significant numerical difference of difference in mortality with BMS and PTA with BMS being slightly higher, so we wanted to give you an example of a non-drug related study where we also saw this ascertainment bias as an example.”
Following responses from all industry presenters, Richard Lange notes, “So what I’m seeing is in all the companies is an improved follow up, there was still a change, it was just not quite as big.”
Speaking to the point of US- versus non-US populations, Yu Zhao points to data for several trials: ZILVER PTX, LEVANT and IN.PACT data all showed the trend of a “generally sicker” population in the USA, Zhao says.
Responding to a question from LoGerfo on how bias in the timing of TLR is avoided, and why patency was not used instead, Dan Claire says: “These trials are designed to try and be set up to evaluate the effect on patients. Stenosis has an effect on us as clinicians, TLR has an effect on patients in terms of what they’re subjected to.” He continues, “I agree with you, it might be much easier to standardize how you evaluate stenosis with duplex criteria, but it’s a lot easier to get a sense of what the impact on a patient is by looking at TLR.”
Peter Schneider and William Gray both present comments on the Medtronic and Philips data, respectively, to show that quality of life “improves significantly with fewer reinterventions” using DCBs.
Panel member Gary Jarvis summarises the day’s work, saying “We know what we know now, we know what we don’t know and don’t have, and we’re going to discuss here in a minute where we’re going to go”. He adds that following the publication in JAHA last year, “everybody has been talking about this”, and cooperation between industry, societies and regulatory panels has been significant. “And that is one thing I hope that industry does, is to continue this collaboration beyond this meeting”, Jarvis says.
Panel member Patricia Daigle, representing consumers, says “as I consumer, my concern is the consumer choices. I think the consumer has the right to be aware of the risk-benefit, but ultimately the choice should be up to the consumer. […] The consumer has a right to have a qualitative and quantitative life, and it’s their choice to decide which type of life they would like to live.”
20 June, 18:30 BST
The potential relationship between paclitaxel dose and mortality is assessed by the panel largely as “inconclusive”, as the data is limited and “unclear”, and insufficient to establish any dose-response relationship. Krucoff notes that “the other important thing from my point of view is that this is not a dose assigned, this is a dose-driven largely by anatomy, by lesion length, etc. So I think the dose-response relationship here is fundamentally confounded, in the data—and the data available don’t make it simple.”
Summarising the thoughts of the panel, Lange says: “it is inconclusive based upon the data, it’s complicated by patient variables including length of lesion, and there’s a concern about high tissue levels intraarterial and intraluminar as well.”
20 June, 18:40 BST
Discussing preclinical models, Krucoff says “in this type of safety signal exploration that anything and everything we can learn from preclinical models we should maximize our efforts to adding knowledge rather than having to explore human risk to change ignorance into knowledge.”
Bram Zuckerman underlines Krucoff’s point, adding human trials are both time consuming and expensive. However, Joaquin Cigarroa argues that while he “wholeheartedly agrees” with the statements of Krucoff and Zuckerman, “as designed, the current approach to preclinical animal studies will be unable to adequately address the question of is this signal associated with a biological plausible model.”
Do you feel additional preclinical studies would be helpful? While a majority on the panel voted yes, Todd Rasmussen says “this would be going backwards. […] I don’t think there’s no use to animal studies, I’m not trying to be argumentative, but I just offer the balance that, when we have something that is acknowledged now as a standard of practice.”
20 June, 18:50 BST
Benefit-risk consideration regarding paclitaxel devices is discussed amongst the panel. Citing a significant number of sources and data demonstrating clear benefit, with the meta-analysis “on the other side of the scale” demonstrating risk, Todd Rasmussen maintains that while the meta-analysis was “extremely well done and is highly important, […] continued marketing of the paclitaxel-coated devices for patients with symptomatic SFA disease should be allowed.”
Joaquin Cigarroa similarly argues that paclitaxel provides a proven “very consistent and clinically profound benefit” to a patient population that greatly needs it. Krucoff adds to this point that the patient perspective is at the centre of this discussion of weighing up the benefits and the risks. He says, “how to clarify the risk and what the risk really is—I think that conversation really needs to go forward.” Several comments across the panel agree that the conversation with patients clarifying these risks and guiding them to weigh up short-term and long-term impacts effectively, underlining that patient agency and choice should be available. Philip Posner further highlights that from his personal perspective, “when you talk to the patient, you have to have the patient learn what the risk really is, what can be done to modify that risk, and then what is the reward.”
Nevertheless, John Hirshfeld argues that the FDA “cannot just walk away from this and say it is ok”, but rather provide some real guidance and continue to collaborate on this issue.
John Somberg states “I don’t think anyone is talking about taking the device off the market. The question most concerning the signal is the risk-benefit ratio.”
20 June, 19:30 BST
With regards to post-market studies and surveillance, the FDA panel reviews the recommended objectives of future trials, what data should be collected, study endpoints and study design.
Karla Ballman emphasises to this point, “I do not think the registries that are in place or the Medicare data are adequate for assessing sort of the signal long term, just because of all the biases in there.” Panel members further stress the importance of intervening in ongoing trials, to highlight the importance of follow-up to five years rather than a one-year endpoint.
“I think there are 21st century way of going forward”, Krucoff says, “is collaboratively using registry-based prospective randomization if that was the best fit. That would ease the burden, increase the speed, reduce the cost, even share the cost, and whatever device is used, let it be used.”
John Somberg points to SWEDEPAD and the potential significant data this trial could provide, once enrolment resumes. Karla Ballman and Mitchell Krucoff both put forward that the quickest, most cost-effective way to gain more insight is by pushing for current ongoing prospective registry trials and other studies to attempt to close the gap of missing data.
Richard Lange summarises, there are data that are available already which has some limitations, from randomised controlled trials. In addition, “there are studies that are either just initiated or ongoing, and I would push those studies to get the information we need, primarily mortality data is what we’re interested in, so long-term follow up. I’ve heard the word collaboration from everybody in the panel. And from industry as well. Because I don’t think anyone wants to tackle this or can tackle it by themselves.”
He adds that importantly, the opinion on the value of registry-derived data is varied across the scientific community.
20 June, 19:50 BST
Discussing potential modifications to labelling of approved paclitaxel devices, Bram Zuckerman asks, “how can we update the labelling, in a transparent fashion that will be of use to practicing physicians and patients who read the label?”
Joaquin Cigarroa responds, the labelling must incorporate the sentiment that “there may—not that there is—a late mortality signal, should be included.” John Somberg contends, however, that a long and non-unidirectional message showing the totality of data would not be read by physicians, and not understood by patients. Instead, Somberg states “if we think there is a signal”, the label should read “something simple in layman’s terms that uses the word ‘may'”.
20 June, 20:00 BST
The panel discusses specific study designs to better evaluate paclitaxel devices for PAD. Firstly, the panel agrees that studies “should not end at 12 months”, but rather continue to collect data out to three or five years.
Zuckerman clarifies, “What we’re asking is for a new PMA device, given what you said, you would wait until we have five years safety results for a new paclitaxel drug-eluting stent.” Ballman responds that while one year is acceptable to determine benefit and efficacy, safety needs to be assessed with long-term follow-up. Cigarroa adds, “I would follow under one year for efficacy, with additional teeth, and attention to the detail of ascertainment to subsequent clinical events with a methodology and an adjudication process that we can feel confident through five years.”
To this point, Lange underlines the “teeth” required, to ensure the data is collected and distributed rigorously to regulatory bodies.
Furthermore, the Todd Rasmussen suggests that as dosing mechanism understanding is evolving, future studies may need to separate DCBs from DES. Kevin Kip meanwhile states that “Any new study must place a premium on paclitaxel exposure prior to the index procedure, and after the index procedure, so that you know that over the course of time and follow-up, who was exposed and who wasn’t.” Kip further adds that adjudication must be added into budget consideration, as it is a time-consuming and costly, but important, effort.
Bram Zuckerman states, “Unfortunately, we have a signal here that remains undetermined. One of the reasons why is that the death adjudication uniformly in these FDA trials was poor.” He summarises, “going forward, mortality will be given a higher priority, and we will need to think about how it can be best assessed and adjudicated.”
Finally, Zuckerman suggests, “I think the basic thing that we’re looking at in this question is a whole rethink of the clinical trial design and execution in this field potentially making it more uniform, which should add efficiencies and better understanding of the data.” Todd Rasmussen agrees “we need to think of new creative ways to do clinical studies in the future”, and produce common data elements.
20 June, 20:25 BST
Based on the available data, the panel discusses whether their recommendations may be applicable to paclitaxel devices with other indications for use. Responding, John Somberg reiterates the importance of analysing efficacy at one year and safety follow-up of three to five years.
With regards to dialysis and CLI patients, the panel suggests that benefit-risk considerations “may be different” for these populations, either because of mechanism or because of longevity of the patient populations affecting risk tradeoffs. Nevertheless, Lange underlines that providing thorough information to the patient is essential to informed consent and patient choice.
Concluding the meeting, Bram Zuckerberg states that the two-day meeting and presentation has been “extremely helpful” for the FDA, who will now consider the analysis of the panel, and “look forward to continued collaboration in this field.”
The US Food and Drug Administration (FDA) has granted 510(k) clearance for the Impede-FX embolization plug (Shape Memory Medical). This device is available in three sizes, the largest having an expanded diameter of 12mm. In 2018, the Impede-FX received CE mark approval in Europe, where it has been available through a limited commercial release in Germany and The Netherlands.
According to Shape Memory Medical, the device is an adjunct to the company’s Impede embolization plug, which previously received FDA clearance, and is indicated to obstruct or reduce the rate of blood flow in the peripheral vasculature.
The Impede product family features the company’s Shape Memory Polymer (SMP) technology. SMP is a porous polymeric material capable of changing from a smaller, catheter-deliverable shape to a “memorised” larger, conformable shape when delivered into a blood vessel.
The halted BASIL-3 study now plans to resume enrolment of patients into the randomised controlled trial, which is comparing balloon angioplasty versus stenting for severe ischaemia in the legs of patients with peripheral arterial disease (PAD). Two of the three trial arms use paclitaxel-coated or -eluting devices.
The update from the investigators summarises the decision to move forward with the trial, stating: “The BASIL-3 team and the HTA met on the 4th June to discuss the future of the trial and the new statement from the MHRA. The Trial Steering Committee, patients and the HTA have all expressed support in re-opening BASIL-3 to recruitment.
“In light of this, we are planning to re-open BASIL-3 to recruitment following ethics approval by mid to late September of this year. We will keep you informed of all new information and actions as to how we will progress with the trial.”
Giving the background for this decision, the update states the trial was suspended to recruitment in December 2018 following a meta-analysis published in the Journal of the American Heart Association, which indicated a trend to increased mortality for PAD patients receiving paclitaxel-coated and -eluting devices. The BASIL-3 statement points out that 89% of the patients in the meta-analysis had intermittent claudication, and not critical limb ischaemia.
“As of the 4th June 2019, the independent Expert Advisory Group (EAG) established by the MHRA released a report stating that the use of paclitaxel-coated balloons and paclitaxel-eluting stents should still be considered in patients with limb threatening ischaemia and specifically states the BASIL-3 trial should consider resuming recruitment,” the BASIL-3 update notes.
“The MHRA have agreed with the EAG, as per the Medical Device Alert (MDA) (MDA/2019/023) released on 4thJune 2019 confirming the use of these devices is still an appropriate option in accordance with NICE guidance for patients with critical limb ischaemia.”
Lastly, the BASIL-3 update also points to the Global Vascular Guidelines, which have released new guidelines on the management of critical limb ischaemia, and in particular highlights a statement from the guidelines on the safety of paclitaxel-eluting devices:
“…the risks and benefits of treatment for CLTI, including drug-eluting devices, need to be examined with appropriately controlled prospective studies that are specific to the CLTI population, the execution of randomised controlled-trials involving PTX-eluting devices in CLTI, with appropriate safety monitoring and regulatory oversight are important to the vascular community.” Page 104S, Conte et al, GVG on management of CLTI June 2019
The Global Vascular Guidelines document is endorsed by the Vascular Society of Great Britain and Ireland (VSGBI) and British Society of Interventional Radiology (BSIR). Andrew Bradbury, principal investigator of the BASIL trials, is also one of the three co-editors of the guidelines, representing the World Federation of Vascular Societies.
The methodology underpinning the conclusion by Konstantinos Katsanos (Patras, Greece) et al that there is a positive dose-response relationship between paclitaxel and mortality is flawed, argues Andrew Holden (Auckland, New Zealand) and colleagues in a paper published in the Journal of Endovascular Therapy (JEVT). Holden and co-authors list the limitations they see in the summary level meta-analysis published in December 2018 in the Journal of the American Heart Association (JAHA), and call for physicians to “significantly modify the way vascular device trials are performed in the future”.
In the JAHA meta-analysis, Katsanos et al linked paclitaxel-coated balloons and paclitaxel-eluting stents to all-cause mortality, reporting a significant increase in deaths at two and five years in the cohort of femoropopliteal disease patients exposed to the drug compared to those treated who were not. Holden et al write: “Although no plausible mechanism of action was identified, the authors postulated that the excess mortality was caused by paclitaxel”.
However, Holden and colleagues do not find this correlation with paclitaxel levels and mortality, and thus claim there is no causative link between dose and death.
On 15 March 2019, the US Food and Drug Administration (FDA) released an updated letter to healthcare providers detailing that while the results of their preliminary review of the JAHA meta-analysis data was ongoing, they had “identified a potentially concerning signal of increased long-term mortality in study subjects treated with paclitaxel-coated products compared to patients treated with uncoated devices”. The statement also noted that each of the trials used “all-cause” mortality calculation methods that differed significantly and had the potential to influence the way those results were interpreted.
The three pivotal premarket trials evaluating paclitaxel-coated products for the treatment of peripheral artery occlusive disease that informed this statement—Medtronic IN.PACT SFA I and II; Cook Zilver PTX; and BD LEVANT 2 randomised controlled trials—each used a different methodology to calculate mortality. “To facilitate a direct mortality comparison between the three trials”, Holden and colleagues write that they “asked each of the companies to provide five-year mortality using the same proportional methods as used by Medtronic [calculated as the number of patients who died divided by the number of patients followed up to five years]”.
Explaining the rationale behind this strategy, Holden et al say: “This consistent methodology allowed for a direct comparison of product dose to test the dose-response theory proposed by the meta-analysis. The highest five-year mortality was found to be associated with the lowest paclitaxel dose device (Zilver PTX), while the lowest mortality was associated with the highest dose device (IN.PACT). It is our view that this directly refutes the causal relationship theory between paclitaxel dose and all-cause mortality.”
Using this proportional method, the investigators report no significant difference in the five-year mortality between paclitaxel-coated balloons compared to controls in the Medtronic IN.PACT and BD LEVANT 2 trials. The Zilver PTX DES displayed a significant difference (p=0.008) between the arms. When the Zilver PTX randomised controlled trial five-year data are reanalysed by an intention-to-treat analysis, the mortality of the paclitaxel-eluting stent remains the highest (22.7%) of the three paclitaxel devices, but the mortality difference compared to the control arm (18.5%) loses its significance (p=0.45).
As patients previously lost to follow-up are contacted and potentially added into the analysis, the proportional calculation may differ (as the denominator, number of patients follow-up to five years, will increase), though the study authors do not think this will change the outcome. Commenting on these findings, Holden and colleagues say: “We believe it is likely, even with more complete patient follow-up, that the lack of correlation between paclitaxel dose and mortality will persist”. They suggest a Kaplan Meier survival plots could be calculated in the future, if more data were collated.
As Holden et al believe the causation theory behind paclitaxel and mortality “now appears unlikely”, they suggest several alternative hypotheses to explain the original JAHA meta-analysis results, including performance and detection bias, trials being inadequately powered for mortality, significant target lesion crossover from the control to treatment arms, and patients lost to follow-up.
They conclude: “Perhaps the most important lesson from this paclitaxel debate may be the need to reconsider and significantly modify the way vascular device trials are performed in the future. We believe there should be an additional emphasis placed on adherence to guidelines-based medical therapy of all enrolled patients as well as safety endpoints such as mortality. Greater effort must be made to reduce subjects lost to follow-up and properly classify the mortality status of those subjects who withdraw.
“It is only with well-conducted safety evaluations that we will completely clarify this issue regarding paclitaxel. Given the known and undisputed benefits of paclitaxel coating on stents and angioplasty balloons, we owe it to our patients to pursue that truth before we restrict these devices from use.”
The medical community awaits an individual patient data meta-analysis to provide greater clarity regarding the alleged link between paclitaxel and mortality.
The methodology underpinning the conclusion by Konstantinos Katsanos (Patras, Greece) et al that there is a positive dose-response relationship between paclitaxel and mortality is flawed, argues Andrew Holden (Auckland, New Zealand) and colleagues in a paper published in the Journal of Endovascular Therapy (JEVT). Holden and co-authors list the limitations they see in the summary level meta-analysis published in December 2018 in the Journal of the American Heart Association (JAHA), and call for physicians to “significantly modify the way vascular device trials are performed in the future”.
In the JAHA meta-analysis, Katsanos et al linked paclitaxel-coated balloons and paclitaxel-eluting stents to all-cause mortality, reporting a significant increase in deaths at two and five years in the cohort of femoropopliteal disease patients exposed to the drug compared to those treated who were not. Holden et al write: “Although no plausible mechanism of action was identified, the authors postulated that the excess mortality was caused by paclitaxel”.
However, Holden and colleagues do not find this correlation with paclitaxel levels and mortality, and thus claim there is no causative link between dose and death.
On 15 March 2019, the US Food and Drug Administration (FDA) released an updated letter to healthcare providers detailing that while the results of their preliminary review of the JAHA meta-analysis data was ongoing, they had “identified a potentially concerning signal of increased long-term mortality in study subjects treated with paclitaxel-coated products compared to patients treated with uncoated devices”. The statement also noted that each of the trials used “all-cause” mortality calculation methods that differed significantly and had the potential to influence the way those results were interpreted.
The three pivotal premarket trials evaluating paclitaxel-coated products for the treatment of peripheral artery occlusive disease that informed this statement—Medtronic IN.PACT SFA I and II; Cook Zilver PTX; and BD LEVANT 2 randomised controlled trials—each used a different methodology to calculate mortality. “To facilitate a direct mortality comparison between the three trials”, Holden and colleagues write that they “asked each of the companies to provide five-year mortality using the same proportional methods as used by Medtronic [calculated as the number of patients who died divided by the number of patients followed up to five years]”.
Explaining the rationale behind this strategy, Holden et al say: “This consistent methodology allowed for a direct comparison of product dose to test the dose-response theory proposed by the meta-analysis. The highest five-year mortality was found to be associated with the lowest paclitaxel dose device (Zilver PTX), while the lowest mortality was associated with the highest dose device (IN.PACT). It is our view that this directly refutes the causal relationship theory between paclitaxel dose and all-cause mortality.”
Using this proportional method, the investigators report no significant difference in the five-year mortality between paclitaxel-coated balloons compared to controls in the Medtronic IN.PACT and BD LEVANT 2 trials. The Zilver PTX DES displayed a significant difference (p=0.008) between the arms. When the Zilver PTX randomised controlled trial five-year data are reanalysed by an intention-to-treat analysis, the mortality of the paclitaxel-eluting stent remains the highest (22.7%) of the three paclitaxel devices, but the mortality difference compared to the control arm (18.5%) loses its significance (p=0.45).
As patients previously lost to follow-up are contacted and potentially added into the analysis, the proportional calculation may differ (as the denominator, number of patients follow-up to five years, will increase), though the study authors do not think this will change the outcome. Commenting on these findings, Holden and colleagues say: “We believe it is likely, even with more complete patient follow-up, that the lack of correlation between paclitaxel dose and mortality will persist”. They suggest a Kaplan Meier survival plots could be calculated in the future, if more data were collated.
As Holden et al believe the causation theory behind paclitaxel and mortality “now appears unlikely”, they suggest several alternative hypotheses to explain the original JAHA meta-analysis results, including performance and detection bias, trials being inadequately powered for mortality, significant target lesion crossover from the control to treatment arms, and patients lost to follow-up.
They conclude: “Perhaps the most important lesson from this paclitaxel debate may be the need to reconsider and significantly modify the way vascular device trials are performed in the future. We believe there should be an additional emphasis placed on adherence to guidelines-based medical therapy of all enrolled patients as well as safety endpoints such as mortality. Greater effort must be made to reduce subjects lost to follow-up and properly classify the mortality status of those subjects who withdraw.
“It is only with well-conducted safety evaluations that we will completely clarify this issue regarding paclitaxel. Given the known and undisputed benefits of paclitaxel coating on stents and angioplasty balloons, we owe it to our patients to pursue that truth before we restrict these devices from use.”
The medical community awaits an individual patient data meta-analysis to provide greater clarity regarding the alleged link between paclitaxel and mortality.
Christof M Sommer, Thilo Hackert and Götz M Richter discuss the renaissance of Lipiodol-based lymphangiography following a decline in its use in lymphatic interventions at the start of the millennium. They cite this return to Lipiodol (Guerbet) as being directly connected to an increase in the number of patients suffering from lymphatic leakage caused by complex surgical procedures, labelling the contrast agent “indispensable” in a lymphatic interventions programme. The rise in Lipiodol usage is here to stay, they argue.
Introduction
The story of Lipiodol-based lymphangiography and lymphatic interventions starts in 1901, when the French pharmacist Marcel Guerbet synthesised Lipiodol, an iodinated poppy seed oil, today commercialised as Lipiodol Ultra Fluid. After the accidental discovery of lymphangiography during routine hystersalpingography by Charles Várady, an enormous amount of specific knowledge and skill accumulated. During the 20th century, Lipiodol-based lymphangiography was excessively used as a diagnostic procedure. Around the turn of the millennium, however, the numbers of patients undergoing lymphangiography decreased considerably, most likely since alternative noninvasive imaging modalities such as MRI became available. In the following years, interest in and competence to perform lymphangiography got lost in hospitals around the world. Interestingly, during the last decade, the pendulum swung back, and a high demand for diagnostic and therapeutic lymphangiography was noted. We believe that this phenomenon is directly connected to the increasing number of patients suffering from therapy-refractory lymphatic leakage caused by surgical procedures of great complexity. Today, Lipiodol is indispensable for all institutions with a lymphatic interventions programme.
Patient with a space occupying iliac lymphocele (asterisk) after kidney transplantation (arrowhead) (Figure 1, top left); 29 days after positioning of a percutaneous drainage (arrowhead) (Figure 2, bottom left), conventional lymphangiography was performed with 18ml Lipiodol demonstrating the different morphological signs of lymphatic leakage including lymphopseudoaneurysm (white asterisk) and pathologic lymph vessels with Lipiodol extravasation (white arrowhead) as well as afferent lymph nodes (black asterisk) and lymph vessels (black arrowhead) (Figure 3, top right); CT lymphangiography immediately after conventional lymphangiography is regularly performed in our centre to visualize the lymphatic leakage (arrowheads) (and targets for a potential second-line lymphatic intervention) with best spatial resolution and dedicated 3D image resonstruction (Figure 4, bottom right)
Indications and outcomes
Lipiodol-based lymphangiography and lymphatic interventions can cure different types of highand low-output iatrogenic (for example, chylous ascites after ultra-radical lymphadenectomy) and spontaneous (for example, pulmonary lymphatic perfusion syndrome) lymphatic leakages. Typically, lymphangiography is performed either with the transpedal or intranodal application of Lipiodol under X-ray imaging, with the following outcome parameters: technical success rate of 90–100%, Lipiodol injection volume of 0.5–40ml, Lipiodol injection speed of 0.3–60ml/hour, complication rate of 0–22%, 30-day procedure-related morbidity and mortality rates of 0% and 0%, respectively, and clinical success rate of 51–100% for transpedal lymphangiography and 33–100% for intranodal lymphangiography (according to the literature published between January 2007 and May 2017, and for patients suffering from post-operative therapy-refractory lymphatic leakage). Second-line lymphatic interventions, feasible on the same day as, or a few days after, Lipiodol-based lymphangiography, include many different procedures, such as interstitial embolization or thoracic duct embolization. Outcome parameters include technical success rate of 89–100% for interstitial embolization and 50–100% for thoracic duct embolization, Lipiodol/cyanoacrylatebased medical glue injection volume of 0.5–8ml, Lipiodol/cyanoacrylate-based medical glue mixing ratio of 1:2–20:1, complication rate of 0–22%, 30-day morbidity and mortality rates of 2% and 0%, respectively, and clinical success rate of 80–100% for interstitial embolization and 90–100% for thoracic duct embolization.
In this case, a typical interstitial embolization procedure was performed as second-line lymphatic intervention due to a persistent drainag volume of >100ml/day (Figure 5-7; top left, bottom left and top right); CT before interstitial embolization demonstrating the persistance of Lipiodol within the lymphatic leakage (arrowheads) (Figure 5, top left); after injection of a total amount of 6.5ml cyanoacrylate based medical glue/Lipiodol 1:1 mixture via lymph nodes (and after direct embolization of one fistula point,) optimal distribution of the embolic material within afferent lymph nodes (asterisk) (Figure 6 and 7, bttom left and top right) and afferent lymph vessels (arrowhead) (Figure 6 and 7, bottom left and top right); radiography control two days after second-line lymphatic intervention demonstrating persistent blockage of the afferent lymph nodes (asterisk) and lymph vessels (arrowhead) (Figure 8, bottom right); After documentation of the complete resolution of the lymphocele applying ultrasound and persistance of the drainage volume, the drainage could be removed four days after second-line lymphatic intervention; Up to now (after four months follow-up), the patient presents clinically stable.
Conclusions
Lipiodol plays a key role in lymphangiography and lymphatic interventions. For patients with iatrogenic and spontaneous lymphatic leakage, Lipiodol is the only pharmaceutical drug approved for radiological imaging of the lymphatic system. Following the application of Lipiodol, fluoroscopy, radiography and, in particular, computed tomography enable the precise visualisation of the different types of lymphatic leakages. Looking at published data, in conjunction with our long-standing experience at Stuttgart and Heidelberg—more than 600 transpedal lymphangiographies performed over the last three decades—it becomes evident that Lipiodol unquestionably features not only important diagnostic, but also therapeutic, characteristics. Selective and persistent blockage of the diseased lymphatic vessels and sterile inflammation reactions with subsequent tissue scarring result regularly in the cure of lymphatic leakage. Lipiodol is also mandatory for second-line lymphatic interventions. Doxycycline- or ethanol-based sclerotherapy and EVOH (ethylene vinyl alcohol)-based liquid embolization show non-satisfying outcomes, especially in the setting of high-output lymphatic leakage, and therefore cyanoacrylate-based medical glue is regularly used instead. Not only for X-ray visualisation issues, but also for the specific adjustment of glue polymerisation time, Lipidodol is mixed with cyanoacrylate-based medical glue in different ratios.
Future directions
Lipiodol-based lymphangiography can be performed as a highly standardised and safe diagnostic and therapeutic radiological treatment. Second-line lymphatic interventions are associated with a higher degree of technical failure, complications, and morbidity, but also with a higher degree of clinical success. Currently, lymphangiography and lymphatic interventions are performed only in specialised centres, and not as nationwide primary care. This is the result of limited theoretical and practical knowledge in the radiological and referring community. Optimised radiological strategies, together with interdisciplinary consensus, should be published in the form of guidelines with the intention of promoting the best lymphatic care. The first steps towards achieving the strong evidence base have already been taken, with a prospective, randomised controlled multicentre trial currently being performed in South Korea, comparing interstitial embolization using Lipiodol and cyanoacrylate-based medical glue versus sclerotherapy in the management of symptomatic postoperative pelvic lymphocele. Nevertheless, the optimal pharmaceutical drug for second-line lymphatic interventions has not been developed yet. There have been speculations as to whether different versions of Lipiodol with even higher viscosity or a Lipiodol containing non-adhesive precipitating liquid embolic could further increase safety and efficacy. We have witnessed the successful renaissance of Lipiodol in lymphangiography; however, the reincarnation of Lipiodol in second-line lymphatic interventions is still an important objective. In the future, the number of patients with lymphatic leakage undergoing radiological treatment will dramatically increase, as soon as different problems (such as communication barriers between medical disciplines and the under-reporting of candidates) are solved.
Christof M Sommer is an interventional radiologist at the Clinic of Diagnostic and Interventional Radiology and 1st Siemens European Reference Site for Interventional Oncology and Radiology, Klinikum Stuttgart, Stuttgart, Germany, as well as an assistant professor of radiology at the Clinic of Diagnostic and Interventional Radiology, Heidelberg University Hospital, Heidelberg, Germany. He has received a speaker honourary from Guerbet.
Thilo Hackert is a professor at and deputy head of the Department of General, Abdominal and Transplantation Surgery, Heidelberg University Hospital and section chief at the European Pancreas Center, Heidelberg University Hospital, Heidelberg, Germany. He has no conflict of interest to report.
Götz M Richter is a professor at and medical director of the Clinic of Diagnostic and Interventional Radiology and 1st Siemens European Reference Site for Interventional Oncology and Radiology, Klinikum Stuttgart, Germany. He has no conflict of interests to report.
A publishing agreement between the Society for Vascular Surgery (SVS) and BIBA Medical Ltd has been signed today by the respective directors at the Vascular Annual Meeting (VAM; 12–15 June, National Harbor, MD, USA). This collaboration makes BIBA Medical the new publisher of SVS’ publications—Vascular Specialist and Vascular Connections—from 2020.
Vascular Specialist—an official publication of the SVS—is issued 12 times a year, published on a monthly basis. The magazine is a source of US-relevant news, conference coverage, research review and opinions from thought leaders in the vascular field. Available in print and online, with fortnightly electronic newsletters, its current readership includes vascular surgeons, vascular neurologists, vascular medicine specialists and endovascular surgical neuroradiologists.
Today’s signing of the contract means SVS will continue to own Vascular Specialist and the brand but, from January 2020, subscribers will see BIBA Medical as the new publisher, who will produce, publish and distribute it in the various formats.
In the same spirit, the agreement maintains SVS’ ownership of Vascular Connections—another of its publications—and with BIBA Medical partnering with the paper’s production, printing and circulation from 2020. Providing coverage and highlights of VAM, Vascular Connections is SVS’ annual meeting newspaper and is published concurrently with and distributed at the SVS-hosted VAM.
Kenneth Slaw, executive director of SVS, told Interventional News: “I think this is going to be a tremendous advance for both organisations. Vascular Specialist is very important to us at SVS. This is our way of conveying important news.” He added, “What I’m really excited about is the enhanced and expanded ability that we are going to have to get our message globally, digitally and in a robust manner.”
SVS’ president, Michel Makaroun, agreed: “This is a great opportunity for both of us [SVS and BIBA Medical]. We are all excited about it.”
The alliance extends BIBA Medical’s publishing portfolio of the company’s own eight newspapers, adding to Interventional News and six sister publications—Vascular News, Venous News, NeuroNewsInternational, Spinal News International, Cardiac Rhythm News and Cardiovascular News—along with the recently launched iWounds News.
Stephen Greenhalgh, BIBA Medical’s business development director, enthused: “BIBA Medical is thrilled to have the opportunity to publish the Society for Vascular Surgery’s official newspaper, Vascular Specialist, for the next five years from January 2020. This is the first newspaper in BIBA’s publishing portfolio that exclusively targets the North American vascular community.”
“We are very excited to use the resources of BIBA and make it the best experience,” said Malachi Sheahan, medical editor of Vascular Specialist. “Just really very excited.”
New data presented at the 20th annual new cardiovascular horizons (NCVH) conference (29–31 May, New Orleans, USA) show positive results for VentureMed Group’s FLEX VP system.
The FLEX iDissection study utilised intravascular ultrasound (IVUS) to assess the reduction in the rate and severity of dissections in peripheral arteries when the FLEX vessel prep system (VentureMed Group) was used prior to angioplasty.
Fifteen patients were evaluated by angiogram and IVUS following treatment of femoropoplitealde novo or no-stent restenosis with the FLEX VP system and percutaneous transluminal balloon angioplasty (PTA). The patients had an average median baseline percentage stenosis of 77%; an average lesion length of 64±33mm; 40% had moderate/severe calcified vessels (PACSS score≥3); 40% were diabetic. Claudication was present in 73% of the patients.
Angiogram and IVUS images were obtained at baseline, post-FLEX VP System, and post-adjunctive PTA to evaluate the presence and grade of dissections. There were significantly fewer new dissections, as well as lower gradations in the circumference and depth patterns of new dissections, post-FLEX VP system and adjunctive PTA.
The majority of new dissections post-PTA, following vessel preparation with the FLEX VP system, involved mostly the intima, the innermost layer of the vessel, (78.4%) and were <180° in circumference (81.1%). Vessel preparation involving only the layers superficial to the internal elastic lamina may prevent restenosis.
“Dissections are grossly under-appreciated on angiogram when compared with IVUS. PTA causes dissections and stretching of the vessel to restore blood flow. However, the severity and depth of the dissections can contribute to restenosis,” comments lead investigator Nicolas W Shammas, (Midwest Cardiovascular Research Foundation, Davenport, USA). “This is a positive signal as these results showed a low rate of dissection after using the FLEX VP system with the majority of those dissections being lesser in depth and circumference.”
Also at NCVH, real-world data of 443 femoropopliteal cases reported from 104 operators in 70 health systems treating lesions of varying lengths (less than or equal to 8mm or greater than 8mm) were presented.
Speaking of this comparative review of the FLEX VP system in the treatment of femoropopliteal lesions of different lengths, Jason A Yoho (Heart and Vascular Institute of Texas, San Antonio, USA) says: “These data highlight the importance of the unique FLEX VP mechanism of action that provides acute luminal gain and improved vessel compliance to reduce PTA balloon opening pressures leading to meaningful clinical results. This real-world data on the use of the FLEX VP system is clinically relevant and important as we continue to evaluate options that may help patients achieve better clinical outcomes.”
The investigators found that the mean 28% improvement in luminal gain achieved by the FLEX VP system alone was consistent regardless of lesion length. Low PTA balloon opening pressures (averaging 4.7atm) suggest the FLEX VP system positively improves vessel compliance. A press release states that the FLEX VP system creates an ideal environment for PTA of choice and was shown to safely and effectively facilitate PTA of femoropopliteal stenosis of differing lengths.
Orchestra BioMed and Terumo have formed a global strategic partnership for the development and commercialisation of Virtue sirolimus-eluting balloon (SEB) in the percutaneous coronary and peripheral interventions field.
Virtue SEB is the first and only non-coated drug-eluting angioplasty balloon that delivers a proprietary bioabsorbable, sustained-release formulation of sirolimus, according to a press release, which also states that sirolimus is the gold standard drug for preventing restenosis following a percutaneous interventional procedure. In April, the US Food and Drug Administration (FDA) granted Virtue SEB breakthrough device designation for treatment of coronary in-stent restenosis, a cardiovascular condition that represents more than 10% of total interventional coronary procedures.
In a prospective study of very challenging in-stent restenosis patients, Virtue SEB demonstrated excellent angiographic results at six months as well as positive clinical outcomes out to three years. Orchestra BioMed plans to conduct a near-term US registrational trial for in-stent restenosis.
Under the terms of the agreement, Terumo will make a one-time, up-front payment of US$30 million and an equity commitment of US$5 million to Orchestra BioMed. Terumo will also make substantial future clinical and regulatory milestone payments to Orchestra BioMed.
• Terumo will also make a strong commitment to finance and execute a global clinical programme in collaboration with Orchestra BioMed to gain regulatory approval for commercial sale of Virtue SEB in multiple markets and indications.
• Orchestra BioMed will share meaningfully in future commercial revenues of Virtue SEB through royalties and per unit payments as the exclusive supplier of the proprietary sustained-release sirolimus formulation used in Virtue SEB.
• Orchestra BioMed retains the rights to develop and license technology used in Virtue SEB for clinical applications outside of coronary and peripheral vascular interventions.
Virtue SEB strengthens the current cardiovascular product offering of Terumo Interventional Systems, Terumo’s largest division, which includes a complete, solution-based product portfolio used in advanced coronary and peripheral endovascular treatments, with market-leading solutions for vascular access, lesion access and intervention. Orchestra BioMed and Terumo are seeking to make Virtue SEB the first drug-eluting balloon approved for coronary use in the USA. Orchestra BioMed expects to initiate a US registrational trial for Virtue SEB in in-stent restenosis under an investigational device exemption (IDE) from the FDA within the next year.
Virtue SEB is currently not approved in any market, but Terumo and Orchestra BioMed plan to conduct trials to support global regulatory approvals in indications including in-stent restenosis, small coronary vessels, peripheral artery disease below-the-knee and other indications. Terumo and Orchestra BioMed’s objective is to commercialise Virtue SEB in the USA, Japan, China, and other markets.
Cardiovascular Systems recently announced that the first patient has been enrolled in the REACH PVI study. The purpose of this study is to prospectively evaluate acute clinical outcomes of orbital atherectomy via transradial access for the treatment of peripheral artery disease (PAD) in lower extremity lesions.
According to a press release, the company’s low profile, 5Fr, Extended Length Diamondback 360 Peripheral Orbital Atherectomy System (OAS) and Extended Length Stealth 360Peripheral OAS are the only atherectomy devices that allow radial access for the treatment of peripheral lesions.
National Primary Investigator for REACH PVI, Ankur Lodha, interventional cardiologist at the Cardiovascular Institute of the South in Lafayette, USA, enrolled the first patient.
Lodha said, “When endovascular intervention is necessary, PAD lesions are mostly treated through femoral artery access. However, many PAD patients could benefit from faster ambulation time post procedure that radial artery access offers. In addition, some patients may have comorbidities, such as obesity, that complicate or preclude femoral access.”
Lodha continued, “The benefits of radial access for percutaneous peripheral vascular interventions are well documented. We believe this study will demonstrate that many of these known benefits, such as low complication rates, high cost effectiveness, and short time to ambulation, can be achieved using orbital atherectomy to treat lower limb PAD lesions through radial access.”
Scott Ward, CSI chairman, president, and chief executive officer, said, “CSI continues to innovate and develop medical evidence to improve the care of patients suffering from PAD. The commercialisation of the Extended Length orbital atherectomy systems and our investment in REACH PVI both demonstrate our commitment to physicians and the patients they serve.”
About REACH PVI
REACH PVI is a prospective, observational, single-arm, multicentre post-market study that will enrol 50 patients at up to 10 sites across the USA. The purpose of this study is to prospectively evaluate acute clinical outcomes of orbital atherectomy via transradial access for treatment of peripheral artery disease (PAD) in lower extremity lesions. The study will include CSI orbital atherectomy devices FDA-cleared for treatment of PAD. All subjects will be followed post-procedure through the first standard of care follow-up visit (7–45 days post-procedure).
A new indication for Lipiodol Ultra Fluid (Guerbet) has been approved in Switzerland and in India for chemoembolization (cTACE) of tumours in adults with known intermediate-stage hepatocellular carcinoma (HCC).
HCC is the most common primary liver cancer and is the 4th leading cause of annual cancer death worldwide.
“Guerbet is proud to have received approval for this new indication for Lipiodol Ultra Fluid. This is evidence of our commitment to making cTACE available to as many HCC patients as possible,” says Thomas Bonnefont, Guerbet’s vice president for Interventional Imaging. “Development of these image-guided procedures is a top priority for Guerbet’s interventional imaging franchise as we work to enhance liver cancer patients’ prognosis and quality of life worldwide.”
Lipiodol Ultra Fluid is used for cTACE, a minimally invasive procedure which consists of mixing Lipiodol Ultra Fluid with an anticancer drug, to treat patients with unresectable liver tumours. The mixture is injected trans-arterially in the liver as a loco-regional targeted chemotherapy for unresectable liver tumors (HCC). Lipiodol Ultra Fluid acts as a contrast agent, a drug-eluting vehicle, and a dual arterio-portal transient embolic.
cTACE indication is now approved in EMEA (Austria, Belgium, Czech Republic, France, Hungary, Iran, Ireland, Luxemburg, The Netherlands, Portugal, Switzerland, Turkey), APAC (Cambodia, Hong Kong, India, Mongolia, New Zealand, Philippines, South Korea, Taiwan, Thailand, Vietnam), and Latin America (Argentina, Brazil, Mexico, Peru).
HCC imaging indication is now approved in Canada, Germany and in the USA.
cTACE has been recognised as the gold standard for the treatment of patients with intermediate-stage HCC by several international clinical consensuses. These consensus guidelines unanimously recommend cTACE as the standard-of-care for patients with intermediate-stage HCC. cTACE has strong recommendation and high leave of evidence for patients at BCLC stage B in European guidelines. Consequently, treatment with cTACE is constantly increasing on all continents, with more than 400,000 patients being treated every year, a Guerbet press release states.
Endologix recently announced that the EC Certificate of Conformity (CE mark) for the Nellix endovascular aneurysm sealing system (Nellix system) has been reinstated by GMED, the EU Notified Body for the Nellix system. The reinstatement followed an assessment of clinical evidence.
“We continue to believe that the Nellix system has the potential to transform the treatment of patients with infra-renal abdominal aortic aneurysms,” said Matt Thompson, chief medical officer of Endologix.
He continued: “This therapy continues to generate positive results when used in patients that conform to the anatomical indications for use. We are delighted that the available data supports the reinstatement of our CE mark, and we look forward to utilising this technology to improve the patient experience and drive better outcomes.”
As previously disclosed, the Nellix system will be made available for use at approved centers in a post-market clinical investigational setting outside the USA. Within the USA, the Nellix System remains an investigational device as part of the EVAS2 study.
The company does not expect this reinstatement to impact its previously communicated financial guidance for 2019.
Post-procedural antibiotic use does not significantly affect infectious complication rates following uterine fibroid embolization (UFE), a recent pilot study concludes. Presenting these data at the Global Embolization Oncology Symposium Technologies (GEST; 9–12 May, New York, USA), Omar Chohan (Christiana Care Health System, Newark, USA) told attendees that, in the small study group under investigation, foregoing post-treatment antibiotics did not result in an increased rate endomyometritis.
However, Chohan acknowledges that the cohort is under-powered to demonstrate non-inferiority of the study group, and thus believes that the present pilot study serves as a model for a larger scale study evaluating the necessity of post-UFE antibiotics.
Chohan and colleagues set out to evaluate the necessity of prophylactic post-procedural administration of antibiotics after UFE in the prevention of procedure-related infections. According to Chohan, current guidelines from the Society of Interventional Radiology (SIR) report limited data regarding antibiotic use and state that prophylaxis is at the “discretion of the treating hospital”, though preprocedural antibiotic use is recommended. Cohan also informs GEST delegates that, as cited in multiple studies, the role of post-procedural prophylactic antibiotic treatment is controversial. “There has been no study confirming whether we need it or not”, Chohan claimed.
The study investigators therefore conducted polling of 92 academic interventional radiology practices in the USA to determine whether or not they used post-procedural antibiotics following UFE. Of 27 responses, ten did and seventeen did not. Of the ten centres that did use post-procedural antibiotics, one used Levaquin/ Flagyl, seven used Ciprofloxacin, and two used Doxycycline.
Following this survey, Chohan and colleagues conducted their pilot study. Two-hundred-and-ninety-three patients undergoing UFE at a single community centre between June 2014 and June 2018 were enrolled in a retrospective cohort study, and divided into a control group and a treatment group. In the control arm, 144 patients were given both preprocedural and post-procedural antibiotics (the latter being oral Ciprofloxacin and 500mg BID over seven days). Meanwhile, the 149 patients in the study group were only given preprocedural antibiotics. There were no significant differences regarding patient demographics or procedure details between the two groups.
In adherence with the SIR guidelines, Chohan and colleagues administered a single dose of pre-procedural antibiotics to all patients. The primary endpoint of the study was infection rate (endomyometritis) within 90 days of the procedure. Embolization was performed using either Embospheres (Merit Medical) or Embozene (Boston Scientific). Ninety-day follow-up data were collected.
The difference in infection rates between the two groups was not statistically significant (p=1): one patient (0.7%) in the post-procedure antibiotic group had sepsis nine days after UFE and was treated with hysterectomy; two patients (0.7%) in the study arm had malodorous discharge at 10 and 15 days, respectively, after the treatment, and were subsequently treated with antibiotics.
Contextualising these findings, Chohan said at GEST that most major and minor infectious complications present within the first month following UFE. Minor complications, he commented, which occur in 0.2–5.9% of patients, often do not necessitate hospitalisation, the intravenous administration of antibiotics, or surgical intervention. Major infectious complications include pelvic abscesses (experienced by 0.3% of patients), septicaemia, and emergency myomectomy or hysterectomy (reported in 1.2–2.6% patients).
Chohan argues that this research is timely and important, given the global conversation regarding the risks of over prescribing antibiotics. He commented: “I think the standard of not using those post-procedural antibiotics makes sense, because otherwise you are giving patients an antibiotic that might alter their gut bacteria or you may inadvertently be increasing antibiotic resistance”.
The US Food and Drug Administration (FDA) has approved expanded sizes of the Lutonix 018 drug-coated balloon (DCB) to treat long superficial femoral artery lesions in patients with peripheral arterial disease.
According to a press release, the Lutonix 018 DCB provides clinicians with a variety of longer sizes allowing more options for 7mm diameter vessels. This includes four new lengths: 80mm, 100mm, 150mm and 220mm. The Lutonix 018 DCB is designed to perform over small guidewires, reduce guidewire exchanges and enable alterative access sites.
Lutonix 018 DCB is available in the USA, and is currently undergoing the regulatory approval process in Europe.
A recent publication confirms “the utility of touchless image navigation in the sterile field in facilitating decision-making and resource allocation during endovascular procedures.” The study, published in Minimally Invasive Therapy & Allied Technologies, provides the third clinical review of TIPSO technology (NZ Technologies), a human-computer interaction based platform that allows real-time access to imaging data in the sterile field.
Lead author Behrang Homayoon (Department of Radiology, Surrey Memorial Hospital, Surrey, Canada) contextualises what he sees as the clinical need for this technology, writing: “The inability to have comprehensive access to all pertinent imaging data related to an endovascular procedure in the sterile field is an unmet need, and its absence may have deleterious effects on decision-making, outcomes and workflow. Current image navigation solutions rely on traditional personal computing interfaces which are difficult to use in the sterile field. Innovative technological solutions are needed to address this need.”
In Homayoon et al’s study, the investigators conducted a case-based observational review of the TIPSO technology’s use in the endovascular suite. The study authors report findings that demonstrated the utility of the product in decision-making and resource allocation, “while avoiding the cognitive and workflow disturbances inherent in leaving the sterile field or involving non-scrubbed third persons in the image navigation process.”
They conclude: “Physician engagement and ‘needs-based’ technological innovation is needed to improve human-computer interaction in the endovascular suite, in hopes of positively affecting procedural decision-making, outcomes, and workflow.”
TIPSO technology
According to an NZ Technologies press release, the touchless control capability of TIPSO is enabled by a unique bedside interface designed for touchless interaction with patient images, obviating the need to delegate the task to an assistant, or un-scrub and use an imaging workstation outside the sterile space.
Homayoon comments: “Our study shows that TIPSO significantly improves physician interaction with—and access to—medical images, providing an impressive enhancement to procedures conducted in the endovascular suite. With safety and efficiency in mind, the use of TIPSO contributes to the adoption of best practices, and improves the quality of patient care and outcomes.”
This latest paper joins two others that present the results of an evaluation of the technology in a range of cases. Collectively, the three reports found that the TIPSO technology contributes by improving workflow in a number of different medical procedures by minimising the episodes of scrubbing-out for image review outside the angio suite, thereby reducing overall procedural time. The articles also reported a reduced use of contrast agent, lowered radiation exposure, and increased procedural precision—all advantages that support better patient outcomes.
Future wireless–touchless applications under NZ Technologies
With an increasing amount of equipment and tools in the operating room that require precision control, the future operating room warrants a centralized technology platform that enables on-demand interaction and automation, all while minimizing the clinician’s burden and effort. This would include such routine tasks as raising or lowering the operating bed height, adjusting room light levels, controlling robotics, and managing gas levels. According to Nima Ziraknejad, founder and CEO of NZ Technologies: “We are driven by our vision to revolutionise the way in which clinicians interact with their operative environments. TIPSO is just the beginning of our development of technologies for the operating room of tomorrow, all aimed at delivering automated, touchless control as the standard of care.”
David Liu, (Department of Radiology, University of British Columbia; Vancouver General Hospital, Vancouver, Canada), was senior author of two of the recent TIPSO studies. He explains, “The modern operating theatre has many distractions arising from simultaneous data, imaging and clinical feeds that can affect the concentration of the surgeon or operator, especially while performing technically or mentally demanding manoeuvres. TIPSO helps usher in a new era in which, as operators, we are taking back our mental bandwidth and allowing clinicians to focus on the important work at hand: saving lives and improving the health of patients.”
Four years ago, vascular experts from around the world had a “quixotic quest”, to get all surgeons and providers to agree on the best ways to treat a common and debilitating illness: chronic limb-threatening ischaemia. The goal has come to fruition, the Society for Vascular Surgery (SVS) have announced, with the publication of the new global guidelines, produced by the European Society for Vascular Surgery (ESVS), SVS, and the World Federation of Vascular Societies (WFVS).
Chronic limb-threatening ischaemia (CLTI)—the term now adopted for what is also known as critical limb ischaemia—is the end-stage of peripheral vascular disease. Patients with CLTI are at risk of amputation or even death from the effects of vascular disease.
Co-editors were Michael Conte from the Society for Vascular Surgery, Philippe Kohl from the European Society for Vascular Surgery and Andrew Bradbury from the World Federation of Vascular Societies. Nearly 60 additional authors worked on the project. Participants spanned six continents and represented all specialties that treat CLTI.
The collaboration between expert vascular specialists from around the world has created a unique practice guideline, reflecting the spectrum of the disease and approaches seen worldwide, said Conte. An extensive evidence review was undertaken, directed by a methodologist, to support the writing group’s work.
“This guideline provides a new foundation for describing and treating CLTI, an escalating public health problem around the world that involves a broad array of health professionals,” Conte said. “By improving the staging of CLTI, we believe that optimal care pathways can be defined and based on more accurate clinical and epidemiologic evidence going forward.”
Conte noted with pride that the multi-specialty, international group of vascular experts emphasised the importance of a patient- and limb-centric approach to the care of CLTI.
“With the continuous evolution of vascular technology, we must remain focused on the primary goals of treatment, in contradistinction to a lesion-centric emphasis on technical success,” he said.
Another major change is the name itself. The term “critical limb ischaemia (CLI)” is “outdated and fails to encompass the full spectrum” of patients evaluated and treated for limb-threatening ischaemia, the authors said.
Conte attributes the success of the diverse, international group to a process of consensus development. “A key aspect of our success was broad agreement on the importance of creating a new set point for CLTI around the world. CLTI is one of the most common conditions treated by vascular specialists, and often the most challenging. We also recognized that where evidence is limited the recommendations must be carefully considered to encompass the scope of practice,” he said.
Major recommendations cover the need for comprehensive assessments in patients with suspected CLTI; optimal medical therapy, including a variety of treatments for patients with CLTI; and prompt and effective revascularisation for patients with advanced ischaemia and limb threat. The document also outlines the importance of an individualised approach to improve patient care and reduce limb loss.
Other significant changes include:
Staging Limb Threat and Anatomic Complexity: WIfI and GLASS
The guideline endorses the SVS Threatened Limb Classification System based on grading wound, ischaemia and foot infection (WIfI) in the affected limb. And it introduces the Global Limb Anatomic Staging System (GLASS) to stratify the patterns of arterial occlusive disease in the affected limb. GLASS integrates the complexity of disease along a selected target artery path (TAP) from groin to foot. GLASS stages (1–3) are designed to correlate with immediate technical success and 12-month limb-based patency (LBP) following peripheral vascular intervention.
Decision-Making: Have a PLAN
“Perhaps most notably, the guideline supports a structured approach to decision-making regarding revascularisation based on Patient risk, Limb severity and ANatomic complexity (PLAN), in that order of priority,” said Conte. “The guideline seeks to provide a new foundation for practice but also for data collection to support Evidence-Based Revascularisation in CLTI.”
Beyond improving patient care, identifying key research priorities is an important secondary goal for the guideline. Thus, each section includes such priorities, where efforts and resources should be focused to improve patient care and advance the science.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has released a newly revised interventional radiology (IR) curriculum for medical students. Where the original curriculum from CIRSE, published in 2012, was five pages long, this most recent version is considerably longer, at 24 pages.
A statement from CIRSE reads: “IR has grown continuously over the past decades, with interventional treatments being applied to an ever-increasing number of conditions. Now more than ever, young physicians are showing interest in pursuing a career in IR—an extremely interesting field combining state-of-the-art procedures with clinical practice, patient interaction and multidisciplinary teamwork.
“Due to its innovative nature, patient-centred treatment approach and the ever-increasing applications of interventional procedures, IR has become one of the most interesting career choices for medical students. In order to help students make an informed decision, CIRSE has released a newly revised IR Curriculum for Medical Students describing the most important procedures performed by interventional radiologists.”
It goes on to say that the updated IR curriculum enables medical students “to find out more about IR’s key areas and the most common clinical conditions treated by interventional radiologists”.
This is the second edition of the IR curriculum for medical students published by CIRSE, the first being released in 2012. Christoph Binkert (Institute of Radiology and Nuclear Medicine, Kantonsspital, Winterthur, Switzerland) is the editor-in-chief of the document, and he founded and chaired a CIRSE taskforce dedicated to updating the curriculum. Five editors worked with him on the revised publication: Roberto Cazzato (Department of Interventional Radiology, Hôpitaux Universitaires de Strasbourg, Strasbourg, France), Jan Jaap Janssen (Academisch Medisch Centrum, Amsterdam, The Netherlands), Gregory Makris (Oxford University Hospitals, NHS Foundation Trust, Oxford, UK and chair of the British Society of Interventional Radiology trainee committee), Arash Najafi (Kantonsspital, Winterthur, Switzerland), and Fatemeh Sakhinia (Royal Stoke University Hospital, Stoke, UK).
Speaking to Interventional News, Binkert says that is timely to provide an updated curriculum now as “IR has changed markedly, and has become a true clinical specialty!”. However, he adds that “carrier planning starts early (not many residents change specialty); unfortunately, in many medical schools, IR is not really taught as a dedicated specialty”.
There have been several additions to the revised document. Where the 2012 curriculum makes no mention of embolization, this latest one includes a dedicated section in the “Vascular IR” chapter to embolization for benign conditions; this includes reference to uterine fibroid embolization, prostate artery embolization, gastrointestinal bleeding, and gonadal vein embolization. Under the “Interventional oncology” chapter, liver malignancy embolization is also included in the revised curriculum for the first time. The updated guidelines also include a subsection on access, which is new from the previous report, and an expanded section on musculoskeletal interventions.
Binkert comments on these key revisions since the publication of the 2012 edition: “In order to make the curriculum more reader-friendly to medical students, we went away from a bullet pointed list to a disease-focused document, with increased detail and discussion on clinical presentation, imaging, IR treatments, and follow-up. We hope that this format will help an interested medical student gain a clearer understanding of what modern interventional radiology is all about. In addition to the curriculum, short videos will be available to explain interventional radiology to medical students within two minutes.”
“I think the combination of clinic work, imaging and [performing the] procedures is very appealing to many young doctors”, says Binkert of the attraction interventional radiology holds for medical students.
Do not use paclitaxel drug-coated balloons (DCBs) or drug-eluting stents (DESs) in the routine treatment of patients with intermittent claudication until further notice, a medical device alert (MDA) issued today by the UK Medicines and Healthcare products Regulatory Agency (MHRA) announces, “as the potential mortality risk generally outweighs the benefits”. However, the use of DCBs and DESs may still be considered in patients with critical limb ischaemia, taking National Institute of Care Excellence (NICE) guidance into consideration, in view of their increased risk of restenosis and reduced life expectancy, the MDA accedes.
The MDA makes the following recommendations concerning the ongoing use of paclitaxel-coated balloons and implantable drug-eluting stents in the treatment of patients with peripheral arterial disease (PAD):
1. Do not use paclitaxel drug-coated balloons (DCBs) or drug-eluting stents (DESs) in the routine treatment of patients with intermittent claudication until further notice, as the potential mortality risk generally outweighs the benefits.
2. Use of paclitaxel DCBs and DESs in patients with critical limb ischaemia remains an appropriate option in accordance with National Institute of Care Excellence (NICE) guidance, as the benefits may outweigh the risks. This is because these patients generally have a higher risk of irreversible ischemic damage resulting from restenosis, and a lower life expectancy.
3. Assess the relative risks on an individual patient basis, and if this supports use of a paclitaxel DCB or DES, ensure that:
a) the process of informed consent includes a risk-benefit discussion regarding the uncertainty in long-term outcomes with these devices, and the current evidence which indicates an increased mortality rate
b) the patient receives enhanced life-long follow-up.
4. Ensure local procedures accounting for duty of candour are in place for the continued management of patients who have already been treated with paclitaxel DCBs an DESs. Consider the need for enhanced patient follow-up, and the provision of information and advice to address patient concerns arising from the current uncertainty in long-term outcomes with these devices.
5. Where enhanced patient follow-up is appropriate this may include telephone consultations or review in the community, and any serious adverse events and cause of death should be reported.
6. Report adverse events involving these devices through your local incident reporting system and/or your national incident reporting authority as appropriate: England, Scotland, Northern Ireland, Wales. You should also report directly to manufacturers if your local or national systems do not.
These recommendations are addressed to interventional radiologists and vascular surgeons, and, according to the MHRA announcement, should be actioned by 2 July 2019.
The MDA calls for more data, saying that “A review of results from clinical trials on the use of these devices in patients with arterio-venous fistula remains outstanding. These results should be shared when available to enable assessment of use in this population.”
The announcement adds: “In all cases where paclitaxel DCBs or DESs are used, there needs to be fully informed consent and an enhanced, long-term patient follow-up. Formal long-term surveillance is essential to improve understanding of the safety and performance of these devices following their market approval.”
The MDA states: “It is accepted that the causal relationship between paclitaxel-coated devices and mortality is not yet understood and requires further evaluation. However, having taken account of the EAG’s findings, together with other relevant information and opinions, MHRA considers the current evidence does not support the routine use of paclitaxel DCBs or DESs in patients with intermittent claudication.
“We will review the need to update this advice as further evidence emerges, including the findings of an ongoing meta-analysis using the patient level data from the randomised controlled trials reviewed by Katsanos et al. To build on the current evidence base, the ongoing and completed trials that have reported results from one or two-year follow-up should continue or reopen patient follow-up to try to establish the longer-term mortality status of all patients, up to at least five years post-treatment.
“The risk-benefit profile for patients with other vascular indications may be different to those for intermittent claudication and requires further clinical evidence to be reviewed before conclusions can be drawn.”
The SAVE-US (Surfacer system to facilitate access in venous occlusions—United States) pivotal trial has completed enrollment. The SAVE-US trial is evaluating the safety and efficacy of the Surfacer Inside-Out access catheter system (Bluegrass Vascular Technologies) in thirty patients across seven US centres, and demonstrated positive clinical results by meeting its primary and secondary endpoints.
According to a press release, the Surfacer system is a novel approach to achieving right-sided, upper body central venous access in patients with upper body venous occlusions or other conditions that preclude central venous access by conventional methods.
“I am quite encouraged by the highly positive results demonstrated by the Surfacer system,” states Mahmood Razavi, an interventional radiologist at St Joseph Hospital in Orange, USA, and lead investigator of the SAVE-US study. “I am eager for the system’s commercial approval, and look forward to offering a reliable and repeatable solution to patients with varying occlusion types, halting the devastating impact of central venous occlusive disease.”
Of the thirty patients enrolled in the US IDE SAVE-US trial, 90% met both the primary and secondary efficacy endpoints of facilitated central venous access by the Surfacer system. On average, central venous access was achieved in approximately 12 minutes despite a more complex patient population comprised largely of Type 3 and 4 occlusions (three or more occluded vessels).
“The Surfacer system passed the SAVE-US study with flying colours, confirming the system is a safe, viable option for achieving right-sided central venous access, preserving secondary central veins,” comments Ehab Sorial (Division of Vascular Surgery, Stanford, USA; Santa Clara Valley Medical Center, San Jose, USA), the study’s second highest enroller. Sorial first learned about the Surfacer system while working alongside John Gurley, the system’s inventor, for over a decade at the University of Kentucky, Lexington, USA. “This is a highly anticipated treatment that gives physicians a safe and effective alternative to other less efficacious treatments with higher complication rates. I am looking forward to its commercial approval and implementing it into my day-to-day practice.”
Bluegrass Vascular Technologies anticipate that the Surfacer system will be commercial available to physicians in 2020.
The UK Medicines and Healthcare products Regulatory Agency (MHRA) acted to limit the future use of paclitaxel-eluting stents and paclitaxel-coated balloons in routine clinical care following recommendations from the independent Expert Advisory Group (EAG) on the use of these devices.
The independent EAG was formed following the publication of a meta-analysis published by Konstantinos Katsanos (Patras, Greece) et al late last year in the Journal of the American Heart Association (JAHA) that raised concerns amongst the medical community for reporting an increased risk of death at two and five years after using paclitaxel devices in the femoropopliteal artery. The EAG consists of leading UK clinicians from multiple specialties, including interventional radiology, vascular surgery, toxicology and statistics.
The group reviewed the findings of the Katsanos et al paper, and concluded that the statistical analysis used by the investigators was robust. The EAG also considers that “there is a possible dose dependent effect of the use of paclitaxel-coated/-eluting devices on mortality although no scientific or clinical explanation is currently available.
“There are some established causal links between multiple factors and mortality, but the association of increased mortality and the use of paclitaxel-coated/-eluting devices is established by randomised controlled trials which control for confounding in known factors. There is no evidence to suggest that confounding persisted within these studies. Current knowledge gaps include dose-time relationship, outcomes of paclitaxel coated balloons versus paclitaxel eluting stents, patient factors, effect on patients with claudication compared with those with critical limb ischaemia, peer-reviewed publication of commercial evidence, mechanistic explanation, and biological evidence.”
The EAG was tasked with providing recommendations to the MHRA on the benefits and risks of the use of these devices in the treatment of peripheral arterial disease (PAD).
The expert group recommends that these devices not be used to treat patients with intermittent claudication, saying that this is a condition that may be treated effectively with other devices and therapies. However, for patients with critical limb ischaemia (CLI), the EAG advise that the devices may still be considered “where it is felt that the benefits outweigh the risks and taking NICE guidance into consideration in conjunction with appropriate informed consent and an enhanced patient follow-up”.
After receiving the recommendations, the MHRA has acted to limit the future use of these devices in routine clinical care, until more is known on this issue. Writing on their website, the MHRA encourages “anyone, patient, carer or healthcare professional, who is aware of a safety complication or adverse event associated with a medical device, to report to us via the Yellow Card scheme”.
The EAG recommends that future research is undertaken to evaluate the causal relationship between these devices and mortality. In line with the EAG’s recommendations, the MHRA will consider the available evidence supporting the use of these devices for other conditions.
The EAG also conclude that paclitaxel devices “may still be considered a treatment option within ethically approved trials following appropriate informed consent. In particular, currently suspended RCTs involving patients with CLI should consider resumption in recruitment.” This comes days after the investigators of the SWEDEPAD trials announce their intention to explore the possibility of resuming enrolment.
The US Food and Drug Administration (FDA) is leading a review of patient-level data from clinical trials involving these devices. The MHRA will take this review into account going forward, saying on their website that they “will consider any further information concerning the safety of these devices. It will take any regulatory action and update its guidance where necessary”.
The US Food and Drug Administration have issued a Class I Recall of the SoloPath (Terumo Medical) ballon-expandable transfemoral system and re-collapsible balloon access system, due to malfunction. A total of 14 reports had flagged related incidents of a specific device malfunction, including two injures. No deaths have been reported, the FDA notes.
The malfunction issue, the FDA recall announcement states, is a potential for dislodgement of the fairing tip from the sheath, hindering the smooth transition of the device through the body. This malfunction could make the device unable to transition through the skin to the iliac artery, or cause dissection, false lumen, pseudoaneurysm, haemorrhage, vessel perforation and vessel disruption, which in turn may result in additional interventions, increased procedure time, or death.
In April 2019, Terumo issued a voluntary recall and listed the following recommended actions:
Review the Product Recall Bulletin and the Required Actions.
Assure that all users receive notice of this issue so that required actions can be performed.
Assure that this notice is forwarded to applicable facilities if any affected products were further distributed outside of your facility.
Review your SOLOPATH inventory immediately to identify and isolate affected inventory to prevent future use.
Complete the Medical Device Recall Response Form. The form is required even if you do not have product to return.
If you have product to return, contact Stericycle to obtain a credit and reference event number 10082. Phone Number: 855-205-2627 E-Mail: return to [email protected].
E-mail the Recall Acknowledgement Form to [email protected] to arrange for product to be returned to Stericycle.
Terumo encourages customers to consider alternative suppliers.
The opening Plenary Session of GEST 2019: Masterclass and Materials: Coils and Plugs.
The 2019 GEST (Global Embolization Oncology Symposium Technologies) Symposium took place on 9–12 May in New York, USA, with a new focus this year on trainees and fellows, representing, as co-convenors of the conference Marc Sapoval (Hôpital Européen Georges-Pompidou, Paris, France) and Jafar Golzarian (University of Minnesota, Minneapolis, USA) tell Interventional News, “the future of interventional radiology (IR)”.
This focus was manifested in an increase in trainee attendance and engagement, with 150 medical students from across the globe. New this year, a specific programme dedicated to career development, starting outside the usual conference hours at 7am, was packed. Sapoval enthused about the youth turnout, saying it was “striking to have a room full of people, with an average age of around 25, turning up at that time”. GEST 2019 also played host to a series of case competitions aimed at medical students and trainees. An evening session entitled “Future Meets the Present (…Almost the Past)” saw established interventional radiologists giving their advice to the younger cohort. Justin McWilliams (David Geffen School of Medicine, Los Angeles, USA) spoke about how to approach the first year in practice; Brian Stainken (Stamford Health, Stamford, USA) noted three things he would do differently in his early career were he to start over; Donna D’Souza (University of Minnesota, Minneapolis, USA) outlined her experience of being a successful woman in IR; and Michael Darcy (Mallinckrodt Institute; Washington University, St Louis, USA) detailed what a work/ life balance should look like. These activities and the positive response prompted Golzarian and Sapoval to describe the meeting as “a push for the future” of the specialty.
In addition to an increase in youth turnout specifically, there was a more general increase in attendance this year: a rise of 20%, according to Sapoval. This included approximately 50 new faculty members, meaning the meeting had a faculty more than 150 strong in total. GEST 2019 saw 180 abstracts submitted, and 90 accepted posters. Three of the abstracts received financial prizes, as did the three best posters. There were also three prizes awarded in the case competition aimed at trainees.
The global nature of IR was reflected in the international cohort who attended and organised the GEST meeting. Forty-seven percent of the nearly 1,100 attendees were international (from outside of the USA), and the four committees that help organise the conference programme comprised of a diverse group of volunteers. These committees—focused on research, interventional oncology, training, and workshops—are entirely volunteer-led, and Golzarian and Sapoval thank all those who have invested their time and efforts into GEST 2019: “Their involvement made this meeting our best yet”.
Gary Siskin, Marc Sapoval, Jean-Pierre Pelage and Yasuaki Arai conduct the Masterclass: Particles and New Developments in Microcatheters.
The sessions dedicated to prostate artery embolization (PAE) and portal intervention were attendee favourites. At the end of the PAE Symposium, audience polling revealed that 100% of voters wanted to see the session return next year. Speaking to InterventionalNews, Golzarian claimed that GEST was “the only meeting that covers these two topics to this degree of detail”. The focus on PAE is a stalwart fixture of the meeting, which has featured a dedicated PAE day since 2012.
Sapoval also spotlighted the flow dynamics session as a high point of the conference, saying: “It was an amazing session”. This was only open to registrants, and, in Golzarian’s words, “covered a lot of ground, including what we need to know but do not yet understand”. He said that flow dynamics was an “important topic” as “it is so essential to what we do in embolization”.
Jafar Golzarian presenting at GEST 2019
New this year was the “GEST stress test”, based off the American “Shark tank” or the European “Dragon’s Den” concepts, where three innovative interventionalists presented their novel research ideas to a group of expert panellists, who then judged the entrants’ projects. This sparked “excellent debates” and showcased three very different projects, Sapoval comments. “I think it really helped the investigators to focus on their research and hone in on how they could improve their current projects”, he said.
James Spies (MedStar Georgetown University Hospital, Washington, DC, USA) comments: “GEST continues as the premier embolization meeting in the world. It is unique in the breadth of faculty experts, the detailed review of the tools of embolization and the quality of the presentations. The panel discussions have been expanded, where real life cases and questions can be addressed by the leaders in the field. I never fail to learn new things at GEST and it remains my favourite meeting of the year.”
In the wake of the recent joint statement from the British Society of Interventional Radiology (BSIR) and the Royal College of Radiologists (RCR) advocating for the increased provision of interventional radiology services in the UK (see here), and in anticipation of the publication of the Provision of Interventional Radiology Services (POIRS) document in the summer of 2019, BSIR president Trevor Cleveland writes about why patient access and awareness of interventional radiology (IR) procedures is crucial.
It is important to improve the provision of IR (image guided surgical) procedures across a range of emergency and elective, adult and paediatric services, because they have the ability to treat people with reduced morbidity, and generally have a quicker recovery time. IR as a specialty has evolved within what was originally a diagnostic service, with the expertise in image interpretation as a cornerstone to its effectiveness and success. The situation now is that IR procedures are the “go to” option in a number of emergency and elective scenarios, offering treatment for patients who previously needed more invasive open surgery, or were considered too high risk for those treatments. In many ways, image-guided procedures complement the open options, and extend the range of people who can have effective treatment (including cancer treatments). In other scenarios, the minimally invasive nature of IR procedures has meant that some open surgical side effects and complications can be avoided.
By its very nature, a new specialty develops in a relatively uncoordinated way, with pockets of enthusiasm and expertise being developed. The time has come, and the clinical need exists, for IR to come out of those shadows and be recognised for the specialty that it is, and the great things it can offer patients.
The POIRS and RCR Census tell us that we need more interventional radiologists in training, and that we need to use our current capacity more effectively. We also know that trainees and consultants can be discouraged in taking on IR procedures because of the high emergency commitment (so we need to make that more acceptable to work life balance), the higher risk of litigation, and the low level of recognition of the specialty.
However, it is clear that IR procedures offer great short and long term benefits for patients, to which they deserve to have access in a timely fashion, and for these to be performed by well trained, well-practised and fresh doctors.
Interventional radiologists must take primary responsibility in the patient pathway
It is important that interventional radiologists take primary responsibility in the patient pathway. The techniques, work up, follow up and audit of IR procedures, like all interventions, carry with them benefits and risks unique to the procedures and to individuals. It makes sense for patients and interventional radiologists to meet, discuss and address questions and expectations. Indeed, it is a requirement from the General Medical Council (GMC) that these facilities exist. Perhaps, in the past, where simple imaging was “ordered”, the situation was different. But as the complexity, and the potential risk:benefit analysis becomes more complex, such a situation is not tenable. It can be a very difficult balance, because there are a number of high volume procedures, which are relatively straight forward, and mandating direct face-to-face IR input may result in delay in treatment.
There are two potential ways to address this. One is to have very clear information for patients and other clinical teams, with specific training designed to allow for delegated responsibilities along the consent process. This at least reduces the time pressures required of interventional radiologists directly. The other approach is to significantly increase the IR capacity. Of course the latter is the ideal, but difficult to achieve, particularly in the short term. It is vital that these two strategies run concurrently, to ensure the highest quality service to patients possible.
Alongside this, it is important that patients have the opportunity to have a review with an interventional radiologist after a procedure, to ensure optimised aftercare, to manage any difficulties or complications, and it is essential that interventional radiologists are made aware of outcomes, and are able to record these for audit and quality purposes.
BSIR is addressing challenges facing IR in the UK
One of the challenges for IR, which BSIR is trying to address, is the general lack of understanding of what IR is, and what we can offer. This level of misunderstanding exists in many areas, including amongst patients, commissioners, general practitioners and even fellow hospital clinicians.
BSIR has established a communications team, which includes interventional radiologists alongside communications experts. We have been leveraging a number of areas to try to raise the knowledge and profile of IR, including social media, web site information, newsprint (including Interventional News) and through direct involvement in parliamentary groups.
In addition, BSIR has recognised for a number of years that medical students and junior doctors often have not been exposed to, or understand, IR procedures. To address this, we support a series of essay and case study applications, which, if successful, give the opportunity (with expenses support) for both groups to attend the BSIR annual scientific meeting (13–15 November, Manchester, UK), where there are specific events for them, in addition to the main programme. We also support local meetings of interested groups, as well as training events. These are aimed at increasing the awareness of IR, as well as trying to encourage suitably minded trainees to join the IR specialty.
Trevor Cleveland is an interventional radiologist at the Sheffield Teaching Hospitals NHS Foundation Trust and the Sheffield Vascular Institute, Sheffield, UK.
Three-year results from the ILLUMENATE Pivotal trial and the ILLUMENATE European randomised controlled trial (EU RCT) have been presented in a late-breaking trial session at the New Cardiovascular Horizons Annual Conference (NCVH; 29–31 May, New Orleans, USA) by S Jay Mathews (Bradenton Cardiology Center, Bradenton, USA). The data demonstrated a significant treatment effect with a high safety profile through three years following treatment with the Stellarex (Philips) sirolimus drug-coated balloon (DCB), with no significant difference in mortality compared to plain percutaneous transluminal angioplasty (PTA).
The two trials a are part of a series of five trials evaluating the safety and efficacy of Stellarex .035″ low-dose DCB to restore and maintain blood flow in the superficial femoral artery and popliteal arteries of patients with peripheral arterial disease. The results were evaluated compared to PTA treatment with uncoated balloons, the current standard of care.
Presenting the data, Mathews highlighted the following results:
The ILLUMENATE Pivotal trial results show that at 36 months, 64.2% of the patients treated with DCB maintained blood flow through the treated segment of the diseased artery, compared to 51% of the patients treated with an uncoated balloon, demonstrating continued durability of the procedure.
The ILLUMENATE Pivotal patient pool was the most complex studied in a randomised clinical trial. The pool included patients with the highest rates of comorbidities, such as diabetes and renal insufficiency, while 43.9% also had severely calcified lesions.
The ILLUMENATE EU RCT results show that at 36 months, 67.5% of the patients treated with the DCB maintained blood flow (assessed through blinded core-lab adjudicated patency), compared to 59.9% of the patients treated with PTA.
Through three years, both studies showed no significant difference in mortality compared to treatment with uncoated balloons. The mortality rate of patients treated with Stellarex in the ILLUMENATE Pivotal trial was 10.1%, compared to the mortality rate of patients treated with an uncoated balloon of 11%. The EU RCT showed mortality rates of 9.4% for patients treated with the DCB, compared to 8.5%for patients treated with PTA.
“The three-year data of the ILLUMENATE Pivotal trial and ILLUMENATE EU RCT add to the robust and consistent multi-year data of the Stellarex program,” Mathews said. “The demonstrated durability of Stellarex in the complex patient pool of the ILLUMENATE Pivotal trial, which are patients that are at high risk for restenosis, a recurring blockage, is unique in the industry. Moreover, we continue to see no significant difference in mortality rates between patients treated with Stellarex and those treated with uncoated balloons, which confirms our confidence in the safety profile.”
The results follow a data release from a pooled analysis of 2,300 patients’ patient-level data, presented earlier this year. Sean Lyden (Cleveland, USA) and Fabrizio Fanelli (Rome, Italy) discussed these data with Vascular News at the Leipzig Interventional Course (LINC; 22–25 January, Leipzig, Germany). Watch the video discussion here.
The Interventional Radiology Committee of the Royal College of Radiologists (RCR), in collaboration with the British Society of Interventional Radiology (BSIR), have released a statement for interventional radiology (IR) service provision in the UK to supplement the existing Provision of Interventional Radiology Services (POIRS) document. This supports both longitudinal care and ownership of patients by interventional radiologists, and has been met with approval from the IR community.
In a document entitled “The clinical role of interventional radiology (image guided surgery) in patient care”, the two bodies write: “The Provision of Interventional Radiology Services (POIRS) has been revised, and the second edition is due to be published this summer (2019). This statement has been released by the Royal College of Radiologists (RCR) and British Society of Interventional Radiology (BSIR) to introduce the POIRS document, identify the benchmarks for interventional radiology and to highlight the competencies of interventional radiologists in patient management, both in an inpatient and outpatient scenario, obtained as part of their subspecialty training.”
Speaking to Interventional News about how this joint statement will affect interventional radiologists in the UK, BSIR president Trevor Cleveland (Sheffield, UK) comments: “IR has changed considerably, even between the 2013 version of this document and today. Interventional radiologists are using increasingly complex techniques and treating more complex clinical situations, often in an emergency environment. This includes acute bleeding (associated with trauma and iatrogenic injury) in a number of organ systems. The treatment of sepsis, whilst to some degree a core radiology skill, in more complex situations requires more advanced techniques. As such, interventional radiologists have become essential to the effective functioning of many acute services. This is in addition to an expanding range of elective treatments, including oncology, as well as the more established IR procedures, such as angioplasty and stenting, and more recently stroke treatment and prevention. These are delivered across both adult and paediatric populations.
“Yet there remains a relatively small number of interventional radiologists who can provide this service, in an environment where the emergency commitment is increasing for this group. The POIRS update provides current information, informed by both the BSIR membership and the RCR Census survey, on the present service delivery, and the numbers that need to be included in the workforce planning going forward.
“Key to this is delivering a timely service for patients (making the best use of the IR skills that we have now, including ensuring that IR skills are not unnecessarily lost as a result of the reconfiguration processes and/or an imbalance of emergency commitment) and future planning. Trainees are our future, and we must ensure that we have an environment that encourages enthusiastic young doctors, and the capacity to meet the expanding needs. Add to this the likely loss of IR skills as some of the present community reach retirement (which is compounded by the pension tax laws which mean that, like in General Practice, experienced doctors are being effectively encouraged to leave or to reduce their activity).”
As an “essential part of modern medicine”, the BSIR and RCR joint statement introducing the anticipated POIRS document outlines how interventional radiologists can act to widen the provision of IR services in the UK. There are four conclusions:
IR is a subspecialty of clinical radiology requiring an additional year of training, compared to diagnostic radiology (six years total) to be certified by the General Medical Council (GMC) IR Certificate of Completion of Training.
IRs receive training appropriate to their scope of practice, enabling them to clinically manage patients under their direct care, throughout the patient pathway, and provide clinical advice for patients under the care of other clinical specialties.
To deliver this clinical care, IRs require appropriate clinical time, infrastructure and support from their employing organisations, including access to outpatient clinics and inpatient beds.
Trusts should be supportive of IRs who wish to deliver high quality longitudinal care on a par with many fellow specialists.
Commenting on these conclusions, and the ramifications she envisages they will have for British IR, Clare Bent, an interventional radiologist at The Royal Bournemouth and Christchurch Hospitals, Bournemouth, UK, says: “The IR benchmarks and a focus on the development of a subspecialty IR curriculum are both key to the provision of a robust, competent IR workforce who can deliver comprehensive, longitudinal, high quality care in both an inpatient and outpatient setting. Ward rounds, outpatient clinics, and admitting privileges with adequate and appropriately trained support staff are all integral factors in the optimisation of patient centred care for the IR specialty.
She continues: “The diverse nature of IR service provision and continual innovations in the specialty mean that trained interventional radiologists are best placed to provide information and consent for such minimally-invasive procedures—which in turn improves patient experience, understanding, and confidence. Formalising the IR clinical role will bring clarity to the doctor-patient relationship for the IR speciality, establish a standardised IR management pathway and will allow allocation of appropriate funding streams. The less invasive approach that IR offers allows rapid recovery, reduced in-hospital stay and reduced morbidity and mortality, with a profound impact on healthcare economy.
“This interim statement is a step forward in supporting interventional radiologists, as clinicians, to deliver high quality patient care to the UK population.”
Cleveland is in accordance, explaining how the document, which “represents a close collaboration between BSIR and RCR”, provides “as representative a statement as possible, including engagement from Members and Fellows of both organisations.” He goes on to explain that, as such, “it provides a framework for change and development, and serves as guidance to the wider healthcare community including interventional radiologists, radiologists more generally, commissioners, NHS England and Health Education England. We hope that it will act as a useful support for the real and effective changes that need to take place to ensure a high quality and equitable service, which patients deserve.”
In advance of the publication of the POIRS document this summer, Cleveland stresses its significance: “The POIRS document is an enormously important one, which provides information on IR procedures, and guidance for future planning. It seems highly likely that the attractiveness, for patients and healthcare services alike, of IR procedures will result in a continued expansion. Innovation and equipment development are also likely to continue, with further techniques and applications being identified on a regular basis. Key to these is the expert interpretation and training in imaging that IRs have. Whilst it may be appealing to split off some of these activities for short-term reasons, IRs offer a skill set that extends across a wide range of clinical scenarios and teams. The major challenge facing us at the moment is delivering an emergency service, in a timely equitable fashion, whilst maintaining and developing a sustainable workforce. This requires an elective practice that underpins the emergency service. The issues raised and recommendations made in the POIRS document are key to achieving this for NHS patients.”
Investigators of SWEDEPAD have announced the conclusion of their safety committee analysis, which recommends the halted trials resume enrolment.
This decision to consider resuming enrolment in the SWEDEPAD trials came twelve days after a dedicated session called “Paclitaxel: The last word” took place at the Charing Cross Symposium (CX; 15–18 April, London, UK). At this meeting, Mårten Falkenberg (Gothenburg, Sweden) provided an update on the status of the SWEDEPAD trials. Speaking on 16 April, he told the CX audience that the decision to halt enrolment was predicated on the findings of the Katsanos et al meta-analysis published in the Journal of the American Heart Association (JAHA) late last year, which suggested that there is an increased risk of death at two and five years following the use of paclitaxel-coated balloons and stents in the femoropopliteal artery. He added that, despite keeping up with the ongoing international conversation, at the time of his presentation the investigators were still trying to determine the best course of action, and that no obvious consensus had emerged at the time.
However, whilst the SWEDEPAD investigators have since reached the conclusion to begin the process of recommencing their trial in the weeks following CX, at the time of publication, there has been no update from the BASIL-3 trial—this is the only other randomised controlled trial investigating drug-eluting devices to halt in response to the Katsanos et al meta-analysis published late last year. Indeed, at CX, the decision to stop enrolment in BASIL-3 was explained by statistician Jon Deeks (Birmingham, UK) as being based on the assumption that the signal seen in the Katsanos et al meta-analysis could be real.
The SWEDEPAD announcement
Writing on their website, the investigators of the SWEDEPAD trials announced (originally in Swedish): “Decision made to investigate possibilities of commencing inclusion in SWEDEPAD! On 28 April, 2019, SWEDEPAD’s Security Committee (DSMC) carried out a new analysis of mortality among patients randomised into SWEDEPAD 1 and 2. Based on this, the DSMC recommended the trial to resume inclusion.”
In their recent announcement indicating that enrolment will recommence, the SWEDEPAD triallists explain: “This means that our currently available data do not support the conclusions of the meta-analysis published in December 2018 on increased late mortality among patients treated with paclitaxel-treated balloon or stent. After meeting in SWEDEPAD’s steering group on 2 May, and after open discussion during the Swedish vascular meeting in Båstad on 10 May, we have decided to investigate the possibilities of resuming inclusion in SWEDEPAD.
“We will first (1) update patient information, (2) send a supplementary application to the ethical review board, and (3) share our information with regulatory authorities. So the plan is to resume, but a lot of work remains before that can be realised.”
It is imperative that every medical institution has an interdisciplinary CLI team, argues Jihad Mustapha. Here, he exhorts the benefits of working in such a multidisciplinary team, and outlines how the circle of care concept can be applied to reduce rates of unnecessary major amputation.
The most effective critical limb ischaemia (CLI) multidisciplinary team structure is comprised of multiple layers or groups of providers from a variety of areas, including surgical and endovascular revascularisation, podiatry, wound care, endocrinology, primary care, orthopaedics, cardiology, infectious disease and physical medicine. The action of each group is reactive to the immediate need of the CLI patient. The course of action in the treatment cascade is not linear; instead, it is both repetitive and reactive. To transform the potentially catastrophic event of a CLI diagnosis into a patient with a successful outcome, the team must act in harmony and initiate the reactive cycle of therapy when a CLI patient receives treatment at the level that is most critical at any single point in time (Figure 1). A provider will refer the CLI patient to the next most critical continuum for the secondary issue to be addressed (cascade of care). The CLI team must always be aware of and acknowledge that the CLI patient’s therapy is not conclusive, and that the chance of recurrent disease is high. Therefore, heightened awareness and strict follow-up evaluation are required. Once a recurrent CLI event is discovered, the repetitive cycle must be initiated. For a patient with active CLI disease, there should never be a period of time where no form of therapy is being delivered. The average time it takes for a CLI patient to receive any type of first treatment or diagnostic testing has been reported to be nine days. This is unacceptable. Too much can happen in nine days to result in a poor outcome for a CLI patient. Therefore, the repetitive phase must be initiated as early as possible.
Any member of the CLI team can and should trigger the repetitive treatment cascade in the presence of:
Recurrent rest pain
Absent doppler pulse
Occluded target vessel and lack of progression of wound healing
Regression of wound healing
Infection or sepsis. Note: Amputation is not always the answer here. Revascularisation and intravenous antibiotics must be tried first, unless the patient is in shock and the limb is not salvageable. Only then should amputation be performed without an attempt at revascularisation.
Once a CLI patient has been treated and has reached a stable form of the disease, such as wound healing, rest pain resolution and/or return to activity, the preventive phase of CLI therapy (in the circle of care) should be initiated by the CLI team. The CLI team members must each provide their recommended medical treatment based on their specialty. Most importantly, the circle of care (preventive phase) should never be stopped. In fact, prevention should be started in the pre-CLI phase for patients who are Rutherford 1–3. Any form of peripheral arterial disease (PAD) should be preventively treated as early as possible to prevent the catastrophic outcomes that we know can happen to those patients that reach the CLI phase. Hence, there is an extreme need for a multidisciplinary CLI team to exist in every institution in the USA and around the globe.
Jihad Mustapha
CLI centres are a new concept, and have adopted the strategies discussed above. The success of any CLI centre is dependent upon the harmony of the members of the multidisciplinary CLI team. CLI centres’ outcomes have been shown to produce excellent outcomes with impressive reductions in major amputation.1,2 The future of effective CLI therapy lives in a cohesive and functional multidisciplinary team.
Jihad A Mustapha is the associate clinical professor of Medicine at Michigan State University COM, E Lansing, USA. He is also the CEO of Advanced Cardiac and Vascular Centers for Amputation Prevention, Grand Rapids, USA.
References 1. Mustapha JA, Saab FA, Diaz-Sandoval LJ, Beasley R, McGoff T, Finton S, Heaney C, Adams G. The Peripheral RegIstry of Endovascular Clinical OutcoMEs (The PRIME Registry): Interim Analysis of the First 328 Subjects With Critical Limb Ischemia. Vascular Disease Management. 2017;14(3): E55-67. 2. Raymond Dattilo, Alexandra Dattilo, Shawn Colby. Outcomes of Patients Treated for Critical Limb Ischemia in an Outpatient Endovascular Center. Vascular Disease Management 2018;15(6):E49-E52.
ControlRad has announced that the US Food and Drug Administration (FDA) has granted 510(k) clearance for its ControlRad Trace. The company has initiated its commercial launch. The ControlRad Trace is the only technology that can be integrated into existing mobile C-arms to reduce radiation in any fluoroscopic imaging procedure.
“Radiologists and our teams have grave concerns about the long-term effects from radiation exposure,” says John A Carrino, vice chairman of Radiology, Hospital for Special Surgery (New York, USA). “I am excited that new technology for mobile C-arms is now available because it has the potential to drastically improve our radiation safety while maintaining image quality so we can continue to effectively diagnose and treat our patients. I believe these new products should become the standard of care for fluoroscopic procedures.”
Fluoroscopically guided procedures with C-arms have allowed for major advances in treating countless diseases, however they expose patients and medical staff to ionising radiation, which may increase a person’s lifetime risk of developing cancer. For example, an interventional fluoroscopy procedure is roughly equivalent to the adult effective dose of between 250–3,500 chest X-rays.
“Radiation from C-arm procedures may increase the risk of brain cancer, cataracts, strokes and atherosclerosis,” says Guillaume Bailliard, ControlRad CEO. “It is our mission to dramatically reduce these life-altering radiation health risks to medical personnel and patients. This FDA clearance for ControlRad Trace allows us to provide our valuable radiation reduction technology to all mobile C-arm users looking to provide a safer environment without compromising patient care.”
With its proprietary semi-transparent filter, tablet and image processing technology, the ControlRad Trace solution can be retrofitted on existing C-arms, which, according to a press release, reduce the barrier to adopting the technology in order to reduce unnecessary radiation by up to 89%, without compromising image quality in the region of interest and overall workflow. The medical staff draws a region of interest on a ControlRad tablet, which in real-time optimises image quality in the region of interest while reducing unnecessary radiation in the periphery.
PhD (“push, hold, deliver”) polycarbonate haemostasis control valve
Merit Medical has announced the launch of its PhD (“push, hold, deliver”) polycarbonate haemostasis control valve, now available in the USA.
The dual-seal PhD device allows operators to manipulate the valve with one hand by pressing down on the cap, keeping the other hand free for the insertion and withdrawal of diagnostic/interventional devices, according to a company press release. Its two seals—a primary compression seal and a secondary polyisoprene push and release bleedback seal—help physicians minimise blood loss without restricting device movement. The PhD allows for pressure injections up to 400 psi, accommodates devices up to 7.3F, and features a clear body that provides unobstructed visibility.
The PhD device has been available to European markets since 2014. There, it has seen significant success, with unit sales averaging 34% year-over-year growth. In the USA, Merit will offer the device as a stand-alone or in combination with Merit’s suite of leading inflation devices and custom kits. Merit will also offer optional sidearm extension tubing that creates additional space between the valve and connected devices.
The commercial launch of the PhD device follows the late 2018 reveal of Merit’s basixTAU, a first-of-its-kind inflation device featuring a fold out handle that can increase the speed of inflations and deflations. The basixTAU inflation device provides greater versatility and ease of use, while reducing rotational force by up to 67%. It is also designed with a clear barrel for visibility and an easy-to-read luminescent analogue display suitable for use in low-light procedures. The 20 mL device can achieve a maximum pressure of 30atm.
1. Opacification of the distal part of IMA showing superior rectal arteries (SRA) with right opacification of the corpus cavernosum recti (white arrow). 2. Embolization with coils. 3. Control after embolization of right and left superior rectal arteries: notice the small left SRA still patent. 4. Control after complete embolization.
As a world-leading advocate of the “emborrhoid” technique—the embolization of the superior rectal arteries—and the lead author of the 2015 study demonstrating the procedure’s efficacy, Vincent Vidal provides an update four years on concerning the current status of the technique. In 1994 and 1998, EV Galkin (Krasnoyarsk, Russia) first described a potential interventional radiology treatment for chronic haemorrhoids complicated by haemorrhage. Published in Russian, the audience for these two papers was limited, and Vidal has been a pioneer for the furtherance of this work outside of Russia. With a randomised, comparative evaluation of the emborrhoid technique underway, Vidal hopes to confirm its place as a minimally-invasive, therapeutic alternative for treating patients with haemorrhoidal disease.
With a prevalence of 4–35%, haemorrhoidal disease is the most common anorectal condition. One of the main chronic symptoms is rectal bleeding. Its recurrence can alter the quality of life and, more rarely, cause anaemia. Pain is less common, only occurring in the event of a complication (congestive exacerbation, external haemorrhoidal thrombosis, fissures). The most common treatment involves hygiene and dietary measures, phlebotonics and/or nonsurgical outpatient treatment (infrared photocoagulation, elastic band ligation).
The haemorrhoidal arteriovenous network is a normal vascular formation. Internal haemorrhoids are now thought to result from an increase in arterial blood flow from the rectal arteries into the haemorrhoidal cushion (corpus cavernosum recti).1 Expansion of the vascular network of the anorectal submucosa initiates a negative vicious circle of progressive vascular dilation and venous insufficiency, leading to haemorrhoidal hyperplasia. This hyperplasia causes an increase in blood pressure, arterial inflow and anal pressure in the corpus cavernosum recti. The mechanical function of the corpus cavernosum recti is dependent on the influx of arterial blood from the branches of the inferior mesenteric artery, the superior rectal arteries, but also in 30 to 50% of patients from the unilateral or bilateral middle rectal artery. By contrast, the lower part of the rectum and the anal canal are supplied with blood by the inferior and middle rectal arteries, both of which have origins at some distance from the inferior mesenteric artery (pudendal artery, iliac network).2
Ten years ago, proctologists developed a new concept of treatment: elective transanal Doppler-guided haemorrhoidal artery ligation (DGHAL). The DG-HAL technique involves the identification and ligation of the superior rectal arteries under transanal Doppler guidance. Ligation of the superior rectal arteries provides a significant reduction of arterial blood flow to the haemorrhoids, and is effective in treating haemorrhoid disease.3
We have suggested that arterial ligation can be performed with coils in the terminal branches of the superior and middle rectal arteries via the endovascular route.
The advantages of emborrhoid and DG-HAL technique versus surgery are that it maintains the haemorrhoidal tissue in place, preserves anal continence, has no rectal wounds (meaning no local care is necessary), there is significantly less pain, and the complications of open surgery are avoided, thus allowing a faster return to activity.
Emborrhoid embolization is performed using a right femoral route. The inferior mesenteric artery is catheterised using a Simmons or Sidewinder catheter. The superior rectal arteries are then catheterised with a microcatheter. Coils used for the embolization are 0.018’’, from 2–3mm in diameter. Distal opacification of the superior rectal artery may depict a direct anastomosis with a dominant middle rectal artery in 30 to 50% of cases. In this situation, the middle rectal artery should be also embolized after catheterisation of the anterior trunk of the hypogastric artery.
The technical success of the emborrhoid technique has been reported to be up to 90%. Meanwhile, the clinical success is also impressive: the literature reports between 74 and 83% of patients treated with the emborrhoid technique as having no complications.2,6
The main advantages of emborrhoid technique are:
Patients have absolutely no pain.
No major complications have been related to the emborrhoid technique, and especially no ischaemic or continence complications.
This technique is available in an outpatient setting.
The patient can return to activity the day after embolization.
Embolization does not close the door to a complementary treatment if mandatory.
The technique is easy to perform in an hour or less, especially if there is no need for middle rectal artery embolization.
There are many benefits of endovascular treatment, including the complete visualisation of all the branches of the superior rectal arteries and anastomoses with middle and inferior rectal arteries.7 With the DG-HAL technique, it is possible that not all arteries are detected, which can lead to incomplete treatment, especially if there are anastomoses. Obviously, embolization eliminates the risk of direct anorectal trauma. There are many patients who suffer from haemorrhoids but do not complain to physicians because they refuse to have an endorectal treatment. If we can offer a treatment for outpatients without pain, we believe more patients will seek treatment for this condition.
Vincent Vidal
We have demonstrated that distal coil embolization of the superior and middle rectal arteries to stop chronic bleeding is safe and effective. Many clinical studies are ongoing in Europe, Asia and America. We are now building a randomised, comparative evaluation with DG-HAL to confirm the role of the emborrhoid technique as a minimally invasive therapeutic alternative for haemorrhoidal disease.
Vincent Vidal is the head of the Interventional Radiology section in the Department of Medical Imaging at the University Hospital TIMONE in Marseilles, France.
References 1. Aigner F, Bodner G, Conrad F, Mbaka G, Kreczy A, Fritsch H. The superior rectal artery and its branching pattern with regard to its clinical influence on ligation techniques for internal hemorrhoids. Am J Surg 2004; 187:102–108 2. Moussa N, Sielezneff I, Sapoval M, Tradi F, et al. Embolization of the superior rectal arteries for chronic bleeding due to hemorrhoidal disease. Colorectal Dis. 2016 Jun 24. doi: 10.1111/codi.13430. 3. Infantino A, Altomare DF, Bottini C et al. Prospective randomized multicentre study comparing stapler haemorrhoidopexy with Doppler-guided transanal haemorrhoid dearterialization for third-degree haemorrhoids. Colorectal Dis 2012; 14:205–211 4. Vidal V, Louis G, Bartoli JM, Sielezneff Y. Embolization of the hemorrhoidal arteries (the emborrhoid technique): a new concept and challenge for interventional radiology. Diagn Interv Imaging 2014 95:307–315 5. Vidal V, Sapoval M, Sielezneff Y, De Parades V, Tradi F, Louis G, Bartoli JM, Pellerin O. Emborrhoid: a new concept for the treatment of hemorrhoids with arterial embolization: the first 14 cases. Cardiovasc Intervent Radiol 2015; 38:72–8 6. X. Sun a, y, J. Xub, y, J. Zhang a, Y. Jina, Q. Chen. Management of rectal bleeding due to internal haemorrhoids with arterial embolisation: a single-centre experience and protocol. Clinical Radiology 2018; 73:985.e1-6. 7. Bilhim T, Pereira JA, Rio Tinto H, et al. Middle rectal artery: myth or reality? Retrospective study with CT angiography and digital subtraction angiography. Surg Radiol Anat 2013; 35:517–522
Proximo Medical has announced that it has been selected as the marketing and commercial partner for Walk Vascular, a medical device company that has developed JETi, a novel peripheral thrombectomy catheter.
Proximo Medical is a fractional commercial organisation for start-up medical device technologies that delivers market validation, an experienced workforce and scalability to deliver accelerated revenues, a press release states.
Walk Vascular has just released its new JETi 88 device, which employs an internal jet, located inside its catheter mouth, capable of engaging large thrombus volumes through a miniature lumen, rapidly clearing peripheral vessels that would prove difficult and frequently clog standard aspiration devices.
Last autumn, Jean Cournoyer-Rodrigue (Centre Hospitalier de l’Université de Montréal Research Center in Montreal, Quebec, Canada) presented data from a study assessing the safety and efficacy of the JETi thrombectomy system at CIRSE 2018, the Cardiovascular and Interventional Radiology Society of Europe annual meeting (22–25 September, Lisbon, Portugal).
The system was tested in 23 venous thromboembolism cases with an 83% rate of technical success, defined as restoration of antegrade flow with the elimination of any obstructing lesion without overnight post-procedural lytic infusion via catheter-directed thrombolysis.
“This percentage of ‘single session’ efficacy, with a mean total procedure time of 73 minutes, is quite remarkable relative to the existing literature. Using devices that require adjunctive procedures, intensive care unit stays, is not a win for anyone in the healthcare value chain, especially the patient. Single session devices offer great promise of a new treatment paradigm,” states Cournoyer-Rodrigue.
“By partnering with Proximo Medical we can hit the ground sprinting, with high quality direct sales representatives that start-ups generally cannot afford without the need for additional funding,” comments David Look, president and CEO of Walk Vascular. “Proximo provides a crucial next step absent of most technology developers. Their ability to quickly de-risk commercial viability, confirm reordering patterns and document the salesforce’s ramp time provides huge value to both the developer and potential future acquirer.”
“We are pleased to be working with Walk Vascular and the JETi technology, a proven solution that safely and effectively restores blood flow in coronary and peripheral interventional procedures,” says Brett Martin, Proximo Medical CEO. “With more than 75% of medical device start-ups failing prior to commercialisation, we are proud to partner with innovators like Walk Vascular to provide insights, marketing strategy, and a top-tier salesforce to ensure commercial success and clinical adoption.”
Interventional News speaks to Jemianne Bautista-Jia about her research on uterine fibroid embolization (UFE). “Being in the same demographic as my patients allows me to realistically consider what I would want in their situation,” she says. Bautista-Jia calls for interventional radiologists to become better at marketing themselves, as she believes increasing awareness of the minimally-invasive possibilities offered by interventional radiology will foster the greater multidisciplinary collaboration necessary to best serve patients with uterine fibroids. She also acknowledges that more work needs to be done to collect data on the plausibility of pregnancy follower UFE.
What did you learn from this study?
Firstly, that UFE is safer than surgery with a lower rate of post-procedure blood transfusions. I think this is primarily due to the more invasive nature of the procedure [myomectomy], resulting in greater blood loss compared to UFE. Other studies corroborate our results such as the retrospective study published by Narayan et al in the Journal of Vascular and Interventional Radiology (JVIR) in 2010.
One of our most surprising findings was that UFE resulted in a much higher rate of improvement in menorrhagia when compared with myomectomy. Seventy-five percent of patients in our UFE group reported an improvement in menorrhagia, versus only 50% in our myomectomy group—menorrhagia is the most common symptom that patients present with. Being a woman myself, I think that if I had symptomatic fibroids, I would rather have a procedure where you do not have a large incision, and you avoid the complications that can come with surgery such as blood loss and the development of adhesions which put you at risk for complications in the future.
Why do you think so many potential patients do not know about UFE, and what role can interventional radiologists play in spreading the word?
Firstly, a patient’s primary care physician is normally an internal medicine specialist or an obstetrician gynaecologist. Those are the doctors that patients see consistently, whereas interventional radiologists are specialists only seen by referral, at least in the USA. Those physicians are the gateway to get to interventional radiology, and may not be aware of this procedure. Maybe this lack of awareness is on us for not being more vocal about this procedure, and for publishing in journals that are specifically read by interventional radiologists. We need to be more proactive in letting other specialties know about this procedure, so they know it is an option to offer to their patients.
Additionally, if patients are seeing obstetricians and gynaecologists for their problems, and obstetricians and gynaecologists are the ones performing myomectomies, of course they are more familiar with that procedure, and are probably more inclined towards keeping those patients and providing comprehensive care.
We also need to be more vocal about what our specialty is and what procedures we do, to reach patients directly, and to educate the wider public on what it is that interventional radiologists do. We have to be better at marketing ourselves and our procedures.
Another reason may be, as studying fibroids is a relatively young branch of research, there is not enough data yet proving the safety of UFE in terms of pregnancy outcomes after the procedure. I think the most important thing interventional radiologists can do is to build a registry of patients who had UFE and who attempted to conceive following the procedure, so we can see whether it is safe or not. Being able to assuredly offer a minimally invasive treatment to patients with uterine fibroids who want to later get pregnant would be hugely valuable. We need to have more data for how UFE affects the plausibility of pregnancy post-procedurally.
The late Dr Pisco’s recent research in patients receiving conventional or partial UFE suggested that the procedure may actually aid in fertility. Particularly partial UFE in which only the arteries feeding the fibroids were embolised appeared to reduce the risk of infertility. These findings should be further explored.
Why do you think it is important to work with obstetricians and gynaecologists?
I think it is of the utmost importance, you have to have good relationships with all the physicians in your hospital, because of course everyone has something important and valuable to contribute to patient care. In specific situations, other specialities’ inputs and experiences may be more important for a patient and can help you to look at the situation from a different point of view. If any group is working in isolation, that is a disservice to the patient, because the treatment options are limited.
However, many women are not receiving fibroid embolizations- a study published by NEJM found that, in the USA, just a few thousand patients receive UFEs each year, compared to around 200,000 who have hysterectomies. Some of these hysterectomy patients likely could have been treated with UFE and had their uteruses preserved, so the collaboration is clearly not as strong as it could be in an optimal scenario. We still have a way to go.
Vicki Marx (2018–19 SIR president) awards Alan Matsumoto the Charles Dotter Lecture Award
Interventional radiologists must work as a group to make the practice of medicine more patient-centric and efficient, said Alan H Matsumoto, professor and chair of the department of radiology and medical imaging at the University of Virginia, Charlottesville, USA, who delivered the Society of Interventional Radiology’s (SIR) 2019 Dr Charles T Dotter Lecture during SIR’s annual scientific meeting (23–28 March, Austin, USA).
“By providing timely and accurate diagnoses and performing minimally invasive procedures with less morbidity and faster recovery times for patients, interventional radiologists are well positioned to address the triple aim of healthcare: better patient care, improving the health of populations and reducing per capita costs,” said Matsumoto.
“We must have the will and fortitude to employ patience while we adapt and create mutually viable practice models for all members of our specialty. Interventional radiology can go so much further together, as one, in our efforts to grow the specialty and serve our patients,” he said. “We must grow our relationships with patients to transition from being a doctor’s doctor to being a patient’s doctor. Our patients can and will become some of our biggest advocates and allies, as long as we put them at the centre of our care models.”
Matsumoto based his lecture on four facts that he believes are impacting the practice of medicine and IR in the USA. In his words, these are:
US healthcare is the most expensive in the world, yet ranks last amongst developed countries.
Consumerism is starting to drive healthcare.
Information is doubling every 73 days.
Healthcare is changing so quickly, that being adaptable is now a requisite for health systems and providers.
The US healthcare system is expensive
Elaborating on the expense and inefficiencies of the US healthcare system in his Dotter lecture, Matsumoto quoted an international study from 2014 that looked at 11 different healthcare factors in developed nations, including efficiency, access, quality, and infant mortality, where the USA ranked last. “Despite that”, he said, “comparing the life expectancy amongst these 36 different developed countries, the USA ranks just 31st. Life expectancy in the USA was 78.6 years in 2016. In 2018, it decreased a little more.”
He continued, “Despite the fact that our quality is lagging, and our life expectancy is below other developed countries, the cost of US healthcare is still going up. It is averaging US$12,000 per person, per year. What that translates into is that the cost of healthcare in the USA is more than two times the cost in any other developed country, and translate to about US$3.3 trillion a year, which is about 18% of the US GDP and more than the entire GDP of the United Kingdom.”
“Consumerism is driving healthcare”
Speaking to Interventional News, Matsumoto expanded on the role of consumerism in driving healthcare. “Consumerism has hit the marketplace in healthcare. At the same time, industry has changed how they are approaching healthcare”, he said. “There is a lot of money in healthcare, so when the business sharks smell the blood in the water, they go to it. Retailers, payers, pharmacies, private equity firms and venture capital groups are becoming more involved in the delivery of care. They are forming US$100–200 billion corporations and partnerships and vertically-integrated health system networks to affect and control where patients receive their care. Mega-mergers, acquisitions, partnerships and corporatisation of medicine are more commonplace, such that the era of healthcare disruption is here and is causing many hospitals to close because they can no longer compete.”
Considering the purchasing power and impact of these large, transnational companies, as compared to smaller health systems or to the amount of individual hospitals, Matsumoto asked the audience to “Imagine the influence these companies can have on our healthcare marketplace.”
Showing a graph of changes in healthcare premiums between 1999 and 2015, he demonstrated that healthcare premiums have increased more than 200%, whilst earnings had only increased 56% in the same timeframe. Noting this, he said that “This financial divergence is creating a major problem for patients and employers, so many folks are choosing large deductible plans and higher co-pays, which ultimately transfers the costs down to the patient.”
“In addition, the growth in household spending between 2008 and 2016 grew on average about 1.6%, yet expenditures related to items like apparel, entertainment, housing and transportation have grown less than 1.2%, while the cost of health care and health insurance increased 5.6% and 8.4%, respectively. Healthcare costs have risen so much that patients are not able to make their payments, causing bad debt to rise 500%, increasing from to 1% to 5% over that same eight-year period. Therefore, increasing healthcare costs alone has effectively wiped out any significant income gains for the average family.”
“It has also led many politicians and patients to advocate for a single payer system. Indeed, the CEO of Walgreens was quoted in The New York Times as saying, ‘The patient as a consumer will expect, and have increasingly seamless access to, care when, where, and at the value that they want’. The need for price transparency and more affordable care are really driving consumerism.”
He went on to use the example of the cost for a total knee replacement in various geographies in California. The average cost of this surgery was US$22,000 more, according to Matsumoto, on the Monterey coast than in the San Joaquin Valley. “This variability in cost without demonstrated difference in outcomes has led to the development of online shopping sites; further driving consumerism,” he told the SIR audience.
Summing all these difficulties, Matsumoto stated: “All of these headwinds in the healthcare industry are leading to disaggregation of health care services, failing practices, and hospital closures.”
Information is doubling every 73 days
“In four years, we will be dealing with one million times the information we are dealing with today”, Matsumoto informed delegates. “An inflection point in business occurred around 2005,” he went on to say. “Empowered by an exponential growth in computational capabilities, industry seized the opportunity to use this information to usher in the digital age of business and social media. Over the next few years, Google introduced Android and acquired YouTube. Twitter was launched. Virtual Machine (VM) software soon appeared—which made it possible to run multiple systems and applications simultaneously, which eventually enabled cloud computing. The development of IBM Watson, a cognitive computer which used machine learning and artificial intelligence algorithms, was also initiated. The ultimate disruptor, the Apple iPhone, was also introduced. Technology was changing the world, and with it, health care.“
“The rapid pace of data generation and information sharing has made it difficult for systems and people to manage and adapt to this accelerating pace of change.” Matsumoto said.
Being adaptable is a prerequisite of working in the US healthcare system: The opportunity for IR
When asked how interventional radiologists can adapt to this changing environment, Matsumoto explained to this newspaper: “Because of the nature of our specialty, IR is well-positioned to help in managing this healthcare conversation.” He cited a paper authored by Donald Berwick, a former administrator of the Centers for Medicare and Medicaid Services, and colleagues, in which they outlined the “triple aim of healthcare”. These were, in Matsumoto’s words, “Better health for patients, with improved quality, access, and outcomes; enhanced population health; and reducing the costs of healthcare, or at least bending the cost-curve for health care.”
However, the rate of change is accelerating, making it feel as if we are in the middle of a disruptive health care tornado, resulting in fragmentation and disaggregation of patient care, while at the same time creating a sense of urgency to fix things. In addition, most organisations and people adapt to change on a linear scale, making it difficult for them to adapt to the exponential rate of change that is occurring, which is further aggravating the health care equation. In this environment, interventional radiologists are very well-positioned to help address the triple aim of health care because of the innovative and creative nature in which interventional radiologists address patient care dilemmas by using minimally-invasive procedures. It is in this current environment that the specialty of IR and its tendency to attract providers with a high adaptability quotient also come into play. Interventional radiologists are better suited than most providers to adjust to the accelerating rate of change in medicine. Therefore, my message is: patients and patience—by keeping patients as our ‘true north’ and remembering that patients are our reason for being, while we exercise patience in making decisions and developing solutions going forward. It is also the perfect time for interventional radiologists to evolve from being a doctor’s doctor to being the patient’s doctor.”
Emphasising his take-home message, Matsumoto said: “The biggest message I have is that unity and purpose are essential, not only for our patients, but also for our specialty. With the fragmentation that is occurring in healthcare, if the specialty of IR is not unified and segments of IR go off separately, our collective voice will become a whisper, such that the policy makers, legislators, payers, health systems, and most importantly patients, will not hear us. They will not recognise the value and special skills we bring to the equation during this disrupted and fragmented period in health care.”
Ending on a positive note, he said to Interventional News: “I wanted to convey that we are much stronger together than apart, and the sum of the whole is greater than the individual parts.” He ended his Dotter lecture with a take home message quoting an old African proverb: “If you want to go quickly, go alone; if you want to go far, go together.”
The Dotter Lecture, supported by SIR Foundation, is an annual event named in honour of Charles T Dotter, considered universally to be the founding father of interventional radiology. SIR says that the annual lecture spotlights an outstanding interventional radiologist who has greatly contributed to the field and to the society.
“Dr Matsumoto’s commitment to patient-centred care is representative of what the future of interventional radiology will be,” commented SIR president M Victoria Marx, an interventional radiologist at Keck Medicine of USC, and professor of clinical radiology and diagnostic radiology residency program director at Keck School of Medicine of USC, Los Angeles, USA. “His call for unity and a shared purpose among interventional radiologists is a model for us to follow to make a change in the wider health care community.”
A University of Virginia faculty member since 1991, Matsumoto has helped train more than 200 diagnostic radiology residents and 100 vascular and interventional radiology fellows. His patient-centred and collaborative working style has led to the multidisciplinary care of many patients. Matsumoto is a past-president of SIR and former programme chair of the annual scientific meeting; he has been involved with SIR for 31 years.
Eluvia DES is the only technology that uses polymer-based drug delivery to treat Peripheral Artery Disease (PAD). Its polymer ensures that the majority of drug is delivered to the tissue while minimizing downstream particulates. Boston Scientific has more than 20 years of expertise developing and commercializing stents that elute paclitaxel via a polymer across coronary and peripheral vessels. Eluvia’s safety results combined with a holistic review of all Boston Scientific’s long-term clinical data on coronary polymer-based paclitaxel eluting devices showed no difference in all-cause mortality when compared to non-coated devices.
This video was filmed and sponsored by Boston Scientific. It is being distributed in association with Interventional News.
Top: Fragment of green suture (size 2) inserted into a 4 FR catheter. Middle: Fragment of purple suture (size 2) inserted into a microcatheter. Bottom: Blue particles roughly cut with scissors. Image courtesy of Vincent Vidal.
Vincent Vidal (Marseille, France) and colleagues have demonstrated the in vivo feasibility of arterial embolization with permanent and absorbable suture fragments, leading them to propose what they have termed the “FAIR-Embo” concept to the wider interventional radiology (IR) community. Writing in Cardiovascular and Interventional Radiology (CVIR), they conclude: “Embolization by absorbable and non-absorbable suture is a feasible and effective treatment, which opens up the possibility of global use of this inexpensive and widely available embolization agent”.
Speaking on this topic for the first time at GEST (Global Embolization Oncology Symposium Technologies; 9–12 May, New York, USA), Vidal presented the results of the preclinical study to attendees, calling this “the first step” towards his ambitions for the FAIR-Embo initiative. In this initial preclinical study, the investigators used a porcine model to test the feasibility and safety of arterial embolization with absorbable and non-absorbable suture fragments.
Their publication reports that the embolization with these agents was a technical success. As described in the CVIR paper, an interventional radiologist embolized the target artery by inserting a suture fragment into the lumen of a 5ml syringe, and then pushing it through the catheter, along with contrast agent. Once a complete occlusion of the artery was achieved, the embolization was finished. The maximum suture fragment diameter corresponded with the inner catheter and microcatheter diameter: for example, when using a 4F catheter, the largest compatible suture fragment diameter was 0.9mm.
Dubbing this method the “FAIR-Embo technique”, Vidal and coauthors state: “The FAIR-Embo technique is similar to a torpedo gelatine embolization. In our study, the selective catherisation, along with an operator, has resulted in selective embolizations without any off-target embolizations.”
They continue: “FAIR-Embo is a concept based on the hope [of using] interventional radiology in emerging countries, by the development of safe, available and cheap embolic material. “This work [the preclinical study] is a proof of concept of the feasibility and safety of the FAIR-Embo procedure, using homemade suture fragments—made from a globally available suture material—with the aim of making arterial embolization available in the greatest number of countries.”
FAIR-Embo ambitions
“Interventional radiology is very powerful for treating a vast range of different indications”, Vidal said at GEST. Showing an image of a well-kitted out angiography suite replete with multiple screens and bright, clinical lighting, he continued: “This is what we think when we think of interventional radiology in our country. In emerging countries, this is not the case.”
Elaborating to Interventional News, he explained: “We have the knowledge, skill, and materials to save lives through interventional radiology, but these are unequally distributed around the world. In certain countries with emerging economies, physicians cannot perform embolizations, as they lack the embolic agents necessary. This can be for two reasons: firstly, the embolic agent may be too expensive; secondly, the material may not be available in that country, as the manufacturer does not distribute in that region. In both these cases, we can potentially offer a solution, if further testing proves that embolization with absorbable or non-absorbable sutures is safe and effective.”
Afshin Gangi, CIRSE vice-president, is enthusiastic about FAIR-Embo, commenting: “Even if this concept is not adapted for all cases, if this material becomes clinically available [as an embolic agent], it will be a game changer for developing and even for industrial countries.”
Detailing why he thinks this, Gangi says to Interventional News: “Traumatic, post-partum or post-surgical bleeding is a major cause of mortality. Until the late 1970s, operative management was considered the only legitimate course for blunt and penetrating abdominal and extremity vascular injuries. Interventional techniques first popularised in the early 1970s now offer a wide range of solutions, principally using transcatheter arterial embolization. Various embolic agents (for example, coils or gelfoam) and particles may be used to stop or control bleeding. All theses agents used individually or in combination can save lives by stopping life-threatening bleeding.
“An embolization performed by a well-trained interventional radiologist is essential in all centres dealing with bleeding—trauma centres, maternity wards, surgical units where high blood loss is common, to name a few. In developing countries, training interventional radiologists to safely perform embolization is key. However, regardless of IR training or the presence of an angiosuite with high resolution C-arm fluoroscopy capabilities, availability of the embolic agent is an issue. The idea of having an efficient embolic agent which is available anywhere and is cost-effective is very attractive.
“The idea underpinning ‘The FAIR-Embo Concept’, which demonstrates the feasibility and efficacy of using non-absorbable and absorbable sutures, is about making a cheap embolic agent available everywhere. In addition to this availability, the benefits of this material are that it is inexpensive, can be temporary or permanent, that it leads to mechanical obstruction, and that suture fragments are easy to work with.”
Where FAIR-Embo started and next steps
Vidal, though he describes a conversation in Alexandria, Egypt, with Jafar Golzarian (University of Minnesota, Minneapolis, USA), a co-convenor of GEST, as catalytic. Allegedly, Golzarian and he were talking of many nations’ inability to afford the cost of materials for interventional radiology procedures. When asked about this conversation, Golzarian tells Interventional News: “We were talking about the cost of stents, and if it would be possible to create cheaper stents for use in countries that do not have much money. With this in mind, Vincent [Vidal] started to think about what we could do for embolization, and then he realised we have these absorbable and permanent suture materials that he could cut and use as an embolic agent. It is very smart.”
Currently, Vidal and his team are working on a second preclinical study. This will also use small fragments of sutures (non-spherical, non-calibrated particles, as in the first preclinical study presented at GEST and published in CVIR), but this time Vidal explains to his newspaper that the aim is to investigate their safety and efficacy when treating benign and malignant tumours. “That means we can have a range of embolizations, which is important”, he states. Vidal hopes to have completed this work and have the results before the end of the year.
The next step will be to run a clinical study, where the feasibility of the FAIR-Embo technique can potentially be demonstrated in humans. Vidal informs Interventional News that, dependent on favourable outcomes in the second preclinical study, he hopes the clinical study can begin at the start of 2020. “We need to move as quickly as possible,” Vidal urges. “My goal is for everyone in the interventional radiology community to play their part; I want to give this idea to everyone. If we get good clinical results next year [2020], I would like to create a foundation to collect money to develop the FAIR-Embo project.”
Vincent Vidal
An international effort
Ultimately, Vidal would like FAIR-Embo to be an international effort, with interventional radiologists from developed countries working with those in more resource-poor settings to provide these cheaper, safe embolic agents.
He stresses that this is an opportunity to spread interventional radiology practices across the world, offering these minimally-invasive, image-guided procedures to all countries. The target regions are Africa, South America, South-East Asia, and some countries in the Middle East, such as Iran and Iraq.
However, Vidal stresses that “it is important to understand that this community [of interventional radiologists] do not want to do the job for physicians in the emerging country.” He says: “We plan to provide the tools for them to do these procedures and build the interventional radiology practices themselves. This will give them the opportunity to do other kinds of interventional radiology procedures in the future.”
The opportunities this endeavour represents for industry is something emphasised by multiple proponents of the FAIR-Embo initiative. Speaking with Interventional News, Golzarian said: “This certainly offers an opportunity to developing countries, in terms of physician education and patient outcomes, but also for industry. If these emerging countries start to perform embolizations, they will be able to attract more interventional radiologists, to train a younger group of physicians, and this will help grow interventional radiology and thus the market these companies operate in.”
Marc Sapoval (Hôpital Européen Georges-Pompidou, Paris, France), co-convenor of GEST with Golzarian, lent his support to the project, enthusing: “If we could do fibroid embolization like this, it would be amazing”.
Marc Sapoval presents at GEST during the PAE Symposium
Marc Sapoval presents at GEST during the PAE Symposium
Current evidence supports the use of prostate artery embolization (PAE) as a safe, effective, and minimally-invasive treatment for the symptoms of benign prostatic hyperplasia (BPH) in appropriately selected patients. This is the conclusion of a multisociety consensus position statement on the use of PAE in the treatment of lower urinary tract symptoms attributed to BPH. The document has been published in the May edition of the Journal of Vascular and Interventional Radiology (JVIR) and outlines recommended standards of practice. The multisociety and multidisciplinary position statement comes from the Society of Interventional Radiology (SIR), the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Société Française de Radiologie (SFR), and the British Society of Interventional Radiology (BSIR).
However, the interventional radiology (IR) community is still working to convince their urology colleagues to adopt the procedure as one treatment option. An SIR-sponsored research consensus panel for PAE has convened with urologists from the American Urological Association (AUA) to map a path towards PAE gaining acceptance in the urologists’ own guidelines. This meeting was chaired by Clifford Davis (Medical College of Virginia, Richmond, USA) and Jafar Golzarian (University of Minnesota, Minneapolis, USA). Golzarian informed Interventional News that one of the key takeaways from this meeting was understanding the importance urologists place on sham studies. Currently, a study comparing PAE with a sham procedure is underway; many in the IR community are hopeful that the publication of this data will support their case for the recognition of PAE as an effective, minimally-invasive procedure by urologists.
The recommendations of the multisociety consensus position statement
The multisociety release, penned by Justin McWilliams (David Geffen School of Medicine, Los Angeles, USA) et al, advises PAE be used as a “valuable minimally invasive option for patients who cannot tolerate or who have failed medical therapy, and those who are poor surgical candidates or refuse invasive surgery.” The document makes the following eight recommendations:
PAE is an acceptable minimally invasive treatment option for appropriately selected men with BPH and moderate to severe lower urinary tract symptoms.
PAE can be considered as a treatment option in patients with BPH and moderate to severe lower urinary tract symptoms who have very large prostate glands (>80cm3), without an upper limit of prostate size.
PAE can be considered as a treatment option in patients with BPH and acute or chronic urinary retention in the setting of preserved bladder function as a method of achieving catheter independence.
PAE can be considered as a treatment option in patients with BPH and moderate to severe lower urinary tract symptoms who wish to preserve erectile and/or ejaculatory function.
PAE can be considered in patients with haematuria of prostatic origin as a method of achieving cessation of bleeding.
PAE can be considered as a treatment option in patients with BPH and moderate to severe lower urinary tract symptoms who are deemed not to be surgical candidates for any of the following reasons: advanced age, multiple comorbidities, coagulopathy, or inability to stop anticoagulation or antiplatelet therapy.
PAE should be included in the individualised patient-centred discussion regarding treatment option for BPH with lower urinary tract symptoms.
Interventional radiologists, given their knowledge of arterial anatomy, advanced microcatheter techniques, and expertise in embolization procedures, are the specialists best suited for the performance of PAE.
In addition to the four societies that authored the guidelines, these recommendations are endorsed by the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR), the Canadian Association for Interventional Radiology (CAIR), the Chinese College of Interventionalists, the Interventional Radiology Society of Australasia, the Japanese Society of Interventional Radiology, and the Korean Society of Interventional Radiology.
Speaking recently at GEST (Global Embolization Oncology Symposium Technologies; 9–12 May, New York, USA), lead author Justin McWilliams addressed the audience on the status of international recommendations for PAE. “These recommendations are very supportive of PAE, and I think are reflective of the data and literature that are currently out there. With the endorsement of multiple international IR societies, my co-authors and I reviewed all articles published between 2010 and 2018 relevant to PAE—some 280 articles, which were whittled down to 67 after duplicate cohort, case reports and technical papers were excluded—and summarised their findings.” Of the 67 included articles, three were randomised controlled trials, a further three were non-randomised comparative trials, and 17 were unique cohort studies. There were also multiple reviews and meta-analyses, in addition to miscellaneous papers focusing on factors such as cost and radiation exposure. In total, over 2,200 patients from eleven countries were reviewed in these studies.
“The overall findings were of no surprise to anyone in this room”, McWilliams said to the attendees of the GEST PAE Symposium, all interventional radiologists, “and are similar to the findings of prior meta-analyses. PAE is definitely effective; IPSS [International Prostate Symptom Score] improvement, depending on which study you look at, is between 10 and 18 points, and quality of life improvement ranges from two to four points. Just as importantly, PAE is very safe, with a low major complication rate and no change in erectile function. Ejaculatory dysfunction is still an open question; that was originally thought to be very uncommon, but some more recent studies have shown higher than expected rates of either reduced ejaculation or dry ejaculation. Radiation dose seems to be similar to other complex embolizations, such as gastrointestinal haemorrhage or pelvic arteriovenous malformation embolization. In certain specific clinical scenarios, PAE is also effective. Definitely so in very large prostates, and catheter independence can be achieved in approximately 80% of patients with a Foley catheter. Haematuria of prostatic origin can almost always be stopped immediately.”
Calling this “a landmark document”, Marc Sapoval (Hôpital Européen Georges-Pompidou, Paris, France), a co-author of the statement, voices his support to this newspaper: “At this point in 2019, we can say that PAE can be used safely and effectively in patients as an alternative to other treatments. This is strongly stated and supported by IR societies all around the world. I think this is very important for IR, to give us confidence in our support of PAE.”
Speaking to Interventional News of the importance of these guidelines, Sandeep Bagla (Vascular Institute at Virginia, Woodbridge, USA), a co-author of the document, says: “We as a community are proud to have seen these guidelines come to fruition, after many years of having our initial guidelines out. It is a very difficult and tedious process to update a position statement. Along with many other important co-authors, including lead author Justin McWilliams, who really was the energiser behind this project, we were able to pull together a collaborative document representing the evidence-based view of many societies around the world. The value of this document is multi-fold. It is a rather big step for SIR to put forth this document with recommendations; it mirrors the actions of other large societies, such as the American Heart Association, where the guidelines are presented in a similar manner, based on level of evidence and the strength of recommendation. That is important, because many guidance documents just release recommendations based on panel agreement, not based on a review of data, and without using a universally accepted grading system, like we do in these recommendations.”
History of benign prostatic hyperplasia treatment recommendations
Prostate artery embolization is a minimally-invasive treatment for lower urinary tract symptoms attributed to BPH. More than 70% of men aged over 70 are affected by BPH, and a quarter of men over 70 have moderate to severe lower urinary tract symptoms that impair their quality of life. This has led McWilliams et al to call BPH and ensuing lower urinary tract symptoms a “significant health issue affecting millions of men”.
The lower urinary tract symptoms caused by BPH have historically been treated by medical and surgical methods. Medical therapies, such as α-1 blockers and 5-α reductase inhibitors, are the mainstay of treatment for mild to moderate lower urinary tract symptoms, while the more invasive transurethral resection of the prostate (TURP) and simple prostatectomy are considered the gold standards for patients with severe symptoms.
After initial reports on PAE in humans from João Pisco (Lisbon, Portugal) and Francisco Carnevale (University of Sao Paulo Medical School, Sao Paulo, Brazil), McWilliams described the AUA as “unimpressed”, after their 2010 guidelines for the management of BPH failed to mention PAE. An initial review by the UK National Institute for Care Excellence (NICE) concluded in 2013 that more research was needed to establish the safety and efficacy of the procedure. McWilliams authored an initial SIR position statement in 2014, with multiple other interventional radiologists, though he says that “at that time, the data was not yet mature. We also concluded that additional investigation was needed before we could accept PAE into routine therapy.”
However, “a lot has changed over the last five years”, he says. To date, more than 2,000 patients have been studied in PAE-pertaining publications, and there have been three randomised controlled trials comparing PAE to TURP. The longest duration of follow-up now exceeds five years. An FDA review in 2017 concluded that “the probable benefits outweigh the probable risks for this indication”, and in June the same year, the indication of Embosphere microspheres (Merit Medical) was expanded through the FDA’s 513(f)(2) de novo classification to include PAE. In 2018, the product was approved for the same indication by a 510(k) pathway. Embozene microspheres (Boston Scientific) also gained an expanded indication in 2018, with the US FDA granting approval for its on-label use in PAE treatment in the USA via the 510(k) pathway.
In the UK, NICE determined last year that the evidence on the safety and efficacy of PAE for BPH was adequate to support the use of this procedure on the National Health Service (NHS). This decision came after BSIR and the British Association of Urological Surgeons (BAUS) worked together to coordinate the UK ROPE study. The study compared embolization to conventional prostate surgery. It found embolization provided a clinically and statistically significant improvement in symptoms and quality of life for men with enlarged prostate.
Also last year, in the USA, the updated AUA guidelines briefly mentioned PAE, where they did not recommend the procedure’s use outside of a clinical trial. During a debate at GEST on the topic this May, no one in attendance said they thought PAE should be restricted to clinical trials only. Indeed, during the PAE Symposium hosted by the conference, Riad Salem (Northwestern University, Chicago, USA), another co-author of these multisociety guidelines, said that, with the FDA approval of the Embosphere and Embozene microspheres, interventional radiologists “should not assume that PAE can only be performed as part of a clinical trial. In fact,” he added, “most cases are not. I think that is an important nuance.” However, he also said that “the most powerful data you can generate for your institution is the data generated internally”, and urged any audience members who performed PAE to collect data from their own patients. This is something done by an interventional radiologist attending the GEST PAE Symposium, who shared that he contacts all of his PAE patients one, three, six and 12 months’ post procedure.
In the most recent guidelines from 2018, the AUA calls for additional sham trials to account for possible placebo effect, and, in McWilliams’ words, “remain unconvinced of the efficacy and safety of the technique”. Tiago Bilhim announced that he is working on a study that will compare PAE against a sham procedure, and that he hopes for the results to be published later this year. This work was started with his colleague Pisco, who passed away in March this year.
Ari Isaacson presenting at GEST 2019, with the PAE panellists
“We will have a lot more success if we collaborate with urology”
As NICE approved PAE in the UK in 2018, Tarun Sabharwal (Guy’s and St Thomas’ Hospital, London, UK), a co-author of the guidelines and a GEST panellist, says that the collaboration between urologists and interventional radiologists in Britain acts as an example of how this relationship can benefit patients. He tells this newspaper: “These guidelines are significant in that they highlight to the American urological community what interventional radiologists can safely offer. Currently in the UK, with NICE approval for PAE, we have a good collaboration between urology and IR. We are able to offer our patients a broad spectrum of choices for their prostate outlet obstructions that include embolization, so it is an alternative to surgery for them.”
“For me, the issue I have with this therapy is that the response I get from urology is not a scientific response, it is an emotional response,” Salem tells the GEST audience during the PAE Symposium, speaking of the reaction he sees from urologists to PAE. “Even when you highlight the limitations of current therapies for BPH, and you highlight the tremendous work that has been done over the last ten years on PAE, the calibre of new studies that are being performed, the robustness of the findings, the attempts to recognise what you can and cannot do in a randomised setting, the post-hoc analyses, independent analyses by NICE—all the data triangulate to their being an important role for PAE in BPH. I think we have to get away from the emotionality of the subject.”
This sentiment is echoed by Marc Sapoval (Hôpital Européen Georges-Pompidou, Paris, France) and Golzarian, also authors of these recommendations. Speaking to Interventional News, Sapoval comments: “I think this document demonstrates to urologists that IR is organised as an international community, and has an academic rigour equal to that of other specialties. We are taking PAE seriously, because we believe the evidence points to the procedure as a safe and effective one. I do not believe urologists are taking us seriously at this point, though I hope that changes—it is the patients who are currently missing out.”
Golzarian adds, “PAE clearly works and helps patients—it is here to stay. In my opinion, the urologists’ guidelines are biased; they are mostly led by a few urologists that are personally very involved with urologic material development for BPH. Despite asking persistently, there was also no involvement of any IR society in the making of these guidelines [the most recent AUA guidelines, from 2018]. My strong recommendation is that SIR and AUA work hand-in-hand to identify which patients will benefit most from PAE. As a physician, our goal should only be to provide the best care for our patients; anything else is secondary.”
Understanding the demand from the IR community for a closer collaboration with urology, one interventional radiologist who recently met with the AUA describes this conversation: “What we discussed was the lack of level I evidence, [which is needed] for any therapy to make it into the guidelines. I think they [AUA] have a very strong stance on this. Having said that, they are not very rigid in terms of their guidelines, because, for example, they are flexible in using bipolar TURP or using GreenLight laser for large glands, which is not what the guidelines state. The guidelines only state [you should use] monopolar TURP or perform open prostatectomy, but that is not the standard of practice.
“However, we do have an SIR [multisociety] position statement, which details when to use this procedure [PAE] in specific settings, but PAE is not in the AUA guidelines. The AUA guidelines are important in terms of reimbursement for the procedure.” Insurance coverage for PAE currently varies across the USA.
In order to convince urologists that interventional radiologists are knowledgeable and skilled when it comes to PAE, Insausti Gorbea (Clínica Universidad de Navarra, Navarra, Spain), a panellist at the PAE Symposium hosted by GEST, stressed how important he believed it was to select patients carefully, saying “I think trials now should not be comparing PAE to surgery or TURP any longer; trials should be just to find out who are the good responders to this treatment. I think the technique is mature enough for this. Then we can say to urologists, ‘I know my limits’.” This comment was met with agreement by Bilhim, who added that for those first starting out performing PAE, they should begin with straightforward cases. Also in accordance, an audience member commented: “It does take some experience, so you should have five to seven years’ experience with basic embolization before moving on to PAE.”
Riad Salem (Chicago, USA) tells Interventional News at the SIR annual scientific meeting that removing a key step—the MAA scan to determine lung shunting—in a select subset of patients undergoing multistep Y-90 procedure can bring down the skin-to-treatment time to around 60 minutes.
Salem, who delivered the Honorary Lecture at the recent GEST 2019 meeting, clarifies that it would be premature to entirely eliminate the MAA scan for primary liver cancer patients, in whom, he says, the scan is “mandatory” to prevent shunting to the lung.
However, in UNOS stage 1 and stage 2 transplant patients with limited disease, where radiation segmentectomy is indicated, the procedure can be shortened considerably.
Sandeep Bagla (chair of Interventional Radiology at the Vascular Institute at Virginia, Woodbridge, USA) presented the results of an initial clinical study detailing his positive experience treating 20 patients with geniculate artery embolization (GAE) for mild to moderate knee osteoarthritis and moderate to severe pain at the annual scientific meeting of the Society for Interventional Radiology (SIR; 23–28 March, Austin, USA) earlier this year. This is the prelude to a second, ongoing, randomised controlled trial focusing on GAE—a larger cohort has just been approved by the US Food and Drug Administration (FDA). With this wealth of data on the horizon, an embolization registry is being launched with the hope of utilising artificial intelligence (AI) to predict patient outcomes.
Describing the initial pilot study to Interventional News, Bagla believes the results are promising: “We found that the vast majority of patients were responders, so 19 out of 20 patients demonstrated a significant improvement in pain. The average reduction in pain was around 65%. The improvement in disability and the improvement in physical function paralleled the change in pain scores.” All 20 patients were followed up to six months post treatment, and were assessed for pain, disability, and physical function. Imaging was also compared before and after embolization.
Sixty per cent of patients reduced their medications following the procedure. Bagla explains that “these patients were on a variety of medication— NSAIDS or opioids—and as the majority of patients were able to reduce these, I think this could have a big impact on the opioid crisis.”
“In terms of safety”, Bagla further comments, “there were a number of minor adverse events, the most common being transient skin discolouration, which occurs as a result of non-target embolization to cutaneous arteries. Two of our patients developed transient plantar numbness. Both of those patients were treated with a smaller sized particle, at 75 microns, so at that point we upsized our particle size to 100 microns, and we did not experience that [complication] further. Both of them resolved spontaneously in under two weeks, but they were eye opening in terms of us understanding what the potential complications could be.”
The investigators used a permanent embolic, Embozene (Boston Scientific), in this initial clinical study. Bagla says that this decision was informed by previous work in this space from Yuji Okuno and colleagues in Tokyo, Japan. Okuno et al used either the resorbable antibiotic imipenem/ cilastatin sodium or 75μm calibrated Embozene microspheres as the embolic agent in the transcatheter arterial embolization of 11 and three patients, respectively, suffering from mild to moderate knee osteoarthritis. “For us”, Bagla says, “the first natural step was to replicate and expand on what he had done, in terms of [using] a permanent embolic.”
However, a second, follow-up study is underway, with enrolment just completed, that will use a resorbable embolic, Optisphere (Medtronic). This is a randomised controlled trial comparing GAE against a placebo, with a scheduled 12-month follow-up. Twenty-one patients are enrolled, with 2:1 randomisation—14 patients will undergo embolization, and seven will have a sham angiogram procedure with catheterisation. After one month, if the patients who received the sham procedure have reported no improvements, they will be allowed to cross over to the embolization arm of the study and be embolized. “As those seven patients can be unblinded and receive the treatment, in reality, all 21 patients could potentially receive the treatment”, explains Bagla.
The US investigators have additionally recently received approval from the US Food and Drug Administration (FDA) for a much larger cohort study, which will roll out after the second study of 21 patients.
Desiring to make best use of this imminent wealth of data focusing on GAE and embolization as a whole, Bagla and his team are launching a global embolization registry. This registry will cover embolization for osteoarthritis as well as other forms, such as prostate artery embolization and uterine fibroid embolization. Bagla enumerates the benefits he believes a registry provides, saying that “Clinical trials can be criticised for their lack of ability to replicate the data in the real world. Many clinical trials are very well controlled, and have very strict inclusion and exclusion criteria, meaning that many patients are screened out. Registries allow practioners like myself, and others around the world, to collect real world data, so patients do not necessarily have to meet very strict criteria for enrolment and can be treated as part of their standard of care, where you are collecting information for all outcomes and adverse events. A registry also allows for large cohorts of patients. Now, you can get large cohorts of data from Asia, Europe, America, and pull the data together to perform more detailed analyses on subsets of patients. This enables you to determine which groups of patients do better.” He also hopes that data pooled in a registry will drive insurance coverage for the procedure.
The registry will be sponsored by JiggleMed, a software company that Bagla heads as CEO. JiggleMed is partnering with the artificial intelligence company Surgeri to collect, annotate and analyse the data. “Ideally”, Bagla enthuses, “this data will help us to predict which patients will do better. The future of our field is to gather this data in one place, and to use it to predict how individual patients will do. Annotating the data is a time-intensive process, but it is a project we are dedicated to.”
Data presented at EuroPCR today indicates that renal denervation with the Symplicity system (Medtronic) is associated with a reduction in subclinical atrial fibrillation in high-risk patients with hypertension over a median follow-up of two years.
In the study, 80 patients were randomised to undergo renal denervation or a sham procedure. Over two years, subclinical atrial fibrillation developed at a lower rate in the group of patients who received renal denervation than in the group who received the sham procedure (19% vs. 47%). Implantable diagnostic technology (Medronic) was used to monitor the occurrence of atrial fibrillation.
Marshall J Heradien (Stellenbosch University, Cape Town, South Africa), the principal investigator, says: “In this high-risk cohort of patients with hypertensive heart disease, who are at risk for atrial fibrillation and cardiovascular death, this study suggests there may be an important benefit provided by renal denervation. Consistent with previous studies, these data show that the renal denervation procedure offers a lasting, positive effect that may translate into improved clinical outcomes.”
He added that the “observed benefits are likely mediated by reducing sympathetic tonic”. However while the criteria for superior blood pressure lowering were met in the study, there were no significant differences between the sham procedure group and the renal denervation group at the six-month follow-up point.
New three-year data from the Global SYMPLICITY Registry were also presented at EuroPCR. The Global SYMPLICITY Registry is the largest registry to document the long-term safety and effectiveness of Medtronic renal denervation systems in a real-world setting in patients with uncontrolled hypertension. To date, the registry has enrolled more than 2,600 patients treated with renal denervation and includes three-year follow-up for more than 2,300 patients.
The latest outcomes indicate that significant and clinically meaningful reductions in both office and ambulatory blood pressure that were sustained out to three years’ post-procedure (16.5mmHg office systolic blood pressure and 8.9mmHg 24-hour systolic ambulatory blood pressure monitoring). The findings were consistent and sustained across various high-risk patient subgroups, including those with diabetes, isolated systolic hypertension, chronic kidney disease, resistant hypertension and those aged 65 years and older.
Dave Moeller, vice president and general manager of the Coronary and Renal Denervation business, which is part of the Cardiac and Vascular Group at Medtronic, comments: “As demonstrated by these studies presented at EuroPCR, new data continue to demonstrate that renal denervation is a safe and useful complement to manage uncontrolled hypertension, with patients experiencing meaningful blood pressure reductions out to several years and in the setting of daily clinical practice. Results from these studies will add to the robust growing body of evidence supporting renal denervation and may be important for consideration with patients suffering from uncontrolled hypertension.”
The long-awaited Global Vascular Guidelines for chronic limb-threatening ischaemia have been finalised, with the comprehensive guideline set to be published shortly. The news were announced by the Society for Vascular Surgery, one of the societies participating in the international effort to produce the document.
The Journal of Vascular Surgery is publishing the guideline, with 113 specific recommendations, as a supplement to the June edition. It will be made available online before late May, according to the Society for Vascular Surgery’s newspaper, Vascular Specialist.
The Society for Vascular Surgery (SVS) reports the the guideline “creates a new conceptual framework for treating chronic limb-threatening ischaemia, the end-stage of peripheral arterial disease. The document encompasses nomenclature, disease staging and a platform for evidence-based revascularisation that will allow for future evolution and quality improvement in the field.” Furthermore, a notable change is a purposeful move from the term critical limb ischaemia (CLI) to chronic limb-threatening ischaemia (CLTI): a name which the authors explain is a better reflection of the full spectrum of the disease.
Michael Conte of the Society from Vascular Surgery, Philippe Kolh of the European Society for Vascular Surgery and Andrew Bradbury of the the World Federation of Vascular Societies co-edited the guidelines document, with close to 60 additional authors. All specialties treating CLI were represented among the authors, the SVS notes, with participants from six continents. Highlighting the thorough and methodical work of the writing group, the finalised document is “a unique practice guideline, reflecting the spectrum of the disease and approaches seen worldwide,” Conte told the SVS.
The SVS further discloses that major recommendations will cover the need for comprehensive assessments in patients with suspected CLTI; optimal medical therapy, including a variety of treatments for CLTI patients; and prompt and effective revascularisation for patients with advanced ischaemia and limb threat. The document also outlines the importance of an individualised approach to improve patient care and reduce limb loss. Other significant changes include a standardised classification system with endorsement of the SVS Threatened Limb Classification System based on grading wound, ischaemia and foot infection (WIfI) in the affected limb, as well as introducing the Global Limb Anatomic Staging System (GLASS) to stratify patterns of arterial occlusive disease.
“Perhaps most notably, the guideline supports a structured approach to decision-making regarding revascularisation based on Patient risk, Limb severity and ANatomic complexity (PLAN), in that order of priority,” Conte comments in the SVS announcement. “The guideline seeks to provide a new foundation for practice but also for data collection to support evidenced-based revascularisation in CLTI.”
Philips has announced the launch of its new IntraSight interventional applications platform. According to a press release, the secure, application-based platform offers a comprehensive suite of clinically proven instant wave free ratio (iFR), fractional flow reserve (FFR), intravascular ultrasound (IVUS) and co-registration modalities to simplify complex interventions and speed routine procedures.
In image-guided treatments of the heart and peripheral blood vessels, there is an increasing trend to use advanced catheters and pressure wires that are capable of producing ultrasound images of the interior of blood vessels (IVUS) and perform blood pressure measurements (FFR and iFR). There is a growing body of clinical evidence that the use of such technologies in conjunction with interventional X-ray improves patient outcomes.
“IntraSight has made an immediate impact in our lab,” says Rasha Al-Lamee, a clinical academic interventional cardiology consultant at Imperial College Healthcare NHS Trust, London, UK. “It is so simple and intuitive to use that it took us no time at all to get used to it. It has made using physiology and imaging even quicker and easier, which is a great advance for us and for our patients.”
Philips IntraSight optimises lab performance with tableside touchscreen control, systems integration, data management and remote service diagnostics. The combination of IntraSight and Azurion, Philips’ image-guided therapy platform, provides an unmatched level of diagnostic insight and intuitive tableside control that enables clinicians to provide cardiac and peripheral vascular patients with superior care. IntraSight delivers an outstanding user experience with a modern, intuitive interface that minimises learning curves and increases workflow confidence.
A significant advance in Philips’ portfolio of systems, smart devices, software and services in image-guided therapy, the scalable IntraSight platform is based on Philips’ common software and hardware architecture.
Further providing seamless integration in the interventional lab, Philips SyncVision, available on IntraSight, advances patient care by mapping both the pressure profile and IVUS measurements of the whole vessel onto the angiogram. With iFR pullback and co-registration and IVUS co-registration, physicians can identify the precise locations causing ischaemia, plan stent length and placement with a virtual stent, and predict physiologic improvement.
iFR is an innovative pressure-derived index proprietary to Philips, allowing a simplified hyperaemia-free physiological assessment of coronary blockages. It continues to be adopted into clinical practice, states a Philips’ press release, with mounting evidence that this technology contributes to reducing costs, improving outcomes and enhancing the patient experience.
IntraSight will be showcased at the Society for Cardiovascular Angiography and Interventions (SCAI) 2019 scientific sessions (19–22 May, Las Vegas, USA) and EuroPCR (21–24 May, Paris, France).
Until recently, creation, maintenance and restoration of vascular access function was entirely performed by open surgical methods. However, it is becoming apparent that endovascular management is a valid treatment option and a comparable alternative to the open surgical one, write Panagiotis M Kitrou, Konstantinos Katsanos and Dimitrios Karnabatidis from Patras, Greece, who are organising the first EVA meeting on the topic on 21–22 June 2019, in Patras, Greece.
Vascular access constitutes the “lifeline” for haemodialysis patients. Until recently, creation, maintenance and restoration of function (when thrombosis occurred) was performed by open surgical methods. However, it is becoming apparent, verified even in the most recent surgical and interventional guidelines for vascular access, that endovascular management is a valid treatment option and a comparable alternative to the open surgical one.1–3
(L to R) Dimitrios Karnabatidis, Konstantinos Katsanos and Panagiotis M Kitrou
In the last decade, there has been a continuous development of novel endovascular tools and devices (some of which were initially tested in the arterial vascular bed) that have made the endovascular approach faster and more appealing. Different types of wires and catheters, low profile devices, high-pressure balloons, drug-coated balloons, scoring balloons and covered stents have improved patency rates, and in many cases circuit survival.4 Each of these devices offers an additional option to the operator. High-pressure balloons have revolutionised vascular access treatment, mainly because stenosis in this specific vascular field is characterised by an aggressive fibromuscular thickening that needs high pressures of up to 40atm, in many cases, to enable treatment. Drug-coated balloons have allowed for more extensive use of high-pressure balloons by decelerating the effect of restenosis.5,6 Covered stents offer a valid bail-out option in cases of persistent stenosis or elastic recoil; pseudoaneurysms; and ruptures—and there is Level 1 evidence supporting their use as a primary option for the treatment of venous graft anastomotic stenosis.7
When thrombosis occurs, endovascular treatment with thrombolysis, thrombectomy or, in many cases, a mix and match of these procedures offers quick, safe and efficient ways of blood flow restoration. It also allows the patient to return immediately to haemodialysis without the need for central venous catheter placement.8 Several thrombectomy devices are available on the market and there is already extensive clinical experience with these devices. An important benefit of endovascular treatment is that it offers the ability to perform, in the same setting, both declotting and treatment of the underlying stenosis, which in the majority of cases is the reason for thrombosis.
“EndoAVF”, a major advancement
Lately, there has also been a major advancement in the vascular access field with the endovascular creation of AVF. This innovation occurs in a scenario where the gold standard (open surgery) has a failure rate of more than 50%. With two systems already available on the market (WavelinQ [BD] and Ellipsys [Avenu]) and with evidence detailing their benefits beginning to mount, patients will have the opportunity to have their fistula created without the need for surgical cut-downs, incisions and sutures, which are largely responsible for failure of maturation and future stenosis. Being available via a 4F radial or “wrist” access or under ultrasound guidance, these fistulas are created in the deep venous system. “EndoAVF” provides additional vascular access creation sites (two when WavelinQ is used and one when Ellipsys is employed) and could conceivably become the primary option for fistula creation. The reason for this is that “endoAVF” does not implicate the superficial venous system, which is the system used in the open surgical fistula creation. Additionally, in case of failure, conditioning of the superficial outflow veins of the arm may occur facilitating faster surgical fistula maturation.
Even though there is a growing role for endovascular vascular access management, centres performing these procedures remain low. We believe it is important for all specialties involved to understand the benefits that endovascular approaches provide to haemodialysis patients. Meetings on the specific subject remain highly “open surgery oriented and those with broader audiences sometimes combine vascular access treatment with venous disease. We feel that there is a need to help disseminate education and awareness in this area, particularly among nephrologists on the endovascular pathway/service they can provide to their patients. Endovascular therapists, either interventional radiologists, vascular surgeons or interventional nephrologists would also gain from staying current with developments in the field with a view to improving the care available to haemodialysis patients. In light of the current developments in this field, hospital multidisciplinary team meetings should involve endovascular specialists and congresses on the specific subject should be geared towards a multidisciplinary approach. It is in this context that the EVA (Endo Vascular Access) Meeting was created—its content is specifically designed to focus on the treatment options that the endovascular approach offers to haemodialysis patients. From EndoAVF, trial updates and treatment of symptomatic central venous stenosis to central venous catheters and background development, the EVA Meeting presents a multidisciplinary faculty of physicians from around the globe. The first EVA Meeting will be held in Patras, Greece on 21–22 June 2019.
Panagiotis M Kitrou and Konstantinos Katsanos are assistant professors of interventional radiology and Dimitrios Karnabatidis is a professor of interventional radiology, Patras University Hospital, Patras, Greece. They are also directors of the EVA meeting.
References
Dariushnia SR, Walker TG, Silberzweig JE, et al. Quality improvement guidelines for percutaneous image-guided management of the thrombosed or dysfunctional dialysis circuit. J Vasc Interv Radiol. 2016;27(10):1518–30.
Ibeas J, Roca-Tey R, Vallespin J, et al. Spanish clinical guidelines on vascular access for haemodialysis. Nefrologia. 2017;37 Suppl 1:1–191.
Schmidli J, Widmer MK, Basile C, et al. Editor’s Choice – Vascular Access: 2018 Clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55(6):757–818.
Kitrou P, Papasotiriou M, Katsanos K, et al. Recent developments in endovascular interventions to sustain vascular access patency in haemodialysis patients. Nephrol Dial Transplant. 2018.
Trerotola SO, Lawson J, Roy-Chaudhury P, Saad TF, Lutonix AVCTI. Drug coated balloon angioplasty in failing AV fistulas: A randomized controlled trial. Clin J Am Soc Nephrol. 2018;13(8):1215–24.
Kitrou PM, Papadimatos P, Spiliopoulos S, et al. Paclitaxel-coated balloons for the treatment of symptomatic central venous stenosis in dialysis access: Results from a randomized controlled trial. J Vasc Interv Radiol. 2017;28(6):811–7.
Haskal ZJ, Trerotola S, Dolmatch B, et al. Stent graft vs. balloon angioplasty for failing dialysis-access grafts. N Engl J Med. 2010;362(6):494–503.
Kitrou PM, Katsanos K, Papadimatos P, et al. A survival guide for endovascular declotting in dialysis access: Procedures, devices, and a statistical analysis of 3,000 cases. Expert Rev Med Devices. 2018;15(4):283–91.
Boston Scientific has announced results from sub-analyses of the IMPERIAL clinical trial for the Eluvia Drug-Eluting Vascular Stent System. Data demonstrated that the efficacy and safety performance of the polymer-coated Eluvia drug-eluting stent does not appear to be affected by challenging lesions, defined as being severely to moderately calcified or completely blocked within the superficial femoral and proximal popliteal arteries.
One of the analyses from the global, randomised, controlled IMPERIAL trial, which evaluated the Eluvia Stent System in patients with symptomatic peripheral artery disease, assessed outcomes of patients diagnosed with moderate to severely calcified lesions. Highlights of the findings include:
A primary patency rate—a measure of the target vessel remaining unobstructed at 12 months—for patients diagnosed with moderate to severe lesion calcification of 89.2%
A low rate (2.8%) of target lesion revascularisation in study participants with moderate to severe lesion calcification at 12 months;
A low rate of stent thrombosis (1.1%) for patients treated with the Eluvia stent who were diagnosed with moderate to severe lesion calcification.
“Our analysis demonstrated the Eluvia stent is a highly effective treatment option for some of the most complex lesion classifications commonly associated with femoropopliteal disease,” said Frank Vermassen, Ghent University Hospital, Gent, Belgium, an investigator in the IMPERIAL trial. “The findings underscore the ability of this stent to successfully treat varying lesion characteristics, and its performance will continue to be observed in ongoing patient follow-up.”
Investigators also analysed the safety and performance of the Eluvia Stent System for patients diagnosed with having 100% blockage—or chronic total occlusions—at the target lesion and found that these patients experienced 83.9% primary patency at 12 months.
“The data adds to the clinical evidence supporting the Eluvia Stent System as a viable first-line treatment option for patients suffering from debilitating peripheral artery disease,” said Ian Meredith, executive vice president and global chief medical officer, Boston Scientific. “Designed with a controlled release of the lowest possible drug dose to seek the best clinical outcomes, we believe the Eluvia stent can become a preferred therapy option and look forward to continued clinical successes with this product.”
iD3 Medical has announced that it has received approval in Belgium to initiate a randomised controlled trial, BIOPACT-RCT: a physician-initiated multicentre trial evaluating the safety and efficacy of Biotronik’s Passeo-18 Lux drug-coated balloon (DCB) for the treatment of peripheral arterial disease (PAD) in the upper leg compared to the IN.PACT Admiral DCB (Medtronic). The first patient was enrolled by Roel Beelen in the OLV-hospital (Aalst, Belgium).
BIOPACT-RCT will be led by Koen Deloose (AZ Sint-Blasius Hospital, Dendermonde, Belgium) as principle investigator. The trial will enrol up to 302 patients. Six Belgian sites already have their approval. iD3 Medical also expects approval in Switzerland (four centres, co-principal investigator Christoph Binkert), Austria (two centres, co-principal investigator Marianne Brodmann) and France (four centres, co-principal investigator Yann Gouëffic). Included patients, Rutherford classification 2 to 4 with a max study lesion length of 18cm in the femoropopliteal arteries, will be randomised 1:1 to undergo treatment with either the Passeo-18 Lux or the IN.PACT Admiral DCB. The primary efficacy endpoint is freedom from clinically-driven target lesion revascularisation at 12 months, defined as any reintervention at the target lesion due to symptoms, drop of ankle-brachial-index (ABI) of more than 20% or a drop of 0.15 compared to the post-procedure ABI. The primary safety endpoint is a composite of freedom from device- and procedure-related death through 30 days post-index procedure, freedom from major target limb amputation (above-the-ankle) through 12 months post-procedure and clinically-driven target vessel revascularisation through 12 months post-index procedure.
IN.PACT Admiral DCB (Medtronic)
In iD3 Medical’s press release, Deloose comments: “Although we have already a lot of safety and efficacy data available on the Passeo-18 Lux through the BIOLUX P-I, P-II and the ongoing BIOLUXP-III trial, a more in depth, head-to-head comparison with today’s market leading DCB will offer more answers about the relative performance of DCBs and potential class effects. Especially related to the ongoing debate on DCBs safety concerning a signal of increased long-term mortality with paclitaxel-coated devices, based on the publication of Katsanos et al in the Journal of the American Heart Association, and the FDA- and CIRSE-statements here about additional patient level data, also in the longer run, are essential. Adapted patient informed consents, data safety monitoring board and clinical event committee instructions, and prolonged patient follow up procedures for the BIOPACT-RCT are already implemented in the Belgian approval and waiting for approval in the other countries.”
Deloose continued: “Also in this BIOPACT-RCT, patient safety is number one priority and an even closer monitoring of all the enrolments, can contribute to the clarification in this critical time for peripheral arterial disease endovascular therapies.”
Embolx has announced the commercial availability of the new Sniper K-tip in the USA and Europe. The sniper balloon occlusion family of microcatheters now includes the new K-tip, a 45-degree angled tip designed to enhance tracking and vessel access capabilities. This extension to the sniper family offers physicians the ability to customise treatment with an array of different balloon microcatheter lengths and tip options.
“The Sniper K-tip marks the first pre-shaped tip on a balloon microcatheter and has shown remarkable performance in accessing target locations previously too challenging to reach,” says Michael Allen, president and CEO of Embolx. “For interventional radiologists, the K-tip provides an additional option to handle complex anatomies so they can achieve improved results.”
The sniper microcatheters are now available with two tip options—straight tip or K-tip—and in three lengths: 110cm, 130cm and 150cm. The K-tip offers interventional radiologists better control and torqueability through hard-to-navigate vessels to deliver targeted embolization treatment, a press release states.
“Sniper has changed the way I do both chemoembolization and radioembolization. With sniper, I am able to infuse a higher volume of embolic agent into a smaller, focused area. This allows me to treat tumours more aggressively with less impact on normal liver tissue,” comments Brian Kouri, associate professor in interventional radiology at Wake Forest Baptist Medical Center, Winston-Salem, USA. “My initial case experience with sniper’s new K-tip design has been great in every respect. It allowed me to access some pretty small vessels quickly and navigate an over 180-degree vessel turn into the right gastric artery. The tip performance is impressive as it easily tracks inside vessels and torques on a one-to-one basis allowing the sniper to make sharp vessel turns.”
The sniper microcatheter alters blood flow‐dynamics by controlling pressure to increase therapeutic agent delivery into target areas. It is currently used for the treatment of cancerous tumours in the liver and other organs, enlarged prostate (benign prostatic hyperplasia), and uterine fibroids. This therapy allows the delivery of drugs and embolic agents to only targeted treatment areas, while protecting surrounding healthy tissues.
The sniper balloon occlusion microcatheter has been used in over 2,500 cases in hospitals within the USA and Europe to date.
Boston Scientific has won FDA approval for its Vici Venous Stent System for the treatment of iliofemoral venous obstructive disease.
The device received CE mark in 2013, and was developed by Veniti, one of the many companies Boston Scientific acquired last year. The company paid US$108 million for Veniti last August, and FDA approval of the Vici Stent System satisfies one of the milestones for up to another US$52 million.
Iliofemoral venous obstructive disease occurs when the flow of blood through the veins located deep in the pelvic region becomes blocked by a blood clot or compressed by anatomical anomalies. Endovascular treatment for venous obstructive disease is focused on restoring the normal flow of blood from the legs back to the heart. Because the iliofemoral veins are located deep in the pelvis, they may be subject to significant crushing forces from other anatomical structures such as the right common iliac artery. To help solve for this, the Vici stent system was designed to be uniformly strong and crush resistant, capable of restoring blood blow by creating a cylindrical, patent vessel.
FDA approval was supported by data from the VIRTUS study, a prospective, multi-centre, single-arm study with 170 patients. The VIRTUS study evaluated the stent in relation to pre-defined objective performance goals in patients with a clinically significant obstruction in the illiofemoral venous outflow tract. It met its primary safety and effectiveness endpoints.
According to Mahmood Razavi (St Joseph Hospital, Orange, USA), venous obstructive disease can cause quality of life issues without optimised treatment options.
“With the approval of the Vici stent, clinicians now have access to a stent that was purposely developed and engineered to resist the vessel compression and anatomical tortuosity commonly found within the iliofemoral venous system, enabling our ability to deliver best outcomes for our patients,” Razavi says.
Boston Scientific note that venous obstructive disease affects nearly 40% of the US population and can be caused by conditions such as deep vein thrombosis, post-thrombotic syndrome, and compressive diseases such as May-Thurner syndrome. In patients with venous obstructions, blood may pool in the legs, resulting in pain, swelling, and skin ulcers.
Within the context of liquid biopsy’s rising clinical application, Bruno Damascelli and Vladimira Tichà propose a means of improving this analytical technique through selective venous sampling. They argue that by drawing blood from a site nearer to the area affected by the malignancy, the sensitivity and specificity of the diagnosis would be enhanced. They present two illustrative cases that, according to the authors, “reinforce the interest for liquid biopsy”, a procedure they describe as “an important tool for the molecular definition of cancer and for its precise treatment”.
Incidence rates for malignant melanoma are currently rising more than those of any other malignancy. Predisposing factors are not fully known, except for the phenotype with fair complexion and light hair and eyes. A family history of melanoma accounts for 10% of all cases. Diagnosis is difficult because melanoma presents as a pigmented lesion, usually in a person with several cutaneous nevi. Electronic dermatoscopy has improved melanoma diagnosis, but excision of the skin lesion is normally conservative because staging is post-surgical unless there are distant lymph node metastases. Clinical-pathological staging is based on excisional biopsy, wide local excision, and sentinel lymph node biopsy. The American Joint Committee on Cancer (AJCC) melanoma committee strongly recommends sentinel lymph node biopsy because of the great difference in five-year survival rates in patients with negative lymph nodes. The sentinel lymph node must be removed for lesions with a Breslow thickness of 0 or >1mm, and those with spontaneous ulceration or with a mitotic rate of 1/mm2. This means planning at least three separate procedures: (1) excisional biopsy, (2) wide excision, and (3) selective lymphadenectomy (SLN).
It is now known that the DNA released by tumour cells (ctDNA) can be detected in blood even in an early stage of disease. This analytical technique, known as liquid biopsy, is increasingly finding clinical application. The limitation of liquid biopsy lies in the minimal amount of tumour DNA, which is masked by the prevalent amount of cell-free DNA (cfDNA) produced by the body’s normal tissue turnover. One or more mutations related to a certain tumour confirms the diagnosis with some certainty, as is the case when circulating tumour cells (CTCs) are found in blood samples. If blood is sampled in proximity to the venous drainage of the area affected by the malignancy, it is possible that a larger amount of tumour DNA will be obtained, with an increase in the sensitivity and therefore of the specificity of the liquid biopsy. Two cases presented here by way of example suggest that selective venous sampling should be considered in early-stage melanoma.
Case one
Figure 1 (Left): 53-year-old man—Histological examination of melanoma on left arm. Figure 2 (Right): Intraparenchymal metastasis, diameter 1mm, in sentinel lymph node.
Fifty-three-year-old man with nevus on left arm and a diagnosis on excision of superficial melanoma, with a Breslow thickness of 0.7mm, Clark level 3, non-brisk tumour-infiltrating lymphocytes (TILs), no ulceration or regression, mitotic rate of 2/mm2, no vascular and perineural invasion, and negative lateral and deep margins. The indication for SLN was marginal. Peripheral liquid biopsy was negative. Selective liquid biopsy via transfemoral catheterisation of the left subclavian vein showed fragmented circulating DNA with a p.Y1021S mutation in codon 1021 of the PiK3CA gene. No mutations were found in the KRAS, BRAF and NRAS genes. On SLN, melanoma metastases were found in one of two sentinel lymph nodes in the left axilla, as well as two intraparenchymal micrometastases, the larger measuring 1mm (Figures 1 and 2). Radical lymphadenectomy with 27 lymph nodes was negative, as was two-year follow-up of the patient.
Case 2
Figure 3 (Left): Seventy-nine-year-old man—Pigmented nevus on left arm, suspected melanoma. Figure 4 (Right): Right transbrachial catheterisation of left subclavian vein for selective liquid biopsy blood sampling.
Seventy-nine-year-old man with nevus on left arm, suspected to be melanoma (Figure 3). Selective liquid biopsy with sampling from the left subclavian vein (Figure 4) at the same time as peripheral sampling was suggested. Mutation p.Q61R of the NRAS gene in exone 3 was found, leading to a diagnosis of melanoma and wide excision (Figure 5) with sentinel lymph node lymphoscintigraphy and biopsy (Figure 6). Histological diagnosis confirmed melanoma with horizontal growth, no vertical growth, Breslow thickness of 0.9mm, Clark level 3, non-brisk TIL, no ulceration or regression, pigmentation present, mitotic rate 0, no perineural invasion, associated nevus present, and negative lateral and deep margins. Molecular tissue analysis confirmed the NRAS gene mutation. SLN biopsy was negative, as was liquid biopsy molecular analysis six months after surgery.
Figure 5 (Left): Wide local excision of nevus. Figure 6 (Right): Sentinel lymph node identification at time of wide local excision.
Bruno Damascelli and Vladimira Tichà are interventionalists at the Department of Interventional Oncology EMO GVM Centrocuore Columbus in Milan, Italy. Their work is sponsored by the Falciani Foundation. The authors report no disclosures pertaining to this article.
Jonathan Beard (Sheffield, UK) discusses the current medico-legal issues in the field and explains how interventionalists can become “the fall-guy for the inadequacies of other clinicians”. Beard touches on how the threshold for informed consent has changed “dramatically” in recent years which has led to “the death of medical paternalism”. He also talks about how doctors can protect themselves from the increased risk of litigation and why a signed consent form “is not consent”. Beard emphasises that when paclitaxel devices are used, patients must be told there “may be an increased risk of mortality”.
Hester Scheffer (Amsterdam, The Netherlands) advocates for the use of combined irreversible electroporation (IRE) and other immune stimulatory therapies to achieve greater overall survival in patients with pancreatic cancer. At the 2019 European Meeting on Interventional Oncology (ECIO), Scheffer presented the preliminary results of the first clinical proof of evidence study for an IRE-induced T cell specific immune response in pancreatic cancer in humans.
The presented work was a small side study of the recently completed PANFIRE trial, with the investigators conducting immune monitoring on 10 patients. Scheffer told the ECIO audience that this meant this “pilot study was therefore not powered for statistical significance”, and that they had carried it out for “exploratory purposes”. However, she said that the results were “interesting” nonetheless, and illuminating for the direction of future research.
The problem: Pancreatic cancer can “escape the immune system”
Pancreatic cancer is particularly aggressive, Scheffer explained, due to its ability to “escape the immune system”. The cancerous tumour is capable of this evasion through two mechanisms: its suppression of the tumour microenvironment, and the rarity of spontaneous apoptosis in pancreatic cancer cells.
Pancreatic cancer suppresses its microenvironment by releasing suppressive cytokines into the surrounding tissue, which upregulate immunosuppressive T cells (regulatory T cells and myeloid-derived suppressor cells [MDSCs]). These, in turn, downregulate effector T cells, which directly effectuate the immune response. The tumour is therefore not recognised by the immune system, and “T cell tolerance against the tumour develops”, Scheffer said.
The second way in which a pancreatic tumour limits the immunogenic potential is due to the low spontaneous apoptosis rate amongst pancreatic cancer cells: when a cell undergoes apoptosis, it breaks up into immunogenic epitopes that are taken up by antigen-presenting cells and transported to the lymph nodes, where a systemic, adaptive anti-tumour immune response can be elicited. This does not occur in pancreatic cancer.
The potential solution: shifting the balance “from immunosuppressive to immunostimulative”
Hester Scheffer presenting at ECIO 2019
Understanding these molecular machinations, Scheffer stated: “To improve the survival of pancreatic cancer patients, the cytokine balance needs to change from immunosuppressive to immunostimulative”. She and her colleagues hypothesised that IRE may be capable of altering this balance. As IRE reduces the tumour mass, it also leads to a reduction in the secretion of suppressive cytokines, which ultimately results in reduced T cell tolerance. Additionally, the apoptosis induced by the IRE treatment triggers the sequence of events that stimulates the systemic, adaptive, anti-tumour immune response not otherwise witnessed in pancreatic cancer patients. Scheffer added that “hopefully, memory T cells will then induce anti-tumour immunity and delay or maybe even prevent the development of metastases. Through this way, IRE could in fact be a type of in situ tumour immunisation.”
To test this hypothesis, Scheffer and colleagues sampled the venous blood of their patients three times: directly before IRE treatment, again two weeks after IRE treatment to investigate the immediate immune response, and then lastly three months post-IRE treatment, to investigate the durable immune response. White blood cells were isolated immediately after blood sampling and cryopreserved for later analysis. None of the patients in the pilot study had received pre- or post-IRE chemotherapy.
Speaking at the conference, Scheffer explained: “When we had collected the blood of all 10 patients, we broadly performed two different tests. In the first test, we determined the type, frequency and activation status of the circulating immune cells using flowcytometry. We investigated the MDSC and the T-cell subsets, and also activated PD-1 T-cells. But this only told us the number and the activation status of the circulating immune cells; it does not say anything about whether they were acting against pancreatic tumour specifically.”
To test the targeted immune response to the cancerous cells, the team performed tumour specific T-cell monitoring. They took the Wilms’ tumour 1 (WT1) epitope, which is expressed exclusively on the cell membrane of the pancreatic tumour, and coated it with an interferon-gamma (IFN-у) antibody so it could be detected. The investigators then combined the white blood cells collected from the patients with the Wilms’ tumour 1 epitope, and counted how many interferon-positive white blood cells—and thus Wilms’ tumour 1 positive white blood cells—there were. These represented tumour-specific T-cells, so tumour cells that were aggressive towards the pancreatic tumour.
The Dutch researchers reported a significant and a near-significant decrease in the immunosuppressive cells (the regulatory T cells [p=0.03] and the MDSCs [p=0.09]) two weeks after IRE. Scheffer said: “We also found a near-significant increase in the immune-effector cells [p=0.08]. So, the observed reduced immune suppression did seem to allow for the effector T cells to develop, just as we hypothesised.
“We also saw a significant de novo activation of PD-1 cytotoxic [p=0.04] and helper T-cells [p=0.01] two weeks after IRE, whereas the expression of the other immune checkpoints remained low and unchanged.”
Turning their attention next to the tumour-specific T cell monitoring, the investigators found an immune response against the Wilms’ tumour antigen, and thus against the pancreatic tumour, in five out of the 10 patients. Scheffer elaborated: “This Wilms’ tumour 1 response correlated with the reduced immune suppression. Most interestingly, the patients who had a positive, tumour-specific T-cell response had a higher median overall survival than patients who did not have this Wilms’ tumour 1 response [p=0.055].”
Scheffer summarised: “We found a temporary alleviation of the tumour-induced immune suppression, which created a window for anti-tumour T cell activation that was in turn associated with better overall median survival. These results advocate for the combination of IRE with other immune stimulatory therapies to further enhance this effect and achieve an even better overall survival.”
Future work, Scheffer said, will look at the possibilities of further stimulating the immune response through a combination of IRE and immune modulatory therapies: this is the remit of the PANFIRE III trial. Ideas included performing a PD-1 blockade to additionally suppress regulatory T cells (as the investigators reported an upregulation of the PD-1 antigen), and the intratumoural delivery of Toll-like receptor ligands.
According to Scheffer, the PANFIRE III trial will treat patients with oligometastatic pancreatic carcinoma—patients with between one and five liver metastases that are stable on four regimens of folforinox. “The patients will be randomised in three groups of six patients, and they will all receive PD-1 blockade, because we found upregulation of PD-1, so we think that is a very good thing to add,” Scheffer outlined. One arm will receive PD-1 blockade and IRE; one arm will receive PD-1 blockade and an intratumoural injection of Toll-like receptor ligand, and one arm will receive all three—PD-1 blockade, IRE, and the Toll-like receptor ligand. The PANFIRE III trial has just received full funding, and will begin recruiting patients in the coming months.
Hugo Rio Tinto (Lisbon, Portugal), one of the panel moderators, said that this was “an interesting result”, commenting: “Maybe in the future we can regulate this immune response to a greater degree. Though I think the most important thing is patient selection”, something Scheffer agreed with.
Martijn Meijerink
Rio Tinto also asked about the plausibility of predicting which patients would most benefit from this combined treatment, querying if Scheffer and colleagues will study factors that will predict patient outcomes, such as immune markers: “There are some immune types that are responding better to this therapy than others,” he said, “How will you identify these [possible] predictive factors?”. As half the patients showed the Wilms’ tumour 1 response, and half did not, Scheffer said at ECIO that this was something to consider. Speaking to Interventional News after the conference, Scheffer and Martijn Meijerink (Amsterdam, The Netherlands), panel moderator and senior author of the PANFIRE trial results, disclosed: “In our future study, we aim to perform NanoString sequencing and proteome analysis on pancreatic tissue pre IRE treatment. This will hopefully provide us with information about more than 700 oncogenes and just as many proteins and could possibly bridge the gap between cancer genome information, the observed cancer phenotype and the patient response to combined treatment with IRE and immunotherapy.”
Fielding a question from the audience regarding whether or not the investigators were targeting the primary pancreatic tumour itself or the metastases, “which are more easy to puncture”, Scheffer said: “We are lowering the pulse protocol because we want to induce apoptosis as we want the antigen release, but we do not need to destroy the tumour completely, because obviously there are also metastases, so we will never achieve complete elimination. Hopefully we will not find any complications with this less invasive protocol. We chose the primary tumour because of the lymph drainage directly around it; the antigens have to be taken to the lymph nodes. For now, we think that will give the highest chance of a response, and if we only treat one metastasis, there might be fewer lymph nodes that can pick up the antigens. It is just a hypothesis, but we had to make a choice.”
The use of mixed reality will enable interventionists to see 3D anatomy ‘in 3D’, as a hologram (as opposed to on a 2D screen). “Having holography that I can reach out, grab and move around like a virtual object is going to be amazing as we get to do new interventions,” says Atul Gupta (Philadelphia, USA), an interventional radiologist and chief medical officer of Philips Image-Guided Therapy.
Gupta spoke to Interventional News at SIR 2019 after a session on virtual reality and mixed reality.
Kevin Seals (San Francisco, USA) and Andrew Taylor (San Francisco, USA) talk to Interventional News at SIR 2019 about the current and future use of smart speaker technology in the angiosuite, which allows interventional radiologists to access critical digital information almost instantly. Smart speakers, such as the Amazon Echo and Google Home, offer a conversational voice interface that allows interventional radiology (IR) physicians to ask questions and retrieve information needed for their patient treatments without breaking sterile scrub.
Seals, who believes the technology is “a really excellent fit” for doctors performing procedures in a sterile environment, looks at the benefits of the technology and some of the pitfalls as well. One particular issue Seals delves into is that the current speakers available are not HIPAAA compliant and that “working through those issues is absolutely critical” prior to these tools being used clinically.
Taylor, meanwhile, talks about the current working prototypes the team are developing and touches on the importance of voice recognition and how it can work in conjunction with augmented reality (AR) and virtual reality (VR) technologies. Combined, the technology offers the ability to “interact, listen and gather information without having to look away from what you’re doing”, says Taylor.
Acute Stroke Challenges session during the CX Symposium
In the closest debate of the Acute Stroke Challenges session that took place on the first day of the Charing Cross (CX) Symposium (15–18 April, London, UK), Jan Kovac (University Hospitals of Leicester NHS Trust, Leicester, UK) and Andrew Clifton (St George’s University Hospitals NHS Foundation Trust, London, UK) discussed whether intracranial thrombectomy should be limited to neurointerventionists.
Kovac, a cardiaologist, whose proposition was that intracranial thrombectomy should not be limited to neurointerventionists, won the debate with 57% of the vote, but a substantial minority (43%) supported Andrew Clifton’s arguments that the procedure should be limited to neurointerventionists.
While Clifton argued that experience and proper training leads to “appropriate patient selection [and] faster, safer procedures with fewer complications”, Kovac said that, given the magnitude of the potential clinical and economic benefits of mechanical thrombectomy, a “collaboration of various interventional specialists is desirable to deliver this therapy to a wider population”.
Kovac argued that “Mechanical thrombectomy is the best evidence-based therapy for acute ischaemic stroke if provided in a timely manner by an experienced, multidisciplinary team.” He went on to say: “There is currently a hiatus between evidence and its implementation into practice across the world, with practice varying significantly within and between countries. For several logistical, practical and economic reasons, collaboration of various interventional specialists is desirable to deliver this therapy to a wider population.”
Indeed, he concluded that, “Given the magnitude of the potential clinical and wider economic benefits from mechanical thrombectomy, it should now be a key priority to address the substantial infrastructure and workforce obstacles impeding rapid and widespread implementation in the UK, Europe and beyond.”
Watch a video here of Martin Radvany (Little Rock, USA) and Joan Wojak (Lafayette, USA) explaining to Interventional News that, as there is a shortage of physicians trained to perform stroke thrombectomy, it is vital for interventionists to acquire the education, training and technical skills specific to stroke therapy.
Intracranial thrombectomy
The debate on intracranial thrombectomy was part of a whole session dedicated to the procedure. Hugh Markus (Cambridge, UK), who was chairing the session, called intracranial thrombectomy “one of the huge advances in stroke care at the moment”. Outlining its significance, he said “for every three patients we treat, we can cure one, so it is a massive treatment effect. It has transformed stroke care.”
In a keynote lecture, David Hargroves (Kent, UK) reviewed what thrombectomy trials “really tell us”, and how the findings can be implemented into routine clinical practice. In light of the DAWN and DIFFUSE-3 trials, he said that there is a strong evidence basis for thrombectomy and that this treatment should be available to all patients. Additionally, Hargroves posited that regional and countrywide networks are required to deliver and achieve its 10% potential reach. However, he said, caution is needed when reorganising stroke services, so as not to destabilise the ‘core’ business and therapeutic benefit of organised care, closest to home.
Virtual reality for training purposes may elucidate “who can do the procedure”
Thomas Liebig (Munich, Germany) looked at the use of virtual reality in thrombectomy training. He described his own training as similar to that of learning to drive a car, and contrasted it with the simulator experiences of pilots who must demonstrate their competencies in a virtual environment. Liebig pointed out that skilled performance is difficult to characterise, and then outlined his work with University College Cork (Republic of Ireland) to develop surrogate parameters for performance metrics that can be used in a simulator. The findings, he said, “have the potential not only for training purposes” but, in a nod to the earlier debate on intracranial thrombectomy, could also allow us to “discriminate between a person who can do the procedure and those who should be doing something else”.
The US Food and Drug Administration (FDA) has given 510(k) clearance to the ZOOM aspiration system (Imperative Care), a family of products designed to facilitate clot removal during ischaemic stroke.
The ZOOM aspiration system includes the ZOOM reperfusion catheters, ZOOM aspiration pump, ZOOM canister, and the ZOOM aspiration tubing. The ZOOM reperfusion catheters are designed with the TRX tip to navigate complex anatomy and optimally engage blood clots, a press release states. The ZOOM reperfusion catheters come in four sizes (0.071”, 0.055”, 0.045”, and 0.035” internal diameter) and are designed to enable smooth tracking through challenging vasculature.
The ZOOM reperfusion catheters complement Imperative Care’s line of access catheters. According to a company press release, these access catheters enable smooth, consistent navigation deep into the blood vessels of the brain, which can be challenging because of the brain’s highly complex and tortuous vasculature.
“Aspiration procedures have provided a true breakthrough for treating stroke by removing clots with a high rate of first pass success,” comments Aquilla Turk, physician at Greenville Health System and chief medical officer and founding clinical advisor to Imperative Care. “Treatment options have significantly improved over the last decade, but the need for improved effectiveness and efficiency still remains. Imperative Care’s products are designed to enable first-class navigation and may improve clot ingestion, and I am excited to see the full line of products in use.”
The ZOOM aspiration system is for use in the revascularisation of patients with acute ischaemic stroke secondary to intracranial large vessel occlusive disease (within the internal carotid, middle cerebral—M1 and M2 segments, basilar, and vertebral arteries) within eight hours of symptom onset. Patients who are ineligible for intravenous tissue plasminogen activator (IV t-PA) or who fail IV t-PA therapy are candidates for treatment.
Imperative Care is planning to launch the company’s portfolio of products later this year.
Implementing a method of heparinisation guided by activated clotting time (ACT), with a goal of 200–220 seconds, provides a “promising” increase in safety and may decrease risk of thromboembolic events, while not increasing bleeding complications. Presenting the findings of the pilot ACTION trial, Arno Wiersema (Amsterdam, The Netherlands) stated he and his colleagues “believe it is time to upgrade one of the foundations of vascular surgery to optimise patient care and to prove that ACT-guided heparinisation results in far fewer thromboembolic complications.”
“The success of open and endovascular arterial interventions depends on a delicate balance between coagulation and anticoagulation”, said Wiersema in the first Aortic Podium 1st Session at Charing Cross (CX) yesterday. “Ever since its introduction in clinical practice 70 years ago, unfractionated heparin has been administered during these non-cardiac arterial procedures to prevent thromboembolic complications. A major disadvantage of this use of heparin is that it could increase bleeding complications, as extensive surveys have shown that almost all vascular surgeons and interventional radiologists use a standardised bolus of 5,000IU of heparin during non-cardiac arterial procedures.” This is in sharp contrast to cardiac interventions, noted Wiersema, where heparin is used in higher dosages. “As surprising as it may seem, only one randomised controlled trial (in 1996) has been performed on the benefit of heparin, comparing a group with heparin to a group without heparin as prophylactic antithrombotic.” The fact that no other study has since been performed on this subject despite the wide uptake of heparinisation is, to Wiersema and his colleagues, reportedly “astonishing”. For this reason, the ACTION trial was designed, to examine the benefits of heparinisation guided by ACT, with the hypothesis that less thromboembolic complications and no increase in bleeding complications would be observed.
“The final goal of ACT to strive for”, commented Wiersema, “was set at 200 to 220 seconds. To reach those ACT values, a starting bolus of 100 units per kilogram was used and additional doses were set at 60 or 30 units, depending on the actual ACT.” He added that a protocol was instituted for the use of protamine at the end of the procedure, to decrease the incidence of bleeding complications.
In terms of the results, “ACT-guided heparinisation ensured the vast majority of the patients of adequate and safe anticoagulation. Almost all patients reached an ACT of more than 200 seconds after the first bolus.” The mean dose of heparin needed to maintain this optimal anticoagulation was roughly twice the bolus of 5,000 units. While the incidence of bleeding complications was not increased, a “promising trend” of decrease in thromboembolic complications was observed, falling from 11% to 6%.
Wiersema emphasised the importance of establishing the added value of ACTguided heparinisation “once and for all”, stating: “We are on the verge of receiving a large grant to perform an international randomised controlled trial. This trial is starting in The Netherlands, Hamburg (Germany) and Copenhagen (Denmark), and we are more than happy to include other major vascular centres around the world. We need only 748 patients in five years to prove a reduction for the combined incidence of thromboembolic complications and mortality from 19% to 11%. If this method is proven to be better during open aortic aneurysm repair, it can be directly incorporated for all our other procedures.”
Concluding, Wiersema said “the ACTION pilot showed that ACT-guided heparinisation increases patient safety and looks very promising as a method to decrease thromboembolic complications, without a relevant rise in bleeding complications.”
Marianne Brodmann outlines follow-up and surveillance protocols after endovascular treatments for peripheral arterial disease (PAD), arguing for a standardised approach to ensure best practice for patients who have gone through peripheral endovascular procedures.
Endovascular procedures have become a key element of treating patients with PAD, either with intermittent claudication or critical limb ischaemia. Nevertheless, there is currently no standardised approach and no general- or guidelines-derived recommendation for how to do this. The follow-up after these procedures is often dependent on facility resources, such as available manpower and equipment, or geography (urban versus rural).
What is the rationale of surveillance after endovascular procedures? It is important to accurately implement preventative strategies to avoid other cardiovascular events and disease progression in a patient cohort with a high risk of morbidity and mortality, while also avoiding recurrence of symptoms and the need for repeat revascularisation. The importance of this is amplified by the fact that we are facing an increasing disease burden of PAD patients needing treatment. In 2008, >98,000 endovascular procedures and >86,000 surgical revascularisations were performed for lower limb arterial disease in Germany alone, illustrating the burden of peripheral revascularisation interventions in Europe.
For a standardised approach to surveillance, we need to discuss several questions. What should we offer and how should we do it? Is follow-up with anklebrachial index (ABI) alone enough, or should we also perform duplex ultrasound? What are the timeframes to do this? Another important question is, who should perform the follow-up? One simple key element is the clinical follow-up. This also means that we should create awareness among patients about the symptoms that occur in revascularisation failure, and when immediate contact to vascular specialists is indicated.
With regards to imaging techniques, which help us to detect restenosis either in the immediate or long-term follow-up, duplex ultrasound is the most applicable. It is non-invasive and widely available, and can be repeated over time to detect subclinical and abnormalities. It has therefore become the first-line technique for follow-up. Duplex ultrasound surveillance has been reported to predict severe in-stent restenosis with a specificity of >90%.
Functional tests such as ABI or toe-brachial index (TBI) can further help to optimise surveillance of the lower limbs. Computed tomography angiography (CTA) and magnetic resonance angiography are mostly limited to the confirmation and investigation of duplex ultrasound findings, but can be performed straight away in urgent cases.
In cases of recurrent claudication, treadmill test with post-exercise ABI can assess the functional severity.
However, ensuring follow-up after endovascular procedures will also serve to prevent disease progression. Regular monitoring for risk factor modification, exercise training and medical therapy is a must. Even in patients with intermittent claudication, disease progression to chronic limb threatening ischaemia may be underestimated. In a meta-analysis of studies conducted between 1990 and 2015, 21% of patients with intermittent claudication were diagnosed with chronic limb threatening ischaemia during a five-year follow-up period, and 4%–27% of them suffered amputations.
How often should we do it?
There should be an immediate postprocedural follow-up the day after the procedure, to gain insight into the procedural success achieved. To detect early restenosis, the next follow-up should be performed one month later, and thereafter in a six month period up to one year. Long-term follow up should be performed annually. As for who should carry out the followup, this should be performed by the people taking care of patients with vascular disease, whether they are general practitioners or cardiovascular specialists, such as cardiologists, vascular physicians or vascular surgeons. The appropriateness of who carries this responsibility will vary according to the management of patients in different countries.
Marianne Brodmann is a vascular specialist at the Medical University of Graz, Austria.
The National Institutes of Health (NIH) National Heart, Lung and Blood Institute has awarded a US$2.8 million grant to support the development of an intravascular steerable robotic guidewire. Jaydev Desai, a professor in the Wallace H Coulter department of Biomedical Engineering at Georgia Tech and Emory University (BME) and director of the Georgia Center for Medical Robotics (GCMR) and his lab are the recipients of the grant.
The NIH ranked Desai’s grant application with its highest degree of confidence, a one percentile score. Commenting on this, Desai says: “That is highly encouraging. It clearly demonstrates how critical and challenging the clinical problem is and why innovative engineering solutions need to be developed to address it.”
The project features the first use of intravascular steerable robotic guidewire capable of forward-looking ultrasound imaging and image-guided navigation through vasculature and occluded vessels.
Quoted on the Georgia Tech website, Desai explains that the ability to steer, visualise, and navigate the guidewire is highly novel and will eventually result in improvement of clinical workflow and patient treatment outcomes. “Think of a plumber’s snake,” he says. “And this is all about steering the tip of the long snake with visualisation of where to go with ultrasound imaging.”
Desai’s collaborators include Brooks Lindsey (Coulter Department), Stanislav Emelianov (Coulter Department and School of Electrical and Computer Engineering), and from Emory, Muralidhar Padala (cardiothoracic surgery), Khusrow Niazi (interventional cardiology) and Zachary Bercu (interventional radiology).
Desai’s team plan to address three specific aims:
Design and develop a robotically steerable, 0.014-inch diameter guidewire (0.355mm) system to accommodate a 0.350mmx0.350 mm ultrasound transducer at its tip, and can be steered with image feedback from the transducer.
Design and build a forward-looking transducer for the robotically steerable guidewire and an algorithm to reconstruct an image of the encountered occlusion.
Iteratively optimise the ultrasound-steerable guidewire design using 3D printed, patient-specific models of chronic total occlusions (CTOs), realistic human cadaver limbs with CTO, and a live animal model of CTOs.
“The clinical challenge is well recognised in the community,” Desai adds. “Since endovascular approaches are increasingly utilised over conventional approaches, there is an urgent need to develop new technologies to meet this critical need!”
The designed system, Desai says, “will have significant societal impact through improved patient outcomes, reduced radiation exposure for the physician and the patient, reduced rate of procedural failures, and lower healthcare costs.”
National Health Service (NHS) England have announced that selective internal radiation therapy (SIRT) using yttrium-90 (Y-90) microspheres will now be routinely commissioned for NHS patients with advanced colorectal cancer that has spread to the liver and is not responding to standard chemotherapies.
The use of SIRT in the NHS was assessed by NHS England from January 2014 to March 2017, as part of their Commissioning through Evaluation (CtE) scheme and the results of the assessment were published by the National Institute of Care Excellence (NICE) and NHS England in October 2017.
The findings were also published online as a scientific paper in the Journal Clinical Oncology by consultant radiation oncologist Ricky Sharma (chair of radiation oncology, University College London, London, UK) and his colleagues in September 2018, which confirmed that the real-world experience of SIRT in the NHS is consistent with the published literature.
Since 2017, NHS England has been considering the case for routine commissioning of SIRT, and they have reached the conclusion that the evidence base on SIR-Spheres resin microspheres (Sirtex) is sufficient to offer SIRT as a routine treatment for patients with colorectal cancer that has spread to the liver who meet certain criteria.
In the Clinical Commissioning Policy paper: Selective Internal Radiation Therapy (SIRT) for chemotherapy refractory/intolerant metastatic colorectal cancer (adults), NHS England recommends that adults with chemotherapy refractory or chemotherapy intolerant unresectable, liver-only metastatic colorectal cancer that meet all of the eligibility criteria will be able to be treated with SIRT using Y-90 microspheres.
Patients with advanced bowel cancer will have to meet certain criteria to be eligible for the treatment on the NHS. Specialist liver centres in England which satisfy the criteria specified by NHS England will be able to routinely offer this procedure.
“The decision by NHS England to locally commission SIRT from April [2019] is an enormous relief for patients with bowel cancer that has spread to the liver. These patients often need disease control within the liver and have limited treatment options. As long as patients meet NHS England’s clinical criteria for SIRT, treated in expert liver centres—there is likely to be benefit in controlling the liver spread,” comments Harpreet Wasan, consultant in medical oncology (London, UK). Wasan was co-chief investigator for the FOXFIRE trial of SIRT in liver metastases.
The liver metastases should be inoperable, and the disease should not be responding to standard chemotherapies. For patients with other cancers that may benefit from SIRT, such as primary cancers of the liver, the policy proposals are still being reviewed.
Patients who do not qualify for this treatment by the NHS criteria may be able to receive SIRT by participating in a clinical trial, by submitting Individual funding requests via their oncologist, or pay for it privately.
“In specialist centres we have the possibility to treat patients with innovative treatments such as SIR-Spheres Y-90 resin microspheres, which is a unique way to treat liver tumours with internal radiation therapy without damaging the healthy liver. It is great news that we now have the possibility to discuss this treatment option during the multidisciplinary team meetings for all patients who could benefit from it (meeting eligibility criteria)” states Jon Bell, consultant interventional radiologist at the Christie NHS Foundation Trust, Manchester, UK.
Sharma says: “We are delighted by this announcement. Our study has confirmed that the real-world experience of SIRT as a cancer treatment in the NHS is consistent with the published data from other countries. There is still scope for improving access to this specialist treatment for patients with a variety of cancers, not just bowel cancer, and across all the nations of the UK, not just England.”
“The NHS England decision to fund internal radiation therapy to treat liver tumours is a significant development that offers new hope for patients with aggressive bowel cancer. We were very concerned for those patients who needed the treatment but who were unable to fund it privately or raise funds to receive it. Patients in England with liver cancer that has spread from their bowel and who have exhausted other treatments, now have access to a therapy which can extend their survival so that they can spend extra time with their loved ones and enjoy more life. These patients have very few treatment options, so this is a really important step,” says Vanessa Hebditch, director of policy at the British Liver Trust.
SIR-Spheres Y-90 resin microspheres are approved for use in Argentina, Australia, Brazil, the European Union (CE Mark), Switzerland, Turkey, and several countries in Asia for the treatment of unresectable liver tumours. In the USA, SIR-Spheres Y-90 resin microspheres have a Pre-Market Approval (PMA) from the US Food and Drug Administration (FDA) and are indicated for the treatment of unresectable metastatic liver tumours from primary colorectal cancer with adjuvant intra-hepatic artery chemotherapy (IHAC) of FUDR (floxuridine).
Surmodics has announced it has received US Food and Drug Administration (FDA) 510(k) clearance for its Sublime guide sheath.
The highly flexible, proprietary Xtreme braid-reinforced Sublime sheath is designed to resist kinking and maximise strength while retaining a low profile. The sheath will be available in 5F and 6F diameters, and 120cm and 150cm lengths. The entire working length of the guide sheath is Serene hydrophilic coated to provide a lubricious surface. It is preloaded with a dilator and has a haemostasis valve with side arm for flushing. The dilators are available with .018” and .035” guide wire compatibility.
“Surmodics continues to make progress in the development of clinically important and innovative technologies,” said Gary Maharaj, Surmodics president and CEO. “Our Sublime guide sheath will set a new standard for performance and enable the delivery of lower extremity interventions from the radial artery.”
Radial artery access has been widely adopted for use in coronary procedures where devices have been developed to accommodate that need. The Sublime guide sheath is intended to introduce therapeutic or diagnostic devices into the vasculature, excluding the coronary and neuro-vasculature. Radial access offers many benefits relative to femoral access including reduced puncture site bleeding complications, earlier ambulation, reduced length of hospital stay, and lower healthcare costs.
The development of the Surmodics Sublime guide sheath is a step forward in the company’s strategy to be a provider of whole-product vascular solutions, including a family of radial access products. Surmodics has complete capabilities for design, development and high-volume manufacturing of a wide variety of highly differentiated balloon catheter and specialty catheter solutions.
Surmodics has announced the company has now resumed patient enrolment into its TRANSCEND clinical trial, and is nearly 75% of the way to its goal of 446 randomised patients.
Patient enrolment in TRANSCEND, the pivotal clinical trial for the SurVeil drug-coated balloon (DCB), was temporarily paused following the March 15 publication of a US Food and Drug Administration (FDA) letter to physicians. The letter included an update on the Agency’s preliminary analysis of a potentially concerning signal of increased long-term mortality with paclitaxel-coated devices and recommended that physicians consider alternative treatment methods until additional analysis has been performed.
“Immediately following publication of the March 15 FDA communication, we reached out to the Agency seeking guidance on the recommendations and the impact on TRANSCEND,” says Gary Maharaj, Surmodics president and CEO. “Following multiple conversations, we have taken several actions in response to the Agency’s recommendations, including updates to investigator communications, patient Informed Consent Forms (ICF), and data safety review and patient follow-up procedures. A number of our trial sites have already secured IRB or Ethics Committee approval of the updated ICF and are actively enrolling and randomising patients.”
FDA Recommendations:
Surmodics Action:
Follow device recommendations from March 15 letter
Communicated FDA recommendations to trial investigators
Update patient informed consent form (ICF)
Initiated process to update ICF at sites worldwide
Include ongoing independent Data Safety Monitoring Board (DSMB) review
Ongoing Clinical Events Committee (CEC) and DSMB reviews were initiated at trial onset
Take measures to increase follow-up with patients
Establishing an aggressive patient follow-up program for both new patient randomisations and those already treated
The TRANSCEND randomised trial will evaluate the SurVeil DCB for treatment of peripheral arterial disease (PAD) in the upper leg compared to a commercially available DCB treatment. The results of the trial will also include long-term, patient-level data out to five years. The company continues to assess the impact of the March 15 FDA communication on its expectations regarding the timing of completion of patient enrolment in the TRANSCEND clinical trial and related regulatory approvals for the SurVeil DCB.
“Patient safety is the top priority in every study, so pausing trial enrolment while implementing the recommendations from the FDA was in the best interest of both our patients and this trial,” said William Gray, the national co-principal investigator of the TRANSCEND study. “We are pleased to see many sites enthusiastically resuming enrolments. The TRANSCEND trial comes at a critical time in the endovascular field and will provide important safety and efficacy data for the next generation SurVeil DCB as it compares to the Medtronic IN.Pact DCB and will ultimately be useful for physicians and the patients that they treat.”
Standard microcatheter, positioned in the artery
irrigating the tumor: the embolization microspheres
travel not only downstream (desired effect) but also
upstream (undesired effect), in an artery irrigating
healthy tissues that need to be preserved.
Left: Standard microcatheter, positioned in the artery irrigating the tumor: the embolization microspheres travel not only downstream (desired effect) but also upstream (undesired effect), in an artery irrigating healthy tissues that need to be preserved. Right: Anti-reflux microcatheter: the anti-reflux technology sends all the embolization microspheres downstream into the area to be treated. The healthy tissue continues to be irrigated by blood free of microspheres.
SeQure and DraKon (Guerbet), two novel microcatheters for peripheral embolization procedures, are set for commercial launch in Europe. The devices have received the CE mark for the delivery of intra-arterial therapy and embolic materials into all peripheral vessels.
The SeQure microcatheter is a reflux control microcatheter that, according to a press release, uses flow dynamics to create a fluid barrier designed to deliver more treatment to the target vessel and reduce the risk of non-target embolization, for less potential damage to surrounding tissue. It consists of side slits specifically sized to allow the outflow of contrast media, Guerbet describe, creating a fluid barrier around the microcatheter to reduce microspheres reflux and assist delivery to the target vessel.
The DraKon peripheral microcatheter is the same as SeQure but without the side slits. A press release claims it has been designed to optimise “pushability, flexibility and torqueability for improved trackability and highest performance standards”.
Guerbet obtained both microcatheters as part of their acquisition of Israeli company Accurate Medical Therapeutics, announced in January 2018. The SeQure and DraKon microcatheters received FDA clearance on January 26, 2018 and are currently commercialised on the US market. They are also registered in Hong Kong, New Zealand and Thailand. The registration plan includes Australia, China, India, Japan, Korea, Singapore and Vietnam within the next two years.
SeQure and DraKon are class IIb medical devices intended for use by interventional radiologists and interventional oncologists for the infusion of contrast media into all peripheral vessels and for drug infusion in intra-arterial therapy and infusion of embolic materials. They should not be used in cerebral vessels.
The move comes a month after the US Food and Drug Administration (FDA) said that its preliminary review of long-term follow-up data found a “potentially concerning signal” of increased long-term mortality in people with peripheral artery disease who were treated with paclitaxel-coated devices compared to those treated with bare devices.
Cook Medical said that it was releasing the data to encourage further collaboration with researchers to improve treatment of peripheral arterial. The company website states: “In the spirit of full transparency, Cook Medical is providing our extensive long-term data on Zilver PTX, our drug eluting stent. Zilver PTX is a paclitaxel-coated stent that was approved by the FDA in 2012 through the premarket approval process.”
The Zilver PTX randomised, controlled trial followed 479 patients over five years in the USA, Germany and Japan.
Cook Medical touted that it is the first company with paclitaxel devices to make its de-identifiable patient-level data publicly available.
“We will continue to support our customers and their patients by sharing what we have discovered from our research and data in the area of paclitaxel,” vascular division vice president Mark Breedlove said in a press release.
Last September, Cook Medical said that it won FDA approval for a smaller-diameter version of its Zilver PTX peripheral drug-eluting stent.
Spatial frequency domain imaging. Image courtesy of Modulim.
New evidence supports the utility of spatial frequency domain imaging (SFDI) for identifying compromised circulation in patients at risk of peripheral arterial disease (PAD). These data were published in the Journal of Vascular Surgery, in a study that describes SFDI-based technology from Modulim as a promising non-invasive optical imaging method for rapidly assessing compromised circulation in tissue in the lower extremity of patients with and without diabetes.
The study examined the ability of SFDI, a new method that uses structured illumination combined with visible and non-infrared light to characterise sub-surface tissue beneath the skin to evaluate lower extremity circulation in 94 limbs (47 patients).
In the first-of-use study in PAD, lead researchers Craig Weinkauf (University of Arizona, Tucson, USA) and David Armstrong (University of Southern California’s (USC’s) Keck School of Medicine, Los Angeles, USA) compared SFDI outputs to current non-invasive testing standards, including the ankle-brachial index (ABI), toe-brachial index (TBI), pedal pulses, and Doppler waveforms. Existing assessment tools have been shown to be unreliable and/or limited in their ability to detect local tissue perfusion due to their high subjectivity, time consumption, and vessel stiffening (for example, atherosclerosis), which is common in patients with diabetes, the authors write.
“We demonstrated that SFDI was able to produce reliable measurements of local haemoglobin perfusion and oxygenation in subjects with and without diabetes,” says Weinkauf. “Evaluating both the tissue oxygen saturation and local haemoglobin in patients with diabetes gives us new insight into the compromised circulation in this population, which is at a particularly high risk for PAD.”
The results showed that SFDI revealed a distinct perfusion profile of the diabetic foot. The recruited subjects with diabetes had significantly elevated tissue oxygen saturation (StO2) and lower superficial haemoglobin (HbT1) supplying the capillary beds compared to subjects without diabetes. These findings suggested that, in patients with diabetes, oxygen was not appropriately extracted by the tissue due to capillary dysfunction.
“The phenomenon of arteriovenous (AV) shunting associated with vascular dysfunction (diabetic neuropathy) has been observed in diabetes patients, but SFDI gives us a non-invasive and objective method to validate the compromised circulation due to this aetiology,” comments Armstrong.
Finally, an SFDI-derived index of HbT2 (haemoglobin in the reticular dermis)/HbT1 (haemoglobin in the papillary dermis) was found to differentiate between diabetes patients with and without PAD.
“The early results of the current study suggest that SFDI technology could potentially overcome the shortcomings of existing methods that are confounded by vessel stiffening,” Weinkauf shares. “That is why we are expanding our study and continuing our evaluation of SFDI technology.”
The study was completed in collaboration with Modulim and researchers from the University of Arizona, Icahn School of Medicine and USC. SFDI is an advanced imaging technique co-invented by Modulim’s CEO and CTO David Cuccia, and his colleagues at UCI’s Beckman Laser Institute. Both Cuccia and Amaan Mazhar, Modulim’s vice president of research and development, are co-authors of the current study.
Following the latest information presented at the Charing Cross (CX) International Symposium related to the meta-analysis of paclitaxel-coated devices (Katsanos et al), hear from a multi-specialty panel of global experts who are discussing their current practice and the way they inform patients.
Vascular News speaks to Giovanni Torsello (Münster, Germany), Andrew Holden (Auckland, New Zealand), Alan Lumsden (Houston, USA, and Yann Gouëffic (Nantes, France).
At the Charing Cross International Symposium, Gary Ansel (Columbus, Ohio) moderates a global panel that includes Thomas Albrecht (Berlin, Germany), Peter Schneider (San Francisco, USA) and Eric Secemsky (Boston, USA). The panel outlines the value of paclitaxel devices in the treatment of peripheral arterial disease patients; examines new evidence on the safety of paclitaxel devices; and determines where the vascular community goes from here.
Albrecht reports on the findings of a pooled analysis of four randomised controlled trials that ultimately showed no correlation between mortality and paclitaxel, while Secemsky discusses real-world data that showed no difference in survival for drug-coated devices vs. non-drug devices.
The panel comments on future steps including the planned independent patient-level meta-analysis of pooled data from the US randomised controlled trials by the VIVA group.
There were calls for greater transparency and sharing of the available randomised controlled trial data of paclitaxel-coated devices at theCX 2019 Highlight Session, Paclitaxel: The Last Word. The session also emphasisedthe need for a meta-analysis of individual patient-level data going forward.
Cook Medical has just announced the release of de-identifiable patient-level data for the ZILVER PTX randomised controlled trial.
Vascular News spoke to Michael Dake (Tucson, USA), Gary Ansel (Columbus, USA) and Aaron Lottes (West Lafayette, USA) about why this is an important step, and the highlights of the Zilver PTX five-year safety and mortality data.
For more information about Zilver PTX, and to request the patient-level data, visit cookmedical.com
Delegates voted overwhelmingly against the notion that there was a demonstrable danger in any organ of the body attributed to circulating paclitaxel. These polling results, with a 67% majority, came after vascular pathologist Elena Ladich (Hollywood, USA) presented insights from new analysis on the effects of paclitaxel in the body. A CX Symposium Highlight Session explored the ramifications and possible resolutions four months on from the Katsanos et al meta-analysis published in the Journal of the American Heart Association(JAHA). The session was chaired by Roger Greenhalgh and moderated by CX Executive Board members Gunnar Tepe, Andrew Holden and Thomas Zeller. Experts, representatives of regulatory bodies (US FDA and UK MHRA) and other stakeholders scrutinised the current controversy surrounding paclitaxel-eluting devices over the course of four hours.
Additional polling at the close of the session revealed that 85% of CX delegates believed “no danger has been demonstrated in any organ of the body that is attributable to circulating paclitaxel”. This conviction was further consolidated, when attendees were asked: “Have we established that there are substantial levels circulating in arteries used for reducing restenosis”—68% of respondents said no.
Ladich, whose presentation closed the session, spoke on the effects of paclitaxel on the artery wall, drawing from her practice with human autopsies. She explained that a proportion of the drug and excipient coating of paclitaxel-eluting devices are known to embolise distally. While she says she “does not know the answer”, Ladich stresses the importance of asking whether or not we should be concerned with “the potential shower of drug into the end organ”. In her experience, “rare case reports have described aneurysms, localised hypersensitivity, downstream vasculitis and panniculitis following drug-coated balloon treatment”. However, she also notes that “to date, there are no published reports of autopsy findings or specific organ toxicity in humans treated with drug-coated balloons”. Additionally, to her knowledge there are “no causal links or mechanisms to explain the reported association of paclitaxel in the lower limbs and patient mortality”. Ladich clarified that despite this lack of evidence in both the literature and her experience, “this does not mean a potential damaging effect to organs does not exist”.
The Highlight Session began with a summary of the key messages from last month’s Vascular Leaders Forum (VLF; 1–2 March, Washington, DC, USA) by Gary Ansel (Columbus, USA). He told CX delegates that a central discussion point was whether a “protective benefit” with plain percutaneous transluminal angioplasty (PTA) could explain the higher mortality seen with paclitaxel devices in the meta-analysis. Ansel commented there was “no mechanistic signal to date” for such a benefit but, potentially, risk factors may be more frequently identified—and thus modified—in PTA patients because they are seen more often and undergo more interventions than those who receive paclitaxel devices.
“This [peripheral arterial disease] population dies at a very high rate during the five years after a procedure. We should be focused on how we stop these patients from dying. From my standpoint, these patients should be followed much more closely for their general medical condition. We have to make sure these patients are not having infections or different oncology problems. We need to change this mortality rate with much more aggressive risk factor modification,” Ansel noted.
The lack of mechanistic signal was one main criticism levelled at the Katsanos et al meta-analysis findings. Defending his methodology and conclusions, Konstantinos Katsanos (Patras, Greece) told CX delegates that the increased risk of death reported in the meta-analysis following the application of paclitaxel-eluting devices in the femoropopliteal artery was consistent and significant across multiple statistical analyses.
“We are mathematically 99% certain of this significance”, Katsanos stated emphatically, pointing to results of a trial sequential meta-analysis. He added, “every trial is only as good as its methodology. […] The key message here is not a smoking gun—it is the consistency of the findings. You see here the consistency of the mortality signal, and this I would say is the main take-home message.”
Mårten Falkenberg (Gothenburg, Sweden), investigator of the SWEDEPAD registry-based randomised controlled trial, reported on the status of the trial which ceased enrolment in the wake of the JAHA meta-analysis. He told the CX audience that despite keeping up with the ongoing international conversation, the investigators were still trying to determine the best course of action, but no obvious consensus has emerged. Answering the question, “Do you agree with BASIL-3 and SWEDEPAD to recommend stop using paclitaxel products at this moment?”, a slight majority of 52% agreed. Furthermore, a similar split was seen as 53% voted for the motion “Do you suspect that the finding of Dr Katsanos is correct?”.
Jonathan Michaels (Sheffield, UK), chair of the steering committee for the BASIL-2 and BASIL-3 trials, spoke about the halting of enrolment into the latter trial, which was set to expand on BASIL-2’s investigation of paclitaxel treatments for claudicants by examining the therapy in patients with critical limb ischaemia (CLI). However, BASIL-3 enrolment ceased following the Katsanos et al meta-analysis in order to review the ethics of continuing to treat patients with this drug. Michaels queried if there was an “innocent explanation” for the mortality signal. Like Ansel, he suggested a “plausible” reason for the observed increased mortality may be related to a greater follow-up frequency in patients treated with PTA, for whom potential comorbidities may be more likely to be diagnosed. Meanwhile, both Michaels and principal investigator Andrew Bradbury (Birmingham, UK) expressed their hopes to restart recruitment, although the unanswered questions surrounding paclitaxel present “serious challenges” for the triallists. Speaking from the floor, Bradbury further argued that a distinction “must be made” between claudicants and CLI patients as the risk profile varies drastically between the two. “For claudicants, treatment is about enabling the patient to walk further.” With CLI, Bradbury added, “the risk weigh-up” instead hinges on improving quality of life in end-stage peripheral arterial disease (PAD), for which effective treatment may be worth a potential increased late mortality risk.
Responding directly to Bradbury’s comments concerning CLI, Zeller noted that teasing out an association of increased mortality would be more difficult in a CLI patient cohort, due to the “higher background noise” caused from greater overall mortality rate in this patient population compared to less ill patients. Bradbury further said “we cannot assume that Katsanos’ findings apply to CLI patients.” Expressing his personal view, he told attendees that the BASIL and SWEDEPAD trials “represent a unique opportunity to settle the question with regard to CLI”. Indeed, speaking to this point, US FDA representative Misti Malone (Silverspring, USA) suggested that regulatory bodies may be able to make such a distinction between claudication and CLI, and pointed out that the FDA has currently not recommended the halting of paclitaxel trials.
The methodology and statistical validity of the meta-analysis outcomes were comprehensively described by statisticians and regulatory authorities. Overview of the meta-analysis’ statistical analysis was provided by Jon Deeks (Birmingham, UK), statistician of the BASIL-3 trial, and Sue Duval (Minneapolis, USA), one of the two independent, academic statistical advisors to the VIVA independent patient data (IPD) review. Deeks suggested that many of the studies used in the meta-analysis by Katsanos et al were “inadequate” in terms of the raw data, and that the reporting of the trials was “suboptimal”. However, Deeks acknowledged “statisticians are never satisfied with the data”. Polling following this statistical discussion showed a slight shifting in favour of believing that there is statistical evidence currently indicating a real increased mortality from the use of paclitaxel on a balance of probabilities: 57% to 43%.
Malone gave the FDA position, and announced the IPD review panel to take place on 19–20 June this year. This will be a meeting of the FDA’s Circulatory System Devices Panel of the Medical Devices Advisory Committee, and will take place from 8am to 5pm 19 June and 8am to 3pm 20 June in Gaithersburg, USA.
Hazel Randall (London, UK) of the UK Medicines and Healthcare Products Regulatory Agency (MHRA) relayed the working process of the expert advisory group created last month, which is due to release its final recommendations for paclitaxel use “in the next few weeks”. Both regulatory bodies received considerable support from audience polling, with 68% believing the authorities were “reacting appropriately”. This result was quite decisive in comparison to the less unifying answers of previous polling.
Lessons from the paclitaxel pioneers and other disciplines
CX delegates heard from Ulrich Speck (Berlin, Germany), who spoke of his early work to enable the drug to coat the balloon, resulting in the plethora of devices available today. It was evident from Speck’s account that from the outset, the cell-killing effects of paclitaxel were known. “Of all the drugs tested in the swine model, none were as effective as paclitaxel”, Speck stated.
Speaking on the pharmacokinetics of paclitaxel, Lindsay Machan (Vancouver, Canada) gave a description of the early application to stents, which was incorporated to address the issue of instent restenosis. The choice of paclitaxel was reliant upon its observed “powerful” ability to inhibit cytokine-induced migration of cartilaginous cells, which Machan explained cannot grow when more than 2mm away from a capillary.
Providing an oncological perspective, Erica Mayer (Boston, USA) detailed the use of paclitaxel as a primary therapy in cancer care. Notably, Mayer referred to paclitaxel as “one of our most commonly used treatments” in breast cancer patients, and even reported its safe, effective use in the second and third trimester of pregnancy. “We think it is safe enough to give to our pregnant patients”, Mayer told the CX audience. Furthermore, she pointed to the significant difference in dosing: a higher-dose drug-coated balloon reportedly providing 0.55% of an average dose given in a weekly breast cancer regimen over 12 weeks.
Finally, Bruno Scheller (Homburg/ Saar, Germany) outlined the lessons learned from paclitaxel use in coronary arteries, comparing the drug to its alternatives, sirolimus and everolimus. Referring to a similar controversy over a decade ago, in which a potential association with increased mortality was discussed for paclitaxel in the coronary arteries, Scheller said this 2006 “firestorm” is the “perfect blueprint” for the current paclitaxel debate. Ultimately, however, Scheller reported that the coronary community concluded that the stent design and coating technology is “more important” than drug selection in these arteries, and drug-eluting devices are in continued use.
Commenting on these lessons, Greenhalgh summarised that the early users of paclitaxel were “fully aware that the drug was cytotoxic, is has been used in oncology since”, iterating that its use in vascular applications was “always known to damage the artery wall in some way, which discouraged the restenosis process”. At this stage, 85% of the audience agreed with this sentiment, answering the poll: “Do you think that those who used paclitaxel in the early days were quite aware that paclitaxel kills cells?”. A follow-up question elaborated: “If you accept that the pioneers knew that paclitaxel would kill cells, do you think that they always aimed to have a balance between achieving less restenosis in the patients’ interest without increasing mortality?”. The result of this query was 72% in favour, capturing the audience support for the idea that there may exist a trade-off in the use of paclitaxel. “On the one hand,” Greenhalgh summarises, “paclitaxel contributes to greater patency in the lower limbs, but on the other hand, there is an alleged increase in death.” Extensive discussion followed on whether there exists a causative action as the drug circulates within the body, or whether this is “merely an association”. Overall, there was near unanimous support from speakers, audience and the regulatory bodies on the position that while an association may exist, further investigation is required.
New data from the MIMICS-2 trial show the BioMimics 3D stent, which mimics natural vascular curvature, remains safe and effective for patients with symptomatic atherosclerotic disease of the femoropopliteal arteries two years after implantation.
Principal investigator Timothy Sullivan (Abbott Northwestern Hospital, Minnesota, USA) presented the two-year findings at this year’s Charing Cross Symposium (CX; 15–18 April, London, UK) in a Podium 1st session. He explained: “We know that swirling flow creates increased wall stress in the arterial wall, which is atheroprotective, and this is especially important in the superficial femoral artery where, under normal circumstances, shear stress is quite low. The use of a helical stent produces swirling flow and increased wall shear stress.”
MIMICS-2 is an international investigational device exemption (IDE) study to evaluate the safety and efficacy of the BioMimics 3D stent system (Veryan Medical) in patients undergoing endovascular intervention to relieve obstructive or occlusive disease in the femoropopliteal artery. The three-year, prospective, single-arm trial is tracking outcomes in 271 subjects with a mean age at baseline of 68.4 years, across 43 sites in the USA, Germany and Japan.
About 50% of patients had diabetes mellitus, and the majority were in Rutherford categories 3 and 4: “These were patients with significant clinical symptoms related to lower extremity arterial claudication and a baseline ankle-brachial index of 0.7, representing patients that we all would treat in our clinical practice, typically with lower extremity intervention following a trial of exercise therapy.”
Device and technical success was 100%. The primary safety endpoint of freedom from major adverse events (death, major amputation, or clinically-driven target lesion revascularisation [CD-TLR]) at 12 months was achieved for 99.6% of subjects.
At 24 months, freedom from CD-TLR was 84.2% and “compares quite favourably to that at 12 months, which was 89%,” said Sullivan. “The [Kaplan-Meier] curve really starts to flatten out at about 360 days, without much loss in clinically driven-TLR.”
This performance at two years is similar to that of drug-eluting stents (DESs) and drug-coated balloons (DCBs), despite the MIMICS-2 subject cohort including a greater proportion of challenging cases than those in pivotal DES/DCB trials. Imaging confirmed there were no cases of stent fracture in any of the MIMCS-2 subjects, including those who have reached three-year follow-up.
Sullivan concluded: “Swirling flow with this BioMimic stent creates increased shear stress at the vessel wall, which is atheroprotective without the use of an antiproliferative drug.” The positive outcomes were achieved independent of lesion complexity—at the start of MIMICS-2, 45.9% of subjects had moderate to severe legion calcification. The Kaplan-Meier estimate of survival from CD-TLR at 24 months for those in this group was 85.5%. Sullivan told Interventional News: “What these data tell me is that, in complicated patients with very calcified lesions […] when a device becomes available for general clinical use in the USA, I will be using it for long or calcified lesions, […] in which I might otherwise have used one of the other treatment algorithms, with the confidence that restenosis is going to be minimal. The results shown are pretty amazing after two years.”
The other MIMICS-2 principal investigators are Thomas Zeller (Bad Krozingen, Germany) and Masato Nakamura (Tokyo, Japan).
Office-based lower extremity arterial interventions are feasible, safe, and cost-effective, and provide high levels of patient satisfaction. Enrico Ascher (Brooklyn, USA) presented data that “challenge the dogma that high-risk patients should not be offered office-based endovascular infrainguinal arterial procedures”, while providing a US perspective on ambulatory interventions at the Charing Cross Symposium (CX; 15–18 April, London, UK).
Ascher cited studies that show patient satisfaction levels with outpatient care of 99%, and listed its other advantages as improved physician efficiency, due to multitasking, better reimbursement levels, and increased independence for practitioners because hospital administrators are “cut out of the equation”.
He also highlighted his own data series, collected from 2014–2018 and based on 8,336 cases. There were no procedure-related deaths, and only one case required an emergency transfer. The complication rate was 1.3%, and death rate at one month was 0.15%. Among the patients excluded were those who weighed >180kg, had advanced chronic obstructive pulmonary disease (COPD) or disabling spine stenosis (and therefore could not remain supine), as well as unstable psychiatric patients.
From 2014–2018, there were 576 arterial interventions, with zero cases of embolisation, retroperitoneal bleed, and acute stenosis, and six cases of puncture site stenosis.
A review of the arterial patient selection criteria revealed that lesion type or location did not play a factor in patient selection, and that eligible patients were given a choice to have their procedure done in the office or in the hospital. Ascher pointed out: “You would think that we would select patients with easy lesions, but that was not true.”
The data were then further evaluated by comparing findings in high-risk patients with those of more average risk. The risk factors analysed were age ≥80 years old, serum creatinine ≥2mg/dL or end-stage renal disease, ejection fraction (EF) ≤39%, and American Society of Anaesthesiologists (ASA) classification of 3 and 4.
For patients who were ≥80 years old, the reintervention rate at one year was 21% vs. 38% in the younger group (p=0.04). Of these, 18% were office-based and 1.4% were hospital-based for older patients, compared to 29% office-based (p=0.03) and 4% hospital-based reinterventions (p=0.18) among those of a younger age. No patients required a bypass.
A comparison between those with renal impairment and those with adequate renal function found a reintervention rate of 12% among high-risk patients, and 36% in the lower-risk group (p=0.01). All patients at higher risk had the repeat procedure performed in hospital, while only 4% of patients with adequate renal function were hospital-based (p=0.21); 14 of the 297 reinterventions in the low-risk group required a bypass.
Reintervention rates for patients with impaired cardiac function—defined as an EF ≤39%—was 31% compared to those with adequate function at 34% (p=0.44). Only one of five reinterventions was office-based for those with impaired cardiac function, versus 84 of 105 cases among lower-risk patients (p=0.22). Two patients with EF ≤39% had a bypass vs. 12 of those with EF function ≥39%.
Outcomes for patients with an ASA classification of 3 and 4 were compared to those with a classification of 2, and showed a reintervention rate of 12% among those at higher risk vs. 34% among the lower-risk group (p=0.44). Numbers of bypasses were the same in each group as for those among the high and low-risk cardiac function patients. The mortality rate was zero and there were no major amputations among any of the groups selected for comparison.
Limitations of the data analysis were that it was retrospective and single-centre, and based on a single surgeon performing >15,000 endovascular arterial procedures. However, Ascher concluded: “Appropriately selected high-risk patients can benefit from office-based endovascular arterial procedures,” adding, “ideally, office-based arterial endovascular procedures in high-risk patients should be further validated by a large multicentre prospective randomised study.”
Interventionists can confidently use lower profile drug delivery platforms, based on data that show 0.018-inch guidewire devices are noninferior to 0.035-inch guidewires. In a Podium 1st presentation at the Charing Cross Symposium (CX; 15–18 April, London, UK), Andrew Holden (Auckland, New Zealand) said: “At 90 days, we can see that the 0.018-inch IN.PACT Pacific device is certainly noninferior to the [0.035-inch] IN.PACT Admiral device—the device with so much five-year follow-up data. What this means is we can have confidence transposing all the published data from 0.035-inch technologies to these newer low-profile 0.018-inch devices.”
Randomised controlled trials and real-world registries have established a patency advantage in the femoropopliteal segment for drug-coated balloons (DCBs) with an 0.035-inch guidewire compatible platform. But Holden pointed out: “There are a lot of clinicians who would like to use lower profile, 0.018-inch guidewire compatible devices,” and he listed the clinical advantages. “The profile is smaller and that reduces access sheath size and bleeding risk,” he said. “And that is often very relevant, particularly in elderly female patients with small calibre vessels. Lower profile means we have better deliverability and crossing ability, and we can just use one guidewire to cross lesions above and below the knee.”
Researchers created arterial injuries in swine models using angioplasty and stenting, and treated 30 days later with a DCB or drug-eluting stent. They then assessed restenosis rates using quantitative vessel analysis (QVA) and optical coherence tomography (OCT) imaging at 60, 90 or 120 days post-treatment, and also measured tissue levels of drug at the terminal timepoint.
Firstly, the performance of two 0.035-inch compatible guidewire devices, the IN.PACT Admiral (Medtronic) and the Stellarex (Phillips), were compared: “At various timepoints, both 60 and 90 days, there is a significant reduction in restenosis with the IN.PACT Admiral compared to the Stellarex, and this is not surprising given the higher input dose with the IN.PACT Admiral. The tissue concentrations that were obtained at the terminal timepoint also showed that there was higher tissue dose of paclitaxel with the IN.PACT Admiral.”
The investigators also looked at two 0.018-inch guidewire compatible devices—the Pacific (Medtronic) and the Ranger (Boston Scientific); this comparison extended the timepoint to 120 days. “The Pacific was trending towards a lower restenosis rate with QVA and OCT compared to the Ranger at 60 and 120 days. It did not reach statistical significance, but there was a positive trend.”
Holden told Interventional News that the lower stenosis rates found with Pacific compared to Ranger could also be explained by the higher input dose for the Pacific balloon. The dissolution rates with paclitaxel for all the devices are pretty much the same so if you have a higher input dose at the start you are likely to see a pronounced, more prolonged restenosis effect. However, “both platforms performed extremely well in terms of preventing restenosis,” Holden said.
A comparison between the IN.PACT Pacific and the IN.PACT Admiral—the 0.018-inch and the 0.035-inch devices from the same company—by QVA and OCT found comparable performance in terms of restenosis. Holden said: “This implies that the data we have from the 0.035-inch database can be translated to the 0.018-inch platform.”
He concluded: “We certainly could show that the 0.018” guidewire devices were noninferior to the 0.035” devices. Although this is a preclinical study, it is one that really does have clinical relevance.”
Graphic of two NanoKnife disposable electrodes positioned around ablation zone
Graphic of two NanoKnife disposable electrodes positioned around ablation zone
The US Food and Drug Administration (FDA) have approved AngioDynamic’s investigational device exemption (IDE) application for NanoKnife Irreversible Electroporation “Direct IRE Cancer Treatment” clinical study (DIRECT).
The DIRECT Study supports a proposed expanded indication for the NanoKnife system in the treatment of stage III pancreatic cancer. In January 2018, the FDA granted the company’s NanoKnife system a breakthrough device designation under the 21st Century Cures Act.
According to a press release, the NanoKnife system is a next-generation ablative technology that physicians have identified as an innovative treatment for pancreatic cancer. AngioDynamics state that this is evidenced by the 42 publications that document more than 800 patients who have been treated for stage III pancreatic cancer with NanoKnife technology from 2012 to 2019.
The NanoKnife system received 510(k) clearance from the FDA for the surgical ablation of soft tissue in 2008. Unlike other ablative technologies, the NanoKnife system utilises low-energy, direct-current electrical pulses to permanently open pores in target cell membranes and does not rely on thermal effects, the press release explains. These permanent defects in the cell membranes result in cell death. The treated tissue is then removed by the body’s natural processes in a matter of weeks, mimicking natural cell death.
AngioDynamics state that their DIRECT study will feature a “comprehensive data collection strategy” that will provide meaningful clinical information to healthcare professionals, support a regulatory indication for the treatment of stage III pancreatic cancer, and facilitate reimbursement for hospitals and treating physicians. The study is classified as a Category B IDE by the FDA, allowing participating sites to obtain coverage for procedures performed as well as related routine costs.
The DIRECT study comprises a randomised controlled trial at up to 15 sites and a real-world evidence, next-generation registry (RWE) at up to 30 sites, each with a NanoKnife system treatment arm and a control arm. AngioDynamics expects each NanoKnife arm to consist of approximately 250 patients with an equal number of control patients. The primary endpoint of the study is overall survival.
The randomised controlled trial component of the DIRECT study will illustrate the promise of the NanoKnife system by isolating variables in a controlled setting, says the press release. Recognising that results from a hyper-controlled setting do not always translate to clinical practice, the study also includes a RWE component to provide clinicians, patients, and payers with data generated in a real-world setting.
As part of the DIRECT clinical study, AngioDynamics is launching AngioDIRECT.com to facilitate the enrollment of participants. The online platform will provide patients and their families with information about pancreatic cancer and details about the study. It will also feature a physician locator to help prospective participants and referring healthcare professionals identify clinical study locations.
“Existing evidence that has accumulated over the last 10 years has shown that irreversible electroporation is an effective adjunctive treatment for patients with locally advanced pancreatic cancer,” comments Robert C G Martin, co-principal investigator of the DIRECT study and surgical oncologist at the University of Louisville, Louisville, USA. “We anticipate that this trial will demonstrate how the NanoKnife system can be utilised to enhance the quality of life for patients with stage III pancreatic cancer.”
“I have had promising experience utilising irreversible electroporation as a treatment option for pancreatic cancer patients,” says Govindarajan Narayanan, co-principal investigator of the DIRECT study and chief of Interventional Oncology at the Miami Cancer Institute. “We expect that the results of this trial will lead to a widely available alternative treatment option for advanced pancreatic cancer patients.”
There are approximately 57,000 new cases and 46,000 estimated deaths from pancreatic cancer in the USA annually. Total deaths due to pancreas cancer are projected to increase dramatically to become the second leading cause of cancer-related deaths before 2030. The mortality rate is high due to the aggressive nature of the disease and lack of early warning signs, and less than 20% of patients are candidates for surgical resection at time of diagnosis. Approximately 35–40% of patients will present with stage III and 45–55% with metastatic disease. Regardless of the stage of pancreatic cancer, it is one of the least survivable cancers, and survival rates have not improved substantially for more than 40 years. For all stages combined, the five-year relative survival rate is 8% and, for those with advanced disease at the time of diagnosis, the five-year survival rate remains at 3%.
There are limited treatment options for stage III and IV disease, with chemotherapy and/or radiotherapy considered the standard of care. There have been advancements in both techniques, but this has come at the cost of greater toxicity, limiting the number of patients that are candidates for treatment.
A recent taskforce report charged by the American Society for Bone and Mineral Research (ASBMR) concluded that current evidence does not support the routine use of vertebroplasty for the treatment of pain from vertebral fractures. However, as someone who strongly believes the evidence supports the use of this procedure to alleviate pain, Douglas Beall has significant concerns about the impact this report will have on patient numbers.
This article published in the Journal of Bone and Mineral Research (JBMR) is dangerous and puts patients at an increased risk of morbid injury and death. The manuscript focuses on recommendations by a task force from the American Society for Bone and Mineral Research (ASBMR). Most of the taskforce do not even perform the procedure they are writing about (vertebral augmentation) and the ones that do it still do it after writing negative articles about it. I would never continue to do a surgery or procedure that I found to be ineffective, but it is well documented that authors of this trial do. One can only conclude that either they do not believe their own recommendations, or that they perform the procedure for reasons other than clinical effectiveness. I would also never write any article, especially a highly critical one about a technique that I did not personally do, but the taskforce is filled with authors from the departments of Internal Medicine, Clinical Sciences, Epidemiology and Human Metabolism that have never seen the inside of an operating room in their current professional positions.
So what is dangerous about these recommendations? The task force says there is insufficient evidence to recommend vertebral augmentation. This will assuredly decrease the number of patients treated. This situation has been seen previously after two vertebroplasty versus sham trials were published in the New England Journal of Medicine (NEJM) in 2009. What happened afterwards was recently described by Kevin Ong (Philadelphia, USA) et al who documented the decreasing number of patients treated and estimated that 75,452 patients were at higher mortality risk and that 6,814 lives were lost due to the downward trend in treatment. The inevitable increase in patient morbidity and mortality is not even been addressed by the task force despite the fact that this has been studied by many authors from many countries in the USA, Europe and Asia. If the ASMBR taskforce has their way, they would like to ban a procedure that is demonstrably life-saving and life prolonging.
The taskforce states that there is “insufficient evidence to support kyphoplasty over non-surgical management, percutaneous vertebroplasty, vertebral body stenting or Kiva” but is apparently unaware of a large kyphoplasty randomised control trial (RCT), the FREE [Fracture Reduction Evaluation] trial published in 2009 provided Level 1 evidence supporting kyphoplasty over non-surgical management and a recent meta-analysis by Ioannis Papanastassiou (Rimini, Greece) that showed prominent pain, function and quality of life improvements with vertebral augmentation. The meta-analysis examined 1,587 articles in the English language including 27 Level I or II articles compared to the task force’s five articles.
Why only five articles? They only examined the vertebroplasty versus sham trials. Despite this severely limited dataset this didn’t stop the taskforce from making recommendations about implant augmentation and kyphoplasty which has been shown to be highly effective. The taskforce incorrectly stated that “a sham procedure means that local anaesthetic was administered to the skin and the procedure was simulated”, which is only true for one of the positive trials, not the three negative ones. The negative studies use a sham that involved injecting anaesthetic onto the bone in the location of the medial branch of the dorsal ramus, a technique that has Level I evidence supporting its efficacy in significantly decreasing back pain. Not only is this not a sham, it is an active treatment that significantly decreases back pain. This active treatment called a sham by the authors of VERTOS IV decreased the pain by a massive 4.75 points on the numerical rating scale. So how does this rate? If you accout for their calculations for significance, this is better than spine injections, radiofrequency ablations, cervical discectomy, total hip arthroplasty and virtually everything we do in medicine. Yes, even the gold standards in spine and orthopedic surgery—the cervical discectomy and fusion and the hip arthroplasty—are nowhere close to as good as the fake surgery for the authors of VERTOS IV.
The fundamental problem is that by comparing mean pain scores, as was inadvisably done in VERTOS IV, the authors created an impossibly high benchmark for comparison that almost nothing significantly outperforms, except for, ironically, kyphoplasty. In the largest clinical trial ever done on kyphoplasty with 354 patients, the pain decreased by an average of 6.3. The world’s largest registry recently completed in the USA showed real world results on data collected from sites around the country and featured a mean pain score reduction of 6.7 points and a median pain reduction of 9 points. These two data sources are the largest real world post-market data sources in the world for vertebral augmentation but were not even mentioned by the ASBMR task force.
The bottom line is that we know better than to produce recommendations like this that are completely divorced from the reality of today’s treatment of vertebral compression fractures and we know better to recommend something that has been shown to result in increased morbid suffering and death. The best way I can describe these recommendations is that they are shameful.
Douglas Beall is the chief of Radiology Services at the Clinical Radiology of Oklahoma in Oklahoma City, USA.
Kallmes DF, Comstock BA, Heagerty PJ, Turner JA, Wilson DJ, Diamond TH, Edwards R, Gray LA, Stout L, Owen S, Hollingworth W, Ghdoke B, Annesley-Williams DJ, Ralston SH, Jarvik JG. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 2009; 361:569–579.
Buchbinder R, Osborne RH, Ebeling PR, Wark JD, Mitchell P, Wriedt C, Graves S, Staples MP, Murphy B. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med 2009; 361:557–568.
Firanescu CE, Vries J,Lodder P, Venmans A, Schoemaker M, Smeet A, Donga E, Juttmann J, Klazen C, Elgersma O, Jansen F, Tielbeek A, Boukrab I, Schonenberg K, van Rooij W, Hirsch JA, Lohle PNM. Vertebroplasty versus sham procedure for painful acute osteoporotic vertebral compression fractures (VERTOS IV): randomized sham controlled clinical trial. BMJ 2018;360:k1551. http://dx.doi.org/10.1136/bmj.k1551
Beall DP, Tutton SM, Murphy K, Olan W, Warner C, Test JB. Analysis of Reporting Bias in Vertebral Augmentation. Pain Physician. 2017 Nov;20(7):E1081–E1090.
Ong KL, Beall DP, Frohbergh M, Lau E, Hirsch JA. Reply to “At what price decreased mortality risk?”. Osteoporos Int. 29(8), 1929–1930. 2018 May 3., doi: 10.1007/s00198-018-4551-4.
Edidin A, et al. Mortality Risk for Operated and Non-Operated Vertebral Fracture Patients in the Medicare Population. JBMR, 2011: Feb 9. DOI: 10.1002/jbmr.353
Chen AT, Cohen DB, Skolasky RL. Impact of nonoperative treatment, vertebroplasty, and kyphoplasty on survival and morbidity after vertebral compression fracture in the Medicare population. J Bone Joint Surg Am. 2013 Oct 2;95(19):1729–36. doi: 10.2106/JBJS.K.01649.
Zampini JM, White AP, McGuire KJ. Comparison of 5766 vertebral compression fractures treated with or without kyphoplasty. Clin Orthop Relat Res. 2010 Jul;468(7):1773–80. doi: 10.1007/s11999-010-1279-7.
Park J, Park S, Lee HJ, Lee C, Chang B, Kim H. Mortality following benign sacral insufficiency fracture and associated risk factors. Arch Osteoporos (2017) 12: 100. https://doi.org/10.1007/s11657-017-0395-3
Lange A, Kasperk C, Alvares L, Sauermann S, Braun S. Survival and Cost Comparison of Kyphoplasty and Percutaneous Vertebroplasty Using German Claims Data. Spine 2014;39:318–326
Edidin AA1, Ong KL, Lau E, Kurtz SM. Morbidity and Mortality after Vertebral Fractures: Comparison of Vertebral Augmentation and Non-Operative Management in the Medicare Population. Spine (Phila Pa 1976). 2015 May 27.
Kanis JA, Oden A, Johnell O, et al. Excess mortality after hospitalisation for vertebral fracture. Osteoporos Int 2004;15:108–112
Lin JH, Chien LN, Tsai WL, et al. Early vertebroplasty associated with a lower risk of mortality and respiratory failure in aged patients with painful vertebral compression fractures. Spine J 2017
Wardlaw D, Cummings SR, Van Meirhaeghe J, Bastian L, Tillman JB, Ranstam J, Eastell R, Shabe P, Talmadge K, Boonen S. Efficacy and safety of balloon kyphoplasty compared with non-surgical care for vertebral compression fracture (FREE): a randomised controlled trial. Lancet. 2009. PubMed PMID: 19246088.
Papanastassiou ID, Phillips FM, Meirhaeghe JV, et al. Comparing effects of kyphoplasty, vertebroplasty, and nonsurgical management in a systematic review of randomized and non-randomized controlled studies. Eur Spine J DOI 10.1007/s00586-012-2314-z
Noriega DC, Rodrίguez-Monsalve F, Ramajo R, Sánchez-Lite I, Toribio B, Ardura F. Long-term safety and clinical performance of kyphoplasty and SpineJack procedures in the treatment of osteoporotic vertebral compression fractures: a pilot, monocentric, investigator-initiated study. Osteoporos Int. 2019 Mar;30(3):637–645. doi: 10.1007/s00198-018-4773-5. Epub 2018 Nov 28.
Wilson DJ, Owen S, Corkill RA. Facet joint injections as a means of reducing the need for vertebroplasty in insufficiency fractures of the spine. European radiology 2011;21:1772–8.
Im TS, Lee JW, Lee E, Kang Y, Ahn JM, Kang HS. Effects of Facet Joint Injection Reducing the Need for Percutaneous Vertebroplasty in Vertebral Compression Fractures. Cardiovasc Intervent Radiol 2016;39:740–5.
Nath S, Nath CA, Pettersson K. Percutaneous lumbar zygapophysial (Facet) joint neurotomy using radiofrequency current, in the management of chronic low back pain: a randomized double-blind trial. Spine 2008; 33:1291–7.
Tekin I, Mirzai H, Ok G, Erbuyun K, Vatansever D. A comparison of conventional and pulsed radiofrequency denervation in the treatment of chronic facet joint pain. Clin J Pain 2007; 23524–9.
Lakemeier S, Lind M, Schultz W, Fuchs-Winkelmann S, Timmesfeld N, Foelsch C, Peterlain CD. A comparison of intraarticular lumbar facet joint steroid injections and lumbar facet joint radiofrequency denervation in the treatment of low back pain: a randomized, controlled, double-blind trial. Anesth Analg 2013; 117:228–235.
Fischgrund, J. S., Rhyne, A., Franke, J., Sasso, R., Kitchel, S., Bae, H., et al. (2018). Intraosseous basivertebral nerve ablation for the treatment of chronic low back pain: a prospective randomized double-blind sham-controlled multi-center study. European Spine Journal, 1–11.
Manchikanti L, Cash KA, McManus CD, Pampati V. Fluoroscopic caudal epidural injections in managing chronic axial low back pain without disc herniation, radiculitis, or facet joint pain. J Pain Res. 2012;5:381–90. doi: 10.2147/JPR.S35924.
Kapural, Leonardo, Cong Yu, Matthew W. Doust, Bradford E. Gliner, Ricardo Vallejo, B. Todd Sitzman, Kasra Amirdelfan, DonnaM. Morgan, Lora L. Brown, Thomas L. Yearwood, Richard Bundschu, Allen Burton, Thomas Yang, Ramsin Benyamin, and AbramH. Burgher. “188 Randomized Controlled Clinical Trial Evaluating the Safety and Effectiveness of 10 KHz High-Frequency and Traditional Low-Frequency Stimulation for the Treatment of Chronic Back and Leg Pain.” Anesthesiology Pain Med Newly Published on 07 2015: doi:10.1097/ALN.0000000000000774
Rolfson O, Dahlberg L E, Nilsson J A, Malchau H, Garellick G.Variables determining outcome in total hip replacement surgery. J Bone Joint Surg Br 2009; 91(2): 157–61.
Beall DP, Chambers MF, Thomas SM, Amburgy J, Webb JR, Goodman B, Datta D, Easton R, Linville D, Talati S, Tillman JR. Prospective and Multicenter Evaluation of Outcomes for Quality of Life and Activities of Daily Living for Balloon Kyphoplasty in the Treatment of Vertebral Compression Fractures: The EVOLVE Trial. J of Neurosurgery 0:1–11, 2018 DOI:10.1093/neuros/nyy017.
Beall DP, Shonnard NH, Berven SH, Anderson PA, Norwitz J, Wagoner D, Khor S. Registry Outcomes of Cement Augmentation for Osteoporotic Vertebral Compression Fractures. (Abstract Accepted) Society of Interventional Radiology, Austin, USA, 23–28, 2019.
The lessons learned from a recent research article were outlined in a presentation by interventional radiologist Maxime Ronot (Beaujon University Hospital, Paris, France) at the European Conference on Interventional Oncology (ECIO; 8–11 April, Amsterdam, The Netherlands). The article under scrutiny was ‘Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: a multicentre observational study’, which was published by Wang et al in the Journal of Hepatology in 2019.
Transarterial chemoembolization (TACE) is the standard of care for patients with Barcelona Clinic Liver Cancer (BCLC) intermediate stage B hepatocellular carcinoma (HCC) and for patients with unresectable BCLC stage A HCC. It can also be used as a bridge before liver transplant.
When attempting to predict patient outcomes after TACE, Ronot reported, “individual factors have been described in many research papers as predictive of response to TACE, whether favourable or not, such as the size of the tumour, the number and location of lesions, and the way the tumour is enhanced or not after contrast injection.
“You can also find many studies that try to include features and parameters about liver function or the status of the patient, and you end up with a lot of prognostic models with a lot of prognostic systems, and it is very hard to know which ones we should use, and how, and in which context,” he continued.
Ronot also noted that, “most of these prognostic models have been described and derived from small series and from monocentric studies, and they lack external validation. Many are also derived from cohorts of patients receiving TACE in a broader setting beyond the usual recommendations. This is where this paper comes in.”
In their study, Wang et al included patients receiving conventional TACE for HCC from 24 tertiary Chinese centres. They used strict inclusion criteria so their target population was made up of “recommended” or “ideal” candidates of TACE who were treatmentnaïve, had well preserved liver function with a Child-Pugh score of A5-B7 and had at least one measurable lesion >1cm.
They screened 3,810 patients for eligibility. After exclusions, a total of 1,604 patients (87% male; 85% with hepatitis B virus) were randomised into training (n=807) and validation (n=797) cohorts in the study.
“The authors’ first message,” said Ronot, “was that the patients’ median overall survival was rather high at more than 32 months and they explained that this was because of the strict inclusion/ exclusion criteria.”
They produced two different models to see which was better at predicting patients’ overall survival: one with a simple addition of tumour size and number and a second which used an adjusted tumour size and number and included alpha-fetoprotein. Ronot stated that “the second model was not significantly better than the first model so they chose to stick with the first model.
“The researchers proposed new criteria: the six–12 criteria, which we could use to stratify patients into three strata: the sum of the largest tumour and the number of tumours will be lower than six, between six and 12 or larger than 12. They showed how this could stratify in terms of patients’ overall survival in the derivation and validation cohorts,” he explained.
They then compared the performance and discriminative ability of this model with existing models. Ronot described how “for every scenario they found the accuracy of their model was higher, at the upper range of the discriminatory ability of all the models.”
They also provided “a nice easy numbergram where you can plot the probability of one-, two- and three-year survival, as well as median survival, using the six–12 criteria. This is very useful and very easy to do.”
Ronot outlined the strengths of the study, “which is clearly multicentric, as the data were from 24 centres, it has a clear endpoint of overall survival which is easy to understand, there is validation, the model was compared with other models and the model gives a continuous result.” He also noted some limitations: “As an observational study, the risk of bias is not completely absent, there was a high rate of HBV, as is common in Asia, and they did not look at the way treatment response reacted and changed with this model.”
Ronot concluded that some important points can be taken from this study, “It underlines the importance of tumour burden that we frequently observe in HCC. It has demonstrated that survival can be quite long for patients at intermediate stage or with unresectable tumours—close to 33 months’ overall median survival is interesting. But most important for interventional radiologists, when I read this paper, I realised there was room for wide differences in the type of drug and dose used, whether gelatine sponge or polyvinyl alcohol foam particles were introduced, how tumour feeding vessels were embolized and so it is hard to believe that these differences will not have an impact on patient survival or response. I therefore believe that we need to start collectively working on a standardisation about the way we report procedures and the way we do the procedures.”
Jens Ricke (Department of Radiology, University Hospital LMU Munich, Germany) presented the latest evidence about Y-90 radioembolization in hepatocellular carcinoma (HCC) at the 2019 European Conference on Interventional Oncology (ECIO; 8–11 April, Amsterdam, The Netherlands).
He outlined the latest recommendations from the European Society for Medical Oncology (ESMO) for treating HCC according to Barcelona Clinic Liver Cancer (BCLC) stage. “The figure summarising the treatment options has changed recently. What has changed is the position of radioembolization (selective internal radiation therapy; SIRT). In BCLC stages 0–A, SIRT is listed along with stereotactic radiation therapy (SBRT) and brachytherapy as alternative treatment. SIRT is also listed as an alternative treatment for BCLC stage B cancers, but not for BCLC C anymore.”
A study by Salem et al in 2016 that compared conventional transarterial chemoembolization (cTACE) with Y-90 radioembolization in a small group of patients with HCC of BCLC stages A or B found that Y-90 treatment provided a significantly longer time to progression than cTACE. Ricke elaborated: “The response is probably totally similar between Y-90 and TACE, but the time to progression is much better with radioembolization than with cTACE—this needs further validation.”
The palliative substudy of the SORAMIC trial compared patients with advanced stage liver cancer treated with SIRT and sorafenib or with sorafenib alone. There was no significant difference in patients’ overall survival rates between the two groups but in some patient subgroups there were some possible survival benefits with the addition of SIRT.
Ricke noted that “these are hypothesis-generating data and might affect how we treat these particular groups of patients in the future. We observed a survival benefit in patients with no cirrhosis (22 vs. 10 months, HR=4.46) and those with non-alcoholic aetiology (15 vs. 11 months, HR=4.63). We understand these results may be due to liver function. We also found a survival benefit in patients younger than 65 years (18.5 vs. 11 months, HR=4.65).”
To understand why younger patients might fare better, Ricke described albumin-bilirubin (ALBI) development in these patients: “We see that with the addition of Y-90 to systemic treatment, in younger patients the ALBI score is fairly consistent, but in patients over 65 it gets out of hand.”
In PP patients with Child Pugh points ≤6 and tumour size and lesions ≥7 (patients who are well compensated) overall survival with SIRT/sorafenib is 15 months vs. 11 months in patients treated with sorafenib (HR=4.82). Ricke compared this result with the same patients who were previously treated with TACE: “Liver function gets lost in the TACE group. If you apply Y-90 after TACE you may therefore run a risk of losing the patient’s liver function early—somewhere between four and eight months.”
A study by Chow in 2018 compared SIRT and sorafenib in patients with HCC and overall survival did not differ significantly between the two groups, though it initially looked better in patients treated with SIRT. Ricke explained, “Our hypothesis is that radiationinduced liver disease (RILD) is happening later than we are used to, so you lose those patients who are not well enough compensated or when there are no measures to prevent liver function. Liver prevention from RILD is key for radioembolization.”
The preventive effects of a combined drug regimen (ursodeoxycholic acid, pentoxiphylline and enoxaparin) on focal radiation-induced liver injury (fRILI) in patients with HCC were illustrated by a 2014 study by Seidensticker et al. Patients underwent radiotherapy and one group was given the combined drug regimen. After six weeks, the combined drug group had a significantly higher minimal mean hepatic threshold dose than the no drug group (19.1Gy vs. 14.6Gy, p=0.011) and fRILI was found in 45.5% of patients in the combined drug group compared with 90.9% of the no drug group (p=0.022).
Another study by Seidensticker et al in 2019 assessed the effect of RILD prophylaxis in patients with breast cancer. Ricke summarised the multivariate analysis, “The only post-therapeutic issue that would influence survival is intensified prophylaxis. The Kaplan Meier curves for survival analysis calculated from the date of radioembolization also show that intensified prophylaxis improves the probability of survival. This needs further validation but indicates that there is something we can do against RILD.”
Ricke reported that a number of studies being carried out in intermediate-stage HCC combine immunooncology with something interventional such as Y-90: “Some of these studies will have an arm with immunotherapy only in BCLC stage B.”
The immunological impact of Y-90-radioembolization was examined in a study by Chew in 2018. Ricke noted that “a prediction model applying the immune response after Y-90 is the absolute best discriminator for overall survival. If you have immune response afterwards you will survive.”
The AROMA study, which involves SIRT treatment of HCC, is collecting baseline biopsies and biopsies before a second intervention is given. Ricke explained, “you then have target tissue from abscopal untreated tumour four to six weeks after radioembolization. Four weeks after SIRT you can see extensive lymphocyte infiltration, which may be prognostically valuable. It is intriguing in terms of future combination with immunooncology.”
Ricke concluded: “In SIRT, sequential and selective approaches must be mandatory—I urge you to be very selective, even in Y-90—and strict patient selection must be carried out according to risk group definitions. Preventive measures need more validation but appear to be quite hopeful. In the future treatment will require combination with immuno-oncology.”
Avinger has announced that the company received 510(k) clearance from the US Food & Drug Administration (FDA) for its Pantheris SV (small vessel) image-guided atherectomy system.
Avinger is a developer of image-guided, catheter-based systems for the diagnosis and treatment of patients with peripheral arterial disease (PAD). Pantheris SV, a product line extension of the company’s Lumivascular image-guided atherectomy platform, is expected to expand the available market for the product line by up to 50% and allow the company to address a larger portion of the estimated US$500 million atherectomy market. Designed with a lower profile and longer length than Pantheris, the small vessel device is indicated for the diagnosis and treatment of PAD in small vessels (2mm–4mm in diameter). The new device incorporates key improvements introduced to the platform with the launch of the next-generation Pantheris system in June 2018, including a stiffer shaft for increased pushability, a refined OCT imaging system, and an enhanced cutter design.
Pantheris SV received CE Marking in October 2018 and the first patients were treated with the device in Germany in November. The company intends to initiate a limited launch of the device in several sites in the USA when commercial product is available. Distribution is expected to be expanded as the company gains additional clinical experience, builds product inventory, and receives purchasing approvals in new Lumivascular sites.
“We are excited to receive US pre-marketing clearance for Pantheris SV, which we believe could expand our addressable market for atherectomy procedures by as much as 50%,” says Jeff Soinski, Avinger’s president and CEO. “With the clearance of this new device, we are well-positioned to build on the positive momentum we have seen in our Pantheris business since the introduction of the next-generation system in 2018. Following our anticipated limited launch, we plan on leveraging our growing commercial infrastructure and installed base of Lumivascular accounts to efficiently scale up the introduction of Pantheris SV and drive growth of the product family in the second half of 2019.”
Jaafer Golzar, Avinger’s chief medical officer and a highly experienced interventionalist treating patients with small vessel disease, comments, “This product line extension represents a significant advancement for patients with PAD, in particular those suffering from the complications of small vessel disease. Treating small vessels presents a number of challenges and physicians have had a limited set of minimally invasive tools that can provide safe and effective outcomes for this high-risk patient population. Pantheris SV uses a combination of directional atherectomy with onboard image-guidance to provide several potential clinical advantages, including an enhanced safety profile, the ability to maximise luminal gain without causing vascular injury, and precise vessel measurement capabilities.”
Atherectomy is a minimally invasive treatment for PAD in which a catheter-based device is used to remove plaque from a blood vessel. Lumivascular technology allows physicians, for the first time ever, to see from inside the artery during an atherectomy procedure by using an imaging modality called optical coherence tomography, or OCT, that is displayed on Avinger’s proprietary Lightbox console. Physicians performing atherectomy with other devices must rely solely on X-ray as well as tactile feedback to guide their interventions while treating complicated arterial disease. With the Lumivascular approach, physicians can more accurately navigate their devices and treat PAD lesions, thanks to the real-time OCT images generated from inside the artery, without exposing healthcare workers and patients to the negative effects of ionising radiation.
Reflow Medical has announced the completion of enrolment in its Wing-IT investigational device exemption (IDE) trial; a prospective, multicentre, nonrandomised study evaluating the ability of the Wingman catheter to cross chronic total occlusions (CTOs) in peripheral lesions after failed guidewire attempts.
Eighty-five patients with advanced peripheral artery disease enrolled in the Wing-IT trial were evaluated at 12 centre in the USA, Germany, and Austria. John R Laird of Adventist Heart and Vascular Institute, St. Helena, USA, is the principal investigator for the study.
“We would like to express our gratitude to the participating patients, physician investigators, research staff and employees. Their efforts have made it possible for us to reach this major milestone,” says Laird.
The Wingman Crossing Catheter uses an extendable beveled tip that creates a channel to help penetrate, or cross, the occlusion. This enables further treatment of the lesion with therapeutic devices.
Isa Rizk, chief executive officer of Reflow Medical, commented, “Our goal is to expand the physician’s ability to treat CTOs, which often develop in patients with advanced peripheral arterial disease. Facilitating CTO crossings helps physicians avoid amputations or bypass surgery, which directly correlates to better long-term outcomes.”
Biotronik has launched the Carnelian support catheter, designed to improve the access for treatment of tortuous and highly calcified lesions. Carnelian support is indicated for the exchange and support of guidewires into peripheral vasculature.
The launch of the Carnelian support marks the start of a partnership between Biotronik and Tokai Medical Products. Whilst the catheter is from Tokai Medical Products, it is commercially available in most European countries through Biotronik.
Up to 40% of patients with symptomatic peripheral artery disease present with a chronic total occlusion (CTO), a press release states. If just a guidewire is used to cross the CTO, the release continues, there is a risk it will buckle once it encounters resistance by atherosclerotic plaque, stopping it from advancing further. Carnelian support is designed to prevent this buckling by enhancing guidewire control and allowing CTO crossing.
Carnelian support comes in five models and has a low tip profile of 1.6 and 1.8 French. Its tungsten braided shaft and platinum marker contribute to high kink resistance and excellent radiopaque visibility. According to the company, the catheter’s multi-segment shaft design provides a smooth transition from the soft distal tip allowing trackability to the stiffer proximal part that ensures additional push.
“I was impressed by the Carnelian support and Japanese crossing technique that enable the treatment of very complex lesions, as I recently had a chance to demonstrate in live cases at CLIC [Critical Limb Ischemia Course] 2019,” explained Marco Manzi, (Policlinico Abano Terme, Italy). “The Carnelian support catheter is the right tool to tackle the most challenging crossings even in below-the-ankle arteries.”
Figure 1. Professor Pisco (centre) and the interventional radiology team from Saint Louis Hospital in Lisbon, Portugal. Left to right: Nuno Vasco Costa, Keith Pereira (visiting from the USA to learn about prostatic artery embolization), João Pisco, Tiago Bilhim, Lúcia Fernandes.
Tiago Bilhim remembers Professor João Bexiga Martins Pisco, who passed away on 26 March 2019, during the annual meeting of the Society of Interventional Radiology (Austin, USA): “He was very accessible and kind, fond of teaching and enthusiastic about all types of minimally-invasive image-guided interventions.” Bilhim reflects on the “legacy” Professor Pisco leaves behind, following a life-time of pioneering research.
Professor Pisco was a renowned physician, both in his home country of Portugal and worldwide, and was especially esteemed amongst the radiology and interventional radiology community. He leaves behind a legacy, his work a major influence within the Portuguese radiology community. Professor Pisco had an immense interest in image-guided interventions, and his career tracked the evolution of interventional radiology from its beginnings in the 1970´s until the end of his life in 2019, by which time he was a landmark figure for interventional radiology throughout the globe.
He graduated in medicine in Coimbra, Portugal, and completed the radiology residency in Lisbon, Portugal (1972–1975). Between 1975 and 1976 he undertook a fellowship in cardiac radiology in the National Heart Hospital in London, United Kingdom. Afterwards, he continued his international career as a fellow, instructor and consultant radiologist at the University of Louisiana, USA (1977–1980). These three years in the USA had a profound effect on his whole career, shaping the way he approached medicine and patient care. He decided to pursue interventional radiology, embracing teaching and scientific research simultaneously. Those who learned from him knew his very practical and “American” way of working: “See one, do one, teach one”. He was very accessible and kind, fond of teaching and enthusiastic about all types of minimally-invasive image-guided interventions. With this in mind, Professor Pisco returned to Portugal in 1980, and became one of the great pioneers in interventional radiology. During his further 40 years of practice in Portugal, he was responsible for the dissemination of interventional radiology within our country. He was the director of the Radiology Department of the Santa Marta Hospital between 1980 and 1998. Later, he was the director of the Radiology Department of the Pulido Valente Hospital from 1998 through to 2005. He then became head of the Interventional Radiology Unit from Saint Louis Hospital in Lisbon, a position he held from 1998 until his death.
Those who knew him experienced his enthusiasm for all interventional radiology procedures, and how he always highlighted the huge impact they had on patients’ lives; offering many different treatment options, alternatives to surgery with lower morbidity and mortality. He was responsible for the implementation of many different interventional radiology techniques within Portugal, such as: percutaneous transluminal angioplasty; intra-arterial fibrinolysis; arterial and venous stent placement; arterial embolization; intra-arterial chemoembolization; inferior vena cava filter placement and sclerotherapy of varicocele and pelvic venous congestion syndrome. He became known worldwide for his scientific research regarding arterial embolization for pelvic tumours in the 1980s at the Santa Marta Hospital, but is mainly recognised for the research he developed at Saint Louis Hospital on uterine fibroid embolization from the late 1990’s and, since 2009, on prostatic artery embolization. He truly put Saint Louis Hospital in Lisbon on the map from the perspective of the interventional radiology community. This small hospital received hundreds of interventional radiologists and urologists in the last decade that came in to learn about prostatic artery embolization (Figure 1). During his lifetime work at Saint Louis Hospital, we performed over 2,100 uterine fibroid embolizations and 1,500 prostatic artery embolizations, with a huge impact in all of these patient’s lives. He was married to Beatriz (Figure 2) and they had a daughter, Joana, who is following Professor Pisco’s passion for interventional radiology (Figure 3).
Figure 2. Professor Pisco with wife Beatriz and daughter Joana.Figure 3. Professor Pisco with his daughter Joana after finishing a uterine artery embolization procedure.
Besides these clinical activities, Professor Pisco was a dedicated teacher and scientific researcher. He completed his PhD thesis in interventional radiology at the Nova Medical School in 1990 (Figure 4). His chosen research topic was the vasa vasorum changes following percutaneous transluminal angioplasty and stent placement in experimental arterial stenoses in a canine model; this was published in the Journal of Vascular and Interventional Radiology (JVIR) in 1993 and 1994. Many of the publications and scientific research in the 1980´s and 1990’s included case-reports and retrospective cohort studies of the first patients treated in Portugal with percutaneous transluminal angioplasty, stent-placement and arterial or venous embolization. From 2008, most of the work developed at Saint Louis Hospital in uterine fibroid embolization and prostatic artery embolization started to appear in all of the major international radiology journals, including Radiology, European Radiology, JVIR and Cardiovascular and Interventional Radiology (CVIR), amongst others. He published over 200 research manuscripts, participated in over 400 presentations during scientific meetings, published six books and 78 book chapters, and received many awards for his scientific research in prostatic artery embolization (Figure 5). He was a devoted teacher, becoming the head of the Radiology Department at the Nova Medical School from 1997 to 2011. He taught all medical students during that time-period, introducing them to the fundamental role of radiology in medicine and of interventional radiology in patient care. He would invite the best medical students to pursue interventional radiology, letting them perform the simplest procedures first, and guiding them through many subsequent interventions. He was also responsible for the post-graduate courses in radiology and interventional radiology that were held in Lisbon every other year; 22 overall (Figure 6). He would have national and international renowned faculty and approximately 200–300 attendants. Through all of this exhausting work, he shaped the present and future of radiology and interventional radiology not just in Portugal, but worldwide.
Figure 4. Professor Pisco after completing his PhD.Figure 5. Professor Pisco and Tiago Bilhim before receiving an award from Bial in Portugal in 2014, one of the most prestigious awards in medicine from his native country.
Professor Pisco kept his “American” influence and was an entrepreneur and pioneer. He always tried to maintain the bond between clinical practice and scientific research, and his constant eagerness for new studies and publications made him a frequent participation in all European and American interventional radiology meetings (in particular the annual meetings of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR)). During the last 20 years, one can finger-count the number of CIRSE or SIR meetings where Professor Pisco was not there presenting the most up-to-date results from our group on uterine fibroid embolization and prostatic artery embolization. He was very active during the latest CIRSE meeting in Lisbon (22–25 September 2018), and was present at the last SIR in Austin, USA (23–28 March 2019). Those who knew his passion for interventional radiology meetings are not surprised that he passed away during one—this was his “home away from home”. He died after a full day of prostatic artery embolization sessions, where he participated both as presenter and commenter. Late in the afternoon he received an award from the JVIR regarding one of our group’s publications from 2018; he was notably happy (Figure 7). Professor Pisco loved the recognition from his peers, loved SIR and CIRSE, and received three prizes from the JVIR during the last 10 years in the field of prostatic artery embolization. This was a perfect ending—already in the clouds after receiving another award even before passing away. He left us, certain that future generations touched by his passion for interventional radiology will keep alive all minimally-invasive, image-guided therapies—embolization and angioplasty—as alternative treatment options to surgery.
Figure 6. Professor Pisco (at the speaker’s podium) in the opening ceremony of the last post-graduate radiology course he organised in Lisbon, Portugal.Figure 7. Professor Pisco (third from right) receiving an award from JVIR 2018 editor’s honourees clinical studies. Photo taken a few hours before he passed away during the 2019 annual meeting of the Society of Interventional Radiology (SIR), on 26 March in Austin, USA.
For all of the patient’s lives that he helped to save, all of the medical students he taught, all of the radiologists and interventional radiologists that he taught—thank you! I hope to see you someday again.
Tiago Bilhim is an interventional radiologist in Lisbon, Portugal.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has released a statement on the use of paclitaxel-coated balloons and stents in the treatment of peripheral arterial disease (PAD) following the paper published late last year by Konstantinos Katsanos (Patras, Greece) and colleagues in the Journal of the American Heart Association.
The statement from CIRSE reads:
“Recent debates at various global meetings, corrections to original papers and an FDA [US Food and Drug Administration] update suggest that there is a safety signal associated with the use of paclitaxel-coated balloons and stents in PAD patients. A preliminary review by the FDA of the three pivotal randomised controlled trials (975 patients with five-year follow-up data) comparing paclitaxel-coated balloons or stents with standard balloon angioplasty or uncoated stents has confirmed a higher mortality in patients treated with paclitaxel products. There was an approximate 50% increased crude risk of mortality in patients treated with paclitaxel products.
“Clearly, these results are preliminary and should be interpreted with caution. The trials involved mainly claudicants, and involved exclusively femoropopliteal lesions and not below-the-knee lesions.
“Moreover, a specific cause and mechanism of the increased mortality is unknown, few trials have long term follow-up data and it will take more time and possibly new trials to determine the veracity of the increased safety signal.
“In the meantime, and until more information is available, CIRSE sees no alternative but to take the position that:
In the majority of patients undergoing lower limb recanalisation therapies, alternatives to drug-eluting devices should be used.
For some individual patients at particularly high risk for restenosis, clinicians may decide that the benefits of using a paclitaxel-coated device may outweigh the risks.
Drug-eluting devices should only be used after a full informed consent process that has discussed the mortality implications from the Katsanos meta-analysis.
All patients who have already received paclitaxel-eluting devices should be followed up to assess for a potential effect on mortality.”
Update from the SVS paclitaxel safety task force
In response to the updated letter to healthcare providers from the US Food and Drug Administration (FDA), the Society for Vascular Surgery (SVS) also released the a letter, signed by the SVS president, Michel Makaroun, and Kim Hodgson, chair of the SVS paclitaxel safety task force and president-elect of the SVS. The Society formed the paclitaxel safety task force earlier this year.
The SVS letter states that since their initial communication announcing the formation of the task force, “two additional developments regarding paclitaxel-delivering devices have prompted this member update.”
Martin Radvany (Little Rock, USA) and Joan Wojak (Lafayette, USA) tell Interventional News that there is a shortage of physicians that are trained to perform stroke thrombectomy and to look after patients after the procedure. It is vital for interventionists to acquire the education and training specific to stroke therapy, and the required technical skills before performing stroke thrombectomy safely. Both physicians opine that these are skills cannot be acquired “on a weekend course”; but specialty or pedigree, should not be a barrier to acquiring them, they say. The Society of Interventional Radiology (SIR) has just completed an update to its 2009 training guidelines for intra-arterial catheter-directed treatment of acute ischaemic stroke, and the document is currently undergoing revision, Radvany says.
Laura Findeiss, (Atlanta, USA) president of SIR, talks to Interventional News about the society’s efforts to improve access to interventional radiology (IR) in communities across the globe. Findeiss touches on the issues that hinder the widespread adoption of IR, including lack of infrastructure, training, and government recognition. India and Egypt, Findeiss explains, are two countries where SIR is seeing increased collaboration around accreditation and recognition of the specialty. Findeiss spoke to Interventional News at the 2019 SIR Annual Scientific Meeting in Austin, USA (23–28 March).
Alan Matsumoto (Charlottesville, USA) talks to Interventional News about the disruption and fragmentation that is causing a “tornado in healthcare”. He expanded on how interventional radiologists should show “unity in purpose” in the face of disaggregating forces such as consumerism, Big Business and Big Data, to centrally focus on the two things that matter most: patients who need care, and patience that allows for that care to be delivered wisely and well. Matsumoto delivered the annual Charles T Dotter Lecture at the 2019 SIR Annual Scientific Meeting (23–28 March, Austin, USA).
The SVS letter states that since their initial communication announcing the formation of the task force, “two additional developments regarding paclitaxel-delivering devices have prompted this member update.”
The developments are outlined as the following:
Two recent industry notifications indicate that data contrary to previous reports throw additional doubt on results
After their own preliminary analysis of long-term follow-up data from the IDE trials revealed a similar mortality signal, the FDA issued a recommendation that surgeons consider “alternative treatment options” to paclitaxel devices for most peripheral arterial disease (PAD) patients until the science is further clarified. That communication came just two months after the FDA had advised no significant changes in clinical practice other than close surveillance and discussing the issue with patients.
The letter continues: “As previously communicated, the SVS is concerned about the recent publication in the Journal of the American Heart Association suggesting higher rates of two- and five-year mortality in patients with PAD treated with paclitaxel-delivering devices.
“As you may recall, several weeks ago the Society announced a new SVS Paclitaxel Safety Task Force, whose mission is to facilitate the performance and interpretation of an individual patient data (IPD) meta-analysis using patient-level, randomised controlled trial data from our industry partners.
“While the decision of how to treat is always up to the physician, the cloud over paclitaxel has darkened with these new findings and advisories. At bare minimum a documented discussion with the patient and a detailed description of the perceived benefits of a paclitaxel device are prudent if one is to be used in this climate.
“Given the conflicting conclusions about a paclitaxel dose effect, even proceeding but choosing a lower dose device seems unsubstantiated.
“The SVS continues to believe that only an independent patient data meta-analysis—as we are planning—will yield the conclusive answers we need. We remain troubled by the recent reports of re-analyses of existing datasets, pooled analyses of randomised controlled trials and other ‘series,’ as we believe that the findings of these statistically inferior analyses bring no additional clarity, cannot be relied upon for guidance and distract us from the analysis that needs to be performed.
“While debate about a possible mechanism for, or even existence of this effect continues, knowledgeable trialists have concluded that clarification will only be possible by performance of such an IPD meta-analysis of combined trial data. We will keep you apprised of our progress in this endeavour.”
A prototype wearable device, tested in animal models, can continuously collect live cancer cells directly from a patient’s blood. Proposed as an alternative to biopsy, the system allows for the analysis of larger blood volumes, leading its developers to write in Nature Communications that “this technology could potentially be used to analyse larger number[s] of circulating tumour cells to facilitate translation of analytical information into future clinical decisions”.
Developed by a team of engineers and doctors at the University of Michigan (Ann Arbor, USA), it could help doctors diagnose and treat cancer more effectively.
“Nobody wants to have a biopsy. If we could get enough cancer cells from the blood, we could use them to learn about the tumour biology and direct care for the patients. That is the excitement of why we are doing this,” says Daniel F Hayes, the Stuart B Padnos professor of breast cancer research at the University of Michigan Rogel Cancer Center and senior author of the Nature Communications paper.
Cancerous tumours can release more than 1,000 circulating tumour cells (CTCs) into the bloodstream in a single minute. These have become an established biomarker for prognosis in patients with various carcinomas, with elevated levels of CTC isolated from a single blood draw being indicative of metastatic breast, colorectal, prostate, or lung cancers. Current methods of capturing CTCs from blood rely on samples from the patient—usually no more than a tablespoon taken in a single draw. Some blood draws come back with no cancer cells, even in patients with advanced cancer; an average 7.5mL sample from a patient with metastatic breast cancer contains no more than 10 cancer cells, identified within the context of billions of erythrocytes and millions of leukocytes.
Over a couple of hours in the hospital, the new device—a portable aphaeretic system—could continuously capture CTCs directly from the vein, screening much larger volumes of a patient’s blood. In animal tests, the cell-grabbing chip in the wearable device trapped 3.5 times as many cancer cells per millilitre of blood as it did running samples collected by blood draw.
“It is the difference between having a security camera that takes a snapshot of a door every five minutes or takes a video. If an intruder enters between the snapshots, you would not know about it,” explains Sunitha Nagrath, associate professor of chemical engineering at the University of Michigan, who led the development of the device.
The wearable device measures roughly 2×2.75×1 inches, with the cancer cell-capturing chip mounted on top. The catheter connecting to the patient runs through the hole in the top left corner.
Research shows that most cancer cells cannot survive in the bloodstream, but those that do are more likely to start a new tumour. Typically, it is these metastases that are deadly, rather than the original tumour. This means CTCs captured from blood could provide better information for planning treatments than those from a conventional biopsy. Indeed, the investigators of the present proof-of-principle study hypothesised that “CTC evaluation might be used for early detection of malignancy, if an assay with sufficient sensitivity and specificity could be developed.”
The team tested the device in dogs at the Colorado State University’s Flint Animal Cancer Center (Fort Collins, USA) in collaboration with Douglas Thamm, a professor of veterinary oncology and director of clinical research there. They injected healthy adult animals with human cancer cells, which are eliminated by the dogs’ immune systems over the course of a few hours with no lasting effects.
Inside the wearable device, the blood pump sits in the upper left corner while the heparin injector runs the length of the near side of the box. The green circuit boards control the blood pump, heparin injector and provide display data.
For the first two hours’ post-injection, the dogs were given a mild sedative and connected to the device, which screened between 1–2% of their blood. At the same time, the dogs had blood drawn every 20 minutes, and the cancer cells in these samples were collected by a chip of the same design.
The device shrinks a machine that is typically the size of an oven down to something that could be worn on the wrist and connected to a vein in the arm. For help with the design, the engineering team turned to Laura Cooling, a professor of clinical pathology at the University of Michigan and associate director of the blood bank, where she manages the full-size systems.
“The most challenging parts were integrating all of the components into a single device and then ensuring that the blood would not clot, that the cells would not clog up the chip, and that the entire device is completely sterile,” comments Tae Hyun Kim, who earned his doctorate in electrical engineering in the Nagrath Lab and is now a postdoctoral scholar at the California Institute of Technology (Pasadena, USA).
Each component of the device is integrated into a compact 3D printed, portable structure, and is controlled through a custom built mobile application via wireless communication. The system consists of four major parts: a micro-controller, peristaltic pump, heparin injector, and a CTC capture module that contains a microfluidic CTC capture chip.
The investigators developed protocols for mixing the blood with heparin, to prevent clotting, and sterilisation methods that killed bacteria without harming the antibodies on the chip. Kim also packaged some of the smallest medical-grade pumps in a 3D-printed box with the electronics and the cancer-cell-capturing chip.
The chip itself is a new twist on one of the highest-capture-rate devices from Nagrath’s lab. It uses the nanomaterial graphene oxide to create dense forests of antibody-tipped molecular chains, enabling it to trap more than 80% of the cancer cells in whole blood that flows across it. The chip can also be used to grow the captured cancer cells, producing larger samples for further analysis.
In the next steps for the device, the team hopes to increase the blood processing rate. Then, led by Thamm, they will use the optimised system to capture cancer cells from pet dogs that come to the cancer centre as patients. Chips targeting proteins on the surfaces of canine breast cancer cells are under development in the Nagrath lab now.
Hayes estimates the device could begin human trials in three to five years. It would be used to help to optimise treatments for human cancers by enabling doctors to see if the cancer cells are making the molecules that serve as targets for many newer cancer drugs.
“This is the epitome of precision medicine, which is so exciting in the field of oncology right now,” says Hayes.
After coming across interventional radiology in a “fortunate accident”, the 2019–2020 Society of Interventional Radiology (SIR) president Laura Findeiss talks to Interventional News about her career, the future of the discipline, and the importance of working across disciplines to foster the creative thinking necessary in difficult cases.
You started your residency in surgery, but then changed to interventional radiology (IR). Why?
Lots of factors. For one thing, I found myself burned out. That was before work hour restrictions, and there was a different culture in surgical training programmes. When I lost my originally deep compassion for patients, I realised that I could not do it anymore. I loved operating, but even this lost its lustre. After I left my residency, I spent a year working in rural hospital emergency departments (really, emergency rooms) in Tennessee, and this was a great experience for me, learning true clinical independence and gaining an understanding of what rural medicine is really like—how isolated some of these places are even now. Ultimately, choosing a radiology residency was a process of exclusion and was not particularly deliberate. I enjoyed the imaging very much, but was like a fish out of water without the hands-on patient care. When I “discovered” IR, it really was a perfect combination of the beauty of imaging and the ability to care for patients in a creative and technically challenging way. When you have cared for lots of patients recovering from surgery and see the difference our techniques make, you see how truly impactful it is.
Have you had important mentors throughout your career? What have they taught you?
Yes! So many. The chief of IR at my residency programme, Ellen Hauptmann, was so committed to doing the right thing for patients, and she was such a role model for me. Her compassion, knowledge base, imaging skills and true technical ability were part of what really attracted me to the specialty. I learned about what it means to be a great colleague from her, as she was so collaborative with all the referring specialties. The chief of IR in my fellowship, Torre Andrews, was great at talking to patients at their level, and that was great to observe. He became a true sponsor, as he was the one who got me involved on committees in the SIR, and it was that early engagement that got me energised and networked in the society. He was one of a core group of SIR members pushing the clinical practice paradigm early on, and his passion about this issue reinforced my own. Finally, Scott Goodwin, who gave me a great opportunity when he hired me at the University of California at Irvine as section chief, was a great mentor in that he let me execute my vision with guidance and trust. He really stood back and supported me in the background while I ran the section in the direction our team wanted to go, and that was just a fantastic leadership experience that gave me the confidence to move on to other roles. It also taught me about leading by supporting others.
In several of your workplaces, access to IR services has been limited. What are some common barriers to access, and how can these be overcome?
This topic is really important to me. I think the biggest barrier to access in many places is the lack of an IR in a community or hospital. Recent literature looking at the distribution of providers of image-guided interventions throughout the USA validates this perspective; the availability in communities is dismal. This applies, unsurprisingly, to extremely rural locations, but I think the big shock is how even suburban and not-so-remote areas suffer from this lack of availability.
I see this as an amazing opportunity for our specialty. We have a generation of IRs emerging from training now, more independent and clinically-minded. From my point of view, so many of the communities that would benefit from the presence of an IR are great places to live and grow diverse practices. Talking to young IRs who have had an opportunity to take advantage of these availability gaps, I am amazed at the high-quality practices they have built, and how rewarding this process has been for them.
One barrier that has been raised with regard to growing an IR practice in communities has been the “exclusive contracts” issue in the USA, whereby IRs may be ineligible to get hospital privileges if they are not affiliated with the hospital’s radiology group, but may find that they are unable to practice the way they wish to, in a more clinical fashion, within a radiology group. We have members advocating on both sides. SIR is actively working to find common ground on this topic through collaboration with the ACR’s IR Commission and the General, Small, Emergency, and Rural (GSER) groups Commission, as these issues are a mutual concern.
As a self-described “systems operations geek”, how does thinking systemically aid you in your work?
In my current role as chief of Service for Radiology at Grady Memorial Hospital, a large public safety net hospital in Atlanta, I am working to improve our systems and operations to provide better efficiencies in care to create more access without increasing costs. We are relatively under-resourced due to our mission of caring for a largely self-pay, county-funded, and Medicaid-funded population. On top of emphasising process improvement methodology, I am focusing on change management principles, since all of this requires significant cultural reorientation and generation of buy in on multiple levels. I love the challenge of navigating all of this with the promise of better access to higher quality care for our patients. Before this role, using the same kind of systems thinking was really important for some of the structural changes I have participated in in other places: leading institutional change around procedural sedation standards, creating best practices in the IR area, negotiating a hospital contract focused on aligning incentives to achieve common goals. I think backing up and establishing the target state and thinking systematically about how to achieve the goals is always a best practice.
As the president-elect of the SIR, what are your aims for the society over the next 12 months?
We have already touched on a major theme: access to care. I truly believe that there are significant disparities in patient outcomes related to lack of access to IR. I also think that our burgeoning clinical IR workforce is a great match to this challenge. If we can navigate, through our collaborative work with the ACR, the current challenges in creating avenues for clinical IR practices within or alongside radiology practices, we can create a win-win(-win) for radiology practices, IRs, and communities.
Another topic that is very important to me is that of promoting and supporting diversity in our specialty. The SIR has a goal of creating an inclusive environment. I hope to make progress on this front over the next year, particularly with respect to establishing venues for engagement and solidifying the platform from which specific, member-driven efforts can launch. The SIR should be a place where all IRs can find a sense of belonging.
You are an advocate for multispecialty collaboration within healthcare. How can this be improved?
I firmly believe patient outcomes are better, and care is more efficient, when there is open and respectful communication between different specialties. In so many places we find ourselves in conflict with other specialists over areas of mutual expertise, configured as turf battles or even just ego battles, and patients are the losers. Physicians can easily get distracted from best patient care in these kinds of environments—watching your back instead of watching the patient. It is just another systems thing, in that reducing friction between specialties will help us to use institutional and system resources better and reduce cost, improve efficiencies, and optimise outcomes. Modifying incentives, of which monetary rewards are only a part, can help. To improve collaboration for the benefit of patients will ultimately take strong institutional and systemic leadership focused on reducing the incentives to compete and increasing incentives for collaboration.
Would you describe a particularly memorable case?
One of the most rewarding cases I did was early in my career. I had a patient referred for evaluation for a spontaneous portosystemic shunt. She had presented to our hospital comatose from severe hepatic encephalopathy and she had suffered from medication refractory bipolar disorder and schizophrenia starting early in adolescence. She had been institutionalised for many years, and had reportedly displayed psychotic behaviour. There is a lot in the veterinary literature about congenital portosystemic shunts in dogs, who demonstrate bizarre behaviours that can resolve with surgical occlusion of the shunts. We wondered if this was in play. Then we learned that the antipsychotic and other medications she was on are dependent on hepatic metabolism—the metabolites are the active agents. After a lot of multidisciplinary discussion, I ultimately occluded her shunt and psychiatry modified her medications. She ended up being discharged home to self-care after a few months with the support of her adult daughter. In follow-up, she thanked me for giving her a relationship with her daughter. This case is a reminder to think outside the box, something I think IRs are really good at.
What is the biggest challenge in IR at the moment?
We are in a major transition with the training pathway, and this is bringing learners with different perspectives and expectations into the specialty. I think this will be good for patients and the specialty if they can execute on the promise of a new kind of practice model. It is going to be disruptive, though, to radiology, and I am glad we are starting to talk about this at the SIR-ACR level.As a society, our imperative is to help get our members the tools they will need to navigate the changing landscape through productive negotiations with radiology practices, hospitals, payors, health systems, or whatever entities they need to work with to build the practices that make the most sense in their local environments. One big challenge is how different local environments are from each other in our health system, so the approach cannot be one size fits all.
Outside of your own research, what has been the most interesting paper that you have seen in the last 12 months?
Rosenkrantz et al, “Generalist versus Subspecialist Workforce Characteristics of Invasive Procedures Performed by Radiologists”, in Radiology online. An incredible take home point from the article was that only 347 counties throughout the USA have access to an IR, and only 869 counties have access to a generalist radiologist who performs procedures. This clearly shows that a large part of the country is un- or under-served from the standpoint of IR and we need to look at how to address these access disparities.
What do you anticipate being the most disruptive technology in IR over the next 10 years?
Targeted molecular therapies. In addition to immunotherapy, I see a lot of promise in the theranostic arena, with molecularly-targeted imaging/radiotherapy agents for diagnosis, treatment, and monitoring of response to therapy. I can actually see IR playing a big role in the transarterial delivery of these agents to tumors, since intravenous administration is fraught with problems from a dosimetry point of view. These applications are just a one-off from what we already do with SIRT [selective internal radiation therapy]. It is another reason to make sure we maintain our ability to achieve AU status, and the molecular therapy piece is an important reason for IR’s to engage in bench research.
How has the field changed since you started your career?
There is the obvious answer of case mix—early in my career my whole practice was abdominal and then thoracic endografts, renal artery stenting, carotid stenting, and CLI [critical limb ischaemia] intervention. I had to strive to start programmes for chemoembolization, UAE [uterine artery embolization], and TIPS [transjugular intrahepatic portosystemic shunt]. That landscape continues to change and can always be expected to change, since our talent as a specialty is figuring out how to treat disease in different, less invasive, innovative ways, and if we do not see procedures migrating out and new ones migrating in then we are not innovating.
Even more important is the change in the understanding of what it means to practice clinically. Early in my career I was, I think, in great company, but in the minority as far as beating the drum on having to have a dedicated clinic model and practice like any other procedural specialty. It is great to see how this concept has been embraced and is now at the core of our training programmes.
What are your interests outside of medicine?
A lot of individual sports: skiing, snowboarding, road cycling, mountain biking, rock climbing, wake boarding. I started triathlon recently, and have been learning how to telemark. I love to travel, and enjoy ballet and a good book (but these days most of my books are sitting on a shelf staring at me, reminding me they want to be read).
Appropriately trained interventional radiologists performing endovascular thrombectomy in technically complicated stroke cases achieve similar reperfusion and clinical outcomes to those reported in the published literature. This is the conclusion of Andrew Hines, an interventional radiologist at Northeast Charlotte Radiology, Charlotte, USA, presenting his data at the annual meeting of the Society of Interventional Radiology (SIR; 23–28 March, Austin, USA).
“There is a lot of political pressure right now amongst other subspecialties, and they feel that we are not appropriately positioned to perform stroke thrombectomies, so it is even more important for those of us in this room to make sure that our data is extremely robust,” he said to SIR attendees.
Hines said that, although he believes interventional radiologists are doing a good job at demonstrating their technical ability at performing M1 occlusions, the most common type of large vessel occlusion, they must demonstrate that capability in more technically challenging stoke cases to assuage “critics of interventional radiology”. Tandem occlusions are occlusions of the internal carotid artery in addition to occlusions of some of the inter-cerebral vessels and, according to Hines, there is very little literature focusing on gauging how well interventional radiologists are performing these procedures specifically.
“Interventional radiology is not new to this [stroke cases]”, he informed delegates; “75% of the patients in the MR CLEAN study were performed by interventional radiologists, and that was actually the first of the five landmark trials, so we certainly have been here since the beginning.” The other four “landmark” trials he mentioned are ESCAPE, EXTEND IA, SWIFT PRIME, and REVASCAT.
Comparing published studies looking at tandem occlusions specifically, Hines said that “they all have a low patient sample size, ranging from two patients to about 100”. He also noted that both the technical outcomes and the TICI 2B/3 [Thrombolysis In Cerebral Infarction scale; an evaluation of angiographic intracranial flow] varied widely, both “from 50 to 100%”.
Several of the investigators from the five “landmark” trials have conducted subanalyses of their data to look at tandem occlusions. Showing the SIR audience an ESCAPE trial subanalysis, Hines said “In this series, in their tandem occlusions the TICI 2B/3 was 69% for technical success in revascularisation, and their mRS 0–2 at 90 days was 60%. So this sets the bar, I think, as to what we interventional radiologists should be trying to achieve.”
Turning to his own data, Hines then asked the question “So, how well did we do?”. Going through his results, he explained, “With tandem occlusions, we achieved a TICI 2B/3 of 86%—that is almost as good as our M1 data. Our mRS 0–2 at 90 days was 43%, compared to 48.7% [in his M1 data]. Importantly, our complication rate was only 2.7%, and our mortality rate was 24%.
“If you squeeze this data into the various retrospective series”, he continued, “you can see that we are definitely in the top quartile of all of the published series, especially when you look at the series that have more than 30 patients.”
The key takeaway Hines stressed to the audience was that, when appropriately trained, interventional radiologists are proficient at performing these complicated procedures, and that the clinical outcomes are comparable with published data from other specialties who perform these tandem occlusions as part of stroke care.
BD has announced the launch of their UltraScore 014 Focused Force percutaneous transluminal angioplasty (PTA) Balloon. This marks the first scoring balloon with sheath compatibility as small as 4F on the US market.
The UltraScore balloon is intended to dilate stenoses in the iliac, femoral, ilio-femoral, popliteal, infra-popliteal and renal arteries and for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulae. This device is also recommended for post dilatation of balloon expandable stents, self-expanding stents, and stent grafts in the peripheral vasculature. UltraScore is designed to longitudinally fracture plaque at lower inflation pressures compared to standard PTA and may allow for more controlled plaque fracture and less vessel recoil, even in calcified lesions. With the addition of the 0.014” guidewire platform, the device is available in both 0.014” and 0.035” solutions with sizes ranging from 2mm to 8mm in diameter and up to 300mm in length.
“The deliverability, ease of use and expansion of the vessel with UltraScore Focused Force PTA Balloon are excellent,” commented William Bachinsky, director of the Cardiac and Vascular Interventional Program at UPMC Pinnacle. “The addition of UltraScore 014 Focused Force PTA Balloon will fit right in with our treatment algorithms for popliteal and infrapopliteal lesions.”
Both UltraScore 035 and UltraScore 014 devices are CE-marked and have received 510(k) clearance by the US Food and Drug Administration (FDA).
The FDA has cleared an expanded indication of Embosphere microspheres (Merit Medical) for the embolization of blood vessels to occlude blood flow in the peripheral vasculature to control bleeding or haemorrhaging.
The Embosphere microspheres are the first spherical embolic devices to be cleared for this use.
According to Merit Medical, Embosphere microspheres have now received more indications for use than any other spherical embolic on the market.
With this approval, Embosphere microspheres are now indicated for use in embolization of arteriovenous malformations, hypervascular tumours, symptomatic uterine fibroids, prostatic arteries for the relief of symptoms related to benign prostatic hyperplasia, and for controlling bleeding or haemorrhaging in the peripheral vasculature.
A new global registry from Ethicon (part of Johnson & Johnson medical device companies) has been launched to collect and analyse real-world data on patients with soft tissue liver lesions ablated with the company’s Neuwave microwave ablation system. Ethicon announced this registry at the Society of Interventional Radiology (SIR) annual meeting (23–28 March, Austin, USA).
The multicentre, observational registry will follow approximately 1,500 patients worldwide for a total of five years from the date of their first liver ablation procedure with the Neuwave system.
Real-world data will be collected from up to 30 centres throughout the world on the technical aspects of the procedure, including ablation time under varying liver tissue and lesion conditions. Efficacy and other outcome data will also be documented and assessed at various time points over the course of the study.
“The goal of the registry is to systematically and comprehensively develop ablation parameter guidance for the microwave ablation of liver lesions with the Neuwave system,” says Paul Laeseke, an interventional radiologist at the University of Wisconsin School of Medicine and Public Health (Madison, USA), who consulted on the design of the registry. “Microwave ablation is an important treatment option that is increasingly being utilised throughout the world, and this data may provide new insights into factors that are critical for successful outcomes across a range of patients, clinical settings and health care providers. The registry will be an important contribution to our understanding of microwave ablation and support its further adoption.”
The registry will also include data from consenting patients enrolled in other Ethicon-sponsored studies on microwave liver ablation with the Neuwave system in Korea and China, as well as a multicentre study that is evaluating the device using Neuwave’s ablation confirmation software, which, according to a press release, helps physicians identify ablation targets, assess appropriate probe placement and confirm the technical success of each procedure.
“Microwave is the fastest growing ablation modality and as this treatment grows, Ethicon is committed to working with clinicians throughout the world to generate robust clinical evidence for the innovative Neuwave microwave ablation system. This will help inform treatment decisions and improvements in procedural efficiency and patient outcomes,” comments Piet Hinoul, global head medical and clinical franchise lead for Ethicon.
The Neuwave system, which Ethicon claim is the microwave ablation market leader in the USA, is a minimally invasive system that enables physicians to effectively tailor ablations for lesions of varying shapes and sizes with consistency and control. A press release states that studies have shown microwave ablation has strong efficacy and a favourable complication profile, with most patients leaving the hospital the same day with a bandage at the probe insertion site.
Daryl Goldman, Suroosh Marzban, and Robert Rosen highlight the use of catheter-based techniques for the treatment of Parkes Weber syndrome in children. Summarising their recent work, presented at the Society for Interventional Radiology 2019 conference (SIR; 23–28 March, Austin, USA), Goldman et al detail how it demonstrates the feasibility and safety of embolization for treating arteriovenous malformations associated with the disease, and expands on the key role paediatric interventional radiology has to play in the multidisciplinary management of this rare disorder.
Parkes Weber syndrome (PWS) is a rare congenital vascular disorder characterised by high-flow arteriovenous malformation, limb hypertrophy, and port wine stain. PWS was first described by Frederick Parkes Weber in 1907, who reported on two patients with limb hypertrophy, port wine stain, and vasculature with pulsatile thrill. The etiology is not well understood, but PWS has been associated with mutations in the RASA1 gene, which codes for various growth factor receptor signals involved in proliferation, migration, and survival of vascular endothelial cells. The exact prevalence of PWS is unknown, and PWS carries an associated mortality rate of approximately 1%.
Arteriovenous malformations are often the most debilitating of the PWS triad, causing a wide variety of clinical features such as pain, fatigue, ulceration, and high-output congestive heart failure. Unfortunately, arteriovenous malformations remain a significant challenge to treat given a high recurrence rate and the morbidity associated with surgical resection. Catheter-based techniques have emerged as the preferred mode of therapy. Catheter-based techniques for treatment of high-flow arteriovenous malformations consist of embolization with various types of embolics including acrylic adhesives, EVAL, sclerosing agents including ethanol, coils, and microspheres. The arteriovenous malformations of PWS are not completely curable given the diffuse nature of the disease with multiple areas of small vessel shunting. They also tend to recruit new collateral vessels that contribute to the recurrence of symptoms. Therefore, the goals of management are to improve symptoms and slow disease progression from childhood, including the development of heart failure and limb hypertrophy. The clinical manifestations can be unusually severe in PWS compared to other AVMs, with a significant incidence of tissue loss (ulceration, amputation) and high output states.
The purpose of our study, presented at the SIR conference in Austin, was to describe the safety, feasibility, and efficacy of catheter-based therapy for the treatment of high-flow arteriovenous malformations in paediatric patients with PWS. A retrospective review was performed from January 2004 to January 2018 to identify patients with PWS who underwent diagnostic angiography of arteriovenous malformation. Nine paediatric patients were included in this study (mean age: eight, range: five to 16; four male, five female). Treatment response (relief of symptoms), technical success, lesion characteristics, procedural details, and adverse events were recorded.
Two of nine patients (22.2%) were affected in the upper extremity and seven of nine (77.7%) in the lower extremity. Presenting symptoms included pain (in 100% of patients), edema (in eight of the nine patients, 88.8%), ulcer (in three of nine patients, 33.3%), difficulty ambulating (in four patients, 44.4%), and high-output cardiac failure (in five patients, 55.5%). Three (33.3%) patients were found to have diffuse arteriovenous communication without a discrete arteriovenous malformation nidus and thus were not treated with embolization. Six (66.6%) patients were treated with transcatheter embolization of the arteriovenous malformation’s arterial inflow. Four (66.6%) required multiple inflow embolization procedures (median, four; range, one to 10). Twenty-seven arterial inflow embolization procedures were performed in total. N-Butyl cyanoacrylate (nBCA) adhesive was used in 19 cases (70.3%), microspheres in seven (25.9%), and a combination of coils and adhesive in one (3.7%) case. Two patients (22.2%) also had interventions to treat the venous component of the malformation. Median follow-up time was 67 months (range, 0-97). Technical success (decreased arteriovenous shunting) was 100%. One (16.6%) patient treated with embolization experienced no response and five (55.5%) experienced a partial response (reported improvement in symptoms). There were no periprocedural complications.
The arteriovenous malformations associated with PWS are often debilitating. Management requires a multidisciplinary approach, including both surgical and endovascular interventions. Interventional radiology plays a crucial role in the treatment of these patients. Transcatheter and direct embolization are feasible techniques for treatment of arteriovenous malformation’s in patients with PWS with a favorable treatment response, safety profile, and high technical success rate.
Even in a practice such as ours consisting primarily of treating vascular malformations, Parkes Weber Syndrome remains one of the most challenging situations, due to the diffuse nature of the shunting and lack of a clear cut nidus. These are the patients who have the highest incidence of tissue loss, non-healing ulceration with associated pain, and high output cardiac states, including cardiac failure in the most severe cases. The goals of treatment are thus directed at reducing the shunting to improve the local symptoms as well as reducing the cardiac workload—real “cure” is an unrealistic goal in most of these patients. The best hope in the future may be pharmacologic, as our understanding of the molecular basis of angiogenesis is constantly advancing.
Daryl Goldman is an interventional radiology integrated resident at Icahn School of Medicine at Mount Sinai, currently doing her intern year in General Surgery at Lenox Hill Hospital, New York, USA.
Suroosh Marzban is a vascular surgery resident at Lenox Hill Hospital, New York, USA.
Robert Rosen is an interventional radiologist at Lenox Hill Hospital, New York, USA.
The Society of Interventional Radiology (SIR) announced the establishment of the Grants for Education of Medical Students (GEMS) programme at its 2019 annual scientific meeting (23–28 March, Austin, USA). Alan H Matsumoto, former SIR president, introduced the programme during his acceptance speech for the SIR Gold Medal Award (for which he was one of three recipients). The GEMS programme aims to support diversity within interventional radiology (IR) by providing travel grants for medical students participating in an IR clerkship outside of their home institution.
“With IR now being recognised as its own medical specialty, we have a wonderful opportunity to engage medical students, whilst also focusing on the diversity within our specialty,” Matsumoto said. “We all know that once medical students are exposed to IR, they often fall in love with it. So it is really about giving them a chance to see and experience how IR really is early enough in their career so they can make the appropriate choice.
“The purpose of the GEMS programme is to grow the diversity in IR by providing a travel grant to medical students who identify as either being from a gender, racial, or ethnic group underrepresented in IR, or who identify as LGBTQ, and who are seeking to be first generation physicians in their families, as well as students from a socioeconomically disadvantaged background, regardless of their gender or ethnicity, by providing them a travel grant as a way to encourage them to explore the specialty of IR as a career. Up to 10 US$15,000 travel grants per year will be awarded to medical students who have applied to participate in the GEMS programme, to participate in a four week IR clerkship outside of their home institution.”
The funding for the GEMS programme comes through donations from the Matsumoto family, the SIR Foundation, Boston Scientific, Cook Medical, Penumbra, Siemens Healthineers, and WO Gore.
On the SIR Foundation’s website, the society state: “The clerkships to which the students are applying must devote at least 50% and up to 100% time to IR, with any remaining time devoted to diagnostic radiology (DR), nuclear medicine or a subspecialty area within DR. The clerkship must be at least four weeks in duration.”
For IR programmes interested in participating, the SIR Foundation has said that it will “identify IR programmes from around the country” who are committed to assisting the eligible groups of medical students “to gain exposure to the field of IR” and will provide this listing on the SIR Foundation website.
In his announcement speech, Matsumoto elaborated on the programme’s purpose: “The intent of the programme is to eliminate any financial barrier that might have prevented a medical student from exploring an IR clerkship. The rationale for encouraging students to participate in an IR clerkship different from their home institution is to provide them with the opportunity to be exposed to a different institution in an IR programme, to have a more personalised learning experience about the specialty of IR, to become more comfortable in a new environment, as a prelude to the residency application and interviewing process, and to potentially develop an early mentoring relationship in IR and broaden their professional network.
“Not only does the programme offer opportunities for medical students, but hopefully will also encourage IR training programmes to contribute to the promotion of diversity in our specialty.”
The GEMS programme began accepting applications from 1 April 2019.
Matsumoto concluded: “It is really the goal and sincere hope of my family, Boston Scientific, Cook Medical, Penumbra, Siemanns Healthineers, Gore, the SIR and the SIR Foundation that the GEMS programme will help to expand the diversity of thought, and personnel of our specialty, so we may better serve the growing diversity of patients for whom we provide care.”
This sentiment was echoed by then SIR president Victoria Marx (Keck School of Medicine of the University of Southern California, Los Angeles, USA), who commented: “SIR and SIR Foundation are incredibly grateful to Dr Matsumoto, his family and our inaugural industry sponsors—Boston Scientific, Penumbra, Siemens Healthineers, Gore and Cook—for supporting this important initiative to engage diverse groups of medical students in interventional radiology.”
A first-in-human trial finds that gallbladder cryoablation to be a promising alternative to long-term cholecystostomy tube drainage for the treatment of cholecystitis in non-operative patients. Presenting this research at the Society of Interventional Radiology (SIR) annual conference (23–28 March, Austin, USA), Hugh McGregor (University of Arizona, Tucson, USA) informed attendees that the minimally invasive treatment may facilitate safe cholecystostomy tube removal in this patient population.
“Gallbladder cryoablation is something we have been working on over the past five years. We have been able to take the idea from conception to animal models, and finally [now] into the clinical realm,” McGregor said.
Gall stone disease affects 20 million patients in the USA, with over 300,000 cholecystostomies performed each year nationally. McGregor explains that “unfortunately, complication rates in elderly and infirm patients can be as high as 31%, and this necessitates percutaneous cholecystostomy as an alternative treatment. This itself is not definitive, with a recurrence rate of calculous cholecystitis up to 46% following tube removal. This leaves high risk patients with gall stone disease with three options: they undergo high risk cholecystectomy, they have their tube removed with a moderate to high risk of recurrent cholecystitis, or they have a tube for life. We all know this [a tube] needs constant, regular changes, and is not good for quality of life. There is definitely a need for a novel treatment option for these patients.”
This was therefore the aim of McGregor et al’s study: seeking an alternative treatment option. Following successful pre-clinical trials in swine models, which proved the safety and efficacy of gallbladder cryoablation, the Arizona investigators set out to determine the procedure’s safety and efficacy in humans.
The first patient treated was a 71-year-old man with obesity, chronic obstructive pulmonary disease, diabetes and ischaemic heart disease. He was admitted for acute calculous cholecystitis and, following surgical consultation, was given a cholecystostomy tube, placed under CT guidance. He was discharged after four days in hospital, and a week after discharge was seen by the interventional radiology team. Twenty-four days after his initial discharge, he underwent CT-guided gallbladder cryoablation with moderate sedation.
This gallbladder cryoablation was successfully performed under CT guidance using three PCS-24 cryoprobes. Two 19-gauge Yueh needles were inserted percutaneously under CT guidance to facilitate hydrodissection of the transverse colon and duodenum. A total of 1,260ml of normal saline was used for hydrodissection. A 10-8-10 minute freeze-thaw cycle with intermittent CT was used to ablate the gallbladder and achieve 5mm ablation margins. The cholecystostomy tube was removed immediately after the procedure, and the patient was discharged one day after the cryoablation with a 10-day course of moxifloxacin.
According to McGregor, laboratory values on post-procedure day 28 were notable for a mildly elevated alkaline phosphatase of 167IU/L, which normalised by three months. An MRI enhanced with the contrast agent eovist at 28 days’ post-procedure demonstrated a thick gall bladder wall with a persistent lumen, a patent common bile duct, and no filling of the cystic duct. MRI at three-months’ post-procedure showed partial collapse of the gall bladder, with early and delayed enhancement suggestive of ongoing inflammation and fibrosis. McGregor described how the imaging at six-months follow-up “really nicely demonstrated the continued involution of the gall bladder”, which then had no lumen: “it is just a completely involuted, collapsed structure, really a scar”. The patient was asymptomatic at all follow-up times.
Summarising this clinical work, McGregor said to the SIR audience: “This is one case, but we feel it may be a promising option for high-risk, tube dependent patients with gall stone disease. Our imaging follow-up demonstrated cystic duct occlusion, as well as involution of the gall bladder, and clearly studies are need to establish the safety and efficacy of the procedure, particularly in patients with bulky gall stone disease. Those are in the pipeline.”
Recently, McGregor and colleagues performed gallbladder cryoablation on a woman with a single large gall stone, and one-month imaging (the latest follow-up imaging available) is promising, with the patient currently asymptomatic. McGregor said at SIR that he is “looking forward to her further follow-up imaging”. To date, the investigators have performed gallbladder cryoablation on five patients, though only the first patient’s experience was presented at SIR.
The procedure involved the off-label use of an FDA approved device, and McGregor disclosed that several authors of the study have a patent pending for a cryoablation device.
Fielding a question from the audience asking how the patient felt following the procedure, McGregor explained: “He [the first patient] was a pretty stoic guy. According to him, he felt great. He was hungry, he wanted to eat immediately afterwards; we kept him in NPO [nil per os] because we were a little concerned about that duodenum there on the first case. But he felt great. We followed him up every day for a week afterwards, and really, there were no complaints.”
The Society of Interventional Radiology (SIR) presented its highest honour, the SIR Gold Medal, to Alan H Matsumoto, Daniel Picus and James B Spies during its 2019 Annual Scientific Meeting (23–28 March, Austin, USA). These awards acknowledge distinguished and extraordinary service to SIR or to the discipline of interventional radiology.
“The 2019 Gold Medallists exemplify the innovative and collaborative spirit of interventional radiology through their research, mentorship, dedication to the advancement of the quality of medicine and patient care,” says SIR 2018–2019 president M Victoria Marx, interventional radiologist at Keck Medicine of USC, and professor of clinical radiology and diagnostic radiology residency programme director at Keck School of Medicine of University of Southern California (USC), Los Angeles, USA.
Alan H Matsumoto
Matsumoto is professor and chair of the department of radiology and medical imaging at the University of Virginia, Charlottesville, USA, where he has been on faculty since 1991 and helped train more than 200 diagnostic radiology residents and 100 vascular and interventional radiology fellows. He has published 300 articles and book chapters, given more than 300 invited and scientific talks, and served as the site principal investigator for 24 clinical trials. He developed and ran the core lab for the trial that led to the first US Food and Drug Administration (FDA)-approved abdominal aortic stent graft in 1999. A past-president of SIR and programme chair of the 2004 SIR Annual Scientific Meeting, Matsumoto has also served as an American Board of Radiology examiner, in committee and council chair positions at the American Heart Association, and as a member of the American College of Radiology Council Steering Committee and Board of Chancellors.
Daniel Picus
Picus is a professor of radiology and surgery at the Mallinckrodt Institute of Radiology (MIR) at Washington University School of Medicine, St. Louis, USA. There he established the interventional radiology section, serving as its first chief from 1987–2000. He then took on the role of division chief for diagnostic radiology until 2018. During his career, Picus’ interest in coding and reimbursement led him to become a member of the American Medical Association’s Current Procedural Terminology (AMA CPT) Editorial Panel. He has authored more than 130 peer-reviewed publications, as well as multiple textbook chapters and scientific exhibits. Picus delivered the Dr Charles T Dotter Lecture at the 2013 SIR Annual Scientific Meeting and has served SIR in many roles, including both Education and Annual Meeting Councillor, first editor of the Society of Cardiovascular and Interventional Radiology (SCVIR, now SIR) newsletter, and first deputy editor and second editor-in-chief of SIR’s Journal of Vascular and Interventional Radiology.
James B Spies
Spies is a professor of radiology at Georgetown University School of Medicine and chair of the department of radiology at MedStar Georgetown University Hospital in Washington, D.C, USA. Spies is recognised as an international authority on uterine artery embolization (UAE) for fibroids. He maintains an active UAE clinical practice, has performed extensive research in that area and continues to actively research outcomes from a range of fibroid therapies. He has published more than 100 scientific studies and given more than 400 invited presentations. In addition to serving as a trustee of the American Board of Radiology (ABR) for interventional radiology since 2016, Spies has served SIR in many roles, including SIR president from 2014–2015, SIR Foundation chair from 2006–2008, and as a member of numerous SIR committees.
Immersive virtual reality (VR) may enable interventional radiologists to improve treatments using real-time 3D images from inside a patient’s blood vessels. New research presented at the Society of Interventional Radiology’s 2019 annual scientific meeting (23–28 March, Austin, USA) shows that the interactive technology could provide faster, more efficient treatment, with less radiation exposure and greater precision, ease and confidence.
“Virtual reality will change how we look at a patient’s anatomy during an IR treatment,” asserts Wayne Monsky, a professor of radiology at the University of Washington (Seattle, USA) and lead author of the study. “This technology will allow physicians to travel inside a patient’s body instead of relying solely on 2D, black and white images.”
The purpose of the study is to demonstrate the feasibility of using a catheter with electromagnetic sensors projected onto a VR headset to see and steer the catheter through the anatomy to certain blood vessels.
Using a CT angiography scan, researchers created a 3D-printed model and a holographic image of blood vessels in a patient’s abdomen and pelvis. Monksy’s team of radiologists guided hi-tech catheters through the 3D-printed model while the tracking system showed the image from the catheter through the VR headset. They compared the time taken to steer the catheter from the entry point of the femoral artery to three different targeted vessels versus the time the process took using conventional fluoroscopic guidance, as well as time taken in similar real-life clinical angiographic procedures.
In 18 simulated procedures, researchers found the mean time to reach the three targeted vessels using VR was much lower than in fluoroscopy, the standard practice that uses an X-ray image. In the first vessel, virtual reality took 17.6 seconds versus 70.3 seconds using the standard practice on the model and 171.2 seconds in the real-life procedure.
With the improved efficiency, the researchers believe VR technology will create safer treatments by reducing the amount of radiation exposure to both patient and physician. They say it would also increase access to IR treatments.
“Currently, the life-saving potential of IR is limited to hospitals and areas with the resources to invest in image-guided technology,” says Monsky. “There are three billion people worldwide in rural areas who do not have this access. This technology could allow for portability and accessibility so that these procedures are brought to rural areas using nothing more than a suitcase.”
Researchers also surveyed the practitioners who had tried the technology, and they reported that VR improved the ease, precision and efficiency of the treatment. Additionally, the users said they felt more confident in their abilities.
The VR software was developed through a University of Washington business incubator that supported development of a start-up, Pyrus Medical, of which Monsky serves as the chief medical officer. The researchers are continuing to conduct research in 3D models, as well as animal studies, as they begin the regulatory process to apply for approval from the US Food and Drug Administration.
Uterine fibroid embolization (UFE) effectively treats uterine fibroids with fewer post-procedure complications compared to myomectomy, according to new research presented at the Society of Interventional Radiology’s 2019 annual scientific meeting (23–28 March, Austin, USA). Women who received this minimally-invasive treatment also had a slightly lower need for additional treatment than those who underwent surgery.
UFE is a minimally-invasive treatment for uterine fibroids that is less painful, preserves the uterus, and allows women to get back to their lives sooner than surgical options. However, past research suggests US women, a majority of whom will experience uterine fibroids by age 50, are largely unaware of UFE despite more than 30 years as an evidence-based treatment.
“Women have options for treating their uterine fibroids. UFE and myomectomy are procedures with similar efficacy and durability for treating fibroids, but UFE has fewer complications and shorter hospital stays,” says Jemianne Bautista-Jia, radiology resident at Kaiser Permanente (Los Angeles, USA) and lead author of the study. “There are important factors women should consider when choosing between the procedures. These factors include risk of bleeding, possibility of infections, and recovery time.”
In the retrospective cohort study, researchers analysed treatment outcomes of 950 uterine fibroid patients from 1 January 2008 through to 31 December 2014. Half of the patients underwent UFE, a non-surgical treatment that eliminates the blood supply to fibroids, causing them to shrink or disappear. The other half were treated surgically through myomectomy, a procedure that removes existing fibroids.
After an average seven-year follow up, the study found that women who underwent myomectomy had a higher rate of post-procedural complications, including a 2.9% rate of blood transfusion, which was significantly higher than the 1.1% rate for those who were treated using UFE. Patients in both treatment groups demonstrated a significant increase in haemoglobin one year after the initial procedure due to reduced bleeding. The two methods were comparably effective based on the rate at which secondary interventions—including UFE, myomectomy, and hysterectomy—were needed. Second interventions were completed in 8.6% of women who received an initial UFE compared to 9.9% for women who initially underwent a myomectomy.
This study also showed similar rates of miscarriage for women who underwent either UFE or myomectomy. Future research should explore the impact of all uterine-sparing fibroid procedures on pregnancy, which remains still poorly understood.
See the interview with Jemianne Bautista-Jia here.
Training interventional radiologists to perform endovascular thrombectomies results in positive outcomes for patients experiencing stroke, according to a study presented at the Society of Interventional Radiology annual scientific meeting (23–28 March, Austin, USA). Expanding access to this treatment provides patients timely access to this gold-standard treatment.
“With a limited availability of providers, thrombectomy is only available to 2–3% of eligible patients in the USA,” says Kelvin Hong, associate professor and division chief of interventional radiology at Johns Hopkins University, Baltimore, USA. “Patients do not plan where and when they have a stroke. Our model of training board-certified interventional radiologists can expand access to quality, evidence-based care, and reduce the lifelong disability associated with stroke.”
Thrombectomy increases the survival rates among those suffering an acute ischaemic stroke, reduces the likelihood of resulting disabilities, and speeds function recovery. However, to gain these benefits, thrombectomies must be initiated and performed quickly. Many hospitals do not have providers available to perform these treatments and must transfer patients to a facility where they can get this care, losing valuable time.
To determine an efficient and sustainable way to expand access to thrombectomy, researchers from Johns Hopkins University developed an interventional radiology stroke team at Suburban Hospital, a community hospital in Montgomery County, Maryland, a suburb of Washington, DC. The team consisted of four interventional radiologists who were specially trained by a neurointerventional radiologist for six months. The entire team was available 24 hours a day, seven days a week with the neurointerventional radiologist helicoptered to the hospital for every case during this training period.
“We looked to change the dynamic in stroke care, where instead of transporting medically fragile patients, we brought in a specialist to perform this care and build the infrastructure necessary to provide this treatment to a community with limited stroke care resources,” comments Ferdinand Hui, a neurointerventional radiologist and associate professor of radiology and radiological science at Johns Hopkins University. “In a situation where every minute counts, we wanted to design our programme to provide the training and organisation necessary to bring 24/7 highly trained stroke interventionalists online as quickly as possible.”
Once the interventional radiologists were conducting the treatments independently, researchers measured the technical success of the thrombectomies performed by the newly trained physicians in 35 stroke cases using the Thrombolysis in Cerebral Infarction (TICI) scale, and found no significant differences compared to the 2016 HERMES meta-analysis of endovascular thrombectomy outcomes performed by other practitioners, such as neurointerventional radiologists and neurosurgeons. Additionally, 14% mortality in the first 90 days after the procedure was similar to 15.3% 90-day mortality among patients at stroke centres evaluated through the Journal of the American Medical Association-published HERMES trial. The median interval from symptom onset to the point when blood flow was restored was 325 minutes, compared to 285 minutes in previous research.
Researchers plan to further evaluate the technical outcomes and time metrics in a second-year study with a goal of further reducing the time to treat each patient by improving efficiency and optimisation year over year.
A limitation of the study may be in whether hospitals of varying sizes and resources can reproduce the programme with the same outcomes, the study authors accede. The research team plans to re-evaluate the programme after two years of data collection.
BrightWater Medical has announced that the US Food and Drug Administration (FDA) has cleared the company’s ConvertX biliary stent system for the treatment of biliary obstructions.
Patients with severe duct blockages or difficult anatomies—such as gastric bypass or liver transplant patients—face serious complications including infection, sepsis, biliary cirrhosis or injury to the liver. Today, most of these patients will either need to undergo two separate one-hour interventional procedures for stent placement or, if considered poor candidates for the staged stent procedure, undergo a drain placement instead. If the biliary blockage is managed with a drain, the drain must be exchanged for a new one every two to three months, for life.
The ConvertX system is the first to provide interventional radiologists with a percutaneous plastic biliary stent option. The system is designed to eliminate the need for the second invasive procedure and the associated risk, cost, and time. Rather than a drain-to-stent exchange, the ConvertX system itself enables stent release in less than one minute during an in-office visit or at bedside without the need for sedation or repeated drain insertions, a press release explains.
“Before this, we have had to treat these serious cases without having the right tools,” explains Saher S Sabri, director of Interventional Radiology at MedStar Washington Hospital Center and professor of Radiology at MedStar Georgetown University Hospital (Washington, DC, USA). “The ConvertX is a significant paradigm change that enables the interventional radiologist to be involved in percutaneous temporary plastic stent placement for benign and malignant biliary disease. It allows us to treat with one less invasive procedure for the patient, reducing radiation exposure for the patient and staff.”
Biliary obstructions may be caused by tumours, gallstones, enlarged lymph nodes, cysts or strictures. Interventional radiologists treat biliary obstructions that are more severe or anatomically challenging, such as in patients with gastric bypass or liver transplants, through two separate one-hour interventional procedures for stent placement.
“The biliary stent system was designed by interventional radiologists for interventional radiologists,” comments ConvertX system developer Bob Smouse, founder and CEO of BrightWater Medical and professor of Radiology and Surgery at the University of Illinois College of Medicine (Chicago, USA). “It is simple to use and deliver with standard interventional techniques and does not require additional physician training. Before the ConvertX, the absence of a percutaneous plastic stent was a huge product gap in the device armamentarium of the interventional radiologist. According the American College of Radiology practice guidelines, a temporary plastic stent is the device-of-choice in eight out of nine bile duct blockages and now the interventional radiologist has that stent option.”
The ConvertX biliary stent system is part of BrightWater Medical’s ConvertX stent family, which includes the company’s ConvertX Nephroureteral stent system cleared by the FDA for treatment of ureteral obstructions. That system enables the interventional radiologist to eliminate a second invasive interventional procedure in treating patients with severe ureteral blockages.
Tennis elbow, the painful chronic condition that affects up to 3% of the US adult population, can be effectively treated through transcatheter arterial embolization (TAE), according to research presented at the Society of Interventional Radiology’s 2019 annual scientific meeting (23–28 March, Austin, USA).
“Tennis elbow can be difficult to treat, leaving many patients unable to perform the simplest tasks, such as picking up their children, cooking dinner, or even working on a computer. With this frustration, many patients turn to invasive major surgery after years of failed physical therapy and medication use,” comments Yuji Okuno, founder of the Okuno Clinic in Tokyo, Japan, and lead author of the study. “We were interested to see if this technique, already in use in other areas of the body, would be effective for this common, debilitating condition and help people immediately regain a range of motion that many of us take for granted in our everyday tasks.”
Okuno’s team conducted a prospective study in 52 patients with tennis elbow who did not find relief from other forms of treatment. The patients received TAE between March 2013 and October 2017 and were followed for up to four years after the treatment. The researchers said they found statistically significant reductions in pain-rating scores, using methods including the quick disability of the arm, shoulder and hand scores; visual analogue scale pain rating scores; patient-rated tennis elbow evaluation scores; and pain-free grip strength. Additionally, images taken in 32 patients two years after undergoing TAE showed an improvement in tendinosis and tear scores.
The treatment can be completed in approximately one hour, and requires access via the radial artery in the wrist under local anaesthesia. A catheter is moved through the wrist to the elbow where the inflamed blood vessels are embolized, preventing excessive blood flow to the affected part of the elbow. The treatment is safe and effective and does not require physical therapy, the researchers say. No adverse events were observed and no patients experienced negative effects to the surrounding bones, cartilage or muscles.
Smart speakers that are customarily used in your living room can be programmed to act as an aid to physicians in hospital operating rooms, according to new research presented at the Society of Interventional Radiology’s 2019 annual scientific meeting (23–28 March, Austin, USA). Smart speakers, such as the Amazon Echo and Google Home, offer a conversational voice interface that allows interventional radiology (IR) physicians to ask questions and retrieve information needed for their patient treatments without breaking sterile scrub.
“During treatment, IRs rely on nuanced medical information delivered in a timely manner. When you are in the middle of a procedure, you need to remain sterile, so you lose the ability to use a computer,” says Kevin Seals, a fellow in interventional radiology at the University of California, San Francisco (UCSF; San Francisco, USA) and lead author of the study. “This smart speaker technology helps us to quickly and intelligently make decisions relevant to a patient’s specific needs.”
The researchers at UCSF developed a device-sizing application for the Google Home smart speaker. The application processes questions from a human voice and provides recommendations on the precise sizing of medical devices. For example, if an IR needs to know what size sheath to use to implant a stent in a patient’s blood vessel, the smart speaker can quickly and accurately communicate the correct size based on the specific circumstances, which helps the physician in making a final decision.
“There are hundreds of devices, with more being introduced every day, making it difficult to determine the correct sizing or materials needed in every circumstance. This technology allows physicians to concentrate more closely on the care of their patients, devoting less time and mental energy to device technicalities,” explains Seals.
In developing the application, size specifications were acquired using literature reviews for 475 IR devices, such as catheters, sheaths, stents, vascular plugs and others. Natural language processing was implemented using Dialogflow, which extracted the information of interest from an input query. Logic operations and other data processing were performed using a Python script deployed to the cloud.
The researchers plan to continue to build on this technology and expand its scope to include information on material costs and inventory databases. Having this information readily available will make treatments more efficient, cost-effective and beneficial to patients. Further research will look to yield information for physicians in other specialties and provide information from electronic health records and patient clinical data, such as allergies or prior surgeries.
Endovascular therapy training provider Mentice has signed an agreement to donate its virtual reality-based simulators to humanitarian organisation Rad-Aid for use in interventional radiology (IR) procedure training in various resource-constrained regions of the world.
Under the agreement, the Gothenburg, Sweden-based Mentice pledges to contribute simulator software, hardware and expertise to RAD-AID IR educational teams.
Commenting on the agreement, Mentice CEO Göran Malmberg says “RAD-AID is doing an amazing job bringing the benefits of IR to disadvantaged communities around the world. It is a great honour and a privilege to be working with RAD-AID helping improve patient care access and outcomes in these underserved communities.”
Launched in 2008, RAD-AID is a 501c3 non-profit organisation committed to bringing radiology and imaging technologies and solutions to developing countries and medically underserved communities. “It is easy to forget,” adds Malmberg, “that for many people, even relatively cost-effective X-ray imaging remains a luxury. We at Mentice can make a real contribution by helping improve access and IR performance.”
RAD-AID is active in over 30 countries worldwide, and encompasses over 10,000 volunteers from 100 countries, 73 university-based chapter organisations, and an annual conference on global health radiology. “RAD-AID programmes are multidisciplinary and bring together innovative technology, infrastructure-planning, and educational initiatives. Such multidisciplinary cooperation is essential, and by working with Mentice, we can help bring effective IR programs to some of the world’s neediest patients,” says Daniel Mollura, founder and CEO of RAD-AID International.
Interventional radiologists earned higher salaries in the USA in 2018 than their colleagues in diagnostic radiology, according to the latest data from AuntMinnie.com’s SalaryScan survey on medical imaging compensation.
With an average annual salary of US$411,345, interventional radiologists had higher annual compensation than diagnostic radiologists, regardless of the latter’s modality subspecialisation, according to the SalaryScan data. The top salary for diagnostic radiologists was for those who subspecialise in computed tomography (CT), with an average annual salary of US$396,907, followed by magnetic resonance imaging (MRI) subspecialists at US$395,328.
The lowest-paid radiology subspecialty was mammography, with an average annual salary of US$375,514.
The survey also broke down salaries by region in the USA. Radiologists living in the US West North Central region had the highest average annual salary, at US$445,945, compared with an average annual salary of US$394,034 for North American radiologists of all experience levels, organisation types, and modality specialisations.
The second-highest earners were radiologists living in the US West South Central region, with an average annual salary of US$424,061. The lowest salaries were pulled in from radiologists working in the US New England region, with an average annual salary of US$363,264.
For radiologic technologists, the salary hierarchy by subspecialty was slightly different. Interventional radiology technologists earned an average base salary of US$79,368 per year, compared to an average base salary of US$72,351 a year for technologists with no subspecialisation. Nuclear medicine technologists were the best compensated, with an average annual salary of US$80,779, and mammography technologists earned the lowest average annual salary, at US$69,382.
According to AuntMinnie.com, SalaryScan is based on data acquired from the website’s members in the USA from January to February 2019. They do not say how many people took part in this survey.
The US Food and Drug Administration (FDA) has granted 510(k) clearance to the company DOSIsoft to market its Planet Onco Dose software, for its oncology and Yttrium-90 (Y90) microsphere selective internal radiation therapy (SIRT) 3D dosimetry components.
According to a company press release, Planet Onco Dose is a comprehensive software platform dedicated to medical diagnosis aid, therapy response assessment aid, contouring for radiotherapy, and internal dosimetry computation, using molecular imaging modalities.
It is a modular software suite comprised of two main elements: an oncology module (Planet Onco) and a dosimetry module (Planet Dose). The former, the oncology module, has the core system features: comprehensive reviewing of multimodal molecular image series (CT, MRI, PET, SPECT), fusion and registration, automatic and semi-automatic contouring of regions of interest, tumour segmentation, quantification, tumoural activity monitoring, and therapy response assessment. The dosimetry module includes 3D personalised voxel-based internal dosimetry computation dedicated to molecular radiotherapy (MRT).
CE marked since March 2016, Planet Onco Dose is the first fully integrated imaging and personalised 3D dosimetry platform for radionuclide-based therapies, the company states.
Planet Onco Dose is intended to assist the user in the diagnosis, quantification and verification of radiation doses received by tissues as a result of administering permanent Y90 microsphere implants, as well as in therapy response follow-up.
Planet Onco Dose provides tools for post-treatment absorbed dose calculation and evaluation on PET and SPECT images. The following functions are available to allow dose calculations for patients after they have received a treatment using permanent Y90 microspheres:
3D liver-lung shunt assessment
Voxel-based dosimetry based on Y90-microspheres-PET (or SPECT Bremsstrahlung) series
Dose computation models: local deposition method and voxel S value dose kernel convolution approach
Analysis down to any liver sub region: healthy liver, lobes, tumors, toxicity regions
Advanced and interactive dosimetry quantification (profile, dose-volume histograms, statistics)
Ability to scale to known activity
Compatible with PET images acquired with another radioisotope (correction of branching ratio and decay parameters)
The Medicines and Healthcare products Regulatory Agency (MHRA) in the UK and the Food and Drug Administration (FDA) in the USA have both recently issued new statements on the use of paclitaxel-eluting devices. While the FDA release preliminary analysis results from their ongoing review of data, the MHRA announced they have formed an independent Expert Advisory Group, which has now “begun the process of reviewing the available, but highly complex information on these medical devices.” Following preliminary analysis, the FDA meanwhile recommend that “alternative treatment options to paclitaxel-coated balloons and paclitaxel-eluting stents should generally be used until additional analysis of the safety signal has been performed.”
MHRA launches Expert Advisory Group
An MHRA press release states, the group is made up of leading UK clinicians from specialist societies, including interventional radiology, vascular surgery and scientists with toxicology, medicines and statistical expertise. The group has been formed in response to recently published findings by Katsanos et al “raising concerns over the use of paclitaxel eluting balloons and stents in the treatment of patients with peripheral arterial disease (PAD) and in particular the femoropopliteal artery in the leg. […] The publication suggests a possible increased mortality rate from 2 up to 5 years in PAD patients treated with paclitaxel-coated balloons and paclitaxel-eluting stents. This is compared to patients treated with non-coated balloons or bare metal stents. A causal relationship for this observation has not been identified and may reflect limitations in the way the data were analysed, but this has yet to be determined.”
The MHRA add, “Patient safety is our highest priority and we take information questioning the safety of any medical device very seriously. Since the publication we have been collecting and analysing information from a range of sources to try to understand the significance of the findings for future patient treatment options.
“The devices in question have valid CE certificates and remain on the UK market. The outcome of our investigation will determine if new advice is required or if we need to undertake any other regulatory action. The Expert Advisory Group has been asked to consider whether the publication’s findings and device-specific clinical study results are statistically robust and whether there is any evidence of a causal relationship between the drug, paclitaxel, and increased mortality.
“There are a number of other publications which put forward different results and opinions taking into account other factors such as the overall health of the patient. To assist them they have been provided with the full spectrum of source material available to MHRA, together with all relevant published information we have gathered. The aim is to provide a greater understanding of the potential benefits and risks to patients and will help to guide any possible future MHRA action. The Expert Advisory Group has agreed to undertake and complete their review, including reporting their findings to MHRA, within the next few months.
“Additionally, we are collaborating with the major clinical and regulatory stakeholders, including the British Society of Interventional Radiology (BSIR), the UK Basil-3 trial and NICE, as well as other European and global regulatory authorities.”
If you are worried that you might be affected by this matter, we advise you to contact your GP or specialist.”
FDA issue updated letter to healthcare providers with preliminary analysis results
The FDA recently released an update to their January letter to healthcare providers, in which the Administration “promised to communicate as new information became available”.
“We have now conducted a preliminary analysis of long-term follow-up data (up to five years in some studies) of the pivotal premarket randomised trials for paclitaxel-coated products indicated for peripheral arterial disease”, the FDA writes. “While the analyses are ongoing, our preliminary review of this data has identified a potentially concerning signal of increased long-term mortality in study subjects treated with paclitaxel-coated products compared to patients treated with uncoated devices. Of the three trials with five-year follow-up data, each showed higher mortality in subjects treated with paclitaxel-coated products than subjects treated with uncoated devices. In total, among the 975 subjects in these three trials, there was an approximately 50% increased risk of mortality in subjects treated with paclitaxel-coated devices versus those treated with control devices (20.1% versus 13.4% crude risk of death at five years).”
The FDA add that these data should be “interpreted with caution for several reasons. First, there is large variability in the risk estimate of mortality due to the limited amount of long-term data. Second, these studies were not originally designed to be pooled, introducing greater uncertainty in the results. Third, the specific cause and mechanism of the increased mortality is unknown.
“Paclitaxel-coated balloons and stents are known to improve blood flow to the legs and decrease the likelihood of repeat procedures to reopen blocked blood vessels. However, because of this concerning safety signal, we believe alternative treatment options should generally be used for most patients while we continue to further evaluate the increased long-term mortality signal and its impact on the overall benefit-risk profile of these devices. The FDA intends to conduct additional analyses to determine whether the benefits continue to outweigh the risks for approved paclitaxel-coated balloons and paclitaxel-eluting stents when used in accordance with their indications for use. The FDA will also evaluate whether these analyses impact the safety of patients treated with these devices for other indications, such as treatment of arteriovenous access stenosis or critical limb ischaemia.”
Because of concerns regarding this issue, the FDA states it will convene an Advisory Committee meeting of the Circulatory System Devices Panel to:
Facilitate a public, transparent, and unbiased discussion on the presence and magnitude of a long-term mortality signal;
Discuss plausible reasons, including any potential biological mechanisms, for a long-term mortality signal;
Re-examine the benefit-risk profile of this group of devices;
Consider modifications to ongoing and future US clinical trials evaluating devices containing paclitaxel, including added surveillance, updated informed consent, and enhanced adjudication for drug-related adverse events and deaths; and
Guide other regulatory actions, as needed.
Further details concerning the timing and location of the Advisory Committee meeting will be announced in the coming weeks.
Based on the preliminary review of available data, provided healthcare professionals with the following recommendations, until further information is available:
Continue diligent monitoring of patients who have been treated with paclitaxel-coated balloons and paclitaxel-eluting stents.
When making treatment recommendations and as part of the informed consent process, consider that there may be an increased rate of long-term mortality in patients treated with paclitaxel-coated balloons and paclitaxel-eluting stents.
Discuss the risks and benefits of all available PAD treatment options with your patients. For most patients, alternative treatment options to paclitaxel-coated balloons and paclitaxel-eluting stents should generally be used until additional analysis of the safety signal has been performed.
For some individual patients at particularly high risk for restenosis, clinicians may determine that the benefits of using a paclitaxel-coated product may outweigh the risks.
Ensure patients receive optimal medical therapy for PAD and other cardiovascular risk factors as well as guidance on healthy lifestyles including weight control, smoking cessation, and exercise.
The FDA further continued to recommend that health care providers report any adverse events or suspected adverse events experienced with the use of paclitaxel-coated balloons and paclitaxel-eluting stents. Voluntary reports can be submitted through MedWatch, the FDA Safety Information and Adverse Event Reporting program. Device manufacturers and user facilities must comply with the applicable Medical Device Reporting (MDR) regulations. Health care personnel employed by facilities that are subject to the FDA’s user facility reporting requirements should follow the reporting procedures established by their facilities. Prompt reporting of adverse events can help the FDA identify and better understand the risks associated with medical devices.
As interventional radiology evolves as a distinct specialty from diagnostic radiology, the central and ongoing role of diagnostic radiologists in performing certain invasive radiological procedures could have important patient access implications. A recent study, published online in the Journal of American College of Radiology (JACR), characterises longitudinal changes in radiology trainees’ exposure to invasive image-guided procedures.
“Using national Medicare claims data over two decades as a surrogate measure of the changing relative distribution of services rendered by radiology trainees overall, we observed that radiology trainees now spend a smaller fraction of their overall work effort performing invasive procedures than in the past,” says Andrew Rosenkrantz, professor and director of health policy in the department of radiology at NYU Langone Health (New York, USA) and a Neiman Institute affiliate research fellow (Reston, USA). “Previously, a variety of invasive procedures accounted for approximately one third of radiology trainees’ relative work effort. Trainees’ relative invasive procedural work effort has now declined to approximately one half of that.”
Rosenkrantz and team used Physician/Supplier Procedure Summary Master Files from 1997 to 2016, and identified Medicare services performed by radiology trainees in approved programmes by extracting information on services billed by diagnostic radiologists and interventional radiologists reported with “GC” modifiers. Services were categorised as (1) invasive procedures, (2) non-invasive diagnostic imaging services, or (3) clinical evaluation and management services. Relative category trainee work effort was estimated using service level professional work relative value units.
Nationally from 1997 to 2016, invasive procedures declined from 34.2% to 14.3% of relative work effort for all Medicare-billed radiology trainee services. Radiology trainees’ non-invasive diagnostic imaging services increased from 65.1% to 85.4%. Clinical evaluation and management services remained uniformly low (0.7% to 0.3%). Diagnostic radiology and interventional radiology faculty supervised 81% and 19%, respectively, of all trainee invasive procedures in 1997, versus 68.3% and 31.7%, respectively, in 2016. Despite declining relative procedural work, trainees were exposed to a wide range of both basic and complex invasive procedures in both 1997 and 2016.
“Radiology trainees’ relative invasive procedural work effort has declined over time as their work increasingly focuses on CT and MRI,” states study senior author Richard Duszak, professor and vice chair for health policy and practice in the department of radiology and imaging sciences at Emory University (Atlanta, USA) and senior affiliate research fellow at the Neiman Institute. “As diagnostic radiology and interventional radiology/diagnostic radiology residency curricula begin to diverge, it is critical that both diagnostic radiology and interventional radiology residents receive robust training in basic image-guided procedures to ensure broad patient access to these services.”
A new paper looking specifically at mortality has found no difference in deaths between paclitaxel-coated balloons and uncoated balloons when used in the femoropopliteal artery. These data, a pooled analysis of four randomised controlled, multicentre trials, were published in Cardiovascular Interventional Radiology.
In light of the recent meta-analysis by Konstantinos Katsanos (Patras University Hospital, Rion, Greece) et al—writing in the Journal of the American Heart Association (JAHA)—reporting significantly increased mortality at two and five years following angioplasty with paclitaxel-coated devices in peripheral arteries, Thomas Albrecht (Vivantes Klinikum Neukölln, Berlin, Germany) and colleagues performed a two-year, patient-level mortality analysis based on pooled, original data of four randomised, controlled trials (RCTs): THUNDER, FEMPAC, PACIFIER and CONSEQUENT.
This study included 185 patients in the control group (plain angioplasty), and 184 patients in the paclitaxel-coated balloon group, followed up to two years. At two-year follow-up, 13 of 185 patients had died in the control group and 16 of 184 in the paclitaxel-coated balloon group. Corresponding mortality rates were 7% and 8.7% of available patients, respectively (p=0.55). Kaplan–Meier statistics for freedom from all-cause death also showed no difference between groups (p=0.54).
“All this is new, important patient-level data contradicting the paper of Katsanos,” Albrecht tells Interventional News.
Causes of death similar between paclitaxel-coated balloon arm and control arm
Causes of death were split into cardiac (heart failure, acute myocardial infarction, cardiac arrhythmia, and sudden cardiac death), malignancy (of the liver, pancreas and lung), sepsis (pneumonia and perforated duodenal ulcer and peritonitis), and other (which includes chronic obstructive pulmonary disease). The most common causes were cardiac, responsible for the deaths of six patients in the control group and four after paclitaxel-coated balloon use, and malignancy: one lung cancer and one liver cancer in the control group, and one lung cancer and two pancreatic cancers in the paclitaxel-coated balloon group. Causes of death only seen in the paclitaxel-coated balloon group were stroke, major amputation, thrombosis, multiple organ failure, brain haemorrhage and trauma (one patient each). “Overall, causes of death were well balanced between the treatment groups with no obvious pattern or trend towards an increase in any specific causes of death in the paclitaxel-coated balloon group”, write Albrecht et al.
“Even if one assumed that these deaths might have been influenced by the use of paclitaxel-coated devices,” they muse, “it would be extremely difficult to explain what common toxicological mechanism might have played a role in such very different diseases, especially if one considers the extremely low doses of paclitaxel on paclitaxel-coated balloons.”
Study finds no association between paclitaxel dose and increased mortality
Patients who underwent paclitaxel-coated balloon angioplasty and died during the 24-month follow-up did not have a higher paclitaxel dose compared to those who did not die. Indeed, the mean dose per patient was numerically lower in patients who died. The mean delivered paclitaxel doses were 5.3±4.224µg in patients that died during the two-year follow-up, and 6.248±4.629µg in those who did not die (p=0.433).
Speaking of the JAHA meta-analysis findings, Albrecht and colleagues say that Katsanos et al’s “postulated causality was on the foundation of theoretically-derived paclitaxel doses, which in turn were based on a number of assumptions.” According to Albrecht et al, these assumptions included the lesion length and vessel diameter representing the exposed tissue surface, irrespective of the used drug delivery platform (stent or balloon). Conversely, Albrecht et al based their calculation of paclitaxel dose on measurements of residual paclitaxel left on the balloons catheters after use in every patient.
Whilst paclitaxel dosage was not found to be associated with increased mortality, a patient age of 75 years or more was. This was the only significantly associated risk factor for two-year mortality observed by Albrecht and colleagues. They report that all other tested patient and lesion variables had no significant association with mortality. Treatment groups—uncoated balloon or paclitaxel-coated balloon—were not a predictor for mortality (p=0.53) in this analysis.
Armed with these results, Albrecht and colleagues conclude: “We could therefore not confirm the findings of significantly increased mortality after paclitaxel-coated devices in the recent meta-analysis by Katsanos et al.”
Perceived limitations of the Katsanos et al meta-analysis
This present study was designed to overcome several objections Albrecht and colleagues have to the methodology used by Katsanos and team.
Albrecht et al write: “One inherent limitation of the meta-analysis by Katsanos et al is the lack of access to original patient data. Instead, published summaries of data were used. None of these publications focused on mortality, and neither was mortality the primary endpoint of the included studies, nor were the studies designed or powered for long-term analysis of mortality. (Primary endpoints were usually late lumen loss or patency at six or 12 months.)”.
They continue: “Furthermore, for several included studies, the mortality data used in the meta-analysis were calculated based on the number of originally included patients and not on the number of patients with follow-up which was available at the relevant time points. In other words, patients lost to follow-up could not be appropriately considered. Last but not least, causes of deaths were not available to Katsanos and colleagues for most included studies, so that they could not provide any causative explanation, as to why more patients might have died after the use of paclitaxel-coated devices and what the underlying toxicological mechanism might be.
“These limitations potentially challenge the results of Katsanos et al, and the authors acknowledge the urgent need for further investigation into the subject”. This last comment references one of the closing remarks of the JAHA paper, where the authors conclude that “Further investigations are urgently warranted”.
Paclitaxel kills the cells in the artery wall; sirolimus simply stuns them. So says Peter Gaines (Sheffield, UK) at VLF 2019 while commenting on the modes of action of these two agents that have been used in drug-coated devices in both the coronary and peripheral vessels. Sirolimus is likely to have fewer systemic problems [than paclitaxel] and is much less likely to have local toxic effects on the arteries, he says.
Current evidence does not support the use of vertebroplasty for the treatment of pain from vertebral fractures, concludes a recent task force report charged by the American Society for Bone and Mineral Research (ASBMR) aimed at examining the efficacy and safety of vertebral augmentation. Although lead author of the report, Peter R Ebeling (Monash University, Melbourne, Australia), and colleagues surmise that this conclusion is “likely to apply to other augmentation procedures”, such as kyphoplasty, they maintain throughout the report that high-quality evidence from placebo-controlled trials remains absent. However, lead authors of the VAPOUR trial, which reported a benefit with the use of vertebroplasty in fractures of less than six weeks’ duration, have published their concerns in the BMJ Evidenced-Based Medicine regarding the statistical methodology underpinning the ASMBR report.
“The recommendations by this task force are designed to help provide a foundation for advancing the research and clinical care of patients with painful acute vertebral fractures”, write the authors. They stress that clinicians will need to balance the “limited findings” on the safety and efficacy of other nonpharmacological interventions with good clinical judgement, when it comes to making quality, informed patient care decisions.
The rationale behind the commissioned report encompasses the lack of consensus amongst clinicians on whether to use percutaneous vertebroplasty or kyphoplasty to reduce pain in patients with vertebral fractures. This disparity in opinion, as well as the high prevalence of vertebral compression fractures in patients with osteoporosis, led the ASBMR to commission a task force to address key questions on the efficacy and safety of vertebral augmentation and other nonpharmacological approaches, such as spinal bracing or exercise, for the treatment of pain after vertebral fractures.
Ebeling and colleagues explain that vertebral augmentation was introduced into practice before high-quality evidence establishing its efficacy and safety was published, yet remains—in some settings—part of standard routine care. Although the authors acknowledge that balloon kyphoplasty is currently more expensive and is performed almost three times more commonly than percutaneous vertebroplasty in the USA, they write: “No placebo-controlled trials of balloon kyphoplasty have been performed and the evidence of the value of this procedure is reliant on low-quality evidence from trials that have compared kyphoplasty with usual care or head-to-head comparisons with vertobroplasty”.
Ebeling and colleagues performed a systematic review of the existing literature and meta-analyses of an array of outcomes in order to test the efficacy and safety of vertebral augmentation and other nonpharmacological treatments for painful vertebral fractures. Randomised controlled trials (RCTs) and quasi-randomised trials that enrolled adults older than 40 years with acute nontraumatic vertebral fractures, directly comparing percutaneous vertebroplasty or balloon kyphoplasty with any treatment comparator group, were included. In terms of nonsurgical interventions, Ebeling and colleagues included RCTs and quasi-randomised trials of bracing or exercise interventions with similar enrolment criteria.
The ASBMR task force first addresses the efficacy and relative effectiveness of vertebral augmentation therapies and their ability to improve pain, posture, physical function and quality of life. Based on “moderate to high” quality evidence for percutaneous vertebroplasty from five randomised placebo-controlled trials, Ebeling and colleagues find that percutaneous vertebroplasty provide no demonstrable clinically important benefit when compared with placebo or sham. Moreover, they report that subgroup analyses in the updated Cochrane review indicated that the result did not differ according to duration of pain. However, the sensitivity analyses indicated that open trials comparing percutaneous vertebroplasty with standard medical care are likely to have overestimated any benefit of percutaneous vertebroplasty.
William Clark (St George Private Hospital, Sydney, Australia) and colleagues submitted complaints to the authors of the aforementioned Cochrane review of vertebroplasty, claiming that its conclusions were inaccurate, and advocating for the use and efficacy of this procedure in patients with acute pain of under three weeks’ duration.
In terms of balloon kyphoplasty, Ebeling and colleagues write: “There is insufficient evidence to support kyphoplasty over nonsurgical management, percutaneous vertebroplasty, vertebral body stenting, or KIVA”. Although the authors found that kyphoplasty was associated with improved pain, back-related disability, and quality-of-life outcomes compared with nonsurgical management, they acknowledge that these results were derived almost solely from a single trial. Further, the investigators write: “Any apparent benefits of kyphoplasty over nonsurgical management appeared to decrease over time, and, based on available data, it was not possible to determine whether these between-group differences were clinically meaningful of the extent to which they were accounted for by sham effects or study bias.”
Ebeling and colleagues went on to address the potential harms and possible risk of new vertebral fractures with vertebral augmentation. Prior to the task force report, limited evidence was available on these risks. In relation to both percutaneous vertebroplasty and balloon kyphoplasty, the authors found that adverse events—including risk of death, incident vertebral fracture, cement leakage, adjacent fractures, vasovagal reactions, cord compression requiring decompression, hypoxia and respiratory failure—were rarely systematically reported. According to the authors, compared with nonsurgical management, kyphoplasty was not associated with a statistically significant increased risk of incident vertebral fracture, although it was associated with nearly twice the risk of any adverse event within 30 days of intervention. Yet, Ebeling et al alluded to the high risk of bias present in the trials and they write “it is uncertain whether any benefits of kyphoplasty versus nonsurgical management of vertebral fracture outweigh potentials harms”.
Finally, the efficacy and safety of other nonpharmacologic treatments—spinal bracing and exercise interventions, was investigated. Based on the current evidence, Ebeling and colleagues report that for patients with painful vertebral fractures, there is low quality evidence that spinal bracing improves pain, trunk muscle strength, kyphosis, pulmonary volume and quality of life at six months. Furthermore, although the authors note that, following exercise interventions, the “magnitude of effects on mobility were small”, they surmise that exercise interventions have significant positive effects on mobility and may improve pain, fear of falling, as well as back extensor strength or endurance.
Yet, the aforementioned study biases and methodological flaws present in the literature that Ebeling and colleagues acknowledge throughout the report led them to address these gaps in the literature. The authors report on future research that is required to improve patient outcomes in managing osteoporotic vertebral fractures, in relation to both vertebral augmentation and other nonpharmacologic approaches. While a rigorous trial design to minimise the potential for bias was recommended in order to examine all therapies, specific recommendations were also detailed.
“No further trials of vertebroplasty should be performed, unless they are adequately powered to alter the conclusions of the current body of evidence”, write Ebeling and colleagues. If further trials are to commence, the authors state that participants of these procedures, as well as ethics committees, should be fully informed about the current body of evidence. Regarding balloon kyphoplasty, the authors recommend that “further studies are needed to resolve whether kyphoplasty increases the risk of future vertebral fractures or adverse events, which should be systematically collected”, while “any future trials should carefully characterise the timing and severity of vertebral fracture among study participants [and] should have a placebo control group.”
For spinal bracing and exercise interventions, Ebeling et al maintain that more research is needed in general, including clearly defined participant selection criteria and study protocols. Specifically, more data is needed on serious adverse events, in both the intervention and comparator groups, and on the efficacy of exercise after acute vertebral fracture. Lastly, they note that “future exercise trial designs should account for low adherence and attrition in sample size calculations”.
Based on the findings outlined in the report, the ASBMR task force detailed guidelines for the clinical management of patients with vertebral fracture. Maintaining that the optimal management of vertebral fracture remains uncertain, Ebeling and colleagues put forward that when vertebral augmentation is used, patients should be fully informed about the evidence.
In light of the findings, they conclude: “It is critical that anti-oseoporotic medications are started, continued or changed in patients with recent vertebral fracture”. Further, the task force highlights that while the use of bracing in reducing pain immediately after vertebral fracture was not supported by current evidence, exercise may improve mobility and may reduce pain and fear of falling.
Authors of the VAPOUR trial submit complaint about the Cochrane vertebroplasty review
Interventional radiologist William Clark (St George Private Hospital, Sydney, Austrialia) reached out to Interventional News to say that a section of the ASBMR report takes its findings directly from the Cochrane review. Clark and fellow authors of the VAPOUR trial have submitted a complaint to the chief editor of the Cochrane Library about alleged irregularities in the Cochrane Vertebroplasty Review (CVR) of April 2018. They asked that the review be withdrawn from the Cochrane Library, writing “we believe that the report provides a biased analysis of the VAPOUR trial, contains inappropriate statistical analysis and errors in data presentation.”
CVR authors issued a new November 2018 version of CVR to correct errors in analysis 8.1/2, but according to its critics left the bulk of the review unchanged. Clark and colleagues subsequently published their criticism of the CVR in the BMJ Evidence-Based Medicine. Their allegations against the CVR include bias against the VAPOUR trial, breach of protocol, improper use of meta-analysis and other methodological errors.
While the CVR authors conclude that the benefits from vertebroplasty in the VAPOUR trial are “clinically irrelevant and consistent with the negative results of their trials”, Clark and colleagues write that “this assertion is false”.
Indeed, Clark told Spinal News International that “The same criticisms of the Cochrane review apply directly to the ASBMR report, which draws its conclusions directly from the Cochrane review, which includes the flawed Cochrane meta-analyses.
BD has announced that the US Food and Drug Administration (FDA) has granted premarket approval for the Venovo venous stent, the first stent indicated to treat iliofemoral venous occlusive disease.
The Venovo venous stent is a flexible nitinol stent specifically designed to reopen blocked iliac and femoral veins in order to maintain adequate blood flow. The stent is designed with a balance of radial strength, compression resistance and flexibility needed for the treatment of symptomatic post-thrombotic and non-thrombotic iliofemoral lesions. Additionally, the broad stent sizing allows clinicians to treat large diameter veins and long lesion lengths.
“The unique attributes of the Venovo stent make it particularly well-suited to treat iliofemoral occlusive disease,” says Michael Dake (University of Arizona, Tucson, USA), the principal investigator for the Venovo investigational device exemption (IDE) trial. “Most importantly,” says Dake, “it is purpose-built for application in veins, and engineered to address the special challenges of venous lesions that are very different than those posed by arterial narrowing.”
Iliofemoral venous occlusive disease occurs when there is impaired blood flow in the iliofemoral vein caused by acute or chronic deep-vein thrombosis, post-thrombotic syndrome, iliofemoral vein compression including May-Thurner Syndrome or a combination of these diseases. Symptoms include swelling of the legs, pain when standing, skin discoloration and ulcers.
One-year results from the prospective, multicentre single-arm VERNACULAR trial involving 170 subjects demonstrated the safety and effectiveness of the venous stent for the treatment of symptomatic iliofemoral venous outflow obstruction. The data were presented by Dake at the 2018 Vascular InterVentional Advances meeting (VIVA; 5–8 November, Las Vegas, USA).
The clinical findings showed a weighted primary patency rate of 88.3%, with a 96.9% patency rate in non-thrombotic lesions and an 81.3%t patency rate in post-thrombotic lesions at 12 months, exceeding the performance goal of 74%. In addition, patients treated with the venous stent reported a statistically significant reduction in pain symptoms and improvement in quality of life (assessed by CIVIQ-20) at 12 months from baseline. The stent was also deployed successfully to the target lesion and showed adequate coverage in all cases, and there were no fractures seen at 12 months.
“The FDA premarket approval of the Venovo venous stent represents a significant advance for interventionalists treating iliofemoral venous occlusive disease, an underrecognised condition,” said Steve Williamson, worldwide president of Peripheral Intervention at BD. “We designed the Venovo venous stent in collaboration with clinicians to enable them to treat both post-thrombotic and non-thrombotic lesions. Clinicians will now have access to the broadest range of stent sizes in the USA for these difficult-to-treat lesions.”
The Venovo venous stent is commercially available in the USA, Europe, Argentina, Australia, Brazil, Egypt, India, Israel, Mexico, Russia, Saudi Arabia, Singapore and Taiwan.
Patients have a strong preference for transradial access, a recent study published in the Journal of Vascular and Interventional Radiology finds. Lead author Lisa Liu, Rush Medical College, Chicago, USA, and colleagues write: “With transradial access, patients experienced less periprocedural pain and shorter recovery times without significant differences in radiation exposure or procedure length.
The study investigators set out to determine patient preference for these two different access sites during hepatocellular carcinoma (HCC) radioembolization procedures after experiencing both. They explain that “The use of transradial access as the preferred approach over transfemoral access in interventional radiology has steadily increased, owing in part to numerous trials by cardiologists demonstrating fewer access-related complications, greater patient satisfaction, and lower cost with transradial access compared with transfemoral access in coronary interventions.”
Thirty patients with HCC under going MAA (macroaggregated albumin) mapping and transarterial radioembolization (TARE) were enrolled to experience one transradial access and one transfemoral access procedure each, with randomisation of which access approach was experienced first. Previous studies have also found a patient preference for transradial access, though, to Liu et al’s knowledge, no earlier study measured potential reasons for patient preference, “such as associated pain, recovery time, or quality of life after the procedure”, the present study authors write. An additional aim of the present study therefore was to “objectively assess the impact of access site on patient comfort and satisfaction.”
The authors cite a retrospective review assessing the safety and feasibility of the trans-radial approach in the first 1,500 non-coronary interventions to use trans-radial access at a single institution published in 2016 by Raghuram Posham (Icahn School of Medicine at Mount Sinai, New York, USA) et al that demonstrated a safety profile of 98.2% technical success rate and <3% complications, most of which were defined as minor complications.
This prospective, randomised, single-institution, controlled crossover trial of 30 patients (28 men; mean patient age of 66 years) reported that 22 (73.3%) patients indicated preference for radial access. Four (13.3%) patients indicated preference for femoral access, and four (13.3%) indicated no preference. Liu and colleagues deem this a “strong preference for transradial access”, drawing attention to the fact that more than five times as many patients prefer transradial to transfemoral access.
The authors also note that no acute minor or major adverse events were identified on physical examination at the day of procedure at a 30-day follow-up appointment. They write: “No access-site bruising and/or haematoma, radial artery occlusion, or any other minor or major complications were documented.” Fourteen patients self-reported superficial bruising following radial procedures in surveys given out during follow-up; for patients commenting on trans-femoral access, 17 patients reported bruising (46.7% vs. 53.3% for transradial and transfemoral access, respectively; p=0.4074). All 14 patients who reported bruising following transradial access were amongst the 17 to also report bruising following transfemoral access. Amongst the total patient cohort, 10 were taking anti-coagulants: seven of these patients reported bruising after transradial access, and nine after transfemoral access.
To greater elucidate the association between the self-reported bruising rate for transradial versus transfemoral access and the use of anticoagulants, the study authors call for future studies on the incidence of bruising after transradial versus transfemoral access to “control for anticoagulation and antiplatelet medication use.”
Surveys assessing pain and quality of life were administered after each MAA mapping and TARE procedure. Patients were contacted via e-mail, phone, or in person to complete a survey on demographics, occurrence of self-reported bruising, and numerical pain rating scale. This scale ranged from no pain at 1 to worst pain at 10 in four different contexts: during the procedure overall, during the procedure at the access site, after the procedure in the recovery room, and after the procedure at home. Patients also completed a modified 12-item Short Form Health Survey to assess quality of life.
Patients experiencing transradial access recorded, on average, significantly lower overall pain during the procedure, significantly lower pain at the access site during the procedure, and significantly lower pain after the procedure in the recovery room compared with transfemoral access (p=0.0046, p=0.0004, p=0.0357, respectively). No significant difference was observed for average pain reported after discharge at home between transradial and transfemoral procedures (p=0.4235). Liu and colleagues write that “These results suggest that the reduced pain and increased comfort associated with transradial access are short-term benefits limited to the perioperative time period during the procedure and immediately after in the recovery room before discharge.”
Furthermore, the authors report no significant differences between quality of life scores after transradial access versus transfemoral access.
Average fluoroscopy time—a measure of radiation exposure—and total recovery time were also not significantly different between the two access types (p=0.1442 and p=0.1496, respectively). For TARE procedures, the authors note that “radial access cases [both MAA mapping and TARE] were associated with significantly shorter recovery times on average compared with femoral access cases (108 minutes for transradial access, 153 minutes for transfemoral acess; p=0.0193).”
Summarising their results, Liu et al write: “Overall, patients reported significantly less pain with transradial access compared with transfemoral access during the procedure and afterward in the recovery room. Additionally, transradial access was associated with shorter recovery times for both MAA mapping procedures and TARE procedures, with a significant difference observed for TARE procedures.” Liu and colleagues postulate that “the lack of corresponding significance for MAA mapping procedures may be attributed to having overall shorter recovery times compared with TARE (118.9 minutes vs. 130.7 minutes), and perhaps a significant result may have been reached in the MAA mapping group with a larger sample size.
“Additionally,” they add, “the significant difference in recovery time achieved in the TARE group should be considered with caution, as patients receiving trans-femoral access underwent a conservative two-hour bedbound protocol after AngioSeal (Terumo) deployment rather than the recently US Food and Drug Administration (FDA)–approved 20-minute early ambulation protocol.”
Commenting on the significance of this finding, the study investigators comment: “The findings of this study support considering radial access as a default patient-centred approach to radioembolization procedures for patients eligible for both radial and femoral access approaches.”
A positive response from interventional radiologists
Commenting on these results on Twitter, Naveed Rajper, an interventional cardiologist based in New York, USA, wrote: “Trials are not necessary to prove this. Radial first is tried and tested. Let us cross-pollinate advancements like this between procedural specialties, be open to change, and focus on even bigger things.”
Responding to this remark, Aaron Fischman, an interventional radiologist also from New York, USA, and an author on this study, said, “You would be surprised the conversations we have at interventional radiology meetings about this concept. There are some things that have to be proven in a rigorous way to move the needle. Patient preference specific to interventional oncology is an important step in that direction.”
Darren Klass, another advocate for the transradial approach, and an interventional radiologist in Vancouver, Canada, agrees with Fischman, writing online in direct response to the latter ’s comment: “Agree. Patient preference is one. Nursing intensity post-procedure, complications, discharge time, radiation dose to patient and operator, done or in midst of publication for interventional radiology, yet we still face the apathetic objectors.”
Generally commenting on the study, Klass said on social media that this publication is “cementing what radial first operators all experience.”
The study authors do acknowledge some concerns with transradial access. One “potential concern” of transradial access for noncoronary interventions “is longer procedure times and subsequent greater patient radiation exposure owing to the greater anatomic distance from access site to treatment site.” However, they note that trials from interventional cardiology have not found significant differences in fluoroscopy time.
Liu et al also note that the subjectivity of surveys and of pain scales as research tools acts as a limitation to the present study. In addition, they acknowledge that as four of the 30 patients in the trial had experienced a prior intervention using radial or femoral access, there was the possibility of introducing a preconceived bias into their results. However, they write that “the effect of this limitation is expected to be minimal considering the small percentage of patients with prior transradial access or transfemoral access [experience], and no pattern of bias was observed in analysis of this subset of patients and their choice of access preference.”
Encouraging results from Y90 (yttrium-90) radioembolization of pancreatic cancer support a possible role for it in the management of the disease, with initial small scale studies suggesting it provokes a disease response; however, the benefits may vary for different patient subgroups.
Although evidence is still limited, Alexander Kim, chief of Vascular and Interventional Radiology at Medstar Georgetown University Hospital (Washington DC, USA), said: “The data suggest that we can get promising disease response with radioembolization, with response rates from 20–40% in various groups. Patient selection, obviously, is key.” He was speaking at the Spectrum conference (1–4 November, Miami, USA), outlining a possible role for Y90 in the management of pancreatic cancer metastasis.
In 2018, 55,440 new cases of pancreatic cancer were diagnosed, with 44,330 deaths. The five-year survival is 8.5%, dropping to 2.7% in patients with distant metastases. The current standard of care, drug regimens of either FOLFIRINOX or gemcitabine abraxane, has shown an overall survival of about eight to 11 months in trials.
Kim explained the rationale for adding Y90 radioembolization to standard chemotherapy treatment: “Overall, there is a poor prognosis for these patients, so there is a need to find different treatments that may potentially augment survival in a subgroup of these patients. And, there are data that show that liver metastases are a negative independent prognostic factor of survival, causing death in about 50% of these patients.” The radiosensitivity of pancreatic adenocarcinoma suggests Y90 could provide an alternative option.
But there have been very few studies looking at its efficacy; Kim assessed the small number available. The largest study, of 19 patients, was from Germany: “Response rates in the liver are pretty impressive, with about nine of the patients showing a partial response to treatment, and overall survival of nine months from the time of radioembolization, and 19 months from initial diagnosis.”
He also told delegates about the findings from his own study of 16 patients, in which Y90 radioembolization was incorporated into systemic therapy, describing the treatment strategy as “a little unique”.
“We strategised to incorporate Y90 into systemic treatment. We treated those patients with half dose gemcitabine in the cycle prior to radioembolization, then performed whole liver radioembolization for patients, but then gave them a half dose again for the following chemotherapy cycle, and then they went back to a regular dose of systemic treatment.” Overall survival from time of diagnosis was 22 months, and from time of radioembolisation was 12.5 months.
His group have also recently completed a multicentre retrospective study of 33 patients, published in the March issue of Journal of Vascular and Interventional Radiology. It recorded a disease control rate of 81%, and disease response in 42% of patients. The median overall survival from the time of Y90 radioembolization was 8.1 months (95% CI 4.8–12.5), with a median overall survival from diagnosis of 20.8 months (95% CI 14.2–29). “Our toxicity levels were pretty mild, with three patients having Grade III toxicities, and no grade IV or V toxicities in the 33 patients.”
Only one prospective study has been conducted: an open label, phase II, two-centre trial in Australia, which was published in 2015. “The primary objective was to assess progression free survival in the liver. They enrolled 15 patients in the study, everyone had bilobar liver disease. They received whole liver treatment in a lobar fashion using resin Y90. The tumour response rates were generally pretty impressive. You can see the change in CA 19-9 levels decreasing pretty dramatically for the majority of these patients.”
Progression free survival was 5.2 months for the liver, and 4.4 months at any site. But overall survival was only 5.5 months, raising the question, Kim said, of “whether radioembolization actually benefits in the frontline setting. The prospective phase II data would argue against incorporating Y90 in this patient population; the patients overall survival was really unchanged from standard survival that you would expect to see with gemicitabine based treatment.”
He stressed the importance of patient selection. At Georgetown, Kim and other researchers have incorporated Y90 as a consolidated treatment for particular groups of patients, including those who have been treated with frontline therapy for four to six months and have demonstrated good tumour biology.
“The second group we have treated are patients who have developed systemic toxicity with chemotherapy—generally patients who develop toxicity from gemcitabine, and they will either have to switch their regimen or titrate down on their dose. There is a concern that their liver disease will flare after the change in regimen, so we have started to incorporate Y90 for this patient population.”
He said Y90 treatment needed further assessment, including the Georgetown strategy of consolidation and maintenance, to see whether it leads to a survival benefit. And, he added, “there is a lot of interest in assessing the synergistic effect of radioembolization and immunotherapy. That is another area that needs more investigation in the pancreatic cancer patient population.”
Cryoablation increases the clinical efficacy of treatment with the oral multi-target antitumour drug sorafenib for advanced renal cell carcinoma (RCC), a new study published in the International Journal of Hyperthermia has found. Joint first authors Changfu Liu and Fei Cao (both Department for Interventional Treatment, Tianjin Medical University Cancer Institute and Hospital, Tianjin, China) conclude that combining cryoablation with sorafenib can reduce tumour load, improve anti-tumour immunosuppressive status, increase survival, and maintain quality of life in patients with RCC that cannot be surgically resected.
This is the first publication investigating the safety and efficacy of cryoablation combined with sorafenib for the treatment of this disease, but previous work has shown the combined treatment to be better at prolonging survival than sorafenib alone in patients with hepatocellular carcinoma (HCC).
The present study is observational, and followed 156 patients with advanced RCC who were unsuitable candidates for surgical resection. Participants received cryoablation and sorafenib (n=67), or sorafenib only (n=89), and all patients were followed up to at least seven months, with a mean follow-up time of 28.8 months (and a maximum of 67 months).
Of the 156 patients enrolled in the study, 87 were men (56%), and the median age was 65 years (with an age range of 48–84 years). A total of 184 tumours were recorded, with diameters ranging from 3.8cm–14cm, and were classified as clear cell carcinoma (92.95%), papillary carcinoma (5.13%), or chromophobe RCC (1.92%). All patients presented with stage III or IV tumours. There were no statistically meaningful differences between the two treatment groups at baseline.
Improved survival with cryoablation and sorafenib compared to sorafenib alone
“The combined therapy had a clear advantage in terms of efficacy,” the study authors write.
Both progression-free survival and overall survival were statistically significantly higher (p<0.05) in the group treated with a combination of cryoablation and sorafenib than the cohort treated with sorafenib alone, indicating that cryoablation and sorafenib together can more significantly prolong these survival metrics than sorafenib alone can. Progression-free survival was 20 months in the combined group, versus 12 months in the sorafenib only group, and overall survival was 36 months in the former cohort compared to 29 months with just sorafenib.
Additionally, Liu and Cao et al report a higher progression-free survival and overall survival in patients who underwent complete cryoablation (n=25, 38.81% of the patients treated with cryoablation) than the patients who only had a partial cryoablation. Stratification analysis revealed a progression-free survival of 23 months for those patients who had a complete cryoablation; progression-free survival was 17 months for those participants with a particle cryoablation. This trend was the same for overall survival: 41 months in complete cryoablation recipients, versus 32 months in partial cryoablation recipients.
Based off these results, Liu and Cao et al recommend complete cryoablation for advanced RCC with relatively small tumour diameters, and further cryoablation treatments for tumours with larger diameters to achieve complete ablation.
Cryoablation and sorafenib together lower the proportion of patients with disease progression
The combined treatment group had a higher proportion of complete response and stable disease than the group treated with sorafenib alone. The study authors used these metrics to calculate the overall response rate and disease control rate. These measures provide further clarity when assessing the efficacy of the different treatment options for RCC.
The overall response rate was higher for patients treated with cryoablation and sorafenib than sorafenib alone (p<0.05). The overall response rate is calculated by adding the number of patients with a complete response following treatment and the number who exhibited a partial response, and dividing the sum by the total number of patients. In the combined cryoablation and sorafenib arm, a complete response was observed in five patients, and a partial response in 43. In comparison, a complete response was seen in just one patient the sorafenib only group, and a partial response in 16. This yields an overall response rate of 71.64% in the combined cohort, and 19.10% in the sorafenib group.
The researchers also calculated the disease control rate: the total sum of the number of patients with a complete response to treatment, a partial response to treatment, and a stable disease condition after treatment, divided by the overall number of patients. The number of patients with a stable disease condition following treatment was 12 (17.91%) in the combined arm, and 58 (65.17%) in the sorafenib only arm. A progressive disease condition was reported in seven patients (10.45%) in the combined treatment group, and fourteen patients (15.73%) in the single treatment group.
Therefore, the disease control rate was significantly higher when both cryoablation and sorafenib were used together, at 89.55%, than when sorafenib was used alone, 84.27% (p<0.05).
The significantly higher survival rates in the cryoablation and sorafenib group could be explained by a couple of different concepts, Liu, Cao and colleagues suggest. They first propose that cryoablation can effectively reduce tumour load within a short time, thereby increasing overall response rate and disease control rate, and effectively controlling tumour progression in patients with advanced RCC. Secondly, they explain how cryoablation results in the necrosis of a large number of tumour cells in the target area, and “may increase the permeability of tumours and surrounding tissues, thus increasing the sensitivity of residual tumour cells to target drugs.” They continue: “Hyperthermia has been shown to enhance drug delivery, so the changes induced by cryotherapy may improve the uptake of sorafenib, although this association requires further investigation.”
A third reason given by the study authors for the improved disease control rate and survival scores is predicated on the knowledge that the kidney is an immunogenic organ. Liu and Cao et al speculate that “cryoablation may influence the immunogenicity and drug resistance of residual tumour cells, thereby changing or prolonging the effective time of targeted drug therapy.”
In terms of safety, the authors note that cryoablation did not increase the risk of side effects of targeted drugs; there was no significant difference between side effects experienced by patients in either arm of the study.
Enhanced antitumour immunity: A new treatment strategy for advanced RCC
Liu, Cao and colleagues report that the combined therapy of cryoablation and sorafenib “may enhance the body’s antitumour immunity, and effectively prolong progression-free survival and overall survival without compromising patient quality of life, thus representing a new treatment strategy for advanced RCC.”
The antitumour immunity is particularly important, as the authors note that, “similar to other targeted drugs for tumour treatment, […] patients develop resistance to sorafenib, leading to disease progression and death.”
The study investigators therefore analysed serum indicators related to immune function in both the combined treatment group and the sorafenib only group. In the combined treatment arm, the proportion of Treg cells was significantly decreased, and the proportions of several T lymphocytes were significantly increased after treatment compared to before treatment. This was not the case in the sorafenib only group: in this cohort, no significant difference in Treg cells or T lymphocytes was observed before and after treatment.
Explaining this finding, Liu, Cao and colleagues write that these data “suggest that cryoablation enhanced tumour immunity more than sorafenib alone.”
The authors summarise: “As a potential new treatment strategy for advanced RCC, cryoablation combined with sorafenib, therefore, requires further investigation in future randomised controlled trials.”
Endovascular denervation can improve pain in patients with abdominal cancer and may offer a new approach to palliative care, according to a study recently published in the Journal of Vascular and Interventional Radiology. The study investigators, Qi Zhang, Gao-Jun Teng (both Center of Interventional Radiology and Vascular Surgery, Zhongda Hospital, Nanjing, China) and colleagues, conclude that the procedure is safe and effective for the alleviation of pain caused by cancer.
The study enrolled seven patients (two men and five women) with diagnoses including pancreatic cancer (n=3), cervical carcinoma (n=2), cholangiocarcinoma (n=1), and oesophageal cancer with retroperitoneum lymph nodes invasion (n=1) from April 2017 to February 2018.
A surface electrode was placed on the back of each patient and connected to the denervation device. Denervation was carried out at the abdominal aorta close to the origin of celiac artery and superior mesenteric artery with the use of a multi-electrode radiofrequency ablation catheter with the time and temperature settings respectively at 120 seconds and 60°C.
The authors report that all patients experienced pain relief after treatment, meeting the primary endpoint of improvement in pain score. At one, two, four, eight, and 12 weeks after the procedure pain scores, measured by visual analogue score, decreased significantly compared with baseline (p<0.001). All patients experienced a greater than four-point score reduction.
Secondary endpoints included changes in quality of life, intake of narcotics, and the safety of endovascular denervation.
Narcotics use was significantly reduced within the first three months after treatment, and quality of life scores were improved significantly (p<0.005) with better sleep. There were no severe treatment-related adverse events or major complications reported.
Speaking to Interventional News of how these results will influence clinical practice, corresponding author Gao-Jun Teng, president of the Zhongda Hospital, Southeast University, Nanjing, China, says “Our report presented the preliminary results in a small number of patients, but it showed very promising and encouraging results. It will certainly inspire further research using endovascular denervation. I would not be surprised to see endovascular denervation become a useful tool in pain management in the very near future.”
Writing in the Journal of Vascular and Interventional Radiology, the authors conclude: “Cancer pain management is a formidable problem for physicians and may result in a substantial burden to the public health care system. Opioid analgesics are often required to control cancer pain. Adverse effects from opioids are debilitating and worsen as larger doses are administered,” the authors write. “This preliminary trial demonstrated that endovascular denervation is a promising and safe method for the palliation of pain caused by abdominal cancers. It could be a new approach for management of cancer pain.”
A new approach to palliative care
“This may give interventional radiologists a brand-new approach to treating pain”, Teng adds, “thus [acting to] solidify their place in the field of pain management. Endovascular denervation provides interventional radiologists a new and big territory for treating non-hypertension diseases, which has previously been considered a procedure performed by cardiologists.”
Teng believes it is important to find a new approach to palliative care, telling this newspaper: “It is well known that cancer pain has significant impacts on patients’ quality of life, as well as their prognosis. Traditional management uses narcotics, sometimes in large quantities, which often result in severe side effects such as impairment of judgement and respiratory suppression. Interventional neurolysis under CT/US [computed tomography/ultrasound] is a traditional interventional radiology procedure, which involves the deep puncture of a needle and injects chemical (alcohol, phenol) agents. Accurate needle localisation may be a challenge for inexperienced interventional radiologists. The outcomes vary from the operator’s skill, and the degree of diffusion of the neurolytic agents is sometimes out of control, which may cause serious complications.
“New approaches—especially nonopioid methods—in pain management are still in need clinically. Due to the ubiquitous nature of the vascular network and anatomical accompany of nerves and arteries, endovascular denervation could be a great approach in pain management. It has the advantages of being minimally invasive, [enabling] easy access to any part of the body, and having fewer side effects.”
However, Teng also states that the mechanism for endovascular denervation on uncontrollable cancer pain is “still unclear”, and that more work is required to elucidate the procedure’s machinations. He is the principal investigator in a large scale clinical trial currently ongoing in China and involving more than 10 national medical centres. Speaking of this trial, and what it means for the future of endovascular denervation, he says: “We are exploring different ablation sites for controlling cancer pain in other parts of the body. We are also working to expand the application of the technique to manage pain caused by other diseases.”
The National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF KDOQI) provides evidence-based clinical practice guidelines for haemodialysis vascular access and related complications, and has done so since 1997. The latest guidelines, published in 2006, no longer reflect the most recent evidence for the management of vascular access, causing the haemodialysis and vascular access community to eagerly await the revised recommendations, currently in the external review process and due in Spring 2019.
With more than a decade between the last guidelines and the imminently anticipated ones, the time elapsed is reflected in numbers: the new guidelines will have over 160 statements, compared with the 130 statements of the 2006 guidelines. For the upcoming guidelines, approximately one-third of these statements are based on a rigorous review process, and two thirds predicated on expert opinion. In contrast, the previous guidelines—where the strength of the recommendation was given a letter grade, with A being backed by the strongest evidence—had <20% grade A statements, and the remainder grade B or expert opinion.
Charmaine Lok (University of Toronto, Toronto, Canada), chair of the KDOQI guidelines for vascular access 2018, gave a talk at the Controversies and Updates in Vascular Surgery conference (CACVS; 7–9 February, Paris, France) to provide a glimpse of the upcoming guidelines. When asked by an audience member if the 13 years between guidelines meant there was “a big risk of having an outdated practice in-between” the publications, Lok agreed, telling delegates: “Absolutely. That is why it took us so long to develop the guidelines, because there was such a significant amount of evidence that had to be reviewed. The benefit of having a long time between each is that it allowed time for studies to be conducted, so we could actually learn from them to help develop the next guidelines, but I agree with you.
“There has actually been a study on the ideal time-frame between guidelines: four years. We need to keep these guidelines ongoing. This was a complete renewal of the guidelines, so hopefully the next ones will truly be an update, to make them much more frequent, because the time lapses are far too great.”
Conceptual shifts
Lok told CACVS attendees that there had been several key conceptual shifts involved with this endeavour, to ensure the finished publication best mirrors the changes to the field in the intervening 13 years.
Expanding on one of these ideological changes at CACVS, Lok said: “Here is one of the biggest changes in concept: what we are trying to do is emphasise the end-stage kidney disease (ESKD) life-plan. Everybody is well aware that chronic kidney disease has five stages, and we typically think about reaching stage V, which is ESKD, as the end. However, I really want you to rethink it. When a patient reaches stage V, that is the beginning of the patient’s ESKD life on dialysis or transplant. The beginning of their ESKD life-plan.”
Lok went on to explain that the endstage kidney disease life-plan concept centred around the paradigm of attaining: “The right access, in the right patient, at the right time, for the right reasons”. This, Lok said, means thinking of and planning for the patient’s continued care across their entire ESKD lifetime. She demonstrates this with an example of two patients, a teenager whose ideal treatment would be a preemptive transplant, and an obese comorbid adult man, who “may have a different trajectory.”
In addition to reconfiguring the approach to end-stage kidney disease treatment to encompass the complete patient timeline, the new guidelines consider and encompass more than the focused “fistula first” concept that Lok describes as emphasised since the 2006 recommendations. Instead, Lok asked the attending physicians to focus on a four-step PLAN (Patient Life-plan, Access Needs).
The first step of the PLAN involves considering the patient first, and what their ESKD life-plan looks like. Is the first ESKD modality choice haemodialysis or peritoneal dialysis? Or transplant? Given that it is haemodialysis, next, consider their access needs. Secondly, what is the access creation plan; for example, who will create the access, where (location) and when (timing). Thirdly, the physicians are asked to come up with an access contingency plan, so they have a remedial plan for when the access becomes problematic; for example, before creating the fistula, or to consider the plan of action if it fails to mature. Finally, Lok urged the CACVS audience to think about an access succession plan, before creating an access: it’s not just thinking about fistula first, but what access is next. This takes into account the patient’s life-plan and the longer-term plan. Lok said that it was “especially important to think cleverly about this for younger patients, who have a whole life ahead of them.”
Changes to definitions
A further change outlined by Lok in her CACVS presentation, more pedantic than the overarching conceptual changes described above, is the editing of several definitions. One such changed definition is “catheter dysfunction”. Previously, this had focused on blood pump speed, and was defined in 2006 to include the “failure to attain and maintain an extracorporeal blood flow of 300ml/min or greater at a prepump arterial pressure more negative than 250mmHg.” The new guidelines will define catheter dysfunction thus: “Failure to maintain the prescribed extracorporeal blood flow required for adequate haemodialysis without lengthening the prescribed HD treatment.”
Lok explained: “In some situations as in Tassin, France or for patients receiving nocturnal haemodialysis, these patients undergo longer duration dialysis, at prescribed low blood pump speeds (<300 ml/min) and the patient’s catheter is fine—you would not say it is malfunctioning. So with these guidelines, we looked at innovation in [the] dialysis [field], and how we might be able to keep definitions current.”
The CASSINI trial found that treatment with rivaroxaban did not significantly reduce the incidence of thromboembolism or death caused by thromboembolism in high-risk ambulatory patients with cancer during the 180-day study period. However, during the study’s intervention period, there was a significantly lower incidence of venous thromboembolism and death due to thromboembolism among patients treated with rivaroxaban, and there was a low incidence of major bleeding. The results of the trial were reported by Alok A Khorana (Department of Hematology and Medical Oncology, Cleveland Clinic, Cleveland, USA) and colleagues in the New England Journal of Medicine (NEJM).
It is known that cancer and cancer treatment put patients at risk of venous thromboembolism, but guidelines do not recommend routine thromboprophylaxis for patients with cancer even though it is possible that such treatment could improve their outcomes. The study investigators therefore sought to “assess the efficacy and safety of rivaroxaban thromboprophylaxis in patients with a solid tumour or lymphoma who had a Khorana score of two or higher and were initiating in a new systemic cancer regimen”.
The CASSINI trial was a double-blind, multicentre, randomised trial, which randomised high-risk ambulatory patients with cancer to receive either 10mg rivaroxaban or placebo daily for a period of up to 180 days.
The primary efficacy endpoint—a composite of deep vein thrombosis, pulmonary embolism or death from venous thromboembolism—was assessed for up to 180 days. The same endpoint was similarly assessed during the intervention period, which was the time from first receiving treatment or placebo to the last treatment plus two days. The primary safety endpoint was major bleeding.
Of 1,080 patients originally enrolled in the trial, 49 (4.5%) were found to have thrombosis during screening and 190 had other reasons to be excluded. A total of 841 patients who were all assessed as having a higher risk of venous thromboembolism (Khorana score ≥2 at baseline) and an expected survival of more than six months were included in the randomisation: 420 patients were assigned to the rivaroxaban group and 421 to the placebo group.
The mean intervention period—the time when patients actually received treatment—was 4.3 months, with 43.7% of patients in the rivaroxaban group and 50.2% of those in the placebo group stopping treatment before the end of the trial.
During the study period up to day 180, the primary endpoint occurred in 25 patients receiving rivaroxaban (6%) and 37 patients receiving placebo (8.8%; hazard ratio=0.66; 95% confidence interval [CI]=0.40–1.09; p=0.10). During the intervention period, the primary endpoint occurred in 11 patients receiving rivaroxaban (2.6%) and 27 patients receiving placebo (6.4%; hazard ratio=0.40; 95% CI=0.20–0.80). Major bleeding occurred in eight patients receiving rivaroxaban (1.9%) and four patients receiving placebo (1%; hazard ratio=1.96; 95% CI=0.59–6.49).
Khorana et al comment: “Although the primary endpoint occurred in a lower percentage of patients who had been randomly assigned to the rivaroxaban group in this analysis, the difference was not significant”. However, they note that “in a prespecified supportive analysis involving the same population but assessing the more conventional period of during the intervention, we found a difference of four percentage points in favour of rivaroxaban over placebo with regard to the primary composite endpoint of venous thromboembolism and venous thromboembolism-related death.”
Arterial and isolated distal thromboembolism, which are common in patients with cancer, were found in lower rates among the rivaroxaban-treated patients than in the patients receiving placebo. According to Khorana et al, this “could further increase the net benefit of prophylaxis for patients”.
A limitation of this study is the large percentage of patients who stopped the trial regimen prematurely, but this is not surprising in patients who mostly have advanced cancer.
The investigators conclude: “The results of the CASSINI trial provide important information regarding the baseline prevalence and incidence of thromboembolism among high-risk ambulatory patients with cancer”. However, they were unable to confirm the benefits of treating these patients with rivaroxaban in their trial “because the between-group difference in the prespecified primary efficacy endpoint up to day 180 was not significant”.
Khorana noted to Interventional News that there was a second confirmatory trial in the same issue of the NEJM by Marc Carrier (Ottawa, Canada) et al investigating the same patient population as observed in the AVERT trial. In an accompanying editorial addressing both studies, Giancarlo Agnelli (Perugia, Italy) stated that both trials together “showed a significant benefit of direct oral anticoagulants for the prevention of venous thromboembolism, with a low incidence of major bleeding” and the data are “quite compelling”. Khorana agrees with this editorial leaning.
With “an indisputable association between depression and peripheral arterial disease (PAD)”—nearly a third of PAD patients experience comorbid depression or depressive symptoms—Joel Ramirez and Marlene Grenon here call for vascular interventionalists to take a more active role in their patient’s mental health: increasing the awareness of the links between these two conditions, recognising the symptoms of depression, and referring patients to a mental health specialist where appropriate.
Peripheral arterial disease (PAD) is a major global health problem that has been estimated to affect more than 200 million people worldwide with an increasing incidence.1 PAD has been associated with an increased risk of limb amputation, adverse cardiovascular events, and mortality, as well as impaired quality of life, which have collectively resulted in a high economic burden on society.2 Despite widespread campaigns to improve cardiovascular health, the prevalence of PAD is expected to increase with the ageing world population. Given the large impact that PAD has, it is important that as interventionalists we are able to adequately identify, prevent, and treat modifiable risk factors for PAD.
Although not commonly recognised by interventionalists, the incidence of depression has been rising, particularly in young adults. Depression is a leading cause of disability worldwide,3 and has become a well-recognised risk factor for the development and progression of coronary artery disease (CAD). In fact, depression has been formally recognised by the American Heart Association (AHA) as a risk factor for CAD incidence and adverse outcomes, which has resulted in the creation of guidelines for depression screening in this patient population.4 Given the overlap between risk factors for CAD and PAD, investigators have recently begun to examine the association between depression and PAD.
My colleagues and I have dedicated our recent research efforts to the problem of depression and PAD. Our understanding of the risk factors for the development and progression of PAD used to be narrower, as we primarily only considered traditional risk factors such as smoking, hypertension, hyperlipidaemia, and diabetes, among others. We now have a more comprehensive understanding of this disease and have recognised that mental illness, specifically depression, may play a role in the development of PAD and adverse outcomes among patients with PAD.
It has been reported that nearly a third of patients with PAD have comorbid depression or have experienced depressive symptoms.5 Among patients with PAD, depressive symptoms have been associated with worse claudication, decreased patency after peripheral revascularisation, and increased incidence of major amputation, adverse cardiac events, and mortality.6 From a pathophysiological perspective, our findings support mechanistic pathways linking depression to PAD. We have shown that worse depressive symptoms are correlated with higher levels of inflammation,7 which may mediate the development of PAD and adverse outcomes. Aside from its pro-inflammatory properties, we recently reviewed6 a tremendous body of evidence that suggests that depression can dysregulate the metabolic system, the hypothalamic-pituitary-axis, and the coagulation pathway, all of which are crucial to the proper functioning of the cardiovascular system. Although the relationship between depression and PAD is convincing, there are currently a paucity of reports examining how antidepressants or behavioral therapy alters the risk of PAD incidence or outcomes in this patient population. However, a recent study by Arya et al has observed that among patients with PAD and depression, the absence of antidepressant use was associated with an increased risk of limb loss.8
The scientific evidence supporting a relationship between depression and PAD is growing. To address this new burden of disease, we need to generate innovative solutions and engage leaders in vascular medicine and surgery. The first step in addressing the role of depression in PAD is increasing awareness of the relationships that have been reported.6 While outside the comfort zone of most interventionalists, understanding the role that depression plays in PAD could provide additional insight into opportunities to improve outcomes in this patient population. We have a responsibility to address the well-being of our patients, by enabling open dialogue about mental health and by ensuring that our patients are receiving proper screening and treatment for mental illness. Although most interventionalists are uncomfortable treating or managing mental illness, as the impact of depression on PAD becomes more clear, it is essential that we recognise the signs and symptoms of depression, and refer patients to mental health specialists or primary care physicians for appropriate diagnosis and treatment.
Our understanding of the pathophysiology that implicates depression with the development of atherosclerosis is largely based upon CAD animal models and patients with CAD. Although CAD has a similar pathophysiology to PAD, there are some differences, and research specific to PAD will be necessary to better understand the relationship between depression and PAD. Furthmore, our understanding of the clinical impact that depression has on PAD is currently limited to a few studies.6 We strongly encourage that investigators conduct basic science, translational, and clinical research examining the association between depression and PAD. For clinical and translational research studies, we recommend collecting data related to depression and/or eliciting a brief psychiatric history, documenting antidepressant medications or utilisation of behavioral therapy, and screening for depression using validated questionnaires, such as the Patient Health Questionnaire-9 or Geriatric Depression Scale Short Form. These variables can also be easily collected for secondary aims in other studies of patients with PAD. Additional research investigating the impact of depression on incidence, progression, and outcomes of PAD is necessary, in order to clarify the mechanisms linking these diseases. As research examining the relationship between depression and PAD becomes more robust, we hope that screening and treatment guidelines will be created in order to influence everyday clinical practice. Given that there are similar guidelines from the AHA that exist for depression and CAD, this seems reasonable.4
Furthermore, innovative digital health solutions that aim to approach the treatment of depression in ways that are more adapted to the needs of our population (such as telehealth and on-the-go apps) are becoming more available. Utilising these technologies may allow for improved identification and management of depression in patients with PAD. We encourage vascular clinicians and investigators to engage with this rapidly evolving landscape of innovation and digital health, where disruption may help improve the care that patients with PAD receive.
There exists an indisputable association between depression and PAD. Although our understanding of this relationship is currently limited by existing research, we should increase the awareness of the importance of depression among patients with PAD and those at high risk for PAD, as well as refer patients to mental health specialists or primary care physicians for screening, diagnosis, or treatment when appropriate. Additionally, when designing studies of PAD, we strongly recommend collecting information on mental health and specifically depression. Lastly, we call for vascular interventionalists to become more engaged in innovative digital health solutions that are becoming increasingly available for the treatment of chronic diseases and mental health.
Joel Ramirez is a vascular surgeon in the Department of Surgery, Division of Vascular and Endovascular Surgery, University of California, San Francisco, USA.
Marlene Grenon is a vascular surgeon in the Department of Surgery, Division of Vascular and Endovascular Surgery, University of California, San Francisco, USA, and at Evry Health, Dallas, USA.
References:
1. Fowkes FG, Rudan D, Rudan I, et al Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet 2013; 382: 1329-1340. 2013/08/07. DOI: 10.1016/S0140-6736(13)61249-0.
2. Morley RL, Sharma A, Horsch AD, et al Peripheral artery disease. BMJ 2018; 360: j5842. 2018/02/09. DOI: 10.1136/bmj.j5842.
3. Ferrari AJ, Charlson FJ, Norman RE, et al Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med 2013; 10: e1001547. 2013/11/14. DOI: 10.1371/journal.pmed.1001547.
4. Lichtman JH, Bigger JT, Jr., Blumenthal JA, et al Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association. Circulation 2008; 118: 1768-1775. 2008/10/01. DOI: 10.1161/CIRCULATIONAHA.108.190769.
5. McDermott MM, Greenland P, Guralnik JM, et al Depressive symptoms and lower extremity functioning in men and women with peripheral arterial disease. J Gen Intern Med 2003; 18: 461-467. 2003/06/26.
6. Ramirez JL, Drudi LM and Grenon SM. Review of Biologic and Behavioral Risk Factors Linking Depression and Peripheral Artery Disease. Vasc Med 2018; In Press.
7. Hernandez NV, Ramirez JL, Khetani SA, et al Depression severity is associated with increased inflammation in veterans with peripheral artery disease. Vasc Med 2018; 23: 445-453. 2018/07/24. DOI: 10.1177/1358863X18787640.
8. Arya S, Lee S, Zahner GJ, et al The association of comorbid depression with mortality and amputation in veterans with peripheral artery disease. J Vasc Surg 2018 2018/03/29. DOI: 10.1016/j.jvs.2017.10.092.
Eric Secemsky (Boston, USA) takes Interventional News through the main highlights of his recently published analyses of a US Medicare claims dataset that examined the association between drug-eluting devices and mortality in peripheral arterial disease patients. Secemsky spoke at the Vascular Leaders Forum, hosted by Vascular Interventional Advances (VIVA), and states that these analyses did not find an association between drug-eluting devices and mortality.
The renal denervation bubble collapsed due to a single trial—SYMPLICITY HTN-3, but this trial’s findings went against the grain, Horst Sievert (Frankfurt, Germany) tells Interventional News at CRT 2019. Sievert shares early results of alcohol-mediated renal denervation, which were presented as a late-breaking abstract at the conference.
Clinicians are calling for increased collaboration between computer scientists, biomedical engineers and interventional radiologists as machine learning is posited to play a more prominent role in interventional radiology (IR) procedures, from informing the initial diagnosis, through to patient selection and intraprocedural guidance. In a recent primer published in The Journal of Vascular and Interventional Radiology (JVIR), Brian Letzen, Clinton Wang and Julius Chapiro, all of the Yale School of Medicine, New Haven, USA, outline the clinical applications of machine learning for IRs, and visualise a future where artificial intelligence (AI) enables the elevation of the discipline to become, in Chapiro’s words, “the epitome of personalised medicine”.
Letzen and colleagues outline their vision of AI in IR: “By integrating machine learning into diagnosis, treatment, and management, AI can empower physicians to provide the highest-quality personalised care in an efficient manner that meets the demands of modern clinical practice. Whereas medicine has traditionally focused on incremental hypothesis-based research, AI allows for a new paradigm where ‘big data’ can be rapidly analysed, uncovering new insights that may otherwise have required decades of prospective trials.”
The annual meeting of the Society of Interventional Radiology [SIR] this year features its first machine learning in interventional oncology session, and the BOLD-AIR summit initiated by Stanford and NYU (24 April, New York, USA) will tackle regulatory and ethical issues pertaining to data use for AI research.
In an editorial for this newspaper last year, Chapiro and Aaron Abajian, also at the Yale School of Medicine, New Haven, USA, detailed the results of an early experiment in applying AI and machine learning as a decision support system in interventional oncology to illustrate its potential to overcome rigid staging and scoring systems in the locoregional treatment of liver cancer.
When presenting his argument in favour of the imminent adoption of machine learning in a session dedicated to the topic at Spectrum (1–4 November, Miami, USA), Chapiro told conference attendees: “The age of AI is already here, and with it, IR has the chance to become the epitome of personalised medicine, and to be everything we want it to be as the fourth pillar of cancer care.”
Structuring large datasets for use in AI
AI makes use of large datasets, and the Society of Interventional Oncology (SIO) is currently working on a “high-quality, well annotated, multi-institutional” database for liver interventions, the first data repository to serve such research. According to Chapiro, such data is “difficult to obtain, especially for industry partners that are developing most such tools and instruments.” Chapiro adds that “It will be up to academic institutions and professional societies to collect such data and make it available for academic and industry-sponsored research.” He told Interventional News that other high-quality databases are likely to follow on from that being built by the SIO. Having high-quality, annotated data is an imperative for incorporating machine learning methods into any sort of research, Raul Uppot, of Massachusetts General Hospital in Boston, USA, explained to this newspaper. According to Uppot, this is the biggest challenge facing those advocating the implementation of AI into clinical practice. He comments: “AI requires a large dataset. If you are going to use AI and apply it to tumour board recommendations, or intraprocedural imaging guidance, or physician workflow, you need large quantities of data to feed into the machine in order for the software to analyse the information provided, to identify a pattern, and to then apply it to practice.
“Right now,” he continues, “we are collecting and structuring the data to feed into the deep learning software. The data we have now is mostly in an unstructured format, which is not useable for deep learning algorithms.”
Researchers at Massachusetts General Hospital, Uppot’s institution in Boston, USA, are exploring the potential use of natural language processing tools to help with this essential data structuring. Explaining this technology, Uppot says: “There are software tools that can read a report and identify key words to be pulled out that can then be used to create a structured report.” Ultimately, Uppot believes this structuring of data should be automated. Hypothesising to Interventional News, he comments: “I think the best application of deep learning is to use it to reach the point where the structured data you are collecting is constantly being fed into the machine, and the software is constantly evaluating the variables that are being put in to generate outcomes. This enables constant learning. Ultimately, that means that as the machine gets smarter, it could learn from and identify patterns retrospectively across, say, 30 years’ worth of data, and recognise trends impossible for humans to uncover.”
However, Uppot also stresses that he believes “a human dynamic” will always be essential. Using the example of tumour board recommendations, he describes how, if data of a specific patient is fed into a machine learning algorithm, and the software recommends an ablation, for example, there may be other factors that come into play that rely on human intervention. In this hypothetical case, he says “there may be a situation where the person cannot lay flat on the table, and therefore an ablation is not the best option. I think machine learning will be a supplementary add-on, which I think will be very useful, but will not replace radiologists.”
In fact, one positive use of AI Uppot foresees is the addition of an “objective voice” in the room when tumour boards convene to discuss the optimal treatment strategy for a particular patient. He sees the potential for a machine learning-generated recommendation to reduce “turf tensions” between IRs, radiation oncologists, and surgeons.
Using machine learning for HCC recommendations
Uppot went into greater detail on this use of machine learning at Spectrum. There, Uppot said that hepatocellular carcinoma (HCC) tumour board recommendations could benefit from the complex data processing AI enables. He commented: “Tumour board decisions carry great responsibility, and it is very important to be objective in these decisions. Machine learning is one way in which we can make all these decisions objectively amongst a group of physicians. Multidisciplinary team decisions could then be made by machine learning.” The idea for this use is not new, but the concept of tumour board recommendations being predicated on algorithms rather than expert opinion and discussion remains in the realm of prospective testing at single institutions.
Back in 2017, Uppot and colleagues fed a machine learning algorithm data from 76 HCC patients, ran a random forest algorithm, and then did prospective testing on the results to determine if the output of this AI system—ideal procedural choice—could rival radiologists’ assessment of the best treatment modality. The input data included a range of different patient, lesion and study characteristics, and after running the programme multiple times to create a decision tree analysis, the study investigators reported that the size of the tumour, its location, and the age of the patient were the most important determinants of the final procedural recommendation. Armed with this knowledge, the investigators then gave the machine learning algorithm new cases, to assess its ability to recommend the optimal treatment option. The recommendations that came out of the algorithm’s machinations largely tallied with those of the tumour board: in the first case Uppot described, for example, the predictive model made by the machine learning system recommended a bridge TACE 44% of the time for that particular patient, which matched the recommendation of the multidisciplinary tumour board. However, Uppot did also warn of limitations to the machine learning-based approach. In one case, the tumour board and the algorithm disagreed, with the radiologists favouring the use of stereotactic body radiation therapy (SBRT). The algorithm did not suggest any treatment involving radiation, but in this particular instance, the radiation programme was very strong in that institution, a factor not taken into account by the AI model.
Currently, Uppot and colleagues are collecting and structuring their data to replicate this test with a greater number of HCC training datasets. However, he iterates to Interventional News the importance of expanding the data set: “If we want this to be clinically useful and clinically viable, it needs thousands of cases, and not just from Massachusetts General Hospital, but from all of the major hospitals in the USA and around the world. In order for the machine learning software to be smart enough to make recommendations, it needs to be able to compute data independent of one institution.”
In addition to potentially providing objective tumour board recommendations, Chapiro posits a wide range of future clinical uses of AI. These include new imaging and combined clinical or radiological biomarkers for decision support and improved therapy choice, intraprocedural navigation support and improvements of intraprocedural cone beam CT image quality, applications for advanced image guidance in robotic-assisted ablations, and assessment tools for tumour response on imaging. He postulates that using supervised machine learning to predict treatment response to intra-arterial therapies for HCC will be “a first possible application” of this technology, saying, “I expect that some of it will penetrate preprocedural and intraprocedural imaging as soon as within two to three years.”
Telling of his own institution’s involvement in this field, Chapiro comments, “The Yale Interventional Oncology research group is part of a multi-disciplinary network at Yale in close collaboration with [the] Biomedical Engineering, the Yale Smilow Cancer Center and the Liver Center. We tackle the full breadth of clinical problems and apply AI-based algorithms, mostly machine learning and deep learning methodologies to find solutions for automated lesion detection, characterisation, diagnosis and outcome prediction after locoregional therapies such as TACE [transarterial chemoembolisation]. A lot of credit goes to our biomedical engineers who are truly leading the effort here and collaborate with us closely on this vision.” Most of this work is National Institute of Health-funded.
Marketing AI
“Ultimately, we must strongly advocate for AI from a patient’s perspective”, Chapiro explains to this newspaper. “In most of medicine, AI is being marketed and frankly overhyped for its capability to improve workflows and productivity. This is a one-sided narrative and tarnishes good intentions. Data ‘scandals’ and misunderstood knee-jerk reflexes from patient advocacy groups will be the logical consequence and it is our fault. We must explain to the patients that AI will first and foremost improve patient care, make it more affordable and certainly also improve therapy outcomes, help us avoid ill-informed clinical decisions and streamline medicine towards more personalised healthcare.”
When pitching ideas to translate AI research into clinical practice to General Electric, prior to their recent selling off of their healthcare division, Uppot noted that the company’s interest had been piqued largely by the prospect of outsourcing the “brain of an academic centre” to a community hospital which may have fewer resources or fewer specialised IRs.
At Spectrum, it was mentioned that a large proportion of machine learning companies working in the interventional oncology space were based in China or Israel. Chapiro notes that the geography and local culture “matter a lot” in terms of the development and use of AI in healthcare. He says: “The USA is behind in this respect and we may lose the global contest for the most effective and rapid implementation of those cutting-edge technologies for the benefit of patient care. China benefits from a strong centrally regulated agenda and a more ‘flexible’ approach to protected health information and access to it. In my opinion, this should not be a role model for the western world.
“Israel, however, punches above and beyond its demographic weight and has truly become the world power of AI. This is mostly due to a long-standing educational policy which facilitates the creation of the necessary manpower and the strong reliance on high-tech as part of the regional geopolitical needs. This results in a highly developed academic and military-industrial complex geared towards rapid development and implementation of cutting-edge technology, which in turn trickles down into the healthcare sector. Those circumstances meet a socialised healthcare system and flexible, but still ethically defensible, data policies. In order to compete and win, we [the USA] need to cut regulations and bureaucracy, and possibly even fund a centralised national data registry that would facilitate collection of high-quality data for AI research. The current administration already gave the right impulse by supporting AI research but words must be followed by investments. With the Israeli model by our side, America can still become the global leader in AI.”
The New Zealand-based Adept Medical has launched an overhead arm support designed to support the patient’s arms intraoperatively. The overhead arm support eliminates shoulder flexion, allows abdominal access, and removes artefacts when imaging with C-arm or CT machines, according to a press release.
The winged design of the device can support one or both arms, and according to Adept Medical will accommodate a wide range of patient sizes. In a press release, the company state that the overhead arm support facilitates improved patient comfort, procedural outcome, and repeatability.
“A more comfortable and secure supporting device would mean the clinicians could set the patient up once and leave them there for the duration of the procedure. We also discovered that this position is common for diagnostic and interventional procedures using conventional CT scanners. Clinicians described to us various methods of trying to support the arms in this way, using pillows [or] towels, but none that provided a quick, easy and comfortable solution” says Mike Oxborough, Adept Medical senior product designer.
Designed for use with existing laboratory and imaging equipment, the overhead arm support wings have been engineered to fit inside the bore of standard CT machines and can be used with any C-Arm imaging centre.
Soft, pliable, latex-free polyurethane straps may be used for additional patient security and comfort. The straps are easily installed and adjusted to loosely contain the patient’s arm, according to Adept Medical. Two strap mount locations for each arm ensures that the patient’s arms are fully supported, reducing the risk of arm displacement and aiding patient assurance and comfort.
The overhead arm support is crafted from high-performance engineering plastics for enhanced rigidity, durability and resistance to chemical attack. It weighs 1.5kg, and will be available commercially from 1 April 2019.
A meta-analysis published in the Journal of the American Heart Association (JAHA) late last year by Konstantinos Katsanos (Patras, Greece) and colleagues, suggesting an increased risk of death at two and five years following the use of paclitaxel-coated balloons and stents in the femoropopliteal artery, has generated months of debate amongst the international interventionalist community. The conversation is still ongoing, with every key vascular conference of 2019 to date hosting discussion on the future of paclitaxel-coated and paclitaxel-eluting devices. Since then, prominent physicians have pointed out flaws in Katsanos et al’s methodology. Patient-level data published after the JAHA meta-analysis by industry have revealed no increased mortality associated with the use of paclitaxel-releasing devices. Medtronic and Cook Medical have also announced corrections to their published data. Meanwhile, the continued investigation by the US Food and Drug Administration (FDA) indicates that the story is not yet over.
Speaking from the floor of the Vascular Leaders Forum [see our live coverage here] (VLF; 1–2 March, Washington, DC, USA), hosted by Vascular Interventional Advances (VIVA), FDA investigator Donna Buckley, who has “reviewed most of these devices and recommended them to be approved”, explained the regulatory body’s perspective: “Our first response to the meta-analysis was, I think, similar to everybody else’s: we were a little bit surprised. Nonetheless, it was compelling information that we took very seriously.”
The ongoing FDA evaluation is focusing primarily on US-based randomised controlled trials with data the regulatory body can validate. The FDA’s preliminary evaluation confirmed the mortality signal reported by Katsanos et al. Speaking at VLF, Buckley said the FDA’s own analysis of five US pre-market approval (PMA) trials has “converged to where we feel like it [the meta-analysis findings] is not a statistical glitch—but we still have all this incongruous information as well with all the statistical analysis that we have gone through.”
Also at VLF, Peter Schneider (Honolulu, USA) called the process that the FDA is undertaking to review the data “judicious, straightforward and spot on”.
Indeed, the FDA issued a letter to healthcare providers in January stating that it was evaluating the “recent information regarding the potential for increased long-term mortality” following paclitaxel-coated balloon or paclitaxel-eluting stent treatments in the femoropopliteal artery for patients with peripheral arterial disease (PAD). The agency said that whilst the data review was ongoing, the FDA recommends “continued surveillance” for patients treated with paclitaxel. The regulatory body stated in the letter that it believes the “benefits continue to outweigh the risks” for approved devices within their indications.
At the CRT summit (2–5 March, Washington, DC, USA), which directly followed the release of the FDA’s preliminary evaluation at VLF, polling of panellists in the drug-coated balloon (DCB) safety townhall indicated that the majority of voters believed there to be a “mortality signal” in the femoropopliteal arteris (detailed polling results below).
Katsanos et al’s JAHA meta-analysis
In the original JAHA paper, published 6 December 2018, Katsanos et al conducted a systematic review and meta-analysis of 28 randomised controlled trials investigating paclitaxel-coated balloon angioplasty or paclitaxel-coated metal stents in the femoral and/or popliteal arteries. In all, 4,663 patients (89% intermittent claudication) were analysed. The primary safety measure was all-cause patient death, analysed at different time points.
Previous randomised controlled trials have evidenced that paclitaxel-releasing balloons and stents significantly reduce the rates of vessel restenosis and target lesion revascularisation after lower extremity interventions.
At one year, all-cause patient death (28 randomised controlled trials with 4,432 patients) was similar between 17 paclitaxel-coated devices and control arms (2.3% vs. 2.3% crude risk of death). All-cause death at two years (12 randomised controlled trials with 2,316 patients) was significantly increased in case of paclitaxel vs. control (7.2% [101 deaths in 1,397 patients] vs. 3.8% [35 deaths in 919 patients] crude risk of death, number-needed-to-harm [NNH]: 29 patients [95% CI: 19–59]). Long-term risk of all-cause death up to five years (three randomised controlled trials with 863 patients) increased further in case of paclitaxel (14.7% [78 deaths out in 529 patients] vs. 8.1% [27 deaths in 334 patients] crude risk of death NNH: 14 patients [95% CI: 9–32]).
Katsanos and colleagues wrote that meta-regression showed a significant relationship between exposure to paclitaxel (dose-time product) and absolute risk of death (0.4±0.1% excess risk of death per paclitaxel mg-year; p<0.001). “Trial sequential analysis excluded false-positive findings with 99% certainty (2-sided alpha, 1.0%),” they said.
These data led the authors to conclude that there is increased risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery. “Further investigations are urgently warranted,” they wrote.
This finding prompted the cessation of patient enrolment of three randomised controlled trials within days of its release: SWEDEPAD 1, SWEDEPAD 2, and BASIL 3. At the date of publication of this newspaper, the status of the SWEDEPAD trials is still uncertain, with principal investigator Mårten Falkenberg (Gothenburg, Sweden) saying at the recent VLF: “We are at the moment struggling to make up our mind on how to proceed.”
Industry respond that their data do not support the potential association of increased mortality with paclitaxel use
Several large industry players presented their own patient-level analysis at the Leipzig Interventional Course (LINC; 22–25 January, Leipzig, Germany), unanimously concluding that they could find no association between paclitaxel dose and mortality.
An independent, third party, pooled analysis of all the IN.PACT Admiral DCB (Medtronic) clinical programmes, published in the Journal of the American College of Cardiology and including 1,980 patients, demonstrated that at five years, there is no statistically significant difference in all-cause mortality between the DCB and the control arm (9.3% vs. 11.2% respectively, p=0.399).
Ranger (Boston Scientific) SFA randomised trial three-year data from 105 patients showed no significant difference in all-cause mortality between DCB and control (13.8% vs. 10.7%, respectively), according to the presentation given at LINC with CEC-adjudicated cause of death.
Results from a Cook Medical press release also demonstrated the safety of their drug-eluting stent, the Zilver PTX. Patient-level data found no increased mortality at five years with Zilver PTX compared to non-coated stents and balloons (18.7% vs. 17.6% respectively, p=0.53).
A pooled analysis of patient-level data from Philips also demonstrates the “strong safety profile” of the company’s Stellarex DCB in above-the-knee studies, according to a company statement at LINC. The independent, third party pooled analysis evidenced low mortality rates through three years after the treatment with no device-related deaths.
Five-year data from 1,189 patients in the LEVANT 2 trial within the Lutonix DCB (BD) programme showed no statistically significant difference in all-cause mortality between the DCB and the control group (14.2% vs. 10.6% respectively, p=0.22), as described at LINC.
However, Medtronic and Cook Medical have since issued corrections to their published data regarding the safety of their devices, the IN.PACT Admiral DCB and the Zilver PTX drug-eluting stent, respectively. Medtronic announced they have revised IN.PACT post-market study data due to a “programming error,” and Cook Medical noted a mistake made during data publication: that two mortality figures were “inadvertently reversed”.
According to Medtronic, mortality data were inadvertently omitted from the summary tables included in the statistical analysis of their data presented at LINC. These deaths were, however, previously included and reported in Medtronic’s database, captured in the appropriate study exit forms and adjudicated by an independent clinical events committee, a press release issued by the company said. Immediately upon learning of this error, Medtronic notified the FDA and the study authors. The company added in the release that while a component of the recent patient-level meta-analysis will need to be updated, it has found the revised analysis still supports earlier conclusions.
Cook Medical announced that in a paper published in Circulation in 2016 assessing the clinical effectiveness of their Zilver PTX stent, the mortality figures for the Zilver PTX arm and the percutaneous transluminal angioplasty (PTA) arm were inadvertently swapped. Responding to this error, Circulation state: “When high-resolution files were requested during production, an incorrect version of Figure 1 was mistakenly provided. Subsequently, the published version of the flow chart in Figure 1 contained incorrect numbers. The authors now provide the corrected version of Figure 1.
“The following sentence from the ‘Safety’ section of the paper is incorrect: ‘The five-year all-cause mortality rate was 13.6% (10.2% for the primary DES group and 16.9% for the PTA group, p=0.03), and no deaths were adjudicated as procedure or device related.’ […] The sentence should read: ‘The five-year all-cause mortality rate was 13.6% (16.9% for the primary DES group and 10.2% for the PTA group, p=0.03), and no deaths were adjudicated as procedure or device related.’”
Polling results and informed consent
Polling of 14 panellists at CRT revealed that the majority of voters (10) believed there is “a mortality signal” in the meta-analysis. While none voted against, four responded that they “did not know” if there was a signal or not. In an additional poll, the panel voted eight to six not to change or restrict device labelling. Three voted to restrict and three voted to change labelling. The CRT panel voted unanimously to discuss the Katsanos et al meta-analysis findings with patients during conversations of informed consent. The final poll at CRT showed that the majority of the panel believed the industry patient-level data are poolable for definitive analysis. Nine voted for, one against, and four said they did not know.
Polling from the 31st International Symposium on Endovascular Therapy (ISET; 27–30 January, Hollywood, USA) and from the more recent VLF indicate that the majority of physicians will not change their use of paclitaxel devices following the Katsanos et al meta-analysis. At VLF, 60% (21/35) of the polled audience said they would not be more conservative in recommending drug or device combinations for claudication following the discussion around the JAHA meta-analysis, and 86.5% (32 out of 37 responders) of those polled said they would not change their clinical practice as a result of the meta-analysis findings.
In addition, following a morning-long session at ISET, 79% of the audience responded to an anonymous poll to say that they do not believe the Katsanos et al findings are sufficient to change practice. Sixty-nine per cent of respondents said they would continue to use paclitaxel devices as they always have, with the remaining 31% saying they would use paclitaxel devices less.
However, several physicians voiced concerns, at ISET and since, regarding litigation due to the FDA’s continued investigation into the use of paclitaxel in the femoropopliteal artery. Speaking in general on informed consent regarding the use of paclitaxel-releasing devices at VLF, Paul Rudolf (Washington, DC, USA) said he did not want to trivialise the findings by Katsanos and colleagues, and commented: “Even if the data in the meta-analysis are true, at five years only one out of 14 patients would be affected by the mortality signal, which means that 13 out of 14 patients you would be treating with a drug-eluting stent or balloon would still do just fine and not be affected by that.”
Rudolf also said that 40–45% of malpractice lawsuits hinge on an inadequate discussion of the complications of the procedure prior to treatment. He emphasised that in the case of treatment with paclitaxel, informed consent is the most important factor to consider when thinking about the legal implications. As doctors treating patients with paclitaxel devices in the lower leg already have “complicated informed consents” due to the risk of amputation and recurring disease, Rudolf explained that, from his perspective, “I am not sure how different the informed consent will be. In my view, this is just something that is added on to what is already there.” Rudolf clarified that his comments were made in a general discussion of informed consent during the summit, and were not official legal advice given to practising physicians.
Rudolf suggested physicians stay up to date on device manufacturer information, FDA recommendations, and practice guidelines.
The commissioner of the US Food and Drug Administration (FDA), Scott Gottlieb, has unexpectedly resigned after serving just shy of two years in the post.
Gottlieb announced his intention to stand down in a letter to Alex Azar II, the secretary of the Department of Health and Human Services, the FDA’s parent agency, on 5 March. Gottlieb says the decision is due to the fact that he wants to spend more time with his family.
Speaking in an interview with The Washington Post, Gottlieb says “It was a very hard decision”, calling this posting “the best job I will ever have. He continues: “I am leaving because I need to spend time with my family. I get home late Friday, work on weekends and come back to Washington on Sunday. I did the job 100%.”
Gottlieb took up the position in May 2017, and has presided over a number of important initiatives, including the development of the new 510(k) pathway for device clearances.
No successor has been named. A new commissioner must be approved by the US Senate.
“All of us at the Department of Health and Human Services [HHS] are proud of the remarkable work Commissioner Gottlieb has done at the FDA,” Health and Human Services Secretary Alex Azar comments in a statement. “He has been an exemplary public health leader, aggressive advocate for American patients, and passionate promoter of innovation. I will personally miss working with Scott on the important goals we share, and I know that is true for so many other members of the HHS family.
“Scott’s leadership inspired historic results from the FDA team, which delivered record approvals of both innovative treatments and affordable generic drugs, while advancing important policies to confront opioid addiction, tobacco and youth e-cigarette use, chronic disease, and more. The public health of our country is better off for the work Scott and the entire FDA team have done over the last two years.”
The first geniculate artery embolization (GAE) to take place in the UK to treat osteoarthritis pain in the knee has been performed by Mark Little at the Royal Berkshire Hospital in Reading, UK. Little is the lead investigator in the GENESIS study, investigating the use of GAE in UK patients.
A previous Japanese study found a 75% reduction in pain over a four-year period. Yuji Okuno (Tokyo, Japan) and colleagues found that, in a small cohort of patients, GAE for mild to moderate knee osteoarthritis was feasible, rapidly relieved resistant pain, and restored knee function.
Currently in Europe, osteoarthritic patients are given painkillers, and knee-replacement surgery is conducted in severe cases. GAE is therefore posited as a potential minimally invasive alternative for patients with mild-to-moderate osteoarthritis pain for whom painkillers have not worked.
Little, who is leading the study, comments: “If the results of this study and future studies confirm the Japanese data, then geniculate artery embolization is a potential game changer for the treatment of osteoarthritis. Performed under only local anaesthetic, the procedure takes about one hour and patients go home the same day. It is truly minimally invasive. If you can get patients off high-dose painkillers who are struggling with mobility and unable to work, it has a massive impact on their health and quality of life.”
Speaking to Interventional News, Little elaborates about the ideal GAE patient: “Osteoarthritis of the knee is a hugely common problem. Whilst knee replacement is a good treatment, it is not a perfect treatment, and talking to orthopaedic surgeons, they do not want to operate on the patients who are 40 to 55 because they are young. Some of these patients have conservative treatment (physiotherapy, joint injections), and some will benefit from that for a period of time, but some will not. There is this real middle band of patients that have got significant symptoms from their knee osteoarthritis that are severe enough to affect their quality of life, but which are not severe enough to merit having knee replacement surgery. I think that is where GAE has a massive role to play, if it is proven long-term. As a scientist and as an interventional radiologist, I think we have to get together as a community and study this treatment, as we have done with prostatic artery embolization (PAE), and as we have done with uterine fibroid embolization (UFE). We need good quality data so we can say with decisiveness that this is a good option for our patients.”
Against the backdrop of the current opioid epidemic, in both Europe and North America, Little further emphasises the positive role GAE may play in these patients’ lives by calling the procedure a “big opportunity” to lessen the dependence on painkillers. Whilst deliberate in not over-stating the present role of GAE in this regard, Little does say that “GAE has the potential to be game-changing”. More data are needed to confirm this hope.
Through his work on GAE, Little has been working with orthopaedic surgeons. Of this experience, he says: “The multidisciplinary collaboration is very good. As these patients have failed conservative treatment, but are not suitable candidates for joint replacement, the orthopaedic surgeons are delighted to refer these patients. To be able to offer a potential new treatment for these patients is really very beneficial. There is a huge demand for a treatment in this space—that is why we are having no trouble at all with referrals for the GENESIS study.”
The GENESIS study has nearly completed enrolment, with 38 of 50 anticipated patients currently on board. Little reports a high patient referral rate for this study, and tells Interventional News that he anticipates enrolment to be complete within a few weeks of this newspaper going to press. Preliminary data will be presented at the annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 1–10 September, Barcelona, Spain), and Little says that though this will be based on “incomplete data”, and therefore will not provide “the full story”, he believes that “we will still be able to draw some early meaningful conclusions, as we have a number of patients already with up to six months’ follow-up”.
The GENESIS study, which will follow all patients up to two years, is being conducted in collaboration with the University of Reading, UK. It has funding from Merit Medical and support from the National Institute for Health Research (NIHR). An additional multicentre, randomised controlled trial investigating GAE against a sham procedure has been submitted by Little and collaborators for approvals in the UK through the Health Technologies Assessment (HTA) process, and an “ambitious international project” focusing on the procedure is underway.
Enthusing about the potential of this work, Little comments: “Interventional radiologists are great innovators, and we need to combine that creativity with performing very good, high calibre research. By doing that, musculoskeletal embolization and image-guided intervention may have a huge role to play in the future. There are certainly lots of patients out there, so we just need to prove that it works.”
The first GAE case in the UK: The patient response
The 65-year-old patient, Linda Skilton, underwent the procedure on 29 January, and reported positive results. Quoted in a press release from the Royal Berkshire NHS Foundation Trust, she says that before the procedure “I was having problems with my left knee; a lot of swelling, a lot of fluid, limited mobility.
“I was given cortisone injections, which made it settle for a while, but it flared up again a year later when I was using some equipment in the gym. For the past couple of years, I have not been able stand for too long because it got so sore and swollen and I could not keep it bent or straight for any length of time either, which made sleeping difficult.
She continues to describe the procedure: “I only felt the initial cut to get to the artery, which was no worse than a paper cut. I was expecting some feeling of pushing and pulling, but I did not feel anything at all.
“Since the procedure, I can feel day-to-day that my knee is improving. I can easily walk up the stairs for the first time in years. I am delighted with the outcome.”
Commenting specifically on this patient’s response to the procedure, Little says “Linda is clearly very active and if we can keep her playing golf, then that will have a profound impact on her social interactions with friends, improve her happiness, and well-being, and give her back her independence.”
However, while he hopes that every patient has a reaction as positive as this, Little stresses that “n=1 does not mean that this is going to be the panacea. I will reserve getting carried away until we have data up to two years. Hopefully, we get consistently good results, but we need to take an analytical approach and compare all of our results before we can be categorical in our conclusions.”
You can read an article on this topic authored by Sandeep Bagla (The Vascular Institute of Virginia, Woodbridge, USA), the first to perform this procedure in the USA, here.
The procedure
The patient is treated as a day case procedure. They have a pre-procedural contrast-enhanced MRI scan, where Little says the radiologist is “looking for synovitis and capsular enhancement”.
During the procedure, in the majority of patients the interventional radiologist performs an antegrade puncture in the common femoral artery. The interventionalist then navigates the catheter under X-ray guidance down the affected leg into the geniculate arteries.
Little says “We are looking for an abnormal contrast blush in the region of the degenerative change that correlates with the pre-procedural MRI scans”. Next, the IR uses angiography to select the vessels that correspond to those areas with abnormal vascularity. “Once we are in there,” Little says, “we will confirm through an on-table cone beam CT, and then once we are happy with everything, we will embolize the geniculate arteries. We use diluted Embosphere (Merit Medical) particles to embolize the abnormal regions”.
The Peregrine System infusion catheter (Ablative Solutions) has demonstrated 100% procedural success in the Peregrine post-market clinical trial, new data presented during a late-breaking session at the 2019 Cardiovascular Research Technologies (CRT) meeting (2–5 March, Washington, DC, USA) attests.
The Peregrine post-market study is a European multicentre, open-label trial that evaluated the safety and performance of the CE marked Peregrine System infusion catheter using alcohol as a neurolytic agent in 45 patients with systemic hypertension.
The efficacy endpoint of the study was met, with a reduction in mean systolic 24-hour ambulatory blood pressure of 11mmHg (±14 mm Hg, p<0.001) at six-month follow-up. Additionally, the average reduction in systolic office blood pressure was 18 mmHg (±21 mmHg, p<0.001). Antihypertensive medications were unchanged in 73% and reduced in 23% of patients at six months. The study demonstrated 100% procedural success, and the safety endpoint was met in 96% of patients. Two patients had major adverse events of periprocedural access site pseudoaneurysms, with major bleeding in one patient. There were no deaths or instances of myocardial infarction, stroke, or transient ischaemic attack.
“The Peregrine post-market study showed efficient nerve ablation with the CE marked Peregrine catheter, resulting in significantly sustained reduction in both systolic and diastolic blood pressure at six months, with the vast majority of patients not requiring an increase in the number of anti-hypertensive medications during this time,” says Felix Mahfoud, of Saarland University Hospital, Homburg, Germany.
The Peregrine system infusion catheter has received a Certificate of Conformity and has been CE marked for the infusion of a neurolytic agent (for example, alcohol) to achieve a reduction in systemic blood pressure in hypertensive patients. Designed to be performed in a short and straightforward procedure with minimal sedation required, the Peregrine catheter is engineered to target nerves known to influence the body’s regulation of blood pressure. The delivery of a neurolytic agent—dehydrated alcohol in this study—directly to the space outside of the renal artery is intended to block the overactive signalling of the sympathetic nerves, a press release explains.
The investigational Peregrine kit, which includes the Peregrine system infusion catheter (Peregrine catheter) and Ablative Solutions dehydrated alcohol, will be investigated in the TARGET BP clinical programme, which comprises two clinical trials. The global TARGET BP I trial in centres in the USA and EU is a blinded, randomised, sham-controlled study which will evaluate the safety and efficacy of the Peregrine kit in the treatment of patients with uncontrolled hypertension and who are taking two to five anti-hypertensive medications. Patient enrolment in the Target BP I trial is anticipated to begin soon. The recently initiated TARGET BP OFF-MED trial in Europe is a proof-of-concept, blinded, randomised, sham-controlled study evaluating the safety and effectiveness of the Peregrine kit for the treatment of patients with uncontrolled hypertension who are not taking anti-hypertensive medications.
“Based on early clinical results using the CE-marked Peregrine catheter, we are excited to be embarking upon the pivotal TARGET BP I Clinical trial of the investigational Peregrine kit to evaluate safety and efficacy when used in the treatment of patients with uncontrolled hypertension in conjunction with antihypertensive medications,” says David Kandzari, coprincipal investigator of the TARGET BP I trial, and director of Interventional Cardiology and chief scientific officer at Piedmont Heart Institute in Atlanta, USA.
Ablative Solutions recently announced a US$77 million financing to complete clinical trials in support of US and European regulatory submissions for the company’s minimally invasive renal denervation technology.
The Society for Vascular Surgery (SVS), the premier scientific organisation devoted to the treatment of vascular disease, is concerned about a recent article in the Journal of the American Heart Association (JAHA) by Konstantinos Katsanos et al suggesting higher rates of two- and five-year mortality in patients with peripheral arterial disease (PAD) treated with paclitaxel delivering devices.
Clarification of data is a matter of critical importance to patients afflicted with vascular disease, the physicians who treat them and our industry partners who develop and market these devices, the SVS states in a press release.
As such, the SVS has established a Task Force on Paclitaxel Safety to evaluate all available data related to paclitaxel use in patients with PAD.
Led by SVS President-Elect Dr Kim Hodgson, the task force is soliciting the participation of all industry partners who have conducted randomised controlled trials of paclitaxel devices in patients with PAD in a “mega” analysis of combined patient-level data.
“Only with this enhanced statistical analysis can a valid answer be found for surgeons and patients,” says Hodgson. “This report has created uncertainty about the safety of what has been considered ground-breaking technology. We need to analyse all the data collectively to get valid answers, as single trial analyses are inadequate.”
“Drug-eluting stents (DES) are important additions to the armamentarium of devices used for peripheral artery revascularization, associated with decreased rates of restenosis and target vessel revascularization”, Eric Secemsky (Boston, USA) and colleagues write in the Journal of the American College of Cardiology today.
They penned an editorial in response to the recent meta-analysis, published in The Journal of the American Heart Association (JAHA) and authored by Konstantinos Katsanos (Patras, Greece) and colleagues, which reported an association between peripheral paclitaxel-coated devices and increased long-term mortality. Secemsky et al write: “These findings have not been replicated in other data sources with extended follow-up.”
In their own analysis of patients admitted to US Centers for Medicare and Medicaid Services (CMS) with a principal diagnosis of peripheral arterial disease (PAD), Secemsky and colleagues did not find a statistically significant difference in mortality rates between those treated with a bare metal stent (BMS) and those with the Zilver PTX paclitaxel-coated balloon (Cook Medical). In fact, they conclude that they could find no evidence of increased long-term mortality following peripheral artery revascularisation with DES compared with BMS among CMS beneficiaries, which they suggest indicates “the safety of these devices in routine practice”.
The study investigators collected data from 1 December 2012 through to 30 September 2015. ICD-9-PCS codes were used to identify peripheral drug-eluting stent (DES) and BMS placement. For patients with repeated procedures, only the first procedure was included.
Plotting the temporal trends of BMS and DES overly quarterly time periods, Secemsky and colleagues found that the cumulative incidence of death had similar mortality through 4.1 years (51.7% for DES vs. 50.1% for BMS; log-rank=0.16), and that “this relationship persisted after stratification by critical limb ischaemia (CLI).”
Furthermore, there was no association between stent type and mortality after multivariable adjustment (hazard ratio [HR] for DES vs. BMS: 0.98; 95%CI 0.93–1.03; p=0.53). In addition, there was no adjusted relationship between stent type and death among patients with CLI (HR: 0.97; 95%CI 0.92-1.03; p=0.32) or ALI (HR: 0.99; 95%CI 0.81-1.21; p=0.95).
The authors write: “We observed a gradual uptake of DES use and found no difference in mortality between DES and BMS through the end of follow-up. This finding remained after multivariable adjustment, and among patients with CLI or acute limb ischaemia (ALI). Peripheral artery revascularisation has been challenged by high rates of restenosis and need for re-intervention. The first DES indicated for femoropopliteal artery revascularisation, the paclitaxel-eluting Zilver PTX, was approved in November 2012 after demonstrating improved patency at 12 months compared with balloon angioplasty and BMS. Follow-up data through five years have shown persistent efficacy over these other devices, supporting their routine use.”
However, the authors do acknowledge that the long-term safety of these devices has not been well-established, writing that this is “mainly due to their limited duration on the market”. Regarding the Katsanos et al meta-analysis, which they cite as the motivator for their current analysis, they caution: “Due to the significant implications of these findings and the increasing use of peripheral DES, investigation of this relationship [between mortality and paclitaxel dose] in other data sources is needed urgently.”
Listing the limitations of their study, Secemsky and co-authors write: “This analysis is limited by an inability to localise the lesion of interest, possible misclassification due to use of claims codes, lack of data on outpatient procedures and DCBs (no ICD-9-PCS code), the potential influence of unmeasured confounding, and the inability to determine specific causes of death. In addition, this CMS population was older and had more comorbidities, including CLI, compared with the Katsanos et al meta-analysis.”
The Vascular Leaders Forum is currently taking place in Washington DC, USA (1–2 March 2019), where participants are discussing the use of paclitaxel-coated and –eluting devices following the Katsanos et al publication. Follow updates from our live blog here.
The Charing Cross International Symposium (CX) continues its three-year cycle of raising vascular and endovascular controversies in order to challenge the available evidence and be able to reach a consensus after discussion with an expert audience.
CX will, as always, deliver a world-class programme, and this year with even more exciting, innovative features such as virtual reality live cases. There will also be special sessions dedicated to give the last word on the paclitaxel controversy, as well as exploring the possible impacts of the draft UK NICE guidelines for aortic aneurysms.
Experience live cases like never before
Due to its immersive nature, virtual reality has strong potential for advancing procedural medical training—it allows viewers to experience the entirety of a medical procedure and the associated environment. Awareness of the environment—which can include, for example, fluoroscopy findings, assistants’ actions, team behaviour, and haemodynamic assessments—forms an essential aspect of education and learning for interventional and endovascular procedures. Through the immersive environment provided by virtual reality, this important aspect becomes available in a way that is not possible in a standard educational video or simulator. Virtual reality allows repeatedly returning to the content to observe and review different aspects of the procedure.
CX 2019 will host ground-breaking, first-ever virtual reality live aortic and peripheral arterial cases. The audience will partake in the virtual reality experience of these live cases via 360 video streaming and projection.
Special sessions highlight major topics at CX
An open discussion of the paclitaxel controversy will also be a key feature at CX 2019. The recent meta-analysis of Katsanos et al, published in the Journal of the American Heart Association (JAHA), suggested the need for a reappraisal of paclitaxel-coated balloons and paclitaxel-eluting stents. CX 2019 will undertake an in-depth and independent review of the benefits of paclitaxel in reducing restenosis versus the concerns of increased mortality raised by Katsanos et al.
The future of endovascular aortic intervention is under review following the publication of the draft UK NICE guidelines on abdominal aortic aneurysms. Roger Greenhalgh, principal investigator of the UK EVAR trials on which the draft NICE abdominal aortic aneurysm guidelines are largely based, will propose a new follow-up method to avoid secondary sac rupture and death in a novel way that makes the case for EVAR as the cost-effective standard of care.
Finally, a special session is dedicated to discussion on the Stroke from Thoracic Endovascular Procedures (STEP) study, and the latest findings on reducing the risk of stroke following complex thoracic endovascular procedures will be shared by the study investigators.
New iWounds interdisciplinary programme and workshop
CX 2019 will also introduce a new iWounds village, which features hands-on activities covering wound management for wounds caused by vascular (venous and peripheral arterial disease) and nonvascular conditions (diabetes). With the aim to reduce the number of lower limb amputations due to conditions underlying chronic wounds, this new interdisciplinary initiative will feature three days of iWounds activities, with dedicated iWounds sessions in the Venous and Peripheral programmes, and the main iWounds programme running across half a day.
According to a new survey of European interventional radiology (IR) departments published in Insights into Imaging, five steps should be taken to improve provision of IR procedures in Europe.
While the use of IR procedures is growing as an alternative to surgery, the field is not as healthy in Europe as it should be, the report, written by Lorenzo Derchi (Genoa, Italy) and Afshin Gangi (Strasbourg, France), summarises. The survey was a collaboration between the European Society of Radiology (ESR) and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE).
The survey was commissioned in May 2017 in an effort to understand how European radiology departments on their use of IR practices in their facilities. A total of 98 radiology department heads completed the survey, making up a response rate of 8.3%.
The researchers found a number of challenges facing European interventional practices, all of which had a common theme: not enough interventional radiologists are being trained to meet the growing demand.
Based on the results, the authors recommended five steps to improve the provision of interventional radiology in Europe:
All acute care hospitals should prioritise offering 24-hour IR coverage. In Europe, about 60% of radiology departments can cover interventional emergencies, a percentage that the study authors believe is too low. If a hospital does not have enough interventionalists on staff for 24-hour coverage, hospitals within regions could form networks to share resources.
IR should be promoted to medical students early in their training as a viable career option. Research in the USA has shown that far fewer medical students were exposed to IR compared to diagnostic radiology; this can hamper recruitment to the specialty. Only by attracting more trainees can IR overcome the personnel shortages that are restricting its broader use.
More women must be recruited into IR. While about half of diagnostic radiologists at European hospitals are women, they make up a “small minority“ at facilities dedicated to IR, the researchers found (they note this is also an issue in the USA). They attributed the gender imbalance to concerns about call responsibilities and the lack of role models, which they believe could be counterbalanced by increasing the number of women in interventional faculty and chair positions.
Radiology should recognise the full clinical role of IR. This could be through the allocation of enough day-case beds to accommodate interventional procedures, for example, or through recognition of the administrative responsibilities involved in the full episode of care for patients treated with interventional procedures, such as patient examinations.
Diagnostic radiologists should take a more active role in IR. This could include actions such as recommending referrals to interventional colleagues in radiology reports when appropriate and sharing knowledge with diagnostic radiologists about interventional procedures.
The Vascular Leaders Forum (VLF, 1–2 March, Washington DC, USA), hosted by the non-profit organisation VIVA Physicians, is a special consortium which was called in the wake of the meta-analysis published by Katsanos et al late last year, and the discussion of paclitaxel-eluting devices which ensued. The event was live-streamed on the VIVA Physicians website, and Vascular News provided live updates throughout with highlights from the sessions.
2 March, 17:00 GMT
Gary Ansel (Columbus, USA) states that the discussion and consensus reached over the past two days will be communicated in a paper and published “fairly rapidly”.
Christopher White now begins the conclusion of the VLF summit, asking: where do we go from here? “I am so reassured,” White says, “and very proud of us. Our practices get challenged by a meta-analysis that is not the strongest of meta-analyses and yet, instead of being in denial, we are protecting a self-interest, we recognise the validity of this signal, and we commit to solving this problem.”
To Zeller’s previous point (below), White advises “also to remember that the other side of that coin was that the follow-up to ascertaining mortality was greater in the experimental arm, as opposed to the control group. So not only do the patients not get followed up or get the treatment that they maybe need, but then we find out they died more. We are looking at something that is almost like a perfect storm.”
2 March, 16:55 GMT
Thomas Zeller (Bad Krozingen, Germany) says one insight for him from the VLF meeting was that “I underestimated the compliance issue of our patients when we are enrolling patients in studies which are aiming to prove superiority in technology, whether this is a drug or a device. We knew a long time that patient compliance to undergo a follow-up angiogram is lower in the cohort which is doing well, as compared to those who have got symptoms again. What I did not realise, which has been shown here, is that follow-up compliance for any kind of follow-up visit—even non-invasive—is low in those who are doing well. This is a potential bias I personally underestimated in the past, and may have contributed to the outcome of this meta-analysis. We need to really have a look at that as one of the topics of what can be improved.”
2 March, 16:30 GMT
Donna Buckley of the FDA, who has “reviewed most of these devices and recommended them to be approved”, says “Our first response to the meta-analysis was, I think, similar to everybody else’s: we were a little bit surprised.” Given she herself had reviewed the devices and found no cause for concern in the data, Buckley underlines her personal surprise but states, “nonetheless, it was compelling information that we took very seriously.”
Focusing primarily US-based RCTs with data the FDA can validate, Buckley says they have “converged to where we feel like it [the meta-analysis findings] is not a statistical glitch—but we still have all this incongruous information as well with all the statistical analysis that we have gone through.”
Peter Schneider (Honolulu, USA) calls the process that the FDA is undertaking to review the data “judicious, straight-forward and spot on”.
2 March, 16:07 GMT
An audience polls finds 35 of 36 VLF respondents were “surprised by the JAHA meta-analysis suggesting increased mortality in patients treated with paclitaxel-coated devices.” The next poll, however, finds 14 of 35 respondents would be “more conservative” with their recommendations of drug/device combinations for claudication, based on the discussions at VLF.
When a new endovascular strategy is approved and reimbursed in the USA, 24 of 38 attendees respond that their adoption of that strategy “depends on the strength of the data”. “Data rules in this academic group of clinical experts”, says Michael Jaff.
To the question whether respondents have had “unexpected mortality events” in patients they have treated with paclitaxel-coated peripheral devices, 20 (50%) say they do not know, while 17 respondents say they have not. Only three responded affirmatively.
Has your hospital/outpatient centre talked to you about continued use of paclitaxel-coated peripheral devices since the JAHA meta-analysis was published? In the VLF audience, 30 of 39 say they have not. A “resounding” 30 of 39 respond there should not be local restrictions with these devices—only five opting for the answer, “we need more data”.
In response to three attendees who answered a poll with a call for another RCT to clarify the mortality risk, Michael Jaff says “not in my lifetime will that happen”. A majority of 27 out of 40 answered they would need to see merged patient-level datasets from all manufacturers.
Finally, 32 of 37 say “current trial enrolment in claudicants” should continue, while five say it should stop, and only 5 of 37 plan to change their clinical practice as a result of the meta-analysis.
2 March, 14:50 GMT
Michael Jaff (Massachussets General Hospital, Boston, USA) describes reading the Vascular Newsbreaking story of the Katsanos meta-analysis on his phone, as he is about to walk into a consultation with a patient. In a talk titled “Public hysteria and potential adverse impact on patients: Is there a better way to publish data?”, Jaff discusses the manner in which data should be released, and the “leak that lead to a frenzy even before the paper was published”.
“This meta-analysis was leaked to media outlets well before the paper actually came out”, Jaff says, adding “that leak lead to a frenzy even before the paper was published”. Pointing to the JAHA embargo rules, Jaff says that the rules are subject to some degree of interpretation.
While acknowledging that “all of us [researchers]” have given early interviews or data release to the media, and a paper released in press simultaneous to its presentation or journal publication is a “great feather in the cap of any academic researcher”, Jaff nevertheless states: “as far as I am concerned, unless the authors felt that there was an immediate risk to public health and safety—in which the leak should have been to regulatory authorities—it should not have been leaked to media outlets to be discussed at meetings weeks before the paper came out.”
Highlighting a sentence in the meta-analysis conclusion which reads “Further investigations are urgently warranted”, Jaff argues this wording “was interpreted by many to mean there is a serious threat to public health. And, given we have just spent the last day trying to figure out what the heck is going on […] it is hard to say that ‘urgent’ was was warranted. That alarmist comment, I think, added to the frenzy that we are all dealing with today.”
2 March, 13:50 GMT Paul Rudolf (Washington DC, USA) now discusses “informed consent” regarding the use of paclitaxel-coated and -eluting devices, and expands on the legal implications of the Katsanos et al meta-analysis.
“Yesterday, I was really struck by the patient that was up here. The patient basically said ‘If I trust a doctor, and I have confidence in the doctor, and I believe what the doctor tells me, then I am fine.’ I think that has been the experience of most physicians, and statistically, patients that trust their doctors just don’t sue them. I think it is a case of doctor’s gaining the trust of their patients, which is nothing new to anyone in this room, but was just something that really stuck me yesterday.”
He continues, “The other thing I was struck by is that, as usual, we always find that medicine is an art, not a science. Everything we do is informed by scientific evidence, but at the end of the day we have to make informed decisions with out patients, and those are always individualised decisions.”
Saying he did not want to trivialise the findings by Katsanos et al regarding the mortality signal, Rudolf says: “Even if the data in the meta-analysis is true, at five years only one out of 14 patients would be affected by the mortality signal, which means that 13 out of 14 patients that you would be treating with a drug-eluting balloon or stent would still do just fine and not be affect by that.”
Rudolf also says that 40-45% of malpractice law suits hinge on an inadequate discussion of the complications of the procedure prior to treatment. He emphasises that in the case of paclitaxel, informed consent is the most important factor to consider when thinking about the legal implications of treatment with paclitaxel devices, and also says that as it is mortality that is being discussed, physicians should bear in mind that any possible legal case would be bought by the patient’s estate and family.
As doctors treating patients with PAD in the lower leg indicated for use with paclitaxel devices already have “complicated informed consents” due to the risk of amputation and recurring disease, Rudolf says that, from his perspective, “I am not sure how different the informed consent will be. In my view, this is just something that is added on to what is already there.”
One difference in informed consent between before the Katsanos et al meta-analysis was published and since is that, if medical therapy is a good treatment option for patients, then that should be included to a greater extent in the discussion with patients.
The most important piece of advice Rudolf has for physicians is to stay up to date on device manufacturer information, FDA recommendations (which he says “should be followed, but are not binding”), and practice guidelines.
Informed consent should be patient specific, Rudolf adds. So disucssio of this mortality signal may be more pertinent to a 50 year old patient than to an 88 year old patient, he says, and previous exposure to paclitaxel devices may also heighten the significance of discussing the meta-analysis results.
2 March, 13:42 GMT Marianne Brodmann (Graz, Austria) takes to the stage to discuss how the meta-analysis is being dealt with in Europe.
“You have already heard how we have a more hetergeneous approach in Europe than the USA, because you have heard that the SWEDEPAD and BASIL trials are on hold. What I am talking about is the general approach in Europe, mainly the central European approach,” she begins.
“We have a great tradition in Europe with DCBs and with large RCTs”, Broadmann says.
From early data, Broadmann says that the main concern with DCBs in Europe is of the local effect of paclitaxel (aneurysm risk).
She says that the FDA letter of 17 January 2019 saying that the regulatory body were starting their own investigation caused some concern amongst European peripheral interventionalists.
“We still think it is a safe technology we can use,” Broadmann says of paclitaxel-coated and -eluting devices, following a summary of patient-level data presented at the Leipzig Interventional Course (22-25 January 2019, Leipzig, Germany).
However, despite this cautious optimism, Broadmann says that she saw this morning a headline in a German newspaper, the Frankfurter Allgemeine, reading [translated]: “Within a hair’s breadth of a scandal.” See image below.
From the German newspaper the Frankfurter Allgemeine, the translated headline reads: “Within a hair’s breadth of a scandal.”
However, Broadmann says the content of the article is not as “hard” as the headline, and includes statements from the German Society of Angiology, but that “we never know how patients will respond to such articles.”
2 March, 13:34 GMT
Yoshiaki Yokoi (Osaka, Japan), of the IN.PACT Admiral (Medtronic) SFA Japan trial, explains the ramifications of the JAHA meta-analysis in Japan.
“In Japan, every trial conducted in the USA we have to repeat, to get approval [in Japan]. We have a delayed approval process,” he explains. Based on the IN.PACT Admiral SFA Japan trial, the DCB was approved. However, the US and Japanese approval differed slightly in their indications: whilst in the USA the IN.PACT Admiral paclitaxel-coated balloon could be used in de novo, restenotic, or in-stent restenotic lesions with up to 360m in SFA, in Japan the device could be used in de novo or restenotic lesions, with up to 200mm in SFA. There was no indication in Japan for in-stent restenosis, “a unique regulation”.
Looking at paclitaxel-coated balloon use in his own hospital since the publication of the Katsanos et al meta-analysis in JAHA, Yokoi says, “Fortunately, no obvious paclitaxel-related death was found in our hospital.”
Yokoi says he believe analysis should be separated between DCBs and DESs, and the “paclitaxel dose is 20 times more [for DCB] than in the DES.”
“There us a concern about what the long-term, downstream effect of paclitaxel is”, Yokoi says.
To be “hopefully published soon”, Yokoi tells the VLF audience that he and his colleagues have analysed the cause of deaths in the Japanese cohorts of the IN.PACT Japan trial, the LUTONIX Japan trial, the Zilver PTX trial, and the Eluvia trial up to five years.
Speaking of these results, Yokoi informed delegates that the LEVANT Japan and IN.PACT Japan trials did not show any significant increase of mortality in the DCB arm. Bases on these data, the DCB was accepted by regulatory bodies in Japan, and use started from January 2018. The maximum dose of paclitaxel indicated for use in Japan is 30–40mg. Yokoi says that “A slow flow after DCB use is observed, and there is concern about downstream effects of paclitaxel. We are under investigation of previous Japanese RCTs in regards to mortality and paclitaxel-related complications.”
His personal view is that in most DCB studies, primary patency was systematically used as the primary endpoint, and that this metric may be misleading for the evaluation of real clinical outcome. He concludes by stressing, again, that the downstream effect should be thoroughly investigated.
1 March, 13:20 GMT
Mårten Falkenberg (Gothenburg, Sweden), of the SWEDEPAD study, gives a talk entitled “A clinical trial paradox: Reaction by EU and American investigators to this analysis”.
The SWEDEPAD trials address the “Achilles heel” for endovascular treatment of PAD. Falkenberg says “I think we all agree drug-eluting technology is the most promising new tool” for PAD treatment, but also says that “randomised trials are underpowered to address patient-entered clinical endpoints.” He says there is a need for an independent, large clinical trial with patient-centred endpoints to address these limitations.
“In order to have patient-centred important outcomes, we decided to split the trial.” Falkenberg says. SWEDEPAD 1 will enrol patients with CLI, and SWEDEPAD 2 will entol patients with intermittent claudication. Currently, 1,480 are included in SWEDEPAD 1, and 810 patients are enrolled in SWEDEPAD 2, meaning enrollment is approximately two thirds complete.
Both studies halted enrolment following the publication of the Katsanos et al meta-analysis. “We are at the moment struggling to make up our mind on how to proceed”, Falkenberg concludes.
2 March, 13:00 GMT
Misti Malone, chief of the peripheral interventional group at the FDA, provides FDA insight of the paclitaxel mortality signal. She thanks audience members for participating in this collaboration, and explains that, as is understood in the Food Drug and Cosmetics Act, safe does not mean risk free when it comes to medical devices, but that it is important to gain greater clarity on the mortality signal Katsanos et al reported in their meta-analysis.
Factors to consider when assessing a mortality signal:
Likelihood of the event
Quality of data
Strength of causal relationship
Risk severity
Risk duration
Risk reversibility
Benefit magnitude
Mitigations
Patient vulnerability
Alternative therapies
Implications for related devices
The FDA is in the process of replicating the meta-analysis, using both similar and alternative statistical methodologies to those used by Katsanos and colleagues. This analysis will include all 28 RCTs in the original meta-analysis.
Speaking of this investigation, Malone says: “Following preliminary review of the data, we believe that a signal still persists, and that this warrants additional investigation. We acknowledge that this may impact other disease states, such as AV and CLI.”
The FDA recognises limitations of the available data. According to Malone, these include a lack of standardised categorisation and adjudication of death; unknown causes of death and co-morbidities; treatment with other devices; trial period and ever-changing medical practice.
Malone says that the FDA will use this information to assess the risk for future recommendations, “including a potential advisory panel which may suggest potential modifications to trial design, such as informed consent and labelling, and/ or additional post-market data collection.”
1 March, 20:16 GMT
Thomas Zeller (Bad Krozingen, Germany) says that after his talk on the THUNDER trial and long-term follow-up, “I believe we will understand the potential flaws of the Katsanos study.”
Naming the THUNDER trial and the FEMPAC trials as the beginning of the paclitaxel story, Zeller describes the importance of understanding what happened in the THUNDER trial with regards to mortality: “At five years, we found no late catch-up with regards to clinical efficacy, favouring the DCB concept. …It is important to note, at two years we excluded patients who underwent more than one TLR. This could have been endovascular reintervention or bypass surgery.” By five years, this number of excluded patients rose to 25, 11 of which were in the paclitaxel cohort—”and that is the follow-up bias, basically,” Zeller says, “which is important to realise, but was not included in the Katsanos analysis.”
Regarding the risk ratio, when adjusted to take into account the lesser number of patients available for follow-up at five years, “the end of the story is that the risk ratio is significantly lower when patients where you really have the appropriate clinical information,” says Zeller, adding this is “one of the flaws in the Katsanos study, and I believe this is not only true for the THUNDER trial.”
Summarising his critique of the meta-analysis as it relates to the THUNDER study, Zeller argues: “paclitaxel-coated balloons are more effective than POBA, individual plasma concentrations vary, a constant dose to clinical response correlation does not exist in my opinion, and the risk of five-year mortality depends on the statistical method applied.”
1 March, 18:30 GMT
William Gray (New York, USA) now takes to the #VLF2019 stage to present a critical appraisal of the JAHA analysis.
He summarises: “The pharmacokinetics and toxicity of paclitaxel is well studied and characterised, and there are no prior data that indicate that very, very low doses that are present as part of DCB and DES use produce a mortality effect. Therefore, in order to claim otherwise, and describing a novel, and grave, paclitaxel toxicity, never been described in the history of the world, one would need to present Level 1 evidence: prospective, randomised, and appropriately sized.
“A non-patient level meta-analysis with multiple flaws—many fatal—will likely not suffice.”
He lists several flaws of the meta-analysis:
Katsanos’ paper assumes a random-distribution model, which he says is “appropriate”, in its statistics, but “did not make adjustments for a non-parametric (skewed) distribution. This is inappropriate.”
There is a selection bias due to the lack of a complete follow-up. One year outcomes in the combined 28 studies show no differences in mortality. Two- and five-year data includes a subset of 12 and three trials, respectively, of the original 28. A more appropriate time-to-event analysis cannot be performed and could not be performed on the data available to Katsanos. At one year, trials included with long-term data show a mortality effect, whereas the trials without long-term data show no mortality effect
“The dose-time product is problematic.” He says the selection bias “plays out here as well”, and that the variable “Time” in the dose-time calculation is disproportionately available for the longer-term follow-up studies and worse mortality, biasing the calculation. He adds: “Once the study population is divided by DCB length and size, adjustments for possible differences in population cardiovascular risk factors would need to be made. It’s no longer a randomised application or trial. It is now a trial of sub-setted patients using different sizes of balloon. That needs to be back-adjusted, and it was not.”
The need for—and promise of—meta-analysis is not the assessment of low frequency events that are not typically individually powered. In the case of DCB and DES studies, death was part of a composite safety endpoint. According to unnamed statisticians Gray spoke to, “A prospective study to independetly assess mortality in DCB/ DES for PAD would need to enrol between 2,000 and 6,000 patients to avoid the risk of Type 1 error.” Whilst the meta-analysis begins with 4,663 patients across 28 RCTs, at two years, there are 2,316 patients across 12 RCTs, and at year five, there are 863 patients acrss three RCTs.
The lost-to-follow up are not properly accounted for in this trial; Gray does some back of the envelope calcuations to show that taking the lost-to-follow up patients into account, the relative risk from the five year RCTs included in the study is lower than cited in the Katsanos meta-analysis.
Gray claims the PTA group is likely not paclitaxel naive for the entirety of the analysis. This is because paclitaxel device approvals in Europe and the USA preceded almost all of the one year period of TLR experienced in the PTA arm. “That is, the trial finished, and by the time the one year TLR arm was finished, there was available paclitaxel in the world.” Gray says that as most of his practice uses paclitaxel to treat restenosis, “I think the authors would need to recognise this, and perform some sliding scale analysis of the impact of variable proportions of paclitaxel usage in the TLR patients. Without that, I think this whole analysis blows up, because this assumes that these patients are paclitaxel naive for the duration, rather than move them into the column of paclitaxel mortality.”
1 March, 18:15 GMT
Konstantinos Katsanos (Patras, Greece) presents “The Why, The How and the Results” of the JAHA meta-analysis, saying “I guess most of you have already read the paper.”
“We only looked at randomised controlled studies—exactly to try to tease out only the effect of paclitaxel,” Konstantinos explains, “considering that ideally in a well-designed randomised study, all the other confounders are supposedly accounted for.”
“The tissue half-life of paclitaxel being administered by a DCB or DES seems to be in the order of several weeks, if not months. Above all, I was sort of surprised to find out but there has been recently identified a drug-drug interaction of the metabolism of clopidogrel and paclitaxel—and remember now we are referring to PAD patients.”
Katsanos directs attention to a dataset he finds “highly important”—the IN.PACT SFA suvival analysis: “The hazard ratio of the two arms on the log scale from the beginning up to five years, and you can see that those are non-proportional hazards. The curves are diverging, and then they are converging again. So hazard ratios may not be showing, and may not be documenting the full picture.”
“I think we should not contaminate randomised studies with individual patient data of single arm registries”, Katsanos argues, “before we make sense of the randomised studies. I think what would be a mistake—and this seems to be the avenue taken by the industry—to try to contaminate randomised studies with the inclusion of single-arm registries. These single-arm registries have different follow-up, different characteristics. We need to stick to randomised evidence and we need to agree on the proper way to analyse this evidence.”
1 March, 16:29 GMT
Elazer Edelman, who is the director of the MIT Institute for Medical Engineering and Science and professor of medicine at Harvard University, gives an overview of drug-delivery kinetics and tells the panel: “It does not make any sense to indict the drug for having an effect at five years. […] I do not think we can indict the drug because there is no mechanism that I can envision, that would account for mortality. It does not mean there is not a mortality signal and it does not mean we should not be doing more studies, but at the end of the day we need more data, and we need more people to support the pre-clinical and non-clinical work.”
1 March, 14:16 GMT
Ramon Varcoe (Sydney, Australia) kicks off the second session of VLF 2019 with an overview of “Unintended consequences of various trial designs and their potential effect on mortality and outcomes”.
Considering how trial design can affect outcomes and specifically mortality, Varcoe notes that as randomised controlled trials for interventional studies—as opposed to drug trials—are not as easily blinded, several types of biases can be hard to avoid. “Outcome assessors (for mortality, this is usually study coordinators or investigators) may unconsciously or intentionally alter their assessment”, Varcoe notes.
“How can we determine whether the mortality in the Katsanos review was due to paclitaxel or to trial design?” Varcoe asks, noting that all the studies in the meta-analysis had a “high risk of bias” in this area. Performing an identical meta-analysis of RCTs in the SFA, but excluded all drug-coated devices, to check whether an association was still found. With 22 studies vs. the 28 reviewed by Katsanos et al, and approximately half the subjects (2,451 vs. 4,432), at 12 months Varcoe and colleagues found “a higher risk ratio which favoured the control groups in terms of mortality outcomes—and this was highly statistically significant”.
At two years, the control review by Varcoe dropped to half the amount of studies and about a third of the study subjects, rendering the findings underpowered. However, Varcoe noted, “there if a definite trend” which leads in the same direction, and continues out to five years.
“It is my view that these findings cast some doubt as to the causal link of the association between paclitaxel and mortality.” Instead, Varcoe suggests, “it is much more likely” that this association is due to the introduction of bias, more tenacious follow-up of subjects in the experimental arms, and higher rates of medical interaction in RCT arms with more frequent target lesion revascularisations.
1 March, 13:35 GMT Josh Beckman (Nashville, USA) speaks on variables that may affect mortality in patients with PAD.
“My talk is really simple”, Beckman says, listing four factors that “are enough to tell us about the variables that affect mortality”:
How bad is the PAD?
What are the risk factors that cause PAD?
What is the atherosclerotic burden doing?
What can the patient tell you themselves about how they feel?
“I think, actually asking people how they are doing is a way to integrate every aspect of their problems.” Pointing to a 2006 study by P Garg et al, Beckman notes in this study, to predict twice the risk of mortality, “all you had to do was ask: do you leave your house? So functional capacity is a nice way to integrate everything we are talking about, in terms of risk factors, disease severity, and polyvascular disease.”
“In summary, the primary cause of mortality in PAD is cardiovascular, followed by cancer. […] Prior revascularisation per se did not affect mortality.”
1 March, 13:26 GMT Raghu Kolluri (Columbus, USA) takes to the podium to talk about mortality rates in randomised vascular device trials. Sticking to the femoropopliteal studies, Kolluri begins by saying: “Mortality is not reported in most of the trials, and we don’t have enough long-term data—this is evident from the Katsanos paper itself. At two years, you have twelve studies to compare, and at five years you have only three studies to compare.”
Speaking of the 2016 Circulation paper where the mortality data in the treatmentarm (treatment with the Zilver PTX paclitaxel-eluting stent from Cook Medical) and the control arm (percutaneous transluminal angioplasty [PTA]) were inadvertently swapped, Kolluri says: “When I looked at the numbers, the Katsanos analysis actually included the flipped numbers, so I don’t think this would have mattered in this situation.”
Kolluri cites several recent patient-level analyses which fail to find a statistically significant difference in all-cause mortality between DCB treatment and a control. These include the pooled analysis of all IN.PACT Admiral DCB clinical programmes (from Medtronic), the RANGER SFA randomised three-year data (Boston Scientific), the Zilver PTX data (Cook Medical), and the Philips’ Stellarex data, all reported at the Leipzig Interventional Course (LINC; 22-25 January, Leipzig, Germany).
“The biggest issue I had with this question that the organising committee [of VLF] put to me [What are the mortality rates in the published randomised vascular device trials?] is that mortality was not reported in many trials, and mortality was not the primary endpoint,” Kolluri says.
“The other interesting study that is important to note is the VIBRANT study. VIABAHN compared to the BMS [bare metal stent] showed [a] higher death rate—almost three times—which does not make sense in regards to how that can happen […] I am intrigued. None of these [deaths] were related to the device, it is important to note that.”
Talking of the COMPASS trial, Kolluri notes that the all-cause death rates at 21-months were 5% in each arm, even without any intervention.
In summary, Kollui says: “The paclitaxel, at two years, demonstrated a 7.2% [mortality rate].” He goes on to list the mortality rates of: bare metal stent (4.4% to 9.8%), atherectomy to three years (12.5%), atherectomy (6.9% to 12.5%), PTA (0% to 12.2%), and medical management (0% to 4%).
He concludes: “Honestly, I don’t know why this is happening, I am intrigued, and I am here to learn.”
1 March, 13:10 GMT
An audience poll finds that out of 40 attendees at the VLF, 28 respond they are “concerned about the potential link between paclitaxel-coated devices used in PAD interventions and mortality”.
1 March, 13:00 GMT Gary Ansel (Columbus, USA) opens VLF meeting with an introduction to the goal of the event. Providing a background, Ansel says “all VLF symposium are funded solely and entirely by the VIVA organisation.”
“With the recent JAHA meta-analysis that suggests increased risk of mortality from commonly utilised endovascular devices, we felt strongly that physicians needed to assume a leadership in investigating this potential risk in as transparent, high-level and inclusive a method as possible. To this end, this meeting is being live streamed, so that all those interested may observe the proceedings.”
Ansel says the “most important part of this Vascular Leaders Forum is the hours of open discussion.”
“We are all here to ensure that what we do is best for our patients—after all, that is why we do what we do.”
1 March, 12:30 GMT
First session set to begin at 13:00 GMT.
At the MWC (25–26 February, Barcelona, Spain), formerly the Mobile World Congress, Philips unveiled a unique mixed reality concept developed in partnership with Microsoft for the operating room of the future. Based on Philips’ Azurion image-guided therapy platform and Microsoft’s HoloLens 2 holographic computing platform, the companies will showcase novel augmented reality applications for image-guided minimally invasive therapies. The technology allows wearers of the HoloLens 2 headset to access a virtual screen displaying data from the Azurion system, updated in real time, during procedures.
The Philips and Microsoft augmented reality concept, built for HoloLens 2, brings live imaging and other sources of vital data currently displayed on large 2D screens into a 3D holographic augmented reality environment that can be ergonomically, easily and intuitively controlled by the physician. The concept is being used to gather further clinical insights to support the development of future commercially-available augmented reality solutions for use in image-guided procedures.
“The transition from open surgery to image-guided procedures has driven a seismic shift in improving patient outcomes and reducing costs—not least by dramatically reducing the length of time a patient stays in a hospital after their procedure,” said Atul Gupta, chief medical officer for Image Guided Therapy at Philips and a practicing interventional and diagnostic radiologist. “On our Azurion platform we seamlessly integrate a range of data sources in a way that is intuitive to understand and control. By collaborating with Microsoft and HoloLens 2 we can take it to the next level, immersing the physician in a tailored augmented reality environment. This concept allows me to see the real world superimposed with the live data and 3D medical imagery needed to guide our precision therapy, and importantly also lets me control Azurion with voice recognition, eye tracking and advanced gestures. It is all about keeping our focus on the patient.”
“Mixed reality is giving people new ways to interact with the digital and physical world, bringing the benefits of the digital revolution to entirely new experiences across the globe,” said Alex Kipman, technical fellow, AI and Mixed Reality at Microsoft. “I am thrilled to see companies in a broad range of industries achieve more using the products that we build with our partners and ecosystem. Mixed reality holds great potential in healthcare, and our collaboration with Philips shows how that potential is already beginning to be realised.”
Microsoft unveiled HoloLens 2 during the previous day of the conference. HoloLens is a self-contained holographic computer that enables hands-free, heads-up interaction with three-dimensional digital objects.
Since its global launch in February 2017, over half a million patients have been treated in more than 80 countries using the Azurion platform, which is powered by Philips’ proprietary ConnectOS and combines technical innovations in both software and hardware. ConnectOS allows the integration of advanced digital innovations on the Azurion platform.
A total of 143 free papers including 43 oral papers, 77 e-posters and nine walking posters were presented during the meeting. APSCVIR president Andrew Holden (Auckland, New Zealand) tells this newspaper that “The meeting was extremely well planned by [president-elect] Prijo Sidipratomo [Jakarta, Indonesia] and his organising committee, and continued the proud tradition of an excellent academic programme combined with wonderful social occasions in an exotic location. The four-day schedule involved plenary and concurrent sessions, involving 120 world-class international and regional experts covering a wide range of vascular, oncology and other interventions.”
Andrew Holden, APSCVIR president, with Robert Morgan, CIRSE president
In a press release, the society stated: “APSCVIR enjoyed the commitment and support by various global interventional radiology societies including CIRSE [Cardiovascular and Interventional Radiological Society of Europe], SIR [Society of Interventional Radiology], SIO [Society of Interventional Oncology], SPIR [Society for Paediatric Interventional Radiology] and ISVIR [Indian Society of Vascular and Interventional Radiology] that brought together world-renowned leaders in the different subspecialties of interventional radiology at the meeting, galvanising the bonds with these societies.
“The above academic pursuits would not have been possible without the continued generous support from our 20 industry partners who contributed nine educational sessions during the meeting.” Holden iterated this, saying: “Strong industry support provided a busy trade display area and excellent interaction during session breaks.”
During the awards ceremony held at the Cultural Fest Gala Dinner, three society members received the 2019 APSCVIR Gold Medallist Award: Abdul Samad Bin Sakijan (Kuala Lumpur, Malaysia), Gao Jun Teng (Nanjing, China), and Masatoshi Okazaki (Fukuoka, Japan). Jim Reekers (Amsterdam, the Netherlands), Ziv Haskal (Charlottesville, USA), and Brian Stainken (Stamford, USA) were also presented APSCVIR Honourary Memberships “for their long, untiring support and outstanding contributions to [the] field of cardiovascular and interventional radiology”.
APSCVIR president and APSCVIR president-elect Prijo Sidipratomo, convenor of APSCVIR 2019, pour the champagne to open the Presidents’ Reception
Speaking to Interventional News, Haskal refers to the Honorary Membership as a “career highlight”, adding: “I have been a decades-long attendee and supporter of the APSCVIR, firm in the belief that it brings together a unique group of attendees, ones with expertise that has always broadened my interventional practice and approach. Things are simply different in different parts of the planet, and diversity creates new ideas, opportunities and advances. I think the APSCVIR is one of the most important IR societies, and I would encourage all interventional radiologists to put its meetings firmly on their potential travel calendars.”
Echoing these sentiments, Reekers comments: “The Asian Pacific society for IR covers a very broad area and has a great diversity in members. Additionally, in Asia interventional radiology is a fast growing medical specialty. It is a great honour to be recognised as somebody who has contributed to the development, growth and spread of interventional radiology, also in the Asia Pacific part of the world. It only shows that interventional radiology is truly an international specialty and that IR education and science have no borders. Many of the APSCIVR members visit the CIRSE annual meetings, and it is always a great pleasure to interact there in many ways. Therefore, the honorary membership of APSCIVR means a lot for me personally and I am very grateful for my election. The fact that I have always been a great lover of the Asia Pacific region makes it even more valuable for me to be in this position. I am sure that my ties to this group and region will even be more strengthened.”
Young IRs awarded their grants at the Gala Dinner
Additionally, 15 interventional radiologists below the age of 40 received the young interventional radiologist sponsorship awards, and were provided with a grant to assist with travel. Holden says this continues “the tradition of supporting young interventionalists from developing countries in our region to attend the meeting”.
He adds: “We look forward to welcoming you to the 15th APSCVIR in 2020 in Taipeh, Taiwan—an event that is sure to carry on the fine traditions of our Annual Scientific Meeting”.
Both Medtronic and Cook Medical have issued corrections to published data regarding the safety of their paclitaxel-coated devices. While Medtronic have revised IN-PACT post-market study data due to a “programming error,” Cook Medical have noted a mistake made during data publication, and that two mortality figures were “inadvertently reversed”. Both companies had recently emphasised the gravity of published data on the safety of their devices, following the December 2018 meta-analysis of Katsanos et al, which associated paclitaxel-coated devices with a higher risk of death.
In a statement, Medtronic said that the company “recently became aware of a programming error in the clinical data reporting isolated to the two- and three-year follow-up periods in our IN.PACT Global post-market study, part of the IN.PACT Admiral clinical programme for the treatment of femoropopliteal artery disease. Preliminary results of this study were first released at the Leipzig Interventional Course (LINC) and Medtronic issued a press release summarising the results on January 22, 2019.”
According to Medtronic, due to a programming error, mortality data were inadvertently omitted from the summary tables included in the statistical analysis. These deaths were, however, previously included and reported in Medtronic’s database, captured in the appropriate study exit forms and adjudicated by an independent clinical events committee. In addition, the company stated, the deaths were previously recorded in Medtronic’s complaint system, and MDR/Vigilance reporting has been completed in compliance with the company’s Quality Systems, which are governed by external regulatory requirements.
Immediately upon learning of this error, Medtronic notified the FDA and the study authors. The company stated that while a component of the recent patient-level meta-analysis will need to be updated, it has found the revised analysis still supports earlier conclusions that: there was no statistically significant difference in all-cause mortality between the IN.PACT Admiral drug-coated balloon (DCB) and plain balloon angioplasty at five years; there is no correlation between paclitaxel dosing and long-term survival in the studied population; and, there was no difference in mean nominal dose of paclitaxel between overall survival in patients treated with DCB and those who died.
The data update impacts the publication of the IN.PACT Global two-year data in the Journal of the American College of Cardiology: Cardiovascular Interventions (JACC CI), and the IN.PACT paclitaxel safety analysis, which is in print with the Journal of the American College of Cardiology (JACC). Medtronic has confirmed no other IN.PACT studies are affected by this error, and it is important to note this discrepancy is limited to deaths after the one-year time-point.
Respecting the scientific process, the revised analysis is currently moving through the appropriate peer-review with the study authors and JACC so the manuscripts can be appropriately corrected.
Medtronic also notes a related study published on February 12, 2019 in JAMA Cardiology, “Association of Survival With Femoropopliteal Artery Revascularisation With Drug-Coated Devices.” The study authors concluded: “In this large nationwide analysis of Centers for Medicare and Medicaid Services beneficiaries, there was no evidence of increased all-cause mortality following femoropopliteal artery revascularization with drug-coated devices compared with non-drug-coated devices.”
Zilver PTX mortality data
The authors of the paper by Dake et al, “Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery 5-year results of the Zilver PTX randomised trial,” have issued corrections to the text published in 2016 in Circulation.
According to Circulation, “when high-resolution files were requested during production, an incorrect version of Figure 1 was mistakenly provided. Subsequently, the published version of the flow chart in Figure 1 contained incorrect numbers. The authors now provide the corrected version of Figure 1.”
Additionally, the journal informed, the following sentence from the ‘Safety’ section was incorrect: “The five-year all-cause mortality rate was 13.6% (10.2% for the primary DES group and 16.9% for the PTA group, p=0.03), and no deaths were adjudicated as procedure or device related.” The authors regret that the numbers for the two groups were inadvertently reversed. The sentence should be read: “The five-year all-cause mortality rate was 13.6% (16.9% for the primary DES group and 10.2% for the PTA group, p=0.03), and no deaths were adjudicated as procedure or device related.”
These corrections have been made to the current online version of the article.
Bringing interventional oncology (IO) and radiation oncology (RO) closer together would yield more than important logistical gains for IO; it would open up a wealth of possibilities for patients. Andy Adam (London, UK; an interventional radiologist) and Lizbeth Kenny (Brisbane, Australia; a radiation oncologist) make the case for closer collaboration at CIRSE 2018.
The Trans-Tasman Radiation Oncology Group (TROG), which has embraced this concept, will feature the inaugural, two-day Clinical Interventional Oncology Symposium during its annual scientific meeting in March.
Gary Ansel (Columbus, USA) tells Vascular News at VEITHSymposium 2018 about how drug-based therapies have become a mainstay in femoropopliteal revascularisation and how interventionalists should be using best medical therapy “more than we do [currently]”. He also shares his approach to making the choice between using a drug-coated balloon and a drug-eluting stent.
Canon Medical Systems USA recently introduced its next generation of interventional systems—the Alphenix platform. The new platform of systems incorporates all-new features that enable clinicians to deliver images with clarity and precision without compromising workflow and while prioritising low dose.
With the launch of the Alphenix family, Canon Medical is also unveiling its new Alphenix Hi-Def Detector (High-Definition Flat Panel Detector), which is available on the all-new Alphenix Biplane and Alphenix Core + systems. Made up of what Canon calls the world’s first high-definition detector—with 76 micron resolution—for resolving fine details, the hybrid 12 x 12-inch panel is combined with high-definition flat panel technology that results in resolutions of 2.6 lp/mm (Standard) and 6.6 lp/mm (Hi-Def Detector). The Alphenix Hi-Def Detector technology helps clinicians see finer details during complex interventional procedures such as stent positioning and stent apposition, wire and catheter navigation through the stent struts, and observation of coil deployment.
In addition to the new Alphenix Hi-Def Detector, the Alphenix family includes the following new features:
Next-generation Illuvis technology to reduce image noise with less lag time, and provide clearer images at steep angles while delivering a decreased frame rate that can help reduce dose;
Real-Time Auto-Pixel Shift to automatically correct misalignment between the contrast image and mask image during digital subtraction angiography and 2-D roadmapping utilization; and
(Optional) Tablet touch-screen to optimize tableside workflow with simplified control functions and the option to assign “favorites” to customize the interface, per physician.
Canon showcased the new Alphenix and Alphenix Hi-Def Detector technology, available with the Alphenix Biplane and Alphenix Core + systems, at the 2018 Radiological Society of North America (RSNA; 25–30 November, 2018, Chicago, USA).
In the arterial space, VIVA 2018 focused on the fact that there is an increasing awareness of limb threatening ischaemia coupled with an increase in interventional tools, but no clear defined pathway for treatment. There is also uncertainty about the metrics that matter to patients. In the venous world, there is still a need to define the appropriateness and timing of intervention. So said John Kaufman (Portland, USA; and president of VIVA) and Raghu Kolluri (Columbus, USA; chairman of the VEINS at VIVA meeting) who outlined the critical issues facing vascular specialists. They also looked forward to the trial data that they hope to see in 2019.
Jihad Mustapha (Grand Rapids, USA) explains how the Temporary Spur stent system (Reflow), which is a spiked self-expanding stent is intended for use in conjunction with a drug-coated balloon, works to help deliver drug to the media or subintima of the vessel wall. In a first-time presentation at LINC 2019, he shared initial experience with the DEEPER FIH trial obtained with the system in the infrapopliteal arteries.
Nicholas Inston (Birmingham, UK) tells Vascular News at LINC 2019 about the exciting field of percutaneous arteriovenous fistula (AVF) creation, the main devices and trials in the space and the lack of long-term evidence showing AVFs created percutaneously “are still working” at two to three years. He also elaborates on how surgically created “high flow” fistulas are different from those created percutaneously.
At the EKOS symposium at LINC 2019, Nils Kucher (Zurich, Switzerland), Houman Jalaie (Aachen, Germany) and Mert Dumantepe (Istanbul, Turkey) share their experiences in treatment of pulmonary embolism, acute and chronic deep venous thrombosis (DVT) using acoustic pulse thrombolysis.
This video was filmed by BTG onsite at LINC 2019 and is being distributed in association with Vascular News.
The efficacy and safety of a novel catheter delivering liquid paclitaxel for the prevention of restenosis in below-the-knee lesions has been confirmed by study investigators across 17 sites in the USA. This is the conclusion of the COPPER BTK trial (Occlusion Perfusion Catheter for Optimal Delivery of Paclitaxel for the Prevention of Endovascular Restenosis—below-the-knee), presented by Pradeep Nair of the Cardiovascular Institute of the South Houma (Los Angeles, USA) at the 31st International Symposium on Endovascular Therapy (ISET; 27–30 January 2019, Hollywood, USA).
The occlusion perfusion catheter (Advanced Catheter Therapies) is a universal drug-delivery device. According to an Editor’s note in Vascular Disease Managementwritten by Nair in his capacity as New Technologies Section Editor for the publication, this catheter “allows for delivery of antiproliferative drug[s] to a targeted treatment area, demonstrates exceptional medial layer drug uptake, and can be re-used for multiple treatment sites. Additionally, the outer occlusion balloons prevent downstream washout of antiproliferative agent[s]. Ongoing trials will help establish its role in peripheral arterial disease intervention for both above- and below-the-knee applications.”
The prospective, non-randomised, open-label, multicentre study presented by Nair at ISET aimed to evaluate the efficacy of the occlusion perfusion catheter after atherectomy and percutaneous transluminal angioplasty (PTA) in treating de novo and restenotic below-the-knee lesions, as determined by primary patency at six months. The safety profile of the device was also assessed, defined as freedom from major adverse events at one month. Major adverse events included target lesion revascularisation, major amputation, and target limb related death. A total of 35 patients enrolled in the study, with a mean lesion length of 119.1±80.4mm, and a diameter stenosis of 93.7±8.81%. All patients were in Rutherford class 2–5.
At six months, primary patency was 88%, and the study investigators reported 96% freedom from clinically-driven target lesion revascularisation. There was no target lesion revascularisation, target limb related death, or major amputation in the target limb. The Rutherford classification also improved on average over the course of the study: at baseline, the average Rutherford score was 3.6±0.8, and at six months, the average Rutherford score was 1.8±1.2.
These positive data drew Nair to summarise: “The delivery of liquid paclitaxel using the occlusion perfusion catheter under controlled pressure was technically achievable without procedural complications. The feasibility and initial efficacy of this device provide encouragement for this new technique, with the potential as an alternative approach for infrapopliteal revascularisation. In particular, the ability to treat very long or multi-vessel lesions with a single device could provide a more economical option.”
In addition, he added: “The safety profile in this small cohort study is particularly favourable, and focuses treatment at the target lesion with minimal drug loss that can occur with drug-coated balloons (DCBs).”
Nair acknowledges that longer term follow-up and larger clinical studies will be needed to support the initial findings of this technology with head-to-head comparisons with DCB and balloon angioplasty (with and without atherectomy).
As is common knowledge amongst the interventional community, the optimal strategy for below-the-knee arterial disease remains uncertain. Treatment is impeded by the high incidence of long chronic total occlusions and calcified lesions, meaning previous interventionalists have experienced high restenosis rates and poor-long term clinical patency when treating these difficult lesions. PTA is most commonly employed as a treatment regimen, but, Nair explained at ISET, “often yields non-durable results”. He cited a primary patency of 63% at one-year, less than three-quarters of the six-month primary patency rate observed in the present study with the occlusion perfusion catheter.
Nair noted that DCBs in below-the-knee arteries have historically yielded mixed results, but that several randomised clinical trials in the below-the-knee space evaluating DCBs and scaffolds are ongoing. The main difference between DCBs and the occlusion perfusion catheter used in the COPPER BTK trial is that, while DCBs store antiproliferative agents in the intima, the catheter delivers these therapeutic agents directly to the medial wall.
Occlusion perfusion catheter design
The occlusion perfusion catheter is a multi-lumen catheter designed to temporarily occlude the target lesion from blood flow, flush the blood from the treatment chamber, and then locally deliver the therapeutic agents into the artery. It has two compliant occlusion balloons (one proximal and one distal), which define the treatment chamber. The catheter also has one centre space-occupying balloon, which does not contact the vessel wall. Treatment chamber pressure is measured in real-time during infusion of the therapeutic agent via a sensor located within the chamber connected to an external pressure monitor.
Therapeutic agents are infused through the treatment inflow under continuous pressure injection; treatment time is two minutes. The average paclitaxel dose per placement is 6.15mg. Radiopaque markers are located on both side of the occlusion balloons to define the treatment chamber and assist in catheter placement under fluoroscopy.
The occlusion perfusion catheter has FDA 510(k) clearance, and is a 0.014” guidewire compatible, 5Fr device, with an outer diameter of 1.67mm. The device has existed since the establishment of Advanced Catheter Therapies in 2008.
The COPPER BTK study was sponsored by Horizons International Peripheral Group.
Medtronic has issued the following statement regarding revised clinical study data:
Recently, Medtronic became aware of a programming error in the clinical data reporting isolated to the two- and three-year follow-up periods in our IN.PACT Global post-market study, part of the IN.PACT Admiral clinical programme for the treatment of femoropopliteal artery disease. Preliminary results of this study were first released at the Leipzig Interventional Course (LINC) and Medtronic issued a press release summarising the results on January 22, 2019.
Due to a programming error, mortality data were inadvertently omitted from the summary tables included in the statistical analysis. These deaths were, however, previously included and reported in Medtronic’s database, captured in the appropriate study exit forms and adjudicated by an independent clinical events committee. In addition, the deaths were previously recorded in Medtronic’s complaint system, and MDR/Vigilance reporting has been completed in compliance with the company’s Quality Systems, which are governed by external regulatory requirements.
Immediately upon learning of this error, Medtronic notified the FDA and the study authors. While a component of the recent patient-level meta-analysis will need to be updated, Medtronic has found the revised analysis still supports earlier conclusions that: there was no statistically significant difference in all-cause mortality between the IN.PACT Admiral drug-coated balloon (DCB) and plain balloon angioplasty at five years; there is no correlation between paclitaxel dosing and long-term survival in the studied population; and, there was no difference in mean nominal dose of paclitaxel between overall survival in patients treated with DCB and those who died.
The data update impacts the publication of the IN.PACT Global two-year data in the Journal of the American College of Cardiology: Cardiovascular Interventions (JACC CI), and the IN.PACT paclitaxel safety analysis, which is in print with the Journal of the American College of Cardiology (JACC). Medtronic has confirmed no other IN.PACT studies are affected by this error, and it is important to note this discrepancy is limited to deaths after the one-year time-point.
Respecting the scientific process, the revised analysis is currently moving through the appropriate peer-review with the study authors and JACC so the manuscripts can be appropriately corrected.
Medtronic also notes a related study published on February 12, 2019 in JAMA Cardiology, “Association of Survival With Femoropopliteal Artery Revascularisation With Drug-Coated Devices.” The study authors concluded: “In this large nationwide analysis of Centers for Medicare and Medicaid Services beneficiaries, there was no evidence of increased all-cause mortality following femoropopliteal artery revascularization with drug-coated devices compared with non-drug-coated devices.”
Philips Zenition, a new mobile C-arm imaging platform from Philips, has launched in the USA, Germany, Austria and Switzerland. It is being introduced into these countries over the next six months, and is set to penetrate other markets in the second half of 2019.
Mobile C-arms are X-rays systems that are brought into the operating room to provide live image guidance during a wide range of surgeries, including orthopaedic, trauma and vascular procedures. According to a company press release, the Zenition mobile C-arm platform brings together innovations in image capture, image processing, ease-of-use and versatility pioneered on Philips’ earlier Azurion platform.
The scope and complexity of surgical interventions—especially in the rapidly growing area of image-guided minimally invasive surgery—continues to increase, as does the number of patients requiring treatment. In order to treat more patients at a lower cost, Philips say in a company statement, hospitals require a versatile fleet of C-arms with varying capabilities that easily adapt to the needs of different types of surgery and different operators. Philips claim that Zenition mobile C-arms are easy to move between operating rooms, simple to position around the patient and intuitive to operate.
“The Philips Zenition is a user-friendly system that is intuitive to use for both surgeons and nursing staff,” says Nikolaos Bonaros, associate professor of Cardiac Surgery at the Medical University of Innsbruck, Austria. “Its simplified workflow means that we can convert a room from a conventional operating room to a high-quality interventional room more quickly. At the same time the system provides high image quality at the level required for hybrid operating room procedures.”
Philips Zenition has a tablet-like user interface and this, coupled with the “Unify” workflow, mean that once an operator has learned to use one system on the platform, it is easy for them to operate them all, a press release states. The company also claim that the compact design of the device, as well as its ability to capture images at the periphery of the image intensifier or flat detector, reduce the need for C-arm repositioning by 45%.
The Zenition C-arm systems incorporate the same image processing algorithms used on Philips’ Azurion platform. Additionally, the platform features Philips’ MetalSmart software, which automatically adjusts the contrast and brightness of images to aid image quality, purportedly useful when metal objects such as implants are present in the field of view.
Philips’ Zenition C-arms are CE marked and have received 510(k) clearance from the US Food and Drug Administration (FDA). They will be showcased at the 2019 European Congress of Radiology (ECR) Exhibition (28 February–3 March, 2019, Vienna, Austria).
BD has announced the 510(k) clearance from the US Food and Drug Administration (FDA) for the WavelinQ 4F endoAVF system earlier this month. The endoAVF system is the company’s most recent innovation in endovascular arteriovenous fistula (endoAVF) creation technology, which allows for the creation of an arteriovenous fistula in either the ulnar artery and ulnar vein or the radial artery and radial vein, expanding upon the current indication for the the WavelinQ 6F system.
In the USA alone, there are more than 440,000 patients with end-stage renal disease (ESRD) who are surviving on haemodialysis. EndoAVF systems provide clinicians with a minimally invasive arteriovenous fistula (AVF) creation alternative to open surgery. The WavelinQ 4F, with a slim profile, increases the anatomical AVF location options and enables additional venous wrist access points (ulnar vein or radial vein), providing increased procedural flexibility for physicians while reducing risk of scarring or arm disfigurement for patients compared to open surgical AV fistula creation.
“With BD WavelinQ 4F endoAVF system, I can provide my ESRD patients with two additional fistula location options compared to a surgical fistula,” said Paul Kreienberg, Albany Medical Center, Albany, USA. “These additional AV fistula sites and a minimally invasive procedure can increase the likelihood that patients will get a usable AV fistula.”
“People living with ESRD are an underserved patient population with very limited treatment options available to them,” said Steve Williamson, worldwide president of Peripheral Intervention at BD. “We are excited to add BD WavelinQ 4F endoAVF system to our portfolio of technologies that create, restore and/or maintain AV access for patients on haemodialysis. Endovascular specialists now have an additional tool that enables the flexibility needed to support AV fistula creation for their patients.”
According to recent research from Reto Bale and colleagues, multi-probe stereotactic radiofrequency ablation with intraprocedural image fusion represents an efficient invasive therapy for hepatocellular carcinoma (HCC), as confirmed by histopathologic examination in explanted human livers. Therefore, it may be an attractive candidate for the initial treatment option even in patients with tumours larger than 3cm. Here, Bale speaks to Interventional News about the importance of this work, and advocates for the inclusion of image fusion into guidelines outlining standard of care.
What are the advantages of stereotactic radiofrequency ablation (SRFA) over standard radiofrequency ablation (RFA)?
For successful ablation, it is crucial to ablate the complete lesion, including a sufficient safety margin of at least 0.5cm. The short axis of the ablation zone with one RFA or microwave ablation (MWA) probe is limited to 1.5–4cm, depending on the ablation technology and probe design. Thus, even with the latest generation of MWA probes, only lesions up to a maximum diameter of 3cm can be effectively ablated with one single probe position. Therefore, for lesions larger than 3cm, overlapping ablation zones are required. This task is very difficult if only conventional US- and CT- [ultrasound and computed tomography] guidance is used for probe placement.
Stereotaxy allows for precise 3D planning of multiple probe positions, and then for precise probe placement intraprocedurally according to the plan. In addition, integrated image fusion allows for immediate and precise evaluation of probe placement and of the result during the intervention. Due to the ability to plan and introduce multiple needles with high precision, very large tumours can be completely devitalised. The largest mixed hepatocellular carcinoma (HCC)–intrahepatic cholangiocellular carcinoma (ICC) treated by our group (in 2014) had a diameter of 18cm. In a recent control CT four years after the initial SRFA, the lesion is still local recurrence free.
What are the clinical ramifications of this research?
In international guidelines, resection is recommended as a first line treatment in HCC larger than 2–3cm. If these large lesions are not resectable, a combination therapy of thermal ablation and transarterial chemoembolization (TACE) is proposed.
This work clearly shows that even large hepatocellular carcinomas can be completely devitalised (A0 in analogy to R0) by thermal ablation only. Therefore, SRFA challenges resection as first-line treatment not only in small lesions, but also in lesions greater than 3cm. Moreover, the combination therapy (thermal ablation and TACE) can be replaced by SRFA only, with excellent results, as confirmed by histopathologic examination.
Furthermore, the question arises whether liver transplantation can be replaced or at least postponed in patients with normal liver function by the application of SRFA and follow-up imaging.
What are the challenges presented by HCC treatment, and more specifically with ablative treatments?
Most HCCs develop in patients with liver cirrhosis, which is associated with impaired liver function. This has to considered if large ablations are performed. The remaining liver volume after local treatment has to be larger than in patients with a healthy liver tissue. In addition, many patients have a high portal vein pressure and an impaired coagulation function, which increases the risk of bleeding.
Why is it important to be able to treat larger tumours?
Due to its minimal invasiveness, SRFA has the potential to replace resection even in large lesions where an A0 ablation can be achieved. In my opinion, more than 90% of resections in primary and secondary liver tumours may be replaced by sophisticated thermal ablation procedures, even in large and very large lesions.
Why do patients drop out of the liver transplant waiting list? How will this potentially change?
Tumour progression beyond conventional transplant criteria during the waiting period for transplantation may result in patient dropout rate from the waiting list. Major risk factors include initial tumour load and waiting time. Using sophisticated and effective thermal ablation methods, patients may remain on a waiting list for an extended time.
What is the future of image fusion and SRFA?
Image fusion is key for immediate treatment evaluation and should be mandatory for every ablation procedure. It should be used in combination with standard CT- or US- guidance. Future guidelines should include image fusion as a standard of care and should propose stereotactic and other sophisticated planning and guidance techniques. As we stated in the paper, we strongly believe that our results justify specialised training in stereotactic techniques as well as additional costs related to infrastructure. Other centres should adapt stereotactic planning, image guidance, and image fusion in order to improve the outcome of ablation techniques even in large tumours.
Reto Bale is an associate professor of Radiology in the Department of Radiology at the Medical University Innsbruck in Innsbruck, Austria.
Two-year data on the Passeo-18 Lux drug-coated balloon (DCB; Biotronik) continue to validate its safety and effectiveness in intra-inguinal arteries. Gunnar Tepe from the Klinikum Rosenheim in Germany presented 24-month results for the first time from the full cohort of the Passeo-18 Lux all-comers registry on behalf of the study group at the Leipzig Interventional Course (LINC; 22–25 January, Leipzig, Germany).
Tepe described the finding of 88.8% freedom from clinically-driven target lesion revascularisation (CD-TLR) as a “really good result in this challenging cohort”. The study also found 83.9% freedom from major adverse events, and 92.7% freedom from major target limb amputations with “a high number of patients which did not need to be amputated”. Despite a target lesion calcification rate of more than 76%, Tepe reported that only 15.7% of lesions treated required a stent.
Biolux P-III is a prospective, global, multicentre all-comers trial of almost 900 patients to further investigate the Passeo-18 Lux DCB efficacy and safety in infra-inguinal arteries. It is conducted across 47 sites in 16 countries in the EU, Australia, and Asia. The DCB has a special excipient and comes with a safety guard insertion device which helps the drug to remain on the balloon, and prevents its loss on the sheath. Tepe described the study as the only real-world registry in infra-inguinal arteries, and it is the world’s second largest all-comers DCB registry.
Outcomes were freedom from major adverse events at six months, and freedom from CD-TLR at 12 months. Inclusion criteria were a lesion or lesions in the infra-inguinal arteries suitable for endovascular intervention treated with or scheduled to be treated with the DCB. Exclusion criteria were failure to successfully cross the target lesion with a guidewire. There were no patient or lesion characteristic limitations, and the use of additional devices was allowed.
“The special thing about the trial is that almost every patient could be enrolled, below-the-knee arteries as well as critical limb ischaemia (CLI) patients who may be excluded from other trials”, noted Tepe, with “42.1% CLI patients seen in the patient cohort and below-the-knee arteries were treated in almost 20% of the patients. In addition to that, [there were] high numbers of long lesions with C or D TASC classifications (32.6%), as well as a lot of patients with moderate to heavily calcified arteries (44.6%).”
Most patients were treated by pre-dilatation (72.3%, 784/1085), and the technical success rate was 98.4% (1068/1085).
At 24 months, the full cohort demonstrated 88.8% freedom from CD-TLR, “a very high number of freedom from TLRs”. Tepe suggested the large proportion of CLI patients in the study contributed to the major limb amputations rate. The mortality rate was 11.9%, with no increase over time, and the long-term rate remained the same at 180 days.
“We have to also acknowledge that there were a lot of patients enrolled in this study who have a higher likelihood to die—CLI over 40%, diabetes almost 50%, and patients being enrolled with previous cancer rates at almost 12%. This is not a prospective randomised trial comparing two percutaneous transluminal angioplasties (PTA) arms, so we cannot really compare to a control group, but what we can do is to look into mortality data and to look at one versus two years. There are not any major differences, nothing which strikes us and leads to the conclusion that this DCB is a risk or cause of mortality,” Tepe said.
The mortality rate among participants who are not CLI patients was lower: 2.9% (13/451) at 12 months and 5.5% (25/451) at 24 months. Other predictors of mortality were age, diabetes, and renal disease, and no significant differences in the distribution of cause of death between the first and second year were detected.
Feeding into the recent debate around paclitaxel use and late mortality, Tepe pointed out that dose of paclitaxel was not found to be a predictor of mortality in the Biolux P-III study. Although the low numbers within certain cohorts mean that dose dependency cannot be completely ruled out, Tepe observed “there are no signs that this drug-coated balloon is leading to mortality”, and concluded: “Biolux P-III … continues to confirm the safety and effectiveness of the Passeo-18 Lux DCB after 24 months.”
Tepe thus maintained that evaluated patient-level data showed no significant differences in the distribution of causes of death during the first year compared to the second year, and that no dose dependency of the mortality rate in the full cohort was observed.
CLI subgroup demonstrates low freedom from CD-TLR
Marianne Brodmann (Medical University of Graz, Austria) presented 24-month results from the largest CLI population enrolment in a real-world all-comer registry. Freedom from major target limb amputation was reported at 85.4%, and freedom from CD-TLR at 88.2%. The results also showed a crude mortality rate of 16.2% in the CLI subgroup.
Diabetes subgroup analysis reveals strong results in a challenging population
Focusing on a complex population of patients with diabetes, Johannes B Dahm (MVZ Herz- und Gefäßzentrum HGZ-Göttingen, Krankenhaus Neu Bethlehem, Göttingen, Germany) presented the results of 460 diabetic subjects from the registry with 53.1% CLI and 23.4% BTK lesions. In this subgroup, Dahm reported 87.5% freedom from CD-TLR and 87.4% freedom of major target limb amputation at two years.
Biotronik is extending the follow-up of paclitaxel-coated balloon studies to include long-term five-year patient data retrospectively on randomised control trials (Biolux P-I and P-II) and prospectively in the currently running all-comers registry, Biolux P-III.
A recent US-wide, multicentre analysis has found no evidence of increased all-cause mortality associated with the use of paclitaxel-coated devices compared with non-drug-coated devices for femoropopliteal artery revascularisation. The study, published in JAMA Cardiology, sought to evaluate differences in all-cause mortality between patients treated with and without drug-coated devices for femoropopliteal artery revascularisation. It follows the Katsanos meta-analysis published late last year that reported a higher incidence of death in the long-term with paclitaxel device use in the leg. The study investigators do acknowledge limitations of the present study, recognising that the median follow-up of 389 days was several years shy of the five years’ follow-up included in the Katsanos meta-analysis, and admit that “it is possible that the risks of drug-coated devices could become apparent over greater follow-up.” In a subsequent commentary, Jay Giri suggests some “key principles” for monitoring post-marketing safety of endovascular devices, to allow for “more informed decision making by patients and physicians”.
This retrospective cohort study evaluated 16,650 patients, who were Centres for Medicare and Medicaid beneficiaries, admitted for femoropopliteal artery revascularisation in 2016. It found that the cumulative incidence of all-cause mortality was lower among those who were treated with drug-coated devices when compared to those treated with non-drug-coated devices through 600 days’ follow-up post-procedure (32.5% vs. 34.2%, respectively; p=0.007).
The study investigators, Eric Secemsky (Boston, USA) and colleagues, surmise: “Among Centers for Medicare and Medicaid services patients, we found no signal for increased all-cause mortality following femoropopliteal artery revascularisation with drug-coated devices.” However, the study authors call for a patient-level meta-analysis of randomised clinical trials with survival methods to confirm their conclusions.
Going into more detail on their results, Secemsky et al explain: “When stratified by the type of device used for revascularisation, similar survival trends were observed for patients who were treated with drug-coated balloon (DCB) angioplasty (p=0.06), and drug-eluting stent (DES) vs. bare metal stent (BMS; p=0.56).” In addition to device type, the study investigators also analysed whether their conclusion held when adjusted for patient, procedure, and hospital characteristics. Their findings were consistent in all cases.
This trend was also observed in patients in a more severe condition; among patients with critical limb ischaemia (CLI), there was a lower mortality rate of 38.1% in the group treated with drug-coated devices, compared to 40.1% for those treated without drug-coated devices (p=0.04). The authors note that patients with CLI represented a minority of patients included in the Katsanos et al meta-analysis.
In response to the Katsanos meta-analysis findings
Citing the recent Katsanos meta-analysis published in JAHA, Secemsky and colleagues enumerate “limitations that mitigate its implication”, notably the use of summary-level data. Following the meta-analysis publication, there has been a swell of papers from industry based on individual-level data concluding that there is no association between increased mortality and paclitaxel treatments.
The Katsanos et al meta-analysis found that all-cause mortality rates at two and five years were greater among patients treated with paclitaxel devices, though gave no mechanism of death. Potential candidates suggested by the authors are increased risks of infection, pulmonary disease, and malignancy. These results raised enough concern within the community to halt two ongoing clinical trials, SWEDEPAD and BASIL III, and for the US FDA to initiate an urgent internal safety review with all companies that produce drug delivery technologies for femoropopliteal disease.
However, Secemsky and colleagues add that, in Katsanos’ study, “Mortality rates were estimated using the trial enrolment population, which fails to account for patient withdrawal and loss to follow-up.” Due to the lack of patient-level data in the meta-analysis, Secemsky also notes that summary-level trial data “cannot account for missing data at the individual level, and may lack up-to-date follow-up information. As such”, he continues, “the significance of this harm signal requires replication in other populations to substantiate or alleviate the perceived safety risk.”
Further, as the present study was observational, the treatment effect was non-randomised, meaning the authors “cannot account for treatment selection bias by operators or residual unmeasured confounding.”
Patient characteristics
In this present study, of the 16,560 patients who underwent femoropopliteal artery revascularisation at the 1,883 hospitals under scrutiny, DCB use alone accounted for 16.4% of the treatments (2,709 patients). Percutaneous transluminal angioplasty (PTA) was used as the only treatment in 35% of patients (5,796); DES with DCB in 5.1% (851 patients); BMS with DCB was used in 4.4% of cases (727 patients); DES alone was used in 10.3% of cases (1,702 patients); and just a BMS was used in 28.8% of cases (4,775 patients).
The mean patient age was 72.9 years, and the total population cohort was 46.7% men, 73.9% white, and 49.7% current or previous smokers. Additionally, 59.3% had diabetes, and 51% had CLI—two conditions understood to complicate treatment.
There were no significant differences at baseline between the two arms of the study: those treated with drug-coated devices, and those treated without drug-coated devices. However, patients who were treated with drug-coated devices were more often men, and had a higher prevalence of congestive heart failure, diabetes, hypothyroidism, and anaemia, the authors write.
However, Secemsky and colleagues note that as their analysis was based on Medicare fee-for-service beneficiaries, the population was older and had a higher rate of comorbidities, such as CLI, than in the cohort under scrutiny in the Katsanos et al meta-analysis. They write: “The higher rates of mortality observed in our study likely reflect these differences in patient characteristics. As our analysis could not differentiate cause-specific mortality, we were unable to account for the competing risk of death between cardiovascular and non-cardiovascular causes, or evaluate for associations between drug exposure and specific causes of death.”
Comment: Key principles of a “modern approach” to monitoring post-marketing safety
In a commentary on the results of this study, Jay Giri remarks that there is “insufficient evidence to place a blanket moratorium on the use of PEB/PES out of concerns for long-term safety.” However, he adds that “a careful risk-benefit discussion with patients about the uncertainty in long-term outcomes with these devices is warranted in the context of their greater efficacy with regard to revascularisation outcomes.”
Giri suggests that a “modern approach to monitoring post-marketing safety of endovascular devices might be guided by the following key principles: [1] using administrative data sets for predefined raw looks at device performance [the study by Secemsky et al fits into this category]; [2] mandating public availability of individual patient data for all trials that are cited to support either the European Conformité Européene mark or US Food and Drug clearance or approval; and [3] facilitating linkage of disease and device-specific registries to a broad array of administrative data that will allow for inexpensive, long-term patients follow-up for major adverse events.”
He concludes that “the promise of the modern era of data science is predicated on making this data available to trained researchers in forms that can be used to allow for more informed decision making by patients and physicians, while providing more certainty for device manufacturers.”
A first-in-human, phase I clinical trial using stem cells to prevent venous stenosis formation in arteriovenous (AV) fistulas yields promising results. Sanjay Misra (Mayo Clinic, Rochester, USA) presented these results at the 31st annual International Symposium on Endovascular Therapy (ISET; 27-30 January 2019, Hollywood, USA), and won the award for best poster for the same research.
This was the first time this research had been presented at a meeting, and generated much buzz about the potential of autologous adipose-derived mesenchymal stem cells (AMSCs) for increasing maturation and preventing venous stenosis formation in AV fistulas used for haemodialysis.
To contextualise the importance of this research, Misra says: “At one year, nearly 60% of AV fistulas will develop a malfunction, often due to venous stenosis formation, and nearly 40% fail to mature. Pathologically, AV fistulas fail due to venous neointimal hyperplasia caused by an increase in pro-inflammatory gene expression, including monocyte chemoattractant protein-1 and tissue necrosis factor-1 alpha.”
Recognising that with the primary patency of surgical creation of AV fistulas being between 60–70% means there is a high failure rate of approximately 30%, Misra became interested in using stem cells derived from patients as their own therapy or drug.
Following preliminary research conducted in mice, the research group was granted an IND [Investigational New Drug application] from the US Food and Drug Administration (FDA) to pursue the study, which was a phase I safety trial. “Our primary concern was around safety. Would these cells be creating more infections? Will they be less irritating with respect to fevers? So we did a randomised trial comparing patients who received stem cells or no cells and followed them for one year,” Misra explains.
In the phase I, single centre, prospective, blinded, randomised trial, the study investigators reported no adverse events related to stem cell delivery, and a success in terms of maturation rate with the stem cell cohort compared to the control arm. Crucially, the team at Rochester also reported no safety issues with respect to the cellular delivery.
One month after periadventitial delivery of the autologous AMSCs to the outflow vein of the AV fistula, the maturation rate for radial-cephalic fistulas was 100% in the stem cell arm, versus 66% in the control group. For brachial-cephalic fistulas, the maturation rate was 100% in both the stem cell and the control cohorts (there were four patients in each group).
Nine patients were followed up to 12 months’ post-procedure. At this last follow-up, patients in the control group were receiving more interventions than those in the treatment arm: three patients in the control cohort (one brachial-cephalic and two radial-cephalic) underwent five fistulograms with four percutaneous transluminal angioplasties of the cannulation zone, compared with one patient in the stem cell group. “So we are seeing an effect related to the cells, less frequency of interventions,” says Misra.
The Rochester-based team are continuing to enrol patients in this prospective, phase I trial, and a future study is being planned to help determine the efficacy of this therapy. To date, 16 patients have been enrolled (11 men and five women). Patients have an average age of approximately 65 years and an average BMI of 37.99. All of the 16 patients in the study were hypotensive, 10 had a history of diabetes mellitus, five were on haemodialysis, six had a history of coronary artery disease, and 11 had dyslipidemia.
Misra indicated that a possible future direction of this work could be its use in conjunction with angioplasty for stenotic AVF. He told delegates at ISET that there was interest from the cardiothoracic surgeons at Rochester in using this therapy in coronary artery bypass grafting (CABG), and concluded by remarking that “Obviously, we can start to think about using this in the lower extremity as well.”
He and his colleagues are in the process of filling an IDE for using this stem cell therapy with angioplasty and periadventitial catheters.
The US Food and Drug Administration (FDA) has given premarket approval (PMA) for the MANTA vascular closure device from Teleflex. This device is the first commercially available biomechanical vascular closure device designed specifically for large bore femoral arterial access site closure.
The device is indicated for closure of femoral arterial access sites while reducing time to haemostasis following the use of 10–20F devices or sheaths (12–25F OD) in endovascular catheterisation procedures.
The SAFE MANTA IDE clinical trial, the largest US prospective multi-centre, single-arm trial of a purpose-designed large bore femoral access site closure, demonstrated that the MANTA device successfully achieves fast reliable biomechanical closure with rapid haemostasis, with all primary and secondary endpoints met. With its innovative design, the MANTA device has the potential to reduce bleeding complications and offset other procedural costs.
“I am very encouraged by the results of the SAFE MANTA IDE clinical trial. The clinically proven major complication rate (as defined by the study protocol) of 5.3% and VARC-2 major vascular complications rate of 4.2% compare very favourably to suture mediated devices, and the 24 second median time (65 second mean time) from deployment to haemostasis was impressive,” says Zvonomir Krajcer, lead enroller and co-principal investigator of the SAFE MANTA IDE clinical trial and co-director of the Peripheral Vascular Disease Service at the Texas Heart Institute in Houston, USA. “We have been patiently waiting for this approval, are eager to use the MANTA device commercially, and look forward to the efficiencies it can provide.”
According to a company press release, with this device, clinicians and hospitals can achieve successful large bore closure with a device that does not require pre-closure, low complication rates for biomechanical closure with rapid haemostasis, and reproducible results.
Alvimedica has announced the company has received CE mark for the Cre8 EVO 2.0mm, a polymer-free Amphilimus-eluting stent.
In a press release, Alvimedica states it is now able to offer more extensive treatment coverage for all those patients with complex coronary artery disease: Cre8 EVO 2.0mm embeds the unique technologies of Cre8 and Cre8 EVO drug-eluting stents (DES), extending their clinical benefits to small vessels up to 2.0mm.
In recent decades, small vessel disease has become more frequent due to a worsening of the clinical profile of the patients undergoing percutaneous coronary intervention (PCI): the population needing DES to treat coronary artery disease is increasingly older, often with diabetes mellitus and other comorbidities. These clinical conditions increase lesion complexity and consequently also the need of implanting DES in coronary arteries smaller than 2.25mm, which is usually the smallest available diameter in a DES coronary portfolio.
The Cre8 EVO small vessel DES has a dedicated design which maximises device performance in this clinical setting. The ultra-thin total stent struts of only 70 micron minimise metal volume in small coronaries, while the dedicated design matches the specific requirements of 2.00mm vessels in terms of device deliverability, conformability to the vessel and mechanical performances. Cre8 EVO for small vessel is a “physician-friendly” device with no compromises. Its unique cell geometry allows this DES to be implanted in challenging conditions like tapered and tortuous vessels that can also involve clinically impactful side-branches.
Leyla Alaton, president and CEO of Alvimedica, comments: “We are taking the challenge to develop devices that answer the real everyday clinical un-met needs in a global scenario. The patient population suffering from coronary disease increases every year, as well as its clinical need may be different according to the clinical conditions, disease location and geographical area. Alvimedica wants to be on the edge of innovation to help providing these patients the safest and most effective solutions”.
InspireMD has announced positive interim results from the SIBERIA trial, an investigator-initiated study of the CGuard embolic prevention system (EPS). The data were presented at the Leipzig Interventional Course (LINC; 22–25 January, Leipzig, Germany).
Andrey Karpenko and Pavel Ignatenko from the Siberian Federal Biomedical Research Center, Russia, presented the interim data from their first 50 patients in an independent, randomised clinical trial designed to ultimately include 100 consecutive patients with symptomatic and asymptomatic carotid artery disease. The patients are randomly assigned (1:1) into two treatment groups. Fifty patients will receive the CGuard EPS MicroNet mesh covered stent and the other 50 patients will receive a conventional carotid stent. The primary endpoints are the incidence and volume of new lesions within the brain after carotid stenting using diffusion weighted magnetic resonance imaging (DW-MRI) peri-procedurally and at 30 days.
At the protocol-mandated interim analysis, after recruiting the first 50 patients in the study, the results at one month show that, despite having patients with higher risk factors in the CGuard group compared to the conventional carotid stent arm, the CGuard-treated patients had a significantly lower incidence of multiple lesions in the brain (16% vs. 44%), and a lower incidence of large cerebral lesions (24% vs. 40%). Finally, major adverse clinical events after 30 days occurred in the conventional carotid stent arm but not in the CGuard EPS-treated patients (12% vs. 0%).
Karpenko commented, “We are excited that despite the higher-risk patient profile in the CGuard group, the interim results show a significant reduction of cerebral embolisation while patient outcomes suggest a clinically-relevant benefit of the CGuard EPS. This mandated interim analysis gives us confidence to continue enrolling patients in this trial and extending the data-set in this potentially important advancement in the stroke prevention field.”
Biotronik has presented the company’s Pulsar-18 T3 stent system for the first time during the Leipzig Interventional Course (LINC; 22–24 January, Leipzig, Germany).
The Pulsar-18 T3 system is a unique combination of three technologies for an improved implantation procedure, a company press release states. The 4F low profile decreases the risk of access site complications and reduces the need for closure devices compared to 6F, while the tri-axial shaft design facilitates stable and accurate implantation of the clinically proven Pulsar stent. The intuitive and ergonomic wheel-operated handle simplifies handling during the procedure for physicians.
The superficial femoral artery (SFA) requires a stent that conforms to the natural vessel movement and provides sufficient support in complex and long lesions. The new device unifies proven technologies for efficient delivery of stents up to 200mm to the challenging SFA. The thin struts, low chronic outward force (COF) and high multidirectional flexibility of the Pulsar stent ensure conformability and support to the vessel in all natural vessel movements.
“Pulsar-18 T3 is a unique innovation; this is the first time physicians have access to a self-expanding stent system that combines the benefits of 4F with the accurate deployment of a tri-axial system,” stated Alexander Uhl, senior vice president of Corporate Marketing at Biotronik. “Pulsar-18 T3 represents Biotronik’s dedication to providing effective therapies which minimise burden and reduce risks to patients.”
While introducing the new features to enhance deployment, the new stent system builds on the established Pulsar-18 stent. Recent data highlighted the long term safety and efficiency of Pulsar-18 by showing a freedom from target lesion revascularisation rate of 92.4% at 24 months.
The 4F delivery system offers a number of benefits, including clinically proven lower access site complication rates and a reduced need for closure devices compared to 6F stents. With its low COF and thin struts of 140µm, Pulsar-18 is proven to cause less vessel injury and inflammation, provide faster endothelialisation and lower the risk of restenosis.
Pulsar-18 T3 is indicated for use in patients with atherosclerotic disease of the superficial femoral, proximal popliteal and infrapopliteal arteries and for the treatment of insufficient results after percutaneous transluminal angioplasty (PTA), e.g. residual stenosis and dissection.
The FDA has granted approval to include the use of atherectomy for lesion preparation in its ongoing US pivotal study of the Chocolate Touch drug-coated balloon (DCB; QT Vascular) and the addition of subgroup analysis related to the use of atherectomy.
The Chocolate Touch device is the drug-coated version of the company’s Chocolate percutaneous transluminal angioplasty balloon, which was acquired by Medtronic in January 2018 and is commercially available in the USA.
The prospective, randomised Chocolate Touch pivotal study is being conducted in up to 50 centres in the USA, and selected centres in Europe and New Zealand. The study’s co-principal investigators are Mehdi Shishehbor (Cleveland, USA) and Thomas Zeller (Bad Krozingen, Germany).
In the company’s press release, Shishehbor comments: “The inclusion of atherectomy in the study is a unique element that expands the potential use of Chocolate Touch, both in hospitals and out-patient–based labs. The study will provide an important data set that is consistent with real-world practice, especially at [out-patient–based labs] where more and more patients are getting treated.”
The study is evaluating patients with disease in the superficial femoral and popliteal arteries in the legs. Patients are randomised 1:1 to the Lutonix DCB (BD). The study evaluates acute endpoints such as procedural successes and freedom from bail-out stenting, and long-term endpoints such as patency and target lesion revascularization among others.
The Chocolate Touch DCB is not commercially available in the USA, and can only be used in the investigational device exemption clinical study. The device received CE mark in August 2015 and is available in the European Union and other countries.
Dierk Scheinert (Leipzig, Germany) talks to Vascular News at LINC 2019 about the importance of vessel preparation with adjunctive therapies such as the use of the dedicated scoring balloon, ULTRASCORE (BD), prior to the use of a drug-coated balloon (DCB), such as the Lutonix DCB. The ULTRASCORE Focused Force balloon is an effective and easy-to-use device, designed to fracture plaque at low inflation pressures, he says.
The PreludeSYNC DISTAL compression device (Merit Medical) is now available in US, European, Middle Eastern, African, and Asia-Pacific markets. The device is the first product specifically designed to achieve haemostasis of the radial artery during procedures where access is gained via the distal radial artery.
Designed, according to a company press release, “with a comfortable band and a large window for site visibility”, the PreludeSYNC DISTAL compression device is applied over the arteriotomy, allowing the clinician to slowly inflate the balloon with air while simultaneously removing the sheath. It then maintains pressure at the site to allow the access wound to achieve patent haemostasis.
Merit is also answering demand for distal access training through its ThinkRadial course, with the next one taking place on 9 February 2019. The course will feature a dedicated three-hour session specific to distal radial access, which will be streamed live online and available to interventional cardiologists and radiologists who want to learn the distal technique. Additional information about other ThinkRadial courses, including registration, may be found on the programme’s website.
The live streaming event features Ferdinand Kiemeneij from Amsterdam, The Netherlands, widely considered the “father of transradial intervention”; Sandeep Nathan, an interventional cardiologist in Chicago, USA; and Darren Klass, an interventional radiologist based in Vancouver, Canada.
Sean Lyden (Cleveland, USA) and Fabrizio Fanelli (Rome, Italy) discuss the safety and future of drug-coated balloons (DCB) in light of the latest pooled analysis of patient-level data of over 2,300 patients treated with Philips’ Stellarex DCB in above-the-knee studies.
The independent, third party pooled analysis, presented by Lyden at LINC 2019, demonstrated low mortality rates through three years after the treatment with no device-related deaths.
Renowned experts expressed confidence in the continued use of paclitaxel-coated devices after independent patient-level data presented at LINC 2019 did not show correlation between paclitaxel exposure and mortality.
Findings from Baim (formerly Harvard Clinical Research Institute) are now published in the Journal of the American College of Cardiology (JACC) and are available online.
Speaking to Interventional News, Comerota expressed his gratitude: “This is one of the greatest honours that one can have given. This meeting, ISET, is one of the elite educational programmes in the world, and to be recognised by the directors of ISET, and to be given a career achievement award obviously is exceptionally special, and an enormous honour. I am eternally grateful.”
When asked how the meeting had shaped his career, Comerota said: “I do not know that there is a better meeting that addresses the current issue of vascular disease from all specialities, from medical management, to interventional management, surgical management—it covers all the bases. So it is a wonderful investment of time, and it is a wonderful educational experience.”
Recipients of the career achievement award is voted on by the ISET programme directors. In his introduction, Barry Katzen (Miamia, USA) says that ISET has been awarding the award for approximately 25 years.
Born in Newark, USA, Comerota was the director of Vascular Services at Temple University Health System, Philadelphia, USA, and was professor of surgery from 1989 to 2002 and chief of Section of Vascular Surgery from 1984 to 2002. He then moved to Toledo, USA, to the Jobst Vascular Institute, where he was director from 2002 to 2006. He was also an investigator of the ATTRACT trial. Comerota has previously been profiled by Vascular News, a sister publication of Interventional News.
Described by Katzen as “an academic giant”, Comerota is a journal reviewer in over 15 high impact, peer-reviewed journals, and has trained 46 fellows in Vascular Surgery.
Comerota was an early adopter of multidisciplinary models and collaborative practice, and was one of the first to work closely with interventional radiology. In his speech, Katzen told the ISET audience how Comerota pioneered venous research, diagnostics, surgery, and endovascular therapy.
Katzen finished by saying: “I have done a lot of introductions, and it is very hard to do justice to a man of his distinction and character. It is a great honour to recognise such a man with this career achievement award.”
The editors-in-chief of major cardiovascular journals—of both US and European societies—have come together to “sound the alarm” about the dangers of medical misinformation that has been disseminated through the internet, social media, and other platforms. They claim that this misinformation is dangerous because it leads to patients’ refusing medication, such as statins, that have documented life-saving benefits.
Joseph A Hill (Department of Medicine, University of Texas, Southwestern Medical Center, Dallas, USA) and others write in Circulation and in several other international cardiovascular journals that medical misinformation “hyped through the internet, television, chat rooms, and social media” has caused many patients to think that the risks of statins are far worse than they actually are and, as a result, refuse to take the drugs. “Most patients do not recognise that the benefits of statin use are invisible (‘I didn’t have a heart attack or stroke this past year’) whereas the small and typically reversible risks (e.g. muscle pain) are readily apparent,” they add. The authors note that patients rejecting statins is just one example of the effects of medical misinformation, and that another is parents not letting their children be vaccinated following an infamous—and now widely discredited—paper that linked autism to the MMR vaccine.
Furthermore, Hill et al say that some celebrities, actors, activists, and politicians promote false or misleading medical ideas and claim “not uncommonly” there are people acting with “purely venal motives”. According to Hill et al, “the strident alarms” by well-known people “speaking in absolute terms” exacerbate the problem of medical misinformation because their words resonate better with the general public than the “nuanced voices” of scientists. The authors state that scientists “appropriately couch their statements in statistical terms, which may come across to the public as equivocation”.
Hill et al, therefore, have written their editorial to “sound the alarms that human lives are at stake” and call on the media to “do a better job” at avoiding sharing medical misinformation. “It is unacceptable to posit false equivalents in these discussions [such as the risks and benefits of statins], often done to foster debate and controversy. It is easy to find a rogue voice but inappropriate to suggest that this voice carries the same weight as that emerging from mainstream science,” they comment.
In particular, given misinformation tends to travels faster through social networks than does the truth, Hill et al write that the “purveyors of social media must be responsible for the content they disseminate” and it is no longer acceptable for these purveyors to “hide behind the cloak of the platform”. They explain that, as editors-in-chief, they “reach out to thought-leading experts to evaluate the veracity of each report” they receive and “challenge social media to do the same”—“to leverage the ready available of science-conversant expertise before disseminating content that may not be reliable”.
“Without exaggeration, significant harm, to society and individuals, derives from the wanton spread of medical misinformation. It is high time that this stop, and we lay at the feet of the purveyors of the internet and social media content the responsibility to fix this,” Hill et al conclude.
Hill told Cardiovascular News: “The internet and social media platforms are replete with false information, which does real harm to individuals globally. We charge the purveyors of these media to take first steps in addressing this enormous problem, and we, in the academic medical community, stand ready to help.”
As well as being published in Circulation, the editorial was also published in the European Heart Journal, Journal of Electrocardiology, and the International Journal of Cardiology among others.
A pilot study of edetate disodium-based chelation in diabetic patients with critical limb ischaemia (CLI) has positive results, leading the study investigators to “cautiously support” the design of a chelation trial in peripheral arterial disease (PAD). This conclusion was presented in an e-poster at the 31st International Symposium on Endovascular Therapy (ISET; 27-30 January, Hollywood, USA) by Francisco Ujueta, and as an oral presentation by Gervasio Lamas (both Mount Sinai Medical Center, Miami, Florida), who has dedicated 20 years of his professional life to the study of chelation therapy.
The study authors note that the National Institute of Health (NIH)-funded trial to assess chelation therapy (TACT) demonstrated a reduction in cardiac events in diabetic patients receiving edetate disodium-based chelation. As CLI carries a high annual risk of death, major amputation and/or myocardial infarction, the investigators tested TACT infusions in 10 patients with both diabetes mellitus and CLI (the latter defined as Rutherford category 4 or 5, with ≥75% stenosis in two or more infra-popliteal arteries, as well as a skin perfusion pressure of 40mmHg in the affected limb) to see if they could improve quality of life and limb salvage.
In this open-label trial, up to 50 TACT infusions were given over one year, plus oral vitamins. Infusions contained up to 3g of edetate disodium, 7g of vitamin C, B vitamins, magnesium, and other electrolytes. Lamas acknowledged at the start of his talk that “until recently, [chelation therapy] has been considered quackery”, but set out to change the audience’s mind through sharing his experiences with the treatment and the positive results of the present study.
In a multi-centre, randomised trial of 1708 post-myocardial infarction patients, patients were given either 40 3g dose of disodium-EDTA, or 40 placebo infusions. Overall, there was a modest reduction in recurrent cardiac events in the active chelation group. Lamas reports that most of the benefit seen in the investigational arm was in the 633 diabetic patients. Over the course of five years, the study investigators witnessed a 41% decrease in major adverse cardiac events (MACE). Breaking this result down, Lamas specifically points to the detected 43% reduction in relative risk of death, in his words the “holy grail of clinical trials”, and to an approximately 50% reduction in risk of recurrent myocardial infarction.
Toxic metals are a known atherosclerotic risk factor. The aim of chelation therapy is to reduce this risk via the removal of toxic metals from the body through the urine. Following chelation therapy, huge increases in the urinary cadmium and lead concentrations are observed, indicating the flushing out of these materials from the body. On average, there is a nearly 4,000% increase in urinary lead and a 700% increase in urinary cadmium after an initial chelation infusion, representing excreted body stores of these vasculotoxic metal pollutants. (see figure 1).
Figure 1
Supplementing this multi-centre data with the story of particular cases in a subsequent, pilot study, Lamas describes the desperation of some diabetic patients with CLI. He told ISET attendees how one patient, after experiencing multiple unsuccessful revascularisation attempts through interventional and surgical means, was scheduled for a below-the-knee amputation. According to Lamas, the patient’s wife found out about Lamas’ open-label experiment in 10 patients and “insisted” that he give chelation a try. After 48 infusions, and no other intervention, the patient was no longer at risk of amputation, and the foot ulcerations and pain had disappeared (see figure 2). Of the pre-treatment and post-treatment images, Lamas said: “These are the kinds of pictures that led me to believe we need to look at this as an adjunct to everything that is being done at this conference [ISET]”.
Figure 2
Lamas informed delegates that the patient’s wife refused to stop chelation treatment, and so he has been getting ongoing treatments from a chelation practitioner.
The poster presented at ISET shows these same results. Ujueta and colleagues conclude: “These findings suggest that TACT infusions in diabetic CLI patients are safe, increase excretion of vasculotoxic metals, may improve quality of life, and might improve clinical outcomes.”
Lamas concurred at the end of his presentation: “Toxic metals are a modifiable atherosclerotic risk factor, and that this may be an idea whose time has come.”
The study was funded by Mount Sinai Medical Center and the James Carter Memorial Fund.
Philips launches its Azurion with FlexArm to aid patient imaging and positioning during image-guided procedures.
During increasingly complex interventions, clinicians need to quickly and easily visualise critical anatomy and identify changes to the patient during the procedure. Azurion with FlexArm is designed to allow the clinician to perform imaging across the whole patient in both 2D and 3D. As the clinician moves the system, the image beam automatically maintains alignment with the patient, allowing more consistent visualisation and enabling them to keep their focus on the treatment.
The range and complexity of diseases that can be treated with minimally invasive procedures continues to expand. Correspondingly, the procedures themselves are also becoming more complex, requiring more physicians from different disciplines to be at the patient’s tableside, working together in a highly coordinated way. As a result, the clinical team is required to carry out increasingly challenging procedures in a highly constrained environment.
Azurion with FlexArm’s innovative design provides exceptional flexibility and intuitive control. Powered by a kinematic engine, the system moves on eight different axes, all controlled with its single ‘Axsys’ controller. Simulation tests with clinicians have demonstrated the system’s potential to significantly reduce the repositioning of the patient, staff and equipment to improve access for minimally invasive procedures, including those that enter the body through the patient’s wrist (‘radial access’), and to reduce the risk of unintentional pulling of wires and tubes, as well as significant time savings.1 The system is ideally suited for Hybrid ORs that cater to multiple specialties in one room, such as a combination of surgical and endovascular procedures.
Azurion with FlexArm is the latest addition to Philips’ portfolio of systems, smart devices, software and services in image-guided therapy. As the range of diseases that can be treated with minimally invasive procedures continues to expand and the procedures themselves become more efficient, the patient’s treatment experience continues to improve. They experience less trauma, and as a result their stay in hospital can be dramatically reduced—often returning home after one night in hospital, and for some procedures even leaving the hospital on the same day.
Since its global launch in February 2017, over 450,000 patients have been treated in more than 80 countries using a Philips Azurion system. The Philips Azurion 7 C20 with FlexArm is CE marked and has received 510(k) clearance from the US Food and Drug Administration (FDA).
Barry Katzen moderating the paclitaxel town hall panel at ISET 2019. Photo Credit: Pierce Harman Photography for ISET/HMP
The discussion around the use of paclitaxel-coated and eluting devices continues at the 31st International Symposium on Endovascular Therapy (ISET; 27-30 January 2019, Hollywood, USA). Organisers hosted a paclitaxel town hall to consider whether or not the recent meta-analysis from Katsanos and colleagues—concluding that there is a higher risk of death at two and five years following the use of paclitaxel-coated balloons and stents in the femoropopliteal artery—was concerning enough to alter current standards of practice.
Seventy-nine per cent of the ISET audience did not believe that the findings from the Katsanos et al (Journal of the American Heart Association; JAHA) meta-analysis were sufficient for them to change practice. Although James Benenati (Miami, USA) drew attention to the interesting fact that 31% of respondents said they would use it less, with the remaining 69% answering that they will use these devices as they always have. This result may reflect physician concerns of litigation or a class action, an opinion voiced repeatedly by ISET attendees to Interventional News following the FDA’s recent announcement that it was launching its own investigation into the findings and the pausing of two ongoing paclitaxel trials (SWEDEPAD and BASIL III) until further investigation has been conducted.
Barry Katzen (Miami, USA) contextualised the discussion, saying: “It has been an unusual time over the last couple of months in our space, where a manuscript has come out in a highly reputable journal [JAHA] with some highly significant implications, that could potentially change the practice in our field. There has been a lot of discussion at meetings and… it seemed appropriate that we try and delve into this issue and its implications. We have heard all sorts of responses to this manuscript [the Katsanos meta-analysis], including pulling devices off shelves of inventory, and concerns about the use of devices associated with paclitaxel delivery.”
Paclitaxel dose not biologically relevant after 30 days
Providing a review of the pharmacology and paclitaxel’s mechanism of action, Juan Granada (New York, USA) reminded the ISET audience that paclitaxel is a cytotoxic drug and that the drug-coated balloon (DCB) pharmacokinetics depend on both the concentration and solubility of the paclitaxel. He explained that paclitaxel is a cytotoxic drug that may induce a constellation of toxicities that are usually dose and schedule dependent. However, he further explained that even at its highest dose, compared to systemic use, DCB use results in lower systemic exposure by several orders of magnitude. According to Granada, the transient multi-organ distribution of paclitaxel results in tissue concentrations approaching zero at 30 days. Granada told attendees that he wanted to emphasise this because, in his opinion, the paclitaxel concentration in tissues was “grossly overemphasised, and actually mistakenly overemphasised, by Katsanos”. Granada concluded that “systemic tissue concentrations remain below the therapeutic threshold and are unlikely to exert a sustained biological effect, especially at five years”.
Time-to-event data not used in Katsanos et al (JAHA) meta-analysis
In his review of the Katsanos et al (JAHA) meta-analysis, Jihad Mustapha (Grand Rapids, USA) noted that “metrics such as number of withdrawals, number of patients remaining at risk and timing of deaths were not considered in these calculations. Mortality rates drawn from time-to-event data are preferred in meta-analyses.” He stated that not using time-to-event data led to reporting of very different five-year mortality rates of patients treated with the Zilver PTX drug-eluting stent (DES; Cook Medical) versus controls compared with the original study.
ISET 2019 paclitaxel town hall. Photo Credit: Pierce Harman Photography for ISET/HMP
Don’t start a “paclitaxel panic”
Gary Ansel (Columbus, USA) presented insights from the patient-level data from the IN.PACT DCB and Zilver PTX programmes. Ansel concluded that these data showed that there was no difference in mean paclitaxel dose by survival status, no difference in survival between paclitaxel dose level (low, mid or high) and paclitaxel dose was not identified as a predictor of mortality. Thomas Zeller (Bad Krozingen, Germany) stated that this is not time to start a paclitaxel panic: “Is it time to panic? No. One single bad publication can damage a valuable treatment modality. We have seen this with renal denervation, we have seen this with renal stenting. If papers are published in very big journals, they are taken as truth, and may really bias and impact out treatment of patients,” he said.
Zeller sought to differentiate the systemic effects of paclitaxel from the local effects. He presented a case of a 76-year-old female patient who was treated with the IN.PACT DCB (Medtronic) in 2011, and was still a patient five years later. An aneurysm grew to 5cm following treatment with the device. Zeller mused that while local vessel wall damage such as this has been reported, it is not understood in much detail. However, he concluded that “systemic toxicity with low dose paclitaxel release via DCB or DES seems to be unlikely but warrants further observation.”
No signal for cancer
As the Katsanos meta-analysis indicated a signal for increased mortality risk at two years following the use of paclitaxel devices in femoropopliteal lesions, since its publication there has been interest in the causes of increased mortality at two years, which remain to be elucidated. Juan Parodi (Buenos Aires, Argentina) asked the panel if there was a link with cancer. However, William Gray (Wynnewood, USA) said this was not supported as a cause of death, referring to patient-level data presented at the Leipzig International Course (LINC; 22-25 January, Leipzig, Germany) that showed no signal for cancer.
Also critiquing the meta-analysis, Andrew Holden (Auckland, New Zealand) told delegates that study investigators need to consider the way patients are randomised in trials. However, he began by saying that “I think we need to congratulate Katsanos; I think it takes some courage and, while there are some reasonable concerns about the methodology, at least this has got us considering some very important findings.”
He continued: “Overall, though, I think we are struggling, because the finding is illogical, in that, as we know, the drug dose is much lower than the systemic dose of paclitaxel, the duration is very limited, and given that very limited duration, why would the mortality be different at one year and different at two years? There is also no mechanistic explanation, which we need to find.
“One point I would like to raise, having done a lot of these randomised trials, is the mechanism of randomisation. I think we really need to look at this, as well as looking at the overall use of meta-analyses, and particularly the abuse of meta-analyses we have seen in recent years. What actually happens when you randomise a patient is essentially you go online, and you have some demographic data, primarily lesion length, lesion complexity, patient age and gender—but there is very little data on cardiovascular risk factors. The way the programmes are run, they tend to favour the control arms slightly over the investigational arm. What you do not want in a trial is to find that lesions were more simple in the investigational arm, and what that means is, it is likely that patients in the investigational arm have a higher incidence of risk factors than those in the control arm. We have seen that time and time again. I think we need to evaluate the way we randomise patients, because essentially I think we are randomising patients in trial arms that have slightly more comorbid findings, and that may result in more mortality.”
Holden concluded by saying: “I am not convinced by the finding. I am convinced by the superior patency that we get with drug-eluting technologies, and until we get more information, in New Zealand anyway, we are going to keep using these devices.”
Patient consent at the forefront of interventionalists’ minds
Through the audience discussion, it was evident that patient consent for procedures involving a paclitaxel-eluting or coated device is now at the forefront of many physicians’ minds. Speaking from the panel, Richard Neville (Fairfax, USA) said: “This has had more of an impact on my patients than any paper I can recall recently. I actually had a patient come to the office recently with her family, who had heard about this, and asked if I was going to use ‘that balloon that will kill’ their father. I do not think I have seen a publication that I can recall in recent memory, despite many of the advanced devices that we all use, that has created quite the controversy and the awareness that this has had in patients.”
Holden reiterated this patient response, commenting how he had also seen patients bring up concerns based on the results of the meta-analysis.
Describing how, upon seeing the meta-analysis for the first time, he had felt conflicted about whether or not to inform his patient of the findings, Michael Jaff (Boston, USA) asked the ISET audience if they would have mentioned the publication to a patient who would potentially be receiving treatment involving a paclitaxel-eluting or –coated device. Over half of the audience (52%) indicated that they would not have informed their patient, 29% of respondents said they were “uncertain”, and 19% of patients said “yes”, they would tell their patient. When asked by an audience member which option he chose, Jeff informed delegates that he had told the patient that he “just seen this alert on his phone”, but that he “needed to read more about it”. He reassured his patient that “this was not an urgent situation” and said to give him more time to review this—Jaff is in fact due to see this same patient the week following the ISET meeting, and is hoping to use the clarity gained through discussion to guide his practice going forward.
Review of patient-level data at upcoming conferences
As reported in TCTMD, Granada described how the next steps involve reviewing the existing data: “Everyone is reviewing again all the experimental data, to look at the systemic exposure of these devices. I think that is going to be number one.”
VIVA [Vascular Interventional Advances] has assembled an invite-only special session of the Vascular Leaders Forum series on the topic “Drug elution in peripheral arterial disease (PAD): A critical analysis from a multidisciplinary consortium” (1-2 March, Washington, DC, USA). Following this analysis and discussion, the Charing Cross symposium (CX; 15-18 April, London, UK) will have a highlight session to independently review whether or not paclitaxel usage is beneficial or detrimental to the patient, which aims to have the final word on this controversy.
Experts from the Society for Cardiovascular Angiography and Interventions (SCAI) have reviewed the recent meta-analysis by Katsanos and colleagues and have concluded that the methods are appropriate and within constraints of trial-level meta-analysis. However, the society statement says “it is important to note that SCAI believes the associations are hypothesis-generating and require further investigation with patient-level data.”
The Katsanos meta-analysis, published in the Journal of the American Heart Association (JAHA), revealed an increase in long-term mortality with paclitaxel-coated balloons and paclitaxel-eluting stents. The study evaluated 28 randomised controlled trials across 12 devices for the treatment of femoropopliteal disease.
The SCAI statement summarises the findings of the meta-analysis, before highlighting some limitations of the study. It identifies the following limitations:
There is no mechanistic explanation for the study findings.
A post-hoc analysis did not include patient-level data to adjust for clinical and angiographic differences between those who died and those who did not.
There is evidence of discrepancy in some of the reported numbers.
The study findings could be by chance—a type-1 error due to multiple testing.
Less than 50% of the trials report data beyond one year and only 3% at five years.
The equation to assess the paclitaxel dose/time relationship may have overestimated drug exposure and its effect over time.
Recently, the US Food and Drug Administration (FDA) issued a letter to alert physicians to the meta-analysis findings. The agency has asserted that the benefits of paclitaxel-coated devices outweigh the risks when used as indicated. However, the SCAI point out that the FDA urged healthcare providers to report any adverse events or suspected adverse events with paclitaxel-eluting devices through its MedWatch programme.
The SCAI indicate several recent, large trials with patient-level data presented by investigators at the Leipzig Interventional Course (LINC; 22-25 January 2019, Leipzig, Germany). Data from these trials show comparable mortality rates among patients treated with paclitaxel-coated or -eluting devices compared to plain angioplasty or bare metal stents.
Secondly, the SCAI statement points to the RANGER SFA randomised trial three-year data from 105 patients. This showed no significant difference in all-cause mortality between DCB and control (13.8% vs. 10.7%, respectively).
Five-year data from 479 patients enrolled in the ZILVER PTX randomised trial showed no statistically significant difference in all-cause mortality between ZILVER PTX and the control group (18.7% vs. 17.6% respectively, p=0.53).
A three-year pooled analysis of 2,521 patients from RCTs and non-RCTs from the Stellarex DCB programme (2,351 DCB and 170 controls), showed no statistically significant difference in all-cause mortality between Stellarex and the control groups (7.9% vs. 9.9% respectively, p=0.78).
Five-year data from 1,189 patients in the Levant 2 Trial within the LUTONIX DCB programme showed no statistically significant difference in all-cause mortality between DCB and the control group (14.1% vs. 10.6% respectively, p=0.22).
The SCAI concludes: “We expect further details from these meta-analyses to be examined in peer reviewed journals in the near future. Additional patient-level analyses are underway by [the] FDA, independent physicians, and industry, and SCAI is closely monitoring this evolving situation.”
“At present, SCAI concurs with [the] FDA that the benefits of paclitaxel devices continue to outweigh any potential risks,” says SCAI president, David Cox. “However, we strongly encourage our members to discuss the findings of the meta-analysis with their patients and to report any safety concerns to [the] FDA.”
The IN.PACT Admiral drug-coated balloon (DCB; Medtronic) exhibits a consistent and durable treatment effect in “a more complex patient demographic than typically seen in other DCB pivotal trials”, Osamu Iida (Kansai Rosai Hospital, Hyogo, Japan) informed the audience at the Leipzig Interventional Course (22–25 January, Leipzig, Germany). These are the first reported outcomes from an independently-adjudicated, randomised, single-blind trial evaluating DCB use in Japanese patients through to three years, providing level I evidence in favour of the device’s use.
The study investigators set out to assess the safety and efficacy of the IN.PACT Admiral DCB for the interventional treatment of de novo and non-stented restenotic lesions in the superficial femoral artery and the proximal popliteal artery as compared to treatment with standard percutaneous transluminal angioplasty (PTA).
The trial met both its primary effectiveness and primary safety end-points at one year, and continued to demonstrate safety and efficacy at three years. The primary effectiveness end-point was primary patency at 12 months, defined as freedom from clinically-driven target lesion revascularisation (TLR) and freedom from restenosis as determined by duplex ultrasound-derived peak systolic velocity ratio (PSVR) less than or equal to 2.4.
Three-year primary patency by Kaplan-Meier estimate was significantly better in the DCB arm than the PTA arm: 68.9% compared to 46.9%. At one year, this difference was even more marked, with a primary patency in the DCB arm of 93.9%, compared to a primary patency of 46.9% in the PTA arm at the same time point.
The time to clinically-driven target lesion revascularisation was also significantly greater in the DCB arm, nearly four times longer in fact, at an average of 613.2±243.1 days (range: 235–910 days), compared to just 168.2±65.4 days (range: 57–247 days) amongst the PTA cohort (p<0.001). In addition, although not statistically significant, the three-year freedom from clinically driven TLR was slightly better in the DCB arm, at 84.4% versus 81.3% in the PTA group.
The primary safety endpoint was freedom from device- and procedure-related death through 30 days, and freedom from target limb major amputation and clinically-driven target vessel revascularisation within 12 months’ post-index procedure.
Iida told the LINC audience: “The 36-month major adverse event rate was very low in the DCB arm, just 20.9% [14 out of 67 patients], compared to 31% [9 out of 29 patients] in the PTA arm.” The primary safety composite score was 83.6% for the DCB cohort, and 75.9% for the PTA cohort. All-cause death was low in both groups: 6% (four out of 67 patients) in the IN.PACT Admiral group, and 6.9% (two out of 29 patients) in the angioplasty group.
Iida also emphasised that these results in the IN.PACT Japan trial are consistent with those of the previous IN.PACT Global and IN.PACT SFA studies. The primary patency through to three years in the IN.PACT Admiral cohort of the Japan trial closely matches the 69.5% primary patency observed in the DCB arm of the IN.PACT SFA trial. Clinically-driven target lesion revascularisation was 14.9% in the Japanese trial, compared with 15.2% in the IN.PACT SFA trial and 23.5% amongst the global clinical cohort.
A complex patient cohort
Iida described the patient cohort used in this trial as “a more complex patient demographic than typically seen in other DCB pivotal trials.” The average age in the DCB arm was 73.3±7.4, and the incidence of diabetes mellitus was high: 58.7% in the treatment group (40 out of 68 patients). In the PTA arm, the baseline characteristics were not statistically significantly different, with an average age of 74.2±6.1, and with 56.3% of the 32 patients being diabetic.
“This population is older, and has a higher proportion of diabetic patients, than is typically seen in other DCB clinical trials,” Iida said.
Lesion characteristics were also the same between the two arms of the study. The mean lesion length was 9.15±5.85cm in the 68 patients treated with the DCB, and 8.89±6.01cm in the 32 patients treated with angioplasty—“one of the longest [average lesion lengths] in any DCB trial”, according to Iida. The difference in mean lesion length between the DCB and PTA arms was not statistically significant (p=0.838).
Unique to this trial, the study investigators used intravascular ultrasound (IVUS) to evaluate the ideal diameter for balloon selection. Iida explained that “IVUS is generally used by the Japanese physician as a part of daily practice.”
He added, “We observed a very low provisional stenting rate of 4.4% in the DCB arm, versus 3.1% in the PTA arm.”
New 12-month data from the VIRTUS trial demonstrate that patients who were treated with the Vici venous stent system (Boston Scientific) for iliac and femoral vein obstructions exhibited a high rate of patent, or open, target lesions. Primary safety and efficacy results from the trial were presented as a first-time data release at the Leipzig Interventional Course (LINC; 22–25 January, Leipzig, Germany) by principal investigator Mahmood Razavi (St Joseph Heart and Vascular Center, Orange, USA).
The VIRTUS trial evaluated the Vici stent in patients with clinically significant obstructions in the illiofemoral venous outflow tract resulting from post-thrombotic syndrome (PTS) or compressive diseases such as May-Thurner syndrome.
“The primary safety and efficacy endpoints were very successfully met, with very low p-values”, Razavi told the audience at LINC. The trial’s primary effectiveness endpoint saw a primary patency rate of 84% at 12 months, which was greater than the predefined performance goal (PGE) of 72.1% (p<0.0001).
“Nearly all the patients treated with the stent, 98.8%, were free from major adverse events at 30 days post-procedure, thus surpassing the predefined safety performance goal (PGS) of 94%.
The VIRTUS investigational device exemption (IDE) trial, submitted in June of 2018, is a prospective, multicentre, single-arm, nonrandomised study that enrolled 170 patients with chronic disease; 75% (127) of whom were diagnosed as having post-thrombotic lesions and the remaining 25% (43) were diagnosed with non-thrombotic lesions (i.e., May-Thurner syndrome). Venography, Doppler ultrasound and intravascular ultrasound (IVUS) were performed pre- and post-stenting, as well as at 12-month follow-up.
“In treating patients with venous obstruction, the primary goal is to restore and maintain vessel patency to ensure the return of blood flow to the heart,” said Razavi. “In these results, the Vici stent demonstrated excellent performance outcomes in a difficult to-treat patient population, which translates to improvement of long-term symptoms and enhanced quality of life in these patients.”
In terms of clinical severity, Razavi reported a Vascular Clinical Severity Score (VCSS) decrease of 4.4 points at 12 months, with a median VCSS of 10 in 146 patients falling to 5.6 in 132 patients followed up to 12 months. At baseline, 65.8% of patients presented in the category of most severe VCSS of eight or more, which decreased to 33.3% at six months and further fell to 27.3% at one year.
Two adverse events (1.2%; n=169) were seen in the cohort at 30 days, both of which were described as “arterial or venous injury at the tar get vessel segment and/or target lesion location or at the access site requiring surgical or endovascular intervention”. There were no instances of device-related or procedure-related death, major bleeding at target or access site, acute deep vein thrombosis outside target vein segment, clinically significant pulmonary embolism or embolization of the stent at 30 days.
“Physicians who select endovascular treatment options for their patients with venous disease are not only faced with challenging disease states but must also account for the unique anatomical presentation of these deep veins that are subject to chronic obstruction and compression,” said Ian Meredith, executive vice president and global chief medical officer of Boston Scientific, in a company press release.
“The results from the VIRTUS trial demonstrate the importance of having a therapeutic option that is specifically designed for venous application, thus helping patients avoid recurrent pain, swelling and other debilitating aspects of acute and chronic venous disease.”
The stent system was approved for use in Europe and other geographies that recognise CE mark in 2013. In the USA, the stent is an investigational device and is not available for sale. The device was developed by VENITI, which Boston Scientific acquired in August of 2018.
New results suggest that the Tigris vascular stent (Gore) is a safe and effective device that can be incorporated into a modern “leave-nothing-behind” treatment algorithm that reserves stent usage for more challenging patients. These findings were recently presented at the Leipzig Interventional Course (LINC; 22–25 January 2019, Leipzig, Germany).
Gore has also announced the launch of its Fracture-Free Assurance Program for the device in the United States. Under the programme, the company will provide a refund for device fractures within 10 years of implantation.
The prospective, physician-sponsored registry study evaluated the safety and efficacy of the Gore Tigris vascular stent in treating SFA and PPA occlusive lesions of 100 patients at a single site in Austria. At 12 months, the device met its primary endpoint demonstrating 93% primary patency and 100% secondary patency. Patients with the device had 95% freedom from target lesion revascularisation (TLR) and an improved ankle brachial index (ABI) was observed with an average ABI improvement of 0.21 (from 0.69 at baseline to 0.90 at the 12-months follow-up).
Additionally, zero stent frame fractures were observed at 12 months. This and other studies showing a lack of stent frame fractures led Gore to create the new Fracture-Free Assurance Program confirming its confidence in the stent. All devices were successfully implanted with no device related complications at the time of implant or within the 30-day implant window.
“Peripheral arterial disease in distal anatomy was previously very difficult to treat effectively via stents because the region behind the knee led to high fracture rates. At Gore, we tackled this challenge head on by designing a stent that flexes with the knee while remaining strong to prevent stent frame fractures,” commented Eric Zacharias, Vascular Leader at Gore.
A new pooled analysis of patient-level data from Philips demonstrates the “strong safety profile” of the its Stellarex drug-coated balloon (DCB) in above-the-knee studies, according to a company statement. The independent, third party pooled analysis evidences low mortality rates through three years after the treatment with no device-related deaths.
Sean Lyden, chairman of the Department of Vascular Surgery, Cleveland Clinic (Cleveland, USA), presented these data at 2019 Leipzig Interventional Course (LINC; 22–25 January, Leipzig, Germany) during a symposium focusing on the long-term safety of drug-eluting technologies in the leg.
This latest data contrasts the findings of Katsanos et al’s summary-level meta-analysis published in December 2018 reporting an increased risk of death at two and five years following the use of paclitaxel-coated balloons and stents in the femoropopliteal artery. Medtronic and Cook Medical also announced data at LINC iterating the safety of their devices, the IN.PACT Admiral DCB and the Zilver PTX drug-eluting stent, respectively.
“The LINC session provided important new patient-level data regarding mortality in patients with peripheral arterial disease receiving paclitaxel devices—stents or DCBs—to restore and maintain blood flow in the superficial femoral and popliteal arteries in their legs,” says William Gray, president of the Lankenau Heart Institute (Wynnewood, USA) and investigator for the Stellarex clinical trials. “The data from the Stellarex clinical trial programmes were strong, and represented over 2,300 patients. When the three-year-outcomes were examined, there were no cardiovascular or non-cardiovascular mortality differences between the groups treated with Stellarex and the control arm. This is very reassuring, and this patient-level data will be amalgamated with other paclitaxel device data in order to complete the analysis. These efforts are already underway, as is a publication specifically regarding these Stellarex results.”
“Based on this latest patient-level analysis, we remain confident in the safety and performance of our unique Stellarex low-dose DCB,” comments Chris Barys, business leader, Image Guided Therapy Devices at Philips. “We will continue to communicate any relevant findings we obtain, to ensure our physicians have the most current information on our technologies for optimal treatment of their patients.”
The Stellarex DCB is designed to restore and maintain blood flow to arteries in patients with peripheral arterial disease and is FDA approved and CE marked in the USA and Europe.
Determining the potential role of interventional radiologists in obesity treatment is increasingly important, as the global number of obese patients has long since swollen to pandemic proportions. In this commentary, Alberto Alonso discusses the importance of having a multifactorial approach to obesity treatment, focusing on the unique needs of specific patients. Left gastric artery embolization has been proposed as a promising strategy to treat obesity due to the procedure’s ability to suppress the production of “the hungry hormone” ghrelin, but Alonso argues that the procedure alone is not enough to act as the curative treatment some have hailed it as.
Obesity is defined as a state of increased adipose tissue of enough magnitude to produce adverse health consequences, and is associated with increased morbidity and mortality. Obesity is a pandemic health problem involving genetics, the environment, other diseases, drugs and psychological factors. Treatment for obesity should never be considered “unilateral”—not even a surgical approach should be seen as a standalone option. Obesity always requires a multidisciplinary and tailored approach, focusing on caloric reduction and increased physical activity. Considering a single intervention as an adequate “curative treatment” for obesity is arrogant and most likely will not work.
Lifestyle and dietary changes are probably the best focus for obesity treatment. However, these have proven ineffective in the long-term for the most obese patients. Anti-obesity medications are not without significant side effects, and they are expensive. Gastric volume reduction remains the most effective mechanism currently available to control obesity.
The mechanisms dictating food intake and appetite are complex and, mainly, not well known. Many hormones (such as ghrelin, leptin, obestatin, and insulin) are involved through neural pathways in the “simple” act of eating. Ghrelin, the “hunger hormone” is a peptide hormone produced by ghrelinergic cells in the gastrointestinal tract that functions as a neuropeptide in the central nervous system by regulating appetite, but also plays an important role in regulating the distribution and rate of energy usage. It acts on hypothalamic brain cells to increase hunger: ghrelin is secreted when the stomach is empty, and secretion stops when the stomach is full.
Left gastric artery embolization
Left gastric artery embolization (LGAE) has been proposed as an alternative to bariatric surgery for weight loss due to its effects on the ghrelin hormone. In theory, by reducing the blood supply to the fundus of the stomach via LGAE, the release of ghrelin should decrease and relieve the feeling of hunger, ultimately resulting in the patient eating less. Theoretically.
However, ghrelin also plays an important role in regulating reward perception via dopamine levels in central nervous system neurons, also linked to processing sexual desire, reward, and reinforcement, as well as in developing addictions. Paradoxically, ghrelin plasma levels in obese individuals are lower than those in leaner individuals, suggesting that ghrelin does not contribute to obesity (except in the cases of Prader-Willi syndrome-induced obesity). However, it has also been reported that consumption of “food for pleasure” increases peripheral levels of both ghrelin and the endocannabinoid 2-arachidonoyl-glycerol in healthy humans. This should then also be considered as an underlining psychological factor in any patient with severe obesity, where anxiety and depression are concomitant entities in many cases. Reducing obesity only to “over-eating” and this to a “ghreling secretion” is probably an extremely simplified, and incorrect, point of view.
After LGAE, ghrelin levels initially decrease, then increase at three and six-months’ follow-up to a wide range of values; the same variation is seen in weight loss following LGAE. This may be due to revascularisation of the gastric fundus but also, more interestingly, to the return of appetite after gastric recovery from ischaemic injury, where ischaemic ulcers are widely observed after LGAE.
Evidence of long term reduction in levels of the ghrelin hormone after LGAE has not been confirmed due to limited experience; data regarding the potential role of LGAE for weight loss is scarce. In fact, no clinical trial with long-term follow-up and a relatively large sample size has been reported. Even if it is mainly produced by stomach fundus cells, there are also ghrelin-secreting cells in the proximal intestine, pancreas, pituitary gland, and colon. Those should increase ghrelin secretion after LGAE.
LGAE is effective on its own—probably more due to ischaemic gastric ulcers than to ghrelin secretion—but its efficacy may be enhanced if performed in combination with other therapies, lifestyle modifications, and/or pharmacotherapy. This focus has not been described.
Almost any intervention that leads to a caloric deficit in a severely obese patient will be followed by an initial benefit. In fact, the literature reports that for patients treated with LGAE, glycated haemoglobin (HbA1c) levels were under control following the procedure, and a 10% weight loss had been observed. As in any dietic intervention, the crucial question is: for how long do these benefits last?
The ideal candidate
Identifying the best candidates for the procedure is still a work in progress, as is discerning the long-term outcome. Defining obesity as having a body mass index (BMI) greater than 30kg/m2 is common in published work. BMI is the most frequently used measurement for diagnosing obesity, because of its simplicity and reliability. Excess adiposity but not excess body weight is the real culprit of obesity-associated complications. However, in comparison with techniques involving the direct measurement of adipose, BMI underestimates the prevalence of obesity by 50%; its relationship with adiposity is influenced by age, sex and race. Lean body mass (LBM) is a component of body composition, calculated by subtracting body fat weight from total body weight. LBM has been described as a superior index to total body weight for prescribing proper levels for assessing metabolic disorders. When papers only attend to BMI and absolute weight loss, how can we determine how LGAE affects LBM? Has it been improved or worsed by LGAE? This point should be clarified before considering LGAE as standard treatment.
The ideal embolic agent for LGAE is still uncertain, where agent penetration, devascularisation and revascularisation are the key features. Is a temporary occlusion desired or better than a definitive embolization? Several different types and sizes of embolic agents and spherical particles have been used. The ideal endpoint for embolization also needs to be clarified.
Finally, LGAE reduces future options for an established surgical bariatric procedure. The idea of a gastric volume reduction with a previous devascularised area could be considered as a contraindication for surgery in many of the working groups. Adjustable gastric banding may then be the only option, even when this cannot be considered an adequate second bariatric option.
So, when should LGAE be used? Not as an alternative to surgery, and neither as a bridge to surgery—and definetively not as a solo treatment for obesity. LGAE should be restricted to those patients with a concious and complete refusal of surgery and as an initial starting point for weight loss. But we should always bear in mind that LGAE is only capable of causing a temporary effect.
Alberto Alonso is an interventional radiologist at the Clínica Universidad de Navarra in Madrid, Spain.
References: 1. Zhong BY, Abiola G, Weiss CR. Bariatric Arterial Embolization for Obesity: A Review of Early Clinical Evidence. Cardiovasc Intervent Radiol (2018) 41: 1639. 2. Shoar S, Saber AA, Aladdin M, et al. Bariatric manipulation of gastric arteries: a systematic review on the potential concept for treatment of obesity. Int Jo Surg. 2016;36:177–82. 3. Angrisani L, Santonicola A, Vitiello A, Ferraro L, Iovino P. Reply to Letter to the Editor “Left Gastric Artery Embolization for Weight Loss-a Dead-End Procedure”. Obes Surg. 2018;28(11):3627-28. 4. Fink JM, Martini V, Seifert G et al, Marjanovic G. Left Gastric Artery Embolization for Weight Loss-a Dead-End Procedure. Obes Surg. 2018;28(11):3623-24. 5. Saeed Shoar, Alan A. Saber, Mohammaed Aladdin et al. Bariatric manipulation of gastric arteries: A systematic review on the potential concept for treatment of obesity, International Journal of Surgery. 2016; 36, 177-182. 6. Weiss CR, Akinwande O, Paudel K et al. Clinical Safety of Bariatric Arterial Embolization: Preliminary Results of the BEAT Obesity Trial. Radiology. 2017;283:598-608. 7. Syed MI, Morar K, Shaikh A, Craig P, Khan O, Patel S, Khabiri H. Gastric Artery Embolization Trial for the Lessening of Appetite Nonsurgically (GET LEAN): Six-Month Preliminary Data. J Vasc Interv Radiol. 2016;27(10):1502-8
The findings published by Konstantinos Katsanos and colleagues in JAHA quickly sparked wide-spread debate across the vascular community, as the meta-analysis’ implications and questions raised for use of paclitaxel-coated devices are discussed. The data had a near-immediate impact on practice, as the SWEDEPAD 1 and 2 trials stopped enrolment within days of the publication. Shortly thereafter, the BASIL-3 trial similarly paused recruitment, stating there were concerns about patient safety following the outcomes of the meta-analysis of randomised controlled trials using paclitaxel treatments.
SWEDEPAD
The halted trials were aiming to evaluate various paclitaxel devices for patients with peripheral arterial disease. The SWEDEPAD (Swedish drug-elution trial in peripheral arterial disease) project is designed to test the hypothesis that drug-eluting technology is superior to conventional endovascular treatment in terms of important clinical outcomes, when applied on infrainguinal (femoropopliteal and/or infrapopliteal) obstructive vascular lesions. The SWEDEPAD project consists of two separate parallel studies, SWEDEPAD 1 and SWEDEPAD 2, each defined by the severity of peripheral arterial disease. As noted on clinicaltrials.gov, “patients with critical limb ischaemia are allocated to SWEDEPAD 1 and patients with intermittent claudication are allocated to SWEDEPAD 2.” SWEDEPAD 1 has a planned enrolment of 2,400 patients and SWEDEPAD 2 of 1,333 patients.
An update on the trial website states there is currently a “temporary haltof recruitement” to both trials. The statement reads: “Following the recent publication of a meta-analysis by Katsanos et al, the SWEDEPAD data safety and management committee (DSMC) did an interim safety analysis of SWEDEPADs prespecified safety variables. The results of the metaanalysis, and of our own interim safety analysis, prompted us to on December 10, 2018 temporarily halt recruitment of patients to SWEDEPAD 1 and 2.
“We are now conducting a thorough in-depth analysis of all patients randomised in SWEDEPAD 1 and 2 with respect to this safety warning. This will require additional data and it is therefore decided to prolong the temporary halt of inclusions at least until early February 2019.”
To date, SWEDEPAD 1 has randomised 1,480 patients and 810 have been randomised in SWEDEPAD 2.
Recruitment halt follows steady decline in BASIL-3 enrolment rates
BASIL-3 had already been experiencing difficulties with recruitment, and investigators struggled to reach their enrolment milestone targets throughout. At the Vascular Societies’ Annual Scientific Meeting 2018 (VSASM; 28–30 November, Glasgow, UK), BASIL lead investigator Andrew Bradbury (Heart of England NHS Foundation Trust in Birmingham, UK) warned of difficulties with enrolling patients to the study, saying he was “rather worried about BASIL-3”. Bradbury called on the community of vascular and endovascular surgeons to “explore why it has become difficult to recruit to a trial that actually should be pretty easy— three endo options in a very common procedure, and a very big patient population”.
The research is a joint initiative from University Hospitals Birmingham, the University of Birmingham Clinical Trials Unit (BCTU), and the National Institute for Health Research (NIHR).
“It should be an easy trial, really, because lots and lots of people have femoropop-endo for critical limb ischaemia and, from a patient experience point of view, the three arms are virtually identical,” he said. “We started at the beginning recruiting ahead of target, so why things have fallen off quite so badly in recent times is kind of difficult to understand.”
BASIL-2 is randomising patients with critical limb ischaemia who require infrapopliteal intervention either to vein bypass first or best endovascular treatment first. “Best endovascular treatment can be whatever it is you want to use,” said Bradbury.
Meanwhile, the BASIL-3 trial has no surgical arm. Participants are patients receiving femoropopliteal intervention for critical limb ischaemia and for whom it has already been decided that they will receive endovascular treatment rather than a bypass. They are randomised to either percutaneous transluminal angioplasty with a bailout bare metal stent (BMS), angioplasty with a paclitaxel drug-coated balloon (DCB) with or without a BMS, or to a paclitaxel drug-eluting stent with or without a BMS.
The original target for BASIL 3 was 861 patients. Three years after enrolment began investigators have now randomised 407 patients, less than 50% of the desired amount. Before the newly published data raised questions about paclitaxel treatments and caused the BASIL-3 enrolment to be put on hold, Bradbury acknowledged: “[Patient numbers were] quite a long way below what we had hoped for [for some months], but nevertheless pretty steady. But, since the summer, there has been a bit of a fall off. We have almost stopped recruiting to this trial, and I am not quite sure why that is. But it is quite a big problem, and I do not think any of us really want this to happen to the BASIL trial.”
A renowned panel, moderated by Dierk Scheinert (Leipzig, Germany), comprising Peter Schneider (Honolulu, USA), John Laird (St Helena, USA) and Thomas Zeller (Bad Krozingen, Germany) expressed confidence in the continued use of paclitaxel-coated devices after individual patient-level data were presented at LINC 2019 that did not show correlation between paclitaxel exposure and mortality.
Schneider and colleagues have authored a paper that is currently in press with the Journal of the American College of Cardiology (JACC) highlighting these data.
Martin T Rothman has been appointed as chief medical officer of Vascular Dynamics, effective 1 January 2019.
Rothman is a pioneer in interventional cardiology, as evidenced by his clinical practice spanning several decades, his extensive pre-clinical and clinical research presented in over 200 publications, his success within the cardiovascular industry as a founder of several start-up companies, and his leadership roles at Medtronic.
Recently, Rothman was chief medical officer and vice president of Medical Affairs for the Coronary, Structural Heart, and Renal Denervation Division at Medtronic. In this role, he was involved in evidence development strategies and guided new product development teams for a wide indication spectrum including coronary and vascular disease, resistant hypertension, and minimally invasive and percutaneous mitral valve replacement and repair. Also, following the announcement of the failed HTN-3 study, he was instrumental in the interpretation of renal denervation data and working with others on new strategies for the development of RDN as a treatment option for hypertension patients.
“As a clinician, researcher, and industry participant, I have followed closely the development and initial positive clinical evidence reported for the EVBA approach using the MobiusHD device,” said Rothman. “I am excited about its potential as a viable treatment option for the many patients facing the dire prognoses of resistant hypertension and the potential in other unmet cardiovascular challenges. I look forward to being a part of the Vascular Dynamics team as we advance new breakthrough solutions for these patients.”
Vascular Dynamics is currently sponsoring the CALM-2 (Controlling and lowering blood pressure with MobiusHD) clinical trial, designed to establish the safety and efficacy of the novel endovascular baroreceptor amplification (EVBA) procedure using the unique MobiusHD device as a treatment for drug-resistant hypertension.
MobiusHD is the first minimally invasive technology to use the body’s natural baroreceptor mechanism of regulating blood pressure to address uncontrolled hypertension. Early results of the proof-of-concept CALM-FIM trial are promising, with reductions in blood pressure through six months that were significant and greater than those reported to date for alternative devices used to treat uncontrolled hypertension. These encouraging results, combined with lessons learned in previous clinical trials of device-based approaches, led to the rigorously designed CALM2 study, which began in the second half of 2018.
The BIBLIOS trial has received Ethics Committee (EC) approval, and enrolled its first patient. This announcement comes from Wouter Lansink, who will be treating this first patient at the Vascular Center ZOL Genk in Belgium.
BIBLIOS is a Belgian-Italian prospective, single-arm, multicentre study to evaluate the efficacy and safety of below-the-knee treatment with the Luminor paclitaxel-coated percutaneous transluminal angioplasty balloon catheter (iVascular) with critical limb ischaemia. One hundred and fifty patients will be enrolled from six Italian and Belgian centres.
As stated by Koen Deloose (AZ Sint-Blasius, Dendermonde, Belgium), the trial’s principal investigator, “the benefits of DCBs for critical limb ischaemia are still to be confirmed. Preliminary below-the-knee data with Luminor DCB are promising; therefore, we are looking forward to the results of BIBLIOS, which is set to be representative of real-world population in such [an] indication.”
The primary efficacy endpoint of the BIBLIOS trial is freedom from major adverse limb events at six months. For assessing safety, the primary endpoint of the study is freedom from major adverse limb events or peri-operative death at 30 days.
The secondary endpoints of the BIBLIOS trial include: target vessel functional flow assessment; freedom from clinically driven target lesion revascularisation; amputation free survival; limb salvage; procedural success; wound healing status; and wound healing time, all at six and 12 months.
Donald Clark III Image courtesy of the American Heart Association
African Americans who smoke cigarettes are more likely than those who do not smoke to develop peripheral arterial disease (PAD), according to new research published in the Journal of the American Heart Association, the open access journal of the American Heart Association/American Stroke Association.
African Americans are disproportionately affected by PAD, nearly twice as much as non-Hispanic Whites. While cigarette smoking is a recognised PAD risk factor, little is known about its specific impact on African Americans.
“Peripheral arterial disease is a major disease burden in the African American population,” comments Donald Clark III, assistant professor of medicine at the University of Mississippi Medical Center (Jackson, USA). “Establishing a clear association between smoking and peripheral arterial disease in this particularly vulnerable population can help guide our efforts to lower their risk and to help them improve their health.”
To learn more, researchers analysed medical records of 5,306 participants, aged 21 to 84 years, enrolled in the Jackson Heart Study, the largest single-site cohort study investigating cardiovascular risk factors in African Americans. Among the participants who self-reported, smoking status was 68% who never smoked (3,579 individuals), 19% (986) past smokers and 13% (693) current smokers.
To determine evidence of PAD, the researchers looked at measures of peripheral arterial disease, including the ankle-brachial index, which compares blood pressure in the arteries of the extremities, and computer tomography (CT) scanning to identify calcium build-up in blood vessels, which can indicate the presence of artery-blocking plaques.
In addition to being twice as likely as non-smokers to have subclinical PAD in their lower extremities, current smokers were eight times more likely to have high calcium build-up in the aorta.
The researchers also found an association between the number of cigarettes smoked and the likelihood of PAD. Participants who smoked 20 or more cigarettes a day had significantly higher odds of PAD compared to those who smoked less than 20 cigarettes each day.
The study was conducted through the support of the American Heart Association’s (AHA) Tobacco Regulation and Addiction Center, as part of a multi-year grant initiative from the US Food and Drug Administration (FDA) and the National Institutes of Health (NIH). The aim of the initiative is to conduct research to document the adverse cardiovascular effects of tobacco products that can inform the FDA’s regulation of these products, to learn more about the attitudes and behaviours associated with tobacco use, and to help shape effective communication about the health effects of tobacco products. The AHA’s centre has focused on vulnerable populations in an effort to promote health equity.
“The findings from this study give us strong evidence of the specific debilitating and life-threatening risks African American smokers face, especially the more they smoke,” says Mariell Jessup, chief science and medical officer of the American Heart Association. “This type of research can be useful in the development of clear messages targeted to our African American population to underscore the real physical costs of tobacco product use.”
Writing of the clinical implications of this research, the study authors say: “These findings support the evaluation of smoking‐cessation efforts to reduce the impact of peripheral arterial disease in this population.”
The CE Mark for the Nellix endovascular aneurysm sealing system (Endologix) has been suspended by its Notified Body, GMED, following a voluntary recall and Field Safety Notification (FSN) issued by Endologix on January 4, 2019.
“The notification from GMED is a regulatory action and is not in response to any new information beyond our recent FSN,” explains Matt Thompson, Chief Medical Officer of Endologix. “This action is consistent with our previously articulated plans for the Nellix system and does not affect other Endologix products. We remain steadfast in our commitment to patient safety and believe in the transformational potential of Nellix.”
Earlier this month, Endologix announced that the Nellix system will for the foreseeable future be made available only for use at approved centres in a clinical investigation setting, with all cases pre-screened by a physician panel and supported by Endologix to ensure use in accordance with the current indications and optimal clinical outcomes.
Suspension of the CE Mark means that Endologix may not affix the CE Mark and sell the Nellix System in the European Union during the term of the suspension.
Endologix does not expect this action to impact its previously communicated financial guidance for 2019.
This is the headline result of the IN.PACT DCB paclitaxel safety analysis, an independent, patient-level survival analysis inclusive of all IN.PACT DCB clinical programmes, presented at the Leipzig Interventional Course (LINC) in Leipzig, Germany (22–255 January 2019) following clinical discussions around the safety of paclitaxel-coated and eluting technologies in the treatment of PAD. A Medtronic press release states that these data reiterate the company’s commitment to patient safety and data transparency.
A manuscript detailing outcomes from the IN.PACT DCB paclitaxel safety analysis was also accepted and is in press with the Journal of the American College of Cardiology (JACC).
Key data highlights include:
At five years, there was no statistically significant difference in all-cause mortality between the DCB and PTA arms (9.3% vs. 11.2% respectively, p=0.399)
Data found no correlation between paclitaxel dose and long-term survival. Patients treated in the DCB arm were classified by upper, mid, and lower dose ranges. Freedom from all-cause mortality based on Kaplan-Meier estimates was 91.7% in the upper range, 90.6% in the mid-range, and 90% in the lower range (p=0.700).
Data demonstrated no difference in mean nominal dose of paclitaxel between overall survival in patients treated with DCB (n=1,696) and those who died (n=140). Mean nominal paclitaxel doses were 11,829.8μg±7,347.6μg and 11,419.6μg±7,414.8μg respectively (p=0.529).
Patient-level safety analysis
Peter Schneider, vascular surgeon at Kaiser Permanente Clinic in Honolulu, USA, presented data from the IN.PACT safety analysis at LINC. The independent, patient-level analysis evaluated the relationship between nominal dose of paclitaxel and mortality in all 1,837 DCB patients enrolled across the IN.PACT Admiral clinical programme, including IN.PACT SFA, IN.PACT SFA Japan, IN.PACT SFA China, and IN.PACT Global. The analysis was independently performed by the Baim Institute for Clinical Research (formerly the Harvard Clinical Research Institute) and led by Gheorghe Doros, professor of Biostatistics, Boston University School of Public Health and director, Statistical Consulting, Baim Institute of Clinical Research, Boston, USA.
“This independently adjudicated analysis includes 1,837 patients treated with IN.PACT Admiral and followed long-term,” explains Schneider. “In contrast to a recently published summary-level meta-analysis—which included 28 trials with different devices, designs, levels of monitoring, and follow-up periods—the findings from this study showed neither paclitaxel use, nor dose had any effect on mortality at five years.”
The analysis evaluated all-cause mortality across IN.PACT studies. This included device- or procedure-related death through five years and paclitaxel-related events through 12 months. Upon review of other endovascular therapies in published literature, it was found that the mortality rates across IN.PACT DCB studies are comparable to or lower than what would be expected in similar patient populations. Authors also found no significant difference between nominal dose in those with overall survival through five years. Furthermore, patients who died were older and shared a statistically higher level of co-morbidities at baseline, including coronary artery disease, diabetes, and chronic kidney disease, versus those with higher overall survival rates. Across all studies, results were reviewed and adjudicated by an independent clinical events committee.
“Individual patient data meta-analysis (IPD-MA) offers several advantages over the aggregate data meta-analysis (AD-MA) that renders it as a more powerful statistical approach, allowing for more thorough and more appropriate analyses,” comments Doros. “The advantages are realised by being able to utilise more accurate outcome data, such as time of event and time of drop-out, individual patient covariates, such as paclitaxel dose, patient comorbidities, as well as lesion and procedural characteristics, and more sophisticated statistical models, such as frailty Cox regression and inverse probability of treatment weighting (IPTW).”
“In light of recent discussions around the safety of paclitaxel-coated and -eluting technologies, it is now more important than ever for Medtronic and our industry peers to be forthcoming with all our clinical data,” says Mark Pacyna, vice president and general manager of the Peripheral business, which is part of the Aortic, Peripheral, and Venous division at Medtronic. “The evidence presented today at LINC underscores our ongoing commitment to patient safety, improved long-term outcomes, and data transparency.”
IN.PACT SFA Japan three-year results
New data from the IN.PACT SFA Japan study were also presented by Osamu Iida, of Kansai Rosai Hospital, Amagasaki, Japan. The data demonstrated continued safety, durability, and efficacy compared to PTA at three years. The study enrolled 100 patients across 11 sites in Japan and randomised treatment to either DCB (n=68) or PTA (n=32). Results showed a consistently low clinically-driven target lesion revascularisation (CD-TLR) rate and high patency rate.
IN.PACT SFA Japan demonstrated a 68.9% primary patency in the DCB group compared to 46.9% in the PTA group at three years based on Kaplan-Meier estimates (p=0.001). The three-year freedom from CD-TLR rates based on Kaplan-Meier estimates were 84.4% in the DCB group compared to 81.3% in the PTA group (p=0.451). In IN.PACT SFA Japan, major adverse events were also lower in the DCB group at three years with a rate of 20.9% compared to 31% in the PTA group (p=0.306), with no major target limb amputations in either study arm. The mortality rate was also lower in the DCB arm at 6%, versus 6.9% in the PTA group.
“We stand behind IN.PACT Admiral DCB, which is well supported by evidence from our robust clinical programme,” says Simona Zannetti, vice president, Clinical Research, Medical Affairs, and Education, Medtronic Aortic, Peripheral, and Venous. “In line with our commitment to timely data dissemination—and the physicians and patients we serve—it is critical that we continue to review, report, and publish our findings.”
Findings presented at the Leipzig Interventional Course (LINC; 22–25 January 2019, Leipzig, Germany) contradict the results of a meta-analysis published in the Journal of the American Heart Association in December 2018 linking paclitaxel-coated devices and increased mortality. Several presentations to LINC attendees showed data supporting the use of paclitaxel-coated devices to help the more than 200 million patients globally who have peripheral arterial disease (PAD).
Data were presented on specific paclitaxel-eluting devices. Michael Dake, the principal investigator for the Zilver PTX randomised controlled trial and a paid consultant for Cook Medical, presented results demonstrating the safety and effectiveness of the Zilver PTX drug-eluting stent (Cook Medical). The trial amassed data on 479 patients in a five-year follow-up randomised controlled trial. A separate, recently released Japanese five-year post-market study on Zilver PTX showed positive long-term safety and effectiveness outcomes in challenging real-world patients.
After reviewing all patient level data in the Zilver PTX five-year follow-up, Dake stated that “Cook’s patient level data demonstrate no increased mortality rates at five years with use of a Zilver PTX paclitaxel-coated stent versus the use of non-coated stents and balloons.”
Zilver PTX is indicated for improving luminal diameter for the treatment of de novo or restenotic symptomatic lesions in native vascular disease of the above-the-knee femoropopliteal arteries having reference vessel diameter from 4mm to 7mm and total lesion lengths up to 300 mm per patient.
“We believe industry-wide discussion on topics related to patient safety and long-term patient outcomes are critically important. In the case of paclitaxel, we have studied this drug for more than 20 years and tens of thousands of patients have been treated with Zilver PTX,” comments Mark Breedlove, vice president of Cook Medical’s vascular division. “The recently published meta-analysis linking paclitaxel-coated devices and increased mortality didn’t include patient-level data.”
Women are equally as productive as men in terms of number of publications, citations, and grants, a recent study investigating the impact of women in academic interventional radiology (IR) concludes. The study, published in the Journal of Vascular and Interventional Radiology, found that women are also proportionately represented in the literature, and that female authorship is in fact increasing.
The study investigators, Nicholas Xiao (Department of Radiology, Section of Interventional and Vascular Radiology, Northwestern University, Chicago, USA), Diego Oliveira (Department of Chemical and Biological Engineering, Northwestern University, Chicago, USA), and Ramona Gupta (Department of Radiology, Section of Interventional and Vascular Radiology, Northwestern University, Chicago, USA) set out to determine the representation of female IRs, and to elucidate possible gender-specific disparities.
They analysed 4,884 original, peer-reviewed articles from 2006–2017 in the Journal of Vascular and Interventional Radiology and Cardiovascular and Interventional Radiology. The first author and the senior author were then the subjects of scrutiny to assess gender, citations and grants.
Xiao and colleagues write: “We found that 84% of first authors and 91.4% of senior authors were male (P<0.01)”. Additionally, there was no significant difference in author gender collaboration combinations (P=1).
The study also reported an increasing number of articles authored by women within the 11-year time-frame. Each year, there was a 0.3–0.4% increase in the number of articles with a female first author (P=0.05) or senior author (P=0.01). Furthermore, citations and grants received by female authors increased each year.
The lack of data indicating collaborative or citation/ grant discrimination prompt Xiao, Oliveira and Gupta to believe that “the academic IR community is inclusive of its female constituents, and equally respects their research contributions.”
They conclude: “Based on the statistically significant increases in female authorship observed in this 12-year study, this article reports encouraging trends for the future of women in interventional radiology.”
Figure from the article originally published in the Journal of Vascular and Interventional Radiology
Speaking to Interventional News, Xiao explains that he and his co-authors were not expecting this result. He says: “There are recent papers published in other academic disciplines showing significant bias against female authors in the literature, especially in highly male predominant fields. While we were certainly not expecting IR to reproduce this discrimination, we were pleased to discover that the data did not suggest any type of gender bias, despite IR being one of the most gender imbalanced fields in medicine. I was surprised at the high percentage of women as first authors as compared to the percentage of women in the field. As first authors are frequently the team members whom really drive the project forward, and are often junior to the senior author, this finding, to me, meant that more and more women are entering IR and contributing productively to the literature! This was further supported by trends showing a steady increase of women in the field.”
Research from December 2016, conducted by Mikhail Higgins (Division of Vascular and Interventional Radiology, Department of Radiology, University of Virginia, Virginia, USA) et al and published in the same journal, found that women and minority ethnicities were underrepresented in the IR academic physician workforce relative to the US population. Similar conclusions from other studies, coupled with personal experiences of female IRs, has led to an increased acknowledgement in recent years of gender disparities in healthcare, leading to campaigns advocating for greater equality, such as #ThisIsWhatASurgeonLooksLike on Twitter.
Xiao highlights the importance of social media as a way to promote inclusivity within IR, saying, “I personally follow a number of prominent interventionalists on Twitter, and they are vocal advocates for all minorities in IR and actively engage in mentorship. I believe that the aforementioned candid recognition that biases (gender or otherwise) exist and vocal leadership calling attention to these issues causes a trickle down/ compounding effect and fosters a culture of inclusion.”
Amongst the backdrop of underrepresentation within the field, this recent research demonstrates that in this particular academic context, gender disparity does not come into play.
Delineating why this finding is important, Xiao comments, “I hope that it is encouraging to all women in the field, especially medical students considering the field and young trainees conducting research or pursuing academic careers. While it certainly does not fix the gender gap in IR, I hope that it at least shows that women in the field are respected by their male IR colleagues, and that they can be judged by their merits and not be negatively impacted by their gender in this regard. While there are a number of factors that influence the low number of females in the field, this data should be encouraging to those who have reservations about entering the field or pursuing an academic career due to gender biases in publication.”
Preliminary in vitro data on Anaconda Biomed’s advanced thrombectomy system showed that the reperfusion rates with this novel system outperformed competing mechanical thrombectomy devices at first pass and after three passes. These results were presented by Tommy Andersson, (professor of Neurointervention, AZ Groeninge, Kortijk, Belgium, and senior consultant in Neurointervention, Department of Neuroradiology, Karolinska University Hospital, Stockholm, Sweden) at the 39th ABC-WIN meeting in Val d’Isère, France.
The in vitro study compared the use of the advanced thrombectomy system in conjunction with a stent retriever (Solitaire, Medtronic) to a balloon-guide catheter with a stent retriever (BGC and Solitaire), and to an intermediate distal access catheter with a stent retriever (DAC and Solitaire).
The study results demonstrated that, as compared to the other device combinations, the advanced thrombectomy system achieved statistically significant improvement in revascularisation rates at both first and third pass. In fact, using the system, operators were able to achieve complete recanalisation [Thrombolysis in Cerebral Infarction (TICI) grade of 2b/3] in 100% of cases, with an average of 1.06 passes. Operators also found that the system’s design enabled complete local flow restriction and allowed for a safe exit.
“Mechanical thrombectomy techniques and devices have improved significantly over the years, but limitations remain. These range from difficulties with distal blood flow arrest and clot fragmentation to no or low reperfusion at first pass,” Andersson remarks. “In the in vitro model, with the advanced thrombectomy system, operators were able to overcome these challenges. Assuming these results can be replicated clinically, I believe this system has tremendous potential for fast, effective yet safe endovascular treatment of patients suffering from a major stroke.”
Anaconda’s advanced thrombectomy system consists of a delivery catheter, a unique, funnel-shaped aspiration catheter and a stent retriever. When deployed, the funnel self-expands and directly conforms to the artery diameter up to 5mm, locally arresting flow and allowing full thrombus extraction without fragmentation.
The company are currently planning future clinical studies for the advanced thrombectomy system.
Enrolment of the first patients in the BELONG study—benefit of arterial vessel preparation by arterial by longitudinal micro-incisions before drug-eluting balloon angioplasty of the superficial femoral and popliteal arteries—has been announced by VentureMed Group.
The primary objective of this clinical study is to evaluate lumen patency at 12 months obtained by preparation of vessels with the FLEX vessel preparation system prior to conventional endovascular recanalization of the superficial and popliteal arteries. According to a press release, the FLEX system creates long parallel, linear micro-incisions in all plaque morphologies to prepare an ideal vessel environment to facilitate drug-coated balloon angioplasty. The dynamic micro-incision technique of the FLEX system safely facilitates the treatment of difficult, diseased vessels, improving vessel compliance and acute lumen gain.
This prospective, single arm, non-randomised study will enrol up to 150 patients in Switzerland. Patients will exit from the study at the completion of their twelve-month follow-up. The primary investigator and co-investigator are Daniel Périard and Rolf Engleberger (both HFR- Hôpital Cantonal Fribourg, Villars-sur-Glâne, Switzerland).
“We believe preparing arterial vessels by delivering parallel longitudinal micro-incisions with the FLEX system prior to drug-coated balloon angioplasty has the potential to demonstrate long-term clinical benefits for patients. Our early results have shown that arterial vessel preparation with the FLEX system resulted in improved lumen expansion and vessel compliance after drug-coated balloon angioplasty, with a corresponding reduction in the rate of dissection,” says Périard.
Daniel Hayoz, head of the medical clinic at HFR- Hôpital Cantonal Fribourg, Villars-sur-Glâne, Switzerland, introduced the BELONG study at the 45th VEITH annual symposium (13-17th November 2018, New York, USA) in a presentation titled “Arterial preparation improves outcomes of drug-coated balloon angioplasty.” A poster outlining the concept and inclusion status of the BELONG study won Best Poster at the 2018 Union of Vascular Societies of Switzerland (UVSS) meeting in Lugano, Switzerland (24–26 October, 2018).
Périard will be presenting the recruitment status and early results of the BELONG study at the Leipzig Interventional Course (LINC) on 22 January 2019 in Leipzig, Germany.
The impact of the 2018 meta-analysis of randomised paclitaxel-device trials, published in the Journal of the American Heart Association by Konstantinos Katsanos et al, continues to travel through the vascular world. As industry starts to respond to the conclusions made by Katsanos and colleagues, which highlighted an association between higher mortality rates in the long-term and use of paclitaxel-coated devices in the legs, the US Food and Drug Administration (FDA) has begun to evaluate its recommendations for the treatment. While the review of data is ongoing, “continued surveillance” is recommended for patients treated with paclitaxel, and the agency believes the “benefits continue to outweigh the risks” for approved devices used within their indications.
In a letter to healthcare providers, the FDA states that it is evaluating the “recent information regarding the potential for increased long-term mortality” following paclitaxel-coated balloon or paclitaxel-eluting stent treatments in the femoropopliteal artery for patients with peripheral arterial disease (PAD).
“The [meta-analysis] suggests a possible increased mortality rate after two years in PAD patients treated with paclitaxel-coated balloons and paclitaxel-eluting stents compared to patients treated with control devices (non-coated balloons or bare metal stents)”, the FDA states, adding “the specific cause for this observation is yet to be determined.”
While the FDA evaluate the data, in a review that it says “will focus on causes of death, the paclitaxel dose delivered, and patient characteristics that may impact clinical outcomes”, it recommends only that healthcare professionals continue to monitor patients who have received treatment with paclitaxel, to report any adverse events through the MedWatch reporting systems, and to discuss potential risks and benefits with patients during clinical decision-making for PAD. In fact, for currently approved paclitaxel devices, the FDA states that it believes “the benefits continue to outweigh the risks” when drug-eluting technology is used in accordance with the indications for use.
Impact on industry
An equity research report published by investment banking company Goldman Sachs predicts only limited risks for Philips, BD and Medtronic, as a result of the meta-analysis as drug-coated balloons (DCBs) and drug-eluting stents (DESs) represent only a small fraction of these companies’ total revenue.
FDA worker Photo posted by Scott Gottlieb on Twitter
The US government shutdown means the country’s Food and Drug Administration (FDA) cannot accept new user fees, which means the agency cannot accept new medical product applications.
FDA commissioner Scott Gottlieb took to Twitter to highlight agency employees who are working unpaid to perform mission-critical activities. The FDA cannot legally accept any new medical device or drug submissions until the government shutdown ends because the user fees that are collected with these submissions cannot be processed during the lapse period. The agency is able to support activities funded by carryover user fee balances from the fiscal year 2018, but medical device user fee programmes only have about two months to three months left, and pharmaceutical user fee programmes have less than that.
The agency said it is continuing vital activities that are considered critical to ensuring public health and safety in the USA. These activities include: maintaining core functions to handle and respond to emergencies; supporting high-risk food and medical product recalls; pursuing civil investigations when public health is believed to be imminently at risk and pursuing criminal investigations; screening food and medical products imported to the country; and surveillance for significant safety concerns with medical devices and other medical products.
“You are valued each day,” Gottlieb tweeted to FDA staff. “But it is even more the case that in moments of challenge, when some of our work stops, that your critical role becomes so obvious. FDA cannot achieve its full mission without each of you; whether you are exempt, excepted, or on furlough. We are one FDA.”
“Thank you for your understanding and support,” replied a Twitter user with the handle Larry Stringer. “I am stuck at home, furloughed and reading your tweets. I cannot even look at e-mail to see what I am missing. I want to come back to work. I love my job and believe in our public health mission.”
Gottlieb warned: “It is not business as usual at FDA.”
Philips launches its Azurion with FlexArm platform to aid patient imaging and positioning during image-guided procedures.
Azurion with FlexArm allows clinicians to intraoperatively visualise patient anatomy in both 2D and 3D. As the clinician moves the system, the image beam automatically maintains alignment with the patient, allowing consistent visualisation and enabling them to keep their focus on the treatment.
“With FlexArm, Philips’ engineers have overcome near-impossible geometric and mechanical barriers to enable clinicians to achieve clinical excellence in image-guided therapy,” says Barry Katzen, founder and Chief Medical Executive of the Miami Cardiac & Vascular Institute, Baptist Health South Florida, USA. “FlexArm enables us to dramatically optimise procedures around the patient: we can get the optimal view of what is going on inside the patient without encumbering all of the clinicians that are working around the table. The result is an innovation that is not only clinically important, but also very simple and intuitive to use—a critical factor in the heat of a complex procedure.”
The range and complexity of diseases that can be treated with minimally invasive procedures continues to expand. Correspondingly, the procedures themselves are also becoming more complex, requiring more physicians from different disciplines to be at the patient’s tableside, working together in a highly coordinated way. As a result, the clinical team is required to carry out increasingly challenging procedures in a highly constrained environment.
Azurion with FlexArm’s innovative design provides flexibility and intuitive control, a company statement declares. Powered by a kinematic engine, the system moves on eight different axes, controlled with its single Axsys controller. According to Philips, simulation tests with clinicians have demonstrated the system’s potential to significantly reduce the repositioning of the patient, staff and equipment to improve access for minimally invasive procedures, including those that enter the body through the patient’s wrist—radial access— and to reduce the risk of unintentional pulling of wires and tubes, as well as saving time. The system is suited for Hybrid operating rooms that cater to multiple specialties in one room, such as a combination of surgical and endovascular procedures.
Azurion with FlexArm is the latest addition to Philips’ image-guided therapy portfolio. As the range of diseases that can be treated with minimally invasive procedures continues to expand and the procedures themselves become more efficient, the patient’s treatment experience continues to improve. They experience less trauma, and as a result their stay in hospital can be dramatically reduced—often returning home after one night in hospital, and for some procedures even leaving the hospital on the same day.
Since its global launch in February 2017, over 450,000 patients have been treated in more than 80 countries using a Philips Azurion system. The Philips Azurion 7 C20 with FlexArm is CE marked and has received 510(k) clearance from the US Food and Drug Administration (FDA).
New research published in Radiology reports that CT-guidance is just as effective a tool for allowing interventional radiologists (IRs) to perform lumbar spinal injections as fluoroscopy-guidance, but exposes the physician to a lower radiation dose. However, the Swiss research team found that radiation exposure was greater for the patient when CT-guidance was used.
Both fluoroscopy- and CT-guided techniques are utilised by IRs to facilitate the administration of steroid therapy due to their proven ease of use and reliability, notes lead author Tobias Dietrich (Department of Radiology, Orthopedic University Hospital Balgrist, Zurich, Switzerland) and colleagues. The study investigators sought to compare the radiation exposure for patients and interventionalists, as well as the outcomes, between fluoroscopy-guided versus CT-guided lumbar spinal injections.
In their prospective, non-randomised observational study, Dietrich et al analysed the results of 1,446 patients who received transforaminal epidural injections or facet joint injections under fluoroscopic or CT guidance between October 2009 and April 2016. They measured radiation exposure for interventionalists with dosimeters at the body and wrist, and followed the “as low as reasonably achievable” (ALARA) concept for radiation dose.
There was no clinically significant difference in patient outcome as measured by the Patient Global Impression of Change (PGIC) scale, a patient-reported measure of pain used in this instance to evaluate efficacy at one day and one month post-procedural intervals. However, radiation dose to patients was higher with CT than fluoroscopy, as discerned through student t and χ2 tests.
The mean effective patient dose for fluoroscopy-guided lumbar transforaminal epidural injections was 0.24mSv±0.22, compared with the higher mean effective radiation dose of 0.33mSv±0.1 for CT-guided injections (P<0.003). This difference was more pronounced in effective radiation doses for lumbar facet joint injections: 0.1mSv±0.11 with fluoroscopy guidance, versus 0.33±0.13 for CT guidance (P<0.001).
However, the authors report interventionalists experiencing a reversal of this dose difference, with fluoroscopy-guided injections exposing physicians to more radiation than CT-guided ones: 0.42×10–3mSv recorded on body readings for the former versus 0.11±x10–3mSv±0.44 for the latter. Radiation exposure of the wrist for the interventionalist was higher during fluoroscopy-guided compared with CT-guided lumbar facet injections as well: 0.46×10-3mSv±0.93 vs. 0.06×10-3mSv±0.24, respectively (P<.006).
Overall, physicians’ radiation exposure was 3.7 to 10 times lower during CT-guided spinal injections than it was during fluoroscopy-guided injections (P<0.03). However, CT guidance required a statistically significant increase in patient radiation dose by a factor of 1.4 for epidural injections and 3.3 for facet joint injections, compared with fluoroscopy (P<0.003).
The benefits of CT-guided spinal injections, according to the study investigators, include less radiation exposure to the IR, and improved needle steering and manipulation without the need to constantly confirm the needle’s location. On the other hand, fluoroscopy-guided injections require real-time image guidance that increases radiation exposure to clinicians but decreases effective radiation dose for patients.
Clinicians also have the option of using other imaging techniques, such as ultrasound, MRI, and augmented reality, to guide lumbar injection therapies, the authors note. However, they add that physicians tend to feel less confident using these newer modalities, but propose that additional training and experience may enable them to further reduce the risk of radiation exposure.
Honoured as the Royal College of Radiologists (RCR)/ British Society of Interventional Radiology (BSIR) travelling professor for 2017–2018, Alex Barnacle delivered the Graham Plant lecture at the BSIR annual meeting (14–16 November 2018, Bournemouth, UK). Titled “Paediatric IR: The adolescent years”, she detailed the years’ successes. Here, she expands on this topic, advocating for the continued growth of paediatric IR as a subspecialty.
Paediatric IR is fast becoming one of our most exciting interventional subspecialties, attracting growing interest from trainees to institutions as a service with a central role in delivering modern healthcare to children.
For too long, it has been considered a highly niche area of medicine, providing supra-specialist care in tertiary paediatric centres but being of little relevance in most other settings. It is thrilling to see the tide turning, with both radiologists and industry recognising that minimally invasive procedures can and should be offered to children, too.
All the factors that make interventional radiology a relevant and exciting specialty apply just as much to children, if not more so. Children and families much prefer ‘keyhole’ treatment options that seem less frightening and allow them to get home sooner. More importantly, minimally invasive image-guided approaches decrease the risks of collateral organ or vessel damage, which is critically important in children with 60 or 70 years of life ahead of them. Our adult IR skills are all applicable in children. But paediatric IR challenges us to take things even further. It forces us to think hard about how to adapt adult kit to fit into small bodies and how to modify our techniques to decrease or avoid radiation burden and shorten procedure times. Examples include the use of carbon dioxide as a contrast agent for abdominal angiography [Figure 1]. This technique allows us to keep both fluid volume and iodinated contrast dose to a minimum in small children. A 4kg baby with a circulating blood volume of only 300ml cannot tolerate much in terms of saline flush volumes or contrast pump injections. The use of CO2 gives diagnostic images for initial angiography and allows us to save iodinated contrast for the selective runs. To control radiation burden, paediatric IRs have become adept at using only ultrasound for many procedures, from mediastinal biopsy to most cryoablation procedures. Such innovation is what attracted many of us into IR in the first place and paediatric IR is a field where, for now at least, the innovative directions seem endless.
Conversely, not everything is so different in children. A baby’s femoral artery can usually tolerate a 4Fr sheath perfectly well and it is rare for us to have to use a 3Fr system for angiography or embolization. In fact, sometimes small is not better. For percutaneous nephrolithotomies, large-calibre tracks (24Fr) allow urologists to achieve complete renal stone retrieval more quickly in small children, minimising procedure times and the associated risks of significant blood loss and hypothermia.
Four day old child with a hypervascular rapidly involuting congenital haemangioma (RICH) of the liver and high output cardiac failure. CO2 angiography via the hepatic artery from a left axillary approach delineates the lesion’s vascular anatomy well without fluid overload or iodinated contrast use. Iodinated contrast was then used for the selective runs and embolisation.
What is different about paediatric IR is the underlying disease processes. As with adult IR, it is critical that we become skilled clinicians and try to understand our patients’ pathologies as thoroughly as the paediatricians and surgeons do. Vascular disease is rare in children but it does exist [Figure 2]. The spectrum of oncological disease is very different to that in adults and it is vital to know which lesions require biopsy, which can be diagnosed from sampling nodal disease and how much tissue is required. The complex genetic abnormalities in neuroblastoma, for instance, mean that 15–20 core needle samples are routinely needed for the complex histological and cytogenetic testing required for risk stratification and treatment planning for these children. Complex congenital diseases expose us to a range of new challenges. Technologies such as intravascular ultrasound and optical coherence tomography allow us to investigate structural abnormalities at a new level and push diagnostic boundaries [Figure 3].
The rewards of paediatric IR are huge. Children rarely complain and once they know they are in a safe environment, they make the most fun and trusting patients. Post-operative rounds are often conducted in the playroom or over a plate of jelly, chips and chocolate. Glitter is an occupational hazard. Adult IRs often tell me it is the thought of the parent interactions that is the most daunting. Sure, conversations with anxious parents can be tough, but so are consults with anxious adult patients and their relatives, and these are skills we can learn with a little practice. I usually find parents to be straightforward and as sympathetic to our concerns as we are to theirs. Their gratitude makes paediatric IR immensely rewarding; it is a great honour to be trusted with their children’s lives. The walls of our offices are littered with ‘first day at school’ photos and news of our small patients’ journeys to adulthood [Figure 4]. Knowing you have given a child the chance of a long, full and healthy life is an extraordinary and frequent privilege.
Paediatric IRs come from a variety of backgrounds. There is only one training number in the UK so, as with adult IR many years ago, training programmes need to be far-sighted, flexible and inventive. Here in the UK, it is more common for paediatric diagnostic radiologists to incorporate IR into their paediatric training to subspecialise in paediatric IR, rather than for those with an adult IR background to turn to paediatrics. There are probably several reasons for this, not least the fact that until recently, most trainees on an IR pathway would have little awareness of any paediatric IR career options. Paediatric diagnostic radiologists have already overcome the fear of working with children, and they know the immense rewards of being involved with children’s care. To them, the world of paediatric IR must seem a little less daunting than it might to, say, an adult vascular radiologist, but I believe this can and will change. In North America, paediatric IR is an increasingly mainstream speciality and one that is now highly competitive, with over 20 specialist paediatric IR training schemes in the USA and Canada. The Society for Pediatric Interventional Radiology is an enthusiastic and highly professional organisation, drawing the paediatric IR community together from all around the globe. This year’s meeting is in Amsterdam and I would encourage IRs to attend.
There are currently fewer than 15 consultant radiologists in the UK who have paediatric IR as a major part of their job plan. But it would be naïve to suggest that paediatric IR is only delivered by those few. A high proportion of those reading this will have been involved in paediatric cases in their career, from relatively routine drain insertions through to emergency embolisations in desperate circumstances. It would be unrealistic to expect all IR procedures in children to be delivered by subspecialists and it is vital that we develop a network of education and support so that all IRs know who to call for advice and support when a challenging case arises. In parallel, it is imperative that we drive forward the development of a wider paediatric IR service in this country. The Royal College of Radiologists (RCR) and the British Society of Interventional Radiologists (BSIR) are taking this challenge seriously; together with the other Colleges, we are surveying services across the UK to identify areas of greatest need and then lobby for more jobs and greater funding.
I had the honour of being the RCR/BSIR travelling professor for 2017–2018. It was a fantastic year. I visited 15 training schemes, from Aberdeen to Plymouth, and met an extraordinary number of trainees fired up by the possibilities of paediatric IR. Many have subsequently come to visit our centre and I have absolute confidence that most will follow it through to develop and shape rewarding careers with a paediatric IR focus. Only a few years ago, our paediatric IR fellowship post lay unfilled, but now we have trainees clamouring for similar posts around the UK. Over the last couple of years, it has become increasingly clear that a forum is needed to feed trainees’ interest and to grow a support network for both adult and paediatric IRs working in this challenging and emotive field. A Paediatric IR UK meeting grew out of this and at our inaugural meeting in November 2018, we welcomed 78 trainees, IRs and industry representatives for a memorable day of paediatric IR teaching and sharing that we will be building on in June 2019. Follow us on Twitter @PaediatricIR for details.
I have watched with pride and excitement as its influence has grown over the last ten years and I have no doubt that its future here in the UK is very bright indeed.
Alex Barnacle is a consultant paediatric interventional radiologist in the Department of Radiology at Great Ormond Street Hospital for Children (GOSH), London, UK. She is on Twitter as @BarnacleAlex.
The first-in-human case using the new deep vein thrombosis (DVT) device Vetex thrombectomy catheter (Vetex Medical) has recently been completed in a multicentre study. The device has the potential to reduce hospital stays and costs associated with DVT treatment, a press release announces.
According to Vetex Medical, the Vetex thrombectomy catheter is the first device to combine rotational and grasping action to “quickly and gently” remove large volumes of wall-adherent clot in a single session, without thrombolytic drugs.
The first patient was treated by the study’s principal investigator Stephen Black, Narayan Thulasidasan, and their team at Guy’s and St. Thomas’ NHS Foundation Trust in London, UK.
“The Vetex device was surprisingly effective at removing wall-adherent clot on the first pass and was easy to use in our first procedure. Existing devices can remove fresh thrombus but have difficulty creating a larger lumen through more organised material on the vessel wall,” says Black. “This device shows the potential to start and finish the procedure in one catheter lab session, avoiding intensive care unit/high dependency unit time and a prolonged hospital stay, and thereby saving staff time and hospital costs.”
The multicentre, non-randomised VETEX trial is a feasibility study of 30 patients with acute iliofemoral DVT treated with the Vetex device, with the primary outcome being procedural success, defined as SIR grade II lysis with freedom from procedural related adverse events.
DVT treatment expert Michael Lichtenberg (Klinikum Hochsauerland GmbH in Arnsberg, Germany), who was involved in the study, comments: “DVT technology is not there today to deliver reliable or reproducible results every time. As physicians, our goal is to evolve treatment to be safer for patients, faster and more cost effective, and the Vetex device shows the potential to deliver all three.”
The goal of the current study is to confirm the design of the device; it offers a purely mechanical approach to removing wall-to-wall clots, avoiding the use of thrombolytic drugs due to the associated bleeding risk, according to Vetex Medical CEO Mark Bruzzi. At present, the Vetex thrombectomy catheter is in the early clinical trial phase.
Vetex Medical plans to seek FDA 510(k) clearance for the device. Eventually, the company also plans to expand the patient population to include not just patients with acute DVT, but also those with subacute DVT without the use of thrombolytic drugs.
Today’s DVT treatment
Currently, anticoagulation is the most widespread therapy for DVT, but interventional treatment has demonstrated the potential for better outcomes in some patients. Interventional DVT options on the market today include the use of thrombolytic drugs to dissolve a clot, with or without the use of a mechanical device, or purely mechanical devices that use fragmentation and/or aspiration to create a core through the clot. Because thrombolytic agents thin the blood, they present a bleeding risk for many patients and can require prolonged hospital stays. Without effective treatment, up to 50% of patients with symptomatic DVT will develop post-thrombotic syndrome within two years, which involves chronic limb pain, swelling, heaviness, fatigue, and in extreme instances, limb ulceration.
Speaking to investors at the JP Morgan healthcare conference in San Francisco, executives from Medtronic and Boston Scientific said their data do not show the safety risks cited in Katsanos (Patras, Greece) et al’s published analysis.
According to the Star Tribune, the companies stated that they are not backing away from drug-eluting devices used in blood vessels in the legs, despite the recent JAHA (Journal of the American Heart Association) meta-analysis linking the devices to a significantly increased risk of death at two and five years following the use of paclitaxel-coated balloons (DCBs) and stents in the femoropopliteal artery.
Katsanos and colleagues concluded their study by saying that “further investigations are urgently warranted”, but also claimed that their findings were backed up by strong statistical evidence; the paper synthesised the results of 28 randomised controlled trials of stents and DCBs (including Medtronic’s In.Pact Admiral and Boston Scientific’s Ranger DCB) used above the knee in the legs. Boston Scientific’s Eluvia drug-eluting stent also contains paclitaxel, though was not used in the analysis.
However, looking “deeply” at their own internal data, Medtronic and Bostin Scientific officials claimed they could find no support for an association between paclitaxel and higher death rates.
As reported in the Star Tribune, the Medtronic cardiac and vascular group president Mike Coyle told investors: “We have generated a tonne of clinical evidence: 1,800 patients, we have data out to five years, randomised controlled study for the USA, randomised controlled clinical study for Japan, global registry data. And all of these data have been analysed. We have not seen this safety signal in our data”. These data are likely to be published in coming months.
Boston Scientific global chief medical officer Ian Meredith said meta-analyses like the paclitaxel-device study in JAHA sometimes reach findings that are not replicated in subsequent studies. The Star Tribune also reports that Meredith noted that the broad, population-level data offered no explanation for the potential mechanism behind the deaths.
A statistical observation which generates important questions, not an answer
“I think at this stage, good clinical studies are appropriate,” Meredith said. “There does not seem to be a plausible mechanism to understand how a dose that is imperceptible in plasma or tissue at 30 days could actually really affect mortality two years and beyond.”
In response to the industry push-back, Katsanos commented in an email to the Star Tribune: “I do understand the scepticism of the industry, but at the end of the day, the statistical signal is too strong to be ignored by reasonable doubt”.
Speaking to Interventional News, Peter Schneider (Kaiser Permanente, Honolulu, USA) echoes Meredith’s concern, stating: “The recent meta-analysis associating paclitaxel with late mortality yields a statistical observation. In my opinion, there is a mismatch between the available data and the conclusion. The study generates several important questions but does not propose a mechanism and does not provide a definitive answer.
“The following factors should be carefully considered as we analyse this study. All reported mortality data in superficial femoral-popliteal DCB and drug-eluting stent (DES) studies are within the range of reported results for mortality in other vascular device trials and expected results from population-based studies of peripheral arterial disease patients. The meta-analysis assumes that paclitaxel is present for the length of patient follow-up, and there is much evidence that contradicts this assumption. Some of the data from studies included in the meta-analysis are inferred from the published papers, rather than actual event numbers. It combines DCB and DES data to assess mortality, but this is probably not scientifically valid based upon the very different preparation and mechanism of delivery between DCB and DES.
“Only three studies have extended to five years and would be potentially reliable sources for information on long-term mortality. Although the paclitaxel treatment groups (DCB and DES) are garnering a lot of attention, we must also look at the angioplasty (PTA) control groups. The PTA groups are small at five years and none of the studies were powered to evaluate mortality, especially long-term mortality; 109 patients for DCB (IN.PACT and THUNDER) and 121 patients for DES (ZILVER PTX). By chance, the PTA group in IN.PACT had among the lowest mortality ever reported in a vascular study. The PTA group in THUNDER had 46% lost to follow-up. It is not clear whether PTA groups were followed with the same tenacity as the paclitaxel groups, especially after a patency end point was reached, and this happened significantly more often in the PTA groups than in the paclitaxel treatment groups. Another possibility that needs investigation is whether PTA patients, who underwent many more target lesion revascularisations, also received better medical management in association with more frequent encounters? When deaths were adjudicated by clinical events committees, as in the IN.PACT and ZILVER PTX trials, there was no clustering around any particular cause or timeline.
“In summary, we have a mathematical observation based upon heterogeneous data that prompts many questions but does not answer any.”
Meredith noted that oncologists have more than two decades of experience with paclitaxel as a chemotherapy agent, at much higher doses than used on a stent or balloon, and have found no similar increased risk of death. Katsanos and colleagues wrote in their JAHA article that whereas paclitaxel for chemotherapy is solvent-based and has a half-life of about six hours, the paclitaxel on medical devices has a half-life of weeks to months.
Multi-probe stereotactic radiofrequency ablation (SRFA) with intraprocedural image fusion represents an efficient minimally invasive therapy for hepatocellular carcinoma (HCC), even with tumour sizes larger than 3cm, and without the need to combine its use with additional treatments, concludes Reto Bale (Department of Radiology, Medical University Innsbruck, Innsbruck, Austria) and colleagues, writing in Hepatology.
In their recent single-institution, retrospective study of prospectively collected data, Bale et al found that the stereotactic ablative treatment had a 97.3% success rate, with 183 of 188 treated lesions exhibiting no residual vital tissue post-intervention.
While the authors acknowledge that liver transplantation represents the only curative option for both HCC and underlying chronic carcinogenic liver disease, long waiting lists for transplants mean that tumour progression often advances beyond the conventional transplant criteria, leading to high patient drop-out rates. To remedy this, physicians offer neo-adjuvant locoregional therapy with the aim of down-staging tumours and decreasing the waiting list drop-out rate for liver transplant. However, previous studies have reported that the presence of partial necrosis following locoregional therapy is a major risk factor for tumour recurrence post liver transplantation. Therefore, Bale and co-authors propose SRFA has an alternative option to neo-adjuvant locoregional therapy before liver transplantation. Watch a video of Reto Bale and colleagues performing SRFA here.
A success for image fusion
Typically, radiofrequency ablation (RFA) is the first choice of HCC treatment for very early stage tumours, smaller than 2cm, due to its “great potential for local curative tumour control”, according to the study authors. However, while the therapeutic response in these small tumours is comparable to surgical resection, larger tumour size comes with an attendant increased risk of recurrence in conventional ultrasound- and computed tomography-guided (US- and CT-) single probe RFA. Indeed, univariate analysis has confirmed that increasing size is an indirect predictor of incomplete response to treatment.
Bale and team advocate for the added use of image fusion to lower this risk for larger tumours. The median tumour size in this study was 2.5cm, with the largest being 8cm, and including 52 lesions with a diameter greater than 3cm. Larger needles necessitated the use of more coaxial needles: the median number of needles per lesion was three for all HCCs, but when focusing only on lesions greater than or equal to 3cm in diameter, this number rises to five.
H&E stained liver cells
SRFA was able to overcome the “well-known” limitation of US- and CT-guided single-probe RFA. The authors write: “Using the stereotactic approach with intraoperative image fusion even in lesions greater than or equal to 3cm [in diameter], complete tumour cell death was achieved in 50/52 (96.2%) [of lesions]. In contrast to previous reports about conventional RFA, no correlation between residual tumour and tumour size was found (p=0.5)”.
Long-term survival following SRFA of different cancers—cholangiocellular carcinoma, colorectal liver metastases, breast cancer liver metastases, melanoma liver metastases—has previously been found to be comparable to resection. Listing the advantages of image fusion, the investigators write that 3D-navigation systems “allow for a more sophisticated 3D planning of multiple overlapping ablation zones, precise probe placement and intraoperative assessment of the results by means of image fusion”.
They sought to determine if the implementation of high-end stereotactic techniques—the triumvirate of 3D planning, 3D guidance, and image fusion—could improve the results of thermal ablation. Their findings evidenced that this was the case.
Even with the additional efforts related to the stereotactic approach, Bale and co-authors conclude: “In our opinion the results justify specialised training in stereotactic techniques as well as additional costs related to the infrastructure. We therefore encourage other centres to adapt 3D planning, 3D image-guidance and image fusion to improve the outcome of ablation techniques.”
Results
Seventy-six patients with 131 HCCs between them underwent radiofrequency ablation only, while 51 tumours in 16 patients received RFA after unsuccessful transcatheter arterial chemoembolization (TACE). In 125 sessions, five major complications occurred (4% rate), including one event, respectively, of: liver failure, pulmonary embolism, diaphragmatic injury, bleeding, and pleural effusion.
The authors state that the ultimate goal of thermal ablation is “the induction of irreversible tumour cell destruction”. The absence of residual tumour tissue is therefore an indicator of success. In this study, five out of 188 treated lesions evidenced residual tumour tissue; thus, ablative treatment was considered successful in the remaining 183 lesions (97.3%). In a total of four patients, new manifestations of the disease were observed following treatment.
Statistical analysis revealed that recurrence did not correlate with tumour size (p=0.5), tumour stage (p=0.81), location (p=0.61), sex (p=0.32), or age (p=0.8).
The use of TUNEL staining improved the histopathological analysis
The present study offers the largest patient cohort documented in the medical literature where SRFA outcomes have been histopathologically evaluated using TUNEL staining (terminal deoxynucleotidyl transferase dUTP nick end labelling).
Using TUNEL analysis, freshly apoptotic cell areas show a distinct nuclear staining; in more advanced lesions the cytoplasm of the tumour cells depicts a positive reaction as well. In a 2006 study by Adrian Martin (Baylor Regional Transplant Institute, Dallas, USA) and colleagues, a histological examination of explanted livers utilising both H&E (haematoxylin and eosin) and TUNEL staining yielded a 19.6% higher percentage of tumour cell death than when the HCCs were assessed by H&E staining only.
Whenever the viability of the treated HCC could not be ruled out in conventional H&E sections in Bale et al’s analysis, an additional TUNEL assay was performed. The investigators write: “In contrast to previous studies, and most likely due to the additional use of the TUNEL assay, histopathologic examination correlated well with radiologic imaging prior to liver transplant. To the best of our knowledge, these results are superior to all results published so far on conventional thermal ablation, including similar histopathologic studies with additional TUNEL staining”.
For more information on SRFA, Bale encourages “all interested interventional radiologists” to attend the 3rd European School of Interventional Radiology (ESIR) course on “Reliability in Percutaneous Thermal Ablation”, held 12–13 December 2019 in Innsbruck, Austria. He says: “This workshop will cover an SRFA live case, and all relevant topics that are important for successful thermal ablation. An international distinguished faculty will train the participants in sophisticated planning, guidance and image fusion. Register as soon as possible because the number of participants is limited and the last two courses were sold out soon.”
One of the 22 questions included in the ACR survey
The results of an American College of Radiology (ACR) survey find that small hospitals and rural communities experience greater difficulty recruiting and retaining interventional radiologists (IRs) and meeting IR service demands compared with their non-rural counterparts. The data were published recently in the Journal of the American College of Radiology in an article authored by Eric Friedberg (Department of Radiology and Imaging Sciences, Emory University School of Medicine, Atlanta, USA) and colleagues.
The study investigators worry that these data evidence a “potential subspecialist manpower crisis”, with geographic factors playing an important role in determining patient access to IR services. Upon evaluating the survey results, the authors conclude the “data suggest that small and rural hospitals will be disproportionally affected by future predicted physician shortages, resulting in difficulty meeting both general and subspecialty radiology service needs”.
Friedberg and colleagues sought to capture information regarding the current status of IR staffing across the USA, and to evaluate the perspectives of radiologists across the nation regarding their ability to recruit and retain interventionalists. Via email, they sent out a 22-question survey—finalised by an ACR intercommission workgroup comprised of members from the Commissions on General, Small, Emergency, and/or Rural Practice and the Commission on Interventional and Cardiovascular Radiology—to 15,463 ACR members who self-identified in the ACR Practice of Radiology Environment Database as a “group practice leader,” “general radiologist,” “interventional radiologist,” or “abdominal radiologist.” However, the response rate was low; the conclusions are based on the answers given by the 1,005 email recipients who completed the survey.
Rural radiology practices have more difficulty meeting local demand for IR services
Compared with non-rural equivalents, the study finds that rural radiology units experience more difficulty meeting local demand for IR services, both at the hospital level and the regional hospital catchment area.
A statistically significant greater proportion of responders from rural hospitals compared with non-rural hospitals, the latter defined as those serving an estimated population of 250,000 or more, answered that their group falls far short of the demand for IR services: 6% of rural answers, compared to just 0.9% of non-rural ones. A further 23.1% of rural responders believed that the hospital they work at falls short of the demand for IR services. In comparison, only 13.4% of non-rural IRs thought this about their workplace.
In addition, a greater proportion of non-rural IRs said that their group meets the demand for IR services: 48.2% of rural responders, compared to 60.8% of non-rural survey participants.
The authors also note the relevance of having an exclusivity clause in IRs’ contracts. A greater proportion of responders from both rural and non-rural hospitals where they were able to meet most requests for IR procedures indicated that they did have an exclusivity clause in their contract. In comparison, in hospitals where there was a desire for IR procedures that could not be delivered, i.e. where local demand for IR services was not being met, a greater proportion of responders from both rural and non-rural areas did not have an exclusivity clause in their contract.
In addition, when respondents believed catchment area demands were being met, they more often responded that the IR physicians in their group do not take diagnostic radiology call. Similarly, physicians who reported not meeting IR needs more often reported having primary diagnostic responsibilities.
Rural radiology practices experience more difficulty recruiting IRs
More survey respondents from rural areas had trouble recruiting IR physicians to their practice than non-rural workers did; 59.2% of rural IRs reported this difficulty, compared to 32.8% of non-rural answerers. According to Friedberg et al, “Of rural respondents who perceived they had difficulty recruiting IR physicians to their practice, 58.7% believed that ‘IR physicians do not want to do diagnostic work’ was a factor, which cumulatively accounted for 24% (20.0%, 28.6%) of all responses. Of rural respondents who perceived they had difficulty recruiting IR physicians to their practice, 58.2% believed ‘IR physicians do not want to work in a small or rural setting’ was a factor, which accounted for 29.8% (19.8%, 28.4%) of all responses. Together, these two reasons accounted for 47.8% of all rural respondents’ answers.”
It is harder for rural radiology practices to retain IRs
Over 38% of respondents from rural hospitals reported difficulties with retaining IR physicians in their practice, as opposed to 23.5% of non-rural IRs experiencing the same issues. “IR attending perceived inadequate complexity of case mix” was the largest explanatory factor listed among rural responders, with 67.5% listing this as the top reason for the low retention rate. As expected by the study investigators, fewer non-rural responders, who nevertheless also thought they had difficulty retaining IRs in their own teams, cited this as an issue, with just over half citing inadequate case mix complexity as the number one source of low IR retention in their practice.
The number of available cases was also seen as a contributing factor to a reduced ability to retain IRs for rural responders, but not so much amongst non-rural answers. Two-thirds of rural responders believed an inadequate number of cases to be a contributing factor, whereas fewer than one-third of non-rural responders did. Cementing this difference, 18.1% of non-rural answers claimed that an inadequate number of IR cases was not a contributing factor at all.
The study authors hypothesise: “The overall subjective trend in responses may reflect an underlying desire by IRs to exclusively practice “high end” IR—a trend that may be exacerbated as a large of integrated pathway graduates soon begin entering the workforce”.
New integrated training pathways approved
The American Board of Medical Specialties has recently approved new integrated training pathways for IRs. There are now 78 integrated IR residency programmes currently accredited by the US Accreditation Council for Graduate Medical Education (ACGME), which Friedberg et al describe as “supplanting traditional diagnostic radiology residencies for those who seek highly specialised IR practices”.
However—despite the aim of increasing subspecialisation being to foster a more focused discipline with a greater commitment to longitudinal clinical care—thought leaders have expressed the fear that introducing more niches may exacerbate evolving patient access issues. Friedberg and colleagues write: “Specifically, questions remain around whether this trend will increase the risk that small and rural hospitals will have difficulty recruiting and retaining IRs who no longer seek to provide diagnostic radiology services, potentially leading to hospital administration, referrer, or patient dissatisfaction—as well as endangerment of future radiology contractual relationships”.
The authors go on to comment: “The inability to provide adequate IR services may be a contributor to hospital and referrer dissatisfaction, as well as to patient care underperformance in rural and small areas—a situation that is likely to worsen amidst superimposed training pathway changes, healthcare system consolidations, and projected physician shortages. Respondents to this specific survey consistently indicated that IR services stabilise groups and add value beyond revenue.
They conclude: “Given the value of IR services to patients and the ongoing geographic access challenges to those services as the practice of IR services becomes increasingly subspecialised, professional societies, such as the ACR and the Society of Interventional Radiology, are likely to play a critical role in developing plans and solutions to guide radiology practices. Potential solutions include managing expectations for new pathway trainees, development of additional training opportunities for general radiologists to provide a broader range of at least less complex interventional procedures, novel contractual and practice organisational options for IRs, illumination of the ‘downstream revenue’ value in IR, and synergistic partnering or alliance with other subspecialties or larger institutions”.
Gregory Makris (fourth from right) with collaborators in Uganda
It is time to change patient care for an entire country, writes Gregory Makris. After travelling to Uganda and learning that the country’s 40 million strong population had no access to interventional radiology services, Makris felt the scale of the difficulties besetting healthcare providers in such a resource limited environment, and the urgency of introducing these life-saving procedures to those in need. Here, he gives a first-hand account of how he has been working with the Uganda-UK health alliance and other national and transnational organisations to establish an interventional radiology service in the East African nation.
It is almost 9am and we have just landed in Entebbe international airport after 12 hours of flying through the night. I am a bit tired, but the nice warm breeze of the tropics is welcoming and definitely a pleasant change from the cold and rainy weather of London. The drive to Kampala, capital of Uganda, takes around an hour and half and, having never been to East Africa before, I am slightly nervous. The scenery around us is beautiful; we are in the middle of the rainy season and everything is green and colorful. Lake Victoria, source of the world’s longest river, the Nile, is right next to us, and a quick swim in the cool waters is tempting…
As we approach Kampala, the traffic becomes heavy, providing the first idea of how busy this city of one and half million people is. Boda-bodas—small motorbikes that constitute the main means of transportation in the city, sometimes seemingly dangerously loaded with several passengers—weave amongst the bustle. As we get deeper and deeper into Kampala, the scenery changes considerably, developing a more urban look with open markets everywhere. The packed city’s populous are very friendly, and always more than happy to help. This is despite the large number of people still living in extreme poverty following the long civil war between the North and the South which racked the country, from which its 40 million inhabitants are still recovering.
Uganda became independent from the British in 1962, but has maintained strong links to the UK since. The Uganda-UK health alliance is a great example of this relationship. In 2013, the Uganda-UK health alliance was launched in Kampala as a partnership of UK- and Uganda-based organisations that share a common interest in health developments in Uganda. Initially hosted by the University Hospital of South Manchester NHS Foundation Trust (UHSM), the alliance was underpinned by a Memorandum of Understanding signed by 31 UK-based and 17 Uganda-based public and third-sector organisations, as well as the Ugandan Ministry of Health. One of these organisations is the global engagement division of Health Education England (HEE), which, under the leadership of Professor Ged Byrne (Manchester, UK), has been contributing to the improvement of health care standards in the region. It was when I first met Professor Byrne during a trip for another project that I realised an entire country of 40 million people had absolutely no interventional radiology (IR) service. I was shocked—something had to be done about it, and thankfully HEE and the Uganda-UK health alliance were incredibly willing to help.
Uganda has around 50 radiologists, which is roughly one radiologist for every million people. This scarcity of specialists is a common problem for most African countries. For context, according to the Royal College of Radiology, the average ratio in the UK is 48 radiologists per million people, a number considered small in comparison to EU standards. At the same time, Uganda has one of the worst records of both post-partum haemorrhage and road-traffic related morbidity in Africa. These are areas where good clinical imaging and IR services can make the difference between life and death. The local doctors in Kampala are well aware of this, but the lack of local experts to train the country’s first cohort of interventional radiologists, in combination with the lack of experience in organising a proper supply chain and procurement mechanism for IR consumables, makes this task extremely difficult for Ugandan healthcare professionals to achieve alone.
Dr Rosemary Byanyima is one of the most senior radiologists in Kampala, and was one of the first local radiologists to understand this problem and push for change. Thanks to Dr Byanyima and her team, we were able to organise the first assessment visit to understand how things work in the Mulago National Referral Hospital (MNRH). This is the largest public hospital in the country, with 1,500 beds. In 2014, an average of 80–100 babies were delivered daily, in the hospital’s three maternity wards. The Uganda Heart Institute and the Women’s Hospital are also nearby, and in combination with the Uganda Cancer Institute represent the spearhead of Uganda’s health-care system.
The next three days in Kampala were very intense: trying to get as much information as I could from the local key stake-holders, and assessing the available infrastructure and the existing supply chain and procurement mechanisms. We had meetings with representatives from the Ministry of Health, the Uganda Heart Institute (that houses the only angiography suite in the country), the Medical School of the Makere University, and of course the MNRH administration team. It was great to see that everybody was on board with understanding the potential of developing an IR service in the country, with its main primary focus being the management of acute haemorrhage during post-partum complications or after road traffic accidents. During my invited lecture for the medical personnel of the MNRH regarding the expanding role of IR in modern medicine, everybody seemed to be fascinated about how much can now be done through a pinhole and under image guidance, and of course there was a lot of enthusiasm from the local radiology trainees to learn more about this new dynamic specialty.
Before I realised it, I was on my way back to rainy London. I could not help but think of how many lives in Uganda could be saved or improved if a proper IR service was established. Interventional radiology and clinical imaging should not be considered luxury services any more. We would never consider having hospitals without CT and MRI scanners in the UK, and of course we would not accept a tertiary medical centre with no acute IR service provision. We have come a long way in Europe in terms of that, but in Africa there are still huge parts of the continent without appropriate image-guided clinical services. Uganda unfortunately is not an exception to the rule in Africa; it is just another example.
Organisations like RAD-AID international are setting a great example of how imaging services can be improved in a limited resource environment, and are already doing some great work establishing an IR service in Tanzania using volunteer IRs from all over the USA.
We hope that in this effort to improve access to IR services in Uganda, we will not be alone. If this project is going to be successful, it will need collaboration between local and international partners; it will require collaboration between academic institutions and industry in order to bring together the “know-how” as well as the equipment necessary to build a sustainable IR department in a low income country. Of course, it will also require interventional radiologists who are happy to engage and volunteer their expertise to train more IRs in Africa. Interventional Radiologists have always been adventurous and creative. This project, with all its challenges, can be another opportunity to prove how we can use these qualities to achieve something that might initially look impossible.
I am talking about changing patient care for an entire continent.
So: who is up for the challenge?
Gregory Makris
Gregory Makris is a Vascular and Interventional Radiology Fellow at Oxford University Hospitals, NHS Foundation Trust, Oxford, UK. He is also chair of the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) European Trainee Forum, as well as chair of the British Society of Interventional Radiology (BSIR) trainee committee.
IZI Medical Products (IZI) has acquired select soft tissue biopsy and breast localisation needle assets from Cook Medical. The acquired portfolio of products is commercially marketed under the Quick-Core Biopsy Needle, MReye Breast Localisation Coil, and the Kopans and X-Reidy Lesion Localisation Needles.
This represents IZI’s third add-on acquisition in the last 18 months, including another acquisition from Cook in 2017 (the line of Osteo-Site needles).
“IZI is strategically focused in diagnostic and therapeutic areas with imaging modalities, which will allow them to have a closer relationship with the diagnostic and interventional physicians that are performing the procedures,” commented Mark Breedlove, vice president, Vascular Division at Cook Medical. “We were looking for a company that could invest more resources and continue to support these product families, the patients that benefit from them, and the physicians that use them.
“We have worked with IZI in the past and determined that they would be the ideal partner moving forward, and we are pleased to support the transition as IZI prepares to manufacture these products. This agreement will benefit patients, customers, and hospitals alike.”
Cryoablation shows early indications of effectiveness in treating women with low-risk breast cancers, according to research presented at the annual meeting of the Radiological Society of North America (RSNA; 25–30 November, Chicago, USA). Researchers said that over the four years of the study, there has only been one case of cancer recurrence out of 180 patients.
“If the positive preliminary findings are maintained as the patients enrolled in the study continue to be monitored, that will serve as a strong indication of the promise of cryotherapy as an alternative treatment for a specific group of breast cancer patients,” said study lead author Kenneth R Tomkovich, radiologist at Princeton Radiology and director of Breast Imaging and Interventions at CentraState Medical Center in Freehold, USA.
While cryoablation has been used to treat cancers in the kidneys and lungs, it has yet to become an established treatment for breast cancer. Tomkovich began studying it for that indication more than 10 years ago, as imaging advances in mammography and ultrasound and the development of tomosynthesis enabled the detection of more low-risk cancers. These small, early-stage cancers have the potential to become invasive and life-threatening without treatment. But treatment options have not kept pace with imaging advances.
“We are finding smaller and smaller breast cancers, but we are still treating them the same way we did 30 years ago,” Tomkovich said.
Cryoablation represents a potential new weapon in the arsenal against breast cancer. The tumour-killing procedure takes less than an hour, and patients are able to return to their normal activities shortly thereafter.
As part of the Ice 3 Trial, Tomkovich and colleagues at 18 centres across the USA have been studying cryoablation as a primary treatment for breast cancer without surgical lumpectomy. Starting in 2014, the researchers began performing cryoablation on women ages 60 and over with biopsy-proven, low-risk breast cancer. The patients undergo the procedure and then are followed for recurrence with mammography at six and 12 months and then annually for five years.
As of now, the researchers have three-year follow-up data on about 20 patients and two-year follow-up data on more than 75 patients. The preliminary results have been very promising. The procedure was successfully completed in all patients, and no serious adverse events have been reported. Only one patient experienced a recurrence, giving the procedure a 99.4% success rate so far.
“Lumpectomy is 90–95% effective at removing cancer,” Tomkovich said. “We were going for something close to that, but our preliminary results have been even better. We are getting the same results at 18 centres around the country.”
Advocates claim that cryoablation has advantages over thermal ablation techniques, which use heat to destroy tumours. Additionally, there is preliminary evidence from studies on mice that cryoablation can stimulate an immune system response against cancer cells in the body.
Final results of the study will be published when five-year follow-up data is available for all the women who were treated.
“If it is proven that cryoablation works, then some women might be more inclined to opt for it over surgery,” Tomkovich said.
Kenneth Tomkovich is a consultant for Scion Medical Technologies, and is on the Scientific Advisory Board for IceCure Medical.
The first commercial use of the Tack Endovascular System (Intact Vascular) has taken place in multiple hospitals within Germany. A novel therapy for dissection repair following balloon angioplasty, the Tack implant is a first-of-its kind device for patients with peripheral arterial disease (PAD) and/or critical limb ischemia (CLI).
“The Tack System provides a much needed therapeutic option for treating dissections in the superficial femoral or popliteal arteries following balloon angioplasty,” says Christian Wissgott, assistant director at Westküstenklinikum Heide in Heide, Germany. “I am very pleased with my experience using the implant and I am excited to incorporate this technology into my above and below the knee treatment algorithms going forward.”
Patients treated with balloon angioplasty frequently suffer from dissections. Often overlooked, undiagnosed and untreated, dissections can lead to acute thrombosis and arterial occlusions, which lower long-term patency rates and require repeat procedures. Designed to resolve these dissections while leaving minimal metal behind, the Tack implant is designed to preserve vessel integrity, minimise vessel inflammation and enhance blood flow.
“With the Tack System, balloon angioplasty results are improved regardless if it is drug-eluting or not,” notes Michael KW Lichtenberg, chief of the Angiology Clinic and Venous Center in Klinikum Arnsberg, Germany. “Based on my initial experience, I am confident this new paradigm of focal dissection repair will become standard of care for patients undergoing PAD interventions.”
This follows the recent news that the Tack Optimised Balloon Angioplasty II below-the-knee (TOBA II BTK) clinical trial has successfully completed enrolment, ahead of schedule.
QuiremScout (Quirem Medical) has received CE mark, making it available for clinical centres throughout Europe. QuiremScout is designed to advance the SIRT (selective internal radiation therapy) work-up procedure. It does this by improving the accuracy of predicting lung shunting and the intrahepatic distribution, which aims to optimise SIRT patient selection and treatment planning. QuiremScout will be exclusively distributed by Terumo.
“The commercial introduction of QuiremScout is an important next step towards what we believe will be a true paradigm shift in SIRT,“ says Peter Coenen, president of Interventional Systems Terumo EMEA. “QuiremScout paves the road for increasing confidence in SIRT patient selection and to allow for personalised treatment planning based on each patients’ individual needs. QuiremScout completes our SIRT portfolio, which is built around QuiremSpheres and Q-Suit.”
Until QuiremScout, Tech-99m-MAA (99mTc-MAA) has been used for SIRT work-up procedures around the world, in the absence of any alternative. The limited predictive value of 99mTc-MAA has been recognised by some in the field, leading to the development of QuiremScout.
“QuiremScout has the potential to truly improve the accuracy of the SIRT work-up procedure. It leverages the unique features of Holmium-166 PLLA-microspheres,” Frank Nijsen, Chief Scientific Officer of Quirem Medical and associate professor of Interventional Nuclear Medicine at the Radboud University Medical Center, The Netherlands, explains. “Holmium microspheres emit primary gamma photons and can therefore be imaged in low concentrations using SPECT. Because the scout dose particles are identical in terms of size, weight and shape as those used for QuiremSpheres therapy, the scout dose gives an improved prediction of the post-therapeutic lung shunt. We expect QuiremScout will also lead to improved prediction of the extrahepatic deposition and intrahepatic absorbed dose distribution.”
“QuiremScout has improved our clinical SIRT practice,” Marnix Lam, Head of Nuclear Medicine at the University Medical Center Utrecht (UMCU) says. “Based on data from more than 80 patients, we have demonstrated that QuiremScout is safe in this population and is a better predictor for lung shunting than 99mTc-MAA. As a result, we really feel that we have optimised our SIRT patient selection. In addition, we have established that QuiremScout is also a better predictor for the post-treatment intrahepatic distribution when compared to 99mTc-MAA. Notably, QuiremScout in combination with 99mTc-MAA-colloid enables Dual-Isotope SPECT/CT technology allowing for rapid auto-segmentation of the healthy liver tissue. In our experience, QuiremScout microspheres outperforms 99mTc-MAA. Therefore, we have decided to completely switch to QuiremScout for all QuiremSpheres work-up procedures.”
Unrestricted sales and use of the Nellix System (Endologix) will cease immediately, in order to ensure optimal outcomes for patients, according to Endologix. The product will only be available for use under clinical protocol with pre-screened patients that adhere to the current indications.
“We monitor the performance of the Nellix System through clinical trials, our complaint monitoring system, physician interaction and available publications,” says Matt Thompson, Chief Medical Officer of Endologix. “Our independently adjudicated data from the EVAS1 IDE [Investigational Device Exemption] clinical trial indicates that the Nellix System has performed well when used consistently with the current indications. However, data from recent Nellix publications leave us concerned that outcomes are suboptimal when the system is used outside current instructions for use.”
To ensure optimal clinical outcomes, the Nellix System will, for the foreseeable future, only be available for use under clinical protocol with pre-screened patients that adhere to the current indications. All cases will be pre-screened by a physician panel and supported by Endologix clinical specialists to ensure adherence to protocol. Compassionate use requests will be reviewed in accordance with the process established by the company and associated national competent authorities. The existing inventory will be voluntarily recalled. These actions are described in a Field Safety Notification (FSN) issued on 7 January 2019.
“Ensuring patient safety and optimal clinical outcomes is our top priority, and the current level of off-label use of the Nellix System cannot continue if we are to protect and preserve the potential for transformative EndoVascular Aneurysm Sealing (EVAS) therapy,” explains John Onopchenko, Chief Executive Officer of Endologix. “Taking these actions aligns with clinical practice standards, allows us to control off-label use and will help us ensure appropriate application of the therapy.”
This decision is one of several actions taken by Endologix following a new management mandate in August 2018 to ensure the most appropriate use of each of its devices and is in alignment with a recent publication by the European Society for Vascular Surgery (ESVS). Endologix has been in contact with regulatory authorities regarding the Nellix System recall and related matters to help ensure patient safety and continued appropriate access to the Nellix System.
Endologix refined the technical procedure of EVAS and delivered clinical practice updates and advisories regarding use of the Nellix System through a series of FSNs developed in collaboration with regulatory authorities worldwide. Nevertheless, Endologix has determined that off-label use is occurring at an unacceptable level, with the consequence of sub-optimal results. The company is taking action to ensure optimal outcomes for patients, a press release states.
EVAS therapy was designed to overcome the durability issues of conventional EndoVascular Aneurysm Repair (EVAR) that have led to high rates of aneurysm related mortality when compared with surgical interventions. “When used as indicated, EVAS is associated with low rates of aneurysm sac growth, Type 2 endoleaks and all-cause mortality,” says Onopchenko. “Our actions are intended to preserve and advance this therapy. Clinical data drives our decision making and is our basis for competing in the marketplace. Limiting the use of the Nellix System to only those cases rigorously adjudicated by a review board and performed under clinical protocol will ensure that high integrity data is generated and will enable us to deliver on the promise of this potentially disruptive therapy.”
Medtronic has issued the following statement regarding revised clinical study data:
On 15 February, 2019, Medtronic issued a statement regarding a programming error in the clinical data reporting isolated to the two and three year follow-up periods in our IN.PACT Global post-market study, part of the IN.PACT Admiral clinical programme for the treatment of femoropopliteal artery disease.
As we noted in our previous statement, this programming error impacted the IN.PACT paclitaxel safety analysis, which recently presented at the Leipzig Interventional Course [LINC; 22–25 January] in Leipzig, Germany and published online in the Journal of the American College of Cardiology (JACC).
The revised analysis has been accepted by JACC. Prior to publication of the revised manuscript, the authors of the study have issued a correction letter addressing key revisions to the data. The updated analysis will also be presented by Peter Schneider at the VIVA Physicians Vascular Leaders Forum (VLF) from March 1–2, 2019 in Washington, DC [USA].
It is important to reiterate that the initial conclusions from the patient level meta-analysis remain intact:
Data found no correlation between paclitaxel dose and long-term survival.
Data demonstrated no difference in mean nominal dose of paclitaxel between overall survival in patients treated with DCB and those who died.
At five years there was no statistically significant difference in all-cause mortality between the drug-coated balloon (DCB) and plain balloon angioplasty (PTA) arms.
In addition to the full cohort, a standard cohort has been included by the authors in the JACC analysis. This was done to correct a baseline imbalance between DCB and PTA by identifying a subgroup of DCB patients who met the inclusion criteria for the pivotal studies from the IN.PACT clinical programme, including IN.PACT SFA, IN.PACT Japan, and IN.PACT China. When only the subjects that mirror the baseline variables in the control PTA group are included, we observe a smaller difference in mortality. When adjusted for these baseline imbalances, all-cause mortality between DCB and PTA was 13.2% vs. 11% (p=0.188).
In line with our commitment to transparency, we have shared all our patient-level data with FDA in support of their paclitaxel safety analysis and will plan to do the same to support the upcoming independent VIVA Physicians analysis. Following publication of the revised JACC manuscript, we will also work to correct all impacted materials that live in the public domain.
Ablative Solutions has announced the first close of its US$77 million Series D funding round. The round was led by new investor Glide Healthcare, and co-led by exiting investor BioStar Ventures, as well as an undisclosed new strategic corporate investor. Existing investors, including Michigan Accelerator Fund, Novus Biotechnology, and other individual investors, also participated in the Series D funding round.
Funds from the round will be used to complete clinical trials in support of US and European regulatory submissions for the company’s minimally invasive renal denervation technology designed to help reduce blood pressure for people with uncontrolled hypertension, while taking antihypertensive medication.
“BioStar Ventures focuses on transformational health care investments, and we believe Ablative Solutions fits that model perfectly,” says Michael Fulton, senior managing director of BioStar Ventures, an investor in the company since its Series A round in 2012.
Ablative Solutions’ alcohol-mediated renal denervation procedure is performed using the investigational Peregrine system kit, which is engineered to target nerves known to influence the body’s regulation of blood pressure. The Peregrine kit delivers dehydrated alcohol in small doses directly to the space outside of the renal artery to block the overactive signalling of the sympathetic nerves.
“Hypertension creates a significant burden on the healthcare system, increasing the risk of serious cardiovascular events and stroke,” comments Gilde Healthcare’s Geoff Pardo. “We see tremendous potential for Ablative Solutions’ approach and believe the team has a solid plan for building the clinical data through the TARGET BP clinical programme.”
Ablative Solutions’ CEO and CMO Tim Fischell enthuses: “We are excited to have the support of this thoughtful and high-powered group of investors, which will allow the company to complete the studies required to seek regulatory approvals in Europe and in the USA.”
The Tack Optimised Balloon Angioplasty II below-the-knee (TOBA II BTK) clinical trial has successfully completed enrolment, ahead of schedule. This study, sponsored by Intact Vascular, is the first pivotal trial investigating a permanent vascular implant in arteries below the knee.
The study will examine the safety and efficacy of the Tack endovascular system (Intact Vascular) when used to repair dissections in the arteries below the knee following percutaneous transluminal angioplasty as a treatment for critical limb ischaemia (CLI).
“Patients with CLI experience painful symptoms and are at increased risk of amputation. Unfortunately, therapeutic options are very limited, and no scaffolding solutions are currently FDA-approved for BTK interventions,” commented George Adams, director of Cardiovascular and Peripheral Vascular Research, UNC Rex Hospital, Raleigh, USA, and co-principal investigator for the TOBA II BTK study. “The potential to have a treatment option that maintains vessel integrity and improves blood flow will have a significant clinical impact for treating patients with below-the-knee disease.”
With enrolment completed at 41 US and European sites, the TOBA II BTK trial is a single arm, prospective study to investigate the safety and efficacy of the Tack endovascular system for the repair of post-angioplasty dissections in the mid/distal popliteal, tibial and peroneal arteries. All 233 patients enrolled suffered from CLI, underwent standard balloon angioplasty, and consequently experienced at least one dissection requiring repair.
“Dissections are an expected consequence from balloon angioplasty, yet can have significant implications for patients,” states Patrick Geraghty, professor of Surgery and Radiology at the Washington University School of Medicine in St Louis, USA and co-principal investigator for the TOBA II BTK trial. “Early results with the Tack implant are promising, and I look forward to integrating this technology into my below-the-knee treatment algorithm.”
“Reaching full enrolment for our TOBA II BTK study is an important milestone for below-the-knee interventions,” comments Peter Schneider, a vascular surgeon, and co-founder and Chief Medical Officer of Intact Vascular. “As the first dissection repair device purpose-built for use in these small vessels, we are excited to provide a solution for patients suffering the painful and debilitating effects of CLI and who currently do not have adequate treatment options available. The Tack implant is a novel adjunct therapy that should diminish the chance that these patients will require an amputation.”
The Tack endovascular system is designed to be used in conjunction with peripheral balloon angioplasty in the treatment of peripheral arterial disease. The system is pre-loaded with six self-expanding nitinol devices for above-the-knee interventions, or four for below-the-knee, and can be deployed to treat multiple dissections using a single catheter.
Intact Vascular is sponsoring three clinical trials to evaluate its Tack endovascular system: TOBA II, TOBA II BTK and TOBA III. TOBA II is investigating the combination of the Tack implant with plain angioplasty balloons and the BD Lutonix DCB in arteries above the knee, and successfully achieved both primary and secondary endpoints, as reported at VIVA (5–8 November, Las Vegas). TOBA II BTK is investigating the combination of the Tack implant with plain balloon angioplasty in the arteries below the knee. TOBA III has completed enrolment in Europe and is investigating the combination of the Tack implant with the Medtronic IN.PACT Admiral DCB, inclusive of long lesions.
The original TOBA BTK study in 2016 reported positive six-month results, with a primary patency at that time-point of 87.1%.
The FDA has granted approval for BD’s 0.018-inch guidewire-compatible Lutonix 018 drug-coated balloon (DCB) for the treatment of long superficial femoral artery lesions in patients with peripheral artery disease.
The Lutonix 018 DCB is now available for sale in the USA. In Europe, the device is pending CE Mark approval, advises BD.
Interventional radiologist Constantino Pena (Miami, Florida) commented in the company’s announcement, “By virtue of its lower profile and compatibility with smaller guidewires, the Lutonix 018 DCB will allow physicians to treat more complex lesions from more access sites without the need to exchange to an 0.035-inch guidewire.
“Combined with the 220mm lengths, this represents a significant improvement in our ability to efficiently and effectively deliver a proven drug technology.”
A pooled analysis of four randomised controlled trials finds drug-coated balloon (DCB) angioplasty superior to plain angioplasty in patients with femoropopliteal artery disease, irrespective of their demographics, cardiovascular risk factors, comorbidities or lesion characteristics. This conclusion was recently published in Cardiovascular and Interventional Radiology by Thomas Albrecht (Vivantes Klinikum Neukölln, Berlin, Germany) and colleagues.
Whilst this pooled analysis looked primarily at late lumen loss, it also evaluated secondary endpoints, such as target lesion revascularisation, amputations and all-cause death at 24 months. The rate of target lesion revascularisation was significantly lower in the drug-coated balloon group: 16.3% compared to 40.4% in the plain angioplasty arm (p<0.001). There was no significant difference in amputation rate between the two groups: 2.3% for the plain angioplasty treated patients vs. 2.8% in the paclitaxel-coated balloon cohort (p=0.742).
Most importantly, there were no significant differences in all-cause death rates at 24 months between the plain angioplasty and the drug-coated balloon groups (5.5% and 7.9% respectively; p=0.317).
A recent meta-analysis by Konstantinos Katsanos (Patras, Greece) et al, published in the Journal of the American Heart Association, had contradictory conclusions, reporting an increased risk of death at two and five years following the use of paclitaxel-coated balloons and stents in the femoropopliteal artery.
Whilst the Katsanos meta-analysis analysed data, where it was available, at five years, this pooled analysis references data to two-years post-intervention. However, this present study does offer patient-level data, where the Katsanos meta-analysis did not, and Albrecht believes this at least partially accounts for the different findings.
Explaining these contradictory results, Albrecht elucidates: “We did not see a significant influence of paclitaxel coated balloons on mortality [like Katsanos et al did]. The big advantage of our study is that we had the original individual patient data available for our analysis. This is particularly relevant with regards to patients lost to follow-up, since most published papers used by Katsanos [and colleagues] do not report on how they dealt with these patients—many of which may have died. Furthermore, our cohort is homogenous, consisting only of patients treated with drug-coated balloons and a paclitaxel dose of 3mg/mm2, while Katsanos included drug-coated balloons with different paclitaxel dosages and paclitaxel-eluting stents with very different drug release properties.”
Of the future of paclitaxel-coated devices, Albrecht is cautiously optimistic, admitting that further investigations are needed, but also emphasising the historic safety and efficacy of these drug-coated devices. He says: “Paclitaxel-coated technologies have been proven to be highly effective in reducing the rate of restenosis in the superficial femoral artery and the popliteal artery, so far with virtually no side-effects. The report of Katsanos et al on increased mortality needs to be taken seriously, despite methodological flaws. We will have to review the original data of the previous studies carefully to assess if the observation can be confirmed or not. The future of the field will be dependent on the results of these analyses.”
Katsanos also said that his findings necessitated further investigations into these commercially available devices.
The pooled analysis finds angioplasty with drug-coated balloons superior to plain angioplasty
Albrecht and co-authors surmise that “Our results suggest that all patients and lesions benefit to a similar degree from the use of drug-coated balloons. Drug-coated balloon percutaneous transluminal angioplasty should therefore be preferred to plain balloon angioplasty in all patients with steno-occlusive femoropopliteal lesions of the superficial femoral artery and popliteal artery, irrespective of lesion types and patient risk factors or comorbidities.”
Six-month angiographic data from 355 patients across the THUNDER, FEMPAC, PACIFIER and CONSEQUENT trials were pooled to assess the impact of patient, lesion and procedural characteristics on late lumen loss. All four studies were designed, organised and analysed by the same core research group and recruited patients between 2006 and 2016 in several German centres. All the balloons used across these trials were coated with the same dose of paclitaxel (3µg/mm2).
Intra-study comparisons of baseline data did not reveal any statistically significant differences, meaning the patient cohorts and lesions treated in all four trials were comparable.
Late lumen loss significantly lower after drug-coated balloon angioplasty
“Mean late lumen loss was highly dependent on the treatment used”, the authors write, concurring with earlier published results finding that late lumen loss was significantly lower after drug-coated balloon angioplasty compared to after plain angioplasty.
Albrecht tells Interventional News that these positive results for drug-coated balloons are expected. “On the whole,” he says, “we expected these results. In clinical practice, we have treated all different kinds of patients and superficial femoral artery/ popliteal artery lesions—including calcified ones—with drug-coated balloons for many years, with apparently similar results. Our study confirms this clinical impression, which is very reassuring.”
Patient variables did not affect late lumen loss in the drug-coated balloon arm of this analysis. Notably, the authors report no negative effect of diabetes or coronary artery disease on angiographic outcomes following drug-coated balloon use, contrary to previous reports. The results are in accordance with previous research by John Laird (Adventist Heart & Vascular Institute team, St Helena Hospital, St Helena, USA) and colleagues, who also found no significant impact of patient gender, age, diabetes or Rutherford stages on primary patency in their subgroup analysis of the INPACT SFA study.
The only lesion characteristics that impacted late lumen loss were lesion length and bail out stenting: late lumen loss increased with lesion length in both treatment groups, but drug-coated balloon use outperformed plain angioplasty in any lesion length category. Bailout stenting did not improve late lumen loss in the drug-coated balloon group, but did so in the plain angioplasty group.
Albrecht and colleagues could not account for the fact that their pooled analysis detected a lower late lumen loss in smokers within the drug-coated balloon group (0.10±1.05; p=0.02), saying this finding is “counter-intuitive” and, given the sufficiently balanced groups (61 smokers were included in the analysis and 100 non-smokers), “appears to be a finding to be explored further.” Regardless, both smokers and non-smokers experienced lower late lumen loss when amongst the drug-coated balloon patient population compared to the plain angioplasty one.
Study limitations
Albrecht and colleagues acknowledge several limitations of their pooled analysis. Firstly, they say their study was “a post hoc subgroup analysis of prospectively collected data over a considerable time span which coincided with the overall learning curve to use drug-coated balloons.”
Furthermore, the authors note that different drug-coated balloons were used in three of the four pooled studies. In THUNDER and FEMPAC, the device used was a Cotavance prototype (Bayer Schering/ Medtronic). In PACIFIER, the InPact Pacific (Medtronic) was under investigation, and the SeQuent Please OTW (B Braun) was studied in the CONSEQUENT trial. However, Albrecht et al add that each of the individual studies showed a significant reduction in late lumen loss, irrespective of the device used.
A third limitation identified by the study investigators is the use of a binary scoring of lesion calcification, and finally, the authors understand that the follow-up is constrained to six to eight months’ post-intervention.
Otsuka Medical Devices, a 100% subsidiary of Otsuka Holdings Co., Ltd., and Veryan Medical have announced the completion of the acquisition of Veryan by Otsuka Medical Devices through its UK subsidiary Otsuka Medical Devices UK Ltd.
Veryan’s BioMimics 3D peripheral vascular stent received approval from the US Food and Drug Administration (FDA) in October 2018. Following the acquisition, Veryan and Otsuka Medical Devices plan to collaborate in developing Swirling Flowstents for use in the treatment of vascular disease. As part of the acquisition, Veryan’s operations in Galway, Ireland, will be retained by Otsuka Medical Devices and will play a key role in the continued development of the Swirling Flowtechnology.
Chas Taylor, CEO of Veryan, said: “We are delighted to become part of Otsuka Medical Devices. This will allow Veryan to build on the strong clinical data with the BioMimics stent and realise the potential to significantly advance the treatment of peripheral vascular disease.”
Noriko Tojo, CEO of Otsuka Medical Devices commented: “Veryan’s stent technology represents an excellent fit with our existing activities and has considerable future development potential.”
Otsuka Medical Devices Co., Ltd. focuses on the development and commercialisation of endovascular devices that provide new therapeutic options in areas where patient needs cannot be met through pharmaceutical or other conventional treatment.
Thoracic endovascular aortic repair (TEVAR) demonstrates a one- and five-year survival advantage over the current “gold standard” practice of medical therapy in the treatment of uncomplicated type B aortic dissection, a recent study concludes. In light of these data, lead author James Iannuzzi (currently on staff at University of California San Francisco Medical Center) and senior author Virendra Patel (Division Chief of Vascular surgery at Columbia University Irving Medical Center) and colleagues call for a paradigm shift in the acute management of aortic dissection in favour of early TEVAR.
Citing a paucity of data regarding the impact of acute treatment of uncomplicated type B aortic dissection on long-term survival in a real-world cohort, the study investigators set out to compare TEVAR to open repair and medical therapy.
In their retrospective analysis of a prospectively collected Californian administrative database analysing 9,165 acute uncomplicated type B aortic dissections, 76% of those treated with TEVAR survived to five years’ post-treatment, compared with an inferior five-year survival rate of 67% in open repair patients, and a survival rate of 60% for medical therapy recipients.
The authors hypothesise that the mechanism by which TEVAR may have a favourable impact on survival is “by covering the entry tear, leading to false lumen thrombosis and prevention of aneurysmal degeneration.” They go on to explain: “Evidence from complicated type B aortic dissections treated with TEVAR demonstrates 63% to 88% partial or complete false lumen thrombosis. TEVAR for complicated type B aortic dissection has also been associated with decreased aortic diameter; however, this remains controversial as it has not been demonstrated consistently. By prevention of aneurysmal degeneration, initiation of false lumen thrombosis, and prevention of recurrent dissection, TEVAR may improve long-term survival, as demonstrated in this study and others.”
Iannuzzi and colleagues conclude that TEVAR for uncomplicated type B aortic dissection is a relatively safe and effective approach, associated with longer survival, but note that further study is necessary to determine longer term outcomes for these patients.
Major complications were lower in TEVAR and medical therapy cases than for open repair, with 49% of patients treated with medical therapy experiencing a major complication, and 55% of TEVAR patients, compared to a major complication rate of 72% in open repair cases. Paraplegia rates were also similar between TEVAR and medical therapy (3.4% and 2.9%, respectively), but where found to be highest in the open repair group (9.3%).
Speaking to Interventional News about the clinical ramifications of this finding, Patel comments, “Medical therapy has historically been the gold standard in the management of uncomplicated acute type B aortic dissection, however this work and others call that strategy into question as TEVAR treated patients are associated with better long term survival. This will not be a strategy to treat all patients; however, patients with excellent anatomy and young or healthy patients with expected long term survival should be considered for treatment in experienced centres or referral to aortic centres for TEVAR within the critical window of opportunity to stimulate beneficial remodelling, reduce late aortic events, and improve survival.”
Previous small, randomised controlled trials have found similar results. For example, the Investigation of Stent Grafts in Aortic Dissection (INSTEAD) trial, which randomised patients to optimal medical therapy or TEVAR for treatment of subacute to chronic uncomplicated type B aortic dissection, did not demonstrate a survival benefit at one year (as published in the Journal of Thoracic Cardiovascular Surgery in 2010), but did find that patients treated with TEVAR had improved aorta-specific survival at five years’ follow up. Iannuzzi and colleagues’ study included nearly four times as many TEVAR patients as the INSTEAD trial, and had concordant results.
Explaining the difference between the present study and the INSTEAD trial, the authors write: “A major difference between INSTEAD and this retrospective administrative study is timing of repair. The INSTEAD trial included healthier patients overall with a younger age (mean age of 60 years compared with 66 years), fewer diabetics (6% in INSTEAD vs. 12% in this study), and fewer smokers (17% in INSTEAD compared with 30% in this study). Whereas INSTEAD was a landmark study, corroboration in the real-world setting is imperative, and this study helps validate the INSTEAD findings that long-term survival is improved in patients treated with TEVAR.”
A proponent of stenting more uncomplicated subacute dissections, interventional radiologist Darren Klass, Vancouver, Canada, told Interventional News: “Type B aortic dissection carries a five-year mortality of 20–45%. Since the pivotal trials including STABLE and INSTEAD XL, the question of TEVAR for complicated dissection requires no discussion and patients progress with medical therapy alone. The IRAD demonstrated patients who survive a type A dissection and are discharged from hospital have a plateau in mortality, however patients with type B dissection have a mortality of 25% at three years. These patients therefore constitute a group of so-called ‘uncomplicated dissections’; it is this group, where medical therapy alone is clearly failing—as demonstrated yet again in the recent study by Iannuzzi et al.
“I am convinced we should be treating more uncomplicated type B dissection but two questions remain. 1) What is the ideal timing interval for intervention, and 2) Which patients should be treated?
“We have multiple studies quoting risk factors for aortic progression (entry tear, false lumen and overall aortic size) as well as risks for significantly higher mortality (more than three anti-hypertensive medications), however are these the only surrogates for a more complex disease we do not fully understand? Desai et al (Division of Cardiovascular Surgery, Perelman School of Medicine, University of Pennsylvania, USA) demonstrated a significantly lower complication rate if TEVAR occurred two to six weeks post event. If we could demonstrate reliably an extremely low periprocedural complication rate with an agreed method for TEVAR (PETTICOAT or stent grafting to the celiac), is it possible all uncomplicated dissections would be treated with TEVAR? We do not have the answer yet, but I know if I was unfortunate enough to become a patient, regardless of risk factors for progression, I know what treatment I would demand. Retrospective data or not, I know which Kaplan-Meier curve I want to be on, and it is not the medical therapy one.”
TEVAR twice as expensive as medical therapy in the USA
However, TEVAR was twice as expensive as medical therapy. Costs averaged US$58,000 for medical therapy, compared with US$133,000 and US$200,000 for TEVAR and open repair, respectively. The present study is the first to include cost data when comparing these treatment options in type B aortic dissections, and no prior cost-effectiveness analysis has evaluated TEVAR for uncomplicated dissection. The price tag associated with TEVAR differs dramatically between countries, though, as is expected from vastly differing healthcare systems. Whilst the cost in this US study is not comparable with medical therapy, in a recent Canadian trial, TEVAR cost as little as CA$61,000, less than half of the US expense. Furthermore, a German study of complicated aortic dissection demonstrated TEVAR to be more cost-effective than open repair.
Despite the initial increased cost of TEVAR compared with medical therapy, and the post-therapy surveillance costs incurred by both treatment modalities, the study authors postulate that over a longer time period, the former procedure may demonstrate an improved cost-effectiveness, “given the 25% to 40% increased risk for aneurysmal degeneration over time” present in medical therapy.
Merit Medical has acquired substantially all of the assets of Vascular Insights, based in Quincy, USA. Vascular Insights’ primary assets are the ClariVein IC and ClariVein OC specialty infusion and occlusion catheter systems, which have been utilised in more than 120,000 cases to treat superficial venous disease, particularly below the knee, and venous leg ulcers.
The ClariVein systems address a US$700 million global market. The ClariVein IC system has 510(k) clearance from the FDA, the ClariVein OC system is CE-marked, and the systems are covered by 43 patents issued worldwide.
The purchase price was US$40 million plus additional milestone payments that could amount to an additional US$20 million if certain sales targets are achieved.
“We have had our eye on these products for some time,” comments Fred P Lampropoulos, Merit’s chairman and CEO. “These products complement our existing peripheral intervention sales platform, add to our capability to provide many existing Merit products, such as our micropuncture and vascular access products, and increase our ability to customise the entire procedure for our customers. Additionally, our global sales footprint allows for expansion of sales in previously underserved areas.”
“We are excited to reach this agreement with Merit,” says James Draper, CEO of Vascular Insights. “This acquisition will allow ClariVein to reach more patients in more ways and in more places with the commitment to treat venous disease.”
“I am thrilled that Merit and ClariVein will bring transformative relief to millions of venous disease sufferers worldwide, especially those suffering from debilitating venous leg ulcers,” says Michael Tal, inventor of the ClariVein systems and co-founder of Vascular Insights.
The European Society of Radiology (ESR) and GE Healthcare are partnering on artificial intelligence for the upcoming European Congress of Radiology (ECR; 27 February–3 March, 2019, Vienna, Austria). The partnership includes joint sessions on artificial intelligence and a 300m² dedicated space on GE Healthcare’s 850m² booth where visitors can experience the AI transformation through interactive tools, a press release states.
The average hospital generates 50 petabytes of data annually, including clinical notes, lab tests, medical images, and genomics, yet less than 3% of it is used. Artificial intelligence has the potential to make sense of the data and to generate actionable insights that help improve provider efficiency, increase diagnostic accuracy, personalise treatment, improve patient experience, and enable remote and predictive maintenance. GE Healthcare has over 200 imaging applications and is working with partners like Nvidia, Microsoft, Amazon, and Intel to embed analytics, cloud capability, and artificial intelligence into devices, workflows, and technologies already used by healthcare providers today.
“Artificial intelligence will be one of the leadings topics at next year’s ECR and this exclusive partnership with GE Healthcare is a major step in making ECR 2019 the leading event on artificial intelligence for radiologists and related medical professionals. Through our joint efforts congress participants will be able to witness artificial intelligence excellence at the highest level, making next year’s exhibition an event no one should miss”, said ESR president Lorenzo E Derchi (Genoa, Italy).
“We are honoured to partner with the European Society of Radiology for the leading European radiology event. Artificial intelligence is one of the most exciting developments in healthcare today and a key enabler to achieve precision health. Done right, it can be the technology of the decade, perhaps the century, in healthcare. But there is still much work to do, sound data science and eliminating data siloes are key. Europe and the European radiology community have a key role to play in the artificial intelligence transformation”, comments Catherine Estrampes, president and CEO of GE Healthcare Europe.
An analysis ATTRACT has just been published in the journal, Circulation in which the authors examine the effect of pharmacomechanical catheter-directed therapy (PCDT) in ATTRACT patients with iliofemoral DVT.
Interventional News spoke to Mark Garcia (Wilmington, USA), Jacob Cynamon (New York, USA) and Mahmood Razavi (Los Angeles, USA) about new developments in deep venous thrombosis (DVT) intervention and in the world of mechanical thrombectomy at VEITHsymposium, where the ATTRACT subanalysis was presented.
Twelve-month data from the multicentre prospective MedLift study of the Urolift system (NeoTract, a Teleflex subsidiary) for benign prostatic hyperplasia (BPH) involving a median lobe obstruction provided clinical evidence to support the safety and efficacy of the treatment. Results were published in Prostate Cancer and Prostatic Diseases.
Median lobe obstructions are present in a subset of men with BPH. Results from this study led to the recent US Food and Drug Administration (FDA) clearance of an expanded indication for the UroLift system, making patients who have an obstructive median lobe eligible to receive the UroLift System treatment for BPH symptoms.
“New options are needed for men with an obstructive median lobe, as treatment can be particularly challenging. This condition can cause a higher risk of urinary retention and result in a high failure rate of medical therapy for lower urinary tract symptoms due to BPH,” comments Gregg Eure from Urology of Virginia in Virginia Beach, USA, a lead investigator and co-author of the MedLift Study paper. “The outcomes of this study, which showed significant and rapid improvements in BPH symptoms and quality of life measures, demonstrate the safety and effectiveness of the UroLift System for these patients.”
The MedLift study revealed that patients who were treated for an obstructive median lobe with the UroLift System experienced significant improvements in IPSS (International Prostate Symptom Score), Qmax (peak flow rate), and quality of life scores. The IPSS improved from baseline by at least 13.5 points (p<0.0001) over the course of the study. Quality of life and BPH impact index scores were also improved, by more than 60% and 70% respectively, at three, six, and 12 months (p<0.0001). The mean Qmax improvement ranged from 90–129% (p<0.0001). At one month, 80% of men reported being “much better” or “very much better”, and 89% would recommend the procedure. Bother due to ejaculatory function improved rapidly and remained modestly improved at one year (p=0.001). No patient reported de novo sustained ejaculatory or erectile dysfunction.
“The MedLift Study provides additional evidence of the UroLift system’s utility for the treatment of a broad range of men with BPH, allowing more patients to benefit from this minimally invasive technology,” said Dave Amerson, president of the Teleflex Interventional Urology business unit. “The data from this study, among the many supportive findings from a number of clinical and real-world studies of the UroLift system, have helped the UroLift system become a standard of care treatment for patients with BPH. Treatment with the UroLift system remains the only BPH procedure shown to alleviate BPH symptoms without causing new onset, sustained erectile or ejaculatory dysfunction.”
The outcomes from this study were consistent with those found in the five-year pivotal LIFT study of the UroLift system for patients with lateral lobe enlargement, demonstrating rapid, significant, and sustained improvements in symptoms and quality of life for patients who have an enlarged median lobe, while also preserving their sexual function with no instances of new, sustained erectile or ejaculatory function. No differences were observed in symptom relief based on the size of median lobe protrusion, and the majority of patients required only one additional UroLift permanent implant in the median lobe to achieve lasting relief from BPH symptoms.
The Prelude Ideal hydrophilic sheath introducer (Merit Medical) has launched in European, Middle Eastern and African markets.
The Prelude Ideal is designed primarily for use in radial access procedures, and is an option for use with a wide range of anatomy, including in patients with small and thin vessels. The narrowness of the device wall means that the sheath body inner diameter is larger than the Prelude Ideal’s predecessor’s, translating into more working room for catheters and other devices.
It is constructed with proprietary flat wire braiding technology that provides 23% more resistance to kinking and 124% more resistance to sidewall compression compared to the leading competitor’s sheath, a Merit Medical press release states. The Prelude IDeal utilises a hydrophilic coating to the tip of the sheath tubing. Hydrophilic coatings have been proven in clinical studies to reduce the risk of radial artery spasm.
“The Prelude IDeal really exemplifies Merit’s solutions-oriented approach to innovation. We heard from interventional practitioners that there was a need for a sheath introducer that was designed to reduce risk of compression and kinking while still facilitating easy passage of catheters and other devices,” said Fred Lampropoulos, chairman and CEO of Merit Medical.
The Prelude IDeal hydrophilic sheath introducer was launched in the USA earlier in 2018 and is one of the company’s fastest growing products.
A press release reports that Abiomed is to invest US$15 million in Shockwave Medical and the two companies will collaborate on a training and education programme in the USA and Germany focused on the benefits of complementary use of their respective technologies.
The press release states that Shockwave’s intravascular lithotripsy (IVL) technology employs sonic pressure waves to safely crack vascular calcium within the vessel wall, which enables arteries to expand under low pressure and become more compliant. It adds that Shockwave markets its Shockwave M5 Peripheral Intravascular Lithotripsy Catheter in the USA and Europe, but notes that the Shockwave M5 catheter is increasingly being used in patients with heavily calcified Iliac arteries in order to facilitate the transfemoral delivery of sophisticated devices with catheters, including transcatheter aortic valve implantation (TAVI) and Abiomed’s Impella. IVL enables this patient group to benefit from these life-saving therapies when they would otherwise be ineligible for the procedure or would be at increased risk for procedural complications. In Europe, Shockwave also markets its coronary catheter—Shockwave C2—which is used to treat severely calcified de novo coronary artery disease.
Doug Godshall, president and CEO of Shockwave Medical, states: “While we are still early in our commercial scaling both in the US and Europe, I am pleased with how positively our Shockwave technology has been received and how many different types of patients and vessels our customers are able to safely treat with our IVL system. We are delighted to be able offer patients our solution in combination with Abiomed’s Impella technology using a minimally invasive approach, which should meaningfully improve outcomes. With Abiomed’s best-in-class approach to training and education, Shockwave will be able to more efficiently increase awareness and introduce IVL to customers, which we believe will help them better treat their most challenging patients. We are encouraged to see the positive clinical response we have witnessed to date.”
Interventional News has learned that inclusion into the SWEDEPAD studies, that are examining benefits of drug-eluting technology for peripheral arterial disease patients, has been halted.
As outlined in the public domain, the SWEDEPAD (Swedish drug-elution trial in peripheral arterial disease) project is designed to test the hypothesis that drug-eluting technology is superior to conventional endovascular treatment in terms of important clinical outcomes, when applied on infrainguinal (femoropopliteal and/or infrapopliteal) obstructive vascular lesions. The SWEDEPAD project consists of two separate parallel studies, SWEDEPAD 1 and SWEDEPAD 2, each defined by the severity of peripheral arterial disease. As noted on clinicaltrials.gov, “patients with critical limb ischaemia are allocated to SWEDEPAD 1 and patients with intermittent claudication are allocated to SWEDEPAD 2.” The trials had a planned enrolment of 3,800 participants.
An update on the SWEDEPAD website (when translated into English) reads: “Inclusion in SWEDEPAD studies stop! On the occasion of the Katsano’s [sic] systematic literature review published today, the study management has today met with the Data Safety Monitoring Committee (DSMC) in SWEDEPAD. After DSMC performed an interim safety analysis of the study’s prespecified and monitored safety variables (occlusion rate, amputation rate and mortality by 30 days and one year) distributed on treatment allocation, the recommendation from DSMC is to promptly pause further inclusion in both SWEDEPAD 1 and SWEDEPAD 2.
“The study management is of the same opinion as DSMC and has today decided to stop inclusion in both substudies. On Monday, [10 December 2018], SWEDEPAD’s steering committee meets and discusses the state of progress and further actions that need to be taken in response to this.”
The first European Society for Vascular Surgery (ESVS) guideline on treatment of abdominal aortic aneurysm (AAA), published in the European Journal of Vascular and Endovascular Surgery in 2011,1 has had a major impact on clinical practice and research. However, due to the rapid developments of the field it has become outdated. In 2015, the process to update the ESVS AAA guideline was initiated. A writing committee consisting of 16 vascular surgeons from all over Europe worked out a comprehensive document, comprising 97 pages, including 790 references with a total of 125 recommendations. For the first time, ESVS Guidelines were written in collaboration with patient representatives. The document has undergone three review rounds by 13 external reviewers from Europe, the USA, Asia and Australia, as well as by the 10 members of the ESVS guideline committee. The resulting “European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysm” were presented at the ESVS annual general meeting (25–28 September, Valencia, Spain), published online in November 2018, and will appear in the January 2019 issue of the printed journal.2
Here we summarise some news of importance to vascular specialists as well as policy makers, and briefly discuss notable differences between the ESVS guidelines and other contemporary guidelines; the Society for Vascular Surgery (SVS) AAA guidelines published in 2017,3 and the draft of the upcoming National Institute for Health and Care Excellence (NICE) aortic guideline targeting England and Wales.4
Figure. The recommendations in the ESVS guidelines are based on the European Society of Cardiology (ESC) grading system.
Service standard
The management of AAA has changed profoundly with the introduction of endovascular treatment. Studies have convincingly shown the benefit of endovascular aneurysm repair (EVAR) in both elective and emergency AAA repair in patients with suitable anatomy. At the same time, it is evident that some patients are not suitable for standard EVAR, or more complex endovascular treatment options, but should be offered open surgery. Consequently, one technique cannot entirely replace the other. Compromising the anatomical requirements for standard EVAR, using complex and partially experimental endovascular techniques to avoid established open surgical solution at all cost, or solely offering major open surgery when there are proven minimally invasive techniques, just because it is outside office hours, is not in accordance with good clinical practice. Thus, today it is not acceptable to perform abdominal aortic interventions without the ability to offer both endovascular and open surgical technologies 24/7 (Recommendation 2; Class I, Level B).
The firm evidence of a volume-outcome relationship of surgery in general, and AAA repair in particular, makes it necessary and justifiable to make a recommendation on minimal surgical volume. No clear threshold was possible to identify in the literature, however. Various cut-off levels have been suggested, and other aspects have to be taken into account, such as population density and geographical distances. Based on the literature the ESVS guideline writing committee (ESVS-WC) concluded that there is enough evidence for a rather weak recommendation on a desired minimum hospital volume of at least 30 cases annually (Recommendation 3; Class IIa, Level C) while a stronger recommendation can be issued on a minimum yearly case load of at least 20 repairs to perform aortic surgery at all (Recommendation 4; Class III, Level B). This is essentially in line with what the SVS recommends (an annual minimum volume of 10 cases for each open surgical repair and EVAR), and justifies a continued centralisation to medium and high volume centres. The NICE guidelines draft does not address this topic.
There are limited data concerning a reasonable waiting time for treatment once the threshold for repair has been reached. Although there is no strong evidence to support exact timings, it is reasonable to adopt a similar approach as for other life threatening diseases, such as cancer. Based on the rupture risk, as well as the psychological consequences, a suggested upper limit for the total pathway from referral to treatment is eight weeks, once the intervention threshold is reached. This applies, however, only to standard AAA cases, whereas in more complex aneurysms or comorbid patients a longer planning and/or work-up time is justified. Correspondingly, a shorter timeframe should be pursued for larger AAAs (Recommendation 5; Class I, Level C). Those of us who fail to meet this requirement should promptly develop routines for fast-track preoperative imaging and work-up. Modern cancer care often has well-structured treatment pathways with clearly defined deadlines, and may serve as a role model.
Elective AAA repair
Due to the rapid technological and medical development, the existing randomised controlled trials comparing open surgical repair (OSR) and EVAR are partly outdated and thereby not entirely relevant for today’s situation. The evidence from RCTs also has the limitation that they mainly apply to patients <80 years of age, whereas today the greatest increases in AAA repair is among those >80 years. This group has also seen the most pronounced improvement in outcome after AAA repair, likely related to the preferential use of EVAR for treatment among octogenarians. It is therefore necessary to also include more recent case series and registry studies in the overall evaluation of the evidence base. Thus, despite data from multiple RCTs and meta-analysis, representing the highest level of evidence, we rate the existing level of evidence as mediocre (Level B). Overall, evidence suggests a significant short-term survival benefit of EVAR over OSR, with similar long-term outcome up till 10–15 years of follow-up. Thus, in patients with suitable anatomy and reasonable life expectancy, EVAR should be considered as the preferred treatment modality (Recommendation 60; Class IIb, Level B). Yet, there are indications that increased rate of complications may occur after eight to 10 years with earlier generation EVAR devices and an uncertain durability of current devices, particularly the low profile devices. Thus, although EVAR should be considered the preferred treatment modality in most patients, it is reasonable to suggest an OSR first strategy in younger, fit patients with long life expectancy, i.e. >10–15 years (Recommendation 61; Class IIa, Level B).
These recommendations, which more clearly than before favour EVAR over OSR in most scenarios, differ significantly from the NICE guideline draft, where EVAR is not recommended at all in the elective setting. It is obvious that the ESVS guidelines writing committee has interpreted the literature completely differently, taking into account the fact that the RCTs comparing open surgical repair and EVAR are outdated, while the NICE committee has not done the same assessment. The SVS recommend the use of a perioperative mortality risk scoring system to guide the choice of surgical technique, emphasising the importance of patient involvement.
Ruptured AAA repair
When pooled together, the one-year results of the three recent RCTs (IMPROVE, AJAX, ECAR) suggest that there is a consistent but non-significant trend for lower mortality post EVAR. The IMPROVE trial found faster discharge with better quality of life post EVAR, which therefore was cost effective. The recently published three-year results of the IMPROVE trial suggest that, compared with OSR, an endovascular strategy for suspected ruptured AAA was associated with a survival advantage, a gain in quality of life adjusted years, similar levels of reintervention, reduced costs, and this strategy was cost effective. These findings, together with observational studies and registry data, support a strong recommendation of an EVAR first strategy for ruptured AAA repair (Recommendation 74; Class I, Level B). This recommendation—a major change from the previous ESVS guidelines—is in agreement with both the SVS guidelines and the NICE guideline draft.
New devices
In recent years, manufacturers have developed new stent grafts and delivery systems with lower profiles to allow an endovascular approach even in patients with small access vessels. Although there are some series reporting favourable midterm outcomes for last-generation low-profile stent grafts compared to standard profile stent grafts, more experience and longer-term outcome data, especially about the durability, are needed to confirm those findings. Therefore, when upgrades of existing platforms are used in clinical practice, the need for long-term follow-up should be recognised, and evaluation in prospective registries with complete follow-up is strongly recommended (Recommendation 57; Class I, Level C).
Novel new techniques and treatment concepts, such as endovascular aneurysm sealing with polymer-filled endobags (EVAS) has only been commercially available for a limited time, and their effectiveness and durability are still under investigation. We issue a strong negative recommendation of its use in clinical practice outside studies approved by research ethics committees and with informed consent from the patients, until adequately evaluated (Recommendation 58; Class III, Level C). This approach is supported by recent alarming reports of higher-than-expected rates of leaks around the implant, device movement, and aneurysm enlargement after EVAS.
Neither the SVS guidelines, nor the NICE guideline draft, address this topic, which we consider of great importance given the continued rapid industry driven technical development. CE marking (or approval) is a certification mark for products sold within the European Economic Area (EEA), i.e. European Union (EU) and European Free Trade Association (EFTA). Unlike the rigorous evaluation of efficiency and safety required for Food and Drug Administration (FDA) approval in the USA, CE marking has nothing to do with efficiency or safety. Thus, the role for several new innovative CE marked technologies on the market is still unclear and further data are needed before these can be recommended to be used in routine clinical practice.
Follow-up after EVAR
Due to the risk of graft-related complications and rupture after EVAR, regular imaging follow-up has been regarded as mandatory. The true value of prophylactic regular follow-up imaging after EVAR is uncertain, however. Routine surveillance seldom identifies significant findings requiring reintervention, and most patients who require re-intervention after EVAR present with symptoms. Compliance with annual prophylactic imaging guidelines is suboptimal and lack of adherence to follow-up does not seem to affect long-term mortality or post-implantation rupture rate. Thus, annual imaging after EVAR for all patients is neither evidence-based nor feasible.
An early postoperative clinical and imaging follow-up after EVAR is required to assess the success of the performed intervention (Recommendation 91; Class I, Level B). Recent data suggest that patients considered at low risk for endovascular aortic repair failure after their first postoperative computer tomography angiography, i.e. no endoleak, anatomy within IFU, adequate overlap and seal of ≥10mm proximal and distal stent graft apposition to arterial wall, may be considered to be stratified to less frequent follow-ups, with delayed imaging up till 5 years after repair (Recommendation 92; Class IIb, Level C). Patients who do not meet these requirements should be assessed for the need for reintervention or continued frequent monitoring.
In contrast to the above approach with risk stratification, the SVS guidelines recommend continued annual imaging follow-up for all patients post EVAR. While the NICE guideline draft does not indicate a specific frequency for follow-up, it supports that it should be guided by the individual patients estimated risk of graft related complications.
Juxtarenal AAA
Given the rarity and complexity of JRAAA treatment centralisation to specialised high volume centers that can offer both open and complex endovascular repair seems justified and is recommended (Recommendation 94; Class I, Level C).
Complex endovascular techniques have emerged as promising alternatives, or complement, to OSR for the treatment of JRAAA. However, reliable comparative and health-economic studies are still missing. Consequently, decision making is complex and should be tailored to each individual patient and local health economies. Stratification of cases by anatomy and surgical risk may be useful in patients with JRAAA (Recommendation 95; Class IIa, Level C). OSR with an anastomosis below the renal arteries and short renal clamping time may be a preferable and durable option for fit patients with a short aortic neck. With more complex anatomy or high surgical risk due to comorbidities an endovascular solution may be preferable.
Despite limited data, it is the ESVS-WC assessment that fenestrated technology has a small advantage over parallel graft technique when it comes to proven feasibility and durability, as there are more multicenter reports and longer follow-up data available, and thus it should be the preferable endovascular technique for elective JRAAA repair (Recommendation 96; Class IIa, Level C).
Parallel graft techniques may, however, be considered as an alternative technique in the emergency setting or as a bailout (Recommendation 97; Class IIb, Level C), but one should then aim for a proximal landing zone of at least 15 mm, ensure a proper stent graft-oversizing of 30%, and use a maximum of two chimneys.
As for standard AAA repair, novel new techniques and treatment principles, such as EVAS, Endostaples and in-situ fenestration are not recommended in clinical practice for JRAAA repair but should be limited to studies approved by research ethics committees and with informed consent from the patients (Recommendation 98; Class III, Level C).
Data is even more scarce for ruptured JRAAA, but the risk aversion is lower in such an immediate life threatening and complex situation. Therefore, in patients with ruptured JRAAA open repair or complex endovascular repair (with physician modified fenestrated stent grafts, off-the-shelf branched stent graft, or parallel graft) may be considered based on patient status, anatomy, local routines, team experience and patient preference (Recommendation 99; Class IIb, Level C).
JRAAA is not covered by the SVS guidelines, while the NICE guideline draft clearly recommend against any use of complex EVAR outside randomised clinical trials. Again, a big difference with potential huge clinical impact compared with the recommendations made in ESVS guidelines, and our views of the current knowledge are remarkably different. With today’s rather extensive experience of complex EVAR (especially fEVAR), showing generally good results, and the ability to offer treatment to many patients less suitable for major open surgery; it is difficult to motivate a strong preference for OSR over complex EVAR for JRAAA. Instead, we favour a more pragmatic approach, with OSR and EVAR complementing each other.
Conclusion
We encourage everyone to carefully read the new ESVS aortic guidelines in its entirety. It is an extensive document but offers many more recommendations of clinical importance (including recommendations on medical management, screening, iliac aneurysms, mycotic and inflammatory aneurysms, concomitant malignant disease, etc.) and a comprehensive supporting text that summarises the literature and motivates our positions. We hope you will find the document relevant and useful for your practice.
Anders Wanhainen is chair and corresponding author of the ESVS AAA Guideline Writing Committee. He is also professor of Surgery, Department of Surgical Sciences at Uppsala University in Uppsala, Sweden.
Gert J. de Borst is chair of the ESVS Guidelines Committee and professor of Vascular Surgery, Department of Vascular Surgery at University Medical Center Utrecht in Utrecht, the Netherlands.
References
Moll FL, et al. European Society for Vascular Surgery. Management of abdominal aortic aneurysms clinical practice guidelines of the European society for vascular surgery. Eur J Vasc Endovasc Surg 2011;41:S1e58.
Wanhainen A, et al. European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms, European Journal of Vascular and Endovascular Surgery (2018), https://doi.org/10.1016/j.ejvs.2018.09.020
Chaikof EL, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018 Jan;67(1):2-7
A new study, recently published online in the journal Circulation, reports on outcomes from a subgroup of 391 patients with acute iliofemoral deep venous thrombosis (DVT) in whom pharmacomechanical catheter-directed thrombolysis (PCDT) was evaluated within the ATTRACT trial.
The authors, Anthony Comerota and colleagues, reveal that in patients with acute iliofemoral DVT, “PCDT does not influence the occurrence of the post-thrombotic syndrome (PTS) or recurrent venous thromboembolism (VTE) through 24 months.” However, as reported in the journal, the authors write: “In patients with acute iliofemoral DVT, PCDT does appear to provide greater reduction in acute leg pain and swelling through 30 days’ follow-up, as well as reduced PTS severity, reduced moderate-or-severe PTS, and greater improvement in venous disease specific quality of life through 24 months.”
As outlined in the journal, the clinical implications note that these findings support early use of PCDT in patients with acute iliofemoral DVT who have severe symptoms, low bleeding risk, and who attach greater importance to a reduction in early and late symptoms than to the risks, costs, and inconvenience of PCDT.
Suresh Vedantham, Mallinckrodt Institute of Radiology, Washington University in St. Louis, USA, and national prinicpal investigator of ATTRACT told Interventional News: “At all evaluated time points during the 24 months of follow-up, the symptoms and signs of venous disease were reduced in the patients with acute iliofemoral DVT who received early thrombus removal with PCDT. Given the absence of a PTS-prevention effect and the known risks of thrombolytic therapy, the first-line use of PCDT for iliofemoral DVT may be best considered on an individual basis for patients with low bleeding risk and severe leg symptoms causing functional limitations. When this is done, thanks to the ATTRACT investigators, it will constitute evidence-based therapy for the first time in the 25 years since catheter-directed DVT therapy was introduced. Further studies will help us better understand the magnitude and clinical importance of the long-term treatment effects.”
Comerota and colleagues outline the methods used: “Within a large multicentre, randomised trial, 391 patients with acute DVT involving the iliac and/or common femoral veins were randomised to PCDT with anticoagulation vs. anticoagulation alone (No-PCDT) and were followed for 24 months to compare short-term and long-term outcomes.”
The main results are summarised as follows:
PTS incidence
The researchers note that between six and 24 months, there was no difference in the occurrence of PTS (Villalta scale >5 or ulcer: 49% PCDT vs. 51% No-PCDT; p=0.59).
PTS severity
PCDT led to reduced PTS severity as shown by: lower mean Villalta and venous clinical severity scores [VCSS] (p<0.01 for comparisons at six, 12, 18, and 24 months; and fewer patients with moderate-or-severe PTS (Villalta scale >10 or ulcer: 18% vs. 28%; 0.021) or severe PTS (Villalta scale >15 or ulcer: 8.7% vs. 15%, p=0.048; and VCSS >8: 6.6% vs. 14%; p=0.013).
Leg symptoms
From baseline, PCDT led to greater reduction in leg pain and swelling (p<0.01 for comparisons at 10 and 30 days) and greater improvement in venous disease specific quality of life (QOL) (VEINES-QOL unit difference 5.6 through 24 months, p=0.029), but no difference in generic QOL (p>0.2 for comparisons of SF-36 mental and physical component summary scores through 24 months).
Major bleeding
In patients having PCDT vs. No-PCDT, major bleeding within 10 days occurred in 1.5% vs. 0.5% (p=0.32), and recurrent venous thromboembolism over 24 months was observed in 13% vs. 9.2% (p=0.21).
Contego Medical has announced that the US Food and Drug Administration (FDA) has granted 510(k) clearance for its Vanguard IEP Peripheral Balloon Angioplasty System with Integrated Embolic Protection. Contego Medical is a medical device company developing and commercialising a suite of next-generation devices that address unmet needs in neurovascular, coronary and peripheral vascular disease.
The Vanguard IEP System uniquely incorporates a peripheral angioplasty balloon and distal embolic filter on the same catheter. The system protects the lower limbs during angioplasty without the need for additional devices or exchanges. The Vanguard IEP System has an over-the-wire design with a sheathless integrated 150-micron pore filter distal to the angioplasty balloon. Contego Medical’s filter is the first to feature in-vivo adjustability to suit varying vessel sizes and maximise capture efficiency. Vanguard IEP was evaluated in the ENTRAP 112-patient post-market registry in Europe in which 100% of patients met primary safety and efficacy endpoints at discharge and 30 days.
“The Vanguard IEP System is designed to protect patients at high risk for embolisation during peripheral angioplasty, such as those with acute limb ischaemia, severe calcification, and chronic total occlusions if crossed intraluminally. It is also well suited to protect patients at high risk for complications should embolisation occur, such as those with poor distal run-off,” said Professor Thomas Zeller, director of the Department of Angiology at Unversitaets Herzzentrum, Freiburg in Bad-Krozingen, Germany and principal investigator of the ENTRAP Study. “In our experience, the device has performed exactly as intended and we are impressed with the ease of use of the system, with no more exchanges required than in a typical angioplasty procedure.”
“Securing FDA clearance for Vanguard IEP represents a major milestone for Contego Medical,” said Ravish Sachar, founder and CEO of Contego Medical. “As the patient population with peripheral arterial disease continues to expand and become more complex, we believe our technology will play a critical role in protecting vulnerable patients from embolic events and thus improve procedural outcomes.” Contego Medical now has two FDA cleared devices dedicated to improving the safety profile and outcomes of interventional procedures.
The Vanguard IEP Peripheral Balloon Angioplasty System with Integrated Embolic Protection is indicated for percutaneous transluminal angioplasty (PTA) and capture and removal of embolic material during angioplasty, for the femoral, iliac, popliteal and profunda arteries. The system is not intended for use in the renal, cerebral, coronary or carotid vasculature.
Treating hepatocellular carcinoma (HCC) with microwave ablation is safe in the elderly population, the first study investigating the efficacy and safety profile of this procedure in over 75 year olds reports.
Shicheng Zhou (Yong Loo Lin School of Medicine, Singapore) presented this research at the 2018 British Society of Interventional Radiology annual meeting (BSIR; 14–16 November, Bournemouth, UK), concluding that chronological age was not a predictor of longer hospital stay, postoperative complication rate, or of poorer overall survival.
In Singapore, HCC is the third and fourth most common cause of cancer-related death in men and women, respectively, and globally, it is the fifth most common cancer worldwide. Commenting on these figures, Zhou outlined the need for this work: “This is certainly cause for concern, and for good treatment options to be available. Percutaneous thermal ablation is an established curative treatment with a high technical success rate and good tumour control.”
An aging population in Singapore—and many other nations—also necessitates research specifically evaluating how the elderly population responds to different treatment options. The coupling of an increased life expectancy and a growing number of HCC screening programmes in Singapore has led to earlier detection of this cancer, and subsequently a greater number of patients undergoing curative treatment. The study investigators therefore set out to compare the outcomes of elderly and non-elderly patients undergoing curative percutaneous microwave ablation.
Zhou and colleagues conducted a retrospective review of 59 patients undergoing thermal ablation between 2013 and 2018. The data included treatment naïve HCC patients, and excluded those with metastases, suboptimal ablation, or tumour recurrence. Of the 59 patients included in the study, 18 were over 75 years old, and thus classified as elderly. Zhou et al evaluated patient demographics, tumour characteristics, and post-procedural outcomes, before analysing the data using the software SPSS.
There was no significant association between the age of the patient and the outcome of the procedure, indicating that, elderly or not, comorbidities do not predict a worse outcome in terms of percutaneous ablation. Cumulative survival at one year was 94.4% for the elderly population, and 92.7% for the non-elderly. At three-years, the survival was 66.7% for the elderly and 56.1% for the non-elderly population. After five years, cumulative survival was 50% in the elderly population, compared to 24.4% in the non-elderly population.
The finding that there was no significant difference between elderly and non-elderly patients in terms of procedural outcomes, length of hospital stay, complication rates and local recurrence rate was not necessarily expected. An older patient cohort is more likely than those under 75 to have a number of comorbidities and liver degenerative potential, possibly putting them at a higher risk of adverse effects post-procedure—the results of this study did reveal a higher incidence of hyperlipidaemia and hypertension in the elderly population.
However, Zhou also noted that, “Interestingly, the non-elderly population had a higher incidence of portal hypertension.” He continued: “We also found that the non-elderly population group actually had a worse pre-procedural liver function test, evidenced by the higher Bilirubin and aspartate transaminase levels [25.2µmol vs. 16.7µmol and 55.3U/L vs. 36.6U/L, respectively], and a longer prothrombin time [14.9 seconds vs. 13.8 seconds].”
Acknowledging this as a limitation of the study design, Zhou commented, “This [poorer pre-procedural liver function in younger patients] probably reflects the way a tumour is selected in our institution, and we recognise that this could be a potential source of selection bias. Perhaps older patients with better liver function and younger patients with poorer liver function were selected for ablation techniques.”
Zhou continued, “While not significant, the non-elderly population actually had a shorter survival. Conversely, the older population showed a longer survival period than our non-elderly population group. Perhaps our pre-procedural liver function rather than age itself predicts mortality.”
Additionally, the study investigators understand that as a retrospective, single centre study with a relatively small sample size, further work is needed with a larger cohort to increase the statistical clout of their conclusions.
Previous studies investigating the efficacy and safety of radiofrequency ablation in elderly HCC patients have reported mixed results. Hirokazu Takahashi and colleagues (Department of Internal Medicine, Saga Medical School, Saga, Japan) concluded in 2010 that radiofrequency ablation treatment might be safe and effective in both elderly and non-elderly patients, but Wei-Yu Kao et al (Taipei Veterans General Hospital, Taipei, Taiwan) found younger HCC patients to have a better prognosis after percutaneous radiofrequency ablation, as reported in 2012. Prior to Zhou et al’s work, to the authors’ knowledge, no study looked into microwave ablation in this patient cohort.
Konstantinos Katsanos (Patras, Greece) tells Interventional News about new data from a meta-analysis that has been published in the Journal of the American Heart Association (JAHA) that suggest there is an increased risk of death at two and five years following the use of paclitaxel-coated balloons and stents in the femoropopliteal artery.
This video interview was conducted at the VEITHsymposium 2018 and was under embargo until publication of the study by JAHA.
New data, just published in the Journal of the American Heart Association (JAHA), suggest that there is an increased risk of death at two and five years following the use of paclitaxel-coated balloons and stents in the femoropopliteal artery. While the authors, Konstantinos Katsanos (Patras, Greece) and colleagues, write in JAHA that this meta-analysis provides good statistical evidence to back these findings, some leading physicians state that it lacks individual patient-level data from the randomised controlled trials.
In the JAHA paper, the investigators write that several randomised controlled trials have already shown that paclitaxel-coated balloons and stents significantly reduce the rates of vessel restenosis and target lesion revascularisation after lower extremity interventions.
The investigators conducted a systematic review and meta-analysis of randomised controlled trials investigating paclitaxel-coated balloon angioplasty or paclitaxel-coated metal stents in the femoral and/or popliteal arteries. In all, 28 randomised controlled trials with 4,663 patients (89% intermittent claudication) were analysed. As reported in JAHA, they last screened medical databases, online content and regulatory authority filings in August 2018.
The primary safety measure was all-cause patient death, analysed at different time points. “Risk ratios and risk differences were pooled with a random effects model,” the authors write.
At one year, all-cause patient death (28 randomised controlled trials with 4,432 patients) was similar between 17 paclitaxel-coated devices and control arms (2.3% vs. 2.3% crude risk of death). All-cause death at two years (12 randomised controlled trials with 2,316 patients) was significantly increased in case of paclitaxel vs. control (7.2% [101 deaths in 1,397 patients] vs. 3.8% [35 deaths in 919 patients] crude risk of death, number-needed-to-harm [NNH]: 29 patients [95% CI: 19–59]). Long-term risk of all-cause death up to five years (three randomised controlled trials with 863 patients) increased further in case of paclitaxel (14.7% [78 deaths out in 529 patients] vs. 8.1% [27 deaths in 334 patients] crude risk of death, NNH: 14 patients [95% CI: 9–32]).
Katsanos and colleagues further write that meta-regression showed a significant relationship between exposure to paclitaxel (dose-time product) and absolute risk of death (0.4±0.1% excess risk of death per paclitaxel mg-year; p<0.001). “Trial sequential analysis excluded false-positive findings with 99% certainty (2-sided alpha, 1.0%),” they say.
These data led the authors to conclude that there is increased risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery. “Further investigations are urgently warranted,” they write.
Katsanos told Interventional News about the key data from the JAHA paper. “My colleagues and I have performed a meta-analysis of 28 studies comprising more than 4,600 patients (nearly 90% of these were claudicants) who were randomly allocated to either receive a paclitaxel-coated device (balloon or stent) in the femoropopliteal segment or a control non-drug-coated treatment. Our meta-analysis was restricted to well-designed randomised controlled trials alone to avoid comparing ‘apples’ with ‘oranges’. Statistical inference has identified an alarmingly higher rate of death after the first year in the case of the paclitaxel-coated device group; risk ratio 1.68 at two years and risk ratio 1.93 at four to five years of follow-up. Our findings were robust on multilevel sensitivity and subgroup analyses and we calculated that one out of 14 patients is expected to die because of paclitaxel up to five years (NNH=14).
“Overall, we would welcome collection and reporting of longer-term follow-up in case of all commercial clinical studies to help confirm, or refute our findings. It is also imperative to perform individual patient data time-to-event analysis for each individual device beyond the first year in combination with an in-depth query of potential confounders and predictors. To paraphrase one of Sherlock Holmes’ quotes: ‘When you have eliminated the impossible, whatever remains, however improbable, must be the truth’,” he said.
Interventional News collected early reaction on the dataset from key opinion leaders in the field.
Can the mortality risk be broken down by device type and make?
Robert Morgan
“The authors seem to have conducted a well-designed meta-analysis and subsequent statistical analysis of the incidence of mortality after the use of paclitaxel-coated stents and balloons in the lower extremity arteries. The authors’ findings are surprising, but on the evidence presented suggest that there may be an increased risk of death in the long term after patients have been treated with drug-coated devices. It would be interesting to know whether the authors found a significant difference in mortality between drug-coated balloons and stents. Also, did the authors find a relationship between mortality and the different types of devices? For example, how did the mortality risk play out with the Lutonix drug-coated balloon (DCB; BD) vs. IN.PACT DCB (Medtronic)?” questioned Robert Morgan (St George’s University Hospitals NHS Foundation Trust, London, UK, and president of the Cardiovascular and Interventional Radiological Society of Europe [CIRSE]).
“It is an obvious flaw of the data that causes of death were not uniformly recorded in the studies analysed. Despite the author’s rigorous statistical evaluation, there must still be a risk that the apparent increased mortality with these devices is due to other factors unrelated to paclitaxel. Clearly, the author’s findings suggest that more investigation is warranted into the potential mortal effects of paclitaxel-coated devices in the peripheral arteries. It is a matter of discussion whether all ongoing and future trials involving drug-eluting devices may require long-term, and even, life-long follow-up to look at the potential effects on mortality of these devices. It is a matter for conjecture whether if this were to be the case, the effect on industry’s enthusiasm to fund such trials might be tempered,” Morgan added.
Observation requires serious efforts to explain, but causes of death are crucial missing data
John Kaufman
John Kaufman (Oregon Health and Science University, Oregon, USA, a past-president of the Society of Interventional Radiology [SIR] and the president of Vascular Interventional Advances [VIVA]) told Interventional News: “This is an observation that requires serious efforts to explain in the randomised controlled trials and examine in the real world, where these technologies are used with far greater frequency in critical limb ischaemia than the 11% represented in the trials. As the authors acknowledge, causes of death are the crucial missing data in the studies that were analysed; this information is necessary to determine whether there is causation in patients with claudication, and if so, to modify practice. As with everything we do, these still relatively new technologies should be used in a thoughtful manner in informed patients.”
Does this statistical mining of data bring to mind the fate of the COX-2 inhibitors?
Ziv Haskal
Ziv Haskal (University of Virginia School of Medicine, Charlottesville, USA and editor-in-chief of the Journal of Vascular and Interventional Radiology [JVIR]) emphasised the importance of numbers. “Sometimes certain truths may only be suggested with the power of numbers. Katsanos et al have pooled and mined prospective comparative data on nearly 4,500 patients who underwent lower extremity revascularisation with and without local paclitaxel by balloon or stent. The stunning new observation of this sophisticated analysis is a nearly doubled rate of increased death at two and five years after intervention. This alarming finding brings to mind the similar means by which COX-2 inhibitors were first linked to increased cardiovascular mortality—notably, statistical findings were dismissed early on when they suggested a painful truth about these high value (and high margin) drugs. Now those medications have been withdrawn, or are used with very stringent consideration. As healthcare providers and scientists, we cannot fall prey to the urge to simply dismiss Katsanos et al’s findings and then focus on the next-presented, exciting, drug-coated device trial abstract. Long-term follow-up data must be mandated in all paclitaxel device trials, mechanistic studies must be undertaken, and replicative analyses considered. In the meanwhile, all physicians must consider the potential longer-term implications for their patients, when making treatment choices,” he said.
Investigate thoroughly—we have an earnest responsibility to inform and provide counsel to the patients we serve
Michael D Dake
Michael D Dake (University of Arizona, Tucson, USA and secretary of the SIR Executive Council) said: “The finding that paclitaxel-coated devices used in the femoropopliteal arteries of patients with peripheral arterial disease are associated with an increased risk of death after one year is surprising and clearly unanticipated. The most important response to this unexpected report is: why? In the absence of patient-level data from the randomised trials included in the meta-analysis, we are left grasping for explanations as to potential correlations and possible aetiological theories behind the stunning increase in all-cause death at two and five years in patients treated with paclitaxel-coated balloons and stents. The only sensible response is to join the authors’ concluding plea to support further investigations. These follow-up studies must include not only evaluations of the cause of death in the existing studies, but a thorough review of the meta-analysis methodology employed by the authors. Whenever shocking revelations challenge consensual understanding—especially when the unexpected reports concern serious issues of patient safety—the medical and regulatory communities have an obligation to move expeditiously in a coordinated manner to investigate the findings thoroughly and an earnest responsibility to inform and provide counsel to the patients we serve.”
Seeking a plausible mechanism for a possible link between the drug and mortality remote from the procedure
Gary Ansel
Gary Ansel (OhioHealth Heart and Vascular Physicians, Columbus, USA) told Interventional News: “As a physician and a scientist, I take patient safety very seriously. The authors certainly raise an important question using a meta-analysis in an attempt to link mortality rates to drug toxicity. The meta-analysis is handicapped by lack of patient-level data. Having been an investigator on many non-drug-based trials, it is curious that this association is being made with mortality rates that are very similar to those of the non-drug based technology trials (i.e, bare metal stents, control arms, uncoated percutaneous transluminal angioplasty). The current authors want an ‘urgent’ closer scrutiny of the devices included in the meta-analysis. Having presented on these devices to the Centers for Medicare and Medicaid Services (CMS) and the US Food and Drug Administration (FDA) I know that these agencies and the sponsors who develop and sponsor these technologies (i.e, Cook Medical, Medtronic and other companies) also take patient safety very seriously. I am somewhat surprised that the authors seem to ignore that an independent Clinical Events Committee reviewed all of the deaths in the IN.PACT SFA at the two-year follow-up point and found no link with the use of the paclitaxel-coated drug-coated balloon. As co-national principal investigator for the ZILVER PTX drug-eluting stent trial, a similar process was used for all patient deaths at five-years. The authors also do not offer any plausible mechanism for a possible link between the drug and mortality remote from the procedure. This underscores the importance of sponsors publishing the entirety of their data, at all follow-up periods, and making patient-level data available for independent analyses. These types of efforts should continue to have us look at long-term patient-level results for our procedures and I hope that the close evaluation will be the rule and not the exception.”
Watch the video interview with Konstantinos Katsanos on these breaking news findings.
The Katsanos et al meta-analysis reports an increased risk of mortality beyond one year across randomised studies of paclitaxel-coated balloons (DCB) and paclitaxel-eluting stents (DES). These observations are of great interest to the vascular specialist community. Even if these results are indeed alarming, as they suggest a paclitaxel-related excess mortality for patients with femoropopliteal artery disease, these findings must be interpreted with caution before the use of DCB and DES—which are the most effective interventional tools to date for femoropopliteal artery revascularisation—is discouraged.
I am concerned with the conclusion that there is an association between all-cause mortality and paclitaxel with no clear causal explanation of a pathophysiological mechanism of action. The authors spend no time exploring other potential hypotheses for the observed trends and the lack of patient-level data is a clear limitation to being able to draw these conclusions. As one of the investigators in several of the studies cited here—in particular of those with five-year follow-up (THUNDER, IN.PACT SFA randomised controlled trial, ZILVER PTX randomised controlled trial)—it is important to note that the observed trend is not new. In fact, we published two- and three-year results showing a statistically significant frequency of all-cause mortality between DCB and plain balloon agioplasty arms of the IN.PACT SFA study. We have subsequently presented on the four- and five-year data, showing no significant difference in mortality. Events in the trial were reviewed by an independent Clinical Events Committee and none were related to the device, or paclitaxel.
Clinical pharmacokinetic data of paclitaxel-releasing DCB and DES demonstrated that detectable systemic exposure does not persist longer than a month before drug elimination drives blood concentrations below the level of detection (usually within a couple of weeks). In such circumstances, it is difficult to conceive of a scenario where such drug levels could produce severe and significant systemic events.
For readers not versed in statistical models and meta-analysis, the authors do not take the time to explain the assumptions that went into the analysis nor the assumptions for the equation. For example, the equation suggests that the input dose of paclitaxel persists at the same rate over time. This is clearly inaccurate, as the authors stated paclitaxel is detectable only for weeks to months.
If the authors looked at randomised controlled trials of non-drug eluting endovascular devices trials, they would find a similar trend in mortality, showing an increased mortality rate in the active comparator arm of these trials.
Importantly, the mortality rates observed in the paclitaxel device trials are consistent with rates reported in epidemiological studies of peripheral arterial disease patients and in populations outside the clinical trial setting. Therefore, I question the leap to an association between paclitaxel and mortality. This likely reflects the natural progression of disease in these patients, who are known to present with concomitant comorbidities.
Finally, the authors do not differentiate between continents (America, Europe and Asia). Local differences in clinical follow-up programmes may also drive differences in all-cause mortality.
This meta-analysis highlights the need for additional long-term and patient-level data. Without this, the Katsanos et al conclusion is premature.
Thomas Zeller, Universitaets-Herzzentrum, Bad Krozingen, Germany, is also a member of the Charing Cross Symposium Peripheral Arterial Executive Board.
“There are simply not enough trained specialists to treat stroke patients [with emergent large vessel occlusion, by embolectomy] in the US. We need to recruit physicians with endovascular skills—interventional cardiologists, interventional radiologists and vascular surgeons—to train them appropriately so that they can help deliver endovascular treatment for appropriate stroke patients,” says Thomas A Haldis (Fargo, USA), who is an interventional cardiologist. He spoke to Interventional News at the VEITHsymposium 2018.
The world’s first bioconvertible IVC filter commercially offered in the USA (Sentry; from BTG) has been successfully implanted into the first patients outside of a clinical trial.
The Sentry filter is designed to provide protection from pulmonary embolism for the period of transient risk and then bioconvert to leave a patent, unobstructed IVC lumen, eliminating the need to retrieve and addressing the typical filter-related complications associated with conventional IVC filters, a press release reports.
Ayad K M Agha, Director of Interventional Radiology and an interventional radiologist at Cardiovascular Interventional Radiology Centers in Phoenix, USA, who performed the procedure on one of his patients, said: “Traditional IVC filters are sometimes associated with a variety of concerns. Placing the Sentry filter gives me confidence in reducing potential complications seen with conventional filters. Using the Sentry IVC filter only requires one visit which means my patient does not have to worry about coming back to make sure the filter is retrieved. This is better for the patient and their families and removes the risk of any complications that may arise on a follow up procedure”
The Sentry bioconvertible filter is supported by two years of data available through the SENTRY trial, recently presented on podium at the Vascular Interventional Advances conference (VIVA; 5–8 November, Las Vegas, USA) and demonstrated no instances of filter tilt, migration, embolization, fracture or IVC perforation through 24-months of imaging-intensive follow up.
“We are excited to see this novel filter now available for patients and are confident that it will make a real difference in the management of pulmonary embolization—much like what we have seen in our SENTRY trial data,” says John Sylvester, Chief Commercial Officer for BTG.
EmboCube Embolization Gelatin (Merit Medical) has been granted 510(k) approval for use in embolization of hypervascular tumours.
The uniformly cut cubes of gelatin foam have been specifically designed to address preparation concerns and inconsistent particle sizes associated with using traditional gelatin foam sheets as an embolic, a press release states. EmboCube is preloaded in a Medallion syringe for smooth delivery with minimal to no resistance.
Using traditional gelatin foam sheets as an embolic agent requires the physician to manually prepare the gelatin foam before use, which can be messy and time consuming, and can result in inconsistently sized particles that may clog the delivery catheter or lead to nontargeted embolization.
“I have witnessed many times physicians preparing gelatin foam for endovascular use. They often use a scalpel to cut the gelatin foam, which can be dangerous, and no matter how carefully cut, the particle sizes are inconsistent,” says Fred Lampropoulos, chairman and CEO of Merit Medical. “We designed EmboCube to make the process of using a gelatin embolic faster, easier and more efficient so the physician can focus on the patient.”
EmboCube Embolization Gelatin is available in two sizes: 2.5mm and 5mm. The 2.5mm EmboCube is compatible with the EmboCath Plus and Merit Maestro microcatheters with a 0.024” (0.62 mm) or larger inner diameter. The 5mm EmboCube can be delivered through catheters with a 0.040” (1.02mm) or larger inner diameter. EmboCube is intended for use with an EmboCube Delivery Kit (Merit Medical) that includes two injection syringes (one mL and three mL) and a three-way stopcock for added convenience.
The US FDA has announced plans to modernise its 510(k) clearance programme for approving medical devices for the US market. Data show that about 20% of current 510(k) devices are approved on trials that compare novel devices to predicate devices that are more than 10 years old. With its revised programme, the agency wants to ensure medical devices coming to market account for advances in technology or demonstrate that they meet more modern safety and performance. The announced changes follow a report from the International Consortium of Investigative Journalists (ICIJ) that heavily criticises how medical devices are approved for use.
Under the existing 510(k) clearance programme, a medical device can be approved for market if (according to a study) it shows comparable safety and efficacy to a similar device that is already on the market. However, a limitation of this programme is that a substantial amount of devices (20%) are compared with devices (or predicates) that are more than 10 years old. In a statement, Scott Gottlieb (FDA commissioner) and Jeff Shuren (director of the Center for Devices and Radiological Health) comment: “Older predicates might not closely reflect modern technology embedded in new devices, or our more current understanding of device benefits and risks”. They stress that they are not suggesting these older devices, or the devices that are compared to them, are unsafe but note “we believe encouraging product developers to use more modern predicates would give patients and their doctors a choice among older and newer versions of the same type of device, promote greater competition to adopt modern features that improve safety and performance, and help make sure that newer devices reflect more modern technology and standards that can improve patient care and outcomes”.
Therefore, the FDA is proposing to list devices on its website that have demonstrated substantial equivalence to older predicate devices, with predicates that are more than 10 years old as a starting point. However, before going ahead with this plan, Gottleib and Shuren state that the agency is seeking public feedback on “whether we should make public those devices or those manufacturers who make technology that rely on predicates that are more than 10 years old, whether other criteria should inform our point of reference, and whether there are other actions we should take to promote the use of more modern predicates”.
Additionally, early next year, the FDA intends to finalise guidance establishing an alternative 510(k) pathway that will allow manufacturers of certain well-understood device types to rely on objective safety and performance criteria to demonstrate substantial equivalence as a way to make the pathway more efficient and to adopt modern criteria as the basis for the predicates that are used to support new products. “We are planning to rename this new approach the ‘Safety and Performance Based Pathway’ to reflect its focus on advancing improved safety and performance of new products. Through this new path, a company would demonstrate a novel device meets modern performance-based criteria that have been established or recognised by the FDA and reflect current technological principles,” Gottleib and Shuren comment. They add that “eventually” they would like this new pathway to replace the practice of comparing a new device to “a specific and, sometimes old, predicate device”.
As well as announcing the changes to the 510(k) clearance programme, in their statement, Gottleib and Shuren highlight the work that the Center for Devices and Radiological Health (CDRH), a subset of the FDA, has done (since 2009) to eliminate the use of the 510(k)-cleared predicates when the devices have raised safety concerns that “warrant treating them as high-risk technologies”. They explain that through a process called “up-classifying”, the FDA relabels such a device as “Class III”—meaning it requires “premarket approval, “our most stringent review pathway”, before it can remain on the market.
After discussing other proposed revisions, Gottleib and Shuren conclude their statement by saying: “We are proud of the work CDRH staff are doing to make sure that the devices we regulate are safe. We will continue to take new actions to strengthen the device programme for years to come.”
Report heavily criticises medical device industry
A few days prior to the FDA announcing its changes to the 510(k) programme, the ICIJ published deeply critical report of the medical device industry. The report—the result of a year-long investigation by the ICIJ—highlights several case examples of patients being harmed by medical devices (from a mesh implant to treat incontinence to implantable cardioverter defibrillators). It claims that the medical device industry may be “unnecessarily putting millions of patients at risk of serious harm in its quest for profit”, calling into question how devices are regulated and approved for market. According to the report, governments in “dozens of countries” in Africa, South America, and Asia “do not regulate medical devices at all, instead placing their trust in European authorities or in the US FDA”. Furthermore, while the report acknowledges that the FDA “is generally considered to provide more robust oversight than any other heath agency in the world”, it states “even that oversight is lacking, with complex devices approved too quickly by American authorities and troublesome ones not pulled from hospital shelves fast enough, patient advocates and health experts say”.
At present, there is not a global resource for recalls and safety notices; therefore, to address this issue, the ICIJ has built the “International Medical Devices Database”. The report explains the database “gathers recalls, safety alerts and field safety notices (more than 70,000 from 11 countries) to create a searchable portal that anyone can access to help discover whether a device was flagged for official safety concern”. It adds the database shows that, over the past decade, there have been “more than 2,100 ‘Class I’ recalls in the USA for defects deemed to pose a ‘reasonable chance’ of ‘serious health problems or death’”. “Some of these could be addressed easily, with a quick software update or change of wording in the instructions, while others involved devices implanted in millions of patients that spurred thousands of surgical removals,” the report comments.
Responding to the ICIJ report, the Advanced Medical Technology Association (AdvaMed)—the foremost US trade group for the device industry—accuses it of “magnifying the stories of only a few individuals” and, thus, overlooks the “overwhelming positive experiences of millions of others”. “We take seriously all reports of patient impact, and though the medical community can never completely eliminate risk, we always strive to improve our technologies and delivery care,” the AdvaMed statement adds.
More than ever before, arterial hypertension represents one of the greatest health threats and challenges for both patients and treating physicians. With the new adjustment and narrowing of blood pressures targets for antihypertensive treatment, the number of patients with uncontrolled hypertension is increasing. Importantly, despite advances in drug therapy, reality proves that adherence to medication is very limited, worsens with increasing number of drugs and is difficult to predict. Consequently, non-pharmaceutical, interventional treatment options bear the hope of adding a “one-stop-always-on” therapy to the vast but still not efficient armoury against hypertension. In this commentary, Philipp Lurz reviews the latest evidence for renal denervation and whether it is starting to live up to its initial promise
Renal denervation is one of several innovative device-based interventional therapies, that is aiming for better blood pressure control. It is safe, minimally invasive, and does not leave any implants behind. The effectiveness of this procedure, however, is still subject to fierce debate and controversy.
The available evidence
Recently, the SYMPLICITY ON/OFF MED (Medtronic) and RADIANCE SOLO (ReCor Medical) trials indicated a significant reduction in ambulatory blood pressure with renal denervation (with the Sypral and Paradise systems respectively) vs. a sham procedure. These trial programmes were influenced by the painful experience of the neutral SIMPLICITY HTN-3 trial, which failed to show an efficacy benefit with the first-generation Symplicity system, and show substantial similarities in study design and patient selection.
Most importantly, both programmes implemented a very thorough protocol—including a roll-in period, witnessed pill intake, serial ambulatory blood pressure monitoring (ABPM) measurements, screening for drug adherence, and inclusion of drug-naive patients. These protocol specifications were implemented to reduce major confounding effects of changes in antihypertensive medication and to minimise effects such as regression to the mean or Hawthorne. Consequently, in these recent trials, very little blood pressure reduction was observed in the sham procedure group and the reduction that did occur was significantly less than that seen in the renal denervation groups, supporting the overall concept of the procedure.
These positive results were achieved in both drug-naive patients and patients on one to three antihypertensive drugs. A truly therapy resistant population is being investigated within the RADIANCE TRIO trial (standardised medication using a three-combination polypill) and the results of this study are eagerly awaited (due 2019). Until then, the question of who represents the ideal target for renal denervation remains unanswered. A previous analysis suggested that renal denervation is less effective in isolated systolic hypertension than in combined systolic and diastolic hypertension, leading to exclusion of patients with isolated hypertension in the latest trials. However, there is evidence that subgroups of such patients can benefit from renal denervation equally. A randomised controlled trial focusing on patients with isolated systolic hypertension is needed to clarify the role of renal denervation in these patients.
In summary, there is sound evidence about the effectiveness of renal denervation in drug-naive patients with probable mild and early stage hypertension—a group of patients with projected low cardiovascular risk—but there are still some uncertainties in patients with truly resistant hypertension (RADIANCE TRIO cohort). In the meantime, patients with uncontrolled hypertension despite the intake of some antihypertensive drugs (Symplicity ON MED cohort) and an intermediate cardiovascular risk should represent the most appropriate target for renal denervation.
Current technology
The technology and technique used for renal denervation needs consideration when interpreting study results. Currently, denervation is either performed using radiofrequency energy (Symplicity, Medtronic) or ultrasound energy (Paradise, ReCor Medica). The latter is believed to achieve a penetration depth of 6mm, which is the expected location of sympathetic nerves in the adventitia of the main renal artery. In contrast, the procedural specifics applied in the SPYRAL HTN-OFF MED and ON-MED trails included the use of a spiral catheter with ablations delivered in the main and branch renal arteries, based on the finding that sympathetic nerves run closer to the lumen within the branch renal arteries and therefore more amenable to renal denervation.
Results of recent trials suggest that both strategies are effective and safe, however, comparisons of different techniques and technologies are scarce. At the 2018 Transcatheter Cardiovascular Therapeutics (TCT) meeting (21–25 September, San Diego, USA), I presented the results of the RADIOSOUND trial. This study compared radiofrequency main renal artery ablation vs. radiofrequency main and branch renal artery ablation vs. ultrasound ablation in the main renal artery only. With all three approaches, a significant reduction in blood pressure was achieved. Endovascular ultrasound based renal denervation was found to be superior to radiofrequency ablation of the main renal arteries only, whereas a combined approach of radiofrequency ablation of the main arteries, accessories and side branches was not. Numbers in this trial are small (40 patients in each treatment arm) and no definite recommendations about the preferred technology and technique for renal denervation could be given. Overall, the positive results of the second-generation trials helped renal denervation to resurrect as a hopeful therapy for hypertension. Important tasks for the future include refinements in patient selection and technique as well as establishing a measure of procedural success for renal denervation, which at present is still an interventional unknown.
Philipp Lurz is at Department of Cardiology, Heart Center Leipzig, University of Leipzig, Leipzig, Germany
CT-guided pulsed radiofrequency is safe and effective in people with acute lower back pain that have not responded to conservative treatment, according to a study presented at the annual meeting of the Radiological Society of North America (RSNA; 25–30 November, Chicago, USA).
Conservative treatment options for herniated disks range from over-the-counter pain medications to injections of corticosteroids directly into the affected area of the spine. Those who do not respond may require surgery. In some cases, the entire disc must be removed and the vertebra fused together for stability.
CT-guided pulsed radiofrequency applies energy through an electrode to the portion of the nerve responsible for sending the pain signals.
“Pulsed radiofrequency creates a nerve modulation, significantly reducing inflammation and its associated symptoms,” said study senior author Alessandro Napoli, professor of interventional radiology at Sapienza University (Rome, Italy).
Napoli and colleagues studied the approach in patients with back pain from lumbar disc herniation that had not responded to prolonged conservative treatment. In 128 patients, the pulsed radiofrequency treatment was delivered directly under CT guidance to the root of the nerve. The treatment was applied for 10 minutes.
For comparison, a group of 120 patients received one to three sessions of CT-guided steroid injection on the same anatomical target with no pulsed radiofrequency.
The one-year outcomes demonstrated that CT-guided pulsed radiofrequency was superior to the injection-only strategy. Patients who received pulsed radiofrequency saw greater overall improvement in pain and disability scores during the first year. Relief of leg pain was faster in patients assigned to pulsed radiofrequency, and they also reported a faster rate of perceived recovery. The probability of perceived recovery after one year of follow-up was 95% in the pulsed radiofrequency group, compared with 61% in the injection only group.
“Given our study results, we offer pulsed radiofrequency to patients with herniated disk and sciatic nerve compression whose symptoms do not benefit from conservative therapy,” Napoli said.
The results of the study are superior to those typically reported for usual care strategies and injections and may help a substantial number of patients with sciatic disc compression to avoid surgery, Napoli added.
The use of pulsed radiofrequency also could improve outcomes for patients set to receive corticosteroid injections.
“We learned that when pulsed radiofrequency is followed by steroid injection, the result is longer lasting and more efficacious than injection only,” Napoli explained. “The effect of pulsed radiofrequency is fast and without adverse events.”
Today, therapy for spine disorders allows for definitive treatment of symptoms and conditions using different techniques and technologies.
“Of the different therapies available, pulsed radiofrequency is among the least invasive,” Napoli commented. “Treatment lasts 10 minutes, and one session was enough in a large number of treated patients.”
Integrated interventional radiology has been listed among the American Medical Association’s (AMA) seven most competitive medical specialties in 2018.
“The National Resident Matching Program considers the most competitive specialties those that match with the highest percentage of US medical school graduates,” read a post written AMA staff writer Brendan Murphy. “In 2018, seven specialties with at least 25 positions offered were filled with at least 85% US medical school graduates.”
The total number of 2018 national medical school applicants for integrated interventional radiology was 217 students, though only 35 students matched. The statement noted the percentage of medical school seniors filling the positions was more than 97%.
“While 91.8% of US seniors matched to their preferred specialty, interventional radiology had the lowest rate of students—58.3%—who matched to it even though it was their preferred specialty,” Murphy wrote.
Integrated interventional radiology was one of four disciplines that did not have enough positions to accommodate all US seniors who preferred that specialty. The others included orthopaedic surgery, neurological surgery, and plastic surgery.
Other specialties in the AMA list included: otolaryngology, dermatology and thoracic surgery.
Sharing the news on Twitter, the British Society of Interventional Radiology (BSIR) commented, “The BSIR are working hard to expand the interventional radiology family this side of the pond.”
Left gastric artery embolization leads to the loss of both fat and muscle, according to a new study presented at the annual meeting of the Radiological Society of North America (RSNA; 25–30 November, Chicago, USA). Researchers said the loss of muscle mass is concerning, and underscores the importance of proper nutritional counselling after the procedure.
Obesity is a major health issue worldwide, linked with several serious conditions such as heart disease, cancer and diabetes. First-line treatments such as diet and exercise often do not work, leading many patients to opt for gastric bypass surgery. The surgery, which reduces the size of the stomach, has been effective in treating obesity, but carries with it significant costs and potential complications.
Currently under investigation in clinical trials, left gastric artery embolization is a less invasive option to surgery. By blocking blood flow to the stomach, the embolic agents reduce the production of ghrelin, a hormone that stimulates hunger. Early studies have shown that embolization is effective in helping people lose weight, but information is lacking on how it might change a patient’s composition of muscle and fat.
“There has been lots of research focused on the efficacy of gastric artery embolization for weight loss,” said the lead author of the study, Edwin A Takahashi, vascular and interventional radiology fellow at the Mayo Clinic (Rochester, USA). “However, there has been no data on what is contributing to the weight loss, whether the patients are losing fat, as desired, or muscle mass, or some combination of the two.”
To learn more, Takahashi and colleagues studied CT scans of 16 overweight or obese patients who had undergone left gastric artery embolization to treat gastrointestinal bleeding. The scans were done before and approximately one and a half months after the procedure. The results were compared to those of a control group of 16 outpatients who did not undergo left gastric artery embolization but had CT scans at two different time periods for nonspecific abdominal pain. The investigators used the CT scans to measure body composition based on the differing densities of fat and muscle.
All 16 individuals experienced significant weight loss after the embolization procedure, losing an average of 6.4% of their body weight over one and a half months. Body mass index (BMI) dropped by 6.3%.
While the weight loss was not surprising to the researchers, the changes in body composition were. The skeletal muscle index fell by 6.8%. Loss of skeletal muscle can impair physical function and metabolism and put a person at higher risk of injury.
“The significant decrease in the amount of skeletal muscle highlights the fact that patients who undergo this procedure are at risk for losing muscle mass and need to be managed accordingly after procedure,” Takahashi said. “We must make sure they receive adequate nutrition to minimise the amount of muscle tissue they lose.”
As expected, the patients also lost a significant amount of body fat. Their overall body fat index dropped by an average of 3.7%. However, much of the fat loss was subcutaneous. Visceral fat, the more dangerous fat surrounding the organs and associated with serious health problems like heart disease and diabetes, did not decrease significantly over the course of follow-up.
The researchers plan to expand their studies in the future to include people who are specifically undergoing embolization as a treatment for obesity.
Two-year results for the SENTRY trial were presented at the Vascular Interventional Advances conference (VIVA; 5–8 November, Las Vegas, USA). The prospective, multicentre trial of the Sentry (BTG), a bioconvertible IVC filter, found that in addition to providing protection against pulmonary embolism during the transient risk period, the device also had zero instances of tilt, perforation, migration and embolisation through two years of imaging-intensive follow-up.
“The trial shows no device-related pulmonary embolism and zero stability complications. Physicians can have the peace of mind that they are protecting their patients from the devastating consequences of PE while reducing complications often associated with IVC filter retrieval. This device eliminates the need to retrieve and that truly makes it a next-generation device,” says BTG chief commercial officer John Sylvester.
The findings were presented by principal investigator Michael Dake (Stanford, USA). In the long-term data, 85 patients were followed for 24 months using computed tomography (CT) or CT venography imaging. The rate of freedom from new symptomatic pulmonary embolism through 60 days was 100% and there continued to be no cases of device-related new symptomatic pulmonary embolism through 24 months.
The results, as reported at VIVA, showed that there were no instances of filter tilt, migration, embolisation, fracture or IVC perforation through 24-months. Two patients developed symptomatic caval thrombosis during the first month, however neither experienced recurrence after successful interventions and no further instances of symptomatic caval thrombosis occurred at 24 months. Filter bioconversion was successful for 95.7% of patients at six months, 96.4% at 12 months, and 96.5% at 24 months. No IVC stenosis was reported.
For three decades, the International Symposium on Endovascular Therapy (ISET) has been providing clinicians with premier endovascular education. In 2019, ISET is investing in new programme enhancements to proactively address the growing need for highly specialised, interactive, and practical education for today’s endovascular and vascular specialists.
ISET’S hallmark live cases, which showcase the practical application of cutting-edge endovascular techniques by top operators across the globe, will be expanded to include an additional 90 minutes of case time. Over 15 cases will transmit from several new sites across the USA and around the world, including: Houston Methodist Hospital (Houston, USA), Miami Cardiac & Vascular Institute (Miami, USA), University Hospital Leipzig (Leipzig, Germany), and Wellmont CVA Heart Institute (Kingsport, USA).
The programme will now feature dedicated tracks with interactive sessions woven throughout the course of the meeting, allowing attendees to customise their endovascular education. These tracks will be focused on critically relevant topics, including peripheral arterial disease (PAD), critical limb ischaemia (CLI), complex aortic and iliac interventions, clot management, venous interventions, and embolotherapy.
Late-breaking clinical data with a focus on promising new technologies will also be featured, along with the opportunity to earn 26.75 CME/CNE credits and gain invaluable insight from 70+ experts during 300+ lectures.
Messages from the ISET course directors
An expanded, multidisciplinary slate of distinguished course directors now guide the meeting’s programming and they cannot help but share their excitement for the enhanced programme. Several discuss why ISET 2019 is a must-attend meeting below:
“ISET 2019 is interesting, novel, immediately relevant, and highly interactive. Join us for expanded clinical live cases at live case sites that offer the greatest amount of unbiased, multidisciplinary, practical teaching. Engage in dynamic town halls and late-breaking topic discussions every morning; then dive into one of our three focused tracks each afternoon,” enthuses interventional radiologist Constantino Peña (Miami, USA).
Vascular surgeon Daniel Clair (Columbia, USA), a new ISET course director for 2019, says: “ISET offers clinicians insight into a vast array of treatment methods used by multidisciplinary experts, supplying them with a broad armamentarium for dealing with patients. This year, “deeper dives” into areas of controversy and of particular interest to participants will provide them with heightened practical knowledge. I am honoured to be a part of a meeting that highlights collaboration, collegiality, and critical appraisal of care.”
A live case at ISET 2018
Jihad Mustapha (Grand Rapids, USA), another new ISET course director and an interventional cardiologist, comments: “The ISET faculty possesses deep knowledge of the very latest endovascular therapies. Working together, we help attendees from around the world leave the meeting confidently equipped with multiple solutions to complex obstacles they may face in daily practice. The education at ISET brings us closer to our common goal: better outcomes for our patients.”
Concurring with his colleagues, vascular surgeon Richard Neville (Washington DC, USA) adds, “ISET is an outstanding meeting that emphasises a multidisciplinary approach to vascular therapy in a collegial, but scientific, atmosphere. There is a real cross-fertilisation of ideas and information that simply isn’t available at other meetings.”
Interventional cardiologist D Chris Metzger (Kingsport, USA) contributes his thoughts on the meeting: “ISET has been a longstanding leading forum for interdisciplinary vascular intervention education. It continues to evolve further by featuring current hot topics focused on changing landscapes and innovations and expanding live case venues worldwide. This year promises to take ISET to new levels.”
Agreeing with his fellow ISET course directors, interventional radiologist James Benenati summaries: “Endovascular medicine is a fast-evolving field. Innovation is rapid and new technology developments are constant. ISET provides a fertile environment for multidisciplinary collaboration and sharing of research, innovation, techniques, and new ideas.”
Visit iset.org to learn more and register for ISET 2019.
Figure 1: Stenosis (white arrow) at the anastomosis of a graft (black arrowhead) with a vein (white arrowhead) and a second stenosis (black arrow). Venous tributaries are filled with backflowing contrast medium (white stars). The wire in place can help separating the AVG from the venous tributaries.
This case report has been sponsored by BD.
Panagiotis M Kitrou, consultant interventional radiologist, and Dimitrios Karnabatidis, professor of Interventional Radiology, both at Patras University Hospital, Patras, Greece, report on a case in which they successfully used a COVERATM Vascular Covered Stent (Bard, now BD) in combination with a high pressure balloon to treat two significant stenoses.
A 62-year-old patient with a brachio-axillary arterio-venous graft (AVG) was referred from his dialysis center with signs of inadequate dialysis. The patient’s venogram revealed a significant stenosis at the graft-vein anastomosis and a second stenosis just distal with presence of extensive venous-tributary network (Figure 1).
A 7mm diameter, 80mm length DORADO® High Pressure Balloon (BDPI, Tempe, Arizona, USA) was used to “beat” the stenosis. A flared 8mm diameter 80mm length COVERA™ Vascular Covered Stent was placed to cover both lesions. The final result is shown in Figure 2.
Figure 2: COVERA Vascular Covered Stent deployment at the site of stenosis (white arrow). The synthetic graft can now clearly be seen (black arrowhead) due to complete absence of venous tributaries.
More than 50% of stenosis in AV Access Grafts present within 1cm around the venous anastomosis.1 Therefore, most new technologies have been tested and evaluated in this specific AV Graft segment. A study of paramount importance, published by Haskal et al in 2010, demonstrated a significant patency improvement over plain balloon angioplasty in both Access Circuit and Target Lesion when the FLAIR® Endovascular Stent Graft was used.2 Since then, several studies supported the above mentioned results showing consistency of data.3, 4 Until today, stent grafts are the only devices to provide significant atency improvement at six months compared to plain balloon angioplasty in multicentre randomized controlled trials.
The COVERA™ Vascular Covered Stent is used in our department for the treatment of venous-graft anastomotic stenosis. With our experience of more than 100 devices, the COVERA™ Covered Stent has proven to be an excellent and durable solution for the treatment of those resistant and frequently re-occurring lesions. Additionally, the ease of the deploying mechanism is an advantage because it can be controlled by fellows that have limited interventional experience. Data from the AVeVA study (prospective, multicentre, non-randomised, single-arm clinical study) showed a freedom from primary safety events rate of 96.4% and a six-month target lesion primary patency rate of 70.3% for the COVERA™ Covered Stent.
Our algorithmic approach suggests using a Covered Stent at the venous-anastomotic stenosis as a primary treatment in grafts older than 18 months and for patients with symptoms recurring within a short period of time (<3 months) after balloon angioplasty.
References 1. Kanterman RY, Vesely TM, Pilgram TK, Guy BW, Windus DW, Picus D. Dialysis access grafts: anatomic location of venous stenosis and results of angioplasty. Radiology. 1995;195(1):135-9. 2. Haskal ZJ, Trerotola S, Dolmatch B, Schuman E, Altman S, Mietling S, et al. Stent graft versus balloon angioplasty for failing dialysis-access grafts. The New England journal of medicine. 2010;362(6):494-503. 3. Haskal ZJ, Saad TF, Hoggard JG, Cooper RI, Lipkowitz GS, Gerges A, et al. Prospective, Randomized, Concurrently-Controlled Study of a Stent Graft versus Balloon Angioplasty for Treatment of Arteriovenous Access Graft Stenosis: 2-Year Results of the RENOVA Study. Journal of vascular and interventional radiology: JVIR. 2016;27(8):1105-14 e3. 4. Karnabatidis D, Kitrou P, Spiliopoulos S, Katsanos K, Diamantopoulos A, Christeas N, et al. Stent-grafts versus angioplasty and/or bare metal stents for failing arteriovenous grafts: a cross-over longitudinal study. Journal of nephrology. 2013;26(2):389-95.
The opinions and clinical experiences presented herein are for informational purposes only. The results from this case study may not be predictive for all patients. Individual results may vary depending on a variety of patient specific attributes. The physician has been compensated by BD for the time and effort in preparing the above case study for BD’s further use and distribution.
Figure 1. The ZeroGravity radiation suite in use during a branched endovascular aortic repair at Uppsala University Hospital.
Addressing the importance of radiation protection for the modern interventionist, Kevin Mani writes about the need for knowledge and training in radiation protection for vascular surgeons and interventionalists, and radiation protection as an integrated part of training.
The majority of vascular surgical procedures are today performed with endovascular techniques. The massive increase in the number of endovascular procedures, as well as the increasing complexity of these procedures, necessitates that specific attention is paid to the risks associated with radiation exposure in relation to endovascular surgery.
The repetitive exposure of modern interventionists to high radiation doses is of major concern. Several pioneers in the vascular surgeon interventionalist community have paid a high price for the developments made in endovascular surgery during their time in practice due to excessive radiation exposure, with development of radiation induced cataract as well as neoplasms. Although knowledge regarding the true risks with occupational radiation exposure is still scarce, recent studies indicate that measurable DNA damage among operators occurs already after a simple EVAR procedure.1 Additionally, there are indications of higher prevalence of left-sided brain tumours among physicians with occupational exposure to interventional radiation.
Strategies
Measures to reduce occupational radiation exposure during endovascular procedures are twofold: 1) reducing the radiation dose, and 2) applying adequate protection to reduce scatter radiation. Reduction of radiation dose adheres to the “as low as reasonably achievable” (ALARA) principle, which mandates medical use of X-rays to be limited to the lowest possible dose. In endovascular surgery, this is based on cautious and meticulous X-ray technique. Measures to reduce radiation dose include application of adjusted low dose programmes with minimum pulse frequency and radiation energy which are tailored for the type of endovascular procedure being performed. Such targeted fluoroscopy and angiography algorithms can be developed together with interested hospital physicists in collaboration with the major providers of imaging equipment. Adequate use of beam collimation, digital image magnification, 2D-3D fusion and image overlay are other methods proven to reduce the exposed field and required radiation.2 Reduction of the radiation dose has important benefits both for the patient as well as for the personnel. Real-time dosimeters used by the operating room personnel offers a possibility for direct feedback regarding radiation exposure, in order to increase awareness and modify behaviour.
Adequate protection
In addition to the reduction of radiation dose, use of adequate protection is key to reduce occupational radiation exposure during endovascular procedures. Radiation protection measures can be classified into two groups: 1) radiation shields placed close to the patient, reducing scatter radiation from the patient in general, and 2) radiation protection placed close to or worn by the personnel. Ceiling suspended shields, table mounted shields and disposable radiation-absorbing surgical drapes such as RadPad all encompass radiation protection close to the patient. A properly used combination of these shields can successfully reduce scatter radiation with >80%. The functionality of shields placed close to the patient is however highly dependent on adequate positioning of the shields. Challenges to correct use of these protective shields during complex endovascular surgery include collision of ceiling mounted shields and operating light or flat panel detector, lack of adequate shielding during lateral projection fluoroscopy/angiography, and lack of protection on the patient’s left side during interventions performed, e.g. from left brachial or axillary access.
Basic protective shielding for personnel includes the use of a lead apron and thyroid shield, complemented with protective glasses. Considering that the eye lens is the most radiation sensitive organ, eye protection should be a key element for all endovascular operators. Interestingly, experimental data suggest that the dose reduction effect of protective eye glasses varies significantly between different models, with the majority of the commercially available eye glasses offering a moderate 10–15% dose reduction at left eye. The dose reduction effect is highly dependent on the size of the gutters between the protective glass and the skin. Therefore, protective glasses should be tailored to each operator, with close fit and large protection area.
Additional risk and options
Even with standard lead apron and eye glasses, significant body areas including the arms, shins and head remain unprotected to scatter radiation, which may pose a risk especially for the primary operator closest to the source of scatter radiation. The landmark study by El Sayed et al showing radiation-induced DNA damage in EVAR operators could also verify that DNA damage can be reduced by additional use of radiation-protective shin guards. Optimal radiation protection would include protection for all exposed body areas. However, additional shielding may also be cumbersome and result in excessive weight, potentially with negative effects such as back pain and lumbar hernias. The suspended lead suit radiation protection system (ZeroGravity radiation suit) is an attempt to offer near to full radiation shielding without additional weight on the operator’s body. The system is based on a thick lead suit with a curved lead-acrylic head shield that is suspended either from a ceiling mounted monorail, repositionable floor unit, or a hinged swing arm. The ZeroGravity system offers excellent radiation protection for the primary operator, with significant reduction of the radiation exposure to the head, upper arms, and legs, in addition to what is today achieved with standard lead apron, Figure 1. In a recent assessment of the system in neuro-endovascular intervention, the suspended lead suit resulted in an additional 75% reduction in the operator-received total dose compared to standard protection including lead apron, glasses, ceiling and table-mounted shields.3 There is, however, still potential for further development. In our experience, the weight of the floor mounted ZeroGravity system may hinder repositioning possibilities. Additionally, a relatively high cost of acquiring the system may limit its use to high-volume endovascular centres.
Awareness
Kevin Mani
The increasing number of endovascular procedures in the field of vascular surgery is likely to continue in the future. This results in a need for knowledge and training in radiation protection for modern interventionists, and radiation protection is increasingly an integrated part of vascular surgical training. Although basic protection is achieved with adherence to the ALARA principle and the use of regular protective shields, the risk of repetitive occupational radiation exposure for interventionists remains a concern. Further innovation in endovascular surgery and radiation protection will play an important role in achieving the ultimate goal of zero radiation exposure during these procedures.
Kevin Mani is associate professor of vascular surgery at the Department of Surgical Sciences, Uppsala University, Uppsala, Sweden.
References 1. El-Sayed T, Patel AS, Cho JS, Kelly JA, Ludwinski FE, Saha P, Lyons OT, Smith A, Modarai B, Guy’s and St Thomas’ Cardiovascular Research C. Radiation-Induced DNA Damage in Operators Performing Endovascular Aortic Repair. Circulation. 2017;136:2406-2416.
2. Hertault A, Maurel B, Midulla M, Bordier C, Desponds L, Saeed Kilani M, Sobocinski J and Haulon S. Editor’s Choice – Minimizing Radiation Exposure During Endovascular Procedures: Basic Knowledge, Literature Review, and Reporting Standards. Eur J Vasc Endovasc Surg. 2015;50:21-36.
3. Haussen DC, Van Der Bom IM and Nogueira RG. A prospective case control comparison of the ZeroGravity system versus a standard lead apron as radiation protection strategy in neuroendovascular procedures. Journal of neurointerventional surgery. 2016;8:1052-5.
President of the Interventional Radiology Society of Australasia (IRSA) and European Board of Interventional Radiology (EBIR) examiner for Australia and New Zealand, Gerard Goh emphasises the expanding transnational Interventional Radiology landscape, with “greater international collaboration” between major societies. Here, he speaks to Interventional News about how he knew he had found his calling in the “demanding yet rewarding” discipline of interventional radiology, the need to balance innovation with evidence-based clinical research, and how his passion for fast cars led to a stint as a Formula 1 doctor.
What initially attracted you to interventional radiology?
Throughout medical school and when I was a junior doctor I wanted to be a surgeon. I loved the technical aspects of procedural work and operations, and the way in which surgery offered patients life changing procedures. As a surgical registrar, I soon discovered that interventional radiology (IR) too offered patients many life changing procedures by using minimally invasive techniques whilst offering quicker recovery times and less morbidity than many surgical operations. In addition, the rate at which innovation in IR was making leaps and bounds inspired me like no other specialty had before. At that moment I knew I had found my calling.
Today, what is it you enjoy most about interventional radiology?
Being able to make such a big difference in a patient’s life and sometimes offering lifesaving procedures gives me great satisfaction as an IR. When I see how patients and their families’ lives are changed by IR, even receiving a simple ‘thank you’ makes me feel proud that we can make such a lasting impact on so many people. I could not do any of this without the support of the great teams of radiographers, nurses and administration staff that I have worked with in both London and Melbourne and I am fortunate to have such great colleagues.
Have you had important mentors throughout your career? What have they taught you?
There have been several IRs who have been mentors to me.
Professor Michael Lee from Dublin helped start my journey in IR. Professor Lee not only taught me many of my skills in IR, but he also taught me the importance of being a clinician. Taking an active role in patient management and having a clinical presence in the wards was much more important than being just a ‘technician’ performing a procedure.
When I was a junior IR at St George’s Hospital, London, I was greatly influenced by my colleagues Anna-Maria Belli and Robert Morgan. Belli and Morgan taught me the importance of leadership, research, and teaching. Research and innovation is an important area in IR, as sound clinical research leads to better patient treatments and outcomes. Teaching IR at all levels from medical students, radiology registrars, IR fellows and even IR peers ensures that knowledge and experience is shared for the advancement of IR overall.
You have worked for most of your career in Australia, but spent four years in the UK. How does the Australian healthcare system compare with the UK healthcare system, in your experience?
Healthcare and IR in Australia and the UK are very similar in many ways, such as the disease processes (although there are many more kangaroo related injuries in Australia), the provision of universal healthcare, as well as the way that medicine is practiced. However, the systems are also different in many ways. A particular strength of the UK system is NICE (the National Institute for health and Care Excellence), for which I was an advisor. NICE provides national guidance and advice for healthcare by using evidence-based assessments and analysis. Even in Australia NICE guidance is often considered at government levels. Australia offers a supportive framework for early clinical and pre-clinical research. The ethics and governance processes for performing first in-human trials as well as early safety and efficacy trials are well established, which facilitates running this kind of research in Australia. It is exciting to be able to assess new technologies and devices and to see how these can offer solutions to challenges we have as IRs in treating patients. We are also able to influence the development and direction of many of these devices and companies to improve the technology. We have been involved with several first inhuman trials as well as safety and efficacy trials, in addition to many other trials, here in Australia. In the UK there are more challenges to performing first in-human trials and early clinical research and although it is not impossible to do so, it is a much more involved process. An interesting observation is that when new technologies are ready for market release, they are often prioritised for approval for use in Europe and the USA, followed by larger countries such as China and Japan first, largely due to corporate sales and marketing strategies. It takes a while for many of these devices to become available in Australia so often a device we have conducted a first in-human trial takes many years before it is available for clinical use, even though we were the first to use it!
Could you explain your current research interests?
I am involved with quite a few different research projects being the head of Radiology Research at my hospital. We are currently heading and involved with several first in-human trials for which I am unable to disclose any details! We are involved with several commercial global studies in some spaces, such as drug coated balloons and inferior vena cava (IVC) filters to name a few. In addition, we have several investigator-initiated projects running that include pancreatic and prostate irreversible electroporation (IRE). We have also recently completed some studies on IVC filters, radiation protection, artificial intelligence in IR and education in IR that are currently being finalised for submission.
Could you describe a particularly memorable case?
I will always remember a minor procedure I performed on a female patient who happened to be a major international entertainment celebrity. The reason why this was so memorable was that although I was treating someone who was famous, escorted by a bodyguard and had to use an alias to avoid unwanted attention, in the IR lab all social barriers were broken down and we were doctor and patient. Even though the procedure was relatively minor and was not a highly stressful life and death situation, at the end of the procedure she was very grateful, commented on how comfortable the experience was, and left with a big smile on her face. It made me realise that Interventional Radiology can make a big impact on anyone regardless if they are an ‘ordinary’ person or someone famous.
As President of the Interventional Radiology Society of Australasia (IRSA), what is your main goal for the society?
My main goal is to work towards recognition of IR as a specialty or sub-specialty in Australia and New Zealand. In our region IR is a reasonably well established specialty amongst our peers; however, we still have much work to do to achieve national recognition similar to that in many other countries, such as in Europe, the USA, and Canada. There is much work to be done in this space and we are working with the Royal Australian and New Zealand College of Radiologists (RANZCR) to achieve this goal. This process will undoubtedly last longer than my term as IRSA president, however I hope that I can guide our society in the right direction towards achieving this goal.
One of the initiatives undertaken in 2014 was when IRSA adopted the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) European Board of Interventional Radiology (EBIR) as a certification of recognition of IR training and an international IR certification for our region. In conjunction with CIRSE and RANZCR, IRSA has held the EBIR exam in Australia and New Zealand annually for the last four years, and this partnership has always been strong. The Australian/New Zealand EBIR sitting is open to all candidates internationally with many candidates taking the exam here instead of in Europe. We have over 75 EBIR holders from Australia and New Zealand and this number continues to grow year by year. The EBIR has helped many IRs in our region show their skills and expertise in IR.
You are an Associate Editor for Journal of Medical Imaging and Radiation Oncology and have been a peer reviewer for many other titles. What do you think makes a good research paper?
A good research paper is one that clearly defines an objective, has a robust methodological approach in investigating this objective, and follows with a thorough detailed critical analysis. Whilst novel research is always exciting, not all research needs to be completely novel, as one can always improve on existing research and expand knowledge. When submitting research to a journal it is always recommended to do some investigating about the journals one intends to submit to. You will be able gauge what kind of research papers a particular journal accepts and tailor your submission accordingly. For those who are new to research I recommend finding a mentor, as their guidance will be invaluable and they will be able to help you improve and build on your research capabilities.
How has the field changed since you started your career?
The most noticeable change I have seen is the greater international collaboration between international IR societies around the world. This helps facilitate the spread of knowledge, and helps IRs network with one another across borders.
CIRSE continues to reach out to non-European IR societies, with many who have joined as group members, IRSA included. As mentioned earlier, IRSA is holding the EBIR in conjunction with CIRSE, offering candidates the chance to sit the exam outside of Europe: a prime example of international IR collaboration. The Society of Interventional Radiology (SIR) is also reaching out to international societies with international group affiliation. The Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR), for which I am an executive committee member, continues to mature as an organisation and has been running outreach programmes where IRs, from regions where IR is well established, travel at their own expense to countries with developing IR programmes (for example Myanmar) to teach IR techniques and share knowledge. This is helpful as not all IRs from these countries have the opportunity to attend international conferences or to gain hands on experience abroad. This year APSCVIR invited delegates from SIR and CIRSE to be involved with the outreach programme for 2019.
Outside of your own research, what is been the most interesting paper that you have seen in the last 12 months?
Although it feels like this was published a long time ago, the ATTRACT trial (pharmacomechnical catheter-directed thrombolysis for deep vein thrombosis) published in the New England Journal of Medicine in December 2017 was probably the most interesting paper I have read in the last year. I like papers that provoke discussion and challenge IRs to do further research. The ATTRACT trial has certainly had its share of controversy and discussion around the world, and many IRs are now looking towards further research in treating Ilio-femoral deep vein thrombosis and May Thurner lesion stenting.
In your opinion, what are the most exciting new developments in interventional radiology that we can expect in the next five to 10 years?
I believe that interventional oncology will continue to grow over the next decade and there will be many developments in both intra-arterial and percutaneous techniques. The technologies will be refined and improved over time and larger scale clinical trials well help guide practice. An area to keep an eye on is immunotherapy, as this is a promising area where modulating the immune system in combination with chemotherapy may help to increase the effectiveness of cancer treatment. This is battling cancer on a molecular level and I believe IR will have role to play in this by helping to deliver or administer treatments.
What is the biggest challenge in interventional radiology at the moment?
The biggest challenge facing Interventional Radiology is to keep up in producing high quality robust clinical evidence for the procedures we perform whilst keeping up with the rapid pace of innovation. If innovation progresses too quickly without the proper research, then it creates many problems, such as inadvertently treating patients with techniques and therapies that may cause more harm than good as well as weaken the credibility of IR. Throughout my career there have been many technologies and innovations that seemed at the time to be revolutionary or evolutionary; however, the subsequent clinical trials have demonstrated that there has been little or no clinical benefit to patients. As we are such a dynamic and innovative specialty we need to be able to produce high quality research that keeps up with the pace of change of technology to ensure that we are able to practice the best medicine for the best interests of our patients.
What advice would you give to someone wishing to start their career in interventional radiology?
Interventional radiology is an exciting, demanding but highly rewarding specialty. IR training will give you a great breadth of knowledge across many different disciplines of medicine and surgery and often IRs will be able to offer treatment when there are little or no options left for patients. An IR will never stop expanding their knowledge. IR allows you to embrace the rapid pace of innovation, but remember that good clinical research is what ensures patients receive the best treatment possible. Most importantly, a good IR needs to be a competent clinician and leader.
What are your interests outside of medicine?
I have a black belt in Kung Fu and was previously an instructor for around 16 years. I am currently learning Brazilian Jiu Jitsu. Fast cars are another passion of mine; I currently own a Mercedes AMG, used to do amateur car racing and am a big Formula 1 fan (at one stage I was a Formula 1 doctor). I love travel, having visited 39 countries so far, and I have an Instagram travel blog @funkytyper. I also collect Japanese whisky, with my favourite whisky being 18-year-old Yamazaki.
Fact File:
Current appointments
2014–Present: Consultant interventional and diagnostic radiologist, The Alfred Hospital, Melbourne, Australia 2014–Present: Co-director of training, clinical director of Research, Radiology Research Department, The Alfred Hospital, Melbourne, Australia 2014–Present: Adjunct senior lecturer, Department of Surgery, Monash University, Melbourne, Australia
Current society positions (selected) 2017–19: President, Interventional Radiology Society of Australasia (IRSA) 2017–Present: Executive committee member, Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) 2015–20: Council member, European Board of Interventional Radiology, Cardiovascular and Interventional Radiological Society of Europe (CIRSE)
Appointments (selected) 2010–14: Consultant interventional and diagnostic radiologist and head of Trauma Radiology, St George’s NHS Foundation Trust, London, UK 2012–14: Honorary senior lecturer and Teacher, St George’s NHS Foundation Trust, London, UK 2009–10: Fellow and clinical lecturer in Interventional Radiology, Royal College of Surgeons in Ireland, Beaumont Hospital, Dublin, Ireland
Awards, grants and prizes (selected) 2017: Alfred Health senior medical staff prize for Clinical/Public Health Research 2015: Outstanding service award, Cardiovascular and Interventional Radiology Journal (CVIR)
“I used to sneak away to the arcade at seven years old to play pacman and asteroids; our goal with augmented reality really is to prove my mother wrong when she told me not to play video games as they would never be useful,” Brad Wood, National Institutes of Health, Bethesda, USA, jests.
He speaks to Interventional News about how technologies in gaming and graphics processing transformed into a vision for the future of interventional oncology, with augmented reality assisted procedures aimed to meet clinical needs with the goal of potentially improving patient outcomes.
Augmented reality (AR) is the superimposition of digital features into the real world – unlike virtual reality, which involves a completely simulated environment. In interventional oncology (IO), AR can be used to display deep internal anatomy on top of the patient’s skin. Here, Wood speaks of the pitfalls and promise of this technology, emphasising that an AR revolution is imminent.
What is the current status of augmented reality in the IO space?
Augmented reality is in the developmental phase, which is an exciting time because it has a lot of potential. The hard part now is figuring out exactly how it will be useful; proving a clinical utility is the next step. Several options are possible: from pre-procedural planning to intra-procedural navigation and monitoring, to post-procedural feedback and verification. I envision AR making its first in-road in pre-procedural planning, as it is easy to do and does not change the procedure at all. However, intra- and post-operative uses would be more impactful, in my opinion. Intraoperatively, the interventionist could use AR technology to gain information about the procedure in real time when the patient is on the table. Information is power, and knowing when you have a needle or catheter in the correct location in a patient is the most valuable clinical knowledge for me. After the procedure, AR could be used to monitor and verify outcomes. For example, AR could be used to visualise a pre-treatment and post-treatment tumour fused side by side, enabling a three dimensional comparison, and identification and display of tumor tissue at risk for under-treatment..
With all the excitement surrounding AR today, do you think any aspects of the technology are over-hyped?
All sexy ideas have the potential to be over-hyped, and AR is no exception. The development of surgical robotics was partially driven by billboards and hype, and not strictly science. The perception that it is definitely better to be operated on by a robot than a human allowed that technology to proliferate and penetrate practices perhaps before all of the major questions had been answered concerning when to use them, and when and how they help.
New technology always exists on a dynamic spectrum: it is a continuum between innovation on one side, and robust, evidence-based medicine on the other. To quote Aldous Huxley: “at their first appearance innovators have generally been persecuted, and always derided as fools and madmen.” The introduction of new technologies is a dynamic process, and there will always be a tension between experimental technological change and market acceptance. The best window of opportunity to study AR is now, right at the beginning of its clinical use. We want to define when to use it, how it is going to add value, and when it is going to be cost-effective. We are doing a clinical trial on the use of AR in biopsy and ablation, focusing on the monitoring and navigation of needles. We are also looking into software options, trying to figure out the practicalities of the technology: what it will look like in a clinical setting, when to use it during a procedure, where the information gaps are in current practice, and how to make it user-friendly and cost-effective.
What hardware would you need for AR?
It all depends on what you are doing. Most work is focused on goggles, of which a number are currently commercially available. The goggles are tracked, so it knows where the physician is looking at all times, and images can be superimposed over the physician’s field of view. However, in our initial experience, we think it is going to be more useful to use a smartphone or tablet that interfaces directly with the CT console or workstation, so would be part of the workflow. We can then hijack the smartphone’s gyroscope and camera to visualise the anatomy below the skin without the need for goggles. This sounds more user-friendly, ergonomic, and less disruptive to the workflow.
Outside of medicine, what can interventionists learn from other disciplines currently using AR?
Presently, we are taking technology developed for gaming and trying to apply it to a problem in IR or IO. There is a precedent for this: GPS and multi-modality navigation were both originally developed for purposes outside of the medical field. Nvidia hosts a computer science technology meeting which has been a purely graphical congress focusing solely on gaming graphics and processing. Recently, though, it has expanded to include all sorts of exciting new imaging science technologies: artificial intelligence systems, autonomous driving vehicles, and a host of medical applications, including augmented reality offerings. There is nothing wrong with borrowing technology from other disciplines; we just need to ensure that we have a plan for the use of AR in IR to maximise its potential within the clinical space in a cost-effective fashion. The window of opportunity is wide open now.
The world-first collaboration between interventional oncology (IO) and radiation oncology, embraced by the Trans-Tasman Radiation Oncology Group (TROG), continues to bear fruit, with the inaugural Clinical Interventional Oncology Symposium to be held in Melbourne next March. The two-day event will feature in the TROG annual scientific meeting at the Melbourne Cricket Ground on 14–15 March 2019, Melbourne, Australia.
The inaugural clinical Interventional Oncology Symposium will be a dedicated workshop on all aspects of clinical oncology relevant to interventional radiologists. Internationally renowned oncology experts Constantinos Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA), Andreas Adam (Guy’s and St Thomas’ Hospital, London, UK) and Lizbeth Kenny (Royal Brisbane and Women’s Hospital, Brisbane, Australia) will join with local expert medical oncologists, radiation oncologists, pathologists, surgeons and interventional radiologists to present a wide-ranging syllabus that will highlight the importance of high-quality clinical practice in IO.
IO is a dynamic and ever-expanding profession, and practising interventional radiologists (IRs) must be up to date across a wide range of clinical and technical skills. These sessions will emphasise the need for interventional radiologists to assume responsibility for the clinical care of their patients, and to develop a pattern of practice similar to that of all other oncological disciplines. In turn, this will help IRs to take image-guided interventions into the “mainstream” of oncology.
Teaching will include overviews of tumour biology, pathology, treatment options, clinical algorithms and the critical role that IO has to play in the diagnosis and clinical management of cancer. Sessions will also focus on clinical skills relevant to IR, including procedural sedation, post-procedure analgesia, how to establish and grow an IO clinic, and future IO research areas.
Unlike other IO workshops, the Clinical IO Symposium will not focus on expert technical explanations about how to perform procedures or “hands-on” displays. Instead, the symposium aims to educate IRs about how the IO techniques they perform fit into treatment algorithms, when they should be considered, and how to assess oncology patients.
Kenny, TROG Interventional Oncology Interest Group co-chair, said she was excited to participate in what is another world-first development involving interventional oncology and radiation oncology. “To the best of our knowledge, this is the first time that an IO workshop has been wholly dedicated to imparting purely clinical aspects of interventional oncology,” Kenny commented.
“Whilst quality assurance around how an interventional radiologist performs a procedure is critically important, it is equally necessary for IRs to be able to assess patients clinically and to know when certain interventions are appropriate.
“I am thrilled that radiation oncology and interventional oncology, both using image-guided focal therapy, are coming together in this way. We have so much to learn from each other,” added Kenny.
Adam, a well-known advocate of interventional oncology in Australia and New Zealand, was impressed by the unique approach. “Interventional oncology can by practised safely only as a clinical discipline. If interventional oncologists do not assume primary clinical responsibility for the patients they treat, they cannot ensure optimal care and run the risk of errors. For example, if follow-up of patients undergoing percutaneous ablation is delegated to the referring physician, delays in the diagnosis of recurrent or residual tumour can occur, and potentially treatable disease can become untreatable.
Adam added: “Interventional oncology is already making a significant contribution to contemporary cancer care, but has enormous unrealised potential, which can be harnessed only by its practitioners becoming fully-fledged clinicians. Interventional oncologists should take pride not in their technical expertise, which should be assumed and taken for granted, but in being ‘proper doctors’, like all other oncologists. This is the main value of this innovative workshop.”
“Interventional radiologists need good clinical training to support their technical skills,” said Nicholas Brown, overall symposium convenor, co-chair of the IO Interest Group and chair of the of the RANZCR Interventional Radiology Committee. “We hope that by emphasising the clinical aspects of interventional practice the workshop will help IRs to fulfil their role as clinicians, and develop IO into the mainstream.”
Susan Goode, TROG Cancer Research CEO, said her organisation was delighted to once again incorporate interventional oncology into its annual meeting and was excited about exploring the potential for further collaboration on education, training and research. “This will be the second year that IO has been integrated into the TROG Cancer Research programme, and based on the great response in 2018, next year is promising to be even more successful,” said Goode.
In a plenary address in the main scientific programme, Constantinos Sofocleous will outline the important role of interventional radiologists in modern oncology, and will explain how collaboration between oncological disciplines can benefit patients.
Interventional radiologists at any stage in their career are encouraged to attend and learn more about important concepts in clinical oncology for the modern interventional radiologist. This course is also highly recommended to registrars, fellows and interventional radiologists wanting to develop their practice in IO.
The symposium is supported by an educational grant from Terumo Interventional Systems.
Michael Jaff (Newton, USA) outlines the major recent developments in best medical therapy that will impact the treatment of peripheral arterial disease (PAD) at VEITHsymposium 2018.
Ralf Langhoff, chief, Angiology/Vascular Medicine, Sankt Gertrauden-Krankenhaus, Berlin, Germany, reports on a case in which his team used a novel 0.035” UltraScore™ Focused Force PTA Balloon (Bard, now BD) as an adjunctive therapy with the LUTONIX® drug coated balloon (DCB) to recanalise a chronic total occlusion (CTO) in the superficial femoral artery (SFA).
A 68-year-old female was referred to our vascular center for intermittent claudication primarily in the right leg (Rutherford category 3). She is a current smoker with additional risk factors for atherosclerosis, which are arterial hypertension and dyslipidemia with high cholesterol levels. She had a pain free walking distance below 50 meters, with an Ankle Brachial Index (ABI) of 0.63 on the right side.
After the referring angiologist performed a duplex examination, the test revealed a diseased SFA from the origin of the artery with an occlusion at the distal end. The total length of the diseased segment was 260mm (Fig. 1).
To avoid long segment stenting and to prepare the vessel for better drug-uptake, we intended to intraluminally cross the occlusion and follow with a dedicated scoring balloon for percutaneous transluminal angioplasty (PTA) and vessel preparation.
We used a cross-over access from the left transfemoral with a 6F Fortress Introducer Sheath, 45cm length (Biotronik) and passed the lesion with a 0.035” GLIDEWIRE®, 260cm length (Terumo). As support, we used a 4F multi-purpose catheter, TEMPO AQUA® (Cordis, now Cardinal Health).
Subsequently, vessel preparation was performed with the novel UltraScore™ 5mmx200mm scoring balloon (Bard/BD), which runs on a 0.035” wire (Fig. 2). The intention of vessel preparation is to minimize the risk of dissections, and maximize luminal gain to prepare the vessel for local drug delivery and/or stents.
The balloon was inflated slowly, which allowed the wires to provide concentrated force on the diseased vessel wall. This focused force dilatation led to a controlled plaque fracture, improved luminal gain. Additionally, the objective was to limit risk of major dissections (SOGA 2018) as severe dissections are related to negative long-term outcomes in femoro-popliteal interventions (FUJIHARA 2017). After seeing a very good and promising result after the use of the UltraScore™ balloon, we decided to use DCBs to deliver paclitaxel to the entire lesion.
Figure 3
Furthermore, there is the idea that by using scoring elements during vessel preparation the drug-uptake of DCBs can be increased and optimized (CREMERS 2013). We used two 5mmx150mm LUTONIX® DCBs (Bard/BD) with a 1cm overlap to avoid a geographical miss. We chose a longer balloon inflation time of three minutes because we revealed a short, minor dissection in the former occluded part of the lesion. We decided against provisional stenting because results of the large DCB trials reported strong effects of positive remodeling after application of paclitaxel to the vessel wall via a balloon (TEPE 2013).
Control angiography demonstrated a very good result, with a small minor dissection which was not flow limiting in several projections.
The intervention was finished without any complications and a good outflow (Fig. 3). We used a MYNXGRIP® device (Cordis/Cardinal Health) for hemostasis and vessel closure.
After the case, the patient was free of any ischemic pain while walking.
References 1. Soga Y, Ando K. Effect of an NSE PTA balloon in experimental lesion models. Cardiovasc Interv Ther. 2018 Jan;33(1):35–39.
2. Fujihara M, et al. Angiographic dissection patterns and patency outcomes after balloon angioplasty for superficial femoral artery disease. J Endovasc Ther. 2017;24:367–75.
3. Cremers B, et al. Inhibition of neo-intimal hyperplasiain porcine coronary arteries utilizing a novel paclitaxel-coated scoring balloon catheter. Catheter Cardiovasc Interv. 2014 Dec 1;84(7):1089–98.
4. Tepe G, et al. High-grade, non-flow limiting dissections do not negatively
impact long-term outcome after paclitaxel-coated balloon angioplasty:
an additional analysis from the THUNDER study. J Endovasc Ther. 2013;20:792–800.
Described by her supervisor Glen Schlaphoff (Sydney, Australia) as “a perfect example of a young up and coming interventional radiologist”, Sindhura Nirmalarajan is a Radiology registrar at the Prince of Wales Hospital, Sydney, Australia. At the 2018 annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 22–25 September, Lisbon, Portugal), she was honoured with the Magna cum Laude e-poster award for her work on prostate artery embolization. Here, she discusses this research with Interventional News, as well as why she is excited for the future of interventional radiology (IR).
What is your reaction to winning the prestigious e-poster award at CIRSE?
I submitted this project through the CIRSE trainee support programme and was very excited to hear the poster was accepted for presentation alongside many high calibre projects. Receiving the Magna cum Laude award took me completely by surprise and I feel incredibly honoured by this recognition. I am grateful for the opportunity to have presented this work and for the support of my supervisor Glen Schlaphoff (South Western Sydney Clinical School, Sydney, Australia).
Would you summarise the findings of the research presented in your e-poster?
Prostate artery embolisation (PAE) is emerging as an effective treatment option for lower urinary tract symptoms caused by benign prostatic hyperplasia. One of the technical challenges of this procedure is accurately identifying variant pelvic arterial anatomy. We reviewed the angiograms of 202 pelvic sides and classified the branching pattern of the internal iliac and prostate arteries using the framework of existing angiographic classification systems. We found the incidence of anatomical variants in our series from a single Australian institution (Liverpool Hospital, Sydney) to be comparable to the incidence reported in previous studies. Despite the high degree of variability, the origin of the prostate artery could be classified into one of four types in 96% of our cases.
How will these findings influence clinical practice?
This poster serves as an educational resource that provides a systematic approach to understanding and identifying complex and variable pelvic arterial anatomy. In particular, it provides a pictorial overview of the range of arterial variants related to PAE and potential intra/extraprostatic anastomoses. Ultimately, this awareness improves technical success, reduces fluoroscopy time and minimises the risk of non-target embolization.
Why is this an exciting time to be involved in interventional radiology?
IR is founded on creativity and innovation and this enables the specialty to meet the increasing demand for minimally invasive treatment options, which are effective, safe and have reduced recovery times. There has been a shift in the practice of IR in the modern day, with an increasing recognition that technical expertise is only one component of the larger clinical skill-set of an IR. The continued progression of IR into an increasingly integrated clinical specialty combined with the development of new technical innovations makes this an exciting time to be involved in IR.
You currently practice in Sydney, Australia. How does the Australian healthcare system help and/or hinder your work and how would you describe the IR scene in Australia for up and coming radiologists?
Australia is fortunate to have one of the world’s leading healthcare systems. The availability of universal healthcare means that IR services in public tertiary centres are highly accessible.
IR is embedded in the multidisciplinary healthcare system and there is constant collaboration with other specialties, such as in the settings of oncology, trauma, paediatrics, and many others. As an Australian trainee, this provides a diverse and robust mix of cases and exposure to the breadth of interventional radiology.
There is a widespread recognition of the importance of achieving subspecialty status for IR in Australia. An essential step in this complex process is increasing the clinical focus of IR. This has seen a shift towards the establishment of outpatient clinics, primary clinical responsibility for patients, and collaboration with other disciplines to provide care for a larger number of increasingly complex patients. Furthermore, the need for standardisation of training is recognised and has resulted in many Australian IRs undertaking the EBIR [European Board of Interventional Radiology] certification. For trainees in Australia, this is a great time to be involved in helping to shape the future of this dynamic specialty.
There still exists a gender imbalance in this field, with more male IRs than female. Why do you think this is and what do you think should be done to address/change this?
There is a growing focus on the disproportionately small number of female IRs compared to the numbers of female medical graduates and trainees in other traditionally male-dominated specialties. Several studies have explored the reasons for this disparity and have highlighted multiple contributing and inter-related factors including: the relatively few women in leadership roles, an entry pathway via diagnostic radiology, and the misconceptions surrounding radiation exposure.
Personally, I feel that a potential avenue to address this gender disparity and also recruit individuals (both male and female) who are motivated to pursue a career in IR would be to increase the profile of IR in medical schools and set out a clearly structured IR training programme that builds clinical and procedural expertise alongside diagnostic training. I believe that cultivating an interest in IR at the medical school level could result in a more balanced proportion of female IRs that is more reflective of the numbers of female medical graduates.
I hold this belief because I found that an early exposure to IR in medical school was pivotal in forming my interest in this field. I completed a diagnostic Radiology term at Johns Hopkins Hospital in my third year of Medicine and returned for an IR elective in my sixth year. The elegant solutions to tricky scenarios, the broad scope of practice and the effective, precise treatments that IR could provide were a revelation to me. There were several female IRs working in the department at the time and, looking back, I believe it was this early exposure to IR and the diversity of the team that helped me to see this field as a future career path.
What do you think the next generation of IRs will bring to the discipline?
I think the strength of the next generation of IRs will be to enter the training programme directly from our clinical foundation years and to maintain and build our clinical acumen throughout our training.
I believe that bringing in new perspectives with a steady influx of young trainees and increasing collaboration between IRs and other disciplines will keep the specialty progressing at the cutting edge of medicine.
With traumatic injuries caused by traffic accidents on the rise, Miguel Angel de Gregorio provides an overview of interventional radiologists’ role in performing embolization procedures to help the increasing number of trauma patients. De Gregorio also summarises the work presented at the Cardiovascular and Interventional Radiological Society of Europe 2018 meeting (CIRSE; 22–25 September, Lisbon, Portugal) on the Embolization for Trauma panel.
Despite preventative measures, no one can doubt that many technological advances have brought a considerable increase in the incidence of serious accidents that manifest themselves in incapacitating and even fatal injuries. This increase in accident rates is closely linked to traffic accidents. According to the National Transportation Society Board (NTBS), in the year 2016 in the USA, more than 40,000 deaths were due to traffic accidents—involving a mean of 12.4 people per 100,000 inhabitants. The measures of prevention and control of road safety, together with an improvement in the social conscience of drivers and workers, should reduce the rate of any type of accidents as well as their mortality.
Life support measures, coupled with emergency surgery, play an important role in the management of injured patients who arrive at hospitals. Through embolization procedures, interventional radiology can contribute to the good management and stabilisation of these serious patients in a simple and safe way.
The CIRSE 2018 (Cardiovascular Interventional Radiological Society of Europe) Congress held on 22–15 September in Lisbon, Portugal, included the presentation and discussion of several papers covering trauma and vascular embolization.
Sanja Stojanović and myself moderated the session Embolization for Trauma, in which Christian Scheuring-Meunkler (Berlin, Germany), Michele Citone (Florence, Italy), Dimitrios Karnabatidis (Patras, Greece) and Gary Siskin (Albany, USA) discussed the management of trauma of the spleen, liver, pelvis, and kidney, respectively.
In general, after life support measures, radiological imaging plays an important role in the diagnosis and extension of patients’ trauma. Computed tomography (CT) is the most important imaging technique, enabling a simple, safe and rapid way for the diagnosis of affected organs, as well as for detecting the presence of active bleeding. The image data and clinical assessment establishes the severity of the trauma and also helps to classify the trauma.
The World Society of Emergency Surgery (WSES) assesses four types of closed or open traumas depending on the intensity of the trauma and the anatomical lesions observed. The Organ Injury Scaling Committee for the American Association for the Surgery of Trauma (AAST) divides the type of lesions according to the degree of anatomical lesion (IV grades). Patients with severe trauma—WSES type IV and an AAST grade of AAST (ranging from I–V)—and haemodynamic instability require surgical management (operative management), while in other degrees and levels, haemodynamic stability can be managed without surgery; this is non-operative management. In these latter types, patients are graded as WSES type I–II trauma. If angioCT and, most importantly, angiography establish vascular injury, embolization should be considered the treatment of choice.
There are many types of embolization agents, such as: absorbent gelatins, particles, gel foam, glues, coils, plugs alone or in combination. Embolization requires expertise, and interventional radiologists need to carefully decide which technique to use, such as distal, proximal embolization or combined, depending on the type of injury and the vascular anatomy of the organ or structure to be treated. Clinical results depend on the type of injury and the affected organ with few complications if the technique is adequate.
Endovascular techniques play an increasingly important role in the management of open and closed traumas with extensive vascular bleeding and injury; either to stabilise the patient, or to solve the problem. Hybrid operating rooms near hospital emergency centres can improve the results by reducing intervention times, as well as allowing surgery before, during, or after embolization without mobilising the patient.
Miguel Angel de Gregorio is a professor at the University of Zaragoza, Zaragoza, Spain, and a member of the Minimally Invasive Techniques Research Group (GITMI), Government of Aragon, Spain.
Addressing the audience at the 33rd annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 22–25 September, Lisbon, Portugal), Sanjiv Sharma asks: “If you can have a drug-eluting stent, why can’t you have a stem cell-eluting stent?” Here, Sharma argues that a paradigm shift in the management of critical limb ischaemia is on the horizon, with stem cell therapies proving safe, effective, and less costly than surgical or endovascular revascularisation.
Management strategies for critical limb ischaemia (CLI) are constantly evolving due to issues and challenges with the image morphologies in below-the-knee vessels and rapidly changing device technologies, mostly with unmet long-term outcome expectations. Many times, a strategy for surgical or endovascular revascularisation may not be feasible due to an anatomically irreparable disease. New endovascular techniques and devices may improve short-term outcomes but fail progressively with time, and eventually are not much better than conventional techniques over the long-term, despite major cost escalation.
Therapeutic angiogenesis using cell-based (stem cell) therapies has emerged as a new frontier in this treatment, and has the potential to rewrite the treatment algorithms in patients with critical or chronic limb ischaemia.
Stem cell characteristics
These stem cells have three characteristic properties that make them well suited for this treatment: plasticity, homing and engraftment. Stem cells derived from early human embryos are pluripotent and can generate all committed cell types. These generated cells are higher in number, and have better expansion potential and differentiation abilities when compared with stem cells from adult tissues, but have issues related to adverse effects and ethical concerns. Hence, the clinical experiences are largely restricted to the use of autologous adult stem cells in various disease states. The migration, differentiation and growth of stem cells are mediated by the nature of the tissue, degree of injury and the type of stem cells involved. Damaged tissue releases factors that induce homing of these cells to the site of injury.
In ischaemic tissues, endogenous biochemical agents are released, stimulating angiogenesis. The angiogenesis is developed by vascular cell proliferation and new capillary formation. Pre-clinical studies have shown that angiogenic growth factors promote the development of collateral arteries, a process that is termed therapeutic angiogenesis. This angiogenesis can be achieved either by growth factors or genes encoding these proteins. Endothelial progenitor cells in the CD34+ stem cell fraction of adult human peripheral blood and bone marrow cells also take part in postnatal neo-vascularisation after mobilisation from bone marrow, and contribute to this angiogenesis.
Stem cells can be extracted from various sites, including the bone marrow, peripheral blood and adipose tissue. These can be administered to the affected area by intra-arterial or intra-muscular delivery. Both these routes of delivery have shown clinical benefit in multiple studies.4–6 Preclinical studies have proven the safety of this treatment method and a variable efficacy n terms of relief of induced ischaemia. Current research
revolves around establishing the most suitable source of autologous stem cells, the optimal route of delivery, the right dose of cells, as well as the role of single versus multiple injections for the desired clinical outcomes, the optimal method for assessment of clinical and imaging outcomes, and the role of adjunct therapies in potentiating the effects of cell-based therapies.
Stem cell treatment proven safe and effective in “no option” patients
We conducted a pilot project using graded doses of stem cells in a group of patients with CLI and showed that a benefit, in terms of relief of rest pain and healing of ischaemic ulcers, was seen in all patients in the treatment arm. This benefit was not dependent on the dose of injected stem cells beyond a threshold dose. Whereas in the control arm, no improvement was seen in any patient; CLI improved in all patients in the treatment group who received three graded doses of stem cells. No adverse effects related to the treatment were seen in any patient.
Subsequently, we conducted a randomised first in-human placebo controlled double blind clinical trial that included 80 patients with no option CLI not suited for any form of revascularisation. There was a 1:1 randomisation in control and treatment arms, and the patients were followed for at least six months after this treatment. All patients received an injection, either of stem cells, or a sham injection indistinguishable from the stem cells. Both the operator and the physician who evaluated the patients during follow-up were blinded to the mode of therapy. This trial was recently concluded and the results have established the safety and efficacy of autologous stem cell therapy for limb salvage in these patients. Evidence of therapeutic angiogenesis as evidenced by a demonstrable increase in collateral density after stem cell therapy and 0% amputation rates in the treatment arm was observed.
There is some evidence to suggest that the effect of this therapy may be more pronounced in Berger’s disease than in atherosclerosis.4 The barriers to the development of stem cell therapy relate to the autologous cell population that is often heterogeneous and may lead to varied responses. Also, to obtain the large cell numbers needed for transplantation, ex vivo cell expansion may be required, which leads to regulatory concerns and increased cost and time. Advanced disease also has the problem of cytokine resistance. Furthermore, the cell engraftment efficiency is typically low upon transplantation and may require multiple injections.
The potential of gene therapy
The therapeutic potential of stem cells may be enhanced by combining this treatment with gene therapy. This is likely to overcome insufficient paracrine release, poor cell survival upon engraftment, and lack of cell homing by controlling cell behaviour at the intracellular signalling level.7 To reduce the occurrence of in-stent restenosis, stents have been reshaped and improved in many aspects with the development of drug- and growth-factor eluting stents. Stem cells as a source of seeding cells for coating the stents have also been reported.8 In a recent study, mesenchymal stem cells derived from the bone marrow of New Zealand white rabbits were used as seeding cells and the authors observed that intimal hyperplasia and in-stent restenosis were significantly inhibited by the mesenchymal stem cell coated stent.
Although proof from large randomised trials for the above therapies is still inconsistent, these treatments have shown the ability to improve perfusion in selected patients. We have established the safety and efficacy of autologous stem cells in the treatment of “no-option patients” with critical limb ischaemia. Pre-clinical studies utilising a combination of cell and gene therapy have also shown encouraging results. This may be an alternative option to address the limited number and function of progenitor cells in elderly patients, those with co-morbidities, and the challenge of cytokine resistance. Further research will define their role in suitable patients. The evidence for cell-based therapies is encouraging. There is a need for optimised trials to define the treatment algorithms in these patients.
Sanjiv SHarma is a professor and head of the Department of Cardiovascular Radiology and Endovascular Interventions at the All India Institute of Medical Sciences, New Delhi, India.
References: 1. Chochola M, Pytlik R, Kobylka P, Skalicka L, Kideryova L, Beran S, et al. Autologous intraarterial infusion of bone marrow mononuclear cells in patients with critical leg ischemia. Int Angiol. 2008;27(4):281-90.
2. Matoba S, Tatsumi T, Murohara T, Imaizumi T, Katsuda Y, Ito M, et al. Long-term clinical outcome after intramuscular implantation of bone marrow mononuclear cells (Therapeutic Angiogenesis by Cell Transplantation [TACT] trial) in patients with chronic limb ischemia. Am Heart J. 2008;156(5):1010-8.
3. Amann B, Luedemann C, Ratei R, Schmidt-Lucke JA. Autologous bone marrow cell transplantation increases leg perfusion and reduces amputations in patients with advanced critical limb ischemia due to peripheral artery disease. Cell Transplant. 2009;18(3):371-80.
4. Fadini GP, Agostini C, Avogaro A. Autologous stem cell therapy for peripheral arterial disease metaanalysis and systematic review of the literature. Atherosclerosis. 2010;209(1):10-7.
5. Rigato M, Monami M, Fadini GP. Autologous Cell Therapy for Peripheral Arterial Disease: Systematic Review and Meta-Analysis of Randomized, Nonrandomized, and Noncontrolled Studies. Circ Res. 2017;120(8):1326-40.
6. Bura A, Planat-Benard V, Bourin P, Silvestre JS, Gross F, Grolleau JL, et al. Phase I trial: the use of autologous cultured adipose-derived stroma/stem cells to treat patients with non-revascularizable critical limb ischemia. Cytotherapy. 2014;16(2):245-57.
7. Makarevich P, Rubina Rubina KA, Diykanov Diykanov DT, Tkachuk Tkachuk VA, Parfyonova Parfyonova YV. Therapeutic Angiogenesis Using Growth Factors: Current State and Prospects for Development. Vol. 9_2015. 2015. 59 p.
8. Bompais H, Chagraoui J, Canron X, Crisan M, Liu XH, Anjo A, et al. Human endothelial cells derived from circulating progenitors display specific functional properties compared with mature vessel wall endothelial cells. Blood. 2004 Apr 1;103(7):2577–84.
9. Wu X, Zhao Y, Tang C, Yin T, Du R, Tian J, et al. Re-Endothelialization Study on Endovascular Stents Seeded by Endothelial Cells through Up- or Downregulation of VEGF. ACS Appl Mater Interfaces. 2016 Mar 23;8(11):7578–89.
At the third Capitol briefing from the Society of Interventional Radiology (SIR), Susan Sedory, executive director for SIR, along with a panel of experienced interventional radiologists, presented the case for interventional oncologists to become more involved with mainstream cancer treatment, emphasising the need to educate policy makers, financiers, and patients alike on the evolution of targeted cancer and pain medicine offering minimally invasive options. “The advent of these image-guided, organ-sparing procedures that are done through a tiny pin hole on the skin have changed the landscape of how we treat cancer,” summarised William Alago, panellist and interventional radiologist at Memorial Sloan Kettering Cancer Center, New York, USA.
Alago and Sedory, as well as fellow panel members David Prologo (Emory School of Medicine, Atlanta, USA), Alexander Kim, and Theresa Caridi (both Medstar Georgetown University Hospital, Washington, USA) advocated for increased Capitol support of interventional oncology as a discipline through breifing the audience on the Enhancing Opportunities for Medical Doctors Act.
The bill, also known as HR 1167, was introduced to the House in 2017. According to Sedory, the bill looks to support three areas: new primary education in certain medical fields, of which interventional radiology is one; rural hospitals, which desperately need more physician opportunities to fill open positions; hospitals associated with any brand new medical school. Of importance, Sedory stated that this bill does not seek to increase graduate medical education funding, but instead seeks the opportunity to reallocate unused money.
“As interventional radiologists, we are not having trouble filling our spots, in fact, we are over-subscribed. What we want to do—instead of creating new spots—is to assign some of these unspecified positions to the new dedicated pathway trainees in interventional radiology”, Prologo explained.
Interventional oncology has “an identity issue”
Yet the primary ambition of the SIR briefing—alluded to time and time again throughout the panel’s discussion—encompassed the issue of education: all five speakers agreed that there is currently a lack of knowledge regarding minimally invasive therapies, and patient access to these techniques is suffering as a result.
such minimally invasive treatments to cancer were available for everyone, Alago replied: “No, they are not unfortunately, and part of the mission of our society is to educate [the public] as well as our own referring oncologists about the effectiveness of some of these procedures. As we grow as a speciality, we have seen that more people are actually demanding these type of treatments because of their nature. At large academic centres it has been easier to get the message across so patients can access the care and options that are available; at smaller centres, it has been more of a struggle. I think as people become more aware, inevitably, the breadth and scope of our procedures will grow, and there will be more access for patients who need them.”
In agreement, Kim stated that patient access to interventional oncology procedures is the biggest limitation within this field of medicine today. He commented: “The biggest barrier is patient’s understanding that interventional radiologists can provide therapy that could relieve them of their pain. We need to spread the word of other therapies available outside of the standard medical fields that people may be familiar with.”
Caridi alluded to a particular question that was raised at a previous SIR session: “If I am a patient, what should I ask when I go to my doctor?” She said that although the key phrase is “minimally invasive”, simply for the patient to understand that there is a less invasive option to surgery, and to ask accordingly, is half the battle.
“The majority of patients have never heard of the minimally invasive therapeutic options that are available.“
In terms of patients on pain medication that are seeking other treatment options, Caridi said: “For a lot of patients, it is not about opioid addiction, it is the side effects that come alongside pain medication. Although I am not doubting how miraculous they can be, opioids are known to cause severe constipation, and the patient is uncomfortable for other reasons. So, while pain medication can be very effective, it can be utilised in conjunction with what we do.” Certainly, in the context of the opioid epidemic, the panellists are in accordance that the sooner patients can stop taking pain medication, the better. Stressing the independence from opioids that minimally invasive procedures afford was one of their key messages, and one of the most persuasive arguments in terms of gaining audience approval.
Summarising the issue of patient access and education concerning an awareness of interventional radiology, Kim said: “We have an identity issue. Unless you are a savvy patient who does a lot of internet research and can look into specific diseases and treatments, the majority of patients have never heard of the minimally invasive therapeutic options that are now available.
“The reason that this bill is so important is that it will allow us […] not only to increase the number of interventional radiologists in areas that are relatively under served, but also to have a bigger voice within medicine, giving people the opportunity to become more familiar with the therapeutic options that they have today,” Kim noted.
Minimal cost of interventional oncologic procedures an attractive argument for gaining potential financiers’ support
When questioned by an audience member on the costs of these minimally invasive procedures, Prologo explained two major areas in which interventional radiology most significantly affects cost. “The amount of money that we spend on inpatients […] can be extremely expensive, but we can save hundreds-of-thousands of dollars by decreasing the pain to a manageable level in one short outpatient procedure,” said Prologo. Furthermore, as minimally-invasive therapies offer an alternative to surgery, he said: “We can cure someone of their cancer using a needle through a small puncture site that gets covered by a band aid—which is a lot cheaper than the pain medication, the potential complications, and the hospitalisations that can be associated with surgery.”
Speaking specifically about the beneficial economic impact of interventional radiology, Alago added: “In the advent of these procedures, people can get back to work, even some of the people that do heavier work, it is amazing.”
However, Caridi alluded to an example where the treatment option is not drastically less expensive compared to surgical options—the minimally invasive treatment of uterine fibroids. Irrespective of cost, she noted that an advantage of interventional techniques is that they remain patient-centred, as she stressed the importance of patient satisfaction regarding utilisation of the least invasive option available to a patient.
With regards to how interventional radiology has impacted the treatment of cancer specifically, Caridi described the array of minimally invasive techniques used today. She defined embolization for the audience—“essentially blocking the blood supply to the tumour”—and explained how it can be done by delivering chemotherapy directly to the tumour via small catheters in the blood stream, emphasising that it is a relatively pain free procedure. Further techniques mentioned included ablative therapies (usually with a curative intent), and irreversible electroporation.
“It is quite amazing, after 19 years of practice, I have seen the landscape transform itself into something that is so powerful and able to change the lives of cancer patients in a minimally invasive fashion,” enthused Alago of the evolution he has witnessed over his career.
Sedory concluded the briefing, highlighting that the society’s aim remains to spread awareness of this evolving medical field, and to educate patients on exactly what treatment options are available to them. However, she noted that the health systems are very supportive and understanding of the current array of minimally invasive therapies as they continue to evolve in a specialty that has been around for 50 years. Lastly, she stressed the importance of the bill: “Although the exact number of unspecified spots [able to be reallocated] is unknown, it remains around 1,300; a number that would certainly be impactful.”
Boston Scientific has announced it has reached an agreement on the terms of a recommended offer to acquire BTG, a company headquartered in the United Kingdom, which develops and commercialises products used in minimally-invasive procedures targeting cancer and vascular diseases, as well as acute care pharmaceuticals.
The transaction has been unanimously approved by the boards of directors of Boston Scientific and BTG. Under the terms of the transaction, holders of BTG’s common shares would receive cash consideration of 840 pence per share. The total cash consideration for 100% of BTG’s equity is approximately £3.3 billion, or U.S.$4.2 billion. The transaction is intended to be effected by way of an English court-sanctioned scheme of arrangement, and is expected to close in the first half of 2019, subject to receipt of required regulatory approvals and the approval of BTG’s shareholders and the UK court.
BTG has three key businesses, the largest of which is its Interventional Medicine portfolio, which encompasses several peripheral interventional product lines. The interventional oncology franchise includes the TheraSphere Y-90 radiotherapy microspheres and the GALIL cryoablation system, used to treat patients with liver, kidney and other cancers. More than 840,000 people are expected to be diagnosed with liver cancer in 2018, and that number is expected to grow to 1.1 million by 2030. Kidney cancer is among the 10 most common cancers in both men and women.
The company’s Interventional Medicine business also has a highly-differentiated vascular portfolio, including filters, crossing catheters, microfoam and the EKOS Endovascular System. The EKOS system, in combination with clot-dissolving drugs, breaks down blood clots to restore blood flow in patients with pulmonary emboli, deep vein thrombosis and peripheral arterial occlusions, and was the first device cleared by the Food and Drug Administration for the treatment of pulmonary embolism.
The BTG portfolio also includes a pharmaceutical business comprised of acute care antidotes to treat overexposure to certain medications and toxins, and a licensing business that receives royalties relating to products subject to BTG intellectual property and license agreements.
Boston Scientific has received irrevocable undertakings to vote in favour of the transaction from BTG’s three largest shareholders, covering an aggregate of approximately 33% of BTG’s outstanding shares, as well as from all of BTG’s directors, who hold an additional 0.3% of BTG shares. The transaction would be funded with a combination of cash on hand and proceeds from debt financing entered into by Boston Scientific. The full terms of the proposed transaction, including the full terms of the undertakings from BTG’s shareholders and directors, are set forth in an announcement made by Boston Scientific, Bravo Bidco Limited, a wholly-owned Boston Scientific subsidiary formed to effect the proposed transaction, and BTG in accordance with Rule 2.7 of the UK’s City Code on Takeovers and Mergers. Boston Scientific has entered into a bridge financing facility providing for its receipt of £3.3 billion of committed financing, which satisfies the certain funds requirements of the UK Takeover Code.
The transaction is expected to be two to three cents accretive to Boston Scientific adjusted earnings per share in 2019, and increasingly accretive thereafter. On a GAAP basis, the transaction is expected to be dilutive in 2019, and less dilutive or increasingly accretive thereafter, as the case may be, due to amortisation expense and acquisition-related net charges.
Barclays and Shearman & Sterling are acting as financial and legal advisors, respectively, on behalf of Boston Scientific.
Six-month outcomes of a multicentre randomised controlled trial using the Lutonix 014 drug-coated balloon (BD; DCB) has demonstrated the DCB is safe to use in peripheral lower limbs, below the knee. The primary safety endpoint of freedom from major adverse limb events and all-cause perioperative death at 30 days was met, and a Kaplan-Meier analysis indicated “no significant difference” in safety between the DCB and the plain percutaneous transluminal angioplasty (PTA) arms of the study.
The data were presented at the Vascular Interventional Advances annual conference (VIVA; 5–8 November, Las Vegas, USA) by Jihad Mustapha of Advanced Cardiac and Vascular Amputation Centers, Grand Rapids, USA. Mustapha said the study provide the “largest randomised controlled dataset on DCB versus PTA that is available to us as of today”, adding, “This is the first level 1 endovascular therapy treatment involving a multicentre, blinded randomised BTK trial.”
The clinical study is a prospective, global, multicentre, randomised, controlled trial comparing the Lutonix 014 DCB to standard angioplasty for the treatment of narrowed or obstructed arteries below the knee. The study used both proportional/binary and Kaplan Meier analyses to assess safety and efficacy. The primary safety endpoint—freedom from composite all-cause death, above ankle amputation or major reintervention of the treated limb through 30 days—was met showing statistically significant safety equivalence between the Lutonix 014 DCB and standard PTA catheter, in both the proportional/binary and Kaplan Meier analyses.
Mustapha expressed his hopes for the impact of these data, and excitement about the outcomes, stating: “The six-month clinical data from the Lutonix BTK trial represent the beginning of a paradigm shift in the treatment of patients with critical limb ischaemia (CLI). The initial results are extremely encouraging and give new hope to patients with CLI.”
“Previously published DCB BTK trials have generated concern,” Mustapha said, “regarding amputation rates with DCB use—this is why we looked beyond 30 days, and saw no difference in primary safety at six months between DCB and PTA. The numbers were very close: 97% versus 95%.”
The primary efficacy endpoint was assessed using a composite measurement of freedom from target limb occlusion, above ankle amputation, and clinically driven target lesion revascularisation, to define primary patency. Proportional/binary analysis revealed an improvement in primary efficacy of 10.2% (DCB: 73.7% and PTA: 63.5%, p=0.0273, not-significant) at six months. The more commonly used Kaplan Meier analysis of the primary efficacy endpoint demonstrated a significant difference of 14.6% (DCB: 85.3%, PTA: 70.7%, p<0.001). Additional analyses are planned for 12-, 24- and 36-month follow-ups.
The trial included 442 participants of which 91% had CLI. “Patients with BTK CLI are the most complex subset of peripheral arterial disease in general,” Mustapha said, highlighting the high rates of amputation estimated at around 25–33%, and an approximate US$95 billion cost in the USA per year to treat this patient population.
The amputation rate specific to each arm of the study was not available at the time of presenting, however Mustapha emphasised the notably low overall rate of amputation, comparing the 3.8% figure at six months to double-digit rates in previous trials. “We did not see any increased rate of amputation in the DCB arm,” Mustapha clarified, “but in general actually the number of amputations was less than 4% in the entire cohort—PTA and DCB.”
At baseline, 71% of all patients enrolled had diabetes, 92% had hypertension and close to 60% of patients were smokers. Within the 91% with CLI, the majority were Rutherford category four and five. Addressing baseline demographic risk factors, Mustapha noted that Rutherford categories were balanced across both arms, however the DCB arm had 40% more TASC C and D lesions than the PTA group, and mean lesion length was longer. “The DCB group had more severe lesions concerning calcification and chronic total occlusions with 40.4% more than in PTA.”
Mustapha suggested it is important to note that this is the first global randomised trial to demonstrate safety of a DCB in BTK use, as “generally, in this very sick patient population, with an extremely challenging vascular bed, it is important to put this safety issue to rest: to know that you can use DCB in these severely diseased patients.”
The device has been submitted to the US Food and Drug Administration (FDA) for this indication.
The IN.PACT SFA trial’s co-principal investigator John Laird, from the Adventist Heart and Vascular Institute in St. Helena, USA, has presented the five-year outcomes at the Vascular Interventional Advances annual conference (VIVA; 5–8 November, Las Vegas, USA). The results demonstrate the maintained durability, safety and efficacy of the IN.PACT Admiral drug-coated balloon (Medtronic; DCB) in patients with peripheral arterial disease.
Using time-to-event survival analysis, the IN.PACT Admiral DCB continued to outperform the percutaneous transluminal angioplasty (PTA) control arm in freedom from clinically-driven target lesion revascularisation (CD-TLR) over the five-year follow-up period. The Kaplan-Meier estimate was 74.5% in the DCB group versus 65.3% in the PTA group (p=0.0196).
Long-term safety benefits included low rates of major target limb amputation (0.5%) and thrombosis (2.2%) in the DCB arm, and no device or procedure-related deaths through five years across the DCB and PTA arms.
Speaking at VIVA, Laird stated, “This is the bottom line: at five years, there was sustained benefit with regards to freedom from clinically driven target lesion revascularisation (CD-TLR), with a freedom from CD-TLR rate at 74.5% with drug-coated balloon, versus 65.3% with standard balloon angioplasty: a delta benefit of 9.2%.”
Beneficial outcomes for this patient cohort have been reported over the five years, with patency last presented at three years, and the CD-TLR endpoint at four and five years. While these benefits are indeed sustained in the long term, Laird noted that “we clearly see a narrowing of that benefit over time”.
He added that patients in the two groups were “well-matched with regards to their baseline characteristics. These were primarily claudicants, with moderate to severe claudication, and only 5% of patients had ischaemic rest pain. 20–26% had total occlusions, and only a minority had severe calcification—this was by trial design.”
“We tried hard to avoid provisional stenting in this trial, and were mostly successful: it was a 7.3% provisional stent rate in the DCB arm of the trial, and 12.6% in the PTA arm of the trial—this likely reflected some operator bias.”
Commenting on the low rate of reintervention, Laird maintained that “this is truly remarkable considering the complexity and progressive nature of PAD. For these patients, it means we are providing them with a long-term, durable solution that reduces the need for frequent reinterventions, leading to a potential improvement in their quality of life.”
Laird concluded by reiterating the long-term safety and efficacy of the DCB indicated by this trial’s results. He added, “this is the first independent adjudicated blinded randomised trial to demonstrate superior effectiveness of a drug-coated balloon through five years. […] There were no device procedure- or paclitaxel-related deaths through five years, and also very little thrombosis rates through five years. This trial demonstrated there is durable effectiveness of this particular drug-coated balloon for the treatment of femoropopliteal occlusive disease, and supports the fact that DCB can be considered a first-line therapy for this treatment area.”
Clinicians based at the Royal Stoke University Hospital (Stoke-on-Trent, UK) have developed a new protocol for uterine fibroid embolization (UFE), introducing a day case service option for these patients. Despite a body of opinion convinced that the immediate post-procedural phase is too painful to treat UFE patients on an ambulatory care basis, the study investigators report a near perfect success rate in the small initial patient cohort discharged on the same day as embolization.
Of the first ten patients to follow the new Stoke protocol, nine were discharged before 8pm and had no complications after 48 hours, as determined by a nurse-led follow-up phone call. One patient did progress to an overnight stay, but this was due not to any pain or complications, but to the fact that she had failed to disclose that there would be no adults at home to care for her overnight, a prerequisite of same day release from hospital.
David Wells (University Hospitals of North Midlands NHS Trust, Royal Stoke University Hospital, Stoke, UK) and co-authors conclude: “Using a collaborative, evidence-based approach, tailored to the specific needs of patients undergoing UFE, we were able to formulate a safe, effective and validated strategy for a day case procedure. We do expect some patients to be re-admitted for pain control. This should not be seen as a failure of day case, [but] rather a safety net for some patients.”
In a healthcare system under the strain of in-patient bed shortages, Wells and colleagues decided to review standard practice in order to “find ways of delivering effective therapy to patients in more efficient ways.” They worked with patients, anaesthetists, gynaecologists, and day case and surgical assessment units to provide women with the option of a day case procedure.
The adoption of a trans-radial arterial approach was crucial in facilitating this conversion of UFE treatment to a day case procedure for the Stoke team. Compared with a trans-femoral approach, Wells and colleagues found trans-radial access to dramatically reduce the risk of significant access site haemorrhages, and the approach allowed patients to mobilise immediately.
Describing their methods, the authors comment: “Closure of the radial arteriotomy is achieved using a variable compression wrist device. Once this radial band is removed (which takes on average 40 minutes) and the discharge protocol parameters met, the patient can be safely discharged. The only issue to manage then is pain.”
In 2017, the then current day case analgesia practices for patients undergoing gynaecological day case surgery were reviewed. Prior to revision, the strategy for managing patient’s ischaemic pain from embolizing the uterine arteries at the Royal Stoke University Hospital relied on preoperative anti-inflammatory medications and patient controlled anaesthesia during the procedure and overnight stay. However, patient controlled anaesthesia resulted in a significant number of patients with opioid related nausea and constipation—these were the main complaints seen in follow-up. Delays in taking down the patient controlled anaesthesia set-up led to significant discharge postponement for patients following an overnight stay.
Therefore, the study investigators researched other strategies for pain relief. They found that, given preoperatively, gabapentinoids provide anxiolysis for patients, and the authors cite evidence that this class of drugs significantly reduces opioid consumption in the postoperative period.
The authors give a detailed description of the development of this day case service, as well as the pain relief regimen and its rationale, in an article published in the New Journal of One Day Surgery.
John Kaufman, chair of the Department of Interventional Radiology and director of the Dotter Interventional Institute at the Oregon Health and Science University in Portland, USA, discussed this change in exhibitor space and what it means for the rising profile of IR in medical practice in the ITN [Imaging Technology News] podcastHear and Now: Intervention Rising.
“For many years, I think IRs have had a sense that there is not a lot for me here, particularly on the exhibit floor,” Kaufman said. “The programming has really developed beautifully. [There has been a] big emphasis on oncology and other aspects of IR. But the floor for the interventionalist has not been as interesting.”
He continued: “It supports the whole concept that we have been trying to promote of this really tight relationship [between mainstream diagnostic radiology and interventional radiology]”, a change exemplified by the RSNA’s dedication of a part of the exhibit floor to interventional products. Kaufman added that recent changes in certification by the American Board of Radiology (ABR) support this burgeoning relationship.
The ABR has recently created a new certification, called Interventional Radiology/Diagnostic Radiology (IR/DR). IR/DR joins just three other specialties certified by the Board—Diagnostic Radiology, Radiation Oncology and Medical Physics. The resulting new residency options available to medical students have created “tremendous interest” in IR.
iVascular has announced the completion of enrolment of patients in its T.I.N.T.I.N. (Treatment with the Luminor DCB and the iVolution self-expanding stent) study.
The effectiveness of drug-coated balloons (DCB) to inhibit restenosis in symptomatic superficial femoral artery (SFA) lesions has been proven in many studies. However, the longer and the more complex these lesions are, the more bailout stenting or spot stenting is necessary. Regarding self-expanding stents, the main advantage is the achievement of maximum arterial lumen gain. Nevertheless, the increase of restenosis in long-term results has been demonstrated in several studies, iVascular states in a press release.
The release adds, “What if we combine both therapies resulting in perfect treatment for complex lesions? A combination between the properties of Luminor, the DCB with the best outcomes in SFA and popliteal arteries, and the iVolution self-expanding stent, known for its high flexibility and radial force, can be the solution to avoid bailout stenting and restenosis in long-term results.”
The T.I.N.T.I.N. study aims at evaluating the 12-month outcomes of a combination therapy of the Luminor DCB and iVolution stent, in long TASC C and D femoropopliteal lesions. This prospective, multicentre, physician-initiated study is focused on the following endpoints:
Primary endpoint:
Freedom from clinically-driven target lesion revascularisation (TLR) at 12 months.
Secondary endpoints:
Primary patency rate at six- and 12-month follow-up
Technical success
Freedom from clinically-driven TLR at six-month follow-up
Clinical success at follow-up
Serious adverse events.
Koen Deloose (AZ Sint Blasius Dendermonde, Belgium), T.I.N.T.I.N. study principal investigator states, “The enrolment has just been completed, and we expect outstanding results from this trial, as both Luminor DCB and iVolution self-expanding stent are products that have proven their safety and efficacy in previous studies.”
The enrolment of 100 patients has been completed and the first outcomes of the study will be presented at LINC 2019.
The first patients in Germany have been treated with its Stealth 360 Peripheral Orbital Atherectomy System (OAS; Cardiovascular Systems Inc). The German cases represent the first commercial use of Peripheral OAS in Europe.
Tobias Achenbach, head of the Radiology Department at the St Vincenz Hospital, Cologne, Germany, where the first patients in Germany were treated, says, “CSI’s minimally invasive orbital atherectomy technology allows physicians to gently modify calcified plaque and enables peripheral revascularisation for patients with severely calcified arteries. The introduction of orbital atherectomy in Germany greatly improves the treatment options for my patients suffering from peripheral arterial disease.”
Dierk Scheinert, head of the Department of Medicine, Angiology and Cardiology, Park-Krankenhaus Leipzig, and Head Department of Angiology, University Hospital Leipzig Heart Center, Leipzig, Germany says, “Of those suffering from peripheral arterial disease, many progress to critical limb ischaemia, the most severe and potentially deadly form of peripheral arterial disease. If left untreated, critical limb ischaemia can lead to amputation. The unique ability of orbital atherectomy to safely treat calcified peripheral lesions, both above and below the knee, will allow physicians in Germany to help a very challenging patient population.”
In July 2018, CSI announced that it had signed an exclusive international distribution agreement with OrbusNeich to sell its coronary and peripheral OAS outside of the USA and Japan.
The first peripheral arterial disease (PAD) patient with disease in the superficial femoral and popliteal arteries has been successfully enrolled in the FORTEZ study. The single centre, single-arm non-randomised, prospective study will investigate the treatment of atherosclerotic lesions in the superficial femoral and/or popliteal arteries using the FLEX dynamic scoring catheter (VentureMed Group) plus drug-coated balloon (DCB).
The FORTEZ study is being conducted at the St Joseph Hospital in Fort Wayne, USA. The objective of the study is to assess safety and efficacy of the FLEX catheter in patients with atherosclerotic peripheral artery disease in the superficial femoral and popliteal arteries.
The FLEX catheter creates long parallel linear micro incisions in all plaque morphologies to prepare the vessel environment to facilitate angioplasty. Its dynamic technique safely scores difficult, diseased vessels, providing vessel compliance and acute lumen gain, a press release states.
“There are an increasing number of cases where vessel preparation before drug-coated balloon angioplasty is necessary to deliver the best outcomes. The FLEX catheter is showing potential to change the current practices,” says Lou Lopez, director Cardiac Catheterization Lab, Allen County Cardiology, St Joseph Hospital. Lopez adds, “We are excited to be part of the FORTEZ study and look forward to validating the many possible benefits of this potential clinical advancement.”
The first US patient has been enrolled in the Stellarex ILLUMENATE below-the-knee (BTK) investigational device exemption (IDE) study, led by principal investigators Bill Gray and Mahmood K Razavi. This global, prospective, randomised, multicentre trial is designed to assess safety and effectiveness of the Stellarex 0.014 drug-coated balloon (DCB) versus percutaneous transluminal angioplasty (PTA) in patients with critical limb ischaemia (CLI).
The trial will enrol 354 patients at 45 sites in USA, Europe and Australia in the next 12–18 months. The first patient in the USA was enrolled by Craig Walker at the Cardiovascular Institute of the South in Houma, Louisiana, USA.
“Several studies have shown the safety and durability benefits of the Stellarex balloon,” says Mahmood K Razavi, St Joseph’s Hospital in Orange, USA and principal investigator of the ILLUMENATE BTK study. “This study will look at findings that continue to demonstrate the benefits of the Stellarex 0.014 DCB for BTK peripheral arterial disease (PAD) and its safety and durability for patients. Given the challenging chronic nature of BTK PAD, we are hoping to find that through sustained patency using Stellarex, we can improve healing, and reduce target lesion revascularisation and major amputation.”
The Stellarex 0.014” OTW drug-coated balloon is designed to restore and maintain blood flow to arteries in patients with peripheral arterial disease. The Stellarex 0.014 drug-coated balloon is CE marked and available in Europe.
The FDA have given Medtronic approval to begin a clinical trial to evaluate the Symplicity Spyral renal denervation system in patients with hypertension who are already prescribed anti-hypertension medications. A press release states that the SPYRAL HTN-ON MED trial is the latest prospectively powered, randomised, sham-controlled study within the broader SPYRAL HTN global clinical programme, and that the study will evaluate a patient population comparable to what physicians typically encounter in daily practice—patients with uncontrolled blood pressure taking multiple antihypertensive medications.
The press release adds that the design of the ON MED trial builds on the randomised sham-controlled SPYRAL HTN-ON MED pilot study that was published in The Lancet earlier this year; this 80-patient pilot study demonstrated statistically significant and clinically relevant reductions in both office and 24-hour systolic blood pressure in patients who had uncontrolled hypertension despite receiving optimal medication. Notably, those blood pressure lowering effects were observed not only throughout the daytime, but also during the night time and early morning periods when myocardial infarction and stroke risk due to hypertension are highest, resulting in the observation that renal denervation is “always on”.
The ON MED trial is a 2:1 randomised, sham-controlled study and will randomise up to 340 patients at 55 centres in the USA, Japan, Europe, Australia and Canada. Patients will be followed out to three years. Primary safety endpoints will include major adverse events at one month and new renal artery stenosis at six months. The primary efficacy endpoint is 24-hour ambulatory blood pressure at six months. Patients will be prescribed a stable regimen of up to three antihypertensive medications, including diuretics, calcium channel blockers, ACE/ARB inhibitors or beta blockers.
David Kandzari (Piedmont Heart Institute, Atlanta, USA), principal investigator and member of the SPYRAL HTN Global Clinical Program Executive Committee, says: “A broad range of patients have hypertension today, many of whom remain uncontrolled despite being prescribed a variety of medications; the consequences of uncontrolled hypertension represent both a substantial impact to public health and a large unmet need in medicine for new approaches. This trial will add yet another critical piece to the renal denervation evidence basis and is designed to build on the success of our pilot study, which showed a benefit for renal denervation in an on-med patient population.”
Dave Moeller, vice president and general manager of the Coronary and Renal Denervation business, which is part of the Cardiac and Vascular Group at Medtronic, comments: “Medtronic is committed to building a robust global renal denervation clinical program with results from several randomised, sham-controlled, prospectively-powered, blinded clinical studies, in both the absence and presence of prescribed medications. Results from the ON MED trial will add to the growing body of evidence supporting renal denervation and is intended to support clinicians in making treatment decisions for patients who might benefit from this procedure.”
Further research into the use of percutaneous irreversible electroporation (IRE) in the treatment of pancreatic cancer is essential, according to Govindarajan Narayanan, chief of Interventional Oncology at the Miami Cancer Institute, and professor of Radiology at Florida International University (USA). He made this call at the Spectrum conference (1–4 November, Miami, USA).
“We now see a signal towards possible survival benefits, so a registry and probably a randomised controlled trial to really understand the role of IRE in pancreatic cancer is definitely an unmet need,” he told conference attendees. He added that a comprehensive mechanism for follow-up criteria and protocols for locally advanced pancreatic cancer patients who have had radiotherapy should also be developed and validated.
Until recently, treatment options for pancreatic cancer were surgery, for which only 10–20% of patients will qualify, radiation or chemotherapy, or a palliative treatment algorithm. Narayanan assessed the role of percutaneous IRE to see whether it can be performed in a minimally invasive and reproducible fashion, and what its impact has been on the signal to survival benefit. “After using this technology in the pancreas for the last nine years,” he said, “there are a few things we have learned.”
He ran through the trials to date that have looked at the safety and efficacy of the procedure. The first two he cited were from his own centre. In 2012, his group did a retrospective series on 14 patients looking at percutaneous IRE for down-staging and control of unresectable pancreatic adeonocarcinoma. They followed this with a further retrospective study in 2017, on percutaneous image guided IRE for the treatment of unresectable locally advanced pancreatic adenocarcinoma. This single centre study of 50 patients, all of whom had biopsy-proven unresectable pancreatic cancer, assessed the safety profile, with a secondary objective of determining overall survival. All patients had had chemotherapy, and 60% had also had prior radiation therapy; follow-up was computed tomography (CT) at one month and every three months thereafter.
The median time from diagnosis to IRE was 11.6 months, and there were serious adverse events in 10 of 50 patients (20%)—seven suffered abdominal pain, and one each had pancreatitis, sepsis, and a gastric leak. Narayanan described the finding of 27 months from time of diagnosis and 14.2 months from IRE as “a healthy median overall survival”. There were no treatment-related deaths, and no 30-day mortality.
“We did a multivariate analysis to see if there was any different predictor that helped with overall survival. We found that tumour size <3cm had significantly longer overall survival than tumour sizes that were >3cm.”
Also in 2017, Hester Scheffer (Amsterdam, The Netherlands) et al published the findings of the PANFIRE study, which looked at ablation of locally advanced pancreatic cancer with percutaneous IRE. “The purpose of this study was to investigate the safety,” explained Narayanan, “but also to look at the quality of life, pain perception and efficacy in terms of time to local progression, event free survival, and overall survival. It found that percutaneous IRE for locally advanced cancer is generally well tolerated, although there were some major adverse events. And preliminary survival data were encouraging.”
An Italian study from Maria Belfiore (Naples, Italy) et al in 2017 outlined the preliminary experience of using percutaneous CT-guided irreversible electroporation followed by chemotherapy as a novel neoadjuvant protocol in 20 patients with locally advanced pancreatic cancer. No major complications occurred—although two patients died three and four months after treatment, this was due to rapidly progressive disease. In the remaining 18 patients, six-month imaging follow-up showed a volumetric decrease in the lesion size of 42.8%, and three patients underwent R0 resection. The investigators concluded that IRE followed by chemotherapy is safe, feasible, and effective in producing short-term control of locally advanced pancreatic adenocarcinoma (LAPC) with a possible down-staging effect to resectable lesions.
In the UK, Edward Leen (London, UK) et al conducted a retrospective review from 2011 to 2016 of 75 patients who had unresectable pancreatic carcinoma and underwent percutaneous IRE after chemotherapy using computerised tomography guidance under general anaesthesia.
Post-procedural immediate and 30-day mortality rates were both zero, and all grade adverse events were 25%. The median in-patient stay was one day, described by Narayanan as “typical of percutaneous IRE; you have a significant advantage there, one to one and a half days stay in the hospital.”
The median overall survival and progression free survival rates post-IRE for LAPC were 27 and 15 months, respectively—“very similar to other results that have been achieved”.
Narayanan pointed out: “Prospective and retrospective studies have established the safety of this procedure, and studies from different centres around the world have shown that this technique is reproducible, with a positive signal towards survival benefit. The US Food and Drug Administration has recently provided a breakthrough designation for IRE in pancreatic cancer.”
He said that further developments would follow, and promised: “We are hoping to have more exciting news in this space very soon.”
A study presented at VIVA 2018 (5–8 November, Las Vegas, USA) by Maureen Kohi, associate professor of Clinical Radiology, University of California, San Francisco, USA, has found similar patency outcomes in women and men after treatment with the Stellarex DCB and calls for further research in the area.
The purpose of the trial was to evaluate sex-related differences in the outcomes of the Stellarex drug-coated balloon (DCB, Philips) for the treatment of femoropopliteal arterial disease. A subgroup analysis of the DCB cohort of the Europe and US ILLUMENATE trial was performed. The study endpoints included primary safety and efficacy at 12 months and were compared between men and women. To identify predictive factors for patency, a multivariable predictor analysis was performed.
The study included a total of 418 patients with 269 men (64%) and 149 women (36%). The female subgroup was significantly older compared to men. The mean reference vessel diameter was significantly smaller and the lesion length was significantly longer in the female subgroup compared to the male subgroup.
There was no significant difference in the 12-month primary patency rate or clinically driven target lesion revascularisation rate between men and women. The multivariate analysis demonstrated that reference vessel diameter, lesion length, previous intervention in study limb, severe calcification, and geographic miss were predictors of patency.
Based on this study, despite older age, more comorbidities, and worse vessel and lesion characteristics, women had similar patency outcomes compared to men after treatment with the Stellarex DCB. As a result, Kohi said that further evaluation of the efficacy of DCBs is necessary to understand the disparate nature of the disease progression and to optimise treatment outcomes in women with peripheral arterial disease.
Data from the PREVEIL early feasibility study of the SurVeil drug-coated balloon (DCB, Surmodics) were shared in a late-breaking clinical trial presentation at the Vascular Interventional Advances conference (VIVA; 5–8 November, Las Vegas, USA). PREVEIL is a prospective, US, multicentre, single-arm trial designed to assess the safety and feasibility of the SurVeil DCB in the treatment of patients with symptomatic peripheral arterial disease (PAD) due to de novo lesions of the femoral and popliteal arteries.
Twelve-month data from the study show that acute success measures of safety were achieved in 100% of patients. No patients required re-intervention of either the target lesion or the target vessel at 12 months (100% freedom from clinically driven target lesion revascularisation and target vessel revascularisation (CD-TLR or CD-TVR)). The results also demonstrate continued significant improvement in Rutherford classification, resting ankle brachial index (ABI), and walking impairment questionnaire (WIQ) including walking distance, walking speed and stair-climbing scores at 12 months.
As was presented with the six-month results, median paclitaxel plasma concentration peaked immediately post-procedure (Cmax 1.07ng/mL) and was undetectable at 30 days. Secondary technical, device, and procedure success criteria were achieved. The SurVeil DCB is not yet approved for sale in the USA.
“The ongoing positive results from this study demonstrate that the SurVeil DCB has the potential to be a next-generation DCB with improved efficacy of drug transfer,” said Kenneth Rosenfield, section head, Vascular Medicine and Intervention at Massachusetts General Hospital, and US co-principal investigator for the TRANSCEND trial. “These 12-month data continue to support the functionality and safety of the device.”
Data presented include 12-month results from 13 patients (Rutherford class 2 to 4) at three clinical sites who were treated with the SurVeil DCB. Average lesion length was 56mm. Clinical assessments for the study include primary patency and late lumen loss through six months, plasma paclitaxel levels, and changes in Rutherford classification, ABI/TBI, six-minute walk test, and WIQ at one, six, 12, 24 and 36 months. Key secondary safety endpoints included freedom from major vascular complications, evidence of paclitaxel toxicity, or thrombolysis in myocardial infarction (TIMI).
In July 2017, Surmodics received an investigational device exemption (IDE) from the US Food and Drug Administration (FDA) to initiate a pivotal clinical trial of the SurVeil DCB, and the first patient was enrolled in October 2017. The randomised trial, TRANSCEND, is designed to evaluate the SurVeil DCB for treatment for PAD in the upper leg compared to the Medtronic IN.PACT Admiral DCB.
VentureMed Group has announced the initiation of a new study to determine if the FLEX Dynamic Scoring Catheter reduces dissections and the need for bailout stents in peripheral arteries. The study entitled “Arterial Dissections Following FLEX Scoring and Adjunctive Balloon Angioplasty: Intravascular Ultrasound Assessment and Correlation with Angiographic Findings” will utilise intravascular ultrasound (IVUS) to identify the health of the vessel after treatment.
Nicolas W Shammas, founder and director of the Midwest Cardiovascular Research Foundation in Davenport, USA is the principal investigator for the study. This study is the second iDissection study performed by Shammas. The first study revealed that after atherectomy, in the peripheral arteries, significant dissections are more visible by a ratio of 6:1 when using IVUS in comparison to the typical angiogram. Deducing that the presence and severity of dissection after atherectomy may have been underestimated, especially for deeper dissections which are associated with recurrent restenosis, recoil, and possibly acute closure.
“After the indicative results of the initial iDissection study, I am motivated to look for vessel prep devices that further reduce the need for provisional stenting,” says Shammas. “I am optimistic about the ability of the FLEX Catheter to reduce the rate of high-grade dissections and looking forward to the evaluation.”
Using IVUS, the new study will evaluate the dissection rates of 15 patients following treatment of femoropopliteal de novo or no-stent restenosis by the FLEX Dynamic Scoring Catheter and plain old balloon angioplasty (POBA).
The Tack Optimized Balloon Angioplasty II (TOBA II) clinical trial has successfully achieved both primary and secondary endpoints. One year results from the TOBA II study were presented in the late-breaking scientific session by William Gray, system chief, Division of Cardiovascular Disease at Main Line Health, president, Lankenau Heart Institute and principal investigator for the TOBA II trial at VIVA (5–8 November, Las Vegas).
The first peripheral vascular study to enrol patients with 100% dissected vessels, the TOBA II study, was conducted at 33 US and European sites to investigate the Tack Endovascular System (Intact Vascular) for the repair of post-angioplasty dissections in femoropopliteal arteries. All patients enrolled (n=213) suffered from peripheral arterial disease (PAD), underwent balloon angioplasty with either plain or drug-coated balloons, and consequently experienced at least one dissection, with 69.4% being classified as severe.
Results presented from this first-of-its-kind study demonstrated 92.1% complete dissection resolution within a clinically challenging patient population, along with 79.3% K-M vessel patency and 86.5% K-M freedom from clinically driven reintervention at 12-months. Additionally, the TOBA II study validated the Tack implants as stable and durable, with zero implant fractures, 99.9% freedom from migration, and a 0.5% bailout stent rate.
“The TOBA II study is unique in that it is the first large scale pivotal evaluation in peripheral arterial vessels that are 100% dissected following initial angioplasty and treated with a precisely targeted implant,” commented William Gray. “This study introduces a new therapeutic paradigm, demonstrating that we can repair dissected arteries, leaving minimal metal behind to preserve future treatment options for our patients, and producing excellent 12-month outcomes.”
“As presented today, the TOBA II data further augment the growing body of evidence supporting the idea that a purpose-built implant for dissection repair can enhance the clinical results of balloon angioplasty,” said Bruce Shook, Intact Vascular’s president and CEO. “The Tack Endovascular System is also well aligned with a primary goal of endovascular operators: to leave as little metal behind as possible.”
Results from an aggregated data analysis of the use of the Zilver PTX drug-eluting peripheral stent (DES; Cook Medical) in challenging patient populations concluded that risk factors such as Rutherford classification, sex, calcification and diabetes did not have a significant impact on the target lesion revascularisation (TLR) rate in patients treated with the Zilver PTX stent.
“It is generally thought that sex, calcification and diabetes may have an impact on TLR, but these data demonstrate that these factors do not,” said Mark Breedlove vice president of Cook Medical’s Vascular division. “In this global analysis of Zilver PTX patients, these characteristics did not have a significant impact on TLR.”
The global data analysis on the world’s first drug-eluting stent in the superficial femoral artery (SFA) included nearly 2,400 patients from 16 countries who participated in one of five Zilver PTX studies. This included three pre-market studies in North America, Asia and Europe and two post-market studies in the USA and Japan. The study sought to identify the impact of patient and lesion factors on freedom from TLR at one year. The results indicated that factors typically impacting reintervention rates did not have an impact on the reintervention rates for patients treated with the Zilver PTX stent.
“With an unrivaled five years of data gathered from these studies, Zilver PTX has shown long-term benefits in real-world outcomes. This is a significant amount of data that informs how we continue to work alongside physicians to fight this disease,” said Breedlove. “We’re committed to helping patients who deal with the impact of PAD on their lives.”
Zilver PTX5 was the first DES in the USA used in the treatment of PAD and is the only drug-eluting superficial femoral artery stent with five-year data. As previously published, patients treated with the Zilver PTX stent achieved a higher percentage of freedom from TLR compared to standard of care endovascular treatment, resulting in 91% freedom from TLR at one year and 76% at five years. Zilver PTX has been shown to cut reinterventions by nearly half through five years compared to both bare metal Zilver stents and a combination of bare-metal Zilver stents and percutaneous transluminal angioplasty (PTA).
The five-year and final results from the pivotal IN.PACT SFA Trial and one-year all-subjects results from the Total IN.PACT Pooled Analysis of the IN.PACT Admiral drug-coated balloon in patients with peripheral arterial disease (PAD) in the superficial femoral (SFA) and popliteal arteries were presented in two late-breaking clinical trial presentations at the Vascular Interventional Advances conference (VIVA; 5–8 November, Las Vegas, USA).
IN.PACT SFA Trial
John Laird, medical director of the Adventist Heart and Vascular Institute and co-principal investigator for the IN.PACT SFA Trial presented the first, five-year clinical outcomes for a commercially available DCB, further demonstrating the durability, safety, and efficacy of IN.PACT Admiral DCB in patients with PAD.
Using time-to-event survival analysis, IN.PACT Admiral DCB continued to outperform the percutaneous transluminal angioplasty (PTA) control arm in freedom from clinically-driven target lesion revascularisation (CD-TLR) over the five-year follow-up period. The Kaplan-Meier estimate was 74.5% in the DCB group versus 65.3% in the PTA group (log-rank p= 0.0196). The data also showed the long-term safety benefits of IN.PACT Admiral, with low rates of major target limb amputation (0.5%) and thrombosis (2.2%) in the IN.PACT Admiral DCB arm, and no device or procedure-related deaths through five years in both the IN.PACT Admiral DCB and PTA arms.
“With the data presented today at VIVA, we continue to see sustained clinical benefit of IN.PACT Admiral with three quarters of DCB patients in the study not requiring a reintervention through five years,” said Laird. “This is truly remarkable considering the complexity and progressive nature of PAD. For these patients, it means we are providing them with a long-term, durable solution that reduces the need for frequent reinterventions, leading to a potential improvement in their quality of life.”
Total IN.PACT Pooled Analysis: All-Subjects
Mehdi Shishehbor, director of the Heart and Vascular Institute, University Hospitals Cleveland Medical Center, presented one-year all-subjects data from the Total IN.PACT Pooled Analysis-the largest collective, independently adjudicated DCB series to-date. The data showed that IN.PACT Admiral DCB demonstrated consistently superior safety and freedom from clinically-driven target lesion revascularisation (CD-TLR) compared to standard PTA alone.
The all-subjects analysis evaluated all 1,837 DCB and 143 PTA patients from across IN.PACT Admiral clinical programmes, including IN.PACT SFA, IN.PACT Global, IN.PACT SFA Japan, and IN.PACT SFA China studies. Results showed that IN.PACT Admiral DCB outperformed the PTA control arm in freedom from CD-TLR with a Kaplan-Meier estimate of 93.8% in the DCB group versus 80.2% in the PTA group (log-rank p<0.001). Additional safety and effectiveness outcomes from the DCB arm also included low rates of thrombosis (2.5%), major target limb amputation (0.2%), and all-cause mortality (3.1%) through one-year in a large PAD patient population.
“With Total IN.PACT, we are able to show that IN.PACT Admiral is the first DCB to demonstrate strong and consistent efficacy in lesions up to 360mm,” said Shishehbor. “The data from the all-subjects analysis also confirm IN.PACT Admiral DCB’s superior safety and freedom from reintervention rate at one year, while offering important information to help enhance treatment decisions. These one-year data, combined with the five-year data also presented today, provide physicians with additional confidence in using IN.PACT Admiral DCB as a primary therapy over PTA.”
Clinical outcomes from the IMPERIAL Long Lesion Sub-study were presented at VIVA (5–8 November, Las Vegas, USA) demonstrating that the Eluvia drug-eluting vascular stent system (Boston Scientific) is safe and effective in treating patients with long, complex, calcified lesions within the superficial femoral and proximal popliteal arteries.
The global randomised controlled IMPERIAL trial, which evaluated the Eluvia Stent System in patients with symptomatic peripheral arterial disease (PAD), included a single-arm analysis of 50 patients with femoropopliteal artery lesions 140–190 mm in length. Baseline characteristics of the patients included an average lesion length of 162.8±34.7mm, with 70% of lesions classified as moderately to severely calcified and 32% with chronic total occlusions. Due to the severity of their disease, these patients were also experiencing claudication.
The study results demonstrate that the primary patency rate, a measure of the target vessel remaining unobstructed at 12 months, was 87.9%. Study participants also experienced low rates of target lesion revascularisation (TLR), at 6.5%, indicating a reduced need for repeat procedures at one year. Additionally, these patients reported significant improvement in the decrease of their leg pain and discomfort.
“The lesion lengths, disease complexity and the baseline characteristics presented in this sub-study is more representative of what clinicians see on a daily basis when treating patients with severe cases of peripheral artery disease,” said William Gray, system chief, Division of Cardiovascular Disease at Main Line Health, president of Lankenau Heart Institute in Wynnewood, USA, and co-principal investigator of the IMPERIAL trial. “The results from this long lesion sub-study, combined with those observed in the global randomised controlled IMPERIAL trial, MAJESTIC and other studies suggest that the Eluvia stent, with its sustained drug release design, is a highly effective treatment option for femoropopliteal disease even in more complex lesion types.”
In the IMPERIAL trial, the first randomised head-to-head trial comparing two different drug-eluting stent systems for the treatment of PAD, the Eluvia stent demonstrated superior results as patients experienced significantly greater 12-month primary patency of 88.5%, compared to 79.5% in patients treated with the Zilver PTX Stent System from Cook Medical (p=0.0119). In addition, patients treated with the Eluvia stent had half the target lesion revascularisation rate of Zilver PTX at 12 months, a 4.5% TLR rate for Eluvia versus 9% TLR rate for the Zilver PTX cohort.
As a result of the IMPERIAL Long Lesion Sub-study findings, the Eluvia stent received approval from the US Food and Drug Administration (FDA) to treat long lesions within the superficial femoral and proximal popliteal arteries, up to 190mm in length, in patients with peripheral arterial disease. The Eluvia stent received approval from the FDA in September of 2018 and CE Mark in February of 2016.
Rivaroxaban (brand name Xarelto, Bayer) has received approval from the US Food and Drug Administration (FDA) and the European Commission to reduce risks in peripheral arterial and chronic coronary disease patients. The oral anticoagulant is indicated in combination with aspirin, and is now the first and only Factor Xa inhibitor approved for patients living with these conditions.
Both approvals are based on results from the landmark COMPASS trial, which showed a significant 24% reduction of the risk of major CV events in patients with chronic coronary arterial disease (CAD) and/or peripheral arterial disease (PAD) with a 2.35mg vascular dose of rivaroxaban twice daily plus aspirin 100mg once daily, compared to aspirin alone. This finding was driven by a 42% reduction in stroke, 22% reduction in cardiovascular (CV) death, and 14% reduction in heart attack. The risk of major bleeding was significantly higher in patients taking the rivaroxaban/ aspirin regimen compared to aspirin alone, with no significant increase in fatal or intracranial bleeds.
Derek Connolly, consultant interventional cardiologist at Birmingham City Hospital (Birmingham, UK) and COMPASS trial investigator commented: “Cardiovascular diseases are one of the leading causes of death in the UK, and coronary artery disease and peripheral arterial disease represent a major public health burden—despite many advances in the area of cardiovascular care, CAD and PAD have remained an area of unmet need. Even with currently available treatments for secondary prevention, patients remain at an unacceptably high risk of thrombotic events which can lead to disability, loss of limb and death. This was the biggest study of rivaroxaban to date, and now that it is licensed for these conditions, it provides UK clinicians with a new option for treating CAD and PAD.”
Lars Bruening, CEO Bayer UK & Ireland, said: “The story and momentum behind the COMPASS data continues to grow—from the study being stopped one year early for overwhelming efficacy, the presentation of the results themselves at the European Society of Cardiology congress last year, and now to this exciting news from the European Commission. Ten years ago this October saw Bayer just starting out on the Xarelto journey with the first indication in orthopaedics—and this year we welcome our eighth indication for the management of patients with CAD and PAD in the UK. It is especially exciting to see the continuing impact that Xarelto will have on patients with PAD, most of whom have concurrent CAD, as it has been many years since a new medical therapy has been proven in this high risk patient population.”
Following the license approval across Europe,the new indication will be submitted to the National Institute for Health and Care Excellence (NICE) and the Scottish Medicines Consortium (SMC) for review for routine reimbursement across the UK.
“Despite the use of guideline-recommended therapies, patients with chronic CAD and/ or irreversible CV event,” said Paul Burton, vice president, Medical Affairs. “The new Xarelto vascular 2.5mg dose, when used with aspirin, represents a true breakthrough for patients with chronic CAD and PAD.”
“Treating patients with aspirin only is simply not enough to address the underlying thrombotic risk that comes with chronic CAD and PAD,” said Kelley Branch, associate professor in Cardiology, University of Washington, Seattle, USA. “As we saw in the COMPASS trial, the dual pathway approach of aspirin and the 2.5mg, twice-daily dose of Xarelto can help significantly reduce the risk of CV events in these populations.”
In a joint, global position statement, the Society of Interventional Radiology (SIR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE) and the Interventional Radiology Society of Australasia (IRSA) have committed to providing necessary stroke training to interventional radiologists in order to alleviate the shortage of physicians trained in endovascular stroke therapies.
The ability for patients to access thrombectomy care remains stymied by geography and a shortage of interventional physicians, despite the American Heart Association’s and multiple international stroke organisations’ recommendations that endovascular thrombectomy (EVT or clot removal) be the standard of care for patients suffering acute ischaemic stroke caused by blocked arteries.
“The shortage of physicians and comprehensive stroke centres providing EVT has been confirmed by the stroke neurology community, who recommend that patients be treated locally rather than having long transfer delays,” the joint statement said.
“Appropriately trained interventional radiologists can evaluate stroke patients and provide emergent EVT with good outcomes; especially where neurointerventional physicians are not available.”
Interventional radiologists can also help provide 24/7 care in partnership with neurointerventional physicians where they are available, the statement said.
Endovascular thrombectomy is proven to save lives and improve outcomes for patients suffering acute ischaemic strokes. Patients who undergo these clot-removing treatments not only survive in greater numbers, but also have fewer resulting disabilities and are able to recover functions faster than best medical therapy.
“Reversing symptoms from these strokes requires rapid and safe removal of the occluding thrombus,” the societies said in the statement. Allowing interventional radiologists to join their neurology, neurointerventional and neurosurgeon colleagues on care teams and allowing them to be part of certified stroke centres will greatly increase access to this critical treatment, they said.
SIR is already revising its current stroke training guidelines to support expanded patient access to interventional stroke treatment. The training pathway will reinforce Joint Commission and American Heart Association requirements for physicians operating in thrombectomy-capable stroke centres and comprehensive stroke centres. In September, the Joint Commission and American Heart Association announced they would hold a dialogue with provider organisations to discuss requirements as the organisations work to update certification criteria for both thrombectomy-capable and comprehensive stroke centres.
Back in February 2018, the Joint Commission announced revised eligibility requirements for the Thrombectomy-Capable Stroke Centre (TSC) certification program. The revised eligibility included a requirement for all primary neuro-interventionists (i.e., those who routinely take call to perform emergency mechanical thrombectomy) to either be certified by the Committee for Advanced Subspecialty Training (CAST) or to meet similar criteria, including education, training, and experience performing 15 mechanical thrombectomies over the past 12 months or 30 over the past 24 months. In the May 2018 edition of Perspectives, the Joint Commission announced that this same requirement would be applied to Comprehensive Stroke Centres.
Since the publication of these revised eligibility criteria, a number of individuals and organisations have raised concerns about the individual physician training requirement for CAST certification or the equivalent. First, many expressed that the requirement is overly stringent and is not necessary to ensure that patients at TSCs and CSCs receive high quality mechanical thrombectomy because CAST certification requires training and ongoing experience in a number of procedures other than mechanical thrombectomy (e.g., interventions for aneurysms and arteriovenous malformations).
Second, the training requirement excludes many highly qualified individuals, i.e., interventional radiologists who have training and experience in neurovascular interventions and have been performing mechanical thrombectomy successfully for years. The Joint Commission originally thought these individuals could become CAST certified through the Practice Pathway; however, this is not possible for them because they are not doing other neuroendovascular procedures required for individual CAST certification.
SIR president M Victoria Marx, an interventional radiologist at Keck Medicine of the University of Southern California, USA, said, “SIR strongly believes that interventional radiologists have a current and growing role in the care of patients with ischaemic strokes. We stand committed to advocate for policy changes and provide the cognitive and technical skills and resources necessary for interventional radiologists to provide high-quality care.”
Thirdly, limiting eligibility with these requirements could adversely affect access to mechanical thrombectomy. One health care system said they had no physician in their system that met the training requirement. The system provided data showing that the clinical outcomes for their eight interventional radiologists were similar to those reported in clinical trials.
In addition, the Society of Interventional Radiology sponsored an independent analysis of which specialties were performing mechanical thrombectomies for Medicare patients. Of the 5,914 claims, 37% were performed by physicians who identified themselves as diagnostic radiologists, 27% by neurosurgeons, 20% by neurologists, and 16% by interventional radiologists.
Concerns have also been raised pertaining to the individual physician volume requirement of 15 mechanical thrombectomies over the past 12 months or 30 over the past 24 months, adopted by the Joint Commission based on CAST requirements. Analyses conducted by one healthcare system showed that only three of the eight interventional radiologists in their system were at or near this benchmark.
The CAST volume requirement was adopted by the Technical Advisory Panel of the Joint Commission because it was a concrete benchmark used by a national organisation.
However, the panel acknowledged that there were no adequately powered studies available to determine a distinct threshold for a physician volume-outcome relationship.
In addition, SIR sponsored an independent analysis of the 2016 Centers for Medicare and Medicaid Services (CMS) Physician Supplier and Provider Services (PSPS) files and Provider Utilization File (PUF). Of the 995 physicians who billed under code 61645 (percutaneous arterial transluminal mechanical thrombectomy and/or infusion for thrombolysis, intracranial, any method, including diagnostic angiography, fluoroscopic guidance, catheter placement, and intraprocedural pharmacological thrombolytic injections), 842 (85%) billed for 10 or fewer procedures. For the 153 (15%) physicians who performed more than ten procedures, the median number of procedures was still only 15.
This analysis is limited because it does not include procedures billed to private insurers or Medicare advantage plans, the procedures under the target billing code are heterogeneous, and the data are from 2016 when the indications for mechanical thrombectomy were more restrictive than current ones. Despite these limitations, the data raise important questions about whether the current individual physician volume requirements for the TSC and CSC certification programmes would exclude too many qualified individuals.
The Joint Commission and the American Heart Association believe that additional dialogue is needed with national stakeholder organisations to discuss individual physician training and volume requirements.
For these reasons, the Joint Commission suspended the individual physician training and procedure volume requirements for both the TSC and CSC certification programmes, in September 2018. The facility volume requirement of 15 mechanical thrombectomies per year will still be in force for both certification programmes, however. In an Autumn statement, the Joint Commission said: “We hope to establish new, more appropriate individual physician requirements within the next six months.”
Stroke affects 16.9 million worldwide each year, with 795,000 new cases in the USA annually. Approximately 100,000 of the US cases are eligible for EVT treatment, yet only a fraction are treated due to the shortage of thrombectomy-capable stroke centres. To meet that volume, the USA would need 500 endovascular stroke centres and 2,000 physicians. It currently has 231 thrombectomy-capable stroke centres.
Raman Uberoi (Oxford, UK) tells Interventional News at CIRSE 2018 in Lisbon, Portugal, that offering any treatment for abdominal aortic aneurysms, be it endovascular aortic repair (EVAR), open surgery, or best medical therapy, should depend on putting the patient at the heart of the decision-making process. Even though he is an endovascular enthusiast, Uberoi calls for surgery to be used in the cases for which it is the more appropriate option. “Just because we can perform EVAR, does not mean that we should,” he states while outlining the anatomical features of the aneurysmal neck that need to be considered before the decision to perform an EVAR is made.
Eximo Medical has announced it has received 510(k) clearance from the US Food & Drug Administration (FDA) for its B-Laser atherectomy system for peripheral arterial disease (PAD). B-Laser is a transformative 355nm wavelength laser technology designed to address unmet clinical needs for treating multiple vascular indications. The specific indication cleared by the FDA is: “The B-Laser atherectomy system is intended for use in the treatment, including atherectomy, of infrainguinal stenoses and occlusion, including in-stent restenosis (ISR).”
“This clearance represents a significant milestone for Eximo, as we can now offer the B-Laser atherectomy system for PAD in the USA. This is the first 355nm laser system cleared in the US for this purpose and, according to the clinical results and the feedback that we received from physicians, it seems that this wavelength provides significant advantages over traditional 308nm excimer lasers in term of safety, efficacy, cost and ease of use,” said Yoel Zabar, CEO of Eximo Medical. “We also plan to leverage our B-Laser platform technology to develop additional devices to address significant unmet needs in other vascular indications, including lead extraction (for which we have completed a proof of concept), coronary artery disease, thrombectomy and venous disease. Additionally, we are developing an add-on diagnostic tool and disruptive medical device for interventional gastrointestinal procedures.”
Clinical evaluation of the B-Laser device in the intended population was performed in a prospective, single-arm, multicentre, open-label, non-randomised pilot clinical study in 50 subjects in Europe, as well as in a pivotal, prospective, single-arm, multicentre, open-label, non-randomised IDE clinical study in 97 subjects in USA and Europe.
In the pilot clinical study, the results presented 100% success in crossing the target with no device related peri-operative clinically significant adverse events and no complications requiring intervention. There were no major adverse events (MAE) at one month or six months following the procedure, and only two cases (4.3%) of target lesion revascularisation among 46 subjects who completed the one-year post procedure follow-up. In the pivotal study, the safety and efficacy primary endpoints were achieved with high margins and the six-month data was consistent with the pilot study results.
“I used the B-Laser in challenging procedures during the pivotal study and found the device easy to set up and use, and a valuable addition to our treatment portfolio,” said the national PI, John Rundback, interventional radiologist and director of the Interventional Institute at Holy Name Medical Centre, Teaneck, USA. “The enrolment in both US and Europe was quick (6.5 months), and the study results up to six months have been very impressive despite treating diverse lesions such as calcium, thrombus, and restenosis (including in-stent restenosis), both above and below the knee.”
Humacyte has announced the initiation of a US phase II vascular trauma clinical trial of Humacyl, its investigational human acellular vessel, for vascular replacement or reconstruction in patients with life- or limb-threatening vascular trauma.
The phase II vascular trauma study was initiated last month and will be conducted at six sites in the USA. The trial will evaluate approximately 40 adult patients with life- or limb-threatening vascular trauma that require surgical repair. Enrolment in the trial has begun and will continue for 24 months. The initial patients were enrolled at Rutgers University Hospital in Newark, USA and R Adams Cowley Shock Trauma Center in Baltimore, USA; other sites expected to enrol patients include Johns Hopkins University in Baltimore, USA; Marcus Trauma Center in Atlanta, USA; Ryder Trauma Center in Miami, USA; and Rocky Mountain Regional Trauma Center in Denver, USA.
“As pioneers in regenerative medicine and vascular research, we believe we have a unique and compelling solution to reduce the significant loss of life related to traumatic vascular injuries of civilian victims of violent crimes, automobile accidents, industrial incidents and more,” says Jeffrey Lawson, president and chief executive officer of Humacyte. “Humacyl has the potential to be a first-in-class therapy for long-term blood vessel restoration or reconstruction of traumatic vascular injuries, and the advancement of our phase II study represents a significant milestone to investigate the potential of Humacyl in clinical vascular trauma.”
“A tremendous medical need exists for patients with traumatic injuries who are in need of vascular reconstruction both in the civilian and military populations,” says Michael Curi, chief, Division of Vascular Surgery with Rutgers University. “Advancements in tissue engineering, such as Humacyte’s bioengineered vessel, have the potential to be a game-changer for both patients and the brave members of our armed forces who may experience this critical need. Rutgers University is thrilled to participate in this significant investigational phase II vascular trauma clinical study as part of our ongoing commitment to improve the lives of every patient, every day.”
“As a world leader in trauma research, we are constantly exploring new and innovative approaches to treating life threatening injuries,” says Thomas Scalea, Francis X Kelly Distinguished Professor of Trauma, University of Maryland School of Medicine and physician-in-chief, R Adams Cowley Shock Trauma Center, University of Maryland. “We look forward to evaluating this bioengineered blood vessel in the treatment of appropriate patients requiring vascular surgical repair.”
The first patient in this phase II vascular trauma study was enrolled in the USA in September 2018, and has now surpassed 30 days in the study. Humacyte anticipates top line patient data from this investigative study to be available in late 2020.
Vascular trauma remains a major cause of morbidity and mortality. In October 2017, Humacyte announced that the company received a Broad Agency Announcement (BAA) contract award from the United States Department of Defense (DoD) to help support the addition of clinical sites for this investigative trial.
Humacyte’s Humacyl is also currently in a phase III pivotal trial in the USA and Europe as a conduit for haemodialysis in patients with end-stage renal disease. The company plans to seek regulatory approval in both regions upon completion of the trial. The company is also conducting a US phase II clinical trial of the human acellular vessel as a bypass graft in patients with peripheral arterial disease.
Avinger, a developer of treatments for peripheral arterial disease (PAD), has announced Conformité Européenne (CE) Marking approval of Pantheris SV (Small Vessel), a product line extension of the Lumivascular atherectomy system. CE Marking allows for distribution of Pantheris SV in the European Union (EU) and certain other countries that recognize the CE Marking. Pantheris SV is not available commercially in the USA at this time.
Designed with a lower profile and longer length, Pantheris SV is intended to expand the addressable market for Pantheris by allowing physicians to treat lesions in smaller diameter vessels (2 to 4 millimeters) and more distal regions of the vasculature. Pantheris SV incorporates key improvements from the next generation Pantheris launched in the US market in June 2018, including a stiffer shaft for increased pushability, a refined OCT imaging system, and an enhanced cutter design.
”We believe that Pantheris SV represents a substantial market expansion opportunity for our technology, and having CE Marking for the device represents an important first step towards broader commercialisation,” commented Jeff Soinski, Avinger’ president and CEO. ”The longer length and smaller profile of this new device should increase the number of lesions available for treatment by Pantheris, and we believe the safety profile enabled by our image-guidance system should enhance the confidence of physicians applying directional atherectomy to smaller vessels.”
Jaafer Golzar, Avinger’ chief medical officer, noted, ”Pantheris SV represents an important new option for physicians to treat small vessel disease. Given the potential consequences of an adverse event during peripheral interventions in this challenging area of the vasculature, a device with a high safety profile is of paramount importance. With real-time OCT visualisation, we believe physicians will have the information they need to safely perform an intervention while maximising the size of the channel restoring blood flow to the extremities, which should lead to better outcomes for patients with small vessel disease. We are excited to initiate our first clinical experiences with Pantheris SV in Europe in the near future.”
Atherectomy is a minimally invasive treatment for PAD in which a catheter-based device is used to remove plaque from a blood vessel. Lumivascular technology allows physicians, for the first time ever, to see from inside the artery during an atherectomy procedure by using an imaging modality called optical coherence tomography, or OCT, that is displayed on Avinger’ proprietary Lightbox console. Physicians performing atherectomy with other devices must rely solely on x-ray as well as tactile feedback to guide their interventions while treating complicated arterial disease. With the Lumivascular approach, physicians can more accurately navigate their devices and treat PAD lesions, thanks to the real-time OCT images generated from inside the artery, without exposing healthcare workers and patients to the negative effects of ionising radiation.
The US Food and Drug Administration (FDA) has approved Valiant Navion thoracic stent graft system (Medtronic) for the minimally invasive repair of all lesions of the descending thoracic aorta, including thoracic aortic aneurysms, blunt thoracic aortic injuries, penetrating atherosclerotic ulcers, intramural haematomas, and aortic type B dissections.
Until now, patients with small iliac arteries were considered ineligible for thoracic endovascular aneurysm repair (TEVAR) or required adjunctive procedures to accommodate calcification and tortuosity concerns. Medtronic states in a press release that Valiant Navion allows for the potential for more patients to receive a percutaneous procedure and overcome these anatomical concerns, enabling a less invasive approach to treatment compared to surgical cut-down (open) procedures.
The Valiant Navion system is a lower-profile evolution of the market-leading Valiant Captivia thoracic stent graft system, which has treated more than 100,000 patients globally. Valiant Navion is built on the design philosophy of the Valiant Captivia system for improved performance and increased patient applicability. The system also features both CoveredSeal (proximal covered) and FreeFlo (proximal bare metal) stent configurations, providing physicians with two graft options to treat varying patient anatomies and pathologies.
“A significant reduction of the delivery system profile enables physicians to better facilitate the endovascular treatment of patients with smaller, tortuous, and calcified access vessel arteries,” says Ali Azizzadeh, the US principal investigator for the Valiant Navion IDE study. “Furthermore, the challenging anatomical and comorbid baseline characteristics and resulting clinical evidence of the global investigational device exemption (IDE) subjects support this design.”
Approval was based on 30-day primary endpoint analysis of 87 patients consecutively enrolled in the international, multicentre, prospective investigational device exemption (IDE) study analysing the safety and efficacy of Valiant Navion in patients with thoracic aortic aneurysms and penetrating atherosclerotic ulcers. The study included a challenging real-world patient population with 37.9% female enrolment and 71.3% patients with severe to life-threatening systemic disease (ASA physical status classification III/IV). The results demonstrated efficacy, with:
FreeFlo configuration implanted in 74.7% of procedures with no instances of access or deployment failures at implant in the full study cohort.
The new CoveredSeal proximal configuration implanted in 25.3% of procedures with no instances of access or deployment failures at implant in the full study cohort.
The majority of procedures (50.6%) were performed through a percutaneous access approach, leading to operational efficiency with mean procedure and fluoroscopy times of 88.7±53.4 minutes and 12.2±8.8 minutes, respectively.
Through 30 days, data showed low rates of peri-operative mortality at 2.3% (2/87) and secondary procedures at 2.3% (2/87). The rate of Type Ia endoleaks was 1.2% (1/87) at one-month imaging follow-up.
Research presented at the European Society for Vascular Surgery’s annual meeting (ESVS; 25–28 September, Valencia, Spain) has shone a light on the potentially high cumulative radiation exposure associated with certain venous procedures. Addressing the issue, Stephen Black (Guy’s and St Thomas’ Hospital, London, UK) called for further studies to identify strategies that can reduce radiation exposure, and highlighted the need for increased awareness among interventionalists.
Black indicated that there has been an increase in treatment options for deep vein thrombosis (DVT) in particular and for chronic venous patients over the last few years. While the advances are exciting, it is easy to forget that they come with potentially harmful side effects. Black compared modern venous procedures with endovascular aneurysm repair (EVAR), drawing particular attention to the young age at which venous patients typically require treatment, corresponding with a much longer lifetime of follow-up and potential reintervention procedures.
“It is important to highlight the potential for harm in this patient group who are an average age of 30–40 years, as opposed to the older patients who typically undergo EVAR, for example. The EVAR 1 trial reported an increased incidence of malignancy in patients treated endovascularly after 15 years follow-up. Patients who need thrombolysis or inferior vena cava (IVC) reconstruction are often younger than those with arterial problems and may also require long-term surveillance and secondary interventions, exposing them to further radiation,” Black pointed out.
To investigate the radiation exposure associated with venous procedures, Black and colleagues conducted a retrospective cohort study of patients with symptomatic ilio-femoral deep vein thrombosis and chronic IVC reconstruction, followed for a minimum of one year in order to capture reintervention data. Estimated radiation exposure from the related preoperative, index and postoperative interventions were measured in dose-area product and fluoroscopy time.
At St Thomas’s Hospital, Black explained that all procedures are performed in either the hybrid vascular theatre or in the angiosuites. Default background settings are used with a fluoroscopy pulse rate of 7.5/second in the hybrid operating theatre, 3.0/second in the angiosuite and two frames per second for digital subtraction angiography acquisitions for all rooms.
The 39 patients enrolled in the study were a median age of 35 years (range=18–73) and 27 were male. Nineteen patients were treated for lower extremity DVT and 20 for upper extremity DVT, and these two groups were looked at separately to observe any differences.
In terms of the configuration of stents for IVC reconstruction and the level of disease, three patients had unilateral iliac stents into the IVC, but the dominant group were either to the suprarenal component or a stent extension to the hepatic confluence.
The cumulative radiation exposure to patients undergoing IVC reconstruction was predictably higher, Black reported, with a mean dose-area product of 81,131Gy-cm2. Additionally, fluoroscopy time was long, with some procedures taking up to six hours. Level of radiation exposure also depended on the region which was stented.
“If we look at the difference between the two, it is clear that the stents that extended into the hepatic segment were associated with significantly more radiation exposure than those that remained below the infrarenal component. The cumulative radiation exposure, if we include all the follow-up, remains relatively similar in both the acute and chronic IVC stent extension patients. Further, we found that in patients with upper extremity DVT, the procedure was far quicker and therefore associated with far less radiation than lower extremity DVT. The same applies for cumulative dose-area product and fluoroscopy time for all the reinterventions that occurred in the year after the initial procedure and the surveillance,” Black reported.
Comparing radiation dose measurements for IVC reconstruction with other vascular procedures, Black noted that it is significantly higher than lysis, for example, which has a median radiation exposure of 9Gy-cm2 and 981 seconds of fluoroscopy time compared with 60.8Gy-cm2 and 2,846 seconds for IVC. Compared to procedures such as EVAR and thoracic EVAR (TEVAR), however, the venous treatments do remain lower—especially complex procedures which have been associated with 287Gy-cm2 dose-area product and 4,152 seconds fluoroscopy time—but Black maintained that there should still be concern for the amount of radiation venous intervention patients are exposed to.
“This does not really change the story for venous patients. We can see that IVC reconstruction does have a high dose of radiation exposure, with cumulative radiation over 40–50 years of a patient’s life really needing to be taken into account. The initial procedure for acute DVT is relatively low, but it is not insignificant, and these patients really are much younger than the arterial population and we need to be much more aggressive in reducing their exposure early on,” Black stated.
At his hospital, he said that they have moved to using magnetic resonance (MR) venogram instead of computed tomography (CT) scan in all of these patients for their initial work-ups, so as not to expose them to additional radiation dose. In particular, he added, the use of intravascular ultrasound (IVUS), helps to reduce radiation exposure in the form of contrast-enhanced runs, and is one of the main strategies he uses to reduce dose.
“As interventionalists, we have to learn that often we use another run as time to think about how to proceed, and we have to start getting out of these habits that expose not only ourselves but the patients to more radiation,” Black said.
He concluded, adding that more needs to be done to raise awareness about the importance of reducing radiation dose wherever possible, and maintained that more strategies, such as the use of IVUS, need to be identified and put into practice.
A single-use, high-definition miniature camera has been hailed as a “breakthrough innovation” in intravascular surgery, as Cambridge Consultants announced the device’s launch. Called Leap, the technology allows a digital view inside veins and arteries for the first time.
Leap builds on the latest generation of sub-millimetre cameras, enabling surgeons to visualise parts of the anatomy that are currently inaccessible with today’s imaging techniques. With the potential for even smaller cameras on the horizon, this highly miniaturised ‘chip-on-tip’ architecture features a 400×400 pixel image—0.16 megapixels
as a standard capability—an order of magnitude improvement over standard fibre-optic angioscopes. Chip-on-tip refers to the location of the imaging sensor at the distal end of the endoscope, in contrast to traditional fibre bundles which transmit light to large, external processing towers.
According to a press release, in the future, Leap technology could be combined with Cambridge Consultants’ ‘super-resolution’ image processing to increase the resolution further to 1600×1600 pixels (2.6 megapixels). This state-of-the-art proprietary technique harnesses deep learning to enhance low resolution images without the blurring associated with traditional up-scaling and will ultimately provide visualisation for the most challenging cardiovascular surgery, the company claim.
Despite the ability to provide unique predictive information, current surgical endoscopes are not widely used in angioscopy due to poor flexibility, a limited field of view, and low resolution. At 1.35mm in diameter, the Leap early prototype can be used in a procedure such as intracoronary angioscopy. Leap increases the information available to surgeons with new functionality, such as enabling tissue classification or direct imaging of non-standard vascular occlusions. Moving beyond the traditional endoscope, inspection with a Leap device could be paired with today’s leading technologies, such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), enabling enhanced diagnostic techniques during surgery.
Cambridge Consultants say that while existing endoscopes carry an elevated risk of infection and device damage due to inadequate sterilisation between procedures, a single-use endoscope Leap can be operated from a standard computer, so is not reliant on the availability of large and expensive operating room infrastructure. The falling costs of chip-on-tip technology means that the expense associated with traditional endoscope systems is set to significantly reduce. This is achieved with the introduction of an economical, reposable device, removing the need for sterilisation and maintenance.
Leap in model arm
“We have combined our intravascular device experience with our knowledge of microoptics, systems engineering and artificial intelligence, in conjunction with external manufacturing partners. The result is an economically viable, disposable camera system that is small enough to fit into the working channel of a typical vascular catheter,” says Simon Karger, head of Surgical and Interventional Products at Cambridge Consultants. “For the first time, Leap offers practical, direct visualisation in the procedure room and a platform for integration of new configurations, sensor types and imaging modalities (such as spectroscopy). This can enable a new level of advanced imaging in intravascular procedures and an unparalleled surgical experience” he adds.
Treating severely calcified arteries by endovascular means is still a challenge, although atherectomy, stents and lithotripsy are all techniques that are employed. Lithotripsy (also called Lithoplasty) seeks to microfragment the calcium seen in the vessels of peripheral arterial disease patients by using soundwaves. The procedure could improve the outcomes of endovascular treatments, Gunnar Tepe (Rosenheim, Germany), tells Interventional News at CIRSE 2018 in Lisbon. He believes one of the main benefits of lithotripsy is that it reduces the use of stents in treatment.
Tepe is the European principal investigator of the DISRUPT PAD III study. This is a multicentre, single blind, randomised study of lithotripsy with the Shockwave system used in combination with a drug-coated balloon (Medtronic’s IN.PACT Admiral) vs. standard balloon angioplasty used in combination with drug-coated balloon to treat moderate and severely calcified femoropopliteal arteries.
Fred Lampropoulos, chairman and chief executive officer of Merit Medical, spoke to Interventional News about building a business with lasting value in mind. He attributes the company’s success in developing and acquiring (recent acquisitions include Argon Critical Care, DFINE, Bard’s divestment assets and BioSphere Medical) a product portfolio that spans the breadth of interventional radiology to vision, planning and never putting himself ahead of his employees.
What makes Merit Medical unique in the healthcare industry?
Planning is an important part of what we do. Our biggest single advantage is that we wrote a 100-year business plan. That goes back to my military background as a US military officer and combat officer— I fought an enemy that was willing to fight for 100 years. If you look at our products, our programmes, and our global presence, these came about because we thought about them for a long time. We are now 30 years into the 100-year plan. We are not sellers; we are builders, dedicated to building something of lasting value. And that must be communicated and explained to employees, so that they know that they are safe, there is a future, they are not going to be bought out, and then made redundant. That is a powerful idea. Other key factors are being visionary and disciplined, and understanding the industry.
As a medium-sized company, how do you maintain a diverse portfolio in niche areas?
Last year, we introduced 22 new products. We are able to achieve this through a combination of internal research and development as well as strategic and tactical acquisitions. When we make those acquisitions, we invest in them the same as any other part of the company. We start research projects to enhance the new company, and maintain their facilities and people, thus retaining know-how and tribal knowledge, because that is key to success. People are the key to success.
How do you choose which therapeutic areas you operate in when deciding on acquisition?
We started out in cardiology with a simple polycarbonate control syringe. Then we went on to a digital inflation device. Today, we are the world leader in inflation devices that deploy stents or blow up balloons, even though we do not have a stent. People using the tools want stability, and to be familiar with them. Technology has moved from bare metal stents, on to self-expanding stents and drug-delivery stents, but the tools that deliver them are constant.
Innovation is also important. Most companies have one inflation device; Merit has six. We always have active research and development projects, and have moved from cardiology into interventional radiology, which candidly is now the largest part of our portfolio.
The equipment for cardiology is also used in interventional radiology, but on a bigger scale, because it works in the heart, feet, legs, liver, kidneys, and lungs, as well as in neural pathways and dialysis and PICC lines, There was a lot of room for improvement and innovation, and because it was so fragmented it meant that we could compete in this arena. Later, we looked at oncology and bought BioSphere Medical and its EmboSphere microspheres product line in 2010, and we have doubled the size of that company in the last two years with our focus on poly vinyl alcohol (PVA) and gelfoam and a number of embolics that we will bring out in the future.
Where do you see the most interesting growth opportunities in Merit’s product portfolio?
Without revealing any trade secrets and without sharing intelligence, Merit specialises in five areas — endoscopy, critical care, interventional oncology, the peripheral spine, and cardiology. We look for cross capabilities, points of sale that we can be active in and that we have knowledge of. There are common threads that go through all of our specialties. We also look at areas where other companies had given up, or there was underinvestment, or markets were fragmented. We tie common threads, where there are opportunities for cross-germination, and the things that we know about into products that we believe can be competitive.
In 30 years none of our product lines have ever failed – even though, usually, economic cycles eventually decline. Emerging economies are doing some of the things that were being done in the US 10 to 15 years ago; they use products that are still very good but they are further back in the learning curve. China is one of our fastest growing areas, and we believe it will continue to grow.
Recently, our market cap hit a record high of US$2.4 billion. Within three to four years, it will be $5 billion dollars. We started out as a penny stock.
We have R&D going on in numerous locations – in Singapore, China, and India. Another thing that distinguishes us from other small- to medium-sized businesses is the way that we have grown. The US business accounts for almost 50%, but we are also in Central South America, South Africa, North Africa, Iraq, Iran, Syria, Egypt, Lebanon, and Algeria.
What are the main drivers of the healthcare industry at this time of transformation?
It is always innovation, not being afraid of being a global company with a global perspective, understanding the regulatory environment – and not complaining about it.
It is also important to understand emerging trends via an understanding of demographic issues. All of South East Asia is growing rapidly, so we have expanded there.
Another driver is being able to sort through therapies and make decisions about what to invest in. In Europe and Japan, 80 to 85% of procedures are performed through radial artery access, but the USA was slow to adopt it—five years ago it was at 5%, today it is approaching 45%. We have moved a lot of our procedures and training to the USA so as to develop the products and bring about changes in the thought processes in the USA.
In politics, the saying is that you should act globally but think locally; doing that is different everywhere. For instance, people are smaller in Asia; therefore you cannot necessarily sell the same product to someone in Japan that you would in northern Europe. You have to adapt to the local market. This is part of our strategy and the tactics that support it.
What will the future of physician education look like?
Education is essential and it is a long process. Merit has educational and awareness programmes such as ThinkRadial (an educational platform for clinicians and patients focused on the radial approach), ThinkPAE (an educational course for prostrate artery embolization) and ThinkAccess where physicians are trained by physicians. If you provide training for procedures, and supply the products, service those products, and put support structures in place, people stick with what they know, and with companies that support them.
What is Merit’s approach to supporting online education and live events?
We provide a certain amount of online education but we need to do a lot more. We are relatively inexperienced at this point, but we do not intend to remain so, and there will be more investment and academic input into that process in the future.
On a related note, Merit is also involved in developing a bipartisan bill being introduced to the US Congress that will bring more funds into the training of interventional radiologists. We are involved politically and not just interested in selling products, we are interested in building the industry. Interventional radiologists understand patients from head to toe, but they do not control the patient. That is the real challenge—getting more people trained, and then doing a better job of raising awareness, through social media, word of mouth, and advertising, that men and women can choose to have procedures such as a prostate artery embolization or uterine fibroid embolization (UFE). Given that choice, patients will always go for the minimally invasive option.
Individual evaluation of each patient, and each aorta, is key to durable repair
“The instructions for use (IFU) are not a clinical guideline, so trainees should really think about what the main considerations are when they are implanting devices in the aorta to create a durable repair,” said Tara Mastracci (Royal Free Hospital, London, UK) at the London Aortic Symposium 2018. Mastracci told Interventional News about how clinicians’ practices are being tested on the durability of aortic repair and how it is vital for operators to audit and evaluate their own data.
Coil embolization of hepatic arteries to induce redistribution of blood flow and microspheres has a mediocre success rate, concluded a recent study presented by Ahmed Alsultan (University Medical Center, Utrecht, the Netherlands) at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (22–25 September, Lisbon, Portugal). The data further led Alsultan to advise physicians—when dose planning for a patient—to take into account that the radiation dose in the dependent regions is lower in general.
Alsultan acknowledged that variations in hepatic vasculature can pose a problem for patients undergoing radioembolization. Such variations may require one or more extra injection locations for radioembolization. Yet, according to Alsultan, redistributing the flow by coil-embolizing the problematic artery may be a way of overcoming this issue; eliminating the need for extra injection locations. Therefore, preexisting intrahepatic collaterals would be expected to take over the distribution of blood to a particular area, although Alsultan reported that in practice, himself and his colleagues have observed mixed results.
This led the investigators to carry out a retrospective study in order to screen all radioembolization patients in their affiliated institute, including patients that had a closure of the tumour-feeding artery. By doing so, Alsultan and colleagues aimed to evaluate the effect of coil-embolization of tumour-feeding vessels on the redistribution of blood flow in radioembolization.
To visually assess the effect of redistribution of the microspheres, post-therapy nuclear medicine images were taken from the PET (positron emission tomography) scans—subsequently analysed by two nuclear medicine physicians. The effect of redistribution was quantified by comparing the relative dose to the coil-embolized (dependent) segment relative to the other (non-dependent) segments and to the tumour in that segment on posttreatment PET and SPECT (single photon emission computerised tomography) scans using Simplicit90Y (Mirada Medical) software.
Alsultan pointed to a particular case: a segment four artery that could not be targeted with an injection to the left hepatic artery. The investigators decided to coil this artery and to inject the microspheres proximally to those in the left hepatic artery. According to Alsultan, the nuclear medicine image displayed very good redistribution of the blood flow, while the dosimetry data showed promising ratios: the segment ratio being 1.88 and the tumour ratio 1.21; indicative of good redistribution.
However, he noted that in other instances, less promising outcomes were observed. He discussed another case of a phrenic artery (that supplied three tumours) that was also coiled. Yet in this case, the nuclear medicine image from the PET scan depicted poor distribution and very low tumour rates (segment ratio of 0.93, tumour ratio 0.33).
Of the 37 cases in total, 32 were available for dosimetric analysis and 35 for visual analysis. Regarding the visual analysis, Alsultan reported that around 70% of patients had good redistribution of blood flow (with good interrater agreement, kappa=0.82).
To determine the level of blood redistribution, Alsultan and colleagues came up with three cut-off values: 0.9, 0.8 and 0.7, that correspond to a decrease in the absorbed dose of ten, 20 and 30 per cent, respectively. Therefore, a 30% success rate was observed for the 0.9 cut-off values, and a 55% success rate was observed for the more “liberal” cut-off value of 0.7.
In terms of the segment analysis, the success rate ranged from 46–69%. The median ratios of the dose to the dependent segment and the non-dependent segments were 0.88 (range 0.26 – 2.05) and 0.79 (range 0.19 – 1.62) for dependent tumours compared with non-dependent tumours.
In light of these data, Alsultan concluded that coil embolization of hepatic arteries can be used to redistribute the blood flow and the microspheres. However, he stressed that physicians should keep in mind that the radiation dose in the dependent region is lower in general, which should be taken into account when dose planning.
A recent session at CIRSE 2018 sought to go beyond the headline findings from a number of recent randomised controlled trials (RCTs) in interventional oncology to define the future research directions for selective internal radiation therapy (SIRT; also called radioembolization), particularly with regard to dosimetry and patient selection.
Jose Ignacio Bilbao (Clinica Universidad de Navarra, Pamplona, Spain), presenting on the SARAH (Sorafenib vs. radioembolization in advanced hepatocellular carcinoma) trial from France also compared it with data from the randomised controlled trial SIRveNIB (selective internal radiation therapy vs. sorafenib) study from Asia, that dealt with a similar research question.
The SARAH trial directly compared the efficacy of SIRT using yttrium-90 (Y-90) resin microspheres (Sirspheres, Sirtex) to sorafenib (Nexavar; Bayer). SIRveNIB compared the safety and efficacy of radioembolization and sorafenib in patients with locally advanced hepatocellular carcinoma. The primary endpoint of both trials was overall survival.
Results from SARAH showed that local treatments of SIRT did not lead to a planned superiority difference in overall survival, compared with standard-of-care systemic therapy with sorafenib. However, SIRT had far fewer side-effects and patients who received this treatment had a significantly better quality of life. Very similar data emerged from the SIRveNIB trial, which also failed to meet its primary endpoint.
“This has led to the most recent EASL Practice Guidelines (Journal of Hepatology, 2018) to recommend that radioembolization should not be used to treat hepatocellular carcinoma [in this setting], so this is not good news,” Bilbao said.
Looking more carefully at the data beyond the headline findings, Bilbao stated that in the per-protocol analysis of SARAH, 26.6% of patients did not receive the intended treatment of SIRT and 7.2% of patients did not receive sorafenib. Similarly, in SIRveNIB, 28.6% of patients did not get the intended treatment of SIRT and 9% of patients did not get sorafenib. “This is an important bias in my opinion,” Bilbao said, while also showing that there were some patients in the SARAH trial who were enrolled despite their poor condition. Others, he said, were also undertreated.
Despite these shortcomings, Bilbao described SARAH as “a very positive study” that has shown the benefits of SIRT in certain subgroups of patients such as those with under 25% tumour burden, good liver function as measured by ALBI grade and those that had greater than or equal to 100Gy tumour absorbed doses.
Pointing to what can be learned from the outcome of these trials, Bilbao stated that both SARAH and SIRveNIB had been designed to show the superiority of SIRT. “There is no information regarding non-inferiority of the therapy that can be gleaned from these studies,” he said.
Speaking in particular about the Technetium-99m macro-aggregated albumin scan and refined dosimetry, Bilbao asked: should a bad uptake exclude patients for Y-90 treatment? Is it useful just for the evaluation of lung shunting? How can the activity be accurately evaluated for a personalised treatment?
“SIRT has clear local efficacy with regard to tumour response, and progression within the liver. It should be indicated in locally advanced hepatocellular carcinoma with a better patient selection and treatment optimisation. Refined dosimetry will have a role to play,” Bilbao concluded.
SIRFLOX, FOXFIRE and FOXFIRE Global trials
Thomas Helmberger (Klinikum Bogenhausen, Munich, Germany) analysed the SIRFLOX, FOXFIRE and FOXFIRE Global trials.
“The combination of chemotherapy plus a biological agent is standard first-line therapy in colorectal cancer. The liver is the dominant target site for metastatic colorectal cancer and hepatic metastases are the main cause of tumour-related death. Radiotherapy is a potent therapy in cancer,” he said to explain the rationale behind the use of SIRT and the design of these trials.
The FOXFIRE, SIRFLOX and FOXFIRE Global randomised studies evaluated the efficacy of combining first-line chemotherapy for metastatic colorectal cancer with SIRT using yttrium-90 resin microspheres in patients with liver metastases. The combined analysis comprised data from the SIRFLOX study and data from FOXFIRE and FOXFIRE Global. However, data from the combined analysis showed that there was no statistically significant difference between the overall survival of patients who received SIRSpheres plus standard first-line chemotherapy and those who received chemotherapy alone.
Outlining some of the new questions that the analysis provoked, Helmberger asked: did the study protocol tend to promote the inclusion of patients with potential extrahepatic disease and potential progressive disease? Is reducing the hepatic tumour load by SIRT as liver-directed therapy also reducing extra hepatic progression? Is failure to improve overall progression-free survival really a failure of systemic chemotherapy since extrahepatic disease is targeted by this treatment? Is RECIST 1.1 systematically underestimating the therapeutic effects resulting in deterioration of results?
SIRFLOX is the largest randomised controlled trial in the world with a medical device in interventional oncology; it was well constructed and monitored; reflected an up-to-date chemotherapy regimen—and included more than 1000 patients said Helmberger in outlining the strengths of the study.
Commenting on its weaknesses, Helmberger alluded to the unusually large number of patients who were at high-risk for poor outcomes in the SIRT arm (such as the nearly 36% of those who had extrahepatic metastases, or the over 50% who had the primary tumour in situ). In addition, there was also a significantly intensified systemic chemotherapy regimen in the non-SIRT arm that may have contributed to an imbalance treatment between the two arms of the trial which might have led to the control arm seeing better results, he pointed out.
“The impact of study design and patient stratification is crucial. Comprehensive registry data may provide more robust information in complex scenarios compared to randomised controlled trials,” Helmberger stated.
SORAMIC trial
Roberto Iezzi (Catholic University, Rome, Italy) presented on the phase II SORAMIC trial, a large investigator-initiated randomised controlled trial that evaluated sorafenib in combination with local microtherapies (either radiofrequency ablation in a curative group, or SIR-Spheres in a palliative group) for the treatment of unresectable hepatocellular carcinoma (HCC), and guided by Primovist-enhanced magnetic resonance imaging (MRI). The primary endpoint of the curative arm was time to recurrence whereas for the palliative arm it was overall survival.
“SORAMIC combines the most promising novel diagnostic and therapeutic approaches in HCC treatment available to date: diagnosis with hepatocyte specific contrast agent Primovist; microtherapy with SIRT or radiofrequency ablation; and systemic treatment with tyrosinekinase inhibitor sorafenib,” Iezzi explained.
Results from the palliative group presented earlier this year revealed that SIRT in combination with sorafenib did not provide a significant survival benefit compared with sorafenib alone in patients with advanced hepatocellular carcinoma.
However, although the overall survival rates in the total patient population did not differ significantly between treatment groups, subgroup analyses suggested possible survival benefits with adding SIRT to sorafenib in some patient groups. It was these subgroups that Iezzi emphasised at CIRSE.
“There was a survival benefit in younger patients, those with a non-alcoholic aetiology of the cirrhosis, and those with no cirrhosis at all,” he said.
Furthermore, this trial confirmed that the addition of SIRT to sorafenib is safe and feasible with a toxicity similar to sorafenib alone. Summing up, Iezzi pointed out that these results could justify and encourage the combination of SIRT with also other systemic anticancer treatments, such as immunotherapy. In particular, continuous tumour radiation delivered by SIRT may have immunomodulative effects so that, combined with immune checkpoint inhibition or T cell therapy, could potentially result in improved clinical outcomes.
Further, as this was a palliative study, there was no post-treatment imaging required and therefore, there was potentially no informations on tumour response, downstaging, total time to progression and progression-free survival, Iezzi noted. These parameters could demonstrate the superiority of combined group.
“My take-home message is that we have to perform really tailored treatments based on the indications and appropriate selection of patients. This trial highlighted that liver function clearly is the key. The evaluation of SORAMIC data is still ongoing so this is a continuing discussion,” he said.
Daniel Sze (Stanford, USA) tells Interventional News that the focus on diversity is not just about social justice. “It is really about bringing the many good ideas and innovations that will come from women and underrepresented minorities to the table in order to advance the field of interventional radiology,” he says at CIRSE 2018 in Lisbon, Portugal. Sze is also the Program Chair for the Society of Interventional Radiology Annual Scientific Meeting that will take place in March 2019 in Austin, Texas.
Interventional radiologists must become involved in the multidisciplinary development of phase III randomised controlled trials (RCTs) to further assess the role of radiofrequency ablation in treating colorectal liver metastases. This view was expressed by Gianpaolo Carrafiello (Department of Diagnostic and Interventional Radiology, University of Milan, Italy), when he addressed the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) at the annual congress (22–25 September, Lisbon, Portugal).
Speaking at a focus session outlining the lessons from the CLOCC (Chemotherapy and local ablation versus chemotherapy) trial, Carrafiello acknowledged that RCTs in interventional radiology are difficult to perform, but said they would help to persuade oncologists to work more closely with radiologists.
“We have many problems,” he says, elaborating: “The first one is that many of our procedures are operator dependent. The second one is we use different devices, and also the strategy is not always the same. And, we use different modalities of guidance, so maybe there are too many biases.”
Worldwide, one million people are diagnosed annually with colorectal cancer, up to 50% of whom will develop liver metastases. Only 10 to 15% will be able to undergo surgery, with five-year survival rates between 31% and 58% is carefully selected patients. For non-resectable disease, the standard treatment is systemic therapy, prolonging survival for about two years. Radiofrequency ablation (RFA) has been used to clear tumours from the liver, either alone or in combination with resection, but data on efficacy and survival were lacking until 2012, when the first results from the CLOCC trial became available. Longer-term findings were reported in 2017, and as a result, said Carrafiello, “radiofrequency considered from ESMO (the European Society for Medical Oncology), in addition to surgery, to eradicate visible metastases in liver sites.”
CLOCC was a phase II study of patients with unresectable colorectal liver metastases (CLM), randomised between RFA (with or without surgical resection) plus adjuvant systemic therapy (FOLFOX with or without bevacizumab) versus systemic therapy alone (FOLFOX with or without bevacizumab).
The trial was performed in 22 centres in Europe where 119 patients were randomised; 60 patients to the experimental arm, and 59 to the control arm. The primary endpoint of the first study was a 30-month overall survival rate higher than 38% in the combined modality arm, with secondary endpoints progression free survival, overall survival rate, and health-related quality of life.
By 2017, patients in the combined modality arm had a statistically significantly longer overall survival than patients in the systemic treatment arm, with three-, five-, and eight-year overall survival rates at 56.9%, 43.1%, and 35.9%, compared to 55.2%, 30.3%, and 8.9% in the control group.
Progression free survival was statistically significantly prolonged in the combined modality arm as compared with the systemic treatment arm, with three-, five-, and eight-year rates of 27.7%, 24.2%, and 22.3 in the experimental group, against 11.9%, 5.9%, and 2% in the systemic treatment arm.
But the study’s findings are limited by the fact that it was originally designed as a phase III trial which was downsized to a randomised phase II trial due to a smaller than planned sample size.
Carrafiello said at CIRSE: “A larger sample size would have offered better protection against possible risks of imbalances between treatment arms, and better reassurance of the external validity of the results. And although the effect of RFA on progression free survival was significant, the effect on overall survival is still lacking.”
Still, the legacy of CLOCC had been to enhance understanding of the combined treatment effects, Carrafiello said: “We have new technologies, we have new energy modalities of ablation, we have moved sometimes from radiofrequency to microwaves, and we have new imaging guidance systems. And we can also improve the effects of systemic therapy.”
A new direction for RFA is use in combination with immunotherapy. Carrafiello suggested two mechanisms that potentially have an impact on the efficacy of immunotherapy when used with radiofrequency: “There are mechanical changes in the tumour microenvironment and inflammatory mediated changes in immune-phenotypes. And the use of PD-1 [programmed cell death protein 1] and PD-1 blockade can boost the radiofrequency ablation immune response against tumours.”
Acessa Health has announced that the company has received US Food and Drug Administration (FDA) 510(k) clearance for its third generation Acessa ProVu radiofrequency ablation system intended for use in treating symptomatic uterine fibroids.
The company, based in Austin, USA, says the newly cleared system features ultrasound visualisation and a guidance mapping system, and that it is intended to provide a safe alternative to hysterectomy procedures for women suffering from uterine fibroids.
“The FDA clearance of Acessa ProVu is a significant step forward in terms of offering patients more minimally invasive options to address their fibroids,” former US Surgeon General Regina Benjamin comments in a press release.
“Acessa Health is delighted to usher in our next phase of innovation with the introduction of Acessa ProVu. Each phase of innovation—the original Acessa system, Acessa guidance system and now the Acessa ProVu system—represent a significant improvement in performance and the opportunity to further support our physician partners who help women suffering from uterine fibroid symptoms,” president and CEO Kim Rodriguez states.
In February, Acessa Health announced that 32 US state Medicaid programs now provide access to the company’s Acessa procedure designed to treat uterine fibroids using radiofrequency ablation.
The FDA initially granted clearance to the first generation Accesa system in 2012, when it was a brand new medical technology used in the treatment of uterine fibroids. The announcement of this first market clearance was during the opening session of the Association of Gynecological Laparoscopists (AAGL) Global Congress on Minimally Invasive Gynecology.
Leeann Essai has joined Guerbet’s executive team as North American head of marketing.
In this role, Essai will report to Massimo Carrara, Guerbet vice president for North America, and will lead US and Canadian marketing for Guerbet’s diagnostic imaging offerings in contrast media, medical devices, and digital services, including the deployment of Contrast & Care and the Imalogix partnership. She will also be responsible for the development and execution of marketing strategy for Guerbet US in close collaboration with the company’s sales partners and internal stakeholders.
“We are delighted to welcome Leeann to our North America executive team,” comments Carrara. “Leeann brings more than twenty years of global healthcare marketing and management experience to Guerbet. Her deep healthcare IT knowledge makes her a valuable addition to our team in this exciting time of expanding our digital services offerings and continuing to increase Guerbet’s visibility and growth as a leading player in medical imaging worldwide.”
Essai joins Guerbet from Siemens Healthineers, where she was a global product marketing manager responsible for the worldwide product marketing of radiology imaging IT products in the digital health services portfolio. She also held successive roles of responsibility within Siemens Health Services. Prior to Siemens, Essai served in various marketing management roles at healthcare companies, including Cerner Corporation and MedQuist Inc. (now M*Modal), where she established that company’s marketing department and directed all external marketing efforts and internal communications.
Essai holds a Master of Business Administration from Pennsylvania State University, as well as a Bachelor of Arts in Journalism from the University of South Carolina.
In a complex patient population with advanced, symptomatic below-the-knee peripheral artery disease, treatment with the Lutonix drug-coated balloon (BD) led to excellent freedom from all primary safety endpoints, including 30-day all-cause death, above-ankle amputation, and major reintervention. These interim real world data of the Lutonix global drug-coated balloon registry at 12 months, were presented by Dierk Scheinert (Leipzig, Germany) at the Cardiovascular and Interventional Radiological Society annual meeting (CIRSE; 22–25 September, Lisbon, Portugal).
In the prospective, multicentre, single arm Lutonix global registry, 371 infrapopliteal lesions were treated with the Lutonix drug-coated balloon (DCB). Patients were Rutherford category 3, 4 or 5; two-thirds were diabetics, three quarters suffered from critical limb ischaemia (CLI), and 65% were Rutherford category 5. Mean lesion length was 12cm, with over 20% exhibiting severe calcification.
The interim data presented by Scheinert at CIRSE is highly promising. Out of 244 patients, only 5.4% had a major amputation within one year, a result which Scheinert describes as “very reassuring for this complex patient population.” All-cause mortality was around 12% after one year of follow-up, and there were no unexpected device related events reported. Furthermore, there was 99.7% freedom from re-intervention for distal embolization in the patient cohort.
Improvement in Rutherford clinical category (RCC) was also marked: 80% of patients exhibited a clinical improvement by≥1 RCC, and almost two-thirds demonstrated an improvement by≥3 RCC.
“As the clinical outcome is of utmost importance for the patient,” Scheinert says, “I was most surprised by the excellent clinical results with improvement of Rutherford clinical category in 80% of patients. Further, the observed 80% freedom from target lesion revascularisation rate at one year is very promising, as patency failures are observed frequently after infrapopliteal interventions, in particular in diabetics and CLI patients.”
Speaking to Interventional News of the results’ significance, he states, “Patients with below-the-knee (BTK) disease suffer from high failure rates with currently available treatment modalities, as standard balloon angioplasty for long, complex infrapopliteal lesions is limited by high restenosis rates. As innovations are urgently needed, the Lutonix DCB could become a new tool to improve outcomes in this special patient population. Of course, the results of the Lutonix below-the-knee randomised trial are highly anticipated, and final results of both studies could have a major impact on clinical practice.”
The Lutonix DCB is coated with excipients polysorbate and the endogenous metabolite sorbitol, as well as paclitaxel at a density of 2μg/mm2. Extensive in vitro and in vivo testing has previously demonstrated an excellent downstream particulate safety, with minimal risk of embolization. Scheinert explains how this is particularly important in BTK interventions, where compromised outflow to the foot arteries is often present. He further explains how “a good balance was achieved between adhesion of the coating to the balloon during handling and advancement to the lesion and release of the coating to the vessel wall upon deployment”.
According to Scheinert, patients with long infrapopliteal lesions may benefit most from treatment with the Lutonix DCB, “as restenosis rates are high, especially in diabetics.” Importantly, he notes that target lesion revascularisation rates were comparable for diabetics and non-diabetics.
Recruitment for BTK studies is typically difficult, as patients are often older, suffering from multiple co-morbidities. Ensuring follow-up is also a major challenge, lending greater significance to the results of the present study.
Scheinert also emphasised the importance of using real world registries, arguing “results from real-world patients are important to ensure safety and efficacy of new devices for all treated patients”.
So far, an extensive clinical trial programme showed the benefit of using a Lutonix DCB in the treatment of obstructive lesions in the superficial femoral artery, while confirming minimal risks with the addition of the drug compared to standard balloon angioplasty. Now the same formulation is under investigation for BTK patients and the vascular community eagerly awaits the results of the Lutonix randomised trial, anticipating a potentially major impact on current standard care. Based on his presentation Scheinert summarises: “As these first results are promising, we hopefully can add the Lutonix DCB to our armamentarium for below-the-knee interventions soon.”
In a study evaluating the efficacy of a drug-coated balloon (DCB) in inhibiting restenosis and ensuring long-term patency in patients with arteriovenous fistulae (AVF), the paclitaxel DCB did not show superiority to a placebo high pressure balloon at 12 months’ follow-up. Manuela Moreno-Ramírez (Department of Nephrology, Juan Ramón Jiménez Hospital, Huelva, Spain) presented these results of the EffPAC trial at the Cardiovascular and Interventional Radiological Society of Europe annual meeting (CIRSE; 22–25 September, Lisbon, Portugal).
The trial was an investigatorinitiated, prospective, multicentre, double blind, randomised study conducted across four Spanish hospitals. One hundred and seventy-eight dialysis patients included in the study were divided into two groups: those treated with a paclitaxel DCB—the CE-marked Passeo-Lux 18 (Biotronik)—and those treated with an uncoated high pressure balloon, who were recipients of a placebo. The placebo involved the use of a safe and biocompatible non-hydrophilic excipient called butyryl-tri-hexyl (BTHC) that facilitates the delivery and absorption of the drug from the vessel wall.
Moreno-Ramírez emphasised the need for new procedures to treat stenosis, telling the CIRSE audience that “Difficulties with vascular access are an important source of morbidity and mortality in haemodialysis patients. Stenosis could be treated with percutaneous transluminal angioplasty (PTA), but the primary patency rate is only 40–50% at one year—hence, new procedures are needed.” Thus, the study investigators were interested in researching the paclitaxel DCB as a possible alternative treatment strategy.
However, neither the primary nor the secondary endpoints of this study were met, with the paclitaxel DCB failing to demonstrate superiority over the placebo. In addition to the primary endpoints of safety and efficacy, Moreno-Ramírez and colleagues sought to determine differences in survival rates. They found none. Despite the mean survival in the DCB group being higher, at 265 days versus 237, this was not statistically significant. There were therefore no statistically significant differences in survival at 12 months’ follow-up in terms of stenosis location, type of arteriovenous fistulae, or previous angioplasty. Moreno-Ramírez summarised: “We think this result is not clinically relevant.”
This finding is the same as that of another multicentre clinical trial with a significant sample size, conducted by Scott Trerotola and colleagues (Department of Radiology, Perelman School of Medicine of the University of Pennsylvania, Philadelphia, USA). Trerotola concluded in 2018 that, despite finding a slight improvement in survival using the Lutonix DCB (BD) compared to a placebo at six months’ follow-up, the difference was not statistically significant. However, several other previous studies, such as the IN.PACT trial by Panagiotis Kitrou (University of Patras, Patras, Greece) and colleagues—investigating at the In.Pact Admiral DCB (Medtronic) versus a placebo—contradict this conclusion, finding a definite improvement in survival with a DCB compared to uncoated alternatives.
However, Moreno-Ramírez does believe it is important to note that the global survival rates in her team’s study at 12 months are superior to that in previous published studies, at almost 60%. Moreno-Ramírez attributed this to the use of a high pressure balloon for angioplasty. Clarifying her methodology, Moreno-Ramírez explained that for every patient enrolled in the present study, both those in the DCB arm and the placebo arm, the first angioplasty utilised a high pressure balloon. Next, Moreno-Ramírez and colleagues carried out a fistulography to discover if the first angioplasty had been effective. Allocation into the two different randomised groups occurred then, before a second angioplasty with DCB.
The Covera vascular covered stent (BD) has a superior six-month primary patency rate than standard balloon angioplasty, with an equivalent safety at 30 days, when used in the treatment of stenotic lesions in arteriovenous (AV) fistula patients. Data from AVeNEW, the first level-one clinical trial on the use of a covered stent to treat these patients, were reported at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 22–25 September 2018, Lisbon, Porugal).
Principal investigator Bart Dolmatch (Department of Radiology, Palo Alto Medical Foundation, Mountain View, USA) told delegates: “The primary endpoint was six-month target lesion primary patency, and in the covered stent group the primary patency was 78.7%, whereas in the angioplasty group it was 47.9%; that is greater than 30% difference at six months, with a P value that was highly significant at <0.001.”
The primary safety endpoint was measured by freedom from an event resulting in intervention, hospitalisation, or death at 30 days. The study found that use of the vascular covered stent was non-inferior to percutaneous transluminal angioplasty (PTA) alone.
Dolmatch said: “You can see a comparable safety profile for both the covered stent group and the angioplasty group, with a high significance for showing non-inferiority of the Covera stent graft compared to angioplasty.”
The prospective, international multicentre study randomised 280 patients (1:1) to receive either balloon angioplasty or angioplasty plus the Covera stent graft for the treatment of stenotic lesions in the venous outflow of upper extremity AV access circuits in patients dialysing with an autogenous fistula. The Covera vascular covered stent is a polytetrafluoroethylene- (ePTFE) covered selfexpanding stent. Patients were treated at 24 centres in the USA, Europe, Australia, and New Zealand, and exhibited greater than 50% stenosis in the venous outflow of the AV access circuit, with clinical or haemodynamic evidence of fistula dysfunction.
Dolmatch explained: “The study included the typical sort of dialysis patients we see across the globe, with a mean age of about 62 to 63 years, slightly more weighted towards males than females, and about 30% of patients had a BMI [body mass index] that was… in the obese or heavy range. The patients had typically brachial cephalic or brachial basilic fistulae.”
Secondary measures included access circuit primary patency and the number of reinterventions needed to maintain patency. The number of target lesion reinterventions for the covered stent group was 0.3 for the six-month period, compared to 0.8 for the angioplasty group. Acute technical and procedural success rates were also high in the stent group, at 100% and 98.6%. “Overall,” said Dolmatch, “the procedure was extremely successful, with a very low complication rate.”
He added: “All of the stent graft sub-analyses showed superior outcomes compared to balloon angioplasty—for instance, the use of treatment in the cephalic vein arch, with much better outcomes with the stent graft group compared to angioplasty.” The vascular covered stent had a success rate of 78.7% in the cephalic vein arch versus 38.3% for PTA alone, a difference of 37%. Target lesion primary patency was maintained in 86% of de novo lesions and 77.7% of restenosed lesions in the stent group, compared to 65.6% and 40%, respectively, for angioplasty alone.
The most commonly used diameters of stent graft used in the study were nine and 10mm, and stent graft lengths were typically between 40 and 60 diameters.
Follow up in the AveNEW trial is ongoing for two years, and Dolmatch expressed his optimism about future results. “The divergence [in primary patency] is really starting at about 60 days and continuing on to 180 days. This is six-month data. We are looking forward to seeing 12-month, 18-, and 24-month data showing the superiority of stent graft treatment of the stenoses in fistulae, compared to angioplasty.”
Balt International has announced receiving the CE mark for Magic Glue, its next generation of cyanoacrylate liquid embolic agent. Magic Glue is indicated for the embolization of arteriovenous malformations.
Magic Glue is a class III implantable medical device which is described as an arterial and venous embolization implant due to its haemostatic action, and is applicable in the fields of neuroradiology and interventional radiology. This medical device is applied in solution with a contrast agent.
“We are excited to enlarge our offer in the treatment of arteriovenous malformations with Magic Glue. This cyanoacrylate glue offers new features compared to the historical glues on the market such as delayed polymerisation and less adhesion to the microcatheter. These characteristics will facilitate and expand cyanoacrylate indication in the neurovascular and peripheral fields,” said Nicolas Plowiecki, president of Balt.
“Balt is again expanding its embolization portfolio with a new cyanoacrylate solution that provides another treatment option for neurovascular and peripheral physicians. We were among the first to enter the arteriovenous malformations market with the Magic flow-dependent microcatheter. Thirty years later, BALT keeps on delivering innovative solutions for better patient treatments,” commented Pascal Girin, CEO of Balt and president of Balt International.
A new, spherical resorbable gelatine embolic agent, GelBead, has been shown to be “very effective” for uterine fibroid embolization (UFE). Nigel Hacking (Department of Clinical Radiology, University Hospitals Southampton, Southampton, UK) presented this result at the 2018 annual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 22–25 September, Lisbon, Portugal).
This embolic agent is already available in the USA under the name GelBead (Vascular Solutions/ Teleflex; distributed by Medtronic), and is due for commercial release in Europe soon, where it will be called Optisphere.
GelBead is a purified porcine skin derivative (Hacking noted: “Interestingly, gelatine sponge and even trisacryl microspheres come from pigs. Gelatine products have been used for decades”), and has good mechanical strength. Hacking detailed the embolic agent to the CIRSE audience, saying, “This product does degrade, unlike most of the polymer or plastic embolic agents, in around four to nine weeks, and in animal studies it had completely gone at 12 weeks.
“Those of you who have young children will know that plastics are bad, microplastics are worse, and this is one of the first non-plastic or polymer agents we have used. Not to say that the plastics cause any trouble—I do not think they do—but it is interesting that we may be moving towards resorbable agents in the future.”
Hacking and colleagues first conducted a pilot study, before enrolling a larger scale study evaluating GelBead in UFE in comparison with five established and commonly used embolic agents. GelBead compared very favourably to the existing agents. Those also under investigation for comparative purposes were: Gelfoam slurry (Spongostan Special: J&J Medical), trisacryl gelatine microspheres (Embospheres, Merit Medical), Beadblock (Biocompatibles), Embozenes (Celonova), and particulate PVA (Contour, Boston Scientific).
Twenty-five women with symptomatic fibroids participated in the study, and all had a gynaecological assessment prior to treatment. The investigators took an MRI at baseline, and again three months’ postprocedure, to assess uterine size, number and position of fibroids, and size of dominant fibroid. Concerning the decision to have a three-month follow-up period, Hacking explains, “We know that three month MRI predicts beautifully what will happen in the future. You will get good symptomatic improvement. If you can kill all the fibroids, they will not come back. If you only kill some of them, they will come back. So you do not need more than three months.”
Describing the assessment criteria of the study, Hacking said that he and his team did “something that is not all that common in these [types of] trials; we wanted to look at ovarian function, and whether this resorbable agent was more gentle on the ovaries, perhaps. So we looked at the anti-mullerian hormone (AMH) to assess ovarian reserve, and our endpoint was percentage fibroid devascularisation.”
Hacking reported a 95% dominant fibroid complete devascularisation. “We had three groups: 100% [fibroid devascularisation], 90–99%, and less than 90%. We considered less than 90% a failure,” he said. Dominant fibroid devascularisation was below 90% for all the other embolic agents investigated, except for PVA, which had very similar results to GelBead. The other four agents were between 70% and 85%. However, Hacking noted that this study “is not a randomised controlled trial (RCT)”, saying “I respect the RCT data.”
Looking at total fibroid devascularisation data, Hacking comments “If you have got five fibroids or 25 fibroids, to get the 100% [fibroid devascularisation] you have to kill every last bit of every last fibroid, so that is quite a challenge.” When using GelBead, 80% of all fibroids had complete devascularisation. Of this, Hacking said, “GelBead did very well, slightly less well than PVA [85% of fibroids had complete devascularisation in this group], but there was no statistical difference with GelBead any of these other embolic agents investigated, so it is working well. It is reducing the uterus volume, it is reducing the dominant fibroids, which you would expect, and of course the symptoms have improved.”
Moreover, there was no increased permanent uterine artery occlusion, meaning that repeat procedures in cases of future fibroid regrowth are possible. The study investigators found that 75% of patients in the GelBead cohort had bilateral uterine artery patency on MRI at three months. “Our temporary agent, Gelfoam, that we have used for decades, has a bilateral occlusion rate, at least in my hands, of just over a half, a unilateral occlusion rate of 40%, and only 5% with bilateral patency—very strange. If you look at the others though, bilateral patency even with Embospheres is only 55%; remember it is gelatine based. Bead block, Embozenes and PVA are all better [with a bilateral patency result of 94%, 85% and 75%, respectively]. GelBead is pretty good.”
However, Hacking also acknowledges that he changed his technique slightly: “I pushed the GelBead a bit deeper into the uterus, so I think I am cheating slightly compared to the Gelfoam, but those are still quite impressive figures.”
No reduction in ovarian function
Of these results, Hacking commented: “We got good uterine and dominant fibroid reduction [37% and 46%, respectively] and no significant drop in the AMH levels, representing no significant drop in ovarian function.” All of the patients in this study were over 40, so no conclusions can be drawn concerning fertility from this work, and Hacking advised further studies in younger women be conducted. Noting that this was “pure conjecture”, Hacking nevertheless proposed that the idea behind using a completely bioresorbable embolic agent is that “if you do not damage ovarian function, the younger women that we might be able to treat, might not only be able to conceive, but might be able to carry a healthy pregnancy.”
There was a mean reduction in the symptom score as well over the course of the study. At three months’ followup, the average UFS symptom score was 17, compared with 63 at baseline. Additionally, the majority of patients experienced significant improvements in their quality of life, with most of the 25 women involved in the study saying the treatment was “life changing”. However, speaking of the change in quality of life observed in these patients, Hacking emphasised that this particular finding is not new: “We sort of know this already with all the embolic agents.”
Researchers report the use of ultrasound to detect embolization in real time for patients undergoing treatment for benign prostatic hyperplasia (BPH). Richard Owen (University of Alberta, Edmonton, Canada) presented these results at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (22–25 September, Lisbon, Portugal), demonstrating the clear visibility of the embolic agent Occlusin 500 Embolization Microsphere (OCL 503) within 24 hours of the prostatic artery embolization (PAE) procedure.
The study investigators set out to evaluate the safety and effectiveness of the embolic product OCL 503 in PAE for the treatment of men with BPH. The trial was small; 10 patients with moderate to severe lower urinary tract symptoms secondary to BPH were treated in this open label, single centre pilot study. A standard embolization technique in PAE was used: bilateral embolization using a 2.8F microcatheter. “A 2.8F microcatheter was required, because the embolic product is not compressible, and does not pass through a smaller microcatheter,” Owen said of this choice. The catheter position was confirmed with a cone beam CT at the time of the procedure.
Patients were imaged using a Philips Model IU22 ultrasound imaging system with a transabdominal approach before the procedure, within 24 hours of PAE, and at three months’ follow up.
Owen commented: “These particles [the embolic agents] are clearly visible in all of these patients, in the prostatic tissue, within 24 hours of embolization. A blinded observation of the ultrasound images was able to identify patients that had a bilateral or unilateral embolization by the presence of these particles. Qualitative assessment of the signal intensity within 24 hours of PAE correlated with the number of microspheres delivered to the prostatic tissue. As part of this study, we knew how many microspheres we delivered, and we knew in which patients ,of course. Within three months, none of the particles were visible.
“I am not sure what the clinical role will be, but it [the embolic agent] is clearly visible in the embolized prostate, and it is in fact visible in other tissues,” Owen continued. “I am not at liberty to discuss this here, but it is visible in other embolized tissues, as you would expect. That relates to the density; the density is higher than that of normal soft tissue, and that is why you get such a profound reflection from ultrasound.”
According to the study investigators, the echogenicity relates to the amount of embolic delivered. Owen explained at CIRSE: “It [ultrasound imaging] may well provide a useful tool at the time of embolization to confirm the entirety of embolization. We used to use some other measures post-procedure, CT, for example, in post-procedure imaging, to see where the emboli are, but we could do a real time ultrasound here to see if we have reached an adequate endpoint—but it would require more work.”
Owen concluded his talk by expressing his gratitude to his mentor: “I did visit Portugal several years ago, and I learnt this technique from professor Martin Pisco (Hospital Saint Louis, Lisbon, Portugal), so thanks to him for starting the ball rolling in much of the world.”
A CIRSE attendee asked Owen if he had any experience with contrast enhanced ultrasound, which the questioner claimed to find “extremely useful” in the immediate monitoring of embolization. Owen replied: “You can do that, of course, although it requires the addition of a different agent; the intravenous injection of a contrast. However, there could be other factors, for example spasm in the vessel, that might affect that endpoint [immediate imaging of emboli]. The use of OCL 503 and ultrasound imaging is not affected by those endpoints; it would reflect the actual embolic material in the tissue.”
The embolic agent
OCL 503 is a biodegradable microsphere, comprised largely of poly (lactic-co-glycolic acid) or PLGA, a bioresorbable suture material. It is a Class II medical device approved by the US FDA for use in hypervascular tumours, and is currently pending CE mark approval, as well as clearance for use in Canada. Owen described the microsphere: “It comes as a dry powder, similar to other embolics, and it is reconstituted with contrast—Isobuoyant with Omnipaque 240 in this case.” OCL 503 is eliminated from the body in three to six months, as has been evidenced in a previous animal study published in Cardiovascular and Interventional Radiology. The microspheres degrade to carbon dioxide and water, and have a density of 1.1g/ml (in comparison to the 1.03g/ml of liver tissue, and 1g/ml of water).
This research forms part of an ongoing trial investigating the OCL 500 series in PAE and uterine artery embolization, sponsored by IMBiotechnologies. Owen is also a recipient of the Alberta Innovative Grant, and is a part-time consultant for Cook Medical.
Five-year results from a Japanese post-market surveillance study aimed at evaluating the Zilver PTX drug-eluting stent (DES) in a real-world population show consistently positive outcomes. The findings were presented for the first time at the Cardiovascular and Interventional Radiological Society of Europe 2018 meeting (CIRSE; 22–25 September, Lisbon, Portugal), by Kimihiko Kichikawa, Nara Medical University Hospital, Kashihara, Japan.
According to Kichikawa, the use of the Zilver PTX DES (Cook Medical) in treating patients with femoropopliteal lesions have so far elicited favourable outcomes. Therefore, Kichikawa and colleagues took a multicentre, prospective approach to the post-market surveillance study that evaluated the DES in a real-world patient population.
A total of 904 patients with 1080 lesions were enrolled in 95 institutions in Japan and consecutively treated. Comorbidities were present in the patient population, including a high incidence of diabetes (59%), chronic kidney disease (44%), and critical limb ischaemia (21%).
Stent integrity was assessed by radiography, with site-reported fractures were reviewed by a radiographic core laboratory for classification of fracture type. The investigators noted any clinically driven target lesion revascularisation, defined as re-intervention performed for ≥50% diameter stenosis after recurrent clinical symptoms of peripheral arterial disease. Furthermore, clinical benefit was defined as freedom from the following; persistent or worsening claudication, rest pain, ulcers, or tissue loss.
The investigators found that lesions were complex; their average length at 14.6mm, with 44% found to be totally occluded and an additional 19% involving in-stent restenosis. Clinical follow-up that occurred through five years was obtained for >90% of eligible patients.
The five-year outcomes indicated that the rates of freedom from target lesion revascularisation were 74.2%, while the clinical benefit indicated for the patient population was 68.2%. Speaking to the CIRSE audience, Kichikawa said these figures were indicative of: “Consistently good results in challenging patient population including those with diabetes, renal failure, long lesions, in-stent restenosis, no runoff or critical limb ischaemia.” The ankle-brachial index and Rutherford scores further indicated that clinical improvement was maintained over-time, after the rapid increase in Rutherford scores one year into the trial.
In conclusion, Kichikawa said: “Patient population and lesion characteristics become more challenging in real-world, all-comer studies”. However, he reiterated that the results of the study continue to show positive long-term outcomes and demonstrate the benefit of the Zilver PTX DES across a broad patient population.
Twelve-month data prove that intravascular lithotripsy; a novel approach using pulsatile sonic pressure waves to modify intimal and medium calcium in stenotic peripheral arteries, is a safe and effective treatment option. This is the result of the Disrupt PAD II trial, presented by Andrew Holden, Auckland Hospital, Auckland, New Zealand, for the first time at the Cardiovascular and Interventional Radiological Society of Europe annual meeting (CIRSE; 22–25 September 2018, Lisbon, Portugal).
Speaking to the CIRSE audience, Holden explained that acute results were strong, with compelling safety data showing a final residual stenosis of 24.2%, with a high acute gain of 3mm and minimal vascular complications. In addition, Holden implied that the primary safety profile was “very good”, given that the only major adverse event though to 12 months was a dissection that occurred at the time of procedure.
DISRUPT PAD II was a non-randomised, multicentre study that enrolled 60 patients with complex, calcified peripheral arterial stenosis at eight sites. Patients were treated with the peripheral intravascular lithotripsy system (Shockwave Medical), and followed out to 12 months.
Calcium burden was significant, with 85% of the patient cohort exhibiting severe calcification involving both sides of the arterial wall (using the PARC definition; 50% of patients had severe calcification using the pre-defined Core Lab definition) and an average length of calcium of 98.1%.
The study investigators report high acute gain (following low pressure) in terms of the reduction of pre-procedural severity of stenosis, as well as cross-sectional area gain. This resulted in low dissections and minimal use of stents in this calcified population.
Additionally, 12-month primary patency was 54.5%, with a freedom from target lesion revascularisation rate of 79.3% in a stand-alone therapy. Primary patency outcomes were shown to improve by optimising the procedural technique: appropriate balloon sizing and intravascular lithotripsy therapeutic coverage resulted in the increased primary patency of 62.9% at 12-months follow up, with freedom from target lesion revascularisation being 91.4%.
Target lesion patency; the primary effectiveness endpoint of the study, defined as freedom from ≥50% restenosis, was found to be 69.8% (30/43 patients), as measured by duplex ultrasound. Clinically, improvement in functional outcomes were sustained through to 12-months, in terms of both the ankle-brachial index and the Rutherford score.
In conclusion, the Disrupt PAD II trial remains the first and only core lab adjudicated study to exclusively enrol and follow out to 12-months, heavily calcified lesions. Furthermore, Holden maintained that when intravascular lithotripsy is utilised as a stand-alone therapy in this complex patient population, primary patency outcomes improve.
Regarding the next steps in clinical development, Holden stated: “Importantly, the Disrupt PAD III trial is recruiting… a much larger, 400 patient trial looking to evaluate the role of intravascular lithotripsy in the setting of drug coated therapy.” Specifically, patients have been randomised to intravascular lithotripsy in combination with the IN.PACT drug coated balloon (DCB; the treatment arm) or plane balloon angioplasty and DCB (the control arm), in order to address plaque modification in heavily calcified arteries. “This will be a very important trial to establish the benefit of intravascular lithotripsy in the DCB era,” Holden concluded.
Tobias Steinke (Dusseldorf, Germany) reported on the Lutonix Global arteriovenous (AV) Registry at CIRSE 2018 in Lisbon, Portugal. Lutonix Global AV Registry data add to real-world outcomes of using Lutonix DCB in AV access.
Straight after the presentation, Steinke tells Interventional News about the promising results achieved with the Lutonix AV drug-coated balloon (DCB) in extending the intervention-free interval for patients and about how the results stack up against the results of the Lutonix investigational device exemption (IDE) trial. In the registry data, the target lesion primary patency achieved with the DCB at six-months is around 75%.
The Lutonix Global AV Registry is a prospective, multicentre, single-arm registry investigating the clinical use and safety of BD’s Lutonix (DCB) for the treatment of dysfunctional (AV) fistulas and grafts. Enrolled patients are treated with the Lutonix DCB and followed clinically for a year.
Data from a study seeking to determine the impact of severe calcification and 12-month outcomes of femoropopliteal disease treatment using the Stellarex drug-coated balloon (DCB; Phillips) were presented by Fabrizio Fanelli, Careggi University Hospital, Florence, Italy, at CIRSE (Cardiovascular and Interventional Radiological Society of Europe) 2018 meeting (22–25 September, Lisbon, Portugal). Remarkably similar outcomes were achieved with the device in severely calcified lesions that were amenable to pre-dilation, versus those without severe calcium.
“We know that calcium is the enemy for all endovascular procedures,” noted Fanelli. He acknowledged that although the implications of severe calcification are known—in relation to the occurrence of suboptimal dilation and the ability of calcium to act as a barrier for drugs—the impact of calcium on DCB performance has yet to be fully examined. For instance, previous trials have demonstrated calcium to be a potential barrier to optimal drug absorption; circumferential calcium being the strongest contributor, resulting in the reduction of patency rates.
The authors carried out a prospective study in which patients were pooled from the ILLUMENATE Global (full cohort of the single-arm study; n=371) and ILLUMENATE Pivotal (DCB arm of the randomised trial; n=200). Patency, determined by duplex ultrasound, was assessed at 12 months. Both trials included independent oversight by a Clinical Events Committee and core laboratories analysed angiographic and duplex ultrasound images.
At 12-months, primary patency rates were similar between groups; 82% in the non-severely calcified group compared with 80% in the severely calcified group (log-rank p=0.06). Additional outcomes mirror this similarity; freedom from primary safety events was 93% and the rate of clinically-driven target lesion revascularisation (TLR) was 7% in both cohorts. The rate of 12-month major adverse events was 7.3% and 7.8% (in non-severely and severely calcified lesions, respectively).
Regarding the procedural characteristics, pre-dilatation maximum pressure was higher (9.5 vs. 8.8 atm, p=0.005) and the total DCB inflation time was longer (3.4 vs. 3.9 minutes, p=0.005) in the severely calcified group. Additionally, dissection (>grade C) and provisional stenting rates were found to be similar between groups.
Overall, 556 patients were included in the study, with 242 severely calcified and 314 non-severely calcified lesions. No significant demographic differences were observed in the two groups. However, patients with severely calcified lesions were older and tended to have a higher rate of comorbidities. Severe calcification, prior to contrast injection or digital subtraction angiography, was prospectively defined as “radioopacities noted on both sides of the arterial wall and extending more than one cm of length”.
In light of the findings, Fanelli concluded that similar 12-month outcomes can be achieved with the Stellarex DCB in severely calcified lesions that are amenable to pre-dilatation. The study also confirmed that severe calcium requires longer and stronger inflation, and by doing so, similar stenting rates can be achieved regardless of whether a lesion is severely or non-severely calcified.
Speaking to the CIRSE audience about reasons for the similar patency rates that were observed, Fanelli said: “This can be attributed to the better preparation of the vessel [and] to the characteristics of the balloon itself”.
Darren Klass (Vancouver, Canada) tells Interventional News that social media is helping spread the word about the back hand approach for distal radial access. Klass also elaborates on the technique’s advantages and his team’s experience with it.
Sneak preview: Anna Maria Belli (London, UK; right in video), who was awarded the CIRSE Gold Medal at the 2018 meeting in Lisbon, Portugal, and Tze Min Wah (Leeds, UK) tell Interventional News that addressing the concerns about radiation and enabling flexible working will go a long way towards attracting women into interventional radiology. Full video coming soon…
Christoph Binkert (Kantonsspital, Winterthur, Switzerland) tells Interventional News at CIRSE 2018 in Lisbon, Portugal, that the transradial approach is rapidly gaining momentum in Europe for use in visceral embolization, but that it needs longer lengths of tools before it can be used as effectively in the treatment of peripheral vascular disease.
Robert Morgan, St George’s University Hospitals NHS Foundation Trust, London, UK, discusses the role of interventional radiologists (IRs) in trauma embolization; and whether other clinical specialties with aspirations to perform these techniques should be involved in offering this treatment. Working at a major trauma centre, Morgan, who sees between 100 and 200 traumatic haemorrhage cases a year, highlights the difficulty of the embolization techniques, and explains how important it is that only specialists with proper training should perform these procedures.
At the recent Global Embolization Cancer Symposium and Technologies (GEST) US meeting (9–12 May, Miami, USA), there was a discussion on the topic of embolization and turf. What recent developments suggest that trauma embolization is the next battleground for IRs?
GEST (US) is a North American meeting, and it may be the case that there are more concerns about turf issues in embolization in North America than there are in Europe. However, that is not to say that European IRs should be complacent about this. I think that there are potential issues regarding inadequately trained non-IRs performing embolization procedures, certainly in the trauma field. I am aware that this already occurs in some centres in Europe. In some European hospitals, non-IR trauma specialists advocate that they should be able to perform the full range of treatments for trauma, and that this should include embolization for haemorrhage. These individuals have stated that this approach would be better for patients, without any real evidence base for it.
From my point of view, I disagree with the view that embolization for traumatic haemorrhage is a technique that can be learnt relatively easily by other specialties with no formal training in catheter/guidewire/embolization techniques. I know that our vascular surgical colleagues perform some embolization procedures in connection with EVAR such as plug embolization of the internal iliac arteries and in a few European centres, embolization of endoleaks. However, I do not think that there is a growing enthusiasm from vascular surgeons to take this to the next level and perform embolization of haemorrhage using microcatheters. In the main, I do not see the likelihood of non-IRs performing embolization of haemorrhage as an imminent problem in the UK, and also probably in Europe. However, this is not to say that IRs should be complacent about their role in embolization for haemorrhage.
In my opinion, it is difficult to say that certain specialists cannot perform specific procedures that other specialists do, such as embolization. We have already experienced turf issues between IRs and other specialties in terms of the endovascular treatment of lower limb peripheral vascular disease. From this experience, I do not consider that it is productive to state that one specialty cannot do a procedure that another specialty does. We have to rely on best practice, and ask the question whether the person who wants to take on that procedure is trained to do it sufficiently well enough, according to published professional Standards of Practice guidelines for that specific procedure. It is evident from prior experience with other clinicians who want to perform procedures performed by IRs (for example, uterine artery embolization, or dialysis interventions) that this may not always be the case.
How important is embolization in treating trauma patients?
Embolization is very important for haemorrhage management in trauma. Certainly, not all cases of traumatic haemorrhage require management by embolization. However, there is a subset of patients with haemorrhage from certain abdominal organs, where the standard of care is focused on embolization rather than surgery. Therefore, embolization is integral to the management of some patients with traumatic haemorrhage.
In an interventional radiology list of seven to 12 cases, maybe one or two of those cases will be embolization procedures. In terms of embolization for trauma, maybe one case in 30 to 50 cases. A typical scenario is the patient who has been involved in a road traffic accident and has sustained splenic trauma, usually in the middle of the night.
What constitutes adequate training to perform trauma embolization?
Trauma embolization is just one of the spectrum of cases that are treated by embolization. The procedures are often challenging, requiring endovascular access to small vessels in tortuous arterial territories. Therefore, you need to acquire the skills to be able to access the site of haemorrhage using standard catheters and microcatheters, and standard wires and microwires. You also need to have knowledge of the different types of embolic agents, in which situations to use them and the skills to be able to use them safely. These are not easy skills to acquire. The catheter and guidewire skills necessary to manipulate catheters and guidewires around the relevant arterial territories take time to acquire, and are a considerable step up from the ability to manipulate catheters into relatively large visceral arteries such as renal arteries. Some people never acquire these advanced skills. To master the smaller and more challenging tools that are used for embolization also takes a considerable time.
Embolization of haemorrhage is one of the most challenging tasks in vascular interventional radiology. In terms of how long these skills take to acquire, this will depend on the individual’s endovascular abilities. In terms of absolute numbers at least 50, and probably more than 100, embolization cases using microcatheters would be necessary to acquire the skills to perform embolization of haemorrhage, safely and effectively. To maintain these skills once learned, you would need to be doing between three and five embolization procedures a month. It is not just the catheter and guidewire skills that are essential, it is also the pattern recognition skills of small and large vessel arterial territories on CT angiography and catheter angiography and also the appearance of haemorrhage on these imaging modalities that need to be acquired and maintained.
Finally, embolization for haemorrhage in major trauma patients needs to be done as quickly as possible. Trauma patients usually have skeletal or other injuries that may require urgent surgical management after the bleeding has been stopped by embolization. Therefore, the interventionalist performing an embolization procedure in these critically ill patients needs to work under time pressures, with constant interruptions calling for the patient to be sent elsewhere for other procedures. In these situations, the interventionalist doing the embolization must be highly experienced and able to perform the procedure quickly and successfully under these difficult circumstances.
There is an understanding that non-IR specialties are undertaking simple embolization procedures, in some cases perhaps without adequate training…
I am aware that vascular surgeons undertake embolization in some abdominal arteries as a part of the EVAR (endovascular aneurysm repair) procedure and some surgeons also embolize endoleaks. Many vascular surgeons spend time working in interventional radiology departments, so that they are able to acquire the skills required in those situations. I would reiterate that I do not say for a minute that other specialties should not do those procedures, only that people need adequate training to do them safely and effectively.
As long as there is a recognition by doctors and also hospital administrators that certain procedures should be done by the specialty most suited in terms of training and experience to do them, embolization for haemorrhage will be performed successfully and with minimal procedural complications. In view of the extensive time that IRs spend in acquiring the skills required to use microcatheters and embolic agents, in the vast majority of hospitals IRs should be the specialists who are called upon to perform embolization for traumatic haemorrhage.
In many hospitals, the skills of interventional radiologists in trauma embolization are well-recognised and, as in my hospital, IRs are an important component of the protocols in place for the management of major trauma patients.
What are the key considerations when making the choice between embolization and surgery for traumatic haemorrhage?
The condition of the patient—the patient may be in extremis and may be better off going straight to the operating room for surgery. The patient must be fit enough to come to the angiosuite for the embolization procedure, and anaesthetic support is usually required. Patients must be able to lie flat and immobile throughout the embolization procedure.
Time is important. You need to have enough time to do the embolization procedure—patients with very rapid bleeding need immediate haemorrhage control and should be treated surgically.
The area of haemorrhage that you want to embolize needs to be suitable for embolization, and not more suitable for treatment by any other cause; for example, somebody who is bleeding from a lacerated femoral artery requires surgery, and does not require embolization. Large vessel trauma requires surgery or endovascular stent grafting. Therefore, there is only a small subset of patients with traumatic haemorrhage who are actually suitable for, or require, embolization. Most of these patients will have sustained solid organ abdominal trauma, most commonly the spleen. Pelvic trauma often requires embolization, and occasionally the liver and kidney.
In summary, IRs have the requisite training and experience for the embolization of traumatic arterial haemorrhage and should be an integral part of the team involved in the management of trauma. National government agencies involved in healthcare provision should ensure that sufficient IRs are in place at each hospital that manages trauma to provide a comprehensive embolization service for these patients. Ensuring that there is sufficient cover by a well-staffed interventional radiology service is preferable to an ad hoc service provided by other non-IR clinicians, who seldom have the required skills, training or experience to perform embolization for these challenging and critically ill patients.
Cook Medical have announced that a new 5mm diameter version of Zilver PTX was approved by the US Food and Drug Administration (FDA). It is the first 5mm drug-eluting stent in the USA with lengths available up to 140mm that is indicated to treat vessels as small as 4mm in diameter. The range of Zilver PTX stent diameters now available will address treatment of vessel sizes from 4–7mm in diameter. The new diameter is better sized for smaller anatomy than previous sizes of the stent and provides an additional option to treat patients with lesions in their superficial femoral arteries (SFAs).
“We spend a lot of time listening to physicians to understand their clinical needs. Time and time again, they ask for more treatment options for peripheral artery disease,” said Mark Breedlove, vice president of Cook Medical’s Vascular division. “We’re excited to continue to develop the Zilver PTX line to answer those needs and help more patients around the world.”
The new size is the only 5mm drug-eluting stent on the US market for peripheral artery disease (PAD) and provides another treatment option for lesions in patients with smaller superficial femoral arteries.
Zilver PTX1 was the USA’s first drug-eluting stent used in the treatment of PAD and is the only drug-eluting SFA stent with five-year published data. Zilver PTX has also been shown to cut re-interventions by nearly half through five years, compared to a combination of bare-metal Zilver stents and percutaneous transluminal angioplasty (PTA).
The largest prospective, independently-adjudicated study of drug coated balloons (DCBs) in a broad range of lesions in real-world patients confirms the safety and performance of the IN.PACT Admiral DCB (Medtronic) in the treatment of femoropopliteal artery disease. This is the conclusion presented by Gunnar Tepe, professor of Radiology at the Academic Hospital RoMed in Rosenheim, Germany,during the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (22–25 September 2018, Lisbon, Portugal).
This three-year real-world data shows that freedom from clinically-driven target lesion revascularisation (CD-TLR) was achieved in 76.9% of patients, indicating that this global trial continues to confirm the safety of the IN.PACT Admiral DCB for treatment of femoropopliteal artery disease.
IN.PACT Global was a prospective, multicentre, single arm study conducted at 64 international sites. A total of 1,535 patients, with 1,773 lesions between them, were enrolled in this trial. A wide variety of lesions were included in this study, including: bilateral disease, multiple lesions, TASC (Trans-Atlantic Inter-Society Consensus Document), de novo in-stent stenosis, long lesions (≥150mm), and chronic total occlusions (≥50mm).
The primary safety endpoint that was measured at 12-months showed that no major adverse events were attributed to the DCB itself. Additionally, major limb amputation only occurred in 10 patients out of the entire cohort.
Tepe pointed towards the importance of subgroups to validate findings. For example, the data showed that diabetics (comprising 39.9% of patients in the study) treated within the IN.PACT trial demonstrated “consistent and durable results” through three years, with freedom from CD-TLR at 74.7%, similar to the rate of non-diabetics (78.4%).
The majority of patients in this study (67.8%) were male, and the mean age was 68.6±10.1 years. The mean lesion length was 12.09±9.54cm, including 18% in-stent stenosis, 35.5% total occlusions, and 68.7% calcified lesions.
Back in January 2019, data presented at the Leipzig Interventional Course (LINC; 20 January–2 February, Leipzig, Germany) demonstrated the durability and consistency in clinical outcomes of the IN.PACT Admiral drug-coated balloon. Thus was the result of the two-year MDT-2113 study (IN.PACT SFA Japan), as well as data from a critical limb ischaemia subgroup analysis of the IN.PACT Global study.
In Germany earlier this year, vascular surgeon Michel Reijnen (Rignstate Hospital, the Netherlands) presented the one year results from the critical limb ischaemia subset of the IN.PACT Global study: data showed comparable effectiveness with a freedom from CD-TLR based on Kaplan-Meier Estimate of 86.6% (Rutherford category four), and 85.5% in Rutherford category five (p<0.001).
This present data is an extension of the IN.PACT Global study, and corroborates the earlier findings of the subgroup analysis presented at LINC. Tepe maintained that the data presented so far greatly “reflects the clinical reality,” and noted that follow-up is due to continue for a further two years; allowing for five-year outcomes to be measured.
Andrew Holden (Auckland, News Zealand) interviews Stefan Mueller-Huelsbeck (Flensburg, Germany) to distil the key findings of the IMPERIAL trial one-year data that were presented for the very first time at CIRSE 2018 in Lisbon.
In the randomised controlled trial, Eluvia, which utilises a drug-polymer combination to offer sustained release of the drug paclitaxel, showed higher rates of primary patency at 12 months. Patients in the Eluvia arm of the study also experienced higher rates of freedom from target lesion revascularisation when compared to those treated with Zilver PTX.
The Eluvia drug-eluting vascular stent system (Boston Scientific) shows superior primary patency compared to the Zilver PTX drug-eluting stent (Cook Medical), concludes the 12-month follow-up of the IMPERIAL randomised controlled trial. These data were presented for the first time at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2018 meeting (22–25 September, Lisbon, Portugal).
The data were also presented at the TCT conference and are accompanied by simultaneous publication in The Lancet.
The IMPERIAL trial was a prospective, randomised, single-blinded, multicentre global study aimed at comparing the effectiveness and safety of the Eluvia with Zilver PTX for treatment of symptomatic femoropopliteal artery lesions (lesion length 30–140mm, Rutherford category 2–4).
Presenting the results, Stefan Müller-Hülsbeck (Flensburg, Germany; the European primary investigator) told the CIRSE audience: “Clinical outcome rates were similar between groups, but with half the revascularisation rate for Eluvia.” For instance, the Eluvia stent had a target lesion revascularisation rate of 4.5%, in contrast to 9% observed within the Zilver PTX cohort.
Additionally, the Eluvia stent was found to be more effective than the Zilver PTX, with a primary vessel patency of 88.5% at 12-months versus 79.5% after the same time-frame. Primary vessel patency is defined as a core lab-assessed duplex ultrasound peak systolic velocity ratio of ≤2.4 in the absence of clinically-driven target lesion revascularisation or bypass of the target lesion.
Both the Eluvia stent system and the Zilver PTX—which are designed to restore blood flow in the superficial femoral and proximal popliteal arteries—feature a drug-polymer combination intended to allow for the sustained release of paclitaxel. This drug can prevent restenosis of the vessel.
However, the presence of a polymer (a biostable fluorinated polymer matrix) contained within the Eluvia stent allows for a lower dose of paclitaxel, which is indicative of the main difference between the two stents.
Speaking to the CIRSE audienceabout the reasons for the findings, Müller-Hülsbeck alluded to the presence of the polymer being the “key to success”.
“These impressive clinical outcomes suggest that sustained elution of paclitaxel, delivered by the Eluvia stent, better matched the timing of restenosis in the SFA that can occur months later, thereby reducing the need for repeat interventions,” said William Gray, co-principal investigator of the IMPERIAL trial. “Based on these findings, we believe that the Eluvia stent can be a preferred therapy option when treating patients with arterial blockages in the superficial femoral or proximal popliteal arteries.”
Off the back of data from the MAJESTIC trial, which evidenced long-term freedom from revascularisation at three years, the Eluvia stent system received the CE mark in early 2016. With a primary patency rate of more than 96%, the MAJESTIC trial results represented the highest 12-month primary patency reported for an interventional treatment of femoropopliteal artery lesions among comparable trials, according to Boston Scientific.
The Zilver PTX drug-eluting stent also has a wealth of strong clinical data supporting its efficacy. In 2009, the device was the first CE mark-approved drug-eluting stent designed specifically to treat severe blockages in the superficial femoral artery. Five-years results from the largest and longest-running clinical trial of a drug-eluting stent for treating peripheral arterial disease, published in 2014, evidenced long-term patency for patients treated with the Zilver PTX. This 2014 study compared the Zilver PTX with a bare metal stent, and confirmed the “sustained benefit” of the paclitaxel-eluting stent.
Data from the European Board of Interventional Radiology (EBIR), as presented by O M van Delden at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 22-25 September, Lisbon, Portugal) reveals that only 8% of EBIR-holders and 10-20% of CIRSE members are female.
This gender gap in interventional radiology (IR) has recently been attributed to “imposter syndrome.” Speaking to the CIRSE audience, Tze Min Wah, a consultant radiologist at the University of Leads, UK, said that in relation to IR, imposter syndrome has become a global phenomenon, affecting both males and females. However, this feeling of inadequacy despite evident success is likely to occur more in the underrepresented group of women involved currently in IR.
In relation to overcoming this imposter syndrome, Wah suggested that recognising its existence, mentoring schemes and peer support will be beneficial. Further addressing the gender gap in IR, van Delden pointed to how the EBIR can promote women in IR, as female EBIR-holders and contributors can be role models for IR.
Furthermore, Anna Maria Belli, who was earlier awarded the Gold Medal for her contribution and “fundamental source of inspiration for female IRs though her active leadership role”, alluded to a worldwide misconception involving the perceived dangers of performing IR procedures during pregnancy. She pointed out that although there is sufficient evidence present in the Annals of the International Commission on Radiological Protection that suggests that working in IR during pregnancy is safe, the perception of radiation dangers continues to prevail.
M Victoria Marx, an interventional radiologist at Keck Medicine of USC, Los Angeles, USA, has been appointed president of the Society of Interventional Radiology (SIR) for 2018–2019.
Marx tells Interventional News: “My main goal is to continue the momentum that we have this year on several fronts. The one I am most closely tied to is the development of interventional radiology as a primary medical specialty and the associated development of a robust graduate medical training process in the USA and I am very proud of where we stand with that.
BTG has announced the global launch of its ICEfx cryoablation system. This is an evolution of the existing Visual ICE system, and according to Peter Pattison, head of Interventional Oncology at BTG, “offers predictable, reliable performance with seamless therapy delivery and exceptional ease of technical operation.”
ICEfx enables interventional radiologists to perform cryoablation procedures, facilitating precise and effective treatment without the need for surgery or repeated radiation treatments.
“The ICEfx cryoablation system is a new, more compact design that simplifies the procedure through a set of user-friendly on-screen prompts” explains interventional radiologist AJ Gunn (University of Alabama, Birmingham, USA). “It is easy for my technicians to set up, operate, and shut down. Importantly, this updated version is designed to work with the current line of BTG cryoablation probes, meaning that physicians can still create the reliable ablation zones they have come to expect.”
Pattison comments: “We continue to invest in both new product innovations and clinical research. Building on our commitment in interventional oncology (IO), BTG has added the most advanced cryoablation technology to its portfolio of minimally invasive therapies and is currently supporting a number of active clinical research studies in bone, kidney, lung, pain and prostate. We strive to provide health care professionals with easy access to innovative product choices, our BTG IO portfolio allows them to select and tailor each clinical solution to match a specific patient need.”
The ICEfx cryoablation system will be launched at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) meeting (22–25 September, Lisbon, Portugal).
Cardiovascular Systems Inc. (CSI), a medical device company developing and commercialising interventional treatment systems for patients with peripheral and coronary artery disease, has announced that the first patient in Hong Kong has been treated with its Stealth 360 Peripheral Orbital Atherectomy System (OAS). The Hong Kong case is the first commercial use of Peripheral OAS outside of the USA.
Bryan Yan, associate professor, Chinese University of Hong Kong, who treated the first patient in Hong Kong, said, “Patients with severely calcified peripheral arteries can be difficult to treat due to the limitations of traditional angioplasty or stenting. This can also place patients at risk for subsequent complications including repeat interventions and amputation. The commercialisation of the Stealth 360 OAS in Hong Kong provides physicians with a minimally invasive treatment option for this complex patient population. I am very satisfied with the procedural outcome for my patient because I was able to avoid implanting a stent in the distal superficial femoral artery and I look forward to continuing treatment of similar patients with this technology.”
Scott Ward, chairman, president and CEO of CSI, said, “We are pleased that the first patient treated with OAS in conjunction with our international distribution partner, OrbusNeich, was a success. This positive outcome demonstrates our mutual mission to support physicians in treating patients with peripheral artery disease.”
Scott Addonizio, senior vice president and chief operating officer of OrbusNeich, concluded, “Our experienced sales force is thrilled to bring CSI’s orbital atherectomy technology to Hong Kong. This first procedure occurred only two months after becoming CSI’s international distribution partner. We look forward to introducing CSI’s atherectomy technology to physicians in new markets in the months and years ahead.”
In July 2018, CSI announced that it had signed an exclusive international distribution agreement with OrbusNeich to sell its coronary and peripheral OAS outside of the USA and Japan.
Additionally, in January 2018, CSI announced that it was the exclusive US distributor for OrbusNeich balloon products. Ultimately, CSI will offer a full line of semi-compliant, non-compliant and specialty balloons for both coronary and peripheral vascular procedures. OrbusNeich PCI balloons include the Sapphire II Pro, the first and only 1mm coronary balloon available in the USA.
Merit Medical Systems has announced the expansion of its biopsy portfolio, with the release of five new manual bone biopsy systems. According to a company press release, each of the systems has been specifically designed to optimise diagnostic yield in specialised settings, and, collectively, they provide multiple options for use in a wide variety of applications.
Featured in the new line-up are the Madison and Huntington bone biopsy systems. The direct access Madison features a trocar-tip stylet that can be introduced through the cannula to assist with initial bone entry. The cannula also supports the use of a drill insert that helps traverse hard bone for small cortical abnormalities in axial and appendicular cases. The Huntington is designed with a tri-angled tip and longitudinal groove that both maintains accuracy even in oblique approaches and functions as a collection channel for tissue evacuation upon first contact in hard bone procedures and sclerotic lesions.
The patented perforating cannula included in the Madison and Huntington systems facilitates greater accuracy of placement through dense bone tissue. The stylet of these systems can easily be exchanged for a drill insert without losing the introducer cannula’s place in the bone; when used in conjunction with a drill, the edges of the perforating cannula simultaneously cut around the drill as the tip bores through the bone.
“The range of biopsy systems allows the physician to choose the needle best adapted to the bone density prior to or during the procedure,” says Jean-Denis Laredo, chief of the Radiology Service, Lariboisière Hôspital, and professor of Medicine at the Public Hospital of Paris, University of Paris-Diderot, France. “Having a Seldinger-inspired guide wire approach to the spine assists both experienced and younger radiologists in safely placing a larger needle. The biopsy is almost achieved once the introducer needle is against the target. This also provides a better anaesthetic for the patient, and less radiation caused by repeat scanning.”
In addition to the Madison and Huntington systems, Merit is also introducing the Madison Mini for small rounded bones that have little soft-tissue surroundings; the Westbrook, designed to reach superficial lesions in soft- or normal-density bone; and the Kensington bone biopsy system, which was created for deep bone, upper spine and narrow access procedures. The Kensington is used with the Seldinger-inspired guide wire approach.
All of the systems utilise the Preston bone biopsy needle, which is constructed with clockwise-cutting trephine teeth to support true cylindrical tissue retrieval and use even in sclerotic and blastic lesions. The systems also offer comfortable-grip handles that lock together to allow for more manual pressure if necessary, and depth stoppers to give a visual guide for biopsy needle protrusion beyond the introducer.
“The expansion of our biopsy portfolio allows us to better serve the needs of our customers and underscores Merit’s belief that offering a wide range of products gives practitioners a fuller set of options for instrument selection,” comments Fred Lampropoulos, chairman and CEO of Merit Medical.
Cook Medical has announced that it received a close-out letter from the US Food and Drug Administration (FDA) resolving a 2014 warning letter for processes related to the quality system at the company’s manufacturing facility in Bloomington (Indiana, USA). A company press release states that the resolution was a direct result of the company’s employees’ efforts to improve Cook Medical’s quality system over the last four years.
The 2014 letter issued by the FDA to Cook Medical stated that an inspection “revealed that your firm’s devices are adulterated within the meaning of section 501(h) of the Act, 21 U.S.C. § 351(h), in that the methods used in, or the facilities or controls used for, their manufacture, packing, storage, or installation are not in conformity with the current good manufacturing practice requirements of the Quality System regulation found at Title 21, Code of Federal Regulations (CFR), Part 820.”
“Receiving critical feedback from the FDA in 2014 was tough, but beneficial. After a lot of thoughtful discussion, our leadership team decided this feedback was an opportunity to slow down and take a hard look at our company,” says Pete Yonkman, president of Cook Group and Cook Medical. “As a result, we established a plan to not only address the issues in the warning letter, but transform our entire company.”
A key part of that transformation was the recent realignment of the company’s business into two divisions, Vascular and MedSurg. Other critical changes that are underway include improvements to accelerate the company’s product development process, to elevate the level of customer service, and to upgrade the company’s IT infrastructure. Cook also recently purchased a million-square-foot abandoned factory in Bloomington to provide room to redesign its manufacturing processes.
Yonkman now comments: “As we have focused on resolving the warning letter and improving our company over the last four years, we have, at times, disappointed our customers. For example, adding new systems slowed our production capabilities, and we experienced shipment delays. We are not finished yet, but our teams have worked hard to improve our delivery times, and we thank our customers for sticking with us.
“One of the benefits of being a family-owned, privately held company is that we were able to take the long view and invest in our company and our employees. We still have work to do, but we are proud of the progress our employees have made to get us to this important milestone. Our transformation is making us a better, stronger company so that we can continue to fulfil our mission of improving the lives of patients around the world.”
Thirteen neurointerventional societies have released new guidelines outlining the criteria for Level 1, 2 and 3 stroke centres that provide acute ischemic stroke interventions (ASISs) to stroke patients. The standards are published in the September issue of the Journal of NeuroInterventional Surgery.
Acute ischemic stroke caused by emergent large vessel occlusion (ELVO) is the leading cause of adult disability in the world. Recent studies have shown that neuroendovascular stroke surgery significantly improves outcomes in ELVO patients, especially if the patient receives the surgery in a timely fashion. To ensure positive patient outcomes, it is critical to ensure that facilities can provide the proper care to stroke patients in a safe and timely manner.
For the first time, the societies have specified criteria for Level 1, 2 and 3 stroke centres—terminology they believe will help health providers and the public better understand the capabilities of stroke treatment facilities. Level 1 centres need to offer the full spectrum of neuroendovascular services, including neuroendovascular stroke surgery. In addition to other requirements, these centres need to treat a minimum of 250 stroke patients per year and perform a minimum of 50 thrombectomies per year.
“ELVO patients should be taken to Level 1 stroke centres. Establishing guidelines for Level 2 stroke centres gives patients a chance at the best possible outcome in underserved regions,” says Adam Arthur, president of the Society of NeuroInterventional Surgery (SNIS), and a neurointerventionalist at the Semmes-Murphey Clinic in Memphis, USA. “These guidelines, issued by this eminent group of organisations, will help facilities around the world maintain the highest standard of care for stroke patients.”
The guidelines recommend that Level 2 stroke centres see a minimum of 100 stroke patients per year and perform a minimum of 50 thrombectomies per year. Each neurointerventionalist in a Level 2 centre should perform a minimum of 15 acute intracranial thrombectomies per year.
The guidelines recognise the challenges that newly created Level 2 stroke centres could face in meeting the minimum volume criteria for procedures. They allow for these centres to operate below the minimum threshold numbers as long as they expect to hit their volumes within 12 to 24 months.
The purpose of these guidelines is not to serve as a substitute for existing national and regional guidelines, but rather to outline the best recommendations based on expert opinions and the most current evidence available in stroke care around the world.
The following societies contributed to the development of these guidelines:
Asian-Australian Federation of Interventional and Therapeutic Neuroradiology (AAFITN)
Australian and New Zealand Society of Neuroradiology (ANZSNR)
American Society of Neuroradiology (ASNR)
Canadian Society of Neuroradiology (CSNR)
European Society of Minimally Invasive Neurological Therapy (ESMINT)
European Society of Neuroradiology (ESNR)
European Stroke Organisation (ESO)
Japanese Society for NeuroEndovascular Therapy (JSNET)
Ibero-Latin American Society of Diagnostic and Therapeutic Neuroradiology (SILAN)
Society of NeuroInterventional Surgery (SNIS)
Society of Vascular and Interventional Neurology (SVIN)
World Stroke Organization (WSO)
World Federation of Interventional and Therapeutic Neuroradiology (WFITN)
Embolx, a new medical device company out of Silicon Valley, has been given the European CE mark for its latest Sniper balloon occlusion microcatheters. The devices are used to help deliver embolic agents in various procedures, including the treatment of tumours, uterine fibroids, and enlarged prostate.
The Sniper balloon occlusion microcatheters were recently cleared in the USA, gaining Food and Drug Administration (FDA) approval earlier this year.
The device occludes the vessel to alter blood flow-dynamics using pressure-directed embolization. It is currently used for the treatment of cancerous tumours in the liver and other organs, enlarged prostate (benign prostatic hyperplasia), and uterine fibroids.
“Our next generation devices incorporate experience from more than 1,000 Sniper balloon occlusion microcatheters used to date,” says Michael Allen, president and CEO of Embolx. “Now, interventional radiologists can do everything they would do with standard microcatheters, but with the added benefits of balloon occlusion. This is a big step forward and provides physicians with the most advanced transarterial delivery system for tumour and prostate treatment.”
The Sniper comes in three lengths—110cm, 130cm, and 150cm—enabling access to femoral and radial arterial sites. Improvements in the microcatheter’s atraumatic tip allow for smooth entry and easy visualisation thanks to the radiopaque material, a press release informs. The Sniper is also compatible with conventional diagnostic catheters, guidewires, and embolic agents, so physicians do not require additional accessories.
This European clearance follows the news in April this year that the US National Institute of Health (NIH)’s National Cancer Institute awarded a US$2 million small business innovation research grant to Embolx to fund further research and development of the company’s Sniper balloon occlusion microcatheter.
Boston Scientific has announced that it has entered into a definitive agreement to acquire Augmenix, a privately-held company which has developed and commercialised the SpaceOAR system, a therapy used to reduce common and debilitating side effects that men may experience after receiving prostate cancer radiotherapy. The transaction consists of an upfront cash payment of US$500 million, and up to US$100 million for reaching sales-based milestones.
Each year, more than 1.1 million men are diagnosed with prostate cancer worldwide and approximately 400,000 men will undergo prostate radiotherapy.One of the most common complications of treatment is rectal radiation injury, due to the rectum’s proximity to the prostate and the resulting high doses of inadvertent radiation exposure. Prior to radiation therapy, the SpaceOAR hydrogel is injected to create additional space between the rectum and prostate during treatment, thereby reducing rectal radiation dose and associated side effects.
The SpaceOAR hydrogel is CE marked, cleared by the FDA, and has been used in more than 30,000 patients worldwide. As a result of commercial adoption, expanded US reimbursement and a total addressable market valued at US$750 million, product sales are estimated to reach US$50 million in 2018, and approach US$90 million in 2019.
“The acquisition furthers our category leadership strategy in urology and the SpaceOAR hydrogel is a crucial addition to our growing prostate health treatment portfolio of products that improve the quality of life and clinical outcomes for men with prostate cancer and benign prostatic hyperplasia,” says Dave Pierce, president, MedSurg, Boston Scientific. “The injection of this hydrogel during a minimally-invasive, in-office procedure can reduce the unwanted and unintended side effects of prostate radiation and provide substantial peace of mind for patients and their treating physicians.”
Clinical trials in Europe and the USA have demonstrated that the space created by the hydrogel significantly reduces the amount of radiation delivered to the rectum. Additionally, the randomised SpaceOAR hydrogel US clinical trial demonstrated that patients who received the hydrogel spacer reported significantly less rectal pain during prostate radiotherapy and had significantly less severe long-term rectal complications, including zero incidence of grade 2 rectal toxicity versus a 5.7% rate experienced by patients without the spacer.
A single injection of the SpaceOAR hydrogel is designed to maintain the space between the rectum and prostate for three months—within the duration of a standard radiation treatment schedule. The absorbable hydrogel is gradually reabsorbed by the body within six months of injection.
“We are proud of the clinical and commercial outcomes we have been able to achieve for SpaceOAR hydrogel thus far, and are excited to drive accelerated adoption leveraging Boston Scientific’s urology and pelvic health expertise,” says John Pedersen, chief executive officer, Augmenix. “The company also has the additional resources needed to further explore expansion of indication to other organs throughout the body that could benefit from space creation—such as gynaecological and pancreatic cancers.”
The transaction is expected to be immaterial to adjusted earnings per share in 2018 and 2019, accretive in 2020 and increasingly accretive thereafter. On a GAAP basis, the transaction is expected to be less accretive, or more dilutive as the case may be, due to amortization expense and acquisition-related net charges. The acquisition is projected to close early in the fourth quarter of 2018, subject to customary closing conditions.
BTG has announced it has acquired Novate Medical, a medical device company focused on the prevention of pulmonary embolism in patients at high risk of venous thromboembolic events.
Novate has developed Sentry, the first bioconvertible inferior vena cava filter, which has recently been granted 510(k) regulatory clearance in the USA. Sentry’s 12 month clinical trial data demonstrated no new symptomatic pulmonary embolism and no evidence of device migration, tilt, fracture, perforation or embolization, complications which have been associated with some other inferior vena cava filters. The unique bioconversion feature eliminates the need for an additional interventional procedure to retrieve the device.
BTG plans to launch Sentry in the US in the second half of FY2018/19 and will sell the device through its existing vascular sales force.
“This bolt-on acquisition further enhances BTG’s strength in the vascular space.” said Louise Makin, BTG’s CEO.
“Novate’s unique inferior vena cava filter offers our existing customers a highly complementary product in the management of pulmonary embolism.”
BTG paid US$20m in cash to acquire Novate and may be required to pay additional cash considerations up to US$130m if certain commercial and sales-related milestones are met.
Vascular Dynamics has revealed that enrolment of the first patients in an FDA-approved and best-in-class pivotal clinical trial has started. The CALM-2 study is designed to establish safety and efficacy of the novel endovascular baroreceptor amplification (EVBA) procedure using the unique MobiusHD device as a treatment for drug resistant hypertension.
A press release reports that Vascular Dynamics is developing the first minimally-invasive technology designed to use this natural blood pressure control system to address uncontrolled hypertension. It adds that the MobiusHD is a flexible, self-expanding device that reshapes the carotid sinus following endovascular implantation. It is intended to amplify the baroreflex while maintaining pulsatility.
Results published in The Lancet, from an open-label, proof-of-concept trial (CALM-FIM) using the EVBA approach to treat patients with resistant hypertension were positive—showing significant reductions in blood pressure through six months, greater than the 24-hour ambulatory blood pressure reductions reported to date for alternative devices used to treat hypertension. These results led to the design and development of a rigorous pivotal clinical trial intended to generate conclusive evidence confirming the safety and efficacy of this unique device for resistant hypertension patients.
The CALM-2 (Controlling and lowering blood pressure with MobiusHD) pivotal trial is a prospective, randomised, sham-controlled, double-blinded study targeting patients with drug-resistant hypertension. Lessons learned from numerous clinical trials of first-generation device-based approaches to hypertension were incorporated into the CALM-2 study protocol to provide a best-in-class clinical trial design. The CALM-2 trial is targeting enrolment of up to 300 patients at leading institutions across the USA and Europe. The first patients were enrolled in July 2018 at the Center for Clinical Research at Southern Illinois University Medicine and The Lindner Research Center at The Christ Hospital Health Network.
Gregg Stone (Columbia University Medical Center/New York-Presbyterian Hospital, New York, USA), co-principal investigator of the CALM-2 trial, comments: “Enrolling the first patients in the CALM-2 trial is an important step toward offering a new treatment option for this large patient population with resistant hypertension and the associated health risks.”
Bryan Williams (University College London, London, UK), who is the co-principal investigator of the trial and chair-elect of the European Council on Hypertension of the European Society of Cardiology, comments: “I am optimistic that device-based treatments, such as EVBA with the MobiusHD implant, may be able to provide effective solutions for patients who have not benefited from drug-based treatments.resist
With the graduation of the first ever interventional radiology residents from a US university, Wael Saad and Minhaj Khaja discuss the importance of having a dedicated IR residency programme.
The evolution of the interventional radiology (IR) residency hit a milestone this year with the graduation of the first two IR residents in the USA, both from the University of Michigan. Nishant Patel and Michael Cline completed their IR residency training in June 2018.
The creation of an integrated primary residency in IR has long been in the works. However, a handful of programmes (at the University of Virginia, the University of Rochester, the University of Pennsylvania, and the University of Michigan, all USA) did have focused IR training programmes prior to the establishment of the IR residency at the University of Michigan. Perhaps the most consistent legacy programme of these is the University of Virginia (UVA) programme, established by Alan Matsumoto and John Fritz Angle (both of the Department of Radiology and Medical Imaging, UVA, Charlottesville, USA).
Since the approval of the IR residency in 2014 by the Accreditation Council for Graduate Medical Education, the educational paradigm in vascular and interventional radiology has been evolving at a rapid pace. Under the leadership and direction of Reed Dunnick (chair), Janet Bailey (diagnostic radiology programme director), Wael Saad (IR Division director), Bill Majdalany (IR Fellowship programme director) and Minhaj Khaja (Clinical Pathway programme director and graduate), the collaborative team strategically established the Vascular and Interventional Radiology (VIR) Clinical Pathway at Michigan in 2013, with the plan to transition to the IR residency. The VIR Clinical Pathway was established in such a way that the trainees could easily transfer into the IR residency programme of the future, and were therefore poised to be pioneers. It was modelled after the UVA-programme which we, having attended that university, were very familiar with. It should be noted that the key to this success was the collaborative relationship between IR training (Minhaj Khaja), the diagnostic radiology training (Janet Bailey), and the surgery internship training. This collaboration not only enabled the Michigan programme to be one of the first in the nation, but was noted by the Radiology Review Committee (RRC) site visit.
The first IR residency programmes were approved by the Accreditation Council for Graduate Medical Education in spring of 2015, with the first match that same year. There were only eight resident positions and a handful of programmes involved in the first year. Today, there are over 75 programmes and 130 positions each year. Having been among the first programmes approved for the IR residency and having a pre-established VIR Clinical Pathway, Michigan’s residents were able to easily transfer into the IR residency and the training paradigm of the future. The Michigan IR residency integrated programme, now with a tailored, linked surgical preliminary year, has two graduates and 16 trainees in the programme, spanning all six years of the curriculum. The latest recruited years have three integrated IR residents per class.
Cline has remained on staff at the Ann Arbor Veterans Administration Hospital, and is a faculty member at the University of Medicine and Health Sciences, Basseterre, St. Kitts & Nevis. Patel has moved out west to Denver to begin his career at Radiology Imaging Associates, USA. I am sure the entire IR community can join us in congratulating them in representing our future as pioneers and torch-bearers. We thank all of those who were vital to making this a reality at our institution, as well as nationally.
Wael Saad is a professor of Radiology, Vascular and Interventional Radiology at Michigan Medicine, the University of Michigan, Ann Arbor, USA. Minhaj Khaja is an assistant professor of Radiology at Michigan Medicine, the University of Michigan, Ann Arbor, USA.
Daniel Sze (Stanford University, Stanford, USA), presenting at the European Conference on Interventional Oncology Annual Meeting (ECIO; 22–25 April, Vienna, Austria), calls for a synergy between gene therapy and interventional oncology, saying that delivery efficiency can be improved by interventional oncologic procedures, cutting costs on treatments which currently cost up to US$1,200,000 per patient.
Speaking in the session entitled ‘Immunotherapy in 2018’, Sze tells the ECIO audience: “Even after we have talked about this for 45 years, there are still few approved gene therapies for human disease.” The first gene therapy to be approved was in 2003, when the drug Gendicine was granted clearance in 2003 to treat head and neck squamous cell carcinoma (HNSCC). Since then, only a handful of gene therapies have been approved; most recently, in 2017, the US Food and Drug Administration (FDA) granted marketing authorisation to two CAR (chimeric antigen receptor)-T cell therapies: Kymriah (Tisagenlecleucel, Novartis) for B-cell acute lymphoblastic leukaemia and Yescarta (axicabtagene ciloleucel, Kite) for diffuse large cell lymphoma.
“Even though interventional radiology is expensive, gene therapy is even more expensive”, Sze explains. “For instance”, he continues, “those CAR-T cells that were approved last year, Yescarta and Kymriah, cost US$500,000 per patient. Strimvelis [another gene therapy; GlaxoSmithKline] is US$800,000, and Glybera [uniQure] costs US$1.2 million per patient to be treated. In fact, Glybera is going off the market right now, because in the six years since it has been approved, it has only been used to treat one patient, because only one patient could afford the cost.
“So we have to decide, as a field and as a society, where to spend the money. There is the cost of manufacture of these genetic therapies, as well as the cost of administration.”
If, instead of pumping money into the manufacture, Sze argues, the financiers spend slightly more money on the treatment’s administration, then the overall cost of future gene therapy could be significantly reduced. Currently, gene therapy is so expensive in part because scientists need to grow billions or even trillions of vectors to transfect the host cells and express the desired protein product. Transfection can occur either in vivo, where the patient is injected with the viral vector, or ex vivo, where host cells are removed, the viral vector is added, and the transgenic host cells are reintroduced to the patient’s body. Either method requires multitudinous vectors, which all need to maintain the ability to transfect cells, and if transfection occurs ex vivo, sterile, viable human cells need to be grown on a large scale.
“I propose we could spend a little bit more money on the administration. We could perhaps have the manufacturers manufacture a little bit less vector, and we inject it directly into the organ of interest. Likewise, we could have them grow a few fewer cells, and we could inject them into the region of interest,” Sze suggests.
Vector efficiency: “Let the experts have a crack at it”
“Delivery (in vivo); let the experts have a crack at it” reads the slide behind Sze as he advises utilising the skills of interventional oncologists in improving vector efficiency. A literature review in Anticancer Research cites a variety of possible routes for the administration of viral vectors: intravenous, intra-arterial, intra-tumoural, intra-portal, intra-biliary, intra-splenic. Listing these, Sze says, “Of course, this is focusing on the liver, since the liver is the factory of the body. Of all of these, anyone can do intravenous, but these other types of administration are all in the purview of interventional radiology. So the virologists should work on choosing and engineering optimal vectors, the cancer biologists should focus on choosing optimal genes, but the interventional radiologists should work on the optimal delivery.”
Sze and colleagues have looked at some standard interventional radiology practices, and found that many are readily adaptable to gene therapies, and there are even some specificities for tumour cells over normal cells. For instance, Sze used a wedged retrograde hepatic venous delivery in pigs and baboons of a non-viral vector encoding human factor IX, resulting in expression of the human gene, though the expression was not durable.
Writing recently in Cardiovascular Interventional Radiology, Oliver Pellerin and colleagues (Hôpital Européen Georges-Pompidou, Paris, France) provide an example of interventional oncologic methods applied to a gene therapy treatment. They report the successful intra-arterial injection of a rabbit VX2 hepatic tumour with engineered mesenchymal stem cells. These cells are transgenic, possessing a gene that metabolises the prodrug cyclophosphamide 13 times better than the wild type. Following injection with the engineered cells, the investigators administered intravenous cyclophosphamide. While cyclophosphamide alone did suppress tumour growth, the addition of the genetically engineered mesenchymal stem cells helped to metabolise the drug and enhanced efficacy.
Sze concludes: “After nearly 50 years of study, only a few gene therapies are approved for human use, in part because multigenic diseases such as cancer are very challenging. Interventional oncologic methods, however, may improve efficacy and reduce toxicity, as well as reduce costs, due to locoregional delivery of reduced doses.”
Penumbra, a global healthcare company focused on innovative therapies, has announced it has closed on the acquisition of a controlling interest in its joint venture, MVI Health Inc. After closing the transaction, Penumbra increased its ownership to 90% of the equity of MVI Health for US$20 million in upfront cash consideration.
MVI Health, originally formed in May 2017, is a joint venture between Penumbra and Sixense Enterprises, a leader in virtual reality software and tracking solutions for enterprise. Since its founding, MVI Health has been developing virtual reality technology for healthcare applications.
MVI Health, headquartered in Alameda, USA, is supported by investments from Penumbra and licensed intellectual property and other resource contributions from Sixense Enterprises.
Penumbra has announced US commercial availability of the Penumbra JET 7 and Penumbra JET D Reperfusion Catheters powered by the Penumbra ENGINE aspiration source. The Penumbra JET 7 and JET D Reperfusion Catheters deliver deep vacuum aspiration power of the Penumbra ENGINE to enable physicians to extract thrombus effectively and safely in acute ischaemic stroke patients.
The Penumbra JET 7 is the Penumbra System’s seventh generation reperfusion catheter for proximal large vessel occlusions, and JET D Reperfusion Catheter is designed specifically for distal occlusions. JET 7 Reperfusion Catheter has a large 0.072” lumen for deep vacuum aspiration and is designed for trackability and navigation, featuring 20 transitions from the proximal shaft to distal tip, a progressive distal coil wind for superior flexibility and Quad-Wire technology in the proximal shaft for enhanced pushability. JET D brings deep vacuum aspiration power to distal occlusions with a smaller profile.
“The JET 7 Reperfusion Catheter with its advanced tracking technology and large 0.072” aspiration lumen is the most advanced device for stroke. In my clinical experience, I was able to easily and quickly navigate the JET 7 through tortuous anatomy to the face of the clot and achieve full revascularisation after a single pass,” said Alejandro M Spiotta, Medical University of South Carolina, Charleston, USA. “We know from our own published experience that increases in aspiration lumen size have led to faster recanalisation times and higher likelihood of success at first pass without compromising safety. I eagerly await collecting and publishing our clinical experience with JET 7.”
“The JET 7 and JET D along with the new ENGINE provide a suite of tools to effectively address both proximal and distal occlusions,” said Ian Kaminsky, Radiology Imaging Associates/Swedish Medical Center, Englewood, USA. “In our initial case experience, we saw the easy tracking of the JET 7 and JET D in a range of tortuous conditions and vessel locations that, combined with the deep vacuum of the ENGINE, offer the potential to increase our rate of complete first pass revascularisation while decreasing procedure times.”
Avinger, a developer of treatments for peripheral artery disease (PAD), has announced the Company submitted a new 510(k) application to the US Food & Drug Administration (FDA) for the Pantheris SV (Small Vessel) Lumivascular Atherectomy System.
Pantheris SV is a line extension of the Pantheris family of catheters, the first and only image-guided atherectomy devices for the treatment of PAD. Designed with a lower profile and longer length, Pantheris SV is intended to expand the number of addressable procedures for Pantheris by allowing physicians to target lesions in smaller diameter vessels and more distal regions of the vasculature. Pantheris SV incorporates key improvements introduced to the platform with the clearance of the next generation Pantheris system in May 2018, including a stiffer shaft for increased pushability, a refined optical coherence tomography imaging system, a more robust nosecone, and an enhanced cutter design.
“Effective tools to address lesions in smaller vessels represent an important unmet clinical need in the treatment paradigm for PAD,” said Jaafer Golzar, Avinger’s chief medical officer. “There is a lack of long-term durability noted with other treatment options in this area of the vasculature. However, the concept of pairing onboard image-guidance with a directional atherectomy system could provide a number of significant clinical advantages, including an enhanced safety profile, the ability to maximise luminal gain without causing vascular injury, and a potential enhancement in the uptake of anti-restenotic drug therapy,” Golzar continued.
Jeff Soinski, Avinger’s president and CEO commented, “This submission represents an important milestone in positioning the company for growth in 2019. We are hopeful that this filing will lead to US market availability of Pantheris SV by early 2019, which we believe would allow us to address a significantly larger portion of the estimated US$500 million atherectomy market. We are excited to get this next generation small vessel device into the hands of Lumivascular physicians.”
Atherectomy is a minimally invasive treatment for PAD in which a catheter-based device is used to remove plaque from a blood vessel. Lumivascular technology allows physicians, for the first time ever, to see from inside the artery during an atherectomy procedure by using an imaging modality called optical coherence tomography, or OCT, that is displayed on Avinger’s proprietary Lightbox console. Physicians performing atherectomy with other devices must rely solely on X-ray as well as tactile feedback to guide their interventions while treating complicated arterial disease. With the Lumivascular approach, physicians can more accurately navigate their devices and treat PAD lesions, thanks to the real-time OCT images generated from inside the artery, without exposing healthcare workers and patients to the negative effects of ionising radiation.
AngioDynamics has provided a corporate update and acknowledged a recent, favourable US District Court ruling that impacts its vascular access business.
A press release states that in May of 2017, AngioDynamics filed a lawsuit against CR Bard (Bard) for violating United States antitrust laws with its practice of illegally tying tip location system sales to its line of peripherally inserted central catheters (PICCs). On Monday, 6 August, the US District Court for the Northern District of New York rejected—in its entirety—CR Bard’s motion to dismiss AngioDynamics’ lawsuit against it.
As a result of last week’s ruling, AngioDynamics’ antitrust lawsuit against Bard will proceed.
Tip location systems are devices that can be used to aid healthcare professionals in the bedside placement of a PICC. The lawsuit claims that Bard has a dominant position in the tip location system market and will only sell the proprietary stylet necessary to operate its tip location systems preloaded in its PICCs, not separately, which would allow any type of PICC to be used with the tip location systems. By doing so, customers who want to buy Bard’s tip location systems must also buy Bard’s line of PICCs, which prevents hospitals and other medical providers from purchasing BioFlo PICCs from AngioDynamics’ vascular access business.
The press release adds that AngioDynamics’ lawsuit seeks to end Bard’s violation of the antitrust laws and to recover treble damages for losses due to Bard’s violations, as well as attorneys’ fees and other costs. AngioDynamics is represented by Philip Iovieno and Anne Nardacci of the law firm of Boies Schiller Flexner LLP.
Xarelto, co-administered with aspirin, is indicated in the EU for the prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral arterial disease (PAD) at high risk of ischaemic events.
The European Commission (EC) has approved a combination of Xarelto (rivaroxaban) 2.5mg twice daily plus low dose aspirin (acetylsalicylic acid/ASA) once daily for the prevention of atherothrombotic events in adult patients with coronary artery disease (CAD) or symptomatic peripheral arterial disease (PAD) at high risk of ischaemic events.
The EU approval is based on data from the COMPASS study, the largest phase III study with rivaroxaban (27,395 patients), which showed that the rivaroxaban vascular dose, 2.5mg twice daily, plus ASA 100mg once daily reduced the risk of the composite of stroke, cardiovascular (CV) death and heart attack by 24% (relative risk reduction, ARR: 1.3%) compared with ASA 100mg once daily alone in patients with CAD and/or PAD.
Derek Connolly, consultant interventional cardiologist at Birmingham City Hospital, (Birmingham, UK) and COMPASS trial investigator commented: “Cardiovascular diseases are one of the leading causes of death in the UK, and coronary artery disease and peripheral artery disease represent a major public health burden—despite many advances in the area of cardiovascular care, CAD and PAD have remained an area of unmet need. Even with currently available treatments for secondary prevention, patients remain at an unacceptably high risk of thrombotic events which can lead to disability, loss of limb and death. This was the biggest study of rivaroxaban to date, and now that it is licensed for these conditions, it provides UK clinicians with a new option for treating CAD and PAD.”
Lars Bruening, CEO Bayer UK & Ireland, said: “The story and momentum behind the COMPASS data continues to grow—from the study being stopped one year early for overwhelming efficacy, the presentation of the results themselves at the European Society of Cardiology congress last year, and now to this exciting news from the European Commission. Ten years ago this October saw Bayer just starting out on the Xarelto journey with the first indication in orthopaedics—and this year we welcome our eighth indication for the management of patients with CAD and PAD in the UK. It is especially exciting to see the continuing impact that Xarelto will have on patients with PAD, most of whom have concurrent CAD, as it has been many years since a new medical therapy has been proven in this high risk patient population.”
Following the licence approval across Europe, the new indication will be submitted to the National Institute for Health and Care Excellence (NICE) and the Scottish Medicines Consortium (SMC) for review for routine reimbursement across the UK.
Gynesonics announced that it has received 510(k) clearance from the US Food and Drug Administration (FDA) to market its Sonata sonography-guided transcervical fibroid ablation system.
The Sonata System combines a breakthrough integrated technology, and is the first and only intrauterine ultrasound system with a proprietary radiofrequency ablation device, providing a transcervical, incision-free, uterus-preserving treatment for uterine fibroids, a press release from the company states.
With an estimated volume of more than one million annual global fibroid procedures, Gynesonics projects a US$3 billion–$4 billion global market opportunity for its Sonata System for the treatment of uterine fibroids, including a market opportunity of more than $1 billion in the USA alone.
“We are excited to announce FDA clearance of our Sonata system. This is an essential milestone for Gynesonics in our mission to bring this transformational technology for the treatment of uterine fibroids to women,” says president and CEO Christopher Owens. “The patient outcomes achieved with Sonata demonstrate its potential to become a new standard of care in fibroid treatment, providing important patient benefits as compared to invasive surgery. Clinical trial outcomes show that Sonata provides a significant and durable improvement in symptoms with more than half the women returning to normal activities within 24 hours.”
In a survey published in the American Journal of Obstetrics and Gynaecology, of 968 women affected by fibroids, 79% of women want to avoid invasive surgery. The same study found that affected women wait an average of 3.6 years before being treated, and that most women, regardless of desire for future fertility, want to preserve their uterus.
“The published survey results show that women are looking for new options to address this widespread condition, they want to preserve their uterus and they wish to avoid invasive surgery, including hysterectomy,” Owens adds. “Sonata is the only system that can treat the vast majority of all fibroids with a transcervical, incision-free, uterus-preserving approach. Current transcervical options are limited to treatment of a small portion of the total fibroid market by comparison.”
According to medical literature, about 70–80% of women in the USA will develop uterine fibroids by age 50, with a significant proportion of women having symptoms, many of which can be severe and debilitating. In addition, according to the New England Journal of Medicine, approximately 200,000 hysterectomies are performed in the USA each year because of symptomatic fibroids.
Owens added that the company exceeded the FDA-specified 12-month primary endpoint performance requirements for the Sonata System in the SONATA pivotal IDE clinical trial used to support the FDA regulatory 510(k) filing. The co-primary endpoints included a significant reduction in bleeding and a high rate of freedom from surgical re-intervention due to heavy menstrual bleeding. The safety outcomes were also favourable, including zero device-related adverse events reported in the 147-patient trial.
Catheter-based sclerotherapy is a safe and effective treatment for endometrial cysts and could help preserve fertility in patients, according to a study published in the journal Radiology. endometriosis
Endometriosis is a common condition that affects about 10% of women of reproductive age. When endometriosis involves the ovaries, fluid-filled cysts called endometriomas may form, causing pelvic pain and abnormal uterine bleeding.
Surgery is a common treatment for endometriomas, but it carries risks, including the removal of healthy ovarian tissue, which can affect fertility. Needle-based sclerotherapy is a less-invasive option that involves inserting a needle into the cyst under ultrasound guidance and then withdrawing the cystic fluid through a needle. The cyst is then washed with a solution of ethanol. However, the needle-directed approach has limitations, says study co-author Man-Deuk Kim, professor at Severance Hospital, Yonsei University College of Medicine in Seoul, South Korea.
“Endometrial cyst content can be incredibly thick and sticky. A 16- or 18-gauge needle, which is commonly used for needle-directed sclerotherapy, is sometimes not large enough to completely evacuate the cyst,” he says. “This may reduce the efficacy of sclerotherapy and increase the possibility of needle displacement during aspiration.”
Kim and colleagues studied a sclerotherapy technique that replaces the needle with a catheter, a flexible tube used for removing fluid from cavities in the body. Along with draining cystic fluid more easily, a catheter allows for positional changes during the procedure, which helps maximise the ethanol’s effectiveness by enabling it to contact the cyst wall evenly. The catheter also reduces the risk of spillage into the peritoneal cavity of the abdomen.
The researchers evaluated catheter-directed sclerotherapy with 95% ethanol in 14 women between the ages of 20 and 44 with ovarian endometriomas.
After about one year, the cysts had decreased on average from 5.8cm in diameter to 1.1cm. Pain was relieved in all patients, and blood tests indicated well-preserved ovarian function. There were no procedure-related complications.
There were no endometrioma recurrences, even in patients with internal septation, or division, within their cysts. The multiple compartments of septated cysts can be difficult to puncture with a needle, which may lead to incomplete sclerotherapy. In catheter-directed sclerotherapy, once the endometrioma is punctured, clinicians can manipulate the guidewire and catheter to break down internal septations, allowing for more effective treatment.
“In our study, the recurrence rate of catheter-directed sclerotherapy was 0%, which is very encouraging given that endometriomas measuring up to 13.5cm diameter or those that had internal septation were included in the study,” Kim says.
The results suggest that catheter-based sclerotherapy could lead to better short-term clinical outcomes in women with endometrial cysts while preserving ovarian function and improving future fertility, he notes.
The researchers plan to conduct a study to see how catheter-directed sclerotherapy compares with surgery in terms of fertility, cyst recurrence and improvements in clinical symptoms.
Roberto Iezzi provides an overview of ablative therapies, and what interventional radiologists can expect from ablation procedures in the near future. Amongst the emerging technologies discussed are molecular-targeted agents, improved imaging-guided modalities, and the combining immunotherapy with ablative strategies.
In the last years, local ablative therapies have increased in the clinical practice, playing an important role not only as a curative option in the treatment of localised primary and secondary cancers, but also as an alternative when palliation is desired, local control is needed, or surgical resection is not feasible, principally due to the longer survival of patients with metastatic disease.
In the above clinical scenario, thermal ablation technology has evolved rapidly with substantial technical and procedural improvements that can expand clinical indications, improve clinical outcomes and better safety profiles.
The future perspectives of ablation are mainly based on the attempt to overcome ablation intrinsic limitations, mainly represented by the higher rate of local tumour progression (LTP) compared to surgical resection that can occur due to an incomplete ablation at the periphery of the tumour, and the absence of an ideal tool to precisely guide and monitor the ablative procedures. In detail, the creation of a larger ablation volume in a reasonable time frame without technical complexity is necessary to achieve a complete ablation, significantly reducing the rate of local tumour progression. It is well known that this aim can be obtained using multiple electrodes to switch from monopolar to bipolar/multipolar modes, or by using different energy sources, including microwave, laser, high intensity-focused ultrasound (HIFU) and cryoablation. However, in the last few years the concept of combined treatment has strongly emerged; this can be referred to as multimodality, such as in combined ablation and chemoembolization, and also to intermodality, a combination of ablative procedures, percutaneously or intra-arterially driven, with three-dimensional conformal radiotherapy (3DCRT). In detail, the development of three-dimensional conformal radiotherapy (3DCRT) has enabled high dose radiation to be directed to a tumour with a frank sparing of the non-tumour surrounding liver parenchyma without restriction due to tumour topography and size, presence of peri-tumourous satellite nodules, or associated segmental portal vein thrombosis.
Furthermore, the recent development of molecular-targeted agents in the treatment for hepatocellular carcinoma (HCC) has also prompted synergies between locoregional tumour ablation and systemic chemotherapy.
Other emerging technologies are represented by imaging-guiding modalities and assistive techniques for percutaneous treatment. In particular, recent technical advances of imaging fusion have enabled the overlay or side-by-side display of real-time ultrasound images combined with the established fusion of CT/MRI-acquired images, but also PET (Positron Emission Tomography) during an interventional procedure. Like fusion imaging, contrast-enhanced ultrasound increases radiofrequency ablation performance in terms of localisation and targeting of a tumour. Applying these techniques to tumour ablation enhances the identification of target lesions and the feasibility of the intervention.
Finally, there is a growing interest in combining immunotherapy with ablative strategies, but little data are available to guide if and how these modalities should be combined.
What is clear is that thermal ablation cannot be considered solely as a locoregional therapy. The resultant inflammatory response, though at present limited and unpredictable, paves the way for an expanded role of thermal ablation as a stimulant to the immune system. Ablation, however, is a two-edged sword, and causes of and solutions to its oncogenic effects need to be investigated. What we strongly need is to optimise the timing of immunotherapy and thermal ablation; that is crucial for the creation of a curative therapy. Recent studies seem to demonstrate that a primed ablation protocol can enhance treatment response with a high tumour burden. Also, as a result of mechanical and immunologic changes in the tumour microenvironment following local ablation, it seems to be a window of opportunity for employing immunotherapy, after which the ablation may actually limit the efficacy of immunotherapy. Sequential immunotherapeutic strategies after ablative therapies seem also to show a great potential for the prevention of post-ablation tumour recurrence and for generating durable and powerful antitumor immunity to achieve optimal tumour control. The prospect of manipulating the immune system toward the rejection of established cancers as part of the standard of care for patients is becoming closer to reality, even if more data are still needed to further verify its efficacy.
All these technical and procedural aspects will be discussed in the fourth edition of MIOLive 2019 (Mediterranean Interventional Oncology;28–29 January 2019, Rome, Italy). The meeting will be a forum for discussion for all those who are interested in interventional oncology, as well as locoregional treatments. It will be a practical interactive meeting based on live cases integrated by short presentations and lectures where professionals from various Mediterranean countries can share opinions, experiences, research projects and knowledge, under the guidance of several international experts. It is the best place for obtaining networking opportunities, listening to experts, and learning and sharing best practices.
Roberto Iezzi is an interventional radiologist at Policlinico A Gemelli, Rome, Italy.
Percutaneous CT-guided radiofrequency thermal ablation is a safe and effective alternative treatment option in patients with pulmonary metastases from hepatocellular carcinoma (HCC) that cannot be considered potential candidates for surgery. This is the result of a retrospective study by Italian investigators, presented at the European Conference on Interventional Oncology Annual Meeting (ECIO; 22–25 April, Vienna, Austria) by Giulia Lassandro (University Federico II, Department of Advanced Biomedical Sciences, Naples, Italy).
The study investigators performed a retrospective evaluation of overall survival, local tumour progression, complication rates and early outcomes of percutaneous CT-guided ablation of pulmonary metastases from HCC. HCC is the most common primary tumour in the liver, representing about 90% of primary liver malignancy, and is the third leading cause of cancer-related mortality worldwide. The most common site for HCC metastases is the lungs. In fact, Lassandro informed the ECIO audience that pulmonary metastases occur in 55% of cases via haematogenous dissemination to the pulmonary capillary network.
From February 2012 to September 2017, a total of 23 patients underwent CT-guided radiofrequency thermal ablation treatment as a first line therapy. There were 13 males and 10 females, with a mean age of 62 years. There was a total of 38 lung lesions, treated in 36 CT-guided ablation sessions (two patients had two metastases treated during the same procedure).
Of the 23 patients treated in this study, overall survival observed at one year was 87%, 67% at three years, and 44% at five years. If HCC is untreated, the average survival rate is less than six months. The investigators also report a low complication rate for radiofrequency thermal ablation. The most frequent complication observed in their patient cohort was subtle pneumothorax, which occurred in six of the 38 lung lesions (16%). Just one patient experienced a pneumothorax requiring pleural drainage tube insertion. The most dangerous complication observed was a relapse on a treated lesion, which occurred in one patient who died of extensive HCC occurrence in the liver.
Lassandro comments, “In general, patients with pulmonary metastases may benefit from surgical therapy, but current usual practice for metastasectomy is limited to a specific subset of patients, meaning that the vast majority of them are not suitable for resection. As an alternative, these patients could be treated with minimally invasive therapies like radiofrequency ablation, microwave and cryoablation, that preserve an effective lung parenchyma and have already been used in the treatment of lung lesions.
“In our experience, radiofrequency thermal ablation improves survival and quality of life in selected patients when used in addition to medical therapy.”
Fielding questions from the ECIO audience, Lassandro was asked how she was able to convince the oncologists in her hospital to allow her to perform ablation in metastatic HCC patients. Lassandro answered: “I am very lucky, because at my centre we have a tumour board, including oncologists, pneumologists, gastroenterologists, diagnostic radiologists, interventional radiologists, and also a surgeon. So generally, we treat these type of patients—selected ones with no sign of hepatic disease—with radiofrequency ablation. But it is not a rule for us, because generally oncologists want to treat them [metastatic HCC patients] with Sorafenib. But we do not stop Sorafenib during the RFA treatment, so generally we accord with our oncologists to do this type of treatment in patients with continuous medical therapy. So we agree with each other on this type of treatment on our tumour board.”
Study details
The mean size of the pulmonary metastases was 14mm, with a size range of 30–40mm. None of all 23 patients had active HCC foci in the liver, and no more than three metastases in the lung at the time of radiofrequency thermal ablation treatment. Follow up visits were scheduled at one, three, six, 12, and 24 months after treatment, and each follow-up appointment included a physical examination, protein assay, liver function tests, and also a tumour recurrence monitoring by CT scan.
According to the Barcelona clinic liver cancer (BCC) flow chart, all of the patients included in this study were metastatic, and were classified as advanced stage C. They were treated with Sorafenib in addition to radiofrequency ablation. Every patient was also classified as Class A in the Child-Turcotte-Pugh score, as they had not sign of advanced hepatic disease and no alteration in functional liver tests.
To evaluate treatment effectiveness, the study investigators used contrast CT to detect enhancement and dimensional changes in the lesions. Over the five-year study period, Lassandro and colleagues used three different devices to perform the ablation procedure.
Mermaid Medical Group, a privately-owned international provider of minimally invasive medical devices, acknowledged a product line addition to its vascular business. As part of its strategic focus for expanding their vascular product portfolio, Mermaid Medical Group announced the acquisition of the Angel Catheter technology from Bio2 Medical Inc.
The acquisition immediately establishes Mermaid Medical’s presence in the vascular business, adding a clinically proven and current commercialised product. The Angel catheter can minimise the incidence of pulmonary embolism (PE) by utilising a “temporary” catheter with an attached nitinol basket placed in the femoral vein. Bedside placement allows for easier, quicker, placement while minimising hospital costs.
The Angel catheter offers a safe, effective alternative for catching potential thrombus due to trauma and various underlying patient disease states. The Angel catheter will be utilised throughout the hospital where patients are at risk of a pulmonary embolism.
“The addition of the Angel catheter with its present indication and extensive related portfolio of intellectual property will add significant value to our company” said Lars Vinther, president and CEO of the Mermaid Medical Group. “It will also enhance our strength going forward supporting our upcoming Mechanically Thrombectomy System D-Clot, and will also open new doors at the Trauma units.”
Approved by the FDA in June 2015, the Angel catheter became commercially available in January 2017. The Mermaid Medical Group will immediately begin supporting the current Angel customer base worldwide, with plans to expand the product offering to additional existing Mermaid Medical global markets.
Gore have announced the first implant in conjunction with the Gore ARISE study of the Gore Ascending Stent Graft, an investigational device and the only endovascular stent graft specifically designed to treat type A dissections of the ascending aorta. The successful procedure took place on August 14, 2018 at Memorial Hermann Medical Center in Houston (USA), by Anthony Estrera, and Bruce Tjaden, as part of the Gore ARISE study.
ARISE is the first multicentre, early feasibility study approved by the US Food and Drug Administration (FDA) to investigate the use of a minimally invasive device to treat type A dissection. The national principal investigator is Michael Reardon, from Houston Methodist Hospital, (Houston, USA). The study initially investigated the use of the Gore Tag Thoracic Branch Endoprosthesis (aortic extender) in type A dissection, which is also being evaluated in its own pivotal study to assess safety and effectiveness in treating lesions of the aortic arch and descending thoracic aorta. The new purpose-built Gore Ascending Stent Graft will be used for the remainder of the study to allow investigators to gain a better understanding of how new technology can advance treatment options for this condition.
The Gore Ascending Stent Graft features a precise delivery system that is designed to allow for accurate, controlled deployment in complex anatomies. The delivery system features unique angulation control that gives physicians the option to angulate the device to achieve orthogonal placement to the ascending aorta.
Type A aortic dissection is a tear in the lining of the ascending aorta, above the heart, that creates a second channel of blood flow. It is an emergent condition that requires immediate surgery upon diagnosis. The current standard of care for these patients is open surgery involving a sternotomy—cracking the chest and spreading the two halves of the rib cage apart to gain access to the heart and ascending aorta. This is a very invasive and involved surgery that includes temporarily stopping the heart to prevent blood flow during the surgical repair.
“There is a great need for a less-invasive treatment option for type A dissections, which are fatal for nearly half of all sufferers within 48 hours of onset,” Estrera said. “I’m excited that Gore is breaking ground in this area with the development of the first endovascular device specifically designed to meet the anatomical, curvature, and deployment precision requirements unique to the ascending aorta. This device, upon approval, could provide a treatment option for type A dissection patients who are not suitable for open surgery and a less-invasive treatment for all patients with this condition.”
Not all patients with type A aortic dissection are suitable for open surgery. The average sufferer of ascending aortic dissention is male and in his early 60’s, although it can also affect females and a wide age range and age groups. Risk factors that may complicate open surgery include previous thoracic surgical repair, visceral malperfusion, neurologic deficit, presentation with a concurrent myocardial infarction, cardiac tamponade, obesity, advanced aged, and poor renal, cardiac, or pulmonary function. The Gore study will investigate how an endovascular stent graft, delivered via catheter, may be used to line the dissected portion of the ascending aorta as a less-invasive alternative to open surgical repair. Similar endovascular therapies have proven to reduce the risk of complications and recovery times.
Gore has announced FDA 510(k) clearance, approval from the Japanese Ministry of Health, Labour, and Welfare, and receipt of CE mark for the innovative Gore moulding and occlusion balloon, a compliant polyurethane balloon catheter designed in close collaboration with clinicians to assist in the expansion of self-expanding stent grafts or to temporarily occlude large-diameter vessels. The new device meets all endovascular aortic repair (EVAR) procedural requirements—a single balloon that replaces the need for multiple moulding and occlusion balloons.
The device’s proven radial expansion force across the range of EVAR device sizes enables physicians to consistently seat and seal grafts with confidence. This more efficient graft seal may reduce procedural time and the risk of type I endoleaks. The device is also engineered with the lowest profile to reduce the potential of access-related complications, and its excellent pushability and trackability offers enhanced control with uncompromised inflation and deflation time.
“We have worked closely with clinicians to engineer a single balloon that truly changes both the physician and the patient experience,” said Eric Zacharias, Gore vascular business leader. “This milestone is one of several in our ongoing dedication to treating the entire aorta, and to helping physicians offer the best patient experience possible.”
The new device is supplied in a single catheter length of 90cm to enable use with current Gore Excluder devices as well as future Gore devices while still being compatible with a 180cm length guidewire.
Besides adding value through consistently reliable technical success and patient experience, the use of a single balloon allows for efficiency and inventory optimisation. “We know our physicians are concerned with both technical performance and with economic value to their practices,” Zacharias said. “Use of a single moulding and occlusion balloon during an EVAR case reduces intraoperative waste, minimising overall instrument cost per procedure. The potential to reduce operating room and catheter lab time may contribute to faster room turnover and more on-time procedural starts.”
Interventional radiologists issued a red alert warning over staff shortages in Scotland as the only full-time specialists based in the Scottish Highlands step down. The Scottish Government has been urged to answer for “unacceptable failings”.
From mid-August 2018, one health board will no longer have a substantive consultant interventional radiologist in post and plans to send emergency patients out of the area for treatment.
In a letter to local MSP Edward Mountain, the NHS Highland chair, David Alston, confirmed that there would be “no full time substantive consultant interventional radiologist based at Raigmore [Hospital in Inverness, Scotland] from the middle of August following a retiral and a resignation from the existing establishment of two consultants”.
Grant Baxter, Royal College of Radiologists in Scotland chairman, called on the government to boost the number of trainees to avert major problems after pledges were made for an extra 50 over five years.
Speaking to BBC Scotland, Baxter said: “We are on red alert. There is absolutely no doubt about this. If we do not address this issue now, there simply won’t be a service in the next three, four, five years. When radiology does well, your health service will do well. When radiology fails, the health services fail because every patient will come through an imaging radiology department. This situation is simply unsustainable and has resulted in thousands of studies currently lying around unreported, with all the safety issues that entails. Treatment regimes for cancer patients are almost entirely imaging based—therefore treatment decisions are being delayed.”
A spokeswoman for the health board explains that, for patients with immediate life-threatening conditions requiring intervention, there are arrangements in place to transfer to NHS Tayside or NHS Grampian.
There is an international shortage of radiologists, who are in increasing demand. However, an applicant for a substantive interventional radiologist post at NHS Highland will be interviewed at the end of the month. A locum is due to start in autumn and a retired radiologist will return one day a week from October.
A global recruitment drive was launched for nine boards across Scotland in February. Adverts in Western Europe, India, Australia, the USA and Canada sought to fill 32 radiologist vacancies.
Cabinet Secretary for Health Jeane Freeman said: “Despite an international shortage of radiologists affecting health services worldwide, since 2007 we have increased the number of clinical radiology consultants by 41% and increased radiography staff by 24.4%. We will also create an additional 50 specialist training places for clinical radiologists over the next five years.”
Nicola Strickland, president of the Royal College of Radiologists, expressed “grave concerns” about the workforce crisis in NHS Highland.
Guerbet has announced a commercial partnership with Imalogix, a company focusing on artificial intelligence process and workflow solutions. The commercial partnership combines Guerbet’s diagnostic and interventional imaging with the cloud-based human and machine-intelligence capabilities of Imalogix to proactively identify areas that impact care delivery to reduce variability and improve the quality, safety and efficiency of care around radiation dose management.
According to a press release, the Imalogix Platform gives healthcare organisations the tools to understand and manage the process, quality and safety related to diagnostic imaging and interventional procedures, and meet evolving regulatory standards surrounding radiation dose management.
“Guerbet is thrilled to deliver an AI-powered solution that brings together data in a meaningful way to evolve the standard of care to patients for managing radiation dose,” says Massimo Carrara, Guerbet Vice President for North America. “By partnering with such a recognised expert in the field, Guerbet remains focused on offering the best in diagnostic imaging in a rapidly evolving industry.”
The Imalogix self-learning neural network enables organisations to understand and benchmark in real-time best practices from the mass learnings across a network of providers to drive continuous improvement. Deep learning recommendations highlight where and how changes can be made to enable organisations to proactively change behaviour down to the scanner, protocol and operator level. Insights into procedure length, utilisation, and workflow help organisations understand how to become more efficient and optimise patient flow.
“We are excited to partner with Guerbet who has an extensive track record of innovation. This partnership further demonstrates their commitment to grow and expand their digital offerings to bring best-in-class solutions to their customers,” says John Heil, CEO of Imalogix.
Two-year outcomes from the LIBERTY 360° study have shown a marked improvement across all Rutherford classes, as well as high freedom from major amputation. The results were presented as a late-breaking presentation at the Amputation Prevention Symposium (AMP; 8–11 August, Chicago, USA).
The LIBERTY 360° study is designed to evaluate the acute and long-term clinical and economic outcomes of peripheral vascular interventions in patients with peripheral arterial disease. With over 1,204 patients enrolled at 51 sites across the USA, it is among the first peripheral arterial disease studies to investigate patients across the spectrum of symptomatic peripheral arterial disease (Rutherford classes 2–6). As an “all comers” study, LIBERTY 360°’s trial design included any endovascular device FDA-cleared for treatment of peripheral arterial disease.
Key endpoints include procedural and lesion success, major adverse events (MAEs), duplex ultrasound, quality of life (QoL), six-minute walk test (6MWT) and economic analysis.
The two-year study outcomes were presented by Jihad A Mustapha, Advanced Cardiac & Vascular Amputation Prevention Centers, Grand Rapids, USA. Mustapha’s presentation highlighted the continued high freedom from major amputation in all Rutherford Classifications (RC) at two years (RC2–3, 99.1%; RC4–5, 94.5%; and RC6, 79.8%).
“LIBERTY 360° represents as close to a real-world experience as possible with various endovascular strategies across Rutherford classes. Following endovascular intervention, we saw a marked improvement across all Rutherford classes at two years, as well as high freedom from major amputation. In particular, LIBERTY 360° provides compelling evidence that peripheral vascular interventions can lead to amputation free survival even in RC6 patients, which showed a 79.8% freedom from major amputation following peripheral vascular intervention,” Mustapha said.
Mustapha also noted that an orbital atherectomy (using Diamondback 360, Cardiovascular Systems Inc) sub analysis of the LIBERTY data indicated high freedom from major amputation in all Rutherford Classes (RC2–3, 100%; RC4–5, 95.3%; and RC6, 88.5%).
Cook Medical has introduced the 140mm-length Zilver PTX drug-eluting peripheral stent in both 6 and 7mm diameters in the USA. The longer length comes after an expanded indication approval by FDA to treat total lesion lengths up to 300mm per patient. In addition, the product also received an extended shelf life of two years by the FDA.
The 140-mm length stents will enable physicians when applicable to treat lesions up to 270-mm with only two stents. In addition to this benefit, the stent has been shown to cut reinterventions by nearly half in 5 years, compared to a combination of bare-metal Zilver stents and PTA.
“We’re happy to continually broaden the Zilver PTX product offering, giving physicians more options when treating superficial femoral artery disease based on the individual patient need,” said Mark Breedlove, vice president of Cook Medical’s vascular division.
The device is the world’s first drug-eluting stent for treating peripheral arterial disease (PAD) in the superficial femoral artery (SFA) and is the only drug-eluting SFA stent with five-year published data.
Boston Scientific has signed an agreement to acquire Veniti, a privately-held company in Fremont, USA which developed and commercialised the Vici venous stent system for treating venous obstructive disease. Boston Scientific has been an investor in Veniti since 2016 and currently owns 25% of the company. The transaction price for the remaining stake consists of US$108 million up-front cash, as well as up to US$52 million in payments contingent upon US Food and Drug Administration (FDA) approval of the Vici stent system.
The self-expanding, nitinol Vici stent system was developed specifically for use in the venous anatomy, which presents different challenges than placing stents in the arterial vascular system. The Vici stent is designed to withstand compression and maintain patency and flexibility over the course of a patient’s life expectancy.
“This stent system was designed with the distinctive demands of the venous system in mind, and built to provide physicians with a high-quality lumen across a variety of venous anatomies and disease states,” said Jeff Elkins, president and CEO of Veniti. “We are excited to see this stent technology become even more accessible to physicians and the patients they treat under the leadership of Boston Scientific.”
The Vici stent system received CE Mark in 2013 and Veniti submitted a pre-market approval (PMA) application to the FDA in June, leveraging results from the recently completed VIRTUS pivotal study. Currently in the USA, there are no stent technologies specifically indicated for use in the peripheral venous system.
“With the unique benefits of this differentiated technology and the strong experience of Boston Scientific in the overall venous market, we believe the Vici stent will become an important choice for physicians who choose stents to treat patients suffering from venous disease,” said Jeff Mirviss, senior vice president and president, Peripheral Interventions, Boston Scientific. “Along with our leading AngioJet thrombectomy platform and venous product pipeline, we look forward to meeting the needs of physicians treating both chronic and acute venous disease.”
The acquisition of Veniti is expected to be immaterial to Boston Scientific adjusted earnings per share (EPS) in 2018 and 2019, and accretive thereafter. On a GAAP basis for 2019 and subsequent years, the transaction is expected to be less accretive, or more dilutive as the case may be, due to amortisation expense and acquisition-related net charges. For 2018 on a GAAP basis, the transaction is expected to be accretive due to a one-time gain on prior investment. The completion of this transaction is imminent, subject to customary closing conditions.
In the USA, the VICI Stent System is an investigational device and is not available for sale.
“Innovation has driven my life in interventional radiology—and what a ride it has been,” said Barry Katzen, founder and chief medical executive of Miami Cardiac and Vascular Institute and clinical professor of Radiology and Surgery, Miami, USA.
Katzen, a pioneer, thought leader and innovator, delivered the plenary lecture titled “My life in interventional radiology” at the 2018 Asia Pacific Society of Cardiovascular and Interventional Radiology meeting (APSCVIR; 8–11 March, Auckland, New Zealand).
“Interventional radiology in the USA has become a true and defined discipline of medicine and there are no limits to where our imaginations can take us, as long as we remain focused on improving the status quo and making changes to improve patient care,” Katzen said.
Tracing the beginning of interventional radiology with Charles Dotter’s first therapeutic use of the catheter in 1964, followed by his description of balloon angioplasty as a new technique, Katzen noted that it was in the decade after, i.e. in the 70s, that Katzen himself finished medical school, an internship in internal medicine and completed his radiology residency. “There was no CT, ultrasound, or cross-sectional imaging. Angiography was the ‘definitive’ diagnostic test, short of sugery, and exploratory laparotomy was the most common procedure. People were leaning more and more about how to navigate the body with what would today be considered very primitive tools. Interventional radiology did not exist; fellowships were few, but available in ‘angiography’ or ‘cardiovascular radiology’,” he said, commenting to Interventional News that “there was clearly a lot of room to improve healthcare”.
Katzen also showed a picture that is important to him, even today (photo 1). “One thing that I learnt as a medical student holds true to this day: the answer is always at the bedside. In this era of high-tech medicine when people cannot think without a CT scan, it shows that it is the patient who has the answer, hidden within him/her. So being close to the patient and listening to the patient can be extraordinarily revealing,” he said.
In an era when it was atypical for radiologists to actively seek patient contact, while other radiology residents used to moonlight doing extra radiology work, Katzen used to moonlight doing house calls by covering for general practitioners. “This led to my belief in ‘high-tech, yet high touch’ care in which patient contact is central,” Katzen said. Rejuvenated in Rome Life did not always go as Katzen envisaged and before his fellowship, he was turned down for a job in private practice that he applied for due to lack of experience. However, this led to other opportunities and Katzen went on to do a fellowship in cardiovascular radiology and carried on in academic practice in New York. This in turn, led to a fellowship in Rome, Italy, with the technically brilliant Plinio Rossi (photo 2), who had recently left St Vincent’s Medical Center in New York to return to Italy after building one of the largest angiographic departments in the USA.
“In 1974, I started in July at St Vincent’s Hospital and Medical Center as a fellow who was in line to become the next section chief. In September, I left for Rome for a three-month ‘fellowship’. This decision was perhaps the single most impactful event in my professional life, because I learnt from Plinio Rossi, a truly unique individual, not just technical skills but also his respect for tissue. We did several procedures together that were firsts and it was at this time that I embraced using the catheter as a surgical instrument,” described Katzen. It was also in that warm Roman Autumn (photo 3) that Katzen lost his fear of the unknown “as I understood that all progress needed to be driven by improving patient care and outcomes. I also met Andreas Gruentzig who later became the first person to successfully use balloon angioplasty in the coronary arteries. Gruentzig’s success resulted in a transformative technology, but his dream, which was the catheter-based percutaneous treatment of vascular disease in alert, awake patients was equally thought-provoking. Here was an internist who was also an interventionalist, and I began to think, I too, could be a radiologist/proceduralist who was a clinician,” explained Katzen.
Time in the Italian capital yielded another valuable insight with Katzen mulling on the idea of a practice model that would “serve as a base for the rest of my career. I returned to New York a different person; the ‘passion’ had found a purpose,” he said.
The Alexandria years
On his return to the USA, Katzen left New York and began working as a radiologist at the Alexandria Hospital in Virginia with Arina van Breda (photo 4) as his partner. Almost at once, he began advocating clinical practice for interventional radiology. He also rapidly expanded his practice to full-time interventional radiology. The establishment of the non-invasive vascular lab saw Katzen perform his first balloon angioplasty in 1974 and a series of US firsts including the first renal angioplasty. He also wrote and published on the use of embolization to stop bleeding and he also wrote the first text book on interventional radiology in 1980 that revealed the broad scope of the discipline.
Katzen also established a fellowship training programme and developed a sense of urgency around training radiologists ‘quickly’ (photo 5). This naturally led to beginning live case education which started off as tutorials in angioplasty, once per month. Interest in teaching people and disseminating the message of less invasive medicine also led Katzen to pioneer the use of sophisticated video and audio technology to enhance the process of education for practitioners.
He is also credited with being the first to use “live patient demonstrations” in the USA, which became the benchmark for procedural education in endovascular therapy, and many other procedural areas of medicine. Jeffrey L. Rodengen author of The Ship in the Balloon: The Story of Boston Scientific and the Development of Less-Invasive Medicine writes: “Gruentzig’s demonstration style was adopted and championed by Barry Katzen. John Abele, founder of Boston Scientific, who participated in many of these courses is quoted as saying: ‘It was really a revolution in education. Doctors would fight to get to these courses and watch these live cases. The video would zoom in and let them seen things they could not see even when they were in the operating room. And it was no-holds barred: the good and the bad were shown, and that has really changed the face of medicine.’” Katzen received a lifetime achievement award from Transcatheter Cardiovascular Therapeutics (TCT) in 2007 for originating live case teaching.
In the late 80s interventional radiology had gained significant ground by providing alternatives to surgery in many different conditions. In parallel was the development of interventional radiology practice and the demand for acknowledgement that the interventional radiologists needed to be equal partners in patient care, a viewpoint that Michael Dake, a close colleague and Ernie Ring, a longtime friend shared with Katzen (photo 6).
Katzen was prescient at predicting turf battles that could lead to the demise of radiology involvement in endovascular procedures without clinical practice. This was all driven by the disruptive technology of transluminal balloon angioplasty.
“As-yet turf was not an issue because surgeons simply saw angioplasty as ‘mickey mouse’ care, without real benefit, but I could see that we were headed on a collision course between different disciplines. It was not just proceduralists, we would soon be using the same technique to treat the same disease everywhere in the body. However, different specialties would be doing so and nobody was really talking to each other,” he said. Therefore, Katzen reasoned multidisciplinary models, and patient-centred care needed to be approached as an alternative practice method. During this time he also developed a ‘white paper’ on building an integrated institute based on a collaborative organisational model.
The Miami years
In 1986, Katzen left a well-established programme at Virginia to create something new, which was not possible in Alexandria. “I had bold ideas of integrated care with interventional radiology at the centre of clinical care, and as an equal clinical partner in care. The new organisational model was based on collaboration and mutual benefit, rather than traditional silos and had at its heart, the advancement of less-invasive medicine. It was also built on a philosophy of teamwork.” (Photo 8)
In the first year at Miami, Katzen focused on clinical work, building bridges and getting multidisciplinary support. In the second year, he began a new educational programme with live cases that ultimately expanded into the International Symposium on Endovascular Therapy (ISET).
Innovations during this time saw the expanding of the definitions of image-guided therapy including accessing a beating heart in the angiosuite, but procedures were getting more complex and further change was was called for. Galvanised by the idea of changing the definition of the angiosuite, in 2008, Katzen and his team developed an expansion strategy to create optimal planning and support for the future of image-guided therapies. Fundamental to the plan was that inclusivity leads to resources. Since then, developments at MCVI have included a US$120 million expansion project that has seen the building of interventional suites of the future: there are two new endovascular suites that have glass walls and a video system allowing people to sit in a theatre-style chair outside of the suite and control what they are watching using an iPad. “It is all about being open, transparent and practicing in the sunshine. Fittingly, in many cases, it is well-known patients who have been very generous in their philanthropy and fundraising efforts.”
Katzen acknowledged the vital role played by Judith Katzen, noting that his lifetime partner who has shared his journey (and love of boats) since they were in high school is the secret of his success (photos 9 and 10). “I have been part of, and witness to one of the greatest movements in medical history: the move towards less invasive therapy, to which I have a lifelong commitment. Right from its early beginnings, from seemingly minor procedures, there were big concepts that have changed the landscape of medicine,” Katzen concluded.
Katzen’s principles of success
Integrity is the key
Be an instrument of change rather than a victim of it
Never be satisfied with the status quo: continually try to improve care for our patients
No one can go it on their own: engage and involve others, and create ‘win-win’ situations and outcomes
A vision without execution is a hallucination, you need to do the work to makes things happen
Know your own strengths and weaknesses, because sure as sure can be, everyone else will
I have a lifelong commitment to less-invasive therapy
A prospective US FDA-approved investigational device exemption (IDE) study has demonstrated significant improvement in lower urinary tract symptoms secondary to benign prostatic hyperplasia and reduction in total prostate and central gland volumes in patients treated with prostate artery embolization.
The study was published online on 20 July 2018 in the journal, Urology.
The triallists, including Riad Salem and colleagues from Northwestern University, Chicago, USA, enrolled 45 men with prostate volume greater than 40g. The patients enrolled were classified as having an International Prostate Symptom Score (IPSS) of greater than 13; peak flow rate (Qmax) of less than or equal to 12mL/; and voided volume greater than or equal to 125ml.
“We must all strive to raise the level of evidence with interventional therapies. Prostate artery embolization is no exception. Our group was intrigued by initial reports from pioneers of the procedure in Portugal, Brazil and the USA. As a result, we embarked on a truly multidisciplinary prospective phase 2 study. It is with such prospective investigations that the entire field moves forward and the scientific level of dialogue is raised,” Salem told Interventional News.
Patients were evaluated with questionnaires (IPSS, quality-of-life [QoL]), International Index of Erectile Function (IIEF), and Male Sexual Health Questionnaire for Ejaculatory Dysfunction (MSHQ-EjD)] and clinical measures (post-void residual volume [PVR] and Qmax at baseline, one, three, and 12 months after prostate artery embolization.) Baseline and six-month total prostate and central gland volumes were obtained.
Prostate artery embolization results
As reported in Urology, 45 patients with a mean prostate volume of 99cc (range: 30–214g) were treated over the course of the three-year study. At one month, there were significant improvements in IPSS (p<0.0001), quality of life score (p<0.0001) and Qmax (p<0.0001) that were sustained at the three-month follow-up. At six months, there were significant improvements in IPSS (p<0.0001) and QoL (p<0.0001) that were sustained at one-year follow-up.
Further results from the study showed that there were reductions in post-void residual volume that reached significance at certain time points including at the six-month and one-year marks. Median decreases in total prostate volume and central glad volume were 18% (p=0.0001) and 27% (p=0.0001), respectively. These findings of prostate size reduction will soon be published in a separate analysis in Abdominal Radiology.
The authors reported self-limited adverse events that included dysuria (n=13), haematuria (n=6), haematospermia (n=2), urinary frequency (n=3) and retention (n=2). There were no severe adverse events, non-target embolization, or adverse effects on erectile function or sexual health.
“We were able to complete all 45 patients without non-target embolization or any other significant adverse events. Most importantly, there were no adverse effects on sexual function. It is exciting to be generating data that validate those of ROPE UK and other publications. In my opinion, there has now been sufficient data to support embolization as a legitimate treatment option in selected patients. It is time to start offering embolization as one of many standards of care to patients afflicted with benign prostatic hyperplasia,” Salem told Interventional News.
Percutaneous ablation can be successfully used to treat many cases of early-stage renal cell carcinoma, a new study published in the Annals of Internal Medicine, led by a team at Weill Cornell Medicine and New York-Presbyterian, suggests.
The study was an observational cohort analysis evaluating the outcomes of 4,310 early-stage kidney cancer patients aged 66 and older with tumours under 4cm in a large national registry. The investigators found that percutaneous ablation is associated with fewer complications and lower rates of renal failure for older patients compared with radical nephrectomy (where the kidney is removed). Radical nephrectomy is the standard of care in these older patients.
“For older patients with this type of early-stage kidney cancer, percutaneous ablation should be considered as an alternative to radical nephrectomy,” says lead study author Adam Talenfeld, an assistant professor of clinical radiology at Weill Cornell Medicine and a radiologist at New York-Presbyterian/Weill Cornell Medical Center (New York, USA).
The study authors conclude, “For well-selected older adults with T1a renal cell carcinoma, percutaneous ablation may result in oncologic outcomes similar to those of radial nephrectomy, but with less long-term renal insufficiency and markedly fewer periprocedural complications.”
Kidney tumours are often detected incidentally when doctors obtain imaging studies on patients for other medical reasons. Most of these tumours are classified as stage T1a, being golf-ball sized or smaller—about a third of a normal kidney length in size—and not having yet grown outside the organ.
The first treatment choice for T1a kidney tumours is a surgery, partial nephrectomy, that removes the tumour, but spares most of the affected kidney. However, partial nephrectomy is a more complex procedure with a higher risk of bleeding and other complications. For older patients, doctors sometimes opt for the simpler radical nephrectomy, even though that effectively halves kidney function.
“Older patients, who are already at increased risk for chronic renal failure, should not always have to get their kidney taken out for a golf-ball or smaller sized tumour,” Talenfeld says. “There really has been a need for better alternatives.”
The study investigators found that, compared with partial nephrectomy, percutaneous ablation may be associated with slightly shorter renal cell carcinoma-specific survival, and fewer periprocedural complications.
Over the past decade, doctors increasingly have used percutaneous ablation as a treatment option for stage T1a kidney cancers, but much less frequently than the two main surgical options, in part due to the lack of comparative clinical study data. Comparing outcomes in clinical trials of early-stage kidney cancer treatments has been challenging, since these tumours tend to grow very slowly.
For the study, Talenfeld and his team analysed information from a large patient registry kept by the National Cancer Institute and linked with each patient’s Medicare claims. Their analysis, involving 4,310 kidney cancer patients, found that survival five years after percutaneous ablation was very similar to survival after radical nephrectomy: 98% and 95% kidney cancer-related survival, respectively, and approximately 75% survival overall for all patients. However, percutaneous ablation was associated with lower rates of new-onset chronic renal failure within the first year (11% compared with 18%) and much lower rates of other complications requiring emergency department or hospital admissions within 30 days of intervention (6% compared with 30%).
Of those patients who has partial nephrectomy, 10% had intraoperative conversion to radical nephrectomy. Meanwhile, 7% of patients in the percutaneous ablation group received additional percutaneous ablation within one year of treatment.
Percutaneous ablation also resulted in fewer complications than partial nephrectomy, though a conclusive comparison of survival outcomes was difficult since patients receiving partial nephrectomy surgery were typically significantly younger and healthier on average.
The study authors did list as a limitation to this study the fact that findings from an older study population are probably less applicable to younger patients. Notably, though, the average age of diagnosis of kidney cancer is 64.
However, Talenfeld says, “These results are the best evidence we have so far in support of percutaneous ablation for T1a renal cancer. This study suggests that for many older patients requiring surgical treatment, percutaneous ablation should be the next choice after partial nephrectomy.”
Talenfeld and his colleagues now hope to do additional comparative studies of these procedures, using more recent patient data and including cost comparisons.
Reva Medical, a company developing bioresorbable polymer technologies for vascular applications, has announced that its Motiv bioresorbable scaffold is the first drug-eluting bioresorbable scaffold to receive CE mark approval for treatment of below-the-knee peripheral artery disease.
Late last year, Reva announced its plans to expand use of itstechnology in peripheral artery disease. The approval of MOTIV delivers that milestone and for the first time brings bioresorbable technology to this patient population.
Motiv is made from Tyrocore, Reva’s proprietary polymer designed specifically for vascular scaffolds. Tyrocore is inherently radiopaque, making Motiv visible under x-ray to ensure accurate placement in the artery. The company will identify over the next few months select centers to assess the product’s performance, inform future product development activities and determine its complete commercial strategy in peripheral vascular applications. Reva expects Motiv’s first use in patients to be in late 2018 or early next year.
“Reva did not just achieve its own milestone with CE mark of Motiv, we achieved a therapeutic milestone for patients with critical limb ischaemia (CLI),” said Reggie Groves, Reva’s CEO. “Tyrocore and our polymer technology have a broad range of therapeutic applications. This is our first step beyond the coronary arteries, and we look forward to bringing a new treatment option to peripheral artery disease patients and their physicians.”
The most common indication for patients receiving below-the-knee (BTK) revascularisation is CLI. If left untreated, CLI can progress to severe infection and amputation. Patients with CLI below the knee are a substantially underserved population. It is estimated that approximately 1.5 million people are affected by CLI, but only 150,000 interventional revascularization procedures are performed every year.
Research has shown that early-stage intervention is cost-effective and efficacious compared to late stage treatments like amputation. These interventions are intended to restore blood flow to the blocked artery in order to reduce pain and save the limb. Drug-eluting bioresorbable scaffolds such as Motiv present a significant opportunity to improve the treatment of patients suffering from CLI because of the potential to extend drug delivery and to enable retreatment without the risks associated with metal stents.
European Radiology Experimental has recently published a study on a new augmented reality system that is able to accurately guide interventional oncology procedures. A three-step experiment proves this system is precise and reliable enough to facilitate image guidance critical to the success of interventional oncology procedures.
The developers of a new augmented reality system, Endosight, have now published a study in European Radiology Experimental, which finds that this system can be utilised to guide procedures in interventional oncology. Using a back-face camera and a tablet PC to visualise the patient, the system projects 3D images of body structures such as organs, lesions, and vessels on the video image of the patient. The projections are extracted from pre-operative CT and/or MR scans, and 3D change angles depending on the corresponding camera direction of the tablet. This gives the interventional oncologist the experience of seeing through the patient.
“Through specific sensors, this system allows the interventional radiologist to literally see through the patient, and therefore to target lesions in real time without the need for other imaging technologies”, Luigi Solbiati, professor of Radiology from Humanitas University in Milan, Italy, explains.
Reliable and precise
It is a novel finding that the augmented reality system can guide procedures, as precise image guidance is critical to the success of procedures in interventional oncology. The authors concluded that their system is reliable and precise, as extremely high targeting accuracy (below 5mm) was achieved with experiments based on three models—an anthropomorphic trunk model, a porcine model, and a cadaver model. A thermal ablation procedure was simulated on these models, from which it followed that the projections of the augmented reality system very accurately depicted the location of the needle within the organs. The benefit of guiding procedures with augmented reality is that the need for extra real-time intraprocedural imaging such as CT and/or MRI – and thereby exposure to ionising radiation, is avoided. The Milan-based company that develops the Endosight augmented reality system, R.A.W. Srl, employs five of the eight authors of this study, who helped to develop the system.
Luigi Solbiati (Humanitas University, Milan, Italy) speaks to Interventional News speaks about this new augmented reality system.
How does augmented reality work in the context of interventional oncology procedures?
After acquiring cross-sectional (CT or MRI) scans and performing 3D reconstruction, augmented reality allows physicians to visualise patient’s organs and targets just through a pair of googles, in an easy and straightforward way, without the need for any other imaging modality. Augmented reality also allows the precision targeting with conventional needles, electrodes, and antennas of any nodule previously detected by CT or MRI, at any distance from the skin.
What are the main advantages of using augmented reality in this way?
The main advantages of using augmented reality in interventional oncology are the following:
Having the possibility to easily and precisely target the real centre of nodules, thanks to the 3D visualisation in real-time. This is particularly important for ablative procedures, in order to achieve homogeneously thick ablative margins all around the volume of nodules.
Significant shortening of the time needed to perform the procedure, compared to CT or MRI guidance.
Overcoming the limitations of ultrasound guidance: 2D visualisation, impossibility to visualise organs (lung, bones), difficulty or impossibility to visualise nodules located in critical areas (for example, tumours in the liver dome).
Significant shortening of the learning curve of interventional procedures.
No risk of radiation for patients and operators.
Capability to let all the operators, fellows, students, and other users see exactly what the main operator sees and does, given that the images of the procedure can be simultaneously broadcast to an unlimited number of googles in the same interventional room. This can be extremely useful in the teaching of how to perform interventional procedures.
Do you foresee the use of augmented reality becoming standard practice? If so, what do you think the challenges are with implementing this change?
As has always occurred in the history of medicine, it will take time to shift standard practice. There are many reasons for this lag in augmented reality becoming standard practice for the guidance of interventional procedures, such as the need for simplifying and refining the technology itself, and the traditional difficulty of convincing particularly skilled operators to abandon conventional guidance systems (based on 2D visualisation) and move to a totally new modality, based on 3D visualisation. There will certainly be a phase in which traditional guidance modalities will be used side by side with augmented reality in order to verify the precision of targeting before starting ablative procedures. In my opinion, two completely different populations of users (opinion leaders and young operators particularly skilled in the use of new technologies) could lead the remaining majority of operators toward this change.
How do you see augmented reality systems changing interventional oncology?
Enabling a larger number of non-expert clinicians to safely and precisely perform interventional procedures, thus ultimately increasing the number of procedures performed throughout the world.
What are the clinical ramifications of the study published in European Radiology Experimental, concluding that the Endosight augmented reality system is safe, reliable and precise?
In our study, we decided to start testing the Endosight augmented reality system in a very challenging environment at the Simulation Center of Humanitas University in Milan: targeting small hepatic metastases in a cadaver with a ventilator attached to the trachea to induce simulated respiration. We were able to target both metastases with a distance of the needle tip from their geometric centre ranging from 2.5 to 2.8mm. We should soon start a clinical study in human livers and, in addition, experimental studies in other moving organs (the lung) and non-moving organs (such as the prostate and neck), where we expect to run into fewer difficulties.
How does using augmented reality for interventional oncology procedures compare to the current standard practice involving other imaging technologies?
The biggest breakthroughs in the world of guidance modalities for interventional oncology procedures in the last ten years have been image fusion of real-time sonography and pre-acquired CT or MRI and cone-beam CT. However, the first suffers from the low spatial resolution of sonography and the lack of 3D representation, while the second from the risk of ionising radiation and the need for the use of contrast agents. Augmented reality can overcome all these limitations.
What is the future for augmented reality systems in interventional oncology procedures?
This question is particularly challenging and the answer almost impossible: who could have expected only five years ago(!) that we would have shortly been able to look into a patient by simply wearing a pair of glasses?
B. Braun has announced the recent French reimbursement approval for its peripheral drug-coated balloon (DCB) SeQuent Please OTW effective as of July 2018.
As published in the Official Journal of the French Republic, B. Braun’s over-the-wire DCB is now reimbursed under Title V in the list of reimbursable products and services (LPPR).
According to this announcement, hospitals in France receive an add-on reimbursement with SeQuent Please OTW in its 035 version to treat peripheral arterial disease in femoro-popliteal lesions.
SeQuent Please OTW is a peripheral paclitaxel-coated balloon with a nominal dose of 3 µg/mm2 that is integrated into a matrix with resveratrol. This excipient is a naturally occurring, plant based substance with positive anti-inflammatory, antioxidant & anti-hypertensive characteristics.
The basis for the positive opinion for B. Braun’s DCB issued by the French National Commission for the Evaluation of Medical Devices and Health Technologies is the solid clinical evidence of the CONSEQUENT randomised controlled trial. After 24 months the results in 153 patients (1:1 DCB vs. plain balloon angioplasty) with challenging femoro-popliteal lesions (23.5% with TASC C/D lesions, mean lesion length of 14.5cm) demonstrated a significantly higher primary patency rate in the DCB group (72.3 vs. 48.4%; p=0.006) with no further TLR after 14 months.
Furthermore, SeQuent Please OTW is the only DCB available in France with guidewire compatibilities of 0.014”, 0.018” and 0.035” to treat above-the-knee and below-the-knee lesions.
Every year, up to 1.3 million people in Europe suffer a first stroke. Acute stroke treatment strategies such as acute treatment of patients in a stroke unit, intravenous thrombolysis and endovascular treatment significantly improve the outcome for patients with ischaemic stroke and thus reduce its socioeconomic burden. However, reliable data on access to and delivery of acute stroke treatment strategies throughout Europe are lacking.
The European Stroke Organisation (ESO), the European Society of Minimally Invasive Neurological Therapy (ESMINT), the European Academy of Neurology (EAN) and the patient organisation Stroke Alliance for Europe (SAFE) have therefore surveyed stroke experts from 44 of 51 European countries on the best available information regarding national access to and delivery rates of acute stroke unit care, intravenous thrombolysis, and endovascular treatment.
The results of this survey identify major inequalities in acute stroke treatment, with many countries reporting rates that were far below highest country rates. This article shows in which countries patients still have no or obviously inadequate access to appropriate acute stroke treatment.
According to Urs Fischer, Professor for Acute Neurology and Stroke at the University Hospital Bern, up to 226,662 additional patients could be treated with intravenous thrombolysis and an additional 67,347 with endovascular treatment each year. “Many stroke victims in Europe still have no access to acute stroke treatment,” he said. “If stroke unit care, intravenous thrombolysis and endovascular therapy would be routine practice throughout Europe, many more victims could survive their stroke without a major handicap”. According to Fischer, these inequalities not only have a major impact on the patients, but also on their families and the socioeconomic burden. “Recent studies have shown, that acute stroke treatment is highly cost effective – if you treat your patients right, you will not only improve the quality of life of the patient and his family, you will also save money for your society”, he said. Therefore, efforts have to be done to increase the number of stroke units, intravenous thrombolysis and endovascular stroke therapy. “We have to talk to governments, politicians, health care specialists and stroke physicians in order to set up and improve the system in regions, where acute stroke treatment is lacking!”
In May 2018, ESO and SAFE presented the Stroke Action Plan for Europe to set achievement goals for stroke care by 2030. This survey already provided important insights for the Stroke Action Plan authors. The findings from this survey are relevant for future health-care planning in Europe and beyond.
ABK Biomedical, a company dedicated to the research, development and commercialisation of innovative embolic therapies, has announced the appointment of Michael J Mangano as president and chief executive officer.
Mangano will be responsible for leading global business activities, including the rapid development, regulatory approval and commercialisation of ABK’s unique medical device technologies.
Mangano most recently served as president and CEO of ReShape Medical, a US venture-backed company focused on obesity where he increased organizational value and played a lead role in orchestrating the sale of the company to EnteroMedics in October 2017. Prior to ReShape, Mangano was president of the Americas for Sirtex Medical, a leading publicly traded Australian biomedical company, where he grew the business nearly five-fold from US$30million to more than US$140 million while building a team of 17 to more than 130 employees in a period of six years. His leadership resulted in a dramatic increase in the company’s valuation, leading to the recently announced acquisition in progress of Sirtex Medical by CDH Investments for US$1.4B USD, a press release from ABK Biomedical. Prior to Sirtex, Mangano spent 15 years with Boston Scientific in numerous senior management roles, including overseas assignments in Japan and Australia.
Mangano will continue to serve on the ABK board of directors.
“I am excited to join the team at ABK, which has outstanding experience in the medical device industry. The talent at ABK, coupled with an innovative technology platform and pipeline, provide a strong foundation and solid prospects for our future growth and success,” said Mangano. “I especially look forward to working with the interventional radiology and oncology communities to develop and market novel technologies that will help patients and physicians, and want to thank the founders and the board of ABK for their support.”
Bob Abraham, co-founder and former CEO, is a practicing interventional radiologist and will remain with the company as chief medical officer. He will continue to play a key role in product development and the clinical evolution of ABK’s key technology platforms.
ABK Biomedical is organised to research, develop and commercialise breakthrough medical device therapies to improve treatment outcomes and the lives of patients with benign and malignant hypervascular tumours. Specifically, it holds intellectual property in the focus area of inorganic polymer microspheres, targeted at the growing field of embolotherapy within the interventional radiology/interventional oncology medical disciplines.
James B Spines (centre) flanked by Marc Sapoval and Jafar Golzarian, GEST cofounders and directors
James B Spines (centre) flanked by Marc Sapoval and Jafar Golzarian, GEST cofounders and directors
“In this era, it is common for people not to accept basic scientific data. This has now permeated society so much that people feel empowered to discount facts. My goal is to re-orient our group and say we have to look at the facts. We have to look at the science and really be willing to question our own beliefs. A responsible physician does what is best for their patients, and this should be based on evidence, not beliefs,” said James B Spies (Washington, DC, USA) who delivered the Honorary Lecture at the Global Embolization Cancer Symposium and Technologies (GEST US; 17–20 May, Miami Beach, USA).
Speaking on the topic “Preconceived notions, alternative facts
and fake news” Spies, professor of Radiology and chair of the Radiology Department at Georgetown University Medical Center, asked the questions: why do we believe what we believe? What can we do to base our understanding on objective facts? And, how do we evaluate new information about what we believe?
He explained that developing valid comparative trial data with all bias minimised has been an important goal in his career, which started out in public health before moving to the field of interventional radiology. He now believes it is “just as important to analyse how the results of such trials are interpreted and received”.
“We are trying to gather evidence using research to be able to determine what treatments work and what do not. I spent a lot of energy on study design and conducting trials in interventional radiology. But it has dawned on me, over the last several years, that there is the other half of it, which is that you can do the greatest research, but if people do not receive it in the right way, then the message does not get through. So what I tried to focus this talk on was: how is it that we receive these data, and what are our natural, inborn biases that I, and we all, carry, that lead us to question data that we do not agree with.”
Spies pointed to a whole host of biases that influence the acceptance of information. “There is a whole sociology out there regarding how people receive information. There are various types of biases that are at play when we take in information and make decisions. An important one is ‘confirmation bias’ in which we wish for something to be true, but do not know it to be so. Once a view is formed, we only embrace information that confirms that view, while ignoring, or rejecting, information that casts doubt on it. This can lead to the backlash effect, when people strike back when receiving information that challenges their set notions. So my talk also looked at how we use biases that we have in order to support our preconceptions.”
Speaking about how interventionists function, Spies explained: “We believe in what we are doing. We prefer action to inaction, even action with little chance of success is preferred over no action at all. We are also a pragmatic group and see apparent
cause-effect relationships, even in the absence of any theoretical foundation.”
Coupled with these traits is the fact that as a group “we are highly subjective and depend more on ‘gut feelings’ than
on ‘book knowledge’. We emphasise uncertainty in our defence. When things go wrong, it is not our fault. Because we deal with individual pateitns, rather than groups, we cannot rely on epidemiology concepts, or probabilities derived from population statistics. The trouble is we tend to think in anecdotes. How often do we hear ‘one patient that I treated did really well…’ Of course, we are obligated to treat patients one at a time and that is part of it. However, we cannot as a set of societies, pay for everything. We tend to be procedure-oriented people, so when technologies do not work, we should stop doing them. In the aftermath of practice changing trials such as the ATTRACT trial, we have seen this,” Spies reported.
Spies further weighed in to say: “Although these traits usually serve us well, they invite intellectual gerrymandering. So, when the evidence conflicts with our judgment, we tend to resist it, but when the evidence is consistent with our judgment we tend to embrace it. As a result, if there is even a 1% chance that some technologic advance is marginally better than the status quo, we act as if it is a certainty and discount the downside”.
Adopted, touted, doubted and discarded
“We interventionalists share all the above traits,” explained Spies. “We accept positive new trials based on the thinnest of evidence. We expect new interventions to be successful, so we are ‘early adopters’ and we tend to focus on the positive and minimise the negative. This is borne out in our adoption of technologies such as YAG lasers, Simpson atherectomy, bare metal stents for benign biliary strictures, or even angioplasty for chronic cerebrovascular venous insufficiency. These were all adopted, touted, doubted then discarded and in some cases resurrected. Once we adopt something, we believe in it and we defend it,” he commented.
Spies quoted American writer Upton Sinclair, who said: “It is difficult to get a man to understand something, when his salary depends on his not understanding it”, but qualified to say, “I would like to think that that money is not the primary reason that
people are resistant to data that they do not like; there are something like 20 different biases that come into play when we make a decision. Still, it is natural that when your livelihood and
financial well-being are threatened, the tendency is to question the source. To some extent maybe that is also healthy; because when we innovate and disrupt the work of other specialties, they then question us and it makes us do our work more rigorously, his is the positive side of the coin. But clearly a part of this [rejection of new information] is economic self-interest, or protection of what we do. But the truth is no one I know does this purely for money, we believe in what we do. So really, we need to learn more about how we can overcome the obstacles to accepting new facts.”
An open mind
Reiterating his key message, Spies stated: “We resist data that contradicts our beliefs. There is a misconception that your opinions are the result of years of rational, objective analysis. The truth is that your opinions are the result of years of paying attention to information which confirmed what you believed, while ignoring information which challenged your preconceived notions. It takes strong and convincing evidence to change our preconceived notions. And our first reaction to such evidence is to doubt it. Progress is measured by our willingness to change our views based on new evidence, so come to the table with an open mind.”
Collaboration in matters of training, research and clinical practice between radiation oncology (RO) and interventional oncology (IO) could significantly advance research into local therapies, benefit patients and also stand these two disciplines in good stead, urge leading experts from both fields.
Andreas (Andy) Adam, King’s College London, UK, delivered the keynote address at the Trans Tasman Radiation Oncology Group (TROG) annual meeting in Hobart, Tasmania, on 20 March. This event marked the first time an interventional radiologist addressed an organisation mainly focused on research in RO.
Adam has been involved in the transformation of professional societies and medical disciplines. He was one of the architects of the merger between the European Association of Radiology and the European Congress of Radiology, which created the European Society of Radiology. He also led a project that achieved subspecialty recognition for interventional radiology in the UK, when he was president of the Royal College of Radiologists. He has now moved outside his own specialty, by pursuing a project of convergence between IO and RO. He has championed this cause for several years, in partnership with Lizbeth (Liz) Kenny, who is an internationally renowned radiation oncologist and a past president of the Royal Australian and New Zealand College of Radiologists (RANZCR). Adam, who is also one of the editors-in- chief of Interventional News, and Kenny have co-authored several articles on this subject.
Last year, Adam suggested that interventional oncologists should be invited to the annual scientific meeting of TROG, which is a long-established, well-respected professional organisation focusing on research in RO. His proposal was initially received with scepticism. He was told that previous attempts to involve radiologists in TROG had not been succesful. He persisted, explaining that there is a great difference between inviting diagnostic radiologists who would be peripherally involved in RO studies, and inviting interventional oncologists, who would come as equal partners in minimally invasive, imaging-guided methods of treatment of localised cancers. He sought a meeting with the president of TROG, professor Farshad Foroudi, director, Austin Health Radiation Oncology, Melbourne, Australia, to explain the proposal in detail. This resulted in a meeting of minds; TROG supported the proposal, and a small group of interventional oncologists attended the annual scientific meeting in March 2018.
The IO programme for the TROG annual meeting was put together by Kenny and Nicholas (Nick) Brown, chair of the RANZCR Interventional Radiology Committee (IRC), co-chair of the TROG IO Special Interest Group and an active member of the Interventional Radiology Society of Australasia (IRSA). Adam was invited to deliver the keynote address, the title of which was ‘IO: a sister discipline to Radiation Oncology’. In his talk, Adam encouraged “a degree of convergence” between the two disciplines. He suggested that RO and IO are “natural partners”, both being forms of imaging-guided therapy that are also fundamentally different from surgery (the other local tumour treatment). Some procedures, such as brachytherapy for tumours inaccessible via natural orifices and radioembolization, already rely on skills from both disciplines. Commenting that RO and IO were only “superficially different from each other”, he explained that they could be brought even closer by the exploration of common potential research themes, such as the enhancement of outcomes by combining ablation with radiotherapy.
“Health expenditure should be re-balanced in favour of local tumour treatment and a partnership between RO and IO would revolutionise this field,” argued Adam.
A version of this idea is simultaneously playing out in the medical device industry. Adam used Varian’s (intended) acquisition of Sirtex for US$1.3 billion to illustrate the point (there have since been developments in this regard and this acquisition is no longer on the cards.) Delving into the rationale behind the intended acquisition, he noted that Sirtex provides Varian with an opportunity to expand its addressable market into IO and extend its leadership in the field of radiation medicine. He showed data to suggest that Varian expects the IO market to expand by around US$1 billion by 2022. Varian expects to accelerate its revenue by expanding its oncology customer base through its acquisition of Sirtex, Adam hypothesised.
Kenny told Interventional News: “The TROG meeting in Hobart, Australia, was a landmark in the calendar of IO. TROG is the first organisation to formally invite IO into the RO research arena and we are grateful to the TROG president Farshad Foroudi and the TROG office for their support and encouragement. TROG is a highly successful cooperative clinical cancer research group with an impressive track record in sophisticated trials and studies and has a major focus on procedural quality assurance. To have IO as part of the research infrastructure is just wonderful. The enthusiasm amongst both radiation oncologists and the interventional oncologists was palpable and two studies were approved for development, one in renal cancer and the other in lung cancer. I expect this to be the beginning of a very fruitful relationship, benefiting patients as well as our two disciplines greatly. There will be hard work to do over the next twelve months, but we are already looking forward to next year’s meeting in Melbourne.”
Brown elaborated on the strategy behind featuring IO at the TROG meeting. “IO and RO have a lot in common and both have so much to offer in the focal therapy space. It makes sense for two related specialties to collaborate to achieve our shared objectives and help each other overcome similar challenges. In addition, IO has much to learn from RO’s research successes and focus on quality assurance. There is clear potential for the two specialties to work together to achieve better outcomes from targeted treatments for patients, which will come from a combined approach rather than a competitive one,” he said.
Brown points to the fact that IO is rapidly expanding, but, “with the evolution of technology comes the responsibility of properly validating new techniques and understanding their roles in evidence-based treatment algorithms”, he emphasised. He explained that TROG has been designing, conducting and disseminating high-quality research for 30 years, “which has strengthened the role that radiation plays in modern cancer care. IO is playing catch-up in a field where the evolution of technology tends to outpace full clinical validation and stands to benefit enormously from partnering with RO colleagues.”
IO treatments have made considerable headway to establish equipoise in terms of outcomes with surgery in the treatment of various cancers such as small renal neoplasms and in liver cancer. Treatments such as ablation score over surgery with regard to many factors including the use of local, rather than general, anaesthesia; patients not needing overnight stay in hospital; greater sparing of noncancerous tissue; reduced morbidity and the treatment being less costly.
Adam also briefly dwelt on possibly one of the most important revolutions in cancer treatment: immunotherapy, noting that the link between ablation and immunotherapy was of significant current research interest. “Cancer cells that have been ablated act like antigens. Ablation brings tumour antigen in close contact with immune cells/ cytokines and growth factors to generate immunogenic cell death and prime the immune system. When appropriately timed, ablation can enhance tumour response to immunotherapy leading to many interesting areas of future research when coupled with RO, which also has immunogenic potential,” he said. (See more immunotherapy articles on pages 22 and 23).
In this scenario, a partnership between IO and radiation therapy will create a form of cancer surgery in solid organs. However, there is a “need to find a common language” in order to advance research in imaging-guided therapy. Adam emphasised the need for uniformity in assessing response to treatment. “CIRSE plans to develop global criteria and TROG can be a partner in this effort,” he maintained.
Elaborating, Adam commented that the formation of a research partnership between RO and IO would be beneficial. A closer relationship between professional organisations (such as RANZCR and the Royal College of Radiologists [RCR]) is also desirable. “Such a partnership could lead to teaching modules for interventional oncologists on basics of chemotherapy and radiotherapy and teaching modules for radiation oncologists on the effects of cryotherapy and thermal ablation. There could also be joint clinics, joint appointments and the establishment of clinical practice by interventional oncologists,” conveyed Adam.
Brown, explaining the IO content of the TROG programme in 2018 and the plan for 2019, said: “IO successfully pitched two separate research proposals at the TROG meeting involving percutaneous ablation of small renal masses and lung cancers. The projects will collect important data on how these techniques should best be utilised in modern clinical practice and may help to evolve treatment algorithms for renal and lung tumours to ultimately achieve better outcomes for patients. There is also a growing recognition of the importance of patient-centred outcomes in reporting trial data and that traditional endpoints such as overall survival are not the only consideration. In 2019, we will aim to consolidate our efforts from 2018 and make the two initial studies as successful as possible. We will also look to further develop a robust research strategy for IO in Australia and New Zealand and expand the research portfolio to include studies into treating liver and bone tumours”.
Adam made it clear that partnership between RO and IO would be a senior/junior partnership with RO being the more mature discipline, from which IO has much to learn. Particularly, Adam noted, interventional oncologists needed to practise as full clinicians and not as technicians as well as set up more effective planning systems and processes for quality assurance. There was also a need for IO to gather more and better evidence and organisations such as TROG could help with this, Adam said.
Improving the evidence base for interventional radiology is beneficial in other respects. “One of the main aims of the RANZCR IRC is to achieve specialty recognition for interventional radiology in Australia and New Zealand,” said Brown, noting that an important part of this process is the need for a robust evidence base. “As members of the same college there is also great scope for IO to share in some of the RO teaching modules and develop greater depth of training in oncology and tumour biology. As the RANZCR IRC looks to develop an interventional radiology specific training programme and curriculum, making the most of these opportunities will become very important.”
Adam described the opportunities from a partnership between IO and RO. “We would be able to provide curative treatments for most small tumours in solid organs, a wide spectrum of palliative procedures and we could advance research into combined IO and RO procedures.”
Looking ahead to oncology treatment in 2028, Adam said he foresaw a future in which most local tumour treatment in solid organs was delivered by interventional oncologists and radiation oncologists working in partnership, having undergone common core training. On a lighter note, he added, “TROG will also celebrate the 10th anniversary of being the first organisation in the world to embrace research in both disciplines”.
Roche has announced that the US Food and Drug Administration (FDA) has granted Breakthrough Therapy Designation for Tecentriq (atezolizumab) in combination with Avastin (bevacizumab) as first-line treatment for people with advanced or metastatic hepatocellular carcinoma (HCC). The designation is based on data from a phase Ib study assessing the safety and clinical activity of the combination of Tecentriq and Avastin.
Sandra Horning, Roche’s chief medical officer and head of Global Product Development said: “Preliminary data from the combination of Tecentriq and Avastin in this disease are promising and we look forward to working with health authorities to make this potential treatment regimen available to people with hepatocellular carcinoma as soon as possible.”
Breakthrough Therapy Designation is designed to expedite the development and review of medicines intended to treat serious or life-threatening diseases and to help ensure people have access to them through FDA approval as soon as possible. This is the 22nd Breakthrough Therapy Designation for Roche’s portfolio of medicines and the 3rd for Tecentriq, a press release from the company states.
Roche presented data from a phase Ib study in HCC at the American Society of Clinical Oncology (ASCO) annual meeting, in June 2018. These data showed that after a median follow-up of 10.3 months, responses (independent review facility (IRF) per RECIST v1.1) were seen in 15 (65%) of 23 efficacy-evaluable patients. Responses were seen in all subgroups, including on the basis of the cause of their disease (aetiology: Hepatitis B, Hepatitis C, and non-viral), region (Asia excluding Japan or Japan/US), baseline alpha-fetoprotein levels (high/low) or spread of tumour beyond the liver (yes/no). Assessment by investigators (INV) assessed per RECIST v1.1 demonstrated a response rate of 61% (14 out of 23 patients). Median progression free survival (PFS), duration of response (DOR), time to progression (TTP) and overall survival (OS) have not yet been reached after a median follow-up of 10.3 months; results will be presented at a future medical congress when updated data from an expanded cohort are available. In the safety-evaluable population (n=43), 28% of patients (n=12) experienced Grade 3-4 treatment-related adverse events and no treatment-related Grade 5 adverse events were observed. No new safety signals were identified beyond the established safety profiles for the individual medicines. Roche provided additional data per FDA request and the Breakthrough Therapy Designation has been granted based on the totality of these data.
Earlier this year, Roche initiated IMbrave150 (NCT03434379), an open-label, multicentre, randomised phase III study investigating the combination of Tecentriq and Avastin versus sorafenib in people with previously-untreated (first-line) locally advanced, unresectable or metastatic HCC. This study is currently enrolling.
About the phase Ib study (NCT02715531) This phase Ib, open-label, multicentre study is evaluating the safety and clinical activity of a number of cancer immunotherapy combinations in different solid tumours, including Tecentriq and Avastin in patients with advanced, unresectable or metastatic first-line HCC (arm A). Participants in arm A receive Tecentriq (1200mg) and Avastin (15 mg/kg) intravenously (IV) every three weeks until loss of clinical benefit or unacceptable toxicity. The primary objectives of arm A are to assess the clinical activity, based on objective response rate (ORR) assessment by independent review facility (IRF) per RECIST v1.1 and to assess the safety and tolerability of the combination. Secondary efficacy endpoints include objective response rate (ORR) by investigator assessment (INV), as well as progression-free survival (PFS), duration of response (DOR), time to progression (TTP) all by INV and IRF per RECIST v1.1; and overall survival (OS).
Ra Medical Systems has filed a registration statement on Form S-1 with the US Securities and Exchange Commission relating to a proposed initial public offering of shares of its common stock. The number of shares to be offered and the price range for the proposed offering have not yet been determined. Ra Medical Systems has applied to list its common stock on the New York Stock Exchange (NYSE) under the ticker symbol “RMED.”
Piper Jaffray & Co. and Cantor Fitzgerald & Co. will act as lead joint book-running managers for the offering. SunTrust Robinson Humphrey, Inc. will act as lead manager and Nomura Securities International, Inc. will act as co-manager for the offering.
The offering will be made only by means of a prospectus. Copies of the preliminary prospectus relating to this offering, when available, may be obtained from: Piper Jaffray & Co., 800 Nicollet Mall, J12S03, Minneapolis, MN 55402, Attention: Prospectus Department, by telephone at 800-747-3924 or by email at [email protected]; or Cantor Fitzgerald & Co., Attention: Capital Markets, 499 Park Ave., 6th Floor, New York, NY 10022, or by email at [email protected].
A registration statement relating to these securities has been filed with the Securities and Exchange Commission but has not yet become effective. These securities may not be sold nor may offers to buy be accepted prior to the time the registration statement becomes effective.
This press release shall not constitute an offer to sell or the solicitation of an offer to buy these securities, nor shall there be any sale of these securities in any state or jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification under the securities laws of any such state or jurisdiction.
In May 2017, the US Food and Drug Administration (FDA) granted market clearance to Ra Medical Systems for the company’s Destruction of Arteriosclerotic Blockages by laser Radiation Ablation (DABRA) system. The system is intended to deliver a safer, faster and cheaper solution to peripheral arterial disease treatment than the market otherwise offers.
The Symposium on Clinical Interventional Oncology (CIO) will separate from the International Symposium on Endovascular Therapy (ISET) starting from next year. Beginning in 2019, ISET will shift to a four-day format and will take place 27–30 January at The Diplomat Resort (Hollywood, USA), whilst CIO will be held 11–13 October as a standalone conference at the Eden Roc Hotel (Miami Beach, USA).
HMP, a healthcare event and education charity that runs both CIO and ISET, states in a press release that this is “a move designed to proactively address the growing need for highly specialised, interactive, and practical education for today’s endovascular and vascular specialists.”
Traditionally held concurrently with ISET annually in South Florida, the CIO program highlights innovative and viable treatments in interventional oncology. HMP claim in a press release that the move to separate the meetings reflects the ever-growing importance of interventional oncology (IO), the commitment to the clinical practice of IO, and the increased demand for IO education.
According to Constantino Peña and Ripal Gandhi (both Miami, USA), long-time ISET course directors: “We are extremely proud to be leading the way in this rapidly evolving field. After 11 successful years, the course directors have found it critical to grow the meeting in order to continue our vision of innovative and practical IO education delivered by best-in-class, multidisciplinary experts in order to improve the lives of millions of patients with cancer using minimally invasive techniques. By creating a dedicated CIO event, we will have the opportunity to expand the focus on clinical content, accommodate new attendees, and continue to train the next generation of physicians in this growing field.”
ISET’s hallmark Live Cases, representing the practical core of the meeting, will be expanded to include an additional 90 minutes of case time. Cases will transmit from several new sites across the USA and around the world. Late-breaking clinical data with a focus on promising new technologies will also be featured.
In response to the popularity of the “Deep Dive” sessions, the program will now feature dedicated tracks with interactive sessions woven throughout the course of the meeting. These tracks will be focused on critically relevant topics, including Peripheral Artery Disease, Critical Limb Ischemia, Complex Aortic and Iliac Interventions, Clot Management, Venous Interventions, and Embolotherapy.
Created in 1989 by Barry T Katzen (Miami Cardiac and Vascular Institute, Miami, USA), the founder and chief medical executive of Miami Cardiac & Vascular Institute, ISET is the premier educational forum for physicians and allied health professionals who treat patients with peripheral, cardiac, and neurovascular disease. The annual meeting, which features globally recognised faculty who are experts in their field, draws more than 800 attendees from around the world and delivers practical and hands-on education focused on the latest endovascular approaches, techniques, and technologies.
Katzen comments: “For three decades we have been providing clinicians with premier endovascular education. Innovative thinking, determination, and dedication to excellence are hallmarks of our great field, and we recognise that clinician education must continually change as the needs of patients and the healthcare landscape change. Together with my fellow course directors, we have enhanced ISET in response to the needs of our participants, and we believe the new investments we have made and the new approaches we are taking will yield the strongest ISET program yet. We look forward to delivering relevant, real-world endovascular education with a uniquely personal and interactive approach led by globally recognised faculty to a multidisciplinary audience in 2019.”
SonaCare Medical has reported five-year outcomes from a multicentre study of 625 medium to high-risk clinically significant nonmetastatic prostate cancer patients following focal therapy treatment with its Sonablate high intensity focused ultrasound (HIFU) technology.
With a median five-year follow-up, the results from the study showed that failure free survival at one, three, and five years was 99%, 92%, and 88% respectively, equivalent to that achieved with surgery. Metastasis-free, cancer-specific, and overall survival at five years was 98%, 100%, and 99% respectively. The study additionally reports that 98% of men maintained pad-free urinary continence after their procedure and 85% maintained erectile function, both material improvements over that seen with surgery and radiation therapy.
The study concluded that failure free survival with HIFU can be equivalent to that of surgery but with a side-effect profile, far more beneficial to the patient’s quality of life post-procedure. A press release from Sonablate references a recent report from the UK on 1,000 patients who underwent a radical prostatectomy found maintenance of pad-free continence at only 65%. “This suggests that focal HIFU therapy can result in a 97% reduction in the number of men who require pads post-procedure when compared to surgery; ancillary data suggests a similar magnitude reduction in erectile dysfunction with focal HIFU compared to surgery,” the release further adds.
“Focal HIFU is a major shift in treating men with early prostate cancer. Our study shows that cancer control in the medium term is very good and importantly, men can expect a low-risk of side effects such as incontinence and erection problems,” states Hashim Ahmed, chair of Urology at Imperial College London and contributing author to this study. “All men who are suitable for focal HIFU should be told about this treatment option so they might consider it as an alternative to radical prostatectomy or radiotherapy.”
Cagent Vascular has announced the completion of US$11.87 million in Series B funding. The round was led by two strategic investors including one that participated in the Series A financing. Additional participants included Balestier Investments, Ben Franklin Technology Partners1, Synergy Ventures, and other private investors. Proceeds will be used to scale manufacturing and initiate a limited launch of Cagent Vascular’s first product, the Serranator Alto.
Further uses of proceeds include supporting development efforts to build upon existing confirmatory data, expanding indications, and receiving additional regulatory clearances. The next product in the Serranator family of PTA serration balloon catheters will be the Serranator Bass, for use in infrapopliteal arteries.
“The breadth and diversity of the investor base reflects an understanding of the value proposition that this technology delivers,” stated CEO, Carol A Burns.
The Serranator is an angioplasty device with serrated metal strips embedded on a semi-compliant balloon. The Serranator’s unique technology is designed to create multiple longitudinal lines of interrupted micro-serrations within the luminal surface to aid in arterial expansion. The result is predictable and controlled lumen gain. The company’s first device, the Serranator Alto, performed well in the above-the-knee PRELUDE study, especially in a subset of patients with severe calcium. It received FDA 510(k) clearance and CE marking in 2017 and is indicated for the treatment of diseased femoral and popliteal arteries, dysfunctional AV access grafts and AV fistulae.
“The Serranator’s serration technology is unique in that it combines an effective vessel dilatation technology with a highly deliverable system on a single platform. In my experience, it is quite effective in calcified or highly fibrotic lesions where balloon angioplasty has historically fallen short,” explained Mahmood K Razavi, a vascular and interventional radiology specialist at St Joseph Hospital in Orange, USA.
“We believe that the Serranator Alto’s ability to operate even in highly calcified vessels is a significant differentiating factor for the product, which owes its performance to the serrated metal strips that score the lesion and aid in dilatation,” added Carol A Burns. “We are confident that these characteristics will benefit our Serranator Bass product, which is designed for use in diseased infrapopliteal arteries where current treatment options are generally poor due to the diffuse calcified nature of these vessels. Treatment of critical limb ischaemia (CLI) remains an enormous area of interest where we believe the device will shine and will become the new standard of care for below-the-knee interventions.”
The iDissection Classification trial results published in the Journal of Invasive Cardiology have shown that with the use of intravascular ultrasound (IVUS) investigators were able to identify more dissections following percutaneous transluminal angioplasty than with angiography.
Post-percutaneous transluminal angioplasty (PTA) dissections are often overlooked, underdiagnosed and left untreated. These dissections can compromise clinical outcomes in both the short and long term. The use of intravascular ultrasound (IVUS) has been found to help visualise the presence and severity of dissections not typically seen on angiography.
In the iDissection study, 15 patients with femoropopliteal disease were treated with atherectomy and adjunctive PTA. Angiographic and IVUS images were obtained at baseline, post-atherectomy and post-angioplasty and evaluated for the presence and severity of dissections. Dissections seen on angiography were graded per the NHLBI scale, and IVUS images were graded using the iDissection classification. All images were independently adjudicated by multiple core laboratories. While angiography identified eight dissections, IVUS revealed 46 dissections—a ratio of 6:1. The iDissection study reveals that significant dissections may not be thoroughly observed with angiography yet are substantially more visible when using IVUS, potentially altering the course of patient treatment in real-time.
“In this small series of patients undergoing atherectomy, there were significantly more dissections noted by IVUS when compared to cine angiography. Angiography has been the main modality used for evaluating the peripheral arteries, but it has consistently under-estimated the severity of calcium, the presence of thrombus, the true vessel size, and lesion severity. In contrast to the NHLBI classification, the iDissection classification reveals the extent of injury and its depth. Pathologic studies have shown that deeper injuries into the media and adventitia correlate with loss of patency and increase in TLR rate. These deeper injuries were also identified on IVUS. The identification of deeper injury that cannot be seen on angiography may offer an explanatory mechanism for the occurrence of restenosis in otherwise successful procedures as seen on angiography following atherectomy. Although data indicate that atherectomy reduces angiographic dissections and stenting compared to balloon angioplasty, this concept may need to be revisited with IVUS-based imaging,” the writers explain.
“Angiography is a suboptimal test to visualise the peripheral arteries. It underestimates vessel size, the presence and extent of calcium, thrombus and stenosis, and does not give a clear picture of optimal stent expansion and apposition. Moreover, the iDissection data confirm that angiography seriously underestimates the presence and severity of dissections following endovascular intervention,” commented Nicolas W Shammas, Founder and Research Director, Midwest Cardiovascular Research Foundation, Davenport, USA. “The iDissection study validates the need for more sophisticated imaging, such as IVUS, to evaluate acute procedural results.”
EchoNous Vein (EchoNous), an ultrasound-based tool designed specifically for nurses to improve peripheral IV catheter placements, has received US Food and Drug Administration (FDA) approval.
A company release explains that EchoNous Vein provides immediate, clear images at depths from 1–5cm for quickly visualising superficial and deeper veins with just two-button controls. EchoNous Vein will integrate with the company’s existing intelligent medical tool, Uscan, to form the EchoNous platform.
One of the most commonly performed minimally-invasive procedures, peripheral IVs can be challenging due to chronic illness, chemotherapy, obesity and drug abuse; first-attempt IV catheter insertion fails in up to 26% of adults and 54% of children.
“Time is critical, especially when patients need an infusion or antibiotic treatment, and finding the right vein can be challenging. We designed the EchoNous Vein to provide nurses with rapid, clear images of veins to directly improve patient care, satisfaction and HCAHPS scores,” says Kevin Goodwin, CEO of EchoNous. “We wanted to create an easy-to-use tool that would help to reduce failed sticks, as with each failure comes a much higher risk of vessel trauma or infections which can lead to longer stays in hospital and higher medical costs.”
Early feedback from healthcare providers has shown the EchoNous Vein’s unique frequency profile and optimised gain and depth presets have the potential to provide significant advancements in evaluating veins of paediatric patients—a traditionally challenging patient population for IV insertion.
“EchoNous Vein’s simple on-screen controls allows clinicians using ultrasound to clearly identify veins in the centre of the display, helping to not just locate veins, but to evaluate their health and quality prior to peripheral IV placement,” says Nancy Moureau, CEO of PICC Excellence. “As clinicians we know that IV insertion selecting a healthy vein for catheter placement can help to reduce the chance of post insertional complications. To have a tool specifically designed to easily select veins and guide catheter placement is extremely valuable as we’re always looking to improve the patient experience.”
In addition to launching the new vascular access tool, the company also announces its plan to converge its Signostics brand and AI-driven Uscan bladder scanner product under the single EchoNous brand.
Otsuka Holdings, Otsuka Medical Devices, and ReCor Medical have signed a merger agreement pursuant to which Otsuka Holdings will acquire the remaining shares in ReCor from its current holders. The transaction is subject to approval by ReCor’s shareholders.
Otsuka Holdings’ acquisition follows the announcement by ReCor that the US FDA has given its approval to initiate a pivotal clinical study, RADIANCE II, for the evaluation of the Paradise renal denervation system for the safe and effective reduction of blood pressure in patients with hypertension. Previously, data from RADIANCE-HTN SOLO demonstrated a statistically significant reduction in blood pressure with the Paradise sysmte in hypertensive patients.
Following the acquisition, according to a press release, ReCor plans to continue to develop and evaluate the Paradise System in patients with hypertension in preparation for worldwide commercialisation, as well as explore its use in additional clinical applications such as heart failure, kidney disease and metabolic disorders, while also building the Otsuka Medical Devices’ incubation and clinical development hub in the USA and Europe.
Andrew Weiss, president and CEO of ReCor, says: “We are very encouraged by the results of our clinical trials with the Paradise System, which have been conducted in the USA and Europe— none of which would have been possible without Otsuka and the strong relationship between our teams. This transaction demonstrates that tremendous value can be created for companies and venture investors through strategic partnerships.”
Tatsuo Higuchi, president and representative director of Otsuka Holdings, says: “Our decision today reflects not only ReCor’s excellent clinical results, but also the close relationship we have built over the years. Our acquisition of ReCor represents an important step forward for Otsuka’s medical device business, leveraging an innovative technology with Otsuka’s expertise in pharmaceuticals and clinical development.”
Merit Medical Systems has been named the exclusive global distributor of the Q50 Plus Stent Graft Balloon Catheter (QXMédical). The Q50 Plus is used in abdominal and thoracic endovascular aneurysm repair (EVAR) procedures to repair abdominal aortic aneurysms (AAA) and thoracic aortic aneurysms (TAA). It is also suitable for temporary occlusion of large vessels.
The Q50 Plus features a broad balloon diameter range of 10mm to 50mm and is compatible with 12 French introducer sheaths. Constructed from a proprietary polyurethane technology, the balloon catheter is strong yet compliant and also offers exceptional balloon inflation and deflation rates, Merit Medical indicates in a press release.
The Q50 Plus is available with either a 65cm length catheter or a 100cm length catheter and is designed with a unique tapered flexible tip to facilitate device passage.
“This addition of the Q50 Plus Stent Graft Balloon Catheter to our offering allows Merit Medical to fully support vascular surgeons during all phases of their procedures. We anticipate no interruption for existing customers as we take on global distribution of the Q50 Plus, and in fact, Merit’s existing infrastructure will be an asset for seamless, worldwide distribution,” says Fred Lampropoulos, Merit’s chairman and chief executive officer. “With QXMédical we have established a valuable partnership with a company that has compatible corporate values and similar commitment to bringing superior products to market.”
BD (Becton, Dickinson and Company) announced it has completed the acquisition of TVA Medical, a company that develops minimally invasive vascular access solutions for patients with chronic kidney disease requiring haemodialysis including the everlinQ endoAVF System.
The addition of TVA Medical enables BD to offer the everlinQ endoAVF System, a new endovascular arteriovenous (AV) fistula creation technology that adds to the company’s end-stage renal disease portfolio of dialysis catheters, drug-coated balloons, standard angioplasty balloons and endovascular stent graft products. This technology will further improve BD’s ability to serve physicians and their patients by providing a minimally invasive option for creating critical AV fistulas for hemodialysis procedures.
“The addition of TVA Medical allows BD to provide another innovative device to physicians who treat patients suffering from chronic kidney disease requiring haemodialysis,” said Steve Williamson, worldwide president of Peripheral Intervention at BD. “This technology is highly complementary to our Peripheral Intervention offerings, and we will continue to bring new technologies to market that improve our category-leading ESRD portfolio. This is a great example of our continued strategy to use tuck-in acquisitions to advance category leadership.”
EverlinQ endoAVF System to become WavelinQ EndoAVF System
On 22 June, the US FDA announced De Novo marketing authorisation for the everlinQ endoAVF System. The system uses two, thin, flexible, magnetic catheters that are inserted into the ulnar artery and the ulnar vein in the arm through a small puncture. When placed close to each other, the magnets in each catheter attract, pulling the vessels together. After confirming alignment, an electrode from the venous catheter delivers radiofrequency energy to create the connection between the artery and vein. Embolization of the brachial vein is then recommended. The fistula is confirmed with an angiogram (X-ray image of the vascular system) to show that arterial blood is flowing to the low-pressure venous system. The procedure minimises the amount of vessel and skin trauma compared to traditional fistula creation using open surgery. The everlinQ endoAVF System enables an additional AV fistula location for patients than what is typically done surgically. The device is already commercially available in Europe and Canada. The product name will be transitioned to WavelinQ EndoAVF System during integration.
This transaction is not expected to have a material impact on BD results for fiscal 2018 or 2019. Future results for TVA Medical will be reported under the Peripheral Intervention business within the Interventional Segment at BD. The company used cash on hand to finance the transaction. This transaction does not impact the company’s previously-communicated commitment to deleverage as part of the Bard acquisition. Terms of the transaction were not disclosed.
The RADIANCE-II study of the Paradise Ultrasound Denervation System (ReCor Medical) for the treatment of hypertension has been approved by the US Food & Drug Administration (FDA).
Building upon the recent positive results of the RADIANCE-HTN SOLO study, RADIANCE-II will be a randomised, sham-controlled, blinded study in patients with moderate hypertension, powered to demonstrate the safety and efficacy of the Paradise System’s ability to lower blood pressure. ReCor expects to initiate enrolment in RADIANCE-II in October of 2018.
“We have had a very constructive dialogue with the FDA during the past nine months to craft what we believe is a strong study to develop a robust set of clinical data to support the future FDA review for PMA approval,” comments Leslie Coleman, vice president of Regulatory & Medical Affairs. “At the time of PMA submission we plan to have four independently-powered, blinded, sham-controlled, randomised studies of the Paradise System in patients with different stages of hypertension—our SOLO, TRIO, REQUIRE, and RADIANCE-II studies—approaching a total of nearly 500 patients, with outcomes as long as three years.”
“Our Steering Committee and medical advisors have been instrumental in the design of the Global RADIANCE Clinical Program—including the RADIANCE-II pivotal study—for the USA, Europe, Japan and Korea,” adds Helen Reeve-Stoffer, vice president of Clinical Affairs. “Given the recent positive SOLO results, and subsequently the numerous review articles in medical journals, we recognise the potential impact the Paradise System may have in the treatment of hypertension for millions of patients world-wide. Accordingly, ReCor is committed to conduct rigorous, randomised, controlled studies to demonstrate the safety and efficacy of the Paradise System to lower blood pressure, thus helping physicians to evaluate how, in whom, and when to use Paradise for the treatment of hypertension.”
Paradise is an ultrasound-based system for endovascular denervation of the renal nerves Renal denervation is a potential therapeutic option for treatment of hypertension, one of the most prevalent medical conditions. The Paradise System bears a CE mark but is not approved for sale in the USA. ReCor Medical is conducting the RADIANCE-HTN clinical trial under an IDE from the US FDA in the USA and Europe, the REQUIRE trial in Japan and Korea with its partner Otsuka, and recently received approval from the FDA to conduct RADIANCE-II as a pivotal study of the Paradise System.
Results from the DETOUR I trial evaluating the DETOUR System (PQ Bypass) for percutaneous bypass showed promising 12-month durability for patients with extremely long blockages in the superficial femoral artery (SFA). The data were presented as a late-breaking clinical trial session last week at the Society for Vascular Surgery (SVS) Vascular Annual Meeting (20–23 June, Boston, USA).
The trial enrolled lesions longer and more complex than those typically studied in SFA clinical trials, with an average lesion length of 37cm, 100% TASC II C/D, 96% chronic total occlusions (CTO), and 81% with moderate-to-severe calcification.
The DETOUR I trial, a prospective, single-arm, multicentre, core lab-adjudicated study, enrolled and treated 77 patients and 81 lesions. Primary and primary-assisted patency at 12 months in all lesions of the DETOUR I trial was 73% and 80%, respectively. Secondary patency was achieved in 94% of patients. Additional safety and effectiveness outcomes include 100% freedom from amputation, 99% freedom from acute limb ischaemia, and Rutherford improvement of ≥2 classes in 90% of patients.
“The lesions treated in DETOUR I were more than just long, they were extremely long, completely blocked, and severely calcified,” said Dainis Krieviņš, vascular surgeon and director of the Institute of Research at Pauls Stradins Clinical University Hospital. “Endovascular devices currently approved for use on these incredibly challenging lesions have surprisingly low durability in lesions that are half the size of the average DETOUR lesion and fail approximately 40% of the time by the 12-month milestone. This truly highlights the need for the minimally invasive DETOUR procedure for long, complex SFA lesions.”
Percutaneous femoropopliteal bypass (the DETOUR procedure) is an entirely new procedure enabled by the DETOUR System. The DETOUR procedure creates a pathway with PQ Bypass’s proprietary stent grafts, originating in the SFA, travelling through the femoral vein, and ending in the popliteal artery, bypassing the diseased part of the artery. The stent grafts re-direct oxygen-rich blood around the blockage, restoring blood flow to the lower leg and foot of the patient.
“These results represent exciting promise for patients with long, complex SFA lesions, a growing, yet severely underserved population,” said Heather Simonsen, VP of Global Therapy Development at PQ Bypass. “By routing blood around the disease, rather than forcing a way through it, the DETOUR System is designed to treat extremely long lesions that are not well-addressed by current endovascular devices. We look forward to continuing the collection of clinical data in our US IDE to build upon the outcomes observed in DETOUR I.”
In this article, Bijan Modarai outlines recent research on the effects on radiation exposure in high-volume interventionists, why a future with alternative modalities to X-ray guided procedures is an exciting prospect, and what safety measures could make a difference in the meantime.
In recent years, alarming and emotive reports of cancer diagnoses made in high-volume interventionists at a relatively young age have focused attention on the deleterious effects of occupational radiation exposure. The fact that even the low doses absorbed during fluoroscopically guided procedures can induce DNA damage, triggering inherent reparative mechanisms within the cell, are now beyond doubt and our group has shown this to be the case in both patients and operators after endovascular aortic procedures. These studies also suggested the fact that operators may have differential sensitivity to the same exposure dose. DNA repair pathways are error-prone and can lead to genomic instability and cytogenetic damage after chronic radiation exposure. In the absence of long-term studies in large cohorts of health workers, however, a definitive link between exposure and malignant transformation remains difficult to prove.
Our bodies are continuously bombarded by low-dose environmental radiation and in the UK, for example, an individual would accumulate approximately 2mSv of natural background exposure per year. Flying at altitude increases this exposure, with a 10 hour flight accounting for an extra 50μSv. A link between low dose exposure and cancer may be emerging with a recent publication showing an increased incidence of cancer in pilots who have the highest cumulative air hours and large dose exposures before the age of 40. Our recent studies monitoring real-time radiation exposure have measured an average dose of approximately 70μSv to exposed body parts after a complex endovascular aortic repair. A high volume operator, performing 50 cases per year, for instance, would incur a significantly raised dosage over that time. A modern day vascular trainee in their early 30s would be at risk of accumulating the aforementioned yearly dose for more than 30 years, with consequences that are unknown at present but may become apparent as our understanding of the ill effects of chronic exposure improves.
Real-time monitoring has allowed linkage of operator behaviours that account for the highest dose exposure. Protective manoeuvres during digital subtraction angiography (DSA) appear to be particularly important. Left lateral angulation of the C-arm, distance of the operator from the table and the “air gap” between the detection plate and the patient’s body are independent predictors of radiation exposure during DSA. The operators who were studied remained tableside for the majority of DSA runs, significantly increasing their absorbed dose. Perhaps a paradigm shift in strategies that ensure minimal exposure throughout the procedure is required. A non-operating “spotter”, delegated with prompting the operator to instigate optimal protective manoeuvres for themself and the rest of the team, particularly during the more critical steps of the procedure when focus on radioprotection may wane, could prove highly effective in reducing dose.
A definitive link between low-dose chronic radiation exposure and cancer remains to be demonstrated, but the mere fact that exposure can trigger DNA damage should motivate all, and in particular young and training vascular interventionists, to optimally protect themselves. The promise that one day we may circumvent the use of X-rays during procedures, instead using modalities such as electromagnetic guidance, for example, is exciting. Until then, encouraging radiation safety behaviours, ensuring optimal room set up and insisting on maximal shielding is of paramount importance.
Bijan Modarai is a reader/consultant in vascular surgery and a senior fellow at the British Heart Foundation.
In February 2018, the first European case of endovascular aneurysm repair (EVAR) for the treatment of an abdominal aortic aneurysm was performed using a prototype device based on augmented reality by Nyali Swiss, an advisory company based in Lugano, Switzerland, write Anna Maria Lerardi, Mario Petrillo, Salvatore Alessio Angileri and Gianpaolo Carrafiello (pictured), from Milan, Italy.
The procedure was performed in the angiosuite of San Paolo Hospital, in Milan, Italy. In real time, several doctors, residents and students, watched (via live streaming) the procedure above with “the eyes of the first operator”. The “spectators” were in Pisa, Italy, where the first edition of the European Campus in Interventional Radiology took place, dedicated to Italian and European residents.
The prototype device used is based on “space-cognizant” augmented reality that is able to superimpose virtual objects on the surroundings. The “virtual objects” represented in each scenario can have spatial relationships with real objects in 3D space: in our case an external operator was able to draw arrows or annotation on specific points on the patient’s skin or in other locations in the angiosuite.
The result was a strong interaction between the first operator, external consultants and the “spectators” in Pisa. All subjects were able to see and interact with the first operator.
In the meanwhile, the first operator was able to consult some virtual objects located in the angiosuite like the CT scan of the patient and some other documents that were able to help during the procedure. These were all superimposed as holograms in specific areas of his field of view.
Many start-ups are currently using augmented reality technologies for employee training: the aim is to familiarise trainees with different environments or specific scenarios. This approach is derived from the military, which has been experimenting in augmented reality interfaces for years.
It is now being exploited in interventional radiology to enable a consultant to virtually (outside of the operating theatre, at home or anywhere in the world) make suggestions to the first operator to decide on strategies, or issue warnings that are useful for the correct execution of the treatment by sharing the same field of view and the same information. In more and more cases, non expert operators may deal with challenging situations by calling upon help “from home”. This could be a more expert colleague (at home; in another room; or somewhere else in the world entirely) who is now able to see the procedure and suggest real-time operating strategies.
Our experience could be considered a milestone in augmented reality applied to interventional radiology, switching as we were from a virtual scenario to the patient bedside.
We have observed a faster learning curve for novice operators compared with the usual coaching when we have used augmented reality. More students, residents and interested physicians may follow the procedure from outside the operating room.
Our aim is to use augmented reality to help manage the pain and distress associated with a wide variety of interventional radiology procedures by using different strategies focused on integrating analgesia with anxiety reduction. To this end, patients can wear special glasses equipped with immersive virtual reality and dial up a scene from a beach or any other different relaxing scenarios during different interventional procedures (whether they are oncological or not). The aim is to investigate and capture the compliance and experience of patients with and without glasses.
In our department, we routinely perform percutaneous thermal ablation of solid tumours under mild sedation that provides both analgesia and anxiety reduction. We have undertaken a study that was based on the premise that virtual reality glasses can serve to “distract” the patient from the pain of the procedure and preliminary results are showing that a lower dose of benzodiazepine was used in patients who wore glasses. We are also performing the same investigation in a non oncological setting, specifically in the context of interventions to treat low back pain. Every year, we treat almost 200 patients with percutaneous lumbar and cervical disc decompression and our idea is to compare the dose of analgesics administered in patients wearing virtual reality glasses with those who do not. Moreover, a questionnaire to investigate patient compliance during the procedure will be proposed to every patient.
Virtual and augmented reality are new, evolving fields with several applications that need testing in clinic in order to help the technology mature and go beyond just entertainment.
Anna Maria Lerardi, Mario Petrillo, Salvatore Alessio Angileri and Gianpaolo Carrafiello (professor and chief of Diagnostic and Interventional Radiology Unit) are from the University of Milan, Milan, Italy.
For many venous specialists, dedicated venous stents represent the future—and the promise of an ideal venous stent on the horizon is a central topic of discussion. In this article, Rick de Graaf, Friedrichshafen, Germany, reviews the recent history of venous stenting and outlines the questions that need to come next.
Obviously, treatment of deep venous obstructions with stents goes much further back than just five years. The first reports of successful deep venous stenting originate from Germany, Sweden and the USA in the early 1990s. Mainstream attention increased rapidly in the early 2000s, after publications by the Stanford group (O’Sullivan and Dake) and of the bestknown series by Neglen and Raju.
Nevertheless, the last five years may truly qualify as a new era. Deep venous interventions blossomed intensely during this time, with multiple centres in Europe and the USA exploring interest in the endovascular approach. Both physicians and industry sought new innovative techniques and devices and thus, dedicated venous stents were developed. Deep venous treatment became a returning popular theme at major conferences around the world. Thereby, discussions over approach, strategy and devices intensified with a host of questions: Which imaging modality should be used? Is any stent superior over others? Do we need recanalisation devices? Which patient does well after recanalisation and which patient does not? How do we identify the optimal patient for intervention? Why do stents reocclude and how do we prevent it? What is the best antithrombotic strategy— anticoagulation, antiplatelets or both; and how much is needed, how long for, etc. The list goes on and on.
A few major points should be discussed, in order to shed light on the current state of venous stenting procedures. The first dedicated stents came to the market around 2012. At the time, the Wallstent was not considered good enough. Admittedly, the Wallstent caused some problems—in my own experience as well—and some were difficult to solve. Nevertheless, since 2012, I have not seen a perfect stent appear. Every stent has specific pros and cons. Some downsides are so destructive however, that the problems caused by the stent cannot be solved anymore, at least not through endovascular means. Sometimes, it even feels like a step backwards.
Although newer stents may be easier to deploy and can be positioned more accurately, it is important to note that there is no scientific evidence that any of the new stents perform better than the Wallstent. Certainly, new stents will continue to enter the market in the coming years, some with well thoughtout designs that may help to boost clinical success, others with anti proliferating drug coatings or another unsubstantiated smart marketing gimmick. Still, these stents should not be expected to magically shift the patency to 100%.
Naturally, this does not mean we should not continue to look for innovations to support our daily practice and optimise patient outcome. However, if stent design does not fully account for stent patency, what does? As can be extracted from Virchow’s triad, unfavourable haemodynamics or increased coagulability may be additional reasons for stent occlusion. Low flow may cause thrombosis, but we do not know how much flow is enough. I have seen some patients with dreadful flow with patent stents after many years, while others have excellent flow yet still occlude.
Although the need of antithrombotic therapy after deep venous stenting is beyond discussion, the exact concentration, duration and type remain debatable. Direct anticoagulants (DOACs) seem to slowly but surely be surpassing vitamin K-antagonists as primary oral anticoagulants (OACs); however, some interventionalists challenge the superiority of OAC in favour of antiplatelets. Due to the multifactorial nature of stent reocclusions, it will be extremely hard if not undoable to find superiority of one medical treatment over the other. It is important however to scrutinise the optimal antithrombotic strategy for the individual patient. Attention for resistance to certain medications should also be advocated for deep venous interventions; close collaboration with haematologists therefore is recommended. Stent reocclusion is cumbersome to treat and increases the risk of (fatal) pulmonary emboli.
The deal may not be sealed with an open stent however. Why do some patients benefit from an open stent while others seem not to improve? For one, the complaints may not have been venous-related in the first place. So, do we need better or different scoring systems? Although the Villalta scale is most widely used, it has not been published in a peer-reviewed journal and is open for critique. Another reason may be inadequate venous outflow from the leg, either by continued venous insufficiency due to valve destruction or absence of inline flow towards the stents. Previously created collateral pathways may inadequately distribute a significant blood volume away from the stented venous segments. Thus, patent iliac stents do not necessarily prevent venous hypertension in the leg. Maximising complete and fast outflow of the leg into the stents is the prerequisite.
Finally, some patients may not qualify for treatment in the first place. Patient selection should be one of the key points of interest. Extensive post-thrombotic scarring of all major inflow veins may preclude autonomous long-term stent patency. Surely, an arteriovenous fistula can be placed in all of these patients. The stents are likely to stay open—that is, until restenosis by intimal hyperplasia. However, when spontaneous venous blood flow from the leg is compromised it is unlikely that the patient will do better.
In conclusion, the last five years established the bottlenecks of a procedure that nevertheless has proved very successful and safe. Optimisation of antithrombotic therapy and flow enhancement may result in the unchallenged status of deep venous stenting.
Rick de Graaf is director of Radiology, Interventional Radiology and Nuclear Medicine at the Clinical Centre of Friedrichshafen, Germany.
Figure 1. Representative images of arterial embolization in a rabbit kidney with Hydrogel Embolic System. Image panel includes a) baseline angiogram of right kidney, b) hydrogel embolic delivery under fluoroscopy c) digital subtraction angiography confirming stasis and embolization (inlay non-subtracted), and d) microscopic image showing hydrogel embolic (stained with trypan blue) in vessels large and small <25 um.
To become a mainstay liquid embolic for peripheral use, an optimal product should be easy to use, have reproducible and controllable deep penetration for tumour and organ applications, be compatible with aqueous contrasts, drugs and standard microcatheters and not be prone to non-target embolization, writes Suvranu Ganguli, Boston, USA, on the topic of embolic agents that are just around the corner. embolics
Embolic particles and coils are the current mainstay of peripheral embolotherapy. Liquid embolics such as Onyx liquid embolic system (Medtronic) and TruFill (Cordis, now Cardinal Health) are
currently approved for neurological applications in the USA. These two liquid embolics are often used off label for peripheral applications, but they do have limitations with the inability to achieve diffuse distal embolization and challenges in delivery
technique. To become a mainstay liquid embolic for peripheral use, an optimal product should be easy to use, have reproducible and controllable deep penetration for tumour and organ applications, be safe from non-target embolization, and be compatible with aqueous contrasts, drugs and standard microcatheters. This is an overview of some liquid embolics in development, working to deliver this long sought after tool for interventional therapy.
Hydrogel Embolic System
Instylla’s Hydrogel Embolic System (HES) is being designed for both the diffuse embolization of tumours and organs as well as specific segmental embolizations, such as in the setting of haemorrhage requiring proximal vessel occlusion. Instylla is the latest in the Incept family of companies that has been responsible for the development of more than a dozen innovative hydrogel based medical products used in millions of patients worldwide. The HES is a biocompatible, hydrophilic, hydrogel designed to offer controlled, safe and targeted embolization. HES is formed from precursors of functionalised polyethylene glycol that self react to form a hydrogel rapidly. Once delivered, the HES materials polymerise in-situ but with the location of embolization (distal or proximal) reliably controllable through simple adjustments in the rate and volume of delivery, much like techniques used with embolic particles. The HES is formulated to inhibit the gel from forming in non-target branching vessels, limiting non-target embolization. Since the polymerisation is self reacting and not based on precipitation (as in the case of Onyx or glues) the delivery procedure can be paused by the physician to provide an additional aspect of procedure control. The embolization is also blood and coagulation independent. These qualities support significantly reduced embolization procedure times but with safety and control. The resulting hydrogel is soft with a feel much like tissue, but physiologically stable and unaffected by natural thrombolytic processes that may cause recanalisation. Both small and large animal studies have demonstrated rapid and complete embolisation of diffuse vascular beds down to sub 10 microns as well as the ability to create discrete proximal vessel occlusions in a variety of vessel sizes, and in both cases avoiding nontarget embolization. The company is currently expanding its set of published in vitro and in vivo data and preparing for the first human clinical studies with the HES (Figure 1).
Shear-Thinning Biomaterial
A team from Mayo Clinic Arizona and UCLA Bioengineering, USA, is developing a liquid embolic based on shear-thinning biomaterial (STB), a nanocomposite hydrogel containing gelatin and silicate nanoplatelets, to function as an embolic agent for endovascular embolization procedures (Figure 2). STBs are injectable through clinical catheters and needles and have haemostatic activity comparable to metallic coils, the current gold standard. In addition, STBs withstand physiological pressures without fragmentation or displacement in elastomeric channels in vitro, in explant vessels ex vivo and in large animal models. In vitro experiments also indicated that STB embolization did not rely on intrinsic thrombosis as coils did for occlusion, suggesting that the biomaterial may be suitable for use in patients on anticoagulation therapy or those with coagulopathy. Using CT imaging, the biomaterial was shown to fully occlude murine and porcine vasculature in vivo and remain at the site of injection without fragmentation or nontarget embolization.
Figure 2
Given the advantages of rapid delivery, in vivo stability, and independent occlusion that does not rely on intrinsic thrombosis, STBs offer an alternative gel-based embolic agent with translational potential for endovascular embolization. Furthermore, the STB does not generate artifact from imaging allowing visualisation of the embolized vasculature. STB as an embolic agent was the cover story in the November 2016 issue of Science Translational Medicine; research on STB is ongoing with two NIH R01 grants.
GPX
Fluidix Medical’s GPX, a liquid embolic, is based on biomaterials from sandcastle worms. These biomaterials are formulated into a colloidal-rich coacervate which when delivered into blood precipitates out the biomaterials to form the embolic. At high ionic strengths, the embolic coacervates are injectable fluids that can be delivered through long narrow microcatheters. At physiological ionic strength, the embolic coacervates transition into a nonflowing solid morphology. Transcatheter embolization of rabbit renal arteries demonstrated capillary level penetration, homogeneous occlusion, and 100% devascularisation of the kidney, without the embolic crossing into venous circulation. The benign waterborne composition and setting mechanism avoids many of the problems of current liquid embolics, and provides precise temporal and spatial control during endovascular embolization.
Silk Elastin Protein Polymer
Theratarget is developing a liquid embolic using a Silk Elastin protein Polymer (SELP). Theratarget was formed from research on SELP conducted at the University of Utah through the USTAR Initiative. The SELP material is a liquid at room temperature but at the internal human body temperature of 37°C, it transitions into a solid hydrogel capable of vessel occlusion. Since it is a single component system, it can be delivered using standard microcatheters. It is currently in development for chemoembolization with in vitro and animal model in vivo studies performed showing the feasibility of the product.
Suvranu “Shoey” Ganguli is associate chief, Interventional Radiology, Massachusetts General Hospital Harvard Medical School, Boston, USA. He is a consultant to Instylela, Boston Scientific, Medtronic and Sirtex.
An update to last year’s FDA letter, expressing concern over risk of type III endoleaks in relation to endovascular graft systems, now states that the increased risk is specific to one device which was discontinued in 2014.
Endologix’ AFX Strata, an endovascular graft system indicated for endovascular aneurysm repair (EVAR), ceased to be manufactured by the company in 2014. In December 2016, Endologix issued a recall of the “small remaining quantity” of AFX Strata devices remaining in hospital inventories. However, the FDA highlight, the device is still in use in patients who had it implanted prior to discontinuation or recall.
The FDA’s original 2017 letter described an increase in type III endoleaks reported by several sources including the Administration’s own Medical Device Reporting (MDR) system and manufacturers’ Annual Clinical Updates to Physicians. The increased risks were associated with EVAR and endovascular graft systems, but the FDA were not specific as to which systems could be affected, instead recommending reports of adverse events from physicians and manufacturer compliance with MDR regulations and reporting requirements.
Since the 2017 letter, the FDA now write, the increased risks were narrowed down to the AFX Strata based on new information, observing “greater risk for a type III endoleak compared to other endovascular abdominal aortic aneurysm (AAA) graft systems.
Type IIIa endoleaks were, as estimated by Endologix, 0.9% at two years and 5% at five years, while type IIIb endoleak rates were 0.66% at two years and 2.4% at five years. “Because these estimates are calculated using voluntary reporting and units sold, the rate estimates may be low compared to the true endoleak event rates”, the FDA write.
Matt Thompson, chief medical officer for Endologix, says, “The FDA update does not disclose risks beyond those already communicated to health care practitioners in safety notice issued by Endologix in December 2016, which requested that all remaining AFX Strata devices be returned from the field and emphasised the fact that Endologix has not manufactured AFX Strata grafts since 2014.”
“Endologix is committed to working collaboratively with the FDA,” comments John Onopchenko, the company’s chief executive officer. “Our current commercially available versions of the AFX system, the AFX Duraply and AFX2 products, are manufactured using a different ePTFE processing methodology and include additional product improvements. These AFX Duraply and AFX2 products are not the subject of today’s FDA-issued awareness notification. Through our comprehensive system of post-market surveillance, anonymised registry data, and the only randomised trial to compare EVAR systems (the LEOPARD trial), we have a strong, growing evidence base that supports the use of the AFX Duraply and AFX2 systems for patients with AAA. We are proud of, and committed to, advancing our collaborative work with the FDA on behalf of our patients, customers, and the broader clinical community.”
At this time, the FDA advise health care providers monitor affected patients and ensure annual follow-up to monitor for type III endoleaks. “The FDA continues to work collaboratively with Endologix,” they write, “to assess the treatment options for patients with the AFX with Strata device and type III endoleaks, and to provide further instructions in the labelling on this concern.”
The Direxion™ Microcatheter, with its unique shaft design, offers you unrivaled torqueability for improved maneuverability. Further enhancing your ability to access challenging treatment sites are a variety of tip shapes that allow for flexibility and efficiency.
With Direxion’s best-in-class torque response and high-pressure flow rates, now with improved tip shapes and hydrophilic coating, you can reposition the microcatheter tip without a guidewire and obtain clear imaging with power injections up to 1200 psi.
Direxion™ Microcatheters can handle multiple acute turns at artery branches. This is made possible because each microcatheter has over 10,000 laser cuts through the nitinol shaft. Carefully calibrated spacing of these cuts allows us to offer the optimal stiffness profile—achieving a balance of pushability to advance the microcatheter with the softness needed to reach the most distal anatomy. With Direxion™, you’ll get the precision and control you need to get the procedure done.
Direxion™ and Direxion HI-FLO™ Torqueable Microcatheters Indications, Safety, and Warnings Prescriptive Information CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the complete “Directions for Use” for more information on Indications, Con-traindications, Warnings, Precautions, Adverse Events, and Operator’s Instructions INTENDED USE/INDICATIONS FOR USE The Direxion and Direxion HI-FLO Torqueable Microcatheters are intended for peripheral vascular use. The pre-loaded Fathom and Transend Guidewires can be used to selectively introduce and po-sition the microcatheter in the peripheral vasculature. The microcatheter can be used for con-trolled and selective infusion of diagnostic, embolic, or therapeutic materials into the vessel. CONTRAINDICATIONS None known. WARNINGS •Never advance or withdraw an intravascular device against resistance until the cause of resistance is determined by fluoroscopy. Movement of the microcatheter or guidewire against resistance may result in damage or separation of the microcatheter or guidewire tip, or vessel perforation. •This Direxion Microcatheter family is not intended for use in the coronary vasculature or neuro-vasculature. •The Direxion HI-FLO Microcatheter is not designed for the delivery of embolic coils. •Use of excessive force to manipulate the microcatheter against resistance can cause a fracture in the nitinol shaft. Take care not to over-torque the microcatheter, and to relieve any tension before withdrawal by rotating the microcatheter in the opposite direction. PRECAUTIONS •This device should be used only by physicians thoroughly trained in percutaneous, intravascular techniques and procedures. •Do not introduce the microcatheter without guidewire support as this may cause damage to the proximal shaft of the catheter. •Because the microcatheter may be advanced into narrow sub-selective vasculature, repeatedly assure that the microcatheter has not been advanced so far as to interfere with its removal. ADVERSE EVENTS The Adverse Events include, but are not limited to: •Allergic reaction •Death •Embolism •Hemorrhage/Hematoma •Infection •Pseudoaneurysm •Stroke •Vascular thrombosis •Vessel occlusion •Vessel spasm •Vessel trauma (dissection, perforation, rupture)
The annual census of UK consultants and higher speciality trainees—Focus on Physicians 2017–18—indicates that more than half of all consultants and two thirds of trainees reported frequent gaps in trainees’ rotas, with one in five respondents saying these are causing significant problems for patient safety in hospitals.
The report, which has been jointly published by the Royal College of Physicians and Surgeons of Glasgow, the Royal College of Physicians of Edinburgh, and the Royal College of Physicians of London, also shows:
Almost half of advertised consultant posts remain unfilled because of a lack of suitable applicants
Consultants and trainees are working around 10% more than their contracted hours. This equates to trainees working an extra six weeks and consultants an extra month unpaid a year
33% of the current consultant workforce are predicted to reach their intended retirement age in the next decade. Medical student places need doubling now to fill this and the gap left generally by doctors leaving the profession
Satisfaction among consultants and trainees with working in general internal medicine remains significantly lower than with specialty-working.
Commenting on the findings of the census David Galloway, president of the Royal College of Physicians and Surgeons of Glasgow, says: “I am glad that the three Royal Colleges have once again joined together to produce this important piece of work. It is vital that everyone involved in the NHS now reflects on these findings and takes all the action necessary to replicate best practice and address the challenges that this document has highlighted. What is of particular concern is the finding that almost one in five consultants across the UK reported that rota gaps cause significant problems for patient safety in their hospital. This is an unsustainable situation which must be addressed as a matter of urgency.”
He adds that while the colleges welcome the short-term actions that UK governments (England & Wales and Scotland) are taking, they believe “consistent and sustained action” is needed if the situation is to be addressed in the longer term. “Government, patients and the medical profession must work hand in hand if we’re to deliver the best possible NHS for all,” Galloway comments.
Ellipsys Vascular Access System (Avenu Medical) has been granted De Novo marketing authorisation from the Food and Drug Administration (FDA). Ellipsys is a minimally-invasive catheter-based system designed for end-stage renal disease (ESRD) patients requiring haemodialysis.
“Good vascular access makes a tremendous difference in patient outcomes,” says long time kidney patient advocate Terry Litchfield. “This revolutionary non-surgical fistula creation can reduce the pain and suffering associated with traditional fistula surgery, lessen failed surgeries and reduce catheter time for patients.”
Since 1966, the AV fistula has been surgically created in an operating room by sewing a vein and an artery together, usually in the arm. When this is done, blood from the artery will pass through the vein increasing its flow rate and diameter. This makes the vein suitable for the insertion of the needles required for haemodialysis treatment. An AV fistula is the preferred method for vascular access as there is evidence of longer term patency, improved flow rates and fewer complications than other methods of vascular access.
A new innovation for dialysis patients and clinicians, Ellipsys is a less-invasive alternative to the traditional creation of AV fistulas and is designed to be used by a physician under local or regional anaesthesia in all sites of service including hospital outpatient departments, ambulatory surgical centres and physician offices.
According to Avenu, ultrasound is used to guide the Ellipsys catheter through the skin to the pre-determined vascular target. The catheter delivers a small amount of thermal energy that fuses a sutureless and permanent anastomosis, or connection, between the vein and artery allowing the creation of an AVF. Unlike surgery, the Ellipsys System uses a minimally invasive, endovascular approach that leaves the skin without a scar, and the vascular bed undisturbed and intact without leaving any foreign material implanted (including suture). After the procedure, the patient leaves with just a band aid.
Clearance was granted after the FDA reviewed data from a non-randomised, US multicentre study of 103 patients. The study was designed to demonstrate the safety and efficacy of the Ellipsys System for the percutaneous creation of an AV fistula.
“This approval marks a seismic shift for the patients and physicians within the ESRD community. We can now offer a faster, more efficient and less-invasive option for patients requiring vascular access here in the USA and worldwide,” says Mark Ritchart, president of Avenu Medical. “For too long there has been a shortage of dedicated vascular surgeons who can create AV fistulas leading to delays in performing the surgery and requiring expensive, temporary catheter access. Our Ellipsys System has the potential to significantly increase the number of clinicians performing vascular access procedures, thereby reducing these delays. This, in turn, will result in reduced morbidity and the cost associated with temporary catheter access. In short, it represents a quality of life improvement opportunity for this patient community.”
“Using the Ellipsys Vascular Access System is very similar to common procedures such as obtaining venous and arterial access with ultrasound,” says Jeffrey E Hull, director of the Richmond Vascular Center in Richmond, USA. “Most physicians involved in vascular access have the endovascular skills required and will learn to use the Ellipsys System quickly.”
Surgeons Preparing Equipment For Surgery Wearing Hospital Mask Concentrating
An embolization procedure
Shape Memory Medical announced it has received 510(k) clearance from the US Food and Drug Administration (FDA) for the Impede embolization plug. The device is indicated to obstruct or reduce the rate of blood flow in the peripheral vasculature. It is available in three sizes, to treat vessels up to 10mm in diameter.
The Impede embolization plug received CE marking in August 2017 and has been used to treat patients in New Zealand and in several countries in the European Union.
Speaking about the device, Jafar Golzarian, interventional radiologist with University of Minnesota Health, Minnesota, USA, stated, “It is exciting to see the approval of new developments in embolization technology, offering physicians a new alternative to embolization coils.”
Commenting on this regulatory milestone and ongoing clinical usage, Shape Memory Medical’s president and CEO, Ted Ruppel, said, “The Impede embolization plug is an exciting development in embolization technology, expanding the options open to physicians treating conditions requiring occlusion of the peripheral vasculature.”
The devices feature proprietary Shape Memory Polymer (SMP) technology developed at Texas A&M University and Lawrence Livermore National Laboratory. Shape Memory Medical was founded to commercialise stable, predictable embolization solutions for a variety of clinical applications. The SMP technology includes porous polymeric materials capable of changing from a catheter-deliverable shape to a “memorised” larger conformable shape when delivered into a blood vessel. The company continues to develop SMP technology for an expanded range of clinical uses, including neurovascular applications.
With both internally developed and licensed technologies, Shape Memory has 26 issued US patents and multiple patents under review on a worldwide basis. This intellectual property includes the use of SMP for a variety of clinical applications, a press release from the company states.
everlinQ endoAVF System (TVA Medical) is now approved by the US Food and Drug Administration for de novo marketing. This innovative, minimally invasive technology uses magnetic catheters and radiofrequency energy to create an arteriovenous fistula (AVF) for haemodialysis access without open surgery.
“The everlinQ endoAVF System is a significant advance in the management of chronic kidney disease,” says Paul Kreienberg, vascular surgeon at The Vascular Group, Albany Medical College, Albany Medical Center Hospital, Albany, USA. “Hundreds of thousands of Americans require vascular access for lifesaving dialysis, but until now this access has required open surgery that is accompanied by high failure rates and low patient satisfaction. The everlinQ endoAVF System is transforming vascular access using a minimally invasive approach, and I anticipate a high level of interest from both patients and physicians for this compelling endovascular solution.”
According to a company release, more than 400,000 people in the USA receive haemodialysis multiple times a week for end-stage renal disease (ESRD). The current standard vascular access approach uses open surgery to create an AVF for dialysis. Surgical AVFs are associated with failure rates up to 60% and often require frequent revisions. When a surgical AVF procedure is effective, the fistula takes on average over four months to mature before dialysis can begin. In addition, vascular access creates concern and stress for many ESRD patients, including the threat of repeat procedures and disfigurement of the arm, with up to 30% of patients refusing fistula surgery.
“Vascular access issues significantly hinder the delivery of adequate dialysis for patients, and there has been little innovation related to surgical fistula creation in more than 50 years,” adds Kreienberg. “The everlinQ endoAVF System is a significant new vascular access option for these patients.”
The FDA marketing authorisation enables use of the everlinQ endoAVF System as a Class II medical device in the ulnar artery and ulnar vein, to create an endoAVF for haemodialysis use in properly indicated patients. Data from four clinical studies using the everlinQ endoAVF System demonstrated 97% procedural success; 88% fistula maturation (suitable for dialysis) at three months; and 75% successful cannulation at six months with minimal need for re-intervention.
“FDA marketing authorization of the everlinQ endoAVF System is a monumental milestone for dialysis patients who now have an alternative AVF option,” says Adam L Berman, president and CEO of TVA Medical. “Thanks to extensive collaboration with the FDA, clinical study investigators and clinical advisors, we are thrilled to now partner with the US vascular surgery and nephrology communities to offer an innovative endovascular fistula creation approach. Training will begin immediately at select US vascular surgery centres, and a US post-market study is scheduled to initiate before the end of the year.”
The everlinQ endoAVF System was reviewed by the FDA through the De Novo premarket review pathway, a regulatory process for some new medical devices that are low to moderate risk and have no legally marketed predicate device to base a determination of substantial equivalence. The everlinQ endoAVF System received European CE mark in 2014 and Health Canada Medical Device License in 2016 for ESRD patients.
The support of the UK’s National Institute for Health and Care Excellence (NICE) signals that embolization has a unique role in the treatment of benign prostatic hyperplasia, outside of the traditional spectrum of medical and surgical options, write Riad Salem and Samdeep Mouli, Chicago, USA, while reviewing the new evidence in favour of the minimally invasive procedure.
Benign prostatic hyperplasia affects more than half of men over the age of 50 and its incidence increases with age. Enlargement of the prostate gland leads to lower urinary tract symptoms (LUTS), including urinary frequency and urgency, nocturia, difficulty urinating, and incomplete bladder emptying. Together these symptoms lead to a significant impairment to quality of life. Management of these symptoms can be challenging, and must take into account prostate disease burden, pre-existing sexual function, and medical co-morbidities.
Several medical and surgical therapies have been utilised to treat this patient population, but variable efficacy and persistent side effects have driven patients to seek alternative therapies that maximise quality of life. As such, the treatment of these symptoms has evolved over the last several years, moving away from invasive surgical options towards minimally invasive therapies. Concurrently, a greater emphasis has been placed on functional outcomes and quality of life, such as hospital stay, recovery time, and return to work. Prostate artery embolization has been developed to address these limitations of current treatment options. Via imageguided catheter-directed embolization of the prostatic arteries, embolization induces ischaemic necrosis of the gland, with resultant improvement in LUTS.
The initial prostate artery embolization studies focused on understanding arterial anatomy, defining patient selection, and demonstrating technical feasibility. These early studies demonstrated safety and efficacy, with a relatively favourable side-effect profile, mostly limited to mild transient haematuria and dysuria. Critically, multiple studies have confirmed that embolization does not result in the typical urinary and sexual dysfunction issues seen with both medical and surgical treatment options.
Early enthusiasm for this novel therapy was tempered by technical difficulty. Initial variability in clinical outcomes has subsided with refinements in microcatheter technique, embolic agent selection, a clearer understanding of arterial anatomy, as well as the advent of cone-beam CT. Along with these advancements, more mature data has emerged clarifying the role of embolization in the treatment of lower urinary tract symptoms, secondary to benign prostatic hyperplasia.
Within the last year, several studies have demonstrated efficacy across prostate gland sizes, particularly in patients with large prostates (>80 grams), which are often difficult to treat surgically. Additionally, embolization has been successfully employed to treat hyperplasia-related chronic urinary retention requiring long-term foley catheterisation. Several groups have reported 80–90% of patients with chronic urinary retention are catheter-free following embolization. Critically, the procedure has been proven safe and effective in patients who are not surgical candidates due to underlying medical co-morbidities.
Data from the multicentre UK ROPE (Registry of prostate embolization) registry of prostate artery embolization have recently been published by Alistair F Ray and colleagues in BJU International in April 2018. Investigators compared 305
patients undergoing embolization (n=216) vs. the surgical gold standard, transurethral resection of the prostate (TURP; n=89) in the setting of a noninferiority study. While embolization did not outperform TURP, significant improvements in both urinary symptoms and quality of life were observed, without significant complications or effects on sexual function. Additionally, the majority of patients in the embolization arm were treated on an outpatient basis, whereas surgical patients required at least overnight admission. The results of this registry mirror our own US FDA-approved prospective open label trial presented at the Society of Interventional Radiology’s 2018 meeting (SIR; 17–22 March, Los Angeles, USA). In a cohort of 45 men treated with embolization, we observed early and sustained improvements in urinary function and quality of life over a one-year follow-up period. There were no severe complications, and sexual function was not affected throughout the course of the study. These data are currently under review.
These latest studies add to the data proving embolization is both safe and effective for treating lower urinary tract symptoms secondary to benign prostatic hyperplasia. It offers significant and sustained improvement to both urinary function and quality of life. This body of evidence has led the UK’s National Institute for Health and Care Excellence (NICE), the governing body for health and social care, to support the use of embolization in the National Health Service (NHS). NICE does not usually approve new treatments without significant reflection and a critical review of the data; their approval of embolization into the treatment algorithm is sure to set the stage for reimbursement approval in the USA. The support of the UK’s NICE signals that embolization has a unique role in the treatment of benign prostatic hyperplasia, outside of the traditional spectrum of medical and surgical options.
Moving forward, the treatment of benign prostatic hyperplasia and lower urinary tract symptoms will require multidisciplinary collaboration, tailoring treatment to both patient disease burden and functional goals. In this context, embolization should be offered to patients seeking an alternative to current therapies, one which maximises quality of life. In 2014, we predicted that embolization would become one of the standard of care treatments for benign prostatic hyperplasia within three to seven years after data from Portugal and Brazil could be confirmed in independent cohorts. The work of Nigel Hacking and the other UK investigators, has helped to accomplish this feat in four years.
Samdeep Mouli and Riad Salem are both at the Section of Interventional Radiology, Northwestern University, Chicago, USA. They have reported no disclosures pertaining to this article.
Terumo has announced receiving the CE mark for its Kanshas drug-coated balloon catheter used in the treatment of lower extremity peripheral arterial disease.
With a September launch planned in Europe, Terumo is expected to be the first Japanese company to launch drug-coated balloon sales in Europe, and the European launch will be followed with launches in Latin America and Asia, as well.
A drug-coated balloon catheter is a medical device coated with a drug that suppresses cell proliferation on the balloon surface. When the balloon is expanded, it comes into contact with the blood vessel walls, transferring the drug to the vascular tissues, which is expected to suppress restenosis.
Kanshas can be expected to have an enhanced therapeutic effect due to Terumo’s proprietary uniform micro-crystal coating named Unicoat, which has been designed so that the coated drug is less likely to migrate before it reaches the lesion and then transfers swiftly to vascular tissue when the balloon is expanded. Product line-up of long balloon with a range up to 200mm can be treated for long lesions, which are common in the lower extremities.
Terumo is aiming to expand its peripheral vascular intervention business globally and is building up its product portfolio, a company release states. The launch of Kanshas is part of this strategy. Going forward, Terumo is determined to enhance its contribution to medical treatment in the endovascular field, the release adds.
A randomised, open label trial that was published in the BMJ on 19 June 2018 suggests that the improvement in lower urinary tract symptoms secondary to benign prostatic hyperplasia (BPH) seen 12 weeks after prostatic artery embolization (PAE) “is close to that after transurethral resection of the prostate (TURP)”.
However, the investigators report that the non-inferiority of embolization to TURP could not be established in the trial. “Prostatic artery embolization is associated with fewer complications than TURP but has disadvantages regarding functional outcomes, which should be considered when selecting patients,” they write.
Dominik Abt, consultant urologist and a team of colleagues from Switzerland that includes Lukas Hechelhammer, section chief of interventional Radiology, set out to compare prostatic artery embolization with in the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia in terms of patient reported and functional outcomes.
Trial details
The investigators randomised 103 patients aged ≥40 years with refractory lower urinary tract symptoms secondary to benign prostatic hyperplasia to either receive embolization or surgery. In the trial, 48 patients who were treated with embolization and 51 who were treated with surgery reached the follow-up endpoint 12 weeks after the procedure.
The authors report that embolization was performed with 250-400μm microspheres under local anaesthesia vs. monopolar TURP performed under spinal or general anaesthesia.
The primary outcome of the study was a change in international prostate symptoms score (IPSS) from baseline to 12 weeks after the procedure; a difference of less than three points between treatments was defined as non-inferiority for embolization and tested with a one-sided t test. The secondary outcomes included further questionnaires, functional measures, magnetic resonance imaging findings, and adverse events; changes from baseline to 12 weeks were compared between treatments with two-sided tests for superiority.
The mean reduction in IPSS from baseline to 12 weeks was −9.23 points after embolization and −10.77 points after TURP. “Although the difference was less than three points (1.54 points in favour of TURP, non-inferiority of embolization could not be shown (p=0.17),” the authors write.
“Before starting this trial, we did our sample calculations with assumed drop out rates etc. to correctly power this study. Nevertheless, our standard deviations regarding the primary outcomes for both interventions were larger than assumed for the sample calculations. Therefore, this study is underpowered to show non-inferiority of prostatic artery embolization. On the other hand, it does not show that embolization is inferior,” Hechelhammer told Interventional News.
Further, none of the patient reported secondary outcomes differed significantly between treatments when tested for superiority; IPSS also did not differ significantly (p=0.31). At 12 weeks, embolization was less effective than TURP regarding changes in maximum rate of urinary flow (5.19 vs. 15.34 mL/s; p<0.001), postvoid residual urine (−86.36 vs. −199.98 mL; p=0.003), prostate volume (−12.17 vs. −30.27 mL; p<0.001), and desobstructive effectiveness according to pressure flow studies (56% vs. 93% shift towards less obstructive category; p=0.003). Fewer adverse events occurred after embolization than after TURP (36 vs. 70 events; p=0.003).
“Improvement in lower urinary tract symptoms secondary to benign prostatic hyperplasia seen 12 weeks after embolization is close to that after TURP […] Further comparative study findings, including longer follow-up, should be evaluated before embolization can be considered as a routine treatment,” the authors write.
“Due to our results we believe that an ideal candidate for embolization is a man in whom the indication for intervention is primarily based upon symptoms; with a suitable vascular anatomy; and a reasonable volume of the prostate. Embolization can also be used for polymorbid patients not suitable for TURP.
Since embolization shows a less desobstructive effect after 12 weeks, TURP should be preferred in patients with bladder outlet obstruction (BOO) associated complications,” Hechelhammer added.
Veryan Medical has announced completion of enrolment of the 500th patient in the MIMICS-3D pan-European registry, a prospective, multicentre, observational registry to evaluate the BioMimics 3D Self-Expanding Stent System in the treatment of femoropopliteal artery disease.
The registry is evaluating safety, effectiveness and device performance within a real-world clinical population in combination with other therapies, including drug-coated balloons and atherectomy devices, in 25 hospitals across Europe.
The MIMICS-3D Registry principal investigator, Michael Lichtenberg (Arnsberg, Germany) says: “I am delighted that this significant landmark in the MIMICS-3D registry has been reached. The clinical sites have been extremely committed to both the device and the study and the speed of enrolment and quality of the data being collected are impressive. I would like to extend my thanks to all involved for getting us to this stage.”
Veryan’s CEO Chas Taylor adds: “The fact that 500 patients were enrolled in just 18 months is testimony to the commitment of the participating clinical sites. I’d like to thank Dr Lichtenberg the principal investigator for leading this important study and all of the investigators and the research personnel who contributed. To date, the MIMICS clinical programme has gathered impressive data on over 1000 patients in a growing database of clinical experience that is providing significant validation of the unique helical shape of BioMimics 3D and the benefits of Swirling Flow. It is notable that there have been no fractures confirmed in any of these clinical study devices nor, indeed, in any BioMimics 3D device since the first one was implanted in February 2010.”
Humacyte, an innovator in biotechnology and regenerative medicine, has announced that Jeffrey Lawson has been appointed president and chief executive officer. The former chairman and chief executive officer, Carrie S Cox, has assumed the role of executive chairman.
Lawson, an innovator, scientist and vascular surgeon has been involved in the development of Humacyte’s vascular technologies, in collaboration with his career-long research partner and Humacyte founder Laura Niklason, over the past 20 years. Lawson has worked with Humacyte since its founding in 2004 to support the science, preclinical and clinical testing of Humacyte’s novel tissue engineered blood vessels, which are being developed for dialysis access and cardiovascular surgery. He was appointed chief medical officer of Humacyte in 2015 to oversee the clinical development of these vascular technologies as the company initiated phase III clinical trials for dialysis access and expanded clinical programmes in vascular repair and trauma.
Prior to joining Humacyte, Lawson served in leadership roles at Duke University Medical Center, including Professor of Surgery and Pathology, vice chair for Research in Surgery, and director of Clinical Trials for the Department of Surgery. Lawson earned his medical degree and his Ph.D. in Cell and Molecular Biology from the University of Vermont and completed his residency in General and Thoracic Surgery and his fellowship in Vascular Surgery at Duke University Medical Center. Lawson is also an American Board of Surgery certified Vascular Surgeon, a Fellow of the American Surgical Association and the current President of the Vascular Access Society of the Americas (VASA).
“Under Carrie’s leadership, the organisation has delivered remarkable progress in its first product candidate, catching the attention of research institutions, key opinion leaders, clinical sites, and investors all over the world,” says Lawson. “I look forward to continuing that work, along with the world-class team at Humacyte. It will be my honour and privilege to lead the Humacyte team into the future as we continue to develop transformative tissues to improve the lives of dialysis patients and expand our pipeline of product candidates, with the objective of helping patients in need of vascular repair and reconstruction.”
As executive chairman, Cox will serve as a senior, strategic advisor to Lawson and the executive team, helping to develop ongoing strategy for Humacyte as the company works toward regulatory approval and commercialisation for its flagship product, the investigational Human Acellular Vessel (HAV), HUMACYL.
Since joining Humacyte as chairman and CEO in 2010, Cox has led the company through significant business, clinical, regulatory and operational milestones. She has guided the company’s clinical review process, including its ongoing pivotal phase III clinical trials to evaluate the efficacy and safety of the bioengineered blood vessel as a conduit for haemodialysis in patients with End-Stage Renal Disease (ESRD). Most recently, she led the negotiation of a strategic global commercialisation partnership with Fresenius Medical Care, to potentially make HUMACYL available to more patients worldwide following approval of the product.
“Leading Humacyte has been one the most fulfilling and rewarding experiences of my career. I’m impressed by and proud of the incredible achievements of our team, as we strive to make groundbreaking science a reality for patients and physicians,” says Cox. “Our work to transform vascular medicine and tissue therapy has only just begun, and under the leadership of Dr Lawson, I’m confident we are well positioned to further advance the boundaries of regenerative medicine and vascular therapeutics. With a track record of success in our own clinical development, Dr Lawson is uniquely positioned to lead Humacyte through our next stage of growth and pipeline development.”
Prior to serving as Humacyte’s chief medical officer, Lawson served as a consultant and advisor in the development of the investigational HAV. As an investigator in Humacyte’s phase II clinical research programme in haemodialysis, in 2013 he and Niklason, were the first to implant Humacyte’s investigational HAV for vascular access into a patient diagnosed with ESRD. “The development of Humacyte’s first-in-class therapeutics has always required a team that is committed, extremely talented, and visionary. With Jeff’s appointment to the CEO role, we are continuing our great tradition of outstanding leadership as we continue our work to develop transformative and meaningful tissues in the regenerative medicine space,” says Niklason.
Sirtex has announced entering into a binding scheme implementation deed with CDH Genetech (CDH) and China Grand Pharmaceuticals and Healthcare Holdings Limited (CGP). It has also announced the termination the Varian Scheme in relation to the proposed Sirtex acquisition.
Sirtex shareholders will be entitled to A$33.60 in cash for each Sirtex share held if the CDH-CGP Scheme is implemented. The Scheme Consideration represents a 20% premium to the Varian offer price of A$28 per Sirtex share, an announcement from Sirtex states.
Background to the CDH-CGP Sirtex acquisition bid
On 30 January 2018, Sirtex announced it had entered into a binding Scheme Implementation Deed with Varian Medical Systems under which it was proposed that Varian acquire 100% of the shares in Sirtex by way of a Scheme of Arrangement for A$28.00 per share.
Subsequently, on 4 May 2018, prior to the Varian Scheme Meeting to approve the Varian Scheme, Sirtex received an unsolicited non-binding, indicative and conditional proposal from CDH Investments to acquire 100% of Sirtex for a cash price of A$33.60 per share. On 5 May 2018, Sirtex announced the adjournment of the Varian Scheme Meeting.
On 22 May 2018, Sirtex announced it had received an offer capable of acceptance from CDH for the acquisition of all of the shares in Sirtex by way of scheme of arrangement, including a draft scheme implementation deed.
On 14 June 2018, Sirtex announced the termination of the Varian Scheme and that it was entering into a binding scheme implementation deed with CDH and CGP. CDH Genetech is an entity wholly-owned by funds advised by CDH Investments.
The interim chairman of Sirtex, John Eady, said: “The Board has undertaken a comprehensive investigation of the merits and risks of the CDH-CGP proposal, including seeking specialist advice in relation to specific regulatory, legal, funding and other risks. Based on the materially higher offer price and our evaluation of the associated risks, the Board of Sirtex has formed the unanimous view that the CDH-CGP proposal is a superior proposal and is in the best interests of shareholders.”
The CDH-CGP Scheme is subject to independent expert review on behalf of shareholders, shareholder approval, and regulatory and legal approvals.
An announcement from Sirtex notes that the Sirtex board unanimously recommended that Sirtex shareholders vote in favour of the CDH-CGP scheme and intend to vote shares in their control in favour of the proposed CDH-CGP scheme, subject to Sirtex not receiving a superior proposal and the independent expert concluding that the CDH-CGP scheme is in the best interests of Sirtex shareholders.
On completion of the CDH-CGP Scheme, Sirtex will be ultimately owned 51% by funds advised by CDH, and 49% by CGP, the announcement from Sirtex adds.
Varian provides update on proposed Sirtex acquisition
Varian announced on 14 June that it received notification from Sirtex that its board has determined that the proposal from CDH Investments and China Grand Pharmaceutical and Healthcare Holdings Limited (CDH-CGP Proposal) is a Superior Proposal as defined in the Scheme Implementation Deed between Sirtex and Varian (Varian Scheme). Consistent with Varian’s prior announcements, Varian informed Sirtex that Varian will not be providing a counter proposal. Sirtex has consequently terminated the Varian Scheme and confirmed that it is required to pay a Reimbursement Fee of approximately A$16 million to Varian.
“Varian is very disciplined in its business development approach and we do not see value beyond the A$28 price per share we offered for Sirtex,” said Dow Wilson, president and chief executive officer of Varian. “While disappointed with this decision, Varian’s long-term strategy has not changed. We remain focused on becoming a global leader in multidisciplinary, integrated cancer care solutions; expanding the addressable markets that Varian can impact; and growing and creating sustainable value for our company and our shareholders.”
Medtronic has announced that it has received US FDA approval for 200mm and 250mm lengths of the IN.PACT Admiral drug-coated balloon (DCB) to treat long superficial femoral artery lesions in patients with peripheral artery disease.
“As superficial femoral artery disease progresses, we tend to see patients present with longer, more complex lesions. As a result, these lesions become incredibly challenging to treat and often require interventions with multiple technologies to effectively treat the entire segment,” said Gary Ansel, medical director for Vascular Services at OhioHealth Riverside Methodist Hospital in Columbus, USA. “The approval of the IN.PACT Admiral 200mm and 250mm balloons provides physicians with a solution to treat these long, complex lesions with fewer devices, potentially leading to shorter procedure times and reduced procedural cost.”
Challenging lesions can be treated by IN.PACT Admiral
Complex lesions, including those over 150mm, are commonly encountered in clinical practice and remain a significant treatment challenge for physicians. In April of this year, IN.PACT Admiral received approval to treat superficial femoral artery lesions up to 360mm in length. Approval was based on clinical data from the complex lesion imaging cohorts of the IN.PACT Global Study, including long lesion, in-stent restenosis, and chronic total occlusion (CTO) groups with lesion lengths >180mm. Across these groups, a total of 227 subjects with mean lesion lengths of 28.7±7.1cm were analysed. Data showed a one-year patency rate of 89.1% by Kaplan Meier estimate at day 360, and a clinically-driven target revascularisation (CD-TLR) rate of 7.1%.
“In our IN.PACT Global Study, IN.PACT Admiral demonstrated safety and effectiveness in real-world patients with complex lesions, including long lesions,” said Mark Pacyna, vice president and general manager of the Peripheral business in Medtronic’s Cardiac & Vascular Group. “Our new long lesion indication, coupled with the approval of the 200mm and 250mm balloons, furthers our commitment to the clinical community by equipping them with the tools and evidence needed to effectively treat complex cases.”
Amg International, a wholly owned subsidiary of Q3 Medical Devices, announced that it has received CE mark approval for their novel biodegradable biliary and pancreatic stent technology, allowing the company to begin selling the product in Europe and other markets.
Archimedes is the only fully biodegradable biliary and pancreatic stent approved for placement in obstructed biliary or pancreatic ducts. While biliary and pancreatic duct stents are typically made of plastic or metal, the Archimedes stent is made of a combination of dissolving materials permitting different rates of degradation depending on the clinical indication.
The Archimedes stent is designed to completely degrade via hydrolysis in approximately 12 days, 20 days or 11 weeks, depending on its composition. The stent is designed to maintain duct patency, without occlusion as it degrades, due to its patented design. It is intended as an option to avoid repeat procedures to remove traditional non-biodegradable plastic stents, avoiding adding additional cost of care and risk for patients.
“This CE mark approval is a major advancement in the treatment of obstructive biliary and pancreatic disorders and provides physicians such as myself, a truly innovative and advanced treatment option for my patients,” said Sundeep Lakhtakia of the Asian Institute of Gastroenterology in Hyderabad, India. “This is great news, as a fully biodegradable stent has the potential to reduce complication rates and procedural costs typically associated with biliary and pancreatic stenting,” Noted Paul Yeaton, chief of Gastroenterology at the Carilion Clinic in Roanoke, USA.
Biodegradable biliary stent major breakthrough
Eric K Mangiardi, CEO of Q3 said, “The Archimedes biodegradable stent represents a major breakthrough in the treatment of obstructive biliary and pancreatic disorders, and also in the field of biodegradable and bioresorbable materials and their application in medical devices moving forward.” He added, “This technology has numerous benefits for patients, doctors, and healthcare providers as it has the potential to reduce complication rates typically associated with plastic stents and removal procedures.”
In a recent safety and efficacy clinical study, including 53 patients, conducted in India and Malaysia, the Archimedes stent showed zero stent-related complications during the study period.
This educational supplement, sponsored by Guerbet, is intended for readers in the EU only. Guerbet obtained the CE mark for its conventional transarterial chemoembolization (cTACE) mixing and injection system, Vectorio, which is an all-in-one, unique, ready-to-use kit. It could also help to standardise cTACE, say interventional oncology experts.
Multidisciplinary oncology thought leaders discuss the personalisation of SIRT, new and recent evidence for the minimally invasive procedure over sorafenib in advanced HCC, the surgical aspects of SIRT for mCRC and HCC, patient selection, promising results in neuroendocrine tumour treatment and advances in techniques in this educational supplement, sponsored by Sirtex.
In this supplement:
Personalisation of SIRT is the next step
New evidence supporting SIRT over sorafenib in advanced HCC
More evidence to come for patients with advanced HCC
Surgical aspects of SIRT for mCRC and HCC
Could careful patient selection increase earlier use of SIRT in mCRC?
Promising results for SIRT in neuroendocrine tumour treatment
Advances in techniques to deliver SIR-Spheres
This educational supplement has been sponsored by Sirtex.
The opening plenary at the World Conference on Interventional Oncology (WCIO; 7–10 June, Boston, USA) put biopsy, which is considered a mundane procedure by some interventional radiologists, at the heart of cancer diagnosis and personalised treatment. Many experts see that doing a biopsy well could establish a fruitful collaboration with referring medical and surgical oncologists.
The session “Obtaining Tissue in the Age of Precision Medicine” highlighted biopsy as one of “the main inroads” for interventional radiologists to get into the oncology space. Biopsy is seen as a gateway procedure by interventional oncologists. Once interventional oncologists get in the door and do a good job with biopsy, they can then offer other treatments to help manage the disease that was biopsied, delegates heard.
David C Madoff, professor of Radiology, vice chair for Academic Affairs, Weill Cornell Medicine, New York, USA, and programme chair of WCIO 2018, told Interventional News: “One of the most common image-guided procedures done by interventional radiologists is biopsy. Biopsy is seen as a bread-and-butter procedure that is considered by many practitioners as a routine one. Still, it may ultimately have the most impact on anything that we do in interventional oncology. One of the reasons that it is so important is that patients’ treatments are now reliant on the tissue obtained and its typing. It used to be that obtaining tissue was simply for diagnosis, and once a diagnosis was established, patients with a particular cancer would all be treated the same way in a one-size-fits-all manner. However, we know now that tumour tissue is very heterogeneous. This can be within a tumour and there could also be heterogeneity between the primary tumour and metastases. So over the years, interventional radiologists are asked to get much larger volume samples and many more samples in order to guide personalised treatment. With biopsy, interventional oncologists play a critical role in the diagnosis and management of patients with cancer.”
Speaking at the session, Stephen Solomon, chief, Interventional Radiology Service, Memorial Sloan Kettering Cancer Center, New York, USA and president of the Society of Interventional Oncology, noted that in the era of precision medicine, it is essential to provide reliable tissue biopsy. He noted “in-room pathology assessment will lead to improved results. Molecular imaging can provide improved targeting as it recognises tissue heterogeneity. New technology solutions can provide in-room assessment for all hospitals,” he said.
Interventional radiologists are held responsible for the collection of the biopsy sample and it is important to set appropriate expectations on the challenging biopsy, delegates at the session heard.
Alda Tam, associate professor of Interventional Radiology, MD Anderson Cancer Center, Houston, USA, speaking of the role of biopsy in oncology clinical trials said: “[Essentially] what we are looking for is an actionable mutation or an actionable immune biomarker so that a patient’s treatment for cancer can be individualised. In order to do that, biopsy plays a critical role. In addition to this, we are being held to a molecular adequacy standard and what that means could be different for different trials.
“I think as interventional radiologists/oncologists, we need to embrace the need for interventional radiology involvement in clinical trials at the level of which trials are being developed. So you need to write the protocol and review the protocol on how you sample the tissue. At MD Anderson, protocols do not go before the Institutional Review Board unless an interventional radiology collaborator has already signed on. We need communication tools amongst ourselves to ensure that we are in compliance about the number of samples that are being requested for each protocol. Hopefully, at some level, we can move towards a standardisation of the sampling requirements, beyond just the number of cores,” she noted.
Importantly, Tam noted that it was important to weigh the risks and benefits carefully before undertaking challenging biopsies.
“Be a clinician, weigh-in on the risk of the biopsy and lesion selection,” said Tam. “At the end of the day, you want that patient to go to the trial, but if they cannot, they cannot. We ought to be realistic as we are the only ones looking at the imaging and we are the only ones who know how much tissue is going to come out of the lesion being studied. Lastly, collaborate with pathology, because feedback is essential in order to improve quality and improve results,” Tam urged.
Ally Bridge Group (ABG), a cross-border life science investment group, has completed a Series A investment, as the first part of a total of US$50 million raise, in Quantum Surgical, an innovative surgical robotics company in France.
Quantum Surgical is developing next-generation robotic solutions for minimally invasive cancer therapies. Quantum’s predecessor company Medtech SA, a leading French neurosurgical robotics company, was acquired by global orthopaedics giant Zimmer Biomet in 2016 after an investment from ABG in 2015.
“ABG is excited to support again the Quantum Surgical team led by Bertin Nahum in their new venture following our successful investment in—and exit from—Medtech SA. The team has been dedicated to—and has a proven track record—in developing and commercialising innovative surgical robots globally. ABG has been working closely with Quantum Surgical since its inception and our partnership now breaks into new ground in building next-generation surgical robots to facilitate interventional oncology treatment, especially for early-stage cancer patients,” says Frank Yu, Founder, CEO and CIO of Ally Bridge Group. “Quantum Surgical is a natural extension of ABG’s recently led US$300 million investment in GRAIL, a healthcare company whose mission is to detect cancer early, when it can be cured. Early cancer detection must be accompanied by more effective early treatment,” Frank Yu adds.
“Quantum will set new standards for minimally invasive cancer treatment procedures. We are excited to partner up with Ally Bridge Group again, after our successful collaboration in 2015-2016, and to continue to benefit from ABG’s truly global industry perspectives, network and strong financing, capital markets and M&A capabilities,” says Bertin Nahum, Founder and CEO of Quantum Surgical.
Lifetech Scientific, a leading innovative medtech company in China, has also participated in the investment through its joint venture with ABG and will collaborate with Quantum Surgical in China market.
Stephen B Solomon, chief, Interventional Radiology Service, Memorial Sloan Kettering Cancer Center, New York, USA and president of the Society for Interventional Oncology (SIO) talks personalised medicine, immunotherapy and how being a cancer consultant helps make treatment decisions that are not desperation oncology with Interventional News. “Two big challenges [for interventional oncology] are demonstrating clinical data to support our work and ensuring high quality. Compared to other cancer specialties such as radiation oncology, interventional oncology has not been well organised […] this is one of the pressing issues that led to the formation of the SIO,” he explains.
What made you choose interventional oncology?
I love innovation and creativity—interventional radiology is one specialty in medicine that allows practicing clinicians to be both innovative and creative. I have gravitated to interventional oncology, because it is still interventional radiology, but focused on a specific disease state, oncology, which has tremendous opportunity for invention and improvement. For me, the focus on oncology has given me purpose, focus, and mission in my practice of interventional radiology.
In interventional oncology we are a critical part of the cancer patient’s journey and can provide longitudinal care throughout the journey. We are part of the diagnosis (e.g. biopsy), treatment (e.g. TACE), and palliative care (e.g. ascites management). This continuity allows me to have a relationship with our patients rather than simply come in for a procedure and be done.
Finally on a lighter note, interventional oncology has also made answering the cocktail party question of “what do you do for a living?” much easier. When answering “interventional radiology,” there are blank faces, but when answering “interventional oncology” there is a sense of understanding.
What are the three most important considerations when you are a physician treating patients with cancer?
Be a consultant: In the oncology world the interventional oncologist is a consultant and not a technician. Patients are referred to us not just to do procedures but also for our advice. We must understand our procedures and understand the patient’s disease and course. What stage is this patient in? What is their life expectancy? What might my procedure offer the patient? Will the procedure be providing for improved quality of life? For example, if a patient only has one month to live, then putting them through a procedure that keeps them in the hospital for several days is probably not a good idea.
Understand the disease and other treatments: You must understand the interplay between what an interventional oncologist can offer and what other specialists can offer. For example, patients with heavily treated livers with chemotherapy or prior radiation may be at higher risk from an interventional oncology treatment. You also need to understand the literature on other treatments. For example, lobectomy for stage 1 primary lung cancer is considered standard of care, whereas surgeons treat metastatic lung cancer with wedge resection. You must understand staging of cancer. For example, to biopsy a breast cancer distant lytic bone lesion is better than to biopsy an axillary node since it will determine upstage the disease and dictate different treatment.
Show compassion: Many of these patients we see will have a limited life expectancy. They may be quite desperate. It is important to show compassion and empathy, keeping quality of life as a critical part of making decisions. We can offer patients autonomy as individuals, by assisting them in making decisions that are unique to them.
Which innovations have most influenced your career, and how?
I am in awe of the power of CT fluoroscopy. With this imaging tool we can pinpoint and biopsy/ablate 5mm lung nodules in a moving lung! CT fluoroscopy has enabled me to perform percutaneous tumour ablation and successfully cure or palliate hundreds to thousands of patients. While the field began with image-guided ethanol and radiofrequency ablation, it continues to evolve with cryoablation, microwave, high intensity focused ultrasound, and irreversible electroporation. The next step is understanding how these energies interact with human biology. If we can ultimately harness the immune system, we will be able to transition ablation, which is a local treatment, into one that has a systemic effect on metastatic disease.
Why was the Society of Interventional Oncology formed?
Much like the Society of Surgical Oncology is to the American College of Surgeons/European Surgical Association, or the Society of Urologic Oncology is to the American Urological Association/European Association of Urology, the Society of Interventional Oncology is to the Society of Interventional Radiology in the USA or the Cardiovascular and Interventional Radiological Society of Europe (CIRSE). While SIR and CIRSE cover the full range of interventional radiology, the SIO is focused on the subset of interventional oncology. We were formed to make interventional oncology “the fourth pillar of cancer care” along side chemotherapy, surgical therapy, and radiation therapy. The SIO does this through education (in the form of the annual SIO meeting, Fellows courses, and online IO University), research grants and representation (outreach to other oncology associations). We expect our members to also be members of SIR, CIRSE, and APSCVIR. This is where critical governmental issues pertaining to interventional radiology take place. We see SIO as complementary to these other organizations providing foundational oncology research and advocating for the practicing interventional oncologist among the oncology community.
As president of the SIO, what are your key goals for the society in your presidential term?
Build foundational interventional oncology research to show the value of this discipline. This is being accomplished through our research grant programme which has given out over $1 million to the interventional oncology community in the past year. We are also working with SIR and others to create a multi-institutional registry of procedures that will help create additional clinical evidence for interventional oncology.
Globally educate for best practices in interventional oncology. The annual WCIO/SIO meeting and the Fellows courses along with our outreach to China and other parts of the world will educate the future interventional oncology specialists. The online IO University is also a way to enable improved education in this field.
Build representation of interventional oncology specialists in the multi-disciplinary oncology community. We must be represented in the National Comprehensive Cancer Network (NCCN), American Society of Clinical Oncology (ASCO), Eastern Cooperative Oncology Group (ECOG), and European Society for Medical Oncology (ESMO) and other multidisciplinary organisations. We have too often been excluded from guidelines, because we did not have a seat at the table.
In your view what are the biggest developments in interventional oncology today?
Personalised medicine means the recognition that patients have unique cancer gene mutations which must be identified for optimised targeted therapy. This revolution has put the interventional oncologist who performs image-guided biopsy at the centre of cancer care. We should cherish this position and work to improve it. We should also realise that to the oncologist the collection of useful biopsy material is far more important than a chemoembolization procedure. This means that performing biopsies well, can lead to a strong relationship with one of the most critical practitioners in the cancer pathway.
Immunotherapy is the second big revolution in oncologic care. Again, interventional oncology is at the centre of this revolution. Whether we perform ablation or catheter-directed liver therapy, we are creating tumour antigens and a signal to attract the immune response. We have seen in animal models and even some early human studies that these interventional oncology techniques coupled with immune-stimulating drugs can create an enhanced anti-tumour “vaccine.” Further, other advances in oncolytic viruses and nanoparticles are discovering that intra-tumoural delivery has a better result. This intra-tumoural delivery is, again, in the wheelhouse of the interventional oncologist.
We are only beginning to understand the interplay between immunology and the antigen-producing procedures (i.e. ablation or chemoembolization) we perform. It is quite possible that these procedures will be elevated as they develop into a systemic treatment and not just a local one.
What are three early technologies that you are keeping an eye on?
CAR T-cells are having a dramatic effect on the “liquid” cancers (i.e. lymphomas, leukemias), however, the effect has been more challenging in the solid tumours. There is some evidence that intratumoural delivery would aid in the effect on solid tumours and interventional oncologists are well positioned to “drive the CARs” where they need to go.
Oncolytic virus and “cancer eating bacteria” have shown positive results when injected intratumourally. T-VEC is the first approved oncolytic virus. It is approved for injection in superficial melanoma. Studies are now being done with interventional oncologists injecting under image-guidance into deep lesions. Other similar virus and bacteria injections are being investigated.
Interventional oncologists have used anatomic imaging such as ultrasound, fluoroscopy, CT, and MR to perform procedures. However, in oncology, metabolic imaging is oftentimes critical. Tumour heterogeneity and differences in viability after prior treatment can be best distinguished with metabolic imaging. PET guided interventions open a new avenue for interventional oncologists. For example, PET may allow detection of viable cancer cells after ablations enabling retreatment while the patient is still on the procedure table. With advancement in specific cancer radiotracers beyond fludeoxyglucose (FDG) such as prostate-specific membrane antigen (PSMA), there will be additional opportunities for PET-guided interventions.
In the past few years the concept of “personalised medicine” has revolutionised oncology. The interventional oncologist is central to this revolution, as we are the ones often responsible for acquiring the tissue necessary to perform the “personalised medicine.” When we do a poor job, we are the scapegoats, and when we do a good job, we are the heroes. Doing a good job requires good communication with the referring oncologist to ensure that an understanding between the delicate balance of safety and obtaining adequate tissue for molecular analysis is possible. Personalised medicine has put a priority on us doing a high quality job. This is an area for our specialty to work on to ensure that this critical part of the cancer patient’s care is done at a high level. We are doing an ever-increasing number of needle biopsies, and service and quality are paramount.
You have been a prolific inventor of devices in various fields. Could you describe some of these devices?
I love innovation and have spent most of my career focused on creating solutions for problems. I have developed a range of devices spanning cardiology, oncology, pulmonary, urology, and obesity. One of the first concepts I worked on was a Global Positioning System (GPS) electromagnetic sensor for interventional tools. We demonstrated this in the transjugular intrahepatic portosystemic shunt (TIPS) procedure, and with inferior vena cava filters. However, we got the most traction in cardiac electrophysiology. The device is called CARTO sold by Johnson and Johnson and is the standard of care throughout the cardiac electrophysiology world. It uses GPS on a catheter to measure the heart’s electrical signal and position and creates an electrical map of the heart. We then fused the electrical map to MRI/CT images. As an offshoot of this GPS catheter, I put the sensor on the end of a bronchoscope which created the field of electromagnetic navigational bronchoscopy which became the basis for the SuperDimension device now sold by Medtronic. Another device I created was the Aspire Assist obesity device which is on the market for treating morbid obesity. This concept uses a reverse gastrostomy tube to remove calories from the stomach before absorption, and although controversial, is as good as the lap band yet, safer and easily reversible. I created the split-dose concept for PET-guided tumour ablations which uses a small FDG dose to guide ablation needle placement followed by a second larger FDG dose at the end of the ablation to assess for completeness while the patient is still on the procedure room table. At our institution this has become the standard of care for FDG avid liver ablations. I also helped develop the first software for vessel tracking to guide intra-arterial therapies. This software is called LiverCare and is sold by GE Healthcare. Finally, I helped create a venture capital firm through which I was able to contribute and help nurture multiple other technologies.
What are the biggest challenges for interventional oncology in 2018?
Two big challenges are demonstrating clinical data to support our work and ensuring high quality. Compared to other cancer specialties such as radiation oncology, interventional oncology has not been well organised. Radiation oncologists have RTOG (Radiation Therapy Oncology Group), for example, that helps organise clinical trials and provide the infrastructure to recruit patients quickly to allow rapid generation of clinical data. This is one of the pressing issues that led to the formation of the SIO. The SIO hopes to provide similar infrastructure support to allow rapid generation of interventional oncology clinical data. More and more payors and referrers are looking for the clinical evidence to support decisions. Without such formal evidence, we in interventional oncology may suffer. The SIO is working with SIR and others to build the Interventional Oncology Clinical Outcomes Registry (IO-CORE) which will be a multi-institutional registry for interventional oncology procedures.
Another important area for us to emphasise is quality. Again, the SIO through education courses being offered worldwide and through the online IO University are teaching high quality to IO practitioners. It is essential to realise that the procedure is only one component to good care. We need to make sure interventional oncologists understand the disease, treatment alternatives, and where interventional oncology fits in.
Could you describe a memorable case?
One memorable case is that of a 42-year-old woman who had metastatic colorectal cancer. Her disease was controlled except for a few lung metastases. I was able to ablate her lung metastases and give her a “chemo holiday” which was great. That was five years ago. However, what was so memorable about the case was the handwritten letter I received from her young children written in crayon thanking me for keeping their mommy alive. These are the kinds of things that make our careers meaningful and remind us that each patient has a family around them that cares so much about what we do. I remind myself of that letter all the time with each patient I treat.
What are your interests outside of medicine?
My other passion is my family. I have an amazing wife who is a singer, songwriter, and fashion entrepreneur. We have two terrific boys aged three and five with whom we spend as much time as possible introducing them to the fascinating world we live in. On weekends, we take the boys to the Museum of Natural History, classical music concerts, apple picking, kayaking, and golf.
Shown here is a gas embolotherapy scenario. After the droplets were injected intravenously with or without therapeutic agents (e.g., chemotherapeutics or genes) and subsequently transported to the tumor microcirculation by blood flow, bubble formation was induced by ADV on demand. Credit: Dui Qin/Xi’an Jiaotong University
Recently, scientists have explored another version of embolization, called gas embolotherapy. During this process, the blood supply of cancerous tumours is cut off using acoustic droplet vapourisation (ADV), which uses microscopic gas bubbles induced by exposure to ultrasonic waves.
A team of researchers from China and France has discovered that these bubbles could also be used as potential drug delivery systems. The researchers reported their findings this week in Applied Physics Letters.
“We have found that gas embolotherapy has great potential to not only starve tumours by shutting off blood flow, but also to be used as a source of targeted drug delivery,” said Yi Feng, associate professor of biomedical engineering at Xi’an Jiaotong University and first coauthor of the paper.
In gas embolotherapy, researchers inject droplets, from tens to hundreds of nanometres in diameter, into feeder vessels surrounding the tumour. Microscopic gas bubbles are then formed from the droplets through ultrasound, growing large enough to block the feeder vessels (eg, arterioles). ADV is the process of transforming droplets into bubbles.
Gas embolotherapy does more than block blood flow
In previous work, the researchers expected to use ADV to starve the tumour by blocking blood flow in the arterioles. To their surprise, they found that the bubbles not only blocked the arterioles, but other gas bubbles made their way into the capillaries, resulting in vessel rupture and more leaky microvasculature.
In their latest work, gas embolotherapy through ADV was performed to further explore the dynamics of the bubbles inside the capillaries. Testing was conducted ex vivo on rat tissue that attaches the intestines to the abdominal wall. It involved bubble formation in droplets of dodecafluoropentane containing a bovine serum which were injected into the blood flow.
Produced in the dodecafluoropentane through ultrasound, the bubbles accumulated, sometimes merging, as they lodged themselves in the capillaries. At one point, the researchers observed a local vessel invagination (a pouchlike cavity), which they believe was caused by the interaction between the bubble and vessel and led to a capillary rupture.
Their findings could provide a one-two punch for cancer treatment—shutting off blood flow from the arterioles and delivering drugs through the capillaries. In addition, chemotherapy drugs could be kept localised for longer periods of time because blood flow has been shut down, reducing drug dosage.
“In cancer therapy research, scientists are always interested in answering two questions: how to kill the cancer effectively and how to reduce the side-effects of chemotherapeutic drugs,” said Mingxi Wan, professor of biomedical engineering also at Xi’an Jiaotong University and corresponding author of the paper. “We have found that gas embolotherapy has the potential to successfully address both of these areas.”
With an ultrasound imaging method in place, according to Feng, gas embolotherapy has a good chance of becoming a standard practice. Wan and Feng’s team is working with another group of researchers in the same lab, and such an imaging system is being built to apply the ADV gas embolotherapy method in rats.
MicroStent (Micro Medical Solutions), a vascular stent designed to reduce below-the-knee amputations caused by critical limb ischaemia (CLI) resulting from peripheral arterial disease (PAD) has been implanted for the first time in the USA. The company received approval from the Food and Drug Administration late last year to begin a clinical trial evaluating MicroStent’s safety and efficacy.
Co-principal investigator Robert E Beasley performed the first procedure in the trial on 25 April at Mount Sinai Medical Center in Miami Beach, USA. Beasley placed two 3mm x 40mm stents in the anterior tibial artery of a patient with CLI, fully restoring blood flow to a previously occluded vessel.
“We found implanting the MicroStent to be a very safe, quick, easy procedure. Using a retrograde pedal puncture, we used a small 3-French sheath to place two of these very low-profile, easy-to-deploy stents in the anterior tibial artery in about 30 minutes. Post-procedural ultrasound taken immediately, at 14 days and at one month showed a wide-open, unobstructed artery with excellent flow,” explained Beasley. “By returning sufficient blood flow to the lower leg, we were able to ensure adequate oxygenation to the tissue. As a result, a wound on the patient’s toe is now healing, and he is unlikely to require below-the-knee amputation. I’m hopeful that MicroStent will represent another tool to treat the devastating disease of CLI.”
Beasley has since performed four more MicroStent procedures. Craig Walker, co-principal investigator in the study with several cases completed, oversees the MicroStent research site at the Cardiovascular Institute of the South in Houma, USA.
Walker noted, “With CLI, the ability to achieve patency in a vessel is paramount to saving both the vessel and the limb. Use of MicroStent, a self-expanding stent with great radial force and very little chronic outward force, has resulted in patent arteries with low probability of long-term stenosis. In fact, we have seen zero stenosis post-procedure on both ultrasound and angiography, and one patient remarked that dramatic pain relief occurred immediately after the MicroStent procedure. We anticipate that this critically important technology will continue to produce good outcomes and clinical results.”
Micro Medical Solutions CEO Gregory Sullivan added, “Everyone at MMS has been working together toward this achievement. We are very excited not only about this milestone, but also about the progress and momentum we are showing toward approval of MicroStent in the USA. Ultimately, we hope MicroStent will fulfil its purpose to reduce preventable amputations and preserve patients’ freedom and quality of life.”
MicroStent received CE mark approval in Europe in 2017 and continues to be studied internationally, as well as through this clinical trial of MicroStent in the USA.
Countries in the European Union have long been the first to receive new innovations in medical technology, as the EU’s Medical Device Directive (MDD) provided quicker routes to implementation of new devices than its equivalent in the USA, the Food and Drug Administration (FDA). However, on both sides of the Atlantic, the regulatory pace is likely to change over the next few years—in opposite directions.
The EU is moving to replace the MDD with the Medical Devices Regulation (MDR): a more extensive regulatory document, introducing significant revisions to quality and safety standards and the range of regulated devices. The MDR was initiated in May 2017, and a three-year transition period applies. Current MDD certificates remain valid, but cannot be renewed, meaning that from 26 May 2020 onwards, all medical devices brought to market in the EU and Switzerland must conform to the MDR. While increasing demands on the standard of clinical data and safety profiles of new technology, medical device innovation in the EU is likely to see reduced speeds on the road to the CE mark.
Meanwhile, the US FDA has published its strategic priorities for the MDD-MDR transition period of 2018–2020, outlining an aim to “reduce the time and cost of generating clinical evidence, typically the most expensive and lengthy regulatory requirement for marketplace entry.” The FDA states it has adapted their policies and procedures to “facilitate and streamline the development and approval” of clinical trials in the USA, and redistributing the data collection requirements pre- and postmarket. “By striking the right balance between premarket and postmarket data collection we can help assure we get the right data at the right time, thereby creating incentives for timely patient access to high-quality, safe and effective technologies to improve their health and quality of life.”
Speaking on the subject in the CX Innovators Showcase at the Charing Cross Symposium (CX; 24–27 April, London, UK), Veryan CEO Chas Taylor noted that the FDA’s strategic direction is “more open and approachable,” and while it does not change the burden of proof, it “makes the system easier to navigate.” The EU MDR on the other hand, “will increase barriers to entry in Europe” with new regulation, Taylor said.
The panellists of the session, Gido Karges (Wangs, Switzerland) and Jeffrey Jump (Most-sur-Rolle, Switzerland) similarly feared that the pace of innovation in Europe will be diminished, with Jump stating that “the golden age of innovation in Europe is coming to an end.” Jump suggested “CE mark lead approval time will at least double (6–12 months)”, and claimed “the number of innovative medical devices receiving CE mark will drop down by an estimated 30%.”
Karges explained the ramifications: “Expenditures associated with MDR compliance are enormous. Due to these costs, device developers will need to make choices about which areas of their business to remediate first. Some may decide the costs of remediation exceed the business opportunity, choosing to sell or close down certain product lines. As manufacturers decide to discontinue legacy products, suppliers go out of business, dragging other manufacturers who bought from them behind. German and Swiss health authorities predict the extinction of 30% of all medical device manufacturers. They also expect that 50% of all medical devices will be discontinued or fail to meet the requirements. Patients might be at risk—it is a very grim outlook.”
In contrast, Japan’s Pharmaceuticals and Medical Devices Agency (PMDA) is collaborating with the US FDA to allow “globalisation” of approval studies, Taylor highlighted, in an initiative called “harmonisation by doing.” The FDA state that the initiative will see them agreeing with the PMDA, academia and industry on internationally developed standards for global clinical trials related to cardiovascular devices, addressing “regulatory barriers that may delay timely medical device approvals in both countries.”
Jump summarised, “The FDA and other competent authorities have released new regulations and guidelines in order to decrease the burden of getting market access for innovative devices.”
“Europe is now heading in the opposite direction, particularly for innovative products. Due to the uncertainty of MDR implementation and interpretation, increased cost of compliance, fragmented distribution and divergent reimbursement policies, the 40-year old model of ‘go to Europe first’ will be challenged. Europe may have to wait for innovative medical devices to be proven safe and effective in other markets before European patients will have access to improved technologies. I believe innovators will follow the path of least resistance and vote with their feet.”
Aaron Abajian and Julius Chapiro, New Haven, USA, write about results from an early experiment in applying artificial intelligence (AI) and machine learning as a decision support system in interventional oncology to illustrate its potential to overcome rigid staging and scoring systems in the locoregional treatment of liver cancer.
Most patients with hepatocellular carcinoma (HCC) are diagnosed at intermediate to advanced stages of the disease and are no longer amenable to curative surgical or image-guided ablative therapies. In such cases, transarterial chemoembolization (TACE) is the only locoregional therapy that is fully endorsed by guidelines and therapeutic recommendations, such as the most recently updated Barcelona Clinic Liver Cancer (BCLC) staging system by the European Association for the Study of the Liver (EASL).1
Prognostication for therapeutic outcomes in HCC is mostly based on established clinical, laboratory and imaging data points. For practical reasons, such features are mostly organised in scoring systems to help guide therapeutic decisions. As an example, the model for end-stage liver disease (MELD) score, the Child-Pugh classification are commonly used to guide therapeutic decisions, transplant listing as well as to predict long-term outcomes following any intervention.2 Most such scoring systems are based on a regression of basic laboratory or clinical parameters (eg, MELD=dialysis status, creatinine, bilirubin, INR, and sodium; Child-Pugh=bilirubin, albumin, INR, ascites, encephalopathy). In order to arrive at a therapeutic recommendation, individual scoring systems are often combined with clinical performance scores (such as the ECOG performance status score) and imaging data on tumour size to build straight-forward decision support algorithms, such as the BCLC staging system. While such prognostication algorithms have introduced a certain level of standardisation for data collection, they are mostly based on statistically highly variable and cohort-dependent interpretation of retrospectively collected data. As such, there are currently more than 10 different, mostly regionally variable staging systems for HCC, each with slightly different therapeutic recommendations. This circumstance, in and by itself, indicates that none of them is sufficient to provide universally applicable answers for therapeutic decisions. Instead, most such systems merely group patients into rough categories, in some cases mixing highly heterogeneous patient groups into one class with similar treatment recommendations. Interestingly, the recently published BRIDGE study, a global survey on patterns of management and treatment of liver cancer, demonstrated a rampant non-adherence to guidelines across the globe.3 In addition, modern clinical patient workup generates an overwhelming, practically indigestible amount of disparate data such as laboratory and imaging parameters, which adds to the institutional and individual variabilities of multidisciplinary decision-making.
With growing needs for more patient-centred and individualised care, artificial intelligence solutions, specifically machine learning algorithms, may help make sense of the potentially nonsensical. Along the lines of our National Institutes of Health (NIH)-funded effort to introduce more quantitative and data-driven solutions for locoregional therapy of liver cancer, we experimented with the idea of a specific statistical application in machine learning to predict outcomes after TACE before the actual procedure.4 As such, we used AI/machine learning techniques to predict an outcome using observed baseline features. Our study included 36 patients with HCC treated with TACE. We used 25 individual features, including lab parameters, clinical performance scores and 3D quantitative imaging biomarkers for tumour enhancement (qEASL values) to train logistic regression (LR) and random forest (RF) models to predict patients as treatment responders or non-responders. The performance of each model was validated using a so called “leave-one-out” cross-validation where the entire dataset except for one patient is repeatedly used to confirm the applicability of the model to each patient. As a result, our models successfully predicted tumour response with an overall accuracy of 78% (sensitivity 62.5%, specificity 82.1%, positive predictive value 50%, negative predictive value 88.5%). The presence of cirrhosis, high volumes of contrast-enhancing, presumably viable tumour tissue on baseline MR imaging were among the strongest individual predictors. In addition, therapy with Lipiodol rather than drug-eluting beads was associated with a higher response rate.
Our model had several limitations, among others the small cohort size and only a limited set of features that were initially considered for the model. However, this early experiment in applying machine learning as a decision support system in interventional oncology illustrates the potential of such methodologies to overcome rigid staging and scoring systems. Ultimately, if trained on larger datasets, such systems may introduce an element of personalised care where current approaches show gaps.
AI could help overcome disadvantages of staging systems
The obvious disadvantage of currently available prognostication and staging systems is that simple models are limited in the amount of information that they can capture. For instance, it is unreasonable to expect a five-component model like the Child-Pugh to have a high accuracy in predicting the benefit of a complex and multifactorial outcome, such as tumour response to TACE. Tumour board participants routinely consider hundreds of pieces of information before arriving at a therapeutic decision which is ultimately based on their learned professional experience, having seen thousands of cases as a reference. An ideal model would therefore take all patient-centred data as input to predict response to TACE or any other therapy, after being trained on a vast number of previously treated patients with a similar condition. In the future, neural networks will be capable of incorporating much larger numbers of features and extract predictive patterns from data that were previously invisible. However, we are not quite there yet. In order to train an algorithm to “think” like a tumour board member, it must be exposed to thousands of datasets to learn from.
Interventional oncology has been practiced for almost a generation, and while individual clinical trials continue to be mostly underpowered, vast training data is available already. Our next step as a community of interventional oncologists should therefore be to organise, collect and store a well-characterised multi-institutional database which would enable us to introduce and study advanced machine learning based solutions to improve clinical decision making. Similar examples, such as the united network for organ sharing (in short UNOS) database exist and may inspire us to pool the resources necessary for success. Only then will artificial intelligence truly be given a chance to add value to the way we practice interventional oncology.
References
1 European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L: Easl clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol 2018.
2 Asrani SK, Kamath PS: Model for end-stage liver disease score and meld exceptions: 15 years later. Hepatol Int 2015;9:346–54.
3 Park JW, Chen M, Colombo M, Roberts LR, Schwartz M, Chen PJ, Kudo M, Johnson P, Wagner S, Orsini LS, Sherman M: Global patterns of hepatocellular carcinoma management from diagnosis to death: The bridge study. Liver Int 2015;35:2155–66.
4 Abajian A, Murali N, Savic LJ, et al: Predicting treatment response to intra-arterial therapies for hepatocellular carcinoma with the use of supervised machine learning-an artificial intelligence concept. J Vasc Interv Radiol 2018;29:850–7 e851.
Aaron Abajian is a diagnostic radiology resident at the Department of Radiology, University of Washington. He has no disclosures pertaining to this article.
Julius Chapiro is research faculty and interventional radiology resident, Department of Radiology and Biomedical Imaging, Yale University School of Medicine, New Haven, USA. He has received research grant support from Philips Healthcare, Boston Scientific, Guerbet, Rolf W Günther Foundation, German-Israeli Foundation for Scientific Research and is a consultant to Guerbet, Eisai and Philips.
The Society of Interventional Radiology (SIR) debuted the first-ever virtual reality 360 (VR360) training video showcasing an endovascular transjugular intrahepatic portosystemic shunt (TIPS) procedure in practice, during its Annual Scientific Meeting in March in Los Angeles, USA.
“Virtual reality walks you into a new world. A video like this is a transformative, immersive engagement in a procedure that allows you to adopt, learn and proctor in a completely unprecedented fashion. The pure immersive ability, even in early generations of technology, made it clear to me that this was going to have a major role in medicine,” Ziv J Haskal, a professor with the department of Radiology and Medical Imaging at the University of Virginia Health System in Charlottesville, USA and pioneering editor of the Journal of Vascular and Interventional Radiology (JVIR) told Interventional News.
The one-hour multisegment movie was a special project of SIR’s peer-reviewed journal, JVIR, and was funded by an innovation grant from its publisher Elsevier.
Haskal has recently released a first-of-its-kind, ten-part movie that he has likened to “the Falcon Heavy rocket with the Tesla Roadster on top” that will harness the gifts of virtual reality in endovascular interventions. He has filmed an entire procedure of what is still one of the hardest procedures for people in interventional radiology, TIPS, and segmented it into separate videos. “This procedure is something that I have spent decades trying to perfect. The single most effective way to teach this procedure is in a one-to-one apprenticeship fashion. Those who have not been apprenticed in this fashion do not see the same skill transfer. The totally immersive ability of virtual reality technology will enable such procedures to be taught in another way,” he explained.
Still from VR360
“We have spent a lot of time creating an all-enveloping, in-the-room virtual reality film allowing an operating physician to return to any complex segment they wish for learning, review and perspective. The multicamera shoot and floating high-definition inserts offer viewers every perspective of the case, maximising learning. With the procedure I chose to film, I was teaching on the fly and it will appeal to people on multiple levels who will be able to take something from the training that is beneficial and particular to them. I recently showed it to my mentor, Ernest Ring (Professor Emeritus in the Department of Radiology and Biomedical Imaging at the University of California, San Francisco, USA), who taught how me to do this procedure. He put it on his head and described it as amazing; I could not get it off his head,” Haskal reported.
Hurdles
Commenting on hurdles that might limit further uptake of the technology, Haskal commented that “actually getting people to look at it and put the head set on” is a challenge. “To create a media event for five hundred people and put the box on their head is difficult. It has to be a gradual release, because once people experience the virtual reality video, they are instantly drawn in and excited. I am planning a video to show that it is an easy technology to access; there are multiple platforms and even with an entry level box US$5 they are able to fully access all that virtual reality has to offer.”
The video premiered during the Extreme IR session at SIR 2018 and session attendees received complimentary virtual reality viewers to experience the video on their smart phones.
“Virtual reality is a force multiplier, providing expert training to physicians around the world. I think it will be the future of physician and provider training of new technologies and retention of skills. It will also allow interventionalists the ability to ‘gird their loins’ before going into battle to do a difficult procedure. Virtual reality could also prove to be an invaluable tool to re-train in the use of devices that have not been used for sometime and have become unfamiliar, especially if there is no one available for re-proctoring.
“Virtual reality puts you in that practice environment in a way that is not provided by any other means, which ultimately benefits the patient because you start to absorb information without paying attention to the artifice of a cardboard box on your face,” Haskal maintained.
To see the 10-part movie, navigate your YouTube mobile app to: https://bit.ly/2KzvWH7 Start a segment, launch the VR view by tapping the Google Cardboard icon, and placing your phone into your VR viewer, be it Cardboard or Samsung Gear. If you have an Oculus or Vive headset, you will see it in the highest resolution and field of view.
Boston Scientific showed at the Global Embolization Cancer Symposium and Technologies (GEST US; 17–19 May, Miami Beach, USA) meeting that the US Food and Drug Administration (FDA) has approved an expanded indication for Embozene making it on-label for use in prostate artery embolization treatment in the USA.
As conveyed by Boston Scientific to its US customers, the full indication for Embozene is as follows: “Embozene microspheres are intended for the embolization of arteriovenous malformations
and hypervascular tumours, including uterine fibroids and hepatoma, and for embolization of prostatic arteries for symptomatic benign prostatic hyperplasia.”
In addition to the general embolization contraindications, warnings and adverse events, additional contraindications, warnings and adverse events specific to the prostatic artery embolization procedure were also notified.
“Embozene microspheres are spherical, tightly calibrated, biocompatible, non-resorbable, hydrogel microspheres coated with Polyzene-F, a proprietary polymer. The microspheres are compressible to enable smooth delivery through the indicated delivery catheter and colour-coded by size to allow for easy identification,” Material on the company’s website states.
Microspheres are packaged in single syringe units with 2mL of product in 20 mL syringes.
Publically available documents in relation to the US FDA approval reveal that the expanded indication was cleared on the basis that Embozene is substantially equivalent to the legally marketed Embosphere (Merit Medical) microspheres, cleared by the FDA, with regard to indications for use and technological characteristics.
“Both devices are spherical, non-resorbable polymer microspheres which are delivered through a microcatheter to embolize the target vessel. There are differences in actual material composition; however, the materials of Embozene are well-known and widely used in the medical environment and are biocompatible for their intended use,” the documents state.
“The devices are available in similar sizes, Embozene (40–1300 µm) vs. Embosphere (40–1200 µm). The differences in materials and size range of these devices do not affect overall safety or effectiveness as demonstrated by clinical data,” the FDA material that is available online, states.
As you pursue new and innovative procedures within more complex anatomy, you need precision and control like never before. Fathom Steerable Guidewires feature a nitinol hypotube distal segment—a design that revolutionizes the ability to access even the most tortuous vascular beds. Diamond-cutting the nitinol hypotube and creating an alternating pattern of microscopic channels helps transmit turn-for-turn torque control that enhances responsiveness and maneuverability. The platinum-tungsten distal tip is shapeable and is engineered to achieve accurate placement while maintaining tip-shape memory. For more information, visit our Fathom™ Steerable Guidewires page.
Indications, Safety and Warnings Prescriptive Information CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the complete “Directions for Use” for more information on Indications, Contraindications, Warnings, Precautions, Adverse Events, and Operator’s Instructions
FATHOM -14 Steerable Guidewire INTENDED USE/INDICATIONS FOR USE The FATHOM -14 Steerable Guidewire is intended for general intravascular use in the peripheral vasculature. It can be used to selectively introduce and position catheters and other interventional devices within the peripheral vasculature. This device should be used only by physicians trained in percutaneous, intravascular techniques and procedures.
Fathom-16 Steerable Guidewire INTENDED USE/INDICATIONS FOR USE The FATHOM -16 Steerable Guidewire is intended for general intravascular use in the peripheral vasculature. It can be used to selectively introduce and position catheters and other interventional devices within the peripheral vasculature. This device should be used only by physicians trained in percutaneous, intravascular techniques and procedures.
Fathom -14 and -16 Steerable Guidewire Contractions, Warnings and Adverse Events CONTRAINDICATIONS None known. WARNINGS The FATHOM Steerable Guidewire is not intended for use in the coronary vasculature or the neuro vasculature. ADVERSE EVENTS Complications attributed to endovascular procedures are the following: • Vessel trauma • Vessel damage • Embolism (catheter/device, air bubble, plaque, thrombus, air embolism, thromboembolism) • Pseudoaneurysm • Seizure/stroke • Vessel dissection • Hematoma at the puncture site • Nerve injury • Infection • Perforation of the vessel • Vessel spasm • Hemorrhage • Vascular thrombosis • Vessel occlusion • Death • Bleeding • Failed treatment • Inability to position guidewire • Damage to the catheter
A study, evaluating the efficacy and safety of transarterial chemoembolization (TACE) using LifePearl (Terumo) drug-eluting embolic agents in the treatment of hepatocellular carcinoma has just been published in the June issue of the Journal of Vascular and Interventional Radiology. The study included data from 302 patients over a 20-month period of time.
This paper, from lead author F Veloso Gomes, hospital Curry Cabral, Lisbon, Portugal, includes one of the largest patient populations treated with TACE using precisely calibrated LifePearl drug-eluting microspheres in hepatocellular carcinoma.
As reported in JVIR, the median follow-up time was 11.9 months. One-month follow-up CT revealed complete response in 179 patients (63.2%), partial response in 63 (22.3%), stable disease in 16 (5.7%), and progressive disease in 25 (8.8%). The most frequent complications were post-embolization syndrome in 18 patients (6%), liver abscess in five (1.7%), and puncture site haematoma in three (1%). Biochemical toxicities occurred in 57 patients (11.6%). Survival analysis at 12 months showed a progression free survival rate of 65.9% and overall survival rate of 93.5%. Patients who received transplants showed a 57.7% rate of complete pathologic response. Veloso and colleagues concluded that “Chemoembolization with polyethylene glycol (PEG) embolic agents for hepatocellular carcinoma is safe and effective, achieving an objective response rate of 85.5%.”
Crucial role of drug-eluting embolics
Élia Coimbra, senior author and head of Interventional Radiology Unit from the research team, said: “Chemoembolization of hepatocellular carcinoma with drug-eluting embolics plays a crucial role in both our liver transplant candidates, and intermediate stage patients, according to BCLC classification. Our goal is to improve patient outcomes continuously, which is why we are dedicating more resources to research at our Hospital.”
LifePearl microspheres are used in the treatment of primary and secondary liver cancer. They comprise a range of microspheres that are biocompatible, hydrophilic, precisely calibrated and capable of loading and releasing chemotherapeutic agents in a controlled manner, says a press release from the company. This supports the wider use of TACE so that it is reproducible and standardisable as well as providing physicians with another option to treat patients in the early stage of BCLC staging, the release adds.
Since its launch in 2015, LifePearl microspheres have been used in approximately 8,000 TACE procedures in Europe, Middle East and Africa. LifePearl microspheres have now seven publications in various scientific journals and have been the subject of multiple clinical trials and presentations in interventional radiology congresses, continues the release. These data show consistent and promising results, it states.
Transarterial chemoembolization (TACE) is a mainstay of locoregional treatment for hepatocellular carcinoma (HCC) in the intermediate stage. “The technique for this procedure, however, continues to vary, leading to a heterogeneity in the literature and making meaningful comparisons between treatments difficult,” said Jafar Golzarian, Minnesota, USA, at the Global Embolization Cancer Symposium and Technologies (GEST 2018 US; 17–20 May, Miami Beach, USA) reporting on a survey on the topic.
Golzarian, director, Division of Interventional Radiology and Vascular Imaging, University of Minnesota, USA is one of the founders and co-directors of GEST US, reported the main findings from a survey that obtained information on the technical aspects of international TACE practice in an effort to understand current treatment strategies as a first step towards standardisation of the technique.
Golzarian explained that the survey was an anonymous, 18-question, survey distributed via email to practicing members of five interventional radiology societies in English and Chinese. The researchers gathered a total of 1,160 responses from 62 countries.
The survey included questions on the type of practice the interventional radiologist was in (the majority of respondents, 369, was in academic practice) and the most common cytotoxic agent used in the treatment of HCC was doxorubicin (701 respondents reported using it over other agents including epirubicin, cisplatin, irinotecan, idarubicin and others). There were further questions on which procedure was typically performed for a single HCC, to which the majority of respondents (467) stated that they employed drug-eluting beads, while 265 employed conventional TACE. Nearly 175 said that it depended on the extent of disease and its location; very few (30) noted performing bland embolization.
Other questions elicited answers on the amount of ethiodised oil used (the majority of those who used cTACE, said they used more than 10ml) and about how ethiodised oil was mixed with the cytotoxic agent. Interestingly, answers to the latter revealed that 216 practitioners had no preference whatsoever whether this was mixed as oil-in-water (which 87 preferred) or water-in-oil (which 216 preferred).
There was also no consensus on follow-up protocol, but the majority (634) preferred to use CT over MR (307) and other modalities (49). With regard to the criteria employed to determine tumour response, 586 utilised modified RECIST and 224 used RECIST, followed by 61 who used EASL and 49 who reported ‘other’.
Conclusion
“In conclusion practitioners across diverse geographies differ in the way they perform TACE for the treatment of HCC. These differences lead to difficulty in comparing studies in this field. We are driven by the lack of high-level data to guide treatment. Further research and consensus panels are needed to help determine the most effective technical methods to perform TACE,” said Golzarian.
There is no “stereotypical” female interventional radiologist. We are simply as skilled, motivated, committed, and diverse in our interests as our male colleagues. Yet, there are definitely still barriers to women choosing interventional radiology, writes Maria Tsitskari, Greece, who is hopeful that raising these issues will help to change mind-sets.
It is probably fair to say that life for women in the field of interventional radiology is no picnic. But this holds true for men who practice in the field as well. Interventional radiology is a tremendously demanding, yet very exciting, subspecialty. As it is increasingly essential to the delivery of modern emergency and acute setting care, interventional radiology requires extensive training and comes with the assurance of long and unpredictable work hours. Consequently, there is great pressure and interventional radiologists need to draw on cognitive, technical, and leadership skills in sometimes difficult situations.
There are, however, some challenges that are unique to women practising in the field and it is important to consider the issues that women have to face today. We need to examine these challenges in the light of data showing that there are currently extremely low numbers of women in this field.
The most common factors that discourage women from taking up interventional radiology include difficult work-life balance and radiation risks during pregnancy. However, there are sound data to show that being an interventional radiologist is safe and that women can practise interventional radiology, be pregnant and safe. There are also the challenges that women interventional radiologists have to face in relation to child rearing. Finding a balance between work and family is an issue that affects anyone with a high-pressure job and requires good personal help and understanding from all sides of the family.
One of the hardest challenges that I have faced is having to fight for acceptance from other physicians, beginning with male interventional radiologists. There is an enduring belief that women are not capable of delivering the goods when it comes to technically demanding procedures. At this point I would like to refer to an old maxim in surgical training about the attributes needed to be a good surgeon: the eyes of an eagle; the heart of a lion; and the hands of a woman. Technically amazing procedures often need fine and delicate movements and women might even have some advantages on this front. In general, interventional radiology is a specialty that is seeking recognition and acceptance from other physicians. When women in this field also have to strive to gain a basic acceptance of their skills and ability, it adds another dimension to the mix.
One of the most interesting and motivating aspects of my work is that I have received great trust and acceptance from patients. There is a stereotype in our society that the surgeon “has to be a man”. This might be why it is easy for patients to accept that a woman is the proceduralist during minimally-invasive interventional radiology, which is vastly different from open surgery.
In the four years since my interventional radiology fellowship, I have been on an incredibly rewarding journey, during which I have had several testing times and obstacles. This has only made me more determined. When you keep pushing through, no matter what the situation is or how painful the setbacks are, incredible things begin to happen. My work in this field fills me with happiness and satisfaction. Interventional radiology is definitely the profession that I would go into, if I had to choose all over again.
My main message is this: there is no stereotypical female interventional radiologist. We are as skilled, motivated, committed, and diverse in our interests as our male colleagues are. I am hopeful that changing times, the data on radiation safety during pregnancy and shifting attitudes will bring more women into the field, and help them stay on the course of their chosen careers. Until then, I am certain that the small number of us currently practising will continue to make a big impact on our profession and patients.
Maria Tsitskari is an interventional radiologist in Greece.
Guerbet has announced the upcoming launch of SeQure and DraKon, two novel microcatheters for tumour and vascular aneurysm embolization procedures. The company introduced the microcatheters at GEST (Global Embolization Cancer Symposium and Technologies) 2018 US in Miami, USA.
SeQure is designed to lower the risk of non-target embolization with its fluid barrier technology with a unique filter tip designed to increase drug and embolic microsphere delivery to tumours, reducing embolic material backflow enhanced and targeted embolization.SeQure and DraKon microcatheters received US FDA clearance on 26 January 2018 for the use of infusion media into all peripheral of contrast vessels as well as drug infusion in intra-arterial therapy and infusion of embolic materials. They will be available for sale during the third quarter of 2018.
DraKon is a standard microcatheter adapted for conventional transarterial chemoembolization (cTACE) as well as simple embolization cases.
Both SeQure and DraKon offer enhanced intra-arterial navigation to interventional radiologists, with optimal combination of torqueability, pushability, trackability and visibility, and kink resistance enabling access in cases of difficult-to-navigate vascular networks and lesions.
Some examples of use may include vascular tumours and anomalies requiring treatment with catheter embolization, such as liver cancer directed therapies which include cTACE and TACE using drug-eluting beads, as well as renal and lung tumour embolization, preoperative embolization of cancer tumours, presurgical embolization of juvenile angiofibroma, uterine fibroid embolization, prostatic artery embolization for benign prostatic hyperplasia, angiomiolipomas, haemorrhages, and vascular anomalies.
“The launch of SeQure and DraKon microcatheters is an important step as Guerbet accelerates expansion beyond diagnostic radiology into the interventional imaging space. This new range of microcatheters will allow us to help interventional radiology teams deliver a higher quality of care during image-guided embolization procedures,” said Massimo Carrera, Guerbet vice president for North America.
Guerbet obtained both microcatheters in their acquisition of Israeli company Accurate Medical Therapeutics announced in January 2018.
Percutaneous vertebroplasty does not result in statistically significant greater pain relief than a sham procedure, reports a study detailing the results of the VERTOS IV trial, published in the British Medical Journal (BMJ). This study followed patients with acute osteoporotic vertebral compression fractures for 12 months following either a vertebroplasty or a sham intervention.
After the 2009 masked randomised controlled trials published in the New England Journal of Medicine, INVEST (Kallmes et al) and the Australian trial (Buchbinder et al), both found no benefit for vertebroplasty over a sham control, there was an angry backlash from interventionalists who questioned both the trial designs and their findings.
Kallmes, who repeatedly clarified that in the INVEST trial, vertebroplasty worked, just not significantly better than the sham intervention (which also, for some reason, had worked rather well) went on to publically declare himself likely “the most reviled radiologist on the planet”.
A potential upshot of these trials, according to prevailing community opinion, was that vertebroplasty began to be eyed with caution in some quarters and the numbers of these cement augmentation procedure began to dwindle. Then came the results of the 2010 open-label VERTOS II (Klazen et al, The Lancet) and the 2016 masked Australian VAPOUR trial (Clarket al), the results of which gave vertebroplasty a much-needed boost. Many interventionalists felt vindicated that their observations of vertebroplasty ‘done right’ i.e., in acute vertebral compression fractures and using an adequate volume of cement, were finally being borne out. And yet, here are the results of the VERTOS IV group (Firanescu et al) whose data follow the path of the 2009 trials. The question is: what does this mean for the continued clinical role of vertebroplasty?
Patient selection
VERTOS IV is a blinded, sham controlled clinical trial that included 176 patients: 90 participants, with 115 fractures, in the vertebroplasty group and 86 participants, with 108 fractures, in the sham procedure group. Patients referred to four radiology centres for spinal radiographs who were found to have radiographic fractures were administered a questionnaire. Those with a VAS pain score of at least five out of 10 and duration of fracture less han nine weeks were invited to enroll.
Consenting patients were referred for MRI and physician consult and if still deemed eligible underwent the procedure 11 to 13 days later (mean 6.1 weeks). This was an outpatient only trial.
The procedures
All participants received local infiltration with 1% lidocaine (lignocaine) into each pedicle followed by 0.25% bupivacaine.
Next, each participant received two stab incisions at the level of the vertebral body, after which the sealed randomisation envelope was opened—the patient was then assigned to either the vertebroplasty or the sham group.
For both groups, the cement was prepared in close proximity to the patients, who could hear the mixing sound and smell the PMMA in the room. However, while the cement was injected in the vertebroplasty group, the injection was simulated in the sham procedure group using verbal and physical cues. Bone biopsy needles were positioned bilaterally, with the sham intervention involving periosteal placements instead of transpedicular placements. After the procedure, participants in the vertebroplasty group underwent computed tomography, whereas participants in the sham procedure group were subjected to preliminary scout view scanning only.
Findings
First author Cristina E Firanescu (Departments of Radiology and Internal Medicine, Elisabeth TweeSteden Hospital, Tilburg, The Netherlands) and colleagues report that compared with baseline, the reduction in the visual analogue scale (VAS) score over 12 months in both groups was clinically and statistically significant at all measurement points: one day, one week, and one, three, six and 12 months. Firanescu et al write, “This significant reduction was measurable starting at day one after the procedure and remained significant throughout the follow-up.”
The primary prespecified objective of the VERTOS IV trial was to determine the difference between groups in mean reduction of VAS score during 12 months’ follow-up, at one day, one week, and one, three, six, and 12 months after the procedure. The VAS score ranged from 0 (no pain) to 10 (severe pain).
Quality of life improved for both the vertebroplasty and the sham procedure groups. The quality of life questionnaire of the European Foundation for Osteoporosis (QUALEFFO) and physical functioning with the modified Roland-Morris disability (RMDQ) questionnaire scores were used as secondary endpoints of the study.
For both measures, the worse the health related quality of life condition, the higher the score. There was a statistically significant decrease in both the QUALEFFO and RMDQ scores compared to baseline at all time-points measured during the 12 months’ follow-up period.
The mean reduction in QUALEFFO score at the last measurement point (12 months) was 18.32 in the vertebroplasty group (95% confidence interval 18.32 to 23.61) and 18.61 in the sham procedure group (13.02 to 24.2), with a between group difference of −0.14 (95% confidence interval −3.04 to 2.76). The mean reduction in RMDQ score at the last measurement point (12 months) was 7.71 in the vertebroplasty group (5.87 to 9.55) and 7.47 in the sham procedure group (5.56 to 9.38), with a between group difference of 0.12 (−1.11 to 1.35).
The study authors hypothesise, “These results suggest that factors aside from instillation of PMMA might have accounted for the observed clinical improvement after vertebroplasty; for example, the effect of local anaesthesia, expectations of pain relief (placebo effect), natural healing of the fracture, and regression to the mean.”
Speaking to Interventional News, Firanescu pointed to one way of looking at these findings: “Although percutaneous vertebroplasty did not result in statistically significantly greater pain relief than a sham procedure, more patients show secondary fractures and persistent pain in the sham group. A future therapeutic pain strategy could be a combined regimen of periosteal infiltration during natural healing. Additional cement seems indicated only in a selected subgroup of patients with insufficient pain relief after this early phase,” she says.
Recent history of blinded trial evidence
The Kallmes et al and Buchbinder et al trials in 2009, two blinded randomised studies, found no benefit of vertebroplasty compared with sham controls. The VAPOUR (Vertebroplasty for Acute Ppainful osteoporotic fractURes) trial showed that better pain relief was achieved after vertebroplasty compared with sham treatment, as measured by a clinically significant pain reduction at all time points from three days till six months, with the primary endpoint at 14 days. There was also significant reduction in disability, improved quality of life and 30% greater preservation of vertebral body height.
David Kallmes (Mayo Clinic, Rochester, USA), principal investigator of the INVEST trial, tells Interventional News: “Aiming to ‘correct’ numerous apparent deficiencies in patient selection criteria in prior blinded augmentation trials, the VERTOS IV investigators have instead joined those casting doubt on the technique. Notably, the results of VERTOS IV, in which 75% of patients were treated beyond 28 days, are in fact entirely congruent with those of the VAPOUR trial, which demonstrated that fractures three weeks of age and older did not benefit from spine augmentation. If the VERTOS family of trials, with unblinded VERTOS II showing profound comparative benefit of the cement that vanished with blinding in VERTOS IV, has shown us anything it is that effective blinding in spine augmentation trials is essential. VERTOS IV provides additional concrete evidence that the spine augmentation procedure reduces pain and improves function and quality of life, but we must continue to try to understand why some patients experience these benefits without cement.”
Of the contrasting results between the most recent VERTOS IV trial and the VAPOUR trial, William Clark (Department of Radiology, St George Private Hospital, Kogarah, Australia), principal investigator of the 2016 VAPOUR trial, comments, “VAPOUR and VERTOS IV are very different trials. The VAPOUR trial used different patient selection criteria to VERTOS IV, with earlier vertebroplasty (2.8 weeks vs. 6.1 weeks mean pain duration). VAPOUR included hospitalised inpatients and outpatients with severe (NRS≥7/10) pain despite analgesic therapy (including opiates in 90%) and offered vertebroplasty without further delay. VERTOS IV was outpatient only, 34% of patients were taking strong opiates, VAS pain threshold was 5/10 and there was 13-day delay between initial recruitment and vertebroplasty. The benefits of vertebroplasty in VAPOUR were concentrated in patients with fractures ≤ 3 weeks duration, with no advantage over placebo in fractures greater than three weeks. At the time of vertebroplasty 88% of patients in VAPOUR had fractures less than or equal to four weeks duration compared to 25% in VERTOS IV. These differences explain the different trial outcomes. Vertebroplasty should be reserved for patients (including inpatients) with severe, uncontrolled pain despite maximal medical therapy and should be offered early, without undue delay.”
Afshin Gangi (Radiology and Nuclear Medicine, Imagerie Interventionnelle, Strasbourg, France; Oncological Interventional Radiology, King’s College London, Guy’s and St Thomas’ NHS, London, UK) concurs with Clark, saying, “Patient selection is really the key… [this trial is] treating patients too late—we need to treat them faster to reduce the immobilisation and stop spinal deformation and hyperkyphosis. Vertebroplasty stops vertebral collapse and avoids the eventual progression to spinal deformation. They [the VERTOS IV trial investigators] just evaluate the pain.”
Commenting on the importance of the data, Joshua Hirsch, vice chair of Interventional Radiology, service line chief, Interventional Radiology, director, Interventional Neuroradiology, chief, NeuroInterventional Spine, Massachusetts General Hospital, Boston, USA and Harvard Medical School, Boston, who is a coauthor of VERTOS IV, says: “We believe VERTOS IV to be an important addition to the existing augmentation literature. While this trial suggests that there may be a role for the use of high volume periosteal anaesthetic in vertebral compression fracture patients, this approach would require further validation through open label trials. Moreover, it is critical to appreciate that the real-world alternative to augmentation for compression fractures is conservative therapy. Such treatment including opiates, limitation of activities of daily living and bedrest have their own risk profile. Vertebral augmentation results in early mobilisation and sagittal preservation. These are likely important factors leading to the strong evidence for morbidity and mortality benefits associated with augmentation. It is our sincere hope that the results of VERTOS IV are carefully scrutinised leading to thoughtful interpretation and conclusions.”
Med Alliance SA, a company developing and commercialising the first sirolimus micro-reservoir drug-coated balloon (SELUTION DCB) to treat patients suffering from peripheral artery disease (PAD), coronary artery disease (CAD), arteriovenous fistulas (AVF) and grafts (AVG) for end-stage renal disease, has raised US$37 million.
The US$37 million consists of US$22 million equity and US$15 million in non-dilutive licensing agreements for Japan and China. The Investment Round was led by a US$20 million investment by Shenzhen Salubris Pharmaceuticals.
Kevin Ye, chief executive officer of Salubris, highlighted the MedAlliance investment and distribution agreement: “Sirolimus’ combination of anti-restenotic and anti-inflammatory properties have been proven clearly superior to first generation paclitaxel drug coatings on stents, but technical challenges have precluded the transposition of this evolution in stents to the drug-coated balloons used in reperfusion procedures. Salubris is pleased to support MedAlliance progress through this strategic investment, and we look forward working together to commercialise the company’s technology for the benefit of many millions of patients with coronary and peripheral artery disease in China”.
The proceeds from the equity financing will be used to fund European commercialisation, US regulatory approval and support global clinical programs.
In January 2018, MedAlliance announced a strategic agreement with Kaneka Corporation, a leading provider of PTCA balloons in Japan. The agreement involves technical collaboration, product licensing, manufacturing and distribution for the MedAlliance DCB, limited to the treatment of coronary arteries in Japan.
“We are very pleased to have both Salubris and Kaneka as partners. These companies share our belief in providing clear patient benefit demonstrated by strong supporting clinical data”, said Jeffrey B Jump, chairman and CEO of MedAlliance. “The validation from these highly successful, international medical organisations represent a significant endorsement of both our technology and our team.”
The MedAlliance technology includes unique micro-reservoirs made from biodegradable polymer intermixed with the anti-restenotic drug sirolimus. These micro-reservoirs provide controlled and sustained release of sirolimus. Extended release of sirolimus from stents has shown to be highly efficacious in both coronary and peripheral vasculatures. MedAlliance’s proprietary CAT (Cellular Adhesive Technology) enables the micro-reservoirs to be coated onto balloons and adhered to the vessel lumen when delivered via an angioplasty balloon.
Encouraging primary endpoint data from the First-in-Man (FIM) study of the SELUTION DCB was presented at the Leipzig Interventional Course (LINC) in February 2018. Late Loss of the target lesion, as measured by Quantitative Vascular Angiography (QVA) at six months post-index procedure, was 0.19mm. The rate of Target Lesion Revascularisation (TLR) was 2.2%—one of the lowest ever reported in a drug-coated balloon FIM study at six months. There were no incidences of either death or the need for minor and/or major amputations.
Subgroup data presented at CRT and Charing Cross meetings indicated similar performance in patients with long lesions and with moderately severe and severe calcifications.
“We are very encouraged by the FIM data and investor enthusiasm for this novel sirolimus DCB technology”, concluded Jeffrey B Jump.
Late-breaking SPYRAL HTN-ON MED study at EuroPCR indicates renal denervation lowers blood pressure in hypertensive patients in presence of blood pressure medication.
Medtronic has announced first-ever-data from the SPYRAL HTN-ON MED study. Initial results found statistically significant and clinically important blood pressure reductions in hypertensive patients prescribed antihypertension medications treated with the Symplicity Spyral renal denervation system with no major adverse safety events out to six months. The late-breaking trial data, presented at the 2018 EuroPCR Annual Meeting in Paris, was published simultaneously in The Lancet. The Symplicity Spyral system is investigational in the USA and Japan.
At six months, patients randomised to the renal denervation procedure experienced an average 9mmHg drop in 24-hour mean systolic ambulatory blood pressure (ABPM), resulting in a 7.4mmHg difference compared to patients in the sham control arm (p=0.005). For renal denervation patients, 24-hour mean diastolic ABPM also declined 6mmHg, which is 4.1mmHg lower than the sham control arm (p=0.029).
Likewise, average office systolic blood pressure (OBP) in patients in the renal denervation arm declined 9.4mmHg – a 6.8mmHg difference from the sham control arm (p=0.021), and the diastolic OBP declined 5.2mm Hg, a 3.5mmHg difference from the sham control arm (p=0.048).
“Data from the SPYRAL HTN-ON MED study is important for the clinical community and for patients with hypertension as it represents a typical scenario of managing uncontrolled hypertension patients, prescribed up to three blood pressure medications,” said David Kandzari, director of interventional cardiology and chief scientific officer at Piedmont Heart Institute in Atlanta, USA, co-principal investigator in the SPYRAL HTN-ON MED study, and member of the Medtronic Executive Committee that designed and oversees the SPYRAL HTN Global Clinical Program. “With these new results, mirroring those of the parallel SPYRAL HTN-OFF MED trial, we have convincing evidence at six months showing the continued safety and efficacy of renal denervation in both the presence and absence of blood
The SPYRAL HTN-ON MED patients were prescribed a stable regimen of up to three anti-hypertensive medications, including diuretics, calcium channel blockers, ACE /ARB inhibitors or beta blockers. Similar to recent studies of uncontrolled hypertension, drug testing indicated that adherence to prescribed antihypertensive medication was inadequate as only about 60% of patients were found to be taking medications as prescribed. Medication adherence remains a challenge in controlling hypertension in patients resulting in intermittent blood pressure control that can lead to an increased risk for cardiovascular events.
Additional analysis of the cyclical hourly changes in blood pressure demonstrated that the blood pressure lowering effects of renal denervation were distributed throughout the day and, importantly, throughout the night-time period when blood pressure control is even more critical due to higher risks of adverse events like heart attack and stroke caused by hypertension. Blood pressure during sleep is the most significant predictive marker of cardiovascular disease morbidity and mortality, and reduction in asleep blood pressure is associated with highly significant reduction of cardiovascular disease risk.
“We are encouraged by these data showing the procedure may enable a blood pressure lowering effect 24 hours a day. Renal denervation is essentially ‘always on’ even when the effect of medications may be subsiding between doses” said Raymond Townsend, director of the Hypertension Program at the Hospital of the University of Pennsylvania, a professor of Medicine in the Perelman School of Medicine at the University of Pennsylvania, and co-principal investigator in the trial. Townsend is a member of the Medtronic Executive Committee that designed and oversees the SPYRAL HTN Global Clinical Program.”
Drug-coated balloon (DCB) angioplasty devices have been categorised by the US Centers for Medicare and Medicaid Services (CMS) into the same billing code as plain balloon angioplasty, following the expiration of the technology’s transitional pass-through and new technology add-on payments on the 1st of January 2018. The decision not to create a separate reimbursement code for DCBs comes to the surprise and disappointment of a wide range of stakeholders and advocates, from industry to public advocacy groups.
The conflation of the two technologies into the same ambulatory payment classification has caused protests from scientists, physicians, societies, public advocacy groups and industry alike, who argue that the decision will indirectly discourage DCB use despite evidence of superiority compared to plain angioplasty.
A recent viewpoint article published in the Journal of the American College of Cardiology (JACC): Cardiovascular Interventions calls the ruling “arbitrary” and “disappointing”, urging “all who advocate for patients with peripheral artery disease” to engage on CMS decisions regarding payment.
Vascular News spoke to Mehdi Shishehbor (Case Western Reserve University School of Medicine, University Hospitals, Cleveland, USA), first author of the article, who finds the decision both puzzling and alarming. “There is Level 1 evidence from three randomised controlled trials with three different devices, showing clearly that drug-coated balloons compared to angioplasty alone is superior”, he says. “We [Shishehbor and colleagues] are puzzled as to why the CMS would treat DCBs as being the same as angioplasty, because by not giving it a new billing code, the CMS is implying that DCBs and angioplasty are the same. We are just dumbfounded. I have no idea why they believe that.”
Mehdi Shishehbor
Although DCB treatment costs are significantly higher than angioplasty use per-treatment, Shishehbor points to higher long-term costs of reintervention rates and continued care stemming from the lower patency rates of plain angioplasty. Grouping the two under one APC billing code, the fear is that patients who are uninsured or relying on Medicare and Medicaid will not receive DCB treatment, as hospitals pay out of pocket for the higher costs of the device.
The CMS can allow innovative device technologies that are too novel to be included in regular coverage, to instead be covered over a short-term period under the transitional pass-through add-on payment and new technology add-on payment categories. This ensures patients gain access to beneficial new treatments while the CMS gather data to make a decision on its long-term ambulatory payment classification (APC), or billing code. The pass-through phase usually lasts for up to two years, and Shishehbor notes that this period is rarely extended. In the JACC article, Shishehbor et al write that the CMS “should be applauded for approving additional DCB coverage through [add-on payments], recognising the incremental clinical benefits afforded by DCB compared with traditional uncoated angioplasty for patients with peripheral artery disease.”
As the pass-through and new technology add-on payment phase came to an end, however, the decision was made to package DCB device treatment costs into an existing category for angioplasty—surprising professional societies, physicians, public policy organisations and medical centres who argued against the idea “out of concern over unintended patient consequences”, write Shishehbor et al. What should have been done, they argue, was to create a new APC category or assign the device to a “more appropriate APC category”.
The unintended consequences
In the long-term, Shishehbor et al argue that elderly and disadvantaged patients who rely on Medicare and Medicaid will be assigned to suboptimal treatment with plain angioplasty.
“This policy in the USA affects everyone over the age of 65”, Shishehbor told Vascular News, “because the majority of these patients—male or female and regardless of race—get their insurance through the Medicare system. So every single patient over the age of 65 who relies heavily on Medicare as their insurance, which is a majority of the population, may be affected by this. It also affects those who do not have insurance, or rely on Medicaid as insurance.”
“For these patients it is very unlikely that they would receive treatment with a technology that costs 5–6 times more than the other technology, as the hospital would have to pay out of their own pocket in order to use it”, Shishehbor said. He added that in 2018, the uncoated balloon alternative, which physicians are likely to fall back on for these patients, “is not something that is clinically appropriate in most cases—if not all”.
Chairman of the NCVH, Craig Walker, voiced his opposition on the change when it was proposed in 2017, and encouraged physicians to submit public comments. He said at the time that the proposed payment structure (now implemented) “would not adequately reflect the added costs of DCB and could adversely impact access for Medicare beneficiaries given the difference in costs between a plain balloon and DCB. The clinical benefits and cost effectiveness of DCB angioplasty have been well-established through randomised controlled trials and large-scale, population based observational studies. CMS’ approval of both inpatient and outpatient temporary add-on payments for DCB was in recognition that DCBs represent a significant clinical improvement in the treatment of PAD relative to plain balloon angioplasty catheters when compared to drug coated balloon therapy.”
“I believe an appropriate payment structure after the expiration of these add-on payments is important to avoid patient access barriers to a technology that reduces repeat interventions for patients and health care costs to Medicare.”
A fee-for-service system of care
Describing the disconnect described between the evidence of DCB superiority and the failure to designate it to a new APC category, Shishehbor explained it is due to the guidelines which inform CMS’ decisions. “The bigger issue comes down to the fact that this is really not the CMS’ fault. These are rules that are set by Congress and by the government.”
“When CMS wants to give something a pass-through code, the rules say they need to look whether clinically, that technology offers something superior. But for the regular billing code in the second phase, there is no rule that says the CMS need to look at efficacy. They only need to look at cost.”
The CMS responded to the request that a new reimbursement code be created for DCBs, explaining that their decision is based on “a prospective payment system that relies on the principles of averaging, with some cases in an APC being more costly than others (and some being less costly)”.
These principles however, as Shishehbor maintains, are problematic. “What they [the CMS] say is they believe in the concept of averaging”, Shishehbor told Vascular News. “The idea is, sometimes physicians use angioplasty and sometimes physicians use DCBs, and over time the cost kind of averages out. That would be true if DCB and plain balloons were the same, but they are not the same. A drug-coated balloon is much more superior—not only from the standpoint of patency, but also from the standpoint of patient quality of life and even long-term cost, because as patients come back for reinterventions due to their lower patency plain angioplasty, this affects cost to the healthcare system.”
“This principle is outlined by Congress and by the law, and that rule fundamentally is what we need to change if we want to move towards a value-based system rather than a fee-for-service system.”
The role of industry
Not alone in voicing disagreement with the reimbursement code decision for DCB devices, Sheshehbor et al’s call to action is joined by industry actors and stakeholders. Mark Pacyna, VP and GM of the Peripheral business in Medtronic’s Cardiac and Vascular Group, recently released a statement in response to Shishehbor et al, referring directly to the article. “As discussed in the JACC article”, Pacyna says, “DCBs serve as a cost-effective solution to safely and effectively treat femoropopliteal disease, while also reducing rates of reintervention. While the expiration of CMS’ transitional pass-through add-on payment for DCBs was anticipated, data has proven that drug coated balloons offer economic and clinical value.” He concluded, “Medtronic and our collaborating partners will continue to pursue appropriate reimbursement for DCB procedures and ensure access to this proven therapy that improves outcomes and delivers long-term savings to health systems and payers.”
Shishehbor hopes that through collaborative engagements between societies, public advocacy groups and scientists, their concerns can be communicated to the CMS and influence the upcoming reevaluation of DCB reimbursement.
Regarding the role of industry partners in this collaborative response, Shishehbor comments he is aware that industry is engaging CMS on their own, “because they also believe that something has to be done”. To his knowledge however, there is no direct collaboration between industry and people like Shishehbor, “who are advocating on behalf of my patients and on behalf of my profession” rather than for financial reasons. However, he says, “They are fighting on the right side of the isle, fighting for something that I believe as a scientist and as a physician, is the right thing to do. […] Industry obviously wants these devices to be paid for by the government, and we do too.” In this sense, he says, they are aligned.
The first 24-month data from the LUTONIX AV investigational device exemption trial were presented at the Charing Cross Symposium in April. These interim data show a sustained effectiveness benefit for the Lutonix drug-coated balloon (BD) and indicate that it leads to an average time to first reintervention that is four months longer than plain balloon angioplasty.
The randomised, prospective, multicentre Lutonix AV trial was designed to assess the safety and effectiveness of the Lutonix 035 drug-coated balloon in the treatment of native dysfunctional arteriovenous fistulae. The patient cohort was a “real-world” group and the study included secondary non-target lesions, denovo/restenotic lesions, and stents in the access circuit outside of the studied lesions. Investigators in the trial randomised 285 patients at 23 clinical sites. After predilatation to specific requirements with a plain angioplasty balloon, patients who had less than 30% residual stenosis were then enrolled and randomised 1:1 to treatment with either a drug-coated balloon or a standard matched compliant percutaneous transluminal angioplasty balloon.
Kate Steiner (consultant interventional radiologist at East and North Hertfordhsire NHS, Stevenage, UK) reported the latest data from the trial. Emphasising the points that would resonate most with patients, she highlighted that patients in the drug-coated balloon arm had, on average, a reintervention at 11 months (318.7 mean days) as compared to patients in the control arm who had a reintervention at seven months (198.4 mean days). “Four months, or 120 reintervention-free days, is significant to the dialysis patient who already spends three days a week on dialysis,” Steiner commented.
The primary efficacy endpoint of LUTONIX AV was target lesion primary patency at 180 days. While the trial did not show a statistically significant benefit for the drug-coated balloon at this time point, further follow-up revealed that the paclitaxel drug had a significant effect on the lesion patency at later time points. The primary safety endpoint was freedom from any serious adverse event(s) involving the arteriovenous access circuit through 30 days and showed that treatment with a drug-coated balloon was non-inferior to treatment with a plain balloon. Follow-up was clinically driven and took place at one, three, six, nine, 12, 18 and 24 month visits.
Steiner maintained that the long-term data suggest a sustained efficacy benefit through the 24 months. “Nowhere in the patency curve do the lines cross through 24 months,” she said, adding that long-term safety remains non-inferior to plain balloon angioplasty. “The Kaplan-Meier patency curves start to separate around the 90 to 100-day mark and what we see now is that they continue to remain separate; there is no time point at which the curves cross or come together. We see a 36.8% improvement out to 550 days and this continues out to a 30% improvement out to 730 days, or 24 months,” she explained.
Results
Results from the study were adjudicated by a core lab, an Independent Clinical Events Committee, and Data Safety Monitoring Board.
The evidence is emerging for the use of drug-coated balloon use in AV access. “When we combine the LUTONIX AV trial, LUTONIX global registry (n=324), and LUTONIX post-approval study (n=213), we will have well over 800 patients going towards addressing the data deficit in dialysis access. I will predict that as we learn more about the pathophysiology of dialysis access stenosis, we will see more innovation in this area,” Steiner stated.
Vascutek and Bolton Medical, subsidiaries of Terumo Corporation of Japan, have combined into a single, integrated business, Terumo Aortic, which is looking to grow its presence in the global aortic and vascular implants market. Terumo acquired Vascutek in 2002 and Bolton Medical in 2017.
As a combined business, Terumo Aortic aims to become recognised for its focus on individualised treatments that offer clinicians more options than ever before.
Terumo Aortic will have a combined revenue of nearly US$200m and over 1,100 employees worldwide. Its primary research and manufacturing facilities will remain in Glasgow, Scotland and Sunrise, Florida.
The combined offering includes advanced technologies such as surgical grafts for abdominal, cardiothoracic and peripheral applications as well as hybrid and catheter-based stent graft systems for abdominal and thoracic aortic aneurysms. These implants have already helped to save, or improve, the lives of over two million patients in over 100 countries worldwide.
Vascutek and Bolton Medical have been working to consolidate and streamline their complementary offerings for the past year. Significant focus has been placed on creating an integrated research and innovation strategy that will push the boundaries of the aortic and vascular implants market.
Paul Holbrook, president of Terumo Aortic, said: “This coming together of two organisations with highly advanced technologies will be transformative for physicians and the patients they serve.”
“We have woven together the products, services and expertise offered by our teams in Europe and the USA, enabling clinicians to meet the unique needs of their patients and redefine the treatment of aortic disease.”
Medtronic has announced that it has received US Food and Drug Administration (FDA) approval for the IN.PACT Admiral drug-coated balloon (DCB) to treat long superficial femoral artery (SFA) lesions up to 360mm in patients with peripheral artery disease (PAD).
Approval was based on clinical data from the complex lesion imaging cohorts of the IN.PACT Global Study, including long lesion, in-stent restenosis, and chronic total occlusion (CTO) groups with lesion lengths >180mm. Across these groups, a total of 227 subjects with mean lesion lengths of 28.7±7.1cm were analysed. Data showed a one-year patency rate of 89.1% by Kaplan Meier estimate at day 360, and a clinically-driven target revascularisation (CD-TLR) rate of 7.1%.
“Data from the IN.PACT Global Study demonstrate that the DCB is a safe and effective treatment option in real-world patients with lesions beyond 180mm, frequently comprised of in-stent restenosis and chronic total occlusions,” said Daniel Clair, chair of the Department of Surgery for University of South Carolina (USC) and the Palmetto Health-USC Medical Group. “More specifically, these results show maintenance of strong clinical outcomes, including a high primary patency rate and limited need for reintervention in patients exhibiting these complex, long lesions—among the most prevalent cases we see. The FDA’s approval of this expanded indication now offers US physicians a clinically-proven endovascular therapy to address this critical patient need.”
Complex lesions, including those over 150mm, remain a significant treatment challenge for physicians.
“In conversations with physicians, a key clinical challenge raised is the ability to provide a sustainable treatment option for longer length, complex lesions. With this approval, IN.PACT Admiral is now indicated to treat the longest lesions of any commercially-available DCB or peripheral stent in the US, providing physicians with additional confidence in using this DCB as part of their treatment algorithm,” said Mark Pacyna, vice president and general manager of the Peripheral business, which is part of the Aortic & Peripheral Vascular division at Medtronic. “In partnership with the clinical community, we look forward to continued collaboration as we work to address additional treatment challenges in PAD with this device.”
The BATTLE trial comparing a drug-eluting stent (Zilver PTX, Cook Medical) vs. a bare metal stent (Misago, Terumo) for the treatment of intermediate femoropopliteal lesions has failed to the show superiority of the paclitaxel-coated stent at one-year follow-up. The trial highlights a need for further direct comparative data between devices and strategies for treatment of femoropopliteal lesions.
The data were presented for the first time by Yann Gouëffic (Nantes, France) at the Charing Cross Symposium (CX; 24-27 April, London, UK). BATTLE is a French multicentre randomised clinical trial that included 181 patients who were randomised 1:1 into the Zilver PTX drug-eluting stent and Misago bare metal stent arms (n=85 vs. n=86, respectively). Included patients were classed as Rutherford 2–5, with de novo atherosclerotic femoropopliteal lesions of 2–14cm and a reference vessel diameter of 4–7mm.
There are currently several different options for treating TASC A and B lesions, Gouëffic said, including bare metal stents, drug-eluting stent, drug-coated balloons and covered stents. However, few head-to-head randomised trials have been completed so far to compare the safety and efficacy of devices for femoropopliteal lesion treatment.
Data from the Zilver PTX randomised controlled trial indicated that the paclitaxel-coated Zilver PTX fared better compared to a bare metal stent. This comparative data from a second arm of randomization of Zilver PTX trial, Gouëffic explained, led to the hypothesis that Zilver PTX would prove superior to the bare metal Misago stent and subsequently the BATTLE trial was designed as a superiority trial, rather than non-inferiority.
The patient population at baseline showed similar mean lesion lengths and reference vessel diameters, with intermittent claudication present in 79% of patients in the Zilver PTX arm and 82% in the Misago arm. Technical success was 100% in both arms.
At 12 months the primary endpoint—freedom from in-stent restenosis—90.3% in the paclitaxel-eluting stent arm and 85.7% in the bare metal stent arm (p=0.36). The primary endpoint was defined as restenosis of >50%, as well as a peak systolic velocity index of >2.4 at the target lesion.
The trial did show a significant benefit for the paclitaxel-eluting stent with regard to secondary endpoints either. Patency rate was 84.2% vs. 81.6% (p=0.41) for Zilver PTX and Misago, respectively; target extremity revascularisation was 4.9% vs. 3.8% (p=0.52) and notably, target-lesion revascularisation was 8.8% vs. 8.9% (p=0.91), respectively, at 12 months. No difference was seen between the treatment arms in Rutherford stage at baseline or at 12 months. Finally, there was an 88.6% clinical improvement in the Zilver PTX arm vs. 85.3% in the bare-metal stent arm (p=0.56).
Due to the design of the study, Gouëffic explains, they were not able to look at non-inferiority of the Misago stent, as opposed to superiority of the Zilver PTX. “This conclusion is not for all drug-eluting stents,” Gouëffic pointed out, as future generation devices may cause the field to change. “Advantages of drug-eluting therapy in comparison to bare metal stents are still required, to define the strategy for the treatment of intermediate length femoropopliteal lesions,” Gouëffic concluded.
In an exciting session at the Charing Cross Symposium (CX; 24-27 April, London, UK), the audience witnessed the demonstration of a novel treatment strategy with intravascular lithotripsy for calcified arterial stenosis. It will now become a CX tradition to feature live cases to showcase what has been discussed in the presentations, so that the audience can observe the evidence given in practice.
Giving some background to the concept of intravascular lithotripsy, Andrew Holden, Auckland, New Zealand, who performed the first-in-human intravascular lithotripsy procedure, explained, “the basic concept is to create apposition of the angioplasty balloon to the vessel wall at very low pressure to perform lithotripsy, to create microfragmentation of the calcium in both the medial and intimal layers, change the compliance of the artery and then allow the balloon to dilate out to nominal diameter at low pressure and hopefully, with a low instance of residual stenosis or dissection.”
The live case was broadcast from Bad Krozingen, Germany, with operator Thomas Zeller.
The patient was an 84-year-old female with Rutherford stage 3 claudication, with a history of coronary vessel disease and internal carotid artery stenosis. Previously, the patient had an occlusion of the right superficial femoral artery, extending into the popliteal artery, with significant calcification that was treated with lithotripsy and drug-coated balloon angioplasty, after which she had been pain free on her right leg.
In the procedure broadcast at CX, Zeller used lithotripsy to prepare the vessel in the patient’s left leg for drug-coated balloon angioplasty using the protocol from the DISRUPT III randomised controlled trial which is comparing lithotripsy plus drug-coated balloon to drug-coated balloon as standalone therapy.
Providing some tips based on his experience with the lithotripsy device, Zeller placed a lot of importance on the preparation of the catheter. “In every balloon there is still some air trapped and it is important to evacuate the air from the folded balloon before you inflate it and before you try to apply the sonic pressure waves because if there is still air trapped in the balloon, the pressure waves will not be transmitted to the vessel wall,” he said.
Further, pulling from lessons learned in the DISRUPT I and DISRUPT II trials, Zeller advised that the balloon should be slightly oversized in order to improve acute outcomes. “Undersizing leads to inferior outcomes acutely and also in the longer term. Similarly, increasing the dose, i.e. doing more lithotripsy cycles in the same position, does improve the overall outcome of the lithotripsy procedure.”
Describing how the device is used by the operator during the procedure, he explained, “the device has seven markers in total. The markers at the edges represent the proximal and distal balloon shoulders and the five markers in-between are the emitters. It is important to position the emitters in the lesion area and the balloon marker can be outside.”
Watching the case, Holden commented that the lithotripsy is a dose that is delivered to refractory stenoses to try to improve the acute outcome—Zeller then added, “the specific feature of lithotripsy is that you disrupt medial calcification.”
As for his strategy following intravascular lithotripsy, Zeller reported that at his centre, it is followed up with a drug-coated balloon. “That is our general strategy, because, based on what we learned from the pilot study, lithotripsy is a very good tool for achieving good acute outcomes, but in the long-term we still see restenosis development. This leads me to believe the combination of vessel preparation with lithotripsy followed by drug-coated balloon angioplasty is a logical approach to treat these lesions. DISRUPT III will prove whether it is true or not,” Zeller stated.
Polling following the live case showed that 50% of the CX 2018 audience believes that calcified tibial vessels are best managed with a drug-coated balloon following vessel preparation during endovascular procedures. Further, 69% of the CX 2018 audience would not use a drug-coated balloon for a heavily calcified lesion without vessel preparation.
A focus on calcification
Broadening the discussion on calcification, Arne Schwindt, Münster, Germany, weighed in with his personal experience, adding, “lesions that are unresponsive to stenting and high pressure ballooning could be treated. We have seen acceptable clinical and angiographic outcome in rock-like calcified common femoral arteries. Early experience shows promising results of intravascular lithotripsy in highly calcified small mesenteric and celiac branches, and has the potential to make EVAR/TEVAR/TAVI feasible in patients with poor iliac access.”
In her assessment, Renu Virmani, Gaithersburg, USA, called for a “dedicated device for calcified lesions that either cracks or removes calcified areas in order to achieve adequate vessel expansion. Probably, such lesions need drug-eluting stents rather than drug-coated balloons.”
In the end, Fabrizio Fanelli, Florence, Italy, concluded that calcium significantly increases procedural complications and that most studies have excluded severely calcified lesions from endovascular treatments. He said that acute and long-term endovascular outcomes are inferior when severe calcium is present, and that it represents a great limitation of superficial femoral artery procedures due to vessel recoil after balloon dilatation, flow-limiting dissection related to high pressure use and a higher stent implantation rate. “Multiple technologies are available nowadays but ‘the ideal’ is not available yet. Atherectomy devices increase the luminal gain and may also improve drug uptake. Further, vessel preparation with plaque scoring and lithotripsy do not debulk calcium, but are able to increase vessel permeability, drug absorption, and patency rate.”
Stroke is a major concern following TEVAR (thoracic endovascular aortic repair) and Charing Cross delegates heard the results from a collaborative study that pooled practice data from a number of high-volume centres in order to benefit patients undergoing the procedure. A highlight of the session was the transmission of a live complex aortic case from Hamburg, Germany, that illustrated the key learning points from the session. The case was a live endovascular arch reconstruction by Nikos Tsilimparis on a patient with thrombus on the arch.
The STEP (Stroke from Thoracic Endovascular Procedures) study was presented by the STEP investigators Roger Greenhalgh (London, UK), Stéphan Haulon (Le Plessis Robinson, France), Tilo Kölbel (Hamburg, Germany) and Fiona Rohlffs (Hamburg, Germany).
Advisors to the STEP study are Hugh Markus, a neurologist, Simon Redwood, an interventional cardiologist, Heinz Jakob, a cardiothoracic surgeon, and Kyriakos Lobotesis, a neuroradiologist.
“The purpose of this is to share the experience this group is producing. This experience includes over 800 procedures per year broken down into the various zones, and that data is a powerful tool. We also have the facts illustrated by a live procedure that is taking place alongside,” Greenhalgh said.
The STEP study aims to provide best practice for endovascular procedures for the ascending aorta, aortic arch, great vessel branches and high TEVAR to lower the risk of cerebral embolism. It is an independent, all-encompassing, open, interdisciplinary group built to learn from each other and to make TEVAR safer for patients. The STEP collaborators include Frank Arko, Carlos Bechara, Adam Beck, Dittmar Böckler, Matthew Eagleton, Dennis Gable, Stéphan Haulon, William Jordan, Tilo Kölbel, Gustavo Oderich, Jean Panneton, Geert Schurink, Santi Trimarchi, Marwan Youssef and the physicians who were all nominated by the manufacturers of the devices used in the procedure including Martin Czerny, Michael Dake, Ahmed Koshty and Rodney White.
The manufacturers of devices used by the 18 operators were Cook Medical; Gore; Bolton Medical, now Terumo Aortic; Jotec and Medtronic. The STEP study did not seek to compare outcomes based on the device used.
Rohlffs, noting that air, thrombus, particles or plaque can cause emboli during TEVAR, further explained that there was a STEP questionnaire sent out to gather data on experience and current practice. The questions were formulated before the data was collected. “With regard to the experience of the 18 physicians who were surveyed, all key opinion leaders operate on each zone and the survey group has a cumulative 143 years of experience in Zone 0 interventions; 193 years in Zone 1 and 232 years in Zone 2,” Rohlffs said.
STEP results
Illuminating data on the number of procedures performed within each zone per year revealed that there were 171 procedures performed in Zone 0 (21%); there were 135 procedures performed in Zone 1 (17%) and 510 procedures performed in Zone 2 (62%).
Other key findings include data from the preprocedural, intraprocedural and postprocedural phases of TEVAR.
Preprocedural results
Preprocedural findings showed there was 100% consensus that an interdisciplinary team is central to the final decision for treatment strategy in Zone 0. In Zone 1 and Zone 2, this was seen as less necessary.
The physicians unanimously responded “yes” to the question: Do you apply endovascular techniques in urgent or emergency cases? This established that the endovascular approach is undoubtedly utilised among those surveyed in this setting.
There was also 100% consensus to the question of which imaging technique was preferred to visualise the pathology, with all physicians revealing that they preferred CT angiography over MR angiography.
However, there was less consensus on how long before the procedure the imaging could be performed.
Intraprocedural data
With regard to intraprocedural data, there was consensus about anticoagulation and that the procedure should be done under antiplatelet therapy and that the activated clotting time should be above 250 seconds.
There was no consensus on revascularisation of the left subclavian artery, which was either done routinely or selectively and in terms of timing, sometimes in advance, simultaneously or on a case-by-case basis. There was 100% consensus on the use of cardiac output reduction in Zone 0, with less consensus in the other zones. There was no consensus on the technique of cardiac output reduction or embolisation prevention strategies with some physicians using carotid clamping, others using the CO2 flushing technique or minimising arch and device manipulation. There did not seem to be a role for filters here. There was no consensus on adjunctive techniques.
Post-procedural findings
All operators favoured CT angiography to visualise the stent graft at follow-up, but there was no consensus on the timing of the imaging. Again, there was consensus on antiplatelet therapy and postprocedural intensive care unit stay for the Zone 0 patients, but no consensus on the others.
There was no consensus on embolisation prevention techniques with some respondents using carotid artery clamping; others using a CO2 flushing technique and some respondents using other techniques, such as minimising archwire and device manipulation, and pacing.
Simon Redwood, King’s College London, spoke on the topic of reducing cerebral embolisation with transcatheter aortic valve implantation (TAVI) to note that stroke remains an issue and that it is under-reported. “The risk of stroke is up to 4–5% in trials at 30 days. Trials only report major disabling strokes, yet minor strokes or transient ischaemic attack have a two to four increase in mortality. Stroke risk is independent of operator experience and using diffusion-weighted MRI, 68–99% of patients show evidence of embolisation,” Redwood explained. With regard to the timing, stroke is a procedural issue and usually occurs within 72 hours of undergoing the procedure, he said.
Alan Lumsden (Houston, USA) presented useful data on transcranial Doppler being a useful technique for monitoring arch interventions. Transcranial Doppler is a non-invasive technique that uses a pulsed Doppler transducer for assessment of intracerebral blood flow. Cerebral emboli can be recognised by “high-intensity transient signals” (HITS). “Real-time middle cerebral artery monitoring is the gold standard as it relates immediately to intervention. It can be used for troubleshooting established and developing procedures and identifies high-risk manoeuvres,” he said.
Markus made the point that stroke is clinically relevant and it is what matters to the patient. It requires large numbers in studies as there are few endpoints. Surrogate endpoints such as brain imaging, imaging of emboli and cognition is often what counts, he noted.
Operative risk of stroke and death in endarterectomy studies is assessed differently depending on the specialty of the assessor, whether the assessor was the study author or whether it is a surgeon. This was one of the key messages that came out from Markus’ presentation that outcomes need to be assessed independently.
Markus further commented that transcranial Doppler cannot reliably distinguish solid from air emboli—and that the two types of emboli have very different consequences. “Transcranial Doppler emboli detection needs to be used with caution intra-operatively; post-procedure emboli are likely to be solid emboli. It provides additional information on cerebral blood flow,” said Markus.
Rohlffs had spoken earlier in the session on how systematic exclusion of air from unpacking to deployment avoids air embolism, explaining that the amount of air released by stent grafts can by minimised in several ways. Firstly, Rohlffs pointed to the way in which the amount of air released can be influenced by the ‘flushing technique’. Secondly, she observed that the construction of the stent graft system can influence the amount of air released during the procedure. Rohlffs maintained that synergistic effects of different approaches to reduce air release can be used, and concluded that “the amount of released air can be minimised.”
Haulon said that the STEP study has shed light on modern practice in the selected high-volume centres and that the group had learned from each other and were now ready to sit around the table to decide how they should perform these complex procedures. “We have learned about how we should design future studies and monitor results to find out what can be changed to reduce the stroke risk following complex TEVAR,” he said. Kölbel closed the session by saying this was an area in which there was a need for logical outcome measures, as very rough outcome measures had been used so far. “Additionally, it is vital to have independent measurement of outcomes as this has been shown to have a bearing on the data. There may also be some old dogmas to kill and I look forward to further collaboration,” he told delegates.
“We have worked out some of the questions we want to see answered and advances have been made in the areas of obvious consensus. The key next steps will be designing future studies that need to be carried out in order to benefit this group of patients who are inherently at risk of stroke after TEVAR,” Greenhlagh concluded.
Francesco Carnevale (São Paulo, Brazil) speaks on the growing acceptance for prostatic artery embolization. The national regulatory bodies in Brazil and the UK recommending the procedure are “a huge development in the field of embolization”, he tells Interventional News at the GEST 2018 US meeting in Miami, USA.
Embozene microspheres are precisely calibrated microspheres engineered for greater embolization control. Unique colored sizing allows for improved visualization during suspension.
The National Institute for Health and Care Excellence (NICE), which provides national guidance and advice to improve health and social care, has decided that the currentevidence on the safety and efficacy of prostate artery embolization for benign prostatic hyperplasia is adequate to support the use of this procedure on the National Health Service (NHS).
Prostate artery embolization can serve as a bridge between medical therapy and surgery, say experts on the topic. The procedure is a minimally invasive alternative to transurethral resection of prostate (TURP) or laser prostatectomy.
NICE first looked at prostate artery embolization in 2013, but felt that more research was required to determine whether the procedure was effective and safe. Since 2013, NICE has worked with the British Society of Interventional Radiology (BSIR) and the British Association of Urological Surgeons (BAUS) to coordinate the UK ROPE study. The study compared embolization to conventional prostate surgery. It found embolization provided a clinically and statistically significant improvement in symptoms and quality of life for men with enlarged prostate.
In light of this study and other new evidence, NICE has updated its guidance. It now says embolization can be offered to patients. The procedure should be carried out by an interventional radiologist with specific training and expertise.
Nigel Hacking, consultant interventional radiologist at University Hospital Southampton, UK, said: “The UK-ROPE project has taken several years and required extra training of professionals working in 18 centres across England and Scotland.”
The updated NICE guidance notes that patient selection should be done by a urologist and an interventional radiologist and that embolization is a “technically demanding procedure [that] should only be done by an interventional radiologist with specific training and expertise in prostatic artery embolization.”
The potential benefits of prostate artery embolization compared with surgery include fewer complications, avoiding a general anaesthetic and that it may be done as a day case procedure.
The BSIR has issued a press release on NICE’s decision stating that the recommendation from NICE could revolutionise the way men are treated.
“Traditional surgical options for this condition can have significant complications, including surgical bleeding and retrograde ejaculation, which can have upsetting effects on men. Prostate artery embolization, the new alternative, as shown in the UK-ROPE registry headed up by Nigel Hacking, can now be offered to men in the UK as an alternative treatment for men who would prefer to avoid surgical options,” the release states.
The BSIR release further adds:
“This is a significant development for men with moderate to severe lower urinary tract symptoms from their enlarged prostate glands. The new guidelines published on 25 April 2018, approved embolization under ‘Standard’ conditions meaning that this treatment could now become a real treatment option for men in the UK.
“Men will still need to be seen by an urologist to exclude cancer and other causes for their symptoms and working as a close knit team they will then liaise with their interventional radiology colleagues to choose the most suitable candidates for this treatment. Embolization is not going to replace TURP, but it will provide a bridge between medication, once this is ineffective or causing side-effects, and surgery. In some men it will provide a definitive solution, but in others there may still be a need for surgical options, including some less invasive procedures such as the Urolift procedure. Tailoring a patient’s needs to their treatment rather than offering a one-size-fits-all policy is a major advance.”
“An enlarged prostate can have a severe impact on the lives of those living with it and complications related to treatment can effect men for the rest of their lives. It is important patients receive all the treatment options and not just conventional surgery. The BSIR, working closely with BAUS and NICE, are very pleased to promote access to this new option,” said Trevor Cleveland, president of the BSIR.
A novel technique that delivers high doses of radiation to tumours while sparing the surrounding normal tissue shows promise as a curative treatment option for patients with early-stage liver cancer, according to a study published online in the journal Radiology.
Curative treatment options for early-stage hepatocellular carcinoma (HCC), the most common type of liver cancer, include surgery, liver transplantation and radiofrequency ablation. However, many patients are not candidates for these therapies due to the presence of other conditions. In addition, these treatments carry significant costs and potential complications.
Radiation segmentectomy is a minimally invasive option that uses the radioisotope yttrium-90 (Y90) to destroy tumours. The procedure’s name derives from the fact that surgeons divide the liver into a number of segments. Using cone beam CT, interventional radiologists gain a detailed view of the complex liver vasculature and can focus delivery of the Y90 to the relevant segment.
“Cone beam CT has revolutionised our ability to perform segmental injections isolated to very small tumours, sparing the majority of normal tissue,” said study senior author Riad Salem, chief of Vascular Interventional Radiology in the Department of Radiology at the Northwestern University Feinberg School of Medicine in Chicago. “Before cone beam CT, we had the ability to focus radiation, but not with this level of accuracy.”
Salem and colleagues studied long-term outcomes in 70 early-stage HCC patients who had undergone radiation segmentectomy between 2003 and 2016. They analysed the patients’ responses to treatment based on two commonly used sets of criteria.
Based on one criteria, 90% of patients showed positive response to the therapy, of which 59% showed complete response. Based on a second criteria, 71% achieved positive response, of which 16% achieved complete response.
Radiation segmentectomy controlled the target tumour, slowed the time to disease progression and improved survival outcomes at rates comparable to radiofrequency ablation, surgery and transplantation for early-stage HCC patients.
Almost three-quarters of patients had no progression of cancer in the target tumour five years after treatment. Median overall survival was 6.7 years, and one-, three-, and five-year survival probabilities were 98%, 66% and 57%, respectively. One-, three-, and five-year overall survival probability was 100%, 82% and 75% in patients with a baseline tumour size of 3cm or less.
“The results show that we are able to impart curative outcomes to these patients,” Salem said. “Our numbers with radiation segmentectomy match, or outperform those of other curative treatments in terms of tumour control, survival rate and recurrence.”
Radiation segmentectomy is performed on an outpatient basis, is minimally invasive and has a low toxicity profile, Salem said. Given the potency of the radiation, it outperforms transarterial chemoembolization, another minimally invasive procedure in which cancer-killing drugs are injected into the liver’s main artery under imaging guidance and travel to the tumour microvasculature. Transarterial chemoembolization has the additional disadvantage of requiring hospitalisation.
The researchers continue to follow the patients from the study group as they work on ways to optimise the treatment.
“We want to see these outcomes validated in patients over the longer term,” Salem said. “We also want to minimise the time from clinic visit to treatment, and fine-tune dosimetry so that we can find the optimal dose that will kill the tumour. In the right patient setting, radiation segmentectomy can be considered curative.”
The first full results of the Early Venous Reflux Ablation (EVRA) ulcer study were presented at the Charing Cross Symposium (24–27 April, London, UK). The presentation was accompanied by simultaneous publication in the New England Journal of Medicine after the session.
The randomised trial revealed that early endovenous ablation outperforms deferred treatment in healing leg ulcers. It shows early ablation of superficial venous reflux results in faster healing of venous leg ulcers and patients having much more time free from ulcers than deferred ablation does. Early treatment is also cost-effective, which means that the findings of this trial, which provide the first high-quality data backing early ablation, will have global implications for clinical practice and patient care pathways. Nearly 90% of the CX voters agreed with the motion that the EVRA trial will change clinical practice.
“This presentation continues the great tradition of trials to come out from Imperial College at the Charing Cross Symposium,” said chief investigator of the trial, Alun Davies, Imperial College London, UK, who presented the clinical results along with the team at the Late breaking trials sessions yesterday. The EVRA ulcer study was funded by the National Institute for Health Research Health Technology Assessment Programme.
The ESCHAR trial previously showed that surgical correction of superficial venous reflux in addition to compression bandaging does not improve ulcer healing but reduces the recurrence of ulcers at four years and results in a greater proportion of ulcer free time. While compression bandaging is the mainstay of leg ulcer treatment, early intervention has long been taboo in certain circles. EVRA was designed to capture data on the timing of intervention.
EVRA set out to evaluate whether early endovenous ablation can improve venous ulcer healing in addition to compression therapy. The triallists included Manj Gohel (Cambridge, UK), who reported the rationale and study methods; Francine Heatley (London, UK) who provided data on the recruitment and demographics; and David Epstein (Granada, Spain) who reported on the health economics analysis of the trial.
The investigators reported in NEJM that venous disease is the most common cause of leg ulceration. “Although compression therapy improves venous ulcer healing, it does not treat the underlying causes of venous hypertension. Treatment of superficial venous reflux has been shown to reduce the rate of ulcer recurrence, but the effect of early endovenous ablation of superficial venous reflux on healing remains unclear,” they write.
“The usual journey for a patient who presents with a leg ulcer is that they may be seen in primary care, or a wound health care centre. Often, they do not get referred on to a vascular specialist for evaluation to see if their veins can be treated. One of the mainstays of treatment is just use of compression therapy,” Davies noted.
Investigators working in 20 centres in the UK randomly assigned 450 patients with venous leg ulcers and superficial venous reflux to either an ‘early’ group that received compression therapy (with stockings or bandages) followed by endovenous ablation within two weeks (224) patients), or a ‘deferred’ group that received compression therapy followed by deferred ablation i.e. after the leg ulcer had healed, “which often in the UK is regarded as standard practice,” said Davies. The latter group consisted of 226 patients. Of these, 31 patients were lost to follow-up, or withdrew and 12 died leaving 387 patients in the per protocol analysis.
The primary outcome measure was the time to ulcer healing from the date of randomisation. The secondary outcome measures were the rate of ulcer healing at 24 weeks; the length of time free from ulcers (ulcer-free time) during the first year after randomisation; and patient-reported health-related quality of life as measured by Venous Clinical Severity Score (VCSS), Quality of life (AVVQ, EQ-5D-5L, SF36) and cost-effectiveness.
In the trial, treatment modality and strategy was determined by the treating clinical team. Endovenous ablation included the use of foam, endothermal ablation and non-thermal techniques. “The outcomes of all modalities are good, and we are not going to break down the data by technique,” Davies commented.
With a sample size of 450 patients (or 254 leg ulcer healing events), the study was powered to detect 15% difference in 24-week healing rate (60% vs.75%) with 90% power and 5% significance.
Results
Patient and clinical characteristics at baseline were similar in the two treatment groups. The time to ulcer healing was shorter in the early intervention group than in the deferred intervention group; more patients had healed ulcers with early intervention (hazard ratio for ulcer healing, 1.38; 95% confidence interval, 1.13 to 1.168; p=0.001). The median time to ulcer healing was 56 days (95% CI, 49 to 66) in the early intervention group and 82 days (95% CI, 69 to 92) in the deferred-intervention group. The hazard ratio for ulcer free time in the early group was 1.54 (95% CI, 1.07–2.21) p=0.02. At both six weeks and six months, the group that received early intervention had significantly better quality of life scores. With regard to procedure complications, there were more instances of deep vein thrombosis in the group receiving early intervention, than in the group receiving delayed intervention.
“EVRA is the first large randomised trial to confirm that early endovenous ablation accelerates ulcer heaIing. In the UK, and worldwide, it is important to look at whether a treatment is cost-effective. We found the pathway of early intervention was undoubtedly cost-effective. The results revealed an 86–99% probability that early intervention is cost-effective at the UK National Institute for Health and Care Excellence (NICE) threshold,” explained Davies.
Ramifications
“These data highlight the need for a major review of leg ulcer care pathways worldwide so that we can implement a strategy for rapid assessment and ablation of superficial venous reflux for patients with venous leg ulcers. Education of patients, nursing teams, healthcare professionals and commissioners is essential,” Davies stated at the first CX Press Conference.
At the Charing Cross Symposium, Raghu Kolluri, Columbus, USA, commented on the ramifications of the trial to say: “EVRA showed faster ulcer healing, more ulcer free days and cost savings. Several recommendations such as the current Society for Vascular Surgery (SVS)/American Venous Forum (AVF) guidelines are based on evidence at the level of 2C, and we hope that this will change to incorporate EVRA into the treatment algorithm. It is also important to educate all involved in venous leg ulcer care.”
Davies reiterated the point, “We will undoubtedly need to see a rewrite of many of the international the global guidelines but one of the key things is to empower the nurses and people with leg ulcers to actually seek referral to a vascular specialist and to persuade the insurers globally, and commissioners in the UK i.e., those who monitor and dispense healthcare budget that endovenous ablation is a very cost-effective way to treat patients. In the UK, we hope to see patients, rather than languishing in the community, being referred for very early evaluation and early intervention. As you can see from the data, we were unable to randomise over a third of patients because they had their leg ulcer present for more than six months, and there is a large group of people who have chronic leg ulcers who never really get assessed for intervention. Education of patients and those with first contact with patients for referral to a specialist who can carry out the appropriate evaluation and treatment is vital.”
Guerbet has announced that it has signed an agreement to acquire a laboratory-stage technology developed by Occlugel, a French company specialised in the research and development of microspheres used in embolization.
This acquisition is line with the GEAR 2023 strategic plan, and is one of two acquisitions planned by the end of this financial year.
“We are very pleased to integrate this new microsphere technology into our Interventional Imaging research and development programme”, said Claire Corot, Research, Innovation & Business Development vice president.
Under the terms of the agreement and in exchange for the acquisition of this technology, Guerbet has made an initial payment of €3 million, with additional payments conditional on completing the technology transfer and achieving regulatory objectives.
A complementary technology to interventional imaging
The technology will be used in several ranges of microspheres for vascular embolization of benign tumours, for example uterine fibroma and prostate adenoma, and for vascular chemoembolization of malignant tumours, including in some liver, lung and kidney cancers.
This technology will complete the existing range of Guerbet’s Interventional Imaging solutions, and above all create strong synergies with the Accurate range of antireflux microcatheters, acquired recently by Guerbet.
Vascutek and Bolton Medical, subsidiaries of Terumo Corporation of Japan, have combined into a single, integrated business, Terumo Aortic, which is looking to grow its presence in the global aortic and vascular implants market. Terumo acquired Vascutek in 2002 and Bolton Medical in 2017.
As a combined business, Terumo Aortic aims to become recognised for its focus on individualised treatments that offer clinicians more options than ever before.
Terumo Aortic will have a combined revenue of nearly US$200m and over 1,100 employees worldwide. Its primary research and manufacturing facilities will remain in Glasgow, Scotland and Sunrise, Florida.
The combined offering includes advanced technologies such as surgical grafts for abdominal, cardiothoracic and peripheral applications as well as hybrid and catheter-based stent graft systems for abdominal and thoracic aortic aneurysms. These implants have already helped to save, or improve, the lives of over two million patients in over 100 countries worldwide.
Vascutek and Bolton Medical have been working to consolidate and streamline their complementary offerings for the past year. Significant focus has been placed on creating an integrated research and innovation strategy that will push the boundaries of the aortic and vascular implants market.
Paul Holbrook, president of Terumo Aortic, said: “This coming together of two organisations with highly advanced technologies will be transformative for physicians and the patients they serve.”
“We have woven together the products, services and expertise offered by our teams in Europe and the USA, enabling clinicians to meet the unique needs of their patients and redefine the treatment of aortic disease.”
Forge Medical, a US developer of solutions for transradial and transpedal haemostasis and manufacturer of the VasoStat haemostasis device, announced today that the company has entered into a commercialisation agreement with Lokai Medical.
Lokai Medical, based in Phoenix, USA, is a specialty distributor of coronary/cardiovascular and interventional devices throughout the USA.
Timothy Clark, CEO of Forge Medical, said: “Transradial and transpedal approaches are becoming increasingly adopted by interventional cardiologists, interventional radiologists and vascular surgeons. These clinicians demand an effective solution for puncture site management with rapid and patent haemostasis and optimal patient comfort. We are pleased to partner with the talented team at Lokai Medical to provide this unique and innovative haemostasis device to ever growing numbers of US clinicians and hospitals.”
The questions of if, how and when to combine interventional oncological procedures with systemic immunotherapy are on the tip of everyone’s tongue, from multidisciplinary tumour boards to industry executive boardrooms, writes Ryan Hickey, New York, USA.
Immunotherapy has transformed the landscape of cancer care in the last several years. It has not only introduced an entire new class of anti-cancer agents into the treatment paradigms of nearly every cancer, it has also led to an entirely new understanding of the interplay between our immune systems and cancers. As testament to the excitement behind this new mode of cancer treatment, the US Food and Drug Administration has been approving the use of immunotherapeutic agents at an unprecedented rate, in certain circumstance even lowering the threshold for the level of evidence traditionally required to gain approval.
As my co-authors and I discussed in a recent article published in Journal of Vascular and Interventional Radiology (JVIR), the molecular biology driving the efficacy of immunotherapeutic agents, particularly the immune checkpoint inhibitors, suggests that interventional oncologic procedures could offer tremendous potential for synergy with these immunotherapeutic agents.
Immune checkpoint inhibitors, such as the anti-CTLA-4 antibody ipilimumab and the series of antibodies against the PD-1 receptor or its ligands, including pembrolizumab, nivolumab and atezolimumab, function by blocking the “off-switch” of cytotoxic and regulatory immune cells, in a sense “re-activating” the immune system against cancer cells.
The combination of an inflammatory response and tumour antigen exposure results in proliferation of tumour-specific cytotoxic T cells, yet any significant antitumour response is typically impeded by activation of these “off-switches,” either by the tumour cells themselves, or the tissue immediately surrounding the tumour cells (tumour microenvironment). By combining the inflammatory response and antigenic exposure inherent to interventional oncology procedures with a blockade of these immune system “off-switches,” the science suggests that we could achieve far greater results than we might achieve with either modality alone.
Furthermore, as we learn more about the relationship between cancer cells and the cytotoxic and regulatory components of the immune system, we are discovering that our local therapies have important, and possibly detrimental, systemic effects. For example, percutaneous ablation has been shown to change the expression of these very same “off-switches,” not only on lymphocytes, but also on tumour and tumour microenvironment cells far from the site of ablation. An increase in certain circulating cytokines and growth factors has been implicated as a factor in the changing phenotype of these remote cells. Interestingly—and concerning—many of these same cytokines and growth factors are upregulated as a result of transarterial embolotherapies as well.
Radiation is a potent initiator of an immune response, although mechanistically in a different manner than seen with the immediate necrosis effects of percutaneous ablation and hypoxia inducing transarterial embolotherapies. The combination of external beam radiotherapy with immune checkpoint inhibitors has already been shown to provide synergistic effects on certain cancers, such as prostate cancer and melanoma. What effect, therefore, might the brachytherapeutic mechanism of radioembolization have when combined with systemic immunotherapy?
The questions of if, how and when to combine interventional oncologic procedures with systemic immunotherapy are on the tip of everyone’s tongue, from multidisciplinary tumour boards to industry executive boardrooms. There has arguably been no greater opportunity for interventional radiologists to cement interventional oncology as a central pillar of cancer care. We must rise to the challenge, drive the investigation of these questions and own the synergistic treatments that result.
Ryan Hickey is director, Interventional Oncology and Transplant Interventions, NYU Langone Health, New York, USA. He has reported no disclosures pertaining to this article.
File photo of Medtronic’s Solitaire revascularisation device.
Should interventional radiologists up-skill to perform emergency stroke thrombectomy and help deliver stroke services? And if they did, would the increase in the number of physicians who can offer thrombectomy be essential in delivering a round-the-clock, modern stroke intervention programme? A consensus on the rigorous training needed for timely salvage of compromised brain tissue still remains an important, thorny, and politically charged issue. Interventional News finds out more…
“Interventional radiologists have the training to properly select patients for endovascular stroke treatment, the technical skills to perform intra-arterial stroke interventions, and the clinical knowledge to manage these patients. Since they have this intensive training in the clinical management of patients, image-guided endovascular procedures, and the ability to work as part of structured, multispecialty care teams, they provide excellent care to patients with acute ischaemic stroke, with good patient outcomes,” Martin Radvany, chief, Interventional Neuroradiology, University of Arkansas for Medical Sciences, Little Rock, USA, told Interventional News.
Radvany, who is a coordinator of the Society of Interventional Radiology (SIR) Stroke Course, and many other physicians, believe that more interventional radiologists should become part of comprehensive stroke teams. “Rapid access to stroke centres that offer thrombectomy saves lives and reduces disability after stroke, but many hospitals do not have this important capability due to a need for appropriately trained specialists. Time is of the essence in caring for stroke patients, so if more hospitals can be properly staffed, we can avoid transferring patients and delaying treatment. This will save lives and prevent long-term disability. Interventional radiologists are already present in most community hospitals and are currently providing care for stroke patients at some hospitals, either where neurointerventional physicians are not available, or where they have partnered with neurointerventional physicians to provide 24/7 coverage. We need to support these existing programmes and encourage establishment of new ones,” he says.
There is, however, the matter of additional training. “Interventional radiologists can help provide endovascular thrombectomy locally and 24/7, but require additional training to do so. SIR is currently revising its stroke training guidelines. Interventional radiologists need to be expert in patient selection and endovascular treatment, and must track outcomes to be certain that care meets national and international benchmarks,” cautions David Sacks, an interventional radiologist at Tower Health System in West Reading, USA. Sacks is a past president of SIR and is current president of the Intersocietal Accreditation Commission (IAC) Carotid Stenting division.”
In the landscape of current stroke care, there are many recent developments that will have enduring effects on patient care. First, a major new recommendation from the most recent update to US ischaemic stroke guidelines released by the American Heart Association and American Stroke Association in February increases the time window for mechanical thrombectomy to be offered to 24 hours for selected acute ischaemic stroke patients. The new guideline, based on the most recent evidence available, recommends that large vessel strokes can safely be treated with mechanical thrombectomy up to 16 hours after a stroke, in selected patients. Further, under certain conditions and based on advanced brain imaging and key inclusion criteria, some patients may have up to 24 hours for treatment with mechanical thrombectomy, the guidelines state.
Martin Radvany
The previous time limit was six hours. It is widely believed that this new recommendation will likely result in more patients becoming eligible for thrombectomy since more patients will be treated based on clinical presentation rather than a time cut-off alone. Following from this, the US FDA has also expanded the treatment window for the use of clot retrieval devices in certain stroke patients.
But perhaps the most important development of all is that in 2018, large vessel embolectomy undeniably has the backing of the highest quality of evidence and represents the greatest advance in acute stroke management in a few decades. It is
recognised as a game-changer and is the new standard of care therapy for stroke patients. This has created a number of profound challenges internationally as politicians, hospital administrators, patient advocacy groups and stroke care providers are demanding that endovascular stroke treatment be incorporated into practice (effective at once), prompting careful national examinations of existing stroke services and analysis of how a comprehensive roll-out of stroke thrombectomy can be achieved.
Klaus Hausegger, head of Department of Diagnostic and Interventional Radiology, Klagenfurt State Hospital, Austria, and editor-in-chief of CardioVascular and Interventional Radiology (CVIR), comments: “Within a very short time mechanical thrombectomy has become the first-line treatment for patients with acute ischaemic stroke due to large vessel occlusion in the cerebral circulation. Very recently, two randomised trials (DAWN and DEFUSE 3 trials, both published in the New England Journal of Medicine in 2018) have shown that the time window can even be extended up to 24 hours, provided that the infarct size is still limited (as shown by multiparametric imaging) and patients have
a disproportionately high National Institutes of Health (NIH) stroke score. This means that even more stroke patients are
eligible for mechanical thrombectomy, and as a consequence, more dedicated interventionalists are required to provide
a full 24/7 service through the year. While interventional radiologists have the appropriate skills to contribute significantly to this service, those who are not experienced in neurovascular procedures should undergo rigorous training before they enter the field of endovascular stroke treatment. It is my sincere hope that a training programme specifically designed for interventional radiologists will be set up soon throughout Europe.”
Other countries, like Australia, are experiencing a similar demand for adequately trained practitioners. Gerard Goh, consultant interventional and diagnostic radiologist, The Alfred Hospital, acting head of Interventional Radiology and president of the Interventional Radiology Society of Australasia (IRSA) told Interventional News, “In addition to the several landmark papers that have demonstrated the significant benefits of stroke thrombectomy over conventional systemic anticoagulation in certain patients, advances in diagnostic imaging and the creation of dedicated stroke referral pathways are allowing patients to be rapidly assessed and referred for treatment within a time window where intervention can make a difference to outcomes. This has led to a surge in demand for adequately trained practitioners to perform stroke thombectomy.”
In January this year, there was new UK guidance released on training interventional radiologists to speed up the roll out of stroke thrombectomy services. A press release on the issue notes: “Emergency mechanical thrombectomy dramatically increases a stroke patient’s chance of a full recovery. The UK does not have enough skilled doctors to provide the procedure. NHS England plans to roll out the technique nationally, but will need at least another 50 extra specially trained radiologists.” The guidance was produced by The Royal College of Radiologists, the British Society of Interventional Radiology, the British Society of Neuroradiologists and the UK Neurointerventional Group.
The crux: “to combat a UK-wide shortage of interventional neuroradiologists—who normally perform stroke thrombectomy the umbrella group is encouraging hospitals to support existing
interventional radiologists to train in the new technique.”
Trevor Cleveland, president of the British Society of Interventional Radiology, said: “NHS England hopes that around 8,000 patients every year will be able to benefit from stroke thrombectomy, however, currently only a few hundred do so because we need more trained doctors. Training enough radiologists to carry out this specific life-changing technique will not happen overnight, however, we hope to encourage and support clinicians and hospitals to invest their time and expertise to make the promised roll out of stroke thrombectomy services a reality.”
Klaus Hausegger
However, the success of stroke thrombectomy is undeniably dependent on multiple factors, one of which is the training and expertise of the interventionalist delivering the care. And, the training required to perform stroke thrombectomy safely and expertly is one of the more controversial aspects of interventional radiologists performing this therapy.
Patrick A Brouwer, neurointerventionalist, Karolinska University Hospital, Stockholm, Sweden, general-secretary of the European Society for Minimally Invasive Neurological Therapy (ESMINT) and Board member of the World Federation of Interventional and Therapeutic Neuroradiology (WFITN) notes: “Anyone with proper training (as described in the consensus document of 12 international neurointerventional societies worldwide and published in three journals) is welcome to help out.”
The consensus document Brouwer points to is a paper published in October 2016 titled “Training guidelines for endovascular ischemic stroke intervention: an international multi-society consensus document”.
The purpose of the document is to “define what constitutes adequate training for physicians who can provide endovascular treatment for acute ischaemic stroke patients” note the authors and the paper sets out the training requirements, maintenance of physician qualifications and hospital requirement needed to offer this treatment. The paper summarises: “We believe that a neuroscience background, dedicated neurointerventional training, and stringent peer review and quality assurance processes are critical to ensuring the best possible patient outcomes. Well trained neurointerventionalists are a critical component of an organised and efficient team needed to deliver clinically effective mechanical thrombectomy for acute ischaemic stroke patients.”
Left: David Sacks; Middle: Gerad Goh; Right: Trevor Cleveland
Radvany notes: “As with any procedure, if the individuals performing the procedure are not appropriately trained there can be complications. Inadequate training would be a potential pitfall of interventional radiologists performing stroke intervention. The appropriate technical training can be ensured by integrating the training into the interventional radiology residency/fellowship pathway. SIR has created a course that provides the cognitive continuing medical education. Accredited training programmes would be expected to offer appropriate training and thus reduce the risk of harm to patients”.
While many interventional neuroradiologists do not support the idea of interventional radiologists being involved in the offering of stroke thrombectomy, there are several prominent interventional neuroradiologists, says Radvany, “such as Mary Lee Jensen (University of Virginia, Charlottesville) and Joan Wojack (Acadiana Radiology Group, Lafayette) as well neurosurgeon, Adnan Siddiqui (State University of New York at Buffalo), who support interventional radiologists participating in stroke care. I believe these leaders can help persuade the others,” he states.
Goh returns to the importance of training: “It is important that interventional radiologists who wish to provide stroke thrombectomy be sufficiently trained and skilled. They need to be aware that the techniques of stroke thrombectomy are different to peripheral thrombectomy, although this basic skill set provides a great foundation for interventional radiologists to up-skill. There are certain important technical aspects when working in the cerebral space that are similar, but also different to, carotid interventions. Many of the catheters, sheaths, wires and devices are different to those commonly used in the peripheral space.
“In addition, there are several other factors when treating patients with stroke that interventional radiologists need to be aware of and involved with. These include the diagnostic imaging aspects of stroke including CT perfusion imaging and MRI; establishing rapid and efficient stroke care pathways in conjunction with stroke physicians; and to be trained and skilled with the technical aspects of stroke thrombectomy. I would encourage all interventional radiologists who are interested in performing stroke thrombectomy to seek training and upskilling in collaboration with interventional neuroradiologists to help provide a comprehensive service to all patients,” he says.
Medtronic announced the US launch of OptiSphere embolization spheres, a resorbable embolic platform designed for embolization of hypervascular tumours.
OptiSphere offers patients an alternative treatment option, a resorbable embolic, with comparable results to a permanent embolic, a press release from Medtronic states.
Hypervascular tumours can present as malignant or benign and can be found in various anatomical structures. Physicians may choose to treat these tumours with various therapies including, but not limited to, embolization, microwave ablation, radiofrequency ablation, or cryoablation.
“Medtronic continues to seek opportunities to expand the therapies we offer to patients and the physicians who treat them. With increased and better quality of care, the cancer patient population is living longer with the disease and it is important that we continue to introduce therapies that help positively impact and improve their quality of life,” said Jeff Cambra, general manager of the Pain Therapies Interventional business, which is part of the Restorative Therapies Group at Medtronic. “We consider this launch to be a win for both sides of the healthcare pathway, as OptiSphere addresses patient concerns of having permanent implanted spheres left behind while enabling physicians to offer an innovative treatment option in their facilities.”
OptiSphere is manufactured for Medtronic by Vascular Solutions, a subsidiary of Teleflex. Medtronic continues to partner with the company to further innovate the technology. OptiSphere received US Food and Drug Administration (FDA) 510(k) clearance in April 2014.
“Teleflex is very pleased to have Medtronic as a strategic distribution partner for our novel platform of embolic spheres,” said Jake Isenburg, director of Scientific Affairs for Teleflex. “The development of unique resorbable implants, particularly in the field of embolization, has become one of our core technical competencies at Vascular Solutions and Teleflex. By combining this technical expertise with Medtronic’s focus in interventional oncology, Teleflex is excited to collaborate on providing an alternative solution to healthcare professionals who are seeking a resorbable embolization product.”
OptiSphere short-term spheres have shown long-term results and offer an alternative solution for treating hypervascular tumours. The resorbable microspheres begin to degrade starting at four weeks post-procedure with significant degradation noted at nine weeks.
The spherical shape of OptiSphere provides smooth embolic delivery and even, predictable distribution. The product line offers procedural flexibility with two volume options and five size ranges which may be combined in a single procedure as needed to achieve the desired occlusion.
The SORAMIC study, presented at The International Liver Congress, shows that the addition of selective internal radiation therapy (SIRT) to sorafenib in patients with advanced hepatocellular carcinoma was associated with no overall survival benefits compared with sorafenib alone. However, it may offer benefits in some subgroups of patients.
The final results of the palliative cohort of the SORAMIC study in patients with unresectable, locally advanced primary liver cancer have confirmed no clinical advantage to adding SIRT using Sir-Spheres (Sirtex) to standard sorafenib treatment compared with using sorafenib alone.
However, although the overall survival rates in the total patient population did not differ significantly between treatment groups, subgroup analyses suggested possible survival benefits with adding SIRT to sorafenib in some patient groups.
Jens Ricke
‘SORAMIC is the first large, randomised controlled trial to compare the efficacy and safety of combining liver-directed SIRT and sorafenib with using sorafenib alone’, explained study director, Jens Ricke from the Ludwig-Maximilians-University in Munich, Germany.
Ricke presented the results at The International Liver Congress 2018 in Paris, France.
‘Although we were disappointed to find no overall survival benefit of adding SIRT to sorafenib across the entire study population, we did observe a survival benefit in younger patients, those with a non-alcoholic aetiology of the cirrhosis, and those with no cirrhosis at all’.
Sorafenib is the standard, first-line systemic therapy for individuals with advanced HCC1 with the SHARP study demonstrating an increased median overall survival from 7.9 months to 10.7 months with sorafenib treatment compared with placebo in this population.
Study details
The SORAMIC (Sorafenib in combination with local micro-therapy guided by gadolinium-EOBDTPA-enhanced MRI) study was initiated in February 2010 and comprises three separate diagnostic, local ablation, and palliative substudies. The palliative substudy presented randomised 424 patients with inoperable HCC who were not candidates for transarterial chemoembolization (TACE) to receive treatment with either SIRT with yttrium-90 resin microspheres (Sir-Spheres) plus sorafenib (target dose 400mg bid) or sorafenib alone.
The primary endpoint of the study was overall survival in the intention-to-treat population.
As Ricke reported, the median overall survival was 12.1 months (95% CI: 10.6, 14.6) in the SIRT + sorafenib arm (n=216) and 11.5 months (95% CI: 9.8, 13.9) in the sorafenib arm (n=208) (HR: 1.01; 95% CI: 0.82, 1.25; p=0.93). In the per-protocol group, the median overall survival was 14.1 months (95% CI: 10.9, 16.4) in the SIRT + sorafenib arm (n=114) and 11.1 months (95% CI: 9.7, 13.9) in the sorafenib arm (n=174) (HR: 0.86; 95% CI: 0.67, 1.11; p=0.25).
A subgroup analysis of the per-protocol population in this study revealed a survival benefit of SIRT + sorafenib for patients ≤65 years of age (HR: 0.652), those with a non-alcoholic aetiology of the cirrhosis (HR: 0.632), and those with no cirrhosis (HR: 0.465). Adverse events grade three or higher were reported in 115/159 (72.3%) patients in the SIRT + sorafenib arm and in 135/197 (68.5%) patients in the sorafenib arm.
“There remains a significant unmet need for new treatment approaches in patients with unresectable HCC, and SIRT had shown promising results in previous, non-randomised studies,” said Ricke. “We believe our results have generated some very interesting new hypotheses in terms of the types of HCC patients that might benefit from combination therapy of SIRT and sorafenib, and we hope to explore these further in the future.”
“The SORAMIC trial is the first reported randomised controlled trial evaluating the survival benefit of adding SIRT to sorafenib in unresectable, locally advanced HCC not suitable for transarterial chemoembolization,” said Alejandro Forner from the Hospital Clinic Barcelona, Spain, and EASL Governing Board Member. “Regrettably, the study failed to meet the primary endpoint and the addition of SIRT to sorafenib did not show an overall survival that was superior to sorafenib alone. Further studies are needed to identify which specific population might benefit from this treatment approach,” he concluded.
Guerbet has announced a partnership with the Department of Radiodiagnosis and Interventional Radiology of Lausanne’s University Hospital (CHUV) and the Lausanne Center for Experimental Therapies (CTE) to launch a study aimed at evaluating the activating effects of Lipiodol-based conventional transarterial chemoembolization (cTACE) on the immunity of patients with hepatocellular carcinoma (HCC).
cTACE is the reference treatment for patients with intermediate-stage HCC and has been demonstrated to significantly improve patient survival compared to supportive palliative therapy. Nevertheless, and despite progress brought by new medical practices, there is an urgent need to develop new therapies to fight this pathology which has a poor prognosis.
Immunotherapy, aimed at stimulating or restoring the immune responses that specifically fight the tumour, is a new approach that has elicited much interest and is the subject of several clinical trials for HCC treatment. Modern cancer treatment of most types of tumour involves a combination of several therapies used either sequentially or simultaneously, with the aim of obtaining an additive and sometimes even synergistic therapeutic effect. Combining local treatments, such as cTACE, with systemic immunotherapy promises to improve the tolerance and individual effectiveness of treatments.
Study details
In this context, local treatments like cTACE could play an essential role by activating and/or restoring the systemic and/or local immune system which fights patients’ liver tumours. Preliminary results confirm the potential of this technique in terms of “paving the way” for systemic immunotherapy. Additional data are needed to accurately identify the role of cTACE in inducing and/or reactivating an immune response and to determine the possible synergy between this treatment and immunotherapy.
The partners will work together to clarify the immunomodulatory and activating mechanisms induced by a cTACE procedure in 20 patients with HCC, by measuring variations in the expression of different families of genes and of proteins involved in the anti-tumour immune response.
The study, to be conducted on the premises of the CHUV, will be coordinated by Rafael Duran, principal investigator and member of the CHUV Department of Radiodiagnosis and Interventional Radiology, and Lana Kandalaft, co-investigator and director of the CTE, located within the Lausanne CHUV Oncology Department.
“HCC is the second leading cause of cancer-related death worldwide. The innovative immunotherapy approach, which uses the immune system’s anti-tumour capacities, has delivered promising results and is opening up new treatment perspectives for an ever-increasing number of patients,” said Alban Denys, head of the CHUV Interventional Radiology Unit.
“It is essential that we improve our understanding and characterisation of the anti-tumour effects of cTACE and that we study its ability to convert poorly immunogenic tumours, also called ‘immune deserts’, into immunogenic tumours. By reprogramming the tumour microenvironment, we could combine cTACE with immunotherapy,” added Duran from the CHUV Department of Radiodiagnosis and Interventional Radiology.
“We are delighted to announce the launch of this new study, the results of which will provide a solid foundation for explaining the role of cTACE as an activator of patients’ anti-tumour immune systems and pave the way for new combination therapeutic approaches, which represent the future of HCC management,” commented Pierre Desché, Development, Medical and Regulatory Affairs vice president at Guerbet.
The US National Institute of Health (NIH)’s National Cancer Institute has awarded a US$2 million grant to medical device company Embolx. The Small Business Innovation Research (SBIR) grant will fund further research and development of the company’s future generation Sniper balloon occlusion microcatheter, a pressure-directed embolization therapy system.
The Sniper balloon occlusion microcatheter alters blood flow‐dynamics by controlling pressure to increase therapeutic agent delivery into target areas for the treatment of cancerous tumors, benign prostatic hyperplasia (BPH), and uterine fibroids. This therapy allows interventional radiologist physicians to deliver drugs and embolic agents to only targeted treatment areas while protecting surrounding healthy tissues.
“We are excited for the opportunity to further our unique technology and advance minimally invasive cancer and BPH therapy,” said Michael Allen, president and CEO at Embolx. “This NIH grant, and recently completed US$5.5 million Series B financing, will accelerate our efforts to develop high performing medical devices that support better patient outcomes.”
The Phase II portion of the grant will build on completed work done in Phase I to develop an advanced generation of the Sniper microcatheter. With this new advanced device, interventional radiologists will have the capability of monitoring pressure in the vicinity of a tumor, tracking embolization progress in real-time and achieving a quantitative embolization endpoint, thereby improving reproducibility and efficacy of transarterial embolization procedures.
The co-investigator for this grant is Sanjay Gupta, chair ad interim, Department of Interventional Radiology at The University of Texas MD Anderson Cancer Center in Houston, USA.
Society of Interventional Radiology (SIR) publishes guidelines on clinical practice of intra-arterial stroke revascularisation
Revised guidelines for the non-surgical, image-guided interventional treatment of acute ischaemic stroke will ensure patients receive the right treatment at the right time. The updated guidelines, endorsed by the Society of Interventional Radiology (SIR) and 11 other medical societies, were published in the April edition of SIR’s peer-reviewed journal, the Journal of Vascular and Interventional Radiology (JVIR).
This revision updates standards of practice first published in 2013 and establishes 15 metrics on patient care and outcomes, based on findings of recent scientific studies about interventions such as thrombectomy and revascularisation. The 2018 guidelines cover important factors in selecting patients for interventional treatments and ensuring optimal outcomes, such as the time since the patient was “last known well,” preprocedural imaging and clot location.
“The one constant in stroke treatment is time to opening the artery,” noted David Sacks, an interventional radiologist at Reading Hospital/Tower Health in West Reading, and the lead author of the standards. “Seconds count from time of admission to successful treatment. Meeting the outcomes described in these guidelines will ultimately benefit patients by requiring strict adherence to a rapid treatment schedule.”
The benchmarks set in this revised guideline are intended for use in quality improvement programmes to assess and improve processes and outcomes and may also help facilities meet the criteria for accreditation as a comprehensive stroke centre.
“We know from recent studies that rapid access to interventional treatments increases the odds of survival and decreases the occurrence of disability in patients who suffered an acute ischaemic stroke,” said M Victoria Marx, SIR president and professor of clinical radiology at the Keck School of Medicine of the University of Southern California. “Now is the time for these guidelines to be adopted and applied to save lives.”
The societies joining SIR in the guidelines are the American Association of Neurological Surgeons (AANS), American Society of Neuroradiology (ASNR), Canadian Association for Interventional Radiology (formerly the Canadian Interventional Radiology Association), Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Congress of Neurological Surgeons (CNS), European Society of Minimally Invasive Neurologic Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Society for Cardiovascular Angiography and Interventions (SCAI), Society of NeuroInterventional Surgery (SNIS), and World Stroke Organization (WSO).
There were several devices in the New Product Showcase at the Society of Interventional Radiology’s Annual Scientific Meeting in Los Angeles, USA. Among these was Medtronic’s OptiSphere resorbable embolization spheres, which the company introduced at the meeting.
OptiSphere resorbable spheres provide an alternative solution for treating hypervascular tumours, according to the company.
OptiSphere is made from purified porcine skin gelatin and the spherical shape provides smooth embolic delivery and even, predictable embolization. These resorbable microspheres begin to degrade starting at four weeks post-procedure with significant degradation noted at nine weeks, the company states. The product is offered in two volume options and five size ranges designed for reliable, targeted embolization of hypervascular tumours.
Included in a selection of the new products seen by Interventional News was Teleflex’s Octane thrombectomy system, which is intended for the removal of peripheral arterial and deep venous thrombosis. The system consists of a thrombectomy catheter and a hand pump for selective and controlled aspiration. The catheter assembly is a combination of two coaxial catheters with a 6F inner and 8F outer lumen that slide back and forth. This combination is designed to break up and remove thrombus plugging the catheter tip, the company states.
Bard, which is now part of BD, showcased the PowerFlow implantable apheresis IV port, which, the company states, is the only high-flow, power injectable port designed and indicated specifically for therapeutic apheresis.
Another product from the company was the UltraScore focused forced percutaneous transluminal angioplasty balloon. This is an over-the-wire scoring balloon that uses focused force technology to cause plaque fracture at low inflation pressures, even in calcified lesions. Compared to a standard angioplasty balloon, the UltraScore balloon provides 24 times more force when the wire contacts the lesions, material from the company states.
Argon Medical showcased BioPince Ultra, the latest innovation in biopsy technology. BioPince Ultra uses a triaxial core, cut and capture cannula system to harvest diagnostic quality, full core specimens while reducing the risk of crush artifact and tissue fragmentation.
Siemens Healthineers showcased nexaris Angio-CT to individualise treatment with seamless access to multiple imaging modalities in one interventional suite. The nexaris therapy suite provides synergised imaging for planning, guidance and results assessment during a single procedure, material from the company states.
BTG, which acquired Roxwood Medical in October 2017, showcased its range of anchoring catheters and microcatheter obtained from the acquisition. These offer options for physicians in the crossing of complex lesions and arterial blockages.
M Victoria Marx, an interventional radiologist at Keck Medicine of USC, Los Angeles, USA, has been appointed president of the Society of Interventional Radiology (SIR) for 2018–2019.
“Through my new role as president, I will continue to move forward important SIR initiatives aimed at everything from promoting diversity within the specialty to increasing patients’ awareness of the benefits of interventional radiology,” said Marx.
Marx told Interventional News: “My main goal is to continue the momentum that we have this year on several fronts. The one I am most closely tied to is the development of interventional radiology as a primary medical specialty and the associated development of a robust graduate medical training process in the USA and I am very proud of where we stand with that.
“This is an exciting time to be an interventional radiologist. Interventional radiology is recognised as its own specialty and residency programmes are overflowing with a diverse and highly competitive pool of applicants in just their third year,” said Marx. “The future of our specialty is bright, and I am proud to lead SIR during this time of surging interest in the limitless potential of image-guided therapies to improve patient care,” she added.
Marx, who joined Keck Medicine in 1999, is an expert in women’s health, biliary disease and radiation safety. In her clinical practice, she advocates for managing symptomatic uterine fibroids with uterine fibroid embolization, a minimally invasive treatment that avoids hysterectomy. She is also focused on broadening regulatory standards to minimise radiation exposure for patients, physicians and staff.
“I believe that women can practice interventional radiology and be effective, safe, and pregnant. I think the promotion of a stronger universal culture of safety in the world of interventional radiology will make it easier for women to practice through pregnancy; if all interventional suites used optimal safety all the time and this was based on the assumption that every person in the room was pregnant, there would not be a need for special measures during pregnancy,” Marx told Interventional News.
Marx is also a professor of clinical radiology at the Keck School of Medicine of USC, vice chair of education for the Department of Radiology and director of the
In addition to Marx, other incoming officers of SIR’s 2018–19 Executive Council include president-elect Laura Findeiss, Emory Healthcare, Atlanta; secretary Michael D Dake and immediate past-president Suresh Vedantham, Mallinckrodt Institute of Radiology, Washington University, St Louis, USA.
Cryoablation of the posterior vagal trunk, the nerve carrying hunger signals to the brain, may help patients with mild-to-moderate obesity lose weight, according to a study presented at the Society of Interventional Radiology’s 2018 Annual Scientific Meeting (17–22 March, Los Angeles, USA). The treatment was determined safe and feasible in the initial pilot phase.
“We developed this treatment for patients with mild-to-moderate obesity to reduce the attrition that is common with weight-loss efforts,” said David Prologo, an interventional radiologist from Emory University School of Medicine, Atlanta and lead author of the study. “We are trying to help people succeed with their own attempts to lose weight.”
The vagal trunk, located at the base of the oesophagus, is one of several mechanisms that tells the brain that the stomach is empty.
Other interventional radiology procedures such as bariatric artery embolization are also being explored as a treatment option for morbid obesity.
In the study, 10 patients with a body mass index (BMI) between 30 and 37 underwent the procedure and were followed for 90 days. All patients reported decreased appetite and the overall average weight loss was 3.6% of initial body weight and an average decline of nearly 14% of the excess BMI. No procedure-related complications were reported, and there were no adverse events during the follow up.
“Medical literature shows the vast majority of weight-loss programmes fail, especially when people attempt to reduce their food intake,” said Prologo. “When our stomachs are empty, the body senses this and switches to food-seeking survival mode. We are not trying to eliminate this biological response, only reduce the strength of this signal to the brain to provide a new, sustainable solution to the difficult problem of treating mild obesity.”
Following the success of this preliminary safety and feasibility study, more patients are being recruited for a larger clinical trial of the procedure to test the efficacy and durability of the procedure. In presenting the study, the authors note several limitations, including the small sample size and the interim nature of the results.
The study was funded by Healthtronics, a medical technology company that manufactures the ablation probes used for the treatment.
Rendering of patient’s pelvic anatomy from CT. The green portion of the femoral vessels was 3D printed in the study.
A relatively inexpensive 3D-printed model of a patient’s blood vessels is as effective as current commercially available models for training medical students in interventional radiology vascular access, according to a study presented at the Society of Interventional Radiology’s 2018 Annual Scientific Meeting.
“We have come up with a viable method for creating something that is inexpensive and also customisable to individual patients,” said Alexander Sheu, an interventional and diagnostic radiology resident at Stanford University School of Medicine, and lead author of the study. “The current model used to train medical students lacks the ability to replicate a patient’s anatomy. Our 3D-printed model will provide students a more realistic experience, allowing for better preparation before they perform procedures on real patients.”
The researchers tested medical students’ comfort in using a 3D-printed model, compared to commercially available models, to simulate ultrasound-guided access through the femoral artery in the groin.
Thirty-two students were randomised to practice with the 3D-printed model or the commercial model in a simulation experience developed by the authors of the study. Prior to the simulation exercise, 73% of the 3D group and 76% of the commercial-model group indicated that they did not feel confident in performing the procedure. After the training, most of the 3D model and commercial model trainees agreed that their respective models were easy to use (93.3% and 94.1%) and helpful for practice (93.3% and 94.1%). Additionally, confidence in performing the procedure, known as femoral artery access, increased a similar amount in both groups.
“Now that we know that a 3D-printed model is just as effective at training medical students in this type of procedure, this simulation experience can be made available to even more trainees and potentially improve procedural skills for residents, fellows, and attendees,” said Sheu. “We foresee this really making an impact in the world of interventional radiology training.”
Medical simulation exercises are playing an increasingly larger role in medical training; especially in the field of interventional radiology. Many commercially available devices cost between US$2,000 and US$3,000 each, while 3D printing has the ability to produce practice models inexpensively and more realistically, the authors said.
The 3D-printing technology can reproduce a patient’s exact vessels based on a CT scan and produce an ultrasound-compatible vascular access model that is unique to that patient’s anatomy. To adapt the 3D printing technology to their needs, the researchers used a tissue-mimicking material that was durable to withstand punctures, but still felt realistic. This tailoring allows trainees to practice with variations in anatomy before they encounter them during a procedure, which may help to lower complication rates, researchers said.
Advanced stage liver tumours may be safely treated through image-guided injections of an immunotherapy approved for melanoma, according to phase 1 data presented at the Society of Interventional Radiology’s Annual Scientific Meeting.
Researchers found that talimogene laherparepvec (T-VEC)—a genetically modified version of the herpes virus—can be safely administered into active cancer in the liver in order to stimulate the immune system to destroy cancer cells throughout the body.
“Advanced stage liver tumours, including ones that have spread from other locations, have limited treatment options because the patients can be in poor health; further, the complex structure of the organ can make it difficult to target with standard approaches,” said Steven S Raman, professor of radiology, surgery and urology at the David Geffen School of Medicine, University of California, Los Angeles, and lead author of the study. “This minimally invasive treatment offers patients a novel way to directly and indirectly attack the cancer cells.”
Using image-guided needle injections, researchers at centres in the USA, Switzerland and Spain, treated 14 advanced-stage cancer patients with liver metastases, including those with cirrhosis. Patients were given escalating doses of T-VEC, up to the maximum US FDA-approved dose for melanoma. Injection volume was based on lesion size. Researchers found the patients tolerated the treatment well with expected side-effects, including temporary flu-like symptoms.
As part of the study, researchers will follow patients for up to two years, and new trials to investigate the effectiveness of the drug in treating advanced cancer in the liver are being planned. Additional investigation is also planned to test the therapy in combination with a checkpoint inhibitor to activate a stronger immune response.
“Image-guided treatments have expanded the options available for patients with liver cancer from innovative approaches to biopsies to resections to chemotherapy,” said Raman. “This is an exciting way to look to the future, but patients living with advanced liver cancer should understand that this treatment will not be available for several years, except through clinical trials.”
The authors note several limitations of the current study, including the preliminary nature of the results, as well as the number of patients tested.
Amgen, the pharmaceutical company that makes T-VEC, was a sponsor of the trial.
Geniculate artery embolization could improve quality of life for patients with knee pain due to osteoarthritis, according to new research presented at the Society of Interventional Radiology’s 2018 Annual Scientific Meeting (SIR; 17–22 March, Los Angeles, USA).
In the first US clinical trial involving geniculate artery embolization, a minimally invasive procedure that blocks key arteries in the knee to reduce inflammation and pain, a majority of study participants achieved significant pain reduction and improvements in range of motion, avoiding more invasive measures.
“A majority of our patients with osteoarthritis of the knee saw significant pain reduction, not only just a few days after the procedure, but a month after as well, making this an accessible treatment for patients looking to improve their quality of life without surgery,” said Sandeep Bagla, director of interventional radiology at the Vascular Institute of Virginia and lead author of the study. “We are very encouraged by the results and the implications for the millions suffering from this common, yet debilitating condition.”
This prospective, multicentre clinical trial evaluated 13 patients with severe osteoarthritis pain. Each patient’s pain and disability were measured along two scales, with evaluations before and after the treatment. The treatment was successfully completed in all 13 patients, with no adverse events. One month later, researchers followed the progress of eight patients and found that embolization significantly decreased pain (-58mm on the Visual Analog Scale), reduced stiffness and increased physical function (-36.3 on the Western Ontario and McMaster University Osteoarthritis Index). Together the scales represent an 80% improvement in function compared with preprocedure conditions.
“This procedure could have a significant impact in the treatment of osteoarthritis pain as a whole,” said Bagla. “The current mainstay of treatment in patients who have arthritis is pain medication, which comes with significant side-effects and risks. But geniculate artery embolization provides another option for patients struggling with pain and may even allow patients to avoid the painful recovery of knee surgery and the need for the kind of opioid pain medications associated with the dangerous epidemic in the USA.”
This study builds on the growing international research around geniculate artery embolization and osteoarthritis. While preliminary data shows that the treatment does work and is feasible, it has only been used in a clinical trial setting. The study has completed enrolment of 20 patients and final results are expected in summer 2018. A second randomised controlled clinical trial began in February 2018 and will provide further data on what types of patients are the best candidates for this treatment and how it could move toward clinical practice.
Virtual reality (VR) provides interventional radiologists with a 360-degree view of internal anatomy to enhance procedure planning.
Interactive VR brings medical images to life on screen, showing interventional radiologists a patient’s unique internal anatomy to help physicians effectively prepare and tailor their approach to complex treatments, such as splenic artery aneurysm repair, according to new research being presented at the Society of Interventional Radiology’s 2018 Annual Scientific Meeting (17–22 March, Los Angeles, USA).
“Treating splenic artery aneurysms can be very difficult because of their intricate nature and anatomic variations from patient to patient,” said Zlatko Devcic, a fellow of interventional radiology at Stanford University School of Medicine, Stanford, USA and collaborating author of the study. “This new platform allows you to view a patient’s arterial anatomy in a three-dimensional image, as if it is right in front of you, which may help interventional radiologists more quickly and thoroughly plan for the equipment and tools they’ll need for a successful outcome.”
Researchers compared the new VR technology to the use of images from a commonly used visualisation software system that displays images on a standard two-dimensional platform.
VR turns a patient’s preprocedural CT scans into 3D images that the radiologist can virtually move and examine while wearing virtual reality-type glasses. By allowing the operator to manipulate routine, two-dimensional images in an open three-dimensional space, VR provides a look into a patients’ organs and tissues that had not been possible outside of the human body, until now. As a result, the operator is armed with a deeper and intuitive understanding of spatial relationships, such as between an aneurysm and the surrounding arteries.
In the study, three radiologists, using both technologies, independently evaluated 17 splenic artery aneurysms in 14 patients. Researchers measured the radiologists’ accuracy in identifying inflow and outflow arteries associated with the aneurysms with each method. Radiologists in the study also ranked improvements in their confidence on a four-point scale when using VR compared to the standard method.
Researchers found accuracy was similar with both methods, though confidence improved substantially with VR. In fact, 93% of participating physicians who used the VR method indicated higher confidence in their abilities (a score of at least three).
“Preoperative planning is possibly the most important step towards successfully treating a patient, so the value of VR cannot be understated,” Devcic said. “This technology gives us a totally different way to look at that structure and safely plan our approach to patient care.”
Researchers hope that future studies will examine whether this technology will ultimately help reduce the time needed to perform the treatment and as a result, reduce the amount of radiation and contrast exposure to the patient.
Anne Roberts (centre) with Janice Newsome (left) and Erika Ugianskis (right)
Fostering a diverse interventional radiology (IR) workforce is difficult, but vital, because heterogeneous groups can be more innovative, be better at complex problem-solving, achieve superior outcomes and be more successful financially than their homogeneous counterparts, said Anne Roberts at ISET 2018.
Anne Roberts, division chief, Vascular and Interventional Radiology and professor of Radiology, University of California San Diego Health, USA, delivered the annual Charles G Tegtmeyer lecture at the International Symposium on Endovascular Therapy (ISET; 3–7 February, Hollywood, Florida, USA).
Roberts focused on diversity when speaking on the topic “Incorporating new ideas into practice: challenges and solutions for today’s world”.
“Diversity is probably one of the biggest challenges in today’s world and this is reflected in medicine, particularly in interventional radiology. We need policy that encourages tolerance and appreciation for people of different backgrounds,” she said.
Roberts pointed out that there were many aspects to diversity including race/ethnicity, gender, socioeconomic background and sexual orientation. Outlining some of the relevant numbers, particular to radiology in the USA, she noted that under-represented minorities made up about 8% of radiology trainees in the USA compared to 15% of medical school and graduate medical education trainees. When it came to women, just 27% of radiology trainees were women when compared to the 48% who went to medical school and 46% of graduate medical education trainees.
Why embrace diversity?
Roberts referenced Katherine W Phillips’ article, published in Scientific American in 2014, “How diversity makes us smarter” to provide some answers. She noted: “Research shows that socially diverse groups are more innovative than homogeneous groups. They are also better at solving complex, non-routine problems. Simply interacting with individuals who are different, forces group members to prepare better; to anticipate alternative viewpoints and to expect that reaching consensus will take effort.”
Phillips also states that diversity has been shown, in multiple studies, to enhance financial performance. Groups with diversity outperform groups with no diversity, whereas being with similar others leads to thinking that we all hold the same information and share the same perspective. “Diversity jolts us into cognitive action in a way that homogeneity does not,” said Roberts.
On the other hand, Roberts said, members of a homogenous group “tend to feel they will agree with one another, will understand one another’s perspectives and beliefs and will be able to easily come to a consensus. Heterogenous groups anticipate differences in opinion and perspective and assume they will need to work harder for consensus.
“People may not like encouraging diversity because it is harder, but this can lead to better outcomes,” Roberts said.
Intelligent design for diverse organisations
Pointing to lessons that can be learned from other organisations that are looking to achieve greater diversity, Roberts noted that the successful improvement of gender representation and creation of inclusive environments were reliant on plans to support family requirements and salary equality. They also included prominent role models for under-represented minorities.
Roberts explained that professional society attention can help to mentor under-represented minorities and that the Society of Interventional Radiology (SIR) has already budgeted for outreach to these groups. “Institutions are also including specific questions to faculty candidates about their experience with encouraging diversity. For instance, the University of California requires individuals who are applying for faculty positions, or those who are being promoted, to describe what they have done to promote diversity,” she commented.
Barriers
Barriers to diversification in interventional radiology include inadequate specialty exposure; the specialty being perceived as having little patient contact or being less of a direct service to the community. An important barrier is the lack of role models and mentors. Bias can also play a key role, particularly when an equally qualified candidate is ranked lower for a position because of gender, race or ethnicity.
As potential solutions, Roberts proposed that the early exposure programmes to interventional radiology be expanded to student interest groups. “We need to encourage student application to existing summer fellowships and create summer internship programmes to enhance the competitiveness of future applicants. At national meetings, we need to showcase faculty who represent diversity, and who formally mentor students. We also need to improve education and the marketing of radiological professions. It is vital to include new and diverse members on residency selection committees and faculty search/promotion committees.”
She also called attention to other diversity issues such as the lack of appreciation for diversity of medical specialists in medical centres. Additionally, isolation within specialty silos, the lack of interaction between various specialties and within different areas of the hospital all meant there was less co-operation and sharing of experience. The tools and approaches used by one specialty could be applicable to others and interactions could improve all practices, she said.
“One of the challenges with society meetings is that they tend to isolate specialties and the subspecialty meetings tend to include mostly individuals from the specialty. This can result in disseminating a form of specialty “groupthink” by which people seek out and remember information that provides support for their pre-existing attitudes and beliefs,” she noted.
“It is a real credit to ISET and the Miami Cardiac and Vascular Institute (MCVI) that they have worked hard to try and breakdown the silos. ISET, with multiple specialties being involved has been a leader in this approach in conferences. MCVI, with the inclusion of multiple specialties within the institute has also been an example of the value of diversity,” commented Roberts.
“Striving for greater diversity involves leaving our comfort zone and coming together to embrace our differences. Humanity is plural not singular and everybody should be in, with nobody being “out”. Differences are not just to be celebrated, but are essential. We do not see things the same [way] and our power lies in that we do not see things the same,” Roberts concluded.
Reflow Medical announced that the first patients have been enrolled in a prospective, multicentre, non-randomised study intended to evaluate the ability of the Reflow Wingman catheters to cross chronic total occlusions in peripheral lesions.
The Wing-IT study is a non-randomised study evaluating the safety and effectiveness of the Wingman catheter to cross chronic total occlusions in infrainguinal peripheral arteries.
Initial patient enrolments were performed by Nilesh Goswami of Prairie Cardiovascular at HSHS St. John’s Hospital Prairie Heart Institute, Springfield, USA and S Jay Mathews of Bradenton Cardiology Center in Bradenton, USA. The Wing-IT trial is expected to enroll 85 patients at up to 13 centres in the US and Europe. The principal investigator for the study is John Laird of Adventist Heart and Vascular Institute, St. Helena, USA.
“Patients with advanced peripheral artery disease frequently develop chronic total occlusions, which can be difficult to treat with endovascular therapy,” says Laird. “The ability to cross chronic total occlusions is directly related to acute procedural success and favourable long-term outcomes, including preventing the need for either bypass surgery or amputation.”
“Reflow is excited to be conducting this study to support expanded treatment options for physicians,” states Isa Rizk, CEO of Reflow Medical.
Dr. Keren Aviva Bashan-Gilzenrat (left) and Dr. Bryan Morse (center) demonstrate technical aspects of REBOA during the first GREAT class in December 2017. (PRNewsfoto/Grady Health System)
Keren Aviva Bashan-Gilzenrat (left) and Bryan Morse (centre) demonstrate technical aspects of REBOA during the first GREAT class in December 2017.
Grady Memorial Hospital, the first in Georgia, USA, to perform resuscitative endovascular balloon occlusion of the aorta (REBOA), will soon offer trauma specialists around the state and the country the opportunity to learn how to perform the procedure.
“REBOA is a minimally invasive technique that uses a catheter to insert a balloon into the aorta, which temporises a severely haemorrhaging wound when inflated, and buys time for a patient to get to the operating room or interventional radiology. Time is key, and this is another tool in the arsenal to do the best we can for our patients,” said Keren Aviva Bashan-Gilzenrat, assistant professor of surgery, trauma/critical care, Morehouse School of Medicine.
The endovascular surgical skills course called Grady Rescue and Endovascular Approaches to Trauma (GREAT) was developed by Bryan Morse, assistant professor of surgery, trauma/critical care, Emory University School of Medicine, Jonathan Nguyen, assistant professor of surgery, trauma/critical care, Morehouse School of Medicine, and Bashan-Gilzenrat, the team that performed the state’s first REBOA in November 2016.
“As the only nationally verified Level 1 trauma centre in Metro Atlanta, Grady must lead in research and continually pursue innovative ways to treat our patients,” said Morse, who is also the trauma research director at Grady.
“We conducted the first GREAT course in December last year with eight Emory and Morehouse surgeons, who are now trained to perform the procedure at Grady,” Morse said. “We built this course from the ground up, and as a teaching hospital, it is exciting to see how far it will go.”
The course comprises classroom and simulation training using the latest catheter technology to demonstrate technical aspects of the procedure on mannequins and cadavers. The next session is planned for May 2018.
Acuson Juniper is a new ultrasound system with advanced applications and imaging performance while featuring a lightweight, ergonomic design and complete manoeuvrability for use across a wide variety of clinical segments, a press release from the company states.
Siemens Healthineers launched Acuson Juniper at the 2018 European Congress of Radiology (ECR; 28 February–4 March, Vienna, Austria), the annual congress of the European Society of Radiology (ESR).
Though small in size, the Acuson Juniper does not compromise in performance, offering providers a system that is not only powerful, but nimble in design, a press release from the company states.
Siemens Healthineers incorporated feedback from the 365 participants in its largest-ever ultrasound co-creation project to ensure that the Acuson Juniper meets the needs of today’s changing healthcare landscape. The system’s versatility and adaptability makes it ideal for diverse patient anatomies and physiologies. Users can customise the Acuson Juniper based on patient interactions for improved clinical workflow.
“As the healthcare industry evolves, providers need a nimble, versatile ultrasound system like the Acuson Juniper,” says Robert Thompson, head of Siemens Healthineers Ultrasound. “It is the latest example of how Siemens Healthineers evolves with healthcare trends by transforming care delivery as we improve the patient experience.”
Where form meets function
The smallest, most lightweight system in its class, the Acuson Juniper adapts to virtually any exam environment and manoeuvres easily with no trade-offs in performance, the release notes. Sleep and boot-up times of mere seconds allow clinical users to transfer the system within a hospital without sacrificing time with patients. The system has flexible, intuitive, and customisable tilt settings. Five active transducer ports allow for the system’s quick and easy readiness after transfer from department to department, it adds.
The Acuson Juniper’s LED monitor and touch panel are the largest in its segment. The system’s two standard USB ports enable quick transfer of images to patients, eliminating the need for print-out documentation. Further improving the patient experience, the Acuson Juniper is 40 per cent quieter than other ultrasound systems in its class. Additionally, a protective sheet is available for the system’s key pad, to facilitate the reading and use of the controls while in a sterile environment such as the operating room. This protective skin can be disinfected for reuse.
New features
Acuson Juniper is powered by a completely new imaging platform that was designed from the ground up with user needs in mind. Its new front-end engine offers exceptional system sensitivity and specificity as well as high dynamic range for improved tissue differentiation. A new signal processor reduces probe and patient motion artifacts, and enables fast image acquisition. A new back-end engine allows advanced elastography imaging and has a new measurement package. For use across departments, the Acuson Juniper is equipped with 16 transducers and is customisable with advanced imaging applications for use in radiology and interventional radiology, urology, cardiovascular, orthopedic, and obstetrics/gynecological imaging, the press release from the company states.
Immunotherapies promote a sustained T-cell response with tumour kill. Copyright: Professor Vicky Goh
Evasion of the immune system is an important mechanism in the development and progression of cancers. Cancer immunotherapies are a promising class of therapeutic agents that re-engage the immune system in its fight against cancer cells, explained Vicky Goh, London, UK.
Goh was speaking at the press conference of European Congress of Radiology (ECR; 28 February–4 March, Vienna, Austria).
“These therapies use strategies that range from activating innate/adaptive immune effector mechanisms to neutralising inhibitory/suppressive mechanisms. For example, treatment with interleukin 2 (IL-2) or interferon-α (IFNα) stimulates effector immune cells. Conversely antibodies against immune-checkpoint molecules (eg. cytotoxic T lymphocyte-associated protein 4 [CTLA4]-targeted antibodies and programmed cell death 1 [PD1]-targeted antibodies) neutralise immune suppressor mechanisms,” said Goh, chair of Cancer Imaging and head of Department at King’s College London and honorary consultant radiologist and academic lead at the Guy’s and St Thomas’ Hospitals, London/UK.
Immunotherapies have shown to be effective in a number of advanced cancers including melanoma and non-small cell lung cancer where improvement in overall survival has been achieved. For melanoma, ipilimumab (an anticytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) antibody) was approved in 2011, based on results from a phase III trial, in which 20% of patients with melanoma experienced long-term survival. Since then nivolumab and pembrolizumab, antibodies targeting programmed cell-death protein 1 (PD-1), have been associated with response rates of 28–40%.
However, it is important to note that only 20–40% of advanced melanoma patients have durable responses to immune checkpoint inhibitors, said Goh noting that their positive effects need to be balanced against severe off-target immune toxicity and high costs.
Goh alluded to the “the good, the bad and the ugly” about this new treatment option. “The trials have shown that immunotherapies prolong overall survival, may be synergistic and their effects on tumours are different to standard chemotherapy, or targeted therapies, such as antiangiogenics. The response can be slow in onset but prolonged, and there are significant side-effects such as on the skin and gastrointestinal system, most commonly. Up to a third of patients may have to discontinue treatment,” she noted.
Future research directions
Her talk also focused on the role of imaging and considered future research directions. “Predictive biomarkers to select patients with likely clinical benefit from treatment are needed. Can imaging play a part? As immunotherapies generate anti-tumour effects by enhancing tumour-specific T cell responses rather than the direct cell killing, therapy assessment may be challenging by imaging. Response may take longer to be detectable by imaging and standard methods, such as Response Evaluation Criteria in Solid Tumours (RECIST) may be misleading,” said Goh ahead of the ECR press conference.
“The challenge for imaging is how best to assess if therapy is working, or not, given the high likelihood of treatment-related side effects. Further, how best to identify the patients who are likely to benefit from treatment; how best to exploit interventional oncology in the era of immunotherapies and the question of whether interventional oncology can harness the abscopal effect all remain research issues,” said Goh.
The analysis of big data with artificial intelligence (AI) techniques will have an enormous impact on disease prevention, cure and care. By 2030, it will have dramatically changed the landscape of the healthcare system, said Wiro Niessen, Rotterdam, The Netherlands, speaking at the press conference of European Congress of Radiology (ECR; 28 February–4 March, Vienna, Austria).
Niessen, professor in Biomedical Image Analysis, Erasmus MC, Rotterdam, The Netherlands and at the University of Technology in Delft, spoke on the topic “AI and big data in medical imaging” on 3 March at the ECR. He started off by referencing The Economist’s 2016 article “Anything you can do, AI can do better” and asked the question: “should AI be embraced or feared?”
Niessen then went on to provide examples in healthcare where artificial intelligence and big data should be “embraced” as they have the capacity to realise the potential of precision medicine and precision health.
Niessen explained that precision medicine involved taking individual variability into account to optimise diagnosis, prognosis and treatment. In cardiovascular disease, this can involve knowing which patients to treat; in cancer treatment, this can involve predicting which treatment is likely to be successful; and in dementia, this can involve prognosis to support preventive strategies.
“With an ageing society, there is an urgent need to develop new preventive and therapeutic strategies for common, age-related, diseases, such as Alzheimer’s disease, the most common form of dementia,” said Niessen.
“Largescale data analytics in longitudinal population neuroimaging studies, especially when combining imaging with other clinical, biomedical and genetic data, provide a unique angle to study the brain, both in normal ageing and disease,” he said while also discussing the promise and challenges of using state-of-the-art artificial intelligence techniques as deep learning in this domain, to improve diagnostics and prognostics.
“As a second example, radiomics approaches can be used to improve tumour characterisation and therapy selection and guidance in oncology, and here the enormous potential and pitfalls of using artificial intelligence in the interpretation of these data were discussed,” stated Niessen.
Preliminary findings from an initial study with 25 patients have shown that measuring the changes in oxygen concentration at baseline, during, and after endovascular revascularisation, can predict wound healing and functional improvement in critical limb ischaemia patients.
Marianne Brodmann, Medical University Graz, Austria, presented the initial OMNIA study results that used the Lumee oxygen platform (Profusa) as a unique tool to assess and clinical management of critical limb ischaemia patients at the Leipzig Interventional Course (LINC; 30 January–2 February 2018, Leipzig, Germany). The platform is designed to provide immediate feedback on the quality of revascularisation and along the entire course of the patient’s recovery. It uses hydrogel sensors that are injected into the skin of the patient that measure the oxygen concentration in the tissue.
Assessing procedural success in a complex critical limb ischaemia setting is challenging. “When it comes to critical limb ischaemia, we all still struggle with an objective assessment in the management of these patients,” said Brodmann.
OMNIA (Oxygen monitoring near ischemic areas) is a prospective, single-arm, open label, multicentre study designed to understand the relationship between revascularisation success, traditional measures of gross haemodynamic characterisation and Lumee measurement of tissue perfusion. Data were captured to establish feasibility and generate a hypothesis.
Through end of 2017, 21 patients—all Rutherford class five and most who were diabetic—had been enrolled. All but two received endovascular treatment, whilst the others had bypass surgery, after attempted endovascular therapy.
Four Lumee sensors were injected into each patient; three in the foot and one as a reference sensor in the arm. Measurements were performed continuously during the functional assessment tests performed before and after revascularisation, during the endovascular revascularisation procedure at one, three and six months at follow-up visits, explained Brodmann. Traditional clinical metrics sampled throughout visit schedule included arterial duplex, toe and ankle-brachial index (ABI), wound, ischaemia, and foot infection (WIfI) scores, wound characterisation and photographs.
Commenting on the information extracted from Lumee intrasurgically, Brodmann said: “This is called reperfusion modulation, which is defined as the difference in Lumee Oxygen Index (LOI) between baseline and maximum after intervention. Larger values are associated with greater increases in tissue oxygen during the procedure and this data can be averaged across all Lumees or selected from a Lumee of interest”.
Changes in LOI measured during endothelial revascularisation were found to be predictive of wound healing. Describing a case when the endovascular procedure was successful and flow was re-established to the foot, investigators obtained a LOI change that was high. Later functional assessment was positive and the patient’s wound decreased in size, the ankle-brachial index increased and the patient’s Rutherford category changed.
In another case when endovascular treatment was unable to re-establish flow, ie, in a non-responding patient, the LOI change was very low and later functional assessment and follow-up established that the wound did not heal, but that wound area increased.
“These results show that larger increases in LOI were associated with wound healing in our patients. When we observe LOI changes that are larger than 10, this predicts wound healing (as seen in 5/6 patients). When we observed oxygen index changes of less than zero, this predicted non-response, and we saw this in the two subjects who later underwent bypass surgery,” said Brodmann.
Adverse events
“There were 50 adverse events reported, of which 27 were serious and all unrelated to the study device. There were also 23 minor adverse events, of which 22 were unrelated to the study device. There was one mild swelling that resolved at follow-up that was possibly related to the device,” said Brodmann.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) announced that the first patient has been enrolled in CIREL (CIRSE registry for LifePearl microspheres), a Europe-wide observational study that will gather data on transarterial chemoembolization (TACE) using LifePearl (Terumo) microspheres loaded with irinotecan in patients with colorectal cancer and liver metastases.
The pan-European observational study CIREL will enrol up to 500 patients with colorectal cancer and liver metastases receiving TACE using LifePearl microspheres loaded with irinotecan as part of their standard treatment. The study aims to observe and categorise the real-life use of the device in the context of patients’ cancer treatment and will also collect extensive data on the safety, toxicity, efficacy, and quality of life.
Maria José Sousa and Belarmino Gonçalves, interventional radiologists at Instituto Português de Oncologia do Porto, Portugal, are among the first to join CIREL. They pinpointed why they think participation in the registry is important: “Through collaborative effort, we can optimise treatment and standardise procedures to majorly benefit our patients. Positive study outcomes, furthermore, could lead to changes in evidence-based guidelines on locoregional treatments for metastatic colorectal cancer.”
For further information on the CIREL study, please contact: Robert Bauer on [email protected], or visit www.cirse.org/cirel
Cook Medical has announced the leaders of its two new business divisions. Mark Breedlove has been named vice president of Cook’s Vascular division and DJ Sirota (below) has been named vice president of Cook’s MedSurg division.
The new organisational structure that was announced last week impacts more than one-third of the company’s workforce and realigns the former 10 business units into two business divisions.
Breedlove will now lead the new Vascular division, which brings together the former aortic intervention, peripheral intervention, interventional radiology, and lead management business units. He is a 24-year Cook veteran, whose passion is helping physicians treat their patients with innovative technologies while helping healthcare systems manage their supply chain in an efficient manner.
“Having started my career as a sales rep, I understand the importance of empowering your sales teams to make decisions based on the specific needs of their customers,” said Breedlove. “The organisational changes we have made will streamline the way they develop and manage customer contracts. These changes also allow the sales team to be more responsive and have the ability to support a customer more holistically across our entire vascular portfolio.”
He has previously held positions as a regional sales manager, national sales manager, director of marketing and product management and, most recently, vice president and global business unit leader for the peripheral intervention business unit.
DJ Sirota
Sirota will now lead the new MedSurg division, which comprises the six businesses that serve surgery, urology, reproductive health, critical care, endoscopy, and otolaryngology/ head and neck surgery specialties.
“Working together across these six specialties of medicine will allow us to share technologies more efficiently and develop new, innovative products that will continue to make a difference in the lives of patients,” said Sirota. “That is the reason I have been with Cook for over 30 years, because our goal is to do what is best for our customers and ultimately their patients.”
Sirota came to Cook out of college as part of an initiative by Bill Cook to place Indiana University students at the company. He, along with four others from that group who started on the same day in 1987, remain with the company. Sirota spent his first 12 years as a district manager in Pittsburgh, Pennsylvania. Since then, he has served as a marketing manager, product manager, senior global product manager, division leader and, most recently, as vice president and global business unit leader for critical care and interventional radiology.
“Mark and DJ both started their careers at Cook in the field working directly with physicians. Their wide-ranging experience at Cook has prepared them for these positions,” said Pete Yonkman, president of Cook Group and Cook Medical. “They are the right people to lead the divisions because they have the passion, experience and drive to serve physicians and their patients.”
Terumo Corporation has announced that it has entered into an agreement to acquire assets related to the large bore vascular closure device, Xpro System, from Medeon Biodesign, a Taiwanese publicly traded medical device company.
Under the terms of the agreement, Terumo will pay US$20 million upfront and additional payments based on the achievement of future specific development milestones. It will be funded through cash on hand.
In recent years, the number of percutaneous cardiac and peripheral catheterisation procedures that use a large bore device, such as transcatheter aortic valve implantation (TAVI), endovascular aneurysm repair (EVAR) and thoracic endovascular aortic repair (TEVAR), has been increasing. Usage is projected to increase by over 20% per year. The Xpro System is an automated suture-mediated closure device to simultaneously deliver two pairs of sutures, specifically targeting percutaneous large bore procedures via the common femoral artery. It is designed to achieve rapid and reliable haemostasis at the puncture sites.
The device is undergoing evaluation for CE mark certification in Europe.
Terumo supplies a range of minimally invasive vascular access and closure devices. Terumo continues to expand its product portfolio in growing segments through both in-house development and external investment, such as the recent acquisition of Angio-Seal and Femoseal family of vascular closure devices from Abbott in January 2017.
The product’s safety and effectiveness have been successfully demonstrated through a clinical study in New Zealand, Australia, and Taiwan, with patients undergoing percutaneous endovascular procedures utilising 8–18F introducer sheaths via the common femoral artery. The device achieved immediate or rapid haemostasis at the puncture sites with excellent clinical outcomes, including fast ambulation and discharge from hospitals, a press release from Medeon Biodesign notes.
“Access site complications in large bore procedures remain to be a significant concern among practicing clinicians. Leveraging the advantages of the security of suture-mediated closure and built-in safety mechanisms, the closure system provides a better solution for the large bore procedures with excellent outcomes and rapid haemostasis. We are pleased that the closure system’s unique and innovative technology complements Terumo’s vascular closure device portfolio, and we look forward, together with Terumo’s strong expertise in product development and commercialisation, to accelerating the time to market of the closure system in the emerging large bore market and driving further innovation into the hands of healthcare providers,” said Yue-Teh Jang, chairman and CEO of Medeon.
Healthcare centres around Europe are realising a new realm of clinical efficiency with the Infinix-i 4D CT system, which seamlessly integrates interventional radiology and CT. Canon Medical has announced showcasing system at this year’s ECR annual meeting.
The system’s unique merging of the Infinix-i angiography system with the customer’s choice of either the Aquilion One Vision Edition CT or the Aquilion Prime CT, allows clinicians to efficiently plan, treat and verify in a single clinical setting. The following healthcare providers are already using the Infinix-i 4D CT system to help clinicians improve visualisation and workflow:
Hôpital Saint Louis, Paris, France uses the Infinix-i 4D CT for a variety of interventional radiology and oncology procedures. “An amazing system combining CT with an interventional lab, opening new worlds for interventional oncology,” according to Eric de Kerviler.
University Hospital of Montpellier, France, uses the system to perform all kinds of interventional liver related procedures. This unit is dedicated to liver oncology treatment, such as embolization in combination with chemotherapy or radioactive beads destroying tumours with ice or high temperature. “Having the best of all imaging modalities gathered in the same interventional suite is the dream of any interventional radiologists,” said Boris Guiu, leader of the team in Montpellier.
University Hospital Strasbourg, France, uses the system for interventional radiology and oncology, as well as during liver ablations and orthopaedic procedures. “High quality true CT scanning during a complex intervention is key for us,” said Afshin Gangi.
Additional facilities will be installing the Infinix-i 4D CT system this year. The system’s integration of interventional radiology and CT technology into one solution can help clinicians improve visualisation and productivity, while prioritising patient safety.
“Interventional procedures are becoming more and more complex, which could result potentially in an increase in fluoroscopic time. This means that the interventional landscape is looking for new technologies and innovations to help physicians reduce radiation, increase image quality and improve their workflow. During the last two years, we observed a new, double market trend in the interventional landscape. The cone beam CT (CBCT) market segment remains the largest market segment; however, based on new clinical challenges, especially in interventional oncology, trauma, stroke and complex procedures in general, there was a spectacular increase in demand for angio CT concept. Canon is investing a lot in R&D and developing both segments at an extremely high level in parallel. This strategic approach combined with unique and very advanced dose reduction features makes us the preferred partner for many high-profile sites” said René Degros, European sales director, at Canon Medical Systems Europe. Additionally, the system offers a suite of dose management features, like Canon Medical’s AIDR 3D for simplified CT dose reduction and the Dose Tracking System, which is designed to help clinicians minimise X-ray exposure in real time.
Early data from the prospective multicentre AVeVA study that employed a covered stent (Covera; Bard, now BD) to treat stenoses at the venous anastomosis of arteriovenous graft access circuits has shown superior results when measured against predicted benchmark data.
Bart Dolmatch (Palo Alto Medical Foundation, Palo Alto, USA), speaking on behalf of the AVeVA investigators at the Leipzig Interventional Course (LINC; 30 January–2 February 2018, Leipzig, Germany) presented the six-month data from the study that is ongoing to two years.
“It is was widely known that arteriovenous grafts have a high rate of stenosis at the graft-to-vein anastomosis and that post-angioplasty recurrence of this stenosis is common. Most arteriovenous graft failures, whether it is poor flow, ineffective dialysis or thrombosis are related to this stenosis,” Dolmatch explained.
The Covera Vascular covered stent comes in two configurations, either flared or straight to accommodate for diameter differences in arteriovenous access anatomy, and is an ePTFE covered, helical, nitinol stent that is available in various sizes.
The AVeVA study is a prospective multicentre, non-randomised study with 110 patients who were enrolled and treated at 14 investigative centres in the USA. “The objective was to treat stenotic lesions at the graft-vein anastomosis of arteriovenous grafts with the Covera vascular covered stent and assess safety and patency,” said Dolmatch.
There was a clinical events committee that adjudicated safety events. The endpoints were measured against performance goals since there was no comparator control group.
Demographics and lesion characteristics
Data reported at LINC revealed that there were 110 patients of whom just over half were female. Most lesions treated were restenosis lesions. “Most stenoses are treated with balloon dilation and then recur, and these constituted nearly 72% in the study,” noted Dolmatch. The mean lesion length was 24.1±15.5mm; the mean baseline target lesion stenosis was 75.1%±14.8%; and a quarter of the patients had thrombus either at the time of presentation, or within 30 days of presentation.
Endpoints
The primary endpoint was safety through 30 days freedom from protocol (defined as safety events in the arteriovenous access circuit, not including stenosis or thrombosis) with a performance goal of 88% derived from the literature.
Target lesion primary patency (TLPP) at six months was defined as the time from the study procedure until the next clinically-driven reintervention at the treatment site, thrombotic occlusion, surgery, or permanent access abandonment. The control was a performance goal of 40% derived from the literature and pivotal studies.
Secondary endpoints include technical and procedural success; access circuit primary patency (ACPP; the time until the next access thrombosis or clinically-driven repeated interventional anywhere in the access circuit); index of patency function (the time to study completion or access abandonment divided by the number of reinterventions to maintain vascular access).
The upper arm was the access site in the majority of cases (98%) and therefore, the flared configuration of the stent was most commonly used. There was almost no residual stenosis after the procedure, noted Dolmatch.
“A first look at the AVeVA data shows that there was 94.6% freedom from a primary safety event at 30 days, which was superior to the performance goal of 88% (p=0.002).The 70.3% TLPP rate at six months, which was the primary efficacy endpoint, was superior to the performance goal of 40% (p<0.0001). With regard to secondary outcomes through six months, there was a 100% acute technical and procedural success rate and 39.2% six-month ACPP rates. The target lesion intervention rate was 0.41 at six-months and access circuit intervention rate is 1.05 the same follow-up point. The follow up in the AVeVA trials is ongoing through two years,” said Dolmatch.
Whether you are chasing Pikachu in the park or planning an IR procedure, virtual reality is increasingly “part of life” and has huge opportunities in medical education, procedure planning, stroke rehabilitation and more, writes Colin McCarthy, Boston, USA.
Whether you have been walking through the mall, or flying over Google Earth, it is likely you have noticed a surge in interest related to virtual reality (VR) and augmented reality (AR) over the last few years. Although “virtual reality” headsets have been around for some time, recent advances in technology have revolutionised consumer-level head-mounted displays (HMDs).
Indeed, modern smartphones have sufficient processing power to allow users to experience virtual and augmented reality without any additional hardware, apart from perhaps a relatively cheap cardboard viewer.
The terminology surrounding virtual and augmented reality is worthy of a brief discussion. For many, the term “virtual reality” evokes images of a computer-generated world. However, it is now somewhat of a catch-all term for content, be it real-world or computer generated, that can be displayed in an immersive fashion using a headset or similar device. Immersive video content, or 360-degree video, refers to recordings of the real-world, where the viewer is able to control the viewing direction. Finally, augmented reality allows for computer-generated content to be overlayed on real world content.
There are many potential uses for the technology, ranging from gaming, to interior design and of course, healthcare. Early adopters of virtual reality and augmented reality in medicine have by now had a few years to develop applications and test potential uses of the technology.
360-degree camera
At my hospital, we have been recording procedural content using a head-mounted 3D camera and an immersive 360-degree camera for several years. The footage is post-processed for display on a variety of devices, including head-mounted displays and smart phones, with the intention of delivering high quality content to junior trainees, for example. Medical students are another group that have already benefitted from this technology. A collaboration between Microsoft and researchers at Case Western Reserve University has resulted in the development of an impressive anatomy learning tool using the HoloLens.
Virtual reality technology also been used for other purposes, including stroke rehabilitation and pain management. Several hospitals have also started recording their facilities using 360-degree video, allowing both adult and paediatric patients to “visit” ahead of time, which may help with the fear and anxiety associated with undergoing a trip to the hospital.
Elsewhere, the technology is being used to assist with surgical planning. For example, Surgical Theater LLC has developed a platform that can be used to assist with neurosurgical planning, and may also be incorporated into the operating room workflow. This same technology could also offer patients a new perspective on their medical care, by allowing them to experience customised immersive content and facilitate shared decision making, for example.
It is certain that this type of technology could also help an interventional radiologist in preprocedural planning, too. Of particular interest for an interventional radiologist would be the ability to use augmented reality to overlay a DICOM image over a patient undergoing a procedure. Various image fusion applications and navigational tools have been developed over the years, and augmented reality would seem to be a natural extension. However, there are challenges associated with accurate image registration, soft tissue deformation and usability that will keep developers busy for some time to come.
Finally, augmented reality headsets may allow another method of information delivery to medical staff at the point of care. Being able to review laboratory results, imaging studies and other clinical data in real time at the bedside or in the interventional radiology suite certainly sounds appealing, but is not without challenges. In the era of “information overload”, it is possible that using the technology for this purpose would actually be counterproductive, and may serve as more of a distraction than anything else. Similar concerns have been raised with the use of heads-up displays in cars.
As sales of virtual and augmented reality devices continue to rise, so too will the number of potential uses for the technology in interventional radiology. There is no off-the-shelf solution that is easily deployable in a complex environment such as healthcare; separating hype from the potential tangible benefits to patients and physicians will take several more years. Continued research and refinement will maximise the potential for virtual reality and augmented reality in interventional radiology.
Colin McCarthy is an interventional radiologist at Massachusetts General Hospital in Boston, USA. He has reported no relevant disclosures pertaining to this article.
Corindus has announced receiving 510(k) clearance from the US Food and Drug Administration (FDA) for use of the CorPath GRX system in peripheral vascular interventions. The system brings the added benefits of robotic precision and radiation protection to minimally invasive techniques.
The CorPath system is the first and only FDA-cleared medical device to bring robotic precision to both percutaneous coronary intervention and peripheral vascular intervention procedures, a company release states. The advanced CorPath GRX system broadens the capabilities of the CorPath robotic technology platform from exclusively treating coronary artery disease to include peripheral arterial disease, the release adds.
“My colleagues and I have seen first-hand how CorPath GRX can overcome the challenges of manual percutaneous coronary intervention and I am excited to apply the capabilities of robotics to effectively treat peripheral arterial disease patients,” said Alan Lumsden, chief of the Department of Cardiovascular Surgery at Houston Methodist Hospital, Houston, USA. “As a training site for future robotic interventionalists, I look forward to teaching these techniques to further enhance the quality of care for patients with both coronary artery disease and peripheral arterial disease.”
“CorPath GRX enables me to provide transformational treatment options to my patients suffering from peripheral arterial disease,” said Joseph Ricotta, medical director, Vascular Surgery and Endovascular Therapy, Tenet Healthcare, professor of Surgery, Charles E Schmidt College of Medicine, FAU, Boca Raton, USA. “As a long-time adopter of robotics, I am passionate about the opportunity this technology presents to advance endovascular care while providing a safer work environment for healthcare providers.”
Mark Toland, president and CEO of Corindus, stated, “The new indication aligns with our objective to provide more patients access to the benefits of precise robotic treatment while protecting healthcare professionals from harmful radiation during lengthy peripheral vascular intervention procedures.”
The FDA updates the standards for accepting clinical data from clinical investigations conducted both inside and outside the United States
The Food and Drug Administration (FDA) has today issued the final rule on “human subject protection; acceptance of data from clinical investigations for medical devices”.
The rule updates the FDA’s standards for accepting clinical data from clinical investigations conducted both inside and outside the United States to help ensure the protection of human participants, and to help ensure the quality and integrity of data obtained from these clinical investigations.
The final rule amends FDA regulations on acceptance of data from clinical investigations conducted outside the United States to reflect the increasing globalisation of clinical trials and the evolution of clinical trial standards for protecting human subjects.
The new rule requires that sponsors and applicants provide statements and information about how the investigations conform with good clinical practices. This applies to clinical data submitted to support investigational device exemptions, premarket notifications, requests for De Novo classification, premarket approvals, product development protocols, and humanitarian device exemptions.
The FDA believes that the requirements set out in the final rule provide flexibility for medical device sponsors conducting multinational clinical trials by allowing them to describe the standard for good clinical practice they followed.
The final rule also amends the investigational device exemptions, premarket notifications and humanitarian device exemptions regulations for FDA acceptance of data from clinical investigations conducted within the United States to require a statement regarding compliance with FDA regulations for human subject protection, institutional review boards, and investigational device exemptions. This change is intended to provide consistency across different submission or application types.
Robert Morgan, consultant vascular and interventional radiologist, St George’s Hospital, London, chairman of the CIRSE EBIR committee and a deputy editor on CVIR, told Interventional News that it was important to obtain formal qualification in interventional radiology to protect patients and that a table was worth a thousand words for those seeking to publish their work.
Can you describe your journey into interventional radiology?
During my early years, after qualification as a doctor, I was attracted into radiology by the exciting new procedures radiologists started performing such as angioplasty and stent procedures in the vascular, biliary and urological systems. From day one as a radiology trainee, I intended to be an interventional radiologist. After five years of radiology training, I went to University of Texas Medical Branch, USA, to undertake a fellowship in IR working for Eric vanSonnenberg. Initially intending to be a hepatobiliary interventional radiologist, I soon realised that my interests lay mainly in the vascular system. After staying a further year in Texas as a member of the IR staff, I returned to the UK and worked as a lecturer in IR for Andy Adam at Guy’s and St Thomas’s hospitals for 18 months, before taking up a consultant post in IR at St Mary’s NHS Trust, London.
Which innovation in IR shaped your career the most?
My two main areas of interest are the role of endografting for diseases of the thoracic and abdominal aorta, and the role of IR in the management of lower limb arterial occlusive disease. Therefore, I guess you might say that the main innovations were the advent of bare metal stents and endografts for use in the arterial system, including the aorta.
Who do you regard as your mentors in IR, and what advice of theirs do you carry with you, even today?
Andy Adam has always been a major influence in my IR career. I was always impressed with his mantra that anything can be achieved if you have the will and energy to see it through. Other major influences in making me what I am today are Irving Wells in Plymouth who first taught me how to perform angiography, and Eric vanSonnenberg and Eric Walser (also from UTMB, Texas), who never failed to surprise me with new approaches to a thorny clinical problem.
Could you describe a memorable case, and how IR came to the rescue?
Earlier this year, I treated a patient who illustrates the importance of interventional radiology and how as IRs, we can save patients’ lives. A 23-year-old medical student’s wife had a severe torrential postpartum haemorrhage and after losing 23 units of blood, her obstetricians were losing the battle to stop the bleeding and maintain her perfusion. On a Friday night, I was called back to the hospital to perform emergency angiography and embolisation. She arrived in the angiography department, with a blood pressure of 50/0 and close to cardiac arrest. Pelvic angiography immediately identified the two sites of active haemorrhage in branches of her internal iliac arteries. As her condition was so critical, it was necessary to inflate a balloon in the aorta to reduce the rate of bleeding. With her condition stabilised temporarily, after selectively catheterising the arteries supplying the bleeding points, I embolised the vessels with coils. The procedure took less than an hour. Her condition improved and she experienced no further bleeding. She was discharged from hospital five days later. I am in no doubt that without interventional radiology, she would have died.
IR in the UK has just received subspecialty status. What does this mean for the field?
It is a very important development, which will help considerably to promote the importance of interventional radiology and interventional radiologists to our patients, in our hospitals, in our relationship with our clinical colleagues, and finally in our discussions and negotiations with our political masters.
As the deputy editor of CVIR, what writing tips would you give to interventionalists who are looking to submit their work for publication?
The most commonly submitted articles to most journals are case reports. While sometimes interesting, few are truly unique, and there is a trend to reduce the numbers of case reports published in CVIR. In general, interventionalists would be much better off devoting their time to producing scientific papers based on a research project. Articles should be well-written without excessive verbiage. “A table is worth 1,000 words” is an old saying, and is very true! In my opinion, results should be presented in tabular form, if possible. Finally, do not make your article excessively long. Brevity is best!
Is it true that researchers nowadays break up their work into “bite-sized” publishable chunks in order to gain more publications?
This is an unfortunate trend worldwide, which, as the Reviews Editor for Cardiovascular and Interventional Radiology, one has to be aware of and to restrict, if at all feasible. It is a practice that should be discouraged if at all possible, although in reality it is difficult to police.
The first EBIR exam has just taken place—how many people took part, and what is the importance of this qualification?
The European Board of Interventional Radiology (EBIR) examination was launched at the recent CIRSE congress in Valencia, Spain. Twenty candidates sat the first inaugural examination. We plan to hold examinations in Vienna next March, and at the CIRSE congress in Munich in September 2011. Further examinations are already planned to follow the Munich congress as part of an ongoing commitment to enable all IRs who want to take the examination to achieve the EBIR qualification as quickly as possible. The EBIR qualification is important because it is envisaged that it will rapidly become a recognised benchmark of quality, indicating that interventional radiologists holding the EBIR certificate have achieved the level of knowledge and ability required to practise as IRs in Europe.
How do you think IRs should arm themselves to protect patients from other specialities (who are perhaps not adequately trained) who are carrying out IR procedures?
The procedures that interventional radiologists developed are coveted all over the world by other specialities, who wish to perform these procedures, and think they have the right to do so, despite the total absence of structured training. One hears frequent stories about patients who are harmed by non-IR doctors performing established IR procedures without any formal training. For example, gynaecologists may start performing uterine fibroid embolisation, without undergoing formal training in IR, and rename themselves “interventional gynaecologists”, similarly we hear about “interventional neurologists” performing carotid artery stenting and intracranial thrombolysis, and “interventional nephrologists” performing dialysis fistula interventions. The list is almost endless. IRs can protect themselves from this incursion into their territory by admitting patients to their own beds, undergoing recognised IR training, and undertaking formal certification in interventional radiology. This is one of the main reasons the EBIR certificate has been introduced.
What are the current techniques and technologies that you are watching closely?
Branched endograft technology for the treatment of thoraco-abdominal aneurysms is an exciting, relatively new, treatment that will probably replace open surgery for this condition. Similarly, the final frontier for branched endograft usage is the ascending aorta and aortic arch. Although extremely challenging, I think we will see a workable solution to this conundrum in the next five to ten years.
What fascinates you about interventional radiology even today?
Despite all of the procedures that IRs have introduced to the medical world in the last 30 years or so, I never fail to be amazed at the continuous stream of new innovations which we see on an annual basis. Life is never dull as an interventional radiologist!
Cook Medical has announced key changes that simplify its organisational structure to better support customers.
These changes realign the current sales, marketing, research and development, and customer service teams in addition to establishing new distribution channel management and medical education teams. The changes are a direct result of feedback from customers on how the company could improve operations to make it easier to work with Cook.
Pete Yonkman, president of Cook Group and Cook Medical, told Interventional News: “Our approach to how we are realigning ourselves came from our customers and our employees. In the last year and a half or so, we have been really listening intensely to our customers and our teams in the field and what they came back and told us was that we needed to change how we were doing business and how we were servicing our customers. Healthcare has been changing rapidly over the last few years with hospitals getting bigger and physicians working in much more collaborative environments, so we had to make a change [to reflect this]”.
“Healthcare has evolved rapidly over the last several years and we have reset our teams to focus on what our customers need today,” he said in a press release issued by Cook Medical. “We have seen customers change their structure and decision making to focus on delivering better patient outcomes in a more efficient way, and we have realigned our business to help them meet those goals.”
Key changes in Cook Medical’s structure:
Business divisions: Ten strategic business units merged to form two business divisions, MedSurg and Vascular. This change provides the flexibility to align sales teams to specific customer needs. It also creates a more streamlined contracting process for customers.
The Vascular division brings together the former aortic intervention, peripheral intervention, interventional radiology and lead management businesses into one team.
The MedSurg division comprises six teams that serve customers in critical care, endoscopy, otolaryngology/head and neck surgery, reproductive health, surgery, and urology clinical specialties.
Customer Support and Delivery: All global customer support centres and distribution centres are now centralised under one leadership team to improve customer service and develop innovative solutions that create supply chain efficiency.
Distribution Channel Management: A new global team has been established to maintain our commitment to fully compliant and ethical access of Cook Medical products and to work with third party distributors improving distributor support and distribution channels to serve patients globally.
Research and Development: Engineering reorganised to form a dedicated Research and Development team that actively listens to the needs of customers and develops products that improve the efficiency and effectiveness of patient care.
Medical Education: A new global team has been created, pulling expertise from across the company to improve and support Vista, Cook Medical’s comprehensive educational product training programme for customers.
“We are committed to putting the needs of our customers and our employees at the centre of everything we do,” Yonkman continued. “These changes are exciting and will be beneficial for employees, customers, and ultimately patients.”
There will be no layoffs due to these structure changes.
Balt International announced that it has received CE mark for the Squidperi 34 and 34LD liquid embolic agents.
Squidperi is a non-adhesive liquid embolic agent indicated for peripheral embolization. It is composed of ethylene vinyl alcohol copolymer (EVOH) dissolved in dimethyl sulphoxide (DMSO) and with (suspended) micronised tantalum powder for radiopacity.
“We are excited to provide physicians with the ability to widen their treatment options with Squidperi 34 and 34LD. The unique lighter tantalum and more fluid versions offered by Balt in our liquid embolic product portfolio represent significant advances in embolization treatment solutions,” said Nicolas Plowiecki, president of Balt.
“Balt is now able to offer one of the largest portfolio for peripheral solutions, including EVOH liquid embolic agents, embolic coil systems and patented dual lumen balloon devices. Balt will continue to support the peripheral embolization field by adapting innovative solutions in our product portfolio to create clinically significant advancements for the peripheral embolization field,” commented Pascal Girin, CEO of Balt and president of Balt International.
Since it was established in 1977, Balt has worked with neurointerventionalists to treat complex life-threatening conditions such as strokes, aneurysms and arteriovenous malformations. It designs manufactures and distributes the interventional neuroradiology devices such as catheters, stents and coils that are essential in treating such conditions. The company is now entering into the interventional radiology space with a comprehensive portfolio around embolization solutions with liquid embolic agent and coils.
The US FDA’s granting of an investigational device exemption (IDE) allows MagForce to conduct a pivotal clinical evaluating the company’s NanoTherm therapy for intermediate risk stage patients at selected medical centres in the USA.
The purpose of this focal thermal ablation registration study that will enroll up to 120 men in a single arm study is to demonstrate that NanoTherm can focally ablate cancer lesions for patients who have advanced to intermediate risk prostate cancer stage and are under active surveillance. By focally ablating these cancer lesions, it is anticipated that patients will be able to be maintained in Active Surveillance Programs and to avoid definitive therapies such as surgery or whole gland radiation with their well-known side-effects.
In order to conduct the study, MagForce has already installed two NanoActivator devices, magnetic field applicators in which the NanoTherm therapy is performed, at University of Washington Medical Center in Seattle and at Christus Santa Rosa Hospital – Medical Center in San Antonio.
Ian M Thompson, Jr, president of Christus Santa Rosa Hospital – Medical Center and director, Cancer Therapy and Research Center, a National Cancer Institute-designated Cancer Center at the University of Texas Health Science Center at San Antonio, and Dan W Lin, chief of Urologic Oncology and professor in the Department of Urology at the University of Washington School of Medicine in Seattle, have agreed to be co-principal investigators in the focal thermal ablation registration study.
“We are delighted to announce that NanoTherm therapy has been granted FDA IDE approval. This is a significant milestone in the development of NanoTherm therapy for the treatment of prostate cancer patients in the USA and a significant step towards our goal—to supplement the current standard therapy with a less invasive, effective, and well-tolerated form of treatment. Potentially 50,000 to 100,000 men in active surveillance programmes in the US could benefit from this focal therapy after registration,” said Ben Lipps, chief executive officer of MagForce AG and MagForce USA.
NanoTherm therapy has obtained a CE mark in the European Union to treat brain tumours and is already commercially available to brain tumour patients at renowned treatment centres in Germany.
Potential advantage of focal ablation
Prostate cancer is treatable, if detected early. Within the past two decades, Active Surveillance Programs have been developed in the USA to follow the slow growth of prostate cancer in order to avoid the side-effects of definitive therapy (radiation or surgery), for as long as possible. Currently, there are over 250 Active Surveillance Programs in the USA. Active Surveillance is the merging of watchful waiting and active management into a program that is interactive for the patient, ultimately allowing a man diagnosed with prostate cancer to monitor his disease and have the highest quality of life possible while delaying or even completely avoiding invasive treatments.
For the past decade, these Active Surveillance Programs have been seeking a focal therapy which would ablate the small tumours that have progressed to the intermediate risk stage because approximately 60% of the patients in Active Surveillance Programs who have participated in these programmes for an extended period of time require definitive therapy such as whole gland surgery or radiation.
NanoTherm therapy represents a new concept for interstitial hyperthermia of the prostate. This method is based on the controlled transfer of energy from an alternating magnetic field to biocompatible, superparamagnetic nanoparticles injected into the tumour. The resulting amount of heat generated is suitable to directly destroy cancer cells. MagForce expects to ablate these small lesions of cancer with focal NanoTherm therapy with minimal adverse effects. With successful NanoTherm treatment, it is anticipated that the patients can return to Active Surveillance and keep their quality of life.
There in an increasing physician interest in exploring the role of drug-coated balloons in arteriovenous (AV) access. At the Leipzig Interventional Course (LINC; 30 January–2 February, Leipzig, Germany), Panagiotis Kitrou (Patras, Greece) presented the interim six-month outcomes of the Lutonix AV registry and Andrew Holden (Auckland, New Zealand) reported that the IN.PACT AV access investigational device exemption (IDE) study had completed two-thirds of its enrolment target.
Previous studies have shown that the use of drug-coated balloons in failing AV access fistulas results in significantly higher target lesion patency and far fewer reinterventions to maintain patency than standard angioplasty.
Lutonix AV drug-coated balloon
Lutonix AV registry
Kitrou, who presented the interim six-month outcomes of the Lutonix AV registry, explained that this was a prospective, multicentre, single-arm registry investigating the clinical use and safety of the Lutonix drug-coated balloon catheter for treatment of dysfunctional AV fistulas and grafts.
“At 180-days, the safety is consistent with Lutonix DCB reported outcomes. Efficacy outcomes show that target lesion primary patency is 74.9% and access circuit primary patency (ACPP) is 70.9%,” he revealed.
“The registry’s objective is to demonstrate safety and assess the clinical use and outcomes of the Lutonix DCB for treatment of dysfunctional AV fistulae located in the arm in a heterogeneous patient population in real-world clinical practice. Up to 300 patients will be enrolled at up to 30 international sites,” he said.
The primary efficacy endpoint is target lesion primary patency through six months and the primary safety endpoint is freedom from any serious adverse events involving the AV access circuit through 30 days. Clinical assessment is scheduled for patients at six months and clinical or telephone assessment at three and 12 months.
Kitrou reported that the interim data was based on 236 patients who had been enrolled and treated with a Lutonix AV DCB. “With regard to demographics, just over half were male; the mean age was 67 years with nearly 75% who had hypertension and just over 40% who had diabetes. Nearly 27% had dyslipidemia and nearly 8% were current smokers,” he said.
He made the point that the Lutonix AV registry is “the first and only global drug-coated balloon registry to include arteriovenous fistulae, grafts, central veins and restenotic lesions as well as in-stent restenosis. It includes a larger patient population than existing published data”.
IN.PACT Admiral AV
IN.PACT AV access trial
Holden then presented an update from the IN.PACT AV access IDE trial to state that the objective of study is to evaluate the safety and efficacy of the IN.PACT AV access drug-coated balloon compared to percutaneous transluminal angioplasty for treatment of de novo or restenotic obstructive lesions of native arteriovenous fistulae in the upper extremity.
The principal investigators of the trial are Robert Lookstein (USA); Andrew Holden (New Zealand); and Hiroaki Haruguchi (Japan) and recruitment is ongoing in all these geographies.
This trial is a prospective, global, multicentre randomised single-blinded study that will include 330 patients who will be followed for two years. The trial is adopting a 1:1 randomisation model and will include patients who have lesions that are up to 10cm in length.
Inclusion criteria
“The vessel diameter needs to be between 4 and12mm by visual estimate and includes patients with de novo or non-stented restenostic lesions located between the arteriovenous anastomosis and axillosubclavian junction with less than or equal to 50% stenosis. There is the possibility to include tandem lesions as long as certain conditions are met.
Holden commented on the importance of vessel preparation, “Predilation with a high pressure balloon catheter is extremely important so that the residual stenosis is less than or equal to 30% and there is an absence of a flow-limiting dissection or perforation.”
The primary safety endpoint is a serious adverse event rate involving the AV access circuit through 30 days post procedure. The primary efficacy endpoint is primary patency rate through six months defined as freedom from clinically-driven target lesion revascularisation (CD-TLR) or access circuit thrombosis measured at six months post-procedure. Holden explained that the IN.PACT AV access primary patency is measured out to 210 days endpoint rather than 180 days.
There were nearly 64% diabetic patients in the cohort and 40.8% had concomitant peripheral arterial disease, with the vast majority having undergone a previous revascularisation.
“Baseline clinical and lesion characteristics reflect the early recruitment and geographic distribution and are likely to change with full recruitment. Patient enrolment is around 65% completed,” noted Holden.
The study results with the Ekos system (BTG) were presented at the International Society on Endovascular Therapy (ISET; 3–7 February 2018, Florida, USA).
The findings confirm that bilateral pulmonary embolism patients treated in as little as two hours with a total tissue plasminogen activator (tPA) dose as low as 8mg continue to show improvements in right ventricular-to-left ventricular diameter ratio (RV/LV) ratio over the long term with a very low all-cause mortality rate of 2%, an equally low recurrent pulmonary embolism rate of 2%, and continued quality of life improvements. These data further demonstrate the efficacy and safety of the OPTALYSE PE treatment regimens, a press release from BTG states.
“The long term follow-up results reinforce that a new interventional standard is being set for pulmonary embolism treatment,” said principal investigator Victor Tapson, director, VTE and Pulmonary Vascular Disease Research Program, Cedars-Sinai Medical Center, Los Angeles, USA. “The 2% one-year all-cause mortality rate observed in OPTALYSE PE is much lower than the ~8% rate seen in comparable anticoagulation studies. This is important for institutions that are adopting the new low-dose, shorter duration treatments explored in OPTALYSE PE.”
The authors followed the 12-month outcomes of 101 patients at 17 centres who participated in the OPTALYSE PE study in which the patients were randomised to one of four cohorts. These patients were diagnosed with acute proximal pulmonary embolism in at least one main or proximal lobar pulmonary artery and an RV/LV greater or equal to 0.9 on chest CTA. Patients received treatment within 48 hours of diagnosis. The four cohorts ranged from 2–6 hours in treatment duration and 8mg to 24mg total tPA for bilateral pulmonary embolism.
All cohorts saw a significant reduction in RV/LV by approximately 23 to 26% taken via CTA at 48 hours. For follow-up, patients received echocardiograms at four hours, 48 hours, 30 days, 90 days, and at one year post-Ekos therapy. The initial significant reductions in RV/LV continued to improve in all cohorts through one year – with mean RV/LV ratios in the 0.70 range at one year for all cohorts. Multiple quality of life measurements showed valuable improvements between 30 days and 365 days—further demonstrating the long-term benefit of Ekos therapy.
“Ekos is the only device cleared for the treatment of pulmonary embolism. This is the first time that long-term mortality and quality of life data has been reported for an interventional pulmonary embolism treatment, which continues to show our commitment to evidence-based innovation, predictable and cost-effective procedures, and strong safety profiles that improve patient outcomes and help make the most challenging cases easier,” said Ekos vice president and general manager Matt Stupfel.
A separate registry study, KNOCOUT PE, is currently underway to measure how hospitals are adopting and benefiting from the new standard of care. At full enrolment, the KNOCOUT PE study is expected to include as many as 100 centres internationally. Cases will include those from before and after the release of the original OPTALYSE PE study.
Early data from the first randomised controlled trial to compare two drug-coated balloons (DCBs) suggest that the primary patency obtained with the Ranger DCB (Boston Scientific) is “comparable” to that achieved with the IN.PACT DCB (Medtronic) in the treatment of superficial femoral artery lesions.
COMPARE 1 is an investigator-initiated trial that is funded by Boston Scientific and conducted at 15 German centres. Dierk Scheinert, principal investigator of the trial, presented the data at the Leipzig Interventional Course (LINC; 30 January–2 February, Leipzig, Germany).
“This is really the first randomised controlled trial which compares two different paclitaxel-coated balloons with different coating and paclitaxel dose density for the treatment of femoropopliteal disease,” said Scheinert who presented one-year data from the interim analysis of the trial.
While both Ranger and IN.PACT are coated with paclitaxel, the two devices used different doses of the antirestenotic drug. Ranger uses what is often described as a “low” paclitaxel dosing of 2μg/mm2, while IN.PACT Admiral uses a dose of 3.52μg/mm2 of the drug. The two DCBs also use different excipients; Ranger combines paclitaxel with a citrate ester excipient that is highly hydrophobic, while IN.PACT Admiral uses hydrophilic urea.
The first phase of COMPARE 1 was a pilot study involving 150 patients, before the investigating team secured funding for an extension that can involve up to 414 patients to test the non-inferiority hypothesis, Scheinert noted. Patients were stratified by lesion length into three groups and follow-up points were at six, 12 and 24 months. Scheinert noted that patient retention was “quite acceptable” at 12-months.
The study focused on patients with symptomatic peripheral arterial disease who are classified as being Rutherford class 2–4, with stenotic or occlusive lesions, de novo or restenotic lesions. The study excluded patients with in-stent restenosis and severe calcification. Investigators enrolled patients who had had no previous treatment with DCBs or drug-eluting stents in the treated limb and included patients with lesion lengths of up to 30cm.
In the pilot phase study, 150 patients were randomised to either receive treatment with the Ranger DCB (74 patients), or to receive treatment with an IN.PACT DCB (76 patients). The baseline patient demographics and lesion characteristics were well balanced between two groups. “This was a complex real world lesion subset with lesion length of around 12cm and around 40% chronic total occlusion. Bail out stent placement was 25% in both groups,” said Scheinert.
Primary endpoint
In the pilot, phase one cohort, the primary efficacy endpoint was patency rate at 12 months, which was defined as absence of clinically-driven target lesion revascularisation or restenosis evaluated by Duplex ultrasound. Kaplan-Meier estimates at one year showed that Ranger group had a primary patency rate of 84% and IN.PACT group had a primary patency of 89%. At the end of the follow-up window, pre-specified as ±45 days, the primary patency rate for the Ranger group was 84% compared to 62% in the IN.PACT group, which Scheinert clarified saying: “The standard deviation is bigger here due to the missing data points in terms of unreadable duplexes. That is why I would find these results comparable”.
“The first head-to head comparison of two paclitaxel-coated DCB showed excellent efficacy at one year in both arms. There was a similar patency at one year with the low-dose Ranger compared with the higher dose IN.PACT. Recruitment of the full cohort is ongoing and will likely be completed in the second quarter of 2018. The results are anticipated in the next couple of years,” Scheinert concluded.
An international meta-analysis of clinical experience in patients who received an endovascular arteriovenous fistula (endoAVF) for haemodialysis access was presented at Leipzig Interventional Course (LINC; 30 January–2 February, Leipzig, Germany) 2018.
The meta-analysis, which analysed data from 236 patients with end-stage renal disease at 28 centres across seven countries, demonstrated positive clinical results using the everlinQ endoAVF System (TVA Medical).
The everlinQ endoAVF System received European CE mark in 2014 and Health Canada Medical Device License in 2016 for end-stage renal disease patients. It is not available for sale in the United States and is currently under review by the US FDA.
The results were presented by Tobias Steinke, chief of vascular and endovascular surgery at Schoen Hospital in Düsseldorf, Germany. “Our meta-analysis from four clinical studies and real-world experience across three continents supports the use of the everlinQ endoAVF System as a valuable haemodialysis access option without open surgery,” he said.
The meta-analysis included four clinical studies with pooled efficacy and safety data from 157 and 125 patients, respectively, using both the 4F or 6F versions of the everlinQ catheter system, as well as data from 79 commercial cases, using the 6F catheter system. The following results were demonstrated:
Procedure success rates of 96.8% and 97.8% in the clinical study population and real-world cases, respectively, with an acceptable safety profile
Fistula maturation rate of 88% at three months among evaluable subjects from the clinical studies
Successful cannulation by six months of 74.8% of patients from the study population and 90% in the real-world cases
In addition, the following Kaplan-Meier estimates were reported:
Primary patency at 12 months of 74.8% in the clinical study patients
Secondary patency at 12 months of 79% in the clinical study patients
Functional patency, or durability post-cannulation, of 98.2% at 12 months in the clinical study patients.
Following the meta-analysis data presentation, Robert Jones, consultant interventional radiologist, Queen Elizabeth Hospital, Birmingham, UK, presented a recorded patient case he performed using the everlinQ 4 endoAVF System. The everlinQ 4 endoAVF system, which received CE mark in 2017, uses a 4F catheter system to create an endovascular fistula. “I am very pleased with the utility and patient outcomes I have experienced to date with the new 4F everlinQ endoAVF System,” said Jones. “I am excited to have an endovascular option to offer patients.”
Each year approximately three million people worldwide with end stage renal disease are treated with haemodialysis. However, the first step, creating a viable access in the arm, is often a significant clinical challenge. The current standard approach, surgical arteriovenous fistulas, are associated with high failure rates and they require frequent revisions, a press release from the company states.
The company also announced that the US FDA has accepted the company’s proposal to expand the feasibility study by an additional 15 patients and three new sites, bringing the total number of patients enrolled in the feasibility study to 25 US subjects and six US institutions.
“This is the biggest advance I have seen for people at risk of amputation in my 25 years in practice,” said Daniel Clair, chair of the Department of Surgery at the University of South Carolina and the Palmetto Health-USC Medical Group, Columbia, USA, who performed the tenth case in the feasibility study on 25 January. “In the past, the only thing we had to offer these no-option patients was a segmental amputation of parts of their foot, and most patients ended up losing their entire foot. Major amputation has a very poor overall prognosis in terms of mortality and quality of life for patients and must be improved.”
The FDA also accepted the LimFlow System into its Breakthrough Device Program, a designation previously known as the Expedited Access Pathway (EAP). The designation is intended to speed patient access to breakthrough technologies that provide for more effective treatment of life-threatening or irreversibly debilitating diseases, for which no approved or cleared treatment exists or that offers significant advantages over existing approved or cleared alternatives.
“We are excited to be among the first technologies treating lower extremity disease to be granted access to the FDA’s Breakthrough Device Program,” said LimFlow CEO Dan Rose. “Their decision recognises the novelty of our system and the promise it holds in treating the epidemic of critical limb ischemia. Over 100,000 patients in the USA have a major ischaemic lower limb amputation every year and we look forward to closely collaborating with the FDA to soon bring the LimFlow technology to US patients with no good options today.”
To relieve the symptoms of critical limb ischaemia today, patients are often treated with angioplasty or open bypass surgery. In many late-stage patients, however, neither option is feasible due to extensive disease in the target arteries or other anatomical constraints, the press release explains.
The LimFlow System uses proprietary ultrasound-guided catheters and covered nitinol stents designed to restore perfusion to the ischaemic foot by bypassing diseased arteries and diverting blood flow into the tibial vein to vascularise the foot. Achieving tissue perfusion may relieve rest pain, promote chronic wound healing, reduce major amputations and restore mobility for patients, the release concludes.
Two scientific abstracts of a new vascular embolic device, GPX (Fluidx Medical Technology) were presented this week at the 2018 Leipzig Interventional Congress (LINC; Leipzig, Germany). These were titled “A biomimetic, in situ setting embolization agent” and “A novel embolic with minimal catheter adhesion properties”.
“GPX is a biocompatible gel-particle embolic device that transforms from low-viscosity particles in a syringe to a solid particle after injection into a vessel,” said Jihad Mustapha, interventional cardiologist at the Advance Cardiac and Vascular Amputation Prevention Center, Grand Rapids, Michigan, “It is water-based, does not polymerise or precipitate, and is designed to deliver new control and safety for embolization procedures.”
“The data are exciting. Some embolics stick to catheters during delivery and there have been a number of procedures where catheters are accidentally ‘glued’ into the body,” said George Adams, director, Cardiovascular and Peripheral Vascular Research, Rex Hospital and associate professor, Cardiology, UNC School of Medicine. “This GPX data confirmed that a catheter could be left in the body, with embolic material around it, for hours without risk of catheter entrapment. This may bring new precision, flexibility, and safety to embolic delivery.”
Daniel Sze, an interventional radiologist at Stanford, USA, whilst presenting on the topic “Pipeline liquid embolics: glimpse into the future” at the Global Embolization Symposium and Technologies US (GEST US) 2016 meeting described GPX to state that it was based on the chemistry of marine worm tube formation. “This is a proprietary gel-coated particle that increases viscosity at physiologic salinity. All ingredients [found in the embolic] are in other US FDA cleared products,” he said. Sze explained that there were two different viscosity formulations and a toothpaste-like delivery and control. GPX is noncytotoxic, nonhaemolytic, noninflammatory and nonadhesive, he noted at the GEST US conference.
GPX is under development and not US FDA cleared or CE-marked at this time.
Bentley has launched BeGraft Plus, a covered balloon expandable stent indicated for restoring and improving the patency and treatment of aneurysms, acute perforations and ruptures of the iliac and renal arteries in the European markets.
Eric Verhoeven (Nuremberg, Germany) officially launched the stent on 31 January at the Leipzig Interventional Course (LINC) 2018 (30 January–2 February, Leipzig, Germany).
BeGraft Plus stent system and BeGraft peripheral stent system are indicated for the same conditions, however, BeGraft Plus has exclusive stent properties that make it more suitable for complex and demanding endovascular lesions and/or vascular defects – notably its high radial force and remarkable flexibility, a press release from the company states. These features are associated with reliable sealing properties.
“With BeGraft Plus, we see a new generation of covered stents that offer us new options for the treatment of aneurysm disease,” said Eric Verhoeven, Department of Vascular and Endovascular Surgery, General Hospital Nuremberg and Paracelsus Medical University.
Stéphan Haulon, Hôpital Marie Lannelongue, Paris, France, is another early adopter of this product. “Recently, we have used a lot of different stents in our daily work, but the BeGraft Plus is really a different story because it has the highest radial force we have seen so far for covered stents yet remains very flexible, which makes it easy to use in the most complex procedures and complicated lesions,” he remarked.
Novel wall construction
One size of stent does not fit all, and explaining a key development with BeGraft Plus, Verhoeven pointed out that “BeGraft Plus has a sandwich layer in the wall construction, which makes it more suitable for the treatment of complex aneurysmal disease.” The different unique layers of BeGraft Plus comprise an outer and inner stent with an outer layer and an intermediate layer of ePTFE tubing, which ensures reliable sealing properties.
The BeGraft Plus has up to 3.5 times higher circumferential radial force compared to other balloon expandable covered stents in the market, notes the release. “The high radial force ensures a secure connection to the nitinol rings of branched endografts and strong performance in complex lesions,” said Haulon.
After CE mark-approval in February 2017, distribution began at selected European centres but the BeGraft Plus is now available across Europe in lengths such as 27/28mm, 37/38mm and 57/58mm and diameters from 5–10mm. The BeGraft Plus is 7F compatible up to a diameter of 8mm and 8F for diameters of 9 and 10mm. This is one french larger compared to the regular peripheral BeGraft. To date, over 350 patients have been successfully treated with BeGraft Plus in a small selected group of hospitals.
Thomas Zeller (Bad Krozingen, Germany) presented the 12-month results from Veryan Medical’sMIMICS-2, a prospective, single arm, multicentre clinical study to evaluate the safety and effectiveness of the BioMimics 3D helical, swirling flow stent system in the treatment of patients with symptomatic atherosclerotic disease of the femoropopliteal artery.
Zeller, who along with along with Timothy Sullivan (Minneapolis, USA) and Masato Nakamura (Tokyo, Japan) is a co-principal investigator, presented the MIMICS-2 12-month safety and efficacy data at LINC 2018 in Leipzig, Germany. He announced for the first time that both the primary safety and effectiveness endpoints were met; there were no stent fractures; the Kaplan-Meier estimate of freedom from loss of primary patency at 12 months was 81.9% at day 365 and the Kaplan-Meier estimate of freedom from clinically-driven target lesion revascularisation (CD-TLR) at 12 months was 88.8%.
He commented further that these MIMICS-2 results reinforce the results of the company’s earlier MIMICS-RCT study in a larger, more challenging patient population. The BioMimics 3D primary patency result at 12 months is similar to those reported for drug-eluting stents and drug-coated balloons which suggests that natural swirling flow is an alternative to antiproliferative drugs, a press release from the company states.
Conducted under a US FDA investigational device exemption with concurrence of the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) under the FDA/PMDA Harmonisation By Doing collaboration, MIMICS-2 enrolled 271 patients undergoing femoropopliteal intervention across 43 investigational sites in US, Japan and Germany.
The BioMimics 3D stent has a three-dimensional helical shape, designed to impart natural curvature to the diseased femoropopliteal artery, promoting swirling flow and elevating wall shear, which has a protective effect on the endothelium. The helical shape of the BioMimics 3D stent is also designed to facilitate shortening of the stented segment during knee flexion and mitigate the risk of stented segment compression causing localised strains that in a straight stent may lead to stent fracture and chronic vascular injury, the release adds.
Chas Taylor, Veryan’s CEO commented: “The achievement of a successful outcome to our pivotal study, which has provided data for our premarket approval applications in the US and Japan, is a major milestone for Veryan as we build toward global commercialisation of our BioMimics 3D swirling flow stent. We would like to thank the principal investigators of MIMICS-2; and all the investigators and research teams that participated in the study. We are delighted that the MIMICS-2 results reinforce those from our earlier MIMICS randomised clinical trial. The combined results from these studies and other ongoing investigations support our belief that BioMimics 3D offers an important solution for both primary and complementary stenting in the femoropopliteal artery.”
Varian Medical has announced it has signed an agreement to acquire all the outstanding shares of Sirtex Medical for A$28 per share in cash. On a fully diluted basis, this represents a total equity purchase price for the acquisition of approximately US$1,283 million as of the date of this release.
The acquisition has been unanimously approved by the Board of Directors of each company and the Sirtex Board of Directors has agreed to unanimously recommend that Sirtex shareholders approve the transaction, provided that an independent expert, to be retained by Sirtex, considers the transaction to be in the best interests of Sirtex shareholders and in the absence of a superior offer.
This acquisition of a global leader in radioembolization extends Varian’s leadership in radiation medicine, expands Varian’s addressable market into interventional oncology, and is consistent with Varian’s long-term growth and value creation strategy. Varian expects to leverage its capabilities in treatment planning and delivery, image guidance and processing, oncology practice management software, and radiation safety in combination with Sirtex’s interventional oncology platform to provide customers of both companies with a wider range of cancer care solutions.
“This acquisition is the latest step in Varian’s long-term strategy to become a global leader in multi-disciplinary integrated cancer care solutions,” said Dow Wilson, CEO of Varian. “The combination of the two companies will expand the reach of the Sirtex platform by making it more broadly available to the clinical community. Our companies share a common vision of a world without fear of cancer, and we look forward to completing this acquisition and positively impacting more patients’ lives around the world.”
Sirtex’s lead product is a targeted internal radiation therapy for certain liver cancers. Approximately 80,000 doses of SIR-Spheres Y-90 resin microspheres have been supplied to treat patients with liver cancer at over 1,090 medical centres in over 40 countries. It has premarket approval from the US Food and Drug Administration (FDA), the European Union (CE mark) and Australia’s Therapeutic Goods Administration (TGA). Sirtex has manufacturing capabilities in the United States, Singapore and Germany.
Sirtex generated annual revenues of A$234mm in the fiscal year ended June 30, 2017. Sirtex has approximately 300 employees worldwide and maintains sales and distribution operations primarily in the United States, Europe and Asia.
The transaction is expected to close in late May 2018.
Medtronic added to its robust body of clinical evidence supporting the IN.PACT Admiral drug-coated balloon with new presentations that demonstrated durable and consistent clinical outcomes in peripheral artery disease.
The new data presented at the Leipzig Interventional Course (LINC) in Leipzig, Germany, included the two-year results from the MDT-2113 study (IN.PACT SFA Japan) and data from a critical limb ischaemia subgroup analysis from the IN.PACT Global study.
Two-year Japan data
New data from the IN.PACT SFA Japan Study were presented by Osamu Lida, Kansai Rosai Hospital, Japan. The study enrolled 100 patients across 11 sites in Japan and randomised treatment to either drug-coated balloon (n=68) or percutaneous transluminal angioplasty (n=32). The results were consistent with two-year findings from the pivotal IN.PACT SFA study, showing a low clinically-driven target lesion revascularisation (CD-TLR) rate and high patency rate.
“Across superficial femoral artery trials, IN.PACT Admiral has consistently demonstrated superior safety and efficacy compared to percutaneous transluminal angioplasty,” said Lida. “We are pleased to see comparable results in Japan at two-years with durable patency outcomes, low target lesion revascularisation, and no instances of thrombosis. There has been a critical unmet need in Japan for new technologies that safely and effectively treat peripheral arterial disease, and we believe IN.PACT Admiral is well-positioned to meet this need.”
IN.PACT Admiral SFA Japan demonstrated 79.8% primary patency in the drug-coated balloon group as compared to 46.9% in the plain balloon angioplasty group at two years based on Kaplan-Meier Estimate (p<0.001). The two-year results also demonstrated a CD-TLR rate of 9.1% for the drug-coated balloon group compared to 20.7% in the plain balloon angioplasty group (p=0.177) and a freedom from CD-TLR based on Kaplan-Meier estimate of 90.8 for the DCB group compared to 81.3 percent in the PTA group (p=0.114). In IN.PACT SFA Japan, major adverse events were also lower for the DCB at two years (15.2 percent compared to 24.1 percent in the PTA group; p=0.384), with no major target limb amputations. There were no additional safety concerns at two years.
Medtronic’s announcement follows the recent approval of IN.PACT Admiral from the Japanese Ministry of Health, Labor and Welfare (MHLW) for the treatment of peripheral artery disease in the upper leg, specifically, in the superficial femoral arteries) and behind the knee (popliteal arteries). The MHLW also granted reimbursement approval for the IN.PACT Admiral in December of 2017. IN.PACT Admiral is expected to commercially launch in Japan after completing the conditions associated with Shonin approval.
Critical limb ischaemia cohort analysis
Michel Reijnen, vascular surgeon, Rijnstate Hospital, The Netherlands, presented the one-year results from the critical limb ischaemia subset of the IN.PACT Global Study, including data from 156 patients with Rutherford classification categories four and five. IN.PACT Admiral demonstrated consistent treatment effect among this group of patients. Data showed comparable effectiveness with a freedom from CD-TLR based on Kaplan-Meier Estimate of 86.6% (Rutherford category four) and 85.5% (in Rutherford category five) (p=0.6881). The rate of major target limb amputations remained low at 1.4% overall. Additionally, IN.PACT Admiral had a clear impact on improved quality of life as measured by the EQ-5D from baseline to 12 months (p<0.001).
“The treatment of critical limb ischaemia in peripheral arterial disease remains a challenge and has led to the need for more clinical evidence around the safety and efficacy of drug-coated balloon in this population,” said Reijnen. “The data presented are very encouraging in that we were able to confirm IN.PACT Admiral’s strong performance in this clinically complex patient subset, as well as improved quality of life.”
Medtronic has announced the initiation of its investigational device exemption (IDE) study for the Abre venous self-expanding stent system. The ABRE IDE Study will evaluate the safety and effectiveness of the Abre stent in patients with iliofemoral venous outflow obstruction.
The first procedure was performed in December of 2017, by Erin Murphy, director of the venous and lymphatic programme at Carolinas HealthCare System’s Sanger Heart & Vascular Institute in Charlotte, USA, and national principal investigator for the ABRE IDE Study in the USA.
The multicentre, single arm study intends to enrol 200 patients with deep venous disease from up to 35 sites throughout the USA and Europe. The primary efficacy endpoint will evaluate patency at 12 months, which is defined by freedom from occlusion and freedom from clinically-driven target lesion revascularisation (CD-TLR). The primary safety endpoint will evaluate the incidence of composite major adverse events (MAE) at 30 days following stenting of an obstruction in the iliofemoral venous segment. Data from the study will be used to support the Abre stent US pre-market approval (PMA) application for the treatment of symptomatic iliofemoral venous outflow obstruction in patients with venous occlusive disease.
“The launch of the ABRE IDE Study marks the beginning of an important journey to establish new options for the treatment of deep venous disease,” says Murphy. The first procedure was performed at Sanger Heart & Vascular Institute on a patient with Nonthrombotic Iliac Vein Lesion (NIVL) who is doing well post-treatment. We are excited to continue enrolment at our sites throughout the USA and Europe.”
Medtronic estimates deep venous obstruction affects more than 24 million individuals worldwide. Deep venous obstruction occurs when veins in the deep venous system become compressed and restrict blood flow. It can result in discomfort and pain, limit a patient’s mobility, and impair quality of life.
The Abre stent is an investigational device in the USA intended for permanent implant in the iliofemoral vein. It is pre-mounted on a 9 French delivery system and features a nitinol stent with a tri-axial shaft design. The stent utilises an open-cell design with three connection points between the cells that are intended to enable flexibility and conformability. Upon deployment, the Abre stent uses an optimised balance of strength and flexibility to exert an outward force and open the vein.
“Deep venous disease can cause pain, swelling, and blood clots, which can potentially be devastating to patients,” says Stephen Black, consultant vascular surgeon, Guy’s and St Thomas’ Hospital, London and European principal investigator for the ABRE IDE Study. “As a result, there is a critical need for treatment options that are safe, effective, and durable. We look forward to using the Abre stent in the restoration of patency in patients with deep venous disease.”
In the USA, Abre is an investigational device and not yet approved for commercial use. Abre received CE mark approval in April of 2017 and is intended for use in the iliofemoral veins for treatment of symptomatic venous outflow obstruction.
The American Heart Association and American Stroke Association released updated ischaemic stroke guidelines that were published in Stroke, and released during the International Stroke Conference 2018 (ISC; 24–26 January 2018, Los Angeles, USA).
A major new recommendation increases the time window to 24 hours for selected acute ischaemic stroke patients to receive mechanical thrombectomy, a procedure only advisable in clots that block large vessels. The new recommendation will likely result in more patients becoming eligible for thrombectomy since more patients will be treated based on clinical presentation rather than a time cut-off alone.
The new guideline, based on the most recent science available, recommends that large vessel strokes can safely be treated with mechanical thrombectomy up to 16 hours after a stroke in selected patients. The expanded treatment window from six to 16 hours is based on clinical evidence from the DAWN and DEFUSE 3 trials. Under certain conditions, based on advanced brain imaging, some patients may have up to 24 hours for treatment with mechanical thrombectomy, based on the DAWN Trial criteria. The previous time limit was six hours.
The purpose and scope of 2018 American Heart Association/American Stroke Association guidelines were presented by William J Powers, Chapel Hill, USA at ISC.
“The purpose of these guidelines is to provide an up-to-date comprehensive set of recommendations for clinicians caring for adult patients with acute arterial ischaemic stroke in a single document. They address prehospital care; urgent and emergency evaluation; treatment with intravenous and intra-arterial therapies; and in-hospital management including secondary prevention measures that are appropriately instituted within the first two weeks,” said Powers, the guideline writing group chair and professor of neurology, University of North Carolina.
Explaining two of the new recommendations, Powers said: “In selected patients with acute ischaemic stroke within six to 16 hours of last known normal who have large vessel occlusion in the anterior circulation and meet other DAWN or DEFUSE-3 eligibility criteria, mechanical thrombectomy is recommended. In selected patients patients with acute ischaemic stroke within 16 to 24 hours of last known normal who have large vessel occlusion in the anterior circulation and meet other DAWN eligibility criteria, mechanical thrombectomy is reasonable.
“The expanded time window for mechanical thrombectomy for appropriate patients will allow us to help more patients lower their risk of disability from stroke,” he noted, saying “that is a big deal. That is potentially a lot more people who could benefit, and it has completely changed the landscape of acute stroke treatment.”
Another new recommendation broadens the eligibility for administering intravenous alteplase, the only US FDA-approved clot-dissolving treatment for ischaemic stroke. Previously, patients with mild strokes were not eligible for clot-busting treatment, but new research suggests it could help some of these patients. The guideline says doctors should weigh the risks and benefits in individual patients, because the drug can decrease disability when given promptly and appropriately.
The guideline is based on a review of over 400 peer-reviewed published studies. The studies were examined by a group of experts in stroke care and are the most comprehensive recommendations for treating ischemic stroke issued since 2013.
Cerenovus, part of the Johnson & Johnson Medical Devices Companies, today announced the launch of the Galaxy G3 mini coil, its smallest and softest embolic finishing coil, for use in the endovascular treatment of cerebral aneurysms and haemorrhagic stroke. The company received 510 (k) clearance for the device from the U.S. Food and Drug Administration (FDA) in late September 2017.
Galaxy G3 mini coils are about 25% softer than the Galaxy G3 XSFT coils, the company’s other finishing coil and have an ultra-low coil profile with a primary wind diameter of 0.009-inches, the lowest available in the Cerenovus Spectra family oanf coils.
The new coil is the latest addition to the Galaxy G3 microcoil portfolio of filling and finishing coils which all feature stretch resistance technology and a proprietary complex random loop design. The Galaxy G3 mini coil is designed to have a random complex shape which may make the coil conformable and enable them to seek and fill open spaces in cerebral aneurysms to achieve higher packing densities, which have been shown to lower patient retreatment rates.
Brain aneurysms are weak spots on blood vessels that have the potential to rupture and cause bleeding within the brain. They can lead to serious complications, including haemorrhagic stroke, permanent nerve damage or death. According to the American Stroke Association, about 3–5 million people in the United States have cerebral aneurysms.
During a minimally invasive coiling procedure, tiny coils are inserted directly into the aneurysm to induce clotting or embolisation and prevent rupture. The coils may be of various shapes, sizes and configurations and are deployed by the physician based on the anatomy and shape of the aneurysm.
“Now, Cerenovus brings a family of endovascular coils that offers physicians a total procedural solution that can be used from start to finish or from periphery to core,” said Shlomi Nachman, company group chairman of Johnson & Johnson Medical Devices Cardiovascular & Specialty Solutions. “We will continue to work to advance the treatment of cerebral aneurysm and both haemorrhagic and ischemic stroke to help physicians give stroke patients a new lease on life.”
Penumbra announced results of the company-sponsored PROMISE study, demonstrating real-world safety and efficacy of the Penumbra system with ACE 68 and ACE64 reperfusion catheters as frontline treatment in patients with acute ischaemic stroke.
The PROMISE study used the ADAPT (A direct aspiration first pass technique) approach and its results were presented at the International Stroke Conference (ISC 2018) in Los Angeles, USA.
“ADAPT as a frontline approach demonstrated excellent results – both in revascularisation rates and clinical outcomes,” said Peter Schramm, department of Neuroradiology, Universitatsklinikum Schleswig-Holstein, Lubeck, Germany. “In addition, the low mortality rate and strong safety profile indicate that stroke revascularisation with aspiration is safer and more effective with ACE68 and ACE64 than ever before.”
The PROMISE study was a prospective, single-arm multicentre study that enrolled 204 patients across 20 European centres. Core-lab adjudicated mTICI 2b–3 revascularisation was attained in 93.1% of patients, with 39.2% of patients attaining mTICI 3 revascularisation. Clinical independence, measured by modified Rankin Score (mRS) 0–2, was achieved in 61% of patients at 90 days. Key secondary safety related endpoints also demonstrated excellent results: All-cause mortality at 90 days was 7.5%, symptomatic intracranial haemorrhage (sICH) at 24 hours was 2.9% and embolization in new territories was 1.5%. Median procedure time, as measured as groin puncture to mTICI 2b–3 revascularisation, was 31 minutes [20–53].
The post-market, non-interventional, multicentre, non-randomised, single-arm study will enroll approximately 150 patients across 25 sites in Europe and Russia, and will evaluate the safety and performance of a ChEVAR procedure using the Endurant II/IIs stent graft system (Medtronic) in a real-world setting.
The first enrolment at St Franziskus Hospital in Munster, Germany, was led by Giovanni B Torsello, chief of Vascular Surgery and principal investigator for the ENCHANT study.
ChEVAR refers to the use of a parallel graft chimney technique that uses covered renal stents with a standard aortic stent graft. The study is the first to assess the clinical outcomes, safety, and performance of the ChEVAR technique for treating patients with complex aneurysms with short infrarenal neck lengths of greater than or equal to 2mm in a real-world setting.
“We are excited to initiate this study in a real-world population, which will build upon existing clinical evidence for the ChEVAR technique as a standardised approach for treating short infrarenal necks,” said Torsello. “We believe the study marks another significant milestone for patients with complex forms of aortic disease who, until recently, had not been suitable for a minimally invasive endovascular procedure.”
The ENCHANT study’s primary safety endpoint is major adverse events through 30 days post-index procedure. The primary performance endpoint is the proportion of enrolled patients who have technical success at the time of the index procedure and are free from secondary interventions through 365 days, a press release from the company states.
“As the only stent graft company with a ChEVAR indication, we are deeply invested in delivering solutions, in partnership with the clinical community, that are backed by clinical rigour and address the unmet needs of abdominal aortic aneurysm patients,” said Daveen Chopra, vice president and general manager of the Aortic business, which is part of the Aortic & Peripheral Vascular division at Medtronic.
The Endurant II/IIs stent system received CE mark for a ChEVAR indication in December 2016.
This approval also expands the number of chemotherapeutic drugs that can be loaded onto LifePearl to include idarubicin and epirubicin, a press release from the company states.
LifePearl class III device is used in the treatment of primary and secondary liver cancer. It comprises a range of microspheres that are biocompatible, hydrophilic, precisely calibrated and capable of loading and releasing chemotherapeutic agents in a controlled manner.
The recent approval to load additional chemotherapeutic agents onto the LifePearl device provides more treatment options for interventional radiologists performing transarterial chemoembolization (TACE) with drug-eluting microspheres (DEM-TACE). LifePearl is currently the only drug-eluting-microsphere CE marked as a Class III device with the capability of loading four chemotherapeutic agents: doxorubicin, idarubicin, epirubicin and irinotecan, the release adds.
Since its launch in 2015, LifePearl has been used in approximately 8,000 TACE procedures in Europe, the Middle East and Africa. LifePearl has five publications in various scientific journals and multiple presentations in interventional radiology congresses, material from Terumo states.
A recent study demonstrated that amongst 11 anticancer drugs used in TACE, idarubicin is the best in vitro candidate drug for this treatment based on three hepatocellular carcinoma cell lines. Due to its high lipophilicity, idarubicin penetrates cell membranes more efficiently than other anthracycline compounds, notes the release.
Boris Guiu, from CHU Montpellier, France said: “CE mark approval for LifePearl loaded with idarubicin is a first and important step towards an optimised regimen for TACE for hepatocellular carcinoma in daily practice. LifePearl [microspheres] can completely and rapidly load idarubicin and provide prolonged release. This is of particular importance, given the greater efficacy of idarubicin on hepatocellular carcinoma cancer cell lines, as compared to other drugs including doxorubicin and epirubicin”.
Emergency mechanical thrombectomy dramatically increases a stroke patient’s chance of a full recovery. The UK does not have enough skilled doctors to provide the procedure. NHS England plans to roll out the technique nationally, but will need at least another 50 extra specially trained radiologists.
Now interventional radiology leaders have teamed up to produce guidance to help hospitals train more doctors in the technique. They have issued guidance to help hospitals train more specialist radiologists to perform life-changing stroke thrombectomy treatment.
To combat a UK-wide shortage of interventional neuroradiologists – who normally perform stroke thrombectomy – the umbrella group is encouraging hospitals to support existing interventional radiologists to train in the new technique.
Currently, there are only 74 fully-trained interventional neuroradiologists in England, however, official plans to roll out stroke thrombectomy would require at least 120 trained experts in England, with additional interventional neuroradiologist expertise needed across the UK.
The quick guidance document covers topics such as the agreements between doctors and their employer trusts to formalise training arrangements, what interventional radiologists learning stoke thrombectomy need to know about stroke management, and how mentoring and training takes place in practice.
Andy Clifton, president of the British Society of Neuroradiologists, said: “Stroke thrombectomy is a game-changer in the management of acute stroke. It is a technically challenging procedure that is currently carried out by interventional neuroradiologists. There is a shortage of interventional neuroradiologists in the UK and therefore to expedite roll out of this procedure across the UK, BSNR/UKNG has worked with our interventional radiology colleagues to facilitate and encourage trusts to consider appropriate formal training of their current consultant interventional radiologists in this technique.”
Jai Patel, chair of The Royal College of Radiologists interventional radiology committee said: “Stroke thrombectomy can have a huge impact on the outcome and recovery of a stroke patient, but it is a time-sensitive intervention and needs to be performed by expertly trained interventional radiologists. Sadly, the NHS does not have the infrastructure and manpower to deliver this ground-breaking treatment. However, this collaboration between stroke thrombectomy experts and our practical guidance for doctors and hospitals is a great first step to making sure we have the skilled workforce we need so that more stroke victims can benefit.”
Trevor Cleveland, president of the British Society of Interventional Radiology, said: “NHS England hopes that around 8,000 patients every year will be able to benefit from stroke thrombectomy, however, currently only a few hundred do so because we need more trained doctors. Training enough radiologists to carry out this specific life-changing technique will not happen overnight, however, we hope to encourage and support clinicians and hospitals to invest their time and expertise to make the promised roll out of stroke thrombectomy services – at least in England – a reality.”
Szela brings nearly 30 years of progressive leadership experience to Surefire building global billion-dollar brands, advancing pipeline products in the biotechnology, medical products, and pharmaceutical industries, while creating value for stakeholders.
Surefire Medical develops infusion technologies that help physicians deliver therapy deeper into liver tumours while protecting healthy tissue, giving patients greater confidence in their cancer care.
Szela succeeds James Chomas, Surefire’s founder, who has served as CEO and president since 2009. Chomas will remain a director on the company’s board and an active member of the senior management team. In the operations of the company, Chomas will also serve as chief technology and oncology strategy officer with a focus on the discovery and application of oncology drug delivery technologies.
“Immune therapies are reshaping the battle against cancer. The innovative application of technology at Surefire positions the company to become a leading medical device provider in the treatment of cancer,” said Mats Wahlström, Surefire’s chairman of the Board. “Mary brings the leadership capabilities necessary to fulfil the full potential of what Surefire’s technology can do to transform cancer care on a global scale. Her proven commercial track record, coupled with her passion and commitment to patients, aligns with the company’s mission to better deliver quality of life for cancer patients.
Szela previously served as chief executive officer of Novelion Therapeutics, a rare disease company, where she orchestrated the merger of Aegerion Pharmaceuticals and QLT Therapeutics. Additionally, she secured the approval, registration and launch of lomitapide in Japan, oversaw the European filing for metreleptin, and built a clinical development platform to treat multiple diseases using leptin hormone replacement therapy.
A new study has found that a test that identifies circulating tumour cells (CTCs) present in the bloodstream can detect colorectal cancer at an early stage, with accuracy ranging from 84 to 88%. Collection of CTCs from the blood is one form of “liquid biopsy.”
Most prior studies using CTCs have been able to detect late-stage colorectal cancer, and this study is one of the first clinical studies to show that CTCs can be useful for detecting early, more treatable stages of the cancer. These findings were presented at the 2018 Gastrointestinal Cancers Symposium in San Francisco, USA.
CTCs break away from the primary tumour and travel into the bloodstream where they can then form new tumours at distant locations.
“Our study is important because there is still some reticence among patients to use stool-based tests or have an invasive exam like colonoscopy to detect colorectal cancer,” said lead study author Wen-Sy Tsai, assistant professor, Linkou Chang Gung Memorial Hospital, Taipei, Taiwan. “Our results may point to a solution for people who are reluctant to get an initial screening colonoscopy or are not compliant in returning stool-based test kits that they get from their doctors.”
About the study
This study was conducted at Chang Gung Memorial Hospital, Taoyuan, Taiwan. The researchers enrolled 620 people over the age of 20 who were coming to the hospital for routine colonoscopies or had a confirmed colorectal cancer diagnosis. Based on the colonoscopy and biopsy, 438 people were found to have either adenomatous polyps (pre-cancerous growths) or early to late-stage colorectal cancers. The remaining study participants had no signs of a precancerous growth or colorectal cancer (comparison group).
All 620 enrollees had 2ml of blood tested for CTC analysis through a routine blood draw.
The blood samples were processed using CMx, an assay that captures rare CTCs — such as those found in early-stage cancer — on a lipid-coated chip that mimics human tissue. The results of these assays were then compared in a blinded analysis with the colonoscopy results.
In prior studies, this assay was found to be able to detect very small numbers of CTCs, even down to the level of one CTC per billion blood cells found in most polyps.
Key findings
The researchers focused on specificity of the liquid biopsy test, which is the proportion of healthy individuals correctly identified as not having polyps or cancer. “We believe our high specificity results are important because a high number of false-positive results would discourage many people who are considering getting screened for colorectal cancer from doing so,” said Tsai. The specificity values were 97.3%, indicating a very low (less than 3%) probability of a false-positive result.
The study results showed that sensitivity ranged from 77% for detection of CTCs in precancerous lesions, to 87% for stage I-IV cancers. The researchers also calculated the accuracy of the results, which takes into account both sensitivity and specificity, and found that the accuracy of the test was high and ranged from 84 to 88% between pre-cancerous and cancerous samples. The accuracy of this test was superior to that of faecal occult blood testing (FOBT).
Next steps
“Recent surveys have found that over 80% of patients who are reluctant to undergo colonoscopy screening would be receptive to a blood test over stool-based tests,” said co-author Ashish Nimgaonkar, gastroenterologist and Medical Director in the Center for Bioengineering Innovation and Design at Johns Hopkins University, Baltimore, USA. “A number of studies have found that affordability was the number one reason for not being screened, however this test is highly affordable and can potentially cost less than US$100.” Nimgaonkar also noted that colonoscopy would still be the gold-standard diagnostic test and would be needed for tumour or polyp sample removal if an individual had a positive CTC test.
The authors are currently planning to validate the use of CTC testing in the general population in Taiwan and to conduct studies in the USA. According to the authors, the technology used in this study potentially could be used with other solid tumours, such as breast, lung, and prostate cancer.
This study was sponsored by the Ministry of Health in Taiwan and Chang Gang Memorial Hospital.
Surmodics has announced receiving US FDA 510(k) clearance for its Telemark 0.014” coronary and peripheral support microcatheter. The company is making this product available for US distribution in the coming months.
The Telemark support microcatheter offers crossability for complex coronary and peripheral lesions and combines the company’s Xtreme composite shaft technology with a high-performance Pristyne hydrophilic coating that together provide deliverability, kink resistance and lesion crossing, a press release says. The Telemark microcatheter’s tapered profile design has an outer diameter ranging from 2.6F to 1.4F for effective penetration of tough, calcified lesions.
“Our Telemark microcatheter incorporates advanced technology that enables an exceedingly low crossing profile, excellent trackability and resistance to kinking, even in complex coronary and peripheral lesions, where there is still a great market need,” said Gary Maharaj, president and CEO of Surmodics.
The development of the Surmodics Telemark 0.014” support microcatheter is a step forward in the company’s strategy to be a provider of whole-product vascular solutions for its medical device customers. Surmodics has complete capabilities for design, development and high-volume manufacturing of a wide variety of highly differentiated balloon catheter and specialty catheter solutions.
Enrolment is complete in the Lutonix below-the-knee trial with BD planning to submit a pre-market approval application to the US Food and Drug Administration (FDA) in late 2018.
The Lutonix below-the-knee trial is a prospective, multicentre, randomised, controlled trial intended to demonstrate superior efficacy and non-inferior safety of the Lutonix 014 drug coated balloon (DCB) as compared to standard angioplasty balloon catheters for treatment of severe claudication and critical limb ischaemia patients with stenotic or occlusive lesions in the below-the-knee arteries.
The Lutonix below-the-knee trial is the only on-going DCB trial for below-the-knee arteries in the USA and has enrolled more than 450 patients over the past four years.
The Lutonix 014 DCB product for below-the-knee has been commercially available in Europe, Canada and Australia for treatment of the arteries associated with critical limb ischaemia since 2013.
The registry will combine noninvasive, vascular ultrasound testing data with vascular treatment and outcomes data, making it possible to analyse the relationships between diagnosis and care provided to patients with vascular disease.
The Society for Vascular Ultrasound (SVU), the Society for Vascular Surgery (SVS), and Medstreaming-M2S, have announced the development of the Vascular Quality Initiative (VQI) Vascular Ultrasound Registry. The new registry is an expansion of the SVS VQI and will allow more comprehensive analysis and improvements in the care of patients with vascular disease.
Groundbreaking in this registry will be the inclusion of actual ultrasound images which will make future machine analysis and learning possible from the collected registry, which currently does not exist, a press release regarding the registry’s launch notes.
The Vascular Ultrasound Registry’s initial efforts will focus on collection and analysis of data associated with the diagnosis and treatment of carotid artery disease. The development of the registry and ongoing research related activities are being led by a VQI Vascular Ultrasound Registry Task Force, chaired by physicians David Dawson and Gregory Moneta.
It is anticipated that the registry will provide the means and an impetus to promote vascular laboratory standardisation and thereby improve patient care. “Noninvasive vascular testing has evolved to the point where it is being relied upon heavily to direct patient medical management decisions”, said James Wilkinson, SVU executive director. “With the rapid growth and diversification in the number of medical specialties providing testing, there is a lack of standardisation in the delivery of testing and the reporting of results. Targeted, yet broad-based research will significantly contribute to standardisation efforts.”
Fundamental to the VQI Vascular Ultrasound Registry is the ability to link technical data and images to the clinical data collected from the SVS VQI’s existing registries. “The addition of the VQI Vascular Ultrasound Registry, to the existing VQI registries, will further aid the VQI’s mission of improving vascular care by enhancing the data we can make available to our members. We are also pleased that this registry expands the reach of the VQI to include vascular technologists, sonographers and other professionals in the vascular laboratory setting. The VQI has long embraced a team-approach to care with 59% of VQI membership coming from specialties outside of vascular surgery, including cardiology and radiology,” said Jens Eldrup-Jorgensen, medical director of the SVS Patient Safety Organisation.
Efficient data capture
A key to the success of any registry is providing means for efficient data capture. The VQI Vascular Ultrasound Registry leverages the infrastructure of the preexisting registry with linkages to ultrasound images from the vascular laboratory. “Medstreaming-M2S’s specialty based workflow solutions, along with its clinical data management system for structured data aggregation can be used for uploading of data and images,” noted Wael Elseaidy, Medstreaming-M2S CEO. Initially, only a select number of current VQI sites will participate, but Vascular Ultrasound Registry participation is expected to be broadly available in the next phase of the programme, along with an increase in registry content and scope of projects.
“Unique to the VQI Vascular Ultrasound Registry is the inclusion of an imaged based registry component, which will include the actual ultrasound images acquired during patient studies. When combined with powerful analytics and potential for machine learning, we foresee opportunity to normalise ultrasound image data submitted from different sites, develop new benchmarking standards, further explore and promote utilisation of all the information embedded in the images,
A new study suggests thoracic endovascular aortic repair (TEVAR) may be appropriate in uncomplicated Type B aortic dissection (TBAD) based on several anatomic criteria determined by CT imaging.
Historically, the standard of care for uncomplicated patients with TBAD has been medical management because of favourable one-year survival rates compared with open replacement of the descending thoracic aorta.
But medical management alone is associated with a 40% incidence of aneurysmal dilation of the outer wall of the false lumen in the first five years. There has been little data on which patients benefit from early TEVAR.
Aortic dissection is the most common catastrophic event affecting the aorta with an incidence of 3.5 per 100,000 person-years. Stanford Type A dissection, involving the ascending aorta and arch, is treated by emergent replacement of the ascending aorta to protect from coronary artery obstruction and/or cardiac tamponade.
Conversely, Stanford Type B dissection, involving the aorta distal to the left subclavian artery, has been traditionally treated with aggressive antihypertensive medication as prior study has revealed no significant survival advantage of surgery over medical therapy.
More recent data suggest that TEVAR coverage of the proximal entry tear in acute TBAD complicated by persistent pain, impending aortic rupture and/or distal aortic branch malperfusion, results in superior 30-day mortality over medical therapy. Further, it appears that aortic remodelling occurs along the stented segment of the aorta preventing aneurysmal degeneration.
As reported in the January 2018 edition of the Journal of Vascular Surgery, researchers from the Massachusetts General Hospital, led by vascular surgeon Mark F Conrad, retrospectively reviewed their experience treating 254 patients presenting with uncomplicated TBAD from 2000–13 and followed with serial CT imaging. The goal of the study was to identify clinical and anatomic factors associated with the need for late (defined as greater than 180 days from presentation) aortic intervention in patients presenting with uncomplicated TBAD.
At a mean follow up of 6.8 years, they found that 38.2% of patients underwent aortic intervention, mainly for aneurysmal degeneration, with a 6.2% 30-day operative mortality. Two-thirds involved open surgical intervention and the remainder endovascular therapy. After dividing their series into those who required intervention versus those who did not, they found no difference in the groups based on demographics (age, gender, race, presence of co-morbidities).
Four anatomic predictors for intervention included:
An entry tear >10mm
Total aortic diameter >40mm at presentation
False lumen diameter >20mm
An increase in total aortic diameter >5mm between serial imaging studies.
The researchers did note that complete thrombosis of the false lumen was protective against late operative intervention.
“It is clear from the literature that TEVAR is effective in managing patients with acute complicated TBAD by improving aortic remodelling,” notes Conrad. “It is intuitive that this therapy may be beneficial for uncomplicated cases if we can understand who is at high risk for future aortic-related complications. This study suggests that patients whose aortas meet these anatomic criteria may benefit from elective TEVAR 14 to 90 days after presentation.”
While this retrospective study cannot fully define the role of TEVAR in uncomplicated acute TBAD, it provides evidence for use of anatomic criteria in decision making in these complicated cases.
The Riptide aspiration system is intended for use in the revascularisation of patients with acute ischaemic stroke secondary to intracranial large vessel occlusive disease (within the internal carotid, middle cerebral—M1 and M2 segments, basilar and vertebral arteries) within eight hours of symptom onset.
The system is designed to retrieve thrombus through the Arc catheter and restore blood flow in patients experiencing ischaemic stroke. It adds a valuable tool to the acute ischaemic stroke product portfolio, a press release from the company states.
Patients who are ineligible for intravenous tissue plasminogen activator (IV t-PA) or who fail IV t-PA therapy are candidates for treatment.
“While I primarily use the Solitaire revascularisation device to treat patients with acute ischaemic stroke, I utilise a direct aspiration approach as my first line treatment strategy in select circumstances such as basilar artery thromboembolism and in select anterior circulation cases,” said Daniel Sahlein, interventional neuroradiologist, Goodman Campbell Brain and Spine, assistant professor of clinical neurology in the department of Neurological Surgery, Indianapolis University-Purdue University, Indianapolis, USA. “The Riptide Aspiration System will provide me with another proven Medtronic product to utilise when treating stroke patients.”
The Riptide aspiration system includes the Arc catheter, Riptide aspiration tubing, Riptide aspiration pump and Riptide collection canister with intermediate tubing. The Riptide aspiration system is a foundational platform for future aspiration catheters, currently in development.
“Medtronic is committed to developing services and solutions that address healthcare needs by improving clinical and economic outcomes,” said Stacey Pugh, vice president and general manager of Medtronic’s Neurovascular business which is part of the Restorative Therapies Group. “We believe that the Riptide aspiration system and Solitaire revascularisation device provide our customers with a comprehensive suite of products to choose from. Medtronic is committed to being a complete solutions provider in the treatment of acute ischaemic stroke market.”
The upcoming annual meeting of the European Society of Radiology (ESR; 28 February – March 4, 2018, in Vienna, Austria) has adopted the motto ‘Diverse and United’ and will feature a brand new programme format titled “Interventional Radiology at the Cube”.
In 2018, the most spectacular of the new ECR entrants will be “Interventional Radiology at the Cube”, a press release from ESR states. The new programme is intended to introduce young radiologists to the fascinating subspecialty of interventional radiology, and to provide enhanced knowledge to radiologists who need the subspecialty in their everyday professional life. Lectures and hands-on workshops will focus on interaction with the participants, simulating clinical routine and concentrating on practice-oriented contents. For the new project, rooms in a nearby church have been rented and a contemporary architectural cube has been created, which gives rise to the name.
The press release also draws attention to The “Coffee and Talk” sessions are another new format. In a relaxed atmosphere in one of the Austria Center’s stylish lounges, short lectures and discussions will be offered on topics such as clinical decision support, challenges for department chairs, undergraduate teaching of radiology, radiation protection, and imaging biobanks. Participants are welcomed and encouraged to stop by and contribute to the informal discussions while sipping their coffee or tea.
Another format, the ‘My Thesis in 3 minutes – MyT3’ sessions provide a platform for residents and young radiologists who would like to present their thesis as a first author, in a dynamic and entertaining scientific session. For this format a new location, the Sky High Stage, overlooking the Austria Center and providing a magnificent view of Vienna from the top of the nearby Saturn Tower, has been made available.
ECR 2018 will put the focus on the latest and hottest topics in radiology as well as on basic knowledge and training at the highest level.
“The current hot topics in radiology are big data; challenges and risks when dealing with ever larger amounts and varieties of data; artificial intelligence; and radiomics. These are exciting issues that we have to deal with in the near future by recognising the potential these developments have for us in terms of improving the quality of our work and patient care. We need not fear them as threats – I firmly believe that radiologists will always have a pivotal role in both diagnostic and interventional therapeutic patient management. Moreover, I also firmly believe that our specialty will benefit from these developments. Innovations mean advancement – a case in point in radiology is hybrid imaging, which will be another focus at ECR 2018,” ESR President Professor Bernd Hamm from the Charité, Berlin.
To make it more widely accessible, the ECR will again broadcast nearly every lecture via live web streams on ECR Online, a service delegates have used increasingly since its introduction four years ago. Lectures will also be available to watch on demand afterwards. This option will make it possible for delegates who are not able to attend a session in person to catch up on its content afterwards.
Viz.ai has announced the CE mark of its direct-to-intervention system, ContaCT, a novel approach to stroke care that automatically analyses brain CTs and notifies a specialist that a suspected large vessel occlusion has been identified.
Viz.ai CEO and co-founder Chris Mansi said, “Today’s stroke care is indirect, with lengthy time to treatment. Direct-to-intervention care provides the right information to the right doctor at the right time, greatly expediting the assessment and treatment process. Our direct-to-intervention system represents a paradigm shift in stroke care, one which promises to speed workflow and increase access. When every minute matters, there is a compelling advantage in being able to identify and transfer patients faster. This approach could potentially save countless lives, greatly reduce disability and decrease the cost burden to healthcare systems.”
Viz.ai’s direct-to-intervention system utilises deep learning algorithms to automatically identify large vessel occlusions that are responsible for the most devastating of strokes, and involves a stroke specialist in the care of that patient earlier than possible through conventional means.
Viz.ai’s approach recognises the importance of timely intervention by stroke specialists as supported by the American Stroke Association’s updated guidelines. From the latest STRATIS registry, current workflows can result in a door-to-treatment time of several hours resulting in poor patient outcomes. Viz.ai’s software has demonstrated its potential in a clinical trial, where it was able to correctly notify stroke specialists of a suspected large vessel occlusion in a matter of minutes thus potentially reducing the time to intervention.
Guerbet has announced that it has entered into an agreement under which it will acquire Israeli company Accurate Medical, which specialises in the development of microcatheters used in interventional radiology.
Accurate Medical has developed a range of microcatheters for embolization procedures of tumours and vascular aneurysms. These products are currently being registered with the US and European health authorities.
A press release from Guerbet states that this range includes two series of microcatheters.
The first series was designed and developed to propose an optimisation of microcatheters for intra-arterial navigation, even in case of tortuous vascular network and hardly accessible lesions.
The second series possess the same optimised navigation qualities, while also incorporating unique anti-reflux technology. This effect is achieved thanks to side holes located in the terminal part of the catheter, which create a fluid barrier preventing the reflux of embolization microspheres. This new technology makes it possible to administer more embolization microspheres to the targeted treatment area while also preventing them from refluxing upstream to arteries irrigating healthy tissues (non-targeted areas that need to be preserved; see picture above).
“This acquisition will fuel Guerbet’s growth in interventional radiology and will round out its current portfolio. This new range of microcatheters will allow us to help interventional radiology teams deliver a higher quality of care during image-guided embolization procedures” said Yves L’Epine, Guerbet’s CEO.
Agreement details
Under this agreement, Guerbet will acquire 100% of Accurate’s capital share, with an initial payment of 19.5 million euros and additional payments spread over several years depending on the achievement of regulatory and commercial objectives. The transaction is expected to start generating sales by the end of this year and be accretive from the 4th quarter of 2019. Accurate, founded in 2015, will retain its structure in Israel and will continue to be led by its inventor, co-founder and CEO Eran Miller.
A prospective, randomised single-centre study that set out to compare the safety and efficacy of vascular plugs and fibred platinum coils for embolization in pelvic congestion syndrome has shown that while both devices resulted in successful embolization, plugs were associated with decreased fluoroscopy time and radiation dose
In the study, recently published in the Journal of Vascular and Interventional Radiology (JVIR), embolization resulted in pain relief in 90% of patients. The authors reported that the group treated with coils had a significantly longer fluoroscopy time and significantly higher radiation dose (p<0.001).
Miguel A De Gregorio, Universidad de Zaragoza, Zaragoza, Spain and colleagues, from the Research Group of Minimally Invasive Techniques enrolled 100 women with pelvic congestion syndrome from January 2014 to January 2015. They randomly assigned patients to one of two groups: patients in one group were embolized with Nester coils (Cook Medical; n=50) and in the other, they were embolized using Amplatzer vascular plugs II (St Jude Medical; now Abbott; n=50).
Results
Results from the study showed that clinical success and subjective improvement were not significantly different between the groups at one-year follow-up. On average, there were around 18 devices used per case in the group embolized using coils. In the group embolized with vascular plugs, on average around four devices were used. There were three instances of coils migrating to the pulmonary vasculature and one instance of a plug doing the same. These migrations occurred approximately three to six months after the procedure, and all migrating devices were retrieved without complications, reported the authors.
As reported in JVIR, the average age of patients was just over 42 years, and their average visual analog scale (VAS) score for pelvic pain before treatment was about 7.4. The primary outcome of the study was defined as clinical success at one year using the VAS score. The investigators also compared the number of devices used; procedure and fluoroscopy times; radiation doses; costs; and complications. Patients were followed at one, three, six, and 12 months.
Canon and Canon Medical Systems Corporation have announced the official name change of Toshiba Medical, which was acquired in 2016, to Canon Medical Systems Corporation.
Since joining the Canon Group in December 2016, Canon Medical Systems has been undertaking the procedures for obtaining regulatory approval for integration with the Canon Group and change of the company name under the relevant national or regional laws concerning pharmaceuticals and medical devices. Canon announced that such procedures have been completed, and that the change of the company name enters into effect on 4 January 2018.
A press release from the company notes that since its establishment in 1930, Canon Medical Systems has introduced a number of “first-in-Japan” and “first-in-the-world” medical systems in cooperation with its customers worldwide.
Canon first entered the medical equipment business in 1940 with the development of the first domestically produced indirect X-ray camera, and utilising its advanced imaging technologies, currently produces equipment such as digital X-ray imaging systems and optical coherence tomography ophthalmic devices, the release adds.
Virtual reality has tremendous potential in healthcare
Penumbra has announced that it has entered into a joint venture called MVI Health, for the purpose of exploring healthcare applications of virtual reality technology with Sixense Enterprises.
“We have long believed in the tremendous potential of immersive, full-presence virtual reality to help improve lives though better healthcare and Penumbra is the perfect partner for us to collaborate with in this vision,” said Amir Rubin, CEO and founder of Sixense Enterprises. “We believe that by combining our unique immersive computing platform with Penumbra’s innovative approach to development and commercialisation of medical products, MVI Health can establish itself as a leading digital health platform.”
“We are excited about the potential of the Sixense technology and its ability to improve patient experiences across broad areas of healthcare and wellness,” said Adam Elsesser, chairman and CEO of Penumbra and CEO of MVI Health. “We look forward to collaborating with healthcare professionals and institutions to address a wide variety of medical conditions that can impact a vast number of people.”
MVI Health will be headquartered in Alameda, and will be supported by investments from Penumbra and license, intellectual property and other resource contributions from Sixense Enterprises.
W L Gore and Associates has announced the first implant of the Gore Excluder conformable abdominal aortic aneurysm endoprosthesis in the USA. The procedure took place on 19 December 2017 at Maimonides Medical Center in New York by Robert Rhee, chief of Vascular and Endovascular Surgery, and national principal investigator.
This endovascular aneurysm repair (EVAR) device, which is the first to feature angulation control, is part of an investigational clinical study approved by the US FDA. The clinical study will assess the safety and effectiveness of the device in treating infrarenal abdominal aortic aneurysms in patients with challenging anatomy. The clinical study consists of two sub-studies, each assessing the device for a different range of patient anatomies. The implantation by Rhee is part of the short neck substudy to assess the device in aortic neck angles of 0 to 60 degrees and aortic neck lengths of 10mm or greater. The high neck angulation substudy will evaluate proximal aortic neck angles of 61 to 90 degrees and aortic neck lengths of 10mm or greater.
“Patients with extreme proximal neck anatomies often do not qualify for EVAR. Regardless of device flexibility, current delivery systems make it difficult to achieve conformability during deployment,” said Rhee. “The angulation control in the new delivery system for the Gore Excluder conformable endoprosthesis device is intended to allow physicians a greater level of control to angle or bend the device to achieve orthogonal placement to the aortic blood flow lumen.”
The Gore Excluder conformable AAA device debuts the Active Control System into the abdominal aorta. This delivery system includes angulation control, giving physicians the option to angle or bend the device to achieve orthogonal placement to the aortic blood flow lumen and to maximise the conformability and seal of the device. It also offers the ability to reposition the device if needed after initial deployment to achieve optimal device placement.
The Global Medtech industry is moving together to enhance compliance practices across Europe, China, the Middle East, North Africa and Asia-Pacific, announces a statement released by AdvaMed, APACMed, Mecomed, and MedTech Europe.
“AdvaMed, APACMed, Mecomed, and MedTech Europe represent manufacturers of medical devices and diagnostics around the world. Our organisations promote high ethical standards in interactions between our member companies and healthcare professionals and healthcare organisations. We strive to achieve timely patient access to safe and effective products to help patients live longer, healthier lives around the world,” the statement adds.
It further adds that “collaboration and interactions with healthcare professionals and healthcare organisations must be transparent, and must be balanced against the need for healthcare professionals to make independent decisions regarding patient care and treatment.
Codes of ethics revised
“For these reasons, our organisations are instituting policy changes that affect how medical technology companies support healthcare professionals training and education around the world: Our industry has revised its codes of ethics in China (the AdvaMed China Code), in Europe (the MedTech Europe Code), in the Middle East and North Africa (the Mecomed Code), and in the Asia-Pacific region (the APACMed Code) to strengthen our collective commitment to training and education of healthcare professionals, and to ethics and integrity,” the statement informs.
It specifically points to “one of the key revisions” in codes of ethical practice: the elimination of “direct sponsorship” of healthcare professional attendance at third-party educational events, such as medical conferences and congresses, effective 1 January 2018. “’Direct sponsorship’ means those situations in which a company selects and pays for an individual healthcare professional’s registration fee, travel, lodging, and meals/hospitality to attend a third-party educational event,” the statement clarifies, noting that this means that effective 1 January 2018, “companies will no longer select or influence the selection of specific healthcare professional attendees at third-party educational events; directly arrange or pay for attendees’ travel, accommodation and/or registration; or reimburse the expenses of specific healthcare professional attendees at third-party educational events.”
“Importantly, these changes do not diminish companies’ commitment to healthcare professionals training and education; rather, what will change is how companies support third-party educational events. Companies may offer educational grants and sponsorship to third-party conference organisers, healthcare institutions, and/or professional associations to enable them to select healthcare professionals to attend third-party educational events. Companies will also continue to host and support robust technical product and procedure training, and educational meetings, which instruct healthcare professionals on how to safely and effectively use our companies’ complex, life-saving products. With the end of direct sponsorships, we anticipate that companies will have more resources to devote to high-impact training and education opportunities based on companies’ individual educational strategies,” the statement clarifies.
The announcement explains that this change is the result of extensive industry discussions and dialogue with key stakeholders over a number of years. “It follows a global trend that began to move away from direct sponsorship some time ago, as in the USA, Australia, and other countries such as Sweden and Russia,” it says.
Teleflex has announced that it has completed its previously announced senior leadership transition with Liam Kelly succeeding Benson Smith as president and chief executive officer effective 1 January 2018.
Kelly previously served as Teleflex’s president and chief operating officer.
Smith, who was re-elected to the Teleflex Board of Directors in May 2017 for another three-year term, will continue to serve as non-executive chairman of the Board, a press release from the company states. In addition, he will provide transition support to the company on a consulting basis through 31 December 2019.
“I am delighted to be assuming the role of CEO at such an exciting time for Teleflex,” said Liam Kelly. “The other members of Teleflex’s executive team and I join the Board in thanking Benson for his strong leadership over the past seven years, and we look forward to continued success as we position Teleflex for future growth.”
The first results from the UK-ROPE multicentre registry, presented at CIRSE 2017 in Copenhagen, Denmark, reveal that prostatic artery embolization is highly effective in reducing lower urinary tract symptoms in men with benign prostatic obstruction.
When compared directly with a matched cohort of men undergoing transurethral resection of the prostate (TURP), embolization was almost as effective as resection. Patients who underwent minimally invasive embolization stayed significantly fewer days in hospital compared to those who underwent TURP.
Nigel Hacking, a consultant interventional radiologist at University Hospital Southampton NHS Foundation Trust, Southampton, UK, presenting the results at the CIRSE annual meeting, said: “We have shown that prostatic artery embolization is safe and efficacious and [this procedure] really wins out on length of stay. The median length of stay after embolization is zero days compared with a median of two days with TURP. So for men who would rather avoid surgery, embolization is an excellent first option with likely economic benefits due to the day case nature of the procedure.”
UK-ROPE (Registry of prostate embolization) is the first multidisciplinary registry of prostatic embolization. It aimed to compare two cohorts of patients who underwent different treatments for lower urinary tract symptoms following benign prostatic hyperplasia: prostatic artery embolization and resection. The embolization arm had 216 patients; the resection arm included TURP (n=89) and holmium laser prostatectomy (HoLEP; n=13). The registry was designed as a non-inferiority study, ie, one that compares a novel treatment to an active treatment with a view to show that it is not clinically less effective with regards to a specified endpoint. The UK registry was jointly funded by the National Institute of Health and Care Excellence (NICE), the British Society of Interventional Radiology (BSIR), the British Association of Urological Surgeons (BAUS) and Cook Medical.
Investigators began recruiting in July 2014 and closed in January 2016. They enrolled 318 patients. The primary endpoint was the International Prostate Symptom Score (IPSS) score at 12 months. There were multiple secondary endpoints including length of stay; complication rates; reintervention rates; prostate volumes; flow studies; and erectile function after the procedures, diagnosed using the International Index of Erectile Function (IIEF-5).
The UK ROPE registry results show a significant improvement in 12 months for both groups. Embolization is clinically effective, producing a median 10-point improvement in IPSS. There was greater IPSS improvement in TURP cases, with a median 15-point IPSS improvement. “Propensity score analysis on 65 closely matched embolization/TURP patient-pairs support these findings. Embolization had “slightly worse” outcomes than TURP, but was still very effective,” said Hacking.
Similarly, the IPSS quality of life score showed that there was significant improvements in both groups at 12 months. There was greater quality of life improvement in TURP cases, “but the urologists and scientists have been very impressed with these results for embolization,” Hacking explained.
Results from the registry
Erectile function as measured by the IIEF-5 (that has a maximum score of 25), went up from a baseline of about 14.5 in both groups to 16.3 after embolization, and 14.8 in the TURP group at one year.
Urinary flow (Qmax) improved from baseline in both groups, but more in the TURP group. At baseline, the median score for embolization was 8.8 and at 12 months, it was 14.1. For TURP, baseline median Qmax was 10.4 and at 12 months, it was 22.3.
Residual volume in the embolization group was 161 at baseline and 129 at 12 months. Baseline values in the TURP group were 263 and at 12 months, they were 80.
There was a reduction in prostate size in both groups, with an average reduction of nearly 30% in the embolization group.
Embolization scored over TURP when it came to the time that patients took to return to normal; on average, this was about five days after embolization, as against 14 days after TURP.
Complications and reoperations
There was one blood transfusion, four haematomas, and one case of sepsis in the group that underwent embolization. This compared with no blood transfusions, or haematomas, but two cases of sepsis in the TURP group.
The reoperation rate for the embolization group was 5% within 12 months and 11.6% when planned operations after the 12-month period are taken into account. In the TURP group, within the 12-month period, the reoperation rate is 3.4% and just 1.1% after the 12-month period. The reoperation rate in the embolization group was slightly higher than reported in some other series. Prostatic artery embolization failures are mainly due to unilateral embolization, median lobe obstruction, or patient dissatisfaction despite IPSS improvement, Hacking said.
Patient reported complications included haematuria, haematospermia, and retrograde ejaculation (24% in the embolization group and 47% in the TURP group). These figures are likely to be inaccurate, due to the nature of a ‘questionnaire-based study’ as on direct questioning many of the men reporting retrograde ejaculation after embolization admitted that this symptom started after oral medication, months or years, before the prostatic artery embolization.
Commenting on the strengths of the data, he noted: “This was the first multicentre study, funded by multiple stakeholders, with an independent medical assessment unit. There was a free choice of embolic, and catheter/microcatheter. Still, this is non-randomised data, and the results would have been influenced by the learning curve for all but two participating centres who were being trained to perform prostatic artery embolization, even as they recruited to the registry as this is a difficult procedure with a clear learning curve. Also, the study had a 12-month endpoint, meaning that outcomes outside of this defined window will not form part of the analysis. We also used the original rather than the PErFecTED technique.”
New EURO-ROPE registry on the cards
Hacking also said that another multidisciplinary, multinational, multicentre registry of prostatic artery embolization, EURO-ROPE, is on the cards, potentially scheduled to begin recruiting in 2018. EURO-ROPE will have support from CIRSE and advice from key members of the European Association of Urology (EAU). It will be industry-sponsored and designed to rapidly collect data from 1,000 patients who will undergo embolization and then be followed for two years. “Participant centres are being trained and proctored in 2017, so that experienced teams of interventional radiologists and urologists will be involved in the data collection,” Hacking concluded.
XableCath has announced its XableCath blunt tip support catheter has received clearance from the US FDA. The blunt tip catheter facilitates true lumen passage of lesions, both above and below the knee, in the peripheral vasculature.
Procedures using the XableCath blunt tip catheters can be performed quickly and safely, allowing physicians to more effectively treat peripheral arterial disease (PAD), a press release from the company says.
“In two clinical investigator-led studies, XableCath was demonstrated to be a safe, effective, and easy-to-use device, enabling therapeutic options for patients with PAD,” said Johannes Dahm, director of Interventional Cardiology and Angiology, Heart and Vascular Center Neu-Bethlehem, Göttingen, Germany. “The XableCath blunt tip catheter is unique in its ability to cross chronic total occlusions quickly while remaining over-the-wire and in the true lumen. XableCath catheters will be powerful tools in the interventional suite.”
The company expects to perform its first US cases in the first half of 2018.
“I am excited to use the XableCath devices in my practice, because I believe it will enhance our ability to treat difficult occlusions and ultimately help our patients,” said James Benenati, medical director, Noninvasive Vascular Laboratory and fellowship program director at the Miami Cardiac and Vascular Institute at Baptist Hospital in Miami, USA. “XableCath addresses an unmet clinical need, and we believe it will allow us to succeed in treating patients with complex occlusive disease.”
XableCath president and CEO, Lisa Dunlea commented, “Different from most interventional devices used to facilitate lesion passage, XableCath was designed to be one of the best support catheters and to facilitate over-the-wire lumen passage, minimising the need for multiple products and exchanges and reducing procedure time. We believe that our catheters will quickly integrate into standard clinical practice to the benefit of both patients and physicians. With the success of our products in PAD, we are excited to apply our innovative technologies to future coronary and atherectomy products.”
BTG has announced that following positive results of its 15-year experience between 2003 and 2017 with TheraSphere, Northwestern University, Illinois, USA, has adopted Y-90 transarterial radioembolization (TARE; also known as radioembolization, or selective internal radiation therapy [SIRT]) with TheraSphere as the primary transarterial locoregional therapy for patients with hepatocellular carcinoma (HCC) limited to the liver.
Northwestern University’s decision to adopt radioembolization with TheraSphere as a first-line therapy or patients with HCC was informed by data prospectively collected and incrementally reported, demonstrating outcomes as expected by the BCLC algorithm for stages A-D, applied as either neoadjuvant or definitive treatment. Compared with TACE, the data confirm that outpatient radioembolization allows for fewer treatments, better quality of life, longer time to progression and versatile application as neoadjuvant locoregional therapy combined with either resection or orthotopic liver transplantation.
Physician comment
“Patients are looking for treatments that are safe, efficacious, have minimal detrimental effects on their quality of life and as pain free as possible,” said Riad Salem, chief, section of Vascular and Interventional Radiology, Department of Radiology at Northwestern University and lead author of the paper “Institutional decision to adopt Y-90 as primary treatment for HCC informed by a 1,000-patient 15-year experience” recently accepted for publication in the journal Hepatology. “The benefit of Y-90 TARE with TheraSphere is that it meets all of these patient needs, and also enables patients to be treated as outpatients, permitting discharge on the same day, reducing the need for lengthy hospitalisations and minimising impact on daily life. We recognise the many approaches to establishing a new standard of care. In our case, we are proud of the controlled, prospective studies we completed over the last decade, each addressing a specific question, and each getting us closer to the unanimous, multidisciplinary adoption of Y-90 as first-line. We are hopeful that when colleagues and peers review the study, the long-term survival outcomes, our rationale and the strength of the evidence, many will follow suit.”
“If you are clinically skilled, achieve a high level of technical training in interventional radiology procedures, have the best audited results for a procedure and a good relationship with your clinical colleagues, you are always going to be busy and have a highly successful career,” Andrew Holden, convenor, Central Organising Committee Members, Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) tells Interventional News. Holden is director of Interventional Radiology, Auckland Regional Public Health Service, and associate professor, Radiology, at Auckland University School of Medicine, Auckland, New Zealand.
What made you choose interventional radiology? What still motivates you in this field?
When I was a junior hospital doctor, I was attracted to radiology because it was a dynamic and rapidly changing specialty. However, I missed direct patient contact and the rewards associated with managing patient problems. Image-guided intervention (or interventional radiology) provided me with great opportunities to combine evolving technology with minimally invasive therapy. The rate of progress has not slowed and continues to challenge and stimulate me.
Who were your mentors and what wisdom did they impart to you?
Everyone has role models and for me two international pioneers who influenced my career (and still do) were Barry Katzen (Miami, USA) and Michael Dake (Stanford, USA). Both interventional radiologists gave me an early understanding of the value of being clinically relevant and contributing to a multidisciplinary approach. Locally, my recently-retired colleague, Alan List, taught me the importance of respecting your patients and colleagues as well as keeping humour in your day.
Which innovation in interventional radiology has most influenced your career?
Without doubt, endoluminal repair of aortic aneurysm disease has had the most profound influence on my career. By good luck rather than good management, I was involved in the first bifurcated endovascular aneurysm repair (EVAR) devices with Michael Lawrence-Brown and David Hartley at Royal Perth Hospital, pioneering a device that would become the Cook TriFlex device. Subsequently, I have had the privilege of being involved in many EVAR “first-in-human” and live case presentations as this technology continues to develop.
The most important change in the last decade has been the development of a quality vascular research programme at Auckland Hospital. We have been involved in over 30 first-in-human device trials over that period as well as multiple multicentre trials and registries. Traditionally, interventional radiology has not been as strong as other specialties in participating in clinical trials that support evidence based practice, but this is changing.
In the new age of big data healthcare, personalised medicine, robotics and specialties coalescing and separating, can you please describe the future of image-guided interventions as you see it?
The future of image-guided, minimally invasive intervention has never looked brighter. The ability to perform procedures under fused or virtual imaging control with the associated reduction in patient and staff radiation is already established and will continue to evolve. Technological advances will facilitate more refined and new procedures. Interventional oncology, in particular, is an area of huge growth potential. In terms of specialties coalescing, I have always taken the approach that the patient benefits most when the skill sets of physicians are combined.
As an interventional radiologist who is at the forefront of vascular interventional practice, how will the development of the endovascular specialist affect the “interventional radiologist” who wants to maintain a thriving endovascular practice?
I believe interventional radiology must embrace the concept of an endovascular specialist. For example, at Auckland Hospital, our interventional radiology fellows are encouraged to spend time in vascular surgery, acquiring relatively simple surgical skills as well as attending outpatient clinics. The vascular surgical fellows also spend time in the interventional radiology suites. The hybrid operating room provides a unique opportunity for multidisciplinary interaction. The distribution of workload should ultimately be decided by the skill set and outcome audit, rather than the specialty background. While most proceduralists perform simple interventions well, the ability to perform complex interventions with excellent outcomes is much more limited. This is particularly true in critical limb ischaemia, where the endovascular specialist must be able to demonstrate high levels of success with crossing chronic total occlusions, retrograde access, etc. My advice to the interventional radiologist who wants to maintain a thriving endovascular practice is to offer a clinical and procedural service, achieve superb technical skills and collect and publish outcomes. If you are clinically skilled, achieve a high level of technical training in interventional radiology procedures, have the best audited results for a procedure and a good relationship with your clinical colleagues, you are always going to be busy and have a highly successful career.
Could you briefly describe how interventional radiology is practised “down under” and in the wider Asia Pacific region?
Throughout the region, interventional oncology procedures are almost entirely performed by interventional radiologists. This will continue to grow, supported by trial evidence and new procedures. Venous intervention is also growing, as is interventional neuroradiology, particularly with the development of acute stroke services in many centres. Like most parts of the world, there are geographic variations in who performs endovascular procedures with interventional radiology playing a major role in many countries in the Asia Pacific.
What are your key goals as the convenor of the upcoming APSCVIR meeting in March 2018 in Auckland?
The APSCVIR is our regional interventional radiology society similar to CIRSE in Europe and SIR in North America. APSCVIR is rapidly developing and has enormous potential, particularly as there are more interventional radiologists practising in the region than any other region globally. APSCVIR 2018 (apscvir2018.com) aims to bring together a superb international and Asia Pacific faculty to discuss the latest developments, focusing on endovascular and interventional oncology topics. Live cases, multidisciplinary discussion forums and many visiting societies should contribute to an excellent learning opportunity. Late summer is also a great time to visit Auckland and New Zealand!
What clinical science are you most excited about showcasing at the APSCVIR meeting?
These are exciting times for interventional radiology with many recent trial results and device developments becoming available. At APSCVIR 2018, we intend to present and debate these results in attempt to provide some consensus on optimum current treatment strategies.
How has research changed in interventional radiology? What do you make of the recent high-profile trials such as ATTRACT and SIRFLOX that have not shown a benefit for interventional radiology procedures?
Quality research has greatly improved and increased over the last decade. It is very important for interventions to be supported by a solid evidence base, particularly in the current cost-conscious environment. The ATTRACT trial is a good recent example and provides evidence-based support for iliofemoral revascularisation in chronic venous insufficiency but not revascularisation below the inguinal ligament. This facilitates clear and consistent decision making. Likewise, recently presented trial data evaluating the role of radioembolization in the management of hepatocellular carcinoma (SARAH/SIRveNIb) and colorectal metastatic disease (SIRFLOX/FOXFIRE) have contributed significantly to understanding how this therapy fits in to the oncology armamentarium.
Which of the trials that you are involved in currently are you most looking forward to the results of?
We are currently involved in over 25 vascular device trials in various stages of recruitment and follow-up. Lower limb arterial trials include drug-coated balloon trials (with devices such as Stellarex [Spectranetics] and Ranger drug-coated balloon [Boston Scientific]) and drug eluting stent trials such as XPEDITE (Cook Medical) and MAJESTIC (Boston Scientific). I am looking forward to the results of the IMPERIAL trial that will provide a head-to-head comparison between two different drug-eluting stent platforms. We are currently involved in a number of trials that embrace different methods of angioplasty and vessel preparation. Shockwave lithoplasty is a fascinating example of this (we are currently recruiting to DISRUPT PAD III) but we are also involved in trials using the Trireme Chocolate drug-coated balloon and the Cagent Serranator device. Bioresorbable scaffolds have been challenging, but we are currently recruiting to the Elixir DESappear trial. On the aneurysm front, we performed the first-in-human experience with the Ovation Alto platform and are involved in the Endologix Nellix FORWARD 2 registry. Other trials we are currently involved in include several embolization and venous device trials. I am lucky enough to be one of the principal investigators in the Medtronic drug-coated balloon in arteriovenous access randomised trial that I hope will support an important advance in dialysis access intervention. Finally, I do hope that the COROLLARY trial gets underway. This is a trial proposed by the CORAL trial investigators who noted that patients with low baseline albuminuria did significantly better with renal artery revascularisation than those treated medically. It may be that albuminuria is the biomarker we have been looking for to assist in selecting patients who will benefit from renal artery revascularisation.
Which early technologies in interventional radiology are you keeping an eye on?
In the peripheral vascular space, the advent of drug-eluting technologies has improved patency but primarily in short to medium length, relatively simple, lesions. The concept of adequate vessel preparation is expanding to allow more complex disease to be successfully treated with these therapies. Many devices that may be considered standalone or vessel preparation devices are currently being evaluated including the Shockwave Lithoplasty system for heavily calcified lesions and the Cagent Serranator device.
In the aortic space, I have long believed that active aneurysm sac management is the key to providing a durable outcome with minimal reintervention. Aneurysm sac filling technologies, either as part of the primary endoluminal device (eg Endologix Nellix) or as an ancillary to conventional EVAR (eg Arsenal Medical) remain of great interest. There are also many technological and procedural innovations in both venous intervention and interventional oncology.
What have been the biggest challenges for interventional radiology in 2017?
As the indications for minimally invasive, image-guided therapy continue to expand, the need for well-trained physicians with excellent procedural and clinical skills also grows. This is the biggest challenge for interventional radiology. It is not surprising that the junior membership of interventional radiology societies such as SIR and CIRSE is at record levels but this must continue if image-guided therapy is to reach its potential.
Could you describe a memorable case?
There are many I could describe but one was a live case broadcast to a European meeting. I was performing the case late in the evening in New Zealand to facilitate time differences. It was a tricky, large main renal artery aneurysm that I was treating with a self-expanding covered stent. The case went very well but was complicated by guidewire induced spasm so I was giving repeated boluses of intra-arterial vasodilator. At the end of the procedure, I was congratulated by the live case panel and could hear the applause from 10,000 kilometres away. Thirty seconds after the live transmission ended, the controlled environment of the interventional radiology theatre turned upside down as the patient collapsed and was unresponsive. Fortunately, it was only a vaso-vagal induced hypotensive episode, probably exacerbated by the vasodilators, and the patient fully recovered. However, it reminded me of the challenges and sometimes good fortune needed to perform live cases.
Andrew Holden
What are your interests outside of medicine?
I have a great family and enjoy spending time with them. We have a beach house and enjoy water sports there—swimming, fishing, snorkelling, etc. I like to keep fit with cycling and running and enjoy most sports although, like most New Zealanders, rugby is a passion.
PQ Bypass has received conditional approval of its investigational device exemption (IDE) from the US Food and Drug Administration (FDA) to initiate the pivotal DETOUR II clinical trial. As the first-ever pivotal trial for percutaneous femoropopliteal bypass, DETOUR II will evaluate the safety and effectiveness of the DETOUR System in up to 292 patients with lower limb ischaemia due to long blockages (>15cm) in the superficial femoral artery (SFA) caused by peripheral artery disease (PAD).
“Patients with life-limiting claudication or critical limb ischaemia typically have lesions longer than 15cm, and we know that lesion length is directly proportional to patency. Until now, endovascular methods of treating these long lesions have not been comparable to open bypass surgery,” said Sean P Lyden, professor and chairman of the Department of Vascular Surgery, Sydell and Arnold Miller Family Heart & Vascular Institute at Cleveland Clinic, and national co-principal investigator of DETOUR II. “The DETOUR procedure is designed to treat patients with severely calcified or long-segment disease. It is essentially a femoropopliteal bypass with polytetrafluoroethylene, but done percutaneously. The DETOUR I trial in Europe demonstrated safety and efficacy in patients with lesions as long as 44cm in length, and we look forward to continuing to study this procedure with the commencement of DETOUR II.”
DETOUR II is a prospective, single-arm, global multicentre trial and will be conducted at up to 40 sites to enable the collection of safety and effectiveness data in support of a pre-market approval (PMA) submission to the FDA. Additionally, to demonstrate health economic outcomes, the trial includes a prospective economic study designed to collect data related to the costs associated with treating PAD in the study population. An economics core lab will lead the collection of quality-of-life outcome measures (collected at baseline, 30 days, six and 12 months), and procedural and follow-up costs, including rehospitalisations, through 24 months.
“We worked closely with the FDA, leading physicians and healthcare administrators to design a trial that we expect to demonstrate the total value of this unique approach to treating severe PAD,” said Richard Ferrari, chairman of the board of directors at PQ Bypass. “DETOUR II is an exciting milestone in the journey toward establishing a potentially transformative future standard of care for these patients.”
Percutaneous femoropopliteal bypass (the DETOUR procedure) is an entirely new procedure enabled by PQ Bypass’ proprietary DETOUR System, which is comprised of the TORUS Stent Graft, DETOUR Crossing Device, and DETOUR Snare. The DETOUR procedure creates a pathway that originates in the SFA, travels through the femoral vein and ends in the popliteal artery, bypassing the diseased part of the artery. This pathway allows TORUS Stent Grafts to be placed in a continuous line and consistently re-direct oxygen-rich blood around the blockage, restoring blood flow to the lower leg and foot of the patient. Unlike existing technologies such as stents and drug-coated balloons, which merely create a channel through the disease and are not designed for extremely long blockages, the DETOUR procedure is a unique solution designed to provide the durability of open bypass surgery but with a minimally invasive approach.
“The DETOUR System features a truly innovative, intuitive design and the trial will investigate its benefits in addressing long lesions that are not well served by existing minimally-invasive approaches,” said Jihad A Mustapha, clinical associate professor of medicine, Michigan State University College of Osteopathic Medicine and national co-principal investigator of the DETOUR II Trial. “We look forward to working with the DETOUR II Trial clinical sites on this important research.”
In March 2017, PQ Bypass received CE mark approval for all three devices that are included in the DETOUR System. In August 2017, Frost & Sullivan recognised PQ Bypass with the 2017 European PAD Interventions Technology Innovation Award for the DETOUR System.
Figure 3: Cluster of two well-preserved tumour cells obtained by left hypogastric artery sampling.
Laboratory techniques that make genetic profiling and mutation monitoring of tumours more readily accessible than by direct tissue biopsy have recently been introduced. These techniques, based on the detection of circulating tumour DNA (ctDNA), have become known as liquid biopsies because they rely on peripheral blood sampling, write Bruno Damascelli, Vladimira Tichà, Elena Repetti and Tshering Dorji, Milan, Italy.
Detection of somatic mutations in circulating DNA is comparable to that obtained from tumour tissue biopsy, but with a direct therapeutic advantage in that the molecular diagnosis can be updated through noninvasive serial sampling. Liquid biopsy also includes detection of circulating tumour cells (CTCs) that can be characterised by immunofluorescence, contributing to a precise molecular diagnosis.
The number of CTCs is small and a peripheral blood sample may contain only one tumour cell for every 600,000 nucleated cells. Likewise, fragmented DNA derived from tumours is found only in small amounts, mixed with DNA resulting from normal cell death, which accounts for at least 90%. Despite these limitations, liquid biopsy is gaining ground and has been internationally validated for non-small-cell lung cancer, melanoma and colorectal cancer.
Laboratory methods are improving daily and target sequencing and target mutation techniques are becoming increasingly effective in detecting a larger number of mutations and identifying single mutations of direct interest for targeted molecular therapy.
Figure 1: Pelvic MRI showing the tumour (arrow).
In just the same way as selective sampling is used for localisation of hormone-producing tumours, we decided to use selective venous catheterisation to overcome, in part, the dilution effect that ctDNA and CTCs undergo in peripheral blood. The circulation draining any part of the body can be reached by percutaneous venous mini-catheterisation via brachial, jugular or femoral puncture, according to standard interventional radiology practice. There are no contraindications to the procedure, which is carried out in an outpatient setting with acceptable invasiveness and can be repeated any number of times.
Figure 2: Selective catheterisation of the left hypogastric artery via contralateral femoral access
In a preliminary clinical series, liquid biopsy carried out in parallel on selective and peripheral blood samples yielded interesting results. In the case of sarcoma of the left gluteus shown by way of example, target sequencing on a peripheral blood sample and on a selective sample from the left hypogastric artery showed a TP53 gene mutation, which can indicate tumour sensitivity to treatment with doxorubicin and ifosfamide. A tumour cell cluster was detected only in the selective sample (Figures 1–3).
Figure 3: Cluster of two well-preserved tumour cells obtained by left hypogastric artery sampling.
Bruno Damascelli and Vladimira Tichà are with EmoGVM Centrocuore Columbus, Milan, Italy. Elena Repetti is with IMPACTLAB, Department of Genetics, Milan, Italy, and Tshering Dorji is with LAMM – IMPACTLAB Group, Department of Pathology, Milan, Italy. None of the authors reported any disclosures pertaining to this article.
Henk Valk (CEO Philips Benelux) and Laurens van der Tang (CEO VitalHealth)
Royal Philips has announced that it has acquired VitalHealth, a provider of cloud-based population health management solutions for the delivery of personalised care outside of the hospital, for example, in regional care networks.
Headquartered in the The Netherlands, VitalHealth’s products and services are being used by more than 100 healthcare networks in various countries including the US, India, China, Sweden, Germany, Belgium and the Netherlands, a press release from Philips states.
Philips also recently acquired CardioProlific, a US-based thrombectomy company.
VitalHealth was founded in 2006 by Mayo Clinic (US) and Noaber Foundation (The Netherlands) and employs approximately 200 employees. Financial details of the transaction were not disclosed.
“This strategic acquisition complements our current offering in population health management, and supports our commitment to deliver integrated solutions for care providers and patients to improve people’s health,” said Carla Kriwet, chief business leader of the Connected Care & Health Informatics Businesses at Philips. “As a pioneer in comprehensive population health management solutions, we are committed to help drive business transformation for providers, health systems, employers, and payers transitioning to value-based care. VitalHealth will help us deliver on that commitment by strengthening our offering for care coordination, outcome management and patient engagement.”
“Population health management is a proactive approach to improving health and reducing costs for entire patient populations. It involves the aggregation of patient data across multiple health IT sources, smart analytics to understand the health needs of the population, navigation and coordination of care within that population, and engagement with each individual patient to improve both clinical and financial outcomes. In line with its strategy to deliver integrated solutions across the health continuum, from healthy living and prevention to diagnosis, treatment and home care, Philips has been expanding its population health management business,” a press release from the company states.
“VitalHealth’s offering will complement Philips Wellcentive’s solution to help improve patient outcomes, as the combined portfolios will enable healthcare providers to better identify and manage high-risk, high-cost patient populations. Moreover, VitalHealth’s platform will strengthen Philips’ HealthSuite digital platform, the company’s digital enabler for the next generation of connected health solutions,” the press release adds.
A study of nearly 62,000 hospitalisations nationwide in the USA has found that more than one in six patients with peripheral arterial disease (PAD) who undergo revascularisation procedures to restore blood flow to blocked leg arteries and other arteries outside of the heart are readmitted to the hospital within 30 days.
Led by researchers in the Smith Center for Outcomes Research in Cardiology at Beth Israel Deaconess Medical Center (BIDMC; Boston, USA), the large-scale analysis determined that 30% of readmissions following peripheral revascularisation were related to complications associated with the procedure, while differences in hospital quality accounted only modestly for readmission risk.
The findings, which were published in the Annals of Internal Medicine on 5 December, suggest that strategies to help prevent readmissions should focus on high-risk patients with PAD, including those who live with other serious health conditions, such as diabetes. Interventions related to post-procedure care might halt the need for readmission, such as early clinic follow-up and post-discharge nursing.
Revascularisation procedures – including surgical bypass operations and endovascular procedures in which balloons and stents are placed in the arteries with catheters to open blockages – can significantly improve patients’ quality of life and disease outcomes. However, limited data from earlier research of older Medicare patients have suggested that, like patients who undergo coronary bypass surgery, patients with PAD who undergo lower extremity bypass surgery are at high risk for readmission.
“With this new study, our aim was to determine the burden of nationwide readmissions following both endovascular and surgical revascularisation procedures for patients with PAD,” said first author Eric A Secemsky, an investigator at the Smith Center at BIDMC and a vascular medicine and intervention fellow at Massachusetts General Hospital. “We also wanted to identify potential causes of readmissions, both at the patient and institutional level, in order to identify areas for intervention and prevention.”
“In recent years, there has been an increased focus on preventing hospital readmissions as a way to improve health care quality and decrease costs,” explained Robert Yeh, the study’s senior author, director of the Smith Center for Outcomes Research in Cardiology at BIDMC and associate professor of Medicine at Harvard Medical School. As part of the federal healthcare reform, The Centers for Medicare & Medicaid Services’ (CMS) Hospital Readmissions Reduction Program (HRRP) financially penalises hospitals for higher-than-expected readmissions for key conditions. “In this new work focused on patients with PAD, we confirmed that not only are readmissions expensive, averaging US$11,000 per patient, but they also leave patients at risk for the development of further complications and potential setbacks to their recovery.”
The authors used the Nationwide Readmissions Database, which includes data from 22 states and represents nearly 50% of all US hospitalisations. Patients with public and private insurance, as well as patients who self-pay, are represented in the database.
“We found that in 2014, there were 61,961 hospitalisations during which a patient with PAD underwent a peripheral revascularisation procedure to treat their condition and were later discharged,” said Secemsky. “We were surprised to find that the 30-day hospital readmission rate was 17.6%, meaning that more than one in six PAD patients – whether they underwent bypass surgery or endovascular intervention – had to return to the hospital following their procedure.”
Further analysis showed that nearly 30% of patients were readmitted due to procedural complications. “Some sort of issue related to the procedure, maybe a related infection or problem with a stent, was causing patients to have to return to the hospital,” said Secemsky. In addition, approximately 8% of patients developed sepsis, a bacterial infection of the bloodstream, and 7.5% of patients were readmitted as a result of complications related to diabetes, a common problem among patients with PAD.
The authors went on to assess whether differences in hospital quality contributed to variations in readmissions risk for patients with PAD. “Using data from the 1,085 hospitals included in this data set, we created a new analytic model to examine readmission rates between institutions that took into account differences in patient populations,” explained Secemsky. These results found that differences in hospital quality accounted only modestly for readmission risk, suggesting that penalising hospitals with greater than expected readmission rates may not be the only effective approach at reducing readmissions.
“Moving forward, as clinicians and researchers, we need to recognise the special needs of the PAD patient population,” added Yeh. “If we can find ways to identify patients at highest risk of readmissions, we can implement practices or develop programmes to help them better manage their condition outside the hospital and avoid the need for readmission.”
This research was supported by the Smith Center for Outcomes Research in Cardiology at Beth Israel Deaconess Medical Center.
InspireMD has announced it has signed Diverse Devices as its exclusive distributor for Australia and New Zealand, and has signed Do Gia Production and Trading JSC as its exclusive distributor in Vietnam. The company’s product line includes the Cguard embolic prevention system (EPS).
Agustin Gago, executive vice president and chief commercial officer of InspireMD, commented: “We are pleased to announce these two additional distributors in the Pacific Rim, which represents the continuation of our planned expansion into the Asian market and further expand our global distribution footprint. Our partners have strong physician networks across all the relevant clinical specialties that treat carotid artery disease in their respective regions. These agreements follow similar announcements in Hong Kong and Taiwan. The Asia-Pacific region represents a sizable and important market given the prevalence of carotid stenting as a preferred alternative to vascular surgery. We look forward to announcing additional partnerships for the region in the coming months.”
The company previously announced the start of patient enrolment in an investigator initiated trial in Russia, seeking to assess the neuro protection and clinical superiority of the minimally invasive interventional procedure with the Cguard EPS vs. Abbott’s RX Acculink carotid stent in patients at high risk for carotid endarterectomy (CEA).
The trial is a single centre randomised trial with two interventional arms comparing Cguard EPS to Acculink. The trial will enroll 100 consecutive eligible patients with 50 patients in each arm. The primary endpoint of the trial will be new ischaemic areas in the brain within 24 to 48hrs post procedure, and new lesion permanence at 30-days as determined by diffusion-weighted magnetic resonance imaging (DWMRI). Each patient will receive clinical and ultrasound follow-up at one year.
The research will be lead by Andrei Karpenko, the head of the vascular surgery department, Center of Vascular and Hybrid Surgery within the Scientific Research Institute of Circulation Pathology in Novosibirsk, associated with Novosibirsk State University.
The majority of patients were pain free after receiving a new image-guided pulsed radiofrequency treatment for low back pain and sciatica, according to a study presented at the annual meeting of the Radiological Society of North America (RSNA; 27 November–1 December, Chicago, USA).
Most back pain is short-term, but about 20% of people affected by acute low back pain go on to develop chronic low back pain lasting a year or more. A compressed and herniated disc is a major cause of low back pain that can radiate to the legs.
“The nerve root is a sensitive structure that when pinched becomes inflamed and causes pain,” said lead investigator Alessandro Napoli, an interventional radiologist at Sapienza University of Rome. “The body reacts with muscle constriction, which decreases the distance between vertebrae, and a vicious cycle is created.”
Study details
The single-centre prospective study included 80 patients experiencing at least three months of low back pain due to a herniated disc that had not responded to conservative treatments including exercise and medication.
The patients underwent minimally invasive pulsed radiofrequency treatment under CT imaging guidance. Even without touching the disc, the interventional radiology pulsation treatment serves to resolve the herniation.
“The probe delivers a gentle electrical energy, so there is no thermal damage,” Napoli said. “The results have been extraordinary. Patients have been relieved of pain and resumed their normal activities within a day.”
Of the 80 patients treated, 81% were pain free one year after a single 10-minute treatment session. Six patients required a second pulsed radiofrequency session. Ninety per cent of the patients were able to avoid surgical treatment.
Figure 1
Following this treatment, inflammation and pain go away. With relaxation of the muscles, the distance between the vertebrae returns,” Napoli explained, noting that no patients experienced side-effects after receiving the minimally invasive outpatient treatment.
“There is a big gap between conservative treatments for disc compression and herniation and surgical repair, which can lead to infection, bleeding and a long recovery period,” Napoli said. “Evolving technologies like this image-guided treatment may help a substantial number of patients avoid surgery.”
The notion of locally destroying a cancer percutaneously with minimal morbidity and mortality has become accepted as part of the modern armamentarium for treating patients with cancer. Thermal ablation technology has evolved rapidly during the past decades, with substantial technical and procedural improvements that can help to improve clinical outcomes and safety profiles, writes Roberto Iezzi, Rome, Italy.
Radiofrequency ablation has become a touchstone of interventional oncology. The beginnings of what we now know as radiofrequency ablation stretch back to nearly 20 years. The future of ablation will rely on expanding clinical indications, creating the potential for larger areas of ablation, attempting to more accurately control the area of ablation, ensuring the safety of the procedure and looking for greater succesful long-term outcomes in the tumours we ablate. Energy-based ablation includes technologies that destroy a tumour either through thermal (hot or cold) or non-thermal mechanisms.
Radiofrequency ablation is currently the ablation modality supported by the largest number of studies, including randomised controlled trials and meta-analyses. Microwave ablation is gaining acceptance in the medical community and the evidence regarding its benefit in comparison with radiofrequency is increasing, although a recently presented randomised controlled trial has failed to demonstrate its superiority over radiofrequency ablation.
Cryoablation destroys tumoral tissue by freezing, or alternating freezing and thawing. Rapid tissue freezing and thawing produces the greatest cytotoxic effects by disrupting cellular membranes and inducing cell death. Its advantages include the ability to monitor the ice-ball formation during the procedure on imaging and the absence of pain when delivering the treatment.
US-guided high-intensity focused ultrasound (HIFU) treatment for patients with hepatic metastasis offers effective local tumour control with minimal adverse effects whereas MR-guided HIFU for liver lesions is still at an early stage due to the limited therapeutic window caused by the thoracic cage and respiratory motion.
Irreversible electroporation is a new ablative technique that uses high-voltage, low-energy direct current to create nanopores in the cell membrane by the passage of electrons through adjacent cells.
Other emerging technologies are represented by imaging-guiding modalities and assistive techniques for percutaneous treatment. In particular, recent technical advances of imaging fusion have enabled the overlay or side-by-side display of real-time ultrasound images combined with the established fusion of CT/MRI-acquired images during an interventional procedure. Like fusion imaging, contrast-enhanced ultrasound increases RFA performance in terms of localisation and targeting of a tumour. Applying these technique to tumour ablation enhances the identification of target lesions and the feasibility of the intervention.
Recently, the crucial role of multimodal or combination treatment for patients with liver malignancies has been emphasised. In particular, it was demonstrated that combination treatment with transarterial chemoembolization (TACE) and radiofrequency ablation has shown promising clinical results in terms of tumour necrosis and disease-free survival. Combining treatments appears to have superior outcomes compared to those obatined with TACE or radiofrequency ablation alone. These synergistic effects may be due to the decreased blood flow into the target lesions with the additional elimination of adjacent micrometastasis. The recent development of molecular-targeted agents in the treatment for hepatocellular carcinoma has prompted synergies between locoregional tumour ablation and systemic chemotherapy.
To conclude, the true extent of the systemic ramifications of thermal ablation is only now beginning to be appreciated. What is clear is that thermal ablation cannot be considered solely as a locoregional therapy. The resultant inflammatory response, though at present limited and unpredictable, paves the way for an expanded role of thermal ablation as a stimulant to the immune system. Ablation, however, is a double-edged sword and the causes of (and the solutions to) its oncogenic effects need investigation.
Roberto Iezzi is an interventional radiologist, Catholic University, Rome, Italy.
MIOLive to showcase state-of-the-art IO
The third edition of MIOLive 2018 (www.miolive.eu) will be held in Rome, Italy, on 29 and 30 January 2018. The meeting will be a forum for discussion for all those who are interested in interventional oncology as well as locoregional treatments. It will be a practical, interactive meeting based on live cases integrated by short presentations and lectures where professionals from various countries in the Mediterranean area can share opinions, experiences, research projects and knowledge, under the guidance of several international experts.
There is no evidence that accumulation in the brain of the element gadolinium speeds cognitive decline, according to a new study presented at the annual meeting of the Radiological Society of North America (RSNA).
Gadolinium-based contrast media were introduced in 1988 as a means of enhancing MRI images and are commonly used today. The contrast agent is injected into the patient’s bloodstream and eliminated from the body through the kidneys.
“It is estimated that approximately 400 million doses of gadolinium have been administered since 1988,” said the study’s lead author, Robert J McDonald, neuroradiologist at the Mayo Clinic in Rochester, USA. “Gadolinium contrast material is used in 40–50% of MRI scans performed today.”
Scientists previously believed gadolinium contrast material could not cross the blood-brain barrier, the semipermeable membrane that selectively filters materials from the bloodstream from entering extracellular fluid in the brain and central nervous system. However, recent studies, including one from McDonald and colleagues, found that traces of gadolinium could be retained in the brain for years after MRI.
On 8 September 2017, the US FDA recommended adding a warning to labels about gadolinium retention in various organs, including the brain, for gadolinium-based contrast agents used during MRI. The FDA highlighted several specific patient populations at greater risk, including children and pregnant women.
Still, very little is known about the health effects, if any, of gadolinium that is retained in the brain.
For this study, McDonald and colleagues set out to identify the neurotoxic potential of intracranial gadolinium deposition following intravenous administration of gadolinium-based contrast agents during MRI.
The researchers used the Mayo Clinic Study of Aging (MCSA), the world’s largest prospective population-based cohort on aging, to study the effects of gadolinium exposure on neurologic and neurocognitive function.
All MCSA participants underwent extensive neurologic evaluation and neuropsychological testing at baseline and 15-month follow-up intervals. Neurologic and neurocognitive scores were compared using standard methods between MCSA patients with no history of prior gadolinium exposure and those who underwent prior MRI with gadolinium-based contrast agents. Progression from normal cognitive status to mild cognitive impairment and dementia was assessed using multistate Markov model analysis.
Study details
The study included 4,261 cognitively normal men and women, between the ages of 50 and 90 with a mean age of 72. Mean length of study participation was 3.7 years. Of the 4,261 participants, 1,092 (25.6%) had received one or more doses of gadolinium-based contrast agents, with at least one participant receiving as many as 28 prior doses. Median time since first gadolinium exposure was 5.6 years.
After adjusting for age, sex, education level, baseline neurocognitive performance, and other factors, gadolinium exposure was not a significant predictor of cognitive decline, dementia, diminished neuropsychological performance or diminished motor performance. No dose-related effects were observed among these metrics. Gadolinium exposure was not an independent risk factor in the rate of cognitive decline from normal cognitive status to dementia in this study group.
“Right now there is concern over the safety of gadolinium-based contrast agents, particularly relating to gadolinium retention in the brain and other tissues,” McDonald said. “This study provides useful data that at the reasonable doses 95% of the population is likely to receive in their lifetime, there is no evidence at this point that gadolinium retention in the brain is associated with adverse clinical outcomes.”
This paper is the winner of the Kuo York Chynn Neuroradiology Research Award.
Dosimetry, within the context of selective internal radiation therapy (SIRT) using Y-90 microspheres, is typically understood to be the measurement and calculation of the absorbed dose in matter and tissue resulting from the exposure to indirect and direct ionising radiation.
Currently, PET or SPECT images are obtained after treatment to verify the distribution of microspheres. Now, absorbed dose from the Y-90 microspheres can be calculated on a voxel-by-voxel basis using the PET or SPECT images.
MIM SurePlan LiverY90 provides timesaving tools for liver and tumour segmentation, deformable registration, and allows patient-specific dose calculation on yttrium-90 (Y-90) PET and Bremsstrahlung SPECT images after administration of permanent Y-90 microspheres, a press release from the company states. The absorbed dose can be calculated for tumours and the liver to help provide important additional information to the clinician.
Three methods are available for dose calculation: Local Deposition Model, Local Deposition Model with scaling for known injected activity, and the Voxel S Value approach based on the schema in MIRD Pamphlet No. 17. All three methods are available for PET while only the Local Deposition Model with scaling for known activity is available for SPECT images that are not in Becquerel per milliliter (Bq/ml).
MIM Software will demonstrate MIM SurePlan LiverY90 at the 2017 Radiological Society of North America (RSNA) annual meeting 26–30 November in Chicago, USA. Attendees wishing to view a demonstration can visit booth 8108.
In October 2016, BTG and Mirada Medical announced CE mark certification for the Simplicit90Y dosimetry software, designed to optimise the planning of Y-90 selective internal radiation therapy and facilitate personalised treatment for patients with liver cancer.
As the evidence mounts showing the benefits of prostatic artery embolization (PAE), there is an explosion of interest in performing the procedure. Siemens’ unique imaging solutions can be specifically utilised in the planning phase and for optimised visualisation of the prostatic vasculature during the procedure. There is also a set of tools employed to try to improve the outcomes of this challenging procedure.
In this supplement:
PAE benefits patients and hospitals
Planning ahead makes all the difference
Use of syngo DynaCT can help avoid complications
Appropriate training vital to ensure effective treatment
Actively reducing radiation dose is important for complex procedures.
This educational supplement has been sponsored by Siemens Healthineers.
Left to right: Lindsay Machan, Rodney Raabe, Aravind Arepally
Timothy Clark, director of Interventional Radiology at Penn Presbyterian Medical Center, Philadelphia, USA and co-founder and chief executive officer of Forge Medical, which has commercialised the Vasostat, radial artery haemostat device, interviews three interventional radiology “serial inventors”: Lindsay Machan (Vancouver, Canada), Rodney Raabe (Spokane, USA) and Aravind Arepally (Atlanta, USA) on their “Eureka!” moments, innovation, the rocky path to successful commercialisation, and current opportunities for inventors.
Biographies
Lindsay Machan is professor of Radiology at the University of British Columbia (UBC) and an unrelenting entrepreneur. He is the co-inventor of the first drug-eluting stent. He co-founded Angiotech (now Surgical Specialties), which developed paclitaxel coating and delivery technologies subsequently licensed to Boston Scientific and Cook Medical for their drug-eluting stent programmes.
Rodney Raabe recently retired from private practice. Throughout his prolific research and publishing career (he was the first to demonstrate a cognitive improvement after carotid artery stenting) he developed many new technologies and devices (eg. the Raabe sheath). He was the first to pioneer adhesive closure technology for treating saphenofemoral insufficiency for which he co-founded Sapheon (later acquired by Covidien/Medtronic).
Aravind Arepally is former associate professor of Radiology at Johns Hopkins University and currently serves as chair of Radiology at Piedmont Health System in Atlanta, USA. He is widely credited as the inventor of bariatric embolization as well as targeted transcaval portal vein delivery for islet cell transplantation. He is the co-inventor of the Surefire antireflux embolization catheter for which he co-founded Surefire Medical; the company’s device is sold and distributed throughout the world.
The treacherous journey from an idea to a product
Timothy Clark, director of Interventional Radiology at Penn Presbyterian Medical Center, Philadelphia, USA and cofounder and CEO of Forge Medical
Interventional radiology colleagues and trainees often ask me about pathways for commercialising their ideas for improved devices, therapies and imaging technologies. It is a challenging process and one which is difficult to balance with the demands of a busy clinical practice or research programme.
My own background includes founding Forge Medical, a company which developed the VasoStat device used in the USA and Japan for radial artery and tibial artery haemostasis. I also spent years designing a high-performance dialysis catheter which reduces platelet activation and thrombosis risk (the Arrow-Clark VectorFlow), developing two push-button torque devices (the SeaDragon and SeaDragon2) and a suture locking device (the SlipNot).
However, the reality is that most of my inventions to date have not been commercialised. A partial list of those which have thus far failed to reach the market (despite exhaustive efforts including extensive prototyping and preclinical validation in animal models) include an inferior vena cava filter designed to prevent caval penetration and retrievable via either jugular or femoral veins, a pulmonary thrombectomy device, an adjustable-flow transjugular intrahepatic portosystemic shunt (TIPS) stent, a biliary benign stricture dilation device, a device for contralateral limb catheterisation during endovascular aneurysm repair (EVAR), and a semiautomated drainage catheter device.
I list these “failures” not to dissuade would-be interventional radiology inventors but only to illustrate that successful commercialisation of ideas is heavily dependent on persistence, timing, and fluctuating clinical needs and market demands. The cost and complexity of securing intellectual property can also be a barrier for many great ideas in interventional radiology.
Innovation is intrinsic to the DNA of interventional radiology. Every interventional radiology procedure that involves a particular challenge, hurdle, complication or failure can be seen as an opportunity to improve upon existing techniques and technologies to make them safer and more effective. I recently interviewed three luminaries who have successfully commercialised innovative ideas that emerged from realising unmet clinical needs in their everyday clinical practices. I asked each of them a series of questions revolving around the innovation process.
Finding three interventional radiologists who have succeeded in the invention process was not difficult as there are so many men and women in our field I know who have successfully done so. However, for this interview I selected three individuals whose contributions were for particularly unique and disruptive innovations.
Interview
Timothy Clark (TC): Was there a “Eureka!” moment for an idea which led to your product?
Lindsay Machan (LM): Actually, there was one. Back then, we were stenting the superficial femoral artery with early self-expanding stents and were seeing a huge problem with restenosis. One day our weekly vascular surgery conference was found to be short of a speaker. A medical student at UBC, William (Bill) Hunter, offered to present his summer research involving targeting inflammation in an animal model of rheumatoid arthritis. This involved the use of paclitaxel and similar agents to target the inflammatory component of joint destruction in what we now refer to as angiogenesis.
As Bill gave his presentation, my “Eureka” moment was the sudden realisation that if paclitaxel could inhibit angiogenesis, then it could potentially reduce restenosis if delivered locally using vascular stents. Bill and I soon teamed up and formed Angiotech. Early on, we saw potential for vascular devices including stents, embolic agents to release paclitaxel as well as a vascular wrap around surgical anastomoses. Obviously this was too broad at first, so we eventually narrowed our focus to developing just a drug-eluting stent.
Rodney Raabe (RR): I was doing a lot of neurointerventional cases at that time. After performing a complex paediatric central nervous system embolization case with another colleague, I got to thinking that glue remained a challenging embolization agent due to its low viscosity. It was a vascular “filler” but not something one could use to treat a very long vascular segment. I was also doing a lot of thermal ablation for greater saphenous vein (GSV) insufficiency. One day while performing a GSV ablation I thought “if glue (n-Butyl cyanoacrylate; NBCA) can be used for a wide range of vascular embolizations, why can’t we just glue the GSV shut? We just need to co-apt the vein walls and figure out the right glue viscosity.”
Aravind Arepally (AA): It was not really a single “Eureka!” moment; it was more of a step-wise process. Jim Chomas, my co-founder of Surefire, and I were contemplating a variety of device technologies around which to form a company. Jim was visiting a high-volume interventional radiology practice which did a lot of interventional oncology. He witnessed reflux resulting in non-target embolization during transarterial chemoembolization (TACE). We discussed this as to how much an issue this was in clinical practice. The more we looked, the more we saw. After I saw additional cases of pancreatitis and gastric ulceration among my colleagues, I knew we were onto something. Wanting to solve that clinical problem led to our antireflux embolization catheter.
TC: How long did you think it would take to commercialisation and how long did it actually take?
LM: We were pretty confident that we could do it in about nine months for less than US$100,000. In reality, it was closer to eight years and cost over US$20 million, including capital invested by industry. It probably would have taken even longer if not for serendipity and the amazing outcome of one particular patient.
He was a grandfather of several young grandchildren who developed dysphagia from advanced oesophageal cancer. He was constantly drooling which frightened his grandchildren. He told his physicians all he wanted was to be able to swallow so that he could play with his grandchildren and eat ice cream. He consented to enroll in a first-in-human trial of a paclitaxel-eluting oesophageal stent we had under investigation at that time. The stent insertion went very smoothly.
The morning after I inserted his stent, I went to his room and found his hospital tray table covered with empty ice cream cups and two of his grandchildren sitting beside him. I gave him a big hug and nearly burst into tears. It was a hugely emotional moment seeing him and his family so happy.
Nearly a year later, when he succumbed to his cancer, he had consented to an autopsy. The histologic findings of how paclitaxel had inhibited his tumour’s ingrowth was so compelling that the US Food and Drug Administration (FDA) allowed it to become part of our submission for eventual regulatory approval.
RR: We thought commercialisation and strategic exit would take a couple of years, and that the cost would be around US$500,000 (£378,000, €426,000). The actual time was closer to seven years and took multiple rounds of investment totaling over US$35 million, US$8 million of which we returned to our shareholders after the sale of the company. It turned out there was a lot of science and iteration needed to impart the right level of viscosity to NBCA and to developing a delivery system that made the embolization material visible with ultrasound. It became a huge undertaking and took us years. At one point we even had a full-time team of chemists.
What helped early on is that we partnered with a technology incubator affiliated with an academic medical centre. They were also able to assist with obtaining seed capital and really get the ball rolling. It turns out that they were independently working on a percutaneous venous ligation device, which really complemented our technology, so that they knew the space and the clinical need.
AA: We thought that we could approach this non-target embolization problem head-on and develop a device with US FDA clearance in one year, from concept to product. In actuality it took about one and a half years, so we were not too far off. Most people are surprised how quickly we did this. What really accelerated the process is that we partnered with a medical device engineering firm early on, and used dedicated engineering workspace within their facilities. As they were also a contract manufacturer of medical devices, they were able to help us navigate us through the design iterations to a commercially-viable design freeze.
TC: Do you think the opportunities for interventional radiologist inventors are better now in the era of consolidation within the medical device industry, or worse?
LM: I think that the recent consolidation in the medical device industry is both an opportunity and a threat. Larger companies present increasing layers of bureaucracy which can make it difficult to navigate. This can be intimidating for a lot of physician inventors. On the other hand as companies merge, realign their business units and move forward, they can become hampered in innovation without ongoing physician input.
You cannot simply task a team of engineers and marketing people to come up with a new type of product line without knowing in depth what the clinical needs are. I also see this happening in academic medical centres who create centres for innovation, often with little to no physician input.
RR: I would advise interventional radiology inventors to remember that we are a unique breed. Our culture of innovation is a big part of why we went into this specialty. Large companies need us, and there are too many people in their business and research and development ranks afraid of getting fired for taking on bold initiatives which do not pan out. This can lead to enormous inertia within their development programmes.
My advice to young inventors is to not give up, just keep on being creative. It also helps to do a small licensing deal or two early on in your career with existing companies. You will not make much money off the royalties but you will learn a lot from the device development process. You will also get a reputation within industry as an innovator.
AA: I think the challenges facing interventional radiology inventors are worse these days with the all of the consolidation going on within the medical device industry. There seems to be less innovation and less willingness to take risks compared to when there were more small and mid-sized companies. The regulatory pathways for US FDA clearance and European CE mark approval are also getting more complex and expensive. However, interventional radiology as a field is full of entrepreneurs, and entrepreneurs will always find a way.
TC: Thank you, gentlemen, for sharing your insight and perspectives. It seems the message to innovators is to accelerate the development of your idea through collaboration and using outside resources such as medtech engineering firms and incubators. If there was one word which summarises what is required to successfully commercialise an idea to a product, what would that be?
Paolo Zamboni, Ferrara, Italy, the proponent of the chronic cerebrospinal venous insufficiency (CCSVI) theory, and his colleagues have reported that the randomised, double-blinded, sham controlled Brave Dreams trial has not demonstrated a benefit for venous angioplasty in the treatment of patients with multiple sclerosis (MS).
Zamboni, presented the results of the Brave Dreams trial at VeithSymposium (14–18 November, New York, USA). The results were also simultaneously published online ahead of print in JAMA Neurology on 18 November.
Chronic cerebrospinal venous insufficiency (CCSVI) is a term that describes compromised flow of blood in the veins draining the central nervous system. According to Zamboni, it is characterised by restricted venous outflow from the brain and spinal cord. “Whether this condition is associated with MS and whether venous percutaneous transluminal angioplasty is beneficial in persons with MS and CCSVI is controversial,” the authors write in JAMA Neurology.
Many MS patients and advocacy groups are disillusioned by the influence of drug companies in their medical treatment regimens and have became passionate torchbearers of CCSVI and venous angioplasty after it was first proposed in 2009. The rapid spread of information regarding the scientifically unproven condition, CCSVI, and also angioplasty as a proposed treatment option via the internet resulted in patients travelling afar to receive this treatment, much before it was rigorously tested. Recent well-designed randomised controlled trials have not shown a benefit for venous angioplasty for MS patients.
As reported in JAMA Neurology, Zamboni and colleagues noted that in the Brave Dreams trial, which included 115 patients with relapsing-remitting multiple sclerosis, venous angioplasty did not increase the proportion of patients who improved functionally nor did it reduce the mean number of new combined brain lesions on magnetic resonance imaging at 12 months. The team further reported that there was a tendency for more patients to become free of new lesions after venous angioplasty, mainly because of a reduction in new lesions appearing six to 12 months after randomisation. These findings led them to conclude that venous angioplasty cannot be recommended for patients with relapsing-remitting multiple sclerosis.
The trial was carried out in six MS centres in Italy from 2012 to 2016. Patients were randomly allocated (2:1) to either venous angioplasty or catheter venography without venous angioplasty, which was the sham arm and the findings analysed on an intention-to-treat basis.
The two primary endpoints assessed at 12 months were: a composite functional measure (ie, walking control, balance, manual dexterity, postvoid residual urine volume, and visual acuity) and a measure of new combined brain lesions on magnetic resonance imaging, including the proportion of lesion-free patients. Combined lesions included T1 gadolinium-enhancing lesions plus new or enlarged T2 lesions.
The authors concluded: “Venous angioplasty has proven to be a safe but largely ineffective technique; the treatment cannot be recommended in patients with MS.”
Intact Vascular has announced that positive single centre twenty-four month results from its TOBA (Tack optimised balloon angioplasty) clinical study were presented at VEITHsymposium 2017 by Christian Wissgott, assistant director, Westküstenklinikum Heide in Heide, Germany.
The multicentre TOBA study enrolled 138 patients with femoropopliteal peripheral arterial disease in Europe. All participants underwent percutaneous balloon angioplasty and repair of any dissections (or tears) resulting from the procedure using the Tack endovascular system. There is currently a below-the-knee investigational device exemption study ongoing with the system in the USA.
The Tack implant is a first-of-its kind device for precision dissection repair following balloon angioplasty, a press release from the company states. The Tack endovascular system is designed to help maintain vessel integrity and maximise blood flow to promote healing, improve outcomes and save limbs. The system leaves a minimal amount of metal in the artery, reduces mechanical stress on the arterial wall and preserves future treatment options. Unrepaired dissections—which are frequent following balloon angioplasty procedures—increase the probability of acute arterial occlusion and may continue narrowing the artery, which leads to lower long-term patency rates.
The 24-month Kaplan-Meier patency results were unchanged from the favourable twelve-month rate of 87.5%. “The Tack implant offers a new paradigm for focal dissection repair in the superficial femoral or popliteal arteries,” Wissgott said. “Zero reduction in vessel patency over twelve months appears to be attributable to the Tack design, which leaves 70–80% less metal behind when compared to traditional stents. In addition, the Tack’s lower chronic outward force minimises vessel inflammation and reduces vessel trauma that can contribute to restenosis.”
Ongoing studies
Intact Vascular is sponsoring three clinical trials to evaluate its Tack endovascular system: TOBA II; TOBA II BTK and TOBA III. TOBA II is investigating the combination of the Tack device with both plain and drug-coated balloon angioplasty in the arteries above the knee, and completed enrolment in February 2017. TOBA II BTK is investigating the combination of the Tack device with plain balloon angioplasty in the arteries below the knee and is actively enrolling patients. TOBA III is currently underway in Europe and is investigating the combination of the Tack device with drug-coated balloon angioplasty; enrolment is nearly complete.
Merit Medical has announced signing an asset purchase agreement with BD (Becton, Dickinson and company) to acquire certain assets which BD proposes to sell in connection with its proposed acquisition of CR Bard. Merit’s proposed asset acquisition is subject to the closing of BD’s proposed acquisition of Bard as well as other usual and customary closing conditions.
The assets to be acquired are soft tissue core needle biopsy products currently sold by BD under the trade names of Achieve programmable automatic biopsy system, Temno biopsy system and Tru-Cut biopsy needles. Merit understands these products are currently sold worldwide through a combination of a direct sales force and distribution partners.
Additionally, Merit proposes to acquire the Aspira pleural effusion drainage kits and the Aspira peritoneal drainage system currently marketed by Bard. Merit understands these products are currently sold primarily in the USA.
Purchase price
The purchase price for the product lines and related assets to be acquired is US$100 million, subject to adjustment for fluctuations in the value of transferred inventory.
“We believe this is a perfect fit for Merit,” said Merit’s chairman and chief executive officer Fred P Lampropoulos. “These products are well established with an installed base and complement Merit’s CorVocet full core biopsy system and our recently-acquired bone biopsy products.”
Clinicians’ use of Philips Azurion at St Antonius Hospital resulted in significant time savings.
Philips has announced the results of a comprehensive, independent, two-year study demonstrating the clinical workflow benefits of its next generation image-guided therapy platform, Azurion.
The study investigated nearly 800 patient procedures to evaluate the impact of Azurion at St Antonius Hospital in Nieuwegein, the Netherlands. The data demonstrated clinicians’ use of Azurion resulted in significant time savings for the hospital, including a 17% reduction of the average interventional procedure time, a 12% reduction of in-lab patient preparation time, and a 28% reduction of post-procedure lab time.
“As the use of image-guided therapies continue to rise, new systems need to be easy and intuitive to use so clinicians can quickly and efficiently move through procedures,” said Marco van Strijen, interventional radiologist, St Antonius Hospital. “With the Azurion system, we were able to change our workflow in such a way that we now can do more patients in a single day, resulting in more patients a week, resulting in more patients per year, with no compromise to patient safety or quality of care.” Read more about Azurion, here.
Overall, the improvements achieved with Azurion will give St Antonius Hospital the ability to treat one more patient per day – on an average of 6 to 8 patients per week, to help hundreds more patients each year. The reduced preparation, procedure and lab time resulted in fewer planned cases finishing after normal working hours and higher employee satisfaction. St Antonius Hospital, treating more than 93,000 patients annually, was among the first hospitals to install Azurion and participated in this comprehensive study to evaluate the impact of the new platform and its clinical workflow on their department.
“Hospitals are facing a hard to predict and growing patient demand and needed a solution that provides impactful clinical and operational improvements,” said Ronald Tabaksblat, business leader Image Guided Therapy Systems. “Less than a year after Azurion’s official launch, we are delighted with these impressive results that clearly demonstrate how Azurion’s state-of-the-art technology and flexible workflows are helping hospitals increase efficiency and optimise patient care.”
The Society of Interventional Radiology (SIR), in coordination with Member of the US House of Representatives (Rep.) from Utah’s 4th district, Mia Love, hosted a panel discussion on the important role of interventional radiologists on trauma teams responding to mass casualty incidents.
The discussion was to observe the International Day of Radiology on 8 November with Capitol Hill briefing on interventional radiology’s role on trauma teams.
In trauma situations, interventional radiologists are frequently called in to stop active bleeding without a single stitch. In the past these patients would be sent to surgery, but now, through embolization, the interventional radiologist stops the bleeding to stabilise the patient so it is safe for a surgeon to go in and repair the damage caused by the trauma.
This procedure was performed on Rep. Steve Scalise, R-La., after he was shot on 14 June while practicing for the congressional baseball game. He discussed his care during the briefing, which can be viewed on SIR’s Facebook page.
Joining Reps. Scalise and Love at the briefing were Matthew Mika, director of government relations at Tysons Food who was also shot on 14 June; Rep. Scalise’s doctor, Arshad A Khan, a senior interventional radiologist at MedStar Washington Hospital Center; Mika’s doctor, Libby Schroeder, a trauma surgeon at George Washington University Hospital; Saher S Sabri, director of Interventional Radiology at MedStar Washington Hospital Center; and Susan E. Sedory, SIR executive director and panel moderator.
“Rep. Scalise is living proof that physicians like interventional radiologists are an essential part of our life-saving healthcare system,” said Rep. Love. “With the growing shortage of graduate medical education residency slots across the nation, I am working to solve this issue so that we can fill the gap in the education of our needed healthcare providers.”
The panel also explored issues that limit access to adequate and timely trauma care, including training gaps in rural and underserved areas. Rep. Love has sponsored a bill, H.R.1167, the Enhancing Opportunities for Medical Doctors Act, to help fill that gap by expanding access to residency slots among rural programs, new medical schools and new primary medical specialties, like interventional radiology.
“Interventional radiology has a vital role to play on the trauma team, but many rural areas do not have access to any interventional radiology care, let alone the 24/7 IR care needed in a trauma center,” said Sedory. “That is why Rep. Love’s bill is so important. Through the reallocation of training slots to new and underserved areas, her bill would create more opportunities for patients to obtain access to critical and necessary care.”
The briefing was held as part of the International Day of Radiology, which commemorates the invention of the X-ray on 8 Nov 1895. This year, the International Day of Radiology was focused on the role of radiology in emergency care, which includes image guidance and minimally invasive procedures pioneered by interventional radiologists.
Janssen Pharmaceuticals has announced that the FDA has approved the 10mg once-daily dose of rivaroxaban (Xarelto) for reducing the continued risk for recurrent venous thromboembolism (VTE) after completing at least six months of initial anticoagulation therapy.
The approval follows a FDA Priority Review and is based on data from EINSTEIN CHOICE, which found that a factor Xa inhibitor, specifically rivaroxaban, demonstrates superior efficacy in reducing the continued risk of recurrent VTE and with major bleeding rates similar to aspirin.
“We believe the availability of the 10mg Xarelto dose will change clinical practice and the management of VTE recurrence,” said Paul Burton, vice president, Medical Affairs, Janssen. “The landmark EINSTEIN programme results yet again demonstrate Xarelto is a safe and highly effective option, not only for the initial treatment of a VTE, but also for the continued prevention of a recurrent event.”
With this approval, the rivaroxaban prescribing information provides instructions for physicians to begin treatment with rivaroxaban 15mg, dosed twice daily, for the first 21 days after a VTE occurrence. On day 22 through at least day 180, the daily dose decreases to rivaroxaban 20mg once daily. After at least 180 days, physicians can prescribe rivaroxaban 10mg once daily in patients at continued risk for DVT and/or PE.
“If anticoagulation therapy is stopped, up to 20% of patients will have a recurrent VTE within three years. To prevent this, physicians have long debated how best to extend anticoagulant use beyond the initial treatment window,” said Jeffrey Weitz, professor, Departments of Medicine and Biochemistry and Biomedical Sciences, McMaster University, and Executive Director, Thrombosis & Atherosclerosis Research Institute. “The FDA’s approval of the 10mg dose of Xarelto for preventing recurrent VTE, along with clinical evidence confirming the superiority of Xarelto over aspirin for extended VTE prevention, means we can finally put this debate to rest.”
The EINSTEIN CHOICE study evaluated patients with VTE who were already treated with six to 12 months of initial anticoagulation therapy and then received rivaroxaban 10mg once daily, rivaroxaban 20mg once daily or aspirin 100mg once daily for up to an additional 12 months of treatment. Patients taking either rivaroxaban dose had significantly fewer recurrent VTE compared to those taking aspirin. Specifically, rivaroxaban 10mg reduced the risk of recurrent VTE by 74% and rivaroxaban 20mg by 66%. All three treatment groups had low rates of major bleeding (0.4% with rivaroxaban 10mg, 0.5% with rivaroxaban 20mg, 0.3% with aspirin).
In September 2017, Janssen’s development partner Bayer announced the Committee for Medicinal Products for Human Use of the European Medicines Agency granted a positive opinion to update the Xarelto label to include the 10mg once-daily dose in the European Union; the European Commission granted approval on 19 October 2017.
New European standards for eye exposure to radiation will come into effect on 6 February 2018
The new European Directive laying down basic safety standards for protection against the dangers arising from ionising radiation exposure will come into effect on 6 February 2018. The most relevant change for interventionists in the occupational exposure section is the new annual limit for the lens of the eyes (20 mSv/year, instead of 150 mSv/year), write Eliseo Vano (Madrid, Spain) and Gabriel Bartal (Kfar Saba, Israel).
With this new radiation safety legislation coming into effect soon, the Radiation Protection Pavilion at the Cardiovascular and Interventional Radiological Society of Europe’s annual meeting in Denmark was a timely and interactive awareness campaign for radiation protection and dose management.
The new European Directive 2013/59/Euratom laying down basic safety standards for protection against the dangers arising from exposure to ionising radiation is expected to have a relevant impact on European diagnostic and interventional radiology. The Directive was adopted by the Council of the European Union (EU) on 5 December 2013. Member States of the European Union are required to complete the transposition of the Directive into national legislation by 6 February 2018. After the transposition, the implementation of the new requirements will represent a serious challenge for the interventional practices in Europe, but is expected to substantially improve the radiation exposure safety for patients, as well as personnel.
The most relevant changes in the new Directive (with impact on interventional practices) in comparison to the existing ones may be summarised as follows: Use and regular review of diagnostic reference levels (DRLs) including interventional procedures; Education and training (not included in the chapter on medical exposures); Responsibilities (involvement of several professionals in optimisation); Role of medical physics experts in diagnostic and interventional procedures; New requirements for equipment; Procedures: optimisation process, clinical protocols and clinical audit; Registry and analysis of accidental or unintended exposures of the patients. The most relevant change in the occupational exposures is the new annual limit for the lens of the eyes (20 mSv/year instead of 150 mSv/year).
New European limits for the exposure to radiation of the lens of eye will come into effect on 6 February 2018
The use and regular review of diagnostic reference levels is a new requirement. Appropriate local reviews are needed whenever diagnostic reference levels are consistently exceeded and require corresponding corrective action without undue delay. The impact of complexity factors when setting diagnostic reference levels in interventional procedures will be a challenge and implemented gradually with the transition to new angiography equipment.
Member States shall ensure that practitioners and the individuals involved in the practical aspects of medical radiological procedures have relevant competence in radiation protection. Appropriate curricula need to be established and corresponding diplomas, certificates or formal qualifications, recognised. Continuing education and training after qualification need to be provided and especially when new techniques are introduced.
With regards to responsibilities, it is stressed that any medical exposure takes place under the clinical responsibility of a practitioner and that the practitioner, the medical physics expert and those entitled to carry out practical aspects of the procedures shall be involved in the optimisation process.
The Directive contains new requirements for equipment: Any equipment used for interventional radiology shall have a device or a feature informing on the quantity of radiation produced by the equipment during the procedure and shall have the capacity to transfer the dosimetric information to the record of the examination (equipment installed prior to 6 February 2018 may be exempted from this requirement). Member States shall ensure that “Information relating to patient exposure forms part of the report of the medical radiological procedure”.
It is also required to give information to the referrer, the practitioner, and the patient or their representative, about clinically significant unintended or accidental exposures and the results of the analysis and to declare them as soon as possible to the competent authority.
Eliseo Vano is a professor at the Department of Medical Physics Service, Radiology Department, San Carlos Hospital, Complutense University Madrid, Spain.
Gabriel Bartal is director, Department of Medical Imaging and Interventional Radiology at Meir Medical Center, Kfar Saba, Israel.
The authors have reported no disclosures pertaining to the article.
European Society of Radiology (ESR). Summary of the European Directive 2013/59/Euratom: essentials for health professionals in radiology. Insights Imaging. Aug; 6(4): 411–417 (2015).
Vano, E. Radiation Protection: Are you prepared for the new legislation in 2018? Hot Topic Symposium. Radiation Protection: Burning Issue. CIRSE 16–20 September, Copenhagen, Denmark. (2017).
L to R: Bijan Modarai, Tamer El-Sayed and Ashish Patel
The health implications of prolonged low dose radiation exposure are frequently a topic of discussion amongst vascular interventionalists, who are performing a growing number of fluoroscopically guided procedures of increasing complexity. Anecdotal evidence points to an alarming pattern of premature, atypical malignancies in high volume operators. However, in the absence of large, prospective registries relating radiation dose to long-term health effects, a causal link with prolonged exposure cannot be established.
The standard method for measuring exposure to the operator employs personal monitors that record cumulative dose in an isolated body area, often not in real time. The safe dose limits set for occupational radiation exposure use a linear no-threshold model that assumes the risk of cancer increases in a linear manner with the exposure. Furthermore, these safe limits are extrapolated from cancers that develop after much higher dose irradiation in survivors of atomic bombs and those exposed to nuclear accidents. In truth, we know very little about the biological effects of chronic, low-dose occupational radiation exposure.
Research, carried out at the St Thomas’ Hospital Campus of the King’s Health Partners Vascular Unit and published in Circulation (B Modarai et al. Circulation 2017; doi: 10.1161/circulationaha.117.029550), shows evidence of cellular DNA damage in operators performing endovascular aneurysm repair (EVAR), particularly those carrying out complex endovascular aneurysm repair (EVAR). Bijan Modarai, Reader and Consultant Vascular Surgeon, and co-workers, Tamer El-Sayed and Ashish Patel, also found that use of shielding—especially leg shielding—seems essential protection during such cases.
DNA damage to operators was quantified by measuring the lymphocyte expression of γ-H2AX; a histone protein created by DNA double standard breaks and phosphorylated ATM (pATM); a DNA damage response marker. Lymphocytes are exquisitely radiosensitive and therefore ideal cells to use for monitoring the biological effects of exposure. Expression of γ-H2AX and pATM on lymphocytes was quantified preoperatively, immediately postoperatively and 24 hours postoperatively.
Screening time was significantly longer for complex EVAR procedures than for standard EVAR, resulting in a higher radiation dose area product (DAP) over the course of the procedure. The study showed that complex EVAR procedures were associated with higher levels of DNA damage, with a marked spike in the immediate postoperative period, before falling back to normal levels within 24 hours. Sampling of operators after standard EVAR showed a milder increase in DNA damage markers immediately postoperatively, while open repair showed no increase.
Radiation exposure to the legs is significant and appears to be a danger. Radiation was measured under a lead apron, over a lead apron, and on the legs during complex and standard EVAR. During standard EVAR, radiation under the lead apron was 0uSv (range 0–3uSv), over the lead was 11uSv (range 4–74uSv), and to the legs was 92uSv (range 43–203uSv). For complex EVAR, radiation under the lead apron was 2uSv (range 0–13uSv), over the lead was 27uSv (range 4–1504uSv), and to the legs was 145uSv (range 16–416uSv).
The induction of γ-H2AX and pATM in operators reflects these high levels of radiation exposure, with a sharp spike post-procedurally without leg pad protection.
In a separate part to the study, blood from six different operators who had not had any exposure to radiation in the previous 48 hours was collected and exposed in vitro to the same radiation dose. The expression of γ-H2AX varied on operators’ lymphocytes irradiated with the same dose, with blood from some individuals consistently producing high levels of this marker of DNA damage.
This is the first study to find evidence of cellular DNA damage in operators after performing EVAR and hints at the potential utility of a biodosimetric approach to measuring the effects of radiation exposure. Directly measuring cellular response rather than conventional dosimetry could identify operators who are prone to radiation damage and who may have a lower “safe” limit than radio-resistant operators. Factors such as age, gender, previous exposure, and diet may also impact the response to radiation. It must be stressed, however, that a greater understanding of the long-term consequences of the raised expression of γ-H2AX and pATM in irradiated lymphocytes is required before conclusions can be reached about its relationship to cancer risk.
Cryoablation is increasingly being used to treat benign soft tissue lesions in adults.
Barnacle and team retrospectively reviewed cases from a prospectively maintained interventional radiology procedural database. The team performed five procedures in four children, three of whom were male. The median age of the patients was 4.5 years (range 1.4–11.1), and weight 17.3Kg (range 6.9 to 40). The anatomical location and biopsy-proven diagnoses were: calf fibroadipose vascular anomaly; thigh venous malformation; shoulder microcystic lymphatic malformation and chest wall hamartoma. Treatment was offered to patients who were experiencing; due to the size of the lesion and to one patient who was failing to thrive.
“We performed all procedures under anaesthesia with ultrasound and/or cone beam CT guidance using the SeedNet Gold ablation system (Galil Medical, now BTG). Each time, the procedure used three probes and two freeze-thaw cycles. The technical success of the procedures was 100%,” said Barnacle.
The in-hospital stay of patients ranged from one to five days. One patient required intravenous analgesia, fluids and nutrition for three days. “We observed a reduction in pain in most cases and also that lesion volume was reduced (by 69–94%, as measured in two patients). The patient who was failing to thrive has gained weight and improved her developmental milestones. Cryoablation is technically feasible for benign soft tissue lesions in children. Our initial experience suggests it is well-tolerated and effective,” Barnacle concluded.
Mercator MedSystems has announced completion of enrolment in the company’s LIMBO-ATX (Lower-limb adventitial infusion of dexamethasone via Bullfrog to reduce occurrence of restenosis after atherectomy-based revascularisation) clinical trial. The primary six-month endpoint data is expected to be available in the second quarter of 2018
LIMBO-ATX is a prospective, multicentre, randomised controlled trial that enrolled over 100 patients with arterial obstructions in arteries below the knee. The trial was designed to use Mercator’s proprietary Bullfrog microinfusion catheter to test a new treatment strategy to potentially improve blood flow and decrease repeat revascularisation procedures in below-the-knee critical limb ischaemia. Current solutions for critical limb ischaemia face many limitations, leaving a significant unmet need for these patients and physicians treating the disease.
“The investigators associated with LIMBO-ATX are very excited to have completed enrolment in this important study. Meaningful results utilising Mercator’s proprietary delivery technique could lead to a change in the standard of care treatment of critical limb ischaemia in the USA,” said George Adams, national co-principal investigator for LIMBO-ATX and director of Cardiovascular and Peripheral Vascular Research at the University of North Carolina, Chapel Hill.
Mercator previously sponsored the DANCE trial, which reached its primary endpoint in early 2017 and demonstrated positive patency outcomes from delivering dexamethasone in combination with angioplasty or atherectomy in above-the-knee endovascular revascularisation.
The European Commission, under the EU Merger Regulation, has approved the acquisition of Bard by BD, subject to conditions. Both US-based companies supply medical devices including catheters, stents, surgical instruments, devices for biopsies, and patient monitoring systems.
The merger is conditional upon BD divesting in its core needle biopsy devices business, and in a tissue marker product that is still in development.
“The conditions we have imposed on this merger will help to ensure that millions of European patients and Member States’ healthcare systems in the EU, will continue to enjoy access at fair prices to a variety of innovative medical devices,” said commissioner Margrethe Vestager, who is charge of competition policy.
The Commission state that they have concerns that the merger would have removed choice and innovation in the area of core needle biopsy devices, as this market faces “limited competitive pressure.”
Similarly, Bard and BD are two of just a few competitors in the field of tissue marker devices for marking a biopsy site. The Commission declared that due to BD’s in-development tissue marker product, the merger may have eliminated a future credible competitor and again reduce innovation in this area.
BD has agreed with the Commission, and has committed to divesting in these two areas of its business so that the merger may proceed.
In April of this year, BD announced its intention to acquire Bard for US$24 billion (£18.2b, €20.3b), an agreement that was unanimously approved by the boards of directors of both companies.
In August, Bard was the first company granted premarket approval from the USA FDA for its Lutonix 035 DCB drug-coated balloon catheter for use in end-stage renal disease (ESRD) patients.
“One of the biggest challenges for interventional radiology in 2017 is that we are in desperate need of outcomes research that documents the value of interventional radiology in modern healthcare,” Matt Mauro, CEO of UNC Faculty Physicians and chairman, Department of Radiology, University of North Carolina at Chapel Hill Education, Chapel Hill, USA, tells Interventional News.
When did you first decide on a career in medicine and why did you choose interventional radiology?
I obtained an engineering degree from Cornell University (Electrical Engineering) with the intent of pursuing a career in that field. It was during a summer internship at an engineering company that I discovered that engineering was not my path, mainly because of the lack of a direct personal connection with people. It was suggested to me that medicine was the integration of science (biological sciences) and direct contact with people. I switched my career choice the summer before entering my senior year at Cornell University.
Who were your mentors and what wisdom did they impart to you?
My interest in imaging and intervention began as a medical student at Cornell University Medical College. I was intending to be a surgeon and had multiple discussions with the chair of surgery at New York Hospital about matching there. It was Joe Whalen, Mort Meyers, and Tom Sos (all Cornell Radiology faculty members) who believed in the power of imaging and the future of image-guided interventions. My early career was particularly influenced by Fred Keller, Barry Katzen, and Bob White—all giants in the field of interventional radiology. They demonstrated the importance of patient interaction and the tremendous impact on patient care that our newly developing specialty could have through their clinical skills.
Which innovations in interventional radiology have most influenced your career, and how?
My first arterial puncture was in 1977. We were making our own catheters from reels of polyethylene tubing—shaping tips, tapering etc. We were performing very detailed diagnostic arteriograms for many disorders since this was the primary method of diagnosis and staging—prior to the evolution of quality cross sectional imaging. Treatment was confined to vasopressin infusions for lower gastrointestinal bleeding and some bland embolotherapy. Innovation and inspiration by many have been responsible for the creation and growth of our specialty. Embolotherapy has been one of my primary interests within the field of interventional radiology, and the development of the vast array of embolic materials and their delivery mechanisms have been particularly important to my career. Other areas of innovation that have particularly impacted me include image guided venous access, venous reconstruction, and the management of aneurysmal disease.
From an interventional radiologist to the CEO of UNC Faculty physicians—how has your outlook changed?
During my career, I have transitioned through three jobs, each with different responsibilities and priorities with respect to interventional radiology. From the beginning of my faculty appointment (1982) to my appointment as chair (2007), I was responsible for the development and growth of this area of practice both at UNC as well as in the field in general. In that role, I introduced each new device, technology, and procedure to our medical centre. Upon becoming department chair, that role fell to my colleagues, and my new responsibility was to the department as a whole. However, I remained very active with two full days per week in the interventional suite, a half-day clinic, and full call. I was careful not to micromanage any of my divisions, including interventional radiology. In 2015, with my appointment to the newly created position of CEO of UNC Faculty Physicians, I have the overall responsibility for a US$500 million enterprise with direct reporting structure to the CEO of the entire UNC Health Care System. In this role, I could no longer maintain an active interventional practice, but I continue to rotate on our vascular imaging service, a component of the interventional radiology division. My primary focus and responsibility now is to the entire UNC medical practice, but I hold the firm opinion that a strong interventional radiology programme is essential and vital to our unified success. It is for example, necessary for lowering our length of stay and the prompt management of a variety of complications generated by other services.
From your perspective as CEO, what does interventional radiology do well and what does it need to improve to stay relevant?
A successful and well-run interventional radiology programme improves the clinical care and efficiency of care to the patients of the medical centre. However, it may go unnoticed because it is not considered a “service line” unto itself. It is actually an important part of multiple service lines (eg. cancer, Heart and Vascular, Abdominal Transplant, Neurosciences), and it should be represented as such. Recognised leaders of these service lines will typically not be interventional radiologists, and, therefore, interventional radiology’s contribution may not be readily apparent to senior leadership. It is important for interventional radiology to be well situated within the service line leadership structure so that its value can be clarified appropriately.
One interesting caveat is that at UNC, senior leadership clearly recognises interventional radiology. However, it is sometimes difficult for me to advocate strongly for interventional radiology for fear of appearing biased.
Specifically, how has the state of research in interventional radiology changed from the early days until now?
Interventional radiology has always struggled with level one data—prospective randomised trials. The trials that were developed have been predominantly industry-sponsored. Our colleagues are data driven, and these new studies are required to show efficacy and value. I would say one of the biggest challenges for interventional radiology in 2017 is that we are in desperate need of interventional radiology outcomes research that documents the value of interventional radiology in modern healthcare.
How has the interventional radiologist changed from the 1980s, when you were a fellow, to now?
Interventional radiology can continually reinvent itself in response to innovations across the medical discipline. In the early eighties, percutaneous biliary interventions were replacing open operative remedies for biliary and gallbladder disease. With the advent of interventional endoscopy, our role has been modified. The success of interventional radiology will be its constant ability to innovate and apply our principles to other areas. When one door closes, another opens. Our innovation will sustain our success, and our minimally invasive methodology will be desired in a world of population health.
Which early procedures are you keeping an eye on?
Management of morbid obesity via left gastric artery embolization—obesity is an American epidemic and bypass surgery has significant complications; continued development of prostatic artery embolization—a very common problem in older men—we have a place in this arena; and targeted cancer therapies.
Interventional radiology has always had close ties to the device industry. How is this relationship best navigated?
Interventional radiology is the marriage of complex imaging and devices—those items that can be placed within the body through small openings and guided by imaging. A healthy relationship with device manufacturers is very important. New and innovative devices advance our specialty, perhaps more than any other factor. The benefits include the development of clinically useful products that are of value to society. The pitfalls arise when personal profit enters into the relationship and clouds our ultimate mission. The relationship is best navigated by maintaining a professional level of understanding that the partnership is focused on advancing clinical care.
Please describe a memorable case…
I will offer two memorable cases.
It was the very early days of transjugular intrahepatic portosystemic shunts (TIPS), and I had given a few presentations to a group of somewhat sceptical transplant surgeons. In the middle of one evening, a Childs C cirrhotic patient presented with uncontrollable variceal haemorrhage with a >60% operative mortality. The chief of our transplant programme personally called me (I was not even on call that evening) and asked if I wanted to try a TIPS on this patient—a test case. I successfully performed our first TIPS procedure in the middle of the night; the patient stabilised and was discharged several days later. Although this violated the general approach that your first case of a new procedure should be performed on a patient with high chance of success, this case solidified the value of TIPS at UNC.
Percutaneous inferior vena cava (IVC) filter deployment had just been published. At that time, IVC filters were inserted by surgical cutdown by our vascular surgery service. I spoke to our chief of vascular surgery who again was sceptical about percutaneously placing a 24F sheath in the vein and deploying this device. He insisted on being present for our test case. As soon as I made the venous puncture, the vascular surgery chief was paged, and he stepped out for several minutes to return the call. When he returned, I was holding pressure on the access site—we had already dilated the access site and deployed the filter.
What are your interests outside of medicine?
I was a multisport athlete in college and continued playing organised soccer and basketball until I was 40.
From ages 40 to 60 I became heavily involved in competitive martial arts (tae kwon do, hapkido and kickboxing).
Nowadays, in addition to spending time in the gym on a routine basis, I enjoy the yard and auto maintenance that comes with car and home ownership; movies; and times with friends and family.
Fact file
Current roles
CEO UNC Faculty Physicians, University of North Carolina at Chapel Hill Education, Chapel Hill, USA
Chairman, Department of Radiology, University of North Carolina at Chapel Hill Education
Ernest H Wood Distinguished professor of Radiology and professor of Surgery, Department of Radiology, University of North Carolina at Chapel Hill Education
Education (selected)
1982
Fellow in abdominal and vascular/interventional radiology, The Edward Mallinckrodt Institute of Radiology, Washington University School of Medicine, St Louis, USA
1981
Fellow in diagnostic and vascular radiology, Department of Radiology, University of North Carolina School of Medicine Chapel Hill, North Carolina
1980
Chief resident in radiology, Department of Radiology, University of North Carolina School of Medicine Chapel Hill
1977
MD, Cornell University Medical College New York, New York, USA
Awards (selected)
2014
Society of Interventional Radiology (SIR) Gold Medal
2009–2013
Chairman, Radiologic Society of North America (RSNA) Scientific Programs Committee
2011–present
Voting/Alternate ABMS assembly representative
2010
American Board of Radiology (ABR), Lifetime Service Award
2010
Charles Tegtmeyer Lecturer, International Symposium on Endovascular Therapy annual meeting
2009
Dotter Lecturer; 25th annual SIR meeting
Society roles (selected)
1999–2000
President, SIR
1999–2000
Executive committee, American Heart Association
2008–2013
Section editor, The American Journal of Roentgenology, American Roentgen Ray Society
International registries will help demonstrate the value of interventional oncology therapies
The primary importance of collecting data from registries would be to establish outcome data to prove the value of the interventional oncologic therapies to healthcare administrations and governments; ie. to establish interventional oncology’s value in healthcare. Further, it could help gather data to confirm that interventional oncology treatments of cancer impact patients’ lives and the quality of their survival.
“There is a strong need for registries, especially for prevalent cancers treated by interventional oncologists: lung primaries, metastatic disease, liver, lung, kidney and bone cancers. These registries would also capture data on the complications of interventional oncology therapies.
“This is a call for more mature, higher quality research within interventional oncology,” said Constantinos Sofocleous, Memorial Sloan Kettering Cancer Center, New York, USA and professor of Radiology, Weill Medical College of Cornell University, New York. He is also a director-at-large of the Society of Interventional Oncology (SIO). Both Sofocleous and Matthew Callstrom, professor of Radiology, Mayo Clinic College of Medicine, Rochester, Minnesota, USA, and scientific programme chair of the World Conference on Interventional Oncology (WCIO) 2017 spoke to Interventional News at the WCIO annual meeting in Boston, USA, in June.
Graeme Poston, professor of Surgery, University of Liverpool, Liverpool, UK, speaking at the European Conference on Interventional Oncology (ECIO; April, Bilbao, Spain) meeting noted that while randomised controlled trials remained the gold standard to underpin evidence based practice, it was well recognised that such trials addressing a surgical/interventional radiology procedure may be difficult to design and recruit to.
“There will be situations where it will not be practically possible to recruit patients to large phase III surgical/interventional radiology randomised controlled trial. Alternative prospective study strategies, including registries, are possible, and although not perfect, should be considered as alternatives to randomised controlled trials,” he said.
David J Breen, clinical director of Radiology, Southampton University Hospitals, Southampton, UK, concurs: “High level trials in interventional oncology are particularly problematic due to the increasing complexity of cancer treatment pathways, multiple competing therapies and not least the ‘transdisciplinary’ nature of many interventions in this field, where perceived clinical equipoise may still be controversial. Registries, whilst representing dirty but real world data, can quickly accrue and prove the technical and to a large extent the oncological merit of a particular intervention.
David Breen says that registries can quickly accrue data to prove the merits of certain interventions
“Renal cancer ablation is a good case in point where attempts at randomised studies against surgery have failed, yet there is considerable activity, and the safety, procedural outcome and recurrence rates of this therapy can be determined in relatively short order. We have great hopes for the European EuRECA and North American ARMOR renal ablation registries which are currently open,” he says.
Govindarajan Narayanan (chairman of Vascular/Interventional Radiology) and Riccardo Lencioni (director of Interventional Oncology Research) from the University of Miami-Miller School of Medicine, Miami, USA, who organise the Synergy Miami meeting, also note that gathering registry data is the way forward. They say: “We strongly believe that interventional oncologists should focus more and more on collecting outcome data in the context of well-designed, multicentre, prospective registries. This is the most powerful tool to be able to produce high-quality data. We should also focus on the ability of these therapies to improve quality of life, a metric that has been finally recognised as a key endpoint for cancer clinical care.”
Sofocleous reiterates the point: “There are a lot of data that we can capture right now even if they are not the gold standard that may never arrive. Thirty years from now, if we do not set up registries and collect data, and prove our value as a specialty, we are not going to exist as a specialty. Other specialties will be doing image-guided intervention. If we do not prove our value and there is an economic change in healthcare reforms such that there is no reimbursement, we will be shut down.
“This is a call for more mature, higher quality research within interventional oncology,” says Constantinos Sofocleous
“Image-guided oncological therapies will then need to go through another cycle of development through other specialties, which would not necessarily mean the extinction of the therapies, however, it will have an impact on the survival of interventional oncology. The value of our treatments is under question when we do not have randomised level one evidence. So what we need is to collect data from prospective registries with well-defined data points. Surgery and radiation oncology have done this; we have not,” he says.
Callstrom adds: “Registries are a way to establish a better foundation of the data across the spectrum of people that do these procedures. This type of data is a notch above single-centre data. In renal tumour ablation, for example, which has good outcomes, with registry data we are going to be able to say to patients, you can go to any of the centres in the country that participate in this registry, and this is going to be your likely outcome. It is a very valid measure.”
Both make the point that valuable prospective registry data will require centres to achieve a high level of performance and appropriate patient selection. In order to participate in the registry, physicians will have to ideally contribute a minimal standard of acceptable data to it. So for example, in a pre-defined prospective registry for liver ablation, the registry would mandate the inclusion of patients that have liver-only disease; patients should have no more than three lesions, each one of them being no more than 3cm. The outcomes obtained would then pertain to this pool of patients.
“Right now we have a lot of dirty data because you are pooling together cases of patients who have 3cm, 5cm and 8cm lesions who were treated by ablation, which may not be what is considered optimal care. This makes the data look worse than it should if appropriate patient selection had been used,” explains Callstrom.
“Right now we have a lot of dirty data,” says Matthew Callstrom
Need for an ICOG group
The Eastern Cooperative Oncology Group (ECOG) is one of the largest clinical cancer research organisations in the USA, and conducts clinical trials in all types of adult cancers. Many thought leaders at the WCIO meeting noted that the creation of an Interventional Cooperative Group (ICOG) would be important.
“We are challenged as a specialty; we do not have an oncology group. If we establish a similar framework, we can rapidly collect prospective data. It does not have to be randomised. At least it gets us to that higher level of evidence. Establishing such a framework to collect that data would be invaluable. We need an organisation that creates registries for all interventional therapists,” Callstrom said.
Sofocleous adds: “What we need is the set-up of a cooperative group, so that we accumulate data that are not based on vendor-type or biased by financial interest of what therapy we are choosing. We want to see the outcome of the different therapies, and then as much as there are subtype differences between devices and tools; that can be a secondary aspect.”
The current IO registries that are running, often tend to be by device type, in a particular region. Sofocleous notes that “ideally, I would like to see disease-based outcomes. I want to see the outcomes of metastatic bone disease treated by ablation, for example. Or, I would like to see the outcomes of renal cell carcinoma treated by ablation. With these data we are going to be able to characterise the treatment to a very high level, if you do a good job in terms of how you establish the data collection.”
One of the current aspects of registries pertaining to interventional oncology is that they are basically vendor oriented. “Vendors have tried to support the use of their devices, which is valid, particularly in the application in which they might dominate, or have investment in. But I think as you move to registries that are broader or generic, you can still collect the information on the device that is used, and potentially even filter data based on this, but these data will provide a very broad perspective of outcome, which is valuable,” said Callstrom.
Interventional oncology experts agree that it is time to do this. “We have to move aggressively to establish the value of what we do, provide objective measures, and collecting registry data is one step in that direction,” says Callstrom.
“I hope we are able to get together all the relevant stakeholders in image-guided intervention in cancer to get this done as efficiently and in an as unbiased a way as possible,” concluded Sofocleous.
A prospective randomised controlled study that compared outcomes between hepatocellular carcinoma patients who were treated by microwave ablation with those who were treated by radiofrequency ablation, did not find a benefit for microwave over radiofrequency.
For local tumour progression and survival at two-year follow-up, “the theoretical benefit of microwave does not translate into clinical benefit for hepatocellular patients with lesions smaller than 4cm. This was a negative trial as microwave failed to demonstrate superiority over radiofrequency,” said Alban Denys, Radiology, Lausanne University Hospital, Lausanne, Switzerland, who presented the results at CIRSE 2017.
Denys reported that this was a prospective, randomised, multicentre study to compare the efficacy of radiofrequency ablation with microwave ablation. The theoretical advantages of microwave include shorter ablation time, higher temperature of ablation, reduction of heat-sink effect and treatment of larger lesions. Previous modelling studies have predicted that microwave ablation is likely to be more effective than radiofrequency ablation, particularly when they are in the proximity of large vessels, where radiofrequency is widely thought to be compromised by the heat sink effect.
“It has also been claimed that the recurrence we observe with radiofrequency around the vasculature of the liver, mainly large vessels, should be reduced with microwave. However, it has not been proven in vivo that one technique is superior to the other,” he added. Denys also noted that a previous study from China that compared these modalities (in which a non-commercial device was used) did not show a benefit for microwave over radiofrequency.
“We found no difference in local tumour progression and survival at two-year follow-up between patients who were treated by radiofrequency ablation when compared to those treated with microwave ablation,” Denys reported.
From 2011 to 2015, the investigators randomised patients with hepatocellular carcinoma who had three, or fewer, lesions that were four centimetres in length or shorter, to treatment with either radiofrequency ablation or microwave ablation. All the patients had chronic liver disease; were unsuitable for surgery; and eligible for thermoablative treatment. The primary outcome was the rate of local tumour progression at two-year follow-up. Secondary outcomes were time to progression; survival; incomplete treatment rate; and safety of the treatment. The investigators used the unpaired T-test and Chi-square test depending of the type of data. They analysed survival using Kaplan-Meier curves.
Final data were analysed from 73 patients (15% female, 73% Child–Pugh A, 104 lesions treated) in the radiofrequency ablation group and 72 patients (17% female, 80% Child–Pugh A, 98 lesions treated) in the microwave ablation group the two patient groups were similar for demographic, biology and tumour characteristics (mean lesion size was 18mm in both groups).
Results
At the two-year mark, there were slightly higher numbers of recurrence in the radiofrequency ablation group, ie, just over 11% cases of local tumour progression, compared to 6% in the microwave ablation group (p=0.32). The average time to local progression in the radiofrequency ablation group was 16 months (6.5 months standard deviation [SD]); in the microwave ablation group, it was 12 months (8.2 SD; p=0.28) This showed, said Denys, that there was late recurrence in the radiofrequency group, for unknown reasons.
The survival rate at two-year follow-up was described as “excellent” in both groups—87% in the radiofrequency ablation group and 88% in the microwave ablation group (p=0.78). The rate of incomplete treatment after one session of thermoablation was similar in the two groups (4% and 5%, respectively; p=0.93).
There were fewer complications in the microwave group, and no major complications in either group. There were two grade four complications—both arterial bleeds that required embolization—in the microwave ablation group. Nearly the same number of patients in both groups went on to have a transplantation.
The US Food and Drug Administration has cleared the first seven tesla (7T) magnetic resonance imaging (MRI) device, more than doubling the static magnetic field strength available for use in the USA. The Magnetom Terra (from Siemens) is the first 7T MRI system cleared for clinical use in the USA.
“The overall image quality of MRI improves with higher magnetic field strength,” stated Robert Ochs, director of the Division of Radiological Health in the FDA’s Center for Devices and Radiological Health. “The added field strength allows for better visualisation of smaller structures and subtle pathologies that may improve disease diagnosis.”
Before this clearance by the FDA, clinical MRI systems in the USA were available in field strengths of 3T and below.
According to a release from the FDA, it reviewed the Magnetom Terra through the 510(k) premarket clearance pathway. The FDA based its clearance on comparison to a predicate device and acquisition of sample clinical images. The agency reviewed the safety of the radiofrequency subsystem through computational modelling, simulations and rigorous experimental validation.
The manufacturer also provided data from a comparative study of 35 healthy patients that compared images of the patients using the 7T device and images using the 3T device. Board-certified radiologists reviewed the images and confirmed that the images acquired on the 7T device were of diagnostic quality and, in some cases, an improvement over imaging at the 3T.
The Magnetom Terra is for patients who weigh more than 66 pounds, and is limited to examinations of the head, arms and legs (extremities).
Vivasure Medical has announced the successful enrolment of the first patient in the Frontier IV clinical study, a non-randomised multicentre international trial, designed to expand the indications of its proprietary PerQseal large arteriotomy closure technology. The patient was enrolled by Peter Crean (Blackrock Clinic, Dublin, Ireland).
Large arteriotomies (12Fr) are vessel punctures created to facilitate endovascular procedures such as transcatheter aortic valve implantation (TAVI), endovascular aneurysm repair (EVAR), balloon valvuloplasty, and ventricular assist devices. A press release reports that PerQseal is the world’s first fully absorbable, patch-based large-bore percutaneous closure technology.
Christoph Naber (Contilia Heart and Vascular Centre, Essen, Germany), who is the TAVI principal investigator of Frontier IV, says: “Driven by clinical and economic outcomes data, percutaneous access-site management has become an increasingly important aspect of TAVI procedures. I strongly believe PerQseal, which is designed specifically to address large arteriotomies, will help improve outcomes for these patients.”
“We are very excited to begin the Frontier IV trial as the next phase in our commitment to build the clinical experience with PerQseal. A percutaneous approach has now become the gold standard for procedures such as TAVR and EVAR, driven by clinical outcomes data. As patient volumes increase, access site management and closure has become an increasingly important aspect of complication and cost reduction. The data from this trial will be used to support our goal of expanding the indication range of the PerQseal technology,” comments Gerard Brett, co-founder and CEO of Vivasure.
Researchers from the University College London (UCL) Cancer Institute, London, UK, and BTG have begun the first clinical trial of an experimental treatment for liver cancer using X-ray imageable microscopic beads loaded with a targeted anti-cancer drug placed directly in the liver.
The trial will evaluate delivering a precisely controlled dose of vandetanib, an inhibitor of multiple tumour growth pathways, directly to the arteries feeding a liver tumour by pre-loading the drug on a radiopaque bead which can be visualised on CT scans. Although still at a very early stage of research, the development programme aims to improve current treatments for patients with primary liver cancer and metastatic colorectal cancer (mCRC).
The current standard of care for liver cancer patients is known as transarterial chemoembolization, (TACE). Despite advances in this procedure, liver cancer remains one of the most common causes of cancer death worldwide.
VERONA study
To improve the treatment of patients with primary liver cancer and mCRC, the beads used in the VERONA study (vandetanib-eluting radiopaque beads in patients with resectable liver malignancies) are preloaded with a multi-kinase inhibitor called vandetanib. Vandetanib targets genetic alterations and cell-signalling pathways that lead to liver cancer growth, recurrence and metastasis. These pathways, including vascular endothelial growth factors (VEGF-A and C) and epidermal growth factor receptor (EGFR), stimulate new tumour blood and lymph vessel growth and aid the development of solid tumours. They may also promote spread of the cancer to other organs and inhibit the body’s own immune response to the tumour. A phase II trial of vandetanib in patients with advanced liver cancer showed some promise, and provided a strong rationale for the locoregional delivery of this drug.
Ricky Sharma, chair of Radiation Oncology at UCL and the study’s primary investigator, said: “The incidence and mortality rates for primary liver cancer continue to climb and it is vital that we explore new treatment approaches. This research is exciting because it is the first time we have been able to preload a targeted cancer drug on to an imageable bead, to deliver the targeted drug in high doses to the cancer and see exactly how well the beads reach the target we have defined. By refining the treatment using information from this clinical trial, we may be able to develop a liver-directed treatment as a superior alternative to the rather poorly tolerated drug treatments we currently offer patients with this type of cancer.”
The vandetanib-eluting bead was developed in collaboration with Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland and Alban Denys, professor at the department of medical radiology at CHUV. Vandetanib-eluting beads use BTG’s recently developed radiopaque bead platform, DC Bead Lumi. Beads that can be visualised with CT or fluoroscopic imaging offer the advantage of providing visible confirmation of bead location during and after the embolization procedure, enabling real-time adjustments to optimise patient treatment.
Eligibility
Patients with primary liver cancer or mCRC who meet the eligibility criteria will be offered participation in the clinical trial at University College London Hospitals NHS Foundation Trust and the Royal Free Hospital NHS Foundation Trust. Patients suitable for the VERONA study are those scheduled to have their liver tumours removed surgically. By studying the resected tissue in great detail, and comparing it to the scans performed before the operation, researchers will be able to assess exactly where the vandetanib-eluting beads have been deposited in and around the tumours, and how much drug has been delivered to the target. In this way, the VERONA “window of opportunity” clinical trial will assess the safety and tolerability of the new treatment and the potential it offers for treating liver cancer, a press release from BTG says.
Six-month results from a prospective, randomised, non-inferiority study presented at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 16–20 September, Copenhagen, Denmark) reveal that prostatic artery embolization is safe and effective in the treatment of benign prostatic hyperplasia (BPH) and that it results in symptomatic improvement for patients based on achieving a decrease in prostate volume.
Ana Sáez de Ocáriz García, Complejo Hospitalario de Navarra, Pamplona, Spain, who reported the results, said: “This clinical trial shows that prostatic artery embolization is a real alternative that is not inferior to transurethral resection. Further, the results show that there are no severe complications related to prostatic artery embolization. We would like to emphasise the importance of teamwork between urology and interventional radiology in furthering this treatment.”
BPH can result in lower urinary tract symptoms (LUTS) which are usually treated with medication at first instance. However, medical treatment often fails in the medium to long term. At this point, the “gold standard” treatment offered to patients is transurethral resection of the prostate (TURP), but there are many alternatives that are being explored such as microwave treatment, laser ablation, and high-intensity focused ultrasound. Supraselective transarterial embolization of the prostate is one such treatment alternative and interventionists hope that it will have the same effectiveness, but with fewer side-effects.
The randomised trial set out to compare clinical and urodynamic results of prostatic artery embolization and TURP in the treatment of LUTS in patients with BPH. The triallists also set out to evaluate early complications related to sexual function and compare the gain in quality of life between the two treatments.
“In our study, we enrolled 80 patients. Twenty one were excluded and then 60 patients were randomised in a 1:1 ratio. We assigned 30 to the embolization group and 30 to the TURP group (however, one patient declined the surgical procedure). There was no substitution mechanism and the treatment allocation was not masked. We collected data on maximum urinary flow rate (Qmax), international prostate symptom score (IPSS), quality of life (QoL), international index erectile function (IIEF), prostate specific antigen, prostatic volume, and post void residual volume in the follow-up visits scheduled for one, three, six and 12-months after treatment. Here, we present the six-month results,” Sáez de Ocáriz García said.
Patients had to be older than 60 years of age, diagnosed with BPH and have moderate or severe obstructive LUTS that was refractory to six months of medical therapy in order to be eligible. They also needed to have a Qmax of less than 10mL/s, and to be able to provide written informed consent. Baseline characteristics between the two groups were comparable.
Exclusion criteria
Patients were excluded if they had severe atherosclerosis and tortuousness of the iliac arteries; unidentifiable prostatic arteries by CT angiography; allergy to iodinated contrast; uretheral stenosis; neurogenic bladder; malignant tumour; glomerular filtration rate of less than 30mL/minute; and any other important and uncontrolled disease that interferes with participating in a trial.
Endpoints
The improvement in maximum urinary flow rate (Qmax) was the main effectiveness endpoint. Secondary endpoints included improvement in IPSS score. Reduction in prostatic volume, no worsening or improvement of erectile function; reduction of PSA and post-void residual volume; and patient satisfaction with the intervention performed.
“One of the most important things is CT angiography that helps to select patients and obtain the imaging needed to perform the procedure. While the origin of the prostatic arteries is very variable, the most important arteries are the internal pudendal, gluteal pudendal, obdurator artery and vesical-prostatic artery,” she noted.
Results
The investigators achieved technical success in 100% of patients with both techniques. At 24-hours, patient satisfaction with embolization was nearly 84%; whereas it was 77% with TURP. Those who underwent embolization reported a mean pain score of 0.5, compared to those who underwent TURP (mean VAS =2.9). On average, embolization was a longer procedure than TURP. On average, those who underwent embolization stayed in hospital for a day, when compared to nearly two days for those who underwent TURP. There were no complications with either procedure.
At six months, there was significant improvement in the Qmax of both groups with the gains being very similar. There was also improvement in the IPSS score in both groups, with TURP appearing to confer a greater benefit. “Most of the quality of life improvement was seen in the first three months after the procedure with some subsequent stability. While post-void residual volume reduction was similar in both groups, the reduction of prostate volume was greater with TURP than embolization,” Sáez de Ocáriz García explained.
Minor complications after embolization included haematuria (two patients); haematospermia (two patients); intermittent claudication (one patient) and radiodermatitis (one patient). There was also one major complication—a rectal ischaemic plaque.
Minor complications after TURP included urinary incontinence (one patient); stenosis of the urethral meatus (one patient); testicular pain (one patient) and urinary urgency (one patient). There was also one major complication of urethral stenosis in one patient.
“The results after six months of embolization were a decrease of 25 points in IPSS, an increase of three points on IIEF, and a decrease of 37.2% in prostate volume. All patients with acute urinary retention could remove the bladder catheter, three weeks after,” the authors reported.
Gerard Goh, Radiology, The Alfred Hospital, Melbourne, Australia, reported results from a comparative study of inferior vena cava (IVC) filters at CIRSE 2017 that examined the effectiveness, safety and complication rates of the Celect, Celect Platinum and ALN vena cava filters.
While all three inferior vena cava filters, Celect, Celect Platinum (both from Cook Medical) and ALN vena cava filter (ALN), demonstrated safety and high rates of retrievability, the incidence of minor complications was quite high, with limb penetration being the most common.
“As far as the authors are aware this is the first data on the Celect Platinum filter. The study was a retrospective review of hospital medical records of patients receiving an inferior vena cava filter in a level one trauma centre and was performed between November 2011 and June 2016,” Goh said.
Two interventional radiologists examined each filter episode with available angiography and CT images. They also examined the patients’ medical notes for each admission and to extract the relevant data.
Results
Goh and colleagues reported that 476 filters were placed (161 ALN; 153 Celect; and 162 Celect Platinum). Of the filters with follow-up imaging, limb penetration was the highest minor complication recorded at just under 65% for ALN and Celect, while it was nearer 35% for Celect Platinum. Malposition (including tilt >15 degrees), was the next most frequent complication with 22% of ALN filters moving out of position followed by 8% of Celect filters and 4% of Celect Platinum filters.
Of the patients with follow up imaging, major complications (including breakthrough pulmonary embolism, migration, fracture, inferior vena cava strictures and pericaval haematoma) were just over 7% for ALN, around 3% for Celect and just over 1% for Celect Platinum filters. Breakthrough pulmonary embolism constituted the largest major complication at nearly 4% for ALN, around 2% for Celect and under 1% for Celect Platinum. Malposition occurred in 22% of ALN filters and in 6–8% of Celect filters.
“Excluding breakthrough pulmonary embolism, the rates of other major complications rates were low. The breakthrough pulmonary embolism rates for each filter, however, were in line with the current literature. Where retrieval was attempted, it was successful in around 98% of ALN filters (although this filter had the highest required rate of advanced retrieval techniques), compared to around 93% of Celect retrievals and over 95% of Celect Platinum filters,” Goh stated.
Scientists have discovered new information about a molecule which is part of the body’s tissue repair system. This finding could help treat non-healing wounds and injuries, such as diabetic foot.
The number of limbs amputated because of diabetes is at an all-time high of 20 each day in England alone. Intense research around the world is being carried out to discover new treatments that could help avoid such life-changing operations and reduce medical costs for society.
A study led by the universities of Exeter and Bath, UK, and published in the journal Antioxidants and Redox Signalling has made great strides in understanding how the molecule deoxyribose-1-phosphate stimulates the formation of new blood vessels.
Angiogenesis
It has long been known that the formation of new blood vessels is critical during the body’s response to tissue damage. Now, thanks to this project jointly funded by Biotechnology and Biological Sciences Research Council (BBSRC) and the Medical Research Council, the understanding of how deoxyribose-1-phosphate works could open new avenues of treatment in encouraging the body to heal- a discipline known as regenerative medicine.
Giordano Pula, of the University of Exeter Medical School, Exeter, led the team. He said: “We are very excited to provide new insights into how this crucial molecule works to stimulate the formation of blood vessels in people. We now hope to be able to use this knowledge to trigger the formation of new blood vessels in patients where this is required for tissue regeneration, such as diabetic foot.”
This study demonstrates that deoxyribose-1-phosphate activates an enzyme called NADPH oxidase 2 (NOX2). This in turn leads to the stimulation of the transcription factor called NFkB, which is responsible for turning on genes specifically involved in the formation of new blood vessels.
Among the genes activated in the chain of events leading to blood vessel formation, the vascular endothelial growth factor receptor 2 (VEGFR2) play a central role. This is a key target in regenerative medicine, and the team hope that this discovery will provide a cost-effective treatment for manipulating blood vessel formation.
Pula’s team is now planning to focus their investigation on the ability of deoxyribose-1-phosphate to stimulate skin repair by increasing the vascularisation of wounds and non-healing ulcers. The team hopes this work will lead to new applications for treating conditions such as diabetic foot.
The first patient was treated in the CONTROL hypertension (HTN)-2 clinical study, the Rox Medical’s pivotal study to evaluate the safety and effectiveness of the Rox Coupler used to create an arteriovenous anastomosis in the iliac vessels, in patients with high blood pressure.
A press release reports that the CONTROL HTN-2 study is a large, multicentre trial that will include up to 30 study sites in the USA. The first procedure was performed at Brookwood Baptist Health Princeton Baptist Medical Center in Birmingham, Alabama, USA, by Farrell O Mendelsohn.
Prior to CONTROL HTN-2, the press release notes, Rox Medical conducted a multicentre randomised trial in Europe. Patients treated with the Rox Coupler experienced a mean drop in blood pressure of 27mmHg which was sustained out to six months. A manuscript has been recently accepted for publication confirming a significant and durable pressure drop at one year.
The Rox Coupler and Flow procedure creates a passage between an artery and a vein in the upper thigh, which redirects a measured amount of arterial blood to the veins. This therapy is intended to reduce peripheral vascular resistance and add a compliant venous element to the arterial system through creation of a therapeutic arteriovenous anastomosis with the Rox Coupler.
Mendelsohn, the principal investigator for the research protocol, says: “Our entire research team at Cardiology, P.C. is excited about implementing this research study for our patients as the ROX Coupler technology may offer an alternative option to treat the global problem of uncontrolled hypertension.”
Rodney Brenneman, chief executive officer of ROX Medical, says: “Sarting the Rox CONTROL HTN-2 study is a crucial milestone in our efforts to help the millions of patients living with uncontrolled high blood pressure manage their disease. We congratulate our colleagues at Brookwood Baptist Health Princepton Baptist Medical Center on being the first to enroll in this important study”.
Catheters for cardiovascular and peripheral arterial disease
BTG today announces it has acquired Roxwood Medical, an innovative provider of advanced cardiovascular specialty catheters used in the treatment of patients with severe coronary and peripheral artery disease.
Roxwood’s anchoring catheters (CenterCross, CenterCross Ultra, MultiCross) and microcatheters (MicroCross) offer options for physicians in the crossing of complex lesions and arterial blockages. By incorporating a self-expanding scaffold that stabilises the delivery of a guidewire, Roxwood’s catheters provide positioning accuracy and support to facilitate the crossing of blockages, mitigating guidewire buckling and enabling treatments such as angioplasty, stenting or atherectomy.
“This bolt-on acquisition continues to build BTG’s strength in the interventional vascular space, further expanding our portfolio of differentiated minimally invasive vascular technologies,” said John Sylvester, BTG’s chief commercial officer. “Roxwood’s products complement our existing business and will be offered through our existing Ekos hospital sales force, providing our customers with options to enable treatment of these patients with complex lesions.”
“This is an exciting new chapter for the team at Roxwood and further testament to the utility of the anchoring and microcatheter platforms,” said Mehrdad Farhangnia, Roxwood’s CEO. “With the expanded commercial and clinical reach of BTG, these minimally invasive tools can help far more clinicians successfully treat patients with severe arterial blockages.”
BTG will pay up to US$80 million in cash to acquire Roxwood, comprising US$65 million paid on closing and up to an additional US$15m should certain future commercial milestones be achieved. The transaction is expected to be accretive to adjusted EPS from the second full year of ownership.
Teleflex has announced the completion of its previously announced acquisition of NeoTract.
Founded in 2004, NeoTract is a privately-held medical device company that has developed and commercialised the FDA-cleared UroLift system, a novel, minimally invasive technology for treating lower urinary tract symptoms due to benign prostatic hyperplasia, or BPH. Performed primarily through a transurethral outpatient procedure, the UroLift system delivers permanent implants that hold open the urethra, reducing the prostate obstruction without cutting, heating, or removing prostate tissue.
Transaction value
On 5 September 2017, the two companies announced a definitive agreement for Teleflex to acquire NeoTract in a transaction valued at up to US$1.1 billion. Under the terms of the agreement, Teleflex acquired NeoTract for an upfront cash payment of US$725 million at closing, and has agreed to pay up to an additional US$375 million upon the achievement of certain commercial milestones related to sales through the end of 2020.
Teleflex will provide additional details on the transaction, including an update to its fiscal year 2017 financial outlook as a result of this transaction, on its third quarter 2017 investor conference call.
iVascular SLU has announced the initiation of the TINTIN trial, evaluating the combined therapy of Luminor drug-coated balloon (DCB) and iVolution self-expandable stent.
The TINTIN study is prospective, investigator-initiated, non-randomised, multicentre trial, investigating the 12-month safety and efficacy of combined Luminor DCB and iVolution self-expandable stent in TASC C and D femoropopliteal atherosclerotic lesions.
“Both Luminor and iVolution have already demonstrated their safety and efficacy in previous studies” stated Lluis Duocastella, CEO of iVascular SLU. “The TINTIN trial is the next step to prove their combined benefit for the patient with the most complex lesions”.
Koen Deloose (AZ Sint Blasius Dendermonde, Belgium), is the TINTIN trial principal investigator. Deloose enrolled the first two patients on 22 September. “We are excited to drive the first multicentre study evaluating the dual therapy DCB with bare metal stent in real-life TASC C and D lesions. Performing this with a drug-eluting balloon that has shown the best results in a randomised controlled trial as of today, and a self-expandable stent that has proven its efficacy in EVOLUTION trial, we expect outstanding results in the most challenging superficial femoral artery lesions” Deloose said.
It is now almost a decade since the first patient underwent catheter-based renal denervation as a participant in a safety and proof-of concept study (SYMPLICITY HTN-1).1 Since then, SYMPLICITY HTN-3 has indicated that renal denervation does not provide benefit for patients with resistant hypertension and the recently published SPYRAL HTN-OFF MED has shown that it does provide benefit for patients who are not receiving antihypertensive medication. In this commentary, Markus P Schlaich reviews the evidence for renal denervation.
The publication of SYMPLICITY HTN-1 triggered substantial interest and enthusiasm in the hypertension community. While relatively small in size, the study suggested that catheter-based renal denervation using a first-generation single electrode catheter appeared safe and was associated with a significant reduction in office blood pressure at six, 12, and 36 months post-intervention, respectively.
The subsequent SYMPLICITY-HTN-2 was designed as a prospective randomised, controlled clinical trial.2 The blood pressure lowering effect observed in this study, in the renal denervation group, was -32±23/12±11 mmHg at six months post-procedure. Sustained blood pressure effects were subsequently demonstrated at 12 months.3
While SYMPLICITY HTN-1 and HTN-2 found a substantial reduction in blood pressure with renal denervation, SYMPLICITY HTN-3—the largest and first study to include a sham control—failed to demonstrate a blood pressure lowering effect beyond that observed in the sham control group.4 Potential shortcomings in the execution of the study, including limited operator experience and insufficient denervation among other factors, are now considered likely contributors to these neutral findings. Also, from a technical perspective, the failure of SYMPLICITY HTN-3 sparked renewed interest and investigations in renal nerve anatomy and physiology, the development of more sophisticated catheter designs, and adjustment of treatment algorithms aimed at achieving more complete and reliable renal denervation.
Against this background and with additional insights obtained from relevant preclinical models, the recently published SPYRAL HTN-OFF MED trial5 was conducted as a renewed proof-of-concept study. It showed a significant difference, at three months, in 24-hour ambulatory blood pressure (the primary endpoint) and office blood pressures from baseline with renal denervation.
Importantly, a more aggressive treatment approach was applied in SPYRAL HTN-OFF MED; both in terms of the average number of ablations performed per patient (43.8±13.1 vs. 11.2±2.8 in SYMPLICITY HTN-3) and in terms of how many arteries were treated (both the main arteries and smaller branches). Therefore the study, with its more aggressive approach, confirms the general safety of catheter-based renal denervation.
Overall, the findings provide unequivocal evidence for biological proof-of-principle for the efficacy of catheter-based renal denervation to reduce blood pressure in patients with hypertension not treated with antihypertensive medications and absence of other confounders. The challenge now is to determine which patient cohorts may benefit most from this approach.6
To this end longer term safety is an important aspect that needs to be addressed to provide more robust assurance that the substantially more aggressive treatment algorithm does not cause major reno-vascular or other adverse consequences. Identification of the most appropriate patient cohort that may benefit from renal denervation, as well as those who may not be suitable candidates for such an approach is crucial. Patients with resistant hypertension in whom sympathetic activity has been shown to be particularly elevated have been studied most extensively, but data on efficacy with the more aggressive treatment approach are scarce. One recent study with a head-to-head comparison of the conventional (main renal artery only) vs a more aggressive (distal main artery + branches ) treatment approach did demonstrate a clear signal for more efficacy with the latter.7 Several studies are ongoing, including the SPYRAL HTN-ON MED trial, which will provide some more insights using renal denervation in the context of resistant hypertension. Patient cohorts characterised by increased sympathetic activation such as those with heart failure, chronic- and end-stage renal disease, and obstructive sleep apnoea accompanying hypertension may be particularly well suited. However, studies in all these patient groups would have to be conducted to assess the potential utility of renal denervation, given that technical advances and the described more aggressive treatment approach have not previously been applied in these cohorts and may provide different results compared to those available from studies using previous generation catheters and less aggressive ablation algorithms.
With SPYRAL HTN-OFF MED renal denervation has been rehabilitated as therapeutic approach to lower blood pressure but the ideal clinical scenarios for its clinical application remain to be determined.
References
Krum et al. Lancet 2009; 373(9671): 1275–81.
Esler et al. Lancet 2010; 376(9756): 1903–09.
Esler et al. Circulation 2012; 126: 2976–82.
Bhatt et al. N Engl J Med 2014; 370(15): 1393–401.
Townsend et al. Lancet 2017. Epub.
Am J Hypertens 2017; 30(9): 847–56.
Pekarskiy et al. J Hypertens 2017; 35(2): 369-75.
Markus P Schlaich is Head of the Dobney Hypertension Centre, School of Medicine – Royal Perth Hospital Unit, University of Western Australia; Departments of Cardiology and Nephrology, Royal Perth Hospital, Perth, Australia; and the Neurovascular Hypertension & Kidney Disease Laboratory and Human Neurotransmitter Laboratory, Baker IDI Heart and Diabetes Institute, Melbourne, Australia.
This video from the Penn Image-Guided Interventions (PIGI) laboratory demonstrates an augmented reality computed tomography-guided lung ablation procedure using the Microsoft Hololens. The PIGI laboratory focuses on translational research for the development of novel imaging approaches and advanced therapeutics in interventional radiology.
“While both radial and femoral accesses are safe and effective for transarterial liver embolization, it is clear that the patients prefer radial access,” said Marcelo Guimaraes, Charleston, USA, who was presenting on the BEST ACCESS trial at the Super Tuesday session during the 2017 CIRSE annual meeting.
The BEST ACCESS trial is a randomised, prospective, single institutional, intra- and inter-patient controlled trial, which compared of radial vs. femoral access in transarterial liver embolization in the treatment of primary or metastatic liver cancer. The trial set out to evaluate patients’ preference, crossing from radial to femoral, effectiveness, safety, advantages, and appropriateness of performing transarterial hepatic embolization of liver cancer via arterial access from the radial artery vs. conventional transfemoral arterial access. The procedures that were used included transarterial chemoembolization, specifically performed for hepatocellular carcinoma, and transarterial bland embolization which is performed for types of liver tumours such as carcinoid tumours or liver metastases.
Randomisation
The researchers randomly, and then sequentially, assigned all patients who underwent at least two interventions so that they underwent one transradial procedure and one transfemoral procedure.
“If a third procedure was needed, the patient selected the access type,” noted Guimaraes, who is director, Vascular and Interventional Radiology and professor of Radiology and Surgery, Medical University of South Carolina, USA.
The primary endpoint of the trial was patient access preference, and secondary endpoints were access-related complications, radiation exposure to operator and patients, contrast volume, procedure time. All patients were assessed the day after the intervention and at 30 days post-intervention. The assessment included a questionnaire and physical exam followed by ultrasound.
Results
The researchers initially randomly assigned 55 patients with liver cancer (31 hepatocellular carcinoma and 24 metastatic disease) to either radial or femoral access. A total of 124 transarterial liver embolizations were performed. Thirty-six patients completed the trial which was terminated early as the primary endpoint was achieved sooner than expected.
After undergoing treatment via both accesses, 81% of patients preferred radial and 19% preferred femoral access (ratio 4:1). There were no major adverse events in either access group, including ultrasound exams arterial occlusion and clinically evident stroke. Thirty seven per cent of patients had minor complications that were mainly bruising and local pain, without any significance difference between the two groups. No difference was found in patient radiation exposure.
“However, the other major finding was the threefold reduction in radiation exposure to the operator when radial access was used. This was possible due to the type of shielding and left arm being positioned open at 70–90 degrees,” Guimaraes concluded.
The world’s largest randomised trial comparing three central venous access devices—peripherally inserted central catheters (PICCs), Hickman-type devices and chest wall ports—should provide definitive results in terms of their relative efficacy and cost-effectiveness, Jon Moss, Glasgow, UK, told CIRSE delegates.
The CAVA (Cancer and venous access) trial is a National Institute of Health Research- funded randomised controlled trial with associated qualitative research of venous access devices that deliver long-term chemotherapy. It is an open, multicentre trial with 17 participating UK sites involving 1,500 patients who received chemotherapy for three months, or more. The trial is currently recruiting and patients will be followed for a year.
“There are four randomisation options available for eligible patients (PICC vs. Port, PICC vs. Hickman, Hickman vs. Port, and PICC vs. Port vs. Hickman). We preferred the third option, but if one device was not suitable for, or refused by a patient, the other two-way comparisons could be used. The PICC vs. Hickman arm was a non-inferiority comparison, and the other options were a superiority comparison,” said Moss, who is a professor of Radiology at NHS Greater Glasgow and Clyde.
The primary outcome measure is complications. Secondary endpoints include venous thrombosis, re-intervention rates (device removal and replacement), interruptions to chemotherapy delivery, time to first complication and quality of life. Health-related quality of life including a novel device specific instrument and a full health economic analysis outcome, including cost effectiveness are being performed.
Baseline characteristics
“To date, we have randomised nearly 1,000 patients, and the Hickman vs. Port comparison has been closed. The baseline patient characteristics are adults who are 18 years of age, or above, with either a solid or haematological malignancy who are scheduled to receive a course of chemotherapy lasting a minimum of three months. The three most common cancer types are colorectal, breast and pancreas, in that order. The trial closes to recruitment in February 2018 with a maximum follow up of 12 months. The results should be available in early 2019,” Moss told Interventional News.
Boston Scientific has announced the three-year results from the MAJESTIC trial for the Eluvia paclitaxel-eluting vascular stent system at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), in Copenhagen, Denmark.
Data demonstrated that in this study, long-term treatment durability was experienced among patients whose femoropopliteal arteries were treated with the Eluvia stent system.
The prospective, single-arm, multicentre clinical trial enrolled 57 patients with symptomatic lower limb ischaemia and lesions in the superficial femoral artery or proximal popliteal artery. Primary patency through two years was 83.5% with 91% of patients experiencing no or mild symptoms associated with claudication, or pain while walking. (Updated primary patency data point of 83.5% at two years reflects adjudicated data as a result of additional patient follow-up at three years, the company states). Previously reported primary patency for MAJESTIC at two years was 78.2%. Results at three years demonstrated a sustained benefit of this therapy, with 85.3% of patients experiencing freedom from target lesion revascularisation (TLR).
“Over the course of the MAJESTIC trial, the majority of the patients, including those with relatively challenging lesions, have remained largely symptom-free,” said Stefan Müller-Hülsbeck, principal investigator at the Vascular Center Diako Flensburg and head of the Department of Diagnostic and Interventional Radiology / Neuroradiology, Academic Hospitals Flensburg, Germany. “The sustained drug release enabled by the polymer-based stent can be credited with reduced reinterventions over a three-year period, as well as establishing a long-term safety profile in the femoropopliteal arteries.”
IMPERIAL trial
In addition to the MAJESTIC trial, Boston Scientific recently completed enrolment of 485 patients in the randomised, head-to-head IMPERIAL trial, which will assess the safety and efficacy of the Eluvia Stent System compared to the Zilver PTX Stent (Cook Medical). Initial results, expected to become available in 2018, will be used to support regulatory submissions in the USA and Japan.
The Eluvia Stent System received CE mark in February of 2016 and is an investigational device and not available for sale in the USA.
Terumo has announced that it has launched QuiremSpheres microspheres in Europe on 18 September.
QuiremSpheres, the next generation of selective internal radiation therapy (SIRT) microspheres are indicated for the treatment of advanced unresectable liver tumours and are the only commercially available microspheres that contain the radioactive isotope holmium-166. They are available in Europe with plans for expansion in areas outside of Europe in the future.
Recent trials have shown the safety and efficacy of holmium microspheres for the treatment of advanced liver cancer.
According to Terumo, unlike the widely adopted Yttrium-90 microspheres, QuiremSpheres can be visualised in low concentrations by means of SPECT and MRI. This allows clinicians to quantitatively assess the distribution of microspheres in the liver, enabling accurate evaluation of treatment directly after SIRT procedure. The half-life of QuiremSpheres is 26.8 hours, which means that more than 90% of the radiation is delivered within the first four days following the implantation procedure.
For further information, please contact Alexandra Vassiliades, group manager, Marketing Communications Terumo Interventional Systems, EMEA on [email protected]
The six-month results from the full clinical cohort of the EffPAC randomised study were presented in the drug-coated balloon (DCB) abstracts session at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2017 conference in Copenhagen, Denmark. The data demonstrate the efficacy of iVascular’s Luminor DCB in patients with peripheral arterial disease (PAD).
EffPAC (Effectiveness of paclitaxel-coated Luminor balloon catheter vs. uncoated balloon catheter in the arteria femoralis superficialis) enrolled 171 patients at 11 German centres who were randomised to treatment with either the Luminor DCB or percutaneous transluminal angioplasty (PTA). The six-month data include a total of 153 patients (77 DCB and 76 PTA).
According to iVascular, Luminor is a paclitaxel-coated balloon with a proprietary coating, using unique nanotechnology for minimised drug loss during navigation and enhanced delivery to the artery wall. A full range is available with 0.014”, 0.018” and 0.035” guidewire compatibility, providing ultra-low profile and fast deflation time.
Ulf Teichgräber, director of the Department of Radiology of the University Hospital Jena, Germany, presented the new, primary endpoint late lumen loss and the clinical six-month results from the full cohort of the EFFPAC study demonstrating the effectiveness of Luminor DCB vs. PTA in the superficial femoral artery.
Results
The study met its primary endpoint (late lumen loss) and secondary endpoints (freedom from target lesion revascularisation; patency; and change of ankle brachial index, Rutherford stage and quality of life with high statistical significance).
Primary endpoint revealed a late lumen loss (LLL) of 0.14mm in the DCB group vs 1.06mm in the PTA group (p<0.001).
Target lesion revascularisation (TLR) was 1.3% (DCB) vs 17.1% (PTA)
Rutherford stages were improved overall for 85.2% patients (DCB) vs. 75% (PTA) (p=0.021), and by three stages for 44.6% patients (DCB) vs. 27.8% (PTA)
There were no amputations, or product-related adverse event in the DCB group.
A comparison with other published data from randomised controlled trials involving DCBs, underlined that Luminor DCB shows higher efficacy than most other available DCBs. In a press release from iVascular, Teichgräber said: “These incomparable outcomes are the result of the innovative coating technology of Luminor DCB, which is shown not only in the patency, LLL and TLR data, but also in significant improvement of patients’ clinical status”.
On 21 September 21 iVascular announced that the Luminor 14m has received the Canadian Medical Device License (MDL). Luminor DCB received the CE mark in 2013 to treat superficial femoral, popliteal and infrapopliteal arteries and is available in more than 50 countries.
Guerbet has announced obtaining the CE mark for its conventional transarterial chemoembolization (cTACE) mixing and injection system, Vectorio.
Designed in collaboration with interventional radiologists worldwide, Vectorio is a unique set of Lipiodol resistant medical devices including syringes, patented stopcock and sampling devices. Vectorio is dedicated for mixing and delivering Lipiodol ultra fluid and anticancer drugs during cTACE procedure in adults with known, intermediate-stage hepatocellular carcinoma (HCC).
Advantages
This medical device offers multiple advantages for healthcare professionals:
24-hour Lipiodol resistance
patented three-way stopcock with four connections offering possibility of “on-table mixing” where interventional radiologists have the possibility of remixing without disconnection from the micro-catheter, thus maximizing the safety during the intervention
unique ready-to-use set with all devices in one set
user-friendly, ergonomic and quick device set-up, improving cTACE procedures for physicians.
“Vectorio has been developed in collaboration with international interventional radiologists to match their medical needs for accurate, user-friendly and safe solution during cTACE procedures. The development of these image-guided procedures is a top priority for Guerbet’s Interventional franchise. We are committed to enhance liver cancer patients’ prognosis and quality of life worldwide” said Yves L’Epine, CEO of Guerbet.
Designed and manufactured in France, Vectorio’s commercial launch will start this fall in European countries, where Lipiodol Ultra Fluid is registered for cTACE. The Vectorio registration programme is also planned in other countries where cTACE is indicated for Lipiodol Ultra Fluid.
The journal was launched at CIRSE’s annual meeting (16–20 September, Copenhagen, Denmark). The new journal has a multidisciplinary and international Editorial Board with leading experts from the field of endovascular treatment. Jim A Reekers, Amsterdam, The Netherlands, is the editor-in-chief.
CIRSE has stated that it wants to offer a podium and publication space for high-quality endovascular papers and research that are going unnoticed through a lack of publication possibilities. “To offer a solution for this and increase the amount of published endovascular papers, CVIR Endovascular will be open access and open peer-reviewed, providing the possibility for all interested in reading the published articles to do so for free. Through open access, CVIR Endovascular will allow articles and research on the newest trends, and hot topics in endovascular treatment to be easily disseminated and have a further reach in the medical community and amongst the public,” a press release from the organisation states.
CVIR Endovascular opened for submission on 16 September when the journal’s Springer website went live. The first published articles are expected in the first quarter of 2018.
Mentice has announced the release of a new simulation training software for transarterial chemoembolization (TACE). The new software was showcased at the 2017 CIRSE congress (16–20 September, Copenhagen, Denmark).
TACE is a challenging procedure that involves various sub-techniques, complex anatomies and variant vasculatures requiring the extensive use of radiation. Success of the procedure and impact on cost is tied to the ability to complete it safely and accurately within the permitted radiation doses.
“Conventional apprentice-based training in the clinical practice is costly, resource-intensive and can have an impact on patient safety,” comments Mentice CEO Göran Malmberg. “Our TACE software provides a safe, effective, repeatable and highly realistic solution—allowing interventional radiologists to have hands-on training outside of the cath lab.”
The Mentice TACE training solution is based on real-life cases, which is essential for successful training and features an integrated radiation safety module, that provides dose monitoring for patient and staff at all times. The software also features output of metrics, enabling objective assessment of trainees’ progress. “Realistic high-fidelity simulation solutions are very effective for procedures such as TACE,” adds Malmberg. “Trainees can acquire the multi-level skills required to perform the procedure in a dose-dependent, time-effective way, reducing overall costs, while maintaining patient safety.”
The European results of the first-in-human trial of Vascular Dynamics’ MobiusHD implant indicate that the device is associated with a reduction in 24-hour ambulatory systolic blood pressure of 21mmHg from baseline at six months after implantation in patients with resistant hypertension. The study was presented at the European Society of Cardiology (ESC) congress (26–30 August, Barcelona, Spain) and published in The Lancet.
The CALM-FIM_EUR study was a first-in-human feasibility study in which 30 patients were enrolled at six European centres between December 2013 and February 2016. All patients had resistant hypertension (defined as office systolic blood pressure above 160mmHg, despite the use of three or more antihypertensives, including a diuretic). The MobiusHD devices were implanted unilaterally in the internal carotid artery. Mean office blood pressure was 184/109mmHg at baseline and was reduced by 24/12mm Hg at six months. Mean baseline 24-hour ambulatory blood pressure was 166/100mmHg at baseline and was reduced by 21/12mmHg at six months despite an observed reduction in hypertensive medication. The investigators reported six serious adverse events, all of which were reported to have resolved without sequelae.
The MobiusHD System—a minimally-invasive system—is designed to capitalise on the ability of the body’s baroreceptor mechanism to regulate blood pressure. Baroreceptors are receptors located in the carotid artery that sense blood pressure and relay that information to the brain. The goal of the implant is to amplify the signals received by the surrounding arterial baroreceptors, and thereby increase the body’s natural response to lower blood pressure through vasodilation.
Lead author of the study, Wilko Spiering (University Medical Center Utrecht, the Netherlands) comments: “These published results of the CALM-FIM_EUR study demonstrate that the MobiusHD device may significantly reduce both office and ambulatory blood pressure among patients on three or more drugs who have been unable to control their hypertension. Our positive experience with the MobiusHD device demonstrates the need for continued investigation in a sham-controlled setting, which is currently running in the Netherlands and is starting up in the USA, UK, and Germany shortly.”
“We are most enthusiastic about the use of radioembolization to treat patients with early stage Barcelona Clinic Liver Cancer (BCLC) A disease. The long time to progression following segmental radioembolization allows most patients to be bridged to liver transplant following one treatment; this therapy can now be delivered on the same day as planning angiography,” write Riad Salem and Robert J Lewandowski, Chicago, USA.
We presented data at the Society of Interventional Radiology annual meeting this year on 1,000 hepatocellular carcinoma (HCC) patients treated with glass microsphere radioembolization (Therasphere, BTG) at Northwestern University in Chicago, USA. Through this large patient cohort, we report on our vast experience with radioembolization that has now become our institutional standard of care and treatment of choice for hepatocellular carcinoma.
Radioembolization was historically employed in those patients deemed unsuitable for chemoembolization; typical patients exhibited multifocal bilobar disease, infiltrating tumours, large tumours, portal vein (tumour) thrombus, elevated performance status, or significant comorbidities. Radioembolization was limited in competitiveness from a clinical adoption standpoint since it was considered only in such advanced disease compared to early disease for chemoembolization. This was our practice until 2005, when we started observing long-term benefits of Y-90: outpatient treatment, excellent response rates, better quality of life, and downstaging to resection and transplantation. A recent prospective randomised trial performed at our institution demonstrated a significantly longer time to progression after radioembolization compared to conventional chemoembolization, reinforcing the knowledge that fewer treatments are required for patients with this therapy.
We view the two recent randomised prospective trials (SARAH and SIRveNIB) positively. While these trials did not meet their primary endpoint of superiority of survival compared with sorafenib, they did bolster what we have known: radioembolization offers similar survival but improved tolerability and quality of life compared with systemic agents for patients with advanced HCC. The potential of radioembolization in advanced stage HCC is particularly evident in patients with portal vein tumour thrombus. The concept of boost radioembolization describes an aggressive use of this therapy in patients with more invasive tumour biology. Targeting tumours with doses >200 gray have yielded survival outcomes not previously seen. Combining radioembolization with systemic therapies, such as immunotherapy, offer much promise with many studies currently underway. We are most enthusiastic about the use of radioembolization to treat patients with early stage Barcelona Clinic Liver Cancer (BCLC) A disease. The long time to progression following segmental radioembolization allows most patients to be bridged to liver transplant following one treatment; this therapy can now be delivered on the same day as planning angiography. Radioembolization has also been shown to have better capacity to downsize tumours to within Milan criteria than chemoembolization, allowing more patients to be considered for liver transplantation Newer applications of radioembolization have the potential to expand the application of curative therapies for patients with unresectable disease. Radiation lobectomy, defined as lobar radioembolization with the intent to facilitate surgical resection in patients with small future liver remnant, has been compared favourably to portal vein embolization by providing hepatic tumour control during the time interval to hypertrophy while also optimizing R0 resection by shifting tumours away from major vessels. Tumour cell death prior to resection may equate to decreased dissemination of viable microscopic tumour cells during surgical mobilisation/manipulation. Radiation segmentectomy, defined as segmental radioembolization with the intent to deliver high dose, ablative radiation doses to the targeted tumour and adjacent surrounding non-tumorous parenchyma has demonstrated excellent tumour response and complete pathologic necrosis in explant specimen in patients with solitary HCC <5cm. Survival outcomes in patients with preserved liver function and small peripheral tumors compare favourably to liver resection and ablation, suggesting that radiation segmentectomy may be considered curative in these select patients.
Over the last two decades, radioembolization has helped move the field of interventional oncology forward and demonstrated tremendous versatility in treating HCC. Early disease patients can be treated with radiation segmentectomy/lobectomy as well as bridged or downstaged to transplantation. Those with vascular invasion can be treated with Y-90, providing similar survival outcomes as systemic agents with fewer side-effects. Overall, Y-90 has become one of the standards of care for HCC and an essential tool for all interventional radiologists.
Riad Salem is section chief, Interventional Radiology and vice-chair, Image-Guided Therapies, Department of Radiology, Northwestern University, Chicago, USA. He is an advisor to BTG. Robert Lewandowski is professor of Radiology, Medicine, and Surgery and director of Interventional Oncology, Department of Radiology at the same institution. He is a consultant to BTG
Medtronic has announced its intent to move forward with a new renal denervation pivotal trial following positive first results from a sham-controlled study in patients with high blood pressure. Investigators of the SPYRAL HTN-OFF MED Study found statistically significant and clinically important blood pressure reductions in the patients treated with renal denervation across both office and ambulatory systolic and diastolic measurements. The data in the first 80 patients enrolled in the study at three months were presented in a late-breaking clinical trial session at the European Society of Cardiology (ESC) meeting in Barcelona, Spain and published simultaneously in The Lancet.
“Based on the clinical results presented at ESC, we are confident that the SPYRAL HTN-OFF MED Study has successfully demonstrated the treatment effect of RDN,” said co-principal investigator and presenter of the data at ESC, Michael Böhm, chairman, department of internal medicine, University of Saarland in Homburg/Saar, Germany. “With consistent and significant drops across ambulatory and office-based blood pressure—including both systolic and diastolic measurements—we are confident to be moving forward with a pivotal trial so that doctors and patients may have an alternative approach to lowering blood pressure.”
The initial three-month data found that patients who underwent renal denervation had their office systolic blood pressure (OSBP) decline an average 10mmHg, resulting in a 7.7mmHg difference with the patients in the sham control arm (p=0.016), and their diastolic blood pressure declined an average 5.3mmHg, resulting in a 4.9mmHg difference with the sham control arm (p=0.008). With a systolic blood pressure difference of 7.7mmHg between the two groups, a recent meta-analysis published in The Lancet associated that decrease with a relative risk reduction of approximately 20% for major cardiovascular events, including heart attack and stroke.
In SPYRAL HTN OFF-MED renal denervation patients, the 24-hour systolic ambulatory blood pressure (ABPM) declined 5.5mmHg, resulting in a 5mmHg difference from the sham control arm (p=0.041), and the diastolic AMBP declined 4.8mmHg, resulting in a 4.4mmHg difference from the sham control arm (p=0.002). Additionally, there were no reported cases of new or worsening renal failure, vascular complications, or other major adverse events, confirming the safety of the renal denervation procedure – even with a revised procedural approach that extended ablations into the kidney’s branch arteries and an increase in total number of ablations compared with previous trials.
“After SYMPLICITY HTN-3, we learned a lot about the procedure itself, medication adherence and which patients may have less response to the renal denervation procedure—these insights have been incorporated into the revised clinical approach in the SPYRAL HTN program,” said co-principal investigator David Kandzari, director of interventional cardiology and chief scientific officer, Piedmont Heart Institute in Atlanta, USA. “With this new approach and protocol design, coupled with new technology that allows more consistent circumferential treatment and easier access into the distal anatomy, based on these compelling results we are confident that we have appropriately addressed the issues in previous renal denervation trials.”
The SPYRAL HTN-OFF MED Study evaluated renal denervation in the absence of any antihypertensive medications compared to a sham-controlled population to isolate its effect on blood pressure reduction. The study enrolled 353 patients who were either drug naïve or willing to discontinue medication for four months, with mild-to-moderate hypertension (OSBP equal to or more than 150mmHg and less than 180mmHg) at 24 centres in the USA, Europe, Japan, and Australia. Prior to randomisation, patients were required to stop taking their antihypertensive medication during a period of three to four weeks, known as a medication washout. During the washout period and the three months following randomisation, patients were monitored to ensure their blood pressure would not exceed 180mmHg.
“These results are extremely encouraging for the more than 50% of hypertension patients who become non-adherent to their medications within one year of initiating therapy,” said co-principal investigator Raymond Townsend, director of the hypertension programme, University of Pennsylvania. “The societal implications are potentially huge as well, as high blood pressure contributes more than 500 billion dollars in direct costs to our healthcare systems globally.”
Unlike SYMPLICITY HTN-3, where patients self-reported adherence, and change in medications occurred among 40% of patients, the SPYRAL HTN-OFF MED study limited that variability, as patients remained off their medication throughout the duration of the study as confirmed by serum and urine testing for antihypertensive medication. Additionally, the aftermath of SYMPLICITY HTN-3 revealed new anatomical insights showing that renal nerves are easier to access when the catheter treats the renal artery segments located close to the kidney. While SYMPLICITY HTN-3 only averaged five ablations in the main renal artery and no ablations in the branch arteries, the unique, flexible design and low profile of the investigational Symplicity Spyral system achieved an average of 10 main renal artery and 13 branch artery ablations per kidney.
“These data confirm our long-held belief that the underlying science behind renal denervation is strong and we are committed to continuing our mission to realize the full potential of this procedure to help address an unmet need for the more than one billion people worldwide living with high blood pressure,” said Sean Salmon, senior vice president and president of the Coronary and Structural Heart division, which is part of the Cardiac and Vascular Group at Medtronic. “We intend to continue consulting with our physician advisors and global regulatory authorities about these results so that we can appropriately move forward with a pivotal trial design to ultimately support regulatory approval in the USA, Japan and other countries where the technology is not currently available.”
Bard’s Lutonix 035 drug-coated balloon PTA catheter (DCB) has been granted premarket approval (PMA) by the US Food and Drug Administration (FDA) for a new indication and is now available for sale in the USA.
With this approval, the Lutonix 035 DCB catheter becomes the first and only drug coated balloon that is FDA approved as safe and effective in end-stage renal disease (ESRD) patients with stenotic lesions in dialysis arteriovenous (AV) fistulae, a Bard press release says. This latest approval adds to the prior FDA indication of the DCB for the treatment of superficial femoral artery and popliteal artery disease.
The FDA approval was based on the results of the LUTONIX AV clinical trial, the first investigational device exemption trial using DCBs in patients with stenotic lesions in AV fistulae. The follow-up results from randomised patients who were treated with the Lutonix DCB catheter demonstrated safety comparable to uncoated balloons.
The Lutonix 035 DCB also demonstrated a sustained clinical benefit compared to conventional angioplasty through 12 months:
71.4% target lesion primary patency (TLPP) at 180 days with superior results at 210 days (DCB 64.1% vs. PTA 52.5%);
31.3% fewer reinterventions compared to PTA at six months;
Nearly two months more reintervention-free days (217 days vs. 163 days) compared to PTA;
31.2% improvement in TLPP through 12 months;
95% freedom from primary safety event, indicating a consistent safety profile to PTA.
“For patients undergoing haemodialysis for kidney failure—who already spend a significant portion of their time undergoing dialysis and other treatments—repeated reinterventions to maintain AV access can be an added burden, with many patients returning as frequently as every other month,” said Scott O Trerotola (Perelman School of Medicine, University of Pennsylvania), principal investigator of the LUTONIX AV clinical trial. “The Lutonix 035 DCB provides another option for physicians. It is intended to offer patients with end-stage renal disease fewer interruptions in treatment and less time undergoing access maintenance, potentially leading to improved patient satisfaction and quality of life.”
American women are largely unaware of uterine fibroid embolization according to results from a new nationwide poll released by the Society of Interventional Radiology (SIR). The data included in the report, “The fibroid fix: What women need to know”, show that 44% of women diagnosed with uterine fibroids say they have never heard of the less invasive treatment option.
The online survey was conducted by Harris Poll on behalf of the SIR in June 2017 among 1,176 US women ages 18+ to better understand awareness of uterine fibroids and women’s knowledge of fibroid treatment options. These results uncover a lack of knowledge that suggests women with fibroids are not being informed by their physicians about all treatment options for this condition, which affects the majority of US women. The survey found a majority of women diagnosed with uterine fibroids note that having their doctor discuss all options with them is the most important factor for selecting a treatment. However, 46% of women diagnosed with uterine fibroids who have heard of UFE did not first learn about the treatment from their obstetrician-gynaecologist.
“Misperceptions about uterine fibroids and the treatments available often lead women to undergo invasive and potentially unnecessary surgery for their fibroids, despite more than 20 years of clinical use supporting uterine fibroid embolization,” said James Spies, a professor of radiology at Georgetown University Medical Center in Washington and an adviser for the report. Spies, a past president of the SIR, is an internationally recognised expert on UFE who has made valuable contributions to primary and clinical research assessing outcomes related to various fibroid therapies. “It is a disservice to women to not provide all the information needed for an informed decision,” he said.
The survey also found:
More than half of US women (57%) do not think they are at risk of developing uterine fibroids.
A majority of women (62%) have never heard of UFE, with 44% of women diagnosed with uterine fibroids reporting that they have never heard of the treatment.
Among women who have heard of UFE, the majority (73%) did not first learn of it from their obstetrician-gynaecologist, the frontline provider of fibroid treatment. These women first learned about the treatment from other sources, including friends or family (32%), their own research (9%) or, particularly for younger women, from advertising (23% for all women 18+ and 38% for women 18–34).
One-fifth of women (20%) think hysterectomy is the only treatment for fibroids, and, of those diagnosed with fibroids, 11%still think hysterectomy is the only treatment option.
“It is remarkable that 62% of women are unaware of UFE and that one in five women (20%) believe the only treatment is hysterectomy,” said Janice Newsome, a physician adviser to the report and associate division director of interventional radiology and image-guided medicine at Emory University Hospital in Atlanta. “Uterine preservation should be an important goal of therapy for fibroids. Yet many women seem unaware of safe and effective treatment options apart from hysterectomy.”
“Physicians need to ensure that women are presented every option for treatment so that patients can make the decision that is right for them,” said Suresh Vedantham, president of the SIR and professor of Radiology and Surgery at the Mallinckrodt Institute of Radiology, Washington University in St Louis. “UFE is an example of an image-guided therapy that has improved the standard of care and quality of life for many women, allowing a minimally invasive treatment with a shorter recovery time, less pain and risk of complications than traditional surgeries for uterine fibroids.”
Methodology
The survey was conducted online within the United States by Harris Poll on behalf of the SIR between 23 and 27 June 2017 among 1,176 US women ages 18+. Because the sample is based on those who agreed to participate in the Harris Poll panel, no estimates of theoretical sampling error can be calculated.
Addition to article on 4 September 2017:
Jim A Reekers, Amsterdam, The Netherlands, a past president of CIRSE and principal investigator on the EMMY trial, tells Interventional News: “The title of this piece should really be women are kept unaware of uterine fibroid embolization. We of the EMMY trial made a conscious decision to publish all our research in the top international gynaecology journals, including the 10-year follow-up results, which showed similar outcomes for uterine fibroid embolization and surgery. All gynaecologists must know about these data, but they appear to be not emphasised to patients. This might relate to financial protection of practice. It seems inexplicable that within Medicare and Medicaid, the number of uterine fibroid embolization procedures is at least four times higher than outside of this coverage. The number of hysterectomies is also very low in this scenario. While there are not many advantages associated with having a low income, access to the most patient-friendly and cheapest treatment for uterine fibroids, ie embolization, maybe one of them.”
BTG and the Society of Interventional Oncology (SIO) have expanded their commitment to the Immuno-oncology /interventional oncology research grant programme, by announcing a second round of funding available to investigators.
Interventional oncology, which includes a range of minimally invasive, image guided, locoregional therapies, and immuno-oncology, using the body’s own immune system to treat cancer, are two areas of scientific interest that have great potential for improving cancer therapy. The SIO grant programme is designed to fund cutting-edge research initiatives to investigate the potential for these therapeutic approaches to work in combination. Specifically, the programme is looking to fund research proposals that:
Evaluate immune stimulation of interventional oncologic therapies
Combination approaches to improve clinical outcome
Improve the understanding of underlying mechanisms as to how different loco-regional therapies influence both adaptive and innate immunity
Earlier this year, four investigators were awarded grants at the World Conference on Interventional Oncology (WCIO) in Boston to further their cutting-edge research in the field. Their project proposals ranged from exploratory pilot projects to prospective clinical trials. The winners were chosen by the SIO Immuno-Oncology / Interventional Oncology Committee, a panel of international experts which includes both interventional radiologists and immuno-oncologists.
With a large number of high quality submissions and the level of interest in the programme to date, BTG and SIO have announced their intention to expand the programme to ensure more collaborative research will be funded and accelerate the pace of scientific advancement in the combination of interventional oncology and immuno-oncology therapies.
“We are very pleased with the ongoing generosity of BTG that will continue to enable the SIO to fund additional meritorious, cutting-edge research that combines the strengths of interventional oncology and immuno-oncology — two disciplines that hold great promise for improving cancer therapy,” said S Nahum Goldberg, SIO Interventional / Immuno-oncology Working Group chair, and vice-chair for Research and head of the Interventional Oncology Unit, Hadassah Hebrew University Medical Center in Jerusalem, Israel.
Melanie Lee, chief scientific officer of BTG, said: “We were delighted by the number of high calibre entries we saw from investigators in response to the original call for proposals, with lots of brilliant ideas of how to best combine locoregional and immunotherapies. We believe such approaches can help new agents to penetrate solid tumour mass, expose tumour specific antigens, and help the immune system to mount a response. Given the high levels of interest, we have decided to double our efforts and provide further funding in 2018 to support additional research in this area.”
To apply for a grant, completed applications need to be submitted online at www.io-central.org/grants by the 15 December 2017. The submission must include a detailed research plan that outlines a one to two year budget proposal and a letter of support from the department chair (for faculty applicants) or fellowship director (for trainee applicants). Grants of up to US$50,000 are available for one year exploratory pilot projects and up to US$100,000 for larger one to two-year projects.
Siemens Healthineers has received the CE mark for the 7 Tesla magnetic resonance (MR) scanner Magnetom Terra, making it the first-ever ultra-high-field MR scanner to be approved for clinical use, a press release from the company says.
Clinicians in Europe can now use the system for neurological and musculoskeletal examinations in routine clinical applications.
“Thanks to our long-standing commitment and experience with ultra-high-field MRI as well as our extensive innovation network of collaboration partners around the world, we are now establishing 7T imaging in the clinical routine with Magnetom Terra”, says Christoph Zindel, senior vice president and general manager of Magnetic Resonance Imaging at Siemens Healthineers. “Having now gained approval for clinical use, we are expanding the scope of diagnostic MRI – 15 years after 3T scanners first became established. With this new clinical field strength, we can achieve a new level of detail in anatomy and function, helping further pave the way for precision medicine,” says Zindel. “I am convinced that Magnetom Terra will help grow the footprint of 7 Tesla in research and clinical application, allowing us to further explore new territories in MRI.”
“This ability to use 7 Tesla technology in the clinical realm is a breakthrough into broader clinical 7 Tesla MR applications. This CE certificate is now well-supported by the remarkable progress with respect to novel radiofrequency technologies and MR methods that will make whole-body MRI at 7 Tesla feasible in the future. It will definitely foster the translation of research into clinical applications,” says Siegfried Trattnig, director of the MR Centre of Excellence at the Medical University of Vienna, Austria, “And, the higher signal to noise ratio, the improved contrast, and non-proton MR at 7T will translate into better spatiotemporal resolution, but even more importantly into enhanced biochemical and metabolic tissue characterisation en route to clinical noninvasive personalised medicine.”
Philips has announced that it has completed the acquisition of The Spectranetics Corporation, a US-based global leader in vascular intervention and lead management solutions. Spectranetics’ financial results will be consolidated as part of Philips’ Image-Guided Therapy business group as of 9 August 2017.
Spectranetics is currently growing double-digits and projects 2017 sales to be approximately US$300 million. The acquisition is expected to be revenue growth for Philips by 2018, a press release says.
“Spectranetics is a highly complementary addition to our Image-Guided Therapy business group and will strengthen its position in a €6 billion growth market,” said Frans van Houten, CEO of Royal Philips. “The completion of this acquisition will accelerate the realisation of our strategic expansion into therapy devices. The combination of Spectranetics’ highly competitive product range and our leading portfolio of interventional imaging systems, devices, software and services will deliver enhanced care for patients by enabling clinicians to decide, guide, treat and confirm the appropriate cardiac and peripheral vascular treatment.”
Spectranetics’ device portfolio includes a range of catheters to treat coronary and peripheral artery disease, and the removal of implanted pacemaker and implantable cardioverter defibrillator leads. The Stellarex drug-coated balloon is a key growth driver in this portfolio. It is a next generation drug-coated balloon that provides proven peripheral artery disease treatment and is backed by robust clinical evidence. The Stellarex drug-coated balloon is CE-marked and recently obtained US FDA premarket approval.
The acquisition of Spectranetics was structured as a merger under Section 251(h) of the General Corporation Law of the State of Delaware following the successful completion of Philips’ previously announced tender offer to purchase all outstanding shares of common stock of Spectranetics for US$38.50 per share in cash, without interest, less any applicable withholding taxes.
A randomised, double-blind, placebo-controlled trial evaluating the efficacy of prophylactic dexamethasone in preventing the most frequent adverse events of transcatheter arterial chemoembolization (TACE) in patients with hepatocellular carcinoma found it to be more effective than a placebo regimen.
Corticosteroids such as dexamethasone can be used to reduce inflammation; lower the immune response and help reduce sickness when having chemotherapy.
The trial was published in Hepatology in late July. Study authors Sadahisa Ogasawara, Department of Gastroenterology and Nephrology, Graduate School of Medicine, Chiba University, Chiba, Japan and colleagues randomly assigned Child-Pugh class A/B patients with HCC and no macrovascular invasion/extrahepatic metastases to either receive a treatment regimen that used intravenous dexamethasone or a placebo regimen with intravenous saline.
As summarised in Hepatology, the primary endpoint was complete response defined as the absence of grade ≥1 fever, anorexia, or nausea/vomiting according to the Common Terminology Criteria for Adverse Events (version 4) and no use of rescue therapy for 120 hours after TACE. A total of 120 patients between October 2010 and June 2013 were randomly assigned to treatment groups. The overall complete response rate was greater with the dexamethasone regimen than with the control regimen (p< 0.001). The cumulative incidences of fever, anorexia and nausea/vomiting were higher in the control regimen group. The authors report that the dexamethasone regimen was generally well tolerated by hepatocellular carcinoma patients including those with well-controlled diabetes mellitus and those with hepatitis B virus infection.
Conclusion
Ogasawara and colleagues concluded that the dexamethasone regimen was more effective than the control regimen in preventing TACE-induced fever, anorexia, and nausea/vomiting in patients with hepatocellular carcinoma.
The ASTER randomised clinical trial that examined the effect of endovascular contact aspiration vs. stent retriever on revascularisation in patients with acute ischaemic stroke and large vessel occlusion in the anterior circulation found that first-line thrombectomy with contact aspiration compared with stent retriever did not result in an increased successful revascularisation rate at the end of the procedure.
As Bertrand Lapergue (Department of Stroke Center and Diagnostic and Interventional Neuroradiology, University of Versailles and Saint Quentin en Yvelines, Foch Hospital, Suresnes, France) and colleagues reported in JAMA in August, the benefits of endovascular revascularisation using the contact aspiration technique vs. the stent retriever technique in patients with acute ischaemic stroke remain uncertain because of lack of evidence from randomised trials.
The ASTER (Contact aspiration vs. stent retriever for successful revascularization) study was a randomised, open-label, blinded endpoint clinical trial conducted in eight comprehensive stroke centres in France (October 2015–October 2016). According to the investigators, patients who presented with acute ischaemic stroke and a large vessel occlusion in the anterior circulation within six hours of symptom onset were included.
The triallists randomised 381 patients (mean age, 69.9 years; nearly 46% women) to either receive first-line contact aspiration (n=192) or first-line stent retriever (n=189) immediately prior to mechanical thrombectomy.
As summarised in the JAMA article, the primary outcome was the proportion of patients with successful revascularisation defined as a modified Thrombolysis in Cerebral Infarction (TICI) score of 2b or 3 at the end of all endovascular procedures. The secondary outcomes included degree of disability assessed by overall distribution of the modified Rankin Scale (mRS) score at 90 days, change in National Institutes of Health Stroke Scale (NIHSS) score at 24 hours, all-cause mortality at 90 days, and procedure-related serious adverse events.
Results
Trial results revealed that 363 completed the trial. The median time from symptom onset to arterial puncture was 227 minutes. For the primary outcome, the proportion of patients with successful revascularisation was 85.4% in the contact aspiration group vs. 83.1% in the stent retriever group p=0.53. For the clinical efficacy outcomes (change in NIHSS score at 24 hours, mRS score at 90 days) and adverse events, there were no significant differences between groups.
Penumbra provided an institutional grant to support the ASTER trial.
The 24-month results of the worldwide experience with Lutonix 035 drug-coated balloon (CR Bard/Beckton Dickenson) were published online in August in JACC: Cardiovascular Interventions. Data revealed that patients with femoropopliteal lesions who were treated with the drug-coated balloon experienced symptom improvement and that low reintervention rates were observed at 24 months, even in patients with difficult-to-treat lesions.
Marcus Thieme, Sonneberg, Germany and colleagues report that outcomes from the registry at two-years confirm Lutonix is a “safe and effective long-term treatment option in real-world patients with peripheral arterial disease with superficial femoral artery lesions.” These outcomes were also achieved in patients with long lesions and in-stent restenosis.
As reported in JACC: Cardiovascular Interventions, the Global SFA registry is a multicentre, prospective study that enrolled 691 patients in 38 centres from 10 countries. These patients were treated with the Lutonix 035 DCB in femoropopliteal lesions. The registry set out to assess safety, clinical benefit, and outcomes of the Lutonix 035 drug-coated balloon in a heterogeneous, real-world patient population at 12 and 24 months.
Freedom from a composite of target vessel restenosis, major index limb amputation, and device- or procedure-related death at 30 days was defined as the primary endpoint. “The primary effectiveness endpoint was freedom from target lesion restenosis at 12 months. Secondary endpoints were acute device and procedural success and clinically assessed primary patency,” the authors write.
Results
The registry results showed a 99.4% freedom at 30 days from the composite safety endpoint. There was 89.3% freedom from target lesion restenosis in the overall population at 24 months. In long lesions up to 50cm, the freedom from target lesion restenosis was 88.2%; in patients with in-stent restenosis this figure was 84.6%. The clinically assessed primary patency was 75.6% and more than 76% of patients showed improvement of at least one Rutherford category.
Editorial comment
In an accompanying editorial comment in the journal, Ivan P Casserly, Dublin, Ireland, writes: “Most endovascular specialists are inherently attracted to the use of drug-coated balloon angioplasty as the primary strategy for revascularisation of the femoropopliteal segment. This is driven by several considerations. Primarily, the greatest concern is to avoid the spectre of in-stent restenosis, for which there is no good therapy. If a durable result can be achieved with drug-coated balloon angioplasty, even if it has lower primary patency rates compared with drug-eluting stent, then this option would generally be favoured. In addition, angioplasty is ‘very straightforward’, resulting in a reasonably predicatable outcome across a broad range of operators.”
According to a new study published online in the journal Radiology, when ultrasound-guided percutaneous irrigation is performed to treat shoulder calcification, the choice of using either one needle or two should be tailored to the type of calcification.
The results of the study will help interventional radiologists determine whether to use one or two needles for an ultrasound-guided treatment for rotator cuff calcific tendinopathy.
Calcific tendinopathy is a condition in which calcium deposits form on the tendons of the rotator cuff, a group of four tendons that stabilises the shoulder joint. The condition, which occurs in approximately 20% of painful shoulders, causes pain and tenderness ranging from low-grade to highly disabling.
“There is still no consensus on how to treat calcific tendinopathy,” said researcher Luca Maria Sconfienza, associate professor at the University of Milan and chair of the Department of Radiology at the IRCCS Istituto Ortopedico Galeazzi. “However, ultrasound-guided percutaneous irrigation is widely performed throughout the world and is currently the first-line treatment for the condition, because it is quick, minimally invasive and has a low complication rate.”
The procedure involves injecting a fluid such as saline solution into the tendon to dissolve the calcium deposits and then extracting the calcium-filled solution.
“The main difference among ultrasound percutaneous irrigation procedures is the use of one or two needles,” Sconfienza said. “Until now, a direct comparison of one vs. two needles has never been performed.”
The study included 211 patients (77 men and 134 women between the ages of 24 and 69) who underwent ultrasound percutaneous irrigation between 2012 and 2014. The patients were randomly assigned to have the one-needle or the two-needle procedure.
Ultrasound exams were performed on each patient to identify the exact location of calcium deposits in the tendons and whether the deposit appeared to be hard or fluid. For patients in the double-needle procedure group, 16-gauge needles were inserted inside the calcification under continuous ultrasound monitoring, and the area was flushed with injections and extractions of saline until the tendon was free of visible calcium. The single-needle procedure utilised an 18-gauge needle for the injection and extraction.
“Procedure times were shorter and the calcium dissolution was easier when using two needles for hard calcifications and one needle for fluid calcifications,” Sconfienza said.
“In terms of clinical outcomes after one year of follow-up, there was no significant difference between single- and double-needle ultrasound-guided irrigation,” he added.
At one-year follow-up, no residual or new calcifications or tendon tears at the site of the initial calcium deposits were detected.
While further refining where radioembolization should optimally lie in current treatment paradigms for the most common liver-confined or liver-dominant cancers is important, a honing of current administration protocols is also possible, writes Suvranu Ganguli, Boston, USA.
Radioembolization using Yttrium-90 (Y-90) microspheres continues to grow in utilisation as a minimally invasive, liver-directed interventional oncology therapy for primary and secondary liver cancers. This steady growth has resulted from a multitude of factors, including increased clinical data and experience within the interventional oncology community, as well as increased awareness among referrers within the oncology community and by patients themselves. However, hurdles to further adoption and utilisation by interventional oncologists and the greater oncology community remain. Aside from further refining where radioembolization should optimally lie in current treatment paradigms for the most common liver-confined or liver-dominant cancers, which will only come with further clinical studies and experience, refinements to current administration protocols are also possible.
The current state for Y-90 administration requires two outpatient procedures, spaced at least one week apart. The first procedure is for pretreatment evaluation and mesenteric mapping in preparation for the Y-90 administration. This diagnostic angiogram maps the hepatic vasculature, determines the vascular treatment distribution, and identifies any possible hepatico-enteric collateral vessels. Embolization of these hepatico-enteric collaterals maybe performed, depending on the treatment distribution. After thoroughly mapping the mesenteric and hepatic vasculature and selecting the vascular treatment distribution for the subsequent Y-90 administration, Technetium-99m macro aggregated albumin (Tc-99m-MAA) is injected with a subsequent nuclear medicine scan. This step is performed to identify and quantify possible extrahepatic deposition, including the percentage that will shunt to the lungs, to minimise the risk of radiation- induced lung disease. The treatment procedure is usually scheduled at least one week after the mapping, to ensure the mapping procedure confirms the patient is still a good candidate with adequate time to cancel the Y-90 dose, if needed.
The current treatment protocol with two procedures over multiple weeks continues to enforce the idea that Y-90 treatments are lengthy, complicated, and costly, both to referrers and patients. Given this perception and with our increased growth, experience and familiarity with Y-90, we introduced a same-day mapping and treatment protocol this year at Massachusetts General Hospital. It remains an outpatient procedure, but the benefits of same-day mapping and treatment with Y-90 translates to treating patients faster with improved patient convenience, and decreasing the myth and perception that Y-90 is lengthy and complicated.
Aside from our normal patient selection parameters for Y-90 treatments, which include preserved functional status and liver function, we offer it more frequently to patients with secondary metastatic disease rather than patients with hepatocellular carcinoma (HCC), given that lung-shunt percentages are usually less with metastatic disease than HCC. We also usually plan for lobar treatments rather than a whole-liver treatment, given that small hepatico-enteric collaterals could be present at the liver hilum. The possible drawbacks of same-day mapping and treatment with Y-90 include a longer day for the patient and the discovery during the mapping that the Y-90 dose cannot be safely administered. However, given our careful patient selection and our thorough prior experience with Y-90, we have treated more than 20 patients thus far and have not had any patients who could not be successfully treated. Furthermore, all patients have all been extremely pleased with the same-day mapping and treatments, including the few that experienced both treatment protocols.
In addition to whether the treatments are safe and effective, the economics of same-day mapping and treatment with Y-90 will require further attention. Whether we will be reimbursed for both procedures, similar to when they are spaced out by more than a week, is still not clear. We have investigated creating a new Current Procedural Terminology (CPT) code for the same-day Y-90 paradigm, although in discussion with interested parties including the Society of Interventional Radiology (SIR), it is apparent that all CPT codes would be revisited if a new CPT code were to be requested. Therefore, although the treatment protocol may improve patient treatments, experience and costs, there is little support to pursue a new CPT code at this time. Lastly, the natural progression from same day Y-90 mapping and treatment may, and should be, a future state where the mapping portion is forgone and/or not required in a large number of patients. With proper patient selection, experience, and likely a clinical trial to prove the safety of it, many patients will forgo the nuclear medicine scan and go right to Y-90 treatment, similar to the treatment paradigm of chemoembolization.
Suvranu “Shoey” Ganguli, is associate chief, Division of Interventional Radiology, co-director, Center of Image Guided Cancer Therapy, Massachusetts General Hospital and assistant professor of Radiology, Harvard Medical School, Boston, USA. He is a consultant to Sirtex, Boston Scientific, Medtronic and, Boston Biomedical Associates.
A new study is underway at Emory Healthcare, Atlanta, USA, to evaluate the use of cryoablation to treat mild to moderate obesity.
The clinical trial, called “Percutaneous image-guided cryoablation of the vagus nerve for management of mild-moderate obesity” will assess the safety of cryoablation of the posterior vagus nerve.
This study seeks to assess the efficacy of cryoablation for the treatment of mild to moderate obesity and test the safety of this procedure. The vagus nerve transmits hunger signals from the stomach to the brain, and in response transmits stomach expansion signals from the brain to the stomach. Investigators believe that by interrupting this communication, participants could experience less hunger and in turn, lose weight.
The two-year study will enrol 20 patients, and participants will serve as their own control group. Patients with a body mass index of 30 to 35 who are unable to lose weight with diet changes or exercise are eligible for inclusion if they have no coagulopathy.
The primary outcome measures include record of the number of adverse events which occur within the first 24 hours following cryoablation; clinical signs or symptoms of infection, haemorrhage that occur outside of the time periods specified for cryoablation procedure events; and significant adverse events include life-threatening adverse events and death upto two years.
J David Prologo, director of Interventional Radiology Services at Emory Johns Creek Hospital, and assistant professor in the Department of Radiology and Imaging Sciences in Emory’s School of Medicine, is the principal investigator of this interventional study.
“We use image guidance to insert a cryoablation probe near the stomach, targeting the nerve that sends hunger signals to the brain,” says Prologo.
The trial will examine patients using self-reported questionnaires regarding physical activity, appetite and living habits as well as data measurement.
Participants will attend five visits for evaluation and doctors will follow their progress for six months after the procedure. The outpatient cryoablation procedure takes about an hour.
Endocare is funding this clinical trial.
For information regarding enrolment, please contact Maria Rivas: [email protected]
The Gore Viatorr TIPS endoprosthesis with Controlled Expansion, a new device configuration developed by Gore, may reduce portal hypertension treatment complications, even when compared to the Gore Viatorr TIPS endoprosthesis, Gore’s legacy TIPS device. The latter has a strong history of patency and proven performance at fixed diameters. These findings were obtained from the abstract presented at The International Liver Congress 2017 in Amsterdam.
The preliminary data at three months also confirmed that hospital readmissions from cirrhosis-related complications, including refractory ascites and sepsis, were significantly reduced using either of the Gore Viatorr TIPS endoprosthesis products compared to bare metal stents.
“The goal in TIPS creation is to shunt as much blood as necessary to reduce portal pressure below the threshold that leads to portal hypertension complications, and as little blood as possible to maintain hepatic perfusion and cardiac output,” said Jonel Trebicka, Department of Internal Medicine, University of Bonn, Germany. “But when a stent is underdilated (less than the device’s nominal diameter), a common technique in pursuing the ideal gradient, the device diameter may increase over time reaching the nominal diameter in as little as six weeks. Since liver stiffness varies, the amount and rate of this passive expansion is unpredictable. As a result, the change in pressure, increase in shunting and increase in hyperdynamic circulation, factors that could potentially induce serious complications, are also unpredictable. The new capabilities of the Gore Viatorr TIPS Endoprosthesis with Controlled Expansion allow us to optimise the shunt diameter (at time of implantation) to achieve and maintain the desired portal pressure. The preliminary data show this forward-thinking attribute may result in direct patient benefits including reduced readmissions and complications such as hepatic encephalopathy.”
The physician-sponsored, case-control study is ongoing at the University of Bonn in Germany and continues to enrol patients in the controlled expansion arm. Preliminary findings were based on 21 patients receiving the Gore Viatorr TIPS Endoprosthesis with Controlled Expansion, and retrospective data of 48 patients receiving the Gore Viatorr TIPS Endoprosthesis and 36 patients receiving a bare metal stent. At three months, the Gore Viatorr TIPS Endoprosthesis with Controlled Expansion group showed significant superiority compared to both other groups in several areas including lower MELD-Na score (p=0.019) and higher blood flow velocity (p=0.002). Both the Gore Viatorr TIPS Endoprosthesis with Controlled Expansion group and the Gore Viatorr TIPS Endoprosthesis group experienced reduced early splanchnic vein thrombosis (p<0.001) compared to the bare metal stent group. Both the Gore Viatorr TIPS Endoprosthesis with Controlled Expansion group and Gore Viatorr TIPS Endoprosthesis group experienced fewer readmissions from sepsis (p=0.034). Gore Viatorr TIPS Endoprosthesis with Controlled Expansion group experienced fewer readmissions from ascites (p=0.006). Importantly, this beneficial effect was only observed after three months of implantation, suggesting that the lasting diameter control of controlledeExpansion may be at least partly responsible for the reduction in this post-TIPS complication.
The study authors suggest that this underlines the importance of stent diameter control in the performing of TIPS. Further studies are necessary to confirm the benefits of lasting diameter control.
The Gore Viator TIPS Endoprosthesis with Controlled Expansion features the same proprietary ePTFE graft lining that minimises transmural permeation of bile and mucin (common causes of patency loss). With the new controlled expansion capability, physicians can start at the smallest diameter (8 mm) and balloon up as needed during implantation to optimise the diameter until the target pressure gradient is reached. Benchtop data on file showed diameter expansion was no more than 0.25mm over a simulated 10-year period at physiological portal pressures. Further, the new device now covers a range of diameters between 8 and 10 mm in a single device, helping to simplify inventory.
The Gore Viator TIPS Endoprosthesis with Controlled Expansion is US FDA approved and CE marked for the treatment of portal hypertension with TIPS procedures.
Merit Medical will partner with internationally renowned interventional cardiologist Ferdinand Kiemeneij to deliver the next generation in educational opportunities for interventional cardiologists and interventional radiologists. Kiemeneij will serve as a co-proctor at the upcoming Advanced Transradial Intervention Education Course for Interventional Cardiologists (13–14 October, Merit Medical Education Cente, Salt Lake City, USA).
Acclaimed as the “Father of Transradial,” Kiemeneij—a Dutch interventional cardiologist—performed the first transradial coronary angioplasty in 1992 at the Onze Lieve Vrouwe Gasthuis in Amsterdam, The Netherlands, followed by transradial stenting in the same year and stenting on an outpatient basis in 1994. A sought-after instructor and lecturer, he serves as the Interventional Cardiology proctor for Merit’s ThinkRadial EMEA course and has trained countless physicians in transradial techniques over the years.
Sandeep Nathan (University of Chicago Medical Center, Chicago, USA), the ThinkRadial Interventional Cardiology Course director and founder, and will co-proctor the Advanced IC training with Kiemeneij.
Fred Lampropoulos, chairman and chief executive officer of Merit Medical, says: “We are excited to partner with Kiemeneij, one of the pre-eminent interventional cardiologists in the world. The advanced training course, which has been designed to help experienced interventional cardiologists continue to grow their practice, is the next logical step in Merit’s ThinkRadial initiative. Hundreds of physicians from across the globe have already attended one of our ThinkRadial training courses. This unparalleled educational opportunity will help attendees elevate their practices to the next generation of radial access.”
In addition to its ThinkRadial training programme, a press release reports, Merit Medical offers a full line of tools for radial procedures, including the PreludeEASEtm Hydrophilic Sheath Introducer. Available in 4Fr to 7Fr sizes, featuring a hydrophilic coating that facilitates easier insertion and removal, specifically up to 30% less insertion force than the leading competitor, the PreludeEASE is suitable for use in a wide range of interventional and diagnostic procedures. It is available in multiple kit configurations and custom options to meet specific procedural needs.
Johnson and Johnson Medical Devices Companies introduced Cerenovus, its new neurovascular business, at the Society of NeuroInterventional Surgery 14th Annual Meeting (SNIS; 24–28 July, Colorado Springs, USA).
Cerenovus, a name derived from the Latin words for ‘new’ and ‘brain’, will focus on delivering innovative therapies for haemorrhagic and ischaemic stroke patients.
According to a press release, the Johnson & Johnson Medical Devices Companies are committed to neurovascular care, having expanded Cerenovus’s product portfolio in the last year with targeted investments. The recent acquisitions of Pulsar Vascular, with a specialty in the endovascular treatment of wide-neck bifurcation aneurysms, and Neuravi, offering extensive expertise and knowledge in acute ischaemic stroke with its EmboTrap Revascularization Platform, greatly extend Cerenovus’s abilities to address unmet clinical needs in these areas.
Johnson and Johnson’s neurovascular business was previously under the name Codman Neuro.
Spectranetics has announced receipt of US Food and Drug Administration (FDA) premarket approval of the Stellarex drug-coated balloon (DCB), designed to restore and maintain blood flow to the superficial femoral and popliteal arteries in patients with peripheral artery disease (PAD).
“The Stellarex DCB has shown safety and efficacy in a cohort of patients which included a higher preponderance of diabetics and core-lab defined severely calcified lesions in the US IDE trial. These results, in combination with the cohort of patients studied in the European randomised controlled trial, demonstrate the Stellarex DCB is safe and effective in diverse patient populations when addressing symptomatic femoropopliteal disease,” stated Prakash Krishnan, ILLUMENATE pivotal trial’s co-principal investigator, Mount Sinai, New York, USA.
Sean Lyden, ILLUMENATE’s co-principal investigator, Cleveland Clinic, Cleveland, USA, added, “The ILLUMENATE pivotal trial treated a challenging patient population with a low paclitaxel drug dose. When considering options, I think most clinicians would prefer to use a lower drug dose if they can also achieve great patency results.”
Throughout the ILLUMENATE trial series, Stellarex DCB’s EnduraCoat technology demonstrates both safety and efficacy with consistently high patency rates and low clinically-driven target lesion revascularisation rates in a range of lesion complexities and patient co-morbidities. The device offers both hybrid paclitaxel crystallinity and a durable excipient to provide efficient drug transfer, effective drug residency with high coating durability and minimal particulate loss.
“The Stellarex DCB delivers top-tier clinical results for common to complex patients. As the only commercially-available DCB with two reported randomised controlled trials, Stellarex has demonstrated durability with consistently high patency rates in a wide range of patients,” said Scott Drake, president and chief executive officer of Spectranetics. “Our customers refer to Stellarex as a no-compromise solution. This next generation DCB provides proven treatment backed by robust clinical evidence.”
“Spectranetics is a provider of proven solutions to manage the challenges of crossing lesions, preparing vessels, and treating even the most complex coronary and peripheral lesion morphologies. We are always focused on better patient care, and with today’s FDA approval, the Stellarex DCB becomes a formidable competitor in the drug-coated balloon market, and a proven solution for those suffering with PAD,” said Scott Hutton, senior vice president and general manager at Spectranetics.
“The choice to become a parent should not prevent an interventional radiologist from having a successful career, nor should a successful career in IR preclude parenthood,” said Meridith J Englander, chair of SIR’s Women in Interventional Radiology section.
To support interventional radiologists with families, SIR encourages institutions and practices that employ IRs to craft policies that provide paid parental leave for new parents, and include the maintenance of full benefits and 100 percent of pay, for at least six weeks.
“Paid leave has clear benefits for both the family and the IR practice,” said Englander, an interventional radiologist at Albany Medical Center in New York, USA, and co-author of the position paper. “By allowing new parents time off to care for their children, paid parental leave reduces infant mortality and improves the health of mother and child. At the same time, it boosts worker morale and increases retention and productivity by encouraging the physician to return to work.”
In this new guidance, SIR advises IR practices to:
Include parental leave policies in all employment contracts.
Exclude from consideration the past or potential use of parental leave when making decisions about employment, benefits, promotion or tenure.
Allow for scheduling flexibility to accommodate prenatal care appointments for the IR or an IR’s spouse or partner.
Keep parental leave separate from vacation time and sick leave.
Not require physicians on parental leave to make up missed call time.
At minimum, adhere to Family Medical Leave Act (FMLA) allowances for protected unpaid leave after the birth or adoption of a child, even if the practice is exempt from FMLA requirements.
“This statement confirms SIR’s strong support for parental leave policies that foster healthy families and a healthy work-life balance,” said SIR president Suresh Vedantham, professor of Radiology and Surgery at the Mallinckrodt Institute of Radiology at the Washington University School of Medicine, St Louis. “Becoming a parent does not make physicians less committed to their professions and parents should not face discrimination as a result.”
Klaus Hausegger, chairman of the Institute of Diagnostic and Interventional Radiology in Klagenfurt, Austria, and president-elect of the Austrian Roentgen Society, will take up a new role as editor-in-chief of the journal CardioVascular and Interventional Radiology (CVIR) in September 2017. He takes over from current editor-in-chief, Dierk Vorwek, chairman of the Department of Diagnostic and Interventional Radiology, Klinikum Ingolstadt, Ingolstadt, Germany, who has been the journal’s editor-in-chief since 2003. Interventional News spoke to Hausegger about his ideas and aspirations for the journal.
In your view what is the role of a peer-reviewed medical journal such as CVIR in today’s world?
Generally speaking, information has become widely and easily accessible via numerous search options and the internet. If you require medical and/or scientific information about a certain topic you just type it into a search engine and you will probably find numerous hits responding to your request. However, many of these hits provide unfiltered and unconsidered information. Therefore, the main role—and even more strongly—it is the duty and responsibility of peerreviewed medical journals to contribute scientifically proven, considered, valid information and knowledge to the vast amount of information and even misinformation that is circulating around. The reader of a peer-reviewed journal should know that he, or she, can rely on the fact that every bit of content from a peer-reviewed journal, such as CVIR, has been rigorously scrutinised for scientific reliability and content by renowned experts in the field.
What are your aims and aspirations for CVIR under your editorship?
CVIR is one of the world-leading journals in the field of interventional radiology. Of course, it is my main goal to further develop this role of CVIR in the international medical/ scientific field. My predecessor, Dierk Vorwerk did an excellent job of developing and promoting the journal—a path that I would wish to continue. Beside the focus on science, I also want to pay attention to education. My team and I plan to provide our readers with the possibility of acquiring continuing medical education credits by working on selected manuscripts and we want to create a link to the European Board of Radiology (EBIR). It may be of interest to provide summarised state-of-the-art knowledge about certain topics; therefore we plan to publish “special issues” on selected topic on a regular schedule. Overall, the journal should be “the voice of interventional radiology”.
What is the type of research that you would like to see interventional radiologists undertaking and publishing?
Of course, we want to read and publish scientifically sound and well-performed studies, ideally prospective, randomised trials which address important clinical issues. However, we all know that conditions under which randomised studies are performed quite often do not reflect clinical practice. This might be better reflected by representative cohort studies, retrospective analyses of case series, or the results of well-documented single- or multicentre registries, which we also want to see published in our journal. New ideas and concepts may be reported in the form of brief communications, technical notes or even outstanding case reports. Basic research from the laboratories may also well contribute to the whole portfolio of the journal. And last but not least, we are living in the world of globalisation and data collection. I would be very happy to receive manuscripts, which deal with the evaluation of the influence of interventional radiology on the global health of large parts of the population, based on the analysis of big data. Just as an example, it should be possible to answer the question to which degree crural artery interventions influence the lower limb amputation rate by comparing large population cohorts before and after the wide availability of this intervention.
What is the most memorable research that you read in 2016–17 in CVIR?
A short selection of my favourites would be a manuscript on perfusion angiography of the foot in patients with critical limb ischaemia; a review article on percutaneous isolated hepatic perfusion in the treatment of unrespectable liver malignancy; a manuscript about the simulation of flow dynamics in aortic type B dissection; a large cohort study on the outcome of peripartal aortic balloon occlusion in patients with placenta praevia; and a meta-analysis on the results of treatment of unresectable hepatocellular carcinoma radioembolization vs. chemoembolization. However, there are many more papers and topics published that are worth reading closely.
The revised syllabus has been widely endorsed by European IR societies and can be downloaded here. This version will serve as the basis for the European Board of Interventional Radiology (EBIR) examination from March 2018, information from the society notes. The first edition of the curriculum and syllabus was published in 2013.
“The revised IR Curriculum and Syllabus is a standardised guideline for training that covers an array of general IR topics and safety concepts with which a well-trained interventional radiologist should be familiar,” CIRSE notifies.
Key additions in the new document include sections on interventional oncology; prostate artery embolization; a blueprint colour coding system to guide physicians who wish to take the EBIR; and core procedures in IR, CIRSE apprises.
Further information highlights that the revised edition of the curriculum and syllabus has an increased focus on clinical practice and safety. The editor-in-chief, Raman Uberoi, Oxford, UK, and editorial board comprising Antonio Basile (Catania, Italy), Anna-Maria Belli (London, UK), Afshin Gangi (Strasbourg, France), Klaus Hausegger (Klagenfurt, Austria), Michael Lee (Dublin, Ireland), Stefan Müller-Hülsbeck Thomas Rand (Vienna, Austria), Dimitrios Tsetis (Heraklion, Greece) and Otto van Delden (Amsterdam, the Netherlands) has reorganised several sections so that therapeutic areas and procedures are more appropriately aligned and excluded procedures that are no longer widely performed.
The European Curriculum and Syllabus is the basis for the European Board of Interventional Radiology (EBIR), which allows physicians who have followed the objectives of the curriculum and mastered the content of the syllabus to prove their professional competence.
Stephen Solomon, chief of Interventional Radiology at Memorial Sloan Kettering Cancer Center in New York, USA, has assumed presidency of SIO, and joins new board officers “to drive strategy and deliver quality resources to medical professionals in the interventional oncology field,” an announcement from the society states.
Solomon has helped pioneer several different technologies to help patients. A majority of his current research is in the field of image-guided tumour ablation and he is exploring ways to augment ablations with immune stimulation and adjuvant therapies. Solomon has been a consultant to the US FDA and a consultant to a number of medical device companies, the announcement informs.
William S Rilling, professor of Radiology and Surgery, at the Medical College of Wisconsin is named president-elect. Rilling is a local and national principal investigator for a number of important interventional oncology (IO) trials and is currently active as a consultant for a number of companies working to improve outcomes in IO.
SIO’s announced list of officers is:
Stephen Solomon, president
William Rilling, president-elect
Riad Salem, treasurer
Further, Alban Denys (Lausanne, Switzerland), Nahum Goldberg (Jerusalem, Israel), Alexis Kelekis (Athens, Greece), Kevin Kim (New Haven, USA) and Costantinos Sofocleous (New York, USA) have been named as the directors-at-large.
The SIO Board of Directors is responsible for governing, supervising and controlling the affairs of the society, in addition to establishing its policies and programmes. Members will work in cooperation with the new officers, other board members, and the society’s staff, the announcement explains.
Gore has announced the first patient implant of conformable thoracic stent graft with Active Control System after receiving CE mark last month. The first implant was performed by Giovanni Torsello and Martin Austermann at St. Franziskus Hospital, Munster, Germany. The new device will be formally launched in European regions later this year.
The thoracic endovascular aortic repair (TEVAR) device is the first to feature a new delivery system that provides the physician with controlled, staged deployment. The system optimises accuracy, angulation, and apposition to treat aetiologies of the descending thoracic aorta including aneurysms, transections, and acute and chronic type B dissections. The new device will be formally launched in European regions later this year.
The Active Control System enhances the exceptional conformability of the stent graft; facilitating the optimised wall apposition that the Conformable Gore Tag device is renowned for even in complex anatomies, such as acute aortic angles. The novel staged deployment feature enables the physician to refine positioning and angulate the stent graft within the body to achieve optimal placement prior to full-diameter expansion. The angulation control capability gives physicians the option to angulate the device to achieve orthogonal placement to the aortic blood flow lumen and maximise conformability and seal. These features enable physicians to more confidently perform endovascular treatment even in anatomies where tortuous vessels might historically have suggested open surgery.
“The enhanced control capabilities this new delivery system allows could reduce many common complications that can occur if the stent graft is not placed correctly during the TEVAR procedure,” said Torsello. “Secondary interventions can be traumatic for patients and costly to the provider. The innovative staged deployment feature of the Gore Active Control System provides a level of precision that has never existed in TEVAR. This level of control in combination with the long-term benefits of the stent graft is a significant advancement for the field.”
The new product offering features the same time-tested stent graft as the conformable Gore Tag device, whose predictable outcomes have been established through its long-term freedom from reintervention (89%) and low serious endoleak (6%) and migration (0%) rates through five years.
The Journal of Vascular and Interventional Radiology’s(JVIR’s) impact factor—one measure of a journal’s influence based on the number of article citations compared to the total number of articles published—increased by 8.2% in 2016.
JVIR earned an impact factor of 2.780 for 2016, an increase from 2.570 the previous year, according to data released in the Journal Citation Reports published by Thomson Reuters. The impact factor, which reflects citations in the previous two years, is often used as a measure of the quality and influence of medical journals within scientific, professional and academic communities.
“The continued growth in JVIR’s impact factor affirms interventional radiology’s global importance and cements JVIR’s reputation as the authoritative source for breakthrough scientific research on minimally invasive image-guided therapies,” said editor-in-chief Ziv J Haskal, a professor of radiology and medical imaging at the University of Virginia School of Medicine in Charlottesville, USA.
JVIR continues to have the highest impact factor among interventional radiology journals. This is an important factor for authors, as are the more than two million media impressions JVIR garners each year, he said. As important, underscored Haskal, is the continued annual growth of manuscript submissions.
JVIR published 451 articles in 2014–2015, earning 1,254 citations of those articles in 2016. Those citations appeared in radiology, nuclear medicine and medical imaging journals and peripheral vascular disease journals.
Twelve-month data from the BIOFLEX-I study demonstrates the
safety and efficacy of the Pulsar-18 self-expanding stent for blocked SFAs, the main arteries in the lower limb. (PRNewsfoto/BIOTRONIK)
Biotronik’s Pulsar-18
Biotronik has announced that 12-month data from the BIOFLEX-I study have demonstrated the safety and efficacy of the company’s Pulsar-18 self-expanding stent for blocked superficial femoral artery treatment.
The study results were presented during a late-breaking session at the 2017 Complex Cardiovascular Catheter Therapeutics Advanced Endovascular and Coronary Intervention Global Summit (C3; 29–30 June, Orlando, USA).
In lesion lengths up to 190mm, clinical findings demonstrated:
7% freedom from major adverse events (MAEs) at 30 days
6% freedom from clinically-driven target lesion revascularisation (TLR) at 12 months
8% primary patency at 12 months
Clinical follow-up for the prospective, international, multicentre, two-arm investigational device exemption (IDE) trial will be for a total of 36 months
Pulsar-18 is the only superficial femoral artery self-expanding stent approved by the US Food and Drug Administration (FDA) with a 4F delivery system, designed to enable simpler, safer and more efficient procedures than larger diameter delivery systems. Procedure times may be reduced because the system can more easily crosses lesions, lower access site complication rates, and requires less compression time without the need for a closure device.
“Superficial femoral artery blockages are often challenging to navigate and treat because of the length of the artery and frequent presence of diffuse disease. Reduced blood flow to the limb can lead to amputation, so it is critical that patients are treated quickly and effectively,” says BIOFLEX-I US principal investigator, Mark Burket (Toledo, USA). “Because of Pulsar-18’s flexibility, small delivery system and thin struts, the stenting procedure takes less time, reduces complications and allows for earlier patient discharge.”
With low chronic outward force and thin struts (140μm), a press release states that Pulsar-18 may reduce vessel injury and inflammation, provide faster endothelialisation and lower the risk of restenosis. The BIOFLEX-I study found improved clinical and quality of life metrics, including ankle-brachial index (ABI), six-minute walk and walking impairment questionnaire (WIQ).
Pulsar-18 received FDA approval in March 2017 and is available in the USA though Biotronik’s distribution partner Getinge.
The UK’s Information Commissioner’s Office (ICO) has found that the Royal Free National Health Service (NHS) Foundation Trust (London, UK) did not adhere to the UK’s Data Protection Act when it provided patient details to Google DeepMind.
The Trust, a press release reports, provided personal data for around 1.6 million patients as part of a trial to test an alert, diagnosis and detection system for acute kidney injury.
According to the press release, an ICO investigation found several shortcomings in how the data were handled—including that patients were not adequately informed that their data would be used as part of the trial. The Trust has now been asked to commit to changes ensuring it is acting in line with the law by signing an undertaking. It has been asked to:
Establish a proper legal basis under the Data Protection Act for the Google DeepMind project and for any future trials
Set out how it will comply with its duty of confidence to patients in any future trial involving personal data
Complete a privacy impact assessment, including specific steps to ensure transparency
Commission an audit of the trial, the results of which will be shared with the Information Commissioner, and which the Commissioner will have the right to publish as she sees appropriate.
Elizabeth Denham, Information Commissioner, says, “There is no doubt the huge potential that creative use of data could have on patient care and clinical improvements, but the price of innovation does not need to be the erosion of fundamental privacy rights.” She adds that the Data Protection Act is not a “barrier to innovation” but that it “does need to be considered wherever people’s data is being used”.
The GET LEAN (Gastric artery embolization trial for the lessening of appetite nonsurgically) study shows promising six-month preliminary data with an average body weight loss of around 20lbs and no serious adverse events. The first diabetic patient was treated using embolization and we saw an improvement in her glycosylated haemoglobin, HbA1c, levels at six months, write Sumeet Patel, Azim Sheikh and Mubin Syed.
GET LEAN is a pilot study designed to collect safety and efficacy data in patients undergoing left gastric artery embolization for morbid obesity in the USA. As a secondary goal, the pilot study seeks to obtain quality of life data. It is not designed to achieve new indications for Bead Block (BTG), which is the embolic agent used in the study. Researchers treated four white patients (three women) with an average age of 41 years and mean weight of 259.3lbs. The patients had a mean body mass index (BMI) of 42.4 kg/m2 underwent a left gastric artery embolization procedure with 300–500μm Bead Block particles via right common femoral or left radial artery approach. As reported last year in The Journal of Vascular and Interventional Radiology (JVIR), the follow-up included upper endoscopy at three days and 30 days if necessary, and a gastric emptying study at three months.
The results of the GET LEAN study at six months reveal an average weight loss of 20.3lbs (n=4; range, -6 to -38lbs), or -8.5% (range, -2.2% to -19.1%). Average excess body weight loss at six months was -17.2%. There were no serious adverse events. There were three minor complications, superficial gastric ulcerations that healed by 30 days, and did not require hospitalisation. The results showed that left gastric artery embolization appears to be safe in the intermediate term for weight loss in morbidly obese patients. The quality of life measures showed a general trend toward improvement. We also found that the radial artery approach appears to be feasible and this may have implications as a safer more convenient access site in this population. All procedures in the study were performed in an outpatient setting.
The first diabetic patient was treated in this study under US FDA investigational device exemption (IDE) clearance and had a weight loss of 28lbs with an associated drop in her HbA1c.
The study has recently received FDA IDE clearance to treat anatomic variants that occur in as many as 15% of the population.
Mubin Syed
Obesity is one of the largest public health concerns in the USA, and indeed, worldwide. In fact, 1/3 of the world population is either obese or overweight according to The Lancet. Obesity predisposes patients to a variety of maladies, including adult-onset diabetes, cardiovascular disease, hypertension, malignancy, obstructive sleep apnoea, venous stasis disease and osteoarthritis. Morbid obesity affects 6.6% of the US population. Bariatric surgery, the standard of care, is often performed for morbidly obese patients. This is because in these patients, conservative weight loss measures such as diet and exercise often fail. Unfortunately, these surgical treatments have known serious complications, including anastomotic leaks, bowel obstruction, deep vein thrombosis, pulmonary embolism, gastrointestinal bleeding, dumping syndrome, and anaesthesia risks that result in morbidity and mortality. The 30-day mortality rate from bariatric surgery is approximately 0.31% as of 2014, which is less than previously reported in 2004. Despite this, the reoperation rate is 7% and the total overall complication rate is 17%. It is estimated that only 1% of eligible patients choose to have bariatric surgery.
Sumeet Patel and Azim Shaikh are with the research team at Dayton Interventional Radiology, Dayton, USA. Mubin Syed is an interventional radiologist, president and coowner of Dayton Interventional Radiology. He received the runner’s up award Editor’s Award 2016 for Distinguished Clinical Study at the SIR 2017 Annual Scientific Meeting in Washington, DC, USA. The authors have reported no disclosures pertaining to this article.
Sirtex has announced the presentation of the SIRFLOX/FOXFIRE Global right-side survival data in metastatic colorectal cancer at the 19th European Society for Medical Oncology (ESMO) World Congress on Gastrointestinal Cancer (WCGIC) in Barcelona, Spain.
Guy van Hazel, clinical professor of Medicine, University of Western Australia and coprincipal investigator on the SIRFLOX study presented the data. The combined SIRFLOX and FOXFIRE Global studies (n=530 and n=209, respectively) showed that for patients with a right-sided primary tumour, median overall survival was significantly improved with the addition of SIRSpheres Y-90 resin microspheres to standard chemotherapy versus chemotherapy alone (22 vs. 17.1 months, respectively; p=0.007;), but not for patients with a left-sided primary tumour.
Importantly, van Hazel also presented the baseline characteristics of the combined patient dataset between the two arms of the study for both left-sided and right-sided patients. There was no statistically significant difference in the baseline characteristics of patients who received SIR-Spheres microspheres plus chemotherapy vs. chemotherapy alone. Patients with a right-sided primary tumour were older (mean: 64.4 vs. 61.6 years) and a higher proportion were female (42.5% vs. 32%), compared to those with a left-sided primary tumour.
Andrew McLean, chief executive officer of Sirtex said “There is now solid scientific evidence to support the observation that for patients whose primary cancer is located on the right-side of the bowel, their prognosis is demonstrably worse, with fewer treatment options and a lower overall life expectancy. The statistically significant 4.9 month overall survival benefit observed in patients who received SIR-Spheres microspheres is clinically meaningful and subject to further confirmatory analyses, coupled with additional supporting evidence of this overall survival benefit from the FOXFIRE study. Collectively, this may support consideration of right-sided liver-only or liver-dominant metastatic colorectal cancer patients for SIRSpheres microspheres treatment.”
“This striking and essentially unexpected finding may bring new hope to metastatic colorectal cancer patients with liver-only or liver-dominant tumours that have spread from the right side of the bowel or colon. These cancers are genetically and structurally different from tumours that start on the left side of the colon. Patients with right-sided primary tumours have a worse prognosis for survival and fewer treatment options. They do not respond well to such biological therapies as cetuximab or panitumumab,” said van Hazel.
Internationally-renowned radiation oncologist, Lizbeth (Liz) Kenny, has received her badge as an Officer of the Order of Australia. The investiture ceremony was on 4 May 2017. The Order of Australia is the principal and most prestigious means of recognising outstanding members of the community at a national level. The award was publicly announced on Australia Day (26 January).
“I received a letter from the Governor General’s office in late 2016, informing me that I had been awarded the Officer of the Order of Australia and this was formally announced on Australia Day,” Kenny, senior radiation oncologist at the Royal Brisbane and Women’s Hospital, Queensland, Australia, told Interventional News.
On being asked how she felt about receiving this honour, Kenny, who became the youngest-ever president of the Royal Australian and New Zealand College of Radiologists (RANZCR) in 2005, said: “I felt completely overwhelmed with the award. I completely understand its significance and importance and feel deeply honoured. My husband, Colin, and children, William and Sophie, were proud and delighted, as were our friends and family. I have been truly humbled by the number of good wishes and genuine happiness expressed from my hospital, my colleagues, bosses and patients. I am aware of the responsibility that goes hand-in-hand with accepting this award. It will not change my day-to-day clinical work or research but it gives me even more enthusiasm. I have the privilege of working with wonderful people, both clinically and with my regional team, who are so dedicated to improving cancer care across Queensland.”
Kenny and her family celebrated the news in style. “We had a fabulous party at our favourite Brisbane restaurant, Moda, along with 70 of our family and friends. We combined this with birthday celebrations for both me and my husband as we both have birthdays around this time. My old boss acted as master of ceremonies and it was just a great night.”
Kenny wears her Officer of the Order of Australia badge
Interventional News asked Kenny about where her continuing motivation to do more comes from and how she balances her rewarding career and rich family life. “I love my work. At the core, caring well for patients drives everything I do professionally, be it one-on-one care with my patients, working with my clinical and research teams, or trying to improve services at a state or national level. I do not have any recipe for a balanced life, in fact I suspect that my family feel that I am a bit unbalanced! My family travel with me as much as possible and this is always wonderful. Seeing our children grow up into such good and independent people makes me think that we must have done something right. Having wonderful personal assistant support at work and at home makes all the difference,” she explained.
Although Kenny is a pre-eminent radiation oncologist, she is a longstanding supporter of interventional radiology, and is a member of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and its Oncology Alliance Subcomittee. When asked about her big picture goals for cancer care, Kenny said: “In my own profession of radiation oncology, the future is very bright for our teams. The combination of wonderful technology, that continues to develop, combined with the very real human face of caring for people with cancer, often at their time of greatest need, drives us all. I would love to see the world refocus on the importance of local treatment and local cure, which brings the greatest gain to patients.
Partnering with interventional oncology and imaging research is a very clear road ahead from my perspective and CIRSE’s commitment to Quality Assurance in interventional oncology will go a long way to facilitating this.” The investiture ceremony took place on 4 May, at Government House in Brisbane. Liz Kenny received the award from the Governor of Queensland, at a glittering ceremony attended by her family. In the evening, she attended a formal dinner hosted by the Governor. Amongst the dozens of congratulatory messages that followed the announcement of the award on the Governor’s webpage, was a wonderful post on Facebook by Sophie, which said: “When I was five years old, I used to think mum was superwoman. Now that I am 22, I realise that I was right all along!”
A retrospective review of single-institution experience, published in July in the Journal of Vascular and Interventional Radiology (JVIR), suggests that percutaneous image-guided ablation is feasible, well tolerated and achieves “acceptable” local tumour control rates.
The investigators, Andrew J Erie, Mayo Clinic, Rochester, USA and colleagues, set out to retrospectively review and report the efficacy and safety of percutaneous image-guided ablation (cryoablation or radiofrequency ablation) in the treatment of oligometastatic prostate cancer.
As reported in JVIR, an institutional registry was retrospectively reviewed and revealed 16 patients with oligometastatic prostate cancer who underwent percutaneous image-guided ablation to treat 18 metastatic sites.
The researchers reported that a subgroup of seven patients with eight metastases were androgen-deprivation therapy-naïve and underwent ablation to delay initiation of this antihormone therapy whose main use is in treating prostate cancer. Local tumour control, progression-free survival, antihormone therapy -free survival, and procedural complications were analysed.
The study reported that local tumour control was achieved in over 80% at a median follow-up of over 25 months. There was local tumour recurrence in 17%, with a median time to local recurrence of 3.5 months. Estimated progression-free survival rates at 12 and 24 months were 56% and 43%, respectively. “In the seven patients who had not had anti-hormone therapy patients, local tumour control was achieved in all metastases, and the median androgen-deprivation therapy-free survival period was 29 months. There were no major procedural complications,” the authors write.
These findings led them to conclude that in this group of patients percutaneous ablation may be particularly useful in patients who wish to delay initiation of androgen-deprivation therapy.
Interventional radiologists at the Emory Johns Creek Hospitals (EJCH), Johns Creek, USA, are using radiofrequency ablation to reduce pain for cancer patients.
Radiofrequency ablation is a minimally invasive procedure in which doctors use image guidance to ablate or cauterise tumours that have spread to the spine in cancer patients.
J David Prologo, director of Interventional Radiology Services at EJCH, and assistant professor in the Emory Department of Radiology and Imaging Sciences, says he uses fluoroscopy (live x-ray) to properly determine where to place the needle to target the pain.
“An electrical current is used to generate heat and destroy the cancer cells,” says Prologo, who is also a member of Emory’s Winship Cancer Institute. “Then, cement is injected to stabilise the bone fragments.”
Historically, cancer patients who have spinal tumours have had very limited options and relied on opioids for pain relief.
The treatment provides patients benefits including: greater range of motion, improved quality of life, shorter recovery time and longer-lasting pain relief.
Spine radiofrequency ablation is an outpatient procedure and allows patients to resume activities almost immediately.
Royal Philips has announced the acquisition of CardioProlific Inc, a USA-based, privately-held company that is developing catheter-based thrombectomy approaches to treat peripheral vascular disease. Financial details of the transaction will not be disclosed.
A company press release states that CardioProlific’s technologies are complementary to Philips’ portfolio of image-guided therapy devices and to the portfolio of The Spectranetrics Corporation, which Philips recently has also agreed to acquire. The acquisition of CardioProlific underpins Philips’ aim “to develop new solutions for clinicians to decide, guide, treat and confirm the appropriate therapy for cardiac and peripheral vascular disease”.
“The acquisition of CardioProlific will further strengthen our innovation pipeline of catheter-based therapy devices,” said Bert van Meurs, Business Leader Image Guided Therapy at Philips. “We are convinced that the development of CardioProlific’s differentiated thrombectomy technologies, combined with our suite of image-guided therapy solutions, will help our customers drive the procedure innovation for the treatment of peripheral vascular disease.”
Philips’ image-guided therapy portfolio comprises interventional imaging systems, planning and navigation software, interventional devices—including catheters for diagnosis and therapy—and a broad range of services, all aimed at helping clinicians to deliver more efficient and effective care to improve the lives of the patients they treat.
Augmenix, a medical technology company that develops, manufactures, and sells proprietary absorbable hydrogels that separate and protect organs at risk during radiotherapy and interventional procedures, announced that the first patients have been treated with SpaceOAR hydrogel at the Chaim Sheba Medical Center in Tel Hashomer, Israel. SpaceOAR hydrogel is an absorbable prostate-rectum spacer that reduces rectal injury during prostate radiotherapy.
“We are excited to offer our patients this new, innovative technology to significantly reduce risks of prostate cancer radiotherapy,” said Zvi Symon, from the Chaim Sheba Medical Center. “SpaceOAR hydrogel will provide meaningful long-term benefits, improving overall quality of life for our patients.”
“We are extremely pleased to bring our innovative SpaceOAR hydrogel to physicians and patients in Israel,” commented John Pedersen, CEO of Augmenix. “Our growing body of clinical evidence demonstrates that SpaceOAR hydrogel significantly reduces the risk of rectal and urinary toxicities and loss of sexual function associated with prostate cancer radiotherapy. SpaceOAR hydrogel is making a significant difference in the lives of men around the world.”
Radiation therapy in the treatment of prostate cancer can cause unintended injury to adjacent healthy tissue, which can lead to bowel, urinary and sexual symptoms that can affect patient health and quality of life. With SpaceOAR hydrogel, physicians can place a hydrogel barrier to separate the prostate from surrounding healthy tissue.
In January 2017, Augmenix announced three-year post-treatment data from a prospective, randomised, multi-centre, patient-blinded clinical trial showing that patients treated with SpaceOAR hydrogel technology prior to prostate cancer radiotherapy demonstrated significant rectal (bowel), urinary, and sexual benefit through three years of follow up. Overall patient wellness at three years was assessed by looking at the percent of patients with clinically significant declines in all three quality of life (QOL) domains (bowel, urinary and sexual). Fully 20% (1 in 5 patients) of men in the control arm had clinically significant declines in all three QOL areas compared to only 2.5% (1 in 40 patients) of men in the SpaceOAR hydrogel arm (p=0.002). Among men who were potent at baseline, the analysis showed that SpaceOAR hydrogel treated men were better able to maintain erections sufficient for intercourse through three years of follow-up (p=0.03). Of the men treated with SpaceOAR hydrogel, 66.7% could achieve erections sufficient for intercourse at three years compared to 37.5% in the control arm, a 77.8% improvement.
Royal Philips and The Spectranetics Corporation announced that they have entered into a definitive merger agreement. Pursuant to the agreement, Philips will commence a tender offer to acquire all of the issued and outstanding shares of Spectranetics for US$38.50 per share, to be paid in cash upon completion.
Philips also acquired CardioProlific, a USA-based, privately-held company that is developing catheter-based thrombectomy approaches to treat peripheral vascular disease.
The Spectranetics merger agreement represents a 27% premium to Spectranetics closing price on 27 June 27 2017. The implied enterprise value is approximately €1.9 billion, inclusive of Spectranetics’ cash and debt. The board of directors of Spectranetics has approved the transaction and recommends the offer to its shareholders. The transaction is expected to close in the third quarter of 2017.
Philips has a leadership position in the €6+ billion image-guided therapy market with a unique portfolio of interventional imaging systems and devices, planning and navigation software, and services, serving a large, global customer base and supported by a global network of leading clinical partners, a press release states.
The acquisition of Spectranetics will further expand and strengthen Philips’ Image-Guided Therapy Business Group. Spectranetics is a leader in vascular intervention to treat coronary and peripheral artery disease, and in lead management for the minimally invasive removal of implanted pacemaker and implantable cardioverter defibrillator (ICD) leads. Spectranetics is currently growing double digits and projects 2017 sales to be in the range of US$293 million to US$306 million.
Spectranetics’ device portfolio includes a range of laser atherectomy catheters for treatment of blockages with laser energy in both coronary and peripheral arteries; the AngioSculpt scoring balloon used to mechanically push a blockage aside in both peripheral and coronary arteries; the AngioSculptX scoring balloon, which is the only drug-coated scoring balloon in the market, and the Stellarex drug-coated balloon, which treats common to complex lesions while inhibiting the recurrence of these blockages. All of these market segments exhibit high growth rates.
The Stellarex drug-coated balloon is a key growth driver in Spectranetics’ portfolio. Stellarex already is CE-marked, and under review by the USFDA for premarket approval in the USA. The drug-coated balloon segment is one of the fastest growing segments in peripheral vascular procedures. Top-tier outcomes in the most complex patient population studied in drug-coated balloon investigational device exemption trials indicate that Spectranetics’ Stellarex has excellent clinical performance with proven results in complex disease.
“Today’s exciting announcement follows a series of bolt-on acquisitions to strengthen our portfolio across the health continuum,” said Frans van Houten, CEO of Royal Philips. “Building on the successful integration of the Volcano acquisition in early 2015, we are now accelerating our strategic expansion into therapy devices with the agreement to acquire Spectranetics. This transaction is expected to be revenue growth and profit accretive by 2018, given the projected revenue and productivity synergies. Spectranetics’ highly competitive product range, integrated with our portfolio of interventional imaging systems, devices, software and services will enable clinicians to decide, guide, treat and confirm the appropriate cardiac and peripheral vascular treatment to deliver enhanced care for patients with better outcomes, as well as significantly boost recurring revenue streams for Philips.”
Cardiolife acquisition
A company press release states that CardioProlific’s technologies are complementary to Philips’ portfolio of image-guided therapy devices and to the portfolio of The Spectranetrics Corporation. The acquisition of CardioProlific underpins Philips’ aim “to develop new solutions for clinicians to decide, guide, treat and confirm the appropriate therapy for cardiac and peripheral vascular disease”.
“The acquisition of CardioProlific will further strengthen our innovation pipeline of catheter-based therapy devices,” said Bert van Meurs, Business Leader Image Guided Therapy at Philips. “We are convinced that the development of CardioProlific’s differentiated thrombectomy technologies, combined with our suite of image-guided therapy solutions, will help our customers drive the procedure innovation for the treatment of peripheral vascular disease.”
Philips’ image-guided therapy portfolio comprises interventional imaging systems, planning and navigation software, interventional devices—including catheters for diagnosis and therapy—and a broad range of services, all aimed at helping clinicians to deliver more efficient and effective care to improve the lives of the patients they treat.
Merit Medical has announced that it has received 513(f)(2) (de novo) classification from the FDA to expand indication for its Embosphere microspheres. The indication now includes prostatic artery embolization for symptomatic benign prostatic hyperplasia.
“Merit’s Embosphere is the first embolic agent to receive FDA 513(f)(2) classification for prostatic artery embolization, providing a non-surgical treatment option for millions of men who suffer from benign prostatic hyperplasia,” said Fred P Lampropoulos, chairman and chief executive officer of Merit.
ATTRACT trial results a catalyst for advance in management of deep vein thrombosis
SIRT significantly better tolerated than sorafenib, but does not increase overall survival in hepatocellular carcinoma patients
Matthew Callstrom: IO updates
Andrew Holden: PAD trials
Profile: Bob Abraham
ATTRACT trial results a catalyst for advance in management of deep vein thrombosis
SIRT significantly better tolerated than sorafenib, but does not increase overall survival in hepatocellular carcinoma patients
Matthew Callstrom: IO updates
Andrew Holden: PAD trials
Profile: Bob Abraham
Canada’s recent recognition as a subspecialty at the national level has helped to raise awareness amongst other disciplines, healthcare policymakers and hospital administrators. “We will use this momentum to promote the value of interventional radiology to these same groups by providing evidence that our interventions reduce longer term hospital and societal costs through reduced hospital stay and patient morbidity while still improving outcomes,” Robert Joseph (Bob) Abraham, president of the Canadian Interventional Radiology Association (CIRA) 2015–17 tells Interventional News. Abraham is a professor in the Diagnostic Imaging and Interventional Radiology Department, Dalhousie University in Halifax, Canada.
When did you first decide on a career in medicine and why did you choose interventional radiology? I was always fascinated by how things work and I loved to tinker and build as a child. I would build go-karts, motorised air planes and the like. I also had a great passion for maths and problem-solving, and really enjoyed working with people. Through my mother, a medical doctor, I learned that medicine offered a career that brought all of my passions together. In medicine, you are dedicated to improving people’s lives by working on the most complex of all systems; the human body. One uses problem solving skills at multiple levels,, and of course there is constant interaction with people. I discovered interventional radiology in my senior year when I followed one of my patients to observe a pulmonary angiogram. I was absolutely fascinated by the skill of the operator and his ability to insert a catheter through a small nick in the skin at the groin and then thread it through the heart and deep into the lungs all the while watching the progress in real time on a monitor. This was video games on steroids with the additional fact that he was making a huge impact on the patient’s life and care. I was absolutely hooked! Even that early in the day, I could envision that the future for interventional radiology was enormous. I thought to myself: “What if we could someday use a catheter to actually remove the clot in the lungs?” It is amazing to see how that has come about, as interventional radiology now plays a major role in the treatment and removal of clots in various conditions including pulmonary embolus.
Who were your mentors and what wisdom did they impart to you? My mother instilled the importance of hard work, perseverance and dedication. She also taught me the value and importance of always listening to your patient and to treat each patient as if they were a family member. The individual who opened my eyes to the world of interventional radiology on the day I watched that pulmonary angiogram was Dave Gordon, who had trained under Ron Colapinto in Toronto. Dave and his partner, Alphonse Johnson, took me under their wing in residency in Dalhousie University, trained me in the fundamentals of catheterisation and showed me the great promise of the subspecialty. My mentor during my fellowship at the Royal Melbourne Hospital in Australia was professor Kenneth Thomson. Ken is a well-known pioneer in our field and is an SIR Gold Medallist and a CIRSE Distinguished Fellow. He showed me the importance of keeping cool under pressure, and how with proper planning and the innovative use of interventional radiology techniques and devices, one can maximise one’s ability to achieve a successful outcome during any procedure. I witnessed some miraculous results in very difficult circumstances because of his skill, innovation and perseverance, and I benefited greatly from his teaching and guidance.
Which innovations in interventional radiology have most influenced your career? We have seen numerous revolutions in our field with new procedures and indications using existing technology as well as incredible product innovations that have revolutionised and enhanced how we perform well-established procedures. It never ceases to amaze me how I can now routinely recanalise complete arterial occlusions extending from the upper thigh all the way down into the foot, and in fact, sometimes navigate through the foot and back up the other side to allow me to significantly improve blood flow to the lower leg. These procedures are saving limbs where amputation is often the only option. I could not imagine being able to do something like this ten years ago. The fact that we can now treat abdominal aortic aneurysms percutaneously using low profile stent grafts is also truly remarkable. The well-known internet video of a patient hopping off the table and waving as he walks off after one of these procedures will stay with me forever.
What is interventional radiology’s place in Canada’s healthcare system? The quality of interventional radiology in our country has always been top notch, and interventional oncology, general embolization, venous access, dialysis fistula intervention and non-vascular interventions predominate. There are also several centres including mine where we treat aortic and peripheral vascular disease.
Market research confirms Canadian interventional radiology has lagged significantly in comparison to all other G7 nations with regards to per capita interventions. That is, interventional radiology is profoundly underutilised in Canada and this relates to multiple barriers to adoption including a lack of awareness of the benefits of interventional radiology amongst other clinical specialities, hospital administrators and healthcare policy makers.
Interventional radiology has been chronically under-recognised and underfunded in our single-payer system where annual department-based hospital budgets hinder adoption of procedures which are considered “expensive” in the Canadian budgetary model due to the higher upfront costs of the technologies being used. As well, providing a minimally invasive outpatient interventional radiology-based alternative for a patient that would otherwise have required surgery does not reduce operating room costs as the operating room time and hospital bed are simply filled by another patient on the waiting list, and so overall utilisation and short-term costs are therefore higher. We need to change this line of thinking and provide health policymakers and administrators with the evidence that interventional radiology leads to improved patient outcomes, decreased morbidities and mortalities, more cost-efficient treatments, shorter hospitalisations, decreased waiting times and, ultimately, reduced costs in the long run. We need to show how valuable interventional radiology is to our healthcare system.
As the CIRA president for 2015–17, what were your goals for the organisation? During my tenure, I wanted to ensure that we have a long-term plan in place to address the challenges faced by Canadian interventional radiologists. To do this, the CIRA Board embarked on a strategic planning process that lays out key action items including promoting and advocating for interventional radiologists amongst other specialities, healthcare administrators, policymakers and the public; supporting our members in the transition to a longitudinal clinical care model; fostering collaborative research across the country; improving communication and interaction between our members; and promoting interventional radiology as a career choice for medical students and residents.
Our recent recognition as a subspecialty at the national level has helped to raise awareness amongst other disciplines, healthcare policymakers and hospital administrators. We will use this momentum to promote the value of interventional radiology to these same groups by providing evidence that our interventions reduce longer term hospital and societal costs through reduced hospital stay and patient morbidity while still improving outcomes.
We are embarking on new clinical-based fellowships across the country that will train our newest recruits under a longitudinal clinical model of care, but will also need to provide education and resources for established interventional radiologists in this regard. We need to encourage all interventional radiologists to take full responsibility for the patients they treat, establish direct referral paths, seek admitting privileges and become comfortable with the overall care of our patients. We have a long way to grow to match other G7 countries and as we grow, we will need to find ways to attract and encourage new physicians to choose interventional radiology as a career in order for there to be enough of us to match the future growth.
Which aspects of interventional radiology do you foresee a strong growth for in Canada? Interventional oncology will continue to grow in Canada, particularly if we remain proactive in building collaborative multidisciplinary teams to care for these patients. I also believe our involvement in the treatment of peripheral vascular disease and aortic diseases will continue to grow as we strive to work with our surgical colleagues and other healthcare workers in collaborative teams. It will take time to forge these relationships, but in the end the patients will benefit greatly from such an approach.
What interventional radiology research from Canada are you most proud of? Ron Colapinto was one of our pioneers and his early technical work with transjugular intrahepatic portosystemic shunt (TIPS) and peripheral intervention has led the way for others here in Canada. It is great to see that his keen interest in furthering our field through research and innovation has continued with the likes of David Liu, Lindsay Machan (both Vancouver) and Gilles Soulez (Montréal) amongst many others. These individuals are true luminaries and great mentors and what they have achieved is nothing short of astounding. The work in Canada has included development of drug coating technology, novel embolic agents, as well as high level clinical research in all areas of interventional radiology. More recently we have seen award-winning outcomes research on the use of drug-coated balloons for peripheral vascular disease coming out of Newfoundland. It is fantastic to see all corners of Canada making a real difference to positively impact our field and improve the care of our patients.
You have a particular interest in radioembolic particles. What are the important developments in the field? We are embarking on a new era in embolization where imageable embolic agents will provide us with information that has not been available before. This will allow us to learn so much more about these treatments thereby allowing us to improve on how these procedures are performed and, in turn, improve patient outcomes. I believe imageable embolic agents will help us to standardise, optimise and personalise embolization treatments, will result in a better understanding of embolization endpoints and allow for confirmation of adequate treatment of a target artery or tumour. With yttrium- 90 (Y-90) radioembolization, there is the potential to quantify the radiopacity of infused radiopaque radioembolic agents within the tumour with radiopacity mapping and then correlate this with radiation dose administered to tumour. Developing new products is not an easy task and I am lucky to be surrounded by a brilliant, highly skilled, dedicated team who all have the same passion for research and innovation as I do.
What are the current interesting research questions regarding radioembolic particles? There has been tremendous research in radioembolic therapy over the past 20 years, but there is still much to learn. Some of the questions I have relate to optimising the treatment as I would like to better understand optimum particle size range, activity at time of administration, distribution in tumour and the like. We also need a better understanding of the additional factors that come into play when dealing with different tumour types. I believe we need different strategies when treating hepatocellular carcinoma vs. treating metastatic neuroendocrine tumours or metastatic colorectal cancer. In addition, we need proper data to allow us to personalise these treatments, not only for different tumour types but also for differing tumour volumes, tumour location and tumour vascularity. I am particularly excited by the promise of radiation segmentectomy and lobectomy and the potential for these treatments to be first-line therapy one day. I believe imageable Y-90 radioembolic microspheres will help us in understanding a lot of the current unknowns and help us develop customised treatment strategies that will improve outcomes.
Interventional radiology has always had close ties to the device industry. What are the some of the benefits and pitfalls of this relationship? Collaboration between interventional radiologists and industry can result in great research and product innovation that ultimately benefits our patients. However, this collaboration must be respectful, professional and beyond reproach. This is best accomplished by ensuring that there is full and complete disclosure of any financial compensation and/or conflict of interest. It is not only reputation and credibility of the interventional radiologist or industry partner that is at risk here, but also the integrity of how we conduct our scientific investigations. Interventional radiologists need to exercise sound judgement throughout, and we and industry representatives need to keep the common goal of improving the care of patients, and maintaining their trust and confidence, at the forefront of any collaboration or interaction.
Please describe a memorable case. I could think of many, but the cases that really have demonstrated the power of interventional radiology have been with embolization. I have performed embolization for patients with severe bleeding who were literally within seconds of death and, similar to the story of raising Lazarus, these patients have been able to stand and walk on their own within a few hours of our embolizing the bleeding site. These incredible life-saving events have occurred after traumatic haemorrhage but, equally, some of the most profound results seen have been with post-partum haemorrhage. Not much can be better than seeing a mother cuddling with her newborn so soon after such a harrowing and potentially catastrophic event.
What are your interests outside of medicine? I do as much as I can with my family—my wife and best friend, Natalie, my daughter Zoe (19), my son Nikhil (15) and our rescue dog, Marlie. They are my biggest fans (even the dog!) and I cannot thank them enough for their huge support, particularly their patience. We all do our best to help improve the world by volunteering for and supporting numerous causes particularly related to human and animal welfare and social justice. We are also huge sports lovers. I played waterpolo for my university, but I would probably drown if I tried to play now. The sport I now love is golf as I find it a wonderful way to enjoy the outdoors while spending time with family and friends. It is a sport where I am constantly trying to improve. It is all about striving to be the best that you can be. I took up guitar later in life and absolutely love it. My family are adept at music with voice, guitar, drums and piano in our domain. In fact, we used to get together in a recording studio each year to make a music album together which was a lot of fun. I really look forward to doing that once again someday soon.
Argon Medical announced in June that it has formalised a Medical Advisory Board comprised of distinguished physicians from institutions across the USA who specialise in interventional medicine. The Medical Advisory Board will continue to provide scientific and clinical expertise to guide the organisation in planning and implementing product development initiatives and marketing programs with the goal of improving the lives of patients and their caregivers, a press release from the company states.
Argon welcomes seven members to the Medical Advisory Board: James F Benenati, Miami Cardiac and Vascular Institute, Miami; Jim Caridi, Tulane University Medical Center, New Orleans; Matthew S Johnson, Indiana University Health, Indianapolis; John A Kaufman, Oregon Health and Science University, Portland; John Moriarty, UCLA Medical Center, Santa Monica; Robert K Ryu, University of Colorado Hospital, Aurora; and David W Trost, Weill Medical College of Cornell University, New York.
“We are very pleased to introduce the founding members of Argon’s Medical Advisory Board. Their knowledge and expertise in interventional procedures provide a unique and unparalleled perspective, which helps us drive innovation to meet customer needs,” said George Leondis, president and CEO of Argon.
In February, Philips announced the global launch of Azurion, its next generation image-guided therapy platform, which forms the new core of its integrated solutions portfolio. Atul Gupta, chief medical officer for Philips’ Image Guided Therapy business has spent more than 15 years as a practicing interventional radiologist. He guides Interventional News through the key features of the new platform.
The Azurion image-guided therapy platform is the result of a multi-year development programme conducted in close collaboration with leading clinicians in the field. It features a state-ofthe-art ergonomic design with an easy-to-use intuitive user interface, enabling clinicians to swiftly and confidently perform a wide range of routine and complex procedures in the interventional lab, a media release from Philips says. With the rapid growth of image-guided therapy procedures, hospitals and health systems are increasingly faced with the need to control costs, while improving their standards of care. Azurion has been designed to address these challenges and is equipped with new workflow options and performance dashboards, as well as an upcoming range of productivity improvement services.
New components, high image quality at ultra-low X-ray dose and real-time image processing on multiple work spots within the interventional lab. From the standpoint of an interventional radiologist, what are the key benefits that Azurion will offer?
Most importantly, it is vital to have superior performance—that is the bottom line. By superior performance, I mean that Azurion offers superb image quality alongside ultra-low dose radiation—that is the heart of the system and it has over 1,000 new components built in to achieve this. If you think about the procedures that we are doing today, they are completely different from those we did 10 or 15 years ago. A decade or so ago, I basically had X-rays to see the device and the patient and that was it. Now, my procedures are far more complex and diverse, so I need to integrate a whole host of 2D and 3D imagery and data together to navigate the procedure.
Atul Gupta
Azurion allows us to connect all of these different information sources into the system. Personally, just like a pilot in a cockpit, I want to have total access to all the information I need at my fingertips. And not just to view it, but also to interact with it. Azurion lets me interact and control things like electronic health records, PACS, ultrasound, haemodynamic monitors, 3D workstations, and so on, all from my table side. So there is the superior performance, there is the interaction and connectivity of the multiple devices, and then, there is the efficiency. One of the ways that Azurion can increase efficiency by its touchscreen capabilities. This is a very intuitive and elegant interface with simple gestures that you and I are already familiar with from our smartphones and tablets, such as zooming in or pinching to collimate the image. The world of intervention has become so complex that systems need to blend into the background. You could have the best tools in the world, but if they are overly complicated, nobody will end up using them. Ultimately we know that these tools improve outcomes, reduce radiation, reduce procedure time, so we want people to use these tools. The only way to get them to use the tools is to make a simple elegant user interface. We just want to be physicians; we are not computer programmers, so these systems really need to feel like extensions of our hands and our minds. We do not want to have to think about how to programme the system, we just want to keep our minds and our eyes on the patient.
All interventionists are now expected to do “more with less”. How will Azurion help achieve this?
Today, we are expected to do many more cases than we were doing 10 years ago. Patients are getting sicker and minimally invasive treatments are markedly expanding. Azurion allows me to do more cases, potentially, per day and also more diverse types of cases. This is especially true if you are sharing the lab with cardiology colleagues or vascular surgery colleagues. In such a scenario, suites need to be capable of doing everything from structural heart disease repairs to aneurysm repairs to interventional oncology procedures.
Today, to get more cases a day completed means that I have less time per case. And I also want to do more cases with less radiation exposure. To be entirely truthful, I also have fewer staff. With hospitals crunching costs, sometimes I may have only one tech – nologist available to me on call, and I need that one technologist to be able to do everything. So how does Azurion solve all of these things? Well, by increasing efficiency in the lab, Azurion allows me to do procedures in less time. We actually did some usability testing with over 60 users. These were not just physicians but also technologists throughout North America and Europe. Over 90% felt that Azurion would allow them to become more efficient in the lab.
So if I can shave of five or 10 minutes a case over the course of a busy day, this could add up to maybe an extra case per day. At the same time, I can also use dose reduction tech – nology and new positioning features built into the system to significantly reduce radiation dose for patients and staff. Azurion allows the technologist to control every aspect of this system from the table side via touchscreen. I think all interventionists have been in the situation where they have technologists who have to take off their gloves to go into a control room, or somewhere else, to operate a piece of equipment before coming back and scrubbing in again, and this process goes on, back and forth, during an acute intervention, simply because you are short on staff. That is now gone because you can now control Azurion and these connected devices, all while scrubbed and directly from the tableside. I think these are just a few ways that Azurion addresses doing more with less.
Who were the thought leaders in interventional radiology who collaborated and contributed to Azurion’s development?
A few of our interventional radiology collaborators for Azurion have been Barry T Katzen, founder and chief medical executive of the Miami Cardiac and Vascular Institute, Baptist Health South Florida (Miami, USA; See Katzen’s article on critical limb ischaemia treatments on page 35); Marco van Strijen, St Antonius Hospital (Nieuwegein, the Netherlands); Ralf-Thorsten Hoffmann chief of Interventional Radiology, Dresden University Hospital (Dresden, Germany); and Otto Elgersma, Albert Schweitzer Hospital (Dordrecht, the Netherlands). Cardiologists, surgeons, technologists and administrators also collaborated with us from 20 sites around the globe.
Azurion is the result of a long development programme and collaboration with leading clinicians in the field. You cannot create these technologies in a vacuum and then put them out there and expect them to be used. We firmly believe that collaboration leads to the best innovation.
A session at the World Conference on Interventional Oncology (WCIO; 8–11 June, Boston, USA), organised by the Society of Interventional Oncology (SIO), identified the most influential publications of 2016–17. The session was moderated by Muneeb Ahmed (Beth Israel Deaconess Medical Center, Boston, USA) and David C Madoff (Weill Cornell Medical Center, New York, USA).
The PREMIERE trial (chemoembolization vs. radioembolization for primary liver cancer); PANFIRE study (feasibility of irreversible electroporation to treat pancreatic neoplasms); and a study of ablation in combination with Tremelimumab for advanced hepatocellular carcinoma were among the top picks from research published in the last year.
PREMIERE trial
Commencing, Riad Salem (Northwestern University, Chicago, USA) reported on the findings from the study PREMIERE (Prospective randomised study of chemoembolization vs. radioembolization for the treatment of hepatocellular carcinoma) trial. The study was published in December 2016 in Gastroenterology. The randomised, phase II study set out to compare the effects of conventional transarterial chemoembolization (cTACE) and Y-90 radioembolization in patients with hepatocellular carcinoma.
“In this study of patients classified as Barcelona clinic liver cancer (BCLC) stages A or B, we found Y-90 radioembolization provided significantly longer time to progression than cTACE. Y-90 radioembolization provides better tumour control and could reduce drop-out from transplant waitlists,” Salem said.
He told WCIO delegates: “Level one evidence shows that Y-90 treatment outperforms cTACE with regard to time to progression. This is a timely finding given the new mandatory six-month wait time prior to transplantation. Y-90 should be considered in the bridge-to-transplantation patient population using the segmentectomy technique. The findings of this study confirm our rationale for Y-90 as our institutional standard of care.”
Immune checkpoint inhibitors and ablation
Then, Tim Greten (National Cancer Institute, Bethesda, USA) spoke on the paper “Tremelimumab, an immune checkpoint inhibitor in combination with ablation in patients with advanced hepatocellular carcinoma” that was published in the Journal of Hepatology in March 2017.
The researchers set out to ascertain whether Tremelimumab could be combined safely and feasibly with ablation. As reported in the journal, Tremelimumab is a fully human monoclonal antibody that binds to cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) on the surface of activated T lymphocytes. Findings from the study led the authors to conclude that Tremelimumab in combination with tumour ablation is a potential new treatment for patients with advanced hepatocellular carcinoma, and leads to the accumulation of intratumoural CD8+ T cells.
Greten said: “The combination of tumour ablation and anti-CTLA-4 therapy is feasible and the treatment is safe. Immune correlates suggest an activation of tumour virus-specific immune responses. Anti-CTLA-4 therapy leads to infiltration of CD8+ T cells in the tumour of the responding patients.”
PANFIRE study
Next under the lens was a study that used ablation to treat pancreatic cancer, with Martijn R Meijerink (VU University Medical Center, Amsterdam, The Netherlands) presenting on a phase I/II study that treated patients with percutaneous irreversible electroporation. Published in Radiology in February 2017, this study investigated the safety of irreversible electroporation in the treatment of locally advanced pancreatic cancer. It also set out to evaluate the quality of life, pain perception, and efficacy in terms of time to local progression, event-free survival, and overall survival.
The investigators concluded that percutaneous irreversible electroporation for locally advanced pancreatic cancer is generally well tolerated, “although major adverse events can occur”. “Preliminary survival data are encouraging and support the set-up of larger phase II and III clinical trials to assess the efficacy of irreversible electroporation plus chemotherapy in the neoadjuvant and adjuvant or second-line setting compared with more widely adopted regimens such as chemotherapy and/or radiation therapy,” they write.
“There is promising survival, especially if neo-adjuvant folforinox can evoke a specific immune response,” said Meijerink. He also alluded to the fact that percutaneous irreversible electroporation is a difficult procedure with a long learning curve. “Further, there is no uniform protocol and there are no comparative studies as yet,” he added.
Local and systemic effects of irreversible electroporation vs. radiofrequency ablation
In the final presentation, Muneeb Ahmed reported on the periablational and systemic effects of two mechanistically different types of ablation: thermal radiofrequency ablation and electroporative ablation with irreversible electroporation in appropriately selected animal models. The study was published in August 2016 in Radiology.
Introducing the topic, Ahmed said: “Thermal ablation (radiofrequency and microwave) is used to treat solid tumours in the liver, lung, kidney and other organs. Complete ablation requires treating a rim of normal parenchyma in all cases, ie. an ablative margin. Recent experimental and clinical evidence suggests that thermal ablation may also [elicit] distant tumour growth. Potential secondary systemic effects from ablation are not completely understood.”
The study set out to compare radiofrequency ablation and irreversible electroporation on periablational changes after ablation; cytokine and growth factor production; and distant tumour growth in two animal models.
The results of the study found there were differences in tissue injury patterns between the two ablative modalities, with vascular patency persisting within the electroporation zone. The post-ablation inflammatory cell response was also different with more robust wound healing seen with irreversible electroporation. The latter modality also resulted in higher systemic release of IL-6. Compared to radiofrequency ablation, hepatic irreversible electroporation stimulated growth of tumours in one specific animal model and also led to growth reduction in distant tumours in another.
Ahmed and colleagues noted that persistent patency of vasculature within the coagulated zone from irreversible electroporation increases the area and accumulation of infiltrative cells that is associated with a higher serum IL-6 level than radiofrequency ablation. These local changes of irreversible electroporation induce stronger systemic effects, including both tumorigenic and immunogenic effects.
BTG has highlighted the results of the ACCESS PTS trial, presented at the Society for Vascular Medicine 28th annual scientific sessions (14–17 June, New Orleans USA). The study found chronic deep vein thrombosis patients with post-thrombotic syndrome can be treated safely and effectively with Ekos therapy.
The ACCESS PTS study is a multicentre prospective single-arm study of 73 patients with iliofemoral deep vein thrombosis, meeting eligibility criteria including a Villalta Score of eight or greater, and who had failed three months of conservative therapy. Patients were treated with anticoagulation drugs followed by Ekos therapy with balloon dilatation.
The study met its primary efficacy endpoint and showed a significant improvement of Villalta Scores of 34% at 30 days across 77 limbs treated among the 73 patients with a p-value of <0.0001. On average, patients treated in the study experienced a symptom reduction from severe down to borderline mild. The study also showed a 21% improvement in patients’ quality of life. There was one bleeding incident and one pulmonary embolism, meeting the study’s safety endpoint.
The ACCESS PTS protocol using Ekos therapy is now the only treatment regimen proven to significantly reduce the signs and symptoms of post-thombotic syndrome and show a significant improvement in quality of life, a press release from BTG says.
“ACCESS PTS demonstrates that Ekos therapy with balloon dilatation is effective and safe in reducing the signs and symptoms of post-thrombotic syndrome for patients suffering from chronic deep vein thrombosis, while improving their quality of life,” said lead investigator Mark Garcia of Vascular & Interventional Associates of Delaware in Wilmington, USA. “Ekos therapy is a useful and important option for physicians treating debilitating chronic deep vein thrombosis and post-thrombotic syndrome.”
TVA Medical has announced the online publication of positive results from the Novel Endovascular Access Trial (NEAT) evaluating its everlinQ endoAVF system. The 12-month data published online in the American Journal of Kidney Diseases (AJKD) demonstrate the potential benefit of the novel approach to create haemodialysis access as an alternative to traditional open surgery.
The everlinq endoAVF system is designed to create an arteriovenous fistula (AVF) for haemodialysis access in an endovascular procedure using catheter-delivered radiofrequency energy.
The article explains that 80 patients were enrolled (20 roll-in and 60 participants in the full analysis set; the latter are reported). Endovenous AVFs were created in 98% of participants; 8% had a serious procedure-related adverse event (2% of which were device-related). Eighty-seven per cent were physiologically suitable for dialysis (eg. mean brachial artery flow, 918 mL/min; endovenous AVF vein diameter 5.2mm [cephalic vein]). Endovenous AVF functional usability was 64% in participants who received dialysis. Twelve-month primary and cumulative patencies were 69% and 84%, respectively.
“The NEAT results show that the everlinQ endovascular approach can produce fistulae for haemodialysis, with an acceptable safety profile,” said NEAT principal investigator Charmaine E Lok, medical director of the haemodialysis programme at the University Health Network-Toronto General Hospital and senior scientist at the Toronto General Hospital Research Institute in Toronto, Canada. “This unique approach offers clinicians and chronic kidney disease patients another option for fistula creation that is minimally invasive.”
The NEAT study is a single-arm, prospective, multicentre study conducted at nine sites in Canada, Australia and New Zealand. The study measured safety, efficacy (defined as endovenous AVF physiologically suitable for dialysis within three months), functional usability of the endovenous AVF to provide dialysis with two-needle cannulation, and primary and secondary patencies.
Each year approximately three million people worldwide with ESRD are treated with haemodialysis. However, the first step, creating a viable access in the arm, is often a clinical challenge.
In addition, an article published this spring in The Journal of Vascular Access showed that patients who received an endovenous AVF in the NEAT study required fewer post-endovenous AVF interventions, with a potential first-year medical cost savings per patient of US$11,240, compared to patients who received a surgical AVF. The propensity score-matched comparison to surgical AVF was calculated using a 5% random sample from Medicare Standard Analytical Files.
The Montpellier University Hospital (Montpellier, France) has inaugurated an avant-garde interventional radiology intervention room in the Department of Interventional Radiology at the St-Eloi Hospital.
The Infinix-i 4D CT room from Toshiba Medical (acquired by Canon in late 2016) is the first in Europe to combine a new generation angiography room, a 640 slice 4D CT scanner moving on a sophisticated rail concept and a widescreen display. This room is the 11th in the world (Seven in Japan, two in Korea, one in the USA) integrating such advanced technology.
“We are extremely pleased with the new Infinix-i 4D CT system. It is a very flexible and user-friendly system with many intelligent tools for dose optimisation”, said Boris Guiu, head of the Department at St-Eloi Hospital. “With this new room we can carry out complex procedures of hepatic interventional radiology, which require all the existing guidance means, such as liver thermoablations. Each year we approximately take care of 1,000 patients in this room in the best conditions of care, safety and comfort.”
“We are very proud to support the oldest faculty of medicine in Europe with our newest interventional clinical concept”, said René Degros, Business Unit manager X-Ray at Toshiba Medical. “The groundbreaking new Infinix-i 4D CT supports our customers in bridging the gap between the interventional lab and CT with one seamlessly integrated solution for the ultimate in patient care. Infinix-i 4D CT eliminates the need to transfer patients back and forth between different rooms, while minimising dose and maintaining patient safety. In this way the system can help save valuable time and gain efficiencies with the ability to plan, treat, and verify in the same room, on a single system.”
Similar concepts have also been chosen by two other centres in France and will be installed soon, making CHU Montpellier the leader in this field, a press release from the company adds.
The treatment can help restore fertility in women with uterine fibroids, according to a new study published online in the journal Radiology.
Uterine fibroids are considered one of the most common causes of infertility and complications related to pregnancy. Previous research has found that one out of every four women with fibroids has problems related to fertility. The standard treatment option for such women is myomectomy, or surgical removal of the fibroids.
However, myomectomy is not always possible or effective and can result in major complications including hysterectomy, according to study co-author João Martins Pisco, Department of Interventional Radiology, Saint Louis Hospital in Lisbon, Portugal.
Despite its less invasive nature, uterine fibroid embolization has yet to be fully embraced in the medical community as a fertility-preserving treatment for women with symptomatic fibroids due to concerns that the procedure may cause inadequate blood flow to the endometrium.
For the new study, Pisco and colleagues assessed pregnancy rates in 359 women with uterine fibroids who were unable to conceive and who underwent either conventional or partial fibroid embolization. In conventional embolization, all uterine artery branches are embolized. However, the partial procedure requires treatment of only the small vessels to the fibroids, leaving the corresponding larger vessels unaffected. Partial embolization may help reduce the risks of infertility associated with the conventional procedure.
After an average follow-up of almost six years, 149 of the 359 women, or 41.5%, had become pregnant one or more times, and 131 gave birth to a total of 150 babies. It was the first pregnancy for more than 85% of the women who gave birth.
The procedures had a clinical success rate of approximately 79% for fibroid-related symptoms. Complication rates were 14.6% for partial uterine fibroid embolization and 23.1% for conventional fibroid embolization. The procedure was repeated in 28 patients whose fibroids had not been fully treated, as shown by MRI, and 11 of those patients subsequently got pregnant.
“Our findings show that uterine fibroid embolization is a fertility-restoring procedure in women with uterine fibroids who wish to conceive, and pregnancy following uterine fibroid embolization appears to be safe with low morbidity,” Pisco said. “Women who had been unable to conceive had normal pregnancies after uterine fibroid embolization and similar complication rates as the general population in spite of being in a high-risk group.”
Pisco suggested that embolization may become the first-line treatment for women with fibroids who wish to conceive, particularly for those with numerous or very large fibroids. Such patients have a fibroid recurrence rate of more than 60% after myomectomy, making embolization an important option.
The researchers are continuing the treatments and compiling data. Since the time of writing, there were 12 additional pregnancies.
“In our study there are now almost 200 newborns following uterine fibroid embolization,” Pisco said. “Our next step will be a randomised study comparing the results of partial and conventional uterine fibroid embolization.”
The Society of Interventional Oncology (SIO and BTG have announced their 2017 Interventional interventional oncology /immuno-oncology research grant recipients.
The interventional oncology /immuno-oncology research programme was established earlier this year to fund initiatives that evaluate how interventional oncology therapies stimulate the immune system; combine locoregional and immunotherapy approaches to improve clinical outcome; and improve the understanding of the underlying mechanisms that cause different therapies to influence adaptive and innate immunity, as well as underlying inflammation and tumorigenesis.
The investigators and project proposals that have been awarded grants are:
Rafael Duran, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, to investigate the immunobiology of hepatocellular carcinoma in patients undergoing Y-90 radioembolization.
Joseph P Erinjeri, Memorial Sloan Kettering Cancer Center, New York, USA, for T-Cell clonality and cancer neoantigen presentation following interventional oncology (IO) therapies: which IO techniques optimally stimulate the immune system?
Florian J Fintelmann, Massachusetts General Hospital, Boston, USA, for a pilot study of cryoablation combined with immune checkpoint inhibitor therapy in patients with PD-1 refractory metastatic melanoma: prospective clinical research and correlative laboratory studies.
Stephen Hunt, University of Pennsylvania, Philadelphia, USA for TAEVax: immunobiologic treatment effects of embolization in a rat hepatocellular carcinoma model.
“We are very pleased that through the generosity of BTG, SIO has been able to fund the most meritorious, cutting-edge research that combines the strengths of interventional oncology and immuno-oncology—two disciplines that hold great promise for improving cancer therapy. The large number of high quality submissions to this grant call attests to the intense interest of interventional oncologists worldwide to continue to advance our field through robust scientific inquiry and clinical study,” stated S Nahum Goldberg, SIO Interventional/Immuno-oncology Working Group chair, and vice-chair for Research and head of the Interventional Oncology Unit, Hadassah Hebrew University Medical Center in Jerusalem, Israel.
Grant recipients were chosen by the SIO Interventional Oncology Immuno-Oncology Working Group, which includes both interventional radiologists and immuno-oncologists. The group plans to publish a white paper later this year to guide further research and clinical practice.
Medtronic has announced recent reimbursement approvals in both France and Belgium.
A Ministerial decree was published in the Official Journal of French Republic to enlist Medtronic’s IN.PACT Admiral drug-coated balloon (DCB) for add-on reimbursement in the treatment of peripheral artery disease in the upper leg. The National Commission for the Evaluation of Medical Devices and Health Technologies (CNEDiMTS) issued a positive opinion and recommended the IN.PACT Admiral drug-coated balloon (DCB) for reimbursement.
This approval makes IN.PACT Admiral the first peripheral DCB approved for reimbursement (as of 7 June 2017) in France for the treatment of peripheral artery disease. This reimbursement approval in France became effective on 19 May.
The IN.PACT Admiral DCB is now not only the first peripheral DCB to receive reimbursement approval in France, but one of the first invasive non-implantable device to obtain this new add-on reimbursement in France under the newly created LPPR Title V legislation.
Medtronic also received reimbursement approval for IN.PACT Admiral in Belgium, effective as of 1 April, 2017. IN.PACT Admiral is the first DCB to be approved for reimbursement in Belgium, based on a body of robust scientific evidence demonstrating significantly superior clinical outcomes and cost effectiveness vs alternatives.
The Belgian Ministry of health specifies that only DCBs which have demonstrated statistically significant reduction in the rate of revascularisation will be eligible for reimbursement in Belgium.
“The reimbursement approvals for the IN.PACT Admiral DCB in France and Belgium mark significant milestones for Medtronic, further confirming the superiority of IN.PACT DCB in the treatment of peripheral arterial disease,” said Mark Pacyna, vice president and general manager of the Peripheral business in the Medtronic Cardiac & Vascular Group. “This decision will ultimately help to improve patient access to the IN.PACT Admiral, which is the only DCB that has demonstrated consistent and durable outcomes out to three years.”
Beyond embolization endpoints under fluoroscopic guidance, the introduction and standardisation of cone-beam CT imaging in the procedure room has allowed Lipiodol (Guerbet) to become a true imaging biomarker for therapeutic efficacy, write Julius Chapiro and Jean-Francois (Jeff) Geschwind.
Hepatocellular carcinoma is the second most common cause of cancer-related deaths worldwide and its incidence is continuing to grow at an alarming rate in Europe and the USA. The clinical management of patients with this disease has greatly evolved over the course of the last three decades. The progress in the field has been mainly driven by innovation in image guidance technology and drug delivery platforms, resulting in substantially improved clinical outcomes. These developments have allowed interventional oncologists to become the primary liaison for patients seeking therapy.
Most newly diagnosed patients cannot be treated by curative surgical therapy; oncologists also acknowledge that no systemic therapy has been shown to improve patient survival, with the notable exception of sorafenib that has conclusively been shown to improve survival in patients with advanced stage disease. In parallel, locoregional tumour therapies such as radiofrequency ablation and conventional transarterial chemoembolization (cTACE), have grown beyond their initial role as niche applications and have been fully incorporated into interdisciplinary guidelines and recommendations across the globe.
The data collected in the GIDEON (Global investigation of therapeutic decisions in hepatocellular carcinoma and of its treatment with sorafenib) registry, the largest observational registry completed in the field, suggest that nearly 50% of all patients with hepatocellular carcinoma undergo transarterial chemoembolization (cTACE) at some point after diagnosis. More importantly, the GIDEON registry reinvigorated the data from two older randomised controlled trials and once again established substantial survival benefits of cTACE over best supportive care. cTACE, a widely used longstanding technique among image-guided cancer therapies, takes advantage of the fact that hepatocellular carcinoma lesions draw their blood supply almost exclusively from the hepatic artery, whereas the remainder of the liver is supplied by the portal vein.
The most widely applied cTACE protocols involve selective intra-arterial infusion of a chemotherapeutic drug cocktail suspended in Lipiodol, an iodinated poppy seed oil–based medium, thereby creating an emulsion that sticks to the cancer cells. This step is followed by embolization of tumour feeding vessels with calibrated particles or gelatin sponge in order to protect the emulsion and prevent its separation, thereby keeping the chemotherapy within the tumour and maximising exposure time. Lipiodol has been widely considered as a unique agent which seems to be preferentially retained by the tumour tissue. While this agent has US FDA approval for imaging, it is not indicated for hepatocellular carcinoma treatment. However, in Europe and other parts of the world, Lipiodol is indicated both for the imaging and treatment of hepatocellular carcinoma. This oily medium works as an effective drug carrier, and tumour-seeking embolic agent, all at once. Most importantly, it is iodinated and can thus be easily visualised using any X-ray based imaging modality such as fluoroscopy or CT. This particular characteristic has become the key advantage with respect to identifying intra-procedural embolization endpoints.
Beyond embolization endpoints under fluoroscopic guidance, the introduction and standardisation of cone-beam CT imaging in the procedure room has allowed for Lipiodol to become a true imaging biomarker for therapeutic efficacy. As such, cross-sectional cone beam CT imaging provides immediate quantitative information on tumour coverage with Lipiodol oil, which can then be used as a key instrument to identify undertreated compartments of the target lesion with the catheter still in place. Such measurements have also been shown to closely correlate with tumour response, as measured on follow-up imaging, which usually occurs after one to two months after cTACE. This relationship establishes Lipiodol as an early indicator of therapeutic efficacy and allows for potential non-responders to be identified directly in the procedure room.
The conspicuity of ethidised oil also allows for an effective detection of non-target deposits, both within the liver and beyond, thus potentially gauging the extent of undesired toxicity. At the same time, Lipiodol causes no signal alteration on MR imaging and causes no interference with contrast-enhanced T1 sequences that are commonly used to assess tumour response. Despite all those benefits, Lipiodol has faced some challenges over the last decade and some practices have favoured the more recently introduced drug-eluting beads as the drug delivery vehicle of choice. However, TACE using drug-eluting beads (DEB-TACE) has yet to fulfill the promise of improved efficacy and its use has not translated into survival benefits for patients. Drug-eluting beads also lack the aforementioned imaging biomarker features of Lipiodol. It will thus be up to the interventional oncology community to resurrect and prospectively validate Lipiodol in the role it has played for almost 30 years ie, as a theranostic agent for the therapy of hepatocellular carcinoma.
Julius Chapiro is an associate researcher with the Department of Radiology and Biomedical Imaging, Yale School of Medicine, New Haven, USA. He has reported no disclosures pertaining to this article.
Jeff Geschwind is chairman, Department of Radiology and Biomedical Imaging and professor of Radiology and Oncology, Yale School of Medicine. Geschwind recieves grants from Philips, BTG, Boston Scientific, Guerbet and the National Institutes of Health. He is a consultant to Boston Scientific, BTG, Philips, Merck, Bristol-Myers Squibb, Guerbet, Terumo and Bayer.
Francisco Carnevale and his father, Jose Angelo Carnevale
This is the story of bonding over a prostate artery embolization. Many times, as physicians we share a closeness with our patients, and form a relationship with them that is based on caring for them at what is often a vulnerable time in their lives. This is a very different story: it is the story of performing a new medical procedure that I believe in, on a man that I am very close to—my father, writes Francisco Carnevale, São Paulo, Brazil.
Looking at it through the prism of clinicians, we have here a patient; a 78-year-old man with severe lower urinary tract symptoms (LUTS) due to an enlarged prostate. This patient is also my father. Benign prostate hyperplasia was affecting my father, Jose Angelo Carnevale. For nearly two decades, he had been taking medication to alleviate his symptoms. While he experienced some periods of improvement, overall, he had a poor quality of life. During his annual visits to the urologist, he had been told that, some day in the future, he would have to undergo a surgical procedure to alleviate his lower urinary tract symptoms. In the early years, transurethral resection of the prostate (TURP) was the only option. Then, newer technologies came along and it was suggested that he could have a laser procedure. However, due to the size of the hyperplasia, a prostatectomy was also mentioned as a treatment option. Faced with that difficult choice, he called me to discuss his final decision: “I will not have a surgery and do not want to be admitted into a hospital. Hospitals are your domain, my son. I have never been admitted to a hospital and I am not about to change that.”
Looking back, I realised that that was a true and accurate statement. By the grace of God, my father had never had to be hospitalised due to any serious disease or injury. Being a workaholic, he even used to squirm at the idea of a vacation. Put simply, my father loves to work, especially since my mother passed away.
Time went by and my father stuck to his decision. But it was not easy. There were some embarrassing episodes: urinary incontinence in a shopping mall; several other times that he needed to urgently get to a toilet while pushing on the brakes of his car. Then, he was removed from an airplane due to lower abdominal pain, and of course, there were the years and years of nocturia. One day, my father called me very early one morning and said (in his trademark soft Italian tones): “I give up. I woke up five times to urinate last night. It is just too much. I am now too tired to work. I cannot even drink a glass of wine or beer, or even water, in the evening… Either you treat me, or I will get my prostate removed.” The message was clear and his tone was final.
Francisco C Carnevale
So, after talking to his urologist, we decided to evaluate and check if he was a good candidate for prostate artery embolization. His results showed lower urinary tract symptoms with International Prostate Symptom Score (IPSS) of 27; normal blood tests, prostate-specific antigen of 5.2ng/mL. Imaging with ultrasound revealed a 95cm3 prostate bladder thickness and post void residual volume of 20mL. MRI showed an enlarged prostate (99.5cm3) with several benign hyperplasia nodules with an enlarged central gland; prominent median lobe; bladder thickness without diverticulum; and no signs of cancer. Urodynamic testing confirmed bladder outlet obstruction with Schafer VI score. So, yes, my father was a good candidate for a prostate artery embolization procedure. Now, we were faced with a decision: who was going to treat him? When presented with his options, his answer was: “My son, of course!” That was the moment I knew that all my studies had paid off, because a father’s recognition is priceless.
That is how on a Thursday morning in August 2014, my father got his prostate artery embolization at Hospital das Clinicas of the University of São Paulo Medical School, under local anaesthesia, using the Foley technique balloon, cone-beam CT. He had the PErFecTED technique (Proximal Embolization First, Then, Embolize Distal) bilaterally with Embospheres (Merit) microspheres. A closure device was used and two hours after the procedure, he was discharged. As per usual, he got medications for post-prostate artery embolization syndrome (dysuria, urethral burning, frequency and urgency). Three days later, during the “Fathers’ Day holiday” he drove his own car to our country house to enjoy a delicious Brazilian barbecue. It was recommended that he wear diapers in case of urinary urgency while driving. When he arrived at our country house, he was presented with an unusual gift from his grandchildren: a pack of diapers! But he has never needed them, because all his symptoms improved a lot and at the two-year follow-up evaluation, he had an IPSS of 2, without urinary residual volume, and a prostate size of 57cm3, which is a 43% prostate reduction by MRI.
But, what about the quality of life index? Well, here is another story. It was about 8pm one night when my cellphone rang and I saw that it was my father. I then heard the unmistakeable sound of beer being poured into a glass. “Now, I can drink without the need to wake up to pee in the middle of the night.” So his quality of life had distinctly improved as well.
Three years on, my father is 81 years old. He is still driving, drinking, and enjoying life with his friends and family. I figured that for all the things that he has done for me, this is the least I could have done for him. So, thank you, dad.
Francisco Carnevale is associate professor of Medicine, University of São Paulo, São Paulo, Brazil, and director, Interventional Radiology Fellowship Programme. He designed the PErFecTED technique and reports no disclosures pertaining to this article.
Avinger has announced positive two-year clinical data from the pivotal VISION study of the company’s Lumivascular technology. Twenty-four-month follow-up results from 89 patients were presented by Patrick Muck, chief of Vascular Surgery at Good Samaritan Hospital in Cincinnati, USA, at New Cardiovascular Horizons (NCVH) in New Orleans, USA. This includes an additional 34 patients beyond the interim data set presented on January 25, 2017.
Data presented remain subject to adjustment based on final statistical analysis and review by the study’s clinical events committee.
The VISION study was designed to evaluate the safety and effectiveness of Avinger’s Pantheris system to perform directional atherectomy while allowing physicians to use real-time intravascular imaging to aid in the removal of plaque from diseased lower extremity arteries. Data from the study, which demonstrated successful achievement of all primary and secondary safety and effectiveness endpoints, was used to support US Food and Drug Administration (FDA) 510(k) clearance of the system in 2016.
Key highlights of the presentation include:
– Kaplan Meier survival probability measured 82% freedom from target lesion revascularisation (TLR) at 12 months by patient (84% by lesion) and 74% freedom from TLR at 24 months by patient (76% by lesion)
– The VISION 24-month Kaplan Meier freedom from target lesion vascularisation at 24 months remained stable between 18 and 24 months
– Statistically significant improvements in ankle brachial index (ABI) and Rutherford classification at 30 days were maintained through 24 months
– A majority of lesions were treated using standalone optical coherence tomography (OCT) guided atherectomy with the Pantheris catheter, with only 9.6% (n=19/198) receiving adjunctive drug coated balloon (DCB) therapy and only 5% (n=10/198) receiving adjunctive stent therapy
“The complete VISION 24-month data demonstrates positive longer-term sustained results for patients treated with Pantheris, and importantly, these patients have largely avoided the need for a repeat procedure in a two-year timeframe,” comments Muck. “Considering that the outcomes were generated at the hands of brand new users with a first-generation clinical trial device, such positive results represent an important step forward for Pantheris in the clinical setting.”
Philips has announced the relaunch of the Pioneer Plus catheter, described as the only re-entry device with intravascular ultrasound (IVUS) capabilities and needle deployment designed to assist arterial vessel intervention.
IVUS captures images of vessels in the peripheral vascular system from inside the artery, allowing physicians to identify a targeted area and place a catheter in a specific location and to help guide the treatment partially or fully blocked arteries.
The Pioneer Plus IVUS-guided catheter helps physicians decide, guide, treat, and confirm true lumen re-entry with speed and precision, a press release from the company says. The device has received US FDA clearance and CE mark approval. It is not indicated for use in the coronary or cerebral vasculature.
The Pioneer Plus catheter is intended to facilitate placement and positioning of catheters within the peripheral vasculature. Commonly used to help treat chronic total occlusions, which are caused by heavy build-up of plaque within an artery that can cause blockages, Pioneer Plus enables a physician to cross the occlusion beyond the stenotic lesion prior to additional interventional treatment of the lesion using interventional techniques. With a successful interventional procedure, patients may avoid having surgery, which is a considerable improvement in patient care and outcomes as chronic total occlusions patients are often at risk for amputation.
The Pioneer Plus catheter also provides a cross-sectional ultrasound image of the arterial area of interest to facilitate placement of guidewires beyond stenotic lesions (eg, subtotal, total or chronic total occlusions) prior to additional interventions. According to a study published by the Journal of Invasive Cardiology, the Pioneer Plus catheter demonstrated a 95% to 100% procedural success rate in procedures affecting the arterial wall, specifically subintimal angioplasty. The study found a rate of 26% of failed re-entry for cases of chronic total occlusion that did not use the Pioneer Plus catheter.
“Pioneer Plus is the only re-entry device that has intravascular ultrasound capabilities. The ultrasound on the tip of the catheter allows physicians to see inside the arterial walls to give them the information they need to properly assess the area of interest,” said Christopher Barys, business leader at Philips Volcano. “We are happy Pioneer Plus is back in our IVUS suite of products, which aim to deliver improved patient and economic outcomes.”
Philips initiated a design modification to the Pioneer Plus catheter in 2015, and proactively removed the device from the market until the modification was complete. The design modification has had no impact to the overall catheter dimensions, performance or the intended use of the device.
SIRveNIB is an investigator-led Asia Pacific Primary Liver Cancer Study to be presented on 4 June 2017 at the American Society of Clinical Oncology (ASCO) annual meeting in Chicago, USA.
The abstract, published online in the Journal of Clinical Oncology, states that the overall survival of patients with locally advanced hepatocellular carcinoma who undergo a single treatment of SIR-Spheres yttrium-90 (Y-90) resin microspheres does not significantly differ from the overall survival of patients who recieve twice-daily oral sorafenib. Selective internal radiation therapy (SIRT) results in significantly better tumour response and fewer and less severe adverse events.
SIRveNIB was designed to compare the efficacy and safety of SIRT with Y-90 resin microspheres (SIR-Spheres; Sirtex) vs. sorafenib (Nexavar; Bayer HealthCare), a systemic treatment that is the current standard of care in advanced hepatocellular carcinoma. The patients in SIRveNIB were ineligible for potentially curative therapies, such as surgical resection, ablation or liver transplantation.
The study was conducted by The Asia-Pacific Hepatocellular Carcinoma Trials Group (AHCC) in collaboration with the National Cancer Centre Singapore (NCCS) and Singapore Clinical Research Institute (SCRI) and supported by the National Medical Council Singapore and Sirtex.
The lead author of the SIRveNIB abstract, Pierce Chow, senior consultant surgeon at the National Cancer Centre Singapore and the Singapore General Hospital said: “Asia Pacific patients with locally advanced primary liver cancer with no spread outside the liver who are treated with Y-90 resin microspheres have a significantly better tumour response rate (TRR) compared to sorafenib, despite 28.6% (n=52) of patients not receiving Y-90 therapy as planned (TRR – 16.5% for Y-90 resin microspheres vs. 1.7% for sorafenib, respectively; p<0.001). Moreover, patients experienced fewer, less serious adverse events when compared with those treated with sorafenib. There were no statistically significant differences in the primary endpoint of overall survival between the two treatments.”
Although the median overall survival in the intent-to-treat group was 8.54 months for Y-90 resin microspheres vs. 10.58 months for sorafenib, respectively (p=0.203), there was a trend in improvement in median overall survival in the treated group for Y-90 resin microspheres (11.27 vs. 10.41 months, p=0.273). While Y-90 resin microspheres were not superior to sorafenib regarding overall survival, Chow, who is also professor and course director at the Duke-NUS Medical School, indicated that “the better tumour response and tolerability of Y-90 resin microspheres offers a compelling treatment alternative for patients with advanced hepatocellular carcinoma, for whom there are limited treatment options available.”
Soo Khee Chee, director of NCCS added: “Each year we are making good progress in treating liver cancer. The deeper we go in our research, the better we are able to understand how the cancer behaves and we are able to widen the treatments options for our patients. The results reinforced our belief that with the right people on the research project, we can get the best results. I am grateful to our partners for collaborating in this study.”
Adept Medical, the Auckland based manufacturer of the STARSystem, has announced the release of its latest product innovation, the I.R. Platform (interventional radiology platform). The I.R. Platform is an over-the-patient work surface, specifically designed for use by interventional radiologists when they are working through the femoral artery.
Adept’s previous experience with the development of the STARSystem, a radial arm support system used by interventional cardiologists around the globe, and the femoral table, a much smaller, lightweight, work surface to aid femoral access procedures in cardiology and neuroradiology, has provided further insights into the clinical environment and requirements of the wider interventional radiology field.
Post market feedback and extensive research identified the need for a longer over-patient work surface that would be useful for clinicians performing ‘over the wire’ procedures and using very long wires of up to 300cm.
One of the key benefits of the I.R. Platform is the improved operational security for equipment on a stable, height and length appropriate surface unaffected by the patient’s legs, a press release from Adept says.
Manufactured from carbon fibre composite and plastic, the I.R. Platform is strong, lightweight, radiolucent and very easy to set up or remove for each patient, the release adds. The Lower (base) board slides under the mattress which allows the platform to fit any procedure table. Then, with the patient lying in a supine position on the imaging table, the platform is simply placed over the patient’s legs to locate in the sockets on the Lower Board.
The height of the platform can be adjusted to suit the specific patient size ensuring the platform’s feathered, front edge can be tuned perfectly adjacent to the femoral access site. With its easy to attach, optional extension, the I.R. Platform can be set at two different lengths according to equipment needs.
The standalone platform (without extension) is well-suited for shorter wire procedures such as ‘rapid exchange catheter systems’ and the extended platform is suited for ‘over the wire catheter systems’ and neuroradiology wires.
Another feature of the I.R. Platform is that the working surface is secured above the patient by locking clips which connect the legs to the Lower (Base) Board under the mattress. This removes the risk that a distressed patient could dislodge the platform off the table.
The US FDA has approved the investigational device exemption (IDE) study to evaluate the safety and efficacy of IN.PACT AV access drug-coated balloon as a treatment for failing arteriovenous fistulas in end-stage renal disease patients.
“We are delighted to enrol and treat the first patient in this significant study of IN.PACT AV access drug-coated balloon in patients with obstructed AV access,” says Jeffrey Hull, principal investigator at Richmond Vascular Center in Richmond, USA. “Maintaining access patency is critical to delivering dialysis treatment, and for salvaging failing AV fistulas. Durable treatment options in these patients are limited.”
“This important clinical study is designed to address the clinical need for new, innovative options for patients with limited AV access,” says Robert A Lookstein, national principal investigator in the US and professor of radiology and surgery, vice-chair of interventional services, and medical director of clinical supply chain at Mount Sinai Healthcare System, New York City, USA. “Drug-coated balloons are supported by clinical evidence in patients with peripheral artery disease in the upper leg. We hope that this study may provide data to support this drug-coated balloon’s use to improve patency and reduce the need for repeat interventions in AV access sites for patients on dialysis.”
The IDE study will evaluate the safety and efficacy of the IN.PACT AV Access DCB for up to two years at approximately 30 sites in the USA, Japan, and New Zealand. In addition to Robert Lookstein, global principal investigators include: Andrew Holden, director of interventional radiology at Auckland Hospital, Auckland, New Zealand, and associate professor of radiology at Auckland University, New Zealand, and Hiroaki Haruguchi, clinic director at Haruguchi Vascular Clinic, Tokyo, Japan.
The study will aim to enrol 330 patients with a 1:1 randomisation to either treatment with IN.PACT AV access drug-coated balloon or standard percutaneous transluminal angioplasty balloon. The primary efficacy endpoint is patency of dialysis fistulas through six months and the primary safety endpoint is serious adverse events through 30 days.
The IN.PACT AV access drug-coated balloon is based on the IN.PACT Admiral technology. IN.PACT AV Access is an investigational device and is not FDA-approved for sale in the USA.
Metastatic colorectal cancer patients treated first-line with SIR-spheres Y-90 resin microspheres more likely to become candidates for potentially curative liver surgery, the REsect study shows.
Surgeons’ blinded assessment of pre- and post-treatment CT scans of patients with previously unresectable colorectal cancer liver metastases treated in the SIRFLOX study were presented at the 12th annual European-African Hepato-Pancreato-Biliary Association meeting in Mainz, Germany (24 May 2017).
Adding selective internal radiation therapy (SIRT) with SIR-spheres Y-90 resin microspheres to first-line FOLFOX-based chemotherapy was associated with a statistically significant gain in potentially curative liver resectability, an independent, international panel of expert liver surgeons has reported.
“We performed a blinded evaluation of the extensive radiological database of the recently-reported SIRFLOX study to compare potential liver resectability at baseline and follow-up,” said Benjamin Garlipp, the principal author of the REsect study and a liver surgeon at Otto-von-Guericke-Universität, Magdeburg, Germany.
“We found that while resectability increased from baseline to follow-up in both the chemotherapy only arm and the chemotherapy + SIRT arm of the SIRFLOX study, the increase was significantly more pronounced in patients receiving the combination treatment, 38.1% of these were resectable on the basis of their liver CT scan at follow-up, compared to 28.9% of the patients receiving chemotherapy only (p<0.0001). This is an important finding because surgical resection is the mainstay of potentially curative treatments for these patients, and there is an increasing body of evidence suggesting that it can prolong their lives, even though most of them eventually recur.”
Of the 472 SIRFLOX study patients whose pre- and post-treatment liver CT scans were evaluable by the REsect surgeons, 228 had received first-line mFOLFOX6 chemotherapy (± bevacizumab), while 244 were treated with the combination of chemotherapy and SIR-Spheres Y-90 resin microspheres. There was no significant difference in the resectability of the patients’ liver metastases at baseline (11% vs. 11.9%; p=0.775). In a second analysis, of the patients who were deemed still unresectable at baseline, significantly more patients in the Y-90 resin microspheres group had resectable liver metastases compared to those who received chemotherapy alone (31.2% vs. 22.7%; p<0.0001).
The REsect study was conducted by a panel of 14 hepatopancreatobiliary surgeons from leading medical centres in Belgium, France, Germany, Italy, The Netherlands, Spain, the UK and the USA. Five surgeons performed independent, blinded analyses of 100 baseline and follow-up scans chosen at random from the 472 cases to be reviewed. Blinded analysis of the remaining scans was conducted of 22–25 cases at a time by three surgeons working independently and chosen at random from the nine other members of the REsect panel. The reviewers were blinded to patient identifiers, visit (baseline or follow-up), treatment and clinical information, as well as being blinded to the other reviewers’ assessments. A patient was deemed to be resectable or unresectable by majority agreement (≥3 of 5 surgeons or ≥2 of 3 surgeons).
“As a surgeon, it is always my aim to offer the option of a potentially curative liver resection to patients with metastatic colorectal cancer. We know that in many patients with metastatic colorectal cancer, the liver is the only organ with cancer deposits, and converting patients from a stage where resection of the disease is not possible into one where potential curative resection becomes an option again has an enormous impact for patients. This retrospective analysis suggests that SIRT with Y-90 resin microspheres could be a means to achieving resection for more of these patients,” Garlipp emphasised.
The FOXFIRE, SIRFLOX and FOXFIRE Global randomised studies evaluated the efficacy of combining first-line chemotherapy for metastatic colorectal cancer with selective internal radiotherapy (SIRT) using yttrium-90 resin microspheres (SIR-Spheres, Sirtex) in patients with liver metastases. The combined FOXFIRE analysis comprises data from the SIRFLOX study, first presented in 2015, and data from two new studies – FOXFIRE and FOXFIRE Global.
The studies were designed for prospective, combined analysis of overall survival. Data from combined analysis showed that there was no statistically significant difference between the overall survival of patients who received SIR-Spheres plus standard first-line chemotherapy and those who received chemotherapy alone. The combined analysis data were published as an abstract by the American Society of Clinical Oncology (ASCO) and will be presented at the society’s annual meeting on 5 June 2017.
As published in the ASCO abstract, the three trials randomised (1:1) chemotherapy-naïve metastatic colorectal cancer patients (performance status 0/1) with liver metastases not suitable for curative resection/ablation. Arm A was oxaliplatin-based chemotherapy (mFOLFOX6/ OxMdG)±investigator-chosen biologically targeted agent. Arm B was the same systemic therapy (oxaliplatin dose modification)+single treatment SIRT with cycle one or two of chemotherapy.
The minimum sample size was 1,075 patients. Secondary outcomes included progression-free survival, liver-specific progression-free survival and response rate. Apart from safety, outcomes were analysed on an intention-to-treat basis using meta-analytic methods of pooled individual patient data.
Secondary analyses of data from SIRFLOX and FOXFIRE Global show a statistically significant nearly five-month improvement in median overall survival in patients with right-sided primary colon cancer favouring the SIR-Spheres plus chemotherapy arm (p=0.007). Patients in this population had a statistically significant 36% reduction in their risk of death, and lived a median of 4.9 months longer when SIR-Spheres were added to chemotherapy compared with when chemotherapy was used alone, a press release from Sirtex states. These data are expected to be presented at the World Congress of GastroIntestinal Cancers in Barcelona, Spain, in June.
Between 2006 and 2014, 1103 patients were randomised in 14 countries. The median age was 63 years; median follow-up 43.3 months. There were 844 deaths. There was no difference in overall survival (p=0.609) or progression-free survival (p= 0.108) between arms. Objective response rate (p=0.001) and liver-specific progression (p< 0.001) were significantly more favourable in arm B. Patients in arm B had higher risk of non-liver progression as first event (p<0.001). Grade three to five adverse events were more common in arm B (74%) than A (66.5%; p=0.009). In health status questionnaires, EQ-5D utility scores were not significantly different between arms at six, 12 or 24 months.
The investigators concluded that despite the higher response rates and improved liver-specific progression-free survival, the addition of SIRT to first-line oxaliplatin-fluorouracil chemotherapy for patients with liver-only and liver-dominant metastatic colorectal cancer did not improve overall survival or progression-free survival.
“While these results are not what we expected, we believe that SIR-Spheres Y-90 resin microspheres will continue to play an important role in the treatment of patients with metastatic colorectal cancer,” said Gary Donofrio, senior vice president Americas, Sirtex Medical. “We are committed to helping people with advanced colorectal cancer and look forward to additional validation of this potentially significant finding to improve survival in patients with right-sided colon cancer in the first-line setting.
“Understanding why patients with right-sided colon cancer do not respond as well to certain drug regimens is currently one of the most actively investigated and controversial conundrums in the gastrointestinal oncology field,” Donofrio continued. “We have known for several years that patients with right-sided colon cancer that metastasises generally have a poorer prognosis than those with left-sided disease. If our initial findings are confirmed, a five-month improvement in median survival in the first line setting could be seen as clinically meaningful in this difficult-to-treat population with liver metastases.”
QT Vascular has announced that it has entered into an asset purchase option agreement with Medtronic, for the acquisition of the non-drug coated Chocolate PTA.
“Chocolate represents a breakthrough in percutaneous transluminal angioplasty design. Its unique nitinol constraining structure is designed to provide atraumatic dilatation in the treatment of blocked arteries. Less trauma translates to better acute results, QT Vascular states on its marketing materials.
Independently, QT Vascular will continue to develop and market its other products including a drug-coated version of Chocolate PTA, Chocolate Touch, which has received investigational device exemption approval from the US FDA and its coronary products portfolio of both drug and non-drug coated products. QT Vascular is based in Singapore with a US subsidiary, Trireme Medical.
QT Vascular develops and commercialises of next-generation minimally invasive products for the treatment of complex vascular disease. It works closely with leading physicians and scientists from around the world to create differentiated devices that improve procedural and clinical outcomes.
According to our results, the physician who performs prostatic artery embolization procedures, even with a ceiling suspended shield, would reach the annual radiation limit for the left eye with just one procedure per week, writes Gustavo Andrade, Recife, Brazil.
Prostatic artery embolization is a minimally invasive treatment of the obstructive symptoms of the lower urinary tract, secondary to benign prostatic hyperplasia. Embolization is slowly but surely gaining worlwide acceptance. Its efficacy is already proven and involved groups are now trying to improve its safety. There is also the important aspect of radiation exposure to be considered. We need to minimise radiation exposure as a way to improve the results of embolization.
We prospectively analysed 25 consecutive prostatic artery embolization cases using direct and indirect measures to evaluate patients’ and radiologists’ exposure. We placed a radiosensitive film designed to measure the peak skin dose under the patient’s pelvis. The interventional radiologist wore nine pairs of very small dosimeters strategically positioned (eyes, glabella, thyroid, chest, hands, knees and feet) that could measure effective and equivalent dose to organs and tissues. Cone beam CT (CBCT) was available and used only when the interventional radiologist judged it to be necessary, not routinely. We found that even when used, the CBCT was the source of less than 10% of the radiation. Digital subtraction angiography was responsible for 71.45% and fluoroscopy for 19.9% of the radiation.
There are very few data available in the literature regarding radiation exposure with prostatic artery embolization. In a few papers, only indirect measures such as fluoroscopy time and dose area product, both easily extracted from the equipment at the end of the procedure, were available. In the largest series (Pisco 2016) with CT angiography previously performed in all 630 patients, the fluoroscopy time was low (19.5 minutes) but the dose area product was high (2,415Gy.cm2) showing that fluoroscopy is not the main source of radiation, and that the equipment needs adjustments in order to respect the ALARA (As low as reasonably achievable) principles.
Our dose area product (450.7Gy.cm2), while amongst the lowest in all series reported (that had at least 10 patients), still represent values above those reported in other complex interventional procedures. This can be explained due to the high number of digital subtraction angiography runs and images obtained in different oblique views to understand the anatomy of the very thin prostatic arteries. The average equivalent dose found for the left eye was 0.378mSv. After several studies reporting a significant increase in radiation-associated eye lens opacities and cataracts among interventional physicians, the International Commission on Radiological Protection (ICRP) reduced the annual limit for equivalent dose for lens of eyes to 20mSv. According to our results, the physician who performs prostatic artery embolization procedures, even with a ceiling suspended shield, would reach the annual limit for the left eye with just one procedure per week.
In the light of this data, we invited the engineer of the imaging system (Siemens) and arrived at a radiological protocol for prostate artery embolization where we are working with about 30% of the dose obtained with the standard protocol. These data will be published soon.
Gustavo Andrade is professor of Radiology in FCMCG and director of Angiorad, Hospital Santa Joana in Recife, Brazil. He has reported no disclosures pertaining to this article.
Peripheral artery disease patients who were treated with an anti-inflammatory steroid injected directly into the tissue surrounding their leg artery showed a significant reduction in inflammatory biomarkers.
Results from the DANCE trial (Dexamethasone infusion to the adventitia to enhance clinical efficacy after femoropopliteal revascularisation) were presented as a late-breaking clinical trial at the Society for Cardiovascular Angiography and Interventions (SCAI) 2017 scientific sessions on 11 May in New Orleans, USA.
Treatment approaches that treat blockages from the inside of the artery can trigger a cycle of inflammation that may contribute to restenosis. Over the course of six to 12 months, a meaningful percentage of patients experience a repeat blockage due to restenosis, a press release from SCAI states.
Researchers in the DANCE trial measured the inflammatory biomarkers in a patient subgroup (n=52 who underwent angioplasty and n=42, who underwent atherectomy) before and after using the Bullfrog microinfusion device to locally deliver dexamethasone (1.6mg/cm of treated artery) after their angioplasty or atherectomy, and a control group (n=12 who underwent angioplasty and n=16 who underwent atherectomy) that did not receive the steroid following the same techniques. Both groups had blood drawn prior to intervention, at 24-hours, and at four weeks post-procedure. Patients treated with the microinfusion device and dexamethasone experienced a significant reduction of two key inflammatory biomarkers that have been linked to restenosis in balloon angioplasty interventions: high-sensitivity C-reactive protein (hsCRP) and monocyte chemoattractive protein-1 (MCP-1).
“This is a novel approach to treating the diseased artery by administering a steroid to the tissue that surrounds it,” said one of the study’s leading investigators Ehrin J Armstrong, VA Eastern Colorado Healthcare System and associate professor of medicine, University of Colorado School of Medicine. “By injecting anti-inflammatory drug directly into the artery wall and the adjacent tissue, as opposed to inside the artery where much of the drug could be washed away by blood flow, the drug is precisely targeted to the site of the inflammatory signals. Thus, the cycle of inflammation that can lead to repeat blockages is controlled, and the healing process is potentially improved.”
In the control group, the average 24-hour increase in hsCRP was 280% with angioplasty or 138% with atherectomy as compared to 55% with angioplasty or 14% in the atherectomy group in treated patients. Additionally, a 24-hour mean rise in MCP-1 of 19% or 14% was seen in the non-treated group, while treated patients experienced a reduction of 39% or 52%.
Armstrong noted, “The way we address a blockage in the leg artery now is to initially restore blood flow and any limitation to the blood flow dynamics using a balloon or stent to mechanically open the artery back up. The idea behind the addition of a steroid to the procedure is to change the underlying biology associated with these techniques so that the intervention is more durable over time. The DANCE study has provided insight that the measurement of the levels of the inflammatory biomarkers for individual patients may be a beneficial strategy in predicting outcomes and lead to improvement by personalising our therapy for each peripheral arterial disease patient.”
Pill that shrinks uterine fibroids gathers early data
Lutonix AV results provide tailwind for drug-coated balloons in dysfunctional arteriovenous fistula treatment
Michael Dake: TEVAR’s dirty secret
Goetz Richter: MIRACLE I demonstrates high tumour control rate for drug-eluting microspheres
Profile: Suresh Vedantham
Pill that shrinks uterine fibroids gathers early data
Lutonix AV results provide tailwind for drug-coated balloons in dysfunctional arteriovenous fistula treatment
Michael Dake: TEVAR’s dirty secret
Goetz Richter: MIRACLE I demonstrates high tumour control rate for drug-eluting microspheres
Profile: Suresh Vedantham
The Canadian Interventional Radiology Association (CIRA) Board of Directors has announced the appointment of Daniel Lapointe as CIRA’s new executive director on the association’s website.
Lapointe is a seasoned association executive and has served as chief staff officer at a number of associations, notably Katimavik, the Canadian Institute of Actuaries and the Canadian Hemophilia Society, the announcement notes. “In his role with these associations, Daniel has helped define and achieve their strategic goals with regards to membership growth, revenue diversification and branding. He has also been instrumental in influencing public policy on behalf of these organisations,” it adds.
“Since 2012, Daniel has worked as a consultant, a teacher and an author, helping not-for-profit organisations improve their governance and achieve their development goals. Daniel is an instructor at Université de Montréal, where he teaches two courses on association management. He is also the author of two acclaimed books, published in 2013 and 2016, on fundraising and good governance in the not-for-profit sector. Daniel holds an MBA at HEC Montréal and a Master’s of political science at Université du Québec à Montréal,” the announcement outlines.
The announcement further explains that Lapointe brings pragmatic decision-making and tremendous management experience to CIRA. “He is a well-known expert in not-for-profit association governance and operations. The CIRA Board is quite excited about the future of our organisation under Daniel’s leadership and his experience and expertise will be a great asset to the organisation,” the notice says.
Guerbet has announced that the Bundesinstitut für Arzneimittel und Medizinprodukte (BfArM; The German Federal Institute for Drugs and Medical Devices) has now approved Lipiodol Ultra-Fluid for use after intra-arterial catheterisation of the hepatic artery for the visualisation and localisation of hepatocellular carcinoma in the intermediate stage in adults.
Hepatocellular carcinoma is the most common primary liver cancer and is the second biggest cause of death due to cancer worldwide.
“Guerbet is proud to be granted approval for this new indication for Lipiodol Ultra-Fluid, this reflects a strong positive endorsement from German liver cancer doctors” commented Maximilian Hudl, general manager of Guerbet in Germany. “The additional indication approved by BfArM is a major milestone on the ambitious approach taken by the company to keep the product accessible for German patients to assist in the management of this devastating disease”, he said. This indication is already approved in the USA.
Lipiodol has a high affinity for primary hepatic tumours and optimises visualisation of hepatocellular carcinomas compared to the surrounding liver parenchyma. Lipiodol-associated to radiofrequency ablation allows the successful treatment of small hepatocellular carcinoma. Most of ultrasound-invisible hepatocellular carcinomas, including tumours in unfavourable locations could be successfully treated using this technique, a press release from Guerbet says.
Two new sub-analyses from the IN.PACT Global Study of the IN.PACT Admiral in patients with peripheral artery disease have been reported at the annual 2017 Charing Cross Symposium (CX) in London, UK, one of the world’s largest educational meetings specialising in vascular and endovascular disease management.
In a “Podium First” presentation at the conference, Gary Ansel, system medical director for Vascular Services at OhioHealth Riverside Methodist Hospital in Columbus, USA, presented one-year results analysing outcomes in patients from the IN.PACT Global study with complex lesions. The analysis compared standard usage patients (n=281) who met similar inclusion criteria for the IN.PACT Superficial Femoral Artery pivotal trial, an investigational device exemption (IDE) study, compared with use in a broader spectrum of patients (n=1125) who had wider inclusion criteria reflecting more real-world patients.
Results in both groups demonstrated consistent and positive outcomes with IN.PACT Admiral at one year. In the standard IN.PACT Global study group, clinically-driven target lesion revascularisation (CD-TLR) was 3.4%, which was comparable to 2.4% in a similar population in the IN.PACT Superficial Femoral Artery pivotal trial. CD-TLR for the group with complex lesions was 8.5%, despite the disease complexity observed in these patient types. These results were also consistent with the full clinical cohort for the IN.PACT Global Study (n=1406), in which one-year CD-TLR was 7.5%.
Results of the primary safety endpoint were generally consistent across the cohorts and no safety signals were observed.
“These sub-analyses show that IN.PACT Admiral continues to deliver durable and consistent results across our more typically treated patient populations,” comments Ansel. “Notably, the data in this study highlight that the IN.PACT Admiral drug-coated balloon can be safe and effective when used in our patients with complex peripheral artery disease, such as those with challenging calcified lesions and with significant co-morbidities.”
Additionally, Fabrizio Fanelli, professor of radiology at the Sapienza University in Rome, Italy, shared results of a new subset analysis of patients with complex, calcified lesions from the long lesion and chronic total occlusion imaging cohort of the IN.PACT Global Study.
The analysis included long lesion and chronic total occlusion patients defined as having moderately severe or severely calcified lesions (n=72). Calcium levels were assessed by the site according to protocol and confirmed by core laboratory assessment. At one year, patients achieved primary patency rates of 88.8 percent as calculated by Kaplan-Meier analysis. Primary patency is the ability for the treated artery to remain open over time. The analysis also demonstrated a CD-TLR rate of 8.5%. Consistent with other data sets, no safety signals were observed. In 51.4% of subjects, provisional stenting occurred.
Positive results from the RANGER SFA trial for Boston Scientific’s Ranger paclitaxel-coated percutaneous transluminal angioplasty (PTA) balloon catheter have been presented at the 2017 CX Symposium in London, UK. Data demonstrated that the drug-coated balloon (DCB) exhibited both a high rate of primary patency and freedom from target lesion revascularisation at 12 months, reducing the need for re-interventions to re-establish flow in previously blocked blood vessels.
The prospective, randomised, controlled trial, comparing the Ranger DCB to uncoated PTA balloons, included 105 patients with femoropopliteal lesions, at ten centres in Europe. Results demonstrate 86% primary patency and 91% freedom from target lesion revascularisation; both findings statistically significantly higher than the control arm of patients treated with an uncoated balloon. Patency was assessed by duplex ultrasound at 12 months post-procedure. Eighty-four per cent of patients in the Ranger DCB group presented either with no or mild symptoms associated with claudication, or pain while walking. There were no target limb amputations.
“The rates of primary patency and freedom from target lesion revascularisation are amongst the highest observed in this type of first-in-man trials at one year,” says Dierk Scheinert, chairman Division of Interventional Angiology, University Hospital Leipzig, Germany, and principal investigator of the RANGER SFA trial. “As a clinician, it is important to have a treatment option…that exhibits consistent performance and outcomes; for patients, these attributes impact their quality of life such as alleviating pain and discomfort, as well as reducing the probability of repeat procedures.”
To expand upon these findings, Boston Scientific recently received approval to commence enrollment in the RANGER II SFA study, a randomised United States Food and Drug Administration Investigational Device Exemption trial designed to evaluate the safety and efficacy of the Ranger DCB versus standard PTA balloons. Anticipated enrolment will include up to 400 patients in 70 centres in the USA, Canada, Europe, Japan and New Zealand. Data from the RANGER II SFA trial is expected to support regulatory submissions in the USA and Japan.
The Ranger drug-coated balloon received CE mark in June 2014.
BD (Becton, Dickinson and company) has definitively agreed to acquire Bard for US$317 per common share in cash and stock, for a total consideration of US$24 billion.
The agreement has been unanimously approved by the Boards of Directors of both companies.
Vince Forlenza, BD’s chairman and chief executive officer, says, “Combining with Bard will accelerate our ability to offer more comprehensive, clinically relevant solutions to customers and patients around the globe, creating a strong partner for healthcare providers who are increasingly focused on delivering better outcomes at a lower total cost.”
Tim Ring, Bard’s chairman and chief executive officer, says, “We are confident that this combination will deliver meaningful benefits for customers and patients as we see opportunities to leverage BD’s leadership, especially in medication management and infection prevention.”
BD recently announced that, in connection with the previously announced acquisition of CR Bard, BD has commenced offers to exchange any and all outstanding notes issued by Bard as set forth in the table below for up to US$1,149,820,000 aggregate principal amount of new notes issued by BD and cash.
The 459-patient randomised controlled SARAH study shows that local treatments of advanced or inoperable hepatocellular carcinoma with selective internal radiation therapy (SIRT) did not lead to a planned superiority difference in overall survival compared to standard-of-care systemic therapy with sorafenib. However, SIRT had far fewer side-effects and patients who received this treatment had a significantly better quality of life.
The investigator-initiated SARAH (Sorafenib vs. radioembolization in advanced hepatocellular carcinoma) study directly compared the efficacy of SIRT using yttrium-90 [Y-90] resin microspheres (Sir-spheres, Sirtex) vs. sorafenib (Nexavar; Bayer). The trial was launched in December 2011 and concluded enrolment in February 2015, with 237 patients receiving SIRT. The primary endpoint of the study was overall survival and secondary endpoints included progression-free survival, time to radiological progression at any site and in the liver as the first event, tumour response, quality of life, and safety and toxicity.
Valérie Vilgrain, Department of Radiology, Beaujon Hospital, Assistance Publique – Hôpitaux de Paris (AP-HP) and Université Paris Diderot, Sorbonne Paris Cité, France, principal investigator of the SARAH study, said: “Neither sorafenib nor SIR-Spheres Y-90 resin microspheres produced a statistically significant difference in overall survival of the patients we studied. Despite 26.6% of patients in the SIRT arm not receiving Sir-spheres per protocol, the primary endpoint of overall survival by intention-to-treat [ITT] was not significantly different (median 8 vs. 9.9 months; p=0.18).Moreover, if we look at the patients who received Sir-spheres or sorafenib according to the SARAH protocol, median overall survival was identical (9.9 vs. 9.9 months; p=0.92).”
Patients with advanced or inoperable hepatocellular carcinoma who usually received one or two treatments of SIRT had similar survival compared to patients who received standard twice-daily systemic treatment with sorafenib, but with less than half the number and significantly fewer severe treatment-related adverse effects and significantly better quality of life. Almost 70% of the patients in the SARAH study had advanced hepatocellular carcinoma (Barcelona Clinic Liver Cancer stage C), with portal vein thrombosis and no extrahepatic spread. Most of the other patients had failed two cycles of transarterial chemoembolization.
Vilgrain presented the data at The International Liver Congress 2017, Amsterdam, The Netherlands, and also at the European Conference on Interventional Oncology (ECIO) in Bilbao, Spain.
The trial further demonstrated that the cumulative incidence of radiologic progression in the liver as the first event was significantly lower in the SIRT group compared to the sorafenib group (p=0.014), and the response rate was significantly higher in the SIRT group compared to the sorafenib group (19% vs. 11.6%, p=0.042). Median progression free survival was 4.1 months and 3.7 months in the SIRT and sorafenib groups, respectively (p=0.765). Overall, there were 1,297 and 2,837 treatment-related adverse events including 230 and 411 grade 3, in the SIRT and sorafenib groups, respectively. Both the side-effect profile and quality of life scores were significantly better over time in the SIRT group compared to the sorafenib group (p=0.005).
“Patients with advanced or inoperable hepatocellular carcinoma have a poor prognosis, often with underlying cirrhosis, and the treatment option currently available, sorafenib, has a high level of toxicity. As cohort studies have demonstrated the efficacy of SIRT with Y-90 resin microspheres, we set out to compare the efficacy of this treatment vs. the current standard of care,” said Vilgrain.
The difference in the frequency and severity of side effects of patients treated with SIRT vs. sorafenib is clear. Significantly fewer patients treated with SIRT had any treatment-related side effects at all (76.5% vs. 94.0% for sorafenib; p<0.001), and these were also less severe (≥ grade 3; 40.7% vs. 63.0%, respectively; p<0.001). Moreover, those patients treated with SIRT who reported treatment-related side-effects experienced a median of only five such events over the course of the SARAH study, compared to a median of 10 events in those who received sorafenib (p<0.001).
General treatment-related symptoms such as fatigue (42% vs. 65%; p<0.001), abdominal pain (20% vs. 29%; p=0.032), nausea or vomiting (12% vs. 23%; p=0.001) and infection (4% vs. 11%; p=0.007) were also significantly less frequently reported and less severe for patients receiving Sir-spheres microspheres, compared to sorafenib.
Fewer patients receiving SIRT experienced treatment-related diarrhoea (13% vs. 68% for sorafenib; p<0.001), hand-foot skin reaction (0.4% vs. 21%; p<0.001), anorexia (13% vs. 32%; p<0.001), weight loss (6% vs. 21%; p<0.001) and alopecia (0% vs. 16%; p<0.001), as well as infections (4% vs. 11%; p=0.007), hypertension (3% vs. 13%; p<0.001) and non-gastrointestinal haemorrhage (3% vs. 10%; p=0.002).
The results of quality of life surveys filled out by SARAH participants at three month intervals after their initial treatment showed that patients treated with Sir-spheres maintained their health status over the duration of the SARAH study, whereas patients receiving sorafenib reported a significant and sustained decline in quality of life (group effect: p=0.005; time effect: p<0.001; between group difference increase over time: p=0.045).
There were few potential SIRT-associated treatment-related complications and, importantly, no radioembolization-induced liver disease (radiation hepatitis) experienced.
“In terms of what matters for patients, the findings from this first large head-to-head comparison of liver-directed SIRT and systemic chemotherapy with sorafenib also show clearly that liver-directed procedures with Sir-spheres result in a significantly better tolerance of treatment and quality of life,” Vilgrain stated. “I believe this consideration should be a critical factor in selecting first-line treatment for this patient population in the future.”
Getinge is proud to announce the launch of the Advanta V12 32mm length balloon expandable covered stent at the Charing Cross International Conference. This is a much needed addition to the Advanta V12 product offering and will allow clinicians additional treatment options for optimal patient outcomes, a press release from the company says.
With over 200 clinical publications and close to 500,000 patients successfully treated worldwide, this latest product line extension will add to the rapidly growing body of evidence supporting the safety and efficacy of Getinge’s covered stent technology.
The Advanta V12 covered stent is a low profile, premounted balloon expandable covered stent made of a radial expandable 316L stainless steel that is completely encapsulated with a patented one-piece polytetrafluoroethylene (PTFE) covering technology. Getinge’s proprietary covering technology creates a microporous PTFE layer that completely encapsulates the stainless steel stent and allows for uniform expansion without ridges or folds in the material being formed. V12 is customisable with the ability to post dilate to meet each patient’s anatomical needs.
Getinge will also host, at Charing Cross, in partnership with Vascular International, a series of masterclass workshops in which participants will have hands-on experience using the new Advanta V12 32mm and learn the latest techniques from the experts. ‘It is extremely important to provide appropriate training and guidance to the medical community and these workshops allow not only hands-on experience on training models but also provide the participants with the opportunity to network and build relationships with medical experts” says Markus Stirner-Schilling, vice president, Marketing and Academy, Getinge, Europe, Middle East and Africa.
Two patients were treated for hepatocellular carcinoma and one patient was treated for malignant colorectal cancer metastasised to the liver.
DC Bead Lumi is the first commercially available radiopaque drug-eluting bead in the EU which can be loaded with doxorubicin or irinotecan for the local treatment of tumours in patients with hepatocellular carcinoma and metastatic colorectal cancer, respectively. DC Bead Lumi is a next-generation development of DC Bead.
At the Istituto Oncologico Veneto, Padova, Italy, Camillo Aliberti, director of Radiology, and his team performed transarterial chemoembolization (TACE) procedures using DC Bead Lumi, enabling real-time, visible, lasting confirmation of bead location during and after embolization of tumours in the liver.
“We are very pleased with the results from treatment in our patients, and DC Bead Lumi offered clear, real-time evidence on the treatment of the target lesion while the long-term radiopacity means not only can we see where we are delivering the treatment during the procedure, but we can also identify areas of successful treatment—or under treatment—in follow-up scans,”Aliberti said.
“DC Bead Lumi provides the opportunity to individualise a patient’s treatment and bring a new level of control to TACE procedures. At the same time, the lasting radiopacity allows you to see rather than assume the location of the beads, providing reassurance to patients that the treatment is getting to where it needs to be,” commented Duncan Kennedy, BTG head of Interventional Oncology.
DC Bead Lumi gained class III CE mark certification in early March, 2017.
The 2017 edition of the annual PAIRS meeting was held in Dubai 15–18 March and reflected the growing enthusiasm of the interventional radiology community in the Middle East, writes Hicham T Abada.
We are also going to witness some changes: the acronym PAIRS, which used to stand for Pan Arab Interventional Radiology Society will now stand for Platform of Advanced Interventional Radiology Solutions, reflecting the more inclusive and global nature of the upcoming conference in 2018. In January, we also launched an open access journal for interventional radiologists, the Arab Journal of Interventional Radiology (AJIR), with biannual issues. This will represent another asset to be utilised by the young generation of interventional radiology to fully contribute not only clinically but also academically in order to expand the community of the region.
Minimally invasive treatments are gaining widespread acceptance in the local population. This is essentially because patients want to be actively informed about the most modern treatment options and are actively seeking out different media sources for clear answers about outcomes.
This year, we were able to implement a comprehensive programme that addressed dedicated sessions on critical limb ischaemia with a special focus on the diabetic foot, multiple lectures on venous interventions and varicose veins, a full day for aortic disease and extensive sessions on embolization and interventional oncology that continue to be very popular. In addition we had a designated neurointerventional radiology track as well.
It was also refreshing to observe that some centres in the region have initiated advanced programmes on prostate artery embolization and are even reporting preliminary data of the endovascular approach for the treatment of bleeding in patients with haemorrhoids. These treatments are limited to few established and experienced centres in North America and Europe, so it was exciting to see data emerging from the Middle East.
If we reflect a moment on market analysis reports, they have clearly shown that growth in North America is primarily driven by the increase in the prevalence of chronic diseases and an aging population. Although the population in the Middle East is much younger, there is a prevalence of diabetes, obesity, and kidney disease that has already significantly impacted the Middle East.
For instance, the World Health Organization’s most comprehensive report on diabetes shows there are now 422 million people with the disease worldwide. This includes about 43 million from the Eastern Mediterranean region, with nearly a million of those being solely from a single country of the Gulf Cooperation Council (GCC)—the UAE, which has a population of 9.1 million inhabitants. The importance of interventional radiology in the management of those patients is irreplaceable. There is no doubt about the increased need for interventional radiology in the region and it is imperative that interventional radiology curricula are implemented to fulfill patients’ needs.
Being involved in the annual meeting of the PAIRS programme for the last two years, I have witnessed an unprecedented momentum from young interventionalists in the whole region. Some of them have already initiated, or established high-quality programmes in their respective countries in the region. The PAIRS meeting has become a valuable and established platform to promote high standards of interventional radiology expertise and facilitate collaboration between physicians both within the region as well as international faculty.
Hicham T Abada is chief of Interventional Radiology, Cleveland Clinic Abu Dhabi, Abu Dhabi, UAE. He is also the programme chair of the annual PAIRS meeting in 2018.
Merit has showcased a new radial compression product, Preludesync, on its website.
The Preludesync devices assists in achieving vascular haemostasis. It features a large area with clear, unobstructed site visibility of the access site. The device can personalise the patient’s recovery experience with an exciting random assortment of designs provided in each box. It is constructed from a soft material that lies against the patient’s skin while providing an outer layer that is easy to clean and the balloon was designed to comfortably achieve patent haemostasis, information provided on the website states. Further, Merit notes that band attachment was designed with a material that provides adjustable, secure placement of the device.
Preludesync is available in two sizes—24cm and 29cm. It is available with the safety and convenience of a specialised connection device and syringe. It is also available with a standard luer device and standard syringe.
The Society of Interventional Radiology (SIR), the American Society of Hematology and 23 other medical societies have released a statement in support of the March for Science on 22 April.
Here is the text of the statement:
“As the world’s leading organisations representing clinicians, laboratory researchers, and physician-scientists committed to improving patient care, we support the March for Science and its nonpartisan call for the appreciation of scientific evidence, education, and investment. Science has no political agenda but gives us the tools to find the truths about our world and then implement informed policies to enrich our communities.
“Fundamental appreciation for scientific evidence is vital, and it begins with access to science education that highlights critical thinking and evidence-based decision-making. Americans need access to education that inspires them to question the world around them and develop new technologies and solutions.
“Science is vital to our health, as an understanding of human biology is essential to stimulating discoveries that lead to cures for devastating diseases. Every day, physicians make the best patient-care decisions they can by relying on science-based tools. Clinicians prevent disease by administering immunisations, and they manage disease by providing therapies that have been thoroughly and scientifically vetted for optimal outcomes. This science-based care saves lives, decreases human suffering, and reduces unnecessary costs.
“Therefore, it is critical that we protect federal investment in our health. Over the past several decades, research supported by the National Institutes of Health (NIH) has yielded significant advances across all fields of medicine. Today, diseases with previously grim prognoses are treatable. We have powerful therapies that engage the patient’s own immune system to conquer cancers and non-malignant diseases. And, genome editing is showing early promise in curing and even preventing debilitating genetic conditions.
“We rely on evidence from the Agency for Healthcare Research and Quality (AHRQ) to address patient safety, quality of care, efficiency, and access in our health care system. Research supported by the agency has prevented the spread of infections in hospitals and improved access to health care for patients in rural areas. And, through its surveillance programs, the Centers for Disease Control and Prevention (CDC) has played an important role in preventing and controlling inherited and communicable disease as well as dangerous outbreaks. Without the CDC, outbreaks would spread, food-borne illness would go undetected, and chronic diseases would have a higher human and monetary cost.
“Scientific progress and support of vital federal research programmes have led to major advances in our health. We hope patients, their families, and everyone committed to advancing healthcare will join us in celebrating the value of scientific evidence in our everyday lives.”
A study published online ahead of print in CardioVascular and Interventional Radiology (CVIR) has demonstrated that at one year, uterine fibroid embolization significantly improves all aspects of sexual function and quality of life for patients who undergo the minimally invasive treatment.
Investigators on the EFUZEN study, Hélène Vernhet Kovacsik, Marc Sapoval and colleagues from the French Society of Interventional and Cardiovascular Imaging (SFICV) research group, set out to evaluate sexual function before, and a year after, fibroid embolization.
As reported in CVIR, the secondary goals of the study were to evaluate the quality of life before, and one year after embolization, and to determine any correlation or relationship between imaging findings (MRI data) before and three to six months after embolization to changes in sexual function and quality of life.
EFUZEN was a prospective, multicentre observational study that enrolled 264 consecutive symptomatic women who underwent uterine fibroid embolization. The women were treated using Embozene (Celonova/Boston Scientific) from March 2012 to May 2013.
Vernhet Kovacsik and colleagues calculated the sexual function score and the quality of life score using the previously validated Female Sexual Function Index (FSFI) by Rosen and UFS-QOL by Spies, respectively, before and one year after the interventional procedure.
They also performed MRI before and three to six months after embolization recording the uterine and main fibroid volume and percentage of fibroid enhancement after injection of gadolinium. They also looked for a relationship between the imaging data before and after embolization, sexual function scores and quality of life scores.
The investigators obtained Female Sexual Function Index data in 170 women. They also obtained quality of life data in 192 women. One year after embolization, 78.8% saw an improvement of sexual function score; at the same time point, 90.2% of women saw an improvement in quality of life scores. Nearly 85% saw an improvement in symptom severity. However, the study was unable to establish a relationship between reduction in the main fibroid, or decrease of fibroid enhancement and quality of life and sexual function scores.
Pancreatic Cancer Action Network (PanCAN) grantee George Miller, head of the Cancer Immunology Program at Perlmutter and vice chair for research in the Department of Surgery at NYU Langone and his research team have discovered a novel and potentially targetable way that pancreatic cancer cells hide themselves from the immune system. The findings, published online in the journal Nature Medicine, have the potential to broach a new era of effective immunotherapies for pancreatic cancer.
“Though valuable research has been done in the area of pancreatic cancer immunotherapy, patients have not yet experienced significant clinical benefits,” said Lynn Matrisian, chief science officer at the Pancreatic Cancer Action Network. “Our hope is that this novel research discovery can be quickly translated and evaluated in the clinical setting, with an ultimate goal of improving patient outcomes.”
According to NYU, researchers involved in this study uncovered a critical pathway by which pancreatic cancer cells turn off the immune system charged with attacking them. In addition, scientists found that targeting this pathway could enable efficacy for checkpoint-based immunotherapies, which have failed so far in clinical trials in pancreatic cancer.
The research team believes that these findings will introduce a new type of strategy leading to effective immunotherapies in pancreatic cancer, and they hope to bring new drugs targeting these pathways to the clinic soon.
The study, conducted in mice and including analyses of human cancers, found very high levels of two proteins – dectin-1 and galectin-9 – in pancreatic tumours. Their interaction prevented first-responder immune cells, called macrophages, from triggering reactions that kill cancer cells. Related analyses of human patient data linked elevated levels of galectin-9 to reduced survival in pancreatic ductal adenocarcinoma (PDA), although larger, confirmatory studies are needed, say the authors.
Perlmutter researchers used a mouse model of PDA, a disease that is usually fatal in patients within five years of diagnosis. They compared mice with pancreatic cancer that made dectin-1 against a group engineered to not make the protein, and determined that the mice without dectin-1 lived longer. The research team also found that treating mice with an antibody that blocked the galectin-9/dectin-1 interaction dramatically reduced tumour size and increased survival.
“Pancreatic cancer cells are deadly because they programme nearby immune cells to permit the tumours to survive and grow,” said Miller. “Our study reveals a previously unknown mechanism that we might be able to block to make tumours ‘visible’ again to attacking immune cells, perhaps in combination with other immunotherapies,” he added.
PinnacleHealth CardioVascular Institute has enrolled the first US patient in a trial assessing the safety and effectiveness of a new type of approach for blockages in the leg artery.
DISRUPT PAD III is the largest ever multicentre randomised study to exclusively enrol patients with calcified peripheral artery disease. The objective of the trial is to assess the optimal therapy to dilate heavily calcified lesions by comparing the Shockwave Medical Lithoplasty system vs. traditional angioplasty, with a primary goal of achieving less than 30% residual stenosis without the need for stenting. In addition, all patients who do not receive a stent will be treated with a drug-coated balloon. The trial will enrol 334 patients in up to 45 global sites. William Bachinsky, medical director of vascular services at PinnacleHealth CardioVascular Institute, serves locally as principal investigator at PinnacleHealth.
“We are very excited to be the first to treat a US patient in the global study of this cutting edge technology for patients with claudication or pain in the legs due to leg artery blockages,” says Bachinsky. “The Shockwave Medical Lithoplasty device, if proven as a result of this clinical trial, will be a “game changer” in the treatment of patients with peripheral artery disease, allowing for low pressure, controlled expansion of blocked artery and potentially less risk for internal tearing of the artery and need for implanting permanent metal stents.”
Lithotripsy uses high-speed pressure waves to disrupt calcium and has been used for years in treating patients with kidney stones. Lithoplasty technology delivers localised lithotripsy for the treatment of calcified arteries in patients with peripheral artery disease. Built on an angioplasty balloon platform, each catheter incorporates multiple lithotripsy emitters activated with the touch of a button while the integrated balloon is inflated, according to a company release. Once activated, these emitters produce therapeutic sound waves that are inherently tissue-selective, passing through the balloon and soft vascular tissue, preferentially disrupting the calcified plaque by creating a series of micro-fractures. Once the calcium has been disrupted, the vessel can be effectively dilated using low pressures thereby enabling even historically challenging peripheral artery disease patients to be treated effectively and with minimal injury to the vessel.
Codman Neuro has announced the acquisition of Neuravi. This acquisition comes after the company’s recent acquisition of Pulsar Vascular, expanding its products for stroke therapy. DePuy Ireland Unlimited Company, an affiliate of Codman Neuro, is the acquiring entity. Financial terms of the transaction were not disclosed.
Founded in 2009, Neuravi has invested extensively in scientific research on the varieties of clots that cause acute ischaemic stroke, and has translated learnings into its EmboTrap Revascularisation Platform. The EmboTrap device is engineered to restore blood flow to the brain by retrieving a clot with its proprietary dual-layer stent-like structure, and it has already been used to treat over 3,000 patients in Europe.
Globally, stroke is the second leading cause of death after the age of 601, and ischaemic strokes, caused by blockages in vessels supplying blood to the brain, account for 87% of all strokes. According to the European Journal of Neurology, the number of stroke events in Europe is projected to rise from 1.1 million in 2000 to 1.5 million per year by 2025, while the American Heart Foundation estimates someone dies of a stroke every four minutes. In the USA alone, the economic burden of stroke is estimated at US$33 billion annually, including the cost of health care services, medications, and lost productivity.
“Rapid restoration of flow is of utmost importance when treating stroke patients,” says Shlomi Nachman, Company Group Chairman of Johnson & Johnson Medical Devices Cardiovascular & Specialty Solutions. “The EmboTrap platform was designed to address this critical need and we are excited to combine Neuravi’s expertise in clot research with Codman Neuro’s global resources to accelerate innovation in acute ischaemic stroke treatment.”
The EmboTrap and EmboTrap II Revascularisation Devices are commercially available in Europe and have been available in the USA for investigational use only under the ARISE II clinical trial, which will support a US Food and Drug Administration (FDA) submission planned for later this year.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has launched its CIRSE Registry for LifePearl Microspheres (CIREL), a new European-wide observational study that will gather data on patients with colorectal adenocarcinoma and liver-only or liver-dominant metastatic disease, treated with transarterial chemoembolization (TACE) using LifePearl microspheres (Terumo) loaded with irinotecan in specialist hospitals across Europe.
The study aims to observe and categorise the real-life use of the device in the context of patient’s cancer treatment and will also collect extensive quality-of-life data to learn more about the palliative aspect of TACE. Previous research on LifePearl microspheres included only pre-clinical and pharmacokinetic studies.
Philippe L Pereira, speaking on behalf of CIRSE as co-chairperson of the CIREL Steering Committee, states that “CIREL will greatly contribute to the collection of scientific knowledge and clinical data in one of interventional radiology’s most dynamic and promising fields and help us understand better what could be the potential indications to treat patients with TACE”. Pereira is head of Radiology, Minimally Invasive Therapies and Nuclear Medicine at Klinikum am Gesundbrunnen, Heilbronn, Germany.
Gillian Jessurun (Treant Zorggroep, Scheper Hospital Emmen, The Netherlands) has enrolled the first patient in the investigator-initiated MASTER DAPT (Management of patients post bioresorbable polymer stent implantation with an abbreviated DAPT regimen) study, launching the global investigation.
Jessurun says, “Having the privilege of enrolling the study’s first patient reflects our team and Treant Zorggroep, Scheper Hospital’s commitment to research.”
The major new MASTER DAPT study is set to compare within current guidelines abbreviated versus prolonged dual anti-platelet therapy (DAPT), following implantation with Terumo’s Ultimaster DES, a drug-eluting bioresorbable polymer stent, in patients presenting with high bleeding-risk features. Patients (4300) will be randomly assigned to one of the treatment options in 130 hospitals across 34 countries in Europe, Asia, Australia and Latin America. The study primary end-points are non-inferiority for net adverse clinical events; superiority for bleeding; and non-inferiority for ischaemic endpoints of abbreviated versus prolonged DAPT, at one year.
Peter Smits, Head of Intervention Cardiology, Maasstad Hospital and study co-principal investigator says, “This new trial is an important step towards gathering robust evidence to define the safest DAPT regimen in this sizable proportion of patients treated in contemporary percutaneous coronary intervention practice. It is great that The Netherlands is the first of 34 countries worldwide to contribute to this important scientific work.”
Co-principal investigator Marco Valgimigli, prof of Cardiology and director of Clinical Research, Inselspital Universitätsspital Bern, Switzerland, says, “We have been working on this study for a long time, so it is a very rewarding moment to see it get underway with our first patient enrolled. We have an ambitious target but I am optimistic that with the support of many highly motivated centres and investigators across the globe we will get there.”
All patients in the study will have the Ultimaster stent implanted in the context of routine care.
Following a mandatory one month of DAPT treatment, patients will be randomised to either continue DAPT, or transition to APT monotherapy. The Ultimaster DES is designed to promote optimal vessel recovery and therefore hypothesised to facilitate a shortened DAPT regimen.
The study is sponsored by the European Cardiovascular Research Institute (ECRI, Rotterdam, The Netherlands) and supported with an unrestricted grant by Terumo Corporation.
Ivascular has announced the product range extension of its self-expandable stent, iVolution, to 200mm length, in various diameters.
Ivolution is a nitinol endovascular stent, combining high flexibility and conformability, together with increased radial strength. Its mechanical properties have been independently evaluated by the Paris Institute of Technology.
Lluis Duocastella, iVascular CEO said: “The addition of the 200mm iVolution to the iVascular portfolio, is a major step to improve therapy in the most complex indications such as TASC C and D femoropopliteal lesions. We are excited to provide such new references to physicians, without any compromise on the French size compatibility, stent features or ease of use”.
A Sheffield healthcare company has announced a strategic ‘buy out’ from its parent company, BD (Becton, Dickinson and Company), a deal which will see the company independently trade once again as UK Medical Ltd.
UK Medical supplies a range of interventional medical devices to the UK’s National Health Service (NHS) and the private healthcare sector. The company specialises in products used in minimally-invasive image-guided procedures to diagnose and treat diseases in various organs of the body.
UK Medical’s products, which include devices in breast radiology, urology, interventional radiology and cardiology, are designed to meet individual patient needs and help clinicians deliver positive clinical results, a press release from the company says.
Going forward, UK Medical will continue to serve BD as the UK distributor for the same soft tissue and bone marrow biopsy products that UK Medical was selling before the ‘buy out’.
Speaking at the announcement Ian Aaron, managing director of the company, said: “This is a great deal for both companies and we look forward to a continued and long partnership. Alongside our biopsy range we will also have an exciting range of other innovative interventional products. We want to partner with the NHS by supplying products that add value, improve patient care pathways and at the same time provide excellent value. We are very excited to be making a difference to patients and to the NHS.”
In 2012, UK Medical was purchased by CareFusion, a medical technology company, which BD acquired in 2015. UK Medical will now run independently from its Sheffield headquarters.
Terumo Europe NV has announced the first commercial clinical case using Quiremspheres—the next generation radioembolization microspheres for advanced unresectable liver cancer.
Quiremspheres are the only commercially available microspheres that contain the radioactive isotope holmium-166. In recent trials, holmium microspheres have been shown to be safe and effective for the treatment of advanced liver cancer, a press release from Terumo says.
Unlike the widely adopted yttrium-90 microspheres, Quiremspheres can be visualised in low concentrations by means of single-photon emission computed tomography (SPECT) and MRI. This allows clinicians to quantitatively assess the distribution of microspheres in the liver, enabling accurate evaluation of treatment directly after the radioembolization procedure.
Quiremspheres have been used for the first time outside of a research setting, in clinical practice at the University Clinic Carl Gustav Carus in Dresden, Germany. A multidisciplinary team, consisting of R T Hoffmann and J Kotzerke and their dedicated teams performed the radioembolization procedure on a patient with metastatic colorectal cancer in the liver.
Hoffmann, head of Interventional Radiology at the University Clinic Carl Gustav Carus said: “As a radiologist, I value the unique imaging capabilities of Quiremspheres. SPECT and MR-imaging opens new opportunities that we look forward to exploring. This will give us the confidence we need to start individualising treatments.”
In addition to the unique imaging capabilities, Holmium-166 also has a shorter half-life than Yttrium-90. Kotzerke, head of the Nuclear Medicine department at the University Clinic Carl Gustav Carus commented: “The short halftime of holmium-166 results in a high initial dose rate. Therefore, we expect to see an improved radiobiological effect.”
In reflection of the physician-led collaboration for the development of this treatment, Marnix Lam, heading the Nuclear Medicine department of the University Medical Center Utrecht in the Netherlands said “I am excited to see this treatment, which has been developed at our hospital, now becomes available for patients across Europe.”
Peter Coenen, president of Interventional Systems Terumo EMEA said: “We are grateful for the confidence that the Dresden clinical team places in us and QuiremSpheres. We strongly believe that the unique imaging capabilities of Quiremspheres can be a game changer in the field of radio-embolization and this first patient treatment is an important milestone towards realising its full potential.”
Jan Sigger, CEO of Quirem Medical BV, the manufacturer of Quiremspheres said: “We are excited that, after more than 15 years of research, Quiremspheres has become available for clinical use. Through our strategic partnership with Terumo, liver cancer patients across Europe can now benefit from the next generation microspheres for radioembolization.”
For any questions, please contact Alexandra Vassiliades, group manager, Marketing Communications Terumo Interventional Systems, EMEA: [email protected]
A study recently published in Cardiovascular and Interventional Radiology has, for the first time, identified adenomatous-dominant benign prostatic hyperplasia as a predictor of clinical success following prostate artery embolization.
The investigators, Mark W Little, and CR Tapping from the Department of Radiology, Churchill Hospital, Oxford University Hospitals NHS Foundation Trust, Oxford, UK, set out to investigate the clinical impact of performing prostate artery embolization on patients with adenomatous-dominant benign prostatic hyperplasia.
Twelve patients from the ongoing STREAM (Prostatic artery embolization for the treatment of benign prostatic hyperplasia) trial were identified as having adenomatous-dominant benign prostatic hyperplasia. The condition was defined as two or more adenomas within the central gland of ≥1cm diameter on multiparametric MRI. These patients were age matched with patients from the STREAM cohort, without adenomatous-dominant benign prostatic hyperplasia. Patients were followed up with repeat multiparametric MRI at three months and one year. International prostate symptom score (IPSS), international index for erectile function (IIEF), and quality of life assessment from the IPSS and EQ-5D-5S questionnaires were recorded before embolization, at six weeks, three months, and one year.
The mean age of patients was 68 years and all had embolization as a day-case procedure. The technical success in the cohort was 96%. There was a significant reduction in prostate volume following embolization with a median reduction of 34% in the group with adenomatous-dominant benign prostatic hyperplasia, compared to a mean volume reduction of 22% in the other group (p=0.04). There was a significant reduction in IPSS in the group with adenomatous-dominant benign prostatic hyperplasia group following embolization when compared with the control (p=0.01). IPSS quality of life scores significantly improved in the adenomatous-dominant benign prostatic hyperplasia group compared to the control group (p=0.007). There was no deterioration in sexual function in either group after the procedure.
“Adenomatous dominant benign prostatic hyperplasia is more responsive to embolization due to the increased vascularity of these benign lesions within the gland, resulting in preferential embolic flow into the adenomatous tissue,” Little told Interventional News.
Goetz Richter, Clinic for Diagnostic and Interventional Radiology, Stuttgart, Germany, presented breaking data from the Miracle 1 multicentre hepatocellular carcinoma trial at The Symposium on Clinical Interventional Oncology (CIO, 4–5 February, Hollywood, Florida). He spoke to Interventional News on the role of drug-eluting particles in interventional oncology.
What are the key findings from the MIRACLE 1 trial?
MIRACLE I study results demonstrated a high tumour control rate and few serious adverse events among patients with locally or clinically unresectable hepatocellular carcinoma treated with Embozene Tandem (Boston Scientific) microspheres loaded with 150mg doxorubicin. Specifically, complete response was achieved in nearly half of the patients (48%) treated; 19% had a partial response; 29% had stable disease; and disease progression was observed in only one patient (5%). No specific safety concerns were associated with the small 75μm microsphere size used in the study, and systemic toxicities were minimal with no myelosuppression and only one patient developing mild alopecia.
Although the study was relatively small with 25 patients enrolled, it was fairly representative of a “real world” situation of hepatocellular carcinoma interventional treatment: around 40% of the patients had ascites and, furthermore, almost 40% had an advanced stage of liver disease besides the tumour burden (Child B and C stage).
These study results support the safety of transarterial chemoembolization (TACE) procedures using drug-eluting beads performed with small (75μm) calibrated microspheres.
Additionally, these small microspheres loaded with doxorubicin provided good local tumour control. We never encountered pulmonary complications indicating that choosing a size of 75μm for drug-eluting particle embolization does not entail systemic (shunt) risk as compared to Y-90 therapy.
What is the role of drug-eluting particles in interventional oncology?
The role of drug-eluting particles is growing. As the body of evidence demonstrating procedural safety, tumour response, and a lack of systemic effects grows, it builds support for drug-eluting embolic therapy as an option for patients with hepatocellular carcinoma and other cancers that have few or no other treatment alternatives.
What were some of the limitations of MIRACLE 1?
The study sample size was small with 25 patients and, as with many studies of hepatocellular carcinoma treatment, patient characteristics such as tumour burden and severity of liver disease varied widely. Furthermore and theoretically, it would be conceivable to use 40μm or 100μm sizes for drug-eluting bead embolization in hepatocellular carcinoma. This was not tested in this study.
In general, what are the trends you see with regard to embolic particles in interventional oncology?
Embolic particles are very versatile and the ability to load drugs further adds to their therapeutic potential. This potential will not be restricted to its use in hepatocellular carcinoma alone. Research is ongoing to test the safety and efficacy of particle embolization in liver metastastic disease. There is also interest in combining the use of embolic particles with thermal ablation in a variety of organs to enhance safety and efficacy.
“Cryoablation of metastatic breast cancer is a safe and effective method that allows local control of the disease,” Claudio Pusceddu told delegates at the European Congress of Radiology (1–5 March, Vienna, Austria).
Pusceddu, who is director of Interventional Radiology, Hospital Oncology, Cagliari, Italy, presented on his team’s initial experience of using cryoablation as a local therapy for patient with metastatic breast cancer.
With cryoablation, noted Pusceddu, several observational studies have demonstrated a higher survival rate among patients with stage IV breast cancer in whom the primary tumour is completely excised at the time of diagnosis. He also emphasised that breast cryotherapy offered several advantages compared to other techniques: it is performed under local anaesthesia (an advantage for elderly patients and those with comorbidities); the procedure results in little, or no post-procedural pain; it is possible to monitor the ice-ball in real-time; there is minimal or absent post-ablation syndrome; and the procedure entails a short hospitalisation that usually consists of one day.
Pusceddu and colleagues set out to evaluate the safety and efficacy of breast cryoablation. They treated 39 breast lesions, mean size 2.1 cm (range 1–6.7cm) in 29 consecutive patients with a mean age of 51 years. All patients had core-needle biopsy-proven breast carcinoma. All patients included in this study presented with metastases at the beginning of disease. Twenty-three patients had one lesion; four patients had two lesions; one patient three lesions and one patient had five lesions.
The tumour and surrounding breast tissue were ablated with percutaneous CT-guided cryoablation under local anaesthesia. Cryoablation consisted of two cycles each of 10 minutes of freezing followed by a four minute active and four minute passive thawing phase for each one. Twenty-four patients underwent one cryoablation session, four patients underwent two cryoablation sessions and one patient underwent three cryoablation sessions.
All cryoablation sessions were successfully completed and all the tumours in the breast were ablated. There were transient and mild ecchymotic changes and post-procedural oedema seen in ten cases. The therapeutic outcomes were evaluated using contrast-enhanced CT or MRI at two-, six-, 12-, and 18-month intervals. The absence of tumour enhancement on CT or MR image was considered as indicating complete tumour necrosis. During the mean follow-up of 15 months (six to 28 months) 26 patients had shown complete response to the treatment. Only three patients out of 29 (10%) showed relapse close to the treated lesion. These patients were treated with a second cryoablation procedure.
“Cryoablation of the breast is a safe and effective procedure capable of obtaining complete destruction of the tumour without significant consequences. This method can effectively be used with good local control of the disease in patients who present with metastases at the beginning of the disease,” concluded Pusceddu.
In a new study published in JCI Insight, UC Davis researchers have shown that combining high-intensity focused ultrasound with two immunotherapies (a PD-1 checkpoint inhibitor and TLR9 agonist) can produce excellent response rates in mouse models of epithelial cancer. They also found that, for the combination to be effective, immunotherapies must come first.
“These combination protocols can achieve a complete response in a large fraction of solid tumours,” said Katherine Ferrara, professor of the UC Davis Department of Biomedical Engineering and senior author on the paper. “We found that we could achieve responses in distant lesions, but the specific protocol is really important.”
High-intensity focused ultrasound is a relatively new approach to eliminating or reducing malignant tumours. An ultrasound beam heats up tumour tissue, killing cancer cells in minutes. However, the effect is purely localised. The UC Davis team hoped that by combining it with immunotherapies they could gain more systemic tumour control.
On the immunotherapy side, the PD-1 inhibitor takes the brakes off cytotoxic T-cells, releasing them to fight cancer with greater intensity. The TLR9 agonist boosts dendritic cells and other immune components.
With the ultrasound, researchers were relying on the “abscopal effect,” which is often observed in patients who receive radiation. As cancer cells die, they release antigens that kick up the immune response, focusing T-cells on the tumour and turning a local effect into a systemic one. Ultrasound also contributes by shrinking the tumour, making it more vulnerable to immune attack.
In the study, the team tested the immunotherapies both before and after ultrasound to determine which protocol was more effective. They found that priming the immune response before ultrasound was the best approach, leading to complete responses in 80% of mice after 90 days.
“We were surprised the protocol made such a difference,” said Matthew Silvestrini, first author of the study. “For the immunotherapy to be successful, it is particularly important to start it first. We found the focal therapy could have negative consequences if the immunotherapy was not started first.”
The study showed that early immunotherapy both expanded the T-cell population and primed them to respond.
“You get the immune response going, and then you deliver the focal therapy,” Ferrara said.
When given in the correct order, the therapies had a profound impact on tumours, controlling systemic lesions, as well as those being targeted with ultrasound. In addition, treating multiple tumour sites sequentially with ultrasound following immunotherapy was more effective than immunotherapy alone.
The researchers acknowledge they need to better understand why some tumours respond differently than others. They are in the process of developing imaging probes that will help them track a therapy’s effectiveness and quickly hone in on the most beneficial protocols.
“We know we need to personalise these therapies,” said Ferrara. “We are developing the tools that will help us do that.”
Angiodynamics has announced it has received CE mark certification for the Solero microwave tissue ablation system. Solero and its accessories are indicated for the ablation of soft tissue during open, laparoscopic or percutaneous procedures. The Solero system is not intended for cardiac use.
“The Solero microwave tissue ablation system is a significant addition to our portfolio of oncology/surgery products and allows physicians to maximizs the volume of tissue ablated in the shortest period of time,” said Rick Stark, senior vice president and general manager of the Oncology/Surgery division of AngioDynamics. “Solero is a single applicator system able to complete upto a 5cm ablation in six minutes at maximum power.”
The Solero system features the Solero microwave generator and the specially designed Solero applicators. The solid state Solero microwave generator with a 2.45 GHz operating frequency can power up to 140W for optimised power delivery and fast ablations. The Solero applicator’s optimised ceramic tip diffuses energy nearly spherically, and its patented cooling channel with thermocouple provides real-time monitoring to help protect non-targeted tissue ablation. In addition, the Solero system offers physicians scalability with a single applicator designed for multiple, predictable ablation volumes by varying time and wattage.
Mirabilis has announced CE mark authorisation to market the Mirabilis System in the European Union. The system combines high-speed therapeutic ultrasound technology with an advanced robotic system for uterine fibroid treatment.
The company simultaneously announced receiving approval from the US FDA to begin a clinical study of the Mirabilis System in the USA.
Approximately 25% of all women suffer from symptomatic uterine fibroids at some point in their lives, with annual US spending on fibroid treatment exceeding US$2.1 billion according to the National Institutes of Health. Over 40% of all hysterectomies are performed to treat fibroids.
Current treatments for uterine fibroids typically involve an invasive surgical procedure that can include endometrial ablation, myomectomy, and hysterectomy. In addition to the cost, surgical risk, and recovery time of such procedures, they often result in infertility.
The system treats uterine fibroids non-invasively by focusing ultrasound energy into the fibroids from outside the body; there is no incision involved. The procedure is performed by a physician placing the system on a woman’s abdomen, locating the fibroid using built-in ultrasound imaging, and selecting the area of the fibroid to be treated. Under physician control, the device then automatically treats the fibroid using a robotic motion system. Proprietary Mirabilis technology allows typical treatments to be completed in less than ten minutes in a medical office, as opposed to several hours in a hospital for some alternatives.
“The Mirabilis System has been in development for nearly ten years, and it is very exciting to now be able to bring this technology to market,” said Jens U Quistgaard, president and CEO of Mirabilis. “This technology holds the promise of helping a large number of women worldwide, and we’re very pleased to be able to begin making it available.”
The Mirabilis System is currently restricted to investigational use in the USA, however, the company expects to begin a clinical study later this year intended to lead to US marketing approval. The Mirabilis DIANA study is planned to be conducted at 12 clinical sites in the US, Canada, and Europe.
Metactive, an early-stage company focused on developing embolization devices for the treatment of peripheral vascular and neurovascular diseases, has announced the issuance of US patents 9,572,697 and 9,572,698 covering its Blockstent Microcatheter for embolization of peripheral arteries and veins and Ballstent Microcatheter for embolization of cerebral aneurysms. These proprietary microcatheter devices deliver a compressed gold metal implant over a 0.014” guidewire to treatment sites, where the implant is expanded and then detached to permanently stop blood flow.
“We designed the Blockstent and Ballstent devices to provide an ideal solution for embolization. These devices are low profile, easy to use, and can quickly be placed with a high degree of precision, resulting in immediate, complete, and lasting cessation of blood flow,” said F Nicholas Franano, president and CEO of Metactive.
The new patents are part of an intellectual property portfolio that also contains numerous additional patent applications to which Metactive has exclusive rights in the US and major international markets. The portfolio covers four major patent families and includes methods of treating aneurysms, arteries, and veins, as well as related embolization devices.
Metactive also announced the closing of US$1.5 million of additional Series A financing, co-led by Mid-America Angels, with the participation of a family office and additional individual investors. Metactive previously raised $7.5 million in Series A funding, bringing the total funding raised to $9 million.
“This new funding provides Metactive with the resources to continue the development and testing of its novel embolization devices,” said Franano. “Our preclinical study results show that both devices routinely provide immediate, complete, and durable occlusion, something that market leading coils, flow diverting stents, and mesh vascular plugs cannot deliver. We look forward to a time when standing in the interventional suite wearing heavy lead protective garments, placing multiple devices, and performing serial angiography waiting for a vessel to occlude will no longer be required to complete an embolization procedure.”
The new meta-analysis, presented as a poster by researchers from the University of Texas Health Sciences Center, San Antonio, USA, during the 2017 American College of Cardiology meeting on 19 March, included data from nine studies comparing the use of RenalGuard to conventional volume expansion. Six were randomised controlled trials using RenalGuard in the treatment of patients undergoing various cardiovascular diagnostic and therapeutic interventions. Primary outcomes in the analysis included the incidence of contrast-induced acute kidney injury and relative risk. Secondary outcomes included the incidence of mortality, major adverse cardiovascular events, and the need for post-procedure dialysis.
The investigators found RenalGuard therapy to be associated with a significant risk reduction in contrast-induced acute kidney injury compared to the control therapy (Relative risk: 0.409; 95% CI: 0.282-0.591; p<0.001).
RenalGuard measures a patient’s urine output and automatically infuses hydration fluid based on that urine output. The system is designed to induce high urine rates, which have been shown to protect the kidney from a range of insults. A number of studies have demonstrated RenalGuard’s ability to protect patients from AKI following catheterisation procedures when compared to the standard of care.
“We are very pleased that independent analysis of the growing clinical data continues to support the potential of RenalGuard to significantly reduce the serious health risks associated with acute kidney injury related to cardiac interventional procedures,” said Andrew Halpert, president of RenalGuard Solutions. “In doing so, we believe RenalGuard offers the potential to safely bring the important benefits of such medical interventions to more patients, especially those who have been considered at too high risk due to their reduced kidney function.”
Halpert further noted that a US pivotal clinical trial of RenalGuard was currently on track to complete at the end of 2017, and if positive, the company planned to seek US marketing approval from the FDA in 2018.
Unfors RaySafe has introduced the RaySafe i3, to its suite of real-time dosimetry products, at the European Society of Radiology in Vienna, Austria.
The RaySafe Real-Time Dosimetry solution, introduced in 2012, helps physicians and clinical staff visualise X-ray exposure in real time using easy-to-read bar graphs displayed on a monitor. The instant feedback empowers medical staff to adapt their behaviour around radiation, to help minimize unnecessary exposure.
“The improvement in radiation protection has been more than dramatic at the URMC. There is no substitute for a constant and real-time reminder of the dose being received,” said Labib H Syed, of University of Rochester Medical Center, Rochester, USA.
The RaySafe i3 is designed to improve wearability, prolong life cycle and increase measurement accuracy. The RaySafe i3 can be used in low dose procedures and in hybrid OR environments.
“RaySafe i3 helps keep the medical staff in-the-know, at all times, about the level of radiation exposure, for themselves and their colleagues, in real-time,” said Bart Leclou, personal dosimetry business area manager for RaySafe. “The decision to implement the RaySafe i3 shows a commitment and dedication by a department to keep their staff safe from excessive radiation exposure.”
The new Acuson Freestyle Elite ultrasound system can now be combined with the Artis angiography systems to enable fast and easy-to-use ultrasound guidance during interventional procedures. With this combined solution, referred to as Artis Freestyle Access, Siemens Healthineers supports a more convenient, less time-consuming, and safer workflow, a press release from the company says.
Acuson Freestyle Elite is a member of the new generation of wireless ultrasound systems from Siemens Healthineers. Its cable-free transducers utilise an ultra-wide band frequency to wirelessly transmit imaging data from the probe to the system, freeing the ultrasound user from distracting cables. With the Artis Freestyle Access solution, the antenna receiver is positioned on top of the Artis Display, and the Acuson Freestyle ultrasound unit is mounted at the rear of the display, which results in a completely cable-free solution in the room. This not only saves space and increases workflow flexibility, it also promotes a hazard-free work environment in the interventional suite.
In many labs, the ultrasound system often has to be brought into the angio suite when ultrasound guidance is required. The patient’s name then has to be registered on the system and the transducers have to be draped. In order to make any changes in the ultrasound parameters during the examination, a second non-sterile staff member is required to intervene and operate the buttons on the ultrasound system. Artis Freestyle Access helps to eliminate the extra time needed for these steps.
The combined solution is available for immediate use and only requires patient registration once on the angiography system, because when prompted, the ultrasound unit automatically receives the patient information registered on the Artis angiography system. This provides seamless registration on the ultrasound system and shortens the time needed to begin the ultrasound exam. With its custom-fitted sheaths, the cable-free probes can be more quickly and easily draped compared with cabled probes on conventional ultrasound systems, and on-probe controls give the user direct control of the ultrasound features and eliminate dependency on other staff members. During the procedure, the ultrasound images are shown directly on the Large Display. At the end of the procedure, the ultrasound images are automatically sent to PACS, with no need for further user interaction. That’s how Artis Freestyle Access in tandem with the Acuson Freestyle Elite ultrasound system facilitates the use of ultrasound in interventional suites during interventional procedures.
The use of ultrasound guidance plays an important role in vessel punctures, for example, of the femoral artery. It helps decrease the likelihood of complications while increasing the likelihood of first-attempt success, as shown by a meta-analysis study published in the Journal of Invasive Cardiology. Therefore, the ability to quickly and easily use ultrasound in the angiography suite, as enabled by Artis Freestyle Access, can help reduce puncture-related complications during endovascular procedures.
Simplified procedure planning and catheter navigation for liver embolization
With the new version of the syngo Embolization Guidance software, automatic feeder-detection and colour-coded visualisation of tumour-feeding vessels facilitates the location of the optimal treatment position for each tumour nodule. This means that syngo Embolization Guidance can support a complete embolization of the entire tumour in transarterial chemoembolization (TACE) procedures, for example. The interventionalist simply needs to mark the treatment area(s) by drawing a line describing the diameter of each lesion with just one click. Then the software fully automatically detects the catheter and identifies the vessels between the treatment area(s) and the catheter. By automatically calculating a safety margin of a few millimetres around the lesion, the algorithm is also able to identify vessels that feed the surrounding environment of the tumour where non-visible singular tumour cells are suspected. This feature helps support targeted embolization where the malignant tissue is completely covered by treatment while as much healthy tissue as possible is preserved. “The principle of selective microcatheter placement in chemoembolization aims for accomplishing complete tumour coverage while at the same time preserving healthy liver tissue from unnecessary treatment. Syngo Embolization Guidance automatically extracts essential tumour feeder information from DynaCT datasets during the intervention, resulting in a simplified process for the interventionalist when choosing optimized treatment positions”, explains Bernhard Meyer from Hannover Medical School Germany.
The interventional radiologist can easily adjust the vessel tree by pruning, removing, or adding vessels manually. As in the previous version, the software also allows for segmentation and determination of tumour nodule volume based on syngo DynaCT, CT, or MRI datasets. The new features support an efficient, standardised and safe treatment of liver tumours, either from the control room or right at tableside. The interventionalist may no longer need to stop and leave the interventional room during the procedure. This innovation from Siemens Healthineers aims to enable customers to increase their treatment efficacy and workflow efficiency while also reducing costs.
Venoplasty is not effective in treating multiple sclerosis, according to the first presentation of interim data from a randomised, double blind clinical trial of jugular and azygous venoplasty in multiple sclerosis. Lindsay Machan, University of British Columbia (UBC) and Vancouver Coastal Health, presented the data at the Society of Interventional Radiology’s annual scientific meeting in Washington, DC, USA.
“In our study, we found no difference in subjective or objective changes between patients who had sham angioplasty or balloon venoplasty,” Machan told Interventional News.
These data concerning the “liberation therapy,” which thousands of people with multiple sclerosis have undergone since 2009, do not support the claim that multiple sclerosis patients can achieve dramatic improvements from a one-time medical procedure.
The multicentre prospective randomised blinded sham-controlled trial of jugular venoplasty in multiple sclerosis study set out to compare the clinical efficacy of balloon venoplasty vs. sham angioplasty of jugular and azygous vein stenoses in patients with multiple sclerosis 48 weeks post procedure.
“I do believe this to be the most rigidly scientifically conducted assessment of chronic cerebrospinal venous insufficiency (CCSVI) to date. These results constitute a mid-term report of our study. We have seen highly respected practitioners of our specialty observe marked improvement in some patients and although in this mid-term report we did not observe differences in outcome between sham and balloon venoplasty, I await with interest the final dataset when we will compare the results in individual patients,” Machan explained.
“After week 48, all patients underwent a crossover procedure (those who had the sham procedure at week 0 had balloon angioplasty and vice versa). All patients have now had their crossover procedures and are being followed for another 48 weeks after that. We expect the final report sometime in Autumn,” he added.
“We hope these findings, coming from a carefully controlled, ‘gold standard’ study, will persuade people with multiple sclerosis not to pursue liberation therapy, an invasive procedure that carries the risk of complications, as well as significant financial cost,” said Anthony Traboulsee, a UBC associate professor of Neurology and director of the MS Clinic at the Djavad Mowafaghian Centre for Brain Health. “Fortunately, there are a range of drug treatments for multiple sclerosis that have been proven through rigorous studies to be safe and effective at slowing disease progression.”
Multiple sclerosis patients, including relapsing and progressive, from four academic clinics, recruited after clinical and ultrasound screening were blinded by deep conscious sedation. If catheter venography confirmed jugular or azygous vein stenosis, they were prospectively randomised 1:1 intra-procedure by sealed envelope to receive balloon or sham venoplasty of all stenoses.
The study was “double-blinded”: Neither the patients nor the physicians who evaluated them knew who was receiving the actual treatment or the sham procedure. The study had some people undergo a “sham” procedure. All 104 participants had a catheter inserted into their blocked veins, but only 49 had venoplasty.
Patient questionnaires were given at baseline, 24 hours and 12 weeks, physical exam at the baseline and at weeks 12, 24, 36, and 48, and MR at baseline and weeks 24 and 48. Safety outcomes including serious adverse events, venous thrombosis, and restenosis were monitored by an independent data safety monitoring board, and clinical trial monitors provided trial oversight. Patients initially randomised to venoplasty received a sham procedure one year later, and vice versa. Extensive efforts were made so the patient experience was the same for both procedures.
A year later, the venoplasty group’s results were statistically the same as those in the sham group, as measured by brain imaging, standard assessments of multiple sclerosis symptoms and the patients’ own self-assessments.
The researchers found no statistically significant difference between the treatment group and the sham group in patient symptoms, either as reported by the patients or as determined by physicians, three days after the procedure and a year later. Both groups showed slight but equal improvements a year later in the patients’ own assessments; physician assessments showed no improvement in either group.
MRI of their brains was used to count the number of new lesions in their myelin, and researchers found no difference between the treatment group and the placebo group at six months and one year later.
The researchers are now preparing an article, based on the US$5.4-million study, jointly funded by the Canadian Institutes of Health Research, the MS Society of Canada, and the provinces of British Columbia, Manitoba and Quebec, for publication in a peer-reviewed journal.
Using venoplasty as a multiple sclerosis treatment was first put forward by vascular surgeon Paolo Zamboni of Italy, who asserted that narrowing of the veins in the neck could be causing iron to accumulate in the brain and spinal cord, triggering an autoimmune response. He called his theory chronic cerebrospinal venous insufficiency (CCSVI), and cited several dozen cases of patients who improved after undergoing venoplasty performed by him.
Many patients in Canada and Europe, upon learning of those anecdotal results through the news media, asked for imaging of their veins and subsequent venoplasty. But almost all Canadian physicians, citing the lack of supporting evidence, would not perform it, prompting some patients to seek the treatment in the USA, Latin America and Eastern Europe.
This is the second study to be led by the UBC and Vancouver Coastal Health team and involving researchers from across Canada that aimed to seek more evidence on the CCSVI theory. The first study, published in The Lancet in 2013 and supported by the MS Society of Canada, sought to determine if narrowed veins was a distinct feature of multiple sclerosis and found that narrowing was just as common in people without the disease.
“Despite the negative findings of that diagnostic study, many patients wanted to know if the venous dilation procedure could help,” said Machan. “We were committed to meticulously evaluating this treatment with robust methods and patient-focused outcomes.”
Interventional radiologists at the University of California at Los Angeles (UCLA), Los Angeles, USA, are using technology found in self-driving cars to power a machine learning application that helps guide patients’ interventional radiology care, according to research presented today at the Society of Interventional Radiology’s 2017 annual scientific meeting (4–9 March, Washington, DC, USA).
The researchers used cutting-edge artificial intelligence to create a “chatbot” interventional radiologist that can automatically communicate with referring clinicians and quickly provide evidence-based answers to frequently asked questions. This allows the referring physician to provide real-time information to the patient about the next phase of treatment, or basic information about an interventional radiology treatment.
“We theorised that artificial intelligence could be used in a low-cost, automated way in interventional radiology as a way to improve patient care,” said Edward W Lee, assistant professor of Radiology at UCLA’s David Geffen School of Medicine and one of the authors of the study. “Because artificial intelligence has already begun transforming many industries, it has great potential to also transform healthcare.”
In this research, deep learning was used to understand a wide range of clinical questions and respond appropriately in a conversational manner similar to text messaging. Deep learning is a technology inspired by the workings of the human brain, where networks of artificial neurons analyse large datasets to automatically discover patterns and “learn” without human intervention. Deep learning networks can analyse complex datasets and provide rich insights in areas such as early detection, treatment planning, and disease monitoring.
“This research will benefit many groups within the hospital setting. Patient care team members get faster, more convenient access to evidence-based information; interventional radiologists spend less time on the phone and more time caring for their patients; and, most importantly, patients have better-informed providers able to deliver higher-quality care,” said co-author Kevin Seals, resident physician in Radiology at UCLA and the programmer of the application.
The UCLA team enabled the application, which resembles online customer service chats, to develop a foundation of knowledge by feeding it more than 2,000 example data points simulating common inquiries interventional radiologists receive during a consultation. Through this type of learning, the application can instantly provide the best answer to the referring clinician’s question. The responses can include information in various forms, including websites, infographics, and custom programmes. If the tool determines that an answer requires a human response, the programme provides the contact information for a human interventional radiologist. As clinicians use the application, it learns from each scenario and progressively becomes smarter and more powerful.
The researchers used a technology called Natural Language Processing, implemented using IBM’s Watson artificial intelligence computer, which can answer questions posed in natural language and perform other machine learning functions. This prototype is currently being tested by a small team of hospitalists, radiation oncologists and interventional radiologists at UCLA.
“I believe this application will have phenomenal potential to change how physicians interact with each other to provide more efficient care,” said John Hegde, resident physician in radiation oncology at UCLA. “A key point for me is that I think it will eventually be the most seamless way to share medical information. Although it feels as easy as chatting with a friend via text message, it is a really powerful tool for quickly obtaining the data you need to make better-informed decisions.”
Prostate artery embolization maintains its effectiveness for at least three years after patients undergo the therapy, according to research presented at the Society of Interventional Radiology’s 2017 annual scientific meeting. The study was awarded as the “Abstract of the Year”.
This study of 1,000 men is the largest of its kind to evaluate the long-term effectiveness of prostate artery embolization.
Researchers also found that embolization is especially effective in men with benign prostatic hyperplasia who also have acute urinary retention or the inability to voluntarily urinate and in patients with very large prostates who are normally treated with open surgery.
“Prostate artery embolization gives men with benign prostatic hyperplasia a treatment option that is less invasive than other therapies and allows them to return to their normal lives sooner,” said João Martins Pisco, an interventional radiologist at St Louis Hospital in Lisbon, Portugal, and the study’s lead author. “Time and time again, I see patients who are relieved to find out about prostate artery embolization because they are not able to tolerate medications for benign prostatic hyperplasia due to their side-effects. These men also do not want traditional surgery because it involves greater risks, has possible sexual side-effects, and has a recovery time that is relatively long compared to prostate artery embolization, which is generally performed under local anaesthesia and on an outpatient basis.”
Between March 2007 and March 2016, Pisco and his team performed prostate artery embolization on 1,000 men with the average age of 67 years. All patients were evaluated in the short term (one, three, and six months); 807 patients were seen through the medium term (every six months between six months and three years), and 406 patients were evaluated long term (every year after three years).
During each evaluation, the men’s symptoms were measured by the International Prostate Symptom Score (IPSS), which tests for the blockage of urine flow, and the International Index of Erectile Function (IIEF), which assesses erectile dysfunction. Researchers also measured the size of the prostate and the amount of urine left in the bladder after urination. They also evaluated the peak urinary flow rate and the prostate-specific antigen (PSA) level, a test used to screen for prostate cancer.
The data from these measures revealed at the short-term mark that the treatment had an 89% cumulative success rate—measuring the success across all variables through the given testing period.
The 807 men evaluated at the medium-term mark had an 82% success rate. And of the 406 patients measured at the long-term mark, 78% were considered cumulative successes.
“Our results demonstrate that this minimally invasive treatment is successful in the long term and should always be presented to patients who are exploring options to resolve their benign prostatic hyperplasia,” remarked Pisco.
In an additional analysis, researchers found that among 112 patients who also suffered acute urinary retention before undergoing embolization, 106 or 94.6% had their catheter removed between two days and three months after treatment. At medium-term and long-term follow-up, 95 of the 112 (84.8%) and 89 of the 112 (78.5%) did not experience any recurrence of their acute urinary retention.
The team also performed prostate artery embolization in 210 patients who had limited treatment options due to extreme enlargement of the prostate (larger than 100cm³). Of these men, 84% experienced cumulative success at short-term evaluation and 76.2% at medium- and long-term. The normal size of a prostate is 15–30cm3.
While this research demonstrated that prostate artery embolization was highly successful, Pisco noted that the treatment may not be appropriate for all patients, such as those with advanced arterial atherosclerosis that may be due to smoking or diabetes.
As a next step, researchers are now conducting a study comparing the effectiveness of prostate artery embolization to a sham—or placebo—treatment to address any possible placebo effect that may have occurred during Pisco’s research with these 1,000 patients.
BTG has received Class III CE mark certification for DC Bead Lumi, the first commercially available radiopaque drug-eluting bead (DEB) in the EU which can be loaded with doxorubicin or irinotecan for the local treatment of tumours in patients with hepatocellular carcinoma and malignant colorectal cancer metastasised to the liver. According to a company release, for the first time, DC Bead Lumi provides real-time visible and lasting confirmation of bead location.
The visibility of DC Bead Lumi, both during and after embolisation, is intended to provide the opportunity to individualise a patient’s treatment, by enabling real-time evaluation of the completeness of tumour treatment and enhanced endpoint determination. The incorporation of a tri-iodobenzyl moiety is designed to offer inherent long-term radiopacity of DC Bead Lumi, allowing informed decision-making for future treatment plans as DC Bead Lumi is still visible in follow-up scans, identifying areas of treatment and under-treatment.
“The ability to see bead location during transcatheter arterial chemoembolization procedures is a key step in enhancing the quality and potentially minimising complications of the procedure, and can help improve treatment outcomes compared to current techniques,” says Tobias Jakobs, The Hospital of the Order of St John of God, Munich, Germany. “More importantly, the lasting radiopacity of DC Bead Lumi means I can show patients that treatment has been placed exactly where it is needed.”
Bluegrass Vascular has announced that it is entering into a strategic relationship with Merit Medical. The agreement will streamline European distribution of the recently CE mark approved Surfacer inside-out access catheter system and will provide funding to support the company’s efforts to secure FDA clearance for product sales in the USA.
“The Surfacer System is an innovative inside-out approach to restore access to the right internal jugular vein and to preserve treatment options in haemodialysis patients with occluded veins,” stated Fred Lampropoulos, chairman and CEO of Merit. “This unique approach addresses an unmet need in haemodialysis care and aligns with Merit’s interventional portfolio, which includes the Hero graft, a complementary device designed to reduce catheter-associated complications and costs. We are very excited to bring this novel technology to market.”
Central venous obstruction occurs in roughly 40% of instances where haemodialysis is being received by a central venous catheter. While permanent arteriovenous fistulas are the preferred form of vascular access for haemodialysis patients, central venous catheters continue to serve as an important bridge to securing long-term access for life-saving haemodialysis treatment. The current approach for most patients with central venous occlusions is to use an alternative vein, which reduces the ability to place and mature a functioning fistula, resulting in increased catheter days and costs.
The Surfacer inside-out access catheter system provides reliable, efficient and repeatable central venous access to the right internal jugular vein, the optimal location for placing a central venous catheter. By securing safe and repeatable central venous access to this vein, the Surfacer System allows physicians to “avoid going left”, thereby protecting arteriovenous fistulas placement for better patient outcomes and improved health economics for both hospitals and haemodialysis providers.
Data from the randomised controlled ATTRACT trial revealed that the addition of catheter-based intervention to standard-of-care anticoagulation failed to significantly decrease the occurrence of post-thrombotic syndrome in patients who received this treatment strategy when compared to its occurence in patients who received anticoagulation alone. While there is disappointment at the headline findings of this landmark trial, experts have called the data both illuminating and hypothesis-generating.
The National Institutes of Health (NIH)-sponsored, phase III, multicentre ATTRACT (Acute venous thrombosis: thrombus removal with adjunctive catheter-directed thrombolysis) trial set out to determine if the use of pharmacomechanical catheter-directed thrombolysis added to standard care for above-the-knee proximal deep vein thrombosis prevents the post-thrombotic syndrome from developing over two years.
The primary outcome measure was the cumulative occurence of post-thrombotic syndrome between six and 24 months after randomisation, as measured by the Villalta scale. Secondary outcomes include safety, general and venous disease-specific quality of life, relief of early pain and swelling, post-thrombotic syndrome severity and cost-effectiveness.
ATTRACT data on the long-term effects of pharmacomechanical catheter-directed thrombolysis showed that 46.7% of the group that received interventional therapy went on to develop post-thrombotic syndrome, whilst 48.2% of those who received anticoagulation alone went on to develop post-thrombotic syndrome (p=0.56).
“Whilst ATTRACT results show no difference in the development of post-thrombotic syndrome in the two groups, there is a suggestion that getting the clot out is associated with a reduced severity of post-thrombotic syndrome,” Suresh Vedantham, the national principal investigator of the trial, told delegates at the Society of Interventional Radiology’s annual scientific meeting in Washington, DC, USA, where he presented the results for the first time today. Vedantham is professor of Radiology and Surgery, Mallinckrodt Institute of Radiology, Washington University School of Medicine in St Louis, USA.
Short-term data captured from the trial showed that the effects of pharmacomechanical catheter-directed lysis resulted in more major bleeds in the interventional arm (1.7%) than in the in the control arm, (0.3%; p=0.049). There were also significantly more instances of any bleeding (4.5%) in the interventional arm vs. 1.7% in the control arm (p=0.049). There were no fatal or intracranial bleeds in either arm of the trial indicating that few patients will be harmed as a result of thrombolytic therapy.
“Pharmacomechanical catheter-directed thrombolysis does not prevent post-thrombotic syndrome, and does increase bleeding. The ATTRACT data suggest that most deep vein thrombosis patients can avoid an [adjunctive] unhelpful procedure. Data also suggest that we need a better understanding of the pathogenesis of post-thrombotic syndrome. However, pharmacomechanical catheter-directed thrombolysis reduces early deep vein thrombosis symptoms and post-thrombotic syndrome severity. [As such] The open vein hypothesis is likely relevant to post-thrombotic syndrome progression and there is a suggestion that targeting this therapy to patients with iliofemoral deep vein thrombosis based on the high risk of post-thrombotic syndrome [might be beneficial],” Vedantham added.
The results suggest that pharmacomechanical catheter-directed thrombolysis should not be routinely used to prevent post-thrombotic syndrome in patients with symptomatic proximal deep vein thrombosis above the popliteal vein as there is no added benefit to exposing them to the risks and costs of additional catheter-based thrombolysis. The current standard therapy for patients with acute proximal deep vein thrombosis consists of anticoagulation and compression bandages.
However, data from subgroups and secondary analyses suggest that catheter-directed thrombolysis may have a benefit in patients who have acute iliofemoral deep vein thrombosis. The data also showed a trend towards greater treatment effect for catheter-based interventions with patients who present with more severe symptoms. However, triallists emphasise that ATTRACT was not statistically powered to draw definitive conclusions from these secondary analyses and outcomes and that the treatment effect seen in these should be seen as trends only and springboards for future research.
The triallists enrolled approximately 692 patients with acute proximal deep vein thrombosis involving the femoral, common femoral, and/or iliac vein into the ATTRACT study at 56 centres. They randomised 337 catheter-directed thrombolysis and 355 to anticoagulation alone.
The devices used in the trial to achieve pharmacomechanical catheter-directed thrombolysis were the AngioJet thrombectomy system (Boston Scientific); the Trellis-8 Peripheral Infusion System (Medtronic. This device is no longer on the market); or catheter-directed rt-PA infusion for up to 24 hours via a multisidehole infusion catheter.
“The limitations from this study are that there were losses to follow-up and that it was a medium-sized study. It was also not designed to evaluate specific methods of pharmacomechanical catheter-directed lysis,” Vedantham said.
An expert panel convened after the presentation pointed to the fact that this is a complex dataset because iliofemoral deep vein thrombosis has a different prognosis and natural history from femoropopliteal clot. Yet, these two different disease entities were grouped together in this trial for various valid reasons and because it was reasonable to evaluate if the open vein hypothesis might apply to both.
Mahmood Razavi, director, Center for Clinical Trials and Research, Heart and Vascular Center, St Joseph Hospital, Orange, California, USA, who is on the steering committee of the trial told Interventional News: “First, Suresh Vedantham deserves huge credit for undertaking the monumental task of running this trial. His contribution to the field of deep vein thrombosis research is immense and must be acknowledged. Second, interventional radiologists have long existed in a ‘pre-facts’ world and this trial provides the first rigorous dataset for catheter-directed lysis in deep vein thrombosis. When spinning the results of this trial, the purists will emphasise the statistical analysis and focus on the fact that the trial failed to meet its primary endpoint. However, pragmatists looking at the same data might interpret it differently and focus on the direction of treatment effect seen for catheter-based interventions in specific subgroups. For those of us who have been performing venous interventions for a long time, these data confirm what we have observed in clinical practice. From the practical standpoint, the data are encouraging for those patients with acute iliofemoral deep vein thrombosis. Also, if you look at clinically relevant measures such as a moderate to severe Villalta score and Venous Severity score, there is a signal there. However, it is important that these are clearly understood to be signals and tested further in an appropriate manner. There are very good clues from the ATTRACT data to further identify patients who would benefit from catheter-based treatments. We see from the data that there is a strong likelihood that certain groups of patients are helped more than others with additional catheter-based thrombolysis. In my view, the ATTRACT data are fantastically illuminating and hypothesis-generating. This is just the beginning of our research and activities in deep vein thrombosis.”
The panel of multidisciplinary experts including Michael Jaff (Massachussetts, USA) Timothy Murphy (Rhode Island, USA), Anthony Comerota (Toldeo, USA), Clive Kearon (Hamilton, Canada) and Susan Kahn (Montreal, Canada) convened immediately after the presentation, discussed the implication and impact of the findings. Some members opined that these results would see venous thromboembolism guidelines hardening to restrict the use of catheter-directed thrombolysis in deep vein thrombosis patients. Others felt the study provided a starting point in the identification of patient subgroups that would benefit from the treatment.
Razavi also called attention to the parallels between the ATTRACT trial results and trials in the world of stroke interventions. “The initial NIH-sponsored IMS- III (Interventional management of stroke III) trial showed no benefit for endovascular therapy after the use of intravenous thrombolysis over intravenous thrombolysis alone in the treatment of acute ischaemic stroke. This was due to older devices being used and for various other reasons. However, after these results came out, industry, propelled by the investigators’ belief that getting the clot out helps patients, took it upon themselves to carry out the definitive studies in the appropriate patients and we then saw a host of high quality trials (such as MR CLEAN, ESCAPE, EXTEND IA and SWIFT PRIME) that clearly demonstrated the benefit of endovascular treatments for large vessel occlusions in acute ischaemic stroke. Similarly, we are looking forward to ATTRACT being the start of the next phase of deep vein thrombosis research,” he said.
A large US nationwide study shows that the uterine fibroid embolization is vastly underutilised, compared to hysterectomy—especially in rural and smaller hospitals.
In fact, there were more than 65 times as many hysterectomies performed than embolizations, despite data showing that the minimally invasive procedure results in substantially lower costs and shorter hospital stays than the surgical option, the study reveals.
The research was presented today at the Society of Interventional Radiology’s 2017 annual scientific meeting (4–9 March, Washington, DC, USA).
“These findings suggest there is a lack of awareness about this safe, effective and less invasive therapy for uterine fibroids,” said Prasoon Mohan, the study’s lead author and assistant professor in the Department of Interventional Radiology, University of Miami Leonard M Miller School of Medicine, Miami, USA.
“Interventional radiologists urge healthcare professionals to present patients with all available treatment options so that the patient can make an informed decision. Patients need to know about the major differences between surgical treatments and uterine fibroid embolization, especially that this is a non-surgical treatment that preserves the uterus and has a much faster recovery time compared to hysterectomy.”
According to the National Institutes of Health, a majority of women—almost three out of four—will develop uterine fibroids by the age of 50. Women are at increased risk for developing fibroids if they are overweight, African-American, over the age of 40, have high blood pressure, have had no children, and have first-degree relatives with fibroids.
Fibroids develop from the uterine muscular wall and vary in size from a quarter of an inch to larger than a cantaloupe. In most cases, women are not aware that they have fibroids because they do not have symptoms. Symptoms when they occur include heavy menstrual bleeding, pelvic pressure or pain, abdominal enlargement, pain with intercourse, constipation and frequent urination.
This study included an analysis of data from the 2012 and 2013 Nationwide Inpatient Sample (NIS), the largest all-payer inpatient healthcare database in the country. Using billing codes that identified hysterectomies and embolizations completed for the treatment of uterine fibroids, researchers compared how women were treated for this condition, the costs of the treatments, and the outcomes.
The data revealed that over this period, 165,000 more hysterectomies were performed than embolizations (167,650 vs. 2,470, respectively) nationwide. Further, researchers found that only 0.4% of fibroid embolizations were performed in rural hospitals compared to 9.4% of hysterectomies in the same setting; and 7.9% of embolizations were performed in small hospital systems compared to 67.4% in large hospital systems.
“The fact that so few women undergo uterine fibroid embolization in rural and small hospital settings shows a healthcare access and education disparity in who receives this treatment. It is important that we continue to educate patients about choice and determine ways to increase access to this effective, less invasive therapy,” said Mohan.
The data also showed that embolization resulted in shorter hospital stays (2.16 for vs. 2.32 days), and was less expensive than a hysterectomy by about US$12,000 (US$21,583 vs. US$33,104). Further, the women who elected to undergo embolization had more chronic conditions than found in the patients who received a hysterectomy.
Navigation systems have been developed to increase target accuracy, reduce procedure time, reduce procedure cost and, if, possible to reduce radiation exposure, writes Miltiadis Krokidis, Cambridge, UK.
The overall concept behind navigation systems is to localise an object and the exact relationship that the object has with its surrounding structures. Navigation systems in medicine were initially introduced in neurosurgery and orthopaedics and their use has been considered a significant milestone, comparable to the use of general anaesthesia or the use of microscopes as they offered surgeons the possibility to reach targets that were otherwise not visible, to avoid adjacent organs and to be oriented in the absence of anatomical landmarks.
In interventional radiology, imaging offers all that. Tissue targets are visible, adjacent organs can (mostly) be avoided and there is always perception of needle position in relationship with the surrounding anatomical organs. So what could be the added value of navigation systems and why have they been developed for interventional radiology applications?
The quintessence of interventional radiology is accurate device manipulation under image guidance to target specific tissue. Percutaneous image-guided interventions offer a minimally invasive solution for a variety of conditions and their number has exponentially increased in the last decades. Image-guided biopsies, drainages and tumour ablation have an established role in the management of complex patients. Accurate needle placement is of paramount importance to achieve treatment and to avoid complications. In the past, tissue targeting depended exclusively on the talent, the stereotactic perception and the experience of the operator. As the complexity of percutaneous interventions increased the necessity for accuracy and reproducibility has also increased. Navigation systems have been therefore developed aiming to increase target accuracy, to reduce procedure time, to reduce procedure cost and if possible to reduce radiation exposure.
The main system categories that have been developed for interventional radiology navigation are computed tomography (cone-beam CT [CBCT]) systems, electromagnetic tracking systems and optical navigation devices.
CBCT systems may be used alone or in a hybrid setup with fluoroscopy. In the latter, the needle trajectory is planned after CT pictures are obtained and the path is fused onto real time fluoroscopy pictures. Such systems appear to increase technical success rates of needle placement procedures. The main drawback is the radiation exposure that is required for real time needle placement and the fact that patient respiratory motion may impair registration and decrease accuracy. Significant reduction of radiation may be achieved with the use of electromagnetic systems. These are based on the use of sensor coils with differential magnetic fields and offer a significant advantage in ablation procedures and lung biopsy.
Optical navigation devices use a stereoscopic camera that emits infrared light and can determine a 3D position of reflective marker spheres. This allows for real-time tracking of the position of the marker spheres. A free line of sight is required between the camera and the markers. Systems that use fusion imaging combined with optical navigation have been also developed. The CAS-One navigation system (Cascination) is based on this principle. The system uses four to six reflective spheres that are positioned in a predefined array in the line of sight of the infrared camera. The patient is positioned in a vacuum fixation system in order to limit potential movement. A CT scan of the target region with 1mm slice reconstruction is obtained and the images are fused with the registration information obtained from the optical markers. The position of the markers is confirmed on fusion imaging. Three further optical markers are placed in a mechanical arm that is used for needle placement. When the needle trajectory is defined, the mechanical arm is locked and the needle can be potentially inserted without image guidance, significantly reducing radiation exposure.
The system was recently introduced in the UK and the first two cases were performed in Cambridge University Hospitals for the ablation of two kidney tumours with excellent results.
Navigation systems inevitably come with an added initial cost that is not negligible. Nevertheless, in the long term, the standardisation of procedures, the predictability of the result, the reduction of procedure time and the lower morbidity/ mortality are expected to offer a reduction of the overall cost. More precise needle placement will lead to more accurate tissue sampling for biopsies; increase the range of lesions that may be considered as suitable for drainage; and permit the placement of multiple ablation electrodes with specific distance and array configuration. Furthermore, with the use of fusion imaging, lesions that are not visible on standard imaging modalities may be detected and targeted, therefore, increasing the range of lesions that may be treated percutaneously.
As technology evolves, navigation systems will be further integrated into interventional radiology procedures. The use of optical navigation systems with integrated fusion imaging and no requirement for continuous screening appears to open new perspectives for percutaneous interventions.
Miltiadis Krokidis is a consultant vascular and interventional radiologist, Cambridge University Hospitals, Cambridge, UK. He has reported no disclosures pertaining to this article.
Y-90 radioembolization is a promising locoregional therapy for a devastating disease with few available treatment options. Ongoing and future clinical trials will help to determine if Y-90 radioembolization can safely be integrated with systemic chemotherapy, writes William Rilling, Milwaukee, USA.
Often overshadowed by hepatocellular carcinoma, cholangiocarcinoma is frequently referred to as “the other liver cancer”. This is a rare but devastating malignancy with poor five-year overall survival rates of <5%. Surgical resection is the only standard curative treatment. However, only 20–30% of patients present with resectable disease and intrahepatic recurrence is common even after an R-0 surgical resection. Transplant is performed in very highly selected patients who undergo a rigorous pretransplant protocol and the long-term results of liver transplant for this disease are still somewhat uncertain.
The overall management of intrahepatic cholangiocarcinoma and extrahepatic cholangiocarcinoma differ significantly. Extrahepatic cholangiocarcinoma is managed surgically when possible, occasionally aided by transhepatic biliary stents for hilar cholangiocarcinoma. Adjuvant chemoradiation is sometimes employed post-resection. Y-90 radioembolization does not play a role, at this time, in the treatment of extrahepatic cholangiocarcinoma, but there is growing evidence of its benefit in the treatment of intrahepatic cholangiocarcinoma.
Despite its aggressive nature, chemotherapy for cholangiocarcinoma has had limited success. Current standard of care chemotherapy includes gemcitabine and cisplatin with reported median survival of 12 months and progression free survival of eight months in a phase III trial published in the New England Journal of Medicine in 2010. Both National Comprehensive Cancer Network (NCCN) and European Society of Medical Oncology (ESMO) guidelines do not endorse any specific second line chemotherapy regimen.
Multiple retrospective single centre series have been published reporting the safety and efficacy for Y-90 radioembolization in unresectable intrahepatic cholangiocarcinoma. Median overall survival ranging from nine to 22 months were reported in some of the initial single-centre reports. The majority of these patients were treated in a salvage situation following progression on systemic chemotherapy. Overall response rates to Y-90 radioembolization show progressive disease in the liver in only 15–25% of patients with disease control obtained (combination of partial response and stable disease) in 75–80% of patients. Another clear advantage of Y-90 radioembolization is the excellent tolerance of the therapy and low toxicity. The incidence of high-grade adverse events in all published series is rare. Most patients require only one or two treatment sessions, preserving quality of life in this patient population with limited survival.
A recent pooled analysis of Y-90 radioembolization for intrahepatic cholangiocarcinoma was published in the European Journal of Surgical Oncology in 2015. The analysis included 298 patients in 12 studies. Overall median survival was 15.5 months. Tumour response rates were partial response in 28% and stable disease in 54% at three months post treatment.
Other liver-directed therapies, primarily chemoembolization, have also been shown to be effective in intrahepatic cholangiocarcinoma. In a recent multicentre review, 198 patients with unresectable intrahepatic cholangiocarcinoma reviewed were treated at five institutions over 20 years in the USA. The majority of patients in this review (128) have been treated with conventional chemoembolization and with 46 patients treated with Y-90 radioembolization. There was no significant difference in the overall survival between these two therapies in this retrospective review.
These data have prompted NCCN to include locoregional therapy as one of the treatment options for unresectable and recurrent intrahepatic cholangiocarcinoma. The ESMO guidelines also endorse locoregional therapy including Y-90 radioembolization for second line treatment of locally advanced or metastatic intrahepatic cholangiocarcinoma.
Based on the reported success of these early studies, a prospective phase II trial has been initiated to study the safety and efficacy of combining Y-90 radioembolization with gemcitabine and cisplatin for unresectable intrahepatic cholangiocarcinoma. The study will be using Y-90 resin microspheres and is currently enrolling and additional phase III studies are planned.
In summary, Y-90 radioembolization is a promising locoregional therapy for a devastating disease with few available treatment options. Ongoing and future clinical trials will help to determine if Y-90 radioembolization can safely be integrated with systemic chemotherapy. Future research is needed to further define the role of different locoregional therapies in this disease, which is increasing in incidence worldwide.
William Rilling is professor of Radiology and Surgery, Vascular and Interventional Radiology and vice chair, Clinical Operations, Department of Radiology, Medical College of Wisconsin, Milwaukee, USA. He is a consultant for BTG and receives research support from Sirtex for clinical trials.
An amputation due to critical limb ischaemia is directly associated with loss of function and death, writes J A Mustapha, Wyoming, USA.
Amputation. A common term we have been using for centuries to describe the loss of a limb. When people most think of amputation, they envision young patients who have undergone a traumatic amputation due to accident or war that are rehabilitated and go on to live a functional life. But ischaemic amputation, which is a major epidemic today, lends a different perspective to the patient and his/her family.
An amputation due to critical limb ischaemia is directly associated with loss of function and death. The TASC II update in 2007 showed that after amputation, 25% of patients are dead within one year and 20% of those patients who survive continue to struggle with the disease.1 The majority of patients over 75 years of age who receive an amputation do not ever walk again. Amputation is a very traumatic event that impacts the life of the patient and family in a profound and critical way.
Historically, much awareness has focused on many other less deadly diseases that have 10% of the mortality in comparison to critical limb ischaemia, including breast cancer and colon cancer. A patient diagnosed with breast cancer has an almost 90% chance of surviving five years. A patient who is diagnosed with colon cancer has a 65% chance of surviving five years.2 Critical limb ischaemia patients who undergo amputation have a less than 20% chance of five-year survival. So let us discuss the obvious. There is a clear and present lack of critical limb ischaemia awareness among all healthcare providers. A disturbing 2012 publication by Goodney et al showed that 54% of major ischaemic amputations were performed on patients without a prior diagnostic angiography or intervention during the year prior to the amputation.3
I feel strongly that patients and their families need to learn there are options today that can prevent amputation. Avoiding amputation, in most cases, can delay or prevent death. Because of the serious consequences of amputation, I feel compelled to describe the course that critical limb ischaemia tends to run through. Due to this aggressive course, frequent and regular surveillance must occur to achieve sustainable amputation-free survival. As shown in Figure 1, the majority of patients diagnosed with critical limb ischaemia without their course of therapy adjusted are likely to either receive a major amputation within 12 months or, worse yet, die. Whereas, in Figure 2 the same patients, but with an adjusted course of critical limb ischaemia therapy, can experience completely different outcomes. The majority of them are alive and without a major amputation at 12 months. It is time for us to take action, educate others and ourselves about the seriousness of this illness, and not allow a single amputation to take place without a detailed vascular work up and exhaustive attempts at revascularisation. Consider joining the Critical Limb Ischemia Global Society (www.cliglobalsociety.org) whose awareness and advocacy efforts are aimed at raising public, patient and health professional awareness of treatments to prevent unnecessary amputations.
J A Mustapha is director of Cardiovascular Research, Metro Health University of Michigan Health, Wyoming, USA. He is also clinical associate professor of Medicine, Michigan State University College of Osteopathic Medicine, East Lansing, USA.
References
Jaff MR et al. An update on methods for revascularization and expansion of the tasc lesion classification to include below-the-knee arteries: a supplement to the inter-society consensus for the management of peripheral arterial disease (TASC II): The TASC Steering Committee. AnnVascDis. 2014; 8(4): 343–57
The surveillance, epidemiology, and end results (seer) program of the national cancer institute (http://seer.cancer.gov/statfacts/
Goodney PP et al. CircCardiovascQualOutcomes. 2012; 5(1): 94–102
The NEAT (Novel endovascular access trial) study demonstrates the possibility of using a catheter-based system to create an endovascular arteriovenous fistula (endoAVF) in patients requiring haemodialysis as a first-line reliable option, without the need for open surgery, writes Dheeraj Rajan, Toronto, Canada.
With around three million patients receiving haemodialysis annually, reliable vascular access is mandatory to facilitate adequate therapy. An arteriovenous fistula is the
preferred vascular access for these patients. However, high thrombosis rates, access maturation failure with multiple interventions, and patient refusal plague access usability. Failing access is the leading cause of hospitalisation for patients undergoing haemodialysis and is responsible for US$2.9 billion in annual costs.
The everlinq endoAVF system (TVA Medical) creates a fistula without open surgery or vessel dissection, eliminating trauma to the vessels to minimise the neointimal hyperplasia responsible for failures with surgical fistulas. The procedure uses two magnetic catheters placed in an artery and adjacent vein (venae comitantes) in the ulnar artery/ulnar vein or radial artery/radial vein. When the catheters are inserted, the magnets align the catheters holding the vessels together. Then, radiofrequency energy is delivered from the venous catheter in the vein to the artery, creating a side-to-side anastomosis and the catheters are removed. As a final step, the entry brachial vein is embolised to divert flow to the superficial veins, which are later cannulated for haemodialysis.
NEAT is a prospective, single-arm, multicentre study designed to evaluate the safety and efficacy of the everlinQ endoAVF system to create an endoAVF in patients with end-stage renal disease who require haemodialysis vascular access. The main inclusion criteria were: target vein and artery diameters ≥2mm; life expectancy >1 year; absence of central or ipsilateral upper extremity venous stenosis; or ineligibility for a distal forearm fistula. Patients were followed for 12 months with duplex ultrasound and physical exam. Key outcomes included procedural success, percentage suitable for dialysis by physiologic criteria (brachial artery flow >500ml/min and vein diameter >4mm), functional usability (received dialysis with two-needle cannulation of endoAVF for at least 2/3 of sessions over four weeks), primary, secondary and functional patency, and adverse events (as adjudicated by an independent Clinical Events Committee).
Eighty patients were enrolled at nine centres in Canada, Australia and New Zealand (20 roll-in and 60 participants in the evaluable cohort). EndoAVF was created in 98% of participants; 91% were physiologically suitable for dialysis within three months with mean brachial artery flow of 918ml/min and vein diameters 5.2mm in cephalic, 5.9mm in median cubital and 6mm in basilic veins. EndoAVF functional usability was 67% in participants who received dialysis, with only 12% of usable endoAVF requiring an intervention to achieve usability. The 12-month primary and cumulative patencies were 68.6% and 83.5%, respectively, with functional patency of 89.4%. There was one serious device-related event that occurred in one patient (1.7%). When compared to a propensity-score matched Centers for Medicare and Medicaid cohort of surgical AVF, the endoAVF required fewer post-creation procedures (0.6 per patient year vs. 3.4), with fewer event rates for angioplasties, thrombectomies, catheter placements, arteriovenous graft creations, new surgical AVF creations, and vascular access-related infections.
The NEAT study demonstrates the possibility of the endoAVF as a first-line reliable AVF creation option for patient without the need for open surgery. Given the cutoff 2mm vessel sizes and unique locations of the endoAVF, more patients may be candidates for the procedure compared to those meeting surgical criteria. Furthermore, the roll-in patient group demonstrated that a physician with endovascular skills can easily learn the procedure. Most importantly, outcomes of endoAVF are higher when compared to other reported studies for surgically created fistulas: maturation (91% vs. 53–76%) and patency (83.5% vs. 68–72%) with a statistically lower post creation intervention rate. These clinical outcomes may translate into lower long-term costs, improved patient acceptance and a fundamental change in current standards of practice.
Dheeraj Rajan is head and professor, Division of Vascular and Interventional Radiology, Department of Medical Imaging, University of Toronto, Toronto, Canada. He is an equity holder at TVA Medical.
References
Liyanage, et al. Lancet. Epub March 2015;10.1016/S0140–6736
US Renal Data System. USRDS 2010 Annual Report
Robbin et al. Radiology, 2016; 279:620–9
McGrogan, D. et al.J Vasc Surg 2015;62:1652–7
Al-Jaishi, et al.Am J Kidney Dis. 2014; 63(3):464–478
There is a recent story about a UK-based private insurer potentially no longer recognising interventional radiologists as primary practitioners for the treatment of varicose veins that is doing the rounds. While this story is unconfirmed, it acts as a wake-up call and a reminder that we have to remain vigilant in order to protect our professional rights, writes Gregory C Makris, Oxford, UK.
There are many potential future risks for our specialty. Everybody has the right to train in endovascular techniques in a recognised training centre and in a regulated environment. This means that if you have obtained the necessary skills through the required years of training then you should be able to perform certain endovascular tasks independently and be given the chance to compete on an even footing.
We should accept the fact that like in any other market, if you have the skills and you can provide a high quality and safe service, then you should be allowed to compete for a place in that market, whether that is called peripheral arterial work or varicose veins.
The market law of “demand and supply” is usually very efficient at providing the environment that allows a healthy competition that in the end benefits the patient. However, what we should not accept are attempts to manipulate the rules of healthy competition so that we are no longer able to compete. Interventional radiologists have all the necessary skills and training required to be independent providers of endovascular treatments for the management of varicose veins and any attempt to keep us out of the contention for this work is a real threat and should not be accepted.
A case in point of such an attempt, in my opinion, is the wide variation in the status of admitting rights. How can we be expected to compete when we are not able to admit our own patients in our own hospital beds? The introduction of interventional radiology day units in some hospitals has provided a partial solution to this, but more needs to be done in order to ensure a fair environment for healthy competition. Despite the fact that I recognise that every organisation has the right to run its business the best way they see fit, when it comes to damaging the rules of competition and limiting the choices that patients have, then there should be a justification based on facts. In cases like these it is becoming obvious how important it is to have strong national and European professional societies and possibly this is the real “take home” message from this story.
The aforementioned story is an example of what potentially poses the most serious risk to our profession. It is not competition from other specialties but our exclusion from being able to compete on equal grounds for the provision of endovascular services. Once a fair competitive environment has been established, interventional radiologists have nothing to be afraid of since we have the skills and qualities necessary to provide excellent services for our patients and the other specialties we work with.
Gregory C Makris is a vascular and interventional radiology fellow, Oxford university hospitals, NHS Foundation Trust, and clinical entrepreneur fellow at NHS Innovation England, UK
Frequently, instructions for use (IFU) parameters published by device manufacturers are not adhered to in order to increase patient candidacy for endovascular aneurysm repair (EVAR). In a multicentre study of patients undergoing elective EVAR for abdominal aortic aneurysm, we examined whether IFU nonadherence was related to a worse mid-term outcomes. The primary outcome in our study was a composite endpoint of graft-related adverse events and included aneurysm-related death, sac growth, endoleak (except type II), endoleak intervention, limb occlusion, device migration or rupture.
Our study population included 461 patients with an IFU non-adherence rate of 43.8%. Patients with IFU non-adherence were less likely to be men (90% vs 78.7%) and more likely to have peripheral vascular disease (7.3% vs 12.4%). Iliac and neck diameter non-adherence (21.4% and 15.2%, respectively) occurred the most frequently. Graft-related adverse events occurred at a rate of 12.8% during the study period with endoleak and sac growth occurring the most frequently (8.5% and 8.1%, respectively). On survival analysis, freedom from graft-related adverse events was significantly higher in patients with IFU adherence compared to those with non-adherence (p=0.031). When considering neck IFU non-adherence in isolation, freedom from graft-related adverse events remained significantly higher in IFU adherent patients compared to non-adherent (p=0.003). On adjusted Cox regression, IFU non-adherence, age ≥80, peripheral vascular disease, and use of the Talent graft (Medtronic) were significant predictors of graft-related adverse events in both any IFU non-adherence and neck-only IFU non-adherence models.
IFU non-adherence in the literature ranges from 38–53%, which is similar to our own results.2–6 The relationship that exists between IFU non-adherence and negative outcome is not clear. Many studies have found that IFU non-adherence appears to be associated with lower mid-term survival and that freedom from graft-related adverse events was significantly lower in the IFU non-adherent group.2,3 Neck anatomy that falls outside of IFU parameters have also been found to be associated with a higher rate of type I endoleak but showed no significant difference in survival or graft patency.4 Several studies have found no difference in mortality, aneurysm-related mortality, sac enlargement, need for reintervention, or endoleaks in grafts placed within and outside of the IFU.5,6 However, there are several limitations in the published literature. Many of these studies employed solitary outcomes with low event rates as their primary outcome instead of using a composite endpoint as we did in this study. Consequently, these studies did not attain power and any signal of association between IFU non-adherence and outcomes may have been lost. As well, some studies used generic IFU parameters rather than device-specific parameters, which may not accurately predict graft performance. Finally, many of the survival analyses have rapid loss of follow-up (patients at risk), which decreases the robustness of the analysis.
Since its inception nearly 25 years ago by Juan Parodi, commercially available endovascular grafts have undergone multiple design modifications to overcome constraints imposed by complex anatomy. Lower profile delivery systems are now available as small as 14F providing EVAR access vessel suitability for 90% of men and 70% of women.7,8 Uncovered stents, suprarenal fixation, radial force from self-expanding stents, and increased columnar strength have been some additions commonly found in modern grafts to maximise neck apposition and reduce migration. More recently, sealing rings filled with radio-opaque polymer have allowed for reliable sealing of short neck (≥7mm) aneurysms, however, the long-term results of these devices are still unknown. An FDA-approved device for short necks <10mm has had some success however type I endoleak rates still remain higher than conventional neck lengths and long-term results are not yet known.
Chimney and snorkel adjunct offers an alternative to complex neck anatomy that falls outside the IFU for standard available endografts but are associated with high rates of gutter leaks9 that are exceedingly complex to treat. Caution should be used before considering these procedures since they require advanced endovascular skills to safely perform and both the endografts and the covered and uncovered stents employed to create the snorkel or chimneys are being deployed outside their respective IFUs. There is some favourable published short-term outcome data from experienced centres related to these procedures, although the durability of chimneys and snorkels is currently not known.
More complex solutions such as custom branched EVAR and fenestrated EVAR remain promising solutions to complex neck aneurysms. As they become more accessible to US centres, many are touting these custom grafts as the solution to complex anatomy. However, the four- to six-week custom order waiting period, the requirement of advanced endovascular skills, excessive coverage of the normal aorta, considerable procedural times and potential inadvertent branch vessel occlusion associated with custom grafts creates impracticality and makes them less appropriate for small-volume centres.
Custom grafts have been available in Canada for approximately 15 years and are commonly used in most academic centres. Through the time period of our study, custom grafts were available as an alternative for complex anatomy cases at the study centres, one of which also offers a complex aortic endovascular programme and fellowship. And yet, a relatively high rate of IFU nonadherence was still found in this series. It is likely that because of the impracticality of applying custom techniques to a high rate of abdominal aortic aneurysms that are outside of IFU parameters and for the other above-listed issues, that surgeons continue to elect to push the limits of device capabilities for standard endografts. It is our belief that this will also hold true in the US market and fail to solve the complex anatomy issue. Finally, let us not forget how abdominal aortic aneurysm repair began; open repair remains a viable and reliable solution for many of these cases.
Our study would indicate that offering EVAR repair in patients whose anatomy is not compliant with IFU parameters must be done with caution. Widespread aggressive application of EVAR in non-IFU adherent patients must be limited and other endovascular and open options must be considered. In some comorbid patients this may still remain the lowest-risk option for abdominal aortic aneurysm repair. Other patients may be willing to accept the higher risk of graft-related adverse events in order to avoid a laparotomy or complex open repair. In these instances, a patient must be properly advised and consented for these risks. At the very least, if patients are treated using standard EVAR devices outside IFU, these patients warrant very rigorous follow-up imaging. Further device development and creative solutions in EVAR technology may someday yield a universal device for complex anatomy, but for now we must use all the options available to provide the best care for patients.
References
JC Parodi, JC Palmaz, HD Barone. Ann Vasc Surg 1991; 5: 491–9
TA Abbruzzese, CJ Kwolek , DC Brewster, et al. J Vasc Surg 2008; 48(1): 19–28
KP Donas, G Torsello, K Weiss, et al. J Vasc Surg 2015; 62(4): 848–54
AF AbuRahma, M Yacoub, AY Mousa, et al. J Am Coll Surg 2016; 222(4): 579–89
J Walker, LY Tucker, P Goodney, et al. J Vasc Surg 2015; 61(5): 1151–9
WE Beckerman, RO Tadros, PL Faries, et al. J Vasc Surg 2016; 64(1): 63–74
Percutaneous arteriovenous fistulae creation may allow greater patient access to fistula formation as more physicians will be able to create these channels, thus potentially reducing waiting times for surgery, writes Gerard Goh, Melbourne, Australia.
The creation and maintenance of dialysis access is a large healthcare issue that challenges physicians worldwide. Dialysis is usually delivered via peritoneal dialysis catheters, percutaneous dialysis catheters or surgically created arteriovenous fistulae.
The advantages of surgically created arteriovenous fistulae over alternative dialysis access is well established. Studies have shown that surgically created arteriovenous fistulae have lower rates of three-year mortality for patients than if they receive an arteriovenous graft or central venous catheter for haemodialysis.1 Furthermore, surgical fistulae have also been shown to have lower infection rates, re-operation rates and be economically less expensive per year.2 However surgical fistulae often require multiple interventions to maintain functionality. Central venous catheters have been associated with central venous stenosis, possibly due to superior vena cava barotrauma and/or local irritation and inflammation of the venous wall. Should a central venous stenosis develop this may lead to further complications, such as occlusion, necessitating further interventions and possibly impacting on future upper limb dialysis access options.
A novel alternative method to create arteriovenous fistulae is by percutaneous endovascular means. Two companies that have developed percutaneous devices to create arteriovenous fistulae are TVA medical with the EverlinQ system and Avenu Medical with the Ellipsys system.
The EverlinQ device is a dual catheter device that received CE marking in 2014. Retrograde access into the brachial artery and brachial vein is achieved under ultrasound guidance with a micropuncture kit. Wires are placed and 6 and 7F vascular sheaths are placed in the artery and veins respectively. 0.018” wires are manipulated into the interosseous artery and vein and the EverlinQ catheters are inserted. The catheters have rare earth magnets so that once they are aligned appropriately, these catheters are activated holding the artery and vein together. A small radiofrequency electrode is deployed and activated creating a fistula between the artery and vein. The catheters are then removed and the brachial vein is embolized with a coil to redirect venous blood into the superficial systems. The as-yet unpublished NEAT trial, incorporating centres from Canada and Australia, recently preliminarily reported a primary technical success of creating an arteriovenous fistula of 98.3% (59/60 patients) and at three months 91.3% (57/60 patients) had a physiologically usable fistula (defined as a brachial artery flow rate ≥500ml/min and a cephalic/basilic/medican cubital vein diameter of ≥4mm or a successful dialysis with two needles).
The Ellipsys system is a single catheter electrocautery device. A retrograde puncture and access of the median cubital vein is performed and over the wire, a needle is used to enter the perforating vein. The needle is then directed towards and advanced to puncture the adjacent radial artery under ultrasound guidance. A 6F sheath is inserted. The Ellipsys device is then introduced and the sheath retracted back, positioning the distal tip of the electrocautery device within the radial artery and the proximal tip in the perforating vein. The device is engaged closing the electrocautery tips which hold the artery and vein together. The device is activated and an electrocautery is performed creating the fistula (see article below).
Percutaneous arteriovenous fistulae creation may allow greater patient access to fistula formation as more physicians will be able to create arteriovenous fistulae, thus potentially reducing waiting times for surgery. Early research seems to indicate that there may be a quicker maturation time of arteriovenous fistulae over surgically created ones; however longer term research with larger patient numbers is needed. This should be an interesting space to watch.
Gerard S Goh is an interventional radiologist at The Alfred Hospital, Melbourne, Australia. He has reported no disclosures pertaining to this article
References
Perl J et al. Hemodialysis vascular access modified the association between dialysis mortality and survival. J Am Soc Nephrol. 2011 Jun; 22(6):1113–1121
Woo K et al. Influence of vascular access type on sex and ethnicity-related mortality in hemodialysis-dependent patients. Perm J. 2012 Spring; 16(2):4–9
Extensive research has shown that intermittent compression and rubber tourniquets help to dilate superficial veins after fistula placement. The Fist Assist device is an external, medical wearable that can apply intermittent pressure on a specific arm vein to help dilate the vein after fistula placement in a simple non-traumatic way, writes Tej M Singh, Los Altos Hills, USA.
Unfortunately, many renal failure patients progress to end stage renal disease, requiring dialysis. Dialysis options include central catheters, peritoneal dialysis or haemodialysis via fistulae or grafts placed in the arms. Autogenous fistulae are preferred, but development and maturation of these fistulae is a slow process that may lead to chronic catheter placement and extra costs to do interventions to help mature the fistulae. Many patients are instructed to do arm and hand exercises. Unfortunately, many of these exercises are never implemented or successful.
It is hard to predict which veins will enlarge to the appropriate size for dialysis. Unfortunately, many arm veins fail to dilate and enlarge. Some patients are told that their veins are too small, or the fistula does not have appropriate flow to dilate. This results in more inconvenience, more procedures, frequent readmissions, delayed care and increased costs in caring for renal failure.
Extensive research has shown that intermittent compression and rubber tourniquets help dilate superficial veins after fistula placement via mechanisms such as increases in wall tensile stress or nitric oxide release. Recently, a novel noninvasive device called the Fist Assist was developed and created to help study the role of pneumatic compression on fistula dilation. The first feasibility study of the device was done at MS Ramaiah Medical Center in Bangalore, India under the guidance of Sanjay Desai, chief of Vascular Surgery.
One week after arteriovenous fistula creation, Fist Assist was applied 15cm proximal to the fistula in order to apply cyclic compression (50mmHg).Twelve patients with an arteriovenous fistula were enrolled in an institutional review board-approved study to test vein maturation at baseline and with Fist Assist. The device was applied during dialysis three times per week in seven patients for a maximum of 90 days postoperatively. The five patients who were controls did not have any application of Fist Assist. Vein size was measured and recorded at zero, 30 and 90 days by duplex measurement. Clinical results (percentage increase) were recorded and tested for significance.
In the study, no patients experienced thrombosis or adverse effects. Patient compliance and satisfaction was high. No significant, immediate early vein maturation was seen after 30 days in either group. After three months, the mean percentage increase in vein diameter in the Fist Assist treatment group (159.5%) was significantly larger (p=0.05) than controls (76.7%) in the first 5mm segment of the fistula. Comparing three-month average per cent increase: the mean for the treatment group (123.2%) seems to be statistically greater than the control group (66.2%; p=0.03). All fistulae treated with Fist Assist are still functional with no reported thrombosis or extravasations.
Early application of an intermittent pneumatic compression device may assist in arteriovenous fistula maturation and success. Novel, noninvasive devices like Fist Assist may have clinical utility to create functional fistulae development and decrease costs as they may assist in maturation.
There is a need to provide improved vein dilation methods and devices to sufficiently and/or effectively dilate a vein for haemodialysis, help mature fistulae, and help insure that placed fistulae reach their optimal size without extra delay and extra procedures.
The Fist Assist device is an external, medical wearable that can apply intermittent pressure on a specific arm vein to help dilate the vein after fistula placement in a simple non-traumatic way to ensure vein enlargement and dilation. Larger studies continue to test the device in patients with fistulae.
Tej Singh is the president and CEO, Fist Assist Devices, Los Altos Hills, USA
This is an exciting time for vascular access. Minimally invasive anastomosis devices have been developed and are being utilised in the creation of percutaneous arteriovenous fistulae (pAVF) in the upper extremity, writes Jeffrey Hull, Richmond, USA.
The vision for haemodialysis access is to evaluate end-stage renal disease patients in the office with clinical exam and Doppler ultrasound mapping. In appropriate patients, we can now create a percutaneous arteriovenous fistula in the office-based lab with the Ellipsys vascular access system (Avenu Medical). Fistula follow-up, maturation and maintenance are also done at the office-based lab establishing a valuable continuity of care.
This approach was successfully applied in the pivotal US clinical trial where 117 patients were enrolled at five sites across the USA. All the procedures were done in the office-based lab, using ultrasound guidance. The results of this study, designed to demonstrate the safety and efficacy for the percutaneous creation of arteriovenous fistulae, will be forthcoming in the next few months. Avenu Medical has received CE mark approval for the commercial sale of Ellipsys vascular access system in Europe.
The current anastomosis device takes advantage of the unique anatomy in the ante-cubital fossa. An anastomosis is created between in-situ arteries and veins that are side by side. The Ellipsys catheter creates an anastomosis between the proximal radial artery and the perforating vein. The resultant fistulae are multi-vein outflow with filling of the cephalic and basilic veins in the upper arm. The central advancement of the Ellipsys anastomosis device is the development of an image-guided, catheter-based procedure that creates an anastomosis without an implant or foreign body.
The exciting part for practicing interventionists adopting one of the anastomosis device technologies will be to develop methods of practice that suit the needs of their patients and facilities. Academic practices will have the opportunity to thoroughly test the anastomosis devices, and develop the best practices and evidence based recommendations for their use. Appropriate methods of practice need to be developed for patient selection, imaging guidance, procedure venue, anatomic location of anastomosis, anatomic location for dialysis cannulation, and fistula maintenance. The cycle of innovation to practice invigorates our specialty.
It is been 50 years since Brescia-Cimino described the first modern arteriovenous fistula using the surgical technique. While there have been numerous advancements in surgical fistulae, the basic principles have remained the same. A vein is identified as suitable for fistula creation, the vein is dissected free and then attached to an adjacent artery with a sutured anastomosis. Typically the attached vein is a single vessel matured for dialysis. This has been the safest and most cost-effective method of providing haemodialysis. Despite being the best current access for haemodialysis there are problems providing patients with a functional fistula. From 30–60% of fistulae created fail to mature into functioning fistulae, leaving patients on catheter dialysis. The reasons for non-maturity are varied and include early thrombosis, intimal hyperplasia and inadequate vein development. The pAVF may help overcome the problems with surgical fistulae. The pAVF is more easily monitored and more amenable to treatment in the early postoperative period due to lack of incisions and tenderness. The pAVF is not limited to a single pre-selected outflow vein.
A related problem in dialysis access is that 80% of patients initiate dialysis with a catheter, a percentage that has not changed over the last 10 years. This is due to lack of patient education, lack of payment, and resistance to surgical procedures. The minimally invasive percutaneous arteriovenous fistula will allow a larger number of physicians to create high quality fistulae.
The committed interventionalist can join a multidisciplinary group of committed vascular access surgeons and nephrologists in the care of end-stage renal disease patients. Increased manpower with minimally invasive and cost-effective options for creating fistulae will help interventional radiologists, surgeons, nephrologists, patients, and underwriters of healthcare become more proactive in using fistulae for haemodialysis, ultimately, reducing the morbidity, mortality and cost of catheter dialysis.
Jeffrey E Hull is director of the Richmond Vascular Center in Richmond, USA. He is a founder, stockholder and consultant to Avenu Medical
By Alexandre Laurent, Laurent Bédouet and Laurence Moine
Chemoembolization with sorafenib (Bayer and Onyx Pharmaceuticals) is a promising technique for the treatment of hepatocellular carcinoma (HCC) because, administered orally (400–800mg daily), it is associated with increased three-month survival.1 Also, the combination of sorafenib and transarterial chemoembolization (TACE) has been shown to increase the time to progression and patient survival compared with TACE alone.2 Sorafenib has been approved for treatment of advanced HCC since 2008, but local delivery of the therapy is a new concept. Alexandre Laurent, Laurent Bédouet, and Laurence Moine review the data for sorafenib in this context.
Local delivery of sorafenib has been studied in animal models. In a rabbit study, Lip-TACE with lipiodol emulsions of sorafenib was found to be technically feasible and increased the concentration of drug in healthy liver by several times compared to the therapeutic drug concentrations (2–10μg/mL) observed in plasma during oral treatment.3 In a VX2 tumour model, Lip-TACE concentrates the drug in the tumour compared to the healthy liver, before a rapid clearance of the drug (5.2 hour half-life) and an important systemic exposure of 58μg/mL.4
An extemporaneous loading of sorafenib by ionic mechanism as for doxorubicin on microspheres, such as LC Bead (BTG) or Hepasphere/Quadrasphere (Merit Medical), is difficult for two reasons. First, sorafenib is devoid of any cationic function, precluding its ionic attraction; and second, sorafenib is a hydrophobic molecule having low-water solubility. Its loading on LC Bead has been attempted but two days in highly diluted conditions (20μg/mL) are required to achieve a loading of 10mg/mL and the release occurs quickly (50% is released in vitro within one hour).5 Today, new materials and new loading procedures are necessary for sorafenib delivery.
Degradable microspheres for sorafenib delivery
A degradable microsphere could have three advantages over non-degradable microsphere. First, the degradable carrier allows a complete drug delivery, thus avoiding the risk of toxicity that could come from a long-term delivery of infra-therapeutic doses of drug. Second, a complete arterial recanalisation allows you to repeat the chemoembolization procedures. Third, the re-opening of the lumen could reduce the post-embolization angiogenesis and the risk of post-embolization syndrome.
We studied the loading of sorafenib on a degradable microsphere (PEG-MS, Occlugel) composed of polyethyleneglycol monomer cross-linked with a degradable PEG-PLGA triblock crosslinker.6 Previously, we have shown different size ranges of PEG-MS (300–500μm, 500–700μm, and 700–900μm) that degrade in one day, occlude pig renal arteries according to their size and give way to full recanalisation after one week.7
The particular composition of the PEG-MS, comprising both hydrophilic and hydrophobic moieties, is prone to favour the loading of a neutral drug such as sorafenib by weak interactions, different from ionic attractions. Our first in vitro trials were positive. Sorafenib could be loaded in less than one hour, simply by mixing it with the PEG-MS (size range of 50–100μm) at room temperature in a medium composed of water and dimethyl sulfoxide (DMSO). The maximum sorafenib load was around 13mg/mL of microspheres, with an efficacy of loading of 70%. The loading of the hydrophobic sorafenib on the PEG-MS did not induce aggregation of the PEG-MS and did not hinder their deliverability through a microcatheter. Interestingly, the drug release in saline medium occurred without a burst and was gradual and proportional to the microsphere degradation. The delivery was complete when the PEG-MS were fully hydrolysed. This sustained release suggests an efficient interaction between sorafenib and the microsphere. In vitro, the viability of HepG2 cells was reduced by sorafenib eluted from PEG-MS, showing that the drug activity was not modified by its loading.
Our preliminary results are promising: hydrophobic and neutral sorafenib can be promptly loaded at a significant concentration on a degradable PEG-MS. Its delivery is proportional to the rate of degradation of the embolic and it is complete. It could be interesting to investigate the optimal delivery time (microsphere degradation time) with regard to anti-tumour efficiency and recanalisation.
References
Llovet et al. N Engl J Med 2008; 359(4): 378–90
Bai et al. J Dig Dis 2013; 14(4): 181–90
Gaba et al. J Vasc Interv Radiol 2013; 24(5): 744–50
Parvinian et al. Diagn Interv Radiol 2015; 21(3): 235–40
Lahti et al. J Vasc Interv Radiol 2015; 26(2): S80–S81
Louguet S et al. Acta Biomater 2013; 10(3): 1194–205
Maeda N et al. J Vasc Interv Radiol 2013; 24(9): 1391–98
Alexandre Laurent is at AP-HP Hôpital Lariboisière, Department of Neuroradiology, Paris, France; Laurent Bédouet is at Occlugel SAS, Jouy en Josas, France; and Laurence Moine is at Institut Galien Paris-Sud, CNRS, Univ. Paris-Sud, Université Paris-Saclay, Châtenay-Malabry, France. AL is a founder and member of the scientific board of Occlugel. The authors are co-inventors in a patent on the resorbable microsphere discussed in the article
Nearly 10 years have passed since Aravind Arepally et al published data from the first gastric artery chemoembolization preclinical trials for the treatment of obesity. Since that time, preclinical trials with bland embolic microspheres rather than chemoembolization have shown the most promise in terms of safety and efficacy. This once radical obesity treatment idea (bariatric artery embolization) is now becoming more widely accepted as early human clinical trials at several sites are showing promising preliminary results.
The mechanism through which bariatric artery embolization is thought to trigger weight loss is through modulation of the ghrelin hormone. Ghrelin is a 28-amino-acid peptide hormone produced and secreted predominately by mucosal X/A cells lining the gastric fundus in humans. Ghrelin is thought to be the principal appetite-inducing stimulus in humans and has an influential role on caloric energy balance. Following embolization, decreased serum ghrelin levels and suppression of appetite resulting from ischaemia may be responsible for the weight loss observed in both preclinical and early human trials.
The history of transarterial obesity treatments explored in preclinial trials includes some caustic agents: belomycin A5 hydrocloride and sodium morrhuate have both been used as chemoembolics, while calibrated microspheres down to 40μm in size have been used as bland embolics. However, in spite of the preclinical success of some of these agents, the use of yttrium-90 (Y-90) radioembolization in a procedure similar to bariatric artery embolization might initially seem contraindicated. This is largely due to the perceived hypersensitivity of the gastrointestinal tract to radiation—a fallacy commonly promoted among interventional radiologists. In fact, data from external-beam radiation therapy tells us that the gastrointestinal tract is probably less radiosensitive than normal liver tissue, where Y-90 radioembolization is most commonly used as a treatment for liver cancer.
Figure: A) Haematoxylin and eosin stained section of fundus with mucosa, submucosa and a large area of fibrosis labeled.Y-90 microsphere clusters are visible in both the submucosa and deep mucosa (white arrows). B) Radiation dose profile showing rapid dose decrease toward the lumen resulting in sparing of superficial mucosa. Fibrosis and radiation burden is highly targeted to deep mucosa where the majority of ghrelin producing cells are found.
While a potential complication in radioembolization for treatment of liver cancer is gastrointestinal ulceration following non-target embolization of hepatoenteric collateral vessels, both bland and chemoembolization can also result in such ulceration.
A recent paper from our group in the Journal of Vascular and Interventional Radiology has described a bariatric arterial radioembolization procedure using Y-90 microspheres in a preclinical model. While the goal of bariatric arterial embolization is to use ischaemia to initiate a change in orexigenic hormone levels and energy balance, using radioembolization is associated with minimal tissue ischaemia. Instead, it uses a localised radiation burden to affect ghrelin hormone production.
Further, preclinical data suggested that weight loss may also be achieved through a restrictive component to this therapy resulting in decreased stomach size and volume. Both a strength and a weakness of Y-90 bariatric radioembolization therapy compared to ischaemic bariatric artery embolization is that the former may allow for more precise targeting of ghrelin-producing cells. Immunohistochemistry of the gastric fundus has shown that the greatest concentration of ghrelin producing cells is deep in the fundal mucosa. The goal of bariatric arterial radioembolization studies was to eliminate as many ghrelin-producing cells as possible, while sparing superficial gastric mucosa to avoid potential ulceration and side effects. This was accomplished through pretreatment planning using an injectable radiopharmaceutical as a Y-90 microsphere surrogate, similar to established techniques in hepatic radioembolization. Careful dosimetry based on pretreatment planning combined with suitable sizing of the microsphere allowed for deposition in the sub-mucosa for complete ablation of the deep mucosa, including ghrelin-producing cells. At the same time, a rapid fall off in radiation dose ensured that superficial mucosal integrity was maintained.
Of course, while this planning process led to an elegant targeted solution, the technical complexity greatly exceeds that of conventional bariatric arterial embolization. Critics of Y-90 bariatric artery embolization have pointed out potential radiation risks associated with this use of radiation therapy in the treatment of benign disease. However, morbid obesity can hardly be called a benign disease. Like bariatric artery embolization, bariatric artery radioembolization is not a potential intervention for patients wishing to lose a few pounds to look better in their swimsuit. It is a potential therapy for morbidly obese individuals that are refractory to diet and exercise and for whom bariatric surgery is the only remaining intervention.
While radiation is associated with increased probability of future neoplasia, this risk is substantially less than the 30-day mortality associated with traditional surgical obesity intervention, which can exceed 1%. Where this therapy will fit among the numerous transarterial approaches that have been attempted in animal models for the treatment of obesity is uncertain. However, even if this therapy is never attempted in a human, it strengthens the argument that left gastric artery embolization with a variety of therapeutic embolic agents is a realistic and potentially safe treatment modality for morbid obesity. Initial investigations into Y-90 bariatric artery radioembolization also have had important implications regarding the use of radioembolization in the treatment of liver cancer. We now have a much better understanding of the microscopic changes that occur in gastrointestinal tissue following radioembolization.
In particular, Y-90 radioembolization may not be as toxic to the gastrointestinal tract as was once thought as we have recently described in the Journal of Nuclear Medicine. While gastrointestinal damage may occur with substantial Y-90 non-target embolization, excessive prophylaxis is probably unnecessary since small doses are not likely to result in clinical sequelae.
Alexander S Pasciak is a clinical associate professor of Radiology at the University of Tennessee Graduate School of Medicine, Knoxville, USA. He received grant funding from Sirtex in support of a preclinical study in the use of SIR-Spheres for the treatment of obesity.
“Interventional radiology has always been characterised by its innovative spirit. We are now seeing progress with new procedures being developed to create percutaneous arteriovenous fistulae. I am impatiently awaiting the results of the NEAT (Novel endovascular access trial) study,” Gireesh Mukund Warawdekar, consultant interventional radiologist at several leading hospitals in Mumbai, India, and 2014–16 president of the Indian Society of Vascular and Interventional Radiology (ISVIR), tells Interventional News.
When did you first decide on a career in medicine and why did you choose interventional radiology?
I grew up with a father who, in addition to being a practising radiologist, was also extremely keen on teaching and exploring radiophysics at the Atomic Energy Institute, Mumbai, India. He would spend many happy hours focused on the theoretical and experimental study of radiation; its emission, propagation, and interaction with matter.
His interest in radiology and radiation probably led to my decision to study medicine. During my residency I had the privilege of working in interventional radiology and I realised, quite clearly, that this was the field I wanted to pursue.
Who were your mentors and what wisdom did they impart to you?
I was taught the basics and finer nuances of interventional radiology by Dr Vimal Someshwar, my guide. He always emphasised that the patient should be a physician’s primary focus, and said that the best treatment for him/her with the least likelihood of complications, is the way one should practice medicine. It was never a teacher-student relationship; rather, he was like a friend who showed me the way ahead.
Gireesh Mukund Warawdekar
Which innovations in interventional radiology have most influenced your career?
During my training period, when interventional radiology was at a nascent stage in India, we had absolutely no access to medical devices—we used to make coils out of guidewires and catheters out of Kifa tubing. Unsurprisingly, our crossing rate of stenoses and occlusions used to be 20–30%.
Similarly, we did not have access to vascular sheaths either. Until we started acquiring sheaths and most importantly the Glidewire (Terumo), our practice in India was quite limited. However, what we lacked in terms of devices, I think we made up for in ingenuity. The Glidewire revolutionised our interventional radiology practice and our crossing rate of occlusions/stenoses went up to nearly 95–98%.
Could you please briefly describe interventional radiology’s place in Indian healthcare? What procedures are widely performed and what are some of the challenges that it faces?
India is a vast nation made up of some 30-odd states. We always say of India, that diversity and change are the only constants. The practice of interventional radiology is similarly very variable depending on the state in question. I believe that the practitioner who begins practicing first, tends to dominate the market. In Mumbai (in the state of Maharashtra), where I practice, interventional radiologists were the first to carry out both vascular and non-vascular interventions, so we dominate the practice.
However, the situation is different in the other regions where it is dominated by the other medical specialties such as cardiologists, or vascular surgeons, depending on the specialty that began performing these procedures first. When interventional radiologists are in charge, the entire gamut of interventional radiology procedures is usually performed. On the other hand, in situations where other specialties dominate, interventional radiologists predominantly perform embolization and other non-vascular procedures including image-guided biopsies, ablations and management of venous insufficiencies.
As president of the ISVIR 2014–16, what are your goals for the organisation in your term?
Until now, we have had no formal training programme for interventional radiology as a subspecialty in India. We have just got approval to start two superspecialty programmes, ie. the post-doctoral certificate course (DM) and Fellowship of the National Board (FNB) in interventional radiology which we will start in early 2017. The only way forward for interventional radiology is to train more young and enthusiastic radiologists to take it up as a full-time profession. This can only be achieved if we have a well-structured training programme in place, which I think we have achieved. This credit goes to the entire Executive Committee of ISVIR that has worked so hard to achieve this goal.
Interventional radiology is such a wide-ranging speciality that turf wars seem almost inevitable. How is this challenge tackled in India?
It does seem like turf wars are here to stay. In India, we had the problem that there were not enough interventional radiologists to take up the challenge. The way to overcome this is to have more interventional radiologists available to do the job, fill any current lacunae and deliver results. Finally, if interventional radiologists are better trained and so more competent to perform procedures, the other specialties automatically will become irrelevant. I believe that these new super-specialty programmes will deliver the goods. This model has worked in Mumbai and I see no reason that it will not elsewhere in the country as well.
Which aspects of interventional radiology do you forsee a strong growth for in India?
Interventional oncology is and will always remain our forte. I have seen a quantum leap in the number of procedures being performed. The number of centres carrying out these procedures has grown as well. I anticipate that vascular interventions too will follow suit.
Which early technologies are you keeping an eye on?
Interventional radiology has always been characterised by its innovative spirit. We are now seeing progress with new procedures being developed to create percutaneous arteriovenous fistulae. The NEAT data are certainly to look out for. I am impatiently awaiting these results, which are expected to come out by the end of this year, or early next year. If the results are favourable, then this will add a new dimension to the venous access field.
What research from India are you are most proud of?
So far, research opportunities in India whose results will alter the course of practice in interventional radiology have been few and far between. The good news is that we are about to embark on a trial that may result in a paradigm shift in the treatment of superficial femoral artery and tibial lesions.
What are the biggest challenges for interventional radiology in 2016?
We need to increase awareness about interventional radiology and the safety and efficacy of our treatments. We need to educate not only the medical fraternity but also our potential patients. I think this can be achieved by starting our own outpatient departments so that the patients can walk in directly to the interventional radiology department rather than being referred to us by other specialists.
Could you please describe a memorable case?
A case that was referred to me after being refused by three cardiovascular and thoracic surgery units for an iatrogenic post-aortic valve replacement pseudoaneurysm of the ascending aorta is one that stays with me. Re-exploration was refused by all the three surgeons at these units and we finally treated this female patient with a patent ductus arteriosus closure device, percutaneously for this infrequent but well-recognised and potentially fatal complication after cardiac surgery.
What is your key message to young interventional radiologists?
Interventional radiology is a very demanding, but rewarding specialty. The young interventional radiologist must be clinically trained, focused and utterly competent in order to comprehensively treat patients. There might be a latent period before you get busy in your practice, but during that time you should use your time to pursue research and publish your work in order to be relevant in the field.
What are your interests outside of medicine?
I love spending time with my family and our pets (we have rescued a dog and a cat). I also love my Sunday morning round of golf which I call my weekly fix. Besides that, I enjoy sports such as cricket and soccer. I thoroughly enjoy travelling and exploring new places and local cuisines. I confess to listening to “retro” music quite a lot!
Fact file
Current role
Consultant interventional radiologist at Lilavati Hospital and Research Centre, Holy Family Hospital, Cumballa Hill Hospital and Heart Institute, Breach Candy Hospital, Fortis Hospitals, Asian Heart Institute, Jupiter Hospital, Dr Namjoshi’s Criticare Hospital, Hinduja Hospital, Dr LH Hiranandani Hospital and others.
Residency and fellowships
1992–1994 Senior resident, Departments of Ultrasound, General Uroradiology, and Vascular and Interventional Radiology, Bombay Hospital Institute of Medical Sciences, Mumbai, India
1994–1995 Senior resident, Department of CT Scanning, Bombay Hospital Institute
of Medical Sciences
August–October 1998 Fellowship in endoscopic ultrasound and interventional radiology, Georgetown University Medical Centre, Washington, USA
1998 Fellowship in Endoscopic ultrasound and interventional radiology, Universität Krankenhaus Eppendorf, Hamburg, Germany Achievements (selected)
1992 First to perform fallopian tube recanalisation in Mumbai, India
1996 First to perform carotid stenting in Mumbai
1998 First to perform transjugular liver biopsies in Mumbai
1998 First to perform endovascular repair of abdominaland thoracic aortic aneurysms in Mumbai
1998 First to start using endoscopic ultrasound at Bhatia Hospital in Mumbai
2002 First to perform intracranial stenting in India
2000 Approved panel physician by Boston Scientific for “Carotid Angioplasty Center of Expertise” programme
Society memberships
2002–04 Joint secretary, Indian Society of Vascular and Interventional Radiology (ISVIR)
2014–present Executive member of ISVIR, president, ISVIR
A minimally invasive treatment for migraine headaches used for adults is also proving to be a safe and effective treatment for children and teenagers. Further, it only takes minutes for a child to feel relief, according to new research being presented today at the Society of Interventional Radiology’s 2017 annual scientific meeting (4–9 March, Washington, DC, USA).
Migraines are a common medical condition among youth and adults, affecting 12% of people ages 12 and older. They can be especially debilitating in teenagers and often disrupt everyday activities, such as school, music and sports.
A sphenopalatine ganglion block does not involve needles touching the patient. Instead, a small flexible catheter is inserted into each nostril and local anaesthetic is administered to the sphenopalatine ganglion, a nerve bundle thought to be associated with migraines, located at the back of the nose. Briefly disabling the sphenopalatine ganglion can disrupt and reset the headache circuit, breaking a cycle of severe migraines and reducing the need for medication. The minimally invasive block takes almost immediate effect with relief potentially lasting for months, researchers said. Ssphenopalatine ganglion blocks are not a frontline treatment. A child only qualifies for the therapy if he/she has been diagnosed with a severe migraine that has not responded to first-line treatments.
“This treatment, performed in an outpatient setting by an interventional radiologist, can safely relieve a child’s migraine quickly,” said Robin Kaye, section chief, interventional radiology, Department of Medical Imaging, Phoenix Children’s Hospital, and a co-author of the study. “By reducing the need for medications that come with serious side-effects or intravenous therapies that may require hospital stays, children do not have to miss as much school and can get back to being a kid sooner.”
Kaye and her team conducted 310 treatments in 200 patients aged seven to 18 at Phoenix Children’s Hospital. Patients’ pain levels before the intervention were recorded on a scale of one to 10. Ten minutes after the treatment, patients were asked to compare their pain level, using the same scale. The researchers saw a statistically significant decrease in the headache scores, with average pain score reduction of just more than two points on the 10-point scale.
“While it is not a cure for migraines, this treatment has the potential to really improve the quality of life for many children,” said Kaye. “It can be performed easily, without complications, and gives quick pain relief, which is important to parents who want to see their children happy, healthy and pain-free again. If needed, we can also repeat the treatment if or when the migraine returns.”
Daniel Sze, speaking at the ninth annual Symposium on Clinical Interventional Oncology (CIO; 4–5 February 2017, Hollywood, USA), noted that immunotherapy is a “huge opportunity” for interventional oncology.
Sze, professor of Radiology, Stanford University, USA, was speaking on the potential role of immunotherapy in interventional radiology. “The immune system is the natural defense against cancer and plays a role in surveillance, recognition, attack and vigilance. It is important to understand at least the following checkpoints: cytotoxic T lymphocyte-associated protein 4 (CTLA-4); programmed cell death protein 1 (PD-1); and its ligand (PD-L1),” he said.
Immunotherapy involves stimulating the cancer patient’s immune system so that it can robustly fight the disease. Sze used the analogy of a military defense strategy to counter insurgencies to elaborate on the rationale behind immunotherapy: “Instead of sending in more US marines, teach the local militia to expel the insurgents,” he said alluding to how immunotherapy works.
As reported in the June 2016 cover story in Interventional News, experts now believe that there could be a time when interventional radiologists no longer perform procedures to destroy tumour tissue alone—they might be ablating or embolizing to provoke the patient’s immune system to powerfully destroy cancer cells.
Sze then drew attention to a variety of immunotherapy agents such as ipilimumab, pembrolizumab, nivolumab, and atezolizumab. Ipilimumab was US FDA approved in 2011 and saw US$1 billion sales in 2015. Indicated for late stage melanoma, or as an adjuvant therapy, this monoclonal antibody may result in autoimmune toxicity and costs around US$150,000 for four infusions. PD-1/PD-L1 inhibitors pembrolizumab and nivolumab were approved in 2014 and have both gone on to see huge sales. Pembrolizumab has US FDA indication for late stage melanoma and added indications for non-small cell lung carcinoma (NSCLC) with overexpression of PD-L1 and for head and neck squamous cell carcinoma. Nivolumab is approved for melanoma, NSCLC, renal cell carcinoma, Hodgkin lymphoma, and urothelial carcinoma.
Sze emphasised the high cost of immunotherapy agents and noted that health agencies in some countries had halted their routine use in the healthcare system on the basis that they have not been shown to be cost-effective. In addition, systemic administration may result in life-threatening autoimmune toxicity, leading to warnings from the US FDA, he noted.
There are also other types of immunotherapies such as cell-based therapy which involves the introduction of new components of the immune system which have been engineered or manipulated outside of the body, taught to recognise cancer, and reintroduced into the patient. In addition, oncolytic immunotherapy uses engineered viruses to selectively infect cancer cells. Infected cells undergo lysis, releasing antigens, and the ensuing stimulation of the immune system promotes attacking of cancers throughout the body.
“Sorafenib taught medical oncologists to keep their patients, avoid referral to tertiary care, and avoid referral to interventional radiology. We cannot allow systemic immunotherapies to repeat this history. We must re-establish interventional radiology as a key player in cancer care. This will not be handed to us—we must generate the data,” urged Sze.
“Interventional radiology must identify the unmet needs within immunotherapy: many therapies are systemically toxic and some cannot penetrate tumour microenvironments. The response rates are still low and cancers are a biochemical moving target. We must devise interventional radiology solutions and administer these locoregionally. We must disrupt tumours and uncloak antigens. We must select patients based on tumour genetics and track changes in biochemistry,” he concluded.
Guerbet has announced that the Thailand FDA has given approval of a new indication for Lipiodol Ultra-Fluide for selective hepatic intra-arterial injection for visualisation, localisation and vectorisation during transarterial chemoembolization of tumours in adults with known, intermediate stage hepatocellular carcinoma.
Hepatocellular carcinoma is the most common primary cancer and is the second biggest cause of death due to cancer worldwide.
“Guerbet is proud to be granted approval for this new indication for Lipiodol Ultra-Fluide, this reflects a strong positive endorsement from Thailand liver cancer doctors,” commented Eam-Maly Nam, Guerbet ASEAN Distribution Manager. “The development of these image-guided procedures is a top priority for Guerbet’s Interventional Radiology and Theranostic Business Unit as we work to enhance liver cancer patients’ prognosis and quality of life in Thailand and worldwide.”
Lipiodol Ultra-Fluide is used for conventional transarterial chemoembolization (cTACE), a minimally invasive procedure which consists of mixing Lipiodol Ultra-Fluide with an anticancer drug. The mixture is injected transarterially in the liver as a locoregional targeted chemotherapy for unresectable hepatocellular carcinoma tumours. Lipiodol Ultra- Fluide acts as a contrast agent, a drug-eluting vehicle, and a dual arterioportal transient embolic.
This indication was recently approved in Japan, France, Austria, The Netherland, South Korea, Turkey, Czech Republic, Hungary, Peru, Mongolia, Argentina and Vietnam. It has been submitted to many other European and Asian countries and other registrations are still pending. These steps follow approval of the indication by the US Food and Drug Administration (FDA) in April 2014 for “selective hepatic intra-arterial use for imaging tumours in adults with known HCC “.
Guerbet Lipiodol Ultra Fluide is used in conventional cTACE procedures for the treatment of patients with inoperable liver tumours. cTACE has been published in over 100 clinical studies, of which five were international randomised controlled trials, out of a total number of more than 10,000 patients with intermediate stage hepatocellular carcinoma who have been reported on in the peer-reviewed scientific literature.
cTACE has been established as the gold-standard for the treatment of patients with intermediate stage hepatocellular carcinoma by several international clinical consensus guidelines in Japan, Europe and the United States. These consensus guidelines unanimously recommend cTACE as the standard-of-care for patients with intermediate stage hepatocellular carcinoma. These recommendations were made with a Level of Evidence 1iiA and a Grade of Recommendation 1A in the European guidelines.
These guidelines stipulate that these patients present a median survival of 16 months only whereas cTACE extends the survival of these patients to a median of 20 months, ie four additional months. Additionally, the shortest survival reported is 14 months for the worst case scenario of untreated candidates whereas the longest survival reported is 45 months for the best responders to cTACE, i.e. a 31 month differential, according to a press release from Guerbet.
Consequently, the release adds, treatment with cTACE is constantly increasing in all continents, with more than 500,000 patients being treated every year.
Surefire, the developer of site-specific delivery devices for the interventional oncology market, has announced the first closing of a US$12.8 M Series D financing round.
Surefire Medical will use the round, led by Ori Healthcare Fund and with continued support from previous funders, to:
Expand sales and marketing in the USA and Europe
Initiate sales and clinical trials in the multibillion dollar China market
Complete the 170-patient randomised controlled QED clinical trial (NCT02748161)
Pursue promising opportunities in the US$66 billion immunotherapy market, focusing on site-specific delivery to solid tumours
Surefire’s unique infusion system uses an expandable tip that increases infusion pressure within the tumour. The increased pressure overcomes barriers to drug delivery, delivering significantly more therapy into the tumour than older, less efficient end-hole catheters. Simultaneously, the expanding microcatheter tip protects healthy tissue by blocking backflow during infusion.
“ORI Healthcare Fund focuses on disruptive technology platforms that will lead to new standards of care, “ says Simone Song, senior partner, ORI Healthcare Fund. “We are fortunate to be able to invest in Surefire’s technology, which will change the standards of care in liver embolization and immunoncology approaches requiring direct-to-tumour delivery. We will leverage our resources in China to help penetrate the Chinese market, which has the highest and fast-growing liver cancer incidence.”
Growing body of significant clinical data
In a randomised trial, the Surefire catheter was shown to improve tumour uptake by 68% while simultaneously decreasing non-target delivery by 58%. Additionally, a multicentre registry found use of the Surefire Precision Infusion System in the treatment of primary liver cancer (hepatocellular carcinoma) was associated with a 68% complete tumour response and 92% objective tumour response. These response rates are considerably higher than the average response rates seen in the literature for this patient population.
New clinical data to be presented at the 2017 Society of Interventional Radiology’s annual scientific meeting this month reinforces previous findings. In a retrospective case-controlled comparison, the use of Surefire infusion technology achieved a 79% objective response rate in the treatment of primary liver cancer (hepatocellular carcinoma) in transarterial chemoembolization procedures (TACE) vs. 37% with a standard microcatheter.
“We plan to have the Surefire Infusion System become the standard of care in liver embolization,” says Surefire Medical president and CEO James Chomas. “We are very pleased to welcome the ORI Fund. This series D financing supports our core liver cancer business by expanding to large untapped markets as well as expanding our business model through partnerships with biotechnology companies developing immunotherapies for solid tumours.”
Mentice has announced the release of the world’s first simulation training software module for prostatic artery embolization. The software, created from real patients’ data, will allow interventional radiologists to train for the procedure.
The software has been developed together with two of the world’s leading prostatic artery embolization authorities: Shivank Bhatia, associate professor, Interventional Radiology and Urology, University of Miami Hospital, Miami, USA, and Marc Sapoval, professor of Radiology, Hôpital Européen George-Pompidou, Paris, France.
“The Mentice software, created from real patients’ data, will allow interventional radiologists to train for prostatic artery embolization, and will help reduce the steep learning curve associated with this technically challenging and complex procedure,” says Bhatia. “Collaborating with Mentice has resulted in a training innovation that I am personally very proud of.”
Prostatic artery embolization is a novel procedure that was first presented at SIR 2011. A minimally invasive endovascular procedure, it has been shown to be safe and efficacious. The procedure scores highly in terms of patient satisfaction, and dramatically reduces length of hospital stay compared to transurethral resection of the prostate.
“Prostatic artery embolization,” said Sapoval, “is a demanding procedure performed by experienced interventional radiologists. The anatomy is highly variable, the microcatheter and microwire skills required are advanced, and a high degree of technical competence in various areas is essential. Simulation training aims to facilitate the learning curve for performing prostatic artery embolization.”
Mentice formally released and demonstrated the simulation training software at Society of Interventional Radiology’s 2017 annual scientific meeting (4–9 March, Washington, DC, USA).
“War (as in turf war) is an emotional word because, in wars, people get hurt. I believe we truly care about the patients we serve and the last thing we want is for patients to get hurt. […] By and large, we have found that approaching role extension issues through discussion is preferable to confrontation,” Gregory John Slater, president, The Royal Australian, and New Zealand College of Radiologists (RANZCR), tells Interventional News. Slater is a radiologist at Queensland X-Ray, Brisbane, Australia, and a visiting medical officer at several private hospitals. He enjoys the outdoors, and like any true blue Aussie, loves throwing a shrimp on the barbie.
What made you choose interventional radiology?
I wanted to be a medical doctor at around 10 or 11 years of age. After that, there was no time to be wasted, it was simply a matter of getting on with it.
Having arrived in medicine, it took me much longer to yield to the siren call of interventional radiology. I was very curious about the wide spectrum of medicine and explored several specialties. I did enjoy performing procedures like cesarean sections or being a member of an open-heart surgery team, but not enough to commit to a lifetime. Then, a decade after graduating as a doctor, I resolved to commence radiology specialty training and voilà, a treasure trove of opportunity lay before me. These years were the heyday of interventional radiology as new techniques and procedures sprung everywhere. And the excitement has not waned…
Who were your mentors and what wisdom did they impart to you?
In this specialty, which relies so much on personal guidance and inspiration, mentors loom large over all our careers.
The first person to turn me on to interventional radiology was John Harper, the head of intervention at the Princess Alexandra Hospital in Brisbane. He set himself high personal standards for even simple procedures, emphasising patient safety and demanded the same from his trainees.
Ken Thomson from Royal Melbourne Hospital is a truly inspirational interventional radiologist who has had a profound effect on the lives and careers of a generation of young physicians across the Asia-Pacific region and around the world. He was truly dedicated and would never give up. I remember seeing him do a vascular case despite being badly troubled by back pain that would have confined most mere mortals to bed. Ken was so determined that he designed a frame to bear the weight of the lead gown that allowed him to work beneath the frame from the sitting position as he was unable to stand.
I was extremely fortunate to gain a two-year fellowship in abdominal imaging and intervention with Peter Mueller at Massachusetts General Hospital (MGH) in Boston, USA. Peter is one of the most inspiring teachers you would ever meet and is rightly recognised as a giant in the field.
Of all the great young interventional radiologists I met in Boston, Michael Lee, Dublin, Ireland, stands out as one who would go on to achieve great things as an innovator, teacher and leader. He has served CIRSE mightily and I will feel proud to see him awarded the Gold Medal at this year’s meeting.
Could you describe interventional radiology’s place in Australia’s healthcare system?
On the whole, interventional radiology is well established and accepted in the Australian healthcare system.
Healthcare outcomes and longevity in Australia are amongst the world’s best, yet our costs fall in the middle of the band of Organisation for Economic Co-operation and Development (OECD) countries. By and large, the health system works well.
Interventional radiology is widely available in both public and private hospitals and we generally perform similar procedures to those available overseas. For example, prostate artery embolization is now being performed at several centres, with results in line with those being achieved elsewhere. We are fortunate to have good access to medical devices without the onerous restrictions of some other countries. We have been innovative over the years and procedures such as endovascular aortic repair (EVAR) and selective internal radiation therapy (SIRT) have emanated from this country.
Many routine arterial interventions are now performed by vascular surgeons, but procedures such as embolization and thrombolysis are usually done by interventional radiologists. Interventional radiologists carry out nearly all venous interventions, except for areas such as varicose vein ablation which is shared with other specialties. Neurointerventional radiologists do almost all neurointerventional procedures in Australia.
As the 2016 president of the RANZCR, what are your goals?
At our recent Board and Faculty Council meetings, we have decided to establish a standing committee of interventional radiology. This is our highest-level committee and aims to advance the role and place of interventional radiology in Australia and New Zealand. It aims to promote interventional radiology to the highest levels of government and the community and I expect it will seek to establish the discipline as a recognised subspecialty in our countries.
With the evidence for endovascular stroke therapy growing, I have been working with our jurisdictions and societies (Interventional Radiology Society of Australasia [IRSA] and the Australian and New Zealand Society of Neuroradiology) to determine arrangements for delivery of these services. This is a challenge in countries with relatively sparse and widely dispersed populations.
I attended the recent European Board of Interventional Radiology (EBIR) examinations held in Queenstown, New Zealand. This is the second examination series we have held, under a joint agreement between RANZCR, IRSA, and CIRSE. The examination was a great success and we are grateful to CIRSE for its support and supervision. At present this is the only EBIR examination that is held outside Europe, and we certainly aim to build on its success.
How is the challenge of turf wars tackled in Australia?
War is an emotional word because, in wars, people get hurt. I believe we truly care about the patients we serve and the last thing we want is for patients to get hurt.
The best outcome for patients is achieved when their procedure is performed by the operator with the most knowledge, training, and experience. This person will often be an interventional radiologist, but it is not automatically so. We should be aware that we do not own procedures or patients. It is inevitable that some of our procedures will be adopted by other specialty groups, and we should be proud that the procedure is sufficiently worthwhile and robust to have redefined the standard of care. It is futile to try to prevent change and sometimes it is better to be an active part of change than to rail against it.
By and large, we have found that an approach to role extension issues through meeting and discussion is preferable to confrontation. For example, we have maintained cordial relations with vascular surgeons by being involved in their conversion to endovascular surgical techniques. As long as they have the patients, it is inevitable that this would happen, but we have maintained dialogue and professional interaction going forward.
We are well aware that standards of training and certification are paramount in the definition of quality and patient outcomes. We do not accept that other operators with less skill or experience should take over a procedure, as patient outcomes would be expected to suffer. In addition to standards of training, logbooks and audit are fundamental to the defence and evaluation of our interventions. We have not always performed well here.
Finally, some of our subspecialty groups have not taken a cooperative stance with each other in role management. We should find it much easier to agree with radiologists than other specialists as we have all come through the same training programmes and have the same fundamental training and beliefs. Time wasted in internal disputes will allow other entrants to focus their resources and potentially steal a march on us.
Which aspects of interventional radiology do you foresee a strong growth for in Australia?
I am tremendously excited about the advent of interventional oncology and how it will benefit our patients. It offers the potential to stand alongside our medical, surgical and radiation oncology colleagues. It is a once-in-a-lifetime opportunity but will need to be carefully and actively managed. We will need to energetically commit to patient consultations, daily ward rounds, admitting rights, multidisciplinary teams, social media, evidence base, research, audit, and other less-familiar areas if we are truly to be regarded as clinicians. There is much we can learn from our colleagues in radiation oncology who are experts in targeting cancer.
Ablative therapy will continue to increase. There is a desperate need for robust data to support their growth potential.
Interventions for varicose veins, while quite common now, have a lot of growth potential still.
Uterine fibroid embolization has a certain following, but is much underused in Australia and New Zealand. There is a growing expectation that gynaecologists should discuss all treatment options with their fibroid patients, but this is not happening yet.
As any interventional radiologist who regularly performs percutaneous vertebroplasy knows, it is extremely effective in properly selected patients. The procedure had funding withdrawn in Australia following the trials published in the New England Journal of Medicine (NEJM) in 2009, but new evidence will hopefully restore it to being more widely used.
Musculoskeletal interventions, such as joint and bursal injections and spinal interventions for pain relief, have undergone massive growth in the last decade but are expected to grow further. Again, there is a dearth of high-quality evidence to justify large growth rates and these will come under increasing scrutiny by funders.
Prostate artery embolization should have a huge future. With the obesity epidemic, there could be a future for bariatric interventions, if they stack up.
What interesting trial data have you come across recently?
At the recent IRSA meeting in Queenstown, William Clark presented the results of the VAPOUR trial. These have just been published in The Lancet. This is an important randomised double-blinded controlled trial that provides strong evidence of the significant beneficial effects of percutaneous vertebroplasty in recent vertebral crush fractures and significant pain, both in the short-term and long-term (See Clark’s article, here).
Also at the IRSA meeting, Gerard Goh presented early experience with percutaneous arteriovenous fistula creation using two devices (everlinQ and Ellipsys). He presented the early findings of the NEAT (Novel endovascular access trial) study taking place Australia, New Zealand and Canada. The ability to successfully create an arteriovenous fistula for dialysis is a very interesting concept that could potentially have wide applicability, and the findings to date are promising.
The SIRFLOX, FOXFIRE, and FOXFIRE Global trials are prospective, open-label, multicentre randomised controlled trials comparing Y-90 spheres plus chemotherapy vs. chemotherapy alone as first-line therapy in patients with liver metastases from primary colorectal cancer, with results expected around June 2017. These, and other ongoing studies, will add further information about the value of radioembolization, and may increase its penetration.
What is the research you have carried out that you are most proud of?
The large Hypertension Unit at Greenslopes Hospital where I have worked since 1996 has a particular interest in primary aldosteronism. In radiology, we are called upon to perform large numbers of adrenal vein samplings. My colleague, Nick Daunt, and I have performed around 1,700 of these procedures between us, the largest number in the world. I hope that the published findings on technique and tips that have allowed us to increase our success rates will make the procedure a little less challenging for those who are inexperienced in it, as it can be technically difficult and has a long learning curve.
Please describe a memorable case that you treated
Of course, there are many including the patient who returned my precordial thump at the commencement of cardiopulmonary resuscitation (he was only sleeping!).
But one that stays is a female patient in her 40s with hereditary haemorrhagic telangiectasia. She had multiple nasopharyngeal telangiectases and a 30-year history of recurrent severe epistaxis and nasopharyngeal bleeds. Her life was misery as she bled for several hours each day. She required frequent hospitalisations and had required blood transfusion on hundreds of occasions. Multiple ear, nose, and throat specialists had been consulted and she had undergone many nasal cauteries and packings, but she was told that “nothing more could be done”. Remarkably, embolization had never been considered. Obviously, this was in the days before Google!
I performed a three-pillar embolization, perfectly straightforward, and she had a marvellous result. Her bleeding almost completely ceased and her life was transformed. She had a durable response and sent me a Christmas card for many years afterwards.
What is your key message to young interventional radiologists?
If this is your calling then embrace it and go hard.
Never abandon the patient if the outcome is suboptimal; they need your extra support and often will be very grateful for it.
Do not skimp on research, do all you can and build relationships with your mentors.
Remember the three “A”s that guarantee success: Able, affable and available.
Above all, do the EBIR!
What are your interests outside of medicine?
I have always enjoyed the outdoors, and enjoy camping and fishing, although my fishing boat has been sitting forlornly in the driveway for way too long.
Snow skiing has been a great love of mine since student days and has continued since my knee reconstruction 30 years ago after a fall on the long skis. Hiking is now more age-appropriate; my wife and I enjoyed walking the Routeburn Track in New Zealand earlier this year—spectacular even in the rain.
In spectator sports, I support the Wallabies rugby team, even though we lose a lot. I also follow Australian drivers in Formula One.
My love of the ballet began when doing my fellowship in Boston; it was not all work! I have a share in a small winery in the mountains with some friends and it is great to visit, pick the grapes or help the winemaker. And like any true blue Aussie, I love to throw a shrimp on the barbie!
Factfile
Education
MBBS University of Queensland
Fellow of The Royal Australian and New Zealand College of Radiologists (RANZCR)
Postgraduate training (selected)
1989–93 Registrar, Radiology, Princess Alexandra Hospital, Brisbane
1993–95 Clinical fellow in Abdominal Imaging and Interventional Radiology, Massachusetts General Hospital, Boston, USA
1995–2000 Visiting radiologist, Princess Alexandra Hospital, Brisbane
2006–07 Visiting radiologist, Princess Alexandra Hospital, Brisbane
First Class Honours, Medical School of the University of Queensland
Private Practice Research and Education Trust Fund Scholarship, Princess Alexandra Hospital, Brisbane
46th Baker Fellowship Award, Royal Australasian College of Radiologists, for further training in the field of abdominal imaging and intervention at the Massachusetts General Hospital
Honorary membership, American Roentgen Ray Society
Memberships of professional societies:
Australian Medical Association
Royal Australian and New Zealand College of Radiologists
Interventional Radiology Society of Australia
Cardiovascular and Interventional Radiology Society of Europe
Suresh Vedantham, professor of Radiology and Surgery, Mallinckrodt Institute of Radiology, Washington University School of Medicine in St Louis, USA, is scheduled to present the final results of the landmark ATTRACT trial on 6 March at the Society of Interventional Radiology’s annual scientific meeting in Washington, DC, USA. The trial’s results will then be discussed by a panel of experts.
Vedantham is the national principal investigator of the ATTRACT trial and the 2017 incoming president of the SIR. (Get behind the trial data and read his profile in the next issue of Interventional News, available at our booth at the SIR meeting next week).
ATTRACT (Acute venous thrombosis: thrombus removal with adjunctive catheter-directed thrombolysis) set out to determine if the use of pharmacomechanical catheter-directed thrombolysis can prevent the post-thrombotic syndrome in patients with deep vein thrombosis, with acceptable safety and costs.
The trial is a National Institutes of Health-sponsored, phase III, multicentre, randomised, controlled clinical trial. It is a major international collaborative effort among leading North American researchers of diverse subspecialty.
“[At the time this publication goes to print] I am not yet free to discuss the trial’s findings, but I do believe this trial achieved its main objective of telling us which acute deep vein thrombosis patients should, or should not, receive endovascular intervention,” Vedantham, professor of Radiology and Surgery, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St Louis, USA, and the 2017 incoming president-elect of the Society of Interventional Radiology (SIR) told Interventional News ahead of the presentation.
Here is a teaser (and a few outtakes from the interview), available exclusively on our website.
Could you comment on the importance of multidisciplinary collaboration and its value in the running of large-scale clinical trials such as the ATTRACT trial?
First, interacting with other providers enables one to understand the disease in a broader context that goes beyond one procedure or category of intervention. It pushes you to challenge your own groupthink. We tend to forget that our view on a disease is shaped by many factors: the clinical setting in which we see patients; the mindset of our colleagues; and (both for better and for worse) the effect of industry (the drug industry for internists and the device industry for endovascular physicians) upon all of it. Training matters too—internists view deep venous thrombosis as basically an imbalance in the clotting system; whereas we view it from anatomical and physiological perspectives. Only when we share these camera angles with each other can we see a fuller picture.
Second, collaborating recruits skills that one would not have otherwise. What I have learned from ATTRACT is pretty humbling. Despite being considered a “research leader”, the truth of the matter is that I am first and foremost a well-trained clinician who does research on the side. But many of the other leaders in the ATTRACT trial are professionally trained researchers, and believe me it shows. The trial could never have been designed, funded, and completed without all kinds of different expertise being brought to bear on it.
Third, your potential to have real clinical impact, and stave off challenges to your study, is multiplied manyfold by collaborating. My best advice to young researchers would be that you need to be able to speak the language of multiple subspecialties around the condition you are studying. That means knowing their literature, guidelines, and culture. Only when they see that you appreciate their perspectives can they reach beyond them to understand yours. And, do not be put off by bumps in the road; they are inevitable. The amazing thing I have seen with ATTRACT is that over 10 years, our steering committee members have actually grown together in their individual perspectives on deep venous thrombosis, learning from each other along the way.
As a member of various writing groups on the treatment of venous thromboembolism, what are the most important changes in the latest guidelines?
Recently developed guidelines include updated quality improvement guidelines for interventions from SIR (2014); the first guideline to focus on the diagnosis, prevention, and management of post-thrombotic syndrome from the American Heart Association (AHA, 2014); the Anticoagulation Forum’s practice-oriented chapters on venous thromboembolism management (2016); and of course, the 2016 Chest Guidelines update. Important changes include recommendations supporting the use of new oral anticoagulants for venous thromboembolism care, the weakening of recommendations for compression stockings in acute deep venous thrombosis patients (due to the results of the rigorous SOX trial which were negative), slightly more attention to chronic sequelae of venous thromboembolism including post-thrombotic syndrome, and the continued need for clinical trial evidence to guide recommendations on endovascular care options.
From your 2007 paper “Myths, misconceptions, and incorrect interpretations of the deep venous thrombosis literature”, which of these hold true ten years later?
I would say it continues to be important to consider deep venous thrombosis and post-thrombotic syndrome as “diseases” with multifactorial aetiologies. It continues to be important to ensure quality anticoagulation for deep venous thrombosis. One thing that has changed since 2007 is that compression therapy has been found in a recent rigorous, double-blind, multicentre randomised trial not to prevent post-thrombotic syndrome. It continues to be important not to draw outsized inferences from observational associations and data from low-quality studies. We need to keep pushing the envelope by completing multiple highly rigorous studies to drive us forward.
BTG has announced that US FDA 510(k) clearance has been granted to the Ekos control unit 4.0.
The Ekos system includes an ultrasonic device that uses acoustic pulses, powered by the new Control Unit 4.0, to quickly and safely dissolve blood clots and restore blood flow in patients with pulmonary embolism, deep vein thrombosis, and peripheral arterial occlusions.
The Ekos control unit 4.0 was specifically designed to support a new standard of pulmonary embolism treatment – allowing physicians to use one control unit to treat both pulmonary arteries. The colour touchscreen allows physicians to easily monitor and independently manage two Ekos devices simultaneously, simplifying bilateral pulmonary embolism treatment. With new functionality and workflow-based intelligence, the Ekos control unit 4.0 is designed to support a medical team’s ability to perform at a high level – from cath lab to transport to intensive care unit.
“Currently the only device cleared for the treatment of pulmonary embolism, Ekos has been in a leadership position in the pulmonary embolism treatment market since the beginning” said BTG vice president and general manager Matt Stupfel. “Now, BTG is further solidifying our leadership position with the Ekos control unit 4.0. This new platform will allow for further device innovation to simplify treatment for clinicians and improve outcomes for patients.”
The Ekos system uses acoustic pulses to unwind and thin fibrin to expose drug receptor sites, allowing the drug to reach deeper into the clot, accelerating absorption and helping to dissolve the clot faster and with less thrombolytic.
There is an explosion of interest in transradial access within interventional radiology. With the twitterverse abuzz with hashtags such as #radialfirst and #transradial and physicians stating that the best way to a person’s heart is through their radial artery, Interventional News spoke to two proponents of the radial revolution, Darren Klass and Aaron Fischman, about what we need to know in 2017.
Klass is an interventional radiologist at Vancouver Imaging, Vancouver, Canada and Fischman is an interventional radiologist with the Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, USA.
“Radial intervention is not a religion; the patient is central, not the procedure. [But] This is a technique that should be practiced by all interventional radiologists, because it is better for patients,” Klass said.
What is the most interesting piece of research you have come across recently about radial access?
Darren Klass
DK: The most interesting research in my opinion is within the cardiology literature; however, the findings are extremely important and pertinent to our specialty. PROPHET II was a randomised controlled trial of 3,000 patients comparing patent haemostasis with and without ipsilateral ulnar artery compression. The rates of radial artery occlusion at 30 days were significantly lower in the group where patent haemostasis and ulnar artery compression was used. This has changed my practice and although our centre, after over 1,200 cases, has an extremely low asymptomatic occlusion rate, my aim with every access is to ensure, as much as possible, that the vessel is spared for subsequent interventions. The theory of ulnar artery compression during patent haemostasis allows increased flow through the radial artery thus decreasing occlusion rates. The ulnar artery is not accessed and, therefore, temporary compression does not cause occlusion.
Within the interventional radiology space, Marcelo Guimaraes (Medical University of South Carolina) is conducting an extremely interesting prospective study assessing patient preference for transarterial chemoembolization (TACE), and I eagerly await the result.
AF: The PROPHET II study by Pancholy et al. was very interesting because in a randomised fashion they were able to show a significant decrease in radial artery occlusion with prophylactic ipsilateral ulnar compression during radial artery haemostasis. The primary endpoint of 30-day radial artery occlusion was 0.9% with ulnar compression vs. 3% in the control arm. Despite the fact that this is a cardiology study, I think this has implications for interventional radiology. Radial artery occlusion is not very common in my practice, but does occur in small numbers. This technique could virtually eliminate that in certain high risk cases.
What is the most interesting radial access research that you are carrying out?
DK: We have just completed data analysis of a rapid haemostasis protocol named PROTEA (Percutanous radial haemostasis using a truncated deflation algorithm), which will be presented at SIR 2017. This protocol uses a proprietary haemostasis pad (Statseal, Biolife) to aid with haemostasis during deflation of the balloon. The protocol decreases the haemostasis time to 25 minutes (from an hour, or more) in patients undergoing procedures with a 7F sheath or less and no more than 5000IU heparin. This has dramatically improved patient discharge times, and our centre now has an 85% TACE out-patient service where patients are discharged within 90 minutes of coming off the angiography table.
Aaron Fischman
AF: Right now, we are designing a randomised trial for interventional oncology patients. Specifically, quality of life (QOL) and patient satisfaction is of great interest to me. We plan to take a patient population that has multiple procedures in a short period of time such as Y-90 and randomise them to femoral or radial access and then use the opposite technique for their second procedure. Using validated survey mechanisms, we are going to determine if patients are more satisfied with radial or femoral access. QOL is something that is provable in interventional radiology with smaller numbers of patients.
Within the interventional radiology world, what is the response to hands-on learning and workshops in this area?
DK: The response has been excellent and I believe this is echoed by all of my colleagues who train interventional radiologists in this technique. The most important message is that this is not just an access procedure and it involves the training of paramedical staff and having tools to be able to complete cases and tips for challenging cases. I am asked all the time if it is necessary to attend a course before offering this service; I think it is absolutely necessary. The training provides not only access and haemostasis, but also addresses complications, pitfalls and inventory needed for complex cases. You can learn this yourself but I do not believe if you have access to training, that patients should be put at risk while you work things out for yourself when you can be provided all the tools to do this.
I have given advice to many interventionists once they begin using this approach. The most common questions are often around difficult cases or non-specific symptoms after the case, where patients may present with pins and needles in the hand and operators are unsure as to the approach to deal with these issues. The answer is often a simple one, but you need the tools to be able to manage these issues and the courses and workshops provide them.
AF: I have organised and co-ordinated many hands-on workshops regarding radial access over the years. They are often well attended and of great interest to the interventional community. The radial approach is not a new concept but for interventional radiologists it can be intimidating if the tips and tricks are unfamiliar. When I teach these courses I tend to focus proper technique. If proper technique is followed from the beginning, success rates are much higher.
What would be your most compelling argument to a staunch femoralist about radial access?
DK: This is a procedure that is better for patients. It allows them to ambulate much faster and is more comfortable. For oncology procedures, keeping a patient in overnight just because of a femoral puncture is not good patient care. These patients often have a few months to live and taking away a night from their loved ones just because you do not think radial access is worth learning is doing the patient a disservice.
For operators doing many peripheral vascular procedures, the argument of percutaneous brachial is not an argument. Performing a procedure on a patient with a complication rate of 12% (of which 50% require surgery) is unforgivable. It is 2017—use the radial artery.
AF: All femoralists should consider this: interventional radiology has always been about innovation, creative thought and high technical skill. Many of the procedures we do are not unique to us. What can differentiate us from other specialties is the desire to make our procedures less invasive, more patient friendly, low cost and low morbidity. The data support radial access over femoral access in all of those categories. As we create more data on the radial access technique in interventional radiology, I am confident that we will be able to easily demonstrate the value of radial access. Even the most staunch femoralists realise that there are situations where radial access is needed regardless of operator preference. It will only serve us well in the future to make sure our trainees are well versed in both techniques allowing for optimised patient care.
Are there any devices missing from the market currently?
DK: The biggest current issue is the lack of guiding catheters longer than 100cm. We need at least 115cm or 120cm guiding catheters to allow for more complex visceral work. The stent and balloon delivery systems need to be at least 150cm to allow for work through 120cm Sheathless guiding catheters and either rapid exchange systems or longer wires. Lower profile balloons and stents with technology acquired from coronary devices would be beneficial and important to allow work through as small delivery systems as possible.
AF: We are beginning to see longer diagnostic catheters ranging from 110–125cm in our labs. Microcatheter systems are generally well suited at the 150cm lengths. However, guiding catheters typically max out at 100cm length and this can be a problem when planning more complex interventions. Also, guiding sheaths are not typically hydrophillic all the way to skin entry point and this is as huge safety problem when using them in complex interventions requiring covered stents or distal peripheral arterial disease interventions. These are currently in development. Newer closure bands taking into account the findings of the PROPHET II study and others would be of tremendous value. Lastly, distal peripheral arterial disease interventions are not yet ready for primetime. Longer stent, balloon and atherectomy delivery systems would be extremely valuable in developing the peripheral arterial disease radial technique. This is currently underway and is something I am very excited about.
Darren Klass (seated) proctors interventional radiologists and Ferdinand Kiemeneij (standing second from left), regarded as the father of transradial interventions, proctors cardiologists.
Radial “MasterKlass” with Darren Klass
Essential devices
Always use a sheath designed for the radial artery, there are multiple options and all come with an access needle and wire, a femoral sheath cannot be used. I use a single catheter for all of my visceral work (Ultimate 1; Merit Medical) and a 45-degree angled catheter for everything else.
The Ultimate 1 shape is mirrored by other manufacturers and is essential for visceral work. The more important aspect is catheter length. I have both 110cm and 125cm 4F and 5F radial catheters on my shelf which I use for all my cases including pelvic work (trauma, gastrointestinal bleeds and uterine fibroid embolization) and also keep a 4F and 5F 45-degree, 150cm catheters on the shelf for taller patients for pelvic work as well as proximal superficial femoral artery work. A 150cm microcatheter is also an essential.
An indispensible piece of equipment is the sheathless guide catheter range (Asahi-INTECC), which allows the operator to use large bore guiding catheters for complex procedures without having to use large sheaths. This allows for up to 8.5F guiding catheters to be used in the radial artery and opens a platform for stenting using covered self-expanding and balloon expandable stents, as well as complex balloon occlusion or multicatheter embolic protection techniques.
New radial access technique
I am working on a new technique of accessing the dorsal branch of the radial artery, proximally in the anatomical snuffbox. This technique has been well-described in Russian literature, and appears to be more comfortable for patients with an even lower rate of haematoma and bleeding than conventional radial artery access. The haemostasis is simpler and faster than conventional access, given the anatomy of the dorsal radial artery.
Radial access in five years
I hope it will have the same trajectory as radial access in cardiology in Europe and Asia. If 50% of centres are doing radial that will be a huge achievement. I would like to qualify that by saying radial intervention is not a religion; the patient is central, not the procedure. What I mean is this should be a technique practiced by all interventional radiologists, because it is better for patients. However, the femoral artery is still essential in our everyday work. I still access the femoral artery all the time, but if I have the choice, I choose radial.
Klass’ top tips for beginners
Attend a course; it is invaluable for setting up a service and making sure your nurses and technologists are engaged.
Take time to make sure the room set-up is optimal for you and your team.
Plan complex cases well so you have the correct inventory available. A common misconception with inexperienced operators is thinking 100cm catheters are long enough; they more often are not.
Always perform an ultrasound of the radial artery to assess size and anatomy. This will ensure you do not overstretch the vessel and ensure you do not cause unnecessary spasm or complications due to a missed radial loop or aberrant anatomy.
Always remove the catheter over a wire; although it may be unnecessary in many situations, removing a catheter with an unprotected tip through the radial artery can cause discomfort for the patient, or worse (spasm, dissection and thrombosis).
Engage with your cardiology colleagues; they have tremendous experience and are a great resource (you will not spontaneously combust!).
Cook Medical has rounded out the Universa line with the introduction of two new sets for percutaneous urinary drainage.
Each set includes a catheter and accessories for specific procedures. These sets streamline Cook’s offering of percutaneous drainage products.
The Universa set options now available are introductory sets for initial catheter placement; and suprapubic sets for suprapubic drainage.
The Universa brand of urinary drainage products also includes ureteral stents and Foley catheters, available in multiple sizes and configurations to meet patient needs and physician preference.
“With the Universa line, we are providing our customers with a full line of products for their drainage procedures,” said Jean-Marc Creissel, vice president and global leader of Cook Medical’s Urology division. “Grouping our percutaneous drainage products into these convenient sets helps us serve customers better through a streamlined ordering process and improved management of inventory and stock.”
Penumbra has announced the presentation of the results of the ASTER trial, the first independent, prospective, randomised trial comparing the use of Penumbra’s aspiration system to stent retriever, in the opening plenary session at the International Stroke Conference in Houston, Texas.
The results provide additional evidence of Penumbra’s aspiration system as an effective frontline thrombectomy approach for acute ischaemic stroke as part of the ADAPT (A direct aspiration, first pass technique).
The ASTER (Adapt vs. stent retriever) trial is a prospective, randomised controlled study that compared the safety and efficacy of the Penumbra aspiration system used frontline as part of the ADAPT technique vs. stent retrievers. The primary endpoint was end of procedure revascularisation (TICI 2b/3). The study enrolled 381 patients at eight centres in France over 12 months beginning in October 2015. Penumbra provided an institutional grant to support the ASTER Trial.
“The ASTER study provides evidence that starting with Penumbra aspiration first as part of the ADAPT technique is similar to the stent retriever technique,” said Michel Piotin, principal investigator and interventional neuroradiologist at Rothschild Fondation Hospital in Paris. “The ADAPT technique offers the possibility to easily add a stent retriever following Penumbra aspiration if needed, leading to time savings.”
The data showed that the ADAPT technique compared favourably: 85.4% of patients treated with Penumbra’s aspiration system achieved the primary endpoint of TICI 2b/3 at the end of the procedure compared with 83.1% of patients treated with stent retrievers (p=0.53). Moreover, 63% of patients treated with Penumbra’s aspiration system achieved the secondary endpoint of TICI 2b/3 after frontline treatment compared to 67.7% with stent retrievers (p=0.33).
“The ASTER trial shows no significant difference in revascularisation rate and safety using either thrombectomy technique – Penumbra aspiration and stent retrievers – for acute ischaemic stroke patients with large vessel occlusions,” said Bertrand Lapergue, Division of Neurology, Stroke Center, Foch Hospital, University Versailles Saint-Quentin en Yvelines (France) and scientific coordinator for the study. “The broad eligibility criteria achieved in the ASTER Trial make the results generalisable to the majority of stroke patients with large vessel occlusions.”
Secondary safety endpoints presented, including embolization in new territory (ENT) and symptomatic intracranial hemorrhage (sICH), were not statistically different between the two arms.
“The ASTER Trial builds on the results of the 3D trial, providing additional evidence supporting the use of Penumbra System direct aspiration devices as a first-line treatment for acute ischaemic stroke patients,” said Adam Elsesser, chairman, chief executive officer and president of Penumbra. “The ADAPT technique with the Penumbra System as a frontline approach together with complementary adjunctive devices when needed offers a cost-effective solution for treating stroke patients, which is critical as patient access to mechanical thrombectomy is further expanded.”
Philips has announced the global launch of Azurion, its next generation image-guided therapy platform, which forms the new core of its integrated solutions portfolio for the fast growing image-guided therapy market.
Following the acquisition of Volcano in 2015, via which Philips has become a leader in advanced catheters for diagnosis and therapy, the company is now further cementing its overall leadership in the €5 billion image-guided therapy market with one of its largest global product launches in recent years. Philips’ Azurion image-guided therapy platform for interventional labs is the result of a multi-year development program conducted in close collaboration with leading clinicians in the field. This next generation platform features a state-of-the-art ergonomic design with an easy-to-use intuitive user interface, enabling clinicians to swiftly and confidently perform a wide range of routine and complex procedures in the interventional lab, a media release says.
With the rapid growth of image-guided therapy procedures, hospitals and health systems are increasingly faced with the need to control costs, while improving their standards of care. Azurion has been designed to address these challenges and is equipped with new workflow options and performance dashboards, as well as an upcoming range of productivity improvement services.
The Azurion platform also features over 1,000 new components, including an enhanced flat-panel detector, and Philips’ newly developed ConnectOS operating system for the seamless integration of real-time information from all relevant technologies in the interventional lab. All of these components work together to deliver high image quality at ultra-low X-ray dose and real-time image processing on multiple work spots within the interventional lab. Parallel working enables the team of clinicians to complete different tasks simultaneously in the interventional lab, saving valuable time without compromising quality of care. Azurion features procedure cards that allow clinicians to pre-program routine tasks and user preferences, helping to minimize preparation errors and further reducing preparation and procedure time.
Philips has pioneered a steady stream of innovations in planning and navigation software for areas such as vascular surgery (VesselNavigator), interventional cardiology ( EchoNavigator), interventional oncology (EmboGuide), and interventional neuroradiology (AneurysmFlow). All these advanced interventional tools integrate seamlessly into the Azurion platform to support the clinical workflow.
Driven by their benefits for patients and care providers, minimally-invasive therapies, such as the catheter-based treatment of certain tumours, aneurysms, obstructed blood vessels, heart rhythm disorders and defective heart valves, continue to grow fast. In addition to reduced patient trauma and shorter recovery times, such procedures also have the benefit of allowing the treatment of patients who would not be able to withstand the trauma of open surgery. However, during such procedures, clinicians cannot directly see and feel the organs they are working on. Effective imaging, measurement and navigation technologies are therefore key to guiding minimally-invasive procedures. At the heart of the interventional lab, these technologies allow identification and visualization of target organs and tissues, the operation of interventional devices, and the placement of implants, leading to improved chances of therapy success.
“For over 30 years, we’ve pioneered minimally-invasive treatments that help our patients get back to their daily lives,” said Barry T Katzen, founder and chief medical executive of the Miami Cardiac & Vascular Institute, Baptist Health South Florida, USA. “The imaging environment is critical to perform such procedures efficiently and effectively. As an interventionalist, we want to be in the cockpit, similar to a pilot in an airplane, where we have control of everything we need and have all the relevant functions at our finger tips. Philips’ next generation image-guided therapy platform just takes it to a whole other level and allows interventionalists to accomplish the procedures quicker and more efficiently, which benefits the patient.”
Teleflex Incorporated has completed its previously announced acquisition of Vascular Solutions.
On December 2, 2016, the two companies announced a definitive agreement for Teleflex to acquire all of the issued and outstanding shares of Vascular Solutions common stock for US$56.00 per share, in cash.
Vascular Solutions focuses on developing clinical solutions for minimally invasive coronary and peripheral vascular procedures. Teleflex hopes that the combination will accelerate the growth of the company’s vascular and interventional businesses by its entry into the coronary and peripheral vascular market, as well as increased cross-portfolio selling opportunities to both Teleflex and Vascular Solutions customer bases.
Some research data suggest there could be a synergistic effect between immunotherapy and minimally invasive procedures. Tumour types that do not respond to checkpoint inhibitors – so called “cold tumours” – could “turn hot” after treatment with locoregional therapies, writes Melanie Lee, London, UK.
Recent advances in cancer immunotherapy have led to an explosion of interest in the field. (See Interventional News article) Commentators have described it as a revolution in the treatment of cancer and some even see it as possibly offering a cure for a portion of cancer patients. Although using the immune system to fight disease is not a new concept, the excitement has been driven by regulatory approvals of monoclonal antibodies against immune system checkpoints, such as cytotoxic T lymphocyte-associated protein 4 (CTLA-4), programmed death ligand 1 (PD-L1) and its receptor (PD-1). Soon, we will also have data about chimeric antigen receptor T cells (CART). While very exciting, none of these therapies on its own can offer a silver bullet.
These new agents have only been shown to be effective in certain tumour types, such as melanoma, renal cell carcinoma and non-small cell lung cancer. Even in these indications, many patients treated with checkpoint inhibitors do not respond to monotherapy. These therapies are also associated with immune-related side-effects which differ from the known toxicities of traditional chemotherapy, further complicating their use.
It is now thought that immunotherapy will need to be used in combination with other agents or therapies to expand the proportion of cancer patients who could benefit. Researchers are therefore turning their attention to combining different checkpoint inhibitors, or combining checkpoint inhibitors with other cancer treatments, like radiation therapy.
Jump-starting the immune system
Combining immuno-oncology therapies with image-guided, minimally invasive therapies is one approach that is starting to attract interest from oncology physicians. Sometimes called locoregional therapies, these procedures deliver a treatment precisely where it is needed, aiming to destroy tumour cells without causing damage to healthy tissue. For example, interventional radiologists may insert a cryoprobe directly into an area to destroy a tumour with freezing, use beads to embolize specific blood vessels that feed a tumour, or use radioactive microspheres to give a localised dose of radiation to a tumour.
Some research data suggest there could be a synergistic effect between immunotherapy and these minimally invasive procedures. A number of clinical trials are already underway to study the safety and effectiveness of immune checkpoint inhibitors in combination with locoregional therapies.
Tumours use a variety of mechanisms to suppress the patient’s immune system and evade attack from T cells. The goal of checkpoint inhibitors is to take the brakes off the cancer-immunity cycle by turning off signals that can inhibit the ability of T cells to kill cancer cells. But some tumours are more immunogenic than others, and other factors in the local tumour microenvironment may affect whether or not a patient will respond to treatment with a checkpoint inhibitor.
How could using locoregional therapies help? First, these therapies debulk the tumour, which makes it easier for the immune system to tackle what remains. Second, there is also evidence that some locoregional therapies may induce a tumour-specific immune response, or in situ vaccination, by releasing tumour antigens. Further evidence indicates they induce cytokine production, stimulating the immune system and helping to create an antitumour microenvironment. If combined with a checkpoint inhibitor, these effects could enhance overall outcomes. There is even the possibility that tumour types that do not respond to checkpoint inhibitors – so called “cold tumours” – could “turn hot” after treatment with locoregional therapies, perhaps helping make immunotherapy more successful for a broader patient population.
Safety and cost are also important considerations when selecting an agent or treatment to combine with checkpoint inhibitors that are known to have immune-mediated side effects and are relatively expensive. As locoregional therapies are generally well tolerated, combining them with a checkpoint inhibitor is unlikely to substantially add to the side-effect burden and their cost-effectiveness may ease adoption of this combination approach.
Multidisciplinary approach
BTG has large a growing portfolio of minimally invasive therapies used by interventional radiologists across a variety of tumour types, including tumours in the liver and kidney. The therapies represent different modalities that could potentially have a synergistic effect if used in combination with immune checkpoint inhibitors.
For example, our bead products block the arteries that feed liver and other hypervascularised tumours, depriving them of blood and nutrients, while our selective internal radiotherapy product delivers radiation directly to liver tumours. Our cryoablation solutions use ultra-thin needles cooled to extremely low temperatures to freeze and destroy diseased cells in bone and soft tissue, kidney, liver, lung and prostate. While the potential for using locoregional therapies in combination with immunotherapy shows promise, many questions remain unanswered.
BTG has announced a partnership with the Society of Interventional Oncology (SIO), organisers of the annual WCIO conference, to fund new research in this area. Under the agreement, a working group will develop a white paper to direct research of locoregional therapies alongside immunotherapies, and SIO will award research grants to investigators advancing science in this area.
The complexities of manipulating the cancer-immunity cycle to fight tumours demand a multidisciplinary approach. By bringing together oncologists, immunologists and interventional radiologists, the partnership with SIO is fostering a collaborative environment across disciplines, which will be key to making progress as we explore these new combinations.
Image-guided, minimally invasive therapies already bring many benefits to physicians and their patients, and their use as a treatment approach for cancer is growing. We are hopeful that by better understanding the science of how these locoregional therapies could work in combination with immuno-oncology agents, we can help expand the number of cancer patients who might benefit from the immuno-oncology revolution.
Melanie Lee is the chief scientific officer of BTG
BTG has announced a collaboration with the Society of Interventional Oncology (SIO; a global organisation working to nurture and support interventional oncology worldwide) to explore the role of interventional oncology alongside immuno-oncology.
Recent advances in cancer immunotherapy have led to an explosion of interest in immuno-oncology. Newly approved treatments, such as checkpoint inhibitors, have been shown to prolong overall survival but only for a limited proportion of cancer patients, and only in certain tumour types. Combining immuno-oncology agents with the minimally invasive, locoregional therapies of interventional oncology has the potential to expand the number of cancer patients who could benefit. Further research is needed to understand the potential of these combinations.
SIO and BTG have established a working group to determine how best to explore the role of interventional oncology alongside immuno-oncology in the fight against cancer. This group, which includes interventional radiologists and immuno-oncologists, will identify unmet clinical needs and the critical areas of science that require further dedicated research. The working group plans to publish a white paper to guide research and clinical practice later this year.
This collaboration also establishes an independent research fund that will enable SIO to offer grant funding to independent investigators to address the critical unanswered questions for this combination therapy. SIO plans to fund collaborative research ranging from exploratory pilot projects to prospective clinical trials.
“SIO was founded to provide an optimal and necessary vehicle to nurture and support interventional oncology as the fourth pillar of cancer therapy worldwide. This research collaboration with BTG will help provide the resources necessary to further uncover how interventional oncology procedures may work synergistically when combined with another of the most cutting edge oncologic strategies – immunotherapy,” stated S Nahum Goldberg, vice-chair for Research and Head of the Interventional Oncology Unit, Hadassah Hebrew University Medical Center in Jerusalem, Israel and SIO Interventional/Immuno-oncology Working Group Chair.
Melanie Lee, chief scientific officer of BTG, commented “As a leader in interventional oncology therapies, we believe this is an excellent opportunity to work with the scientific community and invest in generating new knowledge. Our portfolio includes embolic beads, radioactive microspheres, and cryotherapy solutions and this research will answer important questions about whether these minimally invasive therapies can expand the benefits of immuno-oncology drugs.” See Lee’s feature article on the topic, here.
How locoregional therapies might help
Checkpoint inhibitors turn off signals that can inhibit the ability of T cells to kill cancer cells, but different tumours present different immunological challenges with responses also dependent on factors in the local tumour microenvironment. Locoregional therapies, such as cryotherapy, embolization or selective internal radiation therapy, debulk the tumour, which may make it easier for the immune system to tackle what remains. There is also some evidence that locoregional therapies can also induce a tumour-specific immune response, releasing tumour antigens, and can help create an antitumour microenvironment. If combined with a checkpoint inhibitor or other immunotherapy, these effects could help make these agents more effective in a larger patient population. As locoregional therapies are generally well tolerated, using them in combination is less likely to complicate the side-effect profile—an important consideration given the immune mediated side-effects commonly experienced with checkpoint inhibitors.
Medtronic has announced that the US FDA has cleared an expanded indication for the OsteoCool radiofrequency (RF) ablation system.
Originally cleared for use in the spine, the FDA now allows the marketing of the OsteoCool system for palliative treatment of metastases in all bony anatomy—such as ribs, sacrum, extremities, and hip—in patients who have failed, or are not candidates, for standard therapy. The system uses targeted radiofrequency energy to ablate malignant metastatic bone tumours.
“Patients with metastatic bone cancer may be treated with conventional therapies such as opioids, chemotherapy or radiation therapy for pain palliation,” said Sandeep Bagla, an interventional radiologist with the Vascular Institute of Virginia in Woodbridge, USA. “With the expanded indication for the OsteoCool system, I now have the option to ablate these patients’ painful bone tumours when conventional therapies are considered ineffective, too slow-acting or cause unacceptable side effects.”
Metastatic bone disease has been reported to occur in 60–80% of cancer patients, most frequently among patients with primary malignancies of the breast, prostate, liver, and lung. More than 80% of bone metastases are found in the axial skeleton, which includes the skull, spine, and ribs.
Medtronic acquired the OsteoCool technology and associated intellectual property from Baylis Medical on 16 December 2015 and partnered with the company to further innovate the system.
The OsteoCool system is the only cooled radiofrequency ablation technology that offers simultaneous, dual-probe capabilities providing for procedural flexibility and predictable, customised treatment, a press release from Medtronic states. The system is temperature controlled and uses internally water-cooled probes to prevent overheating of surrounding tissue during the procedure, it adds.
The device also has a CE mark for the ablation of benign bone tumours such as osteoid osteoma and palliative treatment of metastatic malignant lesions involving bone, including the vertebral body. This indication is not available in the USA.
Most complications related to Y-90 therapy may be prevented or mitigated with appropriate patient selection, careful pretreatment planning, meticulous procedural technique, and optimisation of dose with use of dose reduction strategies when appropriate, writes Ripal T Gandhi, Miami, USA.
Transarterial yttrium-90 radioembolization is an accepted modality for treatment of both primary and metastatic liver malignancies and has become incorporated into several National Comprehensive Cancer Network (NCCN) guidelines. Although radioembolization is generally a safe and effective procedure, adverse events may occur and it is critical that the procedural physician is familiar with strategies to both prevent and manage potential complications.
Toxicities can be divided into three main categories: those related to non-target deposition of the radiomicrospheres (gastric or duodenal ulceration, oesophageal injury, pancreatitis, skin damage, and cholecystitis; compromised liver function due to radiation induced parenchymal damage (radioembolization-induced liver disease); technical complications related to angiography and embolization (groin haematoma, dissection, contrast-induced nephropathy).
Gastrointestinal ulcers occur in <5% of cases due to inadvertent delivery of radiomicrospheres to the gastroduodenal artery (GDA), right gastric artery, left gastric artery, or supraduodenal artery. Ulcers can be prevented with meticulous planning angiography and utilisation of cone beam CT. Factors that increase risk of ulcers include stasis during delivery, distal origin of the gastroduodenal artery, proximal administration of Y-90 (even in the setting of prior coil/plug embolization), and young patient age. We no longer routinely embolize the gastroduodenal and right gastric artery for both glass and resin microspheres as the development of collateral vessels can often complicate subsequent radioembolization. A paper from the Stanford group demonstrated that 34% of patients required 31% adjunctive embolization procedures for hepaticoenteric vessels at time of Y-90 administration even when all hepaticoenteric vessels were embolized at mapping angiography. Despite re-embolization, 7.1% of patients still developed a gastric or duodenal ulcer.
Patients who develop gastrointestinal ulcers typically present hours to days after radioembolization with abdominal pain, anorexia, nausea, vomiting, and/or gastrointestinal bleeding. In one study, mean time to diagnosis was 3.2 months. Suspicion for ulcer should be confirmed with endoscopy and aggressively treated as they can be difficult to heal due to injury arising from the serosal surface. In our practice, we prophylactically prescribe proton pump inhibitors at the time of mapping angiography and continue for three months. Patients who develop ulcers are treated with proton pump inhibitors, sucralfate, sodium bismuth, and motility agents. Pentoxifylline and alpha-tocopherol (vitamin E) have also been shown to be beneficial. Chemotherapy and especially biologic agents may have to be temporarily withheld as these may interfere with ulcer healing. Ulcers refractory to medical management may require surgery. Radiation-induced cholecystitis is rare, occurring in <2% of patients. When feasible, it is our approach to deliver the Y-90 distal to the cystic artery. In patients with a particularly large cystic artery in whom distal delivery is not possible, distal split dosing may be considered. We do not typically coil embolize the cystic artery given the low incidence of radiation-induced cholecystitis, however, we do use prophylactic antibiotics following radioembolization if the gallbladder is in the radiation field. Most cases of cholecystitis can be managed conservatively with antibiotics, hydration, and pain control. Surgery or cholecystostomy may be necessary in severe cases.
Radioembolization-induced liver disease (REILD) occurs in <4% of patients and can be potentially fatal. Patients typically present one to two months after radioembolization with jaundice and ascites with elevated bilirubin and alkaline phosphatase (aspartate transaminase/alanine transaminase may be normal) in the absence of tumour progression or biliary obstruction (Figure 1). Risk factors include patients with abnormal liver function, cirrhosis, exposure to multiple lines of chemotherapy, prior radioembolization or external beam radiation, and single session whole liver Y-90 administration. Biopsy of normal liver may be needed to confirm diagnosis; pathologic hallmark is veno-occlusive disease. Steroids are the mainstay of therapy. Since the underlying pathophysiology involves veno-occlusion, defibrotide and anticoagulation may be considered. Radioprotectants such as ursodeoxycholic acid and pentoxifylline may also be beneficial.
Figure 1: A patient with hepatocellular carcinoma presenting with radioembolization-induced liver disease six weeks after radioembolization. The patient developed jaundice and ascites with elevated bilirubin and alkaline phosphatase without tumour progression.
Radiation pneumonitis is extremely rare with an incidence of <1%. It is important that dose to the lungs is <30Gray in a single Y-90 administration and <50Gray cumulative during lifetime to minimise risk. It is reasonable to be more conservative in patients with COPD, prior lung resection or other disease with compromised pulmonary function. High lung shunts are typically seen in tumours with vascular invasion (such as hepatocellular carcinoma), large tumour burden, and infiltrative disease (Figure 2). Clinical presentation typically occurs one to six months after radioembolization with non-productive cough, low grade fever, and progressive exertional dyspnoea. Classic imaging feature is patchy consolidation with peripheral sparing (aka bat-wing appearance). Radiation pneumonitis is managed with steroids and bronchodilators. Pentoxifylline may also be considered as it is radioprotective and prevents early and late pulmonary toxicity.
Figure 2: High lung shunt (30%) demonstrated on planar scan following Tc-MAA administration in patient with hepatocellular carcinoma and hepatic vein invasion.
Hepatobiliary infection (liver abscess or cholangitis) may occur after radioembolization, typically in patients with biliary-enteric anastomosis, sphincterotomy, or biliary stent/drain across the ampulla. The risk is significantly lower with Y-90 than with chemoembolization, likely due to the less embolic nature of radioembolization. Liver abscess is treated with antibiotics and percutaneous drainage. Given the significant morbidity of infection, patients with prior biliary instrumentation should be prophylactically treated with an aggressive antibiotic protocol (with or without bowel preparation) before and after Y-90 administration to decrease the risk.
Most complications related to Y-90 therapy may be prevented or mitigated with appropriate patient selection, careful pretreatment planning, meticulous procedural technique, and optimisation of dose with use of dose reduction strategies when appropriate.
Ripal T Gandhi is an associate clinical professor, FIU Herbert Wertheim College of Medicine, Miami Cardiac & Vascular Institute, Miami, USA. He is a consultant to Sirtex Medical and BTG
The Radiological Society of North America (RSNA) held its 12th Clinical Trials Methodology Workshop 7–13 January in San Diego, USA. This programme offers intensive training in clinical trial design and statistics for academic radiology faculty from around the world and is a phenomenal resource to grow the cadre of rigorously trained clinical trialists in interventional radiology, writes Michael Soulen, Philadelphia, USA.
The workshop offers morning didactic sessions, followed by small group sessions in which each “student” transforms a concept for their own clinical trial into a complete protocol, ready for submission upon return to their home institution. With a 1:1 faculty to student ratio, the trainees have ample opportunity to interact with all the faculty both within and outside of their protocol groups. The yield from this programme is rewarding: by three years, half the students have done a trial; half have received grant funding; and all have multiple publications. More importantly, the skills acquired enable trainees to continue to develop future trials. In addition, the week-long immersion provides an intimate environment for networking among young academicians.
The majority of interventional radiology literature still consists of retrospective single institution studies. Interventional radiology needs to up its game to match the standards of our colleagues in oncology and vascular disease. For the past few years I have been encouraging colleagues at major academic interventional radiology centres in North America and Europe to send junior faculty to the workshop, and it really paid off. Six of the 24 students (25%) at the 2017 workshop were interventional radiologists, and another two were accepted to the programme but were unable to attend.
Topics were varied. Frederic Deschamps from Institut Gustave Roussy in France developed a phase1/2 trial for a new percutaneous screw/cementoplasty device for pelvic fixation. Vamshi Kotha from Calgary, Canada wrote a multicentre randomised trial of bare metal aortic stenting after hybrid arch repair of type 1 dissections. Sailendra Naidu from Mayo Clinic, USA, designed a phase 1/2 study of prostate artery embolization for high-risk non-surgical candidates. There were multiple interventional oncology projects from the USA, including immune checkpoint therapy Nivolumab, with transarterial chemoembolization (TACE) for unresectable hepatocellular carcinoma (Stephen Hunt, University of Pennsylvania), TACE for paediatric hepatocellular carcinoma (Matthew Lungren, Stanford University), and quality of life in Barcelona Clinic Liver Cancer (BCLC) C patients treated with TACE, sorafenib, or both (Resmi Charalel, Cornell University). The workshop ends with a poster reception of all the students’ projects:
The Clinical Trials Methodology Workshop is a phenomenal resource from RSNA to grow the cadre of rigorously trained clinical trialkists in interventional radiology. If we keep training a half-dozen interventional radiology faculty each year, we will soon see the payoff with publication of prospective controlled trials, improving the level of evidence for interventional radiology therapies, and increasing the impact factor of our journals.
Michael Soulen is professor of Radiology at the Hospital of the University of Pennsylvania, Philadelphia, USA. He is the interventional radiology faculty and chair-elect for the Clinical Trials Methodology Workshop.
Scott Trerotola presented the first release of eight-month data from the Lutonix AV IDE trial at the Leipzig Interventional Course (LINC; 24–27 January, Leipzig, Germany) and showed that drug-coated balloons (Lutonix 035 AV from Bard) are linked with a significantly higher target lesion patency and far fewer reinterventions to maintain this opening in a wide variety of failing arteriovenous fistulas than standard angioplasty.
Commenting on the significance of the data, Trerotola (University of Pennsylvania Medical Center, Philadelphia, USA) said: “This is the first trial in the 51 years since fistulas have been created to look at an intervention for lesions within native fistulas in a prospective, randomised, multicentre fashion. A lot of things [different technologies] have been tried; this is the first one that has worked.” See video interview.
The Lutonix AV study is a prospective, global, multicentre, randomised, controlled study designed to evaluate the safety and effectiveness of the Lutonix 035 AV drug-coated balloon catheter compared to a standard percutaneous transluminal angioplasty catheter in treating patients presenting with clinical and haemodynamic abnormalities in native arteriovenous fistulae located in the upper extremity. The investigators randomised 285 patients at 23 clinical sites and Trerotola noted that this was the trial incorporated a wide variety of lesions and fistula types.
The primary safety endpoint was freedom from any serious adverse events involving the arteriovenous access circuit through 30 days. The primary effectiveness endpoint was target lesion primary patency at six months.
The results at 240 day demonstrated that the procedure, when the drug-coated balloon was used, was as safe as the control procedure, percutaneous transluminal angioplasty. “The target lesion primary patency, showing the effect of the drug, was 61.6% for the drug-coated balloon as compared to 49.4% for percutaneous transluminal angioplasty (p=0.02). The number of interventions required to maintain target lesion patency at 240 days was 66 in the drug-coated balloon group and 94 in the plain angioplasty group (p=0.024) meaning that there were 29.8% fewer interventions required to maintain target lesion patency in the drug-coated balloon arm than the control arm,” Trerotola told delegates.
Interestingly, the 180-day target lesion primary patency was not significantly different between the two treatment groups and a convergence of curves were seen at that point. As this was the primary endpoint, Trerotola noted that it was not met, but clarified that this was a “statistical blip” as the curves continue to clearly diverge by the 240-day mark.
“The most important finding is that starting at about 60 days, there is a divergence in the curves with a sustained benefit that reaches statistical significance at 240 days for the drug-coated balloon compared to the control arm. In addition to that, the number of interventions to maintain target lesion patency was significantly fewer than in the control arm,” Trerotola added in an interview with Interventional News.
There were 141 patients who were treated with the drug-coated balloon and 144 who were treated with plain balloon angioplasty. The patients were evenly matched in both groups with baseline demographics between the two groups being similar. There were over 95% in both groups being hypertensive and around 60–65% being diabetic. Fistulae that were treated reflected an American population and were in the upper arm, antecubital fossa and forearm. The treated vessel locations included the cephalic vein, basilic vein, median cubital vein and subclavian vein.
With regard to lesion characteristics, there were 30.5% de novo lesions and 2.8% tandem lesion in the group treated with drug-coated balloon and 27.1 de novo lesions and 7% tandem lesions in the group treated with plain balloon angioplasty. The target lesion length was 28.4±15.09mm in the drug-coated balloon group and 29.5±18.69 in the plain balloon angioplasty group.
Barry Katzen, Miami, USA, announced the establishment of a new society, the Critical Limb Ischaemia (CLI) Global Society, whose mission is to improve quality of life by preventing amputations and death due to the condition.
He made the announcement at the International Symposium on Endovascular Therapy (ISET; 4–8 February, Hollywood, USA). Katzen is founder and chief medical executive of Miami Cardiac & Vascular Institute, and one of the course directors of ISET.
“We are the only professional membership-based medical society focused on advanced peripheral arterial disease and critical limb ischaemia,” said Katzen, who is also the current president of the new society. Members contribute to the scientific study, research, literature and education of critical limb ischaemia and the society will serve as an alliance and advocacy for the prevention of unnecessary amputation, according to the society’s website.
“In terms of advocacy, there are opportunities to get involved with a strong unified community of physician, healthcare and industry leaders with a focused goal of critical limb ischaemia education. The society has a commitment to raise public, patient and health professional awareness of critical limb ischaemia treatments to prevent unnecessary amputations,” the website notes.
Katzen told Interventional News: “The announcement also focused on the direction of resources towards the creation of a true definition around critical limb ischaemia from a regulatory and payment point of view. In the USA, and most countries, there is no diagnostic code for critical limb ischaemia and a lot of confusion in terminology which leads to limitations on determining actual event rates, outcomes and payment. Early on, we are applying resources to try to resolve this challenge.”
While drug-eluting devices, be they balloons or stents, use chemotherapeutic agents (usually paclitaxel) to reduce the build-up of scar tissue inside the arteries, a microinfusion device that applies the anti-inflammatory agent, dexamethasone, to the outside of arteries to enhance healing, is seeing largescale early positive results.
Clinical trial data from the DANCE (Delivery of dexamethasone to the adventitia to enhance clinical efficacy after femoropopliteal revascularization) trial that uses the Bullfrog microinfusion device (Mercator MedSystems) were recently presented at two conferences.
Mahmood Razavi and George Adams, the national co-principal investigators of the DANCE trial, each presented comprehensive 13-month data from the trial during late-breaking sessions at the International Symposium on Endovascular Therapy (ISET; 4–8 February, Hollywood, Florida) and Leipzig Interventional Course (LINC; 24-27 January, Leipzig, Germany) respectively.
The Bullfrog microinfusion device was used in the trial to deliver a generic anti-inflammatory steroid, dexamethasone, along with radio-opaque contrast to visualise distribution. The drug was delivered to the tissues around femoropopliteal arteries after undergoing endovascular intervention which forcibly opened obstructions. The data demonstrate a high level of durability of the revascularisation, low occurrence of major adverse limb events, and no device or drug-related adverse events.
“We attribute the success seen in the DANCE trial to the Bullfrog device and its ability to efficiently deliver drug in difficult-to-reach anatomy,” said Razavi. “Technologies such as drug-coated balloons or drug-eluting stents use chemotherapeutic agents to reduce the risk of scar tissue build-up inside the arteries. Alternatively, we have proposed that the delivery of an anti-inflammatory agent to the outside of the artery enhances the healing process and interrupts the cascade leading to scar formation and restenosis. Overall, we have found the therapy in DANCE to be intuitive, safe and effective.”
The 13-month data from DANCE were separated into two groups based on method of revasculariaation: atherectomy was performed in 157 limbs, while 124 limbs received angioplasty without atherectomy. For both groups, the primary safety endpoint revealed no post-operative death within 30 days, with major adverse limb events prior to a revascularisation reported as 1.6% in the atherectomy group and 0.9% in the angioplasty group. The per-protocol primary efficacy endpoint of primary patency did not widely vary between groups, with 83.6% at 12 months and 80.0% at 13 months in the atherectomy group, and 80.2% at 12 months and 78.2% at 13 months in the angioplasty group.
Primary patency was defined as the lack of clinically-driven target lesion revascularisation (CD-TLR) or narrowing detected by a duplex ultrasound peak systolic velocity ratio (PSVR) greater than 2.4. Freedom from CD-TLR was 89.6% at 12 months and 88.7% at 13 months in the atherectomy group and was 89.1% at both 12 and 13 months in the angioplasty group. No broad disparities were reported among results by gender, with 13-month primary patency of 79.3% in men and 77.9% in women, or by diabetic status, with 13-month primary patency of 79.5% in diabetics vs. 78.8% in non-diabetics.
DANCE is a prospective, multicentre, single-arm study designed and sponsored by Mercator. The trial is being conducted in 35 centres. The Mercator Bullfrog is a FDA 510(k)-cleared and CE-marked system designed to infuse therapeutic and diagnostic agents directly, non-systemically and safely through blood vessel walls into adventitial tissues. The Bullfrog device is tipped with a balloon-sheathed microneedle, and is compatible with 0.014” guide wires and 5 to 7 French introducer sheaths. The closed balloon provides a protective covering for a tiny, perpendicular-oriented injection needle as it is guided safely through the vasculature to target vessels with diameters of two to eight millimetres.
Argon has announced that it has completed the sale of its Critical Care Unit including a manufacturing facility in Yishun, Singapore and related commercial operations in Europe and Japan, to Merit.
The sale of the Critical Care Unit allows Argon to focus solely on its interventional business worldwide, a press release from the company says.
The Argon interventional product portfolio consists of the Option Elite retrievable inferior vena cava filter, CleanerXT and Cleaner15 rotational thrombectomy systems, BioPince full-core biopsy instrument, TLAB transjugular liver biopsy instrument, Atrieve vascular snare, Skater drainage systems and T-Lok bone marrow biopsy needles.
A press release from Merit on 6 February states that it has acquired certain products from Argon Medical Devices and Catheter Connections. “The combined revenues of the two acquired product lines were approximately US$46 million in 2016. The transactions were financed with a combination of cash and existing credit facilities, which totalled $48 million,” the release added.
Cardiovascular systems (CSI) presented six-month data from its LIBERTY 360 degrees post-market study in a presentation at the 29th International Symposium on Endovascular Therapy (ISET; 4-8 February, Hollywood, USA). The study is evaluating the acute and long-term clinical and economic outcomes of peripheral vascular interventions in treating patients with symptomatic lower extremity peripheral artery disease.
Physicians were able to use any US Food and Drug Administration (FDA)-approved device, including CSI’s Diamondback 360 peripheral orbital atherectomy system. Findings continue to demonstrate that peripheral vascular interventions can be successful in treating patients in all Rutherford Classes and suggest that “watchful waiting” for patients in Rutherford Class 2-3 and “primary amputation” for patients in Rutherford Class 6 may not be necessary.
Six-month study outcomes were presentedby William Gray of Main Line Health, Wynnewood, USA.
Findings suggest that on average peripheral vascular interventions can restore Rutherford 4-5 patients with critical limb ischaemia status (eg. limb pain at rest, cold and/or numbness in feet, open or non-healing wounds on toes or foot) to moderate claudicant status (eg. limb pain during movement)
Through six months, these data demonstrate on average peripheral artery disease patients (Rutherford 2-6) post-peripheral vascular interventions have maintained good outcomes and positive changes in Rutherford classification
Change in Rutherford Classification Following Endovascular Intervention
Baseline
30 Days
6 Months
RC 2-3
2.8
1.3
1.4
RC 4-5
4.5
3.1
2.3
RC 6
6.0
5.5
4.6
Table 1: All Rutherford Classes show improvement in RC from baseline to 30 days. RC4-5 and RC6 show continued improvement from 30 days to six months while RC2-3 maintains improvement at six months.
Gray said, “Following endovascular intervention, we saw a marked improvement across all Rutherford Classes at six months: Rutherford 4-5 and Rutherford 6 patients showed continued improvement from 30 days to six months, while Rutherford 2-3 patients maintained improvement at six months. We also saw a high freedom from major adverse events (MAE) across all classes. This suggests that endovascular intervention is an alternative treatment option in place of watchful waiting or even primary amputation.”
Rutherford Classification
RC 2-3
RC 4-5
RC 6
Freedom from (FF) MAE (6-month)
92.6%
81.2%
73.7%
FF Major Amputation
99.8%
96.8%
87.1%
FF Target Vessel Revascularisation (TVR)
93.0%
83.1%
85.1%
FF Death
97.1%
95.3%
85.1%
Table 2: High freedom from MAEs at six months across all Rutherford Classes. Kaplan-Meier method used to estimate event-free rates. MAE defined as death (≤30 days after the procedure), major amputation of the target limb, and TVR.
According to VascuQoL, a patient-reported, peripheral artery disease-specific health-related quality of life questionnaire, patients in the LIBERTY 360° study reported improved quality of life across all Rutherford Classes, including such measures as physical activity, symptoms and pain.
During a concurrent session at ISET, Jihad Mustapha (Wyoming, USA) explored the importance the LIBERTY 360° Rutherford 6 data will have on the endovascular field. He stated, “LIBERTY 360° is novel in that it addresses all Rutherford Classes, including Class 6, representing some of the most challenging and life-threatening PAD cases. Six-month data suggests that these patients can be treated successfully with endovascular interventions—a significant step in establishing a new standard of care for this difficult-to-treat population.”
Additionally, it was shared that the recently released 2016 Guidelines on the Management of Patients with peripheral artery disease from the American Heart Association/American College of Cardiology support this data, stating:
Revascularisation is a reasonable treatment option for patients with lifestyle-limiting claudication and an inadequate response to medical management and exercise; and
An evaluation for revascularization options should be performed by an interdisciplinary care team before amputation in the patient with critical limb ischaemia
Society of Interventional Radiology (SIR) president Charles E Ray Jr has issued the following statement in response to US president Donald J Trump’s executive order suspending entry into the USA of nationals from the countries of Iraq, Iran, Libya, Somalia, Sudan, Syria and Yemen.
“The SIR is a global organisation dedicated to the limitless potential of interventional radiology to solve the toughest medical problems. We represent more than 6,100 interventional radiology professionals worldwide and a global medical specialty that improves lives using innovative, minimally invasive, image-guided treatments.
“Interventional radiology relies on academic discourse, innovation and continuing medical education to deliver quality patient care. As such, limiting the movement of active physicians, researchers and healthcare professionals puts such advances in jeopardy by constraining collaboration, education, research and innovation that contribute to optimal patient outcomes.
Moreover, it is critical for nationals who are pursuing medical training and research in interventional radiology to be allowed to come to the USA to study and share their work, and for US-based attending physicians from the banned nations who are traveling overseas—including travel for medical missions, research or conferences—be allowed to return to their patients in the USA.
“From 4–9 March, the SIR Annual Scientific Meeting in Washington, DC, will bring together more than 5,000 physicians, researchers, medical associates and students from more than 35 countries to discuss the latest advances in interventional radiology. The diversity of our attendees, their expertise and ideas constitute the very backbone of our meeting. This ban is discouraging and disruptive to the medical education, sharing of scientific research and corporate innovation that benefits all attendees and participants in our meeting as they strive to improve health outcomes worldwide.
“We are also concerned that limiting the travel of physicians from banned countries may also have detrimental effects on the international health care community, particularly in areas that suffer from a lack of medical infrastructure due to ongoing strife.
“SIR stands committed to promoting diversity and inclusiveness and welcomes collaboration from all interventional radiology professionals. We call on our national leaders to eliminate barriers to scientific exchange and medical education.”
Former US Senate majority leader Tom Daschle will headline a special 9 March symposium “IR Economics, Quality and Value: Are You Ready For MACRA?” at the Society of Interventional Radiology’s 2017 annual scientific meeting in Washington, DC, USA.
Daschle will provide insight on healthcare reform, federal policy, and the healthcare priorities of the incoming Trump administration, information from the society states.
In addition, Rep. Brett Guthrie, R-Ky., will deliver a lunchtime keynote offering a congressional perspective on the Trump administration’s healthcare reform agenda. Guthrie serves on the House Energy and Commerce Committee Health Subcommittee.
This special symposium aimed at preparing interventional radiologists for Medicare payment reform will also provide attendees a detailed overview of the new IR Registry, reporting under the new Merit-based Incentive Payment System (MIPS) and proven tools for interventional radiology practice management.
Registration is independent of SIR 2017 registration. To register for the meeting and the symposium, please visit sirmeeting.org.
Guerbet has announced that as of 1 February 2017, Methapharm will promote and distribute all Guerbet products in Canada.
“As a result of our excellent experience with Methapharm over the past four years, we have expanded the range of Guerbet products in their care for promotion and distribution,” says Massimo Carrara, vice president North America, Guerbet. “We are confident that our successful partnership with Methapharm will continue to flourish with this expanded product line.”
Guerbet is committed to partnering with local associates to support Canadian patients and practitioners and to fostering local production in Canada at its Guerbet fill and finish plant in Montreal.
Guerbet solutions distributed by Methapharm will now span the full range of the company’s products registered in Canada. This includes contrast media products (including Lipiodol, Patent Blue V, OptiRay, Conray and Telebrix); injectors and consumables.
With these developments, Guerbet continues to extend its footprint in North America. Guerbet previously solidified its position as a global leader with the acquisition of US-based Mallinckrodt’s Contrast Media and Delivery Systems (CMDS) business in 2015.
Gore has announced that the Gore Viabahn VBX balloon expandable endoprosthesis has received US FDA approval for treatment of de novo or restenotic lesions found in iliac arteries, including lesions at the aortic bifurcation.
This marks the availability of the only balloon expandable stent graft with an indication for the iliac artery.
“The VBX stent graft demonstrated notable immediate and nine-month safety and efficacy in treating patients with iliac occlusive disease which can be attributed to the exceptional device design,” said Jean Bismuth. He continued: “Overall, there were multiple clinical benefits observed, including no median change in the device length upon deployment and a 100% technical success rate with no occurrences of stent dislodgement or significant residual stenosis. The study device performed well in disadvantaged lesions, including occlusions, which speaks to its trackability, radial strength, conformability, and stent retention.”
FLEX clinical study
Of the patients in the Gore VBX FLEX investigational device exemption clinical study (n=134), 32% presented with TASC II type C or D lesions, 18% required contralateral access to the lesion, and 42% involved kissing stents at the aortic bifurcation. Clinical data from study conducted for US FDA approval reflected that the design components of the VBX stent graft were resilient both during stenting procedures and over time:
100% success rate in device delivery and coverage of target lesions in all patients
100% success rate in reducing the target lesion to less than or equal to 30% of the original stenosis
Zero change in median length of the device upon deployment; and
96.9% primary patency at nine-months, including a 95.3% primary patency rate in those patients with TASC II C or D type lesions.
Further, there were no reported incidences of device dislodgement, failures in stent integrity, or device-related serious adverse events through the primary endpoint follow up, meaning no additional costs incurred for either endovascular or surgical stent removal. The VBX stent graft does not require predilation, which reduces the number of balloons required, and the longer lengths available reduce the need to use multiple stents for extensive lesions, both of which also contribute to procedural cost savings.
The VBX stent graft was developed utilising the small diameter, ePTFE stent graft technology from the Gore Viabahn Endoprosthesis. The VBX stent graft is available in a range of diameters from 5–11mm and lengths of 15, 19, 29, 39, 59, and 79mm to cover a wide variety of treatment needs.
The Karolinska Institute-sponsored, prospective, observational MAVERRIC study aims to demonstrate that a strategy of first line local microwave ablation of colorectal liver metastases is not inferior to liver resection in terms of survival rates at three years.
Jacob Freedman, principal investigator of the study told Interventional News: “The lack of data that compare local ablative treatment with resection for liver metastases prompted us to undertake this study. Ablative treatment has, for many years, been used as an adjunct to resection and as an alternative when major surgery is contraindicated because of comorbid conditions. It has been clearly shown that ablative treatment is easier for the patient, resulting in far fewer complications and a much shorter length of hospital stay, but whether survival, the most important variable, is on par with surgery has not been shown despite a decade of speculation.”
Freedman is associate professor, Karolinska Institutet, Department of Clinical Sciences, Danderyd University Hospital, Division of surgery, Sweden.
The study has set out to enroll a cohort of 100 patients who will be treated with CT-guided microwave ablation (performed with any generic microwave ablation system cleared for clinical use). In order to be eligible for enrolment patients should have one to five metastases of less than 31mm in size. All lesions need to be amenable to CT-guided percutaneous microwave ablation, and the patient also needs to be deemed “resectable” and be so evaluated at a multidisciplinary tumour board meeting. The outcomes of ablative treatment will be followed and compared with propensity scored matched controls from the Swedish liver surgery registry (SweLiv).
The study is a multi-institutional effort by the hepatopancreaticobiliary units in Stockholm (Sweden), Bern (Switzerland) and Groningen (the Netherlands).
“The study is in full swing recruiting patients from all three centres since December. We now have 33 of the planned 100 patients treated and hope to close the study in early 2018,” Freedman explained.
The secondary endpoints outlined are: survival at five and ten years; interventional complication rates; length of stay; precise measurements of ablation; need for further interventions; and health-economic analysis.
Commenting on the choice of ablation modality, Freedman said, “We chose microwave because it has clearly been shown that it has benefits, although these are small, compared to radiofrequency ablation. The energy is delivered faster which reduces heat-sink problems and shortens anaesthesia times. There is no charring of tissue and no problems with conductivity [with microwave]. Larger lesions can be ablated with a single antenna.
“All procedures are CT guided with computer assisted guidance using the CAS-one system (CAScination). We are not using ultrasound because we want to have optimal documentation of each antenna placement for future reference, if there are recurrences. I am convinced that fused ultrasound would have been as good in most situations, but retrospective review is much more difficult with ultrasound images,” he concluded.
Sirtex has announced that the SARAH (Sorafenib vs. radioembolisation in advanced hepatocellular carcinoma) randomised controlled study results will be presented at the upcoming European Association for the Study of the Liver (EASL), International Liver Congress (ILC) in Amsterdam, the Netherlands (19–23 April 2017).
The study will be presented on Saturday, 22 April 2017.
SARAH is a phase III multicentre prospective randomised open-label study for patients in France that directly compared the efficacy and safety of Sir-spheres Y-90 resin microspheres with the current standard-of-care systemic therapy, sorafenib (Bayer) in patients with advanced non-resectable primary liver cancer. Unless embargoed, the study abstract will be released on 5 April, a press release from the company states.
Patients with advanced hepatocellular carcinoma (Barcelona Clinic Liver Cancer [BCLC] stage C) with or without portal vein thrombosis and no extrahepatic spread, or patients with early/intermediate hepatocellular carcinoma (BCLC stage A or B) whose disease has progressed or recurred after previous therapies; and who are ineligible for surgical resection, ablation or liver transplantation were recruited to participate.
The primary endpoint of the SARAH study is overall survival. Secondary endpoints include safety, progression-free survival at six months, quality of life, and healthcare costs. The study completed enrolment of >460 patients in March 2015.
SARAH is the largest randomised study ever to compare selective internal radiation therapy using Sir-spheres microspheres against the standard-of-care systemic therapy in the treatment of hepatocellular carcinoma, the release adds.
Following Health Canada regulatory approval, BTG is to launch its polidocanol injectable foam (Varithena), a drug/device combination product used to treat varicose veins, in Canada. The product is intended for use in adults with clinically significant venous reflux as diagnosed by duplex ultrasound.
Polidocanol injectable foam is indicated in Canada for the treatment of incompetent great saphenous veins, accessory saphenous veins, and visible varicosities of the great saphenous vein system, above and below the knee.
Polidocanol injectable foam is a uniform, low nitrogen, microfoam dispensed from a proprietary canister device. A physician injects a small amount of the foam into the malfunctioning vein of a patient through a catheter or a needle. It displaces the blood from the vein to reach and treat the vein wall; the diseased vein should then collapse and blood flow is diverted to healthy veins nearby.
“BTG has done a great job preparing the medical community with teaching materials and helpful protocol details,” says Douglas Hill, principal of The Vein Treatment Centre in Calgary, Canada, and president of the Canadian Society of Phlebology.” Polidocanol injectable foam holds great promise to effectively treat varicose vein networks in just one visit and is able to treat large diameter great saphenous veins that may not respond to other extemporaneous foam treatments.”
Medtronic has received an investigational device exemption (IDE) from the US Food and Drug Administration (FDA) to initiate a study of the In.Pact Admiral drug-coated balloon for a potential new indication in patients with end-stage renal disease.
The randomised study will evaluate the In.Pact Admiral drug-coated balloon as a treatment for failing arteriovenous fistulas in these patients as compared to plain balloon angioplasty. The IDE approval enables Medtronic to initiate the study and gain safety and effectiveness data for the device in this investigational indication.
“In the past, when the arteriovenous access site became narrowed, the only option was use of a standard percutaneous transluminal angioplasty balloon to re-open and regain access for dialysis. This would often result in restenosis and high rates of reintervention,” says Andrew Holden, director of interventional radiology at Auckland Hospital and associate professor of radiology at Auckland University, Auckland, New Zealand. “Patients on dialysis need alternatives to help reduce and manage stenoses of their arteriovenous access sites. It is important to effectively evaluate options such as this drug-coated balloon, which already has clinical evidence in patients with peripheral artery disease in the upper leg. ”
The IDE study will evaluate the safety and efficacy of the In.Pact drug-coated balloon for up to two years at approximately 30 sites in USA, Japan, and New Zealand. Principal investigators include: Holden, Robert Lookstein, professor of radiology and surgery, vice-chair of interventional services, and medical director of clinical supply chain at Mount Sinai Healthcare System, New York City, USA, and Hiroaki Haruguchi, clinic director at Haruguchi Vascular Clinic, Tokyo, Japan.
The study will aim to enrol 330 patients with a 1:1 randomisation to either treatment with In.Pact Admiral drug-coated balloon or standard balloon angioplasty. The primary efficacy endpoint is patency of dialysis fistulas through six months and the primary safety endpoint is major adverse events through 30 days. Additional endpoints include reducing access circuit related events including repeat procedures.
TVA Medical has provided clinical updates involving its everlinQ endoAVF system at the 2017 Leipzig Interventional Course (LINC; 24–17 January, Leipzig, Germany).
Scientific data were presented this week at LINC including a main arena discussion by Tobias Steinke, chief of Vascular and Endovascular Surgery, Schoen Hospital, Dusseldorf, Germany.
“The promise of the everlinQ endoAVF system as a viable alternative to surgical arteriovenous fistulae procedures, demonstrated in clinical trials and real-world cases, is very exciting,” states Steinke. “Patients deserve more options, and an endovascular solution is extremely appealing.”
One-year data presented from the single-arm, prospective, multicentre Novel Endovascular Access Trial (NEAT) study in patients with end-stage renal disease showed high fistula maturation (91%); high patency (84%); low thrombosis (10.5%); and low interventions (0.46 per patient year).
At two centres in Germany reporting real-world experience with the everlinQ endoAVF system, physicians achieved 100% procedural success; dialysis initiation in 86% of patients within 56 days; and a low rate of interventions.
In addition, data were reported from a preclinical feasibility study using the everlinQ endoAVF system for peripheral artery disease. The cadaver study demonstrated the feasibility of creating an endovascular in situ vein bypass—in place of a surgical distal autologous vein bypass—for below-the-knee revascularisation, without stents, couplers or other foreign material.
Results were also presented from a study evaluating the everlinQ 4 endoAVF system, which is designed to enable other access sites like the wrist, using a 4F (vs. 6F) catheter system. The prospective, single arm, single-centre trial showed 97% procedural success and fistula maturation in 81% of patients within 30 days.
“This technology has the potential to revolutionise dialysis access. The clinical results using the 4F everlinQ endoAVF System, which may benefit additional dialysis patients, are consistent with positive clinical results seen with the innovative 6F system,” comments Todd L Berland, vascular surgeon, NYU Langone Medical Center, New York City, USA.
The everlinQ endoAVF System has European CE mark and Health Canada Medical Device License for end-stage renal disease patients who need haemodialysis, and commercialisation has begun at select centres in Europe. It is not commercially available in the USA and is currently under review by the US Food and Drug Administration.
Each year approximately three million people worldwide with end stage renal disease are treated with haemodialysis. However, the first step, creating a viable access in the arm, is often a significant clinical challenge. The current standard approach, surgical arteriovenous fistulas, are associated with high failure rates, often as high as 60% and they require frequent revisions, resulting in increased morbidity and unnecessary costs.
New data presented at the 2017 Leipzig Interventional Course (LINC) have demonstrated strong efficacy and consistent outcomes for Medtronic’s In.Pact Admiral drug-coated balloon across multiple patient populations. The data represent real-world outcomes from regional cohorts of the IN.PACT Global Study in Asia and Belgium.
Donghoon Choi from the division of cardiology at Severance Cardiovascular Hospital, Seoul, South Korea, presented one-year results from the Asian subset of the IN.PACT Global Study, including data from 114 patients at six sites in South Korea and Singapore.
In this subset analysis, the low clinically-driven target lesion revascularisation at one year (3.8%) was consistent with the results in the complete cohort of 1,406 patients in the IN.PACT Global Study (7.5%). Results of the primary safety endpoint in the Asian cohort were also consistent with results from the full Global Study cohort, with 96.2% of patients achieving positive outcomes.
In a separate presentation of results from the IN.PACT Global Study, Koen Deloose from the vascular surgery unit at AZ Sint Blasius, Dendermonde, Belgium, presented data on 305 patients from seven sites in Belgium. Belgium was the first country to enrol patients in the study and remains the largest enrolling country. At one year, patients experienced positive outcomes based on both efficacy and safety measures, consistent with overall findings from the IN.PACT Global Study.
In this patient subset, the low clinically-driven target lesion revascularisation at one year (7.6%) was also consistent with the results in the complete cohort of patients in the IN.PACT Global Study (7.5%). Results of the primary safety endpoint in the Belgium cohort were also consistent with results from the full study, with 90.6% of patients achieving positive outcomes.
Interim data presented at the 2017 Leipzig Interventional Course (LINC; 24-27 January, Leipzig, Germany) has demonstrated encouraging results for Biotronik’s dedicated lower limb intervention portfolio.
“Currently available clinical evidence shows that the Passeo-18 Lux drug-coated balloon has similar efficacy to drug-eluting stents when used standalone or in combination with Pulsar self-expanding bare metal stent,” comments Jos van den Berg, Regional Hospital of Lugano, Switzerland, symposium moderator. “One crucial advantage of using drug-coated balloon with Pulsar bare metal stent in the superficial femoral artery, however, is that it may reduce the metallic implant load due to its thin strut design.”
Advantages of combining the Passeo-18 Lux drug-coated balloon with the Pulsar-18 bare metal stent were discussed as part of Biotronik’s Response-adapted combination therapy (REACT) to treat superficial femoral artery disease. “The REACT approach offers physicians versatility when deciding exactly how much metallic support is necessary, based on each vessel’s unique anatomy and lesion characteristics,” adds van den Berg.
The REACT approach is designed to allows physicians to effectively treat superficial femoral artery disease with full-lesion paclitaxel coverage offered by a drug-coated balloon and either spot stent or full-lesion stenting, depending on the lesion response to an initial angioplasty. The latest interim data (203 patients) from the superficial femoral artery disease cohort of the BIOLUX P-III registry, presented by Koen Keirse (Regional Hospital “Heilig Hart”, Leuven, Belgium) investigating Passeo-18 Lux in an all-comers population, demonstrated 12-month primary patency of 82.1% and freedom from clinically-driven target lesion revascularisation of 94%.
Biotronik Pulsare-18 bare metal stent
The bailout stenting rate within BIOLUX P-III was 14.5%. Further data and subgroup analysis, including TASC D and heavily calcified lesions, are ongoing. In addition to the data from BIOLUX P-III, the BIOFLEX PEACE all-comers registry, presented by Michael KW Lichtenberg (Clinic Arnsberg, Germany) shows that the Pulsar-18 self-expanding bare metal stent alone—and also in combination with drug-coated balloon therapy—continues to be an effective treatment option in the superficial femoral artery. The primary patency rate of 74.3% and freedom from target lesion revascularisation of 92.6% confirm the results shown in previous Pulsar studies.
Interim data (90 of 120 patients) on the intentional combination approach using Passeo-18 plus Pulsar-18, from the multicentre investigator-initiated BIOLUX 4EVER study, presented by Koen Deloose (AZ Sint-Blasius Hospital, Dendermonde, Belgium), demonstrated primary patency at 12 months of 88.9%, and a freedom from target lesion revascularisation of 92.5%. Previously, the prospective, investigator-initiated DEBAS4 study showed a similar (94.1%) rate of primary patency at 12 months.
The final 12-month results of the Stellarex (Spectranetics) drug-coated balloon ILLUMENATE Global Study have found high primary patency and freedom from clinically driven target lesion revascularisation results.
The ILLUMENATE Global Study is a prospective, multicentre, single-arm study designed to assess the clinical performance of the Stellarex drug-coated balloon in the superficial femoral and popliteal arteries.
The results were presented by Thomas Zeller, professor of Angiology, Albert-Ludwigs University of Freiburg, and head of the Department of Angiology, Universitäts-Herzzentrum Freiburg, Bad Krozingen, Germany, at the Leipzig Interventional Course (LINC) in Leipzig, Germany.
The ILLUMENATE Global Trial enrolled 371 patients. The treated lesions were highly complex, including a high proportion of chronic total occlusions (31%) and severe calcification (41%), as reported by an independent angiographic core-laboratory. The key results, per Kaplan-Meier survival estimates at day 365, include:
– Primary patency was 81.4%
– Freedom from clinically-driven target lesion revascularization (CD-TLR) was 94.8%
“In a real-world setting, ILLUMENATE Global validates the earlier ILLUMENATE US Pivotal results, achieving best-in-class 12-month primary patency rates in a patient cohort with the highest rate of severe calcium yet studied. These results are significant because severe calcium has been one of the greatest challenges in our drug-coated balloon practice,” says Zeller.
Medtronic has been granted CE mark approval for the HawkOne directional atherectomy system in a lower profile size for treating patients with peripheral artery disease. The new HawkOne 6 Fr provides an effective and easy-to-use treatment option for patients with peripheral artery disease both above and below the knee with a single device. The HawkOne system is designed to remove plaque from the vessel wall and restore blood flow.
“Directional atherectomy is an established treatment modality for patients with complex peripheral artery disease to restore patency, maximise luminal gain and preserve future treatment options,” says Thomas Zeller, head, Department of Angiology, Universitäts-Herzzentrum Freiburg, Bad Krozingen, Germany. “The new smaller HawkOne 6Fr size is an advanced option to treat patients with multi-level peripheral artery disease, addressing lesions of various length, morphology, and location, particularly those below the knee.”
The HawkOne system is also designed to enable physicians to treat severe calcified lesions more efficiently with no increase in cut depth. The system can treat calcified lesions up to two times more effectively than the TurboHawk device, according to a company release. The HawkOne system has a preloaded flush tool, which improves cleaning time by up to 55% when compared to the TurboHawk high efficiency cutter. The 6F size is designed to simplify device selection and provide easy set-up with no capital equipment.
“We are excited to announce CE mark approval for HawkOne 6F shortly after receiving FDA clearance for the system in October,” says Mark Pacyna, vice president and general manager of the Peripheral business, which is part of the Aortic & Peripheral Vascular division at Medtronic.
Terumo has announced that it has completed its acquisition of certain assets owned by Abbott and St Jude Medical on 20 January 2017 (North American Central Standard Time).
Terumo has acquired the Angio-Seal and FemoSeal vascular closure product lines and Kalila Medical, a company developing next-generation access technologies, the first being the Vado steerable sheath, used in cardiac electrophysiology procedures. The acquisitions enhance company offerings in the interventional access device business.
The acquired assets become part of Terumo Interventional Systems, a division of Terumo Corporation. By building on Terumo’s existing infrastructure and competencies, the acquisition will enable Terumo to maximise the value of the acquired businesses and contribute to supporting safe and efficient interventional procedures.
The financial impact will be included on a consolidated basis, starting with the fourth quarter of the fiscal year ending 31 March 2017. The impact of the acquisition on Terumo’s business performance is being examined. Further details regarding the impact of the acquisition will be disclosed as needed, once the analysis is completed.
Researchers who developed a safe and effective procedure to remove thick clogs in children’s airways are now reporting similar success in adult patients. In this rare condition, called plastic bronchitis, patients develop thick, caulk-like casts that form in the branching paths of their airways.
The researchers developed new imaging tools and a minimally invasive catheterisation technique, lymphatic embolization, to treat a form of plastic bronchitis caused when abnormally circulating lymphatic fluid dries into solid casts.
“In some cases, the cause of this condition is unknown, but this new study suggests that most adult patients with plastic bronchitis have abnormal pulmonary flow of lymphatic fluid that we can safely treat,” said study leader Maxim G Itkin, an interventional radiologist at Children’s Hospital of Philadelphia (CHOP) and the Perelman School of Medicine at the University of Pennsylvania.
Itkin and his co-author Yoav Dori, a paediatric cardiologist at CHOP and Penn Medicine, co-lead a specialised team at the Center for Lymphatic Imaging and Interventions jointly operated by CHOP and Penn. They collaborated on the current study with pulmonologist Francis X McCormack, of the University of Cincinnati, in a paper in the October 2016 issue of the Annals of the American Thoracic Society.
The study reports on seven adults with a mean age of 50 years old who presented with branching bronchial casts, associated with chronic cough and/or asthma. Using a customised type of magnetic resonance imaging called dynamic contrast-enhanced MR lymphangiography (DCMRL), the team found that six of the seven patients had abnormal lymphatic flow, which they now propose designating as pulmonary perfusion syndrome, as distinct from idiopathic plastic bronchitis, in which the cause is unknown.
The team treated the six patients with lymphatic embolization, which involves inserting a combination of glue and coils through catheters to halt the flow of lymphatic fluid. Five patients reported immediate and complete resolution of symptoms, and the sixth patient reported significant partial improvement. Four patients had minor abdominal pain, which resolved after treatment with painkillers. The average follow-up was 11 months after initial treatment.
Earlier this year, Itkin and Dori reported a retrospective case study of 18 children who had plastic bronchitis as a complication of palliative surgery for single-ventricle heart disease. While rare, plastic bronchitis can cause life-threatening respiratory distress in children. In adults, the condition may go undiagnosed for years in patients who may initially be diagnosed with asthma or chronic cough. Plastic bronchitis has a long medical pedigree—the Greek physician Galen described a form of it in the second century.
“This was a small study, and a first report of this treatment in adults with lymphatic plastic bronchitis,” said Dori. “Longer follow-up will be needed to confirm the long-term risks and benefits of this procedure.”
An interventional pioneer, Josef Rösch made monumental contributions to medicine through his research and development of numerous minimally invasive, image-guided procedures. This video from the Interventional Initiative tracks his life and works.
Terumo Corporation has announced that it has entered into a definitive agreement under which it has agreed to acquire Bolton Medical from its parent company. Bolton Medical is a leading innovator in thoracic and abdominal stent graft systems.
“The acquisition will enhance Terumo’s existing product portfolio in the global stent graft market and our vascular graft business will be further strengthened in the US, in what is the largest stent graft market today,” said Shinjiro Sato, president of Cardiac and Vascular company, Terumo Corporation.
The transaction is expected to close in a few months and it will be funded through cash on hand and debt. The closing is subject to antitrust clearance and other customary closing conditions. The impact of the acquisition on Terumo’s financial is currently being scrutinised.
WCIO has announced via email communication that the board of directors of the organisation, a non-profit association that supports and promotes the field of interventional oncology (IO), has established the Society of Interventional Oncology (SIO), effective 17 January. The society’s annual IO conference will maintain its name of WCIO.
“As an established society, SIO serves as the only membership-based organisation dedicated wholly to the emerging field of IO, working to further promote the mission originally put forth by WCIO. SIO will offer four membership categories: Active, Affiliate, Resident/Fellow, and Student,” the WCIO communication adds.
Further, the email notes: “SIO benefits vary by membership level within the organisation. Primary benefits include discounts on the WCIO conference, access to online education through IO University, the opportunity to apply for research grants, and voting rights (contingent on level). Secondary benefits include first choice for Early Career Workshop at WCIO, free abstract submission for WCIO, access to Case of the Week sample cases, access to the IO Insights enewsletter, and inclusion in the member directory.”
Ulipristal acetate is the first oral therapy to demonstrate efficacy and safety for uterine fibroids in two US pivotal studies, a press release states.
Allergan and Gedeon Richter announced positive results from Venus II, the second of two pivotal phase III clinical trials evaluating the efficacy and safety of ulipristal acetate in women with abnormal bleeding due to uterine fibroids. A new drug application filing for ulipristal acetate is planned for the second half of 2017.
Venus II was a multicentre, randomised, double-blind, placebo-controlled clinical trial in premenopausal women in North America between 18 and 50 years old with cyclic (22 to 35 days) abnormal uterine bleeding in ≥4 of the last six menstrual cycles, menstrual blood loss ≥80 mL as measured by the alkaline hematin method over the first eight days of menses, ≥1 discrete uterine fibroid of any size and location observable by transvaginal ultrasound, follicle-stimulating hormone ≤20 mIU/mL, and uterine volume ≤20 weeks by exam. Eligible patients were randomised to ulipristal acetate 5mg, 10mg or placebo for two separate 12-week treatment courses followed by a 12-week treatment-free follow-up period.
The study included 432 patients with 162 patients randomised to ulipristal acetate 5mg, 157 patients to receive 10mg, and 113 patients to placebo. The average age of patients enrolled was 41 years and 67% of enrolled patients were Black/African Americans. The study met all the co-primary and secondary endpoints with both ulipristal treatment arms achieving statistically significant results over placebo (p<0.0001). The co-primary efficacy endpoints were percentage of patients with absence of uterine bleeding and time to absence of uterine bleeding on treatment during Treatment Course One (12-week duration). Significantly more patients in the 10mg group (54.8%) and the 5mg group (42%) achieved absence of bleeding compared to placebo (0%).
The secondary efficacy endpoints were the percentage of patients with absence of uterine bleeding from day 11 to end of the first treatment course; the percentage of patients with absence of uterine bleeding after the second treatment course; time to absence of uterine bleeding on treatment during treatment course two; and the change from baseline in the UFS-QOL revised Activities subscale at the end of the first treatment course. The UFS-QOL is a validated fibroid-specific symptom and health-related quality of life questionnaire.
More patients in the 10mg group (55.4%) and the 5mg group (34.6%) achieved absence of bleeding within 10 days after treatment initiation in the first course of treatment compared to placebo (0%). Significantly more patients in the 10mg group (57.3%) and the 5mg group (40.5%) achieved absence of bleeding compared to placebo (8%) in the second course of treatment. The improvement from baseline in the UFS-QOL revised activities subscale was significantly greater in the 10mg group (56.7%) and the 5mg group (48.3%) compared to placebo (13%).
The most common adverse events (≥5%) on ulipristal acetate treatment were hot flush, headache, fatigue, and nausea in the combined period of first course of treatment and first off-treatment interval. The most common adverse event (≥ 5%) on ulipristal acetate treatment was headache in the combined period of the second course of treatment and second off-treatment interval.
Ulipristal acetate is an investigational drug for the medical treatment of uterine fibroids. It is a selective progesterone receptor modulator (SPRM), which acts directly on the progesterone receptors in three target tissues: the endometrium (uterine lining), uterine fibroids, and the pituitary gland. Ulipristal acetate exerts a direct effect on the endometrium (suppressing uterine bleeding) and direct action on fibroid size by decreasing the formation of new fibroid cells and promoting fibroid cell death. The safety and efficacy of ulipristal acetate has been evaluated in two phase III US studies of more than 589 adult women of reproductive age. Ulipristal acetate is protected by a patent that expires in 2029. To date, more than 310,000 women have been treated with ulipristal acetate for fibroids in over 65 countries worldwide.
The European Society of Radiology (ESR) and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), have joined forces to address the future of diagnostic and interventional radiology with a special focus on improving patient care.
The decision to enhance collaboration was taken in a meeting between the leaderships of both societies in July 2016. The first step will be a joint survey on the state of the art and current practice of interventional and diagnostic radiology with the aim to identify synergies and ultimately optimise patient care. The questionnaire is planned to be sent out in early 2017.
“This partnership intends to fortify the position of diagnostic and interventional radiology and to attract more clinically oriented medical students to radiology. We want to support medical students and radiology residents in their ambitions to become interventional radiologists or radiologists with a special focus and experience in interventional radiology and we want to shape future training models to make sure that our future colleagues embrace clinical responsibilities and feel comfortable to pursue the clinical management of patients. Last but not least, we should concentrate on establishing and improving functioning referral routines in hospitals, which could prove very valuable for both interventional and diagnostic radiology,” said Elias Brountzos, current CIRSE president.
One of the ESR’s successful projects in the field of education is the establishment of the European Training Curriculum for Radiology, designed to provide a valuable template for training radiologists and enhance the quality of care for patients throughout Europe. The ESR has added further clinical and patient-care related aspects of interventional radiology to its Curriculum for Undergraduate Radiological Education and will include an update of CIRSE’s input in its subspecialisation curriculum. Revised versions of both curricula will be released on the ESR website on the occasion of ECR 2017.
In 2013, CIRSE has established the first edition of the European Curriculum and Syllabus for Interventional Radiology. This document, which provides guidance for radiologists wishing to specialise in IR (www.cirse.org), is currently being updated and the second edition will be released in early 2017. The European Curriculum and Syllabus for Interventional Radiology is the blueprint for the European Board of Interventional Radiology (EBIR), a certificate of competence, providing a benchmark for European Interventional Radiology practice, which is officially endorsed by the ESR.
“CIRSE is at present involved in the ESR’s annual congress (ECR), which is reflected by a broad selection of interventional and vascular radiology sessions, in the European Diploma in Radiology (EDiR – an initiative of the ESR dedicated to continued education and certification for general and sub-specialised radiologists), ESR’s EU and International Affairs, in EuroSafe Imaging, the ESR’s quality and safety campaign, as well as the European Institute for Biomedical Imaging Research (EIBIR). I believe that the increased commitment of both societies will greatly benefit patient care and the radiological community,” said Katrine Riklund, chairperson of the ESR Board of Directors, from Umeå, Sweden.
Future plans include increased collaboration with the ESR’s EU and International Affairs department, as well as joint courses and society booths at major radiology events to further communicate that diagnostic and interventional radiology belong together. The ESR and CIRSE will work together on strategic issues to promote the subspecialty of interventional radiology, and will meet on a regular basis to improve communication and further deepen their ties.
Furthermore, CIRSE’s application to become a member of the European CanCer Organisation (ECCO) was fully supported by the ESR, which joined ECCO in May 2016. ECCO is a multidisciplinary federation which upholds the right of all European cancer patients to the best possible treatment and care, promoting interaction between all organisations involved in cancer care at the European level.
Robert Califf is to step down as US Food and Drug Administration (FDA) commissioner upon the inauguration of Donald Trump as US President on 20 January 2017. Democrat Califf, who was appointed to the post in September 2016 by Barack Obama, is required to resign along with other presidential appointees.
Califf, a cardiologist and researcher, had received endorsement from The American College of Cardiology, the New England Journal of Medicine and the American Heart Association, as well as others.
Califf’s tenure was not without controversy, with his ties to the pharmaceutical industry questioned by US senator and former presidential candidate Bernie Sanders. Senator Edward Markey expressed concern that Califf “did not give [him] confidence” that the FDA would act appropriately to quell the growing US opioid epidemic under his sterwardship.
Current deputy commissioner Stephen Ostroff is likely to serve as commissioner on a deputy basis, as he did between Califf’s appointment and former commissioner Margaret Hamburg’s departure.
According to Politico, venture capitalist Scott Gottlieb—a past FDA deputy commissioner—is likely to take over the position on a long-term basis. Other names suggested by the Wall Street Journal include Jim O’Neill, managing director of Mithril Capital Management and Balaji Srinivasan, founder of Counsyl, a genetic-counselling firm.
A study, published in the Journal of Vascular and Interventional Radiology suggests that percutaneous image-guided irreversible electroporation of unresectable locally advanced pancreatic adenocarcinoma is associated with a satisfactory safety profile.
The research, which included 50 patients (23 women), set out to assess the safety profile of irreversible electroporation and as a secondary objective, to determine the overall survival of patients who were treated with the procedure.
Irreversible electroporation uses short, repetitive, non-thermal high-energy pulses of electricity to destroy cancer cells. It has been reported to have been used intraoperatively, laparoscopically or percutaneously
All patients included in the study had biopsy-proven, unresectable locally advanced pancreatic adenocarcinoma and received computed tomography (CT)–guided irreversible electroporation. They all had had prior chemotherapy (one to five lines), and 60% of patients had had prior radiation therapy. Follow-up included CT at one month and at three-month intervals thereafter.
Govindarajan Narayanan, chairman, Department of Interventional Radiology, University of Miami, Miller School of Medicine, Miami, USA, and colleagues reported that there were no treatment-related deaths and no 30-day mortality. However, serious adverse events including abdominal pain, sepsis and gastric leak occurred in 20% of the patients.
The investigators also reported that the median overall survival was 27 months from time of diagnosis and 14.2 months from time of receiving the interventional radiology procedure. Patients with tumours that were smaller than 3cm (n=24) had significantly longer median overall survival when compared to patients with tumours that were larger than 3cm: 33.8 vs. 22.7 months from time of diagnosis (p=0.002) and 16.2 vs. 9.9 months from time of irreversible electroporation (p=0.031). Tumour size was confirmed as the only independent predictor of overall survival at multivariate analysis, they further reported.
Most drugs that we use are only required to work at one specific point in the body and yet we administer them in a completely systemic manner so that they affect all sites within the body. If a drug is quite toxic, or has a very narrow therapeutic window, as with, for instance, chemotherapeutic compounds, many undesirable side-effects can be experienced alongside the beneficial effects at the site of concern due to drug distribution in healthy tissues. Methods of giving drugs that are only activated at the desired site of action are therefore highly desirable to minimise side-effects (which may in some cases be very severe) and allow patients to remain relatively well whilst receiving maximum therapeutic effect from the drug.
It is now possible to chemically engineer nanosized liposomal particles to encapsulate and carry a variety of drug payloads around the body without the drugs having an action in the circulation. The liposomal drug particles can be further engineered to be heat sensitive so that when the temperature is raised by a controlled amount, the liposomes become porous and release their drug contents. Controlled non-interventional heating of a deep area of the body where we require a therapeutic effect can be achieved using high intensity focused ultrasound which can be either ultrasound- or MR-guided. Using this combination, it is possible to deliver chemotherapy just to the cancer site rather than to all areas of the body which potentially can greatly decrease the morbidity and complications seen with many types of chemotherapy which are such a problem for many patients.
We have demonstrated this approach clearly in small animals showing that tumours can be rapidly treated with this combined focused ultrasound and liposomal drug nanoparticle approach. The advantages of this approach however do not stop at this point. We have discovered that the uptake of the chemically engineered liposomes from the circulation is much greater when the area in question is heated than would otherwise be expected suggesting that this mild hyperthermia during this process opens up blood vessel permeability allowing a much greater concentration of the circulating liposomesto be delivered into the target site with a very large increase in overall tumour concentration of the drug. This is exciting in itself but we have managed to further engineer our focused ultrasound pulse delivery so that we not only heat the target site with non-invasive focused ultrasound at the time of the drug circulation in its 1st pass but repeat this thermal mild hyperthermia 30 minutes later. Using this further recipe of repeated focused ultrasound short hyperthermia pulses we have found that there is a new, huge increase in the overall concentration of the activated chemotherapeutic agent released from the thermally sensitive liposomes at the target site. In some instances we were able to increase the concentration of active current chemotherapeutic agents at the site of therapy by several hundredfold.
The potential of this type of approach to allow treatment with few side-effects but with much greater local action is very exciting. Not only will we be able to decrease side-effects from conventionally utilised chemotherapy, but we may be able to utilise very effective but very toxic drugs which are otherwise unusable to now treat just the designated target lesions.
We have also combined MR contrast agents with the chemically engineered liposomes so that the area of deposition can potentially be visualised with MR imaging to further control and follow the therapeutic effect.
Wladyslaw Gedroyc is consultant radiologist at St Marys Hospital, Imperial College Healthcare NHS Trust, London, UK
The first Hong Kong-based patients diagnosed with pulmonary embolism have been treated using the newly available BTG EKOS system. The EKOS system includes an ultrasonic device that uses acoustic pulses to quickly and safely dissolve blood clots and restore blood flow in patients with pulmonary embolism, deep vein thrombosis, and peripheral arterial occlusions.
According to a press release, the EKOS system uses acoustic pulses to unwind and thin fibrin on clots to expose drug receptor sites, allowing the drug to reach deeper, accelerating absorption and helping to dissolve the clot faster and with less thrombolytic.
Luk Wing Hang, consultant radiologist at the Princess Margaret Hospital, Kwai Chung, Hong Kong, performed the procedure on one of the patients. He comments, “Prevalence of fatal pulmonary embolism was 0.21% (1964-74), 1.08% (1975-79), 1.83% (1980-84), 2.77% (1985-90), and 4.7% (1990- 94) and the trend has been found to be increasing year after year with the percentage approaching western countries’ occurrence rate.” According to Luk, the patient treated with the EKOS system was clinically stabilised with no desaturation or shortness of breath, and their blood pressure was back to normal.
Later, in the same week, another case of submassive pulmonary embolism was treated just eight miles away at the Prince of Wales Hospital, Sha Tin, where interventional cardiologist Bryan P Yan was treating physician. “The EKOS system enables much lower and safer doses of thrombolytic drugs to be used which significantly reduces the risk of major bleeding. The device is currently the only US FDA-cleared, minimally invasive endovascular therapy for pulmonary embolism. Our patient’s condition was improved significantly after 12 hours of ultrasound assisted thrombolysis with the system. His breathing and blood pressure were improved and his grossly dilated right heart returned to nearly normal size and he was successfully discharged home,” adds Yan.
Ask4UFE has announced the #LoveYourUterus campaign to encourage women with painful fibroids to share their stories of health and healing. Uterine fibroids often result in women having hysterectomies because they are unaware of uterine fibroid embolization (UFE), which is a less invasive procedure.
Lynne Haze, a prominent radio personality in Dallas, USA, chose to share her recent experience with UFE so that other women in similar situations know that there is another option when dealing with painful fibroids. Suzanne Slonim, Precision Vascular and Interventional, recently performed the UFE procedure for Haze.
UFE provides relief from symptomatic fibroids, while also allowing women to avoid the higher risks and much longer recovery from surgery. Most importantly, with UFE, women keep their uterus, which is a significant and often unappreciated advantage over hysterectomy due to the prevalent consequences many women suffer post-hysterectomy.
“I want women to know that they have a choice, that there is a choice that you do not have to spend six weeks of your life laid up in bed,” says Haze. “That there is a choice that this could be something where if you still want to have children, you can have children. You do not have to have your uterus removed.”
Teleflex has announced that its Arrow VPS Rhythm device with optional TipTracker technology has been issued 510(k) clearance so that the device can be commercialised in the USA.
Arrow VPS Rhythm device is a simple and versatile solution that provides electrocardiogram-based tip confirmation in a highly portable and lightweight design, a press release from the company says.
The device assists in placement and confirmation of a catheter tip in the superior vena-cava-cavoatrial junction; it may be used with a broad range of catheter types and brands. Intravascular P-wave changes are saved as the catheter approaches the superior vena-cava, helping to identify the lower 1/3 of the superior vena-cava, near the cavoatrial junction, eliminating the need for confirmatory chest X-ray or fluoroscopy in adult patients. When paired with the single-use TipTracker stylet for insertion of peripherally-inserted central catheters (PICCs), the Arrow VPS Rhythm device provides real-time visual navigation by tracing the catheter pathway with a blue line on a colour screen. The device has an expansive sphere of visual navigation to provide easy navigation of the PICC during insertion.
“This clearance positions us to provide catheter tip placement solutions that meet customer’s unique therapeutic and budgetary needs,” said Jay White, president and general manager, Vascular Division of Teleflex.
Abbott announced on 4 January 2017 that it has completed the acquisition of St Jude Medical.
“Abbott has a strong track record of successfully integrating dozens of businesses on a global scale and accelerating growth,” said Miles D White, chairman and chief executive officer, Abbott. “The addition of St Jude Medical strengthens our global medical device leadership while offering innovative products to address more areas of care, in more physicians’ offices and hospitals around the world.”
Pursuant to the terms of the Merger Agreement, upon completion of the acquisition, St Jude Medical became a wholly-owned subsidiary of Abbott.
St Jude Medical’s strong positions in fast-growing areas such as atrial fibrillation, heart failure, structural heart and chronic pain complement Abbott’s leading positions in coronary interventions and mitral valve disease. Together, the company will compete in nearly every area of the $30 billion cardiovascular market and hold the No. 1 or 2 positions across large and high-growth cardiovascular device markets.
Abbott will have a powerful pipeline across cardiovascular and neuromodulation patient care ready to deliver next-generation medical technologies and offer improved efficiencies for healthcare systems around the world.
NICE’s Scientific Advice programme will work with companies looking to attain both FDA approval and payer coverageThe UK’s National Institute for Health and Care Excellence (NICE) has announced its participation in the US Food and Drug Administration (FDA)’s Payer Communication Taskforce. This programme aims to accelerate US patient access to new technologies by gathering evidence of clinical effectiveness in an attempt to encourage US insurers to fund new treatments, post FDA-approval.
“To help companies overcome this hurdle, NICE’s Scientific Advice programme has joined forces with the FDA in the Payer Communication Taskforce.” explains Leeza Osipenko, head of the NICE Scientific Advice programme, in a press release. “Early engagement should help medical technology makers to design their development programmes better to produce the data needed both to obtain regulatory approval and to persuade the payers of the value of their product.”
The FDA already requires the demonstration of certain evidence before it will approve a product for commercialisation in the USA. However, many insurance companies require supplementary evidence, demonstrating the value of diagnostic tests or medical devices, before they will consider providing funds for such products.
“In their efforts to get a product to market, companies can get caught out,” explains Osipenko. “Although [companies] often do enough [evidence] to win FDA approval, they need additional evidence to prove to the organisations who would actually pay for those devices that they are cost-effective and clinically-effective.”
The NICE Scientific Advice programme—a fee-for-service consulting branch of the organisation—offers advice to life sciences technology companies on “evidence generation on economic and clinical effectiveness.” According to the release, NICE may review evidence, provide advice pre-FDA submission, and produce “formal, written advice.”
Companies seeking advice from the organisation are encouraged to notify both the FDA and NICE.
DC Bead Lumi is also called LC Bead Lumi in other geographies
BTG International Canada has announced the commercial launch of DC Bead Lumi in Canada. The launch represents the first market commercialisation of DC Bead Lumi in the world, with regulatory clearances and launches planned for additional markets worldwide.
DC Bead Lumi is sometimes also called LC Bead Lumi in other geographies. The company received Health Canada approval for DC Bead Lumi in August 2016.
DC Bead Lumi is the first available radiopaque embolic drug-eluting bead that can be loaded with doxorubicin for the treatment of hepatocellular carcinoma, the most common type of primary liver cancer or with irinotecan for the treatment of malignant colorectal cancer metastasised to the liver (mCRC).
The unique visibility of DC Bead Lumi helps optimise patient treatment by enabling real-time visible confirmation of bead location during and after the embolization procedure. This provides interventional radiologists more control, while at the same time facilitating discovery of regions of under-treatment, allowing precise evaluation of the completeness of tumour treatment and enhanced end-point determination, with long-lasting radiopacity to support follow-up management.
Sunnybrook Health Sciences Centre in Toronto, Canada was the first institution to perform transarterial chemoembolization (TACE) using the new device.
“The Lumi TACE beads really delivered. They were what one hoped for; it was easy to see under fluoroscopy, single shot and cone beam CT,” said Chris Dey, staff vascular/interventional radiologist, Sunnybrook Health Sciences Centre and assistant professor, Faculty of Medicine, University of Toronto. “You can appreciate actual bead deposition in the liver for the first time, flow patterns much more reliably and make intraprocedural adjustments or determine endpoints more precisely.”
“DC Bead Lumi allows for the personalisation of liver cancer treatment like never before, providing the vision, precision and assurance that the treatment is getting where it needs to be,” added Frank Maiorino, director, Marketing at BTG International Canada.
Researchers at Mayo Clinic (Rochester, USA), Harvard Medical School and the Massachusetts Institute of Technology (both Boston, USA) are developing a biomaterial that has potential to protect patients at high risk for bleeding in surgery.
Embolization is often accomplished by inserting metallic coils through a catheter into a vessel, which induces clotting to prevent further bleeding.
Rahmi Oklu, a vascular interventional radiologist at Mayo Clinic’s Arizona campus, explains shear-thinning biomaterial offers many advantages over metallic coils.
Do you know what scanxiety is? Or scanticipation? As clinicians who look after patients with cancer, interventional oncologists must realise the impact that a diagnosis of cancer, and the course of treatment, has on patients. Jim Caridi, professor of Vascular and Interventional Radiology, Tulane University, New Orleans, USA, outlines what really happens when a person travels on that difficult journey of being treated for cancer. And how, even as a physician, the most compelling advice on being a cancer warrior comes from other patients on the front lines. This is what led him to set up the oneIAM club.
It is said that a picture is worth a thousand words, but occasionally the contrary is also true. A few words can be worth a thousand pictures or images. Just ask any individual who hears the dreadful words: “You have cancer.” The typical response is a total shutdown of sensory input. While you are sitting there petrified, the word “cancer” engenders images of childhood, family, holidays, travel, hospitals, IVs, doctors, vomiting, diarrhoea, funerals, and, worst of all, life without you in it. Unrelenting images cloud your senses, and when you temporarily focus on the individual delivering the news, you see lips moving but nothing has registered. If you are fortunate, you are accompanied by someone who can recall the information you have missed.
We know that this scenario is typical, but we as providers of care must realise this sensory deprivation and take measures to ensure that any vital messages are passed on and clearly understood.
After the initial shock, you realise life as you knew it is now over. You have joined a subset of society made up of people who spend the majority of their time and efforts simply focusing on staying alive. Previous hardships and annoyances are now a mere nuisance. They have been replaced with regimented appointments, tests, scans, medication, side-effects and complications. Even if things work out in your favour, the albatross of cancer is omnipresent.
Scanziety and scanticipation are the words that come to mind. The results of one test or scan can change one’s life instantaneously. It is not unusual for affected individuals to become anxious days or even weeks prior to definitive tests. If things happen to go as planned, it is then followed by the waiting game for the results and the next course of action. This can amount to weeks of apprehension. The anticipation and waiting game is bad enough, but any disruption of this sequence—for example, a cancellation of scheduled exams—subjects the patient to even greater hardship and anxiety. This can be devastating to the patient’s psyche, and as caretakers we should ensure that these planned events and their results go unimpeded.
It is readily apparent that those with cancer live by a separate set of rules and conditions, and their main focus is to be that “one in a million” who beats the odds. Regardless of how sensitive, knowledgeable or understanding healthcare workers may be, it is difficult for them to slip their feet completely into the cancer warrior’s shoes. The most compelling advice and experiences come from those with personal exposure. The oneIAM club or one in a million club was created to instantly open lines of communication among those with cancer so they can communicate experiences, tricks, strategies and ideas that combat the isolation, confusion and negativity that typically go along with a diagnosis of cancer. It also provides a forum for support, comfort and encouragement. It lets those affected know they are not alone and that the path they are about to travel has been walked by many. And if they heed what the many have to say, their travels will be less stressful and more agreeable.
In this regard a unifying one in a million logo was created to include all cancers. Although cancers may vary in type and location, they share many of the same problems and hurdles and the approach to success is usually the same. The oneIAM club’s logo and intent—whether in person or on social media (the club has a Facebook page)—is to identify and recognise members of the club, thereby providing an instant forum for camaraderie and the exchange of useful information and experiences. This is particularly relevant now when medicine has relegated much of its role to computers and ancillary personnel. They cannot and do not replace personal experiences. Such aids as B vitamins for neuropathy, ice for mucositis, turmeric for liver dysfunction and exercise for fatigue and depression come from the experience of members and are often not communicated by medical personnel.
As a member of the oneIAM club, I am well aware of the pain, misfortune and hardships experienced by many of its members. I am also aware that I am not alone and that there is strength in numbers. The sharing of positive experiences, successes, strategies, reassurance and support can result in a more positive and even fruitful journey. Because of the assistance of other members before me I have been able to persevere, remain positive and return the favour to others.
The oneIAM members may not have asked to join this club but together we can change and influence the lives of those with cancer for a more encouraging, optimistic and productive journey.
Jim Caridi is professor of Vascular and Interventional Radiology, Tulane University, New Orleans, USA, and creator of the oneIAM club
Sebastian Mafeld who can be found Tweeting at @SebastianMafeld
Sebastian Mafeld who can be found Tweeting at @SebastianMafeld
Sebastian Mafeld, interventional radiology Fellow at NHS and co-founder of UK Endovascular Trainees (UKETS) tells Interventional News about how a three-dimensional (3D) printed model of an aorta is a valuable training tool for endovascular interventions and how printing unique catheter shapes and patient-specific devices might be around the corner.
What is 3D printing and how does it work?
Three-dimensional (3D) printing is a manufacturing process whereby an object is created by sequentially printing it in layers. A 3D printer is guided by a computer file, typically in STL (surface tessellation language) format. This manufacturing process is also referred to as “additive manufacturing”. There are several additive manufacturing technologies but one of the most common ones is Stereolithography; this works by sequentially solidifying a light-sensitive liquid compound (photopolymer) layer by layer.
One of the reasons why this manufacturing process is important is that traditionally manufacturing processes have been ‘subtractive’ (in its simplest form, imagine wood carving; pieces are removed from a block of wood until finally the model is created). 3D printing, on the other hand, is additive, this means incredibly complex designs can be created which were not possible previously with traditional manufacturing methods.
3D printing is suddenly becoming accessible. Why?
3D printing has been around for decades but has only expanded rapidly over the past few years. Peter Diamandis gives a great explanation in his book Bold on why this may have occurred. He states: “an exponential technology does not really become disruptive until a powerful, user-friendly interface exists”. While 3D printers have been around for decades, user-friendly software for designing 3D printable models has not. Now that this software is available to virtually to anyone with a computer and combined with easier access to 3D printers (just google “3D printing + your city) these factors play an important role in the evolution of this technology.
A 3D-printed model of an aorta and its branches produced by Mafeld and his team
Can you comment on the key findings from your study presented at CIRSE 2016. What did the feedback from physicians who used the 3D printed vascular model suggest?
We 3D printed a scale model of the entire aorta along with its major branches in a transparent material for the purposes of endovascular simulation training. This project was undertaken together with Materialise, a 3D printing company based in Leuven, Belgium. A 6F sheath was inserted into a predesigned hole in each common femoral artery and the model was filled with regular tap water. This allowed the use of normal catheters/wires/balloons inside the model. We thought this may give a user a better understanding of how common endovascular tools behave whilst experiencing enhanced haptics including pushability, torquability, and trackability.Ninety-six physicians in training trialled the model under the supervision of an experienced interventional radiologist. Common endovascular tasks eg accessing the visceral vessels were performed. Candidates then rated their agreement with 12 statements regarding their training experience on a standard five-point Likert scale. The data from this was presented at CIRSE 2016 in Barcelona, Spain. Our data shows a trend towards “strong agreement” that this 3D printed model was a valuable learning tool for training in basic endovascular skills. Candidates also generally agreed that catheterisation of vessels and manipulation of the guidewire was “realistic” inside the model.
Where does 3D printing fit into the healthcare setting?
Despite a lot of excitement about 3D printing in healthcare, its exact role in healthcare has yet to be established. There are countless reports for unique uses of 3D printing, most of which centre around printing structures for improved anatomical understanding. Other areas include the printing of implants for craniofacial/skeletal surgery. As medicine is shifting towards a “personalised” instead of population-based approach, 3D printing reflects this theme by allowing patient specific products to be created.
How can 3D printing impact procedure planning/ simulation? Are there any data to suggest improved treatment outcomes from using 3D printing technology?
From an endovascular standpoint, 3D printing may be useful in procedural planning and device testing. For example, in the treatment of complex aneurysms, 3D printing can allow visualisation of an aneurysm and evaluation of stent graft suitability. The ability to physically test critical parts of an endovascular procedure using a 3D printed model might lead to reductions in procedure time and radiation exposure or improvements in outcomes and patient safety. However, at present, I am not aware of any large scale published data which demonstrates improved treatment outcomes from using 3D printing in endovascular practice or any other field of medicine. Biglino et al have published some data showing that the 3D printing of patient-specific models of congenital heart defects can improve communication between cardiologists and parents. It is imperative that data is obtained to establish the potential impact 3D printing can have on procedures in all areas of medicine.
Mafeld and teams’ 3D printed model aorta in action
Specifically, what endovascular applications are there for 3D printing?
In terms of implantable 3D printed devices, endovascular practice lags behind its orthopaedic and maxillofacial counterparts. While there have been many reported cases of 3D printed bone implants, I am not aware of any 3D printed implanted endovascular devices. Currently, the endovascular applications for 3D printed have mainly been focussed on creating models for procedural planning and device testing. In is possible that patients have benefitted from 3D printed vascular models as companies and physicians have been able to better test their devices prior to deployment.
What are the challenges for 3D printing in the healthcare setting?
3D printing faces the same challenges as many technologies in medicine; regulation, time, technical skill, cost, and validation.
As 3D printing in medicine is a rapidly evolving field but currently lacks large-scale evidence, regulation is challenging. The FDA, however, has released draft guidance in 2016 entitled “Technical considerations for additive manufactured devices” – which marks a step towards regulating this area.
Being able to accurately 3D print a medical model from imaging data requires detailed anatomic understanding and the ability to use software. If we are going to base treatment decisions on 3D printed models then we need to be confident about the software and printer’s ability to accurately reproduce the anatomy in question. Patient safety is always paramount, therefore robust validation systems are needed to ensure accuracy.
The speed of 3D printing is also highly variable, small models can be produced relatively quickly while, for example, our model took 96 hours to print as it was made up of over 5000 layers. The time taken to produce the STL file necessary for 3D printing must also be considered in an era where healthcare professionals are increasingly overstretched.
Anecdotal evidence from case reports or small series may support the value 3D printing, but is not enough to understand whether it will remain a novelty or become a necessity. Large scale data are necessary to determine the impact of 3D printing on medical procedures, and to establish a cost:benefit analysis.
Mafeld and team with their aorta model
What does the future of 3D printing in endovascular practice look like?
In the short term, I think we will start to see more patient-specific devices being produced. For example, in challenging anatomies we might be able to print unique catheter shapes to facilitate procedures. In the longer term, the 3D printing of endovascular stent grafts or other implantable devices may be possible. If we look even further to the hypothetical future, rather than departments keeping large stocks of multiple device sizes, companies might instead provide a 3D printer which can produce a patient-specific device on-demand. 3D bioprinting of blood vessels is also an evolving area which may have unique endovascular applications. Overall, I remain optimistic about the technology’s future in endovascular practice.
Since prostate artery embolization was started as a treatment option for benign prostatic hyperplasia in March 2009, many distinguished Portuguese urologists have been invited to watch the procedure. However, only four have accepted the invitation, João Martins Pisco, Hospital Saint Louis, Lisbon, Portugal, tells Interventional News.
Where does the story begin?
Prostate artery embolization was started at St Louis Hospital in Lisbon in March 2009 after approval by an Ethics Committee. The medical team involved in the procedure includes a urologist who is the director of the Department of Urology and professor of Urology at the New University of Lisbon. Ever since we began carrying out these procedures, we have invited several distinguished urologists in Portugal to watch the procedure, however, only four have accepted the invitation.
In 2008, a local newspaper published news about prostatic artery embolization and stated that 27 cases were already performed. At that time, the urologists reacted and tried to stop prostatic artery embolization being performed through the College of Urology. Nonetheless the College of Urology has decided that there are no substantial reasons to abolish this innovative procedure.
What has happened since?
Shortly afterwards, in 2012, a lawsuit was filed against the medical team carrying out prostatic artery embolization and the St Louis Hospital by some urologists in Portugal. They stated that there were not enough validated data to support the efficacy of this technique when compared with other treatment options already being performed by urologists. Meanwhile, other reports supporting this innovative procedure have been published and presented in international medical conferences by our interventional radiology team in Portugal and others worldwide. The efficacy of the procedure and the outcomes being reported are quite similar.
The fact that the procedure is well-known and enthusiastically supported by international interventional radiology societies and that it has good mid-term published outcomes has strengthened the case for the efficacy of the procedure. Eventually, these legal processes begun by the urologists were dismissed without prejudice.
How is enrolment in the randomised trial progressing?
In 2014, we began a randomised sham trial to determine whether prostatic arterial embolization is an effective and safe treatment compared to a sham procedure, for the treatment of benign prostatic hyperplasia in patients with severe lower urinary tract symptoms not adequately controlled by medical therapy with alpha-blockers. The effectiveness and safety will be assessed by the International Prostate Symptom Score (IPSS) after six months. Patients will be randomised in a 1:1 ratio to either embolization or a sham procedure and evaluated at one, three and six months through several different imaging, biochemical and functional exams and through international validated questionnaires.
Two years ago, when the sham trial started, the College of Urology and the Portuguese Association of Urology were informed of the inclusion and exclusion criteria. However, we have had no patients referred to the trial by them. The patients enrolled in our trial were mostly self-referred, or referred by other previously-treated patients.
What is the current situation?
In March 2015, we reached the milestone of 1000 cases of prostatic artery embolization procedures at St Louis Hospital. There was extensive coverage from our national media on this occasion and a popular newspaper and TV channel came to our hospital and reported on the procedure’s success. The Portuguese Association of Urology then asked for an official statement from the College of Urology regarding prostatic artery embolization. We also asked for an official report from our national College of Radiology. In addition, statements and data from several distinguished interventional radiologists regarding prostatic artery embolization was collected as well as a report from CIRSE and SIR on the procedure.
The report from the Portuguese College of Urology is based on the fact that the fundamental action of prostatic artery embolization is not well known. In addition, they state that there are only a few prospective studies that evaluate the results of the procedure. Moreover, the Portuguese College of Urology notes that the actual published evidence for the efficacy and safety of prostatic embolization is not of high enough quality and that there are but few studies on the subject. The document draws attention to the single, prospective and randomised study, from China, comparing prostatic artery embolization and transurethral resection of the prostate (TURP) outcomes. It mentions the better results obtained by TURP in all parameters of the study, except hospitalisation time, which is not supported by the presented data.
We do not know what the next step of the Portuguese urologists who do not accept prostatic artery embolization will be—the future will tell us.
Sirtex has announced that SIR-Spheres Y-90 resin microspheres have been included as a Category 2A recommended treatment in the latest National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology for colon cancer and rectal cancer. This designation denotes that there is uniform consensus among the NCCN panel that selective internal radiation therapy (SIRT) with yttrium-90 microspheres is an appropriate option in patients with liver dominant, chemotherapy resistant colorectal disease. This recommendation places SIR-Spheres Y-90 resin microspheres at the same designation as the recommended mCRC systemic chemotherapeutic regimens. SIRT can also be carried out using glass microspheres. BTG’s TheraSphere is currently FDA-cleared only for hepatocellular carcinoma treatment in the USA, but approved for liver neoplasia in other geographies.
Nearly 140,000 Americans are diagnosed with colorectal cancer every year, more than 50% of whom will see the cancer spread to their liver. “The NCCN Guidelines aim to assist medical teams, patients and their families in making informed treatment-related decisions with the goal of optimal cancer care,” said Kevin Richardson, chief executive officer for Sirtex Americas.
“The 2A designation represents a very important milestone for SIR-Spheres resin microspheres and provides further validation for the role of our medical device as an important treatment option for unresectable, liver dominant metastatic colorectal cancer. We also have positive signals in the first-line setting through the results to date of the pivotal SIRFLOX study and eagerly anticipate the overall survival results in more than 1,100 patients from the SIRFLOX, FOXFIRE and FOXFIRE Global studies which we expect to be available in the first half of 2017.” These findings are also supported by the landmark MORE study, a large retrospective analysis conducted in the USA with SIR-Spheres Y-90 resin microspheres in more than 600 mCRC patients. The MORE study helped to increase the understanding of SIRT as a treatment option for patients who have failed multiple lines of chemotherapy while highlighting the positive aspects of the safety and efficacy of the protocol for patients of all ages.
“Clinical research has shown that SIRT brings patients with colorectal liver metastases improved and prolonged quality of life,” said lead investigator of the MORE study, Andrew S Kennedy, director, Radiation Oncology Research, Sarah Cannon Research Institute, Nashville, USA. “We look forward to expanding access to this outpatient procedure, which has demonstrated minimal side effects, to improve outcomes for this population of patients and advance the standard of care.”
SIR-Spheres Y-90 resin microspheres are the first and only microspheres with FDA premarket approval for colorectal cancer that has metastasised to the liver, a press release from Sirtex adds.
Terumo has reached an agreement with Abbott and St Jude Medical to acquire certain products owned by both for a total of US$1.12 billion.
Based on an agreement in principle previously announced by Terumo, Abbott and St Jude Medical on October 18, 2016, Terumo will acquire St Jude Medical’s Angio-Seal and FemoSeal vascular closure product lines and Abbott’s Vado steerable sheath. The total annual sales of the businesses to be acquired is approximately US$268 million.
The acquisition remains subject to antitrust regulatory approvals and successful completion of Abbott’s proposed acquisition of St Jude Medical.
10-year EMMY results show majority undergoing embolization for symptomatic fibroids can avoid hysterectomy
Percutaneously created AV fistulae need far fewer post-creation interventions than those made by traditional surgery
Raman Uberoi: 24/7 IR services
Jim Caridi: Talking about cancer
Gerard Goh: Percutaneous AVF
Profile: Gireesh Mukund Warawdekar
10-year EMMY results show majority undergoing embolization for symptomatic fibroids can avoid hysterectomy
Percutaneously created AV fistulae need far fewer post-creation interventions than those made by traditional surgery
Raman Uberoi: 24/7 IR services
Jim Caridi: Talking about cancer
Gerard Goh: Percutaneous AVF
Profile: Gireesh Mukund Warawdekar
BrightWater Medical has announced that the US FDA has cleared the company’s innovative ConvertX nephroureteral stent system for treatment of ureteral obstructions.
Patients with obstructions preventing urine in the kidneys from draining to the bladder face potential pain, infection, and long-term damage, necessitating immediate treatment. In severe cases referred to the interventional radiologist, the ConvertX is the only device that enables the interventional radiologist to eliminate a second invasive interventional procedure to treat the patient, a press release from the company says.
In the two traditional procedures, the interventional radiologist first implants a nephrostomy catheter to externally drain urine and in the second procedure exchanges the nephrostomy catheter for an internal ureteral stent to circumvent the blockage. The ConvertX system, in contrast, is implanted only once and converts from a catheter to a stent in a brief office procedure without the need for radiation or sedation, in less than one minute. The ConvertX stent then remains implanted in the patient like a standard internal ureteral stent.
“Ureteral blockages due to kidney stones, tumours or scarring from previous surgeries must be treated quickly so urine can be voided,” explained ConvertX system developer Bob Smouse, founder and CEO of BrightWater Medical, and professor of Radiology and Surgery, University of Illinois College of Medicine. “The ConvertX System saves the patient the risk and discomfort of an additional second interventional procedure and may reduce healthcare costs, free up the hospital’s angiosuite for other procedures and save the interventional radiologist procedural time that can be devoted to care of other patients.”
“The ConvertX system is the kind of technology advancement that we require to meet the dual goals of improving patient care and reducing the financial burden to the healthcare system,” explained James F Benenati, clinical associate professor of Radiology at the University of South Florida College of Medicine. “Interventional radiology enables patients with severe ureteral blockages to be quickly treated, and technologies like the ConvertX platform provide the interventional radiologist with simpler, more cost-effective solutions.” Benenati is also medical director of the Peripheral Vascular Laboratory, Miami Cardiac & Vascular Institute, and past president of the Society of Interventional Radiology.
In addition to the FDA clearance, BrightWater recently received its medical device manufacturing license from the California Department of Public Health. The company is submitting an application for the ConvertX System to the European Union for CE marking and is developing additional ConvertX-based products for other staged procedure treatments in interventional radiology.
“There is no easy fix with current endovascular tools and strategies and a default realisation is that it is easier and more definitive to treat aortic dissection early,” Michael D Dake, Stanford, USA, told Interventional News about the Achilles’ heel of thoracic endovascular aneurysm repair (TEVAR) management for uncomplicated type B dissection.
“At present we are armed with a tool box of largely unproven and often complicated multi-step therapies and a ‘wait and see’ approach that satisfies no one. Future success will require new ideas and creative thinking,” he said while talking about TEVAR’s dirty little secret. The paradigm for treatment might need to be radically re-thought, he added.
Dake received the British Society of Interventional Radiology (BSIR)’s Honorary Fellowship at the society’s annual meeting (15–17 November 2016, Manchester, UK). Dake is the Thelma and Henry Doelger Professor (III), Department of Cardiothoracic Surgery, Stanford University School of Medicine, Falk Cardiovascular Research Center. He delivered a lecture on aortic dissection, speaking on the topic “Endovascular Management of Aortic Dissection: What We Know, Think We Know and Need to Know”.
There are three main strategies for uncomplicated type B aortic dissection: medical management alongside a “wait and watch” approach for complications to occur, after which treatment is undertaken; early endovascular treatment for all patients; and early endovascular treatment only for patients at high-risk of complications.
“In all initially uncomplicated type B dissections, should we look for high risk features that predict early progression or just plan to treat all except those in whom the procedure may be difficult or at risk of complication?,” Dake questioned.
The clinical course of type B uncomplicated aortic dissection is not entirely benign. Early TEVAR will benefit some high risk patients who can be identified by predictive factors. Accumulating evidence may favour even more liberal early TEVAR in type B dissection, but the timing of the intervention and its cost-effectiveness still remain questions, Dake told attendees.
“We are not providing a definitive treatment for dissection. In some fraction of patients after TEVAR, we know that there is going to be persistent false lumen perfusion from abdominal branches that can, not only continue to provide a risk for the patient in terms of rupture, but also lead to dilatation and false lumen aneurysm formation. Trying to really excommunicate the false lumen aneurysm in a chronic state is really difficult to do with our current toolbox,” Dake informed Interventional News.
“I think we need to think about this differently. Yes, we now have stent grafts in the tool box and we can use these even in the branches, but it is very difficult to achieve good results in a chronic state. Even experts who have a lot of experience using branched grafts in chronic dissections understand that endoleaks still exist and that branch vessel grafts still occlude. There has got to be a way to deal with this upfront and definitively so as not to have a long tail of potential complications and so that the false lumen does not have the opportunity to be a bad actor in the chronic state. With the current tools that we have, we just do not have the opportunity to do that. People have tried many kinds of gizmos and gadgets to plug the false lumen, but these seem to only work in the acute setting when the lamella is thin and weak. In the chronic setting some combination technologies such as the use of extreme tapers and reverse tapers with distal cutting that seek to rupture the dissection septum could be risky. I think we need to think of a new paradigm that will probably include stent grafts at some level, but it may have to be radically rethought. First, there needs to be the understanding that what we are providing in a subgroup of patients, is inadequate. With that realisation, which shows that that stent grafts are not a panacea, we can move ahead and truly create a more definitive solution without constant surveillance and the risk that there is going to be late progression.”
The challenge of undertaking dissection trials
“Because dissections are relatively rare, in order to obtain data from a large number of patients, the trial will need to have a large number of participating centres who are interested in aortic disease and experienced in both open and endovascular treatments. When you have that many institutions participating, there are going to be expenses and the issue is who is going to foot the bill. Trials that are being reported are basically industry-sponsored. Industry has to do these trials to get approval for their devices so funding these trials is part of a business strategy. However, once approval is obtained, industry really does not have the same motivation or incentive to fund the trials that we need to have done for the doctors and patients. In the climate of decreasing resources for research it takes a lot of coordination to muster the resources to carry out these trials,” Dake concluded.
Selective internal radiation therapy (SIRT) has been available since December 2013 to a defined group of patients with liver metastases in England on the National Health Service (NHS) via a special Commissioning through Evaluation scheme from NHS England. However, NHS England has now decided to stop funding SIRT at the end of March 2017 while it analyses the data obtained so far.
The British Society of Interventional Radiology (BSIR) and many interventional oncologists believe that this decision is unfair to patients who will be unable to access SIRT on the NHS during the data analysis period and fear that the hiatus might result in the de-skilling of SIRT multidisciplinary teams that include interventional radiologists. There is also growing concern that referral networks for the treatment could be lost in the analysis period when SIRT will be unavailable to patients.
Materials available at the BSIR annual meeting (15–17 November, Manchester, UK) note that according to the Health Minister, the data analysis, which includes a cost-effectiveness analysis, “could take up to two years”.
Many interventional radiologists maintain that there is already substantial evidence supporting the benefits of SIRT in patients with liver metastases from bowel cancer and that the planned gap in provision is unfair to patients. “In the light of the evidence, a conclusion that NHS patients should not have access to SIRT from April 2017 on the basis of insufficient evidence appears inconsistent with the published studies,” the material from BSIR further adds.
Interventional oncologists emphasise that it will cost the NHS both in terms of time and money to decommission services and then re-skill clinicians at a later date, if SIRT funding is lost for 12–18 months while the data is analysed. All these factors have led to the BSIR asking NHS England, as a matter of urgency, to allow for continuity of service provision from April 2017 onwards.
Brian Stedman, consultant interventional radiologist at University Hospital of Southampton, Southampton, UK, and chair of the BSIR communications committee told Interventional News: “SIRT is a complex treatment that needs collaboration between interventional radiology and nuclear medicine and centres need to invest in equipment and staffing to get this treatment underway. It took about a year to get the 10 centres who were delivering SIRT treatments in England up and running. Over the last 18 months, most of these have been running at the level of activity that we have been expecting. Having developed this service and expertise, our anxiety is that we are going to be left with no funding mechanism for these patients. If there is an 18-month hiatus, we are going to lose the skill base in these 10 centres. If there is a positive analysis from the data, we will then have to re-skill these centres and this will be at a significant cost to the NHS. We are seeking some form of interim funding so that patients are not disadvantaged, and skills are maintained while the data is analysed.”
Stedman added: “In this scenario, we are talking about patients who have failed two or more lines of chemotherapy and these patients are looking at few, or no, treatment options despite having a good quality of life. These patients are not going to be cured by SIRT, but our aim is to prolong life and maintain quality of life. I strongly believe that liver-directed therapies have a real benefit for our patients. Unlike with drugs, when it comes to innovative device technologies, we are struggling to get clear funding pathways. Prior to the Commissioning through Evaluation scheme, SIRT was regionally available through the Cancer Drugs Fund. My issue is with the slightly ad hoc funding of these technologies and this is a difficulty that we need to address as an interventional oncology community.”
In June 2013, NHS England agreed to fund 660 NHS patients who had failed, or were intolerant to chemotherapy, to receive SIRT for the treatment of liver metastases from bowel cancer and biliary tract tumours in the liver at 10 NHS hospitals in England. The funding is scheduled to stop after an estimated 520 patients will have been treated.
We need to find other physician groups to support neuroradiologists in the delivery of mechanical thromebectomy. But are interventional radiologists, as those who regularly perform procedures with similar technologies to those used for mechanical thrombectomy, the right group to support this initiative? Trevor Cleveland, Sheffield, UK, details some of the challenges.
Stroke is a major cause of death and disability, for which the UK Department of Health formulated a strategy in 2007. A significant part of that strategy was the acute treatment of stroke, recognising that “time is brain”, and gave recommendations for the use of thrombolytic agents. The National Clinical Guidelines for stroke on 2012, published by the Royal College of Physicians, emphasised the importance of early treatment with the benefits of starting treatment after 4.5 hours being unproven. The intention of thrombolysis is to re-establish blood flow to the brain, before there has been irreversible ischaemic damage. More recently, a series of randomised trials have been published which show that there is an additional benefit of mechanical thrombectomy in patients with large artery occlusion strokes.
The question now facing many healthcare systems around the world is how best to implement a service maximising the use of such techniques?
In common with many other situations, the translation of trial results into everyday clinical practice is not an easy one. Randomised clinical trials are performed in very defined and controlled circumstances. The trials investigating mechanical thrombectomy were done with specific case selection and procedures performed by teams of experienced neurointerventionalists. Replicating identification of relevant patient groups is relatively easy; it is however, much more problematic to get patients to a place where intervention can be undertaken, and to deliver the procedures in a timely fashion.
In the UK, patients can present to any acute hospital, be considered for thrombolysis, and transferred to the nearest Hyper Acute Stroke Unit (HASU). However, few of these units have a 24-hour interventional neuroradiology service.
To deliver mechanical thrombectomy in a robust fashion will require teams (including doctors able to make the diagnostic decisions and deliver the mechanical thrombectomy, radiographers, nurses, anaesthetic support, postoperative care, etc). These teams will need to be rapidly available both in, and out, of hours. It will also crucially need patients to be transferred to the places where such services are available. It would seem unlikely that a patient could be transferred into a HASU and then a further transfer to a centre with mechanical thrombectomy availability, within the time constraints. Therefore, such services will need to be available in sufficient numbers and locations to allow a consistent level of care across the population, with primary transfer to those centres.
At the moment, in the UK, there are very few centres able to deliver a 24/7 neurointerventional service. The options therefore would seem to be to either try to rapidly train a cohort of interventional neuroradiologists, or to identify a group who have sufficient transferrable skills, who can relatively quickly gain experience in mechanical thrombectomy, sufficient to provide a service with outcomes that deliver benefit to patients.
Training a large enough cohort of neuroradiologists would take a number of years, and would also require a considerable financial commitment to support such a scheme. In the present climate it seems difficult to believe that this would be forthcoming, particularly in the timeframe necessary to deliver a service within the next few years.
That means, we need to find others to support neuroradiologists. Are interventional radiologists the right group to support this initiative?
Interventional radiologists regularly perform procedures with similar technologies to those used for mechanical thrombectomy. They perform super selective catheterisation of many arteries (although notably, rarely the cerebral circulation) and use coaxial systems and microcatheters for a variety of elective and emergency procedures. As trained radiologists they also have the background skills that would translate into the interpretation of the imaging that underpins the selection of patients who may benefit from mechanical thrombectomy.
Thus it would seem that interventional radiologists are probably the group most suited to support neuroradiology in the delivery of mechanical thrombectomy.
However, this is not without practical difficulties. Many interventional radiology acute services are under pressure with an estimated shortfall of around 200 interventional radiologists in the UK. The concept of additional emergency workload is one that may not meet with enthusiasm or financial support (a funding stream to support mechanical thrombectomy for both neuroradiologists and interventional radiology seems unclear at present). Further, interventional radiologists will need to be given sufficient time and support to enhance their neuroradiology diagnostic skills, to refamiliarise themselves with the cerebral circulation, and learn the use of the mechanical thrombectomy devices. A mentoring process would seem to be suited to this. Even in such circumstances, it is uncertain if sufficient numbers of interventional radiologists (in suitable locations) would be willing to take on mechanical thrombectomy. This would also need appropriate governance arrangements to allow for their experience/training to be monitored, and to ensure that their outcomes would be sufficiently reliable to deliver the benefits shown in the mechanical thrombectomy trials.
There seems little doubt that mechanical thrombectomy has the potential to offer patients with stroke a significant improvement in prognosis. The practicalities of how best to achieve this remains unclear, but interventional radiologists have the potential to offer significant expertise. This will need efficient patient pathways, alongside a well-supported national strategy.
Trevor Cleveland is a consultant vascular radiologist, Sheffield Vascular Institute, Sheffield Teaching Hospitals, Sheffield, UK. He has reported no disclosures pertaining to this article
“Patient safety must come first, alongside the recognition of the essential role interventional radiology plays in the provision of modern medical care,” Raman Uberoi, consultant interventional radiologist and honorary senior lecturer, John Radcliffe Hospital, Oxford, UK, and current president of the British Society of Interventional Radiology (BSIR) tells Interventional News. Uberoi also outlines some of the challenges of providing a 24/7 interventional radiology service in the UK and calls for major investment in interventional radiology nationally to train and appoint more consultants and allied health staff.
What is current situation with 24/7 provision of interventional radiology services?
Every acute trust has a duty to ensure that there are formal arrangements to secure provision of elective and emergency interventional radiology services. Several surveys have shown that this is not occurring. In the most recent survey, around 2/3 hospitals had some form of cover either internally or networked for nephrostomy and endovascular interventions; just over half had cover for haemorrhage control; and less than half had cover arrangements for post-partum haemorrhage. This, of course, means there is huge post code lottery with some centres having excellent provision, while others have none, or minimal, cover arrangement.
What medical conditions does the 24/7 provision currently cover?
The major indications for treatment with interventional radiology is haemorrhage control ie trauma bleeding, gastrointestinal haemorrhage, post-partum haemorrhage, aortic dissections and ruptures (both thoracic and aortic) using stent grafts, sepsis control (ie nephrostomy, biliary drainage and abscess drainages), acute peripheral and visceral ischaemia due to arterial occlusions that require thrombolysis. Bowel obstruction is another area where interventional radiologists can improve patients’ overall condition using urgent colonic stenting prior to definitive surgery. Acute stroke treatment is another focus area where there is a desperate need for a national strategy with the development of acute thrombectomy centres. Interventional radiologists will be key members of the team potentially delivering this service (See Trevor Cleveland’s article on page 41.)
What are the goals of the BSIR in this regard?
We aim to put patient safety first, recognising the essential role of interventional radiology in the provision of modern medical care. We are working on recognising the resources and manpower required to provide a 24/7 interventional radiology service. It is of extreme importance to be clear and transparent regarding the local provision of interventional radiology services and decide what is, and what is not possible to provide, in and out of hours.
We aim to enter into discussions with healthcare authorities and other trusts in the region to make arrangements which ensure robust and coherent regional interventional radiology service provision 24 hours a day, seven days a week.
We would want there to be either a local on-call or networked on-call solution with a minimum of six consultant interventional radiologists on a 24/7 call rota with similar rotas for our allied health staff, ie, nurses and radiographers to provide safe and sustainable 24/7 emergency care.
What are some of the challenges with regard to providing 24/7 services?
The key factors in this regard are adequate infrastructure and support. There is a significant shortage of staff to run this service, particularly of consultants. As things stand, we are short of around 220 interventional radiology consultants, and see similar shortages of nursing and radiography staff. How can they be met? There needs to be a recognition that in the absence of provision of interventional radiology services, patients will be placed at risk. There needs to be an immediate-, medium- and long-term strategy to deal with this staffing shortfall. In all healthcare trusts, there should be an exploration of ways in which a comprehensive service may be offered by internal reorganisation, maintenance of core skills, additional funding/training/appointments, or external networking.
There should be clarity within the trust and among referring clinicians and service commissioners about what interventional radiology services are available and when they are available. If a service is not available at all, within or outside routine working hours, for example, embolization for acute haemorrhage, this should be known to the clinical governance authorities. Where there is an unmet clinical need, it is the responsibility of the clinical and medical director to have made all reasonable attempts to ensure these interventional radiology services are available to all patients 24/7 and discussions should take place about purchasing appropriate services from another trust. It should be clear which particular interventional radiology services are being purchased.
Clear pathways should also be in place for treating patients appropriately when the interventional radiology service is not available. The trust’s clinical governance process and relevant referring clinicians need to be aware of the situation. This will allow discussion about planned patient pathways when the service is not available, for example, default to surgical treatment, and also document an area of possible need for service development. When a service is not provided on a 24-hour basis, and if this usually results in patients being transferred to other trusts, this pattern of referral requires clarification with the clinical governance processes and agreement on the part of the receiving trust. There should be formal contractual arrangements for patient transfer, including appropriate clear protocols for patient transfer in a timely fashion, lines of clinical responsibility, patient repatriation and funding.
In the medium to long term there is a need for major investment in interventional radiology nationally to train and appoint more consultants and allied health staff.
There needs to be a significant increase in training numbers to increase interventional radiology consultants for the future. We need to ensure that there are good training opportunities for clinical interventional radiologists. Vascular procedures form the bedrock of training for all the key areas of emergency and urgent interventional radiology and training centres need to have access to a range of vascular and nonvascular procedures to learn the core skills that are required to carry out these important procedures.
What do you aim to achieve in your presidential term?
I want to ensure that we are training sufficient numbers of clinically focussed interventional radiologists. We need to increase training opportunities and the numbers of trainees to meet the current and future challenges of providing a high quality, safe and sustainable 24/7 interventional radiology service. This means not just having a strategy to increase training numbers, but having an appropriate curriculum which focusses on training clinicians who can assess and manage patients as well as have the knowledge and skills necessary to carry out complex procedures. I want to ensure that interventional radiologist have sufficient clinical time to provide a high quality, safe and sustainable service, which requires time for clinics, ward rounds, patient follow-up, audit, and research to demonstrate the huge benefit of interventional radiology.
I want to ensure that the value of having a good interventional radiology service is clearly recognised, both clinically and financially. This can only be achieved by having good effectiveness data and a sound financial platform for trusts to support our services with appropriate interventional radiology tariffs that cover the range of procedures we undertake.
Many suspect that medical tribalism is economically motivated and the most common answers from clinicians on why inter-speciality tension exists are “money” and “ego.” Rather, the primary driver of medical tribalism seems to be underappreciated value differences across specialities, write Eric J Keller and Robert L Vogelzang.
Uterine fibroid embolization was first described in 1995 and has been shown to be safe and effective with high patient satisfaction.1-4 Nevertheless, many interventional radiologists feel this less-invasive option is underutilised by gynaecologists despite extensive research and efforts to advertise the procedure. For example, we found that fibroid embolization referrals have remained constant at our institution over the last decade while the use of laparoscopic hysterectomy and myomectomy increased,5 and a recent study found that 38% of women who received a hysterectomy were not counselled on alternative treatments.6
However, these studies do not answer the critical question of why practice variation exists, only that it does. This is because “why” is more of a qualitative question than a quantitative one. As such, we embarked on a journey into the social sciences and found a well-validated technique called grounded theory that was initially designed in the 1960s to explore patients’ and providers’ perceptions of end-of-life care. We have now spent the last two years becoming budding medical anthropologists while using this method to answer long-standing questions such the one represented in this article’s title.
Many suspect that medical tribalism is economically motivated. In fact, the two most common answers we receive from clinicians for why inter-speciality tension exists are “money” and “ego.” Certainly these can exacerbate underlying tension, but we have found that tension persists across practice environments. Rather, the primary driver of medical tribalism seems to be underappreciated value differences across specialities.
When asked about their practices, interventional radiologists tend to define themselves by the procedures they offer. Patients are either candidates for procedures or not and treatments are valued primarily in terms of their non-invasiveness. Because of this, interventional radiologists tend to emphasise the high technical success rate of uterine fibroid embolization and shorter recovery times compared to hysterectomy. When a gynaecologist prioritises hysterectomy over embolization, this is viewed sceptically as subjecting patients to an unnecessarily invasive procedure, and since the interventional radiology professional identity is based on procedures, this choice not only implies that the gynaecologist devalues fibroid embolization but interventional radiology in general.
Gynaecologists however define themselves by their patient populations, eg, “I primarily treat women with fertility concerns.” As such, the value of treatments is primarily understood in terms of “definitiveness,” the ability to address the patient’s chief complaint(s) long-term. The choice of one procedure over another has little to do with gynaecologists’ professional identity, and as such, they tend not to perceive any tension. In fact, multiple gynaecologists have told us that studying medical tribalism may be fruitless because turf wars do not exist.
Where does this leave us? We are repetitively impressed by how distinct but underappreciated speciality value differences are in healthcare. Some may conclude that differences should be discouraged, but we disagree. As put by one interventional radiologist, “friction creates energy… We need people to think differently. We need people to challenge others”7. Practices where interventional radiologists and gynaecologists or cardiovascular radiologists and cardiologists collaborate more are not where there are less value differences but where clinicians are more aware and appreciative of such differences to better respond to them.
Thus, we have come to believe that better understanding speciality-specific values is critical for inter-specialty collaboration and better patient care. In regards to uterine fibroids, interventional radiologists could instead emphasise the definitiveness of uterine fibroid embolization and how it may address patients’ specific concerns. Gynaecologists could be more sensitive to the connotation communicated to interventional radiology if they continually choose hysterectomy or myomectomy over embolization. However, beyond this issue, we believe medical anthropology has much to offer the field of interventional radiology, helping interventional radiologists to grow shared territory with other specialists rather than competing for the same slice of the pie.
Eric J Keller is a medical student at Northwestern University, Chicago, USA. Robert L Vogelzang is the Albert Nemcek Education Professor of Radiology, Northwestern University, Chicago, USA. The authors have reported no disclosures pertaining to this article
References
1 Cain-Nielsen AH, Moriarty JP, Stewart EA, Borah BJ. Cost-effectiveness of uterine-preserving procedures for the treatment of uterine fibroid symptoms in the USA. Journal of Comparative Effectiveness Research. May 30 2014:1-12.
2 Gupta JK, Sinha A, Lumsden MA, Hickey M. Uterine artery embolization for symptomatic uterine fibroids. The Cochrane database of systematic reviews. 2012;5:CD005073.
3 Scheurig-Muenkler C, Koesters C, Powerski MJ, Grieser C, Froeling V, Kroencke TJ. Clinical long-term outcome after uterine artery embolization: sustained symptom control and improvement of quality of life. Journal of Vascular and Interventional Radiology Jun 2013;24(6):765-771.
4 Toor SS, Jaberi A, Macdonald DB, McInnes MD, Schweitzer ME, Rasuli P. Complication rates and effectiveness of uterine artery embolization in the treatment of symptomatic leiomyomas: a systematic review and meta-analysis. American Journal of Roentgenology. Nov 2012;199(5):1153-1163.
5 Keller E, Vogelzang R, Chrisman H. Fibroid treatment options: A ten year analysis of utilization and referral patterns. Society of Interventional Radiology Annual Scientific Meeting; 2015; Atlanta, USA.
6 Corona LE, Swenson CW, Sheetz KH, et al. Use of other treatments before hysterectomy for benign conditions in a statewide hospital collaborative. American Journal of Obstetrics and Gynecology. Mar 2015;212(3):304 e301-307.
7 Keller EJ, Vogelzang RL, Freed BH, Carr JC, Collins JD. Physicians’ professional identities: a roadmap to understanding “value” in cardiovascular imaging. Journal of Cardiovascular Magnetic Resonance 2016;18(1):52.
Spectranetics has announced that its Stellarex 0.014” drug-coated angioplasty balloon has received the CE mark. The device is designed to treat small vessels, below-the knee disease, and challenging critical limb ischemia in patients.
The combination of the currently available Stellarex 0.035”and the new 0.014” line available in Europe expands Spectranetics’ comprehensive portfolio of next generation drug-coated balloons to treat complex disease states across the lower extremities. “Now available on a 0.014” balloon platform, Stellarex represents a latest generation drug-coated balloon backed by compelling evidence in the femoropopliteal arteries. It holds strong promise to deliver safety and efficacy in the notoriously challenging infrapopliteal district,” said Dierk Scheinert of Universitätsklinikum in Leipzig, Germany.
Spectranetics president and chief executive officer Scott Drake states, “Spectranetics is committed to providing specialised and innovative tools and compelling clinical data to improve our patients’ quality of life. Stellarex 0.014” exemplifies these important elements and augments our existing product portfolio, which now includes clinically differentiated treatment for both above and below-the-knee disease. The Stellarex 0.014” drug-coated balloon is a significant advancement in our effort to eradicate restenosis and amputation.”
Cook Medical has completed enrolment in the first clinical study of an iliofemoral venous stent conducted in the USA under a US FDA-approved investigational device exemption.
The VIVO clinical study is a prospective, non-randomised, multicentre study intended to evaluate the safety and effectiveness of the Zilver Vena venous stent in the treatment of symptomatic iliofemoral venous outflow obstruction.
A total of 243 patients with acute or chronic symptomatic iliofemoral venous outflow obstruction were enrolled in the VIVO Clinical Study, which has a one-year primary endpoint. The study is being conducted in 29 active sites throughout the US as well as one in Taiwan.
A press release reports that Cook Medical recently completed a similar first-of-its-kind study in the European Union on the safety and performance of the Zilver Vena stent. Gerard O’Sullivan (Galway University Hospitals, Galway, Ireland) presented data from the VIVO-EU study at CIRSE 2016 and VEITHsymposium.
Anthony Comerota (Jobst Vascular Institute, Toledo, USA), one of the study’s principal investigators, comments: “I view the completion of enrolment for this trial as an important milestone in development of options for managing patients with proximal venous obstruction. I am excited to see the full enrollment of the first FDA-approved venous stent trial.”
This has the opportunity to help many patients,” agreed Lawrence “Rusty” Hofmann (Stanford University Hospital, Stanford, USA), co-principal investigator, agreed.
Terumo Europe has entered into a distribution agreement with New Zealand company Adept Medical to make the STARSystem available to clinicians working across Western Europe. A press release reports that the support for transradial angiography and revascularisation (STAR) system is a combination of the STARBoard and STARTable. It adds that STARBoard is a forearm and hand support that is designed to make performing transradial procedures quicker and easier.
According to the press release, the STARBoard is ergonomically designed with fully articulating arms and friction joints and aims to provide excellent patient comfort and ease of use for clinicians. STARSupport connects to the STARBoard, facilitating left arm procedures. Additionally, the STARTable provides a stable work surface and support for catheters, wires and other equipment as well as additional X-ray scatter reduction. The STARBoard vertical shield reduces X-ray scatter at neck height by 80%.
Peter Coenen, president of Terumo Interventional Systems EMEA, said he was delighted to be bringing the STARSystem to Europe and anticipated strong interest from clinicians. He comments: “Seeking partnerships of this kind in addition to investing in our own research and development means we continue to lead the field in transradial access solutions for interventional cardiology and peripheral intervention. By making the world’s best equipment available to our customers we help them to perform at their best, ultimately helping achieve the best outcomes for patients.”
The press release states that weighing 1kg, the STARBoard is extremely lightweight, compact and very easy to handle for cath lab staff. It also states that the unique, one-piece, “foldaway” design of the device takes up minimal storage space.
Adept Medical is New Zealand’s leading specialist plastics manufacturer to the medical market and a subsidiary and specialist medical business unit of the award winning design and manufacturing company Adept Limited.
Merit Medical Systems has received 510(k) clearance for the SwiftNinja steerable microcatheter, covering peripheral and coronary applications.
With the exception of Japan, Merit has global distribution rights for the SwiftNinja.
“For the past several months we have been marketing this unique product with great success in Europe,” said Fred P Lampropoulos, Merit’s chairman and chief executive officer. “Physician response relating to range, convenience and overall cost, when compared to the use of multiple devices, has validated our initial expectations.”
The SwiftNinja is scheduled to be launched simultaneously with the Corvocet biopsy system, which also recently received 510(k) clearance.
“We believe these two patented and transformative technologies will provide substantial momentum and enthusiasm amongst our sales force and customers as we prepare for 2017,” Lampropoulos said.
For the upcoming MIOLive symposium, we had the idea of introducing a special “ten commandments” session for ablation, chemoembolization, and radioembolization, to create a practical handbook for the interventional radiologist who approaches liver interventions, write Roberto Iezzi, Rome, Italy and Laura Crocetti, Pisa, Italy. They give Interventional News readers a preview of the first five commandments.
The second edition of Mediterranean Interventional Oncology Live (MIOLive 2017) symposium is to be held 30–31 January, Rome, Italy.
Discuss your case in a multidisciplinary tumour board
The indication for ablation of a liver lesion should come from a multidisciplinary tumour board discussion and should be clearly decided in a shared manner by an interventional radiologist, oncologist, hepatologist and liver surgeon. Multidisciplinary evaluation will take into consideration the specificities of the patient beyond liver tumour burden, such as comorbidities, compliance to treatment, general performance status, and history of the disease. These features are of growing importance considering that oncological patients often share a very long history of disease. In fact multiple therapies, including locoregional and systemic ones, should be applied and combined, always in line with the view that every patient really is unique.
Be up-to-date with the literature
You will likely encounter colleagues saying that what you are doing is not proven or that there is something else that works better. Know the current guidelines and results of high-impact studies—this will help you to support your work. Moreover, this will prevent you, especially at the beginning of your practice, from treating the wrong patients. These could include patients with disease that is too advanced, or those with histotypes of tumours that will not benefit from ablation. It is very important to have good results, not only for the patients, but to also support and spread ablation techniques.
A successful case is the best advertisement
Do not start liver ablation with a difficult case. If you are starting your ablation training or testing a new ablative technique, choose easy cases at first. If the first cases go wrong, it will be difficult to continue. If you are doubtful about selecting a case, ask for advice from more experienced colleagues. Companies are also willing to provide beginners with proctors so that you can adequately prepare in order to be successful.
Remember that you are part of a team
When performing an ablation you need to cooperate with the anaesthesiologist, the nurse and the technician. You need to confer with the anaesthesiologist and outline exactly what you need, ie., general anaesthesia or deep intravenous sedation, depending on whether you need the patient to be cooperative at the beginning of the procedure or to sleep through the duration. The technician and nurse should be trained by the physician and experienced colleagues to be ready to provide assistance in all the phases of the procedure.
Consider the possible complications
The knowledge of possible complications will help you to avoid them. Each ablative technique, especially thermal ablative techniques, can lead to complications. The rate of puncture-related complications can be reduced by checking the coagulation status of the patients and choosing the most appropriate path to safely reach the nodule. Thermal energy-related complications can be avoided in most cases by using adjunctive procedures (ie., hydrodissection) to protect the organs or structures at risk of damage by heating.
We have disclosed five of the 10 commandments for ablation—for the rest, we welcome you to Rome.
Roberto Iezzi is an interventional radiologist, Catholic University, Rome, Italy and Laura Crocetti is an interventional radiologist, University of Pisa, Pisa, Italy. MIOLive 2017 will focus on liver-directed therapy for hepatic malignancies. It will be a practical, interactive meeting based on live cases and short presentations and lectures, in which professionals from various countries from the Mediterranean area will have the opportunity to share experiences, research projects and valued mentoring from international experts
A preliminary analysis suggests that thermal ablation may be effective in selected patients with local small cell lung cancer without adjuvant therapy. The research from Brown University, Providence, USA was published in the Journal of Vascular and Interventional Radiology (JVIR).
Aaron WP Maxwell and colleagues, including Damian E Dupuy, from the The Warren Alpert Medical School of Brown University set out to evaluate outcomes in a small cohort of patients with local or disseminated small-cell lung cancer who received percutaneous thermal ablation.
About 12% of lung cancers diagnosed are small cell lung cancer and this type of cancer is usually caused by smoking. Small cell lung cancer often spreads early on and chemotherapy, rather than surgery might be recommended for it.
Percutaneous ablation has become an accepted treatment option for patients with non-small cell lung cancer and published literature has shown it to be both feasible and safe in nonsurgical candidates.
In this study, the investigators retrospectively evaluated 10 biopsy-proven small cell lung cancer tumours in nine consecutive patients. As reported in JVIR, the average tumour sizes were 1.8cm ± 0.5 in patients with local disease and 2.6cm ± 1.2 among patients with disseminated disease. The physicians treated five tumours with microwave ablation and five with radiofrequency. None of the patients received adjuvant therapy following thermal ablation. Median follow-up duration was 16 months (range, 2–48 months).
When Maxwell and colleagues compared median and one-year overall survival for patients in the local and disseminated disease groups, they found that both these measures were better among patients treated for local small cell lung cancer compared with disseminated disease. Further, they found that pneumothorax occurred in five patients (55.6%), and three patients received successful outpatient thoracostomy tube placement. No patients were hospitalised, and there were no major complications.
InspireMD has announced 12-month follow up data from PARADIGM-101 study of the CGuard Embolic Prevention System (EPS), which were presented at the Transcatheter Cardiovascular Therapeutics symposium (TCT 2016, 29 October–2 November, Washington, DC, USA).
Piotr Musialek, Jagiellonian University Department of Cardiac and Vascular Diseases, Krakow, Poland, reported 12-month follow up data from PARADIGM-101, an investigator-led clinical study evaluating the use of CGuard in 101 consecutive patients with carotid artery stenosis.
Key findings from the presentation included:
Zero device-related adverse events at 12 months
Device and procedure success were each 99.1%.
Vessel narrowing was reduced from 83±9% to only 6.7±5% (p < 0.001) by independent core lab analysis
Periprocedural death/major stroke/myocardial infarction was 0%.
One periprocedural event was adjudicated by the Clinical Events Committee as a minor stroke (0.9%), with no change in NIH Stroke Scale or modified Ranking scale and no clinical sequelae
At 12 months the device showed a normal healing profile, and the patency of the external carotid artery was normal
“These data further reinforce the strong safety and efficacy profiles reported in previous trials of the CGuard EPS, and validate the system as an important option for endovascular management of patients with carotid artery disease,” said Musialek.
“Importantly, the very low incidence of peri- or post-procedural complications and stroke create a positive risk-benefit profile for CGuard EPS in patients with asymptomatic carotid artery disease. These patients are frequently denied intervention due to fear of the complications associated with conventional intervention, and are left with a substantial risk of stroke when treated only with medication. Our study found that CGuard EPS is applicable in up to 90% of all-comer patients with carotid stenosis. These data indicate that CGuard EPS may fundamentally alter the paradigm for managing patients with carotid artery disease, whether they have symptoms or not,” he added.
CGuard EPS is CE marked and not approved for sale in the US by the Food and Drug Administration at this time.
Shockwave Medical has announced plans for DISRUPT PAD III—what it claims is the “largest ever” multicentre randomised study to exclusively enrol patients with calcified peripheral artery disease.
Previous DISRUPT PAD studies utilised Lithoplasty as primary therapy, demonstrating safe, effective and consistent revascularisation of calcified lesions while maintaining future treatment options. To date, the potential benefit of combination therapy in these patients has not yet been evaluated.
DISRUPT PAD III will study use of the Shockwave Medical Lithoplasty system in combination with drug-coated balloon therapy to assess short- and long-term outcomes compared to those achievable using traditional balloon angioplasty prior to drug-coated balloon in a calcified patient population.
“Most contemporary randomised studies in peripheral artery disease have excluded calcified lesions. The available data on this difficult-to-treat patient cohort largely comes from post-hoc, subset analyses of single-arm registries. DISRUPT PAD III will be an important study because it will provide physicians foundational Level I evidence to guide treatment of this difficult-to-treat patient cohort,” said William Gray, principal investigator of DISRUPT PAD III and system chief, Division of Cardiovascular Disease at Main Line Health and president, Lankenau Heart Institute, Wynnewood, USA. “Today, there is no clear standard of care for interventional treatment of calcified peripheral artery disease.”
“Modifying calcium is the first step in any successful treatment of this patient cohort,” said Daniel Hawkins, chief executive officer of Shockwave Medical. Lithoplasty technology has been shown to effectively and consistently modify calcium, enabling successful revascularisation of these patients while keeping subsequent treatment options open. With the multiple treatment approaches being used in peripheral artery disease intervention today, and the absence of a consistent standard, understanding the benefits of using Lithoplasty in combination with other therapies is important to advancing the data on the treatment of calcified peripheral artery disease.”
In September, the Lithoplasty system received clearance from the US Food and Drug Administration (FDA) for use in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, infra-popliteal, and renal arteries.
Six-month follow up data from the DISRUPT PAD Study, presented last month at the VIVA 16 Conference, demonstrated that Lithoplasty is safe and the results are consistent and effective in the treatment of patients with calcified lesions. The 95-patient single-arm study evaluated Lithoplasty as a stand-alone, primary therapy.
DISRUPT PAD III will compare the safety and effectiveness of Lithoplasty followed by drug-coated balloon versus drug-coated balloon with standard pre-dilatation for the treatment of moderately and severely calcified femoropopliteal arteries. The study will enrol up to 300 patients at 45 global centres in the USA, Europe and New Zealand. The IN.PACT Admiral drug-coated balloon will be used in both treatment arms. Drug-coated balloons have historically been shown to be effective in non-calcified lesions, but results are far less favourable as calcification levels of increase. The DISRUPT PAD III study is designed to assess the impact of Lithoplasty on outcomes of drug-coated balloon use in calcified lesions. The primary endpoint of the study will be acute procedural success absent the need for stents and the secondary endpoint will be primary patency at 12 months.
“We are very pleased with positive, consistent DISRUPT PAD data and the durability of outcomes out to six months thus far,” said Todd Brinton, clinical associate professor of Medicine at Stanford and co-founder of Shockwave Medical. “The data to date demonstrates that Lithoplasty is a viable primary therapy for revascularisation of calcified peripheral artery disease. However, the combination of peripheral Lithoplasty to treat calcification and reduce the need for stents, in conjunction with a drug-coated balloon to reduce long-term restenosis may be a highly attractive therapeutic option for patients with calcified peripheral artery disease.”
DISRUPT PAD III will begin enrolment in early 2017.
The US Food and Drug Administration (FDA) has granted staged approval for Intact Vascular’s investigational device exemption (IDE) application to begin its TOBA II BTK (Tack optimised balloon angioplasty II below the knee) clinical study. The study will examine the safety and efficacy of the Tack endovascular system when used to repair dissections in the arteries below the knee following percutaneous transluminal angioplasty as a treatment for critical limb ischaemia.
Patrick J Geraghty, professor of Surgery and Radiology at the Washington University School of Medicine of St Louis, USA, and George Adams, director of Cardiovascular and Peripheral Vascular Research, UNC REX Hospital, Raleigh, USA, are national principal investigators for the study.
The TOBA II BTK study is designed to enrol 232 subjects at up to a total of 50 US and international sites. Patients experiencing symptoms from advanced peripheral artery disease below the knee will be eligible. Study subjects will be treated with the Tack endovascular system following standard balloon angioplasty in the popliteal or tibial arteries when a dissection occurs.
Bruce J Shook, president and chief executive officer at Intact Vascular, stated, “The TOBA II BTK clinical study represents an exciting opportunity to bring the first vascular implant to the US market for the treatment of critical limb ischaemia patients. We are thrilled with the level of enthusiasm from the clinical community and look forward to collaborating with them on this important advancement for critical limb ischaemia care.”
In July 2016, 12-month results from the TOBA study, which examined use of the Tack implant to treat dissections above the knee, were published in the Journal of Vascular Surgery. The 12-month results from the TOBA BTK pilot study were also released at the Society for Cardiac Angiography and Interventions (SCAI) 2016 annual meeting (4–7 May, Orlando, USA). Both of these studies demonstrated the potential of the Tack implant to improve arterial healing following angioplasty above and below the knee.
Geraghty stated, “Critical limb ischaemia is a debilitating condition for many patients with serious downstream consequences such as amputation and loss of independence. The disease is growing rapidly, especially with the increasing incidence of diabetes, creating an urgent need for more effective treatments. The TOBA II BTK study represents an exciting opportunity to improve the long-term results associated with angioplasty, which is our primary, minimally invasive treatment for critical limb ischaemia. This study is the first pivotal trial ever conducted in the USA supporting the FDA approval of an implantable device for critical limb ischaemia treatment.”
Adams added, “We are very enthusiastic about the commencement of the TOBA II BTK clinical study. The Tack endovascular system is uniquely tailored for use in arteries below the knee. These arteries are small in diameter, so the minimal metal burden associated with the Tack implant and the implant’s ability to adapt to the diameter of the artery are both ideal for dissection repair in this part of the leg.”
St Jude Medical has announced that, based on the preliminary voting results from St Jude Medical’s Annual Meeting of Shareholders held on 26 October, St Jude Medical shareholders approved the merger agreement under which Abbott will acquire St Jude Medical.
Based on preliminary vote results, approximately 99% of voting St Jude Medical shareholders cast their vote in favour of the merger, representing approximately 74% of St Jude Medical’s outstanding stock as of the record date. The final vote results, including the other proposals’ results, will be available on a Form 8-K that St Jude Medical plans to file with the Securities and Exchange Commission later this week.
Michael T Rousseau, St Jude Medical president and chief executive officer, commented, “Today our shareholders voted overwhelmingly in favour of the merger with Abbott. This acquisition brings together two industry leaders with a shared passion for patients, innovation, and culture. The combined organisation will create one of the world’s premier medical device companies and will provide customers a broad portfolio of products across cardiovascular diseases, chronic pain and movement disorders.”
The companies continue to expect the transaction to close by the end of the year, subject to regulatory approvals and satisfaction of customary closing conditions.
Cancer pain matters and it is likely to matter even more in the coming years. Treatment advances have increased life expectancy for cancer patients, leaving them exposed to pain for longer, whereas pain management strategies have remained virtually unchanged for years, writes Bruno Damascelli, Milan, Italy.
In 2014, the American Cancer Society forecast that annual deaths due to cancer of the pancreas, liver, bile ducts, stomach, bowel, uterine cervix, bladder and prostate would total 176,000. A portion of these patients will develop visceral and neuropathic pain, of which 20% will become refractory to opiates and to all their possible combinations with steroids, non-steroidal anti-inflammatory drugs and neuroleptics. Between 5% and 7% of patients with intractable pain experience a severe deterioration in their quality of life, leading to a negative impact on social and family life and an increased burden on health services.
In recent years invasive pain management (neurolysis) has been introduced. These procedures are managed mainly by anaesthetists, gastroenterologists and neurosurgeons and aim to interrupt conduction of visceral and neuropathic pain signals from the structures affected by cancer to the higher nerve centres. As imaging methods have evolved, interventional radiologists have become involved and have begun to perform coeliac and upper hypogastric plexus blocks and neurolysis independently. The chemical and physical agents used are ethanol, phenol, heat (radiofrequency) and cold (cryoablation), which are difficult to apply and can give rise to significant complications. Up to 30ml of ethanol may be needed for coeliac plexus or coeliac ganglion block. It is unthinkable for such a large volume to remain confined to a small anatomical area after percutaneous infiltration.
Ablation of the nerve fibres that run in the artery wall became a reality a few years ago with the introduction of endovascular renal artery denervation for resistant hypertension. When applying this technique with the EnligHTN system (St Jude) we noticed that when the procedure was repeated in non-responders, it was not accompanied by the usual intense pain. It therefore seemed possible to apply the same method to other vascular districts such as the coeliac artery and the hypogastric arteries to obtain the same result as percutaneous neurolytic procedures based on infiltration of ethanol or phenol or application of radiofrequency.
The same electrodes and ultrasound probes already certified for renal artery denervation are used for ablation of the sympathetic nerve fibres that run in the walls of the coeliac and hypogastric arteries. Neurolysis occurs when the heat generated by ultrasound or radiofrequency is applied to the endothelium. The artery wall reaches a temperature of 70°C, which leads to degeneration of the nerve fibres. Introduction of the instruments is to all intents an angiographic percutaneous arterial catheterization procedure that can be performed under local anaesthesia via the femoral artery. At present the only exclusion criterion is anatomical inaccessibility. The reproducibility and safety profile using either radiofrequency or ultrasound are comparable to those reported for renal sympathetic denervation.
We have treated more than 20 patients with intractable cancer pain with radiofrequency to an average of 10 sites along the endoluminal surface following transfemoral catheterisation. The analgesic effect of this procedure has been assessed on a Visual Analog Scale (VAS) and mean score recorded for each patient during follow-up.
To date, in patients undergoing endovascular coeliac or hypogastric denervation for palliation of refractory abdominal cancer pain, the procedure has proved effective in durably reducing pain, particularly end-of-dose or breakthrough pain, and also in cutting down opiate consumption. We were particularly struck by a message from an anaesthetist whose father underwent endovascular coeliac neurolysis for pancreatic cancer pain, who said: “It is a month since you performed the procedure and, although my father is not doing well from a general point of view, he is doing well as far as pain is concerned and has almost stopped taking opiates”.
Bruno Damascelli is with the Department of Interventional Oncology, GVM Emocentrocuore Columbus, Milan, Italy. He has reported no disclosures pertaining to this article
Medtronic has received US FDA 510(k) clearance for the HawkOne directional atherectomy system in a new size for treating patients with peripheral artery disease. The HawkOne system is designed to remove plaque from the vessel wall and restore blood flow. The new HawkOne 6F provides an effective and easy-to-use treatment option for patients with peripheral artery disease both above and below the knee with a single device at a lower profile.
“Considering the complex disease pattern seen in below-the-knee peripheral artery disease, traditional treatment options such as placement of permanent stents or treatment with a balloon, may not be ideal for achieving long-term results. Directional atherectomy, on the other hand, is an established intervention that not only restores patency but also maximises luminal gain while keeping future treatment options open,” said Brian DeRubertis, associate professor of surgery at the David Geffen School of Medicine at UCLA. “The new, smaller HawkOne 6F device further adds to the versatility of this directional atherectomy system and enables us to treat a larger set of patients with more complex lesions, including patients with challenging calcified lesions.”
The HawkOne 6F size is an advanced option to treat patients with multilevel peripheral artery disease both above and below the knee, addressing lesions of various length, morphology, and location.
Key benefits of the system include:
Treating calcified lesions: The HawkOne system enables physicians to treat severe calcified lesions more efficiently with no increase in cut depth. The system can treat calcified lesions up to two times more effectively than the TurboHawk device.
Ease of use: The HawkOne system has a preloaded flush tool, which improves cleaning time by up to 55% when compared to the TurboHawk high efficiency cutter. The 6F size is also designed to simplify device selection and provide easy set-up with no capital equipment.
Irreversible electroporation to treat prostate cancer
A new study presented at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE 2016, 10–14 September, Barcelona, Spain) meeting finds that the treatment of prostate cancer with irreversible electroporation is efficacious and safe.
Michael K Stehling, professor of Radiology, Prostate Center, Institut für bildgebende Diagnostik, Offenbach am Main, Germany, and colleagues reported an impotence rate of 15% and zero incontinence observed in the study.
“Irreversible electroporation is suitable for prostate cancer recurrences after any previous treatment. MRI is a powerful tool for diagnosis and follow-up, but should be combined with 3D biopsy for optimal treatment planning. Irreversible electroporation has the potential to become the new standard of care in the treatment of prostate cancer,” Stehling told the CIRSE audience.
As reported by the authors, “Irreversible electroporation is a novel tissue ablation modality which selectively destroys cells whilst preserving non-cellular tissue. It has low toxicity on critical anatomical structures and may thus be an ideal therapy for prostate cancer, since it has the potential to avoid side effects of surgical/radiation treatment of prostate cancer such as impotence, incontinence and rectal damage.”
The investigators treated 300 patients with T1–T4 and recurrent prostate cancer with irreversible electroporation in the last five years. All treatments were based on multiparametric magnetic resonance imaging, while in 136 patients, additional transperineal 3D biopsy was performed.
Patients were treated under general anaesthesia and deep muscle relaxation. The physicians placed the probes by means of transrectal ultrasound guidance. All patients had follow-up MRI 24 hours post-treatment and further follow-up by MRI and prostate-specific antigen testing at three, six and 12 months, and then annually.
“The initial ablation of cancerous tissue was successful in all patients. We report recurrent disease in 5% of all cases during follow-up. No life-threatening and four medically significant adverse events occurred. Potency was transiently reduced in 15.2% and persistently reduced in 8.4% of surveyed patients. Continence was preserved in all cases,” Stehling reported.
In December 2015, in a Radiological Society of North America (RSNA) press release on treating prostate cancer with irreversible electroporation, Stehling commented: “Treating prostate cancer with minimal pain and minimal risk of impotence and incontinence, even in patients with advanced and recurrent cancer, with a one-time, one-day treatment, until recently, was unthinkable. The cutting edge technology of irreversible electroporation makes this a reality.”
Most people have heard about personalised medicine. How about personalised medical devices? Northwestern’s McCormick School of Engineering researchers Guillermo Ameer and Cheng Sun have teamed up to use 3D printing to develop flexible, biodegradable stents that are customisable to suit a specific patient’s anatomy.
“Right now, the vast majority of stents are made from a metal and have off-the-shelf availability in various sizes,” said Ameer, professor of biomedical engineering in Northwestern’s McCormick School of Engineering and professor of surgery in the Feinberg School of Medicine, Chicago, USA. “The physician has to guess which stent size is a good fit to keep the blood vessel open. But we are all different and results are highly dependent on physician experience, so that is not an optimal solution.”
Supported by the American Heart Association, their research is published online in the journal Advanced Materials Technologies. Robert van Lith, a postdoctoral fellow in Ameer’s laboratory, and Evan Baker, a graduate student in Sun’s laboratory, are co-first authors of the paper.
When ill-fitting stents move in the artery, they can ultimately fail. In these cases, physicians have to somehow re-open the blocked stent or bypass it with a vascular graft. It is a costly and risky process.
“There are cases where a physician tries to stent a patient’s blood vessel, and the fit is not good,” Ameer said. “There might be geometric constraints in the patient’s vessel, such as a significant curvature that can disturb blood flow, causing traditional stents to fail. This is especially a problem for patients who have conditions that prevent the use of blood thinners, which are commonly given to patients who have stents. By printing a stent that has the exact geometric and biologic requirements of the patient’s blood vessel, we expect to minimise the probability of these complications.”
To create these customised stents, Ameer worked with Sun to adapt a 3D printing technique, called projection micro-stereo-lithography, to fabricate stents using a polymer previously developed in Ameer’s lab. The technique uses a liquid photocurable resin or polymer to print objects with light. When a pattern of light is shined on the polymer, it converts it into a solid that is then slowly displaced to cure the next layer of liquid polymer. The printing technology allows the team to fabricate a stent that precisely matches desirable design characteristics.
Although current stents are made with metal wire mesh, Ameer used a citric-acid based polymer previously developed in his lab. The resulting stent is flexible, biodegradable, and has inherent antioxidant properties. Drugs can also be loaded onto the polymer and slowly released at the implantation site to improve the healing process in the blood vessel wall. Ameer has previously shown that the polymer can be engineered to inhibit clot formation when applied to vascular grafts. The stent is strong and biodegradable, allowing it to exercise its mechanical function during the vessel’s initial dilation and slowly dissolve as the re-opened blood vessel recovers.
“In theory, it’s safer because the patient doesn’t have permanent foreign metal devices in the body,” Ameer said. “If, for any reason in the future, the surgeon needs to go back in to that location in the vessel, they can. There is not a metal stent in the way.”
Current biodegradable stents are made from plastics similar to those used for sutures. They are not as strong as wire mesh and can take longer than metal stents to fully expand when deployed. To compensate for this weakness, the plastic stents are strengthened by increasing the thickness of their struts relative to that of a metal stent. Ameer’s 3D printed stent, however, can be fabricated with the thinner profile of traditional metal wire stents, so it is more compatible with the body.
Ameer and Sun, associate professor of mechanical engineering, imagine a future process whereby the dimensions of a patient’s vessel are obtained using standard imaging techniques available at hospitals, and a stent is then printed on site to exactly fit the vessel’s dimensions, packaged, and given to the surgeon for implantation. Next, Ameer plans to investigate how long it takes for the biodegradable stent to break down and absorb into the body. His team also aims to investigate innovative stent designs to improve their long-term performance.
Abbott and St Jude Medical have announced an agreement in principle to sell certain products to Terumo Corporation.The agreement is an important step toward completion of Abbott’s acquisition of St Jude Medical. Abbott’s acquisition of St Jude Medical is expected to close by year-end.
The transaction reflects a purchase price of approximately US$1.12 billion and is subject to the successful completion of Abbott’s acquisition of St Jude Medical and antitrust regulatory approvals. Abbott, St Jude Medical and Terumo are bound by the terms of an exclusivity agreement.
The divestiture is an all-cash transaction and will include the products globally for St Jude Medical’s AngioSeal and Femoseal vascular closure products and Abbott’s VadoSteerable Sheath. Abbott will retain its vascular closure products, which include the Perclose ProGlide suture-mediated closure system, StarClose SE vascular closure system and Prostar XL percutaneous Vascular Surgical System.
Abbott expects to mitigate any impact to its adjusted earnings per share projections related to the sale of these assets to Terumo.
Liver cancer researchers from France and Singapore collaborate on a prospective meta-analysis of two studies of Y-90 resin microspheres vs. sorafenib in patients with unresectable hepatocellular carcinoma.
Researchers from Assistance Publique – Hôpitaux de Paris (AP-HP) and The Asia-Pacific Hepatocellular Carcinoma Trials Group (AHCC), National Cancer Centre Singapore (NCCS) and Singapore Clinical Research Institute (SCRI) announced that they will collaborate on a prospective meta-analysis that will combine the impending results of two large, randomised controlled studies of Y-90 resin microspheres vs. sorafenib. The two studies, which have completed patient recruitment, enrolled approximately 800 patients with advanced primary liver cancer.
The French HCC study, called SARAH, sponsored by AP-HP with the financial support of the company Sirtex, and the Singapore HCC study, called SIRveNIB (AHCC protocol 06), which also received financial support from Sirtex, use similar research designs to compare the efficacy, safety profiles and quality of life of selective internal radiation therapy (SIRT) with liver-directed Y-90 resin microspheres and sorafenib, a systemic chemotherapy treatment that is the current standard of care in advanced hepatocellular carcinoma. Hepatocellular carcinoma patients enrolled in SARAH and SIRveNIB were ineligible for potentially curative therapies, such as surgical resection, ablation or liver transplantation and had either failed or were unsuitable for treatment with transarterial chemoembolization.
Pierce Chow, principal investigator of the SIRveNIB study, and senior consultant surgeon at the National Cancer Centre Singapore and the Singapore General Hospital, explained: “As we stated when we first announced completion of enrolment in SIRveNIB, the search for more effective and better tolerated treatments of hepatocellular carcinoma is important because so few proven treatment options currently exist. Our study enrolled more than 360 patients from 27 specialist centres in 10 Asia-Pacific countries. While our data will be reported independently, the opportunity to combine these data in a prospective meta-analysis with the results of the French SARAH study presents a compelling scientific undertaking across a much larger patient population that will significantly increase the data available for various pre-planned statistical analyses, including overall survival. This should provide physicians who treat hepatocellular carcinoma with even greater certainty of the applicability of our results in the treatment of this increasingly common and deadly cancer.”
Valérie Vilgrain, principal investigator of the SARAH study, head of Department of Radiology, Beaujon Hospital AP-HP, and professor at the Université Paris Diderot, Sorbonne Paris Cité, France, said: “The SARAH study was conducted in more than 25 specialist centres throughout France and is expected to report results in the first half of 2017. While we will also report the results of SARAH independently, we believe a prospective meta-analysis of our findings combined with those of the SIRveNIB study may be very compelling. Hepatocellular carcinoma in France and most of Europe is found in patients whose livers have become cirrhotic primarily from the Hepatitis C virus and alcohol misuse, while the majority of hepatocellular carcinoma cases in Asia are triggered initially by the Hepatitis B virus. Thus, our prospective meta-analysis will provide safety and efficacy data on patients who presented with a full range of the major hepatocellular carcinoma aetiologies, potentially increasing the clinical applicability of the study results.”
Results of the prospective meta-analysis are expected to be available in 2017. In the interim, further details regarding the methodological and statistical approach to the meta-analysis are to be published in a peer-reviewed journal.
BTG and Mirada Medical announced CE mark certification for the Simplicit90Y dosimetry software, designed to optimise the planning of Y-90 selective internal radiation therapy and facilitate personalised treatment for patients with liver cancer. CE mark certification follows approval for Simplicit90Y in Canada.
BTG, in collaboration with Mirada Medical, have developed Simplicit90Y to be a customised, easy-to-use, dosimetry software developed for rapid Y-90 selective internal radiation therapy workflow. Simplicit90Y provides digital processing, review and reporting of medical images with unique options for data display, quality control, image manipulation and quantification analysis. Together, these features allow for more standardised and consistent dosimetry planning and post-treatment validation, and the ability to personalise treatment for each patient.
“Dosimetry can be a time intensive and complex process and Simplicit90Y simplifies both dosimetry planning and post-treatment validation,” said Etienne Garin, chair and professor of Nuclear Medicine, Cancer Institute, Centre Eugene Marquis Rennes, France. “Knowing you can use this intuitive software to help deliver a more personalised treatment for each patient, achieving the best dose of Y-90 radiation to the tumour while minimising exposure to healthy tissue, gives physicians more confidence.”
Highlights: -Vertebroplasty trumps placebo in treatment of painful spinal fractures -Two-year randomised data a shot in the arm for stent graft use in arteriovenous access treatment -Jeff Geschwind: Tumour treatments -David Breen: Fusion confusion -Profile: Gregory Slater
Coils and plugs are among the most commonly employed tools for vessel sacrifice and aneurysmal occlusion. In practice, these tools must be catered to each individual patient as each case will bring unique challenges to the operator, say Rahul S Patel and Richard Tapnio, New York, USA.
With so many products on the market for use in transcatheter vascular embolization, the plethora of tools and techniques can create unnecessary stress and confusion for the interventionalist. Before starting any case, the interventional radiologist has to be familiar with the particular armament of tools at his or her disposal. We have outlined a few general tips and tricks to be considered.
Using the proper catheter
Before planning any embolization, it is important to choose your delivery platform to ensure the appropriate catheters and embolic materials are available in your inventory before the procedure. Fortunately, the large number of coils and plugs available allow for flexibility regardless of the type of catheter or microcatheter system being used for the case. Each type of microcoil has its own catheter size requirements, and checking to make sure that you have a compatible coil-catheter system preprocedure will avoid any unnecessary headaches during the procedure. When using vascular plugs, remember that Microvascular Plugs (MVP, Medtronic) are tailored for use in 0.021” to 0.027” microcatheter systems depending on size, while Amplatzer Vascular Plugs (AVP, St Jude Medical [under purchase by Abbott]) can be used within a 0.038” system for the AVP 4 or within a 5–9 French guide catheter for the AVP and AVP II depending on plug size.
Packing density
An important measure to keep in mind for embolizing aneurysms with microcoils is achieving sufficient packing density. The packing density of an aneurysm refers to the fraction of aneurysmal volume occupied by a deployed microcoil. While aneurysmal volume can be estimated using the ellipsoid volume equation (4π/3×L/2×W/2×H/2) and coil volume is estimated as (π×(D/2)2×L×10), packing density is simply defined as the number of coils, multiplied by coil volume over aneurysm volume. Online tools, such as AngioCalc (www.angiocalc.com), can facilitate these calculations. A packing density of less than 24% is associated with higher rates of coil compaction and recanalisation. In addition to coil size, it is important to keep coil softness in mind to prevent catheter kickout. Finally, while fibred microcoils do not add significant volume to packing density, hydrogel from coated hydrocoils (Terumo) expands within the aneurysm sac, resulting in increased filling of the aneurysm.
Cost-effectiveness
Given increasing scrutiny on procedural costs in both inpatient and outpatient settings, choosing the appropriate embolic agent can help to significantly reduce overall expenses. Estimated costs will depend on target size and indication for coil embolization, whether it be for aneurysm filling or vessel sacrifice. In addition, significant cost variability between microcoil systems can result in cost differences of several thousands of dollars for even small aneurysms. Check your inventory price list, and keep in mind that the cost of using a single vascular plug for vessel occlusion may be comparable to or even less than deployment of multiple microcoils.
Length is as important as width for plugs
If a vessel occlusion is planned with vascular plugs, remember that some of the devices will lengthen depending on how much the plug is oversized for the target vessel—in an inverse proportion to the diameter of the vessel. This factor is particularly important when embolizing a vessel with a short trunk length, such as the gastroduodenal artery. While plug elongation is only minimal (up to 2.2mm for an 8mm AVP 4 plug), this small difference may be critical in tight spaces. Finally, each of the vascular plugs has a unique occlusive zone. For example, while the AVP 4’s tapered bilobed shape results in a smaller central occlusive zone allowing for easier navigation, the AVP II has multiple large points of contact with the vessel wall, making the device more suitable for high-flow vessels.
Device sizing is specific to each coil and plug
Oversizing is an important concept in vascular embolization that helps ensure the plug or coil remains seated in the desired location without kickback. However, there is large variation in manufacturer-recommended device sizing among plugs and coils, from zero oversizing with Ruby (Penumbra) and Azur CX (Terumo) coils, to 10–20% oversizing with Interlock (Boston Scientific) and Concerto (Medtronic) coils, and 30–50% oversizing with AVP vascular plugs. Be sure to read each product’s brochure before deciding on which device size to employ in your case.
These five points should be reviewed before starting any vascular embolization case with plugs or coils. By becoming comfortable with a variety of devices and keeping these points in mind – you will minimise any unneeded stress while keeping costs to a minimum.
Rahul S Patel is an assistant professor, Radiology and Surgery, Mount Sinai, New York, USA. Richard Tapnio is a resident at Mount Sinai Beth Israel, New York, USA. The authors have reported no disclosures pertaining to this article.
NEAT (Novel endovascular access trial) data presented at the Vascular Interventional Advances (VIVA) 2016 meeting (18–22 September, Las Vegas, USA) suggest that endovascular arteriovenous fistula creation using everlinQ technology (TVA Medical) is associated with almost six-fold fewer post-creation interventions and may be approximately US$11,000 cheaper than surgical fistula creation.
Over the past two decades, there has been more than a 150% increase in dialysis treatment worldwide. Currently, 20-60% of traditional surgically created fistulae are not suitable for dialysis and require an average of two to three interventions to facilitate and/or maintain use, explained Charmaine Lok, University of Toronto, Toronto, Canada. Mean maturation time ranges from four to nine months and occlusions (thrombosis) rates have been reported as high as 17–25%, while the cost of the first year of arteriovenous fistulae intervention ranges from US$15–20,000. This, Lok said, represents a “significant unmet need, and there needs to be another option for fistula creation and maintenance”.
At the 2015 VIVA meeting, Lok presented the endovascular everlinQ system as a potential alternative to traditional fistula creation. The system uses an arterial and a venous catheter, aligned using magnets, with the fistula created by a radiofrequency electrode.
The 12-month prospective, non-randomised multicentre study—NEAT—enrolled 60 patients in Canada, Australia and New Zealand to evaluate the safety and efficacy of everlinQ to create arteriovenous fistulae with a primary efficacy endpoint of three-month fistulae maturation (defined as the proportion free of stenosis or thrombosis with a brachial artery blood flow ≥500mL/min and vein diameter ≥4mm). Patency and post-creation intervention rates were also included as additional study endpoints.
Lok and colleagues also used a cohort of Medicare patients treated with traditional surgical arteriovenous fistulae creation to see how their post creation intervention rates and costs compared with everlinQ endovascular creation. Propensity score matching was used to create the surgical comparator, and balance was achieved with no significant differences between the two groups for all baseline patient characteristics.
By three-month follow-up, over 90% of endovascular fistulae were physiologically mature. Technical success was 98%, procedure/device-related severe adverse event was <10% and the mean blood flow was >900mL/mm. The intervention rate by patient year was almost six times higher for traditional, surgically created fistulae compared with endovascular fistulae. This difference in intervention rates was reflected in associated costs, with endovascular treatment found to be approximately US$11,000 cheaper than traditional surgical fistulae creation—approximately US$1,800 Vs. US$13,000.
“NEAT demonstrates that the everlinQ technology is a promising technology for facilitating arteriovenous fistulae creation for both pre-dialysis and dialysis chronic kidney disease patients,” Lok told the VIVA audience.
Timothy P Murphy, MD
Diagnostic Imaging
Rhode Island Hospital
2012
Timothy P Murphy
Timothy P Murphy, Vascular Disease Research Center, Rhode Island Hospital, Providence, USA, and one of the investigators on the CORAL study, told delegates at CIRSE 2016 in Barcelona, Spain, that a low urine albumin:creatinine ratio could be used to help identify a large group of patients with renal artery stenosis who might benefit from stenting.
“These patients might experience improved event-free and overall survival after renal artery stent placement plus optimal medical therapy compared with optimal medical therapy alone,” he said.
“Randomised clinical trials that have used various clinical endpoints have not shown an additional clinical benefit for renal artery stent placement over optimal medical therapy alone. We sought to examine the effect of baseline albuminuria on clinical outcomes after renal artery stent placement,” Murphy explained.
The CORAL (Cardiovascular outcomes in renal atherosclerotic lesions) study was a multicentre, open-label, randomised, controlled trial that compared medical therapy alone with medical therapy plus renal-artery stenting in patients with atherosclerotic renal-artery stenosis and elevated blood pressure, chronic kidney disease, or both.
The study randomised 947 patients with ≥60% renal artery stenosis to receive medical therapy only or medical therapy plus stenting. Enrolled patients, whose average age was 69 years, had renal artery stenosis and either systolic blood pressure of 150mmHg or higher while taking two or more drugs or stage three (moderate) chronic kidney disease. The primary endpoint was a composite of major cardiovascular or renal events (death from renal or cardiovascular causes, stroke, myocardial infarction, hospitalisation for heart failure, progressive renal insufficiency, and permanent renal replacement therapy).
In 2014, results from the study, published in the New England Journal of Medicine, showed that stenting of the renal artery appears to offer no significant improvement when added to medication-based therapy.
The investigators stratified the CORAL study population (n=826) based on the median baseline urine albumin/creatinine ratio and analysed for the five-year incidence of the primary composite endpoint (myocardial infarction, hospitalisation for congestive heart failure, stroke, renal replacement therapy, progressive renal insufficiency, or cardiovascular- or kidney disease-related death) and overall survival. They compared longitudinal systolic blood pressure between the treatment groups.
Murphy and colleagues found that when baseline urine albumin/creatinine ratio was less than, or equal to, the median value (22.5mg/g), renal artery stenting was associated with a significantly better event-free survival with respect to the primary composite endpoint (73% vs. 59% at five years, p=0.02), cardiovascular disease-related death (93% vs. 85%, p=<0.01), progressive renal insufficiency (91% vs. 77%, p=0.03), and overall survival (89% vs. 76%, p=<0.01). They also reported that there was no benefit with stenting when baseline urine albumin/creatinine ratio was greater than the median value.
The investigators further found no significant difference in longitudinal systolic blood pressure based on the treatment group for baseline urine albumin/creatinine greater than 22.5mg/g, but borderline significance favouring stent treatment was observed when the ratio was less than 22.5mg/g (p=0.052).
“These data raise the question about whether millions of people with atherosclerotic renal artery stenosis could benefit from renal artery stent placement,” Murphy told Interventional News.
New European Society of Medical Oncology (ESMO) biliary cancer guidelines indicate yttrium-90 (Y-90) therapy as an option for post-chemotherapy treatment of intrahepatic cholangiocarcinoma.
Sirtex has announced that ESMO has indicated the use of radioembolization, also called selective internal radiation therapy, using Y-90 microspheres, as an option in for the treatment of intrahepatic cholangiocarcinoma.
Sirtex is conducting a randomised controlled study in the setting of first-line treatment for intrahepatic cholangiocarcinoma. The SIRCCA (SIRT in cholangiocarcinoma) study is examining the role of Sir-spheres Y-90 resin microspheres followed by the standard-of-care first-line chemotherapy in Cholangiocarcinoma, compared to chemotherapy alone.
The new ESMO guidelines on biliary cancers were published in September 2016 as a supplement to the Annals of Oncology. The lead author of the publication, Juan Valle, department of medical oncology, Christie NHS Foundation Trust, University of Manchester, UK, states that selective internal radiation therapy “may be considered in patients with inoperable intrahepatic cholangiocarcinoma, usually after first-line chemotherapy.”
The ESMO inclusion of selective internal radiation therapy for the treatment of intrahepatic cholangiocarcinoma was based on ESMO’s review of a pooled analysis of 12 studies totalling 298 patients that was published in the European Journal of Surgical Oncology in 2015, by D P Al-Adra of the University of Edmonton, Canada and others. These data showed a median overall survival of 15.5 months and treatment response rate of 28% in patients treated with selective internal radiation therapy.
In addition, the new ESMO guidelines on biliary cancers call special attention to a subset of studies in the pooled analysis, stating that “importantly, 7/73 (10%) patients in three selected studies were converted to resectable disease, highlighting the importance of reassessment of patients in the multidisciplinary team in the event of a good response to any treatment.”
David Cade, chief medical officer of Sirtex, said that “We are delighted to see Sir-spheres Y-90 resin microspheres cited in the new ESMO guidelines as an important post-chemotherapy option for patients with locally advanced or metastatic intrahepatic cholangiocarcinoma, given no current standard of care exists beyond first-line treatment with cisplatin and gemcitabine chemotherapy in these patients. We believe that these are the first international clinical guidelines to indicate selective internal radiation therapy as a treatment option for patients with intrahepatic cholangiocarcinoma.”
Most intrahepatic cholangiocarcinoma patients are diagnosed relatively late in the course of their disease, and therefore are not immediately eligible for potentially curative surgical resection. The fact that even a small proportion of these patients may become surgically resectable after chemotherapy suggests that selective internal radiation therapy may offer real hope for them, a press release from Sirtex states.
SIRCCA is being conducted in some 30 centres in Australia and several European countries, including Belgium, France, Germany, Italy, Spain, The Netherlands and UK.
Teleflex has announced that it has received US FDA 510(k) clearance to market its Arrow JACC with Chlorag+ard technology and TightTrack tunneler.
Arrow JACC with Chlorag+ard technology is a long-term, tunneled, small french size antithrombogenic and antimicrobial central venous catheter designed to meet the needs of patients throughout their course of therapy or illness.
The catheter is also designed for use with high-pressure injection for diagnostic studies. The Arrow JACC with Chlorag+ard technology protects against catheter occlusion, phlebitis, and intimal hyperplasia for up to 30 days. The Arrow JACC with Chlorag+ard technology will enable caregivers to effectively and economically preserve vessel access, and care for millions of end stage renal disease patients.
“At Teleflex, we are committed to providing the right line for the right patient at the right time,” said Jay White, president of the Vascular Division. “We are proud to add the tunneled Arrow JACC to our line of vascular access products. By providing an antithromogenic and antimicrobial catheter that protects against catheter occlusion, we are offering a technology that no one else can. This is especially important in patients with end stage renal disease where vessel health and preservation is essential to provide a future dialysis vascular access.”
Bio2 Medical has announced that the Angel catheter, a new device for the prevention of pulmonary embolism, was placed in two patients at St Mary’s Medical Center in West Palm Beach, USA, by Lawrence Lottenberg and Robert Borrego on 29 September. This is the first commercial usage of the device.
The Angel catheter received 510(k) clearance from the US FDA as the first ever, prophylactic indication for a medical device to protect critically ill patients at high-risk for pulmonary embolism and contraindicated for anticoagulation.
The first patient was at high risk for pulmonary embolism due to traumatic brain injury post craniotomy. The second patient had prolonged immobilisation due to a cervical spinal cord injury and quadriplegia. Both patients were contraindicated to prophylactic anticoagulation for 7–10 days. The Angel catheter was placed at the bedside in the trauma intensive care unit, without the need for fluoroscopic guidance, allowing Lottenberg and Borrego to provide their patients with immediate pulmonary embolism prophylaxis.
Lottenberg stated: “The Angel catheter provides an unmet need for a prophylactic indication for the prevention of pulmonary emboli. Unlike traditional filters, the Angel catheter cannot migrate from its deployment position, and it is easily inserted and easily removable for patients who cannot be prophylactically anticoagulated during the immediate and early phases of injury. There are none of the complications seen in the many currently available inferior vena cava filters. This makes the device unique and one of a kind. The recognition of the value of this technology to patient safety and patient care by the Tenet Healthcare System and St Mary’s Hospital in bringing this technology to our level one trauma cannot be overstated.”
Borrego provided the following statement: “The placement of the Angel catheter at the bedside is a safe and efficient way to protect patients at high risk for pulmonary embolism, who cannot be anticoagulated for seven to ten days therefore protecting them from additional morbidity/mortality due to pulmonary embolism in high risk patients.”
Intended use of the Angel catheter
•The Angel catheter is intended to provide the combined functions of an inferior vena cava filter and a multilumen central venous catheter.
•The Angel catheter is intended for short-term use for the prevention of clinically significant pulmonary embolism in critically ill patients at high risk for pulmonary embolism or recurrent pulmonary embolism, and recognised contraindications to standard pharmacological thromboprophylaxis therapy.
•The Angel catheter is also intended to provide access to the central venous system.











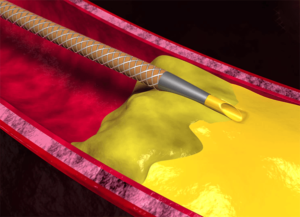




 The US
The US 




 Cerus Endovascular receives FDA approval for its first microcatheter. The 021 microcatheter will be offered with three different distal configurations, and commercial sales are expected to begin during the second quarter of 2020.
Cerus Endovascular receives FDA approval for its first microcatheter. The 021 microcatheter will be offered with three different distal configurations, and commercial sales are expected to begin during the second quarter of 2020.












 clearance")










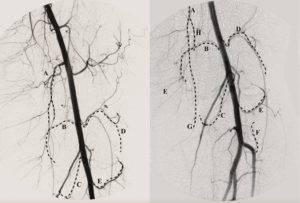






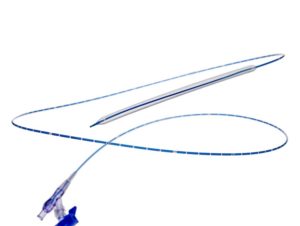







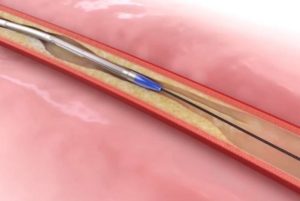

 Stratus Medical, a new company created to focus on advancing radiofrequency (RF) ablation treatment for chronic pain, has announced that it completed a private placement to acquire the assets of NimbusRF from Biomerics and provide growth capital funding to support the continued global expansion of the Nimbus RF Multitined Expandable Electrode for chronic pain. The investment was led by Med Venture Holdings.
Stratus Medical, a new company created to focus on advancing radiofrequency (RF) ablation treatment for chronic pain, has announced that it completed a private placement to acquire the assets of NimbusRF from Biomerics and provide growth capital funding to support the continued global expansion of the Nimbus RF Multitined Expandable Electrode for chronic pain. The investment was led by Med Venture Holdings.



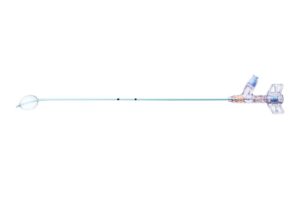














 Addressing the audience at the
Addressing the audience at the 





























 Several reports emerged last year concerning issues with MRI safety.
Several reports emerged last year concerning issues with MRI safety.



























 The first UK clinical trial site for the treatment of diabetic patients with chronic limb-threatening ischemia (CLI) using a novel patient-specific regenerative therapy has opened for patient recruitment at the University Hospital of Wales in Cardiff, UK. The site will be evaluating
The first UK clinical trial site for the treatment of diabetic patients with chronic limb-threatening ischemia (CLI) using a novel patient-specific regenerative therapy has opened for patient recruitment at the University Hospital of Wales in Cardiff, UK. The site will be evaluating 



 Philips has announced a major clinical trial to assess the impact of a direct-to-angiosuite workflow on stroke patient outcomes. The study will assess whether with Philips’ advanced image-guided therapy platform it is possible to diagnose, plan and treat stroke patients in the interventional suite without requiring an initial CT or MRI exam. The multicentre, prospective, randomised, controlled, open-label, blinded-endpoint trial will be run across eight sites and over 460 patients globally. It will begin in the first half of next year and is expected to be completed in 2022.
Philips has announced a major clinical trial to assess the impact of a direct-to-angiosuite workflow on stroke patient outcomes. The study will assess whether with Philips’ advanced image-guided therapy platform it is possible to diagnose, plan and treat stroke patients in the interventional suite without requiring an initial CT or MRI exam. The multicentre, prospective, randomised, controlled, open-label, blinded-endpoint trial will be run across eight sites and over 460 patients globally. It will begin in the first half of next year and is expected to be completed in 2022.










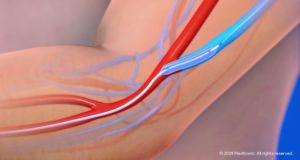













 Establishing the first Interventional Radiology department in Argentina, Ricardo García-Mónaco is a pioneer of minimally invasive, image-guided therapies in South America. Looking back on a career that spans more than three decades, he discusses how establishing interventional radiology (IR) as a clinical discipline rather than a technical one is crucial for the field’s survival and success, and recalls a particularly memorable case where IR intervention in a two-day-old baby saved the patient from amputation and enabled her to go on to become the healthy, active teenager she is today.
Establishing the first Interventional Radiology department in Argentina, Ricardo García-Mónaco is a pioneer of minimally invasive, image-guided therapies in South America. Looking back on a career that spans more than three decades, he discusses how establishing interventional radiology (IR) as a clinical discipline rather than a technical one is crucial for the field’s survival and success, and recalls a particularly memorable case where IR intervention in a two-day-old baby saved the patient from amputation and enabled her to go on to become the healthy, active teenager she is today.


 Since founding the
Since founding the 





























 The first patient has been enrolled in the
The first patient has been enrolled in the 





















 The National Institute for Health and Care Excellence (NICE) has published the final appraisal determination (FAD) recommending the use of
The National Institute for Health and Care Excellence (NICE) has published the final appraisal determination (FAD) recommending the use of 










 Luminor 18 and Luminor 35 drug-coated balloons (DCB; iVascular) are now listed on the French LPPR list for de novo lesions of the femoropopliteal arteries.
Luminor 18 and Luminor 35 drug-coated balloons (DCB; iVascular) are now listed on the French LPPR list for de novo lesions of the femoropopliteal arteries.

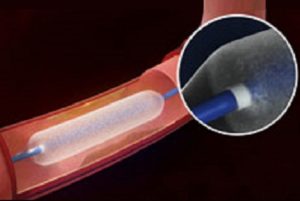
























 Following the publication of
Following the publication of 















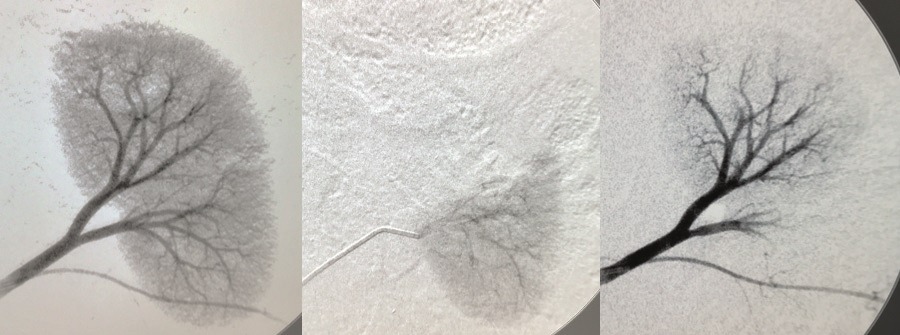

 Medtronic has announced the first-ever results from the IN.PACT AV access clinical study comparing the investigational IN.PACT AV drug-coated balloon (DCB) to percutaneous transluminal angioplasty (PTA) in patients with de novo or non-stented restenotic arteriovenous (AV) fistulae lesions. The study met primary safety and effectiveness endpoints and data were presented today at the
Medtronic has announced the first-ever results from the IN.PACT AV access clinical study comparing the investigational IN.PACT AV drug-coated balloon (DCB) to percutaneous transluminal angioplasty (PTA) in patients with de novo or non-stented restenotic arteriovenous (AV) fistulae lesions. The study met primary safety and effectiveness endpoints and data were presented today at the 




 Foundation trainees’
Foundation trainees’ 









 SIR 2020 is expected to attract more than 5,000 attendees from around the globe to Seattle, a city known for germinating new technologies and bold scientific thinking. Researchers who are accepted will have the opportunity to grow the field of image-guided interventions by sharing their discoveries, device and procedure innovations, clinical outcomes, and breaking research in areas that address many of today’s most challenging medical problems, including cancer, vascular disease, and men’s and women’s health.
SIR 2020 is expected to attract more than 5,000 attendees from around the globe to Seattle, a city known for germinating new technologies and bold scientific thinking. Researchers who are accepted will have the opportunity to grow the field of image-guided interventions by sharing their discoveries, device and procedure innovations, clinical outcomes, and breaking research in areas that address many of today’s most challenging medical problems, including cancer, vascular disease, and men’s and women’s health. About the Society of Interventional Radiology
About the Society of Interventional Radiology










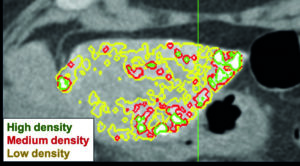







 Boston Scientific has announced the completion of its acquisition of BTG, pursuant to the
Boston Scientific has announced the completion of its acquisition of BTG, pursuant to the 



























 Ablation costs are significantly less than those of transarterial chemoembolization (TACE) and Yttrium-90 (Y-90), according to a comparative cost analysis of the three procedures at a tertiary care centre. These results were presented at the
Ablation costs are significantly less than those of transarterial chemoembolization (TACE) and Yttrium-90 (Y-90), according to a comparative cost analysis of the three procedures at a tertiary care centre. These results were presented at the 















 When new rules capped training hours for medical residents at 80 hours per week in 2003, critics worried that the change would leave physicians-in-training unprepared for the challenges of independent practice. New research, published today in the British Medical Journal (BMJ) and led by scientists in the Department of Health Care Policy in the Blavatnik Institute at Harvard Medical School, shows that these warnings were largely unjustified.
When new rules capped training hours for medical residents at 80 hours per week in 2003, critics worried that the change would leave physicians-in-training unprepared for the challenges of independent practice. New research, published today in the British Medical Journal (BMJ) and led by scientists in the Department of Health Care Policy in the Blavatnik Institute at Harvard Medical School, shows that these warnings were largely unjustified.













 “Deep in my heart, I knew interventional radiology (IR) had a tremendous future,” Alex Tang tells Interventional News. Looking back at his career, Tang talks of setting up IR services in his native Malaysia, and, as the convenor of the
“Deep in my heart, I knew interventional radiology (IR) had a tremendous future,” Alex Tang tells Interventional News. Looking back at his career, Tang talks of setting up IR services in his native Malaysia, and, as the convenor of the 








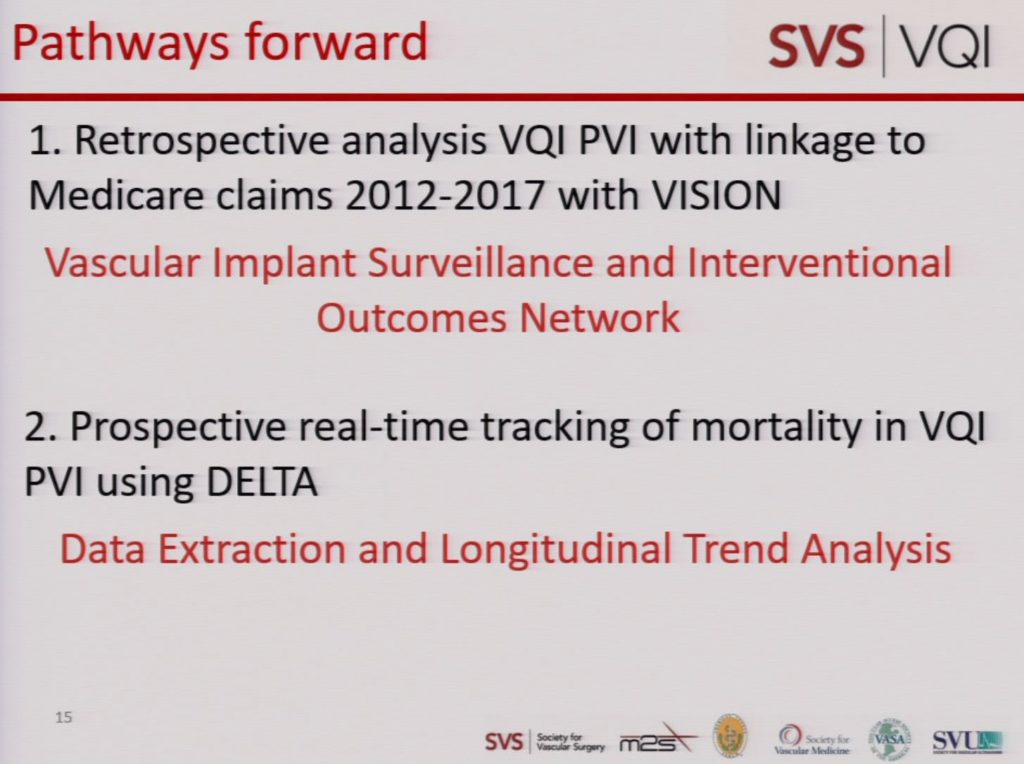






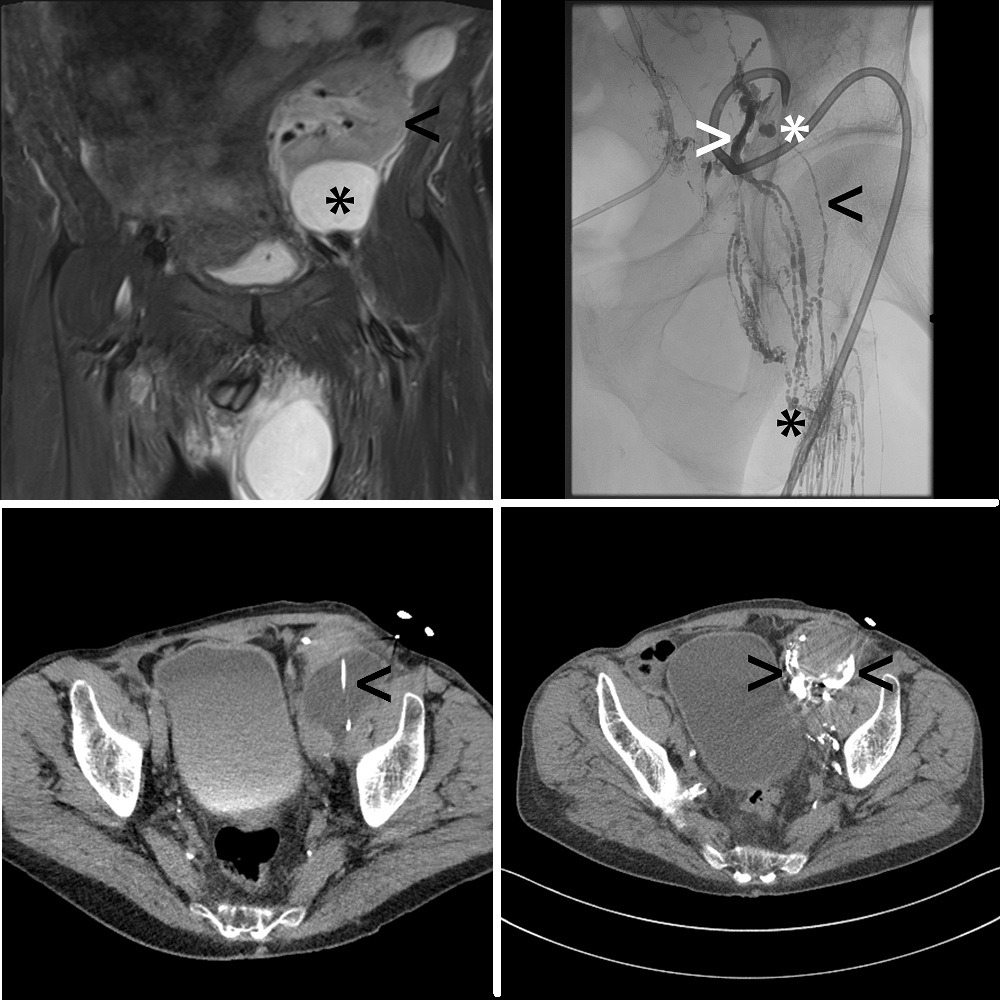
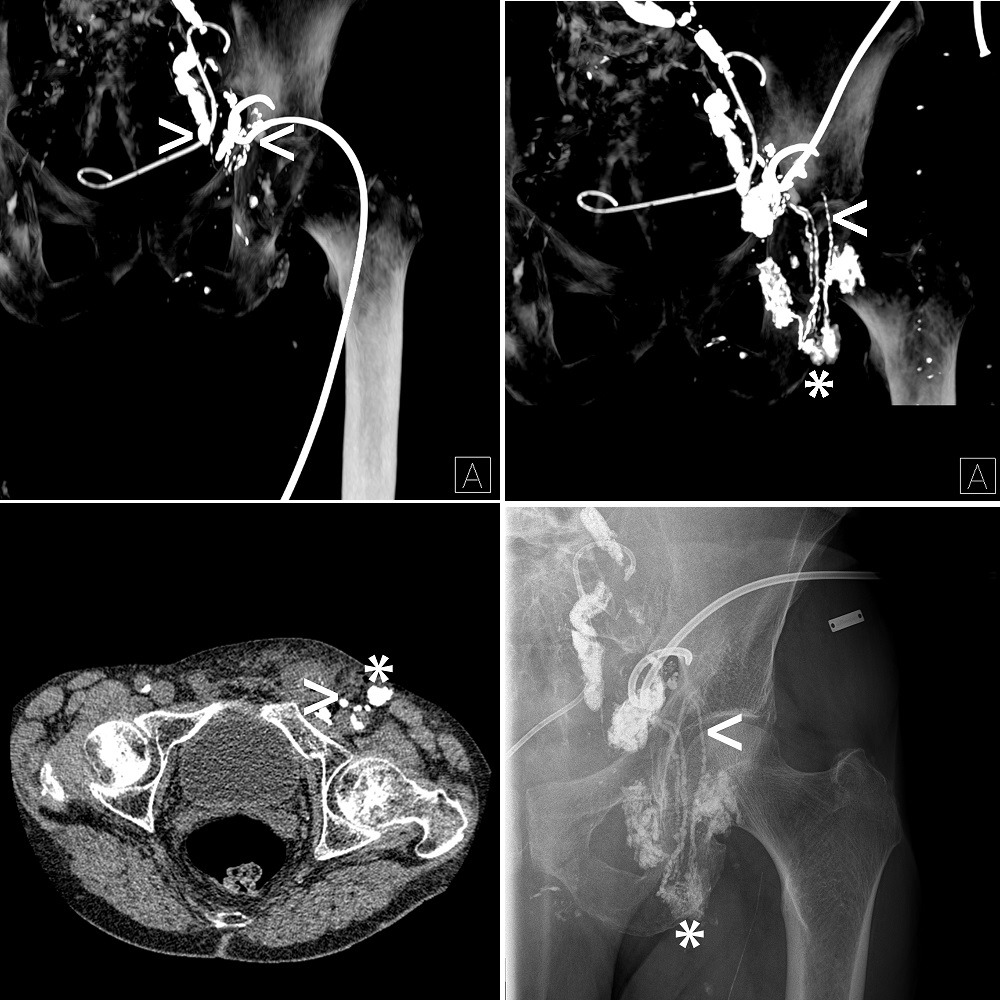




 Orchestra BioMed and
Orchestra BioMed and 

 Post-procedural antibiotic use does not significantly affect infectious complication rates following uterine fibroid embolization (UFE), a recent pilot study concludes. Presenting these data at the Global Embolization Oncology Symposium Technologies (
Post-procedural antibiotic use does not significantly affect infectious complication rates following uterine fibroid embolization (UFE), a recent pilot study concludes. Presenting these data at the Global Embolization Oncology Symposium Technologies (
 The US Food and Drug Administration (FDA) has approved expanded sizes of the
The US Food and Drug Administration (FDA) has approved expanded sizes of the 
 A recent publication confirms “the utility of touchless image navigation in the sterile field in facilitating decision-making and resource allocation during endovascular procedures.” The study, published in Minimally Invasive Therapy & Allied Technologies, provides the third clinical review of TIPSO technology (NZ Technologies), a human-computer interaction based platform that allows real-time access to imaging data in the sterile field.
A recent publication confirms “the utility of touchless image navigation in the sterile field in facilitating decision-making and resource allocation during endovascular procedures.” The study, published in Minimally Invasive Therapy & Allied Technologies, provides the third clinical review of TIPSO technology (NZ Technologies), a human-computer interaction based platform that allows real-time access to imaging data in the sterile field.

 The
The 













 ControlRad has announced that the US Food and Drug Administration (FDA) has granted 510(k) clearance for its ControlRad Trace. The company has initiated its commercial launch. The ControlRad Trace is the only technology that can be integrated into existing mobile C-arms to reduce radiation in any fluoroscopic imaging procedure.
ControlRad has announced that the US Food and Drug Administration (FDA) has granted 510(k) clearance for its ControlRad Trace. The company has initiated its commercial launch. The ControlRad Trace is the only technology that can be integrated into existing mobile C-arms to reduce radiation in any fluoroscopic imaging procedure.


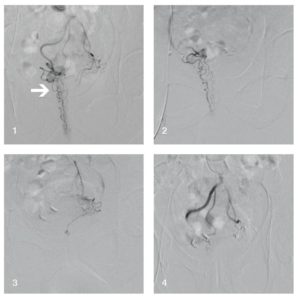

















 iFR is an innovative pressure-derived index proprietary to Philips, allowing a simplified hyperaemia-free physiological assessment of coronary blockages. It continues to be adopted into clinical practice, states a Philips’ press release, with mounting evidence that this technology contributes to reducing costs, improving outcomes and enhancing the patient experience.
iFR is an innovative pressure-derived index proprietary to Philips, allowing a simplified hyperaemia-free physiological assessment of coronary blockages. It continues to be adopted into clinical practice, states a Philips’ press release, with mounting evidence that this technology contributes to reducing costs, improving outcomes and enhancing the patient experience.



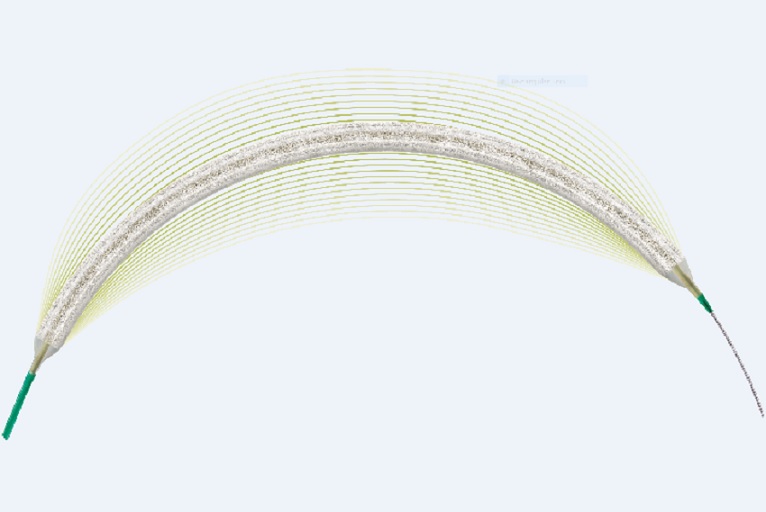






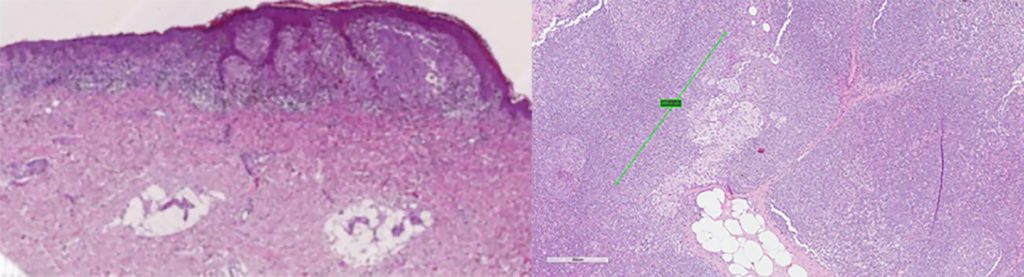

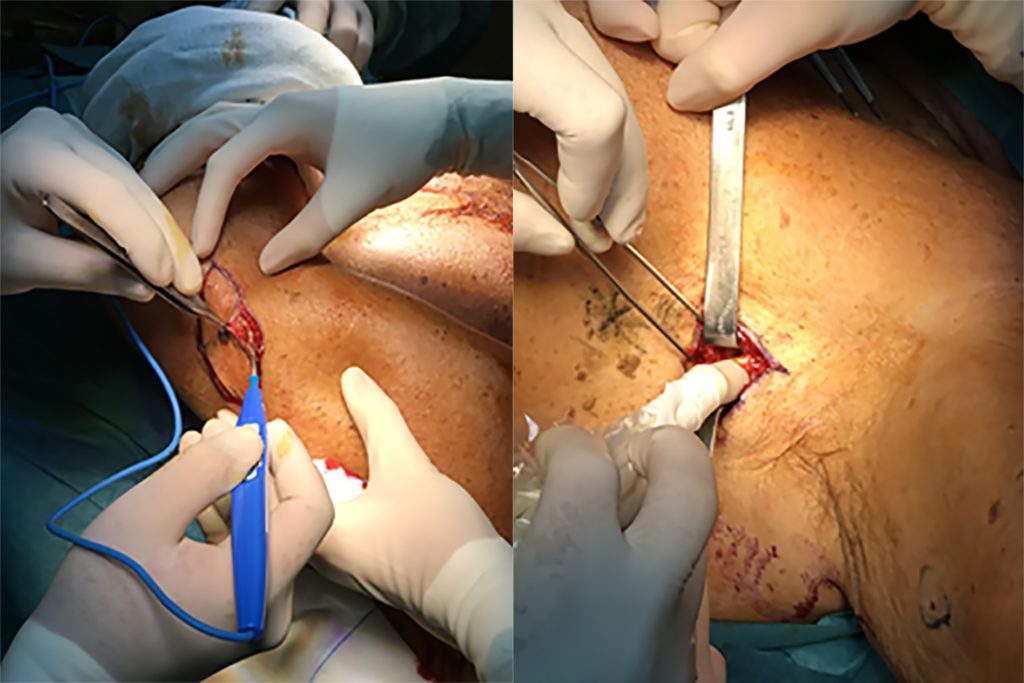


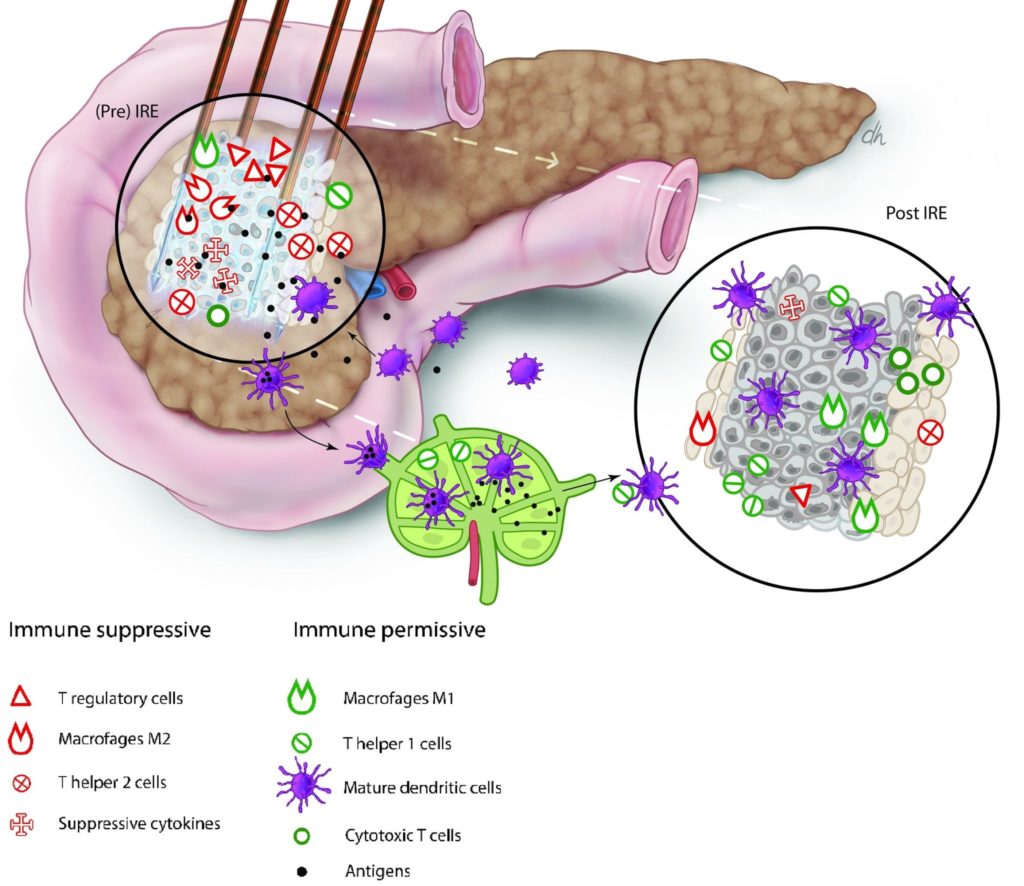








































")















 After coming across interventional radiology in a “fortunate accident”, the 2019–2020
After coming across interventional radiology in a “fortunate accident”, the 2019–2020 
 Appropriately trained interventional radiologists performing endovascular thrombectomy in technically complicated stroke cases achieve similar reperfusion and clinical outcomes to those reported in the published literature. This is the conclusion of Andrew Hines, an interventional radiologist at Northeast Charlotte Radiology, Charlotte, USA, presenting his data at the annual meeting of the Society of Interventional Radiology (
Appropriately trained interventional radiologists performing endovascular thrombectomy in technically complicated stroke cases achieve similar reperfusion and clinical outcomes to those reported in the published literature. This is the conclusion of Andrew Hines, an interventional radiologist at Northeast Charlotte Radiology, Charlotte, USA, presenting his data at the annual meeting of the Society of Interventional Radiology (










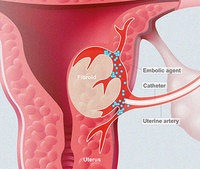




 clearance to software suite for molecular imaging and molecular radiotherapy dosimetry")
 The US Food and Drug Administration (FDA) has granted 510(k) clearance to the company DOSIsoft to market its Planet Onco Dose software, for its oncology and
The US Food and Drug Administration (FDA) has granted 510(k) clearance to the company DOSIsoft to market its Planet Onco Dose software, for its oncology and 





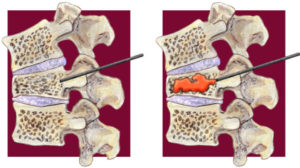







































 clearance of WavelinQ 4F endoAVF system")






































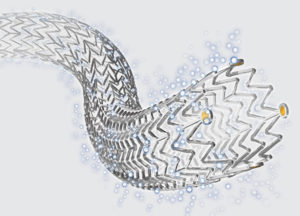





 The impact of the
The impact of the 














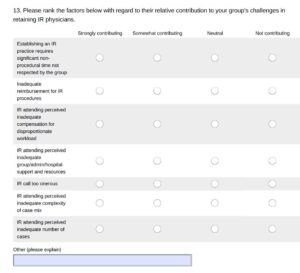


 Dr Rosemary Byanyima is one of the most senior radiologists in Kampala, and was one of the first local radiologists to understand this problem and push for change. Thanks to Dr Byanyima and her team, we were able to organise the first assessment visit to understand how things work in the Mulago National Referral Hospital (MNRH). This is the largest public hospital in the country, with 1,500 beds. In 2014, an average of 80–100 babies were delivered daily, in the hospital’s three maternity wards. The Uganda Heart Institute and the Women’s Hospital are also nearby, and in combination with the Uganda Cancer Institute represent the spearhead of Uganda’s health-care system.
Dr Rosemary Byanyima is one of the most senior radiologists in Kampala, and was one of the first local radiologists to understand this problem and push for change. Thanks to Dr Byanyima and her team, we were able to organise the first assessment visit to understand how things work in the Mulago National Referral Hospital (MNRH). This is the largest public hospital in the country, with 1,500 beds. In 2014, an average of 80–100 babies were delivered daily, in the hospital’s three maternity wards. The Uganda Heart Institute and the Women’s Hospital are also nearby, and in combination with the Uganda Cancer Institute represent the spearhead of Uganda’s health-care system.




 The Tack Optimised Balloon Angioplasty II below-the-knee (
The Tack Optimised Balloon Angioplasty II below-the-knee (
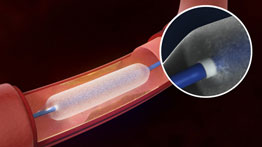 The FDA has granted approval for BD’s 0.018-inch guidewire-compatible Lutonix 018 drug-coated balloon (DCB) for the treatment of long superficial femoral artery lesions in patients with peripheral artery disease.
The FDA has granted approval for BD’s 0.018-inch guidewire-compatible Lutonix 018 drug-coated balloon (DCB) for the treatment of long superficial femoral artery lesions in patients with peripheral artery disease.

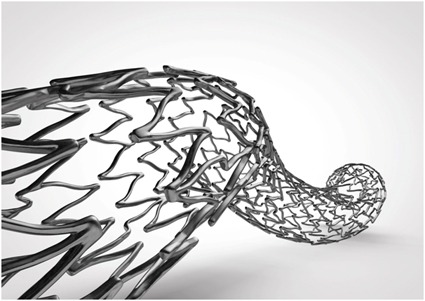





 The European Society of Radiology (ESR) and GE Healthcare are partnering on artificial intelligence for the upcoming
The European Society of Radiology (ESR) and GE Healthcare are partnering on artificial intelligence for the upcoming 







 Figure. The recommendations in the ESVS guidelines are based on the European Society of Cardiology (ESC) grading system.
Figure. The recommendations in the ESVS guidelines are based on the European Society of Cardiology (ESC) grading system.

 clearance for Vanguard IEP system")











 clearance programme")









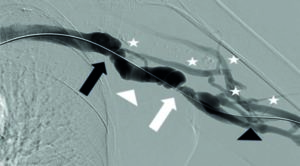
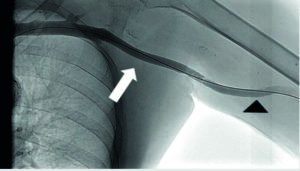




 President of the Interventional Radiology Society of Australasia (IRSA) and European Board of Interventional Radiology (EBIR) examiner for Australia and New Zealand, Gerard Goh emphasises the expanding transnational Interventional Radiology landscape, with “greater international collaboration” between major societies. Here, he speaks to Interventional News about how he knew he had found his calling in the “demanding yet rewarding” discipline of interventional radiology, the need to balance innovation with evidence-based clinical research, and how his passion for fast cars led to a stint as a Formula 1 doctor.
President of the Interventional Radiology Society of Australasia (IRSA) and European Board of Interventional Radiology (EBIR) examiner for Australia and New Zealand, Gerard Goh emphasises the expanding transnational Interventional Radiology landscape, with “greater international collaboration” between major societies. Here, he speaks to Interventional News about how he knew he had found his calling in the “demanding yet rewarding” discipline of interventional radiology, the need to balance innovation with evidence-based clinical research, and how his passion for fast cars led to a stint as a Formula 1 doctor.





























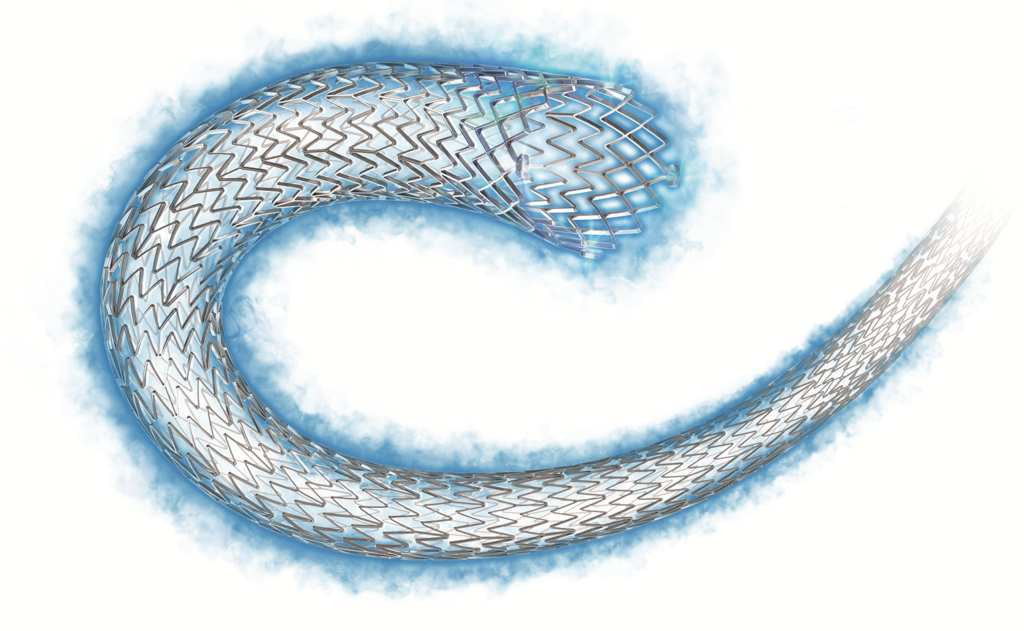


 In a joint, global position statement, the Society of Interventional Radiology (SIR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE) and the Interventional Radiology Society of Australasia (IRSA) have committed to providing necessary stroke training to interventional radiologists in order to alleviate the shortage of physicians trained in endovascular stroke therapies.
In a joint, global position statement, the Society of Interventional Radiology (SIR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE) and the Interventional Radiology Society of Australasia (IRSA) have committed to providing necessary stroke training to interventional radiologists in order to alleviate the shortage of physicians trained in endovascular stroke therapies.



 The US Food and Drug Administration (FDA) has approved Valiant Navion thoracic stent graft system (Medtronic) for the minimally invasive repair of all lesions of the descending thoracic aorta, including thoracic aortic aneurysms, blunt thoracic aortic injuries, penetrating atherosclerotic ulcers, intramural haematomas, and aortic type B dissections.
The US Food and Drug Administration (FDA) has approved Valiant Navion thoracic stent graft system (Medtronic) for the minimally invasive repair of all lesions of the descending thoracic aorta, including thoracic aortic aneurysms, blunt thoracic aortic injuries, penetrating atherosclerotic ulcers, intramural haematomas, and aortic type B dissections.

 In terms of the configuration of stents for IVC reconstruction and the level of disease, three patients had unilateral iliac stents into the IVC, but the dominant group were either to the suprarenal component or a stent extension to the hepatic confluence.
In terms of the configuration of stents for IVC reconstruction and the level of disease, three patients had unilateral iliac stents into the IVC, but the dominant group were either to the suprarenal component or a stent extension to the hepatic confluence.




















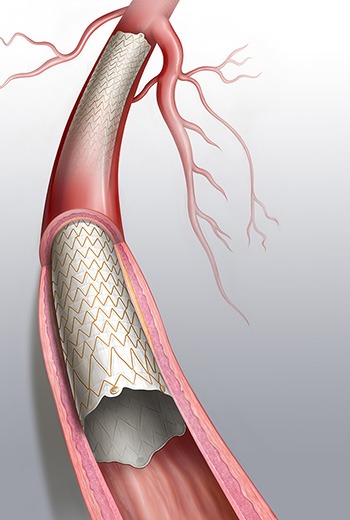





 Five-year results from a Japanese post-market surveillance study aimed at evaluating the Zilver PTX drug-eluting stent (DES) in a real-world population show consistently positive outcomes. The findings were presented for the first time at the Cardiovascular and Interventional Radiological Society of Europe 2018 meeting (CIRSE; 22–25 September, Lisbon, Portugal), by Kimihiko Kichikawa, Nara Medical University Hospital, Kashihara, Japan.
Five-year results from a Japanese post-market surveillance study aimed at evaluating the Zilver PTX drug-eluting stent (DES) in a real-world population show consistently positive outcomes. The findings were presented for the first time at the Cardiovascular and Interventional Radiological Society of Europe 2018 meeting (CIRSE; 22–25 September, Lisbon, Portugal), by Kimihiko Kichikawa, Nara Medical University Hospital, Kashihara, Japan.
 Twelve-month data prove that intravascular lithotripsy; a novel approach using pulsatile sonic pressure waves to modify intimal and medium calcium in stenotic peripheral arteries, is a safe and effective treatment option. This is the result of the Disrupt PAD II trial, presented by Andrew Holden, Auckland Hospital, Auckland, New Zealand, for the first time at the Cardiovascular and Interventional Radiological Society of Europe annual meeting (CIRSE; 22–25 September 2018, Lisbon, Portugal).
Twelve-month data prove that intravascular lithotripsy; a novel approach using pulsatile sonic pressure waves to modify intimal and medium calcium in stenotic peripheral arteries, is a safe and effective treatment option. This is the result of the Disrupt PAD II trial, presented by Andrew Holden, Auckland Hospital, Auckland, New Zealand, for the first time at the Cardiovascular and Interventional Radiological Society of Europe annual meeting (CIRSE; 22–25 September 2018, Lisbon, Portugal).








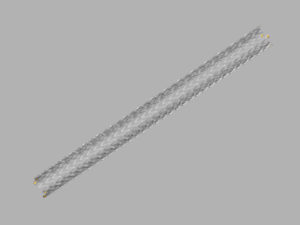 Cook Medical have announced that a new 5mm diameter version of
Cook Medical have announced that a new 5mm diameter version of 



 Data from the European Board of Interventional Radiology (EBIR), as presented by O M van Delden at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 22-25 September, Lisbon, Portugal) reveals that only 8% of EBIR-holders and 10-20% of CIRSE members are female.
Data from the European Board of Interventional Radiology (EBIR), as presented by O M van Delden at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 22-25 September, Lisbon, Portugal) reveals that only 8% of EBIR-holders and 10-20% of CIRSE members are female. 






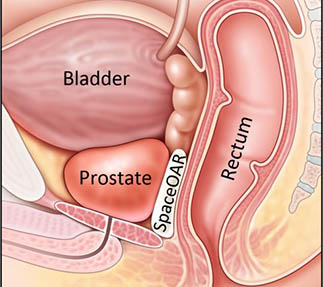








 Avinger
Avinger










 Gore have announced the first implant in conjunction with the Gore ARISE study of the Gore Ascending Stent Graft, an investigational device and the only endovascular stent graft specifically designed to treat type A dissections of the ascending aorta. The successful procedure took place on August 14, 2018 at Memorial Hermann Medical Center in Houston (USA), by Anthony Estrera, and Bruce Tjaden, as part of the Gore ARISE study.
Gore have announced the first implant in conjunction with the Gore ARISE study of the Gore Ascending Stent Graft, an investigational device and the only endovascular stent graft specifically designed to treat type A dissections of the ascending aorta. The successful procedure took place on August 14, 2018 at Memorial Hermann Medical Center in Houston (USA), by Anthony Estrera, and Bruce Tjaden, as part of the Gore ARISE study.


 Interventional radiologists issued a red alert warning over staff shortages in Scotland as the only full-time specialists based in the Scottish Highlands step down. The Scottish Government has been urged to answer for “unacceptable failings”.
Interventional radiologists issued a red alert warning over staff shortages in Scotland as the only full-time specialists based in the Scottish Highlands step down. The Scottish Government has been urged to answer for “unacceptable failings”.


























 EchoNous Vein (EchoNous), an ultrasound-based tool designed specifically for nurses to improve peripheral IV catheter placements, has received US Food and Drug Administration (FDA) approval.
EchoNous Vein (EchoNous), an ultrasound-based tool designed specifically for nurses to improve peripheral IV catheter placements, has received US Food and Drug Administration (FDA) approval.











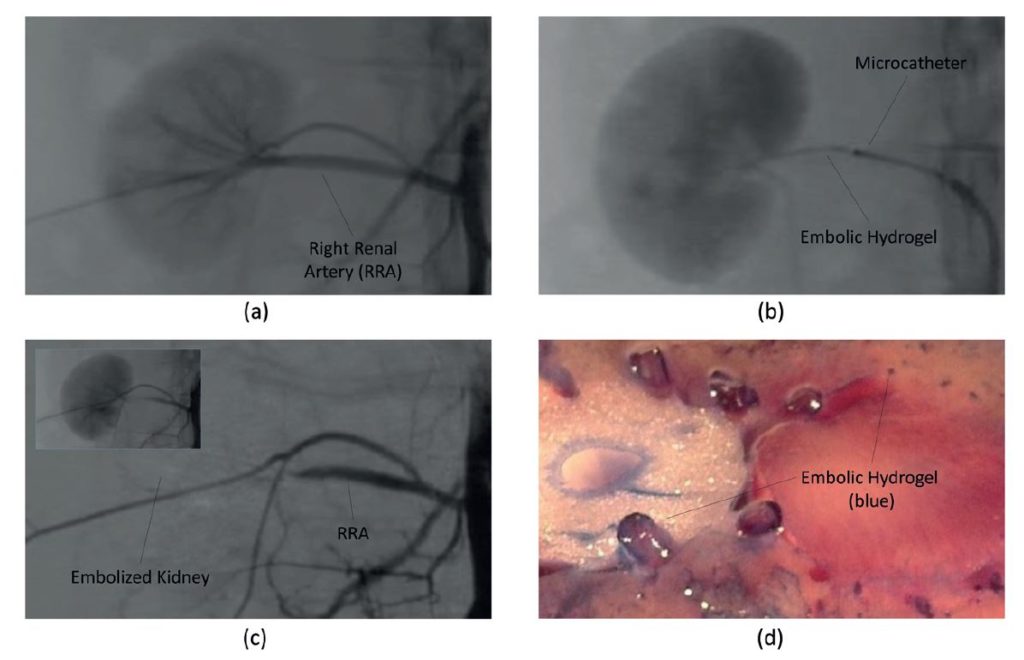
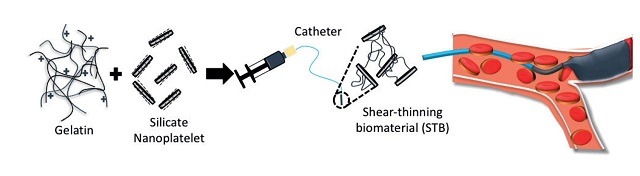







 Terumo has announced receiving the CE mark for its Kanshas drug-coated balloon catheter used in the treatment of lower extremity peripheral arterial disease.
Terumo has announced receiving the CE mark for its Kanshas drug-coated balloon catheter used in the treatment of lower extremity peripheral arterial disease. 












 The opening plenary at the World Conference on Interventional Oncology (WCIO; 7–10 June, Boston, USA) put biopsy, which is considered a mundane procedure by some interventional radiologists, at the heart of cancer diagnosis and personalised treatment. Many experts see that doing a biopsy well could establish a fruitful collaboration with referring medical and surgical oncologists.
The opening plenary at the World Conference on Interventional Oncology (WCIO; 7–10 June, Boston, USA) put biopsy, which is considered a mundane procedure by some interventional radiologists, at the heart of cancer diagnosis and personalised treatment. Many experts see that doing a biopsy well could establish a fruitful collaboration with referring medical and surgical oncologists.
 Stephen B Solomon, chief, Interventional Radiology Service, Memorial Sloan Kettering Cancer Center, New York, USA and president of the Society for Interventional Oncology (SIO) talks personalised medicine, immunotherapy and how being a cancer consultant helps make treatment decisions that are not desperation oncology with Interventional News. “Two big challenges [for interventional oncology] are demonstrating clinical data to support our work and ensuring high quality. Compared to other cancer specialties such as radiation oncology, interventional oncology has not been well organised […] this is one of the pressing issues that led to the formation of the SIO,” he explains.
Stephen B Solomon, chief, Interventional Radiology Service, Memorial Sloan Kettering Cancer Center, New York, USA and president of the Society for Interventional Oncology (SIO) talks personalised medicine, immunotherapy and how being a cancer consultant helps make treatment decisions that are not desperation oncology with Interventional News. “Two big challenges [for interventional oncology] are demonstrating clinical data to support our work and ensuring high quality. Compared to other cancer specialties such as radiation oncology, interventional oncology has not been well organised […] this is one of the pressing issues that led to the formation of the SIO,” he explains.














 Guerbet has announced the upcoming launch of SeQure and DraKon, two novel microcatheters for tumour and vascular aneurysm embolization procedures. The company introduced the microcatheters at GEST (Global Embolization Cancer Symposium and Technologies) 2018 US in Miami, USA.
Guerbet has announced the upcoming launch of SeQure and DraKon, two novel microcatheters for tumour and vascular aneurysm embolization procedures. The company introduced the microcatheters at GEST (Global Embolization Cancer Symposium and Technologies) 2018 US in Miami, USA.


 Drug-coated balloon (DCB) angioplasty devices have been categorised by the US Centers for Medicare and Medicaid Services (CMS) into the same billing code as plain balloon angioplasty, following the expiration of the technology’s transitional pass-through and new technology add-on payments on the 1st of January 2018. The decision not to create a separate reimbursement code for DCBs comes to the surprise and disappointment of a wide range of stakeholders and advocates, from industry to public advocacy groups.
Drug-coated balloon (DCB) angioplasty devices have been categorised by the US Centers for Medicare and Medicaid Services (CMS) into the same billing code as plain balloon angioplasty, following the expiration of the technology’s transitional pass-through and new technology add-on payments on the 1st of January 2018. The decision not to create a separate reimbursement code for DCBs comes to the surprise and disappointment of a wide range of stakeholders and advocates, from industry to public advocacy groups.






























 “Now that we know that a 3D-printed model is just as effective at training medical students in this type of procedure, this simulation experience can be made available to even more trainees and potentially improve procedural skills for residents, fellows, and attendees,” said Sheu. “We foresee this really making an impact in the world of interventional radiology training.”
“Now that we know that a 3D-printed model is just as effective at training medical students in this type of procedure, this simulation experience can be made available to even more trainees and potentially improve procedural skills for residents, fellows, and attendees,” said Sheu. “We foresee this really making an impact in the world of interventional radiology training.”
















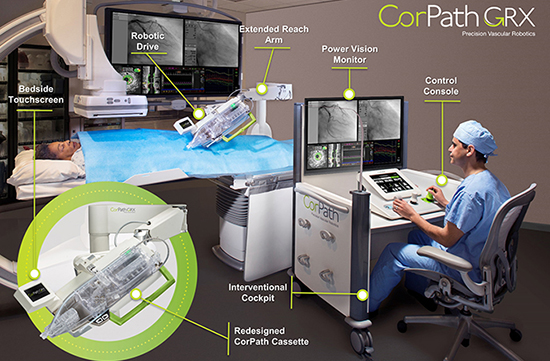





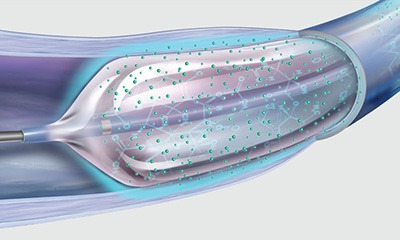












 The post-market, non-interventional, multicentre, non-randomised, single-arm study will enroll approximately 150 patients across 25 sites in Europe and Russia, and will evaluate the safety and performance of a ChEVAR procedure using the Endurant II/IIs stent graft system (Medtronic) in a real-world setting.
The post-market, non-interventional, multicentre, non-randomised, single-arm study will enroll approximately 150 patients across 25 sites in Europe and Russia, and will evaluate the safety and performance of a ChEVAR procedure using the Endurant II/IIs stent graft system (Medtronic) in a real-world setting.





 The registry will combine noninvasive, vascular ultrasound testing data with vascular treatment and outcomes data, making it possible to analyse the relationships between diagnosis and care provided to patients with vascular disease.
The registry will combine noninvasive, vascular ultrasound testing data with vascular treatment and outcomes data, making it possible to analyse the relationships between diagnosis and care provided to patients with vascular disease.


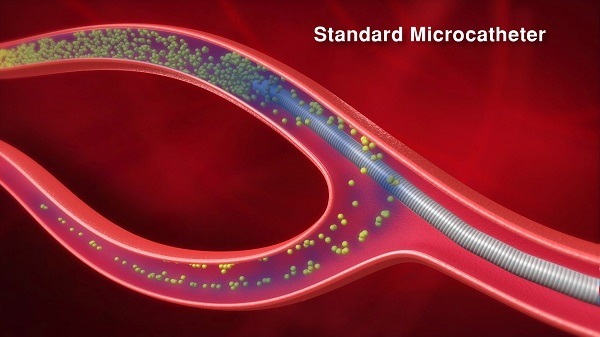
 The second series possess the same optimised navigation qualities, while also incorporating unique
The second series possess the same optimised navigation qualities, while also incorporating unique 




 The Global Medtech industry is moving together to enhance compliance practices across Europe, China, the Middle East, North Africa and Asia-Pacific, announces a statement released by
The Global Medtech industry is moving together to enhance compliance practices across Europe, China, the Middle East, North Africa and Asia-Pacific, announces a statement released by 



 “If you are clinically skilled, achieve a high level of technical training in interventional radiology procedures, have the best audited results for a procedure and a good relationship with your clinical colleagues, you are always going to be busy and have a highly successful career,” Andrew Holden, convenor, Central Organising Committee Members, Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) tells Interventional News. Holden is director of Interventional Radiology, Auckland Regional Public Health Service, and associate professor, Radiology, at Auckland University School of Medicine, Auckland, New Zealand.
“If you are clinically skilled, achieve a high level of technical training in interventional radiology procedures, have the best audited results for a procedure and a good relationship with your clinical colleagues, you are always going to be busy and have a highly successful career,” Andrew Holden, convenor, Central Organising Committee Members, Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) tells Interventional News. Holden is director of Interventional Radiology, Auckland Regional Public Health Service, and associate professor, Radiology, at Auckland University School of Medicine, Auckland, New Zealand.




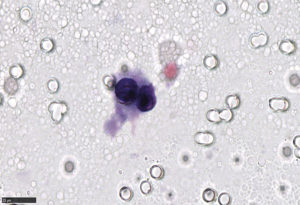


 The authors went on to assess whether differences in hospital quality contributed to variations in readmissions risk for patients with PAD. “Using data from the 1,085 hospitals included in this data set, we created a new analytic model to examine readmission rates between institutions that took into account differences in patient populations,” explained Secemsky. These results found that differences in hospital quality accounted only modestly for readmission risk, suggesting that penalising hospitals with greater than expected readmission rates may not be the only effective approach at reducing readmissions.
The authors went on to assess whether differences in hospital quality contributed to variations in readmissions risk for patients with PAD. “Using data from the 1,085 hospitals included in this data set, we created a new analytic model to examine readmission rates between institutions that took into account differences in patient populations,” explained Secemsky. These results found that differences in hospital quality accounted only modestly for readmission risk, suggesting that penalising hospitals with greater than expected readmission rates may not be the only effective approach at reducing readmissions.




 The notion of locally destroying a cancer percutaneously with minimal morbidity and mortality has become accepted as part of the modern armamentarium for treating patients with cancer. Thermal ablation technology has evolved rapidly during the past decades, with substantial technical and procedural improvements that can help to improve clinical outcomes and safety profiles, writes Roberto Iezzi, Rome, Italy.
The notion of locally destroying a cancer percutaneously with minimal morbidity and mortality has become accepted as part of the modern armamentarium for treating patients with cancer. Thermal ablation technology has evolved rapidly during the past decades, with substantial technical and procedural improvements that can help to improve clinical outcomes and safety profiles, writes Roberto Iezzi, Rome, Italy.

 clearance for post-treatment dosimetry of yttrium-90 microspheres")






 Intact Vascular has announced that positive single centre twenty-four month results from its
Intact Vascular has announced that positive single centre twenty-four month results from its 
 Merit Medical has announced signing an asset purchase agreement with BD (Becton, Dickinson and company) to acquire certain assets which BD proposes to sell in connection with its proposed
Merit Medical has announced signing an asset purchase agreement with BD (Becton, Dickinson and company) to acquire certain assets which BD proposes to sell in connection with its proposed 







 The new European Directive laying down basic safety standards for protection against the dangers arising from ionising radiation exposure will come into effect on 6 February 2018. The most relevant change for interventionists in the occupational exposure section is the new annual limit for the lens of the eyes (20 mSv/year, instead of 150 mSv/year), write Eliseo Vano (Madrid, Spain) and Gabriel Bartal (Kfar Saba, Israel).
The new European Directive laying down basic safety standards for protection against the dangers arising from ionising radiation exposure will come into effect on 6 February 2018. The most relevant change for interventionists in the occupational exposure section is the new annual limit for the lens of the eyes (20 mSv/year, instead of 150 mSv/year), write Eliseo Vano (Madrid, Spain) and Gabriel Bartal (Kfar Saba, Israel).




 “One of the biggest challenges for interventional radiology in 2017 is that we are in desperate need of outcomes research that documents the value of interventional radiology in modern healthcare,” Matt Mauro, CEO of UNC Faculty Physicians and chairman, Department of Radiology, University of North Carolina at Chapel Hill Education, Chapel Hill, USA, tells Interventional News.
“One of the biggest challenges for interventional radiology in 2017 is that we are in desperate need of outcomes research that documents the value of interventional radiology in modern healthcare,” Matt Mauro, CEO of UNC Faculty Physicians and chairman, Department of Radiology, University of North Carolina at Chapel Hill Education, Chapel Hill, USA, tells Interventional News. Fact file
Fact file






























 Mentice has announced the release of a new simulation training software for transarterial chemoembolization (TACE). The new software was showcased at the 2017 CIRSE congress (16–20 September, Copenhagen, Denmark).
Mentice has announced the release of a new simulation training software for transarterial chemoembolization (TACE). The new software was showcased at the 2017 CIRSE congress (16–20 September, Copenhagen, Denmark).




 Bard’s Lutonix 035 drug-coated balloon PTA catheter (DCB) has been granted premarket approval (PMA) by the US Food and Drug Administration (FDA) for a new indication and is now available for sale in the USA.
Bard’s Lutonix 035 drug-coated balloon PTA catheter (DCB) has been granted premarket approval (PMA) by the US Food and Drug Administration (FDA) for a new indication and is now available for sale in the USA.
 American women are largely unaware of uterine fibroid embolization according to results from a new nationwide poll released by the Society of Interventional Radiology (SIR). The data included in the report, “The fibroid fix: What women need to know”, show that 44% of women diagnosed with uterine fibroids say they have never heard of the less invasive treatment option.
American women are largely unaware of uterine fibroid embolization according to results from a new nationwide poll released by the Society of Interventional Radiology (SIR). The data included in the report, “The fibroid fix: What women need to know”, show that 44% of women diagnosed with uterine fibroids say they have never heard of the less invasive treatment option.


 Philips has announced that it has completed the acquisition of The Spectranetics Corporation, a US-based global leader in vascular intervention and lead management solutions. Spectranetics’ financial results will be consolidated as part of Philips’ Image-Guided Therapy business group as of 9 August 2017.
Philips has announced that it has completed the acquisition of The Spectranetics Corporation, a US-based global leader in vascular intervention and lead management solutions. Spectranetics’ financial results will be consolidated as part of Philips’ Image-Guided Therapy business group as of 9 August 2017. 







 The Gore Viatorr TIPS endoprosthesis with Controlled Expansion, a new device configuration developed by Gore, may reduce portal hypertension treatment complications, even when compared to the Gore Viatorr TIPS endoprosthesis, Gore’s legacy TIPS device. The latter has a strong history of patency and proven performance at fixed diameters. These findings were obtained from the abstract presented at The International Liver Congress 2017 in Amsterdam.
The Gore Viatorr TIPS endoprosthesis with Controlled Expansion, a new device configuration developed by Gore, may reduce portal hypertension treatment complications, even when compared to the Gore Viatorr TIPS endoprosthesis, Gore’s legacy TIPS device. The latter has a strong history of patency and proven performance at fixed diameters. These findings were obtained from the abstract presented at The International Liver Congress 2017 in Amsterdam.
 Spectranetics has announced receipt of US Food and Drug Administration (FDA) premarket approval of the Stellarex drug-coated balloon (DCB), designed to restore and maintain blood flow to the superficial femoral and popliteal arteries in patients with peripheral artery disease (PAD).
Spectranetics has announced receipt of US Food and Drug Administration (FDA) premarket approval of the Stellarex drug-coated balloon (DCB), designed to restore and maintain blood flow to the superficial femoral and popliteal arteries in patients with peripheral artery disease (PAD).
 Klaus Hausegger, chairman of the Institute of Diagnostic and Interventional Radiology in Klagenfurt, Austria, and president-elect of the Austrian Roentgen Society, will take up a new role as editor-in-chief of the journal CardioVascular and Interventional Radiology (
Klaus Hausegger, chairman of the Institute of Diagnostic and Interventional Radiology in Klagenfurt, Austria, and president-elect of the Austrian Roentgen Society, will take up a new role as editor-in-chief of the journal CardioVascular and Interventional Radiology (
 The
The 







































































 PinnacleHealth CardioVascular Institute has enrolled the first US patient in a trial assessing the safety and effectiveness of a new type of approach for blockages in the leg artery.
PinnacleHealth CardioVascular Institute has enrolled the first US patient in a trial assessing the safety and effectiveness of a new type of approach for blockages in the leg artery.
 Codman Neuro has announced the acquisition of Neuravi. This acquisition comes after the company’s recent acquisition of Pulsar Vascular, expanding its products for stroke therapy. DePuy Ireland Unlimited Company, an affiliate of Codman Neuro, is the acquiring entity. Financial terms of the transaction were not disclosed.
Codman Neuro has announced the acquisition of Neuravi. This acquisition comes after the company’s recent acquisition of Pulsar Vascular, expanding its products for stroke therapy. DePuy Ireland Unlimited Company, an affiliate of Codman Neuro, is the acquiring entity. Financial terms of the transaction were not disclosed.



 A Sheffield healthcare company has announced a strategic ‘buy out’ from its parent company, BD (Becton, Dickinson and Company), a deal which will see the company independently trade once again as UK Medical Ltd.
A Sheffield healthcare company has announced a strategic ‘buy out’ from its parent company, BD (Becton, Dickinson and Company), a deal which will see the company independently trade once again as UK Medical Ltd.










 Mirabilis has announced CE mark authorisation to market the Mirabilis System in the European Union. The system combines high-speed therapeutic ultrasound technology with an advanced robotic system for uterine fibroid treatment.
Mirabilis has announced CE mark authorisation to market the Mirabilis System in the European Union. The system combines high-speed therapeutic ultrasound technology with an advanced robotic system for uterine fibroid treatment.
 Metactive, an early-stage company focused on developing embolization devices for the treatment of peripheral vascular and neurovascular diseases, has announced the issuance of US patents 9,572,697 and 9,572,698 covering its Blockstent Microcatheter for embolization of peripheral arteries and veins and Ballstent Microcatheter for embolization of cerebral aneurysms. These proprietary microcatheter devices deliver a compressed gold metal implant over a 0.014” guidewire to treatment sites, where the implant is expanded and then detached to permanently stop blood flow.
Metactive, an early-stage company focused on developing embolization devices for the treatment of peripheral vascular and neurovascular diseases, has announced the issuance of US patents 9,572,697 and 9,572,698 covering its Blockstent Microcatheter for embolization of peripheral arteries and veins and Ballstent Microcatheter for embolization of cerebral aneurysms. These proprietary microcatheter devices deliver a compressed gold metal implant over a 0.014” guidewire to treatment sites, where the implant is expanded and then detached to permanently stop blood flow.



 The new Acuson Freestyle Elite ultrasound system can now be combined with the Artis angiography systems to enable fast and easy-to-use ultrasound guidance during interventional procedures. With this combined solution, referred to as Artis Freestyle Access, Siemens Healthineers supports a more convenient, less time-consuming, and safer workflow, a press release from the company says.
The new Acuson Freestyle Elite ultrasound system can now be combined with the Artis angiography systems to enable fast and easy-to-use ultrasound guidance during interventional procedures. With this combined solution, referred to as Artis Freestyle Access, Siemens Healthineers supports a more convenient, less time-consuming, and safer workflow, a press release from the company says.


 Interventional radiologists at the University of California at Los Angeles (UCLA), Los Angeles, USA, are using technology found in self-driving cars to power a machine learning application that helps guide patients’ interventional radiology care, according to research presented today at the Society of Interventional Radiology’s 2017 annual scientific meeting (4–9 March, Washington, DC, USA).
Interventional radiologists at the University of California at Los Angeles (UCLA), Los Angeles, USA, are using technology found in self-driving cars to power a machine learning application that helps guide patients’ interventional radiology care, according to research presented today at the Society of Interventional Radiology’s 2017 annual scientific meeting (4–9 March, Washington, DC, USA).















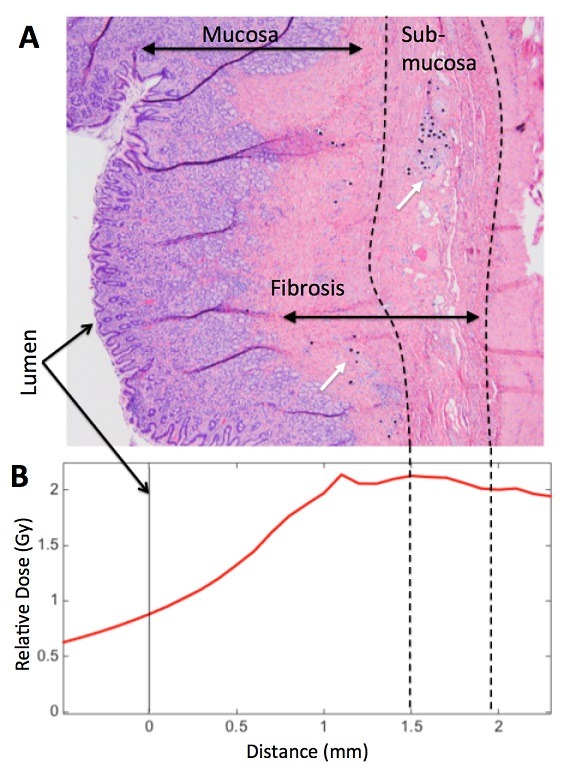









 “Prostatic artery embolization,” said Sapoval, “is a demanding procedure performed by experienced interventional radiologists. The anatomy is highly variable, the microcatheter and microwire skills required are advanced, and a high degree of technical competence in various areas is essential. Simulation training aims to facilitate the learning curve for performing prostatic artery embolization.”
“Prostatic artery embolization,” said Sapoval, “is a demanding procedure performed by experienced interventional radiologists. The anatomy is highly variable, the microcatheter and microwire skills required are advanced, and a high degree of technical competence in various areas is essential. Simulation training aims to facilitate the learning curve for performing prostatic artery embolization.”
 “War (as in turf war) is an emotional word because, in wars, people get hurt. I believe we truly care about the patients we serve and the last thing we want is for patients to get hurt. […] By and large, we have found that approaching role extension issues through discussion is preferable to confrontation,” Gregory John Slater, president, The
“War (as in turf war) is an emotional word because, in wars, people get hurt. I believe we truly care about the patients we serve and the last thing we want is for patients to get hurt. […] By and large, we have found that approaching role extension issues through discussion is preferable to confrontation,” Gregory John Slater, president, The  At our recent Board and Faculty Council meetings, we have decided to establish a standing committee of interventional radiology. This is our highest-level committee and aims to advance the role and place of interventional radiology in Australia and New Zealand. It aims to promote interventional radiology to the highest levels of government and the community and I expect it will seek to establish the discipline as a recognised subspecialty in our countries.
At our recent Board and Faculty Council meetings, we have decided to establish a standing committee of interventional radiology. This is our highest-level committee and aims to advance the role and place of interventional radiology in Australia and New Zealand. It aims to promote interventional radiology to the highest levels of government and the community and I expect it will seek to establish the discipline as a recognised subspecialty in our countries.
 Suresh Vedantham, professor of Radiology and Surgery, Mallinckrodt Institute of Radiology, Washington University School of Medicine in St Louis, USA, is scheduled to present the final results of the landmark
Suresh Vedantham, professor of Radiology and Surgery, Mallinckrodt Institute of Radiology, Washington University School of Medicine in St Louis, USA, is scheduled to present the final results of the landmark 






 Penumbra has announced the presentation of the results of the ASTER trial, the first independent, prospective, randomised trial comparing the use of Penumbra’s aspiration system to stent retriever, in the opening plenary session at the International Stroke Conference in Houston, Texas.
Penumbra has announced the presentation of the results of the ASTER trial, the first independent, prospective, randomised trial comparing the use of Penumbra’s aspiration system to stent retriever, in the opening plenary session at the International Stroke Conference in Houston, Texas.
 Philips has announced the global launch of Azurion, its next generation image-guided therapy platform, which forms the new core of its integrated solutions portfolio for the fast growing image-guided therapy market.
Philips has announced the global launch of Azurion, its next generation image-guided therapy platform, which forms the new core of its integrated solutions portfolio for the fast growing image-guided therapy market.







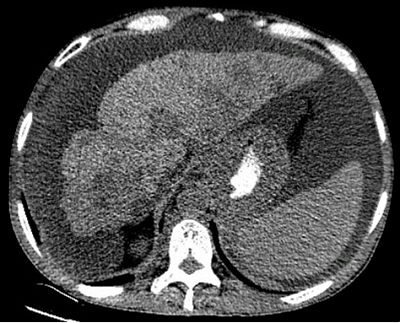












 Medtronic has received an investigational device exemption (IDE) from the US Food and Drug Administration (FDA) to initiate a study of the In.Pact Admiral drug-coated balloon for a potential new indication in patients with end-stage renal disease.
Medtronic has received an investigational device exemption (IDE) from the US Food and Drug Administration (FDA) to initiate a study of the In.Pact Admiral drug-coated balloon for a potential new indication in patients with end-stage renal disease.








 Terumo Corporation has announced that it has entered into a definitive agreement under which it has agreed to acquire Bolton Medical from its parent company. Bolton Medical is a leading innovator in thoracic and abdominal stent graft systems.
Terumo Corporation has announced that it has entered into a definitive agreement under which it has agreed to acquire Bolton Medical from its parent company. Bolton Medical is a leading innovator in thoracic and abdominal stent graft systems.
 Robert Califf is to step down as US Food and Drug Administration (FDA) commissioner upon the inauguration of Donald Trump as US President on 20 January 2017. Democrat Califf, who was appointed to the post in September 2016 by Barack Obama, is required to resign along with other presidential appointees.
Robert Califf is to step down as US Food and Drug Administration (FDA) commissioner upon the inauguration of Donald Trump as US President on 20 January 2017. Democrat Califf, who was appointed to the post in September 2016 by Barack Obama, is required to resign along with other presidential appointees.



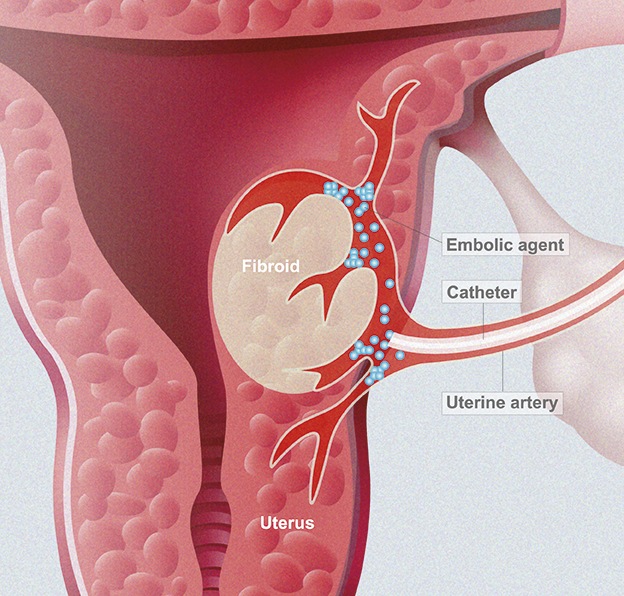






















 clearance for the SwiftNinja steerable microcatheter")


 For the upcoming MIOLive symposium, we had the idea of introducing a special “ten commandments” session for ablation, chemoembolization, and radioembolization, to create a practical handbook for the interventional radiologist who approaches liver interventions, write Roberto Iezzi, Rome, Italy and Laura Crocetti, Pisa, Italy. They give Interventional News readers a preview of the first five commandments.
For the upcoming MIOLive symposium, we had the idea of introducing a special “ten commandments” session for ablation, chemoembolization, and radioembolization, to create a practical handbook for the interventional radiologist who approaches liver interventions, write Roberto Iezzi, Rome, Italy and Laura Crocetti, Pisa, Italy. They give Interventional News readers a preview of the first five commandments. Roberto Iezzi is an interventional radiologist, Catholic University, Rome, Italy and Laura Crocetti is an interventional radiologist, University of Pisa, Pisa, Italy. MIOLive 2017 will focus on liver-directed therapy for hepatic malignancies. It will be a practical, interactive meeting based on live cases and short presentations and lectures, in which professionals from various countries from the Mediterranean area will have the opportunity to share experiences, research projects and valued mentoring from international experts
Roberto Iezzi is an interventional radiologist, Catholic University, Rome, Italy and Laura Crocetti is an interventional radiologist, University of Pisa, Pisa, Italy. MIOLive 2017 will focus on liver-directed therapy for hepatic malignancies. It will be a practical, interactive meeting based on live cases and short presentations and lectures, in which professionals from various countries from the Mediterranean area will have the opportunity to share experiences, research projects and valued mentoring from international experts
 A preliminary analysis suggests that thermal ablation may be effective in selected patients with local small cell lung cancer without adjuvant therapy. The research from Brown University, Providence, USA was published in the Journal of Vascular and Interventional Radiology (JVIR).
A preliminary analysis suggests that thermal ablation may be effective in selected patients with local small cell lung cancer without adjuvant therapy. The research from Brown University, Providence, USA was published in the Journal of Vascular and Interventional Radiology (JVIR).