Synchron has announced that the medical journal JAMA Neurology has published peer-reviewed, long-term safety results from a clinical study in four patients with severe paralysis implanted with the company’s first-generation Stentrode neuroprosthesis device. The study found that it is possible to use the neuroprosthesis device to transmit neural signals from inside a blood vessel in the brain over a long-term period without any serious adverse events related to the device.
The SWITCH (Stentrode with thought-controlled digital switch) trial—a first-in-human study—evaluated four patients implanted with Synchron’s Stentrode. Patients participating in the study completed a 12-month follow-up with no persistent neurological deficits. There were no clots or migrations of the device, a Synchron press release reports, and signal quality remained stable with no evidence of significant deterioration.
In addition, each participant successfully controlled a personal computing device with the brain-computer interface (BCI). They were able to use the implant to generate digital switches under intentional control for routine digital activities, such as texting, emailing, personal finance, online shopping, and communication of care needs, the release adds.
The study was led by Peter Mitchell, the neurointerventionist who performed the procedures, and vascular neurologist Bruce Campbell (both University of Melbourne, Melbourne, Australia). The procedures were performed in a neurointerventional angiography suite.
“We carefully conducted this first-in-human study with a primary focus on safety. The patients all tolerated the procedure well and were typically discharged home within 48 hours,” said study co-principal investigator Mitchell. “The widespread availability of the angiography suite for this procedure could promote a rapid translation of BCI for people with paralysis.”
As a Synchron press release notes, paralysis may result in a loss of control of muscles in the body, while the brain can remain intact. Motor intent is the brain signal underlying the physical will to move, and a BCI is designed to restore the lost motor intent signal transmission associated with paralysis. The device is implanted in the motor cortex of the brain via the jugular vein in a minimally invasive endovascular procedure. Once implanted, it detects and wirelessly transmits motor intent in order to control personal digital devices.
In the SWITCH trial, motor intent was detected using a robust decoder that searches for power changes in certain frequency bands. The digital switches were executed under the volitional control of frequency band shifts by the users.
Synchron’s first-generation system was developed in partnership with Ripple LLC and utilised Ripple’s neural sensing technology to provide core signal acquisition, data telemetry and signal processing capabilities, the release also states.
“This technology holds great promise for people with paralysis who want to maintain a level of independence,” added co-principal investigator Campbell. “The Stentrode enables a form of motor restoration, with individuals able to use the switches to communicate and engage with their digital world.”
“The SWITCH study is an early demonstration of safety in a low number of participants using a commercial grade BCI. The decoder was simple and robust, meaning that patients did not have to train hard to execute switches,” said Tom Oxley, CEO and founder of Synchron. “Our view is that a motor neuroprosthesis should be safe and easy to use. Digital switches controlled by motor intent could translate into a meaningful restoration of motor capability for patients with paralysis and the return of things we take for granted, like texting loved ones or turning on a light.”
The publication of this study follows Synchron’s announcement of ongoing patient enrolment in the COMMAND trial at Carnegie Mellon, the University of Pittsburgh and Mount Sinai Hospital in the USA to assess safety and explore quantified efficacy measures of Stentrode. Three out of six participants have been enrolled in the COMMAND trial, with the clinical trial sites still actively looking for the next participants.
Fluidx Medical has released information regarding the success of the IMPASS Embolic Device in in vivo research related to middle meningeal artery (MMA) embolizations which can be used to treat chronic subdural haematomas (CSDH) on the surface of the brain.
CSDH is a common pathology that can result in death and/or disability in patients. The typical treatment of CSDH involves drilling a hole in the skull and draining the blood. Minimally invasive catheter-based MMA embolization can be an alternative to surgical treatment.
“We have been listening to clinicians and they need better tools to treat CSDH,” says Danny Smith, vice president of research and development for Fluidx. “We designed the IMPASS embolization device to work with standard embolization catheters and embolize microvasculature in the MMA. Our results are encouraging and the IMPASS product could be a great solution to unmet patient needs.”
MMA embolization is a promising option to address CSDH and is particularly appealing for elderly patients and others who cannot undergo invasive surgical procedures. Hundreds of thousands of patients with CSDHs may benefit from this minimally invasive procedure. During the procedure, a small catheter is navigated into the MMA located within the dura mater which covers the brain, then an embolic material is delivered into the vessel to block arterial flow.
The Fluidx embolic platform is expected to bring simple preparation and controllable material delivery to a range of applications. The IMPASS device is packaged in a ready-to-use syringe, can be prepped tableside by the clinician in about 30 seconds, and may be delivered through standard microcatheters (no complex mixing systems or special delivery catheters are necessary).
Speaking to Interventional News at the recent Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain), Arthur Rocha (São Paulo, Brazil), from professor Carnevale’s team, shares the development of an optimised imaging workflow—which consists of “cone-beam computed tomography (CBCT) from the internal iliac artery as the main imaging and the use of embolization planning and guidance software such as Embo ASSIST (GE HealthCare) to improve anatomy assessment and prostate artery embolization (PAE) planning and navigation.
Arthur Rocha outlines some of the advantages of CBCT with software such as Embo ASSIST compared to digital subtraction angiography (DSA), noting that it helps “avoid misleading identification of the origin of the prostatic artery, which would make navigation difficult, as well as identify secondary prostatic arteries which, if not embolized, may lead to symptoms recurrence”.
He examines past literature on PAE and how it relates to a recently conducted study which showed that CBCT helped find almost four times more secondary arteries than previously described based on DSA only. “We recommend routine use of CBCT imaging with augmented planning and guidance software to improve PAE outcomes,” concludes Arthur Rocha.
Lydus Medical is pleased to announce that the Vesseal has received US Food and Drug Administration (FDA) 510(k) clearance. The Vesseal is a microvascular anastomosis suture deployment system, for standardised omnivessel anastomoses, enabling simple, fast, safe, and effective procedures.
An anastomosis is one of the most complicated steps of microvascular surgery and fundamental to the success of these demanding surgical interventions. Varied clinical fields require microvascular anastomosis, including breast reconstruction; head and neck reconstruction; surgical lymphoedema treatment; and vascular access for haemodialysis.
Until now, microvascular anastomoses have been performed manually. Manual microanastomoses are time- and labour-intensive, require a long learning curve, a unique skill set and great surgical dexterity. The Vesseal is designed to mimic the skill set and dexterity needed to deliver quality patient care in microsurgical anastomoses. It provides, simple, accurate, dependable and consistent results through symmetrical placement of eight microsutures at the anastomosis site.
“FDA clearance of the Vesseal is a significant milestone both for innovation in microvascular anastomoses, and for Lydus Medical. It is common knowledge that there are large clinical unmet needs around microvascular anastomosis,” said Jessica Weiss, CEO of Lydus Medical. “Clinicians who used the Vesseal stated that it shows a significant advantage over the manual anastomosis and provides more consistency in the procedure. We believe that the Vesseal will support enhanced outcomes in microsurgical procedures, as well as improved patient care.”
Paula Novelli, who is associate professor of interventional radiology (IR) at the University of Pittsburgh Medical Center (Pittsburgh, USA) put her own spin on a British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) presentation titled ‘Women are more likely to work part-time’. The ‘myth-busting’ session as a whole saw speakers weigh in on how gendered perceptions and, in some cases, realities, can impact women interventional radiologists’ careers. Novelli in particular, bringing the perspective of ‘the only girl in the gang’—the gang being her IR team at Pittsburgh—left delegates with the salient message that “on all levels”, women are not overinvesting in education, despite the fact that, in the USA, “women practise fewer total hours than men due to significant household responsibilities.”
Novelli began her presentation remarking that, based on a 1970s survey of 97 male and 95 female doctors, 59% of the female respondents and 87% of the men had been working full-time from graduation, with 17% of the women not working due to taking on a traditional ‘female’ role instead. The prevailing thought at the time was that medical education of women in the USA was a poor investment due to the likelihood of women practising fewer hours over their professional lifetimes. Yet, despite these figures, Novelli conveyed that the findings demonstrated “women spent 90% as much time in medical work as did men, accounting for childbearing responsibilities.” This points to the idea of the “superwoman”, the presenter elaborated—female doctors may be working fewer overall hours, but they work with increased productivity.
More current than the previous data, Novelli then highlighted a British Medical Journal (BMJ) op-ed from 2008, which professed the opinion that women doctors were concentrated in “family-friendly” specialties, including paediatrics, psychiatry and family medicine. This was considered to be a “ticking timebomb” since women are more likely to work part-time, and this “feminisation” of these family-friendly specialties would mean that the specialties would disproportionately suffer the implications of part-time working and maternity leave, such as lack of continuity of care and resource use.
However, recent data on the state of women in academic medicine from the Association of American Medical College (AAMC) Novelli countered, while “difficult to interpret” because of varying definitions of what percentage of full-time work part-time constitutes, suggests that among part-time doctors, there is an almost equal male-female split. The figures she cited were 50.1% of male part-time medical faculty, versus 49.9% women.
The “leaky pipeline” in IR
Bringing the focus to IR specifically, Novelli noted that radiology and surgery are “up there” when it comes to the specialties in which the aforementioned part-time doctors are concentrated, but that, as shown by the statistic, this is not due to a higher number of women faculty members in these specialties.
Yet, according to a Journal of the American Medical Association (JAMA)-published study of parental status among early-career physicians, the object of which was to determine which factors influence doctors’ decisions to work part-time or full-time, 75% of female participants said they were considering reducing their hours. Novelli underlined the importance of this “early gap” in hours practised between men and women, reaffirming the definite gender imbalance in this regard with anecdotal evidence: “I have never worked with another female IR [interventional radiologist] in my entire 18-year [IR career]”. The leaky pipeline will perpetuate the gender imbalance in medicine for the foreseeable future, Novelli posited.
The mental “toll” on women in IR
Novelli then brought burnout among interventional radiologists into the picture, flagged how, as found in a recent Society of Interventional Radiology (SIR) questionnaire, burnout was “significantly higher” than among diagnostic radiologists, and, pertinent to the current discussion, also among women over men. Similarly, Novelli added, another JAMA study assessing depression among doctors just post-medical school found that the rate was also higher among the female respondents.
A theory Novelli brought to explain this phenomenon was that, perhaps, women need to work harder: “I do believe that we need to work harder in any academic setting just to prove ourselves.” This “toll” medicine takes on women is multifactorial, the presenter furthered, stating that female doctors are more likely to be reported, have fewer advancement opportunities, and less likely to become full professors or academic leaders. “We are not really learning from the past,” Novelli lamented, explaining that since the seventies, there have been calls for women to receive more flexibility and respect to foster their advancement. “We need to eliminate biases and harassment,” was one of Novelli’s own calls regarding how to successfully support women in their medical careers.
Women are currently supported to some extent, Novelli acknowledged, mentioning the BSIR’s pamphlet that informs women of the scope for flexibility around training and provides guidance on radiation exposure for those of childbearing age who may be concerned about this aspect of an IR career.
Investment in women in medicine not misplaced
“Today, the total training cost per diagnostic radiology resident is US$99,000 a year on top of the half-a-million that they pay to become a physician academically,” was Novelli quantifying for the audience members the extent to which embarking on becoming a radiologist in the USA is a significant financial undertaking. Be this as it may, she opined that women are not “overinvesting” in their medical education, as their practices, even if they do not work full-time hours, provide the same level of patient care.
Novelli’s parting words were that “as the only girl in the gang” she has been “called into the principal’s office” many times—this refers back to how it is harder to be a woman in medicine, how the standards to which women are held are higher. “But I have been able to maintain the support of family and work/life responsibilities,” she celebrated. Novelli then admitted that she is “still waiting for her ‘Me Too’ moment and is “not sure” that her 16-year-old daughter should pursue a career in medicine as “there is still a lot of work to do.”
Subsequent discussion around the subject of Novelli’s presentation drew out the sentiment that her point about not necessarily encouraging her daughter to go into medicine was “[disheartening]”. This then raised the question of whether women could be the predominant source of negative comments dissuading fellow female doctors or trainees from pursuing IR. Mentorship was suggested as an antidote for women’s reticence about entering into a field which may have seemed, traditionally, not to be a good “fit” for women. “[The mentor need not] be a woman,” was Shilpi Pal’s (Ninewells Hospital, Dundee, UK) view—“[just] someone who has been in your shoes”.
Interventional News covered a whole range of the specialty’s news during 2022, but readers’ attention was most piqued by acquisitions (Boston Scientific’s of Obsidio and Bentley’s of the GoBack catheter); study results from meetings that highlighted the “potential” and “promise” of both renal denervation and prostatic artery embolization (PAE); and the launch of a first-in-human trial of a sirolimus drug-coated balloon (DCB) for peripheral indication.
In August, Inari Medical announced planned enrolment of the DEFIANCE randomised controlled trial (RCT), which is designed to compare the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only.
Also in August, Boston Scientific shared the news of the acquisition of Obsidio, a privately held company that has developed the Gel Embolic Material (GEM) technology used for embolization of blood vessels in the peripheral vasculature.
Late-breaking trial data presented at EuroPCR 2022 (17–20 May, Paris, France) underscored the potential of renal denervation as an adjunctive therapy to treat hypertension, complementing existing first-line treatments including lifestyle modifications and medication, attendees of the conference heard.
Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) presented during the Scientific Paper session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), and won the award of best abstract for his and co-authors’ ‘Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia’.
Again in August, BD announced the start of enrolment in the PREVISION first-in-human trial, a prospective, multicentre, single arm, non-randomised study designed to evaluate the safety of the BD sirolimus DCB in the treatment of peripheral arterial disease (PAD) in the femoropopliteal arteries.
In November, Otsuka Medical Devices and ReCor Medical, a subsidiary of Otsuka, shared the news that they had filed a pre-market approval (PMA) application to the US Food and Drug Administration (FDA) for the Paradise ultrasound renal denervation (uRDN) system in the treatment of uncontrolled hypertension.
September also saw Medtronic share that it received CE mark for its Radiant balloon-expandable covered stent, the first and currently, only, covered stent indicated for use in chimney endovascular aneurysm repair (ChEVAR) with the Endurant II/IIs stent graft system.
AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases and advance development and preclinical work on a PIVL device for coronary cases.
BioStar Capital, the lead investor in the company’s Series A round, also led the Series B round. BioStar Capital is focused on transformational investments in medical technologies with an emphasis on cardiovascular and orthopaedics.
“AVS is one step closer to offering a new treatment solution for patients with severely calcified peripheral arterial disease and progressing toward preclinical studies for coronary cases,” said Mark Toland, managing director for BioStar Capital and executive chairman/CEO of AVS. “Patients in this disease state too often face the prospect of limb amputation due to a lack of treatment options. We see a significant opportunity to address that need and advance the intravascular lithotripsy space through minimally invasive technology in both peripheral and coronary therapy.”
AVS’s novel balloon-based platform, the Pulse IVL system, shatters calcium with pressure waves in frequent bursts and expands calcified arteries, all with a single device.
“We are proud to support AVS in both its successful Series A and Series B funding rounds,” said Louis Cannon, founder and senior managing partner of BioStar Capital. “The preclinical results of the Pulse IVL System have shown the potential to raise the standard of care and significantly impact the wellbeing of patients with calcified arterial disease. We are excited to partner with AVS as it looks to future clinical trials and development.”
In September 2022, AVS announced enrolment, successful treatment, and positive 30-day follow-up data of the first patients in its POWER PAD I clinical trial, a first-in-human study. Jon George (University of Pennsylvania Health System, Philadelphia, USA) an interventional cardiologist at the and medical advisor to AVS, assisted in trial cases in the Dominican Republic.
“Our early trial results showed that we can successfully treat patients with multiple lesions using a single device,” said George. “We saw patients report a reduction in leg pain, increase in blood flow to the leg, and improvement in their ability to walk in our initial study. This is a patient population that needs easier access to advanced therapies and this platform has the potential to provide that access.”
Cardiovascular Systems (CSI) announced that Innova Vascular (Innova) has submitted a 510(k) premarket notification to the US Food and Drug Administration (FDA) for its thrombectomy devices intended to treat peripheral vascular disease.
CSI intends to acquire and commercialise each of the novel thrombectomy devices from Innova targeting peripheral vascular disease. Commercialisation of the thrombectomy devices will be complementary to CSI’s broader portfolio of advanced technologies used in the treatment of cardiovascular disease.
Sanjay Shrivastava, CEO of Innova, said, “the FDA submission of the thrombectomy devices for use in the peripheral vasculature marks an important milestone in our commitment to develop innovative technologies targeting large, underserved markets. We are excited to partner with CSI, which has been serving the interventional cardiology, interventional radiology, and vascular surgery communities that will be the primary users of this thrombectomy system.”
Pending regulatory clearance in the USA and completion of the acquisition of the first Innova system, CSI could begin to commercialise a portfolio of aspiration catheters and clot retrieval devices for use in peripheral vasculature in approximately six months. The portfolio and corresponding indications for use will be expanded to include the treatment of deep vein thrombosis and pulmonary embolism following completion of the respective clinical trials and subsequent 510(k) clearances. These trials are expected to begin enrolling later in 2023.
Scott R Ward, chairman, president and CEO of CSI said, “CSI’s strong commercial presence, with over 150 peripheral sales representatives, will make thrombectomy an excellent fit as we seek to reach more patients and drive increased revenue through our sales channel beginning later this year.”
Under the terms of the agreements signed with Innova, CSI has provided financing to Innova for the development of the thrombectomy devices. Under an acquisition option agreement, upon Innova’s completion of key technical, regulatory and clinical milestones in the development program, CSI will have exclusive rights to acquire the thrombectomy devices, subject to the satisfaction of closing conditions set forth in the agreement.
IceCure Medical, developer of the minimally-invasive ProSense System for cryoablation, which destroys tumours by freezing, today announced interim results from the ICESECRET study for the treatment of patients with small renal masses (SRM) who cannot be offered kidney-preserving surgery. Data were presented at the Urological Association Conference (14 December, Eilat, Israel). The presentation, titled “Renal Mass Cryoablation – Interim Analysis ICESECRET Study”, was delivered by Nasir Said (Bnai Zion Medical Center, Haifa, Israel).
According to the presentation, out of the 115 patients enrolled, 107 patients (112 lesions) returned for follow-up with a mean duration of 22.8 months and a range 12-60 months. In a subgroup of patients with no previous history of kidney cancer on the same kidney and a lesion ≤3cm, an 89.5% recurrence-free rate was observed at a mean follow-up time of 22.2 months when the procedure protocol was followed.
The recurrence-free rate was 85.1% for the 107 patients (91 patients, including 13 patients who underwent a second cryoablation), at a mean follow-up period of 16.5 months. Five serious adverse events were reported, four of which were of mild severity and were treated conservatively and resolved within one to five days, with one severe complication of a new onset of ipsilateral hydronephrosis seven months after the cryoablation procedure that led to nephrectomy.
Cryoablation time and hospitalisation time were relatively short, up to approximately 25 minutes and two days, respectively. The presentation concluded that, based on these interim results, cryoablation is safe and effective for treating renal masses under five centimetres.
According to the American Journal of Roentgenology, small renal masses, which may be malignant or benign tumours in the kidney, have been rising in incidence over the past two decades. According to the American Cancer Society, in 2022, in the US, an estimated 79,000 new cases of kidney cancer will be diagnosed, with about 14,000 dying from the disease. Globally, there were more than 430,000 new cases of kidney cancer in 2020 and about 180,000 deaths according to World Cancer Research Fund International.
“These impressive interim results demonstrate the value of ProSense for urologists and interventional radiologists as a therapeutic alternative when patients are not eligible for surgery,” stated IceCure’s Chief Executive Officer, Eyal Shamir. “We believe the findings will support further use of ProSense in the jurisdictions in which our cryoablation system is approved for use with benign and malignant tissues of the kidney. The growing body of data on ProSense’s efficacy and safety across a broad range of indications supports commercialization momentum, particularly in facilities that benefit from one device that can be used across multiple specialties.”
ICESECRET, a prospective, multicentre, single-arm clinical trial is being performed at Bnai-Zion Medical Center, Haifa, Israel, and Shamir Medical Center, Zerifin, Israel, and led by principal investigator Halahmi Sarel (Bnai Zion Medical Center, Haifa, Israel). The trial included 115 patients (138 lesions) with localized SRM of ≤5cm who were treated with ProSense cryoablation under computed tomography (CT) guidance. Full engulfment of the renal lesion, including a safety margin of 0.5cm was achieved in approximately 96% of the procedures where there was no anatomical limitation. Follow-up visits are performed 6 weeks, 6 months, 1 year, and then annually up to 5 years after the procedure. During the follow-up visits, data related to local recurrence, based on CT imaging, is collected. Safety was determined by monitoring procedure-related adverse events throughout the study.
ReCor Medical and its parent company Otsuka Medical Devices have announced the appointment of Lara Barghout as president and chief executive officer of ReCor.
Barghout will lead the ReCor business strategy and organisation in the global commercialisation of ReCor’s Paradise ultrasound renal denervation system for the treatment of hypertension. She brings more than 20 years of experience leading global businesses in the medical device industry, joining ReCor from Siemens Healthineers, where she was senior vice president and head of advanced therapies, leading the image guided therapy business in North America. Prior to Siemens Healthineers, Barghout held several roles at Terumo Cardiovascular.
“I am honoured to lead the extraordinary team at ReCor at an exciting time in the company’s growth,” said Barghout. “High blood pressure is a leading contributor to cardiovascular disease burden worldwide, resulting in increased patient risk and higher costs to health systems. I look forward to leading our focus to advance ultrasound renal denervation as a treatment for hypertension and the global commercialisation of the Paradise ultrasound renal denervation system. We believe our Paradise ultrasound renal denervation technology to be a true game changer in improving hypertension therapy, with the potential to offer a new option for physicians to help improve blood pressure outcomes for their patients on a global scale.”
“We are delighted to name Ms Barghout President and CEO of ReCor. She is a highly experienced leader with a track record of commercial success across a range of medical device businesses, coupled with extensive experience in global leadership,” said Noriko Tojo, executive director of Otsuka Holdings and president of Otsuka Medical Devices. “We are very excited for Ms Barghout to lead ReCor into its next phase of global growth. Her deep commercial experience and adept leadership make her ideal to build on the technology development and clinical trial successes of the ReCor team, guiding the business to realise its therapeutic and commercial potential. I would like to thank Andy for his outstanding leadership and countless contributions over the past 10 years.”
The Paradise system bears the CE mark for the treatment of hypertension in Europe and is an investigational device in the USA and Japan.
Lung nodule biopsies performed with new robotic bronchoscopy technology may be safer and more effective than those done by traditional methods, a study by researchers at the University of Texas Southwestern (UTSW; Dallas-Fort Worth, USA) suggests.
UTSW was among the first in the country to use robotic-assisted bronchoscopy (RAB) to biopsy pulmonary lesions. Paired with advanced imaging that provides real-time 3D visuals, the technology enables UTSW’s Interventional Pulmonology team to navigate an ultra-thin, ultra-flexible tube with light and camera capabilities into a patient’s lungs to pinpoint and test suspicious abnormalities.
The increased dexterity of the steerable tube makes it possible to safely reach areas in the lungs that could not be accessed through traditional bronchoscopy and other sampling tools.
A retrospective analysis of 200 of those procedures found that shape-sensing, robotic-assisted bronchoscopy (ssRAB), when combined with technologies such as intraprocedural cone beam computed tomography imaging (CBCT) and radial endobronchial ultrasound, offers high diagnostic accuracy, sensitivity, and specificity with an excellent safety profile. The findings were published in Lung.
“The goal of advanced bronchoscopy is to diagnose lung nodules and perform mediastinal staging in a single procedure, while achieving a comparable diagnostic yield to percutaneous biopsy and at the same time, minimising complications,” said Kim Styrvoky, assistant professor of internal medicine in the Division of Pulmonary and Critical Care Medicine at UTSW, and Muhanned Abu-Hijleh, professor of internal medicine in the Division of Pulmonary and Critical Care Medicine.
“The diagnostic yield of current bronchoscopic techniques is limited, and there is about a one-in-four chance of pneumothorax, or collapsed lung, with percutaneous biopsy,” Styrvoky said. “Our study showed that this new technology provided accuracy of 91.4%, on par with traditional biopsy methods, while reducing the risk of pneumothorax complication to 1%.”
Lung cancer remains the leading cause of cancer-related deaths for both men and women in the USA. Each year, between 1.5 million and two million pulmonary nodules are identified through diagnostic imaging. UTSW is using robotic bronchoscopy in cases where traditional biopsies present a higher risk of complications, including patients with lesions deep in the lung, near major blood vessels, or adjacent to a portion of diseased lung.
This was UTSW’s first reported study detailing the usage of ssRAB-CBCT, but other trials focusing on various aspects of robotic bronchoscopy are underway.
If further studies confirm the findings, ssRAB-CBCT has the potential to become the standard of care for targeted lung sampling, Styrvoky and Abu-Hijleh said.
RF Medical is a Korean thermal ablation system manufacturer and the creator of the Mygen M-3004 generator and specialised electrodes including Myoblate. Both of these products have been cleared by the US Food and Drug Administration (FDA) and are now commercially available in the USA.
RF Medical’s chief executive officer Mike Jun imparted that the company is delighted to extend some of its finest medical equipment to the American market. Jun is confident that Mygen and Myoblate will empower US-based medical facilities and practices, and will modernise the standard of care for minimally invasive practices in the USA.
According to Jun, RF Medical’s commitment to developing effective, affordable, and minimally invasive medical devices is embodied in its latest inventions, communicating the following:
“The world’s medical device market is showing remarkable growth driven by cutting-edge minimally invasive technology and its industrial value is limitless. RF Medical is working diligently in an effort to keep pace with the advanced medical market. Improving the health and safety of mankind is our top priority and we are dedicated to carrying our mission as a leading medical device company through continuous investments in superior workforce and research and development.”
The Mygen M-3004 is a medical device that enables a combination of monopolar and bipolar modes. In addition to delivering radiofrequency energy more effectively, it also supports optimised algorithm modes for use in a variety of lesions depending on their size and shape.
The clearance of the Myoblate system is expected to bring another option to women suffering from uterine fibroids. A recent study showed that approximately 70-80% of women will experience this condition at some point; the Myoblate system will then be a less invasive, and more patient-friendly alternative to hysteroscopy or myomectomy.
Myoblate electrodes are intended for soft tissue coagulation and ablation to treat fibroids in a minimally invasive manner.
Myoblate utilises radiofrequency ablation to safely treat fibroids individually while keeping the uterus intact. According to Ben Ovenden, Business Director of RF Medical, USA, “Myoblate is the only RFA system for the treatment of uterine fibroids that utilises a wide range of approaches, unlike existing ablation technology.”
VentureMed Group, a privately held medical device innovator in access management for arteriovenous (AV) fistulas and grafts and vessel preparation for interventional treatment of peripheral arterial disease (PAD) announced data presented at the VEITHsymposium, (15–19 November, New York, USA). Overall, the data presented demonstrated that Flex vessel prep used prior to balloon angioplasty improves 12-month outcomes both in PAD and AV fistulas and grafts.
“AV Access management is a critical component of successfully treating AV patients over time,” said John Aruny (Dialysis Access Institute, Orangeburg, USA), primary investigator of the Flex Vessel Prep AV registry clinical study, the 12-month outcomes of which he presented at VEITH. “The FLEX AV Registry 12-month outcomes shows that utilising Flex vessel prep provides more time between interventions and continues to excel in the very difficult cephalic arch lesions.”
The study was a single arm, prospective study conducted in eight centres in the USA with 114 real world patients.
The Flex AV Registry 12-month outcomes demonstrate sustained patency across most patients and particularly good results specifically in the cephalic arch.
49% patency for all AV fistula patients (comparable historical data 26%)
59.7% patency for cephalic arch lesions (comparable historical data 0–33.9%)
AV grafts had average time to target lesion revascularisation of 228 days (41.2% patency at nine months)
No observed serious adverse events.
“Vessel preparation has become a necessary step for better patient outcomes,” said Eric Secemsky, director of vascular intervention, Beth Israel Deaconess Medical Center (Boston, USA), who presented the 12-month results of the Belong study with Flex vessel prep system prior to drug-coated balloon (DCB). “Vessel preparation in PAD with Flex creating longitudinal microincisions prior to DCB therapy had impressive freedom from clinically driven target lesion revascularisation and looks to improve outcomes by lowering balloon inflation pressures and potentially enhancing drug delivery.”
The Belong study was a single-centre, single-arm, prospective study conducted with 41 patients in Fribourg, Switzerland.
12-month efficacy results:
97.5% (39/40) freedom from clinically driven target lesion revascularisation
84.2% (32/38) freedom from target lesion restenosis via duplex
Corindus has been rebranded to Siemens Healthineers Endovascular Robotics and will sit as a dedicated business within the Advanced Therapies area of Siemens Healthineers, the company has announced.
This brand unification is the final step of the company integration process that commenced in 2019 with the acquisition of Corindus by Siemens Healthineers, the company says in a press release. The aim of the Endovascular Robotics business is to advance interventions with robotics and change the way that care is delivered through innovations that enhance physician technique and bring precision to interventional procedures, the press release adds.
Siemens Healthineers Endovascular Robotics says it will continue to offer the CorPath GRX system to support endovascular procedures while working to revolutionise treatment of emergent conditions by developing technologies to provide specialised and timely medical care to more patients around the world.
Wayne Markowitz, worldwide executive vice president of Siemens Healthineers and head of endovascular robotics, said: “The completion of our brand evolution marks the final step to becoming a united company and we remain focused on pioneering breakthroughs for everyone, everywhere. Our flagship product, the CorPath GRX system, is designed to support endovascular interventions, and we look forward to working with our customers as Siemens Healthineers Endovascular Robotics while fuelling our vision to connect more patients to advanced care.”
Efemoral Medical has today announced the closing of its US$4.9 million preferred Series A1 round. Supported by existing investors as well as an experienced cohort of new investors, the proceeds will further Efemoral’s device development and expand enrolment in its ongoing first-in-human clinical trial, EFEMORAL I, investigating the Efemoral vascular scaffold system (EVSS) with FlexStep technology.
The new funds will also complement Efemoral’s recently announced phase II Small Business Innovation Research (SBIR) grant award, which will support pre-clinical studies.
The EVSS with FlexStep technology offers a new approach to treating peripheral arterial disease (PAD) by addressing the specific anatomical challenges and complex biomechanics of patients with athero-occlusive disease in the leg, Efemoral states in a press release. Through the use of inter-scaffold spaces, the patented FlexStep technology combines flexibility with support to accommodate tortuosity and skeletal movement, while the balloon-expandable deployment system is designed to open vessels and sustain healthy blood flow. The novel bioresorbable scaffold with long-term Sirolimus elution aims to restore normal vessel diameter at the time of the procedure, deliver therapeutic benefits across all lesion lengths and morphologies, prevent restenosis, and maintain patency while leaving no permanent implant behind, the company’s statement adds.
“The implantation of strong, balloon-expandable, drug-eluting stents has conclusively been shown to be the best therapy for diseased human arteries. Their results in the coronary arteries of the heart have been no less than spectacular,” said Lewis B Schwartz, co-founder and chief medical officer (CMO) of Efemoral Medical. “However, these rigid devices cannot be safely implanted into the arteries of the legs because they would be crushed as the patient walks or sits. The EVSS uses a unique design of alternating dissolvable scaffolds and spaces that, for the first time, allows the long arteries of the legs to be treated with the same, effective, balloon-expandable technology proven to be successful in other human vascular beds.”
“The initial clinical experience in EFEMORAL I has demonstrated that the EVSS has the potential to be a highly effective treatment for femoro-popliteal disease,” said Christopher Haig, co-founder and chief executive officer (CEO) of Efemoral Medical. “This new funding will allow us to build additional confidence in our device by taking it to multiple hospitals and enrolling more patients. We remain committed to advancing the science behind our device and are excited about the potential of our technology to offer a durable clinical solution to patients and physicians.”
Cook Medical announces John A Kaufman (Cook Medical, Bloomington, USA) will be joining as its chief medical officer, effective July 2023. With Kaufman’s expertise and new appointment to this position, Cook is taking a significant step in its clinical and product-related goals.
Kaufman is an interventional radiologist with 30 years of experience. In 1982, he earned his doctor of medicine from the Boston University School of Medicine. He interned at the hospital of the University of Pennsylvania. Then, he finished a residency at Boston University/Boston City Hospital, later becoming chief resident in radiology, completing a fellowship in vascular and interventional radiology there as well.
Throughout his career, his research has focused on aortic aneurysms, venous diseases, vascular malformations and image guide treatment of liver cancers and uterine fibroids. Then, in 2010, he earned an MS degree in healthcare management from the T.H. Chan School of Public Health at Harvard. Kaufman is the inaugural chair of the Dotter Department of Interventional Radiology, director of the Dotter Interventional Institute and the Frederick S Keller professor of Interventional Radiology at the Oregon Health & Science University (OHSU) in Portland, Oregon.
In addition to practicing medicine and being a professor, Kaufman has been involved in many societies. He is active in the American Heart Association, American Board of Radiology, American College of Radiology, American Roentgen Ray Society and Radiological Society of North America. As a long time fellow of the Society of Interventional Radiology (SIR), Kaufman served as SIR president. SIR named him as the 2012 Dotter lecturer. Additionally, he is a fellow of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE). Both SIR and CIRSE awarded Kaufman gold medals for his research and his passion for education.
“We are honoured to have Kaufman join Cook Medical and add his unique expertise to our leadership team. We’ve followed Kaufman’s work for years and it’s evident that we share the same value of putting patients first. He will bring a unique insight into the needs of clinicians, patients, and scientists as we work together to move the practice of medicine forward,” said Pete Yonkman, president of Cook Medical and Cook Group.
In his role as chief medical officer, Kaufman will represent the company to regulatory and legislative agencies, advise on the educational needs of the clinical community and patients, serve as voice of the patient to ensure understanding and promote the future of minimally invasive interventions within Cook. The chief medical officer will also serve as clinical resource for engineers, marketing and ethics and compliance officers, as well as provide strategic input on current devices and programs.
“I look forward to sharing my perspective from the front lines of patient care,” said Kaufman. “One thing I am particularly passionate about is education. Teaching and learning have been staples in my career, and medical education is integral to Cook’s product philosophy. Most importantly, joining Cook is a beautiful opportunity to be a liaison between the scientific community and patients as we learn together how we can improve patient lives.”
Kaufman will continue his clinical practice part-time at OHSU.
Boston Scientific has announced that it will make a partial offer to acquire a majority stake, up to a maximum of 65%, of shares of Acotec Scientific, a Chinese medical technology company that offers solutions designed for a variety of interventional procedures.
The proposed price is HK$20 per share, which represents a total upfront cash payment consideration of approximately US$523 million for the 65% stake at current exchange rates.
Acotec is a leader in medical solutions, including drug-coated balloons (DCBs), which are used in the treatment of vascular and other diseases. In 2016, the company launched the first peripheral DCB in China after receiving approval from the National Medical Products Administration. The Acotec portfolio also includes radiofrequency ablation technologies and thrombus aspiration catheters, as well as more than 20 other products in various stages of development across a range of specialties. In the 12-month period ending June 30, 2022, Acotec generated sales of RMB 339 million (approximately US$53 million), growing 25% year-over-year in the first six months of 2022 with strong double-digit growth in each of the two years prior.
“Acotec is a profitable, fast-growing company with a strong portfolio and innovative pipeline of medical technologies, and we believe this investment will generate growth opportunities for both companies,” said Art Butcher, executive vice president and group president, MedSurg and Asia Pacific, Boston Scientific. “We expect completion of the partial offer to further strengthen our presence in China and create the potential for commercialisation of Acotec products globally, providing an increased number of physicians and patients access to our robust and complementary product portfolios.”
Boston Scientific expects the impact to adjusted earnings per share to be immaterial in 2023 and the impact to generally accepted accounting principles (GAAP) earnings per share to be less accretive, or dilutive, as the case may be, due to amortisation expense and acquisition-related net charges.
The completion of the transaction, which is anticipated in the first half of 2023, is subject to acceptance and approval by Acotec shareholders and other conditions set forth in related filings.
Europe’s health commissioner, Stella Kyriakides, has announced that proposals to extend the transition period for the implementation of the European Union’s (EU) Medical Device Regulation (MDR) will be put forward in early 2023.
Kyriakides informed health ministers from the EU’s 27 member states of the plan at a meeting of the Employment, Social Policy, Health and Consumer Affairs Council in Brussels on Friday (9 December), where the council members discussed the current status of the implementation of the MDR.
The regulation—which changes the way that medical devices are certified for use in the European market—first came into effect in 2021 with an initial three-year transition period, having been delayed by one year in 2020 due to the onset of the COVID-19 pandemic.
Concerns have been raised over the impact of the transition to the new regulatory regime, with the European Society of Cardiology (ESC) last week calling upon ministers to act to prevent a “shortfall of essential medical devices for cardiovascular patients”, which the Society warned could include diagnostic and ablation catheters and some stents.
At Friday’s meeting, Kyriakides informed ministers that she will propose an extension to the transition period for the implementation of the MDR in early 2023—with the measure then to be voted upon by the European Council and Parliament.
“Patients rightly expect to have safe and high-quality medical devices,” Kyriakides told journalists at a press conference that followed the council meeting, where she acknowledged it is now a “crucial time” for the transition to the new rules.
“We have been following the progress achieved towards this goal very closely in the past months and, while the number of notified bodies have increased and actions have been taken to prepare manufacturers, this is not enough,” Kyriakides added. “In addition, we are now experiencing supply shortages on the global market. We are still feeling the impacts of the pandemic, and now also the Russian war in Ukraine, where several manufacturers of devices are located. This is creating additional complications.
“This is why I announced today to ministers that we will propose to extend the transition period to mitigate any short-term risks. This targeted amendment will take into account the risk class of different devices and address the sell-off date. At the same time, we will work on medium- and long-term solutions to address the more structural issues that have arisen with the new rules.
“Our citizens do not only expect medical devices to be safe, they also expect them to be available. We will do everything in our power to ensure that this transition does not create any disruptions.”
Reto Bale (Innsbruck, Austria) talks to Interventional News at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain) about some of the key benefits of using navigation and robotics during interventional radiology and oncology procedures, such as the ability to “increase reliability and reproducibility” and “improve workflow”.
Bale discusses his initial experience of using an early robotic system for cone beam computed tomography (CBCT)-guided procedures for bone interventions, noting that, with this technology, “you can precisely reach nearly every target in the body from head to toe”.
One of the major strengths of the Micromate robotic system (Interventional Systems) “is that it is very flexible” states Bale, who concludes that “it is a very interesting tool to do all types of CT-guided procedures, including radiofrequency ablation”.
This video is sponsored by Interventional Systems.
Interventional News’ most popular stories last month included news of a US Food and Drug Administration pre-market approval submission of an ultrasound renal denervation system, as well as that of receipt of aforementioned approval for a drug-coated angioplasty balloon for peripheral artery disease; and a report of a British Society of Interventional Radiology presentation on the state of genicular artery embolization practice in the UK.
Otsuka Medical Devices and ReCor Medical have announced the filing of the pre-market approval application to the US Food and Drug Administration for the Paradise ultrasound renal denervation system in the treatment of uncontrolled hypertension.
The first trial participant has been treated as part of GENESIS II, a study of Embozene microspheres for genicular artery embolization as treatment of mild-to-moderate knee osteoarthritis.
The US Food and Drug Administration (FDA) has approved the Chocolate Touch drug-coated balloon (DCB) percutaneous transluminal angioplasty catheter for the treatment of patients with peripheral artery disease in the superficial femoral artery and the popliteal artery.
The Sundance (Surmodics) sirolimus drug-coated balloon (DCB) has an “excellent” safety profile in a “challenging, real-world, predominantly CLTI [chronic limb-threatening ischaemia] population,” and has a primary patency rate of 80% at 12 months in a per-protocol analysis population.
The British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) featured a presentation on the existing body of evidence for GAE’s safety and efficacy and the roadmap for growing this further in order to gain UK National Institute of Health and Care Excellence (NICE) recommendation.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (10–14 September, Barcelona, Spain) discussion participants underlined that while vying to make your voice heard at multidisciplinary team meetings is vital, this should not be motivated by ego, rather, by the common goal of what is best for the patient based on clinical effectiveness and patient outcome.
The Society of Interventional Radiology (SIR) published a position statement deeming endovascular thrombus removal “an acceptable treatment option in selected patients with acute iliofemoral deep vein thrombosis [DVT].”
The latest results from CLOUT and a propensity score-matched analysis of CLOUT versus ATTRACT bolster the evidence base for mechanical thrombectomy in the field of deep vein thrombosis (DVT) management.
Delcath Systems announced the publication of a retrospective analysis of patients who underwent a percutaneous hepatic perfusion procedure (PHP) with Chemosat for the treatment of either inoperable intrahepatic cholangiocarcinomas (iCCA) or extrahepatic cholangiocarcinoma (eCCA) with liver metastases.
Sixteen of the 17 patients were evaluable for response as one patient died without follow-up imaging 13 weeks after the first PHP with no identifiable relationship to the PHP treatment. After the first PHP, one patient (6%) presented with a complete response (CR). Three patients (18%) had a partial response (PR) in the first follow-up exam and seven patients (44%) presented with stable disease (SD). Five patients (31%) had progressive disease (PD), one of which was limited to extrahepatic progression only. In total, in 17 treated patients had an overall response rate (ORR) of 25% and a disease control rate (DCR) of 75% was achieved. Two patients with PR, six patients with SD and the patient with PD limited to extrahepatic progression received further PHP treatments. In the subsequent follow-up exams, the overall best therapy response in these patients was PR in 78% and SD in 22%. One patient was treated in total with eighy PHP treatments within 30 months.
The median progression-free survival (PFS) was 3.5 (95% CI:2.2–7.4) months with a similar median hepatic PFS of 3.6 [95% CI: 2.6–9.5] months. Calculated from first diagnosis of iCCA (or CCA liver metastases), the median survival was 27.6 [95% CI: 16.5–37] months. From first PHP, a median survival of 9.9 [95% CI: 3.8–21] months was observed, with a one-year survival rate of 41%. For context, the authors noted that for inoperable CCA, the treatment options are limited and a median survival of 2.5–6 months is to be expected, which can be extended to approximately 12 months under first-line chemotherapy with gemcitabine and cisplatin. In this study all patients were previously treated with at least systemic therapy and the authors note that the results of their analyses confirm the potential for survival extension by PHP treatment even after the exhaustion of systemic therapies.
The authors highlighted the increasing importance of locoregional forms of therapy in the treatment of CCA and that the new edition of the German S3 cancer guideline ‘Diagnostics and Therapy of Hepatocellular Carcinoma and Biliary Carcinomas’ now includes PHP with melphalan for the treatment of inoperable iCCA or eCCA liver metastases. Based on the results of this study, the authors concluded that for patients with inoperable, treatment-refractory iCCA and CCA liver metastases, PHP is an effective and safe treatment option that has the potential to prolong life in a palliative setting.
Data have been presented for the first time at the Paris Vascular Insights (PVI) conference (23–25 November, Paris, France) from the ABISS trial, which compared drug-coated balloon (DCB) with plain-balloon angioplasty for arteriovenous fistula (AVF) stenosis.
ABISS was a physician-designed prospective, randomised, double-blind trial that included 12 centres in France. The study enrolled 150 adult patients who had a native autologous AVF stenosis already punctured for haemodialysis. Following predilatation, patients were randomised 1:1 between DCB (Lutonix, BD) and placebo balloon application. The study was mainly funded by the French government clinical research programme (PHRC).
The primary outcome of the study was cumulated incidence of loss of primary patency of AVF at six months. The study authors, led by Raphaël Coscas (Ambroise Paré Hospital and Paris-Saclay University, Paris, France) found in an intention-to-treat analysis DCB was superior to plain-balloon angioplasty at six months but not in a statistically significant way, with a p value of 0.09. It was however statistically significant at three months (p=0.002). In a prespecified per-protocol analysis, the DCB was superior to a statistically significant degree at the intervals of three (p=0.0004), six (p=0.008) and 12 months (p=0.029) for the main outcome. There was no difference in terms of mortality or rates of adverse events between the groups. Coscas noted that the secondary outcomes, which included dialysis circuit patency, restenosis, and thrombosis, will be presented in future meetings.
The presenter drew attention to the difference between the intention-to-treat analysis results and those of the per-protocol analysis. He said that “the way data of the study were analysed will need to be discussed because, in the intention-to-treat analysis, patients lost to follow-up or who waived consent were imputated to the worst-case scenario (loss of patency if DCB arm and patency if placebo arm),” suggesting a “disadvantage” for the DCB in the intention-to-treat results. “This was less the case in the per-protocol analysis—I think we will discuss that later on”. He added that post-hoc analyses based on similar criteria of other major DCB in AVF trials are ongoing.
Egg Medical, a medical device company commercialising technologies to reduce scatter radiation exposure during interventional angiographic procedures, has announced that it has achieved CE mark for the EggNest XR radiation protection system. The EggNest protects the entire interventional team in hospital X-ray labs (cardiac catheterisation, electrophysiology, interventional radiology, and operating rooms) from the harm of long-term exposure to scatter radiation.
“Occupational exposure of hospital staff to X-rays during medical procedures is an important workplace risk. Almost everyone in the interventional cardiology and radiology profession knows someone with a radiation-related illness. There have been minimal improvements in X-ray shielding over the past 30 years, leaving the medical teams working in these environments exposed to scatter radiation every day,” said Robert Wilson, Egg Medical CEO. “The EggNest platform addresses the problem of hospital personnel radiation exposure for everyone working in these environments by reducing scatter radiation by an average of 91 per cent.”
With the CE mark certification, Egg Medical will continue expansion into all markets recognising the CE mark.
“At Egg Medical, our belief is that everyone deserves protection, meaning the entire interventional team,” said Wilson. “With CE mark approval of the EggNest platform, we are bringing this protection to more interventional teams worldwide.”
Royal College of Radiology (RCR) president Kath Halliday (Nottingham University Hospitals, Nottingham, UK) gave a presentation to the British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) exploring how new technologies and infrastructural reforms can improve outcomes for patients under interventional radiology (IR) department care. Drawing attention to the problems with IR practice in the National Health Service (NHS), particularly with regard to capacity, she suggested harnessing artificial intelligence (AI), collecting data and recourse to dedicated day case units and hybrid theatres could reduce waiting times and drive more effective interventions.
She drew attention to the fact that “there are no data” widely available on IR procedures. The Getting It Right First Time (GIRFT) programme reviews services and procedure outcomes across the NHS but, Halliday said, provides little in the way of information on the outcomes of IR procedures. “We need to be able to identify IR procedures from our radiology codes,” she argued, stating that these in turn need to link to the codes used in Hospital Episode Statistics (HES), a database of NHS admissions records covering comorbidities, length of stay and outcomes.
According to Halliday, a similar problem exists in informing patients of their options around IR procedures, as those who present the information are often not radiologists themselves. Often, this is due to a lack of a dedicated area within radiology departments in which to see patients. Integrating IR procedures into a more comprehensive data management system means interventional radiologists and their patients can make more informed decisions about procedures. This will also require improvements to NHS IT infrastructure, Halliday suggests.
Capacity was another focus of Halliday’s talk. She described how “lack of capacity too often results in poor outcomes for patients,” adding that “for instance, some people wait so long for angioplasty that they end up with amputation,” then referring to the situation in some hospitals where capacity is so limited that radiologists are forced to come in to perform procedures when they are not on call. Improving capacity is difficult because those radiologists required to teach trainees are already overworked, she argued. It would also require creating a more hospitable workplace in terms of morale and working hours to encourage radiologists to stay in the field. For a technology-driven solution Halliday pointed to procedure simulators, which are still underused in training new radiologists. AI would also be useful for diagnostics in IR—though she said she did not believe robots would be performing procedures any time soon.
Halliday concluded the question and answer that followed her presentation by advocating for expanded IR training.
A minimally invasive treatment for carpal tunnel syndrome provides complete and long-term relief to patients without the use of corticosteroids, according to research presented at the annual meeting of the Radiological Society of North America (RSNA; 27 November–1 December, Chicago, USA).
Carpal tunnel syndrome is a form of nerve entrapment neuropathy, involving the pressing or squeezing of a peripheral nerve. It occurs when the median nerves and tendons inside the carpal tunnel, a narrow and rigid passageway that runs from the forearm to the palm of the hand, are being pressed or squeezed at the wrist. This results in tingling, numbness and/or weakness of the fingers and hands. Carpal tunnel syndrome is the most common and widely known form of entrapment neuropathy, affecting about 3% of the USA’s population.
Surgery is often required to treat carpal tunnel syndrome when non-surgical methods, such as physical therapy or corticosteroid injections, are insufficient. The most common and widely used surgical method involves cutting the carpal ligament to reduce pressure on the median nerve. This method requires making an incision into the wrist.
The study’s findings show that a technique called hydrodissection effectively treats nerve entrapments without the need for surgery or corticosteroids. It involves the injection of a liquid, usually saline, into a nerve to separate it from the surrounding tissue. Ultrasound guidance is used to accurately identify nerves.
Lead author Anindita Bose (University College of Medical Sciences, Delhi, India) comments “previously, the studies that have been done on ultrasound-guided hydrodissection for carpal tunnel syndrome have used corticosteroids either alone or as a part of the injection, making it difficult to assess whether hydrodissection alone was beneficial, or if it was due to the effect of the steroids.”
For this randomised controlled trial, Bose and colleagues enrolled a total of 63 patients suffering from carpal tunnel syndrome. Researchers used the Boston Carpal Tunnel Questionnaire (BCTQ), the Visual Analog of Pain (VAS), and cross-sectional area ultrasounds of the median nerve to assess patient pain and symptoms before and after the procedure. The 63 patients were divided into three groups. Group one received ultrasound-guided hydrodissection with just a saline injection. Group two received ultrasound-guided hydrodissection with an injection mixture of saline and corticosteroid. Group three received just an ultrasound-guided corticosteroid injection with no hydrodissection.
Follow-up was done at four weeks, 12 weeks and six months. At the four-week mark, all three groups of patients showed a reduction in pain. By the 12-week and six-month mark, both groups that received ultrasound-guided hydrodissection showed further improvement while the group that received just a corticosteroid injection reported a recurrence of symptoms and an increase in BCTQ and VAS scores.
Additionally, ultrasounds showed a significant reduction of median nerve cross-sectional area in both hydrodissection groups. Group one showed a reduction of 43%, and group two showed 46%. Group three showed only an 11% reduction.
The procedure is short, requiring only 10 to 15 minutes, which can reduce costs for treatment facilities. Anupama Tandon (University College of Medical Sciences, Delhi, India) a co-author of the study notes, “it came as a pleasant surprise when this simple procedure of ultrasound-guided hydrodissection provided patients with long-term relief.” She continues, “the patients were highly satisfied, as the cost was low, no anaesthesia or hospitalisation was needed, and they could go back in an hour’s time and resume their routine work.”
Neurologica, a subsidiary of Samsung Electronics, has announced that its head-to-toe trauma imaging solution—the BodyTom 64 point-of-care mobile computed tomography (CT) scanner—has received 510(k) clearance from the US Food and Drug Administration (FDA) for commercial use in the USA.
Based on customer feedback, the company designed the BodyTom 64 to enhance the user experience and improve clinical workflows through revisions to both the software and the data acquisition system (DAS), a press release states. Such revisions include incorporating Linux as the operating system and having the ability to generate up to 64 cross-sectional CT images of a patient’s body, versus the 32 images produced by the predicate BodyTom Elite system.
A Neurologica press release also details that, with indications for both paediatric and adult imaging, the BodyTom 64 is a multi-departmental imaging solution that can be utilised for various needs, including:
Neurosurgery/surgery—when combined with any radiolucent skull fixation device, it can transform an operating room into an intraoperative neuroimaging suite to enhance neuro-navigation and surgical outcomes, including clinical utility for extracranial procedures
Trauma/emergency room (ER)—its unique combination of internal lead shielding and battery operation allows any standard trauma bay to be transformed into an advanced CT imaging suite
Interventional radiology (IR)—it can also help optimise workflows by remaining ready to rescan for each stage of needle guidance, and bring the power of multi-slice CT to the interventional suite
“We are thrilled to build off our expertise and elevate point-of-care imaging with our BodyTom 64, which can transform any room in a hospital into an advanced imaging suite,” said Jason Koshnitsky, senior director of Global Sales and Marketing at Neurologica. “This full-body 64-slice CT scanner is an upgraded version of the BodyTom Elite CT scanner, providing enhanced functionality with the same high-resolution imaging capabilities.”
“In contrast, for patients with RCCs smaller than 3cm, either cold-based or heat-based therapy is just as effective in reducing cancer-specific mortality,” comments lead author Gabriele Sorce (San Raffaele Scientific Institute, Milan, Italy). “The findings may help us to better tailor the choice of ablation technique for patients with small RCCs.”
Lower risk of cancer death with cryoablation versus heating
Renal cell carcinoma is the most common type of kidney cancer. For patients with early-stage RCCs smaller than 4cm, an increasingly popular treatment option is destroying the cancer by freezing it or heating it. For these clinical stage T1a RCCs, ablation can provide high survival rates without the need for more extensive kidney surgery.
However, the outcomes of ablation appear “less favourable” for a subset of patients with clinical stage T1a RCCs: those whose tumours are between 3 and 4cm in size. Current European guidelines recommend cryoablation over thermal ablation for these cancers measuring 3 to 4cm, while US guidelines state that either treatment can be used. Both sets of guidelines state that either freezing or heating can be used for T1a RCCs measuring 3cm or smaller.
To clarify the issue, an international research group analysed patients with stage T1a RCCs treated with freezing or heating between 2004 and 2018. Patients were drawn from the US National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program. The study focused on two matched groups of patients with cancers measuring between 3 and 4cm: 757 treated with cryoablation and 388 treated with thermal ablation.
Median age at treatment was 71 years. Follow-up data on cancer-specific mortality were available for 422 patients treated with freezing and 238 treated with heating.
Eight years after treatment, estimated cancer-specific mortality among patients with RCCs measuring 3 to 4cm was 8.5% for patients treated with cryoablation versus 12.9% for those undergoing heat-based thermal ablation. With both treatments, about 40% of patients died from causes other than cancer.
Implications for treatment decisions in ‘small, potentially curable’ kidney cancers
After adjustment for non-cancer-related death and other characteristics, patients undergoing thermal ablation for RCCs between 3 and 4cm were twice as likely to die of kidney cancer. In contrast, for patients with cancers smaller than 3cm, estimated cancer-specific mortality was similar between groups: 6.8% after cryoablation and 6.1% after thermal ablation.
The study is one of the first to directly compare clinical outcomes for freezing versus heating in patients with stage T1a RCCs measuring between 3 and 4cm. The results suggest that thermal ablation has “a highly statistically significant and clinically meaningful” disadvantage in terms of the long-term risk of death from kidney cancer, compared to cryoablation.
“Conversely, in patients with tumours 3cm or smaller, either ablation technique is equally valid,” says Sorce. “We believe our findings have important implications for clinical decision-making and informed consent for patients with these small, potentially curable kidney cancers.”
The Swiss Federal Assembly has voted in favour of accepting medical devices with US Food and Drug Administration (FDA) marketing authorisation in Switzerland.
A motion for ‘more freedom of action in the procurement of medical products for supply of the Swiss population’ was discussed and put to a vote in the country’s parliament on Monday 28 November, with many industry groups, including Swiss Medtech, supporting the acceptance of FDA-approved devices.
In a press release, Swiss Medtech described this as a “necessary and urgently needed decision”, and stated that it is “essential” for this order to now be implemented swiftly and pragmatically. It further draws on Australia and Israel as examples of countries in which “efficient procedures” to recognise FDA approvals in parallel with the CE mark have “proven successful”, and “can be achieved in an uncomplicated manner”.
“Swiss Medtech very much welcomes the policymakers’ important and forward-thinking decision,” added Peter Biedermann, managing director of Swiss Medtech. “It is a response to circumstances that could no longer be ignored. Specifically, problems with the implementation of the new European Medical Device Regulation [MDR], and the negative consequences concerning availability, product range and quality of medical devices throughout Europe. As innovations are increasingly being introduced first to the market in the USA, new products reach Europe with a delay, at best.”
The Swiss Federal Council—the executive body of the country’s federal government—opposed this proposition, citing the administrative burden that would be brought about by this regulatory shift, and patient safety concerns caused by risk classification discrepancies between the USA and Europe.
On 30 May 2022, the potential acceptance of US FDA products was voted on by the 46 members of the Swiss Council of States (the upper house of the country’s Federal Assembly), with 23 voting to accept and 12 voting to reject.
Shortly following this decision, the Federal Council asserted in a press release that there was no need to accept non-CE-marked medical devices, such as US FDA-approved devices, at that time—describing the extension of simplified market access to other countries outside of the EU as “disproportionate”—before noting that it would re-evaluate this situation at the end of 2024. It added that the supply of safe medical devices in Switzerland was “currently guaranteed”, referencing various backup measures it took back in 2021 to ensure this “even without an updated MRA [Mutual Recognition Agreement]”.
The parliamentary vote that took place earlier this week was borne out of the introduction of the European MDR on 26 May 2021, with the MRA and all related trade-facilitating effects for medical devices between the EU and Switzerland also ceasing to apply from the same date.
And, while devices ‘in conformity’ with the MDR can be certified and placed on the market until 25 May 2024, marketed devices must be certified directly under the MDR from the following day (26 May) onwards. With this deadline drawing ever closer, concerns have been raised regarding regulatory challenges, supply chain gaps and device shortages, and the impact this could have on patient care and industry alike.
As a statement from Swiss Medtech notes, “more than 1,000 of the approximately 5,000 foreign manufacturers have already stopped supplying Switzerland with their products—they are not prepared to meet the additional requirements for the limited Swiss market, and patients in Switzerland are the ones to suffer”.
The motion to accept US FDA approval of devices in Switzerland was brought up to the 200-seat Swiss National Council (the lower house of the country’s Federal Assembly) on Monday, with 100 votes in favour and 79 against being cast. As such, both chambers of Switzerland’s national parliament have now voted to adopt the initiative, and will instruct the Swiss Federal Council to adapt legislation to allow devices with US FDA clearance onto the market.
Details of this new system and the logistics of implementing it, as well as when it will come into effect, are yet to be confirmed.
Otsuka Medical Devices and ReCor Medical, a subsidiary of Otsuka, announce the filing of the pre-market approval (PMA) application to the US Food and Drug Administration (FDA) for the Paradise ultrasound renal denervation (uRDN) system in the treatment of uncontrolled hypertension.
The Paradise uRDN system is designed to reduce sympathetic nerve activity by denervating nerves which surround the renal arteries with the goal of reducing blood pressure, and uses a combination of ultrasound energy to denervate the renal nerves and a water-filled balloon to protect the renal artery. The system employs an interventional procedure in which a catheter is placed in each of the main renal arteries, following which two to three seven-second ultrasound emissions are delivered to denervate the surrounding renal nerves, thereby reducing blood pressure.
Since 2009, ReCor has been focused on developing and testing the Paradise uRDN system to treat hypertension safely and effectively. ReCor has three global, independently powered, sham-controlled randomised clinical trials of the Paradise uRDN system in more than 500 patients with uncontrolled hypertension: RADIANCE-HTN SOLO, RADIANCE-HTN TRIO and RADIANCE II. Each RADIANCE trial met its prespecified primary efficacy endpoint of blood pressure reduction, with positive safety.
RADIANCE II is the USA FDA’s investigational device exemption (IDE) pivotal trial. In September 2022, ReCor and Otsuka Medical Devices announced that the trial successfully reached its primary efficacy endpoint. Results showed a reduction in daytime systolic ambulatory blood pressure of -7.9 mmHg in those treated with uRDN and a difference between uRDN and sham of -6.3 mmHg (p <0.0001). The results from the all three RADIANCE clinical trials have been included in the submission for approval to the FDA.
The uRDN system bears the CE mark for the treatment of hypertension in Europe and is an investigational device in the USA and Japan.
L to R: Clare Bent, Peter Littler, Robert Morgan, Raman Uberoi (at BSIR 2022)
L to R: Clare Bent, Peter Littler, Robert Morgan, Raman Uberoi (at BSIR 2022)
In the opening session of the British Society of Interventional Radiology (BSIR) annual scientific meeting 2022 (2–4 November, Glasgow, UK) titled ‘What’s up, Doc?’, four faculty members spelt out for attendees what they consider to have been the most noteworthy advancements in the specialty of late, as well as their forecasts for interventional radiology’s (IR) direction of travel. Advances from the vascular, interventional oncology (IO), non-vascular, and non-clinical spheres featured in the session, with the latter consisting of a call to encourage trainees into IR to meet the current workforce shortfall.
In Robert Morgan’s (St George’s Hospital, London, UK) vascular-focused presentation, he first drew attention to a paperthat had reported favourable results of the use of paclitaxel-coated balloons below the knee for patients with peripheral arterial disease (PAD) including no risk of death. He reminded the audience that a previous meta-analysis of studies involving paclitaxel-coated devices had suggested an increased risk of all-cause death, which had been ascribed to paclitaxel-coated device use. During his presentation, he stated that no study published since 2018, looking at single-cause mortality and involving the use of paclitaxel-coated devices above or below the knee, had found an increased risk of death associated with paclitaxel-coated devices.
Morgan also described the IMPERIAL randomised study comparing the Eluvia (Boston Scientific) and the Zilver PTX (Cook Medical) drug-eluting stents (DES), which had concluded that there was no significant difference in patency at two years between the two DESs. However, there was a slight benefit in target lumen revascularisation rate for the Eluvia DES, which just reached significance.
Morgan discussed the positive results of the randomised controlled trial DISRUPT PAD III, which compared Shockwave Medical’s peripheral lithoplasty system plus drug-coated balloon (DCB) for treating moderate and severely calcified femoropopliteal arteries with standard balloon angioplasty. He described the findings as “providing proof of concept for intravascular lithotripsy” as a treatment for heavily calcified femoropopliteal occlusive lesions.
Robert Morgan presenting at BSIR 2022
Another study that Morgan referenced was an analysis of Medicare data from 2011 to 2019 published in the Journal of Vascular and Interventional Radiology (JVIR) in November 2022. This study examined clinicians’ use of medical devices including drug-eluting balloons (DEBs), DESs and atherectomy in treating PAD patients in the USA. Morgan described an attached commentary as being relatively “scathing” of existing practice with excessive non-evidence based used of atherectomy compared with DEB/DES. Morgan concluded by stating that the evidence supports much more widespread use of DCBs and DESs compared with atherectomy devices, although the two techniques may be complementary in selected patients.
Peter Littler’s (Freeman Hospital, Newcastle upon Tyne, UK) focus was on IO, detailing advances in the techniques used in selective internal radiation therapy (SIRT), noting that for the first time, this type of cancer treatment has been included in international guidelines. Advanced catheters like the SWIFTNinja steerable catheter (Merit Medical) and personalised dosimetry, where individual cancer patients can be given amounts of radiation catered to the nature of the tumour, are among the developments in SIRT. Littler cited a study in The Lancet that evidences considerable improvements in survival rates after such tailored treatment.
Advances have also been made, Littler said, in ablation. Littler, who carries out ablation procedures on the liver, noted the benefits of stereotactic needle guidance technology. He then shared details of the novel ablation technology histotripsy, a non-invasive, ultrasound-based technique that works “like 3D sculpting” that is currently only being used in the HOPE4LIVER trial. Littler offered the suggestion that many of the technologies he detailed would be more widely available in the immediate future.
Clare Bent (University Hospitals Dorset, Bournemouth, UK) then gave her take on the “exciting new interventions and applications” in the benign non-vascular world of IR—an area that is “expanding at a fast pace”.
Clare Bent presenting at BSIR 2022
Musculoskeletal (MSK) embolization has grown as a discipline, Bent informed the BSIR audience, with genicular artery embolization (GAE) having the largest evidence base. Experimental studies have demonstrated a link between angiogenesis and pain, shown as hyperaemia on angiographic imaging, Bent detailed, enabling targeted therapeutic embolization. Bent also described several other applications including embolization of plantar fasciitis, with reductions in both plantar fascial thickness and pain following treatment. The next step for MSK embolization, she advised, is for the IR community to secure investment into further scientific research, the results of which may then help move these techniques from “marginal” to “mainstream”.
Bent also gave an overview on the use of glue, over coil, embolization to reduce cost, radiation dose and increase durability of the embolic endpoint, using pelvic vein and prostate artery embolization as examples of where this alternative technique may be advantageous. Moreover, and despite its “slow uptake in the UK”, radiofrequency ablation for benign symptomatic thyroid lesions has been endorsed by many societies worldwide. News of National Institute of Health and Care Excellence (NICE) guidance stating that microwave ablation can be used provided standard arrangements are in place for clinical governance, consent, and audit has been released since Bent gave her presentation.
“Expanding on existing techniques can change lives,” Bent concluded, adding cryotherapy for Morton’s or amputation stump neuromas to her list of novel IR applications.
Raman Uberoi (Oxford University Hospitals, Oxford, UK) rounded off the first session of the meeting by addressing the non-clinical side of IR, choosing to home in on recruitment of interventional radiologists in line with achieving a fit-for-purpose national service specifically as worthy of focus. He began by outlining the “huge range and complexity – has grown and grown, is exploding” of IR procedures, and how this has seen interventional radiologists branch into different subspecialties. However, the small numbers in these subspecialties make providing a 24/7 IR service challenging, the audience heard. Therefore, Uberoi incited delegates to “think carefully” about how the “next generation” of interventional radiologists can and should work.
Raman Uberoi presenting at BSIR 2022
The speaker made some suggestions as to how the specialty can “make things better for future interventional radiologists”. Among these was the adoption of specific IR training and formal assessment, as the subspecialty increasingly diverges from diagnostic radiology, Uberoi explained. The European Board of Interventional Radiology (EBIR) examination is an example of an accreditation model that has been proven to work worldwide, with a dedicated curriculum to match the exam content.
Future improvements to training, the presenter went on to note, could include in non-operative, more “human factors that are pertinent to our practice”, as well as coverage of day-to-day catheter skills.
Although the IR workforce has, on average, grown by 4% year on year over the last five years, Uberoi underlined the “unacceptable risk for patients” that the insufficient number of interventional radiologists in the UK is causing—50% of UK trusts were “unable to provide adequate 24/7 IR services in 2021,” Uberoi stated.
Therefore, the presenter left the audience on a to-do list for future-proofing IR services, involving increasing advertising to attract more IR trainees, protecting time for specific IR training, and ensuring trainees are exposed to ‘on-call’ earlier—“you should not be doing your first independently once you have become a consultant”.
“There are opportunities to collaborate across the spectrum,” Uberoi concluded, highlighting stroke as an area that lends itself to cross-disciplinary working. However, he emphasised how “we [in BSIR] have to drive the changes” and “work with the [Royal College of Radiologists]” so that improved patient quality of care is the outcome.
This article was amended on 30th November to correct an error.
Findings from a recent prospective study show promising safety and patient outcomes data for locally advanced and borderline resectable pancreatic cancer treatment using ablative stereotactic magnetic resonance imaging (MRI)-guided on-table adaptive radiation therapy, also known as SMART. Approximately 25% of the study’s participants were patients treated at the Henry Ford Pancreatic Cancer Center (HFPCC; Detroit, USA).
“As a pioneering institution in the field of MRI-guided adaptive radiation therapy, Henry Ford Health is thrilled to have led this novel study, which was the largest international study of ablative radiation for pancreatic cancer in the world,” said Ben Movsas, Medical Director of Henry Ford Health Cancer and Chair of Radiation Oncology. “Henry Ford was first in the world to treat a patient using the MRIdian MRI-Guided Radiation Therapy system back in 2017. Since then, we have treated many cancer patients with MRI-guided radiation therapy.”
The primary endpoint outcomes from the study were presented at the 64th annual meeting of the American Society for Radiation Oncology (ASTRO; 23–26 October, San Antonio, USA) by Parag Parikh, the principal investigator of the study and Director of Gastrointestinal Radiation Oncology and MR-Guided Radiation Therapy at Henry Ford Cancer.
“In this study, 136 patients were treated with ablative MRIdian SMART at 13 international centres,” said Parikh. “The study’s primary outcome measured grade 3 or higher gastrointestinal toxicity, such as nausea, vomiting or abdominal pain, in the first 90 days after treatment. The study’s primary safety objective was met, with zero incidence of acute grade 3 or higher gastrointestinal toxicity definitively related to SMART treatment.”
Secondary measures of the study include overall survival, local control, distant progression-free survival, and changes in patient-reported quality of life, Parikh explained. While study patients are still early in the follow-up period, preliminary clinical outcomes data of one-year local control and distant progression-free survival were 82.9% and 50.6% respectively. One-year overall survival from diagnosis was 93.9%.
NOTE: This video is ONLY available to watch in selected countries and geographies
Lambros Tselikas (Villejuif, France) speaks to Interventional News about a recent retrospective study evaluating Liver ASSIST Virtual Parenchyma—the results of which he presented at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain).
The software simulated the perfused parenchyma from a virtual selective injection point on the proximal cone-beam computed tomography (CBCT). It was compared to the corresponding selective CBCT considered as the ground truth.
“You can have very easily the vascular extraction, tumour-feeding vessels, and more interestingly, you can now test multiple injection points and simulate the associated liver parenchyma,” says Lambros Tselikas.
“If it were easy, this session would not be here.” These are the words of Jens Ricke (University Hospital Munich, Munich, Germany), who drew attention to the self-evident nature of the difficulties involved in multidisciplinary collaboration during an expert roundtable discussion at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual meeting (10–14 September, Barcelona, Spain). Titled ‘If you are not at the table, you will be on the menu’, the discussion participants, who presented perspectives on multidisciplinary work from their various societies, kept returning in the subsequent question and answer section of the session to one key message. They underlined that while vying to make your voice heard at multidisciplinary team meetings is vital, this should not be motivated by ego, rather, by the common goal of what is best for the patient based on clinical effectiveness and patient outcome.
Eric Verhoeven
Raman Uberoi (John Radcliffe Hospital, Oxford, UK) began the discussion with a question for vascular surgeon Eric Verhoeven (General Hospital Nuernberg, Paracelsus Medical University Nuernberg, Nuernberg, Germany) and Stefan Müller-Hülsbeck (Academic Hospitals Flensburg, Flensburg, Germany) on the “stresses and strains” that arise from multidisciplinary collaboration. “You have both made the point that we ‘forget patients’—how much do you think that is driven by egos?” Verhoeven was first to acknowledge that a little bit of ego may not be a bad thing, pointing out that “without that [type of] personality”, it can be difficult to convey your specialist perspective effectively and persuasively. He recounted how he was able to influence the clinical setup at his hospital, so as to have “the whole personnel working together in the same location”—this includes radiologists, vascular surgeons, and nurses and technicians specially trained in radiology and endovascular techniques. Emphasising the “big benefit” this approach affords their patient-centric service, Verhoeven went on to share how they have a daily “vascular patient meeting”—even the name puts the focus on the patient, as opposed to the interdisciplinary makeup of the clinical team behind the care.
Raman Uberoi
Müller-Hülsbeck picked up the discussion to label this multidisciplinary way of working as “an ideal playground”, which should be harnessed to “put the patient first”. Collaboration can yield highly successful outcomes, which, at Müller-Hülsbeck’s centre, takes the following form: “if we need, for certain reasons, surgical cutdown, we call the vascular surgeon, and vice versa, if they need help from the interventional radiologist”. This collaborative way of operating is how they go about treating thoracic and abdominal aneurysms in Nuernberg and Flensburg, delegates heard, with a strong emphasis on “speaking a clear language” to facilitate cross-specialty communication for the benefit of the patient.
Part of this clarity when communicating, Müller-Hülsbeck detailed, is establishing “clear rules that are defined in advance”. This is so that the answer to the question of “who does what with the patient?” is not dictated by egos, or other factors that may render patient outcome a secondary consideration. In contrast, Verhoeven relayed how, at his hospital, “it is completely irrelevant who is doing what”, elaborating on this to say that “we decide together as a team who is the best suited” for taking on each individual case. This statement then gave way to Ricke making the point that different people’s definitions of collaboration will be different, and that what multidisciplinary involvement looks like in a particular hospital needs to be defined— ‘involved’ does not necessarily mean doing the procedure, as he added that it could mean only taking part in decision-making beforehand.
Stefan Müller-Hülsbeck
In addition to keeping the patient at the forefront of a procedure and “[putting] ego aside”, as Valérie Vilgrain (Assistance Publique-Hôpitaux de Paris, Paris, France) drove home in her presentation, Ricke summed up another takeaway from the session as a whole: “What I have learned today is that we need communication training in medical school.” He went on to contextualise this by making clear that “Nuernberg is not the rule” and that collaboration may not occur in a multidisciplinary manner as effectively in other hospitals. His hope, therefore, is that by starting early, the next generation of clinicians can learn while still at medical school to communicate in a way that is conducive to collaborative, yet patient-centred work.
Jens Ricke
Antonin Krajina (Charles University Hospital, Hradec Kralove, Czechia) then called upon the societies, such as those represented round the discussion table, to “take responsibility for interdisciplinary education.” Examples of this already occurring were heralded throughout the session, including the European Society for Minimally Invasive Neurological Therapy’s (ESMINT) theoretical stroke course (EXMINT).
Valérie Vilgrain
Stroke treatment and by whom it is delivered formed a further part of discussion during the session, with the panel shining a light on the differences in stroke thrombectomy services between the UK and The Netherlands in particular. Beyond the theory, as courses such as EXMINT teach, there is a question of how much training an interventionalist should be required to do before they can independently carry out thrombectomies for stroke patients. Wim van Zwam (Maastricht University Medical Center, Maastricht, The Netherlands) explained how “in The Netherlands, we have a requirement that if you want to do thrombectomies, you have to do at least 25 under the guidance of an experienced interventionalist, and your centre has to do at least 50 thrombectomies per year. These are very simple and straightforward guidelines.” However, Van Zwam acknowledged that, while there are more centres that can and want to do stroke thrombectomy than the country needs in The Netherlands, such is not the case in the UK. Uberoi labelled the latter as a “chicken and egg situation”, whereby “until you start doing the procedure, how can you have enough cases to train in it.”
Wim van Zwam
Van Zwam followed up to ask whether a solution could be to allow adequately trained cardiologists to perform stroke thrombectomy, to which Uberoi responded: “I do not really think the patients care who does their procedure], as long as it gets done and it is a safe service. Ultimately, you want the best trained person, but there has got to be a reality check in terms of what is achievable. Do you want zero service, or could a ‘silver’ or ‘bronze’ service be good enough to improve outcomes without compromising safety? That is the kind of balance I feel we need to look at in the UK.”
The session closed with all participants agreeing that “the clinical aspects of patient care are the same whether you are a vascular surgeon, interventional cardiologist or interventional radiologist.” This can, therefore, be a unifying motivation in multidisciplinary collaboration scenarios, and, as Vilgrain summarised, “we are better doctors when we work together”. This necessitates leaving egos at the door and working communication skills into education for medical students and trainees.
Hospices Civils de Lyon (HCL; Lyon, France) has acquired Epione, the robotic platform developed by Quantum Surgical (QS) that is designed to enable minimally invasive ablations of tumours in the abdomen. This was announced by QS in a press release.
This partnership between HCL and QS will allow more patients to benefit from Epione, a platform allowing clinicians to plan, target, deliver and confirm ablation treatment in a more secure and precise manner. Epione is currently used to target liver and kidney tumours but will be expanded to the treatment of lungs and bones as radiologists at HCL expand their robotic interventional oncology practice.
HCL is the second hospital in the world to offer this platform. The first Epione robot was acquired by Institut Gustave Roussy (Villejuif, France) in January 2022 and the team is approaching their 100th robotic procedure.
“This new acquisition of Epione is a major step for QS and a full validation of the key benefits that Epione offers. It is a great honour to have our robotic system acquired by one of the top medical institutions in France. The most exciting part of this story is that patients will now have a powerful new technology that can offer curative treatments by robotically navigating to destroy tumours while sparing surrounding healthy tissue,” explains Bertin Nahum, QS chief executive officer.
“Epione is a unique percutaneous robotic solution […] Currently, only few expert radiologists perform these treatments. Robotics will allow us to standardise these treatments and more radiologists will thus be able to perform these cases, especially the more complex ones, on tumours that would not be treated. This will allow us to help and cure more patients,” underlines Laurent Milot, deputy head of medical and interventional imaging department at HCL.
Varian, a Siemens Healthineers company, announced today that the first trial participant has been treated as part of GENESIS II, a study of Embozene microspheres for genicular artery embolization (GAE) as treatment of mild-to-moderate knee osteoarthritis. GENESIS II is the largest randomised clinical trial of GAE to assess pain relief from this condition.
GENESIS II is being conducted at the University Department of Radiology, Royal Berkshire NHS Foundation Trust, in Reading, UK. The trial targets mild-to-moderate osteoarthritis (OA) of the knee joint, a common condition and a leading cause of chronic disability. GAE involves a small catheter being advanced into the genicular arteries and Embozene microspheres are delivered through the catheter to reduce the blood supply to the areas of greatest inflammation in the knee, with the goal of reducing pain.
In the GENESIS II clinical trial, patients with knee OA will either receive treatment with the Embozene microspheres or a sham control; they have the option to receive Embozene treatment later in the clinical trial. This clinical trial design allows more accurate assessment of pain relief from the new treatment.
In October 2021, the US Food and Drug Administration (FDA) granted breakthrough device designation for Embozene microspheres for GAE for OA. Currently, Embozene is used to treat hypervascular tumours, arteriovenous malformations, uterine fibroids, and benign prostatic hyperplasia. Embolics are not yet authorised for marketing anywhere for GAE.
Mark Little, consultant diagnostic and interventional radiologist at the University Department of Radiology at the Royal Berkshire NHS Foundation Trust, is the principal investigator of the GENESIS II study. “In GENESIS, our previous 38-patient prospective study, GAE in patients with mild-to-moderate knee OA was found to be safe and effective at early follow-up,” Little noted. “We are excited to build upon this foundation with GENESIS II, which has the potential to improve our understanding of the clinical applications for the procedure. Including a sham-treated group provides the opportunity to validate the findings of GENESIS as well as to gain insight into longer-term follow-up and patient quality of life.”
“Varian is committed to supporting research that has the potential to improve outcomes and enhance the quality of life for patients around the world, and we view the GENESIS II study as an important opportunity to do this,” said David Hahn, chief medical officer, Interventional Solutions, at Varian. “Interventional radiology is defined by minimally invasive techniques, and we believe the treatment of chronic pain is a natural fit for this specialty, particularly given the World Health Organisation’s guidance on this subject. We look forward to better understanding the possible role of GAE in addressing a pressing challenge for care providers and patients.”
The Sundance (Surmodics) sirolimus drug-coated balloon (DCB) has an “excellent” safety profile in a “challenging, real-world, predominantly CLTI [chronic limb-threatening ischaemia] population,” and has a primary patency rate of 80% at 12 months in a per-protocol analysis population. Ramon Varcoe (Prince of Wales Hospital, Sydney, Australia) presented these findings from the SWING first-in-human study at the VEITHsymposium 2022 (15–19 November, New York, USA).
Varcoe, who is co-lead investigator of the trial, added that the research team observed no major amputations, “very low” rates of major adverse events, and “impressive” luminal gain, which was sustained out to six-month angiogram. In addition, Varcoe reported that Rutherford category and the functional outcome measures were improved.
“The Sundance sirolimus-coated balloon is a novel device,” Varcoe informed VEITH attendees. He elaborated: “It has a microcrystalline surface, but also a very sophisticated proprietary excipient, which, rather than using nanoparticles or microreservoirs uses chemistry to deliver the drug into the blood vessel wall and have it retain that much more so than the other devices on the market.”
The presenter noted that SWING is a prospective, multicentre, single-arm feasibility study that looked at patients with stenotic or occluded lesions. The researchers enrolled 35 patients over eight sites in Australia, New Zealand, and also in Europe.
Noting some key inclusion criteria, Varcoe detailed that patients had to be either Rutherford 4 or 5. He added the caveat that Rutherford 3 patients were included, but numbers were capped at 20% of the total cohort. Furthermore, patients had to have de novo or restenotic lesions and at least 50% stenosis by visual estimate of the investigator. They could have up to two distinct lesions in the same or different below-the-knee (BTK) artery, and had to have successfully treated inflow, as well as an unimpaired outflow artery in continuity to the ankle or foot.
The investigators performed both an intention-to-treat and a per-protocol analysis, Varcoe informed the audience. “The reason for that was because [the trial] was conducted over the COVID-19 pandemic period, so we lost seven patients to the primary endpoint of angiography,” he noted, adding that there were also three post-protocol deviations. For these reasons, the research team focused on the 25 patients who had the per-protocol analysis.
The presenter stressed that the patients included represent a “real-world” population, including a high proportion of patients who are smokers and have diabetes, as well as a majority of patients with Rutherford 4 or 5 disease. “They also had high proportions of moderate-to-severe calcification in excess of 18%, and around a third of these patients had total occlusions,” he added.
The study had two primary endpoints. The first was a safety primary safety endpoint—freedom from major adverse limb event (MALE) and perioperative death at 30 days following the index procedure. The primary efficacy endpoint was the rate of late lumen loss at six months, as assessed by quantitative vascular angiography. Both primary endpoints of the SWING trial were achieved, Varcoe revealed.
Varcoe reported that, in the per-protocol population, there were no major amputations, no major reinterventions, and complete freedom from perioperative death, “so it was a safe device”.
The team also saw a rate of all-cause death that was 0%, target lesion amputations were 0%, and a “very low” rate of clinically driven target lesion revascularisation at 8%.
Varcoe added that the minimal luminal diameter at the end of the procedure was “very high”, which he thinks “represents modern-day angioplasty techniques”, and reported a late lumen loss of 1mm at six months—results that compare “very favourably” to other equivalent DCB trials below the knee, he remarked.
As six months, the researchers observed a primary patency of 88.5%. Varcoe noted that primary patency was retained and consistently retained out to 12 months at 80%—a figure that he said is “very good for this part of the vasculature”.
Varcoe added that, “pleasingly,” the team also saw improvement in Rutherford Becker classification, which was sustained and improved out to 12 months. Regarding quality of life, he noted that patient-reported outcome measures were again consistently improved out to that 12-month endpoint.
In closing, Varcoe shared his belief that the Sundance device has “great promise” and “warrants evaluation in a large-scale pivotal trial” based on these latest findings.
Amanda Smolock (Medical College of Wisconsin, Milwaukee, USA) discusses how her practice operates, using microwave ablation nearly exclusively for primary and metastatic liver tumours targetable under ultrasound (US) and/or computed tomography (CT) guidance.
Patients are typically discussed at a multidisciplinary liver tumour conference and referred to the interventional radiology (IR) clinic for evaluation. At consultation, a full history and physical exam is completed along with updated laboratory studies, including complete blood count, liver function studies, and coagulation tests. Patients with good performance status and preserved liver function are considered appropriate for percutaneous liver ablation. Contrast-enhanced (CE) CT images or magnetic resonance images (MRI) are obtained within one month of evaluation and procedure. US assessment is performed at the clinic visit to ensure sonographic visibility and percutaneous approach for ablation. The approach is communicated with the procedure team and helps to streamline preparation on the procedure day.
Procedures are scheduled for general anaesthesia in the interventional CT suite and proper patient positioning for the procedure is a team effort: a posteriorly located tumour may require oblique positioning of the patient, and safe positioning of arms overhead improves CT image quality.
Non-contrast and multiphasic CE-CT are typically obtained prior to probe placement. This helps to review anatomy pre-procedure, confirm tumour location and size, and optimise the percutaneous approach. When possible, probes are placed under direct US guidance. Few cases have tumours visible only on CT or only after lipiodol staining with transarterial chemoembolization (TACE). In these cases, CT navigation software is used to optimise probe placement, which is often best in double oblique approaches to maximise both safety and efficacious tumour treatment. Respiratory manoeuvres in concert with the anaesthesiology team are utilised as needed to accurately and precisely target tumours with ablation probes. A non-contrast CT is obtained to confirm and document probe position. Hydrodissection and/or biopsy, if being performed, are done after securing ablation probe position(s). CT and US are complementary imaging to confirm appropriate tumour targeting and predict ablation zone coverage. Activated probes and ablation zone formation are monitored in real time with US and intermittent CT. This allows for confirmation of ablation zone formation and coverage.
Another CE-CT is obtained at the conclusion of the ablation. Total contrast volume is split between pre- and post-ablation CE-CT, not to exceed 150–200ml of iodinated contrast agent. Post-ablation CE-CT assesses ablation zone coverage of the tumour with adequate margins and also evaluates for any complications. If margins are inadequate, additional ablation can be performed at this time.
A recent addition to our practice is MR-guided cryoablation. This technology allows ablation of small liver metastases that are visible only on MRI. Patient positioning and tumour targeting require additional considerations to maintain safety in the MR environment.
Patients receive a check-up telephone call from a nurse the day after the procedure and are then seen one month post-procedure in clinic along with CE-CT/MR. Follow-up with imaging occurs every three months, which may be extended to every six months after one year of documented complete response.
Amanda Smolock is assistant professor at the Division of Vascular and Interventional Radiology, Department of Radiology, Medical College of Wisconsin (Milwaukee, USA).
Relevant disclosures: consultant/speaking faculty and grant recipient/research support, Neuwave Medical.
Terumo Europe has announced in a press release that it welcomes the guidance released by the National Institute for Health and Care Excellence (NICE) mentioning that microwave ablation can be used provided standard arrangements are in place for clinical governance, consent, and audit. This has the potential to broaden access to minimally invasive alternatives to surgery available to patients with symptomatic benign thyroid nodules.
The guidance describes ultrasound-guided percutaneous microwave ablation for symptomatic benign thyroid nodules as a minimally invasive procedure that can be performed in an outpatient setting using local anaesthesia. The aim is to reduce symptoms and improve cosmetic appearance by making the nodule smaller while preserving thyroid function, and with fewer complications than surgery.
This guidance is part of NICE’s interventional procedure programme which considers whether interventional procedures are safe and work well enough for wider use in the NHS. A comprehensive review of the literature and consultations with clinical experts and patient representatives informed the decision.
This is a positive endorsement of the treatment and a complement to the 2020 European Thyroid Association clinical practice guideline for the use of image-guided ablation in benign thyroid nodules.
The NICE document also reports that using uncooled microwave ablation devices means thinner needles can be used.
“Nowadays microwave technology is widely used in liver, lung, and kidney ablation” says Eduardo Crespo, chief of the radiology department at Hospital Universitario Fundación Jimenez Diaz (Madrid, Spain). “So far, the main gap to approach thyroid ablation has been the lack of thinner and shorter probes, to avoid potential damage to the adjacent nerves, which could lead to complications. Within the TATOpro antennae range, Terumo Interventional Systems introduced a dedicated thyroid antenna as thin as 18G with a length of 8 cm, to be used at limited power. Moreover, a 17G antenna is also available to treat larger nodules in one session, avoiding the need for patients to come back for multiple treatments.”
Soundbite Medical Solutions announced that it has entered into an exclusive license agreement with VFLO Medical (VFLO).
Pursuant to the agreement, Soundbite has granted VFLO an exclusive license for certain proprietary products including its SoundBite crossing system and the Active microcatheter system. Under the Agreement, VFLO is entitled to manufacture, develop, and commercialise the products in mainland China, Hong Kong, Macau, and Taiwan. Soundbite is, in return, entitled to receive an upfront fee, subsequent milestone payments, plus royalties from sales of such products. The terms also allow cross-licensing on future improvements of the products, aligning both companies’ focus on innovation.
“The growing prevalence of atherosclerotic vascular disease burdened by calcium has become a serious public health problem in China. We are excited to partner with the Soundbite team and look forward to bringing the unique technology and portfolio of treatment solutions to patients in Greater China that suffer from calcified arterial disease,” commented Dong Wu, president and CEO of VFLO.
“We are thrilled to work with VFLO to bring our revolutionary shock wave technology to patients in China, opening a key market for our company with an experienced partner like VFLO. Bringing non-dilutive capital to our shareholders provides us with the opportunity to build meaningful value while serving patients in the growing Chinese market,” said Lori Chmura, president and CEO of Soundbite.
VentureMed Group has announced new data presentations on the treatment of peripheral arterial disease (PAD) with drug-coated balloon (DCBs) in addition to 12-month AV Registry Data. These presentations will be given as part of the VEITH Symposium Annual Scientific Meeting 2022 (15–19 November, New York, USA).
Data presented will cover the use of FLEX Vessel Prep System in both PAD treatment with DCB and also in arteriovenous (AV) access interventions. The AV Access presentation will expand the six-month AV Registry data presented at VASA in June with 12-month results.
The first of two presentations will be titled “Late Breaking Trial with FLEX Vessel Prep and DCBs Show Better 12-Month Results With FemPop” and be presented by Eric A Secemsky (Beth Israel Deaconess Medical Centre, Boston, USA).
The second is titled “FLEX Vessel Prep System: Clinical Outcomes and Utility in HD Access Practice—AV Registry 12-Month Study Results,” and will be shared by primary investigator John E Aruny (Dialysis Access Institute, Orangeburg, USA).
Interventional News’ most popular content last month featured a report on the need for greater interventional radiology (IR) service coverage in rural areas of the USA; news of a US Food and Drug Administration (FDA) premarket approval (PMA) submission by Endologix; new restorative haemodialysis access graft data from Xeltis; and the release of three-year effectiveness data for the Abre stent (Medtronic).
A new report from a joint taskforce of the American College of Radiology (ACR) and the Society of Interventional Radiology (SIR) recommends improved access to interventional radiologists in small and rural areas.
Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.
Roberto Luigi Cazzato speaks to Interventional News about the emergence of IR outpatient clinics (IROCs) and his view that IR hospitalisation clinics (IRHCs) will soon begin being established too.
XACT Robotics announced that its ACE Xtend remote control unit received US FDA clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room.
Medtronic has announced the 36-month final results from the ABRE clinical study, the puropse of which was to evaluate the safety and effectiveness of the Abre venous self-expanding stent system, intended for the treatment of symptomatic iliofemoral venous outflow obstruction.
In the USA, atherectomy use in peripheral vascular interventions (PVIs) “more than doubled” from 2010 to 2019, with office-based procedures a “major driver” of this increase. This is according to published US data from the Vascular Quality Initiative (VQI).
Mark Little (Royal Berkshire Hospital, Reading, UK) brought delegates up to speed on genicular artery embolization (GAE) for knee osteoarthritis over two sessions at the recent British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK). Little led audience members through the existing body of evidence for GAE’s safety and efficacy, before outlining the roadmap for growing this further in order to gain UK National Institute of Health and Care Excellence (NICE) recommendation.
“We set up the first European study [GENESIS] back in 2017 and the interim analysis was published in CVIR [CardioVascular and Interventional Radiology] last year.” Little began his presentation by offering the BSIR audience background to his research. The participants in the study, he explained, were “patients with mild-to-moderate knee osteoarthritis [OA]”, numbering 38, and who “had to have had at least an attempt at conservative treatment in the six months preceding referral.”
Regarding the method and materials used, Little shared that for GENESIS, he used 100–300-micron Embosphere particles, and “skin-to-skin”, the embolization procedure took “about an hour”.
For both GENESIS and the now-enrolling GENESIS II studies, Little stated the primary outcome as being knee pain and function, assessed according to the Knee Injury and Osteoarthritis Outcome Score (KOOS). The measure of technical success, the presenter elaborated, was carrying out the embolization, which, according to the GENESIS interim analysis was 84%.
Posing the rhetorical question “Why was it not 100%?”, Little gave by way of an answer that they did not embolize six patients. The reasons in each case varied among a “risk of non-target embolization to the skin, anastomotic communication between the genicular and popliteal arteries posing an unacceptable risk of non-target embolization, and a lack of hyperaemia”.
Interim results show “initial improvement sustained to follow-up”, Little declared, before alluding to the fact that, for the one-year data, due for publication in 2023, “the trends are the same”.
Little then addressed the NICE appraisal for GAE that he undertook 18 months ago. NICE recommend research preferably in the form of randomised controlled trials against sham or current best practice. Patient-reported outcome data will also be key, Little reported.
Brain scans and a neuropsychometric questionnaire were also included in the GENESIS trial to evaluate the impact of chronic pain on procedure outcomes. The finding, Little relayed, was that “there is a strong signal between patient catastrophising and poor outcomes” in terms of pain.
Rounding off his coverage of GENESIS, Little concluded that the trial demonstrated that GAE for mild-to-moderate knee OA is “safe with potential efficacy” and has “good scientific rationale”. To prove efficacy and heed NICE’s request for more data, there is GENESIS II, to which the presenter then turned.
This trial began two weeks ago, and is using the same KOOS primary endpoint, with a placebo comparison, the presenter outlined. Patient-reported outcome data will constitute a secondary endpoint, Little added. GENESIS involved a patient questionnaire, from which the results showed that “75% [of participants] would be more than happy to have [the procedure] again”.
Session chair Rob Morgan (St George’s Hospital, London, UK) asked Little whether anyone in the field had gathered data over more than a year—“there are Japanese data to four years,” the presenter replied, following up by affirming that “the effects [are] maintained”.
In the second session of GAE coverage, Little spoke to deepened understanding of knee OA anatomy that has come in the last decade, citing discoveries about vessel formation as “pivotal”.
Pre-empting the question of where GAE fits into the treatment strategy, Little asserted that the majority of knee OA patients are treated by their general practitioner but that many of those will fail conservative therapy, including injections and physiotherapy. Moreover, the presenter went on, “there is a treatment gap between those [whose conservative treatment has] failed and those who are eligible for joint replacement surgery—orthopaedic surgeons do not like to operate on young patients, [for example].”
The current ideal patient, Little communicated, is one with mild-to-moderate knee OA, as these are the individuals in whom the procedure has been trialled to date. There is good data concordance despite slight differences in technique and embolic agent across various centres—“patients get better and then there is a plateau”.
Conrad von Stempel (University College London Hospitals, London, UK) put the question to Little, following his presentation, of how to convince orthopaedic colleagues to refer patients for GAE. According to Little, “these are difficult to treat patients as they will have failed conservative treatments but are not surgical candidates”. Orthopaedic colleagues “are delighted” to have another potential treatment option in the form of GAE. “It is a completely different mindset to traditional turf wars,” Little emphasised.
The Society of Interventional Radiology (SIR) published a position statement deeming endovascular thrombus removal “an acceptable treatment option in selected patients with acute iliofemoral deep vein thrombosis [DVT].” The position statement is published online on the Journal of Vascular and Interventional Radiology (JVIR) website.
SIR convened a multidisciplinary writing group that conducted a comprehensive literature review. The group used evidence from 84 studies—including randomised trials, systematic reviews and meta-analyses, prospective single-arm studies, and retrospective studies—to develop 17 recommendations to guide the use of endovascular venous intervention for the care of patients with acute iliofemoral DVT.
Among the key recommendations were for physicians to quickly identify DVT and provide prompt and adequate anticoagulation, symptom control and functional recovery at the time of diagnosis. For those with anatomically extensive and clinically severe DVT and low bleeding risk, a form of catheter-directed thrombolysis (CDT) is reasonable to use in carefully selected patients after evaluating their comorbidities and personal preferences.
“Endovascular management has been used to treat select patients with acute iliofemoral DVT for more than 25 years, but newer and better designed studies have shown us that such interventions are most effective and safest when applied to younger patients with severe DVT symptoms,” said Suresh Vedantham lead author and an interventional radiologist with the Washington University in St Louis (St Louis, USA).
“Most DVT patients will benefit from anticoagulation alone, and can be spared anything more invasive, but for those who are suffering from severe symptoms or are at the highest risk of developing lifestyle-limiting post-thrombotic syndrome, catheter-directed therapies are appropriate and effective in reducing symptom severity early and late,” said Vedantham.
Vedantham was the primary investigator on the ATTRACT trial, the findings of which were published in 2017 and informed the new recommendations. Vedantham lauded the efforts of the international thrombosis research community in conducting several pivotal randomised trials to enable well informed guidelines, and the strong support of the SIR Foundation in the development and conduct of ATTRACT.
Based on the findings of the ATTRACT trial, the position statement authors recommend against the use of CDT for most patients with DVT that is limited to the tibial, popliteal, and femoral veins, for patients with clinical factors that confer a moderate or high risk for bleeding, and for patients with only mild lower extremity symptoms.
“Patient selection is the most important factor for success in the application of interventional treatments,” said, Kush R Desai, chair of SIR’s Venous Disease Clinical Specialty Council, a co-author of the statement, and an interventional radiologist with Northwestern Medicine (Chicago, USA). “Our recommendations follow the evidence so those who may benefit from endovascular treatment options are quickly identified to receive care and ensure positive outcomes.”
“Timing of intervention for acute deep vein thrombosis is important to optimise outcomes,” said Ronald S Winokur, vice chair of SIR’s Venous Disease Clinical Specialty Council, co-author of the statement, and an interventional radiology with Weill Cornell Medicine (New York, USA). “Clear guidance on patient selection including an understanding of extent of disease and accounting for flow dynamics helps patients receive the best treatment at the right time.”
As further research proceeds, SIR believes that adherence to the recommendations in the position statement allow for the use of endovascular therapy in a manner that optimises benefit and minimizes harm.
“SIR is dedicated to the evidence-based practice of interventional radiology and ensuring our position statements and guidelines reflect the findings of the latest science so patients receive the best possible care,” said SIR President Parag J Patel, an interventional radiologist with the Medical College of Wisconsin (Milwaukee, USA). “Thank you to the authors for their time and energy to ensure that DVT patients have access to the care appropriate for their case and medical history.”
The Chocolate Touch drug-coated balloon angioplasty balloon
Genesis MedTech Group announced that the US Food and Drug Administration (FDA) has approved the Chocolate Touch drug-coated balloon (DCB) percutaneous transluminal angioplasty (PTA) catheter developed by TriReme Medical for the treatment of patients with peripheral artery disease (PAD) in the superficial femoral artery (SFA) and the popliteal artery.
The Chocolate Touch DCB was shown to have statistically superior patency and non-inferior safety at 12 months as compared with Lutonix DCB based in a head-to-head, randomised trial of patients with symptomatic femoropopliteal disease.
The Chocolate Touch showed statistically superiority in its primary efficacy endpoint of 12-month true DCB success—a measure of the target vessel remaining patent without the need for bail-out stenting. Primary patency by Kaplan-Meier (KM) estimate was 83.3% for the Chocolate Touch and 73.0% for Lutonix DCB at 12 months.
The primary safety endpoint of 12-month freedom from major adverse events (MAEs) was 88.9% for those treated with the Chocolate Touch versus 84.6% for Lutonix DCB.
Additionally, Chocolate Touch results reported the lowest all-cause KM mortality value as compared to reported mortality for FDA-approved DCBs in pivotal studies. Mortality rates for Chocolate Touch using KM estimates at three years were 6.7% for the Chocolate Touch and 11.1% for the Lutonix DCB.
“I am very excited to see the Chocolate Touch, a next-generation DCB, is now available for patients across the USA. This technology is an important tool in the armamentarium for the treatment of patients with PAD,” stated Mehdi H Shishehbor, interventional cardiologist at University Hospitals Harrington Heart and Vascular Institute (Cleveland, USA) and the Chocolate Touch trial’s co-principal investigator.
Chocolate Touch is designed to open in small sections using pillow-like structures coated with a therapeutic agent with the goal of providing patients suffering from PAD with an alternative treatment to traditional DCB angioplasty.
“This next-generation paclitaxel DCB is based on the chocolate mechanism of pillow-and-groove formation resulting in an increased balloon surface facilitating effective drug release to the vessel wall and potentially reducing the need for permanent implants. The recently completed randomised, controlled study demonstrated excellent primary results, with statistical superior effectiveness as compared to the control DCB. The Chocolate Touch is a DCB category of its own,” commented co-principal investigator Thomas Zeller of Universitaets-Herzzentrum (Bad Krozingen, Germany).
Xeltis announced today the initiation of a pivotal trial with the “first-ever” restorative synthetic haemodialysis access grafts, dubbed ‘Axess’.
The first two patients have been successfully implanted as part of the AXESS European pivotal trial at AZ Sint-Jan Brugge-Oostende AV (Bruges, Belgium) by vascular surgeon Jan De Letter, and discharged from hospital.
The AXESS EU pivotal trial is a prospective, single-arm study to evaluate the safety and performance of Axess in patients with end-stage kidney disease who need haemodialysis. The study will enrol 110 patients at up to 25 centres in Europe and will follow them for five years.
The Axess graft has been previously successfully implanted in 20 patients, as part of the AXESS first-in-human (FIH) trial, which completed enrolment in September 2022. AXESS FIH full cohort data are expected in 2023.
“A device that enables immediate use, as seen with the existing synthetic ePTFE [expanded polytetrafluoroethylene] grafts, and turns into a living blood vessel that recovers promptly after puncturing from each dialysis session may become the safer and longer-lasting solution that patients on haemodialysis need,” explained De Letter, who also has previous experience with Axess, having implanted it during the FIH trial. “We are encouraged by the promising preliminary experience with this device from the FIH trial, and confirmation in a larger trial involving more patients and implanting sites is an important next step.”
The Axess graft is a restorative, synthetic, electrospun blood vessel for arteriovenous haemodialysis access. Once implanted, its porous microstructure gets colonised by the patient’s own tissue cells through the body’s natural healing process, turning into a living vessel made of their own tissue over time.
“Life for patients on haemodialysis means multiple hospital visits each week, involving puncturing, bleeding, waiting, healing and risk of infections from all of the above, in addition to poor renal function,” added An De Vriese, head of Nephrology and Infectious Diseases at AZ Sint-Jan Brugge-Oostende AV, and one of the coordinating investigators of the AXESS EU pivotal trial. “If a novel device can spare part of this burden through reduced bleeding, prompt coagulation and healing, lower infection risks and longer durability, it would be a life-changing experience for most patients.”
HYBRID - fluorescent Neon tube Sign on brickwork - Front view - 3D rendered royalty free stock picture. Can be used for online banner ads and direct mailers.
Chris Titze Imaging/stock.adobe.com
Chris Titze Imaging/stock.adobe.com
Year three of the COVID-19 pandemic and yet much now feels unrestricted and ‘back to normal’. This can certainly be said of meetings—at least in Europe and the USA—which, throughout 2020 and some of 2021, took place online, but have returned to in-person in recent months. However, transatlantic, intra-European and American travel, though possible and permitted, has not been plain sailing (flying?), even this year. Therefore, many societies, within interventional radiology (IR) or otherwise, for 2021/2022, have opted for a hybrid setup, where delegates have had the choice of accessing sessions, or to travel to the physical venue. Several society spokespeople relay to Interventional News their plans for the hybrid and in-person evolution of some of the IR calendar’s main meetings, based on how those from the last couple of years have panned out.
Parag J Patel (Medical College of Wisconsin, Milwaukee, USA), president of the Society of Interventional Radiology (SIR), provides the perspective of a society that has, deliberately, not offered hybrid attendance options. The reason being, he explains, that “this allows us to provide a consistent experience to all who participate, ensuring valuable learning, interactions with speakers, and connection to the materials.” So, this year’s Society of Interventional Radiology annual meeting (SIR; 11–15 June, Boston, USA) was in-person only, and 2021’s exclusively online, after the 2020 meeting, scheduled for late March, was cancelled. However, Patel notes, the SIR 2022 plenary sessions were available via livestream, and saw 230 viewers tune in.
This reflects where the society stands on the question of a hybrid future for meetings right now, and Patel details how the hybrid model has, by no means, been discounted by SIR, which is “exploring the possibility of deploying hybrid models at future meetings to allow more IRs to participate in the way in which they prefer to or are able to attend. We know that travel and time off can be a challenge, and hybrid models enable accessibility from an attendance standpoint.”
In contrast, the European Society of Radiology (ESR)’s director of communications David Zizka tells Interventional News, that his society has taken a hybrid approach to its annual meeting, the European Congress of Radiology (ECR) since 2013 when it started streaming educational content. “Our participants are used to having the option to attend the event either onsite or online, but in many cases, they choose to attend in both ways,” Zizka notes, qualifying this statement with the following: “What we have learned this year is that there is no strict distinction between an onsite or online visitor anymore, as many of our participants visit us in Vienna, but not for the entire five days, and then continue their ECR experience online.”
Concerns for superiority of in-person experience not universal
Patel expresses concerns that moving away from in-person only, may not be solely positive for the SIR meeting—as the rationale for not offering SIR 2022 in a hybrid format suggests. “We want to ensure that what we deliver does not create silos in the audience based on the format through which the attendee chose to participate. There is a risk with a hybrid approach that one group receives a lesser experience because they are not in the audience,” Patel acknowledges, before highlighting what underpins this reservation. “We do not just want to broadcast content to a passive audience. We want to actively engage our audience in discussion and learning, whether in-person or online.”
Zizka appears not to share such concerns, stating that “we are stepping away from differentiating participants according to [whether they are online or onsite attendees], as ECR is not a single event anymore but a year-long one with a variety of ways of participating.” He expands upon this assertion, pointing to the fact that “watching sessions on-demand during the actual congress period and especially afterwards for the rest of the year has become very popular amongst our participants.”
Adding his voice to the discussion, the Radiological Society of North America (RSNA) associate executive director for meetings services and corporate relations John Jaworski, whose opinion comes from the position of having 40% of RSNA attendees come from outside of North America, is therefore aware of the constraints that prevent people from travelling to the physical event space. Luckily, he acknowledges that “RSNA is fortunate to have a great team able to support both [the in-person and virtual] events,” which enables the society to fulfil the important objective of “[reaching] a greater number of healthcare professionals across the globe and providing them with important educational content to assist in patient care.”
Shared observations of post-pandemic attendance upswing
Patel underlines that all societies are having to consider how to keep optimal engagement from attendees the foremost priority. Interestingly, Zizka underlines that there was already “a regressive trend in onsite meeting attendance before COVID-19”, but that a reduction in appetite for attending in person may have been “accelerated” by the pandemic. In the eyes of the ESR spokesperson, “onsite attendance must be a special experience for the participant [if the meeting has a remote attendance option], something that adds unique benefit in comparison to online-only participation,” justifying this with the point that offering hybrid meetings means “you will see a decrease in onsite participation.”
But, right now, in the immediate aftermath of lockdowns, Patel recounts witnessing “a chorus of excitement and eagerness to be completely in-person,” at SIR 2022. “Screen fatigue is real,” Patel adds, attributing the “[palpable] desire to continue to meet in person” to this fact. Jaworski has observed the same enthusiasm for the in-person RSNA annual meeting: “Currently, our in-person registration is up 54% from this time last year, while our virtual meeting is on a par with 2021,” he relays to Interventional News. This follows an RSNA 2021 meeting for which attendance was “in line with our expectations”—30,000 attendees, of whom 6,000 attended virtually.
ECR received similarly positive feedback about their 2022 meeting, including from those who made last-minute decisions to attend remotely instead of in Vienna, and vice versa. “A big benefit of our registrations system is that every ECR ticket allows for full onsite and online access,” Zizka emphasises, “so participants can make that decision at any time without any bureaucratic efforts.”
Priorities for a bright future of IR meetings
Quizzed on how SIR plans on fulfilling the aforementioned goal of maintaining high levels of engagement, Patel refers to the possibility that SIR 2023 will livestream “at least some in-person sessions and in ways to ensure that any online audiences are actively engaged in the lessons happening on site in Phoenix.” After the fact, an on-demand library will enable attendees to revisit sessions, or view those they missed, Patel adds, stating that this “will also be available for purchase after the meeting for those who could not attend in person.”
The priority for the RSNA meeting logistics-wise, Jaworski brings to Interventional News’ attention, is to “better connect the virtual attendee to the in-person meeting.” For him this means “[looking] at almost every session like a TV studio and [considering] what the virtual attendee will be seeing and hearing.” One example of a simple but pivotal consideration in this regard is checking that in-room microphones are switched off during breaks “so personal conversations are not broadcast virtually”. Jaworksi adds that the RSNA is also “working on a way to better connect the virtual attendee with the speaker during session question and answer sessions, which will require some re-training of session moderators.” Finally, he alludes to the longer-term goal of RSNA “[improving] virtual networking between attendees and engagement opportunities with virtual exhibitors.”
Patel appears optimistic about the future of SIR meetings, in whatever variation on a hybrid form they may take, based on the 4,000-strong attendance at the 2022 meeting. Even if in-person attendance is set to decrease, as Zizka predicts, he believes that the strategies the ESR is adopting will mitigate this, at least in part, with “state-of-the-art online participation possibilities that live up to the latest technical trends, and [by reinventing] our event every year [to make it] a unique experience […] that people are always drawn to take part in onsite.” Jaworksi sees the meetings trend going the way of fewer attendees overall “in the short-term”, before increased comfort with travel leads to an uptick in attendance once more. “Nothing is better than face-to-face meetings for connecting with colleagues and developing relationships,” he professes, suggesting too that “competition from virtual meetings will lead to better in-person meetings […] with experience and engagement opportunities for attendees, such as interactive and hand-on experiences.”
ReCor Medical and its parent company, Otsuka Medical Devices, announced consistent and significant blood pressure-lowering results across a range of patients with uncontrolled hypertension, including across differences in age, sex, baseline blood pressure, medication level and ethnicity. The results come from analysis of the pooled data from ReCor’s RADIANCE global clinical trial programme: three prospectively powered, randomised and sham-controlled clinical trials which evaluated the endovascular Paradise ultrasound renal denervation (uRDN) system in patients with uncontrolled hypertension.
The results were presented at the 2022 American Heart Association (AHA) annual meeting (5–7 November, Chicago, USA) by Ajay Kirtane, professor of medicine at Columbia University and an interventional cardiologist at New York-Presbyterian/Columbia University Irving Medical Center (both New York, USA).
The RADIANCE pooled analysis includes data from more than 500 patients randomised in the three studies from ReCor’s RADIANCE global programme: RADIANCE-HTN TRIO, which studied patients with resistant hypertension, and RADIANCE-HTN SOLO and RADIANCE II, which studied patients with mild-moderate hypertension. The combined dataset showed an overall reduction in daytime ambulatory systolic blood pressure in the uRDN group of -8.5mmHg (p<0.0001) with a difference between treatment and sham at two months of -5.9mmHg (p<0.0001), favouring uRDN. Blood pressure results were similarly positive in the 24-hour, nighttime, home, and office measures. A favourable safety profile was consistently observed following uRDN treatment across the studies.
“Pooling the data from the RADIANCE programme demonstrates that treatment with the Paradise uRDN System results in a consistent reduction in blood pressure across differing severities of hypertension. The consistent and clinically meaningful blood pressure reduction across multiple patient groups increases our interest in the use of uRDN as a potential therapeutic option, when added to lifestyle modification and medications for our patients with uncontrolled blood pressure,” said Kirtane, study co-principal investigator.
“It is very important that the RADIANCE pooled analysis demonstrated a consistent blood pressure reduction in patients across a range of hypertension and both with and without antihypertensive medication, thus broadening the potential applicability of uRDN. Just as important, more than 50% of patients treated with uRDN in the pooled analysis either achieved daytime ambulatory blood pressure control or had a greater-than-10mmHg decrease in daytime ambulatory systolic blood pressure at two months, showing the potential benefits of uRDN as an element of a treatment regimen for patients with uncontrolled hypertension,” said study principal investigator Michel Azizi, professor of medicine at Université Paris Cité, Hôpital Européen Georges Pompidou, Paris, France.
The RADIANCE global programme is an international, multicentre initiative designed to explore the benefits of ultrasound renal denervation in hypertension. The RADIANCE studies are double-blind, randomised, sham-controlled trials designed to provide information about the ability of the Paradise uRDN System to treat high blood pressure. All three studies in the RADIANCE global programme were individually powered for efficacy with a primary endpoint of daytime systolic ambulatory blood pressure at two months, and all three met their primary efficacy endpoint with statistical significance at two months.
If maintained in the long-term, the blood pressure reductions demonstrated in the RADIANCE pooled analysis correlate to a potential 25% reduction in cardiovascular risk as shown in a meta-analysis of the cardiovascular benefits of antihypertensive medications.
Medtronic has announced the six-month results from the full cohort of the SPYRAL HTN-ON MED clinical trial. The late-breaking data were presented at the American Heart Association (AHA) Scientific Sessions 2022 (5–7 November, Chicago, USA). With this news, Medtronic has submitted the final module of the Symplicity Spyral premarket approval (PMA) package to the US Food and Drug Administration (FDA) for review and approval.
Subjects who were prescribed antihypertensive medications and were treated with the Medtronic Symplicity Spyral renal denervation (RDN) system had a statistically significant and clinically meaningful reduction in office-based systolic blood pressure (OSBP), a key secondary endpoint, compared to subjects in the sham control group. However, in the primary endpoint, RDN did not demonstrate a statistically significant reduction in 24-hour ambulatory systolic blood pressure (ABPM) due to increased medications in the sham control group and the potential impacts of the COVID-19 pandemic on the clinical trial environment. The study also included win ratio, a pre-specified secondary endpoint that combines reduction in blood pressure with reduction in medication burden, which enables assessment of the overall beneficial effect of RDN. The win ratio demonstrated significance in favour of RDN versus a sham procedure. Finally, the study met its primary safety endpoint, with a low incidence of procedure-related and clinical adverse events.
“The ON MED study demonstrated significant reductions in office-based blood pressure, the most commonly used measure in clinical practice. Additionally, we saw reductions in absolute blood pressure that were consistent with earlier RDN studies,” said David Kandzari, chief, Piedmont Heart Institute and Cardiovascular Services (Atlanta, USA) and SPYRAL HTN-ON MED principal investigator. “Surprisingly, 24-hour ABPM declined with RDN but did not differ from the sham group, and the primary endpoint was not met. More than 80% of patients in the ON MED expansion group experienced follow-up during the COVID-19 pandemic. Compared with patients enrolled before the pandemic, significant differences in baseline 24-hour ABPM were observed that may reflect changes in patient behaviour and lifestyle during the pandemic. Additionally, patients treated with the sham procedure increased the amount of medication they were taking compared to those treated with RDN. These factors likely contributed to the smaller-than-expected differences in ABPM.”
SPYRAL HTN-ON MED is a global, randomised, sham-controlled trial investigating the blood pressure-lowering effect and safety of RDN with the radiofrequency (RF)-based Symplicity Spyral RDN system in hypertensive patients who have been prescribed up to three antihypertensive medications, including diuretics, calcium channel blockers, ACE/ARB inhibitors or beta blockers. A total of 337 patients with uncontrolled hypertension were enrolled at 42 sites across the USA, Europe, Japan, Australia, and Canada, and were randomised 2:1 to RDN (n=205) versus sham control (n=132). Results were as follows:
The primary Bayesian efficacy endpoint of 24-hr systolic ABPM reduction was not met, with a 51% probability of superiority for the RDN group versus those who received a sham control procedure. However, nighttime systolic ABPM reduction was statistically significant.
6.5 mmHg 24-hr systolic ABPM reduction in the RDN group versus 4.5 mmHg in the control group (treatment difference of -1.9 mmHg, p=0.119)
6.7 mmHg nighttime systolic ABPM reduction in the RDN group versus 3.0 mmHg in the control group (treatment difference of -3.7 mmHg, p=0.01)
The study met the prespecified secondary endpoint, which was the change in OSBP from baseline to six-month follow-up between the RDN group (n=199) and the sham control group (n=126).
Statistically significant 9.9 mmHg OSBP reductions in the RDN group versus a 4.9 mmHg reduction in the sham control group (treatment difference of -4.9 mmHg, p=0.001)
The study met the primary safety endpoint, evaluating major adverse events at one month post-procedure, and renal artery stenosis at six months, pooled across the SPYRAL HTN-ON and OFF MED studies (p<0.001)
RDN demonstrated a low incidence of procedure-related and clinical adverse events at six-months in the SPYRAL HTN-ON MED study specifically.
The win ratio demonstrated significance in favour of RDN versus a sham procedure (p=0.005).
Overall burden of medications was higher in the sham control group at six months (p=0.04).
L-R: Alik Farber, Matthew Menard, and Kenneth Rosenfield
L-R: Alik Farber, Matthew Menard, and Kenneth Rosenfield
The first results from the BEST-CLI randomised controlled trial (RCT) of 1,830 patients show that surgical bypass with adequate single-segment greatsaphenous vein (GSV) is a more effective revascularisation strategy for patients with chronic limb-threatening ischaemia (CLTI) who are deemed to be suitable for either an open or endovascular approach. Researchers also found that both strategies can be accomplished safely and are effective for treatment for CLTI.
Further, the triallists urge that patients with CLTI who are candidates for limb salvage should undergo an evaluation of surgical risk and conduit availability. “Bypass surgery with adequate single-segment saphenous vein should be offered as a first-line treatment option for suitable candidates with CLTI as part of a fully informed shared decision-making. Level one evidence from BEST-CLI does not support an endovascular-first approach to all patients with CLTI. In patients without a suitable single-segment saphenous vein, both surgical and endovascular strategies are effective in treating patients with CLTI, so we believe that there is a complementary role for both revascularisation strategies in these patients,” they say, bringing the “quality of vein” back into the centre of discussion on revascularisation strategy.
The co-principal investigators—Alik Farber (Boston Medical Center, Boston, USA), Matthew Menard (Brigham and Women’s Hospital, Boston, USA), and Kenneth Rosenfield (Massachusetts General Hospital, Boston, USA)—note that this is the largest RCT comparing revascularisation treatment strategies in patients with CLTI and will provide important information regarding the management of these patients.
BEST-CLI (Best endovascular versus best surgical therapy for patients with CLTI) randomised patients with CLTI and infrainguinal peripheral arterial disease (PAD) to receive either infrainguinal bypass or endovascular intervention. The trial consisted of two parallel trials: Cohort 1 included patients with single-segment great saphenous vein; Cohort 2 included patients who lacked single-segment GSV and therefore alternative autogenous vein or prosthetic was used in those randomised to the open arm.
According to Farber, the best way to evaluate whether a patient has single-segment GSV—one he says needs to be at least 2.5mm in diameter, but ideally above 3mm, and must be free of thrombus—is by using duplex ultrasound. Speaking to Vascular News on this topic, Menard notes that while assessment of the vein is common practice for vascular surgeons, it is not for other specialties. In the wake of BEST-CLI, he suggests that evaluation of the GSV—a “very important” part of the assessment for treatment—should be included in the guidelines.
Farber tells Vascular News: “We are not claiming to bring down the 10 commandments here; all we are saying is that we are introducing some level one data into a space that has almost no Level one data.[…]. Here is another study that says the endovascular-first [approach] is a great thing for some people, but [it is not] for everybody. So, if a patient is a candidate for surgery and [..] has a good single-segment saphenous vein, there should be a conversation about surgery, for that individual.”
Key results
The investigators found that surgery was more effective than endovascular therapy in the Cohort 1 patients. At AHA, Farber revealed that there was a reduced rate of major adverse limb event (MALE) or all-cause death—the primary endpoint—in patients with good single-segment GSV who underwent open surgery, as well as fewer major reinterventions, at median follow-up of two point seven years. The maximum follow-up time in these patients was seven years.
Going into the details, Farber noted that Cohort 1 included 1,434 patients with single-segment GSV who were randomised 1:1 to either surgical or endovascular treatment. At median follow-up, the rate of MALE or all-cause death was 42.6% in the surgery arm compared to 57.4% in the endovascular arm (hazard ratio, 0.68; 95% confidence interval [CI], 0.59 to 0.79; p<0.001). In terms of secondary endpoints, he revealed that 10.4% of patients in the surgery arm underwent above-ankle amputation of the index limb versus 14.9% in the endovascular arm, in addition to rates of 9.2% vs. 23.5% for major reintervention on the index limb and 33% vs. 37.6% for all-cause death for patients in the open and endovascular arms, respectively.
In patients who did not have adequate saphenous vein, i.e. those in Cohort 2, there were no significant differences in the primary endpoint. Farber detailed that that this group included 396 patients who were randomised 1:1 to either surgical or endovascular treatment. The median follow-up was 1.6 years and maximum follow-up, 5.1 years. Farber reported that the rate of MALE or all-cause death in this cohort was 42.8% vs. 47.7% in the open and endovascular arms, respectively (hazard ratio, 0.79; 95% CI, 0.58 to 1.06; p=0.12). The corresponding figures for the secondary endpoints were as follows: 14.9% vs. 14.1% for above-ankle amputation of the index limb; 14.4% vs. 25.6% for major reintervention on the index limb; and 26.3% vs. 24.1% for all-cause death.
Farber added that there were no differences in perioperative mortality or major adverse cardiovascular events (MACE), and that mortality and MACE were similar between treatment strategies over the course of follow-up.
The presenter concluded that surgery with adequate saphenous vein “should be offered as a first-line treatment option for suitable candidates with CLTI, as part of fully informed, shared decision-making”. He added that level one evidence from BEST-CLI “does not support an ‘endovascular-first’ approach to all patients with CLTI,” and instead supports a “complementary role” for both revascularisation strategies. He noted that further studies are needed to better elucidate the comparative outcomes in subsets of patients.
While the primary focus of the trial was clinical outcomes in the comparison of open surgery versus endovascular therapy, Menard tells Vascular News that the investigators planned two “very important” ancillary assessments: cost-effectiveness—which the team is yet to conduct—and quality of life. With regards to the latter, he noted that the team used a number of different metrics for this, including the vascular disease-specific VascuQoL, as well as the EQ-5D and the SF-12.
According to Menard, the baseline scores for quality of life speak to the impact of CLTI on patients’ everyday lives: “The quality of life for all patients at baseline on entry into the trial was extremely poor and low, and that is consistent with what is known about the devastating impact of CLTI on patients’ overall function, the mental status, their physician limitations, and their high degrees of pain.”
Menard reports that both revascularisation strategies resulted in “significant gains” across every metric studied, noting also that there was not any significant difference between the two treatment arms.
Making the case for the benefits of the endovascular approach, Rosenfield emphasises: “This is the first trial that really shows that when you compare ‘endo’ to surgery, certainly in the disadvantaged vein group, they both actually had durable outcomes. A lot of us had questions about how durable outcomes for the ‘endo’ approach would be. And it should be clear that it is an approach, because sometimes touch-ups are needed on both sides and those are not considered MALE events. You really had to have a major reintervention to reach an endpoint of MALE, or an amputation. But I think that this for the first time shows that, in a head-to-head trial, that both are durable and that, on the ‘endo’ side, once you achieve successful technical outcome, it is comparable even in the group that had reasonable vein in cohort one.”
BEST-CLI meets “astronomic” need for high-quality, practice-changing data
At AHA, Farber noted that data from the Vascular Quality Initiative (VQI) from centres of excellence in North America revealed “tremendous” centre-specific variability in treatment strategy in the use of bypass versus endovascular for CLTI patients, which BEST-CLI national trial manager Michael Strong tells Vascular News attributes to the lack of evidence-backed guidelines in the space.
Speaking to this newspaper, the investigators express their confidence that the results of BEST-CLI will change practice and impact the Global Vascular Guidelines published in 2019. Menard believes there is “no question” that guidelines will change, partly because the current guidelines are “riddled with gaps”. He notes that anywhere from 10–15% of current guidelines are based on level one data—a “miserably low” figure in his opinion. “The need for quality data that the BEST-CLI represents is astronomic,” he says.
Rosenfield remarks that the trial will “definitely change practice” as it provides the clear message that “surgery is not dead, in fact it is very much alive and well for the appropriately selected patients”. He stated that the data “should be described to patients—simple as that,” and that patients “should have the option of deciding, but they should be knowledgeable that they will do better with surgery [in selected cases], and that is an appropriate response to [these results].”
Farber concurs, noting that there is now level one evidence to support the role of bypass in certain patients. “It supports a body of literature that is not as strong, and so I think [guidelines] will change,” he comments.
“I think it is nice for us to have all these arrows in our quiver to treat CLTI patients, and that is what this is; it is about saying this arrow does work and it should be used in some situations,” Farber summarises. “That is a great thing to add because, before BEST-CLI, the data were not as strong.”
“The first step”
While the investigators agree that BEST-CLI will be practice changing, they acknowledge that it represents “the first step” in a long trajectory of future investigations and discussions in CLTI research.
At AHA, Farber noted some limitations of the trial, including selection and operator bias in enrolment and intervention, the fact that equipoise and eligibility were determined locally and were variable, and that anatomic complexity is yet to be evaluated. In addition, cohort 2 was likely underpowered, anatomic complexity yet to be evaluated, percentage of female patients lower than targeted, and use of paclitaxel balloons or stents affected by the Katsanos meta-analysis during enrolment, they elaborate.
“We need to dig deeper,” Rosenfield says. He describes the trial as a “game-changer in many respects,” but stresses that “this field is still a moving target” and so BEST-CLI must be seen as “the first foray into developing very solid level one evidence”. Specifically, he notes that techniques will “continue to improve and get better”. Looking ahead, Rosenfield believes that those who treat CLTI will “learn a lot more over the course of the next couple of years as we peel back the layers of the onion”.
According to Menard, the trial stimulates two topics that will take centre stage in the “great discussions that are going to be had” in the coming months. “We are all trying to figure out exactly how we are going to interpret the results for our own practices, and in order to do that, you really need to understand the patients enrolled into the trial, and that is a big focus of the future work—defining what their anatomy was […] and a bit more about overall demographics. You can have selection bias, but you cannot imply or in any way get around the fact that at that institution they were deemed appropriate for both [open and endovascular strategies],” he tells Vascular News.
Farber stresses that further investigation might also elucidate how an operator decides between adopting an open or endovascular approach in certain patients. “We all know that if it is an easy ‘endo’, then of course the patient should have an ‘endo’, there is no equipoise, and then on the other extreme there are cases where everything is blocked from the groin to the foot and somebody might say of course surgery is the way to go, and then there is everything in between,” he says. What remains, according to Farber, is for the investigators and others in the field to “dig deep” into these data to answer the question of how to define appropriateness for a certain treatment.
For now, Rosenfield notes that the investigators are “really excited” about analysing the “treasure trove” of data that BEST-CLI provides and seeing what they can learn. Looking beyond this, Menard expresses the team’s hope that “many more trials will come along and build on what the trial has laid as a foundation”.
Two datasets presented during the late-breaking clinical trials session at The VEINS (Venous Endovascular Interventional Strategies) 2022 (30–31 October, Las Vegas, USA)—the latest results from CLOUT and a propensity score-matched analysis of CLOUT versus ATTRACT—bolster the evidence base for mechanical thrombectomy in the field of deep vein thrombosis (DVT) management. However, discussion at the meeting pointed to the need for further, high-quality data to solidify the role of this treatment modality.
The latest analysis from the now fully-enrolled CLOUT registry demonstrates the “excellent safety profile and effective thrombus removal” of mechanical thrombectomy with the ClotTriever system (Inari Medical) in a “real-world” DVT population of 500 patients. This is according to David Dexter (Sentara Vascular Specialists, Norfolk, USA), who presented in-hospital and 30-day outcomes from this multicentre, prospective registry at The VEINS 2022. Steven Abramowitz (MedStar Washington Hospital Center, Washington DC, USA) also presented data on the ClotTriever system, sharing results of a propensity score-matched analysis of early clinical outcomes from the CLOUT and ATTRACT studies.
The CLOUT (ClotTriever outcomes) registry is an all-comer, multicentre study evaluating patient outcomes following treatment of proximal, lower extremity DVT with the ClotTriever system, and, according to Dexter, represents the largest mechanical thrombectomy study in the field of DVT. All-comer patients were enrolled, irrespective of symptom duration, thrombus age, prior failed treatment of the current DVT, or bilateral disease. The primary endpoint was complete or near-complete (≥75%) thrombus removal, assessed by an independent core laboratory.
Dexter reported that the primary endpoint was achieved in 91.2% of limbs, and the 30-day device-related severe adverse event rate was 0.2%. Nearly all procedures were single session (99.4%), median estimated blood loss was low (40mL), and only 2.2% of patients received overnight post-thrombectomy intensive care unit monitoring, he added. Furthermore, patient symptoms (e.g. pain and oedema) were significantly reduced at discharge and showed sustained improvement through 30 days.
The presenter also revealed recovery of vessel flow and compressibility as measured by duplex ultrasound, improvements in revised Venous Clinical Severity Score and EuroQoL five dimensions quality-of-life score, median 5.5-point reduction in Villalta score, and <10% of patients with a moderate or severe Villalta score (≥10).
A question from the panel probed what is next for the field of mechanical thrombectomy in light of these results. Dexter pointed to the need for more studies, and also stressed what the focus of future research should be: “We need to show a real, long-term result on post-thrombotic syndrome”.
CLOUT versus ATTRACT
Steven Abramowitz at The VEINS 2022
In Abramowitz’s presentation of the propensity score-matched analysis, the presenter summarised that CLOUT patients showed better thrombus extraction and improvement in 30-day Villalta scores than ATTRACT patients. Specifically, the presenter revealed that nearly two times more CLOUT patients had complete thrombus removal, and that 13% fewer CLOUT patients had Villalta scores ≥5 at 30 days.
Abramowitz explained that ATTRACT is a reference trial evaluating interventional treatment for DVT that showed no added benefit compared to anticoagulation. “New interventions have emerged since the completion of ATTRACT, and their comparative effectiveness is unknown,” he said. Using propensity score-matched data, the investigators compared outcomes from the CLOUT registry with those from the treatment arm of the ATTRACT trial.
To adjust for differences in study design, patients with bilateral DVT, symptom duration >4 weeks, or incomplete case data were excluded. Propensity score matching (1:1) on 11 baseline covariates (age, sex, body mass index, sidedness, prior venous thromboembolism, race, symptom duration, DVT location, presence of provoked DVT, Villalta score, and Marder score) was performed between the remaining CLOUT and ATTRACT patients, resulting in 166 matched pairs.
No significant differences in baseline characteristics remained after matching, the presenter noted. Rates of stenting and venoplasty were similar between the groups and, as expected based on differences in mechanism of action, rates of thrombolytic use (0% vs. 100%, p<0.0001), single-session treatment (98.2% vs. 25.3%, p<0.0001), and postprocedural hospital overnights (mean, 1.7 vs. 3.4, p<0.0001) were significantly different.
Abramowitz reported that thrombus extraction as measured by core laboratory-assessed Marder scores was 22.3% better in CLOUT patients (p<0.0001), and 22.2% more CLOUT patients achieved ≥75% thrombus clearance (p<0.0001). Similarly, 12.7% fewer CLOUT patients had Villalta scores ≥5 at 30 days (p<0.05). Logistic regression on ATTRACT showed that 30-day Villalta scores significantly predicted post-thrombotic syndrome at six months, one year, and two years (odds ratios, 1.37, 1.32, and 1.43; p<0.0001), which the presenter said highlights the potential long-term effect of these differences.
Closing his presentation, Abramowitz echoed Dexter’s call for more data, noting that randomised controlled trials such as the recently announced DEFIANCE trial “will further clarify the role of the ClotTriever system in treating DVT”.
The first of four presentations was delivered by Rosario Grasso (Campus Biomedico University Hospital Foundation, Rome, Italy), who argued that percutaneous thermal ablation approaches like radiofrequency ablation (RFA) or cryoablation are an option for the management of patients with clinical-stage T1 renal lesions—primarily in masses <3cm in size, but potentially for larger masses in select patients too.
Grasso stated a belief that percutaneous ablation represents a safe and effective alternative to surgery in treating T1a renal cell carcinomas due to the “excellent” functional and technical outcomes seen with the procedure. The “very low” complication rate these procedures hold also compares favourably to those associated with nephrectomy, he added.
The speaker concluded that there is currently Level C evidence that, in selected patients with suspected T1a renal cell carcinoma, percutaneous thermal ablation should be offered over active surveillance owing to the “acceptable” long-term oncological and survival outcomes it has demonstrated to date. Grasso also said RFA, cryoablation and microwave ablation are all appropriate treatment modalities, and claimed that the choice of ablation method “should be left to the discretion of the operating physician”.
Treatment planning
Arian van Erkel (Leiden University Medical Center, Leiden, The Netherlands) followed this by discussing treatment planning in renal ablation—a “well-established” treatment for small T1a tumours. He posited that the first step here is to choose between surgery, ablation or active surveillance, and that this decision is an individualised one influenced by patient preference, age and life expectancy, renal function, the location and size of the tumour, and multiple other factors.
“Planning the treatment of your RFA is very important in getting complete ablation, with a sufficient margin, and in avoiding complications,” van Erkel asserted. “This planning involves image guidance, the ablation modality and protective measures.” He further claimed that axial diameter, bowel proximity, adjacency to the ureter, and several other characteristics of the tumour, should be taken into account.
“An immediate CT [computed tomography] after ablation is, of course, important, to evaluate your complications and your ablation margins especially,” van Erkel concluded. “And, there is software on the market that can help you make these estimations in a more scientific and exact way.”
Different modalities
A closer look at the different approaches to percutaneous ablation for renal cell carcinoma was then provided by Esther Gálvez González (Hospital Severo Ochoa, Madrid, Spain). The speaker corroborated many of her colleagues’ earlier points, noting that ablative treatment is as effective as surgery in T1a tumours—adding that it can also help to preserve renal function, and is associated with low complication rates.
Gálvez González further asserted that a key advantage held by RFA is the wealth of experience and high volume of published papers associated with the technique, but also noted two important limitations: thermal tissue conductivity and the ‘heat sink effect’. In contrast, she continued, bigger tumours can be ablated more quickly, and at higher temperatures, with microwave ablation, while its relative insensitivity to the heat sink effect allows it to be used in target areas located closer to larger blood vessels. The major limitation of microwave ablation, however, is the increased risk of complications in more central locations, which restricts its use to peripheral lesions, she added.
The speaker also touched on the various advantages and limitations of two other approaches—cryoablation, and a non-thermal technique (on which there are minimal published data) called irreversible electroporation—stating that both are essentially unaffected by impedance and the heat sink effect, but are limited by smaller ablation volumes and longer procedure times as well. Gálvez González concluded by asserting the importance of selecting the correct approach based primarily on the size and location of the target tumour.
Combined therapies
The session’s final talk was given by Marco van Strijen (St Antonius Hospital, Nieuwegein, The Netherlands), who outlined several combined treatments in cryoablation. “Combined treatment in renal cryoablation, in my opinion, consists of either embolization—which is a safe treatment but for which scarce literature is available—or thermoprotection by liquid; air or CO2 dissection; or pyeloperfusion,” he stated. Homing in on the former technique, the speaker said that, despite the limitations around previous studies and a lack of prospective data, percutaneous embolization is considered a safe procedure that is “most effective” in reducing periprocedural blood loss, and holds potential benefits in local tumour control and procedural visibility.
Van Strijen went on to highlight two further, more recently introduced tools that he also considers among the options for combined approaches: robotic needle placement, and the use of integrated controls and augmented reality to perform ablations virtually with the aid of a HoloLens device (Microsoft). In concluding his presentation, van Strijen added: “Robotic needle placement is currently one of my favourite techniques.” Here, he cited the fact it is “very simple”, and enables steep angulations, as well as reducing radiation exposure and speeding up the procedure “considerably”.
Concept Medical has announced the successful completion of enrolment for the SIRONA randomised controlled trial (RCT) investigating the use of its Magic Touch PTA sirolimus drug-coated balloon (DCB) versus paclitaxel DCB angioplasty for the treatment of peripheral artery disease in the femoropopliteal vessel segment.
The prospective, multicentre, head-to-head, corelab adjudicated RCT enrolled a total of 480 patients across 28 sites in Germany and Austria. The target patient was enrolled on September 23, at Hanusch Hospital Vienna (Vienna, Austria) by principal investigator (PI) Martin Werner and team.
Coordinating principal investigator, Ulf Teichgräber, said: “I am thrilled to work with 28 highly dedicated and motivated study sites that have managed to complete enrolment much earlier than expected. SIRONA represents a breakthrough head-to-head RCT with the potential to usher in a new era of sirolimus DCB in peripheral arterial disease (PAD) to replace an old technology.”
SIRONA will be a game changer trial, considering its bold design and the direct comparison against paclitaxel, say Concept Medical. The trial enrolled all patients with a disease in the superficial femoral artery (SFA) segment, whether de-novo or restenotic, falling into Rutherford classes 2–4, and experiencing intermittent claudication to critical limb ischaemia (CLI).
The 12 month results will feature patency (defined as the absence of target lesion revascularisation (TLR) or restenosis), and the primary safety endpoint is assessed as the composite of freedom from device or procedure-related death at 12 months as well as major target limb amputation.
The University Heart Center (Bad Krozingen, Germany) topped the enrolment under the lead of Thomas Zeller.
“It is exciting that enrolments into the first head-to-head comparative study between a sirolimus coated DCB and a variety of marketed paclitaxel coated DCB for femoropopliteal indication could be finished in such a short time”, said Zeller. “The study has sufficient size and the power to demonstrate if there is at least equivalent performance between the Magic Touch DCB and a range of paclitaxel coated DCB and if so, if there are potential lesions which may even benefit from the use of a sirolimus coated DCB,” he added.
Magic Touch PTA has already been granted a breakthrough device designation by the US FDA for below-the-knee indication.
Gerd Grözinger (Tübingen, Germany) chats with Bernhard Gebauer (Berlin, Germany) at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain) about some of the difficulties associated with treating patients with pulmonary embolism (PE) and deep vein thrombosis (DVT). Gebauer states that “the options we have at the moment with either anticoagulation or lysis are very limited”. One of the problems with systemic thrombolysis for example, explains Gebauer, is that “you could have some complications” with the high dose, in addition to the fact that lysis “is contraindicated in a lot of patients”.
Grözinger agrees with Gebauer that the age of the thrombus is very important. Asked about the perfect time window to treat those with DVT, Grözinger states that “in the old days we had to tell our patients that beyond two to four weeks there is no chance of getting rid of the clot”. However, “this strict timeframe can be overcome with new technology like the ClotTriever (Inari Medical) which can address thrombus of various ages” and ultimately “extend our treatment window”, he adds. The pair conclude by discussing which patients benefit most from interventional treatment for DVT or PE.
Synchron has announced that enrolment in the COMMAND trial has commenced at the University of Pittsburgh in Pittsburgh, USA.
The COMMAND trial is an early feasibility study funded by the National Institutes of Health (NIH) that will primarily assess safety while beginning to explore quantified efficacy measures of Synchron’s brain-computer interface (BCI) technology—the Stentrode—in severe paralysis patients, with the goal of enabling them to control digital devices, hands-free.
COMMAND is being conducted under what Synchron claims is the first investigational device exemption (IDE) awarded by the US Food and Drug Administration (FDA) to a company assessing a permanently implanted BCI. This new site at the University of Pittsburgh marks the second approved COMMAND trial location, joining Mount Sinai in New York, USA, where patients are also currently being enrolled, a company press release notes.
“Synchron’s Stentrode has the potential to restore functionality to the millions of people worldwide suffering from paralysis,” said Raul Nogueira, director of the University of Pittsburgh Medical Center (UPMC) Stroke Institute. “Giving patients the option to receive this device without the need for open brain surgery may open endless possibilities into the application and scalability of this promising technology.”
“This exciting technology may open up the possibility for patients with paralysis to use digital devices to communicate with loved ones again, and restore independence back into their lives,” said David Lacomis, COMMAND principal investigator and chief of the University of Pittsburgh’s Neuromuscular Division. “Something as simple as surfing the web or doing online grocery shopping can seem mundane to some, but it can change the world for someone who previously had those fundamental abilities taken away.”
The Stentrode is implanted within the motor cortex of the brain via the jugular vein in a minimally invasive endovascular procedure. Once implanted, it detects and wirelessly transmits motor intent, restoring a capability for severely paralysed patients to control personal devices hands-free with ‘point-and-click’. COMMAND will assess the Stentrode’s impact on tasks like texting, emailing, online shopping and telehealth services. The US FDA granted Breakthrough Device designation to Synchron in August 2020 and an IDE in July 2021 for this trial.
“Today marks an important milestone in our mission to advance technology access for the millions of people who have lost the ability to use digital devices,” said Tom Oxley, CEO and founder of Synchron. “We are excited to expand the COMMAND trial with enrolment at the University [of Pittsburgh] as we look to advance a scalable BCI solution to market.”
Transit Scientific has announced that the XO RX 2.2Fr and XO RX 3.8Fr platform has received US Food and Drug Administration (FDA) clearance to crack, break and dilate stenoses in peripheral arteries and arteriovenous dialysis fistula-associated lesions.
“We have demonstrated XO’s rotating strut technology can crack, break, and dilate intimal and medial calcium,” said Jihad Mustapha (Advanced Cardiac and Vascular Centers for Amputation Prevention, Grand Rapids, USA). “The new 3.8Fr XO RX has a low profile and accommodates 20cm balloons, making it a good option for PAD [peripheral arterial disease] and CLI [critical limb ischaemia] disease. The lower-profile 2Fr version helps address gaps in treatment options currently available for BTK [below-the-knee], tibiopedal and pedal loop stenoses.”
XO RX and XO OTW (over-the-wire) exoskeleton devices include up to 22 rotating struts that slide onto a broad range of off-the-shelf angioplasty balloons, according to a press release from Transit. During balloon inflation, the struts rotate 90 degrees to crack, break and dilate calcified stenotic atherosclerotic lesions, and intimal hyperplastic lesions, and can be used for vessel prep for other treatment options.
“We have seen good results in PTA [percutaneous transluminal angioplasty]-resistant intimal hyperplastic and elastic venous lesions in patients with dialysis fistulas with the XO at low nominal or near-nominal pressures,” said Richard Saxon (Tri-City Medical, San Diego, USA). “The new XO RX presents a unique and versatile option for prepping and dilating longer lesion types in patients with severe PAD during limb salvage procedures.”
The XO RX and XO OTW technology is designed to reduce shear and facilitate balloon rewrap by counter-rotating 90 degrees upon deflation. Clinicians can deliver fluids from the hub to the balloon before, during or after inflation with XO OTW. No consoles, new capital equipment, or complex learning curve are required, the release adds.
“The XO RX platform sets new standards for low-profile, flexibility and performance,” said Jennifer Arnold, Transit’s chief operating officer. “Patients and clinicians need more tools to crack, break and dilate occlusive lesions in patients with cardiovascular disease. XO RX allows clinicians to add XO technology to hundreds of angioplasty balloons covering a wide range of diameters and lengths with just a few SKUs [stock-keeping units].”
The XO RX PTA system is intended to be used in conjunction with a PTA balloon to facilitate dilation and apposition of the scoring surface to the stenotic material in the iliac, femoral, ilio-femoral, popliteal, infra-popliteal, and renal arteries, and for treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulas. However, it is not for use in the coronary or neuro vasculature, according to Transit.
XO RX is available in 2.2Fr and 3.8Fr sizes, which accommodate 1.5–7mm outer diameter standard PTA balloons of lengths from 20–200mm, reducing inventory requirements, the release also notes.
Matthew Gibson (Royal Berkshire Hospital, Reading, UK) will be delivering this year’s British Society of Interventional Radiology (BSIR; 2–4 November, Glasgow, UK) Wattie Fletcher Lecture ‘Survive and thrive in interventional radiology [IR]’. Interventional News spoke with Gibson to glean some of the details of his talk, in which he will address the “psychological and non-medical stresses and strains of being an interventional radiologist and even suggest some things we can do to improve the situation.”
From Gibson’s preview, it would appear that he intends to underline in the lecture how “just trying to get through to the next day is not enough” as an interventional radiologist. A self-professed enthusiast who, from personal experience, knows the value of enjoyment and laughter at work, Gibson makes a compelling case for thriving over mere survival in IR.
“I have an interest in several areas of IR, for example below-the-knee angioplasty, dialysis access, and deep venous intervention but I am sure there are plenty of people better qualified than me to talk on these topics,” Gibson begins, talking through how he chose his lecture topic. He wanted to make it relevant and interesting to a wide audience. In a career of 25 years as a consultant interventional radiologist, he has “retained his enthusiasm for the job and IR in general”. This has surprised his contemporaries and younger colleagues, who have seen stress and burnout lay claim to many medical professionals’ enjoyment of their job. He felt he was well placed to produce a talk on the all-too-common stresses of IR, rather than a more specific procedure or medical talk about a certain area of IR.
Before delving into burnout and the many contributing factors that make this a reality for many interventional radiologists, Gibson states his keenness to work discussion of serious adverse events (SAEs) into his lecture. Namely, he expresses a desire to examine beyond the important impact of SAEs on the patient’s safety: the effect involvement in a SAE can have on medical professionals. “It is something we do not talk about enough, but SAEs produce a definite adverse effect on medical staff”. This can result in, according to Gibson, damage to confidence and self-esteem and anxiety about making another mistake and, he adds, “you are more likely to be involved in another adverse event if you have already had one.”
“Death by 1,000 arrows” is the metaphor Gibson uses to characterise how the UK healthcare system investigates adverse events. “Although it is supposed to be a no-blame medical culture, being under investigation at any level can be damaging and upsetting. Anyone can refer a doctor to the General Medical Council [GMC], which can be extremely stressful,” Gibson relays, emphasising that doctors have taken their own lives after being referred.
Opening the issue of stress and burnout back up, Gibson again suggests that “[he does] not think we have talked about it enough in IR”, suggesting that this “[may be because] some of us think we are immune to it.” However, “we are all at risk”, he counters, moving on to list multiple explanations for this. Paperwork, emails, directly looking after our own patients”, work-life balance and “time poverty”. In addition, the public’s attitude plays a role, Gibson notes—“the medical profession is less respected than previously and patients and relatives may not understand the subtleties of why mistakes occur and the effect making mistakes, and being the subject of complaints, can have on the medical staff involved.”
In addition, lack of professionalism and rudeness at work “can make your IR team dysfunctional and negatively impact on patient care”.
Yet, there are positive steps that can be taken to mitigate the strain of working in modern medicine and IR, Gibson points out. “Governments, employing organisations, managers, interventional radiologists and their team members can take steps to redress work-life imbalance, time poverty, improve resilience and, hopefully, reduce the risk of burnout and also improve patient safety.”
Interventional radiologists would also stand to gain from understanding that “being vulnerable is not a weakness,” Gibson advises, labelling this as “a real issue for us—we are expected to be invulnerable, to ride into high-stress situations and know what to do with no doubt in our mind.” Be this as it may, “you probably also need to be vulnerable at times in order to have a caring, empathetic relationship with your patients,” Gibson admits, elaborating on the importance of “shedding this armour”. Being invulnerable also “spills over into your private life—doctors can have issues with depersonalisation and desensitisation and thus cut themselves off from their loved ones.”
“Having a laugh with staff and patients might seem frivolous because medicine is a serious business, but it can have some very positive effects,” Gibson offers as part of the explanation for his having staved off burnout 30 years into his IR career.
“I cannot pretend that I have all the answers but stress and burnout are very much with us now and are probably only going to get worse.” This is what he expects the BSIR’s first survey into burnout among interventional radiologists to show and is why “it can be quite difficult to convince junior doctors or medical students how much of a privilege it is to care for patients.” Such, Gibson says, is his “humble opinion”, but he is convincing in how he conveys a need to address the issues that will form the basis for his lecture.
Above: Roger Greenhalgh, Tilo Kölbel, Markus Steinbauer, Heinz Jakob; Below: Jans Heyligers, Michele Antonello
Above: Roger Greenhalgh, Tilo Kölbel, Markus Steinbauer, Heinz Jakob; Below: Jans Heyligers, Michele Antonello
The second day of the CX Aortic Vienna 2022 Digital Edition (24–26 October) saw presentations on dynamic computed tomography angiography (CTA), a device with the potential to bring hologram guidance to vascular procedures and an edited case highlighting the role of intravascular ultrasound (IVUS) intraoperatively in thoracoabdominal branched endovascular aneurysm repair (BEVAR). The multidisciplinary moderating panel, which included a cardiac viewpoint from Heinz Jakob (Essen, Germany), questioned these technological developments for imaging in the post-presentation discussions—in terms of the limited access to them for cost reasons, and whether the reduction in radiation exposure the technologies offer can justify hospitals assuming the financial burden.
The first presentation came from Alan Lumsden (Houston, USA), who demonstrated why dynamic CT imaging might be considered the “new gold standard” for diagnosis and interventional planning. “It is obviously important to choose the right diagnostic tool at the right phase of the treatment modality,” the presenter began, declaring CT as a “very flexible” modality. This means that it can lend itself to dynamic imaging, Lumsden explained—static imaging and the single “view” it offers is sometimes akin to “no view” at all.
Lumsden then detailed how and why time-resolved CTA, developed for cardiac imaging, can be advantageous for use in endovascular aneurysm repair (EVAR) follow-up. The approach involves “moving the patient in and out the scanner, taking snapshots”, which can then be “put together” to form a three-dimensional composite image over time, Lumsden relayed, likening it to a “movie”. This allows the surgeon to see the contrast dye’s flow pattern and how long it takes to “arrive”, meaning “you can work out what type of endoleak you have.”
Furthermore, the presenter asserted that there is no radiation exposure increase as compared to triphasic CTA. His concluding remarks were that dynamic CTA can be applied to “guide subsequent interventions” and can be “widely performed on conventional scanners”.
It was whether this imaging approach can, in fact, be “widely performed” that featured in the discussion that followed. Moderator Markus Steinbauer (Regensburg, Germany) acknowledged its potential as a “valuable tool”, but that he does not currently have access to it in his practice. Anchor Roger Greenhalgh (London, UK) concurred—“we encourage the concept, but it needs to be more widespread”.
Another point the discussion raised was whether the reduced radiation exposure facilitated by dynamic CTA warrants shouldering the financial cost of implementing the requisite technology. For this reason, moderator Tilo Kölbel (Hamburg, Germany) posited that it would “take a while until this is standard practice”.
The result from the interactive audience poll suggested that dynamic CTA could indeed become the gold standard for diagnosis and interventional planning, with 88% of respondents voting in the affirmative.
The edited case presented by Michele Antonello (Padua, Italy), which shed light on intraoperative intravascular ultrasound (IVUS) in thoracoabdominal branched endovascular aneurysm repair (BEVAR), also yielded noteworthy discussion. Fellow presenter Jan Heyligers (Tilburg, The Netherlands) again posed a question on radiation exposure to Antonello—“is it mainly a reduction of radiation that you are aiming at?”—to which the response was that IVUS can “reduce contrast [use] by 30%”. Kölbel queried the impact IVUS has on procedure time, highlighting that this is also a factor when evaluating the cost-effectiveness of the approach as compared to the standard of care.
Heyligers’ own presentation demonstrated the scope for holographic augmented superposition of patient-specific imaging. The device in question, Heyligers suggested, could, with further development, solve the “problem” in vascular surgery of having to interpret three-dimensional information from a two-dimensional display. With smart glasses projecting directly onto the exact location on the patient, Heyligers shared with delegates that thus far, the technology has proved promising in static applications such as in a foot or wrist. Future iterations will be “smarter”, and capable of assisting in a “moving environment”, such as the vasculature, the presenter ventured.
Once more, the hologram technology elicited lively discussion, with Kölbel keen to hear how this could work in endovascular procedures. Heyligers underlined that other technologies could be harnessed “once inside vessels”, reiterating that the holographic capability to “recognise patient-specific surroundings” can help fulfil the “ambition” to have “faster, more precise” procedures, with “less radiation”.
Steinbauer pointed to the potential for applying the technology in educational settings, such as to project guidelines onto a patient to show where and where not to operate. This was an idea with which Heyligers agreed— a “remote experience” is possible, he added, thanks to the device’s internet connectivity, which could allow a seasoned surgeon “to help younger colleagues out” even if they are not in the room.
The thread running through this session on thoracic imaging was that practising at the forefront technological and procedural advancements in vascular surgery does not come without significant financial cost, ultimately constituting a barrier to entry for many centres. The moderating panel emphasised that radiation reduction is a priority when considering whether or not to implement a new procedure and shoulder the cost of the technology required to perform it.
“The spine is an area where interventional radiologists play a crucial role in both diagnosis and therapeutic management of a variety of pathologies”.
Dimitrios Filippiadis is associate professor of diagnostic and interventional radiology (IR) at the National and Kapodistrian University of Athens (Athens, Greece) whose practice centres around musculoskeletal (MSK) interventions and diagnostics, and interventional oncology (IO) and cancer pain management. Beyond this, he is passionate about IR education, which has seen him, this year, take up the position of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Online Education Committee chair. From his research on discomanometry, to personal experience at the forefront of adopting ablation procedures within Greece, Filippiadis speaks to Interventional News about the “intrinsic rewards” and “lifelong memories” that being an interventional radiologist has given him in his decorated career thus far.
What attracted you to a career in IR?
When I started my residency in diagnostic radiology, I had a lot of second thoughts about sitting in front of a computer monitor dictating reports. Then, a fellow resident came to me and suggested I register for a postgraduate course in IR, which was organised by Professor Dimitrios Kelekis in Greece. From the introductory courses onwards, I knew that this was the clinical career path I wanted to follow. Some years later, a visit to Strasbourg on a CIRSE grant made me realise that interventional oncology (IO) and pain management would be my specialist practice.
Who are, or were, your mentors?
I was fortunate enough to have had wonderful mentors early on in, and throughout, my career. During my residency, Alexis Kelekis introduced me to spinal and MSK procedures and influenced me greatly. Elias Brountzos taught me that providing patient care is one aspect of our work, with the other being to bolster the IR community by volunteering our time and expertise to help our specialty to flourish further. Nikolaos Kelekis gave me the opportunity to work almost exclusively in the field of ablation and I will always be grateful to him for this chance. Last but not least, even though I have never worked with him, Loukas Thanos, a Greek pioneer in the field of ablation, has had a great influence on my career.
Could you describe a particularly memorable case of yours?
I will never forget the first time I treated a paediatric cancer patient. He was 16 years old with a history of right paraganglioma and right nephrectomy due to renal cell carcinoma (RCC) and presented with an endophytic RCC lesion in the lower pole of his left kidney. The stress obtaining the parents’ consent and preparing for the ablation was unbearable, at least for me. The night before the ablation, I was not able to sleep, imagining only the worst-case scenario. However, after the procedure, when I informed the parents that everything had run smoothly, that we had totally ablated the tumour without any adverse events, they started crying. It is a moment I will never forget.
What led you to pursue your PhD in quantitative discomanometry? How is it complementary/relevant to your role as an interventional radiologist?
The spine is an area where interventional radiologists play a crucial role in both diagnosis and therapeutic management of a variety of pathologies. Specifically for intervertebral disc herniation, what I have always found fascinating is the fact that the success rate of percutaneous decompression techniques is around 80% no matter which technique you use. Discomanometry could serve as a diagnostic tool to escalate patients, leading to an improved patient-specific, or even better, hernia-specific, approach.
Your paper on pain management in cancer patients, recently published in Current Oncology Reports, is one of many you have authored on the subject—what innovations do you see on the horizon in this area?
Management of cancer pain is one of the most interesting topics in my everyday clinical practice. We have published numerous papers on the topic, but myself and the rest of the co-authors are actually particularly proud of this publication, which has been included in the National Comprehensive Cancer Network 2021 guidelines for adult cancer pain. As far as innovations in the field of pain management are concerned, I am convinced that cryoneurolysis is the ideal technique for pain palliation, as it offers more confined and more organised nerve regeneration alongside pain reduction. Although, at present, there is no standardised ablation protocol, given the wide range of variables that affect intraprocedural temperature at the ablation site, a more palatable solution will be a new device with information-gathering capabilities, to form and perform individual cryoneurolysis protocols.
You were appointed to the position of associate professor of diagnostic and interventional radiology at the National University of Athens Medical School—what has changed the most about your practice since your early senior consultant days over a decade ago?
Being an educator offers intrinsic rewards and brings with it lifelong memories. Providing real-life clinical experiences and context to medical students is an essential part of today’s medical education—whereas I had only very minimal obligations towards medical students and teaching when I started as a senior consultant. Integrating the role of medical students into the healthcare system provides added value, both to clinical care and medical education. You need to change your workflow in order to allow students to contribute before, during, and after visits, and to engage them holistically in patient care. Last but not least, you need to strike a balance between apprenticeship and an academic model, and choose which approach works best for whom.
You were at the forefront, at your centre, when it came to integrating microwave and navigation-guided ablation into IR services, yours being the first in Greece to adopt both procedures—why do you think it is important to lead the charge in adopting new techniques and procedures?
New techniques and procedures go hand in hand with IR, which is a discipline born of innovation; adopting new technologies is essential for the growth and flourishing of our specialty. Early adoption results in improved efficacy, ability to offer what no one is offering at the moment, and empowering practice with new and improved systems that make for better services. From our first experience with microwaves in 2008 to today, it has been evident for us that this technology offers unique advantages and has a role in today’s ablation practice. Ideally, when it comes to locoregional therapies, we want to have all the ablation techniques available in our armoury and to be able to take a lesion-tailored approach. Application of navigation tools as well as simulation and verification software significantly contribute to standardisation of ablation; I strongly believe that in the near future, these tools and software will be part of all interventional radiologists’ everyday practice. The tools will prove their value by allowing for better comparison of percutaneous ablation to surgical and radiation oncology.
In (also) becoming the first Greek hospital to enrol in the International Accreditation System for Interventional Oncology Services (IASIOS), what has the impact on your practice and patients been?
Even though the second department of radiology is in the process of acquiring the IASIOS accreditation, the benefits for patients and in terms of practice performance are more than evident. The whole process of patient care and treatment is improved. During the IASIOS accreditation process, we have analysed our service, improved its coordination and monitoring, and the end result is improved delivery of high-quality IO care, with the patient receiving the best possible treatment for an optimal, individual clinical outcome. This improvement has been throughout the department, affecting not only IO but all IR services.
You recently became the CIRSE Online Education Committee chairperson—what do you hope to do in this role that has not been done before?
Education extends beyond practical knowledge. Educated physicians develop thinking and skills, which help them make good decisions for the benefit of the patients. The Online Education Committee deals with the CIRSE Library, Academy and Webinars as well as with everything included in these three main pillars of virtual and online education provided by our scientific society. To leave your own footprint on this position I must admit is a very difficult task, since my predecessor Stefan Müller-Hülsbeck has done a superb job in organising almost everything from scratch. I am positive though, that along with my deputy chairperson Julien Garnon and all the members of the Committee, we will rise to the challenge and structure education in order to foster a love of learning among our IR community.
What are your hobbies and interests outside of medicine?
Before and during my medical studies, I worked as a DJ. What I have left from these days and nights are thousands of vinyl records and CDs of all kinds of music, which I love listening to in my free time. Apart from listening to music, I love reading books, especially historical novels (Bernard Cornwell, Wilbur Smith and Ken Follett are my favourite authors). My other main hobbies are playing basketball and swimming, especially on my beloved island of Lefkada where we have a beach house.
1-3) Preoperative CT scan views. The lateral left lung lesion is clearly visible; 4) Definition of the planned needle path. The red contour corresponds to the borders of the segmented lesion; 5) Alignment of Micromate to the planned needle path under live imaging; 6) Insertion of the biopsy needle through the guidance needle and tissue harvesting.
This advertorial is sponsored by Interventional Systems.
Marco van Strijen
Marco van Strijen is an interventional radiologist at St Antonius Ziekenhuis (Nieuwegein, The Netherlands) who specialises in non-vascular interventions and interventional oncology. Image-guided procedures feature heavily in his practice, Van Strijen tells Interventional News, enabling him to “[draw] needle paths, [define] targets and [introduce] needles”. Micromate(Interventional Systems) provides robotic assistance for these tasks, Van Strijen reports, detailing how “it is three years that we have been using Micromate”, following on from a successful stint with the early prototype that “functioned so well” that “the rest was history”.
On how Micromate fulfils its role within his practice, Van Strijen begins by acknowledging that for any percutaneous biopsy “it is very important to have a stable needle”, and therefore, “a device that helps you keep the needle stable while advancing the device through the skin to the desired target,” such as Micromate does, is valuable. “This is especially true in […] areas where there is not that much overlying skin or soft tissue [to] hold your needle while you are trying to centre it in the direction of your target,” Van Strijen adds, before exemplifying how unwieldy some of the former approaches to intraprocedural needle stabilisation were: “we were using our own hands, sterile towels draped around the needle insertion point, or sterile forceps, making adjustments until we had the needle in a holding position, but these were not that stable, especially when you have a patient who is still breathing or maybe even starts to move because of their discomfort on the table: you always have the risk of dislodging the needle.”
Van Strijen then enumerates the precise advantages of having a completely stable needle, as achieved with Micromate—“not only will it help in reducing the number of [needle] re-positionings, but it reduces the need for imaging, as you can advance the needle as quickly as possible. And this is [of…] benefit in reducing the amount of radiation, not only for the patient but also for yourself as the operator.” Furthermore, Van Strijen speaks of the procedural time reduction that this results in, and, consequently, the discomfort the patient is subjected to on the table.
In a particular case of Van Strijen’s—that of a percutaneous lung biopsy close to the pleura in a 52-year-old patient referred with suspected rectal carcinoma—in which Micromate was used under live imaging, the procedure time was 43% faster than previously reported, Interventional Systems states. The radiation level decrease measured 70%. Greater needle stability facilitates greater procedural accuracy, which, Van Strijen shares, makes “[working] in areas that rely on needles being positioned to millimetre or sub-millimetre accuracy” possible. For example, this could be “in the vicinity of critical structures such as the neck or the face or close to the major vessels of the thorax”. Van Strijen asserts that “this is where this type of robotic device comes in very handy.”
1-3) Preoperative CT scan views. The lateral left lung lesion is clearly visible; 4) Definition of the planned needle path. The red contour corresponds to the borders of the segmented lesion; 5) Alignment of Micromate to the planned needle path under live imaging; 6) Insertion of the biopsy needle through the guidance needle and tissue harvesting.
To the question posed by Interventional News of how Micromate reduces complications in lung biopsy cases, such as the aforementioned, Van Strijen states that “a quick in-and-out is the ideal strategy”, and with Micromate, the biopsy is possible “during one single breath-hold”. The incidence of pneumothoraces, which Van Strijen notes is the “most encountered complication in this procedure”, is “[reduced] significantly” by virtue of being able to avoid unnecessary pleura punctures. Where the needle is less stable, the necessary multiple attempts and sometimes, leaving the needle in, can cause tears in the pleura, Van Strijen explains.
Micromate may be responsible for something akin to his team becoming victims of their own success, Van Strijen then admits—”I think that by having this type of technology available, we are challenged quite a bit by our referring clinicians who are asking for more and more challenging lesions to be biopsied.” In practice this means “trying to get histology from a lesion of just a few millimetres,” in contrast to a decade ago, when, Van Strijen says “a two- or three-centimetre lesion was common”.
Likewise, because of the development of robotic technology, Van Strijen now carries out biopsies “next to very challenging structures—close to major vessels, close to the beating heart”.
Van Strijen is also keen to mention a further advantage of Micromate and the impact it has in his teaching hospital. “This type of device should be very easy to use, one that any user immediately understands without a lot of training—after only one or two demo cases,” he opines. And, with Micromate satisfying such an expectation, Van Strijen sees it as “[bridging] the gap between inexperienced and experienced users […] Young doctors are challenged in trying to perform the same procedures as their tutors,” but, as Van Strijen informs Interventional News, “one of the things I find very helpful [about Micromate]” is how doctors of different levels of experience can use it successfully.”
In the USA, atherectomy use in peripheral vascular interventions (PVIs) “more than doubled” from 2010 to 2019, with office-based procedures a “major driver” of this increase. This is according to published US data from the Vascular Quality Initiative (VQI), which also revealed wide regional variability in the use of atherectomy.
According to authors Tonga Nfor (Aurora St Luke’s Medical Center, Milwaukee, USA) and colleagues, small, older studies have indicated that the use of atherectomy devices has become common in PVIs despite what they describe as the “paucity of strong clinical guidelines”.
The study, published in the Journal of Vascular Surgery (JVS), was a retrospective analysis of prospectively collected data from the VQI registry, which the investigators say provides a “unique opportunity” to fill knowledge gaps in this field of research using “real-world” data originating from across the USA. The team identified all patients who had undergone endovascular PVIs for occlusive lower-extremity arterial disease from 2010 to 2019. Procedures in which an atherectomy device had been used as the primary or secondary device were classified as the atherectomy group, Nfor et al write.
In the study period, the authors note that 205,377 PVIs were performed for 152,693 unique patients. They report in JVS is that, during the 10-year study period, 16.6% of the PVIs had used atherectomy, with the data showing that use “significantly increased” from 8.5% in 2010 to 19.7% in 2019.
Geographic variation was evident in the study results, with Nfor and colleagues stating that they found a significant difference in the prevalence of atherectomy use across 17 geographic regions, ranging from 8.2% to 29%. These regions were further split into North, East, South, and West, the authors write, revealing that the observed frequency of atherectomy use in PVIs during the 10-year period was highest in the South at 22.5%, followed by the West (19.9%), North (17.3%), and East (12.6%; p<0.0001).
The 10-year VQI data also clarified predictors of atherectomy use. According to the study authors, the strongest predictor of use was performance of PVI in an office setting (odds ratio [OR], 10.08; 95% confidence interval [CI], 9.17–11.09) or ambulatory centre (OR, 4; 95% CI, 3.65–4.39) versus a hospital setting. Furthermore, the geographic trend in atherectomy use followed the distribution of the proportion of office-based PVI procedures—South (6.1%), followed by the West (4%), North (3.9%), and East (0.5%).
They note that the presence of severe (OR, 2.6; 95% CI, 2.4–2.85) or moderate (OR, 1.5; 95% CI, 1.4–1.69) lesion calcification was also predictive of atherectomy use, as well as some other factors including elective status, insurance provider, lesion length, prior PVI, claudication symptoms, and diabetes mellitus.
The researchers also examined the reimbursement aspect of the atherectomy discussion, highlighting differences in compensation levels for hospital-based versus office-based procedures, and for angioplasty versus angioplasty with atherectomy. For angioplasty performed in a hospital, the physician total relative value units (RVU) was 12.94, averaging about US$466, they report. For the same procedure performed in an office-based laboratory [OBL], the total RVU was 100.68 (procedure total), translating to US$3,628. Nfor et al further reveal that, when angioplasty was performed with atherectomy in a hospital, the physician RVU was 17.61, averaging US$635. However, when atherectomy with angioplasty was performed in an OBL, the reimbursement increased to 345 RVU— approximately US$12,444. The authors, however, point out that these total RVU reimbursement figures for office and ambulatory centre procedures includes the technical and facility fees.
“To provide patients with the highest quality of care, physicians must allow their decision-making to be guided only by the clinical factors and the best interest of the patient, and should be mindful of any biases that might influence their practice, including the reimbursement structure and financial incentives,” the researchers stress.
Despite the financial incentives that exist, the authors acknowledge that clinical considerations “play an important role in interventional decisions that guide patient care”. For example, they note that patients in the hospital setting will tend to have more acute disease with greater urgency and a greater risk of complications. “It follows naturally that operators might want to avoid long, complicated procedures that will subject patients to more risk, which might partly explain the lower use of atherectomy,” the investigators remark.
There are a number of limitations to the present study which the authors address in their discussion. For example, while the VQI database offers researchers a “large sample of patients from multiple regions,” they acknowledge that a selection bias could still occur because the nature of the database is “dynamic” and different centres were added cumulatively over time.
Despite this and other drawbacks, Nfor and colleagues claim that, to the best of their knowledge, the present study was “the largest to investigate specific clinical and non-clinical predictors of atherectomy use and also to examine the trend and geographic distribution”.
Routine use of atherectomy for infrainguinal PVI called into question
Caitlin Hicks
In a commentary on Nfor and colleagues’ report, Caitlin Hicks (Johns Hopkins University School of Medicine, Baltimore, USA) underscores the “overwhelming message” of the analysis: that atherectomy is being overused in the USA.
“This is not an attack on physicians who work in OBLs,” Hicks stresses at the outset of her commentary—titled ‘Atherectomy overuse is a real problem’—but rather a “statement of the facts,” of which she assembles four from this latest addition to the available research:
Atherectomy use for infrainguinal PVI has been “increasing rapidly” in the USA
No high-quality evidence that atherectomy improves outcomes compared with alternative endovascular therapies is available
Atherectomy is much more frequently used in OBL settings than in hospital-based settings
Reimbursement for atherectomy procedures is substantially higher than that for stenting and balloon angioplasty in the outpatient setting
“Based on these facts, the routine use of atherectomy for infrainguinal PVI is suspicious at best,” Hicks remarks. She acknowledges that cases exist for which atherectomy has proven beneficial—calcific disease, popliteal lesions that cannot or should not be stented, and recalcitrant lesions, for example. However, Hicks also notes that the data have shown the use of atherectomy in up to 100% of cases by some physicians—a fact that is “not right” in her view.
Hicks concludes: “As a field, vascular surgeons need to come together and unite on this issue. If we do not police ourselves regarding the appropriate use of high-cost technologies, the Centers for Medicare and Medicaid will most certainly do it for us.”
Cordis is a global interventional vascular technology company
Cordis today announced its acquisition, subject to customary closing conditions including regulatory approvals, of MedAlliance.
A press release notes that the agreement includes an initial investment of US$35 million and US$200 million payment upon closing in 2023, regulatory achievement milestones up to US$125 million and commercial milestones up to US$775 million through 2029. Cordis will immediately begin co-promotion of MedAlliance’s Selution SLR drug-eluting balloon in markets where it is commercially available.
The Selution platform leverages spherical MicroReservoirs made from biodegradable polymer mixed with the drug to control the sustained release of sirolimus. The continuous manufacturing process produces millions of precisely formed, miniature drug delivery systems. According to Cordis, Selution SLR is the only drug-eluting balloon using MicroReservoirs and is designed to provide the longest and most effective pharmacokinetics release profile of any device on the market.
“Nearly twenty years ago, Cordis introduced Cypher, the first drug-eluting stent, transforming cardiovascular treatment for patients around the world,” said Shar Matin, Cordis CEO. “Today, we are furthering that legacy of innovation and market disruption with MedAlliance and the first MicroReservoir sirolimus drug-eluting balloon, Selution SLR.”
Duke Rohlen, executive chairman of Cordis added: “The acquisition of MedAlliance illustrates our vision to maximise patient impact by pairing highly innovative growth drivers with Cordis’ trusted brand and extensive global commercial capabilities.”
Jeffrey B Jump, chairman and CEO of MedAlliance, commented: “When looking for a partner to bring our ground-breaking Selution SLR technology to market, Cordis was the perfect fit with its proven record in the industry. Our sirolimus drug-eluting balloon programme provides a flagship product that complements Cordis’ existing portfolio and will benefit greatly from its deep marketing and distribution expertise.”
Selution SLR received CE mark approval for the treatment of peripheral arterial disease in February 2020 and for the treatment of coronary artery disease in May 2020. In addition, MedAlliance has obtained investigational device exemptions for peripheral below-the-knee (BTK) and superficial femoral artery (SFA) interventions. Two IDE clinical studies are already underway.
“I have had the privilege to meet with clinical experts around the world and review hundreds of angiograms demonstrating the impact of Selution SLR in both cardiovascular and peripheral vascular patients,” said George Adams, chief medical officer for Cordis. “The clinical outcomes are remarkable, to say the least—especially for patients with few if any other treatment options.”
CSI notes in a press release that the 2.00 Max Crown is uniquely designed to enable simultaneous modification of both intimal and medial calcium. The device features an increased 70-micron diamond coated crown that creates more efficient engagement in mixed plaque, helping to achieve optimal luminal gain in mild to moderately calcified lesions above the knee.
Amit Srivastava (Bay Area Heart Center, St Petersburg, USA), who was one of the first physicians in the USA to incorporate the 2.00 Max Crown into his practice, commented: “The new 2.00 Max Crown greatly expands the lesions that can be treated with CSI’s orbital atherectomy. This device delivers exceptional luminal gain in mixed morphology lesions above the knee.”
Scott R Ward, chairman, president and chief executive officer of CSI, said: “The full commercial launch of the 2.00 Max Crown represents another important product launch for CSI as we broaden and diversify our product offering. Our peripheral orbital atherectomy systems can now treat a wider range of plaque morphologies throughout the leg. Combining this new device with our full line of interventional support devices, we continue to advance the ability of physicians to improve outcomes for patients undergoing peripheral interventions.”
Medtronic has announced the 36-month final results from the ABRE clinical study. The purpose of the ABRE clinical study was to evaluate the safety and effectiveness of the company’s Abre venous self-expanding stent system, intended for the treatment of symptomatic iliofemoral venous outflow obstruction.
The study results were presented in a late-breaking clinical trial session at the American Vein and Lymphatic Society (AVLS) 2022 annual meeting (13–16 October, New Orleans, USA). Stephen Black (Guy’s and St Thomas’ Hospital, London, UK), co-principal investigator for the ABRE study, presented the data.
“The 36-month ABRE data have continued to demonstrate the long-term durability of interventions in patients suffering from deep venous disease,” Black said. “The results show a sustained result in both technical aspects, but more importantly, in patient outcomes.”
The ABRE study included a complex set of patients. Within this patient group:
47.5% of patients were categorised as having post-thrombotic syndrome (PTS),
35.8% of PTS patients presented with a complete venous occlusion confirmed by the core lab
Mean lesion length of patients was 112.4mm
44% of patients had stents that extended below the inguinal ligament.
Of note, the study results showed:
Overall, effectiveness following treatment with the Abre venous stent was sustained through 36 months as evidenced by a Kaplan-Meier estimated primary patency rate of 81.6% and a Kaplan-Meier estimated freedom from clinically driven target lesion revascularization (CD-TLR) rate of 89.3%.
No stent fractures or delayed stent migrations were reported through 36 months.
Sustained and clinically meaningful improvements were observed through 36 months compared to baseline as measured by EQ-5D and VEINES-QoL quality of life.
Sustained and clinically meaningful improvements through 36 months as measured by Villalta and VCSS venous functional assessments indicates less severity of PTS disease and venous disease overall.
“Medtronic is strongly committed to the deep venous market. As the 36-month results show, the Abre venous stent system safely and effectively treats venous disease,” said Dave Moeller, president of the Peripheral Vascular Health Operating Unit at Medtronic. “This study included many patients with highly challenging cases, showing that Abre is meaningfully able to improve patients’ quality of life—including those with severe disease—for a long period.”
Interventional radiology (IR) was officially born on January 16, 1964, when Charles Dotter performed the first arterial angioplasty at the Department of Radiology at Oregon Health and Science University (Portland, USA). We still can see the prescription Dotter received from the referring physician, which stated: “VISUALISE BUT DO NOT TRY TO FIX!!!” Roberto Luigi Cazzato speaks to Interventional News about the emergence of IR outpatient clinics (IROCs) and his view that IR hospitalisation clinics (IRHCs) will soon begin being established too.
The above phrase summarises what interventionalists are—dreaming souls looking for innovation. For this reason, it is not surprising that in the last few decades, IR has evolved so rapidly that today, at least one type of IR procedure can be done on any and every organ. Moreover, devices and imaging guidance are becoming so sophisticated and precise that new interventions and clinical outcomes are presented yearly. Therefore, as interventional radiologists, we are succeeding in providing innovation in healthcare.
Our willingness for innovation is not only due to our love for novelty and technology. In our minds, innovation has a purpose, and it is a noble one—to serve our patients! For this reason, we stay in close contact with patients before and after interventional procedures.
It is not a surprise that in the last decade, IR initiatives intended to increase contact with our patients and improve their care have flourished. From this perspective, two main measures can be adopted: the IROC for consulting patients before and after the intervention; and on the other side, the IRHC, which provides hospital beds for patients undergoing challenging interventions.
Both of these solutions are desirable for the development of our specialty. However, the clinical, administrative, and financial input to establish IROCs versus IRHCs differs— it is much less costly to establish an IROC compared to an IRHC. In the last decade, newly built IROCs have flourished, with IRHCs less of a priority. The creation of IROCs is the first step, but we are confident that IRHCs will soon become more common.
In the meantime, we can analyse the performance of the IROC so far. In a paper published in CardioVascular and Interventional Radiology (CVIR), the addition of an IROC at the University Hospital of Strasbourg (Strasbourg, France) has had a positive effect on patient care. The results have been quite surprising:
The total number of consultations steadily increased from the first to the last year of the study period (from 693 consultations performed in 2011, to 1595 consultations performed in 2019, which accounts for an increase of 130%); the rate of unattended consultations remained stable throughout the entire study period (around 7%); in the 2018–2019 period, the cumulative procedure conversion rate, namely, the rate of first consultations that led to an IR procedure, was higher than 85%; among the 159 patients being surveyed to evaluate their satisfaction with the IROC, 99.2% highly appreciated their IROC experience, and pointed out that the main aspects they took into account to evaluate their IROC experience were the quality of secretarial and medical services.
These results represent another successful chapter for IR in its so far short, but bright, history. This study points out that as interventional radiologists, we are succeeding in taking care of our patients and that our clinical role is being affirmed, which may pave the way to establishing IRHCs in the near future.
Nevertheless, with patients looking for high-quality secretarial and medical services, these results also show that specific training is required for the employees involved in running the IROC.
The entire IR community is becoming increasingly interested and focused on developing this topic; for this reason, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) dedicated a lecture to ‘How to establish and run an outpatient clinic’ at its annual meeting (10–14 September, Barcelona, Spain).
Roberto Luigi Cazzato is associate professor at the Department of Interventional Radiology, University Hospital of Strasbourg (Strasbourg, France).
Disclosures: The author declared no relevant disclosures.
Interventional News’ most popular content last month included news of the acquisition of a new catheter by Bentley, the announcement of the final patient enrolled in a liquid embolic study, latest data from the SAVAL trial of a drug-eluting stent, and a video discussion of the current landscape of deep vein thrombosis (DVT) treatment.
Bentley announced that it has acquired the rights of the GoBack catheter from Upstream Peripheral Technologies. The catheter will simplify crossing and re-entry in occluded arteries.
Medtronic announced that it has recently received CE mark for its Radiant balloon-expandable covered stent, the first and currently, only, covered stent indicated for use in chimney endovascular aneurysm repair (ChEVAR) with the Endurant II/IIs stent graft system.
Stryker has announced in a press release that its OptaBlate bone tumour ablation system (OptaBlate) has received 510(k) clearance from the US Food and Drug Administration (FDA). The addition of the OptaBlate technology to Stryker’s Interventional Spine (IVS) portfolio expands on its core competencies in vertebral augmentation and radiofrequency ablation and completes its portfolio of treatment options for metastatic vertebral body fractures.
Andrew Wigham (Oxford, UK) and Rick De Graaf (Friedrichshafen, Germany) discuss the current state of DVT treatment at the Leipzig Interventional Course (LINC) 2022 (6–9 June, Leipzig, Germany), with both noting that “a massive problem” in Europe is the lack of awareness around treatment.
Fluidx Medical announces completion of trial enrolment for its GPX embolic device. In this multicentre trial, GPX was used to treat a variety of primary and metastatic tumours, renal adenoma tumours, and a range of other arterial and venous applications.
Philips announced new milestones in the development of the world’s first spectral detector angio computed tomography (CT) solution— Philips Spectral Angio CT suite—bringing the company’s breakthrough spectral CT imaging technology into an integrated hybrid angio CT suite.
Penumbra and Asahi Intecc, a Japanese medical device manufacturer, announced that they will collaborate to introduce Penumbra’s Indigo Aspiration System into the Japanese market upon regulatory approval.
Reto Bale (Medizinische Universität Innsbruck, Innsbruck, Austria) gave a presentation titled ‘Stereotactic thermal ablation—can it break the current limits?’ at the 2022 European Conference of Interventional Oncology (ECIO; 24–27 April, Vienna, Austria). A key takeaway was that the stereotactic procedure yields “excellent” results.
Ablation is used to destroy or shrink tumours in the liver, lung, kidney, bone, and other organs. In recent decades, image-guided ablation has become integral to modern cancer therapy with curative or palliative intent. Although a promising treatment option, the main challenge is the accurate and safe positioning of the ablation probes to achieve complete tumour coverage, especially in difficult-to-access localisations.
XACT Robotics announced that its ACE Xtend remote control unit received US Food and Drug Administration (FDA) clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room. The first-of-its-kind feature for computed tomography (CT)-guided percutaneous procedures is designed to improve physician workflows while limiting physician and other users’ exposure to radiation, and to reduce physical strain.
“The XACT ACE Robotic System has already allowed users to make percutaneous procedures, such as ablations, drainages and biopsies, more accurate, consistent and efficient,” said Shai Meltzer, chief executive officer of XACT Robotics. “The addition of ACE Xtend has the potential to further increase efficiencies for the care team with a streamlined workflow that helps reduce the time during which physicians and other users are exposed to harmful radiation during standard procedures.”
“Interventional radiology is among the medical specialties that are facing a physician shortage in the coming years and technologies that can improve their efficiencies are crucial,” said Jeffrey Solomon, vice president of Medical Affairs at XACT. “By equipping different users with tools that can standardise the procedure and potentially shorten procedure times, we can maximise the number of patients they see.”
The comprehensive XACT ACE Robotic System combines image-based planning and monitoring with patented S-Drive technology, which enables the system to quickly adapt from a linear to a non-linear trajectory with its robotic insertion and steering of instruments during interventional percutaneous procedures.
The XACT ACE Robotic System has been proven to achieve 1.7mm tip-to-target average accuracy upon first insertion based on data obtained from company clinical studies for biopsy procedures. By providing accurate and actionable results for medical diagnosis, the system aims to enhance early detection and improve patient outcomes.
Six-month data from the Surmodics SWING first-in-human (FIH) study of the company’s Sundance sirolimus drug-coated balloon (DCB) were shared at the 2022 Amputation Prevention Symposium (AMP; 9–11 October, Lugano, Switzerland).
The SWING study is a prospective, multicentre, single-arm feasibility study to evaluate the safety and performance of the Sundance sirolimus DCB when used to treat occlusive disease of the infrapopliteal arteries.
The study’s primary safety endpoint data showed no perioperative deaths or major amputations at 30 days and just one major reintervention was reported among the 35 trial subjects, a Surmodics press release reports. Data for the primary efficacy endpoint show a late lumen loss (LLL) of 1mm (±0.79mm) across 35 lesions at six months, indicating that the large luminal gain achieved immediately after the procedure was sustained six months post-treatment.
“At six months we observed a consistent improvement in Rutherford category and functional measures, as well as an excellent primary patency of 88.5%, which compares favourably to other DCBs used in the infrapopliteal circulation,” said SWING trial co-lead investigator Ramon Varcoe, vascular surgeon at the Prince of Wales Hospital and associate professor of vascular surgery at the University of New South Wales (Sydney, Australia).
The SWING trial enrolled subjects with stenotic or occluded lesions of the infrapopliteal arteries, a reference vessel diameter (RVD) of 2mm to 4mm, and a total lesion length of ≤230mm for treatment with the Sundance sirolimus DCB at eight sites in Australia, New Zealand, and multiple locations in Europe. They will be followed for 36 months following the index procedure.
“The novel coating on the Sundance sirolimus DCB was evaluated in a challenging, predominantly CLTI [chronic limb-threatening ischaemia] population with a high proportion of diabetes and moderate-severe calcification,” said trial co-lead investigator Andrew Holden, director of interventional radiology at the University of Auckland (Auckland, New Zealand). “This first-in-human study demonstrates that the Sundance sirolimus DCB could be a safe and promising treatment for occlusive disease of the infrapopliteal arteries.”
The Sundance sirolimus DCB utilises a “next-generation” coating technology consisting of microcrystalline sirolimus and a proprietary excipient to maximise drug transfer, which, according to Surmodics, enhances sirolimus delivery and sustains therapeutic levels in the artery.
In a press release, Surmodics notes that sirolimus is a potent anti-inflammatory and anti-proliferative compound, has been used successfully in coronary drug-eluting stents. “The delivery of sirolimus to the vessel wall during mechanical dilatation provides an ancillary action of inhibiting the proliferation of cells, with the intended purpose of reducing restenosis,” the company adds. Surmodics advises that the Sundance sirolimus DCB is not available for sale anywhere in the world, and currently is for investigational use only.
A new report from a joint taskforce of the American College of Radiology (ACR) and the Society of Interventional Radiology (SIR) recommends improved access to interventional radiologists in small and rural areas. The taskforce was formed to explore strategies for recruitment and retention of interventional radiologists in rural areas, which have the greatest challenges with access to interventional radiologic care.
“Interventional radiologists play a key role in improving patient health outcomes and creating healthier communities,” said Alan H. Matsumoto, vice chair of the ACR Board of Chancellors and a member of the joint taskforce. “The recommendations should be beneficial for practices in small and rural areas that hope to recruit interventional radiologists and provide the care patients deserve.”
“Access to an interventional radiologist’s care can be the difference between life and death.”
The taskforce focused on improving training opportunities, creating templates to help radiology practices and hospitals provide interventional radiology (IR) services in small and rural communities, and developing appropriate financial models to recruit interventional radiologists to these areas and retain their services.
“Access to an interventional radiologist’s care can be the difference between life and death, yet millions of Americans living in rural communities do not have access to the image-guided treatments interventional radiologists perform to literally save life and limb,” said SIR President Parag J. Patel, professor of radiology at the Medical College of Wisconsin (Milwaukee, USA). “Access to IR services improves the care offered within a hospital or health system. The recommendations outlined in this paper will help practices attract IR talent and expand IR services where they are often needed the most, eliminating IR deserts and improving patients’ access to the care they need.”
The report was published online in the Journal of the American College of Radiology (JACR).
Endologix has announced the submission of a premarket approval (PMA) application requesting approval for the Detour system to the US Food and Drug Administration (FDA).
The Detour system, which earned FDA Breakthrough Device Designation, is a unique therapy that allows the creation of a fully percutaneous femoropopliteal bypass that is routed through the femoral vein. The Detour system uses the Endocross Device and Torus Stent Graft to treat patients with moderate to severe peripheral arterial disease with long blockages of the superficial femoral artery (SFA).
The PMA application includes the results of the DETOUR2 IDE study, which were presented at the 2022 Annual Meeting of the Society for Vascular Surgery (SVS; 15–18 June, Boston, USA). Sean Lyden (Cleveland Clinic, Cleveland, USA), one of the study’s principal investigators presented results that included 12-month primary patency of 72.1% in SFA lesions with a mean length of 32.7cm. The trial demonstrated technical success of 100% in 202 patients, with a 30-day major adverse event rate of 7%.
“This submission is a significant milestone in our mission to expand our therapeutic products into the large peripheral vascular market opportunity. Patients with long SFA blockages have compromised treatment options at present due to high rates of failure with conventional endovascular techniques and the morbidity associated with open femoropopliteal bypass surgical procedures,” said Matt Thompson, president, and chief executive officer of Endologix. “Once approved, offering a fully percutaneous femoropopliteal bypass, will provide a disruptive, innovative therapy to physicians for the treatment of long-segment SFA disease and expand the treatment options available for these patients.”
Thomas Rand (Klinik Florisdorf, Vienna, Austria) recently presented on the preliminary results to 12 months of the Motiv bioresorbable scaffold (Reva Medical) postmarket trial at the recent Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain). With the objective of evaluating safety and efficacy for the treatment of patients with rest pain or minor tissue loss due to the presence of lesions of a maximum length of 100mm at the level of the below-the-knee (BTK) arteries, Rand shared in a FIRST@CIRSE session that at 12 months, primary patency—the efficacy endpoint—was 88%, and the technical success rate, 99%.
The MOTIV BTK study is a prospective, single-arm, multicentre trial, in which 58 patients with BTK artery lesions of a maximum length of 100mm have been enrolled. The study is being carried out on 60 limbs with 76 Motiv scaffolds, Rand specified. The Motiv scaffold has been approved for use in Europe since 2018 when, according to Reva Medical, the device became the first bioresorbable scaffold to receive CE mark for use below the knee.
“The special thing with the Motiv scaffold,” Rand opined, “is that it is sirolimus-eluting and bioresorbable, so you have two good things.” The presenter noted that this is in keeping with the ‘leave nothing behind’ concept. “The scaffold itself is made from TyroCore, which is derived from tyrosine amino acid,” Rand then detailed, and this design is responsible for “low inflammation and irritation during degradation and [no calcification].” The thin struts “have been evaluated as best-in-class,” Rand supplemented.
Moving on to address the preliminary study outcomes, Rand described them as “really very good, [with] a 99% technical success in all patients.” Primary patency at six months was 90%, and the 12-month preliminary result 88%. The limb salvage rate until now at 12 months, as conveyed by Rand was 97%, and the 14% (n=8) death rate was entirely unrelated to the device or procedure. The freedom from clinically driven target lesion revascularisation (CD-TLR) was “a very nice” 98.3% at 12 months, Rand also underlined, with a “decline in Rutherford stages observed during this time.”
“As a conclusion, already, we can say with the Motiv scaffold we had excellent tracking and visibility and a problem-free delivery.” Rand proceeded to emphasise the scaffold’s ease of use and the 90% vessel patency rate, before sharing that the CD-TLR and limb salvage rates remained stable from six to 12 months.
“The major concept behind this study, which I really like, is the ‘nothing left behind’ concept, and this is really fulfilled in this study,” Rand finished by informing delegates.
Enrolment in MOTIV IDE clinical trial begins
In the weeks following CIRSE 2022, Reva Medical announced that enrolment in the MOTIV pivotal trial has been initiated at clinical centres in both the USA and Europe. The study, which is being conducted under a US Food and Drug Administration (FDA) investigational device exemption (IDE), will evaluate the use of the Motiv sirolimus-eluting bioresorbable vascular scaffold for treatment in patients suffering from chronic limb-threatening ischaemia (CLTI).
The MOTIV study is a global, randomised controlled trial (RCT) that was designed to evaluate the safety and efficacy of the Motiv scaffold for the treatment of infrapopliteal lesions in patients with CLTI by randomised comparison with standard balloon angioplasty. The study, led by co-principal investigators Ehrin Armstrong (Adventist Health, St Helena, USA) and Andrej Schmidt (Universitätsklinikum Leipzig, Leipzig, Germany) will follow up to 292 patients at approximately 35 clinical centres in the USA and Europe.
Schmidt recently recorded a live case using Motiv scaffolds that was shown at the 2022 Transcatheter Cardiovascular Therapeutics (TCT) conference (16–19 September, Boston, USA). During the procedure, Schmidt implanted three 60mm Motiv scaffolds in a patient with CLTI below the knee, and the patient has demonstrated positive postoperative results.
“The absence of an approved device as a dedicated treatment option for the estimated 20 million patients worldwide suffering from CLTI is a significant unmet need,” commented Jason Ricci (Bellin Health Cardiology Associates, Green Bay, USA), the physician who enrolled the first US patient. “I am delighted to play a role in this important trial and evaluate its potential to advance the science and therapies available to this highly complex patient population.”
“The Motiv scaffold has a demonstrated history of positive clinical results, and I am honoured to have performed the first procedures with the device in this trial,” stated Henrik Schröder (Ihre Radiologien MVZ, Berlin, Germany), who enrolled the first European patients. “The scaffold was easily delivered, and the procedure was aided by visibility of the device under fluoroscopy, which is beneficial to confirm proper placement.”
Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.
The company has also reported that enrolment in the trial is now complete, with 20 patients having been successfully implanted with the Axess graft.
During haemodialysis, the Axess device demonstrated 100% cumulative primary and secondary patency, with an average follow-up time of 5.8 months and no device-related complications, in patients implanted by Matteo Tozzi and his team at the University of Insubria (Varese, Italy)—one of six European sites participating in the trial.
These data will be presented at the Porto Vascular Conference (PVC; 7–8 October 2022, Porto, Portugal), organised by the European Society of Vascular Surgery (ESVS). To date, Axess has enabled more than 1,200 haemodialysis sessions in just over a year as part of the AXESS FIH trial. Sixty of these sessions have taken place in Varese, a Xeltis press release states.
“Our initial clinical experience with Axess is very promising, from implanting to puncturing, and the data on functionality observed so far are very encouraging,” Tozzi commented.
Xeltis’ Axess device is a synthetic, bio-restorative vessel graft that enables early puncturing needed to connect to the haemodialysis machine. Unlike any currently available options—according to Xeltis—it is also designed to turn into a patient’s own living blood vessel, like an arteriovenous fistula, as its porous structure gets gradually colonised by patient’s own tissue cells.
According to the experience in Varese, Axess improved compliance over time, which may result from new tissue forming in the device.
After the disappointment of a few failed randomised controlled trials (RCTs), transarterial radioembolization (TARE) is finally back in the spotlight. And interventional radiologists (IRs) are learning from these past failures to shape the future.
Despite negative results, former trials have taught us that TARE is a highly effective treatment option if some essential rules are respected. Firstly, thoughtful selection of patients, with careful evaluation of the liver function reserve. Secondly, adequate arterial vascularisation, with a preference for no harm caused by prior therapy. The third rule is to carry out personalised dosimetry tailored to the vascular anatomy, tumour type and extension, the patient’s characteristics and the goal of treatment.
Irene Bargellini
Learning from the past, the current decade has finally started with successful trials, showing the efficacy and safety of TARE in primary tumours (such as the DOSISPHERE-01 [Boston Scientific], TRACE and LEGACY [Boston Scientific] trials for hepatocellular carcinoma (HCC) in advanced, intermediate and early stages, respectively) as well as metastatic lesions (such as the EPOCH [Boston Scientific] study in second-line colorectal cancer metastases).
Personalised dosimetry has become a central focus of investigation in an attempt to identify the most adequate administered activity for achieving tumoricidal tumour-absorbed doses without harming the surrounding liver parenchyma. With high tumour-absorbed doses, complete tumour necrosis may be achieved, translating into a durable response, conversion to surgery and ultimately significant survival advantage. However, obtaining a high tumour-absorbed dose implies limited dose to the non-tumoral parenchyma— in other words, a high tumour-to-liver ratio. If all or almost all the activity is concentrated selectively in the tumour cells, there is, potentially, no limit to the radioactivity level we could administer!
But what do IRs have to do with this? There is no doubt that good dosimetry starts with a good angiographic work-up, by understanding anatomy, flow distribution and haemodynamics, so that the tumour can be targeted selectively. Over the years, the preliminary angiographic work-up has adapted to increasingly refined dosimetry calculations. From whole-liver and hemi-liver treatments, in which the main challenge was the identification of extrahepatic vessels, we are moving towards selective and super-selective treatments and, where these are not possible, we are learning how to exploit and modify the arterial flow.
While selectivity can be relativity easy to obtain when dealing with hypervascular lesions, and well demarcated and limited tumour burden, it becomes challenging in patients with infiltrative lesions, hypovascular tumours and multifocal extensive disease. How can we obtain a selective intratumoral concentration of particles in these cases?
Several computational studies have shown that even minimal modifications in injection parameters and position, shape and orientation of the supporting catheters and of the microcatheters may have a meaningful impact on the distribution of flow in the target volume. As an example, when the catheter is close to an arterial bifurcation, a preferential flow into one of the two branches is frequently observed, influenced by the size of the distal vessels, their area of distribution, and the morphology and the orientation of the catheter’s tip. The challenge for the operator is to select the most appropriate position for the catheters and, if needed, exploit specific pre-shaped microcatheters, to obtain a homogeneous flow distribution in the entire target liver volume.
The capacity of the arterial branches to receive the right quantity of spheres is another matter of concern, particularly in tumours with multiple feeding vessels and in pre-treated patients with impaired arterial vascularisation. Minor tumour-feeding vessels may require coil embolization to promote flow redistribution. However, redistribution requires an in-depth knowledge of the possible intra- and extrahepatic arterial connections; it may be tricky and unpredictable, varying by specific vascular anatomy, the tumour type and tumour location. The success of flow redistribution has been reported to be lower in certain conditions, such as when parasitised arteries are embolized proximally, or when it is difficult to predict which vessels are going to be recruited after embolization— in centrally located tumours if unilobar treatment is planned, and in hypervascular bulky lesions. As a result, flow redistribution is now recommended only when strictly needed.
Specific microcatheters, such balloon and anti-reflux microcatheters, have recently become available, and through different mechanisms, they are able to modify the haemodynamics and flow distribution, potentially enhancing the intratumoral uptake and reducing the risk of reflux and non-target embolization. These tools may be of particularly useful for treating hypovascular lesions and multifocal disease. How effective they are for radioembolization is still being investigated.
In conclusion, we have learned over the years that, to be successful, radioembolization requires a high level of expertise—it is a truly multidisciplinary treatment modality. Dosimetry is key to success; yet, personalised dosimetry requires personalised angiographic planning based on flow analyses and where possible, flow modification, to achieve selective tumour uptake.
Irene Bargellini works within the Division of Vascular and Interventional Radiology at Florence University Hospital (Florence, Italy).
Disclosures:Bargellini declared having received an institutional research grant from Boston Scientific; consulting fees from AstraZeneca, EISAI, GE Healthcare, Guerbet, Merck, Sirtex, Terumo; honoraria for lectures from AstraZeneca, Bayer, Boston Scientific, Eisai, Guerbet, Merck, Sirtex, Sobi, Terumo; having been part of the Independent Data Safety Monitoring Board for AstraZeneca.
Results of the FLASH registry demonstrate the “excellent safety profile” of the FlowTriever system (Inari Medical) in 800 “real-world” patients. This is according to Catalin Toma (University of Pittsburgh Medical Center, Pittsburgh, USA), who presented outcomes for the full US cohort of FLASH at the 2022 Transcatheter Cardiovascular Therapeutics meeting (TCT; 16–19 September, Boston, USA). The results were simultaneously published in EuroIntervention.
Toma reported a 1.4% major bleeding rate and 0.4% rate of other major adverse events (MAEs) in what the presenter described as the largest prospective interventional study in pulmonary embolism (PE). All-cause mortality was <1% at the 30-day visit in this “real-world” population with prevalent baseline predictors of mortality, the presenter added, noting also that haemodynamics improved on-table, acute vitals and right ventricular (RV) strain normalised, and clinical recovery continued through six months.
The presenter noted that acute all-cause mortality following PE has remained high (>10%) over two decades, adding that, following PE, the 30-day readmission rate is nearly 25%, and up to half of patients report persistent dyspnoea, exercise intolerance, and/or functional limitations at three to six months.
According to Toma, guidelines suggest considering advanced therapies, including mechanical thrombectomy, when thrombolytics fail or are contraindicated, or haemodynamic deterioration occurs. However, he said, major bleeding risks with thrombolytic-based treatment strategies remain a concern, and their use is limited by corresponding contraindications and consequent intensive care unit (ICU) monitoring.
Mechanical thrombectomy can rapidly extract thrombus and relieve RV strain without thrombolytics, the presenter informed the TCT audience, stating that “additional data on the risk-to-benefit ratio could shift the standard of care”. One example of a mechanical thrombectomy device is FlowTriever, he highlighted, noting that this system is 510(k)-cleared by the US Food and Drug Administration (FDA) and CE mark-approved for the treatment of PE.
FLASH is a prospective, multicentre, single-arm registry designed to evaluate the safety and effectiveness of the FlowTriever system for treatment of PE through six months, with the decision to intervene being at the discretion of treating physicians or local PE response team (PERT). The primary endpoint is an MAE composite endpoint of device-related mortality within 48 hours, major bleeding within 48 hours, and intraprocedural device- or procedure-related adverse events.
At TCT, Toma reported outcomes for the full US cohort. In terms of the primary outcomes, he relayed a primary MAE rate of 1.8% (14/788), which combined a 0% rate of device-related deaths (0/788), 1.4% rate of major bleeding (11/788), and 0.4% rate of intraprocedural adverse events (3/788). The presenter also communicated all-cause mortality data, noting rates of 0.3% at the 48-hour visit (2/794), 0.8% at the 30-day visit (6/734), and 5% rate at the six-month visit (28/588). Importantly, the procedure led to significant improvement in invasive haemodynamics with decreased pulmonary pressures and improved cardiac output. Finally, Toma revealed that the rate of all-cause readmissions at the 30-day visit was 6.2%, with 1.4% related to PE treatment (10/711) and 4.8% unrelated to PE treatment (34/714).
Looking ahead, Toma highlighted that “data from the ongoing PEERLESS randomised controlled trial will provide important evidence regarding the safety and effectiveness of FlowTriever mechanical thrombectomy compared with catheter-directed thrombolysis”.
Paediatric interventional radiologist Alex Barnacle (Great Ormond Street Hospital, London, UK) gave the Josef Roesch Lecture at the Cardiovascular and Interventional Radiological Society of Europe 2022 meeting (CIRSE; 10–14 September, Barcelona, Spain), choosing to present on the subject of ‘Developing excellence in interventional radiology (IR) for our youngest patients’.
The presenter used various case examples to demonstrate to non-paediatric interventionalists that they “still need to think about [paediatric IR]—children grow up and graduate into adult practice”. A take-home message from Barnacle was how cross-specialty collaboration on issues such as establishing standards of practice, especially with the wider IR community, will help paediatric IR grow and “[change lives]”.
Barnacle’s presentation began with the story of a patient of hers, who was the first to receive orbital sclerotherapy at Great Ormond Street Hospital. Highlighting the life-changing impact of the treatment on her patient, Barnacle also underlined the importance of her network in providing the care her patient required—“[David Lord] talked me through [the procedure] over the telephone and we did [it].” This success is proof of the value of tapping into “the very small pool of expertise around the world”—Lord is based in Sydney, Australia—however “if we do not know each other, we cannot share our expertise and data,” Barnacle acknowledged.
How crucial cultivating a network within paediatric IR is, is complemented by the need to communicate and work together with other specialties so that they better recognise where paediatric IR can play a key role in patient care. “Just as with IR […] paediatric IR is massively under-recognised by other specialties,” Barnacle stated, going on to explain the impact this has—”we get late referrals because other teams do not know what we can do”. An example of where increased awareness and implementation of paediatric IR expertise could make a difference to current practice is, as illustrated by Barnacle, central venous access. “We all know that children should not need to be going through repeated painful, distressing cannulations […] that will mentally and physically scar them and their families for the rest of their lives.” What is a “bread and butter” procedure for a paediatric interventional radiologist will enable their patients to “get on with dealing with [everything else] that they need to, without having to think about those repeated cannulations.”
Barnacle presenting her Josef Roesch Lecture at CIRSE 2022
In contrast to the day-to-day roles paediatric interventional radiologists can play, such as by providing central venous access, Barnacle touched on the “supportive care” that they can give patients with rarer conditions, including those with rapidly involuting congenital haemangioma, and those who have swallowed button batteries, and may require dozens of interventions to “get through”.
Protocols and guidelines are also a factor in limiting the extent to which paediatric IR can fulfil its potential in such cases, as Barnacle also flagged. The presenter illustrated her point with a trauma case example, which saw the 15-year-old patient requiring a partial splenic embolization bypass a major trauma centre, as protocol would not allow (non-paediatric) interventional radiologists to carry out the treatment. “[It] just feels wrong”, Barnacle admitted, before suggesting that, as with the “limited” existing standards of practice for paediatric IR, “we need more”. As a potential solution to the paucity of paediatric IR-specific practice guidelines, the presenter offered the approach of adding paragraphs to existing guidelines on how to nuance well established adult practice for children.
A further barrier to widespread recourse to paediatric IR that Barnacle brought to the audience’s attention was the increase in paediatric contraindications for some devices—“we have had to change the inferior vena cava [IVC] filter we use,” the presenter lamented. This is symptomatic of a “small toolbox that is being emptied very quickly,” which, in addition to affecting paediatric IR practice, also has a knock-on effect for training, as device companies feel obliged to pull out of events such as the hands-on device training offered at meetings.
Nevertheless, Barnacle rounded off her presentation on a positive note, taking stock of the increasing interest in paediatric IR, of which there is ample evidence. The scope of the paediatric IR programme at CIRSE was one example Barnacle drew upon, including a sell-out hands-on session in spite of one company pulling out for the aforementioned reason of contraindications. “Things are changing,” according to the presenter, proceeding to celebrate the fact that CVIR Endovascular’s most downloaded paper of the past year was on paediatric IR, and how the remote Society of Paediatric Interventional Radiology annual meeting in 2020 saw attendees from 43 different countries.
Key now, Barnacle believes, is to “build on this interest”, which, she believes, extends to trainees looking for more of a “human side” to their work and “greater job satisfaction”—requirements that, she opines, being a paediatric IR can meet. As relayed throughout her presentation, efforts to grow paediatric IR, and interest and awareness of it, can take the form of establishing clearer guidelines and protocols, drawing on professional networks to aid innovation and optimal patient care, and working with colleagues in other specialties “so that children get referred to us sooner—this is better than picking up the pieces,” Barnacle concluded. “[After all], we are all here because we believe that minimally invasive procedures are the way to go” was the presenter’s salient final remark.
Terumo Medical Corporation has announced late-breaking data showing the safety and efficacy of radial to peripheral (R2P) interventions with the R2P Misago self-expanding peripheral stent in lower extremity endovascular interventions via a radial approach. The results were presented at this year’s Transcatheter Cardiovascular Therapeutics (TCT) conference (16–19 September, Boston, USA).
Presented by Yulanka Castro-Dominguez (University Hospitals’ Harrington Heart & Vascular Institute, Cleveland, USA), the study results showed that using a radial approach in treatment of complex lower extremity peripheral arterial disease (PAD) allowed 92.3% of patients to be discharged the same day. In addition, there were no serious access site complications for any of the patients enrolled in the study.
“In the invasive management of patients with PAD, the ‘radial first’ approach is beginning to gain momentum,” said Michael Martinelli, chief medical officer of Terumo Medical Corporation. “Radial artery access has been shown to minimise bleeding and vascular complications, lessen mortality rates, reduce costs, and shorten length of stay compared to femoral access in patients undergoing percutaneous coronary intervention (PCI), and we are now seeing growing evidence for similar benefits in peripheral arterial intervention. Our study contributes significantly to this expanding body of evidence as it clearly demonstrates the safety and efficacy of radial access in PAD intervention.”
The study was a prospective, multicentre, core-lab reviewed, clinical endpoint committee (CEC) adjudicated, single-arm study aimed at evaluating the safety and feasibility of radial access when used in the treatment of complex lower extremity PAD. A total of 120 PAD patients with Rutherford classification 2–5, from eight medical centres from across the USA were enrolled from 29 June, 2020 to 24 June, 2021 and followed up to one year.
In the final analysis, the primary safety endpoint included evaluation of radial access related complications, to include: access site bleeding, hand ischemia, hematoma, nerve damage, perforation, pseudoaneurysm, radial artery occlusion, embolic stroke or transient ischemic attack (TIA). Based on CEC adjudication, primary safety events categorized as serious access site-related adverse events did not occur in any patient. Radial access was successfully achieved in 100% of patients.
Patients who received R2P Misago self-expandable bare metal stent were later followed up to 12 months and the reintervention on the target lesion was required only in two patients.
The study was sponsored by Terumo Medical Corporation. Dedicated Terumo radial devices used in this study included: R2P Destination Slender guiding sheath, R2P Metacross RX percutaneous transluminal angioplasty (PTA) balloon dilatation catheter, R2P Crosstella RX PTA balloon dilatation catheter, R2P Misago self-expandable bare metal stent and TR Band radial compression device.
Truveta announced a strategic collaborative agreement with Boston Scientific to improve long-term patient care and gain insights into healthcare disparities. Through this collaboration, Boston Scientific researchers will be able to access data from Truveta, which contain de-identified medical records from more than 65 million US patients.
“Truveta will enable us to gather insights on a breadth of devices and disease states, including peripheral artery disease (PAD), venous thromboembolic disease, and segments of interventional oncology,” said Michael Jaff, vascular medicine specialist and chief medical officer and vice president, Medical Affairs, Innovation and Technology, Peripheral Interventions, Boston Scientific. “The first analysis will focus on gaining a deeper understanding of the long-term patient outcomes relating to the use of our products indicated for treatment of PAD.”
According to the US Centers for Disease Control, PAD affects approximately 6.5 million people aged 40 and older in the USA. This month is PAD Awareness Month, and Truveta recently shared new insights from its de-identified data, including findings that of the more than 11,000 PAD patients who received revascularisation procedures, Black or African American patients with PAD (1.0%) were less likely to undergo revascularisation than white patients diagnosed with PAD (2.6%). Of those who are treated with an interventional procedure, Black or African American patients were also less likely to receive drug-eluting stents than their white counterparts. Additionally, insights into major adverse outcomes, like lower-limb amputation, were discovered. For example, patients treated with drug-eluting stents had lower rates (4.8%) of amputation compared to all patients who received revascularisation (8.5%).
“Device manufacturers realise it is critical to have data on the clinical outcomes for patients treated with their devices following regulatory approvals, yet those data can be messy, fragmented, and difficult to obtain and analyse,” said Terry Myerson, chief executive officer of Truveta. “Truveta solves this problem, empowering researchers with real-world data on how any drug or device is currently being used every day across the USA.”
Truveta data provide the most up-to-date picture of US health across age, race, ethnicity, geography, socioeconomic factors, and more. Data are updated daily and include the full Electronic Medical Record (EMR), including device-specific data, not just the medical bill from claims data, all de-identified and aggregated
These clinical data are linked across providers and with medical claims when care is provided outside Truveta’s network. Every patient record is enhanced with comprehensive socioeconomic data and daily mortality data for a complete picture of each patient’s health journey without risk of re-identification.
“The COVID-19 pandemic put a spotlight on the importance of data to inform and improve patient care. It also put a glaring spotlight on the inequities in accessing and receiving equitable healthcare that are prevalent among people of colour and low-income communities throughout the USA,” said Debbie Salas-Lopez, Community and Population Health at Northwell Health and Truveta Ethics and Health Equity Board of Governors member.
Guerbet announced that the US Food and Drug Administration (FDA), after priority review, has approved Elucirem (Gadopiclenol), a new macrocyclic gadolinium-based contrast agent (GBCA) for use in contrast-enhanced magnetic resonance imaging (MRI).
Elucirem (Gadopiclenol) is a new macrocyclic GBCA with high relaxivity indicated for use in adults and children aged two years and older, for contrast-enhanced magnetic resonance imaging (MRI). The product is used to detect and visualise lesions with abnormal vascularity in the central nervous system and the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system).
Gadopiclenol, the active substance of Elucirem, has been designed with two sites for water molecule exchange to increase relaxivity and contrast, allowing it to be used at half the conventional dose of gadolinium compared to other non-specific GBCAs.
The efficacy and safety of Gadopiclenol have been assessed as part of Guerbet’s clinical development plan, with marketing authorisation being targeted worldwide (cf. phase III trial results below).
The FDA is the first health authority to have approved Elucirem. It is currently in the process of examination by the European Medicines Agency via a centralised procedure.
“As a pioneer in MR imaging, thanks to the success of our first gadolinium-based macrocyclic contrast agent, we are delighted with the FDA approval of Elucirem. This approval allows patients and practitioners to benefit from the innovations brought by Elucirem,” said David Hale, chief executive officer of Guerbet Group.
Phase III clinical trials for Elucirem
The approval was primarily based on data from two phase III studies completed in March 2021 which demonstrated that Elucirem leads to non-inferior results in brain and body MRI at half the gadolinium dose of Gadobutrol. The endpoints were met in terms of the diagnostic benefit of injecting Gadopiclenol (0.05 mmol/kg) during MRI examinations, based on two criteria:
The superiority of the examination with Gadopiclenol compared to the examination with no contrast agent
The non-inferiority of Gadopiclenol (0.05 mmol/kg) compared to Gadobutrol (0.1 mmol/kg) for the visualisation and detection of lesions of the central nervous system and in the other anatomical areas studied
No major safety signals were reported during the development of Gadopiclenol, and the adverse reactions reported during the two phase III studies were similar for both products administered.
Penumbra and Asahi Intecc, a Japanese medical device manufacturer, announced that they will collaborate to introduce Penumbra’s Indigo Aspiration System into the Japanese market upon regulatory approval.
“By bringing together our newest innovations with Asahi’s leadership and expertise in the Japanese medical device market, we can provide physicians in Japan with technology that has been proven highly effective, helping patients to return home quickly and in good health,” said Adam Elsesser, president and chief executive officer of Penumbra.
Penumbra’s Indigo Aspiration System can be used to remove emboli and thrombi from vessels of the peripheral arterial and venous systems, and for treatment of pulmonary embolism. A minimally invasive device, Indigo enables the restoration of blood flow in such cases as acute limb ischaemia and venous thrombus.
Penumbra’s newest generation offering combines hypotube-based Indigo Aspiration Catheters with Lightning Intelligent Aspiration, a unique computer-aided clot detection technology that can differentiate between clot and blood, designed to reduce blood loss and the need for clot-dissolving drugs, which may lower the risk of bleeding complications.
“Our companies share the mission of helping expand the available treatment options for serious conditions that impact an increasing number of people in Japan,” said Masahiko Miyata, president and chief executive officer of Asahi Intecc. “We believe that, together, we are able to provide physicians with the latest innovations that best meet their patients’ needs and help advance patient care.”
Penumbra’s neurovascular thrombectomy and neurovascular and peripheral embolization devices will continue to be distributed by its long-time partner, Medico’s Hirata. This includes the latest RED reperfusion catheters, which are designed with optimised trackability and aspiration efficiency to help navigate the complex anatomy of the brain and deliver efficient aspiration for the removal of blood clots in a broad range of stroke patients.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual meeting (10–14 September, Barcelona, Spain) saw presenters explore artificial intelligence (AI), its current role in interventional radiology (IR), and how the two will evolve together to shape innovative practice in a session named “IR: The most tech of the medical specialties”. Among the key takeaways was reassurance that AI will not “replace” human interventional radiologists, rather that it is a question of understanding how AI can be useful in IR, learning how best to harness it as a tool for improving practices, and combining it with the knowhow and abilities of interventional radiologists to achieve ‘hybrid intelligence’.
Discussion of virtual reality (VR) and augmented reality (AR) also featured in the session, as well as wider commentary on what it takes to become a technological innovator in the IR space.
AI can lead to “truly patient-focused, individualised medicine”
The first speaker, Fernando Gómez Muñoz (Netherlands Cancer Institute, Amsterdam, The Netherlands; Hospital Clinic and Hospital Sant Joan de Déu, Barcelona, Spain), provided a comprehensive overview of how AI is currently being applied in IR and how he predicts this landscape will look in the coming years. Referring to the results for ‘artificial intelligence interventional radiology’ that a pubmed.gov search yields, the presenter demonstrated that AI in IR has been a topic of growing research focus—in 2016 there were 16 publications on the subject, and in 2021, 290.
Fernando Gómez Muñoz presenting at CIRSE 2022
Defining AI as “a combination of algorithms to provide machines with the capability to solve problems in a similar way to humans”, and machine learning as “a subtype of AI that uses computer algorithms to build predictive models,” Gómez Muñoz gave the example of how the latter can be used to predict type 2 endoleaks. The importance of this capability is, he shared with delegates, that “if you can predict [these], you can embolize the vessels that may cause the endoleak beforehand, avoiding a more complex procedure later, or an aneurysm rupture, which can happen if there is no adequate follow-up”.
Among the other applications of AI is in predicting local tumour progression post-thermal ablation, classifying peripheral arterial disease (PAD) in conjunction with computed tomography (CT) angiography, 3D planning for ablation procedures, as well as intraprocedural verification. The presenter then spoke to the advantages that AI offers for limiting unnecessary radiation exposure, such as during fluoroscopy-guided endoscopic procedures. Gómez Muñoz relayed his experience using verification software after ablation of liver tumours. It can “lead to early retreatment in some situations”, he explained, and can “dramatically reduce the recurrence rate of colorectal liver metastases”.
A further take-home message from Gómez Muñoz’s presentation was that he sees haptic perception in robots as a key area of future development with relevance to IR procedures. “Pressure, vibration, temperature and viscosity” are among the types of perception that the presenter hopes to see in robots used in IR settings, bringing the interventional radiologists who will make use of these innovations in a position to practise, increasingly, “truly patient-focused, individualised medicine”.
VR: the potential to reduce radiation exposure
Bradford Wood (National Institutes of Health Center for Interventional Oncology, Bethesda, USA) focused on VR in IR now, and its future directions. An important message he had for delegates was regarding the precise ways in which VR can benefit IR, which “can be poor” when reproducibility is concerned: by standardising practice and “equalising” the care patients receive. VR also has the potential to reduce interventional radiologists’ and patients’ radiation exposure through providing real-time mapping during cases, such as in conjunction with cone beam CT, to increase accuracy. This will also, in turn, reduce procedural complications and the time the given procedure takes. Related to this, VR can track patient movements so registration—the matching of images to the patient—remains accurate throughout the procedure.
Bradford Wood presenting at CIRSE 2022
However, Wood admitted that there are hurdles to adopting VR technologies in an IR practice. For example, goggles—a common means of accessing VR for use in a procedure—can bring on cybersickness, which discourages its use. However, handheld and projector-based tools can be a way around this ergonomic issue—Wood cited a smartphone app that can aid precise needle placement, even for interventional radiologists who are less experienced. Cost-effectiveness, Wood explained, is another barrier to healthcare providers incorporating VR into IR procedures, even though the benefits of increased accuracy and therefore reduced radiation exposure and intraprocedural complications, as Gómez Muñoz outlined, are highly valuable.
Technological innovations at lower cost
Luigi Solbiati (Humanitas University, Milan, Italy) gave his presentation on technological innovations in IR, what it takes to get them off the ground, and the obstacles that innovators can come up against in trying to do so. Solbiati also covered the benefits and pitfalls involved in developing these types of innovations and what he foresees the next disruptive IR technologies being. In terms of the latter, Solbiati cited histotripsy as already showing significant “world-changing” potential as a non-invasive, non-thermal, non-ionising procedure, where high-intensity focused ultrasound (HIFU) has been less successful.
Luigi Solbiati (image credit: CIRSE)
Image fusion technology, which came into being around 20 years ago, was an example Solbiati gave of game-changing technology innovation in IR—“nowadays, we have wonderful rooms where you can do [ultrasound, angiography, CT and cone beam CT] together”.
However, he was keen to acknowledge the lack of accessibility of these types of advancements throughout the world, due to the cost involved. Therefore, Solbiati concluded, “we should find alternative solutions”. Among these, he listed “the fusion of real-time ultrasound (US), contrast-enhanced CT and positron emission tomography (PET) in the US room,” which he qualified by stating that it is “a simple and significantly lower-cost alternative to interventional PET-CT rooms.”
The presenter also opined that robots that facilitate remote needle placement will be a crucial future development in AI for IR, and that ablation confirmation software that should become mandatory after every ablation.
Solbiati himself, as highlighted by his co-presenters, has successfully created technology that can thermally ablate liver tumours using AR alone, and no radiation. One of the ideas behind this is to solve the aforementioned issue of the high cost associated with installing sophisticated multifunction CT suites.
To round off the session, moderator Laetitia Saccenti (Hôpital Paris Saint-Joseph, Paris, France) asked a question on behalf of those who may be concerned about AI capabilities exceeding those of interventional radiologists, and thus reducing or eliminating the scope of human practitioners’ roles in IR. “You cannot change the way things are going, you just have to surf the wave […] the more you learn, the more useful [a tool] it will be,” Gómez Muñoz answered.
Wood reiterated that “[AI and VR] will not replace” interventional radiologists. Certainly, a key takeaway from all three speakers was that technology will evolve to complement the work of interventional radiologists; enhancing what they are able to achieve and far from rendering their role obsolete.
Comparing the Saval drug-eluting stent (DES) below-the-knee (BTK) vascular stent system (Boston Scientific) and percutaneous transluminal angioplasty (PTA) in the infrapopliteal lesions of chronic limb-threatening ischaemia (CLTI) patients, the trial failed to meet its primary effectiveness and safety endpoints.
The primary objectives of the SAVAL study were to evaluate one-year primary vessel patency and safety following use of the Saval DES, which is designed specifically for BTK interventions, Van Overhagen asserted. The stent is made of nitinol and polymer-coated, with paclitaxel.
The presenter then explained that the SAVAL trial is a prospective, multicentre, randomised superiority trial of patients with symptomatic infrapopliteal artery lesions and Rutherford category 4–5 CLTI. The patients were assigned 2:1 to treatment with Saval DES or PTA.
The primary safety endpoint (non-inferiority) is 12-month major adverse event (MAE)-free rate, defined as a composite of above-ankle amputation of the index limb, major reintervention and 30-day mortality, the presenter elaborated.
Providing further details of the study, Van Overhagen stated that a total of 201 patients were enrolled and randomly assigned to treatment (n=130 DES, n=71 PTA) at 39 study centres in Belgium, France, The Netherlands, the USA, and Japan.
In terms of primary results, Van Overhagen reported a high technical success rate of 100% in the DES group and 98.7% in the PTA group.
However, “the primary effectiveness endpoint of superior 12-month primary patency was not met,” the presenter relayed—the figure was 68% in the DES group and 76% in the PTA group. “The primary safety endpoint of non-inferior 12-month MAE-free rate was [also] not met,” Van Overhagen supplemented, citing the results of 91.6% and 95.3% respectively for the DES and PTA groups, while freedom from all-cause mortality was 92.2% versus 89.9%.
Van Overhagen shared the rationale behind conducting the study: CLTI is a condition with “few effective endovascular options for infrapopliteal artery revascularisation” and DESs have yielded positive results in previous studies. This reflects what Van Overhagen highlighted in an earlier presentation he gave on DESs—both an endovascular approach and revascularisation are key to optimal treatment of CLTI.
In view of the primary results, Van Overhagen told delegates that “patient follow-up will continue through three years in-office with vital status assessment through five years, as specified in the study protocol […] We believe that given the impact of CLTI on limb and life, continued innovation to provide minimally invasive treatments is needed”.
In another PAD day session, Van Overhagen presented on the devices currently available and evidence to support the use of DESs specifically.
Van Overhagen began his first presentation of the day by underlining that the “cornerstone” of CLTI is revascularisation—”we try to get unobstructed blood flow all the way into the foot and avoid amputation”. The presenter went on to acknowledge that “we all know that endovascular treatment is less invasive. This is why, where possible, we use an endovascular approach”.
The presenter then proceeded to explain the origin of drug-eluting balloons (DEB) and DES: “[they] have been introduced in order to try to reduce restenosis […] we try to diminish the amount of intimal hyperplasia”. The Dutch PADI trial, for which Van Overhagen was principal investigator, compared PTA with bare metal stents (BMS) to DES and, at two-year follow-up, there were almost twice as many major amputations in the former group, a trend which was also observed at five years.
“Our initial conclusions were that DES BTK in CLTI achieved improved patency, a trend towards fewer major amputations [and indicated] a need for dedicated self-expandable and longer stents,” Van Overhagen reported. Further analysis out to ten years has also shown DES BTK to be safe and cost-effective, the presenter concluded.
Stryker’s first bone tumour ablation system with patented microinfusion technology
Stryker has announced in a press release that its OptaBlate bone tumour ablation system (OptaBlate) has received 510(k) clearance from the US Food and Drug Administration (FDA). The addition of the OptaBlate technology to Stryker’s Interventional Spine (IVS) portfolio expands on its core competencies in vertebral augmentation and radiofrequency ablation and completes its portfolio of treatment options for metastatic vertebral body fractures.
“Stryker’s new bone tumour ablation (BTA) system is a significant improvement on existing technology and builds on Stryker’s IVS portfolio,” said Anthony Brown, a vascular and interventional radiologist at Radiology Imaging Associates (Englewood, USA).
As Stryker’s first interventional oncology technology, OptaBlate optimises all aspects of the procedure, from set-up to ablation. Featuring four probes and Stryker’s patented microinfusion technology, OptaBlate allows physicians to customise their procedure and reduce ablation time by three minutes.
Specific key features of the system include:
Treatment of two vertebral body levels at once using a bipedicular approach
Quicker, more consistent ablation
Microinfusion technology, which keeps the zone hydrated, reducing impedance errors and preventing charring
“The collaboration has helped us to develop a more efficient bone tumour ablation system to address their unmet needs,” said Greg Siller, vice president and general manager, interventional spine business, Stryker. “OptaBlate will help our customers provide another treatment option for those suffering from painful metastatic cancer.”
Medtronic announced that it has recently received CE mark for its Radiant balloon-expandable covered stent, the first and currently, only, covered stent indicated for use in chimney endovascular aneurysm repair (ChEVAR) with the Endurant II/IIs stent graft system.
Used together, the Endurant II/IIs stent graft and Radiant covered stent offer a standardised, fully on-label, off-the-shelf solution for short-neck, juxtarenal abdominal aortic aneurysms (AAA). This enables safe and effective endovascular repair in both urgent and elective juxtarenal AAA cases.
The Radiant product’s design offers predictable, accurate delivery and deployment, while providing the flexibility and radial strength necessary for a chimney covered stent.
The covered stent is intended to maintain perfusion to the renal arteries when used in combination with the Endurant II/IIs stent graft system for AAA patients with inadequate sealing zones.
With this CE mark, Medtronic will roll out a comprehensive training programme and continue to invest in clinical data to optimise ChEVAR outcomes for physicians and the patients they treat.
“Having a stent graft specifically approved for ChEVAR reflects a milestone towards standardisation of the technique and the materials used. In combination with the strict preoperative protocol regarding planning and sizing, ChEVAR will stabilise its role and approach in the existing endovascular alternatives to treat aneurysms with inadequate infrarenal sealing zones,” Konstantinos Donas, head of the Department of Vascular Surgery and director of the Research Vascular Centre, Asklepios Clinic Langen, University of Frankfurt (Frankfurt, Germany) said of the Radiant stent graft.
In partnership with Getinge
The Radiant product comes from the long-term collaboration between Medtronic and Getinge, leveraging Getinge’s proven Advanta V12 design and eight sizes of the Getinge (Atrium Medical) stent portfolio. It will be produced by Getinge and distributed by Medtronic.
“To support this business expansion, Getinge has invested in doubling our stent production capacity in order to provide all of our global customers with the devices needed to treat patients,” the company’s senior director of Global Marketing and Product Management, Vascular Systems, Patty Burns, said of the partnership.
Findings from the RADIANCE II randomised pivotal trial, presented at the 2022 Transcatheter Cardiovascular Therapeutics meeting (TCT, 16–19 September, Boston, USA), “confirm that ultrasound renal denervation lowers blood pressure across the spectrum of hypertension”.
RADIANCE II—results of which were described as “important data for the field” by discussants—was the first of two major renal denervation trials reporting results at TCT 2022, with the treatment having seen a renaissance following successive sham-controlled trials showing statistically significant and clinically meaningful in blood pressure.
The trial’s primary result was presented during a late-breaking clinical science session by Ajay Kirtane (Columbia University Irving Medical Center New York-Presbyterian Hospital, New York, USA). Kirtane reported that ultrasound renal denervation using the Paradise (Recor Medical) system was superior at lowering blood pressure when compared to a sham procedure.
Patients with hypertension (seated office BP ≥140/90 mmHg and <180/120 mmHg) on no more than two anti-hypertensive medications underwent a four-week observation time during which they were taken off all hypertension medications. Those who remained clinically stable after the observation period and whose blood pressure remained elevated with daytime ambulatory systolic blood pressure (ASBP) greater than or equal to 135/85 mmHg but less than 170/105 mmHg underwent anatomic screening with CTA/MRA. Those with qualifying renal artery anatomy proceeded to renal angiography, and if angiography re-confirmed suitability for ultrasound renal denervation, they were then randomised 2:1 to receive bilateral uRDN of the main and accessory (≥3 mm) renal arteries or a sham procedure.
Between March 2019 and May 2022, a total of 150 patients received the renal denervation procedure and 74 underwent a sham procedure. Baseline characteristics including ambulatory blood pressure and the number of anti-hypertensive medications were similar between both groups.
The primary efficacy endpoint was the change in ambulatory systolic blood pressure at two months. The change in ambulatory systolic blood pressure was -7.9 mmHg for the ultrasound renal denervation group compared to -1.8mmHg for the sham group. The between group difference was -6.3 mmHg (95%CI, -9.3 to -3.2, p<0.0001. In addition, the secondary efficacy endpoints of change in 24-hour, nighttime, home, and office systolic blood pressure showed statistically and clinically significant reductions (∆5-7 mmHg versus sham). There were also no major adverse events in either group through 30 days, Kirtane reported.
Kirtane’s presentation preceded the delivery of long-term results from the SYMPLICITY HTN-3 trial, assessing radiofrequency renal denervation using Medtronic’s Symplicity system.
Deepak Bhatt
Investigator Deepak Bhatt (Brigham and Women’s Hospital Heart & Vascular Center and Harvard Medical School, Boston, USA) commented that the findings indicate that durable blood pressure reductions with radiofrequency renal denervation in combination with maximal medical therapy can be safely achieved.
In the primary report of the SYMPLICITY HTN-3 trial, at six months, renal denervation was found to be safe but did not show any significant incremental blood pressure lowering benefit compared with a sham procedure. The present analysis reports long-term blood pressure changes in both initially treated renal denervation patients as well as in a composite control group consisting of sham-treated patients as well as sham-treated patients who crossed over to renal denervation after six months (but using blinded, pre-crossover data as the control).
Eligible patients had an x ≥160 mmHg and 24-hour ambulatory systolic blood pressure ≥135 mmHg. In addition, they were on stable, maximum tolerated doses of three or more antihypertension drugs.
A total of 535 patients at 88 sites in the USA were randomised 2:1 to renal denervation using the Symplicity Flex catheter (n=364) or sham control (n=171). Unblinding occurred after six months, and eligible control patients could crossover to renal denervation. For the 101 patients who crossed over and received renal denervation, their most recent blinded pre-crossover BP measurement and medication data were used as controls. Treatment differences were adjusted for baseline blood pressure.
At 12 months, renal denervation patients had significantly greater office systolic blood pressure reductions compared with sham control after crossover imputation (-18.9 mmHg vs -6.3 mmHg, p<0.0001, respectively). In addition, the number of antihypertension drugs were similar between patients in the RDN and control groups (4.7±1.4 vs. 4.7±0.9, p=0.22). The office systolic blood pressure reductions continued each year following the procedure, and at 36 months, the reduction in blood following renal denervation was -26.4 mmHg compared with -5.7 mmHg for the control group (p<0.0001). Similar results were observed in other measures of blood pressure (office diastolic blood pressure, 24 hour systolic and diastolic blood pressure).
Sirtex Medical announced that the Brazilian National Agency of Supplementary Health (ANS) approved SIR-Spheres Y-90 resin microspheres for the treatment of intermediate- and advanced-stage hepatocellular carcinoma (HCC) in Brazil.
In an update to its List of Health Procedures and Events, ANS recommends SIR-Spheres for use in selective internal radiation therapy (SIRT), a minimally invasive treatment that delivers high doses of radiation directly to tumours while sparing surrounding healthy liver tissue. Sirtex received product approval from the Brazilian Health Regulatory Agency (ANVISA) for SIR-Spheres in 2014.
“This milestone represents the close collaboration we have fostered with Brazilian colleagues, interventional radiologists and respected regulatory entities like ANS over the last six years,” said Kevin R Smith, chief executive officer of Sirtex. “We celebrate the recognition of SIR-Spheres to advance care for HCC patients, and we also reaffirm our commitment to global growth and partnership for more effective cancer treatment worldwide.”
The proposals for incorporation into the ANS List of Health Procedures and Events underwent broad social participation and careful technical analysis by the ANS, using the methodology of health technology assessment, similar to England, Canada, Australia and Germany.
“The ANS recommendation of SIR-Spheres solidifies it as a valuable treatment option, especially since 76% of HCC patients in Brazil are diagnosed at an advanced stage when treatments of curative intent are no longer an option,” said Joaquim Maurício da Motta Leal Filho (Universidade de São Paulo, São Paulo, Brazil), president of the Brazilian Society of Interventional Radiology and Endovascular Surgery (SOBRICE). “As we continuously strive to improve outcomes for patients, we are proud of this achievement and feel gratitude to the many people who contributed to this decision.”
In addition to Brazil, SIR-Spheres are approved for use in Argentina, Australia, Switzerland, Turkey, and several countries in Asia for the treatment of unresectable liver tumours. In the USA, SIR-Spheres Y-90 resin microspheres have a Pre-Market Approval (PMA) from the US Food and Drug Administration (FDA) and are indicated for the treatment of unresectable metastatic liver tumours from primary colorectal cancer with adjuvant intrahepatic artery chemotherapy (IHAC) of FUDR (floxuridine).
L-R: Rainer Bregulla, director R&D; Sebastian Büchert, CEO; Thomas Morawek, Arnold Schwarzenegger double; Hartmut Grathwohl, director Operations; Andrew Brabner, director Finance & IT; Christian Bader, director Quality & Market Access
L-R: Rainer Bregulla, director R&D; Sebastian Büchert, CEO; Thomas Morawek, Arnold Schwarzenegger double; Hartmut Grathwohl, director Operations; Andrew Brabner, director Finance & IT; Christian Bader, director Quality & Market Access
Bentley today announced that it has acquired the rights of the GoBack catheter from Upstream Peripheral Technologies.
“The acquisition of the GoBack catheter marks the start of inorganic growth for Bentley,” said Sebastian Büchert, Bentley’s CEO. “We launched our first of six existing product families to the market in 2012 and have experienced significant growth since then. Now, only 10 years later, we are able to acquire this very innovative product. This strategic move further completes our product offering to hospitals and physicians to the benefit of our joint patients.”
The GoBack catheter will simplify crossing and re-entry in occluded arteries. A press release notes that the product’s unique feature is a curved nitinol needle that can be manipulated by the physician using the device handle. Thanks to its small profile, the device can even be used in the smaller arteries in the lower leg.
“Bentley acquiring the GoBack makes me feel proud. I am sure that with Bentley’s global footprint more physicians will have access to the catheter,” said Dan Rottenberg, CEO of Upstream Peripheral Technologies. “Our vision is to save limbs and reduce the number of amputations. With Bentley’s strong network more patients will have access to such treatment.”
The GoBack catheter is CE marked and US Food and Drug Administration (FDA) cleared. Launched in 2019, the device is now available in 23 countries. It is Bentley’s intention to extend the global availability to all of the 80 markets in which the company is already active, the press release details.
Martijn Nugteren, director Sales & Marketing, Bentley, says, “We will be really busy in the months ahead. Not only because we want to make the product commercially available in additional markets, but also due to the fact that we are going to rebrand the GoBack to BeBack. This is to make sure that our new product will be recognised as another leading product underneath Bentley’s brand umbrella.”
Currently produced in Israel and initially shipped from there, a production transfer to the Bentley production facility in Hechingen, Germany, will be completed by 2025.
Merit Medical Systems has announced the US commercial release of the Prelude Roadster guide sheath. The Prelude Roadster is the newest addition to the Merit Vascular-Peripheral Access portfolio, which includes introducers and other products, including access kits, vessel dilators, and accessories.
The device is designed for deliverability, visibility, and resilience in tortuous peripheral vasculature anatomies. Indicated for use in a variety of procedures, the device will also help deliver devices used to diagnose and treat the large patient population who suffer from peripheral artery disease (PAD).
“Patients with peripheral vascular disease often have complex vessel anatomies that make treatment challenging,” said Sandeep Nathan, interventional cardiologist and director of the Coronary Care Unit at the University of Chicago Medicine (Chicago, USA) and a consultant of Merit Medical. “The Roadster sheath is designed to help physicians deliver the diagnostic and therapeutic devices needed to achieve successful outcomes.”
“The Prelude Roadster is an example of Merit’s commitment to understanding, innovating, and delivering products to meet the needs of physicians. After decades of offering vascular access products, we are always searching for ways to help physicians diagnose and treat successfully, improving the lives of patients worldwide,” said Fred P Lampropoulos, Merit Medical’s Chairman and CEO.
ABK Biomedical has announced US Food and Drug Administration (FDA) 510(k) clearance of Easi-Vue embolic microspheres for the treatment of patients suffering from arteriovenous malformations and hypervascular tumours.
Aravind Arepally, chief medical officer of ABK Biomedical said: “The evolution of embolic therapies to treat these complex disease states has been notable in recent years. Now, with Easi-Vue embolic microspheres, interventional radiologists have a highly calibrated, see-and-do technology capable of visually targeted placement using conventional X-ray and fluoroscopy systems. This microspheres technology and proprietary controlled-concentration delivery system have the potential to improve patient outcomes.”
“We are excited to achieve FDA 510(k) clearance for this new technology that has the potential to advance the field of embolic therapies”, said Gary Donofrio, chief business officer of ABK Biomedical. “This represents a major milestone for ABK as our team continues to execute our product development objectives. We will partner with key physicians to understand the range of clinical utilisation and optimisation of Easi-Vue therapy. Additionally, ABK continues to significantly advance the development programme of our Eye90 microspheres radioembolic technology that is being investigated for the treatment of patients with unresectable hepatic cellular carcinoma (HCC). Easi-Vue embolic microspheres share core technologies and design characteristics with Eye90 microspheres. Both devices continue to add to our knowledge base regarding the clinical experience of the first glass radiopaque embolic microspheres therapy.”
Interventional News’ popular stories last month included acquisitions by Boston Scientific and Gore, studies of deep vein thrombosis and peripheral arterial disease treatments and, on the subject of the latter, research into the racial disparities affecting patients who receive peripheral vascular interventions. Stories covering data presented at two of the summer’s meetings—Society of Interventional Radiology (SIR) and the European Conference on Embolotherapy (ET)—also garnered ample views.
Boston Scientific has announced the acquisition of Obsidio, a privately held company that has developed the Gel Embolic Material (GEM) technology used for embolization of blood vessels in the peripheral vasculature.
Inari Medical has announced planned enrolment of the DEFIANCE randomised controlled trial (RCT), which is designed to compare the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only.
BD has announced the start of enrolment in a first-in-human trial of a peripheral sirolimus drug-coated balloon (DCB). The PREVISION trial is a prospective, multicentre, single arm, non-randomised study designed to evaluate the safety of the BD sirolimus DCB in the treatment of peripheral arterial disease (PAD) in the femoropopliteal arteries.
Fluidx Medical disclosed study results examining extent of vessel filling using the GPX embolic device compared to microspheres, a common treatment for many types of tumours.
A database study titled ‘Unplanned 30-day readmissions and in-hospital outcomes for the management of submassive and massive acute pulmonary embolism: Catheter-directed versus systemic thrombolysis’ has produced results that could provide some of the evidence base for preference of catheter-directed over systemic thrombolysis in treating the more severe cases of pulmonary embolism (PE).
Mark Little (Royal Berkshire NHS Foundation Trust, Reading, UK) described the emergence of, and advancement within, musculoskeletal (MSK) embolotherapy as “fast-paced” during a presentation at this year’s ET (22–25 June, Nice, France). The take-home message was that the “signs are encouraging” when it comes to MSK embolotherapy’s integration into more mainstream practice.
Ramona Gupta (Northwestern University, Chicago, USA) addresses the issue of recurrent varicose veins, highlighting in particular the “multiple tools” now at physicians’ disposal to treat the problem.
Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.
Interventional News spoke to Eric A Secemsky and Anna K Krawisz (Smith Center for Outcomes Research in Cardiology, Beth Israel Deaconess Medical Center, Boston, USA)—about the motivations for carrying out their study into racial disparities in peripheral vascular interventions, the results it yielded, and where this research might lead.
Concept Medical has announced the initiation of the LIMES trial, which has enrolled 15 patients to evaluate the safety and efficacy of the company’s Magic Touch sirolimus-coated percutaneous transluminal angioplasty (PTA) balloon for the treatment of peripheral arterial disease (PAD).
This advertorial is sponsored by Interventional Systems.
At the onset of the COVID-19 pandemic in early 2020, healthcare systems across the globe were forced, almost overnight, to adapt to a new reality. No corner of the healthcare landscape has been left untouched, and the ripple effects of the pandemic have changed the financial reality for care providers everywhere.
“Capital equipment sales are always a long-term process, with budgeting and approval processes,” Scott Peairs, vice president of Global Sales at Interventional Systems, tells Interventional News. “The pandemic made that worse with a diversion of capital assets towards the treatment of COVID-19 patients.”
This has prompted a realignment in the way that hospitals and healthcare facilities approach the procurement of new technologies and devices, and creates a potential hurdle to investment in cutting-edge treatment solutions. For Interventional Systems, the developer of Micromate—a table-mounted medical robot for interventional procedures—this represents a particular challenge as hospitals refocus their spending priorities, and capital expenditure on new technologies becomes more difficult.
Micromate suite
“Only equipment that was broken or was desperately needed was being purchased under the capital price,” comments Peairs, adding that since the start of the pandemic, many providers have become wary of making capital investments, seeking more flexible solutions instead. “We are starting to come out of that cycle now and hospitals are starting to get back on more of a standard capital cycle, but we are probably another year away from normal.”
As a result of this, hospitals may be missing out on the opportunity to access new technologies that will smooth workflows and improve outcomes for patients through high-quality care. To address this, Interventional Systems has sought to deliver a service that will allow hospitals to still have the opportunity to offer the innovative Micromate robotic system to their patients, albeit without the initial capital outlay that is usually involved in this kind of procurement.
“We wanted to offer a way that, if the hospital does not have the budget but wants to use a robotic system, we can offer them a subscription model,” Peairs explains. The subscription model—which Peairs says is relatively unique to the healthcare technology setting—works in a similar way to how users purchase software packages.
“Microsoft or Adobe are the best examples,” he explains. “You used to have to go and buy the software, it was loaded to a hard drive on a computer, and then you would have to go and buy an upgrade for it. The software companies have completely moved to the subscription model, where it is virtual. You get the free upgrades, it is accessible, and you can turn it on and off when you want to.”
A flexible option
One of the potential advantages of this model is, according to Peairs, the fact that healthcare providers will have the flexibility to incorporate an emerging technology into their practice, without the long-term outlay that comes with a commitment to capital expenditure on new equipment. And, with a subscription-based service, getting hold of a robotic system may be a more streamlined process, Peairs says, as the subscription may not fall into the capital expenditure category, meaning that the physician can incorporate the cost into the budget that they already control.
Scott Peairs
“The idea is that we want to give them access to it,” Peairs tells Interventional News. “They can have a system and they are not obligated for the long term, that gives the physician access to it. From there, they can explore internally if it adds value to the procedures within their facility.” Additionally, without the initial outlay of the capital cost of the system, hospitals can potentially reap the efficiency gains that can be achieved by deploying the Micromate system, quicker.
Interventional Systems offers three different subscription models that are structured depending on the volume of procedures to be performed using the robotic platform and the duration that the healthcare provider wishes to sign up to. The centre pays a fixed amount per month, which covers the disposable components that are needed for each procedure, as well as software updates that may occur during the subscription time and technical assistance during the first cases.
As these core services are essential, they are covered within each of the three packages on offer, however, customers can opt to get access to more whenever needed, and have the option to upgrade or downgrade their subscription at any time. Furthermore, the system requires no preventive maintenance and the customer pays for service only outside warranty, and when needed. “To go back to the Microsoft analogy—it updates itself, you do not have to do service, you do not have to do training—it is all included in that subscription,” says Peairs.
Setup and training are also important aspects of the provision, which are delivered to clients at the outset of the subscription. Interventional Systems offers service support to troubleshoot any issues that may arise, and can centrally access the system via a remote interface. If hardware repairs are needed, Interventional Systems offers a “swap-out” facility whereby faulty components are replaced to reduce downtime.
Learning curve
As Micromate is a system that can be used in a number of different procedures on different organs, Interventional Systems says that there are several factors that will affect how long it may take to master the system. “A lot of it depends upon the type of procedure that they are doing,” says Peairs, adding that learning to use the platform in lung, kidney or liver tissues—the primary interventional radiology target areas—may have different requirements. From experience, and though it changes from physician to physician and centre to centre, five procedures is generally a good rule of thumb for getting to grips with the system, that he describes as a “third arm” for the operator.
“Some of the interventional radiologists have told us that they would use it on the hard cases because that is where they would think they would have the need,” Peairs adds, commenting on the learning curve involved in mastering the robot. “Now the mindset has shifted and several of them have told us that they are going to use it on every case, even the simplest of biopsies, because of its fast setup.
“They want to use it on easy cases so the staff know the workflows and the setup using the robot, so that once they get to the hard cases that is not a stressor. I really see that is where a subscription model is going to help, because it is going to allow them to use it on all cases,” he says.
The subscription model will be available to Interventional Systems’ customers in the USA and Europe from Autumn 2022.
The European Society of Cardiovascular and Interventional Radiology (CIRSE) will host its 38th annual meeting in Barcelona from September 10 until September 14. Around 5,000 healthcare professionals from around the world are expected to attend more than 400 lectures in person, while a custom-built online platform will allow full digital access to all lectures and symposia for those unable to make it to Barcelona.
Living up to its motto “Science for people”, CIRSE 2022 will have two main foci: increasing the evidence base for interventional radiology, and continuing to make interventional radiology (IR) a clinical, patient-centred discipline. Two FIRST@CIRSE session will contribute to IR’s evidence base with the largest number of data releases of IR studies to date—one session focusing on studies in peripheral arterial disease treatment and a second session presenting data releases on other treatments.
Other session highlights will include those comprising PAD Day, the Interdisciplinary Endovascular Aortic Symposium (IDEAS), as well as various sessions focusing on paediatric interventions.
The CIRSE 2022 Local Host Committee headed by Mariano Magallanes Bas (Hospital Ribera Povisa, Vigo, Spain) has organised a patient information exhibition with the title “The medicine of today”, which will take place throughout the congress in the nearby shopping mall Diagonal Mar with the aim of increasing popular awareness of the specialty. Using laymen’s terms and appealing images, the exhibition will give the general public an introduction to the wide array of conditions that can be treated by interventional radiologists, from uterine fibroids to benign prostate hyperplasia, highlighting both the state-of-the-art nature of IR treatments as well as the specialty’s human, clinical side.
The Micromate robot for percutaneous interventions
The Micromate robot for percutaneous interventions
Interventional Systems haslauncheda newsubscription servicefor Micromatewith three package levelsofferingthe miniature robotic system including the latestplanning and navigation station, as well as disposable accessories and specialised services. The subscription fee is fixedand there are nomandatory service agreements, making the costs as predictable and low as needed.
“The cost of technology is responsible for half of the increase in healthcare–related costs worldwide. This can help explainwhy only up to 3% of surgeries and interventions are performed with robotic assistance, despite its obvious advantages”, says Pedro Costa, chief product officerat Interventional Systems.“The word democratisation is ubiquitous in brochures, publications,slide decks,and websites. Every new player in MedTech democratises something, just to proceed by charging you a million euros for a robot, disposables that cost you thousands,and mandatory service agreements of at least 8% capital cost. Our understanding is different. We want to ensure true access to every physician and, ultimately, patient.”
“Healthcare providers are looking for more flexible solutions”, adds Scott Peairs, vice president of global sales at Interventional Systems. “With a subscription–basedservice,they canhavetherobotic systemfor as long and as many procedures as they need.And because they are spending each month only a fraction of the capital cost of the robot, they can also leverage the increase in efficiency to generate profits faster and get a better return on investment.”
The Micromate subscription is available in the USA and Europe as of September 12022, with plans to expand globally.
Penumbra announced today that its RED reperfusion catheters have secured a CE mark and are now commercially available in Europe. The catheters are part of the company’s Penumbra system, which is a fully integrated mechanical aspiration thrombectomy system designed to restore blood flow in acute ischaemic stroke patients.
“When addressing stroke, our goal is to remove the blood clot as quickly as possible for patients to have the best outcome,” said Saleh Lamin (Queen Elizabeth Hospital, Birmingham, UK). “With RED catheters, we will be able to get up to the clot quickly and efficiently remove it, most of the time within a single pass. Restoring blood flow promptly is key as it is associated with less damage to the brain and better outcomes.”
The RED family of catheters is engineered with the latest technology in trackability and aspiration to address a wide range of large vessel occlusions via mechanical aspiration thrombectomy, a Penumbra press release notes.
The RED catheters feature the company’s REDglide technology—which enhances the trackability of the catheters as they navigate the challenging vessel anatomy of the brain while also maximising aspiration efficiency to remove blood clots. Additionally, the RED catheters have a full-length polytetrafluoroethylene (PTFE) liner designed to maintain their true lumen size under powerful vacuum, the release adds.
“Penumbra’s commitment to advancing technology allows us to have one of the most expansive aspiration stroke portfolios on the market, enabling physicians to have the latest innovations with the most options to provide the best care to their patients,” said Joan Kristensen, vice president and head of the Europe, Middle East and Africa region for Penumbra. “With enhanced trackability and powerful aspiration, initial data have shown that Penumbra’s RED catheters can restore blood flow quickly across all clot types, which would potentially have a significant impact on patient outcomes here in Europe.”
Royal Philips today announced new milestones in the development of the world’s first spectral detector angio computed tomography (CT) solution— Philips Spectral Angio CT suite—bringing the company’s breakthrough spectral CT imaging technology into an integrated hybrid angio CT suite. By combining its Spectral CT 7500 system and the image-guided therapy system—Azurion with FlexArm—in a fully integrated interventional suite solution, Philips aims to give physicians immediate access to these two key imaging modalities in a single room, enabling innovation in minimally-invasive procedures in areas such as oncology, stroke, and trauma care.
Expanding Philips’ clinical network
Leiden University Medical Center (Leiden, The Netherlands) has joined Philips’ global network of clinical partners to investigate how its spectral detector angio CT solution could offer new treatment opportunities and improve patient care.
“We are excited to co-create an innovation that could play a defining role in improving patient care in the space of interventional oncology,” said Mark Burgmans, head of Interventional Radiology at Leiden University Medical Center. “Adding spectral CT imaging to the interventional suite will enable us to offer new treatment opportunities, avoid moving patients from one imaging suite to another, and offer the unique benefits of spectral CT information when you need it.”
Philips is also working on its innovation with Mayo Clinic (Rochester, USA) and Baptist Health’s Miami Cardiac & Vascular Institute (Miami, USA).
Philips Spectral Angio CT suite combines the company’s latest diagnosis and treatment technologies. Philips Azurion with FlexArm is the company’s next-generation image-guided therapy platform, integrating best-in-class imaging systems, software, and specialised diagnostic and therapeutic devices to support exceptional treatment for the most complex procedures. The addition of Philips’ award-winning Spectral CT 7500 system means physicians only need one scan to capture all the spectral information required to differentiate and quantify different tissues. Spectral CT enables improved detection, delineation, and quantification of lesions, leading to better-informed planning for minimally invasive procedures and more precise interventions.
It has already demonstrated higher sensitivity in detecting malignant findings and improved readings of incidental findings. With its ability to improve tissue characterisation, the Spectral CT 7500 offers significant benefits over conventional CT, the company states.
Research results show better targeted biopsies using spectral CT guidance
At this year’s Cardiovascular and Interventional Radiological Society of Europe Annual Meeting (CIRSE 2022; September 10–14, Barcelona, Spain) Filippo Piacentino, interventional radiologist at the University of Insubria (Varese, Italy), is giving a presentation on the value of spectral CT imaging guidance for performing high-confidence tumour biopsies. The results being presented illustrate the potential for Philips’ spectral CT technology to better guide biopsies by distinguishing between active and non-active regions in a tumour.
“With conventional CT, large masses may appear as a largely uniform mass, making highly targeted biopsy difficult,” said Filippo Piacentino. “By fusing images from Philips’ XperGuide live needle guidance with images from spectral CT, that are colour-coded based on the effective atomic number of tissues, and provide a large amount of additional information, we can now investigate the possibility of obtaining better defined biopsy targets with a fewer number of inconclusive biopsies.”
New clinical collaboration on reduction of the risk of tumour recurrence
Philips also announced a research collaboration with the University of Pennsylvania (Philadelphia, USA) to study the practicality of using spectral CT-based tissue temperature mapping to provide real-time feedback during tumour thermal ablation procedures to confirm its effectiveness before the patient leaves the room. This will potentially reduce the risk of localised tumour recurrence.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) recently incorporated transarterial chemoembolization with degradable starch microspheres (DSM-TACE) into its guidelines for hepatic transarterial chemoembolization.¹ In addition to society backing, experts are also in favour of this treatment modality, underlining its role as a game-changing addition to the liver cancer care paradigm.
Speaking to Interventional News, Roberto Iezzi, associate professor of Radiology at the Catholic University of Rome (Rome, Italy) and Christiane Kuhl, head of the Department of Radiology at Aachen University (Aachen, Germany), share their clinical experiences with EmboCept® (PharmaCept®) and how the European guideline update solidifies its place in liver cancer treatment by TACE.
Roberto Iezzi
“EmboCept consists of a suspension of starch microspheres that are rapidly and completely degradable within 90–120 minutes² (in vitro half-life time 30–40 minutes) from the arterial infusion, allowing a temporary occlusion of the arterial microcirculation at the tumour level,” Iezzi explains, giving an overview of EmboCept’s mechanism of action. This, he says, improves the therapeutic effect by reducing the immediate wash-out of the cytostatic agent, and decreasing the risk of systemic toxicity and post-embolic syndrome.
EmboCept is also characterised by a cross-linked, partially hydrolysed starch matrix that allows the interventionalist to obtain a ready-to-use solution with different chemotherapeutic drugs being mixed with them. Iezzi recalls how this feature positively impacted his practice: “This option allowed us to open the door in the last few years for new indications, for liver metastases from lung, breast and gynaecological tumours, for example. You can now use EmboCept with any cytostatic that can be given intra-arterially, allowing [the interventionalist] to be much more flexible and broadening the range of indications.”
Christiane Kuhl
Kuhl notes that the current CIRSE recommendation reflects the current level of evidence, but is still conservative regarding the patient cohort included. She states: “Maintaining liver function is decisive for a patient’s treatment as well as survival. A patient needs a working liver, both to survive, but also because an adequate liver function is a prerequisite for most systemic treatment protocols.” In patients with metastatic solid tumours, metastatic overgrowth of the liver can thus become the driver of a patient’s prognosis. Kuhl highlights that interventionalists now have the tools to help the liver fight against this metastatic overgrowth in addition to systemic treatment. “With systemic treatment, often in the liver, the dose is simply not high enough to stop the cancer,” she says, stressing that in these patients, palliation of liver function through local treatment is key, and is the major goal of liver-directed treatment. “This is similar to the local treatment of osseous metastasis to a vertebral body, where the intention is to palliate the static function of the bone,” Kuhl adds. “Similarly, in patients with secondary liver cancer, the aim is to palliate the liver. We are able to do that with EmboCept-driven transarterial chemotherapy”.
In the field of embolic agents, both interventionalists are in agreement that EmboCept holds its ground, providing a solid treatment option and in some cases offering advantages over alternatives. “I think the most obvious advantage of EmboCept compared with other embolic agents is the fact that it only causes a temporary occlusion, maintaining the route to the tumour,” Kuhl opines. She believes this is crucial in the treatment of liver cancer other than hepatocellular carcinoma (HCC), where the main method of action may not be devascularisation, but in bringing the chemotherapeutic agents into the tumour. Kuhl elaborates: “Everywhere we want to treat chemo-sensitive cancer in the liver, these agents must be applied not only once, but repetitively—just as is usual practice with their systemic use. In such patients, temporary occlusion of vessels by degradable starch microspheres allows one to keep the route to the tumour patent for several courses of transarterial chemotherapy.” Such TACE should only temporarily occlude the vessels to avoid passage of the chemotherapeutic or cytotoxic agent through the tumour, but ideally keep it inside the tumour.” This is what EmboCept achieves in a perfect way,” Kuhl remarks.
According to Iezzi, DSM-TACE can offer benefits where other TACE options, namely drug-eluting bead TACE (DEB-TACE) and conventional TACE (cTACE), are not indicated. “DSM-TACE is safe, without side effects or worsening of liver function. It is also safe in advanced HCC patients, with the worst clinical conditions (Child-Pugh>B7), vascular invasion (portal vein thrombosis), high bilirubin level or ascites—patients in whom DEB or cTACE could be contraindicated,” he relays.
Overall, however, it is Iezzi’s opinion that DSM-TACE is not necessarily in competition with DEB or cTACE, but provides another treatment option that interventionalists can offer to their patients, thereby widening clinical indications and improving disease prognosis overall. Iezzi adds that DSM-TACE “could also be used as a bridge to other locoregional or surgical options as it is effective and repeatable (so called bridging and downstaging) being able to maintain vessel patency”.
Figure 1. Preprocedural (A, B) and postprocedural (C, D) CT images of a 68-year-old patient with unresectable multinodular bilobar HCC treated successfully with DSM-TACE. The patient showed >6 hepatic lesions, the largest of which was 7cm (A and B). DSM-TACE procedures were performed with a selective lobar catheterisation and with a coaxial technique placing a 2.7Fr microcatheter in the right or left hepatic artery that was feeding the tumour lesions. A solution of 450mg in 7.5ml of EmboCept S mixed with 50mg of Doxorubicin and non-ionic contrast medium was slowly infused. The patient experienced no adverse events, with dismission after 24 hours, without any pain or periprocedural complications. Since the CT follow-up performed after three months showed an almost complete response with necrosis of almost all multinodular liver lesions (C, D), the patient received two more DSM-TACE sessions. (Case: R. Iezzi)
CIRSE’s approval of DSM-TACE has solidified its place as “an important pillar of tumour treatment,” says Kuhl. In recent years, a number of papers have been published that highlight the role of DSM-TACE in HCC, and all of these have contributed to the acceptance of DSM-TACE in the CIRSE guidelines. For example, Iezzi was part of a team that recently published a multicentre European study confirming that DSM-TACE is well tolerated with no major clinical adverse events and only limited major laboratory events.³ He tells Interventional News that preserved liver function was observed after repetitive DSM-TACE treatments in this study. “Our results confirm that repetitive DSM-TACE is a safe, well tolerated and effective treatment option for HCC patients with high tumour burden, ineligible for, or failing other palliative therapies,” said Iezzi, relaying the key take-away message from the paper.
“Guidelines are what drive clinical patient care,” Kuhl states, underlining the significance of the CIRSE update. DSM-TACE is now an accredited treatment option and this, according to Iezzi, “widens indications for locoregional treatments and gives new opportunities to patients”. In addition, he believes that the guideline update might convince all interventional radiologists, hepatologists and oncologists who were doubtful of the important role of DSM-TACE in the treatment of liver cancer.
References 1. Lucatelli P, Burrel M, Guiu B, et al. CIRSE standards of practice on hepatic transarterial chemoembolisation. Cardiovasc Intervent Radiol. 2021; 44 (12): 1851–1867. DOI: 10.1007/s00270-021-02968-1. 2. Wiggermann, P, Heibl M, Niessen C, et al. Degradable starch microspheres transarterial chemoembolisation (DSM-TACE) of HCC: dynamic contrast-enhanced ultrasonography (DCE-US) based evaluation of therapeutic efficacy using a novel perfusion software. Clin. Hemorheol. Microcirc. 2012; 52 (2–4): 123–129. DOI: 10.3233/CH-2012-1590. 3. Ludwig, JM, Iezzi R, Theysohn JM, et al. European multicenter study on degradable starch microsphere TACE. The digestible way to conquer HCC in patients with High tumor burden. Cancers. 2021; 13 (20).
Andrew Wigham (Oxford, UK) and Rick De Graaf (Friedrichshafen, Germany) discuss the current state of deep vein thrombosis (DVT) treatment at the Leipzig Interventional Course (LINC) 2022 (6–9 June, Leipzig, Germany), with both noting that “a massive problem” in Europe is the lack of awareness around treatment.
Wigham highlights some of the major challenges associated with treating this patient population, including that “traditional devices have a limited window of effective treatment of acute DVT”, as well as “limited operating room time and bed availability” due to the COVID-19 pandemic, and “significant bleeding risk to the patient” with thrombolysis. “We are really in need of solutions to address these issues”, he adds.
“We do not want to do thrombolysis anymore,” states De Graaf, when questioned on his preferred treatment modality. “We went through all the devices out there and my major problem was always that I could not get all the thrombus out,” he says, adding that “thankfully now I am finally very confident that I have a device [ClotTriever, Inari Medical] that takes out all the thrombus.” Wigham himself adds that ClotTriever is “a very effective device that helps us to clear the thrombus and potentially limit the amount of stents we are using in a young patient cohort.”
Wigham goes on to say that one of the principle advantages of the device is that he has found it to be “effective out beyond six weeks”. De Graaf adds that this is “a huge benefit that we see as well”, with the pair concluding that the device is a real “gamechanger” for the treatment of DVT.
This video is sponsored by Inari Medical.
Rick de Graaf and Andrew Wigham will be sharing their experiences with ClotTriever® for the treatment of deep vein thrombosis during the Inari symposium at CIRSE 2022 (Sunday, 11th September, 1pm–2pm, room 114).
Fluidx Medical announces completion of trial enrolment for its GPX embolic device. In this multicentre trial, GPX was used to treat a variety of primary and metastatic tumours, renal adenoma tumours, and a range of other arterial and venous applications.
“We are pleased to announce the enrolment of the final patient in the trial and look forward to participating in future trials using this promising technology,” stated the trial’s principal investigator, Andrew Holden (Auckland City Hospital, Auckland, New Zealand.) “In the trial, GPX showed significant potential to advance liquid embolics, penetrating very distally, providing profound embolization, and demonstrating excellent radiopacity which helped to avoid non-target embolization and preserve healthy adjacent tissue.”
GPX has shown promising results for tumour embolization and other uses where there is a desire for distal vessel bed penetration. Embolization is a procedure in which arterial or venous blood supply to an organ, malformation, aneurysm, bleed, tumour, and/or other abnormal area of issue is blocked.
L: baseline image of contract flowing through tumour-feeding vessels of pelvic tumour. R: GPX embolization of a pelvic tumour’s largest feeding vessel.
Interim results of the GPX study have been presented at recent annual congresses including Global Embolization Symposium & Technologies (GEST), Society of Interventional Radiology (SIR), and Leipzig Interventional Course (LINC).
Holden concluded, “We’ve only touched on some of the applications. Further trials will provide opportunities to look at broader applications of this product. We believe it will be an exciting addition to the embolic portfolio for interventionalists.”
GPX is an innovative embolic designed for simple preparation and controllable material delivery. The device is packaged ready-to-use in a syringe, can be prepped tableside by the clinician in about 30 seconds, and may be delivered through standard microcatheters (no complex mixing systems or special delivery catheters are necessary). GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolus upon delivery without polymerisation or dimethyl-sulfoxide (DMSO) precipitation.
Inari Medical has announced planned enrolment of the DEFIANCE randomised controlled trial (RCT), which is designed to compare the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only.
The trial will enrol 300 patients at up to 60 centres worldwide. DEFIANCE is Inari’s second RCT and it will run in parallel to the PEERLESS trial. PEERLESS commenced earlier this year and compares FlowTriever to catheter-directed thrombolytics in pulmonary embolism.
“Anticoagulation is still the predominant therapy used in the management of DVT and in some studies has been associated with post-thrombotic syndrome (PTS) in up to 50% of patients,” said Steven Abramowitz (MedStar Health, Washington, DC, USA), co-principal investigator. “PTS is a debilitating condition with symptoms including swelling, difficulty walking, skin changes and poorly healing open wounds. Research has shown PTS quality of life scores can be as low as those of patients suffering from heart failure or cancer. Mechanical thrombectomy procedures, using technology like ClotTriever, rapidly remove large volumes of DVT and may thereby reduce the risk of PTS.”
“DEFIANCE is the first RCT to compare mechanical thrombectomy to anticoagulation for the treatment of DVT,” said Xhorlina Marko (Beaumont Health, Dearborn, USA), co-principal investigator. “The primary endpoint for the trial is a hierarchical composite of treatment failure and PTS severity at six months. The trial has the potential to influence guidelines and change the standard of care.”
“Physicians need to know in which patients to use our devices and what outcomes to expect. This is our basic responsibility,” said Thomas Tu, Inari’s chief medical officer. “We have studied over 2,000 patients, published 250 peer reviewed publications, and DEFIANCE marks our sixth major clinical study. These high-quality studies will establish a new standard of care for patients and further distance us from competition.”
Ablation is used to destroy or shrink tumours in the liver, lung, kidney, bone, and other organs. In recent decades, image-guided ablation has become integral to modern cancer therapy with curative or palliative intent. Although a promising treatment option, the main challenge is the accurate and safe positioning of the ablation probes to achieve complete tumour coverage, especially in difficult-to-access localisations. The CAS-One® IR system (CASCINATION AG) and its AblaSure®margin assessment software aim to improve the reproducibility, reliability and accuracy of ablation procedures for liver, lung, pancreas, kidney and bone. It enables more patients, and those whose cases are more challenging, to be treated, and to reduce rates of recurrence and procedural complications.
Quality Ablation with the CAS-One IR System
Martin Hoffmann (St Claraspital, Basel, Switzerland) and Shaheen Noorani (Hampshire Hospitals NHS Foundation Trust, Basingstoke, UK) have experience using CAS-One IR with AblaSure to ablate advanced tumours where single or multiple electrodes are required to treat the tumour adequately. They believe that lesions can be targeted more accurately using the navigation system compared to the traditional manual ablation. Hoffmann and Noorani spoke to Interventional News about their experiences using CAS-One IR with AblaSure and contextualise these in the broader landscape of ablation, as well as detailing how, and for which patients, the CASCINATION offering yields advantageous ablation results.
Hoffmann begins by stipulating that he has around five years’ experience with CAS-One IR, which contrasts with Noorani’s more recent incorporation of it into her practice. Hoffmann recalls being asked, when he started in his current hospital, whether he could find some way of treating large kidney- and liver-dominant tumour masses? This stemmed from the fact that, as Hoffmann elaborates, “we would see patients [who could not be treated systemically] declined from our surgical services.” So, CAS-One IR provides a solution for treating these “more challenging lesions in challenging locations” as Noorani puts it, illustrating that the pair share motivations for using the technology. Both Hoffmann and Noorani spoke of the advantage of achieving standardised ablation that is consistent from one patient to the next, and also from one interventional radiologist (IR) to the next.
Martin Hoffmann
Asked about the challenges involved in using conventional ultrasound or computed tomography (CT) freehand ablation, Hoffmann reframes his response from the outset: “it is not so much a limitation of CT or ultrasound,” but the ablation modalities. He then explains that “one of the prerequisites of [using NanoKnife electrodes] is that they must be arranged parallel around the tumour,” which is very challenging manually. The CASCINATION system also has the advantage of allowing the use of “an un-bordered array of microwave antennae” that work in tandem “to cover a large tumour volume, [ablating] section by section” in many different positions during the same procedure. Similarly, Noorani points to the issue of having “[to eyeball] the targeted ablation zone and needle position” when carrying the procedure out manually, which means that the “technical ability” of the IR is a “huge factor” in dictating how successful the outcome is. Furthermore, IRs encounter the issue of not being able to see the “invisible lesions” on CT that do show up on magnetic resonance imaging (MRI) scans—ablation of those lesions freehand is, consequently, impossible. Yet, Noorani clarifies that CAS-One IR resolves this problem, “[fusing] the MRI scans to the CT images.”
Shaheen Noorani
While CAS-One IR is versatile and usable with all ablation modalities and suitable for liver, kidney, lung, bone and other organs, it is AblaSure that adds value for patients, Noorani then shared, as being able to do margin assessment alongside the ablation means “we can re-treat on the same day, rather than bringing the patient back.”
Continuing in a similar vein, Noorani outlines where CAS-One IR holds potential economic value for healthcare providers. “Patients with deep-seated lesions would, in the past, have had a hepatectomy,” she begins, but as there is now the option for ablation with CAS-One IR, “[there will be fewer large operations, which] will ultimately mean reduced length of stay, [less] need for intensive care beds, and reduced wait for open theatre procedures.” Workflow can also be managed better in a hospital with the length of procedure time being shorter and less variable, as “more challenging lesions can be done in a timelier manner,” and the increased accuracy of ablation with CAS-One IR means that, in time, Noorani “[hopes] to see a reduction in patients having repeat ablations.” Moreover, “a larger cohort of patients can be treated with curative intent,” to the same end.
A case from Noorani: Trajectory plan, needle verification, AblaSure confirmation
On the hot topic of attaining sufficient margin, Hoffmann emphasises that there is, indeed, “huge demand for safety margin verification and that can only be achieved with a navigation system, such as CAS-One IR.” Image overlay, which is the means of verifying margins without such a system, is flawed, Hoffmann continues: “it can torque the kidney and liver,” and only works where there are “very advanced algorithms” at play. Noorani concurs, adding that post-ablation assessment is also “becoming more and more important […] economically to reduce re-ablation rates.”
A summarising remark from Noorani is that CAS-One IR allows for targeting lesions “at angles not previously achievable,” and this advantage is supplemented those conferred by the fusion software capabilities. Hoffmann’s own parting message is that, where in the past, ablation may have been prized by its practitioners as an art form, what IRs want now is to have “reproducible and accurate results.” Backing up his assertion with anecdote, Hoffmann stated that he finds it “embarrassing to go to a multidisciplinary tumour board meeting and be presented with evidence that there is a new tumour growing at the back of the ablation scar.” CAS-One IR is a means to avoiding such unsavoury scenarios, he concludes.
You can read more about Quality Ablation and CAS-One IR at www.cascination.com
Alban Denys is a French-Swiss interventional radiologist who was one of the founding members of the Society of Interventional Oncology (SIO). He has held the position of chairman of the European Conference on Interventional Oncology (ECIO) and developed and patented a chemoembolization method that includes anti-angiogenic agents. Passionate about mentorship and giving up-and-coming interventional radiologists quality fellowship opportunities, Denys is head of diagnostic and interventional radiology (IR) at the Centre Hospitalier Universitaire Vaudois (CHUV) in Lausanne, Switzerland. Interventional News spoke to him about his career highlights, research interests, and what is required to succeed as an interventional radiologist.
What attracted you to a career in IR?
I actually discovered IR by chance during my residency. I was lucky enough to be working at the Gustave Roussy Institute (IGR) under the supervision of Alain Roche with a bunch of other young fellows. At the IGR, I discovered a brand new field of medicine where image guidance could facilitate effective, yet less minimally invasive treatment. I had also found myself a little frustrated by diagnostic radiology, where there is not much close patient contact. IR was a way to be more directly involved in patient care.
Who were your mentors?
I am lucky to have had fantastic radiology mentors. Alain Roche in Paris and Michel Lafortune in Montreal have really impacted my work. Both are extremely patient-centred and are highly respected both in and outside of their specialty. Michel Lafortune has also shown me that academic medicine—coming up with ideas, and designing a study, and then publishing it—can bring me a lot of joy. I also love the interventional oncology (IO) family that I have met over the years: Bradford Wood, Riad Salem, Ricardo Lencioni, Patrick Chevallier, Thierry de Baere, Afshin Gangi, they are more than colleagues; we have had this shared adventure in the development of IR and IO. I have also welcomed fantastic fellows to Lausanne—the stars of today and tomorrow—including Rafael Duran and Boris Guiu, who are working together on CIRSE’s (Cardiovascular and Interventional Radiology Society of Europe) Interventional Oncology for Immuno-oncology (IO4IO) initiative.
Could you describe a particularly memorable case of yours?
The day that my oldest daughter came to the world, I received a call from my chief nurse whose daughter-in-law had just given birth to twins in a small clinic in a Parisian suburb. She had had a very severe form of postpartum haemorrhage, and she also had a coagulation disorder. The obstetrician had already left for the weekend and the ambulance could not transport her to the hospital because she was so haemodynamically unstable. I ended up embolizing her successfully in a very basic radiology room without any angiographic facilities, in the small clinic she was in. This was probably the most emotionally intense day of my entire life— there was the extreme happiness I felt at the arrival of our newborn, and then the stress of this intervention. I have kept a ‘basic embolization kit’ in my car ever since.
What are the most challenging aspects of using IR techniques to diagnose and treat liver cancers?
The real challenge is to develop an oncologic approach; to work out when best to perform an IO treatment, you actually have to develop skills and knowledge in both surgery and oncology. Our techniques have had to demonstrate their validity through strong medical evidence, too. Designing a trial, finding the money to run the trial and recruiting patients, all of these are tricky tasks.
Alban Denys
This year’s ECIO featured the first IO foundation course—what is the significance of this for the future of IO and its practitioners?
This brings me back to my previous comment. We have to have an open dialogue with the oncologists we work with. This means understanding how they work and seeing things from their perspective, to then offer our solutions for the patients, at the right point in their treatment. But we should also be able to challenge oncologists’ decisions sometimes. And you can only do this if you have an in-depth knowledge of oncology. The IO foundation course is intended to equip our younger colleagues with this knowledge.
You patented chemoembolization composition including anti-angiogenic agents, which was then licensed for use in the VERONA study, now completed. What was the patent process like from your researcher’s standpoint?
Developing a new therapeutic concept, and building the preclinical evidence was extremely challenging. However, this was a lot of fun, even if finding money for experiments, going through the process of patenting, and then trying to license the product, was as exciting as it was difficult. In the end, the product licensed to BTG was approved for use in a clinical trial, which yielded interesting results. I also learned a lot from my exchanges with the industrial partners. Unfortunately, the project was not considered enough of a priority to be continued.
You recently published, in the Journal of Hepatology, a report on your experience with portal vein recanalisation? What do you think your results brought to the medical community?
This is actually the first large single-centre study of portal vein recanalisation in symptomatic chronic portal obstruction. This study reflects 15 years of practice in this rare and often misdiagnosed disease and demonstrates that this technique can be offered even after decades of portal obstruction. It leads to symptom and clinical improvement in 70% of cases and improves the nutritional status of patients. On the other side of the Atlantic, Riad Salem developed another treatment for the same disease. Time will tell whose is better.
During your professorship at CHUV Lausanne, what would you say the biggest shift in IR practice has been, both in your hospital and more widely? How has this impacted interventional radiologists’ approaches to cases and the consequent patient outcomes?
In 2018, we acquired an angiosuite combined with a computed tomography (CT) scanner in the same room. This kind of interventional suite has been used in Japan for years under the leadership of Professor Arai, but not much in Europe. This has been a game-changer in our practice for all procedures that require both angiography and percutaneous intervention. Of course, cone beam CT is also an option, but it has the disadvantage of being way more limited in term of imaging quality. We use our combined angiosuite and CT everyday and it has made us feel more secure and confident in our techniques, and probably also improved our clinical results.
Mentorship was the subject of this year’s Charles T. Dotter lecture at the Society of Interventional Radiology (SIR) Annual Meeting—why is this so important in IR and how can interventional radiologists seek to be better mentors?
Mentorship in every interventional or surgical activity is crucial; it is so important to be at young colleagues’ sides in the angiosuite. The transmission of all the tips and tricks of IR can only be done this way. The development of phantom and robotic IR will certainly change this approach in the near future, just like it did for laparoscopic surgery.
What are your hobbies and interests outside of medicine?
One of my main hobbies is biking, either in the Swiss mountains or in my beloved Normandy where we have a beach house. I also try to listen to live jazz music whenever I get the chance and I love reading books (particularly modern American authors like Jim Harrison). I am lucky enough to have been married for 30 years now, to a painter, and we enjoy visiting the museums and galleries in the places we visit on our travels, often with our children too.
Indrajeet Mandal, a second-year radiology registrar at Oxford University Hospitals NHS Foundation Trust (Oxford, UK), speaks to Interventional News about the interventional radiology (IR) awareness initiative that he co-founded in 2019—IR Juniors.
Mandal along with Niall Burke (NHS Lothian, Edinburgh, UK), Sachin Modi (Royal Free London NHS Foundation Trust, London, UK) and Navin Nagesh (Oxford University Hospitals NHS Foundation Trust) under the guidance of Gregory Makris (Guy’s and St Thomas’ NHS Foundation Trust, London, UK) and further support by Jim Zhong (Leeds Teaching Hospitals NHS Trust, Leeds, UK), launched the website to further awareness of the specialty. IR Juniors is now partnered with the British Society of Interventional Radiology (BSIR). The group aims to educate those at the start of their medical career about how they can pursue IR, become involved in the initiative’s affiliated research collaborative (UNITE) and embark on an elective in IR abroad—and much more besides.
Q: How did you end up as a radiology trainee with a passion for IR?
A: Just one day of a vascular surgery placement I did as a medical student was in IR, and that day changed my life. The consultants there probably do not know that they inspired me this much, but I am going to namedrop them anyway—Nick Woodward and Neil Davies at the Royal Free Hospital in London. I just had a fantastic experience—they let me scrub and explained exactly what IR was. Before, I had thought that it was just cardiologists who did stents, and this showed me a whole other world. Independently of that, I then did a placement in radiology towards the end of medical school and my supervisor happened to be an interventional radiologist. I really got inspired by the concept of ‘minimally invasive procedures under image guidance’—there is no other specialty like it.
Q: Why do you think that there tends not to be much awareness of IR among medical students? What specifically led you to set IR Juniors up?
A: In my opinion, the medical school curriculum is already very congested, and IR does not really fall among the priorities, which was fair enough a few decades ago. However, it has now become such a vital cog of healthcare. Even with some medical school teaching, it is hard to get a full grasp of what radiologists do, and this was partly the ‘why?’ for IR Juniors. It was also personal—before my IR elective I was searching for a basic website or book to help me prepare and I felt like there was a gap. We hope IR Juniors, as a solution to this, is accessible and not too advanced.
Q: UNITE—National IR Trainee REsearch Collaborative—is IR Juniors’ affiliated research group, which you also set up. Why was encouraging research involvement among students and trainees a priority?
A: Education is important, but research is too—IR has been one of the most innovative specialities. There are not that many avenues in the UK to explore IR research, and while not everyone is going to be an investigator or a researcher, it is still key to show that a career in research in IR is possible.
Q: You have carried out COVID-19-related projects through UNITE, among others—what has come from this research so far?
A: Our first project was on the impact COVID-19 had on IR training and services. As a trainee-led research collaborative, it was important to start with this. We found that, while a lot of surgical services had to stop because of the anaesthetic risk during the pandemic, a lot of IR services carried on, which highlights the importance of IR in the patient pathway. The next project was a multicentre study on the outcomes of cholecystostomy and over 30 centres collaborated—that work was presented at the BSIR meeting in 2021. It was great proof that we could mobilise trainees across the country, which had been done in other specialties, but never until then in IR. The papers from this study have now been accepted for publication.
Q: The Global IR section of IR Juniors shows your commitment to widening access to all that IR has to offer, for clinicians and patients alike—what does this look like in practice?
A: As a specialty, IR has always been collaborative—among different specialties but also countries—and we wanted to show that as an IR, you are part of a huge network around the world. There are two parts to the Global IR section, the first being highlighting opportunities for training in countries such as Canada and Australia. You can learn new techniques during these fellowships, while sharing how things are done in the UK too. Secondly, IRs can help set up training programmes and infrastructure in less developed countries. Road2IR is a great initiative as part of which trainees from the UK and USA go to Uganda to set up an IR training programme. This teaches participants that the specialty is not just about fancy, expensive equipment.
Vascular Therapies has announced that the first patient in the ACCESS 2 clinical trial was enrolled by Nikhil Kansal at Harbor-UCLA Medical Center in Torrance, USA.
The Phase 3 prospective randomised ACCESS 2 study will enrol 120 patients from centres in the USA and UK. The study is being conducted to validate an encouraging subgroup analysis from the first Phase 3 (ACCESS) study that showed that Sirogen use in end-stage renal disease (ESRD) patients 65 years and older resulted in clinically meaningful improvement in arteriovenous fistula (AVF) maturation and durability.
Kansal commented: “We are excited to participate in this randomised clinical trial that addresses an important unmet clinical need. The elderly population is the fastest growing segment of the haemodialysis population and these patients urgently need a solution to improve AV fistula maturation.”
Sriram Iyer, chief scientific officer of Vascular Therapies commented: “Initiating enrolment of the ACCESS 2 clinical study is an important milestone for Vascular Therapies. We would like to thank our investigators and their research teams for their interest in Sirogen and desire to evaluate a new potential therapy for haemodialysis patients.”
Vascular Therapies advises that the Sirogen drug development programme has received Fast Track status from the US Food and Drug Administration (FDA).
Reto Bale (Medizinische Universität Innsbruck, Innsbruck, Austria) gave a presentation titled ‘Stereotactic thermal ablation—can it break the current limits?’ at the 2022 European Conference of Interventional Oncology (ECIO; 24–27 April, Vienna, Austria). A key takeaway was that although the 3D planning and other elements of the stereotactic procedure may require more effort than conventional ultrasound (US)- and computed tomography (CT)-guided ablation approaches, the results that it yields are “excellent.“
His presentation covered an explanation of stereotactic thermal ablation, the logistical challenges of implementing it, and the outcomes it can achieve. Bale underlined to Interventional Newsthat “interventional oncology must become reliable and reproducible,” and that this is what underpins the stereotactic approach.
Bale’s stereotaxy workflow, he detailed, begins with “precise planning of multiple overlapping ablation zones”, to determine isotherms and to cover the whole tumour plus a safety margin. The next step, Bale relayed, is to place needles/probes in accordance with the plan, using respiratory triggering.
Planning CT showing colorectal liver metastases in segment VIII with 3cm diameter
Bale expanded on his previous explanation, conveying how a stereotactic approach is key when dealing with tumours greater than three centimetres, as, larger than this, and ablation from a single-probe position may not be possible, hence the need for multiple needles, and the careful 3D planning that precedes their use.
Since his very first stereotactic radiofrequency ablation (SRFA) in 2001, Bale has used the image fusion software of the stereotactic navigation system to superimpose the intraoperative contrast-enhanced control CT to the planning CT for verification of complete coverage of the tumour by the ablation zone. With regard to obtaining the results of the procedure, image fusion enables the interventional radiologist to see the results of stereotactic thermal ablation before the patient even wakes up. This intraoperative verification is an advantage that stereotaxy has over radiation therapy, which necessitates waiting until long-term follow-up imaging has been completed.
Planning of eight needle trajectories
Speaking to the outcomes of treating his patients with stereotactic thermal ablation, Bale stated that they very obviously demonstrate how “the additional efforts” necessary in order to conduct 3D planning, stereotactic needle placement and image fusion “lead to excellent results”. He expanded upon this assertion, explaining that his team treated more than 3,500 tumours in this way between 2001 and 2020, in more than 1,100 patients, and that even patients with multiple lesions and lesions greater than 10cm respond well. The complication rate after 2011, Bale underlines, was 0.5% mortality and 6% major complications. Of particular note is that more than half of these major complications “could be treated in the same session by the interventional radiologist.” The same is true when treating multiple lesions—they can often be treated simultaneously, in a single session.
Verification of precise coaxial needle placement by image fusion
Referencing histopathological evidence of the treatment’s success, Bale acknowledged the results of his study, which evaluated 188 hepatocellular carcinomas (HCCs) in 96 patients—the residual tumour rate was 2.7%. In lesions greater than three centimetres, the residual tumour rate is still as low as 3.8%, Bale added.
Consequently, Bale concluded, SRFA is now regarded the first-line treatment by the Innsbruck Tumour Board for most patients with primary and secondary liver tumours, encouraging clinicians first to ask themselves whether ablation could be an alternative to resection in HCC and colorectal liver metastasis patients. The advantages of the additional use of stereotaxy and image fusion are that it enables the interventional radiologist to treat more patients more consistently, with curative intent, minimally invasively, and while sparing tissue. Moreover “the beauty of the technique,” Bale emphasised, that “it is easy to teach” and that “training of three-dimensional needle trajectory planning can be done in your own lab on virtual patient datasets.”
Final contrast enhanced CT showing large ablation zone with sufficient margin as confirmed by image fusion
The logistical obstacles that stand in the way of more widespread current rollout of the treatment, Bale concedes, are the need for general anaesthesia, more than three hours per patient in the CT suite, the stereotactic neuronavigation system, and “there is still a problem, also, with reimbursement.”
Bale left the audience on the note that he hopes his excellent results will encourage those responsible for reimbursement guidelines to make changes to improve the accessibility of SRFA.
ŌNŌCOR has announced in a company press release that the ŌNŌ endovascular retrieval system was used to remove a large central-line-associated thrombus from the right atrium in a teenage patient.
The team at Children’s Hospital Los Angeles (CHLA; Los Angeles, USA) led by Darren Berman, Director of Congenital Interventional Catheterisation with CHLA’s Heart Institute, percutaneously removed a large fibrotic thrombus from a 14-year-old patient using a combination of ŌNŌ, endovascular snares, and electrocautery.
“This procedure was inspired by the Seattle procedure recently performed at the University of Washington, and represents the first time that a large haemodynamically problematic thrombus was captured and removed non-surgically, and without fragmentation or distal embolization of particulate matter,” said Berman. “The ŌNŌ was key to securing the mobile mass and subsequently removing it from the vasculature atraumatically.”
Berman continued, “Intra-atrial thrombus formation associated with indwelling central lines is a common problem. Typically, the approach is to treat with anticoagulants in the hopes that the clot reabsorbs. When this doesn’t work, and the thrombus burden remains substantial, it represents an ongoing risk for pulmonary and systemic emboli.
“Our patient today is representative of a clinical dilemma that we often face. Up until this point, the only options that we had were ‘watchful waiting’ or open-heart surgery,” said Berman.
The ŌNŌ designed to receive, align, compress, and remove material (non-biologic and biologic) from the vascular system. ŌNŌ is intuitive to use and is compatible with commercially available vascular sheaths, endovascular snares and other graspers.
“We are delighted that ŌNŌ was able to help the team at Children’s Hospital Los Angeles,” said Mark Piper, CEO of ŌNŌCOR. “ŌNŌ was designed to help safely remove material from the vascular system, so it’s rewarding to hear that the patient in Los Angeles has done well and recovered nicely from this procedure.”
Teleflex has announced a new agreement with FundamentalVR, a company providing virtual reality (VR) integration for medical simulation. The agreement will provide Teleflex with a VR training platform to accelerate the effective use of the company’s UroLift 2 system, a technology for treatment of benign prostatic hyperplasia (BPH), commonly known as enlarged prostate. The VR training platform integrates tactile feedback and a digital representation of the UroLift 2 system to provide urologists with a ‘hands-on’ VR experience that can accelerate their learning.
By leveraging the capabilities of FundamentalVR’s Fundamental Surgery platform, Teleflex aims to increase access and standardisation of clinical training of the UroLift 2 system in the USA and around the world, including Japan, where the UroLift 2 system was recently approved for use. The customised solution from FundamentalVR will enable urologists globally to practice the procedure remotely in a virtual environment.
Teleflex showcased the Fundamental Surgery platform at the company’s UroLift system booth at the 2022 American Urological Association (AUA) meeting in New Orleans.
“We are delighted to offer our customers this leading VR platform for surgical and procedural education which offers advanced, realistic graphics to help demonstrate the ease of use of the UroLift 2 system in a variety of prostate anatomies,” said Kevin Hardage, president and general manager of Teleflex Interventional Urology. “FundamentalVR’s Fundamental Surgery platform is versatile and scalable, making them an ideal supplier to meet our customers’ needs for training for the UroLift 2 system around the world.”
Chris Scattergood, co-founder at FundamentalVR said, “We are delighted that Teleflex, a market leader in urology, has chosen FundamentalVR as their partner for their future vision. Integrating extended reality education solutions can have a positive impact on surgeons and patients.”
A study recently published in the World Journal of Surgery claims to be the first to provide comprehensive population-level data on the epidemiology of lower extremity amputation (LEA) in a Latin American low- and middle-income country (LMIC). The investigators write that their data, which focus on the Brazilian state of Sao Paulo, are “crucial to plan strategies to reduce the burden of LEA”.
“Lower limb amputations represent a high social, economic and health burden,” Rodrigo Bruno Biagioni (Hospital do Servidro Público Estadual de São Paulo, São Paulo, Brazil) et al write. According to the authors, most lower limb amputations are preventable, and reflect areas for improvement in healthcare. For these reasons, they stress that it is “essential” to know the epidemiology of these amputations, underscoring the rationale behind their study.
The investigators detail that LEA rates are “highly variable” across the world and that LEA trends are “conflicting”. These factors, they say, necessitate population-based studies in particular, “not only to truly know the local epidemiology of LEA, which reflects the quality of the health system, but also to build a global panorama in order to establish standards and goals.”
According to the authors, several countries in Europe, North America and Australasia have reported their amputation epidemiology, with most data coming from high-income countries (HICs). “Data from [LMICs] are scarce,” they write, noting that in Latin America no such study existed before the present analysis, to the best of their knowledge. “The paucity of data on LEA in LMICs is of particular concern,” the researchers note, “as the burden of PAD and [diabetes mellitus] is increasing in rates higher in LMICs than those observed in HICs.”
Biagioni et al’s study was a retrospective, population-based, cross-sectional analysis on all lower limb amputations performed in public hospitals in Sao Paolo—the most populous Brazilian state—between 2009 and 2020. The authors relay that they used a public database to evaluate types, rates and trends of the amputations performed, main aetiologies leading to the indication for amputation, hospital length of stay and in-hospital mortality rates, demographics of the amputees and procedure costs.
The study included data on 180,595 lower limb amputations and surgical revisions of amputations, with toe amputations (45%) and major amputations (33%) being the most frequent types of surgeries. Biagioni and colleagues report a significant increase in the rates of both of these procedures. They add that peripheral arterial disease (PAD) was found to be the most frequent underlying diagnosis for LEA, followed by diabetes mellitus, with an increasing trend for both over the last 12 years. Furthermore, they also observed seasonality in procedure rates, with peaks in August in all years.
The authors also reveal that most patients were male (69.3%), Caucasians (55.6%) and elderly. Other findings included a 6.6% rate of in-hospital mortality and lower limb amputations and total of US$67,675,875.55 reimbursed by the government.
Based on these findings, the authors propose some preventive strategies—namely foot ulcer screening, multidisciplinary diabetic foot care, and encouraging revascularisation procedures, which, they claim, have not significantly increased in the city of São Paulo, the capital of the state of Sao Paulo, since 2008.
In the discussion of their results, the research team considers some possible explanations for PAD being the main underlying diagnosis for all LEA in Sao Paulo, one of which is that Brazil is “late in the epidemiological transition concerning LEA”. They predict that it is likely Brazil will reach similar statistics to those found in most recent nationwide studies—which point to diabetes mellitus as the most common underlying cause of LEA—in the coming years, as the prevalence of smoking is reducing and that of diabetes mellitus is rising.
Furthermore, Biagioni et al address the finding that August showed the highest number of amputations in all years of their study. They write that, although this contrasts a previously reported finding from Hong King of higher LEA frequency due to diabetes mellitus during the summer, in this study the main underlying diagnosis was PAD, and it is possible there may be a worsening in PAD during winter. They elaborate: “Even though impaired circulation of lower limbs is documented for venous insufficiency, it is reasonable to think it may also play a role in arterial insufficiency.”
The authors recognise there are some limiting factors to their study, including the accuracy of their findings being “susceptible to inherent miscoding or data entry errors,” as with any database-driven study. In addition, they acknowledge that their data represent only the state of Sao Paulo, which depends solely on the public health system. “An integrated database covering data from public and private health systems would be more comprehensive,” they note.
Speaking to Vascular News, corresponding authors Louzada and Nelson Wolosker (Hospital Israelita Albert Einstein, São Paulo, Brazil) comment on the study findings: “Knowledge of the data is essential for decision-making by public policy managers. Knowing the real amputation rates, increased investment in risk factor controls, and increased access to revascularisation become the most obvious attitudes. Soon, adopting such attitudes, amputation rates will probably decrease. This way, Brazilian society can evolve, an example for other countries.”
The first US patient has been enrolled in the US Food and Drug Administration (FDA) SELUTION4BTK (below-the-knee) clinical trial evaluating Selution SLR, MedAlliance’s novel sirolimus-eluting balloon. This follows investigational device exemption (IDE) approval in the USA in May 2022, with enrolment of the first patient occurring in Germany one week after approval.
“We are very excited to finally have drug-eluting technology in the USA to treat this difficult patient population,” commented the trial’s principal investigator (PI) Ehrin Armstrong (University of Colorado, Denver, USA). “We are encouraged by the positive early outcomes with this novel Selution SLR sirolimus drug-eluting balloon (DEB) in Europe and Asia. We hope this FDA IDE trial will demonstrate significant benefit for patients who currently have limited treatment options.”
The aim of the SELUTION4BTK clinical trial is to demonstrate the superior efficacy and equivalent safety of Selution SLR compared to plain (uncoated) balloon angioplasty in the treatment of BTK arteries in chronic limb-threatening ischaemia (CLTI) patients. The trial is a prospective, multicentre, single blinded, randomised study.
377 subjects are being randomised 1:1 to either Selution SLR or control treatment. This is the first study of its kind where ‘real-world’ patients with CLTI can be included. Patients are being enrolled at approximately 40 sites across the USA, Europe and Asia. This first US patient was enrolled at Vascular Solutions in Cary, USA, by Siddhartha Rao.
“We are very pleased to be participating in this ground-breaking study,” said Rao. “We hope that this promising technology will fulfil a huge need for our patients with CLTI, saving life and limb. We look forward to the rapid enrolment of this trial.”
“We were the first company to be granted Breakthrough Device designation for a DEB by the FDA and are proud to enrol the very first US patient in a sirolimus DEB study,” added Jeffrey B Jump, MedAlliance chairman and CEO. “Many companies have been trying for years to bring sirolimus to the USA and we are very pleased with our team for achieving this significant milestone. US patients will now have an alternative to paclitaxel DEB, addressing the concerns expressed by the FDA.”
MedAlliance advises that Selution SLR is available in Europe and all other countries where the CE mark is recognised.
BD has announced the start of enrolment in a first-in-human trial of a peripheral sirolimus drug-coated balloon (DCB).
The PREVISION trial is a prospective, multicentre, single arm, non-randomised study designed to evaluate the safety of the BD sirolimus DCB in the treatment of peripheral arterial disease (PAD) in the femoropopliteal arteries.
A company press release notes that BD initiated this trial to determine the viability of sirolimus as a future treatment option for patients with PAD. The first patient was successfully treated by principal investigator Andrew Holden at Auckland City Hospital (Auckland, New Zealand).
“It is an honour to enrol the first patient in the PREVISION study,” said Holden. “The burden of PAD continues to impact patients and challenge physicians around the globe. A continued focus on developing next-generation technology is important for the patients suffering from PAD.”
PREVISION is being conducted across multiple sites in Australia, New Zealand, and Singapore. The trial will enrol and follow-up on approximately 50 patients over the coming months.
Building upon “pioneering work” at University of Texas Southwestern (UTSW) Medical Center (Dallas, USA), investigators recently reported the results of a clinical trial exploring the role of stereotactic ablative radiation therapy (SAbR) for patients with a handful of metastases, or so-called oligometastatic disease.
As per a UTSW press release, the study represents the first clinical trial for patients with untreated oligometastatic kidney cancer.
“There has never been a clinical trial for these patients. It is unclear whether these patients should be treated with medication, surgery, or another approach. This represents an unmet medical need,” said Raquibul Hannan (UTSW, Dallas, USA), lead author of the study along with Robert Timmerman and James Brugarolas (both UTSW).
As per the release, kidney cancer encompasses a wide spectrum and can present with extensive metastases, or just a handful. However, today, all patients are treated the same way—with medication. Metastatic kidney cancer is typically treated with immunotherapy agents or targeted drugs, which are toxic and diminish quality of life. For most patients, the disease ultimately progresses, necessitating a change in treatment, until patients exhaust their options. When metastatic, most patients eventually succumb to the disease, and the quality of their remaining lifespan is negatively impacted by the cancer drugs.
The phase 2 clinical trial tested SAbR, a treatment that delivers potent, narrow beams of radiation to tumours, in 23 kidney cancer patients with oligometastases (up to five metastases) at UTSW and the affiliated county hospital, Parkland Health. Patients received SAbR to metastatic tumours at the outset and while the disease remained oligometastatic. Overall, 57 metastases were treated.
The primary goal was to control the metastatic cancer in at least 60% of patients at one year. The study was successful, with more than 90% of patients demonstrating disease control at one year without systemic therapy.
“It appears that most patients will be free of systemic therapy for at least two years,” said Hannan.
None of the patients experienced serious side-effects either, the release notes, and periodic questionnaires showed no negative impact on quality of life. A large, phase 3 randomised clinical trial evaluating SAbR for oligometastatic kidney cancer has now been approved by the National Cancer Institute and will also be led by Hannan.
“If successful, this phase 3 trial will establish, for the first time, a standard of care for patients with oligometastatic kidney cancer,” added Brugarolas. “The hope is that the treatment will help patients by delaying progression while preserving their quality of life.”
A new imaging device at University of Texas (UT) Southwestern (Dallas, USA) is making complex aortic repairs safer for patients and operating room staff by dramatically reducing their exposure to radiation. The device, known as Fiber Optic RealShape (FORS; Philips), uses light to visualise blood vessels, nearly eliminating the need for X-rays typically used during minimally invasive vascular procedures.
“Complex aortic repairs tend to be long operations that require frequent in-procedure imaging. Every time a surgeon presses on the X-ray pedal, the patient and staff including assistants, nurses, scrub techs, anaesthetists, and X-ray techs gets a dose of radiation,” said Carlos Timaran, professor of surgery at UT Southwestern. “The safety of each of these individuals is paramount, so reducing radiation exposure during these procedures is an important goal.”
UT Southwestern was one of about a dozen medical centres in the USA and Europe chosen to participate in the early implementation of FORS. Timaran has completed more than 300 fenestrated endovascular aortic repairs as part of his physician-sponsored investigational device exemption study, in which a patient-specific graft is used to support the aorta and its main branches.
As an alternative to conventional imaging, the FORS device uses light travelling through hair-thin optical fibres built in specially designed catheters and wires to display its position and shape inside the body. Once this device is placed within a blood vessel, the strain on the optical fibres changes the light’s pathway. By analysing how light reflects back along the fibres, a computer algorithm reconstructs and visualises the full shape of the device. The result is a real-time, three-dimensional view of the blood vessel that surgeons can overlay on computed tomography images taken before the procedure, providing a roadmap that surgeons can view in any angle to guide the surgery. Timaran said that far fewer X-rays are necessary when using FORS, significantly reducing patients’ and staff’s exposure.
He expects FORS use to expand to other vascular procedures over time. “This technology could potentially be used for any cardiovascular procedure,” he said. “This will eventually be the goal.”
Iodinated contrast media agents, namely Omnipaque (iohexol) and Visipaque (iodixanol), are frequently used in imaging studies for both diagnosis and treatment. GE Healthcare, the manufacturer, had to shut its plant in Shanghai, China, due to local COVID-19 policies, which created a domino effect in the supply chain, as seen in recent months. In May and June of 2022, clinicians were offered guidance on alternative imaging methods for interventional radiology procedures
Speaking to Interventional News about hers and colleagues’ article, which was published in the Journal of Vascular and Interventional Radiology (JVIR), lead author Nikki A Keefe (Department of Radiology, University of North Carolina at Chapel Hill, Chapel Hill, USA) outlines the current iodinated contrast media supply situation, and what the response to her recommendations has been among radiologists.
Taking the American College of Radiology (ACR) Committee on Drugs and Contrast Policy’s guidelines statement as a starting point, Keefe and her co-authors recommended using a priority matrix to help manage radiology services in the face of the contrast media shortages. The matrix should encompass the following types of procedures: those requiring iodinated contrast media versus procedures that can be deferred; those that can be performed with alternative imaging modalities such as intravascular ultrasound; and those that can be performed with an alternative contrast media.
Keefe first underscores to Interventional News the impact of the shortage on radiology services: there were many cancellations and delays for non-emergent procedures, and alternative agents used. “Many procedures were transitioned,” she expands, citing how the traditional gastrostomy tube placement replaced the balloon-assisted gastrostomy tube placement, non-contrasted computed tomography (CT) replaced sinogram, and ultrasound-guided saline injections replaced fluoroscopy-guided contrast injections for tube placements.
The article’s lead author also relays how she, personally, “received many questions about using gadolinium, gastrografin and carbon dioxide in unique methods such as within angioplasty balloons.”
From a patient point of view, Keefe details how they were often “not familiar with the cases performed in the usual manner”, so remained largely unaware of procedural changes caused by the shortage, such as the employment of different imaging modality. Many, however, were acutely aware of the delays in imaging and their procedures.
“It would be interesting to see how radiation doses changed during this period, as perhaps patient doses decreased due to increased utilisation of ultrasound,” Keefe muses, while also contemplating how doses may actually have increased “if interventionalists were less familiar with alternative contrast agents and therefore the procedure was made more challenging and lengthier”
Regarding the current state of contrast media availability, Keefe asserts that it seems to be at “pre-shortage levels”, owing to Bracco’s increased production and importation to the US market and GE Healthcare’s production having returned “to normal”.
However, “it may be prudent to continue to utilise some of the mitigation strategies full-time,” Keefe advises, citing that nephrology colleagues of hers are in support of such an approach. “Use of air, carbon dioxide, and intravascular ultrasound where applicable can decrease both patient and provider radiation dose during the procedure,” the lead author suggests. Keefe goes on to say that “this may not increase procedural time but perhaps [even] decrease it, while providing [higher-quality] diagnostic imaging in certain situations.”
In a study recently published in Circulation, researchers found that Black adults underwent significantly more endovascular peripheral vascular interventions (PVI), were treated for more advanced disease and were also more likely to experience adverse outcomes following PVI procedures, including amputation and death. Interventional News spoke to two of the authors—Eric A Secemsky and Anna K Krawisz (Smith Center for Outcomes Research in Cardiology, Beth Israel Deaconess Medical Center, Boston, USA)—about their motivations for carrying out the study, the results it yielded, and where this research might lead.
Asked what led them to study race-related disparities in PVI treatment and outcomes, Secemsky and Krawisz explain that the Vascular Research section at the Smith Center is “deeply invested in improving care for patients with peripheral artery disease (PAD).” This, they assert, means “confronting the healthcare disparities that are prevalent in the vascular field.” PVI is now a common means of revascularisation and, therefore, the authors state their desire to “to understand whether racial disparities exist in different aspects of PVI”, knowing, as they do from their study, that “Black adults have a higher prevalence of PAD than white adults and they are more likely to have adverse outcomes such as amputation.” Moreover, the authors sought to identify what underpins the differences in outcomes for Black versus white patients.
Eric A Secemsky
Secemsky and Krawisz relay their findings as follows— Black race was associated with worse one-year outcomes following PVI, with adjustment for age and sex, owing, in large part, to the “disproportionate burden of advanced comorbidities among Black adults.” A further finding, the authors communicate, was that Black adults have more advanced PAD than white adults when they are referred for PVI.
“These results were not necessarily surprising,” they admit, but it is nonetheless, “critically important” that the vascular community be aware of them, given how much PVI is used to manage symptomatic PAD. However, what did surprise them was how few patients, regardless of race, received guideline-directed medical therapies following PVI—”we would have expected that medical therapy would be optimised prior to moving towards revascularisation,” they state.
The authors’ hope for their findings is that the vascular community better understands how “critically important” it is to detect, and effectively treat, comorbidities early. This is particularly crucial in Black adults, they affirm, so as “to reduce health disparities and improve limb outcomes.”
Regarding where this research will lead, Secemsky and Krawisz convey that they “continue to untangle the interplay between many types of disparities that impact care and outcomes in PAD, including poverty, gender, regional wealth, and geographic location.” Krawisz will give special focus to better understanding why women, like Black patients, tend to present for treatment with more advanced PAD, and why, when they require amputation, it is, generally, “more proximal”. Her research programme, she explains, will centre around PAD management for female patients. She reports that clinical trials in PAD “tend to underrepresent female patients”.
CX Aortic Vienna returns in October for its third edition (24–26 October, Digital), bringing together world-leading specialists from the cardiac and vascular fields to discuss all facets of aortic care from selection to investigation, diagnosis, techniques and technologies. The meeting will showcase the latest approaches—open and endovascular—for the treatment of complex aortic problems spanning the aortic valve to the iliac arteries.
Having attracted a global, online audience during its first two editions, CX Aortic Vienna will continue to reach out to the worldwide aortic surgery community. The 2022 edition features three days of high-quality digital programming, to be broadcast live from 24–26 October for the wider global audience, delivering a total of 15 hours of aortic education, which will also be available on-demand to registered attendees after the event.
The format for the digital edition will follow the CX style of short talks, debates, and audience interaction, presented live via broadcast. The programme includes open and endovascular aortic techniques and technologies, including edited aortic cases.
For the first time, the meeting will also offer an in-person component from its home city, Vienna, Austria, where CX Aortic Vienna has been invited to provide two 90-minute primetime cutting-edge English-language sessions for attendees of the Dreiländertagung—the joint meeting of the Austrian Society of Vascular Surgery (ÖGG), the Swiss Society for Vascular Surgery (SGG) and the German Society of Vascular Surgery (DGG)—on Thursday, 20 October.
World-leading faculty
The full programme has been curated by a Vascular, Endovascular and Cardiothoracic Executive board comprised of leaders in the field of aortic care including CX Aortic Vienna founding chair Roger Greenhalgh (London, UK), alongside Tilo Kölbel (Hamburg, Germany) who will moderate the in-person session at Dreiländertagung, Afshin Assadian (Vienna, Austria), Roberto Chiesa (Milan, Italy), Martin Grabenwöger (Vienna, Austria), Stéphan Haulon (Paris, France), Gustavo Oderich (Houston, USA), Markus Steinbauer (Regensburg, Germany) and Alexander Zimmermann (Zürich, Switzerland).
“This is, as always, a focus upon the aorta as managed by cardiac aortic surgeons, open vascular surgeons and endovascular surgeons; from the aortic valve at one end, to the iliacs at the other end,” says Greenhalgh of the event’s 2022 edition. “CX Aortic Vienna, for those of you who have been to it before, is for all of those who manage the aorta,” he adds. “This is not just the surgeons, but the physicians—we have radiologists, imaging experts, vascular scientists and vascular nurses. All who manage aortic patients are welcome to come and join us for the digital edition on 24, 25 and 26 October this year.”
“October is the time for aortic disease and to discuss newest trends, technologies and features in aortic therapy,” comments Kölbel. “We are focusing on both open and endovascular techniques and we are inviting the cardiovascular and vascular communities to come to CX Aortic Vienna, with a presence during the Dreiländertagung, and very much to the virtual event that happens a few days later.”
Multidisciplinary approach
The importance of multidisciplinary aortic approaches will be a key strand running through CX Aortic Vienna’s content and discussion, and the 2022 event will continue its mission to bring together specialists of all skills—be they cardiac, vascular or endovascular—to provide a comprehensive overview of cutting-edge aortic treatment.
“CX Aortic Vienna is the unique chance to get together with cardiac surgeons and all kinds of vascular specialists that are treating the aorta,” says Zimmermann, discussing the importance of the multidisciplinary focus at the heart of CX Aortic Vienna. “The problem is that we have a transition zone in the arch and we—as vascular surgeons—move further and further into the ascending aorta with our endovascular techniques. This can only be done with the support of the cardiac surgeons, and this is the reason why we really look forward to CX Aortic Vienna because everyone comes together addressing this complex field.“
Talking points
The programme encompasses discussion and debate spanning key talking points in the aortic space including aortic arch interventions, thoracic dissection, thoracic imaging, thoracoabdominal techniques, juxtarenal, abdominal aortic and iliac artery therapies.
“I have had the honour and the privilege during my career to treat the aorta from the aortic valve all the way to the femoral arteries,” notes Joseph Coselli (Houston, USA), who has been among the expert speakers to have participated in previous editions of CX Aortic Vienna and is returning in 2022. “The entire history of aortic surgery, and vascular surgery to the same extent, has been one of technical and clinical evolution.”
Coselli adds: “The Charing Cross meetings are among the best with regard to the broad spectrum of technology and clinical information and sharing among experts. I would invite everyone to take the opportunity to learn a lot about vascular and aortic surgery at CX Aortic Vienna.”
From 2023 onwards, CX Aortic Vienna will be held annually in October as a hybrid meeting in-person in Vienna whilst simultaneously livestreaming globally.
Boston Scientific has announced the acquisition of Obsidio, a privately held company that has developed the Gel Embolic Material (GEM) technology used for embolization of blood vessels in the peripheral vasculature.
Recently cleared by the US Food and Drug Administration (FDA), the GEM technology is a semi-solid, proprietary material packaged in a ready-to-use form, thus reducing the preparation time required for many embolization procedures. Physicians deliver the GEM agent through a catheter, and its gel-like composition enables controlled placement within patient anatomy. Unlike solid and liquid embolics that can take time to form an obstruction to blood flow, once placed, the GEM technology conforms to the targeted vasculature, immediately creating a barrier.
“The GEM technology combines benefits of currently available embolics, such as precise control of a solid and malleability of a liquid, to create a unique technology that offers procedural efficiency and a more personalised therapy for patients,” said Peter Pattison, president, interventional oncology and embolization, Peripheral Interventions, Boston Scientific. “This acquisition strengthens our interventional oncology and embolization portfolio with a differentiated solution for physicians and their patients suffering from haemorrhages, cancer and other debilitating conditions.”
Ramona Gupta (Northwestern University, Chicago, USA) addresses the issue of recurrent varicose veins, highlighting in particular the “multiple tools” now at physicians’ disposal to treat the problem.
Superficial venous insufficiency and varicose veins affect approximately 23% of adults worldwide. Treatments have significantly evolved from surgical ligation and stripping to less invasive endovascular ablative procedures. However, recurrent varicose veins are common with both surgical and endovascular techniques. Durability is an important long-term outcome measure. Recent studies have examined recurrences following endovenous procedures and delineated the rates of recurrence, the patterns of recurrence, and factors associated with recurrence.
Recurrence rates following endovenous ablation procedures has consistently proven lower in long-term studies when compared to ligation and stripping. Multiple studies have confirmed durable closure rates approaching 95% after five years with the thermal and non-thermal ablative technologies. Recurrent rates after ligation and stripping have been described ranging from 20–80% with incidence increasing over time.
Importantly, the recurrence patterns following endovenous ablation are significantly different from those following ligation and stripping. The REVAS (Recurrent varices after surgery) study evaluated a large cohort of patients and found that 20% of recurrences were due to saphenofemoral neovascularisation, 19% of recurrences were secondary to incorrect junctional ligation and 55% of recurrences originated from perforator reflux. Neovascularisation after endovenous ablation is rarely seen. Instead, the majority of recurrences are due to recanalisation of a segment of previously treated vein or new reflux in an accessory saphenous vein or alternate truncal pathway. Specifically, recanalisation of a previously treated great saphenous vein (GSV) or reflux in the anterior accessory great saphenous vein (AAGSV) are common causes of recurrent disease in patients.
Treating these patterns of recurrence often involves employing non-thermal techniques. Recanalised short segment GSV can be effectively treated with ultrasound-guided foam sclerotherapy (USGFS) with special attention to newly refluxing perforator veins frequently noted in the thigh. Recurrent disease with new reflux in the GSV below the knee can be treated with cyanoacrylate adhesive closure or USGFS to avoid nerve injury. The AAGSV frequently becomes superficial, tortuous and outside the sheath after only a few centimetres. Endovenous laser ablation is successful in treating to the saphenofemoral junction although tumescing outside the sheath and achieving adequate depth to prevent a skin burn can be difficult. Cyanoacrylate adhesive closure requires 10cm of straight segment to treat. USGFS is an option but has routinely demonstrated lower closure rates. The short saphenous vein is also a common culprit for disease recurrence and can be successfully treated with most of the newer technologies, thermal or non-thermal.
Factors related to varicose vein recurrence after endovenous ablation include: 1) obesity with increased abdominal pressure increasing the likelihood of venous reflux, 2) increase in the diameter of the vein to be treated and 3) treated refluxing venous segment below the knee.
While awareness of these factors is important, they rarely cause me to alter my treatment or post-treatment plan. However, I do council patients that recurrence may be more likely in these situations and I encourage vigilant use of compression in the immediate- and long-term post-treatment period.
In my practice, recognising and treating recurrent disease is an important factor in overall long-term leg health and patient satisfaction. Our practice does not routinely bring patients back at one year for follow-up ultrasound so most recurrences are noted solely due to return of symptoms or new visible varicosities. In addition, recurrences can be a significant cause of morbidity as seen in the case below.
Figure 1. Map of a patient treated with endovenous radiofrequency ablation of the GSV at an outside clinic five years prior to her presentation in Gupta’s clinic.
Figure 1 is the map of a patient who was treated with endovenous radiofrequency ablation of the GSV at an outside clinic five years prior to her presentation in my clinic. Her standing duplex ultrasound examination demonstrates several important patterns of recurrence: perforator reflux and new small saphenous vein (SSV) reflux. Moreover, she had a large non-healing wound at the medial malleolus, which had been present for six months (Figure 2).
Figure 2: Ulcer at left medial malleolus at presentation.
I treated her in a single session with endovenous laser ablation of the SSV and USGFS of the refluxing varicosities in the thigh and calf. She followed a strict regimen of compression and wound care following the procedure. At six months, the wound showed significant healing and the patient reported meaningful improvement in her swelling and heaviness (Figure 3).
Figure 3: Ulcer six months post treatment.
While recurrent varicose veins can be frustrating for the patient and the physician, rates of recurrence are low with newer techniques and patterns of recurrence are easily recognisable. Physicians have multiple tools available to treat these new refluxing veins and are able to achieve excellent clinical outcomes.
Ramona Gupta is associate professor of radiology at Northwestern University in Chicago, USA.
Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.
Jeffrey Lawson and Shawn Gage from Duke University School of Medicine’s Department of Surgery (Durham, USA) have developed the InnAVasc device, which is specifically designed to allow for safe, easy, reproduceable and durable access for dialysis treatment of patients with graft circuits.
The investigational InnAVasc device is designed to protect the graft from backwall punctures and reduce the damage associated with frequent needle sticks which occur over the lifespan of a dialysis graft. This can lead to circuit failure and shortened circuit life. “To be stuck with two needles three times a week for haemodialysis for 52 weeks, that’s 312 times a needle goes into a patient’s graft each year,” said Stephen Hohmann, vascular surgeon at Texas Vascular Associates (Dallas, USA). “So having a graft that has the ability to decrease risk potential and long-term injury is definitely something that would be a game-changer.”
“Backwall punctures and damage due to excessive needling are painful and can cause unwanted bleeding, delay or stoppage of treatment, and reduced graft durability,” said Prabir Roy-Chaudhury, professor of medicine at the Division of Nephrology and Hypertension at the University of North Carolina (Chapel Hill, USA). “I greatly appreciate how this technology is intended to be so patient-centric, addressing this important interface need, for both clinicians and home caregivers.”
“We see an array of synergies working with Gore. The company is well recognised for its advanced material capabilities. [It has a] long history of designing graft solutions […] used in dialysis access procedures today, and we are excited to collaborate on future innovations,” said InnAVasc CEO Joseph Knight.
Royal Philips today announced an important milestone in the evolving standard of care for treating patients with peripheral vascular disease: the establishment of the first-ever global consensus for the appropriate use of intravascular ultrasound (IVUS) in lower extremity arterial and venous interventions.
Published in the August 2022 issue of the Journal of the American College of Cardiology: Cardiovascular Interventions, the new consensus document from 30 global vascular experts recommends routine use of IVUS as a preferred imaging modality in all phases in many peripheral vascular disease procedures.
“The voting panellists considered a variety of clinical scenarios and based on their extensive experience, arrived at a strong consensus,” said lead author Eric A Secemsky (Beth Israel Deaconess Medical Center, Boston USA). “They recommend routine use of IVUS as a preferred imaging modality in all phases for many peripheral interventions, both diagnostic and therapeutic, as it enables such exquisite visualisation of the target vessel and lesion. Their recommendations, which withstood the rigour of peer review, can now be considered in the formulation of clinical guidelines for the diagnosis and treatment of peripheral vascular disease.”
Peripheral vascular disease affects an estimated 200 million people worldwide, including approximately 40 to 45 million Americans, according to the American Heart Association. The authors noted that minimally invasive approaches for peripheral vascular disease interventions are increasingly common, but traditional imaging techniques like angiography have limitations, including two-dimensional projections of three-dimensional vasculature, which can complicate diagnosis and intraprocedural optimisation.
“As the global leader in providing vascular solutions to physicians and the patients they serve, we especially value the rigour and independence of this cross-specialty expert consensus,” said Heather Hudnut Page, general manager and business leader for peripheral vascular image guided therapy devices at Philips. “It is exciting to know that this initiative has the potential to standardise the use of IVUS in peripheral interventions and guide clinical decisions to further improve the quality of care procedures for patients.”
Supported in part by research grants from Philips and Boston Scientific, the study was conducted and analysed independently by Smith Center for Outcomes Research, gathering a wide spectrum of vascular expert opinion to ascertain the role of intravascular imaging in contemporary clinical practice.
Delcath Systems has announced the publication of a retrospective analysis of patients who underwent a percutaneous hepatic perfusion procedure (PHP) with Chemosat at three European centres, one in the Netherlands and two in Germany, between February 2014 and December 2019. The study, published in CardioVascular Interventional Radiology (CVIR) involved 101 patients who completed a minimum of one PHP procedure for the treatment of unresectable uveal melanoma (UM) liver metastases.
The study by T. M. L. Tong, et al, included a total of 212 PHP procedures for the 101 patients included in the study. Of the 101 patients, 66 received PHP as first-line treatment and 33 had received prior therapy (status of two patients was unknown). Approximately 50% of patients had greater than nine metastases. Seventy-seven patients underwent at least two procedures and 25 patients received more than two PHP procedures. After a median follow-up time of 15 months, a complete response (CR) was reported in five (5.0%) patients; partial response (PR) in 55 (54.5%), and stable disease (SD) in 30 (29.7%), resulting in an objective response rate (ORR) of 59.4% and a disease control rate (DCR) of 89.1%.
The median progression-free survival (PFS), liver progression-free survival (LPFS), and overall survival (OS) were 9.0 months (95% CI 7.7–10.3); 11.0 months (95% CI 9.0– 13.0); and 20.0 months (95% CI 13.7–26.3), respectively. Twelve patients who were lost to follow-up were censored in the survival analyses. The study also found statistically significant differences in median PFS, median LPFS, and OS between patients who had CR, PR, or SD; and patients with progressive disease (PD). For example, for patients with CR or PR the median OS was 27 months (95% CI 17.5–36.5); for patients with SD the median OS was 21 months (95% CI 11.2–30.8); and 8 months (95% CI 5.7–10.3) for patients with PD.
Although the study did not find a statistically significant difference in either median PFS and LPFS for patients treated with two or more PHP procedures compared to patients treated with one PHP procedures, the study did find a statistically significant difference in OS (20 months vs. 8 months) for patients who had two or more PHP procedures compared to patients who were treated with one PHP procedure.
The safety analysis was conducted on the first treatment cycle (183 PHP procedures). The most common adverse events were haematological toxicities which were grade 1/2 and self-limiting in the majority of patients and consistent with previous reports on PHP. Other adverse events were thromboembolic in nature. The mortality rate was 1.1% within 30 days after PHP.
AngioDynamics recently announced that it has received US Food and Drug Administration (FDA) 510(k) clearance of an expanded indication for the Auryon atherectomy system to include arterial thrombectomy.
The FDA recently cleared the expanded indication for the Auryon system’s 2mm and 2.35mm catheters to include adjacent thrombus aspiration when treating stenoses in native and stented infrainguinal arteries. Both catheters have aspiration capabilities as atherectomy devices, including in-stent restenosis (ISR).
“AngioDynamics is pleased to have received these expanded indications for the Auryon atherectomy system,” said Scott Centea, senior vice president and general manager, Global Endovascular Therapies. “Since launching commercially in September 2020, the Auryon atherectomy system has become an essential tool for providers across the USA in the treatment of peripheral arterial disease (PAD) and related conditions. These expanded indications further validate the extensive capability and effectiveness of the Auryon technology offering our providers an advanced and efficient treatment option for PAD.”
The Auryon laser can be used to treat all infrainguinal lesion types, including above-the-knee (ATK), below-the-knee (BTK), and ISR, and to date, has been used to treat more than 21,000 patients in the USA, a company press release reports.
“Combining the 2mm and 2.35mm Auryon laser atherectomy with the aspiration capability has changed our practice. We now treat acute limb ischaemia in a single session where we remove the acute component as well as treat the underlying lesion. Patients are now discharged in less than 24 hours without the need for an ICU bed or overnight lysis,” said Carlos J Guevara (Washington University School of Medicine, St Louis, USA).
Fluidx Medical disclosed study results examining extent of vessel filling using the GPX embolic device compared to microspheres, a common treatment for many types of tumours.
“GPX is demonstrating deep distal vessel penetration,” said Ryan O’Hara, interventional oncologist at the University of Utah (Salt Lake City, USA). “The ability to fill the smallest tumour-feeding vessels and reach distal vessel beds is very important in effective treatment of hypervascular tumours and in other therapeutic embolic procedures.”
Embolizing blood supply to tumours is a high-growth procedure to block blood supply to certain tumours. Transarterial chemoembolization (TACE) includes delivering chemotherapy with embolization. Tumour embolization may also be performed prior to resection.
“GPX exhibited effective and thorough embolization throughout the renal cortical vasculature,” according to a pathology assessment conducted by study pathologist James Stanley. “GPX filled the smallest arteries/arterioles of the distal cortex which was not observed with 40-micron microspheres.”
GPX and microspheres were studied in selected small branches of renal arteries. The GPX embolic device was found to fill vessels more completely and penetrate deeper into smaller vessel beds than the smallest microspheres commonly used for tumour treatments.
“The extent of distal penetration of GPX, combined with its potential as a drug-loadable oncology solution, make this a unique technology with an exciting future in advancing cancer care,” said Danny Smith, Fluidx Medical vice president of research and development.
Selution SLR, MedAlliance’s sirolimus-eluting balloon, has received conditional US Food and Drug Administration (FDA) investigational device exemption (IDE) approval to initiate its pivotal clinical trial for the treatment of occlusive disease of the superficial femoral artery (SFA).
This comes only a few months after the company received IDE approval for Selution SLR in the treatment of below-the-knee (BTK) indications (May 2022).
Enrolment will begin in the SELUTION SLR IDE SFA study later this year. It will be conducted at over 20 centres in the USA and an additional 20 centres around the world. This study will enrol 300 patients to demonstrate superiority over balloon angioplasty (POBA). The principal investigator of this study is George Adams, the director of cardiovascular and peripheral vascular research at Rex Hospital (Raleigh, USA).
“We are very excited that US patients suffering from PAD [peripheral arterial disease] will have the opportunity to receive this novel sirolimus drug coated balloon technology. This is yet another advancement in the field of treating vascular disease and we are confident that this study will enrol quickly,” Adams commented.
“This is a significant milestone for MedAlliance: we are the first non-paclitaxel drug coated balloon to receive IDE approval, and now the first to have two applications approved. This is the culmination of a multi-year research and development programme to provide the comprehensive non-clinical data required to satisfy the very high standards expected by the US FDA,” added Jeffrey B Jump, MedAlliance chairman and chief executive officer. “We are very pleased with the rapid level of sales growth we are experiencing in Europe, Asia and South America and very much look forward to entering the US market.”
Selution SLR was awarded CE mark approval for the treatment of PAD in February 2020 and for the treatment of coronary artery disease in May 2020. The US FDA has awarded Selution SLR with four breakthrough designations: for the treatment of atherosclerotic lesions in native coronary arteries; coronary in-stent restenosis; peripheral below-the-knee and AV-fistula indications.
In August 2021, the first of over 3,000 patients was enrolled in a ground-breaking coronary randomised controlled study comparing Selution SLR with any limus drug-eluting stent [DES]. This is the largest drug-eluting balloon (DEB) study ever initiated.
MedAlliance’s DEB technology involves MicroReservoirs made from biodegradable polymer intermixed with the anti-restenotic drug sirolimus. These MicroReservoirs provide controlled and sustained release of the drug for up to 90 days. Extended release of sirolimus from stents has been proven highly efficacious in both coronary and peripheral vasculatures. MedAlliance’s proprietary CAT (Cell Adherent Technology) enables the MicroReservoirs to be coated onto balloons and adhere to the vessel lumen when delivered via an angioplasty balloon.
Shape Memory Medical announced today that its 1,500th patient has been treated, marking a significant milestone for the company’s portfolio of shape memory polymer embolotherapy devices—the Impede embolisation plug family and the TrelliX embolic coil. The patient was treated by Thomas Maldonado (NYU Grossman School of Medicine and NYU Langone Health, New York, USA).
“We were excited to perform our first case using shape memory polymer technology, and in this particular case for the occlusion of the internal iliac artery for prevention of post-EVAR [endovascular aneurysm repair] type II endoleak,” said Maldonado.
According to a company press release, shape memory polymer is a new concept in medical devices, built on 25 years of polymer research and expertise initiated at Lawrence Livermore National Laboratory (LLNL; Livermore, California) and further developed at Texas A&M University (College Station, USA). Shape memory polymer features a porous, compliant polyurethane embolic material that enables conversion to organised thrombus followed by gradual healthy tissue formation. In 2009, Shape Memory Medical was formed to develop and commercialise devices for use in the peripheral and neurovascular embolisation markets. An emerging alternative to traditional, bare metal embolisation devices, shape memory polymer is soft and conformable, and the material is radiolucent which improves visibility of the surrounding anatomy during and after the procedure.
“This milestone is especially significant for Shape Memory Medical,” said Ted Ruppel, chief executive officer. “This accomplishment is only the beginning of our plans for this emerging technology, with a product pipeline focused on the development of shape memory polymer solutions for aortic aneurysms and aortic dissection.” The company is also pursuing research and development and corporate licensing partnerships for potential applications across multiple therapeutic areas such as aortic therapies, structural heart, biopsy, and drug delivery.
Since the launch of the Impede embolisation plug family in the USA, Europe, and Japan and the TrelliX embolic coil in Europe, these novel devices have been used by vascular surgeons and interventional radiologists in over 25 countries. The growing body of evidence presented from the podium and in the literature has raised physician awareness and interest in the Impede and TrelliX devices, including data from the TrelliX APEX study and the IMPEDE EMBO postmarket surveillance study. The Impede-FX RapidFill device is also currently being evaluated in a first-in-human safety and efficacy trial for a potential new indication for abdominal aortic aneurysm (AAA) sac management during elective endovascular aneurysm repair (EVAR). “Early AAA-SHAPE results are encouraging,” said Michel Reijnen (Rijnstate Hospital, Arnhem, The Netherlands), principal investigator, AAA-SHAPE Netherlands. “Shape memory polymer technology has the potential to improve post-EVAR sac regression, reduce secondary interventions, and reduce the burden for our patients as well as for healthcare systems.” The AAA-SHAPE trial is ongoing, with one-year results expected to be announced in 2023.
Prostate conditions and their treatment proved popular reading topics during the month of July. Interventional News reported on this subject from various angles—from an award-winning abstract on prostatic artery embolization for benign prostate hyperplasia (BPH) and the US Food and Drug Administration (FDA) 510(k) clearance of a new high-flow microcatheter, to new data to support a minimally invasive procedure to treat BPH, and a US FDA investigational device exemption for high-intensity ultrasound therapy for prostate cancer.
Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) won the award of best abstract for his and co-authors’ ‘Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia’ at this year’s European Conference on Embolotherapy (ET; 22–25 June, Nice, France).
Embolx, a company developing microcatheters for arterial embolization procedures to treat cancerous tumours, benign prostatic hyperplasia, and uterine fibroids, has announced that the company has filed a 510(k) to the US FDA for its new line of high-flow microcatheters, Soldier.
Merit Medical has announced the successful enrolment of the first patient in its WRAP registry study, which will evaluate the clinical benefits associated with the use of the Wrapsody cell-impermeable endoprosthesis in patients receiving haemodialysis that experience stenosis or occlusion of blood vessels required for dialysis.
The University of Texas at Arlington (UTA; Arlington, USA) announced in June 2022 that Kytai Nguyen, a UTA bioengineering professor, had received National Institutes of Health (NIH) funding to develop a dual-capability biodegradable nanoparticle for use in treating peripheral arterial disease (PAD).
As part of the ‘Trauma and Emergencies’ session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), conference deputy chairman Otto van Delden (Amsterdam University Medical Centers, Amsterdam, The Netherlands) presented blunt abdominal trauma cases to delegates “to underscore the teaching points” that these types of clinical scenarios offer.
Ra Medical Systems has announced receipt of US FDA 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. The catheter features enhancements including a six-month shelf life.
Instylla, a company developing liquid embolics for peripheral vascular embolotherapy, recently announced two publications that evaluated the Embrace hydrogel embolic system (HES) in preclinical porcine haemorrhage models.
Teleflex has announced the results of several research studies that further support the safety and efficacy of the UroLift system for men living with enlarged prostate, benign prostatic hyperplasia (BPH), or those who have a wide range of prostate sizes and/or a median lobe obstruction.
Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US FDA clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser atherectomy catheter.
Insightec, a global healthcare company dedicated to using acoustic energy to transform patient care, announced that it has received US FDA approval for an investigational device exemption (IDE) for a clinical comparative study of the Exablate Prostate system used to treat diseased prostate tissue.
Study team at the University Hospital Münster Germany
Study team at the University Hospital Münster
Concept Medical has announced the initiation of the LIMES trial, which has enrolled 15 patients to evaluate the safety and efficacy of the company’s Magic Touch sirolimus-coated percutaneous transluminal angioplasty (PTA) balloon for the treatment of peripheral arterial disease (PAD).
A Concept Medical press release elaborates that LIMES is a prospective, multicentre, randomised controlled trial (RCT) that is designed and aimed to evaluate the Magic Touch balloon 0.014” and 0.018” versus standard angioplasty in a head-to-head comparison (1:1).
Initiated by the University Hospitals Jena and Leipzig in Germany and led by principal investigator (PI) Ulf Teichgräber (Jena University Hospital, Jena, Germany) alongside co-PI Thomas Zeller (University Heart Center Freiburg-Bad Krozingen, Bad Krozingen, Germany) and Dierk Scheinert (University Hospital Leipzig, Leipzig, Germany), the trial kicked off with the index patient enrolled on 31March 2022 by Nassan Malyar at the University Hospital Münster in Münster, Germany.
LIMES RCT is set to enrol 230 patients in 19 centres across Germany and Austria. The patient population will include patients presenting with documented chronic limb-threatening ischaemia (CLTI) in the target limb defined as Rutherford clinical category 4, 5 or 6 aged ≥18 years. The study evaluates patients with a reference vessel diameter (RVD) ≥2 and ≤4mm and total occlusions (100% stenosis) of the target lesion. There is no minimal lesion length required, no lesion length limitation and no limitation in number of used devices. Follow-up will be per in-house visits at 30 days, six, 12, 24 and 36 months.
The RCT will measure the efficacy of sirolimus-coated balloons in a complex setting (CLTI) of the PAD segment (located below the P3 segment of the popliteal artery to the tibiotalar joint) against the current standard of care. The study’s primary endpoints are the composite of limb salvage and primary patency through six months. The key secondary safety endpoint is the composite of major adverse limb events and perioperative death at 30 days. A blinded core lab will assess patency at six, 12 and 24 months by duplex ultrasound and quantitative vascular angiography in case of any target lesion revascularisation.
In the press release, Teichgräber commented on why the RCT is valuable in terms of DCB intervention in infrapopliteal occlusions: “BTK [below-the-knee] revascularisation deals with the most challenging vascular territory in very sick patients. LIMES will solve the question if sirolimus balloon angioplasty has the potential to become the future standard of care in BTK interventions.”
Mark Little (Royal Berkshire NHS Foundation Trust, Reading, UK) described the emergence of, and advancement within, musculoskeletal (MSK) embolotherapy as “fast-paced” during his presentation on the trends and developments in the field, delivered at this year’s European Conference on Embolotherapy (22–25 June, Nice, France). Featuring in the meeting’s Joints session, the presentation’s take-home message was that the “signs are encouraging” when it comes to MSK embolotherapy’s integration into more mainstream practice.
Among the opening statements from Little was the “[importance of discussing] agents”—“different territories need different embolic agents,” he informed delegates. For osteoarthritis of the hand or tendinopathy in the foot, “you would not want a permanent embolic”, which is where the “antiquated” antibiotic imipenem, in combination with cilastatin, comes in. It acts as a temporary embolic agent, Little explained, and it has “rapidly emerging potential.”
For example, for plantar fasciitis, which is “really difficult to treat” and “extremely painful”, imipenem/cilastatin (I/C) can be injected into the posterior tibial artery, resulting in reduced pain and plantar fascia thickness. Sports medicine, Little went on, is “a real growth area” for MSK embolotherapy, as hyperaemia that cannot be treated conservatively may be resolved with agents such as I/C. However, a current limitation, Little acknowledged is the fact that I/C is not approved for embolotherapy in many countries, and the UK and USA are not among those where approval is granted.
Nevertheless, Little conveyed the significance of the fact that MSK embolotherapy has the potential to treat “a breadth of conditions,” listing tennis elbow, for which surgical options are limited, and adhesive capsulitis, which is increasingly prevalent as a result of the increasing prevalence of diabetes.
Little then turned to his area of specialism—genicular artery embolization (GAE)—which has the “largest evidence base to date” of all MSK embolotherapies. “We have done a lot of work looking at GAE and how we can refine the treatment,” he supplemented.
By way of example, Little referred to imaging from one of his own cases—medial compartment knee osteoarthritis, which “[showed] a large area of abnormal synovitis.” The approach for this patient was to cannulate the superior medial genicular artery, Little detailed, but, crucially, “to maintain the normal in-flow vessel.”
This is “very different” to the endpoint for prostate arterial embolization—”we are not wanting to completely block the in-flow vessel”, the result of which could be necrosis. Instead, Little “[prunes] the area of abnormality while maintaining normal osseus blood flow.”
To further illustrate the potential of MSK embolotherapy, Little referenced a small study of I/C to treat chronic lower back pain that had not been responsive to conservative therapy. However, given the size of the cohort, “we still have a lot more work to do”, he admitted.
Moving on the address the scientific rationale for MSK embolotherapy, Little described how the conditions are “underpinned by [an] area of hyperaemia.” New abnormal blood vessel formation “results in the release of cytokines” followed by “[hypersensitisation] of the nerves” and “pain”.
Next on the agenda for Little was to outline how “new” pain as a symptom to treat actually is within interventional radiology (IR)—typically, the means of assessing pain-related outcomes of treatment has been limited to the visual analogue scale. But, “what if your pain goes from a 10 to a 5?” Little asked rhetorically, “what does that mean in patients’ daily lives?” This is where minimally clinical important difference as a measure of pain outcome has a role to play—except that what that looks like for GAE is, “right now, anybody’s best guess.” Hence, this should be an area of focus in the field, Little advised. An “interesting area of future research” will be “the interplay between the brain and the knee”, as “how patients view pain impacts their progress,” Little then asserted.
The presenter summarised the scope for MSK embolotherapy’s more widespread use as “encouraging”. Recent National Institute for Health and Care Excellence (NICE) guidelines want evidence for its effectiveness, Little shared, in the form of “randomised controlled trials [RCTs] against sham procedure or best current practice,” with more patient-reported outcomes. GENESIS 2—an RCT against sham procedure—is, therefore, a study to watch. Little sees longer-term data and multicentre studies following on from this.
Fielding questions from the audience following the presentation, Little responded to an enquiry into whether use of antibiotics as temporary embolic agents could lead to patients developing resistance. “A good question—I have no idea”, Little admitted, going on to say “one would intuitively think, yes.” He then acknowledged that the main issue with antibiotics for this indication is the “East/West divide”—“we [in the UK] are very much limited”, as a result of the temporary agent I/C’s lack of availability.
A follow-up question on his preferred embolic material saw Little state that the MSK community is “crying out for imipenem” and all of its “mystical, magical properties” when it comes to treating hands and feet. For knees, he continued, “there is good data for permanent embolics”.
2Fr XO Cross 14 microcatheter shown with a 0.014” guidewire
2Fr XO Cross 14 microcatheter shown with a 0.014” guidewire
Transit Scientific has reported multiple successful peripheral vascular procedures with the XO Cross catheter platform utilising pedal retrograde access.
The non-tapered 2Fr XO Cross 14 microcatheter in 90cm, 135cm, and 175cm lengths is designed to facilitate guidewire support, guidewire exchange, and contrast media injection during complex peripheral vascular interventions.
“2Fr 014 catheter-guidewire systems are an important tool for pedal and below-the-knee interventions,” said George Adams (UNC REX Healthcare, Raleigh, USA). “The XO Cross incorporates a non-tapered torquable shaft design which supports a smaller and less invasive access site from below. Tools like these can help broaden options for approaches and access techniques in CLTI [chronic limb-threatening ischaemia] patients.”
According to a Transit Scientific, the XO Cross catheter platform introduces new levels of pushability, trackability, flexibility, and torque response to access challenging lesions and complex anatomy. XO Cross’s non-tapered, metal-alloy and polymer construction delivers high fatigue resistance against tough lesions found in late-stage peripheral arterial disease (PAD) and CLTI, the company claims.
Richard Saxon (Tri-City Medical Center, Oceanside, USA) shared: “A patient presented with trifurcation disease and severe calcifications in the superficial femoral artery (SFA), popliteal, and the posterior tibial artery. The low-profile and pushability of the XO Cross 14 enabled pedal retrograde access following failed crossing and wire from above. A second XO Cross 14 (135cm) was used from above to support a flossing technique and subsequent angioplasty treatment. The unique non-tapered design of the XO Cross lends itself well to challenging limb salvage procedures that often require multiple access sites and different approaches to achieve a good outcome.”
Transit Scientific’s XO Cross platform features 24 US Food and Drug Administration (FDA)-cleared devices including 2Fr XO Cross 14 microcaths, 2.6Fr XO Cross 18 microcaths, and the 3.8Fr XO Cross 35 support catheters for use with standard 0.014”, 0.018”, and 0.035” guidewires in 90cm, 135cm, 150cm, and 175cm lengths.
A database study titled ‘Unplanned 30-day readmissions and in-hospital outcomes for the management of submassive and massive acute pulmonary embolism: Catheter-directed versus systemic thrombolysis’ has produced results that could provide some of the evidence base for preference of catheter-directed over systemic thrombolysis in treating the more severe cases of pulmonary embolism (PE).
Osman Ahmed, who is author of the study and associate professor of radiology at the University of Chicago (Chicago, USA), met with Interventional News at the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11–16 June, Boston, USA) to discuss his research. The abstract was also presented by Waseem Wahood (Dr Kiran C Patel School of Allopathic Medicine, Fort Lauderdale, USA) during the meeting’s pulmonary embolism session.
Ahmed began by outlining his clinical background and what led him to pursue this research on PE treatment. Clinically, he explained, one of his main interests is venous thromboembolism, but being the co-chair of the SIR Comparative Effectiveness Research Committee—an arm of the society whose goal is to develop “evidence-based data to compare interventional radiology [IR] services and procedures with their medical and surgical alternatives”—he wanted also to incorporate this area of focus into a study.
The first question posed to Ahmed was regarding the existing PE treatment landscape and what determines whether a given patient will receive catheter-directed or systemic thrombolysis. Ahmed dubbed this “a great question” to which the answer lies in the fact that “PE in general is a heterogenous disease, with different levels of severity”—massive, submassive and low-risk. “Fortunately,” he continued, “most patients are low risk”. Expanding on this, Ahmed specified how it is the massive and submassive patients who “require hospitalisation and often follow-up intervention,” which is, “where IR comes into play.”
One of the key advantages of the catheter-based approach is that it is minimally invasive, Ahmed pointed out, however, “most society guidelines [for PE treatment] outside of IR […] do not recommend what we do.” Ahmed asserted his nonetheless widely shared belief that catheter-based thrombolysis is “safe.” Studies carried out before his, while smaller, showed “a similar rate of effectiveness” between catheter-based and systemic treatments, but the former saw “lower rates of bleeding.” Ahmed referred to this existing, promising evidence as motivation for doing his database study.
Asked then why he choose to approach the study from the angle of side effects, Ahmed offered by way of explanation the “very high chance of recurrence” with PE. “If you survive [the rate can be between] 30 and 40%”. Furthermore, Ahmed underlined, the nature of the treatment means that “if you give too much of the [PE] medication, the risk of bleeding is high, but too little and you do not clear the PE.”
Bleeding was “a big problem” in the patients from the database who had received systemic over catheter-based treatment, which often resulted in rehospitalisation—problematic in that it depletes resources and beds for patients with other conditions, Ahmed highlighted.
Moving on to discuss the results of his study—whether or not they were as expected—Ahmed conveyed how he had been surprised by how they were “very, very consistent with what we thought”. This was the case for “every metric [and even with] propensity matching.” Ultimately, rates of intra-abdominal and intracranial bleeding, as well as hospital readmissions were “all one to two times higher with systemic thrombolysis.” Ahmed acknowledged that it was an outcome that “almost felt too good to be true,” especially since the patients at higher risk of bleeding are often those who receive catheter-directed treatment. “If we were going to see no difference,” Ahmed admitted, he would have expected it to be as a consequence of the sickest patients receiving this less evidence-based treatment.
Finally, conversation turned to next steps regarding the picture of PE treatment and research in the future. “Trials […] take a lot of time and cost a lot of money,” Ahmed emphasised, which, in turn, accentuates “the beauty” of his study, conducted with a 36,000-strong patient base. “We really need [more] trials,” Ahmed affirmed, expressing his hope that the promising results his research has yielded will “pave the way” for increased government funding assigned to future PE research.
Yet, of note, is the fact that even without these prospective trials and the inclusion of catheter-directed thrombolysis in the majority of PE treatment guidelines, there has been, of late, a “tenfold increase” in the recourse to catheter-directed treatment. Ahmed ended on the following note—”We are hoping that [our study] helps provide the framework” to include catheter-directed thrombolysis in guidelines more widely.
Biotronik recently announced that it has received US Food and Drug Administration (FDA) approval of its Pulsar-18 T3 peripheral self-expanding stent system. Full US commercial launch of the device, which will begin in early August, according to the company.
Biotronik states that the Pulsar-18 T3 stent system uniquely combines three technologies. A 4 French low-profile delivery system may decrease the risk of access site complications and reduce the need for closure devices when compared to 6 French devices, the company claims. It adds that the triaxial system with braided shaft design facilitates stable and accurate implantation of the clinically proven Pulsar stent and, with its thin struts and low chronic outward force (COF), the Pulsar-18 stent contributes to a reduced mean area of restenosis.
The redesigned Pulsar-18 T3 stent system offers physicians an “intuitive and ergonomic” wheel-operated handle for one-handed stent release enhancing the ability to control deployment, according to Biotronik.
“I was immediately impressed by the new concept of the Pulsar-18 T3 system,” said Koen Deloose (AZ Sint Blasius Hospital, Dendermonde, Belgium). “The combination of having a very ergonomic handle combined with a triaxial system and also everything in a 4 French concept was, for me, quite unique.”
“The Pulsar-18 T3 stent system is an innovative solution that delivers clinically proven performance—providing effective therapy that is easy to use for physicians while minimizing metal burden and may reduce the risk of restenosis for patients,” stated David Hayes, chief medical officer, Biotronik.
Biotronik will offer the Pulsar-18 T3 in up to a 200mm stent length for treatment of long lesions, the company advises.
Biotronik details that the Pulsar-18 T3 stent system is indicated for use to improve luminal diameter in patients with symptomatic de novo, restenotic or occlusive lesions located in the superficial femoral or proximal popliteal arteries, with reference vessel diameters from 3–6mm and total lesion lengths up to 190 mm.
Instylla, a company developing liquid embolics for peripheral vascular embolotherapy, recently announced two publications that evaluated the Embrace hydrogel embolic system (HES) in preclinical porcine haemorrhage models.
In a Journal of Vascular and Interventional Radiology (JVIR)publication, Gandras et al evaluated the ability of Embrace HES to achieve haemostasis in a porcine mesenteric artery haemorrhage model that replicates injury in humans. Results demonstrated that Embrace HES achieved complete, rapid, and durable embolization in 100% of the injured arteries with a mean delivery time of 5.3 minutes. There was no angiographic evidence of non-target embolization.
“Embrace was effective in achieving haemostasis in an animal haemorrhage model without evidence of non-target embolization. This next generation liquid embolic has tremendous potential to play an important therapeutic role in a wide variety of clinical applications including haemorrhage and interventional oncology,” commented Eric Gandras, associate chief of vascular and interventional radiology at North Shore University Hospital, (Manhasset, USA) and lead author of the study.
In an independent study conducted by Kauvar et al, splenic injury and resulting haemorrhage were induced in swine models. A comparison was made between a control group having no embolic treatment to treatment groups that received embolization with Embrace HES, gel foam slurry, or coils. Under coagulopathic conditions, Embrace HES showed improved survival time and a significant reduction in bleeding compared to the control group, gel foam slurry, and coil treatments.
Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US Food and Drug Administration (FDA) clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser atherectomy catheter.
This is the first time the FDA has awarded a 510(k) clearance for reprocessing this type of atherectomy catheter.
The device is used to treat peripheral arterial disease (PAD) and emits high-energy ultraviolet light to vaporise blockages inside the vessels.
Chief executive officer and and founder Craig Allmendinger discussed what this means to the company, saying, “It is validating to receive this clearance from the FDA after all the work our team undertook to meet the standards of earning a 510(k). The team at the FDA pushed us hard, and rightfully so, to prove that our methods and processes created an equivalent device to the original after reprocessing.”
He went on to say, “There is no doubt now that what we are doing is helping redefine the medical device landscape as we add another device type to our reprocessing portfolio. As we continue to expand our device types and reach, we look to further help the office-based lab physician and never compromise on patient safety.”
The company has said that it will have an additional announcement soon regarding when the 0.9mm over-the-wire Turbo-Elite laser atherectomy catheter device will be available for sale.
ReCor Medical and Otsuka Medical Devices have announced that the RADIANCE II US Food and Drug Administration (FDA) investigational device exemption (IDE) pivotal trial evaluating the Paradise ultrasound renal denervation (uRDN) system as a treatment for hypertension met its primary efficacy endpoint, demonstrating a statistically significant reduction in daytime ambulatory systolic blood pressure between treatment and a sham procedure measured at two months.
The RADIANCE II US FDA IDE pivotal trial is a randomised, sham-controlled clinical trial of the ReCor Paradise uRDN System for the treatment of patients with uncontrolled hypertension. 224 patients with mild-to-moderate uncontrolled hypertension, previously treated with up to two medications, were randomised while off medications at more than 60 study centres in eight countries.
“Despite the truly formidable challenges of conducting a complex clinical trial in the throes of the COVID-19 pandemic, we are thrilled to observe these positive results of RADIANCE II, especially in light of those we have previously reported from RADIANCE-HTN SOLO and TRIO,” said study principal investigators Ajay Kirtane (Columbia University, New York, USA) and Michel Azizi (Hôpital Européen Georges Pompidou, Paris, France). “We cannot adequately convey our thanks to the patients, coordinators, and study physicians for their collective efforts, and we very much look forward to being able to present and publish the complete study details in the near future.”
“We at Otsuka are very pleased with the positive outcome of the RADIANCE II study,” said Kazumichi Kobayashi, executive deputy president of Otsuka Medical Devices. “With three successful clinical trials of the Paradise uRDN system, we believe even more strongly that the Paradise system can become an important treatment option for patients and physicians struggling to control blood pressure.”
“ReCor is thrilled that the RADIANCE II trial met its primary efficacy endpoint. Following the positive SOLO and TRIO clinical trials, RADIANCE II adds to the evidence for the Paradise system as a potential future treatment for patients with uncontrolled hypertension,” said ReCor president and CEO, Andrew M Weiss. “We would like to express our gratitude to the principal investigators, steering committee and all investigators for their efforts throughout this important trial.”
RADIANCE II is the third and largest component of ReCor’s RADIANCE Global Program—randomised and sham-controlled studies evaluating the Paradise uRDN System in patients with hypertension. The first two studies in the series are the previously reported RADIANCE-HTN SOLO (conducted in patients with mild-to-moderate hypertension) and TRIO (conducted in those who remained hypertensive despite being on antihypertensive therapy). Both studies met their primary effectiveness endpoints.
About 6.5 million Americans over the age of 40 suffer from peripheral arterial disease (PAD). In the USA, Black adults in their 50s are at least twice as likely to suffer from PAD as their white counterparts, a disparity that continues to increase with age.
In a new paper published in Circulation, researchers at the Richard A and Susan F Smith Center for Outcomes Research in Cardiology at Beth Israel Deaconess Medical Center (BIDMC; Boston, USA) conducted a large, nationwide analysis of Medicare beneficiaries to document racial differences in revascularisation treatment for PAD, and outcomes for patients with PAD. The team found that Black adults underwent significantly more endovascular peripheral vascular interventions (PVI), were treated for more advanced disease and were also more likely to experience adverse outcomes following PVI procedures, including amputation and death.
“Black race was significantly associated with worse one-year outcomes after revascularisations, after adjusting for age and sex,” said senior corresponding author Eric Secemsky, director of Vascular Intervention at BIDMC, as well as section head of Interventional Cardiology and Vascular Research at the Smith Center for Outcomes Research at BIDMC. “This link persisted after we adjusted for individual and regional socioeconomic factors. However, the association between Black race and worse outcomes was no longer apparent after we adjusted for comorbidities, suggesting that the well documented Black-white disparities in the prevalence of PAD risk factors, including hypertension, diabetes and end-stage renal disease, explain the disproportionate development of PAD among Black adults.”
The analysis included 215,320 patients who underwent the gold-standard revascularisation procedure—PVI—between 2016 and 2018. Black adults had a higher incidence of treatment, with 0.86 percent of Black Medicare beneficiaries undergoing the procedure, compared to 0.51 percent of white Medicare beneficiaries. What is more, a greater proportion of Black adults were treated for more severe arterial disease, while more white patients were treated for a milder form of PAD. Despite their relatively greater severity of disease, a lower percentage of Black adults were prescribed key cardiovascular medications.
“Structural racism perpetuates these health disparities,” said Secemsky, who is also an associate professor of Medicine at Harvard Medical School (Boston, USA). “One important way in which these systemic and structural factors lead to worse outcomes in Black patients is through comorbidities. This suggests a critical need for targeted, upstream intervention to reduce the disproportionate burden of PAD in the Black population.”
Co-authors included Sahana Natesan, Rishi K Wadhera, Siyan Chen, Yang Song, and Robert W Yeh of the Smith Center at BIDMC; Michael R Jaff of Harvard Medical School; and Jay Giri and Howard Julien of the Perelman School of Medicine, University of Pennsylvania (Philadelphia, USA).
Monica Webb Hooper, deputy director of the National Institute on Minority Health and Health Disparities (Bethesda, USA) works to help reduce healthcare disparities and improve minority health. Among the subjects of her presentation at the second plenary of the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11—16 June, Boston, USA) was the “relationship between racial discrimination and health,” of which a key takeaway was that there is “well documented evidence [that] racism worsens health,” and that therefore it is incumbent upon healthcare professionals to take steps to redress the imbalance.
Webb Hooper began her talk by clarifying that “characteristic differences between population groups, [such as sickle cell disease and colour blindness]” are not the same as health disparities. In contrast to the former, which are determined by genes or biology, the latter result from “disadvantage at multiple levels”. However, the nature of these “systemic obstacles” that racial minority groups face is such that they are “modifiable, by definition.”
Listing some “considerable” disparities when it comes to racial and ethnic minority health, Webb Hooper included overall shorter life expectancy, infant mortality, cardiovascular disease, lung cancer, sexually transmitted infections, mental health difficulties, dental ill-health and COVID-19. Webb Hooper then delved into the reasons why this is the case, beginning by highlighting how Black or African American, American Indian or Alaska Native, and Hispanic or Latino populations are all less likely to be diagnosed early with lung cancer. Consequently, they receive less treatment. Underpinning these inequities, Webb Hooper posited, it is “the assumption” among physicians and scientists “that genetics are responsible” for health issues among these groups, based on which may be less motivation and perceived necessity to intervene medically.
“Race is a sociocultural construct that has varied over time,” Webb Hooper then relayed, but that what has been constant is the “discrimination and chronic stress” to which racial and ethnic minority groups have been subjected. This is why, she noted, it is important to understand “what happens outside the body and how it affects what is going on inside the body.” A further key message for delegates was that “population differences are not the same as health disparities,” and it is believing that they are that hampers “further investigation” into the causes of these health disparities.
Conveying the degree to which racial and ethnic minority groups receive inferior care as a result of ill-founded beliefs around race and health, Webb Hooper asserts that “irrespective of socioeconomic status, [these groups] are more likely to be denied pain medication and opportunities to take part in clinical trials.”
Webb Hooper then took time to reiterate how we must accept the following commonly held belief as flawed: that health disparities either stem from biology, and therefore are not modifiable, or they have cultural underpinnings, and thus the onus lies with the members of said culture to change. There are “clear indicators” of the effects of personal, institutional and structural racism on health, which cannot be ascribed to biological nor cultural factors.
Webb Hooper then discussed the longstanding need to increase the representation among members of racial and ethnic minority groups in clinical trials. Webb Hooper’s first recommendation for how to achieve this is to “focus on setting standards for inclusion a priori.” This may mean making adjustments to inclusion criteria so as to include a sample of racial and ethnic minority individuals that reflects the wider population—this is 19% Hispanic or Latino in the USA, Webb Hooper offered by way of example.
The second recommendation she gave was to “focus on individuals’ motivations for participating in a clinical trial,” and once identified, turn those motivations into active participation. Thirdly, it is necessary to “address the reasons for low participation” among racial and ethnic minority groups. “Research teams must be willing to change their enrolment process,” she averred, suggesting that to inform this, community groups are consulted to gain on-the-ground insight into current attitudes around clinical trials. It is a case of asking more racial and ethnic minority patients to participate and recognising that they are just as willing to, Webb Hooper underlined.
Labelling these groups as “hard to reach” is an excuse, Webb Hooper concluded.
As part of the ‘Trauma and Emergencies’ session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), conference deputy chairman Otto van Delden (Amsterdam University Medical Centers, Amsterdam, The Netherlands) presented blunt abdominal trauma cases to delegates “to underscore the teaching points” that these types of clinical scenarios offer. In the course of his presentation, he addressed key questions an interventional radiologist (IR) may have regarding the treatment of blunt abdominal trauma, including “which embolic agent and technique [you should] choose for the most frequently encountered injuries.”
A noteworthy feature of this session overall was audience interaction; with each case presented, the speaker posed the question of whether to embolize and, if so, which agent to use, to the floor, before commenting on how closely the consensus from the room aligned with their preferences and choice in the real-life scenario about which they were speaking. Van Delden’s presentation gave him opportunity to convey his feeling that “blush” on a computed tomography (CT) image—indicative of vascular injury—is not a solely sufficient reason for embolizing, but that when it does not “resolve itself”, and the IR has also taken into account “age, coagulopathy and fragility”, it can be a good approach.
In both the cases van Delden put to the audience, opinion was split down the middle on whether or not to embolize, highlighting the multifaceted decision-making involved in intervening in these trauma situations. Van Delden summarised for the audience that, if they themselves are faced with the question of whether or not to embolize, the factors to consider are the extent of organ injury, haemoperitoneum, and vascular lesions, which can be seen on CT. Expanding on this, van Delden listed some of the vascular lesions, in the presence of which, embolization may be indicated: active extravasation outside or within the organ, and false aneurysm. If high-grade organ injury or enlarging haemoperitoneum show on a CT scan, then these are “predictors” of an embolization, van Delden also noted.
Coils were the most popular means of embolization among audience members for the cases van Delden presented, with 71% of the vote for the splenic injury case, which was one of those detailed by the presenter. Although coils may be a favoured choice, “you need to choose the size carefully,” van Delden cautioned, as it is essential not to occlude too much vessel, nor to have the coil move within it.
Then addressing the question of proximal or distal embolization, van Delden acknowledged that “there is no consensus” on which is best, and that it can be down to IRs’ preferences as individuals and “multiple different variables.”
“Tortuosity of vessels” and “time pressure” also come into embolization-related decisions, the presenter added, reinforcing his earlier point that embolization for trauma can divide opinion and resist consensus. “Although coils are the mainstay for treating liver injury,” a little over the majority of voting delegates would have chosen a gelfoam agent in the instance shown on screen by Van Delden, who conceded that depending on coagulopathy, a non-coil embolization may be more suitable.
The University of Texas at Arlington (UTA; Arlington, USA) announced in June 2022 that Kytai Nguyen, a UTA bioengineering professor, had received National Institutes of Health (NIH) funding to develop a dual-capability biodegradable nanoparticle for use in treating peripheral arterial disease (PAD).
The US$2.1 million grant will allow Nguyen, in collaboration with Jian Yang, a Penn State University (University Park Pennsylvania, USA) bioengineering professor, and Ralph Mason, a professor of radiology at UT Southwestern (Dallas, USA), to investigate the potential applications of a drug-delivering, fluorescent polymer. Nguyen discussed her project with Interventional News, shedding light on key aspects of this research.
Nguyen opened the conversation by recounting the emergence of nanotechnology: “I began working at UTA in 2005,” she relayed, “and at this time, nanotechnology was still new. I was interested in whether I could apply [a] nanoparticle as a drug carrier and an imaging agent.”
It was not in the PAD space that Nguyen initiated her research, however. She explained that “at first, we worked with cancer, and cardiovascular and lung disease.” The motivation for entering into this area of research stemmed from the fact that drug delivery to treat these conditions often results in side-effects for patients, she outlined. “When you deliver a drug, it will go all over the body […] Many drugs are effective, but toxic to the body.” This is where nanoparticles come in, she proceeded to detail, as they can be more specifically targeted within the body. In turn, this has “the potential to reduce side-effects.” This would amount to an improvement on existing treatments for PAD, as, like those for cancer, and cardiovascular and lung disease, drugs, as they are delivered currently, cannot always be targeted with desirable accuracy.
Then probed about the dual capabilities of both drug delivery and imaging compatibility, Nguyen shared how the polymer she is researching is naturally fluorescent. This means, she expanded, that “we can use multiple imaging modalities,” of which ultrasound is one, to determine “the location and quantity of the particle delivered.” This speaks to the shortcomings of current drug delivery methods, which lie in the fact they cannot be as easily localised. With the drug “encapsulated” inside the very polymer that facilitates precise imaging, there is no need for a separate “toxic quantum dye” in addition to the drug, to highlight where in the body the drug has travelled. “We can chase this polymer [over time],” Nguyen summarised. For PAD specifically “we want to focus on the muscle and where [within it] the nanoparticle ends up.”
Next on the discussion agenda was the significance of the polymer’s biodegradability: “We want [it to be] biodegradable so it will leave the body and not accumulate,” Nguyen stated. It is crucial, she went on, to be able to re-administer the drug “many times” when treating PAD, but drug carriers, some of which contain metals, can become toxic to the body in the long term. Her nanoparticle, however, can be “cleared by the body,” while allowing the drug it contains to act where it is targeted.
Nguyen ended by casting her mind forward to the next five years, and the milestones that await them in this project. As far as the here and now is concerned, research is at the in vitro study stage, Nguyen elucidated, underlining that “much more work” will be necessary before they can test on humans. “We are testing on mice […but] hopefully, if everything is successful, we will move on to larger animals.” Clinical trials are likely to be at least five years away, Nguyen advised.
Embolx, a medical device company developing microcatheters for arterial embolization procedures to treat cancerous tumours, benign prostatic hyperplasia, and uterine fibroids, has announced that the company has filed a 510(k) to the US Food and Drug Administration (FDA) for its new line of high-flow microcatheters, Soldier. It uses the same ultra-thin wall (UTW) technology initially developed for its flagship product Sniper.
UTW technology allows microcatheters to be smaller in outer diameter yet maintain the largest possible internal lumens. UTW, in combination with Soldier’s unique design, enables it to display best-in-class tracking, torquing, and flow rates. Currently available in Europe, Soldier’s arrival on the US market is expected to shift the paradigm and set a new standard for both high-flow microcatheters and micro-microcatheters.
“Soldier is a superior microcatheter by all measures of performance,” said Michael Allen, president, and chief executive officer of Embolx.”Using our proprietary and patented technology we are expanding our best-in-class catheter products for use in the peripheral vasculature and neurovasculature.”
The Soldier microcatheter will be available in 2.0Fr and 2.5Fr and will come in three lengths—130cm, 155cm, and 165cm. The 2.0Fr offers an 0.022″ lumen and the 2.5Fr offers an 0.027″ lumen.
The addition of the Soldier product line will expand the use of Embolx products for all types of embolization, immunotherapy, and drug-delivery procedures.
Subtle Medical, a key provider of artificial intelligence (AI) solutions for medical imaging, and Siemens Healthineers have officially announced the integration of Subtle Medical’s SubtleMR image-enhancement software into the new reconstruction pipeline of Siemens Healthineers, Open Recon. The launch was communicated in a Subtle Medical press release.
SubtleMR offers deep learning post-processing for denoising and increased sharpness on faster magnetic resonance imaging (MRI) sequences, enabling improved image quality, optimised workflow, and a better patient experience.
SubtleMR will be available on Siemens Magnetom Sola, Solafit, and Altea scanners with NX VA51. The software works with major contrasts, including T1, T2, T2 FLAIR, T2 (2D, 3D) and is compatible with the majority of MRI procedures. It is compatible with all downstream quantitative and diagnostic applications.
The Open Recon interface of Siemens Healthineers is designed to enable third-party image reconstruction and post-processing solutions to be directly integrated in the reconstruction pipeline. This way, no additional image export step is necessary, and the results are directly available on the scanner console. The reconstruction including post-processing with SubtleMR is now selectable in the user interface.
“We are proud to become the first AI technology company Siemens Healthineers has entrusted with their innovative new Open Recon interface,” said Ajit Shankaranarayanan, Chief Product Officer at Subtle Medical. “This milestone marks how powerful collaborations are between AI innovators and scanner manufacturers in order to provide the most robust imaging solutions to providers and the best care possible to patients worldwide.”
Subtle Medical’s suite of clinically validated AI-powered software solutions, SubtleMR and SubtlePET, increase the efficiency of image capture by improving the quality of both accelerated and low-dose imaging. Subtle’s solutions are compatible with all scanner models and field strengths.
Cordis has announced the start of the RADIANCY premarket clinical study in Europe.
A press release details that RADIANCY is a prospective, multicentre, single-arm study to assess the safety and efficacy of the S.M.A.R.T. Radianz vascular stent system intended for treatment of lesions in the iliac, superficial femoral, or proximal popliteal arteries via radial artery access through 30-day follow up.
The first procedure was performed by Mercedes Guerra (University Hospital of Guadalajara, Guadalajara, Spain) using the Brite Tip Radianz guiding sheath and Saberx Radianz percutaneous transluminal angioplasty (PTA) balloon catheter to facilitate delivery of the S.M.A.R.T Radianz self-expanding stent in an iliac lesion.
Upon completion of the procedure, Guerra said: “My colleagues and I are pleased to have the opportunity to perform the first case in this significant clinical study. We applaud Cordis for pursuing the technological innovation to meet the need for radial access solutions in lower extremity interventions. We look forward to contributing our findings to the global endovascular community as part of the RADIANCY clinical study.”
The RADIANCY study, led by principal investigator Raphaël Coscas (Ambroise Paré Hospital, Boulogne-Billancourt, France), is planned to enrol 159 patients at approximately 15 sites across seven European countries. “The RADIANCY study initiation marks a new course for the future management of patients with peripheral arterial disease (PAD) by expanding their treatment options from current conventional femoral to radial access,” Coscas said.
Coscas also highlighted the era of practice evolution in this space: “As the gold-standard approach in coronary interventions, radial is in its exciting inception phase for PAD and offers unequivocal patient-centric advantages in terms of early mobility and comfort, critical in both in-patient and out-patient practice settings.”
The S.M.A.R.T. Radianz vascular stent system, specifically engineered for radial access, was approved by the US Food and Drug Administration (FDA) earlier this year, and successful first-in-human procedures were performed in June 2022 by Jihad Mustapha (Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, USA).
George Adams, Cordis chief medical officer, said: “Cordis is committed to developing tools to treat complex PAD patients. Understanding the real-world, 10-year S.M.A.R.T. vascular stent system data combined with the innovation of a radial approach allows the interventionalist to treat PAD safely, efficaciously, and cost effectively. Mirroring this innovation with research and a strong educational program to advance the field is truly at Cordis’ core.”
SoniVie today announced that on 30 May this year the first patient was treated with its renal artery denervation Tivus therapeutic intravascular ultrasound technology,as part of the recently US Food and Drug Administration (FDA) investigational device exemption (IDE)-approved REDUCED1 pilot study to treat hypertension.
A company press release details that the procedure was successfully performed with Tivus at the Kaplan Medical Center (Rehovot, Israel) by Michael Jonas, principal investigator of the REDUCED1 study.
Jonas commented: “We were able to use the Tivus catheter to rapidly and efficiently perform ultrasound-based renal denervation in our patient suffering from uncontrolled hypertention. The Tivus catheter’s excellent ease of use and its ability to denervate at significant depth of the perivascular space allowed for a short, simple and straightforward procedure. We will closely follow our patient and look forward to continuing enrolment in this exciting trial.”
Renal denervation with Tivus is a minimally invasive procedure that uses high-frequency non-focused ultrasound energy to ablate nerves in the renal artery, SoniVie advises in the press release. This causes a reduction in the nerve activity, which may decrease blood pressure. The procedure is designed for patients who suffer from resistant hypertension.
“Millions of people worldwide suffer from resistant hypertension which substantially increases the risk of heart attack, stroke and kidney failure. We are genuinely happy for this important step forward. There is a lack of effective therapeutic solutions for these patients” says Christian Spaulding, CMO, SoniVie.
“This procedure represents a great fulfilment for SoniVie team, whose expertise and achievements have been focusing on developing Tivus technology for the renal denervation indication, both providing a promising treatment to the hypertensive patient and a high performing, easy to use device to the physician”, says Tomaso Zambelli, CEO, SoniVie.
A prospective, multicentre study involving the Covera vascular covered stent (BD) has confirmed the benefits of immediate, post-percutaneous transluminal angioplasty (PTA) placement of the device in treating arteriovenous graft (AVG) venous anastomotic stenosis when anatomically and clinically suitable. Writing in the Journal of Vascular and Interventional Radiology (JVIR), Bart Dolmatch (Palo Alto Medical Foundation, Mountain View, USA) and colleagues report a 30-day freedom from safety-related events of 96.4% and a six-month target lesion primary patency (TLPP) of 70.3% with the Covera stent.
The authors begin by noting that, as per three prospective, multicentre, randomised trials, placement of a covered stent has previously led to statistically superior TLPP rates compared to PTA alone in restoring flow and maintaining haemodialysis access.
They add that the current study, AVeVA (Arteriovenous stent graft in the treatment of stenosis at the graft-vein anastomosis of AV graft circuits), examined a self-expanding nitinol covered stent (Covera) that is more flexible than the device used in two of those prior studies (Flair, BD).
AVeVA study
Between August 2016 and February 2017, 110 patients were treated by investigators across 14 US centres in AVeVA—a single-arm, investigational device exemption (IDE) study without a concurrent control. Dolmatch and colleagues note that, because prospective trials of previous-generation covered stents had been completed and published, and the devices had been approved by the US Food and Drug Administration (FDA) for the indication being studied, pooled mean values from these trials as well as additional published data on the use of PTA alone for haemodialysis graft stenosis were used to develop safety- and patency-related performance goals for AVeVA.
The primary safety endpoint was 30-day freedom from an adverse event involving the access circuit resulting in additional intervention, surgery, hospitalisation or death. The primary efficacy endpoint was six-month TLPP, or the interval following treatment until the next clinically driven reintervention at the site of the target lesion or until the AVG was abandoned. Prespecified secondary endpoints included acute technical and procedural success, access circuit primary patency (ACPP), cumulative patency, number of reinterventions, index of patency function (IPF), and adverse events through two years.
Of the 181 patients who gave informed consent to participate, 71 did not meet the study eligibility criteria—with 75% deemed not to have angiographic evidence of ≥50% stenosis and clinical evidence of graft dysfunction—meaning 110 patients (mean age=64.3 years, 54.5% female, mean body mass index [BMI]=28.7kg/m2) were ultimately enrolled and treated with the Covera device. The vast majority (98.2%) had an upper-arm AVG.
New Covera data
The authors detail that the mean anastomotic lesion stenosis at the time of treatment was 71.5%, decreasing to a mean residual stenosis of 21% following PTA predilation. One covered stent was used to treat each study lesion, meaning 110 stents were deployed, and all but two of these were postdilated. The mean residual stenosis at procedure completion was 0.9%, Dolmatch and colleagues report. In all cases, the covered stent was deployed to the intended location and eliminated preprocedural symptoms of access dysfunction—constituting a technical and procedural success rate of 100%. All but two patients (98%) resumed dialysis after the procedure using their AVG.
At 30 days, freedom from adverse events was 96.4%. Four patients (3.6%) required additional reintervention and one patient (0.9%) underwent required/prolonged hospitalisation. The primary safety endpoint was therefore adjudged to be superior to the performance goal of 88% derived from prior studies and existing literature.
A total of 102 patients (92.7%) were available for the six-month primary efficacy analysis. TLPP at six months was 70.3% among these patients, the authors detail, and this was deemed superior to the prespecified performance goal of 40%. The only observed difference in patient subgroup analyses related to thrombosed AVGs, as those who presented with thrombosis within 30 days of the index procedure and/or at the time of the procedure demonstrated inferior TLPP rates at six months to those in non-thrombosis groups. Dolmatch and colleagues note that reasons behind this are unknown, but the fact this was observed in their study supports the “long-suspected belief” that a thrombosed AVG is more likely to fail due to TLPP loss, even when treated with a covered stent.
Noting secondary endpoint data, which they say should be considered observational and were calculated at predetermined intervals through the end of the study, the authors state that the Kaplan-Meier survival estimates for TLPP were 54.2% at 365 days and 36.9% at 730 days after the procedure, while Kaplan-Meier survival estimates for ACPP were 40.4%, 16.7%, and 7.8%, at 180, 365 and 730 days, respectively. A total of 91 adverse events across 53 patients (48.2%) were reported through 24 months, and 18 patients experienced device- or procedure-related events, meaning 86.3% were free from such events at 24 months.
Concluding messages
The Covera stent did an “adequate job” of maintaining target lesion patency over time, they add, but the “marked” and “ongoing” loss of ACPP (7.8% at 24 months) indicates that—regardless of TLPP improvement with a covered stent—some AVGs may be prone to recurrent stenosis or the development of new stenoses elsewhere in the circuit. The authors state that the 24-month cumulative circuit patency rate of 73.6% further supports this notion, and the finding that TLPP was “acceptable” with covered stent placement. The mean number of reinterventions to maintain patency was 1.6 at the treatment site and 3.6 in the access circuit at 24 months.
Dolmatch and colleagues conclude their JVIR report by noting that AVeVA was designed as “a first-in-human look at the Covera covered stent” in treating AVG venous anastomotic stenosis—and it demonstrated rates of freedom from major adverse events at 30 days (96.4%) and TLPP at six months (70.3%) that were both superior to literature-devised performance goals.
They also note, however, that AVeVA is not directly comparable with other, similar trials like FLAIR Pivotal, RENOVA and REVISE, and outline limitations of the current study, such as the inclusion of thrombosed AVGs and nontarget stenoses (rather than a more homogenous AVG group), and the potential for an “inherent bias” being created by its single-arm design and the selection of historical studies. “A comparative, powered, randomised study would be needed to determine patency differences between different covered stents within the same demographic population,” the authors add.
Biotronik announced the presentation of two studies on the performance of its drug-coated balloon (DCB) catheter Passeo-18 Lux at the Leipzig Interventional Course (LINC) 2022 (6–9 June, Leipzig, Germany).
The BIO REACT study was designed to better understand when and where a stent is needed following DCB for the treatment of femoropopliteal artery lesions in patients with peripheral arterial disease (PAD). Principal investigator Michael Lichtenberg (Arnsberg Vascular Center at Karolinen Hospital, Arnsberg, Germany) revealed the 12-month outcomes of this pilot study at LINC 2022.
While the use of intraoperative duplex ultrasound in this small cohort did not improve the identification of flow-limiting dissections, according to a company press release, the presented data showed that Biotronik Response Adapted Combination Therapy—combining Passeo-18 Lux DCB with Pulsar-18 T3 thin-strut stents when and where needed—is a safe and effective treatment of femoropopliteal lesions, while leaving less metal behind.
In the press release, Biotronik reports the following outcomes from BIO REACT:
Twelve-month freedom from clinically driven target lesion revascularisation (fCD-TLR): 94.8%
Twelve-month primary patency: 81.5%
Twelve-month survival: 97.2%
No major target limb amputation
“Identifying when to place a stent remains a complex issue, but the 12-month outcomes of the BIO REACT pilot study demonstrate that the Passeo-18 Lux DCB is an effective standalone therapy with a fCD-TLR rate of 94.0%,” Lichtenberg commented.
In another LINC presentation, Marianne Brodmann (Medical University Graz, Graz, Austria) reported the results of the Passeo-18 Lux DCB long lesion cohort, which combines the BIOLUX P-III all-comers registry’s long lesion subgroup and the BIOLUX P-III Spain study evaluating device performance in TASC C and D lesions >15cm.
In this pooled analysis, 159 patients with long and complex femoropopliteal lesions were treated with Passeo-18 Lux DCB. At 12 months, Biotronik reveals, the Passeo-18 Lux DCB showed good results in this real-world, challenging patient population (40.3% diabetes mellitus, 32.7% chronic limb-threatening ischaemia), with 84.4% fCD-TLR, 83.9% freedom from major adverse events, 98.6% freedom from major target limb amputation and 93.3% amputation-free survival.
The press release adds that, consistent with the results presented from the BIO REACT study, the Passeo-18 Lux DCB was shown to be an effective standalone treatment for complex lesions, with 60% of lesions not needing bailout stenting despite the long lesion length (mean lesion length, 24.9cm). “The treatment of long, complex TASC C and D femoropopliteal lesions with Passeo-18 Lux DCB as a standalone therapy is clearly shown to be safe and effective,” remarked Brodmann.
Biotronik advises that randomised controlled trials and all-comers registries have investigated safety and efficacy of Passeo-18 Lux DCB in the treatment of over 1,900 patients with PAD in the infrainguinal arteries.
Access Vascular, Inc. (AVI) has shared initial findings from a retrospective review of patient records according to a press release. These demonstrate an increase in dwell times compared to other commercially available devices and no complications when using AVI’s consistently hydrophilic materials for midline catheters.
As a result of a three-month retrospective evaluation of 29 HydroMID midline catheters at a long-term, acute care US hospital conducted in early 2022, AVI’s biomaterial-based catheters were found to have an average dwell time of 15.8 days. Furthermore, there were no incidences of phlebitis, occlusion, deep vein thrombosis (DVT), or bloodstream infections.
Traditional, polyurethane-based midline catheters have a median dwell time of only six days and an incidence of phlebitis of up to 35%, exhibit up to 7% rate of DVT, a 0.88% incidence of catheter-related bloodstream infection and an average occlusion rate of 22%.
“Midlines are an essential vascular access tool, but clinicians have been hampered for years by polyurethane-based catheters that must continually be replaced or that lead to unnecessary and frequent complications,” said Access Vascular, Inc. chief executive officer James Biggins. “These new data show that choosing the right catheter can make all the difference, giving clinicians the trust and competence they desire from their vascular access devices. We are confident that new, ongoing studies will demonstrate even longer dwell times for AVI’s biomaterial-based catheters.”
AVI’s patented hydrophilic biomaterial catheters mimic the body’s chemistry to significantly reduce the most common and costly complications associated with vascular access procedures. Given the high utilisation and complication rates of standard catheters, the use of AVI devices may meaningfully improve patient outcomes.
Philips has announced that its SmartSpeed artificial intelligence (AI)-powered magnetic resonance (MR) acceleration software has received US Food and Drug Administration (FDA) 510(k) clearance. It is one innovation within the portfolio of smart Philips MR systems showcased at the 2022 European Congress of Radiology (ECR; 13‒17 July, Vienna, Austria).
Adding advanced AI data collection algorithms to Philips’ existing Compressed Sense MR acceleration engine, Philips SmartSpeed delivers higher image resolution with scan times that are three times faster, and with virtually no loss in image quality, representing a major step forward in diagnostic confidence and MR department productivity.
With personalised treatment for complex diseases such as cancer increasing the need for high-confidence precision diagnoses, coupled with soaring caseloads due to aging populations and high levels of clinician burnout, radiology departments are under increasing pressure to improve performance, productivity, and profitability.
“Philips’ AI-based SmartSpeed reconstruction is the new benchmark among acceleration techniques for us. It improves on the company’s existing Compressed Sense in all aspects and allows a reduction in scan times with excellent image quality and diagnostic confidence,” said Grischa Bratke, radiologist and expert in musculoskeletal imaging at the University Hospital of Cologne, Cologne, Germany.
Philips SmartSpeed, the latest addition to Philips’ expanding portfolio of AI-driven, smart, connected imaging and smart workflow solutions, helps achieve the quadruple aim of improving diagnostic outcomes, enhancing patient and staff experiences, and reducing healthcare costs overall.
This latest AI-powered MR software increases resolution up to 65% and achieves up to three times faster scanning times compared to conventional MR scans. Coupled with its support for 97% of current clinical protocols – including advanced contrasts and diffusion-weighted imaging, and even quantitative imaging, Philips SmartSpeed helps increase diagnostic confidence in a wide range of cases, including those that are more complex.
The unique deep learning technology of Philips SmartSpeed is applied at the source of the MR signal and integrated with Philips’ Compressed Sense speed engine to deliver higher resolution and high signal-to-noise ratio needed for detailed images, small lesion detection and enhanced diagnosis.
Robert Jones (Birmingham, UK), Interventional radiologist and president of the Vascular Access Society of Britain and Ireland (VASBI), tells Renal Interventions at the Endovascular Access meeting (EVA; 24–25 June, Patras, Greece) that there are still significant untapped areas for research and education in the endoAVF field.
“Patient selection is a great example,” he says, noting that most of the focus to date in this area has been on vessel mapping and size criteria and the presence of the perforator. More understanding of whether pre-dialysis patients or those already on dialysis will benefit the most from endoAVF is another good example. And recognising recent studies in surgical fistulas that have demonstrated major differences in fistula use and success between ethnic groups, he points out: “We do not have this data for endoAVF.”
Inconsistencies in endpoint definitions are abundant in the literature, he warns. “I think there does need to be some consistency with definitions moving forward so we can make some meaningful comparisons between all these different studies.”
Jones also calls for more focus on cannulation. “[…] that is what is important to the patient. At the end of the day, they are the end user, and whilst we talk about the scientific side of things, there needs to be more focus, understanding and education around cannulation”.
Ra Medical Systems has announced receipt of US Food and Drug Administration (FDA) 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. A company press release details that the catheter features enhancements including a braided overjacket design that is intended to improve deliverability and kink resistance when navigating tortuous anatomy, as well as a six-month shelf life.
“While we are pleased to receive this regulatory clearance, it comes as our board continues its evaluation of strategic alternatives to optimise our company’s path forward in the current challenging economic environment,” said Will McGuire, Ra Medical Systems CEO. “As we have previously announced, the Dabra 2.0 catheter represents an interim step in our work to develop a guidewire-compatible version of the Dabra catheter, and at this time we have no plans to commercialise the Dabra 2.0.”
On 16 May 2022 Ra Medical Systems disclosed that its board of directors is reviewing strategic alternatives with the goal of maximising shareholder value. In conjunction with this review, on 6 June 2022 the company filed a report on Form 8-K with the Securities and Exchange Commission (SEC) announcing initiation of a reduction in force under which approximately 65% of the company’s full-time employees were terminated. Non-terminated employees were offered conditional retention arrangements for a period of approximately 60 days from the date of the filing to allow for evaluation and monitoring of the company’s near-term personnel needs based in part on the company’s financial status and the board’s review of strategic alternatives. The purpose of the reduction in force is to preserve capital with the goal of maximising the opportunities available to the company during the board’s review of strategic alternatives, Ra Medical Systems advises.
Konica Minolta Healthcare Americas has announced that the company’s Dynamic Digital Radiography (DDR) technology, enabling the visualisation of anatomy in motion, will be available on the mKDR Xpress mobile X-ray system. The mobile system will also be compatible with the newest technology in wireless flat panel X-ray detectors, the AeroDR glassless high-definition detector. These new advancements in X-ray technology will be introduced at the Association for Medical Imaging Management (AHRA) 2022 Annual Meeting (10–13 July, Phoenix, USA).
DDR is the next evolution in X-ray, enhancing diagnosis and management of pulmonary diseases and orthopaedic conditions. DDR enables clinicians to visualise the dynamic interaction of anatomical structures, such as tissue and bone, with physiological changes over time. DDR is a series of individual digital images acquired at high speed and low dose. In the same study, clinicians can acquire static and dynamic images. The resulting cine loop delivers up to 40 seconds of anatomy in motion in a diagnostic-quality view with a simple acquisition performed on a conventional system.
“Pairing DDR with the high-performance mKDR Xpress enables clinicians to elevate patient care with mobile X-ray at the point of care in a hospital,” Guillermo Sander, the company’s marketing director for digital radiography explained.
The mKDR Xpress delivers exceptional imaging performance in a small footprint at the bedside or in the emergency department, operating theatre, or intensive care unit. On-board charging for two detectors and front and back storage for detectors and accessories help technologists meet the most demanding mobile X-ray imaging needs. A tube-mounted graphical user interface and image preview function help ensure clear images are visible quickly, improving efficiency.
“Konica Minolta is imagining more possibilities with diagnostic radiography and mobile X-ray to help clinicians meet their most demanding imaging needs, providing solutions that redefine what radiography can do,” Sander added. “We envision a world where advanced X-ray capabilities provide the immediacy of information that clinicians need, at a lower cost than other imaging systems, so they can make better decisions, sooner.”
Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal) presented during the Scientific Paper session at this year’s European Conference on Embolotherapy (22–25 June, Nice, France), and won the award of best abstract for his and co-authors’ ‘Long-term outcome of prostatic artery embolization for patients with benign prostatic hyperplasia’.
Bilhim et al conducted this single-centre retrospective study in 1,072 patients with follow-up over a 10-year period to assess the outcomes of prostatic artery embolization (PAE) for, as stated in paper’s title, benign prostatic hyperplasia (BPH), in patients with lower urinary tract symptoms (LUTS). The authors were able to deem PAE a “safe and effective treatment option for patients with BPH” following the study’s completion, but that various further studies can deepen understanding of the BPH and PAE landscapes.
The authors begin the paper by outlining some of the pre-existing research in the area of PAE for BPH— data have shown that compared to prostatic surgery, PAE can achieve “similar LUTS improvements with a lower adverse event profile.” However, surgery leads to improvement in all BPH objective measurements and data suggest that re-treatment rates for patients who underwent prostatic surgery may also be lower.
In his presentation, Bilhim reported that the study ran from March 2009–19, and the 1,072 patients who were studied excluded those who did not have follow-up (11% of the original study population), the 1% in whom PAE was a technical failure and the 3% who were diagnosed with prostate cancer during follow-up.
Bilhim went on to detail how each patient was evaluated for International Prostate Symptom Score (IPSS) and quality of life (QoL), prostate volume (PV)—measured with transrectal ultrasound—prostate-specific antigen (PSA), peak urinary flow rate (Qmax) and postvoid residual (PVR) volume. Follow-up appointments took place yearly and also evaluated use of prostatic medication, reintervention rates and repeat PAE and prostatectomy rates.
In terms of embolic agent, Bilhim proceeded to explain that over the ten years, various embolic agents were used. These were non-spherical polyvinyl alcohol (PVA) particles, measuring 100–300 micrometres and spherical PVA microspheres, measuring 300–500 micrometres. Some patients received treatment with trisacryl gelatin microspheres measuring 100–500 micrometres, or 250-400 micrometres polyzene-coated hydrogel microspheres. Notably, the first group treated within the study remit received PVA particles, so their follow-up was longer. Mean follow-up time was 4.39±2.37 years.
Adverse events were determined according to Cardiovascular and Interventional Radiology Society of Europe (CIRSE) criteria, and Bilhim stated that they did not consider frequency, urethral burning sensation or slight pelvic pain lasting for one to three days post-PAE as being in category, but rather as post-PAE syndrome. Reintervention, IPSS over 15, or QoL >3 were all considered ‘clinical failure,’ with need for prostatic medication registered but not counted as failure.
Bilhim then proceeded to relay his results to delegates in the audience: at the final follow-up appointment, mean IPSS and QoL improvements were -10.14±8.34 (p<.0001) and -1.87±1.48 (p<.0001) points, mean PV reduction was -6.82±41.11 cm3 (p=0.7779), mean PSA reduction was -1.12±4.60ng/mL (p=0.9713), mean Qmax increase was 2.72±6.38 mL/s (p=0.0005), mean PVR reduction was -8.35±135.75mL (p=0.6786) and mean IIEF-5 improvement was 0.18±7.40 points (p=0.4546).
The number of patients who required prostatic medication after PAE was 335, or 31.3%. The reintervention and repeat PAE rates were 3.4% and 2.3% at one year, 21.1% and 9.5% at five years and 58.1% and 23.1% at 10 years, respectively. Prostatectomy rates were 1.1% at one year, 11.6% at five years and 35.0% at 10 years, Bilhim reported.
The presenter also noted that the study saw a 90% acute urinary retention resolution rate, with the other 10% having to have surgery, and the rate of post-PAE syndrome was 23%.
In terms of difference in outcomes among the different embolic agent groups, the paper acknowledges that PVA led to lower rates of penile skin lesions, haematuria and rectal bleeding after PAE compared to the other spherical embolic agents. A possible explanation for this could be that PVA offers a lower permanent vessel occlusion.
Other trends observed during the study were that unilateral PAE was a significant predictor of clinical failure and reintervention and that those who received a repeat PAE (n=25, 25.8%) were more likely to undergo prostatectomy compared to those who only received one PAE procedure.
Bilhim et al were able to draw the conclusion that PAE gives patients lasting and long-term LUTS relief and that reintervention rates are 20% in the first five years, rising to between 30 and 60% >five years post-PAE. Addressing the ET audience, Bilhim declared PAE a “safe and effective treatment option for patients with BPH.” The study yielded “promising” findings, the presenter added, among which was that 74% of patients remained prostatectomy-free, demonstrating the potential for repeat PAE to ensure treatment effectiveness durability.
Bilhim showed his awareness of his study’s “many limitations”—namely that it was carried out retrospectively with no controls and that they “lost patients during follow-up.” Comparing the embolic agents also made the study more difficult because of different follow-up times for each group, but they did control for this factor with multivariable Cox regression analyses, Bilhim clarified.
He admitted that “we need more long-term data to keep on proving that PAE is a good alternative treatment to prostatectomy/transurethral resection of the prostate (TURP).” Studies with large cohorts are also necessary, Bilhim added, to “fill this gap in the knowledge” around BPH treatment and PAE. Future trials should compare PAE with other minimally invasive surgical treatments (MISTs), as well as look more closely at the differences in outcome when using various embolic agents, Bilhim suggested. Long-term reintervention rates also mean that the benefits of PAE in terms of faster recovery, it being less invasive with fewer adverse events and better at preserving ejaculation, “must be viewed with caution,” Bilhim advised.
Session moderator and meeting deputy chairperson Otto van Delden (University Medical Centers Amsterdam, Amsterdam, The Netherlands) asked Bilhim after he had finished presenting whether “[you can] use [whatever agent] you want.” Bilhim responded in the affirmative, before explaining the following: “What I have seen is that when you do PAE repeatedly, even though I could not prove this, [there seems to be] more recanalisation of the native prostatic artery with PVA than with spherical particles.” Nevertheless, Bilhim asserted, he has seen “no big clinical difference” among the different embolic agents—“all patients will have revascularisation from different origins.”
Regarding the frequently asked question of how PAE compares to other procedures, Bilhim sought to clarify that “you cannot compare recovery and morbidity between PAE and [surgical resection].” It is more appropriate and beneficial to draw comparisons between PAE and other MISTs, such as those which are commonly carried out in the USA.
Rounding up the post-presentation discussion, Bilhim concluded that these study data are “good” for him—” I can tell [patients] about 10-year likely outcomes.”
This study presents the largest PAE cohort with the longest follow-up data so far, with over 900 patients with follow-up data from 1–3 years, over 300 patients with available data at five years and 150 patients up to 10 years. This will be a relevant addition to the existent PAE literature as it presents the first study looking at reintervention rates up to 10 years post-PAE.
Among the most popular pieces from last month are reports on papers delivered at the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11–16 June, Boston, USA), two stories of innovations in pain management, and a write-up of a call to action regarding limiting radiology staff lead exposure.
‘Surface lead contamination on personal lead radiologic protective apparel’ is a recent report published by Kieran Murphy et al (Toronto Western Hospital, Toronto, Canada). The subject of the report is free lead dust on lead aprons: the study involved testing aprons at a Toronto university hospital, which yielded the finding that 60% of aprons and thyroid shields have free surface lead.
‘Multivessel pelvic embolization during caesarean hysterectomy for placenta accreta spectrum: A single-centre experience and comparison to internal iliac artery balloon occlusion’ was presented at SIR.
The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist, SD-101, and the proprietary Pressure-Enabled Drug Delivery (PEDD) method of administration to overcome critical treatment barriers.
“I do not want interventional radiology to be a treatment for the rich, nor for those who live in the wealthiest countries.” Yasuaki Arai was, until recently, executive advisor to the president at Japan’s National Cancer Center in Tokyo, where he is currently a member of the interventional radiology centre.
Four of the abstracts submitted were declared ‘Abstract of the Year’ by Society of Interventional Radiology (SIR) scientific chairs. The prizes were conferred during the final plenary session of the meeting, and, according to SIR, reward the ‘best scientific work’ in terms of ‘overall quality, timeliness and content’.
An experimental formulation of a hydrogel injected into spinal discs proved safe and effective in substantially relieving chronic low back pain caused by degenerative disc disease (DDD), according to new research.
M.I.Tech is the creator of the HANAROSTENT technology, a family of conformable, non-vascular, self-expanding metal stents, which have been distributed by Boston Scientific in Japan since 2015.
Shimadzu Medical Systems USA introduced the new Trinias system, which uses artificial intelligence deep learning to improve the visibility of medical devices while using lower X-ray doses than previous models, at SIR 2022.
Damaged nerves can be regenerated with the application of a frozen needle using an advanced imaging technique called interventional cryoneurolysis, which is performed by an interventional radiologist and can offer hope to patients in persistent pain following a traumatic injury, according to an SIR press release.
The first patient has been enrolled in the US Food and Drug Administration (FDA) investigational device exemption (IDE) below-the-knee (BTK) SELUTION4BTK clinical trial involving SELUTION SLR, MedAlliance’s sirolimus-eluting balloon.
Merit Medical has announced the successful enrolment of the first patient in its WRAP registry study in a press release. This study will evaluate the clinical benefits associated with the use of the Wrapsody cell-impermeable endoprosthesis in patients receiving haemodialysis that experience stenosis or occlusion of blood vessels required for dialysis.
Globally, over two million patients with advanced kidney disease receive dialysis. Haemodialysis, the primary approach used for dialysis, requires long-term vascular access that is typically achieved through the surgical creation of an arteriovenous fistula (AVF) or placement of an arteriovenous graft (AVG). However, complications, such as stenosis and/or occlusion within the dialysis outflow circuit of an AVF or AVG, can impair vascular access which compromises the ability to provide adequate dialysis treatment. The Wrapsody cell-impermeable endoprosthesis was created to help overcome this challenge by maintaining the integrity of the dialysis outflow circuit.
Dean Huang, consultant diagnostic and interventional radiologist at King’s College Hospital in London, England, enrolled the first patient in the WRAP Registry. “The patients being treated with the Wrapsody cell-impermeable endoprosthesis have historically had few clinical options,” Huang said. “These patients have typically faced frequent reinterventions to maintain vessel patency resulting in multiple procedures and hospitalisations. The WRAP study will add to the growing body of evidence on Wrapsody’s ability to achieve durable outcomes for this vulnerable patient population.”
The WRAP registry study will enrol up to 500 patients with outflow circuit stenosis or occlusion who are receiving haemodialysis at medical facilities throughout Europe, South America, Australia, and New Zealand. Clinical outcomes of patients after the initial placement of the Wrapsody cell-impermeable endoprosthesis will be evaluated over a two-year period in accordance with the instructions for use associated with its CE Mark.
The Wrapsody cell-impermeable endoprosthesis is an expandable nitinol stent frame fully enveloped by an external layer of expanded polytetrafluoroethylene (PTFE) and an internal layer of spun PTFE with an interposed cell-impermeable layer. The Wrapsody cell-impermeable endoprosthesis system is being studied under an investigational device exemption (IDE) in the USA.
Teleflex has announced the results of several research studies that further support the safety and efficacy of the UroLift system for men living with enlarged prostate, benign prostatic hyperplasia (BPH), or those who have a wide range of prostate sizes and/or a median lobe obstruction. The data were presented at the 37th Annual European Association of Urology (EAU) Congress in Amsterdam (1—4 July) and virtually.
Key findings include:
Pooled outcomes of over 300 controlled subjects from five clinical studies revealed most men shifted to lower international prostate symptom score (IPSS) symptom severity after treatment with prostatic urethral lift (PUL). The majority of subjects (79%) improved by three points or more, and 66% of those patients moved into a lower IPSS severity grade 12 months post-treatment.
Comparative evaluation of real-world and controlled trial outcomes of PUL demonstrated that symptom improvement is not correlated with prostate size and shape. The study examined PUL outcomes in differing gland sizes and morphologies, comparing controlled trial results from BPH6 for patients with small prostate sizes and MedLift for patients with obstructive median lobes. At 24 months, all groups demonstrated significant and sustained IPSS improvement.
An analysis of US healthcare claims revealed higher de novo prescription rates after transurethral resection of the prostate (TURP) and photoselective vaporisation of the prostate (PVP) compared to PUL. The study revealed that post-surgical medication usage was significantly higher for BPH patients who were treated with more invasive surgical procedures as compared to those treated with the UroLift system.
“The UroLift system is the most well studied minimally invasive surgical therapy for BPH. In a combined analysis from five controlled studies, we found that the majority of men who had received the procedure demonstrated measurable improvement in their BPH symptoms, flow rate, and quality of life. Subjects [also] preserved their sexual function,” said Claus G Roehrborn, urologist at the University of Texas Southwestern Medical Center (Dallas, USA) and a lead author on the paper.
“The evidence presented at EAU means that urologists can further help their BPH patients make an objective, data-driven, and informed decision based on real-world evidence, particularly when faced with prostate sizes and shapes that fall outside of the range of randomised clinical trials. Our research showed not only rapid, but also durable improvement,” said Christian Gratzke, medical director, urology clinic, University Hospital, Freiburg (Freiburg, Germany).
Cydar Medical, in partnership with King’s College London, has initiated the ARIA study—a randomised controlled trial to assess the clinical, technical and cost-effectiveness of a cloud-based, artificially intelligent image fusion system in comparison to standard treatment to guide endovascular aortic aneurysm repair.
Endovascular aneurysm repair (EVAR) is an alternative to open aortic surgery due to perceived advantages in patient survival, reduced post-operative complications and shorter hospital lengths of stay.1 Despite these potential advantages, there is still significant variability in preoperative planning and sizing, problems associated with imprecise visualisation and device positioning intraoperatively, and inconsistent patient outcomes, a Cydar Medical press release states.
Rachel Clough, principal investigator of the ARIA study and clinical senior lecturer at King’s College London, said: “Our central hypothesis is that digital technology—specifically cloud-computing and artificial intelligence—can be used to assess and learn from large volumes of data to inform clinical decision making and has the potential to improve the predictability of individual patient outcomes and the consistency of outcomes in the NHS.”
The randomised trial will enrol 340 patients in 10 sites across the UK with a clinical diagnosis of abdominal aortic or thoracoabdominal aortic aneurysm suitable for endovascular treatment. The trial will follow patients for one year and assess the effect of Cydar EV Maps on clinical-, technical- and cost-effectiveness in comparison to standard treatment in endovascular aortic aneurysm repair, used for both standard and complex devices.
The study was initiated with the first patient enrolled at the Liverpool University Hospitals NHS Foundation Trust. “Cydar EV Maps is a game-changing technology for vascular navigation. The ARIA study provides a unique opportunity to demonstrate the benefits like reduced procedure time and reduction to radiation exposure, although some of the more subtle benefits related to procedural quality and reduced operator fatigue may never be directly measured but are obvious as an operator,” added Dr Simon Neequaye, Principal Investigator at the Liverpool University Hospital NHS Foundation Trust.
Cydar EV Maps is currently available in the EU, UK and US. It is certified software-as-a-medical device with an EU CE mark and US Food and Drug Administration 510(k) clearance.
References:
Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial. Lancet. 2004;364(9437):843-8.
Insightec, a global healthcare company dedicated to using acoustic energy to transform patient care, announced that it has received US Food and Drug Administration (FDA) approval for an investigational device exemption (IDE) for a clinical comparative study of the Exablate Prostate system used to treat diseased prostate tissue. This study will evaluate the safety and efficacy of focal treatment using high-intensity focused ultrasound when compared to active surveillance in men living with prostate cancer.
The Insightec Exablate Prostate system uses soundwaves to ablate targeted tissue in the prostate. The treatment is performed under magnetic resonance imaging (MRI) guidance for high-resolution visualisation of the patient’s anatomy for precise targeting and real-time temperature monitoring. The single-session treatment does not require incisions and allows patients to return to normal activities quickly, with minimal complications.
“We are excited to continue this important research that can impact on the standard of care for prostate cancer treatment,” said Behfar Ehdaie, a urologic surgeon at Memorial Sloan Kettering Cancer Center (New York, USA), and principal investigator for the study. “Exablate Focused Ultrasound has been shown to provide an accurate, safe, and effective option to engage the prostate gland directly in selected patients based on two-year biopsy outcomes.”
A previous Insightec-sponsored clinical trial led by Memorial Sloan Kettering Cancer Center for the Exablate Prostate system reported minimal damage to adjacent structures and low rates of impact on potency and continence, supporting function and quality of life for patients. The new comparative study builds on the evidence of this clinical trial and aims to further enhance prostate treatment options and improve clinical outcomes.
The Insightec Exablate Prostate system received 510(k) FDA clearance in November 2021, making way for the system to be offered to patients in a commercial facility and for further clinical studies. In January 2022, the system was used to treat prostate disease in its first US commercial patient.
Results from the new study will define the role of focal therapy to delay and avoid radical therapy for men with prostate cancer and support expanded clinical adoption of the technology and increased access for patients through insurance reimbursement.
Transit Scientific's XO Score inflated with a standard off-the-shelf PTA balloon
Transit Scientific’s XO Score inflated with a standard off-the-shelf PTA balloon
Transit Scientific had shared via press release successful outcomes on multiple fistula and graft cases using its XO Score sheath platform, a first-of-its-kind metal-alloy scoring, cutting, and constraining structure (CS) device, along with off-the-shelf percutaneous transluminal angioplasty (PTA) balloons.
XO Score can be used in significant chronic dialysis fistula and graft cases using low-pressure inflation, in some cases after high-pressure PTA treatment failed.
“A patient presented with a high-grade stenotic lesion in a brachiocephalic fistula restricting venous outflow. The lesion was resistant to initial treatment using a high-pressure PTA inflated to 40 atmospheres. The lesion was then treated with the XO Score device and followed by effacement of the stenosis with standard balloon PTA inflated to nominal pressure (nine atmospheres). There was no residual stenosis and the fistula was no longer pulsatile on exam,” Jeffrey Hoggard, an interventional nephrologist at Raleigh Access Center (Raleigh, USA), shared. “XO Score presented a great treatment option for us where high-pressure PTA failed.”
Traditional PTA cutting, scoring, and constraining structure (CS) technologies are manufactured with metal or polymer wires, struts, blades, or grooves wrapped around, or fused to, the outside of the angioplasty balloon. These wires, struts, blades and/or grooves expand with the balloon to provide focal force in calcified, hyperplastic, and/or resistant lesions to prevent dissection, dilate resistant lesions, and/or prep the vessel for other intervention. Traditional systems can be bulky, difficult to use, cost-prohibitive, and require significant inventory.
The XO Score is a thin one-piece metal alloy exoskeleton sheath, with up to 22 struts/grooves, that slides over off-the-shelf angioplasty balloons. When the angioplasty balloon is inflated, the struts/grooves expand with the balloon and rotate 90° to apply focal force to the vessel. When the balloon is deflated, the XO struts/grooves rotate 90° back to an atraumatic position and the XO structure assists in balloon rewrap for removal.
XO’s technology can also be optimised to constrain balloons and prevent torsional and longitudinal shear during angioplasty balloon inflation.
The XO Score system is US Food and Drug Administration (FDA) and CE-Mark cleared to dilate stenotic material in iliac, femoral, iliofemoral, popliteal, infrapopliteal, and renal arteries and for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistula.
Kytai Ngugen
Credit: University of Texas at Arlington
Kytai Nguyen Credit: University of Texas at Arlington
A University of Texas at Arlington (UTA; Arlington, USA) bioengineer is leading a project that will develop biodegradable nanomaterials that will take pictures and deliver medicine to combat peripheral arterial disease (PAD), the university announced in a press release.
Kytai Nguyen, a UTA bioengineering professor, is the principal investigator in the four-year, US$2.1 million National Institutes of Health (NIH) grant-funded project. She is collaborating with Jian Yang, a Penn State University (University Park Pennsylvania, USA) bioengineering professor and former UTA faculty member, and Ralph Mason, a professor of radiology at UT Southwestern (Dallas, USA).
“What is important in this project is that the technology carries fluorescent and ultrasound imaging capabilities, which will provide patients and doctors with more detailed information,” Nguyen said. “It also gives patients more targeted medicine, making it more efficient.”
PAD, more commonly known as either atherosclerosis, is a condition commonly found in the elderly. It affects more than 200 million people worldwide and is associated with high rates of morbidity and mortality.
The research aims to develop novel biodegradable nanoparticles to deliver therapeutic agents that specifically protect cells under stress conditions, facilitate the formation of blood vessels under hypoxia and allow noninvasive multimodal imaging methods.
One impact of the research is to use these new nanoparticle platforms to deliver any therapeutics locally, treat the disease effectively and monitor the treatment noninvasively by imaging. “The overall goal is to reduce complications and improve the quality of life for PAD patients,” Nguyen said.
Michael Cho, chair of the UT Arlington Bioengineering Department, said Nguyen’s innovative research could greatly help those who live with PAD.
“This cutting-edge technology has a chance to change our protocols on how to deal with atherosclerosis,” Cho said. “When you are able to target localised lesions for treatment, that is so much better for the patients and much less invasive than current treatment.”
Nguyen, who has been at UTA since 2005, received Cancer Prevention & Research Institute of Texas grants in 2010, 2016, and 2021. She also has received funding through the NIH, National Science Foundation, American Heart Association, and US departments of Education and Defense, among others.
Investigators provide clinicians with guidance on alternative imaging methods for interventional radiology procedures and strategies to maintain the short supply for emergencies, a press release announced. The guidance has been published in the Journal of Vascular and Interventional Radiology(JVIR).
“As interventionalists, adaptation is at the core of our specialty, and this situation has proved no different,” said lead author Nikki A. Keefe, Department of Radiology, University of North Carolina at Chapel Hill (Chapel Hill, USA) and her co-authors. “We have developed an initial approach to case prioritisation, and we also looked at short-term strategies for the management of existing supply to optimise utility and minimise waste.”
In response to this shortage, the American College of Radiology (ACR) Committee on Drugs and Contrast Policy has published a guidelines statement. Using these guidelines as a foundation, Keefe and her co-authors offer a set of practical solutions for dealing with the current situation.
The authors recommend creating a priority matrix covering the following categories: procedures that require iodinated contrast media versus procedures that can be deferred; those that can be performed with alternative imaging modalities such as intravascular ultrasound; and those that can be performed with an alternative contrast media.
With maximum dose recommendations, gadolinium (Gd) can be used in the vascular system even for patients with renal insufficiency. Carbon dioxide has been used as a safer alternative to iodinated contrast media in patients with renal dysfunction or allergy, although there are some associated risks. To prevent ischaemia, dosages should be timed one to two minutes apart. While alternate contrast agents have limitations in defining the anatomy of large diameter vessels such as the aorta, digital stacking of images may improve visualisation.
Intravascular ultrasound has an established role in vascular procedures, and it can obviate the use of contrast media and decrease radiation exposure and procedural times. With appropriate training, clinicians can apply intravascular ultrasound for procedures such as inferior vena cava filter placement and transvenous biopsy.
GE Healthcare recently announced that it has been able to reopen its Shanghai facility, but distribution and other supply chain issues may linger. “That being said,” Keefe and co-authors cautioned, “with China’s zero-COVID-19 policy, a shutdown may unfortunately happen again, and it would be prudent to have a plan in place should shortages recur.”
As interventional radiology (IR) evolves and expands, so too does the role of anaesthetic support to get these patients safely through their procedures. Where previously anaesthetic support was reserved for only the most acute and complex patients, now, some centres have regular anaesthetic lists supporting elective, urgent and emergency work.
Maintaining standards
Anaesthesiologists’ experience in the traditional ‘theatres’ means they can bring that knowledge across, setting standards for anaesthesia, such as recommended emergency airway equipment, a go-to box for anaesthetic emergencies like malignant hyperpyrexia, and stockage of appropriate medication. Having a regular anaesthetist also means these standards are regularly reviewed and revised.
It also brings across a culture of theatres, championing morning huddles or team briefs; completion of the WHO [World Health Organisation] checklist and debriefing sessions; efficient turnaround time between cases and better list utilisation overall.
The presence of anaesthetists within the IR suite permits the teaching of skills critical to safe patient management, airway management skills, for example, and the transfer of knowledge that will enhance patient satisfaction. Postoperative pain management is an example of such knowledge, the importance of which will be seen in years to come as the repertoire and complexity of IR procedures continues to grow.
Patient population
Studies have shown that the mean age of patients in IR is 3.5 years higher than those having surgery. With increasing age, you see increasing co-morbidities.
Certainly, in the surgical population there has been a significant increase in patient complexity as reflected in their American Society of Anaesthesiologists (ASA) Physical Status grade. Previously, ASA 1 patients made up 35% of the surgical population whereas now they make up just 15%. Naturally, the percentage of ASA 2, 3 and 4 patients has increased, and overall, patients have increased numbers of health conditions and poorer control of existing conditions.
Certain subsets of IR patients may demonstrate this heightened risk more clearly than others. A recent three-month audit of patients presenting on the anaesthetic list for lower limb angioplasty at a major teaching hospital in London, revealed that 23% of patients were octogenarians, 23% were ASA 4 and above, and 17% were not for resuscitation in the event of a cardiac arrest. Many of these patients present as urgent cases—best practice national guidance recommends that they should be revascularised within five days of their admission to hospital.3 Strict adherence to this practice leaves little time to optimise them prior to their procedure.
The nature of IR means that the patient considered too high-risk for a surgical procedure, or an open technique, is referred for a minimally invasive one instead. High-risk refers to the anticipated surgical insult associated with major surgery, which the team intend to mitigate through a minimally invasive technique, thus reducing physiological stress on the body. However, there remains an associated risk from anaesthesia, which is independent of the surgical or procedural approach. This anaesthetic risk may be significantly prolonged, in some cases, with procedures taking many hours to complete.
When anaesthetising patients in IR, it is important to strike the right balance between anaesthetic approach, procedural technique and patient risk factors. Often “a less is more” approach suits the high-risk patient better.
Type of work
The challenge comes when anaesthetists are unfamiliar with the nature of the procedure, particularly the approach and the duration. Additionally, the type of work in IR is often a mixture of elective, urgent and emergency work, meaning it is a hybrid of a traditional elective lists and emergency lists from theatres: a combination of stable patients having minor procedures, like sclerotherapy and unstable patients having life-saving procedures like embolization. A flexible and adaptable mindset is therefore needed when working in IR.
The challenge, and possibly the enjoyment, of anaesthetic lists in IR is that no two lists are alike. Patient demographics differ wildly from one to the next and procedures vary significantly from gastrointestinal procedures to vascular work.
Education and training
Anaesthetic training has not kept pace with the growth in demand for anaesthetic involvement in delivering care in the IR environment. Remote-site anaesthesia is given consideration within the anaesthetic curriculum, however, the concentration of IR services, mainly in larger teaching institutions, and the relative lack of specific focus on this subject in the training syllabus, means that most anaesthetic trainees have little to no exposure to IR until their final years of training, or until they become consultants.
The knowledge and experience gap that needs to be crossed, as a consultant, is therefore significant. The initial learning curve is steep and there is a lack of resources to support the education and training of anaesthetists who are interested in this field. It may take months to years for consultants to become comfortable with IR procedures and practices, and to acquire the mindset and techniques required to operate effectively within the IR environment. A wholesale change in thinking is needed to address this, from the teams who create the training curriculum, to the rota makers who assign trainees to theatre lists. Going forward, training lists in IR need to be seen as mandatory rather than just a tick-box option.
Location and space
One of the obstacles that face anaesthetists who work in IR is the unfamiliar environment. IR suites are often in a remote location in the hospital and away from the main theatre complex. The anaesthetic support that can be found in main theatres is not available in IR and the anaesthetist must work closely with their anaesthetic assistant to deliver care. In an emergency, help from a fellow anaesthetist is not close at hand. This much is also true for the IR anaesthetist who needs relief for a lunch break or to review a patient.
In addition, the configuration of IR suites has often not taken the needs of the anaesthetic team into consideration, with limited space for the anaesthetic machine, which can be far from the head end of the table. Access to an anaesthetic room is preferable but again with limited space, a luxury that the IR suite cannot always afford.
A combination of the above challenges breeds a reluctance in anaesthetists to deliver regular anaesthetic lists in IR.
Safety
The lack of regular anaesthetist-supported lists has led to many procedures being completed under local anaesthetic or “vocal anaesthetic”, when ideally, they should have anaesthetic involvement.
There is much debate over whether procedures, such as oesophageal dilatations, should be done under “vocal anaesthetic” with (or without) radiologist-delivered sedation, or under general anaesthetic. Centres all across the country use a different approach and each have their merits. The benefits of anaesthesia delivered by an anaesthetist is that the radiologist and their team can focus on the procedure, whilst the anaesthetist can focus on the patient, ensuring they are adequately analgised, anaesthetised and monitored.
This is ever more important when dealing with sick patients. Regular exposure to emergency work, and benefitting from formal training in intensive care medicine, anaesthetists are well versed in the management of medical emergencies that may be encountered both inside and outside of the operating theatre. Their leadership qualities come to the fore when dealing with the unstable or deteriorating patient.
Summary
Anaesthetists are uniquely placed to collaborate with IR teams on patient safety and maintaining the same standards of practice as theatres to ensure effective care is delivered.
Though there are many unique challenges to providing care in this setting, with increase in workload, it is certain that more and more centres will recognise the value of regular lists. Supported by the Society of Anaesthesia and Radiology, undoubtedly some of these challenges, like a lack of familiarity with the environment and procedures, will be rectified.
Overall, as a speciality, consideration needs to be given to adopting a surgical theatre approach to delivering care and at the centre of this is anaesthetic support.
Authors Nazia Khan and Pele Banugo are consultant anaesthetists at Guy’s and St Thomas’ NHS Foundation Trust, London and Sanya Patel is an anaesthetic trainee at Lewisham and Greenwich NHS Trust, London, UK.
Primary paediatric liver cancer is a rare disease, accounting for 1–2% of childhood cancers, or about 150 new diagnoses of paediatric liver malignancy per year in the USA. These include hepatoblastoma (HB), hepatocellular carcinoma (HCC), undifferentiated embryonal sarcoma of the liver (UESL), and rhabdoid tumour of the liver (RTL). Surgical resection is the foundation of cure for all paediatric liver tumours; however, only one-third of patients have resectable disease at diagnosis.
Allison Aguado
While chemotherapy is effective in making two-thirds of initially unresectable patients with HB resectable, effective standard-of-care chemotherapeutic regimens that render HCC, UESL, or RTL resectable have yet to be described.
Recent reports suggest that orthotopic liver transplant may be required in 20–30% of newly diagnosed paediatric liver tumours who will require lifelong medical therapy with potential episodes of rejection and occurrence of post-transplant lymphoproliferative disease.
The primary staging system used for paediatric liver tumour is PRETEXT (pre-treatment extent of tumour) classification which describes the extent of tumour in the liver based on Couinaud segmental anatomy and is used to predict overall survival. It is a pre-therapy assessment of HB and HCC but is intended to be applicable to all primary malignant liver tumours of childhood. PRETEXT annotation factors include venous involvement, extrahepatic disease, multifocality, tumour rupture, and metastatic disease. This is used to create the risk stratification system used for the Pediatric Hepatic International Tumor Trial (PHITT) which is based on PRETEXT, metastases, age, α-fetoprotein (AFP), annotation factors, and resectability.
TARE with Yttrium-90 (TARE-Y90) has demonstrated an emerging role in the treatment of primary paediatric liver tumours in several small studies. It was initially used in heavily pretreated children with HB, HCC, and transitional liver tumours (showing features of both HB and HCC) where it showed that it was feasible, safe, and demonstrated anticancer effects by imaging and decreased tumour markers. It has since been used as a component of curative therapy in two paediatric patients with HB who responded to TARE-Y90 with decreased tumour size, decreased tumour marker levels, hypertrophy of the future liver remnant, the facilitation of conventional hepatectomy, and complete remission. It has also been used as part of curative therapy in two paediatric patients with HCC, who were downstaged to hepatic resection; one is alive with no evidence of disease 18 months post-completion chemotherapy and one is alive with evidence of disease 13 months post-resection.
Earlier integration with combination therapies may offer an important option and strategy to improve survival, result in less chemotherapy delivered, decrease rates of orthotopic liver transplantation (OLT), and present potentially curative options for patient with refractory and recurrent disease. While early results are encouraging, more research is required to determine the efficacy of TARE-Y90 in children and to define the clinical scenarios where there is likely to be greatest benefit.
Allison Aguado is a paediatric interventional radiologist at Nemours Children’s Hospital, Wilmington, USA.
Interventional radiology (IR) is a growing, dynamic field, still working to define its professional identity— who we are and where we are going as a specialty. I believe an important part of that maturation rests on our ability to articulate our collective values as a professional group, particularly in regard to challenging questions that arise in our work. Through my ethics graduate education and medical training, I have come to view ‘ethics’ as just that— the collective values of a group of people. So, to help IR establish itself as a clinical specialty, we need to define and articulate the ethics of IR.
Unfortunately, many common approaches to ethics tend not to feel particularly practical or helpful in day-to-day clinical practice. Ethics often feels abstract and verbose and tends to treat clinicians as a monocultural group, assuming that the ethical issues and solutions for IR are the same as internal medicine or gynaecology. Although there are certainly common issues across healthcare, medical specialties have remarkably distinct cultures, workflows, and ways of thinking. As such, my hypothesis has been that the salient ethical issues and means of navigating
them probably vary in important ways across specialties. To make ethics feel more practical and useful, I decided to test out an applied, specialty-specific approach to ethics in IR. Instead of starting with ethical theory and a top-down approach, I work bottom-up, starting with an understanding of how people in IR are approaching an ethical issue and why, and then using that understanding alongside ethical theory to design practical approaches and tools to better navigate those issues. The ultimate goal is to foster an ethics consciousness in IR, a common understanding of our shared values and how best to navigate the sticky situations we face as a specialty.
To do this, I founded a multi-institutional working group of faculty and trainees focused on research, education, and public relations using this new approach. Creating something new always comes with challenges and setbacks, but we now have approximately 30 people affiliated with the group, and since being founded in 2019, we have published over 20 manuscripts, given multiple invited lectures at major IR conferences, and have a column in Seminars in Interventional Radiology called the ‘Ethics Corner.’ We have found that IRs face a wide array of ethical issues in their work; the vast majority consider these to be important issues but state that they often feel limited by a lack of tools and specific guidance for navigating them. Common issues include differentiating palliative from futile care, managing complications, consent and surrogate decision-making, conflicts of interest and research ethics, tribalism and medical business ethics, and social media ethics.
For example, consent is a ubiquitous part of our daily workflows and right at the core of our relationships with patients and families. Nevertheless, studies suggest that consent practices tend to be limited in quality and completeness across healthcare. This is important not only ethically, but because poor periprocedural communication and understanding is a common source of medical mistakes and lawsuits. We first completed an exploratory study of consent in IR, finding that the dynamic nature of IR practices and limited baseline public awareness can make truly informed consent particularly challenging in our specialty. To improve consent practices, we have not only been working to develop more engaging educational resources on ideal consent practices for IR, but also better patient decision aids (PDA).
PDAs are handouts, videos, or other tools that present balanced information on the risks, benefits, and alternatives of a healthcare decision, ideally at the average reading level (seventh grade in the USA), using patient-friendly, plain language. Unfortunately, current PDAs for image-guided procedures tend to be limited in quality and consistency, so we partnered with a not-for-profit called The Interventional Initiative to create better PDAs via an extensive vetting process. We then trialled them at two institutions where people were randomised to receive a PDA or not, while waiting to talk to their clinician. This way, clinicians did not have to do anything differently; rather, we took advantage of dead time in the patient flow, which is ideal for sustained adoption. We found that the people who received a PDA were not only more likely to have better understanding and satisfaction, but were also more likely to feel that their clinician had spent enough time with them and answered all their questions.
This is one example of our applied approach. Rather than writing a 50-page analysis about how interventional radiologists should ‘do better’ at consent, we instead assume that people are doing their best, try to understand current barriers, and construct environments and workflows that support better consent practices in IR without requiring more time or energy.
We are always looking for collaborators and partnerships to help establish our collective values as interventional radiologists.
Eric J Keller is a resident physician at Stanford University, Stanford, USA and founder of the Applied Ethics in IR working group.
Disclosure: Keller is a board member of The Interventional Initiative.
At the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11-16 June, Boston, USA), four of the abstracts submitted were declared ‘Abstract of the Year’ by the society scientific chairs. The prizes were conferred during the final plenary session of the meeting, and, according to SIR, reward the ‘best scientific work’ in terms of ‘overall quality, timeliness and content’.
Erica Emmons
Erica Emmons (Vanderbilt University Medical Center, Nashville, USA) was one of the winners, for her paper ‘Survival outcomes and toxicities following yttrium-90 (Y90) radioembolization of colorectal cancer metastatic to the liver: 498-patient analysis from the RESiN registry.’ The purpose of the study was to report on the outcomes of 498 patients from a prospective, multicentre, observational registry of Y90 resin microspheres as treatment for colorectal liver metastases. The outcomes measured were treatment characteristics, survival, and safety.
The patients on whom Emmons et al’s study reports were treated from 2015-2020 and the cohort was 40% female (n=200) and 60% male (n=298). The median age was 60 years old.
Regarding tumour burden, it was <10% in 210 (47%), 11–25% in 115 (26%) and >26% in 125 (28%) patients. Treatment was bilobar in 257 (52%) and unilobar in 241 (48%) patients. At baseline, 180 patients (38%) had extrahepatic disease. Eastern Cooperative Oncology Group (ECOG) status was between zero and one in 441 patients (93%).
There was variation in whether Y90 was used as part of first-line therapy (17%), second line therapy (41%) and third line or beyond in 43% of patients. Fourteen per cent of patients had undergone hepatic resections before treatment with Y90, another 14% had received ablation, 6%, and 2% of patients had undergone portal vein embolization.
The median OS among the patients was 15 months after Y90 (95% confidence interval [CI], 13.2-16.9). One-, two- and three-year OS was 60%, 29%, and 19% respectively. Median OS by line of therapy was 13.9, 17.4 and 12.5 months for first-, second- and third-line. PFS across the whole group was 7.4 months (95% CI 6.4-9.5). Median PFS by line of therapy was 7.9, 10, and 5.9 months for first, second and third.
Six months after treatment, hepatic function toxicities were available in 327 patients. Sixty grade three or four hepatic function toxicities developed with bilirubin (in 29 patients), albumin (13), and aspartate aminotransferase (12) toxicity being the most common. The incidence of hepatic function toxicity at grade three or higher significantly increased with multiple lines of therapy, with bilirubin in 6% of patients after first-line, 7.8% after second-, and 10% after third-; p=0.01). Albumin was 4.2% after first-, 3.1% after second-, and 4.7% after third-line; p=0.008). Five patients (1%) died of liver failure, which was able to be attributed to radiation-induced liver disease.
Emmons’ and her co-authors’ conclusion is that Y90 resin microsphere embolization contributed to 15 months OS after treatment, with patients with the longest OS having received the treatment as part of second-line therapy.
Kieran Murphy
Kieran Murphy (Toronto Western Hospital, Toronto, Canada) also won the award, for his report on a non-inferiority, prospective, randomised controlled trial, which compared intradiscal oxygen-ozone chemonucleolysis to microdiscectomy for lumbar disc herniation radiculopathy.
Murphy’s objective was to compare the non-inferiority treatment status and clinical outcomes of the two aforementioned types of treatment in patients with refractory radicular leg pain due to single-level contained lumbar disc herniations.
The study was multicentre, carried out across three European hospital spine centres. Forty-nine patients with a mean age of 40, of whom 17 were females and 32 males, were studied. All had a single-level contained lumbar disc herniation and had been experiencing radicular leg pain for more than six weeks, as well as being resistant to medical management.
Patients were randomly assigned one of the two treatments, with 25 given intradiscal oxygen-ozone and 24 the microdiscectomy. Eighty-eight per cent (n=43) received their allocated treatment and constituted the as-treated (AT) population.
The primary outcome was overall six-month improvement in leg pain, compared to baseline. Secondary outcomes included back numerical rating pain scores (NRS), Roland Morris Disability Index (RMDI) scores and EuroQol (EQ)-5D, which were collected at baseline, one week, and one, three and six months.
In terms of the study’s results, primary analysis found the overall six-month difference between treatment groups in leg pain improvement using the AT population was -0.31 (standard error [SE]=0.84) points, favouring in microdiscectomy. Using the intention to treat (ITT) population, the difference was 0.32 (SE=0.88) points in favour of oxygen-ozone. The difference between oxygen-ozone and microdiscectomy did not exceed the non-inferiority 95% confidence lower limit of treatment difference in either the AT (95% lower limit, -1.72) or ITT (95% lower limit, -1.13) populations.
Both treatments resulted in rapid and statistically significant improvements over baseline in leg pain, back pain, RMDI, and EQ-5D that persisted in follow-up, and no outcome differences were statistically significant between the two groups.
Murphy’s conclusion is that intradiscal oxygen-ozone chemonucleolysis for single-level lumbar disc herniations that are unresponsive to medical management, met the non-inferiority criteria to microdiscectomy on six-month mean leg pain improvement. Moreover, both treatment groups achieved similarly rapid, significant and persistent clinical improvements. The study also found that 71% of patients who were randomised to the oxygen-ozone group were able to avoid having further surgery.
Bela Kis
Bela Kis (Moffitt Cancer Center, Tampa, USA) received the prize for the second time in two years. In 2020, his winning abstract was ‘Transarterial chemoperfusion treatment of unresectable pleural mesothelioma—interim results of a phase two prospective study’. This year, he won with ‘Radioembolization with Y90 glass microspheres as first-line treatment for unresectable intrahepatic cholangiocarcinoma—a prospective phase two clinical trial’.
Kis explained that patients with unresectable intrahepatic cholangiocarcinoma (IHC) have a dismal prognosis; without treatment the expected survival is three to six months. Standard-of-care first-line treatment with gemcitabine and cisplatin demonstrated improved median overall survival (OS) of 11.7 months. However, this therapy was complicated by severe adverse events in 70% of patients. Prior retrospective studies demonstrated survival benefit of Y90 radioembolization as a first-line treatment in IHC with minimal side effects. The recent phase two clinical trial (MISPHEC) of a combination of Y90 radioembolization plus chemotherapy (cisplatin and gemcitabine) as a first line-treatment in ICC showed median OS of 22 months, but 71% of patients had severe, grade three and four, adverse events. In view of these prior reports, Kis’ study aimed to evaluate the safety and efficacy of Y90 glass microsphere radioembolization as first-line treatment without chemotherapy for unresectable IHC.
Twenty-five eligible patients were enrolled in Kis’ institutional review board-approved phase two study. Eligibility criteria were absence of evidence of extrahepatic metastasis, Childs-Pugh A or B, without main portal vein thrombus, bilirubin <2mg/dL, ECOG performance status of zero to two, and not having chemotherapy, liver embolization, or radiation therapy for IHC. The primary endpoint was progression-free survival (PFS) and secondary endpoints, OS and toxicity.
Two patients were excluded from the study on the basis of unrecognised lung metastasis at the time of Y90 treatment, and right hepatectomy four weeks after Y90, respectively. Twelve women and 11 men were included, of whom the median age was 76 years.
The patients received a median dose of 136Gy radiation from the Y90 treatment. Median PFS was 5.5 months (95% CI: 3.9–7.1 months). Median OS was 27.2 months (95% CI: 8.5–4.9 months) from diagnosis and 19.4 months (95% CI: 4.6–34.1 months) from Y90 treatment.
Univariate and multivariate analyses were performed to find prognostic factors associated with PFS and OS, but none were identified. Furthermore, Kis states that, patients tolerated the radioembolization treatment well, with only two incidences of grade-three toxicity (radiation capsulitis and gastric bleed) reported. At three months, there was one grade three biochemical toxicity (elevated bilirubin).
Kis concludes that first-line treatment of IHC with radioembolization is promising from an OS and toxicity standpoint. When compared to published data on IHC, radioembolization appears to be at least as effective as systemic chemotherapy, but with a much better toxicity profile. This prospective trial suggests that radioembolization can be considered a first-line treatment for unresectable IHC, and can be a stepping stone to initiate large, multi-institutional randomised trials to compare radioembolization to chemotherapy as a first-line treatment of unresectable IHC.
Amy Deipolyi
Amy Deipolyi (Charleston Area Medical Center, Charleston, USA) was another presenter whose abstract ‘Immune activation markers and response to radioembolization of breast cancer liver metastasis: Pilot study’ won the prize. Her purpose in carrying out the study was to ascertain whether radioembolization (RE) of breast cancer liver metastasis (BCLM) activates immune function, as well as to identify the markers of immune function that are associated with RE response. RE was found to be associated with immune activation, as seen within the tumour microenvironment and peripherally. The results also suggest that peripheral markers of inflammation, including monocytes, MDSCs, and ILs may indicate a poor response to RE.
Bluegrass Vascular Technologies recently announced the publication of a paper featured on the cover of the June 2022 issue of the Journal of Vascular Surgery (JVS). The paper reports the use of the company’s Surfacer system to perform an ‘Inside-Out’ procedure and obtain central venous access in a haemodialysis patient presenting with severely symptomatic superior vena cava (SVC) syndrome.
The procedure was performed by Alexandros Mallios (Hôpital Paris Saint-Joseph, Paris, France) and his team.
“Our paper is the first to report on a fully extraanatomical, minimally invasive approach resulting in the bridging of a functioning upper extremity access to the SVC,” stated Mallios. “The use of the Surfacer system enabled us to quickly and efficiently obtain central venous access after two previous attempts to recanalise the central vein occlusion using other approaches were unsuccessful.”
“The case report presented by Dr Mallios and his colleagues further demonstrates the broad clinical utility of the Surfacer system to help facilitate gaining venous access in patients with central venous obstructions,” said Gabriele Niederauer, CEO and president of Bluegrass Vascular. “We congratulate Dr Mallios and his team on having a featured covered story in JVS associated with this interesting case, which included the use of the Surfacer system.”
This follows an announcement from April 2022 in which Bluegrass Vascular highlighted a paper, published in the Journal of Vascular Access, that detailed the use of the Surfacer system to perform the Inside-Out procedure via a transcollateral approach.
Earlier this year, the company also closed US$5 million in convertible debt financing to support the commercial expansion of its Surfacer system.
TriSalus’ clinical leadership team presented new preclinical data at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA). The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist, SD-101, and the proprietary Pressure-Enabled Drug Delivery (PEDD) method of administration to overcome critical treatment barriers that can prevent immunotherapeutic uptake in hard-to-treat tumours.
In one abstract presentation, TriSalus highlighted data that suggest the PEDD method was more effective in delivering SD-101 into liver tissue than direct needle injection. To further support these findings, TriSalus is collaborating with Massachusetts General Cancer Center (Boston, USA) on an investigator-initiated clinical trial to evaluate whether PEDD improves the delivery of radioactive microspheres during radioembolization treatment for liver cancer, compared to a standard microcatheter.
In a second abstract presentation at SIR 2022, TriSalus highlighted new data on the development of a transvenous approach for the regional treatment of pancreatic tumours, called pancreatic retrograde venous infusion (PRVI). This preclinical data are the first of their kind to demonstrate that the PRVI approach can improve uptake and tumour response for pancreatic tumours. Unlike the liver, using the arterial systemic for drug delivery in the pancreas poses significant anatomic challenges. TriSalus has developed a novel approach to leverage the PEDD method in venous branches using a new US Food and Drug Administration (FDA)-cleared device designed for highly targeted intrapancreatic delivery of SD-101.
“Patients with liver and pancreatic tumours can experience poor outcomes due to tumour-induced immunosuppression and high intratumoral pressure that often prevent therapeutics, such as immunotherapy drugs, from reaching their targets. Existing treatment approaches, including direct needle injections and intravenous immunotherapy alone, often fail to address these barriers in a comprehensive way. By engineering new approaches to meet these challenges, we may be able to improve the treatment paradigm for liver and pancreas tumour patients,” said Steven C Katz, chief medical officer at TriSalus.
University Medical Center Utrecht (Utrecht, Netherlands) recently published the latest results from the HEPAR Primary study, which evaluated the safety and efficacy of Holmium-166 (QuiremSpheres holmium-166 microspheres) Selective Internal Radiation Therapy (SIRT) for hepatocellular carcinoma (HCC) patients (Barcelona Clinic Liver Cancer stages B and C) without curative options.
HEPAR Primary showed an acceptable toxicity profile and demonstrated an objective response rate of 54% (14/26 patients) at three months after mRECIST evaluation of target liver lesions. The news was shared by Terumo Interventional Systems, the company behind the technology.
“We are very excited about the safety and efficacy results of our HCC study, in which we have been using QuiremScout for the work-up and QuiremSpheres for the SIRT treatment. At the start of our study, we did not have the opportunity to use the pre-treatment planning functionalities of the Q-Suite imaging software (launched in September 2020),” said author, Marnix Lam (University Medical Center Utrecht, Utrecht, Netherlands). “Looking towards the future, I strongly believe that we can achieve even better clinical outcomes by truly individualising the treatment of each patient using the entire Holmium platform. Therefore, we are currently recruiting patients in a new multi-centre iHEPAR study to further demonstrate the importance of individualising SIRT in HCC using the full Holmium platform.
The Holmium platform consists of three integrated products, QuiremScout holmium-166 microspheres, QuiremSpheres holmium-166 microspheres and Q-Suite imaging software, that allow healthcare professionals to select patients with confidence, deliver treatment with precision and plan and verify with accuracy.
“We are delighted with the results of the HEPAR Primary study, which demonstrate the benefits of Holmium SIRT in the treatment of primary liver cancer. This study is an additional demonstration of the value of our Holmium platform and using QuiremScout and QuiremSpheres together. We are confident this will continue supporting the adoption of the Holmium platform,” said Laurent Domas, global vice president of strategy and therapy development, Interventional Oncology Terumo.
The findings of a collaborative research project at the University of California San Diego, San Diego, USA were presented in an abstract titled ‘Multivessel pelvic embolization during caesarean hysterectomy for placenta accreta spectrum: A single-centre experience and comparison to internal iliac artery balloon occlusion’ at the Society of Interventional Radiology (SIR) 2022 Annual Meeting (11–16 June, Boston, USA).
This collaboration among interventional radiology, obstetrics and gynaecology, and maternal foetal medicine teams aimed to compare how intraoperative pelvic embolization performed to reduce blood loss during surgical management of placenta accreta spectrum (PAS) versus internal iliac artery balloon occlusion (IIABO). The abstract’s lead author, Christine Boone, explained to Interventional News ahead of the presentation her surprise at the extent of blood loss reduction with embolization compared IIABO, alongside some of the other aspects of her research.
Regarding the study’s results, Boone first outlined her prediction that blood loss would be “similar or better” among the embolization group. “But what surprised me was by how much [embolization improved outcomes],” Boone went on to acknowledge. In the IIABO group, she noted, median blood loss was 2.5 litres, where any amount over one litre in a caesarean section delivery is considered a haemorrhage. “It was a lot more before [occlusion], and people had to get blood transfusions,” Boone said, contextualising the benefit that IIABO intervention brings. Yet, the median blood loss, she then noted, with embolization, was only 675ml “which is not even considered a haemorrhage by the criteria for caesarean [delivery].” In this group, no patients needed transfusions, which was not the case for the occlusion group. Boone labelled this “a really striking difference,” accounting for her surprise at her study’s findings. Of note, the comparative procedure times for IIABO and embolization, which were an average of 35 and 64 minutes, respectively, Boone admitted that the duration of the procedures is an important consideration. While the longer duration of the embolization procedures did not present issues in the context of the study, it may in some cases.
Christine Boone
The abstract was also recognised as ‘exceptional’ among those presented at the meeting. Additionally, Boone received the SIR Foundation Resident Research Award during the meeting’s award ceremony plenary session on Monday 13 June.
Boone began by relaying to Interventional News how she was inspired to study the applications of interventional radiology (IR) in women’s health after “[repeatedly] hearing about how maternal mortality was increasing in the USA” as she was finishing medical school. “I thought this was so strange,” she admitted, given “how we pay so much for healthcare in this country.”
Expanding on what drew her into women’s health and IR, she conveyed her passion for being “able to intervene, especially in postpartum haemorrhage situations” and that “that was the thing that would often kill women in childbirth.” Boone went on to underline how haemorrhage management can be achieved in “as little as 15 minutes,” and that this is one of the reasons why she sees her area of research as a “really exciting opportunity to help.”
Learning more about placenta accreta spectrum disorders, Boone highlighted as “fascinating”, not just from a treatment point of view, but also from a scientific standpoint. “The more I read about it, the more I learned that it was almost like a malignancy […] it does not respect boundaries […] and behaves like a cancer.” Spreading greater awareness about the disease is, therefore, something about which Boone feels strongly.
Quizzed on the two treatment options compared in her research project, Boone first conveyed how there is, currently, no standard of care regarding PAS treatment. Different clinicians may choose different approaches, including hysterectomy, as well as leaving the placenta in place to manage bleeding (the latter, however, brings with it risk of infection). IR provides a further swathe of treatment options, such as embolization and balloon occlusion, Boone detailed.
According to Boone, this application balloon occlusion “came earlier”, but that it is not necessarily used more often than embolization nowadays, as there isn’t data available on this. Nevertheless, the fact remains that there is more research on the former type of treatment. Aortic balloons are used in trauma situations, and so are widely seen as an effective method for stopping blood flow, hence the recourse to them in a PAS treatment scenario, Boone proceeded. She then detailed how aortic balloons have, in fact, been used for PAS cases during surgery, but that this threatens limbs and other organs by stopping blood flow to everywhere below where the balloon is inflated. Consequently, “the benefit of the [IIABO] is that it is more selective […]—the internal iliac artery [supplies] blood to everything in the pelvis, but the legs are excluded”.
Despite this advantage of IIABO, Boone then shared her thoughts on why embolization may work better still: “The placenta in PAS does not respect [anatomic] boundaries, including its vascular supply and so it can pull blood from the abdominal wall [for example].” This may mean that, in certain cases, the IIABO’s role is insufficient, as it is not stopping blood flow to additional vessels in question. Embolization is favourable in these cases, Boone outlined, expanding on this point with the following explanation: “[with embolization], we are looking for collaterals […] we can adapt the therapy to the unique situation of the patient and where the blood is coming from.”
The discussion then turned to the specific particles one can use for embolization to treat PAS. Boone began by conceding that no study to date has compared particle types for this indication. There can be different approaches to embolization and the type of particle is an important consideration in this strategy. Studies to determine optimal embolization strategies and embolic type would be a significant next step. Another “good future direction” for research would be subgroup analysis, as the study is ongoing. Boone explained, however, for now, the number of patients is too low for this to be possible. “There is definitely something to be said for gravidity [and there also could be] for the number of caesarean sections a patient has had,” Boone stated.
In conclusion, Boone told Interventional News how she sees these results as “huge”, and she is excited to see the impact they might have for PAS care. She also took the opportunity to give insight into her other area of research. Currently used in the treatment planning of pelvic venous disease at the University of California San Diego, Boone shared her interest in taking 4D flow magnetic resonance imaging (MRI) into the area of PAS, to see if it could aid in identifying where the placenta is drawing blood from in each specific patient’s case, ahead of the procedure, which could make treatment faster.
Peripheral arterial disease (PAD) produces a global health burden and remains a leading cause of disability, limb loss and reduced quality of life. PAD is also a proxy for cardiovascular and cerebrovascular death. Endovascular therapies have become widely used among symptomatic patients refractory to medical and exercise therapy alone, including stents, drug-eluting balloons, atherectomy, and vessel modification devices.
Our current understanding of the biologic mechanisms of these devices remains incomplete. Endovascular practitioners need a deep understanding of the vascular biology and biomechanics of endovascular therapies to enable critical appraisal, identify gaps in existing knowledge and define unmet needs for their current and future patients.
Chronically occluded lower extremity arteries, particularly long-segment TASC-C and -D lesions, were long considered untreatable with percutaneous approaches and amenable only to surgical bypass. Endovascular techniques which intentionally create an intramural channel within the arterial media, followed by angioplasty with or without stent placement, were first described by Bolia but have since evolved to encompass a wide array of dedicated technologies. This approach, known as subintimal recanalisation, has now become routine for many interventionalists. What is remarkable is that the vascular remodeling following subintimal recanalisation almost completely replicates the histologic elements of a native artery.
Understanding the remodelling changes after this approach can guide selection of subsequent use of other endovascular techniques to maintain vessel patency and limb preservation.
Angioplasty balloons and stents as delivery platforms for anti-proliferative drugs to the therapeutic targets of fibroblasts and smooth muscle cells within the media and adventitia have become widely utilised in endovascular therapy. Interventionalists need to distinguish cytostatic from cytotoxic drugs, understand their pharmacokinetics and mechanisms within the cell cycle. Perhaps as importantly, various coating and polymeric delivery systems (excipients) differ greatly in efficiency and efficacy and are significant determinants of clinical benefits of these therapies.
Timothy Clark
Bioabsorbable scaffolds offer enormous potential to provide a stent-like scaffold to optimise arterial remodelling, while resorbing over time to leave no permanent implant behind. These devices gained rapid, nearly global adoption in the coronary vessels until the risks of late thrombosis were recognised and led to their near-abandonment. In the peripheral vascular applications, bioabsorbable scaffolds face a demanding list of attributes: high radial force, predictable resorption without particulate embolization or thrombosis, and sufficient radio-opacity to enable precise deployment within heavily calcified vessels. Despite these challenges, several promising technologies may soon yield these devices for the periphery with favourable effects on vascular remodelling.
Atherectomy is a widely utilised technique in endovascular therapy, but randomised trials dating back to first-generation plaque excisional devices have consistently struggled to show a compelling, cost-effective clinical benefit of this therapy. A wide array of atherectomy systems have since evolved, however the extent to which these devices remove significant quantities of plaque, thrombus, or cellular/fibrotic deposits remains insufficiently understood. Vascular remodelling after atherectomy is variable and often unpredictable, and intraprocedural risks of embolic debris worsening underlying limb ischaemia remain an ongoing concern. A broader understanding of the vascular biology behind the purported mechanisms of various atherectomy systems is needed.
Vessel preparation techniques employ devices to score, cut, sonicate, or create microfenestrations in a vessel wall prior to subsequent angioplasty or stent placement. These techniques are considered beneficial when peripheral arteries are highly calcified or extremely stenotic. It is key to understand the vessel wall modifications that occur with these ‘vessel prep’ devices and to what extent these modifications confer a benefit in sustaining vessel patency.
Lastly, self-expanding nitinol stents, including bare-metal, drug-eluting and polytetrafluoroethylene-covered, are widely used in the femoropopliteal artery. The femoropopliteal artery experiences among the highest levels of torsion and compression within the body. These stents are typically laser-cut, electropolished nitinol tubes which are shape-set to undergo prescribed expansion upon delivery within a vessel. Specific stent design features may be less prone to strut fractures and thereby, intimal hyperplasia and thrombosis. Certain stent designs
can create spiral laminar flow, which may reduce wall shear stress and platelet activation.
Each of these topics were explored within a Categorical Course at the Society of Interventional Radiology Annual Scientific Meeting (11–16 June, Boston, USA). By understanding the biology of vascular remodelling, which occurs following endovascular interventions including angioplasty, subintimal recanalisation of chronic total occlusions, stent placement and atherectomy, we hoped to provide further insight to vascular interventionists to distinguish existing endovascular devices based on design, mechanism and performance.
Timothy Clark is director of interventional radiology at Penn Presbyterian Medical Center, University of Pennsylvania, Philadelphia, USA, and professor of clinical radiology in the Department of Radiology at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, USA.
Disclosures: Clark is a consultant for BD, Boston Scientific, Teleflex, B. Braun and Baylis Medical, and receives royalties from Teleflex and Merit Medical. He is founder of Forge Medical and NeuRx Medical.
The 2022 European Congress on Interventional Oncology (ECIO) took place 24–27 April in Vienna, Austria. Interventional News spoke to chairman Philippe Pereira (SLK-Kliniken, Stuttgart, Germany) to hear his thoughts on the new addition to the meeting programme for this year: the foundation interventional oncology (IO) course.
Q: Why is the launch of this course such a landmark event? What will it mean for the area of IO and its trainees going forward?
A: IO is rapidly continuing to establish itself as the fourth pillar of cancer care alongside medical, surgical and radiation oncology. To the advantage of the right patients, IO can be combined with surgery, systemic treatment and, in some instances, with radiation therapy. Moreover, IO procedures can be hugely beneficial not only for the recovery times of the patient, but they are often far more cost-effective when compared to other therapies. The most effective way to increase the possibilities for patients to benefit from minimally invasive oncology treatments is for interventional oncologists to practise as fully fledged clinicians rather than simply as technicians, holding outpatient clinics and participating fully in discussions at multidisciplinary team meetings. In order to do this successfully, they must learn the basics of oncology in relation to the conditions they treat, so that they can engage in meaningful discussions with other clinicians and patients.
During ECIO 2022, we had the first foundation course in IO ever to have been held in Europe. The foundation course is for interventional radiologists who are not yet familiar with minimally invasive oncological procedures, and this day-long foundation course on the basics of oncology, including all surgical disciplines and radiation therapy offers a fantastic opportunity to get started in this field. The course came into being based on a very important concept, namely the recognition that interventional oncologists must be educated as true medical doctors (oncologists), and not just carry out the role of a technician.
The goal of the course is, ultimately, to improve cancer care by increasing clinicians’ knowledge of multidisciplinary and multimodal treatment strategies: IO offers safe and effective treatment for patients with a variety of malignancies. In recent years, potentially curative interventional radiology (IR) procedures have also emerged, making an increasingly significant contribution to the treatment of cancer patients. And this does not only hold true in a palliative setting. These developments are what is responsible for establishing IO as the fourth pillar of cancer care, alongside medical, surgical and radiation oncology, as I mentioned. IO procedures, when applied to the right patients, achieve excellent oncological results with fewer complications and shorter hospital stays than conventional surgery. As a result, they are less expensive and more cost-effective than surgery.
Despite these advantages, many countries do not have the infrastructure and provisions for carrying out IO procedures, and this even includes those countries where IR is well established. Across the globe and within Europe too, the spectrum of available IO procedures varies substantially, making it difficult to offer this service to patients in a reliable manner. This variation also makes it harder for tumour boards to make recommendations as to the best multidisciplinary IR treatments for patients.
Q: What were some of the meeting highlights for you?
A: It is a bit difficult to answer this question as the chairman of the meeting (!), but I would say, maybe, the sessions that focused on combined treatments were a highlight, as this is a field that is continuously evolving. The contents of the sessions gave insight into some of the developments we will see in the future, underlining that multidisciplinary approaches can achieve some of the best results for lung and metastatic cancer patients in particular. The take-home message here is that no single clinician or oncological specialty alone has the solution for cancer patients. Other highlights were the clinical research sessions that will establish IO in future treatment algorithms, the place of artificial intelligence in IO, but also emergencies in IO as well as and the session on IO in paediatrics, without forgetting the famous ‘Morbidity and Mortality’ session.
Q: What is your impression of how the course went?
A: This course was the first multinational event after COVID-19. Nevertheless, the course was packed, and there were numerous enthusiastic comments from some of the younger attendees, and also from the experienced clinicians on the faculty.
The best question or comment (even if we did not allow enough time to discuss it at length) was from a young participant: “…but who decides on the treatment of a cancer patient, the oncologist, the surgeon, the radiotherapist or the interventional radiologist?” This, I felt was especially pertinent as it was asked without any preconceptions, and it best reflects the need for this kind of course.
In the USA, liver transplantation continues to be the best chance at long-term survival for patients suffering from the sequelae of end-stage liver disease. However, recent data from the Organ Procurement and Transplant Network (OPTN) suggest that there are 13,000 patients in the USA who are listed for liver transplant at any given time. Of that number, a high percentage of patients will either pass away while waiting for liver transplantation or be delisted due to complications of liver disease making transplantation difficult or impossible. For many of these patients, we have found that interventional radiology (IR) and the techniques we are able to offer can help prolong patient survival on a waiting list or reduce the number of delistings due to technical limitations.
With that said, many of the patients who do go on to receive a successful liver transplant, will end up with post-transplant liver complications. This could be as many as 30% of patients, and a significant number can benefit from endovascular or percutaneous intervention. The benefit of a multidisciplinary approach and, specifically, the use of endovascular techniques for many peritransplant vascular complications, is the ability to avoid major surgery or revisions.
Although peri-liver transplant patients comprise such a complex group, of whom many could benefit from these IR services, there are data to suggest that a large number are still not being offered interventional services in both a pre- and post-transplant setting. Some of the contributing factors are lack of awareness among referring providers regarding the services we can provide; lack of patient awareness; and lack of consensus among interventional radiologists themselves about the best treatment plans for these
complex patients.
Our own experience has been that when patients are offered interventional radiology services, the outcomes of liver transplantation for our centre as a whole improves. Formal incorporation of IR into the Multidisciplinary Liver Transplant group (including representation on the Liver Selection Committee), and establishment of an IR and hepatology-led multispecialty portal venous thrombosis clinic are some of the ways in which our IR team has provided access to many of the advanced techniques that should be offered to the Liver Transplant patient cohort. Indeed, use of advanced portal vein recanalisation techniques, pretransplant large portosystemic shunt embolization, and optimisation of liver graft arterial flow through hepatic artery stenting and splenic embolization for portal hyperperfusion are examples of how IR can maximise liver transplant centre outcomes.
Given the current issues facing pre- and post-hepatic transplantation vascular management, we proposed the ‘Advanced IR hepatic and splenic vascular interventions in peritransplant patients’ course as a new forum for the recent Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting, Boston, USA. This session provided a forum for experts in the field to discuss these complex cases in a format that generated robust discussion and questions.
Muneeb Ahmed is chief of the division of vascular and interventional radiology and vice chair for interventional services at Beth Israel Deaconess Medical Center, Boston, USA. He is also associate professor of radiology at Harvard Medical School, Boston, USA.
Vijay Ramalingam is co-director of interventional radiology for the Mesenteric Venous Thrombosis Program at Beth Israel Deaconess Medical Center. He is also an instructor at Harvard Medical School.
SoniVie recently announced that on 5 May 2022 the US Food and Drug Administration (FDA) granted investigational device exemption (IDE) approval for its REDUCED1 pilot study to treat resistant hypertension patients with renal artery denervation using the company’s therapeutic ultrasound ablation system (TIVUS).
“We are very pleased that the FDA has approved the REDUCED1 (Renal denervation using ultrasonic catheter emitted energy) study. Sites initiation has started, and many clinical teams have responded very favourably about participating in the study. There is a significant number of patients that may benefit from our technology and we are happy to announce this important step towards the introduction of TIVUS in the USA. There is a lack of effective therapeutic solutions for patients suffering from resistant hypertension, and physicians are looking forward to a safe, effective and easy to use device treatment,” says Christian Spaulding, CMO, SoniVie.
“This is a significant US regulatory milestone for SoniVie, starting the feasibility study using the ultrasound ablation platform in the USA for the renal denervation indication. This is a major step and priority in the company’s history,” says Tomaso Zambelli, CEO, SoniVie.
The REDUCED1 study will further expand the company’s clinical experience based on two clinical trials in renal denervation performed using the earlier generation of the TIVUS.
According to SonieVie, renal denervation with TIVUS is a minimally invasive procedure that uses high-frequency non-focused ultrasound energy to ablate nerves in the renal artery. The company claims that this causes a reduction in the nerve activity, which may decrease blood pressure. This procedure is designed for patients who suffer from resistant hypertension.
Shimadzu Medical Systems USA introduced the new Trinias system, which uses artificial intelligence deep learning to improve the visibility of medical devices while using lower X-ray doses than previous models, at the Society of Interventional Radiology Annual Meeting (SIR 2022; 11–16 June, Boston, USA).
This is the first time AI has been incorporated into the image-processing engine of an angiography system, the company declared in a press release.
The new Trinias system also offers an extensive new feature set to simplify workflow, allowing a more efficient clinical operation in any medical setting, the company reported. Shimadzu has also launched a subscription service that ensures software can always be updated to the current version, making the Trinias system a more sustainable product designed for long-term use.
Angiography systems are used to perform angiographic examinations, where the physician inserts a catheter through a blood vessel in the patient’s wrist or inguinal region to a specific site and observes an area of disease or concern, and to perform catheterisation procedures, where a therapeutic device is inserted in the patient and used to dilate blood vessels or perform other interventional procedures.
Medical facilities are increasingly operating angiography systems at low radiation levels to reduce X-ray doses, but low radiation levels also lead to X-ray noise that reduces device visibility. To support the low-dose operation of angiography systems by medical facilities and ever-smaller therapeutic devices that reduce the burden on patients, Shimadzu has developed SCORE Opera, a new image-processing technology that uses AI to ensure catheterisation procedures are safe even at low radiation doses.
Cordis recently announced the first-in-human use of the Radianz radial peripheral system by Jihad Mustapha at Advanced Cardiac & Vascular Centers (ACV) Grand Rapids, USA.
The Radianz radial peripheral system solution includes Brite Tip Radianz guiding sheath used to optimise lower extremity lesion access, the Saberx Radianz percutaneous transluminal angioplasty (PTA) catheter to facilitate treatment, and the S.M.A.R.T. Radianz vascular stent system to help maintain patency for lasting favourable outcomes.
The system is purposely engineered for radial access, which, the company claims, is proven to produce fewer vascular complications and higher patient satisfaction than femoral approaches.
Mustapha, chief executive officer and director of endovascular intervention at Advanced Cardiac & Vascular Centers (ACV) for Amputation Prevention, commented: “My colleagues at ACV and I are pleased to have successfully performed the first procedures using the Radianz radial peripheral system. We believe this portfolio represents true innovation in meeting the need for radial access solutions for lower extremity intervention.”
“We are extremely pleased with the positive feedback from Dr Mustapha and proud that these first-in-human cases were performed so successfully and by such a highly esteemed physician,” said Cordis CEO Shar Matin. “When used as a comprehensive treatment solution for vascular disease, we believe the unique capabilities of the Radianz radial peripheral system have the potential to positively impact outcomes and improve quality of life for patients.”
According to a company press release, multiple studies have demonstrated overwhelming patient preference for radial versus femoral access. Studies also show that patient ambulation time can be reduced from hours to minutes, and that patients experience improved mobility and comfort from the outset, the release continues.
In addition to the clinical benefits of the Radianz radial peripheral system, Cordis claims that radial access can reduce the total cost of care. The company references a systematic review of 14 randomised controlled trials that found radial access lowered hospital costs in the USA by up to US$1,116 per procedure in duration-of-stay costs compared to femoral access.
The Radianz radial peripheral system portfolio is expected to launch later this year in the USA and in the near future in Japan, the company advises.
Artio Medical today announced the closing of US$28 million in oversubscribed Series A2 and Series A3 financing, bringing the total amount raised by the company to date to US$74 million.
Funds will be used to support US commercialisation efforts for the recently cleared Solus Gold embolisation device and to accelerate the development of Artio’s broad portfolio of products, including expanding the company’s engineering and manufacturing capabilities, a press release details.
Artio is currently developing 10 products for the peripheral vascular market, including the Solus Gold and Solus Flex embolisation devices for peripheral vessel occlusion and the Amplifi vein dilation system—which is designed to prepare haemodialysis patients for successful arteriovenous fistula vascular access site creation.
Artio is also currently developing four products for the neurovascular market, including the Endura embolisation system comprising a detachable balloon and coils for the treatment of saccular brain aneurysms.
“We would like to thank our existing investors for their continued strong support and also welcome a new group of investors to Artio,” stated Joseph McConnell, vice president of Finance and Business Operations at Artio. “We have the opportunity to do something really special here, to bring a new generation of medical devices to market with the potential to save lives, reduce disability, and improve the quality of life for millions of people. This new capital will help Artio expand our team and scale our operations to deliver on that mission.”
M.I.Tech is the creator of the HANAROSTENT technology, a family of conformable, non-vascular, self-expanding metal stents, which have been distributed by Boston Scientific in Japan since 2015. The agreement consists of a purchase price of KRW 14,500 per share, which represents a total of KRW 291.2 billion or approximately $230 million at current exchange rates, subject to closing adjustments.
Non-vascular gastrointestinal and airway stents are used to help clear occlusions or strictures in various areas of a patient’s anatomy, including the biliary tree, pancreatic duct, oesophagus, colon and duodenum. In many cases, stent placement is minimally invasive and may aid faster patient recovery compared to surgery.
The HANAROSTENT technology features a unique hook-cross nitinol design intended to provide a natural and flexible fit within a patient’s anatomy, as well as flared ends to help prevent stent migration.
“M.I.Tech is an innovator in non-vascular stent development, with product offerings that complement our existing stent portfolio, including the differentiated AXIOS stent and Electrocautery enhanced delivery system and the flexible and conformable Agile oesophageal stent system,” said Art Butcher, executive vice president and group president for medical surgery and Asia Pacific, Boston Scientific. “We are committed to investing in technologies that advance care for patients around the world and are eager to work more closely with M.I.Tech to expand their international footprint.”
The company expects to complete the transaction in the second half of 2022, subject to customary closing conditions. The impact to generally accepted accounting principles and adjusted earnings per share is expected to be immaterial in 2022.
Cordis Names George Adams, MD as Chief Medical Officer
George Adams
Royal Philips today announced the latest results from the Tack optimised balloon angioplasty (TOBA) II below-the-knee (BTK) clinical trial, demonstrating that the Philips endovascular system—Tack (4F)—provides a sustained treatment effect and positive impact on quality of life for patients with chronic limb-threatening ischaemia (CLTI) out to three years of clinical follow-up. The Tack 4F is the first and only device of its kind approved by the US Food and Drug Administration (FDA), according to a company press release.
The TOBA II BTK trial studied the safety and efficacy of post-angioplasty dissection repair using the Philips Tack endovascular system in patients with CLTI and infrapopliteal disease. Philips details that the Tack endovascular system is a unique specialised implantable device to optimise the treatment of dissections in patients with CLTI. Endpoints included rates of major adverse events, target lesion revascularisation (TLR), target limb salvage (TLS) and quality of life (QoL) metrics.
“Based on 36-month follow-up in the TOBA II BTK trial, which is following 233 patients at 41 sites internationally, the Tack endovascular system offers a new standard in repairing below-the-knee arterial dissections,” said co-principal investigator George Adams (UNC Rex Hospital, Raleigh, USA), who presented the results at the New Cardiovascular Horizons (NCVH) conference (31 May–3 June, New Orleans, USA).
Adams added: “The device stands to significantly benefit patients with CLTI whose treatment with balloon angioplasty often leads to this particular complication, which typically goes untreated and unaddressed, to the detriment of long-term clinical outcomes.”
The three-year analysis of TOBA II BTK results includes the following clinical insights on the Tack endovascular system:
93.9% target limb salvage in CLTI patients at three years
69.6% freedom from clinically-driven target lesion revascularisation across all patients at three years
Sustained improvement in established clinical classification systems including the Rutherford clinical category and haemodynamics in ankle- and toe-brachial indices
Sustained improvement in patient-reported quality-of-life and mobility measures
“In treating peripheral arterial disease below the knee with balloon angioplasty, dissections of the popliteal, tibial and peroneal arteries occur with considerable frequency,” explained Chris Landon, business leader of Image Guided Therapy Devices at Philips. “With the Tack endovascular system from Philips, interventionists can reliably repair below-the-knee arterial dissections – and in doing so, improve major amputation rates and quality of life.”
Philips has previously reported data from the TOBA II and III studies, which evaluated the Tack endovascular system for superficial femoral and proximal popliteal artery dissection repair following uncoated balloon angioplasty and/or drug-coated balloon (DCB) angioplasty. These multicentre, global and European studies demonstrated that the use of the Tack endovascular system resulted in dissection resolution following uncoated or DCB angioplasty.
In TOBA II, which involved uncoated and drug-coated balloons, dissection repair with the Tack System resulted in 89.6% and 86.5% 12-month primary patency (uncoated balloon group) and freedom from CD-TLR
In TOBA III, which involved drug-coated balloons, dissection repair with the Tack endovascular system resulted in 95.0% and 97.5% 12-month primary patency and freedom from CD-TLR
There were no major adverse events reported through 30 days in either study.
Together, the TOBA II, TOBA III and TOBA II BTK trials support the safety and efficacy of the Tack endovascular system for post-PTA dissection repair in above- and below-the-knee arterial disease. According to Philips, the 36-month TOBA II BTK data reported at NCVH adds to the “robust” body of clinical evidence supporting the safety and effectiveness of the Tack Endovascular System in both vessel beds.
Philips Tack endovascular system is currently available for sale in the USA and some EU countries. Further information, including safety information, is available here.
Damaged nerves can be regenerated with the application of a frozen needle under advanced imaging guidance, according to new research to be presented at the Society of Interventional Radiology Annual Scientific Meeting (SIR; 11–16 June, Boston, USA).
The technique, called interventional cryoneurolysis, is performed by an interventional radiologist and can offer hope to patients in persistent pain following a traumatic injury, according to an SIR press release.
“The idea that we can induce regeneration of damaged nerves simply by placing a cold needle through the skin under imaging guidance is extremely exciting,” said the lead author of the study, J. David Prologo (Emory University School of Medicine, Atlanta, USA). “This research answers the call from United States legislators and specialty medical societies to develop alternatives to opioids for the management of pain.”
Researchers at Emory University treated eight patients with chronic nerve pain related to a prior trauma with computed tomography (CT)-guided interventional cryoneurolysis. CT-guided cryoneurolysis uses imaging to place a needle and freeze damaged nerves, causing them to degenerate and lose function. “What happens next is almost magical,” Prologo says. “If the nerve is exposed to the correct amount of cold, over the correct area, for the right amount of time, it will regenerate—replacing the previously damaged nerve with a healthy one.”
In this study, the average time from traumatic injury to the procedure was 9.5 years. There were no procedure related complications or adverse events, and all patients returned to their baseline strength over time—confirming regeneration of the targeted nerve. In six of the eight patients, pain symptoms dramatically improved following regeneration—reflected as a collective decrease of 4.6 points in Visual Analog Scale pain scores. The average time from the procedure to the final contact point was 1.9 years.
Prologo believes that the interventional radiology skillset applied to nerve freezing has many applications for treatment of complex pain. “We are using this regeneration technique not only to manage nerve pain induced by trauma—but also for pudendal neuralgia, post-mastectomy pain, post-surgical pain, and many other conditions historically managed with narcotics,” says Prologo. “Interventional radiologists can place these needles safely in precise locations all over the body, allowing access to pain generators that were previously unreachable and giving hope to patients who struggle with pain.”
An experimental formulation of a hydrogel injected into spinal discs proved safe and effective in substantially relieving chronic low back pain caused by degenerative disc disease (DDD), according to new research to be presented at the Society of Interventional Radiology Annual Scientific Meeting (SIR; 11–16 June, Boston, USA). Hydrogels have been used for a number of years to treat DDD, but the current study is the first test of this particular gel in humans, according to an SIR press release.
After six months, all participants in this small study reported significantly less low back pain—declining from an average self-reported pain level of 7.1 down to 2.0 on a scale of zero to 10. They also experienced greatly improved physical function, with average scores falling from 48 to six on a questionnaire to gauge the impact of low back pain in preventing patients from the ability to perform normal activities.
“If these findings are confirmed in further research, this procedure may be a very promising treatment for chronic low back pain in those who have found insufficient relief from conservative care,” said lead author Douglas P. Beall (Clinical Radiology of Oklahoma, Edmond, USA). “The gel is easy to administer, requires no open surgery, and is an easy procedure for the patient.”
The gel used in this study, Hydrafil, is a second-generation hydrogel developed by ReGelTec, Inc. In 2020, it received US Food and Drug Administration (FDA) breakthrough device designation, which allows expedited review when early evidence suggests an experimental product may provide more effective treatment than current options for treating a serious condition.
The research team enrolled 20 patients, aged 22 to 69, with chronic DDD low back pain. Each described their pain as four or higher on the 10-point scale. None had found more than mild relief from conservative care, which includes rest, analgesics, physical therapy, and back braces.
Patients were sedated for the procedure, and the gel was heated to become a thick liquid. Guided by fluoroscopic imaging, researchers used a 17-gauge needle to inject the gel directly into the affected discs, where the gel filled in cracks and tears, adhering to the disc’s centre and outer layer.
“We really have no good treatments for degenerative disc disease, aside from conservative care,” said Beall. “Surgery is statistically no more effective than conservative care and can potentially make things worse; nerve ablation is appropriate for only a few patients; and existing hydrogels are inserted through an incision as a soft solid, which can pop out of place if you’re not highly skilled in placing it.”
“Because this gel is injectable, it requires no incision, and it augments the whole disc, restoring its structural integrity, which nothing we have currently can do,” he said.
Degenerative disc disease is the leading cause of chronic low back pain, one of the world’s most common medical conditions. Healthy discs cushion the spine’s vertebrae, facilitating movement and flexibility. With normal aging, though, they can become dry, thin, cracked or torn, causing pain or loss of motion. By age 60, most people have at least some disc degeneration.
A simple diagnostic procedure, followed by an interventional radiology treatment known as fallopian tube recanalisation, could allow a high percentage of women struggling with infertility from blocked fallopian tubes to conceive with less involved or, in some cases, no further invasive fertility procedures, according to new research to be presented at the Society of Interventional Radiology Annual Scientific Meeting (SIR; 11–16 June, Boston, USA). Researchers said in a press release that most women with with blocked fallopian tubes could have their condition easily corrected.
“This procedure and treatment can help women make an informed decision about infertility treatments. And for many, it can actually give them the chance to conceive naturally,” said Lindsay Machan (University of British Columbia, Vancouver, Canada), a lead author of the study. “As women increasingly desire more thorough discussions of available options and input into their medical care, they appreciate detailed information to help them make choices. This is especially true with fertility treatments.”
Researchers at the University of British Columbia Hospital (Vancouver, Canada) studied cases from 2015 to 2021 involving 956 women with infertility who had previously been diagnosed as having one or both fallopian tubes blocked based on the standard diagnostic procedure used to assess the openness of fallopian tubes, known as hysterosalpingogram (HSG). The women then underwent a selective salpingography to confirm their HSG diagnosis and, if needed, underwent fallopian tube recanalisation. In many cases, researchers said, the purported blockage was only a piece of mucus that was easily removed.
The diagnostic examination known as selective salpingography showed that nearly one in four (23.8%) had been mistakenly told they had one or both fallopian tubes blocked. Of those with a blockage, over half (56.7%) were unblocked using a fine wire in the fallopian recanalisation process, researchers said. In summary, 80.5% of women in the study who had previously been told they had tubal blockages left the same day with both fallopian tubes open after a simple outpatient procedure. In an additional 15.9%, a more precise diagnosis of significant tubal disease was made that in many cases, potentially altered treatment options.
Selective salpingography uses X-ray guidance to insert a tiny catheter through the cervix and into the opening of the fallopian tubes. A contrast dye is then injected to assess whether the tubes are open or blocked. The interventional radiologist, in many cases, is then able to perform recanalisation which opens the tube using a fine guidewire. The procedure is performed as an outpatient under light sedation and typically takes under 30 minutes.
Machan said the research suggests that selective salpingography should be offered more broadly in assessing and treating female infertility. “Fertility treatments can be expensive and out of reach for many women,” he said. “Infertility is also an emotional, often heart-breaking journey, so having this diagnostic procedure and treatment available could be life-changing.”
May’s top 10 stories on Interventional News include a report of long-term data on the safety of femoropopliteal endovascular treatment with paclitaxel-coated devices, FDA clearance of a new fibred detachable coil, and coverage of two developments in the use of robotics for performing interventions with increased accuracy.
Magneto Thrombectomy Solutions (Magneto), a medical devices company developing thrombectomy solutions for the treatment of ischaemic stroke and pulmonary embolism, presented successful first-in-human (FIH) results showing safety and feasibility of the eTrieve system, a catheter based on electric fields for removing blood clots, in patients with acute pulmonary embolism (PE).
The Royal Australian and New Zealand College of Radiologists (RANZCR) has issued a statement addressing the Australian and global shortage of iodinated contrast media.
New long-term data from the SAFE-PAD (Safety assessment of femoropopliteal endovascular treatment with paclitaxel-coated devices) study were presented as late-breaking clinical research at the Society for Cardiovascular Angiography & Interventions (SCAI) 2022 Scientific Sessions (19–22 May, Atlanta, USA).
Shockwave Medical announced that long-term data from the Disrupt PAD III trial found that superior vessel preparation with intravascular lithotripsy (IVL) led to excellent long-term outcomes out to two years with preservation of future treatment options compared to percutaneous transluminal angioplasty (PTA) in the treatment of calcified peripheral arterial disease (PAD).
The new addition to Micromate makes it possible for physicians to rely on pre- and intraoperative scans to plan the intervention, the company behind the robot Interventional Systems, announced in a press release. These planning capabilities can then be leveraged to navigate and guide instruments to the trajectory automatically with submillimetre accuracy.
Interventional Systems recently announced a new collaboration with Johns Hopkins University (Baltimore, USA) in a company press release. The research team at Johns Hopkins, led by Axel Krieger and Lidia Al-Zogbi, will not only investigate ways to improve the Micromate system but leverage the platform nature of the robot and identify new anatomical locations or applications, whose accuracy or safety issues could be addressed by using a robot.
Boston Scientific has received US Food and Drug Administration (FDA) 510(k) clearance for the EMBOLD Fibered Detachable Coil, which is indicated to obstruct or reduce the rate of blood flow in the peripheral vasculature. The first procedure using the device was performed recently at the University of Alabama (Birmingham, USA).
CLS Americas announced it will debut its office-based, magnetic resonance (MR)/ultrasound (US) fusion-guided, TRANBERG Thermal Therapy System for high-precision focal laser ablation of soft tissue, such as prostate cancer tumours, at the American Urological Association (AUA) 2022 Conference (May 13–16, New Orleans, USA).
Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.
TriSalus Life Sciences announced the enrolment of the first patient in its Pressure-Enabled Regional Immuno-Oncology (PERIO-02) clinical study in a press release.
‘Surface lead contamination on personal lead radiologic protective apparel’ is a recent report published by Kieran Murphy et al (Toronto Western Hospital, Toronto, Canada). The subject of the report is free lead dust on lead aprons: the study involved testing aprons at a Toronto university hospital, which yielded the finding that 60% of aprons and thyroid shields have free surface lead. Murphy et al draw on their results to make recommendations for addressing this professional occupational health issue. The contents of the report will be presented at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA).
The purpose of the study, the authors outline in their abstract, was to evaluate the extent of surface lead dust contamination on lead radiation protection apparel (RPA) used in Toronto-based university teaching hospital radiology departments. They then compared these results with those from pre-existing reports that point towards lead RPA being a biohazard in and of itself, despite its crucial role in protecting radiologists and other technicians during diagnostic and interventional procedures.
Murphy et al state having surveyed a convenience sample of RPA, which was kept mounted on the wall outside the angiography and emergency departments. As part of the sampling, the team recorded the following information about each specimen: lead equivalency, manufacturer, quality of lead, year of purchase and product type (i.e. lead apron, thyroid collar, or garments combining the two). A combination of visual inspection, fluoroscopy and the use of LeadCheck rapid testing was used to assess both the condition of the RPA and the extent of surface lead contamination.
Of the 69 RPA items surveyed, one failed a radiological quality inspection check, and eight items were in poor condition—the majority of all garments were over five years old and made from a lead/tin-composite material that had a 0.5mm lead equivalency. The authors also break down the RPA items in the report by their type: lead aprons (n=11); lead aprons with thyroid collars (n=25); and separate thyroid collars (n=8). The key finding is as follows: “The overall prevalence of surface lead contamination on RPA surfaces based on LeadCheck sampling was 60.9% (95% confidence interval [CI]: 49.1%, 71.5%). Surface lead contamination was significantly (p=0.0035) higher on thyroid collars (78.8% [95% CI: 62.2%, 89.3%]) than on lead aprons (44.4% [95% CI: 29.5%, 60.4%]).”
Murphy et al then proceed to discuss the significance of their own clinical findings, drawing the conclusion that they support what previous studies conducted in the USA, Europe, Taiwan and Canada have shown: surface lead dust is “[highly prevalent]” in radiology departments. Two studies referenced in the authors’ report went as far as to look at the potential toxicity of lead dust exposure, sampling blood and hair. On the basis of the sum of these investigations (which found the presence of lead in the technologists’ hair, thus indicating ingestion risk), the authors make recommendations for improving conditions for the continued use of lead RPA, in order to reduce risk to personnel wearing the garments.
Firstly, the authors highlight that their recommendations are all the more necessary as there are no current regulations in place to mandate risk assessment for lead exposure from RPA in workplaces with radiation exposure. Moreover, Murphy et al underline that all the RPA they surveyed had passed radiologic quality control tests, but that this does not preclude the presence of surface lead dust. The conclusion from this is that “stringent protocols” must be formulated and followed in terms of cleaning RPA, as well as the shielding structures made of lead. In addition, the authors accentuate the importance of further studies into the toxicity impact of long-term lead exposure among personnel.
Alongside their recommendations, the authors draw attention to the limitations of their investigation, which evaluated “only a small sample of lead aprons and thyroid collars for surface lead dust contamination at a single institution.” They also point to the inexpensive LeadCheck test as yielding less reliable results than may have been achieved with other methods. Murphy et al add to the limitations the fact that the RPA they surveyed was made exclusively of a lead composite material; for this reason, they suggest that their results may not be wholly applicable to solid lead RPA. Lastly, they acknowledge that, when comparing their results with previous studies’, they may not have included all relevant literature, leading to potential omission of key findings which could have produced a different conclusion.
A final note from the authors in their report is that “there is no established safe level of lead” and, therefore, surface lead dust contamination should be continuously monitored where RPA and lead room shields are being used. Likewise, personnel and those responsible for workplace risk assessment should be aware of any defective equipment which may need to be taken out of use to reduce exposure to lead dust.
“I do not want interventional radiology to be a treatment for the rich, nor for those who live in the wealthiest countries.” Yasuaki Arai is an interventional radiologist who was, until recently, executive advisor to the president at Japan’s National Cancer Center in Tokyo, where he is currently a member of the interventional radiology centre. He founded the Japan Interventional Radiology in Oncology Study Group (JIVROSG) and is a prolific physician-inventor, including of the tip-deflecting microcatheter. He answers some of Interventional News’ questions.
What attracted you to a career in interventional radiology (IR)?
IR attracted me because it was an area where I knew that my enthusiasm, skills, ideas and efforts could improve patient distress directly and quickly. No other medical specialty ever really appealed to me as much, but prior to deciding to become a doctor, I did think I would like to be a chef.
Who are, or were, your mentors?
When I started in IR, the specialty did not exist in Japan yet. So, I did not have a mentor. I learned angiography from a book, but I did the rest while thinking for myself. For me, my patients may have been a kind of mentor, as it was their conditions and also the patients themselves that would tell me whether the procedure I had done was right or wrong, good or not so good for them.
Could you describe a particularly memorable case of yours?
Selecting one case is not easy, but doing novel procedures that no one anywhere in the world has done before is always memorable. For example, the implantation of a catheter and port system via the left subclavian artery for hepatic arterial infusion chemotherapy; extra-anatomical shunt creation between the hepatic vein and the ascites cavity, the portal vein and the splenic vein, between biliary
trees, and so on.
You founded the JIVROSG: what prompted you to set this group up?
I learned the importance of clinical trials and evidence in discussion with medical oncologists when I presented the results of hepatic arterial infusion chemotherapy for liver metastasis at a conference. It was one of the international conferences of loco-regional treatment that took place during the 80s in Europe. The oncologists I met taught me that randomised controlled trials (RCTs) are necessary for proper scientific evaluation of emerging treatments. It made sense to me then that conducting clinical trials and presenting evidence is something that we should be doing in Japan too.
And what are some of the most exciting findings to come out of the JIVROSG?
There are two purposes of JIVROSG clinical trials. One is to answer clinical questions in IR. Another is to be able to use evidence to obtain approval for IR devices that, until that point, did not have sufficient evidence to support approval. In the case of the former, the positive results of an RCT of palliative IR procedures such as percutaneous vertebroplasty for painful bone metastases and percutaneous transoesophageal gastric tubing (PTEG) to relieve patients of the pain associated with standard nasogastric tubes were very exciting. An example of an exciting finding of the latter variety was a clinical trial of conventional transarterial chemoembolization (cTACE) for hepatocellular carcinoma (HCC) in collaboration with scientists in South Korea. With this clinical trial, lipiodol for TACE was approved in Japan, and then approved all over the world. Similarly, a clinical trial of the liquid embolic material N-butyl 2-cyanoacrylate (NBCA) is due to be approved in Japan. We hope it will go on to have an even wider-reaching impact on the world of IR.
What are the most challenging aspects of using IR techniques to diagnose and treat cancers?
Progress in IR happens at a rapid pace and sometimes this is even too fast for the evidence to be recognised by physicians outside of IR. As a result, sometimes IR procedures are not recommended, even when the patient is a good candidate for IR treatment. This is probably one of the most challenging aspects of using IR to diagnose and treat cancers. We will need to put in continual effort to make IR a standard treatment in modern medicine.
You have been involved in research and development to bring a number of medical devices to market such as the implantable port and the tip-deflecting microcatheter. What is an example of a cutting-edge device that is currently transforming how you treat patients in your field?
There are many fascinating, unsolved problems. Of most interest to me is how we treat stenotic lesions of the small intestine. With advances in endoscopy, the gastrointestinal tract and bile ducts are becoming less the domain of the interventional radiologist, and more the field of endoscopists. However, the small intestine, which the endoscope cannot reach, remains the realm of IR. I hope to establish techniques and devices to treat stenotic lesions of the small intestine percutaneously.
As former executive advisor to the president at Japan’s National Cancer Center, what are your hopes for the future of interventional radiology in oncology?
The recent progress of systemic medical treatments with molecular target agents and immunotherapies is tremendous. However, I feel that the importance of regional treatments such as surgery, radiation therapy and IR are sometimes forgotten about. There are not many cancers that can be completely treated with systemic medical therapy alone. So, I think it is very important to work on establishing guidelines for the appropriate combinations of systemic therapy and IR for particular types of patients. I hope that IR will, before too long, be recognised as one of the undisputed standard therapies in oncology.
You were named a distinguished fellow at Cardiovascular and Interventional Society of Europe (CIRSE) 2017. What would you like to see the 2022 meeting’s programme include?
Unfortunately, there is a big gap within the world of IR, not only between IR and other specialties. It is the gap between the economically rich and less rich countries. The progress of IR is great, but the costs involved are also growing rapidly. I do not want IR to be a treatment for the rich, or those who live in the wealthiest countries. I think it is very important to enable patients who live in poorer countries to be treated with IR. It will not be easy, but it would be great if we could start discussing how we go about bringing ‘cheaper IR’ into worldwide medical practice.
This year, the Japanese Society of Interventional Radiology (JSIR), the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR), and the International Symposium of Interventional Radiology (ISIR) are holding a joint meeting. What are the most common issues facing IR in the widespread geographical region that is Asia and the Pacific?
The area of Asia is very large, and the economic situation, medical systems and social attitudes are very different country to country. So, the biggest problem with IR in Asia is that it is difficult to all come together as professionals working in diverse countries to make unified recommendations or establish common practices. However, more IR doctors than ever before will participate in APSCVIR 2022, which is a step in the right direction. Also, APSCVIR has been playing a central role in promoting educational programmes through webinars, and this has allowed IR professionals to share ideas and practices across geographical, cultural and economic borders.
What are your hobbies and interests outside of medicine?
Mountain climbing, playing music and cooking are some of my favourite pursuits. Mountain climbing and cooking are similar to IR, because I must make decisions quickly in order to achieve the best results; the results will clearly reveal whether my decision was a good one or not. As for music, I perform in a live ‘Beatles Night’ concert with professional musicians every four months. I play bass, piano and do vocals, and I think that music is more difficult than my work as an IR.
The first patient has been enrolled in the US Food and Drug Administration (FDA) investigational device exemption (IDE) below-the-knee (BTK) SELUTION4BTK clinical trial involving SELUTION SLR, MedAlliance’s sirolimus-eluting balloon.
Michael Lichtenberg, chief of the angiology department at the Klinikum Hochsauerland (Arnsberg, Germany), said: “I am excited to begin an important trial which will establish the evidence that this novel technology benefit patients suffering from critical limb threatening ischaemia (CLTI).
“So far nothing has worked consistently in this patient population. The early clinical data from SELUTION SLR registries are encouraging and I have seen the performance of this new technology in my routine work. This study is designed to prove that SELUTION SLR is more effective than the current standard of care in this difficult patient population”.
The start of enrolment in the study follows IDE approval in the US one week ago. The BTK indication for SELUTION SLR was granted breakthrough device designation by the FDA in 2019.
The aim of the SELUTION4BTK clinical trial is to demonstrate the superior efficacy and equivalent safety of SELUTION SLR compared to plain (uncoated) balloon angioplasty (POBA) in the treatment of BTK arteries in CLTI patients. The trial is a prospective, multicentre, single blinded, randomised study.
A total of 377 patients will be randomised 1:1 to either SELUTION SLR or the control. According to MedAlliance, this is the first study of its kind where real-world patients with critical limb ischaemia can be included. Patients are being enrolled at approximately 40 sites across the US, Europe and Asia.
“I am very proud of the MedAlliance team which has been able to initiate this study so quickly and have the first patient enrolled only a week after receiving IDE approval”, added Jeffrey Jump, MedAlliance chairman and CEO. “This is a great achievement and a major milestone for MedAlliance.”
SELUTION SLR was awarded CE Mark approval for the treatment of peripheral artery disease in February 2020 and for the treatment of coronary artery disease in May 2020. The US FDA has awarded SELUTION SLR with four breakthrough designations: for the treatment of atherosclerotic lesions in native coronary arteries; coronary in-stent restenosis; peripheral below-the-knee and AV-Fistula indications.
Arjo has announced the development of a new intraoperative Doppler system that includes a single-use, sterile intraoperative probe and Dopplex DMX Vascular Doppler.
This latest system provides immediate evidence of a successful vascular reconstructive procedure by capturing the bloodflow waveforms with the surgical probe and displaying it on the high-resolution colour display of the DMX Doppler, say Arjo, adding that the Doppler results can then be stored on the micro SD card for later review or transfer to a computer.
The company add that bloodflow sound is also improved with the Dynamic Digital Noise Reduction (DDNR) system that eliminates background noise when moving the probe. The probe is single-use and provided sterile to reduce the risk of infection during surgery. By providing quality assurance of blood flow intraoperatively, time and costs of a potential re-operation can be avoided and ischemic time can be significantly reduced. The Dopplex single-use intraoperative probe and DMX Doppler can assist in the performance of safe surgery, it claims.
Simon Larsen, managing director of Arjo, said: “Quality control is vitally important in performing surgery, if secondary intervention and re-operation are to be avoided. Our Dopplex Single Use Intraoperative system enables surgeons to perform an Intraoperative Doppler ultrasound assessment with sound and waveform display and allows for storage in the Electronic Medical Records for documentation. The system brings high level quality assurance to patients and healthcare providers.”
Cardio Flow has announced it recently received US Food and Drug Administration (FDA) clearance for the company’s FreedomFlow peripheral guidewire.
According to a company press release, the FreedomFlow guidewire features a stainless steel core-to-tip design with a fixed distal-spring coil which was developed to provide support for diagnostic and therapeutic devices used in treating plaque blockages in arteries both above and below the knee.
The newguidewire features a silicone-coated spring coil along with a silicone coating on the distal 200cm that eases the crossing of difficult blockages, the release adds. Furthermore, it states that the 0.014-inch core-to-tip design provides interventionists superior torque transmission and precise control when delivering therapeutic devices.
Cardio Flow has also revealed that Jihad Mustapha (Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, USA) recently completed the first commercial case with the new guidewire on a patient presenting with complex multi-vessel disease with blockages below the knee, requiring a pedal loop.
Mustapha was impressed with the trackability and versatility of the FreedomFlow guidewire, the company reports, noting, “I was able to deliver three PTA [percutaneous transluminal angioplasty] balloons, one IVUS [intravascular ultrasound] catheter, and a therapeutic device across the single guidewire—all glided easily along the FreedomFlow wire. This new product has the potential to save time and costs in the endovascular lab, given its versatility in crossing occlusions and ability to deliver multiple interventional devices on a single guidewire.”
Outlining Adept Medical’s process for identifying and solving ergonomic issues in the cath lab.
With technological advancements over the last 10 years rapidly changing the scope of atrial treatment, radial has quickly become the access point of choice for clinicians globally. Between 2011 and 2018, radial access adoption for diagnostic angiograms increased from 17.5% to 60.4%, and from 14% to 51.8% for percutaneous coronary intervention (PCI) procedures¹, and this trend is set to rise.
This change of technique has led to clinicians having to adapt the interventional lab environment, making improvements to patient set-up for the radial approach, protecting the clinician, and considering workspace ergonomics. As designers of advanced patient supports, Adept Medical has been collaborating with industry-leading experts to address identified needs in improving the interventional lab working environment.
Adept Medical first launched the STARBoard as part of the STARSystem in 2013. After seeing the need for a device to facilitate ease of radial access during interventional cardiology procedures, the company developed a solution alongside experts in the interventional cardiology field, allowing for quick, effective presentation of the patient’s wrist for radial access. Since its launch in 2013, Adept Medical has successfully placed upwards of 2,600 units of the STARBoard in market globally and experienced a positive uptake for a device to provide ongoing procedural repeatability in the cath lab.
After surveying existing users, spanning from New Zealand to the UK, Adept Medical has gathered insight into the benefits the STARSystem has provided clinicians in the cath lab, when compared to their previous way of working.
The Adept Medical STARSystem offers an ergonomic procedural position for the safe wire/device manipulation
Wire/device manipulation and security
When first witnessing procedures without a device to manage radial access, Adept Medical noticed that often the equipment and wires would be placed over the patient, causing concern of the wires kinking during advancement, or dislodgement of wires from the access site completely. When using the Adept Medical STARSystem, clinicians can easily position and place the wire for ease of manipulation on the work surface of the STARTable.
In a recent study, completed by Adept Medical, the company found that users of the STARSystem had an 87% satisfaction rate with the ergonomic procedural position of wire/device manipulation and an 83% satisfaction rate with wire/device security when using the STARSystem, compared to not using it.
Ergonomic procedural position for the clinician
Without correct positioning of the patient, the clinician is often left having to bend over to gain radial access and complete wire manipulation, particularly in instances when left-arm access is required. Using a rigid arm board or rolled towels offers little flexibility when considering patient management, and often leaves the clinician restricted in movement throughout the procedure.
The STARSystem has been designed to improve the clinician’s posture by having a rotatable arm board that can be positioned correctly to their working preferences. The left arm support allows radial access to be gained on the left-hand side, with the patient’s arm then able to be draped across the abdomen so the clinician can continue to work as normal on the right-hand side. This allows for better working ergonomics for the clinician, eliminating the need of having to bend over the patient and consequently causing back issues.
In a recent study conducted by Adept Medical, it was discovered that users of the STARSystem have an 81% satisfaction rate in the ergonomic procedural position of back straightness using the device, compared to when not using it.
The Adept Medical STARSystem handle design provides reassurance for the patient, limiting movement during radial access procedures
Managing patient restlessness and movement
During procedures where the patient is under conscious sedation, the risk of restlessness and movement is a concern for clinicians who manage patient safety and imaging outcomes.
After understanding the requirements of the clinician, Adept Medical noticed that patients often need a security reminder to avoid excess restlessness and movement. The handle design of the STARSystem allows the patient to grip an object which provides reassurance throughout the procedure and therefore limits movement compared to not using any methods of patient security. The concaved channel also assists with forearm containment preventing it rolling sideways.
In Adept Medical’s recent study, the company found that clinicians had a 81% satisfaction rate in the STARSystem’s ability to control patient restlessness and movement when compared to their previous method.
Gaining hyperextension of the wrist for access
One of the STARSystem’s key features is its ability to present the patient’s wrist quickly and effectively for proximal radial access when hyperextension is required for ease of puncture. The STARSystem handle is designed to be manipulated to rotate the patient’s wrist from a medially rotated position to a hyperextended position, allowing the radial artery to be presented for puncture. This can often be a cumbersome process without having the degree of manipulation and rotation that the STARSystem provides.
In Adept Medical’s recent study, clinicians had an 85% satisfaction rate in the STARSystem’s ability to hyperextend the patient’s wrist using the device, when compared to their previous method.
Product set-up time when performing left and right arm radial access
Having to create custom solutions for each procedure to set the patient up for radial access is less than ideal. Rolling towels for support, or taping patients to homemade arm boards is a lengthy process for the clinical team, affecting the time to set-up and procedural repeatability. These solutions offer less procedural flexibility, which can also cause delays in gaining access to begin the procedure.
The length of the STARSystem adapts to each patient’s size once they grip the handle. Adept Medical designed the STARBoard to allow for multiple levels of adaptability to comfortably suit most patient sizes.
Clinicians in Adept Medical’s study rated their level of satisfaction with product set-up time when performing right arm and left arm radial approach at 77% and 75% respectively using the STARSystem compared to their previous method.
The Adept Medical STARSystem presents the patient’s wrist effectively for proximal radial access when hyperextension is required for puncture
The solution
Adept Medical’s development journey of designing a complete radial solution for left and right access has been one derived from strong clinical input. With Adept Medical adopting a solution when radial access was first gaining traction, it allowed the company to understand pain points and offer benefits to a technique that was novel for many clinicians.
According to the company, its findings show that the STARSystem forms a complete and effective ergonomic solution that offers benefits to the clinician during radial access for both patient management and clinician workflow and comfort.
All of Adept Medical’s patient positioning equipment and operator supports are proudly designed and manufactured at the company’s site in New Zealand.
References:
1. Doll, J, Beaver, K, Naranjo, D, et al. 2022. Trends in Arterial Access Site Selection and Bleeding Outcomes Following Coronary Procedures, 2011–2018. Circulation: Cardiovascular Quality and Outcomes.
Global Embolization Oncology Symposium Technologies (GEST; 19–22 May, New York, USA) provided delegates and faculty alike with the opportunity to hear about worldwide approaches to hepatocellular carcinoma (HCC) treatment. The dedicated session comprised discussion of various curative-intent therapies, how to define this as a concept, and how the scope of it might be expanded beyond that which achieves recurrence-free survival. A key takeaway from the session was that the next generation of interventional radiologists hold radiation segmentectomy in high regard, with its advantages now playing out in the form of clinical data.
The session began with Donna D’Souza’s (University of Minnesota, Minneapolis, USA) presentation titled ‘(Thermal) ablation is the only curative-intent therapy for early-stage HCC’. However, she immediately offered the disclaimer that, in reality, she does not believe that it is the only way to treat with curative intent, especially now that we are in “the era of radiation segmentectomy”. Robert Lewandowski (Northwestern University, Chicago, USA) followed on the subject of the latter.
D’Souza started by explaining that the updated 2022 Barcelona Clinic Liver Cancer (BCLC) guidelines still recommend ablation for unresectable, small HCC, with the new addition of transarterial chemoembolization (TACE) or radioembolization as a second-line therapy if ablation is not feasible.
Regarding the definition of ‘curative-intent’, D’Souza described it based on a comparison with surgical resection, which is widely viewed as “the gold standard” for curative-intent therapy for HCC. She elaborated that the rate of complete pathologic necrosis (CPN) after ablation is also of importance in determining local cure rates.
D’Souza proceeded to detail recent data, including randomised controlled trial data out of Hong Kong, which allocated 109 patients to surgical resection and 109 to radiofrequency ablation (RFA). The paper, published in 2017, comprised data gathered over a median follow-up period of 7.7 years, and showed no difference in local recurrence rate, disease-free survival, and survival to 10 years, between ablation and resection, even for larger lesions. D’Souza highlighted the significance of these findings: “traditionally, surgery outperforms ablation for lesions between three and 5cm”. Moreover, the SURF randomised controlled trial, of which some of the results were published in 2021, demonstrated that there was, again, no difference in recurrence-free survival, nor overall survival, at five years.
In conclusion, D’Souza underlined how “ablation is the most evidence-based curative-intent treatment modality for HCC for interventional radiologists”, and also highlighted the high complete pathologic necrosis rates that have been achieved in
recent studies.
Lewandowski then pivoted to explore the curative-intent capacity of ablative, segmental transarterial radioembolization (TARE), using the case of a 95-year-old female who survived two years after undergoing ablative radiation segmentectomy for HCC. Lewandowski explained that the definition of ‘curative intent’ can and should be expanded beyond its current status: achieving a comparable degree of CPN to surgical resection. The implications of a broader scope of the term could be that it comes to encompass treatments that facilitate bridging or downstaging to transplant, namely TARE.
Lewandowski emphasised the role of dosimetry, citing his awareness of threshold doses: targeting HCC with 190 Gray sees almost three times the rate of CPN when compared to lower doses, and targeting a threshold dose of 400 Gray has yielded 100% CPN explant in a retrospective study.
Finally, given the opportunity to field questions from the audience and each other, the panel touched on cryoablation and its performance relative to that of thermal ablation. “There are some pretty good data out there showing that it is effective [and can] outperform RFA,” D’Souza outlined. She also responded to Lewandowski on the topic of SBRT: “in some centres it is becoming more common,” while the existing literature still favours RFA. Panel moderator Nadine Abi-Jaoudeh (University of California Irvine, Irvine, USA) corroborated D’Souza’s “last-resort” approach to using SBRT, but made the point that “younger radiation oncologists are excited about the therapy’s potential.”
Medtronic has announced approval from the US Food and Drug Administration (FDA) for the IN.PACT 018 paclitaxel-coated percutaneous transluminal angioplasty (PTA) balloon catheter, a drug-coated balloon (DCB), indicated for the interventional treatment of peripheral arterial disease (PAD) in the superficial femoral and popliteal arteries.
“The IN.PACT 018 DCB will allow physicians to better address challenging cases, such as those with narrow lesions or complex anatomies,” said Prakash Krishnan (Icahn School of Medicine at Mount Sinai, New York, USA), who also serves on a scientific advisory board for Medtronic. “The available long-term data [from the IN.PACT Admiral studies] on its benefits gives physicians another effective treatment for PAD in complex anatomies.”
The IN.PACT 018 DCB uses the same drug coating formulation and is built upon equivalent technology to the IN.PACT Admiral DCB, which is compatible with 0.035” guidewires. The IN.PACT 018 DCB is indicated for PTA of de novo, restenotic, or in-stent restenotic lesions with lengths up to 360 mm with vessel diameters of 4‒7 mm. It is engineered to cross tight lesions, provide better deliverability and is compatible with 0.018″ guidewires, Medtronic states in a press release.
The IN.PACT 018 DCB will be the only commercially available DCB with a 200cm over-the-wire (OTW) catheter length, providing physicians the option to treat via femoral or radial access. This is in addition to the to the 130 cm OTW catheter length.
“Medtronic is committed to offering physicians a suite of products to treat patients with PAD. Based on feedback from our clinical community and the need for an 018” guidewire compatible DCB, Medtronic is excited to bring this technology to market in the U.S,” said David Moeller, president of the Peripheral Vascular Health Operating Unit at Medtronic. “The addition of the IN.PACT 018 DCB further reinforces Medtronic’s commitment to being the market leader in drug-coated balloons.”
MedAlliance’s Selution SLR drug-eluting balloon (DEB) has received investigational device exemption (IDE) approval from the US Food and Drug Administration, making it the first limus DEB to be available to US patients, the company announced in a press release.
The Selution SLR (sustained limus release) is a novel sirolimus-eluting balloon that provides a controlled sustained drug release, similar to a drug-eluting stent (DES). The device was granted breakthrough device designation by the FDA in March 2019 and further in September 2019 for below-the-knee (BTK) indications in peripheral artery disease.
“This is a major milestone for MedAlliance,” the company states in its press release. MedAlliance has announced it will begin enrolment in the below-the-knee (BTK) IDE randomised clinical trial (RCT) SELUTION4BTK immediately outside of the US and early this summer in US centres. Principal investigators of the study are Ehrin Armstrong (Adventist Heart and Vascular Institute, St Helena, USA), Marianne Brodmann (Medical University of Graz, Division of Angiology, Austria), and Tjun Tang (Singapore General Hospital, Singapore).
Selution SLR was awarded CE mark approval for the treatment of peripheral artery disease in February 2020. The device has shown early promising clinical results in treatment of patients with chronic limb threating ischemia (CLTI) and below-the-knee artery disease.
In the PRESTIGE study which was presented as a late breaking trial at VIVA 2021 (5–7 October, Las Vegas, USA) by Tang, use of Selution SLR in complex BTK lesions resulted in sustained safety and efficacy outcomes out to 18 months. An additional 75 patients with BTK disease and Selution SLR treatment have been studied in the PRISTINE registry and the results are scheduled to be presented at LINC 2022 (6–9 June, Leipzig, Germany).
Based on the early data following the use of Selution SLR in treatment of BTK disease, MedAlliance has moved forward with the design of the SELUTION4BTK RCT to further investigate the safety and efficacy of this device and prepare for US FDA approval.
Selution SLR’s technology involves unique MicroReservoirs made from biodegradable polymer intermixed with the anti-restenotic drug sirolimus. These MicroReservoirs provide controlled and sustained limus release (SLR) of the drug. Extended release of sirolimus from stents has been demonstrated highly efficacious in both coronary and peripheral vasculatures.
MedAlliance’s proprietary CAT (cell adherent technology) enables the MicroReservoirs to be coated onto balloons and adhered to the vessel lumen when delivered via an angioplasty balloon.
Selution SLR is available in Europe and all other countries where the CE mark is recognised.
VentureMed Group recently announced that it has completed enrolment of a randomised controlled trial (RCT) titled ‘Flex Vessel Prep prior to PTA for the treatment of obstructive lesions in the native AVF’. This RCT was conducted to assess primary patency at six months when using Flex Vessel Prep system prior to percutaneous transluminal angioplasty (PTA) versus PTA alone for the treatment of obstructive lesions of native arteriovenous fistulas (AVFs) in the upper extremity.
The FLEX RCT was a prospective, multicentre, randomised study conducted in seven sites across the USA. Seventy-five patients were enrolled and includes 30-day, three-month, and six-month follow-up.
“Although fistula are the preferred access for haemodialysis, fistula dysfunction and failure remains a significant issue in AV dialysis access care. Balloon angioplasty considered the gold standard by most, still has its limitations due to the resistant and recurrent nature of these hyperplasic lesions, often requiring the use of high-pressure balloons,” said Sanford Altman (Open Access Vascular Access, Miami, USA). “These high-pressure balloon treatments can cause vessel wall damage accelerating restenosis and shortening the time between interventions. By utilising the Flex Vessel Prep prior to angioplasty, we are hoping to see improved vessel compliance, reducing the need for high-pressure balloons while reducing the barotrauma to the vessel wall thereby extending the primary patency and time between interventions.”
“This RCT builds upon the rich and diverse data we are gathering for the Flex system. The rapid enrolment of these 75 patients at seven US centres during a COVID-19 surge is encouraging”, said Denis Harrington, president and chief executive officer of the VentureMed Group. “We are excited to report our previous study, the FLEX AV Registry, will be presented at the VASA 2022 Symposium (6–9 June,Charleston, USA). 2022 is becoming a very impressive year for Flex Vessel Prep”.
Shockwave Medical and Genesis MedTech Group announced today that they have successfully obtained approval from China’s National Medical Products Administration (NMPA) to market and sell the Shockwave intravascular lithotripsy (IVL) system with the Shockwave C2 coronary IVL catheters and the Shockwave M5 and S4 peripheral IVL catheters in China.
A joint venture between Genesis MedTech and Shockwave was formed in March of 2021 as a partnership to distribute Shockwave’s products in China and to leverage Genesis MedTech’s Wuxi research and development and production base to accelerate the manufacturing of Shockwave’s products for the local Chinese market.
The Shockwave M5 and S4 IVL catheters, which are used for the treatment of peripheral arterial calcification lesions, are approved in the USA, the European Union, and other select international jurisdictions and have been used to help treat more than 50,000 patients globally who suffer from peripheral arterial disease (PAD). The Shockwave C2 coronary IVL catheters, which are used for the treatment of coronary arterial calcification lesions, are approved in the USA, the European Union, and other select international jurisdictions, and have been used to help treat more than 70,000 patients globally who suffer from coronary artery disease.
In July 2021, Yundai Chen of the Chinese People’s Liberation Army General Hospital (Beijing, China) led a team to perform the first clinical IVL procedure in China to treat a patient with severely calcified coronary artery lesions. “Shockwave IVL technology is an innovative solution for treating coronary artery calcification, especially when the calcium is deep in the artery. The technology is easy to use, which is good for increasing access,” commented Chen.
In August of 2021, Weiguo Fu and Zhihui Dong, both of Zhongshan Hospital (affiliated to Fudan University, Shanghai, China) led their team to successfully complete the first clinical IVL procedure in China on severely calcified lesions in peripheral arteries. Fu said: “Shockwave IVL provides a powerful solution to calcified lesions that could not be effectively treated in the past. It is a promising and indispensable approach for the future.”
With an ageing population, there is an increasing incidence of calcified vascular disease in China. According to the Chinese Expert Consensus on the Diagnosis and Treatment of Calcific Coronary Lesions 2021 (Expert Consensus Statement 2021), the risk of developing coronary artery calcification increases with age, with an incidence rate of about 50% in people aged 40–49 years and about 80% in people aged 60–69 years. Calcification is also a common problem in patients with PAD. According to Statistica, China had a population of over 1.4 billion in 2020, 50% of whom were over the age of 40.
“Approval in China represents another milestone in the international expansion for Shockwave’s IVL technology. We are very appreciative of the work and the quick regulatory approval by the NMPA—despite the difficult conditions in China in the past months—and its recognition of IVL’s clinical value for patients in China,” said Doug Godshall, chief executive officer of Shockwave Medical. “Genesis MedTech is a perfect partner for Shockwave in China and this accomplishment underscores the value of their established infrastructure and local relationships. We look forward to our continued relationship as we bring IVL to physicians and patients in China for treatment of arterial calcification.
Adept Medical says it has responded to the call from interventional radiologists for a device to comfortably support and manage a patient in the prone position with the launch of its new Prone Support solution, which will be available from 23 May 2022.
The Prone Support is the ideal solution for supporting and managing a prone patient, providing comfortable patient positioning during C-arm image-guided procedures, according to Adept. It is a versatile device designed to support a patient in the prone position for multiple procedure types and is stably held for the duration of a procedure by the patient’s weight.
“Optimal patient positioning is one of the key steps for a successful procedure. The Adept Medical Prone Support allows for a posterior approach for imaging-based diagnostic and guided interventional procedures. We worked closely with local interventional radiologists and other medical professionals to develop a product that allows for a consistent and comfortable patient experience. A driving goal was to produce a solution that maintains the balance of simplicity and complexity when providing functional adjustability that could accommodate a wide range of patients. We believe the Adept Medical Prone Support will be very well-received and become the state-of-the-art device for prone patient positioning,” said James Kember, lead product design engineer, Adept.
The arm supporting surface is cantilevered out from the imaging table, accommodating a variety of patient sizes and mobility ranges comfortably. The elevated cushioned face support provides additional comfort with clearance through the centre to reduce any anxiety experienced from being contained and providing space for nasal oxygen prongs.
The head-supporting assembly can also be removed completely to suit specific patient or case needs, according to Adept. The Prone Support can be simply placed underneath the mattress using the baseboard design, allowing for efficient set-up and removal on most C-arm imaging tables.
New long-term data from the SAFE-PAD (Safety assessment of femoropopliteal endovascular treatment with paclitaxel-coated devices) study were presented today as late-breaking clinical research at the Society for Cardiovascular Angiography & Interventions (SCAI) 2022 Scientific Sessions (19–22 May, Atlanta, USA). The analysis found no meaningful difference in survival between patients treated with a paclitaxel drug-coated device and those treated with a non-drug-coated device for up to six years after the index procedure, regardless of the patient’s mortality risk and device type.
The SAFE-PAD study was created in collaboration with the US Food & Drug Administration (FDA) to evaluate the long-term safety of paclitaxel-coated devices compared with non-paclitaxel-coated devices for femoropopliteal artery revascularisation among a broad, real-world population of patients with peripheral arterial disease (PAD).
The study included Medicare beneficiaries ≥66 years treated with a drug-coated device or non-drug-coated device from 1 April 2015 to 31 December 2018. Non-inferiority between devices was evaluated for mortality through 21 July 2021. A number of prespecified subgroups, including a cohort at the lowest risk of mortality defined as those aged 66–70 with no chronic limb-threatening ischaemia (CLTI) and ≤2 comorbidities, were evaluated.
“Our goal is to give patients the most durable treatment possible that will keep them out of the hospital and living their lives. Patients with PAD tend to be of lower socioeconomic status, more likely to be underserved minority populations and often need to travel long distances or take time off work to seek treatment,” said Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA). “Not having access to important treatment options known to reduce the risk of repeat intervention can have a substantial influence on our PAD patients, ultimately impacting their outcomes and quality of life. The findings presented today add to the growing body of evidence showing these devices are safe for use.”
Of 168,553 patients, 70,584 (41.9%) were treated with a drug-coated device. Median follow-up was 3.52 years. The weighted cumulative incidence of mortality at 6.3 years was 63.6% with non-drug-coated devices and 62.5% with drug-coated devices (p<0.0001). Findings were consistent among all subgroups. In particular, there was no difference in risk among those at lowest risk of mortality (n=4,212; weighted hazard ratio [HR], 0.98; 95% confidence interval [CI], 0.87–1.10).
Researchers note that were will future several reports from the SAFE-PAD study with a final report published in the next two years.
Shockwave Medical announced today that long-term data from the Disrupt PAD III trial found that superior vessel preparation with intravascular lithotripsy (IVL) led to excellent long-term outcomes out to two years with preservation of future treatment options compared to percutaneous transluminal angioplasty (PTA) in the treatment of calcified peripheral arterial disease (PAD).
As previously published, IVL at 30 days demonstrated superiority over PTA in the primary endpoint analysis, defined as procedural success with a residual stenosis less than or equal to 30% without flow-limiting dissection, prior to drug-coated balloon (DCB) or stent, with a rate of 65.8% vs. 50.4% (p=0.0065) as determined by an independent angiographic core lab. Additionally, PAD III showed that IVL achieved a reduction in frequency and severity of flow-limiting major dissections (1.4% vs. 6.8%, p=0.03), a reduction in stent implantation rate (4.6% vs. 18.3%, p<0.001) and no distal embolisation or perforation events.
These new long-term results found that the powered secondary endpoint of primary patency (defined as freedom from clinically-driven target lesion revascularisation [CD-TLR], restenosis determined by duplex ultrasound and provisional stenting) favoured IVL over PTA at one year (80.5% vs. 68.0%, p=0.017) and remained favourable through two years (Kaplan-Meier estimate: 74.4% vs. 57.7%, p=0.005), respectively.
“Prior to the PAD III study, there were limited long-term data available to provide treatment guidance for this challenging population since patients with severe calcification have historically been excluded from endovascular trials,” said William Gray (Main Line Health, Wynnewood, USA), co-principal investigator of PAD III who presented the long-term results. “The primary endpoint at 30 days showed IVL to be a superior vessel preparation strategy by demonstrating stenosis resolution with significantly fewer complications including severe dissections and the subsequent need for bailout stent implantation. Avoiding unplanned stent implantations allows interventionalists to preserve all their future treatment options should reintervention be necessary. These new long-term data show that vessel preparation with IVL followed by DCB result in excellent efficacy and durable patency out to two years, and taken together the acute and long-term results reinforce IVL as a preferred vessel preparation strategy for calcified femoropopliteal disease.”
Disrupt PAD III was a prospective, multicentre, randomised study designed to demonstrate the safety and effectiveness of IVL as a vessel preparation procedure in moderate to severely calcified superficial femoral and popliteal lesions, followed by a DCB or stent. The study enrolled 306 patients randomised between IVL and PTA at 45 sites in the USA, Germany, Austria, and New Zealand. In the IVL arm, 82.9% of patients were classified by the angiographic core lab as having severe calcification, with an average calcified lesion length of 129.4mm. Joining Gray as co-principal investigator of the study was Gunnar Tepe (RoMed Clinic Rosenheim, Rosenheim, Germany).
The Royal Australian and New Zealand College of Radiologists (RANZCR) has issued a statement addressing the Australian and global shortage of iodinated contrast media.
The release explains that GE Healthcare—the manufacturer of Omnipaque and Visipaque and the primary supplier of contrast media in Australia—has recently faced supply issues due to the current outbreak of COVID-19 and subsequent lockdown in Shanghai, China, affecting the company’s manufacturing plant.
“RANZCR is liaising with the Therapeutic Goods Administration (TGA), which is seeking alternative supplies of contrast to address the shortfall,” the statement reads, noting that updates can be found on the TGA website.
The release continues: “RANZCR recommends that medical practitioners considering referring a patient for a CT during this time consult with a radiologist for advice on alternative imaging modalities or other strategies that could be used to diagnose and manage their patients.”
In addition, RANZCR communicates that it endorses the recommendations of the American College of Radiologists (ACR) Committee on Drugs and Contrast Media that radiology practices and hospitals implement a range of strategies to conserve current supplies of contrast to manage patient care. These recommendations include “utilise alternative studies to answer the clinical question such as non-contrast CT, MRI with or without gadolinium-based contrast media, ultrasound with or without ultrasound contrast agents, nuclear medicine, or PET-CT, when feasible,” and “look for alternative versions of contrast agents, which may be marketed under a different brand name or intended clinical use”.
Finally, the release notes that RANZCR further endorses the recommendations in the recent article by Joseph Cavallo and Jay Pahade (both Yale School of Medicine, New Haven, USA), titled “Practice management strategies for imaging facilities facing an acute iodinated contrast media shortage” published in the American Journal of Roentgenology, which provides details to support practice management during this contrast shortage.
Late-breaking trial data presented at EuroPCR 2022 (17–20 May, Paris, France) underscore the potential of renal denervation as an adjunctive therapy to treat hypertension, complementing existing first-line treatments including lifestyle modifications and medication, attendees of the conference heard.
Day one of the four-day international interventional cardiology meeting, which has returned to an in-person format in Paris for the first time since 2019, saw the release of data from three clinical studies assessing the use of renal denervation as a treatment for hypertension—the Global Symplicity Registry, SPYRAL HTN-ON MED and an analysis of ultrasound renal denervation from the RADIANCE HTN SOLO and TRIO trial cohorts.
Speaking in a press conference ahead of the presentation of the data, Felix Mahfoud (Saarland University Hospital, Hamburg, Germany) told attendees that renal denervation represents a device-based treatment option to tackle the problem of hypertension.
“Despite all advances in care we still have a significant proportion [of patients] that are either undiagnosed or not sufficiently controlled to target blood pressure, and that holds true for almost all regions and geographies around the world,” he told assembled press, pointing out that the release of the data also coincides with the 2022 World Hypertension Day, which carries an aim to communicate to the public the importance of hypertension and its serious medical complications, and to provide information on prevention, detection and treatment.
“We know from large meta analyses and prospective randomised clinical trials that reducing blood pressure is impactful for patients,” he added. “The problem is not that we do not know that blood pressure is an issue and is serious, the problem is that we have available drugs that work quite well but patients do not like them and patients do not take them.
“There is obviously an unmet need, and renal denervation represents a device-based treatment option to tackle that problem,” he said.
Mahfoud then previewed data to be released later in the day during a hot-line session at EuroPCR, the three-year Global Symplicity Registry results, assessing blood pressure and major adverse cardiovascular events (MACE) after renal denervation using Medtronic’s Symplicity system.
The results show that a 10% time in target range increase in the first 12 months reduces the odds of MACE events in the following 24 months and led to the conclusion that sustained blood pressure reduction after renal denervation predicts a meaningful reduction in clinical events. In this large, global registry, which involved 3,077 patients, those who underwent radiofrequency renal denervation spent a greater amount of time in target blood pressure range and had less cardiovascular events including cardiovascular death, myocardial infarction, and stroke.
The presenter commented that, though the data come with some limitations, they are “encouraging” and show for the first time patients with a higher time in target range have reduced events. “That should convince people that lowering blood pressure with renal denervation translates into improved outcomes,” he remarked.
David Kandzari
Also presenting data during the same EuroPCR session, David Kandzari (Piedmont Heart Institute, Atlanta, USA) offered three-year data from the SPYRAL HTN-ON MED trial, investigating Medtronic’s Symplicity Spyral renal denervation system, giving an overview of the impact of renal denervation on long-term time in target blood pressure range compared with sham control.
Time in target therapeutic range has become an established and validated measure of control for chronic disease conditions, Kandzari said in his presentation, adding that specific to hypertension, time in target range is an independent measure of blood pressure control and is an independent predictor of cardiovascular events.
Kandzari noted that early results from the pilot study showed that patients who underwent renal denervation while on antihypertensive medications had lower blood pressure when compared to the sham control group, the effect of renal denervation on blood pressure burden over time had not been established.
With this latest report, a time in target therapeutic range analysis was performed using data comparing the two groups over three years and showed that the renal denervation and AH group had significantly higher time in target therapeutic range with more time in the blood pressure target range at two and through to three years as compared to the sham group, thus affirming the sustained efficacy of renal denervation over late-term follow-up.
Also presenting alongside Mahfoud and Kandzari, Ajay Kirtane (Columbia University Irving Medical Center/NewYork Presbyterian Hospital, New York, USA) offered findings of a patient-level pooled analysis of ultrasound renal denervation in the RADIANCE HTN SOLO and TRIO trials.
The analysis examined data tracking the use of ultrasound renal denervation using the Paradise (Recor Medical) system in a drug resistant population (three years or more of antihypertensive medications) taken from the RADIANCE-HTN TRIO study, and from RADIANCE-HTN SOLO, in a population with mild to moderate hypertension (controlled on 1-2 antihypertensive medications or uncontrolled on 0-2 medications).
The results of the analysis showed that there was no heterogeneity in effect on blood pressure reduction and medication burden. Those results looking at a mixed population over a six-month period favoured ultrasound renal denervation over the sham population and the pooled analysis of the RADIANCE-HTN trials suggests “the response to ultrasound renal denervation is similar in the presence or absence of medications and consistent across the whole spectrum of hypertension.”
Vivasure Medical has announced the closing of the first tranche of €22 million (US$23 million) as part of its Series D financing round that could reach up to €52 million (US$54 million) in total.
The company states that the financing, led by a multinational strategic corporation, includes an option to buy Vivasure upon certain milestones. Other participants in this Series D financing round include a second strategic corporate investor as well as existing investors, Fountain Healthcare Partners, Orchestra BioMed, LSP Health Economics Fund managed by the EQT Life Sciences team, Panakès Partners and Evonik Venture Capital.
The financing will support the US and European clinical development and regulatory approval of the company’s portfolio of fully absorbable, patch-based large-bore percutaneous vessel closure devices for transcatheter endovascular and cardiovascular procedures, a press release details. These devices include PerQseal and PerQseal+ for arterial closure and PerQseal Blue for venous closure.
Vivasure’s PerQseal technology consists of a proprietary bioabsorbable intravascular patch that seals the vessel from the inside, returning the artery or vein to its natural state without leaving behind the remains of any materials such as collagen, metal implants or sutures commonly used in other closure technologies.
According to Vivasure, the PerQseal device is the first sutureless and fully absorbable synthetic implant for large-bore arterial vessel punctures and is available to physicians in Europe for use in transcatheter endovascular procedures, including transcatheter aortic valve replacement (TAVR), thoracic endovascular aortic repair (TEVAR) and endovascular aneurysm repair (EVAR).
The company communicates that its next-generation PerQseal+ device has an enhanced bioabsorbable patch designed to address more complex patient anatomies and is currently under clinical evaluation in Europe and the USA.
Vivasure is also developing PerQseal Blue, designed exclusively for sutureless and fully absorbable large-bore venous vessel closure following percutaneous cardiovascular procedures, such as transcatheter mitral valve repair or replacement (TMVR), transcatheter tricuspid valve repair or replacement (TTVR) and leadless pacemaker implants. The company claims that, currently, there are no sutureless options available for vessel closure following large-bore venous procedures.
“While tremendous progress has been made for minimally invasive structural heart procedures, vascular issues related to the closure of the procedure remain the most common complication of these interventions,” said Azeem Latib, section head and director of interventional cardiology and director of structural heart interventions at Montefiore Health System (New York, USA). “The novel PerQseal technology is designed to address these shortcomings and has tremendous potential to improve patient outcomes and enhance procedure efficiency.”
Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.
At its heart is the CATHISsimulator, which is fully functional with all standard software systems including every iOS system and Oculus VR (virtual reality).
The training is supported by a structured curriculum, delivered by specialist endovascular instructors with many years‘ clinical experience. The programme is targeted at specialist trainees in every year of their course, medical students on a condensed course, and interested interventionists. The scope of the package includes endovascular aneurysm repair (EVAR) for carotid, renal, iliac, femoral and tibial artery angioplasties. In addition, the curriculum includes training on emergency vascular cases such as ruptured aneurysms and visceral bleeding and trauma.
“The importance of periodical continuous education, training and structured curricula of interventional procedures has been confirmed by numerous clinical experts around the globe“, noted CATHI managing director of marketing and sales Manuela Werner. “With this joint venture between VSS and our company we are combining top-level expertise with our near-to-reality simulation systems.“
Consultant vascular surgeon Abdullah Jibawi (Ashford and St Peter’s Hospital NHS Foundation Trust, Chertsey, UK), who is involved with delivering the new programme, added: “We have built our curriculum with the end user in mind in every minute detail. We want to answer the real need for training by allowing a layer-by-layer build-up of skills and decision-making […] Our programme introduces the ability to train interventionists over a specified period of time, followed by a customised exposure to a specified product line to fine-tune their experience as needed.“
CLS Americas announced it will debut its office-based, magnetic resonance (MR)/ultrasound (US) fusion-guided, TRANBERG Thermal Therapy System for high-precision focal laser ablation of soft tissue, such as prostate cancer tumours, at the American Urological Association (AUA) 2022 Conference (May 13–16, New Orleans, USA).
The system is designed to work with multiple MR/US fusion image guidance systems for precise and accurate ablation in a minimally invasive setting, while preserving healthy prostate tissue.
“CLS is pleased to introduce its office-based, fusion-guided TRANBERG Thermal Therapy System at this year’s AUA conference,” stated Michael Magnani, president of CLS Americas. “We are commercialising this innovative technology so that patients can benefit from being treated with focal laser ablation in a urology office or clinic instead of a hospital.”
“While treating prostate cancer tumours successfully is the primary goal, some current treatment options expose patients to unacceptably high risks of complications such as erectile dysfunction or urinary incontinence,” said Fernando J Bianco, investigator-in-chief for the Urological Research Network, and principal investigator of the Phase I clinical study running at Urological Research Network, Miami Lakes, USA. “Based on my initial clinical trial experience with the TRANBERG laser, I believe that partial gland fusion ablation provides the precision to successfully treat the cancerous lesions while offering patients a superior side effect profile. The ongoing study will provide us with more information on this.”
Interventional Systems recently announced a new collaboration with Johns Hopkins University (Baltimore, USA) in a company press release. The research team at Johns Hopkins, led by Axel Krieger and Lidia Al-Zogbi, will not only investigate ways to improve the Micromate system but leverage the platform nature of the robot and identify new anatomical locations or applications, whose accuracy or safety issues could be addressed by using a robot.
Johns Hopkins University has always been at the forefront of numerous innovations in robotic-assisted surgery, more recently with the development of a robotic platform capable of performing laparoscopic surgery on the soft tissue of a pig without the guiding hand of a human, on a significant step toward procedure automation.
Through this agreement, Interventional Systems strengthens its strategy of close cooperation with leading academic institutions.
“These partnerships are extremely important for us”, shares Interventional Systems chief product officer Pedro Costa. “They allow the crosspollination of ideas and technologies between the industry and the academy, allowing us to design better, safer, and more innovative products, and brings research and students closer to what is actually happening on the market. This benefits the patient and, ultimately, the entire healthcare system. We are excited to get started and are sure that Interventional Systems will learn immensely throughout this process. We hope we can teach as much”.
A report from the American Venous Forum (AVF) 2022 meeting (23–26 February, Orlando, USA) on the comparative merits and demerits of dedicated and non-dedicated stents heads the list of Interventional News’ April top 10 articles. Some of the other most read pieces include the latest profile on Karim Valji, a conversation with Robert Hinchliffe, and a debate covering some of cancer treatment’s current controversies.
Venous stenting was a hot topic at the recent American Venous Forum (AVF) annual meeting (23–26 February, Orlando, USA). Catching the audience’s attention, Lilian Tran highlighted a head-to-head study of dedicated versus non-dedicated stents.
Medtronic recently voluntarily recalled a subset of its IN.PACT Admiral and IN.PACT AV paclitaxel-coated percutaneous transluminal angioplasty (PTA) balloon catheters due to the potential for pouch damage resulting in a loss of sterility.
Karim Valji is professor of radiology at the University of Washington (Seattle, USA) and professor Emeritus at the University of California, San Diego (USA) and speaks to Interventional News about his career.
Looking ahead to the CX Symposium, (which has now taken place: 26–28 April, London, UK) Robert Hinchliffe (University of Bristol, Bristol, UK) dubs the session on the “hurting leg” a highlight.
Alucent Biomedical announced in a press release that it has enrolled the first patient in ACTIVATE II, an Australia-based first-in-human clinical trial to evaluate the safety and efficacy of its natural vascular scaffolding (AlucentNVS) technology.
Truvic Medical shared via press release that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for the Prodigy thrombectomy system, designed for the treatment of peripheral vascular thrombus.
One of the key takeaways from the debate session at this year’s Society of Interventional Oncology (SIO) meeting (24–28 March, San Francisco, USA) was that radiation oncology has seen much innovation, and that this must continue in order to provide the best outcomes for patients into the future.
Cydar Medical recently announced it has entered a strategic collaboration with Medtronic. Under the pilot arrangement, Cydar’s EV Maps software will be introduced to up to 40 new global sites, combining Cydar’s augmented intelligence technology with Medtronic’s services and case support.
An analysis showed benefit of XARELTO plus aspirin in reducing thrombotic hospitalisations for peripheral arterial disease (PAD) patients with and without chronic kidney disease (CKD).
TriSalus Life Sciences announced the enrolment of the first patient in its Pressure-Enabled Regional Immuno-Oncology (PERIO-02) clinical study in a press release.
The trial is evaluating SD-101, an investigational toll-like receptor 9 (TLR9) agonist, in adults with locally advanced, metastatic, or unresectable hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC). SD-101 will be administered using the Pressure-Enabled Drug Delivery (PEDD) method in combination with systemic checkpoint inhibitors.
Initiated at The University of Texas MD Anderson Cancer Center (Houston, USA) with additional sites anticipated, the study is the second in a series of clinical trials assessing TriSalus’ immunotherapy platform across multiple indications.
The initial trial using this platform, the PERIO-01 study, is actively enrolling and is evaluating the safety of SD-101 administered by PEDD in combination with checkpoint inhibitors in patients with uveal melanoma with liver metastases.
“Patients with advanced HCC or ICC often have limited options when seeking treatment, as checkpoint inhibitors have had some success in these indications but results are not what we want them to be in most cases,” said Steven C Katz, chief medical officer at TriSalus. “The PERIO-02 clinical trial has potential to advance the scientific foundation required to help address this unmet need, deliver new therapies to improve clinical outcomes, and ultimately, give patients a better chance to respond more reliably to different forms of immunotherapy.”
While immunotherapy has yielded significant advances in cancer treatment, unique properties of liver tumours, including immune response suppression and high intratumoral pressure, can prevent optimal delivery and performance of therapeutics and limit the overall effectiveness of immunotherapy for patients with liver cancers.
“With the PERIO-02 trial, we are striving to enable immunotherapy for the most common primary liver tumours,” said Katz. “The study is implementing a multifaceted approach by testing the integration of an immunotherapeutic, SD-101, with a [US Food and Drug Administration]-cleared delivery device, to hopefully induce the type of immune response that we are so eager to see for patients with HCC and ICC.”
The eTrieve catheter for removing blood clots in patients with acute pulmonary embolism
Magneto Thrombectomy Solutions (Magneto), a medical devices company developing thrombectomy solutions for the treatment of ischaemic stroke and pulmonary embolism, presented successful first-in-human (FIH) results showing safety and feasibility of the eTrieve system, a catheter based on electric fields for removing blood clots, in patients with acute pulmonary embolism (PE).
The data, presented at Biomed Israel 2022, the international life science and healthtech conference in Israel (May 10–12, Tel Aviv), showed a significant reduction in right ventricle/left ventricle ratio and alleviation of PE-associated symptoms.
“Magneto provides intermediate and high-risk PE patients with a unique solution for safely and effectively removing large clots blocking the arteries in the lungs,” said Piotr Musialek (John Paul II Hospital, Krakow, Poland) and an investigator in the study. “The combination of a large-diameter ‘vacuum cleaner’ with electro-mechanical thrombus extraction, allows an immediate resolution of dyspnoea and swift recovery of the cardio-respiratory system.”
The prospective, single-arm, multicentre first-in-human study assessed the initial safety and performance of eTrieve in treating patients with acute PE. The study enrolled 10 participants across three sites in Denmark and Poland. Results show that the procedure, performed under light sedation only, was safe with no device related complications. The primary performance endpoint was also met, with significant reduction of right ventricle to left ventricle volume 48 hours post-intervention. Significant clot volumes were removed, and alleviation of PE-associated symptoms was demonstrated. The catheter removed both fresh and organised clots and successfully removed blood clots of all sizes and types, from locations that could not have been safely reached using other techniques.
Prof. Asger Andersen (Aarhus University Hospital, Aarhus, Denmark), principal investigator of the study, added, “large bore aspiration of central clots with possibility to retrieve segmental clots with the eTrieve catheter, optimises the possibility for complete pulmonary revascularisation in acute PE.”
NOTE: This video is ONLY available to watch in selected countries and geographies
In a late-breaking Podium 1st presentation at the 2022 Charing Cross (CX) International Symposium (26–28 April, London, UK), Andrew Holden (Auckland, New Zealand) revealed that patients treated in the drug-coated balloon (DCB) arm of the IN.PACT AV Access trial remained intervention-free for longer than those who received a standard percutaneous transluminal angioplasty (PTA). Click on the video for the full presentation.
Holden told delegates that end-stage kidney disease patients in IN.PACT AV Access had a median time to reintervention that was 14.7 months longer when they were treated with DCB compared to PTA and that there were no safety concerns. As such, Holden added, these findings represent durable long-term data supporting the use of the IN.PACT DCB as “a standard of care” for AVF maintenance in this patient population.
The Micromate miniature robotic platform for percutaneous procedures
The new addition to Micromate makes it possible for physicians to rely on pre- and intraoperative scans to plan the intervention, the company behind the robot Interventional Systems, announced in a press release. These planning capabilities can then be leveraged to navigate and guide instruments to the trajectory automatically with submillimetre accuracy. All features fit into a one square metre console, with the robot being manoeuvered from afar, and relying on a miniature, table-mounted camera. This substantially reduces radiation exposure to physicians and patients, the number of interoperative rescans, and does not negatively impact the available space in the room.
“For years, we have been discussing making Micromate the control panel of the entire medical workflow. This solution is the first step in that direction”, says Michael Vogele, Interventional Systems’ founder and CEO. “We have developed this planning and navigation system while bearing in mind all constraints related to practicality and cost. Our all-in-one platform integrates seamlessly with the workflow and allows the use of conventional fluoroscopy, computed tomography (CT), and CT navigation, all while still being extremely affordable. We are looking forward to what is to come.”
Reto Bale (Medical University Innsbruck, Innsbruck, Austria) will be one of the earliest adopters of the technology: “Planning and navigation tools are fundamental for successful percutaneous procedures and clinical efficacy depends on them. I’m looking forward to incorporating the Micromate robot in my practice and further developing new applications whose outcomes can be improved with robotics”.
A current user of Micromate at the (Ordensklinikum Linz BHS, Linz, Austria) Alexander Kupferthaler, adds: “Precise image-driven targeting and highest accuracy while reducing radiation exposure are the ultimate goals in interventional radiology procedures. The Micromate all-in-one planning and navigation station with its intuitive handling and seamless integration to the angio-suite or CT workflow is a unique platform to add to patient safety and further perfect my interventions.”
Avail Medsystems, a healthcare technology company whose surgical telepresence platform facilitates real-time, interactive collaboration during live procedures among a network of physicians and medical device industry representatives, announced that it has entered into a partnership with the Stroke Thrombectomy and Aneurysm Registry (STAR).
STAR supports the global tracking and study of health outcomes after endovascular treatment for stroke, brain aneurysm, or other cerebrovascular diseases, with the goal of improving physicians’ precision in choosing effective therapies for patients with these conditions. Researchers at 94 participating institutions across the world use the registry data to publish papers, describing new techniques, devices, and expertise that have the potential to boost neurosurgical acumen and patient care.
STAR principal investigator Alejandro Spiotta (Medical University of South Carolina, Charleston, USA) a STAR registry co-founder, believes that physicians who share experiences with their colleagues are better prepared to improve their skills, adopt cutting-edge ideas, and help patients who previously would have been considered untreatable. Yet, collaboration typically requires travel, and for many physicians, the burdens of cost and time mean that these trips can only happen a few times a year.
To promote STAR members to engage in the collaboration and storytelling needed to advance neurological care, Spiotta decided to implement a technology that would allow STAR members to observe and collaborate during each other’s procedures and offer guidance any time—without leaving their own practices. He selected the Avail system because it allows surgeons immediate, on-demand connection both within the STAR network and across Avail’s broader network of physicians and industry, at the touch of a button through high-definition video, two-way audio, and surgical imaging views.
“Sometimes, we just need to talk a procedure through with a peer or see someone else do it to know it is possible; that’s how we push each other to improve,” stated Spiotta. “The next generation of neuroendovascular surgeons is always smarter than the last because we learn from each other’s stories […] Avail takes storytelling to the next level by allowing us to share live procedural experiences with any of our STAR collaborators in every corner of the world. It breaks down barriers and connects all of us in an international network to a degree that was not previously possible and will help propel the field forward as an experience and knowledge accelerator.”
iVascular has announced the initiation of its first trial with the new generation covered stent iCover—the iliCo study. The study has the objective of evaluating the safety and effectiveness of iCover for the treatment of de novo aorto-iliac atherosclerotic lesions in patients with symptomatic arteriopathy of the lower limbs.
The first iliCo patient was enrolled by Elias Noory (University Heart Center Bad Krozingen, Germany) part of the team of the co-primary investigator of the study, Thomas Zeller (University Heart Center Bad Krozingen, Germany). The case was transmitted live at the 2022 Charing Cross (CX) Symposium in London, UK (26–28 April, London, UK).
The case presented by Noory was a patient with an occlusion in the right common and external iliac artery. Three iCovers were implanted successfully, achieving an excellent flow after the procedure.
The iliCo study is a prospective, multicentre, non-randomised, single-arm observational study led by Co-investigators Zeller and Bahaa Nasr (CHU Brest, Brest, France). The study will evaluate the efficacy and the safety of the iVascular iCover covered stent for the treatment of de novo aorto-iliac atherosclerotic lesions in 214 patients with symptomatic arteriopathy of the lower limbs across 18 sites in Germany, France, Belgium, and Spain.
Patients will be followed up for up to two years. The primary endpoint of the study is primary patency at 12 months. Secondary endpoints include 30-day complications, major amputation at target limb, target lesion revascularisation (TLR), target vessel revascularisation (TVR), and quality of life.
iCover received the CE mark on March 2021 and has demonstrated in different cases and used its unique visibility, conformability, and safety during the procedure, iVascular said in a press release.
“We are excited and honoured to participate in the trial and enrol the first patient of the iliCo trial,” says Zeller. “From our own experience, iCover facilitates the iliac arteries treatment with its radiopaque markers, flexibility, and excellent balloon crimping.”
“The start of iliCo study represents an exciting milestone as iCover is an advancement of aorto-iliac lesions treatment,” adds Nasr.
The iliCo live case and all CX broadcast sessions can be watched on demand by registered viewers.
Boston Scientific has received US Food and Drug Administration (FDA) 510(k) clearance for the EMBOLD Fibered Detachable Coil, which is indicated to obstruct or reduce the rate of blood flow in the peripheral vasculature. The first procedure using the device was performed recently at the University of Alabama (Birmingham, USA).
The newest addition to the Boston Scientific interventional oncology portfolio, the EMBOLD Fibered Coil was designed for use in a variety of embolization procedures. A minimally invasive treatment, it is intended to block one or more blood vessels to obstruct or reduce blood flow. Occlusion in this manner is a technique used to stop haemorrhaging, prevent aneurysm ruptures, reduce the size of certain tumours and to treat a variety of venous abnormalities.
“When performing an embolization procedure, it is essential to have a device that is easy to use from start to finish,” explained Theresa Caridi, director of Division of Vascular and Interventional Radiology from the Heersink School of Medicine at the University of Alabama, and the first physician to treat a patient with the EMBOLD Fibered Detachable Coil. “The multicatheter compatibility of the EMBOLD Fibered Coil provides physicians with […] catheter choice and helps reduce the number of potential device exchanges, which may [in turn] improve procedure efficiency and enable better patient outcomes.”
In addition to the multicatheter compatibility of the EMBOLD Fibered Coil, the device also features a nitinol delivery system that prevents kinks from forming in the device during the procedure: this is intended to reduce treatment complications. These design attributes may also reduce preparation and procedure times by limiting the amount of equipment and additional products required to complete treatment, which may reduce the overall cost of the procedure.
Medtronic announced new randomised controlled data demonstrating the sustained and superior performance of IN.PACT AV drug-coated balloon (DCB) compared to percutaneous transluminal angioplasty (PTA) through 36 months, with no difference in mortality. The data was presented as a Podium 1st at the 2022 Charing Cross (CX) Symposium in London, UK.
“The 36-month data from the IN.PACT AV Access study validates that treatment with the IN.PACT AV DCB can lead to less life disruption and fewer reinterventions for patients for an extended period of time, further reinforcing the results of earlier data milestones,” said Andrew Holden, director of interventional radiology and associate professor of radiology, Auckland University School of Medicine, Auckland, New Zealand. “As the only pivotal DCB study in arteriovenous (AV) access to meet its primary effectiveness endpoint, the IN.PACT AV DCB has shown unrivalled long-term clinical benefits that support its use as the standard of care for AV fistula maintenance in patients with end-stage kidney disease.”
As vessel restenosis limits the ability to use AV fistulas effectively over time, patients often undergo up to three AV fistula maintenance procedures per year to restore function. The need for frequent reinterventions can result in significant disruptions to critical haemodialysis care and increased costs to the healthcare system.
The IN.PACT AV Access study’s three-year data further demonstrates the ability for the IN.PACT AV DCB to extend time to reinterventions from the index procedure by maintaining AV access site patency, therefore maximising a patient’s uninterrupted access to lifesaving dialysis care. Over three years, the IN.PACT AV DCB group demonstrated a continued clinical benefit compared to the PTA control group. Key highlights for this dataset include:
The Kaplan-Meier estimated target lesion primary patency through 36 months was 43.1% in the IN.PACT AV DCB group compared to 28.6% in the PTA control group (log-rank p<0.001).
The Kaplan-Meier estimated access circuit primary patency through 36 months was 26.4% in the IN.PACT AV DCB group compared to 16.6% in the PTA control group (log-rank p<0.001).
The Kaplan-Meier estimated cumulative incidence of all-cause mortality post-vital status update through 36 months was 26.6% in the IN.PACT AV DCB group and 30.8% in the PTA control group (log-rank p=0.709).
“Medtronic is committed to bringing forward technologies that improve the lives of patients undergoing dialysis,” said David Moeller, president of the Peripheral Vascular Health business, which is part of the Cardiovascular Portfolio at Medtronic. “These results demonstrate IN.PACT AV DCB’s ability to significantly reduce the number of reinterventions, as well as the potential to reduce comprehensive care costs.”
Surmodics has announced that its Pounce thrombectomy system achieved 100% technical success in 20 first-in-human (FIH) procedures. The FIH data were presented by Gary Ansel (Columbus, USA) at the 2022 Charing Cross (CX) Symposium (26–28 April, London, UK).
Technical success was defined as the removal of clot to restore blood flow without the use of an additional adjunct thrombectomy device. Ansel, the inventor of the Pounce thrombectomy system and a consultant for Surmodics, also revealed that 19 of the 20 procedures were able to avoid the use of thrombolytics in the target lesion. The FIH cases were performed across six US medical centres, with the first use of the US Food and Drug Administration (FDA)-cleared system occurring in June 2021.
“The Pounce thrombectomy system demonstrated technical success in these early clinical cases, showing an ability to quickly deal with a wide range of clot from soft to organised, including emboli in the peripheral arterial vasculature,” said Ansel. “This fully mechanical thrombectomy device has no power unit or other capital equipment requirement, making it easy to use and efficient for physicians to treat patients with complex peripheral arterial disease (PAD).”
Average procedure time in the FIH cases was 79.6 minutes and the average lesion length measured 109mm (range 5–300mm). Clinical presentation time ranged from one hour to eight months, with 30% of cases involving acute on chronic clot. Chronic clot (25%), acute clot (25%) and subacute (15%) was also removed. Five per cent of cases did not indicate clot classification. The superficial femoral artery was the most common vessel treated (50%) while 40% of the cases involved the popliteal artery.
“The Pounce thrombectomy system has the potential to revolutionise the treatment algorithm for arterial thrombectomy,” said Gary Maharaj, Surmodics CEO. “By providing peripheral interventionalists with an innovative, non-surgical tool for treating arterial thrombotic occlusions with a single session device designed to achieve an on-table result, this device will serve an important clinical need while advancing therapies for PAD.”
The Pounce thrombectomy device is comprised of three components: a 5Fr delivery catheter, a basket wire, and a funnel catheter. The basket wire is delivered distal to the location of the thrombus, deploying two nitinol self-expanding baskets. The baskets capture the clot and are retracted into a nitinol collection funnel. With the clot entrained, the system is withdrawn into a minimum 7Fr guide sheath through which the clot is withdrawn and removed from the body.
New long-term data presented at Charing Cross (CX) demonstrated the safety of BIOTRONIK’s Passeo-18 Lux paclitaxel drug-coated balloon (DCB) for the treatment of peripheral artery disease (PAD) in infrainguinal arteries.
The independent analysis was led and presented by Ron Waksman, Clinical Professor of Medicine, Georgetown University and Associate Director of Cardiology, MedStar Washington Hospital Center, Washington D.C., USA. Individual patient-level data were pooled from three trials in the Passeo-18 Lux DCB clinical programme: the BIOLUX P-I and P-II randomised controlled trials (RCTs) and the BIOLUX P-III all-comers registry. Five-year follow-up data from 943 patients treated with Passeo-18 Lux DCB and 66 patients treated with percutaneous transluminal angioplasty (PTA) were evaluated.
The analysis showed that the use of the Passeo-18 Lux paclitaxel DCB in infrainguinal arteries was not associated with an increase in all-cause mortality at five years compared to standard PTA (33.56% for DCB versus 43.79% for PTA; P=0.47).
“Our recent analysis adds to the body of long-term evidence supporting paclitaxel-coated balloons, which are an essential and safe tool for the treatment of patients with PAD who are presenting with increasingly challenging disease and are often at high risk of restenosis,” commented Ron Waksman on the results. “In line with previous clinical data, the Passeo-18 Lux DCB has been shown to be safe at five years when compared to PTA.”
These results confirm the previous analysis of this dataset, published last year, which reported similar mortality at one year irrespective of the treatment with DCB or PTA and clear reduction in the incidence of the composite endpoint of any amputation and target lesion/vessel revascularisation compared to standard PTA. Other recent data have also shown similar mortality rates in patients treated with paclitaxel-coated balloons compared to PTA.
“We are pleased to contribute evidence that helps to address concerns about the safety of paclitaxel-coated technologies and confirm Passeo-18 Lux’s excellent safety record. We are continuing to invest in DCB clinical research including the upcoming BIOPACT RCT, which will further support evidence-based decision making,” said Alexander Uhl, president of vascular intervention at BIOTRONIK.
The BIOPACT RCT clinical trial, which completed enrolment last year, will provide a head-to-head comparison of Passeo-18 Lux and IN.PACT Admiral DCBs. The primary endpoint will be presented upon completion of 12-month follow-up.
Medtronic has announced that Laura Mauri has been appointed as the company’s chief scientific, medical and regulatory officer. This appointment adds to Mauri’s prior responsibilities as chief clinical and regulatory officer, aligning and integrating the company’s scientific, medical, clinical research and regulatory affairs under her leadership, according to a Medtronic press release.
It also intends to leverage her deep expertise and understanding of the interaction between patients and medical technology to accelerate innovation that puts patients first, the release states. Mauri will continue to serve as a member of the Medtronic Executive Committee as well.
“With this appointment, we are enabling a patient-centred approach to healthcare technology innovation at every stage of the product lifecycle,” said Geoff Martha, chairman and CEO, Medtronic. “Dr Mauri’s expertise and leadership connects medical and scientific intelligence, ensuring we have a clear appraisal of the medical and scientific landscape as we make investment decisions, and helping to deliver effective and reliable innovations for patients and healthcare providers.”
The release adds that priorities for Mauri include delivering a transformative approach to both patient safety and patient engagement. She recently hired Olaf Hedrich—a patient safety, risk and analytics industry expert—to serve as the company’s chief medical safety officer, responsible for leading an independent medical safety organisation that will provide expert input to assure patients safety and quality across Medtronic products.
Mauri will also lead the integration of robust and independent medical expertise into the company’s business processes, including investment decisions, business development, exploration of therapeutic areas, and development of novel technologies.
“Medtronic is fortunate to have world-leading experts across diverse scientific and medical fields who provide unique insights and breakthrough discoveries,” said Mauri. “I am excited to integrate this expertise across our company, to connect technology innovation with better health outcomes for patients. A strong scientific and patient-centred mindset across all stages of device development will enable innovation that saves and improves lives.”
Prior to joining Medtronic, Mauri was a practising interventional cardiologist at the Brigham and Women’s Hospital in Boston, USA for 15 years, and an internationally renowned investigator and professor of medicine at Harvard Medical School. She succeeds Richard Kuntz as chief medical and scientific officer, who previously announced his retirement, effective 29 April.
Scott Trerotola (University of Pennsylvania, Philadelphia, USA), who will be awarded a Society of Interventional Radiology (SIR) Gold Medal in June 2022, raises some issues with the 2019 Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines and interrogates some dubious dialysis access interventions. Trerotola, who is the Stanley Baum professor of Radiology and associate chair and chief, Interventional Radiology, sat down with Interventional News to share his views on the current vascular access landscape.
A first word on the guidelines
Interventionalists need to read the guidelines. Whilst there will soon be several different tools out there that will be easy to digest, such as a YouTube video or a podcast, there is no substitute for reading the guidelines. They are the result of a 25-year process of refinement, iteration, research and opinion, so they are the best thing we have got right now. I love the way that the most recent KDOQI update looks at access as a ‘life plan’—because you cannot take a 99-year-old patient, and compare them to a 25-year-old patient who is going to be on dialysis for many years until they eventually, hopefully, get a transplant. And, if you are practising dialysis access interventions, it behooves you and your patient to read those guidelines. Not doing so really means that you are not practising evidence-based medicine—and you should be.
Good medicine struck down by lack of evidence
Guidelines by their very nature become a research workbook for the next generation. There is a fundamental problem associated with any guideline formation. The fact of the matter is that committees are a victim of the evidence team, which changes, and looks at the exact same evidence with a different eye.
A lot of evidence had changed by the time the KDOQI guidelines were updated in 2019, and it appears that the evidence team tried to really push as hard as they could, even when there was not all that much evidence. In doing so, they backed off on a lot of existing beneficial guidelines. I am not sure that was the right thing to do. One of the most significant examples of this is in the vessel of choice for dialysis catheters and the order in which they should be used. Previously, the guidelines essentially said internal jugular first, then external jugular, and we can all agree on that. But, the subclavian vein was listed as being the absolute last choice and it was made clear that it should not be used except in extreme situations. In the latest update, it was actually moved to the third position, on the basis that there was no high-level evidence precluding this, which is insanity as there will never be a randomised controlled trial of subclavian versus other tunneled dialysis catheter sites. It just makes no sense whatsoever and opens the doors for a variety of complications that we literally have not seen (and for good reason) in 30 years. So, if we now allow interventionists to start putting catheters in the subclavian, the harm that is going to come to this patient population is really significant.
Another important element is that they raised transfemoral above translumbar access to the inferior vena cava. Both of these access types have been studied independently and the infection rate is three times higher for transfemoral; it takes a viable access site and/or potential transplant site and, at least a quarter of the time, destroys it by virtue of venous thrombosis. It is also much more of an issue when somebody develops catheter-related venous thrombosis in a femoral vein. All this just does not happen with translumbar access. Of course, not everyone is suitable for translumbar, but for those who are, it is a much better access route. Now, is this supported by randomised data? No—and it never will be. But, it is supported by level two evidence that the evidence team just seems to have ignored. They essentially seem to have refused to consider lower-level evidence. What we (prior KDOQI teams) did in the past, repeatedly, was to then apply expert opinion, especially when we saw something we felt was good medicine being struck down by lack of evidence. Charmaine Lok (University of Toronto, Toronto, Canada) and team did that here as well such as in surveillance of dialysis access—I just wish they had done that in a few more places, but that is my opinion.
One of the areas that the KDOQI guidelines did not go strongly enough on (in fact, backed off on compared to 2006) was promoting and preserving the concept of over-the-wire exchange for infection. We have toed this line for all of the 20-plus years I have been here at Penn and we simply do not see people who are crippled by a lack of vascular access options such that all of their upper extremity and lower extremity access has been used up and they are on dialysis with a transhepatic catheter. We see very few people in whom all of their upper extremity veins are gone. And, when we do, they are from outside of the health system. Why? Because we are so careful about over-the-wire exchange preservation of venous access sites. It is well-established that over-the-wire exchange is just as effective as removal and replacement. And, yet, we have to fight with infectious disease specialists every single day in our practice. This was an opportunity for the KDOQI team to come out very strongly and really advocate for patients, but it is not as strong as it should be. It is a horrible battle that we should not have to fight, and having this remain clearly spelled out in the guidelines, as it was in 2006, would have helped when communicating with the infectious disease doctors.
Do even well-intended guidelines have inadvertent negative consequences?
Yes, 100%. The ‘Fistula First’ message from the prior guidelines is a great example. We were very strong with that message, which was the right thing to do and I will stand by this to my dying day. A quarter of all US dialysis patients had fistulas at the time of the first guidelines in 1997; patients across the rest of the world had 60–80%, so the USA was a vast outlier. And we needed to fix that. If we had not gone with that message, we would not have gotten the wholesale swing toward us having the 60–70% fistula rate that we have today. But, the pendulum swung a little bit too far, and the guidelines placed a lot of penalties, especially on nephrologists, which caused them to have economic disincentives. Sometimes people could start with a fistula, just for the sake of having a fistula, but it would never get used. So, I do think that the pendulum needed to swing back a little bit from the prior guidelines to say that there are patients in whom grafts are appropriate, and there are patients in whom catheters are appropriate, and the 2019 KDOQI reflects this.
We also did not necessarily want very prescriptive thresholds, and one of the big changes in the current guidelines was that they moved away from thresholds and absolute numbers. The primary reason for that was that, in the USA, our Medicare system uses those guidelines as weapons against those on the front lines. When payers weaponise guidelines, then nobody benefits—patients the least. That is why I think Lok and her team did a very good job of making the update kinder and gentler so that, in the appropriate patient for whom a graft (or catheter) is the right thing to do when it fits with their life plan, they will get that, as opposed to saying, ‘you have to have a fistula first’. So, yes, guidelines can have negative, unintended consequences.
Common misconceptions
There are incredible misconceptions that surround aneurysm formation and high flow. One is that central venous or downstream stenosis causes aneurysms to form, which is simply wrong. The thing that causes aneurysms to form is high flow. And the problem is that the people who are fixing stenoses think that is helping. Indeed, they are only making things worse by increasing flow and thereby exacerbating that vicious cycle of flow that results in aneurysm formation. We need practising interventional radiologists, surgeons and nephrologists to understand the relationship between flow and aneurysm formation in a very visceral way, so that they stop perpetuating the problem now. Gerald Beathard (University of Texas, Austin, USA) has gotten on board here with cephalic arch stenosis—not necessarily related to aneurysm formation, but just broadly related to high flow—and was speaking about not overtreating these stenoses at the most recent Controversies in Dialysis Access (CiDA) meeting in Dallas, USA. I think this is a great step forward because he is such a respected leader in this community. It is vital to recognise that we should not just do a one-size-fits-all stenosis treatment of the terminal arch but, rather, we need to use important tools (such as direct measurement of flow) to dial in the right size of stenosis to fix the clinical problem or not intervene at all.
I think the lack of relationship between central venous stenosis and access dysfunction is another point worth making clearly. We still have people treating asymptomatic central venous stenosis because they think it affects access function, which is frankly just not true. I think the most important thing about stenosis in any circuit is that you need to understand that you should not treat it unless it is symptomatic. If we stopped applying the oculotherapeutic reflex and just treating every stenosis, we would, first of all, treat far fewer stenoses, and we would probably have a lot less restenosis too. So, we absolutely do not want to treat a stenosis that is quiescent. Treatment such as percutaneous transluminal angioplasty should be applied only to stenoses with a matching clinical indicator. We have published studies on these in the interventional radiology literature, but maybe not in the kidney space, and because of this we just need to get different types of specialists starting to answer these big questions.
Common sense and vein preservation
We need to preserve access and I still think we do a terrible job of venous preservation in the USA—and probably the rest of the world. The concept of device-created fistulas (i.e. EndoAVF) is in its infancy, but it is very clear that in the right hands it can make a massive difference and revolutionise the way dialysis access creation takes place. However, it can only get there if it is coupled with the basic techniques of venous preservation. If everybody had a good forearm cephalic vein, we would not be talking about upper arm fistulas; patients would all get forearm fistulas that would last 10 or 20 years. Forearm fistulas require the least amount of maintenance, have the best outcomes, and patients do not generally get high output heart failure with them. I mean, why not have more of those? The reason is because people that have good cephalic veins have them used up indiscriminately by people putting in intravenous (IV) lines.
Device-created fistulas address that to some extent, as some of the deeper veins are still accessible because they have not been torn up. But, ultrasound-guided IVs, while very good for patients, are also tearing up those same veins because, again, they are being used indiscriminately by people who should be exercising venous preservation. It is a big picture thing. I have been promoting and practicing venous preservation for going on 35 years now and you start to see trends. And all the new technology in the world will not help us if we do not practice basic things like common sense and vein preservation. Fortunately, this is an area where the current KDOQI team diverged from the evidence team and kept a strong expert opinion-based statement about vessel preservation in the 2019 guidelines. Indeed, this stance is highlighted as an example of divergence from the evidence team recommendations on page S20 of the document.
Plain balloon angioplasty—the mainstay for access stenosis
In our practice of over 1,000 interventions per year, we use stent grafts in perhaps 5% of cases, and that includes central venous stenosis. Our use of stent grafts is very low. Yet, we have the same outcomes (which have been published repeatedly) as everybody else. If you look at, for example, the control arms in both the drug-coated balloon (DCB) trials—Lutonix AV (BD) and IN.PACT AV (Medtronic)—and you compare them to the treatment arm of, say, the AVeNEW study (BD), which is stent grafts in fistulas vs. percutaneous transluminal angioplasty, they are the same. The control arm in the AVeNEW study has terrible results. Bart Dolmatch (El Camino Health, Mountain View, USA), principal investigator of the latter, told me: “That is real-life angioplasty.” I disagree. I think real-life angioplasty has been properly defined in the two large US DCB trials—it should be judicious and properly executed, maximising the bang for the buck that you get when you open that high-pressure balloon. Prolonged angioplasty, if done correctly, takes time and dedication, but when you do that, as evidenced by these large trials, which were subjected to expert core lab evaluation, the results are outstanding. Using plain balloon angioplasty saves a huge amount of money over stent grafts, and I firmly believe the latter buy short-term patency at the expense of long-term patency.
Thrombectomy using a US$10,000 device is profligate
I am obviously a proponent of mechanical thrombectomy. Unfortunately, after a good, 25-year run, the Arrow-Trerotola percutaneous thrombolytic device (Teleflex) has now been withdrawn from the market—although there are other thrombectomy devices we are using. On the subject of aspiration, I think that using large, expensive suction thrombectomy devices is an utter waste of money when you can get a mechanical thrombectomy device for US$500–600 that will do the job. Suction thrombectomy has been studied many times over the years and decades. The challenge with suction is that the adherent clot material is still there and getting that stuff off the wall is still a problem, which is why wall contact thrombectomy devices are so popular. The bottom line is that there are lots of different ways to do this, as outlined in the literature. The one thing that I will reiterate is that using a US$10,000 device to do a thrombectomy is profligate. When I see it presented at meetings, it makes me cringe.
SIR Gold Medal
I am extremely honoured and humbled to be receiving the SIR Gold Medal. It is a lifetime achievement, and wonderful. When I look back, I am really happy about the paper trail and evidence basis that my colleagues and I have generated. We adopted a philosophy of practising what we preach, and publishing on and disseminating that. We really believe that the best way to get a message out there is to study it and publish a paper about it. I decided to do that a long, long time ago when I was young and I would not change a thing.
EDDA Technology, a provider of advanced imaging-guided precision treatment solutions, announced it has entered into an agreement with the Society of Interventional Oncology (SIO) for its ACCLAIM Trial (Ablation with Confirmation of Colorectal Liver Metastases Prospective Trial for Microwave Ablation as a Local Cure). IQQA-BodyImaging Interventional will be used to provide 3D assessment of the ablation zone and margin for selected colorectal liver metastases.
In this prospective, multicentre, international trial, SIO proposes to establish microwave ablation (MWA) as the preferred treatment option for selected colorectal liver metastases that can be ablated with sufficient margins. The study will be the first global, prospective trial to use an objective and reproducible technical outcome in its study design, which the SIO believes will drive important changes to future treatment guidelines. The ACCLAIM study will estimate disease-free survival of colorectal liver metastases treated with MWA incorporating 3D ablation software (EDDA Technology) margin confirmation intraoperatively and through a subsequent independent review centralised validation process.
The IQQA platform provides comprehensive 3D image analysis using magnetic resonance (MR) and computed tomography (CT), and has been used in over 80,000 cases worldwide for surgery and treatment with substantial time-saving. This solution supports in-depth quantitative volumetry with fast, dependable results and allows for versatility of transplantation, resection, or interventional procedure planning.
“IQQA is a proven innovation to support physicians in providing individualised and optimised treatment solution. Powered by our precision 3D capabilities, IQQA aims to facilitate the next generation of precision surgery and treatment,” said Jianzhong Qian, president and CEO of EDDA Technology. “We’re glad that the IQQA platform was chosen by SIO for this global trial, which will bring important clinical information for the future interventional treatment guidelines.”
Cydar Medical recently announced it has entered a strategic collaboration with Medtronic. Under the pilot arrangement, Cydar’s EV Maps software will be introduced to up to 40 new global sites, combining Cydar’s augmented intelligence technology with Medtronic’s services and case support, with the goal of improving patient care.
The Cydar EV Maps software harnesses the latest in cloud graphics processing unit (GPU) computing, computer vision and machine learning technology to advance surgical visualisation and decision-making in theatre and across the care pathway. This enables clinicians to create detailed patient-specific 3D maps for procedure planning, image-guided navigation, and post-operative review, resulting in less radiation exposure to the patient and the clinical team, reduced procedure time, and increased delivery confidence. This pilot programme will also inform the future development of predictive analytics to support procedure planning, by assessing factors such as the risk of endoleaks, sac regression probability and more.
Medtronic is the first medical technology company to enter a public strategic collaboration in digital endovascular technology to advance aortic patient treatment decisions. The collaboration is part of Medtronic’s ongoing commitment to innovation in aortic care for physicians and their patients.
“Medtronic aims to revolutionise endovascular aortic treatment with digital solutions with this phased approach. By collecting data across the patient journey—before, during and after procedure—our goal is to provide analytic support to make our endovascular stent grafts ‘smart’,” Carolyn Sleeth, a vice president and general manager at Medtronic, explained.
“By collaborating with Medtronic to bring our Cydar EV Maps solution to up to 40 new hospital sites, we are a step closer to achieving our mission to ensure every image-guided endovascular procedure goes exactly as planned,” said Paul Mussenden, CEO of Cydar.
Penumbra has announced that its Indigo aspiration system with Lightning 7 and Lightning 12 have secured CE mark and are now commercially available in Europe. Both technologies are part of Penumbra’s Indigo aspiration system—now with Intelligent Aspiration for mechanical thrombectomy—and are designed for single session arterial and venous thrombus removal, including the treatment of pulmonary embolisms.
“Technology advancements such as Lightning 7 and Lightning 12 are critical to improving patient outcomes and expanding use of mechanical thrombectomy to a broader range of patients,” said Andrew Wigham, interventional radiology consultant at John Radcliffe Hospital, Oxford, UK. “Lightning enables us to remove blood clots in the body quickly and efficiently, often in a single session, while also minimising blood loss and potentially reducing the need for thrombolytics and prolonged ICU stays.”
Powered by the Penumbra Engine, Lightning 7 and Lightning 12 combine the new Indigo system CAT7 and CAT12 aspiration catheters with Lightning intelligent aspiration, a computer-aided clot detection technology that can differentiate between clot and blood. The system designed to reduce blood loss and the need for clot-dissolving drugs, which, Penumbra claims, may lower the risk of bleeding complications.
The company states that the Lightning technology also provides an alternative to other surgical options. “CAT7 is a high-power, low-profile catheter that features laser-cut hypotube technology and circumferential sweep designed for dependable delivery and maximal clot extraction,” a press release details. “CAT12 is a large-lumen aspiration catheter that also incorporates novel laser-cut hypotube-based catheter engineering to provide advanced deliverability and torqueability within the body.”
“The launch of our Lightning portfolio in Europe will provide a much-needed option for physicians to address debilitating blood clots in the body effectively and efficiently,” said James Benenati, chief medical officer at Penumbra. “We have seen our latest advancements in mechanical thrombectomy reduce blood loss while increasing clot removal efficiency in the USA. These innovations may help improve patient care compared to conventional therapy. We are now able to help more patients with this technology by expanding access to physicians in Europe.”
“Blood clots in the body can be difficult to access and are potentially life-threatening. Until now, treatment options have been limited,” said Joan Kristensen, vice president and head of the Europe, Middle East and Africa region for Penumbra. “The introduction of our Lightning portfolio in Europe will expand access of our most advanced clot removal technology for the body, which combines intelligent aspiration and innovative catheter engineering to remove blood clots in a single session. With Lightning, mechanical aspiration technology continues to advance to meet the needs of patients, which is our core purpose at Penumbra.”
Corindus, a Siemens Healthineers company, announced today the opening of its new headquarters at 275 Grove Street in Newton, USA. Siemens Healthineers relocated the Corindus headquarters from its previous location in Waltham, USA to accommodate company growth, doubling the size of the current location from 35,000 to 77,000 square feet, according to a company press release.
The headquarters will serve as the global ‘Centre for Excellence’ for Siemens Healthineers’ endovascular robotic technologies—encompassing development, manufacturing, and administration, the release adds.
“Our new facility is a testament to the commitment Siemens Healthineers has made to metro Boston and Massachusetts as a hub for innovative talent,” said Wayne Markowitz, executive vice president and head of Corindus. “As we continue to advance our robotic-assisted platform, the new facility will support our mission to elevate the standard of care and increase access to cutting-edge treatment for coronary artery and neurovascular disease.”
The new facility marks the first of 15 new offices or major facility expansions that Siemens Healthineers has planned in the USA. It also features a fully equipped ‘Customer Experience Centre’ that simulates the robotic setup in a hospital cath lab and control room that will include remote capabilities over various types of connections, according to the release.
In addition, the new office will provide physicians and cath lab personnel the opportunity to participate in interactive demonstrations of the CorPath GRX system—which the company claims is the first US Food and Drug Administration (FDA)-cleared medical device to bring robotic precision to percutaneous coronary and vascular procedures, and the only CE-marked robotic system for neurovascular use in select markets—and future innovations.
“Siemens Healthineers is an important addition to the Newton community’s growing roster of innovative companies,” said Massachusetts 4th Congressional District Representative Jake Auchincloss. “I am honoured to welcome a leader in the endovascular robotics space and look forward to the company’s continued growth and leadership as a top employer in the area.”
“I took a giant leap of faith and applied for a radiology residency with the sole intention of doing interventional radiology (IR). I was lucky—it turned out to be the perfect specialty for me,” Karim Valji, professor of radiology at the University of Washington (Seattle, USA) and professor Emeritus at the University of California, San Diego (USA) tells Interventional News. Valji is also the former editor-in-chief of the Journal of Vascular and Interventional Radiology (JVIR).
What attracted you to a career in IR?
In medical school, I was drawn more towards the doctors who were ‘thinkers’ rather than ‘doers’. I started an internal medicine residency at UCSF [University of California, San Francisco], but by the end of my internship I realised that I really wanted to work in a procedure-driven field. Ernie Ring and Bob Kerlan were there running one of the premier IR sections in the country, and I watched them do several cases on my patients. Having spent no time whatsoever on an IR service, I took a giant leap of faith and applied for a radiology residency with the sole intention of doing IR. I was lucky–it turned out to be the perfect specialty for me.
Your 2020 Dotter Lecture focused on a fundamental question—why are we doing this procedure? Could you outline recurring scenarios in which this question should be at the forefront of a proceduralist’s mind?
In the busyness of our hectic workday, it is so easy just to do the cases listed on the board without stepping back to consider what we are really doing for every patient. We really need to have a different mindset. Like a surgeon, we must always start by looking at a patient’s clinical problem and consider how IR might benefit him or her. Sometimes it is as simple as deciding that a tunnelled catheter is more appropriate for this person than the port that was requested.
On one end of the spectrum are the referrals that require help with a complex situation. In that scenario, there may be a tendency to get swept up in the details of a proposed procedure—or a desperate patient or provider can make us feel compelled to do something. But we need to stop and ask these questions: Is the procedure likely to help the clinical situation? Are the potential benefits worth the risks? Is there a better option, perhaps even doing no intervention at all? And will it help the patient in the long run?
The polar opposite is the routine elective tube change. The case is totally mundane and so easy to do, but frankly, our responsibility goes beyond just changing out the catheter. We need to advocate for the patient and make sure there is a long-term plan that will, if possible and desired, allow the external catheter to come out. If that is not the case, we need to help the patient and family understand why the device may be in place for the long run. So, we must work with referring providers to advance treatment that will optimise the patient’s ultimate quality of life.
Having been the editor-in-chief of JVIR and having written three textbooks for IR, in 2022, what are ways to best educate the IR community?
Of course, when I started in IR over 30 years ago, the resources for learning the substance of IR were limited. To pick up the basics of interventional radiology, many current residents tell me that they still prefer print textbooks and ‘linear reading’ to study a particular topic or learn the fundamentals of our field more broadly. But frankly, I think many also rely more on various online sites for ‘bites’ of information that are short and well illustrated, and preferably interactive. While those sources are usually more enticing and up-to-date than print books, I do wonder about the accuracy of some of that material.
The quality of research being published in JVIR has never been higher. There is no better authority for learning about the newest advances in our field. However, I think we should always have a healthy dose of scepticism about any new technique or concept that we read about, even in venerated journals. In that same vein, I have found that many interventional radiologists (especially very experienced ones) can get dogmatic about the procedures they do and how they do them. It brings to mind the warning that a former dean at Harvard Medical School gave to an incoming class: “Half of what we are going to teach you is wrong and half of it is right. The problem is we do not know which half.”
What is your advice to a young trainee or interventional radiologist with an interest in academic medicine?
First, find a mentor—a person who can inspire you and guide you as you start doing research or getting involved in some other academic pursuit. It is not necessary to find someone with an international reputation or a CV a mile long. It is much more important to choose a person whom you respect and enjoy working with.
Second, if you have no experience with research, try your hand at a simple case report or short review article. Unfortunately, the sheer act of writing seems to turn off many aspiring young interventional radiologists. But, please believe that with some effort almost anyone can learn to write reasonably well.
Finally, do not reject the idea of academics simply because you think it means years of churning out papers. In many institutions, an interventional radiologist with an aptitude for teaching or an interest in leadership can have a rewarding and successful career as an educator or an administrator with minimal requirements for publication.
In the last few years, what research paper has particularly caught your attention?
In a JVIR article several years ago, my colleague Jeff Chick reported results of a national survey that he conducted to assess burnout among interventional radiologists. The findings were sobering. Burnout is a serious and growing concern for healthcare providers of every sort. Lack of energy, disengagement from colleagues, loss of satisfaction with work, a short temper with staff or even patients—these are some of the signs.
There certainly are a number of strategies for helping prevent or deal with burnout. But the first step is admitting to yourself that there may be a serious problem brewing, and that it should not be taken as a personal failure. Unfortunately, the ‘superman’ ethos that is common among interventional radiologists can make it hard to accept that reality.
At the very least, interventional radiologists concerned about their negativity towards work need to share these feelings with family or with close, trusted peers. And, just as important, all IR groups should confront this issue openly and directly, and make a real effort to identify and support colleagues who seem to be at risk.
What is one important way interventional radiologists can improve the quality of patient care they deliver?
Better communication. Not just with patients and families, but also with other providers who make up the medical team. Many surveys show that poor communication is one of the biggest complaints by the public about the modern healthcare system. We sometimes fail to be explicit about what a patient should expect during and after a procedure. Or, we do not provide clear and thorough information about how to manage a catheter, for example, when the patient is recovering. Or, we do not make it easy to reach us when a patient or family has concerns.
But on a broader level, the many individuals and teams caring for a patient sometimes give mixed or confusing messages about care plans and expectations for the future. The IR doctor gives the patient instructions about nephrostomy catheter management, and the IR nurse tells the family member something different. We do a complex venous reconstruction, but the procedure fails when another provider stops anticoagulation prematurely because the long-term plan was not well communicated. The problem is daunting. But we need to do our best to make the system work for each of our patients.
What gives you the most pleasure from travelling and teaching in different countries?
My most satisfying teaching experiences overseas have involved showing unknown cases to IR residents and fellows. These young trainees are so eager and grateful for teaching from someone from the USA who works in a leading centre for IR. And, any preconceived notions about the quality of training in some less-advantaged countries are quickly dispelled after a short time spent with some of their smart and enthusiastic interventional radiologists-to-be.
What are your interests outside medicine?
I am a voracious reader, gym junkie, and avid theatre-goer. My husband Jon and I spend as much time as we can visiting San Diego to see our two children and grandkids (now aged six, three, and one). And we are both lifelong travel fanatics. We spend hours and hours on Kayak putting together our own trips. We know exotic airport codes like sports fans know players’ stats. And our interests complement one another’s really well. I have made him appreciate all that world cities have to offer, and he entices me to places I could once barely find on a map…The Gambia, anyone?
The March top 10 features news that the US trial of the LimFlow system designed to prevent amputations has completed enrolment. Other highlights include two video interviews addressing the treatment of the superficial femoral artery (SFA), as well as a report of an ECR 2022 session, in which Thomas Helmberger called for a “shift [in] treatment focus from volume to value”.
Enrolment has been completed in the PROMISE II pivotal trial of the LimFlow deep vein arterialisation system designed to prevent amputations in so-called “no-option” chronic limb-threatening ischaemia (CLTI) patients, the eponymous device maker announced today.
Antonio Micari (interventional cardiologist, Italy) gives his thoughts on the EMINENT RCT and whether it may have influenced his decision to use drug-eluting stents and drug coated balloons after a percutaneous transluminal angioplasty.
With cancer cases growing worldwide and an increased number of late-stage diseases in elderly patients, there is an increasing need for an integrated approach. “Through evidence, cost, and acceptance of interventional oncology (IO), we can create value-based care and shift the treatment focus from volume to value”.
Johns Hopkins Medicine researchers have developed and tested a new imaging approach they say will accelerate imaging-based research in the lab by allowing investigators to capture images of blood vessels at different spatial scales.
Koen Deloose (vascular surgeon, Belgium) looks at the evidence needed in order to make the best decisions for his patients when treating the superficial femoral artery (SFA). Deloose dives into the implications on daily practice of the EMINENT RCT results, as well as stenting strategy and the use of paclitaxel in the future.
The VasQ external support device (Laminate Medical) has demonstrated long-term benefits for radiocephalic (forearm) arteriovenous fistula (AVF) creation in a retrospective analysis of 150 consecutive procedures. Robert Shahverdyan (Asklepios Klinik Barmbek, Hamburg, Germany) and Dirk Hentschel (Brigham and Women’s Hospital, Boston, USA) have published these data in Seminars in Dialysis.
Six-month outcomes from the ongoing CLOUT registry demonstrate the “safety and efficacy” of the ClotTriever thrombectomy system (Inari Medical) in a real-world deep vein thrombosis (DVT) population regardless of clot chronicity level, the 2022 annual meeting of the American Venous Forum (AVF; 23–26, Orlando, USA) heard.
A prospective multicentre study has evaluated the safety and efficacy of a polyethylene glycol (PEG)-based liquid embolic in treating hypervascular tumours, according to an Instylla press release.
Cordis recently announced that the US Food and Drug Administration (FDA) has approved the S.M.A.R.T. Radianz vascular stent system, a self-expanding stent purposefully engineered for radial peripheral procedures.
One of the sessions at this year’s Society of Interventional Oncology (SIO) meeting (24–28 March, San Francisco, USA) comprised four debates moderated by David Breen (University Hospital Southampton, Southampton, UK) and William Rilling (Medical College of Wisconsin, Milwaukee, USA). One of the key takeaways from the session was that radiation oncology has seen much innovation, and that this must continue in order to provide the best outcomes for patients into the future. Another was that “response assessment [can be] challenging”.
Peripheral colorectal lung metastases: SBRT vs. ablation
Abraham Wu (Memorial Sloan Kettering Cancer Center, New York, USA) and Thierry de Baere (Institut Gustav Roussy, Villejuif, France) took to the podium in turn—Wu as a proponent of stereotactic body radiation therapy (SBRT), and de Baere of thermal ablation, as a means of treating peripheral colorectal lung metastases.
“SBRT has really ushered in a revolution in radiation oncology.” Wu began his side of the argument by dubbing SBRT a “new standard for early-stage inoperable lung cancer”, citing the therapy as particularly successful in metastatic tumours.
Abraham Wu
Wu proceeded to highlight the non-invasive benefit of SBRT—there is “no cutting, needles, pain, nor a need for anaesthesia.” Furthermore, there are no medical contraindications, with patients free to continue on anticoagulant drugs alongside receiving SBRT. The toxicity profile, Wu assured, is also “favourable”, with “essentially no mortality risk” associated with using the therapy to treat peripheral lesions, including when treating multiple lesions, and retreating the same one.
It is also easily adaptable to large tumour sizes, and complicated tumour shapes and locations, Wu emphasised. The convenience of the therapy is also a draw when it comes to SBRT, now that it is available relatively widely in “most modern radiation facilities”.
Wu’s bottom line is that “high-level control is achievable with a sufficient dose”, which is safe for peripheral lesions. He contended that “SBRT is the preferred treatment” for peripheral colorectal lung metastases, stating that there is a larger and longer-term evidence base when compared to ablation.
Thierry De Baere
De Baere began his counterargument by explaining that he “fully [agreed] with the previous speaker in that what matters is local tumour control”. However, defining local tumour control is another matter entirely. He argued that ablation sees total control in the longer term, when compared to SBRT, which, de Baere suggested “puts some smoke around the tumour”, then making it difficult to have local response criteria. Where it may be tempting to look at imaging for two years post-SBRT and declare a complete response, he underlined the need to “look past two years”, and once one does that, in the case of SBRT, he believes that it is “always the same story”—the tumour is still growing, just very slowly.
One can get a more reliable picture of the ongoing success of treating via ablation, de Baere highlighted, as it can be obtained with pathology, as opposed to the imaging that indicates in SBRT cases whether it is working.
De Baere brought nuance to his side of the debate, acknowledging that different types of cancer, for example, primary vs. metastatic, warranted different treatment approaches. Likewise, the observed success of a particular approach depends on the dosage given. It is perfectly possible, de Baere admitted, that a tumour can continue to grow after ablation, if you “mistarget with cryotherapy” or give “too low a dose”. However, he maintained that while SBRT may seem low-toxicity in the short term, in the middle or long term, “it is a different story” and one starts to see a decrease in lung function.
Given the opportunity to answer his opponent’s comment, Wu thanked de Baere for a “strong and thoughtful response”, agreeing that “response assessment with SBRT is challenging” and that it is a “limitation” of the treatment when compared to other modalities. Wu went on to outline that administering a sufficient radiation dose can resolve the issues with SBRT that de Baere pointed to, but, given his chance for rebuttal, de Baere doubled down on his preference for ablation—that a high enough dose may well “kill the tumour [with SBRT], but maybe you will also kill the patient or the lung.”
Alucent Biomedical announced in a press release that it has enrolled the first patient in ACTIVATE II, an Australia-based first-in-human clinical trial to evaluate the safety and efficacy of its natural vascular scaffolding (AlucentNVS) technology. The therapy is designed to open vessels and maintain patency without the use of permanent implants for the treatment of peripheral artery disease (PAD) of the lower extremities.
The AlucentNVS vessel restoration system with photoactivated linking combines standard angioplasty with linking of the structural proteins in the wall of a blood vessel. The intervention is designed to deliver restoration of the vessel’s lumen and sustained improvement of blood flow, without the introduction of a foreign implant, such as a metallic stent. AlucentNVS photoactivated linking is also designed to mitigate the well-known adverse effects of angioplasty, such as vessel recoil. Sustained, improved blood flow is expected to result in pain relief, limb preservation, and an improved quality of life for patients.
The first patient in the ACTIVATE II study was enrolled by Chris Delaney at Flinders Medical Centre in Adelaide, Australia. In total, the trial will enrol up to 50 subjects at up to 12 research sites, which will include Prince of Wales Hospital in Sydney, The Alfred Hospital in Melbourne, Royal Perth Hospital, and Sir Charles Gairdner Hospital in Perth. The primary endpoints of the study are freedom from composite investigational-device, procedure-related major adverse events, primary patency as assessed by Doppler ultrasound, and freedom from clinically driven target lesion revascularisation (CD-TLR) at one year.
ACTIVATE II follows the completion of enrolment for ACTIVATE I safety study of AlucentNVS in the USA. Pre-clinical testing of AlucentNVS in animal studies has shown acute and long-term safety and patency without the pro-inflammatory and mechanical risks of placing a rigid foreign implant into the blood vessel.
“PAD is a difficult condition affecting so many people worldwide, and its current treatments have significant shortcomings,” said Myles Greenberg, Alucent Biomedical’s CEO. “We want to change that by offering a whole new way to treat these patients with AlucentNVS. Alucent’s novel approach has the potential to change the way PAD is managed in the future.”
Truvic Medical, a subsidiary of Imperative Care, announced in a press release that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for the Prodigy thrombectomy system, designed for the treatment of peripheral vascular thrombus.
“We are excited to receive FDA clearance for our first thrombectomy system. We look forward to working with experts in the field to translate Prodigy’s novel design elements and features into superb clinical outcomes,” said Mike Buck, CEO of Truvic. “This represents our first regulatory milestone as part of our strategy to advance multiple programmes designed to meet patients’ needs and bring more innovative technologies to the market, faster.”
“Imperative Care and Truvic share a culture of innovation and intense commitment to the needs of patients. I am pleased that these common values continue to help propel our development programmes towards elevation of patient care,” Fred Khosravi, chairman and CEO of Imperative Care, added
Truvic is based in Campbell, California, USA and its technology is designed to redefine peripheral vascular thrombus management by enabling single-session thrombus removal without the use of thrombolytics.
Imperative Care is a medical technology company focused on developing the next generation of solutions to address the vast and urgent needs in stroke intervention and peripheral thrombectomy. The company has two FDA 510(k) cleared product platforms, as well as an expansive stroke technology development pipeline.
The findings also show a higher risk of events in patients with underlying conditions (comorbidities), patients with more severe COVID-19, and during the first pandemic wave compared with the second and third waves.
The researchers say these results support measures to prevent thrombotic events (thromboprophylaxis), especially for high-risk patients, and strengthen the importance of vaccination against COVID-19.
It is well known that COVID-19 increases the risk of venous thromboembolism (VTE), the authors write. However, they note that less evidence exists on the length of time this risk is increased, if risk changed during the pandemic waves, and whether COVID-19 also increases the risk of major bleeding.
To address these uncertainties, the researchers set out to measure the risk of DVT, PE, and bleeding after COVID-19.
Using national registries in Sweden, they identified more than one million people with confirmed SARSCoV-2 infection between 1 February 2020 and 25 May 2021, matched by age, sex, and county of residence to more than four million people who had not had a positive SARS-CoV-2 test result.
They then performed two analyses: in the first, they calculated the rates of DVT, PE, and bleeding in COVID-19 individuals during a control period (before and long after COVID-19 diagnosis) and compared it to the rates in different time intervals after COVID-19 diagnosis (days 1–7, 8–14, 15–30, 31–60, 61–90, and 91–180).
In the second analysis, they calculated the rates of DVT, PE, and bleeding during the period 1–30 days after COVID-19 diagnosis in the COVID-19 group and compared them to the corresponding rates in the control group.
The results show that compared with the control period, risks were significantly increased 90 days after COVID-19 for DVT, 180 days for PE, and 60 days for bleeding.
After taking account of a range of potentially influential factors, the researchers found a fivefold increase in risk of DVT, a 33-fold increase in risk of PE, and an almost twofold increase in risk of bleeding in the 30 days after infection.
In absolute terms, this means that a first DVT occurred in 401 patients with COVID-19 (absolute risk 0.04%) and 267 control patients (absolute risk 0.01%). A first PE event occurred in 1,761 patients with COVID-19 (absolute risk 0.17%) and 171 control patients (absolute risk 0.004%), and a first bleeding event occurred in 1,002 patients with COVID-19 (absolute risk 0.10%) and 1,292 control patients (absolute risk 0.04%).
Risks were highest in patients with more severe COVID-19 and during the first pandemic wave compared with the second and third waves, which the researchers say could be explained by improvements in treatment and vaccine coverage in older patients after the first wave.
Even among mild, non-hospitalised COVID-19 patients, the researchers found increased risks of DVT and PE. No increased risk of bleeding was found in mild cases, but a noticeable increase was observed in more severe cases.
This is an observational study, so the researchers cannot establish cause, and they acknowledge several limitations which might have affected their findings. For example, VTE may have been underdiagnosed in patients with COVID-19, testing for COVID-19 was limited, especially during the first pandemic wave, and information on vaccination was not available.
However, results were largely consistent after further analyses, and are in line with similar studies on the association between COVID-19 and thromboembolic events, suggesting that they withstand scrutiny.
As such, the researchers say their findings suggest that COVID-19 is an independent risk factor for DVT, PE, and bleeding, and that the risk of these outcomes is increased for three, six, and two months after COVID-19, respectively.
“Our findings arguably support thromboprophylaxis to avoid thrombotic events, especially for high-risk patients, and strengthen the importance of vaccination against COVID-19,” they conclude.
In a linked editorial, researchers at the University of Glasgow (Glasgow, UK) point out that despite the potential for new variants of concern, most governments are removing restrictions and shifting their focus to determining how best to “live with COVID-19.”
However, they say this study “reminds us of the need to remain vigilant to the complications associated with even mild SARS-CoV-2 infection, including thromboembolism.”
LimFlow recently announced it has closed a US$40 million (€36 million) oversubscribed Series D financing round.
A press release reports that new investors Longitude Capital, Soleus Capital Management, and an undisclosed strategic investor joined the round along with current major shareholders of the company: Sofinnova Partners, through its Crossover Strategy fund; Bpifrance, the French sovereign investment bank; and Balestier, a Singaporean family fund.
The LimFlow system, designated by the US Food and Drug Administration (FDA) as a Breakthrough technology, uses a minimally invasive family of transcatheter products designed to optimise perfusion of the critically ischaemic foot, potentially avoiding major amputation, resolving pain, and promoting wound healing. Proceeds from the Series D financing will fund follow-up for the PROMISE II US pivotal trial necessary to obtain FDA approval and will support the commercialisation of the LimFlow system for deep vein arterialisation, the press release details.
The company recently completed enrolment in PROMISE II, the US pivotal trial of the LimFlow system. It also completed enrolment in CLariTI, a natural history study of high-risk and no-option chronic limb-threatening ischaemia (CLTI) patients, intended to shed light on outcomes from patients treated with the current standard of care. Over the last year, the company also integrated the second-generation of its LimFlow system into its clinical programme and reported positive two-year data from its PROMISE I US feasibility study.
“We are thankful for the support of so many industry-leading investors, both new and existing, who recognise the potential of the LimFlow system to address a major clinical need in saving patients from amputation,” said LimFlow CEO Dan Rose. “We look forward to sharing results from our pivotal trial later this year, and to the prospect of being able to make the LimFlow system commercially available as early as next year to the patients in the USA and Europe who desperately need it.”
“We are truly impressed by the clinical results LimFlow has delivered for patients who have exhausted all other treatment options. We are excited about the technology’s potential to transform the way CLTI patients are treated, and in turn, transform the quality of their lives,” said Maxwell Bikoff, principal at Longitude Capital.
“The LimFlow management team has achieved key milestones and financing needed to successfully bring the LimFlow system to market. We are enthusiastic about continuing to work with the company to help make this game-changing technology accessible to patients in the near future,” said Kinam Hong, partner at Sofinnova Partners.
“Our investment in E2 positions Cordis at the vanguard of innovation in venous interventions,” said Duke Rohlen, executive chairman of Cordis and CEO of Cordis-X, an independent accelerator created to drive innovation and growth for Cordis. “We are proud to support the team’s efforts to define a new standard of care for patients suffering from thromboembolism.”
Cordis is partnering with Santé Ventures and another strategic investor in the E2 transaction, a press release reports.
According to Cordis CEO Shar Matin, “Our investment in E2 meets all the criteria in our strategy to fuel differentiated technology development, expanding our portfolio with innovative and clinically compelling solutions that respond to unmet needs in cardiovascular health. Growing our venous offerings expands our capacity to improve outcomes and deliver better quality of life to more patients around the world.”
“Our new business model leverages the robust global corporate infrastructure and sales capacity of Cordis, and the speed, creativity, and agility of the Cordis-X growth engine,” Matin continued. “DVT and PE affect patients young and old. The investment in E2 supports Cordis’ legacy as a leader in creating lifesaving cardiovascular technologies.”
E2, based in Menlo Park, USA, was founded in 2019 to focus on development of advanced mechanical thrombectomy solutions. CEO Mike Rosenthal said, “The E2 team is thrilled to welcome Cordis and our other investment partners as we join together to help us further the pursuit of developing healthcare solutions that matter. We share a pioneering spirit dedicated to serving patients and physicians in the underserved peripheral indications.”
Shockwave Medical has announced the global commercial availability of the Shockwave M5+ peripheral intravascular lithotripsy (IVL) catheter after receiving both CE mark and US Food and Drug Administration (FDA) clearance.
A company press release details that the Shockwave M5+ catheter is specifically designed to decrease IVL treatment time, provide alternative access options, and expand IVL therapy to patients with larger vessel sizes.
“Shockwave’s new peripheral catheter offers remarkable improvements that enable efficient and effective treatment for some of our most difficult-to-treat patients, some of whom previously could not have been treated with IVL,” said Peter Soukas (Miriam and Rhode Island Hospitals, Providence, USA), one of the first physicians to use the new catheter. “While treating patients with long, severely calcified lesions will always be challenging, the new Shockwave catheter is appropriately sized for larger vessels and has been optimised to expand options for facilitating vessel access, all while decreasing the amount of time needed to perform IVL in the procedure.”
Shockwave M5+ incorporates valued customer feedback to improve IVL efficiency in tackling complex calcified lesions, including quicker cycle time that delivers two pulses per second, an increased catheter length of 135cm, and a new, larger 8mm size, the company communicates. The catheter is specifically designed to treat otherwise difficult-to-treat calcified lesions in the peripheral arterial system of the lower extremities, including the iliac, femoral, iliofemoral, popliteal, infrapopliteal, and renal arteries.
“The launch of Shockwave M5+ is the latest step in our commitment to expanding the applicability of our technology for more diverse patient populations and anatomies,” said Doug Godshall, chief executive officer of Shockwave Medical. “After a very successful limited launch, we are enthusiastic about the global rollout of Shockwave M5+ and the ability to provide our customers with a new tool to advance treatment options—with the consistent reliability and simplicity of IVL that physicians have come to expect when treating patients with Shockwave IVL.”
Shockwave Medical advises that the M5+ catheter is now commercially available in Europe and the USA.
Synchron has announced the results from a study in which four people with amyotrophic lateral sclerosis (ALS) received an implant of the company’s Stentrode device—a small, mesh-like material inserted within a patient’s blood vessel that does not require invasive, open brain surgery. The results were presented on 29 March as part of an exclusive press briefing highlighting breakthrough science at the American Academy of Neurology’s 74th annual meeting (AAN 2022; 2–7 April, Seattle, USA).
Researchers monitored participants for one year and found the device to be safe, with no serious adverse events that led to disability or death, according to Synchron. The Stentrode device also stayed in place for all four patients and the blood vessel in which the device was implanted remained open. Receiving the implant allowed participants to use a computer to communicate by text, and perform daily tasks, such as online shopping and banking, a company press release states.
“People with ALS eventually lose their ability to move their limbs, making them unable to operate devices like a phone or computer,” said study author Bruce Campbell (University of Melbourne, Melbourne, Australia). “Our research is exciting because while other devices require surgery that involves opening the skull, this brain-computer interface [BCI] device is much less invasive. It receives electrical signals from the brain, allowing people to control a computer by thought.”
Rather than drilling through the skull, the Stentrode is fed through a patient’s vein until it reaches the brain. The device, comprised of a net-like material with 16 sensors attached, expands to line the vessel wall. That device is connected to an electronic device in the chest that then relays the brain signals from the motor cortex—the part of the brain that generates signals for movement—into commands for a laptop computer.
“These results are a huge advancement for the field of BCI. We have shown that our endovascular BCI approach is safe, and allows patients to accomplish daily online tasks without invasive brain surgery,” said Thomas Oxley, CEO and co-founder of Synchron. “Years of research and technological development culminated in this moment and, as we continue to develop our technology, it has the potential to change the lives of millions of patients globally who suffer from paralysis, and other debilitating neurological and brain-related diseases.”
An analysis showed benefit of XARELTO plus aspirin in reducing thrombotic hospitalisations for peripheral arterial disease (PAD) patients with and without chronic kidney disease (CKD). A separate analysis demonstrated PAD patients who received XARELTO plus aspirin in addition to statin therapy had the lowest risk of the composite of major adverse cardiovascular events (MACE) or major adverse limb events (MALE) compared to all other treatment groups in the study.
The Janssen Pharmaceutical Companies of Johnson & Johnson recently announced data from new analyses from the Phase 3 VOYAGER PAD clinical trial reinforcing the benefit of the XARELTO (rivaroxaban) vascular dose (2.5mg twice daily plus aspirin 100mg once daily) in reducing severe vascular events in patients with PAD after lower-extremity revascularisation (LER), a procedure that restores blood flow to the legs.
Data from the two analyses demonstrate the role that the XARELTO vascular dose plays in PAD patients with and without CKD and in PAD patients with and without a history of statin therapy. Results will be featured at the American College of Cardiology’s 71st Annual Scientific Session (ACC) 2022 (Washington D.C., USA, 2–4 April).
One lesser known but serious cardiovascular condition is PAD, a common, chronic circulatory condition that causes blood vessels to narrow, thereby reducing blood flow to the limbs, and most often the legs. It is a disease that often goes undiagnosed and undertreated.
While it usually starts asymptomatically, PAD can progress to severe symptoms and require revascularisation—a surgical procedure that restores blood flow after arteries have been clogged—to avoid amputation.
“At Janssen, we are continuing to invest in clinical research to help evolve the standard of care for people living with serious cardiovascular diseases, like PAD, an area of critical unmet need,” said James F. List, Global Therapeutic Area Head, Cardiovascular, Metabolism, and Retina at Janssen Research & Development. “Our research continues to support the use of the XARELTOvascular dose and is a treatment option physicians should consider for patients with PAD or coronary artery disease.”
Nipro Medical Corporation is set to introduce its second-generation Cronus high-pressure (HP) percutaneous transluminal angioplasty (PTA) balloon catheter to the US market.
Cronus HP is indicated for use in popliteal, femoral, iliac, and renal arteries, and in the treatment of arteriovenous fistulas (AVFs), with Cronus HP serving as Nipro’s “go-to choice” for vascular surgeons and interventional nephrologists in the repair and restoration of AVFs in haemodialysis patients—according to a press release from the company.
“Vascular access complications happen, even with the greatest of care,” said John O’Connor, director of Vascular Sales at Nipro. “So, we are here to ensure failed fistulas are transformed into functional fistulas.”
The release adds that the characteristics that are foundational to the Cronus HP include strength, flexibility and durability at high pressures, the ability to aid in using only one balloon during a procedure, facilitating entry across the lesion, and helping to minimise ‘balloon dog-boning’ and address difficult stenoses.
“Cronus HP signifies a unique bridge of two worlds within the Nipro product portfolio—renal and vascular,” said Joe Dawson, executive vice president of Nipro. The release also notes that the company’s vascular division, newly established in April 2021, already features nine products across three categories, including intravascular imaging.
Janssen has announced the launch of ‘Save Legs. Change Lives. Spot Peripheral Artery Disease Now‘, a multi-year initiative aimed at creating urgency and action to address the hidden threat of peripheral arterial disease (PAD)-related amputation, with an initial focus on reaching Black Americans.
Janssen details in a press release that it has joined forces with leading professional associations, healthcare systems, and community organisations to advance equitable care for individuals and communities placed at an increased risk for cardiovascular disease in the USA.
The company states that Black Americans experience disproportionate rates of cardiovascular disease, and—as a result of higher rates of asymptomatic PAD, less access to quality vascular care, and greater risk for delays in care—are up to four times more likely than white Americans to have a PAD-related amputation.
“While health inequities have long existed, the last several years have brought them to the forefront of our collective consciousness. Black Americans are placed at disproportionate risk of losing legs and lives—a reality we all must actively address,” said Pernessa Seele, founder and CEO, The Balm in Gilead, a faith-based organisation engaged in eliminating health disparities. “We believe the most effective way to eliminate the alarming health disparities within Black populations is for intentional, sustained and compassionate action by the healthcare industry, public health and faith communities.”
‘Save Legs. Change Lives.’ has three main areas of focus: driving research, collaborating with powerful partners, and empowering individuals and communities, Janssen states.
Research to break down barriers to PAD screening and increase equitable care
As part of the initiative, Janssen is supporting, sponsoring, and promoting research to uncover systemic bias, identify unmet patient needs, and propel healthcare systems toward change. The company details that research already underway includes a data-based tool to help health systems identify groups of patients with inadequate PAD care and better direct efforts toward those placed at the highest risk of amputation, as well as a series of white papers that highlight best practices of leading limb salvage programmes for people at risk for amputation.
“Everyone deserves a chance to avoid an amputation. I grew up in my dad’s podiatry practice and I saw from a young age what a difference you can make in simply helping people move through the world,” said David G Armstrong, professor of Surgery and director of the Southwestern Academic Limb Salvage Alliance (SALSA), at Keck School of Medicine, University of Southern California (Los Angeles, USA), and president of the American Limb Preservation Society (ALPS). “Limb preservation is of paramount importance, and I believe in the big idea that, together, we can eliminate limb amputations over the next generation. The inspiring thing is that—even with so many factors collectively stacked against our patients, ongoing research, awareness and sharing of best practices is vital to ensure we help people with PAD protect their legs and avoid the devastating consequences of amputation.”
Collaboration to unlock better PAD care and improve outcomes
Janssen notes that it is collaborating with various partners, including universities, health systems, non-governmental organisations, and change makers to break down barriers to equitable and inclusive care, ranging from access and health literacy to healthcare provider diversity.
The company states that it is proud to help support the American Heart Association’s PAD National Action Plan, which aims to reduce PAD-related amputation. Additionally, Janssen is sponsoring the American College of Cardiology Foundation’s ‘Change the FIELD’ initiative, a major multi-year effort to foster inclusivity, equity, leadership, and diversity in the field of cardiology.
Education, awareness and screening to reach individuals placed at greatest risk
Janssen is supporting grassroots PAD awareness, education and screening that empowers individuals and communities to change the trajectory of their health, the company adds in their press release. These efforts include:
Empower PAD: a traveling mobile health unit that brings PAD screening and education directly to communities across the nation;
The Change Network: a steering committee that convenes healthcare thought leaders and patient advocates to fuel discussion and inform the development of patient-friendly PAD resources, including ArteryAware.com;
Healthy Directions: a community education program designed to raise awareness about PAD with Black Americans and in communities of colour; and
The Balm in Gilead: supporting the creation of culturally tailored PAD educational resources and awareness programming for faith-based institutions in the Chicago area serving individuals of African descent with the goals of preventing diseases, improving health outcomes and eliminating health disparities.
“‘Save Legs. Change Lives.’ sets in motion a vision for more relevant, trusted and inclusive care for everyone affected by PAD,” said Avery Ince, vice president, Medical Affairs, Janssen Cardiovascular & Metabolism, Janssen Scientific Affairs. “As part of Johnson & Johnson, Janssen believes that major corporations have the power—and therefore the responsibility—to tackle pressing health challenges and make good health a reality for all people. We hope our efforts will inspire action to reduce amputations among people living with PAD.”
‘Save Legs. Change Lives.’ is part of Johnson & Johnson’s broader initiative, Our Race to Health Equity (ORTHE)—a US$100 million commitment to help eradicate racial and social injustice as a public health threat.
Venous stenting was a hot topic on the agenda of the recent American Venous Forum (AVF) annual meeting (23–26 February, Orlando, USA). Catching the audience’s attention, one presenter highlighted a head-to-head study of dedicated versus non-dedicated stents.
“Iliofemoral venous obstruction when not adequately treated results in chronic debilitating disease and poor quality of life,” said Lillian Tran (University of Pittsburgh Medical Center, Pittsburgh, USA), who noted that deep venous stenting is “increasingly preferred” as the mainstay treatment over medical therapy alone.
According to Tran, this move towards stenting necessitates studies comparing the performance of novel, dedicated venous stents with the more traditional, non-dedicated stents. At AVF, Tran reported the findings of such a head-to-head study at a single centre, detailing that the use of dedicated venous stents was associated with a significant reduction in extension into the inferior vena cava (IVC) without reduced early patency rates compared to non-dedicated stents.
The presenter stressed that outcomes after iliac vein stenting rely on multiple technical considerations and stent attributes. “In addition to adequate sizing and consistency in deployment, […] venous stents must establish a balance between radial force, flexibility and crush resistance,” she informed the audience. Tran detailed that dedicated, nitinol-based stents have been developed to meet these requirements and are now on the market in the USA and Europe. Four of these stents have been approved by the US Food and Drug Administration (FDA) for venous indications, the presenter relayed, noting, however, the fact that the Vici (Boston Scientific) and Venovo (BD) stents were recalled last year.
Outcomes data from investigational device exemption (IDE) trials of the four dedicated venous stents have demonstrated excellent patency rates, Tran communicated. However, she highlighted that head-to-head, comparative performance data against the more traditional Wallstent (Boston Scientific) and other non-dedicated stents are limited.
Tran et al therefore performed a retrospective review of all patients who underwent iliofemoral venous stenting for acute thrombotic, post-thrombotic and non-thrombotic indications at their institution between 2014 and 2021, grouping patients based on the use of novel, dedicated venous stents versus non-dedicated stents during their treatment.
The team measured 30-day stent failure and one-year patency rates as primary outcomes, Tran detailed, adding that secondary outcomes included stent sizing and extension.
A total of 135 patients (186 limbs) were treated in the study, Tran told AVF attendees, specifying that 63 limbs were treated using novel dedicated stents, while 123 were treated using the traditional Wallstent or another non-dedicated stent.
The team noted no preference in stent type in treating acute thrombotic or post-thrombotic lesions at their institution, but they did observe that dedicated venous stents were more likely to be used in non-thrombotic lesions.
Addressing the AVF audience, Tran reported that fewer stents were deployed per limb with the use of novel dedicated venous stents. In addition, she revealed that one patient had a stent fracture without thrombosis, and that there were no cases of deployment failure or stent migration in either group.
Additionally, larger size was observed in limbs using the Wallstent alone compared to dedicated venous stents and proximal stent extension into the IVC greater than 50% was significantly reduced with the use of novel venous stents compared to the non-dedicated devices, Tran detailed.
The presenter relayed some further key outcomes from the study: “Overall, dedicated venous stent use was not significantly associated with differences in early stent patency rates, nor was it a predictor of 30-day stent failure using a logistic regression analysis.”
In addition, she reported that primary patency rates remain comparable between novel venous stents and non-dedicated stents at one year. On subgroup analysis, the researchers did not see any differences between the non-dedicated and dedicated stents in either 30-day or one-year stent patency rates.
Tran acknowledged some limitations of the group’s study, including its retrospective nature, small sample size, short follow-up and no concurrent measurement of clinical improvement.
“In our experience, we found a significant reduction in extension into the IVC, total number of stents deployed and mean stent diameter with the use of novel, dedicated venous stents compared to Wallstents alone,” Tran concluded. In addition, she recapped that there were no significant differences in early outcomes between the two stent types.
Robert Hinchliffe (University of Bristol, Bristol, UK) shares his excitement to attend the upcoming CX Symposium (26–28 April, London, UK). “CX has always represented an unprecedented opportunity to share new techniques and to analyse the latest and best clinical trials across vascular interventions,” the CX 2022 executive board member tells Vascular News. This year, a highlight for Hinchliffe will be a session on the “hurting leg,” which is due to take place on the final day of the in-person and virtual meeting.
“We would all agree that a large component of our practice is patients who present with lower limb problems,” says Hinchliffe, emphasising the significance of the topic. He also highlights the fact that patients are presenting late in many cases—which could well explain high amputation rates. In light of this, he believes that CX 2022 “will be a really fantastic opportunity to assess these really troublesome patients”.
“Hurting legs are a very emotive issue for patients,” Hinchliffe relays, adding that they are a “common problem” for vascular specialists. Unfortunately, however, he highlights that “these problems are not managed particularly well within vascular centres, and it is unclear why this is the case”. Hinchliffe hopes that “CX 2022 will really shine a spotlight on the need to improve evidence in this area, and give an opportunity to share the latest ideas and cutting-edge research”.
In his own practice, Hinchliffe recognises outcome variation between regions and within regions. He points out that while this is “complex problem,” patient engagement is “really quite key”.
Another issue lies in the interdisciplinary nature of patient management, Hinchliffe tells Vascular News. He elaborates that patient management spans primary care, all the way through to more specialist interventions by other vascular surgeons, interventional radiologists, or cardiologists. “We really have not fostered good relationships between professionals,” he says, underlining the problem. Hinchliffe believes that CX 2022 “presents an opportunity to deal with, and shine a light on these problems, providing the opportunity to improve communication and pathways between groups of professionals”.
Finally, Hinchliffe highlights an ongoing need to raise awareness of the hurting leg. He notes that, in other cardiovascular arenas in the UK, a number of campaigns to raise the awareness of stroke, and the timely treatment of stroke, appeared to be “very effective”. “Clearly, there needs to be research to understand how to make the biggest difference and how to reach those hard-to-reach groups,” he urges. “Fundamentally, I think it is a question of raising the awareness both to patients and healthcare professionals and usually in primary care.”
This year, the CX Symposium will be held in person for the first time since 2019. After a two-year COVID-19-induced hiatus, Hinchliffe is keen to get back to face-to-face meetings. “It will be really fantastic to be back at the CX Symposium,” he says, describing it as “an opportunity to meet old friends and hopefully meet some new ones” in addition to its educational offerings.
Researchers at the Wyss Center for Bio and Neuroengineering (Geneva, Switzerland), in collaboration with the University of Tübingen (Tübingen, Germany), have enabled a person with complete paralysis, who cannot speak, to communicate via an implanted brain-computer interface (BCI).
This breakthrough came as part of a clinical case study that has been ongoing for more than two years with the participant—who has advanced amyotrophic lateral sclerosis (ALS)—and the results show that communication is possible with people who are completely ‘locked-in’ because of ALS, according to a Wyss Center press release. Details of the study are published in Nature Communications.
“This study answers a long-standing question about whether people with complete locked-in syndrome, who have lost all voluntary muscle control including movement of the eyes or mouth, also lose the ability of their brain to generate commands for communication,” said Wyss Center senior neuroscientist Jonas Zimmermann. “Successful communication has previously been demonstrated with BCIs in individuals with paralysis. But, to our knowledge, ours is the first study to achieve communication by someone who has no remaining voluntary movement and, hence, for whom the BCI is now the sole means of communication.”
The study participant is a man in his thirties who has been diagnosed with a fast-progressing form of ALS. He has two intracortical microelectrode arrays surgically implanted in his motor cortex. The release details that two microelectrode arrays, each 3.2mm2, were inserted into the surface of his motor cortex. Each array has 64 needle-like electrodes that record neural signals.
The participant, who lives at home with his family, has learned to generate brain activity by attempting different movements. These brain signals are picked up by the implanted microelectrodes and are decoded by a machine learning model in real-time. The model then maps the signals to mean either ‘yes’ or ‘no’. And, to reveal what the participant wants to communicate, a speller programme reads the letters of the alphabet aloud. Using auditory neurofeedback, the participant is able to choose ‘yes’ or ‘no’ to confirm or reject the letter, ultimately forming whole words and sentences.
“This study has also demonstrated that, with the involvement of family or caregivers, the system can, in principle, be used at home,” said Wyss Center chief technology officer George Kouvas. “This is an important step for people living with ALS who are being cared for outside the hospital environment. This technology, benefiting a patient and his family in their own environment, is a great example of how technological advances in the BCI field can be translated to create direct impact.”
Medtronic recently voluntarily recalled a subset of its IN.PACT Admiral and IN.PACT AV paclitaxel-coated percutaneous transluminal angioplasty (PTA) balloon catheters due to the potential for pouch damage resulting in a loss of sterility. This is according to a news alert from the company dated 31 March.
Medtronic communicates that approximately 6,000 IN.PACT Admiral catheters and three IN.PACT AV catheters distributed to customers globally are impacted by this recall. “Medtronic is communicating to customers with affected product on hand to immediately quarantine and return the product to Medtronic, as well as send back a signed confirmation form,” the company details.
The news alert continues: “The pouch damage was discovered during a routine inspection. Upon investigation, a change implemented to one manufacturing line was determined to be the cause. All batches manufactured on this line after that change are being retrieved. The problem on that line was fixed. Additionally, to ensure that no further issues, production on all lines was paused until a follow up packaging inspection was completed. No further errors were discovered.”
According to Medtronic, the company has received zero complaints involving this issue. In addition, they report that there have been zero reports of injury or death related to this issue. “There are no actions required for patients where the affected IN.PACT Admiral and IN.PACT AV catheters were used during a procedure. Patients should continue to be monitored in accordance with the medical facility’s standard care protocols,” the release reads.
The company stresses that, for most regions, there is little or no impact for customers to order replacement product. It advises that customers may reach out to Medtronic Customer service (800-551-5544, selection option “Vascular”) for any questions regarding their return or ordering replacement product.
The company notes that no other Medtronic products are affected by this issue, and that all appropriate regulatory bodies have been notified.
Ra Medical Systems has announced the achievement of a milestone with the enrollment of 100 subjects in the pivotal clinical study, according to a press release. The study is to evaluate the safety and effectiveness of the DABRA excimer laser system as an atherectomy device for the treatment of peripheral arterial disease (PAD). This pivotal atherectomy study is cleared to enroll up to 125 subjects.
“I want to recognize the support from our Ra Medical team and our physician-investigators and staff for their diligence in reaching this significant enrollment milestone, particularly given the daunting challenges that arose from the COVID-19 pandemic,” said Will McGuire, Ra Medical Systems CEO. “Securing clearance for the atherectomy indication is a top priority for Ra Medical as we believe it will expand our addressable market beyond the existing clearance for crossing chronic total occlusions (CTO). Third-party research estimates that the combined CTO and atherectomy markets in the US will approximate $900 million this year.
“Due to the unpredictable nature of the pandemic, we are unable to accurately predict when we will complete study enrollment. However, our goal is to reach full enrollment during the third quarter of this year and to complete a six-month follow-up in early 2023,” he added.
The open-label pivotal atherectomy clinical trial can enroll subjects with symptoms of PAD (Rutherford Class 2-5) at up to 10 sites. Seven sites have been cleared for enrollment and one additional site is in the final phase of qualification. Outcome measures include safety, acute technical success, and clinical success. The trial’s primary efficacy endpoint is the mean reduction in percent diameter stenosis in each patient’s primary lesion as measured by angiography immediately following treatment with DABRA and before any adjunctive treatment. The trial’s safety and clinical success endpoints are major adverse events at 30 days post-procedure and incidence of primary target lesion revascularisation at six months.
Tractus Vascular recently announced the first-in-man use of the Tractus Crossing Support Catheter (Tractus CSC). The Tractus CSC represents a highly novel approach to treating vascular disease, the company states.
Chronic total occlusion (CTO) remains one of the most challenging pathologies encountered by surgeons and interventionalists in performing endovascular interventions. John H. Rundback and Kevin Herman of American Endovascular and Amputation Prevention in West Orange, New Jersey, USA both used the Tractus CSC to treat several patients with challenging cases of critical limb ischaemia, including CTO. Rundback noted, “the Tractus catheter tracked like ice and performed exceptionally well; the cases were all extremely successful.”
The Tractus CSC is US Food and Drug Administration (FDA) 510(k) cleared with 0.014inch, 0.018inch and 0.035inch guidewire compatibility and lengths of 90, 135, 155 and 170cm. While most crossing support catheters are constructed with a braided sheath, Tractus offers its Jigsaw Technology laser cut stainless steel shaft consisting of a continuous helical cut pattern forming interlocking teeth. Distal “gusset cuts” offer a continuous stainless steel tip which extends the attributes of this novel catheter shaft.
In future peripheral arterial disease (PAD) research, clinicians should not consider men and women as a single population and should instead report their data separately. This is the main conclusion of a systematic review and meta-analysis recently published in theEuropean Journal of Vascular and Endovascular Surgery (EJVES), which found that symptoms of lower leg PAD present differently between men and women.
Authors Cindy P Porras (Utrecht University, Utrecht, The Netherlands) and colleagues write that while PAD has traditionally been labelled as a predominantly male disease, recent studies suggest that women are affected at least as often as men. Some of these studies also describe differences in the clinical presentation of lower extremity PAD between the sexes, however the authors note that there has been no systematic review collating this information. Therefore, the present study aimed to collate and pool the available evidence in order to evaluate differences in symptoms between men and women who present with lower limb PAD.
Using PubMed, EMBASE, and the Cochrane Library, Porras et al identified all relevant studies, collecting data on study design, source of data, population characteristics, and the outcome of interest using the Newcastle–Ottawa scale and Cochrane risk of bias tool. The authors note that, using the GRADE methodology, the evidence quality was rated as high, moderate, low, or very low based on the risk of bias, inconsistency, indirectness, and imprecision. In addition, the authors detail that estimates of relative effects were pooled to generate pooled odds ratios (ORs) and the 95% confidence interval (CI) using a random-effects model.
Porras et al relay that only studies reporting on symptomatic PAD were included in their analysis. They specify that studies were eligible if they included patients over the age of 18 with a diagnosis of PAD— established either by questionnaire, ankle-brachial index at rest, treadmill, or duplex—reported symptom prevalence, and presented outcomes. The authors note that review articles and case studies were excluded from their analysis.
Out of the 2,186 studies identified, a total of 21 and 20 studies were deemed eligible for qualitative and quantitative analysis, respectively. The investigators report that, of the qualitative studies, 13 were cross-sectional, six were cohorts, one was a case-control study, and one was a randomised controlled trial. Among the eligible study populations with diagnosed PAD, women represented 43.9%.
The 21 studies eligible for qualitative analysis reported on 1,929,966 patients with diagnosed PAD. According to the authors, the data from these studies show that women presented with intermittent claudication less often than men (25.9 vs. 30.2% with OR 0.78 [95% CI 0.72–0.84]; p<0.001; very low quality of evidence). In contrast, Porras et al communicate that rest pain and atypical leg symptoms were more prevalent in women (12.8% vs. 9.2%; OR 1.4 [95% CI 1.22–1.6]; very low quality of evidence, and 22.8% vs. 19.8%; OR 1.18 [95% CI 0.96–1.45]; very low quality of evidence, respectively).
The authors acknowledge some limitations of the present study. They recognise a “substantial heterogeneity” between the studies, the fact that only studies written in English were analysed, and that not all studies reported outcomes of interest. However, Porras and colleagues express their confidence that these limitations “are unlikely to influence the results significantly” as the lower prevalence of intermittent claudication in women was consistent over several subgroups and in sensitivity analyses.
Looking ahead, Porras et al suggest that future studies are needed to understand the possible reasons for differences in clinical presentation in women and men with PAD, and how this influences diagnosis, treatment, and outcomes.
Artio Medical, a medical device company developing innovative products for the peripheral vascular, neurovascular, and cardiology markets, today announced it received US Food and Drug Administration (FDA) clearance for its Solus Gold embolization device, a next-generation product for peripheral vascular occlusion.
“Current occlusion devices can be difficult to position in challenging anatomy, often require multiple implants, and usually take time to completely occlude the target vessel. This can be a problem when physicians need to control or prevent bleeding and reduce the risk of further complications,” commented Blaise Baxter, the vice president of Neurovascular and Peripheral Vascular Interventions for Artio Medical. “The Solus Gold device aims to overcome these limitations with a single implant designed for precision placement and immediate occlusion, even in high-flow vessels and short landing zones.”
The Solus Gold embolization device is indicated to obstruct or reduce the rate of blood flow in the peripheral vasculature. The delivery system balances flexibility, enabling physicians to navigate tortuous vasculature. Following a controlled expansion and simple mechanical detachment, the non-porous, balloon-like gold implant provides 360° vessel apposition for immediate and complete occlusion, and resists migration and recanalisation, providing physicians with a “one-and-done” solution for peripheral vascular occlusion. As demonstrated in a pre-clinical study, the Solus Gold device achieved immediate occlusion in >90% of cases, including in large and high flow vessels, and demonstrated 0% migration and 0% recanalisation in testing out to 3 months.
“We would like to thank the FDA for providing helpful input to the Artio team through the Q-Submission process, and for the careful and thoughtful review of our 510(k) application. I would also like to thank the talented and dedicated Solus Gold product development team at Artio, our many partners in the industry, and our supportive investors for helping Artio reach this important milestone,” said Nicholas Franano, president and CEO of Artio Medical. “When I first learned to embolize vessels using small metal coils more than 20 years ago, I thought surely someone will come up with a better device for doing that. As we prepare for the market release of the Solus Gold device later this year, I am excited to have the opportunity to provide physicians and patients with an improved peripheral vascular embolization experience.
Malignant ureteric obstruction (MUO) poses several tangible threats to cancer patients—and these threats translate, in turn, to challenges for the interventional radiologist and other treating physicians. Here, Conrad von Stempel and Tim Fotheringham (University College LondoN Hospitals and Barts NHS Foundation Trusts, London, UK) describe a number of alternative techniques to common approaches via percutaneous nephrostomy (PCN) or with polymeric JJ stents, while also assessing currently available evidence in this space.
Ureteric obstruction is a common sequela of genitourinary and other malignancies. Obstruction occurs from direct tumour infiltration, extrinsic compression from lymphadenopathy or tumour mass, and can occur because of malignant fibrosis or surgery. Patients with MUO have a poor overall prognosis with the median life expectancy of less than 12 months.1,2 MUO is a feature of advanced cancer and progressive bilateral obstruction leads to irreversible deterioration of renal function. The development of MUO may also preclude chemotherapy and other cancer therapies.
7mm 12cm Uventa stent
A multidisciplinary approach in the management of patients with MUO is required, as treatment selection is dependent on the prognosis of the patient, and the patient’s performance status combined with available cancer treatment options. Although some MUO can be treated with a retrograde approach, many patients require an antegrade approach by an interventional radiologist. MUO is commonly treated with PCN or with polymeric JJ stents—however, there are other management options available.
Permanent PCN may be required when there is extensive tumour infiltration in the bladder or when the ureteric obstruction cannot be crossed. PCN drainage is a relative contraindication for chemotherapy, requires regular exchanges, and is an undesirable outcome for most patients. Frequent tube dislodgement can occur with PCN, even when using larger-diameter nephrostomy tubes, placing the nephrostomy in a tunnel, or attempting to secure the tube with sutures and dedicated drain-fixation devices. The loop or circle nephrostomy is an alternative in such patients, using a double calyceal puncture. The loop nephrostomy has greater security with less chance of accidental displacement and requires less frequent routine tube changes than standard PCN.3,4
If the bladder still functions, extra-anatomical stenting can be considered through a subcutaneous tunnel and suprapubic access. Extra-anatomic stenting was first described in the 1990s but is seldom offered in PCN-dependent patients with MUO.5 A dedicated device, such as the Paterson-Forrester subcutaneous urinary diversion stent (Cook Medical; 8.5Fr, 65cm) can be placed and exchanged at three monthly intervals under local anaesthetic.
While it is difficult to draw too many conclusions from a limited number of studies, the self-expanding, covered ureteric stents do appear to be more effective in treating MUO, and with better long-term outcomes, compared with JJ stents.
JJ stenting with 6–8Fr polyurethane devices fail to relieve MUO at three months in up to 51% of patients and require regular routine exchange via the retrograde route at three-to-six-month intervals. Stent primary patency is between 40% and 60% at one year.6 An alternative to a polyurethane JJ stent is the Resonance stent (Cook Medical), which is a metal JJ stent made from a cobalt-chromium-nickel-molybdenum alloy and has a maximum indwell time of 12 months before exchange is required. The Resonance has improved primary patency to polymeric stents in some studies with >90% patency at one year, owing to less risk of extrinsic compression and encrustation. In a systemic review, the reported migration is low, at 1%—however, stent obstruction at 17% was seen and patients are prone to the same symptoms of bladder irritation seen with JJ stents.7
Dedicated covered, self-expanding ureteric stents have become available, which can be inserted either retrogradely or antegradely, and offer alternatives to JJ stents requiring fewer exchanges. Devices currently available include Uventa (Taewoong Medical), which is a double-layered, coated, self-expandable metallic mesh stent. The Allium (Allium Medical Solutions) is a fully covered, self-expanding nitinol stent. The entire stent is covered with a biocompatible, biostable polymer, making it a nonpermeable tube, to prevent tissue ingrowth and early encrustation stent. The Hilzo stent (BCM) has a polytetrafluoroethylene (PTFE) cover in spiral configuration—intended to help prevent stent migration. It is designed with soft and smooth ends to minimise hyperplasia.
All of these devices have a delivery size that is suitable for antegrade insertion—10Fr or less—and when deployed the diameter ranges from 7–10mm. The stents can be overlapped at points of tight narrowing, or in very long stricture, and offer focal distension of the diseased portion of ureter and require less frequent reintervention than JJ stents. Removal and replacement of these devices requires endoscopic intervention with graspers to either unwind or collapse the device.
7mm 12cm Hilzo stent
While it is difficult to draw too many conclusions from a limited number of studies, the self-expanding, covered ureteric stents do appear to be more effective in treating MUO, and with better long-term outcomes, compared with JJ stents. Complications seen include occlusion from hyperplasia, encrustation, migration and fistulation. The cost of the devices is offset by the reduced need for reintervention as compared with JJ stents.7–10
In conclusion, there are more options for treating patients with MUO other than PCN and JJ stents. Avoiding permanent PCN is advantageous to the patient, and significantly reduces readmission for either exchanges or managing the arising complications. Interventional radiologists should consider alternatives such as extra-anatomical stents and self-expanding covered stents when dealing with MUO.
References:
Izumi K, Mizokami A, Maeda Y et al. Current Outcome of Patients With Ureteral Stents for the Management of Malignant Ureteral Obstruction. Journal of Urology. 2011; 185(2): 556–61. doi:10.1016/j.juro.2010.09.102
Lienert A, Ing A, Mark S. Prognostic factors in malignant ureteric obstruction. BJU International. 2009; 104(7): 938–41. doi:10.1111/j.1464-410X.2009.08492.x
Noureldin Y A, Diab C, Valenti D et al. Circle nephrostomy tube revisited. CUAJ. 2016; 10(7–8): 223. doi:10.5489/cuaj.3596
Alma E, Ercil H, Vuruskan E et al. Long-term follow-up results and complications in cancer patients with persistent nephrostomy due to malignant ureteral obstruction. Support Care Cancer. 2020; 28(11): 5581–8. doi:10.1007/s00520-020-05662-z
Paterson P J, Forrester A. Extra-Anatomic Urinary Diversion. Journal of Endourology. 1997; 11(6): 411–2. doi:10.1089/end.1997.11.411
Tabib C, Nethala D, Kozel Z et al. Management and treatment options when facing malignant ureteral obstruction. Int J Urol. 2020; 27(7): 591–8. doi:10.1111/iju.14235
Khoo C C, Abboudi H, Cartwright R et al. Metallic Ureteric Stents in Malignant Ureteric Obstruction: A Systematic Review. Urology. 2018; 118(April 2017): 12–20. doi:10.1016/j.urology.2018.01.019
Kim M, Hong B, Park H K. Long-Term Outcomes of Double-Layered Polytetrafluoroethylene Membrane-Covered Self-Expandable Segmental Metallic Stents (Uventa) in Patients with Chronic Ureteral Obstructions: Is It Really Safe? Journal of Endourology. 2016; 30(12): 1339–46. doi:10.1089/end.2016.0462
Moskovitz B, Halachmi S, Nativ O. A New Self-Expanding, Large-Caliber Ureteral Stent: Results of a Multicenter Experience. Journal of Endourology. 2012; 26(11): 1523–7. doi:10.1089/end.2012.0279
Chen Y, Liu C, Zhang Z et al. Malignant ureteral obstruction: experience and comparative analysis of metallic versus ordinary polymer ureteral stents. World J Surg Onc. 2019; 17(1): 74. doi:10.1186/s12957-019-1608-6
Conrad von Stempel is a consultant interventional radiologist at the University College London (UCL) Hospitals NHS Foundation Trust in London, UK.
Tim Fotheringham is a consultant interventional radiologist at Barts Health NHS Trust in London, UK.
The authors declared no relevant disclosures pertaining to this article.
The February top 10 features news of the recent Japanese randomised control trial results, which support the use of mechanical thrombectomy in ischaemic stroke patients. Other highlights include an exploration of innovations in treating and diagnosing small renal masses by Vinson Wai-Shun Chan and Tze Min Wah, as well as Fluidx Medical’s announcement of “very promising” results from the company’s GPX-Clear embolic device in-vivo research.
A new study from Japan has become the first randomised controlled trial to demonstrate the effectiveness of endovascular mechanical thrombectomy procedures in patients who have severe strokes involving clots in one or more large brain arteries.
A recent retrospective analysis published in Melanoma Research has found that percutaneous hepatic perfusion with melphalan for the treatment of metastatic uveal melanoma offers a hepatic response rate of 66.7% and good progression-free survival.
Fluidx Medical Technology has announced the results of the GPX-Clear embolic device in-vivo research which uses the base GPX technology and incorporates an intermediate-term radiopacity agent, as described by the company.
Concept Medical has announced that the SIRONA randomised controlled trial (head-to-head comparison of sirolimus versus paclitaxel drug-eluting balloon angioplasty in the femoropopliteal artery) has completed half the targeted enrolment.
In light of recent and upcoming developments, Vinson Wai-Shun Chan and Tze Min Wah (Leeds, UK) explore the evidence and latest progress in renal tumour biopsy and discuss the treatment of small renal masses more broadly.
An associate professor of Radiology at the Division of Interventional Radiology, Nuovo Santa Chiara University Hospital, Pisa, Italy, Laura Crocetti is also an internationally recognised ablation expert. Here she answers questions posed by Interventional News.
Cerenovus—a neurovascular firm that forms part of Johnson & Johnson Medical Devices Companies—has announced the launch of Emboguard, the next-generation balloon guide catheter to be used in endovascular procedures, including those for patients with acute ischaemic stroke.
Preliminary late-breaking research presented at this year’s International Stroke Conference (9–11 February, New Orleans, USA) shows that mechanical removal of blood clots reduced post-stroke disability in nearly half of “all-comer” real-world stroke patients.
MedAlliance has acquired its partner MDK Medical, a Japanese vascular specialist company. MDK Medical has previously worked closely with MedAlliance in developing Japanese clinical studies for the novel sirolimus drug-eluting balloon—the Selution SLR— for the treatment of peripheral arterial disease.
Inari Medical has announced that the first patient has been enrolled in PEERLESS prospective, randomised controlled trial comparing the outcomes of patients with intermediate-high risk pulmonary embolism treated with the FlowTriever system versus catheter-directed thrombolysis.
With cancer cases growing worldwide and an increased number of late-stage diseases in elderly patients, there is an increasing need for an integrated approach. “Through evidence, cost, and acceptance of interventional oncology (IO), we can create value-based care and shift the treatment focus from volume to value”. This was the main take-home message presented by Thomas Helmberger (Public Hospital, Munich, Germany) at the European Conference of Radiology (ECR) 2022 (2–6 March, virtual).
Starting off the presentation, Helmberger provided some background on the future of patients with malignant diseases, with more patient cases currently in more and in less developed countries. He explained that “this growing number of patients translates to increasing cost and this demographic impact will challenge our healthcare systems”. He went on to explain that for example in colorectal malignomas 20–25% of patients exhibit stage four cancer, with the majority being elderly patients. He pointed out that this, therefore, means that we have to “deal with not only cancer but also comorbidities”. Discussing the “wave” of elderly patients, he explained the “Sisyphus effect”—more elderly expect to be fit and independent into older age, requiring more medical resources, creating more elderly patients.
Discussing the current developments in IO, Helmberger explained that IO techniques are resembling already known techniques, for example, radio-embolic techniques are resembling radiotherapy.
He drew attention to current issues in IO by making reference to an early closed randomised controlled trial (RCT) comparing surgery and percutaneous thermal ablation for hepatic metastases which had just recently illustrated drawbacks such as misconceptions about the eligibility criteria, unconscious bias towards surgery, and a lack of dedicated research nurses to name a few. The currently ongoing COLLISION RCT is dealing with the same comparison, however, it can be questioned to what extent artificial RCTs are still necessary for comparison to real-life data. Numerous studies over the past 15 years pointed to no difference in the overall survival in percutaneous thermal ablation compared to surgery in primary and secondary liver malignancies with diameters up to 3 cm (Otto et al, 2010; Lee et al, 2016). He also explained that combining transarterial therapies such as chemo- and radioembolisation can even enhance the therapeutical benefit of surgical and percutaneous ablative therapies (Hholami et al, 2020).
Helmberger raised the important factor of cost, with healthcare costs presenting differently in each country and between interventional approaches, with local ablation therapies usually costing less. However, in the sense of cost-effectiveness, Helmberger explained it is of limited use to only analyse a single procedure cost, as this does not provide sufficient information on the overall process costs. According to Helmberger, the effectiveness of IO is proven through evidence, cost, but still less acceptance, since “many guidelines and recommendations from professional societies are reluctant to implement interventional radiology techniques”. However, he stressed that IO embedded into interdisciplinary therapy concepts will optimise treatments to be given at the right time during a disease continuum. In doing so, he claims we can create more and more “value-based care”, which remains a central challenge in times of increasingly limited resources.
Fist Assist Devices has announced a three-year affiliation with Regional Health Care Group to commercialise and launch sales of the Fist Assist Model FA-1 device in Australia and New Zealand.
The FA-1 device is a wearable, patent-protected, intermittent compression device that has European CE-mark clearance for use in conditions where vein dilation is desired in patients that will require or have already undergone arteriovenous fistula placement for eventual haemodialysis.
In addition, it is intended to help with infusion arm vein access for chemotherapy, radiology or phlebotomy access support. FA-1 also recently received US Food and Drug Administration (FDA) Breakthrough Device designation for presurgical vein dilation in patients with end-stage kidney disease.
“We are thrilled to combine forces with Regional Health Care Group for the official launch of the Fist Assist Model FA-1 device in Australia and New Zealand,” said Tej Singh, chief executive officer and founder of Fist Assist. “This is a huge milestone, as we now have a committed, dedicated, and exceptional commercialisation arm that is poised to deeply penetrate the Oceania market.”
“We are excited to distribute and commercialise the innovative FA-1 device,” said Scott Clissold, national business development manager of Regional Health Care Group. “We have been watching the Fist Assist technology and patiently awaiting the right time to commercialise a ground-breaking, market-changing and innovative device that will improve the patient journey with renal and cancer care in Australia.”
Enrolment has been completed in the PROMISE II pivotal trial of the LimFlow deep vein arterialisation system designed to prevent amputations in so-called “no-option” chronic limb-threatening ischaemia (CLTI) patients, the eponymous device maker announced today.
“The PROMISE II investigators are very encouraged by our experience using the LimFlow system to treat CLTI patients with no other options. These are likely the sickest patients ever to have been enrolled in a limb salvage trial,” said Daniel Clair, PROMISE II principal investigator, and professor and chair of the department of vascular surgery at Vanderbilt University Medical Center Section of Surgical Sciences in Nashville, Tennessee. “Major amputations have a devastating effect on the lives of patients and their families. We are excited about the prospect of helping improve the lives of more of these patients once this novel technology becomes broadly available.”
PROMISE II is a multicentre, prospective, single-arm study being conducted at sites in the USA of 105 no-option CLTI patients. Endpoints include amputation-free survival at six months, limb salvage and wound healing, with subjects followed out to three years. The no-option patients treated in PROMISE II were determined by an independent physician committee to be no longer eligible for conventional endovascular or surgical therapy to treat CLTI, according to LimFlow.
The company also announced completion of enrolment in the CLariTI study of approximately 200 high-risk and no-option CLTI patients. The prospective, observational, multicentre CLariTI study will track the clinical progression of CLTI and incidence of death, amputation, and revascularisation attempts in patients undergoing standard medical management for the disease over a one-year period.
“Despite suffering from the most advanced form of CLTI, these no-option and high risk patients have been excluded from other trials,” said Anahita Dua, CLariTI principal investigator and assistant professor of surgery at Harvard Medical School in Boston. “Our hope is that the CLariTI study gives us better insights into the reintervention, amputation and death rates in no-option and high-risk patients treated with the current standard of care.”
A prospective multicentre study has evaluated the safety and efficacy of a polyethylene glycol (PEG)-based liquid embolic in treating hypervascular tumours, according to an Instylla press release.
Instylla recently announced the publication of results from the first-in-human (FIH) clinical trial of the Embrace hydrogel embolic system (HES) for the treatment of hypervascular tumours, in the Journal of Vascular and Interventional Radiology (JVIR). This prospective, single-arm multicentre study demonstrated that Embrace HES effectively embolized malignant and benign hypervascular tumours by blocking tumour blood supply with technical success and persistent embolization, as noted in imaging follow-up at 30-days, in all eight patients treated on this study.
“This phase I first-in-human study of Embrace HES in the embolization of a range of hypervascular tumours has shown promising results,” commented Gerard Goh (The Alfred Hospital and Monash University, Melbourne, Australia), lead author on the study. “Embrace HES holds great potential with its ease of use, technical success in all patients, and no tumour revascularisation in the 30-day follow-up imaging.”
Ten embolizations were performed in eight patients with a range of tumour types, including hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (ICC), and angiomyolipoma (AML). Tumour sizes ranged from 2.1–7.5cm and were treated with Embrace HES volumes from 0.4 to 4.0ml, with an average delivery time of 15 minutes.
Jee-Fu Huang (Kaohsiung Medical University Hospital, Kaohsiung, Taiwan) added, “Taiwan has one of the highest age-adjusted incident rates of HCC in East Asia, which is also the second leading cause of cancer-related deaths. This novel liquid embolic, designed to achieve capillary-level embolization, had favourable patient outcomes in the FIH trial, including HCC tumours. We are encouraged by these results. Our centre is currently enrolling in the Instylla HES HVT pivotal study, so I look forward to continuing to assess Embrace HES in treating hypervascular tumours.”
S.M.A.R.T. RADIANZ Vascular Stent System features improved ergonomics and advanced one-handed deployment capability. (PRNewsfoto/Cordis)
PRNewsfoto/Cordis
Cordis recently announced that the US Food and Drug Administration (FDA) has approved the S.M.A.R.T. Radianz vascular stent system, a self-expanding stent purposefully engineered for radial peripheral procedures.
The newly approved vascular stent system joins the Brite Tip Radianzguiding sheath and Saberx Radianz percutaneous transluminal angioplasty (PTA) catheter to complete the Radianz radial peripheral system, a company press release notes.
According to Cordis, the safety and efficacy profile of S.M.A.R.T. vascular stents is validated with a solid foundation of clinical evidence and real-world experience. It claims that the S.M.A.R.T. vascular stents are the only SE lower extremity stents with 10-year follow-up, proven to provide reliable outcomes in over 3,000 patients, and that they have shown comparable one-year revascularisation rates and a significantly lower cost of hospitalisation versus drug-coated stents.
“I am excited that Cordis has committed to delivering new interventional tools that can be utilised in treating patients with cardiac or vascular disorders via a transradial access,” said Craig M Walker, president and founder of the Cardiovascular Institute of the South (Houma, USA). “We have been constrained in the greater utilisation of this important access site associated with greater patient comfort and less major bleeding as our diagnostic and interventional tools that can be delivered via this access have been limited. These lower profile devices should expand the utilisation of radial access in treating patients.”
Cordis advises that the S.M.A.R.T. Radianzvascular stent system features improved ergonomics and advanced one-handed deployment capability, offering excellent placement accuracy and up to 300% greater stability. The product is available in a broad size matrix to support iliac and superficial femoral artery (SFA) lesion treatment, and the rapid exchange delivery system offers more convenient wire management and device exchange compared with over-the-wire (OTW) catheter systems, the company adds.
“At Cordis, we see the Radianz radial peripheral system as a best-in-class option for treating peripheral lesions with the added benefit of reducing the cost of care,” said Matt Muscari, Cordis president, Americas. “Empowered by our legacy, we are now focused on investing in a future of innovation. We are committed to leading the way in radial access to enable the less-invasive procedures that patients prefer.”
The VasQ external support device (Laminate Medical) has demonstrated long-term benefits for radiocephalic (forearm) arteriovenous fistula (AVF) creation in a retrospective analysis of 150 consecutive procedures. Robert Shahverdyan (Asklepios Klinik Barmbek, Hamburg, Germany) and Dirk Hentschel (Brigham and Women’s Hospital, Boston, USA) have published these data in Seminars in Dialysis.
The VasQ device is implanted around the connection between the vein and artery of an AVF to promote maturation into a functional access for haemodialysis. Standard fistulas have reported failure rates to become functional for haemodialysis as high as 60% within the first year, as per a press release from Laminate.
However, the newly published data demonstrate that implanting VasQ resulted in 90% of fistulas being used for dialysis within a median of 41 days, and 84% maintaining secondary patency out to 36 months. The results suggest, according to Laminate, that the addition of VasQ to Shahverdyan and colleagues’ standard of care has helped haemodialysis patients receive more functional fistulas that are durable over the long term.
“I am excited to share these data, which build on my previous publication that demonstrated the short-term benefit of VasQ to reduce my primary failure rate,” Shahverdyan said. “Now, we see the early success with VasQ translated to the long-term benefit of more patients retaining a functional fistula out to three years.”
“I was excited to partner with Robert on this publication,” Hentschel added. “The data supporting VasQ’s use in creating usable fistulas continue to build. I am looking forward to having this technology available for use in US patients.”
Laminate is currently completing a US pivotal study and preparing its submission for market clearance to the US Food and Drug Administration (FDA) for review.
Cardiovascular Systems Inc (CSI) has announced the start of enrolment in a first in-human trial of the peripheral everolimus drug-coated balloon (DCB) being developed by Chansu Vascular Technologies (CVT).
DCBs are a widely accepted percutaneous interventional treatment option for femoropopliteal lesions in patients with peripheral arterial disease. Everolimus, the active drug in CVT’s DCB formulation, acts as a cytostatic agent to reduce tissue hyperplasia and associated restenosis and has a long history of safety and efficacy in coronary drug-eluting stent applications.
The first patient was treated by Benjamin Honton, principal investigator at the Clinique Pasteur, Toulouse, France. The peripheral DCB was used to successfully treat a 69-year-old male with a 7.5cm lesion in his superficial femoral artery (SFA).
“We are honoured to enrol the first patient in the CVT-SFA trial,” said Honton. “We believe this promising new generation of everolimus DCBs could improve patient outcomes for those suffering from peripheral arterial disease.”
CVT intends to enrol 75 patients at a minimum of four sites in France and Germany to support an investigational device exemption (IDE) submission to the US Food and Drug Administration (FDA) and a subsequent US pivotal clinical study.
Jeffery Chambers, CSI’s chief medical officer, said: “Following the announcement of the first in-human experience with CVT’s coronary everolimus DCB in November 2021, we are thrilled to announce the first in-human experience with the peripheral everolimus DCB. We believe these products could become important new therapies in the treatment of peripheral and coronary artery disease.”
Under the terms of the agreements signed with CVT, CSI advises that it is providing milestone-based financing to CVT for the development of coronary and peripheral DCBs. Under an acquisition option agreement, upon CVT’s completion of key technical and clinical milestones in the development programme, CSI will have exclusive rights and obligations to acquire CVT, subject to the satisfaction of closing conditions set forth in the agreement.
Merit Medical announced today that it has received US Food and Drug Administration (FDA) breakthrough device designation for its Embosphere microspheres.
Merit Medical said in a news release that Embosphere microspheres are the most clinically utilised and clinically studied spherical embolic, having been used in more than 250,000 procedures.
“We are pleased with the recognition and partnership of the FDA, making it possible for new and innovative products to reach the market faster,” Merit Medical chairperson and chief executive officer Fred P. Lampropoulos said in the release. “Merit’s embolotherapy platform of products has provided consistent and predictable results for effective embolization. We believe this breakthrough designation allows us to accelerate our programmes to study and obtain FDA clearance for the GAE indication for Embosphere microspheres, ultimately expanding treatment options for patients.”
An embolic device by Fluidx Medical has been used successfully in a variety of complex cancer cases, according to a company press release.
As part of an ongoing multicentre study, Fluidx Medical has released additional information on treating tumours, including a highly vascularised metastatic renal cell carcinoma, with the GPX embolic device.
“We were very pleased with the outcome and the resulting occlusion created by GPX,” said Martin Krauss, head of interventional radiology at Christchurch Hospital (Christchurch, New Zealand.) “In one procedure, the renal cell carcinoma had metastasised to the upper femur/pelvic region. We used a combination of GPX and coils during the case. We treated five different tumour vessel segments with GPX.”
“GPX successfully occluded a variety of vessel presentations from smaller low-flow vessels to larger higher-flowing feeding vessels,” said Christopher Phillips, director of clinical affairs at Fluidx. “GPX was delivered using a range of microcatheters and showed versatility in treating small and large metastatic tumour vessel beds. GPX was delivered through standard microcatheters that were appropriate for each targeted vessel’s size and blood flow.”
The GPX embolic device is designed for simple preparation and controlled delivery. The company advises that the device is packaged ready to use in a syringe, can be prepped tableside by the clinician in about 30 seconds, and may be delivered through standard microcatheters.
Fluidx Medical describes its GPX technology as a low-viscosity, aqueous-based solution in a syringe that solidifies into a durable embolus upon delivery, without polymerisation or dimethyl-sulfoxide (DMSO) precipitation. GPX is designed to occlude blood vessels independent of a patient’s coagulation situation.
Guerbet announces it will more than double its line of microcatheters and launch a new line of guidewires, resulting in a broad range of interventional imaging and embolization solutions becoming available.
The company obtained its original offering of 18 references of SeQure and DraKon microcatheters as part of their acquisition of Accurate Medical Therapeutics in 2018. It received the CE mark in April 2019, and was US Food and Drug Administration (FDA) cleared in 2018.
Guerbet now expands the portfolio, adding 20 versions for a total of 38, and launching a new line of Axessio guidewires with two diameters. A limited market evaluation began in the United States during the fourth quarter of 2021, paving the way for a commercial launch rollout in the second quarter in select markets.
“The positive feedback we have received during the limited market release of our line extension has reinforced Guerbet’s decision to expand available tools to the healthcare professionals for various embolization procedures,” affirms David Hale, chief executive officer. “This year marks our 40th anniversary in interventional radiology. We are proud of that, but we consider it just the beginning. We have never been more dedicated to continuous growth and innovation to help interventional radiology physicians to meet an even greater number of patient needs.”
Both the SeQure and DraKon technologies offer interventional radiologists optimised navigation capabilities which is expected to enable access to difficult anatomies and reach further. Additionally, SeQure is the only reflux control microcatheter enabling a fluid barrier technology for flow-directed embolization. The new models are designed to deliver more targeted treatment and use a wider range of beads, from extra-small to large.
“Innovation means everything to us, because it means everything to our physician partners and to their patients,” explains Jean-François Blanc, Guerbet’s senior VP, for interventional imaging. “The more we see the results, the more we see opportunity to improve lives, and we just want to keep pushing forward. With strategic acquisitions that helped create a unique toolkit of microcatheters and this latest portfolio extension, we are advancing options for the interventional radiology community.”
InspireMD has announced that its CGuard embolic prevention stent system (EPS) will be included as a device option for stenting in CREST-2 (Carotid revascularisation endarterectomy or stenting trial). Following the recent approval of the CREST-2 investigational device exemption (IDE) supplement application from the US Food and Drug Administration (FDA), the company states that it will be evaluating strategic sites to enable expediated access.
Marvin Slosman, chief executive officer of InspireMD, commented: “This approval for use of CGuard EPS in a trial as significant as CREST-2 is proxy to the validation of our technology platform, contributing to this important work. The CREST-2 trial is widely acknowledged as the most significant ongoing trial to scientifically investigate the optimal course of treatment to prevent strokes for asymptomatic patients with significant carotid disease. The opportunity to be a part of CREST-2 is a tremendous milestone for our company, and we look forward to CGuard playing an important role in the stenting results”.
The study first enrolled patients in 2014, as two parallel multicentre randomised, observer-blinded endpoint clinical trials with the purpose of being to determine the best way to prevent strokes in patients with high-grade carotid stenosis but no stroke symptoms related to that blockage. According to an InspireMD press release, the trial will enrol an estimated 2,480 participants who will remain in the study for four years following the start of intervention.
“The CREST-2 executive committee is keenly focused on positioning the results of the trial to be relevant, actionable, and informative to contemporary practices,” said Thomas Brott (Mayo Clinic, Jacksonville, USA), principal investigator of the National Institute of Neurological Disorders and Stroke (NINDS)-sponsored trial. “Over the course of the trial we have continually introduced state of the art medical, pharmacological therapies to reduce the risk of stroke in our randomised patient population. It is critical of any long-term study to remain aligned with evolving technology and relevant devices. After examining the extensive clinical experience with the CGuard stent and the large body of evidence to its effectiveness, the study executive committee felt it appropriate to include this stent as a treatment option. Patients that agree to participate in the CREST-2 trial, depending on accessibility and operator training and discretion, will now have access to this state of the art, carotid stent device.”
According to a press release, CSI intends to acquire and commercialise novel thrombectomy devices from Innova targeting peripheral vascular disease, including deep vein thrombosis (DVT) and pulmonary embolism (PE).
Sanjay Shrivastava, CEO of Innova said: “We strive to bring solutions that are easy to use, safe, and highly effective in treating potentially devastating diseases. We are excited to partner with CSI, which has been serving the interventional cardiology, interventional radiology, and vascular surgery communities that will be the primary users of Innova products. CSI’s commercial presence in this space makes it an excellent fit for accelerating the commercialisation of Innova’s products post regulatory clearances.”
CSI claims that, pending regulatory clearance in the USA, the company could begin to commercialise a portfolio of manual aspiration and clot retrieval devices for the treatment of peripheral vascular disease in 2023. The portfolio and corresponding indications for use are expected to be expanded to include treatment of DVT and PE following the completion of subsequent clinical trials.
Scott Ward, chairman, president and CEO, said: “The commercialisation of these thrombectomy devices will be an important addition to our growing pipeline of products. In total, developing novel drug-coated balloons, intravascular lithotripsy, mechanical circulatory support, and thrombectomy devices target some of the fastest-growing segments within interventional cardiology. Supplementing our core orbital atherectomy devices with these technologies will greatly increase the number of patients we will reach while simultaneously expanding our total addressable market to over US$18 billion in the coming years.”
Under the terms of the agreements signed with Innova, CSI has provided financing to Innova for the development of thrombectomy devices. Under an acquisition option agreement, upon Innova’s completion of key technical, regulatory, and clinical milestones in the development programme, CSI will have exclusive rights to acquire the thrombectomy devices, subject to the satisfaction of closing conditions set forth in the agreement.
David Dexter delivers CLOUT registry data at AVF 2022
Six-month outcomes from the ongoing CLOUT registry demonstrate the “safety and efficacy” of the ClotTriever thrombectomy system (Inari Medical) in a real-world deep vein thrombosis (DVT) population regardless of clot chronicity level, the 2022 annual meeting of the American Venous Forum (AVF; 23–26, Orlando, USA) heard.
David Dexter (Eastern Virginia Medical School and Sentara Vascular Specialists, Norfolk, USA) was delivering the latest subgroup analysis update from the prospective, multicentre study on behalf of the CLOUT registry investigators based on the first 250 patients enrolled at 24 sites. “We were able to meet the performance goal of greater than 75% in all three [chronicity] groups,” Dexter told attendees. “We had remarkably low device-related serious adverse events at one month. And our rates of post-thrombotic syndrome [PTS]—including moderate to severe—at six months were similarly low.”
The data from the registry show 33% of the 250 patients with acute thrombus, 35% with subacute and 32% with chronic.
Almost all procedures were single session, with an average of four passes using the ClotTriever device for all chronicity subgroups, Dexter said. No patients required adjunctive thrombolytics. Adjuvant angioplasty was used in 73% (acute: 70%; subacute: 68%; chronic: 84%) and stents in 47% (acute: 46%; subacute: 42%; chronic: 50%) of cases.
Complete or near-complete thrombus removal was achieved in 85% (acute: 90%; subacute 81%; chronic: 84%) of limbs, including 51% (acute: 54%; subacute: 49%; chronic: 49%) with 100% thrombus removal. The post-thrombectomy median hospital stay was one day for all subgroups.
At six months, 90% (acute: 86%; subacute: 89%; chronic: 96%) of the treated limbs had flow present, and 90% (acute: 84%; subacute: 90%; chronic: 91%) were compressible. Any PTS at six months was about 20% in the acute, 25% in the subacute and 30% in the chronic arms. “Statistically, this has a p value of 0.5—we will see how that holds out in another two years when we have finished enrolment of 500 patients,” Dexter said. On the other hand, moderate-to-severe PTS, “was remarkably low at 5% in the acute arm, and about 10% in the subacute and chronic arms.”
Major adverse events and serious adverse “were similar and also rare,” Dexter added. “All-cause mortality was three patients throughout the first 250.”
Furthermore, in terms of venous clinical severity score (VCSS) scores, at 30 days and six months numbers were “nicely low” at 3 and 2 for the acute group, 4 and 3 among subacute patients, and 4 and 4 in the chronic subset, Dexter pointed out. Pain score numbers were “essentially zero across the board.” The same was true when measuring quality of life, he said. “The average quality of life went back to the patient’s baseline regardless of the chronicity believed to be in the clot for acute, subacute and chronic.”
The CLOUT registry’s follow-up out to two years is ongoing. Total enrolment of 500 patients at up to 50 sites has the intention of probing all-comers—across acute, subacute and chronic clot subgroups.
William Marston delivers data on the early US experience with the BlueLeaf venous valve formation system
An emerging endovenous valve formation system designed to treat patients with chronic venous insufficiency (CVI) with evidence of deep venous reflux has demonstrated continual improvement since US investigators started performing clinical cases with the device 18 months ago, according to recently presented early data.
The BlueLeaf procedure, currently undergoing clinical research worldwide, has shown a rate of 90% technical success among the first 10 patients treated in the USA, William Marston (University of North Carolina at Chapel Hill, Chapel Hill, USA), one of the INFINITE-US early feasibility study investigators, told the 2022 annual meeting of the American Venous Forum (AVF; 23–26 February, Orlando, USA).
These data are part of a total of 30 patients treated at sites worldwide, demonstrating a 93% technical success rate of forming at least one valve, said Marston, who disclosed a consultancy relationship with InterVene, the company behind the BlueLeaf device.
Enrolled patients, classed as C5–6 on the CEAP (Clinical-Etiological-Anatomical-Pathophysiological) classification of disease severity, all had significant deep vein reflux in two main segments between the knee and the common femoral vein, adequate inflow and no acute deep vein thrombosis (DVT), Marston explained.
Thus far, all subjects in the study have had a maximum of two valves formed using the device—most performed on the right leg and all monocuspid valves (US Food and Drug Administration [FDA] approval has now been granted to form bicuspid valves). The patient pool has a mean age of 59, presented with a venous clinical severity score (VCSS) of 15, and 70% had a previous history of DVT (six on the ipsilateral limb).
Marston told AVF attendees how the US investigators had achieved success in nine out of the 10 patients, with the mean number of leaflets formed standing at 1.7. He further noted how procedure time was currently decreasing, explaining how the system requires a period of adjustment as physicians adapt to patient and equipment positioning. Marston pointed out two minor device deficiencies that did not lead to any complications.
In terms of VCSS among the first six subjects with follow-up out to 12 weeks, investigators saw a mean decrease of 2.3, he said, though he cautioned the early-stage nature of the data. Marston reported no major adverse events, one partial valve pocket thrombosis at one day and one partial distal intraluminal thrombosis. Both were asymptomatic and no longer seen after 30 day duplex follow-up, he added.
The process behind the development of the BlueLeaf system—which gained FDA Breakthrough Device designation late last year—”has been under evolution such that we are just starting to do bicuspid valves and, in fact, we are scheduled to do the first one in the USA next week,” Marston said. “The device we are using today is quite different from the one we used 18 months ago.”
The system involves retrograde access; a high-pressure balloon expanded to force the deck of the device up against the vein wall; an advanced needle that enters the vein wall and hydrodissects a flap; and then a nitinol dissector advanced into the flap, expanding and deepening the formation to create a valve cusp.
Improvements made to the latest generation of the device means the valve cusp formed has more depth and a deeper capture of blood after creation, Marston elaborated. Additionally, “the device balloon has been strengthened to help puncture post-thrombotic veins, as most of the patients enrolled are post-thrombotic.”
Marston drew attention to one of the study cases with one year of follow-up to demonstrate the BlueLeaf system’s evolution. The 53-year-old male patient, who had two monocuspid valves created, showed no DVT through 365 days follow up and a VCSS improvement from a baseline of 9 to 6. Marston noted how the valve cusp still showed some motion at one year compared to initial formation. “We would like to see more but this was with a very early version of the device,” he said. “The cusps are now deeper and wider and hopefully will move better at 365 days than we see here. But this patient did have a well-preserved improvement in VCSS.”
Concluding, Marston told the AVF meeting the BlueLeaf procedure “is technically feasible,” capable of forming valve cusps and under “continual improvement.” “The cusps we are forming today are much better than they were a year ago,” he said, pointing to an “exciting” future as study investigators progress into bicuspid valve formation and the hope of greater luminal coverage.
Recently released clinical data has outlined the benefits of the RenovaRP paracentesis management system (GI Supply) for patients with ascites. The study, which was published in the Diagnostic and Interventional Radiology journal by Shane Weber (Dearborn, USA) et al, found that there was a substantially higher fluid flow rate during paracentesis using the RenovaRP system as compared to wall suction.1
The purpose of the study was to investigate if the use of RenovaRP as a treatment for ascites would reduce procedure time compared to standard wall suction without increasing adverse effects, such as hypotension or abdominal pain.2
Procedure room time decreased from 53 minutes with wall suction to 31 minutes with RenovaRP (p<0.001).3 The paper’s authors noted that the RenovaRP pump is portable, simple to use, requires little staff training, and can be used to perform paracentesis outside of interventional radiology. The authors also highlighted that, as a self-contained system, it avoids exposing medical team members to patients’ body fluids, which may occur during exchange of wall-suction canisters.4
Karen Brown (Salt Lake City, USA), a co-author of the research paper, said: “Exposure to a patient’s body fluids is a risk faced by healthcare professionals that must change cannisters or open cannisters to pour in the material that solidifies the removed fluid.”
Brown added that the patient experience “was comparable to conventional wall suction. Patients said they liked Renova better, which might have been due in part to it being a faster procedure”
The study authors also noted that on certain high-volume centres where paracentesis procedures are performed frequently, the RenovaRP pump can be expected to provide superior through-put with relatively minimal added procedural costs. In addition, the pump offers providers and patients substantially faster procedure times without adverse outcomes.5
Rhett Klein, vice president of sales and marketing at GI Supply, commented: “While we anticipated positive outcomes from this clinical study, our team was gratified that the results clearly support the benefits of the RenovaRP system. We are dedicated to enhancing patient safety and satisfaction in a cost-effective system that also supports the needs of medical staff.”
References:
1: Weber S, Al-Dulaimi R, Quencer K, et al. Paracentesis: faster and easier using the RenovaRP® pump. Diagnostic and Interventional Radiology 2022 2: Ibid.
Aidoc, a technology company that provides artificial intelligence (AI) solutions for medical imaging, including in the cardiovascular space, is extending its services beyond the radiologist’s workstation. This is according to the company’s vice president of Innovation, Demetri Giannikopoulos, who spoke to Interventional News at this year’s International Symposium on Endovascular Therapy (ISET 2022; 16–19 January, Hollywood, USA) about the company’s journey and its place in a growing market.
With seven US Food and Drug Administration (FDA) clearances for a variety of pathologies, Aidoc states that its AI algorithms deliver a cross-specialty AI experience for physicians in nearly 600 medical centres across the globe.
Specifically, the company’s suite of solutions includes providing thoracic radiologists triage and notification tools to help identify positive cases of pulmonary embolism (PE). This identification by Aidoc’s AI process is combined with automated right ventricle/left ventricle (RV/LV) ratio calculations, provided by partner company Imbio’s software, to improve patient severity assessment and expedite treatment.
“AI is everywhere,” says Giannikopoulos, who notes that what makes it “transformational” in medicine is its ability to help to shape patient care plans and pathways. The technology can be leveraged to identify the appropriate patients for treatment and bring those patients to the care team in a timely manner, he explains.
Aidoc started in diagnostic radiology. The company’s solutions would automatically flag any positive cases of acute pathologies on the scans, and then prioritise the patients with those positive cases on radiologists’ worklists. “The radiologists would have earlier awareness of the patients with positive acute findings,” Giannikopoulos tells Interventional News.
The company has been extending its AI solutions beyond the radiologist’s work station and connecting radiologists’ findings with the multidisciplinary teams (MDTs) that directly care for the patients, Giannikopoulos reveals. He elaborates: “The focus now is on driving awareness from the radiologist directly to the emergency care physician, directly to the interventionalist, so they know that there is a patient that is worth evaluating immediately.”
“The opportunity for PE patients to fall through the cracks is significant,” says Giannikopoulos, alluding to one of the key reasons why the company endeavours to become more involved in direct patient care. “A lot of times PE is managed by the bedside physician without consulting with the interventional team,” he adds. “We are alerting the team based on the PE identification in the image plus the RV/LV analysis.”
While AI has the potential to improve patient care, Giannikopoulos acknowledges the importance of “pulling the signal from the noise” amidst a growing pool of evidence in the field and fragmented care pathways, and underlines various challenges associated with standing out in a crowded market. He believes that the level of integration Aidoc currently has with the clinical care team sets the company apart, referencing in particular Aidoc’s immediate access to both imaging results and patient information, which can be quickly transferred to team members by their mobile devices.
A still from the visual demonstration of the result of the VascuViz imaging pipeline. Credit: Johns Hopkins Medicine
A still from the visual demonstration of the result of the VascuViz imaging pipeline. Credit: Johns Hopkins Medicine
Johns Hopkins Medicine researchers have developed and tested a new imaging approach they say will accelerate imaging-based research in the lab by allowing investigators to capture images of blood vessels at different spatial scales.
Tested in mouse tissues, the method, dubbed “VascuViz,” includes a quick-setting polymer mixture to fill blood vessels and make them visible in multiple imaging techniques. The approach enables researchers to visualise the structure of a tissue’s vasculature, which in conjunction with detailed mathematical models or complementary images of other tissue elements can clarify the complex role of blood flow in health and disease, say the researchers. The combined images of the blood vessels should not only enhance the study of the biology of diseases that involve abnormalities in blood flow, such as cancer and stroke, but also advance our understanding of the structures and functions of tissues throughout the body, they say.
The report was published on 10 February in Nature Methods.
“Usually, if you want to gather data on blood vessels in a given tissue and combine it with all of its surrounding context like the structure and the types of cells growing there, you have to relabel the tissue several times, acquire multiple images and piece together the complementary information,” says Arvind Pathak (Johns Hopkins University School of Medicine, Baltimore, USA), senior author of the study. “This can be an expensive and time-consuming process that risks destroying the tissue’s architecture, precluding our ability to use the combined information in novel ways.”
Researchers use many different imaging methods, such as magnetic resonance imaging (MRI), computed tomography (CT) and microscopy to study the role of blood vessels in the lab. These images are useful for understanding the dynamics of how tissues develop disease or respond to treatment. However, integrating the data available in these images has remained a challenge because agents used to make a blood vessel visible to one imaging method can make it invisible on other tools. This limits the amount of data researchers can gather from a single sample.
VascuViz overcomes this problem by making the structure of the largest arteries to the smallest microvasculature visible to a variety of imaging tools, which allows researchers to develop a multilayered understanding of blood vessels and related tissue components with less time and effort.
The development of VascuViz is particularly useful in creating computerised visualisations of how complex biological systems such as the circulatory system work, and is a hallmark of the growing field of “image-based” vascular systems biology.
“Now, rather than using an approximation, we can more precisely estimate features like blood flow in actual blood vessels and combine it with complementary information, such as cell density,” says lead author Akanksha Bhargava (Johns Hopkins University School of Medicine). To do this, VascuViz-based measurements are entered into computer simulations of blood flow, such as the cancer models Bhargava studies.
To create VascuViz, Bhargava tested several combinations of existing imaging agents and their suitability for different imaging methods. After multiple iterations, she found that a CT contrast agent named BriteVu and a fluorescently labelled MRI contrast agent called Galbumin-Rhodamine could be combined to create a compound that makes the macro- and microvasculature simultaneously visible when imaging with MRI, CT and optical imaging techniques without interference.
With the compound working in test tubes, the researchers then tested it in a variety of mouse tissues, perfusing it through the vascular system of breast cancer models, leg muscles, the brain and kidney tissues. The resulting images of the tissues acquired with MRI, CT and optical microscopy were then combined to create stunning 3D visualisations of the vasculature and associated components comprising these disease model and organ systems.
Due to VascuViz’s affordability and commercially available components, Pathak and his team hope it is globally adopted by scientists to help shed new light on different diseases involving the vasculature.
Other researchers involved in this study include Benjamin Monteagudo, Priyanka Kushwaha, Janaka Senarathna, Yunke Ren, Ryan Riddle and Manisha Aggarwal of the Johns Hopkins University School of Medicine.
This work was supported by the National Cancer Institute, the National Institute of Dental & Craniofacial Research and NIH Instrumentation grant and the Sidney Kimmel Comprehensive Cancer Center, Quantitative Sciences Pilot Project Grant.
Charing Cross (CX) chair Roger Greenhalgh welcomes the vascular community to this year’s symposium, due to be held 26–28 April in London, UK, and virtually. To read the preliminary programme and register visit cxsymposium.com.
Ra Medical Systems a medical device company focused on developing the excimer laser system to treat vascular diseases, has announced that enrollment has reached 95 subjects in the pivotal clinical trial to evaluate the safety and effectiveness of the DABRA excimer laser system as an atherectomy device for the treatment of peripheral arterial disease (PAD). The company also announces approval from the US Food and Drug Administration (FDA) to increase subject enrollment from 100 subjects to 125 subjects.
DABRA has been cleared by the FDA for crossing chronic total occlusion (CTOs) in patients with symptomatic infrainguinal lower extremity vascular disease and has an intended use for ablating a channel in occlusive peripheral vascular disease. The FDA defines atherectomy to include a prespecified improvement in luminal patency.
The open-label pivotal atherectomy clinical trial can enroll subjects with symptoms of PAD (Rutherford Class 2-5) at up to 10 sites. Outcome measures include safety, acute technical success and clinical success. The trial’s primary efficacy endpoint is the mean reduction in percent diameter stenosis in each patient’s primary lesion as measured by angiography immediately following treatment with DABRA and before any adjunctive treatment. The trial’s safety and clinical success endpoints are major adverse events at 30 days post-procedure and incidence of primary target lesion revascularization at six months.
Perfuze announced today that it has closed a €22.5 million Series A investment round—the proceeds from which will be used to drive the next stage of a US clinical study and regulatory clearance of its Millipede system. The funds will also be used to support ongoing development of new products and to initiate commercialisation of its technology.
The Series A funding was led by new investors LSP, investing from its LSP Health Economics Fund 2, and Seroba Life Sciences. The round was also supported by new investor SV Health Investors, investing from its Medtech Convergence Fund, and existing investors Earlybird, the HBM-MedFocus Fund, Enterprise Ireland and a syndicate of Irish business veterans and stroke physicians, according to a Perfuze press release.
With the closing of this Series A financing round, Anne Portwich, partner at LSP, and Daniel O’Mahony, partner at Seroba Life Sciences, will join the Perfuze board of directors, while Megan MacDonagh, senior associate at SV Health investors, will join as a board observer.
Wayne Allen, CEO of Perfuze, said: “We are delighted to have completed our Series A financing with such experienced investors, and this capital facilitates our continued growth and development. We believe that the Perfuze Millipede system is the next wave of thrombectomy technology in the rapidly growing stroke market and has the potential to positively impact the lives of thousands of stroke patients.”
According to the World Health Organization (WHO), stroke is the second leading global cause of death and a leading cause of disability, the release adds. Perfuze’s next-generation, catheter-based aspiration technology for the treatment of large vessel occlusion (LVO) acute ischaemic stroke aims to provide superior clinical outcomes in shorter procedural times, resulting in safe, cost-effective therapy.
In a press release by Front Line Medical Technologies, the company have announced the expanded availability and distribution of their COBRA-OS (control of bleeding, resuscitation, arterial occlusion system), as more physicians, including interventional radiologists, continue to implement the life-saving aortic occlusion device for various applications.
The COBRA-OS, which is approved by Health Canada and cleared by the U.S. Food and Drug Administration (FDA), is the first 4 French REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) device and has the lowest profile on the market, according to the company. The device is guidewire-free and has a 25mm diameter compliant balloon with a uniquely designed Safety Shoulder Reservoir incorporated into the device to help prevent aortic rupture during inflation. Despite being so small, the device is also strong enough to hold back aortic pressure and allows for permissive hypotension in bleeding areas below the balloon. The device can be deployed quickly, in just over a minute, which is key in emergency situations.
In addition to permitting interventional radiologists the time to perform internal iliac artery embolization in hypotensive patients with unstable traumatic pelvic fractures, the COBRA-OS has been recently used prophylactically to treat a pregnant patient with placenta accreta, significantly reducing the risk to both mother and child.
Adam Power (Victoria Hospital in London, Ontario, Canada), vascular surgeon and co-inventor of the COBRA-OS, has successfully utilized the device with his interventional radiology colleagues in traumatic bleeding cases to help stabilise patients. As the device is so low profile, he has even been contacted to help with pediatric patients with uncontrolled bleeding.
“The COBRA-OS is a versatile tool that can be a swiss army knife for interventionalists. There is no other compliant balloon medical device in the world that goes through a 4 French sheath and can expand to 25mm diameter. I’ve even seen it be used coaxially in larger sheaths to occlude the aorta and allow interventions through the same single sheath which was pretty impressive,” said Power. “Access site complications are the bane of my existence as a vascular surgeon and I want to help lower their incidence, especially in extremely sick patients.”
In light of recent and upcoming developments in the space, Vinson Wai-Shun Chan and Tze Min Wah (Leeds, UK) explore the evidence and latest progress in renal tumour biopsy (RTB), and discuss the treatment of small renal masses (SRMs) more broadly.
The optimal diagnostic pathway and treatments for small renal masses (T1N0M0) is controversial. Due to the lack of tumour markers and inability to determine malignancy from benign pathologies, SRMs are often over-treated. Yet, RTB has not been widely implemented into the diagnostic pathway of SRMs. In terms of treatment, partial nephrectomy remains the gold standard for curative surgery but is associated with significantly reduced renal function and high complication rates. Although high-quality evidence is lacking, percutaneous image-guided ablation (IGA) provides excellent oncological, perioperative, and renal function outcomes.
As a result of increased used of abdominal imaging, the rates of incidentally discovered SRMs have increased over the past decade. However, there is no reliable imaging or tumour markers to determine the lesion’s malignant potential. Further, it was shown that over 20% of these treated masses are benign in histology, suggesting significant overtreatment of patients without malignant disease. A systematic review and meta-analysis have reported that diagnostic core biopsies have a sensitivity and specificity of 99.1% and 99.7%, respectively, for malignancy. Despite the proven accuracy and safety profile of RTB, there is reluctance to implement RTB within the urological community.
The benefits of performing RTB before treatment is at least twofold. First, this can guide patient decision-making on whether to receive treatment. More than 90% of interviewed patients with SRMs have expressed that they believe knowing the mass’ histology status will aid decision-making for the optimal treatment. Secondly, given a malignant result for RTB, an RTB can guide the best treatment for the patient, where low-grade SRMs could opt for active surveillance or IGA; and high-grade SRMs could opt for partial or radical nephrectomy. In fact, the latest study of the EuRECA registry1 showed that, amongst patients undergoing ablation, the pre-cryoablation biopsy rate rose from 42% in 2015 to 72% in 2019 (p<0.001). Subsequently, patients are less likely to be overtreated for benign disease when more biopsies are performed (odds ratio [OR]=0.64, p<0.001).
This has shown promising potential in extending the use of preoperative RTB to other forms of SRM treatment—especially partial nephrectomy—avoiding the significant decline in renal function and high complication rates post-nephrectomy. However, it is important to stratify patients who will benefit the most from biopsies. For example, patients over the age of 70 or who are unfit to undergo definitive treatment for SRM may not benefit from RTB; while those with complex tumours or comorbidities may benefit from RTB to prevent complex, high-risk treatments in these patients.1
Since the introduction of image-guided radiofrequency ablation (RFA) in 1998, the technology of IGA has developed significantly to include multiple different energy sources including cryoablation, microwave, and irreversible electroporation (IRE).2 The advantages of IGA compared to partial nephrectomy are at least twofold. Firstly, IGA is significantly less invasive compared to partial nephrectomy, with significantly reduced complication rates.3 Secondly, IGA is associated with a significantly lesser drop in renal function, which is crucial in patients with bilateral (synchronous or asynchronous) disease, or those who require repeat treatments—such as Von-Hippel Lindau syndrome (VHL) patients.
However, there is a lack of high-quality evidence to support the oncological non-inferiority of IGA compared to partial nephrectomy. This could be due to a few reasons. Firstly, previous recruitment of various trials involving IGA has failed, notably in the SURAB and the CONSERVE studies, which could be a result of patient preferences and lack of evidence at the time to support the recruitment process. Secondly, as pointed out by a review performed by the European Association of Urology (EAU) Renal Cancer working group, the quality of observational studies and systematic reviews on the area is poor, notably affected by severe selection bias whereby younger and fitter patients tend to receive partial nephrectomy, compared to old and frail patients receiving IGA. Similarly, the latest systematic review and meta-analysis, published in the International Journal of Surgery, has suggested the same.3
Based on the limited quality of evidence on T1a SRMs, ablation is associated with similar cancer-specific survival, metastasis-free survival and disease-free survival compared to partial nephrectomy. Local recurrence-free survival is similar to partial nephrectomy patients with a follow-up of more than five years.3 Patients undergoing ablation also experience significantly less postoperative complications (risk ratio [RR]=0.72, p=0.02) and significantly smaller decline in renal function postoperatively (mean difference [MD]= -7.42, p<0.01).
Similarly, the long-term outcomes at our centre from 2003 to 2020 have shown similar outcomes, with overall survival, cancer-specific survival, local-recurrence free survival and metastasis-free survival in IGA at least as good as partial nephrectomy, with significantly better renal function preservation.4 Specifically, IGA is of use in patients with Von-Hippel Lindau syndrome—shown in the 17 patients who underwent IGA for VHL-associated renal cell carcinoma (RCC) and experienced excellent oncological outcome without the need for renal dialysis over 10 years of follow-up.5
The role of RTB and IGA has developed significantly throughout the last two decades; however, further research is required to consolidate the role of RTB and IGA in the treatment of SRMs. Firstly, RTB needs to be implemented in both research and clinical pathways. RTB can act as index tests for future diagnostic studies to facilitate development of new imaging modalities. For future interventional studies of new treatments, RTB will also allow focused research on RCC, rather than undifferentiated SRMs alone to improve the quality of evidence. Secondly, studies reporting outcomes from interventional oncology studies must conform to the CONSORT guidelines to allow for meta-analysis and further discussion of the data. Finally, urologists and interventional radiologists should work closely together to embrace and produce optimal outcomes for patients presenting with RCCs. Upcoming results from the NEST trial comparing the effectiveness of nephron-sparing surgeries and future research studies are highly anticipated.
References:
Chan V W-S, Keeley F X, Lagerveld B et al. The changing trends of image-guided biopsy of small renal masses before intervention—an analysis of European multinational prospective EuRECA registry. Eur Radiol. 2022; 5:1–12.
Wah T M, Lenton J, Smith J et al. Irreversible electroporation (IRE) in renal cell carcinoma (RCC): a mid-term clinical experience. Eur Radiol. 2021; 31:7491–9.
Chan V W-S, Abul A, Osman F H et al. Ablative Therapies versus Partial Nephrectomy for Small Renal Masses—a systematic review and meta-analysis of observational studies. Int J Surg. 2022; 97:106194.
Chan V, Osman F, Cartledge J et al. Percutaneous image guided cryoablation and radio-frequency ablation versus partial nephrectomy for small renal cell carcinomas: A ten-years, single centre observational study. J Urol. 2021; 206(3): 770–1.
Chan V W-S, Lenton J, Smith J et al. Multimodal image-guided ablation on management of renal cancer in Von-Hippel-Lindau syndrome patients from 2004 to 2021 at a specialist centre: A longitudinal observational study. Eur J Surg Oncol. 2021. Doi: https://doi.org/10.1016/j.ejso.2021.10.022.
Vinson Wai-Shun Chan is a final year medical student in the School of Medicine in the Faculty of Medicine and Health at the University of Leeds in Leeds, UK.
Tze Min Wah is a professor, and senior consultant diagnostic and interventional radiologist, in the Department of Diagnostic and Interventional Radiology in the Institute of Oncology at St James’s University Hospital, Leeds Teaching Hospitals NHS Trust, in Leeds, UK.
The authors declared no relevant disclosures pertaining to this article.
Inari Medical has announced that the first patient has been enrolled in PEERLESS prospective, randomised controlled trial (RCT) comparing the outcomes of patients with intermediate-high risk pulmonary embolism (PE) treated with the FlowTriever system versus catheter-directed thrombolysis (CDT).
The first PEERLESS patient was enrolled by Amir Kaki, interventional cardiologist, Ascension St John Hospital, Dearborn, USA. PEERLESS will randomise 550 patients and will also enrol up to 150 patients in a registry cohort for patients who cannot be randomised due to an absolute contraindication to thrombolytics. The trial will include up to 60 centres in the USA and Europe.
“We are excited and honoured to enrol the first patient in this landmark clinical trial,” said Kaki. “From our own experience, the FlowTriever system has the potential to change the way we treat PE patients, safely removing significant clot burden while avoiding thrombolytics and procedure-related ICU stay. Ascension St John’s research team continues to be on the cutting-edge of medical device research and we look forward to contributing and developing the evidence base for the treatment of pulmonary embolism.”
“The start of PEERLESS represents an exciting milestone in the advancement of PE treatment, where randomised clinical data evaluating relevant patient outcomes has been limited,” said global co-principal investigator, Carin Gonsalves, professor of radiology and co-director of the Division of Interventional Radiology at Thomas Jefferson University in Philadelphia, USA. “PEERLESS marks an opportunity to directly compare FlowTriever outcomes to CDT outcomes, addressing current gaps in our understanding of PE and providing critical information to clinicians on the optimal treatment for these patients.”
“The treatment of PE is undergoing a transformation. We have been thrilled by the desire of physicians to move this field forward and generate high-quality data through PEERLESS,” said Thomas Tu, Inari’s chief medical officer. “We are grateful for the collaboration and dedication of our clinical trial investigators on this first of many PE studies to come.”
Takeshi Morimoto (L), Shinichi Yoshimura (R). Credit: Hyogo College of Medicine
Takeshi Morimoto (L), Shinichi Yoshimura (R). Credit: Hyogo College of Medicine
A new study from Japan has become the first randomised controlled trial (RCT) to demonstrate the effectiveness of endovascular mechanical thrombectomy procedures in patients who have severe strokes involving clots in one or more large brain arteries. This preliminary, late-breaking research, which was presented at the International Stroke Conference (ISC 2022; 9–11 February, New Orleans, USA), found that patients who suffer a severe ischaemic stroke may regain far more function if their clots are mechanically removed in addition to standard medical therapy. An increased occurrence of intracranial haemorrhage was, however, also observed in patients who underwent a thrombectomy in the study.
“Our findings confirm that anyone who suffers from stroke should be transferred to a medical facility capable of endovascular therapy as soon as possible,” said senior author of the study Takeshi Morimoto (Hyogo College of Medicine, Nishinomiya, Japan)—who also presented these data at ISC 2022. “The benefit of endovascular therapy is not limited by the severity or region of a stroke. These patients may have the chance to more fully recover from stroke and go back to their previous lives and activity levels.”
In 2018, the American Heart Association (AHA) updated its stroke treatment guidelines to recommend endovascular therapy—which involves clot removal via mechanical thrombectomy—for select stroke patients, with a view to improving their odds of functional recovery. As per an AHA press release, effectiveness of the approach had previously been established for patients whose large-vessel clots disrupted blood flow to fewer areas of the brain. However, clinical experience was mixed for patients with more severe strokes whereby a clot interrupts blood flow to a large area of the brain.
“I have often encountered a dramatic improvement in a patient just after the mechanical clot removal procedure, even when the infarction area was large,” said Shinichi Yoshimura (Hyogo College of Medicine, Nishinomiya, Japan), lead author of the study. “Yet, patients sometimes also experienced severe haemorrhagic transformation [a life-threatening complication that occurs when blood from outside the brain crosses the blood-brain barrier and worsens stroke outcome] after the artery was reopened. So, in Japan, our stroke physicians are always cautious about endovascular therapy when the infarction area is large.”
In this randomised study, which has now also been published in the New England Journal of Medicine, 203 stroke patients (average age of 76 years; 44% women) were treated at 45 hospitals in Japan. Most of these patients (71%) were examined and had magnetic resonance imaging (MRI) or a CT scan of the brain within six hours after stroke symptoms were first noticed—the timeframe that patients are generally considered eligible for endovascular therapy. The other patients were seen between six and 24 hours after symptoms were noticed, and additional imaging showed areas of the brain that might benefit from prompt treatment.
On imaging, all patients were found to have clots blocking a large artery in the brain—either the internal carotid artery, the proximal middle cerebral artery, or both. The strokes were rated as severe (median score of 22 on the National Institutes of Health Stroke Scale [NIHSS], which assesses a patient’s ability to perform normal functions such as speaking and moving) and involved disrupted blood flow to large areas of the brain (about seven out of 10 regions).
After imaging, the patients were randomly selected to receive either standard medical care for stroke—consisting of providing intravenous fluids, controlling blood pressure and other risk factors, and administering clot-busting medications for select patients at lower risk of bleeding—or standard medical care plus endovascular therapy performed within an hour after imaging. Due to bleeding concerns, intravenous clot-busting medications were sparingly administered to select patients in a similar proportion in both treatment groups (27 of those who received endovascular therapy and 29 who received standard care).
Comparing the 100 patients who received endovascular therapy plus standard care with 102 on standard therapy alone, the analysis found:
Patients who received endovascular therapy were 2.43 times more likely (31% vs. 13%) to be able to walk without assistance and to have a residual disability rated as none to moderate 90 days later.
After 90 days, more of the patients (14% vs. 6.9%) who received endovascular therapy were considered functionally independent, meaning they were either able to carry out all their pre-stroke activities or to have a slight disability that did not require daily assistance.
At 48 hours after treatment, more of the patients (31% vs. 8.8%) who received endovascular therapy had major early neurological improvement (improved ability to talk and move limbs).
In addition, several outcomes were compared to evaluate the safety of adding endovascular therapy to medical treatment, with researchers reporting:
Within 48 hours, scans revealed that more of the patients who received endovascular therapy had experienced some bleeding within the brain (with or without symptoms), 58% vs. 31%, respectively.
However, the number of patients who experienced other adverse outcomes was similar in the two treatment groups. The adverse events included brain bleeding within 48 hours that caused a worsening of neurological status (four points or greater worsening on the NIHSS); the need for surgery to relieve pressure on the brain in the first week; death within 90 days; or the recurrence of ischaemic stroke within 90 days.
“The finding of more intracranial bleeding in the patients who received endovascular therapy is very important,” Morimoto added. “However, there were haemorrhages with symptoms and some that caused no symptoms. The haemorrhages with no symptoms were detected on imaging conducted for this study in the endovascular treatment group, not in the standard practice group. Symptomatic intracranial haemorrhage still occurred more commonly among patients in the endovascular group, however, it was not a statistically significant difference from the standard care group.”
The results of this study may not be generalisable to the USA or western countries—because it was conducted in Japan, where there is less use of intravenous thrombolysis than in the USA and other western countries, and where more strokes are imaged with MRI compared to CT, perhaps leading to different estimates of how many brain regions are affected by the stroke, the AHA release states. Due to these differences in treatment protocols, this study’s results may over- or underestimate the effectiveness of endovascular therapy.
The researchers are currently performing sub-analyses to help identify factors that might signal which patients are more likely to have a greater return of function after the treatment. “In addition, tools, devices or rehabilitation methods that could potentially improve the likelihood for similar patients to recover with less disability should be investigated,” Morimoto said.
Cerenovus—a neurovascular firm that forms part of Johnson & Johnson Medical Devices Companies—has announced the launch of Emboguard, its next-generation balloon guide catheter to be used in endovascular procedures, including those for patients with acute ischaemic stroke.
Emboguard is designed to optimise removal of blood clots by controlling blood flow locally during mechanical thrombectomy procedures. Balloon guide catheters increase first pass recanalisation, reduce procedure time, and reduce the odds of clot fragments breaking off and causing distal emboli, according to a Cerenovus press release, which also details that distal emboli in an endovascular procedure can result in new ischaemic events.
“Without timely and effective treatment of stroke, patients can suffer from lifelong disability or dependency,” said David Fiorella (Stony Brook University Hospital, New York, USA). “The benefits of balloon guide catheters are becoming increasingly recognised for their ability to maximise patient outcomes. By adding this innovation to their stroke solutions portfolio, Cerenovus will be arming physicians with the tools they need to better serve our patients, potentially increasing the chances to live a functional and fulfilling life post-stroke.”
Emboguard is the latest addition to Cerenovus Stroke Solutions—a suite of technologies designed with compatibility in mind to assist physicians in performing mechanical thrombectomy procedures. Launched in 2020, it now includes the Embotrap III revascularisation device, the Prowler Ex microcatheter, and the Cerenovus large bore catheter as well as both the Emboguard balloon guide catheter and the Cerebase guide sheath.
The Emboguard balloon guide catheter is set to debut for the first time at the ongoing International Stroke Conference (ISC 2022; 9–11 February, New Orleans, USA).
NovaSignal Corporation has announced the results of a multicentre, prospective, single-arm study indicating that the company’s autonomous NovaGuide intelligent ultrasound is three times more likely to detect right-to-left shunt (RLS)—a recognised risk factor for stroke—than standard of care transthoracic echocardiography (TTE). These results were presented in a late-breaking science session at the International Stroke Conference (ISC 2022; 9–11 February, New Orleans, USA).
“In the stroke population, RLS detection—especially due to a patent foramen ovale (PFO)—is important to reduce the risk of future stroke,” said the study’s principal investigator Mark Rubin (University of Tennessee Health Science Center, Memphis, USA). “We have known for decades that transcranial Doppler (TCD) is exquisitely sensitive for RLS detection, but expertise is scarce. NovaGuide broadens the availability of TCD, allowing any provider to help their patients benefit from the sensitivity of TCD for RLS detection. The BUBL study results underscore the potential for using this diagnostic capability to improve the management of ischaemic stroke patients.”
The BUBL clinical trial assessed use of NovaGuide compared to TTE for RLS diagnosis. The study enrolled adults (≥18 years) who presented with neurological signs and symptoms, which included embolic stroke or transient ischaemic attack, on the differential diagnosis. The primary outcome was the percent shunt detection rate of NovaGuide relative to standard of care TTE.
Among the 129 evaluable participants, RLS detection rate was 63.6% with NovaGuide (82 patients) and 20.9% by TTE (27 patients) for a difference of 42.6% (95% confidence interval [CI]=28.6%–56.7%, p<0.001). Additionally, NovaGuide accurately identified 35 patients (27%) with intervenable shunts (Spencer Logarithmic Scale ≥3), while TTE identified 13 (10%) of these cases for a difference of 17.1% (95% CI=6.9%–27.2%, p=0.002). The primary safety endpoint of adverse events with NovaGuide was 0% (95% CI=0%–2.8%).
“Stroke care has advanced significantly in recent years, but those who have suffered a stroke have a high risk of recurrence,” said Robert Hamilton, chief scientific officer and co-founder of NovaSignal. “RLS is a known risk factor for stroke and these study findings underscore the importance of utilising NovaGuide as a diagnostic technology. It substantially improves detection of RLS compared to current standard of care. The results of this study suggest there may be many undiagnosed patients with RLS who are not receiving appropriate medical management with today’s diagnostic standards.”
Imperative Care has announced the launch of its Zoom POD aspiration tubing—the company’s latest innovation in elevating stroke care.
This is the newest addition to Imperative’s Zoom stroke solution, which is an ischaemic stroke product portfolio also including the Zoom 88 large distal platform for neurovascular access, four Zoom aspiration catheters in various sizes, and the Zoom pump with accessories.
The Zoom POD is the first and only sterile field clot filter device, according to Imperative, enabling faster time to clot capture during critical mechanical thrombectomy procedures for ischaemic stroke patients.
It is integrated into the aspiration tubing, shortening the distance from aspiration to filtration while maintaining full aspiration power. And, because it is positioned within the sterile field, the physician can immediately see the clot as it is extracted from the patient, quickly confirming clot capture and giving them more control over the thrombectomy procedure.
“Stroke care is all about speed. In order to achieve the best possible outcomes for patients, it is imperative to retrieve the clot from the brain quickly,” said Shahid Nimjee (The Ohio State University Wexner Medical Center, Columbus, USA).
“The Zoom POD will allow physicians like myself to visually confirm immediately, right within the sterile field, that the clot has been captured. Additionally, the ability to capture the clot in the Zoom POD allows me to easily take the clot back to the pathology lab, break it down, and analyse it.”
Mechanical removal of blood clots reduced post-stroke disability in nearly half of “all-comer” real-world stroke patients in a global study, according to preliminary late-breaking research presented at this year’s International Stroke Conference (ISC 2022; 9–11 February, New Orleans, USA).
“This study shows how much stroke thrombectomy has advanced,” said lead study author Raul Nogueira (University of Pittsburgh School of Medicine, Pittsburgh, USA). “We saw a wide range of cases, including patients who, not too long ago, would not be considered good candidates for thrombectomy based on older age, pre-existing disability or large size of the stroke on presentation. Our findings in this study expand thrombectomy to be considered for more stroke patients.”
Previous studies have found that stroke patients who received mechanical clot removal had less disability after three months than those who did not. However, according to an American Heart Association (AHA) press release, these studies were performed in carefully selected centres and employed strict clinical and imaging inclusion criteria—which decreases the generalisability of their findings.
To examine the effectiveness of blood-clot removal across a wide range of stroke patients seen in routine daily care, i.e., outside of a clinical trial, the EXCELLENT (Embotrap extraction and clot evaluation and lesion evaluation for neurothrombectomy) trial enrolled 1,000 adult ischaemic stroke patients (average age=70, 52% female) at 36 sites worldwide, from September 2018 to March 2021. The sites were a mix of thrombectomy-capable and comprehensive stroke centres. Patients were treated with a specific mechanical thrombectomy device called Embotrap (Cerenovus) in an unlimited time frame in the trial.
The study was designed to collect real-world treatment and did not exclude patients based on pre-stroke independence level, severity of stroke, location of the occlusion, or time between onset of stroke and treatment, researchers said. As per current guidelines, mechanical thrombectomy treatment can be used within 24 hours of symptom onset in select patients. In addition, the study analysed the characteristics of the removed blood clots and how that impacted stroke recovery.
The EXCELLENT trial found that most of the patients required only one attempt to remove the blood clot. However, it is common to require multiple attempts to completely remove the clot. In nearly half of all patients, clot removal resulted in slight/minimal disability (able to look after own affairs without assistance or no worsening from their pre-stroke condition), as gauged by a standard scale measuring level of disability 90 days after stroke.
The study also found blood clots that were rich in red blood cells and low in platelets resulted in less disability than blood clots composed of less red blood cells, or those rich in red blood cells and high in platelet content. In this study, only 10% of patients whose clots had a higher composition of red blood cell count and a lower composition of platelets died within 90 days, compared to 24% of patients whose clots had a lower composition of red blood cells and platelets. Among patients with higher red blood cell content, 63% with lower platelet content had either slight or no disability, compared to 51% with higher platelet content.
“We knew that fibrin was associated with more difficult clot removal. However, this novel observation that platelets may modify clot properties is very intriguing,” Nogueira added. “The results may have potential implications for technique and device selection when removing clots and the development of better blood-clot removal strategies.”
“I think the future success of ablation was truly unforeseeable, in 1986, when Tito Livraghi published his first paper about ethanol injection in a liver tumour. If we accurately match the energy source, the route of energy delivery, and imaging with the specifics of the lesion, we can treat lesions in almost every organ and anatomical space. Sometimes, it is necessary to enter the operating room together with the surgeon in order to get the best treatment results for the patient, but this should be seen as another opportunity—not an event to escape from,” says Laura Crocetti, associate professor of Radiology, Division of Interventional Radiology, Nuovo Santa Chiara University Hospital, Pisa, Italy. An internationally recognised ablation expert, she is also deputy chairperson of the European Conference on Interventional Oncology (ECIO) for 2022 and 2023.
What attracted you to a career in interventional radiology?
When I was in medical school, I was attracted by minimally-invasive treatments that enabled the possibility of curing patients with minimal damage and discomfort. The other passion I had was for technology and the latest developments on the horizon. So, when I heard of interventional radiology, I immediately realised that represented my future.
Could you share a positive and negative experience you have had as a woman in the interventional field?
I will start with a negative experience: I am a small-framed woman (my son says I am “short”) typically dressed in a non-slim-fit green working uniform and perhaps looking a few years younger than her age. Unfortunately, that is not what most patients expect when told they are scheduled to meet “professor” Crocetti, a “well-known” expert in the field of ablation who will perform the procedure. Still, an empathetic bond is almost always immediately formed, and they feel reassured and protected “in my hands”. Patients often witness their appreciation with very kind messages and emails afterwards.
The first surprise is unfortunately also sometimes observed in older, male leaders and colleagues who do not know you. Interestingly, you can seem transparent or invisible to their eyes. The important thing is that in the long term, I have always been able to convince my colleagues about my professional capacity and am very proud of this.
The positive experience as a woman physician often comes from everyday interactions with my female colleagues: the positive and supportive feeling is immediate and the desire to cooperate and work together is very strong. As female physicians, we are thorough, efficient, and well organised, and our results are usually very good!
What are the most important cancer imaging techniques that you see on the horizon?
I am extremely optimistic about the future of magnetic resonance (MR) and would like to emphasise its as-yet insufficiently explored aspects. Function, metabolism, and vascularisation can all be investigated with this technique. The vast amount of information that magnetic fields can provide is almost infinite. I am fortunate to have a very interesting opportunity to cooperate with the 7T consortium in Pisa (IMAGO 7) and the team really conveys that we are only at the beginning with MR. The application of MR in cancer imaging, for example before and after chemoradiotherapy or interventional radiology procedures, will remain a hot topic in the future.
Where do you see the greatest potential for ablative therapy?
I think the future success of ablation was truly unforeseeable, in 1986, when Tito Livraghi published his first paper about ethanol injection in a liver tumour. The potential of ablative treatments stem from their ductility combined with efficacy. If we accurately match the energy source, the route of energy delivery, and imaging with the specifics of the lesion (its size and location, roughly speaking), we can treat lesions in every organ and anatomical space. Sometimes, it is necessary to enter the operating room together with the surgeon in order to get the best treatment results for the patient, but this should be seen as another opportunity—not an event to escape from.
Do you see different niches for radiofrequency, microwave, and cryoablation?
Each ablative modality has its specificity. Generally speaking, at the moment my workhorse for the liver is microwave ablation, but for kidney, soft tissue, and prostate, I prefer cryoablation. I can see a future of selected microwave devices in thyroid and lung as well, but at the moment I still prefer radiofrequency here. A personalised approach for patient care includes not only choosing an interventional treatment and selecting the correct timing for it, but also picking from all the different energy sources and imaging approaches available to optimise treatment success.
What evidence would you like to see generated in your field of special interest–liver ablation?
Liver ablation is an area where we actually have quite a lot of evidence, especially when compared with other organs. Its efficacy and cost-effectiveness, for example, has been well established in hepatocellular carcinoma (HCC) and it is recognised in the major guidelines. I am very much looking forward to the results of the COLLISION trial, the noninferiority randomised study comparing ablation and resection in ablatable and resectable colorectal liver metastases of less than 3cm.
In the near future, I think we should produce evidence about the role of combination therapies including ablation and immunotherapy.
You have declared the International Accreditation System for Interventional Oncology Services (IASIOS) accreditation to be an important milestone for your hospital. Why?
IASIOS accreditation is a way of demonstrating first to us and then to the global community that the interventional oncology service we provide is of high quality and meets rigorous international standards. It helps to improve the whole process of patient care and treatment and is specifically designed for medical facilities offering interventional oncology. Accreditation already exists for other specialties or services, and it is extremely important to have it already up and running for interventional oncology.
As deputy chairperson for ECIO 2022 (24–27 April, Vienna, Austria), what would you like the programme to reflect?
ECIO is by definition a multidisciplinary meeting and the programme will reflect this special attitude of the congress. All topics will be addressed from multiple points of view and there will also be lots of opportunities to speak about ongoing research and new technologies. It is really a privilege for me to work with Philippe Pereira, the chairperson of ECIO 2022, to prepare the programme (www.ecio.org).
Could you describe a memorable case that has stayed with you?
It is the first liver radiofrequency ablation I performed many years ago, for sure. My heart was beating very fast…but everything went smoothly. I also recall all the difficult cases, those in which I had complications; I remember them all very well. Many of my patients have, fortunately, been able to live with a very long disease history and two of them, in particular, have become family friends. It has been very difficult to say to them that there was nothing further I could offer them and their families from an interventional treatment perspective.
What are your interests outside of medicine?
I love the sea, and particularly enjoy fishing and have a licence for a boat. My other passion is music and I am a conservatory graduate in piano. Hiking with my husband, Francesco, and son, Aurelio, is a family activity we enjoy together.
Figure 1: Schematic of the Delcath Chemosaturation system
Percutaneous hepatic perfusion with melphalan for the treatment of metastatic uveal melanoma (mUM) offers a hepatic response rate of 66.7% and good progression-free survival (PFS). This is the main concluding finding of a recent retrospective analysis published in Melanoma Research—which the authors claim includes the largest number of mUM patients treated in a single centre with melphalan percutaneous hepatic perfusion (M-PHP) to date worldwide.
Co-author Sachin Modi
Carrying a poor prognosis, uveal melanoma (UM) is the most common primary ocular malignancy in adults, according to Sachin Modi and Brian Stedman (University Hospital Southampton NHS Foundation Trust, Southampton, UK) et al. 50% of patients with UM develop metastatic disease, which has a 10‒25% one-year survival rate with no standard established treatment. According to the authors, previous studies have demonstrated M-PHP to be effective for mUM for liver predominant disease, however, it is highlighted that existing research is limited by small sample populations. Modi et al specify that their analysis, therefore, illustrates findings on the safety and efficacy of M-PHP in a sample population of 83 patients, which is the largest number of mUM patients treated in a single centre with M-PHP to date worldwide.
Co-author Brian Stedman
All patients with diagnosed mUM who received M-PHP between August 2012 and September 2020 at the University Hospital Southampton NHS Foundation Trust were included in this retrospective study.
Patients with the non-progressive single-site extrahepatic disease were also included. All patients received 3mg/kg of melphalan, which was delivered with the Hepatic CHEMOSAT Delivery System (Delcath Systems) with the GEN 2 filter (see Figure 1). The authors note that liver function and full blood count were monitored in all patients’ weekly following treatment, with repeat computerised tomography (CT) and magnetic resonance imaging (MRI) every six to 12 weeks to monitor the tumour and overall response, as per RECIST guidelines. The disease control rate (DCR) was calculated as the proportion of patients with complete response (CR) to treatment, partial response (PR), or stable disease (SD) for at least nine weeks. Further M-PHP sessions were planned at six to 10-week intervals, on the presentation of no disease progression.
Figure 1: Schematic of the Delcath Chemosaturation system
A total of 252 treatments with M-PHP were performed across 83 patients (aged 18 to 80), with a median of three M-PHP cycles per patient—two patients experienced a single incomplete treatment, resulting in a total patient number of 81. The median patient age was 59.3 years old (±12.2 years), consisting of 36 (44.4%) males. It is noted that 69 (85.2%) patients presented only intrahepatic disease at the time of workup, however, 12 (14.8%) patients had both intrahepatic and single organ extrahepatic disease.
Modi et al report a median follow-up time of 12.9 months across all patients, with a median time of 13.9 months follow-up time for patients still alive. At the data collection cut-off date (1 January 2021), a total of 15 (18.5%) patients were still alive, three were still continuing M-PHP treatment, with 66 (81.5%) deaths. The overall survival (OS) median was 14.9 months from the first treatment—and OS rates were 62% and 27% at one and two years, respectively.
The authors note that the OS was significantly different (p<0.0001) across hepatic responses, with the overall response rate at 49/81 (60.5%) patients. For CR, the response time was 34.7 months, compared to 16.9 months for PR, 10.6 months for SD, and 7.7 months for progressive disease (PD). A total of 7/81 (8.6%) patients presented the best overall response—CR. A total patient number of 42/81 (51.9%) demonstrated PR, 16/81 (19.8%) for both SD and PD. Hepatic only CR was seen in 10/81 (12.3%) patients and PR was present in 9/81 (11.1%) patients.
In conclusion, the analysis presents an overall response rate of 60.5% (49/81), hepatic disease control rate of 88.9% (72/81), and hepatic response rate of 66.7% (54/81) with M-PHP. The median overall PFS and OS were 8.4 and 14.9 months respectively. The authors report no fatal treatment-related adverse effects (TRAE), however, 43 grade three (n=29) or four (n=14) TRAE occurred in 23 (27.7%) patients, presenting a significant reduction in these events in procedures performed between 2016–2020 vs. 2012–2016 (0.17 vs. 0.90 per patient, p<0.0001). Modi et al suggest M-PHP for mUM exhibits “excellent response rates” and PFS, compared to available treatments.
Stedman said “with such a large series the Southampton team have now demonstrated this treatment can be delivered safely with very few side effects. Patients tolerate the procedure with no impact on performance or quality of life. Having proved the technology works on one of the most chemo-resistant cancers, the team is keen to demonstrate its efficacy in other tumour types.”
“We are happy to report these findings which show impressive response rates with improvement in safety and complications with experience. We hope with this new data and the upcoming data from the international FOCUS study (due to be reported Q4 2022) will lead to better access for this treatment for patients on the NHS and worldwide” added Modi.
Co-author Matthew Wheater
From an oncologist’s perspective, co-author Matthew Wheater (University Hospital Southampton NHS Foundation Trust, Southampton, UK) commented that “metastatic uveal melanoma has been a real challenge to treat, with little response to the agents that have shown such promise in cutaneous melanoma. The randomised data showing a survival benefit for tebentafusp is a significant step forward, however radiological responses to treatment are rare. Our paper shows that melphalan-PHP can induce significant responses in liver metastases, is safe to deliver and well tolerated by patients, providing meaningful quality of life. We eagerly await the final survival results of the Focus trial and hope that if this confirms our findings then melphalan PHP will become a mainstay of treatment for ocular melanoma with wider availability of treatment to benefit more patients.”
Concept Medical lights up NASDAQ in New York's Times Square to celebrate the SIRONA trial achieving 50% enrolment
Concept Medical lights up NASDAQ in New York’s Times Square to celebrate the SIRONA trial achieving 50% enrolment
Concept Medical recently announced that the SIRONA randomised controlled trial (RCT; Head-to-head comparison of sirolimus versus paclitaxel drug-eluting balloon angioplasty in the femoropopliteal artery) has completed half the targeted enrolment.
According to a company press release, SIRONA is the world’s first and largest head-to-head RCT investigating the use of a sirolimus drug-coated balloon (DCB; Magic Touch PTA, Concept Medical) vs. a paclitaxel DCB (CE-certified devices) for the treatment of femoropopliteal occlusive artery disease.
The investigator-initiated and -driven trial, led by Ulf Teichgräber (Jena University Hospital, Jena, Germany) aims to evaluate the safety and efficacy of a sirolimus DCB against a paclitaxel DCB in stenosed or occluded lesions in the superficial femoral artery (SFA) and/or popliteal artery in peripheral arterial disease (PAD) patients with Rutherford class 2–4.
Marianne Brodmann (University of Graz, Graz, Austria) enrolled the 239th patient on 23 November 2021, making the trial halfway towards its target of enrolling 478 patients set to be randomised in 1:1 fashion across 30 sites in Germany and Austria.
Thomas Zeller, site investigator of Universitäts-Herzzentrum Freiburg in Bad Krozingen, Germany, expresses his thoughts on the importance of the trial: “The SIRONA trial substantially contributes to evaluating the effectiveness of an alternative antiproliferative coating (sirolimus) for balloon catheters to treat femoropopliteal stenoses and occlusions compared to the current gold standard of a paclitaxel coating. Especially with regard to the still ongoing safety discussion, SIRONA represents the first head-to-head comparison and therefore is of high scientific and clinical relevance, and is fortunately widely accepted by study patients as the recruitment status demonstrates.”
Teichgräber adds: “I am convinced that SIRONA represents a game-changing trial for PAD.”
Sirtex Medical has announced with Grand Pharmaceutical Group Limited, that SIR-Spheres Y-90 resin microspheres have been approved by the national medical products administration (NMPA) for the treatment of patients with colorectal cancer liver metastases.
According to a recent press release, the NDA approval of SIR-Spheres for the Chinese market is the first therapeutic radiopharmaceutical approved by the NMPA in 2022 and is the only radioactive microsphere product approved by the NMPA based on clinical trial data obtained outside of China. The first procedure of selective internal radiation therapy (SIRT) using SIR-Spheres in China was successfully performed in September 2021, which at that time utilised the pilot implementation policy for commercialised medical devices in Hainan.
According to GLOBOCAN 2020, there were 410,000 new cases of liver cancer with 390,000 deaths in China. Additionally, in 2020, there were over 550,000 new cases of colorectal cancer with more than 280,000 deaths in China. Those morbidity and mortality rates are about twice as high as average global rates.
“The prognosis for patients suffering from liver cancer in China is poor, with the five-year survival rate being roughly 12%,” notes Dr. Tang Weikun, Chairman of the Board at Grand Pharmaceutical Group Limited. “The use of SIR-Spheres to downstage liver tumors to the point where they can be surgically removed has been well documented in other countries. Our hope is that by expanding the reach of SIR-Spheres to China, we will have a similar impact, with improved treatment outcomes and survival rates among patients diagnosed with liver tumors.”
Royal Philips has announced an update to its handheld ultrasound platform—Lumify—adding Pulse Wave Doppler technology to expand the haemodynamic assessment and measurement capabilities of the system.
In a press release, Philips said that the new functionality would enable clinicians to quantify blood flow in a wide range of point-of-care diagnostic applications including cardiology, vascular, abdominal, urology, obstetrics and gynecology.
Pulse Wave Doppler ultrasound provides clinicians with more information, in addition to 2D and colour imaging, to assess haemodynamic patterns to differentiate between arterial and venous blood flow and quantify haemodynamic function, Philips detailed in a press release. An additional update to the system includes obstetric measurements to help in early assessment of gestational age and the identification of high-risk pregnancies.
“By applying Philips’ expertise in cardiovascular care, imaging and patient monitoring to Philips Handheld Ultrasound—Lumify—we are committed to deliver a dedicated, innovative point-of-care portfolio, enabling clinicians to quickly assess haemodynamics—including cardiovascular function, organ perfusion and fetal assessment—in a daily routine, to identify abnormalities and intervene quickly,” said Matthijs Groot Wassink, general manager of Point of Care Ultrasound at Philips. “With the addition of Pulse Wave Doppler and enhanced obstetrics measurements, we have increased the number of markers on which diagnoses can be made, to deliver high quality imaging and enhance the evaluation and effectiveness of treatment in real-time.”
“Having Colour Flow Doppler (CFD) and Pulse Wave Doppler on a handheld device is game changing, allowing clinicians to take point-of-care ultrasound examinations to the next level,” said Robert Jones, professor of Emergency Medicine at the MetroHealth System, Cleveland, USA.
Regio Biosciences, a Hibiscus BioVentures company, recently announced it has entered into an exclusive license agreement with AstraZeneca to further develop REG-101, a novel therapeutic acting on reverse cholesterol transport. Regio expects to initiate a Phase 2a clinical programme evaluating REG-101 in peripheral arterial disease (PAD) during the second half of 2022.
Under the terms of the agreement, AstraZeneca will provide an exclusive license to Regio for further development of REG-101, previously known as MEDI5884, to address patients with high unmet medical needs, including PAD and cardiovascular disease. Regio will be solely responsible for all research, development, and commercial activities of REG-101. Initial financing for Regio’s development activities is being provided via investment by Hibiscus Capital Management (HCM Fund II) and Innoforce.
“The Regio team is thrilled to announce the signing of this license agreement with AstraZeneca to further develop REG-101,” said Chris Jeffers, chairman of Regio Biosciences and CEO of Hibiscus BioTechnology. “We believe that REG-101 could complement the current standard of care as a patient-centric, once-monthly injection for peripheral artery disease.”
“PAD currently has few pharmaceutical options, and without appropriate treatment, symptoms of PAD can progress from pain while walking to gangrene and limb loss,” said Rakesh Dixit, president and CSO of Regio Biosciences. “We believe reducing the size of cholesterol-rich plaque within peripheral arteries using REG-101 has the potential to directly and positively address the underlying pathophysiology of PAD.”
Marc P Bonaca
Regio has partnered with CPC Clinical Research (CPC) and multiple clinical sites in the USA to conduct a phase 2a clinical trial in patients with PAD. “Despite current standard of care therapies that address control of blood pressure, LDL [low-density lipoprotein] cholesterol levels, and clotting risks, there are currently no available pharmacological treatments targeting reverse cholesterol transport to target the plaque that underlies the adverse effects negatively impacting millions of patients,” said cardiologist and vascular medicine specialist Marc P Bonaca (University of Colorado Anschutz Medical Campus, Aurora, USA), who serves as the executive director of CPC Clinical Research and CPC Community Health. “As a clinician, I believe a therapeutic that improves function, reduces the need for recurrent limb interventions as well as other adverse cardiovascular outcomes could provide meaningful improvements for patient quality of life.”
Humacyte today announced results from the first series of compassionate use cases of the company’s investigational Human Acellular Vessel (HAV) for the treatment of chronic limb-threatening ischaemia (CLTI) and vascular trauma.
The HAVs were observed to remain patent and infection free in patients requiring vascular reconstruction, thereby highlighting the potential of the HAV to expand limb salvage options for patients who have exhausted current revascularisation conduit options, a company press release communicates. These results were presented at the 46th Annual Winter Meeting of the Vascular and Endovascular Surgery Society (VESS; 27–30 January, Snowmass, USA).
Humacyte details that their HAVs are engineered replacement vessels being designed to be durable, infection-resistant and off-the-shelf to address long-standing limitations in vessel tissue repair and replacement. The company reports that, under the US Food and Drug Administration’s (FDA) expanded access programme (EAP), the HAV has been implanted in more than 20 patients to address multiple severe vascular repair, reconstruction and replacement conditions when there is not a suitable conduit available for treatment.
The results of eight of these EAP patients were reported at the VESS meeting by Alexander Kersey (Uniformed Services University of the Health Sciences and Walter Reed National Military Medical Center, Bethesda, USA), in a presentation, titled, “Real-world experience with the Human Acellular Vessel: A bioengineered implant for arterial repair that expands limb salvage options.”
Each of the patients had severe peripheral arterial disease (PAD) or vascular injury requiring vascular reconstruction but lacked other treatment options and were at risk for limb loss. In this high-risk group of patients, five of the bypasses performed with the HAV currently remain patent (with follow-up times ranging from four to 20 months after surgery), and no incidences of infection of the HAV were noted. Researchers treating these patients concluded that the HAV may greatly expand opportunities for limb salvage in trauma and urgent vascular reconstruction when patients lack suitable alternative conduits.
“Many patients who require urgent vascular reconstruction due to vascular injury or severe PAD are not candidates for synthetic vascular grafts or autologous vein grafts, and those who have exhausted other treatment methods are at high risk of amputation,” said Kersey. “There is considerable need for a new treatment option to avoid resorting to amputation, and results from these compassionate use cases merit additional research into the role the HAV may play in the future of limb-sparing surgery.”
In addition to infection resistance and durable patency, the presentation highlighted the potential clinical utility of the HAV that can be implanted using normal surgical procedures as a readily available, biological alternative for patients at high risk for amputation.
The HAV is currently being evaluated in late-stage clinical trials in vascular trauma repair, arteriovenous access for haemodialysis, and PAD. Humacyte advises that the HAV is an investigational product candidate and is not currently approved for sale by the FDA or any international regulatory authority.
January’s top 10 features technological advancements, with Cook Medical receiving US Food and Drug Administration (FDA) approval for new drug-eluting stents and Adept Medical launching Lower Leg Support for patients with peripheral artery disease. In addition, Inari Medical announced positive six-month FLASH registry patient outcome data following treatment of pulmonary embolismwith FlowTriever, and Ajax Health has appointed two leadingcardiovascular professionals to Cordis-X.
Cook Medical has received breakthrough device designation from the US Food and Drug Administration (FDA) on a new drug-eluting stent for below the knee. This new stent is designed to treat patients suffering from chronic limb-threatening ischaemia.
Peter Littler (Newcastle, UK) talks to Gerard McLauchlan (Surrey, UK) and Alex Horton (Surrey, UK) regarding veterinary interventional radiology (IR) following a special session titled “All Creatures Great and Small: IR for animals” at the British Society of Interventional Radiology annual scientific meeting (8–10 December, Glasgow, UK).
At this year’s International Symposium on Endovascular Therapy (ISET 2022; 16–19 January, Hollywood, USA), experts presented an array of late-breaking trial results on topics ranging from venous stenting to abdominal aortic aneurysm sac sealing.
There are some very serious risks associated with forgotten ureteric JJ stents. David Maudgil, a consultant interventional radiologist at Wexham Park Hospital, Frimley Health Foundation Trust (Slough, UK), outlines why and when these devices are used, explains the risks a forgotten stent might pose, and provides some guidance on how to mitigate such risks.
A wealth of data emerging in the last 18 months, including from a small multicentre, randomised study of genicular artery embolization for knee pain secondary to osteoarthritis, brings a glimpse of other similar minimally invasive options to treat disability in the entire musculoskeletal system. Embolization, which is rapidly surfacing as a safe and effective procedure for the treatment of patients with osteoarthritis of the knee, has been shown to be technically achievable, with very promising outcomes at early follow-up.
Royal Philips has announced physicians will now have access to advanced new 3D image guidance capabilities through the image-guided therapy mobile C-arm system—Zenition, aiming to improve the outcomes for patients undergoing endovascular treatment. The company has signed a strategic partnership agreement with Cydar, a provider of cloud-based procedure maps software to plan and guide surgery in real-time.
BD (Becton, Dickinson, and Company) has announced the launch and 510(k) clearance from the US Food and Drug Administration (FDA) of the Crosser iQ chronic total occlusion (CTO) recanalisation system, which is designed to cross peripheral artery CTOs intraluminally.
Inari Medical has announced positive acute and long-term interim results from the first 500 pulmonary embolism patients enrolled in the FlowTriever outcomes registry (FLASH).
Ajax Health has announced the appointments of two cardiovascular professionals to Cordis-X, an independent accelerator created to drive innovation and growth to Cordis.
Fluidx Medical Technology has announced the results of the GPX-Clear embolic device in-vivo research which uses the base GPX technology and incorporates an intermediate-term radiopacity agent, as described by the company.
“Our initial in-vivo work with GPX-Clear looks very promising. It has the advantages of the baseline GPX product around ease of use, minimal preparation, and compatibility with standard microcatheters, with the added benefit of radiopacity that dissipates within the first 24 hours,” said Ryan O’Hara, an interventional oncologist at the University of Utah (Salt Lake City, Utah).
According to O’Hara, “There are many instances, particularly in oncology, in which clear visibility of the treated region post-embolisation is critical and can be obscured by radiopacity agents. This is an exciting future product in the GPX line-up and the first product of it’s kind.”
The GPX-Clear embolic device leverages the core GPX technology as well as incorporates a non-artifact-inducing radiopacity agent. The radiopacity agent is trapped within the polymer matrix, providing excellent visibility of the embolic device during and post-embolic delivery—the radiopacity agent then dissipates within 24 hours post-delivery, enabling unobstructed visibility of the treated area.
According to the company, the GPX embolic device is an innovative embolic designed for simple preparation and controlled delivery. The company describes that the device is packaged ready-to-use in a syringe, can be prepped tableside by the clinician in about 30 seconds, does not require dimethyl sulfoxide (DMSO) precipitation, and may be delivered through standard microcatheters. The company note, GPX is therefore designed to occlude blood vessels independent of a patient’s coagulation status.
The GPX embolic device is under development and does not have marketing clearance or approval in any market at this time.
January’s top 10 features technological advancements, with Cook Medical receiving US Food and Drug Administration (FDA) approval for new drug-eluting stents and Adept Medical launching Lower Leg Support for patients with peripheral artery disease. In addition, Inari Medical announced positive six-month FLASH registry patient outcome data following treatment of pulmonary embolismwith FlowTriever, and Ajax Health has appointed two leadingcardiovascular professionals to Cordis-X.
Cook Medical has received breakthrough device designation from the US Food and Drug Administration (FDA) on a new drug-eluting stent for below the knee. This new stent is designed to treat patients suffering from chronic limb-threatening ischaemia.
Peter Littler (Newcastle, UK) talks to Gerard McLauchlan (Surrey, UK) and Alex Horton (Surrey, UK) regarding veterinary interventional radiology (IR) following a special session titled “All Creatures Great and Small: IR for animals” at the British Society of Interventional Radiology annual scientific meeting (8–10 December, Glasgow, UK).
At this year’s International Symposium on Endovascular Therapy (ISET 2022; 16–19 January, Hollywood, USA), experts presented an array of late-breaking trial results on topics ranging from venous stenting to abdominal aortic aneurysm sac sealing.
There are some very serious risks associated with forgotten ureteric JJ stents. David Maudgil, a consultant interventional radiologist at Wexham Park Hospital, Frimley Health Foundation Trust (Slough, UK), outlines why and when these devices are used, explains the risks a forgotten stent might pose, and provides some guidance on how to mitigate such risks.
A wealth of data emerging in the last 18 months, including from a small multicentre, randomised study of genicular artery embolization for knee pain secondary to osteoarthritis, brings a glimpse of other similar minimally invasive options to treat disability in the entire musculoskeletal system. Embolization, which is rapidly surfacing as a safe and effective procedure for the treatment of patients with osteoarthritis of the knee, has been shown to be technically achievable, with very promising outcomes at early follow-up.
Royal Philips has announced physicians will now have access to advanced new 3D image guidance capabilities through the image-guided therapy mobile C-arm system—Zenition, aiming to improve the outcomes for patients undergoing endovascular treatment. The company has signed a strategic partnership agreement with Cydar, a provider of cloud-based procedure maps software to plan and guide surgery in real-time.
BD (Becton, Dickinson, and Company) has announced the launch and 510(k) clearance from the US Food and Drug Administration (FDA) of the Crosser iQ chronic total occlusion (CTO) recanalisation system, which is designed to cross peripheral artery CTOs intraluminally.
Inari Medical has announced positive acute and long-term interim results from the first 500 pulmonary embolism patients enrolled in the FlowTriever outcomes registry (FLASH).
Ajax Health has announced the appointments of two cardiovascular professionals to Cordis-X, an independent accelerator created to drive innovation and growth to Cordis.
MedAlliance has acquired its partner MDK Medical, a Japanese vascular specialist company. MDK Medical has previously worked closely with MedAlliance in developing Japanese clinical studies for its novel sirolimus drug-eluting balloon (DEB) Selution SLR in the treatment of peripheral arterial disease (PAD).
The first Selution SLR study was initiated in July 2020 and involved 134 patients. Enrolment was completed in September 2021. Its objective is to assess the safety and efficacy of Selution SLR in the treatment of lesions of superficial femoral arteries and/or popliteal arteries. The acquisition will facilitate expansion of the Japanese clinical trial programme, which will include diseases of the inferior femoral artery, arteriovenous (AV) fistula access used for kidney dialysis and a drug eluting balloon for the treatment of erectile dysfunction.
“We are very excited to have acquired MDK Medical, as we now have direct access to the Japanese market”, said MedAlliance chairman and CEO Jeffrey B Jump. “We will be focusing on gaining approval for Selution SLR in Japan, one of the world’s most important markets”.
Selution SLR was awarded CE mark approval for the treatment of PAD in February 2020 and for the treatment of coronary arterial disease in May 2020. The US Food and Drug Administration (FDA) has awarded Selution SLR with four breakthrough designations: for the treatment of atherosclerotic lesions in native coronary arteries; coronary in-stent restenosis; peripheral below-the-knee and AV fistula indications.
In August 2021, the first of over 3,000 patients was enrolled in a coronary randomised controlled study comparing Selution SLR with limus drug-eluting stents (DESs). According to MedAlliance, this is the largest DEB study ever initiated and has the potential to change medical practice.
The US Food and Drug Administration (FDA) has issued two final guidances providing recommendations for including patient perspectives in medical device clinical studies.
Describing how device developers, sponsors and industry can voluntarily use patient engagement to improve clinical study design and conduct
Providing examples of approaches to consider when device developers, sponsors and industry wish to incorporate patient advisor input in clinical studies
Describing which patient engagement activities are generally not considered by the FDA to constitute an activity subject to the FDA’s regulations regarding Institutional Review Boards (IRBs)
Clarifying how sponsors can receive feedback from the FDA on plans to voluntarily include patient advisors’ input on their clinical study through the Q-submission process.
According to a press release, Texray radiation protection equipment reduces radiation dose by up to 97% during clinical interventions. This was the main concluding finding of a study led by Felix Bärenfänger (Klinikum Dortmund, Dortmund and University of Witten/Herdecke, Witten, Germany) and colleagues and published in the European Journal of Radiology.
The Texray headband (HeadPeace), and an extended thyroid collar (MindPeace), were evaluated during 20 general radiological and 32 neuroradiological interventions. The clinical evaluation concluded a significant dose reduction of 80–90%, with an average of 81.2±11.1% (general radiology) and 92.1±4.2% (neuroradiology).
It is reported the study revealed a radiation exposure of the head and neck area with cumulative local dose values up to 4.4mSv, in a relatively small sample of procedures. According to the press release, this value is surprisingly high, given that experienced operators performed the interventions, and lead protection shields were used in all procedures.
“We believe that an additional device for the head area is reasonable because usage of the devices yielded effective protection. I was really surprised to see how much scatter radiation is still arriving on the performing physician, although we are already using all these different lead shields and radiation protection devices,” concludes senior author Stefan Rohde (Klinikum Dortmund, Dortmund and University of Witten/Herdecke, Witten, Germany).
We are facing several problems in the field of clinical oncology research, by which I mean that study results are being collected, analysed and reported in many different ways, and we tend not to speak the same language within our discipline, writes Robbert S. Puijk (Amsterdam University Medical Centers and OLVG Hospital, Amsterdam, The Netherlands). These shortcomings are the reason we took the initiative to develop new guidelines regarding preferred clinical outcome measures following image-guided tumour ablation.
Image-guided thermal and non-thermal tumour ablation techniques have become indispensable therapeutic options for a variety of cancer types. For smaller-size malignant tumours, international guidelines have already adopted thermal ablation as a first-line treatment option1-7. The continuing emergence of novel treatment options and growing demand for minimally invasive image-guided tumour ablation techniques have raised the need for evidence-based IO, and with that comes the need for clear documentation of oncologic outcome parameters.
Shortcomings in how to collect, analyse and report data were the motive for our team to develop a modified Delphi consensus project8 in order to provide a framework of key opinion leader recommendations on patient-, procedure-, and tumour-related definitions, starting and ending time definitions, survival time definitions, time-to-event end points, and patient-reported outcome measures. The team consisted of members of the Society of Interventional Oncology (SIO), two independent epidemiologists and Carine Bellera, biostatistician from the French-based Definition for the Assessment of Time-to-Event End Points in Cancer Trials (DATECAN) group.
A total of 62 IO experts from Europe, the United States and Asia, working in 48 centres, eventually joined the evaluating committee. The panellists were asked to rate multiple statements and to provide additional comments whenever desirable. The article can be found online as open access publication in the Radiology journal.
To make the purpose and final results of this project clear, I can provide a few common practical examples which we hope to have solved by now. One of the most straightforward, but misleading, situations is when overall survival, for example for locally advanced pancreatic cancer, is analysed using the date of diagnosis to the date of death in one study and the date of the interventional procedure to the date of death in the other study. In order to compare survival probabilities in terms of Kaplan-Meier estimates and avoid misinterpretations as mentioned earlier, the experts reached consensus on starting and ending time definitions by documenting the time from the date of detection of disease (diagnosis), the date of the start of neo-adjuvant or induction therapy, and the date of the first intervention.
Another confusing situation might occur when different outcome measures are misused or used interchangeably, such as local tumour progression-free survival (LTPFS), primary- or secondary technique efficacy and local control. LTPFS is intended to reflect the effectiveness of the first local treatment, while local control should be used to reflect the final success after additional overlapping (completion) procedures (+/- alternative treatment methods). Furthermore, we tend to merely analyse and report a variety of outcome measures and procedure- or tumour-related outcomes per patient only while results of this article show that this is strictly speaking incorrect. To overcome this issue the experts reached consensus on whether to address outcomes per patient, per session or per tumour. As previously published by Muneeb Ahmed and colleagues, efficacy of a certain ablation device or image-guiding technique to eradicate tumours can best be illustrated by comparing the time to local tumour progression.9 Suppose a situation where a patient has been locally treated for three liver metastases and local tumour progression is being analysed and reported on a per patient basis. In this case, progression of one of the three tumours already counts as an event while the other two tumours where treated successfully, leading to an impractical LTPFS curve while comparing data analysed and reported on a per tumour basis. Therefore, and for the fact that multiple index tumours in one patient cannot be regarded as independent as these tumours are potentially correlated, the experts agreed that one should address and report several parameters both on a per patient and per tumour basis.
Another common issue is related to the fact that, prior to our article, no clear agreements have been made concerning the documentation of complications in the field of IO, as opposed to surgical series where the Clavien-Dindo classification is established to be used.10 Although consensus was not reached for the preferred validated classification system to document, analyse, and report complications and adverse events, the experts have agreed that one should indicate the most recent version of a certain validated classification system so that complications and adverse events can be categorised consistently according to severity, time of occurrence, and likelihood of the event being related to the procedure.
We believe that the clear definitions in these comprehensive guidelines will undoubtedly provide a necessary foundation for scientific reproducibility between randomised and retrospective studies as they will ensure an objective and reliable interpretation of results, allow for accurate comparison of outcomes, and avoid misinterpretations among physicians and researchers. The interchangeable setup of this current consensus document allows us to follow up this project regularly and, hopefully in the near future, helps us to extend these guidelines to regional and systemic cancer treatments to eventually attract the participation of other (inter)national medical societies. Therefore, we encourage all of our colleagues to adopt the recommendations outlined in this proposal in order to facilitate universal communication of scientific advances in the field of clinical oncology research.
Robbert S Puijk is an interventional radiology resident at the OLVG Hospital, (Amsterdam, The Netherlands) and researcher at the Amsterdam University Medical Centers, location VUmc (Amsterdam, The Netherlands)
References:
Meijerink MR, Puijk RS, van Tilborg A, Henningsen KH, Fernandez LG, Neyt M, et al. Radiofrequency and Microwave Ablation Compared to Systemic Chemotherapy and to Partial Hepatectomy in the Treatment of Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. Cardiovasc Intervent Radiol. 2018;41(8):1189-204.
Nieuwenhuizen S, Puijk RS, van den Bemd B, Aldrighetti L, Arntz M, van den Boezem PB, et al. Resectability and Ablatability Criteria for the Treatment of Liver Only Colorectal Metastases: Multidisciplinary Consensus Document from the COLLISION Trial Group. Cancers (Basel). 2020;12(7).
Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301-14.
Xu XL, Liu XD, Liang M, Luo BM. Radiofrequency Ablation versus Hepatic Resection for Small Hepatocellular Carcinoma: Systematic Review of Randomized Controlled Trials with Meta-Analysis and Trial Sequential Analysis. Radiology. 2018;287(2):461-72.
Uhlig J, Ludwig JM, Goldberg SB, Chiang A, Blasberg JD, Kim HS. Survival Rates after Thermal Ablation versus Stereotactic Radiation Therapy for Stage 1 Non-Small Cell Lung Cancer: A National Cancer Database Study. Radiology. 2018;289(3):862-70.
Uhlig J, Kokabi N, Xing M, Kim HS. Ablation versus Resection for Stage 1A Renal Cell Carcinoma: National Variation in Clinical Management and Selected Outcomes. Radiology. 2018;288(3):889-97.
Feng K, Yan J, Li X, Xia F, Ma K, Wang S, et al. A randomized controlled trial of radiofrequency ablation and surgical resection in the treatment of small hepatocellular carcinoma. J Hepatol. 2012;57(4):794-802.
Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311(7001):376-80.
Ahmed M, Solbiati L, Brace CL, Breen DJ, Callstrom MR, Charboneau JW, et al. Image-guided tumor ablation: standardization of terminology and reporting criteria–a 10-year update. Radiology. 2014;273(1):241-60.
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187-96.
The IMPRESSION trial enrolled its index patient on 11 January 2021 to assess the efficacy of the MagicTouch sirolimus-coated balloon (Concept Medical) against a placebo plain balloon in dysfunctional arteriovenous fistulas (AVFs). Since then, the prospective, multicentre, two-arm parallel group RCT has continued enrolling rapidly and has already crossed the 50% enrolment mark in just over 10 months.
The trial—under lead principal investigator (PI) Suai Chieh Tan, head and senior consultant, Department of Renal Medicine, Singapore General Hospital, Singapore, along with site PIs Edward Choke (Sengkang General Hospital, Singapore) and Jackie Ho Pei (National University Heart Centre, Singapore)—targets enrolment of 170 patients with end-stage kidney disease (ESKD) and a matured dysfunctional AVF across these three sites.
The primary aim of the trial is to evaluate primary circuit patency improvement at six months while comparing the MagicTouch AVF and placebo plain balloon in 1:1 randomised fashion.
According to a Concept Medical press release, the trial is doing “exceedingly well”, with 90 patients successfully enrolled so far. And, although the past year was shrouded by COVID-19, and impacted many healthcare institutions, the rate of enrolment has not slowed down.
“I would like to thank all the patients who have participated in the study. I hope that, together, we can find a better treatment to improve your health and many others who are experiencing the same recurring problem of a dysfunctional fistula,” said Tan.
Plain balloon angioplasty has historically been the “go-to” procedure in this area, the release adds. However, its long-term patency is poor, as ESKD patients often experience re-narrowing of their AVF or arteriovenous graft (AVG) due to stenosis. Paclitaxel-coated balloons are also being used to treat dysfunctional AVF—but mixed results have been coupled with safety concerns raised by the US Food and Drug Administration (FDA) regarding paclitaxel, Concept Medical claims.
The sirolimus-coated balloon thus “seems to be a promising option”, the release concludes, as the MagicTouch AVF was granted Breakthrough Device designation by the FDA in 2019, and the IMPRESSION RCT “will provide much-needed data” to reinforce this.
Veryan Medical has confirmed the release of MIMICS-3D EU three-year results by the study principal investigator Michael Lichtenberg (Vascular Center Arnsberg, Klinikum Hochsauerland, Arnsberg, Germany) at this year’s International Symposium on Endovascular Therapy (ISET 2022; 16–19 January, Hollywood, USA).
MIMICS-3D EU is a prospective, multicentre, observational registry to evaluate the BioMimics 3D vascular stent system. The study evaluated safety, effectiveness and device performance within a real-world clinical population of 507 patients enrolled in 23 pan-European sites.
The mean age of enrolled patients was 70 years; 66% were male and 37% were diabetic. Rutherford 0–1, 2–4 and 5–6 were 1%, 82% and 17%, respectively. Mean lesion length was 126mm and 57% of lesions were occlusions. Lesion calcification according to PACSS (Rocha-Singh KJ et al, 2014) was Grade #0—18%; #1—30%; #2—24%; #3—15%; #4—14%. BioMimics 3D placement followed atherectomy in 8% of lesions. Drug-coated balloons (DCB) were combined with BioMimics 3D in 50% of lesions treated.
Technical success for the BioMimics 3D implant procedure as assessed by the operator was 99%, Veryan Medical reports. An independent clinical events committee adjudicated major adverse events (MAE) including death and potential device-related events. The primary safety endpoint was a composite of MAE, comprising death, major index-limb amputation or clinically-driven target lesion revascularisation (CD-TLR) through 30 days. The primary outcome measure for effectiveness is freedom from CD-TLR through 12 months.
A press release details that the Kaplan Meier (KM) estimate of freedom from CD-TLR at one year, two years and three years in the intention-to-treat (ITT) population was 90%, 82% and 78%, respectively. The KM estimate of freedom from loss of primary stent patency (PSVR >2.4) through three years in the ITT population was 71%. There were 4/676 (0.6%) site-reported stent fractures
Lichtenberg commented: “I have been using BioMimics in my daily clinical practice for seven years and it is my ‘go to’ stent for a number of different indications, including long lesions, calcified lesions and lesions located in the distal SFA [superficial femoral artery] and proximal popliteal. I was delighted to be the principal investigator for the MIMICS-3D study and am pleased that the results further validate earlier results from the MIMICS clinical programme, the combined database of which provides significant validation of the clinical benefits of swirling flow.”
Nick Yeo, Veryan’s CEO noted: “I would like to thank Dr Lichtenberg for his significant contribution to the successful running of the MIMICS-3D study, providing invaluable leadership and guidance throughout. I would also like to thank all the other investigators and study coordinators who contributed to the success of the study, and particularly for being so rigorous about the quality of data collected, which is unusual for a typical registry of this type. CD-TLR and patency outcomes in the MIMICS-3D EU study are consistent with those of earlier MIMICS studies and are achieved in longer, more complex lesions. We are excited that these investigations into the postmarket performance of BioMimics 3D support the hypothesis that imparting non-planar curvature onto the femoropopliteal arteries to promote swirling blood flow and increase wall shear stress, results in clinical outcomes that are comparable to those of drug-coated and drug-eluting devices.”
“CLTI is a debilitating disease of growing prevalence around the globe and this is Cook Medical’s latest innovation within our peripheral arterial disease (PAD) programme,” said Mark Breedlove, vice president of Cook Medical’s Vascular division.
He continued: “This new product leverages our deep understanding of stent design and drug elution for lower limb anatomies, and it complements our dedicated portfolio of BTK products for limb preservation. Our goal is to improve the long-term clinical outcomes for CLTI patients.”
The Breakthrough Device designation is granted for devices that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions.
While the product is not commercially available yet, the benefits of the designation include priority review and interactive and timely communication with FDA during the clinical trial and premarket review phases in order to help get lifesaving devices to patients more quickly, a Cook Medical press release details.
The FDA has identified the recall as a Class I—the most serious type in that “use of these devices may cause serious injuries or death.” So far, there have been 163 complaints, 55 injuries and no deaths reported in relation to the device issue, the FDA reported.
HawkOne consists of a catheter and cutter driver, and is used during procedures intended to remove blockage from peripheral arteries. The recall was made “due to the risk of the guidewire within the [system’s] catheter moving downward or prolapsing when force is applied during use,” according to the FDA.
The company distributed an urgent medical device notice to customers on 6 December 2021, requesting they share reports of the defect with all relevant parties, and review both HawkOne’s instructions for use (IFU), and the warnings and precautions listed in the urgent notice letter, before using the product.
“In accordance with our commitment to patient safety, Medtronic recently initiated a voluntary recall to customers related to the risk associated with tip damage caused by guidewire prolapse in its 6 French (6Fr) HawkOne directional atherectomy system,” Medtronic said in a statement. “In our letter to customers, Medtronic noted that a small number of customer reports of tip damage (at a rate of 0.168% when compared to quantity of devices distributed) during the use of the 6FR HawkOne devices. While most of these instances were resolved without patient issue, a small number required endovascular retrieval (0.033%) or open surgical retrieval (0.028%).”
The statement added that there are no product retrievals or disposals requested associated with the recall and no actions required for patients treated with HawkOne.
Should the catheter function as outlined, the FDA reported in a medical device recall advisory, “the catheter tip may break off or separate and this could lead to serious adverse events, including a tear along the inside wall of an artery (arterial dissection), a rupture or breakage of an artery (arterial rupture), decrease in blood flow to a part of the body because of a blocked artery (ischaemia), and/or blood vessel complications that could require surgical repair and additional procedures to capture and remove the detached and/or migrated (embolised) tip.”
Medtronic asked customers to complete a confirmation form enclosed in the urgent notice letter and email them to [email protected].
Peter Littler (Newcastle, UK) talks to Gerard McLauchlan (Surrey, UK) and Alex Horton (Surrey, UK) about veterinary interventional radiology following a special session titled All Creatures Great and Small: IR for animals at the British Society of Interventional Radiology annual scientific meeting (8–10 December, Glasgow, UK).
McLauchlan and Horton discuss some of their most recent interesting cases, with Horton noting that they treat oncological and other conditions such as large arteriovenous malformations in the liver with intrahepatic shunts and other therapies such as prostate embolization and intra-arterial chemotherapy.
He notes that although the “fundamental IR techniques are identical” when it comes to treating humans and animals, there are still some “adjustments” needed and a learning curve with dealing with animals.
McLauchlan says his work with Horton means they can now “offer the animals and their owners a lifeline that they previously would not have had”. He goes on to state that “around 80% of our caseload is oncological so what we now see more than anything is prostate cancer in dogs. It is really uncommon, making up 0.6% of all dog cancers, but we are seeing at least one case a week come to us because we now offer embolization as a treatment.”
They identify some of the interesting and unique problems that arise when working with animals and pinpoint the biggest hurdles as being equipment cost (“four nurses worth of equipment in a cupboard”) and room set-up, particularly in regard to imaging that this available.
Fluidx Medical recently announced that its GPX embolic device was used to effectively devascularise a large tumour with multiple feeding vessels as part of a multicentre clinical trial.
“This could have been a challenging case since it involved a large renal tumour fed by small, low flow, tortuous vessels. We were able to use our standard embolic microcatheter to deliver GPX in a highly controlled fashion. Since we were not worried about catheter entrapment, we could take our time and ensure that we occluded all targeted vessels completely. GPX flowed distally very well, completely filling the targeted region,” said Martin Krauss, head of Interventional Radiology, Christchurch Hospital, Christchurch, New Zealand. “Based on our case experiences, GPX is a great product for effectively filling distal vasculature.”
Fluidx Medical states that the GPX embolic device is an innovative embolic designed for simple preparation and controlled delivery. The device is packaged ready to use in a syringe, can be prepped tableside by the clinician in about 30 seconds, and may be delivered through standard microcatheters (no complex mixing systems or special delivery catheters are necessary), the company adds.
A press release details that GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolus upon delivery without polymerisation or dimethyl-sulfoxide (DMSO) precipitation, a press release explains. According to Fluidx Medical, GPX is designed to occlude blood vessels independent of a patient’s coagulation situation.
“Treating a tumour with multiple feeding vessels in a controlled, thorough manner without risk of catheter entrapment can improve patient care and minimise the need for follow-on procedures,” said Libble Ginster, CEO of Fluidx Medical Technology. “GPX demonstrates improved control and precision. GPX does not require 20+ minutes of preparation time or the clinician to use a special catheter system. The simplicity of GPX preparation makes real-time clinical decision-making possible. We continue to be excited about the GPX portfolio and its future in advancing cancer care.”
The GPX embolic device is under development and does not have marketing clearance or approval in any market at this time, the company advises. It is for investigational use (in New Zealand) only.
BD (Becton, Dickinson and Company) has announced the launch and 510(k) clearance from the US Food and Drug Administration (FDA) of the Crosser iQ chronic total occlusion (CTO) recanalisation system, which is designed to cross peripheral artery CTOs intraluminally.
The Crosser iQ ultrasonic CTO device was developed to help improve CTO crossing predictability to aid clinicians treating these challenging lesions—the CTO crossing device also pairs the Crosser iQ ultrasonic CTO device with the BD recanalization system and the Recon support catheter. The new system utilizes proprietary technology that automatically adjusts the crossing power output to help stabilize the distal tip of the device to assist in crossing through the entire length of the CTO intraluminally.
The BD recanalization system and Crosser iQ ultrasonic CTO device is indicated to facilitate the intraluminal placement of conventional guidewires beyond peripheral artery CTOs, the company claims. The Crosser iQ ultrasonic CTO device is contraindicated for use in carotid arteries.
According to the company, the device utilizes a unique mechanism of action that is specifically designed to vibrate against peripheral arterial CTOs creating an intraluminal channel to facilitate the placement of conventional guidewires.
During the procedure, power from the BD recanalization system is converted into ultrasonic vibrational energy causing microbubbles to expand and implode at the tip of the Crosser iQ ultrasonic CTO device. This breaks the internal structure of the plaque and erodes the solid surface of the CTO, allowing the physician to automatically and selectively ablate plaque, while remaining atraumatic to elastic tissue, advised BD.
A new study reports that watching TV for four hours a day or more is associated with a 35% higher risk of venous thromboembolism (VTE) compared with less than 2.5 hours. The research is published today in the European Journal of Preventive Cardiology, a journal of the European Society of Cardiology (ESC).
“Our study findings also suggested that being physically active does not eliminate the increased risk of blood clots associated with prolonged TV watching,” said lead author Setor Kunutsor of the University of Bristol (Bristol, UK). “If you are going to binge on TV you need to take breaks. You can stand and stretch every 30 minutes or use a stationary bike. And avoid combining television with unhealthy snacking.”
he researchers conducted a systematic review and meta-analysis. The analysis included three studies with a total of 131,421 participants aged 40 years and older without pre-existing VTE. The amount of time spent watching TV was assessed by questionnaire and participants were categorised as prolonged viewers (watching TV at least four hours per day) and never/seldom viewers (watching TV less than 2.5 hours per day).
The average duration of follow-up in the three studies ranged from 5.1 to 19.8 years. During this period, 964 participants developed VTE. The researchers analysed the relative risk of developing VTE in prolonged versus never/seldom TV watchers. They found that prolonged viewers were 1.35 times more likely to develop VTE compared to never/seldom viewers.
The association was independent of age, sex, body mass index (BMI) and physical activity. “All three studies adjusted for these factors since they are strongly related to the risk of VTE; for instance, older age, higher BMI and physical inactivity are linked with an increased risk of VTE,” said Kunutsor. “The findings indicate that regardless of physical activity, your BMI, how old you are and your gender, watching many hours of television is a risky activity with regards to developing blood clots.”
Kunutsor noted that the findings are based on observational studies and do not prove that extended TV watching causes blood clots.
Regarding the possible reasons for the observed relationship, he said: “Prolonged TV viewing involves immobilisation which is a risk factor for VTE. This is why people are encouraged to move around after surgery or during a long-haul flight. In addition, when you sit in a cramped position for long periods, blood pools in your extremities rather than circulating and this can cause blood clots. Finally, binge-watchers tend to eat unhealthy snacks which may lead to obesity and high blood pressure which both raise the likelihood of blood clots.”
Kunutsor concluded: “Our results suggest that we should limit the time we spend in front of the television. Long periods of TV watching should be interspersed with movement to keep the circulation going. Generally speaking, if you sit a lot in your daily life—for example your work involves sitting for hours at a computer—be sure to get up and move around from time to time.”
Clinical decisions approving amputation are frequently made in isolation by a patient’s individual caregivers, a UH press release states. To address this problem, UH Harrington Heart & Vascular Institute created a novel system-wide interdisciplinary team called the Limb Salvage Advisory Council (LSAC) and evaluated its impact on a specific population of patients who were already scheduled for amputation. According to UH, only one quarter (excluding those who died or were lost to follow-up) of the patients formerly scheduled for a major amputation actually lost a limb at 180 days after being managed by LSAC.
“Circulation issues often cause painful cramping, numbness and wounds which can greatly decrease a person’s quality of life. When a doctor suggests amputation to address the pain, patients usually follow that recommendation, yet nearly half of all people with vascular disease will die within five years of an amputation. This is higher than the five-year mortality rates for breast cancer, colon cancer and prostate cancer,” said Mehdi Shishehbor, president of UH Harrington Heart & Vascular Institute, and Angela and James Hambrick chair in Innovation.
Shishehbor leads UH’s limb salvage programme, which uses minimally invasive approaches to restore blood flow to dying limbs and prevent amputation.
The LSAC at UH includes vascular surgeons, endovascular interventionalists, vascular medicine specialists, podiatrists, and wound care experts. Once a patient who is scheduled for a major amputation is identified, the treating physician may elect to notify a designated coordinator who arranges for an urgent virtual LSAC meeting. LSAC members review and discuss available data including comorbidities, functional status, extent of tissue loss, relevant imaging studies and prior interventions with the goal of providing diversified thoughtful inputs. Eventually, the LSAC reaches one of two conclusions: the limb is salvageable and a plan is created to save it, or the patient is approved to proceed with the originally scheduled amputation.
The press release details that, statistically, amputees are disproportionately of lower socioeconomic status, and that African Americans are up to four times more likely to have an amputation than white Americans.
“UH is committed to improving the health of all people by advancing science and human health. All people should have the opportunity to receive the necessary medical resources and support to have a healthier life, regardless of their status in the community or their race,” said Shishehbor. “We believe that broad implementation of this policy nationwide could really help people and significantly reduce amputation rates across the USA.”
A total of 19 patients who were scheduled for major amputation underwent LSAC evaluation between January and September 2019. The patients had a mean age of 63. Three patients were deemed unsalvageable due to extensive tissue loss and proceeded with their originally scheduled amputation, while the other 16 patients were considered for limb salvage. Fifteen patients had successful revascularisation. Nine of them had not undergone major amputation at 180 days and six of them had complete healing or significant reduction in wound size in that time.
UH claims that this is the first study investigating the impact of a novel and proactive interdisciplinary intervention on patients already planned for a major amputation due to CLTI. Two studies have reported on the adoption of multidisciplinary care in CLTI and improved outcomes; however, both were retrospective and had revascularisation proceduralists from a single specialty.
“Our interdisciplinary LSAC is unique because it involves not just multiple teams including endovascular interventionalists and vascular surgeons, but often multiple physicians within the same specialty. This ensures different points of view and more potential options to avoid amputation,” said Tarek Hammad, interventional cardiologist at UH Harrington Heart & Vascular Institute. “It is important to foster a culture of mutual respect and trust within the team and among various specialties to avoid judgement and competition.”
These findings may have significant policy implications if all patients scheduled for major amputation were mandated to receive an evaluation with an interdisciplinary team such as LSAC, UH asserts, adding that widespread implementation of this policy could greatly reduce scheduled amputations. This cause could be further helped by future research exploring how to move the referral to LSAC further upstream allowing for early intervention, the press release concludes.
Ajax Health has announced the appointments of two cardiovascular professionals to Cordis-X, an independent accelerator created to drive innovation and growth to Cordis.
“Since the acquisition of Cordis almost a year ago, we have made substantial investments in R&D, M&A, and strategic partnerships,” said Duke Rohlen, executive chairman of Cordis and CEO of Ajax Health and Cordis-X. “Recruiting Dr John Simpson and Dr Jeremy Durack, two of the greatest minds in cardiovascular science, will help us forge a bold new vision for Cordis.”
Simpson, a cardiologist, is credited with inventing and commercialising the first over-the-wire balloon catheter used for percutaneous transluminal coronary angioplasty (PTCA) and is known for pioneering interventional cardiology as it exists today, an Ajax Health press release details. As senior advisor to Cordis-X, Simpson brings decades of scientific and commercial experience. He has founded and successfully transacted multiple MedTech companies, including ACS and DVI (both acquired by Eli Lilly), CVIS (acquired by Boston Scientific), Perclose (acquired by Abbott), Lumend (acquired by Cordis), and Fox Hollow (acquired by ev3, which is now part of Medtronic).
Simpson received his PhD in biomedical sciences from the University of Texas, his MD from Duke University, and completed his fellowship in interventional cardiology at Stanford University. A member of the American College of Physicians and fellow of the American College of Cardiology, Simpson has published on a wide variety of medical subjects and lectured extensively throughout the world.
Jeremy Durack, an interventional radiologist and former vice-chair of Radiology at Memorial Sloan Kettering Cancer Center, will serve as chief clinical officer for Cordis-X. He is renowned for his work in vascular and interventional radiology, with expertise in a wide range of minimally invasive procedures and particular interest in the treatment of genitourinary cancers and venous thrombosis, the press release communicates.
Durack received his MD from Stanford University School of Medicine and completed his residency and fellowship at UCSF School of Medicine. He has been a leader in the Society of Interventional Radiology and brings a wealth of international research experience to the team.
“The collective capabilities of Ajax Health, Cordis-X, and Cordis are creating a tractor beam for the best and brightest,” said Durack. “It is not just recruiting engineers and physicians motivated to improve how we prevent and treat cardiovascular disease, but also to develop new ways of thinking about fields such as interventional oncology as well as how we can address global health disparities.”
The appointments of Simpson and Durack signal an aggressive effort by Cordis-X to recruit some of the most successful industry innovators to its team.
“I have great admiration for Cordis,” said Simpson. “They created the first catheter I ever used for diagnostic angiography in humans. Cordis products were state of the art, ahead of everyone else. I look forward to helping the organisation push the edges of innovation and create new products we will be talking about decades from now.”
Royal Philips today announced physicians will now have access to advanced new 3D image guidance capabilities through the image-guided therapy mobile C-arm system—Zenition, aiming to improve the outcomes for patients undergoing endovascular treatment. The company has signed a strategic partnership agreement with Cydar, a UK based provider of cloud-based procedure maps software to plan and guide surgery in real time.
As patient numbers rise and procedures become more complex and time-consuming, patient-specific real-time procedure planning and guidance, optimisation of equipment utilisation, and usability have become ever more important. To help overcome these challenges, Philips claims that the image-guided therapy mobile C-arm system—Zenition—brings together innovations in image capture and processing, ease-of-use, and versatility, many of which were pioneered on Philips’ image-guided therapy platform Azurion. Like Azurion, the Zenition mobile C-arm system allows hospitals to maximise operating room performance, enhance their clinical capabilities, and provide staff with a seamless user experience, a press release details.
The integration of Cydar EV Maps software into the Zenition platform now adds extended procedure planning and real-time 3D guidance capabilities.
Cloud-based AI and computer vision
Cydar EV Maps assists in the planning, real-time guidance, and postprocedure review of the endovascular surgery. It brings cloud-based AI and computer vision to mobile surgery, enabling reductions in radiation exposure, fluoroscopy time, and procedure time together with improved ease of use, Philips states. It enables surgeons to create a detailed patient-specific 3D map of the target vasculature to help plan surgery, and then uses these maps to augment intraoperative live image guidance, updating the maps in real time to account for deformations during surgery, such as guidewires and instruments deforming the patient’s blood vessels.
Cydar Maps
Cydar EV also facilitates post procedure outcome analysis. The combined result of this integration of procedure planning, guidance and review is that surgeons can work more accurately and efficiently—enabling an approximate 50% reduction in radiation exposure, a significant reduction in fluoroscopy time and a reduction of procedure times by more than 20%, according to Philips, all while helping achieve better outcomes for patients.
“With Philips’ integrated portfolio, using validated AI and cloud technologies, we can facilitate collaborative care to optimise surgical pathways,” said Karim Boussebaa, general manager Image Guided Therapy Systems at Philips. “Philips has a strong global network of mobile surgery systems and recognises that Cydar’s EV Maps solution can play a key role in further improving our integrated offering for endovascular procedures.”
“By partnering with Philips to bring our Cydar EV Map solution to Philips’ user-friendly Zenition platform of mobile C-arms, we are a step closer to achieving our mission to ensure every image-guided minimally-invasive surgical procedure goes exactly as planned,” said Paul Mussenden, CEO of Cydar. “The benefits of this combined solution, with integrated and enhanced procedure planning and visualisation, include shorter and more predictable procedure times, reduced X-ray exposure to patients and staff, and fewer injections of iodine dye—the leading cause of in-hospital kidney failure.”
Cydar EV Maps is currently in use across the EU, UK and USA. It is certified Software-as-a-Medical Device with EU CE mark and US Food and Drug Administration (FDA) 510(k) clearances.
Royal Philips today announced physicians will now have access to advanced new 3D image guidance capabilities through its image-guided therapy mobile C-arm system—Zenition, aiming to improve the outcomes for patients undergoing endovascular treatment. The company has signed a strategic partnership agreement with Cydar, a UK based provider of cloud-based procedure maps software to plan and guide surgery in real time.
As patient numbers rise and procedures become more complex and time-consuming, patient-specific real-time procedure planning and guidance, optimisation of equipment utilisation, and usability have become ever more important. To help overcome these challenges, Philips claims that its image-guided therapy mobile C-arm system—Zenition—brings together innovations in image capture and processing, ease-of-use, and versatility, many of which were pioneered on Philips’ image-guided therapy platform Azurion. Like Azurion, the Zenition mobile C-arm system allows hospitals to maximise operating room performance, enhance their clinical capabilities, and provide staff with a seamless user experience, a press release details. The integration of Cydar EV Maps software into the Zenition platform now adds extended procedure planning and real-time 3D guidance capabilities.
Cydar Maps
Cloud-based AI and computer vision
Cydar EV Maps assists in the planning, real-time guidance, and postprocedure review of the endovascular surgery. It brings cloud-based AI and computer vision to mobile surgery, enabling reductions in radiation exposure, fluoroscopy time, and procedure time together with improved ease of use, Philips states. It enables surgeons to create a detailed patient-specific 3D map of the target vasculature to help plan surgery, and then uses these maps to augment intraoperative live image guidance, updating the maps in real time to account for deformations during surgery, such as guidewires and instruments deforming the patient’s blood vessels. Cydar EV also facilitates post procedure outcome analysis. The combined result of this integration of procedure planning, guidance and review is that surgeons can work more accurately and efficiently—enabling an approximate 50% reduction in radiation exposure, a significant reduction in fluoroscopy time and a reduction of procedure times by more than 20%, according to Philips, all while helping achieve better outcomes for patients.
“With Philips’ integrated portfolio, using validated AI and cloud technologies, we can facilitate collaborative care to optimise surgical pathways,” said Karim Boussebaa, general manager Image Guided Therapy Systems at Philips. “Philips has a strong global network of mobile surgery systems and recognises that Cydar’s EV Maps solution can play a key role in further improving our integrated offering for endovascular procedures.”
“By partnering with Philips to bring our Cydar EV Map solution to Philips’ user-friendly Zenition platform of mobile C-arms, we are a step closer to achieving our mission to ensure every image-guided minimally-invasive surgical procedure goes exactly as planned,” said Paul Mussenden, CEO of Cydar. “The benefits of this combined solution, with integrated and enhanced procedure planning and visualisation, include shorter and more predictable procedure times, reduced X-ray exposure to patients and staff, and fewer injections of iodine dye—the leading cause of in-hospital kidney failure.”
Cydar EV Maps is currently in use across the EU, UK and USA. It is certified Software-as-a-Medical Device with EU CE mark and US Food and Drug Administration (FDA) 510(k) clearances.
There are some very serious risks associated with forgotten ureteric JJ stents. David Maudgil, a consultant interventional radiologist at Wexham Park Hospital, Frimley Health Foundation Trust (Slough, UK), outlines why and when these devices are used, explains the risks a forgotten stent might pose and provides some guidance on how to mitigate such risks.
Interventional radiologists routinely place large numbers of ureteric JJ stents, for a number of different indications including ureteric blockage or ureteric injury. This is often when retrograde attempts have failed or when there is no available retrograde route from the bladder. The patients who require this come from a wide range of non-urological or nephrological specialties, particularly general surgery, gynaecology and medicine, but will usually require follow up and change of the stent by urologists within three to six months.
Ureteric JJ stent
If the stent is not removed or changed in a timely fashion, there is a high risk of encrustation of stone material around the stent which may not only block the stent but also make it extremely difficult to remove without damaging the kidney, ureter and bladder. There is also a small risk of the stent fracturing within the ureter, causing acute blockage with probable added infection. For these reasons, a forgotten ureteric stent constitutes a “never” event and a serious untoward incident (SUI).
Although guidelines and procedures exist for routine monitoring and change of stents placed retrogradely (by urologists), we did not have a robust system for handing these patients promptly to urology for follow up of their stent (see Box 1 for Healthcare Safety Investigation Branch [HSIB] guidelines).
Box 1 – The UK HSIB published its report: Unplanned delayed removal of ureteric stents in October 2020. They made the following safety recommendations:
Safety recommendation R/2020/091:
Relevant specialties to develop national standards which support electronic and paper-based systems for stent logging/ tracking. These standards should include guidance on monitoring and human oversight.
Safety recommendation R/2020/092:
Review stent patient information leaflets. This should include accessibility and clinical considerations, especially with regards to side effects and complications, and advice on the action to take should concerns arise.
Safety recommendation R/2020/093:
Provide guidance for staff working within the stone care pathway to promote consistent advice to patients as part of discharge planning.
Safety recommendation R/2020/094:
Include information in discharge letters and other communication sent to GPs and patients regarding patients’ stent status, potential complications and the possibility of a retained stent.
We performed an audit showing that of 50 patients in 2019 who had antegrade stents inserted (67% as emergency admissions), 40% subsequently had stents replaced retrogradely, 45% removed, and 15% had extra-anatomical stenting or died before readmission. The mean time from stent insertion to planning removal was 13 days, which appeared unacceptably long and increased the risk of the patient being lost to urological follow up.
These findings were discussed at a joint interdepartmental meeting and we agreed that a logbook should be kept where all antegrade stents would be recorded. Moreover, a standing item at the weekly uroradiological meeting was discussion of every antegrade stent insertion and formulation of an agreed plan for urology to follow up the patient.
Subsequent re-audit three months later showed that all patients had been discussed in a timely manner with mean interval from stent insertion to planning removal reduced to 3.3 days. It was clear that interdepartmental communication regarding these patients was much improved, and that a safe system of working had been developed. This audit, with subsequent significant improvement after discussion, was presented at the the BSIR Annual Scientific Meeting 2021 (8–10 December, Glasgow, UK).
David Maudgil is a consultant interventional radiologist at Wexham Park Hospital, Frimley Health Foundation Trust (Slough, UK).
Adept Medical has today unveiled its Lower Leg Support solution, which is designed to assist with peripheral artery disease (PAD) interventions.
The Lower Leg Support aims to gently immobilise the patient’s leg during fluoroscopy-guided treatment of critical limb ischaemia. The device holds the foot in a slightly plantar flexed position and is endorotation and exorotation capable, providing multiple positioning options to facilitate imaging.
Adept Medical say that the clinician-led, ergonomic design optimally positions the leg to suit the procedural requirements desired during lower limb interventions.
Matt Lazenby, medical product design manager at Adept Medical, said: “Peripheral artery disease is becoming more and more common with over 200 million cases worldwide. We were approached by a number of imaging equipment suppliers, interventional radiologists and vascular specialists requesting a method to keep the leg immobilised whilst treating critical limb ischemia, reducing the requirement for repeat imaging and associated risks.
“This is why we developed the Adept Medical Lower Leg Support. Working with clinicians in the field, we worked hard to provide a solution to comfortably immobilise the leg, aiming to reduce some of the procedural risks for the patient and clinical team. We’re very proud of the result.”
The reversible footplate allows the product to be used on both the left and right foot. The footplate can be removed entirely to enable distal artery access, ultrasound imaging and manipulation of the foot, should it be required during the procedure.
The Lower Leg Support is fitted with a soft foam Leg Pad, providing pressure management for patients who often suffer from painful ulcerations, and soft foam straps to gently immobilise patients under conscious sedation.
Adept Medical say that the Lower Leg Support is compatible with most common table models and is suitable for use with C-arm imaging systems. Resting on top of the table mattress, it can be secured with two table straps equipped with buckles for tensioning and quick release. The Table Straps wrap around the cantilevered table and mattress.
Thrombolex recently announced the results of the RESCUE trial’s prespecified interim analysis, of the first 62 evaluable patients, in a late-breaking clinical trials session at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA).
This PIVOTAL trial is scheduled to enrol at least 100 evaluable patients with acute intermediate-risk pulmonary embolism. This trial is evaluating the efficacy and safety of the Bashir and Bashir S-B endovascular catheters (BECs) in the treatment of acute PE under an investigational device exemption (IDE) from the US Food and Drug Administration (FDA). The Bashir endovascular catheter is intended for the controlled and selective infusion of physician-specified fluids, including thrombolytics, into the peripheral vasculature. It is also now intended for the controlled and selective infusion of physician-specified fluids, including thrombolytics, into the peripheral vasculature, enabling the restoration of blood flow in patients with venous thrombus.
The goal of RESCUE is to achieve an additional indication for use of these devices in the treatment of acute pulmonary embolism.
This prespecified interim analysis was presented by Akhilesh Sista, chief of Interventional Radiology, NYU Langone Health, New York, USA. The analysis included 44 males and 18 females with an average age of 58.5 years; 90.3% had high intermediate-risk pulmonary embolism with both right ventricular dysfunction and elevated biomarkers. Each patient was treated with 7mgs of r-tPA into each pulmonary artery over five hours (a total of 14 mg r-tPA in 58 patients with bilateral pulmonary embolism and 7mg in four patients with unilateral pulmonary embolism) at 18 participating centres in the USA.
Computed tomography (CT) scan at 48 hours after infusion showed that the right ventricular to left ventricular (RV/LV) diameter ratio decreased by 32.1% (0.52±0.38: 95% confidence interval [CI] 0.42–0.62, p<0.0001), and the pulmonary clot burden by Refined Modified Miller Index had decreased by 36.3% (8.4±4.3: 95% CI 7.34–9.5, p<0.0001). The successful device placement rate was 100%, there were no device-related complications and the major bleed rate at 72 hours was zero.
“These interim results from the RESCUE trial are very exciting,” said Sista. “The most notable finding is the core lab-assessed reduction in pulmonary thrombus burden at 48 hours, which may translate to better short- and long-term outcomes pending further research. The reduction in RV/LV ratio and the absence of device- or drug-related adverse events are also salutary outcomes. The expandable infusion basket of the device, with the pharmacomechanical mode of action, appears to restore blood flow promptly. I look forward to the final results of RESCUE and subsequent investigations that will determine the role of this promising novel technology in the treatment of acute pulmonary embolism.” Brian Firth, chief scientific officer of Thrombolex and principal investigator on the Small Business Innovation Research grant from the National Heart Lung and Blood Institute (NHLBI) stated: “The strong support and encouragement that we have received from the NHLBI as we have conducted this trial, especially in the midst of the COVID-19 epidemic, has really made this trial possible.”
Inari Medical has announced positive acute and long-term interim results from the first 500 pulmonary embolism patients enrolled in the FlowTriever outcomes registry (FLASH).
A press release reports that at 48 hours post-procedure, the major adverse event rate and mortality rate were low, at 1.4% and 0.2%, respectively. None of the deaths or major adverse events were device related. Collectively, these pulmonary embolism patients experienced substantial on-table improvements in haemodynamics and symptoms, which translated to six-month improvements in cardiac function, functional status, and quality of life measures. The outcomes were achieved while limiting utilisation of hospital resources, the release adds, with less than 4% of patients receiving adjunctive therapy and a median of zero days in the intensive care unit (ICU) post procedure.
Speaking to Interventional News regarding the growing interest in mechanical thromboaspiration in the treatment of pulmonary embolism patients, Narayan Karunanithy, a consultant interventional radiologist, at Guy’s & St Thomas’ NHS Foundation Trust, London, UK said: “The catheter-based interventional treatments available to treat acute pulmonary embolism have expanded beyond catheter-directed thrombolysis recently to include several percutaneous mechanical thromboaspiration devices. Potential benefits of the latter include the use of the devices in patients with high bleeding risk, when rapid restoration of perfusion to offload the right ventricle is required in high-risk pulmonary embolism and as an alternative to surgical embolectomy in patients with multiple comorbidities. This potentially allows a larger cohort of patients with severe pulmonary embolism to be safely treated. However, at present, there is a lack of robust evidence for these devices demonstrating benefit over standard care. The big research questions are whether high- and intermediate-risk pulmonary embolism patients treated with mechanical thromboaspiration achieve better immediate and long-term outcomes than those managed with standard care anticoagulation and whether the use of the devices is safe. The field is evolving rapidly and in the next few years we are likely to see large-scale studies answer these questions.”
Narayan Karunanithy
FLASH is a prospective, multicentre, single-arm registry evaluating real-world patient outcomes after treatment of pulmonary embolism with FlowTriever. The 500-patient interim results were presented on 27 October via webcast at Transcatheter Cardiovascular Therapeutics (TCT) 2021 by principal investigator Catalin Toma (University of Pittsburgh Medical Center in Pittsburgh, USA.
“These interim results reinforce the strong safety profile of the FlowTriever system in real-world pulmonary embolism patients, with substantial on-table clinical improvements and immediate symptom relief,” said Toma, who added: “We believe these six-month follow-up data suggest that removal of clot burden without the risks of lytics has potential positive long-term implications for pulmonary embolism patients, including strikingly low rates of hospital readmissions, dyspnoea, CTED (chronic thromboembolic disease), and CTEPH (chronic thromboembolic pulmonary hypertension). These data suggest that treatment with FlowTriever may fundamentally improve the natural course of the disease, and that is tremendously exciting.”
In October, Inari Medical also announced planned enrolment in the PEERLESS trial, a new randomised controlled trial comparing the clinical outcomes of patients with intermediate-high risk pulmonary embolism treated with the FlowTriever System versus catheter-directed thrombolysis. PEERLESS is a prospective, multicentre trial that will include up to 700 patients enrolled in 60 centres in the USA and Europe. The study consists of a primary randomisation cohort of 550 patients, and for patients who cannot be randomised due to an absolute contraindication to thrombolytics, a secondary non-randomised cohort of up to 150 patients. The primary outcome for the trial is a hierarchical composite of outcomes including all-cause mortality, major bleeding events, clinical deterioration and/or bailout, and length of stay in the intensive care unit.
“Historically, due to the major bleeding associated with lytic therapy, physicians needed to carefully weigh a patient’s risk of death against the risk of intervention, reserving advanced treatment for only the sickest of pulmonary embolism patients,” said global co-principal investigator, Carin Gonsalves (Division of Interventional Radiology, University Philadelphia, USA). “By offering patients immediate symptom relief upon removal of significant clot burden without the risks of lytics, the potential for bloodless thrombectomy with the FlowTriever System has fundamentally altered the pulmonary embolism treatment landscape, challenging physicians to rethink risk stratification and the goals of intervention.”
In the trial, radioembolization (also called selective internal radiation therapy [SIRT) or sometimes transarterial radioembolization [TARE]) using glass beads (Therasphere; Boston Scientific) containing radioactive yttrium (Y-90) was used as a second-line treatment in combination with standard of care systemic chemotherapy for patients who had disease progression during or after first-line chemotherapy.
The EPOCH trialists, set their sights on determining the impact of radioembolization and second-line chemotherapy in patients with colorectal liver metastases who progressed on oxaliplatin- or irinotecan-based first-line therapy. The international, prospective phase 3 EPOCHpivotal clinical trial randomised 428 patients.
Findings from the trial, which were presented at the European Society for Medical Oncology (ESMO) Congress 2021 in the Autumn and published in theJournal of Clinical Oncology, showed that the addition of SIRT met both its primary endpoints, including progression-free survival (PFS) and hepatic progression-free survival (hPFS) of patients with metastatic colorectal cancer (mCRC) of the liver. The trial did not show significant improvement in overall survival of the patients in the SIRT arm.
TheraSphere treatment
The addition of TheraSphere treatment significantly increased both PFS (p=0.0013) and hPFS (p<0.0001). Patients receiving SIRT with second-line chemotherapy were 31% less likely to show disease progression or death (HR= 0.69) and 41% less likely to show hepatic disease progression or death vs. with chemotherapy alone (HR= 0.59). Median overall survival was 14 and 14.4 months (p=0.7229). There were 68.4% grade 3 adverse events reported radioembolization as compared with 49.3% in those who received chemotherapy alone. Both groups received full chemotherapy dose intensity.
Riad Salem (Northwestern Memorial Hospital, Chicago, USA) and co-principal investigator of the trial, said: “TheEPOCHtrial not only demonstrated positive safety and efficacy data for the patients treated in this study, but underscores the success of integrating a device-based therapy like TheraSphere treatment in the continuum of care with systemic chemotherapy and biologic regimens, thereby providing the rationale and setting the stage for future investigation in other cancer types.
”EPOCH is being hailed as the first positive phase 3 SIRT trial in any disease setting. The data is expected to support Boston Scientific’s regulatory submission to the US Food and Drug Administration (FDA). In the conclusion of the published article, the authors, write: “Further subset analyses are needed to better define the ideal patient population that would benefit from radioembolization.”
A previous phase 3 trial, SIRFLOX, that used a different resin yttrium-90 microsphere platform (SIR-Spheres; Sirtex/China Grand Pharmaceutical and Healthcare Holdings) failed to show significant additive benefits to chemotherapy as measured by progression-free survival at any site (but significantly delayed disease progression in the liver). The trial also did not find additive SIRT when it came to overall survival in a first-line setting. These results and subsequent analyses including a pooled analysis of SIRFLOX-FOXFIRE-FOXFIRE global, which reported some encouraging data for patients with respect to progression in the liver still did not reveal significant benefits with respect to overall survival.
Commenting on the EPOCH trial results, Mary Mulcahy, medical oncologist at Northwestern Memorial Hospital and co-principal investigator of the trial, noted: “In the second line of therapy for metastatic colorectal cancer, with disease isolated to the liver, the addition of TheraSphere with chemotherapy resulted in a significant delay in overall tumour progression. Additionally, chemotherapy-related adverse events were comparable between the trial arms.”Peter Littler (Freeman Hospital, Newcastle, UK) is the 2021 British Society of Interventional Radiology (BSIR) Scientific Programme Committee chair and has a specialist interest in interventional oncology. Speaking broadly on the availability of SIRT in the UK for this patient group, he says: “This study adds important information to existing literature in the area. SIRT availability in the UK for patients with colorectal metastases is limited to small numbers in the palliative setting in relatively few commissioned NHS (National Health Service) centres. Positive phase 3 data in this patient group should inform further evaluation of the technology, enabling greater access to SIRT for more of our patients.”
Mercator MedSystems has recently announced that the DEXTERITY trials research has begun under a technology transfer grant for approximately $300,000 funded by the National Institutes of Health (NIH). Preclinical research performed using the grant resources aims to demonstrate mechanistic effects of local delivery of anti-inflammatory drugs to treat deep vein thrombosis (DVT).
“The formation of DVT appears to begin due to vein wall inflammation, and then as the body’s natural processes work to remove the obstruction, the vein becomes further inflamed,” stated Kirk Seward (president and chief science and technology officer of Mercator, California, USA) “Current treatments to remove the thrombus do not treat this underlying inflammation, which has been tied to the development of new clotting events or dysfunction of the vein and valves. Ultimately, in up to half of DVT patients treated with clot-removing drugs or devices, the damage from the thrombus and the residual inflammation can lead to chronic pain and other symptoms known as post-thrombotic syndrome.”
The NIH grant is being conducted in concert with a team at Massachusetts General Hospital, Harvard Medical School in Boston, Massachusetts, led by Farouc Jaffer (associate professor of medicine at Harvard Medical School and an attending interventional cardiologist at Massachusetts General, Massachusetts, USA), another co-principal investigator for the grant research.
Jaffer commented, “Our team at Massachusetts General Hospital has extensive experience with the development of preclinical models to demonstrate the mechanisms of DVT and restoration of blood flow. In this project, we are measuring molecular, physiologic, and biologic outcomes that will be key to understanding how anti-inflammatory drugs, when delivered locally and precisely to the area around the vein, may work to counteract vein wall injury arising from this disease. We hope that our joint research will help reduce the incidence of the post-thrombotic syndrome, a consequence of DVT that has overburdened the healthcare system for years.”
According to the company, the research covered by this grant is part of a broad effort to treat inflammation related to DVT. In addition to this mechanistic research, Mercator is conducting human clinical trials with the company’s Bullfrog micro-infusion device to deliver the anti-inflammatory drug dexamethasone specifically to areas around affected veins after thrombus removal. The Bullfrog has received US Food and Drug Administration (FDA) clearance and CE Mark approval. Enrollment in the DEXTERITY clinical trials is ongoing.
Akura Medical has announced the closing of its $25M Series A1 financing, which will be used to support the development of its next-generation thrombectomy device.
The financing was led by Cormorant Asset Management, with participation from The Capital Partnership (TCP), PA MedTech VC Fund and Shifamed angel investors.
Amr Salahieh, founder of Shifamed and chairman of the board of Akura Medical, said: “Akura Medical’s mechanical thrombectomy device is designed to simplify the procedure and integrate various mechanisms to efficiently and effectively remove blood clots.
“We are extremely pleased to close this oversubscribed round of financing. The strong interest from investors validates the clear unmet need in this space and we look forward to expanding our world-class team as we drive towards the next development milestones.”
Bihua Chen, founder and managing member of Cormorant Asset Management, added: “Venous thromboembolism (VTE) is a large market that is currently underserved due to limitations of existing treatment options.
“We are excited to lead this round and believe there is ample room for improvement over existing treatments. Akura Medical’s differentiated technology has the potential to overcome these shortcomings with its elegant mechanical thrombectomy solution.”
A wealth of data emerging in the last 18 months, including from a small multicentre, randomised, sham-controlled study of genicular artery embolization for knee pain secondary to osteoarthritis, brings in its slipstream a glimpse of other similar minimally invasive options to treat disability in the entire musculoskeletal system. Embolization, which is rapidly surfacing as a safe and effective procedure for the treatment of patients with osteoarthritis of the knee, has been shown to be technically achievable, with very promising outcomes at early follow-up. It is thought to bring down pain by reducing synovial arterial hypervascularity.
A multicentre, randomised, single-blinded, sham-controlled study published online ahead of print in October 2021 in the Journal of Vascular and Interventional Radiology (JVIR) showed that, in patients with mild-to-moderate knee osteoarthritis, embolization results in symptomatic improvement greater than the sham procedure did, with clinically significant reduction in pain and disability (as measured by the Visual Analogue Score [VAS] and Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC]). In the 21-patient study, all those assigned to the sham group failed to show significant improvements at one month and crossed over to the treatment arm.
“Genicular artery embolization has the potential to be one of the most commonly performed embolization procedures for interventional radiologists in the near future and make a substantial impact in the lives of millions of patients. The data from our study demonstrate that the effect of embolization in reducing pain and improving function is far greater than the effect of a sham procedure or placebo. This study will be useful in convincing potential referrers as well as insurance companies that this procedure should be part of the osteoarthritic knee pain treatment algorithm. What is most exciting is that this procedure may just be the first of many different embolization procedures that will be utilised to treat pain throughout the musculoskeletal system,” Ari J Isaacson, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, USA, and one of the researchers on the sham trial, tells Interventional News.
These investigators further reported statistically significantly greater pain reduction captured by VAS in the treatment group when compared to those undergoing the sham treatment at one month (p<0.01). Disability improvement was also significantly greater in the treatment group (p=0.02).
“Genicular artery embolization has given many of my patients, some of whom have previously given up trying to control their pain, new opportunities to live more fulfilling lives. Often, these patients do not respond to conservative management, but are precluded by their comorbidities from having a knee replacement. Embolization can be performed with permanent particles, which have been shown to be safe, or temporary agents such as an imipenem/cilastatin slurry. The embolization technique itself is also constantly evolving to become safer and more effective. Examples include using ice packs on the skin, which have significantly decreased the rates of cutaneous non-target embolization that results in skin ulcerations. Of course, more knowledge is necessary, and important studies are on the horizon. Nevertheless, we should recognise that we do not yet fully understand the mechanism of action of this treatment. With careful due diligence, however, I think we can help many patients. For instance, I treat with temporary embolics rather than permanent embolics, and tend to treat patients who also have more severe disease and more pain,” says Yilun Koethe, Oregon Health and Science University, Oregon, USA.
Another recent publication that set out to evaluate the safety and efficacy of embolization for the treatment of symptomatic knee osteoarthritis found the procedure to be “effective and durable in reducing pain symptoms from moderate or severe knee osteoarthritis that is refractory to other conservative therapy, with an acceptable safety profile.
”Siddarth A Padia (Division of Interventional Radiology, Department of Radiology, David Geffen School of Medicine at University of California Los Angeles, Los Angeles, USA) and colleagues write that in their 40-patients study, the WOMAC total and VAS pain scores decreased by 61% and 67% at 12 months from a median baseline of 52 (of 96) and 8 (of 10), respectively. Sixty-eight percent of patients had a reduction of ≥50% in both WOMAC total and VAS pain scores.
The prospective, single-centre, open-label US Food and Drug Administration-approved investigational device exemption study was published in October 2021 in the Journal of Bone & Joint Surgery.
Padia and colleagues pointed to transient skin discolouration and transient mild knee pain after the procedure being “common and expected”. Treatment-related adverse events included a groin haematoma requiring overnight observation, self-resolving focal skin ulceration, and an asymptomatic small bone infarct on magnetic resonance imaging (MRI) at three months.
“Other than total knee arthroplasty, treatments for knee osteoarthritis have been limited in effect and duration. Research over the past several decades has failed to improve treatment options for this common ailment. Genicular artery embolization looks to be a promising breakthrough therapy for symptomatic knee osteoarthritis. Our trial showed that embolization demonstrated a marked reduction in pain and improvement in function in 68% of study participants, with minimal adverse events. Moreover, the duration of effect was seen to at least one year. These results will serve as a platform for a large-scale randomised trial, which will hopefully begin in 2022,” Padia told this newspaper.
If the evidence-base carries on being augmented for genicular artery embolization, experts believe that its impact can be widespread. “Knee pain from arthritis affects many people of different backgrounds, genders, ethnicities, and ages. Embolization has the potential to improve the lives of different kinds of patients all over the world,” Theresa Caridi, University of Alabama at Birmingham, Birmingham, USA, contends.
Mark Little, University Department of Radiology, Royal Berkshire NHS Foundation Trust, Reading, UK, commented: “Over the last 18 months, there has been increasing amounts of data within the literature.All studies have reported consistent results; embolization is a safe and potentially effective treatment for patients with osteoarthritis of the knee. The recent study that randomised 21 patients to receive genicular artery embolization or a sham procedure was the first paper to address the placebo effect. Our own interim data from the GENESIS study, which was published in CardioVascular and Interventional Radiology in January 2021, revealed a significant improvement in pain and function at one-year follow-up, in addition to an improvement in synovitis on contrast-enhanced MRI. Embolization for this indication clearly has the potential to offer a unique, minimally invasive treatment to the millions of patients with symptomatic knee osteoarthritis, which could change the way in which we treat the disease! More data are needed to study the long-term outcomes of the procedure, the health economics associated with it, and the ideal embolic agent. Further randomised controlled studies are warranted comparing it to a sham procedure, and best medical therapy, in order to improve data generalisability. My group is extremely excited to commence recruitment for GENESIS II, a large randomised, sham-controlled trial for genicular artery embolization at the beginning of 2022. The future seems vibrant for this procedure.”
Transit Scientific recently announced that its XO Cross platform has been successfully used in challenging peripheral vascular procedures.
A press release details that Jihad Mustapha, interventional cardiologist at Advanced Cardiac & Vascular Center in Grand Rapids, USA, has performed several procedures using 2F XO Cross 14 microcatheters in 90cm and 175cm lengths, designed to facilitate guidewire support, guidewire exchange, and contrast media injection during complex peripheral vascular interventions.
“The 1:1 torque of the XO Cross 14 provided new levels of trackability during the procedures,” Mustapha states. “The XO Cross 14 performed well when treating anterior tibial artery (AT) to posterior tibial artery (TA) pedal loop chronic total occlusions (CTOs), showing uniquely impressive navigation throughout the pedals, saving time and elevating treatment capabilities.”
He adds: “The XO Cross 14 enabled me to effectively cross four chronic CTOs in the pedal loop and then push up into the proximal posterior tibial to treat an additional CTO during a limb-salvage procedure. I would not have been able to access this CTO without the XO Cross 14 catheter.”
AT to PT pedal loop procedures typically involve crossing narrow, tortuous, stenosed, and potentially calcified and/or occluded distal vasculature to facilitate treatment. Penetrating certain narrow lesions can cause guidewires and catheters to buckle, increasing procedure time, requiring device escalation, increasing X-ray exposure, increasing costs, and increasing risk of procedural complications.
“XO Cross technology continues to perform well in difficult anatomy,” says Greg Method, president and CEO of Transit Scientific. “Successfully performing in AT to PT pedal loop procedures further demonstrates how XO Cross technology can help physicians treat diverse disease with better tools.”
Transit Scientific’s XO Cross platform features 24 US Food and Drug Administration (FDA)-cleared devices including 2Fr XO Cross 14 microcatheters, 2.6Fr XO Cross 18 microcatheters, and the 3.8F XO Cross 35 support catheters for use with standard 0.014″, 0.018″, and 0.035″ guidewires in 90cm, 135cm, 150cm, and 175cm lengths.
Interventional News’ top 10 most popular stories of 2021
The top 10 stories of 2021 feature advances in ablation precision, as well as a multicentre, first-in-human prospective study exploring the safety and efficacy of combined renal and common hepatic artery denervation in patients with type 2 diabetes and hypertension. The CAVA trial, which delivered evidence supporting the use of totally implanted ports to supply systemic chemotherapy, also attracted many readers.
Ablation is entering a new era of increased precision and quantification, the interventional radiology community argues. Several clinical trials—including the ACCLAIM, COLLISION, and COVER-ALL trials—are currently underway, and aim to bolster the evidence-base demonstrating favourable patient outcomes from thermal ablation.
Following a successful proof-of-concept study, researchers have embarked upon a first-in-human study to explore the safety and efficacy of combined renal and common hepatic artery denervation in patients with type 2 diabetes and hypertension. Co-principal investigators Gerard S Goh and Markus P Schlaich explain the rationale behind this single-blinded, multicentre, prospective feasibility study—named the MODUS trial—and explore the “pandemic” of cardiometabolic disease.
Trisacryl gelatin microspheres 100–300μm in size can be considered for genicular artery embolization (GAE), a study presented at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online) reported. The presentation covered two-year outcomes of a study comparing Embosphere microspheres (Merit Medical), with imipenem cilastatin for GAE in patients with moderate-to-severe knee osteoarthritis. The particles are comparable in terms of pain reduction and there is a sustained effect out to two-years of follow-up, Shivank Bhatia (University of Miami Miller School of Medicine, Miami, USA) informed delegates.
Despite lower mortality and shorter hospital stays, uterine artery embolization (UAE) is used far less commonly than hysterectomy in the management of clinically significant postpartum haemorrhage. This conclusion, presented at the Society of Interventional Radiology (SIR) annual meeting (20–26 March, online) by Janice Newsome (Emory University Hospital, Atlanta, USA), has led investigators to call for a postpartum haemorrhage response team, akin to a trauma response team. MD candidate Linzi Ardnt, also at Emory University Hospital, is the lead researcher for this work.
From an early understanding in medical school that interventional radiology was “the future”, Parag Patel has dedicated his career to the discipline, notably as a primary investigator of the BEST-CLI and ATTRACT trials, and now as the incoming president-elect of the Society of Interventional Radiology (SIR). He has also been integral to the design and implementation of a universal interventional radiology education curriculum in the USA. In so doing, he has played a large part in shaping that future he once envisioned.
Revisions to current procedural terminology codes in the USA for 2021 overhaul the evaluation and management section, reducing documentation requirements and introducing new rules determining the level of coding. These changes will affect interventional radiologists and radiation oncologists more than they will impact the day-to-day work of diagnostic radiologists, according to Erin Stephens, a senior client manager in education at Healthcare Administrative Partners.
Siemens Healthineers has launched the Somatom X.ceed, a new high-resolution, high-speed computed tomography (CT) scanner. The fastest single-source CT scanner from Siemens Healthineers can assist healthcare providers with their clinical decisions in areas like emergency imaging, cardiac CT, and CT-guided interventions.
Constantinos Sofocleous (Memorial Sloan-Kettering Cancer Center, New York, USA) sat down with Interventional News to discuss how image-guided thermal ablation, when it is deployed with an intent to cure small colorectal liver metastases, can be fine-tuned so that its outcomes match those achieved by open surgery.
“If interventional radiologists wish to become competitive with surgeons, the availability of software enabling the accurate comparison of pre- and post-interventional computed tomography or magnetic resonance imaging scans must become mandatory and routinely employed,” Luigi Solbiati (professor of Radiology at Humanitas University, Milan, Italy) argues.
For most patients receiving systemic anticancer treatment, totally implanted ports (PORTs) are more effective and safer than both Hickman-type tunnelled catheters (Hickman) and peripherally inserted central catheters (PICCs). The CAVA trial’s results, published online in The Lancet, recommended reshaping current guidelines and practice, so that most patients requiring chemotherapy for solid tumours receive a PORT within the UK National Health Service, foreshadowing a pivot in practice that might be “slow to start with”.
December’s top 10 features findings of a retrospective cost-utility analysis published in BMJ Surgery Interventions & Health Technologies. In addition, highlights from the 2021 British Society of Interventional Radiology (BSIR) Annual Scientific Meeting (8–10 December, Glasgow, UK) attracted many readers, alongside an interview with the BSIR former president, Trevor Cleveland (Sheffield, UK).
Two experts in the field of interventional radiology, Bernhard Gebauer (head of interventional radiology at Charité – Universitätsmedizin Berlin in Berlin, Germany) and Ahmed Kamel Abdel Aal (professor of interventional radiology at the University of Texas Health Science Centre in Houston, USA) talk to Interventional News about their experience with SIR-Spheres Y-90 resin microspheres (Sirtex Medical).
A retrospective cost-utility analysis from a UK National Health Service (NHS) perspective finds prostate artery embolization is more cost-effective than transurethral resection of the prostate, the gold standard for the management of patients with benign prostate hyperplasia at one-year follow-up.
Elika Kashef (interventional radiologist at Imperial College NHS Trust, London, UK) addresses the implications of interventional radiology not being equally accessible to people from all walks of life. This has triggered a re-think in the aspirations and nomenclature of the British Society of Interventional Radiology (BSIR) Women and Diversity Committee so that its broader agenda is reflected in its new name: Diversity, Equity and Inclusion Committee.
The British Society for Interventional Radiology (BSIR) has set up an interventional radiology (IR) registry to capture a glimpse of the scope, breadth, and immediate complication rate provided by the service in the UK. In parallel, UK interventional radiologists are bent on building a strong case for IR units to have their own day-case facilities, as these enabled the subspecialty to take pole position during the pandemic as a great resource for image-guided interventions and activity in a COVID-19-secure environment.
“In the last few years, we have seen quite a dramatic increase in patients who present with a structural failure of their stent in the upper gastrointestinal tract, notably the oesophagus, stomach, and duodenum, which has been brought on by the dramatic increase in survival of patients, even with disseminated cancer, Hans-Ulrich Laasch (Christie NHS Foundation Trust, Manchester, UK) tells Interventional News.
Nicholas Inston (consultant vascular access and renal transplant surgeon, Birmingham, UK) discusses the crucial care interventional radiologists provide for renal patients with Ian Mcafferty (consultant interventional radiologist, Birmingham, UK, and immediate past president of the British Society of Interventional Radiology [BSIR]).
Royal Philips has announced that it has signed an agreement to acquire Vesper Medical, a US-based medical technology company that develops minimally-invasive peripheral vascular devices.
Fluidx Medical Technology recently announced the oversubscribed closing of the first tranche of its Series A financing round. The Series A was led by a large multinational strategic investor and joined by the existing investor base as well as several new investors. A press release details that the funding will be used to support prospective clinical trials, including the pivotal trial, as well as preparation for market entry.
Jon Bell (Manchester, UK) outlines the importance of standardisation of selective internal radiation therapy (SIRT) and how this rests on an advanced understanding of personalised dosimetry to achieve optimal outcomes for hepatocellular carcinoma (HCC) patients. “So interventional radiologists, wherever they work, will be treating the same patients in the same way. […] The standardisation is crucial,” he says.
“Young interventional radiologists have got a very exciting future,” Trevor Cleveland (Sheffield, UK, and a former president of the British Society of Interventional Radiology [BSIR]), tells Interventional News. In 2021, Cleveland delivered the Wattie Fletcher lecture at the BSIR Annual Scientific Meeting (8–10 December, Glasgow, UK).
Upstream Peripheral Technologies announced today that its GoBack catheter for crossing and re-entry was proven very effective for patients undergoing complex revascularisations in lower limb arteries. The findings are based on a peer-reviewed study published in the Journal of Endovascular Therapy.
In a single-centre retrospective study led by Andrej Schmidt (University Hospital Leipzig, Leipzig, Germany), researchers reviewed outcomes of 100 consecutive patients who underwent treatment with the GoBack catheter after failed crossing attempts using standard guidewire and support catheter techniques. All lesions were confirmed as either de novo or reoccluded chronic total occlusions (CTOs). The overall technical success rate was 92%.
According to Upstream, the study highlights the versatility and effectiveness of the GoBack catheter as both a crossing and re-entry tool when compared to alternative products, and further outlines the clinical benefits of the GoBack catheter with its robust, retractable needle at its tip.
Dani Rottenberg, founder and CEO of Upstream, remarked, “All patients should have access to the most effective endovascular revascularisation technologies to avoid unnecessary bypass surgeries and amputations. The GoBack helps clinicians achieve such a goal, especially in more complex lesions.”
With these positive results, Upstream plans to make the GoBack available to hospitals and peripheral vascular catheterisation labs throughout the world. Rottenberg explains, “The GoBack helps facilities manage their costs and maximise their lab optimisation by reducing procedure time and using less consumables per procedure.”
A press release details that the GoBack catheter is a single-lumen crossing catheter which features a curved nitinol needle that serves as an effective crossing tool. The needle can be extended straight or to a curved position beyond the GoBack catheter’s tip. The protrusion length is determined by the clinician with a thumb selector on the device’s handle. The GoBack comes in two configurations of 4 French and 2.9 French for above- and below-the-knee procedures. The GoBack has regulatory approval in 30 countries.
Royal Philips has announced US Food and Drug Administration (FDA) de novo clearance for the Philips inferior vena cava (IVC) filter removal laser sheath—CavaClear—to remove an IVC filter when previous methods of removal have failed.
Philips CavaClear IVC filter removal laser sheath is the first and only FDA-cleared solution for advanced IVC filter removal, the company said in a press release. Earlier in 2021, the FDA granted the device Breakthrough Device Designation. Laser has been clinically proven to provide a success rate over 99%, with low complication rates, the press release adds.
IVC filters are used to treat patients with venous thromboembolism, in which blood clots form in the deep veins of the leg and groin, and can travel through the circulatory system. They are placed in the inferior vena cava to capture blood clots from moving to the lungs.
Research has shown that IVC filters may have long-term complications, as the filters can fracture and travel through the bloodstream to other parts of the body. Other identified long-term risks associated with IVC filters include lower limb deep vein thrombosis and IVC occlusion. The FDA recommends that implanting physicians consider removing retrievable IVC filters as soon as they are no longer indicated.
Prior to CavaClear, limited options for removal existed if the filter became difficult to remove, according to Philips. Advanced retrieval tools and techniques are required if the IVC filter becomes embedded in the vasculature. Physicians previously had very few tools to remove the filter when complications occurred and until now there were no FDA-approved devices for this type of advanced removal.
“Today is a historic day. With the approval of CavaClear, physicians now have a device specifically geared remove chronically embedded IVC filters,” said Kush R Desai MD, associate professor of Radiology, Surgery, and Medicine, and director of deep venous interventions at Northwestern University Feinberg School of Medicine (Chicago, USA). “Backed by evidence, this technology can be applied to retrieve IVC filters that are no longer indicated, reducing potential clinical risk for patients and satisfying the FDA’s guidance to retrieve filters when they are no longer indicated.”
“With the FDA’s clearance of CavaClear more than one million patients and their physicians now have access to a safe, effective and efficient option for advanced IVC filter removal,” said Chris Landon, senior vice president and General Manager Image Guided Therapy Devices at Philips. “This clearance demonstrates the commitment of Philips to innovating procedures with physician collaboration to meet unmet needs that can have a critical impact on the lives of patients and their families.”
Fist Assist Devices has announced that it recently received Breakthrough Device designation from the US Food and Drug Administration (FDA) for its Fist Assist Model FA-1 device.
According to the company, the FA-1 is the world’s first wearable device for presurgical vein dilation that promotes arteriovenous fistula (AVF) creation in adult patients diagnosed with chronic renal failure whose preoperative assessment of the venous anatomy suggests that superficial arm vein or perforator vein size is inadequate for the creation of an AVF for haemodialysis access.
Access to the FA-1 device by patients with an end-stage renal disease (ESRD) vein dilation indication is now expedited through the FDA Breakthrough Device programme—which is intended to help patients receive more timely access to breakthrough technologies that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions, such as ESRD.
The programme provides Fist Assist with priority FDA review and interactive communication regarding device development, clinical data, and future indication applications, during the premarket review process, according to a press release from the company.
“As this is a first-of-its-kind wearable device for haemodialysis patients focused on presurgery vein dilation, we are ecstatic to have the FDA recognise this innovative approach to vein dilation and the potential of this therapeutic wearable device that supports the patient’s journey through ESRD,” said Hrishikesh Gadagkar, Fist Assist regulatory advisor and CEO of Idonea Solutions. “We appreciate the FDA’s thorough review of Fist Assist’s Breakthrough Device designation request and look forward to a collaborative relationship as the company develops its FDA de novo classification application.”
The FA-1 device is a wearable, intermittent pneumatic compression device that is worn on the arm to promote vein dilation. The device compresses the outflow vein, which has both biological and physiological benefits, and—because it is automated—the FA-1 device significantly improves patients’ compliance compared to other vein dilation alternatives.
“This designation is another major milestone for Fist Assist Devices. We expect it to change the algorithm for patient care,” said Tej Singh, founder and CEO of Fist Assist. “The recently published data from the FACT trial on stage 4 vein dilation and pFACT trial on perforator vein dilation confirms the value of intermittent vein compression to CKD [chronic kidney disease] patients.
“The FA-1 device benefits patients, physicians and healthcare delivery systems because larger veins give patients more treatment options regarding surgical or endoAVF procedures. Ultimately, our goals are to help patients achieve better outcomes and have more hope. This designation gets us one step closer to accomplishing our goals.”
“Young interventional radiologists have got a very exciting future,” Trevor Cleveland (Sheffield, UK, and a former president of the British Society of Interventional Radiology [BSIR]), tells Interventional News. In 2021, Cleveland delivered the Wattie Fletcher lecture at the BSIR Annual Scientific Meeting (8–10 December, Glasgow, UK).
In discussing the rapid transformation seen in interventional radiology (IR) during his career, Cleveland draws out the revolutions in treatment for gastrointestinal (GI) bleeding, oncology, and trauma that have all been marked by a shift to more minimally-invasive treatments. In his view, the ability for IR to provide a 24-hour service, generate evidence for good patient care, and grasp technological advances have been central to underpin success and “embrace the change”.
“We are very dependent on, and use a lot of high-tech devices. […] One of the reasons we did not treat GI bleeds was because the coils were big, cumbersome, and difficult to deliver. Nowadays, we have got microcatheters and microcoils and we can really get right to work to where the bleeding is a problem,” he explains.
And, on the subject of evidence, Cleveland says, “evidence is king, really, isn’t it?”
Nicholas Inston (consultant vascular access and renal transplant surgeon, Birmingham, UK) discusses the crucial care interventional radiologists provide for renal patients with Ian Mcafferty (consultant interventional radiologist, Birmingham, UK, and immediate past president of the British Society of Interventional Radiology [BSIR]).
Mcafferty asserts that there has been “an evolution” that has seen interventional radiologists poised on the brink of “a primary care role” to deliver therapies such as renal ablation, tumour embolization, and prostatic artery embolization. This shift might provoke the need for a specialised renal or broader, genitourinary, interventionalist. “[These minimally invasive procedures are being] driven by the patients wanting them, rather than traditional surgery,” Mcafferty insists.
Dialysis interventions come in for particular scrutiny with interventional radiologists adding percutaneous arteriovenous fistula creation (EndoAVF) to an armamentarium that has, in the main, consisted of maturation, maintenance and salvage interventions.
The sweeping advances in technology will see interventional radiologists, who tend to be early adopters, really push the field forward, “and this will benefit renal patients”, says Inston, who is also on the executive board of the Charing Cross (CX) Vascular Access Masterclass and editor-in-chief of Renal Interventions.
Jon Bell (Manchester, UK) outlines the importance of standardisation of selective internal radiation therapy (SIRT) and how this rests on an advanced understanding of personalised dosimetry to achieve optimal outcomes for hepatocellular carcinoma (HCC) patients. “So interventional radiologists, wherever they work, will be treating the same patients in the same way. […] The standardisation is crucial,” he says.
“The biggest thing we have seen in the past few weeks is the new Barcelona Clinic Liver Cancer (BCLC) classification, and the importance of seeing radioembolization there for the very first time, and it is there because of LEGACY data,” he says, noting that the dosimetry is a core component of this. It is only when the whole team is familiar with dosimetry that “we going to get the best outcomes for our patients and it is all about patient care at the end of the day,” comments Bell. In parallel, in the UK, the National Institute of Health and Care Excellence (NICE) multiple technology appraisal guidance has granted SIRT reimbursement leading to the treatment gaining ground and a changed landscape.
“We now have great opportunity where we can educate, influence interventional radiologists to go out and promote the therapy and really embed it in the patient pathway,” he says at the British Society of Interventional Radiology (BSIR) Annual Scientific Meeting 2021 (8–10 December, Glasgow, UK).
Janice Newsome (Emory University Hospital, Atlanta, USA), tells Interventional News that she considers herself “a little bit of a global citizen”. “As interventional radiologists, we believe deeply in what we do, every single day—fundamentally, that it improves the health of the patients we treat. And if I believe that, it is only one step further away to see that good healthcare should be available to everyone, everywhere. So, health equity is crucial, both where high-quality healthcare is already being provided, and even more so in places where it is not available, or accessible,” she says.
Janice Newsome
Newsome is also categorical that while she is a strong believer in “interventional radiology”, the desire to take these image-guided procedures to benefit patients in need of them, across the world, means that she is open to looking beyond traditional silos and groups to the broad church of available specialists on the ground. Her sights are set on training really anyone in the healthcare team who can be trained to deliver image-guided procedures, well. “As interventional radiologists, we could never put in all the nephrostomy tubes or all the dialysis catheters that are needed for the population in Tanzania or Rwanda. We really need to be able to partner with the nephrologists seeing these patients; we need to be able to partner with the surgeons that may be already placing subclavian catheters with less-than-optimal outcomes, right? Because again, what we want to do is to advance minimally-invasive procedures. Yes, ideally via interventional radiologists, but really at the end, it is to help with the health of that population and not to really dissect the human body in the way that we have in other parts of the Western world to say that only this specialty can do this here, or only that specialty can do that there. Our goal is to train these skills broadly. And yes, we prefer that these procedures are done by interventional radiologists, but I find that the best way is to find out who else is on this journey.”
Minimally-invasive procedures for maximum impact
Newsome points to one of the smallest procedures performed by interventional radiologists—percutaneous abscess drainage—as having a colossal impact. “People in every country need to be able to have percutaneous abscess drainage. We can actually get a needle into any cavity, or any place in the body and try to drain infected fluid from that body cavity. That simple procedure has done so much to change outcomes. It should be available to any doctor who can use simple imaging to put a tube in the body to prevent the patient from needing another operation, needing anaesthesia, or long hospital stays, or even potentially, dying.” Maternal mortality, especially when related to clinically significant postpartum haemorrhage, is another area in which Newsome seeks to move the needle with interventional solutions. “A more advanced procedure that I do think should be available to every woman, everywhere, and will change the percentages of women that die during childbirth, in large part due to bleeding [complications], is embolization. I believe that any doctor, and I hope it is an interventional radiologist, who can safely perform embolization procedures to stop bleeding can help to save a woman’s life during childbirth. I am really passionate about this, because I believe that giving birth should be something that is quite joyous and no one should die while they are trying to bring a life into the world.” Pain palliation procedures are also singled out as being transformative to populations, be they nerve blocks, or ablation procedures to treat pain. Because pain, in some communities, can change the entire livelihood of a family.
For instance, in farming communities, farmers with degenerative conditions such as arthritis may not be able to provide for their families due to pain. “Pain has a huge impact on lives. Procedures that can alleviate pain and help with degenerative changes in the body should be provided around the world,” she says.
A local and global need
It is generally accepted that lower- and middle-income countries would be able to improve the health of their populations with the wider deployment of image-guided procedures. Newsome contends: “I would say that the need is great locally. And the need is great globally. Low- and middle-income countries tend to be where we focus on when we talk about global health. I have decided myself to concentrate my efforts in Sub-Saharan Africa and to concentrate that effort into training programmes where sustainability is more important. So medical tourism is not the name of the game and medical missions are not the name of the game. Instead, how we assess what is going on locally in that area and provide the care that that population needs [is the real focus].”
Outreach efforts and training
There have been several organisations over the years that have recognised this deficit of minimally invasive procedures in several countries in the world. “Organisations such as Rad-Aid, Partners Health, Doctors Without Borders, have all done incredible work. I can talk specifically about a programme called Road to IR. This organisation decided to take a different approach to set up curriculum training programmes in partnership with universities to provide in-depth training for interventional radiology. It was birthed in Tanzania, and although this programme began many years ago, three years ago we graduated our first fellowship-trained interventional radiologist from Tanzania who eventually moved back to Rwanda, where he originally came from. We are replicating the same programme Road to IR Rwanda through the generosity of one of our industry partners, and the Memorandum of Understanding signed between Emory University and the Ministry of Health in Rwanda. Our goal there is to continue to provide minimally-invasive procedures through an educational programme knowing very well that you can give a person a fish and they will eat fish on that day, but if you teach a person to fish, they will eat fish every day.”
Elaborating, she adds: “If we are able to get in at the university level and start training interventional radiologists, then we are going to be able to blanket whole regions and through societies be able to provide examinations to be able to validate this training, so that people can move freely from one country in Africa to the other and still be able to continue their training and then be able to be in practice.”
Newsome acknowledges that the barriers to widespread adoption of image-guided procedures rests in large part on the high cost of disposables, the time of experts, and language and translation barriers. Of course, COVID-19 was particularly disruptive for training programmes abroad. Still, she remains upbeat. “Even with that disruption, I will tell you that we have still survived and even thrived during COVID-19. One of the things it taught all of us is really how connected our world is; it also forced us to embrace other technologies in medicine. Besides the platforms that allow us to speak to each other, procedural telemedicine was birthed during COVID-19. Even in our lab, we were able to broadcast cases initially through what my partners here call ‘ghetto technology’—having one camera look at another camera or my laptop and five iPads in a room, trying to make sure that our learners are still learning, whether these are learners from right here at Emory or learners that are across the pond or ocean. There has also been an acceleration in the industry development of these technologies. We are going to be way better off in terms of procedural telemedicine or procedural education using these platforms going forward. I am excited about it and there are several of them that are already on the horizons being tested right here,” she says.
Smiling at the margins of progress
What encouraging health equity milestones would bring a smile to Newsome’s face? “I believe that in terms of global health equity, I am going to dance when we are able to have interventional procedure lists deployed in low- and middle-income countries in numbers that are suitable for their populations; I am going to dance when maternal mortality is really changed in the USA, considering that I am also right here in Georgia, a state where this is a huge medical issue. And one single thing that I know from a health equity standpoint that will continue to make me smile is when I see women interventionalists/ women proceduralists taking their rightful role in healthcare. When we are able to break down all those barriers in places in the world where medicine and medical care in the form of minimally-invasive procedures are so male-dominated, I will truly laugh. So, when more women are involved in that space, I believe that we are going to see a lot of change—and I will dance long and hard when those numbers start becoming more equal.”
Emma Hardy, UK Member of Parliament (MP) for Hull West and Hessle and chair of the All-Party Parliamentary Group on Vascular and Venous Disease, outlines pilot efforts steered by National Health Service (NHS) England and the National Wound Care Strategy Programme to improve the care landscape for people afflicted with lower limb wounds in the UK.
This country is facing a crisis in vascular disease made worse by the effects of the COVID-19 pandemic. However, there is a potential answer in the recommendations of the National Wound Care Strategy Programme, being implemented in places like Hull University Teaching Hospitals Trust, but for it to succeed it needs the full commitment and backing of government.
When I was younger my neighbour suffered from vascular disease, although I did not understand at the time. The course of their disease meant an amputation and a life curtailed by pain and disability. I grew up as witness not only to their suffering, but to that of the loved ones and family around them. These memories came rushing back two years ago when I was visiting Hull Royal Infirmary and meeting the vascular service staff, patients, and their families. Suddenly I was reliving this experience through their eyes, and through the eyes of the medical staff who treat this awful disease. The effect on me was immediate and profound.
I learnt that the the most severe form of the disease comes after the tissues have died resulting in foot and leg ulceration, threatening the life of the sufferer. If they do not receive successful treatment to restore blood flow and save their leg, they not only lose it, but face worse survival rates than people with heart failure, stroke, and most cancers.
I was completely unprepared for the scale and the severity of the disease in the UK. Nor was I expecting to hear of the lack of investment in treatment alongside the huge disparities in outcomes depending on where you lived. The General Election was announced shortly after my visit, but the experiences of that day haunted me. Particularly the words of a surgeon, as he showed me images of foot ulcers, that “time is tissue”; that the development of a foot ulcer from something that appears to be small and trivial into something that requires amputation, can be as short as 48 hours.
Many who are not at risk of an amputation must still live with wounds that struggle to heal on their own. Research suggests that around 730,000 wounds of the leg and feet occur each year in the UK. These wounds can be incredibly painful and debilitating, to the point that the person is unable to walk properly and struggles to cope with everyday activities, such as going to the shop or meeting with friends.
Once Parliament reconvened after the election, I joined the All-Party Parliamentary Group on Vascular and Venous Disease and was appointed Chair. As a result, I have had the privilege to meet some of the brightest clinicians and researchers working to revolutionise the way we care for people with these health conditions. Some of this innovative work is taking place right here in Hull.
The National Wound Care Strategy Programme is an initiative to improve the care of wounds, including those on legs and feet. I recently met with the passionate Hull Royal Infirmary and City Health Care Partnership teams who were awarded the opportunity to lead the development of this innovative programme with a national pilot site in Hull. They described the work required to reorganise and integrate the care system to deliver better outcomes for patients. The aim is to make it as easy as possible for people with these health issues to access the right care as soon as possible and the results have been extremely encouraging.
Nurses report that patients’ wounds are healing much better than they did before, and 100% of those treated have rated the new service as “good” or “very good”. I am heartened both by the positive impact this programme has had on patients, and by the fact that Hull is at the epicentre of this national revolution in healthcare.
Although the new systems are having positive effects, the teams are battling with a severe staffing crisis, particularly in community nursing. The Government needs to develop a comprehensive workforce plan to ensure our local NHS services in Hull can meet people’s needs.
Vascular disease is a prime example of how investing in prevention and prompt treatment prevents chronic long-term conditions that ultimately cost far more, both in monetary terms and in human suffering. The cost of wound management in the NHS currently stands at a staggering £8.3 billion a year and the government must understand that if they provide the necessary resources now, our hard-working health professionals can make a real and profound difference to the futures of tens of thousands of people and reduce long-term financial pressures.
Disclaimer
All-Party Parliamentary Group on Vascular and Venous Disease communications are not to be considered official activity from either the House of Commons or the House of Lords. It has not been approved by either House or its committees. All-Party Parliamentary Groups are informal groups of Members of both Houses with a common interest in particular issues. The views expressed in these pages are those of the group.
Elika Kashef (London, UK) addresses the implications of interventional radiology not being equally accessible to people from all walks of life. This has triggered a re-think in the aspirations and nomenclature of the British Society of Interventional Radiology (BSIR) Women and Diversity Committee so that its broader agenda is reflected in its new name: Diversity, Equity and Inclusion Committee.
She talks about the multiple outreach efforts and challenges to ensure that medical students, irrespective of their background, race or gender, are exposed to interventional radiology—an essential requirement to deal with the huge workforce issue that is looming for the subspecialty, simultaneously making certain that the life-saving benefits of interventional radiology are available to all. The new committee will also maintain its focus on retaining women in interventional radiology to up their number from the current 12%, Kashef tells Interventional News at the BSIR Annual Scientific Meeting 2021 (8–10 December, Glasgow, UK).
Alexandros Mallios (Paris, France) and Robert Shahverdyan (Hamburg, Germany) talk to Vascular News about some of the benefits of the Ellipsys™ Vascular Access System (Medtronic), how it compares to more traditional fistula creation techniques, and the key steps for achieving EndoAVF success with the system.
“What I love about Ellipsys is that the procedure is very easy and you can create a very durable arteriovenous (AV) fistula in a short time and with good results,” says Shahverdyan. Mallios outlines that the device is “very simple [to use] and efficacious”. The steps taken when using Ellipsys are “very repetitive” and thus provide a greater consistency in outcomes than those seen with surgically created fistulas, states Mallios, adding that surgery leads to “fairly variable results”. Using Ellipsys can help “minimise these differences so that you get very similar results each time”. Another major advantage of the procedure is that it is “almost painless for patients” and is associated with “better long-term flow results”, he adds.
Shahverdyan and Mallios further compare EndoAVF procedures with traditional surgical techniques, with Shahverdyan noting that the former offers “significantly shorter procedure time with practically no adverse events”. Understanding the anatomy of the patient is “crucial” in order to plan the procedure as well as how to cannulate the fistula, he adds. He also discusses the fistula flow rates obtained with the Ellipsys system and how best to optimise the procedure so that other physicians can “get the great results that we have had”.
Principal investigator of the VOYAGER PAD trial, Marc Bonaca (University of Colorado Anschutz Medical Campus, Aurora, USA) speaks to Vascular News about the latest data from the study, which indicate that patients with claudication are at high risk for adverse limb events and cardiovascular events after undergoing revascularisation. Bonaca highlights the significance of the findings—which he presented the findings at the American Heart Association (AHA) Scientific Sessions (13–15 November, virtual)—and, speaking on what is next for VOAYGER PAD, relays that “there is a lot yet to come”.
What are the key takeaway message from this new subanalysis?
We learned that patients who underwent revascularisation for claudication were severely disabled, with 62% unable to or able to with much difficulty for walking two blocks. We also found that revascularisation was effective in the short term in terms of haemodynamics (ankle-brachial index), patient-reported outcomes (the 62% with disability was reduced to 18%), and in terms of physician assessment (61% with moderate or severe symptoms were asymptomatic or with mild symptoms after the procedure). The benefit on patient-reported outcomes appeared durable out to about two years. With these benefits, however, we saw that the risk of major adverse limb events like amputation and acute limb ischaemia were frequent and increased fourfold on what we see for patients with claudication who have not progressed to needing revascularisation. Finally, we saw a significant benefit of rivaroxaban with regard to irreversible harm events of the heart, limb and brain, with a number needed to treat less than 50, and while there was more bleeding with rivaroxaban, there was a net benefit in this population when looking at events prevented/caused or the net outcome of event-free survival.
Many clinicians may consider patients with claudication at lower risk of adverse limb events and therefore question the risk/benefit of intensive antithrombotic therapy. It was important to understand the risks in the population and the risk/benefit of therapy.
Are there any findings of the that surprised you?
The data on the durability of benefit for symptoms was surprising and encouraging. The data showing the very high risk of adverse limb events was concerning and surprising.
VOYAGER PAD updates always interest our readers—why do think that might be?
VOYAGER PAD was a unique trial. There are very few trials in PAD and this is the largest post revascularisation trial. Beyond the efficacy and safety of rivaroxaban, it serves as an important dataset to learn about PAD as a disease state and how we can better risk stratify and treat this extremely high-risk population.
What is next for VOYAGER PAD?
There is a lot yet to come and in some ways we have just started. We have extensive data on patient-reported outcomes to understand disability in this population. We have analyses understanding how optimal medical therapy (e.g. statin use) impacts the risk benefit of rivaroxaban and overall risk. We have subgroup analyses exploring high risk subgroups like those with chronic kidney disease. We also have limb specific analyses such as validation of the Wound, Ischemia and food Infection (WIfI) classification, and data to come from an angiographic core lab of over 2000 images. Like all trials, VOYAGER PAD was a collaborative effort and many are participating and leading these important analyses.
In our analysis—which I presented for the first time at Transcatheter Cardiovascular Therapeutics (TCT) 2021 (4–6 November, Orlando, USA)—IVUS use made up about 11% of lower extremity arterial interventions, and when used as part of those procedures, was associated with improved outcomes, including decreased risks of amputation and thrombosis. So, although causality is hard to prove in an observational study, that association seems robust when IVUS was used during the peripheral vascular procedures.
Another take-home message is that IVUS use during iliofemoral venous stenting was actually quite high—it was used in over 50% of procedures. I think what this shows is that if you are not using IVUS, you are going to be in the minority when you are performing iliofemoral venous stenting. We have to restrain causal interpretation here, but when IVUS was used as part of a venous procedure, there were fewer hospitalisations for stent embolisation or stent thrombosis, and so we have to assume that IVUS played at least a partial role in those outcomes.
What are the benefits and drawbacks of real-world data?
The strengths of real-world data are that they represent the patients we take care of in clinical practice and the large sample size allows us to look at important subgroups while still analysing a meaningful number of procedures. They also allow us to collect important information on use patterns—so, in this case, how IVUS is being used over time and how it is being used by different providers.
There are limitations as well, and we conduct observational analyses like this one with caution in terms of causal inference. You can gain a good understanding of what outcomes look like between patients who are treated with IVUS versus those not treated with IVUS, but there are certainly important characteristics that we are not able to capture in a claims-based analysis such as anatomical considerations and the reasons why IVUS was used.
With this analysis, we have been able to provide some real-world evidence that IVUS appears to be associated with a beneficial outcome as part of a procedure, and, overall, I think that these are meaningful data to help guide us forward in terms of the continued use of IVUS. However, we must be mindful of some of the limitations associated with real-world data.
This has proven to be a popular story on the Vascular News website—do you have any views on why that might be?
We have increasingly been performing endovascular procedures in the peripheral vascular space, yet our patients are still having adverse events such as venous stent embolisation. I think we understand that we can do something better here, and I think everyone in the field is looking to see how we can improve our outcomes. We have learned a lot from the coronary space where IVUS has been an important adjunctive therapy to improve outcomes, and so I think with that type of experience behind us, as well as some (albeit limited) data out there to support IVUS use in peripheral interventions, and then also our anecdotal experience, more and more people are understanding the value of what IVUS adds to optimise the procedure and achieve better outcomes for our patients.
How does your data compare to previous studies of IVUS in the peripheral space?
We have performed a pretty exhaustive systematic review summarising all the data on IVUS that hopefully will be in press in the near future. There are actually limited data in the arterial sphere, and most are from either from single-centre or small, multicentre, retrospective studies. That being said, the data that are available have primarily shown that IVUS can be beneficial in multiple phases during peripheral arterial intervention. On the venous sides, there are stronger data thanks to the VIDIO study, which was a prospective study evaluating the benefits of IVUS during peripheral venous intervention. Those data are probably the highest-level data we have in the peripheral IVUS space. Overall, I think that all the data out there, including from this latest analysis, are showing consistent findings of benefit.
You announced a new global consensus for the appropriate use of IVUS at Vascular Interventional Advances (VIVA) 2021 (5 – 7 October, Las Vegas, USA)—do these new real-world data inform the recommendations at all?
The consensus document really helps harmonise where experts in the field feel IVUS is beneficial during peripheral interventions. I think it also demonstrates that there is a lot of support for incorporating IVUS routinely into practice and that this is not dependent on the need for more prospective data. These sentiments are already set without the availability of a large-scale randomised trial—ongoing, resulting, or otherwise. I think the take-home message from the global consensus document is that IVUS is an important adjunct to peripheral procedures and this mirrors the growth in IVUS use we observed in the Medicare studies.
What is next for IVUS in peripheral vascular interventions?
Our focus now is on trying to understand other barriers to adoption outside of generating more prospective data. I think that with the results of the consensus document, there is a clear and strong endorsement for using IVUS during peripheral interventions and now we need to understand why people are not using it. One of the reasons will be reimbursement, and that is hard to control, but a lot of it relates to educating practitioners to readily interpret IVUS images and understanding how to build the technology into their workflow without creating delays or extending the length of the procedure.
Do you think it is time for guidelines to advocate the use of IVUS in peripheral interventions, or is there still a way to go in terms of having enough data to back that up?
Based on the consensus of operators and the already increasing use of IVUS—especially in the iliofemoral venous system—I think it should be given a high level of recommendation in any upcoming guidelines. Obviously, there are economic considerations, but from a safety standpoint there is really no harm with these devices. IVUS is meant to improve outcomes, which we and others have shown, and so I think that it definitely deserves inclusion in the guidelines with high support.
Royal Philips today announced that it has signed an agreement to acquire Vesper Medical, a US-based medical technology company that develops minimally-invasive peripheral vascular devices.
Vesper Medical will further expand Philips’ portfolio of diagnostic and therapeutic devices with an advanced venous stent portfolio for the treatment of deep venous disease, the company notes. The transaction, which is subject to customary closing conditions, is expected to be completed in the first quarter of 2022. Financial details of the transaction were not disclosed.
A press release details that Vesper Medical will complement Philips’ current intravascular ultrasound (IVUS) offering in venous imaging by adding a venous stenting solution to address the root cause of chronic deep venous disease. The Vesper Duo venous stent system consists of venous stents intended to treat deep venous obstruction.
“The acquisition of Vesper Medical is another step in our objective to innovate patient treatment with more sophisticated technology and expand our growth in the vascular therapy space,” said Chris Landon, senior vice president and general manager Image Guided Therapy Devices at Philips. “Leveraging our significant procedural expertise, we see strong clinical synergies between Vesper Medical’s innovative stenting solution and our existing peripheral vascular offering. This combined offering will help to better support clinicians to decide, guide, treat and confirm during the procedure, thereby enhancing patient care.”
“I am proud that Philips will become the home for our innovations and our people, joining forces to shape the future of treating deep venous disease,” said Bruce Shook, president and CEO of Vesper Medical. “I look forward to further advance our next generation venous technology and bring it to patients and clinicians globally, together with Philips.”
Vesper Medical was founded in 2016 and is headquartered in Wayne, USA. Upon completion of the transaction, Vesper Medical and approximately 20 of its employees will become part of Philips’ Image-Guided Therapy business.
Many patients are outliving their gastrointestinal (GI) stents, and this can pose particular problems. “In the last few years, we have seen quite a dramatic increase in patients who present with a structural failure of their stent in the upper GI tract, notably the oesophagus, stomach and duodenum, which has been brought on by the dramatic increase in survival of patients, even with disseminated cancer, Hans-Ulrich Laasch (Christie NHS Foundation Trust, Manchester, UK) tells Interventional News.
While much further research is needed, the superalloy, nitinol, that the stents are made of undergoes corrosive failure when exposed to stomach acid so the stents break and fall apart. “We probably have at least one or two stent procedures a week where we have to revise a stent, exchange it and replace it, because the old one is no longer functional,” notes Laasch, who adds that interventional radiologists should be integral to tracking these devices as they have the requisite understanding of the clinical problem, are familiar with how the stents should look, and access to the imaging that shows the changes the earliest.
This interview was filmed at the British Society of Interventional Radiology (BSIR) Annual Scientific Meeting 2021 (8–10 December, Glasgow, UK).
Cleaning and low-level disinfection (LLD) effective against bloodborne pathogens are safe and sufficient procedures for disinfecting ultrasound transducers used in percutaneous procedures—this is according to an intersocietal position statement recently issued by the American Institute of Ultrasound in Medicine (AIUM).
Appearing in the peer-reviewed Journal of Ultrasound Medicine, the statement was issued in an effort to clear up confusion over disinfection practices and ensure that ultrasound equipment remains both safe and available.
Originally published in February 2021, the statement was recently republished with the support of 20 healthcare organisations, together representing more than 790,000 physicians, nurses, infection control professionals, and other healthcare professionals.
Glynis Harvey, CEO of the AIUM, said: “Our hope is that having the support of so many organisations will encourage the widespread adoption of appropriate disinfection practices in clinical and professional settings, bringing significant benefits to patients.”
The position statement was developed to address a growing debate over disinfection practices among practitioners in a wide range of medical specialties, explains Oliver Kripfgans, a medical ultrasound physicist and research associate professor at the University of Michigan (Ann Arbor, USA) who spearheaded development of the statement.
In many advanced medical procedures, ultrasound is used for guiding needles, catheters, and other devices that are inserted through the skin. Such percutaneous procedures include vascular access, arthrocentesis, paracentesis, pericardiocentesis, thoracentesis, lumbar puncture, and the delivery of regional anaesthesia.
The current debate stems from confusion over how ultrasound transducers should be disinfected between such procedures. Some practitioners have supported the use of high-level disinfection (HLD) techniques, which typically involve placing transducers in an apparatus that exposes them to specialised disinfecting chemicals such as glutaraldehyde or a mist of hydrogen peroxide.
Meanwhile, others have maintained that adequate protection is provided by use of a disposable transducer cover followed by cleaning and LLD, which involves wiping the equipment thoroughly with standard disinfectants.
In order to clarify these issues, the AIUM organised an intersocietal taskforce to examine the evidence available in published studies. The taskforce concluded that ultrasound-guided percutaneous procedures can be safely performed in conjunction with cleaning and LLD techniques, noting that transducer covers or other approved mechanical barriers protect the sterility of the procedure. Moreover, evidence showed that rare cases of infection are typically linked to the use of nonsterile or contaminated coupling gels, failure to use a transducer cover, or improper cleaning—but not to the use of LLD techniques.
The taskforce also found that recommendations for HLD are “not evidence-based and will result in unwarranted and unnecessary use of resources”.
Kripfgans said: “There was great concern that we were actually harming patients by requiring high-level disinfection.
With the support of the 20 signatory organisations, the AIUM is now launching an educational campaign to publicise the position statement and encourage the adoption of LLD techniques “to ensure that this invaluable tool remains available to every patient who can benefit from it,” says Harvey.
Teleflex Incorporated have announced that the company has received reimbursement approval from the Central Social Insurance Medical Council of Japan (Chuikyo) for the UroLift System for patients who require treatment for benign prostatic hyperplasia (BPH).
The UroLift System treatment is a minimally invasive approach to treating BPH, commonly known as an enlarged prostate, a condition that causes bothersome urinary symptoms in men. Performed as a same-day outpatient procedure, the UroLift System can help improve quality of life, and offers lasting relief from symptoms with minimal downtime for patients, according to the company.
“The UroLift System is a major advancement in the treatment of BPH and can positively impact patients’ quality of life. We are very excited to have this technology available soon in Japan and look forward to its use in treating our patients,” said Satoru Takahashi, the professor and chairman in the Department of Urology, Nihon University School of Medicine, Tokyo, Japan.
The newly approved reimbursement for the UroLift System in Japan goes into effect 1 April 2022. Teleflex currently plans to enroll Japan’s Pharmaceuticals and Medical Devices Agency (PMDA-mandated), post-market clinical study to expand its already robust clinical data on the efficacy of the UroLift System and support widespread adoption of the UroLift System in Japan.
Cordis Names George Adams, MD as Chief Medical Officer
George Adams
Cordis has announced George Adams as chief medical officer.
“We are delighted to have Dr Adams join our team as we continue to build the new Cordis,” said CEO Shar Matin. “His depth of expertise in the treatment of both complex coronary and peripheral vascular disease will play a vital role in furthering our mission to improve patient care at pace with cost-effective, differentiated solutions that build on our legacy of innovation.”
Adams is globally recognised for his expertise in the treatment of peripheral vascular disease in patients with chronic limb-threatening ischaemia (CLTI) and treatment of coronary artery disease in patients with acute coronary syndromes, a Cordis press release details. He is involved in the development of regional and national systems of care for the treatment of CLTI, ST-elevation myocardial infarction (STEMI), and management of complex coronary and peripheral vascular disease. He has a well-established network of peers and associates who are viewed as key opinion leaders within the global cardiovascular community.
“It is with great honour and excitement that I join the Cordis team as chief medical officer,” said Adams. “I look forward to playing a role in reinvigorating an incredible 62-year legacy. I am grateful to be a part of the future that Cordis is building with integrity and a vision for innovation.”
November’s top 10 features a pilot study regarding cryoablation for the treatment of early-stage, low-risk breast tumours, as well as data indicating that the Ellipsys vascular access system (Avenu Medical/Medtronic) offers an “excellent alternative” to arteriovenous fistula creation via surgical procedures in end-stage renal disease patients. In addition, the declaration of UK interventional radiologists of why to attend British Society of Interventional Radiology (BSIR) (8—10 December, Glasgow, United Kingdom) also attracted many readers.
A pilot study, published in the Journal of Cancer Therapy, reveals that percutaneous cryoablation of early-stage, low-risk breast cancer tumours smaller than 15mm presents a potential substitute for lumpectomy.
The Ellipsys vascular access system (Avenu Medical/Medtronic) can be used to easily and safely create durable percutaneous arteriovenous fistulas (AVFs) for haemodialysis—with new, long-term data suggesting it offers an “excellent alternative” to AVF creation via surgical procedures in end-stage renal disease patients. That is according to Jeffrey Hull, an interventional radiologist and director of the Richmond Vascular Institute in Richmond, USA, who presented five-year results from the Ellipsys US pivotal trial at this year’s American Society of Nephrology (ASN) Kidney Week (2–7 November 2021, virtual).
Hear from Alex Barnacle (London; British Society for Interventional Radiology [BSIR] communications chair), Peter Littler (Newcastle; the 2021 Scientific Programme Committee chair), Ian McCafferty (Birmingham; current BSIR president) and Phil Haslam (Newcastle; incoming BSIR president) about what they are most looking forward to at this year’s meeting.
Six-month outcomes from the randomised RADIANCE-HTN TRIO trial, comparing endovascular ultrasound renal denervation to a sham procedure for treatment-resistant hypertension, demonstrate the additional effects of pharmacologic intervention with maintenance of a blood pressure-lowering effect of renal denervation at six months, according to investigators.
Randomised placebo-controlled trials show consistently that renal denervation provides significant reduction in ambulatory and office blood pressure, the findings of a systematic review and meta-analysis suggest.
XACT Robotics recently announced what it describes as the world’s first remote-controlled robotic instrument insertion and non-linear steering during an interventional oncology percutaneous procedure with ACE Xtend.
Fluidx Medical’s GPX embolic device has released initial results for Oncology Drug Delivery. Fluidx Medical Technology announced that a next-generation, doxorubicin-loaded GPX embolic device was featured at the recent symposium on clinical interventional oncology (CIO) conference highlighting the technology’s potential for oncology drug delivery.
The Society of Interventional Oncology (SIO) has announced the launch of the society’s first clinical trial—Ablation with confirmation of colorectal liver metastases (ACCLAIM) prospective trial for microwave ablation as a local cure. An SIO press release details that this multi-million-dollar trial is funded collectively through grants from Boston Scientific Corporation, NeuWave Medical (part of Ethicon), and Varian, a Siemens Healthineers company.
Royal Philips announced the results of a new large-scale real-world analysis of Centers for Medicare & Medicaid Services (CMS) data on the health outcomes of peripheral vascular interventions guided by intravascular ultrasound (IVUS).
Medtronic today announced findings from a new study of patient preferences for the treatment of hypertension. The findings are set to be presented during the “What’s Novel in Interventional Hypertension” session at the 33rd Transcatheter Cardiovascular Therapeutics annual meeting (TCT 2021, 4–6 November, Orlando, USA and virtual)—the yearly scientific symposium of the Cardiovascular Research Foundation.
Arrow International has recalled its Arrow-Trerotola over-the-wire 7Fr percutaneous thrombolytic device (PTD) kits, which are used to remove clots in adult patients who have arteriovenous fistulas (AVFs) and synthetic dialysis grafts.
The recall has been attributed to the risk of the orange inner lumen of the Arrow-Trerotola PTD catheter’s tip component separating from the device’s self-expanding basket. A statement from the US Food and Drug Administration (FDA) adds that, if this occurs, the lumen may fracture and detach, and block the blood vessel(s) it is being used in.
Resulting health consequences depend upon where the fractured tip component embolises, the FDA statement continues. If the embolisation is local to the treatment target site, retrieval may be attempted, requiring an additional intervention and consequent delay of therapy. In some cases, the embolisation could be central, or possibly even to the heart or pulmonary arteries. This may lead to serious adverse events, such as vessel damage, need for additional medical procedures, or possibly death, the statement adds.
The FDA has identified this as a Class I recall—the most serious type of recall—meaning use of these devices may cause serious injuries or death. To date, there have been seven complaints and no injuries or deaths reported for the Arrow-Trerotola PTD kits.
Arrow, which is a subsidiary of Teleflex, has recalled 3,241 of these devices in the USA following initiation of the recall in August 2021.
More information for healthcare providers or patients who may be affected by the recall can be found here.
Fluidx Medical Technology, has recently announced the oversubscribed closing of the first tranche of the Series A financing round. The Series A was led by a large multinational strategic investor and joined by the existing investor base as well as several new investors. The funding will be used to support prospective clinical trials, including the pivotal trial, as well as preparation for market entry.
Fluidx Medical’s GPX embolic device
“GPX has been quite simple to prepare, deliver and control,” said Andrew Holden (director of Interventional Radiology, Auckland City Hospital, Auckland, New Zealand). “The material is very radiopaque during delivery and has demonstrated excellent distal penetration, particularly important in our tumor embolization cases.”
Embolic devices are widely used to stop blood flow for targeted treatment of hypervascular tumors, vessel malformations, internal bleeds, and other cancer-related uses. Challenges with embolic devices today can include complicated preparation processes, issues with visibility during device delivery, reliance on the body’s coagulation situation, and lack of complete penetration of vessel beds and tumor feeding vessels.
The GPX Embolic Device is an innovative embolic designed for simple preparation and quick material delivery. GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolus upon delivery without polymerization or dimethyl-sulfoxide (DMSO) precipitation. GPX is designed to occlude blood vessels independent of a patient’s coagulation situation. Unlike competitive technologies that require special preparation materials and time, the GPX device is packaged ready-to-use in a syringe, requires less than 30 seconds of tableside preparation by the clinician, and may be delivered through standard catheters or small microcatheters (no complex mixing systems or special delivery catheters are necessary).
The British Society for Interventional Radiology (BSIR) has set up an interventional radiology (IR) registry to capture a glimpse of the scope, breadth and immediate complication rate provided by the service in the UK. In parallel, UK interventional radiologists are bent on building a strong case for IR units to have their own day-case facilities, as these enabled the subspecialty to take pole position during the pandemic as a great resource for image-guided interventions and activity in a COVID-19- secure environment.
Other milestones to mark and challenges to navigate include interventional oncology advances such as the final draft National Institute of Health and Care Excellence (NICE) guidance recommending the use of selective internal radiation therapy (SIRT) for hepatocellular carcinoma (HCC), supporting interventional radiologists who are not formally recognised as paediatric specialists but performing paediatric interventions in “bits and pieces” and getting direct preferencing for radiology registrars into interventional radiology, so that from 2022, they will be “badged as an interventional radiologist, all the way through their training”.
Alex Barnacle (London; BSIR communications chair), Peter Littler (Newcastle; the 2021 Scientific Programme Committee chair), Ian McCafferty (Birmingham; current BSIR president) and Phil Haslam (Newcastle; incoming BSIR president) discuss these developments ahead of this year’s BSIR annual scientific meeting in Glasgow next week (8–10 December, Glasgow, UK).
Two experts in the field of interventional radiology, Bernhard Gebauer (head of interventional radiology at Charité – Universitätsmedizin Berlin in Berlin, Germany) and Ahmed Kamel Abdel Aal (professor of interventional radiology at The University of Texas Health Science Centre in Houston, USA) talk to Interventional News about their experience with SIR-Spheres Y-90 resin microspheres (Sirtex Medical)—which are used in selective internal radiation therapy (SIRT) for certain liver tumours*—and discuss how this advanced technology can help improve survival, boost patient quality of life (QoL) and enable greater flexibility, customisation and speed of treatment.
Ahmed Kamel Abdel Aal
Real-world data
Real-world data from the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Registry for SIR-Spheres Therapy (CIRT)—which was presented at the CIRSE 2020 Summit (12–15 September, virtual)—showed that SIR-Spheres Y-90 resin microspheres were associated with low 30-day mortality (1%) as well as a low incidence (2.5%) of serious adverse events (grade ≥3) within 30 days of treatment. Serious adverse events such as gastritis, gastrointestinal ulcerations, radiation cholecystitis and radioembolization-induced liver disease occurred in less than 0.3% of the total patient cohort.
This large European registry, which included 1,027 patients, was designed to observe the real-life clinical application of SIRT with SIR-Spheres Y-90 resin microspheres and the impact of the treatment in clinical practice. “The strength of CIRT registry data is that they reflect patient and tumour treatment in a real-world scenario, including large treatment centres and smaller hospitals from different countries and healthcare systems,” says Gebauer.
In addition to highlighting low mortality and low serious adverse events, the data also found that median overall survival was 9.8 months (95% CI: 8.3–12.9) in 237 patients with metastatic colorectal cancer (mCRC). These figures from CIRT are “a great result for patients with certain types of cancer who have limited options”, adds Kamel.
Similar findings were reported in the CIRSE Registry for SIR-Spheres Therapy in France (CIRT-FR), the interim analysis of which revealed some interesting data in relation to safety and patient QoL. There were a total of 200 patients (median age 66; 70% male) including 38 mCRC patients in the CIRT-FR registry. As was the case in CIRT, 30-day mortality was 1%. A total of 12% of patients experienced at least one adverse event within 30 days following treatment. In relation to health-related QoL, which was assessed using the EORTC QLQ-C30 questionnaire, the overall global health score remained stable between baseline (66.7%), treatment (62.5%) and the first follow-up (66.7%)
“For heavily pretreated patients, the toxicity of a treatment and QoL are very important”, says Gebauer, adding that “the data show that SIR-Spheres Y-90 resin microspheres are well tolerated and maintain patients’ QoL.” He also explains that, with this technology, patients can be offered a chemo-free interval in order to have the liver treated but without the side effects of a systemic therapy.
Patient selection
Gebauer further discusses which patients can benefit most from this treatment, noting that, in general “SIR-Spheres Y-90 resin microspheres are an option for a broad range of patients.” He also outlines that oncological factors such as tumour size and number of tumours, as well as the functional capacity of the liver “play a great role” in determining the use of SIR-Spheres Y-90 resin microspheres.
“Usually Y-90 treatment using SIR-Spheres is used in patients where the tumours are not resectable or ablatable, either because of tumour factors (tumour too large, adherent to critical organs or structures or invading vascular structures), remaining hepatic reserve limitations (especially if large hepatic resections are planned) or other patient factors or comorbidities that limit larger resections. Specifically, in the first group (tumour factors) Y-90 SIRT could reduce the tumour volume and transfer the patient in a secondary resectable or ablatable state.
“In selected cases, patients might benefit from an earlier treatment with SIRT. SIR-Spheres Y-90 resin microspheres show good response rates in localised liver tumours and offer patients surgical options that were unavailable before SIRT.
“So patients could be transferred into a suitable stage for resection or ablation and transferred into a potentially curative stage. Depending on the location of liver tumours SIRT allows various treatment strategies including segmentectomy, lobectomy and hemiablation with contralateral hypertrophy for resection”, he adds.
“Preinterventional state-of-the-art imaging is essential for therapy planning”, says Gebauer, who adds that “personalised medicine is nowadays the standard of cancer care and therefore the dosimetry should also be so in order to improve the results of SIRT.”
Kamel outlines how it is “important to realise that each disease and each patient is different”. He agrees with Gebauer that, as a result, “treatment should be based on the goal of the therapy, the patient’s liver function, the number and location of the lesions and the prior, concurrent and future treatment(s). Personalised dosimetry is always recommended for all patients receiving Y-90 SIR-Spheres”, he concludes.
Utilisation and customisation
SIR-Spheres Y-90 resin microspheres therapy is a minimally invasive procedure that sees patients usually return home shortly after the procedure is completed. It is currently the only fully US Food and Drug Administration (FDA)-approved Y-90 radiation therapy in the USA for the treatment of colorectal cancer that has spread to the liver. The Y-90 resin microspheres can be delivered in a slow, deliberate manner, thereby helping to achieve an even distribution, thus maximising the number of microspheres delivered and optimising tumour coverage.
Discussing some of the challenges associated with many Y-90 programmes, Kamel states that “outcomes are often variable and not consistent. It can also take some time between the decision for treatment and treatment with Y-90. This can delay other treatments and adds a lot of stress to the patient,” he continues.
However, there is a solution. Helping to address these challenges is Sirtex’s FLEXdose Delivery Programme, which Kamel says has helped optimise his practice. He explains that the FLEXdose Delivery Programme provides physicians with the opportunity to have one-, two- or three-day pre-calibrated vials which contain exactly the same number of microspheres, with different activity per sphere.
“This offers you the flexibility to give the same activity but with either more or fewer microspheres, allowing you the ability to customise treatment based on the tumour burden, lobes and segments of the liver involved, and how selective you are with your catheter,” says Kamel.
“Another advantage is the activity draw, which is really very important in our programme and is very unique to SIR-Spheres. It allows you to administer a tailored and personalised activity for the patient’s specific needs. Imagine that on the day of treatment you wanted a smaller dose or another dose. You can draw the exact dose that you desire from the vial. Being able to change the dose on the day of the treatment means you do not have to keep bringing the patient back again because you do not have the right dose.”
“Previously, the usual sequence of events was to map, do the dose calculation, order the dose and then treat,” notes Kamel. “However, utilising Sirtex’s Order-Map-Treat programme, you get a much faster patient treatment.”
“We know that we can always draw the exact dose we want and that is the beauty of this. It has also really changed the mindset of our referring physicians because we can provide an accelerated treatment timeline that enables patients to be quickly returned to their medical oncologists for further systemic treatment(s)”, concludes Kamel.
*For full indication and prescribing information, please refer to the IFU at www.sirtex.com.
Bernhard Gebauer is head of interventional radiology at Charité – Universitätsmedizin Berlin in Berlin, Germany. He is German board certified in radiology and interventional radiology and specialised in IR cancer treatment.
Ahmed Kamel Abdel Aal is a professor of interventional radiology and the chief of vascular and interventional radiology and the vice chair of radiology at The University of Texas Health Science Center at Houston (UTHealth) in Houston, USA. He is American board certified in radiology and interventional radiology and received his fellowship training in vascular and interventional radiology as well as neuroradiology at the University of Alabama in Birmingham, USA.
Artio Medical has announced that full results from its first-in-human clinical study of the Amplifi vein dilation system were presented at the 2021 VEITHSymposium (16–20 November, Orlando, USA and virtual) by Surendra Shenoy, associate professor of surgery in the Washington University School of Medicine at Barnes-Jewish Hospital (St Louis, USA).
“Data from the first five patients treated with the Amplifi system demonstrated more than a doubling of forearm and upper arm cephalic vein diameters following a mean treatment period of 8.6 days,” said Shenoy. “We were able to successfully create an arteriovenous fistula (AVF) using treated veins in all patients and observed rapid and robust AVF maturation. These data are very encouraging, and I believe this technology has the potential to offer a much-needed solution for increasing AVF suitability and reducing maturation failure.”
The Amplifi vein dilation system is designed to stimulate arm vein enlargement prior to AVF creation to make more patients requiring vascular access for haemodialysis eligible for AVF surgery, reduce the time required for AVF maturation, and increase successful maturation rates, an Artio press release states.
“When physicians create AVFs today, we know there are often vein segments with pre-existing problems, but we do not currently have adequate tools to identify these segments—which contributes to the high rate of AVF maturation failure,” Shenoy added. “The Amplifi system could allow physicians to better identify these segments and either treat them at the time of AVF creation or exclude them from the AVF circuit.
“In this study, three of the five patients had pre-existing problems in the cephalic vein, which were made more apparent by Amplifi system treatment. In one patient, an AVF was made more proximally and, in another, angioplasty was performed, and both patients went on to have successful AVF maturation and use.”
Erdie De Peralta, vice president of clinical and regulatory affairs at Artio, said: “We are pleased to have the data from the Amplifi system FIH [first-in-human] presented at the VEITH conference and look forward to building upon this initial clinical experience with our US IDE [investigational device exemption] trial, which is projected to begin enrolment in 2023.”
Prostate artery embolization (PAE) is more cost-effective than transurethral resection of the prostate (TURP), the gold standard for the management of patients with benign prostate hyperplasia (BPH) at one-year follow-up. However, embolization exhibits a higher reintervention rate, which may reduce the cost-effectiveness in subsequent years following intervention.
There were the concluding findings of a retrospective cost-utility analysis from a UK National Health Service (NHS) perspective, published in October 2021 in BMJ Surgery Interventions & Health Technologies, Sachin Modi, University Hospital Southampton NHS Foundation Trust, Southampton, UK (senior author) and colleagues.
Sachin Modi
The prevalence of BPH increases with age, which, combined with an ageing population in the UK, will create a financial burden on the NHS. With PAE offering a minimally invasive alternative, Modi and colleagues set out to investigate the cost-effectiveness of PAE vs. TURP, in the management of BPH after one-year follow-up. This comparison study, therefore, collected patient data from the UK Register of Prostate Embolization (UK-ROPE) study at one, three, six and 12 months. UK-ROPE holds data on patients treated with embolization or surgical interventions from across 20 U.K centres, and was funded by the UK National Institute for Health and Care Excellence (NICE). In the UK-ROPE study, male patients received either embolization (PAE) (n=133), surgery (TURP) (n=31), open prostatectomy or holmium laser enucleation of the prostate (HoLEP) between July 2014 and January 2016. Patient outcome data was collected on the International Prostate Symptom Score (IPSS), quality of life (QoL) and International Index of Erectile Function (IIEF).
Within the cost analysis, effectiveness was measured as quality-adjusted life years (QALYs) and the costs for both embolization and surgery were taken from University Hospital Southampton data, using 2016 as a reference year. An incremental cost-effectiveness ratio (ICER) was then derived from cost, IPSS values and QALY values associated with both interventions at 12 months.
The original UK-ROPE study outcomes showed no significant differences in patient baseline IIEF, prostate volume or maximum urinary flow rate, however, and it demonstrated that embolization showed a significant statistically improvement in IPSS and QoL post-procedure. However, the improvement in IPSS following surgery was greater.
Within the embolization group, the QALY value was 0.96 (SD=0.03), compared to a surgery QALY score of 0.98 (SD=0.03). The average cost per patient of embolization and surgery was £2,000 and £3,028, respectively. Therefore, the ICER was £64,798.10 saved per QALY lost, making embolization more cost-effective. Within the patient cohort, 36% of those who received embolization reported complications at 12 months, with 84% of surgery patients also reporting complications in the same timeframe.
In conclusion, embolization was deemed to be a more cost-effective intervention in the management of BPH compared to TURP. Shorter patient stays and the lack of necessity for an operating theatre/anaesthesia were major contributing factors to this, however, due to a higher reintervention rate in the embolization group, the authors suggest that this benefit may not be maintained in subsequent years and longer term comparison studies are required to fully evaluate this.
Aopeng Medical’s Allvas endovascular intervention surgical robot has successfully completed a first-in-human clinical evaluation of robot-assisted peripheral artery intervention of an iliac artery in the Department of Vascular Surgery at Shanghai Changhai Hospital.
The procedure was performed by Qing-Sheng Lu and colleagues in the Department of Vascular Surgery at Shanghai Changhai Hospital in Shanghai, China. The endovascular intervention surgical robot, combined with digital subtraction angiography (DSA), precisely evaluated the target lesion and location, and completed a refined operation process to better ensure the safety of the procedure, reduce iatrogenic injury, and reduce the incidence of complications and postoperative reintervention rate, a press release from Aopeng Medical reports.
According to Aopeng Medical, the Allvas endovascular intervention surgical robot is the first platform-robot in peripheral artery intervention with independent intellectual property rights in China. Its core technology covers robot architecture design, robotic arm and actuator process design, force feedback mechanism, software algorithm and automated surgery, and system integration. Aopeng Medical claims that the Allvas is the world’s first universal peripheral artery interventional robot. Early this year, the company completed what it asserts to be world’s first in-human clinical trial of robot-assisted endovascular aortic repair of thoracic aortic aneurysm and abdominal aortic aneurysm.
The traditional surgical treatment has numerous side effects, such as high trauma, high risk, difficulty and multiple complications. In comparison, Aopeng Medical alleges that its endovascular intervention surgical robot, Allvas, can achieve precise positioning through digital technology, which meets specific needs from the individual patient. The company adds that Allvas is also expected to reduce the radiation dose received by the operator by more than 90% and improve the precision of surgical manipulation, thus helping physicians to achieve higher efficiency and more satisfactory effects in clinical practice.
Canon Medical Systems is introducing an all-new size for its high-definition flat panel detector for vascular and interventional radiology (IR) procedures, a press release from the company reports. Canon Medical claims that the 12”×16” high-definition detector provides more than twice the spatial resolution of conventional flat panel detectors, helping clinicians see fine details in complex interventional procedures. The new 12”×16” detector joins the existing 12”×12” high-definition detector to provide clinicians with the ideal size for their unique procedural needs.
Alphenix high-definition detector (Canon Medical)
“All those things which the device does that were impossible to see with conventional flat panel detectors become overly abundant with high-definition detector technology,” said Adnan Siddiqui, director of neurological stroke services, Kaleida Health; CEO of The Jacobs Institute; and professor of neurosurgery at the University at Buffalo, New York, USA).
Now available on Canon Alphenix interventional systems, the 12”×16” high-definition flat panel detector offers the highest resolution in the market, according to Canon Medical. Made up of what the company asserts to be the world’s first true high-definition detector—with 76-micron resolution—for resolving fine details, the hybrid 12″x16″ panel is combined with high-definition flat panel technology that results in resolutions of 2.6lp/mm (standard) and 6.6lp/mm (high-definition detector).
Canon Medical is showcasing Alphenix high-definition detector technology at this year’s virtual Radiological Society of North America (RSNA) annual meeting (28 November–2 December, Illinois, United States). Learn more about the Alphenix’s full suite of technology here.
Cardiovascular Systems has initiated a voluntary recall of unused Wirion embolic protection systems due to complaints of filter breakage during retrieval.
Wirion is a distal embolic protection filter used to capture thrombus and debris that can be associated with all types of peripheral vascular intervention procedures, including atherectomy.
CSI has informed all affected healthcare facilities to discontinue use of Wirion immediately and return unused product to CSI. The US Food and Drug Administration (FDA) has also been notified. To date, CSI has received nine complaints of filter breakage during retrieval. Filter breakage may result in device embolism and possible additional intervention.
The company plans to voluntarily recall all Wirion units currently in customer inventory. In total, 697 devices were distributed in the USA between 22 March and 15 November 2021.
Interventional radiology is regularly characterised as being “a hotbed of innovation”, but the first study to directly evaluate the level of agreement between disclosed financial relationships and open payment data for top-cited image-guided procedures in the USA lays bare that 97% of the studied authors failed to disclose at least one active financial relationship. Importantly, declaring an interest does not equate to resolving potential bias, note authors Lee J Hsieh (University of California San Diego, San Diego, USA) and Mina S Makary (The Ohio State University Medical Center, Columbus, USA). Their research, published online ahead of print in October 2021 in the Journal of Vascular and Interventional Radiology also reignites the debate around how to weed out bias without bedevilling and stifling innovation. Interventional News speaks to the authors of the study to drill down on its findings and implications.
How should the findings of this study influence interventional radiologists to scrutinise published data?
The significance of this work is that it is the first study which directly evaluates the prevalence of conflict of interest (COI) disclosures in US-based interventional radiology (IR) research while evaluating the level of agreement between disclosed financial relationships and open payment data for top-cited image-guided procedure research. Findings from this work should raise the attention of interventional radiologists evaluating published data to this often invisible factor that creates a risk of bias. For example, studies have shown that those with industry sponsorships are more likely to have pro-industry conclusions, and others may publish conclusions inconsistent with the study results. Industry sponsorships may also erode academic freedom and influence research agendas, inadvertently suppressing research that does not further industry’s objectives in science or policy. This potential for bias is the reason expert consensus has emphasised the importance of COI disclosure to help mitigate any potential bias and support data integrity.
What were the leading results from your data?
One of the most interesting findings was that among the 396 authors of 100 US-based, top-cited image-guided procedure publications, 97% failed to disclose at least one active financial relationship, with an average of US$57,937 in undisclosed payments per publication. For comparison, previous studies in other areas of healthcare have found discrepancies in 43–69% of publications, while still others have reported a median rate as high as 81%. Together these trends suggest that conflicts of interest are prevalent in IR, like other areas of healthcare research, and conflicts of interest in top-cited image-guided procedure research are often underreported.
A 30% positive COI rate that climbs to 50% in standards of practice and device-related publications—what needs to be done to help recast these numbers?
To improve disclosure, authors and organisations have advocated for further development and use of open disclosure databases, building upon the successful implementation of ClinicalTrials.gov. Many have noted that relying primarily on self-disclosure is limited and that people may overlook potential biases in themselves that they would otherwise perceive in others. Even authors who are transparent with their COIs may falsely equate disclosure with resolution, assuming that once a potential bias is disclosed, no further action is required. As such, the Committee on Publication Ethics described the importance of a shared responsibility between authors to disclose as well as journal editors to screen for and minimise potential bias. Accurate and complete disclosures may improve author transparency and public trust, but a more comprehensive approach involving public effort, policy change, and institutional support may be needed to address the underlying issues of COIs.
What are the limitations of this dataset? How globally applicable is it?
This work had several limitations. The prevalence of positive COIs in IR was estimated from a single volume of a single IR journal, which reflects only a fraction of a broader body of IR literature. COI disclosures may vary over time and across different journals. The assessment of agreement between disclosed financial relationships and open payment data was limited to studies published after the enactment of the Sunshine Act in August 2013. Since non-domestic financial data are difficult to obtain, only those of US authors were analysed. These all limit the generalisability and external validity of the results, particularly in the global arena.
How do you propose preparing a change?
While relationships between clinicians and industry can have many positive effects, these relationships nevertheless do create a risk of bias that must be mitigated to support the integrity of research. Our collective efforts are necessary to better understand how best to encourage disclosure and reduce bias without stifling innovation, a hallmark of our specialty.
Endologix has completed enrolment in the TORUS 2 investigational device exemption (IDE) clinical study in the USA, a press release reports.
The TORUS 2 study is a prospective, single-arm trial of 188 patients to evaluate safety and effectiveness of the Torus stent graft system in the treatment of peripheral arterial disease (PAD) in the superficial femoral artery (SFA) and proximal popliteal arteries.
The study is led by national co-principal investigators Peter Schneider, professor of surgery, Division of Vascular and Endovascular Surgery at University of California San Francisco (San Francisco, USA), and Ehrin Armstrong, medical director, Adventist Heart and Vascular Institute at Adventist Health St Helena (St Helena, USA). “The development of a new self-expanding covered stent for treatment of the SFA and proximal popliteal arteries represents an important advancement in optimal endovascular therapy of complex lesions,” said Armstrong.
“We especially appreciate the strong efforts of our clinical trial sites to enrol this trial efficiently and with high quality. This is the first time in years that a new and specifically designed stent graft for the femoral-popliteal segment is being evaluated for clinical utility,” said Schneider.
“The completion of enrolment for TORUS 2 is a significant milestone in a clinically challenging area of vascular disease,” said Matt Thompson, president and CEO of Endologix. “The TORUS stent graft is also a pivotal component of the Detour procedure, a totally percutaneous femoropopliteal bypass, currently under clinical investigation. Both systems continue our commitment to expanding the Endologix portfolio of innovative devices and supporting clinical evidence.”
Shockwave Medical has announced the start of the Disrupt BTK II postmarket study to assess the safety, effectiveness and optimal clinical use of the Shockwave peripheral intravascular lithotripsy (IVL) system for the treatment of calcified peripheral lesions below the knee (BTK), including some of the most challenging patients with chronic limb-threatening ischaemia (CLTI).
Disrupt BTK II is a postmarket, prospective, multicentre, single-arm study led by Ehrin Armstrong, medical director and interventional cardiologist, Adventist Heart & Vascular Institute (St Helena, USA), and Venita Chandra, vascular surgeon and clinical associate professor, Division of Vascular Surgery, Stanford Health Care (Stanford, USA). The study is expected to enrol 250 patients across 40 sites globally that will be followed for two years to assess the long-term durability of IVL in this difficult-to-treat patient population. The first Disrupt BTK II patient was enrolled at Midwest Cardiovascular Research Foundation (Davenport, USA) by Nicolas Shammas.
“Patients with severely calcified, diffuse below-the-knee disease, and especially those with CLTI, are often in severe pain with limited treatment options to achieve adequate arterial revascularisation. The unmet clinical need for this population is extremely high,” said Armstrong. “Disrupt BTK II will further evaluate how IVL may be optimally used to treat patients who have historically been excluded from most endovascular treatment trials.”
The primary effectiveness endpoint of Disrupt BTK II is procedural success, defined as ≤50% residual stenosis for all treated target lesions without serious angiographic complications (flow-limiting dissection, perforation, distal embolisation, or acute vessel closure), as assessed by an independent angiographic core lab. The study will assess the absence of major adverse limb events (MALE) within 30 days of the index procedure as a primary safety endpoint.
“More and more patients with CLTI also present with end-stage renal disease, advanced diabetes, or other comorbidities that impact their overall health and our ability to effectively treat their CLTI,” said Chandra. “We already know that IVL can reduce significant dissection as well as reduce the need for provisional stenting over conventional PTA [percutaneous transluminal angioplasty] in peripheral vessel beds, but what makes Disrupt BTK II even more exciting is that we are now isolating the treatment effect to get a clearer picture about what role IVL can offer as a definitive therapy for these very complex patients.”
October’s top 10 features an interview with Maureen Kohi (Chapel Hill, USA), the chair and professor of Radiology (University of North Carolina), and the chief of Interventional Radiology (University of California, San Francisco, USA). The US Food and Drug Administration (FDA) granted Varian breakthrough device designation for its Embozene microspheres for genicular artery embolization (GAE), which has attracted many readers, as has issue 83 of Interventional News.
“I strongly believe that you cannot be what you cannot see. If you want more women or under-represented minorities (URMs) to enter the field and be at the table, then we need more women and URM leaders in the field,” Maureen Kohi (Chapel Hill, USA).
Varian, a Siemens Healthineers company, announced that the US Food and Drug Administration (FDA) has granted the company breakthrough device designation for its Embozene microspheres for genicular artery embolization (GAE) for symptomatic knee osteoarthritis.
Results of the randomised, prospective, multicentre STEP trial show that the FemoSeal vascular closure system (Terumo) is superior to the Perclose ProGlide suture-mediated closure system (Abbott) in peripheral arterial disease (PAD) patients in terms of technical success using a retrograde femoral puncture. Bahaa Nasr (Brest University Hospital, Brest, France) presented the late-breaking data at Paris Vascular Insights (PVI) 2021 (21–23 October, Paris, France), concluding that FemoSeal should be used in PAD patients undergoing lower limb arterial endovascular treatment, especially if they are discharged on the same day as their surgery.
One-year results presented at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA) from the EMINENT trial demonstrated the superiority of the Eluvia drug-eluting stent (DES) system (Boston Scientific) compared to self-expanding bare metal stents for the treatment of patients with peripheral arterial disease (PAD) with superficial femoral artery (SFA) or popliteal artery lesions up to 210mm in length, the principal investigator (PI) said. The study enrolled 775 patients, making it the largest randomised trial of a DES for the treatment of PAD to date, Boston Scientific said in a press release.
Rethink fistula creation and maintenance with Tobias Steinke, Ounali Jaffer, Panagiotis Kitrou and Robert Jones in this four-page advertorial.
This advertorial is ONLY available to read in selected countries and geographies. This advertorial, sponsored by BD, is intended for readers in the EMEA region only.
In the wake of the COVID-19 pandemic, the world of education went virtual. John Rundback (Advanced Interventional & Vascular Services LLP and American Endovascular & Amputation Prevention PC in Clifton, USA), who has been involved in interventional device education for more than 25 years, believes virtual procedural training is here to stay. In this interview, Rundback details how procedural training has adapted and is thriving in its new digital setting, with available systems offering increasingly immersive learning environments available to an international cohort of students. He also predicts an 80:20 split between virtual and in-person training in the future.
Is target lesion revascularisation (TLR) a meaningful clinical endpoint for research or should it be “tossed as a legitimate endpoint for peripheral vascular disease treatment success in US FDA [Food and Drug Administration] approval trials?” Recent keynote presentations and conference debate on appropriate care for peripheral vascular disease leave overuse of interventional therapy, particularly for claudication, staring down the end of a barrel. They also trigger a conversation around TLR becoming a target in and of itself.
Sirtex Medical (Sirtex) has announced that the first procedure of selective internal radiation therapy (SIRT) using SIRSpheres Y-90 resin microspheres in China was successfully performed for a patient with hepatocellular carcinoma (HCC) on 28 September 2021. The milestone was reached with the support of Sirtex shareholder China Grand Pharmaceutical and Healthcare Holdings Limited.
Cryoablation is effective for local tumour control in patients with pulmonary metastatic disease. Within the ECLIPSE study, cryoablation had no significant impact on the patient’s quality of life (QoL), with the patient disease-specific survival rate remaining higher than the overall survival rate at both three and five years of follow-up.
Avinger recently announced that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for a new clinical indication for the Pantheris image-guided atherectomy system. This clearance allows the company to directly market Pantheris for the treatment of in-stent restenosis (ISR) in the lower extremity arteries.
“We are excited to receive FDA clearance for the ISR indication, which expands our addressable market for Pantheris to include a high-incidence disease state for which there are few available indicated treatment options,” commented Jeff Soinski, Avinger’s president and CEO. “Pantheris is now the only directional atherectomy device to have a clinical indication for the treatment of in-stent restenosis, providing a compelling new point of differentiation for the device. By combining real-time intravascular imaging with the precise control and large luminal gain of directional atherectomy, Pantheris enables physicians to visualise stent struts and safely target ISR lesions to restore blood flow to occluded vessels, while avoiding the structure of the previously implanted stent.”
To support the 510(k) submission with the FDA, Avinger provided data generated from the INSIGHT trial, a prospective, global, single-arm, multicentre study to evaluate the safety and effectiveness of Pantheris for treating in-stent restenosis in lower extremity arteries. Sean Janzer, an interventional cardiologist at Albert Einstein Medical Center in Philadelphia, USA, and Glen Schwartzberg, a vascular surgeon in Baton Rouge, USA, served as co-principal investigators of the study. The clinical data from INSIGHT was presented at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA) by Jon George, an interventional cardiologist at University of Pennsylvania Health System in Philadelphia, USA, and were also presented at the 2021 VEITH Symposium (16–20 November, Orlando, USA) by Todd Vogel, chief of cardiovascular surgery at University of Missouri Health in Columbia, USA.
“The Pantheris system’s combination of onboard image guidance and a directional excision mechanism provides significant clinical advantages in treating in-stent restenosis not available with any other therapy,” noted Schwartzberg. “This technology allows the operator to target only the blockage and maximise the channel for restored blood flow while avoiding negative interactions with clearly delineated stent struts. Based on the results of the INSIGHT study and my personal experience with the device, I believe that Pantheris can help physicians safely and effectively treat many ISR patients that previously may not have had other options available and reduce the need for repeat interventions and more invasive surgeries.”
According to a press release, Avinger’s proprietary Lumivascular technology allows physicians, for the first time ever, to see from inside the artery during an atherectomy or chronic total occlusion (CTO) crossing procedure by using optical coherence tomography (OCT) that is displayed on Avinger’s Lightbox console.
Physicians performing atherectomy or crossing CTOs with other devices must rely solely on X-ray and tactile feedback to guide their interventions while treating complicated arterial disease. With the Lumivascular approach, the press release continues, physicians can more accurately navigate their devices and treat peripheral arterial disease (PAD) lesions, due to real-time OCT images generated from inside the artery, without exposing healthcare workers and patients to the negative effects of ionising radiation.
After COP26, it is time for the interventional radiology world to congregate in Glasgow, UK. Diversity, veterinary interventions, sun tan, or single malt–everyone has their own reasons to head there.
Hear from Alex Barnacle (London; British Society for Interventional Radiology [BSIR] communications chair), Peter Littler (Newcastle; the 2021 Scientific Programme Committee chair), Ian McCafferty (Birmingham; current BSIR president) and Phil Haslam (Newcastle; incoming BSIR president) about what they are most looking forward to at this year’s meeting.
The confirmatory EVAS2 clinical study to evaluate the safety and effectiveness of Endologix‘s Nellix endovascular aneurysm sealing system (EVAS) for the treatment of infrarenal abdominal aortic aneurysms (AAAs) contains positive two-year follow-up data, the leading investigator has revealed.
A first study update was presented by principal investigator Jeffrey Carpenter, chairman and chief of the Department of Surgery at Cooper University Health Care in Camden, USA, at the 2021 VEITHsymposium (16–20 November, Orlando, USA).
Carpenter told delegates data from two years of follow-up of patients treated with the EVAS device demonstrate 92% freedom from all-cause mortality, 100% freedom from migration, 100% freedom from saccular enlargement, 98% freedom from type Ia endoleaks, and 98% freedom from type II endoleaks. “We are only at two years of good follow-up,” Carpenter said, explaining that this was the point at which “the signal of problems” emerged in EVAS1. However, he said the study investigators were hopeful of success in the current study as they continue to follow study participants, with data “holding up.”
Carpenter explained that at two years of follow-up in the device’s pivotal investigational device exemption (IDE) trial, “there was a signal of migration and a signal of aneurysm enlargement development.” A root-cause analysis found that thrombus “was playing a big role” in the case of migration, he told VEITH 2021 attendees. Regarding aneurysm enlargement, Carpenter continued, “we were originally employing what turns out to be a plug,” under an understanding that they only needed to fill the aneurysmal portion of the aorta with polymer—but not the seal zones, or “firewalls.” Adjustments were made, resulting in “a revision of the instructions for use (IFU) to make sure that there was able to be sufficient polymer placed into the aneurysm sac to stabilise the stents and that we had good seal zones proximally and distally,” he said.
In 2019, Endologix issued a voluntary recall for the EVAS system in order to ensure optimal patient outcomes through the most appropriate use of the device, with the company noting that it had determined off-label use was occurring at “an unacceptable level, with the consequence of suboptimal results.”
The 333 patients in EVAS1 retrospectively yielded the device IFU, Carpenter explained. Those in this group treated on-label experienced 97% freedom from migration, he added. EVAS2 consists of 92 patients and is an IDE prospective, multicentre, single-arm study with consecutive, eligible subject enrolment at each site. Participants are being followed at 30 days (primary safety endpoint), six months, one year (primary effectiveness endpoint) and annually thereafter out to five years (total follow-up commitment).
Summarising the EVAS2 data delivered at VEITH 2021, Carpenter concluded: “Active sac management of EVAS has shown good freedom from type II endoleak and freedom from all-cause and cardiovascular mortality in all quartiles. Clearly, a second-generation Nellix device is necessary if this is going to be an everyday infrarenal aneurysm repair device.” Data regarding five-year freedom from major adverse events are “encouraging,” he added.
The Society of Interventional Oncology (SIO) has announced the launch of the society’s first clinical trial—Ablation with confirmation of colorectal liver metastases (ACCLAIM) prospective trial for microwave ablation as a local cure. An SIO press release details that this multi-million-dollar trial is funded collectively through grants from Boston Scientific Corporation, NeuWave Medical (part of Ethicon), and Varian, a Siemens Healthineers company.
In this prospective, multicentre, international trial SIO proposes to establish microwave ablation as the preferred treatment option for selected colorectal liver metastases that can be ablated with sufficient margins. The study will be the first global, prospective trial to use an objective and reproducible technical outcome in its study design, which SIO believes will drive important changes to future treatment guidelines. The study will incorporate software to assess the ablation zone and margins and determine if achieving complete margins during an ablation equates to procedural success, where the primary outcome is local disease progression at two-years post-ablation.
Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA) is the principal investigator for the study. “The ACCLAIM trial could impact patient guidelines with regards to the role of ablation as a treatment option for CRC [colorectal cancer] liver metastases. The study is expected to raise the bar for the standard of care, establishing a reproducible method of achieving tumour ablation with local control,” said Sofocleous. “Clinical research is essential for the continued progress of interventional oncology and SIO will continue to drive such important and focused research efforts.”
Despite a favourable safety profile, historically, the inconsistent local tumour progression (LTP) rates after thermal ablation when compared to surgery have limited the widespread adoption of this treatment option in patients with metastatic colorectal cancer to the liver. Suboptimal outcomes and LTP have been attributed to insufficient coverage of the tumour by the ablation zone (tumour and margins). The ACCLAIM study will estimate disease-free survival of colorectal liver metastases treated with MWA incorporating 3D ablation margin confirmation intraoperatively and through a subsequent independent review centralised validation process.
Matthew Callstrom, professor and department chair of radiology at Mayo Clinic (Rochester, USA) is president of the SIO. “It is important to drive what we do as a field forward together, and it takes collaboration and long-term relationships with our industry partners to enable the right studies to be successful,” said Callstrom. “The ACCLAIM industry partners are raising the bar for research investment by making an important commitment to support societies like SIO. Together, we are advancing our vision to establish interventional oncology as the fourth pillar of cancer therapy.”
Participants of the ACCLAIM trial will be patients with a diagnosis of colorectal cancer liver metastases. MWA will be performed using a US Food and Drug Administration (FDA)-cleared, commercially available MWA system and using margin confirmation (visualisation) software. The ACCLAIM study is set to launch in 2022 with an expected three-year enrolment period of 275 participants across sites in the USA and Europe.
XACT Robotics has announced plans to present oral and virtual presentations at the Radiology Society of North America (RSNA 2021, 28 November–2 December, Chicago, USA and virtual) that showcase clinical findings and case studies from leading radiology centres.
Sebastian Flacke (Lahey Hospital and Medical Center, Burlington, USA) will present new data from a multicentre study using the XACT ACE robotic system during percutaneous procedures. His presentation, “Feasibility and accuracy of a hands-free robotic system for CT [computed tomography]-guided percutaneous needle insertion and steering,” will be held on 29 November at 3pm CST.
In a second poster presentation, Gerald Grubbs (Sarasota Interventional Radiology (SIR), Sarasota, USA) will highlight recent clinical experience with the XACT ACE robotic system. His presentation, “Real world use of a hands-free robotic system for percutaneous procedures,” will be held virtually. On-demand access can be obtained by registering through the virtual meeting with RSNA.
RSNA 2021 will also serve as the venue where, for the first time, the company will introduce ACE Xtend, which enables remote activation of the XACT ACE robotic system for CT-guided percutaneous procedures. According to a press release from XACT Robotics, the system’s new capabilities will allow providers to enable precise robotic insertion and non-linear steering of various instruments from outside the procedure room. This, the company claims, will make the procedure more efficient and improve overall safety by reducing the risk of exposure to radiation and other harmful pathogens.
The XACT ACE robotic system features non-linear steering to combine advanced image-based planning and real-time, the company said.
The system received US Food and Drug Administration (FDA) clearance for use during CT-guided percutaneous procedures, as well as CE mark, and commenced commercialisation in October 2020.
The company will showcase the XACT ACE robotic system, including its new ACE Xtend, at the booth (#1557) throughout the RSNA meeting, and at a virtual product theatre on Monday 29 November at 4pm CST.
The UNC Department of Radiology (Chapel Hill, USA) recently named Gloria Salazar, as the department’s next division chief of vascular and interventional radiology (VIR).
Following selection from a competitive pool of candidates nationwide, Salazar began leading the VIR division as an associate professor of radiology in October 2021.
Salazar was recruited to Massachusetts General Hospital (MGH)’s Department of Radiology (Boston, USA) in 2008 as an assistant radiologist, following three years of clinical research and advanced clinical interventional radiology (IR) fellowship training at Beth Israel Deaconess Medical Center in Boston, USA. With over twelve years at MGH, she has built an institutional leadership record, major roles including outpatient IR medical director, Waltham Vein Center (Boston, USA) medical director, fibroids programme co-director, simulation and patient experience officer, and Department of Radiology quality and safety chair.
Salazar is established as a women’s health advocate, subspecialty expert, and practitioner volunteer to the underserved. In collaboration with MGH’s Obstetrics and Gynaecology Department, she co-developed the institution’s programme for fibroids to create a multidisciplinary clinic that improves patient-centred care and informed decision-making for women seeking treatment for fibroids. Her strong belief in outreach to underserved populations led Salazar to join MGH’s Spanish language care medical group during the 2020 COVID-19 pandemic surge to deliver volunteer care to COVID-19 non-English speaking patients. She also served as a faculty proctor and invited speaker at the inaugural Society of Interventional Radiology (SIR) Giveback Program (2019, El Salvador). This programme aims to expand options in minimally invasive procedures in Latin American countries to help underserved women avoid hysterectomies.
As a scholar, Salazar is routinely invited to speak worldwide at conferences and symposia on wide-ranging topics in IR, including quality assurance, procedural treatment, practice quality improvement (IR/general radiology), the value of simulation, and women’s health. She has co-authored multiple publications and book chapters and served as principal investigator (PI) or co-PI of multiple clinical trials and has a strong collaborative record with industry partners in her subspecialty. She is additionally an active SIR member, having served in major leadership roles including:
1) SIR Women’s Health Service line chair
2) SIR Diversity and Inclusion (D&I) advisory board member
3) SIR International Exchange committee member.
Maureen Kohi, UNC Radiology Department chair, noted: “I am confident that Salazar’s exceptional clinical acumen, her national and international reputation as a VIR leader, and her commitment to research and education will continue to elevate our outstanding VIR Division.”
UNC Department of Radiology thanks interim Charles Burke, VIR division chief, UNC Radiology Department, for his dedication and service within the VIR Division and across the department.
Viz.ai has announced the US commercial launch of its AI-powered modules for pulmonary embolism and aortic disease. Debuting at VEITHsymposium 2021 (16–20 November, Orlando, USA), the new modules allow for faster clinical decision making and improved care coordination for patients suffering from these two life-threatening conditions, a press release details.
The new modules leverage advanced deep learning to communicate time-sensitive information, including advanced imaging studies and real time clinical information, to specialists who can more quickly and easily make treatment decisions for the patient, the press release continues. Users can access all aortic and pulmonary imaging from the cloud.
“This technology has changed the way we triage and treat stroke patients, dramatically improving their care,” said Richard Saxon, interventional radiologist at Tri-City and Palomar Health, San Marcos, USA. “In a similar fashion, I believe the Viz.ai PE and Aortic modules will enhance image interpretation with AI [artificial intelligence], dramatically improve the quality and speed of mobile image viewing, and improve caregiver communication. This is truly the care coordination of the future.”
According to Viz.ai, the company has accelerated the time-to-notification of the treatment team by 73% and time-to-treatment by 24%.
“The launch of these two new modules brings the power of the Viz platform to a vast new faction of medical professionals and patients battling life-threatening conditions,” said Chris Mansi, Viz.ai CEO and cofounder. “This is a significant milestone in our mission to fundamentally improve how healthcare is delivered in the world.”
Viz.ai will be showcasing the new AI-powered PE and aortic disease modules at VEITHsymposium Booth #317.
In a pooled analysis of the predictors of drug-coated balloon (DCB) effectiveness, the IN.PACT Admiral DCB (Medtronic) performed well across a broad range of clinical, anatomical, and procedural scenarios. This is according to Prakash Krishnan (Mount Sinai Hospital, New York, USA), who presented key findings of the investigation in a featured clinical research session at Transcatheter Cardiovascular Therapeutics (TCT) 2021 (4–6 November, Orlando, USA).
The analysis combined data from 557 patients treated with DCBs in the IN.PACT superficial femoral artery (SFA) randomised controlled trial (RCT), the IN.PACT Japan RCT and the prespecified long lesion and chronic total occlusion imaging cohorts of the IN.PACT Global study.
The objective of this pooled IN.PACT analysis was to examine the factors contributing to 12-month effectiveness outcomes when DCBs are used for the treatment of femoropopliteal disease. While several studies have evaluated the predictors of DCB efficacy in smaller populations, Medtronic claims that the IN.PACT analysis is the first large-scale collaborative effort to evaluate a broad set of clinical, anatomical and procedural factors using rigorous, core-laboratory-adjudicated data.
Krishnan informed the TCT audience that only residual stenosis >30%, Rutherford category >3, and smaller preprocedure reference vessel diameter were significant multivariable predictors of decreased DCB effectiveness.
He also stressed the importance of vessel preparation, noting that patients with postprocedure residual stenosis <30% had a 4.7-fold higher risk of clinically-driven target lesion revascularisation (CD-TLR; hazard ratio [HR], 5.67; 95% confidence interval [CI], 2.32–13.85) and a 1.7-fold higher risk of binary restenosis (HR, 2.73; 95% CI, 1.6–4.65 through 12-month follow-up compared to patients who had residual stenosis ≤30%.
Other key findings included the following:
Rutherford category >3 was associated with a significantly increased risk of CD-TLR (HR, 4.19; 95% CI, 1.68–10.46) while smaller preprocedure reference vessel diameter was associated with a higher risk of binary restenosis (HR, 1.57; 95% CI; 1.01–2.46) through 12-month follow-up
Longer lesion length, severe calcification, and total occlusion were not statistically significant predictors of DCB outcomes in this multivariate analysis
In his presentation, Krishnan concluded that DCBs work well across a wide range of clinical and anatomical scenarios, adding that patency can be optimised by procedural factors under the operators control, specifically, achieving a postprocedural residual stenosis <30%.
A pilot study, published in the Journal of Cancer Therapy, reveals that percutaneous cryoablation of early-stage, low-risk breast cancer tumours smaller than 15mm presents a potential substitute for lumpectomy.
Investigators, Hinsanoro Kawamoto (Department of Breast Surgery, Breast and Imaging Center, StMarianna) and colleagues report “encouraging short- to mid-term oncology results with good cosmesis outcomes” for the procedure.
They highlight that patients would be able to benefit from local anaesthesia in an outpatient setting and a shorter recovery period.
The pilot study enrolled eight patients and set out to evaluate the feasibility, safety, and cosmetic outcomes of percutaneous cryoablation of breast intraductal carcinoma lesions, as well as post-cryoablation magnetic resonance imaging (MRI) as a follow-up tool for detection of residual malignancies and local recurrences.
“We are excited to see the publication of these data from an independent study which further supports the use of our ProSense cryoablation system to eliminate small malignant lesions in the breast instead of performing breast surgery under general anaesthesia,” commented Eyal Shamir, chief executive officer of IceCure.
A press release from the company states: “The independent study conducted at the St Marianna University Breast and Imaging Center enrolled eight women, 53–72 years of age. Percutaneous ultrasound-guided cryoablation of the breast tumour was performed using IceCure’s ProSense, under local anaesthesia without the need for subsequent resection. The procedure lasted for 40 minutes on average. All patients received radiation and endocrine therapies. The patients were followed using vacuum-assisted biopsy (VAB), mammography (MG), MRI, and Moiré Topography for cosmetic outcomes.”
In September 2021, IceCure announced an Annals of Surgical Oncology publication authored by Richard Fine (West Comprehensive Breast Center, Germantown, USA) and colleagues. The article reported results previously announced at the American Society of Breast Surgeons Annual Meeting, that at a mean of 34.83 months following treatment with the ProSense cryoablation system, only 2.06% (four of 194 patients) experienced cancer recurrence.
The ICE3 trial commenced in 2014 and was conducted at 19 US hospitals, including Columbia University Medical Center and Mount Sinai Beth, Isarel. The trial enrolled and treated 194 patients (average age of 75) with low-risk, early-stage breast cancer tumours measuring up to 1.5cm.
Fine and colleagues conclude: “Breast cryoablation presents a promising alternative to surgery while offering the benefits of a minimally-invasive procedure with minimal risks.” Fine stated that “the three-year ICE3 trial results highlighting the efficacy and safety of the procedure in this patient group are extremely promising for breast cryoablation. Being able to provide a minimally-invasive option for treating appropriate low-risk patients represents a dramatic improvement in care. The procedure is quick, painless and can be delivered with local anaesthesia in doctors’ offices, with minimal recovery time and excellent cosmetic outcomes.”
Rapid Medical today announced US Food and Drug Administration (FDA) investigational device exemption (IDE) approval for what it claims is the first-ever trial to expand interventional stroke treatment to distal regions of the brain.
The DISTALS study is a pivotal, international, multicentre, randomised controlled trial (RCT) to evaluate the safety and effectiveness of distal thrombectomy. This new frontier for ischaemic stroke has been created by Rapid Medical’s development of TIGERTRIEVER 13—the smallest available thrombectomy device—according to a company press release.
“We are especially pleased to receive unprecedented FDA IDE approval for a study with DISTALS focus,” said Jeffrey Saver, professor of neurology and director of the Comprehensive Stroke and Vascular Neurology Program at the University of California Los Angeles (UCLA) in Los Angeles, USA, and the study’s principal investigator. “With the ever-growing benefits of mechanical thrombectomy, we hope to offer better recoveries to a much broader patient population. Rapid Medical has been at the forefront of enabling that progress.”
Currently, less than 10% of ischaemic stroke patients receive mechanical thrombectomy, a well-proven treatment that significantly improves patient outcomes, the release continues. While Rapid Medical’s TIGERTRIEVER 13 has already been used to treat nearly 1,500 patients in Europe and the Middle East, the DISTALS study aims to extend these benefits to an additional 25–40% of stroke patients. It focuses on far territories in the brain, such as M3 blood vessels, and allows intervention within 24 hours from symptoms onset.
“The DISTALS trial is critical for the field of interventional stroke therapy,” said David Fiorella, director of the Cerebrovascular Center at Stony Brook University Medical Center in Stony Brook, USA, and co-coordinating investigator. “It potentially allows us to offer thrombectomy to an additional large group of stroke patients who may benefit substantially.”
The leading investigators of the DISTALS study also include René Chapot, professor and department head of neuroradiology and radiology at Alfried Krupp Krankenhaus in Essen, Germany and Rishi Gupta, director of Neurocritical Care at Wellstar Health System in Marietta, USA. Rapid Medical plans to start the study in Q4 2021 or early in Q1 2022—according to the company’s co-founder and CEO Ronen Eckhouse.
Endologix has announced the appointment of Matthew Thompson as president and chief executive officer. Thompson will also join Endologix’s board of directors. Richard Mott, who previously held the CEO position on an interim basis, will return to his role as executive chairman of the board of directors.
Thompson has been serving as Endologix’s chief medical officer since 2016, and, in that capacity, had oversight of the company’s business development, medical affairs, regulatory, clinical and R&D departments. Thompson also led the April 2021 acquisition and subsequent integration of PQ Bypass. He is a contract staff surgeon in the Department of Vascular Surgery, Heart, Vascular and Thoracic Institute at the Cleveland Clinic Foundation Ohio and visiting professor at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University in Cleveland, USA. Previously he was the professor of vascular surgery at St George’s, University of London and a consultant vascular Surgeon at St George’s Vascular Institute in London, UK.
“I have had the pleasure of working side by side with Matt over the past year and have the utmost confidence in his ability to lead Endologix through this transformative period. Matt embodies the fusion of the entrepreneurial vision and subject matter expertise that we need to successfully accelerate Endologix as a leader in the development and commercialisation of the most innovative devices for the treatment of vascular disease,” said Mott.
“I have been extremely impressed with Matt’s leadership of major company initiatives, including the PQ Bypass acquisition and integration, and the AFX FDA [US Food and Drug Administration] advisory panel meeting, as well as his leadership of major functions within the company,” noted Andrew El Bardissi, Deerfield partner and member of the Endologix board of directors. “I am confident in Matt’s ability to step into the CEO role and guide the company during this important period of growth.”
“I am excited about the opportunity to lead such a dynamic and innovative organisation. I look forward to continuing my close relationship with Rich, the board, and the talented and dedicated team of employees that I have worked so closely with over the past several years,” said Thompson. “I will be completely committed to our physician customers and to the safety and health of their patients, as we continue to work collaboratively with the FDA and other global regulatory agencies to ensure we maintain the highest standards possible. In the next year, we will continue to drive market share gains with our family of AAA [abdominal aortic aneurysm] products and prepare our regulatory submissions for our innovative long-lesion PAD [peripheral arterial disease] products being developed after our acquisition of PQ Bypass earlier this year.”
XACT Robotics today announced what it describes as the world’s first remote-controlled robotic instrument insertion and non-linear steering during an interventional oncology percutaneous procedure with ACE Xtend.
ACE Xtend is the remote-control feature of the XACT ACE robotic system, which the company claims is the “world’s first and only” comprehensive robotic system that integrates image-guided planning and real-time monitoring with precise robotic insertion and non-linear steering to deliver various instruments to a desired target in the body. The procedure using the XACT ACE robotic system with ACE Xtend was successfully completed by the interventional radiology team at Sarasota Interventional Radiology in Sarasota, USA.
“We are very excited about the addition of remote capabilities with ACE Xtend, that can improve workflows, allow us to perform more procedures, and better support our patients and staff,” said Gerald Grubbs (Sarasota Interventional Radiology, Sarasota, USA). “The ability for our interventional radiology team to perform procedures without having to enter the procedure room also increases overall safety by reducing the risk of exposure to radiation and other harmful pathogens.”
In a press release, XACT Robotics said that the XACT ACE system’s features have been proven in over 200 clinical and pre-clinical cases to improve tip-to-target accuracy, efficiency, and consistency in interventional percutaneous procedures. With the addition of ACE Xtend, users can now reduce their exposure to harmful radiation and pathogens by controlling the XACT ACE robotic system from the control room, the company said.
“We are proud to announce this historic event as it shows our commitment to advancing care in interventional percutaneous procedures, and to deliver better outcomes to patients across the world,” said Harel Gadot (founder, executive chairman, and president of XACT Robotics). “With the ability to control the XACT ACE robotic system from outside the imaging suite, we make the procedure more efficient and as such allow more patients to be treated.”
Topping the agenda are the use of drug-coated balloon technology to maintain and treat stenosis in the dialysis access circuit (“the results of at least four large, randomised trials are phenomenally different”); the place for percutaneous arteriovenous fistula creation (“is it ready for prime time?”) and safety and quality in the provision of dialysis access (“who is watching?”). And, they will all come under the scanner at CiDA.
The Ellipsys vascular access system (Avenu Medical/Medtronic) can be used to easily and safely create durable percutaneous arteriovenous fistulas (pAVFs) for haemodialysis—with new, long-term data suggesting it offers an “excellent alternative” to AVF creation via surgical procedures in end-stage renal disease (ESRD) patients. That is according to Jeffrey Hull, an interventional radiologist and director of the Richmond Vascular Institute in Richmond, USA, who presented five-year results from the Ellipsys US pivotal trial at this year’s American Society of Nephrology (ASN) Kidney Week (2–7 November 2021, virtual).
And, speaking to Renal Interventions shortly after this event regarding the role endovascular AVFs now play within access creation strategies, Hull stated: “Once you get past the wrist issue, I would say it could be percutaneous fistula first. If you are a candidate for a fistula, but not a great wrist fistula candidate, then maybe the first possible fistula that should be considered for you is a percutaneous fistula—and I think the data are promising enough to support this.”
Hull began his ASN Kidney Week presentation by briefly demonstrating the procedure through which a proximal radial artery fistula is created using the Ellipsys system—noting the application of pressure and heat to “weld” the target vein and proximal radial artery together. This differs from more traditional, surgical procedures in which suturing is used to create the anastomosis between these vessels, he added. Hull also noted that balloon dilatation is commonly used to relieve spasm in the anastomosis shortly after the procedure.
He went on to provide the audience with an overview of the Ellipsys US pivotal trial, a prospective, multicentre, single-arm study intended to evaluate the safety and effectiveness of AVF creation using the Ellipsys device. It involved a total of 107 patients treated across five outpatient, office-based labs, he reported, adding that—aside from the fact 76 (71%) of these patients were male—the baseline characteristics of these patients were “typical of those seen in dialysis patient populations”, with a mean age of 56.6 years and an obesity prevalence of 50%.
Moving on to discuss one-year data from this trial, Hull reported a technical success rate of 95% (102/107 patients) and a clinical success rate of 95% (98/103 patients), with an average procedure time of 24 minutes also being observed. He added that the target vein was the cephalic vein in the majority of cases (74%), followed by the basilic (24%) and brachial (2%) veins. Discussing methods used to increase blood flow through the anastomoses created in the trial—referred to as maturation procedures—Hull noted that percutaneous transluminal angioplasty (PTA) proximal to the fistula was used in 72% of cases, while branch (35%) and deep (32%) embolisation, cubital vein ligation (31%) and transposition (26%) were also deployed.
Hull then noted that, at one-year follow-up, fistula-related events including thrombosis, stenosis, cannulation-related injuries or difficulties, and steal syndrome, generally looked “very similar” to those seen in surgically created fistulas—something that he stated was “a little disappointing” at that stage. He did add, however, that the Ellipsys US pivotal trial met its primary efficacy endpoint, as 86% (92/107) of fistulas were mature at 90 days, and met its primary safety endpoint, due to there being no serious, device-related adverse events.
Discussing the crux of his ASN Kidney Week presentation, Hull reported that a total of 85 patients were eligible for further follow-up at one year and the trial’s investigators continued to follow up these patients out to five years. Regarding the first of several long-term endpoints—fistula use, assessed by two-needle cannulation—Hull told the audience that 92% (83/90) of these fistulas were used in patients requiring dialysis, describing this as “an excellent outcome” that compares favourably to the 63% rate of two-needle cannulation observed in US patients with surgically created fistulas. He further noted that fistula non-use was low, with 11 of the 24 patients whose percutaneous fistula was unused ultimately not requiring haemodialysis.
Outlining access complications through five years, Hull said 27 patients experienced complications including fistula dysfunction (21.2%), cannulation injury (12.9%), thrombosis (5.9%) and arm swelling (4.7%)—with these being typical of those seen in dialysis patient populations. A total of 91 additional procedures were performed to rectify these issues, he stated, with the most commonly observed types being balloon dilatation (n=71) and thrombectomy (n=12), followed by stent grafting (n=6) and surgical repair (n=4).
Hull also noted, regarding additional procedures per patient per year in the US pivotal trial, that this figure (2.66) was similar to those associated with surgically created fistulas at one year, but that in years two through five a “drastic reduction” in additional procedures per patient per year—ranging from 0.18 to 0.57—was observed. “We attribute that to the low-to-moderate flow in these [percutaneously created] fistulas, averaging 1,000ml per minute, and also the multi-outflow feature of these fistulas whereby, if an injury occurs, the blood will flow around it and keep the fistula operational until it can be repaired,” he reported.
Touching on the final long-term endpoint from the trial, Hull relayed “excellent” primary assisted and secondary patency rates of 74% and 82%, respectively, at five years as per Kaplan Meier estimates, while the functional patency rate was found to be 91.8% through the follow-up period as well. “In summary, this follow-up study has shown us several important things—the first being that high-quality fistulas can be performed by interventional nephrologists,” he concluded. “Secondly, we have expanded the places in which these fistulas can be created, not just in the hospital but now in office-based labs and ambulatory surgery centres too.”
In addition to reiterating the high fistula usage, positive long-term patency outcomes, and low complication rates and subsequent maintenance procedures, seen through five years in the study, Hull ended his presentation by noting that, moving forward, the goal is to reduce the time to two-needle cannulation for the Ellipsys system, with cannulation- and cost-related issues also continuing to be evaluated further.
Royal Philips today announced the results of a new large-scale real-world analysis of Centers for Medicare & Medicaid Services (CMS) data on the health outcomes of peripheral vascular interventions guided by intravascular ultrasound (IVUS).
The study was conducted independently by the Smith Center for Outcomes Research at Beth Israel Deaconess Medical Center (Boston, USA), with the results presented at Transcatheter Cardiovascular Therapeutics (TCT) 2021 (4–6 November, Orlando, USA) by Eric A Secemsky, director of Vascular Intervention and interventional cardiologist at Beth Israel Deaconess Medical Center and assistant professor of Medicine at Harvard Medical School in Boston, USA. The study was supported by Philips.
A press release details that numerous prospective studies have already shown the benefit of IVUS guidance in peripheral vascular interventions, making it a gold-standard imaging modality for this application. The new study results now show that the outcome observations from these prior studies apply directly to a broader patient population and across vascular beds, demonstrating strong support for the use of IVUS during peripheral interventions, the release continues.
“The results of this large-scale study demonstrate favourable long-term outcomes in peripheral vascular interventions when IVUS is used,” said Secemsky. “This analysis, combined with the recent appropriate use consensus on IVUS that was presented at VIVA [Vascular Interventional Advances; 5–7 October, Las Vegas, USA], highlights a clear opportunity to improve health outcomes for millions of patients by broader and more routine implementation of the technology in clinical practice. This is a moment for us to further our efforts in saving lives and saving limbs.”
Peripheral arterial disease (PAD): A 32% reduction in major adverse limb events, including amputations, during lower extremity arterial interventions
The study looked at Medicare beneficiaries aged 65 years or older who underwent lower extremity arterial interventions between 1 January 2016 and 31 December 2019. Among 697,794 interventions, the investigators found a 32% reduction in major adverse limb events, such as amputations, over a median 425 days of follow-up. These findings were consistent across disease states, including chronic limb-threatening ischaemia (CLTI) and non-CLTI, as well as arterial segments such as iliac, femoropopliteal and tibial.
Chronic venous disease (CVD): A31% reduction in repeat intervention, hospitalisation or death during iliofemoral venous stenting
Separately, the investigators examined Medicare beneficiary data for patients treated between 1 January 2017 and 31 December 2019 in multiple clinical settings, including hospital in-patient settings, hospital outpatient centres and private office-based clinics, involving 20,984 individual patients. Of these, 72% underwent stenting guided by IVUS. When IVUS was used, there was a 31% reduction in the composite outcome of repeat intervention, hospitalisation or death. In addition, IVUS use reduced the risk of stent thrombosis, embolisation and stenosis.
“We commend Dr Secemsky and the Smith Center for Outcomes Research for this ongoing study to simplify clinical procedures and improve clinical, economic and patient outcomes,” said Chris Landon, senior vice president and general manager Image Guided Therapy Devices at Philips. “We are committed to supporting evidence-based medical guidelines in pursuit of better patient outcomes. We believe that the ability of IVUS to deliver procedure optimisation and confidence enhances patient and staff experiences and lowers cost of care.”
First-ever global consensus for the appropriate use of IVUS in peripheral vascular disease interventions
In October 2021, a team of clinical experts led by Secemsky established the first-ever global, cross-specialty expert consensus for the appropriate use of IVUS in peripheral vascular disease interventions. This initiative was jointly supported by Philips and Boston Scientific. Today, healthcare providers’ use of IVUS in peripheral vascular disease interventions is not standardised and is therefore inconsistent. The new appropriate-use expert consensus may help establish global standards of care to adopt into guidelines and improve quality of care in peripheral vascular disease, a Philips press release states.
IV stand and monitor (Credit: American Heart Association)
Hispanic adults hospitalised for treatment of symptoms of peripheral arterial disease (PAD) were more likely to access this care by going to the emergency room (ER), and they experienced longer and more expensive hospitalisations than non-Hispanic white patients with PAD, according to preliminary research to be presented at the American Heart Association (AHA) Quality of Care and Outcomes (QCOR) Research Scientific Sessions 2021. The meeting will be held virtually on Monday 15 November 2021 in conjunction with the Association’s Scientific Sessions 2021.
“The Hispanic population is one of the fastest growing ethnic groups in the USA, and prior studies have shown worse outcomes among Hispanic adults with PAD, including higher rates of amputation and fewer revascularisation procedures compared to non-Hispanic white adults with PAD,” said lead study author Kristie Harris, an instructor of Medicine at Yale School of Medicine in New Haven, USA, in a press release from the AHA. “The prevalence of PAD among Hispanic individuals has been difficult to determine because this population often experiences a lack of access to healthcare and is underrepresented in many population-based studies. Our study raises awareness and confirms some of these disparities.”
Harris and her team examined hospital admission data from the 2011–2017 National Inpatient Sample to study differences in the experiences of Hispanic and non-Hispanic white adults treated for PAD symptoms. They investigated whether people sought inpatient PAD care by presenting to the ER or if they came for a planned, elective visit, likely sent by an outpatient care professional.
During the study period, there were 1,018,220 PAD hospitalisations among adults age of 18 years and older in the USA (39% female; 14% Hispanic adults).
The percentage of people who accessed inpatient hospital care via the emergency department increased among both Hispanic adults and non-Hispanic white adults between 2011–2017. The increase was substantial among those who are Hispanic, the AHA press release reports, with the percentage of PAD hospital admissions occurring through the ER jumping from 50% to 70% over the course of the study period.
The researchers found that Hispanic adults with PAD were 80% more likely to access inpatient PAD care by going to the ER for symptoms compared with non-Hispanic white adults hospitalised with PAD. Additionally, Hispanic adults were 12% less likely to undergo elective hospital admissions for PAD.
Among the other findings in the study:
Across all years, 58% of hospital admissions among Hispanic adults began with a visit to the ER, compared with 36.7% for non-Hispanic white adults
The average hospital visit was 4.5 days for Hispanic patients vs. 3.7 days for non-Hispanic white patients, and overall hospital costs were higher, too—US$63,813 vs. US$52,368, respectively
“Our findings reinforce other research that indicates Hispanic individuals often lack a usual source for routine healthcare and frequently defer or avoid care due to costs,” Harris said. “Instead of delaying care, a better way to manage PAD and reduce the risks of future complications is with regular evaluation and follow-up, usually with a primary care doctor or vascular specialist.”
Harris said prevention is key, and as with any other type of cardiovascular disease, people should be encouraged to quit smoking, be physically active and to manage diabetes, high blood pressure or high cholesterol, which all increase the risk for PAD. Individuals who develop pain in their feet or legs with walking not associated with muscle strain should seek medical care early for a comprehensive evaluation.
“This study highlights the importance of better tailoring PAD prevention and management, especially among Hispanic people, which could reduce the need for hospital ER care or hospitalisation,” she said. “Systematic efforts are needed to ensure Hispanic people with PAD have more accessible, affordable and culturally sensitive outpatient care. Efforts should include supports that educate the community regarding the signs and symptoms of PAD and encouragement to seek care early.”
Medtronic has announced its ambition to achieve net zero carbon emissions by fiscal year 2045 across its operations and value chain to accelerate efforts to combat climate change. The announcement comes amidst the 2021 United Nations Climate Change Conference (COP 26), where world leaders are focusing on collectively cutting greenhouse gas (GHG) emissions and limiting global warming to 1.5 degrees Celsius compared to pre-industrial levels.
As published in Medtronic’s new Decarbonization Roadmap, the FY45 milestone builds on the company’s existing goal of reaching carbon neutrality in its operations by fiscal year 2030, to encompass GHG emissions reductions across its entire value chain. To achieve its ambition, Medtronic will pursue setting GHG emission reduction targets across scopes 1, 2, and 3 through the Science-Based Targets Initiative (SBTi) – a multi-year initiative that provides companies a clearly defined path to reduce emissions aligned with the Paris Agreement.
“As a global healthcare technology leader, our goal is to transform industry expectations and behaviour where health and climate change intersect,” said Geoff Martha, Medtronic chairman and chief executive officer. “Our teams across 150 countries are actively working to protect our planet by reducing our energy use, investing in renewables, and now moving toward net zero emissions throughout our operations, supply chain and logistic partners, by pursuing science-based targets.”
Randomised placebo-controlled trials show consistently that renal denervation provides significant reduction in ambulatory and office blood pressure, the findings of a systematic review and meta-analysis suggest.
Findings of the paper, authored by Yousif Ahmad (Yale School of Medicine, Yale University, New Haven) and colleagues, were published in JACC: Cardiovascular Interventionsand presented during an oral abstract session at the Transcatheter Cardiovascular Therapeutics annual meeting (TCT 2021, 4–6 November, Orlando USA and virtual).
In their paper, Ahmad and colleagues note that renal denervation has undergone several blinded placebo-controlled trials, covering the spectrum from patients with drug-resistant hypertension to those not yet taking antihypertensive medication.
The authors performed an updated meta-analysis of randomised placebo-controlled trials of renal denervation and specifically compared the effect of renal denervation in patients taking medications and in those not taking medications. This included latest evidence from the RADIANCE-HTN TRIO trial, presented on the same day at TCT 2021 in a late-breaking trial session.
The study’s primary efficacy outcome was the change in ambulatory systolic blood pressure beyond the effect of the placebo procedure, and analysis was stratified by whether there was background antihypertensive medication use.
Ahmad and colleagues report that there were seven eligible trials, totalling 1,368 patients.
Outlining the results, the study team notes that renal denervation significantly reduced ambulatory systolic (mean difference −3.61mmHg; 95% confidence interval [CI]: -4.89 to -2.33mmHg; p<0.0001), ambulatory diastolic (-1.85mmHg; 95% CI: -2.78 to -0.92mmHg; p<0.0001), office systolic (-5.86mmHg; 95% CI: -7.77 to -3.94mmHg; p<0.0001), and office diastolic (-3.63 mm Hg; 95% CI: -4.77 to -2.50; P < 0.0001) blood pressure.
There was no evidence that the use of concomitant antihypertensive medication had a significant impact on the effect of denervation on any of these endpoints (p-interaction=NS for each comparison).
Ahmad and colleagues conclude that the randomised placebo-controlled trials show “consistently” that renal denervation provides significant reduction in ambulatory and office blood pressure.
“Although the magnitude of benefit, about 4/2mmHg, is modest, it is similar between patients on background antihypertensive medications and those who are not. Denervation could therefore be a useful strategy at various points for patients who are not willing to add antihypertensive agents,” the study’s authors note. “Whether the effect changes with time is currently unknown.”
Six-month outcomes from the randomised RADIANCE-HTN TRIO trial, comparing endovascular ultrasound renal denervation to a sham procedure for treatment-resistant hypertension, demonstrate the additional effects of pharmacologic intervention with maintenance of a blood pressure-lowering effect of renal denervation at six months, according to investigators.
The six-month results were presented during a late-breaking trial session at the Transcatheter Cardiovascular Therapeutics annual meeting (TCT 2021; 4–6 November, Orlando USA and virtual) by Ajay Kirtane (Columbia University Irving Medical Center/NewYork-Presbyterian Hospital, New York, USA). These build upon the presentation of the trial’s two-month findings at the American College of Cardiology’s 70th Annual Scientific Session (ACC.21, 15–17 May, virtual) and also published in The Lancet.
Patients with hypertension require a multi-faceted approach for blood pressure control, Kirtane explained, detailing that in RADIANCE-HTN TRIO, patients with daytime ambulatory systolic blood pressure (dASBP) 135/85mgHg despite a fixed dose combination pill consisting of a calcium channel blocker, angiotensin receptor blocker, and thiazide diuretic, were randomised to renal denervation using the Paradise renal denervation ultrasound system (ReCor Medical, n=69) or a sham procedure (n=67).
The trial’s two-month results found that, in conjunction with the three-drug fixed-dose combination pill, renal denervation reduced dASBP by an additional 8mmHg, a 4.5mmHg greater reduction compared with a sham procedure (–8mmHg versus –3mmHg; median between-group difference–4.5mmHg; adjusted p=0.022).
During months two through five, the addition of a standardised stepped-care antihypertensive treatment (SSAHT) was recommended sequentially with the addition of spironolactone 25mg/d, bisoprolol 10mg/d, full dose of a centrally acting α2 receptor agonist, and an α1 receptor blocker if monthly measured home blood pressure was ≥135/85mmHg, with the goal of achieving blood pressure control in both groups. Adherence to prescribed medications was similar in both groups (71% for renal denervation versus 78% for sham, p=0.41).
The increase in the number of antihypertensive medications at six months following the addition of the SSAHT was 0.7±1 for renal denervation and 1.1±1.1 for sham (p=0.045). The use of aldosterone antagonists at two months was 3% for renal denervation and 11% for sham (p=0.16). At six months, the number increased in both groups but to a lesser extent in the renal denervation group (40% for renal denervation compared to 60.9% for sham, p=0.017).
The addition of the stepped care antihypertensive regimen to the initially randomised therapy further decreased blood pressures in both arms; the overall change from baseline in dASBP was -11.8±14.2mmHg in the renal denervation group versus -12.3±14.2mmHg for sham (p=0.65). Home blood pressure was lower in patients initially randomised to renal denervation when adjusted for baseline blood pressure and number of medications (-4.28mmHg, p=0.027). Safety outcomes were similar for both groups.
“Blood pressure reductions after renal denervation were achieved with a smaller increase in additional medications prescribed and less use of aldosterone antagonists compared with a sham procedure,” said Kirtane. “These results demonstrate the additional effects of pharmacologic intervention with maintenance of a blood pressure-lowering effect of endovascular ultrasound renal denervation at six months.”
During a press conference in which Kirtane presented the latest findings of the study, describing them as “exploratory”, he relayed that the addition of a pharmacologic intervention led to further blood pressure reductions after renal denervation with a smaller increase in additional medications prescribed and less use of diuretics.
In ensuing discussion during the press conference, David Kandzari (Piedmont Heart Institute, Atlanta, USA) described the findings as “welcome” as they add to the totality of evidence around renal denervation. Responding to a question as to whether, given the relative differences in the reduction in blood pressure in both arms, patients would be more willing to undergo an invasive intervention for hypertension, Kandzari noted that reducing medication burden is of “increasing importance” to patients.
He added: “The opportunity to reduce the medication burden in discrete choice experiment studies is one of the key drivers of patient motivation for an alternative therapy or approach like renal denervation.
“Indeed, patients do not typically want to undergo an interventional procedure, but if there is durability with it and if there is a meaningful reduction in blood pressure, which, interestingly by patients’ criteria does not have to be that large of a reduction in blood pressure to be meaningful, and the opportunity to reduce medicines, then it is clinically important to them.”
Roxana Mehran (Icahn School of Medicine at Mount Sinai, New York, USA) questioned if the results demonstrate the “durability” of renal denervation, but described the study as an “exciting next step”. “To me it is opening a window,” she remarked. “Previously the doors might have been closed for renal denervation, but I think the window is opening and it may be a large one!”
Medtronic today announced findings from a new study of patient preferences for the treatment of hypertension. The findings are set to be presented during the “What’s Novel in Interventional Hypertension” session at the 33rd Transcatheter Cardiovascular Therapeutics annual meeting (TCT 2021, 4–6 November, Orlando, USA and virtual)—the yearly scientific symposium of the Cardiovascular Research Foundation.
Medtronic has also announced the initiation of the SPYRAL AFFIRM study, evaluating the long-term safety, efficacy, and durability of the company’s Symplicity renal denervation (RDN) system—which uses a minimally invasive procedure that delivers radiofrequency energy to specific nerves near the kidneys that can become overactive and cause high blood pressure—in real-world patients with uncontrolled hypertension and comorbidities, such as diabetes, isolated systolic hypertension and chronic kidney disease (CKD).
Patient preference for the treatment of hypertension
For the first time, new data presented at TCT 2021 will quantify US patient preferences for considerations of interventional procedures in the treatment of high blood pressure, including treatment mode, effectiveness and risks, according to a Medtronic press release.
The study found that, in exchange for treatment risks, patients on average would require a minimal acceptable benefit of less than 2.5mmHg reduction in office-based systolic blood pressure. Additionally, on average, patients indicated a tolerance of at least 20% risk of adverse events (such as a vascular injury or drug side-effects) in exchange for being able to lower their office-based systolic blood pressure.
These findings suggest that, despite the risks of an intervention, patients may accept lower blood pressure reductions than those observed in published literature of the Medtronic Symplicity Spyral RDN procedure. Additionally, patients may be willing to tolerate risks higher than those observed in peer-reviewed published studies of Symplicity Spyral, the release adds.
The study also concluded that blood pressure reduction was the most important driver of patient preference over all other attributes like medication burden and treatment (including interventional treatment-related) risks.
When applying this model to a patient population that is interested in an interventional procedure without medication, up to 76.5% of patients would be willing to consider an interventional approach like RDN if they achieve a 10mmHg reduction in office-based systolic blood pressure. Including the maximum acceptable risk of 20%:
76.5% of patients would be willing to consider an interventional approach such as RDN with reductions in office blood pressure anticipated at 10mmHg
24.3% of patients would be willing to consider an interventional approach such as RDN with reductions in office blood pressure anticipated at 5mmHg
6.9% of patients would be willing to consider an interventional approach such as RDN with reductions in office blood pressure anticipated at 2.5mmHg, the minimal acceptable benefit
“This novel, patient preference study is particularly valuable for a new procedure like RDN, because it demonstrates that, for patients, lowering blood pressure—even by a small amount—is meaningful,” said Michael Weber, professor of cardiovascular medicine at State University of New York, Downstate Medical Center (Brooklyn, USA). “For the first time, these results give us quantitative insights into hypertension treatment preferences—importantly, patients are very open to considering a medical intervention procedure, such as RDN, with demonstrated improvements in the control of their high blood pressure.”
The study, which was designed based on the US Food and Drug Administration (FDA) Guidance for Patient Preference Information, surveyed 400 individuals in the USA who have high blood pressure (physician confirmed systolic office-based blood pressure greater than 140 mmHg), who were on up to three anti-hypertensive medications, and were not previously involved in a SPYRAL HTN [hypertension] study. The study uses a statistical method called a discrete choice experiment, often used to compare individuals’ preferences among two or more alternatives.
“The patient preference insights, combined with the breadth of real-world and randomised sham controlled trials we have for RDN, are aligned with the recent clinical consensus from the European Society of Hypertension, Society for Cardiovascular Angiography and Interventions, and National Kidney Foundation, that reinforce RDN as a potential treatment option for patients,” said Jason Weidman, senior vice president and president of the Coronary & Renal Denervation business, which is part of the Cardiovascular Portfolio at Medtronic. “Patient preference data will be important to help physicians understand patients’ acceptable benefits and risks related to minimally invasive procedures for the treatment of hypertension.”
SPYRAL AFFIRM study launch
Separately, Medtronic announced that the first patient was enrolled at Piedmont Heart Institute in Atlanta, USA for the SPYRAL AFFIRM clinical study. Using a performance goal, this clinical study will enrol 1,000 real-world patients with uncontrolled hypertension and associated comorbidities, such as isolated systolic hypertension, diabetes, and CKD. SPYRAL AFFIRM will follow these patients for three years. This investigational device exemption (IDE) trial was approved by the FDA in June 2021 and will be conducted at 100 sites globally.
“Through the strong investment in our clinical programme, the AFFIRM study will expand RDN research into a variety of patient groups,” said Weidman. “The AFFIRM clinical study adds to our body of evidence for RDN and will help us further answer questions about the use of this procedure in more complex, real-world patients such as those with isolated systolic hypertension, diabetes and CKD.”
The SPYRAL AFFIRM clinical study is part of the SPYRAL HTN Global Clinical Program, adding to the safety and efficacy data for RDN, the release continues. Along with the real-world data from the Global Symplicity Registry, when combined with commercial experience, there have been more than 20,000 procedures performed with Medtronic RDN technology. The clinical programme is backed by the most rigorous and extensive patient experience studied in the presence and absence of medication, and in patients with high baseline cardiovascular risk.
A press release reports that, at 48 hours post procedure, the major adverse event rate and mortality rate were low, at 1.4% and 0.2%, respectively. None of the deaths or major adverse events were device related. Collectively, these PE patients experienced substantial on-table improvements in haemodynamics and symptoms, which translated to six-month improvements in cardiac function, functional status, and quality of life measures.
The outcomes were achieved while limiting utilisation of hospital resources, the release adds, with less than 4% of patients receiving adjunctive therapy and a median of zero days in the intensive care unit (ICU) post procedure.
FLASH is a prospective, multicentre, single-arm registry evaluating real-world patient outcomes after treatment of PE with FlowTriever. The 500-patient interim results were presented on 27 October via webcast at Transcatheter Cardiovascular Therapeutics (TCT) 2021 by principal investigator Catalin Toma, an interventional cardiologist at University of Pittsburgh Medical Center (UPMC) in Pittsburgh, USA. TCT 2021 will be held in person and broadcast live online 4–6 November in Orlando, USA.
“These interim results reinforce the strong safety profile of the FlowTriever system in real-world PE patients, with substantial on-table clinical improvements and immediate symptom relief,” said Toma.
“We believe these six-month follow-up data suggest that removal of clot burden without the risks of lytics has potential positive long-term implications for PE patients, including strikingly low rates of hospital readmissions, dyspnoea, CTED [chronic thromboembolic disease], and CTEPH [chronic thromboembolic pulmonary hypertension]. These data suggest that treatment with FlowTriever may fundamentally improve the natural course of the disease, and that is tremendously exciting.”
Shockwave Medical has announced that, as part of the calendar year 2022 Medicare Hospital Outpatient Prospective Payment System (OPPS) final rule, the Centers for Medicare and Medicaid Services (CMS) has reassigned the payment for peripheral intravascular lithotripsy (IVL) procedures performed on above-the-knee (ATK) arteries in the hospital outpatient setting. The resulting payment increases will become effective 1 January 2022.
As part of the 2022 OPPS final rule, CMS has announced new Ambulatory Payment Classification (APC) assignments for three Healthcare Common Procedure Coding System (HCPCS) codes that describe peripheral IVL procedures performed in lower extremity arteries in the outpatient hospital setting. The three HCPCS codes affected describe procedures in iliac, femoral and popliteal arteries when IVL is performed by itself or adjunctively with drug-coated balloons (DCB), stents or atherectomy. The new APC assignments will increase the payments hospitals receive for these procedures.
“We appreciate CMS’s collaborative relationship and their swift action in reassigning payment levels for IVL performed above the knee, as the data acknowledge the resources associated with performing IVL in these patients. Importantly, we believe the APC reassignment of these HCPCS codes and subsequent increased payment for IVL procedures performed ATK will further facilitate access to IVL technology for Medicare patients,” said Doug Godshall, president and chief executive officer of Shockwave Medical.
“We would like to acknowledge CMS for making an exception to this year’s standard rate-setting process by considering calendar year 2020 data when determining appropriate payment levels for the new peripheral IVL code set. We are also grateful for the support that came from CMS’ Hospital Outpatient Physician Advisory panel and medical societies during the public comment period.”
Fluidx Medical’s GPX embolic device has released initial results for Oncology Drug Delivery. Fluidx Medical Technology announced that a next-generation, doxorubicin-loaded GPX embolic device was featured at the recent symposium on clinical interventional oncology (CIO) conference highlighting the technology’s potential for oncology drug delivery.
“GPX is easy to prepare, deliver, and control,” said Ryan O’Hara (interventional oncologist, University of Utah, Salt Lake City, USA). “The initial results of GPX as a drug-loadable oncology solution are very promising. GPX would be the first loadable liquid embolic designed for tumour applications.”
Fluidx Medical’s GPX embolic device
Study results presented at CIO included an in vitro characterisation of the loading and drug release profile of the GPX Embolic Material loaded with doxorubicin (GPX-DOX). GPX-DOX provided a zero-order release profile for five weeks and sustained release out to 100 days. The long linear release profile is desirable in drug delivery, as a constant amount of drug is delivered regardless of the concentration within the carrier. These properties are unique in the field of liquid embolics.
GPX-DOX Release Graph
The GPX Embolic Device is an innovative embolic designed for simple preparation and quick material delivery. GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolus upon delivery without polymerization or dimethyl-sulfoxide (DMSO) precipitation. GPX is designed to occlude blood vessels independent of a patient’s coagulation situation. The device is packaged ready-to-use in a syringe, requires less than 30 seconds of tableside preparation by the clinician, and may be delivered through standard catheters or small microcatheters (no complex mixing systems or special delivery catheters are necessary).
“We have not seen other liquid embolic devices that have demonstrated the ability to load and release oncology agents in a sustained manner,” said Libble Ginster, CEO of Fluidx Medical Technology. “The Fluidx team is excited about the future of GPX technology and inspired by bringing new innovations to cancer patient care.”
Fluidx Medical Technology is a Salt Lake City, Utah based company focused on developing the GPX Embolic Device and other innovative medical technologies.
The GPX Embolic Device is under development and does not have marketing clearance or approval in any market at this time. For investigational use (in New Zealand) only. GPX-DOX Embolic Device is under development and does not have marketing clearance or approval in any market at this time.
Varian is excited to announce David Hahn (clinical assistant professor of Radiology, University of Chicago Pritzker School, Chicago, USA) joined the company as vice president of Medical Affairs for Interventional Solutions. As a leading, practicing interventional radiologist, Hahn will bring his extensive experience to Varian to help expand access to personalized, multi-modal cancer care to patient populations worldwide.
“I am so excited to join the team at Varian, and work with such a fantastic group of colleagues as we focus on ways to expand access to new and innovative interventional radiology methods” said Hahn.
This hire reinforces Varian’s ongoing commitment to investing in the future of interventional radiology. Hahn’s extensive experience both in the clinical setting and private sector will bring a unique perspective as Varian works to deliver a portfolio of intelligent solutions and enhance the patient experience at every stage of care.
Based in Chicago, Hahn has held teaching faculty positions at Northwestern University Feinberg School of Medicine, Rush University of Chicago, and the University of Chicago Pritzker School of Medicine, where he is currently a Clinical Assistant Professor of Radiology. He has also authored numerous articles in peer-reviewed journals and has been an invited lecturer and moderator at congresses both nationally and internationally in addition to being a reviewer for the Journal of Vascular and Interventional Radiology since 2006.
There have been several positive expressions regarding Hahn joining Varian. Two quotes are shown below.
“David’s extensive experience in radiology makes him a fantastic addition to our team. I look forward to working together toward our goal of expanding access to personalized, multi-modal cancer care to patient populations worldwide.” Frank Facchini, FSIR, president, Varian Interventional Solutions
“I am thrilled to expand our medical affairs team with the addition of David Hahn. His deep expertise as a world-renowned Interventional Radiologist will be a fantastic resource for our team as we continue to grow and expand to serve new patient populations.” Dee Khuntia, chief medical officer and senior vice president of Medical Affairs, Varian.
Argon Medical Devices, Inc. Logo. (PRNewsFoto/Argon Medical Devices, Inc.)
Argon Medical Devices has announced the launch of two portal vein access sets intended for transjugular liver access in diagnostic and interventional procedures.
The Scorpion portal vein access series addresses the common challenges physicians encounter when placing a transjugular intrahepatic portosystemic shunt (TIPS) or conducting other portal vein access procedures. The Scorpion series includes two sets, Scorpion and ScorpionX, which offer improved visualisation, revolutionary navigation control, and enhanced durability to augment existing procedural techniques, according to Argon Medical.
The Scorpion portal vein access series utilises a patented curve-in-curve system to offer physicians 360-degree range of motion with the needle or stylet used to access the portal vein. Each curved component can work together or independently to accurately steer the device through the liver to the intended target. Existing systems utilise only a single curve limiting the steerability of the needle or stylet. The Scorpion series’ novel design was created by Lowell Kahn, a vascular and diagnostic interventional radiologist located in Springfield, USA, in conjunction with Hatch Medical.
“Establishing access to the portal venous system is often the longest and most challenging part of many procedures. This is particularly true when the liver is diseased, making the anatomy irregular. I designed the Scorpion’s independently controlled dual curves to improve the physician’s ability to navigate through liver parenchyma and reduce the number of attempts necessary to establish access to the portal vein,” said Khan.
“Argon Medical is proud to add the Scorpion Series into our product portfolio. 2021 is our ‘Year of Innovation,’ and we continue to develop and deliver innovative products to the interventional market. Launching Scorpion demonstrates our desire and ability to innovate to improve the lives of our customers and the patients they treat,” said George Leondis, CEO of Argon Medical.
The Scorpion portal vein access sets are currently available in the USA. Scorpion is licensed by Argon Medical and is a trademark of Hatch Medical.
Transit Scientific has announced US Food and Drug Administration (FDA) clearance of new hydrophilic-coated XO Cross microcatheters for guidewire support, exchange, and contrast media injection in the peripheral vasculature.
“The XO Cross devices deliver unique performance and control that make them an excellent tool for crossing above- and below-the-knee lesions,” said Jihad Mustapha, interventional cardiologist at Advanced Cardiac & Vascular Center in Grand Rapids, USA. “The non-tapered XO Cross shaft, lubricious coating, low crossing profile, and 1:1 torque response will be critical for workhorse performance and reducing the need for wire escalation techniques in CLTI [chronic limb-threatening ischaemia] cases.”
Microcatheters are commonly used to provide guidewire support, facilitate guidewire exchanges, access distal anatomy, cross lesions, deliver therapeutic embolics, and inject contrast media, during complex endovascular procedures. Hydrophilic coatings create a lubricious and slippery layer on the outside of catheters for improved navigation and tracking through tortuous vessels and lesions.
The XO Cross platform includes a metal-alloy exoskeleton, non-tapered shaft, proprietary hydrophilic lubricious coating, and large inner lumen for improved 1:1 torque, low-profile, pushability, tracking, crossing, fatigue-resistance, and angiography, a press release details.
According to Transit Scientific, XO Cross microcatheters have been safely and successfully used in challenging peripheral lesions above-the- including but not limited to above-the-knee and below-the-knee chronic total occlusions (CTOs) from contralateral femoral, antegrade femoral, and retrograde pedal access.
This 510k clearance includes new 2Fr XO Cross 14 microcatheters, 2.6Fr XO Cross 18 microcatheters, and 3.8Fr XO Cross 35 support catheters for use with standard 0.014”, 0.018”, and 0.035” guidewires in 90cm, 135cm, 150cm, and 175cm working lengths. The shorter 90cm devices support retrograde pedal and antegrade femoral access while the longer 175cm devices were designed specifically for radial access to peripheral use.
Marie Lannelongue Hospital of Paris Saint-Joseph Hospital Group (Paris, France) and Incepto, a European specialist in artificial intelligence (AI) applied to the medical field, recently announced the creation of ARVA (Augmented radiology for vascular aneurysm), a novel solution for automatic measurement of the maximum diameter of the aorta.
ARVA was developed by surgeons from the Paris Saint Joseph Hospital Group and engineers. According to a press release, this new application is the first solution in the world to fully automate the measurement of aortic aneurysms, providing radiologists and surgeons with a particularly effective aid in the diagnosis and follow-up of aneurysms.
The press release details that ARVA uses a dozen algorithms trained on a base of more than 1,000 scans annotated by experts to generate a pre-filled report in DICOM format that can be integrated into the radiologist or surgeon’s workflow.
“Before ARVA, in order to get accurate measurements of aortic diameter, we had to spend a lot of time analysing the scans. These measurements are complicated because in the presence of an aneurysm, the aorta is often tortuous. The AI we developed with Incepto is a tool that allows us to have precise and reproducible measurements of the diameter of the aorta and therefore to determine whether surgery is necessary,” says Dominique Fabre, surgeon at the Marie Lannelongue Hospital.
ARVA provides automatic measurements of the diameters per segment (S1 to S7) of the entire aorta, from its root near the heart to its division into two iliac arteries in the abdomen, the press release continues. In addition, it adds that ARVA provides a report including a three-dimensional (3D) reconstruction of the aorta, a schematic representation of the aorta by segment, stent detection, measurement of the largest diameter by segment and an oblique section of the largest diameter detected. The release specifies that one of the major benefits of ARVA is the comparison of measurements between different scans performed by the patient, with standardisation of the measurement and time saving for surgeons and radiologists.
ARVA is secure, implemented in the cloud and CE marked class I, according to the release. A first clinical study, published in the European Journal of Vascular and Endovascular Surgery, demonstrated the reliability of ARVA measurements on healthy and pathological aortas with and without stents, showing a median deviation of 1.2mm compared to the measurement performed by an expert. The median deviation between the six other doctors who participated in the study was 1.4mm.
“Since its inception in 2018, we have put forward a worldview of AI solutions rooted in collaboration between data scientists and physicians. Our main goal has always been to develop solutions that concretely help physicians and meet a real need. In line with this ambition, ARVA is the result of exciting work with the outstanding surgeons of the Marie Lannelongue Hospital whose driving force is excellence in patient care,” notes Gaspard d’Assignies, co-founder and chief medical officer of Incepto.
“This first version of ARVA will allow us to be more precise in our surgical indications, to save precious time on a daily basis, and to have at our disposal a document that will allow us to better inform patients. Future versions under development will revolutionise our profession, in particular with the automatic monitoring of aortic volumes. This is just the beginning of the AI adventure in medical imaging”, concludes Stéphan Haulon, head of the Aortic and Vascular Surgery Department at the Marie Lannelongue Hospital.
Twelve-month results from a first-in-human study of the Wrapsody cell-impermeable endoprosthesis (Merit Medical Systems) for the treatment of access circuit stenosis in haemodialysis patients are “very encouraging”. This is according to James Gilbert, a consultant transplant and vascular access surgeon at the Oxford University Hospitals NHS Foundation Trust in Oxford, UK, and president of the Vascular Access Society of Britain & Ireland (VASBI), who presented these data for the first time at the Cardiovascular and Interventional Radiological Society of Europe 2021 summit (CIRSE; 25–28 September, virtual).
Gilbert noted that this first-in-human study—dubbed WRAPSODY FIRST—produced positive results in terms of safety, detailing that no adverse events confirmed as being device-related were observed in 39 patients at one-year follow-up. Regarding effectiveness, he reported promising target lesion primary patency (TLPP) rates at 12 months across all lesion sites, in line with the study’s six-month data, and stated that access circuit patency rates also appear to remain high following treatment with the device. Gilbert went on to detail the pivotal WRAPSODY WAVE trial—a global randomised controlled trial (RCT) that is currently underway to assess the Wrapsody endoprosthesis.
Speaking to Renal Interventions, Gilbert said: “The 12-month effectiveness data, particularly of TLPP, are very exciting because we may have a stent that requires fewer reinterventions to maintain patency at the lesion site and, more importantly, ensures that the access circuit remains functional—which is key for any dialysis patient. The data were also reproducible at all lesion sites treated within the access circuit, from the cephalic arch in a brachiocephalic AVF [arteriovenous fistula] to the graft vein anastomosis site and the central veins. This is suggestive that there is something about the stent’s design, with its cell impermeable middle layer and softened end rows, that is key in minimising edge stenosis at both ends of the stent.
“We recognise that these very encouraging data are only from a small, first-in-human study and so the WRAPSODY WAVE trial will be key in confirming just how good this stent can be. The WAVE study will not only provide a bigger number of patients in which to assess the effectiveness of the stent, it will also provide experiences from a range of expert clinicians globally.”
Addressing the CIRSE audience, Gilbert described the Wrapsody endoprosthesis as a “unique, tri-layered stent graft” that is currently CE-marked for use in Europe and is available in sizes ranging from 6mm to 16mm, making it a viable treatment option for a “huge range” stenotic lesions, including those in the peripheral and central veins of an access circuit.
Wrapsody endoprosthesis
Gilbert went on to detail the design and purpose of WRAPSODY FIRST—a prospective, three-centre, single-arm, first-in-human feasibility study assessing the safety and effectiveness of the device, for which he is the primary investigator. The subject population consisted of dialysis patients with AVFs or arteriovenous grafts (AVGs) in their upper limbs, who experienced stenosis or occlusion within their access circuit. Gilbert reported the primary safety objective as being the proportion of patients without any localised or systemic safety events affecting the access or venous outflow circuit, and resulting in surgery, hospitalisation, or death, while the primary effectiveness objective was TLPP. Follow-up took place at 30 days, three months, six months and 12 months, he added.
Gilbert stated that a total of 46 patients (24 female, mean age=66.7 years) were enrolled in the study, with a cumulative access loss of five patients at the 12-month follow-up point, as well as a further two patients undergoing transplantation, leading to outcome data for 39 patients being available beyond one year. On safety outcomes at 12 months, he reported a total of five adverse events, four of which were adjudicated as being procedure-related, with the access circuit not being salvaged and a lack of imaging data making it impossible to determine if the one remaining event—a thrombosed fistula—was device- or procedure-related.
Touching on effectiveness next, Gilbert described the 12-month TLPP rate of 84.6% as “very encouraging”, and similarly positive to the 97.7% TLPP rate seen at six months, before reporting that reintervention was successful in all problematic cases—resulting in a 12-month assisted TLPP rate of 100%. Further, he noted an access circuit primary patency rate of 65.9% at 12 months. All but five of the remaining access circuits were salvaged via reintervention, he added, leading to a secondary patency rate of 88.6%. These data are also published in the journal CardioVascular and Interventional Radiology (CVIR).
Gilbert concluded his presentation by conveying details of the WRAPSODY WAVE trial, which is a multicentre RCT designed to further assess the Wrapsody endoprosthesis as a treatment option for dialysis access circuit stenoses and support US Food and Drug Administration (FDA) approval of the device. This trial is already underway, and will involve 1:1 randomisation of patients across two study arms—Wrapsody versus percutaneous balloon angioplasty (PTA) in AVF peripheral circuit stenosis (244 patients), and Wrapsody versus PTA in central vein stenosis of AVF and AVG circuits (120 patients)—in addition to a third, registry-based arm that will assess the device’s use at the graft-vein anastomotic site in 113 patients.
This advertorial is sponsored by Argon Medical Devices
Placing a drain is an important, quotidian, “bread and butter” procedure that often has a tremendous impact on patients’ lives. “A drain is a drain until it is not,” says Sean Calhoun, who outlines the benefits of the Skater all-purpose, nephrostomy and biliary drainage catheters (Argon Medical Devices). He hones in on their anti-kinking and locking mechanisms, ease of insertion and transition and compatibility with both alcohol and doxycycline. Calhoun also shares his excitement about the recent commercial launch of the Skater mini-loop drainage catheters in the USA and the European Union, telling Interventional News: “I am hopeful that this will eliminate the problem of losing access to the abscess cavity by having the catheter track smoothly through the wall and into a small cavity. It is also going to be very helpful for external biliary drains.”
“The Skater drainage catheter is consistent, reliable, extremely easy to use and is visualised well under fluoroscopy due to its good radiopacity,” says Calhoun, vice chair of the Radiology Department and an interventional radiologist, Atlantic Health System, Morristown, USA. “Additionally, the locking mechanism is simple, intuitive and designed for patient comfort in that it is not bulky. The break-off tab is very easy to use and very easy to undo when it is time to remove the catheter—these catheters are also perceived to have excellent patency rates, which are the key features for any drainage catheter,” he adds.
Drainage is often seen as a quotidian, relatively routine procedure, with interventional radiologists placing five to 10 drainage catheters a week under different imaging modalities depending on the location. Drains are placed under imaging guidance for a wide variety of indications, including abscesses, biliary and ureteral obstructions, pleural effusions and pneumothoraces, Calhoun, who is also programme director for the Radiology Residency, indicates.
An important point he emphasises is that while a drain is seen as a standard piece of equipment, there are subtle differences that are not appreciated until you have a drain that fails, commenting that “a drain is a drain until it is not”. This is when you really appreciate the differences in the technology and design and the many advantages offered by drains such as Skater, he notes. Calhoun particularly draws attention to the hydrophilic coating, resistance to kinking and accordioning—three things that contribute to the ease of insertion and the reliability of the device.
“During insertion, drains can certainly accordion because the multiple side holes create a relative weakness in the catheter. I have had catheters in the past in which the side holes accordion, particularly in tight biliary strictures. This makes it very difficult to advance the drain. The Skater catheter seems to track very well through firm cirrhotic livers. When using other catheters in the past where there was challenging cirrhotic liver and a tight stricture, I recall going through several catheters that just continually weakened; that has almost never been the case with the Skater line. Those difficult situations now seem like distant memories, because we have been using this product for 10 years.
“The concept of durability and not having the catheter break down necessitates patients having to come in for avoidable changes, particularly when we start using the catheters for things like lymphocoele sclerosis and cyst sclerosis with alcohol, during which some catheters can break down and fragment. I have also seen patients come in with their catheters in all sorts of disarray; they can have kinks, be twisted and become occlusive. While many patients keep them in pristine condition, others do not, and we have observed that the catheter is twisted and wrapped around and coiled under a dressing that has not been well cared for, oftentimes with the catheter not draining in that situation. This might lead the physician to believe that the catheter is occluded, but in fact, there is a kink in the catheter under the dressing; we have seen that with other manufacturers in the past. The Skater catheter appears to be much more resistant to kinking.”
Skater is compatible with both doxycycline and alcohol
One major advantage of the Skater catheter is that it is compatible with both alcohol and doxycycline. Calhoun explains why this dual compatibility is important: “Patients who have undergone drainage of a symptomatic cyst, a symptomatic renal cyst, or a hepatic cyst, or postoperative lymphocoele, will often be sclerosed to avoid cyst recurrence or promote healing. The primary compound that we use is alcohol, but doxycycline is another popular alternative these days with alcohol becoming less available due to manufacturing shortages. Many of the other non-compatible catheters will break down during this sclerosing procedure. You hear horror stories of interventional radiologists chasing catheter fragments in the cyst cavity, and trying to retrieve them can be very difficult. Fragmentation is not only cumbersome, it puts the patient at risk. So, being able to confidently use alcohol, or doxycycline, knowing that the catheter is going to stay intact is huge,” Calhoun elaborates.
He also calls out the flow rates as being important. “The fact that the Skater catheter has a consistent lumen even at the hub means that you avoid the problem of effectively putting in a smaller catheter than what you think you are putting in.”
Biliary drains and occlusions
Biliary drains can frequently be “management headaches” as patients, who are very sick with sepsis and life-threatening infections, can come in with occlusions. Early occlusions are very problematic for patients as they can lead to life-threatening infections. Other times it is just an inconvenience for the patient, notes Calhoun. “If there is poor drainage, it is often due to occlusion of the catheter side holes, so I think the skived side holes of the biliary drainage catheters certainly help to reduce the occlusion rates. All catheters are going to be subject to some rate of reocclusion, but it has been our perception that the Skater catheters have a much lower rate of early occlusion than some of the other catheters that we have used in the past.”
Skater mini-loop launch received with enthusiasm
Commenting on the recent commercial launch of the Skater mini loop catheter, an expansion of Argon’s Skater all-purpose and nephrostomy drainage portfolio, which uses a 40% smaller loop to help secure the catheter and drain fluid from smaller cavities, Calhoun says: “I have often been disappointed with the mini pigtail catheters available because the transition at the tip is unfortunately not ideal to get into a small abscess cavity. In these small cavities, you do not have a lot of guidewire purchase, so you want the catheter to track smoothly and easily through the wall, so that you can situate it without losing purchase. In my experience the transition is much smoother and uniform with the Skater range than the other catheters out there, so I am hopeful that this will eliminate that problem. It is also going to be very helpful for external biliary drains. If it performs the same as the other catheters in terms of drainage and reliability, then we have hit a home run.”
Product support and availability matter
While the pandemic seems to have impacted the availability of product ranges across the board, the Skater device has been relatively unaffected. “My technologists are regularly flagging back orders. Matters can come to a head when a patient is already here, and we have to pivot to find other alternatives. That has not been the case with Skater catheters, or any of the Argon products, which are all manufactured in the USA. They have always been available and the product support has been excellent. We have expanded our Skater inventory as there are multiple sizes and diameters available. We can always count on that catheter being on the shelf and having plenty of stock and it has now become our go-to product,” says Calhoun.
Results of the randomised, prospective, multicentre STEP trial show that the FemoSeal vascular closure system (Terumo) is superior to the Perclose ProGlide suture-mediated closure system (Abbott) in peripheral arterial disease (PAD) patients in terms of technical success using a retrograde femoral puncture. Bahaa Nasr (Brest University Hospital, Best, France) presented the late-breaking data at Paris Vascular Insights (PVI) 2021 (21–23 October, Paris, France), concluding that FemoSeal should be used in PAD patients undergoing lower limb arterial endovascular treatment, especially if they are discharged on the same day as their surgery.
According to Nasr, many studies have compared vascular closure devices (VCDs) for the coronary arteries, while none have compared them for PAD. “We all know that the efficacy of a VCD is different for PAD patients because of the plaque nature in the common femoral artery,” he remarked.
In order to assess this gap in the literature, Nasr and colleagues initiated the STEP trial. “The aim of the study was to perform a direct, head-to-head comparison between ProGlide and FemoSeal,” he relayed, explaining that the FemoSeal is a double polymer resorbable disc, while the ProGlide involves a direct suture in the artery. He noted that the primary endpoint was VCD technical success, assessed five hours post-procedure, and defined as either haemostasis without the need for either an additional VCD or manual compression, or a drop in haemoglobin.
Patients were included in the study if they had received endovascular treatment for PAD with the use of 5–7Fr sheath, Nasr informed the PVI audience. He added that patients who had undergone previous ipsilateral open repair of the common femoral artery, previous stenting at the puncture site, or had either radial, brachial or antegrade femoral punctures were excluded.
Nasr relayed that all patients were treated with a duplex scan-guided, retrograde common femoral artery puncture. He detailed that the resumption of ambulation was assessed five hours after the procedure and that all the investigators were certified and trained for both VCDs.
A total of 230 patients were randomised, with 109 patients undergoing treatment with the assigned device in each group. According to Nasr, the baseline clinical and demographic characteristics were well balanced between the two groups. The presenter highlighted the fact that most of the patients included in the study had intermittent claudication—86% in the FemoSeal group and 85% in the ProGlide group.
The majority of the procedures were performed under local anaesthesia and the most commonly-used sheath was 6Fr diameter, Nasr told PVI delegates. He added that there were no differences in intraoperative antithrombotic regimens, and in fact the only difference between the two groups was the need for a compression dressing, which was higher in the ProGlide group.
Nasr reported that the intention-to-treat analysis showed an 80% technical success rate in the FemoSeal group, which was higher than the 50% rate achieved in the ProGlide group. The difference in technical success could be explained by the need for additional VCDs and a greater need for manual compression in the ProGlide group, the speaker explained. He elaborated: “In the ProGlide group, when taking into account the use of a second VCD, the technical success rate was 90%.”
Postoperative bed rest and hospital stays were similar in both groups, the presenter communicated. The rate of minor access-related complications were higher in the ProGlide group, he added, noting finally that the additional cost per patient valued between 23 and 30% in favour of FemoSeal.
Moderator Marianne Brodmann (Medical University of Graz, Graz, Austria) was “really impressed” that Nasr and colleagues had found the device to be more cost effective, adding a more general comment that it is a “very good idea” to compare two different VCDs for peripheral interventions. In this vein, Brodmann was keen to know if the speaker thought we should conduct more studies and compare more devices in order to end up with one device—“the most cost efficient, effective and safe one”.
“I think we have to talk about other devices,” Nasr replied, noting also that investigators must compare devices with magnet compression and low-profile sheaths.
Speaking from the audience, Eric Ducasse (Bordeaux University Hospital, Bordeaux, France) agreed with Brodmann that it is important to prove a device’s cost effectiveness, but stressed that “we need to go deeper into the comparison”. Data concerning other factors—such as the distance between the artery and the skin, previous fibrotic intervention, the amount of calcification, the position of the plaque, and the wideness of the artery that is punctured—is required, he stressed, in order to “really compare objectively” the different systems.
(A) Pre-procedure axial image from contrast-enhanced CT scan of chest demonstrates a 1 cm solid right upper lobe nodule adjacent to right mainstem bronchus (arrow). (B) Intra-procedural coronal reformatted image shows two cryoablation probes within nodule. (C) 1-month follow-up sagittal chest CT image shows expected post-ablation changes encompassing treated nodule (arrow). (D) 1-year follow-up sagittal chest CT image shows expected involution of treatment zone into flat bandlike scar without residual tumor (arrow).
CREDIT
American Roentgen Ray Society (ARRS), American Journal of Roentgenology (AJR)
USAGE RESTRICTIONS
Image may only be used with appropriate caption or cred
Percutaneous microwave and cryoablation allow for repeat minimally invasive treatment of sarcoma lung metastases with mild complications, according to the conclusions of a study published in the American Journal of Roentgenology (AJR).
“High primary technical success, local control, and overall survival” were the supporting findings, as reported by Florian Fintelmann (Massachusetts General Hospital and Harvard Medical School, Boston, USA) and colleagues. Fintelmann and colleagues’ retrospective cohort study included 27 patients, consisting of 16 women and 11 men, with a median age of 64 years and an Eastern Co-operative Oncology Group performance score of 0–2. The patients received 39 percutaneous computed tomography (CT) guided ablation sessions (21 microwave, 18 cryoablation) with one to four sessions per patient.
(A) Pre-procedure axial image from contrast-enhanced CT scan of chest demonstrates a 1 cm solid right upper lobe nodule adjacent to right mainstem bronchus (arrow). (B) Intra-procedural coronal reformatted image shows two cryoablation probes within nodule. (C) 1-month follow-up sagittal chest CT image shows expected post-ablation changes encompassing treated nodule (arrow). (D) 1-year follow-up sagittal chest CT image shows expected involution of treatment zone into flat bandlike scar without residual tumor (arrow). CREDIT American Roentgen Ray Society (ARRS), American Journal of Roentgenology (AJR) USAGE RESTRICTIONS Image may only be used with appropriate caption or cred
The sessions were to treat 65 sarcoma lung metastases (median 1 tumour per patient, range 1–12; median tumor diameter 11mm, range 5–33mm; 25% non-peripheral) from 2009 to 2021. Ablation modality complications were compared using generalised-estimating equations. Cox hazard methods were also used to evaluate ablation modality, tumour size, and location (peripheral versus non-peripheral) in relation to local tumour progression, with death as a competing risk. Overall survival was also estimated using the Kaplan-Meier method.
The median follow-up time was 23 months (range 1-102 months) and the estimated two-year microwave local control rate was 95% vs. 98% for cryoablation for tumours ≤1cm and 62% and 79% for tumours >1cm. Furthermore, decreased cumulative incidence of local progression was associated with tumour size ≤1cm. Fintelmann and colleagues also noted that ablation modality and tumour location did not affect local progression (p>0.05) and “treatment failure was low, especially for small tumours, with non life-threatening complications for tumours ≤1cm”.
Across 44% of patients, complications (≤grade 3) occurred, resulting in chest tube placement in 23% of these patients. No complications ≥grade 4 occurred and overall survival was 100%, 89%, and 82% at one, two, and three years respectively. Therefore, both percutaneous microwave and cryoablation are suited for the treatment of sarcoma lung metastases, especially in peripheral or non-peripheral tumours ≤1cm, the study’s authors conclude.
An investigational device invented at Sanford Health (Sioux Falls, USA) that helps high-risk vascular disease patients has been granted a Breakthrough Device designation by the US Food and Drug Administration (FDA).
Patrick Kelly, a Sanford Health vascular surgeon, invented the aortic stent graft system designed to treat a thoracoabdominal aortic aneurysm (TAAA). This complex condition can cause dangerous bulging of the aorta extending from the chest down into the abdomen. It typically involves the branch arteries that supply blood to multiple internal organs. Left untreated, the aneurysm can rupture and cause sudden death.
The standard of care is complex open surgery, which is associated with a high rate of complications and mortality, and 40% of patients are not considered candidates for open surgical repair.
Kelly’s concept has the potential to treat more of those people utilising his minimally invasive approach. Under a physician-sponsored investigational device exemption (PS-IDE), he has treated more than 150 patients at Sanford Health over the past nine years who otherwise had no other options.
“This helps move the device through the regulatory pathway,” said Kelly. “It opens the door for more patients to have an option for repair, even the potential for patients with aortic dissections, failed prior repairs and anatomies that were previously thought to be untreatable. The non-anatomical design allows broad applicability of our patient population.”
That unmet need, leaving some patients with no other option, was key to the Breakthrough Device designation, said Katie Pohlson, senior director of innovation and commercialisation at Sanford Health.
“With it, we will receive prioritised reviews, access to senior staff at the FDA and collaboration with the FDA to help with the development of the product,” she said.
The WIfI classification system was developed to stratify the risk of major amputation at one year for patients presenting with chronic limb-threatening ischemia (CLTI). Recently, this system was used to identify patients most likely to benefit from revascularization. WIfI scores were used to define the estimated revascularization benefit quartiles ranging from high benefit (Q1) to questionable benefit (Q4).
“The aim of our study was to evaluate the revascularization benefit quartiles in a cohort of diabetic patients who had presented with critical limb ischemia,” said first author Caitlin Hicks, MD, of Johns Hopkins University.”
As reported in the October issue of the Journal of Vascular Surgery, researchers from the university’s Diabetic Foot and Wound Service, led by Hicks and senior author Christopher Abularrage, MD, evaluated 136 diabetic patients (187 limbs) who underwent lower extremity revascularization between 2012 and 2020 at their institution. The primary outcome of their study was one-year major amputation.
Demographic characteristics of these diabetic patients included:
Age 65 +/- 11 years
63% male
Presentation with ulcer (51%), gangrene (43%) or rest pain (6%)
Revascularization procedures were either endovascular (67%) or open (33%).
The estimated one-year amputation rates for each quartile were:
Q1 7 +/- 4%
Q2 4 +/- 3%
Q3 7 +/- 5%
Q4 26 +/- 8%
Analysis revealed the Q4 group had a significantly greater risk of amputation compared with the Q1 group (hazard ratio 4.3).
For the 137 limbs with greater than one-year follow-up after revascularization, a total of 16 (12%) required amputation. Nine of these were in the Q4 group.
“Overall, our data support the use of the WIfI benefit of revascularization quartiles for estimating the one-year major amputation risk for diabetic patients presenting with critical limb ischemia,” said Hicks. “We did, however, observe our actual amputation rate in the Q4 group was one half of what was expected. This may be explained by the fact that all of our diabetic patients are treated by our multidisciplinary team, which has been previously shown to have robust limb salvage outcomes.”
“Up to one half of the Q4 patients who underwent amputation did so despite patency of their revascularization procedure. This suggests wound size and infection burden are the driving factors behind the elevated risk in this group.”
The decision to perform revascularization in a patient with critical limb ischemia must be made carefully, particularly given their often extensive list of co-morbidities, researchers said. This study supports the use of the WIfI system to predict which diabetic patients with critical limb ischemia might best be served by revascularization and highlights the importance of multidisciplinary teams for complex medical and surgical patients.
A phase 1 clinical trial for the treatment of patients with inoperable mesothelioma, with both pembrolizumab immunotherapy and cryoablation, has begun in New Jersey and New York, USA. Starting 24 September 2021, the trial is expected to be completed by September 2023.
Pembrolizumab immunotherapy enhances the ability of the immune system to detect and kill cancer cells. In patients with inoperable mesothelioma in the chest of the abdomen, researchers are trialing the addition of cryoablation within a phase 1 trial. Cryoablation uses extreme cold applied through the needle into a tumour to break down and kill cancer cells. Researcher Micheal Offin and co-investigators Marjorie Zaudere and Etay Ziv (all Memorial Sloan Kettering Cancer Centre, New York, USA) have therefore begun to investigate the treatment impact of drugs that strengthen the immune system such as pembrolizumab, plus cryoablation for inoperable mesothelioma.
This single group assessment is designed as a single-arm and single-institution study, with an estimated 10 patients recruited. All patients must be over the age of 18 and have pleural or peritoneal mesothelioma that continues to grow despite previous treatment. Eligible patients must be fully capable of self-care, with the exception of carrying out strenuous activities. Patients who have received one previous line of systemic therapy which did not include pembrolizumab, are eligible for the study unless treated one year or more from the trial enrollment. Patients must also present a Karnofsky Performance Score (KPS) of ≤70% with adequate organ function. The criteria for adequate organ function is shown below:
Absolute neutrophil count ≥1.5K/mcL
Platelet count ≥100K/mcL
Adequate renal function as defined as creatinine ≤1.5x upper limit of normal (ULN) or creatinine clearance ≥45ml/min (as calculated by Cockcroft-Gault Formula)
Haemoglobin ≥ 9g/dL (prior transfusion permitted if not within seven days of enrolment)
Total bilirubin level ≤ 1.5 × the upper limit of normal (ULN) range
Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels ≤3.0 × ULN or AST
Eligible patients will receive one cycle of pembrolizumab (200mg/dose) delivered intravenously, followed by image-guided cryoablation of an ablation index lesion which will occur one to seven days prior to the start of cycle two. Cryoablation will treat a lesion with preference given to a lesion that is symptomatic or at risk of causing symptoms. Following institutional standards, complete ablation will be attempted. In addition, pembrolizumab will be continued for up to 24 months, unless disease progression, or intolerable toxicity. The number of patients with an adverse event defined as grade three or higher non-haematologic toxicity within 12 weeks of cryoablation will be the primary outcome measure.
In this penultimate episode of a special five-part series on the history of drug-coated balloons (DCBs), Jos van den Berg (Lugano, Switzerland) is joined by Gunnar Tepe (Rosenheim, Germany) and Thomas Zeller (Bad Krozingen, Germany), with the trio discussing major highlights from the IN.PACT Global real-world study, which showed consistent outcomes with the IN.PACT SFA randomised controlled trial despite including patients with longer and more calcified lesions and those with in-stent restenosis.
Tepe elaborates on some of the key differences between the IN.PACT SFA trial, which had stringent exclusion criteria, to the IN.PACT Global study. The latter, notes Tepe, allows us to “really learn how this DCB works in the real world”.
Zeller compares some of the key findings between the two, noting that at five years freedom from clinically-driven target lesion revascularisation in the SFA trial was 74.5% compared to 69.4% in the IN.PACT Global study. The SFA trial was “very selective”, adds Zeller, with mean lesion lengths of about 8cm compared to the Global study which had a mean lesion length of more than 12cm, and going up to 35cm. The comparable results between the two sets of data show that the device “performs well not only in standard lesions but also in complex lesions”. Overall, this gives Zeller confidence that the IN.PACT Admiral DCB is “very efficient, regardless of what kind of lesion you are treating” and that lesion length only has a “mild impact on overall outcome”.
These favourable outcomes are “related to the unique formulation of a high dose of paclitaxel combined with urea and also the mechanism of action of this balloon,” says van den Berg. He also emphasises the importance of such data, concluding that it “really guides me in my choices in my personal practice”.
Cryoablation is effective for local tumour control in patients with pulmonary metastatic disease. Within the ECLIPSE study, cryoablation had no significant impact on the patient’s quality of life (QoL), with the patient disease-specific survival rate remaining higher than the overall survival rate at both three and five years follow-up.
The multicentre single-arm ECLIPSE study1 prospectively evaluated the feasibility and effectiveness of CA in patients with pulmonary metastatic disease. Patients who had one to five metastatic lung tumours with a diameter of less than or equal to 3.5cm were eligible and treated with cryoablation. Local tumour control was the primary endpoint of this study, with cancer-specific survival, overall survival, and the QoL as secondary endpoints. QoL outcomes were assessed using the Karnofsky Performance Score, the eastern cooperative oncology group performance score, and the short form-12 health survey.
The ECLIPSE study enrolled 40 patients across three sites in the USA and one site in Europe, treating a total of 60 metastatic pulmonary tumours across 48 cryoablation treatments. Patients were followed over a period of five years and their disease status was monitored.
Thierry De Baere, Department of Anesthesia, Surgery and Interventional Imaging, Gustave Roussy
The study elucidated that cryoablation was effective in local tumor control within 87.9% of patients (29 of 33) and 79.2% (19 of 24) per tumour and 75.0% (15 of 20) per patient, at three and five years, respectively. Disease-specific survival was 74.8% at three years, and 55.3% at five years, whereas overall survival at three and five years was 63.2% and 46.7%, respectively. However, during the study, five patients experienced local disease progression. Patient QoL scores did not change significantly (p > 0.05). In the five follow-up years, only 55% of patients had to receive systemic anti-cancer treatment, with 27.5% of patients (11 out of 40) undergoing systemic chemotherapy and 7.5% (3 out of 40) of patients receiving radiation. Therefore, the ECLIPSE study illustrated that cryoablation is an effective method for long-term local tumour control in patients with metastatic pulmonary tumours, does not decrease patient QoL, and lowers the need for systemic treatment.
References
De Baere T. TEMPORARY REMOVAL: The ECLIPSE Study: Efficacy of cryoablation on metastatic lung tumors with a 5-year follow-up. Journal of Thoracic Oncology. 2021 Aug 9.
Rendering of HistoSonics treatment head demonstrating histotripsy delivery and targeted destruction of liver tissue
Rendering of HistoSonics treatment head demonstrating histotripsy delivery and targeted destruction of liver tissue
HistoSonics has revealed that the US Food and Drug Administration (FDA) has granted the company breakthrough device designation for its new histotripsy targeted liver therapy platform which is designed to help provide timely access to non-invasive liver treatment.
HistoSonics say that histotripsy of the liver provides clinicians with the first automated external beam therapy using acoustic energy to mechanically destroy and liquefy tissue in the liver without incisions, ionising radiation or heat.
Mike Blue, president and CEO of HistoSonics, sad: “the breakthrough device designation is a significant milestone for our company and validates our belief that our platform offers significant advantages over existing approved or cleared alternatives, per FDA requirements.
“Early and ongoing clinical results are promising and suggest that our ability to precisely destroy targeted liver tissue, completely non-invasively, and without the challenges associated with ionising radiation or other locoregional therapies, provides advantages to patients and physicians that don’t exist today, and we look forward to working with the FDA to make the technology accessible as quickly as possible.”
The company believes the novel mechanism of action of their proprietary technology may offer significant advantages to patients, including equivalent treatment effect throughout the entire treatment volume resulting in precise and predictable treatment zones. Early clinical and pre-clinical results also suggest that histotripsy largely preserves critical structures such as the liver capsule, and larger vessels and ducts within or adjacent to the treated volume of tissue.
In addition, histotripsy gives the treating physicians the ability to monitor the destruction of tissue under continuous real time visualisation and control, unlike any modality that exists today. The Breakthrough Designation will allow the company to engage with the FDA in a prioritised review during the regulatory market authorisation process, the company adds.
HistoSonics has worked with the FDA for over three years in developing pre-clinical and clinical data required for regulatory market authorisation and intends to continue collaborating with the agency throughout the ongoing Investigational Device Exemption (IDE) study, #HOPE4LIVER US, which is designed to evaluate the safety and technical efficacy of histotripsy in patients with primary and secondary liver tumours.
The company plans to share US and European #HOPE4LIVER study data and results with FDA to demonstrate the benefits of histotripsy in a broad patient population.
The HistoSonics system is investigational and is not available for sale in the United States or Europe. It is limited to investigational use in the approved IDE and European studies.
In support of the Legs Matter Campaign’s awareness week (11–15 October), Sam Everington, a GP at the Bromley by Bow Centre in London, UK, and former British Medical Association (BMA) chair, is calling on GPs, pharmacists and other primary care professionals to adopt a proactive approach towards “preventable,” life-threatening or serious leg and foot problems.
A press release reports that the growing epidemic, costing the UK National Health Service (NHS) up to £8.5 billionannually, affects an estimated 1.8 million people in the UK each year, often linked to obesity and caused by an underlying issue with circulation or neuropathy.
A report published earlier this year revealed that the number of patients with wounds annually has increased from an estimated 2.2 million between 2012/2013 to around 3.8 million in 2017/2018—an increase of 73%, the press release communicates.
Sam Everington said: “The Legs Matter Campaign is rightly focused on patient and public empowerment, identifying the small changes that people need to make to create change. Healthcare professionals providing services in primary care and community pharmacies also need to be at the forefront of this change.
“As GPs and pharmacists, we are there when people seek support for worrying changes or new injuries to legs and feet. We all need to act promptly and provide the right care swiftly so that these wounds do not deteriorate into long-lasting leg or foot ulcers or other serious, chronic conditions. It is simply not necessary and can be prevented.
“I would like to see all primary care professionals adopt a proactive approach to the spiralling number of serious leg and foot problems. If more patients and clinicians work together to address this national issue, we can start to turn the tide on this hidden epidemic.”
As part of the campaign targeting the public and patients; GPs, pharmacists, podiatrists, tissue viability, district and practice nurses are among the healthcare professionals being urged to take action, support the initiative and to sign up for online events during the third nationalweek.
Nurse consultant Leanne Atkin from Pinderfields Hospital in Wakefield, UK, is chair of the campaign, working to increase understanding, awareness and action for serious lower leg conditions, including leg or foot ulcers, swollen legs and cellulitis.
Atkin said: “For this year’s campaign, we want to empower people to be proactive about their own health and we are also asking primary care professionals to take charge of leg and foot problems and ensure that patients have access to face-to-face care, so that any issues can be spotted quickly. Ensuring patients receive the right healthcare at the right time makes a huge difference to both healing times and outcomes.”
Campaigners hope that as part of the week, even more primary care professionals will get involved and help patients to make a positive change using tips and the latest information on the www.legsmatter.org website, including self-management, exercise and having a positive mindset. The site will feature free resources and virtual events, suitable for the public, patients and healthcare professionals, including live Q&A sessions with clinicians and patients.
Former Army medic and disability sportswoman Nerys Pearce is fronting the 2021 Legs Matter Awareness Week campaign—urging others to take positive action and to make a change for better leg and foot health.
After sustaining life-changing injuries, she has received ongoing support from podiatrist and Legs Matter Campaign member Joanne Casey, from The Royal College of Podiatry. Joanne said: “Often with spinal injuries, like those sustained by Nerys, there is a lack of feeling, so it is important for us as health professionals to check the skin on the feet and legs for signs of redness, swelling, bruising, cuts or splits, changes in temperature and deformity. As podiatrists we can quickly identify a problem, suggest treatment and stop it escalating into something which could be life-threatening.”
Supported by NHS England, the Legs Matter Campaign was formed by a group of the UK’s leading lower limb clinicians, who, together with patient partners, are campaigning to make serious leg and foot problems a thing of the past.
Operating under the governance of the charity, The Tissue Viability Society, Legs Matter is also made up of representatives from The British Lymphology Society, Accelerate, The Royal College of Podiatry, The Society of Vascular Nurses, The Lindsay Leg Club Foundation, Foot in Diabetes UK and The Leg Ulcer Forum. It wants to ensure that anyone with a lower leg or foot problem understands their condition and gets the urgent care and support that they need.
One-year results presented at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA) from the EMINENT trial demonstrated the superiority of the Eluvia drug-eluting stent (DES) system (Boston Scientific) compared to self-expanding bare metal stents for the treatment of patients with peripheral arterial disease (PAD) with superficial femoral artery (SFA) or popliteal artery lesions up to 210mm in length, the principal investigator (PI) said. The study enrolled 775 patients, making it the largest randomised trial of a drug-eluting stent for the treatment of PAD to date, Boston Scientific said in a press release.
In the trial, the Eluvia stent exhibited superiority with a primary patency rate of 85.4% vs. 76.3% with bare metal stents (p=0.0087), data presented by EMINENT study PI Yann Gouëffic, from the Department of Vascular and Endovascular Surgery at Paris Saint-Joseph Hospital, Paris, France, showed.
The analysis also showed a significantly greater rate of sustained clinical improvement without reintervention—83% for patients treated with the Eluvia stent compared to 76.6% for those treated with a bare metal stent (p=0.0450). Further, there was no significant difference in major adverse events or all-cause mortality rates between patients treated with the Eluvia stent and those treated with a bare metal stent through one year.
“I am honoured to have been part of this global study, which adds to the robust body of evidence from the IMPERIAL trial and confirms that the Eluvia stent should be considered the stent of choice for treating SFA and [popliteal] lesions of intermediate length,” said Gouëffic. “The superior primary patency rates and greater rates of clinical improvement without reintervention are reassuring for physicians looking to make clinically-based treatment decisions for their patients and reduce the need for repeat procedures.”
A worldwide committee of 40 cross-speciality medical experts achieved the first-ever consensus for the appropriate use of intravascular ultrasound (IVUS) in peripheral vascular disease (PVD) interventions.
Global experts conducted a systematic and comprehensive review of key clinical IVUS scenarios and decision-making processes before voting. The results were shared at a sponsored symposium during Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA). They established clinical consensus to identify optimal use of IVUS and potential gaps in a bid to to set a standard across clinical specialties and drive positive outcomes for patients.
The new consensus and recommendations are aimed at improving quality care in PVD and are based on evidence, expert practice standards, and clinical experience, according to a press release from Philips, the company behind IVUS.
“The results of the cross-speciality expert consensus demonstrate strong support for the use of IVUS during peripheral interventions,” said Eric A Secemsky, an interventional cardiologist at Beth Israel Deaconess Medical Center in Boston, USA. “Future efforts need to focus on improving IVUS implementation into clinical practice and streamlining procedural workflow to help improve our patient outcomes.”
Today, healthcare providers’ use of IVUS in PVD interventions is not standardised and is therefore inconsistent, Philips stated in the press release. “The new appropriate-use expert consensus may help establish global standards of care to adopt into guidelines and improve quality care in PVD,” the company added.
Several subgroups of patients treated with the IN.PACT AV drug-coated balloon (DCB; Medtronic) for arteriovenous fistulas (AVFs) demonstrated a “statistically significant” higher rate of target lesion primary patency (TLPP) compared to those who underwent standard percutaneous transluminal angioplasty (PTA) through 24 months, investigators behind the IN.PACT AV Access study have reported.
Principal investigator Robert Lookstein, executive vice chair in the Department of Diagnostic, Molecular and Interventional Radiology at Mount Sinai Health System in New York, USA, delivered the two-year results from the trial during a late-breaking session at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA).
IN.PACT AV is a prospective, global, single-blinded, randomised controlled trial with 330 participants, with 170 receiving IN.PACT AV DCB and 160 undergoing PTA.
The investigators reported that the primary outcome of TLPP—defined as freedom from clinically-driven target lesion revascularisation—in patients with restenotic lesions, radiocephalic and brachiocephalic AVF types, cannulation zone lesions as well as anastomotic lesions treated with the DCB through 24 months was superior to those who received PTA treatment in all cases.
“Benefits were seen in all other subgroups, though sample sizes were small and the treatment effect was not statistically significant,” Lookstein told VIVA attendees.
The results showed higher TLPP with DCB versus PTA based on time-to-event analyses: restenotic lesions (46% vs. 30.2%), radiocephalic AVFs (53.6% vs. 43%), brachiocephalic AVFs (48.5% vs. 27.3%), anastomotic lesions (48.4% vs. 32.7%), and lesions in the cannulation zone (74.2% vs. 18.9%). The greatest TLPP benefit through 24 months was observed in “lesions treated with the smallest balloon diameter sizes”—those treated with balloon diameters of >6mm showed a TLPP of 52.2% in the case of the DCB group vs. 38.9% among PTA patients. Meanwhile, lesions tackled using balloons with diameters ≤6mm saw TLPP rates of 52.1% (DCB) vs. 32.6% (PTA), the data showed.
“I think this really starts to identify the specific patient population and lesions that are ideally suited for this technology,” Lookstein said. “These durable, long-term data suggest the use of this therapy may be considered stand-of-care for patients with end-stage renal disease [ESRD] at high risk for repeat interventions in their arteriovenous fistulas.”
An interim analysis from the DISRUPT PAD III observational study showed that intravascular lithotripsy (IVL; Shockwave Medical) performs “consistently well” across challenging peripheral vessels, lesions and subgroups of patients, Ehrin J Armstrong, medical director at Adventist Heart and Vascular Institute in St Helena, USA, told a clinical trials late-breaking session at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA).
Analysis of the full data set contained in the study—reputedly the largest angiographic core lab adjudicated real-world evidence for IVL in heavily calcified peripheral arteries according to Shockwave Medical—is due to be presented next year.
Findings from the first 752 patients included in the interim analysis demonstrated that IVL “consistently” showed its ability to safely and effectively modify superficial and deep calcium across multiple vascular beds, lesion types and in patients with chronic limb-threatening ischaemia (CLTI), Armstrong reported. IVL resulted in consistent reduction in the diameter of stenosis with no associated distal embolisation, abrupt closure or thrombotic events at any time, according to Shockwave. IVL outcomes were comparable to the previously reported DISRUPT PAD III randomised controlled trial (RCT) outcomes showing minimal procedural complications and consistent reduction in diameter stenosis. The technology was also successfully used in combination with adjunctive technologies, including specialty balloons and atherectomy, in the treatment of complex calcified lesions, the company further reported.
“Patients with heavy calcification have traditionally been excluded from endovascular treatment trials resulting in little available evidence to provide guidance for treating this challenging patient population,” said Armstrong. “The DISRUPT PAD III [observational study] shows that in common clinical situations that physicians encounter daily, peripheral IVL performs consistently well in a variety of peripheral vessels, lesions and subgroups.”
The observational portion of DISRUPT PAD III is a prospective, multicentre, single-blind study of real-world patients, which augments the DISRUPT PAD III RCT. The interim analysis involves patients enrolled between November 2017 and June 2019 at 18 global sites.
Of the 852 lesions treated in the iliac, common femoral, superficial femoral, popliteal and infrapopliteal arteries, 88% presented with moderate/severe calcification, with an average calcified length of 127mm. The use of IVL in these lesions resulted in a final residual stenosis of 24%, similar to the DISRUPT PAD III RCT finding of 22%, Armstrong told VIVA attendees. Patients also experienced minimal procedural complications, with only 0.9% and 0.1% of patients experiencing final dissections and perforations, respectively. “Notably, there were no instances of embolisation, thrombus, no reflow or abrupt closure.” The observational study completed enrolment in June 2021 with a total of 1,373 patients.
Late-breaking session panellist Benjamin W Starnes, the chief of Vascular Surgery at the University of Washington (UW) in Seattle, USA, commented: “Your one-year follow-up data happened right in the middle of a pandemic—what was it like to conduct a clinical trial in the setting of a pandemic?”
Armstrong said the dynamic of the COVID-19 virus was initially challenging, explaining: “At our own hospital, it was mandated that the research coordinators not interact with patients for the first few months, so I conducted a lot of the follow-up myself. That being said, our patients with peripheral arterial disease [PAD]—because they have such complex issues—in some cases we flexed to doing virtual visits, but we were able to get these patients in in most cases with outstanding follow-up. Which, to me, really demonstrated the versatility of conducting research, despite dealing with all these different complexities in the setting of a pandemic.”
Patients treated with the Ranger drug-coated balloon (DCB; Boston Scientific) sustained “improved primary patency” with fewer reinterventions than those treated with uncoated devices, two-year results from the RANGER II SFA randomised controlled trial have demonstrated, investigators revealed during a late-breaking session at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA).
Principal investigator Ravish Sachar, an interventional cardiologist at North Carolina Heart and Vascular at UNC REX Healthcare in Raleigh-Durham, USA, delivered the data, telling attendees that subgroup analyses—covering women, patients with baseline chronic total occlusions (CTOs) and calcified lesions—also suggest “consistent benefit” of DCB treatment versus standard percutaneous transluminal angioplasty (PTA).
Additionally, the two-year results showed no difference in mortality rate between the groups.
In a press release, Boston Scientific said the data confirmed the safety and efficacy of the Ranger DCB compared to standard PTA for the treatment of patients with peripheral arterial disease (PAD) in the superficial femoral artery (SFA) and proximal popliteal artery. The new findings follow the May 2021 publication of the one-year results of RANGER II SFA in JACC: Cardiovascular Interventions.
Sachar and colleagues found that the Ranger DCB exhibited a higher primary patency rate of 84% compared to 71.4% in patients treated with standard PTA (p=0.0129). Additionally, the subgroup analyses found consistent benefit with greater long-term patency in patients with more complex lesions treated with the Ranger DCB, exhibiting an 89.1% vs. 72.4% primary patency rate in the moderate to severe calcium subgroup (p=0.0052) and a 76.6% compared to a 58.6% primary patency rate in patients with CTOs (p=0.1038).
“These two-year data demonstrate a sustained, high rate of efficacy—including in patients with more complex lesion subtypes, yet another proof point for physicians to consider when determining the best individualised treatment option for their patients with PAD,” said Sachar.
The Ranger DCB also demonstrated a significant reduction in reinterventions at two years, with a freedom from target lesion revascularization (TLR) rate of 87.4% vs. 79.5% observed with standard PTA (p=0.0316). Additionally, there was no significant difference in all-cause mortality: 5.7% for Ranger DCB patients and 3.2% in those treated with standard PTA (p=0.4218). Sachar added that there was no reintervention disadvantage based on gender.
Real-world data drawn from the IN.PACT Global study looking at five-year freedom from clinically-driven target lesion revascularisation (TLR) among prespecified chronic total occlusion (CTO), long lesion and de novo in-stent restenosis (ISR) cohorts “continues to confirm long-term clinical safety and effectiveness” of the IN.PACT Admiral (Medtronic) drug-coated balloon (DCB) in the treatment of complex femoropopliteal lesions.
Results from the study—involving 417 patients—were delivered by Gunnar Tepe, head of the Department of Diagnostic and Interventional Radiology at RoMed, Rosenheim, Germany, during a late-breaking session at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA).
Tepe reported that mean lesion lengths were 22.8±9.7cm, 26.4±8.6cm, and 17.1±10.5cm in the CTO, long lesion, and de novo ISR cohorts, respectively. The majority of lesions were calcified, he said. Kaplan-Meier estimates of freedom from clinically-driven TLR through five years were 69.8% for CTO, 67.3% for the long lesion group and 58% for ISR. The cumulative incidences of the composite safety endpoint were 69.8%, 65.7%, and 56% in the CTO, long lesion and ISR cohorts, respectively, Tepe continued.
The number of major target limb amputations were very low in all three cohorts, with no amputations in the CTO, two in the long lesion, and one in the de novo ISR cohorts, he told VIVA attendees. Kaplan-Meier estimates of five-year freedom from all-cause mortality rates with vital status were 78.2% (CTO), 75.2% (long lesion), and 81.4% (ISR).
“This is the first presentation of prospectively collected five-year data from prespecified in-stent restenosis, long lesion and chronic total occlusion cohorts from a large global DCB study,” said Tepe.
He concluded: “High five-year freedom from clinically driven TLR was demonstrated in all three prespecified cohorts, but it was slightly lower in the de novo ISR cohort, highlighting the challenging nature of ISR lesions. No safety issues were reported in any of the cohorts. All-cause mortality with vital status at five years was 81.4% for de novo ISR, 75.2% for long lesions and 78.2% for CTOs. These data support incorporating the use of the IN.PACT Admiral DCB into clinical treatment algorithms for complex femoropopliteal disease.”
The IN.PACT Global study was a prospective, multicentre, single-arm study conducted at 64 international sites that enrolled 1,535 participants, including some with complex lesions. Assessments through five years included freedom from clinically driven TLR, safety composite and major adverse events.
Preliminary clinical results from a first-in-human study assessing the Amplifi vein dilation system (Artio Medical) were presented at Vascular Interventional Advances (VIVA) 2021 (5–7 October 2021, Las Vegas, USA). Data were presented by Surendra Shenoy—an associate professor of surgery at the Washington University School of Medicine at Barnes-Jewish Hospital in St Louis, USA—during the event’s final late-breaking clinical trial session.
The Amplifi system is designed for percutaneous placement and up to 14 days of use to stimulate arm vein enlargement in haemodialysis patients using rapid, non-pulsatile, venous blood flow. The device includes a wearable, external blood pump, inflow and outflow catheters, and a controller, all of which are removed completely during arteriovenous fistula (AVF) creation. It aims to make more patients eligible for AVF surgery, reduce the time required for AVF maturation and increase successful maturation after AVF creation.
Data presented at VIVA came from the first five patients treated in a prospective, non-randomised, single-arm, first-in-human clinical study with the Amplifi system, and demonstrated that forearm and upper arm mean cephalic vein diameters had more than doubled over an average treatment period of 8.6 days.
AVFs were successfully created using treated veins in all patients. Maturation data are available for the first three patients and show that both the forearm and upper arm AVFs matured quickly with mean outflow vein diameters of 7mm and a mean blood flow rate of more than 1,000 ml/min after a six-week maturation period. No device-related or procedural adverse events were observed.
“Not long after AVFs were first pioneered for haemodialysis in 1966 by doctors Cimino, Brescia, and Appel, concerns were raised about patients who were not suitable for AVF surgery and the high rate of AVF maturation failure,” Shenoy said. “Despite these challenges, AVF remains the preferred option for most patients today. The Amplifi system is the first device I have seen that has real potential to address both of these challenges in a major way, to make good on the promise of providing reliable, long-lasting vascular access sites for this unique and vulnerable patient population.”
In a press release, Artio Medical stated it is planning to set up a US clinical trial of the Amplifi vein dilation system in 2022.
Boston Scientific announced positive results for the EkoSonic endovascular system (EKOS system) during a late-breaking clinical trial presentation at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA). Data from the KNOCOUT PE registry—established to measure institutional adoption of a lower dose and lower-duration thrombolysis protocol for the EKOS system—confirmed the safety and efficacy of the EKOS system for the treatment of patients with intermediate-high and high-risk pulmonary embolism (PE).
“PE remains a life-threatening and complex disease, but these results provide an opportunity to advance patient care by showcasing evidence that proves a lower drug dose and shorter infusion duration of a thrombolytic agent may result in enhanced safety and efficacy,” said Keith M Sterling (Inova Alexandria Hospital, Alexandria, USA), study principal investigator. “The findings in this registry analysis are very reassuring to physicians making critical evidence-based decisions for their patients in what are oftentimes emergent treatment situations.”
The international registry of 489 patients across 83 centres included data from patients treated with the EKOS system who were provided a lower drug dose and shorter infusion duration of a thrombolytic agent than administered in previous studies, reflecting contemporary clinical practice. In the data, there were no intracerebral haemorrhagic (ICH) events, or brain bleeding events, with a low major bleeding rate of 2.5%, compared to the rate previously observed with systemic thrombolysis treatment. Results also demonstrated a 23% post-procedure reduction in the main indicator of heart strain from PE, measured as right ventricular to left ventricular diameter ratio (RV/LV).
“As the largest prospective body of evidence in the interventional PE space to date, the KNOCOUT PE registry provides an accurate modern representation of patients with PE treated with the EKOS system every day,” said Michael R Jaff, chief medical officer and vice president clinical affairs, technology and innovation, Peripheral Interventions, Boston Scientific. “The strong safety and efficacy findings exhibited in this registry add to the existing clinical evidence supporting the EKOS system as a treatment option that physicians can trust, as it is already the most studied interventional device in the PE space.”
The ultrasound technology used by the EKOS system accelerates thrombolysis—the breakdown of the clot—minimising the time it takes to treat a patient and lowering the necessary thrombolytic dose, which can result in optimised outcomes and a lower risk of bleeding.
Eighteen-month results from the PRESTIGE below-the-knee (BTK) study were presented as a late-breaking clinical trial at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA). The objective of this clinical investigation is to evaluate safety and performance outcomes of Selution SLR (MedAlliance), a novel sirolimus-eluting balloon for the treatment of long tibial occlusive lesions (TASC C and D) in patients with chronic limb-threatening ischaemia (CLTI).
Freedom from target lesion revascularisation (TLR) was exhibited by 88% of patients and 79% demonstrated amputation-free survival (AFS). The rate of wound healing was 79% and 79% of the patients improved their Rutherford score by at least one category. The 18-month results have been sustained from the six-month and 12-month data.
PRESTIGE is a prospective, single-centre, physician-initiated clinical study, run at the Singapore General Hospital (SGH) by Chong Tze Tec and Tang Tjun Yip. Twenty-five patients were enrolled with an average age of 64. Eighty-eight had diabetes mellitus and 44% had end-stage renal failure. No patients required bailout stenting. Clinical follow-up was at one, three, six, 12 and 18 months.
“We have observed minimal slow-flow phenomena, seen with other paclitaxel drug-eluting balloons. We have observed several cases of fast wound healing with Selution SLR. It is easy to track and deliver. We are looking forward to gaining further clinical experience with this device,” commented Chong.
“Singapore has a high percentage of diabetics in its population and CLTI therefore constitutes a major challenge among patients seen with peripheral arterial disease (PAD) who may benefit from this technology,” commented Tang. SGH performs over 1,000 interventional procedures a year on patients suffering from CLTI, according to a MedAlliance press release.
Selution SLR was awarded CE mark approval for the treatment of PAD in February 2020 and for the treatment of coronary arterial disease in May 2020. The US Food and Drug Administration (FDA) has awarded Selution SLR with four Breakthrough designations: for the treatment of atherosclerotic lesions in native coronary arteries; coronary in-stent restenosis; peripheral BTK and arteriovenous fistula indications.
LimFlow SA has announced 24-month results from the PROMISE I study of the LimFlow percutaneous deep vein arterialisation system, confirming “excellent and sustained outcomes” for both amputation-free survival and wound healing, a press release reports. The late-breaking data were presented at Vascular Interventional Advances (VIVA) 2021 (5–7 October, Las Vegas, USA).
“The presentation of the PROMISE I 24-month resultsvalidate the benefits of the LimFlow system,” said Daniel Clair, chair of the Department of Vascular Surgery at Vanderbilt University Medical Center Section of Surgical Sciences in Nashville, USA, and PROMISE I principal investigator. “The high percentage of no-option CLTI [chronic limb-threatening ischaemia] patients that remained amputation free at 24-months is a major positive step forward for a condition characterised by high amputation and mortality rates.”
PROMISE I is a multicentre, prospective, single-arm study of the LimFlow system, conducted at seven study centres across the USA. All of the 32 patients enrolled in the study had non-healing wounds on the target foot. The primary endpoints were freedom from amputation, amputation-free survival, and survival overall. There were no amputations after day 75 in the study. At 24-months, freedom from amputation remained at 77% with an amputation-free survival of 59%. Three additional deaths within the second year of study resulted in 77% survival (two non-limb-related deaths; one from sepsis due to a non-healing wound in the non-treated foot). Ninety-two per cent had all wounds classified as healed or healing as adjudicated by an independent core lab. Technical success was reported at 97%.
“The two-year data from PROMISE I US feasibility study are highly encouraging and send a strong signal about the potential of the LimFlow system to strengthen our mission of no limb left behind,” said LimFlow CEO Dan Rose. “We are swiftly advancing our study of the LimFlow system in the ongoing PROMISE II US pivotal study in a patient population which is facing a very poor overall prognosis in terms of mortality and quality of life after major limb amputation. The LimFlow system is designed to help heal wounds and avoid major limb amputation, and we are proud of our mission of ‘No Limb Left Behind’.”
“I strongly believe that you cannot be what you cannot see. If you want more women or under-represented minorities (URMs) to enter the field and be at the table, then we need more women and URM leaders in the field,” Maureen Kohi (Chapel Hill, USA).
What attracted you to a career in interventional radiology?
My ‘a-ha’ moment that drew me into a career in vascular and interventional radiology was during my third year of medical school. I had observed countless prolonged open surgeries, and then scrubbed into one of my first cases of endovascular aneurysm repair of the abdominal aorta. I was moved by the precise and delicate deployment of the stent graft by a ‘vascular and interventional radiologist’ who forestalled a major abdominal surgery and resulted in the patient experiencing a quicker post-procedure recovery, faster hospital discharge, and lower complication rates. I loved the innovation of the field, the efficiency of the procedures, the delicate and yet deliberate procedural dance, and the monumental impact on clinical care provided through a pinhole. I knew I would be destined to become a vascular and interventional radiologist.
Who have been your mentors?
I owe my entire career to my mentors and sponsors along the way, as I truly believe we stand on the shoulders of giants, and I am forever grateful for their support. My most impactful mentor was Ernie Ring, who showed me the glorious world of academic interventional radiology. At the University of California, San Francisco (UCSF), I owe my research and academic success to my research mentors Karen Ordovas and Sharmila Majumdar who taught me how to become a physician-scientist and a research mentor. I also felt so incredibly supported and promoted by my chairman, Ron Arenson, who encouraged me to pursue a leadership career in radiology. During my junior faculty years, I was very fortunate to meet several luminaries who took me under their wing and helped to mentor and sponsor my career. I am forever indebted to Anne Roberts, Barry Katzen, Dan Sze, Jafar Golzarian, Jim Benenati, Jim Spies, Laura Findeiss, Mahmood Razavi, Mike Dake, Mike Darcy, Kathy Krol, Lindsay Machan and Ziv Haskal. During my transition from division chief to department chair, I relied a great deal on support and mentorship from Alan Matsumoto, Bob Ryu, Chuck Ray, Jim Spies, John Kaufman, Matt Mauro, and Reed Omary. Throughout my career, I have been very fortunate to have tremendous women peer mentors and I do not believe I could be where I am without the love and support of Kari Nelson, Theresa Caridi, Nadine Abi-Jaoudeh, Alda Tam, Alex Barnacle, Gloria Hwang, Janice Newsome, Nishita Kothary, Isabel Newton and Tze Wah.
Has COVID-19 provoked new ways of working for the interventional radiologist long-term?
In the clinical realm, we have learned a great deal about telehealth and the ability to offer our services to remote areas. In education, we have learned to leverage virtual platforms for conferences, grand rounds, and guest speakers. However, as good as we have become at assembling virtual meetings, I feel we all crave the in-person experience of socialising and networking. While the virtual component is ‘good enough’, it does not come close to the ideal of in-person meetings. In short, COVID-19 has taught us how to pivot, be nimble, and evolve, but some things are best left in the ‘old world’ such as meeting in-person, without social distancing, and masks. I really hope we can get back to that ‘old normal’ real soon!
Maureen Kohi (USA)
Could you share a positive and negative experience you have had as a woman leader, and how you dealt with both?
As a female leader, I find any interaction where I promote or recruit a woman into the field of radiology or interventional radiology or within its leadership as a positive experience. Most recently, my most positive experience was my privilege to name Gloria Salazar as the very first woman Latin X division chief of Vascular Interventional Radiology at University of North Carolina and also nationwide. I have been fortunate in not having encountered many negative experiences as a female leader. However, the one that comes to mind is being repeatedly mistaken as a medical student, resident, fellow, nurse, or technologist. Once I was written up by a patient who felt I was a resident who placed her chest port when I was a first-year junior faculty. It reminds me of the eternal unconscious bias that as a young-appearing woman interventional radiologist, I look like every other member of the team, except for the attending physician or the leader of the team.
Could you describe your interventional radiology-suite personality?
I am a very efficient and fast-paced person who plans multiple steps ahead and enjoys a brisk procedural dance. I also like to set a relaxed and social procedural environment where I can teach my trainees about how I do a variety of procedures and also use the time to learn more about them. However, when the procedure gets more complicated or things are not going according to plan, I become quieter and more deliberate, knowing that as the attending, I set the cadence in the room. The calmer I am, the more relaxed the environment. The patient is always the focus of our work and the closer and more connected we are as a team, the more successful we will be at delivering excellent patient care.
What is the most exciting way of attracting women and URMs to the interventional radiology table?
I strongly believe that you cannot be what you cannot see. If you want more women or URMs to enter the field and be at the table, then we need more women and URM leaders in the field. We only have one woman interventional radiologist as department chair and currently there are no URM IRs as department chairs. There are no women or URM IRs as deans or CEOs of medical centres. However, we are seeing numerous women IRs become division chiefs and programme directors. This is the first step to bridging the gender and racial gap to ensure we have excellent role models at the table to attract the next generation of leaders, particularly women and URMs into the field.
In the last year, which new research paper has caught your attention?
One of the most interesting manuscripts was the publication of the FEMME (Fibroids with either embolisation or myomectomy to measure the effect) trial, which was a randomised controlled trial comparing quality of life associated with the two treatments among women wishing to avoid hysterectomy. The primary outcome of this trial was the change in the Uterine Fibroid Symptom and Quality of Life (UFS-QOL) questionnaire after two years. This trial was the very first of its kind to have a very diverse population with a large number of African American participants, women with large uteruses, and severe fibroid symptoms. The trial demonstrated that the myomectomy group had a longer hospital stay and almost double the complications than the uterine fibroid embolization (UFE) group. While both groups demonstrated improvement in their UFS-QOL scores after therapy, the myomectomy group demonstrated a slightly higher improvement compared to the UFE group. Overall, the trial demonstrated that UFE and myomectomy are more alike than different. In addition, it demonstrated that compared to myomectomy, UFE resulted in post-embolization syndrome, shorter hospital stay, quicker return to work, fewer severe adverse events, and potentially comparable fertility outcomes.
Could you describe a memorable case?
I was consulted about a 23-year-old female who had presented with massive vaginal bleeding due to a uterine arteriovenous fistula (AVF) following a dilation and curettage (D&C). She underwent UFE with particulate embolization, which was unsuccessful and continued to experience severe vaginal bleeding and was planned to undergo a hysterectomy. I was fortunate to have been consulted to see if there was any way to preserve her fertility. I was able to embolise the AVF by directly puncturing and embolising the nidus using ethylene vinyl alcohol copolymer. She went on to have a quick recovery and then become pregnant and give birth to a healthy baby. The case taught me that the innovative spirit of interventional radiology lives in all of us. In addition, it reminded me that we should not be so quick to recommend hysterectomy. Instead, we should take a step back and think of what else we can offer to preserve fertility and avert hysterectomy. We would never do a nephrectomy for a renal AVF or a pneumonectomy for a pulmonary arteriovenous malformation. So why remove a woman’s uterus because of a fistula? Go direct and obliterate the fistula, retain fertility, and avoid hysterectomy.
What interests you outside of medicine?
I most enjoy spending time with my 11-year-old son, husband, dog and our friends. I also love all things athletic: running, biking, hiking, kayaking, jet skiing, or going to a baseball or basketball game. I am a huge Tar Heel fan, so anything that applies to the University of North Carolina. I am inspired by music and played trombone in the Stanford band. My other interests include baking, travelling, and wine. Reading a book (anything by Jane Austen) at the beach with my feet in the water while my son and husband body surf is a favourite pastime. As I grew up in Northern California, I love wine tasting and learning about how wine is made. Moving to the South my interests have expanded into visiting breweries and distilleries and learning more about Southern cooking.
Left to right: Kim Hodgson, Caitlin W Hicks, Jim A Reekers, Joseph Mills
Left to right: Kim Hodgson, Caitlin W Hicks, Jim A Reekers, Joseph Mills
Is target lesion revascularisation (TLR) a meaningful clinical endpoint for research or should it be “tossed as a legitimate endpoint for peripheral vascular disease treatment success in US FDA [Food and Drug Administration] approval trials?” Recent keynote presentations and conference debate on appropriate care for peripheral vascular disease leave overuse of interventional therapy, particularly for claudication, staring down the end of a barrel. They also trigger a conversation around TLR becoming a target in and of itself.
Kim Hodgson, the 2019–2020 Society for Vascular Surgery (SVS) president, delivered a “delayed-due-to-COVID-19” presidential address at the 2021 Vascular Annual Meeting (SVS VAM 2021; 18–21 August, San Diego, USA and online) laying out a path to champion appropriateness in vascular care. He wasted little time in conveying the message he has long sought to convey to SVS members: that the threat posed to vascular surgery by a small number of “bad actors” carrying out inappropriate procedures is real—and that it is long past time to address the issue.
The day after Hodgson introduced the concept during the Crawford Issues Forum, data were presented by Caitlin W Hicks, associate professor of Surgery at Johns Hopkins Medicine in Baltimore, USA, and colleagues at VAM on the overuse of early peripheral vascular interventions for claudication. Since then, further research has built upon the charge that outliers are performing inordinate levels of certain procedures, including atherectomy carried out in the office-based lab (OBL) setting.
The impact of the explosive growth of atherectomy on patients and healthcare finances is problematic and growing exponentially, Hodgson lamented. He turned to further findings from Hicks showing that of the roughly US$267 million reimbursed by Medicare for first-time femoropopliteal peripheral vascular interventions in 2019, 90% was for atherectomy, “leaving only US$26 million to pay for all of the other therapies that actually have evidence showing that they work.”
Hodgson called out what he called “the enablers” of this type of practice—“people or constructs that encourage or enable negative behaviour in others.” The Centers for Medicare & Medicaid Services (CMS) was one, with “distorted reimbursement incentives” contributing to the problem, he argued.
Another enabler is the FDA, Hodgson said, calling for TLR to be “tossed as a legitimate endpoint for peripheral vascular disease treatment success in FDA approval trials.” Hodgson also called out vascular surgery’s industry partners. He said they should be “the canary in the coalmine for inappropriateness. You are uniquely positioned to spot abuse early—before patients are harmed. You know every one of the outliers in vascular care.”
Jim A Reekers, professor emeritus of Radiology at Amsterdam University, Amsterdam, The Netherlands, is currently the editor-in-chief of CVIR Endovascular and has served as president of several national and international organisations, such as the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the interventional radiology division of the European Union of Medical Specialists (UEMS). He tells Interventional News: “I read with great interest the address of Dr Hodgson during the 2021 iteration of VAM about inappropriateness in care. I fully agree with the content, and I am happy with this initiative for change. I truly hope that his address will mark the start of a new era where the patient will be again the focus of our work and not only the patient’s lesion. As mentioned by Dr Hodgson, there has never been any scientific evidence for atherectomy while there is overwhelming high[1]quality evidence for SET [supervised exercise therapy], and there has been for a long time. Dr Hodgson also touched on the holy grail of TLR, which is instrumental to what he says about inappropriateness in care. TLR is a flawed and constructed pseudo endpoint for peripheral vascular disease treatment success, without any relation to real clinical patient outcome, benefitting only commercial trials (as published by Reekers in The Lancet in 2019). His idea that industry partners are uniquely positioned to spot abuse is true and needs no further discussion.”
Speaking at a separate VAM sponsored session on paclitaxel safety, which drew a mix of sceptical and cautious responses to the latest meta-analysis from interventional radiologist Konstantinos Katsanos and colleagues (Patras University Hospital, Patras, Greece), that reported a heightened risk of major amputation after use of paclitaxel-coated balloons (PCBs) in femoropopliteal and infrapopliteal arteries, Joseph Mills, professor and chief, Division of Vascular Surgery and Endovascular Therapy, Baylor College of Medicine, Houston, USA, and SVS vice president, made the point that there was a real need for studies that are redesigned to look at […] clinically significant endpoints for patients.”
As specialists interested in patency, Mills continued, vascular providers tend to think that if a treated lesion stays patent for a bit longer, then the treatment “has got to be better for the patient. But the actual endpoint for a claudicant would be how far they can walk, what their quality of life is; and, for a chronic limb-threatening ischaemia (CLTI) patient, it is going to be: do they heal? do they have recurrent wounds? Those questions are a little bit different than the actual lesion-specific focus. I think if we can do anything from this, it would be to get industry to start looking at different endpoints.”
In the wake of the COVID-19 pandemic, the world of education went virtual. John Rundback (Advanced Interventional & Vascular Services LLP and American Endovascular & Amputation Prevention PC in Clifton, USA), who has been involved in interventional device education for more than 25 years, believes virtual procedural training is here to stay. In this interview, Rundback details how procedural training has adapted and is thriving in its new digital setting, with available systems offering increasingly immersive learning environments available to an international cohort of students. He predicts an 80:20 split between virtual and in-person training in the future.
What did training look like before the COVID-19 pandemic?
In-person training was the norm before COVID-19. Students would come in to our department to observe cases, to work on projects that we would assign to them and to be involved in live cases. For a live case, we would bring in audio and video crews so that we could broadcast the case for international meetings. There would also be various fellows and residents who would come in and rotate with us. Students had to physically be there, and that was great—you certainly had that personal interaction, but it was also time-consuming in that you had to devote your attention to an individual.
In-person training was dealt a blow due to COVID-19. How did it then transform?
When COVID-19 hit, obviously everything changed. I have been involved in medical education, and specifically interventional device education, for my entire career—more than 25 years now—and so it is part of who I am.
We have now moved towards using virtual platforms. Typically, a virtual platform will feature a video monitor that has several inputs and cameras. What this creates is a remote, immersive environment, and, in many respects, I think it is better than what we used to have. Rather than trying to see what is going on in a busy procedure room, where you are trying to find the optimal positioning to look at the monitors and look at what you are doing, you can now focus more on the patient. In addition, the user can control the inputs, and so there are no wasted efforts in teaching, and this has created a much better flow and a much more curated experience for the people who log in.
There are other advantages as well. Remote learning makes scheduling easier, both for us and for the attendees, who instead of having to set aside a day or longer, they can just log in for specific cases or specific portions of cases, and we can of course record portions of those as well.
Moving forward, I think this is going to be a new paradigm, and we have platforms that are expanding their capabilities with more inputs and more cameras, so we can really make this even more of a comprehensive environment and make the remote user feel like they are in the room.
How do virtual platforms change local training and have they maintained their value when tested for international training as well?
We have actually done some international training already with Avail, the technology that we have chosen for remote virtual training. We have had people who have logged in from Europe so far to watch us during our training and our courses. That is one of the beautiful things about remote learning—by training in a virtual or digital environment, distance is no longer a concern. The challenges of mobilising or disrupting your practice to go and learn, are completely resolved. Furthermore, not only can we potentially educate more people, but from the trainee’s point of view, you can train more often. You cannot necessarily understand everything the first time you go through it but, but remote training gives you the opportunity to participate in a number of different procedures until you reach a comfort level. That would be impossible if trainees had to repeatedly travel to a remote location to try to accomplish the same goal.
What is your lucky guess on the shape of training in the next couple of years?
I think that in the future device and procedural training is going to be 80:20, utilising a virtual platform more often than actual onsite or hands-on training. I think a big part of training is understanding the procedural steps, the cognitive processes behind that and the troubleshooting associated with getting through a case. That is actually 80% of it. Often interventionalists have the skills—the haptic skills, the hands-on skills—and so translating them into your own practice, actually being able to touch the devices and utilise them, is a much smaller part of the training.
In addition, we are increasingly getting a workforce for whom a virtual platform is a familiar and comfortable environment, and actually a preferred way of learning. We are getting people who have been raised during the digital revolution and this is how they interact with the world. So, I think in the future this is going to be the predominant mode of education.
I have heard quite a lot of people talking about this idea of there being a move to a more hybrid model of some being in-person and some being virtual in terms of conferences, and so it is interesting that training will also follow this path, but it does make sense in terms of getting the advantages of physical meetings and also the advantages you get from remote learning.
The reception on the personal interaction during online learning has been lukewarm. Is there a way this can be replicated online?
I think another part of millennial learning is that they very much engage with one another to further their knowledge and to further their comfort level. I think that still happens online. During the virtual live classes there is a conversation that is going on in the background. There is generally a Q&A portal as well so there is interaction there. I know just from my participation that Zoom meetings can be an effective way to share ideas.
Clearly, you lose something in terms of the personal interaction, but again there is the ability for students to see me, if not for me to see them. There was a professor at Harvard who was working in a virtual classroom model where not only could the students see the professor, but there was a video display where the professor could see the students as they spoke. Maybe that would be a nice addition—a separate monitor off to the side so that as people are talking, they can actually have a face-to-face conversation and of course where the students or trainees can also see each other. I think that will be the next evolution as digital advances allow.
Disclosures: John Rundback is a consultant for Avail Medsystems
Despite the well-known obstacles, it is time for a prospective, randomised clinical trial comparing percutaneous ablation (PA) and partial nephrectomy for the treatment of small renal cell carcinomas— and re-thinking the common practice of watching and waiting, rather than intervening, is long overdue, writes Christopher S Morris (Larner College of Medicine, University of Vermont, Burlington, USA).
Current studies with a moderate level of evidence have already confirmed decreased complications and similar effectiveness of PA compared to surgery in treating small renal tumours. Interventional radiologists (IRs) everywhere should be prepared for an increasing influx of patients seeking treatment of their small renal cell carcinomas with PA.
In developed countries, the incidence of renal cell carcinoma has increased over the past 20 years, mainly due to the increase in cross-sectional imaging and improving life expectancies. More than 50% of these tumours are diagnosed incidentally. In 2021, it is estimated that there will be more than 76,000 new kidney cancers diagnosed and almost 14,000 deaths attributed to kidney cancer in the USA alone. Like many solid malignancies, renal cell carcinoma is most effectively treated while small and prior to local and regional invasion, and certainly before the progression to distant metastatic disease.
Although the standard treatment of renal cell carcinoma is nephrectomy and partial nephrectomy, IRs have been treating small T1a (<4cm) renal cell carcinomas with PA, either cryoablation, radiofrequency ablation (RFA), or microwave ablation (MWA) for more than 20 years. Despite the proven safety and efficacy of PA for small renal tumors, less than 10% of these lesions are treated with PA. In addition, studies have shown that patients with small renal cell carcinomas are often surveilled with imaging, rather than treated with PA. Therefore, better awareness of the advantages and utility of PA in treating T1a renal cell carcinomas is needed.><4cm) renal cell carcinomas with PA, either cryoablation, radiofrequency ablation (RFA), or microwave ablation (MWA) for more than 20 years. Despite the proven safety and efficacy of PA for small renal tumors, less than 10% of these lesions are treated with PA. In addition, studies have shown that patients with small renal cell carcinomas are often surveilled with imaging, rather than treated with PA. Therefore, better awareness of the advantages and utility of PA in treating T1a renal cell carcinomas is needed.
Last year, the Society of Interventional Radiology published a Position Statement on the role of PA in renal cell carcinoma, which was endorsed by the Canadian Association for Interventional Radiology and the Society of Interventional Oncology.1 The writing group consisted of a multidisciplinary collection of experts who reviewed the pertinent literature. Although currently there are no randomised controlled trials comparing PA with surgery in renal cell carcinoma, the writing group found many population-based registry studies and systematic reviews of small cohort studies. The writing group concluded that PA is an acceptable treatment option for stage T1a renal cell carcinomas in carefully selected patients and can be offered over active surveillance. Of the three different PA modalities, the writing group found no significant differences in safety and efficacy between cryoablation, RFA, and MWA.
Regarding efficacy, four large database studies have shown that patients with small renal tumours treated with PA had acceptable, but mostly lower overall survival rates than those patients treated with surgery.2,3,4,5 However, when looking at cancer specific survival, two of the four studies showed no significant difference between PA and surgery. One study reported no difference in five-year overall survival between PA and surgery. These results reiterate the necessity for a randomised controlled trial comparing PA and surgery for small renal cell carcinomas, as these database studies may be biased by patient selection and other confounders. Despite the fact that a randomised clinical trial is often hampered by funding restraints, difficulties in recruitment of eligible patients, and political obstacles, it will be essential in further establishing safety and efficacy of PA.
Wind-down “watch and wait”
Multiple database studies have demonstrated the utility of adopting PA in lieu of active imaging surveillance.4,6,7 All studies showed that cancer-specific survival was higher for patients treated with PA than those subjected to surveillance and one study also demonstrated significantly greater overall survival rates for PA over active surveillance. These results seem to argue against the common practice of active imaging surveillance of small renal tumours, which would present large numbers of patients who would be more appropriately treated with PA. One of the greatest advantages of PA compared with surgery is its safety. Simply put, PA is associated with significantly fewer complications than surgery. Multiple cohort, registry-based studies, and systematic reviews have confirmed that complication rates and post-procedure renal function outcomes are better with PA than surgery in treating small renal tumours.3,4,8,9,10
As PA is often performed as an outpatient procedure, the length of stay is shorter for PA than surgery. In the cohort and registry-based analyses, significantly lower complication rates were found for PA than surgery in the treatment of small renal cell carcinomas, with complications following PA ranging from 6 to 21% and the complications from surgery ranging from 29 to 40%. In one study, patients treated with PA had lower rates of acute renal failure when compared to surgery. Acute renal failure associated with PA was 3%, whereas it was 7% with partial nephrectomy and 11% with radical nephrectomy.
A systematic review of 107 studies demonstrated lower rates of urine leak, acute kidney injury, and other urologic complications, as well as shorter median hospital stay and decreased median blood loss in patients treated with PA vs. surgery.9 Another systematic review of 15 studies reported lower perioperative complications with PA than surgery.10 In addition, the surgery (partial nephrectomy) group was associated with decreased renal function at six-month and one-year follow up, compared to the PA patients.
A large registry database study of 773 patients compared outcomes of PA of T1a tumours performed with cryoablation vs. thermal PA (either RFA or MWA)6. No significant difference in cancer-specific survival was found between cryoablation or thermal PA.
The writing group also determined that a biopsy of a small renal tumour should be performed prior to PA at any time, either during the first part of the PA procedure or as a separate prior procedure. In addition, there may be a role for PA in treating some T1b (between 4 and 7cm in diameter) renal cell carcinomas and distant oligometastatic renal cell carcinoma in selected patients.
Overall, PA appears to offer similar cancer-specific survival with fewer complications compared to partial nephrectomy for the treatment of small renal cell carcinomas. In addition, patients with T1a renal cell cancers tend to fare better when treated with PA compared to management with active surveillance. Although a randomised controlled trial is needed to further confirm the promising results of these population-based registry studies and systematic reviews of small cohort studies, IRs should expect a greater demand for PA of small renal tumours in the future.
Christopher S Morris is a professor of Radiology and Surgery at Larner College of Medicine at the University of Vermont, Burlington, USA. He has reported no relevant disclosures.
References:
1: Morris CS, et al. Society of Interventional Radiology position statement on the role of percutaneous ablation in renal cell carcinoma: Endorsed by the Canadian Association for Interventional Radiology and the Society of Interventional Oncology. J Vasc Interv Radiol 2020, 31:189–94 2: Zhou M, et al. SEER study of ablation versus partial nephrectomy in cT1A renal cell carcinoma. Future Oncol 2018, 14:1711–9 3: Talenfeld AD, et al. Percutaneous ablation versus partial and radical nephrectomy for T1a renal cancer: A population-based analysis. Ann Intern Med 2018, 169:69–77 4: Xing M, et al. Comparative effectiveness of thermal ablation, surgical resection, and active surveillance for T1a renal cell carcinoma: A surveillance, epidemiology, and end results (SEER)–medicare-linked population study. Radiology 2018, 288:81–90 5: Uhlig J, et al. Ablation versus resection for stage 1A renal cell carcinoma: National variation in clinical management and selected outcomes. Radiology 2018, 288:889–97 6: Uhlig A, et al. Treatment for localized T1a clear cell renal cell carcinoma: survival benefit for cryosurgery and thermal ablation compared to deferred therapy. Cardiovas Interv Radiol 2018, 41:277–83 7: Larcher A, et al. Population-based assessment of cancer-specific mortality after local tumour ablation or observation for kidney cancer: A competing risks analysis. BJU Int 2016, 118:541–6 8: Larcher A, et al. Mortality, morbidity and healthcare expenditures after local tumour ablation or partial nephrectomy for T1A kidney cancer. Eur J Surg Oncol 2017, 43:815–22 9: Pierorazio PM, et al. Management of renal masses and localized renal cancer: systematic review and meta[1]analysis. J Urol 2016, 196:989–99 10: Hu X, et al. Partial nephrectomy versus ablative therapies for cT1a renal masses: A Systematic Review and meta-analysis. Eur J Surg Oncol 2019, 45:1527–35
Varian, a Siemens Healthineers company, today announced that the US Food and Drug Administration (FDA) has granted the company breakthrough device designation for its Embozene microspheres for genicular artery embolisation (GAE) for symptomatic knee osteoarthritis.
Embozene is a medical device that is FDA cleared for the embolisation of hypervascular tumours, arteriovenous malformations, uterine fibroids and benign prostatic hyperplasia.
According to Varian, Embozene microspheres received the designation due to their potential to offer a more effective treatment for appropriate patients with osteoarthritis of the knee. GAE is designed to reduce the blood flow to the periarticular tissue of the joints, limiting the inflammatory process.
Siddharth Padia, director of interventional radiology at UCLA Santa Monica and the David Geffen School of Medicine at UCLA, Santa Monica, USA, said: “GAE is the first minimally invasive procedure that has demonstrated a significant symptom improvement for a prolonged duration.
“In a 40-patient, prospective study, the procedure resulted in a marked improvement in pain and function, and adverse events were uncommon and mild. I remain excited about the possibilities of this technology and its benefit to patients.” Padia is currently working to initiate a randomised clinical trial and a 400-patient registry.
The FDA breakthrough device program is intended to provide patients with more timely access to medical devices that have the potential to provide for more effective treatment or diagnosis of life-threatening or irreversibly debilitating diseases or conditions. As part of the program, the FDA expedites the traditional review and assessment process to help accelerate the development, assessment and review of the device for possible approval.
Frank Facchini, president of Varian Interventional Solutions, added: “GAE holds great promise in providing clinicians with a new, non-invasive treatment option, which may not only ameliorate pain, but reduce the economic burden of this common disease. Varian’s investigational program for GAE exemplifies our commitment to investing in our core technologies to determine their potential to treat the world’s most debilitating diseases.”
IceCure submitted an amendment to the registration certificate granted for the IceSense3 system by China’s national medical products administration (NMPA), which will allow IceCure to sell the IceSense3 and cryoprobes for commercial procedures in China.
IceCure Medical recently announced the advancement of the regulatory strategy in China with the submission of an amendment to the registration certificate for the IceSense3 system, which was granted by China’s NMPA. The amendment, if approved, will allow the company to sell the disposable IceSense3 cryoprobes for commercial procedures. The company expects the NMPA to evaluate the amendment by the end of 2022 and providing the amendment is approved, the company expects to then launch the commercial sales program for the IceSense3 system in China in early 2023.
“We are excited to announce the advancement of our regulatory strategy for the IceSense3 system in China, as we look to bring our minimally invasive therapy to more cancer patients around the world. With more than 400,000 new breast cancer cases diagnosed in China in 2020, according to the World Health Organization, breast cancer continues to be a significant health concern in China,” commented Eyal Shamir, the chief executive officer of IceCure.
“As Chinese health providers continue to look for advanced technologies, we expect early adopters in China to provide a base for our commercial launch once the IceSense3 cryoprobes receive NMPA regulatory clearance. As part of our strategy to gain greater awareness of our systems and cryotherapy as a cancer treatment more broadly with healthcare providers in the region, we have been supportive of an ongoing independent clinical trial with a site in Hong Kong and a site in Shenzhen. Also, we expect another independent trial to start soon in a leading hospital in Shanghai” said Shamir, illustrating ongoing trail plans.
Sirtex Medical (Sirtex) has announced that the first procedure of selective internal radiation therapy (SIRT) using SIRSpheres Y-90 resin microspheres in China was successfully performed for a patient with hepatocellular carcinoma (HCC) on 28 September 2021. The milestone was reached with the support of Sirtex shareholder China Grand Pharmaceutical and Healthcare Holdings Limited.
“This achievement marks a major step forward in our global growth as a company and in our mission to bring effective treatments to patients with cancer,” said Kevin Smith, chief executive officer of Sirtex. “We are especially excited to advance our efforts in China, given the sizable numbers of colorectal and liver cancer cases in recent years. We thank everyone involved in this accomplishment and look forward to the promising future of SIR-Spheres in China and around the world.”
The procedure was performed by Jiahong Dong (Boao Super Hospital, Hainan, China) and his team. Jiahong is a world-renowned specialist in hepatobiliary pancreatic surgery and liver transplantation and was elected Academician of Chinese Academy of Engineering in 2017.
There are 400,000 new cases of liver cancer in China each year, accounting for more than half of all new cases of liver cancer worldwide. “The successful implementation of the first licensed access to the resin microsphere in the clinical treatment of liver cancer means that China’s liver cancer patients can receive international advanced selective in vivo radiation therapy,” said Jiahong Dong in a press conference. “This is a landmark and milestone in the history.”
Hainan’s first try, first pilot policy allows global new technologies, new ideas, and new products to be implemented through Hainan Hope City. The project of the introduction of SIR-Spheres Y-90 resin microspheres will benefit Chinese patients in China.
In November 2020, the National Medical Products Administration (NMPA) of the People’s Republic of China accepted the Sirtex new drug application (NDA) of SIR-Spheres Y-90 resin microspheres for the treatment of colorectal cancer liver metastases.
The Rotarex™ Atherectomy System is a rotational excisional device that is built to remove and aspirate varying lesion morphologies including plaque and thrombus in the peripheral arteries. The Rotarex™ System, already cleared for use in native arterial vessels, now has the expanded indications to treat within peripheral arteries fitted with stents, stent grafts, and native or artificial bypasses.
Rotarex
BD recently announced it has received 510(k) clearance for expanded indications from the US Food and Drug Administration (FDA) for the Rotarex atherectomy system.
The Rotarex atherectomy system is a rotational excisional device that is built to remove and aspirate varying lesion morphologies including plaque and thrombus in the peripheral arteries. The Rotarex system, already cleared for use in native arterial vessels, now has the expanded indications to treat within peripheral arteries fitted with stents, stent grafts, and native or artificial bypasses.
“The Rotarex atherectomy system is quick and efficient for treating arterial lesions,” said Prakash Krishnan, a cardiologist at the Icahn School of Medicine at Mount Sinai in New York, USA. “With ability to use it for both atherectomy and thrombectomy, it is now a great product to be able to treat in-stent restenosis. Rotarex has been a great device for me to have in my practice, and I am excited about these new indications.”
The FDA clearance of the Rotarex atherectomy system’s new expanded indications follows more than 10 years of real-world clinical experience involving the treatment of thousands of patients globally. Now, physicians can use a proven tool to address some of their most challenging peripheral arterial disease (PAD) lesions, including the treatment of in-stent restenosis.
“I have had the ability to use the Rotarex atherectomy system for over 10 years both within and outside the USA,” said Miguel Montero-Baker, a vascular surgeon at Baylor College of Medicine in Houston, USA. “This indication expansion is exciting and will allow me to utilise a device I trust to care for my complex PAD patients.”
Cardiovascular Systems recently announced that the first patient has been successfully treated with its ViperCross peripheral support catheter.
Billy J Kim (The Surgical Clinic, Nashville, USA), treated the first patient with ViperCross.
Kim remarked: “ViperCross offers the right balance of support and flexibility to successfully navigate tortuous anatomy and cross challenging lesions. In addition, ViperCross provides excellent guidewire support and facilitates easy guidewire exchange.”
Peripheral support catheters are used during peripheral vascular intervention (PVI) procedures for guidewire support to enable lesion crossing, as well as for guidewire exchanges. Physicians use support catheters in approximately 50% of PVIs, primarily in below-the-knee and complex interventions. When calcium is present, lesions can be challenging to cross with an interventional guidewire and often require advanced tools prior to vessel preparation and treatment.
Scott R Ward, chairman, president and chief executive officer of CSI, commented: “With the commercial launch of ViperCross, CSI now offers a complete portfolio of products for the treatment of peripheral arterial disease, including atherectomy, balloon catheters, guidewires, support catheters and embolic protection. Combined, these products advance our ability to help physicians improve outcomes for patients undergoing complex peripheral interventions.”
Siemens Healthineers has launched the Luminos Impulse fluoroscopy system, including features such as a seamless imaging chain, comprehensive dose optimisation, cybersecurity features, and detector-sharing capabilities for radiography.
In a press release, Siemens Healthineers said that the fully digital Luminos Impulse offers high-end features and superior imaging that have not been available at this economical price in the past. “Being able to offer such a compelling product in this price segment makes me really proud of what our team has achieved. We work diligently to bring high-end features to our ‘smaller’ systems while also maintaining their excellent image quality and clinical versatility. Customers can use Luminos Impulse for fluoroscopy and radiography with virtually no limitations,“ says Ronald Fröhlich, head of marketing X-ray Products at Siemens Healthineers.
Luminos Impulse is built for the needs of modern-day fluoroscopy and radiography, the company’s press release said.
Fluoroscopy enables the continuous dynamic observation of moving processes in the human body using pulsed X-rays.
Surmodics today announced the successful first clinical uses of the Sublime radial access 0.018 RX percutaneous transluminal angioplasty (PTA) dilatation catheter.
Ankur Lodha, perfomed the first procedures with the device at Cardiovascular Institute of the South’s office-based catheterisation lab in Lafayette, USA. Subsequently, Imraan Ansaarie, utilised the Sublime radial access 0.018 RX PTA dilatation catheter in cases at Advanced Endovascular Institute of St Augustine in St Augustine, USA. The device is the latest addition to the Sublime radial access platform, joining the Sublime radial access guide sheath and the Sublime radial access 0.014 RX PTA dilatation catheter.
“Sublime radial access RX PTA dilatation catheters will allow physicians to treat the most distal blockages in the foot with just radial access. This will help us perform more complex interventions via this approach which was not possible prior,” said Lodha.
“This Sublime radial access 0.018 RX PTA dilatation catheter is a great addition to the current devices available for minimal arterial access lower extremity intervention procedures,” added Ansaarie.
The Sublime radial access 0.018 RX PTA dilatation catheter, which received US Food and Drug Administration (FDA) 510(k) clearance in June 2021, allows above- or below-the-knee access through a transradial approach by providing the longest working length (220cm) on the market. Outer balloon diameters range from 2–6mm, allowing for treatment in larger vessels, with balloon lengths between 20mm and 220mm. With a proprietary shaft construction incorporating a flexible distal segment, a supportive proximal segment, and a mid-shaft that transitions from supportive to flexible, the Sublime 0.018 RX PTA dilatation catheter is designed to provide improved pushability, trackability and crossability in an RX platform.
The Sublime radial access 0.018 RX PTA dilatation catheter is indicated for PTA dilation of peripheral vasculature stenosis in the iliac, femoral, iliofemoral, popliteal, infrapopliteal, and renal arteries, and for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulas. The device is contraindicated for use in the coronary arteries and the neurovasculature.
Medtronic today announced it has received CE mark approval for its radial artery access portfolio, which includes the Rist radial access selective catheter and the Rist 079 radial access guide catheter—the first catheter specifically designed for the unique demands of accessing the neurovasculature to treat stroke, brain aneurysms and other conditions through the radial artery versus access through the transfemoral artery, according to a company press release.
The Rist 079 radial access guide catheter is 510(K) cleared by US Food and Drug Administration (FDA) and has been in use at limited sites in the USA, receiving strong customer feedback in more than 100 cases on its outperformance in navigability and support for the radial pathway, the release adds.
“With excellent navigability, this first-of-its-kind device will allow clinicians to reach distal locations while still achieving excellent stability to the system,” said Alejandro Tomasello, head of the Interventional Neuroradiology Unit at Vall d’Hebron Hospital in Barcelona, Spain. “The radial artery access portfolio works well in tandem with Phenom PLUS, Phenom 021 microcatheter for stent deployment or Phenom 027 microcatheter for flow diverter deployment, which is a fantastic set up for the Pipeline Vantage embolisation device with Shield technology treatments [all Medtronic].”
Transradial techniques have been the standard of care in the cardiac interventional community since the American Heart Association (AHA) recommended a radial-first approach for acute coronary syndrome in 2018, citing lower bleeding and vascular complications than transfemoral artery access.
Other advantages demonstrated in cardiovascular procedures to radial access include strong patient preference, immediate ambulation and reduced costs, which have led the neurointerventionist community to examine adoption of the transradial approach to their practice, the release also states.
“We are committed to exploring ways to improve outcomes through complication reduction, reducing the cost of care and improving overall patient experience,” said Dan Volz, president of the Neurovascular Therapies business, which is part of the Neuroscience Portfolio at Medtronic. “We believe radial access is a meaningful addition to the clinical armamentarium. The CE mark approval of the Rist radial access portfolio emphasises our focus on driving innovation that gives clinicians who perform neurovascular procedures the broadest product portfolio so they can customise their care based on a patient’s condition and anatomy.”
Biotronik has announced the first patient enrolment in the BIONETIC-I study of the safety and efficacy of the Dynetic-35 cobalt chromium balloon-expandable stent system for the treatment of atherosclerotic peripheral arterial disease (PAD) lesions in the iliac arteries. The study will also evaluate the use of the stent system in association with Biotroniks’s Passeo-35 Xeo peripheral dilatation catheter. The first patient was enrolled by investigator Koen Keirse, vascular surgeon at the Tienen Medical Center in Tienen, Belgium.
The prospective, international, multicentre, single-arm, observational study will evaluate treatment of iliac lesions in approximately 159 patients with up to 60-month follow-up. The primary endpoint is major adverse events (MAEs) at 12 months. MAEs include device- or procedure-related death within 30 days post-index procedure, clinically-driven target lesion revascularisation and major index limb amputation up to 12 months post-index procedure.
“I was impressed by the performance of the latest balloon-expandable iliac stent on the market. The cobalt chromium structure is, to me, very important,” said Keirse. “I am sure that the Dynetic-35 stent’s unique characteristics and fantastic size range—including stents up to 78 mm—will be of added value in many cath labs.”
“I am enthusiastic to collect new clinical data to add to the body of literature regarding iliac artery bare-metal stenting, as we have not had new data in this field for some time,” added principal investigator Marianne Brodmann, head of the Clinical Division of Angiology, Department of Internal Medicine at the Medical University Graz in Graz, Austria.
The next-generation Dynetic-35 iliac stent system, which was launched in the EU and other CE mark-accepting countries last year, is 6Fr compatible across the entire size matrix, and is indicated for the treatment of de novo or restenotic lesions in the iliac arteries.
This advertorial is sponsored by Argon Medical Devices.
Placing a drain is an important, quotidian, “bread and butter” procedure that often has a tremendous impact on patients’ lives. “A drain is a drain until it is not,” says Sean Calhoun, who outlines the benefits of the Skater all-purpose, nephrostomy and biliary drainage catheters (Argon Medical Devices). He hones in on their anti-kinking and locking mechanisms, ease of insertion and transition and compatibility with both alcohol
and doxycycline. Calhoun also shares his excitement about the recent commercial launch of the Skater mini-loop drainage catheters in the USA and the European Union,telling Interventional News: “I am hopeful that this will eliminate the problem of losing access to the abscess cavity by having the catheter track smoothly through the wall and into a small cavity. It is also going to be very helpful for external biliary drains.”
Gore's Viabahn endoprosthesis with Propaten bioactive surface
Gore’s Viabahn endoprosthesis with Propaten bioactive surface
Gore has announced the EMEA launch of the lower profile, large diameter Viabahn endoprosthesis with Propaten bioactive surface.
The device enhancements build on a market-leading stent graft device, which has become an important tool for treating complex vascular disease, Gore said in a press release. According to the company, the device design reduces the delivery profile for larger 9–13 mm diameter stent grafts by up to 3Fr, enabling delivery through smaller sheaths. Smaller introducer sheaths have resulted in a lower risk of vascular access complications in select patient populations.
New radiopaque markers, now also on the larger diameter device configurations, enhance visualisation under fluoroscopy, facilitating positioning and device delivery, as well as precise and predictable placement, the company added.
“In addition to the radiopaque markers that facilitate positioning and deployment, the new lower profile enables use of a smaller sheath, potentially reducing the risk of damage at the access site,” said Manuel Alonso, Vascular Surgeon, Oviedo, Spain. “Combined with the trackability and flexibility this new lower profile offering will become very instrumental for treating complex patients across disease states in my practice.”
“The story of the Gore Viabahn endoprosthesis is a story of physician collaboration across four patient-centric indications and of proving performance over and over,” said Benjamin Beckstead, Gore Vascular category leader.
After a successful introduction of Azurion with SmartCT in 2020, many users have experienced working with the new solution from Philips. Watch the video to learn from our early users how 3D imaging capabilities on their image-guided therapy system has impacted interventional radiology procedures in their facilities.
This video was filmed by Philips and is being sponsored for distribution in association with Interventional News.
Late-breaking trial data has demonstrated improved progression-free survival in patients with metastatic colorectal cancer after treatment with TheraSphere Y-90 Glass Microspheres (Boston Scientific).
Findings from the EPOCH clinical trial, which were presented at the European Society for Medical Oncology (ESMO) Congress 2021 and are to be published in the Journal of Clinical Oncology, showed that the TheraSphere treatment met both its primary endpoints, including progression-free survival (PFS) and hepatic progression-free survival (hPFS) of patients with metastatic colorectal cancer (mCRC) of the liver.
In the trial, TheraSphere treatment—a selective internal radiation therapy (SIRT) comprised of microscopic glass beads containing radioactive yttrium (Y-90) that are specifically delivered to target tumors—was used as a second-line treatment in combination with standard of care systemic chemotherapy (SOC) for patients who had disease progression during or after first-line chemotherapy.
Riad Salem, interventional radiologist at Northwestern Memorial Hospital (Chicago, USA) and co-principal investigator of the trial, said: “The EPOCH trial not only demonstrated positive safety and efficacy data for the patients treated in this study, but underscores the success of integrating a device-based therapy like TheraSphere treatment in the continuum of care with systemic chemotherapy and biologic regimens, thereby providing the rationale and setting the stage for future investigation in other cancer types.”
Peter Pattison, president, Interventional Oncology, Peripheral Interventions at Boston Scientific, added: “EPOCH is the first positive phase 3 SIRT trial in any disease setting and the data is expected to support our regulatory submission to the US Food and Drug Administration (FDA), with the hope that more patients with liver dominant mCRC will gain access to TheraSphere as a treatment option in the future.”
The global, prospective EPOCH pivotal clinical trial is a phase 3 study, designed to assess therapeutic benefit compared to SOC, which randomized 428 patients with mCRC to second line chemotherapy, with or without the addition of TheraSphere treatment. Both primary endpoints were met and included progression-free survival and hepatic progression-free survival, which reflect how long patients live without the disease progressing further, both systemically and within the liver.
The addition of TheraSphere treatment significantly increased both PFS (p=0.0013) and hPFS (p<0.0001). Patients receiving TheraSphere treatment with second-line chemotherapy were 31% less likely to show disease progression or death (HR= 0.69) and 41% less likely to show hepatic disease progression or death versus with chemotherapy alone (HR= 0.59).
Mary Mulcahy, medical oncologist at Northwestern Memorial Hospital and co-principal investigator of the trial, commented: “In the second line of therapy for metastatic colorectal cancer, with disease isolated to the liver, the addition of TheraSphere with chemotherapy resulted in a significant delay in overall tumor progression. Additionally, chemotherapy-related adverse events were comparable between the trial arms.”
Earlier this year, the FDA approved TheraSphere for the treatment of unresectable hepatocellular carcinoma (HCC) and granted breakthrough device designation for expedited review as a treatment of patients with glioblastoma. In the USA, the use of TheraSphere for mCRC is for investigational use only as the safety and effectiveness have not been established, say Boston Scientific.
The development of new research guidelines for interventional oncology that standardise treatment outcomes and the reporting of data represents a major step forward for an increasingly important medical subspecialty, according to a report in Radiology.
Interventional oncology is a fast-growing offshoot of interventional radiology in which treatment is applied directly to the tumour through a catheter. Compared with conventional treatments like surgery and chemotherapy, these minimally invasive image-guided procedures have lower complication rates, superior toxicity profiles and often comparable or superior outcomes—so much so that international guidelines have already adopted thermal ablation, or the destruction of tumours through heat, as a first-line treatment option for certain smaller-sized malignant tumours.
Treatment effectiveness is measured through a variety of means such as disease-free and progression-free survival. A lack of consensus regarding these parameters in oncology-related studies and how to uniformly share these outcomes amongst investigators worldwide has created a host of problems. Issues like different complication-related outcomes reported for the same treatment modality and inconsistencies in the reporting of overall survival data means that study results cannot always be reliably compared.
“Study results are being collected, analysed and reported in many different ways, and we tend not to speak the same language within the field of clinical oncology,” said study lead author Robbert S Puijk, a radiology resident and researcher at the Onze Lieve Vrouwe Gasthuis Hospital and Amsterdam University Medical Centers in Amsterdam, The Netherlands.
To address these shortcomings, an international panel of 62 experts recently convened and developed important recommendations on how to uniformly collect, analyse and report outcomes for patients treated with image-guided tumour ablation.
Among key recommendations, the panel determined that, to compare different treatment techniques, outcomes should be analysed and reported per patient and per tumour. This is because multiple index tumours within one unique patient, such as multiple liver metastases from colorectal cancer, are often treated simultaneously and cannot be regarded as independent.
The panel agreed that parameters like overall survival and disease-free survival should be analysed per patient and not on a per tumour or per procedure basis. Parameters that address both procedure-related side-effects and direct costs such as short-term complications and anaesthesia techniques should be addressed per procedure, the panellists concluded.
The panellists reached several other important agreements, including ones regarding the definitions for recurrence-free, disease-free and progression-free survival.
The new guidelines will boost interventional oncology in a variety of ways, according to Puijk.
“The given definitions in these current guidelines will provide the necessary foundation for scientific reproducibility between interventional oncology studies as they will ensure an objective and reliable interpretation of study outcomes, allow for accurate comparisons of results and avoid misinterpretations,” he said.
Puijk called the participation of a large number of international experts on the panel a key motivating factor to putting the guidelines on paper.
“Together with the help of independent biostatisticians and epidemiologists, it strengthens our methodology and indicates the importance of this project,” he said. “Widespread adoption of these guidelines is another step forward in the professionalisation of our field, interventional oncology.”
The researchers hope to extend these guidelines to regional and systemic cancer treatments and ultimately attract the participation of other medical societies.
The project represented a collaboration between the Society of Interventional Oncology (SIO) and the Definition for the Assessment of Time-to-event Endpoints in Cancer (DATECAN) trials initiative. Martijn R Meijerink, was senior author on the paper.
Biotronik is proud to announce the completion of enrolment of the investigator-initiated BIOPACT randomised controlled trial (RCT). This non-inferiority study evaluates the safety and efficacy of paclitaxel drug-coated balloons (DCBs), comparing the Biotronik Passeo-18 Lux paclitaxel-releasing percutaneous transluminal angioplasty (PTA) balloon catheter to the IN.PACT Admiral paclitaxel-coated PTA balloon catheter (Medtronic).
The study enrolled 302 patients in Austria, Belgium, France and Switzerland and will collect follow-up at one, six, 12, 24, 36, 48 and 60 months. Patients with Rutherford class 2–4 disease were randomized 1:1 to either the Passeo-18 Lux DCB or IN.PACT Admiral DCB for the treatment of stenotic, non-stented restenotic or occlusive lesions in the femoropopliteal artery. A non-inferiority hypothesis will be tested to compare the clinical performance of Passeo-18 Lux to IN.PACT Admiral.
The primary efficacy endpoint is freedom from clinically-driven target lesion revascularisation at 12 months post-procedure. The primary safety endpoint is a composite of freedom from device- and procedure-related death through 30 days post-index procedure, freedom from major target limb amputation and clinically-driven target vessel revascularisation through 12 months post-index procedure. Key secondary endpoints include primary patency, major target limb amputation and all cause of death.
“I am thrilled about this milestone for the BIOPACT RCT and thank all of our investigators for their participation and contribution to the fast enrolment despite the pandemic-induced challenges in patient care over the last year and a half,” said principal investigator Koen Deloose (AZ Sint Blasius Hospital, Dendermonde, Belgium). “Having more head-to-head data is critical to better understand differences in device design and drug dosage and the more data we can add to the safety debate of paclitaxel-coated balloons, the better. We eagerly await the follow-up results of this trial.”
“This head-to-head clinical trial will add to the already extensive evidence supporting our Passeo-18 Lux DCB,” said Alexander Uhl, president Vascular Intervention at Biotronik. “We look forward to these data confirming Passeo-18 Lux’s position amongst the leading DCBs.”
The primary endpoint is intended to be presented upon completion of 12-month follow-up in late 2022.
A large, multicentre cohort study provides a simple, practical method to effectively stratify patients preoperatively into low- and high-risk major amputation categories.
According to lead author Leigh Ann O’Banion (University of California, San Francisco, San Francisco, USA), “traumatic popliteal artery injuries present a serious clinical challenge because they are associated with the greatest risk of limb loss of all peripheral vascular injuries, with major amputation rates of 14–25%.”
Previous scoring systems, such as the Mangled Extremity Severity Score (MESS), attempt to determine a threshold beyond which repair is futile. O’Banion states: “The aim of the present study, unlike the older systems, was to provide an easy to use scoring system that could be used to preoperatively and effectively risk stratify patients with traumatic popliteal vascular injuries for major amputation.”
As reported in the September 2021 issue of the Journal of Vascular Surgery, O’Banion and colleagues from 11 medical centres from the Western Vascular Society retrospectively examined the outcomes of patients who had undergone operative repair for traumatic popliteal arterial injuries from 2007–2018 and identified the factors independently associated with limb loss.
They compared the clinical data between those who ultimately required major (above ankle) amputation with those who did not, and subsequently validated the new scoring system in a random 20% of this population.
Characteristics of the study population (n=355) included:
At a mean follow-up of 69 days, the overall amputation rate was 16%, but those who lost primary patency had a major amputation rate of 46%. These findings underscore the critical need for close follow-up.
Significant preoperative risk factors for amputation included:
Systolic blood pressure <90mmHg (odds ratio [OR] 3.2),
Orthopaedic injury (OR 4.9), and
Lack of pedal Doppler signals (OR 5.5).
Using this information, a Popliteal Scoring Assessment for Vascular Extremity Injuries in Trauma (POPSAVEIT) score was created, assigning one point for blood pressure and two points for both the orthopaedic injury and no Doppler signals.
The study validated the scoring system revealing amputation rates were:
25.5% for a score of 3–5 points vs.
5.9% for a score of 0–2 points (p<0.001).
O’Banion explains: “When evaluating the patient comprehensively, the POPSAVEIT score divides the findings into three critical components: measures of global physiologic insult (blood pressure), musculoskeletal deformity (orthopaedic injury), and ischaemia (Doppler examination).
“This preoperative assessment tool could be used to effectively communicate and risk stratify patients across centres similar to the American Association for the Surgery of Trauma’s injury scoring scales, which are widely accepted and used across trauma centres. Additionally, the ability to risk stratify could be useful in discussing the prognosis and setting expectations with patients, their families, and other providers.”
This study confirms that patients with popliteal vascular injuries are at significant risk for amputation. The POPSAVEIT tool is a valuable tool to assess this risk as soon as the patient enters the emergency room.
Today, Boston Scientific announced an agreement to acquire Devoro Medical, developer of the Wolf thrombectomy platform. The non-console and lytic-free Wolf technology targets and captures blood clots using finger-like prongs that retrieve and remove thrombi in the arterial and venous systems.
“The addition of the Wolf platform advances our efforts to ensure physicians have the right tools to improve procedural efficiencies,” said Jeff Mirviss, executive vice president and president, Peripheral Interventions, Boston Scientific. “Clot management remains a core focus of our business, and upon commercialisation, this highly differentiated technology will complement and expand our offerings to a full suite of interventional strategies for thromboemboli, which also includes the EkoSonic endovascular system (EKOS) and the AngioJet thrombectomy system.”
Boston Scientific has been a strategic investor in Devoro Medical since 2019 and currently holds an equity stake of approximately 16%. As a result, the transaction consists of an upfront payment of approximately US$269 million for the 84% stake not yet owned and up to US$67 million upon achievement of certain clinical and regulatory milestones.
“The Wolf platform is a compelling new option for physicians performing thrombectomy procedures and, importantly, it is designed to target and remove clots without damaging blood vessels, while also minimising blood-loss, which may improve outcomes,” said Michael R Jaff, chief medical officer and vice president of clinical affairs, technology and innovation, Peripheral Interventions, Boston Scientific. “We look forward to accelerating the progress of this platform technology so that we help patients who are dealing with these common, yet challenging health conditions.”
Ten centres have achieved the International Accreditation System for Interventional Oncology Services (IASIOS) accreditation, a benchmark of quality standard and assurance, since 2018. Wesley Medical Imaging has just achieved this recognition to become the first hospital in the Southern Hemisphere to do so. Interventional News speaks to Nicholas Brown (clinical director at I-MED, The Wesley Hospital, Queensland, Australia) on this significant achievement and how it certifies that this hospital is providing the highest standards of interventional oncology (IO) care. “Personally, I am convinced it will bring game-changing renewal and evolution to interventional radiology practice around the world,” he says.
Commenting on the main benefits he foresees as a result of being granted this recognition, Brown says: “The IASIOS accreditation will allow our centre to promote our high standards to patients, referrers and hospital administrators. The process of seeking IASIOS accreditation allowed us to review and critically appraise our existing practices, and to ensure that how we work is aligned with the international standard. The promise of accreditation provided us with the motivation to examine every facet of our practice, including areas where we needed to improve our practices to comply with the IASIOS requirements.”
Brown is categorical about what prompted Wesley Medical Imaging to undergo the rigorous IASIOS accreditation process. “The IO service offered at the Wesley Hospital has always been comprehensive and progressive, and the IASIOS accreditation now provides us with an opportunity to ensure that our practices are benchmarked against an international quality standard. IASIOS accreditation provides us with the confidence that we are providing the highest standard of care, and will allow us to adopt new and evolving technologies within a quality framework. Furthermore, it will provide confidence to patients and referrers that our centre can be trusted to deliver the best possible care.”
The Wesley Hospital (Queensland, Australia)
The IASIOS award, in addition to being the bright line that separates centres that deliver top quality IO care, has wider implications for the growth and development of IO in Australia and New Zealand. Brown elaborates: “Quality assurance and quality control in interventional radiology and IO is critical. ‘Quality’ is the yardstick by which specialty practice is measured and judged by our clinical colleagues, and demonstrates a mature, professional approach to clinical care. The IASIOS system in Australia will help to ensure that quality standards remain a guiding focus as interventional radiology and IO evolve. It particularly demonstrates that specialist IRs can fulfil their potential as equals within the multidisciplinary team environment. Quality assurance is the mark of a true clinical speciality, and an accreditation programme that seeks to uphold standards of practice is a tremendous boost towards promoting these in interventional radiology. IASIOS is an effective tool that legitimises the high standards that we all strive for day-to-day, and provides an easy riposte to any out-dated attitudes from colleagues who doubt the notion of IRs being true clinicians. If ever we needed proof that IRs are clinicians and not just technicians, IASIOS provides it in abundance.”
A challenging process, huge achievement and the team’s unforgettable reaction
The IASIOS process is challenging, as is appropriate for a system designed to set and maintain high quality standards (see box). “It provided a thorough analysis of work practice and required an in-depth review of every part of what we do and how we interact with patients, referrers and the broader hospital setting. The process also takes longer than anticipated. Not all the information required for a successful application will necessarily be readily available, and may have to be reviewed, reproduced or re-written. A critical component—the case audit—is an opportunity to demonstrate the depth of specialty practice but it requires time to compile all the necessary aspects.
The IASIOS process definitely requires a team effort, but also needs one or two local champions who can take responsibility for the process and spearhead progress towards a completed application. A leadership team that involves clinical, nursing and administrative insights is very important.
Nick Brown
An 18-month process, involving hard work and contributions from clinical, nursing, technical, administrative and managerial staff culminated in a successful accreditation. The whole team was absolutely thrilled and rightly proud of this achievement and the recognition that it brings. The affirmation of our high standards of practice is both reassuring and motivates us to continue to improve and evolve. We are also very pleased to be able to share this exciting news with our patients and referrers, as we look to grow not only our practice, but represent the capabilities of the broader interventional radiology profession,” says Brown.
Specifically addressing other global centres who might wish to undertake the accreditation process, Brown says: “It is good to remember that persistence will pay off, eventually. The Accreditation Certificate is just reward for a great effort and lots of difficult work. Attaining and promoting high quality standards in clinical care are important ways of supporting your practice and your profession.
“We are extremely grateful to CIRSE for embarking on the IASIOS journey, and personally I am convinced it will bring game-changing renewal and evolution to IR practice around the world. We are also thankful for the confidence (and patience!) shown to us by CIRSE in having the Wesley Hospital as a pilot site and encouraging us to complete the accreditation programme.”
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) signposts the IASIOS process:
What is the process of IASIOS accreditation?
The accreditation process begins once a facility has registered. By initiating the process, they receive the first seal—that of an IASIOS Enrolled Centre. With the first step, they have shown that they are dedicated to increasing the quality of the patient pathway in their IO service line. The goal of IASIOS is not to make a judgement on the quality of the department at the time of registration, rather it is to help the centre make the necessary adjustments and changes to bring their service to the level outlined in the core requirements of the Standards of Quality Assurance document. The centre can remain an Enrolled Centre for as long as necessary to make the changes and they can utilise the full support of the IASIOS team along the way.
Each application is independently reviewed by two assessors who must both come to the same agreement that compliance has been demonstrated before the seal of IASIOS Accredited Centre has been granted. If there is any doubt on the answers given in the application form, the facility will be able to provide additional documentation or the assessors may request a remote audit for a detailed discussion. After a centre has been an IASIOS Accredited Centre for four years, they have the option of becoming re-certified, or they can ambitiously aim to demonstrate compliance to every single standard outlined in the Standards of Quality Assurance document, which would grant them the IASIOS Centre of Excellence seal.
How does CIRSE guide centres across the globe through the process?
The IASIOS team is readily available for any questions that may arise or obstacles that may be encountered during the application process, whether by email or video call. We have manuals and guidelines that have been developed, and are constantly gathering feedback and information that we can collect and make available to the centres going through the accreditation process so they can learn from the centres that have gone through the process before them. We have been developing a system that is completely online and digitised so it can be easily accessed by multiple people and multiple assessors regardless of time zone or location in the world. Our goal is to create a truly global community of people dedicated to advancing interventional oncology, learning from each other and increasing its quality of care and recognition. As the community grows further, we will be able to offer enrolled centres guidance from council members and consultants in all areas of the world. We received an overwhelmingly positive response from dedicated IO experts worldwide supporting this initiative and joining the IASIOS community as Council Members.
How many centres have achieved accreditation since the 2018 pilot phase?
From the 12 centres that participated in the pilot phase, 10 centres have achieved accreditation and two are undergoing accreditation. These include hospitals from Europe, Asia and the Southern Hemisphere, more specifically: The UK, France, Germany, Switzerland, Italy, the Netherlands, Turkey, Singapore and most recently – Australia.
Since the launch of the scheme in April 2021, eight centres have initiated their enrolment and are awaiting administrative approval from their hospitals. These include hospitals from Canada, Switzerland, Italy, Germany, Austria, Sweden, the UK and the Netherlands.
MedAlliance, with its Japanese partner MDK Medical, has completed enrolment in the clinical study of its novel sirolimus drug-eluting balloon (DEB), Selution SLR, for the treatment of peripheral arterial disease (PAD). This follows the acceptance of a Clinical Trial Notification (CTN) by Japan’s Pharmaceutical and Medical Device Agency (PMDA) in June 2020.
The study involves 133 patients across 13 centres in Japan. Its objective is to assess the safety and efficacy of Selution SLR for the treatment of lesions of superficial femoral arteries and/or popliteal arteries. The study is a prospective, controlled, multicentre, open, single-arm clinical investigation. Its primary endpoint is the primary patency rate at 12 months. Secondary endpoints include major adverse events/target lesion revascularisation (TLR), primary patency, and the change of Rutherford classification/ankle-brachial index (ABI)/walking impairment questionnaire (WIQ).
“We are extremely pleased with the regulatory and quality expertise demonstrated by our partner MDK, and particularly proud that Japanese patients can now benefit from our unique technology. This is the first sirolimus DEB implanted in Japan, where the current paclitaxel coated balloon market generates more than US$100 million in revenue per year”, commented MedAlliance chairman and CEO Jeffrey B Jump.
Selution SLR was awarded CE mark approval for the treatment of PAD in February 2020 and for the treatment of coronary arterial disease in May 2020. The US Food and Drug Administration (FDA) has awarded Selution SLR with four breakthrough designations: for the treatment of atherosclerotic lesions in native coronary arteries; coronary in-stent restenosis; peripheral below-the-knee and arteriovenous fistula indications.
In August 2021, the first of over 3,000 patients was enrolled in a coronary randomised controlled study comparing Selution SLR with a limus drug-eluting stent (DES). According to a press release, this is the largest DEB study ever initiated and has the potential to change medical practice.
Merit Medical Systems has announced positive results from a prospective, observational, first-in-human study to evaluate the safety and effectiveness of Wrapsody—a self-expanding, cell-impermeable endoprosthesis designed for the treatment of arteriovenous (AV) fistula access circuit stenosis and AV graft access circuit stenosis.
The prospective, observational study published in CardioVascular and Interventional Radiology by James Gilbert (Oxford University Hospitals, Oxford, UK) et al, reported 100% target lesion primary patency (TLPP) rate without reintervention through 30 days, with a 12-month TLPP rate of 84.6% and a 12-month access circuit primary patency (ACPP) rate of 65.9%.
The authors state that these results suggest that the Wrapsody endoprosthesis is a safe and effective treatment for AV access circuit stenosis.
The study enrolled 46 subjects with clinically relevant stenosis, who were treated at three centres. The eligible population consisted of patients undergoing haemodialysis through an AV circuit with clinical and radiological evidence of stenosis at the graft-vein anastomosis, in the peripheral outflow veins or in the central veins up to the superior vena cava. The subjects did not have clinically relevant secondary stenosis or thrombus in the access circuit.
The primary safety outcome measure was the proportion of subjects without localised or systemic safety events affecting the access circuit that resulted in surgery, hospitalisation or death during the first 30 days following device placement. All but one subject was free from such a safety event in the first 30 days following device placement (97.8%). The safety event was adjudicated as not related to the device or study procedure. Over the remainder of the study, there was one adverse event adjudicated as possibly device-related.
The primary effectiveness outcome measure for the study was the TLPP rate at 30 days following device placement, which was 100%. At six months following device placement, the TLPP rate was 97.7% and at 12 months following device placement, it was 84.6%.
The six- and 12-month ACPP rates were 84.4% and 65.9%, respectively. TLPP rates were similar regardless of access type and lesion location or whether subjects were treated with a single device or overlapping devices. In all cases, reintervention at the target lesion was successful in maintaining patency (12-month assisted TLPP rate of 100%.)
Primary investigator, Gilbert, said: “Early first-in-human study results show that the Merit Wrapsody endoprosthesis can be safely used to treat stenoses at key sites within a dialysis access circuit
“Even more encouraging are the very promising primary one-year target lesion patency rates of 84.6% and access circuit patency rate of 65.9%. To my knowledge, these are higher than any other published data and suggest that the novel features of the Wrapsody endoprosthesis may have a key role in preserving the longevity of precious dialysis access for our patients.”
Merit is also conducting a large multinational, multicentre study, the WAVE Study, which it plans to use to support a premarket approval application to the US Food and Drug Administration. Enrollment in the randomised WAVE Study comparing the Wrapsody endoprosthesis to percutaneous transluminal angioplasty for treatment of venous outflow circuit stenosis or occlusion in hemodialysis patients began in March 2021. Merit anticipates that the WAVE Study will include 477 subjects.
Fred Lampropoulos, Merit’s chairman and CEO, added: “Merit has built its commercial legacy on innovative products that benefit patients and advance standards of care.
“We are encouraged by the Wrapsody First study’s positive results and excited to help shape the future of arteriovenous access circuit stenosis treatment. We look forward to assessing future study results regarding the Merit Wrapsody endoprosthesis, and to making a positive impact in the lives of patients suffering from kidney disease.”
Bluegrass Vascular Technologies (Bluegrass Vascular) announced today that the Centers for Medicare & Medicaid Services (CMS) has finalised a new Healthcare Common Procedure Coding System (HCPCS) code and New Technology Ambulatory Payment Classification (APC) assignment for use of the Surfacer Inside-Out access catheter system (Surfacer system) procedure.
The new code is C9780, Insertion of central venous catheter through central venous occlusion via inferior and superior approaches (e.g. inside-out technique), including imaging guidance. It is assigned to New Technology APC 1534, with a national average payment rate of US$8,250.50. As a result of this decision, hospitals and ambulatory surgery centres (ASCs) will be able to utilise HCPCS code C9780 to report the Inside-Out procedure when performed with the Surfacer system beginning on 1 October 2021.
The Surfacer system employs a novel Inside-Out approach and is the first US Food and Drug Administration (FDA)-cleared medical device to facilitate upper body central venous access in patients with venous obstructions or other conditions that preclude access by conventional methods.
“The CMS decision to assign a New Technology APC for the Surfacer system is a major milestone and will ensure that our innovative technology will be reimbursed for Medicare beneficiaries. This is a significant development, given the prevalence of thoracic central venous obstruction in patients dialysing via a central venous catheter,” stated Gabriele Niederauer, CEO and president of Bluegrass Vascular. “This decision is a testament to the positive clinical evidence and cost data that support the use of the Surfacer system as a critical, lifesaving technology.”
Thoracic central venous obstruction occurs in roughly 40% of patients where haemodialysis is performed via a central venous catheter, a Bluegrass Vascular press release states. While permanent arteriovenous fistulas are the preferred form of vascular access for haemodialysis patients, central venous catheters continue to serve as an important bridge to securing long-term access for life-saving haemodialysis treatment. The current approach for most patients with central venous obstructions is to use an alternative vein, which reduces the ability to place and mature a functioning fistula, resulting in increased catheter days and costs.
According to CMS, more than 62.4 million Americans are enrolled in the Medicare programme. Approximately 80% of patients on haemodialysis are covered by Medicare fee-for-service as primary payer or by a Medicare Advantage managed care plan. Patients who live with kidney failure represent 1% of the total US Medicare population yet account for 7% of the Medicare costs.
The use of the Surfacer device also avoids left-side catheter placement, better enabling the maturation of permanent arteriovenous access options in the left arm and minimising unnecessary access-related procedures and complications. The National Kidney Foundation’s current Kidney Disease Outcomes Quality Initiative (KDOQI) clinical practice guidelines for vascular access recommend that the ideal access site for haemodialysis catheters is the right internal jugular vein. This preferred right-sided access path is supported by the Surfacer system’s novel “Don’t Go Left” approach.
The Surfacer system received FDA de novo clearance in the USA in February and is CE marked in Europe. The device is available in North America, Europe and other territories.
What are the advantages of using renal denervation to treat hypertension?
In all recent sham-controlled trials there were clinically favourable effects of renal denervation for treatment of uncontrolled hypertension. The great advantage is that the intervention has shown meaningful office and ambulatory blood pressure decrease across multiple phenotypes of patients with mild to moderate as well as more severe hypertension in the presence and absence of medication. This constant reduction in blood pressure over 24 hours—the “always on” impact—of renal denervation differentiates the intervention-induced changes in blood pressure from those by drugs due to the diverse pharmokinetic profiles and dosing regiments along with patient non-adherence.
How does renal denervation compare to other treatment approaches that are available?
According to latest second generation randomised controlled trials and the Global SYMPLICITY Registry (GSR), average blood pressure reduction induced by renal denervation compared to sham ablation is 8-10mmHg in office systolic blood pressure reading and 5-7mmHg in ambulatory systolic blood pressure readings. Other interventional approaches to modulate sympathetic tone by baroreceptor activation is still under investigation.
What do trial data tell us about this approach and its outcomes in the long-term?
The antihypertensive effect of renal denervation is durable and taking into consideration the average drop of 10mmHg in office blood pressure, the renal denervation effect can be translated to significant improved cardiovascular prognosis (approximately 20% reduction in cardiovascular events and 26% in stroke). Renal denervation is also an early and late-term safe procedure with minimal complications based on data from registries and recent sham randomised controlled trials. The observed blood pressure reduction caused by renal denervation is maintained long term with data available up to three years after the procedure.
Are there any unanswered questions to be investigated?
Currently there is an urgent need to define predictors of blood pressure response post renal denervation and there are efforts focusing on diverse parameters both clinical and laboratory. There are data showing that in untreated patients with higher baseline heart rate and plasma renin aldosterone levels renal denervation are associated with better blood pressure reduction. Moreover, the average and standard deviation of night-time ambulatory blood pressure has been identified as a potential robust predictor, which requires further research. Another question is the long-term durability of blood pressure lowering and safety beyond three years as well as safety and efficacy in patients with comorbidities such as renal failure. Further studies are also needed on the renal denervation-induced clinical impact in patients with heart failure, atrial fibrillation and increased overall cardiovascular risk. The cost-effectiveness of the procedure for the health systems is an additional point to be addressed.
Are there any drawbacks to this approach?
Given the established efficacy and safety the only drawback for renal denervation is physicians’ inertia to consider and refer hypertensives for this approach. Additionally, there is a lack of information on the clinical impact of neuromodulation from the stand point of hypertensive patients that limits the implication of the technology to everyday practice.
How should physicians evaluate which patients are suitable for renal denervation treatment for hypertension?
According to the latest evidence, the criteria for considering hypertensive patients for renal denervation is persistent uncontrolled hypertension despite guideline-based therapy including ameliorated lifestyle measures and efforts to increase adherence. Heightened cardiovascular risk (i.e. evident organ damage) or established disease (i.e. coronary artery disease, heart failure) might be pointing towards treatment priority with renal denervation in hypertension. Additionally, patients who are unable or unwilling to take medication might be another renal denervation group, especially in the first stages of the hypertensive disease. The shared decision making process is mostly important for renal denervation and according to patients’ preferences this interventional approach could be selected for diverse phenotypes of hypertension.
Do you see renal denervation as having a significant role to play in the future treatment of hypertension?
Renal denervation constitutes today the most advanced and efficacious device-based interventional approach to treat hypertension, expanding therapeutic options as an alternative and not as a competitive strategy. This would be of important clinical value since approximately half of individuals with hypertension do not meet guideline-directed blood pressure goals. Based on the available evidence, renal denervation is definitely included in the individualised treatment strategy of the future for better hypertension control and reduction of overall cardiovascular disease burden.
Proposed cuts to physician reimbursements could shutter practices and leave thousands of medically vulnerable patients without access to care, the Society of Interventional Radiology (SIR) said in a comment letter submitted to Centers for Medicare and Medicaid Services (CMS) in September.
The letter was submitted in response to the July 13 proposed rule for the 2022 Medicare Physician Fee Schedule (MPFS). Under the proposal, IRs could see an aggregate cut of 13% for all interventional radiology treatments, with certain procedures performed in office-based lab settings experiencing cuts greater than 20%. Treatments with the highest cuts include limb-saving peripheral arterial disease treatments, clot-busting venous treatments, venous stenting and other vascular work.
“The rule represents a perfect storm resulting from CMS’s decision to allow their labour rates and product cost tables to lag behind inflation,” said SIR President Matthew S Johnson, an interventional radiologist and Gary J. Becker Professor of Radiology Research at Indiana University School of Medicine in Indianapolis, USA. “In many cases, practice costs have not been updated in 20 years. Due to purported budget neutrality, CMS made apparently arbitrary cuts rather than reimburse all practices and specialties at their true cost of care.” While CMS c onsiders such cuts “budget neutral” they disproportionately affect procedures performed by IRs in office-based settings, such as treatment of venous ulcers and dialysis access. More importantly, the services most affected treat diseases that disproportionately affect patients of colour, such as peripheral artery disease, venous disease, renal disease and cancer.
“As a result, the profound cuts will negatively affect health equity in communities who have already been particularly hard hit by the COVID-19 pandemic,” said Johnson. “By making it difficult for outpatient, officebased labs to continue to operate, patients seeking care will have to do so in hospital settings, which are still reeling from COVID-19. For some patients, this could mean traveling hours outside of their community to receive treatment.”
Throughout the pandemic, office-based facilities have allowed hospitals to focus on the sickest COVID-19 patients while allowing lifesaving cancer treatments and limb-saving vascular procedures to continue. The cuts may make some practices unsustainable, directly impacting readiness for future COVID-19 surges or new pandemics. In addition, office-based lab facilities deliver quality care to patients far from major hospital centres.
Community-based, outpatient care allows patients to return to their normal lives sooner.
“We must protect patients’ access to that crucial care and prevent private practices from closing down, especially in underserved areas,” said Johnson.
SIR is joining with other healthcare organisations, such as the American Medical Association (AMA), the American College of Radiology, the CardioVascular Coalition and other medical specialty societies, to combat these cuts and plead with CMS and Congress to:
Reverse the cuts.
Suspend sequestration.
Maintain for 2022 the COVID-19 related increase to the conversion factor to ensure that what is reimbursed better reflects the real cost of healthcare in a pandemic world.
Avoid implementing clinical labour pricing revisions at this time. If they must implement it, phase the new rates in over four years to minimise the effects on private practices.
Led by Michel Bosiers (St. Franziskus-Hospital, Münster, Germany) the study is coordinated by the Foundation for Cardiovascular Research and Education and will enrol 70 patients with occlusive disease from sites in Germany, The Netherlands and Italy.
The study aims to evaluate the long-term safety and efficacy of the Solaris vascular stent graft, a flexible and self-expanding endograft which, according to the company, is designed to cover and seal off diseased tissue, providing an endoluminal bypass option for physicians facing complex lesions.
Enrolment started in May 2021 and the final results are expected in May 2023.
The European Society of Hypertension (ESH) has presented an updated position paper on renal denervation (RDN) in a pre-ESH congress satellite symposium (10–11 September, Athens, Greece). The paper was recently published in the September issue of the Journal of Hypertension.
This position paper written by an ESH expert Working Group confirms that RDN is considered a safe endovascular procedure without significant short-term or long-term adverse effects based on data available up to three years.
“In light of the recent publication of several second-generation sham-controlled clinical trials, we thought it was important to provide an updated position paper on RDN and its role in treating uncontrolled hypertension,” said Roland Schmieder, professor of Internal Medicine, Nephrology and Hypertension at the University Hospital Erlangen, Erlangen, Germany and chairman of the ESH Working Group on interventional treatment of hypertension.
RDN is a minimally invasive procedure intended to regulate overactivity of nerves that lead to and from the kidney, which play an important role in controlling blood pressure.
In recent sham-controlled randomised trials and registries, clinically favourable effects of RDN have been consistently demonstrated across a wide spectrum of patients with uncontrolled HTN, in the absence and presence of prescribed antihypertensive medications.
Konstantinos Tsioufis
”RDN represents an evidence-based option to treat HTN, in addition to lifestyle changes and blood pressure lowering drugs. RDN expands therapeutic options to address the first objective of HTN treatment, to effectively reduce elevated blood pressure and achieve blood pressure targets,” said Konstantinos Tsioufis (University of Athens, Athens, Greece), professor of Cardiology and immediate past president of ESH. “Heightened cardiovascular risk such as evident organ damage or established disease like coronary artery disease or heart failure might be pointing towards treatment priority with RDN in hypertension. Additionally, patients who are unable or unwilling to take medication might be another RDN group, especially in the first stages of the hypertensive disease.”
Arterial hypertension constitutes the most prevalent and important risk factor for cardiovascular morbidity and mortality globally despite the availability of pharmacological treatments. In addition, approximately half of individuals with hypertension do not meet guideline-directed blood pressure (BP) goals.
”Many patients with uncontrolled hypertension struggle to adhere to lifelong drug therapy for a variety of reasons and may look to other options that complement traditional treatments,” said Reinhold Kreutz, professor of Clinical Pharmacology and Hypertension at the Charité Universitaetsmedizin in Berlin, Germany and president of ESH. “We believe this advance could help clinicians work with patients to better manage their high blood pressure.”
At the Athens pre-ESH meeting, experts discussed various hypertensive profiles that could benefit from RDN including those unable to achieve BP control despite application of guideline-recommended therapies, and those with high baseline cardiovascular risk or comorbidities or poor tolerance to medications.
Biotronik has announced the expansion of the Fortress reinforced introducer sheath line, which is now available in 7- and 8Fr-compatible sizes in the USA and countries that recognise European CE mark approval.
The Fortress introducer sheaths are intended to provide access and facilitate percutaneous introduction of guidewires, catheters and other devices into the femoral, popliteal and infrapopliteal arteries while maintaining haemostasis during diagnostic and interventional procedures. The sheath is reinforced with a polymer-embedded stainless steel coil to ensure excellent kink and deformation resistance.
“In complex vascular procedures, we as interventionalists need the right tools that simplify our workflows and lower risks for patients,” said Torsten Fuß, head of Internal and Intensive Care Medicine at the Elblandklinikum Radebeul in Radebeul, Germany. “The Fortress 7Fr and 8Fr introducer sheath sizes have a very smooth dilator-to-sheath transition, reducing friction when going over the bifurcation. It is easier to insert compared to other introducers on the market and has excellent pushability in typically challenging access presentations like preoperated and calcified groins.”
The new line extension sizes not only preserve the existing benefits of Fortress introducer sheaths but are designed to offer compatibility with 7Fr and 8Fr devices for endovascular procedures, including the use of covered stents and atherectomy devices. With the addition of these new sizes, the Fortress introducer sheath is now available in a full size range from 4Fr to 8Fr.
“The Fortress introducer sheaths have proven a favourite with interventionalists due to their ease of use and excellent kink resistance,” commented Alexander Uhl, president Vascular Intervention at Biotronik. “The expansion of Fortress introducer sheaths to 7Fr and 8Fr-compatibility allows physicians to use Fortress with a broader range of procedures such as most atherectomy devices and covered stents.”
“Like anything in the medical community, there can be positive and negative,” Agnieszka Solberg (Bismarck, USA) tells Interventional News discussing the impact of social media in the fields of interventional and neuroradiology.
As a founder of the RadChicks movement—an online community for women working in the field of radiology—Solberg believes that social media networks such as Twitter, LinkedIn and Facebook provide vital networking opportunities for women and underrepresented minorities, but warns that physicians must use these platforms with caution, paying particular attention to patient confidentiality, among other potential pitfalls.
Physicians also have an important role in building trust with the public, and should be at the forefront of effort to combat medical misinformation, Solberg argues.
Foreground: A microfluidic 3D model of the human blood vessel has been developed by NTU and TTSH scientists to study atherosclerosis in blood vessels and coronary arteries.
Credit: NTU Singapore
Foreground: A microfluidic 3D model of the human blood vessel has been developed by NTU and TTSH scientists to study atherosclerosis in blood vessels and coronary arteries. Credit: NTU Singapore
A Singapore team of scientists and clinicians from Nanyang Technological University, Singapore (NTU Singapore) and Tan Tock Seng Hospital (TTSH), have developed a three-dimensional (3D) model of the human artery blood vessel wall. Called an “arterial wall-on-a-chip”, it will help researchers study atherosclerosis.
Cardiovascular diseases account for some 32% of deaths worldwide, claiming some 17.9 million lives annually. In Singapore, about 6,990 deaths or about one third of all deaths in 2020 were due to heart disease or stroke.
Using the 3D model, the researchers discovered new knowledge about the early stages of atherosclerosis: as oxidative stress increases, an increase of inflammation happens together with a build-up of plaque.
The team also observed that Vitamin D and a common diabetes medication, metformin, helped to prevent certain key processes leading to the plaque formation. This suggests that their 3D model can be potentially used to screen and test new drug molecules that can treat or prevent atherosclerosis.
Carotid artery surgery and stenting have comparable long-term effects on fatal or disabling stroke in asymptomatic patients with severe carotid artery stenosis. That is the finding of late-breaking ACST-2 data presented in a Hot Line session at the European Society of Cardiology’s 2021 congress (ESC 2021; 27–30 August, virtual) and published simultaneously in TheLancet.
Patients with severe carotid artery stenosis are at elevated risk of stroke and both carotid artery stenting (CAS) and carotid endarterectomy (CEA) can restore patency and reduce the long-term risk of stroke. Nationwide registry data from Germany have shown among asymptomatic patients, CAS and CEA are both associated with an approximately 1% risk of disabling stroke or death. Comparative data are lacking on the long-term protective effects of the two procedures.
ACST-2 was the largest trial to compare the long-term effect of CAS versus CEA on stroke in asymptomatic patients with a severely narrowed carotid artery that had not yet caused a stroke. The trial enrolled patients with severe carotid artery narrowing (60% or more reduction in diameter on ultrasound) found by chance, but with no recent stroke or other neurological symptoms. Participants were thought by their doctor to need CAS or CEA but both doctor and patient were substantially uncertain about which procedure was preferable.
A total of 3,625 patients were enrolled from 130 centres in 33 countries. Participants were randomly allocated 1:1 to CAS or CEA and followed up for an average of five years. The main outcomes were: 1) procedural risks (morbidity and mortality within one month after the procedure); and, most importantly, 2) non-procedural stroke, subdivided by severity.
Regarding procedural risks, 1% of patients in both groups had a disabling stroke or died within 30 days (15 allocated to CAS and 18 to CEA) and 2% had a non-disabling procedural stroke (48 allocated to CAS and 29 to CEA).
The main outcome was five-year non-procedural stroke; fatal or disabling stroke occurred in 2.5% of patients in each group, for a rate ratio (RR) of CAS versus CEA of 0.98 (95% confidence interval [CI] 0.64–1.48; p=0.91), and any non-procedural stroke occurred in 5.3% of the CAS group versus 4.5% of the CEA group (RR 1.16; 95% CI 0.86–1.57; p=0.33). A meta-analysis of this and all other major trials of CAS versus CEA yielded a similarly non-significant result for any stroke (RR 1.11; 95% CI 0.91–1.32; p=0.21).
Principal investigator Alison Halliday (University of Oxford, Oxford, UK) said: “We have shown that, for patients with a severely narrowed carotid artery, stenting and surgery have similar effects on the chances of having a disabling or fatal stroke. The risk from each procedure is about 1%. After that, however, the annual risk over the next five or more years is halved, from 1% down to 0.5% per year.”
Recently released clinical data from the NAVABLATE study has shown that microwave ablation used bronchoscopically—with the Emprint Ablation Catheter Kit with Thermosphere Technology (Medtronic) in conjunction with the firm’s electromagnetic navigation bronchoscopy system—is an option for primary and oligometastatic malignant lung nodules in patients who decline or are not candidates for both surgery and stereotactic body radiation therapy (SBRT).
highlighted the safety and performance of microwave ablation used bronchoscopically with the Emprint Ablation Catheter Kit with Thermosphere Technology (Medtronic) in conjunction with the firm’s electromagnetic navigation bronchoscopy system.
The findings were released at a late-breaking presentation at the European Respiratory Society International Congress (September 5, 2021; virtual).
Kelvin Lau, a consultant thoracic surgeon at St. Bartholomew’s Hospital (London, UK) and a principal investigator for the NAVABLATE study, said: “Patients with malignant lesions in the lung often have limited therapy options due to lesion locations, comorbidities, and treatment side effects.
“The results from the NAVABLATE study explore the potential benefit of a more individualised treatment for patients and offer a new option for surgeons and physicians to provide a minimally invasive, localised treatment of malignant lesions in the lung.”
NAVABLATE is a prospective, multi-centre study that enrolled 30 subjects in the UK and Hong Kong to characterise the safety and performance of the CE Marked Emprint Ablation Catheter Kit. All patients underwent a bronchoscopic ablation procedure using the Emprint Ablation Catheter Kit and were followed for one-month post procedure.
Ablation using the Emprint Ablation Catheter Kit achieved 100% technical success in all 30 subjects immediately post-procedure. One-month imaging showed ‘satisfactory’ ablation of the nodule in 100% of subjects.
The composite rate of adverse events related to the Emprint Ablation Catheter Kit was 3.3% (one subject with mild haemoptysis). There were no deaths or pneumothoraces.
Emily Elswick, vice president and general manager of lung health and visualisation at Medtronic, added: “Despite advances in treatment that can extend survival, the challenges of long-term management of tumours in the lung have been a significant barrier to improving outcomes, quality of life, and extended time with loved ones.
“Medtronic continues to take a broad transformative approach to the care continuum for the treatment of lung disease to improve diagnostics, optimise therapy and accelerate recovery.”
The Emprint Ablation Catheter Kit received Breakthrough Device Designation status from the US Food and Drug Administration (FDA) in April 2021. This device is not approved or cleared by FDA and is not available for sale in the US.
Medtronic say they will continue to study the safety and efficacy of the Emprint ablation catheter kit under an upcoming FDA investigational device exemption (IDE) study, with the intent to submit for device approval or clearance at a future date.
Medtronic has announced the European launch of the 200mm and 250mm IN.PACT Admiral drug-coated balloons (DCBs) following CE mark approval. The product is intended to treat long complex femoropopliteal lesions efficiently in patients with peripheral arterial disease (PAD). The 200mm and 250mm IN.PACT Admiral DCB enables physicians to treat longer lesions using a single DCB instead of multiple DCBs.
Thomas Zeller, director of the Department of Angiology at Universitaets-Herzzentrum, Freiburg-Bad Krozingen, Germany, performed the first case using the new sizes of the IN.PACT Admiral DCB in Europe. He stated, “Patients with SFA [superficial femoral artery] disease often present with longer and more complex lesions as time goes on, which makes it challenging to effectively treat the entire segment. We know the IN.PACT Admiral DCB is effective in providing durable results, and now with the longer sizes, it is a more efficient treatment option for these difficult to treat lesions. Using the new sizes of the IN.PACT Admiral DCB could potentially lead to saving both time and money by using one balloon instead of multiple balloons.”
About the IN.PACT Admiral DCB
The IN.PACT Admiral DCB is a clinically established, primary endovascular therapy, which has been shown to provided durable, consistent and safe outcomes across multiple clinical trials, as well as across complex patient and lesion types. With more than 3,500 patients enrolled in 21 clinical studies and 600,000+ patients treated worldwide, the IN.PACT Admiral DCB is the preferred DCB for treatment of femoropopliteal disease allowing reduced interventions and preserving future treatment options. A DCB’s primary mode of action is physical dilatation of the vessel lumen by percutaneous transluminal angioplasty (PTA), followed by the delivery of paclitaxel. The unique formulation of IN.PACT Admiral DCB with its drug dose, excipient and crystallinity, provides sustained drug residence in the tissue, leading to an effective and durable outcome.
The 200mm and 250mm IN.PACT Admiral DCBs received FDA approval in May of 2018.
R3 Vascular has reported the successful initiation of its first-in-human clinical study evaluating the technical and clinical performance of the R3 Vascular Magnitude bioresorbable sirolimus-eluting scaffold (BRS) in patients suffering of chronic limb-threatening ischaemia (CLTI) due to occlusive below-the-knee (BTK) arterial disease.
A press release details that the R3 Vascular platform incorporates an innovative scaffold design and bioresorbable polymer technology resulting in biomechanical performance comparable to metallic stents. At a 98-micron strut thickness across all its usable range of diameters, the Magnitude BRS device is the thinnest BRS ever tested in this clinical setting, the release adds.
“Given the dire and unmet clinical need of patients presenting with CLTI undergoing BTK revascularisation, we are extremely pleased by the rapid progression of our programme,” said R3 Vascular CEO Kamal Ramzipoor. “Our Magnitude BRS is well-positioned to improve the clinical outcomes of these patients by providing temporary mechanical support and sustained drug delivery while reducing the well-established complications associated with permanent implants.”
“In this early clinical experience, we successfully tested the deliverability and mechanical performance of the Magnitude BRS. Post-procedural angiographic and duplex ultrasound data confirm the mechanical properties and ‘stent-like’ results of the Magnitude BRS device in presence of a high-disease burden. We are looking forward to expanding the patient population cohort and following the clinical results over time,” said Marianne Brodman (Medical University of Graz, Graz, Austria).
Juan F Granada, a strategic advisor to R3 Vascular, added: “In BTK intervention, the prevention of vessel recoil following balloon dilatation is key to prevent negative remodelling and maintain vessel patency over time. BRS offer the best of both worlds by providing vessel support while it is needed and allowing the opportunity for future reinterventions, which is important in this type of patient. The successful validation of this technology may finally offer an effective and durable way to treat patients with this complex medical condition.”
The CardioVascular Coalition (CVC), a coalition of physicians, care providers, advocates, and manufacturers working to improve awareness and prevention of peripheral arterial disease (PAD), has called on Congress and the Centers for Medicare & Medicaid Services (CMS) to address severe proposed cuts to specialty provider services in order to help increase access to care.
CMS recently proposed cutting payments for revascularisation services by approximately 23% in the proposed Physician Fee Schedule (PFS) Rule for CY2022. The proposed cuts, which are being driven by a provision that purports to update clinical labour data, would have a severe impact on cardiology, vascular surgery, venous, radiation oncology, and radiology practices. Though outpatient health services—including revascularisation—are cost-effective and convenient for patients, the proposed cuts would have profoundly negative effects on patient access and health equity. If the proposed cuts are finalised as currently proposed, Medicare beneficiaries will face more serious risks of limb loss.
“As we recognise PAD Awareness Month and the major impact that PAD has on Americans—particularly people of colour—I am deeply troubled by CMS’ flawed proposal to cut vital services like revascularisation by as much as 23%,” said CVC Board member Jeff Carr (Tyler Cardiac and Endovascular Center, Tyler, USA) . “At a time when America is suffering a PAD and amputation crisis on top of the COVID-19 pandemic, it is absolutely critical to ensure patients’ continued access to the services that are proven to help prevent amputations and slow disease progression. Unless Congress and CMS act to address these proposed cuts, I fear that it will be harder for patients to access necessary care, resulting in even more amputations, worse outcomes, and even greater healthcare disparities.”
PAD is exacerbated by conditions like diabetes, chronic hypertension, and renal disease, which are most prevalent in minority populations. Access to revascularisation therapies is especially vital to the African American, Hispanic, and Native American populations who are two to four times more likely to undergo a limb amputation due to PAD because of the increased prevalence of diabetes, obesity, and other risk factors.
“To address the issues of patient access and systemic health inequity in our country, CMS must reverse course and not finalise the clinical labour policy in the 2022 PFS Proposed Rule,” continued Carr. “Further, CMS should work closely with Congress to fundamentally reform the Physician Fee Schedule so that any future unjustified cuts to specialty provider services can be avoided.”
To learn more about PAD and PAD Awareness Month, click here.
Xact Robotics, the developer of the Xact Ace robotic system, recently announced it has successfully completed patient enrolment in the first US study evaluating Xact Ace for use in percutaneous lung procedures including biopsies to confirm the presence of cancer. The Xact Ace robotic system is the world’s first and only “hands-free” robotic system that can help improve targeting accuracy, efficiency, and consistency in computed tomography (CT)-guided percutaneous procedures including ablations, biopsies and targeted drug delivery.
Lung cancer is the second most common form of cancer around the world and millions of percutaneous procedures are performed in the lung each year. When using traditional manual methods to reach areas of interest in the lung, clinicians will sometimes suggest that patients wait until the lesion becomes larger and easier to access. Use of a robotic system may help access areas in the lung earlier, potentially supporting earlier diagnosis and treatment.
“Even among the most skilled radiologists, efforts to reach small areas of interest in the body, especially in the lungs, can be challenging,” said Sebastian Flacke (Lahey Hospital & Medical Center [LHMC], Burlington, USA). “With the completion of this study, we can more precisely assess the ability of the Xact Ace robotic system to help us reach target areas in the lung in a single insertion with a very high level of accuracy.”
During procedures with the Xact Ace robotic system a physician plans the route of an instrument and the robot then inserts and steers the instrument directly to the area of interest, typically reaching the target on the first insertion. In many cases during percutaneous procedures, the area of interest moves during instrument insertion, making it necessary to reinsert an instrument to reach the target. With the Xact Ace robotic system, the advanced algorithm and steering mechanisms can reformulate the insertion pathway to continually remain on route to reach a specific target, even if it moves during the procedure, maximising the rate of success on the first insertion.
The pilot trial primarily looked to evaluate safety of the Xact Ace robotic system when used in percutaneous procedures in the lung. Secondary performance evaluations included the proportion of procedures in which the instrument reached the predefined target based on the physician’s determination and CT imaging confirmation. The study also looked at system accuracy, which was defined as the measured distance from the tip of the instrument to the target location at the end of the insertion.
“The use of the Xact Ace robotic system to help radiologists reach small areas of interest in the lung is another major milestone showing the potential benefits of this technology for patients and clinicians,” said Chen Levin, CEO, Xact Robotics. “The outstanding work of the radiologists at LHMC and Sarasota Interventional Radiology [Sarasota, USA] significantly expands our understanding of the potential of our technology to set the new standard in percutaneous procedures in the lung with the potential to reduce risks for patients while supporting earlier diagnosis and treatment.”
As we start to emerge from the strictures imposed by the COVID-19 pandemic, it is timely to reflect on the delivery of education and training to interventional radiologists (IRs) around the world, especially those living in countries with limited access to the educational opportunities that are generally available to interventionists in the more developed world, writes Robert Morgan (St George’s University Hospitals NHS Foundation Trust, London, UK).
Before COVID-19
Before the COVID-19 pandemic affected populations worldwide, several major international interventional radiology societies (Cardiovascular and Interventional Radiological Society of Europe [CIRSE], Society of Interventional Radiology [SIR] and Asia Pacific Society of Cardiovascular and Interventional Radiology [APSCVIR]) had spearheaded programmes to deliver education and training in several countries around the world. Some medical device companies had also begun their own initiatives sponsoring senior IRs to visit countries to participate in the training of the local IRs. The concept of training IRs travelling to less well-developed countries and systems—i.e. outreach training—had been going on for some years from the start of this millennium. In the last decade, we saw a significant increase in this practice with ever-larger delegations of training IRs visiting a wider number of countries.
These outreach training programmes usually offered exposure to hands-on device training, and in some cases procedural training in addition to more formal teaching through lectures and small group tutorials. Where possible, the local outreach training experience was designed to complement standard training delivered by local senior IRs and online education and attendance at live educational events, where feasible, depending on the financial and political constraints of each country.
Although quality education can be delivered remotely, in-person training such as can be provided by outreach training enables valuable interactions and discussions between training faculty and trainees that are difficult to replicate online. My recent experiences as an outreach training faculty in Myanmar serve to illustrate the benefits of in- person outreach training.
Outreach training pre-COVID-19
In both January 2019 and 2020, I travelled to Myanmar as a member of an intersociety collaborative endeavour to provide training and education in two IR outreach workshops. The workshops were organised by senior members of the Asia Pacific Society of Interventional Radiology (APSCVIR) with participating members from CIRSE and the SIR in collaboration with senior Myanmar IRs.
In each programme, workshops were held in Yangon and in Mandalay General Hospitals. Both hospitals are of moderately large size with over 500 beds each. Each of the radiology departments are well equipped with two or more computed tomography (CT) scanners, at least one magnetic resonance imaging (MRI) scanner, one angiographic machine and general radiographic equipment.
The vast majority of the interventional radiology staff at these hospitals had never had the opportunity to attend a major congress, such as APSCVIR, CIRSE or SIR. All visiting international faculty members were impressed by the enthusiasm of the local staff and trainees to learn about interventional radiology. It was very evident that they were highly appreciative of receiving training from the visiting faculty.
A comprehensive scientific programme was delivered at both workshops covering a wide range of interventional radiology procedures including transarterial chemoembolization (TACE), radiofrequency ablation (RFA) of liver tumours, uterine fibroid embolization (UFE), haemodialysis interventions, central venous access, lower limb arterial interventions, urological interventions, hepatobiliary interventions and abscess drainage. The workshop programme involved lectures, small group teaching and hands-on device training. In addition, there were several live cases performed by the faculty, including myself. Live case topics included TACE, RFA, lower limb arterial angioplasty and stenting, and haemodialysis access angioplasty and stenting.
One less obvious benefit of in-person training was that local IRs strongly encouraged clinicians from other specialties to attend the workshop, particularly specific lectures and live cases that were relevant to their practice. This meant that during each lecture or tutorial, aspects of procedures were highlighted to increase the attractiveness of interventional radiology to these referring clinicians with specific emphasis put on the favourable comparison of interventional radiology procedures with the competing alternative treatments. The desired result of such an interaction would be to increase the number of referrals to interventional radiology by these local clinicians, which in my opinion, was an effective method—and one that is less translatable to an online educational format.
In summary, the main benefits of outreach training included: enabling local IRs without the financial resources to attend in-person congresses to receive a programme of tailored education to their specific requirements and surroundings; and raising the awareness of the potential of interventional radiology among other clinical specialties, which may result in increased referrals of patients for these minimally invasive, typically outpatient procedures.
Where are we now?
Inevitably, as a result of the effect of the COVID-19 pandemic worldwide and the severe restrictions on international travel, these outreach training programmes have come to a halt. In a similar manner to international congresses, which have currently moved almost exclusively to an online/virtual format, some societies have endeavoured to provide outreach training online through webinars and live discussion forums. This method of education has similar drawbacks for the delivery of outreach educational workshops as it does for international meetings. These are relatively obvious but are worth stating nevertheless: reduced impact of online lectures compared with live lectures; a lack of interpersonal interactions for educational and networking purposes; reduced opportunity for small group discussions; and the complete absence of hands-on device or procedural training. Finally, a specific disadvantage of online teaching for less well-developed countries is the dependence on the local information technology (IT) structures and ability of the local IRs and trainees to access the internet adequately for online teaching, which may be demanding in terms of the bandwidth required.
Where do we go from here?
The experiences of the past 18 months have reminded us that the internet is an effective method to deliver education and training. However, the majority of doctors, both trainees and trainers, are firmly of the opinion that virtual methods do not, and must not, completely replace in-person educational methods.
However, the pandemic is a worldwide phenomenon. Although vaccination programmes in many countries, particularly in Europe and North America are well advanced, this is not the case in Asia, South America or Africa where a significant proportion of outreach programmes take place. It is likely that international congresses will return as live educational events in 2022, but they will be restricted by COVID-19 testing and impacted by the country of origin of delegates. Unfortunately, it may be longer before IRs are able to travel to countries with lower vaccination rates to deliver outreach training. However, this is not to say that this form of training must be abandoned or forgotten. International societies such as CIRSE, SIR, and APSCVIR must continue to commit to the concept of outreach training and to make plans for the day when this valuable training format once again becomes feasible to deliver.
In summary, international societies have the ability and an obligation to deliver local education and training to IRs in lower- and middle-income countries. Local in-person outreach training has significant benefits that cannot be provided by the virtual format. Although a return to outreach training workshops may not be feasible for a year or more, this important method of training must not be forgotten and interventional radiology societies must continue to devise schedules for outreach training as soon as this becomes possible again.
Robert Morgan is a consultant and reader in interventional and diagnostic radiology. He is deputy editor-in-chief CVIR Endovascular and a past president of CIRSE. He has reported no disclosures relevant to this article.
From a cost-effectiveness standpoint, primary stenting of the superficial femoral artery (SFA) for the treatment of intermittent claudication can, in many countries, be used as an adjunct to exercise training advice. This is the main conclusion of Henrik Djerf (Sahlgrenska University Hospital, Gothenburg, Sweden) and colleagues, reporting two-year results of a randomised, multicentre trial online in the European Journal of Vascular and Endovascular Surgery (EJVES).
Djerf et al consider what their paper add to the literature: “This examination of the cost effectiveness within a randomised controlled trial for endovascular treatment of the SFA in patients with intermittent claudication adds longer follow-up data than previous studies.”
The authors write that invasive treatment of intermittent claudication is commonly performed, despite limited evidence of its cost effectiveness. In addition, they note that endovascular treatment is performed frequently due to the fact that symptoms of intermittent claudication are mainly caused by atherosclerotic lesions in the SFA. The aim of the present study, Djerf and colleagues relay, was to investigate the cost effectiveness of endovascular treatment versus its non-invasive counterpart.
The researchers randomised 100 patients with intermittent claudication due to lesions in the SFA to treatment with primary stenting, best medical treatment and exercise advice, or to best medical therapy and exercise advice alone (the control group), noting that patients were recruited from seven hospitals in Sweden. For their present analysis of cost effectiveness after two years, the investigators analysed 84 patients with data on quality-adjusted life years (QALYs).
Writing in EJVES, Djerf et al report that the mean cost per patient was €11,060 in the stent group and €4,787 in the control group, resulting in a difference of €6,273 per patient between the groups. In addition, they found that the difference in mean QALYs between the groups was 0.26, in favour of the stent group, which resulted in an incremental cost-effectiveness ratio (ICER) of €23,785 per QALY.
The authors conclude that the costs associated with primary stenting in the SFA for the treatment of intermittent claudication were higher than for exercise advice and best medical therapy alone. They add that, with concurrent improvement in health-related quality of life, primary stenting was a cost-effective treatment option according to the Swedish national guidelines (ICER <€50,000–70,000) and approaching the UK’s National Institute for Health and Care Excellent threshold for willingness to pay (ICER <£20,000–30,000).
In many countries, primary stenting of the SFA is cost-effective and therefore can be used as an adjunct to exercise training advice, Djerf and colleagues summarise. However, they stress that successful implementation of structured exercise programmes and longer follow-up may alter these findings in the future.
Hancock Jaffe Laboratories has announced that promising two-year post-VenoValve implantation data are being presented today at the Society for Vascular Surgery’s Vascular Annual Meeting (SVS VAM 2021; 18–21 August, San Diego, USA and online) by Jorge Ulloa (Fundacion Santa Fe-Universidad de los Andes, Bogota, Colombia), who was the principal investigator for the company’s first-in-human VenoValve trial.
Key highlights from Ulloa’s presentation indicate that:
Reflux decreased from an average of 1.95 to an average of 0.72 (a 63% improvement)
Disease manifestations (measured by revised venous clinical severity score [rVCSS]) decreased from an average of 13.38 to an average of 5.38 (a 60% improvement)
Pain (measured by VAS scores) decreased from an average of 7.25 to an average of 0.5 (an improvement of 93%)
There were no safety issues or venous ulcer recurrences
The data reported are for a group of eight patients who participated in the VenoValve first-in-human study and who agreed to participate in a one-year post-study follow-up. Three additional first-in-human patients elected to not participate in the one-year post-study follow-up, but reported no negative VenoValve-related events during the one-year follow-up period. The average post-VenoValve implantation time for this cohort of patients is two years, and the comparative results are based on pre-VenoValve levels compared to the patients’ most recent office visit.
Marc Glickman, Hancock Jaffe’s senior vice president and chief medical officer stated, “These data are exactly the results that we were looking for as we begin our VenoValve SAVVE [Surgical anti-reflux venous valve endoprosthesis] pivotal trial. Our patients are continuing to benefit from the VenoValve, with no safety issues and no ulcer recurrences. Chronic venous insufficiency [CVI] in the deep venous system has frustrated patients and physicians for decades and our primary investigators for the SAVVE study are as excited and enthusiastic as we are about the upcoming study.”
The SAVVE US pivotal trial for the VenoValve will include 75 patients at up to 20 sites. The primary endpoints for the SAVVE trial will be the same as for the first-in-human trial: the primary safety endpoint is the occurrence of a major adverse event (MAE) in less than 10% of patients at 30 days post-VenoValve implantation, and the primary effectiveness endpoint is improvement of reflux equal to or greater than 30% at six months following VenoValve surgery. MAEs are defined as the composite of all-cause mortality, deep wound infection, major bleeding, ipsilateral deep vein thrombosis (DVT), or pulmonary embolism. Improvement of VCSS and visual analogue scale (VAS) scores are also included in the SAVVE study as secondary endpoints.
Joseph V Lombardi (Cooper University Hospital, Camden, USA) reported long-term outcomes favouring the continued safety and effectiveness of a composite device (proximal covered stent graft plus distal bare stent) deployed for the endovascular repair of acute, type B aortic dissection (TBAD) complicated by aortic rupture and/or malperfusion.
“STABLE II results place freedom from all-cause mortality at 80.3% at one year, and 68.9% at five years [with the use of the Zenith dissection endovascular system from Cook Medical]. Further, there were two procedure-related deaths, and the freedom from dissection-related mortality remained 97.1% at one year through five years,” he told delegates of the Society for Vascular Surgery’s Vascular Annual Meeting (SVS VAM 2021; 18–21 August, San Diego, USA and online).
The Zenith endovascular system includes a proximal covered stent graft to cover the primary entry tear plus a distal bare metal stent, built on a nitinol Z-stent platform, for true lumen support. The bare metal component provides expansible support along the length of the dissected aorta without blocking critical branch vessels to provide a scaffolding to aid adjunctive interventions and facilitate favourable aortic remodelling of the entire dissected aorta.
Outlining the adverse events seen in the study, Lombardi commented that notable adverse events at one year were one instance of aortic rupture, one instance of conversion to open repair and two instances of stroke—there were no instances of paraplegia or paraparesis. “Freedom from secondary intervention was 88.2% in one year, and 70.7% at five years and secondary interventions were used to treat a number of presentations, including distal aortic growth. Aortic growth distal to the stent graft suggests the need for continuous monitoring,” he added.
Study details
STABLE II is a prospective, single-arm, multicentre study that enrolled 73 patients between August 2012 and January 2015 at institutions in the USA and Japan. The mean age of patients was 60.7 years with nearly 66% being male with acute TBAD complicated by malperfusion (78.1%), rupture (27.4%). Patients were treated with either a composite device (proximal covered stent-graft plus distal bare stent, 79.5%) or the proximal stent graft alone (no distal bare stent, 20.5%). Dissections were more extensive in patients receiving the composite device (408.9±121.3mm long, with 47.4% of dissections extending into the iliac arteries) compared with those who did not receive the distal bare stent (315.9±100.1mm long, with 6.7% of dissections extending into the iliac arteries). Five-year follow-up was available for 86.1% of eligible patients.
False lumen thrombosis and the composite device
The researchers also communicated that proximal dissection events were reported in seven patients, including four patients with retrograde progression of dissection and three patients with a new tear/type A dissection. Importantly, Lombardi called out the progressive false lumen thrombosis seen within the stent graft region and the dissected stent region. “Complete false lumen thrombosis rate increased (75% of patients at five-year vs. 51.4% post-procedure), with a higher complete thrombosis rate at five years in patients who received the composite device (81%) compared with the rate in patients who did not receive the distal bare stent (57.1%).
“There were no incidences of device fracture or infolding reported and these five-year data suggest a positive influence of composite device use on false lumen thrombosis,” he summarised.
Bare metal stent necessities
To a question posed on how the decision was made to deploy or not deploy the bare metal stent, Lombardi clarified: “We left that up to our investigators to determine the need for additional stenting using the bare metal stent. A lot of the dissections were very focal on the thoracic aorta and some thought that an additional dissection stent was not needed to support normal aorta distally. So, this was a primary reason why dissection stents were not deployed, but the fact that we did not have dissection stents in a small cohort of patients gave us a nice control group to look at afterwards.
When pressed on recommendations regarding when to use the dissection stent and tips on how far to place it, especially when the dissection was particularly distal, Lombardi explained: “The data is very supportive of the distal aortic remodelling using the dissection stent. And oftentimes, as you saw in the data, secondary interventions are not infrequent, and we will have to go back and reintervene for distal aortic growth to remedy ongoing expansion. The use of the dissection stent in that situation for me and for a lot of our colleagues has been very, very helpful in mitigating a continued false lumen flow. So, I am a believer in using it in all settings, as long as I’m putting it across dissected aorta.”
Poverty and Black race were associated with higher rates of lower leg amputation among people with peripheral arterial disease (PAD) who live in metropolitan areas, according to new research published today in a special issue of the Journal of the American Heart Association (JAHA), an open access journal of the American Heart Association (AHA).
The analysis on PAD-related amputations is one of 16 new research studies highlighting health disparities among people from diverse population groups and published in the special spotlight issue of JAHA.
JAHA senior associate editor Pamela Peterson (University of Colorado Denver, Denver, USA) and associate editor Sula Mazimba (University of Virginia Health System, Charlottesville, USA) note that while management of cardiovascular disease has reduced death rates over time, there are still “striking disparities” in the USA that have widened along racial, ethnic, socioeconomic and geographical lines.
“We hope that this issue of JAHA will reinforce the recent America Heart Association’s presidential advisory statement urging all stakeholders to a committed path towards transforming the conditions of historically marginalised communities, improving the quality of housing and neighbourhood environments of these populations, advocating for policies that eliminate inequities in access to economic opportunities, quality education and health care, and enhancing allyship among racial and ethnic groups,” they wrote.
The study, “Geographic and socioeconomic disparities in major lower extremity amputation rates in metropolitan areas”, by Alexander Fanaroff (University of Pennsylvania, Philadelphia, USA) et al, is an analysis of national Medicare claims data to determine ZIP code-level variation in rates of amputation among Medicare beneficiaries.
“Limb amputation can be delayed and or prevented by timely and aggressive treatment. However, lack of access to specialised care may delay PAD diagnosis and limit efforts to save the limbs if it has progressed to the advanced disease stage,” explained Fanaroff.
Fanaroff and colleagues found that ZIP codes with a higher proportion of Black residents had higher amputation rates than ZIP codes with lower proportions of Black residents. In addition, ZIP codes with lower median household income, more residents eligible for Medicaid and worse scores on the Distressed Communities Index scale (a composite marker of socioeconomic status), had higher amputation rates compared to ZIP codes with higher socioeconomic status, even after adjusting for clinical and demographic characteristics.
“Though amputation rates are generally higher in rural areas, this finding shows that the association between lower socioeconomic status, race and amputation rate extends to major metropolitan areas as well as rural regions,” Fanaroff said. “We found that closer proximity to specialised PAD care within metropolitan areas does not ensure access to high quality care. Strategies targeted to communities with high amputation rates are also needed in urban areas to reduce these disparities.”
A recent AHA scientific statement noted sex and ethnic disparities exist in the diagnosis and treatment of the most severe form of PAD, chronic limb-threatening ischaemia (CLTI).
Another article in the spotlight issue is a retrospective study of more than 425,000 women (ages 12–49; 59% non-Hispanic white women, 31% non-Hispanic Black women and 10% Hispanic women) in South Carolina who gave birth from 2004–2016 and were followed through 2017. The study, “Incident heart failure within the first and fifth year of delivery among women with hypertensive disorders of pregnancy and pre-pregnancy hypertension in a diverse population”, by Angela M Malek (Medical University of South Carolina, Charleston, USA) et al, found racial and ethnic differences in heart failure rates among women who experience hypertensive disorders during pregnancy as well as among women who experience hypertensive disorders both before and during pregnancy.
Non-Hispanic Black women who had hypertensive disorders of pregnancy with and without pre-pregnancy hypertension had a higher incident heart failure risk within five years of giving birth compared to non-Hispanic white women without hypertension (before or during pregnancy). Among women who had pre-eclampsia or other hypertensive disorders during pregnancy, heart failure event rates were substantially higher in non-Hispanic Black women than non-Hispanic white women: 2.28 compared to 0.96 per 1,000 person-years, respectively. In women who had hypertensive disorders of pregnancy with pre-pregnancy hypertension, heart failure event rates were also substantially higher among non-Hispanic Black women than non-Hispanic white women: 4.3 compared to 1.22 per 1,000 person-years, respectively.
“These racial and ethnic differences are important since we already know non-Hispanic Black women experience higher pregnancy-related deaths than non-Hispanic white women,” said Malek. “Clinical and public health prevention efforts are needed to reduce complications and death rates in women who have hypertensive disorders before or during pregnancy as they are at increased risk of heart failure or dying from heart failure within five years.”
Additional research is needed to further examine racial/ethnic differences in maternal incident heart failure after delivery. The clinical and public health implications of this research could inform changes to clinical practice to reduce modifiable cardiovascular risk factors and screening for adverse maternal outcomes in women identified as high risk, according to the study.
Other research featured in the JAHA spotlight issue on health disparities can be accessed in full here.
AAA sac fill (L) with Impede-FX RapidFill implants (R)
Shape Memory Medical has announced the initiation of AAA-SHAPE Netherlands, the company’s prospective, multicentre early feasibility study of the Impede-FX RapidFill device when used for abdominal aortic aneurysm (AAA) sac management during elective endovascular aneurysm repair (EVAR). The Dutch study’s first procedure was performed by Michel Reijnen, vascular surgeon at Rijnstate Hospital in Arnhem, The Netherlands.
Ted Ruppel, president and chief executive officer of Shape Memory Medical said, “We would like to congratulate Michel Reijnen and the clinical study team at Rijnstate Hospital for a successful first AAA-SHAPE case in The Netherlands. The addition of Dutch sites to the AAA-SHAPE programme accelerates our ability to evaluate Impede-FX RapidFill and its potential to improve sac regression in AAA patients following EVAR.” The study will enrol up to 15 patients across three centres in The Netherlands, contributing to the AAA-SHAPE safety study, which is also currently enrolling up to 15 patients in Auckland, New Zealand.
The Impede-FX RapidFill device contains five Impede-FX, 12mm embolisation plugs preloaded into a single delivery introducer for fast and efficient delivery of the embolic material. This high-volume platform incorporates the novel Shape Memory Polymer, a porous, embolic scaffold that is crimped for catheter delivery and self-expands upon contact with blood for rapid conversion to organised thrombus. Preclinical and clinical studies have shown that Shape Memory Polymer offers effective and predictable space filling, stable clot formation for sac embolisation, and progressive healing as the material biodegrades.
“We are excited to contribute to AAA-SHAPE,” said Reijnen, principal investigator for AAA-SHAPE Netherlands. “Patients who develop aneurysm sac shrinkage following EVAR have better outcomes than patients with a stable or growing aneurysm sac. We look forward to learning how the use of Impede-FX RapidFill in combination with EVAR influences sac behaviour,” continued Reijnen.
“We are very pleased to be working together with colleagues from the Netherlands to add to our growing experience with AAA-SHAPE,” said Andrew Holden, interventional radiologist at Auckland City Hospital in Auckland, New Zealand. “Our preliminary experience with AAA-SHAPE has been very encouraging, and the first few patients have shown a reduction in AAA sac diameter at early follow-up,” continued Holden.
The Janssen Pharmaceutical Companies of Johnson & Johnson today announced that the US Food and Drug Administration (FDA) has approved an expanded peripheral arterial disease (PAD) indication for the Xarelto(rivaroxaban) vascular dose (2.5mg twice daily plus aspirin 100mg once daily) to include patients following recent lower-extremity revascularisation (LER) due to symptomatic PAD.
The approval is based on data from the Phase III VOYAGER PAD study. According to a press release, Xarelto is now the first and only therapy indicated to help reduce the risks of major cardiovascular events in patients with coronary artery disease (CAD) and major thrombotic vascular events, such as myocardial infarction, ischaemic stroke, acute limb ischaemia, and major amputation of a vascular aetiology, in patients with PAD, including patients who have recently undergone LER due to symptomatic PAD.
“For more than 20 years, many physicians have used dual antiplatelet therapy after lower extremity revascularisation due to symptomatic PAD with limited data to support efficacy and safety in this setting. Now, the VOYAGER PAD and COMPASS clinical studies have demonstrated the utility of dual pathway inhibition in targeting both platelets and thrombin in patients with PAD. These data provide a new mechanism of treatment using an evidence-based strategy for this vulnerable population,” said Marc P Bonaca (University of Colorado Anschutz Medical Campus, Aurora, USA). “This FDA approval of rivaroxaban plus aspirin is a major advancement for PAD management and sets the stage to evolve the current standard of care for patients with PAD.”
Xarelto now has nine indications in the USA. Today’s approval is based on the Phase III VOYAGER PAD trial, which demonstrated the Xarelto vascular dose (2.5mg twice daily plus aspirin 100mg once daily) reduced the risk of major adverse limb and cardiovascular events by 15% in patients with symptomatic PAD post-LER compared to aspirin alone.The VOYAGER PAD trial saw no significant difference in Thrombolysis in Myocardial Infarction (TIMI) major bleeding between Xarelto with aspirin compared to aspirin alone.
The results from the VOYAGER PAD study complement findings from the landmark Phase III COMPASS trial, which also examined the dual pathway approach of Xarelto with aspirin in CAD and/or PAD patients and further supports this FDA label extension in PAD patients. Data from the Phase III COMPASS trial resulted in FDA approval in 2018 to reduce the risk of major cardiovascular events, such as heart attack, stroke and cardiovascular death in people with chronic PAD and CAD. While there were more major bleeds with the Xarelto vascular dose in COMPASS, there was no significant difference in rates of fatal bleeding, intracranial bleeding or symptomatic bleeding into a critical organ.
Argon Medical Devices has announced the commercial launch of Skater mini-loop drainage catheters in the USA and the European Union.
The Skater mini-loop is a drainage catheter placed through the skin using imaging guidance as a minimally invasive way to remove or drain an unwanted fluid collection. The device, an expansion of Argon’s Skater all-purpose and nephrostomy drainage portfolio, uses a 40% smaller loop to help secure the catheter and drain fluid from smaller cavities.
“The Skater mini-loop drainage catheter is easily inserted and forms a tight loop formation to prevent drainage occlusion. Unlike other drainage catheters in the class, Skater mini-loop is compatible with alcohol and has durability to resist kinking,” says Sujoy Menon (Newark Beth Israel Medical Centre, Newark, USA), one of the first physicians in the USA to use the device.
Argon Medical Devices has introduced several new devices in the biopsy, drainage, and vascular therapy segments in 2020 and is planning on expanding their product list aimed at facilitating interventional vascular and oncology procedures in 2021.
“We are excited to complete our Skater portfolio of drainage solutions and celebrate this next launch in our Year of Innovation [2021],” commented George A Leondis, president and CEO of Argon Medical Devices.
“A strategy of adding rivaroxaban 2.5mg twice daily to aspirin should be considered after lower extremity bypass regardless of conduit type,” concluded Nicholas Govsyeyev (University of Colorado, Aurora, USA) during the William J von Liebig Forum at the Society for Vascular Surgery’s Vascular Annual Meeting (SVS VAM 2021; 18–21 August, San Diego, USA and online). Govsyeyev was giving an update on the VOYAGER PAD trial, addressing the efficacy of rivaroxaban and aspirin in peripheral arterial disease (PAD) patients with venous and prosthetic surgical bypass conduits.
“The optimal antithrombotic therapy following infrainguinal bypass is not known,” Govsyeyev began. He noted that two major trials have examined the role of dual antiplatelet therapy (DAPT) and oral anticoagulation following infrainguinal bypass—CASPAR and DUTCH BOA. While both these trials had neutral results, the presenter detailed, there was significant heterogeneity by conduit type, with the CASPAR trial showing the potential benefit of DAPT in prosthetic conduits and the DUTCH BOA trial demonstrating the potential benefit of anticoagulation in venous conduits. Both trials, however, had a significant increase in major bleeding.
“The VOYAGER PAD trial provides a large, prospective database to further examine the optimal antithrombotic regimen following infrainguinal bypass,” Govsyeyev remarked. This trial randomised 6,554 patients with symptomatic PAD undergoing lower extremity revascularisation and receiving standard of care to rivaroxaban 2.5mg taken twice daily or placebo, with standard of care consisting of aspirin, clopidogrel use per the investigator’s discretion, and the encouragement of statin use.
Govsyeyev summarised the key findings: “The trial demonstrated a 15% reduction in the primary composite endpoint of acute limb ischaemia, major amputation, myocardial infarction, ischaemic stroke, and cardiovascular death; bleeding was increased, but overall incidence was low with rivaroxaban; there was no significant interaction for efficacy or safety on the basis or surgical or endovascular revascularisation; and surgical patients’ risk for primary endpoint events was reduced by 19% with rivaroxaban.”
The objectives of the current study, Govsyeyev explained, were to compare limb outcomes with venous versus prosthetic conduits in VOYAGER PAD patients who underwent bypass, and to evaluate whether the efficacy of rivaroxaban is consistent across conduit types.
In order to assess this goal, the researchers used a multivariate adjusted model to determine the risk of limb outcomes in patients with venous and prosthetic conduits, and Cox proportional hazards to assess for efficacy.
Govsyeyev detailed that a total of 1,448 (66%) patients underwent bypass in the VOYAGER trial. Breaking this down by conduit type, he noted that prosthetic use was slightly more frequent (773 patients; 54%) than venous use (646 patients; 46%).
In terms of baseline characteristics, the speaker communicated that the median age of the venous cohort was 65 (59–70) compared to 66 (61–72) in the prosthetic group, and that the number of female patients in the venous group was slightly lower than in the prosthetic group, at 17 and 22, respectively. Medical comorbidities were not different between the two groups, he added.
With regard to distribution by target artery, Govsyeyev stated that venous conduits were more likely to be used below the knee, whereas three-quarters of prosthetic conduits had an above-the-knee target artery.
Govsyeyev reported that, in the placebo group, the cumulative incidence of unplanned limb revascularisation at three years from randomisation was 29.6% in the prosthetic cohort (n=388) compared to 13.1% in the venous cohort (n=314), with a risk difference of 16.5%. Regarding acute limb ischaemia, the figures were 13.6% and 5.4%, respectively, with an 8.2% risk difference.
The presenter then outlined results related to the efficacy of rivaroxaban on the primary composite endpoint by conduit type. “Prosthetic patients were at higher risk for primary endpoint events, and this was reduced with rivaroxaban, with an absolute risk difference of 6.4%,” Govsyeyev revealed. Among the venous conduits, the data showed an absolute risk difference of 7.9% with rivaroxaban. Govsyeyev added that there was no significant interaction by conduit type and overall bleeding was quite low in the rivaroxaban and placebo groups.
Furthermore, the speaker informed the audience that there was consistent benefit of rivaroxaban on limb outcomes regardless of conduit type. He summarised the results: “Prosthetic conduits had a higher risk for limb outcomes; acute limb ischaemia was reduced in both venous and prosthetic conduits with rivaroxaban, with a particularly strong benefit among venous conduits with a greater than 50% reduction; major amputation was reduced in venous conduits but not in prosthetic; unplanned limb revascularisation was reduced in prosthetic but not in venous; and there was no significant interaction for any limb outcome by conduit type.”
Addressing the VAM audience, Govsyeyev concluded that a strategy of rivaroxaban 2.5mg twice daily reduces irreversible harm events and increases bleeding with a 6:1 benefit risk ratio, and that the magnitude of benefit appears robust in surgical patients. He added that prosthetic conduit patients are at a roughly three-fold risk of acute limb ischaemia and unplanned revascularisation relative to those receiving venous conduits, and that the benefit of rivaroxaban is consistent across conduit types with around a 2% absolute reduction in acute limb ischaemia and around a 6% reduction in primary outcome. Taking all these factors into account, Govsyeyev commented: “A strategy of adding rivaroxaban 2.5mg twice daily to aspirin should be considered after lower extremity bypass regardless of conduit type.”
Fist Assist Devices has announced that data associated with the p-FACT cohort, a subset of the recently completed, non-significant risk Fist Assist clinical trial (FACT trial) that focused on vein dilation in stage four patients with chronic renal failure, show clear evidence that the Fist Assist device dilates the perforator vein.
The p-FACT data derived from the FACT trial evaluated the use the FA-1 device developed by Fist Assist Devices, a novel, intermittent pneumatic compression device, to promote superficial vein dilation in patients with chronic kidney disease to enable creation of all types of arteriovenous fistulas (AVFs) and to ensure the safety of the device in this patient population.
“We are thrilled to announce the results of the p-FACT data. The statistically significant data, with a p value of <0.05, shows that the FA-1 device clearly dilates the perforator vein in stage four chronic renal failure patients” said Tej Singh, chief executive officer and founder of Fist Assist Devices.
“These are very important data as they not only show that the FA-1 device is safe, but also demonstrate that intermittent pneumatic pressure dilates superficial veins including, most importantly, the perforator vein needed for endoAVF success. Condition of the perforator vein is critical for endoAVF planning, and we can now show without a doubt that the Fist Assist FA-1 device can dilate that clinically important vein and have a key role in endoAVF consideration and planning!”
“These are revolutionary data for the ESRD [end-stage renal disease] community, namely the patients, physicians, and companies associated with endoAVF procedures” said FACT investigator John Lucas (Greenwood Leflore Hospital, Greenwood, USA).
“Larger veins not only make vascular access surgery easier and more likely to succeed, but a larger, dilated perforator vein is essential for the endoAVF to mature properly. Both endoAVF technologies presently approved and available for treatment of ESRD utilise the perforator vein as a key component of the procedure. The statistically significant p-FACT data demonstrate that intermittent compression results in a larger perforator vein for stage four patients. Based on the FACT trial p-FACT data, almost every stage four renal disease patient planning to have having an endoAVF procedure should consider using the FA-1 device in preparation for their procedure. Larger veins, especially the perforator vein, will surely improve outcomes! This is very exciting data for all patients and the global ESRD community.”
A research letter published in Circulation: Cardiovascular Quality and Outcomes highlights a “very low” utilisation of supervised exercise therapy (SET) in symptomatic peripheral arterial disease (PAD) patients during the first 19 months after approval by the Centers for Medicare & Medicaid Services (CMS) despite a Class IA guideline endorsement. Authors Sanjay Divakaran (Brigham and Women’s Hospital, Boston, USA) and colleagues write that greater effort is needed to increase SET enrolment across the USA, as well as to improve adherence once enrolled.
In addition to low utilisation of SET and limited participation in therapy following enrolment, the researchers also found that patients referred to SET differed in race, sex, socioeconomic status, and geographic region compared with those unenrolled, suggesting disparities emerging early during implementation.
Divakaran et al detail that SET is recommended in consensus guidelines, based on its proven ability to reduce symptoms of PAD and improve walking performance. A lack of reimbursement for SET was a barrier to access and utilisation up until May 2017, when the CMS determined that that the evidence was sufficient to cover SET for beneficiaries with intermittent claudication. The present study aimed to address a lack of data on utilisation and outcomes associated with SET since the introduction of reimbursement.
The research team included in their study patients with a Current Procedural Terminology code for SET or International Classification of Diseases, Tenth Revision Clinical Modification code for intermittent claudication required by CMS for SET reimbursement between 1 June 2017 (corresponding with CMS’ reimbursement agreement) and 31 December 2018.
Among 129,699 patients with a diagnosis of intermittent claudication, 1,735 (1.3%) were enrolled in SET during the study period, the authors relay in their research letter. The investigators further detail that the median number of SET sessions attended was 16 (interquartile range [IQR], 6–28), and that only 89 patients (5.1%) completed the programme, attending all 36 sessions.
Writing in Circulation: Cardiovascular Quality and Outcomes, the authors report that one-year cumulative incidence of endovascular and surgical revascularisation among patients participating in SET were 11.9% and 2.4%, respectively, adding that no patients undergoing SET underwent amputation during the follow-up period.
Divakaran et al further relay that, in a matched cohort analysis (n=6,940), the use of endovascular or surgical revascularisation was significantly lower among those who underwent SET—endovascular: hazard ratio (HR), 0.49 (95% confidence interval [CI], 0.4–0.6), p<0.001; surgical: HR, 0.27 (95% CI, 0.18–0.42), p<0.001. The researchers add that there were no other differences in outcomes between groups.
Addressing some limitations of their study, Divakaran and colleagues recognise that only a small number of patients were referred to SET and that follow-up time was short. In addition, they acknowledge the possibility of treatment selection bias and residual confounding, the inability to assess severity of symptoms due to the use of claims codes, and the lack of detail regarding SET protocols.
July’s top 10 features a video interview with Jonathan G Moss (Institute of Cardiovascular and Medical Sciences, Glasgow, UK), chief investigator of the CAVA (Central venous access devices for the delivery of systemic anticancer therapy) trial, results of which were published online in The Lancet. A meta-analysis looking at the risk of major amputation after use of paclitaxel-coated balloons (PCBs) in the peripheral arteries has attracted debate, with leading physicians propose that the methodology used needs to be carefully considered and scrutinised before these conclusions are accepted.
VIDEO: For most patients receiving systemic anticancer treatment (SACT), totally implanted ports (PORTs) are more effective and safer than both Hickman-type tunnelled catheters (Hickman) and peripherally inserted central catheters (PICCs). The CAVA trial’s results, just published online in The Lancet, recommend reshaping current guidelines and practice, so that most patients requiring chemotherapy for solid tumours receive a PORT within the UK National Health Service, foreshadowing a pivot in practice that might be “slow to start with”.
“There appears to be heightened risk of major amputation after use of paclitaxel-coated balloons [PCBs] in the peripheral arteries,” findings from a systematic review and meta-analysis of randomised controlled trials (RCTs) published in the European Journal of Vascular and Endovascular Surgery (EJVES) suggest. However, the authors clarify that the level of evidence is graded moderate, not high, due to scarce events in some studies.
A large, single-centre retrospective study has revealed the risk of acute kidney injury (AKI) following pharmacomechanical thrombolysis (PMT) for lower extremity deep vein thrombosis (DVT) is as high as 22%.
Scitech Medical has announced that it has received CE mark approval for the Embosoft microspheres for use in vascular embolization of hypervascular tumours, symptomatic uterine fibroids and prostatic arteries to relieve symptoms related to benign prostatic hyperplasia, as well as for haemostatic embolization.
Endologix announced the company’s ChEVAS (chimney endovascular aneurysm sealing) system has been granted a Breakthrough Device designation from the US Food and Drug Administration (FDA). The ChEVAS system is an investigational endovascular abdominal aortic aneurysm (AAA) sealing therapy designed to combine the Nellix 3.5 endograft with parallel visceral stents to enable treatment of patients with juxtarenal, pararenal, and suprarenal AAA.
Artio Medical announced it has completed enrolment in its first-in-human study evaluating the Amplifi vein dilation system. In the study, five patients were treated by Adrian Ebner, head of the Cardiovascular Department at Sanatorio Italiano Hospital in Asunción, Paraguay.
A population-based study from 2013 to 2015 in Germany has found that nearly one fifth of patients with peripheral arterial disease (PAD) did not receive guideline-based vascular diagnostics three months before incidence amputation. Writing online in the European Journal of Vascular and Endovascular Surgery (EJVES), authors Kristina Hagenström (University Medical Center Hamburg-Eppendorf, Hamburg, Germany) and colleagues say this “reflects an underuse of health services”.
Terumo Medical Corporation has announced the introduction of its Azur vascular plug. The addition to Terumo’s embolisation portfolio is indicated for use to reduce or block the rate of blood flow in arteries of the peripheral vasculature.
Percutaneous Deep Vein Arterialisation (pDVA) with the LimFlow System offers a cost-effective and high-value alternative to traditional therapies or amputation, according to a recent study published in the Journal of Critical Limb Ischemia.
A German claims-based cohort study has revealed that—in 13,204 patients treated with a paclitaxel-coated device for peripheral arterial disease (PAD)—mortality differences were mostly attributable to a female subgroup treated above the knee, while no statistically-significant differences were observed in male patients. These findings were recently published in the Journal of Clinical Medicine (JCM).
MedAlliance has announced completion of patient enrolment in the PRISTINE clinical trial with the Selution SLR 018 drug-eluting balloon (DEB) for the treatment of patients with below-the-knee (BTK) disease. According to a MedAlliance press release, Selution SLR is the first DEB to be awarded Breakthrough Device designation by the US Food and Drug Administration (FDA).
The objective of the prospective PRISTINE trial is to evaluate the safety and efficacy of the Selution SLR sirolimus DEB in the treatment of infra-inguinal occlusive lesions (TASC C and D) in patients with chronic limb-threatening ischaemia in 75 patients over 12 months at Singapore General Hospital in Singapore.
PRISTINE is a follow-up registry to the PRESTIGE trial. The 12-month data from PRESTIGE were presented at LINC 2021 (The Leipzig Interventional Course, 25–29 January, online), showing sustained benefits up to one year. Eighteen-month data is to be presented at VIVA 2021 (Vascular InterVentional Advances; 4–7 October, Las Vegas, USA), where it is anticipated that these benefits will be further sustained. A similar outcome benefit is expected from PRISTINE in a larger real-world population.
“One of the important things to note is that we had few exclusion criteria, unlike many of the randomised controlled trials using drug-coated balloons in the peripheral vasculature, and the data represent real-life lesions that we face every day as vascular specialists in Singapore”, said lead investigator Tjun Yip Tang (Singapore General Hospital, Singapore).
“PRISTINE will offer further insight, leveraging on our initial experience with the PRESTIGE trial, into whether this sirolimus-eluting balloon will become an established device in our angioplasty armamentarium to fight the neointimal hyperplasia effect and restenosis phenomenon that lead to a significant number of clinically driven target lesion revascularisations in the BTK arteries, in this frail and challenging cohort of patients, whose ischaemic foot wounds are difficult to heal.”
In February 2020, MedAlliance received CE mark approval for Selution SLR in the treatment of peripheral arterial disease (PAD) and in May 2020 received CE mark approval for treatment in coronary arterial disease (CAD). MedAlliance has been awarded FDA Breakthrough designation for the Selution SLR for use in BTK and expects to begin the investigation device exemption (IDE) study later this year.
Following its acceptance into Frontiers in Neurology, Phenox has announced the results of a paper exploring the benefit of choosing a longer stentriever for mechanical thrombectomy procedures.
In a paper authored by Carmen Serna-Candel (Neuroradiologische Klinik, Klinikum Stuttgart, Stuttgart, Germany) et al, the outcomes of the pRESET 4×20 and pRESET 5×40 stentrievers (both Phenox) were examined against one another. The results “speak for themselves”, a Phenox press release states, and add to existing evidence that longer stentrievers lead to better patient outcomes.
With the use of the longer stentriever, a significant improvement in recanalisation rates was observed, along with improved mortality rates and fewer passes required to full recanalisation. First pass success was seen in 68.4% of cases with the pRESET 5×40 while the pRESET 4×20 resulted in first pass success in 48.7% of cases.
This led Serna-Candel et al to conclude that “the size of the stent retriever matters in acute M1 occlusions treated with aspiration-assisted thrombectomy”.
“We, in the Phenox engineering team, are delighted to offer to the market another device that will improve the outcomes of patients,” said Ralf Hannes, managing partner of Phenox. “And now, with these data, the 5×40 pRESET has proven its value.”
“We are proud to continue to innovate the neurovascular market and the most important aspect of developing new devices is clinical outcomes,” said Hermann Monstadt, managing partner of Phenox. “This publication is a testament to how we work with feedback from physicians to provide devices to improve patients’ lives.”
At the Society of NeuroInterventional Surgery’s 18th annual meeting (SNIS; July 26–29 2021, Colorado Springs, USA and virtual), Jeffrey Saver, professor of Neurology at the University of California, Los Angeles (UCLA) Medical Center and director of the UCLA Stroke Center (Los Angeles, USA), discussed the various ethical considerations that need to be taken into account regarding robotic applications in neuroendovascular interventions, and remote stroke care, stating that “we all need to work together to make sure patients have the best outcome”.
During a session that also saw multiple presentations demonstrating the potential benefits and new possibilities enabled by these novel technologies, Saver claimed this is an area that brings up “several unique domains of challenging bioethics”—including the ethics of remote care, the ethics of introducing new surgical techniques and training protocols, the ethics of robot-assisted procedures, and even autonomous, artificial intelligence (AI)-powered robotic systems, which are currently physician-supervised but may be unsupervised in the future.
The first specific ethical consideration Saver outlined was “compromised informed consent” on the patient’s part. He emphasised the criticality of full disclosure of the fact many of these procedures are fairly new, and, as such, there is limited evidence on both their benefits and their risks. “There is a general tendency for patients to equate newness with increased benefit—and we have to counter this tendency when we talk with them,” he added. Saver also noted that, while trust in the authority of the interventionist performing the given procedure should be encouraged, “humility”—to reflect their often-limited experience in performing these procedures compared to more traditional surgeries—is important here too.
Saver went on to state that various conflicts of interest on the physician’s side are significant too, and should be fully disclosed to the patient, with these ranging from direct financial benefits and other incentives, and brand loyalty, to the “elevated social status” of being a surgical innovator and bias towards performing a technique in which training has been invested—referring to the phenomenon of “sunk cost” here as well.
He noted that harm to the patient, including increased morbidity and mortality, is the “most important” ethical consideration that may be associated with robotic or remote procedures. “We need stringent QI [quality improvement] and reviews of every case,” Saver added. He went on to state that research burdens should not be placed disproportionately on disadvantaged or poorer communities, despite the fact that patients from these backgrounds may only gain access to advanced care by participating in innovative therapy systems—something he described as a “challenging ethical issue”—and added that these expensive technologies should not take too many resources away from proven care approaches either.
Another factor that Saver claimed is especially pertinent to remote intervention is the notion of a “diminished physician-patient relationship”, whereby the patient has reduced access to the interventionist. “We need to be sure that the interventionist maximises their availability to the patient—not just during the case, but by telemedicine pre and post if they are doing a case remotely,” he stated. Saver noted that there could be a risk for decreased empathy on the part of the physician for patients and families with whom they have never had direct contact too.
On a similar note, he alluded to the “diffusion of responsibility” that may be seen to be associated with these novel surgeries, referring to a “broader network of interdependent care” than is common in medicine. This network involves the remote interventionist, local physicians and nurses, hardware manufacturers, software coders, the AI system being deployed, and more. “We need to make sure we have an active, continuous partnership,” Saver also said.
As well as giving a nod to the more distant future in this ever-evolving space within neurosurgery—that being the ethics of fully autonomous, robotic interventionists—Saver chose to end his presentation on a more positive note. Firstly, he encouraged the attending audience to consider the future of their own patients, but also future generations of patients who, further down the line, stand to benefit from many of the innovations currently being advanced, adding that “a procedural speciality does require a little bit of risk taking”. Saver concluded his talk by addressing the need to consider the wellbeing of the physicians themselves in this debate—noting that the minimised radiation exposure and reduced lead-wearing risks that neurointerventionists may gain via robotic or remote surgical techniques are “a very important ethical goal” as well.
The statement, authored by Michael H Criqui (University of California, San Diego, San Diego, USA) and colleagues, has been published in Circulation.
Lower extremity PAD affects more than 230 million adults worldwide, the authors detail, adding that the condition is associated with an increased risk of various adverse clinical outcomes, including cardiovascular diseases such as coronary heart disease and stroke, and leg outcomes such as amputation.
Despite its prevalence and clinical importance, however, Criqui et al highlight a multifactorial underappreciation of PAD by healthcare professionals and patients, combining limited availability of the first-line diagnostic test—the ankle-brachial index—in clinics, and incorrect perceptions that a leg vascular disease is not fatal and that the diagnosis of PAD would not necessarily change clinical practice. In addition, the authors relay that many patients with PAD are not receiving evidence-based therapies.
The new statement is designed to address these issues by providing an update for healthcare professionals regarding contemporary epidemiology (i.e., prevalence, temporal trends, risk factors, and complications) of PAD, the current status of diagnosis (physiological tests and imaging modalities), and describing major gaps in the management of PAD (i.e., medications, exercise therapy, and revascularisation), Criqui and colleagues write.
In concluding their statement, the authors look to the future: “Orchestrated efforts among different parties (e.g., healthcare providers, researchers, expert organisations, and healthcare organisations) will be needed to increase the awareness and understanding of PAD and improve diagnostic approaches, management, and prognosis of PAD.”
Fist Assist Devices has just announced completion of the FACT trial, which evaluated the use of an intermittent pneumatic compression device, model FA-1, to promote vein dilation in patients with kidney disease. The trial’s results suggest the device could enable an increase in the creation of functional arteriovenous fistulas by enlarging superficial veins. The trial also demonstrates the device’s safety in this patient population.
“This is groundbreaking research that will drive efficiencies in the end-stage renal disease community as it really proves that intermittent compression enlarges superficial veins, and larger veins provide better surgical or endoAVF options and outcomes” said John Ross, director of Regional Medical Center in South Carolina and Inductee in the American College of Surgeons and Academy of Master Surgeon Educators.
The Fist Assist technology is patent protected and focused on developing an intermittent, external wearable pneumatic compression for arm massage and increased vein circulation in the United States, and increased forearm vein enhancement and AV fistula dilation/maturation in India, Canada, Europe, Australia, and New Zealand.
“We are ecstatic to complete FACT and are very thankful to all patients, physicians, and hospitals that worked to complete this trial during the COVID-19 pandemic, which was possible as the device is a patient-centric wearable in the home” said Mary Hammes, primary investigator of the trial and associate professor of Medicine and director, Chronic Hemodialysis, at the University of Chicago, USA. “This is a landmark, global trial evaluating the effectiveness of the FA-1 intermittent compression device on pre-surgery, stage 4 chronic renal failure patients.”
Patients were enrolled in three locations: The University of Chicago Medical Center, Chicago, USA; a medical clinic in Greenwood, USA, under the direction of John Lucas; and MS Ramaiah Medical Center, Bengaluru, India, under the direction of Sanjay Desai.
On preliminary analysis, most enrolled patients showed statistically significant superficial vein dilation (p<0.05) without any safety concerns. A press release from the company states: This will be a gamechanger for the over 40 million stage 4 chronic kidney disease patients in the United States alone because larger veins will help ensure improved arteriovenous fistula creation, whether they are created surgically or by new EndoAVF procedures. “This data is likely to be the foundation for additional indications of use for the Fist Assist device and continues to add more information on novel ways to increase pre-surgery vein size and distensibility for eventual dialysis,” the release adds.
Ross outlines the benefits of larger preprocedural veins: “[…] with the recent focus of fistulas being created percutaneously through EndoAVF technology, this data is critically important as larger, presurgical veins will enable more patients to be candidates for the less invasive EndoAVF procedures. This data could and should even drive CMS reimbursement as larger superficial veins will help improve outcomes, which drastically reduces the cost burden on patients, providers, and the entire healthcare system.”
Boston Scientific has commenced enrolment in the HI-PEITHO clinical trial, a collaborative research study with the Pulmonary Embolism Response Team (PERT) Consortium and the University Medical Center of the Johannes Gutenberg University of Mainz (Mainz, Germany) comparing use of the EkoSonic endovascular system (EKOS) in combination with anticoagulation to anticoagulation alone for the treatment of acute, intermediate-high-risk pulmonary embolism (PE).
The EKOS system uses ultrasound energy in combination with a thrombolytic drug to dissolve blood clots and restore blood flow in patients with PE and peripheral arterial occlusions. According to a company press release, the ultrasound technology used by the EKOS system accelerates thrombolysis, minimising the time it takes to treat a patient and lowering the necessary thrombolytic dose, which can result in optimised outcomes and a lower risk of bleeding.
“I am honoured to be part of this study’s global leadership whose mission is to bring forth guidelines-informing data that will ensure physicians can feel confident in the most appropriate strategy for treating patients with intermediate-high-risk PE,” said Stavros Konstantinides (University Medical Center of the Johannes Gutenberg University of Mainz, Mainz, Germany), study co-lead principal investigator.
The randomised HI-PEITHO trial will enrol up to 544 patients with confirmed acute, intermediate-high-risk PE at as many as 65 sites in the USA and Europe. The trial, which will follow patients for one year, will assess whether treatment with the EKOS system in combination with anticoagulation is associated with a significant reduction in adverse events compared to anticoagulation alone, within seven days of randomisation. The composite primary endpoint is defined as PE-related mortality, cardiorespiratory decompensation or collapse and non-fatal symptomatic and objectively confirmed recurrence of PE.
“Optimal treatment of PE is still poorly understood and there is a need for a coordinated institutional approach to this complex, life-threatening problem,” said Kenneth Rosenfield (Massachusetts General Hospital, Boston, USA), study co-lead principal investigator. “The lead investigators of the trial are pleased to collaborate with the PERT Consortium, which is committed to evidence-driven therapy and is proud to take part in the HI-PEITHO study, aiming to advance the care of patients with PE.”
The Society of Interventional Radiology (SIR) has issued a new position statement on percutaneous lung ablation in the August edition of the Journal of Vascular and Interventional Radiology (JVIR), along with an accompanying quality improvement document, which establishes performance thresholds for patient safety.
Mark Baerlocher, SIR’s standards division councillor and an author of the position statement and quality improvement document, said: “Minimally invasive, image-guided thermal ablation offers patients with early stage, non-small-cell lung cancer, recurring lung cancer, and metastatic disease a safe and effective treatment option.
“The two publications provide physicians with guidance on everything from patient selection to treatment delivery and post-treatment care and follow-up, ensuring high-quality care that improves patients’ lives,” added Baerlocher, an interventional radiologist at the Royal Victoria Hospital in Ontario, Canada.
Lung cancer is the second most common newly diagnosed cancer in the United States, with an estimated 228,000 new cases diagnosed in 2020. It is also the leading cause of cancer-related death.
Interventional radiologists use image-guided thermal ablation to treat primary and secondary lung tumours. Based on the current evidence, the position statement recommends that radiofrequency ablation, cryoablation and microwave ablation are all appropriate forms of image-guided thermal ablation to treat these tumors. The method of ablation should be determined by lesion characteristics and risk mitigation, according to the new document.
SIR president, Matthew Johnson, said: “Evidence-based position statements are important means of improving patient outcomes. Future comparative studies on the use of thermal ablation to treat these forms of lung cancer will help improve the evidence base and allow us to make stronger recommendations to the benefit of patients.”
The position statement was developed by a multidisciplinary group of authors including interventional radiology, medical oncology, thoracic surgery and radiation oncology specialists. It is endorsed by the Canadian Association for Interventional Radiology, the Cardiovascular and Interventional Radiological Society of Europe and the Society of Interventional Oncology.
Abstract submissions are now open for next year’s Society of Interventional Oncology annual meeting (SIO2022), which takes place from 3—7 February in San Francisco, USA.
Abstracts must be submitted by 30 September 2021 at 11.59pm CDT and those submitting for the first time must follow the instructions to create a new account on the submission site.
Successful abstracts will have the opportunity to share their research with more than 600 professionals in the global interventional oncology community. There is no restriction to the number of abstracts that can be submitted.
SIO say that while it does not have a policy that limits prior presentation of data, the reviewing committee gives higher priority for abstracts that have not yet been presented.
Abstracts can be submitted in the following categories:
Basic Science
Education
Genitourinary
Guidance & Targeting
HCC
Imaging
Liver Metastases
Technology
Thoracic
Other
The abstract character limit is 4000 with a minimum of 50 characters, including spaces and any tables and/or graphs. Abstracts may be submitted for an oral or poster presentation and must include objectives, results, and conclusions.
Selected presenters will be notified by November 2021.
For more information or to submit your abstract, click here
Surmodics has announced that J. Michael Bacharach, a vascular interventionalist/cardiologist at North Central Heart, a division of Avera Heart Hospital in Sioux Falls, USA, successfully treated the first patient with the company’s Pounce thrombectomy system.
The procedure involved a patient presenting with increasing pain in the left leg and was diagnosed with an occluded superficial femoral artery (SFA). Three passes of the Pounce device removed 30cm of subacute thrombus and blood flow was successfully restored. Eight additional cases have since been performed in the US with positive outcomes reported following each procedure.
“Despite the challenge presented by this particular case, I could not have asked for anything more. The device’s performance was really amazing,” said Bacharach. “I was able to safely and effectively achieve a positive outcome for this patient with minimal blood loss and without the use of thrombolytics. I’m very excited about the results of this case. I’m a believer in the Pounce system.”
The Pounce Thrombectomy System, which received US Food & Drug Administration 510(k) clearance in September 2020, is a mechanical thrombectomy device intended for the non-surgical removal of thrombi and emboli from the peripheral arterial vasculature.
Depending on the age and magnitude of the occlusion and the viability of the threatened limb, existing treatments for this condition may include catheter directed thrombolysis, surgical embolectomy, and/or percutaneous mechanical thrombectomy. In cases in which the occlusion has caused irreversible damage to the limb, acute limb ischemia can result in the amputation of a lower extremity.
Gary Ansel, founder and former chief medical officer of Embolitech—from which Surmodics acquired the technology and intellectual property behind the Pounce thrombectomy system—said: “I am delighted that the Surmodics team is providing peripheral interventionalists with this innovative tool for treating arterial thrombotic occlusions.
“I also congratulate the company on its continued efforts to advance therapies for patients dealing with arterial thrombosis and peripheral arterial disease while focusing on ease of use and efficiency for the physicians treating these patients.”
Artio Medical announced today it has completed enrolment in its first-in-human study evaluating the Amplifi vein dilation system. In the study, five patients were treated by Adrian Ebner, head of the Cardiovascular Department at Sanatorio Italiano Hospital in Asunción, Paraguay.
“I am very pleased with my initial experience using the Amplifi system,” Ebner said. “The device was simple to implant and well-tolerated by all patients. We observed significant vein enlargement in each enrolled patient and were able to successfully create arteriovenous (AV) fistulas in all patients after treatment, including patients who were poor candidates for AV fistula before treatment.”
The Amplifi system is designed to stimulate arm vein enlargement in haemodialysis patients using rapid, non-pulsatile venous blood flow. After seven days of treatment, the device is removed during surgery to create an AV fistula. The Amplifi vein dilation system aims to make more haemodialysis patients eligible to receive an AV fistula, increase fistula maturation success, reduce maturation time, and prolong the usable life of these fistulas. Amplifi is the first and only medical device intended to dilate and prepare veins prior to AV fistula surgery, according to an Artio Medical press release.
“I am grateful for Dr Ebner and the entire team at Sanatorio Italiano who contributed to the success of this first-in-human study,” said F Nicholas Franano, president and CEO of Artio Medical. “The company looks forward to sharing data on these first five patients in the coming months and building upon this promising early clinical experience. We remain focused on delivering a much-needed solution to the millions of patients worldwide who need haemodialysis.”
Percutaneous Deep Vein Arterialisation (pDVA) with the LimFlow System offers a cost-effective and high-value alternative to traditional therapies or amputation, according to a recent study published in the Journal of Critical Limb Ischemia.
Peter Schneider, professor of surgery at the University of California (San Francisco, USA) and co-author of the published article, said: “The cost-effectiveness analysis builds on recently published 12-month data from the PROMISE I study by showing that pDVA with the LimFlow System can be a high-value therapy alternative to the status quo for no-option CLTI patients.
“This research highlights the health economic benefits of reducing amputations and the need to offer patients a better alternative worldwide.”
The findings highlighted significant and promising data from cost-effectiveness analysis comparing pDVA with the LimFlow System to the status quo treatment for no-option CLTI patients, according to the study authors.
The status quo was defined by a meta-analysis conducted by the Yale Cardiovascular Research Group on no-option patient outcomes from other reputable studies ranging from 2006 to 2018, which is pending publication in the Journal of Critical Limb Ischemia.
The comparative analysis demonstrates that expected outcome improvements with pDVA justify its incremental costs and qualifies it as a “high-value” therapy per established willingness-to-pay thresholds.
Dan Rose, CEO of LimFlow, added: “Avoiding major amputation is a key treatment goal in CLTI due to its associated high costs, loss of functional status and quality of life, and high mortality.
“The analysis using data from PROMISE I demonstrates our technology can provide significant clinical and health-economic value to patients and healthcare providers who are drastically underserved by the status quo.”
“There appears to be heightened risk of major amputation after use of paclitaxel-coated balloons [PCBs] in the peripheral arteries,” findings from a systematic review and meta-analysis of randomised controlled trials (RCTs) published in the European Journal of Vascular and Endovascular Surgery (EJVES) this week suggest. However, the authors clarify that the level of evidence is graded moderate, not high, due to scarce events in some studies.
And, leading physicians propose that the methodology used needs to be carefully considered and scrutinised before these conclusions are accepted.
Barry T Katzen
Clarifying at the outset that he is not an expert on statistical methodology, globally recognised leader in the development of new less-invasive procedures, Barry T Katzen, founder and medical director of Miami Cardiac & Vascular Institute and the president of the CLI Global Society, tells Vascular and Interventional News: “As a physician engaged in multidisciplinary limb salvage with a view to improving quality of life by preventing amputations and death due to critical limb ischaemia, the conclusions from this meta-analysis are of concern, of course, and need to be taken seriously. However, I have in parallel questions about the complex methodologies used in this paper to arrive at a finding that prospective randomised controlled trials have not demonstrated. From a practical point of view, before accepting the conclusion regarding the risk of paclitaxel drug-coated balloon use, there needs to be a significant discussion and analysis of the methodologies employed in this paper. This needs to be undertaken by appropriate statistical experts before these findings change practice, if they do so at all.”
This latest meta-analysis, authored by Konstantinos Katsanos (Patras University Hospital, Rion, Greece) and colleagues with co-authors from France, Germany, Finland and The Netherlands, drills down on the long-term risk of major amputation alone associated with use of PCBs in the lower limbs. The findings point to a significantly higher long-term risk of major limb loss using these devices in the femoropopliteal and/or infrapopliteal arteries.
Anna Maria Belli
Anna Maria Belli, a former consultant radiologist and Professor of Interventional Radiology at St. George’s Hospital and Medical School in London, UK, a past president of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and proponent of evidence-based trials, comments: “It is essential that we have publications such as this interrogating data on new technologies in an unbiased way. There is a natural tendency to believe new technologies will provide better results than old ones. It is only by pooling results from published trials that enough numbers are amassed to detect trends which might be missed by individual trials. Katsanos and colleagues are to be commended for highlighting the increased risk of amputation with PCBs and, as they say, this now needs to be confirmed or refuted by further investigations.”
Commenting on the publication in EJVES, Younes Jahangiri, statistical editor of the Journal of Vascular and Interventional Radiology, says: “The manuscript has used a robust search strategy and meta-analysis techniques. Nevertheless, there are a considerable number of back-calculations and imputations that have been performed for data generation, which might not necessarily fit with real-world data. Additionally, exclusion of studies with no events in both arms, especially if the studies were of high quality and adequate follow-up, might have led to overestimation of the crude risk in both groups and potentially to the statistical significance of between-group differences. Although the meta-analysis itself suggests an alarming signal in a heavily computational way, confirmation of accuracy and adequacy of the signal would still require real-world targeted data.”
The harm signals suggested for paclitaxel devices from previous meta-analyses have not been substantiated by a wealth of real-world datasets that have shown no long-term safety concerns, and instead suggested increased benefits with the use of paclitaxel-coated devices. Importantly, an interim mortality analysis of the SWEDEPAD registry randomised trial did not confirm a heightened mortality risk in cases of paclitaxel treatment, as noted in the EJVES paper.
As reported in EJVES, the investigators performed a literature search last updated on 20 February 2021 to analyse 21 RCTs with 3,760 lower limbs treated nearly equally for intermittent claudication (52%) and chronic limb threatening ischaemia (CLTI; 48%). The median follow-up period was two years. Authors report 87 major amputations in 2,216 limbs in the paclitaxel arm (4% crude risk) compared with 41 major amputations in the 1,544 limbs in the control arm (2.7% crude risk). The risk of major amputation was significantly higher for paclitaxel-coated balloons with a hazard ratio (HR) of 1.66 (95% CI 1.14–2.42; p=0.008, one stage stratified Cox model). The observed amputation risk played out equally across femoropopliteal (p=0.055) and infrapopliteal (p=0.055) arteries. The number needed to harm was 35 for CLTI. In this systematic review and meta-analysis, authors suggest the summary effect demonstrated a 66% higher relative risk of major amputation in the limbs treated with PCBs, and call for further investigations.
Further, Katsanos and colleagues write that there was good evidence of a significant non-linear dose relationship with accelerated risk per cumulative paclitaxel dose (chi square model p=0.007). The results were also stable across sensitivity analyses (clarified as pertaining to different models and subgroups, based on anatomy and clinical indication and excluding unpublished trials).
Ziv Haskal
Ziv Haskal (University of Virginia, Charlottesville, USA), the former editor (2011–2020) of the Journal of Vascular and Interventional Radiology (JVIR) tells Vascular News and Interventional News: “Dr Katsanos and the research team stand, again, to shake-up the PCB planet with a suggested finding of worse amputation—the same goal paclitaxel was intended to make better, and with a dose-dependent effect. Unsurprisingly, it is a rigorous and clear-headed analysis. But there are interpolations, intercalations and imputations, likely to bring out critics, with force. This may be a curtain raiser, but the main play is yet to unfold.”
A large, single-centre retrospective study has revealed the risk of acute kidney injury (AKI) following pharmacomechanical thrombolysis (PMT) for lower extremity deep vein thrombosis (DVT) is as high as 22%.
PMT is an established treatment for selected patients with acute DVT. Despite significant clinical success, haemolysis can lead to AKI with unknown longer-term implications. Researchers in the USA therefore aimed to characterise the rate of AKI after PMT, and identify those patients at the greatest risk.
“Recent evidence has suggested that catheter-direct therapy (CDT) in the setting of acute iliofemoral DVT improves vein patency and post-thrombotic severity with an equivocal risk of bleeding,” said principal author Karim M Salem (University of Pittsburgh, Pittsburgh, USA).
“Catheter thrombolysis can be accomplished by dripping thrombolytic agents through a multiside-hole catheter over several hours, or using PMT devices,” Salem added. “Plenty of evidence has supported the use of PMT over catheter thrombolysis because PMT can achieve fast lytic therapy at a lower tissue plasminogen activator (tPA) dose. Aggressive PMT, however, can cause haemolysis, which can result in AKI.”
As reported in the July 2021 issue of the Journal of Vascular Surgery: Venous and Lymphatic Disorders, Salem’s team studied the records of 137 patients who underwent PMT for acute iliofemoral DVT at the University of Pittsburgh between 2007 and 2018.
The mean age of the 137 patients was 47±17 years, 50% were male, and their preoperative creatinine levels were found to be 0.99mg/dL, on average.
Ultimately, 30 of these patients (22%) developed postoperative AKI, defined as a creatinine 1.5x baseline. According to the report, multivariable analysis demonstrated three significant risks factors for the development of AKI:
Bilateral DVT (odds ratio=4.35, p=0.008)
Single-session PMT (odds ratio=3.05, p=0.046)
Female sex (odds ratio=2.85, p=0.046)
Of the 30 patients who did develop AKI, two progressed to severe renal failure (glomerular filtration rate <30ml/min) and one required long-term haemodialysis.
“Contemporary studies have reported the results of more rapid and aggressive thrombolysis protocols that can be completed in a single session,” Salem noted. “This approach has been associated with a development of acute renal failure owing to the haemolysis caused by the PMT devices.
“Our focus was to identify the preoperative factors that might influence our decision to pursue aggressive single-stage intervention versus multistage CDT. With the results of the present study, we avoid single-stage intervention in women with bilateral extensive DVT to minimise the risk of postoperative AKI.”
This study adds “significant knowledge” to understanding the risks of lytic therapy in patients with iliofemoral DVT, a statement from the Society for Vascular Surgery (SVS) concludes.
Viz.ai has partnered with Avicenna.AI in an effort to enable intelligent care coordination and improve patient triage of patients suffering from pulmonary embolism (PE) and aortic disease.
It is hoped that the collaboration will pave the way for faster clinical decision making and care for patients suffering from these two life threatening conditions.
Avicenna.AI’s FDA-approved algorithms for PE and Type A and Type B aortic dissection (AD), leveraged on the Viz intelligent care coordination platform, aim to empower multidisciplinary care teams to easily coordinate patient care by sending notifications paired with dynamic imaging and detailed patient information to each provider’s desktop or mobile device as soon as a PE or an aortic dissection is detected.
As part of Viz.ai’s commercial aortic module offering, access to imaging and workflows supporting the coordination of care for patients with abdominal aortic aneurysm (AAA), thoracic aortic aneurysm (TAA), rupture, stenosis and transection will be available in addition to the AD algorithm. Similarly, the PE algorithm will be available on Viz.ai’s commercial PE module.
Richard Saxon, interventional radiologist at Tri-City Medical Center (Oceanside, USA), said: “The addition of AI powered workflows should decrease the time from diagnosis to treatment and help to coordinate care for patients suffering from life-threatening PE and aortic disease, as it has in the treatment of ischaemic stroke. It will help to facilitate faster and easier treatment decisions across health systems, and this should improve outcomes for patients.”
Cyril Di Grandi, chief executive officer of Avicenna.AI, said: “We are proud to become a trusted partner of Viz.ai, who is committed to giving access to high-standard healthcare systems worldwide. Thanks to our AI-based solutions, we hope to facilitate an optimal medical response within a short time frame and improve patient care. We look forward to bringing the benefits of our pulmonary embolism and aortic dissection triage tools to the emergency room and beyond.”
PE is a potentially deadly form of venous thromboembolic disease, a common cause of cardiovascular death, and is associated with multiple inherited and acquired risk factors affecting hundreds of thousands of people every year globally. PE occurs when a blood clot gets lodged in an artery in the lung, blocking blood flow to part of the lung. Similar to PE, aortic disease is potentially deadly and can require urgent surgical intervention to prevent death.
Chris Mansi, Viz.ai CEO and co-founder, added: “We’re delighted to partner with Avicenna to bring intelligent care coordination to the peripheral vascular and vascular fields. This will form part of a broader Viz platform, where any patient with life threatening diseases can benefit from AI powered triage, fast mobile communication and synchronized care coordination.
“This partnership will bring the advantages of artificial intelligence to more patients and help hospitals achieve better clinical outcomes.”
The Journal of Vascular and Interventional Radiology’s (JVIR’s) Impact Factor—one measure of a journal’s influence based on the number of article citations compared to the total number of citable articles published—jumped 14% in 2020.
According to the Journal Citation Reports, published by Clarivate Analytics, JVIR’s Impact Factor rose to 3.464 in 2020, up from 3.037 in 2019.
Daniel Sze, editor-in-chief of JVIR and professor of interventional radiology at Stanford University School of Medicine (Stanford, USA) said: “The continued growth of JVIR’s Impact Factor is a testament to the quality of the scientific research we publish and the journal’s authority in the medical community.
“Across the years—thanks to the leadership of editors emeriti Gary Becker; Daniel Picus; Karim Valji; Albert Nemcek; and Ziv J Haskal—JVIR has become a destination journal for IRs around the world to publish their most impactful endovascular research.
“As I take the reins this year, I will aim to build on success of these IR luminaries by expanding our international programs, furthering JVIR’s commitment to evidence-based patient care worldwide.”
The Impact Factor, which reflects citations in the previous two years, is often used as a measure of the quality and influence of medical journals within scientific, professional and academic communities. JVIR citations appeared in radiology, nuclear medicine, medical imaging and peripheral vascular disease journals.
Society of Interventional Radiology president Matthew Johnson, who is also the Gary J. Becker professor of radiology research at Indiana University School of Medicine (Indianapolis, USA), added: “SIR and SIR Foundation are dedicated to building a culture of research within the IR community and JVIR is a key component to demonstrating the clear benefits image-guided treatments have on the lives of our patients.”
Tara Graham (Trillium Health Partners, Toronto, Canada) has become the new president of the Canadian Association for Interventional Radiology (CAIR), assuming the new role at the board’s meeting on June 14th, 2021.
Amol Mujoomdar (London Health Sciences Centre, London, Canada), the outgoing president, will continue to serve on the CAIR executive board in the role of past president replacing Jason Wong (University of Calgary, Calgary, Canada), who will transition into a director position.
.
Alessandra Cassano-Bailey (Health Sciences Centre in Winnipeg, Winnipeg, Canada) will be assuming the role of vice president; and David Valenti (McGill University Health Center, Montreal, Canada) will replace Darren Klass (Vancouver Coastal Health, Vancouver, Canada) as the new CAIR board secretary-treasurer.
A population-based study from 2013 to 2015 in Germany has found that nearly one fifth of patients with peripheral arterial disease (PAD) did not receive guideline-based vascular diagnostics three months before incidence amputation. Writing online in the European Journal of Vascular and Endovascular Surgery (EJVES), authors Kristina Hagenström (University Medical Center Hamburg-Eppendorf, Hamburg, Germany) and colleagues say this “reflects an underuse of health services”. In addition, the researchers report that, in one third of patients who did not receive vascular surgery, major amputation “probably could have been avoided”.
Due to a wider international variance in major amputation, high mortality rates and follow-up, and the “significantly reduced quality of life for patients with amputations,” the authors stress that vascular diagnostics and vascular surgery treatments “are of great importance” for lower limb preservation in patients with PAD. They note that patients with PAD have an increased risk of lower limb amputation, and that the prevalence of PAD and chronic limb-threatening ischaemia (CLTI) is expected to increase due to demographic trends.
The guidelines state that vascular diagnostic and vascular surgical treatments can contribute significantly to the preservation of the lower extremities, and also that early revascularisation can minimise the risk of amputation. In a retrospective longitudinal study, Hagenström et al examined these guideline-based procedures in patients before a first lower limb amputation and PAD.
The researchers analysed data from a large German statutory health insurance (SHI) scheme on patients with first amputation of lower extremities and PAD between 2013 and 2015. They considered pre-defined vascular diagnostic and vascular surgical procedures, as specified by guidelines with inpatients and outpatient care in a defined time before lower limb amputation, Hagenström and colleagues detail.
Reporting their findings in EJVES, the authors relay that the overall estimated incidence of lower extremity amputations in the total population was 0.12% from 2013–2015. Of these patients, they specify, 51.7% had PAD, 81.8% had received at least one diagnostic measure, and 61% a vascular surgery procedure before the lower extremity amputation.
Hagenström et al add that there were only minor variations in the use of diagnostic or surgical treatments between patients with major and minor amputations. “In total, 63.9% of patients had vascular surgery before the incidence major amputation compared with 60% of patients with a minor amputation,” they reveal.
The investigators highlight “noticeable” regional differences in the data, ranging from 91% (Berlin) to 67% (Bremen) regarding diagnostic procedures provided before amputation, and from 83% (Hamburg) to 55% (Saxony-Anhalt) regarding vascular surgery before amputations.
“Timely interventions by specialists and guideline-based treatments could reduce the number of amputations and subsequent costs,” the authors conclude. Commenting on the strengths of their study, they write that its design “permits analyses of a vast and unselected nationwide cohort” and is thus comparable with publications from other countries where population-based data were used. However, they stress that different healthcare systems must be considered.
Hagenström and colleagues also acknowledge some limitations of their study, including the fact that the analysed administrative data are based on only one of several SHI companies in Germany, which limits the transferability of the statements made to the population of Germany as a whole.
Royal Philips today announced the US Food and Drug Administration (FDA) has granted Breakthrough Device designation for a laser-assisted inferior vena cava (IVC) filter removal device. The proposed device is intended for ablating tissue to remove an IVC filter when previous methods of removal have failed.
The failure rate for IVC filter removal is high and limited options for removal exist if the filter has become difficult to remove. Advanced retrieval tools and techniques are required if the IVC filter becomes embedded in the vasculature. Physicians have very few tools to remove the filter when this happens and there are no FDA-approved devices for this type of advanced removal.
Two independent and prospective clinical studies have demonstrated that laser-assisted retrieval was 96–99% effective with a major adverse event rate of 0.7–2%, a Philips press release reports.
“Laser-assisted filter retrieval may be a critical tool for the safe retrieval of filters with extended implantation times,” said Kush R Desai, associate professor of Radiology, Surgery, and Medicine, and director of Deep Venous Interventions at Northwestern University Feinberg School of Medicine (Chicago, USA). “Breakthrough Device designation reflects the potential impact that this technology could have on countless patients where this technology can be applied to safely retrieve filters by an expert physician, thereby reducing their risk of significant filter-related complications.”
“There is a clear need for an innovative device to help physicians more safely perform advanced IVC filter removal and I believe that the Philips excimer laser sheath may greatly enhance the options available to succeed in filter retrieval,” said Atul Gupta, chief medical officer for Image Guided Therapy at Philips and also a practicing interventional radiologist in Philadelphia, USA. “Breakthrough Device designation is an important step for a medical innovation such as this one to help fill an unmet need in patient care.”
For most patients receiving systemic anticancer treatment (SACT), totally implanted ports (PORTs) are more effective and safer than both Hickman-type tunnelled catheters (Hickman) and peripherally inserted central catheters (PICCs). The CAVA trial’s results, just published online in The Lancet, recommend reshaping current guidelines and practice, so that most patients requiring chemotherapy for solid tumours receive a PORT within the UK National Health Service, foreshadowing a pivot in practice that might be “slow to start with”.
The CAVA (Central venous access devices for the delivery of systemic anticancer therapy) trial is a National Institute for Health Research- (NIHR-) funded open–label, multicentre, randomised controlled trial that compared complication rates and costs of the three devices used to deliver anticancer drugs via a central vein.
It is reported to be the largest randomised trial to date to compare all three devices, and set out to establish acceptability, clinical effectiveness, and cost-effectiveness of the devices for patients receiving SACT for three months, or more.
“The bottom line is, for a solid cancer, if you are going to need intravenous chemotherapy for three months or more, you should be offered the option of a PORT. We should try and empower patients so that that this will be something they think will be best for them,” Jonathan G Moss (Institute of Cardiovascular and Medical Sciences, Glasgow, UK), chief investigator, tells Interventional News on the subject of increased PORT take-up.
The paucity of good evidence comparing central venous access devices (CVADs) entails that neither the European Society of Medical Oncology nor the American Society of Clinical Oncology make specific recommendations regarding the type of device to be used.
CAVA showed that PORTs were associated with a reduction in complication rate of about 50% when compared to a PICC line, and when compared with the Hickman line. “There was a fairly strong preference for PORTs, amongst both the patients receiving them and also the healthcare staff who look after them. These were basically felt to be better devices and the only downside is the cost and whether these services are set up and geared to deliver these devices compared to the other two in a timely manner,” he added.
Resetting UK practice may not be a brisk business
With the exception of five patients in the PORT group who received a general anaesthetic, all devices were inserted under local anaesthetic.
Moss outlines that decision-making processes behind the choice of device are “poorly understood” globally. Eye-catchingly, PICC use has been captured to be buoyant. “PICC usage has increased over the past decade and is now the dominant strategy in many western European countries and the USA.” This spike in PICC popularity may be underpinned by the ease of insertion of these devices enabling prompt placement and removal by nurse-led teams, local availability of devices, technical issues such as the avoidance of the vital structures in the neck, and perceived lower up-front costs—but there is a sketchy evidence base behind this uptick, the authors say. “PORTs, by contrast, are the most expensive and least frequently used of the three devices,” Moss emphasises.
On stemming the tide of PICC use, the lead author continues: “Changing policy in institutions like the NHS [UK National Health Service] is never easy. There will be all sorts of reasons why people do not want to change—with costs being one and who is going to be putting in the PORTs [being another], and how quickly they can be put in. […] There are lots of nurse teams at the moment who have been trained to place PICC lines. We need to be able to sell the message to them that we are not saying they should not provide a service for patients but trying to persuade them to put in a different device. I think we need to try and move away from doctors putting in the PORTs and nurses putting in the PICC lines. These are all fairly straightforward procedures to place, and I have great confidence that we can empower nursing teams to place all three devices, but particularly PORTs.”
Moss acknowledges that the complication rates and costs of nurse-led teams placing PORTs was not tested by CAVA, but emphasises that most skill mix is not evidence-tested. “We did not compare different operator groups regarding complication rates as that was not the purpose of the trial. We do know the technical (or periprocedural) complication rates in CAVA were exceptionally low, reflecting well-trained staff using ultrasound guidance. Most of the complications related to these devices arise from their subsequent usage and maintenance. We simply do not have enough events to compare periprocedural complications across operator groups, and have no reason to believe that based on this very low complication rate, that any one group (nurses, anaesthetists or radiologists) was technically better than another. We continue to support the concept of nurse-led vascular access teams in order to make widespread practice change practical to deliver.”
The authors back the challenge “to change the service delivery model so that PORTs can be provided in a more timely and cost-effective manner. There will still be a small group in whom the other devices are preferred. Guidelines should be updated to reflect this new evidence,” they write.
They also probed the issue of cost, which is another factor that will play into service transformation. “We have got to persuade the people that pay for these, the managers, that although the PORT is more expensive at the shop front, at the end of the day, when you look at the total package of care [when dwell time is taken into account], that they actually are no more expensive, or a little bit cheaper. And again, that is sometimes difficult to sell in the NHS because we tend to focus on frontline costs,” explains Moss.
Four-way randomisation in CAVA
CAVA randomised patients with an algorithm taking into account centre, body-mass index, type of cancer, device history, and treatment mode. The trial included adults receiving SACT over a three-month or longer period for solid or haematological malignancy from 18 oncology units in the UK. There were four available randomisation options: Hickman vs. PICCs vs. PORTs (2:2:1), PICCs vs. Hickman (1:1), PORTs vs. Hickman (1:1), and PORTs vs. PICCs (1:1) and these then allowed three 2×2 comparisons, PICC vs. PORT, PICC vs. Hickman and PORT vs. Hickman to be made.
“The primary outcome was complication rate (composite of infection, venous thrombosis, pulmonary embolus, inability to aspirate blood, mechanical failure, and other) assessed until device removal, withdrawal from study, or one-year follow-up,” the authors report in The Lancet.
The triallists screened 2,714 individuals for eligibility, 1,061 were enrolled and randomly assigned (PICC vs Hickman n=424, 212 [50%] on PICC and 212 [50%] on Hickman; PORT vs Hickman n=556, 253 [46%] on PORT and 303 [54%] on Hickman; and PORT vs PICC n=346, 147 [42%] on PORT and 199 [58%] on PICC).
PORTs outpace other CVADs on nearly all fronts
Between 2013 and 2018, 1,061 patients were enrolled and randomly assigned (PICC vs. Hickman n=424, 212 [50%] on PICC and 212 [50%] on Hickman; PORT vs. Hickman n=556, 253 [46%] on PORT and 303 [54%] on Hickman; and PORT vs. PICC n=346, 147 [42%] on PORT and 199 [58%] on PICC).
Similar complication rates were observed for PICCs (52%) and Hickman (49%).
PORTs were superior to Hickman with a complication rate of 29% vs. 43%.
PORTs were superior to PICCs with a complication rate of 32% vs. 47%
Painting a picture of the trial’s main findings, Moss and colleagues report: “There was little difference between PICCs and Hickman in terms of complications. CAVA showed that PORTs reduced the adverse event rate by approximately 50% compared with Hickman and PICCs. A device specific quality of life instrument showed no difference between PICCs and Hickman, but a preference for PORTs. PORTs were associated with the highest total costs; however, after allowing for the dwell time of the devices, there was no difference between PICCs and Hickman, but the cost associated with PORTs was lower when compared with PICCs and Hickman.”
See Moss’ views on the value of randomised controlled trial data:
Scitech Medical, has announced that it has received CE mark approval for the Embosoft microspheres for use in vascular embolization of hypervascular tumours, symptomatic uterine fibroids and prostatic arteries to relieve symptoms related to benign prostatic hyperplasia, as well as for haemostatic embolization.
According to the company, Embosoft’s high rate of viscoelasticity and its hydrophilic surface allow a selective distal embolization that is safe and effective.
Embosoft microspheres are composed of the company’s Polifit 70 material, which guarantees a well-defined spherical shape and a superior compressibility rate. Because of these characteristics, it is possible to reduce approximately 40% of its size during its delivery and will return to the initial spherical shape without fragmentation or deformation in the target vessel, the company stated.
The CAVA (Central venous access devices for the delivery of systemic anticancer therapy) randomised controlled trial (RCT), just published in The Lancet, has revealed that totally implanted ports (PORTs) are more effective and safer than both Hickman-type tunnelled catheters and peripherally inserted central catheters (PICCs). These findings provide important high-quality evidence from more than 1,000 patients to steer choice. Currently, PICCs are by far a dominant strategy in the West, and PORTs the least frequently used of the three devices. “Decision-making processes behind the choice of device are poorly understood globally,” the authors report, but the ease with which PICCs are inserted by nurse-led teams may favour their regular use.
Jonathan G Moss (Institute of Cardiovascular and Medical Sciences, Glasgow, UK), chief investigator of the National Institute of Health Research- (NIHR-) funded trial, tells Interventional News that despite the higher upfront costs associated with PORTs and the fact that they are relatively more difficult to place, most patients receiving systemic anticancer treatment for solid tumours for more than three months should receive a PORT within the UK National Health Service.
A systematic review and meta-analysis has demonstrated that patients undergoing carotid interventions after thrombolysis have a higher risk of periprocedural hazards, compared with those patients who did not have prior thrombolysis. Authors Stavros K Kakkos (University Hospital of Patras, Patras, Greece) and colleagues report their findings in an article published online in the European Journal of Vascular and Endovascular Surgery (EJVES).
“Patients undergoing carotid endarterectomy (CEA) or carotid artery stenting (CAS) after thrombolytic therapy have a higher risk of periprocedural stroke and death, compared with patients undergoing CEA or CAS without prior thrombolytic therapy,” the authors write. However, they note that the difference was statistically significant only for CAS. In regards to other hazards, Kakkos et al note that there was also a higher risk of periprocedural intracranial haemorrhage (ICH) and local haematoma in patients undergoing carotid interventions after thrombolysis.
One of the findings that Kakkos and colleagues state is “of most practical importance” is that periprocedural risks of stroke and death appeared to be higher if CEA was performed in the first few days after thrombolysis. This inverse relationship between timing to CEA and periprocedural stroke/death “mandates careful patient selection and suggests that it may be safer to defer CEA for six to seven days after thrombolytic therapy,” they posit in EJVES.
Using the Medline, Scopus, and Cochrane databases, Kakkos et al identified 25 studies involving patients who underwent either CEA or CAS after thrombolytic therapy to include in their systematic review and meta-analysis. There were a total of 147,810 patients in these 25 studies, 2,557 of whom underwent either CEA (n=2,076) or CAS (n=481) following thrombolytic therapy.
After CEA, the authors report that the pooled periprocedural stroke/death rate was 5.2% (95% confidence interval [CI], 3.3–7.5) and intracranial haemorrhage was 2.4% (95% CI, 1.7–5.6). After CAS, they relay, the pooled perioperative procedural stroke/death rate was 14.9% (95% CI, 11.9–18.2) and ICH was 5.5% (95% CI, 3.7–7.7).
In case control studies comparing CAS outcomes in patients receiving thrombolytic therapy versus no thrombolytic therapy, the authors communicate that periprocedural stroke/death was significantly higher after thrombolytic therapy (5.2% vs. 1.5%; odds ratio [OR] 8.49; 95% CI, 2.12–33.95), as was ICH (5.4% vs. 0.7%; OR, 7.48; 95% CI, 4.69–11.92).
Kakkos and colleagues also detail that meta-regression analysis demonstrated an inverse association between the time interval from intravenous thrombolytic therapy to undergoing CEA and the risk of periprocedural stroke/death (p=0.032). “Perioperative stroke/death was 13% when CEA was performed three days after thrombolytic therapy and 10.6% when performed four days after thrombolytic therapy, with the risk reducing to within the currently accepted 6% threshold after six–seven days had elapsed,” they write in EJVES, communicating the results of their analysis.
The authors acknowledge that a “major limitation” of their systematic review and meta-analysis is that there were no randomised controlled trials to inform clinical practice. “This is especially relevant regarding stratifying procedural risks in stroke patients who do not have any computed tomography (CT)/magnetic resonance imaging (MRI) evidence of infarction post-thrombolytic therapy and for evaluating the benefits of deferring CEA for six-seven days,” they comment.
In addition, Kakkos et al recognise that case control studies have inherent biases because of study design, so that patients receiving thrombolysis “may have had more severe strokes”. This, they note, could explain the worse outcomes observed in their systematic review.
Finally, the researchers state that varying exclusion criteria, timing, and mode of thrombolytic therapy administration, may have caused heterogeneity, and “should be explored in future studies”.
Endologix today announced the company’s ChEVAS (chimney endovascular aneurysm sealing) system has been granted a Breakthrough Device designation from the US Food and Drug Administration (FDA). The ChEVAS system is an investigational endovascular abdominal aortic aneurysm (AAA) sealing therapy designed to combine the Nellix 3.5 endograft with parallel visceral stents to enable treatment of patients with juxtarenal, pararenal, and suprarenal AAA.
ChEVAS is currently being evaluated through the ChEVAS ONE investigational device exemption (IDE) clinical study that is approved to enrol approximately 120 patients at up to 50 clinical sites worldwide. The national principal investigators of the ChEVAS ONE study are Francis Caputo (Cleveland Clinic Foundation, Cleveland, USA); William Jordan (Emory University School of Medicine, Atlanta, USA); Joseph Lombardi (Cooper University Health Care, Camden, USA); and William Quinones-Baldrich (UCLA, Los Angeles, USA).
“The aneurysm sac sealing technology featured in the ChEVAS system is designed to reduce endoleaks, including gutter endoleaks, that are reported after endovascular treatment of complex aneurysms,” said James McKinsey (The Icahn School of Medicine at Mount Sinai, New York, USA), the leading enroller in the ChEVAS ONE IDE study. “Our initial clinical results of this therapy have been promising in a challenging group of patients.”
McKinsey will present his initial experience with ChEVAS at the Eastern Vascular Society Annual Meeting (23–26 September, Charleston, USA).
Terumo Medical Corporation has announced today the introduction of its Azur vascular plug. The addition to Terumo’s embolisation portfolio is indicated for use to reduce or block the rate of blood flow in arteries of the peripheral vasculature.
“The Azur vascular plug represents a balance of properties—stability, accuracy, and reliable occlusion. This technology has unique advantages that truly make it a market first in embolotherapy, in line with Terumo’s ongoing efforts to deliver improved clinical outcomes and economic benefits,” said Chris Pearson, executive vice president, commercial operations, Terumo Interventional Systems.
A Terumo press release details that the Azur vascular plug comes in sizes to treat arterial anatomy ranging from 2.5–8mm, with a short deployment length for increased precision.
Features include a conformable nitinol braid and an expanded polytetrafluoroethylene (ePTFE) and polyethylene terephthalate (PET) inner composite membrane to facilitate mechanical occlusion. Another key element in the plug’s design is its “advanced, predictable” detachment mechanism, the statement reads, which allows for “immediate and reliable deployment with the push of a button”.
The launch of the Azur vascular plug is complemented by the introduction of the PG Pro peripheral microcatheter, which is indicated for the peripheral vasculature for the infusion of diagnostic and therapeutic agents.
The PG Pro microcatheter is designed specifically to deliver all three sizes of the Azur vascular plug. It comes in radial lengths up to 165cm and a 1,200 PSI rating for clearer fluoroscopic imaging. Both are currently only available in the USA.
“Together, these next-generation technologies allow physicians to treat larger, more difficult vessels through smaller delivery options. It is yet another way Terumo is providing the opportunity for operators to take advantage of the benefits of radial access for increasingly complex procedures, while enhancing therapeutic options in the peripheral vasculature with a microvascular plug. It is a welcome addition to our innovative, best-in-class portfolio,” added Michael Martinelli, chief medical officer, Terumo Medical Corporation.
A German claims-based cohort study has revealed that—in 13,204 patients treated with a paclitaxel-coated device for peripheral arterial disease (PAD)—mortality differences were mostly attributable to a female subgroup treated above the knee, while no statistically-significant differences were observed in male patients. These findings were recently published in the Journal of Clinical Medicine (JCM).
Authors Christian-Alexander Behrendt (University Medical Center Hamburg-Eppendorf, Hamburg, Germany) and colleagues note that, while randomised controlled trials have reported excess mortality in patients treated with paclitaxel-coated devices versus uncoated devices, observational studies have reported the opposite. The researches aimed, therefore, to elucidate the underlying factors driving an observed improvement in mortality associated with paclitaxel exposure in patients with PAD.
Behrendt et al studied multicentre health insurance claims data from a large German insurance fund, BARMER. They detail that a homogenous sample of patients with an index of endovascular revascularisation for symptomatic peripheral arterial occlusive disease between 2013 and 2017 was included.
In total, 13,204 patients (54% females, mean age 74±11 years) were followed for a median of 3.5 years. The authors report that female patients were older (77 vs. 71 years), and had less frequent coronary artery disease (23% vs. 33%), dyslipidaemia (44% vs. 50%), and diabetes (29% vs. 41%), as well as being less likely to have a history of smoking (10% vs. 15%) compared with male patients.
In regard to mortality differences, Behrendt and colleagues relay that these were mostly attributable to the female subgroup who were revascularised above the knee (hazard ratio [HR], 0.78; 95% confidence interval [CI], 0.64–0.95), while no statistically significant differences were observed in male patients.
“This study found that female treated above the knee benefitted from paclitaxel-coated devices, while no differences were observed in males,” the authors conclude in JCM. In addition to this fact, which Behrendt et al state has not previously been reported, they found evidence once again for a female patient disadvantage in real-world data. They write: “It appears likely that previously underprivileged female patients benefit from treatment with paclitaxel-coated devices, an association that is moderated through improved optimal pharmacological treatment during follow-up.” However, they note that this subgroup seems to be excluded from previous trials (in Germany)—a fact that would explain a selection bias, they state.
Considering how their findings might impact further research in the area, the authors posit: “Ongoing and future trials should take sex disparities into account”.
In this third episode of a special five-part series on the history of DCBs, Jos van den Berg (Lugano, Switzerland) moderates a Interventional News roundtable discussion where he is joined by John Laird (St Helena, USA) and Peter Schneider (San Francisco, USA).
Study design
Laird examines the context and background to the IN.PACT SFA trial and outlines the study design. He notes that there was a need to change the way superficial femoral artery (SFA) disease was treated, as there were many complications “particularly with the full metal jacket stents…We wanted to create a paradigm and where we could avoid stenting and permanent implants in the SFA,” he adds.
Early expectations through to latest data
Schneider himself notes that in the beginning he was “not at all sure that we were going to be successful” in showing DCB to be superior to percutaneous balloon angioplasty (PTA). Despite having relatively modest expectations, Schneider notes the results were much better than expected, with 75% of patients in the DCB arm reintervention-free at five years. These results were “unheard of” at this time for SFA intervention in lesions up to 18cm. The trial “definitely exceeded my expectations” and “ushered in a new era and a huge advance for our patients,” believes Schneider.
A three-minute balloon inflation
Laird goes on to highlight how a three-minute balloon inflation with the IN.PACT Admiral™ DCB was chosen in order to “achieve the best angiographic and haemodynamic results”, as well as to “maximise drug uptake into the vessel wall” with a “unique formulation of paclitaxel” . The device showed “spectacular results”, at three and five years, he adds.
Safety concerns addressed
Schneider concludes by touching on the paclitaxel safety concerns raised by a meta-analysis and the lessons that have been learnt following its release. There was “ascertainment bias and treatment bias” in the meta-analysis, Schneider says, concluding that the two biases are “why we cannot find a danger signal in the massive amount of data that has been collected since 2018”.
Using selective internal radiation therapy (SIRT) to down-stage hepatocellular carcinoma (HCC) tumours or act as a bridge to surgery is feasible for both small and large growths, regardless of whether or not the patient has undergone portal vein thrombosis. This is the conclusion presented by Lambros Tselikas (Gustave Roussy Cancer Campus, Paris, France) at the European Conference on Embolotherapy (ET; 17–19 June, online).
In his virtual presentation, Tselikas emphasised the importance of dosimetry optimisation, which he said is crucial “to increase the response, to get a high complete response rate, and to increase the FLR [future liver remnant]. Time of surgery [following SIRT] is probably between three months and one year,” he concluded.
When thinking about the reasons why the decision might be made to use radioembolization as a bridge to surgery, Tselikas said simply: “Because we can”.
He cited a review series published in Frontiers in Oncology in 2014 from Arthur J A T Braat (University Medical Center Utrecht, Utrecht, The Netherlands) and colleagues that showed that, depending on the population, it is possible to bridge patients to transplantation. Tselikas also noted that, depending on the selection criteria applied, the percentage of patients that can be staged down varied hugely, from 25–100% of patients, depending on the liver function and the tumour size.
“What is interesting,” the ET speaker continued, “is the relationship between the pathological response you find in the imaging and in the histopathology. These are not very well correlated in some studies. The important message is, depending on the size, when you have complete necrosis on imaging, you will find complete necrosis on pathology.”
Writing in 2014, Braat et al explain the rationale for using radioembolization to downstage tumours: “Inducing significant tumour reduction can downstage patients for resection or, through attaining stable disease, patients can stay on the liver transplantation waiting list. Hereby, radioembolization could make a difference between curative of palliative intent in oncologic patient management. Prior to surgery, the future remnant liver volume might be inadequate in some patients. In these patients, forming an adequate liver reserve through radioembolization leads to prolonged survival without risking post-operative liver failure and minimising tumour progression while inducing hypertrophy. In order to optimise results, developments in procedures surrounding radioembolization are equally important. Predicting the remaining liver function after radical treatment and finding the right balance between maximum tumour irradiation and minimising the chance of inducing radiation-related complications are still challenges.”
Tselikas also presented the positive results of the DOSISPHERE-1 trial, which reported improvement in tumour response rate and overall survival in patients who had HCC treated with Yttrium-90 (Y-90) radioembolization utilising personalised dosimetry. Patients in the DOSISPHERE-1 trial were either given personalised or standard radioembolization; in the personalised group, 35% (10 of 28 patients) went on to have surgery with curative intent, whilst only 4% (one of 28 patients) went on to have surgery with curative intent following standard dose radioembolization.
He also shared the results of the LEGACY (Local radioembolization using glass microspheres for the assessment of tumour control with Y-90) study—a multicentre, single-arm, retrospective study conducted at three sites that included all eligible, consecutive patients with HCC treated with radioembolization between 2014 and 2017. The study aimed to evaluate objective response rate and duration of response. Clinical meaningful response rates and prolonged duration of response were observed in the treatment of unresectable, solitary HCC ≤8cm.
June 2021 saw the publication of issue 82 of Interventional News, and both our cover stories were amongst those most widely-read on our site this month: see our coverage of the Global Embolization and Cancer Symposium Technologies (GEST) 2021 Focus Day on prostate artery embolization (PAE), summarising the passionate discussions that took place concerning PAE’s place in the American Urological Association’s guidelines, and also learn about the latest developments in the COLDFIRE 2 trial, which recently determined that irreversible electroporation (IRE) is an effective and relatively safe treatment for colorectal liver metastases 5cm or smaller that are deemed unsuitable for partial hepatectomy, thermal ablation, or further systemic therapy.
In this Philips-sponsored educational supplement, Interventional News speaks with Hicham Kobeiter, Marc Sapoval, and Wouter Van Den Eynde about their experience on using the Azurion platform with SmartCT to simplify 3D imaging.
The cover story of our latest issue, this story delineating the road to prostate artery embolization (PAE) gaining a recommendation by the American Urological Association (AUA) via inclusion in their guidelines made a splash. The Global Embolization and Cancer Symposium Technologies (GEST) 2021 Focus Day on PAE (6 March, online) sought to open discussion between urologists and interventional radiologists regarding the place of PAE in the treatment algorithm, a topic of heated debate in recent years.
In this video interview, Constantinos Sofocleous (New York, USA) sits down with InterventionalNews to discuss how image-guided thermal ablation, when it is deployed with an intent to cure small colorectal liver metastases, can be fine-tuned so that its outcomes match those achieved by open surgery.
Holmium-166 (166Ho) radioembolization is a safe treatment option for patients with hepatocellular carcinoma (HCC), show results from the prospective, clinical phase I/II HEPAR Primary study, presented at the European Conference on Interventional Oncology (ECIO; 10–13 April, online). Interventional News speaks with Marnix Lam (University Medical Centre Utrecht, Utrecht, The Netherlands) about these latest data, which are anticipated to be published in the coming months, as well as what to expect from the iHEPAR study, which looks at a fully individualised treatment approach, and which Lam claims is the future of HCC treatment. This article is sponsored by Terumo Interventional Systems.
Andreas H Mahnken (Clinic of Diagnostic and Interventional Radiology, Marburg University, Marburg, Germany) enthuses to Interventional News about the potential of degradable starch microspheres (DSM) in transarterial chemoembolization, specifically drawing on his 20 years’ experience with DSM particles (PharmaCept). Indicated for chemoembolization of primary and secondary liver and lung tumours, EmboCept S DSM 50μm are the best-calibrated DSM available, ensuring good vasculature penetration and with a flexible application. This article is sponsored by PharmaCept.
A new study, published online in The Journal of Vascular Access (JVA), suggests that arteriovenous fistulas (AVFs) contribute to higher survival of haemodialysis patients with COVID-19. Authors Ahmet Murt (Istanbul University-Cerrahpasa, Istanbul, Turkey) and colleagues urge that end-stage renal disease (ESRD) patients “should be given the opportunity to have their vascular access properly created,” even in the pandemic era.
Cagent Vascular recently announced the investment of US$9 million by Sectoral Asset Management. Along with the investment, Marc-Andre Marcotte has joined the board of directors. The proceeds will be used to accelerate the commercialisation and scaling of manufacturing for the Serranator below-the-knee (BTK) product. Further uses of proceeds include expanding the product offering to include larger sizes to treat the above-the-knee arteries.
Irreversible electroporation (IRE) is an effective and relatively safe treatment for colorectal liver metastases 5cm or smaller that are deemed unsuitable for partial hepatectomy, thermal ablation, or further systemic therapy, results of the COLDFIRE-2 study, published in Radiology, report. The two-centre, prospective, single-arm, Phase II clinical trial was conducted by Martijn Meijerink, Alette Ruarus (both Cancer Center Amsterdam, Amsterdam UMC, Amsterdam, The Netherlands) and colleagues.
The June 2021 issue of Interventional News was published and distributed this month! Read it online and subscribe here to be sent a free physical copy quarterly.
Chair of the 2022 and 2023 European Conference on Interventional Oncology (ECIO), Philippe L Pereira muses on the status of interventional oncology (IO) in 2021, following more than a year of disruption from the ongoing COVID-19 pandemic. Through his work on various European guidelines delineating cancer care pathways, he has been instrumental in shaping the discipline and flying the flag for IO within multidisciplinary working groups. “Most oncologists recognise the value of our minimally invasive therapies and know very well how to integrate our treatments into the therapeutic armamentarium that currently exists for cancer patients,” he says.
The Roadsaver carotid stent system (Terumo France/Europe and MicroVention Europe) has been reimbursed in France. This follows the positive assessment from the French National Authority for Health (HAS), which highlighted a therapeutic benefit of the device.
“This decision bears out the wisdom of our strategy in the adoption of this technology since its availability in France,” says interventional cardiologist Max Amore (Clinic Louis Pasteur, Essey-Lès-Nancy, France). “We are glad that, now, more carotid patients will have access to Roadsaver, with its advanced design that provides a sustained embolic protection, [and] also after the procedure”.
This is the first dual-layer micromesh carotid stent to be approved by HAS and to be added to the list of reimbursed medical products (LPPR). The approved indication for Roadsaver is the same as for the previously approved “single-layer” platforms. It includes the treatment of symptomatic atherosclerosis when endarterectomy is not an option, or exceptionally in asymptomatic patients.
“The Roadsaver Dual-Layer Micromesh stent is considered a valuable alternative for open surgery in selected patients, based on its safety and efficacy profile, proven in an extended clinical programme,” comments Koen Deloose, director of ID3 Medical and head of the Department of Vascular Surgery at AZ Sint Blasius Hospital, Dendermonde, Belgium.
Terumo’s Roadsaver carotid artery stent system is designed to prevent a plaque protrusion through the struts and provide a sustained embolic protection, a press release explains. Its design incorporates a flexible nickel-titanium (Nitinol) dual-layer micromesh platform. Low crossing 5F profile allows for easy stent delivery in complex anatomies and is compatible with trans-radial approach.
Ghada Farah, SVP of Terumo Interventional Systems EMEA, adds: “We are delighted with this approval, which makes double layer micromesh stents available to all hospitals in France and confirms the robustness of our Roadsaver European registry data, the largest Carotid Artery stenting study in Europe”.
This reimbursement has been granted based on clinical evidence supporting the good safety and performance of Roadsaver carotid artery stent system in both symptomatic and asymptomatic patients, including the interim analysis of a large ROADSAVER observational study, currently being conducted in 13 European countries (52 sites) on about 2,000 patients enrolled.
Chair of the 2022 and 2023 European Conference on Interventional Oncology (ECIO), Philippe L Pereira muses on the status of interventional oncology (IO) in 2021, following more than a year of disruption from the ongoing COVID-19 pandemic. Through his work on various European guidelines delineating cancer care pathways, he has been instrumental in shaping the discipline and flying the flag for IO within multidisciplinary working groups. “Most oncologists recognise the value of our minimally invasive therapies and know very well how to integrate our treatments into the therapeutic armamentarium that currently exists for cancer patients,” he says.
What initially attracted you to a career in interventional radiology?
My mother wanted me to go to law school, my father preferred business, so I decided to become a doctor! No, in actual fact, as far back as I can remember, I have always wanted to be a doctor. That said, I wanted to be a psychiatrist, and I am now on the other side of medicine, the more technical side. Why interventional radiology (IR)? IR, well, because I like the operational side and being able to have an immediate influence on the disease, so as to help patients as soon as possible—the diagnosis alone without the interventional side would never have satisfied me. What we do as interventional radiologists is just incredible.
Who have been important mentors throughout your career?
Alain Roche would be the first one I would like to mention: I did not work with him for very long, but it was his enthusiasm that convinced me that IR was what I wanted to do in my life. The mentor I have learned the most from in the angiographic room was my colleague in Tübingen, Germany, Peter Huppert. One day, he brought back a radiofrequency generator that he had in his office; I quickly recognised the huge potential of this technology, and I have been using this therapeutic modality since 1996. I would also like to thank two other mentors who helped me a lot with their ideas: Fritz Schick, a physicist, and Claus Claussen.
As chair of the 2022 and 2023 ECIO meetings, what are the main takeaways you want for attendees?
First of all, I hope it will be a physical meeting, in person, and a great event to attend. It is a great honour for me that my European colleagues offer me this important position. My main purpose for this meeting is to emphasise the importance of clinical and pre-clinical studies, and to provide all possible support, starting from having the right idea—i.e. the study that will advance IO—then defining the design of the clinical study, right up to its funding. We will also highlight the multidisciplinary nature in the care of cancer patients: we are fortunate to include an oncologist, a surgeon, and a radiotherapist in the scientific programme committee (SPC). We also aim to cover the role that IO can play in combination with new immunological therapies, and to help define the contribution of artificial intelligence (AI) in our daily practice. All this will make ECIO 2022 an exceptional event.
How has the COVID-19 pandemic impacted medical conferences?
At the beginning of the pandemic, I thought that many conferences would become “digital”; I no longer think so. I feel that colleagues need to meet and discuss their latest experiences in person, candidly exploring the latest innovations or their most recent cases, discussing why they did not work as expected or how they achieved such success. Nevertheless, this pandemic has stimulated us, forcing us to find new options to continue education and research. We will probably keep some of these options and make our meetings a kind of hybrid, with sessions that may be live (in person) or half-live (also available digitally).
You are also a member of the Oncologic Alliance subcommittee. What sort of work does this do?
Yes, under the leadership of Andy Adam, this Alliance is addressing, among other things, the recognition of IO, defining international criteria for quality of cancer care, helping to design working groups to explore new and complex aspects of cancer care, and supporting the role of interventional oncology. The list of activities we undertake goes on and on.
You have also been involved with the development of European guidelines related to cancer management. What are the most important considerations when designing new guidelines?
This is a question for which I would need a full journal to answer! When you are working on new guidelines, you need to know all the results of the clinical studies in order to get the best recommendations for the patients. This is a particularly complex job, as you also need to know the results obtained by other medical disciplines as well as those from your own specialty. In cancer care, you have to recognise and support the interdisciplinary aspect: no one has a monopoly on the ideal treatment alone. These collaborations are very important, firstly to define the best treatments for our patients, and secondly to secure (and defend) the position of IR. As we do not have the resources of the pharmaceutical industry for large randomised studies, we need the results of our treatments in large, prospective and controlled registries, which also have the advantage of presenting “real-world” results with a good level of evidence.
What has the experience been like working with the European Cancer Organisation to establish a European network for interdisciplinary research on the diagnosis and treatment of oncologic diseases, and why is this international collaboration so important?
My experience is in fact very positive: IO has found its place in most guidelines, and this is in the interest of the patients. Most oncologists recognise the value of our minimally-invasive therapies and know very well how to integrate our treatments into the therapeutic armamentarium that currently exists for cancer patients.
What developments in IO are you most excited about?
IO is one of the most fascinating and promising specialties in medicine. To mention just a few aspects, I would like to emphasise the extraordinary opportunity that we must seize as interventional oncologists working in what we refer to as “the era of personalised medicine”. There are few medical disciplines that are as patient-oriented as ours. Each therapy is individualised: the application, the doses of drugs that are applied under imaging control, the change of therapies, and the possibility to combine our treatments with systemic treatments, surgery, or even radiotherapy.
Another key development is the enormous interest in new targeted therapies in the immunooncology space. Who can deliver these new therapies more locally than interventional radiologists? Another is to boost the immune response by combining our local treatments with systemic therapies. This is a great opportunity for our specialty. The interventional radiologist can be at the centre of this evolution, at least for some cancers in selected patients, if we are able to participate in preclinical and clinical studies. I say participate and unfortunately not lead because I must admit that we are not the first doctors to be contacted by the pharmaceutical industry.
To achieve this recognition we need first to make IR known to medical students (what could be more attractive than combining minimally-invasive treatments with minimised instruments, intelligent programmes, 3D images, and artificial intelligence). Second, we need to increase our influence in the education of young colleagues, to further the development of experts, and to be able to offer IO services in the same way that surgeons offer surgery: in all hospitals, not just in some specialised centres. Several scientific societies, such as the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), are working hard on this.
What is the greatest challenge currently facing interventional radiologists?
Our position is much better recognised than it was 20 years ago, but there is still a lot to do. The main challenge is to establish IO truly as one of the four pillars of cancer care. It seems to me that it is less necessary to convince oncologists—good oncologists know the benefit we can bring to patients—than it is to inform them of what we can do in the first place. Still too many oncologists are not aware of the wide spectrum of treatments we have to help cancer patients.
Another challenge I would like to mention here is the need to conduct good prospective clinical studies and to stop with retrospective studies on small cohorts that are generally not recognised for guidelines. Again, personalised medicine is a huge opportunity for interventional oncology.
What are your hobbies and interests outside of medicine?
I have a fantastic daughter, Anne-Sophie, of whom I am very proud, and with whom I try to make up for (past) lost time, and my wife, Bettina, with whom I have so many things in common. When I have some spare time, I take one of my electric guitars and play Hendrix, Led Zeppelin, Clapton… or at least I try to! My secondary hobby is definitely sports: tennis, jogging, and rowing, at least twice a week. When it rains, my reading is mostly focused on astronomy, from GNz11 to the acceleration of the universe and the quintessence!
Andreas H Mahnken (Clinic of Diagnostic and Interventional Radiology, Marburg University, Marburg, Germany) enthuses to Interventional News about the potential of degradable starch microspheres (DSM) in transarterial chemoembolization, specifically drawing on his 20 years’ experience with DSM particles (PharmaCept). Indicated for chemoembolization of primary and secondary liver and lung tumours, EmboCept S DSM 50μm are the best-calibrated DSM available, ensuring good vasculature penetration and with a flexible application.
What is DSM-TACE and in which indications is it used?
Besides drug-eluting bead transarterial chemoembolization (DEB-TACE) and conventional transarterial chemoembolization (cTACE), there is a subset of TACE called DSM-TACE, where you use degradable starch microspheres roughly 50μm in size. These microspheres have a half-life of approximately 35 minutes, which means they are only around for a couple of hours at most. This allows you to re-access the same vessel for repeated TACE. The half-life is also short enough to prevent the proliferation of growth factors such as VEGF [vascular endothelial growth factor], which usually enter the bloodstream after a few hours of ischaemia. One of the major advantages of [microsphere] degradability is that you do not have this additional vascular growth. There are actually no limits to the indication within the liver, and you can also use the degradable starch microspheres in the lung for transpulmonary chemoembolization (DSM-TPCE) or in the bronchial arteries, so DSM-TACE has a really broad scope of indications. Our main focus in my department is for liver metastases and primary liver cancer, but we also use it for lung cancer.
What are the differences between DSM-TACE and cTACE/ DEB-TACE?
You have fewer limits. You can combine the procedure with any drug—not only, for example, doxorubicin or epirubicin, but you can really use it with any cytostatic that can be given intra-arterially, also in combinations, so it allows you to be much more flexible. That gives you a broader range of indications.
DSM-TACE also has excellent tolerability, so the patient experiences less pain. You can even perform a whole organ embolization with limited pain, which is pretty advantageous for the patient. It is much better-tolerated by the patient in terms of liver function and degradation, as well as in terms of pain. You can do it even in organs that would be critical for a cTACE or a DEB-TACE, so it gives you more flexibility—that is really the key for me.
If you have a patient with an organ that is already limited, for example a patient with cirrhosis, who then develops multinodular hepatocellular carcinoma (HCC), you may be concerned about having to treat multiple places in the liver. For example, with cTACE, there may be a limit because the function of the organ is not enough to allow treatment of all the tumours, but with DSM-TACE you can embolize all these tumours in a single session, and you will come out with enough remaining liver function to make sure that the patient can tolerate the procedure. In terms of efficacy, it is excellent.
Are there any limitations using DSM-TACE?
To the best of my knowledge there are no limitations. You can even combine it with cTACE; there is a very small prospective randomised trial that combines DSM-TACE with cTACE. That is another opportunity.
What are the future applications of DSM-TACE?
Future applications could include combining DSM-TACE with systemic or even regional immunotherapy—it can be combined with many new drugs. We are living in the time of immunotherapy, and DSM-TACE can be combined with several immune modulators. I feel that this is a really exciting possibility. We have preclinical data that shows us that there is T-cell homing in the tumour after DSM application, so that would be an ideal target for immune modulators, not only interleukins but modern drugs as well. I feel that is one of the greatest potentials DSM-TACE has for the next decade.
Case report
Cholangiocarcinoma is a highly lethal hepatic neoplasm with a median overall survival rate of about 16 months (Waseem 2017). Even after resection, the prognosis is poor, with reported three- and five-year survival rates after resection for perihilar cholangiocarcinoma (pCCA) of around 45% and 30% (Cillo 2019). In unresectable pCCA, common treatment options included chemotherapy with gemcitabine and cisplatinum, and transarterial chemoembolization (TACE).
Patient history degradable
A 78-year-old female patient suffering from unresectable pCCA (Bismuth IV) was referred to our interventional radiology clinic for treatment after failure of first line chemotherapy. Magnetic resonance (MR) imaging revealed progression of the histologically-proven mass-forming pCCA, with multiple new histologies proving the presence of intrahepatic tumours and no extrahepatic tumour (Fig. 1).
On clinical examination, the patient was considered fit for interventional therapy. Laboratory testing showed mild anaemia and a moderately-elevated alkaline phosphatase. Her renal function was normal. She had previously undergone endoscopic biliary stenting, so her bilirubin was normal. We opted for a treatment with TACE and adjuvant capecitabine (Kelley 2020).
Interventional therapy degradable
Our TACE protocol for cholangiocarcinomas includes a so called DSM-TACE with 300mg degradable starch microspheres (EmboCept S DSM 50μm, PharmaCept, Berlin, Germany) combined with intra-arterial application of 75mg/m2 Cisplatinum (PlatiCept, PharmaCept, Berlin, Germany) and Gemcitabine (1,000mg/m2). In addition, a premedication for nausea, pain, and a single shot of intravenous (IV) antibiosis in case of biliodigestive- anastomosis or stenting.
Diagnostic catheter angiography at the beginning of the first treatment session showed a fixed high-grade stenosis of the celiac trunk with subsequent collateral flow from the superior mesenteric artery (Fig. 2). For whole liver treatment, a 2.7F microcatheter was placed in the proper hepatic artery and DSM-TACE with flow-controlled slow infusion of the chemotherapeutics was performed (Fig. 3). Unlike in conventional TACE (cTACE), drugs were infused over a 30-minute period in order to minimise gastrointestinal toxicity in terms of nausea and vomiting. During administration of chemotherapy, EmboCept S DSM 50μm was repeatedly applied under angiographic control via a three-way stopcock. In Germany, PlatiCept is the only available cisplatinum powder. Its major advantage is its good solubility. Therefore, relatively high doses of cisplatinum can be administered with a small injection volume. The latter is considered helpful for maintaining the embolic effect of TACE. With DSM such as EmboCept S DSM 50μm, repeat treatments are feasible, as the target lesion remains accessible. Moreover, the half-life time of about 35 minutes for EmboCept S DSM 50μm minimises systemic expression of proangiogenic growth factors such as vascular endothelial growth factor (VEGF) (Schicho 2016). It moreover reduces side effects such as ischaemic pain, thereby facilitating whole liver treatment.
At six week intervals, the patient underwent three successful DSM-TACE procedures. The procedures were well tolerated, with only a mild one-week fatigue as the only symptom of post-embolization syndrome. The eight-month follow-up MR imaging showed partial response according to RECIST 1.1, with only very little tumour left (Fig. 4). So far, no change on laboratory testing has been seen. Almost two years after the initial diagnosis, the patient feels well without limitations in her daily activity. She is now scheduled for a three-month treatment holiday followed restaging.
References:
1. Waseem D, Tushar P. Intrahepatic, perihilar and distal cholangiocarcinoma: Management and outcomes. Ann Hepatol. 2017 Jan–Feb 2017;16(1):133-139.
2. Kelley RK, Bridgewater J, Gores GJ et al. Systemic therapies for intrahepatic cholangiocarcinoma. J Hepatol. 2020 Feb;72(2):353–363
3. Cillo U, Fondevila C, Donadon M et al. Surgery for cholangiocarcinoma. Liver Int. 2019 May;39 Suppl 1(Suppl Suppl 1):143–155
4. Schicho A, Hellerbrand C, Krüger K et al. Impact of Different Embolic Agents for Transarterial Chemoembolization (TACE) Procedures on Systemic Vascular Endothelial Growth Factor (VEGF) Levels. J Clin Transl Hepatol. 2016 Dec 28;4(4):288–292
Holmium-166 (166Ho) radioembolization is a safe treatment option for patients with hepatocellular carcinoma (HCC), show results from the prospective, clinical phase I/II HEPAR Primary study, presented at the European Conference on Interventional Oncology (ECIO; 10–13 April, online). Interventional News speaks with Marnix Lam (University Medical Centre Utrecht, Utrecht, The Netherlands) about these latest data, which are anticipated to be published in the coming months, as well as what to expect from the iHEPAR study, which looks at a fully individualised treatment approach, and which Lam claims is the future of HCC treatment.
In the HEPAR Primary study, the investigators set out to establish the toxicity profile of 166Ho radioembolization (average liver absorbed dose of 60Gy) in patients with HCC. The primary endpoint was the rate of unacceptable toxicity, defined as total bilirubin increase grade 3 or higher (common terminology criteria for adverse events; CTCAE v.4.03) in combination with ascites and low albumin (radioembolization-induced liver disease; REILD), or any serious adverse event that was related to study treatment. Secondary endpoints included efficacy (according to modified response evaluation criteria in solid tumours; mRECIST), alpha fetoprotein response, dosimetry, quality of life, and liver function. Clinical and laboratory follow-up took place at three and six weeks, and three and six months. Patients included had measurable and liver-dominant disease and no curative treatment options.
Of the 31 patients included in the study, 71% were Barcelona Clinic Liver Cancer (BCLC) stage B, and 29% were BCLC stage C. Most (87%) had multifocal disease, and the median diameter of the largest tumour was 56mm (range 15–195mm). Lam describes this patient cohort as a “real-world” population.
Unacceptable toxicity related to the study treatment occurred in three patients; no REILD was encountered. New or worsened toxicity observed were: fatigue (71%), back pain (55%), ascites (32%), dyspnoea (23%), nausea (23%), and abdominal pain (23%), mostly grade 1. At three- and six- months follow-up, 54% and 84% of the target liver lesions showed complete or partial response. Median overall survival was 14.9 months, and no significant decline in quality of life was observed.
What do the HEPAR Primary study results tell us in terms of the safety and efficacy of the procedure?
Most importantly, the primary endpoint of the HEPAR Primary study was safety. It was a Phase I/II study, in which safety was the primary endpoint and efficacy a secondary endpoint. From the study, we concluded that the toxicity is acceptable. We had pre-defined safety limits: in short, we considered grade III or higher toxicity, which was related to treatment, as unacceptable—but we only found this rate in three out of 31 patients, which confirms the safety in this patient population This result gives us the confidence to move on to further clinical studies of 166Ho-radioembolization in HCC patients.
The efficacy results of the HEPAR Primary study are also very encouraging, both in terms of response rate and in terms of survival for this patient population. This inspires us to continue to investigate this treatment for HCC patients.
I think what is very important for the HEPAR Primary study is the treatment planning involved. We chose an average absorbed dose for the whole perfused volume, so we did not make the differentiation between how many of these microspheres go to the tumour, and how many go to the surrounding liver tissue. For example: in one patient, the microspheres may all end up in the tumour, and none in the surrounding liver tissue (which is ideal, of course, because you hit the tumour hard and you do not damage the surrounding liver), but in another patient, it may be the other way around—you damage the surrounding liver tissue and you do not hit the tumour. So if you choose an average dose, and you treat all patients with a similar number of microspheres and just see where they end up, you are utilising a one-way-fits-all approach. Considering that we used this very rough treatment planning technique, I think the results are even more encouraging, with a lot of room for further improvement.
For every patient, after treatment, we can see the dose that went to the tumour and to the liver, and therefore we can ascertain how that correlates to effect and toxicity. We expect that the harder we hit the tumour, the better the effect, and the same for toxicity. So if we know that correlation, we can say, ‘OK, in terms of safety, the surrounding liver tissue can tolerate this amount of dose as a maximum’, and then in the next study, we will use that for individualised treatment planning.
Why is it important to have these prospective data?
These data are important to establish the safety profile of 166Ho-radioembolization. The HEPAR Primary study is the start of where we want to go with this therapy.
I think it is important to understand that previous studies on radioembolization in HCC—large, Phase III studies—all failed. These particular studies did not use individualised treatment. Because of that, the majority of patients were under-dosed. If you are treating blindly, then of course you need to be careful. I think for us now, it is incredibly important to show that the technique works.
How does the Holmium Platform enable treatment individualisation, and what does the future of HCC treatment look like?
The HEPAR Primary study is really the first step. The second step is showing that individualised radioembolization is feasible and has a benefit. The third step will be to compare it to the standard of care. That is also important—to show that this treatment option has a role to play in the HCC treatment algorithm.
To this end, we are currently working on the iHEPAR (individualised HEPAR) study. In this study, we are using a scout dose as part of the entire Holmium Platform to further individualise the selective internal radiation therapy (SIRT) planning. We have two procedures: the first procedure involves using a limited number of microspheres—enough to visualise where we are going, but not enough to cause damage. That is the scout procedure. We use a scout dose for three reasons:
To determine where exactly the microspheres are going (for example, are they just in the tumour, are some reaching the surrounding healthy liver tissue, or is there a leak to the stomach or elsewhere? We want to avoid that)
To see if the microspheres are remaining in the liver—we want to avoid lung shunting, for example
To understand the distribution within the liver—how many microspheres end up in the tumour, and how many end up in the normal liver?
In the HEPAR Primary study, we did use 166Ho scout dose, but it wasn’t applied to perform dedicated treatment planning. As a result, we treated patients with a one-size-fits-all approach. We used this information to establish the dose-effect relationship, which allowed us to determine the safety threshold dose for the liver. In the iHEPAR study, we will start using the information we obtain from the 166Ho scout dose to personalise the treatment using the entire end-to-end Holmium Platform. For example, if there is a patient where all the microspheres end up in the tumour, we can give him a higher dose.
Another area of future work is investigating the potential of combining 166Ho radioembolization with immunotherapy.
Especially in the era of immunotherapy, combining a locoregional treatment with an immunotherapy treatment is, I think, very interesting. To me, that seems to be the most logical next step: there are already studies underway that combine transarterial chemoembolization (TACE) with immunotherapy, so it seems logical to start combining radioembolization with immunotherapy.
I think that the best candidates for radioembolization are patients with large tumours. Usually, the larger the tumours, the greater the vasculature, so the better they absorb the microspheres, so to speak. This means you are able to target the tumour without damaging the surrounding tissue. So if, for example, you were treating a patient with a very large tumour on the right side of the liver, and multiple small ones on the left, this would be a super interesting candidate for combination therapy. You could hit the big tumour on the right side with 166Ho radioembolization, and then treat the smaller ones with systemic therapy (e.g. immunotherapy).
Cagent Vascular recently announced the investment of US$9 million by Sectoral Asset Management. Along with the investment, Marc-Andre Marcotte has joined the board of directors. The proceeds will be used to accelerate the commercialisation and scaling of manufacturing for the Serranator below-the-knee (BTK) product. Further uses of proceeds include expanding the product offering to include larger sizes to treat the above-the-knee arteries.
The Serranator percutaneous transluminal angioplasty (PTA) serration balloon catheter is an angioplasty device with serrated metal strips embedded on a semi-compliant balloon. The Serranator’s unique technology is designed to create multiple longitudinal lines of interrupted micro-serrations within the luminal surface to aid in arterial expansion. The result is predictable and controlled lumen gain using low atmospheres of pressure.
“Our BTK product launch is going extremely well. Early commercial adoption and clinical outcomes are confirming the positive results seen in the PRELUDE-BTK study. We are delighted to have a high-quality investor like Sectoral join our team. Their deep experience investing and advising device companies focused on peripheral vascular interventions will enable a more rapid expansion of our commercial efforts,” stated CEO Carol A Burns.
Marc-Andre Marcotte, of Sectoral, added, “We have been very impressed by Cagent’s achievements thus far and are excited to partner with them. We are confident that the unique features and high-quality clinical data of Serranator will drive strong market adoption.”
The Serranator’s differentiated mechanism of action is driving adoption. “The BTK space is in desperate need of innovation. These vessels are more challenging in terms of size, lesion length, and calcification and non drug-based balloon angioplasty is still the primary treatment. My experience with Serranator has been excellent and with its novel mechanism of action it has become an important tool in treating BTK disease. In the near future I look forward to using this technology in vessels above the knee to further optimise my angioplasty results,” explained Sarang Mangalmurti interventional cardiology specialist at Bryn Mawr Hospital (Philadelphia, USA).
GEST 2021 PAE panellists. Top row, from left: Shamar Young, Jafar Golzarian, Art Rastinehad. Middle row, from left: Riad Salem, James Spies, Dominik Abt. Bottom row, from left: Mark Little, Philipp Dahm, John Kellogg Parsons.
There are substantial differences amongst guideline recommendations regarding the use of prostate artery embolization (PAE) in the treatment of lower urinary tract symptoms/benign prostatic obstruction (LUTS/BPO), which can be partially explained by different interpretation of the evidence. This is the conclusion presented by Dominik Abt (Klinik für Urologie, Institut für Medizin, Universität St Gallen, St Gallen, Switzerland) at the Global Embolization and Cancer Symposium Technologies (GEST) 2021 Focus Day on prostate artery embolization (PAE; 6 March, online). This virtual meeting sought to open discussion between urologists and interventional radiologists regarding the place of PAE in the treatment algorithm, a topic of heated debate in recent years.
Speaking during the final session of the day, panel chair and co-course organiser Jafar Golzarian (University of Minnesota, Minneapolis, USA) praised the “unique” collaborative attitude of the virtual meeting, where attendees heard from four urology panellists and four interventional radiology (IR) panellists: “This session exploring the level of evidence and directions for future research in PAE is unique in both the IR and urology communities,” he said, “taking a truly interactive and multidisciplinary approach, which is not common practice.” He noted that he hoped this cross-disciplinary collaboration would continue in future meetings.
Speaking first, Mark Little (Royal Berkshire NHS Foundation Trust, Reading, UK) discussed the most important PAE articles published in the last two years. In the last two years, 113 papers on PAE have been published. Of these, five were randomised controlled trials (RCTs), and eight were meta-analyses of systematic reviews.
Regarding the clinical effectiveness of PAE, Little said: “We cannot go beyond the superb sham RCT study that came out of Lisbon.” This was a 2019 study published in European Urology, the official journal of the European Association of Urology (EAU), from João Pisco, Tiago Bilhim (Hôpital Saint-Louis, Lisbon, Portugal) et al that found that the improvements in quality of life measurements and International Prostate Symptom Score (IPSS) in patients following PAE are “far superior” to those due to the placebo effect. Speaking to Interventional News at the time, Bilhim noted that publishing a paper positively describing PAE in a urology journal has historically been difficult for interventional radiologists. He hoped that this publication “might help our way into the urology guidelines with PAE”.
“Anyone who has tried to design a sham trial—which I am trying to do now for genicular artery embolization [GAE]—knows that it is hard work,” Little commented, in praise of the Lisbon group. “On the one hand it is the gold standard study design to refute the placebo effect, but there are a number of ethical dilemmas. So it is an ambitious study design, and one that the Lisbon group did extremely well to set up and running and recruit to.”
In the sham study in question, 80 patients were enrolled, randomised 1:1 to PAE versus a sham procedure with a cross-over design at six months. Summarising their findings, Little relayed: “They found a statistically significant refutation of the placebo effect—PAE does better than sham”. Asking the question, “Is PAE clinically effective”, Little argued that the answer was a definitive “Yes”, based off this Level 1 evidence.
Giving a more practical perspective, Little then turned to covering the evidence for altering clinical practice, focusing on papers dedicated to patients with median lobes and to the question of repeat PAE.
“I remember having conversations at CIRSE [the annual scientific meeting of the Cardiovascular and Interventional Radiological Society of Europe] five or so years ago saying ‘Well, perhaps we should exclude patients with a median lobe, they seem to be difficult to treat’,” he said. Presenting a 2019 publication from Riad Salem (Northwestern University, Chicago, USA) and colleagues in Abdominal Radiology, looking predominately at imaging correlates: “A simple study,” Little opined, “but nevertheless [it] gives the idea and the introduction of where we sit with regard to the technique of embolizing the median lobe.” This cohort study showed that 37% of patients had a median lobe—intravesical prostatic protrusion (IPP)—and that 100% of those IPP-positive patients treated with PAE had a decrease in median lobe size following the procedure.
Marc Sapoval
While this demonstrated that it was feasible to embolize the median lobe, Little asked “What does that mean clinically, do these patients get better?” He turned to a 2021 study from GEST co-founder Marc Sapoval, first author Tom Boeken (both Hôpital Européen Georges-Pompidou, Paris, France) et al that concluded that IPP is “not a prognostic marker of ineffective PAE in men with benign prostatic hyperplasia (BPH)”. Sapoval, Boeken and colleagues also wrote that severe protrusion could lead to a better response to PAE, “though expected prostate height reductions are mild”. They found that the degree of IPP did not limit the efficacy of PAE in patients with lower urinary tract symptoms (LUTS) due to BPH.
Furthermore, a 2020 paper in the Journal of Vascular and Interventional Radiology (JVIR) from Aaron Fischman (Mount Sinai, New York, USA) and colleagues answered the direct question “Should we be treating median lobes?”, Little reported. Stratifying the median lobes by size (patients were categorised as having non-severe IPP if their median lobe was <10mm, as was the case in 17 patients enrolled in the study, and as having severe IPP if their median lobe was >10mm, as was the case in 37 patients), Fischman et al found that both groups had a statistically significant improvement in IPSS and quality of life scores. “So we should not be scared of median lobes in terms of PAE,” Little concluded.
João Pisco (L) and Tiago Bilhim
Concentrating on repeat PAE, Little relayed how approximately 20% of PAE patients could be deemed “clinical failures”, in need of further intervention. “Does that mean one in five need surgery?” he asked. Again turning to work from the Lisbon group, which focused on how these patients failed, Little recounted how patients in the study were categorised into two groups: group A (n=39), those who never showed a response to PAE; and group B (n=69), those who had clinical improvement in the first six months following PAE, but then relapsed. The investigators found that in 75% of patients, the blood flow was coming from the previously embolized prostate artery, perhaps indicating under-treatment, while in the remaining 25% of patients, the blood supply was from collateral vessels. At 24–26 months follow-up, 17% of group A had a clinical benefit from repeat PAE. This led Little to comment: “Effectively, if you have got a patient that does not respond initially, they are unlikely to respond. They [those in group A] probably need to be treated with surgery.” In group B, meanwhile, 52% had a significant clinical benefit from repeat PAE.
AUA guidelines
Little also considered the Society of Interventional Radiology (SIR) consensus panel conclusions, which were the focus of much of the day’s discussion. Published in JVIR and authored by Clifford Davis (College of Medicine and Radiology, University of South Florida, Tampa, Florida) et al, the summary of the SIR consensus panel on PAE regarding the development of a research agenda for the procedure concluded without direction: “Level 1 data are required to be included in the AUA guidelines for treatment of BPH. Because of concerns with all three study designs, the panel did not reach a consensus. Further meetings are planned with the panel to select among these research designs.”
The three research designs mentioned were: i) RCT of PAE versus sham with crossover of the sham group. (ii) RCT of PAE versus simple prostatectomy. (iii) RCT of PAE versus holmium laser enucleation of the prostate/thulium laser enucleation of the prostate.
The SIR consensus panel ultimately recommended a non-industry-funded registry to obtain real-world data.
Currently, the AUA guidelines state that “PAE for the treatment of LUTS secondary to BPH is not supported by current data and trial designs, and benefit over risk remains unclear; therefore, PAE is not recommended outside the context of clinical trials.” The guidelines claim this advice is based on expert opinion.
“I am a UK interventional radiologist,” Little acknowledged, “so I will be as objective as I can be in this argument.” He talked the GEST audience through the guidelines from the perspective of the SIR consensus paper. He noted that the AUA guidelines included RCTs with more than 12 months of outcome data, but that the AUA wanted PAE studies to include a 24-month follow-up “to be equivalent to current data on other surgical therapies for LUTS resulting from BPH”.
Citing a 2020 JVIR study from Iñigo Isausti (Complejo Hospitalario de Navarra, Pamplona, Spain) et al, Little related how the group set out to compare clinical and functional outcomes of PAE with those of transurethral resection of the prostate (TURP) for the treatment of LUTS secondary to BPH. Isausti and colleagues reported: “Reduction of LUTS in the PAE group was similar to that in the TURP group at 12 months, with fewer complications secondary to PAE.”
However, AUA require two-year data. “We are very fortunate to have Dominik [Abt] here,” Little said, “as the lead author of this paper”. Abt (Klinik für Urologie, Institut für Medizin, Universität St Gallen, St Gallen, Switzerland) et al conducted a study comparing the efficacy and safety of PAE and TURP in the treatment of LUTS at two-year follow-up.
They concluded in February 2021: “Inferior improvements in LUTS/BPO [benign prostatic obstruction] and a relevant re-treatment rate are found 2 years after PAE compared with TURP. PAE is associated with fewer complications than TURP. The disadvantages of PAE regarding functional outcomes should be considered for patient selection and counselling.” Their patient summary was: “PAE is safe and effective. However, compared with TURP, its disadvantages regarding subjective and objective outcomes should be considered for individual treatment choices.”
As the reintervention rate was 20% in the PAE group, Little said what treatment these patients should get next is “where the debate now lies”.
“I do not think this paper is a death knell for PAE at all,” he opined. “Actually, I think it shows that it is safe and effective, but, we need a reasonable discussion with our patients about what we can achieve with the technology based on patient selection, anatomy selection, pre-procedural imaging and planning.”
He concluded that PAE is safe and effective, and, in his eyes, gives patient’s a choice, which he believes is “really important”. Citing the sham trial and RCT data to two-years follow-up, Little summarised that there is “lots of level 1 and 2 evidence on PAE, which cannot be argued against in terms of the position statement of ‘Benefit over risk remains unclear’ [from the AUA guidelines].”
He continued: “I am not sure that we can say that with the current evidence case we have,” something fellow panellist and interventional radiologist Riad Salem (Northwestern Memorial Hospital, Chicago, USA) said he agreed with.
James Spies
Going through the AUA guidelines comparing how PAE was assessed compared to alternative therapies, James Spies (MedStar Georgetown University Hospital, Washington, DC, USA) said he thought the recommendation not to perform the procedure outside of clinical trials was “actually a value judgement of one specialty of another” that “seems a little unusual”.
“This is not pointing fingers at the AUA,” he added. “I was former chair of the standards committee of the SIR, and I am a former [SIR] president—clinical practice guidelines really are intended to be evidence-based, and by-and-large they are. The process the AUA use is actually very good. But when it gets down to it, it is difficult to separate our preconceived notions from our review of evidence.”
“Again, this is not a knock on the AUA, but my opinion is that guidelines reflect the opinions of the organisations that create them. That is because it is almost impossible for a group in a room to go beyond what is not comfortable for them. In some ways, the SIR is never going to write a guideline that says PAE is bad, probably, unless we have some definitive data, and the AUA may never write one that says it is good or at least should be on the list. So I would agree we need to increase our data, but I am just not sure we are ever going to be able to get there. This is a benchmark procedure for urologists, and, just like some other specialties that we work with, it can be difficult to get adoption.”
When thanking Spies for his talk, Golzarian noted that Spies is a “pioneer” for uterine fibroid embolization (UFE), a procedure now widely recognised and performed by interventional radiologists: “It is like revisiting history; we are 15 years behind with PAE [compared to UFE], but hopefully we will see the same acceptance,” he commented.
Quality of evidence for PAE: The urologist perspective
Speaking next, urologist Philipp Dahm (Minneapolis VA Medical Center and University of Minnesota, Minneapolis, USA) gave a talk entitled, “Objective rating of evidence: Why it matters and how it applies to PAE”. He recommended the following: “Current best evidence on PAE should be assessed on the basis of a high-quality, protocol-driven systematic review. The focus should be on patient-important outcomes with explicit consideration of clinically important differences [in the case of PAE, this includes IPSS and quality of life scores, adverse events, and retreatment rates; flow rate and prostate volume are deemed “not important for decision-making” by Dahm]. The certainty of evidence rating should be provided on a per outcome basis to qualify how much confidence we have. Lastly, judgements about net benefit need to consider both relative and absolute effect size estimates.”
Dahm is a founding member of the US grading of academic assessment, development, and education (GRADE) network, an informal working group formed in 2000 to develop a new system for rating the certainty of evidence in healthcare and also for making guidelines. Currently, GRADE has over 500 members, and is used by more than 120 organisations.
Unlike the traditional “hierarchy of evidence”—which treats systematic reviews, meta-analyses, and randomised controlled trials at the gold standard—GRADE is based on an alternate hierarchy that Dahm said reflects the flaws in these assessment methods. In particular, he noted that RCTs “can be fatally flawed” in their design, and noted that systematic reviews are only as good as the individual studies they evaluate, so could suffer from a “garbage in, garbage out” scenario. In the GRADE system, systematic reviews are “undocked” from the very top of the triangle in the traditional hierarchy of evidence graphic, and are used as a tool for assessing a body of evidence.
The GRADE system works thus: formulate a question; select outcomes; rate the importance of these outcomes (on a scale from critical, to important, to less important) look at outcomes across studies; create an evidence profile with GRADEpro, which includes a summary of findings and an estimate of the effect for each outcome; rate the quality of evidence for each outcome (from high, through moderate and low, to very low).
“It is really important to provide a certainty of evidence rating that reflects the confidence that we have that an estimate of effect is adequate to support a clinical decision or recommendation,” Dahm said. So a GRADE rating of “high” corresponds to “We are very confidence that the true effect lies close to that of the estimate of the effect”. A “very low” rating translates to “We have very limited confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect”.
He talked the audience through the GRADE summary of findings table for Cochrane review conducted by urologist Jae Hung Jung (Yonsei University Wonju College of Medicine, Wonju, South Korea) and colleagues and published in 2020, which set out to assess the effects of PAE compared to other procedures for treatment of LUTS in men with BPH. Using an updated version from March 2021, Dahm recounted how the GRADE interpretation of the change in IPSS and quality of life scores following PAE is that there is “little or no difference for these outcomes short-term compared to TURP”. In addition, he said that “we are very uncertain” about PAE having a lower major adverse event rate than TURP. Lastly, he noted that the “greatest certainty” the GRADE reviewers had was regarding retreatment rates in the short-term, which they believed were “probably increased” after PAE.
Quality of evidence for PAE: The IR perspective
Riad Salem
Salem offered an interventional radiologist’s perspective, which served as a riposte to Dahm’s previous talk, and detailed the strength of evidence for PAE’s safe and efficacy. While he said he understood the initial scepticism about the success of embolizing the prostate gland, he noted that there have been technical improvements in the procedure since its inception. Furthermore, while attempts at “gold standard” PAE versus TURP trials had failed in the USA, more recent propensity-matched, prospective comparisons of the two procedures and randomised trials of TURP versus sham a procedure are positive indicators that PAE has a positive future.
“More importantly, to Philipp [Dahm]’s point,” Salem commented, “there is a growing patient interest in alternate therapies.”
Following a review of the evidence for PAE, Salem concluded: “In my opinion, no one can say PAE does not work. It does in my opinion satisfy all criteria for a reasonable treatment, and it should be an option presented to patients. At minimum, it should have a limited recommendation for large glands [prostate volumes >80cc], where effectively all of the MISTs [minimally invasive surgical therapies] are ineffective, by the AUA guidelines.
“The AUA guidelines are important, but they are not the final word. Respectfully, no one has a monopoly on the management and the clinical development of managing patients with BPH-LUTS. It should be a team effort. As Philipp said, Level 1 evidence is not the only method of generating high-level, relevant data. Good Phase II data can do that as well—there are ethical and technical challenges with RCTs, as Mark [Little] spoke about.
“Unfortunately, we have been slowed down by—in my opinion—the emotional and polarising reaction by KOLs [key opinion leaders] to evolving PAE data. It is my observation that there is a perceived inconsistency in the manner PAE data are interpreted compared with that [for] MISTs. I think we need to work together, and PAE needs to be offered to the right patient. We need a collaboration between IR and urology, and this collaboration must evolve, not devolve, in a multidisciplinary manner that will benefit patients.”
He ended with a specific request of the attending urologists: “At the end of the day, patients are not satisfied with TURP and MISTs as the only options; they are demanding something else. What I would ask is, given this, what is the pathway for recognition of PAE, at least in a limited scope, [in the AUA guidelines]? If the response is a clinical trial, I would like to know which clinical trial explicitly.”
Offering one urologist’s perspective (with particular emphasis afforded to the “one”), John Kellogg Parsons (Moores UC San Diego Cancer Center, San Diego, USA) took to the virtual podium next. Despite being chair of the AUA BPH guidelines panel, he noted that he was not speaking on behalf of the AUA in any capacity.
He suggested some potential ways forward for interventional radiologists and urologists: “[Look for] other study populations and indications. I think LUTS is unlikely to gain significant traction within the urological community as an indication for performing PAE, so I would encourage you to look for other indications. Haematuria is what I hear constantly as a very compelling indication to investigate, but there are no clinical trials to investigate this. Neoadjuvant therapy, I have heard that hypothesised, I think that is a reasonable avenue to explore; urinary retention and very large prostate, I think that is very reasonable to explore. Always longer term data, and absolutely more multidisciplinary collaboration and coordination.
Addressing his fellow panellists, he said: “I think it is important for this group to know that this field is always rapidly evolving. There is an enormous amount of capital in the private sector in biotech that is investing in newer technologies for BPH. To my knowledge there are at least eight novel urethral stents that are in late phase clinical trials, all with urologists—they come to us when they want to run BPH clinical trials. I would ask you to ask yourselves—the PAE technology, is it static, or dynamic? What kind of future relevance does it have, knowing that this field is constantly evolving with new devices?”
Closing the session, Abt, a principal investigator and sub-investigator in various clinical trials on the treatment of LUTS/BPO (including on PAE, TURP, HoLEP, Aquabeam, and PVP) and a guideline panel member for the Germany Society of Urology document on benign prostatic syndrome, summarised the structural and methodological, problems of guidelines in a bid to understand the reasons for the discrepancies between the SIR and AUA recommendations.
“There are widespread financial and professional conflicts of interest among the sponsors of guidelines, so the societies,” he said, “and also among the authors. Industry funds a network of lobbyists, researchers, and opinion leaders, which then write our guidelines. ‘Panel stacking’ is another problem: if a novel panellist is nominated, they are probably nominated because they believe in the same school of thought, so that leads us to imbalanced guideline panels.”
He commented that the most important part, in his view, is that guidelines often have “highly biased panel compositions”—drawing a “very provocative” comparison, he asked rhetorically: “Which institution would you ask to get the most reliable data on gun violence in the USA? The National Rifle Association (NRA), Americans Against Gun Violence, or a more independent source?
“The same is true for the guidelines for PAE. On the one hand, we have a group of persons that are highly interested in a broad application of PAE, as they work for a society that of course has to represent the interests of their members [indicating the SIR multisociety consensus position statement on PAE for the treatment of LUTS]. The same is absolutely true for the AUA guideline panel.
BPH treatment is a billion-dollar business, and here we have panels where at least some of the people involved have substantial conflicts of interest. In my opinion, it is just plausible that both societies reach different conclusions.”
Abt also touched on the lack of “proper, independent peer-review” prior to the publication of most guidelines, and the idea that recommendations are often provided “despite the data [that form the basis of this advice] being judged as unreliable”.
He agreed with the Institute of Medicine suggestion of removing individuals with a financial conflict of interest from guideline panels, and to implement a limitation on the involvement of clinicians with a professional conflict of interest. “Content experts should be consulted, but not write the guidelines,” he concluded. “Instead, we should use independent statisticians and methodologists, patient representatives, and general practitioners that are interested in the field, but do not earn their money from it.” Abt advocated for the inclusion of a guideline panel review and a checklist to score guidelines ahead of publication, to minimise bias.
This advertorial, sponsored by BD, is intended for healthcare professionals in Europe only.
Michael Lichtenberg
“Improving vessel compliance with focused force longitudinal plaque fracture seems to be a promising strategy instead of standard percutaneous transluminal angioplasty [PTA],” states interventional angiologist Michael Lichtenberg (Arnsberg Vascular Center, Arnsberg, Germany), detailing that the technique avoids “significant vessel damage”. In this case report for Vascular News, Lichtenberg evidences this claim, outlining a case involving the recanalisation of a long superficial femoral artery (SFA) occlusion involving lesion preparation with an Ultrascore™ Focused Force PTA Balloon (BD) followed by angioplasty using a Lutonix™ 018 Drug Coated Balloon PTA Catheter (BD).
An 80-year-old man with severe claudication of the right leg was admitted to our vascular centre. Cardiac risk factors included poorly-controlled diabetes, hyperlipoproteinaemia, and smoking. On duplex ultrasound, a long occlusion of the right SFA from the origin to the popliteal artery was diagnosed (Figures 1 and 2). Ankle brachial index (ABI) on the right side was 0.6. No wounds were present on the right extremity.
Subsequent diagnostic angiography confirmed the long SFA occlusion with diminished contrast flow below the knee and into the foot. For recanalisation of the long SFA occlusion, a crossover approach from the left groin was performed using the new Halo One™ Thin-Walled Guiding Sheath (BD) 70cm, 5 French. This sheath provides a 1 French wall thickness, which reduces the size of the arteriotomy compared to standard sheaths of the same French size without sacrificing inner diameter. The flush occlusion of the SFA (Figure 3) was penetrated with a 0.018” Glidewire Advantage (Terumo Interventional Systems). It was easy to achieve distal re-entry into the true lumen. Next, a two-minute lesion preparation was performed with an Ultrascore™ Focused Force PTA Balloon 5x150mm 5 French with repetitive inflation to 8atm over the whole length of the target lesion. This scoring balloon is designed to longitudinally fracture plaque at a lower inflation pressure. Compared to a standard balloon angioplasty, the Ultrascore™ Focused Force PTA Balloon provides approximately 24 times more force where the wire contracts the lesion. This lesion preparation was then followed by two-minute drug-coated balloon (DCB) angioplasty (Lutonix™ 018 Drug Coated Balloon PTA Catheter 5x220mm and 5x120mm; Figure 4). Subsequent angiographic analysis ruled out a persistent dissection or significant recoil.
After revascularisation, a brisk flow was seen within the whole length of the target lesion, as was a straight flow into the foot (Figures 5 and 6). Follow-up examination of the patient the next day showed an ABI of 0.95 on the right side and a significant improvement in pain-free walking distance with no pain in the target limb during a treadmill test after 500m.
Many options for endovascular revascularisation therapy exist today. Most therapeutic approaches involve PTA as the primary therapy, which consists of adventitial stretching, medial necrosis, and controlled dissection or plaque fracture. Acute vessel damage is frequently seen in non-compliant calcified atherosclerotic vessels and may range from simple plaque rupture to severe flow-limiting dissection, or even local perforations. Dissections can induce pathologic haemodynamic defects, and have been implicated as a contributing factor in acute procedural complications as well as restenosis at the target lesion site. Therefore, improving vessel compliance with focused force longitudinal plaque fracture seems to be a promising strategy instead of standard PTA to avoid significant vessel damage, which may lead to long stent implantation. Reassuringly, the results of the SWEDEPAD interim analysis adds further important safety data on drug-coated devices when used to treat femoropopliteal disease.
A new study, published online in The Journal of Vascular Access (JVA), suggests that arteriovenous fistulas (AVFs) contribute to higher survival of haemodialysis patients with COVID-19. Authors Ahmet Murt (Istanbul University-Cerrahpasa, Istanbul, Turkey) and colleagues urge that end-stage renal disease (ESRD) patients “should be given the opportunity to have their vascular access properly created,” even in the pandemic era.
The Kidney Disease Outcomes Quality Initiative (KDOQI) clinical guidelines recommend arteriovenous access instead of central venous catheters for haemodialysis, the authors state. However, the American College of Surgeon’s case triage guideline for COVID-19 deemed AVF or arteriovenous graft (AVG) operations to be elective and suggested that “postponing should be considered”. Against this background, the investigators sought to analyse the effect of vascular access on the outcomes of haemodialysis patients with COVID-19—a group they note are highly clinically vulnerable.
Murt and colleagues retrospectively analysed 104 haemodialysis patients with COVID-19 from two tertiary care hospitals located in Istanbul. Seventy-two of these patients had AVF as the vascular access, with the remaining 32 patients having had tunnelled catheters. They report that COVID-19 had a high mortality rate in haemodialysis patients (36.5%), with AVFs (odds ratio [OR], 3.36; 95% confidence interval [CI], 1.05–10.72; p=0.041) and using medium cut-off dialysers (OR, 7.99; 95% CI, 1.53–41. 65; p=0.014) being related to higher survival.
In the discussion of their findings, the authors note that those patients with an AVF and those with a catheter were similar for age and comorbidities. “In spite of similarity for COVID-19 severity, peak CRP [C-reactive protein] and ferritin levels were higher for patients in whom catheters were used as vascular access,” they relay, noting that such higher levels in the catheter group point to a higher inflammatory response in catheterised patients.
Murt et al believe that delaying AVF operations “might have socioeconomic, medical, and ethical consequences,” stressing that more frequent use of catheters for haemodialysis will results in more catheter-related complications, requiring longer hospitalisations and, in turn, a higher economic burden.
While the authors recognise that the small sample size may be a limitation of the study, they stress that ESRD patients “should not miss proper vascular access opportunities” based on their findings, especially given that “it does not seem that the pandemic will end in the near future”. They conclude: “Balancing the use of resources with patient-centred decisions should be the approach going forward”.
Constantinos Sofocleous (New York, USA) sits down with InterventionalNews to discuss how image-guided thermal ablation, when it is deployed with an intent to cure small colorectal liver metastases, can be fine-tuned so that its outcomes match those achieved by open surgery.
There are several minimum requirements for ablation to be curative, and Sofocleous outlines these as: adequate imaging to see the target tumour well; tools that allow for optimal placement of the electrode; intraprocedural ability to see the ablation zone and the ability to confirm tumour eradication with adequate margins at the end of the procedure.
Sofocleous also discusses the ACCLAIM trial, of which he is the principal investigator with particular reference to the ablation margins (5mm, and ideally 10mm), stating that when margins are adequately ablated, local tumour control is similar, if not better, than wedge resection for small colorectal liver metastases.
The Society of Interventional Oncology aims to use the trial’s findings to raise the bar and demonstrate that with minimum requirements and standards, ablation can be moved to being a standard of care across different global health care systems.
Irreversible electroporation (IRE) is an effective and relatively safe treatment for colorectal liver metastases 5cm or smaller that are deemed unsuitable for partial hepatectomy, thermal ablation, or further systemic therapy, results of the COLDFIRE-2 study, published in Radiology, report. The two-centre, prospective, single-arm, Phase II clinical trial was conducted by Martijn Meijerink, Alette Ruarus (both Cancer Center Amsterdam, Amsterdam UMC, Amsterdam, The Netherlands) and colleagues.
IRE is a non-thermal ablative technique that uses high-voltage electrical pulses, and, according to the study authors, has shown promise for eradicating tumours near critical structures, including blood vessels and bile ducts. This is exactly why it presents an attractive treatment option to many interventionalists: those patients treated in COLDFIRE-2 were all inappropriate candidates for partial hepatectomy or thermal ablation due to the proximity of their tumours to critical structures. Indeed, up to 70% of patients with colorectal liver metastases are not eligible for surgery because of comorbidities or owing to the number, location, or distribution of the metastases.
Meijerink, Ruarus et al explain that, although most current guidelines consider thermal ablation (radiofrequency and microwave; RFA and MWA) to be the standard of care for small, unresectable colorectal liver metastases, its contraindication for tumours close to large hepatic vessels presents an unmet clinical need that can be catered for by IRE.
The COLDFIRE-1 study (Colorectal liver metastases disease: efficacy of irreversible electroporation, a single-arm, Phase 1 clinical trial) first demonstrated IRE’s ability to eradicate colorectal liver metastases in humans. The COLDFIRE-2 triallists write: “The reported efficacy of hepatic IRE varies widely (45.5–100%) because of the heterogeneity of patient and tumour characteristics, and most studies represent small retrospective cohort studies or case reports with short-term follow-up. The early adaptation of electroporation into the toolbox of ablative methods by the European Society for Medical Oncology in 2016 seems premature given the nonexistence of larger-scale prospective controlled efficacy studies.”
Between June 2014 and November 2018, 50 participants, with 76 fluorine 18 (18F) fluorodeoxyglucose (FDG) PET-avid colorectal liver metastases 5cm or smaller between them, underwent percutaneous or open IRE. Follow-up included tumour marker assessment and 18F-FDG PET/CT imaging every three months for the first year after IRE, and every six months thereafter. The median follow-up after the first, second, and third IRE procedures was 23.9 months, 9.5 months, and 6.3 months, respectively.
The study mets its primary endpoint, which mandated that at least 50% of treated participants had to be alive without local tumour progression at 12 months, defined as local tumour progression-free survival. Per-participant one-year local tumour progression-free survival was 68% (95% confidence interval [CI]: 59, 84) according to competing risk analysis.
Outlining why this primary endpoint measure was used, Meijerink, Ruarus and colleagues explain: “Because the participants in this trial were often heavily pre-treated, overall survival would not properly reflect the efficacy of IRE, and therefore one-year local tumour progression-free survival was chosen as the primary end point.”
The authors go on to say that these results “are in line with those of recent retrospective series”, and conclude: “Thus, we believe that IRE should be accepted as a niche indication for difficult-to-reach colorectal liver metastases, but only in the salvage setting of permanent unresectability and unsuitability for thermal ablation.”
Writing in an accompanying editorial in Radiology, S Nahum Goldberg (Hadassah Hebrew University Medical Center, Jerusalem, Israel) claims the COLDFIRE-2 trial “has the potential to provide a substantial impact on the treatment of this malady and on interventional oncology as a whole”.
Speaking of the trial, he says: “This well-designed and superbly executed effort represents a pivotal clinical trial of IRE for the treatment of intrahepatic colorectal metastases unsuitable for partial hepatectomy, thermal ablation, and further systemic treatments. The authors offer hope for achieving successful treatment for a larger population of difficult-to-treat patients—namely those with centrally located tumours and those with tumours between 3 and 5cm in diameter.”
He continues: “Although the populations were relatively small and will require further confirmation, these data suggest that IRE techniques may enable adequate coverage to expand the range of successfully treated tumours. Some of these benefits may be due to synergistic effects between IRE and the chemotherapy administered in a majority of patients. Combination therapy between thermal ablation and induction chemotherapy—administered systemically or by means of chemoembolization—has demonstrated results that can even outperform surgery.
“Further research and collective experience are warranted if we are to achieve the best clinical results possible. […] The final results of COLDFIRE-2 have been long anticipated and are of great interest to interventional, medical, and surgical oncologists and the patients we serve.”
Secondary endpoints: IRE effective, but depends on operator experience
Secondary aims included safety, technical success, local control allowing for repeat procedures, disease-free status, and overall survival.
The per-tumour one-year local tumour progression-free survival rate was 79% (95% CI: 68%, 88%). Median distant progression-free survival was 5.3 months (95% CI: 2.5, 8.1). The most frequent site of first recurrence was the liver; median extrahepatic progression-free survival was 12.5 months (95% CI: 5.9, 19.1). Median overall survival from was 2.7 years (95% CI: 1.6, 3.8) from the first IRE and 4.8 years (95% CI: 3.1, 6.6) from the date of resection of the primary tumour.
The study authors detail that after repeat procedures, local tumour control was achieved in 74% of participants (37 of 50 patients). They expand: “Six participants were considered unsuitable for local repeat treatment at first local tumour progression because of coexisting distant disease progression, making local treatment futile”.
Local control was not achieved in two participants despite multiple attempts to eradicate the tumours. Recurrences were treated with repeat IRE (n=12), thermal ablation (n=three), stereotactic body radiation therapy (n=three), or selective internal radiation therapy (n=one). In a comparison of the first five versus the next 45 participants, the eventual local tumour progression rate was 80% (four of five) versus 33% (15 of 45) (p=0.06).
Meijerink, Ruarus, and colleagues state that, although this did not reach statistical significance in their study, “the local tumour progression rate of 80% versus 33% in the first five versus the next 45 participants strongly suggests that IRE is dependent on operator experience.”
They determine that, in their opinion, this “underlines the necessity to set up dedicated training programmes and preferably claim minimum volume thresholds” for performing IRE.
Cox regression analysis showed no statistically significant difference in local tumour progression-free survival between small and medium-size tumours (hazard ratio, 1.7; p=0.22). Therefore, Meijerink, Ruarus, et al speculate that technique efficacy may be less susceptible to size with IRE, in which tumours are bracketed by the electrodes, compared with single-probe thermal ablation.
The overall complication rate was 40%: 23 participants experienced a total of 34 adverse events in 25 of the 62 procedures. The most common grade 3 adverse events were de novo biliary obstructions (n=3), periprocedural cardiac arrhythmias (n=4), and portal vein thrombosis (n=3). Two participants experienced a grade 4 adverse event. One participant (2%), who an an infected bilioma after IRE, died fewer than 90 days after the procedure—classified as a grade 5 event. “Our higher complication rate can be partially explained by our prospective study design and allowance for simultaneous procedures during IRE. […] Therefore, not all reported adverse events are likely to be related to the IRE procedure itself,” Meijerink, Ruarus, and co-authors write.
Embolx has announced the launch of its balloon occlusion microcatheter, Sniper, to the European market. Sniper is a delivery system for pressure-directed arterial embolisation therapy and is designed to increase embolic loading and improve tumour response.
The device alters blood flow-dynamics by controlling pressure to increase therapeutic agent delivery into target areas for the treatment of tumors, benign prostatic hyperplasia (BPH), and uterine fibroids. Embolx say that the therapy allows interventional radiologist physicians to deliver drugs and embolic agents to targeted treatment areas while protecting surrounding healthy tissues.
Embolx’s second generation Sniper microcatheter is available in Europe in two tip options–straight tip and K-tip and two lengths 130cm and 150cm–enabling interventional radiologist physicians to access both femoral and radial sites and to navigate torturous arterial anatomy.
Michael Allen, president and CEO of Embolx, said: “I am pleased to offer our technology to the European market, which brings with it the experience of over 5,000 cases completed here in the US
“Now, interventional radiologists can do everything they would do with standard microcatheters, but with the added benefits of balloon occlusion. This is a big step forward and provides physicians with the most advanced transarterial delivery system for tumor and prostate treatment.”
Researchers have found that the AMPREDICT decision support tool (DST) demonstrates “strong usability characteristics and clinical relevance” in amputation level decision making for patients with chronic limb-threatening ischaemia (CLTI). Daniel C Norvell (VA Puget Sound Health Care System, Seattle, USA) and colleagues suggest in an online European Journal of Vascular and Endovascular Surgery (EJVES) article that, following “extensive iterative development and testing,” the tool should now be applied in clinical practice.
The authors describe the AMPREDICT DST as “a novel, web-based, clinical DST that calculates individual one-year postoperative risk of death, reamputation, and probability of achieving independent mobility by amputation level”.
They detail that there are currently a lack of individual patient risk factors informing available evidence on amputation level decision making in patients with CLTI, which instead relies on average population risks. As a result, there is “significant variation of amputation levels across health systems, geographical regions, and time,” the authors state.
While prediction models have been published to hone in on individual patient risk factors, translation to clinical application “has not been undertaken,” Norvell et al write—a gap in the literature this study sought to address. Specifically, the investigators aimed to translate the previously validated AMPREDICT prediction models by “developing and testing the usability of the AMPREDICT DST”.
The investigators explain that a mixed-methods approach was applied to assess the AMPREDICT DST. “Previously validated prediction models were translated into a web-based DST with additional content and format developed by an expert panel,” they explain.
Elaborating on their methods, Norvell and colleagues note that ten clinician end users “from diverse specialities, sex, geography, and clinical experience” assessed tool usability while interacting with the tool using a hypothetical case scenario and an example from their practice. The clinicians engaged in a “think aloud” approach so that investigators could go back and review the interactions. After the interaction, each clinician participated in a semi-structured qualitative interview to evaluate the AMPREDICT DST’s look and feel, user friendliness, readability, functionality, and potential implementation changes. In addition, they completed the Post-Study System Usability Questionnaire (PSSUQ)—a 16-item scale with scores ranging from 1–7, with lower scores indicating greater usability.
Writing in EJVES, the authors report that “most providers said they were eager to use the AMPREDICT DST and some requested to use it as soon as possible”. Furthermore, the qualitative interviews suggested the potential utility of the DST included the following: assistance in counselling patients on amputation level decisions, setting outcome expectations, and use as a tool in the academic environment to facilitate understanding of factors that contribute to various outcome risks. The authors also communicate “favourable” overall and subscale PSSUQ scores, with a mean overall total score of 1.57 (standard deviation [SD], 0.69) and a range from 1–3.21.
Norvell et al acknowledge that the AMPREDICT DST has limitations. For example, they recognise that “the risks produced by the tool are generated from models developed in patients undergoing their first major amputation who did not have severe comorbidities (e.g. coma, paraplegia, quadriplegia, disseminated cancer, tumour of the central nervous system, ventilator dependent) that would put them at high risk of death and more likely a candidate for transfemoral amputation only.
Another issue raised is that the models were developed and validated in a US Veteran population with CLTI, comprising mainly males. Therefore, the use of the DST in other populations “should be considered with caution, since the management and risks of patients in VHA [Veteran Health Administration] hospitals may differ from other populations”.
Despite these drawbacks, the authors stress that the tool is set to move into the next phase of development and evaluation with integration into the VHA electronic health record (EHR). This, they state, will allow for assessment of its impact on physician and patient shared amputation level decision making.
Boston Scientific has initiated the European launch of its SpaceOAR Vue Hydrogel, which is designed to create a temporary space between the prostate and the rectum, minimising the potential side effects of radiation therapy.
The new radiopaque SpaceOAR Vue Hydrogel can be seen on computerised tomography (CT) scans, negating the need for physicians to include magnetic resonance imaging (MRI) in the treatment planning, and accommodating patients who are contra-indicated for MRI
According to the World Health Organisation prostate cancer is the most common cancer affecting men in Europe. More than 400,000 new cases are diagnosed each year, and the the European Association of Urology consider radiotherapy a highly effective treatment.
However, due to the close proximity of the rectum to the prostate, prostate radiation therapy can cause unintended damage to the rectum, which can lead to fecal incontinence issues or other long-lasting side effects.
Clive Peedell, consultant clinical oncologist from the South Tees Hospitals NHS Trust (Middlesbrough, UK), said: “SpaceOAR Vue Hydrogel helps to reduce rectal dose in radiation planning, as well as increase clinician confidence in accurate contouring of the prostate and rectum.
“The increased visibility of the gel also helps in the image-guided targeting of the radiotherapy delivery to the prostate, ensuring treatment accuracy and high-quality care for patients.”
The SpaceOAR Vue Hydrogel perirectal spacer offers the same clinical benefits as traditional SpaceOAR Hydrogel, which was the first FDA-cleared and CE Marked hydrogel perirectal spacer, and has been used in over 100,000 patients worldwide, say Boston Scientific.
In a randomised clinical study of SpaceOAR Hydrogel, at median three years, more patients in the control group experienced declines in bowel (41% vs 14%) and urinary (30% vs 17%) quality of life than in the spacer group.
Additionally, more patients who were potent at baseline and treated with SpaceOAR were able to achieve erections sufficient for intercourse (66.7%, vs. 37.5%) than in the control group.
Miguel Aragon, vice president EMEA, urology and pelvic health at Boston Scientific, added: “SpaceOAR Vue Hydrogel demonstrates our commitment to addressing unmet patient and physician needs with innovations that provide the best possible care.
“SpaceOAR Vue Hydrogel’s design may enable physicians to streamline the department’s procedural workflow by reducing the need for post-procedural MRI scan, while reducing radiation exposure for patients undergoing radiation therapy.”
AngioDynamics recently announced that it has received 510(k) clearance from the US Food and Drug Administration (FDA) for the AlphaVac mechanical thrombectomy system.
According to a company press release, AlphaVac is an off-circuit, multipurpose mechanical aspiration thrombectomy device for the non-surgical removal of thrombi or emboli from the vasculature.
AngioDynamics continues to anticipate the commercial release of the AlphaVac system in the second half of calendar year 2021.
Royal Philips recently announced positive two-year results from the TOBA (Tack optimised balloon angioplasty) II below-the-knee (BTK) clinical trial.
The data show the Philips Tack endovascular system (4F), a first-of-its kind dissection repair device, provides a sustained treatment effect and positive impact on quality of life for peripheral arterial disease (PAD) and chronic limb-threatening ischaemia (CLTI) patients at two years. George Adams (Rex Hospital, Chapel Hill, USA), co-principal investigator, presented the findings at the 2021 New Cardiovascular Horizons (NCVH) conference (1–4 June, New Orleans, USA).
Across all patients in the TOBA II BTK clinical trial at two years, 73.6% had freedom from clinically-driven target lesion revascularisation (CD-TLR) and did not require a repeat procedure for the treated artery segment. CD-TLR is a commonly used indicator of treatment efficacy durability. In the more complex CLTI patient population, which is typically associated with high rates of amputation and mortality, the data showed 94.7% target limb salvage (freedom from major amputation).
“The global endovascular community is diligently working to better understand how to restore blood flow in small limb vessels, promote healing and ultimately preserve limbs for people with CLTI, one of the most vulnerable and critical patient populations,” said Adams. “These positive two-year data reiterate the clinical importance of below-the-knee dissection repair and validates the sustained durability of Tack-optimised interventions.”
The two-year TOBA II BTK data also show sustained improvement in patients’ quality of life. In a patient questionnaire that assesses activity, pain, and overall health, patients report having more control of their health and increased improvement in mobility.
The Tack endovascular system is currently available for sale in the USA and some European Union countries. Further information, including safety information, is available here.
SoundBite Medical Solutions recently announced the use of its novel Active Wire 0.014” platform at a first site in the USA in the successful treatment of patients suffering from chronic limb-threatening ischaemia (CLTI) with heavily calcified lower limb chronic total occlusions (CTO).
The Active Wire was used in procedures at the UNC REX Hospital (Raleigh, USA) by George Adams, who commented: “Peripheral arterial disease (PAD) and CLTI in particular are a threat to life and limb. Our early experience with the 0.014” platform of the SoundBite crossing system in eight patients with severely calcified disease shows impressive CTO crossing efficacy coupled with safety and simplicity”.
He continued: “In several cases, crossing and treatment would not have been possible with standard techniques. With an increased demand for devices to aid in treatment algorithms for calcific plaque morphologies, we look forward to building on our experience with the system. The broader introduction of the SoundBite system holds promise to be game-changing in treating calcified CTOs and enabling better treatment outcomes in a difficult-to-treat patient population suffering from PAD and CLTI,” commented Adams.
The SoundBite crossing System—Peripheral (SCS-P) consists of the reusable SoundBite console, a single-use sterile SoundBite Active Wire, and their respective accessories. SCS-P leverages SoundBite’s proprietary method to produce and safely deliver shock waves via guidewire platforms to selectively “micro-jackhammer” through calcified lesions. SCS-P is now approved in major markets with CE mark, US Food and Drug Administration (FDA) 510(k) clearance, and Health Canada approval in both 0.018” and 0.014’’ platforms.
Two of our top stories this month come from the International Symposium on Endovascular Therapy (ISET; 9–11 May, Miami, USA), which returned as an in-person meeting in 2021: the live and online audiences heard a run-down of new tools on the horizon for the treatment of chronic limb-threatening ischaemia (CLTI), and the Auryon atherectomy system showcased at the conference offered “a new look at laser”. A commentary from Gerard S Goh (Melbourne, Australia) and Markus P Schlaich (Perth, Australia) explored the potential of multi-organ denervation, and, in terms of vascular access coverage, readers were offered insight into a new wearable device for AV fistula remote monitoring that shows promise, but is facing commercial challenges. top 10
“I am going to give you reasons to be excited about your critical limb practice,” Peter Schneider (University of California San Francisco, San Francisco, USA) told delegates attending the International Symposium on Endovascular Therapy (ISET; 9–11 May, Miami, USA), in a talk focusing on innovative tools on the horizon for the treatment of chronic limb-threatening ischaemia (CLTI). “I think critical limb ischaemia has come to the forefront of our practices and of community awareness, and finally now the tools are starting to show that,” he opined.
Following a successful proof-of-concept study, Gerard S Goh and Markus P Schlaich have embarked upon a first-in-human study to explore the safety and efficacy of combined renal and common hepatic artery denervation in patients with type 2 diabetes and hypertension. Here, the co-principal investigators describe the rationale behind their single blinded, multi-centre, prospective feasibility study—named the MODUS trial—and explore the “pandemic” of cardiometabolic disease.
A new wearable device designed to remotely monitor arteriovenous (AV) fistulae function in dialysis access patients uncovered promising data leading one set of researchers to conclude the technology offers hope for improved care and lower costs among a challenging patient population.
Additional randomised controlled data regarding the effectiveness of drug-coated balloons (DCBs) in maintaining arteriovenous (AV) access offers new evidence, but it is freighted with uncertainty. However, specific modelling suggests fewer reinterventions could reinforce economic benefits when the IN.PACT AV device (Medtronic) is used, and sirolimus presents new directions, experts say.
The Auryon atherectomy system (AngioDynamics) “represents an exciting new technology”, John Rundback (Advanced Interventional and Vascular Services, LLP, Teaneck, USA) opined at the International Symposium on Endovascular Therapies (ISET; 9–11 May, Miami, USA, and online), speaking on behalf of the Pathfinder I registry investigators. “I think it has really got a lot of traction; we found it a very useful tool across a wide range of plaque morphologies and vessel beds. Further iterations of this platform will hopefully improve its performance further.”
Volumetric assessment of the periablational safety margin can be used as an intraprocedural tool to evaluate local treatment success in patients with colorectal liver metastases referred to stereotactic radiofrequency ablation (SRFA), a recent study in European Radiology concludes. This could replace the visual, side-by-side evaluation of periablational safety margins, the investigators suggest, which is “challenging, even for experienced radiologists”. Authored by Gregor Laimer, Reto Bale (both Medical University Innsbruck, Innsbruck, Austria) and colleagues from Dresden (Germany), Milan (Italy), Jerusalem (Israel), and Boston (USA), the report offers an objective tool that enables the immediate, real-time determination of the extent and percentage of the safety margin requiring ablation, enabling the reliable prediction of procedural outcome success.
Micro Medical Solutions (MMS) announced this month that the US Food and Drug Administration (FDA) has granted breakthrough device designation for its MicroStent vascular stent. This novel technology is designed to achieve and maintain vessel patency, enhance wound treatment, and improve quality of life and blood flow in order to reduce amputation and mortality for patients with chronic limb-threatening ischaemia (CLTI) resulting from peripheral arterial disease (PAD).
A study has found that bifurcated T-stent reconstruction offers a safe and effective treatment option for hepatic venous outflow obstruction (HVOO) with anastomotic stenoses in orthotopic liver transplantation (OLT) recipients.
Transit Scientific recently announced it has received CE mark clearance in the European Union for the XO Score scoring sheath platform to facilitate dilation of stenotic material in the peripheral vasculature including popliteal, infrapopliteal, and native or synthetic arteriovenous dialysis fistulae. top 10 top 10
In setting up an interventional radiology (IR) COVID-19 response plan, “the most important initial step is to recognise the problem,” stated John A Kaufman (Oregon Health & Science University, Portland, USA) at this year’s European Conference on Interventional Oncology (ECIO; 10–13 April, online). Based on the experience of one US institution, the presenter conveyed various crucial factors, stressing in particular the importance of supporting providers, the impact on whom will be “long lasting”.
“Our response to COVID-19 has evolved over time,” Kaufman began, noting an initial “very inward-facing approach”, focusing on personal protective equipment (PPE), workflow, personnel, and case selection. Subsequently, he explained, the plan became more “outward facing”, involving the wider institution and focusing in more detail on issues such as testing, staffing, hospital case-loads, and policies. Provider support ran parallel to these two main stages, he added, an element of the plan designed to address factors such as stress, income loss, and family concerns.
The first step was to recognise the issue, said Kaufman, noting that this was complicated by the US political environment. He exemplified the atmosphere at the time: “Mask-wearing was a political statement rather than a healthcare concern”. What followed was the founding of a cross-establishment professional leadership group, including physicians, nurses, technologists, and managers, he detailed.
During the “inward-facing” phase of the IR response, PPE was a top priority due to limited supply as well as uncertainty regarding what to wear and when. Testing was another important issue at this stage. Initially, testing was very limited and took a long time. Decisions surrounding workflow, including which sites to keep operational, how many dedicated COVID-19 rooms were necessary, and room turnover for COVID-19-positive patients, were all addressed during this stage. Finally, the team recognised the need to organise personnel. All office and support workers began to work remotely, and prover schedules were adapted to minimise exposure, the presenter recounted.
“Case selection became very important,” Kaufman continued, detailing that it was important for the institution to observe state and national rulings, such as the ban of all elective cases in Oregon that was initiated in March 2020. During the early months of the pandemic, operating room (OR) volume dropped by 90%, compared to a 30% drop in IR volume, the presenter reported, attributing this to there being “few truly elective cases” in IR. Meanwhile, emergent cases, as well as all cancer treatment, continued.
The presenter detailed a “silver lining” of this early phase of the pandemic as being the increased availability of anaesthesia resulting from OR closures. In the discussion following Kaufman’s presentation, session moderator Otto van Delden (Amsterdam University Medical Center, Amsterdam, The Netherlands) remarked that, in Europe, the number of IR procedures performed fell “considerably”, and to a level far lower than in the USA, due to a lack of anaesthesia support. Van Delden was keen to know what impact a good supply of anaesthesia had on case load, with Kaufman responding that the team certainly noted that, as well as IR cases, they were also treating patients who would have, in normal circumstances, been treated surgically.
In terms of written guidance, Kaufman relayed that the team created a COVID-19 standard operating procedure manual. This was updated as needed, including all aspects of hospital and clinical operations relating to IR, and was shared on a public website. Other elements of this initial stage included holding weekly IR leadership meetings and the conversion of all clinics to either telephone or virtual appointments, with in-person consults reserved for acutely-ill patients.
In the “outward-facing” phase of the team’s COVID-19 response, involving higher levels within the institution, the first “big issues” were PPE, testing guidelines, and isolation rules, Kaufman communicated. In addition, staffing shortages became a major issue, with reassignments and travel restrictions having an ongoing impact. The availability of staff, as well as of intensive care unit (ICU) beds, determined elective admissions and saw a shift of cases to partner hospitals.
Finally, Kaufman stressed the importance of provider support in a successful IR COVID-19 response plan. There are numerous factors that needed to be addressed, he detailed, noting a fear of infecting family members, problems finding childcare and the demands of home-schooling, reduced incomes, isolation, the loss of friends and family members, working longer hours, and treating sicker patients.
“Faculty and families may need to adjust priorities,” Kaufman commented, noting for example the need to change jobs to be closer to family. Other important ways in which the pandemic has affected providers included reduced caseload for learners, decreased academic productivity—which he noted has disproportionately affected women—and the proliferation of virtual meetings and conferences. “Keep in mind the impact on providers will be long lasting,” he concluded.
A randomised trial—AB-LATE02—will assess the efficacy of a combination of neoadjuvant atezolizumab, and adjuvant atezolizumab and bevacizumab with radiofrequency ablation (RFA) as a treatment option for patients with hepatocellular carcinoma (HCC). According to the principal investigator Boris Guiu (St-Eloi University Hospital, Montpellier, France), the treatment could improve recurrence-free survival (RFS) at two years, and may reduce the risk of distant recurrence, due to the synergistic effects of the treatment strategies. LATE02
Guiu outlined the rationale for the multicentre randomised trial, taking place in 16 centres across France, during a live “Meet the PI” session at the 2021 European Conference on Interventional Oncology (ECIO 2021, 10–13 April, online). During the session, Guiu was questioned by Philippe Pereira (Academic Hospital of Heilbronn, Ruprecht Karl University of Heidelberg, Germany) and Alban Denys (Lausanne University Hospital, Lausanne, Switzerland).
Ablation has become the first curative treatment for HCC, Guiu told attendees to the session, commenting that its use has increased steadily from 2013 to the present day. Discussing published data looking at RFA, however, he identified two problems. Firstly, the incidence of local recurrence, which occurs in between 5–20% of cases, and predominantly relates to the ability to obtain adequate margins around the tumour. “This is probably more of a technical than an oncological problem,” Guiu said.
Furthermore, he noted that intra-hepatic distant recurrence occurs very frequently—in around 60–80% of cases—and the debate is often whether its origin is a metastases or a de novo HCC. Guiu detailed the publication of a recent paper from his centre, which aimed to look at factors that may explain the presence of distant recurrence, including patient, disease, tumour and disease-related factors.
“We only found two factors associated with distant recurrence,” Guiu said, adding that these were alpha-fetoprotein (AFP) and tumour size. “In a way, these factors reflect the aggressiveness of the tumour and are more in line with the concept of metastases, at least during the first two years.” Further data show that de novo HCC are probably more frequent, Guiu noted.
In the case of a distant recurrence, there is a high risk that the patient cannot be treated using a curative approach, Guiu went on to add, meaning that the need to fight against metastatic escape and tumour growth becomes increasingly important. “There is a drift to palliative care, there is a drift to a palliative prognosis, and this is probably the key time where the patient is losing a good prognosis,” he commented. “We have to fight against this incidence of intra-hepatic distant recurrence and this a very important rationale to support the trial.”
A “new challenger” has recently entered the field of advanced HCC, Guiu said, the combination of atezolizumab and bevacizumab, which he commented show “synergistic effects”. The emergence of this treatment creates a strong rationale to combine immunotherapy and ablation, Guiu added.
AB-LATE02 will assess the treatment of small HCC (<3cm). In the standard arm, patients will be ablated using RFA, with follow-up carried out as normal. In the experimental arm, patients will undergo an induction with neoadjuvant atezolizumab, then ablation, and then treatment with the combination of atezolizumab and bevacizumab for one year.
The trial’s primary endpoint is RFS at two years, which Guiu said the study will aim to extend to 65%, compared to 45% seen in current literature. The study will enrol a total of 202 patients, who will be randomised 1:1 to either the experimental or standard treatment arm.
“What is important is that in addition to the primary endpoint we have to look to overall survival at five years, because we have the chance to change the game in these patients based on the results of this trial,” said Guiu.
The trial will also assess quality of life (QoL), which Guiu said will be important to consider, given the frequency of the treatment in the experimental arm. He explained: “We include QoL in this trial because it is very important to see if there is any impairment. In the experimental arm, we not only have ablation, but every three weeks the patient must go to the hospital to get immunotherapy, and this is something we need to look at and see if the balance, even if the trial might be positive, is positive for the patient.”
Finally, a comprehensive translational study is full part of the trial and notably includes immuno-monitoring, circulating tumour DNA (ctDNA) exome analysis, and peripheral blood mononuclear cell (PBMC) based on serial biological and tissue assessments.
At the time of the presentation, Guiu said that enrolment had already begun in three participating centres, and he anticipated that this would be the case in all 16 centres by the end of April 2021. Results are expected from 2025.
Many individuals with kidney failure have been unable to self-isolate during the COVID-19 pandemic because they require dialysis treatments in clinics several times a week. New research that will appear in an upcoming issue of the Clinical Journal of the American Society of Nephrology (CJASN) highlights the risks faced by these patients and the factors involved.
For the study, Ben Caplin (University College London, London, UK) and colleagues, on behalf of the Pan-London COVID-19 Renal Audit Group, examined information on 5,755 patients who received dialysis in 51 clinics in London. Between 2 March and 31 May 2020, a total of 990 (17%) patients tested positive and 465 (8%) were admitted to hospitals with suspected COVID-19.
COVID-19 risks were higher in patients who were older, had diabetes, lived in local communities with higher COVID-19 rates, and received dialysis at dialysis clinics that served a larger number of patients. Risks were lower in patients who received dialysis in clinics with a higher number of available side rooms and that had mask policies for asymptomatic patients. No independent association was seen with sex, ethnicity, or measures of deprivation.
“Taken together, the findings confirm the high rates of symptomatic COVID-19 among patients receiving in-centre dialysis and suggest sources of transmission both within dialysis units and patients’ home communities,” said Caplin. “The work also suggests that, in addition to isolation of confirmed cases, addressing factors that might reduce transmission from patients without suspected or confirmed disease might provide an additional opportunity to further modify the impact of COVID-19 in this population.”
Medical imaging AI specialist Avicenna.AI has received CE mark certification for its CINA ASPECTS AI tool for stroke severity assessment. CINA ASPECTS automatically processes non-contrast computed tomography (CT) scans and calculates an “ASPECT” score in order to assist radiologists within their existing systems and workflow—according to an Avicenna.AI press release.
“CINA ASPECTS supports stroke physicians and radiologists in the assessment and characterisation of early ischaemic brain tissue injury using CT image data,” said Cyril Di Grandi, co-founder and CEO of Avicenna.AI. “This new tool demonstrates our commitment to providing radiologists with AI solutions that can enhance their capabilities. Securing a CE Mark is a key milestone and we are delighted to be able to start offering the benefits of CINA ASPECTS to our European customers. We look forward to FDA clearance in due course.”
ASPECTS (Alberta Stroke Program Early CT Score) is a topographic scoring system used to quantify the severity of a stroke from a CT scan of the brain. It divides the brain territory affected by a stroke into 10 areas of interest, and provides a score between zero and 10, where 10 is normal and zero indicates widespread ischaemic damage throughout the affected area.
CINA ASPECTS computes a heat map indicating the probability of hypodensity and/or sulcal effacement in the brain, and displays a list of infarcted regions. It also provides tilted and resliced CT images to allow easy comparison of the right and left hemisphere. In addition to assisting clinicians to evaluate the ASPECT score from CT scans, CINA ASPECTS also helps improve the reproducibility of the score, which often varies depending on the radiologist reading the scan.
CINA ASPECTS is part of Avicenna.AI’s CINA Head family of AI tools that support the treatment of stroke and neurovascular emergencies. CINA Head also includes FDA-cleared and CE-marked tools for detecting intracranial haemorrhages (ICHs) and large vessel occlusions (LVOs) from CT scans.
Andrew Holden (Auckland, New Zealand) presents the latest results from the IN.PACT™ AV Access trial (Medtronic), which indicate “outstanding” target-lesion primary patency rates of 52.2% through 24 months in dialysis patients with dysfunctional arteriovenous fistulas (AVFs), offering a “highly-significant advantage” over standard balloon angioplasty procedures. These findings were announced in a podium 1st presentation at the Charing Cross (CX) 2021 Digital Edition (19–22 April, online).
Holden, who is director of interventional radiology at Auckland Regional Public Health Service and the trial’s presenting author, stated that the IN.PACT™ AV drug-coated balloon (DCB) met its primary safety and effectiveness endpoints after 24 months—including demonstrating “absolutely no difference” in all-cause mortality rates between the trial’s DCB and standard percutaneous transluminal angioplasty (PTA) arms.
Presenting the longer-term patency results through 24 months, Holden said it was “very pleasing to see” a flattening of the Kaplan-Meier curves in both the DCB and standard PTA arms of the trial—as well as a target-lesion patency rate of 52.2% in the DCB group. He added that a “highly-significant advantage” was observed compared to the PTA group, which demonstrated a patency rate of 36.2% through 24 months.
Following a successful proof-of-concept study, Gerard S Goh and Markus P Schlaich have embarked upon a first-in-human study to explore the safety and efficacy of combined renal and common hepatic artery denervation in patients with type 2 diabetes and hypertension. Here, the co-principal investigators describe the rationale behind their single blinded, multi-centre, prospective feasibility study—named the MODUS trial—and explore the “pandemic” of cardiometabolic disease.
Cardiometabolic disease has evolved into a pandemic, resulting in substantial loss in quality of life and enormous economic burden on healthcare systems world-wide. Cardiovascular and metabolic regulation is governed by neural signaling from the sympathetic nervous system in critical organs including the heart, kidneys, liver, pancreas, skeletal muscle, and adipose tissue. Increased sympathetic activation is a hallmark of cardiometabolic disease and has been demonstrated in obesity, metabolic syndrome, type 2 diabetes, hypertension, heart failure, chronic kidney disease, and many other relevant conditions. Insulin resistance, non-alcoholic fatty liver disease (NAFLD), and a systemic pro-inflammatory state are key mediators of the adverse consequences associated with cardiometabolic disease. A self-perpetuating cycle develops where sympathetic overdrive contributes to insulin resistance and subclinical inflammation, which in turn maintain increased sympathetic signaling.
Direct therapeutic targeting of the sympathetic nervous system therefore appears as a rational approach to improve both cardiovascular and metabolic control. Indeed, catheter-based renal denervation using either radiofrequency energy or therapeutic ultrasound has now been shown in four sham-controlled trials to be safe and to effectively lower ambulatory blood pressure in patients both treated and untreated with antihypertensive medications (SPYRAL OFF-MED, SPYRAL ON-MED, RADIANCE-HTN SOLO, RADIANCE-HTN TRIO). Additional salutary effects on glucose metabolism have been reported in some renal denervation studies, suggesting that the beneficial effects of selectively targeting the sympathetic nerves may not be limited to the management of cardiovascular disorders, but may also help to restore metabolic homeostasis. This approach would perhaps be most effective if the sympathetic drive to metabolically-active organs such as the liver (gluconeogenesis), pancreas (insulin release), and duodenum could be inhibited directly.
Common hepatic artery denervation. A guide sheath is seen in the the coeliac axis. The balloon catheter is in the common hepatic artery (see 2 radio-opaque markers). Image courtesy of Gerard Goh.
A recent preclinical proof-of-concept study in a porcine model where percutaneous denervation in both renal arteries and the common hepatic artery (CHA) was performed with the iRF Denervation System demonstrated that denervation of both the kidneys and the liver could safely be achieved with reductions in tissue norepinephrine concentration when compared to control animals of 78% and 88% (p<0.001 for both), respectively. Pancreatic and duodenal norepinephrine concentration was also reduced significantly.
Consequently, a first-in-human study has recently been initiated to explore the safety and efficacy of combined renal and common hepatic artery denervation in patients with type 2 diabetes and hypertension.
Renal denervation. Image courtesy of Gerard Goh.
The MODUS trial (Multi-organ denervation to reduce sympathetic drive, a single blinded, multi-centre, prospective feasibility study) is a multicentre randomised trial that is examining the effects of hepatic and/or renal denervation in patients with hypertension, diabetes, and metabolic syndrome. Patients on one or two antihypertensive and oral anti-diabetic drugs within certain BP and HbA1c ranges undergo a ‘wash-out’ phase of four weeks with regular BP and glucose monitoring before receiving a single session denervation therapy. The trial utilises the iRF denervation system (Metavention), which is a radiofrequency balloon-based catheter with internal cooling where the catheter is inserted into the renal and/or common hepatic arteries and denervation performed. Centres in Perth, Melbourne, and Sydney (Australia) are participating in the trial, and the first two patients were recently enrolled at the Alfred Hospital, Melbourne, treated by Gerard Goh and Warren Clements.
Gerard S Goh is head of Interventional Radiology at The Alfred Hospital, Melbourne Australia, and is adjunct associate professor in the department of Surgery at the Monash University, Melbourne, Australia. He is also president of the Interventional Radiology Society of Australasia (IRSA).
Markus P Schlaich is the Dobney chair in Clinical Research and a nephrologist and hypertension specialist at the School of Medicine—Royal Perth Hospital Unit and the University of Western Australia, Perth, Australia.
Disclosures: Gerard S Goh and Markus P Schlaich are co-principal investigators of the MODUS trial, and as such receive research funding from Metavention.
Koya Medical announced today that it has received US Food and Drug Administration (FDA) 510(k) clearance for its active compression therapy system Dayspring for the treatment of lymphoedema and venous diseases that impact lymphatic flow in the lower extremities. The company also announced the appointments of three veteran executives to its leadership team to support commercialisation.
Patients treated with Dayspring receive standard of care active compression therapy with a mobility-enabling wearable device. The system includes a low-profile active garment made of soft, breathable mesh using Koya’s proprietary Flexframe technology; a rechargeable, hand-held controller that can be worn on a lanyard; and a mobile app that allows users or their clinicians to programme custom treatment options. Koya previously received FDA clearance for Dayspring for the upper extremities in June 2020.
Koya Medical also announced the appointments of additional executive leaders to propel commercialisation plans. As head of sales, Rick Biro will be responsible for building and executing Koya’s go-to-market sales strategy. He joins Koya after serving as area sales director, Central USA at PolarityTE where he was part of the commercial leadership team during the company’s most expansive growth period. Prior to joining PolarityTE, Biro spent more than 15 years in the lymphoedema and wound care space where he held a number of leadership positions with Wright Therapy Products, BSN Medical, and Galaxy Medical Products.
As head of market access and clinical affairs, Liesl Oldstone will work to articulate the clinical value of the company’s highly differentiated product and minimise barriers for patients to access. Her leadership in market access, health economics, and reimbursement has spanned more than two decades in both pharma and the medical device industry for industry-leading companies including ResMed, Bristol-Myers Squibb, Covidien (now Medtronic), Cordis (formerly J&J), and Eli Lilly & Company.
Damian Rippole will join as CFO, and brings more than 20 years of financial leadership experience in both private and public medical technology companies. Rippole was most recently CFO at Ebb Therapeutics (acquired in a private transaction funded by leading global investment firm KKR), maker of an innovative FDA-cleared device for treating insomnia. Prior to that, Rippole was corporate controller for Respironics, a global leader in the sleep and respiratory markets that was acquired by Philips for US$5 billion in 2008. Following the acquisition, Rippole led the global finance integration of Respironics into Philips and served as the group controller for Philips Home Healthcare Solutions business.
Exactly 20 years on from his first stereotactic radiofrequency ablation (SRFA) procedure to treat a cancerous liver tumour, Reto Bale (Medical University Innsbruck, Innsbruck, Austria) speaks to Interventional News about the future of this procedure, and warns interventionalists that this may be the next arena for a potential turf struggle: interventional radiologists should start learning now, he urges, as, in his view, “90% of current liver resections could be replaced by SRFA”. At Bale’s institution, proceduralists are able to use up to 36 coaxial needles to ablate tumours, achieving results that rival those of their surgical counterparts, leaving no residual mass behind.
When did you first start using this approach?
The story begins in 1994, when I was using navigation systems in ENT and neurosurgery. Back then, as a student, I developed a few things together with my student fellow Michael Vogele: We had a patent for a navigation device and a head fixation device, amongst other technologies. In 1995 I developed the first aiming device initially for neurosurgical work. I wanted to expand beyond neurosurgery, because I wanted to use navigation not just in the brain, but everywhere. That was why I moved to interventional radiology (IR), and in 1996, as an assistant doctor, I set up the SIP—the Stereotactic Interventional Planning lab in Innsbruck, Austria.
I think stereotaxy is the ideal tool for radiofrequency ablation (RFA). The problem is that there is often a discrepancy between the tumour volume and the ablation volume. This is the reason for recurrence. The simple solution to this is to use multiple coaxial needles. However, although the idea is simple, it is difficult to place multiple coaxial needles in order to ablate the entire tumour volume with conventional ultrasound (US) and computed tomography (CT) guidance. This is why, in my opinion, using stereotaxy is the way to go.
We did the first procedure in the liver in May 2001. I am sure that the way we do radiofrequency ablations has to change—I have always been sure, but when we started this everyone said ‘Oh that crazy Austrian, advancing 10 needles into the body!’ But now, 20 years later, people have changed their minds.
What value does stereotaxy add to radiofrequency ablation?
SRFA helps you not only to guide the needles and visualise placement, but to plan the procedure as well. In most cases, you need multiple overlapping zones in order to ablate the complete volume. Even with microwave ablation (MWA), the maximum short ablation diameter is approximately 3.6cm. So, if a lesion is larger than 2–3cm, it is very difficult to achieve an adequate ablation margin; you need overlapping ablation zones.
How do results from SRFA compare with surgical outcomes?
It [SRFA] is actually better than surgery!
From our results, it is at least as good as surgery in terms of local control rates, and it is dramatically less invasive, of course, and parenchyma-sparing. There is no doubt in my mind: if you can ablate the lesion completely, why would you do a resection? No patient would like you to open them up if there was a less invasive option with comparable outcomes.
In 2019, myself and several colleagues published a retrospective study in Hepatology that evaluated the efficacy of three-dimensional (3D)-navigated, multiprobe radiofrequency ablation (SRFA) with intraprocedural image fusion for the treatment of hepatocellular carcinoma (HCC) by histopathological examination.
From 2009 to 2018, 97 patients were transplanted after bridging therapy of 195 HCCs by SRFA. The rate of residual vital tissue could be assessed in 188 of 195 lesions in 96 of 97 patients by histological examination of the explanted livers using haematoxylin and eosin (H&E) and Tdt-mediated UTP nick-end labeling (TUNEL) stains. Histopathological results were compared with the findings of the last CT imaging before liver transplantation. Complete radiological response was achieved in 186 of 188 nodules (98.9%) and 94 of 96 patients (97.9%), and complete pathological response in the explanted liver specimen in 183 of 188 nodules (97.3%) and 91 of 96 patients (94.8%), respectively. In lesions ≥3cm, complete tumour cell death was achieved in 50 of 52 nodules (96.2%). Residual tumour did not correlate with tumour size (p=0.5).
We therefore concluded that multiprobe SRFA with intraprocedural image fusion represents an efficient, minimally invasive therapy for HCC, even with tumour sizes larger than 3cm, and without the need of a combination with additional treatments. For us, the results justify the additional efforts related to the stereotactic approach.
A very interesting thing about SRFA is that image fusion is part of the procedure. Image fusion is now—now [Bale’s stress]—a key issue. We have been doing this for 20 years.
What developments would you like to see in image fusion?
Firstly, we use image fusion to check the accuracy of needle placement. We do two CT scans: a planning CT, before we place any needles, and a control CT, which is taken with the needles in place. This native dataset is then superimposed onto the planning CT, and onto the virtual pathways we planned. Thereby, we can measure the accuracy of every needle.
The second step is the verification of the ablation zone—we want to know if there is a sufficient ablation margin covering the tumour. This is extremely important, and very helpful. It is better than the pathological report the surgeons receive, for example. One week following surgery, they get a pathology report telling them if they have achieved R0 or R1, whereas we see this immediately, while the patient is still under anaesthesia, and we see it in three dimensions, not only in a two- dimensional rendering. In most cases it is not possible for the pathologists to look at the whole margin under the microscope, it would take far too long! So, they just take a representative specimen. But when we use image fusion, it is a 3D tool, so we can assess the margin in all dimensions.
This allows us to be adaptive intraprocedurally. If we do not achieve the ablation zone, and we have some residual tumour, we can put another needle into the patient.
In our tumour board meetings, the first question used to be “Is it resectable?” Now the first question is – in most cases – “Is it ablate-able?” But this is only at Innsbruck! I hope it will change around the world—this is just the start for SRFA.
What are the barriers to this being adopted at other institutions?
Getting the word out! Our problem is that we do not get refunds for the additional effort. Our department gets money for the ablation probes, like you would need for an US- or CT-guided intervention, which is completely different from SRFA. We need support from insurance companies, and they will only finance this if there are enough data. Currently, we only have data [on SRFA’s safety, efficacy and long-term outcome] from our institution.
We have a prospective database. It includes more than 1000 SRFA patients with more than 4000 tumors treated by SRFA over the last 20 years. It is linked to the hospital’s record of patient files, so it is hard data that is very transparent and auditable. All of our replications are based on this registry.
However, in order to support reimbursement for SRFA, insurance companies need to see prospective, randomised data—my next aim is therefore to conduct a multicentre, prospective, randomised controlled study to obtain these data and hopefully to get reimbursement for the procedure.
What would your advice be for interventional radiologists wishing to do SRFA at their own centres?
Get in touch! I would be happy to assist them to set up a programme. I have done it in Innsbruck, and it works very well, so I would be delighted to assist. It is hard work at the beginning, organising the system and teaching everyone the technical details, but I think it is necessary that more interventional radiologists have this training.
The good thing is that, though it was initially challenging, now we have so much experience. We have many standards of practice; it is much easier to train someone to do SRFA than it is to perform liver surgery, for example. I have a colleague who has completed just three months training, and then he did a procedure completely alone, with great results. My other colleague has been training with me for a year, and he performs extremely complicated procedures that no one else does in the world, outside of Innsbruck.
A very important point: you can do a lot of training without even touching a patient, because we have such extensive datasets, with information (such as CT images) available. So you can train if you want on more than thousand patients before you start with real patients! That is really cool, because the path planning is the most difficult part. It is quite easy to use the navigation system to place a needle; I will turn you into an expert in two weeks, with that, as long as you have some experience with ablation already. But it is difficult to make the path plan; this can be learned in the virtual dataset. My aim is therefore to teach interventionalists with these datasets; I think we could make something big happen here.
It is extremely important that interventional radiologists start now, before it is too late, because I know that otherwise the surgeons will start performing SRFA themselves. In my view, 90% of current liver resections could be replaced by SRFA. If it is possible to completely ablate the tumour and leave no residual mass behind, then there is no argument for a more invasive procedure.
What does the future look like for SRFA?
My hope is that it will become a lot more common practice at several institutions around the world. In addition, at Innsbruck, we aim to make the preprocedural path-planning process at least semi-automatic, through the use of machine learning. We have just recently secured funding for a PhD candidate to get started on this work, so it will be exciting to see what they can achieve.
Histotripsy, which was invented at the University of Michigan, uses pulsed sound waves to destroy tissue. It is a non-invasive and non-thermal mechanism that is currently being studied for its “completely different mechanism for ablating tissue, which […] we will be able to leverage to our advantage in treating cancer”, says Fred T Lee (Madison, USA).Lee, a professor (tenure) of Radiology, Biomedical Engineering, and Urology, The Robert A Turrell Professor of Imaging Science, and the chief of Abdominal Intervention at the University of Wisconsin, asserts that histotripsy could overcome some of the limitations of thermal ablation. More evidence is needed and there is a “still a lot of work to be done”, Lee cautions, while suggesting that in the future, histotripsy could be used as an immune primer in conjunction with checkpoint inhibitors. It might, therefore, be useful in treating patients with very advanced tumours or multiple tumours that “we ordinarily would not be able to treat with ablation”, he says.
The European Union (EU) Medical Devices Regulation (MDR) takes effect from today (26 May 2021).
The Regulation revises quality and safety standards and the range of regulated devices and was first initiated in May 2017, with an initial three-year transition period applied. Implementation was delayed by 12 months due to the COVID-19 pandemic.
According to the European Commission there are over 500,000 types of medical devices and in vitro diagnostic medical devices (IVDs) on the EU market. These have a “fundamental role in saving lives by providing innovative healthcare solutions for the diagnosis, prevention, monitoring, prediction, prognosis, treatment, or alleviation of disease” according to information on the Commission’s website. Separate regulations governing IVDs come into effect in May 2022.
According to the Commission, the new regulations create a “robust, transparent, and sustainable” regulatory framework, that will improve clinical safety and create fair market access conditions for manufacturers.
The new regulations maintain the current grouping of devices into four classes—Class I, IIa, IIb, and III—although certain devices are reclassified and have a wider scope.
The Regulation also clarifies the respective obligations of manufacturers, authorised representatives, importers and distributors, with manufacturers required to put systems in place for risk and quality management, to conduct clinical or performance evaluations, and to draw up technical documentation and keep this up to date. Further to this, the Regulation also requires manufacturers to implement post-market surveillance follow-up plans.
Volumetric assessment of the periablational safety margin can be used as an intraprocedural tool to evaluate local treatment success in patients with colorectal liver metastases referred to stereotactic radiofrequency ablation (SRFA), a recent study in European Radiology concludes. This could replace the visual, side-by-side evaluation of periablational safety margins, the investigators suggest, which is “challenging, even for experienced radiologists”. Authored by Gregor Laimer, Reto Bale (both Medical University Innsbruck, Innsbruck, Austria) and colleagues from Dresden (Germany), Milan (Italy), Jerusalem (Israel), and Boston (USA), the report offers an objective tool that enables the immediate, real-time determination of the extent and percentage of the safety margin requiring ablation, enabling the reliable prediction of procedural outcome success.
“Ablations with [a] 100% three-dimensional (3D) periablational safety margin of 3mm and ablations with at least [a] 90% 3D safety margin of 6mm can be considered indications of treatment success,” the study authors report. They further conclude that their results indicate image fusion of pre- and post-interventional computed tomography (CT) scans with the Ablation-fit software is feasible, and “could represent a useful tool in daily clinical practice”.
SRFA takes a multiple-needle approach, utilising 3D treatment planning, stereotactic needle placement, and image fusion for the intraoperative assessment of the periablational safety margin. According to Laimer, Bale et al, in some centres, this technique can overcome the limitations associated with standard radiofrequency ablation (RFA).
They write: “Several studies have reported that the periablational safety margin, defined as the shortest distance between tumour border and margin of the necrosis zone, independently predicts the local tumour progression in colorectal liver metastases, whereby ablations with safety margins >5–10mm exhibit lower local tumour progression rates [a better outcome]. In conventional CT or ultrasound-guided RFA, the creation of large necrosis zones extending 5–10 mm beyond tumour borders is often hampered by technical limitations, especially for larger tumors (i.e. >3cm), which may result in local tumour progression ranging from 4–70%. In contrast, these limitations have been overcome in some centres with stereotactic thermal ablation.”
In total, 45 patients with 76 colorectal liver metastases between them were treated with SRFA and analysed in this study. During image fusion of pre- and post-interventional contrast-enhanced CT scans, Laimer, Bale et al used a software with non-rigid registration (called Ablation-fit) to assess the percentage of predetermined periablational 3D safety margin and colorectal liver metastases successfully ablated (i.e. with no evidence of residual tumour tissue).
Periablational safety zones (1–10mm) and percentage of the periablational zone ablated were calculated, analysed, and compared with subsequent tumour growth to determine an optimal safety margin predictive of local treatment success.
Presenting their results, Laimer, Bale, and colleagues relayed that the mean overall follow-up was 36.1±18.5 months. Nine of 76 colorectal liver metastases (11.8%) developed local tumour progression; the mean time to local tumour progression was 18.3±11.9 months. Overall one-, two-, and three-year cumulative local tumour progression-free survival rates were 98.7%, 90.6%, and 88.6%, respectively. The periablational safety margin assessment proved to be the only independent predictor (p<0.001) of local tumour progression for all calculated safety margins. The smallest safety margin that was 100% ablated and that displayed no local tumour progression was 3mm, and at least 90% of a 6mm, circumscribed 3D safety margin was required to achieve complete ablation.
“With this work, we confirm prior reports demonstrating the importance of achieving a periablational margin for ablation, as we too established the periablational safety margin as the only significant predictor of local tumour progression in patients with colorectal liver metastases treated with SRFA,” the study investigators write in their discussion. “Apart from the periablational safety margin, no other conventional risk factor such as age, gender, tumour size, tumour location, or previous therapies significantly influenced local tumour progression. Importantly, this observation held true for all calculated 3D safety margins, namely, 1–10mm. Yet, in our study, the smallest safety margin displaying no local tumour progression for ablations with 100% circumscribed 3D safety margin was 3mm (0/55 [0%] target tumours).
“This indicates that an ablation with a 100% circumscribed 3D safety margin of 3mm can be considered successful at the time of the intervention. Given that larger volumes of ablation are more difficult to achieve, this may represent an improvement when considering that previous studies recommend a periablational safety margin of at least 5mm, with better results only seen with a 10mm periablational safety margin for colorectal liver metastases. One possible explanation for this discrepancy might be the exact image fusion and volumetric safety margin assessment achieved with the non-rigid registration software used for this study. Regardless, the small but precise margins in our study may actually represent larger volumes given known tissue shrinkage during ablation.”
Speaking to this newspaper, Bale adds: “Another explanation for this discrepancy may be related to the fact that deformation of the datasets for image fusion during stereotactic thermal ablation (intraprocedural arterial and portal venous phase planning and control CTs) is mimimised by respiratory triggering. This is achieved by temporary disconnection of the endotracheal tube and full muscle relaxation.”
Noting that this study is retrospective in design and is reliant on the experience of a single centre, and also that there is “scarce use of stereotactic approaches in the ablation of liver malignancies” outside of the Medical University in Innsbruck, Laimer, Bale, et al hope that their work aids in generating further interest in this technique.
Transit Scientific’s XO Score device inflated with a standard 4×40 PTA balloon
Transit Scientific today announced that its XO Score scoring sheath platform has been named a winner in the 2021 Medical Design Excellence Awards (MDEA). The MDEA is a premier design competition in the medtech industry, recognising significant achievements in medical product design and engineering that improve the quality of healthcare delivery and accessibility.
“We are honoured that our XO Score platform has been recognised by the MDEA organisation,” said Greg Method, president of Transit Scientific. “We designed XO Score as a novel way to expand angioplasty-based tools available to physicians for treatment of peripheral arterial disease (PAD), chronic limb-threatening ischaemia (CLTI), and end-stage renal disease (ESRD). The award is a testament to the dedication and hard work of the team at Transit Scientific and reflects our commitment to bringing new technologies to market for the advancement of patient care.”
XO Score is a novel scoring sheath that works by fitting over physician selected off-the-shelf percutaneous transluminal angioplasty (PTA) balloons to enable scoring and cutting vessel preparation. The unique balloon-expandable scoring element enables a single XO Score device to work with a large range of balloon diameters and lengths for in-procedure adaptability. XO Score has been used successfully to dilate calcified and fibrous lesions during a multisite, multiuser limited market release.
“XO Score’s proprietary rotating strut design ensures the device remains low profile for tracking to and from the treatment site”, continued Method. “The ability to engage the wall and dilate at a low inflation pressure has yielded great outcomes in a broad range of PTA-resistant lesions.”
The device is currently indicated for treatment of peripheral vascular stenosis including haemodialysis fistulas and grafts.
Concept Medical has released a series of status updates on their head-to-head SIRONA (Sirolimus versus paclitaxel drug-eluting balloon angioplasty in femoropopliteal diseases) randomised controlled trial (RCT).
SIRONA is an investigator-initiated and -driven, prospective, multicentre, corelab-adjudicated trial involving peripheral arterial disease (PAD) patients with Rutherford classification 2–4. The study will enrol a total of 478 patients randomised 1:1 (MagicTouch PTA, Concept Medical: paclitaxel-coated balloon) across 30 sites in Germany and Austria. Led by Ulf Teichgräber (Jena University Hospital, Germany), a press release states that the study is moving “rapidly,” with 20 patients already enrolled.
According to a press release, SIRONA is the world’s first RCT investigating the use of a sirolimus drug-coated balloon (DCB) versus a paclitaxel DCB for the treatment of femoropopliteal artery disease.
The primary objective of the SIRONA trial is to determine the safety and efficacy of sirolimus-coated balloon application in the superficial femoral artery (SFA). The primary endpoint of patency at 12 months has been defined as absence of target lesion revascularisation [TLR] or restenosis and the primary safety endpoint determined as composite of freedom from device- or procedure-related death at 12 months as well as major target limb amputation.
The trial will include all patients with a disease in the SFA segment (either de novo or restenotic) falling under Rutherford class 2–4 and suffering from intermittent claudication to chronic limb-threatening ischaemia (CLTI).
Teichgräber communicates his optimism regarding the trial: “I believe that SIRONA will be a game changer trial by giving new evidence on how to perform PTA [percutaneous transluminal angioplasty] following the principle of nothing leaving behind.”
The US Food and Drug Administration (FDA) have granted breakthrough device designation for the Emprint ablation catheter kit (Medtronic). This is an investigational device not yet approved or cleared in the USA.
The catheter is intended to be used in conjunction with the Emprint microwave generator and lung navigation platform (also Medtronic) to provide a minimally invasive, localised treatment of malignant lesions in the lung, and it can be used together with standard-of-care therapy when indicated.
The FDA breakthrough device programme is intended to help patients receive more timely access to breakthrough technologies that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions. Under the programme, the FDA will provide Medtronic with priority review and interactive communication regarding clinical trial designs through to commercialisation decisions, a press release details.
Current clinical guidelines for the management of malignant lung lesions support a multimodal approach, which may include surgery, radiotherapy, and/or systemic drug therapy, depending on the tumour stage. Because patients with lung malignancies have been shown to have survival benefit from a combination of systemic and local therapy, less invasive local treatment modalities such as the Emprint ablation catheter kit have been developed.Using an endoluminal approach, the Emprint ablation catheter kit will be studied with Medtronic’s lung navigation system to allow for the delivery of microwave energy to the targeted lung lesion(s). Clinical guidelines recommend incorporating local therapies such as thermal ablation, in combination with systemic therapies when suitable.
Though not yet available in the USA, the Emprint ablation catheter kit is CE Marked and the NAVABLATE study completed enrollment of 30 patients in Europe and Hong Kong in 2020.
“This new technology has allowed me to personalise treatment of lung lesions for each patient, particularly lesions that may be challenging to manage,” says Kelvin Lau, a consultant thoracic surgeon at St Bartholomew’s Hospital, London, UK, and principal investigator for the NAVABLATE study.
The Medtronic lung navigation platform enables precise and accurate placement of the ablation catheter within the target lesion, which is critical for the success of this minimally invasive procedure.With 15 years of experience, the navigation platform has been used in more than 200,000 lung procedures.
“At Medtronic, we strive to transform outcomes by taking bold actions to ensure that patients with tumours in the lung receive care sooner, less invasively, and more effectively,” comments Emily Elswick, vice president and general manager, Lung Health and Visualisation, within the Surgical Innovations business, which is part of the Medical Surgical Portfolio at Medtronic. “Breakthrough designation from the FDA is just the first-step in realising our broader commitment to providing less invasive treatment options to patients with lung disease.”
Additional randomised controlled data regarding the effectiveness of drug-coated balloons (DCBs) in maintaining arteriovenous (AV) access offers new evidence, but it is freighted with uncertainty. However, specific modelling suggests fewer reinterventions could reinforce economic benefits when the IN.PACT AV device (Medtronic) is used, and sirolimus presents new directions, experts say.
“DCBs for the prevention of restenosis in haemodialysis fistulas have now undergone rigorous evaluation, arguably more than any other AV access intervention apart from stent grafts for venous stenosis,” write Scott Trerotola (University of Pennsylvania, Philadelphia, USA), Prabir Roy-Chaudhury (University of North Carolina Kidney Center, Salisbury, USA) and Theodore Saad (Christiana Care Health System, Newark, USA) in a May 8 editorial published online in the American Journal of Kidney Diseases (AJKD). They elaborate that it is “perplexing and disappointing” to see conflicting results from a host of DCB studies with similar designs—leading to their claim that more data in this space has not equalled more clarity.
Trerotola, Roy-Chaudury and Saad’s editorial follows in the wake of Yanqi Yin (Peking University First Hospital, Beijing, China) and colleagues’ publication in the same journal in January this year of a multicentre randomised controlled trial evaluating the efficacy and safety of DCBs in preventing fistula restenosis in Chinese haemodialysis patients. The triallists report that, compared to conventional high-pressure balloon angioplasty, DCB treatment achieved superior primary patency defined using ultrasound-measured peak systolic velocity ratio (PSVR) at six months, and superior intervention-free survival of both the target lesion and the target shunt at 12 months, without evidence of greater adverse events.
Importantly, Trerotola and colleagues clarify that the compound, unvalidated endpoint incorporating a “peculiar” patency measure used in this trial confounds the interpretation of the results, as do the procedural differences across the two groups, with both of these factors detracting from the positive results of the study.
These results (obtained with Cardionovum’s Aperto OTW DCB; 3μg/mm2 paclitaxel dose) sit amidst two other previously reported large pivotal trials, the Lutonix AV trial that came within striking distance of achieving its primary endpoint (with BD’s Lutonix AV DCB; 2μg/mm2 paclitaxel dose), and the IN.PACT AV Access trial (with Medtronic’s IN.PACT AV DCB; 3.5 μg/mm2 paclitaxel dose), which was the only trial to successfully do so. A third, as-yet unpublished trial, PAVE, which also used the Lutonix AV DCB, did not demonstrate a benefit to using the antiproliferative. With this conflicting evidence of efficacy, the usual suspects of drug dose, excipient, patient, procedure, fistula and lesion specifics come into the foreground to understand discrepancies in outcome, although Trerotola and colleagues use the Chinese trial results to suggest discounting dose, but not excipient, differences.
But, if the efficacy outcomes of DCBs are mined from the IN.PACT AV Access trial data alone and modelled to demonstrate economic benefit, there are savings gains for systems to be had, investigators maintain.
Robert Lookstein (Mount Sinai, New York, USA), first author of the six-month IN.PACT AV Access trial results, published in the New England Journal of Medicine and showing that DCB angioplasty was superior to standard angioplasty for the treatment of stenotic lesions in dysfunctional haemodialysis AV fistulas, has previously outlined that using the IN.PACT AV DCB can confer economic advantages to healthcare systems.
Lookstein and colleagues used 12-month reintervention rate data from the IN.PACT AV Access pivotal trial within a Budget Impact Model of the US and German healthcare systems to demonstrate cost savings almost immediately. “As those savings were projected out [from 12 months] to 36 months, each individual patient projected out a saving of over €3,000 in the German economic model and over US$3,300 in the US healthcare system”, he stated, elaborating that these numbers—when applied in conservative modelling to the entire end-stage renal disease population in both systems—would demand a lot of attention from payers.
Economic benefits to patients and health systems with DCB use accrue over time
Presenting on the economic outcomes of DCBs in AV access at two years in the US healthcare system, professor of radiology Sanjay Misra (Mayo Clinic, Rochester, USA) reported gains over time for DCB compared to standard balloon angioplasty. The IN.PACT AV access trial one-year results underpinned the calculations used in the analysis with two approaches being used: a primary analysis involving index and reintervention-based costs, and a secondary analysis for comprehensive vascular access costs. The results from the primary analysis showed meaningful reductions in projected reintervention costs. If the DCB cost is US$1,800 or less, the strategy would break even at the two-year mark, and achieve savings of US$1,400 at the three-year horizon, said Misra, noting that “as time goes by, savings become larger.” Even earlier cost neutrality and slightly higher savings at the two-and-a-half-year mark were achieved using the secondary analysis. At a healthcare system level, Misra proposed that Medicare savings to the tune of US$160–250 million could be made at one year, growing to more than US$420 million at three years if half of the 233,000 annual procedures of standard angioplasty were converted to DCB use instead.
Sanjay Misra
Misra said: “Using two independent calculation approaches, treatment with the IN.PACT AV DCB can be expected to lead to substantive per patient and health system savings.” Further, these savings vary by site of service, with the greatest savings being obtained in the in-hospital setting, he noted.
Misra’s recent research has focused on the use of stem cells to aid AV fistula maturation and prevention of venous stenosis. He attributed the patient gains with the use of DCBs to the reductions in reinterventions, which can help reduce patient morbidity and help improve quality of life, but cautioned that these findings were based specifically on data from the IN.PACT AV Access trial and may not apply to other DCB devices.
These data led session moderator Nicholas Inston (Queen Elizabeth Hospital Birmingham, Birmingham, UK) to ask whether DCBs should be rationed and reserved to maintain access in patients who were likely to survive beyond the two-year mark on a cost basis. “I think it is very difficult to determine who is going to live for two years […] so I would be a little hesitant to ration the use of this technology,” responded Misra, noting that things to look out for included determining which patients might thrombose. Co-moderator Domenico Valenti (King’s College Hospital, London, UK) intervened to clarify whether the costs of using high-pressure balloons had been accounted for in the analysis, prompting Misra to explain that these had been bundled within the costs attributed to standard angioplasty.
Exciting new direction for drug treatment accelerates with sirolimus use
The dialysis vascular access circuit is often fated for failure due to neointimal hyperplasia formation, which is widely accepted to be the main pathophysiological reason for vessel narrowing. What man tries to create, nature tries to “take back”, quipped Suai Chieh Tan (Singapore General Hospital, Singapore). The use of sirolimus as an alternative drug coating to paclitaxel to arrest neointimal hyperplasia is advancing, but is still at early stages, he said during the same CX 2021 session on access maintenance.
The two drugs, sirolimus and paclitaxel, are vastly different, Tan made abundantly clear, with the former described as being a cytostatic, immunosuppressant antiproliferative and the latter a cytotoxic, chemotherapeutic agent.
Describing the emerging evidence from Singapore using sirolimus-coated balloons to treat thrombosed AV grafts, which are plagued by abysmal results, Tan drew attention to published results in the Journal of Vascular and Interventional Radiology (JVIR) from last year showing a three-month primary patency of 65% that dropped to 55% at six months—figures he described as encouraging when compared to similar data stemming from the employment of cutting balloons or stent grafts.
Suai Chieh Tan
Turning tack to the outcomes of sirolimus balloons with AV fistulas, he presented data from PLOS One, also from last year, showing six-month circuit access patency rates of 68% and target lesion primary patency rates in the same timeframe of 82.9% with Concept Medical’s MagicTouch device.
Spurred on by these initial data with small numbers of patients, the team at Singapore has embarked on a prospective, multicentre, double-blinded randomised controlled trial and begun enrolling patients with failing AV fistulas from January 2021. The triallists plan to enrol 170 patients who will be allocated to receive either standard angioplasty or treatment with a sirolimus-coated device.
Inston then looked back to the use of sirolimus as an immunosuppressant in renal transplants to seek reassurance that using this potent drug would not eventually lead down a path of “having our fingers burnt” due to impaired wound healing, provoking Tan to reply that these studies were an effort to harness the potential of this drug in slowing down the process of neointimal hyperplasia within the blood vessel being treated.
Tan closed his presentation by noting that the application of sirolimus-coated balloons in dialysis access appears to be safe and effective, but said that larger randomised trials were ongoing to verify these early findings.
This is essentially the same thought Trerotola and colleagues conclude their AJKD editorial on the wider topic of DCB use in failing fistulas with: “[…] nephrologists may be heartened in the knowledge that there are multiple additional large multicentre randomised controlled trials forthcoming, hopefully with commonly used and well-accepted endpoints, which will perhaps provide both more data and more clarity. Only time will tell.”
BoneView, an artificial intelligence (AI) software from French company GLEAMER, provides a gain of 8.7% increase in sensitivity and a 4.1% gain in specificity without loss of reading speed, and thus is an effective aid for radiologists and emergency physicians in the detection and localisation of appendicular skeletal fractures.
The interpretation of radiographs suffers from an ever-increasing workload in emergency and radiology departments, the study investigators write in Radiology, while missed fractures represent up to 80% of diagnostic errors in the emergency department. Lead author Loïc Duron (Adolphe de Rothschild Foundation Hospital, Paris, France) and colleagues therefore set out to assess the performance of BoneView in an effort to improve radiograph interpretation.
“To our knowledge, this is the first study that evaluates the performance of AI‐assisted reading for radiographic fracture detection over the entire appendicular skeleton and on multicentre data, from a variety of imaging systems, some of which were not present in the training database,” comments Duron, who is currently doing a science thesis on AI in medical imaging.
“This study is the result of significant collaborative work between specialists in radiology, data science, biostatistics, and GLEAMER teams to evaluate the clinical performance of BoneView. This is an important step that quantifies and scientifically validates the benefits of this AI solution available to healthcare institutions, in a context where several solutions are marketed without published objective results,” adds Antoine Feydy, osteoarticular radiologist at Cochin Hospital (Paris, France). “Publication in Radiology, a journal with the highest impact factor in the field, reflects on the one hand the rigor of the methodology used but also the magnitude of the obtained results. ”
“We are delighted and proud of the publication in Radiology of our ambitious clinical study with BoneView, whose results are unequivocal on the benefits of the cross‐interpretation of AI and the physician: 30% decrease in the rate of undetected fractures, while reducing the radiographs reading time by 15%, on exams specifically selected for their difficulty, i.e. with so‐called non‐obvious fractures. In 10 years, the number of exams to be analysed by radiologists has doubled, while the number of radiologists has increased by only 20%. We are continuing our developments to improve and enrich our range of AI software to progressively automate the diagnosis of standard radiography to ensure very high reliability of the examination and optimal patient care,” says Christian Allouche, CEO and co‐founder of GLEAMER.
Prior to the study, the BoneView AI system was trained on 60,170 radiographs obtained from trauma patients. For the study, between 2016 and 2018, 600 adult patients in whom radiographs were obtained after a recent trauma, with or without one or more fractures of the shoulder, arm, hand, pelvis, leg, or foot, at 17 French imaging centres, were retrospectively included. Six radiologists and six emergency physicians were asked to detect and localise fractures with and without the help of BoneView software. Sensitivity, specificity, and reading times with and without assistance were compared after averaging the performance of each reader. AI assistance improved physician sensitivity per patient by 12% (and 22% for patients with multiple fractures), and specificity by 5%; it also reduced the average number of false positives per patient by 42% in patients without fractures and the average reading time by 15%. Finally, the stand‐alone performance of a newer version of the AI system was superior to that of all unassisted readers, including osteoarticular expert radiologists.
GLEMER state: “The help of AI improves the diagnostic performance of radiologists and emergency physicians, which will allow better patient management from their first imaging examination. Among the expected consequences, the help of AI should allow to improve the specificity of the complementary exams prescribed after the radiography, to avoid delays in care, and to direct patients into the right therapeutic pathway.”
LimFlow SA recently announced the publication of 12-month data from the full patient cohort in its PROMISE I study of the LimFlow percutaneous deep vein arterialisation (pDVA) system in the Journal of Vascular Surgery.
Results showed sustained positive outcomes for both amputation-free survival and wound healing. The minimally-invasive LimFlow system is designed to bypass blocked arteries in the leg and deliver oxygenated blood back into the foot via the veins in chronic limb-threatening ischaemia (CLTI) patients who are facing major amputation and have exhausted all other therapeutic options.
PROMISE I is a multicentre, prospective, single-arm study of the LimFlow system. It was conducted at seven US centres and enrolled 32 end-stage—or “no option”—CLTI patients, 100% of whom had non-healing wounds on the target foot, 69% of whom had diabetes, and 34% of whom had renal insufficiency. No-option CLTI is defined as being ineligible for surgical or endovascular arterial revascularisation as adjudicated by an independent committee of vascular surgeons.
“The publication of the PROMISE I results in the Journal of Vascular Surgery further validates the benefits of the LimFlow system,” said Daniel Clair, PROMISE I principal investigator and chair of the department of surgery at the University of South Carolina (USC) and Prisma Health-USC Medical Group (Columbia, USA). “The LimFlow pDVA system was effective in treating no-option CLTI resulting in a high percentage of treated patients healing their wounds and surviving free of major amputation at 12 months.”
In the PROMISE I study, 70% of patients achieved amputation-free survival at 12 months following treatment with the LimFlow system, and 75% had all wounds classified as healed or healing at 12 months as adjudicated by an independent core lab. Technical success was reported at 97%.
“Given the unacceptable rates of major amputations globally we are encouraged by the publication of the 12 month PROMISE I data in the prestigious Journal of Vascular Surgery,” said LimFlow CEO Dan Rose. “We are making great strides in our currently enrolling PROMISE II pivotal trial in the USA and Japan, and we look forward to advancing our mission of leaving no limb left behind.”
Researchers have found no statistically significant difference in mortality between patients treated with drug-coated devices and non-drug-coated devices in the SAFE-PAD study. Eric Secemsky (Beth Israel Deaconess Medical Center [BIDMC], Boston, USA) reported this conclusion at the American College of Cardiology’s 70th Annual Scientific Session (ACC.21, 15–17 May, virtual), with results published simultaneously in JAMA Internal Medicine.
At the behest of the US Food and Drug Administration (FDA), Secemsky and Robert Yeh (BIDMC, Boston, USA), designed the SAFE-PAD (Safety assessment of femoropopliteal endovascular treatment with paclitaxel-coated sevices) study to provide information on the safety of paclitaxel-coated devices.
Using claims data from the Centers for Medicare & Medicaid Services (CMS), the researchers evaluated survival following treatment with paclitaxel-coated devices in more than 160,000 leg artery revascularisation procedures conducted between 2015 and 2018.
“Our study of Medicare beneficiaries includes more than 160,000 patients, including more than 30,000 patients with survival data extending past four years, making it one of the largest and most comprehensive evaluations of the safety of drug-coated devices to be published since the initial analysis,” said Secemsky. “Although the 2018 findings [reported by Konstantinos Katsanos et al] raised concerns about the safety of these drug-coated devices, there were many issues with that analysis—including the study’s small size and a lack of complete patient follow-up.”
Secemsky and colleagues’ study included Medicare patients treated with either a drug-coated or non-drug coated peripheral device between 2015 and 2018 at nearly 3,000 hospitals across the USA. Deaths were evaluated through May 2020, and after accounting for any differences in demographics and co-morbidities between the two groups, the investigators found no evidence that drug-coated devices were associated with higher mortality rates through an average 2.7 years of follow-up, with some patients having follow-up through five years.
“We used a number of novel statistical methods to assure these results were accurate, and found consistent results across a number of different patient groups—including among those of lower overall risk, those with more severe disease, and those treated in outpatient centere,” Secemsky said. “We have provided these results to the FDA [US Food and Drug Administration] to make decisions on whether to continue to restrict these drug-coated devices to only those at high risk of needing another leg procedure, or to return to the previous indications where these were used without restriction.”
The current publication is the first report of seven planned biannual reports as part of the SAFE-PAD study, which was designed to continue until all patients in the study had follow-up exceeding five years. As such, Secemsky and colleagues will continue to analyse these Medicare beneficiaries and update their findings until this study completes in late 2023.
“The SAFE-PAD study is a model example for collaboration between industry, academia, and the FDA to carry out rigorously designed, real-world studies to evaluate important medical device safety signals,” said Yeh. “We believe that applying stringent scientific standards to observational studies can create greater confidence in validity of these ‘big data’ approaches to the evaluation of medical therapies.”
Rivaroxaban (Xarelto, Bayer/Janssen), in addition to low-dose aspirin, should be considered as an adjunctive therapy after lower extremity revascularisation to reduce first and subsequent adverse outcomes, analysis from VOYAGER PAD, presented during a late-breaking trial session at the American College of Cardiology’s 70th Annual Scientific Session (ACC.21, 15–17 May, virtual), indicates. The findings were simultaneously published online in the Journal of the American College of Cardiology (JACC).
Rupert Bauersachs, director of vascular medicine at the Darmstadt Clinic (Darmstadt, Germany) and lead author of the study told ACC.21 attendees that the use of rivaroxaban significantly reduced the occurrence of total severe events of the heart, limb or brain and issues related to other vascular complications in patients with symptomatic peripheral arterial disease (PAD) who underwent lower extremity revascularisation. The findings underscore the broad benefits of this strategy in this high-risk patient population, he said.
“To our knowledge, this is the first time that the addition of low-dose rivaroxaban to aspirin has been clearly shown to reduce the occurrence of both first and total adverse events in patients with PAD who have undergone lower extremity revascularisation but remain at high risk for a heart attack, stroke or recurrent arterial blockage in a limb,” Bauersachs said. “The benefits we saw in the trial for total events were statistically significant and entirely consistent with those for first events. Rivaroxaban 2.5mg twice daily with aspirin should be considered as adjunctive therapy after revascularisation to reduce first and subsequent adverse outcomes.”
Recent data have shown that, after lower extremity revascularisation, there is a four-fold risk of acute limb ischaemia, Bauersachs told ACC.21 attendees, adding that this is associated with a high incidence of limb-related complications.
“There is a need for greater awareness that PAD is a distinct disease state and that patients with PAD have a high risk for cardiovascular adverse events and are generally a very vulnerable population, especially in the post-revascularisation setting,” Bauersachs said. “Care for these patients is often fragmented because the surgeon or interventionalist who performs the revascularisation may not follow them for complications or recurrences. They deserve to receive optimal treatment to reduce the risk of recurrences.”
The randomised, double blind VOYAGER PAD trial enrolled 6,564 patients in 34 countries who had PAD and had undergone lower extremity revascularisation. The patients’ median age was 67 years and 74% were men.
Patients were randomly assigned to receive either rivaroxaban or a placebo in addition to daily aspirin. The trial’s primary endpoint was timed to the first event of a composite of acute limb ischaemia, major amputation of vascular aetiology, myocardial infarction (MI), ischaemic stroke or cardiovascular death. Another prespecified endpoint was the total number of vascular events, including recurrent primary endpoint events as well as other vascular events. The median follow-up time was 28 months after revascularisation.
The research team reported in a late-breaking clinical trial presented at ACC.20/WCC that VOYAGER PAD met its primary endpoint, with a 15% statistically significant reduction in the risk of a first major adverse limb or cardiovascular event seen in patients who received rivaroxaban compared with those who received the placebo. The current study reports on the total number of vascular events, with over 4,700 occurring in the 6,564 patients randomised over three years.
“There were 342 fewer adverse events in the rivaroxaban group than in the placebo group, which translates to an absolute reduction in risk of 12.5%,” Bauersachs said. “In a high-risk population, that is a big gain in avoiding the need for patients to come back with vascular complications.”
The 6,564 study participants experienced a total of 4,714 vascular events during the study period with 2,301—or about one-third—experiencing at least one vascular event, Bauersachs said.
“So, during approximately three years of follow-up, about two to three out of six patients with PAD had a vascular event in spite of high utilisation of background medical therapy. This overall rate of vascular events is eye-opening and speaks to the high vulnerability of this patient population,” Bauersachs said. “First events are just the tip of the iceberg.”
A limitation of the study is that the trial was designed to assess the occurrence of first adverse events following lower extremity revascularisation, Bauersachs said. Therefore, in a double blinded trial, patients may come off study treatment or go on to other therapies after an event, which can attenuate the observed benefit. Assessment of the total number of adverse events, however, was a prespecified secondary endpoint and despite this limitation, the findings were statistically significant and robust in absolute terms.
VOYAGER PAD was funded by pharmaceutical companies Bayer and Janssen, who in a press release highlighting the presentation of the results, said that the analysis showed a very high burden of subsequent events and a consistent 14% reduction in both primary endpoint events and total vascular events over a median of 2.5 years.
“The VOYAGER PAD trial is the first and only study of antithrombotic therapy in the past 20 years to demonstrate a significant benefit in patients with PAD after lower extremity revascularisation,” James List, global therapeutic area head, Cardiovascular & Metabolism, Janssen Research & Development, was quoted as saying in the release. “With these new data, we now have a full picture of evidence demonstrating the potential of Xarelto in treating patients through various stages of PAD—chronic, symptomatic, those requiring revascularisation and beyond.”
“Even years after revascularisation, patients with PAD continue to have a markedly high risk for future thrombotic events due to excessive thrombin generation and platelet aggregation,” added Marc P Bonaca, Department of Medicine, Division of Cardiovascular Medicine, University of Colorado Anschutz Medical Campus, (Aurora, USA). “This analysis from VOYAGER PAD looked beyond the first event and found subsequent thrombotic event reduction with rivaroxaban plus aspirin, underscoring the importance of long-term prevention in these high-risk patients.”
Medtronic today announced new clinical data from the Global SYMPLICITY registry (GSR) indicating that renal denervation with the Medtronic Symplicity renal denervation system was associated with clinically significant and sustained blood pressure reductions in a real-world hypertensive patient population through three years. Results from the prospective, single-arm, global, observational study are being presented as a late-breaking clinical trial session atEuroPCR 2021 (18–20 May, virtual).
The study analysed nearly 3,000 patients with uncontrolled hypertension (HTN) and other comorbidities typical in HTN patients (chronic kidney disease, diabetes). Patients were treated with the Symplicity renal denervation system utilising the single electrode Symplicity catheter or the Symplicity Spyral multi-electrode catheter, and their outcomes were analysed up to three years post procedure. RDN with the radiofrequency based Symplicity renal denervation system is a minimally-invasive procedure intended to regulate overactivity of nerves that lead to and from the kidney, which play an important role in blood pressure control.
The GSR study results demonstrated the Symplicity renal denervation System led to significant and clinically meaningful reductions in blood pressure that were sustained out to three years postprocedure. Patients experienced a mean reduction of 16.7mmHg office systolic blood pressure (OSBP) at three years compared to baseline.
Investigators also evaluated the benefit of renal denervation within various patient subgroups using a clinical composite endpoint; a retrospective analysis comprised of both OSBP, 24-hour ambulatory blood pressure (ABPM), and medication burden. They found a consistent benefit of renal denervation in patients with versus without diabetes, chronic kidney disease, or patients who were 65 years and above. The similar clinical composite endpoint was used in a recent EuroIntervention publication that showed patients were nearly three times more likely to benefit from renal denervation compared to remaining on a regime of anti-hypertensive medications alone (Win Ratio=2.78, p<0.001).
“As we continue to expand our clinical data around renal denervation for uncontrolled hypertension management, we wanted to broaden our understanding of the long-term benefits for our patients who suffer from multiple chronic conditions and are typically prescribed multiple medications,” said Felix Mahfoud, cardiologist at Saarland University Hospital in Homburg, Germany and principal investigator in the study. “With this new analysis, we can now help patients continue to see the real-world benefits of renal denervation.”
EuroPCR: New analysis on estimated risk reduction from Symplicity renal denervation system
In addition to the late-breaking clinical trial results at EuroPCR, investigators also reported a new analysis estimating the reduction in clinical events in patients treated with the Symplicity renal denervation system. The analysis used the clinical events observed at three years in the Global SYMPLICITY registry and put these in perspective with a modelled control. The results showed a 26% relative risk reduction in major cardiovascular events (MACE) over three years for the full study cohort treated with renal denervation, and a 34% reduction for patients suffering from resistant hypertension over the same timeframe.
Medtronic expands renal denervation real-world data collection with the new GSR-DEFINE study
Building on the success of GSR and continuing its commitment to providing real-world evidence for the Symplicity Spyral renal denervation system, Medtronic also announced today launch of the GSR-DEFINE study. This new phase of patient data collection aims to enrol an additional 2,000 patients suffering from uncontrolled hypertension, who will be treated with the Medtronic Symplicity Spyral multi-electrode renal denervation catheter. The study will collect data for a subgroup of patients out to five years.
About the Medtronic Symplicity Spyral clinical programme
Along with the GSR and GSR-DEFINE studies, the Medtronic Symplicity global clinical programme also includes the SPYRAL HTN-OFF MED PIVOTAL and SPYRAL HTN-ON MED trials, both prospectively powered, randomised, sham-controlled studies evaluating patients with uncontrolled blood pressure in the absence and presence of prescribed anti-hypertensive medications respectively.
Approved for commercial use in more than 60 countries around the world, the Symplicity Spyral renal denervation system is limited to investigational use in the USA, Japan, and Canada.
In a recent study, Victor Demaerel (University Hospitals Leuven, Leuven, Belgium) and colleagues found that tunnelled haemodialysis catheter (THC) survival in 352 patients was more than 70% after five years. This finding, they conclude, “supports [THC] use for permanent dialysis access”.
The literature is divided about the potential role of THC as a permanent access for haemodialysis and about which patients are at high risk of THC-related complications, the authors write in theJournal of Vascular Access (JVA). They elaborate: “The native arteriovenous (AV) fistula is widely recognised as the optimal vascular access,” noting its association with “excellent” long-term patency and a low complication rate. THCs, on the other hand, “are considered a less reliable permanent access for haemodialysis due to higher rates of infection and thrombosis”.
However, Demaerel et al state, while the THC “definitely has its place”—specifically as a temporary access during AV fistula maturation in patients who need urgent dialysis—it is also “increasingly being considered in the elderly population because of difficulties with maturation of an AV fistula and a potential risk of right heart failure”.
Against this backdrop, the investigators decided to review the incidence and type of THC complications in a large cohort of patients with end-stage renal disease, and also assess the longevity of the THC and factors predicting high risk for complications.
Damaerel and colleagues relay that, between August 2009 and December 2016, a cohort of 538 patients underwent primary THC insertion, detailing that they excluded 67 patients from their analysis who did not have clinical follow-up data available.
The authors report the following results from the 352 patients in whom a THC was inserted in a virgin neck:
THC-related complications were observed in 104 (29.55%) of the patients.
Infection occurred in 38 (10.8%) and malfunction, related to thrombosis or mechanical damage, in 45 (12.78%).
Removal of the THC for the purpose of switching to alternative dialysis methods was planned in 135 (38.4%); the remaining patients were still alive with a functioning THV (n=18; 5.11%) or died (n=95; 27%) with a functioning THC.
The THC survival rate was 82.67%, 78.13%, 74.15%, 72.96%, 71.02%, and 70.63% at six-month, and then one-, two-, three-, four-, and five-year follow-up, respectively.
Gender, Charlson comorbidity index (CCI), age, and site of placement of the catheter were found not to affect the life of the catheter.
The authors acknowledge some limitations of their research. “This is a retrospective, single-centre study,” they recognise, noting that this might prevent generalisation of the conclusions. They do stress, however, that the number of patients included is still “substantial”. They also state that the team did not perform any randomisation or categorisation of types and brands of THC. However, they reference a systematic review and meta-analysis by Xiao-Chun Ling (Taipei Medical University, Tapei, Taiwan) et al, published in the Journal of Vascular Surgery in 2019, in which no catheter type was found to exhibit features that could potentially enhance their suitability for use.
Damaerel and colleagues conclude in JVA that this study “demonstrates the safe and efficient placement of THC under ultrasound and fluoroscopic placement,” and that late complications “mainly include infection and mechanical/thrombotic THC dysfunction”. Patients with more comorbidities, they note, “might be at higher risk of lower catheter survival rates,” and older patients “might experience THC-related adverse events beyond 18 months of follow-up”.
The Auryon atherectomy system (AngioDynamics) “represents an exciting new technology”, John Rundback (Advanced Interventional and Vascular Services, LLP, Teaneck, USA) opined at the International Symposium on Endovascular Therapies (ISET; 9–11 May, Miami, USA, and online), speaking on behalf of the Pathfinder I registry investigators. “I think it has really got a lot of traction; we found it a very useful tool across a wide range of plaque morphologies and vessel beds. Further iterations of this platform will hopefully improve its performance further.”
The Pathfinder registry is a post-market, prospective, multicentre, single arm, all-comers registry of 104 patients with femoropopliteal and tibial stenoses or occlusions or in-stent restenosis (ISR), with peripheral arterial disease (PAD) classified as Rutherford class 2–5. “Lesions of all levels, lesions of all types are included in this real-world registry,” Rundback said.
Patients were treated with either the Auryon atherectomy system or adjuvant therapy. The primary endpoints were acute success (measured as ≤30% final residual stenosis by corelab evaluation) and freedom from peri-procedural major adverse events or complications through 30 days. Long-term results were collected through 24 months, including patency, major adverse events, target lesion revascularisation, and patient-reported outcomes.
Presenting the findings, Rundback said: “These are really important results I think. Across the board, the stenosis reduction or the luminal gain was between 24 and 31%, and this is the laser-cut phenomenon that I think is unique to this laser. In CTOs [chronic total occlusions], there [is an average] 26% luminal gain; [in vessels with] moderate to severe calcium, there was a 27% luminal gain, [in vessels with] ISR, [there was a] 21% luminal gain, and above and below the knee, we see similar levels of luminal gain. So it does not matter what vessel, what vessel calibre, or what the plaque morphology is, this is a very precise, deliverable, controllable, and reproducible result.”
In terms of safety, there was an absence of major adverse events in 99% of lesions. There was one dissection, which was after angioplasty alone, not after laser passage. There were two cases of distal embolization, one of which Rundback said was “probably attributed to the laser”, and one of which was following the treatment of an in-flow lesion that had angioplasty, shockwave, and atherectomy. There were a total of four bailout stents, three of which were for recoil and one of which was for dissection. There was one amputation, which occurred 180 days after follow-up; the patient had Rutherford category 5 disease and gangrene at baseline, and they failed to improve following treatment of their 37cm-long lesion.
The Auryon atherectomy system is a proprietary, solid-state laser with a wavelength of 355nm (different to the currently-available 308nm laser). “What is really unique about this is it is not just the wavelength, but it has a very short pulse duration of 10ns, which results in a very precise, controllable, and reproducible laser energy delivery to the vessel wall,” Rundback explained.
He went on to describe how this particular wavelength (355nm) has a “very high” affinity for atheroma compared to the vessel endothelium, resulting in a reduced risk of perforation. Indeed, in the Pathfinder I trial, no perforations were reported. There is also less overall thermal damage to the vessel wall, he explained, and the laser system is agnostic to the presence of contrast. It also requires minimal warm-up time: “From a practical point of view, it only needs a 15 second warm-up; if you do not like where it is placed in the room, you can pick it up and move it to another spot.” In addition, Rundback claimed the Auryon atherectomy system is optimal for treating all lesion types.
There are four catheters that are used with this system, ranging from a 0.9mm catheter for below the ankle and in the tibial arteries, to a 2.35mm catheter for the popliteal and superficial femoral arteries. There is also a 2mm catheter for the femoropopliteal and tibioperoneal trunk, and a 1.5mm catheter, for tibial and femoropopliteal arteries.
The Pathfinder registry builds on prior investigational device exemption (IDE) and CE studies, which combined investigated 147 patients with 163 lesions. In these previous research, there were no distal emboli events, and no perforations. Of 107 lesions included in the IDE study, there were just 16 graded as minor dissections (grades A or B). In terms of debulking, there was a 34% reduction post-procedure (the FDA threshold for efficacy is 20%). “Clinical results and patient-reported outcomes were very favourable at 12 months,” Rundback stated.
Session moderator Daniel Clair (Vascular Surgery, University of South Carolina (USC) and the Palmetto Health-USC Medical Group, Columbia, USA) praised Rundback for his talk, saying it offered, “A new look at laser”.
Siemens Healthineers launches its Somatom X.ceed, a new high-resolution, high-speed computed tomography (CT) scanner. To support medical staff in their workflows during critical situations, two “companions” for automated user guidance are integrated: myExam Companion guides users through diagnostic procedures; myNeedle Companion supports targeted needle path planning as well as laser-guided insertion across multiple modalities. As a result, the fastest single-source CT scanner from Siemens Healthineers can assist healthcare providers with their clinical decisions in areas like emergency imaging, cardiac CT, and CT-guided interventions.
Somatom X.ceed has an 82cm bore and a “user-friendly” tablet operation, Siemens state in a press release. The integration of myExam Companion allow the system to achieve high-speed and high spatial resolution, key for cardiac, emergency, and spectral imaging.
myNeedle Companion for minimally invasive treatment
CT is one of the most used imaging modalities when cross-sectional image guidance is needed for percutaneous interventional procedures, like biopsies, ablations, or pain therapy. Almost 50% of sites perform at least three CT-guided interventions per day. In these procedures, time and precision are critical. But the time needed, and the success rate, depend greatly on the users and their experience level. Patient cooperation influences the success rate as well. Complex hardware and user interfaces or limited guidance may even increase these challenges and lead to variations in outcome.
Siemens claim that myNeedle Companion simplifies the workflow in minimally invasive treatments. myNeedle Companion is a unique combination of hardware and software designed to greatly reduce the complexity in CT-guided interventions. In addition, it is the first universal solution with a harmonised user interface for the planning and guidance of percutaneous needle procedures across imaging modalities, be it for a CT or an angiography system. Once the workflow is trained on one modality, the training efforts on another modality are expected to be much shorter. This can help to reduce unwarranted variations and minimise training efforts. Familiar user interfaces let the radiologist concentrate on what matters: accurate needle positioning with the help of the unique myNeedle Laser, a powerful, fully-integrated option that projects the needle entry point and insertion angle directly on the body of the patient—even in advanced double-angulated procedures with multiple needle paths.
Emergency and cardiovascular procedures are challenging and growing clinical areas for CT
Emergency radiology is rapidly evolving. In the last 20 years the demand for CT-imaging in emergency departments has increased by 250%. In a busy emergency environment, inefficient workflow can slow down radiologists who need to triage patients and perform multiple, demanding tasks quickly. With the support of myExam Companion, staff members can speed up procedures from patient preparation to image evaluation. Applications powered by artificial intelligence provide ready-to-read results aimed to facilitate diagnostic tasks.
The ability of cardiac CT to rapidly evaluate multiple cardiovascular conditions has allowed CT to become an important diagnostic instrument for steadily rising numbers in cardiovascular diseases (CVD). From 2011 to 2019, CT cardiac procedures more than doubled from 1.4 to 3 million. These procedures, some of the most complex in CT, are now performed routinely by staff of all skills levels. Here, as in emergency imaging, myExam Companion plays a major role in guiding the user towards more standardised results and low dose levels.
“As the number and complexity of radiological procedures increase, demands on staff are reaching heightened levels. This continues to cause unwarranted variation, in both diagnostic and interventional procedures. Somatom X.ceed, together with myNeedle Companion, is a true game changer for CT-guided interventions. After the introduction of myExam Companion last year, reducing the overall complexity of scanner operation in as many aspects as possible was our next logical step,” says Philipp Fischer, head of CT at Siemens Healthineers.
The first patient has been enrolled in DOORwaY-90, a study evaluating the safety and efficacy of selective internal radiation therapy (SIRT) using SIR-Spheres Y-90 resin microspheres (Sirtex) in patients with unresectable hepatocellular carcinoma (HCC).
DOORwaY-90, which stands for “Duration of Objective Response with Arterial Y-90,” is the first prospective, US-based, multicentre, open-label, single arm study of its kind. The study will assess the duration of response and objective response rate of SIR-Spheres. It is being led by co-principal investigators Cheenu Kappadath and Armeen Mahvash (both The University of Texas MD Anderson Cancer Center, Houston, USA). Study enrollment is underway, with the first patient enrolled at Inland Imaging Associates and Providence Sacred Heart Medical Center in Spokane, USA.
“We are thrilled to enroll the first patient in DOORwaY-90,” comments Mark A Turco, global chief medical officer and EVP of research and development for Sirtex. “This clinical trial studying a heterogeneous population of patients with HCC using personalised dosimetry planning has the potential to advance the treatment of HCC patients worldwide. We are deeply thankful to every clinical investigator and patient who will be part of this ground-breaking journey.”
With a planned enrollment of 100 patients across 15 sites both academic and non-academic, DOORwaY-90 is enrolling patients with Barcelona Clinic Liver Cancer (BCLC) Stage A, B1, and B2 who are not eligible for resection or ablation at the time of study entry. The study is unique because it is the first FDA-approved US-based prospective trial to utilise and delineate personalised dosimetry treatment planning and to define actionable post-treatment dosimetric verification for endpoint assessment.
“It is important for physicians to have confidence that their planned Y-90 dose is being delivered in the right amount and to the right place,” says Douglas Murrey, vascular and interventional radiologist at Inland Imaging Associates and Providence Sacred Heart Medical Center in Spokane, USA. “The personalised dosimetry component of the DOORwaY-90 study will provide meaningful insights to advance our practice and patient outcomes.”
HCC is often diagnosed when potentially curative resection or transplantation is not feasible. SIRT has the potential to deliver a lethal dose of radiation to hepatic tumours, while sparing surrounding healthy liver tissue. In countries outside the USA, SIRT has been successfully used to bridge patients to transplantation or downstage HCC to within transplantation criteria or resection.
Transit Scientific recently announced it has received CE mark clearance in the European Union for the XO Score scoring sheath platform to facilitate dilation of stenotic material in the peripheral vasculature including popliteal, infrapopliteal, and native or synthetic arteriovenous dialysis fistulae.
XO Score is a new type of scoring and cutting technology that enables low-pressure lesion dilatation and vessel prep with a broad range of standard off-the-shelf percutaneous transluminal angioplasty (PTA) balloons. Scoring sheaths have the ability to deliver enhanced angioplasty with basic balloons while addressing the cost and performance limitations of traditional scoring or cutting technologies.
“We need novel, safe, and appropriately aggressive vessel prep devices to continue fighting the increasingly difficult stenotic lesions encountered in CLTI [chronic limb-threatening ischaemia] patients,” said Jihad Mustapha (Advanced Cardiac & Vascular Center, Grand Rapids, USA). “XO Score helps fill that unmet need by enabling variable scoring depths and improved pushability which are essential when dealing with tough calcifications.”
The XO Score incorporates a unique one-piece metal-alloy exoskeleton design which adapts to the shape, size, and length of the PTA balloon used inside it. This approach lets physicians select the PTA platform of their choice for use in conjunction with XO Score, potentially reducing inventory and procedural costs. Future ultra-low-profile over-the-wire and rapid-exchange versions are under development for smaller vessel and coronary use.
“The ability to scale this technology down to below 3Fr is especially important for treatment of pedal loop stenosis and deployment in the tibiopedal junction,” continued Mustapha. “This is at the forefront of our fight against CLTI as the disease state continues to worsen.”
This CE mark clearance covers the XO Score platform in 65cm and 125cm working lengths with 0.25mm (0.010″), 0.35mm (0.014″), or 0.50mm (0.020″) scoring or cutting depths to enable precise dilation of calcified and fibrous lesions.
“I am going to give you reasons to be excited about your critical limb practice,” Peter Schneider (University of California San Francisco, San Francisco, USA) told delegates attending the International Symposium on Endovascular Therapy (ISET; 9–11 May, Miami, USA), in a talk focusing on innovative tools on the horizon for the treatment of chronic limb-threatening ischaemia (CLTI). “I think critical limb ischaemia has come to the forefront of our practices and of community awareness, and finally now the tools are starting to show that,” he opined.
Covering developments in assessment (including monitoring, perfusion, and wound evaluation), reconstruction, and medication delivery, Schneider left his audience with an optimistic outlook for the future of CLTI treatment.
Assessment: Wearables, implantables, and artificial intelligence
Turning first to wearables and implantables, which he said “are just around the corner”, Schneider expanded: “[In terms of] implantables, there is a patent application for a stent with a sensor on it, which of course makes sense that someday that is how we will be doing our surveillance.
“Wearables are available now, and are essentially a transfer from other types of technology.” Citing a JAMA Network Open article from late 2020, which looked at the association between wearable device–based measures of physical frailty and major adverse events following lower extremity revascularisation, Schneider said he expected to see “more articles like this one”, adding: “I am sure we are going to have [investigations into the use of wearable devices to assess frailty] for claudication patients on a regular basis as well.”
In addition to wearables and implantables, he also directed the ISET audience’s attention towards the use of artificial intelligence (AI): “A couple of companies have taken it upon themselves to do a digitised wound evaluation, and then use AI to help the programme get smarter over time about identifying the cause of the wound and the progress of the wound. So much of what we are doing is an inexact science: when we think of screening, population management, treatment guidelines, we are thinking about the population as a whole, and just trying to do the right thing, but each of these patients comes having their own code and their own set-up, so the transfer of existing technology I think will help us to individualise the way we would like to.
Reconstruction: Modified balloons, new implants, alternative bypass, below-the-ankle angioplasty
“Below-the-knee [BTK] angioplasty is just sitting there waiting for us to really develop it,” Schneider stated, telling delegates listening in Miami and online that the medical community is now starting to see data showing improved wound healing. However, he noted that the patency data are “still unclear”, and in his opinion needs to be further assessed. “But I think we are really developing [in this arena],” he concluded.
The speaker first highlighted the lithotripsy with Shockwave. Lithotripsy waves travel outside the balloon, and disrupt both superficial and deep calcium. It is a way to improve vessel wall compliance prior to controlled, low pressure dilatation. “The question is how valuable is this going to be in BTK interventions?” Schneider asked. “I think it remains to be seen, but it certainly is a technology for interrupting calcium.”
Another technology Schneider considered was serration angioplasty. Noting his conflict of interest due to his involvement with Cagent Vascular, a developer of serration technology for vessel dilatation in endovascular interventions, Schneider explained how the novel Serranator percutaneous transluminal angioplasty (PTA) serration balloon catheter works: “The idea is that you poke little holes in the artery, and allow a stress relief line along the vessel so that it can be opened. I really believe that BTK angioplasty is due for a makeover by one method or another, and here is just an example of the flexibility of this tool.” The Serranator PTA serration balloon catheter is the first and only angioplasty balloon to receive Food and Drug Administration (FDA) approval and the CE Mark that embeds serration technology into a semi-compliant balloon for treating peripheral arterial disease (PAD). Earlier this year, results of Cagent Vascular’s PRELUDE-BTK study—a prospective, single-arm, multicentre feasibility study investigating the safety and efficacy of serration angioplasty—were presented at the Leipzig Interventional Course (LINC; 25–29 January, online).
Forty-six patients were treated with the Serranator device and 53 lesions were analysed by the core lab. The average final residual stenosis was 21.8%, with an average BTK arterial lumen gain of 1.55mm. These results were achieved with a low average maximum atmospheric pressure of six atmospheres. The bailout stent rate was 1.9%. A subset of lesions (n=10) were imaged with optical coherence tomography (OCT) and intravascular ultrasound (IVUS) and analysed by a core lab. All showed a serration effect. At 30 days, the freedom from primary safety events was 95.7%. Freedom from clinically driven-target lesion revascularisation (TLR) was 97.7%, and there were no serious adverse events related to the device.
Following this discussion on modified balloons, Schneider turned to a new method of post-angioplasty dissection repair: focal dissection repair. He showcased a new implant, the Tack endovascular system (Intact Vascular), the first FDA-approved vascular implant for BTK post-angioplasty dissection repair. Regulatory approval for the device was based on data from Intact Vascular’s Tack optimised balloon angioplasty II BTK (TOBA II BTK) clinical trial, which met all primary endpoints with 100% acute dissection resolution. The TOBA II BTK results demonstrated 95.7% amputation-free survival, 87.3% target lesion patency, with significant improvement in toe-brachial index (TBI), and 92.0% freedom from clinically-driven reintervention at six months.
Schneider mused: “The issue is; do we need IVUS? We know IVUS is more sensitive—all of the trials we did with focal dissection repair were angiographically-driven, however, could the results have been better if we used IVUS routines? Just something to think about as BTK disease gets more sophisticated, what will the role of IVUS be?”
Another implant Schneider explored in his presentation was a bioabsorbable vascular scaffold, the Abbott Esprit. This is an everolimus-eluting device, designed for the superficial femoral artery and iliac arteries. Recently-published data from Ramon Varcoe (Sydney, Australia) and colleagues show “excellent” patency out to five years. The LIFE-BTK randomised controlled trial, where participants will be randomised 2:1 Esprit versus PTA, is now enrolling in the USA.
Lastly in the “reconstruction” portion of his talk, Schneider mentioned percutaneous bypass. “The mean lesion length in the PQ bypass trial is in excess of 30cm, so we have not typically had an option for lesions of that length using percutaneous devices,” he announced. DETOUR II is a prospective, multicentre trial evaluating the Detour system for percutaneous femoral-popliteal bypass in patients with extremely long, complex lesions in the SFA. The study enrolled 202 patients in 36 sites in the USA and Europe, and is assessing freedom from major adverse events (MAE) within 30 days of the index procedure as the primary safety endpoint. The primary effectiveness is primary patency at 12 months.
Speaking to Interventional News about the potential of percutaneous bypass, principal investigator Jihad Mustapha (Advanced Cardiac and Vascular Centers, Grand Rapids, USA) said at the end of 2020: “If percutaneous femoral-popliteal bypass is shown to be safe and effective, similar to the outcomes demonstrated in DETOUR1 study, it could be a game changer for the way we treat complex, long-segment SFA disease today.”
Medication delivery
“We do not have any paclitaxel BTK drug-coated balloons (DCBs) in the USA,” Schneider said. While he noted that there are several paclitaxel DCB trials currently underway in the USA—he showed three of them: IN.PACT DEEP, Lutonix BTK, and BIOLUX P-II—he commented that “nothing is close to being approved”, though some show promise. “In particular, Medtronic has some preliminary data,” he said, before continuing: “My personal opinion is that the paclitaxel issue will fade over time. I think we have had such a hard time finding a danger signal in any subsequent data. Nevertheless, the whole issue has bought forward the concept of limus-based compounds.”
The “paclitaxel issue” he is referring to here is the increased association with mortality reported by Konstantinos Katsanos (University of Patras, Patras, Greece) et al in December 2018 when paclitaxel devices are used in the lower leg, which caused an international furore about the safety of these devices. Since, multiple analyses have failed to replicate this signal, but, as Schneider pointed out at ISET, the publication opened the door wider for research and development into alternative drugs.
“Here is just one,” Schneider said, showcasing the MED Alliance Selution, a sirolimus-coated balloon from Swiss start-up MedAlliance. “This is their SFA device. It uses micro-reservoirs made out of biodegradeable polymer intermixed with sirolimus for sustained and controlled drug release—typically, the slow and difficult uptake has been the problem with sirolimus.” MedAlliance’s planned clinical programme includes specific trials focusing on BTK disease (SELUTION BTK IDE) and CLTI patients (PRESTIGE, PRESITINE, and STEP).
Concept Medical, another start-up, from India, has recently published a first-in-human series from its XTOSI study, demonstrating good six-month primary patency of its MagicTouch PTA sirolimus-coated balloon in the treatment of BTK arterial lesions, in addition to femoropopliteal lesions. In addition, the US-based Surmodics has a BTK DCB (the Sundance DCB) currently in a first-in-human trial.
“There is also a method of administering limus-based compounds using the Mercator Bullfrog catheter,” Schneider said, which has 510(k) clearance. The Bullfrog device delivers generic dexamethasone to the adventitia, reducing inflammation that can be caused by interventional revascularisation. Delivery is confirmed with the co-administration of contrast.
The final technology Schneider mentioned is the “Eluvia-type technology”, seen in the SAVAL BTK drug-eluting stent system from Boston Scientific, which utilises a polymer as well as paclitaxel, and has been successful in SFA trials. It is now being enrolled in BTK trials. The SAVAL BTK stent system was the first CLTI device to be recognised by the FDA breakthrough device programme.
Three of our top 10 stories of April 2021 highlight new data and ideas presented at this year’s Charing Cross (CX) Symposium, Digital Edition (19–22 April, online), covering the potential of Philips’ Fiber Optic RealShape (FORS) technology to reduce radiation exposure, a call on medical agencies to change their paclitaxel recommendations in peripheral arteries, and two-year IN.PACT AV Access results. Last month, the world’s first accreditation programme for interventional oncology also opened for enrolment, and Interventional News readers heard about the latest offerings from Philips Healthcare.
The International Accreditation System for Interventional Oncology Services (IASIOS) is now open for public enrolment, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has announced. Twelve pioneering hospitals from nine countries participated in the IASIOS pilot phase, and the accrediting system, tested and optimised over the past two years, now stands ready to accept applications from facilities offering interventional oncology (IO) services worldwide, regardless of the institution’s size or location.
Opening the CX 2021 Digital Edition, experts deliberated crucial controversies in the abdominal aortic space. Discussion emphasised the potential of Philips’ Fiber Optic RealShape (FORS) technology to reduce radiation and ease technical success, with moderator Gustavo Oderich (Houston, USA) suggesting that “radiation will be a thing of the past” thanks to this new technology. Other key takeaways were a ringing endorsement that endoanchors have a part to play in the treatment of challenging necks, and consensus among the panel that parallel grafts should be used as little as possible in this hostile anatomy.
More than half (58%) of radiology leaders say they do not have enough diagnostic and interventional radiologists to keep patients safe, new data from National Health Service (NHS) trusts and health boards across the UK show. The data, recently published in a Royal College of Radiologists (RCR) report, also show that, despite many imaging doctors staying in the NHS last year to help the coronavirus effort, the NHS radiologist workforce is now short-staffed by 33% and needs at least another 1,939 consultants to meet safe staffing levels and pre-coronavirus levels of demand for scans.
In a Philips-sponsored video, Constantino Peña (Miami, USA) moderates anInterventional Newswebinar focusing on how the SmartCT system (Philips) can “transform” interventional radiology (IR) suites and the importance of 3D imaging within this setting. Peña is joined by two early-users of the technology, Marc Sapoval and Hicham Kobeiter, both from Paris, France.
Addressing representatives from the US Food and Drug Administration (FDA) and UK Medicines and Healthcare products Regulatory Agency (MHRA) directly, Thomas Zeller (Bad Krozingen, Germany) argued at the CX Digital Edition 2021 that “it is time to change the agency recommendations regarding paclitaxel use in peripheral interventions”. Moderators Andrew Holden (Auckland, New Zealand) and Gunnar Tepe (Rosenhein, Germany), Podium 1st presenters Gary Ansel (Columbus, USA) and William Gray (Wynnewood, USA), as well as a 71% majority of the CX audience, supported this view.
Soundbite Medical Solutions has announced US Food and Drug Administration (FDA) 510(k) approval for the SoundBite crossing system—Peripheral (SCS-P) with the 0.014” active wire (14P).
Shivank Bhatia and Vedant Acharya highlight the importance of multidisciplinary collaboration between urologists and interventional radiologists when it comes to forming a successful prostate artery embolization (PAE) clinic, citing a decade of experience at the Miami Miller School of Medicine (Miami, USA).
The results of a two-year study support the continued safety and effectiveness of the Zilver Vena Venous Stent (Cook Medical) in treating symptomatic iliofemoral venous outflow obstruction, according to findings presented at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online).
Last month, Medtronic announced the safety and effectiveness results through 24 months for the IN.PACT AV Access clinical study. The data, which were presented virtually as a Podium 1st at the CX 2021 Digital Edition, demonstrated that the IN.PACT AV drug-coated balloon (DCB) is the first and only DCB to show sustained and superior effectiveness through two years compared to standard percutaneous transluminal angioplasty (PTA) in end-stage renal disease (ESRD) patients with de novo or non-stented restenotic native arteriovenous fistulae (AVF) in the upper extremity.
The results of a recent investigation have revealed no association between infrainguinal bypass tunnelling technique and primary outcomes in patients with limb ischaemia. “Compared to subfascial tunnelling,” write Nallely Saldana-Ruiz (University of Southern California, Los Angeles, USA) and colleagues in the Journal of Vascular Surgery (JVS), “the superficial tunnelling technique is not associated with primary patency or major amputation in limb ischaemia patients undergoing infrainguinal bypass with a single-segment great saphenous vein”.
A new wearable device designed to remotely monitor arteriovenous (AV) fistulae function in dialysis access patients uncovered promising data leading one set of researchers to conclude the technology offers hope for improved care and lower costs among a challenging patient population.
The SmartPatch monitoring system (Alio Medical)—which involves the extraction of real-time data through a series of sensors from a patch placed over an AV fistula, subsequent cloud-based machine learning, and then actionable clinical alerts—is currently undergoing testing in a series of pilot studies aimed at tackling the healthcare burden of kidney failure and vascular access failure.
The first analysed dataset demonstrated the device “has the ability to measure haemoglobin, volumetric flow, and haemodynamically significant stenosis in AV fistulas,” Richard F Neville (Inova Heart and Vascular Institute, Falls Church, USA) recently revealed during the Society for Clinical Vascular Surgery (SCVS) annual meeting (13–17 March, Miami, USA).
Neville and colleagues looked at 128 patients at three dialysis centres, with all study participants wearing a SmartPatch device over an AV fistula either in the upper or lower arm.
“In this particular study, we utilised state-of-the-art optical technology with a particular patented array that allows for better data acquisition,” explained Neville, who disclosed that he serves on the scientific board of Alio Medical. “This took into account position, motion, light, temperature, and pulse of the patient. There was no need for patient interaction. This was all done remotely, and the clinical alerts are in real time.”
The intention of the study was to evaluate the ability of such a device to monitor AV fistula function, degree of stenosis, flow rate and the physiologic parameter of haemoglobin levels as a marker that impacts fluid management.
All participants wore a SmartPatch for a week. Each of the three clinical centres involved focused on one of the three metrics. The location focused on haemoglobin analysis studied 57 patients, the facility looking at volumetric flow looked at 21, and the centre monitoring percentage stenosis evaluated 71 study participants.
For each metric, Neville said, machine training algorithms were developed using the first 116 data streams from the device sensors. The algorithms were subsequently tested and correlated on the next 157 data streams, correlating with haemoglobin standard measurement, transonic flowmeters, and the standard fistulagram, he added.
The resulting data, Neville et al found, showed that haemoglobin was measured with comparative accuracy “and only a standard deviation of 0.41 as compared to haemoglobin measurement using standard techniques.”
The SmartPatch detected low volumetric flow—a potential indicator for access failure—with 100% sensitivity and 75% specificity, Neville continued. “Additionally, the degree of stenosis was also detected, looking at haemodynamically significant stenosis of great than 50%, with 100% sensitivity and 100% sensitivity as compared to subsequent fistulagrams, and arteriographic and angiographic imaging.”
He commented: “Therefore, we concluded in this study that this initial dataset shows us that this remote wearable monitoring system has the ability to measure haemoglobin, volumetric flow, and haemodynamically significant stenosis in AV fistulas. We are also hopeful that this remote monitoring system will allow us—and shows promise to allow us—to improve the care and lower the costs associated with other healthcare factors associated with this patient population.”
Neville said potential future biologic metrics that the device might monitor include oxygen saturation, blood pressure, heart rate, and haemoglobin and sodium levels.
Co-moderating the SCVS session in which Neville delivered his team’s findings, Jean Bismuth (Houston Methodist, Houston, USA) queried how placement of the patch might impact on the reliability of the data collected.
Neville explained that Alio had “spent a lot of time” on the material involved in the patch to ensure it is not injurious to skin, and that it can be used and worn for extended periods of time, among other considerations.
Meanwhile, W Charles Sternbergh (Ochsner Health, New Orleans, USA) who was co-moderating alongside Bismuth, raised the spectre of potential pitfalls toward commercialisation of the technology. Among Medicare patients, Sternbergh said, “evaluation of how their fistula is doing is baked in” to evaluation and management (E/M) services conducted at dialysis centres. “Typically, it is not allowed to have prophylactic testing, and it would even be suggested that that’s fraudulent, as some freestanding centres that do fistulagrams every three months no matter what have found out.”
Sternbergh asked: “How might this device intersect those issues?” Neville admitted this question got to the heart of the studied approach Alio has taken toward commercialisation.
“The technology has evolved rapidly,” he said. “When we first started this project in the animal lab, there was one sensor, a photo acoustic sensor. Now there is an array of sensors, and that is why we are able to generate the variety of information that I showed you.”
But, Neville continued, commercialisation remains an important step yet to be thrashed out. There are number of possibilities, he explained. One option might involve the device being given away for free, with an in-app-based subscription fee then applied for the data. Another would necessitate approaching dialysis companies with the benefits of keeping dialysis access fistulas functioning, and also keeping patients out of the emergency room, Neville said. “There were some initial cost savings shown in a dialysis population in the UK in the national health system [NHS] there, where just monitoring the haemoglobin accurately allowed [doctors] to adjust erythropoietin—which is a very expensive medication—and possibly decrease it, saving money just on the medications that are used on these folks.”
In the end, Neville added, he sees the device incorporated as a value-added part of care for the AV fistula patient population, as large dialysis companies realise close monitoring of access health and physiologic parameters “may actually save the overall cost of the patient in the long term.”
iVascular has received CE mark approval for its balloon-expandable covered stent, iCover, a press release from the company states.
Balloon-expandable covered stents are commonly used for treating arteriosclerotic lesions in renal and iliac arteries, and for the treatment of aneurysms and ruptures.
According to iVascular, iCover can adapt to the most tortuous vessels due to its high flexibility and post-expansion capacity. “It also offers excellent visibility, as it is the only balloon-expandable covered stent with radiopaque markers on the ends of the stent, to facilitate the implantation and the post-expansion,” a company press release details.
iCover is encapsulated with iVascular’s new proprietary technology, CoverTech. This technology attaches the inner and outer expanded polytetrafluoroethylene (ePTFE) layers to ensure a complete encapsulation.
“The first clinical experiences with iCover are remarkable,” states Vicente Riambau (Hospital Clinic of Barcelona, Barcelona, Spain). He adds that “iCover stands out for its excellent navigability and flexibility, while the radiopaque tantalum markers on its ends provide better visibility under X-rays, which enhances precision during implantation. With the launch of iCover, iVascular offers a complete portfolio to treat all type of peripheral lesions.”
Micro Medical Solutions (MMS) recently announced that the US Food and Drug Administration (FDA) has granted breakthrough device designation for its MicroStent vascular stent. This novel technology is designed to achieve and maintain vessel patency, enhance wound treatment, and improve quality of life and blood flow in order to reduce amputation and mortality for patients with chronic limb-threatening ischaemia (CLTI) resulting from peripheral arterial disease (PAD).
“FDA breakthrough device designation is an exciting step forward for MMS and for patients with CLTI, who will have expedited access to MicroStent. We are pleased that the FDA is recognising the importance and severity of CLTI and look forward to collaborating with them as we go through the PMA [premarket approval] process,” said Micro Medical Solutions CEO Gregory Sullivan. “As we remain focused on the completion of our FDA clinical study, STAND, it is gratifying to know we are now one step closer to our goal to help as many CLTI patients as possible live without the trauma of amputation.”
MMS is currently engaged in an FDA randomised, multicentre pivotal clinical study for MicroStent, called STAND (A clinical evaluation of the MicroStent peripheral vascular stent in subjects with arterial disease below the knee), which began in May 2020 and will continue at up to 25 sites across the USA. In addition, the MMS study HEAL (An all-comers observational study of the MicroStent peripheral vascular stent system in subjects with peripheral arterial disease) is currently enrolling patients at centres in the EU.
“Not all Drug-Coated Balloons (DCBs) are created equal”, Juan Granada (New York, USA), tells Vascular News in this second episode of a four-part series on the history of DCBs.
Granada discusses why there are differences in these devices, noting that some have a longer term retention of drug, while some have opted for a more soluble drug so it can disappear more quickly from the tissue. Although many companies are using paclitaxel, the resulting biological effects between the devices may be “quite different”. The IN.PACT™ Admiral™ DCB (Medtronic) originally followed a “different technological principle” compared to other devices, and has a crystalline coating allowing for long-term retention of the drug, says Granada. He adds that this is why coatings and formulations that maintain therapeutic tissue levels over time have a higher chance to have a better clinical result long term.
Local drug delivery in the peripheral field has “changed our lives forever” and “we all need to be grateful that these technologies were aggressively pushed forward and now we have therapies that can really help critically ill patients,” concludes Granada.
A study has found that bifurcated T-stent reconstruction offers a safe and effective treatment option for hepatic venous outflow obstruction (HVOO) with anastomotic stenoses in orthotopic liver transplantation (OLT) recipients.
The findings of this study were presented at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online), and indicated that this interlocking stent construct may also offer advantages in treating complex stenosis involving the hepatocaval junction—while minimising the risk of stent migration or the jailing of hepatic venous (HV) outflow by an inferior vena cava (IVC) stent.
Clinical success, as demonstrated by an improvement in the presenting symptoms of HVOO, was seen in six (75%) of the eight OLT patients included in the study, while the remaining two (25%) patients required repeat intervention, which was performed within two months due to a lack of clinical response in both cases.
The study was presented by Dillon Brown, a medical student at the University of Washington School of Medicine (Seattle, USA), who said: “The bifurcated hepatocaval stent model employed in our study could mean lower rates of complications such as stent migration and hepatic vein jailing for OLT patients experiencing hepatic venous outflow insufficiency. It could also allow the operator to treat more severe anastomotic stenosis, and treat both IVC and HV stenosis simultaneously.”
The study involved a total of eight OLT patients with symptomatic HVOO (six males; mean age: 57.6±7.6 years; range: 48–69 years), all of whom underwent combined IVC and HV bifurcated T-stent placement between 2004 and 2019. Indications observed in these patients included seven refractory ascites (87.5%), four liver function abnormalities (50%), and one hepatic hydrothorax (12.5%) in the setting of hepatocaval anastomotic stenoses, diagnosed using either Doppler ultrasound or computed tomography.
According to Brown, success, adverse events, and stent patency were all assessed, with technical success being defined as intended bifurcated hepatocaval stent placement and clinical success being defined by improvements in presenting symptoms.
All of the patients included in the study underwent technically successful bifurcated hepatocaval stent reconstruction with supra/intrahepatic IVC stent (Wallstent, Wallflex [Boston Scientific] or Gianturco Z-stent [Cook Medical]) placement followed by HV stent (Venovo [BD], Smart [Cordis], or Wallstent [Boston Scientific]) placement through the interstices of the IVC stent. The mean number of stents placed in each patient was 2.3 ± 0.5 (range: 2–3), with a mean IVC stent diameter of 22.6±4.7mm (range: 14–30mm) and a mean HV stent diameter of 12.4±2.2mm (range: 10–16mm).
While no IVC stent migrations occurred over the course of the study, one HV stent migration occurred 18 days after placement, requiring retrieval from within the IVC stent and replacement. One patient also died 66 days after intervention due to graft rejection, according to Brown.
In six of the eight patients included in the study, Brown stated clinical success was achieved at a mean time of 41±28.4 days (range: 7–91 days). For the remaining two patients, repeat intervention was performed within two months due to a lack of clinical response—including angioplasty (n=2) and additional IVC stent placement (n=1) for in-stent stenoses.
All of the stents demonstrated patency at the last follow-up appointment (mean: 2,126 days; range: 32–4,846 days), leading the researchers to conclude that bifurcated T-stent reconstruction offers a safe and effective therapy for HVOO with anastomotic stenoses in OLT.
“The next steps in researching the bifurcated hepatocaval stent construct will be to increase the size of our study by increasing the number of patients who receive this treatment, and also comparing the patient outcomes of patients receiving the bifurcated stents with conventional single-stent therapies,” Brown said.
Vascular Therapies recently announced results from its phase 3 clinical trial in which Sirogen showed encouraging arteriovenous fistula (AVF) outcomes in elderly end-stage renal disease (ESRD) patients. Sirogen is the company’s proprietary sirolimus formulation for intraoperative local drug delivery to reduce surgical stenosis in blood vessels.
Following positive clinical results from a phase 2 clinical study (n=30; two international sites, two surgeons), the company embarked on the ACCESS study, a phase 3, randomised, controlled, multicentre clinical trial. The ACCESS study enrolled 243 patients with ESRD and chronic kidney disease (CKD) from 20 US sites, including 20 nephrologists and 26 surgeons.
The study was designed to evaluate the safety and effectiveness of Sirogen to improve outcomes in patients undergoing the surgical creation of an AVF to provide vascular access for haemodialysis. The primary endpoint of fistula suitability for dialysis at six months was not achieved; however, in exploratory subgroup analyses that reflected the demographics of the enrolled population, the ACCESS study revealed important potential benefits for ESRD patients age 65 and older who required an AVF for dialysis, namely:
Improved overall AVF maturation
Improved radiocephalic AVF maturation
Improved suitability for dialysis at 12 months
Improved secondary patency
Maria DeVita, senior nephrologist at Lenox Hill Hospital in New York, USA, and medical monitor for the study, commented, “The clinical results from the ACCESS study are very encouraging, especially for ESRD patients age 65 and older, who represent 50% of the haemodialysis population in the USA. Additionally, there were no unexpected adverse events, confirming theoverall favourable safety profile of the product.”
Sriram Iyer, chief scientific officer of Vascular Therapies, added, “The findings from the ACCESS study address an important unmet need for elderly dialysis patients. We would like to thank the nephrologists, surgeons, clinical coordinators, and patients for their participation in the study.”
More than half (58%) of radiology leaders say they do not have enough diagnostic and interventional radiologists to keep patients safe, new data from National Health Service (NHS) trusts and health boards across the UK show. The data, recently published in a Royal College of Radiologists (RCR) report, also show that, despite many imaging doctors staying in the NHS last year to help the coronavirus effort, the NHS radiologist workforce is now short-staffed by 33% and needs at least another 1,939 consultants to meet safe staffing levels and pre-coronavirus levels of demand for scans.
Furthermore, half of trusts and health boards (47%) do not have the staff or transfer arrangements needed to run safe 24/7 interventional radiology services, meaning patients are potentially missing out on life-saving procedures. Without more consultants in training, investment in new models of care and better staff retention and recruitment, by 2025 the UK’s radiologist shortfall will hit 44% (3,613 consultants short of real terms demand).
Mark Callaway, radiology workforce lead at The Royal College of Radiologists (RCR), comments: “Our new report has found the NHS needs thousands more radiologists to ensure patients get the safe and effective treatment they deserve, amplified by the first-hand experience of frontline doctors who witness the impact of consultant shortages on patient care on a daily basis.
“The staffing forecast for 2025 makes grim reading, but, even more worryingly, swathes of demoralised radiologists are imminently looking to work less or leave the NHS.”
The RCR’s latest workforce census reveals the NHS needs nearly 2,000 extra radiologists to clear scan backlogs, meet safe staffing quotas, and keep up with demand.
Meanwhile, a recent poll to gauge radiologists’ morale found half intend to cut their hours, and three times as many consultants than normal plan to leave the NHS in the next year.
Waiting lists for hospital treatment have now hit record highs in England and tens of thousands of patients currently face long waits for scans3.
Understaffed radiology departments across the UK are working hard to bring down backlogs caused by last year’s pause in non-urgent hospital work, while having to scan at a slower rate because of infection control and social distancing measures.
The census shows radiologist staffing has reached a tipping point, with imaging leaders warning that shortages pose a serious threat to NHS recovery and that patients facing “long, anxious and inevitable” waits for diagnoses and surgery as a result.
Hospital leaders completing the RCR’s census said radiologist shortages now continually jeopardise patient safety, reporting: “We cannot deliver adequate services for our patients” and “we can no longer provide cancer and acute care safely”.
The report shows the UK now has 4,277 radiology consultants, equating to 3,902 doctors working full-time, an increase of 170 full-time consultants compared to 2019.
Consultant numbers are increasing, but not fast enough to keep up with patient demand. RCR shortfall calculations, which use rota and service demand figures to give a realistic estimate of NHS requirements, show radiologist shortfalls range from 24–38% across the UK.
England now has 146 more full-time imaging experts than it did in 2019. However, it still needs another 1,675 consultants to keep up with NHS demand.
Radiologist numbers in other home nations have barely risen
Northern Ireland gained 19 extra full-time radiology consultants in 2020. Scotland gained five. Wales’ radiologist workforce has stalled and the country has incurred huge patient backlogs for scans during the pandemic. Wales also has the most severe radiologist shortage of any UK nation.
If nothing improves, the RCR predicts the UK’s 33% actual radiologist shortfall will hit 44% by 2025.
Closing the forecast gap between consultant supply and demand would require the number of new radiologists in training across the UK to treble, from 300 to 900 training places per year.
However, shortages could deepen even more quickly than forecast if findings from a recent RCR member survey are realised.
A poll of 1,089 UK radiology consultants at the start of April 20217 found:
41% are moderately or severely demoralised in their jobs post-pandemic
Nearly half (48%) are planning on working less after the past year
A fifth (22%) are now considering leaving the NHS
12% are considering leaving in the next 12 months—three times as many radiologists than would normally leave the NHS each year, equating to potentially losing 735 consultants and trainees across the whole workforce.
Last year, NHS England’s top diagnostics adviser Mike Richards called for a major increase in hospital scanners and radiology staff in England.
On the back of these “stark” staffing data, the RCR is calling for these measures to be urgently realised across the whole of the UK.
The RCR’s radiology workforce lead Mark Callaway says: “The coronavirus pandemic has bluntly contrasted the every-day heroism of NHS teams with the chronic under-funding of services, and the cracks in radiology, as elsewhere, are becoming undeniable.
“Our new report has found the NHS needs thousands more radiologists to ensure patients get the safe and effective treatment they deserve, amplified by the first-hand experience of frontline doctors who witness the impact of consultant shortages on patient care on a daily basis.
“The staffing forecast for 2025 makes grim reading, but, even more worryingly, swathes of demoralised radiologists are imminently looking to work less or leave the NHS.
“Unless hospital imaging capacity is massively improved, the UK will continue to lag behind other countries on cancer survival rates and patients will face worse outcomes for trauma care and all kinds of conditions. The need for investment is urgent.
“The UK’s political leaders have made encouraging pledges around catching up with scan backlogs and implementing new diagnostic pathways and community-based scanning away from hospitals.
“The NHS also came through last year with emergency funding for scanners and private provider support, and we strongly support emerging plans to introduce diagnostic hubs to speed up access to scans, but the vital issue remains—we need more staff.
“Without thousands more radiologists—as well as radiographers, nurses and support staff—patients will inevitably continue to face long, anxious waits for radiology services, missing out on crucial early diagnoses and life-saving image-guided surgery.”
BD announced today that enrolment has begun and the first patients have been treated in the postmarket surveillance study, CONNECT-AV.
CONNECT-AV is a prospective, single-arm, open-label study that will follow patients treated with the WavelinQ endovascular arteriovenous fistula (endoAVF) system for 24 months.
The study’s dual primary effectiveness endpoints are the percentage of subjects dialysing using successful two-needle cannulation for at least 75% of the dialysis sessions over a continuous 28-day period at six months, and the subjects maintaining primary patency at six months.
The primary safety endpoint is freedom from device- and procedure-related serious adverse events through 30 days. The trial is expected to enrol 280 participants in the USA.
“For more than 50 years, medicine has looked for a next-generation haemodialysis access procedure for patients with end-stage kidney disease (ESKD) that can truly change the treatment paradigm,” said Brandon Repko, medical director of nuclear imaging and therapeutic services at Butler Memorial Hospital in Butler, USA, who treated the first patient in the CONNECT-AV trial in March 2021. “The CONNECT-AV trial is the next step in proving WavelinQ endoAVF system’s role in 21st century AVF creation. My colleagues and I are thrilled to be a part of that patient care evolution.”
CONNECT-AV is one of two postmarket studies of the WavelinQ endoAVF aystem. The second study, WAVE-Global is a prospective, single-arm, open-label study that will follow patients treated with the WavelinQ endoAVF system for 24 months.
The WAVE-Global primary endpoints are the number of interventions needed post creation to facilitate and/or maintain AVF use at six months, and the proportion of participants with freedom from Clinical Events Committee adjudicated device- or procedure-related serious adverse events at 30 days. The trial is expected to enrol 150 participants globally (outside of the USA).
“Physicians already have real-world experience using the WavelinQ endoAVF system to create AVFs that make life-preserving haemodialysis possible,” said Panagiotis M Kitrou, assistant professor in interventional radiology at Patras University Hospital in Patras, Greece, and a principal investigator in the WAVE-Global study. “Both of these studies will provide important long-term data on the safety and effectiveness of WavelinQ endoAVF aystem to help make informed decisions about patient care.”
The first patient in the WAVE-Global trial was treated by Kitrou in December 2020 at Patras University Hospital.
Pictured clockwise from top left: Roger Greenhalgh (London, UK); Bijan Modarai (London, UK); Gustavo Oderich (Houston, USA); Marc Schermerhorn (Boston, USA); Konstantinos Spanos (Larissa, Greece); and Enrico Rinaldi (Milan, Italy).
Clockwise from top left: Roger Greenhalgh (London, UK); Bijan Modarai (London, UK); Gustavo Oderich (Houston, USA); Marc Schermerhorn (Boston, USA); Konstantinos Spanos (Larissa, Greece); and Enrico Rinaldi (Milan, Italy).
Opening the Charing Cross (CX) 2021 Digital Edition (19–22 April, online), experts deliberated crucial controversies in the abdominal aortic space. Discussion emphasised the potential of Philips’ Fiber Optic RealShape (FORS) technology to reduce radiation and ease technical success, with moderator Gustavo Oderich (Houston, USA) suggesting that “radiation will be a thing of the past” thanks to this new technology. Other key takeaways were a ringing endorsement that endoanchors have a part to play in the treatment of challenging necks, and consensus among the panel that parallel grafts should be used as little as possible in this hostile anatomy.
FORS addresses “major area of need” in abdominal aortic surgery
Marc Schermerhorn (Boston, USA) gave a presentation on the “disruptive” technology of FORS, which opened a panel discussion on the topic of radiation. Oderich stated that FORS “addresses a major area of need, which is the ability to look at the anatomy on any view we want without being radiated”, highlighting that the technology offers both an ease of technical success and parallel reduction of radiation. Looking ahead, he posited: “Radiation is going to be a thing of the past”.
Following Schermerhorn’s presentation, a Philips’ Meet the Experts session offered a deep dive into FORS technology, with a panel of users and experts discussing latest clinical experience and three-dimensional (3D) catheter agnostic guidance.
Registrants can view Schermerhorn’s presentation on demand here and Philips’ Meet the Experts session here.
Endoanchors in challenging necks come of age
In a Podium 1st presentation, William Jordan (Atlanta, USA) revealed preliminary five-year data from the primary arm of the ANCHOR registry (Aneurysm treatment using the Heli-FX EndoAnchor system global registry). This is a multicentre, prospective study designed to capture real-world usage of the Heli-FX EndoAnchor system (Medtronic) in patients with challenging AAA anatomy, particularly those with hostile aortic neck anatomies. Jordan concluded that, out to five years, patients with hostile necks “may have acceptable durability when the EndoAnchor fixation method is used, particularly at the index operation”.
Registrants can view this presentation on demand here.
Showcasing the practical use of endoanchors in the challenging neck anatomy, Giovanni Pratesi (Genoa, Italy) presented an edited case, with postoperative computed tomography angiography (CTA) showing complete aneurysm exclusion in a challenging proximal aortic neck.
Registrants can view this edited case on demand here.
Audience vote against use of standard EVAR in majority of challenging necks
A CX Debate addressed another pressing issue regarding hostile neck anatomy—that being whether standard endovascular aneurysm repair (EVAR) can be used in most challenging necks. Colin Bicknell (London, UK) stood for the motion, while Vascular Society of Great Britain and Ireland (VSGBI) president Michael Jenkins (London, UK) put forward the counterargument.
“There is significant, successful innovation to ensure short-term sealing and prevent long-term complications,” argued Bicknell, who resolved that EVAR is therefore appropriate for “most” patients with AAA who prefer this approach. Jenkins, on the other hand, contended that standard EVAR cannot be used in most challenging necks “because it does not work”. He elaborated: “It is outside IFU [instructions for use], aortic neck dilatation leads to loss of seal, and sac expansion causes positional change and effacement of seal zone.” He added that while adjuncts may help transiently, they are not durable. “What may have been heroic 10 years ago, perhaps maverick five years ago, now is criminal”, Jenkins concluded.
CX polling results
Following the debate, polling revealed that 71% of the CX 2021 audience disagreed with the motion that standard EVAR can be used in most challenging necks.
Consensus among panel that parallel grafts should be used as little as possible in hostile necks
Also addressing a challenging neck controversy, Alexander Zimmermann (Zürich, Switzerland) gave a presentation on parallel graft use in the anatomy of a hostile neck, focusing in particular on “disappointing” clinical results thus far. He concluded that, in the majority of cases, he aims to “stay away” from using such grafts in challenging necks; the moderators were in agreement, with Ian Loftus (London, UK) voicing that he would only use parallel grafts in “very selective emergency cases” and Roberto Chiesa (Milan, Italy) stating that he uses parallel grafts as infrequently as possible.
Registrants can view this presentation on demand here.
Clockwise from top left: Roger Greenhalgh (London, UK); Andrew Holden (Auckland, New Zealand); Gunnar Tepe (Rosenheim, Germany); Thomas Zeller (Bad Krozingen, Germany); Roopa Prabhakar (MHRA, London, UK); and Sara Royce (FDA, Silver Spring, USA).
Addressing representatives from the US Food and Drug Administration (FDA) and UK Medicines and Healthcare products Regulatory Agency (MHRA)directly, Thomas Zeller (Bad Krozingen, Germany) argued at the Charing Cross (CX) Digital Edition 2021 (19–22 April, online) that “it is time to change the agency recommendations regarding paclitaxel use in peripheral interventions”. Moderators Andrew Holden (Auckland, New Zealand) and Gunnar Tepe (Rosenhein, Germany), Podium 1st presenters Gary Ansel (Columbus, USA) and William Gray (Wynnewood, USA), as well as a 71% majority of the CX audience, supported this view. While there was agreement that it was right to be concerned about the paclitaxel mortality signal raised by Konstantinos Katsanos (Patras, Greece) et al in their December 2018 meta-analysis, there was strong consensus that the evidence is now clear there is no mortality effect when paclitaxel is used in the peripheral arteries. In addition, it was noted that several individual patient-level meta-analyses failed to confirm the high mortality signal flagged by Katsanos and colleagues. There was some discussion surrounding the place of limus as an alternative to paclitaxel, but experts agreed that there is no need to move to another drug—which would have its own set of challenges—given the proven safety and efficacy of paclitaxel. The takeaway message was clear: that, with proper caution and the correct dose, paclitaxel can and should be used in peripheral interventions.
More data find no mortality associated with paclitaxel
Patient safety has been at the centre of CX discussion on the paclitaxel issue since the Katsanos meta-analysis was published. This year, further data were presented that support the conclusion of vascular pathologist Elena Ladich (Hollywood, USA) who two years ago at CX 2019 stated that there are “no causal links or mechanisms to explain the reported association of paclitaxel in the lower limbs and patient mortality”.
Sabine Steiner (Leipzig, Germany) gave the first presentation on long-term paclitaxel data at CX 2021, outlining five-year results of the REAL-PTX study—an investigator-initiated, prospective, European, multicentre randomised controlled trial (RCT) comprising 150 patients with femoropopliteal disease. Patients were randomised to treatment with either a drug-eluting stent (100% Zilver PTX, Cook) or a drug-coated balloon (DCB; 77.3% IN.PACT Admiral/IN.PACT Pacific, Medtronic; 21.3% Lutonix, BD). Steiner reported that mortality rates after five years were “comparable to prior reports investigating long-term outcomes for drug-eluting and non-drug-eluting devices”.
Registrants can view this presentation on demand here.
Also presenting data in support of the safety of paclitaxel, Mårten Falkenberg (Gothenburg, Sweden) gave the latest analysis and interpretation of the SWEDEPAD trial concerning mortality. “It is very unlikely that devices coated with paclitaxel used for the treatment of peripheral arterial disease [PAD] do increase late mortality”, he concluded.
Registrants can view this presentation on demand here.
In a Podium 1st presentation on the topic, Andrew Holden (Auckland, New Zealand), on behalf of co-authors Ramon Varcoe (Sydney, Australia) and Peter Schneider (San Francisco, USA), revealed a five-year meta-analysis update regarding drug-coated technologies in femoropopliteal interventions and all-cause mortality concerns that included the SWEDEPAD update. Holden stressed that there is a “clear benefit of paclitaxel-coated devices in femoropopliteal disease” and relayed that the investigators recommend the continued use of these devices in this patient population. “The time has arrived for regulators to provide updated and clear guidance on these devices for the benefit of patients globally”, he stated.
Registrants can view this presentation on demand here.
Consensus that paclitaxel recommendations need to be changed
With a growing pool of data showing no association between paclitaxel and mortality, representatives from the FDA and MHRA reiterated current agency positions on the topic. Sara Royce, team lead of the plaque modification devices team at the FDA, talked the CX audience through regulatory approaches to the next-generation of drug-coated devices for PAD. Roopa Prabhakar, senior medical devices specialist at the MHRA, offered a UK perspective on paclitaxel device regulation, saying the agency will “continue to assess the significance of any new data in relation to patient safety”.
Registrants can view Royce’s presentation on demand here and Prabhakar’s presentation here.
Following these presentations, Thomas Zeller argued that it is time to change the agency recommendations regarding paclitaxel use in peripheral interventions. “Withholding such devices to patients with severe peripheral arterial occlusive disease may even harm them and result in increased global healthcare costs”, he stated, concluding that “the benefit outweighs the hypothetical risk”.
Registrants can view this presentation on demand here.
CX polling results
Audience polling following Zeller’s talk revealed that 74% of the audience agree it is time to change the agency recommendations regarding paclitaxel use in peripheral interventions.
“What you do not leave behind is a suboptimal result”
In a Podium 1st presentation, Gary Ansel (Columbus, USA) announced results of the IN.PACT Global stented versus non-stented analysis, comprising 353 patients stented and 1,044 non-stented patients. The purpose of this study was to compare outcomes of standalone IN.PACT Admiral DCB usage versus IN.PACT Admiral DCB followed by provisional stenting. Ansel concluded that, in this complex lesion subset from the study, the IN.PACT Admiral DCB “demonstrates durable safety and effectiveness through five years”. He added: “In the event of suboptimal angioplasty results (i.e. persistent residual stenosis >50%, flow limiting dissection), the addition of a stent did not appear to decrease the optimal results through five years”.
In the discussion following Ansel’s presentation, the presenter stressed that, regardless of whether or not you leave a stent behind, “what you do not leave behind is a suboptimal result, just to not leave a prosthetic device in. That is the worst thing to leave behind.”
Registrants can view this presentation on demand here.
Time to look at “the whole patient”
William Gray (Wynnewood, USA) delivered another Podium 1st presentation, giving the five-year results from a patient-level meta-analysis of the ILLUMENATE RCTs. He told attendees how “The Stellarex DCB continues to consistently demonstrate no difference in mortality compared to percutaneous transluminal angioplasty (PTA) year-over-year through five years, both within individual RCTs and pooled analysis.”
When asked by moderator Robert Hinchcliffe (Bristol, UK) if this was “the definitive trial to put the paclitaxel issue to bed”, Gray commented: “When you ask a US physician what puts an issue to bed, that is when the FDA rescinds their statement about danger. In order for them to do that, I think we have to see a high quality, patient-level meta-analysis that includes all the original studies included in Katsanos’ meta-analysis, followed up to five years, plus all the other datasets that have come forward since that time. The key piece here, that we do not talk enough about but we need to recognise, is that the missing data, which were on the order of 20% of the original analysis, even at the patient level, are now only about 5%, as we have gone back and done all the vital statistics. I think that will make a big difference in the ultimate analysis.”
Gary Ansel (Columbus, USA) chimed in to comment on the fact that mortality is largely due to cardiovascular issues or cancer. “I do not think we are really focussed on that,” he said. “Forget the paclitaxel, which has been really put to bed, and let us get back to good patient care and see if we can decrease those cardiovascular and cancer rates.”
Gray agreed, saying that the “major message” was that cardiovascular risk factor modifications (smoking cessation, diabetes and hypertension management) were important to consider, and that it was time to look at “the whole patient”.
Registrants can view this presentation on demand here.
Soundbite Medical Solutions has announced US Food and Drug Administration (FDA) 510(k) approval for the SoundBite crossing system—Peripheral (SCS-P) with the 0.014” active wire (14P).
The SoundBite crossing System—Peripheral (14P) is a recanalisation tool, designed to help physician’s placement of conventional guidewires or treatment devices in the intraluminal space beyond chronic total occlusions (CTOs) in patients suffering from heavily calcified above-the-knee (ATK) and below-the-knee (BTK) peripheral arterial disease (PAD).
The SoundBite crossing system—Peripheral (14P) consists of the reusable SoundBite console, a single-use sterile SoundBite active wire 14P, and their respective accessories. SCS-P leverages Soundbite’s proprietary method to produce and safely deliver shock waves via guidewire platforms to selectively “micro- jackhammer” through calcified lesions. SCS-P is now approved in major markets with CE mark, FDA 510(k), and Health Canada approvals in both 0.018” and 0.014’’ platforms.
The results of a recent investigation have revealed no association between infrainguinal bypass tunnelling technique and primary outcomes in patients with limb ischaemia. “Compared to subfascial tunnelling,” write Nallely Saldana-Ruiz (University of Southern California, Los Angeles, USA) and colleagues in the Journal of Vascular Surgery (JVS), “the superficial tunnelling technique is not associated with primary patency or major amputation in limb ischaemia patients undergoing infrainguinal bypass with a single-segment great saphenous vein”.
Saldana-Ruiz et al detail in JVS that they queried the National Vascular Quality Initiative database infrainguinal bypass module from 2008–2017 in order to address a potential association between tunnelling technique and outcomes. They also communicate that tunnelling type was not associated with primary patency, primary-assisted patency, secondary patency, or major amputation, according to multivariate analyses (p>0.05).
The main exposure variable, Saldana-Ruiz and colleagues relay, was the type of tunnelling—either subcutaneously or subfascially. Primary outcomes were primary patency and amputation, while secondary outcomes included primary-assisted patency and secondary patency. They detail: “We excluded non-greater saphenous vein grafts, grafts using multiple segments, indications of aneurysmal disease, bypass locations outside of femoral to below-knee popliteal artery or tibial arteries, and those missing data on the tunnelling type and limb ischaemia”.
The investigators state that they included a total of 5,497 bypasses—2,835 subcutaneous and 2,662 subfascial—in their study. Writing in JVS, they report the following headline results: “Age, race, graft orientation (reversed/non-reversed), bypass donor and recipient vessels, harvest type, end-stage renal disease, smoking, coronary artery bypass graft, congestive heart failure, P2y12 inhibitor at discharge, surgical site infection at discharge, and indication (rest pain/tissue loss/acute ischaemia) were associated with tunnelling technique,” stating a p-value of <0.05.
Medtronic recently announced the safety and effectiveness results through 24 months for the IN.PACT AV Access clinical study. The data, which were presented virtually as a Podium 1st at the Charing Cross (CX) 2021 Digital Edition (19–22 April, online) demonstrated that the IN.PACT AV drug-coated balloon (DCB) is the first and only DCB to show sustained and superior effectiveness through two years compared to standard percutaneous transluminal angioplasty (PTA) in end-stage renal disease (ESRD) patients with de novo or non-stented restenotic native arteriovenous fistulae (AVF) in the upper extremity.
“A patient who receives haemodialysis will often need to have several reinterventions each year to maintain patency and keep critical access sites open and functioning properly,” said Andrew Holden (Auckland Hospital and Auckland University, Auckland, New Zealand), who presented the results at CX 2021. “Being able to show these results at two years will ultimately impact standard of care for patients undergoing dialysis. For my patients, these durable results translate into fewer reinterventions and a better quality of life.”
Over two years, the IN.PACT AV DCB group demonstrated a continued clinical benefit compared to the PTA control group. Key data highlights per Kaplan-Meier estimates for this dataset include:
Target lesion primary patency through 24 months was 52.2% in the IN.PACT AV DCB group compared to 36.2% in the PTA control group (log-rank p<0.001).
Access circuit primary patency through 24 months was 39.5% in the IN.PACT AV DCB group compared to 25.4% in the PTA control group (log-rank p<0.001).
Freedom from all-cause mortality through 24 months was 82.4% in the IN.PACT AV DCB study group and 82.8% in the PTA control group (log-rank p=0.829).
IASIOS-accredited centres, from L to R: Anadolu Medical Center; Guy’s and St Thomas’s Hospital, NHS Trust; Strasbourg University Hospitals, HUS.
The International Accreditation System for Interventional Oncology Services (IASIOS) has passed its pilot phase with flying colours, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has announced in a press release, and is now open for public enrolment. Twelve pioneering hospitals from nine countries successfully participated in the IASIOS pilot phase. This robust accrediting system, tested and optimised over the past two years, now stands ready to accept applications from facilities offering interventional oncology (IO) services worldwide, regardless of the institution’s size or location.
IASIOS is the world’s only accreditation scheme focussed exclusively on minimally-invasive treatments for cancer. Its main goal is to establish the highest quality standards in IO care throughout the entire service line and patient pathway.
Cancer patients can benefit greatly from IO treatments whose minimally invasive nature is proven to provide numerous advantages, such as less pain, fewer complications, and shorter recovery times than conventional surgery, radiation, or chemotherapy. Furthermore, many IO procedures can be performed on an outpatient basis, increasing efficiency, reducing costs and waiting times, and allowing earlier resumption of normal life. This is especially important in these challenging times, as the pandemic has resulted in backlogs in cancer care which IO could help to substantially reduce.
With the continued growth and recognition of IO as an important clinical discipline and the fourth pillar of cancer care, facilities providing IO therapies must follow appropriate guidelines if the relevant treatments are to be used safely and appropriately. It is likewise essential for patient safety and satisfaction that interventional oncologists have the ability and means to officially prove their value and expertise to patients and hospital administrators, not merely as technicians, but rather as primary clinical healthcare providers. In order to achieve exactly that, the Standards of Quality Assurance in Interventional Oncology, published by CIRSE, were used as a blueprint and set the foundation for developing an accreditation system that will be instrumental in the standardisation of IO services on a global scale.
Chair of the IASIOS supervisory board, Andreas ‘Andy’ Adam (Guy’s and St Thomas’ NHS Foundation Trust, London, UK), provides insight into this global launch, commenting: “IASIOS is the culmination of years of dedicated work by CIRSE. It is exciting to reach this stage, as this pioneering accreditation scheme will help improve cancer care around the world.”
Adam told Interventional News last year that as IASIOS focuses on the entire patient pathway, it is a way of recognising that interventional oncologists are “clinicians, not just technicians”. Speaking in April 2020, he said that the project “will help establish IO as a mainstream clinical discipline, so is very important to IO as a whole”.
Centres that enrol in the IASIOS system become part of a greater worldwide community of top IO centres working together to further develop and promote the practice of IO and raise awareness of the benefits of this discipline amongst both patients and medical providers.
The first patient has been enrolled in the LAVA study to evaluate the safety and effectiveness of the BlackSwan Lava liquid embolic system (LES) for the embolic treatment of arterial haemorrhage in the peripheral vasculature, Sirtex Medical and BlackSwan Vascular have announced in a press release.
The LAVA study, which stands for Liquid embolization of arterial haemorrhages in peripheral vasculature, is a prospective, multicentre, single-arm study of 113 subjects at 20 investigational sites in the USA. The first patient has been enrolled at the University of North Carolina School of Medicine in Chapel Hill, USA, where a clinical team successfully treated a patient with a bleeding hypervascular tumour in the liver using the Lava LES.
“I was able to experience first-hand the impact of embolization with the Lava LES for patient treatment, and I am very pleased with the result,” says Clayton Commander, assistant professor of Radiology at University of North Carolina School of Medicine, who treated the first patient in the LAVA study. “The system has been well studied in pre-clinical testing, and we are thankful to BlackSwan for leading this clinical programme with support from Sirtex that has the potential to bring meaningful advancement to the peripheral vascular field.”
LAVA is led by co-principal investigators Bulent Arslan at the Rush University Medical Center in Chicago, USA, and Mahmood Razavi at St Joseph Heart and Vascular Center in Orange, USA. The study population will include patients with active arterial bleeding from the peripheral vasculature.
“We are thrilled for the launch of the LAVA study, which has the potential to lead to the first US Food and Drug Administration [FDA]-approved liquid embolic for a peripheral vascular application in the USA,” comments Kevin Smith, Chief Executive Officer of Sirtex. “We are proud to partner with BlackSwan on its clinical journey and look forward to the potential expansion of treatment options in the endovascular field for interventionalists and patients in need.”
The LAVA study will assess the primary safety endpoint of a composite of freedom from 30-day major adverse events and the primary effectiveness endpoint of clinical success, defined as absence of bleeding from the target lesion after embolization with the Lava LES, without the need for emergency surgery, re-embolization, or other target lesion reinterventions within 30 days of the index procedure.
“Currently, there is no liquid embolic agent that is indicated for peripheral vascular applications in the USA. Lava has key differentiators of optimised radiopacity, availability in two viscosities, reduced preparation time, and controlled delivery, which can enable treatment of a wide array of peripheral vascular diseases,” says Suresh Pai, Chief Executive Officer of BlackSwan. “Moving the LAVA study forward advances our mission to provide the interventional community with the tools they need that drive safe, effective, and value-based treatments. We are eager to discover the findings.”
The LAVA study enrollment follows the strategic collaboration Sirtex and BlackSwan entered in December 2020. Under the collaboration, Sirtex made a significant equity investment in exchange for preferred shares in BlackSwan, as well as an option to purchase the remaining shares of the company at an agreed price.
“With Varian, Siemens Healthineers has the most comprehensive portfolio in the MedTech sector, which offers the company considerable potential for value creation. With a highly integrated approach, Siemens Healthineers will take the global fight against cancer to a new level,” says Ralf P Thomas, chair of the Supervisory Board of Siemens Healthineers AG.
“With the completion of this transaction, we are now best-positioned to take two leaps together: a leap in cancer care and a leap in our impact on healthcare overall. Together, we are establishing a strong and trusted partner capable of supporting customers and patients along the entire cancer care continuum as well as through all major clinical pathways,” comments Bernd Montag, CEO of Siemens Healthineers AG.
Chris Toth, CEO of Varian, adds: “Through the transformative combination of Varian and Siemens Healthineers, our united company will address the growing need for personalised, data-driven diagnosis and precision cancer care that enables us to fight back against globally increasing cancer rates. By bringing together our unique and highly complementary portfolios and capabilities, we will support oncology clinicians and patients in achieving better outcomes and move even closer to achieving our vision of a world without fear of cancer.”
According to a company press release, the acquisition of Varian will allow Siemens Healthineers to leverage AI-assisted analytics to advance the development and delivery of data-driven precision care and redefine cancer diagnosis, care delivery, and post-treatment survivorship. Through early and accurate detection as well as more efficient diagnosis, increased treatment quality and access, Siemens Healthineers will support and accelerate Varian’s mission to reduce uncertainty for cancer patients and increase the level of cancer survivorship.
Varian’s common stock ceased trading on the New York Stock Exchange prior to the opening of trading today.
One-year findings from B Braun’s CONSEQUENT ALL COMERS observational study were recently published by principal investigator Ralf Langhoff (Sankt Gertrauden Hospital, Berlin, Germany) et al online in Angiology. The data were first presented earlier this year at LINC 2021 (The Leipzig Interventional Course; 25–29 January, online).
In this prospective, single-arm, multicentre observational study, the SeQuent Please over-the-wire (OTW) drug-coated balloon (DCB; B Braun) was used in above-the-knee (ATK) and below-the-knee (BTK) peripheral arterial occlusive disease. The investigators report that, despite the high prevalence of comorbidities, target lesion revascularisation (TLR) and mortality rates were comparable for clinical outcomes of other contemporary DCBs.
Langhoff and colleagues detail that the overall technical success rate of the 1,269 DCBs used was 99.6% (1.6±0.79 DCBs/patient), adding that 12-month TLR rates were 6.3% in patients with chronic limb-threatening ischaemia (CLTI) and 9.6% in claudicants, with a primary patency rate of 89.9% and 87.1%, respectively. They also write that all-cause mortality was 4.3%.
Constantino Peña (Miami, USA) moderates anInterventional Newswebinar focusing on how the SmartCT system (Philips) can “transform” IR suites and the importance of 3D imaging within this setting. Peña is joined by two early-users of the technology, Marc Sapoval and Hicham Kobeiter, both from Paris, France.
Discussing the transition to SmartCT, Sapoval says his team was “very impressed” by the ease of adoption, adding that the “learning curve is quite short”. Kobeiter further states that he is “more comfortable” in the Azurion room with the SmartCT than he was with previous systems.
Asked about improvements to the tableside and workflow, Sapoval says that SmartCT is “very convenient” in that it allows the physicians to conduct all appropriate 3D imaging without leaving the lab and compromising sterility. Kobeiter adds that another advantage is that it helps in teaching others who are outside of the room and gives the user greater control and manipulation of the room. These experiences, says Peña, highlight how the system has made the workflow “more efficient”.
They also highlight advantages of using the system in the current environment with Kobeiter noting that when there is a COVID patient he goes immediately to the room with the SmartCT because “we know that once we step in we do not need to go out”.
The results of a two-year study support the continued safety and effectiveness of the Zilver Vena Venous Stent (Cook Medical) in treating symptomatic iliofemoral venous outflow obstruction, according to findings presented at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online).
The stent met primary safety and effectiveness endpoints at one month, and continued to do so through one- and two-year intervals during the VIVO Clinical Study.
In addition, the Zilver Vena Venous Stent demonstrated high rates of patency by ultrasound, freedom from clinically-driven reinterventions and freedom from reinterventions more generally throughout—all of which were clinical outcomes being assessed in the study.
According to Lawrence “Rusty” Hofmann, professor of interventional radiology at Stanford Medicine (Stanford, USA) and the study’s presenting author, the stent’s integrity was also indicated by the fact there were no core laboratory reports of stent fractures across the two-year study period.
“There has been concern over the years at some centres about stenting below the inguinal ligament,” he said. “In this study, more than 20% of stents extended into this region, and there were not any stent fractures.”
The VIVO Clinical Study took place between December 2013 and October 2016, and enrolled 243 patients (70% female; mean age: 53±15 years) with symptomatic obstruction of one iliofemoral venous segment.
Data assessed during the study included baseline patient characteristics, primary and secondary endpoints—such as 30-day freedom from major adverse events, 12-month primary quantitative patency, and changes in venous clinical severity score (VCSS) from baseline to one month and 12 months—as well as patency, reintervention, clinical outcomes and stent integrity through two years.
The Zilver Vena Venous Stent met primary endpoints for both safety and effectiveness, with a 96.7% rate of 30-day freedom from major adverse events and an 89.9% rate of 12-month primary quantitative patency.
In addition, Hofmann said the mean change (-3.0; p<0.0001) in VCSS from baseline was “significant” at one month and was sustained through 12 months (-4.2), and maintained at two years. Specifically, two-year outcomes included high rates of patency by ultrasound (90.3%±2.2%), freedom from clinically-driven reinterventions (93.2%±1.8%), and freedom from reinterventions (83.4%±2.5%).
“This landmark study moves the ball forward in the treatment of deep venous disease,” Hofmann concluded.
While there is large variability based on the site of insertion, patient characteristics and previous accesses, fluoroscopically-guided insertion of tunnelled central venous catheters (td-CVC) for dialysis can be considered a “low exposure” procedure, according to a report.
The report, which is published in The Journal of Vascular Access (JVA), also concludes, however, that patient exposure to ionising radiation during these dialysis access procedures is “significantly higher” than the levels associated with oncological port-a-cath CVC procedures—and nephrologists should be aware of the administered dose to ensure they comply with the 2013 European Directive on protection against ionising radiation exposure (IRE).
In concluding the report, Andreana De Mauri, the lead author and a researcher in the Nephrology and Dialysis Department at the Maggiore della Carità University Hospital (Novara, Italy), states: “In the next years, nephrologists have to take into account the legal implications, following the directives either of the scientific societies or governments, with regard to the high levels of competences, the clear definition of responsibilities and tasks of all professionals involved in the medical exposure, to ensure adequate protection of patients undergoing medical radio-diagnostic procedures.”
In spite of the indications laid out in the aforementioned 2013 European legislation, existing literature lacks information about the doses associated with fluoroscopically-inserted dialysis td-CVC, according to the report.
And, while td-CVC procedures are used worldwide—either for rescue vascular accesses or a first access in elderly and ill populations—the IRE related to them remains a knowledge gap among nephrologists, and clinical practitioners in general.
The researchers therefore conducted a retrospective study to quantify both the effective dose and the organ dose to relevant organs—including bone marrow, heart, lung, breast, thyroid and skin—in td-CVC, revising these procedures while taking into account radiation risk via dose-per-area product, fluoroscopy timings, and the different anatomical sites of catheter introduction.
The study involved 88 consecutive td-CVCs (Arrow Cannon II Plus, Teleflex), which were placed in 42 male patients (48%) and 46 female patients (52%). The anatomical districts they were used to access included a mix of the right internal jugular vein (RIJV), left internal jugular vein (LIJV), subclavian veins (SVs) and femoral veins (FVs).
Alongside this, the study also retrospectively revised 46 oncological port-a-cath CVC procedures acquired on Philips Healthcare’s Integris 5000 angiographic system, in order to compare the IRE levels in these procedures to those associated with td-CVC.
While the subsequent report concludes that fluoroscopically-guided td-CVC insertion procedures can be considered generally “low exposure”, with a minimal-to-very low risk of fatal cancer induction, it states that large variability and some exceptions exist in this area—mainly driven by the site at which the insertion took place, the characteristics of the patient, and the number of previous accesses carried out.
In addition, it states that the radiological exposure was similar for the LIJV, SV and FV access sites, but all of these were higher than the exposure in the RIJV and, as a result, the latter area should be preferred when the clinical conditions allow it.
The report also claims that, in the select few exceptional cases observed, organ doses are “not negligible” for procedures concerning the heart, lung, breast and bone marrow, and, as such, they should be added to the cumulative dose from all diagnostic and interventional procedures a dialysed patient is undergoing.
Due to the “minimal radiological risk” connected to td-CVC procedures, however, the report states that nephrologists should consider the “definitely superior benefit” deriving from this form of catheter insertion for patient dialysis—especially in patients without arteriovenous fistulae or a prosthetic loop on native vessels who require haemodialysis, as CVCs are mandatory here.
In spite of these minimal IRE-related risks, the report also concludes that these procedures should still be optimised where possible, as the nephrologist or other medical practitioner involved is still required to take part in this process by the 2013 European Directive. For example, it suggests that, depending on single-centre protocols, physicians could choose to insert a CVC using only ultrasound guidance and then perform the necessary radiological checks later via traditional chest radiography, for which the associated IRE is very low, and the related risks are negligible.
The report’s conclusion recommends that the nephrologist or practitioner in question should be aware of the ionising dose administered during a td-CVC procedure, so they can correctly inform the patient and ensure these details are included as part of the final report, as required by the law.
Endologix recently announced it has completed the acquisition of PQ Bypass, a medical technology company pioneering a first-of-its-kind technology that addresses an unmet need for new treatments for severe peripheral arterial disease (PAD).
PQ Bypass’ proprietary Detour platform for percutaneous femoral-popliteal bypass has been designated by the US Food and Drug Administration (FDA) as a Breakthrough Device. The Detour system consists of the TORUS stent graft and the PQ crossing device. The Detour system is currently being studied in a US and European clinical trial, DETOUR2.
“The acquisition of PQ Bypass is a seminal moment in Endologix’s history, building upon our leadership in the treatment of abdominal aortic aneurysm to champion disruptive technologies for the treatment of vascular disease,” said Richard Mott, CEO and chairman, Endologix. “We intend to actively pursue new and innovative vascular technologies that are clinically relevant to surgeons, hospitals, and patients, with a commitment to world-class medical education, clinical research, and excellent procedural outcomes.”
NOTE: This video is ONLY available to watch in selected countries and geographies
Jason Levy (Atlanta, USA) and Elizabeth David (Toronto, Canada) talk to Interventional News about the final cohort data from the OPuS One clinical study, the results of which were awarded as Abstract of the Year at the 2021 annual scientific meeting of the Society of Interventional Radiology (20–26 March, online).
The “compelling” data showed “improvement in pain and quality of life” both at three days and sustained out to 12 months following use of the OsteoCool Radiofrequency Ablation System. It also indicated a “lack of delayed skeletal events” such as fractures or neurologic injuries following the procedure. The fact that there were no skeletal-related events is something “you will never see in a radiation oncology trial” adds Levy.
The “significant decrease” in pain scores that were seen within hours and days of the procedure were “pretty startling”, adds David, who also discusses the use of stereotactic body radiation therapy (SBRT), its limitations and where RFA should sit within the standard of care for patients with cancer-related fractures.
Levy goes on to state that the data “really should move the needle more” towards further utilisation of radiofrequency ablation for this patient population.
Inari Medical has announced the enrolment of the first high-risk pulmonary embolism (PE) patient in the FLAME (FlowTriever for acute massive pulmonary embolism) study. One in 20 PE diagnoses is categorised as high risk and these are associated with a mortality rate of up to 40% at 90 days.
The first FLAME patient was enrolled at the Penn Presbyterian Hospital & Hospital of the University of Pennsylvania (HUP) in Philadelphia, USA, by co-principal investigators Sameer J Khandhar and Jay S Giri. “We are pleased to be the first site to enrol a patient in FLAME,” said Khandhar (Penn Medicine, Philadelphia, USA). “We frequently see on-table normalisation of haemodynamics using FlowTriever to extract large clots in PE patients. We are eager to formally study this effect in high-risk PE patients in whom the immediacy of this impact might reverse the death spiral and save lives,” he added.
FLAME is a prospective, multicentre, parallel-group observational study evaluating treatment outcomes for up to 250 high-risk PE patients. It is the largest ever high-risk PE study of any intervention and its design, informed by evidence development guidance from the American Heart Association (AHA), aims to change the high-risk PE treatment guidelines. “Conservatively managed high-risk PE is associated with high mortality, but there are limited data supporting interventional treatment. We have designed FLAME to prospectively examine all patients at participating centres with high-risk PE, including those not treated with FlowTriever, to maximise generalizability of the study,” said Giri (HUP, Philadelphia, USA).
Beyond FLAME, Inari continues to invest in its clinical study pipeline. Positive long-term late-breaking results were recently presented at VENOUS2021, (17–20 March, virtual), the annual meeting of the American Venous Forum, from both the CLOUT and FLASH studies. FLASH—already the largest prospective haemodynamic study of any PE treatment ever—is being doubled in size to 1,000 patients to collect data from a conservatively managed subgroup and include sites outside the USA. In addition, for the first time ever, 200 patients will be monitored and studied using the Apple Watch.
Royal Philips today announced US Food and Drug Administration (FDA) 510(k) clearance for its Philips SmartCT application software. SmartCT is a key component of Philips’ image guided therapy system—Azurion—providing interventionalists with computed tomography (CT)-like three-dimensional (3D) images (cone beam CT) to support diagnosis, therapy planning, treatment, and follow-up for interventional radiology procedures.
Bringing intuitive touchscreen control of advanced 3D image acquisition, visualisation, vessel/organ segmentation, and quantitative measurements to the table-side, within the interventional lab’s sterile zone, SmartCT helps enhance clinical confidence, smooths workflows, and increases productivity. It includes software applications for angiography, neurology, soft-tissue imaging, and guidewire/catheter navigation, supporting a wide range of procedures such as the treatment of aneurysms, vascular diseases, and liver tumours.
Philips’ latest Azurion image-guided therapy platform integrates essential lab systems and tools needed for complex interventional procedures into an uncluttered laboratory environment in which interventionalists can focus on treating the patient rather than being distracted by the technology. SmartCT brings total control of the Azurion platform to a touchscreen tablet situated alongside the interventional radiology table. This eliminates the need for clinicians to leave the sterile field and step into an adjacent control room, as well as supporting faster and better-informed decision making.
“A key part of our image-guided therapy strategy is to combine high-quality, low X-ray dose imaging with a superior user experience that allows interventional radiologists to diagnose and treat patients as part of smoother, safer and less interrupted workflows,” said Ronald Tabaksblat, general manager Image Guided Therapy Systems at Philips. “Philips SmartCT is a major step forward in 3D imaging, enhancing confidence in the interventional suite and supporting key elements of the quadruple aim of better patient outcomes, enhanced patient and staff experiences, and lower cost of care.”
“Changing to a new technology can be challenging, but if the system itself can show you the way, it makes it much easier to adopt new advances,” Hicham Kobeiter, chief of radiology and interventional radiology, Hôpitaux Universitaires Henri-Mondor in Crétiel, France. “SmartCT leads you through each step of the procedure, bringing us more confidence and more precision across cardiovascular, oncology, and emergency cases.”
“With the new SmartCT interface we can go into more detail more quickly and safely, with fewer staff in the room,” said Marc Sopval, interventional radiologist at Hôpital Européen Georges Pompidou AP-HP in Paris, France. “SmartCT has brought Cone Beam CT to life in everyday practice: all the tools and guidance capabilities are used by the entire team each day.”
With SmartCT, users are guided through the image acquisition process and can review and interact with the acquired CT-like 3D images on the system’s table-side touch screen module using 3D visualisation and measurement tools. These tools have been designed to support procedures in a range of clinical domains, including neurology, oncology, and cardiovascular procedures, and feature intuitive two-point distance measurements on 3D images, the ability to remove structures from the images that obstruct the region of interest, and the ability to select and store optimum projection angles for recall during procedures.
Philips SmartCT image acquisition, visualisation, and measurement software is an integral part of the next-generation Philips image guided therapy system—Azurion—which was launched in September 2020, marking an important step forward in optimising clinical and operational lab performance and expanding the role of image-guided interventions in the treatment of patients. Azurion has achieved rapid global adoption, reflecting the accelerating trend toward minimally-invasive surgery thanks to its benefits in terms of reduced patient trauma, shorter recovery times and hospital stays, and lower healthcare costs.
Atul Gupta (Philadelphia, USA), chief medical officer of Image Guided Therapy at Philips, comments on the SmartCT clinical application software–part of the Azurion image guided therapy platform–which, he notes, makes 3D and CT imaging “really simple”.
Gupta outlines which clinical areas would benefit most from the platform and states that he is “excited” by its use in interventional oncology. Setting up 3D acquisition can be challenging, particularly with new staff or out of hours, notes Gupta, who adds that the built-in SmartCT application simplifies the process “tremendously”.
As well as benefit to interventional oncology, the platform offers physicians full table side control of the 3D images and high-level measuring tools which can offer benefits for procedures like prostate artery embolization, fibroid embolization and stroke.
This video was filmed by Philips and is being sponsored for distribution in association with Interventional News.
Surmodics recently announced the successful first uses in patients for two devices within its Sublime radial access platform: the Sublime radial access guide sheath and Sublime radial access .014 RX percutaneous transluminal angioplasty (PTA) dilatation catheter.
Constantino Pena, Andrew Niekamp, and Brian Schiro, interventional radiologists at Baptist Health’s Miami Cardiac & Vascular Institute (Miami, USA), performed the first set of procedures utilising the Sublime radial access guide sheath earlier this year. In early March, Osama A Ibrahim (Ashchi Heart and Vascular Center, Jacksonville, USA) utilised the Sublime radial access .014 RX PTA dilatation catheter in multiple cases, including a below-the-knee procedure which showcased the benefits of both Sublime products.
“We are thrilled and humbled to be the first facility to use the Sublime .014 RX PTA dilatation catheter, and our initial experience with this PTA catheter and the Sublime radial access guide sheath was outstanding. Delivery of the catheter was easy, even below the knee. The pushability, trackability, and crossability all were exceptional. We performed multiple inflations in the below-the-knee case and the crossing profile of the balloon was impeccable,” said Ibrahim. “Our goal at Ashchi Heart and Vascular Center is to go radial-first for all cases. The Sublime platform products we evaluated could certainly aid us in this effort.”
The Sublime radial access .014 RX PTA catheter, which received US Food and Drug Administration (FDA) 510(k) clearance in August 2020, allows above- or below-the-knee access through a transradial approach by providing the longest working length (250cm) on the market. Outer balloon diameters range from 2–4mm with balloon lengths between 20mm and 220mm. The device is compatible with a 5Fr guide sheath and is designed to provide the performance of an over-the-wire PTA catheter in an RX platform. Its proprietary reinforced shaft technology with flexible, kink-resistant construction and 250cm hydrophilic coating are designed for optimal trackability and push through distal tortuosity.
The FDA-cleared Sublime radial access guide sheath is the industry’s first 5Fr sheath available in lengths up to 150cm and sets a new standard for lower extremity treatment through a transradial approach. Designed to meet the specific demands of transradial access to the periphery, the Sublime radial access guide sheath incorporates a proprietary braiding technology and high metal composition within the shaft to provide a unique balance of kink resistance, flexibility, radial strength, and torque power. The device is also available with a 6Fr outer diameter and 120cm lengths.
The Sublime radial access .014 RX PTA dilatation catheter is indicated for PTA dilation of peripheral vasculature stenosis in the iliac, femoral, iliofemoral, popliteal, infrapopliteal, and renal arteries, and for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulae. The device is contraindicated for use in the coronary arteries and the neurovasculature.
The Sublime radial access guide sheath is intended to introduce therapeutic or diagnostic devices into the vasculature, excluding the coronary and neuro vasculature.
There are some amazing things planned for GEST 2021. Hear from the course directors on why you should attend on April 30–May 2 and the focus days throughout the year. Although the event is virtual, attendees should expect the same level of high-quality, engaging and forward-thinking content that they typically experience during GEST!
Adept Medical first launched its overhead arm support in March 2019, and, following discussions with imaging professionals, is today launching a new, updated version to market. The company say it has made product improvements to the original design, removing metallic components to ensure compatibility with magnetic resonance imaging (MRI) machines.
According to Adept Medical, the overhead arm support is designed to comfortably support the patient’s arms, eliminating extreme shoulder flexion, allows for abdominal access, and removes unwanted artefacts when imaging with MR, C-arm or computed tomography (CT) machines. The overhead arm support has been designed for use with existing lab and imaging equipment and fits within the bore of a 70cm CT and MRI centre, and can be used with any C-arm imaging centre. The wing design can support one or both arms and will accommodate a wide range of patient sizes.
“We had compelling interest from clinical teams and distributors to adapt this product for the MRI application. With the same procedural requirements as C-arm and CT imaging, it seemed like a logical progression for the product. Our challenge has been removing all metal from the product and maintaining the same level of functionality,” comments Matt Lazenby, Adept Medical’s product development manager.
Soft, pliable, latex-free polyurethane straps may be used for additional patient safety and comfort. These can be installed and adjusted to loosely contain the patient’s arm. Two strap mount locations for each arm ensures that the patient’s arms are fully supported, reducing the risk of arm displacement and aiding patient assurance and comfort, a company press release states.
Many of our top 10 stories of March 2021 highlight new data and ideas presented at the annual scientific meeting of the Society of Interventional Radiology (SIR; 20–26 March, online), with our coverage of the Charles T Dotter and InspIRed Lectures, reporting on the two-year outcomes of Embosphere microspheres (Merit Medical) in genicular artery embolization (GAE), and write-up of the Medtronic-sponsored OPuS One clinical trial results garnering attention. Issue 81 of the newspaper was also published this month, featuring a cover story exploring the trend towards increased precision and quantification with ablative procedures in cancer treatments.
Ziv J Haskal (University of Charlottesville, Charlottesville, USA) delivered the 2021 Charles T Dotter Lecture at SIR 2021. He told his virtual audience that the “adrenaline-rush” of seeing or doing an elegant procedure that can alter the course of a patient’s life is often the career-inspiring doorway into interventional radiology. But cautions that, over time, there needs to be a pivot to a different approach—one in which drama and thrill-seeking play second fiddle to perfecting procedural medicine by standardisation and a focus on outcomes, so that satisfaction rests on providing planned, precise, evidence-based, immediate and longitudinal clinical care.
In the cover story for our latest issue, Interventional News spoke to various leading interventional radiologists working to make advance ablation. They argue that ablation is entering a new era of increased precision and quantification, with outcomes that match or surpass those of surgery. Whilst reaching equipoise with their surgical counterparts has been a goal for interventional radiologists since the advent of ablative treatments for cancer, some expert interventionalists claim that the increased precision of modern thermal ablation techniques, coupled with improvements in radiology, mean physicians are often treating smaller volume tumours. This now positions the procedure as the “definitive” treatment for select patients in some cancers.
Trisacryl gelatin microspheres 100–300μm in size can be considered for genicular artery embolization (GAE), a new study presented at SIR 2021 reports. Presenting the two-year outcomes of a study comparing Embosphere microspheres (Merit Medical), which are made of trisacryl gelatin, with Imipenum Cilastatin microspheres for GAE in patients with moderate to severe knee osteoarthritis, Shivank Bhatia (University of Miami Miller School of Medicine, Miami, USA) informed delegates that the particles are comparable in terms of pain reduction, and that there is a sustained effect up to two-years of follow-up.
In this Medtronic-sponsored educational supplement to issue 81 of Interventional news, the OsteoCool RF ablation system is under the spotlight. Elizabeth David (University of Toronot, Toronto, Canada) describes watching a “small Canadian invention” transform cancer care, and offers her insights from working at one of the first centres to use the device. Jason Levy (Northside Hospital, Atlanta, USA) gives the “compelling” OPuS One trial results, detailing how they confirm the role of percutaneous ablation in musculoskeletal metastases. He also authors a case report: Treating expansile L1 breast cancer metastases with the OsteoCool RF ablation system.
Fluidx Medical released details this month on the clinical use of their GPX embolic device, demonstrating its ability to block flow to small microvasculature and large tumour feeding vessels.
Our write-up of Haskal’s 2021 SIR Charles T Dotter Lecture (see 1 on this list for our video interview with Haskal). Speaking to the online audience, he claimed it is time for interventional radiologists to leave behind the “cowboy culture” that was the foundation of the discipline’s early, exploratory days, and to become “legionaries marching in service of data”.
“If interventional radiologists wish to become competitive with surgeons, the availability of software enabling the accurate comparison of pre- and post-interventional CT [computed tomography] or MRI [magnetic resonance imaging] scans must become mandatory and routinely employed,” Luigi Solbiati argues in this opinion piece. He discusses the ablation-confirmation software he has developed with his team in Milan, Italy, and enthuses about the potential of artificial intelligence to refine and improve ablative outcomes in interventional radiology.
Genicular artery embolization (GAE) is “highly effective and durable” in reducing symptoms due to moderate-to-severe knee osteoarthritis that is refractory to other conservative therapy (such as joint injections and medication), and has an acceptably low toxicity profile. So concludes Siddharth Padia (University of California, Los Angeles, USA), in his SIR 2021 abstract presentation.
Treating patients with metastatic bone disease by radiofrequency ablation (RFA) using the OsteoCool system (Medtronic) results in rapid and statistically significant improvement in pain scores, and provides sustained, long-term relief. SIR 2021 attendees were the first to hear the full cohort data from the Medtronic-sponsored OPuS One post-market clinical study in the “Abstract of the year” presentation, delivered by Levy to the virtual audience.
President of the American College of Radiology (ACR) Geraldine McGinty, also a radiologist and the chief strategy officer, as well as the chief contracting officer, at Weill Cornell Medicine (New York City, USA), presented the InspIRed Lecture at SIR 2021. She offered her reflections on “being a first”—in May 2018, McGinty was elected chair of the Board of Chancellors of ACR, the first woman to hold this office in the society’s nearly 100-year history.
Shivank Bhatia and Vedant Acharya highlight the importance of multidisciplinary collaboration between urologists and interventional radiologists when it comes to forming a successful prostate artery embolization (PAE) clinic, citing a decade of experience at the Miami Miller School of Medicine (Miami, USA).
Prostate artery embolization (PAE), an endovascular treatment for benign prostatic hyperplasia (BPH)-related lower urinary tract symptoms (LUTS), was initially performed to control pelvic bleeding of prostatic origin. It was found that the prostate decreased in size. With this insight, the first use of PAE to intentionally treat BPH-associated LUTS was performed in 2000. Larger case series published in 2010–2011 reproduced these initial findings. The presentation of these results at the Society of Interventional Radiology (SIR) 2011 conference [26–31 March, Chicago, USA] led to increasing international interest in studying the effects of PAE.
Over the past 10 years, the PAE landscape has seen a tremendous explosion of research interest.
At the University of Miami Miller School of Medicine, we have developed one of the largest PAE practices in North America. From the outset, we applied a multi-disciplinary approach, working with the department of Urology to better evaluate and identify optimal candidates for PAE. This effort allowed our urology colleagues to evaluate the data regarding PAE’s safety and efficacy and observe, first-hand, the benefit provided to patients who otherwise were not surgical candidates. We have continued to take this multidisciplinary approach by creating data-driven PAE educational materials to build relationships with local urologists and primary care physicians in academia and the community.
At our institution, we have performed more than 850 PAE procedures since 2014, and we currently see over 250 PAEs per year. We have consistently optimised our technique and standardised our preprocedural evaluation and post-procedure follow-up to create a robust clinical practice. Additionally, we have moved to a primarily radial (left wrist) approach. This access is optimal for most patients as it allows immediate ambulation, faster recovery, and features lower risks overall compared to the femoral approach. In addition, we have performed over 250 procedures in a surgery centre with no incidence of need for transfer to the hospital.
Our team is excited to be at the forefront of research in PAE and contribute to the broader interventional radiology and urology communities. The University of Miami Miller School of Medicine hosted Evolution: Miami 2019 [15–17 November, Miami, USA], a multi-disciplinary conference with over 270 attendees, at which PAE best practices and current debates were discussed by international leaders. Over the past decade, we have presented more than 50 manuscripts on PAE at national and international conferences and in peer-reviewed journals. Recognising the necessity of high-quality data to advance the field, we are delighted to be sharing our results in the presentation titled “Prostate Artery Embolization—Single centre experience of 576 patients with five years follow up” at SIR 2021 [20–26 March, online]. To our knowledge, this is the largest series of the patients treated with PAE in North America presented to date.
Brian Malling (Rigshospitalet, Copenhagen, Denmark) et al conducted a meta-analysis and evaluated the clinical outcomes of 1,254 patients who underwent PAE and found that PAE improved International Prostate Symptom Score (IPSS) by 67% at 12 months and reduced prostate volume by 32% at three months. Several high-quality randomised control trials evaluating PAE versus transurethral resection of the prostate (TURP) have shown consistent and reproducible results. Most recently, Gabriel Knight (Northwestern University, Chicago, USA) et al performed a meta-analysis comparing PAE and TURP and found no significant differences between changes in IPSS, IPSS quality of life, and erectile function.
Future developments in PAE include: gaining a greater understanding of the effects of PAE on ejaculatory dysfunction, performing a randomised control trial comparing PAE with Holmium laser enucleation of the prostate (HoLEP; the current gold-standard size-independent prostate procedure), and evaluating the long-term durability of the procedure. We hope that the development of research will provide the American Urology Association (AUA) the required evidence to recommend PAE as a treatment option.
Research on PAE has developed from a small case series to a multicentre international effort over the past decade. We are excited to have built a robust multidisciplinary clinical practice, to have contributed to the literature, and to be a part of further developments to bring this minimally invasive treatment option to more patients with BPH.
Shivank Bhatia is professor of Interventional Radiology and Urology at the University of Miami Miller School of Medicine, Miami, USA.
Vedant Acharya is a fourth year medical student and past Interventional Radiology Research Fellow at the University of Miami Miller School of Medicine, Miami, USA.
Daniel Sze (Palo Alto, USA) recently took the reins of the Journal of Vascular and Interventional Radiology (JVIR) as editor-in-chief.
He plans to extend specific efforts to encourage increased contributions from underrepresented groups such as women, under-represented minorities (URMs), and the LGBTQ+ community to the JVIR ecosystem, and to build on previous international outreach efforts aimed at the Chinese interventional radiology (IR) community, with a similar outreach into the Spanish-speaking world.
Sze also tells Interventional News how expanded and improved graphics may amplify the impact of JVIR content and help to disseminate important IR research on digital platforms.
From an early understanding in medical school that interventional radiology (IR) was “the future”, Parag Patel has dedicated his career to the discipline, notably as a primary investigator of the BEST-CLI and ATTRACT trials, and now as the incoming president-elect of the Society of Interventional Radiology (SIR). He has also been integral to the design and implementation of a universal IR education curriculum in the USA. In so doing, he has played a large part in shaping that future he once envisioned.
What initially drew you to interventional radiology?
I entered medical school with no knowledge of the field. I loved patient care but wanted to be able to treat the pathology as well. All of my medical school research was done within vascular surgery. During my surgery clerkship, we routinely followed our patients for tests or studies. One such patient had a postoperative bleed and I assumed we would go back to the operating room, but instead we ventured down to “Special Procedures” (a thankfully historic term for interventional radiology [IR]). Marc Borge successfully embolized the bleeding source. That was my first exposure to angiography and the opportunities that it provided—I was hooked. That was such a light bulb moment for me. IR was the future. Innovative, elegant, minimally invasive, and, in my mind, the future of medicine. I was all in.
Who have been important mentors throughout your career?
My parents instilled in me a genuine work ethic as well as respect and appreciation of your fellow persons. They gave up so much certainty to provide for me and my brother as immigrants to the USA. Much of who I am today is because of them.
With regards to IR, Marc Borge introduced me to the specialty and fostered a young, naïve, but genuinely interested trainee. Nicos Labropoulos served as a research mentor and emphasised the importance of good science and knowing the data. As a resident, Marc invited me to attend the local Chicago angioclub, which at the time had many leaders in the field that impressed on me the ingenuity and novelty of the specialty. I was fortunate to train at Miami Vascular. Jim Benenati and Barry Katzen led a phenomenal group of faculty that instilled the importance of true clinical practice, exhibiting leadership and grace under pressure. I was privileged to join the group in Milwaukee and continue my growth under the leadership of Bill Rilling, Sean Tutton, Rob Hieb, Eric Hohenwalter, and soon after Sarah White, formed a small but formidable group of interventional radiologists that grew our clinical practice. We supported each other’s research, education, and clinical efforts through a model of shared leadership.
I was very fortunate to receive support from gracious mentors, and can only hope to serve a similar guiding role for other young trainees. This is much of the driving force behind my desire to continue as programme director of our vascular and interventional radiology (VIR) fellowship [that of the Society of Interventional Radiology (SIR)], and now IR residency training programmes.
You have been a primary investigator of the BEST-CLI trial since 2014. Why is this study important?
The BEST-CLI trial (Randomised, multicentre, controlled trial to compare best endovascular versus best surgical therapy in patients with critical limb ischaemia) completed enrolment over a year ago and strives to complete follow-up during the coming year. The study is important as we have very limited high-quality data on the management of critical limb ischaemia (CLI) patients, specifically comparing best surgical versus best endovascular treatments. Our multidisciplinary collaborative practice at the Medical College of Wisconsin (MCW) has routinely followed a shared model of decision making with surgical and endovascular strategies employed in our local practice. Our involvement in BEST-CLI was seen as a natural extension of our practice and may shed light on how to best treat these patients or support how we already practice. Further studies in this space are needed to allow for a more structured and uniform algorithmic approach to be taken in the care of these patients.
As an ATTRACT trial investigator, what did this experience teach you, and how has clinical practice been impacted by these findings?
I learned much from my involvement in ATTRACT (Acute venous thrombosis: thrombus removal with adjunctive catheter-directed thrombolysis), namely, the exhaustive work it takes to consistently beat the drum for screening, enrolment, and follow-up and see a trial through to completion. Much credit goes to Suresh Vedantham for his leadership and effort. We struggled with maintaining clinical equipoise in the trial. We were studying the role of an approved treatment in the hopes of identifying a benefit for our patients long term. Many felt they already knew the best course for their patients and enrolment would prevent proper treatment if they randomised to the non-intervention arm. Nonetheless, the trial did not support routine use of pharmacomechanical catheter-directed thrombolysis (PCDT) for all acute lower extremity deep venous thrombosis (DVT) for prevention of post-thrombotic syndrome (PTS). This has helped inform our practice algorithm, as we no longer offer PCDT for isolated femoropopliteal DVT or in older patients with acute iliofemoral DVT (aside from those with phlegmasia). We will treat younger patients with symptomatic acute iliofemoral or iliocaval DVT in the hopes of improving acute symptoms and minimising the severity of PTS.
As chair of the SIR Residency Essentials Advisory Committee, you have been central to the development of the new online curriculum. What was this experience like?
The Residency Essentials project came about through a strategic planning exercise for the SIR. As Graduate Medical Education Councillor during the time of our IR Residency implementation, I was tasked to champion support for the new training model. The idea of a universal IR education curriculum available for all IR trainees aimed to minimise the significant differences in training experiences across the country. While the technical experiences may vary from institution to institution, the fundamental knowledge base of disease management, role of interventional therapies, and management of these patients could be taught to all trainees nationally. The project was a massive undertaking with cross-divisional collaboration within the SIR and significant staff support. It took over three years and a number of physician volunteers to develop the extensive curriculum outline, identify and curate content (video lectures, timely reviews, and assessment questions), and then neatly package them into modules available on a new learning management system. The project launched in July 2020 to great success. The content will continually be reviewed and periodically updated. The timing of this launch was in the midst of the pandemic and coincided with distance learning mandates across the country. The new Residency Essentials fits this quite nicely as it is an online curriculum. Now that the curriculum is complete, we have the opportunity to support IR education efforts abroad.
You are stepping into the role of president-elect of the SIR. What are your ambitions for the society in the coming years?
SIR, like any big organisation, is a big ship and abrupt changes are not easily handled. I hope to make incremental improvements to the organisation to better serve our members. Namely, we will continue to grow our education and research efforts, and increase awareness of IR treatments to patients and the value of IR to health systems.
What is the greatest challenge currently facing interventional radiologists?
We continue to have much work to do in placing the treatments we provide within the algorithm of management for the diseases we treat. Early on, we struggled with maintaining a hold on our procedures, when maintaining a hold on our patients should have been the focus. If we all agree that minimally invasive, image-guided interventions are the future, then we cannot complain if others adopt this strategy as long as they do it well. I think a bigger concern is why some of our proven therapies still remain outside the standard management guidelines of basic disease entities. This requires a long view with a strategic approach and collaboration amongst our stakeholders to accomplish. I believe we can do it.
What are your hobbies and interests outside of medicine?
Art, architecture, and industrial design. I am also an avid traveller, immersing myself in new cultures and enjoy any time spent in nature. Prepandemic, I have hiked the narrows at Zion National Park, down to the Colorado River at the Grand Canyon, trekked the Inca Trail to Machu Picchu, and am now (hopefully) planning a summit of Mount Kilimanjaro for next year. Family time is a priority, and I enjoy cooking up new recipes with my wife, Mona, or rallying tennis balls on the court with my two daughters, Simrin (age 12) and Siana (age nine). interventional interventional
Nicholas Inston (Queen Elizabeth Hospital Birmingham, Birmingham, UK) speaks to Vascular News ahead of this year’s Charing Cross Symposium (CX), which is being held online 19–22 April. In 2021, the conference will focus on controversies within the vascular and endovascular space.
Could you outline the Vascular Access highlights from the programme you have put together for CX 2021?
The CX 2021 Vascular Access programme as usual covers a lot of ground, but there are some real highlights this year. We are going to start the day by talking about device-created fistulas, and of course we now have the options of surgically-created or device-created fistulas. Where we use these, how we use these, and what are the expected outcomes will be discussed. We are also going to delve into the field of high-flow fistulas. This is an area that has not really been discussed very much in the past and I think this will be the first Masterclass where high-flow fistulas will be in the spotlight. New devices and new evidence is emerging, such as which balloons are best in vascular access, which stents, and where and when they should be used. We aim to explore all of this.
Why should physicians attend the CX 2021 Vascular Access sessions and what do you think they might learn?
I think it is imperative that people keep up their education during this pandemic. The way that we work and the way that patient care is delivered has been hugely disrupted, and there are definitely things that we can learn from the last year. With these changes in practice, it is important to find out what has actually happened to those patients that have not been able to have treatment, or their treatment has been altered. We need to make sure that we learn lessons from each other about new and different approaches to vascular access care.
If you had to pick one controversy in the programme to turn the spotlight on, what would that be?
A topic of controversy that is poorly understood is that of high-flow fistulas. This is a really interesting area and one I think will create a lot of debate. As well as defining a high-flow fistula, the session will address a number of key questions: Does a high-flow fistula have cardiovascular risks? Does it have risks in terms of increasing interventions, increasing problems? Why do we need a fistula that runs at high flow when actually you only need a fistula that runs about a litre a minute?
Why is this controversy important to the global vascular community?
We do not really know how to deal with high-flow fistulas. International practice differences exist in cannulation and dialysis provision with some approaches aiming for fistulas to suit the logistics of dialysis rather than best long-term outcomes for the fistula and the patient. I think this session will raise many questions about vascular access in general and stimulate some interesting discussion.
Representative images of arterial embolization in a rabbit kidney with Hydrogel Embolic System. Image panel includes a) baseline angiogram of right kidney, b) hydrogel embolic delivery under fluoroscopy c) digital subtraction angiography confirming stasis and embolization (inlay non-subtracted), and d) microscopic image showing hydrogel embolic (stained with trypan blue) in vessels large and small <25 um.
The initial patients have been enrolled in the Embrace hydrogel embolic system (HES) global randomised clinical trial for the treatment of hypervascular tumours, Instylla has announced. As demonstrated previously in the completed first-in-human (FIH) study, Embrace HES was effective at embolizing malignant and benign hypervascular tumours by blocking tumour blood supply with complete technical success and persistent embolization as noted in imaging follow up at 30-days.
“I am pleased to be evaluating this new technology for hypervascular tumour embolization,” comments Gerard Goh, head of Interventional Radiology at The Alfred Hospital, Melbourne Australia, and president of the Interventional Radiology Society of Australasia (IRSA). “While participating in the first-in-human study prior to this trial, Embrace showed great promise with good control, favourable patient outcomes, and no tumour revascularisation. We are excited to be the first centre to enrol in this global, randomised trial.”
A hypervascular tumour, which can be found in the liver, kidney, or elsewhere, has an increased number of blood vessels relative to other tissues. These tumours are often associated with low survival rates. Due to the increased risk of bleeding, hypervascular tumours can be challenging to remove. Transcatheter arterial embolization (TAE) and conventional transarterial chemoembolization (cTACE) are established treatments for hypervascular tumours, particularly for patients with limited progressive disease. Embrace HES, an investigational product, is a liquid embolic designed to deeply penetrate the tumour vascular bed, solidify, and stop blood flow. The Embrace HES embolization uses no solvents, does not need sizing to the vessel diameter, and eliminates the possibility of catheter entrapment. Its main components are water and polyethylene glycol (PEG). PEG has a long history of safe use in implantable medical devices, Instylla claim.
“We are thrilled to be the first centre in the USA to treat a patient on this study. Embrace’s predictability helps me embolize the tumour while avoiding non-target embolization,” adds Edgar D St Amour, interventional radiologist from CARTI Cancer Center in Little Rock, USA. “I look forward to continued evaluation of this new advancement in treating hypervascular tumours.”
Fluidx Medical have released details on the clinical use of their GPX embolic device, demonstrating its ability to block flow to small microvasculature and large tumour feeding vessels.
“The versatility of the GPX product has been demonstrated in a variety of interventional oncology uses,” says Andrew Holden, director of Interventional Radiology, Auckland City Hospital, Auckland, New Zealand. “We have seen excellent distal penetration and backfilling of larger vessels in our tumour cases.”
According to Fluidx Medical, the GPX embolic device is an embolic designed “to combine the benefits of other embolics like coils, particles, and liquids with simplified preparation, delivery, precision, and control leading to durable, long-term occlusions”. GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolic material upon delivery without polymerisation or dimethyl-sulfoxide (DMSO) precipitation.
“We saw excellent filling of the distal branches and complete tumour devascularisation,” says Martin Krauss, head of Interventional Radiology, Christchurch Hospital, Christchurch, New Zealand. “The patient exhibited marked decrease in haematuria following the procedure. Since we were not worried about catheter entrapment, we could take our time and ensure that we occluded all the feeding vessels of the tumour.”
GPX is packaged ready-to-use in a syringe, requires less than one minute of tableside preparation by the clinician, and may be delivered through standard catheters or microcatheters, according to Fluidx Medical Technology data on file. Clinicians can decide at time of care to use GPX alone or as a complement to coils or other embolic technologies.
In a recent case at Christchurch Hospital, the GPX embolic device was delivered through long, thin microcatheters, including the 2Fr Terumo Progreat Alpha 130cm length microcatheter with an inner diameter of 0.019 inches (0.48mm).
The GPX embolic device is under development and does not have marketing clearance or approval in any market at this time. It is for investigational use (in New Zealand) only.
During the annual scientific meeting of the Society of Interventional Radiology (SIR; 20–26 March, online), Matthew Hawkins and Raymond Liu jointly hosted a session conveying the value of interventional radiology (IR) services.During the session, the touched on how interventional radiologists can communicate the value their field brings to hospitals and health systems and what other interventionalists can be doing to help move the field forward. Interventional News caught up with Hawkins and Liu for a discussion on the topic.
How can interventional radiologists communicate the value their field brings to hospitals and health systems?
MH: IR has become a specialty that treats a multitude of conditions in nearly every area of the body. Our specialty is an essential component to many revenue-generating service-lines offered by hospitals, such as organ transplant, oncology, stroke care, and trauma. In addition to some of the more complex interventions performed by interventional radiologists, our specialty has become healthcare system experts of central venous access, minimally-invasive biopsies, enteric access management, and percutaneous drainage procedures. But while interventional radiologists are valued for their universal skillsets, it has been difficult for the specialty to communicate how these skillsets translate to the bottom line for hospitals and health systems.
The most important thing interventional radiologists can do is to demonstrate the positive impact they have on generating revenue, containing costs, optimising resource utilisation, and providing high-quality patient care. As it pertains to quality, hospitals/healthcare systems value improved outcomes for patients, shorter lengths of stay (LOS), avoidance of unnecessary admissions, and post-discharge outpatient management to avoid re-admissions and financial penalties. They want to invest in specialties that can deliver on these targets. We know that IR does this, but having robust data and research to support it will be crucial in the future. We hope that interventional radiologists will conduct more research into these areas to further support IR as a value-driven, patient-centered specialty.
How have you personally worked with colleagues across disciplines to provide best patient care? How do you initiate forming an interdisciplinary team—what are the opportunities here?
RL: Interventional radiologists are always open to working in partnership across specialties, and there are more opportunities for partnership with other physicians than many realise. In developing an interdisciplinary team, it starts with identifying the holes within your health system that need filling. Where could your services be most useful in a team environment? Where do you think a team could provide the most value? The next step is to simply reach out to the other physicians within that service-line and have a conversation. Find out if they are interested in forming an interdisciplinary team. Most likely they will be enthusiastic about working together because we all have the same goal—getting patients the best care they deserve. The final step is to get support from hospital leadership. Their backing will help to nurture your team model and even scale it up for the future so it can continue to grow. A great example beyond the well-known oncology model are Hereditary Haemorrhagic Telangiectasia (HHT) teams that draw in specialists such as ENT, haematologists, geneticists, and pulmonologists. And, of course, multidisciplinary teams should not just be considered for clinical issues—at Massachusetts General Hospital, we have created interdisciplinary teams for operational redesign, such as on-time efforts for first case in the operating room, or best practice workflows for anaesthesia support for IR.
A strong team that works across specialties is better for both physicians and patients, so I encourage other interventional radiologists to reach out to their colleagues if they are interested in working in this capacity.
What are the biggest challenges to the spread of IR generally, and how can interventional radiologists work on combating these?
RL: Some of the biggest challenges facing the profession include misperceptions among referring physicians and hospital administrators about what interventional radiologists can do. For a long time, interventional radiologists have been viewed as technicians, but as the field has exploded into other realms of treatment across all areas of the body, other physicians continued to hold the same notions about interventional radiologists’ capabilities. Yes, we can help treat a patient’s complex condition, but we can also provide patients the full clinical spectrum that allow discussions around all treatment options. We need to ensure that other physicians understand that we can be a partner in their patients’ care. Interventional radiologists can change this by strengthening relationships with other physicians in other specialties; by demonstrating to hospital administrators the ways interventional radiologists can help generate revenue, contain costs, and provide patients high-quality care.
I would also say access to IR services is a hurdle our specialty needs to overcome. In some metropolitan areas, there is an abundance of IR specialists that allow many choices for patients. But in many areas, even just a few miles outside major cities, there is a dearth of IR physicians that can address complex conditions and provide best practice treatments. Our specialty needs to identify those geographical areas, as well as improve communication of our services in those locations where there are interventional radiologists, and ensure that every patient has access to an interventional radiologist anytime.
What are biggest misconceptions pertaining to pediatric IR, and how can these be addressed?
MH: As endovascular equipment has continued to get smaller and smaller, it has made many minimally-invasive IR procedures safe for children. Now, rather than open surgical procedures, many paediatric diseases can be treated with minimally invasive, image-guided treatments. Pediatric IR is evolving rapidly and has become an essential specialty in the management of vascular malformations, paediatric organ transplant, and many paediatric benign bone tumors. Paediatric interventional radiologists have also become institutional experts in less-complex, but critical procedures, such as biopsies, enteric access, and central venous access, which are necessary for the care of a wide-array of paediatric diseases. In general, parents are grateful to have minimally-invasive, image-guided alternatives to open surgery.
Thriving paediatric IR practices are generally based out of tertiary referral paediatric hospitals, with an increasing percentage of pediatric interventional radiologists obtaining subspecialised paediatric IR training to supplement their foundational adult IR residency curriculum.
Matthew Hawkins is a paediatric vascular interventional radiologist and associate professor at Emory University and the Children’s Pediatric Institute, Atlanta, USA.
Raymond Liu is an interventional radiologist at Massachusetts General Hospital, Boston, USA. He is a Society of Interventional Radiology (SIR) board member and executive director of Partners HealthCare International (PHI).
Trisacryl gelatin microspheres 100–300μm in size can be considered for genicular artery embolization (GAE), a new study presented at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online) reports. Presenting the two-year outcomes of a study comparing Embosphere microspheres (Merit Medical), which are made of trisacryl gelatin, with imipenem cilastatin for GAE in patients with moderate to severe knee osteoarthritis, Shivank Bhatia (University of Miami Miller School of Medicine, Miami, USA) informed delegates that the particles are comparable in terms of pain reduction, and that there is a sustained effect up to two-years of follow-up.
“Genicular artery embolization has potential to provide midterm relief of pain for patients with mild-to-moderate knee osteoarthritis resistant to conservative management,” he said.
Detailing their methodology, Bhatia described how the investigators conducted a comparative study, assessing a total of ten patients (15 knees) who had a GAE with 100–300μm Embosphere microsphere particles, and comparing them to a subsequent cohort of eleven patients (18 knees) who underwent GAE with Imipenum Cilastatin microspheres. Clinical outcomes were evaluated at six-month and 24-month follow-up and compared to baseline using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire.
Bhatia noted that, at baseline, there were no significant differences in sex, age, body mass index (BMI), duration of pain before the procedure, prior treatment, or Kellgren-Lawrence grade between the two cohorts. Baseline median pain WOMAC and total WOMAC scores were 13 (interquartile range [IQR], four) and 46 (IQR, four) in the Embosphere group and 13 (IQR, three) and 47 (IQR, 28) in the Imipenum Cilastatin group [p=0.875 and p=0.738], respectively.
The median follow-up was 796 days (range, 736–808). Clinical success (measured as 50% reduction in WOMAC pain score vs. baseline) was achieved in 69.23% of the embolized knee joints in both groups (p=1) at six months.
At two-years follow-up, the investigators report clinical success in 61.5% of knees treated with the Embosphere microspheres, versus a 53.8% clinical success rate in the Imipenum Cilastatin group (p=1).
Both embolic materials resulted in a significant decrease in pain WOMAC and total WOMAC scores at six months compared to baseline (p<0.05), and the effect of GAE on pain WOMAC and total WOMAC scores was sustained until the 24-month follow-up visit in both groups (p<0.05).
Relating the adverse events, Bhatia commented: “Minor events included transient cutaneous colour change [in five patients] or transient leg numbness observed in one patient], and was only identified after GAE with Embosphere microsphere particles (p=0.00387), which resolved spontaneously at one-month follow-up (Clavien-Dindo classification grade I).” There were no major adverse events.
Interventional radiologists were often at the frontlines, doing remarkably large numbers of procedures treating COVID-19 patients and among the only specialties that carried on staffing hospitals, providing daily services such as putting in dialysis catheters or treating COVID-19 related pulmonary emboli. “That was a very valuable experience for others to see. We were there, we stepped up – and patients benefitted,” Matthew S Johnson, who took on the Society of Interventional Radiology (SIR) presidency on 23 March 2021, tells Interventional News.
Johnson, who is theGary J. Becker Professor of Radiology Research at Indiana University (Indianapolis, USA), outlines that distilling the lessons learned from the COVID-19 experience and emphasising and building a diverse society membership and leadership form the bedrock upon which SIR aims to employ research as a mature specialty to guide what interventional radiologists do to serve patients better and demonstrate the value of image-guided procedures – to patients, referring physicians and payers.
“We are pushing as a society, as a specialty, for people to become involved in research, to do high quality research and also to join us in [the] Virtex [registry],” he says.
Researchers suggest that, in patients with chronic limb-threatening ischaemia (CLTI), two-dimensional (2D) perfusion angiography is a “reliable tool” when used according to standardised methods. Jetty Ipema (St Antonius Hospital, Nieuwegein, The Netherlands) and colleagues write in the European Journal of Vascular and Endovascular Surgery (EJVES) that theirs is the first study to test the reliability of this method in CLTI patients.
Ipema et al explain that 2D perfusion angiography provides quantitative foot perfusion information from standard digital subtraction acquisitions. In the present study, the investigators aimed to test the reliability of this method in patients with CLTI by investigating repeatability, as well as intra-observer and interobserver agreement.
The team included 20 patients with CLTI and below-the-knee endovascular revascularisation in a prospective, clinical study. Two patients were excluded from repeatability analyses because of major motion artefacts, they note. Prior to treatment, the authors state that two perfusion angiography runs were acquired with a five-minute interval without performing an intervention. In these recordings, regions of interest were selected and time–density curves and perfusion parameters were recorded.
Ipema and colleagues specify that, to investigate intra-observer agreement, one observer performed five measurements on the same acquisition for each patient; to investigate interobserver agreement, three observers performed measurements on the same acquisition for each patient. They presented the results in Bland–Altman plots and as the intraclass correlation coefficient (ICC) per parameter.
Writing in EJVES, the authors report that repeatability analyses of the 18 eligible patients showed excellent correlation for every parameter, with an ICC >0.9 for each. In addition, they relay similarly positive results regarding intra-observer and interobserver agreement for all 20 patients, with an ICC of 1 for every parameter.
Ipema et al note that the study has some limitations. “Although the number of patients was sufficient to show excellent repeatability results,” the authors write, “the Bland-Altman plot shows outliers that could not be fully explained.” They hope that as more data become available in the future, there will be a better understanding of these observations.
Furthermore, they acknowledge that the study only validated the reliability of 2D perfusion angiography. They detail that other aspects of test validation, such as the ability to demonstrate increased blood flow after intervention (responsiveness) and the relationship with clinical outcomes (validity) were not investigated but are “important further research topics”.
Ipema et al conclude that repeatability, as well as intra-observer and interobserver agreement of 2D perfusion angiography in patients with CLTI were excellent. Based on the results of their findings, they suggest that future research can be performed to investigate the relation between perfusion angiography and clinical outcomes.
The adrenaline-rush of seeing or doing an elegant procedure that can alter the course of a patient’s life is often the career-inspiring doorway into interventional radiology. But, over time, there needs to be a pivot to a different approach – one in which drama and thrill-seeking play second fiddle to perfecting procedural medicine by standardisation and a focus on outcomes, so that satisfaction rests on providing planned, precise, evidence-based, immediate and longitudinal clinical care.
So says Ziv J Haskal (Charlottesville, USA), who presented the 2021 Charles T. Dotter Lecture at the Society of Interventional Radiology’s annual scientific meeting titled “The Reluctant Cowboy: Moving Past Myth and Dogma”.
In the lecture, Haskal notes that the problem-solving, lone-ranger cowboy interventional radiology mindset needs to give way to the drumbeat of an army marching in search of, and in support of, evidence. Importantly, sceptical analysis, which must underpin this quest, must turn its sights “at home” with a reappraisal of the common myths and accepted truths that masquerade as evidence – and this can reveal the often shaky ground for decision making in interventional radiology, he says.
“We are not cowboys doing things because we ‘think it makes sense’, rather we must seek to understand the limits of known data, and adhere to science, where it exists,” he tells Interventional News. And, he also talks about skydiving.
President of the American College of Radiology (ACR) Geraldine McGinty, also a radiologist and the chief strategy officer, as well as the chief contracting officer, at Weill Cornell Medicine (New York City, USA), presented the InspIRed Lecture at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online). She offered her reflections on “being a first”—in May 2018, McGinty was elected chair of the Board of Chancellors of ACR, the first woman to hold this office in the society’s nearly 100-year history.
McGinty also highlighted the importance of taking an intersectional approach to mentoring and networking, with several of her key takeaways referencing using your privilege and access to enable opportunities “not just for people who look like you”.
Delivering her InspIRed Lecture on 21 March, McGinty gave ten central lessons for women and other under-represented groups in interventional radiology (IR):
Be thoughtful about the privilege you have on your journey! McGinty encouraged those with power to use it for good.
Everyone is different, and that is a good thing. Acknowledge the different ways people may function, and help power your team more effectively.
You are the one who gets to tell your story. Whether the best part of your day is a clinical case or seeing your favourite show, it is up to you to define that.
You decide what is important. Be thoughtful about where you want to make your effort, and do not leave your value on the table. When you negotiate, it is about more than salary.
You can be authentic. “I have tended to be more successful when I have done that.” But you may need to conform to get to the table.
You have an obligation to pay it forward, and not just for people who look like you.
You will bet on people who will disappoint you, and you may get the most help from where you least expect it. Do not rule out those who do not look like you as mentors.
To quote Reshma Saujani, founder of Girls Who Code: Be brave, not perfect.
Thoughtfully build your network. Seek out people doing interesting work, asking for time with them (perhaps even just a few minutes). You should also have a squad with whom you can discuss issues such as salary and who will support you know matter what.
Think big: “We have to make it okay for us to have ambitious!” You will face criticism, but the work could not be more important. InspIRed
President of the American College of Radiology (ACR), Geraldine McGinty is also a radiologist and the chief strategy officer, as well as the chief contracting officer, at Weill Cornell Medicine (New York City, USA). She presented the InspIRed Lecture at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online) and offered her reflections on “being a first”. In May 2018, McGinty was elected chair of the Board of Chancellors of ACR, the first woman to hold this office in the society’s nearly 100-year history.
McGinty discusses the state of female representation within interventional radiology, how far things have come and what more needs to be done. “We are certainly not where we need to be” in this regard says McGinty, who explains that roughly only 8% of IRs in the US are women.
McGinty outlines some of the main barriers to adoption and notes that a “really powerful deterrent is when you are not seeing women leader and women role models”. She goes on to explain that this is where the Society of Interventional Radiology and the Women in IR group have “done such a terrific job in highlighting pioneering women”.
Attracting more women to IR early in their careers is vital. “We have to connect with students early in their training” says McGinty who adds that having “robust medical outreach is critically important to increasing the diversity of the specialty overall”.
She also draws on her own experience as the first chair of the American College of Radiology, noting that she “wasn’t the first woman who could have done it or should have done it”. “I’d like to think that I’ve opened the doors for other women”, McGinty adds, concluding that it is “not success if it’s just you; you have to help the next woman up”.
The US Food and Drug Administration (FDA) have approved the DOORwaY90 study, a trial evaluating the safety and efficacy of selective internal radiation therapy (SIRT) using SIR-Spheres yttrium-90 (Y-90) resin microspheres (Sirtex Medical) in patients with unresectable hepatocellular carcinoma (HCC).
Unique to other recently published Y-90 studies, DOORwaY90, which stands for “Duration of objective response with arterial Y-90,” is the first prospective, multicentre study to utilise and delineate personalised dosimetry treatment planning and to define actionable post-treatment dosimetric verification for endpoint assessment. The study will assess the duration of response and objective response rate of SIR-Spheres.
Outside the USA, SIR-Spheres are indicated for the treatment of patients with advanced non-operable liver cancer, including HCC.
The DOORwaY90 study is being led by co-principal investigators Cheenu Kappadath and Armeen Mahvash (both University of Texas MD Anderson Cancer Center, Houston, USA). “We are honoured to participate in this important study that could greatly impact the treatment of HCC patients in the USA,” notes Mahvash. “We look forward to working closely with Sirtex in executing and reporting the findings of DOORwaY90.”
DOORwaY90 is a 15-centre, 100-patient, US-based, open label, single arm study run in accordance with Good Clinical Practice. The study population consists of patients with Barcelona Clinic Liver Cancer (BCLC) Stage A, B1, and B2 who are not eligible for resection or ablation at the time of study entry. For each patient, an eligibility review committee will review diagnostic imaging and confirm final eligibility and treatment planning prior to treatment. Enrollment is expected to begin at the start of the second financial quarter of 2021.
HCC is often diagnosed when potentially curative resection or transplantation is not feasible. SIRT has the potential to deliver a lethal dose of radiation to hepatic tumors, while sparing surrounding healthy liver tissue. In countries outside the USA, SIRT has been successfully used to bridge patients to transplantation or downstage HCC to within transplantation criteria or resection.
Ziv Haskal receives Dotter Lecture award from Alan Matsumoto, who gave the 2019 Dotter Lecture
It is time for interventional radiologists to leave behind the “cowboy culture” that was the foundation of the discipline’s early, exploratory days, and to become “legionaries marching in service of data”, Ziv Haskal (University of Virginia, Charlottesville, USA) argued in his 2021 Dotter Lecture, delivered during the Annual Scientific Meeting of the Society of Interventional Radiology (SIR; 20–26 March, online).
“IR knowledge is not atomic: it is complex,” the former Journal of Vascular and Interventional Radiology (JVIR) editor told virtual attendees. “You cannot live with ‘I read the abstract’ or ‘I cruised the conclusion’”, he joked, cautioning SIR delegates against accepting certain ideas as gospel without first scrutinising the data. Indeed, Haskal’s lecture, “The reluctant cowboy: Moving past myth and dogma” deconstructed commonly held interventional radiology (IR) “myths” and dogmatic approaches to practice, and called for a more rigorous culture of data and research.
“We need to be accountable and adopt a sceptical approach that can only be satisfied through repetition and replication,” he said.
In order to do this, he advised his audience to act at various levels: “On a personal level: embrace this constant self-query, self-reflection, scepticism, and patience. Read in detail. Embrace the dialectic.
“On a local level: cheer on developing prospective research; it is five to ten times more effort to write protocols, but they are durable, and impactful, and can be built upon, or will lead to other work.
“On a national level: support initiatives for data that can be congregated, through registries, through standardised reporting, through NIH [National Institute of Healthcare] efforts. Open your pocketbooks with patronage; lend your financial support to societal initiatives.
“And on the big blue planet, think about the large-scale questions, so we can get together with other groups. We have to mine the facts for truth and work daily to be clinical scientists.”
Alan Matsumoto (University of Virginia, Charlottesville, USA), who delivered the 2019 Dotter Lecture, presented the Dotter Lecture award to Haskal on 22 March.
Ziv Haskal giving the Dotter Lecture in a pre-recording
The apodictic versus the apoplectic: Moving beyond a narrow, dogmatic vision in IR
He began his talk by noting that “many or most of us [interventional radiologists] remember that signal case” that led them to pursue a career in IR, which he likens to skydiving due to the “adrenaline thrill”. However, he warned that now is the time for the speciality to turn towards “creating data and our own science”.
Haskal made the distinction between “the apodictic—knowledge we are certain of” and the apoplectic, the “you will do it this way because I was trained this way, and therefore you will be trained this way” school of thought.
He highlighted some specific examples of “apoplectic” thinking “to highlight the types of narrow vision that we have on a daily, or on a field-wise basis”. One such belief he questioned was the idea that pulmonary arteriovenous malformations (PAVMs) less than 3mm do not need to be embolized to prevent stroke. “Are bacteria just too big to fit through a 3mm PAVM?” Haskal asked rhetorically. He traced the origins of this belief to an abstract presented orally at the 1992 meeting of the Radiological Society of North America (RSNA), which did not state that there was no need to embolize smaller than 3mm, but rather found clinically-evident stroke in four patients with feeding artery measuring 2.9–4.5mm. “That is pretty shaky ground for decision-making,” Haskal opined.
“How about gall bladder catheters—they have to be transhepatic, right?” he continued. He cited a 1988 article in the American Journal of Roentgenology (AJR) and a 1994 paper in JVIR that refute this, demonstrating the safety of a transperitoneal route. “If that was not enough, I was recently asked by a plaintiff’s lawyer to be a medical expert on a case in which there was a hepatic bleed, and she insisted the interventional radiologist was negligent because they had gone through the liver, and there was a bleed.”
He also addressed common practice assumptions. “Why do we always get called at night for nephrostomies or arterial lysis?” he asked. But according to a review of cases conducted at the 800-bed University of Virginia Hospital over the course of one year, 84% of nephrostomies and 80% of lysis procedures took place between 8am and 8pm.
According to Haskal, this is due to frequency bias, also known as the Baader-Meinhof effect—after you notice that you have done several night-time lysis procedures, you will notice it more often and believe that it has a high recurrence.
The risks of skimming
In addition to these commonly-held IR “myths”, Haskal also warned his audience of the dangers of “reading light”. Presenting an example, he discussed an “excellently-written, multicentre trial, [conducted] under the auspices of the FDA [the US Food and Drug Administration]”. He published the study, which was an approval trial for a vena cava filter, when JVIR editor. “Here are the conclusions from the abstract,” he read: “The rate of freedom from new symptomatic PE [pulmonary embolism] through 60 days was 100% (n=129, confidence interval [CI] 97.1–100%). [….] There were no cases of PE through 12 months for either therapeutic or prophylactic indications.”
Commenting on this, he said, “So that is pretty good, we want that device,” before adding, “But here is what happens when you read inside [the paper].” A third of the patients were purely prophylactic, “that means they had no DVT [deep vein thrombosis] or PE to begin with”, Haskal said. “That is like taking people with cancer and people who might get cancer, and following them for a year, and then saying ‘Look, we did not have cancer [amongst the total cohort]’. But you put those people in! [Referring to the cohort without any cancer at the start of the study].”
“Papers are this long for a reasons—we have got to read the detail,” he emphasised.
“Three out of four meta-analyses are garbage in, garbage out, cannot be trusted”
Dotter Lecture Award 2021
“Surely meta-analyses are the path to truth?” Haskal posited. “It is the analysis of the analyses, it is integration and power, it is rigour over narrative, it is signal over noise, it is the superman!” he enthused.
However, he showed a meta-analysis that had to pool 95 trials to show that neutropenic cancer patients have lower mortality with antibiotics, saying “even large, individual trials were not enough to pull it together [and reach this conclusion]. That is a life-altering signal.
“But guess what? In one analysis of 7,200 systemic reviews, once you take out the Cochrane analyses, one quarter, 27%, had low risk of bias, compared to 87% of Cochrane analyses. That means that three out of four meta-analyses are garbage in, garbage out, cannot be trusted.
“You have to stay vigilant as a reader,” he advised, counselling his listeners to have a mental checklist when reading papers:
Study question or hypothesis is clearly defined prior to analysis
Study design has been defined before analysis and search is clearly defined
Clear inclusion and exclusion criteria
Methodological quality of the studies has been checked before analysis by a predefined quality standard (and by more than one reviewer)
Publication bias is checked (for example by funnel plot)
Heterogeneity has been properly investigated (graphically or statistically)
A common effect size is used (directly quoted or recalculated) for pooled result
Adjustment for potential confounders has been considered (mainly for observational studies)
Results are clearly reported and properly interpreted
Are statistically significant results also clinically significant?
“We must train scientific methods into the next generation of interventional radiologists”
To stray from the IR echo chamber, Haskal noted, interventional radiologists have to have scientific flexibility.
“The perfect gold standard is not possible in clinical research,” he said. Iteration, reiteration, renewal, and replication is the best that can be done. “We have to have ongoing scepticism and constrain exuberance,” he said.
He closed his lecture with a call to arms: “We must train scientific methods into the next generation of interventional radiologists, and we have to standardise it.”
Writing in JVIR in 2016, Haskal put: “We have new trainees now entering the specialty; we have five years of opportunity to inculcate them with methodical training and research exposure—to methods, critical reading, analysis and study design”.
He continued: “This will require a fundamental and intentional mutation in IT training DNA—potentially a centralised CRISPR insert available to all residencies. We cannot expect that each programme will have the ability to teach this, we need to develop this nationally, and make this available to our trainees [in the USA], and across the planet, because this is our long-game.”
IR and COVID-19: “When diagnostic volumes cratered, […] our volumes went up”
Speaking more broadly of the hardships SIR members and attendees have experienced in the past year due to the ongoing COVID-19 pandemic, and in particular noting how this has affected the SIR meeting, Haskal commented: “On a professional level, 25 years of the Dotter Lecture means sitting in that giant hall, surrounded by thousands of our colleagues, the lights go down, an extraordinary speaker comes out, and something revealing, and visionary, pulls us all together. Instead, we are all separated, watching this on screens, alone.
“But I want to remind everybody what we have done as interventional radiologists this year. Pulling protocols across the planet, trying to figure out how to manage in this plague year; doing all those procedures—PD catheters at bedside, we had not done that before, dialysis catheters, gastrostomy catheters in acute or chronically-ill patients, arterial lysis for hypercoagulability or pulmonary embolism. When diagnostic volumes cratered and people were furloughed and elective surgeries were cut, whether you were in a big metropolitan area or in smaller hospitals hit by COVID patients, our volumes were maintained or went up.”
“We are always going to have the professor Dotter spirit,” Haskal said in his closing remarks. “But we have to embrace the next evolution and work daily to be clinical scientists.”
Matthew S Johnson, an interventional radiologist and Gary J Becker professor of Radiology Research at Indiana University School of Medicine in Indianapolis, USA, assumed the office of president of the Society of Interventional Radiology (SIR) on 23 March, during the society’s annual Members’ Business Meeting.
“COVID has truly placed interventional radiologists on the frontline, which is both a challenge and an opportunity—people are now recognising us as the frontline workers we have always been and seeing what tremendous value we bring to patients and the care team,” Johnson comments. “SIR is committed to provide all interventional radiologists with the tools they need to thrive in their chosen practice setting, to combat burnout and promote wellness, and to foster a more diverse and inclusive specialty, all to the benefit of the patients we serve. Our members can best serve our patients if those interventional radiologists are healthy, happy, and well supported.”
Other incoming officers of SIR’s 2021–2022 Executive Council include president-elect Parag J Patel (Medical College of Wisconsin, Milwaukee, USA), newly appointed secretary Alda L Tam (Anderson Cancer Center, Houston, USA), and immediate past-president Michael D Dake (University of Arizona Health Sciences, Tucson, USA). Interventional radiologists were often at the frontlines, doing remarkably large numbers of procedures treating COVID-19 patients and among the only specialties that carried on staffing hospitals, providing daily services such as putting in dialysis catheters or treating COVID-19 related pulmonary emboli. “That was a very valuable experience for others to see. We were there, we stepped up – and patients benefitted,” Matthew S Johnson, who took on the Society of Interventional Radiology (SIR) presidency on 23 March 2021, tells Interventional News.
New and re-elected members of the SIR Executive Council are:
Derek Mittleider (Miami Cardiac and Vascular Institute, Miami, USA)—SIR councillor-at-large: private practice (four-year term)
Saher S Sabri (MedStar Washington Hospital Center, Washington, DC, USA)—Graduate Medical Education Division councillor (four-year term)
Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA)—International Division councillor (four-year term)
Kelvin Hong (Johns Hopkins University, Baltimore, USA)—Post-graduate Medical Education Division councillor (reappointment: three-year term)
Mark Baerlocher (University of Toronto School of Medicine, Toronto, Canada)—Standards Division councillor (appointment to fill vacancy created by Alda Tam)
The SIR Foundation also appointed the following members to its Board of directors:
Maureen P Kohi—SIR Foundation Development Division chair (three-year term)
Nadine Abi-Jaoudeh—SIR Foundation Clinical Research and Registries Division chair (three-year term)
Shape Memory Medical recently announced that it has received approval from the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) to market its Impede-FX embolisation plug in Japan. Cosmotec championed the approval process in Japan and is Shape Memory Medical’s distribution partner for its peripheral embolisation products.
The Impede-FX embolisation plug is indicated for use in Japan as an adjunct to devices such as stents, coils, and plugs, and the Impede embolisation plug which previously received PMDA approval in 2019. Impede-FX is percutaneously deployed in an artery or vein for obstructing blood flow in abnormal blood vessels like arteriovenous malformation and fistula, aneurysms, bleeding by traumatic vascular injury, tumours, etc. except for intracranial and cardiac vessels. Impede-FX is available in three sizes, with the maximum device having an expanded diameter of 12mm.
Impede embolisation plugs feature the proprietary Shape Memory polymer technology, a porous, embolic scaffold that is crimped for catheter delivery and self-expands upon contact with blood for rapid conversion to organised thrombus. Preclinical and clinical studies have shown that Shape Memory polymer offers effective and predictable space filling compared to traditional coils and plugs, stable clot formation for reduced intradevice recanalisation, and progressive healing as the material biodegrades. To date, nearly 600 patients have been treated worldwide with the Impede embolisation plug family of devices.
LimFlow announced today that the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) has approved its Clinical Trial Notification (CTN) for the Japanese cohort of the ongoing PROMISE II pivotal trial of the LimFlow percutaneous deep vein arterialisation (pDVA) system.
PROMISE II is a multicentre, prospective, single-arm study being conducted in the USA and Japan as part of the Medical Device Harmonization by Doing (HBD) regulatory collaboration between the two countries.
Using an adaptive statistical design, the study plans to enrol 60–120 “no option” chronic limb-threatening ischaemia (CLTI) patients at 25 sites, four of which will be in Japan. The primary endpoint is amputation-free survival at six months; additional endpoints include limb salvage and wound healing. Subjects will be followed out to three years.
The “no option” patients who are candidates for the PROMISE II study are no longer eligible for conventional endovascular or surgical therapy for CLTI, as determined by an independent physician committee.
“Late-stage CLTI patients have a terrible quality of life, where they live with pain and limited mobility. Treatment success with these patients is defined by wound healing and amputation-free survival. The investigational LimFlow therapy has the potential to achieve both—by restoring oxygen-rich blood flow to the ischaemic foot, it may create the conditions for chronic wounds to heal, which may enable patients to avoid amputation and keep their limb,” said Hiroyoshi Yokoi (Cardiovascular Center, Fukuoka Sanno Hospital, Fukuoka, Japan), PROMISE II Japanese principal investigator. “We recently received Investigational Review Board approval to begin the PROMISE II trial at Fukuoka Sanno Hospital and I am enthusiastic about being able to offer a promising new option to my no-option patients.”
Nobuyoshi Azuma (Asahikawa Medical University, Asahikawa, Japan), a PROMISE II investigator said, “In Japan’s ageing society, arteriosclerosis of the lower limbs is increasing, and severe lower limb ischaemia encompassing foot pain, ulceration and necrosis due to impaired blood flow associated with diabetes and dialysis is becoming a major problem. We hope that pDVA with the LimFlow system will be a viable option and we look forward to starting the trial in Japan soon.”
The pivotal PROMISE II clinical trial of the LimFlow system is currently enrolling patients at centers in the USA and Japan.
Cardiovascular Systems recently announced that it has acquired a line of peripheral support catheters from WavePoint Medical.
Peripheral support catheters are used during peripheral vascular intervention (PVI) procedures for guidewire support to enable lesion crossing, as well as for guidewire exchanges. Physicians use support catheters in approximately 50% of PVIs, primarily in below-the-knee and complex interventions. When calcium is present, lesions can be challenging to cross with an interventional guidewire and often require advanced tools prior to vessel preparation and treatment. CSI anticipates it will introduce the acquired catheters as its new ViperCross line in the first half of its fiscal year ending 30 June 2022.
In addition, as part of this transaction, WavePoint will also develop a portfolio of specialty catheters used in the treatment of chronic total occlusions (CTO) and complex percutaneous coronary intervention (PCI) procedures for CSI. CTOs represent a significant and growing segment of PCIs and often contribute to poor patient outcomes. Commercial availability of these specialty catheters is anticipated in CSI’s fiscal year ending 30 June 2023.
Michael Darcy (Washington University School of Medicine, St Louis, USA), David Sacks (The Reading Hospital and Medical Center, West Reading, USA), and Richard Towbin (Phoenix Children’s Hospital, Phoenix, USA) each received an SIR Gold Medal during the third day of the 2021 meeting of the Society of Interventional Radiology (20–26 March, online), in recognition oftheir “distinguished and extraordinary service to the society or to the discipline of interventional radiology [IR]”. The Gold Medal is the highest honour presented by SIR.
In his outgoing presidential address to the virtual attendees, Michael Dake (University of Arizona Health Sciences, Tucson, USA) congratulates the 2021 Gold Medallists: “The 2021 Gold Medallists, through their practice, mentorship, and leadership, have driven interventional radiology to unprecedented heights, and revolutionised patient care through the power of minimally invasive, image-guided medicine.”
Michael Darcy
Known for his expertise in portal vein interventions and interventional management of gastrointestinal bleeding, Darcy has devoted himself to the best interests of the society and the IR community, SIR state in their award ceremony. Darcy served as president of SIR from 2002–2003, and was chair of the SIR Foundation from 2007–2009. He has authored or co-authored over 140 research papers and 39 book chapters, and has been an investigator on all of the major transjugular intrahepatic portosystemic shunt (TIPS) trials in the USA. Darcy was also a founding member of the Association of Chiefs of Interventional Radiology (ACIR), and served as its president from 2016 to 2018. He gave the 2016 Dotter Lecture at that year’s SIR meeting.
David Sacks
Sacks has authored more than 130 peer-reviewed articles, the society says. Sacks served as president of SIR from 2007 to 2008, and has been standards division councillor, chair of the technologies assessment committee, and a member of many SIR and American College of Radiology (ACR) committees. He has been an editorial board member of the Journal of Vascular and Interventional Radiology (JVIR), and was named a JVIR distinguished reviewer in 2019. Sacks is currently chair of the board of the Intersocietal Accreditation Commission, and president of the Intersocietal Commission for the Accreditation of Carotid Artery Stenting Facilities. SIR says that in this latter position, he is “strengthening an important collaborative relationship for the specialty”. Sacks is also one of the founders of SIR’s clots course, designed to train interventional radiologists to treat acute stroke. Sacks was a principal investigator of the KAVIAR trial, comparing vertebroplasty and kyphoplasty, and the National Institute of Health (NIH)-funded ATTRACT trial.
Richard Towbin
Towbin is one of the founders of the Society of Paediatric Interventional Radiology (SPIR), and one of the first full-time paediatric interventional radiologists. He also established the first paediatric interventional radiology (IR) fellowship, and has trained numerous paediatric IR fellows. Towbin has served on both the SIR Executive Council and SIR Foundation board of directors, and has been a member of the Standards committee for over 25 years. According to the society, he was “instrumental” in initiating the paediatric interventional subcommittee. One of his most significant contributions was serving as treasurer for SIR, the society continue. In 2019,Towbin was the recipient of one of the first Gold Medals given by SPIR. He has authored over 375 papers, many of which SIR claim are considered “seminal” to the field of paediatric IR.
Top, L to R: Moderators David Valenti and Susan Shamimi-Noori
Bottom: Speaker David McNiel
Top, L to R: Moderators David Valenti and Susan Shamimi-Noori Bottom: Speaker David McNiel
Delineating the path towards personalised dosimetry in order to “maximise response to therapy”, David McNiel (University of Arizona Health Sciences, Tucson, USA) presented clinical predictors of yttrium-90 (Y-90) uptake in patients with hepatocellular carcinoma (HCC) at the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online). In the presented research, a multiple regression model demonstrated that prior ablation was a significant predictor of an increased tumour-to-normal ratio (T:N) for Y-90 uptake.
“Radioembolization with Y-90 microspheres is a commonly performed procedure for the treatment of HCC,” he began. “Methods for calculating prescribed activity can be divided into two categories: semi-empirical methods and partition model.”
Due to the prior success of the DOSISPHERE-1 trial, which reported improvement in tumour response rate and overall survival in patients who had HCC treated with Y-90 radioembolization utilising personalised dosimetry, McNiel and colleagues conducted a retrospective institutional review board-approved study on all patients who underwent planning angiography with SPECT-CT for radioembolization of HCC between 9 January 2016 and 31 August 2020 (n=106, over a total of 128 angiography procedures). All patients had pre-procedural contrast-enhanced MRI evaluations of the abdomen. According to the speaker, a multitude of patient characteristics were also collected from the electronic medical record for inclusion in analysis.
MR, cone beam CT (CBCT), and SPECT-CT images were exported to SimpliciY90 image-fusion and dosimetry planning software (version 2.2; Mirada Medical) for evaluation.
“Our initial hypothesis with this work was that T to N ratio would be significantly correlated with the aetiology of the patient’s cirrhosis,” McNiel explained. “Surprisingly, however, this was not the case, and despite the apparently diverse group of patients that go on to develop HCC, including patients with NASH-based [non-alcoholic fatty liver disease] cirrhosis, viral aetiologies of cirrhosis, and alcoholic cirrhosis, none of these groups demonstrated significant differences in T:N ratio in our dataset.
“Similarly, clinical factors that we anticipated would likely have correlation with T:N ratio, including Child-Pugh classification, prior surgical resection, and prior systemic therapy also demonstrated no significant differences in T:N ratio in our dataset.”
Turning to the positive results of their study, McNiel detailed how prior intra-arterial liver-directed therapy (including previous Y-90, transarterial chemoembolization [TACE], and/or ablation therapy) demonstrated significant positive correlation with T:N ratio with their dataset.
In addition, tumour volume, while not significantly correlated, showed “a strong negative trend”; larger volumes of tumour took up less macroaggregated albumin (MAA) activity than their smaller counterparts. “This finding is likely artefactual, based on our methodology, as larger tumours are more likely to contain necrotic, poorly-perfused components, and thus, they are likely to take up less relative MAA than their smaller counterparts.”
Patient age was negatively correlated with T:N ratio by univariate analysis. However, with multivariate analysis, the investigators found non-significance between the two variables.
A subgroup analysis of patients who had undergone prior liver-directed therapy “also demonstrated interesting results,” McNiel continued. Patients who had prior liver-directed therapy could be divided into two groups, he explained: those who had undergone intra-arterial directed therapy, in the form of Y-90 or TACE, and patients who had prior ablation therapy.
“Interestingly, patients who had prior intra-arterial therapy demonstrated no significant difference in T:N ratio, whereas patients who had prior ablation therapy demonstrated a strong significant difference in T:N ratio,” SIR attendees heard (mean 3.39 vs. 2.25; p=0.003).
“These findings raise interesting questions,” McNiel concluded. “Is there some different mechanism of ablation therapy versus intra-arterial therapy that affects this activity? Also, is recurrent disease following either of these therapies somehow inherently different in their angiogenesis or their aggressiveness that could explain these findings?”
The US Food and Drug Administration (FDA) have granted approval of the TheraSphere Y-90 glass microspheres (Boston Scientific), developed for the treatment of patients with hepatocellular carcinoma (HCC). The approval expands access to this life-prolonging therapy for a greater number of patients, which, to date, has been utilised under a humanitarian device exemption (HDE)—an FDA classification that required institutional review board approval and limited the number of patients treated with the therapy per year. TheraSphere is now the only radioembolization technology indicated for the treatment of unresectable HCC in the USA.
HCC is one of the most prevalent cancers in the world and the most common type of primary liver cancer, with more than half a million new global cases diagnosed annually. The American Cancer Society estimates that approximately 32,000 new cases of HCC will be diagnosed in the USA in 2021. It is most often treated through surgery, liver transplantation, chemotherapy, or embolization, including both chemoembolization and radioembolization (selective internal radiation therapy [SIRT]). TheraSphere treatment, a type of SIRT with low toxicity, is comprised of millions of microscopic glass beads containing radioactive yttrium (Y-90), which are delivered directly to liver tumours via a catheter and result in minimal exposure to surrounding healthy tissue.
Approval of TheraSphere was based on results from the LEGACY study, designed to evaluate the safety and efficacy of the therapy for the treatment of early and advanced HCC. The study analysed data from 162 patients and met both primary endpoints of objective response rate and duration of response rate (72.2% at four weeks and 76.1% at six months, respectively). Data demonstrated 100% complete or partial patient response up to two TheraSphere treatments—disappearance of all lesions or ≥30% decrease in target lesion diameter —and a 93% overall survival rate in patients with transplant or resection following treatment at three years.
“I am honoured to have spearheaded the LEGACY trial in which we found that patients with early and advanced HCC exhibited very high response rates as well as clinically meaningful durations of response and survival, establishing TheraSphere as a standard treatment for this patient population,” comments Riad Salem, an interventional radiologist at Northwestern Memorial Hospital (Chicago, USA) and principal investigator of the LEGACY trial. “The trial results, which have been accepted for publication in Hepatology, produced one of the most comprehensive databases for TheraSphere, empowering physicians to make informed, data-driven decisions for their patients.”
Treatment with TheraSphere does not require hospitalisation and is typically performed as an outpatient procedure in as little as an hour, potentially alleviating pressure on healthcare systems in an increasingly complex care environment. Recognition of the benefits of SIRT (both to patients and hospitals) were reflected in recently issued guidance from the National Institute for Health and Care Excellence (NICE) when they recommended the use of TheraSphere for the treatment of patients with HCC through the National Health Service (NHS) in England, Wales, and Northern Ireland.
Penumbra today announced US commercial availability of the Indigo system Lightning 7. Lightning 7 expands Penumbra’s offering of the Indigo aspiration system with Intelligent Aspiration for mechanical thrombectomy and is designed for single session arterial thrombus removal.
Offering a new option for physicians to address arterial thrombus removal, the Indigo system Lightning 7 combines the new Indigo system CAT7 aspiration catheter with Lightning Intelligent Aspiration powered by Penumbra Engine. CAT7 is a high power, low profile catheter that features laser-cut hypotube technology and circumferential sweep designed for dependable delivery and maximised clot extraction.
The Indigo system’s proprietary Separator technology is also available with Lightning 7 (Separator 7) and is designed to enable unobstructed aspiration for the duration of the procedure. Lightning Intelligent Aspiration features Penumbra’s proprietary clot detection technology that enables the operator to identify thrombus location and is also designed for blood loss reduction.
“My experience with Lightning 7 suggests that it streamlines clot removal in the peripheral arterial vasculature with low profile access, excellent trackability, and similar power to the CAT8 Penumbra catheter that was previously used for this application. The torquability makes vessel navigation much easier,” said Christopher Metzger (Holston Valley Medical Center, Kingsport, USA). “Penumbra continues to forge ahead with yet another game-changing technology that has the potential to increase single-session thrombus removal and thereby may help improve outcomes.”
“If interventional radiologists wish to become competitive with surgeons, the availability of software enabling the accurate comparison of pre- and post-interventional CT [computed tomography] or MRI [magnetic resonance imaging] scans must become mandatory and routinely employed,” Luigi Solbiati argues. He discusses the ablation-confirmation software he has developed with his team in Milan, Italy, and enthuses about the potential of artificial intelligence to refine and improve ablative outcomes in interventional radiology.
Many studies in the literature have demonstrated that the outcome of any local tumoural treatments (be it surgery, ablation, or radiotherapy) is largely dependent on the technical success achieved, i.e. if the tumour has been completely or partially treated and, when the treatment is complete, if the peritumoural margins of normal parenchyma are sufficiently and homogeneously thick.
Surgeons have always told interventional radiologists that one of the most significant—if not the most significant—differences between surgical resection and thermal ablation is the modality of assessment of technical success. While surgical specimens are sent to a different department (Pathology) to obtain an accurate assessment, for thermal ablation, technical success is monitored by the same interventional radiologist who performed the treatment (or by other colleagues in the same department). This is done through the comparison of pre- and post-interventional CT or MRI scans in side-by side juxtaposition. This method contains many possible sources of error and can be very challenging, even for experienced radiologists. In a recently published study,1 38 radiologists from many different countries (18 with considerable experience in percutaneous tumour ablation and 20 with limited experience) were asked to assess whether technical success and technical efficacy after thermal ablation of nine hepatocellular carcinomas (HCCs) in nine patients with known outcomes had been achieved using the traditional side-by-side juxtaposition of pre- and post-interventional CT scans. As many as 44.1% of cases per radiologist were misjudged and, more importantly, there was no significant difference between the experienced and unexperienced radiologists.
Consequently, if interventional radiologists wish to become competitive with surgeons, the availability of software enabling the accurate comparison of pre- and post-interventional CT or MRI scans must become mandatory and routinely employed. For this reason, over the last few years I have collaborated with colleagues on the development of a software with these characteristics (Ablation-fit; R.A.W. Srl, Milan, Italy). Our software is based on the automatic segmentation of liver parenchyma and major blood vessels, the semi-automatic segmentation and reconstruction of tumoural targets and post-ablation necrotic areas, and the non-rigid, fully automatic registration of pre- and post-ablation CT scans. This allows for the deformation of liver parenchyma section by section, based on the location of intrahepatic blood vessels, enabling us to achieve an extremely precise image fusion regardless of differences in body position, respiratory motion, or liver deformation. In addition, in very short time (just five to 10 minutes), the software calculates the percentages of residual unablated volumes of both the target tumour and the predetermined 3D safety margin.
In a retrospective study on 90 HCCs that have undergone microwave ablation (MWA) with apparent technical success and followed for at least one year, we demonstrated that, if we could have used this software, we would have discovered incomplete treatments at 24-hour CT scan (enabling immediate re-treatment) in 76.6% of the HCCs that actually had local tumour progression at one year.2
In a recently published clinical study on colorectal liver metastases that had undergone radiofrequency ablation (RFA),3 with volumetric assessment of the periablational safety margin performed with this software, it was proven that the safety margin assessment was the only independent predictor of local tumour progression, and that at least 90% of a 6mm circumscribed 3D safety margin was required to achieve complete ablation.
Ablation-confirmation software like this can be used in different modalities. When ablations are performed in sonographic rooms under the control of contrast-enhanced ultrasound (US), potentially integrated with real-time US-CT/MRI image fusion, ablation-confirmation software like this can be used only after the end of the treatment. In this situation, a level of assessment closer to that achieved by pathologists after surgical resection can be obtained, but if incomplete treatment or insufficient ablative margins are seen, the procedure will have to be repeated, just as in surgery. On the other hand, if ablations are performed under ultrasound or CT guidance in the CT room (as is recommended nowadays),4 the software could be used immediately, intraprocedurally, and the treatment could be adapted in order to complete the intervention without the fear of only obtaining partial or insufficient ablative margins. This intraprocedural use represents an advantage even over surgical resection.
In addition, this kind of software can trace out the ideal path to the portion of tumour to be retreated, thus significantly facilitating the completeness of the procedure.
In the near future, it is hoped that such easily usable and extremely fast software will be increasingly employed in interventional departments. We are currently working to extend their applicability also to extrahepatic organs, such as the kidneys, lungs, lymph nodes, and prostate, as well as to MRI scans.
In the end, it is important to point out that there is a perfect integration between the type of software described above, and one of the most attractive (if not the most attractive) incoming modalities for the guidance of any interventional procedure: augmented reality (AR).5 In addition to the already known and much discussed advantages of AR (its low cost, ergonomic feel, diminishment of the learning curve, particularly in younger users, the opportunities this technology provides for educational purposes), it can be particularly helpful for the guidance of interventional devices into incompletely treated tumoural areas, thanks to its ability to define precise trajectory lines that the operator can simply and automatically follow to reach the targets. The association of increasingly accurate and simple ablation-confirmation software and AR is likely one of the milestones of near future interventional radiology.
Luigi Solbiati is an interventional radiologist at the Humanitas University in Milan, Italy. Disclosure: He is a developer of the Ablation fit software.
References
Laimer G, Schullian P, Putzer D, et al. Can accurate evaluation of the treatment success after radiofrequency ablation of liver tumors be achieved by visual inspection alone? Results of a blinded assessment with 38 interventional oncologists. Int J Hyperthermia 2020; 37: 1,362–1,367. doi.10.1080/02656736.2020.1857445
Solbiati M, Muglia R, Goldberg SN, et al. A novel software platform for volumetric assessment of ablation completeness. Int J Hyperthermia 2019; 36: 337–343. doi. 10.1080/02656736.2019.1569267
Laimer G, Jaschke N, Schullian P, et al. Volumetric assessment of the periablational safety margin after thermal ablation of colorectal liver metastases. Eur Radiol 2021. doi.10.1007/s00330-020-07579-x; Online ahead of print
Mauri G, Solbiati L, Orsi F, Monfardini L. Thermal ablation of liver tumours: The crucial role of 3D imaging. Cardiovasc Intervent Radiol 2020; 43(9): 1,416–1,417. doi.10.1007/s00270-020-02560-z
Intra-ablation feedback: software using biomechanical deformable registration volumetric imaging. Image courtesy of Bruno Odisio.
Ablation is entering a new era of increased precision and quantification, the interventional radiology (IR) community argues, with outcomes that match or surpass those of surgery. Whilst reaching equipoise with their surgical counterparts has been a goal for interventional radiologists since the advent of ablative treatments for cancer, some expert interventionalists claim that the increased precision of modern thermal ablation techniques, coupled with improvements in radiology mean physicians are often treating smaller volume tumours. This now positions the procedure as the “definitive” treatment for select patients in some cancers. Several clinical trials including the ACCLAIM, COLLISION, and COVER-ALL trials—are currently underway, and aim to bolster the evidence-base demonstrating favourable patient outcomes from thermal ablation.
“We are now talking about ablation 2.0,” past Society of Interventional Oncology (SIO) president Stephen Solomon (Memorial Sloan Kettering Cancer Center, New York, USA) says. “Ablation 1.0”, in his eyes, is the basic concept underpinning the minimally invasive procedure: put a needle in, use image guidance, burn or freeze the cancerous tissue to destroy it. “But ablation 2.0,” he explains, “means that we are focusing more on precision, on margins, and specifically the road to A0 [where all tumour cells are eradicated].”
When discussing soft and hardware advances in ablation, David Breen (University Hospital of Southampton, Southampton, UK) adopts the framework of “planning, execution, confirmation”. Planning uses preprocedural scans to map out probe positions and angles, along with estimation of the ablation zone—all the steps taken ahead of performing the ablation. Execution is the act of probe positioning, sometimes using guidance tools. The final stage, confirmation, involves determining the adequacy of treatment margins in order to verify complete ablation. “Of these three stages, confirmation and perhaps planning are the two that are beginning to enter a higher level of engineering maturity and reliability. Guidance tools, as they currently stand, must still be used with careful operator insight,” Breen explains.
The upcoming European Conference on Interventional Oncology (ECIO; 10–13 April, online) is hosting a session entitled “Different ways of killing cancer and why we need all of them”, which explores advances in ablation.
In a further sign of the times, several large companies are positioning themselves to buy smaller businesses operating in this space. In 2020, for example, imaging behemoth Siemens Healthineers acquired all shares of Varian, a radiotherapy company, which in 2019 itself acquired Endocare, a company specialising in cryoablation and microwave ablation, and Alicon, a provider of embolic therapy for liver cancer treatment.
Cascination is another company offering an over-arching solution for ablation, with products designed for imaging, planning, navigation, validation, treatment, and treatment verification. Breen believes this is the direction industry is taking, and represents a shift away from a more modular approach where one organisation may only offer products for part of this pathway.
Developing improved planning software
Several different groups around the world are working on developing planning software for ablation treatments with the goal of obtaining a predictable technical outcome. “In order to do this effectively,” current SIO president Matthew Callstrom (Mayo Clinic, Rochester, USA) explains, “it is necessary to have accurate registration software for all phases of the ablation, including planning, intraprocedural evaluation of device placement, and postprocedural measurement of the margins of the ablation. This approach will transition thermal ablation from a subjective technical endpoint to an objective technical endpoint. I think the exciting aspect of this is that many efforts are underway and will become more widely available to proceduralists.”
From the department of Interventional Radiology at the University of Texas MD Anderson Cancer Center (Houston, USA), Bruno Odisio tells Interventional News that he and imaging physicist Kristy Brock have received a National Institute of Health (NIH) grant (Academic-industry partnership–Raysearch Laboratories) for the development of a dedicated liver ablation planning and assessment software. “We are using this software to simulate and evaluate intraprocedurally the treatment endpoint, because we know that when we perform a liver ablation, the most important thing that we can do to improve local tumour control is to effectively cover the tumour with adequate margins in all planes,” he explains.
Odisio and colleagues are enrolling for a phase II trial (COVERALL) to study how well software-aided imaging works in confirming tumour coverage with ablation on patients with liver tumours. The primary objective of the COVERALL trial is “To evaluate if the intraprocedure feedback of a biomechanical deformable registration volumetric image method during percutaneous ablation will increase the minimal ablation margins on a three-dimensional (3D) computed tomography (CT)-generated analysis.”
Clinicaltrials.gov registers: “The current standard for targeting tumour cells and evaluating the outcome of a liver ablation procedure is a visual inspection of the pre- and postprocedure computed tomography (CT) scans. Software-aided imaging systems (such as Morfeus, the one utilised in the COVER-ALL study) may help to improve the accuracy and effectiveness of liver ablation.”
Prior to receiving the NIH grant for the COVER-ALL study, Odisio and Brock conducted a preliminary, retrospective analysis using their software to make a fusion image of the preprocedural and postprocedural CT images. The software utilises a biomechanical model to align the images, which Odisio says allows them to account for patient breathing, positioning, and tissue desiccation associated with the ablation itself. “We noticed that many times, our simple visual inspection of the CT scans before and after the ablation gave us a false sense of confidence regarding covering the entire tumour. In fact, among the patients who had recurrence after the ablation, we noticed based on our software assessment that ablation did not cover the tumour properly in all three-dimensional planes. Also, usually the lack of sufficient ablation margins occurs in an oblique plan between the axials, coronal, and sagittal plans”. He adds: “Based on what we have learned so far, many of the cases we define as tumour recurrence are in fact residual unablated tumour. That was our motivation to use the software.” Using the software with biomechanical modelling negates the issues with trying to decipher simple axial imaging in a complex 3D environment.
He adds that it is very hard to analyse the imaging data intraprocedurally: “You have a constrained timeline; you have too much data for you to run. Our software uses artificial intelligence [AI] and a biomechanical model to analyse the data on probe placement and ablation margins during the liver ablation. We hope that this will solidify the idea that using software really helps to improve treatment endpoints.” This work is part of the Image Guided Cancer Therapy (IGCT) Research Program run through The University of Texas MD Anderson Cancer Center.
Luigi Solbiati and his team at Humanitas University in Milan, Italy, have also developed software to aid ablation (Ablation-fit, R.A.W. Srl). “If interventional radiologists wish to compete with surgeons, the availability of software enabling an accurate comparison of pre- and postinterventional CT or magnetic resonance imaging (MRI) scans must become mandatory and routinely employed,” Solbiati opines.
Describing the software to this newspaper, he comments: “It is based on automatic segmentation of liver parenchyma and major blood vessels, semi-automatic segmentation, and reconstruction of tumoural targets and post-ablation necrotic areas and [employs a] non-rigid, fully automatic registration of pre- and postablation CT scans that allows us to deform the liver parenchyma section by section, based on the location of intrahepatic blood vessels. This allows for an extremely precise image fusion regardless of differences in body position, respiratory motion, or liver deformation. In addition, in very short time (five to 10 minutes) the software calculates the percentages of residual, unablated volumes of both the target tumour and predetermined 3D safety margin.”
In a retrospective study of 90 hepatocellular carcinomas (HCCs) that had undergone microwave ablation with apparent technical success and followed for at least one year, published in the International Journal of Hyperthermia, Solbiati et al demonstrated that, if they could have used this software, they would have discovered incomplete treatments at 24-hour CT scan (enabling immediate re-treatment) in 76.6% of the HCCs that actually had local tumour progression at one year.
In a clinical study recently published in European Radiology of colorectal liver metastases that have undergone radiofrequency ablation (RFA) with volumetric assessment of the periablational safety margin performed using this software, it was proved that the safety margin assessment was the only independent predictor of local tumour progression, and that at least 90% of a 6mm circumscribed 3D safety margin was required to achieve complete ablation.
“Ablation-confirmation software like this can be used in different modalities,” Solbiati says. “When ablations are performed in sonographic rooms under the control of contrast-enhanced ultrasound (US), potentially integrated with real-time US-CT/MRI image fusion, ablation-confirmation software like this can be used only after the end of the treatment. In this situation, a level of assessment closer to that achieved by pathologists after surgical resection can be obtained, but if incomplete treatment or insufficient ablative margins are seen, the procedure will have to be repeated, as it would occur for surgery. If ablations are performed under US guidance (or CT guidance) in the CT room (as would be recommended nowadays), the software would be used immediately, during the procedure, and the treatment could be immediately completed if partial or with insufficient ablative margins. This would represent even an advantage over surgical resection.
“In addition, this kind of software can trace out the ideal path to the portion of tumour to be treated, thus significantly facilitating the completeness of the procedure.
“In the near future, it is hoped that such easily usable and extremely fast software will be increasingly employed in interventional departments, while we are currently working to extend their applicability also to extrahepatic organs (kidney, lung, lymph nodes, prostate) and to MRI scans.”
ACCLAIM and COLLISION: Trial to watch
The SIO is also currently planning a multicentre clinical trial—the ACCLAIM trial—that incorporates software that looks at margins into the ablation, and which will aim to determine if achieving complete margins during an ablation equates to procedural success, assessed through disease progression or recurrence postprocedurally. Constantinos Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA) will be the principal investigator.
“The ACCLAIM trial will be the first liver ablation trial to use a well-defined objective technical outcome measure as a critical aspect of the trial design,” Callstrom tells Interventional News. “We anticipate that this will help drive adoption of this approach as the standard for liver mass ablation”.
Sofocleous comments: “The ACCLAIM trial is a single-arm, prospective, multicentre, international phase II study where thermal ablation will be offered in patients with limited number and relatively small CRC [colorectal cancer] liver metastases. A mandatory requirement for enrolment in the trial is the use of real-time 3D software to assess the ablation zone and show that the target tumour has been completely covered with ideally 10mm and not less than 5mm of minimal ablation margins. The study hypothesis is that if ablation margins are larger than 5mm, local progression-free survival at 12 months after ablation will be over 85%.”
Another hotly anticipated trial is the COLLISION trial. Sofocleous tells this newspaper: “I am very interested to see the results of the COLLISION trial that compares thermal ablation to resection for well-selected small colorectal liver tumours. This trial is now enrolling in The Netherlands, and will address a lot of the questions that exist for the value of ablation. I am particularly interested to find out whether the trial will provide high-level evidence about thermal ablation and whether this treatment can be equally effective and potentially safer than limited resection as a local curative therapy for CRC liver metastases.”
In an additional attempt to further improve margin confirmation, Solomon informs this newspaper that he and Sofocleous are conducting research into performing biopsies around the edges of the tumour intraoperatively, in order to gain a quick pathological assessment of whether or not any cancer cells are left alive. This allows them to be more adaptive during the procedure: “If, during the procedure, we find there is still live tissue, we would do something about it. If the software shows us that the margins are close, maybe we would expand it [the ablation zone] a bit. All of these things allow us to finesse and improve our results.”
Cardiovascular Systems has announced that the first patients in the USA have been treated with the Wirion embolic protection system. Wirion is a distal embolic protection filter used to capture thrombus and debris that can be associated with all types of peripheral vascular intervention procedures, including atherectomy.
Lawrence Garcia, St Elizabeth’s Medical Center, Boston, USA and Nicolas Shammas, Unity Point Health-Trinity Bettendorf, Davenport, USA participated in the WISE LE study where Wirion demonstrated a major adverse event (MAE) rate of 1.9%, which is lower than previously reported rates for other lower extremity embolic protection filters. Importantly, no clinically significant distal embolization was observed when Wirion was used.
Garcia commented: “Wirion represents a critical advancement for distal embolic protection devices. With Wirion, I can use my preferred 0.014” guidewire to cross the lesion and then place the filter anywhere on the wire. As a result, I am able to provide extensive support, individualized to each patient and intervention.”
Shammas added: “Delivery and retrieval of Wirion are easy with a minimal learning curve. Debris capture is very efficient making Wirion exceptionally suited for use with any atherectomy device.”
Scott R Ward, CSI Chairman, president and chief executive officer, said: “We are excited to announce the commercialisation of Wirion. This product will be an important part of our comprehensive portfolio of differentiated products designed to save limbs and improve outcomes for patients undergoing complex peripheral interventions.”
MedAlliance recently announced that it has raised over US$50 million in equity funding. The new investor is Trustar Capital (formerly known as CITIC Capital Partners).
Proceeds from the financing will be used to fund commercialisation of Selution SLR—a novel sirolimus-eluting balloon that provides a controlled sustained release of a limus drug. They will also support global clinical programmes including enrolment of four additional US Food and Drug Administration (FDA) investigational device exemption (IDE) studies this year. The US coronary ISR study is underway and began enrolment in July 2020.
MedAlliance, the first drug-eluting balloon (DEB) company in the world to receive FDA breakthrough device designation status for a sirolimus DEB, was recently awarded breakthrough status for Selution SLR in the treatment of atherosclerotic lesions in native coronary arteries. This was the fourth breakthrough designation awarded to MedAlliance for its sirolimus DEB, following coronary in-stent restenosis, peripheral below-the-knee and AV fistula indications.
In February 2021, MedAlliance enrolled the first patient in SUCCESS PTA, a 700-patient post-market study with Selution SLR for the treatment of peripheral arterial disease (PAD). This is the largest study undertaken to date with the device. Data from the SUCCESS PTA study will be part of the clinical evidence supporting CE mark renewal in 2023/2024 under the new European Medical Device Regulation (MDR).
Selution SLR was awarded CE mark approval for the treatment of PAD in February 2020 and for the treatment of coronary arterial disease in May 2020. It is now available in Europe and all other countries where the CE mark is recognised. The global market for DEB is estimated to be worth over US$1.5 billion.
Treating patients with metastatic bone disease by radiofrequency ablation (RFA) using the OsteoCool system (Medtronic) results in rapid and statistically significant improvement in pain scores, and provides sustained, long-term relief. Attendees of the 2021 meeting of the Society of Interventional Radiology (SIR; 20–26 March, online) will be the first to hear the full cohort data from the Medtronic-sponsored OPuS One post-market clinical study in the “Abstract of the year” presentation, to be delivered by Jason Levy (Northside Hospital, Atlanta, USA) to the virtual audience. This latest dataset follows previous announcements from the OPuS One team also detailing positive results following RFA with the OsteoCool system.
OPuS One is the largest clinical study—with the most meaningful clinical results—considering the OsteoCool technology to date. Principal investigator Sandeep Bagla (Vascular Institute of Virginia, Woodbridge, USA), along with Levy and other colleagues, set out to assess the effectiveness of the OsteoCool RF ablation system. They conducted a global, prospective, nonrandomised, multicentre study of RFA for the palliative treatment of patients with painful osseous metastases.
In addition to pain, osseous metastases can cause fractures and some “pretty debilitating symptoms”, such as spinal cord or neurovascular compression, Levy said.
He continued: “Radiation treatments have been commonly used for this, but they do not always provide pain relief, they can take weeks to occur, and they can set a patient up for fractures down the road. When the effects of their treatment are delayed for weeks, in this population of palliative care patients, that may consist of a significant proportion of that patient’s life.”
The investigators therefore wanted to ascertain the ability of RFA to provide quick and long-lasting pain relief for these patients.
Opining on their results, Levy enthuses: “We are really excited by what we saw. The first thing we noticed is that we had pain relief as fast as three days, which is obviously very significant in this patient population, especially when the standard-of-care treatment right now, radiation, takes four to six weeks.
“In addition, this was sustained. At one year, the majority of patients continued to report pain improvements, which is also a significant improvement over radiation treatment.”
Patients also experienced significant improvement in average pain, pain interference, and quality of life.
“I think the most important outcome from this study is that RFA can give patients a very rapid, improved quality of life within three days, and this is sustained out to 12-months,” Levy reiterated. As the OPuS One trial largely focused on lytic metastases, which are very common, Levy says these results demonstrate that RFA with OsteoCool is a “good option” for a wide range of cancer patients.
“I believe this treatment should be available in the patient paradigm than what we saw in this study, where it was mostly a palliative treatment,” he concluded. “[We should offer it to] more patients where we can prevent future fractures, and prevent pain from lasting a long time.”
Levy and Bagla spoke to Interventional News following the results of the first 100 patients treated in the OPuS One clinical study. The full interview can be viewed here, or below.
Genicular artery embolization (GAE) is “highly effective and durable” in reducing symptoms due to moderate-to-severe knee osteoarthritis that is refractory to other conservative therapy (such as joint injections and medication), and has an acceptably low toxicity profile. So concludes Siddharth Padia (University of California, Los Angeles, USA), speaking at a press briefing in advance of the Society of Interventional Radiology (SIR) annual meeting (20–26 March, online). He will present these results to attendees of the virtual congress.
Padia cites GAE as a “promising therapy” to treat patients with symptomatic knee osteoarthritis by reducing synovial arterial hypervascularity. “As we all know, having arthritis is a very common problem, resulting in pain and physical dysfunction,” he said. Current treatment options for this disease are to “do nothing” and rest up, to take medications (including nonsteroidal anti-inflammatory drugs; NSAIDs), or, if these have failed, to receive a joint injection: “typically a steroid, such as cortisone, or a gel,” Padia said.
“While those can work,” he continued, “they have relatively short-term results. A typical joint injection lasts for anywhere from one to three months, so it is not really built as a long-term solution. Currently, the only long-term solution is a knee replacement, which does work, and is recommended for people with severe, symptomatic osteoarthritis, but the problem, the challenge with total knee replacement is it involves anaesthesia, it involves a hospital stay, and it has a long recovery and rehabilitation time. Many patients are either not candidates, or want to defer their operation to a later date.”
The investigators therefore conducted a prospective, single-centre, open-label, US Food and Drug Administration (FDA)-approved investigational device exemption (IDE) study that aimed to evaluate the safety and efficacy of the minimally invasive GAE procedure for the treatment of symptomatic knee osteoarthritis, with an eye to looking at potential long-term outcomes.
“In theory, if we can reduce the inflammation, we can make people’s pain go away, and make their overall function improve,” Padia explained, justifying the rationale underpinning GAE. “The goal is to normalise or even decrease the blood flow in the knee joint, because right now, in a patient with arthritis, the blood flow is abnormally increased.”
Knee osteoarthritis is age-related, Padia explained, and as such the study enrolled patients aged 49–80 years (median age of 69). All patients had moderate or severe focal knee pain and osteoarthritis on knee radiograph (Kellgren-Lawrence grades 2–4; 18% were grade 2, 43% were grade 3, and 40% were grade 4), no prior knee surgery, and were not candidates or not willing to undergo total knee replacement surgery. Patients had to have failed conservative therapy, including NSAIDs and/or joint injections. Baseline pain (visual analogue scale) and symptom scores (Western Ontario and McMaster Universities Osteoarthritis Index; WOMAC) were assessed. Median body mass index (BMI) was 28 (range 18–44).
After obtaining femoral arterial access, GAE was performed using 100μm particles (Embozene, Varian) of one to three genicular arteries supplying the location of the patient’s pain, as determined by digital subtraction angiography and cone-beam computed tomography (CT). GAE is performed as an outpatient procedure, and not under general anaesthesia, because “the procedure itself is completely painless”.
Over a nine-month period, 40 patients were treated with GAE. The left knee was treated in 25 of the 40 patients (62%), and the right knee was treated in the remaining 15 (38%). Medial knee pain was treated in 27 of 40 patients (68%), and lateral knee pain was treated in 13 (32%). Technical success was achieved in 100% of patients.
WOMAC and pain scores decreased from a median of 52 (out of 96) and eight out of 10 at baseline to 21 out of 96 (60% decrease) and three out of 10 (63% decrease) at 12 months, respectively. “We saw an immediate drop in WOMAC score, from quite a high score at baseline [52 out of 96] to a median of 22 at one month. It further improved with time: at three months, WOMAC score was 15, and it stayed low for the entire duration of the study.”
Padia and colleagues used a cut-off of 50% to consider their procedure a success. In total, 27 out of the 40 patients (68.5%) had a greater than 50% reduction in WOMAC score, and a further 28 patients from the full cohort (70%) experienced a more than 50% reduction in pain score. “A 50% reduction is quite an aggressive threshold to use,” Padia stated. “The orthopaedic surgery literature uses a much smaller cut-off when they define success. When we use a higher threshold, such as a 75% reduction—a 75% reduction in WOMAC score essentially means you are pain free—that was achieved in 43% [of patients]. There are significant improvements in pain in the majority of patients.”
The investigators also noted any adverse events and symptoms scores, assessing these at one week, one month, three months, six months, and one year after GAE. Transient skin discoloration and transient mild post-procedure knee pain were common and expected. Treatment-related adverse events included: one patient with a groin haematoma requiring overnight observation, seven patients with self-resolving focal skin ulceration, and two patients with asymptomatic small bone infarct on MRI at three months.
Despite lower mortality and shorter hospital stays, uterine artery embolization (UAE) is used far less commonly than hysterectomy in the management of clinically significant postpartum haemorrhage. This conclusion, presented at the Society of Interventional Radiology (SIR) annual meeting (20–26 March, online) by Janice Newsome (Emory University Hospital, Atlanta, USA), has led investigators to call for a postpartum haemorrhage response team, akin to a trauma response team. MD candidate Linzi Ardnt, also at Emory University Hospital, is the lead researcher for this work.
Speaking to press ahead of the annual meeting, Newsome expanded on her vision: “When our Ob-Gyn [Obstetrician and gynaecologist] colleagues make the decision to perform a hysterectomy, most of the time the estimated blood loss or the actual blood loss is under-calculated or unknown—so we are in a real dire situation at that point. Interventional radiologists are at many of these hospitals as well. So I believe, in order for UAE to become more utilised in these situations, we need to develop more techniques so we can find out earlier what the actual blood loss is, mobilise a team of people early so that these women can actually have this procedure [UAE] done, before a hysterectomy is chosen at the last minute. We are advocating for forming a postpartum haemorrhage team, so we can train together with our colleagues in Ob-Gyn—I believe that then, we can save more lives.”
Ardnt, Newsome et al picture the postpartum response team consisting of “anyone who cares for mothers and babies”, including anaesthesiologists, interventional radiologists, Ob-Gyns, and in some cases possibly neonatologists.
Contextualising this research, she stated: “Unfortunately, roughly 100,000 mothers will experience significant postpartum haemorrhage, a leading cause of the loss of life associated with childbirth”. The research identified 31 incidences of postpartum haemorrhage per 1,000 live births in the USA, of 9.8 million identified live births in total.
“Additionally,” Newsome continued, “20% of new mothers will have no risk factors. Because postpartum haemorrhage can occur quickly and threaten the life of the mother, the treatment options are sometimes limited. Currently, the most common treatment is just a transfusion [with an average incidence of 116.4 per 1,000 cases of postpartum haemorrhage]. But because physicians must act quickly, in many cases, the mother’s uterus is removed via hysterectomy.”
UAE represents an “underutilised”, less invasive second option, she explained, going on to note that the procedure has the benefit of being uterus-sparing, with quicker recovery times, and fewer adverse events.
The study investigators therefore set out to evaluate the utilisation and comparative effectiveness of hysterectomy versus UAE in patients with clinically significant postpartum haemorrhage requiring blood transfusion.
Using the Healthcare Cost and Utilisation Project Nationwide Inpatient Sample database from 2005 through 2017, they identified all women with live-birth deliveries who experienced clinically significant postpartum haemorrhage (defined as those receiving a blood transfusion only or transfusion plus hysterectomy or UAE). They utilised univariate analysis chi-square testing to determine demographic and clinical predictors of receipt of various therapies. Logistic regression was used to compare mortality and prolonged length of hospital stay (>14 days) for different treatment groups correcting for statistically significant predictors of receipt of various therapies.
The investigators noted that the incidence of hysterectomy to treat postpartum haemorrhage was significantly greater than incidence of UAE (20.4 vs. 12.9; p< 0.001). The following factors predicted the type of therapies received: race, maternal age, year of admission, elderly primigravida, previous or current caesarean section, breech position of foetus, placenta previa, pre-existing hypertension, pre-eclampsia, eclampsia, gestational diabetes, post-date pregnancy, premature rupture of membranes, cervical laceration, uterine rupture, dystocia, forceps delivery and haemorrhagic shock (all p<0.001).
Newsome noted: “We saw this disparity [between the number of hysterectomies and the number of UAEs] across racial lines and geography as well. Hysterectomy was twice as common as embolization in Latinx patients, and also more common in rural and non-teaching urban hospitals, as well as in the South [of the USA], and among Medicare and self-paying patients.
“Additionally, prolonged hospital stays of more than 14 days were twice as likely [2.1 times more likely with hysterectomy than UAE; p<0.001] in patients who had hysterectomies, and the hysterectomy procedure resulted in higher hospital charges—around US$18,000 more than if it were for UAE,” Newsome commented.
On logistic regression, the likelihood of mortality from hysterectomy was 3.1 times that of UAE (p< 0.001).
“Because of the evidence supporting UAE and benefits it provides to patients, we encourage hospitals to provide this treatment option to these women who may be at risk from postpartum haemorrhage. To do this, hospitals can create postpartum haemorrhage teams with an interventionalist, similar to other trauma teams, where we would train together and develop response protocols so they are better able to identify the risk factors o postpartum haemorrhage and ensure that the proper staff is on hand, for any delivery, and to be able to respond quickly, so that we can save mother’s lives before it goes too far, to the point where radical surgery is needed.”
Cardinal Health recently announced that it has signed a definitive agreement to sell its Cordis business to Hellman & Friedman (H&F) for approximately US$1 billion, which includes buyer’s assumption of certain liabilities and seller’s retention of certain working capital accounts. The transaction is expected to close in the first half of Cardinal Health’s fiscal year 2022, subject to customary closing conditions and regulatory clearances.
“Cordis has a long history of innovation in minimally-invasive cardiovascular technology, and we are confident that with H&F as its owner, Cordis will be well-positioned for growth, innovation and success,” said Mike Kaufmann, CEO of Cardinal Health. “Cardinal Health and H&F have a shared passion for delivering high-quality medical products to customers and we are excited about the future for the Cordis business under H&F’s ownership.”
“Our decision to divest Cordis demonstrates our disciplined approach to evaluating our portfolio and focusing our resources in our strategic growth areas where we are an advantaged owner,” Kaufmann continued. “Looking forward, we remain committed to our medical distribution and global medical products businesses.”
“Cordis is an excellent fit with our philosophy of investing in great businesses as a market-leading cardiovascular device manufacturer known for high-quality products, strong physician satisfaction and superb patient outcomes,” said Hunter Philbrick, partner at H&F. “We are excited to invest in the talented Cordis, Ajax and Zeus teams to drive industry leadership, therapeutic innovation and improved patient experiences.”
“We at Ajax Health and Zeus Health are ecstatic about injecting growth into Cordis’ powerful platform, and will do so through investments in the core business and through an independent R&D engine—the ‘Cordis Accelerator’—to develop and commercialise a new pipeline of products exclusively for Cordis,” said Duke Rohlen, CEO of Ajax Health and Zeus Health, partners to H&F in the transaction, and executive chairman-designate of Cordis and CEO of Cordis Accelerator. “We see an unparalleled opportunity to partner with both existing Cordis leadership and H&F to combine a best-in-class innovation engine with a strong and robust commercial chassis. Together, we will establish Cordis as the standard bearer for medical device innovation.”
After closing, most assets and liabilities associated with the Cordis business will transfer to H&F. Cardinal Health will retain full authority for lawsuits related to inferior vena cava filters in the USA and Canada, as well as liability associated with these matters. Cardinal Health estimates that, after completion of the transition services agreement, the divestiture of the Cordis business will decrease Medical segment profit by approximately US$60 million to US$70 million on an annual run-rate basis.
In connection with the entry into this definitive agreement, Cardinal Health will classify the Cordis business as held for sale, which Cardinal Health expects to result in a pretax loss of up to US$120 million in the third quarter of its fiscal year 2021. Additionally, Cardinal Health was authorised to incur costs associated with the planned divestiture of up to US$125 million, primarily in its fiscal years 2021 and 2022.
Shape Memory Medical has announced CE mark approval for the Impede-FX RapidFill device, an expansion of the Impede family of biodegradable peripheral vascular embolisation plugs.
Ted Ruppel, president and CEO of Shape Memory Medical said, “We are excited to introduce Impede-FX RapidFill to the endovascular community in Europe. This is the first device on the market that enables the delivery of multiple embolisation plugs in a single application,which may provide an advantage in cases where the goal is to quickly fill and occlude large spaces such as aneurysms, venous insufficiency, or trauma with reduced procedure and fluoroscopy time, contrast media, and blood loss.”
The Impede family includes the Impede embolisation plug, the Impede-FX embolisation plug, and now Impede-FX RapidFill which consists of five Impede-FX-12 embolisation plugs preloaded into a single delivery introducer. This peripheral vascular platform incorporates the Company’s novel Shape Memory polymer technology, a porous, embolic scaffold that is crimped for catheter delivery and self-expands upon contact with blood for rapid conversion to organised thrombus.
Preclinical and clinical studies have shown that Shape Memory Polymer offers effective and predictable space filling compared to traditional coils and plugs, stable clot formation for reduced intradevice recanalisation, and progressive, intradevice healing as the material biodegrades.
To date, nearly 600 patients have been treated worldwide with the Impede family of devices.
Point-of-care duplex ultrasound (PAD-scan) is a cost-effective test for the detection of peripheral arterial disease (PAD) in patients with diabetes. This is the conclusion of a study recently published online in Annals of Surgery.
Authors Pasha Normahani (Imperial College NHS Healthcare Trust, London, UK) and colleagues write that PAD is a risk factor for cardiovascular disease, diabetic foot ulceration, and amputation in diabetic patients. They state that diagnosis enables optimisation of therapies to manage these risks, and highlight that PAD-scan can be performed by frontline staff and has been shown to be the most accurate bedside test. However, they stress that its cost-effectiveness has not been investigated.
Normahani et al detail that in the present study, a Markov model was constructed to estimate the health outcomes and costs over five years of different testing strategies applied to a cohort of diabetic patients. Bedside tests investigated were PAD-scan, ankle-brachial pressure index (ABPI), toe-brachial pressure index (TBPI), audible and visual Doppler, transcutaneous pressure of oxygen (TcPO2), and pulse palpitation, they specify. The authors note that health outcomes were incidence of new diabetic foot ulcer, major cardiovascular events, amputation, death, and diabetic foot ulcer healing rates.
“PAD-scan was the most cost-effective bedside test with an incremental cost-effectiveness ratio of £11,391/quality adjusted life years (QALY),” the authors communicate, adding that PAD-scan superiority in incremental cost-effectiveness ratio occurred at a PAD prevalence threshold of 0.24. Furthermore, they report that PAD-scan had the highest probability (78.7%) of having the greatest net benefit at a willingness to pay threshold of £20,000 per QALY. Finally, they reveal that the test reduced the number of amputations by 24% and the number of cardiovascular deaths by 10% over five years, compared to TBPI—the next best alternative.
Speaking to Vascular News about the significance of the team’s findings, Normahani commented: “Our results encouragingly suggest that point-of-care duplex ultrasound is accurate, cost-effective, and that its adoption may improve clinical outcomes. These results require external validation but provide a promising target for future research aiming to address the high burden of amputation and mortality in this group of patients.”
Renal artery involvement (RAI) in endovascular aneurysm repair (EVAR) is “highly predictive of the need for postoperative and permanent dialysis,” Anastasia Plotkin (University of Southern California, Los Angeles, USA) and colleagues write in the Journal of Vascular Surgery (JVS). They also report that RAI without revascularisation is associated with lower overall survival.
Plotkin et al detail that revascularisation after intentional or unintentional renal artery coverage “is not always technically successful,” adding that loss of a single renal artery in this patient population may result in the need for postoperative dialysis. In the present study, the investigators aimed to compare outcomes after EVAR stratified by RAI.
The researchers analysed data from the EVAR and thoracic endovascular aortic repair (TEVAR)/complex EVAR modules in the Vascular Quality Initiative (VQI) registry from 2009–2018. The primary outcome was postoperative dialysis, and secondary outcomes were 30-day mortality, dialysis at follow-up, postoperative renal function, and two-year survival.
Plotkin and colleagues detail that repair type cohorts were defined as: 1) no RAI (NRAI); 2) renal artery involvement with revascularisation (RAI-R); and 3) RAI and no revascularisation (RAI-NR). They relay that 25,724 out of 54,020 patients in the EVAR and TEVAR/complex EVAR modules in the VQI met the criteria for inclusion—24,879 NRAI, 733 RAI-R, and 112 RAI-NR.
The investigators report that postoperative dialysis was higher in RAI-NR (0.7% NRAI vs. 2.2% RAI-R vs. 17% RAI-NR, p<0.0001), as were 30-day mortality and dialysis at follow-up. On multivariate analysis, they add, RAI-R (odds ratio [OR], 2.2; p=0.03) and RAI-NR (OR, 5.9; p<0.0001) were independent predictors of postoperative dialysis and remained so after excluding ruptures: RAI-R (OR, 3; p=0.003) and RAI-NR (OR, 22.3; p<0.0001).
Finally, Plotkin et al communicate that other independent predictors of postoperative dialysis were worse preoperative renal function, symptomatic presentation, any preoperative/intraoperative blood transfusion, and larger blood loss (≥200ml).
“These risks should be taken into consideration with planning and performing EVAR and should be weighed against the risks of open repair when considering treatment options,” the authors conclude.
After hepatic artery embolization, preserved flow (≥4 segmental hepatic artery) lowered the risk of hepatic complications regardless of the portal venous flow. This is the conclusion presented by Won Seok Choi, Chang Jin Yoon (both Seoul National University Bundang Hospital, Seongnam, Korea), and colleagues in the Journal of Vascular and Interventional Radiology(JVIR).
The investigators set out to determine the association between hepatic ischaemic complications and hepatic artery collaterals and portal venous impairment after hepatic artery embolization for postoperative haemorrhage.
Between October 2003 and November 2019, 42 patients underwent hepatic artery embolization for postoperative haemorrhage. Hepatic artery collaterals were classified according to hepatic artery visualisation after embolization (grade 1, none; grade 2, 1–4 segmental hepatic artery; grade 3, ≥4 segmental hepatic artery). Transhepatic portal vein stent placement was performed in the same session in five patients (11.9%) with poor hepatic artery collaterals (grade 1 or2) and compromised portal venous flow (>70% stenosis). Hepatic ischaemic complications were analysed for relevance to hepatic artery collaterals and portal venous compromise.
Following hepatic artery embolization, hepatic artery flow was preserved (grade 3) through intra- and/or extrahepatic collaterals in 23 patients (54.8%), and hepatic complications did not occur regardless of portal venous flow status (0%). Of the 19 patients with poor (grade 1 or 2) hepatic artery collaterals (45.2%), segmental hepatic infarction occurred in two out of 15 patients with preserved portal venous flow (10 naïve and five stented; 13.3%). The remaining four patients with poor hepatic artery collaterals and untreated compromised portal venous flow experienced multi-segmental hepatic infarction (n=three) or hepatic failure (n=one) (100%; p<0.005).
“Transhepatic portal venous stent placement seems to be an effective intervention for the prevention of hepatic complications in cases of poor hepatic artery collaterals and compromised portal venous flow,” Choi et al conclude.
Merit Medical Systems recently announced the enrolment of the first patients in its Wrapsody arteriovenous (AV) access efficacy pivotal (WAVE) study of the Wrapsody endovascular stent graft, an investigational device being studied for the treatment of stenosis or occlusion within dialysis outflow circuits. Jeffrey Hoggard (RAC Surgery Center, Raleigh, USA) successfully enrolled the first two subjects with venous outflow peripheral lesions.
“We are pleased to announce the first subjects enrolled into the Merit Medical WAVE study. Stent grafts have a proven track record in dialysis AV access, and we are excited to evaluate the Wrapsody stent fraft in our patients for this clinical trial,” said Hoggard.
Over two million patients with kidney disease worldwide receive haemodialysis. Preferred long-term vascular access in these patients is generally achieved by the surgical creation of an arteriovenous fistula (AVF) or implantation of an arteriovenous graft (AVG). Vascular access circuit dysfunction is a common complication over time in AVFs and AVGs, accounting for 20% of hospitalizations in end-stage renal disease patients. Stenosis or occlusion of these vascular access circuits is most common in the venous outflow segment.
The Wrapsody endovascular stent graft is an investigational device with an expandable nitinol stent frame fully enveloped by an external layer of expanded polytetrafluoroethylene (ePTFE) and an internal layer of spun PTFE with an interposed non-porous fluoropolymer bonding layer.
The multicentre WAVE study comparing the Merit Wrapsody endovascular stent graft to percutaneous transluminal angioplasty (PTA) for treatment of venous outflow circuit stenosis or occlusion in haemodialysis patients plans to enrol 357 patients across multiple sites in the United States, Europe, Canada, and New Zealand. The study has been designed to include a population of 244 patients with AVFs and 113 with AVGs. Merit intends to randomize treatment in patients with AVFs to the Wrapsody stent graft or PTA and follow study subjects for two years postprocedure.
The WAVE study follows successful completion of the Wrapsody FIRST feasibility study which included 46 patients in Europe. The Wrapsody system previously received the CE mark and complements other vascular access products distributed by Merit, including the Hero graft and the Surfacer inside-out access catheter system.
Former Editor of the Journal of Vascular and Interventional Radiology (JVIR) Ziv Haskal (University of Virginia, Charlottesville, USA) has started a petition calling for his interventional radiology (IR) colleagues to pledge to help get their patients vaccinated against COVID-19.
In full, the petition reads: “As interventional radiologists, we see many patients in our clinic who are, by pre-existing conditions, eligible for COVID-19 vaccinations, yet many or most seem unaware or do not know how to seek vaccinations in this turbulent time of vaccine distribution. We have the ability to make every single one of our clinic patients aware of this with counselling at every clinic visit.
“Once you start asking your outpatients about their and their eligible family members vaccine status—prepare to be amazed by how many patients lack the information—or urging to actively seek it—that they need.”
Speaking directly to Interventional News, Haskal explains his motivations for starting this petition. He says, “In the last few weeks of holding my outpatient interventional radiology clinic, I asked every one of my patients if they, or their significant others, had been vaccinated—they are all current candidates due to their underlying conditions or age. With rare exception, the answer was disappointingly low. Patients expressed a desire to be vaccinated but had little idea where to begin and stated that they were waiting to be contacted.
“As endovascular specialists and interventional radiologists, we have first-hand contact with our patients and can help reinforce the message and counsel them about their vaccine candidacy and how to move forward and get vaccinated now.
“I am hoping this campaign will raise awareness so that we can all help our patients step forward, and provide them with the local expertise in how and where to get booked for vaccines appointment today.”
Sharing the petition on Twitter, Haskal put: “Interventional radiologists worldwide: Pledge to counsel & help [get] all our clinic patients COVID vaccinated—fill the gap! Retweet #IRVAX Sign the petition! Act Today.” He is using the hashtag #IRVAX to spread the message on social media.
Humacyte has announced that the clinical results of five-year outcomes in patients receiving the human acellular vessels (HAV) for arteriovenous (AV) access in haemodialysis have been accepted for oral presentation at the Charing Cross (CX) Symposium (19–22 April, online).
On 17 February 2021, Alpha Healthcare Acquisition Corp, a special purpose acquisition company, and Humacyte announced the execution of a definitive business combination agreement along with a fully committed US$175 million PIPE financing agreement.
The presentation will include five-year outcomes on patients who completed the prospective Phase 2 trial and continued routine dialysis utilising the HAV for access to the bloodstream. The results are supportive of Humacyte’s ongoing development program in AV access which includes a Phase 3 trial in AV access to enable haemodialysis in which patients are randomized to receive either an HAV or an autogenous fistula, the current standard of care.
The details of the presentation are as follows:
Title: Update on bioengineered grafts for vascular access Date / time: Tuesday 20 April, 14:00–19:30 GMT (9:00–14:30 ET) Presenting author: Jeffrey Lawson, chief surgical officer, Humacyte
The CX Symposium is the leading global vascular symposium that brings together more than 4,000 vascular specialists from nearly 80 countries to discuss vascular and endovascular controversies. For more information, visit www.cxsymposium.com.
To mark the 20-year anniversary of drug-coated balloons, Bruno Scheller (Homburg/Saar, Germany) and Gunnar Tepe (Rosenheim, Germany), talk to Vascular News about their contributions to the birth and evolution of these devices.
Scheller discusses his work in the 1990s with Ulrich Speck (Berlin, Germany) in the field of contrast media and the early use of paclitaxel, noting that, coupled with the contrast medium, it led to a “long-term biological effect”. However, the problem with the contrast media approach was that “it was not really lesion-specific” in relation to local drug delivery.
Data from early animal testing and first clinical trials, using balloons coated with contrast media and paclitaxel, elicited “strong opposition” from the scientific community, says Scheller. Nevertheless, the researchers were convinced about what they were doing and continued to establish high-quality clinical research. Scheller recalls the unblinding of the first-in-man trial, the PACCOCATH-ISR as “an extremely good moment” because it provided proof that the research direction that had been viewed with scepticism and described “crazy” was “exactly the right way”.
Tepe, who also collaborated with Scheller and Speck in the early days of DCBs, talks about some of the difficulties the researchers encountered in gathering support for the idea. He highlights the THUNDER trial–which examined DCB versus plain balloon angioplasty for the treatment of femoropopliteal artery disease–noting that “expectations for success were really low”.
When he saw the first images of the patients who received drug-coated balloons Tepe was “astonished” because “we could see something different here”. Tepe further outlines his experience presenting the data to a packed auditorium, adding that soon “people started to believe” the results and that ultimately “we could prove that these drug-coated balloons were safe and effective in all patients”.
Tepe alludes to the fact that the involvement of Invatec, that was later acquired by Medtronic, was key to transforming the first home-made balloons into devices that could be widely used in patients and backed by long-term level one evidence. “Only with this support”, says Tepe, “we could prove that these drug-coated balloons are safe and effective in all patients”, adding “we could bring something new and something different to the patients”.
The Royal College of Radiologists (RCR) has called for a fully-costed, long-term funding package to safeguard the future of National Health Service (NHS) radiology and oncology. The calls follow the release of the UK government’s annual Budget, which was predominantly concerned with measures aimed at boosting the UK’s post-coronavirus economic recovery.
The Treasury’s previous Spending Review announced a one-year settlement for the NHS, which included a fund for tackling coronavirus backlogs and £325 million to upgrade aging imaging equipment, and was welcomed by the RCR.
Responding to this most recent budget statement, RCR president Jeanette Dickson said: “Following the autumn spending review—which did grant some welcome funding for parts of the health service—this budget understandably centred on ongoing economic safeguards and stimuli.
“However, the long-term needs of the NHS cannot be ignored forever. The backlogs and delivery challenges caused by coronavirus continue to impact hospital patients and the services that treat them. This statement could have been an opportunity to give much-needed, additional relief to a very tired NHS.
“Imaging and cancer teams are working through recent backlogs but demand only goes in one direction. Even before the immense pressures of COVID-19, the UK radiologist workforce was understaffed by 33%, and the clinical oncology workforce by 19%. There is only so much our stretched medical specialties can do without more resources.
“Treatment waiting lists are now at a record high, and millions of those patients waiting will need some form of radiological diagnosis or treatment.
“At the end of last year, more than 72,000 patients in England were waiting six weeks or more for a CT or MRI scan7, and the most recent COVID-19 winter surge will be hitting waits further.
“Tens of thousands of cancer cases potentially went undiagnosed last year, and front line cancer teams across the UK are telling us that they are seeing more patients presenting with later stage, often less curable cancers.
“To tackle these ongoing care demands, protect against endemic surges of COVID-19, and ensure we can give future patients the high-quality imaging and cancer treatment they deserve, we must have a fully-costed, sustainable funding package from the UK Government that deliberately addresses the equipment, IT and, crucially, workforce needs across NHS radiology and oncology.
“We will work hard over coming months to engage with NHS leaders and training colleagues, and vigorously champion these fundamental long-term priorities ahead of the Treasury’s comprehensive spending round anticipated later this year.”
Our top 10 stories of February 2021: a success story for interventional oncology as intra-arterial delivery of chemotherapeutic agents is shown to improve survival, and a new trial investigating combined radioembolization and immunotherapy for hepatocellular carcinoma (HCC) treatment launches; the vascular community gears up for paclitaxel discussions at the 20–21 Charing Cross Symposium (CX; 1922 April, virtual); and various devices cleared by the US Food and Drug Administration (FDA).
The use of intra-arterial delivery for the treatment of malignant brain tumours is safe and provides clinical benefits in terms of survival when used with the appropriate therapeutic agents, according to a small phase II study presented at the virtual European Conference on Interventional Oncology (ECIO; 24 February, online). Delivering these results, Gérald Gahide (Sherbrooke University Hospital, Sherbrooke, Quebec, Canada) told delegates that while the present study demonstrated the technical feasibility and safety of this application, “there is a dire need for designing multicentre, prospective, phase III studies to properly compare intra-arterial and intravenous treatments”.
The National Institute for Health and Care Excellence (NICE) has issued guidance recommending the use of selective internal radiation therapy (SIRT) for the treatment of patients with hepatocellular carcinoma (HCC), the most common form of liver cancer, with more than 6,400 cases diagnosed annually through the National Health Service (NHS) in England, Wales, and Northern Ireland.
One-year outcomes of patients with chronic-limb threatening ischaemia (CLTI) treated in an outpatient-based vascular limb salvage clinic show an improved rate of major amputation. Authors Andrew Nickinson (University of Leicester, Leicester, UK) and colleagues write in an online European Journal of Vascular and Endovascular Surgery (EJVES) article that their study supports the recommendations of the Global Vascular Guidelines and “provides a reproducible service model that delivers timely vascular assessment in an ambulatory setting”.
An FDA advisory panel has recommended against premarket approval of BD’s Lutonix 014 drug-coated balloon (DCB) for use in below-the-knee (BTK) arteries. In a meeting on 17 February, the majority of the FDA Cardiovascular Devices Panel concluded that the device was likely safe in BTK arteries, but not effective. The benefit-risk ratio also did not appear favourable for the Lutonix 014 DCB, it claimed.
Andrew Holden (Auckland City Hospital; University of Auckland, Auckland, New Zealand) speaks to Interventional News ahead of this year’s Charing Cross Symposium (CX), which is being held online 19–22 April. In 2021, the conference will focus on controversies within the vascular and endovascular space.
Terumo Corporation has signed a definitive agreement to acquire all assets of Health Outcomes Sciences, a specialist in predictive analytics and clinical decision support for healthcare organisations.
The Society of Interventional Oncology (SIO) and Boston Scientific have announced a new multicentre, prospective, randomised trial to study combination therapy of radioembolization and immunotherapy in early and intermediate hepatocellular carcinoma (HCC) patients not eligible for curative treatments: ROWAN.
Rist Neurovascular recently announced that it has received FDA 510(k) clearance to market the Rist Cath Radial Access Long Sheath (Rist Cath) for the introduction of interventional devices into the peripheral, coronary, and neurovascular system.
Tobias Steinke (Düsseldorf, Germany), Matteo Tozzi (Varese, Italy) and Robert Shahverdyan (Hamburg, Germany) give their reactions to the publication in the New England Journal of Medicine of the IN.PACT AV Access clinical trial data, focusing on some of the key data as well as delving into how it has changed their practice and what impact the findings might have in terms of the quality of life for their patients. This video is sponsored by Medtronic.
Driven by an intuitive tablet interface, ControlRad Select optimizes the X-ray beam and image quality to reduce radiation by 85%
ControlRad Select
ControlRad has announced US Food and Drug Administration (FDA) 510(k) clearance to market ControlRad Select, a technology that utilises proprietary semi-transparent filters, a user-interface tablet, and image processing algorithms to reduce radiation exposure during fluoroscopically guided procedures.
The technology is retrofitted onto customers’ existing Siemens Artis zee interventional imaging systems. In preparation for the commercialisation efforts, ControlRad has entered into an exclusive agreement with Boston Scientific to sell the ControlRad Select technology.
“With the FDA clearance and the reach of the global medical device sales team, every cath [catheterisation], EP [electrophysiology], and IR [interventional radiology] lab in the country that has a Siemens Artis zee will now have the opportunity to reduce their radiation dose by 85%1 without compromising image quality,” stated Guillaume Bailliard, CEO of ControlRad.
“The health risks to the medical staff due to lifetime radiation exposure in cath labs have been well documented, including increased incidence of cataracts, atherosclerosis and even left-brain tumours,” stated Simon Dixon, chief of cardiology at Beaumont Hospital, Royal Oak, USA. “We recently completed a clinical trial designed to evaluate how this novel technology might reduce radiation exposure in the cath lab. I have long been passionate about finding innovative ways to improve safety for my colleagues in the lab while they are performing lifesaving procedures for our patients.”
Medtronic has announced the launch of IN.PACT AV drug-coated balloon (DCB) in Japan. IN.PACT AV DCB is indicated for the treatment of obstructive lesions up to 100mm in length in the native arteriovenous (AV) dialysis fistulae in patients with end-stage renal disease (ESRD) undergoing haemodialysis. It is the first DCB to be approved in Japan for this vessel bed.
In Japan, IN.PACT AV DCB received regulatory approval on 23 September 2020 and it became eligible for health insurance reimbursement on 1 February 2021.
According to a press release, IN.PACT AV DCB has the potential to maintain AV access site patency, which can extend the time between reinterventions, therefore maximising a patient’s uninterrupted access to dialysis care has been needed.
In a global clinical trial, patients treated with IN.PACT AV DCB maintained target lesion primary patency longer and required 56% fewer reinterventions to maintain target lesion patency as compared to those treated with standard percutaneous transluminal angioplasty (PTA) through six months.
Mixed reality dose visualisation is expected to improve exposure dose management for interventional radiology (IR) patients and health professionals by depicting invisible radiation exposure in real space, a study published in Journal of Medical Systems reports. First author Takeshi Takata (Graduate School of Medical Care and Technology, Teikyo University, Tokyo, Japan), senior author Jun’ichi Kotoku (Graduate School of Medical Care and Technology, Central Radiology Division, Teikyo University, Tokyo, Japan) et al examined for the first time in the relevant literature the concept and feasibility of an immersive, real-time dose visualisation system using mixed reality for dose management.
Contextualising this research, the study authors write: “For interventional radiology, dose management has persisted as a crucially important issue to reduce radiation exposure to patients and medical staff.” Currently, IR patient dose management generally uses only a displayed dose area product, they continue, saying that this parameter does not identify the exposed position. “For that reason, a dose distribution on the patient’s skin cannot be managed,” they note. Similarly, despite measuring the radiation exposure of the health professionals involved in IR procedures with personal dosimeters, Takata and colleagues explain that the dose is unknown until the dosimeter is read out.
“To optimise exposure for all involved, health professionals must note their exposure dose in real-time according to each situation,” they claim. “An intuitive, real-time dose management system is expected to facilitate management of the dose and to improve patients’ and health professionals’ medical safety.”
Their mixed reality dose visualisation system uses a wearable mixed reality holographic device (Microsoft HoloLens; Microsoft). According to the investigators’ description, the HoloLens uses a simultaneous localisation and mapping algorithm for spatial mapping and detection of the wearer’s position, and provides an accurate three-dimensional holographic representation of digital objects with a full sense of depth. The objects can be viewed by a group of viewers simultaneously from all angles, enabling shared interaction. The display can be flipped up if it gets in the way.
“Projection of the patient’s skin dose onto the patient’s body and estimation of the health professional’s dose requires accurate tracking of their positions and movements in a room,” they explain. “Nonetheless, position tracking using an external tracking system is adversely affected by disturbances such as the movement of staff members and fluoroscopy systems during a procedure. Therefore, an object recognition tracking method is preferred for [our] mixed reality dose visualisation system.” Using a three-dimensional graphics platform and the object detection and tracking functionalities built into a software development kit, they were able to register images in real-time by tracking the relative position and orientation of the real objects using an RGB camera on HoloLens; this positional information was then used to update the transformations within the virtual world for dose projection and estimation. “The optical detection and tracking of a target are useful for real-time high-accuracy registration with no need for an external tracking system,” Takata et al write.
Although HoloLens is a stand-alone device, it lacks sufficient computational power to run the real-time dose simulation, they add. “Therefore, we separated computation of the visualisation and dose calculation, respectively, to HoloLens and an external server.” The patient skin dose distribution and operator eye lens dose were estimated using the Monte Carlo system on an external computer in real time. The estimated doses were transported sequentially to HoloLens and were projected in a real space.
A fast, accurate measure of dose and distribution
The number recognition system accurately recognised all displayed fluoroscopic conditions every 0.2 seconds. In addition, validation of the measured values of the sensor unit (judged based on a comparison with the laser sensor value) revealed that averages of the error were less than 0.18% in three directions between the mixed reality dose visualisation system sensors and the laser displacement sensor.
Average patient skin dose distribution was estimated within three seconds. The dose distribution was visualised with four seconds latency. Takata and colleagues describe how the dose distribution appears in practice: “It is depicted as coloured cubes on the skin. A colour bar shown in the air represents the absorbed dose level. The health professional’s eye lens dose rate was updated continuously. It was indicated as numerical values in the air. [The] mixed reality dose visualisation system has the following functions.”
This led them to conclude: “More than other real-time dose estimation systems for IR, this mixed reality dose visualisation system provides an immersive experience and a detailed depiction of the dose distribution. Although several visualisation systems can be used for dose distributions, our mixed reality dose visualisation system can visualise the dose distribution in three dimensions in front of the user’s eyes. This visualisation mode will help procedures proceed smoothly, because the surgeon need not look at a distant monitor to know the dose.”
The Zenith fenestrated+ endovascular graft (ZFEN+) product (Cook Medical) has received breakthrough device designation from the US Food and Drug Administration (FDA). This designation is granted for devices that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions.
While the product is not commercially available yet, it will now receive priority review, and Cook will engage in “interactive and timely communication” with the FDA during the clinical trial and premarket review phases. The ZFEN+ is the first product from Cook Medical to receive a breakthrough device designation.
The product is intended for use in the endovascular treatment of patients with aortic aneurysms for whom the graft seal zone requires fenestrations and involves one or more of the major visceral vessels: celiac artery, superior mesenteric artery, and/or renal arteries.
The Zenith fenestrated+ endovascular graft includes up to five fenestrations to accommodate the visceral vessels. Cook say in a press release that this extra customisation allows the graft “to be tailored to the patient’s unique anatomy and maximise the seal zone to exclude the aneurysm”. Cook is seeking investigational device exemption (IDE) approval in the coming months with the intention of beginning a pivotal clinical study later this year.
Contrast developer Guerbet has launched OptiProtect 3S, a new range of technical services for its contrast injectors.
OptiProtect 3S offers technical service and support for all Guerbet contrast injectors, ranging from preventive maintenance to equipment protection that includes service continuity. Servicing comes from a team of certified local experts, trained at Guerbet’s centres of excellence in either Lyons, France, or Cincinnati, USA, who renew their certifications every 24 months, Guerbet has said in a statement.
The use of intra-arterial delivery for the treatment of malignant brain tumours is safe and provides clinical benefits in terms of survival when used with the appropriate therapeutic agents, according to a small phase II study presented at the virtual European Conference on Interventional Oncology (ECIO; 24 February, online). Delivering these results, Gérald Gahide (Sherbrooke University Hospital, Sherbrooke, Quebec, Canada) told delegates that while the present study demonstrated the technical feasibility and safety of this application, “there is a dire need for designing multicentre, prospective, phase III studies to properly compare intra-arterial and intravenous treatments”.
Beginning his talk with reference to the “important” primary malignant cerebral nervous system tumours, Gahide explained that both glioblastomas and lymphomas are quite rare (with an incidence of 8.85 out of 100,000 and seven out of 1,000,000, respectively, of the adult population in the USA). Standard treatment for the former tumour is cytoreductive surgery, “meaning you remove as much of the tumour as possible without harming the patient—it is a debulking strategy, used in conjunction with complementary external beam radiation and chemotherapy (mostly with temozolomide)”. The median survival time is 14.6 months. Gahide told delegates: “Unfortunately, it is impossible to remove all of the tumour because it is a very infiltrated disease and relapse is the norm, and five-year survival is less than 10%”.
Commenting on the treatment of cerebral nervous system lymphoma, he said: “The only point that people agree on is that there should be high IV [intravenous] dose of methotrexate (3g/m2) during the induction, but as of today, there is no consensus regarding what other drugs to use for induction or consolidation.”
One of the main reasons explaining the poor prognosis and responses to treatment is the presence of the blood-brain barrier that presents “significant obstacles” to drug delivery, Gahide explained. The blood-brain barrier selectively transports substances into the brain, maintaining the right concentration of essential compounds and protecting the central nervous system from harmful substances. Typically, small (less than 180Da) and lipophilic molecules (oxygen, carbon dioxide, ethanol) diffuse freely and enter a normal blood-brain barrier. Larger hydrophilic molecules need an active transcellular transport to gain access to the central nervous system. According to reports in the literature, 98% of small drugs do not cross the blood-brain barrier.
“Because of these restrictive entities, the role of potentially active chemotherapeutic agents remains marginal in the treatment of malignant astrocytomas,” Gahide said.
Giving an example, he discussed the use of temozolomide in the treatment of primary brain tumours. The intratumoural concentration of the chemotherapeutic agent reaches “only” 20–30% of the serum concentration, he reported, and less than 10% of cerebral metastases reach 10% of the drug concentration measured in the other organs. “So how can we improve that?” he asked.
Intra-arterial drug delivery technique is “quite straightforward”
According to Gahide, the technique used for intra-arterial drug delivery is “quite straightforward”. His team take a femoral approach: “It is a conscious sedation,” he explained, “and we place a catheter in to the carotid or the vertebral artery, depending on the location of the tumour.” Angiography is used to confirm the position of the catheter and the integrity of the cerebral arteries. Patients must have a measurable disease on initial contrast-enhanced MRI scans, and a Kamofsky performance score >50. Chemotherapies are infused with an automated injector: carboplatin, 400mg/m2, 20cc/min; melphalan, 10mg/m2, 20cc/min. Treatment takes place every four weeks (representing one cycle) for up to 12 cycles after a systematic monthly MRI scan.
A history of intra-arterial delivery
In 1950, Calvin Klopp (George Washington University, Washington, DC, USA) reported the first intra-arterial delivery of chemotherapy for nine head and neck tumours, including one glioblastoma.
The rationality behind this approach is that you can increase the local plasma drug concentration via a first pass effect—Gahide noted that it has been demonstrated that you can increase the intratumoural concentration by up to 90% with this approach compared with systemic (IV) delivery.
In addition, despite Gahide recounting how early studies showed severe brain toxicity (including reports of encephalitis and brain necrosis) triggered by chemotherapeutic agents, he reassured the ECIO audience that “we now have a panel of drugs that have demonstrated their efficacy and their innocuity when used intra-arterially for brain tumours treatment.”
Osmotic blood-brain barrier disruption technique can increase intratumoural drug concentration to more than 300 times that of IV
Another way of circumventing the blood-brain barrier is to open it, Gahide said, introducing the concept of osmotic blood-brain barrier disruption (OBBBD). “In order to improve on the delivery obtained with IA [intra-arterial] infusion, the idea of osmotic manipulations for transiently opening the blood-brain barrier has been explored,” he said. “IA infusion of a hyperosmolar agent causes a rapid diffusion of fluid out of the cells, shrinkage of the endothelial cells, and widening of the tight-junctions. Of the many hypertonic solutions with potential to disrupt the blood-brain barrier, mannitol is the typical choice in both preclinical and clinical studies. This increase in blood-brain barrier permeabilisation is transient in the ipsilateral hemisphere and lasts from 30 minutes to two hours.”
Preclinical studies consistently showed higher intratumoural concentrations with OBBBD delivery compared to intra-arterial infusions or systemic administration. It has been reported in the literature that IA infusions with blood-brain barrier disruption increased the intratumoural concentration of carboplatin 18-fold compared with IA administration alone, and 320-fold compared with IV.
“We use it mostly for lymphomas and in young patients with recurrent glioblastomas,” Gahide commented. Patients must have a Kamofsky performance score >50, and the absence of a significant effect on MRI scan. The procedure is performed under general anaesthesia, unlike intra-arterial delivery alone, and Gahide describes how he and his team take a transfemoral approach to the main artery perfusing the tumour. The catheter is placed at the level of C2–C3 for the carotid circulation, and at the level of C3–C4 for the vertebral circulation. The interventionalists obtain angiographic confirmation of the position of the catheter and integrity of the cerebral arteries, and infuse mannitol at high flow for 30 seconds. A second angiogram is taken to ascertain vessel integrity, before chemotherapy is infused at a constant rate with an automated injector to prevent streaming. Like more traditional IA delivery, patients are treated every four weeks for 12 cycles.
Andrew Holden (Auckland City Hospital; University of Auckland, Auckland, New Zealand) speaks to Interventional News ahead of this year’s Charing Cross Symposium (CX), which is being held online 19–22 April. In 2021, the conference will focus on controversies within the vascular and endovascular space. paclitaxel
What can delegates expect from this year’s meeting in terms of understanding the paclitaxel controversy?
This year, we are focusing on controversies. While 2020 was clearly the year of the pandemic, those of us who are endovascular specialists remember 2019 as being the year of the paclitaxel controversy, provoked by a meta-analysis that was published just a month or so before the start of 2019 [in the Journal of the American Heart Association (JAHA) by Konstantinos Katsanos (University of Patras, Patras, Greece) et al]. While it is very import to take reports on safety very seriously, many of us were concerned for patients who, subsequent to this meta-analysis, were not receiving some of the profound benefits of paclitaxel-based anti-restenotic therapies in the lower limb arteries, drug-coated balloons and drug-eluting stents. Clearly, these paclitaxel eluting devices have shown superior patency with lower reintervention rates compared to standard treatment, sustained for many years. Because of that controversy, the use of these devices significantly decreased and there has been real interest in trying to assess if the paclitaxel safety issue was real or due to some other factors, such as trial design, trial patient numbers, and length of follow-up. With that in mind, there has been a huge effort to re-evaluate the data in terms of randomised controlled trials and real-world data, and I am delighted to say that a new meta-analysis with updated five-year data, sheds new light on the paclitaxel mortality issue.
If the paclitaxel mortality issue proves to be incorrect, we need to think about how we integrate paclitaxel into our current practice, and how the regulators in particular deal with this issue. This is important for the global vascular community, because paclitaxel-based products are such a vital component of offering state-of-the-art care for our lower-limb arterial occlusive patients.
I really look forward to joining you in the controversies sections at Charing Cross 2021.
One-year outcomes of patients with chronic-limb threatening ischaemia (CLTI) treated in an outpatient-based vascular limb salvage clinic show an improved rate of major amputation. Authors Andrew Nickinson (University of Leicester, Leicester, UK) and colleagues write in an online European Journal of Vascular and Endovascular Surgery (EJVES) article that their study supports the recommendations of the Global Vascular Guidelines and “provides a reproducible service model that delivers timely vascular assessment in an ambulatory setting”.
While vascular limb salvage services are recommended by the Global Vascular Guidelines to help improve outcomes for patients with CLTI, the authors write that literature on the topic is limited. It was the aim of this study, therefore, to provide data on the effect of treating CLTI patients in an outpatient-based vascular limb salvage clinic on amputation outcomes.
The George Davies Research Group, based at the University of Leicester, undertook an analysis of a prospectively-maintained database, involving all consecutive patients diagnosed with CLTI within the Leicester Vascular Limb Salvage (VaLS) clinic from February 2018 to February 2019.
They compared data with two comparator cohorts, identified from coding data: 1) patients managed prior to the clinic, between May 2017 and February 2018 (Pre-Clinic [PC]); and 2) patients managed outside of clinic, between February 2018 and February 2019 (Alternative Pathways [AP]). Freedom from major amputation at 12 months was the primary outcome.
Writing in EJVES, Nickinson et al detail that 566 patients were included (median age 74 years) in the study. They report that patients managed within the VaLS cohort were statistically significantly more likely to be free from major amputation (90.5%) compared with both the AP (82.1%; adjusted hazard ratio [aHR] 0.52; 95% confidence interval [CI] 0.28–0.98; p=0.041) and the PC (80%; aHR 0.5; 95% CI 0.28–0.91; p=0.022) cohorts at 12 months, after adjustment for age, disease severity, anti-platelets/lipid lowering therapies and presence of diabetes.
Following the publication of these results, Nickinson spoke to Interventional News about their significance: “We are really excited about the publication of these results in the EJVES, the culmination of a great deal of effect by the whole team in Leicester. Our sincere thanks go to George Davies Charitable Trust, who’s generous donation has made the VaLS clinic a reality. Looking forward, a number of centres have now setup similar services across the UK and with the ongoing work of the Vascular Society’s PAD Quality Improvement Programme, it is great to see how interest is building across the UK in improving the outcomes for patients with CLTI.”
The National Institute for Health and Care Excellence (NICE) has issued guidance recommending the use of selective internal radiation therapy (SIRT) for the treatment of patients with hepatocellular carcinoma (HCC), the most common form of liver cancer, with more than 6,400 cases diagnosed annually through the National Health Service (NHS) in England, Wales, and Northern Ireland.
The NICE website states: “After considering the feedback from consultation, the Appraisal Committee has prepared a Final Appraisal Determination (FAD) on Selective internal radiation therapies (SIRT) for treating hepatocellular carcinoma [ID1276] and submitted it to the Institute.”
“The SIRT SIR-Spheres is recommended as an option for treating unresectable advanced hepatocellular carcinoma (HCC) in adults, only if:
used for people with Child-Pugh grade A liver impairment when conventional transarterial therapies are inappropriate, and
the company provides SIR-Spheres according to the commercial arrangement.
“The SIRT TheraSphere is recommended as an option for treating unresectable advanced hepatocellular carcinoma (HCC) in adults, only if:
used for people with Child-Pugh grade A liver impairment when conventional transarterial therapies are inappropriate, and
the company provides TheraSphere according to the commercial arrangement.”
The SIRT QuiremSpheres (Terumo) is not recommended, within its CE marking, for treating unresectable advanced HCC in adults.
SIRT can be used performed an outpatient procedure and typically does not require lengthy hospitalisation, with the potential to alleviate pressure on the NHS. Recent statistics from University College London suggest there could be an additional 18,000 cancer deaths in England due to the COVID-19 pandemic, which Boston Scientific and Sirtex say further highlights the importance for physicians and patients having access to new options.
At the virtual 2020 meeting of the Cardiovascular and Interventional Radiological Society of Europe (12–15 September, online), positive results from the largest European-wide observational study on the treatment of primary and metastatic liver tumours with SIR-Spheres microspheres were presented, demonstrating the product’s safety and showing good overall survival from its 1,027-patient cohort for the first time.
“It is excellent news that NICE has recommended SIRT for the treatment of HCC,” comments Paul Ross, consultant medical oncologist at Guy’s & St. Thomas’ NHS Foundation Trust and clinical lead for HCC at King’s College Hospital (both London, UK). “The expanded options will advance the quality of life for patients and provide meaningful alternatives to existing treatments.”
“The British Liver Trust is delighted that NICE has now approved the use of SIRT as an option for treating unresectable advanced HCC in adults,” says Pamela Healy OBE, chief executive of the British Liver Trust. “HCC is the most common form of liver cancer. It is particularly aggressive and a diagnosis is devastating for patients, carers and their families. Treatment options for patients with advanced liver cancer have been very limited and this decision will make this innovative treatment more easily available and improve options for patients. Evidence shows that outcomes for people with advanced liver cancer are particularly poor so this is a very important step.”
As stated in a Boston Scientific press release, the outcomes of more than 100 clinical studies demonstrate the effectiveness of TheraSphere in improving tumour response across all stages of liver cancer, and in extending and improving the quality of life for patients globally. TheraSphere is a medical device consisting of radioactive yttrium-90 (Y-90) glass microspheres, which are delivered directly to liver tumours via a catheter, resulting in an increased tumour response while preserving surrounding healthy tissue.
Globally, more than 70,000 patients have been treated with TheraSphere, which has been approved for use as an HCC treatment option in 16 other countries. TheraSphere is also indicated for the treatment of metastatic colorectal cancer (mCRC) in patients who have failed second line treatment in the UK . The company plans to further investigate TheraSphere as a treatment for different cancer segments, including prostate and brain cancers.
In a recent meta-analysis, Yang Liu, Huan Lu (Henan Cancer Hospital, Zhengzhou, China), and colleagues found insufficient evidence to prove that inferior vena cava (IVC) filters can reduce pulmonary embolism (PE)-related mortality and overall mortality. However, they did find that IVC filters decrease the occurrence of PE without increasing deep venous thromboembolism (DVT) and major bleeding. Therefore, they conclude: “IVC filters should be considered after balancing the benefits and risks for the patients with contraindications to anticoagulant therapy of high risk for PE.”
Writing in the Journal of Vascular Surgery: Venous and Lymphatic Disorders, Liu, Lu, et al outline the scale of the issue at the core of their analysis: “Venous thromboembolism (VTE), which mainly presents as DVT and PE, is an important and potentially fatal disease with a high incidence and causes a huge burden.”
Considering treatment options, they write that, besides anticoagulation, the application of IVC filters is “commonly used” in patients with contraindications to anticoagulation therapy—for example, those who have been injured or who are at high risk of bleeding—or patients with a high risk of embolism occurrence. “However,” they write, “there is no clear consensus on the benefits and risks of IVCs from randomised controlled trials (RCTs)”.
Liu, Lu, and colleagues elaborate: “Systematic reviews have shown that IVC filters appear to reduce the incidence of subsequent PE, while appearing to increase the chance of DVT, and they have a limited effect on overall mortality. However, data in half of the included trials were not pooled into the effect size (odds ratio), which weakens the evidence of the conclusion.” Due to this lack of clarity on the subject, the researchers performed a systematic review and meta-analysis of RCTs with “more appropriate effect measures and more trials” in order to investigate the effect of IVC filters on PE-related mortality and complications.
The team searched PubMed and Cochrane libraries from inception to 31 October 2019 to identify RCTs for their meta-analysis. They detail that the primary outcome was mortality related to PE; secondary outcomes were overall mortality, occurrence of PE, DVT, and major bleeding.
Overall, the investigators included seven articles, comprising 1,274 patients, in their meta-analysis. They report that there was no significant difference in mortality related to PE between the IVC filter groups and the control group within three months (risk difference, -0.01; 95% confidence interval [CI], -0.03–0; p=0.11) and during the whole follow-up time with low heterogeneity (I2=0%).
However, they relay that the rates of new occurrence of PE within three months and during the whole follow-up period were lower in the IVC filter group than those in the control group (0.81% vs. 5.98%; risk ratio, 0.17; 95% CI, 0.04–0.65; p=0.01; 3.2% vs. 7.79%; risk ratio, 0.42; 95% CI, 0.25–0.71; p=0.0001, respectively).
Finally, Liu, Lu, et al communicate that there were no significant differences in the rates of new occurrence of DVT, major bleeding, and mortality rates during the whole follow-up period between the groups (p>0.05).
The authors acknowledge some limitations of the present study. They recognise, for example, that patients who were recruited in the included trials were “not completely consistent” regarding disease conditions and that performing subgroup analyses was limited because of the paucity of trials. Finally, they state that performance bias was a high risk, which was attributed to the “dramatic difference” in therapy between the two groups. “This made participants and personnel blinding from the intervention strategy impossible, and might have affected the outcomes to a certain extent,” they remark.
Looking forward, Liu, Lu, and colleagues suggest that large RCTs are required “to provide more robust evidence”.
NOTE: This video is ONLY available to watch in selected countries and geographies
Tobias Steinke (Düsseldorf, Germany), Matteo Tozzi (Varese, Italy) and Robert Shahverdyan (Hamburg, Germany) give their reactions to the publication in the New England Journal of Medicine of the IN.PACT AV Access clinical trial data, focusing on some of the key data as well as delving into how it has changed their practice and what impact the findings might have in terms of the quality of life for their patients.
Steinke says he was “really impressed” by the results since “this is the only and first trial that met both safety and effectiveness end points”. He also states that the finding that the use of a drug-coated balloon (DCB) is “superior” to plain balloon angioplasty “really helps us for therapy decisions in our daily practice”, concluding that “we now have scientific proof to justify the use of the DCB.”
Tozzi highlights some of the key data points including the primary patency of the target lesion which was 24.5% higher in the DCB group (72.5%) than the PTA group (48.0%). He further adds that a big advantage with the use of DCBs is the lower number of reinterventions needed, concluding that there is “strong and incontrovertible evidence” that the “DCB must be the gold standard in the treatment of vascular access stenosis”.
Shahverdyan explains that the publication of the IN.PACT AV Access results in the NEJM “changed the way I decide to use balloon angioplasty”. He notes that this data now confirms “that you can and should use a DCB” in the first instance. Shahverdyan also suggests that patients will have “better quality of life” due to the reduction in hospitalisation.
A US Food and Drug Administration (FDA) advisory panel has recommended against premarket approval of BD’s Lutonix 014 drug-coated balloon (DCB) for use in below-the-knee (BTK) arteries. In a meeting on 17 February, the majority of the FDA Cardiovascular Devices Panel concluded that the device was likely safe in BTK arteries, but not effective. The benefit-risk ratio also did not appear favourable for the Lutonix 014 DCB, it claimed.
Prior to the meeting, the FDA released an Executive Summary of the premarket approval application for the Lutonix 014 for the treatment of patients with critical limb ischaemia (CLI) who have obstructive de novo or non-stented restenotic lesions in native popliteal, tibial, and peroneal arteries up to 320mm in length and 2–4mm in diameter.
In the document, they detail results of the Lutonix BTK investigational device exemption (IDE) pivotal study on which they based their conclusions. This was a prospective, multicentre, 2:1 randomised controlled trial comparing the Lutonix 014 DCB (test group) to PTA (control group) for the treatment of BTK arteries. The study was terminated after enrolling 507 of the prespecified 840 vessels.
The FDA summarised the outcomes of the study: “The Lutonix 014 DCB met the non-inferiority primary safety endpoint at 30 days. The primary effectiveness endpoint results did not reach statistical significance, although a 10.5% improvement was noted at six months. However, a durable benefit was not seen at later timepoints, with the KM [Kaplan-Meier] curves converging at 12 months and primary effectiveness event rates favouring the PTA group thereafter.”
Looking in more detail at the benefits and risks, the FDA has not found any safety concerns with this device for this indication from the data provided: “To date, the FDA has not noted any safety concerns associated with the use of the Lutonix 014 DCB that would be expected to exceed those of current standard of care with non-drug containing devices. While a safety signal for increased mortality was noted for the use of paclitaxel-coated devices in the superficial femoral artery, this trend was not evidenced in the current study in the BTK anatomy.”
However, they express concern regarding effectiveness: “A modest benefit in regard to the primary effectiveness endpoint compared to PTA can be seen at six months, but a reversed outcome was noted at 12 months and beyond. Both prespecified and post hoc secondary endpoint effectiveness evaluations did not demonstrate a clear benefit of the Lutonix 014 DCB versus PTA.”
“Overall, the study was terminated early and did not meet the prespecified hypothesis test success criteria. It remains unclear whether the effectiveness differences at six months are clinically meaningful, and that the benefits of the paclitaxel-coated Lutonix DCB outweigh the risks compared to treatment with an uncoated balloon for treatment of atherosclerotic lesions below the knee,” they conclude.
Terumo Corporation has signed a definitive agreement to acquire all assets of Health Outcomes Sciences, a specialist in predictive analytics and clinical decision support for healthcare organisations.
“The acquisition of Health Outcomes Sciences and the ePRISM platform expands Terumo’s presence in the digital healthcare arena and represents a compelling growth opportunity for our company. It further allows Terumo to deliver innovative digital solutions, providing healthcare systems with critical data needed to lower the cost of healthcare delivery while substantially improving patient outcomes,” said Toshi Osada, president of Terumo Corporation’s Cardiac and Vascular Company.
ePRISM delivers a patient’s unique risks to physicians prior to treatment, based upon a calculation that includes their unique disease severity, co-morbidities and demographics. The use of validated predictive models in routine care has the capacity to improve the consistency, outcomes and cost-effectiveness of care across various cardiac procedures and care pathways, Terumo said in a press release.
“When combined with Terumo’s 100-year history and commitment to transforming global healthcare, our ePRISM technology will enable healthcare providers to deliver uniquely focused patient care; improving patient satisfaction, decreasing variability, optimising outcomes and minimising costs. This acquisition provides Terumo with a digital solutions platform that can be scaled globally across multiple healthcare segments,” said John Spertus, founder of Health Outcomes Sciences.
The acquisition is expected to close in February 2021. Following the close, the ePRISM platform will be integrated into Terumo Business Edge, a business unit of Terumo Medical Corporation.
Access Vascular has announced US Food and Drug Administration (FDA) clearance of its HydroMID midline catheter.
A press release from the company states that HydroMID, which is made of Access Vascular’s proprietary biomaterial that has been shown to reduce thrombus accumulation by up to 97% when compared to standard polyurethane catheters, is the second device in its planned portfolio to obtain clearance.
Midline catheters have grown in popularity due to inclusion in the MAGIC (Michigan appropriateness guide to intravenous catheters) guidelines, and the elimination of the need for confirmatory chest X-rays for midline placement. Standard midlines are composed of polyurethanes or silicones, which may lead to protein adsorption. This can result in thrombus accumulation or catheter-related infections.
HydroMID is a 4 French, single-lumen, midline catheter with a maximum usable length of 20cm. HydroMID will be made available over the next few weeks to gain clinical feedback on the usage of this midline catheter.
The company’s expansion into midlines enables healthcare professionals to choose either a midline or peripherally inserted central catheter made of this novel, thrombus-resistant biomaterial, depending on their needs. Midlines, intended for use of up to 30 days, have the advantage of a generally higher level of patient comfort when compared to peripheral intravenous catheters (IVs) due to a fewer number of restarts.5
The release of the midline also furthers the company’s plans to develop a portfolio of thrombus-resistant venous catheters and devices composed of its proprietary biomaterial to address the US$4.4 billion venous access market. The company’s first product—HydroPICC—was FDA-cleared last year and is currently rolling out commercially in the USA with the focus of obtaining real-world clinical data.
“FDA clearance for our second device demonstrates our commitment to a full product portfolio of venous access solutions and our commitment to help clinicians address the thrombus accumulation and catheter occlusion complications plaguing patients,” said Access Vascular CEO James Biggins. “I am proud of our entire team for securing clearance. We look forward to working with clinicians to integrate our devices into their workflow and better understand the benefits that we can bring to patient treatment and care.”
In response to the COVID-19 pandemic reducing medical student presence on clinical services and in classrooms, academic institutions are utilising a virtual format to continue medical student education, Daniel M DePietro (Perelman School of Medicine, University of Pennsylvania, Philadelphia, USA) and colleagues write in Academic Radiology. Appraising this new form of medical education, the authors describe a successful virtual interventional radiology (IR) elective, and claim that this model “provides a framework for others to continue IR medical student education during the pandemic and grow the specialty’s presence within an increasingly virtual medical school curriculum”. They add that it may be modified to improve IR education beyond the COVID-19 era.
The team created a two-week virtual IR elective curriculum, utilising a combination of synchronous and asynchronous learning and a “flipped” classroom educational model. According to DePietro et al, students virtually participated in daily IR resident education conferences, resident-led case review sessions, and dedicated lectures. Asynchronous pre-learning material consisted of text and video correlating to lecture topics. All ten students who participated in the course completed an anonymous pre-course survey, and seven (70%) completed an anonymous post-course survey.
Enrolled students were considering residencies in surgery (50%), internal medicine (40%), interventional radiology (30%), and/or diagnostic radiology (30%). Students’ understanding of what interventional radiologists do and the procedures they perform (p<0.001), when to consult IR for assistance in patient management (p=0.005), and the number of IR procedures students could recall (p=0.015) improved after the course. Case-review sessions and virtual lectures ranked as having the highest education value. Students recommended additional small-group case workshops.
“While the core IR clinical experience comprised of hands-on procedures and patient-care cannot be replaced, the challenges of finding new ways to engage learners and showcase the scope of IR offers opportunities to positively reshape the future of IR medical student education,” the authors write. “The described experience demonstrates that a highly effective virtual IR elective can be created and implemented.”
While the virtual elective was created in response to restrictions imposed on in-person gatherings due to the COVID-19 pandemic, the authors believe it is the start of a trend towards remote or virtual learning. They state: “Interventional radiologists must leverage their ability to embrace technology in order to adapt to the increased emphasis on virtual learning in the wake of COVID-19. This successful initial experience with a virtual IR elective provides a framework for continuing IR medical student education during the pandemic and growing the specialty’s presence within an increasingly virtual medical school curriculum.”
They acknowledge some limitations to their study, notably the small cohort size. DePietro et al add that the generalisability of their institutional experience may be limited by the availability of adequate video conferencing software, ability of IR attendings and residents to participate in synchronous teaching sessions, and access to previously created educational content at other institutions. Furthermore, how participation in a virtual elective impacts student’s abilities to obtain letters of recommendation or impacts their application to IR residency was not evaluated. “Requests to participate in the elective were received from students from outside institutions, however, no institution-approved mechanism for participation of such students were in place during this initial experience,” they say.
Acute kidney injury is a common complication after intervention for peripheral arterial disease (PAD), and is associated with “medium-term mortality” following percutaneous transluminal angioplasty (PTA), a new study in the British Journal of Surgery (BJS) finds. Authored by Emmanuel Katsogridakis (National Institute for Health Research, Leicester Biomedical Research Centre, University of Leicester, Leicester, UK) and colleagues, the paper concludes that while the present work makes evident the fact that the development of acute kidney injury is independently associated with medium-term mortality at two years, the observational nature of the study means the authors “cannot fully elucidate the pathophysiological mechanisms underlying this association”. They call for future research using relevant subclinical markers and mechanistic assessments to shed light on this.
Symptomatic PAD is frequently managed with PTA, particularly in patients with significant co-morbidities, including chronic kidney disease (CKD) and cardiovascular disease. These patients are at risk of developing acute kidney injury after PTA. Postprocedural AKI is not innocuous, the authors write, even for patients with a transient decline in renal function, as it is strongly associated with more complications and a higher financial burden for healthcare providers. As the incidence of, and risk factors for, acute kidney injury after endovascular intervention for PAD are unknown, the study investigators sought to assess the proportion of patients who develop acute kidney injury, and to explore the risk factors.
Their primary aim was to assess the incidence of acute kidney injury after PTA. The primary outcome was therefore the proportion of patients who developed acute kidney injury after PTA, using the Kidney Disease Improving Global Outcomes (KDIGO) reporting criteria. Secondary outcomes were the proportion of patients who died, underwent a major amputation, required dialysis within 90 days of intervention, remained dialysis-dependent after 90 days of intervention, or developed the major adverse kidney events (MAKE) endpoints—death, dialysis, and/or drop in estimated glomerular filtration rate of at least 25%—at 30 or 90 days (MAKE30 and MAKE90, respectively).
Katsogridakis et al prospectively collected and analysed data on 2,041 patients undergoing femoropopliteal endovascular intervention for symptomatic PAD (Rutherford stages III–VI) between 2014 and 2019 across three vascular centres.
Acute kidney injury developed in 239 patients (11.7%), with 47 (2.3%) requiring dialysis within 30 days, and 18 (0.9%) requiring ongoing dialysis. The MAKE30 and MAKE90 composite endpoints were reached in 358 (17.5%) and 449 (22%) patients respectively. Risk factors for acute kidney injury were age, sex, congestive heart failure, chronic limb-threatening ischaemia, emergency procedure, and pre-existing chronic kidney disease. Acute kidney injury, dementia, congestive heart failure, and major amputation were risk factors for medium-term mortality, the authors report.
Commenting on these findings, Katsogridakis and colleagues note: “The acute kidney injury-specific risk factors identified in this series are mostly non-modifiable. Older age, male sex, history of congestive heart failure, CLTI [chronic limb-threatening ischaemia], and preoperative renal function have all been associated with acute kidney injury development previously in a variety of clinical settings, and were strongly associated with acute kidney injury in this study. It is not surprising that these parameters are associated with acute kidney injury in patients with severe PAD. Alongside these findings, the absence of correlation between contrast volume and subsequent acute kidney injury in this series further confirms that acute kidney injury encompasses a plethora of other pathophysiological mechanisms, including perioperative volume depletion, nephrotoxicity, and renal microembolization. Efforts in the prevention of this complex and important complication of endovascular therapy, addressing high-risk groups (elderly, men, CLTI, CKD, and heart failure), are a priority.”
The CLI Global Society is launching the first peer-reviewed academic journal focusing on interventional techniques pertaining to critical limb ischemia (CLI). The new journal, Journal of Critical Limb Ischemia, is launching in the spring of 2021.
According to the CLI Global Society, the goal of the journal is to provide an international forum for the presentation of original ideas and recent results related to all aspects of diagnostic, therapeutic, and pathophysiologic aspects of critical limb ischemia. These articles will likely substantially influence the clinical practice of treating the co-morbidities present in patients presenting with advanced disease, the society states.
Regarding the journal’s content, the society say that priority will be given to original research and on randomised trials and registry studies. In addition, it adds, pharmacological, diagnostic, and pathophysiological aspects of CLI will be given special attention in this online-only journal.
Secretary, treasurer, and co-founding member of the CLI Global Society Jihad Mustapha (Advanced Cardiac and Vascular Centers for Amputation Prevention and Michigan State University College of Human Medicine, Grand Rapids, USA) comments: “The first issue of CLI Global launched in November 2014 to help meet an unmet educational need in CLI. Over the years, the issue has provided data, tips and tricks, and case studies to CLI enthusiasts internationally. The CLI Global Society came into existence in January of 2016 adopting CLI Global as its official publication.
“Over the years, the society worked to bring together a multidisciplinary group of healthcare providers around the globe to discuss contributing factors that create challenges for CLI. Over the past six years we have seen increased awareness for CLI, development of more research in the field, and an increase in the number of dedicated CLI specialists.
“We have seen interest and growth in CLI educational opportunities such as the Amputation Prevention Symposium, which has more than doubled in attendance since the first issue of CLI Global was published.
“We have seen expansion of CLI care into the outpatient arena. I ponder why highly performing physicians who specialise in CLI leave large institutions to focus exclusively on CLI. I believe my story is like many. When we truly look at the CLI patient and the challenges they encounter, we realise the limitations in their care. It takes a very dedicated and passionate provider to work with the patient to coordinate care with their podiatrist, cardiologist, revascularisation specialist, infectious disease physician, nephrologist, and wound clinic. There is a cascade of care for the CLI patient that can start with entry into any one of the specialists listed. CLI is a chronically managed illness that is managed for the lifetime of the patient. And we know that the CLI patient’s prognosis is grimmer than most aggressive cancers. I find great reward in the complex care of CLI patients that require an intricate diagnostic workup, revascularisation, and post-revascularisation surveillance. Starting an outpatient CLI centre of excellence that focuses on leadership, best practices, research, and training all dedicated to CLI has been one of the most rewarding steps in my career.
“However, despite advances in care for CLI patients, we know there is still a long row to hoe. More attention to awareness, research, guidelines, and education must occur. The CLI Global Society board members and members of the society recognise this. With this last issue of CLI Global, the society is taking the next step forward to continue its mission. The society strives to improve quality of life by preventing amputations and death due to CLI by collaborating with like-minded organisations that share an interest in CLI to address treatment, outcomes, coding, and reimbursement to globally improve care.
“I am honoured to report the launch of a new peer-reviewed journal in 2021 that will focus exclusively on CLI. The Journal of Critical Limb Ischemia will bring to light original research from global experts on CLI in a format that will be available internationally. We encourage you to consider submission of your work where it will be reviewed by CLI experts who understand the complex nature of critical limb ischemia.”
There was no increased risk of long‐term, all‐cause mortality associated with paclitaxel-coated device (PCD) use among patients undergoing femoropopliteal peripheral endovascular intervention within the Veterans Health Administration (VHA). This is the conclusion of Jorge Antonio Gutierrez (Duke University Medical Center, Durham, USA) and colleagues, published ahead of print in the Journal of the American Heart Association (JAHA). Theirs was the first study examining the impact of PCD use on mortality with the VHA; they found that in more than 10,000 veterans with peripheral arterial disease (PAD) undergoing femoropopliteal intervention, the rates of two‐year and three‐year all‐cause mortality were similar among patients undergoing revascularisation with PCD (drug-coated balloons [DCB] and/or drug-eluting stents [DES]) and non‐PCD (percutaneous angioplasty balloon and/or bare metal stent) devices.
“The long‐term safety of PCDs for peripheral endovascular intervention is uncertain,” Gutierrez et al write. They therefore used data from the VHA to evaluate the association between PCDs, long‐term mortality, and cause of death, aiming to shed further light on the controversy first sparked in December 2018 by Konstantinos Katsanos (University of Patras, Patras, Greece) and colleagues, who reported in JAHA a potential association between increased mortality and PCD use in the leg.
In the present study, the investigators used the Veterans Administration Corporate Data Warehouse in conjunction with International Classification of Diseases, Tenth Revision (ICD‐10) Procedure Coding System, Current Procedural Terminology, and Healthcare Common Procedure Coding System codes to identify patients with PAD treated within the Veterans Administration for femoropopliteal artery revascularisation between 1 October 2015 and 30 June 2019. An adjusted Cox regression, using stabilised inverse probability-weighted estimates, was used to evaluate the association between PCDs and long‐term survival. They also obtained cause of death data using the National Death Index.
In total, 10,505 patients underwent femoropopliteal peripheral endovascular intervention; 2,265 (21.6%) with a PCD and 8,240 (78.4%) with a non‐PCD (percutaneous angioplasty balloon and/or bare metal stent). Survival rates at two years (77.4% vs. 79.7%) and three years (70.7% vs. 71.8%) were similar between PCD and non‐PCD groups, respectively.
The adjusted hazard for all‐cause mortality for patients treated with a PCD versus non‐PCD was 1.06 (95% confidence interval [CI], 0.95–1.18; p=0.3013). Among patients who died between 1 October 2015 and 31 December 2017, the cause of death according to treatment group, PCD versus non‐PCD, was similar.
Gutierrez et al state: “All‐cause mortality risk related to exposure to PCD was no different when stratified according to claudication or chronic limb-threatening ischaemia (CLTI) presentations. […] After adjustment for treatment assignment, no statistically significant risk in all‐cause mortality was observed between the use of PCD and non‐PCD devices.”
“The endovascular community is now left with difficult decisions regarding when to use PCDs in clinical practice”
Before the reporting of a late mortality signal in the 2018 Katsanos et al meta‐analysis, PCDs were frequently used in femoropopliteal endovascular procedures, as they improved short‐term and intermediate‐term primary patency rates, Gutierrez and colleagues write. The late mortality signal was confirmed by a subsequent analysis from the US Food and Drug Administration of long‐term follow‐up data from pivotal premarket randomised trials for PCD, and most recently by an individual patient data meta‐analysis of US commercially available PCDs.
“However,” the authors of the present study explain, “limitations with these early studies have been recognised, including small sample sizes, substantial amounts of missing data, and poor patient follow‐up”.
They continue: “Nevertheless, PCDs now carry revised package labelling with information detailing the potential for late mortality. Globally, international clinical trials were initially halted (SWEDEPAD [Swedish drug‐elution trial in peripheral arterial disease] and BASIL‐3 [Bypass versus angioplasty in severe ischaemia of the leg]), and the UK Medical and Healthcare Products Regulatory Agency has advised against PCD use in intermittent claudication. The endovascular community is now left with difficult decisions regarding when to use PCDs in clinical practice, leading to wide variability in practice patterns. The Circulatory System Devices Panel and the US Food and Drug Administration acknowledge that additional clinical study data, particularly those evaluating long‐term safety of PCDs, are needed.”
FDA guidance “remains clear” amid developing situation, editorial concludes
An editorial on the new findings were simultaneously published ahead of print in JAHA. Douglas E Drachman and Joseph M Garasic (both Massachusetts General Hospital, Boston, USA) conclude in ‘Paclitaxel-coated devices: Safety and efficacy are in the PVI of the beholder’ that, “For now, the guidance from the [FDA] remains clear: reserve use of PCDs for anatomic and clinical situations where their efficacy may be most advantageous and where their risk is lowest, while participating in shared, individualised consideration of risk and benefit with our patients.”
Considering future directions, they add: “With a growing body of data, including randomised controlled assessments on the horizon, our understanding of the safety and efficacy of PCDs continues to evolve, as will our optimal interventional strategies for the care of patients with symptomatic lower-extremity [PAD].”
PatenSee has initiated a first-in-human clinical trial to assess its machine vision-based surveillance system, a press release from the company reveals. The trial, led by Benaya Rozen-zvi, director of the Institute for Nephrology and Hypertension at Rabin Medical Center (Petah Tikva, Israel), will evaluate the system’s ability to perform contact-free surveillance of fistula stenosis similar to a nurse’s physical exam of haemodialysis patients.
“The clinical data we collect will be the first of its kind and will provide a critical step towards a reliable contact-free early detection tool for fistula stenosis,” explained Rozen-zvi. “Keeping the fistula open is a major clinical need, and early detection of stenosis allows for both simpler treatment and better prognosis for the patient. The non-invasive, contactless nature of PatenSee’s system adds another important benefit for both inpatient settings as well as in homecare in the future. The ability to assess patients effectively at a distance has become particularly important for both patients and clinicians during the worldwide COVID-19 pandemic.”
“The trial initiation is a significant milestone for PatenSee,” said Gal Goshen, CEO of PatenSee. “We are excited to complete all bench testing required to bring the system to the clinical stage and look forward to providing a reliable early detection system for fistula stenosis that can save lives, reduce suffering, and address a challenge currently costing for payers and providers millions of dollars every year.”
The press release states that collaboration with the medical doctors and nurses involved in the trial enabled easy integration of PatenSee’s system into the patient workflow of the dialysis centre. The system is used in the pre-dialysis waiting room with minimal to no intervention of the medical staff and no interruption to the workflow.
One-year findings of the CONSEQUENT all-comers observational study of the paclitaxel drug-coated balloon (DCB) SeQuent Please OTW (B Braun) were reported at LINC 2021 (The Leipzig Interventional Course;25–29 January, online).Principal investigator Ralf Langhoff (Sankt Gertrauden Krankenhaus, Berlin, Germany) relayed low target lesion revascularisation (TLR) and mortality rates.
The prospective, multicentre study evaluates the safety and efficacy of the SeQuent Please OTW in the treatment of de novo and restenotic lesions in peripheral arteries above and below the knee. It includes a total of 784 patients and 879 lesions (almost one third TASC II C/ D lesions, 78.8% calcified and 44.6% occluded).
“We have represented real-world data in this all-comers registry,” said Langhoff. “Many registries are including mostly claudicants. But here, we had a really large group of CTLI [chronic limb-threatening ischaemia] patients—almost 50% had CLTI. Lesion length is also more challenging—13.3±9.3cm in the CLTI group and 10.8±9.1cm in the claudicant group. That is fairly realistic in terms of what we treat every day.”
Twelve-month findings include a TLR rate of 8.1% (CLTI patients, 6.3%; non-CLTI, 9.6%), a patency rate of 88.3% (CLTI, 89.9%; non-CLTI, 87.1%), and an all-cause mortality rate of 4.3% (CLTI, 7%; non-CLTI, 2%). Predictors for TLR included in-stent restenosis at baseline, lesion length, and female gender.
TLR rates were similar above and below the knee, commented Langhoff: “Restenosis rates are generally much higher in BTK [below-the-knee] arteries, but this was just not the case in the CONSEQUENT registry. This is another hint that the SeQuent Please OTW DCB seems to work in BTK arteries”.
The group also carried out additional analysis with respect to mortality in response to the findings of the 2018 meta-analysis by Katsanos et al: “We did not see any difference—as predicted—in all-cause mortality in terms of paclitaxel dose. This is only one-year data, but we didn’t see any correlation so far. Three- and five-year data will be collected and presented later.”
“Using an objective system that discriminates between aetiology and outcome allows a more complete, objective understanding of relative infection risks and outcomes for arteriovenous grafts (AVGs).” This is the conclusion of a review published online in The Journal of Vascular Access (JVA). Authors David Kingsmore (Queen Elizabeth University Hospital, Glasgow, UK) and colleagues suggest that such a system can inform discussions with patients requiring vascular access for haemodialysis.
The authors summarise that AVG infection was not found to be common, that it was caused by a systemic infection in only one-third of patients, did not lead to metastatic infection, and, “importantly,” was treatable without loss of access in one-half of all cases.
“The perception that AVG infection is frequent and severe is not based on contemporary data from large units using modern AVG,” the authors begin. Furthermore, they write that older reports “compounded misperceptions” by using non-standardised reporting that prevents easy comparison against the alternative modalities.
In their review, Kingsmore et al used a recently-published reporting scheme to analyse the frequency, management, and outcome of AVG infection in a large series of sequential early-cannulation AVGs with long-term follow-up. The aim was to assess the application and implications of a standardised reporting system for AVG infection.
The investigators performed a single-centre series analysis of 277 early-cannulation AVGs with a minimum of one-year follow-up. They note that infections relating to the AVG were classified, root-cause analysed, and the outcomes presented.
Writing in JVA, Kingsmore and colleagues report that 16% of all AVGs implanted, representing 51 episodes, developed infection related to the AVG. However, they also relay that more detailed analysis shows that this can be broken down into the following results: primary AVG infection (related to the insertion procedure or within 28 days) occurred in only 3% of AVGs assessed, or nine times; secondary AVG infection (related to AVG in use) occurred 33 times (rate 0.27/1,000) haemodialysis days), at a mean of 382 days; and tertiary AVG infection (in AVG no longer in use) occurred nine times. Finally, they add that only one-third of all AVG infections led to bacteraemia, and that one-half did not lead to loss of functional access.
“Our solution to the limitations of ethanol ablation is the polymer ethyl cellulose,” Erika Chelales (Center for Global Women’s Health Technologies, Duke University, Durham, USA) told delegates attending the abstract presentations at the 2021 meeting of the Society of Interventional Oncology (SIO; 3–6 February, online). In a radiologic-pathologic analysis of a novel ethanol gel formulation involving the ethyl cellulose polymer, Chelales and colleagues found that their newer technique was superior to traditional ethanol for percutaneous ablation in an ex vivo rat liver model.
Comparing a world map of hepatocellular carcinoma (HCC) mortality rates by region and one of human development index (HDI) rates, Chelales showed that countries with lower HDI have higher HCC mortality rates. “This means that the countries with the highest HCC burden have lower income and fewer resources available for treatment,” she commented.
“Many regions lack routine access to safe and affordable standard of care, and can therefore not access [Barcelona Clinic Liver Cancer] BCLC-defined curative treatment options like microwave ablation, radiofrequency ablation, and cryoablation,” she continued. “Unfortunately, ablative therapies are also not easily accessible or affordable in these settings. This is due to inadequate access to supplies, like thermal ablation systems or gas tanks for cryotherapy, as well as cost. Often, the only accessible and affordable ablative therapy in these settings is ethanol ablation.”
Ethanol induces cytosis through cell membrane and cytoplasm dehydration and the disruption and irreversible denaturation of intracellular proteins, resulting in coagulative necrosis. For HCC <3cm, ethanol has comparable five-year survival to RFA, and for HCC <1.5cm, ethanol has comparable overall survival to RFA. But, most importantly, according to Chelales, it is cheaper and more readily-available than RFA. “Although it is low cost, ethanol ablation is still not widely used, and this is due to its limited efficacy,” she said, before saying that its effectiveness is limited by non-target ablation from unpredictable ethanol leak. “Off-target effects result in poor tumour coverage, and then require the patient to return for multiple subsequent treatment sessions. A treatment paradigm involving multiple treatment sessions is not suited for low and middle income settings, where patients are often lost to follow-up.
“Our solution to the limitations of ethanol ablation is the polymer ethyl cellulose”. Ethyl cellulose is an ethanol-soluble but water-insoluble polymer, and induces a phase change from liquid to fibrous gel upon injection into tissue. In the presented study, the investigators sought to compare the spatial distribution of gel, ethanol, and liquid ethanol ablation, and the correspondence of each to the results of necrosis.
“Although we envision ultrasound-guided delivery for use in settings without access to imaging techniques with a large technical footprint, for these validations we used CT [computed tomography] imaging to examine the spatial distribution of ethanol in tissue. This is because ethanol has endogenous CT contrast (pure ethanol is significantly hypodense relative to water),” Chelales explained.
Exploiting the fact that there is a linear relationship between radiodensity and ethanol concentration, the investigators used a two-point calibration equation to provides them with a method of accurately converting radiodensity units from CT images to ethanol concentration in tissue.
They first used this method to determine the optimal gel ethanol formulation in ex vivo rat liver. They injected the target tissue with 100µl of either liquid ethanol or gel ethanol, at various concentrations (6%, 8%, 10%, 12%, or 15%) of the ethyl cellulose polymer at 10mL/hr (n=six). They acquired pre- and post-ablation CT images.
“The CT images show a larger region of low radiodensity corresponding to the injected ethanol in the gel ethanol group compared to the pure ethanol groups,” Chelales noted.
The research team next created maximum intensity projections “to show a clearer picture of cytotoxic ethanol concentrations within the tissue”. For the 12% ethyl cellulose ethanol group, the regions of high ethanol concentration were located centrally within the distribution block, while for the liquid ethanol group, regions of high ethanol concentration were dispersed throughout the tissue, indicating poor localisation.
The research team then quantified the total cytotoxic ethanol volume, and found that liquid ethanol and 12% ethyl cellulose ethanol yielded the smallest and greatest distributed volumes, respectively. They also examined the shape of the distribution by measuring the aspect ratio: a lower aspect ratio was indicative of a more localised distribution, which Chelales said is more desirable for ablation planning, and more comparable to standard-of-care treatment. She reported that all the gel ethanol groups had a better distribution than the liquid ethanol, “indicating improved localisation with the use of ethyl cellulose polymer”. 12% ethyl cellulose ethanol (ECE) yielded a significantly lower aspect ratio than liquid ethanol, and also a significantly greater distribution volume. “Therefore, we determined that 12% ECE was the optimal concentration for use in rat liver tissue,” she said.
Next, the investigators performed a radiologic-pathologic comparison of liquid ethanol (0% ECE) and gel ethanol (12% ECE) ablation in ex vivo rat liver. Post-ablation CT images again showed a larger area of low radiodensity, corresponding to the injected ethanol, for the gel ethanol group compared to the liquid ethanol group. Chelales et al then excised the liver 24 hours after the ablation procedure, and used a dye that would discriminately stain viable tissue over necrotic tissue. In the gel ethanol group, they observed a greater area of necrosis compared to the liquid ethanol.
“We quantified both the distribution and the necrotic volume, and found that both were significantly greater for gel ethanol compared to liquid ethanol ablation,” Chelales summarised. “Therefore, gel ethanol ablation achieves superior CT distribution volume, and increased target treatment. We calculated the average volume of the necrotic volume to ethanol distribution volume, to quantify the correspondence of the distribution as visualised on CT, and the ablative extent. This ratio is closer to one for gel ethanol than for liquid ethanol, although this was not statistically significant. This may indicate that CT imaging provides a more accurate depiction of necrosis for ethyl cellulose ethanol compared to pure ethanol, and a possible explanation for the necessity for the need for multiple treatment sessions with traditional ethanol ablation.
“We determined that 12% ECE achieves minimal leakage and optimal control, and have demonstrated the superiority of 12% ECE ablation to traditional ethanol ablation in an in vivo rat liver model. [As such], ECE is an injectable gel formulation of ethanol that holds promise as a reliable and lower-cost ablative option, and that, compared to thermal ablation, is envisioned to be faster, delivered through a smaller needle with a smaller technological footprint, and can avoid non-target thermal injury for precarious tumour locations.”
Chelales ended by saying that these positive results mean further studies should be conducted in larger animals, and said that the development of ultrasound-based treatment criteria for necrosis is needed.
Soundbite Medical Solutions has announced Health Canada approval for the SoundBite Crossing System – Peripheral (SCS-P) with the 0.014” Active Wire (14P).
The SCS-P (14P) is intended for the treatment of patients suffering from peripheral arterial disease (PAD) with heavily calcified above-the-knee (ATK) and below-the-knee (BTK) chronic total occlusions (CTOs).
“Expanding our technology and product portfolio in Canada is an important milestone for our company in the journey to commercialise the SoundBite system. This is welcome news on the back of our recent positive experience with the system in the EU. We are looking forward to making a positive impact on patients by providing a novel and safe solution around the world,” said Lori Chmura, president and CEO of SoundBite Medical.
The SCS-P 14P system comprises the SoundBite Console and the 0.014” SoundBite Active Wire. SCS-P leverages Soundbite’s proprietary method to produce and safely deliver shock waves via guidewire platforms to selectively ‘micro- jackhammer’ through calcified lesions. SBCS-P has CE mark and Health Canada approval in both 0.018” and 0.014’ platforms; the 0.018” platform has also US Food and Drug Administration (FDA) (510k) approval.
New clinical evidence for the use of the Luminor drug-coated balloon (DCB; Luminor) in complex lesions with long-term follow-up has been presented on the main session of the Leipzig Interventional Course 2021 (LINC; 25–29 January, online). These outcomes show Luminor DCB has “outstanding performance” in the most common peripheral lesions.
Evidence in femoropopliteal arteries: “Amazing” results from EffPac trial at three-and-a-half years follow-up
Ulf Teichgräber (Jena University, Jena, Germany), principal investigator of the EffPac Trial, explained during his presentation at LINC that at three-and-a-half years, a significant clinical and haemodynamic improvement was achieved, with an “amazing” target lesion restenosis (TLR) rate (freedom from TLR: 90.1%). He also remarked that no increased risk of death was detected, and that all-cause mortality was similar to plain balloon angioplasty. Luminor demonstrates “good” efficacy and safety outcomes, even at long-term follow-up, he said.
Evidence in complex and long femoropopliteal lesions: TINTIN trial two years follow-up
Investigating the performance of the Luminor DCB in complex and long femoropopliteal lesions, the newly-released two-year follow-up outcomes of the TINTIN trial corroborate the efficacy of the Luminor DCB. In lesions with a main length of 24.3cm, the combined therapy of Luminor and the iVolution self-expanding stent obtained a primary patency of 90.5% at one-year, and freedom from TLR of 89.4% at two years. Koen Deloose (AZ Sint Blasius, Dendermonde, Belgium), principal investigator of the trial, stated that: “The combination of vessel preparation, DCB, and self-expanding stent is the key to success in real life lesion treatment”.
Endovascular stimulator company CATHI has launched a campaign promoting CATHIS Smart, its portable system, to medical technology and pharmaceutical companies. The system displays all types of endovascular intervention in any medical field, and is designed for neuroradiology, cardiology, radiology, angiology, and pneumology training.
CATHIS Smart is the size of a laptop, and can be customised to individual user needs, such as being set up with specific devices or instruments.
According to CATHI, the system enables sales teams to give “simplified yet high-definition demonstrations of complex products to their customers”. Their company press release states that sales teams can “quickly learn simple-to-follow step-by-step procedures to gain a basic understanding of vessel anatomy, plus the handling of instruments or devices”. CATHIS Smart can also be used by engineers as a tool for aiding product design by facilitating visualisation and the extrapolation of ideas, as well as factoring in ease of operation and a positive user experience.
Users of CATHIS Smart can jump directly to specific steps within the workflow, which the company say is useful for educational purposes.
“Simulators are essential items of equipment for the cath lab, both for initial training and maintaining vital skills,” says Andreas Götte, head of Cardiology at the St Vincenz Hospital, Paderborn, Germany. “But to be effective they must resemble ‘real life’ clinical practice: we must see the coronary artery as it really is, being able to manipulate guide wires as well as catheters and balloons.”
The CATHIS Smart simulator is supported by a range of hardware including a control unit, notebook, and foot pedal.
The sustained release of anthracyclines and durable embolization from LifePearl microspheres (Terumo Europe) makes transarterial chemoembolization (TACE) with these embolic agents a safe and effective treatment option for patients with early and intermediate stage hepatocellular carcinoma (HCC). This was the conclusion presented by Filipe Veloso Gomes (Hepato-biliary-pancreatic and Transplant Center, Hospital Curry Cabral, Centro Hospitalar Universitario de Lisboa Central, Lisbon, Portugal) at the 2021 meeting of the Society of Interventional Oncology (SIO; 3–5 February, online).
Today, TACE is indicated for the treatment of unresectable HCC, according to the latest European Society for Medical Oncology (ESMO) clinical practice guidelines, with level IA evidence for Barcelona Clinic Liver Cancer (BCLC) stage B tumours (intermediate stage tumours), and level IB evidence for tumours categorised as BCLC 0–A (early) stage. TACE is recommended for patients awaiting liver transplants.
Veloso Gomes and his colleagues set out to assess contemporary interventional oncology practice in HCC, and conducted a pooled analysis of patient-level data from more than 550 patients with this liver cancer, enrolled across five different single arm studies and treated with anthracyclines-loaded LifePearl.
Safety was assessed by close monitoring of adverse events, according to the Common Terminology Criteria for Adverse Events (CTCAE). Tumour response was evaluated following hospital practice, according to mRECIST (modified Response Evaluation Criteria In Solid Tumours; used in four studies) and RECIST1.1 (in one study) and analysed as best overall response. Kaplan-Meier analysis was used to estimate event rates for time to event outcomes: progression-free survival, time to un-TACE-able progression, and overall survival.
Of the 586 patients included in the study, 57% were in BCLC 0/A stage, which the presenter said “clearly demonstrates the indication for TACE in a wide spectrum of patients”.
Adverse events were reported in 197 (33.6%) patients; the majority of these (23.3% of all patients) were grade 3. A further 2.3% were grade 4, and 1.5% were grade 5. The most frequent adverse events were related to post-embolization syndrome. Hepatobiliary toxicities were detected in 6.9% of all patients. Veloso Gomes therefore told SIO delegates that there was “a good tolerability and acceptable toxicity” of TACE with LifePearl.
In addition, he commented: “Hepatobiliary toxicities as [assessed by] imaging findings were lower than with other drug-eluting microsphere TACE [procedures] and similar to conventional TACE studies.” He specifically mentioned the recently published, prospective PARIS registry in his talk, which reported a higher hepatobiliary toxicity of 12.9% (in 30 of 233 procedures). Veloso Gomes noted that this 12.9% toxicity rate was still lower than that published in the literature from previous studies of drug-eluting microsphere TACE, and was more comparable to the rate seen in conventional TACE (cTACE) procedures.
He continued: “There was a high tumour response rate [in the pooled analysis that was the key focus of his presentation] that translated into promising progression-free survival, time to un-TACE-able progression, and overall survival. The overall survival observed in this analysis is among the best overall survival observed in recent TACE trials and meta-analyses.”
The presenter also cited some limitations to their methodology, which boil down to the fact that this pooled analysis was not planned prior to conducting the individual studies. Therefore, he said that there was heterogeneity in the populations enrolled, as well as differences in the recording of variables, including frequency, timing, type of imaging, and follow-up duration.
The Society of Interventional Oncology (SIO) and Boston Scientific have announced a new multicentre, prospective, randomised trial to study combination therapy of radioembolization and immunotherapy in early and intermediate hepatocellular carcinoma (HCC) patients not eligible for curative treatments: ROWAN.
Led by investigators Beau Toskich (Mayo Clinic Florida, USA) and Aiwu Ruth He (Georgetown University Lombardi Comprehensive Cancer Center, USA), ROWAN will evaluate the safety and efficacy of TheraSphere Y-90 glass microspheres (Boston Scientific) administered before initiation of durvalumab with tremelimumab compared to treatment of TheraSPhere alone. The study will assess local tumour control, progression-free survival, and the effect of TheraSphere radiation dosimetry on immune response.
Our top 10 stories of January 2021: musings on ethical decision-making during the COVID-19 pandemic, a reflection on the status and future of paediatric interventional radiology, further developments in the ongoing discussion concerning paclitaxel-device use in the peripheral arteries, the future of radioembolization, and new device indications.
In an effort to raise the profile of paediatric interventional radiology (PIR), CVIR Endovascular Editor-in-Chief Jim Reekers (Amsterdam UMC, Amsterdam, The Netherlands) invited Alex Barnacle (Great Ormond Street Hospital, London, UK) and Anne Marie Cahill (The Children’s Hospital of Philadelphia, Philadelphia, USA) to guest edit the journal’s first thematic series on the topic.
Following the publication of the SWEDEPAD interim analysis, Andrew Farb, Misti Malone, and William H Maisel, representatives of the Center for Devices and Radiological Health, US Food and Drug Administration (FDA), authored a perspective piece in the New England Journal of Medicine (NEJM), titled, “Drug-coated devices for peripheral arterial disease [PAD]”.
The European Trainee Forum of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), the Residents, Fellows, and Students section of the Society of Interventional Radiology (SIR), the Society of African Interventional Radiology & Endovascular Therapy (SAFIRE), and Road2IR—a collaborative effort between several partner institutions aiming to build self-sustaining interventional radiology (IR) training programmes in East Africa—published an open letter to the World Health Organisation (WHO) this month in CVIR Endovascular, calling for an increase in the efforts to understand the needs of low income countries regarding image-guided therapies.
Data from the EXRACT-PE trial, published online first in the Journal of the American College of Cardiology (JACC): Cardiovascular Interventions, found that the Indigo Aspiration system (Penumbra) met its predefined safety and efficacy endpoints for the treatment of pulmonary embolism (PE). In this multicentre, prospective study, the Indigo aspiration system was associated with a significant reduction in the right ventricular-to-left ventricular (RV/LV) ratio and a low major adverse event rate in submassive PE patients. Intraprocedural thrombolytic drugs were avoided in 98.3% of patients.
VasQ, a high haemocompatibility biosynthetic vascular device from Laminate Medical Technologies, could be protective against the haemodynamic modifications that occur during arteriovenous fistulae (AVF) creation, a recent article in The Journal of Vascular Access reports. Roberto Palumbo (Saint Eugenio Hospital, Rome, Italy) and co-authors caution that their results, which derive from their clinical experience and are thus representative of a “real-life setting”, should be considered preliminary. They call for further research of the VasQ device in AVF creation, and say that “further effective treatments are needed to prevent or treat AVF failure”.
Personalised treatment selection and planning based on controlled dosimetry will lead to improvements in treatment accuracy. This is the conclusion presented by Marnix Lam (University Medical Center Utrecht, Utrecht, The Netherlands) at ECIO Virtual (27 January, online), a series of afternoon webinars that the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) is hosting in lieu of the 2020 European Conference on Interventional Oncology (ECIO). Lam spoke on the differences between Yttrium-90 (Y-90) and Holmium-166 (Ho-166) radioembolization, and told delegates that it was “very important” to ensure interventionalists conduct a “good” scout procedure with control over selection and planning.
The US Food and Drug Administration (FDA) has granted premarket approval (PMA) for the Woven EndoBridge (WEB) 17 system from MicroVention, a US-based subsidiary of Terumo. This is a new addition to the WEB aneurysm embolization system for the treatment of intracranial wide-neck bifurcation aneurysms.
The US Food and Drug Administration (FDA) has granted Pedra Technology a breakthrough device designation for the periprocedural use of the company’s Pedra Xauron perfusion system in the treatment of critical limb-threatening ischaemia (CLTI).
“Practicing ethical inquiry and reflection may mitigate the moral distress that can arise from ethical dilemmas,” write Michelle Shnayder-Adams, Eric J Keller, and Mina S Makary—and there have certainly been a number of emotionally-challenging ethical dilemmas for healthcare providers treating patients against the backdrop of the COVID-19 pandemic. The authors of this opinion piece discuss the intersection of medical ethics and interventional radiology (IR) amidst this crisis, and propose a framework interventionalists can use to enable decision-making when faced with multiple, conflicting moral obligations, which they say can cause stress and uncertainty.
New data presented for the first time at LINC 2021 (The Leipzig Interventional Course; 25–29 January, online) are positive for the IN.PACT AV drug-coated balloon (DCB) and the Ellipsys vascular access system (both Medtronic). The IN.PACT AV Access study investigated the use of DCB angioplasty versus percutaneous transluminal angioplasty (PTA) for the treatment of dysfunctional arteriovenous fistulas (AVFs). In a second presentation at the virtual congress, delegates were treated to a comparison of surgically-created versus percutaneously-created AVFs.
In a late-breaking trial session at LINC 2021 (The Leipzig Interventional Course, 25–29 January, online), key updates on below-the-knee (BTK) interventions were in the spotlight.
Francesco Liistro (Azienda Usl Toscana Sud Est, Arezzo, Italy) presented nine-month outcomes from the IN.PACT BTK randomised study. He revealed that the IN.PACT 014 BTK drug-coated balloon (DCB; Medtronic) demonstrates efficacy through nine months compared to percutaneous transluminal angioplasty (PTA) in a complex population.
The study was a prospective, multicentre, randomised (1:1) feasibility study. Fifty chronic limb-threatening ischaemia (CLTI) patients with infrapopliteal chronic total occlusions (CTOs) were enrolled at nine sites across five European countries and followed through 60 months.
Focusing on key eligibility criteria, Liistro told viewers that the “most challenging” lesions were purposefully included in the study, comprising single or multiple total occlusions with lesion lengths ≥40mm.
Focusing on nine-month angiographic outcomes, Liistro communicated that sub-segmental late lumen loss was 0.59±0.94 in the IN.PACT 014 DCB group, compared to 1.26±0.81 in the PTA group (p=0.017). In terms of classic late lumen loss, he informed viewers that this was 0.89±0.77 in the DCB group and 1.31±0.72 in the PTA group (p=0.07).
In addition, the presenter detailed that functional flow by duplex ultrasound (DUS) at nine months was 84.6% in the DCB group and 60.6% in the PTA group (0.341). Finally, he reported that 91.3% of patients reached the composite safety endpoint.
“This novel, randomised, feasibility study with a 014 BTK balloon utilising the 3.5μg/mm2 drug formulation and enhanced study design provides an opportunity to affect future BTK studies and treatment algorithms,” Liistro concluded.
ACOART II and ACOART BTK Italy studies support safety and efficacy of Litos DCB
Wei Guo (Chinese PLA General Hospital, Beijing, China) presented 24-month results of the multicentre, randomised ACOART II study. Addressing LINC viewers, Guo described ACOART II as the first randomised BTK trial in China, and—following on from ACOART I—further demonstrates the safety and efficacy of the Litos DCB (Acotec) for the treatment of BTK artery disease.
Regarding 24-month patency, Guo detailed that the rate of clinically-driven target lesion revascularisation (CD-TLR) was 10.3% in the DCB group (6/58) compared to 24.6% in the PTA group (14/57; p=0.042), the rate of wound healing was 90% in the DCB group (27/30) vs. 81.3% in the PTA group (26/32; p=0.342), and the rate of major amputation was 3.4% (2/58) vs. 1.8% (1/57) in the two groups, respectively (p=0.565).
Presenting 12-month results of the ACOART BTK Italy study, Liistro noted their similarity to those of the ACOART II study, and concluded that the Litos DCB “shows efficacy and safety in the treatment of complex BTK lesions in CLTI patients”.
“The strongest message for clinicians is the drastic reduction of reocclusion showed by the DCB in baseline occluded vessels,” he informed LINC viewers, adding that future studies should include only occluded vessels at baseline and that the primary endpoint of these studies should be reocclusion by DUS.
Luminor DCB yields “excellent” results out to 12 months
Also to present in the late-breaking session was Tjun Tang (Singapore General Hospital, Singapore), who outlined 12-month outcomes from the MERLION trial of the Luminor DCB (iVascular) in BTK lesions.
The MERLION trial assessed the treatment of long tibial occlusive lesions (TASC C and D) in CLTI patients, the presenter relayed. A total of 50 patients—94% with diabetes, 50% with end-stage renal failure, and 88% with a Rutherford score of either five or six—were included in the study. The cohort had a total of 66 atherosclerotic lesions with a mean lesion length of 13.7±9.5cm.
Tang reported a 100% technical success rate in conjunction with a low rate of bailout stenting (4.5%). Treatment with the Luminor DCB yielded “excellent” results, he stated, including no deaths within 30 days, and a 12-month amputation-free survival rate of 74%.
In addition, the Luminor DCB proved to be efficacious out to 12 months, with a 69% rate of target lesion primary patency and a 12-month freedom from TLR rate of 82%.
Finally, Tang communicated that wound closure was achieved in 66% of patients and that 60% of patients had improved by at least one Rutherford category at 12 months.
Use of limus-based devices highlighted in four late-breaking trials
Presenting results of the multicentre, dual-blinded, phase II, randomised controlled TANGO study, Ehrin Armstrong (University of Colorado, Aurora, USA) relayed that temsirolimus adventitial drug delivery has provided “robust outcomes” so far, and that a “sizeable effect” has been seen in more complex lesions with temsirolimus delivery.
Twelve-month results from the prospective, single-centre, physician-initiated PRESTIGE BTK study were also revealed. The objective of this clinical investigation has been to evaluate safety and performance outcomes of the SELUTION SLR novel sirolimus-eluting balloon (MedAlliance), for the treatment of long tibial occlusive lesions (TASC C and D) in patients with CLTI.
Presenter Tze Tec Chong (Singapore General Hospital, Singapore) announced that the primary patency rate was 78% and the rate of wound healing was 81%. In addition, freedom from target lesion revascularisation (TLR) was exhibited by 93% of patients and 84% demonstrated amputation free survival (AFS). All these figures have been sustained from the six-month data.
“We have observed minimal slow-flow phenomena and some cases of fast wound healing with SELUTION SLR. It is also easy to track and deliver. We are looking forward to gaining further clinical experience with this device,” commented Chong.
Marianne Brodmann (University of Graz, Graz, Austria) revealed results of the DEEPER LIMUS study—a pilot study examining the performance and safety of the limus-coated Temporary Spur stent system (Reflow Medical), which is for clinical investigational use only, in infrapopliteal arteries.
Broadmann stressed that the Temporary Spur stent system provides localised drug delivery, and may prevent acute vessel recoil and increase luminal gain. In addition, she relayed that the system reduced dissection risk through controlled penetration of the vessel wall, and leaves nothing behind, preserving the natural function of the vessel and allowing future treatment options.
The presenter summarised that there were now “promising” clinical data on the Temporary Spur stent system, not only from DEEPER LIMUS, but also from the DEEPER OUS and DEEPER studies.
Reporting outcomes from the multicentre, single-arm DEEPER OUS trial of the Temporary Spur stent system in conjunction with a commercially available paclitaxel-coated balloon, Michael Lichtenberg (Karolinen Hospital, Arnsberg, Germany) echoed the findings presented by Brodmann.
New data show potential of Limflow system to improve outcomes for no-option CLTI
“Deep vein arterialisation is safe and technically feasible,” stated Peter Schneider (University of California San Francisco, San Francisco, USA) in a presentation on 12-month data from the PROMISE I early feasibility study of the LimFlow system (LimFlow).
Schneider announced that limb salvage for patients with ‘no-option’ revascularisation was achievable in 77% of patients at 12 months, and concluded that lesion from this initial trial will be “incredibly valuable” moving forward. “We continue to gain insights into technical issues and methods to improve outcomes for these patients,” he stated.
Low-pressure XO Score dilation using a standard 6x40 PTA balloon to treat a stenotic haemodialysis fistula
Low-pressure XO Score dilation using a standard 6×40 PTA balloon to treat a stenotic haemodialysis fistula
Transit Scientific has announced the close of its Series A financing round. The round was led by a large multinational investor and joined by previous seed investors.
Transit Scientific achieved US Food and Drug Administration (FDA) clearances and multicentre, multi-user, safe-patient-use of its XO Score angioplasty scoring-cutting platform and separate XO Cross 0.014” and 0.035” microcatheter platform in late 2020.
“XO Score successfully dilated multiple lesions that were resistant to standard or high-pressure balloon angioplasty during our 1st patient uses in haemodialysis fistulas,” said Jeffrey Hoggard (Raleigh Access Center, Raleigh, USA). “It was particularly beneficial to be able to deploy the XO Score device with a standard percutaneous transluminal angioplasty (PTA) balloon in the juxta-anastomotic position and dilate the lesion at low and controlled inflation pressure.”
The XO Score is a novel sheath that converts regular angioplasty balloons into vessel prep scoring and cutting systems. The device is indicated for treatment of peripheral vascular stenosis including haemodialysis fistulas and grafts.
XO Score’s 22 individual scoring and cutting struts rotate 90 degrees to score and cut upon balloon inflation and then rotate 90 degrees back upon balloon deflation to facilitate balloon re-wrap. The technology also allows for infusion at the site of treatment.
“The XO Cross 014, 018, and 035 microcatheter platform adds new torque, pushability and catheter control,” said Richard Saxon (Tri-City Medical Center, Oceanside, USA. “We have used a 014 XO Cross to redirect the guidewire intraluminally while crossing a tibial artery chronic total occlusion (CTO). This would have been very difficult to achieve with other available technology.”
The XO Cross is a non-tapered exoskeleton based microcatheter technology designed to improve torque response, trackability, and control.
Biomodex has announced its partnership with two of the top medical centres in France and a health system in the USA to develop Evias Plus, a training solution for treatment of ischaemic stroke.
“Thrombectomies are very complex in nature and carry a high risk of complications. What is more, these procedures continue to evolve, given the development of new devices and approaches, requiring neuroradiologists to continually advance their skills,” said Francois Eugene, interventional neuroradiologist at the Centre Hospitalier Universitaire, Rennes, France, a partnering medical centre.
Anthony Le Bras, interventional neuroradiologist at the Centre Hospitalier Universitaire, Rennes, France, added, “Biomodex’s solution will not only enable physicians to stay up to date but will also accelerate training of fellows to help ensure we have enough physicians to support this rapidly expanding field.”
According to the company, Evias Plus offers an innovative approach for physician training, particularly fellowship programs. Biomodex adds that the solution for ischaemic stroke enables neurointerventionalists to simulate fluoroscopy-guided procedures in a real-life catheterisation laboratory environment. The company reports that the models come with several realistic, 3D printed blood vessel models or cartridges that plug into a station that simulates systemic flow using Biomodex Bloodsim to replicate blood density and viscosity and other key features include:
A biobased clot, injection system and distal filter for clot collection/validation of retrieval
Femoral access and adjustable aortic arch
Customized tissue-like patient-specific aortic arches, including right and left radial and femoral access accessories
“Mechanical thrombectomy (MT) has revolutionised the neurological outcome of acute ischaemic stroke patients. Nonetheless, still a large proportion of eligible patients are not treated with MT because of a lack of physicians trained to perform this procedure in an emergency. We therefore have an urgent need to train more physicians to offer this treatment to more patients. This new simulation solution offers highly realistic navigation sensations with the possibility to switch within minutes from one anatomy to another,” said Raphael Blanc, co-chief interventional neuroradiologist at the Fondation Adolphe de Rothschild, Paris, France.
“Biomodex’s advanced training system is a significant improvement over traditional training approaches because the models are incredibly realistic and allow us to gain hands-on training for the manipulation of catheters under fluoroscopy. We can also practice navigating realistic aortic arch anatomies ranging from common to complex,” said Ajay Wakhloo, chief of interventional radiology at Beth Israel Lahey Health, Boston, USA.
Cardiovascular Systems (CSI) has partnered with Chansu Vascular Technologies (CVT) to develop novel peripheral and coronary everolimus drug-coated balloons (DCBs).
Under the terms of the agreements, CSI will provide milestone-based financing to CVT for the development of the DCBs. Under an acquisition option agreement, upon CVT’s completion of key technical and clinical milestones in the development programme, CSI will have exclusive rights and obligations to acquire CVT, subject to the satisfaction of closing conditions set forth in the agreement.
CVT, which is based in Sunnyvale, USA, develops peripheral and coronary DCBs using everolimus.
“The CVT DCBs will be designed to capitalise on the proven long-standing anti-restenotic benefits of everolimus for the treatment of patients with cardiovascular lesions,” comments CVT founder Philippe Marco in the company’s announcement. “This collaboration enables us to develop a new class of DCBs that we believe will improve patient outcomes.”
Ryan Egeland, chief medical officer of CSI, states: “This partnership is consistent with our strategic vision to develop an innovative portfolio of new products. We believe these next-generation DCBs will complement our current and growing portfolio of products for the treatment of complex coronary and peripheral disease. We are thrilled to be working with CVT in this partnership and are extremely confident that Dr Marco and his team’s extensive past DCB experience will prove invaluable in developing these next-generation DCBs.”
The Approach Authority Workhorse microwire guide (Cook Medical) is now commercially available in the USA and Canada.
Designed as an 0.018-inch diameter workhorse wire guide, Approach Authority can be used for multiple purposes in the same procedure.
A company press release states that Approach Authority combines “resilient” nitinol tip technology with a hydrophilic coating. This expands the options to physicians placing balloon dilatation catheters during percutaneous transluminal angioplasty (PTA) in peripheral arteries. Physicians can deliver a variety of devices across this wire to offer a broader range of treatment options for patients.
“Cook Medical is proud to introduce this wire to our customers in the USA and Canada. Wire guides have been used in interventions for decades, and we are still innovating,” comments Mark Breedlove, vice president of Cook Medical’s Vascular division.
Fluidx Medical Technology has announced that GPX Embolic Device first patient use cases were presented at LINC 2021 (25–29 January, online).
“This is very promising technology,” said Andrew Holden (Auckland City Hospital, Auckland, New Zealand), who presented the cases at LINC. “The very radiopaque GPX penetrates distally extremely well with excellent control and devascularised the renal tumour entirely.”
According to a Fluidx Medical Technology press release, GPX Embolic Device is an innovative embolic designed to combine the benefits of other embolics like coils, particles, and liquids with simplified preparation, delivery, precision, and control leading to durable, long-term occlusions. The GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolic material upon delivery, without polymerisation or dimethyl-sulfoxide (DMSO) precipitation associated with other embolics.
In the presentation, Holden showed cases in which GPX had successfully embolized the arterial vasculature of a renal angiomyolipoma and in another case, portal vein embolization in a patient with metastatic colon cancer. Of the latter case, Holden said the successful procedure “resulted in complete occlusion of the portal vein branches and excellent visualisation of the target site. At the six-week computed tomography (CT) scan, we can see the branch impact of the occlusion and the patient experienced good left lobe hypertrophy.”
GPX is packaged ready-to-use in a syringe, requires less than one minute of tableside preparation by the clinician, and may be delivered through standard catheters or microcatheters.
The German Institute for Hospital Remuneration (InEK) has renewed the new examination and treatment methods (NUB) Status 1 designation of VasQ external support (Laminate Medical Technologies) for 2021.
NUB Status 1 provides supplemental reimbursement for innovative medical devices that have the potential to improve the standard of care for patients. VasQ external support first received NUB Status 1 in 2017 with 35 participating hospitals and has since grown to 321 participating hospitals to date, which represents the second most among devices that serve the dialysis patient population.
The VasQ external support is implanted around the anastomosis during the creation of an arteriovenous fistula (AVF) to promote more usability without the need for the frequent additional procedures typically required for standard AVFs. AVFs created with the VasQ external support have reported in publications and presentations usability rates as high as 86% or better by six months in seven clinical studies. Growing clinical evidence in support of VasQ as well as the building momentum of usage in InEK calculating hospitals are critical components to support a permanent diagnosis-related group (DRG) code for reimbursement.
“My practice relies on VasQ as our standard of care for creating almost all of our forearm and upper arm surgical fistulas,” stated Robert Shahverdyan, head of Vascular Access Center Hamburg at Asklepios Klinik Barmbek (Hamburg, Germany). “The device has improved my fistula outcomes for my patients, and I am grateful for the NUB designation so my work with VasQ can continue with sufficient reimbursement to cover the additional costs of the device.”
The device is currently being implanted across Europe under a CE mark and has also completed enrolment in an investigational device exemption (IDE) pivotal clinical study to be evaluated by the US Food and Drug Administration (FDA) through the de novo pathway for use in the USA. The FDA has already awarded the device a breakthrough designation based on the breadth of clinical evidence collected so far for VasQ that consistently demonstrates improvement over the standard of care for AVF creation. The designation provides VasQ with the substantiation of clinical improvement required by the Centers for Medicare and Medicaid Services for providing additional reimbursement for new technologies once cleared for the US market.
Cagent Vascular announced the results of its PRELUDE-BTK study at LINC 2021 (25–29 January, online). The PRELUDE-BTK study was a prospective, single-arm, multicentre feasibility study to show the safety and efficacy of serration angioplasty.
The study was led by co-principal investigators, Andrew Holden (Auckland City Hospital, Auckland, New Zealand), who presented the data, and Michael Lichtenberg (Karolinen Hospital, Arnsberg, Germany). Four other centres from Europe participated in the trial which included 30-day and six-month follow-up.
According to a Cagent Vascular press release, the Serranator percutaneous transluminal angioplasty (PTA) serration balloon catheter is the first and only angioplasty balloon cleared by the US Food and Drug Administration (FDA) and CE marked that embeds serration technology into a semi-compliant balloon for treating peripheral arterial sisease (PAD). The device is designed to create multiple longitudinal lines of interrupted micro-serrations to aid arterial expansion.
Forty-six subjects were treated with the Serranator device and 53 lesions were analysed by the core lab. The average final residual stenosis was 21.8%, with an average below-the-knee (BTK) arterial lumen gain of 1.55mm. These results were achieved with a low average maximum atmospheric pressure of six atmospheres. The bailout stent rate was 1.9%. A subset of lesions (n=10) were imaged with optical coherence tomography (OCT) and intravascular ultrasound (IVUS) and analysed by a core lab. All showed a serration effect. At 30 days, the freedom from primary safety events was 95.7%. The freedom from clinically-driven target lesion revascularisation (CD-TLR) was 97.7% with 70% of subjects achieving one or more Rutherford clinical category (RCC) improvement at six months. There were no serious adverse events related to the device.
“Today, we have insufficient data for effective lesion revascularisation in BTK arteries. Based on published plain balloon angioplasty data, especially in calcified lesions, more than 40% of the cases result in complex dissections and significant recoil phenomenon. This ultimately leads to scaffold implantation to stabilise the lumen and prevent diminished outflow. This revascularisation strategy is associated with poor patency outcomes,” stated Lichtenberg.
“The PRELUDE study clearly proved the hypothesis, that haemodynamic and morphologic success in BTK revascularisation is strongly associated with vessel compliance improvement. We need to concentrate first on this aspect, before we can discuss the need for longer-term restenosis prevention with antiproliferative substances. We know that dissections are directly associated with loss of patency and impaired wound healing. Prevention of dissections within a rigid, non-compliant vessel, along with luminal gain can only be successful with a vessel wall modification device that applies low atmospheres. The PRELUDE-BTK study clearly showed that the mechanism of action works well enough that it does not even need additional antiproliferative treatment, as CD-TLR was only 2.3% after six months,” continued Lichtenberg.
The Serranator product offering for the infrapopliteal indication is available in 2.5, 3, and 3.5mm balloon diameters and 40, 80, and 120mm balloon lengths. The company has initiated US and EU sales and plans to expand its commercial efforts later this year.
BD today announced that new clinical data have found robust evidence that using a vascular care solution can help improve outcomes for patients requiring peripheral intravenous catheters (PIVCs).
Results of the CLEAN3 trial, published in The Lancet Infectious Diseases, showed that use of the BD vascular care solution resulted in fewer PIVC failures compared with the standard group (34.8% vs. 47.5%, respectively) and extended the median time between catheter insertion and failure (50.4 hours vs. 30 hours, respectively). PIVC failure was defined as any premature removal of PIVC before end of treatment—other than for routine replacement—and included phlebitis, infiltration, occlusion, dislodgment, local infection and catheter-related bloodstream infection (whichever occurred first).
The CLEAN3 trial also evaluated skin antiseptics with 2% chlorhexidine-gluconate (CHG) 70% isopropyl alcohol (IPA) single use, sterile applicator versus 5% povidone iodine (PVI) 69% ethanol applied with sterile gauze in preventing infectious complications related to the use of PIVCs (catheter colonisation: 0.9% vs. 16.9%, respectively; local infection: 0% vs. 1.2%, respectively).
The trial, which involved approximately 1,000 patients from nine different medical wards within a single university hospital (Poitiers University Hospital, France), evaluated PIVC failure rates by comparing the BD vascular care solution for PIVCs, which included an integrated PIVC (BD Nexiva), a positive displacement needle-free connector (BD MaxZero), a disinfecting cap (BD PureHub) and a sterile prefilled flush syringe (BD PosiFlush)—compared with a standard group, which included a straight safety PIVC (BD Insyte Autoguard BC Winged), extension set three-way stopcock; the PIVCs were continuously infused with saline or polyionic solution, by gravity.
“The findings of the CLEAN3 trial support the use of an integrated solution as the best practice standard when peripheral IV catheter dwell time is expected to exceed 24 hours,” said Olivier Mimoz (Poitiers University Hospital, Poitiers, France), principal investigator of the CLEAN3 trial. “Furthermore, the study shows that the use of 2% CHG-70% IPA single use, sterile applicator should become the first-line antiseptic for skin disinfection prior to PIVC insertion. We believe that the results can be extrapolated to all adult patients admitted to a medical ward requiring a PIVC placement and, by extrapolation, to those admitted to a surgical ward.”
Recent data from the investigator-initiated, randomised controlled trial (RCT), BIOLUX AV, showed that the treatment of patients with dysfunctional haemodialysis access with BIOTRONIK‘s Passeo-18 Lux drug-coated balloon (DCB), is safe and effectively prevents access failure.
Patients (n=120) with dysfunctional haemodialysis access underwent initial high-pressure balloon angioplasty and were randomly assigned for a second angioplasty using either the Passeo-18 Lux DCB or a plain percutaneous transluminal angioplasty (PTA) balloon. Patients were initially followed-up for one year, and quantitative angiography was performed six months after angioplasty.
The one-year data, presented by Eric Therasse (Centre Hospitalier de l’Université de Montréal, Montréal, Canada) at LINC 2021 (The Leipzig Interventional Course, 25–29 January, online) and published in the Journal of Vascular and Interventional Radiology, showed that, in comparison with uncoated balloon PTA, DCB angioplasty was associated with a significantly lower haemodialysis access failure rate and need for reintervention.
Serious adverse events related to HA were less frequent after DCB treatment than after plain PTA. The study principal investigator also stressed that this study, as with previous ones using DCBs in haemodialysis access lesions, did not demonstrate a significant increase in mortality in the DCB group.
Key results from the BIOLUX AV trial publication:
At 12 months, the Kaplan-Meier patency estimate in the DCB arm was 62.6% vs. 35.2% for the plain PTA group (p=0.001).
In comparison with plain PTA, DCB angioplasty was associated with significantly greater time to haemodialysis access circuit failure (mean estimate [95% confidence interval], 267 vs. 209 days; p=0.009) and haemodialysis access target lesion failure (mean estimate [95% confidence interval], 294 vs. 218 days; p=0.001).
Serious adverse events related to haemodialysis access were less frequent after DCB than after plain PTA.
Survival after DCB and plain PTA were not significantly different at 12-month follow-up and through a median follow-up of approximately three years (1,103 days; p=0.31).
“DCBs with paclitaxel have demonstrated variable results to prevent haemodialysis access restenosis in a few RCTs, and, until recently, their effectiveness was unclear,” explained Therasse, BIOLUX AV principal investigator. The study investigators hypothesised that differences in paclitaxel dosages and excipients of DCBs may be responsible for these variable results and that, in comparison to plain PTA, the paclitaxel-coated balloon technology used in the Passeo-18 Lux would significantly decrease the haemodialysis access restenosis rate at the treated site.
“Our results show the clinical benefit of DCBs to prevent haemodialysis access failure. Both haemodialysis access circuit and haemodialysis access target lesion failures were significantly reduced in the DCB group,” summarised Therasse.
Forge Medical has announced the publication of results of an investigator-initiated randomised trial comparing its VasoStat haemostasis device to the TR Band (Terumo Medical) among patients undergoing radial artery coronary and peripheral procedures with planned same-day discharge.
Published in the Journal of Invasive Cardiology, the study authored by Robert L Minor Jr (Billings Clinic, Missoula, USA), the study involved 40 patients without prior radial access undergoing elective coronary, endovascular diagnostic or interventional procedures, who were randomised to receive either VasoStat or TR Band.
The study’s primary outcome was time to haemostasis enabling radial artery compression device (RCD) removal. Minor Jr and colleagues reported significantly shorter times to haemostasis, higher patient satisfaction and fewer device manipulations needed by nursing personnel among the VasoStat group.
All patients were able to be discharged the same day as their procedure, the study reports, adding that Doppler perfusion imaging follow-up within 60 days in all study patients confirmed radial artery patency with no events of radial artery occlusion (RAO) or pseudoaneurysm.
Commenting on the study’s results, Ty Schlander, CEO of Forge Medical, said: “Same-day discharge among elective PCI [percutaneous coronary intervention] and peripheral vascular patients is being used more often by clinicians, hospitals and health systems around the country, with ever higher adoption since the pandemic. We are proud to provide an innovative haemostasis device for radial artery applications differentiated from balloon/band-type devices that enables faster hemostasis and higher patient satisfaction, in alignment with national trends using same-day discharge.”
Forge Medical has announced the publication of results of an investigator-initiated randomised trial comparing its VasoStat haemostasis device to the TR Band (Terumo Medical) among patients undergoing radial artery coronary and peripheral procedures with planned same-day discharge.
Published in the Journal of Invasive Cardiology, the study authored by Robert L Minor Jr (Billings Clinic, Missoula, USA), the study involved 40 patients without prior radial access undergoing elective coronary, endovascular diagnostic or interventional procedures, who were randomised to receive either VasoStat or TR Band.
The study’s primary outcome was time to haemostasis enabling radial artery compression device (RCD) removal. Minor Jr and colleagues reported significantly shorter times to haemostasis, higher patient satisfaction and fewer device manipulations needed by nursing personnel among the VasoStat group.
All patients were able to be discharged the same day as their procedure, the study reports, adding that Doppler perfusion imaging follow-up within 60 days in all study patients confirmed radial artery patency with no events of radial artery occlusion (RAO) or pseudoaneurysm.
Commenting on the study’s results, Ty Schlander, CEO of Forge Medical, said: “Same-day discharge among elective PCI [percutaneous coronary intervention] and peripheral vascular patients is being used more often by clinicians, hospitals and health systems around the country, with ever higher adoption since the pandemic. We are proud to provide an innovative haemostasis device for radial artery applications differentiated from balloon/band-type devices that enables faster hemostasis and higher patient satisfaction, in alignment with national trends using same-day discharge.”
Michelle Shnayder-Adams (L), Eric Keller, and Mina Makary (R)
“Practicing ethical inquiry and reflection may mitigate the moral distress that can arise from ethical dilemmas,” write Michelle Shnayder-Adams, Eric J Keller, and Mina S Makary—and there have certainly been a number of emotionally-challenging ethical dilemmas for healthcare providers treating patients against the backdrop of the COVID-19 pandemic. The authors discuss the intersection of medical ethics and interventional radiology (IR) amidst this crisis, and propose a framework interventionalists can use to enable decision-making when faced with multiple, conflicting moral obligations, which they say can cause stress and uncertainty.
In stressful times, challenges associated with making ethical and honourable decisions become more apparent. The COVID-19 pandemic has placed an immense amount of strain on the medical community, and interventional radiologists are not exempt from this pressure. When ethical norms are disrupted, we have an even greater responsibility as a specialty to bring ethical decision-making to the forefront. This article will highlight: 1) how ethics and IR intersect, 2) how ethical issues have been heightened during the COVID-19 pandemic, and 3) how to apply a framework to ethical decisions pertaining to IR care.
The discipline of ethics helps us to decide how we ought to behave as a standard of behaviour.1 To some, it may not seem obvious to discuss and practice ethical decision-making in medicine as it appears innate. After all, physicians pledge the Hippocratic Oath and vow to “do no harm”. However, conflict arises when ethical principles clash. The COVID-19 pandemic has challenged a number of ethical values, including duty to care, equity, autonomy, and individual liberty. As we continue to practice in a new societal norm filled with personal risk, limited resources, and limited physical contact, we must continue to reflect on our ideals and ethical identities during patient care delivery.
The Society of Interventional Radiology (SIR) Code of Ethics offers guiding principles for IR physicians on societal ethical expectations.2 Respect for human dignity, respect for human rights, and respect for the law are all included. However, these guidelines are not always sufficient when faced with practical matters. Are you obligated to place a central venous catheter in a patient with COVID-19 at a time when personal protective equipment is limited, and other departments have the means to perform this service? Some may argue that a pandemic qualifies as a state of emergency in which physicians must act on the best interest of society. However, in practice, it is much more challenging to jeopardise your own health and the health of your family and colleagues for the sake of professional duty. Physicians have a responsibility to care for patients, but this responsibility must be balanced with a duty to one’s health and one’s family.3,4 We must also resist the urge to deflect risk onto others and should view patient care as a collective responsibility. With thoughtful reflection and support from institutions to ease the moral burden of these difficult choices, IR physicians can weigh their competing responsibilities and come to a solution that balances all the ethical and practical issues at play.5
With the development of the COVID-19 vaccine, resource allocation concerns have shifted from intensive care unit (ICU) bed provision to vaccination distribution priority. How do we decide on a fair system of vaccine distribution? Whether you are a healthcare leader responsible for the development of a vaccine rollout plan or a frustrated IR practitioner awaiting a vaccine, resource allocation and equity affects all healthcare providers. The Center for Disease Control (CDC) has advocated to minimise morbidity and mortality and preserve societal functions.6 With these priorities in mind, some vaccination algorithms have prioritised age over exposure frequency. Without transparency from leaders about their chosen ethical approach, it is reasonable for younger practitioners with frequent exposures to feel betrayed when they observe vaccine prioritisation of older practitioners with lesser patient interaction. There is no absolute right answer when it comes to prioritisation in the setting of scarce resources, but as these ethical dilemmas unfold, it is crucial for healthcare leaders to maintain transparency and robust discussion with their communities to reach more optimal solutions.
Imagine you are running a busy consult service and you are tasked with acquiring consent for a gastrostomy tube placement in a non-English speaking patient with COVID-19 who has been delirious the last few nights. Her son is her power of attorney. Would you risk exposure, call a translator, and attempt to assess the patient’s decision-making capacity, or just call the patient’s son to get consent? From an ethical standpoint, many IR physicians may agree that they would advocate for explaining the procedure and its risks to the patient despite the extra risk, time, and logistic challenges. From a practical standpoint, respecting a patient’s autonomy, while paramount, can be often inconvenient, especially during a pandemic. Despite the challenges, we must keep in mind that assessing a patient’s decision-making capacity is one of our responsibilities as IR physicians, and if needed, there are resources and other departments in the hospital to help with capacity assessments.
Despite being accountable to our individual patients, IR physicians also have a responsibility to the general public. These two obligations may lead to internal turmoil and conflict. Visitor restrictions limit disease exposure for patients, providers, and hospital staff but at the expense of some individual liberty. Limiting a patient’s number of visitors may support a public effort to reduce spread of disease, but the social isolation of patients can lead to psychological distress and worse patient outcomes. 7–9 In balancing these opposing priorities and accepting the restriction of some individual liberties for the betterment of society, interventional radiologists may find that going beyond their usual levels of communication with patients and families may be necessary to preserve the patient-doctor-family relationship during a pandemic.
The COVID-19 pandemic has forced medical professionals, including interventional radiologists, to deal with ethically-ambivalent decisions every day. Many frameworks have been developed to aid in the ethical decision-making process. 1,5,10–12 One such approach is as follows: 1) recognise an ethical dilemma, 2) gather relevant information from all parties involved, 3) scrutinise possible options using various ethical theories, 4) decide how to act, and 5) reflect on the outcome. For example, this framework may be applied to triaging patients. First, we recognise that triaging with limited resources is an ethical issue. Second, we may gather information about the acuity of all patients involved and consider occupancy capacity at nearby facilities. Third, question the correct course of action under a utilitarian, rights, justice, common good, and virtue approach. For instance, under the justice approach, consider which options treats people equally—making sure not to succumb to bias and favouritism. Fourth, decide which patient to treat, and, fifth, consider how your decision impacted those involved. Practicing ethical inquiry and reflection may mitigate the moral distress that can arise from ethical dilemmas.13
Interventional radiologists have started to recognise the importance of ethical discussion in our field. We have an Applied Ethics Committee supported by the Society of Interventional Oncology (SIO) and SIR, and we have growing literature on ethical topics in IR including: complications,14 conflicts of interest,15 research ethics,16 and futility.17–19 The COVID-19 pandemic has highlighted the need for these discussions, and we must continue to provide platforms to discuss how best to act in ethically challenging situations.
Michelle M Shnayder-Adams is an interventional radiology resident at the University of Michigan Hospital, Ann Arbor, USA. @MMShnayderMD on Twitter.
Eric J Keller is an interventional radiology resident at the Stanford University Medical Center, Stanford, USA. @IR_Ethics on Twitter.
Mina S Makary is an assistant professor, interventional radiologist, and the director of scholarly activity and research at the Department of Radiology, The Ohio State University Wexner Medical Center, Columbus, USA. @MinaMakaryMD on Twitter.
References
Markkula Center for Applied Ethics. Accessed January 21, 2021. https://www.scu.edu/ethics/
SIR Code of Ethics. Published online 2018. Accessed June 21, 2020. https://www.sirweb.org/globalassets/aasociety-of-interventional-radiology-home-page/about-us/governance/sir-code-of-ethics_approved-november-2018.pdf
Shnayder MM, Keller EJ, Makary MS. COVID-19 Ethics: What Interventional Radiologists Need to Know. J Vasc Interv Radiol. 2020;31(10):1720-1723. doi:10.1016/j.jvir.2020.07.003
Bakewell F, Pauls MA, Migneault D. Ethical considerations of the duty to care and physician safety in the COVID-19 pandemic. Cjem.:1-4. doi:10.1017/cem.2020.376
Thompson AK, Faith K, Gibson JL, Upshur RE. Pandemic influenza preparedness: an ethical framework to guide decision-making. BMC Med Ethics. 2006;7(1):1-11. doi:10.1186/1472-6939-7-12
CDC. COVID-19 and Your Health. Centers for Disease Control and Prevention. Published February 11, 2020. Accessed January 21, 2021. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations.html
Jago CA, Singh SS, Moretti F. Coronavirus Disease 2019 (COVID-19) and Pregnancy: Combating Isolation to Improve Outcomes. Obstet Gynecol. 2020;136(1):33-36. doi:10.1097/AOG.0000000000003946
Abad C, Fearday A, Safdar N. Adverse effects of isolation in hospitalised patients: a systematic review. J Hosp Infect. 2010;76(2):97-102. doi:10.1016/j.jhin.2010.04.027
Hao F, Tam W, Hu X, et al. A quantitative and qualitative study on the neuropsychiatric sequelae of acutely ill COVID-19 inpatients in isolation facilities. Transl Psychiatry. 2020;10(1):1-14. doi:10.1038/s41398-020-01039-2
Berlinger N, Wynia M, Powell T, et al. Ethical framework for health care institutions responding to novel Coronavirus SARS-CoV-2 (COVID-19) guidelines for institutional ethics services responding to COVID-19. Safeguarding Communities Guid Pract. 2020;2.
A Framework for Making Ethical Decisions | Science and Technology Studies. Accessed January 21, 2021. https://www.brown.edu/academics/science-and-technology-studies/framework-making-ethical-decisions
Ethical Framework for Health Care Institutions & Guidelines for Institutional Ethics Services Responding to the Coronavirus Pandemic. The Hastings Center. Accessed June 18, 2020. https://www.thehastingscenter.org/ethicalframeworkcovid19/
Rushton CH, Kaszniak AW, Halifax JS. Addressing Moral Distress: Application of a Framework to Palliative Care Practice. :9.
Keller EJ. Reflect and Remember: The Ethics of Complications in Interventional Radiology. Semin Interv Radiol. 2019;36(2):104-107. doi:10.1055/s-0039-1688423
Clark JM, Anderson D, Makary MS, Keller EJ. Understanding Bias: A Look at Conflicts of Interest in IR. J Vasc Interv Radiol. 2019;30(5):765-766. doi:10.1016/j.jvir.2019.01.002
Bozorghadad S, Newton IG, Perez AW, Makary MS, Keller EJ. Research Ethics in IR: The Intersection Between Care and Progress. J Vasc Interv Radiol. 2020;31(5):846-848. doi:10.1016/j.jvir.2020.02.014
Clark JM, Keller EJ. Reconsidering Requests—Futility in IR. J Vasc Interv Radiol. 2019;30(6):961-962. doi:10.1016/j.jvir.2019.01.025
Keller EJ, Perez AW, Makary MS. Informed Consent: Beating a Dead Horse or an Opportunity for Quality Improvement? J Vasc Interv Radiol. 2020;31(1):139-140. doi:10.1016/j.jvir.2019.08.010
Keller EJ, Rabei R, Heller M, Kothary N. Perceptions of Futility in Interventional Radiology: A Multipractice Systematic Qualitative Analysis. Cardiovasc Intervent Radiol. 2021;44(1):127-133. doi:10.1007/s00270-020-02675-3
Personalised treatment selection and planning based on controlled dosimetry will lead to improvements in treatment accuracy. This is the conclusion presented by Marnix Lam (University Medical Center Utrecht, Utrecht, The Netherlands) at ECIO Virtual (27 January, online), a series of afternoon webinars that the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) is hosting in lieu of the 2020 European Conference on Interventional Oncology (ECIO). Lam spoke on the differences between Yttrium-90 (Y-90) and Holmium-166 (Ho-166) radioembolization, and told delegates that it was “very important” to ensure interventionalists conduct a “good” scout procedure with control over selection and planning.
Currently, there are three microspheres available for radioembolization treatment in Europe: TheraSphere (Boston Scientific), SIR-Spheres (Sirtex), and Quiremspheres (Terumo). Lam began his talk by highlighting several differences between these microspheres. “Firstly,” he said, “the isotope. This is Y-90 for TheraSphere and SIR-Spheres, and Ho-166 for Quiremspheres.”
Importantly, he said, the different isotopes have different characteristics. Relative embolic effect is lowest for TheraSphere, middling for Quiremspheres, and highest of the three for SIR-Spheres. This is because the number of particles that are injected differs for each microsphere brand: five million for TheraSphere, 50 million for SIR-Spheres, and 20 million for Quiremspheres.
Lam explained: “Typically for Theraspheres, there is a low embolic effect, because we only administer around five million particles. With SIR-Spheres, there is a higher embolic effect, because we administer up to 50 million particles, ten times the number of particles as with TheraSphere. With Quiremspheres, we are somewhere in between, with a medium embolic effect, as we administer around 20 million particles. This means that the specific activity of TheraSphere is much higher: so, the activity per sphere is much higher for Therasphere than it is for SIR-Spheres, and Quiremspheres is again somewhere in between.”
He cited the specific activity for each microsphere as: 1,250–2,500Bq/microsphere for TheraSphere, 50Bq/microsphere for SIR-Spheres, and 200–400Bq/microspheres for Quiremspheres.
“What does this mean?” Lam asked rhetorically. “This is really important to understand”. Pre-clinical work by Alexander Pasciak (Johns Hopkins University, Baltimore, USA) et al in pig livers investigated the use of different numbers of microspheres over the same overall radiation activity (i.e., the same Gy in total; so, when few microspheres were used, they each have a high specific activity, and when large numbers of microspheres were used, they each had a low specific activity). When relatively few microspheres were injected, there was a very heterogeneous distribution pattern. In contrast, when a large number of microspheres were injected into the liver, each with a low specific activity, the distribution pattern was much more homogenous across the organ.
Liver tolerance of the same radiation activity (as measured in Gy), the same absorbed dose, is therefore greater when fewer particles are injected, each with a higher specific activity. The more homogenous distribution of radiation in the high-number-of-microspheres-injected model means that there is a much more limited area of unaffected liver. As Lam explained at ECIO Virtual, in the low-number-of-microspheres group, certain areas of the liver are “super dead”—have a very concentrated radiation dose—and a large swathe of the liver is unscathed.
“This is exactly the difference between TheraSphere [low particle count] and SIR-Spheres [high particle count],” he said. QuiremSpheres are in between.
Expanding on what this means in terms of tolerability, Lam informed listeners that for glass microspheres, a 100Gy radiation dose to the liver results in a 50% chance of toxicity. The same toxicity risk is attained at a 50Gy radiation dose when using resin microspheres, “so half the absorbed dose to the liver, same chance of toxicity, because the distribution is more homogeneous”. The dose thresholds used for treatment planning therefore vary depending on what type of microsphere is used.
Lam commented that this “is a very important message”, and advised the audience “to be very careful when comparing doses between products”.
Interventionalists utilise different imaging modalities for different microspheres
Turning to imaging, Lam explained how, due to differing microsphere characteristics, the imaging modality used for each also varies. Expanding on the clinical implications of this, Lam explained: “The idea of using Ho-166 instead of Y-90 is that Ho-166 has a therapeutic effect very similar to Y-90, but on top of that the element Holmium, like Gadolinium, is chemically a lanthanide, so it is paramagnetic and may be visualised and quantified using MRI [magnetic resonance imaging]. Holmium also emits gamma radiation, that may be used for quantitative SPECT [single photon emission computed tomography] imaging.”
While Y-90 can be imaged using SPECT or positron emission tomography (PET), Lam told ECIO Virtual attendees that the former modality is limited by resolution, and the latter by sensitivity. However, Ho-166 can be imaged at low quantities by MRI or SPECT, meaning that with Quiremspheres, the same particles can be used for the scout dose as for the treatment dose, unlike with Theraspheres and SIR-Spheres. Lam went on to explain the clinical significance of this characteristic of Ho-166.
Typically, ahead of a radioembolization procedure, he explained, the interventionalist will conduct a work-up or scout procedure using Tc-99m MAA (macroaggregated albumin).
The 2017 SARAH trial, an open-label, randomised controlled phase 3 trial investigating the efficacy and safety of selective internal radiotherapy (SIRT) with Y-90 resin microspheres compared with sorafenib in hepatocellular carcinoma (HCC) patients, found no significant difference in survival between the two treatments. In a more recent post-hoc analysis of the SARAH trial, published in Radiology in 2000, Ann-Laure Hermann (Université Paris-Descartes, Sorbonne Paris Cité, Faculté de Médecine, Paris, France) et al showed that when the tumour-absorbed dose is at least 100Gy, there is a clear difference in survival between resin microspheres and SIRT. “I think there is quite a spectacular result when you compare groups over 100Gy tumour-absorbed dose or below 100Gy tumour-absorbed dose,” Lam noted.
“However,” he continued, the same study also demonstrated that the correlation between the Tc-MAA distribution and the post-treatment Y-90 distribution was “good in 53% of patients only”. In 20% of patients, there was a medium correlation, and in “as much as 27% of patients”, a correlation between Tc-MAA and Y-90 distribution was poor.
“This means if we use Tc-MAA for treatment planning, in only 53% of patients the predicted value of Tc-MAA versus post-treatment Y-90 is sufficient for treatment planning. So, this is quite poor,” Lam said. “What we learn from this study is that of course, number one, we have to select patients who will benefit: patients where we can reach a 100Gy absorbed dose, and of course we should plan our treatment accordingly, to make sure we reach that tumour-absorbed dose.
“But what we also learn from this study is that we gain control by having an improved scout procedure, where the work-up is predictive of the final outcome. I believe this is where Holmium steps in, because instead of Tc-MAA, we use the exact same particles for work-up as we use for the treatment procedure. What we gain is control—over the lung-shunt calculation, and also over the intra-hepatic distribution.”
Tomorrow’s treatment planning method: Individualised patient care
Looking to the future, Lam enthused about personalised treatment planning. “Today, we use single compartment modelling at best,” he said, “aiming for an average absorbed dose within a certain perfused volume, but we really want to go towards multi-compartment modelling, differentiating between a tumour-absorbed dose and a normal-liver-absorbed dose in each individual patient. personalised
“We can use the scout dose procedure, the imaging that we gain, by selecting our patients based on a safe normal-liver-absorbed dose and a sufficient tumour-absorbed dose. If we are not able to reach that, we should seek an alternative treatment; so, selection comes first, and, secondly, we should plan our treatment accordingly. This is very important.” personalised personalised personalised personalised personalised personalised personalised personalised
“I consider intravascular ultrasound (IVUS) to be essential equipment in venous interventions,” Rick de Graaf (Clinic of Friedrichshafen, Friedrichshafen, Germany) told viewers of LINC 2021 (The Leipzig Interventional Course; 25–29 January, online). De Graaf was speaking during a session on endovascular procedures for the deep venous system, aiming to answer the question, ‘Is IVUS a fancy tool, or relevant for clinical outcomes?’
“It is hard to say that [IVUS] is fancy,” de Graaf began, noting that this is technology is essentially “just an ultrasound probe on a catheter”. In venous interventions, he noted, the technology is mainly used to indicate stenosis, determine a healthy stent landing zone, to evaluate after stenting, and evaluate after thrombectomy to see if there is any residual thrombus.
Regarding data, de Graaf detailed that there are a number of papers on using IVUS for diagnosis and procedural planning, as well as recent data from the Arnsberg registry, headed by Michael Lichtenberg (Karolinen Hospital, Arnsberg, Germany), that showed IVUS to be an effective option to reduce radiation during deep venous obstruction (DVO) interventions.
De Graaf then summarised the benefits of IVUS in venous procedures, detailing that the technology can identify “subtle yet significant” pathology—even more so than magnetic resonance (MR)-venography, in his view—gives “instant and accurate” three-dimensional (3D) representation, reduces radiation, as different angulations are not necessary and the imaging is more efficient, and reduces contrast.
Moving on to when and how to use IVUS in venous practice, de Graaf expressed his belief that to not use it at all would be “dangerously close to malpractice”. He elaborated: “Sooner or later you are going to miss something, and the patient will suffer.”
De Graaf told the audience that he has IVUS present in all venous cases, because “you never know what you are going to miss,” he said. De Graaf noted that some physicians state they only use IVUS when they need it, but likened this to only wearing a seatbelt when it is needed.
In terms of experience, de Graaf detailed that he started performing venous procedures in 2009 without IVUS, due to the cost. However, he became convinced of its importance after several stent occlusions proved to be related to the lack of IVUS. “I now use IVUS in every venous case,” he reiterated.
De Graaf outlined a specific venous case in which IVUS was crucial. A patient presented with iliac vein thrombosis, but also a distal vena cava thrombosis, he explained. While the speaker noted that he cleared out the iliac vein and stented it, IVUS then showed that there was still thrombus in the inferior vena cava (IVC), which could not be left. “I tried thrombectomy and suction with a large sheath, but I did not get it out,” he relayed. De Graaf then decided to use live imaging with IVUS and was able to remove the thrombus successfully under IVUS guidance.
“IVUS obviously has significant value guiding venous interventions, and real-time IVUS offers further possibilities,” de Graaf concluded.
A key theme among the late-breaking trial data presented at LINC 2021 (The Leipzig Interventional Course; 25–29 January, online) was the emergence of long-term data on paclitaxel devices in the femoropopliteal segment. Results out to five years shows good efficacy and safety.
Thomas Zeller (University Heart Center Freiburg-Bad Krozingen, Bad Krozingen, Germany) presented five-year outcomes of the IN.PACT Global trial, assessing the IN.PACT Admiral drug-coated balloon (DCB; Medtronic), followed by Young-Guk Ko (Yonsei University College of Medicine, Seoul, Korea), who announced results from the IN.PACT Global Asian cohort. Also presenting data out to five years, Marianne Brodmann (University of Graz, Graz, Austria) detailed new findings from the ILLUMENATE randomised controlled trials (RCTs) of the Stellarex DCB (Philips).
The EffPac study of the Luminor DCB (iVascular) now has data out to three and a half years, which Dierk Scheinert (University of Leipzig, Leipzig, Germany) shared with the LINC audience. Finally, Michael Lichtenberg (Karolinen Hospital, Arnsberg, Germany) relayed three-year data from the first-in-human KANSHAS 1 study of the novel Kanshas DCB (Terumo).
“Robust, real-world data”: IN.PACT Global five-year outcomes
First to present was Zeller, who informed LINC viewers that the IN.PACT Global study, “remains the largest and only reported real-world DCB study with independent Clinical Events Committee (CEC) adjudication through five years”. The results demonstrate the sustained efficacy of the IN.PACT Admiral DCB through five years and show evidence of long-term safety.
Zeller noted that patients with complex lesions are usually excluded from randomised controlled trials (RCTs), however, they are reflected in real-world studies. “RCTs and global registries have demonstrated the superiority of DCBs over percutaneous transluminal angioplasty (PTA) for the treatment of peripheral arterial disease (PAD) in real-world patients,” he remarked, adding, however, that long-term evidence in complex real-world patients is limited.
The IN.PACT Global study is a real-world, prospective, multicentre, single-arm, independently-adjudicated femoropopliteal study. A total of 1,416 patients were included across 64 sites in the EU, Middle-East, Latin America, and Asia.
In terms of efficacy, Zeller reported that the five-year freedom from clinically-driven target lesion revascularisation (CD-TLR) rate was 69.4%. He compared this to the rates at one, two, three and four years: 92.%, 83.3%, 76.9%, and 73.4%, respectively. Considering additional efficacy outcomes, Zeller noted that the rate of CD-TRL was 30.6% and that the rate of any TLR was 31.3%.
Regarding the primary safety composite endpoint—which consists of freedom from device- and procedure-related deaths out to 30 days, freedom from major target limb amputation within 60 months, and freedom from clinically-driven target vessel revascularisation (CD-TVR) within 60 months—the rate was 67.4% at five years.
In addition, there was a 78.9% rate of freedom from all-cause mortality out to five years, and 96.4% follow-up was achieved with vital status collection.
Zeller concluded: “Robust, real-world data continue to demonstrate durable results, indicating the IN.PACT Admiral DCB as a viable solution for the treatment of femoropopliteal disease.”
IN.PACT Admiral demonstrates “consistent treatment effect” in complex geographic subset
Honing in on the Asian subset of the IN.PACT Global study, Ko revealed that this subgroup showed more complex baseline clinical and lesion characteristics than the global clinical cohort. However, he also informed the audience that the Asian subset showed a consistently lower CD-TLR rate of 22.9% at five years for complex femoropopliteal lesions, with a mean length of 17.4±12.4cm and 51.4% total occlusions.
“These results demonstrate a consistent treatment effect with the IN.PACT Admiral DCB across IN.PACT studies, including this complex geographic subset,” he concluded.
Five-year ILLUMENATE outcomes show continued efficacy and safety of Stellarex DCB
Brodmann announced the final, five-year results of two RCTs that show no difference in all-cause mortality between patients treated with the Stellarex DCB and those treated with PTA, the current standard of care. Moreover, the studies showed no difference in mortality between the Stellarex DCB and PTA at every 12-month endpoint over the course of the study.
The ILLUMENATE EU RCT and ILLUMENATE Pivotal RCT together comprised approximately 600 patients in Europe and the USA. After five years, the ILLUMENATE EU RCT showed 19.3% mortality among patients treated with the Stellarex DCB compared to 19.4% mortality for those treated with PTA.
The five-year results for the ILLUMENATE Pivotal study also show no statistically significant difference among patients treated with the Stellarex DCB (21.2%) compared to those treated with PTA (20.2%). Both studies had a high vital status follow-up compliance, with the status of over 90% of patients known.
“The five-year final results show favourable overall safety of the Stellarex low-dose paclitaxel DCB, and are applicable within an extensive patient cohort,” said Brodmann. “Every year, the Stellarex programme has demonstrated low mortality rates with no difference in rates between the two patient cohorts.”
Luminor DCB results in “significant haemodynamic improvement” out to 3.5 years in EffPac study
Presenting new findings from the EffPac trial, Scheinert outlined 3.5-year outcomes with the Luminor-35 DCB (iVascular). A total of 166 patients were included in this study; 82 were treated with the Luminor DCB, while 84 were treated with PTA.
He concluded that at the 3.5-year timepoint, DCB angioplasty with the Luminor-35 DCB of medium length superficial femoral and popliteal artery lesions results in a, “significant haemodynamic improvement from baseline,” with a lower TLR rate, and an all-cause mortality rate similar to PTA.
Three-year findings of the first-in-human KANSHAS 1 study demonstrates “good safety and efficacy” of novel Kanshas device
Finally, Lichtenberg presented results of the first-in-human KANSHAS study of the novel Kanshas DCB (Terumo), for which there are results for 31 patients.
The speaker concluded: “Angioplasty using the novel Kanshas DCB for the treatment of de novo femoropopliteal artery lesions displays good safety and efficacy throughout the period of 36-month follow-up.” In addition, he noted that haemodynamic and clinical improvement was maintained in the majority of patients, and that no sign of an abnormal late mortality signal was observed in the studied population, with only a few TLRs noted.
New data presented for the first time at LINC 2021 (The Leipzig Interventional Course; 25–29 January, online) are positive for the IN.PACT AV drug-coated balloon (DCB) and the Ellipsys vascular access system (both Medtronic). The IN.PACT AV Access study investigated the use of DCB angioplasty versus percutaneous transluminal angioplasty (PTA) for the treatment of dysfunctional arteriovenous fistulas (AVFs). In a second presentation at the virtual congress, delegates were treated to a comparison of surgically-created versus percutaneously-created AVFs.
One-year results from the IN.PACT AV Access study demonstrate superior target lesion primary patency outcomes for DCB angioplasty compared to percutaneous transluminal angioplasty (PTA) for the treatment of de novo or restenotic obstructive lesions of native arteriovenous fistulae (AVF) in the upper extremity. So said Andrew Holden (Auckland Hospital, Auckland, New Zealand), addressing attendees virtually.
In a comparison of surgical and percutaneous AVF creation, Robert Shahverdyan (Asklepios Clinic Barmbek, Hamburg, Germany) told LINC 2021 attendees that whilst surgical AVFs have a higher primary patency and fewer re-interventions, percutaneous AVFs with the Ellipsys vascular access system have a higher technical success rate, faster procedure times, higher assisted, secondary patency and maturation rates, faster cannulation times, and fewer abandonments.
Superior target lesion primary patency at 12 months with the IN.PACT AV DCB versus standard angioplasty, new data show
In addition to Holden, Robert Lookstein (Ichan School of Medicine at Mount Sinai, New York, USA) and Hiroaki Haruguchi (Haruguchi Vascular Access Clinic, Tokyo, Japan) are principal investigators of the IN.PACT AV Access investigational device exemption (IDE) study, which evaluated the IN.PACT AV DCB versus PTA.
They conducted a global, prospective, 29-centre, 1:1 randomised, single-blinded study evaluating the safety and effectiveness of DCB angioplasty versus PTA in dysfunctional AVF, following 330 patients out to five years. Each patient enrolled in the study had lesions up to 10cm in length in the native AVF.
The primary safety outcome was measured by the serious adverse event rate involving the AVF access within 30 days of the procedure. The primary effectiveness outcome was defined as freedom from clinically-driven target lesion revascularisation (CD-TLR) or access circuit thrombosis, measured through six months post-procedure.
One year after intervention, target lesion primary patency was 65.3% in the DCB group, and 46.3% in the standard PTA group (p<0.001). Access circuit primary patency was also higher amongst the IN.PACT AV DCB cohort: 55.1% versus 35% (p<0.001).
The subset outcomes of the IN.PACT AV Access trial through 12-months were presented for the first time. Assessing the 12-month data by lesion type, Holden informed the virtual LINC audience that the IN.PACT AV DCB arm demonstrated superior patency in both de novo and restenotic lesions compared to the standard PTA arm. Target lesion primary patency was achieved in 77.5% of de novo lesions treated with the IN.PACT AV DCB (31 of 40), compared to in 61.9% of de novo lesions treated with standard PTA (26 of 42); confidence interval (CI), -4–35.2%. In restenotic lesions, target lesion primary patency was also higher in the DCB group than the standard angioplasty one: 58.4% (59 of 101) versus 35.7% (35 of 98); CI, 9.2–36.2%
Looking at the data by type of AVF type, the IN.PACT AV DCB group achieved better target lesion primary patency at 12-months for all subgroups: radiocephalic (64.5% vs. 47.2%; CI, 1.5–33%), brachiocephalic (63.8% vs. 41.2%; CI, 3.4–41.9%), and brachiobasilic (61.5% vs. 45.4%; CI, -23.5–55.6%). Commenting on these results, Holden told delegates: “Fewer reinterventions are needed to maintain target lesion primary patency in the DCB group compared to the PTA group. We saw a 56% reduction in reinterventions at six months, and a 35.4% reduction in reinterventions at 12 months.
“Through 12 months, sustained superior target lesion primary patency was achieved with DCB in restenotic lesions, and both forearm and upper arm AVF types. Subset analysis of lesion location showed a patency advantage for INPACT AV DCB over standard PTA for all lesion locations in the access circuit but particularly at the arterial inflow, anastomosis and cephalic arch.”
One-year data consistent with positive six-month results
These 12-month data concur with the six-month results of the IN.PACT AV Access study, published in TheNew England Journal of Medicine (NEJM) in August 2020, which also showed that DCB angioplasty is superior to standard angioplasty for the treatment of stenotic lesions in dysfunctional haemodialysis AVFs. Furthermore, it was found to be non-inferior with respect to access circuit-related serious adverse events within 30 days.
The investigators noted last summer that long-term outcomes for standard PTA—the current recommended treatment for dysfunctional haemodialysis fistulas—are poor. They suggested that DCBs delivering the antirestonotic agent paclitaxel may improve outcomes, as evidenced in the present study.
Speaking to Vascular News at the time, Lookstein commented on the clinical implications of the study: “We now have Level 1 evidence of a simple technology that is proven to be safe and effective at improving outcomes for patients with end-stage renal disease [ESKD] on haemodialysis.
“This is the first US Food and Drug Administration [FDA]-approved paclitaxel-based device since the controversy last year, which is a testament not only to the incredible results seen in this trial, but also the significant needs of this population.”
Percutaneous AVF creation with Ellipsys faster, and “easier to salvage” than surgically-created AVFs
In a comparison of surgical and percutaneous AVF creation, Shahverdyan told LINC 2021 attendees that whilst surgically-created AVFs have a higher primary patency and fewer re-interventions, percutaneously-created AVFs with the Ellipsys vascular access system have a higher technical success rate, faster procedure times, higher assisted, secondary patency and maturation rates, faster cannulation times, and fewer abandonments.
Currently, there are two systems available on the market for the percutaneous creation of AVF: the Ellipsys vascular access system and the WavelinQ 4F endoAVF system from BD.
Comparing these two endovascular AVF options with the surgical Gracz technique, the investigators have created over 500 new vascular accesses during the study period in total, from which Ellipsys was used in 116 patients, WavelinQ 4F in 41 patients, and Gracz surgical AVF creation was performed in 90 patients.
Technical success was 100% in the Ellipsys and surgical Gracz groups, and 92.7% in the WavelinQ group.
“Anastomosis is very important,” Shahverdyan said, before sharing that 100% of anastomoses were radial in the Ellipsys group, while 61% were radial in the WavelinQ groups (a further 34.1% were ulnar), and 37% were radial in the Gracz group (an additional 12% were ulnar, and 51% were brachial). Commenting on the fact that half of surgical AVFs were brachial, Shahverdyan noted: “Anastomosis [location] is not only important for the flow, but also after a failed endoAVF, you could still create a brachial artery based anastomosis [surgically]”.
The procedure time was significantly shorter when using the Ellipsys, with a median time of 13 minutes versus 62 minutes in the WavelinQ arm and 69 minutes in the Gracz arm.
“This is where it gets interesting,” Shahverdyan enthused. He shared that maturation at four weeks “is similarly high for Ellipsys and Gracz” (78.4% and 80%, respectively), and that they observed total maturation in 88% of patients for both these groups. Time to cannulation in dialysis patients was shorter for Ellipsys procedures (52 days vs. 69 days in the surgical cohort), and, although there were more interventions in the endoAVF groups, fewer Ellipsys AVFs were abandoned or converted to another fistula (12.3% vs. 36.6% in the WavelinQ group and 15.6% in the surgical group).
At six months, one year, and two years, primary patency was highest in the surgical Gracz group (68%, 53%, and 42%, respectively). The Ellipsys had the second highest primary patency at all time points (50%, 34%, and 27%, respectively), whilst primary patency with WavelinQ was lowest (35%, 27%, and 23%, respectively). However, assisted patency rates at six months, one year, and two years were similarly high for Ellipsys (83%, 77%, and 77%, respectively) and Gracz (84%, 80%, and 78%, respectively) groups, and secondary patency rates were slightly, but not significantly, higher for Ellipsys-group (89%, 87% and 87%) versus Gracz-group (855, 82% and 82%).
“To conclude,” Shahverdyan said, “Ellipsys demonstrates high technical success and faster procedural times compared with both surgical and WavelinQ procedures. It shows similarly high assisted and secondary patency and maturation rates as the Gracz fistula, and especially if you compare it to the proximal radial artery based Gracz AVF, it shows significantly higher secondary patency rates. There are fast cannulation times for Ellipsys AVF, and although there are fewer re-interventions for the Gracz AVF [than with Ellipsys], there are fewer abandonments for Ellipsys percutaneous AVF, so it is easier to salvage.
“Therefore, Ellipsys percutaneous AVF expands the options for a valid, long-term AVF creation in our patients.”
Twelve-month results from the PRESTIGE below-the-knee (BTK) study have been presented as a late-breaking trial at LINC 2021 (25–29 January, virtual). The objective of this clinical investigation has been to evaluate safety and performance outcomes of SELUTION SLR, MedAlliance’s novel sirolimus-eluting balloon, for the treatment of long tibial occlusive lesions (TASC C and D) in patients with chronic limb-threatening ischaemia (CLTI).
The primary patency rate was 78% and the rate of wound healing was 81%. Freedom from target lesion revascularisation (TLR) was exhibited by 93% of patients and 84% demonstrated amputation free survival (AFS). All these figures have been sustained from the six-month data.
PRESTIGE is a prospective, single-centre, physician-initiated clinical study, run at the Singapore General Hospital (SGH) by Tze Tec Chong and Tjun Yip Tang, who are both senior consultants at the Hospital’s Department of Vascular Surgery. Twenty-five patients were enrolled with an average age of 64. Eighty-eight per cent had diabetes mellitus and 44% had end stage renal failure. No patients required bailout stenting. Clinical follow-up was at one, three, six, and 12 months.
“We have observed minimal slow-flow phenomena and some cases of fast wound healing with SELUTION SLR. It is also easy to track and deliver. We are looking forward to gaining further clinical experience with this device,” commented Chong.
Singapore has a high percentage of diabetics in its population and CLTI therefore constitutes a major challenge among patients seen with peripheral arterial disease (PAD). SGH performs over 1,000 interventional procedures a year on patients suffering from CLTI.
In February 2020 MedAlliance received CE mark approval for SELUTION SLR in the treatment of peripheral arterial disease. Both the STEP Pedal Arch study and SUCCESS PTA, a large post-marketing clinical study in PAD, will commence enrolment soon. In the US, SELUTION SLR has received US Food and Drug Administration (FDA) Breakthrough Device Designation Status for a drug-eluting balloon (DEB) in the treatment of peripheral below-the-knee lesions.
Artio Medical recently announced that it has successfully completed the first human use of its Amplifi vein dilation system. The first clinical procedure was performed by Adrian Ebner, head of the Cardiovascular Department at Sanatorio Italiano Hospital in Asuncion, Paraguay.
“Vascular access is a constant challenge for end stage renal disease patients who depend on haemodialysis treatment. Most patients are plagued with interrupted or delayed care due to repeated access site failures and require additional procedures and surgeries to maintain vascular access,” commented Ebner.
“Many also frequently experience access site complications, often resulting in hospitalisation and the need for additional care. I am pleased to be a part of the first human use for the Amplifi system. This is the first technology that seeks to address these challenges by proactively preparing patient’s veins for AVF creation.”
Artio Medical’s Amplifi vein dilation system is designed to stimulate arm vein enlargement in haemodialysis patients using rapid, non-pulsatile blood flow. The innovative system is designed for percutaneous placement and includes a wearable, external blood pump, inflow and outflow catheters, and a controller. The Amplifi system is used for seven to 10 days and removed completely during AVF creation.
“I believe this device has the potential to change the standard of care for haemodialysis patients, allowing more patients to be eligible for AVF surgery and reducing the risk of AVF failure and abandonment,” continued Ebner. “The degree of vein dilation we observed during the treatment period for the first patient was remarkable, and the AVF made with the treated vein matured very rapidly.”
Artio Medical acquired the first-of-its-kind vein dilation technology through the acquisition of Flow Forward Medical in June 2020. The Amplifi vein dilation system aims to address common issues related to vascular access site creation and maintenance for the 2.3 million patients worldwide with end-stage renal disease who require haemodialysis. Artio expects to complete the first-in-human clinical study in the first half of 2021.
VentureMed Group announced today that data from three studies evaluating the use of its Flex Vessel Prep (VP) system were presented during LINC 2021 (Leipzig Interventional Course; 25–29 January, virtual). The Flex VP system is designed to modify plaque and prepare vessels with complex femoropopliteal arterial disease, including in-stent restenotic (ISR) lesions, prior to delivery of the definitive therapy.
“Individually and collectively, these three studies report compelling data,” said J Robert Paulson, Jr, president and chief executive officer of VentureMed. “The data demonstrate that longitudinal, circumferential micro-incisions delivered by the Flex Vessel Prep system safely and consistently modify plaque to improve vessel compliance and increase luminal gain, with minimal trauma to the vessel, which may reduce the need for stenting and facilitate the delivery of drug therapies into the vessel wall. The Flex Vessel Prep system allows physicians to modify plaque and prepare diseased vessels of any length to optimise their choice of definitive revascularisation therapy.”
The following are summaries of the three studies presented at LINC 2021:
12-month results of micro-incision Vessel Prep system showing acute and long-term benefit in superficial femoral and popliteal arteries
This single-centre study assessed the impact of vessel preparation with Flex VP longitudinal, controlled-depth, micro-incisions prior to drug-coated balloon (DCB) angioplasty or percutaneous transluminal angioplasty (PTA) therapy, acutely, and at six and 12 months.
Study findings:
Sixty-three patients with moderate-to-severe symptomatic femoropopliteal peripheral arterial disease (PAD), with lesions averaging approximately 200mm in length, were treated with the Flex VP to create circumferential, controlled-depth micro-incisions prior to delivery of the definitive DCB (paclitaxel) or PTA therapy.
The freedom from target lesion revascularisation (TLR) at six- and 12-months was 98.5% and 93.7%, respectively, with a low provisional stent rate of only 16.9%.
Patterns and number of dissections with atherectomy versus Flex VP: An IVUS assessment
This single-centre, comparative, prospective study was based on published data demonstrating that dissection, not plaque compression, is what opens the lumen of obstructed vessels post-PTA. Published clinical data also has demonstrated that severe dissections per NHLBI classifications (Type C and higher) and dissections involving the adventitia are likely to be associated with worse outcomes after definitive PTA therapy. This study evaluated the differences in dissections between atherectomy and the Flex VP system in femoropopliteal arteries and included de novo and restenotic lesions using intravascular ultrasound.
Study findings:
In lesions with comparable treatment lengths and presence of calcium, there was a pattern of significantly fewer and less severe dissections after Flex VP vessel preparation as compared to atherectomy.
There were no differences in the extent of new dissections following delivery of the definitive PTA therapy.
This data suggests that Flex VP may be less traumatic as vessel preparation.
Lesion modification with a micro-incision Vessel Preparation system enhances balloon-based drug delivery in complex porcine restenotic lesions
This study examined if and how a vessel preparation system delivering micro-incisions could enhance in vivo paclitaxel (delivered from a DCB) retention in a complex porcine ISR lesion model design. Optical coherence tomography (OCT) images of the baseline ISR images confirmed barriers to delivery of DCB therapy. The animals were either (a) imaged by OCT and treated with a DCB and then re-imaged, or (b) imaged by OCT, re-imaged after micro-incisions were delivered by the Flex VP system, treated with DCB and then re-imaged again. The animals were survived to one, 15 or 30 days and the treated arteries then were processed to measure retention of paclitaxel concentrations.
Study findings:
OCT imaging of ISRLs revealed smooth stenotic surfaces posing significant barriers to penetration as evidenced by remarkably low paclitaxel concentrations at one day in standard vessels (<0.9ng/mL).
OCT imaging of the lesions treated with the Flex VP system demonstrated atraumatic micro-incisions along the length and circumference of the vessels, with no dissections, and enhanced tissue retention of paclitaxel as compared to the vessels treated with DCB alone.
Data from two head-to-head trials on drug-eluting technologies in femoral artery treatment were presented during a late-breaking session at LINC 2021 (Leipzig Interventional Course; 25–29 January, virtual)—one-year TRANSCEND and two-year COMPARE results. Both studies point to the non-inferiority of lower-dose paclitaxel devices, prompting discussion on whether these results will see a trend towards using lower-dose devices in practice. Although these results are promising, the panel agreed that more data are needed.
Kenneth Rosenfield (Massachusetts General Hospital, Boston, USA) presented one-year results of the TRANSCEND study, a non-inferiority randomised trial comparing the efficacy and safety of the SurVeil drug-coated balloon (DCB; Surmodics) versus the IN.PACT Admiral DCB (Medtronic), and Sabine Steiner (University of Leipzig, Leipzig, Germany) presented two-year results from the COMPARE trial, assessing the Ranger DCB (Boston Scientific) compared to the IN.PACT device.
All DCBs assessed utilise the anti-proliferative drug paclitaxel. The SurVeil and Ranger DCBs both have a low dose of paclitaxel (2µg/mm²) compared the the IN.PACT Admiral DCB, which has a higher dose of 3.5μg/mm².
TRANSCEND one-year results: SurVeil demonstrates non-inferior efficacy and safety versus IN.PACT Admiral
Rosenfield announced that primary results of TRANSCEND demonstrate the non-inferiority of the SurVeil DCB compared to the IN.PACT Admiral DCB with regards to both safety and efficacy, while delivering a substantially lower drug dose.
In the TRANSCEND trial, the SurVeil DCB was found to be non-inferior to the IN.PACT Admiral DCB in both the primary safety and primary efficacy endpoints. The SurVeil DCB cohort (n=222) exhibited a strong safety profile with 91.7% of subjects demonstrating freedom from device- or procedure-related death within 30 days and freedom from above-ankle amputation or clinically-driven target vessel revascularisation (CD-TVR) within 12 months, compared to 89.6% of subjects treated with the IN.PACT Admiral DCB (n=224).
The SurVeil DCB group also met its efficacy endpoint of primary patency of 81.7% as compared to 85.9% of the IN.PACT Admiral DCB arm. In addition, the number of reinterventions deemed clinically necessary by physicians did not differ between the products.
COMPARE two-year results: Ranger continues to demonstrate similar patency rate to IN.PACT
Two-year results from COMPARE, the first head-to-head comparison of two DCBs with different paclitaxel dosages and coating technologies for femoropopliteal interventions, were also presented.
The study compared the lower paclitaxel dose Ranger DCB to the higher paclitaxel dose IN.PACT Admiral DCB. One-year results of COMPARE were presented for the first time during LINC 2020 (Leipzig Interventional Course; 28–31 January, Leipzig, Germany) and published concomitantly in the European Heart Journal.
At two years, the Ranger DCB, which has a significantly lower drug dose density of paclitaxel continued to demonstrate a similar primary patency rate to the higher-dose IN.PACT DCB with a freedom from restenosis rate of 70.6% for the Ranger DCB (n=207) compared to the 71.4% observed with the IN.PACT DCB (n=207), according to Kaplan-Meier estimate (log-rank p=0.96).
No significant differences were observed for other secondary two-year outcomes, Steiner informed the LINC audience, detailing low all-cause mortality rates at two-years with 3.6% for the Ranger DCB vs. 2.2% for the IN.PACT DCB (p=0.6).
In addition, there was a low clinically-driven target lesion revascularisation (CD-TLR) rate through two years—17.8% for the Ranger DCB vs. 13% for the IN.PACT DCB (p=0.3).
Results for low-dose devices “reassuring,” but more data needed
Subsequent discussion focused on the significance of these results, with moderator Dierk Scheinert (University of Leipzig, Leipzig, Germany) posing the question: “Are low-dose balloons the way to go in the future?”
Rosenfield responded: “I think that this new generation of balloons is going to be better, and the safety data are comparable. If you are going to use multiple balloons in a given patient, I would certainly feel a lot more comfortable using a lower-dose balloon with better transmission of the drug and with less particulates downstream. I believe that this is going to be the way to go. Also, the technology is constantly improving.”
Steiner was in agreement, noting that the results are “reassuring”. While the data from both TRANSCEND and COMPARE point in a similar direction, Scheinert was curious to know if there are any key differences between the datasets. “COMPARE included longer lesions, up to 30cm,” Steiner began, adding that it also included more chronic total occlusions (≈40% CTOs). However, the speaker noted this design came at a price, referring to a much higher bailout stenting rate than TRANSCEND. Steiner also remarked that with the “more typical” design of TRANSCEND, with lesions of up to 18cm only, non-inferiority for a low-dose versus a high-dose balloon was also evident.
Both TRANSCEND and COMPARE assessed low-dose devices to the high-dose IN.PACT Admiral DCB. In the same late-breaking session, Thomas Zeller (Universitäts-Herzzentrum, Bad Krozingen, Germany) had presented long-term data on this device. Scheinert asked for his opinion on the results.
“We have to wait for longer-term follow-up data in order to see whether there will be a difference in terms of future safety endpoints,” Zeller remarked. “However, it is interesting to see that all the data with the first-generation DCB [IN.PACT Admiral] are more or less in line, independently of whether the maker of this device has conducted the trial, or if this balloon was used as a control,” he added, highlighting the strong data available for the device.
In terms of whether this should herald a move towards low-dose devices, Zeller was unconvinced: “I do not see a reason to switch, and I do not know whether it is really necessary.”
Panellist Marianne Brodmann (University of Graz, Graz, Austria) also commented, echoing Rosenfield: “If a low-dose device is as safe and as efficient in the long term as a high-dose device, I think a lot of physicians might feel more comfortable to use a low-dose device.” However, she also stressed that more data on these low-dose devices are needed.
The US Food and Drug Administration (FDA) has granted Pedra Technology a breakthrough device designation for the periprocedural use of the company’s Pedra Xauron perfusion system in the treatment of critical limb-threatening ischaemia (CLTI).
CLTI is a severe form of peripheral arterial disease (PAD) that is defined as ischemic rest pain, tissue loss, or gangrene (tissue death) that develops as a result of chronically poor blood flow to the lower limbs. If left untreated, CLTI can lead to limb amputation or death. The one-year mortality rate of CLTI patients without amputation is 30.3%, and with amputation is 40.4%. At five-years post-CLTI diagnosis, the mortality rate exceeds 50%, which is worse than most cancers.
The breakthrough devices programme at the FDA aims to provide patients and providers with timely access to medical devices that offer for more effective treatment and diagnosis of severe diseases, including a prioritised review of market approval regulatory submissions.
Paul Hayes, vascular surgeon and CMO of Pedra Technology, comments: “With the Xauron device, physicians can at last see real-time perfusion changes during an interventional procedure in the angiographic suite. I am excited about building on our early clinical data and demonstrating that Xauron will save patient lives and limbs.”
Hayes spoke to this newspaper last year at LINC 2020 (Leipzig Interventional Course; 28–31 January 2020, Leipzig, Germany) about the challenges of wound care, in particular assessing the success or failure of endovascular treatment of peripheral arterial disease. At the time, he described Pedra as a novel, portable, tissue-monitoring device that uses laser, and that provides real-time quantitative feedback in the angiosuite about whether the proceduralist has truly achieved improved blood flow to the microcirculation in the foot. Hayes noted that the device does not interfere with the workflow in the cath lab. The full interview can be seen here.“This breakthrough device designation recognises the compelling need for real-time tissue perfusion monitoring during lower limb revascularisation procedures for the treatment of CLTI. To my knowledge, this is the first perfusion monitor for CLTI that has received this designation,” comments Kareen Looi, CEO of PEDRA Technology. “An improvement in microvascular perfusion at the tissue level is necessary for elimination of rest pain, healing of chronic wounds, and for limb salvage. We look forward to developing this important new technology and working closely with the FDA to develop the appropriate clinical programme for market approval.”
Royal Philips has announced the final, five-year results of two randomised controlled trials (RCTs) that show no difference in all-cause mortality between patients treated with the Stellarex drug-coated balloon (DCB) and those treated with percutaneous transluminal angioplasty (PTA), the current standard of care. Moreover, the studies showed no difference in mortality between the Stellarex DCB and PTA at every 12-month endpoint over the course of the study. Results from the two RCTs were presented at LINC 2021 (Leipzig Interventional Course; 25–29 January, virtual).
The ILLUMENATE EU RCT and ILLUMENATE Pivotal RCT together comprised approximately 600 patients in Europe and the USA. After five years, the ILLUMENATE EU RCT showed 19.3% mortality among patients treated with the Stellarex DCB compared to 19.4% mortality for those treated with PTA.
The five-year results for the ILLUMENATE Pivotal study also show no statistically significant difference among patients treated with the Stellarex DCB (21.2%) compared to those treated with PTA (20.2%). Both studies had a high vital status follow-up compliance, with the status of over 90% of patients known.
“The five-year final results show favourable overall safety of the Stellarex low-dose paclitaxel DCB, and are applicable within an extensive patient cohort,” said Marianne Brodmann (Medical University of Graz, Graz, Austria), primary investigator for both trials and a paid consultant to Philips. “Every year, the Stellarex programme has demonstrated low mortality rates with no difference in rates between the two patient cohorts.”
“These study results build on the robust, consistent long-term data of the Stellarex program and confirm the safety and performance of our unique DCB,” said Chris Landon, senior vice president and general manager Image Guided Therapy Devices at Philips. “The Stellarex DCB, with its low drug dose and unique drug coating composition, continues to be an important treatment choice for healthcare providers treating patients with peripheral arterial disease.”
The journal CVIR Endovascular launched its own podcast in December 2020, to discuss endovascular and interventional interventions, and to promote the Cardiovascular and Interventional Radiological Society of Europe (CIRSE)’s open access journal. The podcast, hosted by editor-in-chief Jim Reekers (Amsterdam UMC, Amsterdam, The Netherlands), takes place every other month, and highlights articles published in CVIR Endovascular, as well as features interviews with contributing authors.
Interventional News discusses the new podcast with Reekers, and how he believes it will transform communication and education within interventional radiology through a broadening of the discursive channels available.
Why is it timely to launch a podcast now, and what are your hopes for this platform?
CVIR Endovascular is a platform for interventional radiology (IR) publications, but also for ideas and discussions. Since the postponement of many meetings due to the pandemic, we need a new way to communicate and to exchange our IR narratives, as narratives have always been an important part of this unique and innovative medical specialty. Podcasts are a great way to get our message out, especially to millennials, as you can listen a podcast when you want, and wherever you want.
How will the podcast and the journal complement each other?
They will be complementary in the sense that the podcast will enrich the journal and the publications with additional background information. It will create a community of young interventional radiologists around the journal.
What is it about the medium of a podcast that appeals/ what benefits are there to this format beyond the journal?
Narratives through podcasts are a relaxed way to communicate a message; it does not have the in-your-face nature of social media, you can consume it at your own pace. You can listen whenever you want, commuting, doing the dishes, cooking, just when you want. A podcast is like a friend and not like an aggressive salesperson, it does not speak in headlines. It is thoughtful and contemplative, something we all need in this complex world.
What sort of content can your audience expect from the podcast, and what in the next few months are you specifically excited to discuss with guests?
The podcast will highlight articles published in the journal, as well as hot topics, via interviews with many of our authors and a number of leaders in the field of endovascular interventions. CVIR Endovascular is a journal that promotes directions and ideas through editorials and is therefore a forerunner. The podcast will do exactly the same—it will make you think and sharpen your mind.
What developments in endovascular and vascular interventions are underreported/ explored, and how is CVIR Endovascular giving a platform to these topics?
Endovascular interventions are driven by the hype of the day, for example with all the drug-eluting technologies and the amazing technical skills, but the real core of IR is being a good and thoughtful doctor for your patients. A podcast does away with the dominant visual factor of current IR communications; as such, having a concurrent CVIR Endovascular podcast episode alongside an article will enrich the paper.
What can listeners expect in the future?
Our newest podcast episode is about our special issue of paediatric interventional radiology. I think it is important to become a friend of the CVIR EndovascularPodcast, to reset your mindset, and to step out of the IR roller coaster when you listen.
Bart Dolmatch (Portola Valley, USA) talks to Vascular News about some of the key data highlights from the 24-month AVeNEW trial, which compared the safety and efficacy of the Covera™ Vascular covered stent (BD) against percutaneous transluminal angioplasty (PTA) for the treatment of stenotic lesions in the upper extremity venous outflow of the arteriovenous access circuit.
The data, which was presented at CIRSE 2020, are “very compelling”, says Dolmatch, who notes that that the primary endpoints of safety at one-month and durability at six-months were “superior” for the covered stent compared to angioplasty alone. These results “hold up” at 24-months, he adds, with a greater target lesion primary patency for the covered stent group (N=69) compared to the PTA group (N=25), 41.8% vs. 10.4% respectively – highlighting a “dramatic improvement” at the target lesion site.
He also discusses the importance of circuit patency when treating hemodialysis patients, stating that there is now “robust data” to show that the use of the Covera™ Vascular covered stent is a “great strategy” for cephalic vein arch stenosis. Further sub-analyses showed that the Covera™ Vascular covered stent performed better regardless of the type of arteriovenous fistula, lesion location, de novo or recurrent lesions, concluded Dolmatch.
This video is sponsored by BD
Indication For Use: The Covera™ Vascular Covered Stent is indicated for use in hemodialysis patients for the treatment of stenoses in the venous outflow of an arterio-venous (AV) fistula and at the venous anastomosis of an ePTFE or other synthetic AV graft.
Warnings: DO NOT use in patients with known hypersensitivity to nickel-titanium or tantalum. · Placing a covered stent across a vessel side branch may impede blood flow and hinder or prevent future procedures. · DO NOT place a flared covered stent with the flared end in a straight vessel segment since this may lead to flow turbulences. · Covered stent placement beyond the ostium of the cephalic vein into the axillary/subclavian vein may hinder or prevent future access.
Potential Complications and Adverse Events: Complications and Adverse Events associated with the use of the Covera™ Vascular Covered Stent may include the usual complications associated with endovascular stent and covered stent placement and dialysis shunt revisions.
Please consult product labels and package inserts for indications, contraindications, hazards, warnings, cautions, and information for use.
A recent analysis by finds an association between depression and non-home discharge after revascularisation for chronic limb-threatening ischaemia (CLTI). Authors Joel L Ramirez, James C Iannuzzi (University of California, San Francisco, San Francisco, USA) and colleagues write in an online Journal of Vascular Surgery (JVS) article that these results “provide further evidence of the negative impact that comorbid depression has on patients undergoing revascularisation for CLTI,” and propose that future studies should examine whether treating depression can improve outcomes in this patient population.
“Recent evidence suggests that depression in patients with peripheral arterial disease (PAD) is associated with increased postoperative complications,” the authors begin, noting that problems can include decreased primary and secondary patency after revascularisation and increased risk of major amputation and mortality.
Ramirez et al note that the impact of depression on non-home discharge after vascular surgery remains unexplored, despite this being “an important outcome” for patients. They hypothesised that depression would be associated with an increased risk for non-home discharge following revascularisation for CLTI.
The investigators identified endovascular, open, and hybrid cases of revascularisation for CLTI from the 2012–2014 National (Nationwide) Inpatient Sample, which they explain is “a patient-level administrative claims database that is published annually by the Agency for Healthcare Research and Quality and represents approximately 20% of discharges from US hospitals”.
They write that a hierarchical multivariable binary logistic regression controlling for hospital level variation examined the association between depression and non-home discharge and controlled for confounders meeting p<0.01 on bivariate analysis.
Ramirez and colleagues identified 64,817 cases, of which 5,472 (8.4%) were diagnosed with depression, and 16,524 (25.5%) required non-home discharge. They relay that patients with depression were younger, more likely to be women, white, have multiple comorbidities, a non-elective admission, and experience a postoperative complication (p<0.05).
The authors report that, on unadjusted analyses, patients with depression had a 7% absolute increased risk of requiring non-hospital discharge (32.1% vs. 24.9%, p<0.001). On multivariable analysis, they found that patients with depression had an adjusted 50% increased odds for non-hospital discharge (odds ratio [OR]=1.5; 95% confidence interval [CI]=1.4–1.61; c-statistic, 0.81) compared to those without depression.
After stratification by operative approach, Ramirez et al identified that depression had a larger effect estimate in endovascular revascularisation (OR=1.57; CI=1.42–1.74) compared to open (OR=1.45; 95% CI=1.3–1.62).
Finally, the authors write in JVS that a test for interaction between depression and gender showed that men with depression had higher odds of non-hospital discharge compared to women with depression (OR=1.68; 95% CI=1.51–1.88 vs. OR=1.37; 95% CI=1.25–1.51; interaction p<0.01).
In the discussion of their findings, Ramirez and colleagues recognise that the present study is limited by certain factors. For example, they note that their investigation was based on a large national administrative database, in which all diagnoses are determined based upon billing codes. They acknowledge that use of this particular source “may introduce bias and be susceptible to under-reporting of certain comorbidities”.
The authors summarise that this study found a novel association between depression and non-hospital discharge after revascularisation for CLTI. Considering the wider impact of their findings, they write: “These results provide further evidence that an increased awareness about mental health is fundamental to care for vascular surgery patients and to understand postoperative pathways.”
(A) An enlarged image of the Indigo aspiration catheter; (B) the Indigo aspiration pump producing sustained aspiration power at -28.5mm/Hg.
Data from the EXRACT-PE trial, published online first in the Journal of the American College of Cardiology (JACC): Cardiovascular Interventions, found that the Indigo Aspiration system (Penumbra) met its predefined safety and efficacy endpoints for the treatment of pulmonary embolism (PE). In this multicentre, prospective study, the Indigo aspiration system was associated with a significant reduction in the right ventricular-to-left ventricular (RV/LV) ratio and a low major adverse event rate in submassive PE patients. Intraprocedural thrombolytic drugs were avoided in 98.3% of patients.
EXTRACT-PE stands for Evaluating the Safety and Efficacy of the Indigo aspiration system in Acute Pulmonary Embolism. It is a single-arm investigational device exemption (IDE) trial that enrolled 119 patients at 22 US sites, and is sponsored by Penumbra. Patients with signs and symptoms of acute PE for ≤14 days, computed tomography angiography (CTA) evidence of PE, systolic blood pressure ≥90 mm/Hg with evidence of dilated RV (RV/LV ratio >0.9), and who were 18 years of age or older were eligible for enrollment.
Patients were treated for acute PE with the Indigo aspiration system at each investigational sites. According to Penumbra, the Indigo system is designed to remove clots from arteries and veins in the peripheral vasculature. It was introduced in 2014, and received clearance for the PE indication in January 2020.
The primary efficacy endpoint analysis was the difference between the baseline and the 48-hour RV/LV diameter ratio; it was met if the lower bound of the confidence interval (CI) was >0.2.
The primary safety endpoint was the rate of major adverse events at the 48-hour mark, a composite of device-related death, major bleeding, and device-related serious AEs (SAEs). The primary safety endpoint was met if the upper bound of the CI was <40%. Device-related SAEs were a composite of clinical deterioration, pulmonary vascular injury, and cardiac injury. Secondary safety endpoints at 48 hours included rates of device-related death, major bleeding, clinical deterioration, pulmonary vascular injury, and cardiac injury. Additional secondary safety endpoints were 30-day rates of any-cause mortality, device-related SAEs, and symptomatic recurrence of PE.
Detailing their results, lead author Akhilesh K Sista (NYU Grossman School of Medicine, New York, USA) and colleagues write: “In this prospective study of the Indigo Aspiration device for submassive PE, we found a statistically significant reduction in RV/LV ratio (0.43; 95% CI: 0.38–0.47; p<0.0001), an average reduction in systolic pulmonary artery pressure of 7.9%, and a low major adverse event rate (1.7%) following use of the device. This was achieved with 98.3% of patients receiving no procedural tissue type plasminogen activator (tPA). The rate of major bleeding was 1.7%, and there were no haemorrhagic strokes. Of note, 89.6% (n=103 of 115) of patients had a reduction in RV/LV ratio without an adverse event related to the device, major bleeding, PE-related death, or clinical deterioration.”
This led them to conclude that the Indigo Aspiration system “may be considered by endovascular physicians for use in intermediate risk PE”, and to express the opinion that future prospective studies and randomised trials should focus on which patients (including high-risk PE patients and those with thrombolytic drug contraindications) derive the greatest benefit from aspiration thrombectomy.
New single-centre clinical study data published in the Journal of Neuroradiology claims to support Anaconda Neurovascular Access (ANA) catheter system for the treatment of ischaemic stroke.
Investigators at Hospital Vall d’Hebron, Barcelona, Spain, are participating in the multi-center SOLONDA (“SOL”itaire in combination with the ANA Catheter system manufactured by Anac”ONDA”) clinical trial, a 125-patient, prospective study that will assess system safety and reperfusion measured using the modified treatment in cerebral infarction (mTICI) score.
Hospital Vall d’Hebron investigators followed 35 consecutive patients, with published results as follows:
The primary endpoint, defined as successful reperfusion (mTICI 2b-3) within three passes without rescue therapy, was achieved in 91.4% of patients, with a rate of complete reperfusion (mTICI 2c-3) of 65.7%
The rate of first-pass complete recanalisation (mTICI≥2c) was 42.9%
The rate of sudden recanalisation was 82.9%
The median number of ANA Catheter System passes was one
“The ANA device showed promising high rates of first-pass complete recanalisation,” Alejandro Tomasello (Hospital Vall d’Hebron, Barcelona, Spain), lead author and principal investigator of this study. “We hope that the device completes the regulatory process soon.”
According to a company press release, Anaconda’s investigational ANA catheter system consists of a funnel-shaped delivery and aspiration catheters to be used in combination with a stent retriever. When deployed, the funnel self-expands and directly conforms to the artery diameter up to 5mm. It is designed to locally restrict flow and allow full thrombus extraction without fragmentation. The SOLONDA study aims to validate earlier testing that achieved statistically significant improvement in revascularisation rates at both first and third pass.
“Vall D’Hebron’s early results are fulfilling our expectations for the safety and efficacy of the ANA System,” said Francois Salmon (Barcelona, Spain), CEO of Anaconda Biomed. “Its performance in this study, which was designed with great clinical rigour, is a testament to the system’s potential to benefit physicians and patients.”
Nephrology Associates of Northern Illinois and Indiana (NANI), the largest nephrology group in the USA, is the first practice in Illinois to adopt the Ellipsys vascular access system (Avenu Medical, now part of Medtronic), a technology for patients with end-stage renal disease (ESRD) who require haemodialysis treatments.
In May 2020, interventional nephrologist Gautam Bhanushali first used the Ellipsys system to create an endovascular fistula at NANI Vascular’s Willow Springs Surgery Center in Justice, USA. He has completed nearly a dozen Ellipsys procedures to date, and NANI plans to implement the Ellipsys technology at its other five outpatient vascular access centres in the near future.
“It is a very safe procedure, and research shows that fistulas created with Ellipsys can be used for dialysis sooner than surgically-created ones and that they also work for much longer periods of time,” said Bhanushali. “Patients find this new process much more appealing. Not only are they coming in for a procedure that has a higher likelihood of success, but it requires only a single needle stick instead of surgery, so they walk out with just a band aid on their arm. Our goal is to make the lives of dialysis patients easier, and that is exactly what Ellipsys does.”
For NANI, the use of the Ellipsys System will be a key part of the practice’s participation in the Kidney Care First (KCF) model, part of the federal government’s Advancing American Kidney Care initiative, according to chief executive officer Brian O’Dea. The initiative is designed to improve kidney patient health and quality of life, a large part of which is having ESRD patients begin dialysis with fistulas instead of central venous catheters (CVCs).
“Having a well-informed patient start dialysis with a functional fistula, under the care of a nephrologist, is invaluable,” said O’Dea. “That is what is being incentivised under these programmes, and we are pleased that the Ellipsys technology helps us comply with their guidelines and make a difference for our patients.”
New single-centre clinical study data published in the Journal of Neuroradiology claims to support Anaconda Neurovascular Access (ANA) catheter system for the treatment of ischaemic stroke.
Investigators at Hospital Vall d’Hebron, Barcelona, Spain, are participating in the multi-center SOLONDA (“SOL”itaire in combination with the ANA Catheter system manufactured by Anac”ONDA”) clinical trial, a 125-patient, prospective study that will assess system safety and reperfusion measured using the modified treatment in cerebral infarction (mTICI) score.
Hospital Vall d’Hebron investigators followed 35 consecutive patients, with published results as follows:
The primary endpoint, defined as successful reperfusion (mTICI 2b-3) within three passes without rescue therapy, was achieved in 91.4% of patients, with a rate of complete reperfusion (mTICI 2c-3) of 65.7%
The rate of first-pass complete recanalisation (mTICI≥2c) was 42.9%
The rate of sudden recanalisation was 82.9%
The median number of ANA Catheter System passes was one
“The ANA device showed promising high rates of first-pass complete recanalisation,” Alejandro Tomasello (Hospital Vall d’Hebron, Barcelona, Spain), lead author and principal investigator of this study. “We hope that the device completes the regulatory process soon.”
According to a press release from the company, Anaconda’s investigational ANA catheter system consists of a funnel-shaped delivery and aspiration catheters to be used in combination with a stent retriever. When deployed, the funnel self-expands and directly conforms to the artery diameter up to 5mm. It is designed to locally restrict flow and allow full thrombus extraction without fragmentation. The SOLONDA study aims to validate earlier testing that achieved statistically significant improvement in revascularisation rates at both first and third pass.
“Vall D’Hebron’s early results are fulfilling our expectations for the safety and efficacy of the ANA System,” said Francois Salmon (Barcelona, Spain), CEO of Anaconda Biomed. “Its performance in this study, which was designed with great clinical rigour, is a testament to the system’s potential to benefit physicians and patients.”
Reflow Medical introduces the low-profile Spex LP 0.014 and 0.018-inch reinforced support catheters.
According to the company, the Spex LP is designed with a low-profile tip for accessing and crossing the “tightest and most complex lesions” with a supportive system. The customisable tip can be shaped to the desired angle and is compatible with the physician’s choice of guidewire and procedural technique. The device also features three radiopaque markers that enhance visibility on imaging. Additionally, the Spex LP can be combined with Reflow’s Spex 35 for more robust support, the company notes.
“Using the new Spex LP with the Spex 35 creates a telescoping action for extra support,” comments S Jay Mathews (Bradenton Cardiology Center, Bradenton, USA), one of the first physicians to use the Spex LP, in the company’s press release.
Jihad A Mustapha (Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, USA) adds: “The Spex LP has an extremely low lesion-entry profile and provides unmatched flexibility and trackability, especially in difficult cases.”
The US Food and Drug Administration (FDA) has granted premarket approval (PMA) for the Woven EndoBridge (WEB) 17 system from MicroVention, a US-based subsidiary of Terumo. This is a new addition to the WEB aneurysm embolization system for the treatment of intracranial wide-neck bifurcation aneurysms.
According to the company, the WEB 17 system is designed with microbraid technology, features a lower-profile delivery system compatible with the Via 17 microcatheter, and includes additional device configurations.
“The excellent clinical results we can achieve with intrasaccular flow disruption technology has changed the way we approach the treatment of wide-neck bifurcation aneurysms, and the WEB 17 system expands upon that,” comments Adam Arthur (Semmes Murphey Neurologic & Spine Institute and the University of Tennessee, Memphis, USA), principal investigator of the WEB-IT pivotal trial. “Now, we can deliver WEB devices using a low-profile system, similar to those used for standard coil embolization.”
In April 2019, Arthur et al published the final 12-month results of the WEB-IT trial in Journal of NeuroInterventional Surgery.
MicroVention stated that when placed inside the aneurysm sac, the WEB device’s microbraid technology bridges the aneurysm neck (disrupting blood flow) and creates a scaffold for long-lasting treatment. The WEB system received its first FDA approval in late 2018.
The WEB aneurysm embolization system is indicated for use at the middle cerebral artery bifurcation, internal carotid artery terminus, anterior communicating artery complex, or basilar artery apex for the endovascular treatment of adult patients with saccular, wide neck, bifurcation intracranial aneurysms with dome diameter from 3 to 10mm, and either neck size ≥4 mm or dome-to-neck ratio >1 and <2, advised MicroVention.
The UK Royal College of Radiologists (RCR) has partnered with the Apollo Radiology International (ARI) Academy to create a new exam centre in India.
The move means radiologists in India and surrounding countries will soon be able to sit RCR Fellowship (FRCR) exams locally, reducing travel and expense for candidates and with the aim of expanding RCR exam capacity across the region.
An RCR press release states that, as RCR Fellowship is “an internationally recognised benchmark of excellence”, there is high demand for FRCR exams in India. The press release also notes that RCR Fellowship status makes it easier for overseas doctors to register with the General Medical Council.
Currently, many Indian candidates travel to the UK or to centres in Hong Kong and Singapore to access the exam.
The new venue, which is currently being adapted and equipped with exam stations, is based in the south Indian city of Hyderabad.
Initially, it will host the Final FRCR Part B exam, before rolling out the First FRCR and Final FRCR Part A elements. Capacity will be subject to logistics and scaled up as the centre becomes established. However, the ARI Academy hopes to hold sittings for up to 150 candidates in future.
The RCR and ARI Academy had hoped to host the first Hyderabad exams in spring 2021; however, timelines are now under ongoing review due to the knock on impact of COVID-19 restrictions and logistical challenges.
Welcoming news of the joint agreement to launch the exam centre, RCR Overseas Ambassador for India Venkat Sudigali says: “It is a great initiative from the RCR to establish overseas exams centre in India.
“This exciting development will be of great benefit to many radiologists in India who are keen to attempt the FRCR exam to add to their qualifications, and also for those who potentially want to work in the UK in future, to learn new skills, and gain experience in the NHS.”
The new exam venue builds on recent collaborative work between the RCR and ARI, who worked with education and training partners in 2019 to create a scheme providing three-year placements for Indian radiologists looking to develop their skills working in the UK’s National Health Service (NHS).
Commenting on the Hyderabad exam venue, Sreenivasa Raju Kalidindi, ARI CEO and director of the ARI Academy, says: “It is a privilege to partner with the RCR in working towards a common vision of making FRCR exams more accessible and affordable to radiologists in India and other countries in this region.
“This initiative will set new benchmarks and empower large numbers of radiologists with the knowledge required to achieve higher standards in their practice.”
The RCR and ARI will release more information on the official launch of the centre and first exam bookings as soon as possible.
A trio of vascular experts including Raphaël Coscas (Paris, France), Alexandros Mallios (Paris, France) and Kate Steiner (Stevenage, UK) discuss the key findings of the IN.PACT™ AV Access trial–which was recently published in the New England Journal of Medicine (NEJM)–and what impact its data might have on patients and in clinical practice.
Mallios believes the data is “groundbreaking”, with all physicians agreeing that publication in the NEJM shows that it is a “high-quality” trial. The data itself highlighted a “significant” improvement in patency of the target lesion primary patency with the IN.PACT DCB compared to plain balloon angioplasty.
The experts further delve into what the findings mean for the quality of life of patients, and their own daily practices, with Coscas noting that the benefit of fewer reinterventions and hospitalisations is “huge”. Mallios adds that the data has shown improvement of the entire fistula, not just the primary patency, with the IN.PACT DCB which, for him, is “the most important and most relevant characteristic of this paper”. Concluding, Steiner notes that the IN.PACT AV Access data “adds weight” to the use of DCBs in her clinical practice.
There are several covered stents on the market that are used in an off-label setting as bridging stents for fenestrated and branched endovascular aneurysm repair (F/BEVAR). Currently, there is no consensus on when to use what—no gold standard, no proof, no evidence. According to three experts in the field, however, this is about to change. As trials take place and data begin to emerge, Vascular News speaks to Stéphan Haulon (Hôpital Marie Lannelongue, GHPSJ, Paris, France), Eric Verhoeven (Klinikum Nuremburg, Nuremberg Germany), and Tim Resch (Copenhagen Aortic Center, Rigshospitalet, Denmark), who express their views on the past, present, and future of bridging stents in FEVAR and BEVAR.
Considering the origins of bridging stents in these indications, Haulon explains that they have been used “for years”, but in an off-label sense. Nowadays, however, he relays that specific devices are being developed, and that trials are beginning to specifically evaluate bridging stents for FEVAR and BEVAR.
“I think it is important to stress that bridging stents for fenestrated endografts have different features to bridging stents for branched devices,” Haulon says. “The main difference is that we use bridging stents to connect the fenestration to the target vessel, but usually the fenestration is adjacent or close to the origin of the target vessel, so the bridging stent does not need to cross a large gap or a large aneurysm sac before going into the target vessel. In addition, it needs to be locked to the fenestration […] so there is a flaring process, whereas in branches, you have a long overlap between the bridging stent and the branch, and you have a long gap in most cases to bridge the aortic device to the target vessel,” he explains.
Resch elaborates: “In many cases of fenestrated repair for pathologies such as juxtarenal and pararenal aneurysms, where you have wall apposition of the main body of the device, the fenestrated or branched stent per se is not much for seal, but for direction, to keep patency in these vessels.”
“It means that [the] stent is much shorter and less subjected to difference forces, whereas oftentimes in a branch repair, you are actually traversing an aneurysmal space. It needs to create a whole different seal between the main body of the endograft and the target vessel and traverse a lot of space in between, so those stents are typically longer and need to display more varied properties. They have to be strong and flexible and to withstand forces of a different magnitude than bridging stents in fenestrated grafts,” he adds.
Within this context, Verhoeven highlights the fact that fenestrated and branched procedures require different types of stents. “In fenestrated grafts, or in grafts with fenestrations only, we use balloon-expandable covered stents that we can flare, while in branched grafts, we can use either self-expandable covered stents or balloon-expandable covered stents,” he states, adding that the next step in the branched setting is to have more flexible balloon-expandable covered stents to accommodate the angles between the branches and the target vessel.
Past: Expanding clinical goals and the changing role of industry
Historically, physicians did not have much choice about which stent to use, Verhoeven stresses. Resch echoes this lack of choice, recalling his experience from 15–20 years ago: “It was all about getting a graft in place, so we took whatever device we could regarding trackability and profile, and tried to get it in place.”
Nowadays, they emphasise that the aim is more focused on long-term outcomes. He explains: “Over the years, we have obtained more experience and data on what actually makes the device last, so our aim today is not just to get a device in place and get an aneurysm excluded, but to keep that aneurysm excluded over a long period of time.”
Regarding industry, Verhoeven notes that there used to be only a few companies who had the desire to develop these devices as it was a small market, but that this market has “continuously grown”.
Speaking on this changing role, Haulon remarks that, given the off-label use of these devices, the only way to get better was to combine experiences in order to try and find out which stent worked best in which indication, with little input from industry. “What is changing is that now industry is coming up with dedicated bridging stents and launching trials, so we will have real evidence,” he explains.
More specifically, Verhoeven details which devices he currently uses in his practice. “In fenestrations, we currently use the BeGraft [Bentley], which is a dedicated balloon-expandable covered stent for fenestrations, and we also use the Advanta V12/iCast [Getinge], which we have been using for years. We use both as the ‘new’ Begraft provides all the diameters and lengths we require. For branches, our first covered stent is the balloon-expandable BeGraft Plus [Bentley]. As a bailout with regard to length, we also use the VBX [Gore], because that is the only balloon-expandable covered stent that comes in a length of 79mm.”
Present: Crucially different demands of FEVAR and BEVAR highlight need for trials
The interviewed physicians are keen to stress the importance of differentiating between FEVAR and BEVAR. Recognising the unique demands of the two procedures is “crucial,” according to Resch. “There is still some confusion with regards to that in the marketplace and among users, which sometimes leads to disastrous outcomes,” he explains, using the example of BeGraft (for fenestrations) and the BeGraft Plus (for branches) as examples, stressing that they are “two totally different devices that we use for two totally different things”.
In his consideration of why the two are confused, Haulon underlines the need for data and dedicated stents: “I think the main reason is that we do not have approved bridging stents for the technology. They are being used off-label and that is why we urgently need specific trials.” He elaborates that Bentley is currently actively supporting both a FEVAR and a BEVAR physician-initiated trial with the BeGraft and the BeGraft PLUS as bridging stents that he hopes will bring the data needed to support which stents works well for which indication.
Future: The journey from off-label to on-label continues
Resch sees the gathering of data for these indications as part of an essential part of a wider project. “We have worked on main body stent graft development for many years, and it feels like the mating stents were left a bit behind, so we are very happy now that we are finally taking on the whole package, because the repair itself and its durability is really dependent on the whole graft,” he comments.
“It has been a very long journey,” Haulon adds, noting that it “felt bad” to be using stents off label for so many years. “There was a huge learning curve for everyone, and it was a niche for companies for many years,” he recalls, but adds that the need for data is evident.
“We are moving from pioneering times to a mature technology,” Haulon concluded.
In an effort to raise the profile of paediatric interventional radiology (PIR), CVIR Endovascular Editor-in-Chief Jim Reekers (Amsterdam UMC, Amsterdam, The Netherlands) has invited Alex Barnacle (Great Ormond Street Hospital, London, UK) and Anne Marie Cahill (The Children’s Hospital of Philadelphia, Philadelphia, USA) to guest edit the journal’s first thematic series on the topic.
Barnacle and Cahill commissioned four review articles, which they say “detail the latest evidence for a range of complex interventions in children, demonstrating current best practices in this highly specialised field”.
Musing in an editorial about the lessons learned from these articles, Barnacle and Cahill write: “These reviews illustrate that many of the latest advances in adult IR are applicable in children, despite the concerns of many adult IR practitioners that such interventions may be too risky or perhaps futile. Each paper, however, also highlights the frustrations common to every paediatric interventional radiologist. These include the limited evidence base available to date, the lack of paediatric-sized equipment, and the challenges of developing and maintaining IR competencies with small caseloads, often focussed in only a few specialised centres.”
Whilst they acknowledge these challenges to PIR, they also note that the specialty has come a long way since the early 1980s, when the first paediatric papers were published in the interventional radiology space. According to Barnacle and Cahill, the first PIR workforce survey in 2007 identified “just 110 PIRs practising worldwide, rising to 177 in a follow-up survey 10 years later”. However, in 2020, more than 600 delegates from 22 countries registered for the Society for Pediatric Interventional Radiology (SPIR) annual congress. The editorialists suggest that this is “in part due to the advantages of new online conference accessibility during the COVID-19 pandemic”, but that this “groundswell of interest may be influenced by increasing visibility of the speciality through the work of publications such as this [CVIR Endovascular] and organisations such as SPIR, but we believe it also speaks to a growing interest in a speciality that brings great rewards for those searching for greater meaning in their work. There is immense satisfaction in giving a family real hope for their child and providing care that often means accompanying a child throughout their journey to adulthood.”
They conclude their editorial with a call to action: “It is imperative that we strive to eliminate the inequality that means the vast majority of children even in developed countries are denied modern, minimally-invasive, safe, and highly effective IR procedures that are routinely offered to adults. Significant progress has been made in recent years by a small, highly dedicated PIR workforce, but there is still much more to be done.”
Interventional News spoke with Barnacle about the publication of the CVIR Endovascular guest editorial, to gain insights into the urgency and nature of future PIR work.
What is the significance of having the first CVIR Endovascular thematic series be dedicated to paediatric interventional radiology (PIR)?
This is a real honour for our sub-specialty. This series highlights the breadth and depth of PIR. We hope it will give readers cause to stop and think, and consider what they could perhaps apply in their practice.
What have been the pivotal developments in PIR research and clinical practice since its inception in the early 1980s?
Over time, we have shown that there is far more that is possible in small children than even we could have imagined. PIR has changed the management of a number of diseases and provided minimally invasive options for thousands of children who would otherwise not have been offered treatment or would have undergone far more invasive surgery.
What areas of PIR do you feel are particularly under-researched/ demand greater attention?
It is a real challenge to trial interventional oncology (IO) treatments in children because almost all patients are on protocols that do not include IO options. PIR is where adult IR was 20 or 30 years ago, only being given access to patients who have failed most other interventions. This means that the data are sketchy and our patient cohorts are skewed. In time, we hope to see the oncology organisations show greater confidence in the aims we are pursuing.
What are the biggest challenges to PIR currently, and how can these be overcome?
The biggest hurdle outside of North America is getting hospitals to recognise what PIR can do when it is a fully resourced service. Most centres are not aware of what we can deliver or the benefits we bring. We need more training schemes, more consultant posts, and the commitment to building PIR in several centres in each country, so that children everywhere have access to minimally-invasive, effective IR treatment options.
What message do you want to give to those considering a career in PIR?
PIR is such a rewarding career! Contact a PIR centre near you and ask to visit—you will be amazed by what our departments offer and may be inspired to join us in growing this speciality together.
You can read the full PIR series on CVIR Endovascular here.
Mermaid Medical Group recently announced US commercial availability of the D-Clot HD rotational thrombectomy system. As of 12 January, the company reports 25 successful human cases.
‘‘I am extremely pleased to see dialysis patients who are heavily involved with the healthcare system benefits from the release of D-Clot HD.’’ said Lars Vinther, CEO of Mermaid Medical Group.
A multicentre limited market release evaluation demonstrated the system’s ability to restore flow effectively and safely with no reported complications. The data derives from several institutions where numerous users applied the technology to patients and showed effectiveness across variations in vessel size, access type, and thrombus morphology.
“Today marks a major milestone for the company as we are transitioning to full commercialisation of the product in the USA,’’ stated Lars Vinther. The D-Clot HD will provide an added mechanical thrombectomy option for physicians involved in arteriovenous (AV) access flow restoration.
A recent study concludes that arterial diameter may influence arteriovenous fistula (AVF) aneurysm progression and the interval to surgical revision. “Patients with larger arterial diameters should be monitored closely and referred early after aneurysm development,” authors Alexis M Cahalane (Massachusetts General Hospital, Boston, USA) and colleagues write in an online article in The Journal of Vascular Access (JVA).
Another key finding from the study was that radiocephalic AVFs are more resistant to aneurysm development, and “should be considered the first access option for ESRD [end stage renal disease] patients, especially younger patients,” the authors communicate.
This study included all patients who underwent fistula surgical revisions due to aneurysms between 1 January 2014 and 30 July 2016. From this data pool, the investigators collected patients’ demographics and AVF dimensions based on fistulograms. They identified a control group with non-aneurysmal AVFs who had undergone serial fistulograms between 2013 and 2016.
In this retrospective study, Cahalane and colleagues identified 45 eligible patients in the AVF aneurysm group and 24 in the control group, with the mean age of AVF creation being older in the control group (61.8 vs. 53 years, p=0.03).
Writing in JVA, they report that the mean interval between AVF creation and first fistulogram in the study group was 1,464±282 days, compared to an interval of 263±101 days in the control group (p=0.003). Cahalane et al added that the arterial diameter on first fistulogram (r=0.6, p=0.03) predicted maximum aneurysm diameter on the last fistulogram (r=0.6,p=0.03) as well as the interval between first fistulogram and surgical revision (r=-0.33, p=0.03).
In the discussion of their findings, the authors list some limitations of the present study. They note, for example, that the study group contains only a small number of patients with heterogeneous distribution of AVFs in terms of laterality and location. They explain the reasons behind this: “The overall five-year survival rate for ESRD patients receiving haemodialysis was recently found to be 42%, and aneurysms are a late complication of access, with the average follow-up in our study being 1,324 days. Thus, a small number of patients met the study criteria.”
In this role, Hume will advance SIR’s advocacy, education and policy mission to strengthen and support the practice of interventional radiology and ensure patient access to minimally invasive, image-guided therapies, an SIR press release states.
“I am honoured to join SIR at this exciting time as interventional radiology continues to cement its status as a primary specialty and build a brighter future for patients through minimally invasive medicine,” comments Hume. “Today’s changing healthcare environment presents a variety of new opportunities. I look forward to working with SIR’s physician-volunteers, members, and staff to advance the interventional radiology specialty by transforming the way SIR educates its members and patients, fostering scientific research and innovation, and increasing cross-specialty collaboration.”
Hume previously served as SIR Foundation’s executive director from 2003–2008. He has nearly two decades of executive experience in the healthcare association sector driving strategic program development, regulatory advocacy, organisational growth, and creating sustaining strategic partnerships with healthcare stakeholders, the society state. Hume rejoins SIR following 13 years at the American Society of Plastic Surgeons and the Plastic Surgery Foundation.
“We are thrilled to welcome Keith Hume back to SIR,” says SIR president Michael D Dake (University of Arizona Health Sciences, Tucson, USA). “His understanding of interventional radiology, coupled with his passion for research, quality, and education, will take SIR to new heights as we look forward to transforming IR education, launching our new VIRTEX registry, and growing our research grants and quality improvement programs.”
Hume holds a Bachelor of Science degree from the College of William and Mary (Williamsburg, USA) and a Master of Arts degree, where he focused on autonomic and cardiovascular regulation from the University of Georgia (Athens, USA).
Students took the first fully-remote EBIR exams this week
The first fully remote, online-proctored European Board of Interventional Radiology (EBIR) examination took place on 13 January, 2021, with a 113 participants from 25 countries sitting the test.
EBIR is a voluntary supplemental examination designed to evaluate interventional radiologists’ clinical and technical knowledge, and was first released in 2010 in Valencia, Spain.
According to the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), by taking this examination, “interventional radiologists can certify their expertise and demonstrate their ongoing commitment to pursuing a career in this rapidly evolving discipline”.
“If you are thinking about taking the exam, the CIRSE Library offers hundreds of lectures ideally suited to EBIR preparation,” CIRSE shared on Twitter.
The next EBIR examination will take place on 3 March 2021, and will also be conducted remotely.
In addition to submitting their CV and filling out a competency checklist, applicants for the EBIR examination must also have completed national radiology training. The applicant and the responsible authority listed in the document are also required to confirm that two years of interventional radiology training have been completed or will be completed within a specific time frame. At least one year of this training must be completed after national radiology training.
Applicants must also verify that they have experience as the first operator, performing at least 250 interventional radiology procedures, 150 of which have to be interventions according to chapter 2.2.1 Vascular Diagnosis and Intervention and/or chapter 2.2.5.2 Vascular Interventional Oncology in the European Curriculum and Syllabus for Interventional Radiology.
Following the publication of the SWEDEPAD interim analysis, Andrew Farb, Misti Malone, and William H Maisel, representatives of the Center for Devices and Radiological Health, US Food and Drug Administration (FDA), have authored a perspective piece in the New England Journal of Medicine (NEJM), titled, “Drug-coated devices for peripheral arterial disease [PAD]”.
“Percutaneous revascularisation procedures can improve claudication symptoms, and devices coated with antiproliferative drugs (drug-coated balloons and stents) reduce neointimal proliferation after revascularisation procedures. Pivotal randomised, controlled trials (RCTs) of paclitaxel-coated devices [PCDs] in patients with femoropopliteal PAD reveal significantly reduced repeat-revascularisation rates as compared with use of uncoated devices. Reasonable assurance of device safety and effectiveness at one year has led the FDA to approve six PCDs to date, and their use has become common in symptomatic patients,” they write in NEJM.
“The results of the SWEDEPAD interim analysis provide important and reassuring information on PCDs used to treat femoropopliteal disease,” say Farb et al. “Furthermore, recent analyses of additional data from nonrandomised studies have not identified an increased mortality risk associated with PCDs.”
However, they also add that these newer analyses, “though comforting, are limited by the duration of follow-up”.
“Because of the demonstrated short-term benefits of the devices and the limitations of the available data, the FDA believes that clinical studies of these devices should continue and should collect long-term mortality data. Similarly, the FDA now routinely reviews longer-term data for PCDs for which market authorisation is being sought when they are intended to treat patients with PAD, and the agency requests that trials capture information on adjunctive antithrombotic therapy and medications indicated for patients with atherosclerosis,” they conclude.
VasQ external support (Laminate Medical Technologies)
VasQ, a high haemocompatibility biosynthetic vascular device from Laminate Medical Technologies, could be protective against the haemodynamic modifications that occur during arteriovenous fistulae (AVF) creation, a recent article in The Journal of Vascular Access reports. Roberto Palumbo (Saint Eugenio Hospital, Rome, Italy) and co-authors caution that their results, which derive from their clinical experience and are thus representative of a “real-life setting”, should be considered preliminary. They call for further research of the VasQ device in AVF creation, and say that “further effective treatments are needed to prevent or treat AVF failure”.
According to Palumbo et al, the VasQ device was designed “to improve the outcome of AVF [creation] by optimising the haemodynamics of the flow in the juxta-anastomotic region of the AVFs through tailored external support”. They continue: “The rationale for supporting the implantation of [the] VasQ device is based on the reduction of the turbulent blood flow through the anastomotic site and of the radial stretching of their venous wall, allowing a potential attenuation of hyperplasia and stenosis consequences and, finally, improving AVF-outcomes in haemodialysis patients.”
AVFs are the current gold standard for vascular access during the treatment of optimal chronic haemodialysis patients, due to their prolonged patency and durability, and thanks to their low complication profile. However, there is a high non-maturation rate of native fistulas. The study authors note that a prolonged maturation time, neointimal hyperplasia at the anastomotic site, and a high rate of abandonment are disadvantages associated with AVFs, and state that AVF creation “may cause significant haemodynamic modification in cardiovascular parameters”, potentially leading to adverse cardiac outcomes, such as progressive heart failure.
To establish if the use of the VasQ device would help reduce these haemodynamic modifications, the investigators compared patients who underwent native radio-cephalic AVF creation with and without implantation of the device at their institution between May and September 2019 (15 individuals in each group). Haemodynamic parameters were evaluated pre-operatively, and at one, three, and six months follow-up. The patency and complication rate were also evaluated.
At baseline, there was no significant difference between the treatment group and the control group in terms of mean preoperative arterial flow, vein diameter, preoperative ejection fraction, and cardiac output. Arterial diameter was greater in the treatment group (those where the VasQ device was deployed) at baseline (3.4±0.8mm vs. 2.8±0.5mm), but Palumbo and colleagues dismiss this, writing: “Although the vessel radius is considered a major determinant of the vessel flow, this finding may have reflected only marginally in the clinical results achieved in the VASQ device implanted [in] patients”.
While at one-month follow-up, there was no difference in mean arterial flow between the two cohorts, a significant difference was observed at three months (645±143mL/min in the VasQ group vs. 824±211mL/min in the control group; p=0.02) and six months (714±146mL/min vs. 810±194mL/min; p=0.05).
At six months follow-up, the cardiac output flow was lower in the cohort of patients implanted with the VasQ device: 4,458±928ml/min versus 5,599±1,355mL/min (p=0.05). Palumbo et al suggest that this could mean that the VasQ device “may provide a potential benefit in preventing haemodynamic modifications of the cardiovascular system and preventing the overload of the left ventricle by reducing the altered high cardiac output of haemodialysis patients associated with AVF creation”.
“Of note, no VasQ device complications were recorded,” the authors write. “The VasQ has been well tolerated by the patients, and no patient had poor subcutaneous tissues at the anastomotic site. During surgery, no technical complication occurred.”
At six months, primary patency was 73% in the treatment group and 80% in the control group, respectively. Cumulative patency was 80% and 86%, respectively, in implanted VasQ device patients compared to those in the control group.
“Although our experience is limited to a small group of patients with a relatively short follow-up”, Palumbo and colleagues write, “we confirmed the substantial safety and utility of [the] VasQ device in AVF creation. […] Our experience outlined that the implantation of [the] VasQ device during AVF creation compared to those [who underwent the] standard technique may allow a stabilisation of the high cardiac output of haemodialysis patients.”
Revisions to current procedural terminology (CPT) codes in the USA for 2021 overhaul the evaluation and management section, reducing documentation requirements and introducing new rules determining the level of coding. These changes will affect interventional radiologists and radiation oncologists more than they will impact the day-to-day work of diagnostic radiologists, according to Erin Stephens, a senior client manager in education at Healthcare Administrative Partners.
There are also several other non-evaluation and management code changes affecting interventional radiology for 2021.
Changes to the evaluation and management services section
Under the revised evaluation and management coding structure, physicians may elect to document a visit based either on time spent or on medical decision-making. Level 1 (99201) for new patients has been eliminated, leaving four levels of billing for new patients and five levels for established patients.
Until now, the level of coding has been determined by time spent face-to-face with the patient and by evaluating the three components of an exam:
The patient’s history,
The physical examination, and
The level of medical decision-making
The new system that begins in 2021 will be based only on the following:
The level of medical decision-making or
The total time involved in the service of the patient, including non-face-to-face activities performed by the physician.
For an established patient, a level 1 visit (CPT 99211) might not require a physician to be involved. This could be a nurse visit or blood pressure check. There is minimal medical decision-making and no prescribed time element.
Medicare has approved a new code, G2212, to be used for encounters that exceed the maximum time for a level 5 (99205/99215) visit. Its description is “Prolonged office or other outpatient evaluation and management services (beyond the total time of the primary procedure which has been selected using total time), requiring total time with or without direct patient contact beyond the usual service, on the date of the primary service; each 15 minutes.” This mirrors the language of CPT code 99417 that might be approved by payers other than Medicare.
Other changes: Lung biopsy
The code 32405, “Biopsy, lung or mediastinum, percutaneous needle,” has been replaced by a new code 32408, “Core needle biopsy, lung or mediastinum, percutaneous, including imaging guidance, when performed.” Accordingly, imaging guidance may no longer be billed separately. When more than one core needle biopsy of the lung or mediastinum is performed on separate lesions during the same session on the same day, then 32408 is billed once for each additional lesion along with modifier -59.
Ventricular assist device (VAD) insertion
The coding of these procedures was revised to differentiate between left- and right-heart procedures, encompassing either initial placement or replacement of a percutaneous VAD.
Other changes: Endovascular venous arterialisation
Coding has been available for endovascular revascularisation (37228-37231 and 0505T), but not for arterialisation. A new code (0620T) has been created as follows:
“Endovascular venous arterialisation, tibial or peroneal vein, with transcatheter placement of intravascular stent graft(s) and closure by any method, including:
Percutaneous or open vascular access,
Ultrasound guidance for vascular access when performed,
All catheterisation(s) and intraprocedural road-mapping and imaging guidance necessary to complete the intervention, and
All associated radiological supervision and interpretation, when performed.”
Other changes: Ultrasound ablation of pulmonary arteries
A new code (0632T) has been created as follows:
“Percutaneous transcatheter ultrasound ablation of nerves innervating the pulmonary arteries, including:
Senior authors Miltos Lazarides (left) and George Georgiadis (right)
A recent network meta-analysis shows that, in failing arteriovenous fistulas (AVFs) with outflow stenosis, drug-coated balloon (DCB) angioplasty is “significantly superior” to plain balloon angioplasty, presenting an improved six-month failure rate. However, Gregory Tripsianis (Democritus University, Alexandroupolis, Greece) and colleagues stress that the effectiveness of DCB angioplasty in the long term “deserves further investigation”.
While the 2018 European Society for Vascular Surgery (ESVS) vascular access clinical practice guidelines recommend balloon angioplasty for the treatment of venous outflow stenosis to extend the use of AVFs, the authors note that its effectiveness compared to other endovascular modalities “remains unclear”. In fact, they state more generally that “there is currently uncertainty regarding the ideal treatment to salvage failing AVFs”.
Writing in an online Journal of Vascular Surgery (JVS) article, Tripsianis et al note that it was their intention in this study to investigate the comparative effectiveness of the different endovascular treatments in patients with failing autogenous AVFs with outflow vein stenosis.
The investigators detail that they searched Medline/PubMed and SCOPUS databases for studies that fit the criteria of being randomised controlled trials (RCTs), compared endovascular treatments of autogenous AVF stenosis—including plain balloon angioplasty, cutting balloon angioplasty, and DCB angioplasty—and provided six-month and/or one-year patency data for each group at follow-up.
Inclusion criteria were venous outflow, anastomotic or swing area stenosis, either de novo or recurrent, and exclusion criteria were central vein stenosis or RCTs including open surgical repair or stent/stent graft arms.
Following the literature search, Tripsianis and colleagues performed a systematic review and network meta-analysis of RCTs investigating the effectiveness of plain balloon angioplasty, cutting balloon angioplasty, and DCB angioplasty in autogenous AVFs vein stenosis. They write that they included eleven RCTS in the study, reporting a total of 814 patients, of whom 395 underwent plain balloon angioplasty.
According to the authors, their network meta-analysis showed that DCB angioplasty at six months was “significantly more effective” than plain balloon angioplasty (odds ratio [OR]: 0.39, confidence intervals [CI]: 0.18–0.81) and ranked as the best treatment option, but without having statistically significant difference when compared with cutting balloon angioplasty (OR: 0.65, CI: 0.2–2.12).
Writing in JVS, the investigators also report that statistical significance was not achieved at one year among treatments, and that additional conventional pair-wise meta-analyses did not find significant differences at one year.
Tripsianis et al stress that the results of this review “should be interpreted with caution” due to some limitations. Firstly, they acknowledge that the network geometry did not provide any closed loops and write that “no direct comparison between DCB angioplasty and cutting balloon angioplasty existed, thus it was impossible to assess inconsistency between direct and indirect evidence”.
In addition, they note that there was “a considerable degree of heterogeneity” among the included RCTs and that confounding factors were present. They detail: “There was blending of various AVF configurations, de novo lesions with recurrent ones, high-pressure balloon use in a variable number, different brands of DCBs and paclitaxel dose, differences in patency reports (target lesion versus circuit patency), and difference in methodology of angioplasty regarding predilatation or post-dilatation following DCB angioplasty”.
Finally, they recognise that there was “a high risk of bias” among the included studies, especially those comparing plain balloon angioplasty with cutting balloon angioplasty. Tripsianis et al detail that most of the trials suffered from the “inherently high risk in the domain of blinding,” specifying that all but one of the included studies suffered from bias in blinding or personnel, as this is “almost impossible” in endovascular procedures. However, they note that there was some blinding of the outcome assessment in six studies.
Speaking to Vascular News, Miltos Lazarides (Democritus University, Alexandroupolis, Greece), one of the study’s senior authors, considered the present study in its wider context. He noted that a recently-published RCT had similar findings to those presented here. In the New England Journal of Medicine, Robert Lookstein (Ichan School of Medicine at Mount Sinai, New York, USA) et al found that DCB is superior to plain balloon angioplasty at six months, based on data from 330 patients.
Rapid Medical has announced its Drivewire novel guidewire with a steerable distal top, has received US Food and Drug Administration (FDA) clearance. According to a company press release, Drivewire is the first neurovascular guidewire with a controllable distal end that can change course and shape on-demand for more precise navigation.
Rapid Medical states that, with Drivewire, physicians control the direction and shape of the guidewire’s tip while it is inside the vessel, precisely navigating the neuro and peripheral vasculature. Rapid Medical add that this intravascular steering provides access to difficult anatomical locations, increasing the physician’s ability to treat vascular diseases with less invasive interventional approaches.
The press release states that guidewires are key components for treating intravascular diseases such as ischaemic and haemorrhagic strokes. Rapid Medical claims that currently physicians do not have direct control over the guidewire tip and often remove the guidewire several times to reshape it before reaching the desired location.
Erez Nossek, (NYU Langone, New York, USA), commented: “The development of Drivewire has been an exciting collaboration. I can now easily navigate through complex anatomies by varying the shape of the wire tip inside the vessel, something that cannot be performed with the current neurovascular guidewires.
“I expect this first-of-its-kind technology to benefit patients with challenging anatomies and increase the interventional treatment options available to them.”
The European Trainee Forum of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), the Residents, Fellows, and Students section of the Society of Interventional Radiology (SIR), the Society of African Interventional Radiology & Endovascular Therapy (SAFIRE), and Road2IR—a collaborative effort between several partner institutions aiming to build self-sustaining interventional radiology (IR) training programmes in East Africa—have published an open letter to the World Health Organisation (WHO) in CVIR Endovascular, calling for an increase in the efforts to understand the needs of low income countries regarding image-guided therapies.
In what participants hope marks “the beginning of a great collaboration between the WHO and the IR community”, several letter signatories first met with Adriana Velazquez Berumen, group lead for medical devices and in vitro diagnostics at WHO, online on 23 October to discuss IR and service development in low income countries. Interventional News understands that these remote conversations are ongoing, and that an online petition is in the pipeline “to continue raising awareness and increase the pressure on the WHO to do something about this [lack of IR provision in low-income countries]”.
First author of the CVIR Endovascular letter Yi Yang (Aventura Hospital and Medical Center, Aventura, USA) and colleagues say that the intent of the address is “to initiate a discussion on and collaboration in addressing the dramatic lack of interventional radiology services in low income countries and the lack of associated data”.
The letter is also approved and supported by Andrew Kesselman (RAD-AID International), Susan Jackson (Western Angiographic and Interventional Society), Kartik Ganga and Sreenivasa Raju (both Indian Society of Vascular and Interventional Radiology), Gerard Goh (Interventional Radiology Society of Australasia), Murray Asch and Kevin Shixiao He (Canadian Association for Interventional Radiology), and Karin Euler (Canadian African Health Care Alliance—Tanzania).
The authors write: “Prompt publication of countless dedicated research articles, public education through news outlets and social media on preventive measures, and initiation of vaccine development within weeks of the COVID-19 outbreak highlight the many benefits of global connectivity and collaboration. Yet, these times of fear and stress reveal the persistent chasm of racial inequality, healthcare inequity, and social injustice that have plagued humanity for centuries. These inequalities extend into almost every facet of medicine, but nowhere is the disparity more extreme than in minimally invasive treatment options available to patients in high-income countries and the near-complete lack thereof in most low- and middle-income countries (LMICs).
“[…] There are several hurdles to the implementation of IR in LMICs, including the sparsity of baseline data, limited access to equipment, and lack of training. In order to facilitate effective IR training and adequate supply of IR equipment, there is a critical need for improving and updating the ‘WHO Global Atlas of Medical Devices’.”
Gregory Makris
Speaking to Interventional News about the significance of a collaboration between the WHO and the IR community, immediate past chair of CIRSE’s European Trainee Forum and past chair of the British Society of Interventional Radiology (BSIR) trainee committee, Gregory Makris (Guy’s and St Thomas’ NHS Foundation Trust, London, UK), a senior author of the open letter, comments: “This letter is part of an effort to increase awareness around this very important issue. During the last five years there has been significant effort in increasing the presence of IR in Africa, but we now need more structured support to take these efforts to the next level. We have to make people understand that even standard life-saving procedures like a nephrostomy insertion or a drain of a liver abscess are currently not possible due to the luck of expertise and kit. The scale of the problem, as well as its significance, is massive, and that is why it is important to have a collaboration between international IR societies, the WHO, and the medical devices industry to address the various issues in lack of training, manpower, and supply chain/kit. We are planning to start an online petition within 2021 in order to reach even more people and get people interested in our cause. Introducing IR in Africa can have a major impact in raising health care standards given the multidisciplinary nature of our specialty. We hope for your support.”
Updating the WHO Global Atlas of Medical Devices
The WHO Global Atlas of Medical Devices, the most recent iteration of which was published in 2017, is a report presenting the global status of national medical device policies and the availability of medical device information, regulations, assessments, procurement, and donation guidelines, as well as the density of high cost medical equipment and guidance documents available at country level.
Its authors say that the aim of the publication is “to raise awareness and bring evidence of the indispensable safe and good use of appropriate, affordable, and quality medical devices in health care delivery to achieve better health outcomes”.
Data included in the WHO Global Atlas of Medical Devices come from a 2013 Baseline Country Survey on Medical Devices (to which 177 countries responded), a 2015 global health technology assessment survey (conducted by government or national institutes), and a 2016 study analysing medical devices regulatory frameworks. The information collected by the surveys and studies was then processed into a comprehensive database that includes statistical analyses of more than 100 aspects related to medical devices evaluated with respect to welfare indicators, such as World Bank income groups, health expenditure, Human Development Index and WHO regions.
However, signatories of the recent CVIR Endovascular letter point out that the WHO document does not assess several medical device and equipment categories “that are integral for diagnosis, treatment, and follow-up of patients by minimally invasive means”. Specifically, they request the following be included in future versions of the WHO Global Atlas of Medical Devices:
“1. Ultrasound: As a non-ionising imaging modality, ultrasound is the ideal first-line imaging tool in obstetrics, paediatrics, trauma triage, and is essential for breast cancer diagnosis, biopsy, and follow-up. Ultrasound is used in over 90% of IR procedures to guide percutaneous biopsies, vascular access, and drainage procedures.
“2. Fluoroscopy: As a dynamic, X-ray based, real-time imaging modality, fluoroscopy is the other most essential imaging tool used in IR. With fluoroscopy, interventional radiologists can navigate wires and catheters to almost any place in the body in order to perform embolizations in the setting of haemorrhage, limb salvage from peripheral arterial disease, extract clot in the setting of stroke or pulmonary emboli, and administer radio- and chemotherapy locally. These procedures are often life-saving and significantly less invasive than their surgical alternatives.
“3. Systems for Reviewing Imaging: Determining the availability of PACS (Picture Archiving and Communication System), EMR (Electronic Medical Record), and/or access to a viewing box or written medical records which are paramount for initial evaluation and follow-up of the patient’s medical history, management planning, and disease status over time.”
They expand: “The availability of these data measures will clarify the global distribution of diagnostic and therapeutic imaging and procedural devices. This will allow IR societies, academic institutions, researchers, educators, and non-governmental organisations to strategise and prioritise where and how to best extend and implement minimally-invasive life-saving procedures in LMICs. Additionally, these data will facilitate industry growth and partnerships within the unique context of the LMIC setting.
“We believe that increasing the robustness of the ‘WHO Global Atlas of Medical Devices’ will contribute to increasing access to minimally-invasive procedures in LMICs. We want to be actively involved in this process to support the efforts of the WHO in this matter. For example, as trainees, we can assist with facilitating coordination with consultants and suppliers and lead research efforts in evaluating and guiding implementation. We appreciate your efforts in leading equity in global health and look forward to moving forward in our collective commitment to providing all patients with the care that they need and deserve.”
Exercise can play an important role in treating peripheral arterial disease (PAD), a recent review from Amy Harwood (Centre for Sport and Exercise Life Sciences, Coventry University, Coventry, and the Faculty of Health Sciences, University of Hull, Hull, UK) et al, published in the British Medical Journal (BMJ) Open Sport and Exercise Medicine, shows. The review concluded that, for people with PAD, exercise programmes may help improve walking ability and quality of life by relieving symptoms of leg pain, cramps, and fatigue.
PAD affects 236 million people across the world. While some people with this disease experience no symptoms, approximately 30% experience pain, cramps, numbness, and intermittent claudication. Intermittent claudication is more common in adults over 50, men, and people who smoke.
Currently, PAD treatments focus on managing symptoms and preventing atherosclerotic narrowing of the arteries, which will also reduce the risk of heart disease and stroke. Medications may also be prescribed to reduce cholesterol or treat high blood pressure, which are both risk factors for developing PAD.
Managing intermittent claudication is especially important as people who have it are at a higher risk of other cardiovascular diseases, such as heart disease and stroke. On top of this, the leg pain they experience means people often cannot walk very far. This could lead to lower fitness levels and reduced quality of life. It may also cause depression, as people are no longer as independent as they would like to be in their daily life.
But exercise programmes may offer another treatment approach for people with intermittent claudication, Harwood and colleagues claim. Evidence from their latest review shows exercise can help increase the distance patients can walk pain-free, and may reduce the risk of heart disease and stroke. “We also uncovered what it takes for an exercise programme to be successful,” they write in a press release.
“We found that for people with intermittent claudication, a supervised, walking-based exercise programme is most likely to improve their symptoms. This programme should ideally be done at least three times per week for a minimum of three months. Patients should try to walk at a challenging pace (meaning it causes them to experience strong leg pain) for three to five minutes before resting until the pain goes away. The walk-rest pattern should be repeated for about 30 to 60 minutes.”
This type of exercise programme was shown to significantly improve claudication symptoms, as indicated by an increase in the distance a person can walk without pain. It also increases quality of life and overall fitness levels.
“Revascularisation or drug treatment options should only be considered in patients if exercise training provides insufficient symptomatic relief,” Harwood and co-authors conclude.
For those who cannot access a supervised walking programme, the authors say that exercise can still be done independently, and should also be carried out at least three times a week for 30 to 60 minutes each time. The reviewers recommend people start walking regularly for exercise at their own pace, building up their walking speed and time gradually. “Monitoring how far you walk with an app or smartwatch may be helpful,” they say.
The review also found that resistance exercise (such as lifting weights) can help to improve muscle strength in patients with intermittent claudication. Resistance exercises can be used alongside a walking programme and can be done two to three times per week with each session including exercises for the main muscles of the upper and lower body.
“It is worth noting that people with intermittent claudication should not worry about walking with leg pain, because this pain does not equate to harm being caused,” Harwood et al write. “Claudication pain is thought to be a result of insufficient blood flow to the exercising muscle. Walking while experiencing claudication pain could, over time, stimulate the growth of new blood vessels in the legs and improve symptoms.”
Patients are advised not to exercise if they feel unwell and to seek medical advice if they experience any concerning symptoms when they do exercise—such as chest pain, dizziness, or sickness.
“Our review shows exercise can help manage claudication pain, and may limit the progression of atherosclerotic disease throughout the body. Regular exercise may improve claudication pain in several ways, including improving the way blood vessels work and helping the leg muscles use oxygen more efficiently. Not only can this exercise be done alone or as part of a supervised programme, but it may also have other benefits, including improving cardiovascular health, mood, and sleep.”
The excimer laser sheath technique is safe and effective for removing embedded inferior vena cava (IVC) filters refractory to high-force retrieval, the investigators of a first-in-human escalation trial conclude in the Journal of the American Heart Association (JAHA). “This technique may allow cessation of filter-related anticoagulation and can be used to prevent and alleviate filter-related morbidity,” they write.
This is the largest study to date supporting a new indication for endovascular laser use to remove a variety of embedded IVC filters, regardless of implantation length.
Contextualising this research, lead author William T Kuo (Stanford University School of Medicine, Stanford, USA) and colleagues note that chronic indwelling IVC filters are associated with many potential risks, including non-thrombotic injury, thrombotic events, and the potential need for lifelong anticoagulation. While the US Food and Drug Administration (FDA) recommends that filters be promptly removed once the risk of acute pulmonary embolism has subsided, many filters remain chronically implanted and become refractory to standard retrieval methods. More advanced retrieval techniques (defined as any method other than standard snaring and sheathing) may be effective, but can induce major procedure-related complications due to the use of excessive force. This first-in-human study reports that these complications can be avoided with the use of the excimer laser sheath technique.
Over an 8.5-year period, 500 patients were prospectively enrolled into the study. There were 225 men and 275 women (mean age, 49 years; range, 15–90 years). Indications for retrieval included symptomatic acute inferior vena cava thrombosis, chronic inferior vena cava occlusion, and/or pain from filter penetration. Retrieval was also offered to prevent risks from prolonged implantation and potentially to eliminate the need for lifelong anticoagulation. In total, there were 140 physically symptomatic patients (28%; 140 of 500) with filter-related morbidity, 360 physically asymptomatic patients with filter-related anxiety (72%; 360 of 500), and 78 patients (16%; 78 of 500) receiving filter-related anticoagulation with no underlying thrombophilia.
After retrieval failed using standard retrieval force (6–7lb via digital gauge), treatment escalation was initiated by placing a laser sheath (Spectranetics) connected to a 308-nm XeCl excimer laser generator (CVX-300, Spectranetics), to attempt fibrotic tissue ablation. “We hypothesised that the laser-assisted technique would allow retrieval of more than 95% of embedded filters with less than 5% risk of major complications and with lower force,” Kuo et al put in their abstract.
The three primary study end points were: successful filter retrieval (complete filter detachment from the caval wall and removal from the body, excluding extravascular filter fragments) versus failure; presence versus absence of major procedure-related complications; and the difference in force applied to a patient’s filter both with and without laser assistance during attempted filter removal. Secondary end points were defined as follows: resolution of symptoms in patients with filter-related morbidity, resolution of filter-related anxiety, and further need for filter-related anticoagulation. The primary outcome was successful filter retrieval, and the primary safety outcome was any major procedure-related complication as defined by established guidelines.
Laser-assisted retrieval was successful in 99.4% (497 of 500; 95% CI, 98.3–99.9%). This was significantly higher than the 95% hypothesised by Kuo et al ahead of the study’s initiation (p<0.0001). Three cases that failed retrieval did so because of bulky calcified thrombus (refractory to thrombectomy) within cylindrical-shaped filter components, creating a volume that was too large to be captured within the bore of the existing laser sheath apparatus, the authors explain.
The mean filter dwell time was 1,528 days (4.2 years; range, 37–10,047 days [>27.5 years]), and the median dwell time was 569 days (interquartile range, 260–2,348 days). Successful filter retrieval alleviated filter-related morbidity in 98.5% of cases (138 of 140; 95% CI, 96.5–100%) and allowed cessation of anticoagulation in 98.7% of cases (77 of 78; 95% CI, 93.1–100.0%).
Furthermore, the major complication rate was low: 2% (in 10 of 500 patients; 95% CI, 1–3.6%), with only 0.6% complications from laser. This is significantly less than the 5% threshold (p<0.0005). All complications were successfully treated with either medical management and/or percutaneous endovascular therapy without the need for open surgery.
Discussing the ten complications observed over the study period, Kuo et al say: “As a specialised centre that accepts complex filter cases, our patients were often referred after failed retrieval attempts or when other centres refused to attempt filter removal because of high procedural risks. Indeed, we noted increased variety and complexity of cases encountered throughout the study period. We believe this helps to explain why 10 different combinations of major complications and causes were encountered without duplication. For instance, we accepted cases involving severe filter fractures and penetrations that increased the risk of injury to the IVC and/or adjacent arteries during filter removal. In attempting these cases, we learned that severe filter fractures may lead to asymmetric lasing of fibrous tissue along the vessel wall causing major venous haemorrhage. We also learned that filter components may penetrate through the cava and into adjacent arteries predisposing to organ infarction, major arterial haemorrhage, and arteriovenous fistula formation during filter removal.”
In addition to perhaps seeing more complex cases, another consequence of conducting this study at a single centre specialised in advanced filter removal is that “It is unclear whether the overall safety and efficacy of removing embedded filters as described here [in JAHA] would translate into similar outcomes when performed elsewhere,” as the authors put it. They list this as a limitation of the study, alongside the fact that, although all patients with anxiety reported relief of this symptom, the investigators did not obtain formal psychiatric evaluations or use scoring systems to quantify their anxiety relief post procedure.
Kuo et al also call for a cost analysis study, musing that, although the laser sheath apparatus carries additional device cost, successful filter removal in a single session may decrease overall expense by eliminating the high cost of multiple failed procedures routinely observed before successful laser retrieval.
The laser sheath apparatus is currently not FDA-approved for IVC filter removal; this is an experimental protocol—albeit one that has now been validated in a large cohort of patients.
Corindus has announced today global launch of a new set of automated robotic movements in the technIQ Series designed for the CorPath GRX system. The company received 510(k) clearance from the US Food and Drug Administration (FDA) for new software automation that provides predictable and consistent movements to aid in advanced device manipulation during complex coronary and peripheral procedures.
Jean Fajadet, the co-director of interventional cardiology at Clinique Pasteur, Toulouse, France, performed the first-in-human coronary procedures using the new automated movements, which replicate manual techniques of interventionalists. The procedures demonstrated how the new movements can help to reduce procedure time associated with wire and device manipulation and drive standardisation in quality of care by offering advanced techniques to all physicians.
“This new software algorithm gives the operator new possibilities to advance and facilitate treatment, especially with complex lesions,” said Fajadet. “I am pleased with the success of using the automated moves and am honored to play a role in the advancement of robotic technology that will make interventional procedures more efficient and safer for our patients.”
In 2018, Corindus received CE mark and FDA clearance for an automated technique called Rotate on Retract (RoR). RoR was the first automated robotic movement in the technIQ Series and has demonstrated the potential to significantly reduce wiring time. The latest global introduction and FDA clearance for the technIQ Series provides physicians with four additional automated robotic movements that aid with complex tasks such as crossing lesions, navigating tortuosity, and precisely measuring the anatomy for appropriate device size selection.
“The new technIQ movements mark the next phase in the evolution of robotic-assisted intervention and a vital step toward the advancement of our technology,” said Wayne Markowitz, executive vice president and head of Corindus. “Automating more movements used in cardiovascular intervention will allow physicians to focus their attention on overall case strategy while equipping them with advanced techniques for navigating the vasculature.”
Corindus is a Siemens Healthineers company, following a merger in 2019.
Compared with doxorubicin-loaded drug-eluting embolic transarterial chemoembolization (DEE-TACE), conventional transarterial chemoembolization (cTACE) yielded a higher number of quality-adjusted life years (QALY) at a lower cost, making it the more cost-effective of the two modalities. This is the conclusion reached by a cost-effectiveness analysis published in the Journal of Vascular and Interventional Radiology(JVIR) by Xiao Wu (Yale School of Medicine, New Haven, USA), senior author Nishita Kothary (Stanford University Medical Center, Stanford, USA), and colleagues.
The investigators set out to compare the cost-effectiveness of DEE-TACE versus that of cTACE for patients with unresectable hepatocellular carcinoma (HCC).
They constructed a decision-analysis model that spanned a payer’s entire life; the model simulated the clinical course, including periprocedural complications, additional transarterial chemoembolization or other treatments (ablation, radioembolization, or systemic treatment), palliative care, and death, of patients with unresectable HCC. Describing their methodology, Wu et al explain: “All clinical parameters were derived from the literature. Base case calculations, probabilistic sensitivity analyses, and multiple two-way sensitivity analyses were performed.”
Conventional TACE yielded a health benefit of 2.11 QALYs at a cost of US$125,324, whereas DEE-TACE yielded 1.71 QALYs for US$144,816. In 10,000 Monte Carlo simulations, a mathematical technique used to estimate outcomes of an event, cTACE continued to be a more cost-effective strategy.
The authors report that cTACE was cost-effective when the complication risks for both the procedures were simultaneously varied from 0–30%. DEE-TACE became cost-effective if the cTACE mortality exceeded that of DEE-TACE by 17% in absolute values. The two-way sensitivity analyses demonstrated that cTACE was cost-effective until the risk of disease progression was >0.4% of that for DEE-TACE in absolute values.
“Our analysis showed that DEE-TACE would be more cost-effective if it offered >2.5% higher overall survival benefit than cTACE in absolute values,” Wu and colleagues summarise.
Replying to this journal article as posted on Twitter, Aaron Maxwell (The Warren Alpert Medical School of Brown University, Providence, USA) asked: “If cost effectiveness is being discussed, why not bland embolization alone? No chemotherapy to pay for, and RCT [randomised controlled trial] data with equivalent outcomes to TACE from 2016.”
Co-author Julius Chapiro
Responding, study co-author Julius Chapiro (also Yale School of Medicine, New Haven, USA) wrote on Twitter: “Excellent point! While there is some doubt as to the standard of care for the control arm in the JCO paper (DEB-protocol), I am not at all convinced that chemo adds value to beads. Our experimental studies prove the point, too. We must really think about it in depth.”
He posted a figure from a previous JVIR paper authored by the same team, writing: “Even with smaller calibre beads, the drug (heat map) barely covers the entire tumour. Primarily embolic effect. I will say that my journey so far has really made me doubt the value of chemo.
“We now need to understand the immunological effect of the different materials we introduce and how they may or may not affect the tumour microenvironment and immune response (especially + checkpoint inhibitors). I do not see clear striking evidence for DEBs re outcome. None.”
This prompted Maxwell to reply: “Terrific work. I think it is incumbent upon the IR [interventional radiology] research community to aggressively expand our understanding of the tumour microenvironment if we are to optimise outcomes for catheter-directed locoregional liver therapies.”
Chapiro agreed, exclaiming: “We simply have to aggressively expand our science and transform our therapies to be directed to and tailored for the individual tumour microenvironment!”
Speaking directly to Interventional News, Kothary added: “Data on bland embolization are limited, precluding a robust carcinoembryonic antigen (CEA) test. “DEE-TACE is also associated with a higher need for pain control due to its true embolic nature (I would guess that bland embolization is similar), and pain control often requires overnight hospitalisation that would impact a CEA.”
Guerbet has been granted approval for an indication extension in the UK, where Lipiodol Ultra Fluid is the only oil-based contrast medium indicated for hysterosalpingography (HSG) in women undergoing infertility workup. New clinical evidence showing that an HSG with Lipiodol Ultra Fluid enhances pregnancy rates has been recognised by the UK’s Medicines and Healthcare products Regulatory Authority (MHRA). MHRA’s endorsement of evidence-based clinical practice confirms the benefit of Lipiodol Ultra Fluid in fertility management, a Guerbet press release claims.
One in seven couples face fertility issues in the UK. The fertility workup, during which HSG is performed, is a key step in patient care management.
The technique involves the slow infusion of Lipiodol Ultra Fluid into the uterus, using X-ray monitoring to assess the uterine cavity and tubes.
More importantly, women who underwent an HSG with Lipiodol Ultra Fluid had enhanced pregnancy outcomes:
In a single centre randomised trial: in a group of women with unexplained infertility or endometriosis who received Lipiodol Ultra Fluid (n=73), twice as many became pregnant within six months compared to women who did not benefit from the procedure (n=85). The pregnancy rate was 38.4% and 16.5% respectively (p=0.002).
In a multicentre randomised trial: in a group of women who underwent an HSG with Lipiodol Ultra Fluid (n=554), 37% more became pregnant within six months compared to women who received an HSG with a water-based contrast medium (n=554). The pregnancy rate was 39.7% and 29.1%, respectively (rate ratio (RR): 1.37 [1.16; 1.61]; p<0.001).
In a meta-analysis of randomised controlled trials: in a group of women who underwent an HSG with Lipiodol Ultra Fluid, 42% more became pregnant within six months compared to women who received a water-based contrast medium. The overall odds ratio (OR) for pregnancy was significantly in favour of HSG with Lipiodol Ultra Fluid: odds ratio of 1.42 [1.10; 1.85] when compared to HSG with a water-based contrast medium (six studies, n=2,598).
“This is great news for UK patients experiencing difficulties conceiving, as it brings them additional hope by enhancing their chances of falling pregnant at an early stage of their fertility journey. As with any procedure, patients should be aware of any associated risks,” says Gwenda Burns, chief executive of Fertility Network UK.
“Our clinical experience of Lipiodol Ultra Fluid has showed us that its use is similar to water-based contrast media and does not alter the patient experience during the exam. However, it is noteworthy that long term follow-up studies showed that performing an HSG with Lipiodol Ultra Fluid reduces the median time to pregnancy by around four months, as compared to an HSG with the reference contrast media,” comments Colin Duncan (Royal Infirmary Edinburgh, Edinburgh, UK; chair of the Society for Reproduction and Fertility).
“At Imperial College Healthcare NHS Trust, we have performed more than 10,000 HSGs over the last few decades. The evidence-based results from the H2Oil study encouraged our HSG and fertility teams to use Lipiodol Ultra Fluid for HSG in selected patients. After several months of use, we can confirm that an HSG with Lipiodol Ultra Fluid is an exciting and valuable technique in the management of patients being investigated for fertility issues in our centre. Our teams at Imperial College Healthcare NHS Trust will soon to be involved as investigators in on-going randomised controlled clinical trials evaluating the performance of Lipiodol Ultra Fluid for HSG in extended populations undergoing fertility workup,” adds Anne Hemingway (Imperial College Healthcare NHS Trust, London, UK).
The UK is the sixth European country to grant approval for HSG in women undergoing infertility workup after Ireland, Hungary, The Netherlands, the Czech Republic, and Denmark. Lipiodol Ultra Fluid is also currently approved for HSG in ten additional countries (the USA, including Puerto Rico, Canada, Argentina, Turkey, South Africa, Japan, Taiwan, Thailand, Australia and New Zealand).
In 2016, the Guerbet Group launched its Women’s Health franchise with the ambition to improve the quality of infertility management and breast cancer surgery.
“Not everything that is published is true or important” and “always be critical, but not cynical,” urges Jim Reekers, editor-in-chief of CVIR Endovascular, as he talks about filters that operate in the world of scientific and medical publishing that favour the publication and spread of positive news. He particularly warns against the “silent and very dangerous” trend of unscrutinised, non-peer reviewed papers that are presented as pre-prints with a Digital Object Identifier (DOI) number, enabling the creation of a parallel publishing universe.
“Nobody knows what the truth is anymore, and I think that this the biggest threat to medical science,” he states.
Mårten Falkenberg (left) and Joakim Nordanstig (right)
Mårten Falkenberg (left) and Joakim Nordanstig (right)
An unplanned interim analysis of the registry-based SWEDEPAD clinical trial, in which patients with peripheral arterial disease received treatment with paclitaxel-coated (drug-coated balloons or drug-eluting stents) or uncoated endovascular devices, “did not show a difference between the groups in the incidence of death” during one to four years of follow-up. This conclusion was published today by Mårten Falkenberg, Joakim Nordanstig (Gothenburg University, Gothenburg, Sweden) and colleagues in the New England Journal of Medicine (NEJM).
Falkenberg et al conducted the analysis against a backdrop of “concern about an increased risk of death associated with the use of paclitaxel-coated angioplasty balloons and stents in lower-limb endovascular interventions for symptomatic peripheral arterial disease”. They relay that data for the analysis was from the multicentre, randomised, open-label, registry-based SWEDEPAD (Swedish drug elution trial in peripheral arterial disease) clinical trial.
At the time of their analysis, the authors detail, 2,289 patients had been randomly assigned to treatment with either drug-coated devices (the drug-coated device group, 1,149 patients) or treatment with uncoated devices (the uncoated device group, 1,140). They state that paclitaxel was used as the coating agent for all the drug-coated devices.
Falkenberg et al detail that randomisation was stratified according to disease severity on the basis of whether patients had chronic limb-threatening ischaemia (1,480 patients) or intermittent claudication (809 patients), and that the single endpoint for this interim analysis was all-cause mortality.
Writing in NEJM, the authors communicate that no patients were lost in the mean 2.49-year follow-up period, during which 574 patients died, including 293 patients (25.5%) in the drug-coated device group and 281 patients (24.6%) in the uncoated device group (hazard ratio, 1.06; 95% confidence interval, 0.92–1.22).
At one year, Falkenberg and colleagues write that all-cause mortality was 10.2% (117 patients) in the drug-coated device group and 9.9% (113 patients) in the uncoated device group. During the entire follow-up period, they found that there was “no significant difference in the incidence of death between the treatment groups” among patients with chronic limb-threatening ischaemia (33.4% [249 patients] in the drug-coated device group and 33.1% [243 patients] in the uncoated device group) or among those with intermittent claudication (10.9% [44 patients] and 9.4% [38 patients], respectively).
In the discussion of their findings, the authors acknowledge that this interim analysis “was not a prespecified part of the trial protocol”. They respond to this limitation by noting a twofold rationale behind publishing these total mortality data ahead of completion of the trial: “First, we sought to reduce patients’ and physicians’ concerns regarding the safety of paclitaxel-coated devices, and second, we considered the data to be important to support completion of ongoing trials investigating the efficacy of such devices in peripheral arterial disease.” They add that this analysis was recommended by an independent data and safety monitoring committee “in order to alleviate patients’ and physicians’ concerns” surrounding paclitaxel safety.
Falkenberg and colleagues recognise a number of other limitations to their unplanned interim analysis, including the fact that the open-label design “could have the potential to introduce bias”. However, they point out that the endpoint of all-cause mortality used “is less sensitive to this particular limitation than more subjective outcomes”.
Another drawback the authors recognise relates to the fact that there were few deaths among patients with intermittent claudication, resulting in the confidence interval for that particular group of patients being wide (ranging from 0.72 to 1.93). As a result of this, the investigators write that they “cannot completely exclude the possibility of a difference in mortality in this subgroup”.
Falkenberg et al identify the use of ‘low-dose’ (rather than ‘high-dose’) paclitaxel-coated devices being “relatively common” in the trial as another limitation, which “may have influenced” their results.
In addition, they note that there was variation in the treatment effect among centres, although they write that it “seems likely that this variation is due to chance rather than to variation in centre characteristics”.
Finally, they highlight that no analysis of the efficacy of paclitaxel-coated devices is included in this interim report. They write: “These data are planned to be provided in the final clinical trial report after formal completion of the trial”.
At the end of their discussion, Falkenberg and colleagues stress that the SWEDEPAD trial “was not primarily intended for analysis of total mortality,” pointing out that the main purpose was “to determine whether drug-coating technology ultimately improves the lives of patients with symptomatic peripheral arterial disease by preventing amputation and improving health-related quality of life”.
Because this interim analysis “does not show a significantly higher incidence of death resulting from the use of paclitaxel-coated devices,” the authors conclude with their belief that “equipoise remains,” detailing that recruitment has been resumed with enrolment of patients in both the chronic limb-threatening ischaemia cohort and the intermittent claudication cohort.
The authors write that the trial is funded by grants from the Swedish Research Council, the Swedish Heart-Lung Foundation, and Region Västra Götaland. They also communicate that “all the companies that provide drug-coated balloons and drug-coated stents for patients in Sweden with peripheral arterial disease are supporting the trial by providing price discounts on their devices”.
Sirtex Medical (Sirtex) has announced a strategic investment in BlackSwan Vascular (BlackSwan), a private company developing therapies in endovascular embolization. The investment provides resources for further development of BlackSwan Lava, a liquid embolic system specifically tailored for peripheral vascular target indications.
According to Sirtex, Lava has the potential to be the first liquid embolic for peripheral vascular applications to receive approval in the USA. Its key differentiators, which include optimised radiopacity, availability in two viscosities, reduced preparation time and controlled delivery, can enable treatment of a wide array of peripheral vascular diseases, a press release reads.
“Our investment in BlackSwan marks an important step in Sirtex’s commitment to expand product offerings to the endovascular field and to interventionalists addressing unmet medical needs,” said Mark A Turco, global chief medical officer and executive vice president, research and development of Sirtex. “We look forward to partnering with BlackSwan on its clinical journey and future opportunities to innovate patient care worldwide.”
Under the collaboration, Sirtex made a significant equity investment in exchange for preferred shares in BlackSwan as well as an option to purchase the remaining shares of the company at an agreed price. In addition, Sirtex will appoint an observer member to the Board of Directors.
“We strive to provide the interventional community with the tools they need that drive safe, effective and value-based treatments,” said Suresh Pai, CEO of BlackSwan. “We are excited to partner with Sirtex, a leader in targeted oncology, as an investor and collaborator as we advance our clinical programme and bring much-needed therapy options to patients.”
Hypercoagulability in COVID-19 patients leads to an increase in the malfunction rate of temporary haemodialysis catheters—but heparin locking of the catheters is linked to decreased malfunction rates.
The research sought to address the subset of COVID-19 patients with acute kidney injury who require haemodialysis. With temporary catheters being the mainstay in their treatment and up to 96% of COVID-19 patients experiencing dialysis circuit clotting, the investigators identified a “paucity” of data and guidelines to address the problem.
John J Kanitra, MD (Ascension St John Hospital, Detroit, USA) and colleagues carried out a retrospective cohort study via chart review at their institution—a large urban hospital. The study included patients who needed a temporary catheter placed between 1 February and 30 April, with follow-up for outcomes continued between 1 May 12 May.
A total of 48 patients with a mortality rate of 71% were identified. Malfunction occurred in 31.3% of patients. Thirty-seven patients (77.1%) received heparin locking, 22 (45.8%) received systemic anticoagulation and 38 (79.1%) received venous thromboembolism prophylaxis. The overall rate of malfunction was lower at a trend level of significance with heparin versus saline locking (24.3% vs. 54.6%; p=0.058), Kanitra at al found.
Meanwhile, systemic anticoagulation did not affect temporary catheter malfunction rate (p=0.240). Higher D-dimer levels were related to greater mortality (hazard ratio [HR] 3.28, 95% confidence interval [CI] 1.16–9.28; p=0.025), but were not significantly associated with temporary catheter malfunction (HR 1.79, 95% CI 0.42–7.71; p=0.434).
“The high malfunction rate is likely a result of the hypercoagulability that has been suggested in COVID-19 patients,” the authors write. “Reports describe COVID-19 patients without predisposing factors developing thromboembolic events. The aetiology of this is thought to be endothelial damage driven by the cytokine storm, leading to excess thrombin formation in addition to increased blood viscosity from hypoxaemia.”
The authors noted the need for prospective, randomised studies in order to confirm their findings—chiefly so that locking the temporary catheters with heparin in COVID-19 patients can be recommended. “Increased [venous thromboembolism] prophylaxis suggested a possible association with improved [temporary haemodialysis catheter] patency, though the comparison lacked sufficient statistical power,” they write. “Additionally, the current study found an 71% mortality rate in COVID-19 patients requiring acute haemodialysis, which has important implications for planning and resource delegation for future coronaviral infections.”
Felipe Nasser (São Paulo, Brazil) talks to Interventional News about his experience of the COVID-19 pandemic after contracting the SARS-CoV-2 virus himself, saying that the infection and period of isolation “made me think a lot about my life.” “We are now prepared” and “know how to face a situation like this” in the future, he says, speaking of the capabilities and competencies of his own institution, as well as that of the global medical community as a whole, to responding to public health crises of this scale.
Nasser explains that the rise of the virus has led to a reduction in the number of patients being treated in the oncology department of the São Paulo hospital where he works. “We replaced our normal work with COVID-19 patients”, he says, adding that he has not just been treating oncology patients, but also those with vascular disease.
He goes on to highlight some of the practical modifications his institution has adopted, including the use of an N95 respirator when treating any patient, the separation of catheter labs—there is a specific cathether lab dedicated to COVID-19 patients —and the use of a negative pressure air filtration system. Physicians also now use impermeable scrubs and face shields, and the number of physicians in the room at any one time has been reduced to just one physician and one Fellow.
B Braun has revealed that 12-month results from the LOCOMOTIVE EXTENDED study of the company’s Multi-Loc multiple stent delivery system have been published in Vasa: European Journal of Medicine. The study authors, Klaus Amendt (Diakonissenkrankenhaus Mannheim, Mannheim, Germany) and colleagues conclude that the Multi-Loc “provides promising results concerning target lesions revascularisation and primary patency at 12 months”.
They add that use of the Multi-Loc stent system is both safe and effective for provisional repair of flow-limiting dissections or recoil following plain balloon angioplasty and drug-coated balloon angioplasty of the femoropopliteal artery.
The LOCOMOTIVE EXTENDED (Multi-Loc for flow-limiting outcomes after plain old balloon angioplasty and/or drug-coated balloon treatment in the infrainguinal position with the objective to implant multiple stent segments) study is a prospective, single-arm, multicentre observational study, in which B Braun’s Multi-Loc multiple stent delivery system was used for provisional stenting of the femoropopliteal artery.
Amendt et al enrolled 357 patients with 449 femoropopliteal lesions and a mean age of 71±10 years. The mean lesion length was 16±9.7cm; 44.5% of which were TASC II C/D lesions and 31.4% were chronic total occlusions.
At six and 12 months, the authors report that freedom from clinically-driven target lesion revascularisation was 95.5% and 88.7% and the primary patency rates were 88.7% and 82.3%, respectively.
At 12 months, significant improvements were noted in Rutherford categories and ankle-brachial indices, and in multiple regression analyses, both diabetes mellitus and no distal run-off vessel showed a trend toward worse target lesion revascularisation, while other factors such as drug-coated balloon predilection or the lesion length were not predictive.
Considering future research, Amendt and colleagues write: “Randomised controlled trials are needed to compare the focal stenting strategy to conventional interventions with long stents. Possibly, the efficacy of spot stenting could be further increased by combining it with additional preparation techniques, such as vessel scoring or debulking.”
The European Conference on Interventional Oncology (ECIO) will be held as an online-only event in 2021, and will take place 10–13 April.
Writing to potential attendees, ECIO scientific programme committee (SPC) chairperson Alban Denys and ECIO SPC deputy chairperson Philippe L Pereira write:
“Dear colleagues,
“As 2020 comes to an end, we are hopeful that the promising vaccines developed by various manufacturers will soon provide relief from the pandemic. However, it will take a while until things return to normal and we will once again be able to travel and attend in-person meetings.
“This is why the ECIO leadership has decided to hold ECIO as an online congress from Saturday to Wednesday April 10–13, providing the same high-quality sessions and global platform for research exchange you have all come to expect of our annual meeting in a reliable and safe way.
“The scientific programme committee has been working diligently to create an expansive programme covering the entirety of the interventional oncology spectrum in a convenient, interactive format. Topics will range from clinical subjects and well-established therapies all the way to experimental approaches and the latest study results.”
Pua Uei (Singapore) talks to Interventional News about how Singapore’s interventional radiologists (IRs) in Tan Tock Seng Hospital and National Centre for Infectious Disease (NCID) dealt with the ongoing COVID-19 crisis. Singapore was one of the first countries to register a case outside of China, notes Uei, who adds that as the NCID had previously been on the frontline of the 2003 Severe Acute Respiratory Syndrome (SARS) virus, “preparing for outbreaks was nothing really new to us”.
The “challenge for interventional radiology”, says Uei, was community spread of the virus, which meant that it was no longer possible to effectively identify and segregate COVID-positive and COVID-negative patients. “From past experiences with SARS, it is vital to put a mask on any patient undergoing a procedure to reduce the risk of unprotected contact”, Uei states, adding that such a move was made in Singapore “before masks were made mandatory”.
The second thing that “threw a spanner in the works” early on in the pandemic, as medical facilities were preparing their response to the viral threat, was the existence of asymptomatic spreaders. “We have had to be very responsive,” Uei reflects. “Every time we learn something new about the virus, we have to react to it and put in measures to protect patients”.
He outlines how vital resources were managed: “The moment we knew it was coming, we had stoppages of leave and vacation, and we cancelled academic teaching. As a result there was more manpower than ever. “We were very judicious with regards to the preservation of personal protective equipment (PPE) due to the global supply chain disruption; we had rules on how long you could use a surgical mask and how many times you should reuse an N95 (respirator).”
Uei also touches on the mental health toll caused by the COVID-19 public health crisis, and the fatigue felt by healthcare workers on the frontline. He notes that it is important that experienced physicians, such as those who worked through the SARS epidemic, help provide perspective and support to their more junior colleagues.
Upper row: A large aneurysm with a relatively short neck, treated with a supra renal fixation stent graft with good sealing results. Lower row: An irregular and non-uniform aneurysm neck, but of a good length, which was was treated effectively with an infra renal fixation stent graft.
Mo Hamady discusses developments in aortic stent grafts in recent years, and offers a contemplation on the complications associated with endovascular aneurysm repair (EVAR). Despite advances in stent graft technology, operator knowledge, and physician experience in recent years, he writes that the overall long-term survival remains stable, prompting him to encourage interventional radiologists and vascular surgeons toconsider the most durable and cost-effective intervention and modality when selecting patients for aortic aneurysm repair.
Aortic stent grafts have been through significant developments over the years in terms of mechanical features and material properties.
These changes have refined the performance of stent grafts such as global deformation, profile, navigability, and conformability. The biggest leap in technology was demonstrated mainly between the first- and second-generation grafts.
Have technological changes influenced clinical outcome?
A large retrospective study, published in the Journal of Endovascular Therapy (JEVT) in 2014, comparing the outcomes of old versus new generation stent grafts, showed lower reintervention rates at five and seven years; 86.6% and 83.6% versus 80.3% and 74.2% (p=0.015) in favour of new stent grafts. Similarly, newer stent grafts had better freedom from late conversion and sac growth >5mm (p=0.0001 and p=0.022, respectively). Lower type 1 endoleak (p>0.07) and less grafts migration (p>0.02) were noted in another study featured in the Journal of Vascular Surgery in 2017, assessing the performance of Endurant and Talent stent grafts (Medtronic).
A French Registry of 176 patients reported on the performance of the second-generation Anaconda EVAR (Terumo Aortic) over five years. Although one third of the studied cohort had hostile neck anatomy, there was higher freedom from aneurysm related re-intervention when compared with the reported results of the Dutch DREAM trial: 78% versus 70%. The Italian Registry for the new generation C3 Gore Excluder stent graft of more than 460 patients, all followed for 10 years and treated as per the instructions for use (IFU), showed quite high freedom from reintervention (80%) and freedom from stent-related complications (88%).
The improvement in cloth material and refinement in stent structure have influenced the durability outcomes. Type III endoleak was studied in a large retrospective study of more than 900 patients, published by in the Journal of Vascular Surgery in 2017. Almost 50% reduction of this serious endoleak was noted in the third generation grafts when compared to the first and second generations.
This technological development has been accompanied by a growth in operator knowledge and experience. There is consistent observation in the literature that the use of stent grafts within IFU is accompanied by reduction in early type 1 endoleak, early reinterventions, and late death. In one retrospective study of more than 600 patients, among several other studies, published in the Journal of the American College Surgery in 2016, it was documented that early and late type 1 endoleak, early reintervention, and late death were all significantly higher in the cohort of patients treated outside IFU, despite very high initial technical success. It is alarming that this kind of practice is still widespread and there is a real possibility that the reported results are actually undermining the technological development in this field.
The concept of relation between neck diameter and durability is gathering momentum. Several studies have shown that the smaller the neck diameter, the better the overall results are. The GREAT registry collects data from real life patients treated with C3 Gore stent graft. A study of more than 1,600 patients published in 2018 in the Journal of Vascular and Endovascular Surgery showed that neck diameter of ³25mm was significantly associated with lower freedom from type 1A endoleak, lower freedom from aortic reintervention, and lower freedom from primary composite end point at five years. It is however inconsistent in the literature what the diameter threshold is that defines the desired neck.
Despite the great investment in this technology, the overall long-term survival remains stable regardless of the technology or stent manufacturer. This is perhaps an expected finding in a pathology that frequently presents with several other co-morbidities. This observation should prompt interventional radiologists and vascular surgeons, when selecting patients and/or treatment modality, to consider the most durable and cost-effective intervention.
Future developments
Several outstanding issues are yet to be studied. The new stent designs and new adjuncts such as endostaples should be properly appraised. The optimum neck diameter, together with ideal length (fenestration versus standard EVAR), should be included in the long-term risk-benefit assessment. A reliable and sensitive follow up tool, beyond CT and ultrasound, will be welcomed for the life-long needed surveillance.
Mo Hamady is a consultant interventional radiologist at Imperial College, London, UK, the training programme director for Interventional Radiology at London Health Education England (HEE), and is secretary of the British Society of Interventional Radiology (BSIR). EVAR
“Artificial intelligence [AI] is changing the face of healthcare for all stakeholders, from consumers to providers,” Stephen Hunt (University of Pennsylvania, Philadelphia, USA; co-founder of the Penn Image-guided Interventions Laboratory) told attendees of the virtual 2020 annual scientific meeting of the British Society of Interventional Radiology (BSIR; 1–3 December, online). Speaking during a “State of the Art” session on the future of interventional oncology (IO), Hunt spoke on how “the era of AI” will expand the horizons of interventional oncology.
According to Hunt, the growth of US Food and Drug Administration-approved AI tools in the coming decade “will be exponential”. He urges interventional radiologists to stay abreast of the developments by integrating AI concepts into medical education: “Users must be educated not only on the proper application of these AI tools and on their limitations,” he said, “but on the mechanisms for validating their efficacy. Foundational concepts in statistics and bioinformatics are critical to responsible adoption and use of AI. Collaboration with developers of these tools will improve their clinical relevance and usability to interventional radiology. IO educators and faculty should incorporate AI topics into their curricula and research.”
He defines AI simply: “Really, it is just using computers and software to perform tasks that normally require human intelligence to accomplish. That seems like a very broad definition, and it is—it is somewhat vague on purpose, because it encompasses such a large field.”
Machine learning is a concept integral to AI: it describes the process of a computer learning from experience as it goes through data sets. A machine learning algorithm will learn to make connections between data points or perform some sort of classifier task, such as image recognition, when fed data, and gets better at its designated job the more input it is fed.
“The real breakthroughs for interventional oncology will require assembling and curating larger datasets,” Hunt therefore explained to delegates.
In addition to a large amount of data and a machine learning algorithm (or another tool designed to perform sophisticated calculations, such as a neural network), AI also requires some technical expertise, he continued. The end user has to be able to interpret the output generated by the AI software in order to apply the information to clinical practice.
Hunt provided some examples of AI use in the interventional oncology space.
Intraprocedural spatial localisation
Firstly, he talked the BSIR audience through an example where an interventionalist brings in a patient with a gastrointestinal (GI) bleed. Whilst the imagined patient is lying on the angiography table, the interventional radiologist needs to identify the location of the bleed on a CT scan in order to then stop the blood flow. Hunt suggested that an algorithm could be used in image registration and segmentation: this would enable the fluoroscopy unit to automatically identify the area where it predicts the bleed would appear.
“This kind of technology already exists, it has just not been put to use in clinical practice,” Hunt said. “It has not really been deployed that way.
“In addition, you could take those images [from prior GI bleed angiography studies] and train an AI with them—we have done this in our lab, and other labs have done this too—so automatically you have a classifier that will show you where the bleed is on the image. It is able to learn from some prior database that we made of GI bleed images, and then we can try it on new cases.”
Clarifying this point specifically to Interventional News, Hunt elucidates: “The point is for your angio suite to automatically detect the bleed during angiography and ‘circle it’ or otherwise provide a target sign to point it out to your eye. That way the interventionalist can go to that spot to drop a coil.
“I think within the next five years you are going to see a lot of these tools from the larger venders, like Siemens and Philips.”
CT perfusion imaging during TACE
Giving another example, Hunt next discussed AI in CT perfusion imaging during transarterial chemoembolization (TACE).
“We always have this problem of, during a TACE, how do you know you have full treatment of the tumour? One of the ways would be to do CT perfusion on that patient at the time of TACE. We have one of these image hybrid rooms, we have all the technology there, we have CT perfusion on that CT scanner, which is in the hybrid room of the fluoroscopy CT unit, but it has not been integrated into the workflow, the technicians do not know how to use it—it is these kinds of problems that we have not yet worked out. This is an example where you can have that real-time critical feedback, [as the AI] tells you ‘hey, there is an area of tumour that you have missed’. The CT perfusion would give you that information.
Intraprocedural Augmented reality
A physician using the HoloLens from Microsoft
Turning to an example he said is more in the research and development phase, Hunt then discussed the use of augmented reality intraprocedurally. The HoloLens, from Microsoft, is a set of goggles that the interventionalist could wear that allows them to see virtual projections superimposed over the real world.
There are various methods of registration when it comes to correctly superimposing the projected image on to a patient, which utilises AI. Hunt described how the physician could select a point on the patient’s skin, and a point in the tumour on the projection, and the HoloLens will allow the user to visualise a path that will give them an angle to register their ablation probes. This can be combined with the breathing cycle and cardiac gating, so probe advancement only takes place at the correct time in the cycle. Hunt highlighted work that IMACTIS and XACT are doing in this space, and encouraged listeners to look into these companies.
Thermal lung ablation (TLA) is an effective treatment, resulting in good overall survival with good local control, attendees were told at the 2020 annual scientific meeting of the British Society of Interventional Radiology (BSIR; 1–3 December, online). Elfadil Elmahdi (Royal Liverpool University Hospital, Liverpool, UK) presented his ten-year experience of the non-invasive alternative to surgical resection at a tertiary hospital.
Elfadil and colleagues conducted a retrospective, observational review to evaluate local tumour control, overall survival, and complications of TLA in their centre between 2009 and 2019. While 128 patients in total were treated with TLA during this period, five were excluded from the study for disease progression prior to TLA and no follow-up data. Between the 123 patients analysed in the study, 321 nodules were ablated.
Technical success was achieved in 301 nodules (93.8%). Of the 20 unsuccessful procedures, 14 nodules underwent a repeat ablation.
Showing a Kaplan-Meier graph depicting local recurrence, Elfadil informed his audience that the mean number of years before local recurrence was 10.5 years (±0.234; confidence interval [CI]: 10.07–10.99), with one-, two-, and three-year survival without local recurrence being 90%, 87.5%, and 86%, respectively. A second Kaplan-Meier graph, this time depicting new pulmonary recurrence, showed that the mean time before new tumours developed again was 5.8 years (±0.414; CI: 4.95–6.57), with the one-, two-, and three-year survival rate with no new pulmonary occurrence being 85%, 72%, and 60%, respectively.
Median overall survival was 3.16 years (±0.305; CI: 2.56–3.76). One-, two-, and three-year overall survival was 98%, 82%, and 56%, respectively. These survival rates are comparable to other TLA studies, Elfadil said, “if not slightly better”.
A pneumothorax requiring a chest drain was seen in 50.7% of patients—again, Elfadil told delegates that this was similar to that reported in the literature.
Addressing the limitations of the presented study, he went on to say that the investigators assumed that TLA practice in the Royal Liverpool University Hospital was homogenous between operators over time, co-morbidities that may influence survival were not taken into account, and no correlation was made with the grades of the primary tumour. In addition, there are reservations to what can be achieved with a retrospective study design using data from a single institution. lung ablation
Based on the findings of their first-in-human feasibility study, Joost van Herwaarden (Utrecht University Medical Centre, Utrecht, The Netherlands) and colleagues write in the European Journal of Vascular and Endovascular Surgery (EJVES) that Philips’ Fiber Optic RealShape (FORS) technology “has the potential to improve intraoperative imaging”. Their results show that real-time navigation using FORS technology is safe and feasible in abdominal and peripheral endovascular procedures.
Van Herwaarden and colleagues detail that endovascular procedures are conventionally conducted using 2D fluoroscopy. However, a new technology platform, FORS, has recently been introduced, which allows “real-time, 3D visualisation of endovascular devices using fibreoptic technology,” they explain. This technology functions as an “add on” to conventional fluoroscopy and “may facilitate endovascular procedures”. The present first-in-human study assessed the feasibility of FORS in clinical practice.
The researchers performed a prospective cohort feasibility study between July and December 2018, recruiting patients undergoing either regular or complex endovascular aneurysm repair (EVAR) or endovascular peripheral lesion repair.
Van Herwaarden et al used FORS guidance exclusively during navigational tasks, such as target vessel catheterisation or crossing of stenotic lesions. In EJVES, they write that three types of FORS-enabled devices were available: a flexible guidewire, a Cobra-2 catheter, and a Berenstein catheter. They note that devices were chosen at the physician’s discretion and could comprise any combination of FORS and non-FORS devices.
The primary study endpoint was technical success of the navigational tasks using FORS-enabled devices, and secondary endpoints were user experience and fluoroscopy time.
The authors note that they enrolled 22 patients in the study, comprising 14 EVAR and eight endovascular peripheral lesion repair patients. They detail that, owing to a technical issue during start up, the FORS system could not be used in one EVAR. However, they report that the remaining 21 procedures went ahead without device- or technology-related complications and involved 66 navigational tasks.
Van Herwaarden and colleagues add that in 60 tasks (90.9%), technical success was achieved using at least one FORS-enabled device. In terms of user experience, operators graded FORS-based image guidance “better than standard guidance” in 16 of 21 and “equal to standard guidance” in five of 21 procedures. Finally, regarding fluoroscopy time, the authors report that this ranged from 0 to 52.2 minutes, adding that several tasks were completed without or with only minimal X-ray use.
The authors acknowledge some limitations of the present study. For example, they communicate that, although the operators had experience with the system in preclinical studies, they went through a learning curve during clinical use. Van Herwaarden et al write: “The optimal visualisation settings (regarding viewing angle, magnification, mono- or biplane mode, and optimal overlay) had to be identified for the different types of procedure.”
In addition, they note that workflow improvements, like the optimal positioning of the system, to work from both the groin and the arm, had to be learned during the study. “In this first study, the technical success would probably have been higher if more than two differently shaped catheters had been available,” they posit.
Van Herwaarden and colleagues list a few more limitations for clinical use, including the limited working length of the catheters and guidewire available for this study and also the inability to backload the guidewires. “These issues will be addressed in future releases of the system,” they state.
Finally, they relay that there were technical issues with the FORS equipment during this study. The technology could not be used in one patient, they detail, and using two FORS devices at the same time was impossible in on other patient. They note that these factors “probably affected study results”.
The authors conclude that this exploratory study “demonstrates the feasibility and potential of this technology in clinical practice and forms a foundation for future clinical research.” However, they recognise that comparative studies are needed to “prove and quantify” the benefits and potential radiation reduction for all types of endovascular procedures.
Authors Bruno Damascelli, Vladimira Tichà , Gianluigi Patelli, and Giuseppe Petralia
A combination of liquid biopsy and whole-body magnetic resonance imaging (WB-MRI) could revolutionise cancer diagnostics and monitoring, write Bruno Damascelli, Vladimira Tichà, Gianluigi Patelli, and Giuseppe Petralia. Here, they detail the potential advantages of these non-invasive techniques: “The combination of magnetic resonance and liquid biopsy may potentially solve some diagnostic conflicts and guide new treatments based on molecular diagnosis and its variations as the cancer evolves”.
Modern cancer diagnostics aim to provide improved sensitivity, specificity, and disease localisation, without any risk of biological harm. Liquid biopsy and whole-body magnetic resonance imaging (WB-MRI) are both in an accelerated phase of development as promising, non-invasive methods for early cancer diagnosis and monitoring. A combination of the two methods could prove advantageous.
The genetic profile of a tumour extracted from a blood sample seemed to be the end point for cancer diagnosis, disease monitoring, and selection of targeted molecular treatments. However, liquid biopsy results are not easily reproducible at present because tumours release minimal amounts of fragmented DNA into the circulation in an unpredictable manner. Molecular diagnosis based on biological liquids is complementary to tissue biopsy and cannot replace it. Yet liquid biopsy has unique advantages, such as the ability to demonstrate changes in the heterogeneity of the cancer genome and to detect circulating tumour cells (CTC) with intact DNA, which are prognostically significant.
The most widely used imaging methods in oncology are based on ionising rays, making it undesirable to resort to these methods for screening and for frequent disease monitoring, especially in young patients and women of fertile age. Since its introduction, magnetic resonance imaging has developed surprising abilities to distinguish between normal and tumour tissue without unwanted effects. Diffusion sequences reflect the restricted mobility of water protons that occurs in some tumours because of their greater cell density. The consequent increase in contrast between tumour and normal tissue allows spatial localisation of the cancer. The increased sensitivity and specificity of diffusion-weighted WB-MRI has been demonstrated in cancer patients, but the data on healthy subjects are still preliminary. The possibility of diagnosing cancer in the 1–2% of asymptomatic subjects who undergo screening DWB-MRI makes this test interesting, although findings calling for further investigation may be produced in as many as 30% of those screened, according to published data.
Similarly, liquid biopsy, as conventionally applied in patients without a cancer diagnosis, is unable to provide direct topographical information, although identification of a tumour-related mutation in the blood is of considerable diagnostic significance.
For liquid biopsy, tumour DNA extraction can be improved through enrichment methods currently being developed and through detection of other tumour markers, such as new-generation protein biomarkers, and cancer metabolites identifiable by mass spectrometry. We endeavour to improve the sensitivity of liquid biopsy through selective venous sampling from the vessels draining the district or various districts affected by the tumour, thus reducing the impact of the dilution of fragmented DNA that occurs in the total blood volume.
Case 1
A 46-year-old male with no personal or family history of cancer underwent diffusion-weighted WB-MRI in the context of clinical screening, which revealed enlarged lymph nodes in the left iliac chain. The remaining lymph nodes, spleen, and bone marrow were unremarkable. Given the difficult access for instrumental biopsy, liquid biopsy with selective venous catheterisation was suggested. Only the sample from the left internal iliac vein was positive for the FGFR3 gene mutation, related to lymphoma. Subsequent percutaneous CT-guided biopsy and a video-laparoscopic procedure were both non-diagnostic. Blood tests were normal, while an 18F-FDG PET scan showed positive uptake coinciding with the MRI finding. No progression was seen at follow-up.
Case 2
A 50-year-old male presented with persistent thrombocytopenia. Liquid biopsy performed as a preliminary test showed BRAF gene mutation in selective venous samples as well as in peripheral blood. This mutation is related to lymphoma in 2.23% of cases. Low-grade lymphoma was confirmed by bone marrow biopsy. Chemotherapy led to the disappearance of the mutation in liquid biopsy samples, whereas a repeat bone marrow biopsy confirmed minimal disease. Diffusion-weighted WB-MRI revealed diffuse discrete lesions in the bone marrow, mainly in the spine and pelvis.
Case 3
Liquid biopsy was performed in a 77-year-old asymptomatic female with a close family history of ovarian cancer. The peripheral sample was negative, whereas blood obtained from the inferior vena cava showed the PTEN gene mutation. This mutation is related to ovarian cancer in 3.5% of cases. On DWB-MRI, a right supraclavicular lymph node was enlarged with respect to a previous chest CT scan performed for other reasons. Lymph node biopsy was negative for epithelial cells or lymphoproliferative disease. Gynaecologic examination, transvaginal ultrasound, and abdominal CT scan were all negative. In this case, the liquid biopsy result may be the expression of a tumour clone not destined to develop into progressive ovarian cancer. The finding of the mutation in the sample collected from the blood draining the pelvis nonetheless reinforces the ovarian origin of pathological DNA. Follow-up over time is recommended.
Diffusion-weighted WB-MRI has already earned its place in cancer diagnostics for staging of multiple myeloma and malignant lymphomas, thanks to its ability to depict the bone marrow and skeletal lesions due to solid tumour metastases. In any case, the high contrast resolution of MRI makes it an important alternative for other difficult evaluations, such as peritoneal cancer seeding, for example. The potential value of this imaging method in asymptomatic patients remains to be established. Likewise, liquid biopsy can hardly be accepted as the sole initial diagnostic method in asymptomatic patients and those with no previous history of cancer because tumour-related mutations, which are defined as transient, do not necessarily mean that cancer will develop in that person’s lifetime. On the other hand, the diagnostic and prognostic significance changes when a diagnosis of minimal residual disease or recurrence of disease cannot otherwise be obtained at sites inaccessible to conventional instrumental biopsies. The combination of magnetic resonance and liquid biopsy may potentially solve some diagnostic conflicts and guide new treatments based on molecular diagnosis and its variations as the cancer evolves.
Bruno Damascelli and Vladimira Tichà are interventional radiologists in the department of Interventional Oncology, Emo GVM Centrocuore Columbus, Milan, Italy.
Gianluigi Patelli is the chief of the Radiology Department at Seriate Hospital, Seriate (BG), Italy.
Giuseppe Petralia is director of the Precision Imaging and Research Unit, IEO European Institute of Oncology, IRCSS, Milan, Italy, and is an interventional radiologist in the department of Oncology and Haematology, University of Milan, Milan, Italy, and at Advanced Screening Centers, ASC Italia, Castelli Calepio, Bergamo, Italy.
This work is sponsored by the Falciani Foundation. The authors report no disclosures pertaining to this article.
The Royal College of Radiologists (RCR) and the British Society of Interventional Radiology (BSIR) have created a “myth busting” guide to encourage more women to train as interventional radiologists.
While more than half of medical graduates are female, women are under-represented in interventional radiology (IR).
The RCR’s most recent radiologist census revealed that only one in ten consultant interventional radiologists are women (11%), compared with four in 10 consultant diagnostic radiologists (41%). A 2018 survey by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) found that exposure to radiation, particularly during reproductive years, and the perceived lack of work-life balance has made the subspecialty less attractive to prospective radiology trainees.
To encourage and support more women training in IR, the RCR and BSIR have created “Women in Interventional Radiology: Insights into the Subspecialty”, aimed at interested undergraduates, foundation doctors, and trainee radiologists.
The leaflet features commentary from women in IR working across the UK and at various stages in their careers, addressing common myths and queries about IR training, such as access to flexible training, radiation exposure risks, and working in what has been a traditionally male-dominated medical sub-specialty.
The contributors also give general advice about getting into the subspecialty and the professional satisfaction they have experienced through a career in IR.
Rosemina Ahmad, chair of the BSIR Women and Diversity Committee and one of the guide authors, says: “This is a landmark document in terms of providing a clear focus on and for women in IR.
“The support from the RCR and BSIR has been invaluable in highlighting the importance of recruiting women into IR, so that we have the very best talent and provide doctors that reflect our local communities.
“Role models are incredibly important in shaping career choices and I hope the experiences of women in IR are both motivating and inspiring to readers and highlight that women can and do succeed in this rapidly advancing field of image-guided surgery.”
Michael Robson delivers the PAVE trial data at BSIR 2020 in a pre-recorded presentation. From top to bottom on the right: fellow panellist Isaac Manyonda, BSIR president Ian McCafferty, presenter Michael Robson, session chair Raj Das, and fellow panellist Anna Belli watching live.
There is no evidence of a benefit from additional paclitaxel-coated balloon use compared to standard balloon angioplasty alone in the context of preserving arteriovenous (AV) fistula patency for haemodialysis, the multicentre, randomised controlled PAVE (Paclitaxel-coated balloons and angioplasty of AV fistulas) trial finds. Speaking during the “Trial update” session of the 2020 annual scientific meeting of the British Society of Interventional Radiology (BSIR; 1–3 December, online), Michael Robson (Guy’s and St Thomas’ Hospital and King’s College London, London, UK) informed livestream attendees that there was no indication of an early treatment effect, and that all primary and secondary outcome measures of their trial demonstrated this same conclusion. Robson reported no disclosures relating to the PAVE trial, but noted that BD provided the balloons used. BD played no other role in the investigation, he reported.
Contextualising the PAVE trial, Robson told BSIR attendees: “A fistuloplasty is a good treatment for a blocked arteriovenous fistula before haemodialysis; however, the benefits may be short-term, and a stenosis often occurs. In retrospective series, the post intervention primary patency rate is around 60–70% at six months, going down to 40–50% at one year.”
Drug-coated balloons (DCB) have “a fairly established role” in the peripheral arterial setting and may provide some improvement in patency rates, Robson and colleagues hypothesised. Several small, single-centre studies have suggested a benefit for the use of local paclitaxel delivery in dialysis access, leading the PAVE triallists to design a study that would assess the efficacy of additional paclitaxel-coated balloon angioplasty compared to high-pressure balloon angioplasty only to preserve the patency of AV fistulas used for haemodialysis.
They conducted a double-blind, multicentre randomised controlled trial. Patients were unaware of treatment allocation, as were the majority of the clinical and research team. “It was not possible to blind the radiologists,” Robson explained, “because of the different appearances of the drug-coated balloon and the control balloon.” In total, 212 patients from 20 centres across the UK were recruited, randomised in a 1:1 ratio into the paclitaxel-coated balloon group or the control group, and followed up for a minimum of one year—the trial ended when the last recruited patient had completed one-year follow-up.
There was no statistically significant difference in time to end of target lesion primary patency, the study’s primary endpoint, between the two groups. Time to end of target lesion primary patency was measured when any of the following occurred: a clinically driven reintervention of the treatment segment; thrombotic occlusion that includes the treatment segment; surgical intervention that excludes the treatment segment from the access circuit; abandonment of the AV fistula due to an inability to re-treat the treatment segment.
“We also looked at competing risks, so conducted a sensitivity analysis, and, again, this did not suggest a difference [between the DCB and control arms],” Robson said.
Time to end of access circuit primary patency, one of the study’s secondary endpoints, also was not statistically significantly different between the paclitaxel-coated cohort and the control group.
Time to end of access circuit cumulative patency—when the fistula was abandoned—another secondary endpoint, was again not meaningfully different between the groups.
Continuing the pattern, “there was no suggestion of a difference between groups” when the triallists looked at the angiographic secondary outcomes, late lumen loss and rate of binary restenosis.
Procedural success was “good” in both cohorts, according to Robson said, with no difference between the treatment and control arms of the PAVE trial. There was no difference between the two groups in terms of the number of adverse events.
Lutonix AV clinical trial and IN.PACT AV access study: Randomised controlled trials prior to PAVE
In 2017, data from the first large-scale, randomised controlled trial investigating the clinical use and safety of a DCB catheter (Lutonix 035 AV; BD) for the treatment of dysfunctional AV fistulas and grafts were presented at the Leipzig Interventional Course (LINC; 24–27 January, Leipzig, Germany) and published in the Journal of Vascular and Interventional Radiology (JVIR). The eight-month data presented by Scott Trerotola (Perelman School of Medicine of the University of Pennsylvania, Philadelphia, USA) at the time showed that the drug-coated balloon is linked with a significantly higher target lesion patency and far fewer reinterventions to maintain the opening in a wide variety of failing AV fistulas than standard angioplasty. Two-year data, also published in JVIR in 2020, corroborated this finding.
However, the 180-day target lesion primary patency was not significantly different between the two treatment groups (p=0.06). As this was the primary endpoint, Trerotola noted that it was not met, but clarified at the time that this was a “statistical blip” as the curves continue to clearly diverge by the 240-day mark.
In August 2020, the New England Journal of Medicine published the six-month results of a second large, randomised controlled trial—the IN.PACT AV access study, which used the IN.PACT AV balloon from Medtronic for the treatment of stenotic lesions in dysfunctional haemodialysis AV fistulas. In this study, DCB use was found to be superior to standard balloon angioplasty, and this difference was statistically significant: target lesion primary patency was 82.2% in the former group (n=170), and 59.5% in the latter (n=160; p<0.001).
“So why have we not shown a difference in the PAVE trial, whereas the IN.PACT AV access study did show a difference [at six months]?” Robson asked. “I have not got an obvious answer to that.
“I guess all I can say about the PAVE trial,” he continued, “is that we tried to deliver as robust a trial as we could. We did everything that we could to preserve blinding amongst participants and the research team. Clinically-driven reintervention was called by a different radiologist wherever possible.”
Difference between PAVE trial and IN.PACT AV
There were several differences between the PAVE trial and IN.PACT AV access study: only patients with a single lesion or with tandem lesions that could be treated with a single drug-coated balloon were included in the PAVE trial, whereas IN.PACT analysed data from patients with multiple lesions; AV fistulas with previous thrombosis were included in the PAVE trial, but not IN.PACT; more patients in PAVE were Caucasian, and fewer had had previous revascularisations.
“Whether these explain the differing results I do not know,” Robson said.
Robert Morgan accepts the BSIR Gold Medal in a pre-recorded video while BSIR vice president Phillip Haslam (top), Wattie Fletcher Lecturer Jim Reekers (centre), and BSIR president Ian McCafferty (bottom) watch on the conference livestream
Robert Morgan (St George’s Hospital NH Foundation Trust, London, UK) was awarded the British Society of Interventional Radiology (BSIR) Gold Medal for distinguished service to the specialty and to the society at the BSIR 2020 annual scientific meeting (1–3 December, online).
“It gives me great pleasure to accept this honour on behalf of the society,” Morgan said. He thanked the BSIR council and officers for volunteering him for the award, saying he is “deeply honoured” for the recognition. He also thanked BSIR members for their support, and his interventional radiology (IR) colleagues at St George’s, saying: “without whom this would not have been possible”.
Speaking in a pre-recorded video, Lakshmi Ratnam (St George’s Hospital, London, UK), chair of the BSIR scientific programme committee, said: “Unfortunately, due to COVID, we are unable to do this [present the Gold Medal at a physical meeting] as we usually would, surrounded by colleagues, peers, and family. I am therefore very grateful today to be joined by the chief medical director of St George’s Hospital in London, Richard Jennings, who will present the Gold Medal to this year’s distinguished recipient, Robert Morgan.”
Keeping a distance of 2m as per COVID-19 regulations in the UK, Jennings presented Morgan with his award by placing it on a bench for the recipient to collect. “He is an exceedingly valued clinical leader here at St George’s,” Jennings said, before thanking Morgan for his work. “All of his colleagues think extremely highly of him, and we are very proud to have him working with us.”
Describing her “colleague, mentor, and friend”, Ratnam said of Morgan: “Robert has had an extremely distinguished career in interventional radiology, and has been an IR consultant here at St George’s for 21 years. He has served the BSIR as a member and chair of multiple committees, and has been a secretary of the society. He has represented UK radiology as a member and chair of multiple committees in the Cardiovascular and Interventional Radiological Society of Europe [CIRSE], finally culminating in the prestigious role of president of CIRSE in 2017. Robert is current Past President of CIRSE and is a member of the CIRSE Executive Board. Robert is an officer of the BSIR and is the BSIR council lead for strategy and international relations. He has also held several other roles in national and international societies including the Royal College of Radiologists (RCR), the European Congress of Radiology (ECR), the Society of Interventional Radiology (SIR), the UK Endovascular Forum, and the British Society of Endovascular Therapy.
“His main interest within IR has been in vascular disease, both in the role of endografting for diseases of the thoracic and abdominal aorta, and the role of IR in the management of arterial occlusive disease. During his career, he has been at the forefront of many emerging vascular techniques, and has been a great mentor and teacher to many generations of interventional radiologists, myself included.”
She continued: “Despite his countless and impressive achievements, Rob has always remained approachable, and generous with his knowledge and skills. The growth and achievements of the department here at St George’s are a testimony to the ethos that he has been key to building. He continually champions IR as a subspecialty, and is a great role model for future generations of aspiring interventional radiologists.”
Medical background
BSIR vice president Phillip Haslam (Freeman Hospital Newcastle, Newcastle upon Tyne, UK) introduced Morgan to congress attendees, recounting his education background: Morgan trained at Bristol University Medical School (Bristol, UK), before heading to Plymouth, UK, for three years of radiology training, and then to St George’s Hospital in London, UK, for a further two years. He next completed a Fellowship at the University of Texas (Austin, USA) under Eric Van Sonneberg, specialising in hepatobiliary and vascular interventions. Returning to the UK, Morgan was a Fellow under Andreas ‘Andy’ Adams (Guys’ and St Thomas’ NHS Foundation Trust, London, UK) for 18 months, before becoming a consultant at St Mary’s Hospital, London, UK, between 1996 and 1999. He ultimately returned to St George’s Hospital, where he remains as a consultant interventional radiologist and the clinical director for Diagnostics.
The immediate past president of CIRSE, Morgan was instrumental in the development of the European Board of Interventional Radiology (EBIR), a voluntary supplemental examination designed to evaluate interventional radiologists’ clinical and technical knowledge, first released in 2010 in Valencia, Spain.
“He has a long history of involvement with the BSIR,” Haslam continued, “and is currently a co-opted council member”.
Morgan has written over 160 peer-reviewed articles, authored more than 45 book chapters, and edited multiple textbooks, as well as delivered above 300 lectures to international audiences (including the 2017 BSIR Wattie Fletcher Lecture). His main research interests lie in the endovascular treatment of the aorta and peripheral vascular disease, as well as the use of embolization to control haemorrhage, and the treatment of visceral aneurysms. He is the deputy editor-in-chief of Cardiovascular and Interventional Radiology (CVIR) Endovascular, and has organised many teaching courses throughout his career.
Following the rapid reconfiguration of healthcare practices in response to the COVID-19 pandemic in early 2020, Narayan Karunanithy reflects on the position of interventional radiology (IR) services going into 2021. Citing data demonstrating that the reduction in IR activity during the first national lockdown was far less than that seen in other procedure-centred specialties, such as vascular surgery, urology, and endoscopy, Karunanithy argues that formal incorporation of IR treatments into patient pathwayswouldresult in more efficient care. As many IR procedures can be performed as a day case or in an ambulatory care unit, he writes that interventional radiologists can “hugely support emergency preparedness plans”, which will likely continue to be vital in 2021.
The challenge for healthcare organisations to deliver on the “triple aims” of health system performance has been made many magnitudes more complex in 2020 due to the COVID-19 pandemic (see Table 1).1 The scope and nature of interventional radiology (IR) practice, however, is unusually well-placed to meet these aims, and looks well set to play a more central role in delivery of high quality, safe healthcare in 2021 and beyond.
Table 1: The triple aims of healthcare
At the time of writing, we find ourselves in the midst of the second COVID-19 pandemic wave in the UK, and sadly we are once again already seeing both high infection and mortality rates. The recent promising vaccine results have provided a much-needed glimmer of hope. Whilst vaccines are considered at present our best hope, uncertainty still remains regarding the effectiveness, availability, and impact of those vaccines. Hence, the healthcare strategy—at least for the foreseeable future—will need to incorporate the ability to treat those with COVID-19 and continue to provide timely, safe, effective, and cost-efficient care for everyone with non-COVID related illnesses.
During the first wave, it was impressive and inspiring to see so many IR departments demonstrate a willingness to reconfigure working practice and be available to provide much-needed acute services. One of the models that worked extremely well during the summer/autumn of 2020 was the spatial segregation of services into “low-risk” and “high-risk” sites. This was, in large part, created through partnerships forged with private sector hospitals which enabled IR to maintain access to important treatments such as tumour ablation and uterine fibroid and prostate artery embolization in “low-risk” environments. In parallel, comprehensive cover was provided at “hot” sites for the spectrum of COVID and non-COVID emergencies like embolization, thrombectomy, complex venous access, and percutaneous drainage of obstructed kidneys, bile ducts, and abscesses.2 Published activity data bear this out and have shown that the reduction in IR activity during the first wave of lockdown, by 41% and 25% in outpatient and inpatient volumes respectively, was far less than that seen in other procedure-centred specialties like vascular surgery, urology, and endoscopy.3
Even prior to the pandemic, it was estimated that approximately one in 10 in-patients were treated by IR during their hospital stay, underlining the key importance of IR in the day-to-day functioning of hospitals.4 Formal incorporation of IR treatments into patient pathways and access to IR expertise through ward rounds and clinics would allow far more efficient and streamlined care for those requiring it. Across the spectrum of clinical practice, minimally invasive IR treatments result in quicker recovery, lower morbidity, and shorter hospital stays. Crucially in these times, these procedures can often be performed in a day case or ambulatory care unit. The availability of such units can hugely support emergency preparedness plans. This was illustrated in the first wave of the pandemic, when most endoscopy services ceased and IR stepped in to perform many more radiologically inserted gastrostomies rather than percutaneous endoscopic gastrostomies.
An additional benefit of high-volume IR day case units is the efficient utilisation of resources and an increase in financial income for the organisation. Increasingly, organisations within the UK have come to recognise these clinical and financial benefits, and many centres have invested in such facilities. However, these are not universally available, as highlighted in the recently published Radiology GIRFT [Get It Right First Time] report.5 Alongside this, there is a need for robust workforce planning to ensure there are adequate numbers of IR doctors, nurses, radiographers, and administrative staff to sustain IR services. The skillset that IR staff possess is extremely versatile, and there were many reports of IR supporting the frontline response during the first wave of the pandemic. This included redeploying staff in the critical care setting with the goal of providing bed-side procedures like difficult venous access and ultrasound guided drainage procedures.
Whilst the months ahead will be challenging, there is an opportunity to establish IR practice firmly at the very core of clinical practice through proactive planning and delivery of innovative, effective, and safe care for the benefit of our patients.
I would like to acknowledge the guidance and support from Ian McCafferty (President, British Society of Interventional Radiology [BSIR]) in the preparation of this article.
Stay safe everyone.
Narayan Karunanithy is a member of the Communications Committee, British Society of Interventional Radiology, and is a consultant interventional radiologist at Guy’s & St Thomas’ NHS Foundation Trust, London, UK.
Pendower L, Benedetti G, Breen K, Karunanithy N. Catheter-directed thrombolysis to treat acute pulmonary thrombosis in a patient with COVID-19 pneumonia. BMJ Case Rep. 2020 Aug 11;13(8):e237046
Hashmi A, Parikh K, Al-Natour M et al. Interventional radiology procedural volume changes during COVID-19 initial phase: A tertiary level Midwest health system experience. Clin Imaging. 2020 Nov 10;72:31–36
Shah SS, Tennakoon L, O’Beirne E, Staudenmayer KL, Kothary N. The Economic Footprint of Interventional Radiology in the United States: Implications for Systems Development. J Am Coll Radiol. 2020 Sep 9:S1546–1440(20)30873–5
On the opening day of BSIR 2020 (1–3 December, virtual), Lakshmi Ratnam (London, UK), chair of the scientific programme committee, moderates a special InterventionalNews panel with BSIR president, Ian McCafferty (Birmingham, UK), and vice-president, Philip Haslam (Newcastle, UK).
McCafferty outlines some of the highlights from this year’s programme, which he notes contains a “nice balance between vascular and non-vascular interventional oncology subjects”, adding that he is particularly excited about the lymphatic session.
McCafferty discusses how interventional radiology (IR) has “risen to the challenge” of COVID-19 with the strong message that interventional radiologists have “helped maintain activities in the hospital more than any other group” during the COVID-19 pandemic. He points out that the BSIR has worked closely with the Royal College of Radiologists (RCR), so that interventional radiology could continue to perform procedures throughout lockdown, while the majority of surgery was put on pause. Those interventional radiology departments with their own day case units were the most efficient, he notes, making the point that quick outpatient-style treatment by interventional radiologists is really possible, extremely cost-effective, [generally has] low-morbidity, and is often preferred by patients. Indeed, vitally, it can be carried out in “cold” COVID-free environments outside of the hospital setting.
Haslam, commenting on the symbiotic relationship that industry and many device-using specialties share, states that the BSIR has continued to work closely and collaborate with industry partners to bring about a high-quality virtual event with impactful and useful education. Haslam hopes that COVID-19 will soon “be a thing of the dim and distant past”, which will allow for “a brilliant face-to-face meeting” in Glasgow for BSIR 2021.
Boston Scientific has announced that it has entered into a definitive agreement with Stark International and SERB SAS, affiliates of the European specialty pharmaceutical group SERB, to sell its BTG Specialty Pharmaceuticals business for US$800 million in cash.
Boston acquired BTG in August 2019, an acquisition covering BTG’s three business segments, including an interventional medicine portfolio encompassing interventional oncology therapeutic technologies for patients with liver and kidney cancers, as well as a vascular portfolio for treatment of deep vein thrombosis, pulmonary embolism, deep venous obstruction and superficial venous disease.
The transaction announced today will see Boston divest the pharmaceuticals segment of the business, which develops, manufactures and commercialises antidotes used in hospitals and emergency care settings, including the CroFab, DigiFab, and Voraxaze products. The three franchises are expected to generate approximately US$210 million in revenue for the full year 2020.
SERB, backed by private equity firm Charterhouse Capital Partners since 2017, owns a diversified portfolio of prescription medicines focused on rare and life-threatening diseases.
“This transaction will help the BTG Specialty Pharmaceuticals business enhance its potential as a fully integrated specialty pharmaceuticals platform,” said Anthony Higham, president, BTG, Specialty Pharmaceuticals. “We believe our capabilities and portfolio strongly complement those of SERB, and we look forward to this next chapter as we continue to positively impact the lives of patients and the people who care for them.”
“After acquiring BTG in 2019 for approximately US$3.7 billion net of cash on hand, and following the close of this transaction, we will have divested the two BTG non-medical device portions—Pharmaceutical Licensing royalties in the fourth quarter of 2019 and Specialty Pharmaceuticals announced today—for more than US$1 billion in net proceeds,” said Jeff Mirviss, executive vice president and president, Peripheral Interventions, Boston Scientific. “We continue to be very pleased with the performance of the core Interventional Medicines business, the primary driver of the BTG acquisition, which has delivered strong growth and is expected to exceed our original goal of US$175 million in synergies.”
The Society of Interventional Radiology (SIR) and the American Medical Association (AMA) have sent a letter to the Centers for Medicare and Medicaid Services (CMS) urging them to implement and pay for Current Procedural Terminology (CPT) code 99072 to compensate practices for the additional supplies and new staff activities required to provide safe patient care during the COVID-19 pandemic.
The medical societies of each of the 50 states of America, plus the Medical Society of the District of Columbia, are also signatories, in addition to 76 societies and associations representing different medical specialities at the national level—such as the Society for Vascular Surgery, the American Urological Association, and the Spine Intervention Society. Altogether, hundreds of thousands of physicians are represented by the undersigned organisations.
Addressed to CMS administrator Seema Verna, the letter states that the COVID-19 public health emergency “has placed unprecedented strain on our [the signatories’] physician members, including ongoing threats to their financial viability due to months of lost revenue from practice closures and/or operating at reduced capacity”. According to the letter, in July and August 2020, an AMA survey of 3,500 physicians who provided at least 20 hours of patient care per week prior to the pandemic found that 81% of respondents reported that revenue was still lower than pre-pandemic times, with the average revenue drop being 32%. Compounding the financial stress of lost revenue, practices are also incurring additional costs for heightened infection control protocols and personal protective equipment (PPE).
The letter writers continue: “We recognise and appreciate the significant support and flexibility CMS has provided to physician practices. However, it is imperative that CMS specifically compensate physicians for the additional expenses involved in treating patients during the public health emergency. Practices incur significant costs in implementing the increased infection control measures required to provide safe care during the COVID-19 pandemic. These costs include additional supplies (such as cleaning products and facial masks for both staff and patients), clinical staff time for activities such as pre-visit instructions and symptom checks upon arrival, and implementation of office redesign measures to ensure social distancing.”
The AMA survey from the summer of 2020 describes how practice owners reported an average increase in PPE spending of 57% from February 2020, with 25% of owners saying that PPE expenses have risen at least 75%. Nearly all (99%) surveyed physicians have implemented infection control protocols, such as pre-visit screening phone calls, screening for COVID-19 symptoms/exposure and checking patient temperatures upon office arrival, and limiting the number of patients in the waiting room.
Detailing CMS’ actions, the letter claims that, in order to address the financial impact of these new protocols related to the COVID-19 pandemic, “the CPT Editorial Panel approved CPT code 99072 on 8 September 8 2020. According to CPT guidance, 99072 is used to report the additional supplies, materials, and clinical staff time over and above the practice expense(s) included in an office visit or other non-facility service(s) when performed during a public health emergency, as defined by law, due to respiratory-transmitted infectious disease.”
“Our organisations advocate for CMS to immediately implement and pay for CPT code 99072 with no patient cost-sharing during the public health emergency,” the societies write. “Payment for these additional costs should be fully funded and not be subject to budget neutrality. CMS could use remaining money from the CARES Act funding to pay physicians for these costs and/or recognise the decreased expenditures during the early months of the pandemic to waive budget neutrality. Your support will ensure that physicians receive the critical financial resources needed to maintain intensive infection control measures during the COVID-19 public health emergency.”
Prostate artery embolization (PAE) is a good treatment option for patients with benign prostatic hyperplasia (BPH) with minimal complications, according to the 24-month results of the STREAM (Prostatic artery embolization for the treatment of benign prostatic hyperplasia) trial, which affirms the place of the minimally invasive procedure in interventional radiologists’ arsenal.
This MRI-based study looked to examine factors important in predicting successful PAE using MRI over a two-year follow-up period. The triallists report that while adenomatous BPH does particularly well in the short term when treated with PAE, stromal BPH demonstrates better results at two years. In addition, they conclude that patients with median lobe hypertrophy (MLH) do as well as those without MLH up to 24 months, and that initial prostate volume does not appear to be significant in predicting outcome at two years.
“This study has provided valuable information and allowed a better understanding of which glands respond and how they will respond to PAE,” Charles Tapping (Churchill Hospital, Oxford, UK) and co-authors write in Cardiovascular and Interventional Radiology (CVIR). “It also allows clinicians to provide more information to patients exploring treatment for their BPH. MLH responded as well as non-MLH BPH disease, suggesting this technique may be valuable in treating patients with MLH, especially if some of the other minimally invasive techniques are limited if significant MLH is present.”
STREAM trial data at two years proves the technical and clinical success of PAE
“PAE has established itself as one of the alternative minimally invasive treatments for BPH, and is now accepted as safe and effective,” Tapping et al write. They go on to say that while performing PAE can be technically challenging, with a significant learning curve to perform the technique successfully, it is important to ascertain factors that may aid in predicting which patients would benefit most from PAE. They note that this is a particular imperative for interventional radiologists as there are “a number of robust minimally invasive techniques to treat BPH, such as the Urolift system and water vapour thermal therapy (REZUM)”.
They therefore conducted a prospective cohort study of 50 patients with BPH who were treated with PAE at a single institution. Patients had moderate to severe symptoms of BPH refractory to medical management for at least six months prior to enrolment in STREAM. Patients were imaged with multiparametric MRI imaging pre-PAE, and at three months, 12 months, and 24 months post-procedure. Clinical success was measured with international prostate symptom score (IPSS), international index of erectile function (IIEF), and validated quality of life (QoL) EQ-5D-5L questionnaires.
The technical success rate was 96%—no prostate arteries could be identified intraprocedurally in two of the 50 patients. The study authors report only minor complications arising from PAE: two cases of acute urinary retention and one case of uncomplicated urinary tract infection. While these are positive data for PAE, the authors state that, “Unfortunately, as there was no comparison group or control group in this study, it is not possible to make direct comparisons between different minimally invasive methods for treating BPH.”
Clinical outcomes of the STREAM trial were also positive. The mean IPSS score dropped from a baseline score of 21.1 (range: 16–36) to 7.2 at 12 months, and 8.1 at 24 months. Meanwhile, results from the EQ-5D-5L quality of life questionnaire demonstrated an increased quality of life at three, 12, and 24 months post-procedure. Results from the IIEF showed no significant change in erectile function over the two-year study following PAE. The prostate volume as measured on MRI imaging was significantly reduced from baseline to three months post-PAE. There was then a non-significant volume reduction at 12 and 24 months when compared to baseline.
Greatest improvement in IPSS score seen in patients with adenomatous BPH
“An interesting analysis of the results showed that while adenomatous BPH had an initial greater reduction in their IPSS score, improvement in quality of life, and symptoms (at three and 12 months compared to stromal group), the stromal group had better results at 24 months,” Tapping and colleagues say.
“In fact”, they write, “there was a continued decline in IPSS score in the stromal group over the 24-month study period, with a slight increase in IPSS score in the adenomatous group from 12 to 24 months.”
While the stromal prostate gland volume decreased compared to baseline size at three, 12, and 24 months post-PAE, the adenomatous glands at first rapidly reduced in size, maintained this small volume out to 12 months, and then increased in size again, with a larger volume reported at 24 months.
Discussing this finding, the triallists say: “This adds to the previously perceived literature that suggests adenomatous BPH patients had a better outcome. Angiography of adenomatous masses within the prostate demonstrates that these are highly vascular structures and the more rapid reduction in symptoms and IPSS score can be accounted for by infarction of the adenoma and rapid reduction in pressure on the transition zone of the prostate. Moreover, the more gradual improvement in the stromal group corresponds to typically a less vascular pattern on angiography.”
Patients with median lobe hypertrophy do just as well post-PAE as those without median lobe hypertrophy
No significant difference in IPSS score was observed at any time point between the 19 patients with MLH and those without MLH, according to the STREAM trial findings.
“Typically,” Tapping and co-authors muse, “it has been considered that patients with MLH would not do as well with PAE. However, patients in this cohort did as well as those without MLH. PAE may therefore be a good option for patients with MLH that cannot have alternative minimally invasive forms of treatment for their BPH.”
In addition, there was no significant correlation between initial prostatic volume and the IPSS score at 12 and 24 months post-PAE (p=0.05), the authors note. While previous investigators have suggested that prostate size is associated with clinical success following PAE, Tapping et al consider that in their study, MRI provided extra detail of the internal prostate architecture, meaning that “factors such as adenomatous predominant and stromal dominant disease became more useful”.
They conclude that further studies are needed in order to determine who the most appropriate patients for each minimally invasive BPH treatment are, and to overcome the limitation imposed on this trial by its small sample size.
In their recent systematic review and meta-analysis, Venkata Sai Jasty (University of Arizona, Tuscon, USA) and colleagues found that the risk of ischaemic steal syndrome, “one of the most feared complications in vascular access,” and patency rate are comparable for both tapered and non-tapered prosthetic arteriovenous grafts (AVGs) in dialysis access.
Writing in The Journal of Vascular Access (JVA), Jasty et al detail that end-stage renal disease (ESRD) “remains one of the leading causes of mortality and morbidity”. They note that there are currently three treatment options for ESRD—haemodialysis, peritoneal dialysis, and organ transplantation—but mention that a shortage of organ supply for a rising need has led to “a continued and increased call” for haemodialysis.
Upper extremity arteriovenous access “remains the preferred vascular access for haemodialysis in ESRD patients,” the authors relay, detailing that an arteriovenous fistula (AVF) or AVG are generally favoured over a central venous catheter, “due to lower rates of infection, hospitalisation, cardiovascular events, and all-cause mortality rate”.
They write that prior guidelines recommended AVFs as the initial choice for haemodialysis access due to more durability, higher patency rates, and lower morbidity and mortality compared to AVGs. However, “due to high failure rates of AVF from inadequate maturation and interventions required to achieve and maintain a functional AVF,” they stress that the latest guidelines from the National Kidney Foundation Kidney Disease Quality Outcomes Initiative (NKF KDQOI) “challenge the use of AVFs on certain populations” and recommend AVGs as the “preferable option” for haemodialysis.
Jasty and colleagues note that one of the biggest complications of vascular access placement is ischaemic steal syndrome, where blood is diverted from the hand to the graft, leading to hand ischaemia. To mitigate this problem, they detail that tapered grafts were created. These grafts have a smaller diameter at the arterial anastomosis, they write “which leads to decreased blood flow from the artery to the graft, thus lowering the risk of ischaemic steal”.
“It is unclear whether tapered AVGs are superior to non-tapered AVGs when it comes to preventing upper extremity ischaemic steal syndrome,” Jasty and colleagues state, noting that this gap in the literature led them to evaluate the outcomes of both graft types using a systematic review and meta-analysis.
The investigators performed a literature search in order to identify all English language publications from 1999 to 2019 that directly compared the outcomes of upper extremity tapered and non-tapered AVGs. They evaluated primary patency at one year (number of studies [n]=4), secondary patency at one year (n=3), and risk of ischaemic steal (n=5) and infection (n=4).
Of 5,808 studies screened, Jasty et al identified a total of five studies involving 4,397 patients that met the inclusion criteria and were therefore included in the analysis. They write in JVA that the meta-analyses revealed no significant difference for the risk of ischaemic steal syndrome (pooled odds ratio [OR] 0.92, 95% confidence interval [CI] 0.29–2.91, p=0.12, I2=48%) between the tapered and non-tapered upper extremity AVG.
In addition, they report that the primary patency (OR 1.33, 95% CI 0.93–1.9, p=0.12, I2=10%) and secondary patency at one year (OR 1.49, 95% CI 0.84–2.63, p=0.17, I2=13%), and rate of infection (OR 0.62, 95% CI 0.3–1.27, p=0.19, I2=29%) were also similar between the tapered and non-tapered AVGs.
The authors acknowledge certain limitations of this meta-analysis, including a low number of studies, unknown reasons for surgeons’ preference for one graft over the other, and a low number of patient samples and short follow-up (usually up to one year only) in the included studies.
Jasty and colleagues conclude: “This meta-analysis does not support the routine use of tapered graft over non-tapered graft to prevent ischaemic steal syndrome in upper extremity access”. However, due to the small number of studies and sample sizes, as well as limited stratification of outcomes based on risk factors, they stress, “Future studies should take such limitations into account while designing more robust protocols to elucidate this issue”.
MedAlliance has announced completion of patient enrolment in the ISABELLA clinical trial with the Selution SLR 018 drug-eluting balloon (DEB) for the treatment of dysfunctional arteriovenous (AV) fistulas in end-stage renal failure patients undergoing haemodialysis.
Selution SLR (sustained limus release) is a novel sirolimus-eluting balloon that provides a controlled sustained release of drug, similar to a drug-eluting stent (DES).
ISABELLA (Intervention with Selution SLR agent balloon for endovascular latent limus therapy for failing AV fistulas) is a prospective, single-centre, multi-investigator, non-blinded, single-arm trial investigating the safety and feasibility of the Selution SLR 018 DEB for the treatment of failing AV fistulas in 40 haemodialysis patients.
The objective of this study is to determine the safety and efficacy of the Selution SLR 018 DEB in the treatment of dysfunctional AV fistulas in end-stage renal failure patients undergoing haemodialysis. The anticipated clinical benefit is to improve the target lesion primary patency and reduce the number of reinterventions in stenotic AV fistulas of haemodialysis patients and hence morbidity in this frail patient population compared to conventional balloon angioplasty.
The efficacy endpoint of interest is six-month target lesion primary patency and the safety endpoint is freedom from localised or systemic serious adverse events through 30 days that reasonably suggest the involvement of the AV fistula circuit. The study has recently completed its 40-patient recruitment and will follow them up for a period of two years at Singapore General Hospital (SGH), which performs over 3,000 access salvage procedures annually.
“We are very excited at SGH and eagerly await the results from ISABELLA, which will be the first study to report clinical safety and efficacy data of sirolimus-eluting balloon (SEB) angioplasty using the Selution SLR DEB catheter combined with high pressure conventional balloon angioplasty vessel preparation, for dysfunctional AVF circuits in Asian haemodialysis patients”, said lead principal investigator associate professor Tjun Tang, senior consultant vascular and endovascular surgeon at SGH.
“SEBs are a natural evolution of the current gold standard treatment option of conventional balloon angioplasty for salvaging failing and stenotic AV fistula circuits. Paclitaxel drug-coated balloons have been used with limited success and the data are far from conclusive. The Selution SLR DEB provides therapeutic concentrations of drug within the vessel wall for at least 90 days post-angioplasty, which is a major advantage over other drug-coated balloons in dealing with the extended nature of the NIH [National Institutes of Health] process. Our plan is to follow up patients to two years to define the effectiveness of the studied therapy in the medium term.”
A novel embolization device in the interventional oncology space—the GPX embolic device (Fluidx Medical Technology)—has successfully been used in a patient to therapeutically devascularise a tumour for the first time.
“We are impressed with the GPX embolic,” comments Andrew Holden (Auckland City Hospital, Auckland, New Zealand). “We delivered GPX through a long 150cm 2.4F (0.022inch inner diameter) microcatheter from the patient’s radial artery. GPX was easy to use, precise, and occluded the tumour well. We look forward to using GPX across a broad range of applications to improve patient care.”
The GPX embolic device is an innovative embolic designed to combine the benefits of other embolics like coils, particles, and liquids with simplified preparation, delivery, precision, and control leading to durable, long-term occlusions. The GPX technology is a low viscosity, aqueous-based solution in a syringe that solidifies into a durable embolic material upon delivery, without polymerisation or dimethyl-sulfoxide (DMSO) precipitation associated with other embolics.
According to a company press release, GPX is packaged ready-to-use in a syringe, requires less than one minute of tableside preparation by the clinician, and may be delivered through standard catheters or microcatheters.
“GPX is easy to prepare, deliver, and control,” says Ryan O’Hara (University of Utah, Salt Lake City, Utah USA). “GPX is responsive to the physician and layers well in the vessel during delivery, resulting in improved targeting and control. I see potential for this embolic in interventional oncology and other peripheral vascular and neurovascular uses.”
Therapeutic, super-selective embolization is a high-growth procedure used for minimally invasive, targeted treatment of internal bleeds, tumours, aneurysms, vascular malformations, uterine fibroids, varicose veins, and other uses. A variety of embolic devices (coils, particles, plugs, liquids) are used for these procedures, however many can have issues in terms of ease of use, and controlled, consistent delivery. Some embolics also require specialised catheters and solutions as well as complex and lengthy preparation processes.
“This is a significant milestone for the Company,” adds Libble Ginster, CEO of Fluidx Medical Technology. “GPX is an advanced embolic technology that overcomes the challenges associated with other embolic devices. GPX can be used effectively for distal penetration and occlusion of vessel networks, as well as proximal ‘one-and-done’ use of GPX in conjunction with coiling. We look forward to GPX’s use to help a variety of peripheral and neurovascular patients.”
The GPX embolic device is not available for sale in the USA, and is for investigational use only.
Penumbra today announced US Food and Drug Administration (FDA) 510(k) clearance for expanded indication of the latest iteration of the Indigo aspiration system, Lightning 12.
As part of the Indigo aspiration system, Lightning 12 (Indigo system CAT 12 aspiration catheter with lightning intelligent aspiration) and Separator 12 are now indicated for the removal of fresh, soft emboli and thrombi from vessels of the peripheral arterial and venous systems as well as for the treatment of pulmonary embolism (PE).
“Penumbra continues to strive to bring innovative therapies to the medical community, and this is another important milestone that will help advance pulmonary embolism intervention,” said Adam Elsesser, president and chief executive officer, Penumbra. “COVID has increased the awareness of the need for therapies that remove blood clots, and we are thrilled with the FDA clearance of the PE treatment indication for Lightning 12.”
The Indigo System Lightning 12 is the company’s newest generation aspiration system for peripheral thrombectomy. Lightning 12 combines the Indigo System CAT12 aspiration catheter with lightning intelligent aspiration, enabling physicians to focus on optimising thrombus removal using the system’s unique clot detection mechanism.
CAT12 is a large-lumen aspiration catheter that incorporates novel laser-cut hypotube-based catheter engineering to provide deliverability and torqueability within the body. According to a press release, this combination of intelligent aspiration and large-lumen catheter engineering makes Lightning 12 Penumbra’s most advanced clot removal technology for the treatment of PE.
A novel outpatient procedure—cooled radiofrequency ablation (c-RFA)—offers lasting pain relief for patients suffering from moderate to severe arthritis in their hip and shoulder joints, according to a study presented at the annual meeting of the Radiological Society of North America (RSNA; 29 November–5 December, online). Researchers said the procedure could help reduce reliance on addictive opiates.
People with moderate to severe pain related to osteoarthritis face limited treatment options. Common approaches like injections of anaesthetic and corticosteroids into the affected joints grow less effective as the arthritis progresses and worsens.
“Usually, over time patients become less responsive to these injections,” says Felix M Gonzalez (Emory University School of Medicine, Atlanta, USA). “The first anaesthetic-corticosteroid injection may provide six months of pain relief, the second may last three months, and the third may last only a month. Gradually, the degree of pain relief becomes non-significant.”
Without pain relief, patients face the possibility of joint replacement surgery. Many patients are ineligible for surgery because of health reasons, whereas many others choose not to go through such a major operation. For those patients, the only other viable option may be opiate painkillers, which carry the risk of addiction.
Gonzalez and colleagues have been studying the application of a novel interventional radiology treatment, c-RFA, to achieve pain relief in the setting of advanced degenerative arthritis. The procedure involves the placement of needles where the main sensory nerves exist around the shoulder and hip joints. The nerves are then treated with a low-grade current known as radiofrequency that “stuns” them, slowing the transmission of pain to the brain.
For the new study, 23 people with osteoarthritis underwent treatment, including 12 with shoulder pain and 11 with hip pain that had become unresponsive to anti-inflammatory pain control and intra-articular lidocaine-steroid injections. Treatment was performed two to three weeks after the patients received diagnostic anaesthetic nerve blocks. The patients then completed surveys to measure their function, range of motion, and degree of pain before and at three months after the ablation procedures.
Omar N Kallas
There were no procedure-related complications, and both the hip and shoulder pain groups reported a statistically significant decrease in the degree of pain, with a corresponding increase in dynamic function after the treatment.
“In our study, the results were very impressive and promising,” Gonzalez enthuses. “The patients with shoulder pain had a decrease in pain of 85%, and an increase in function of approximately 74%. In patients with hip pain, there was a 70% reduction in pain, and a gain in function of approximately 66%.”
The procedure offers a new alternative for patients who are facing the prospect of surgery. In addition, it can decrease the risk of opiate addiction.
“This procedure is a last resort for patients who are unable to be physically active and may develop a narcotic addiction,” Gonzalez comments. “Until recently, there was no other alternative for the treatment of patients at the end of the arthritis pathway who do not qualify for surgery or are unwilling to undergo a surgical procedure.”
At last year’s RSNA annual meeting, Gonzalez presented similarly encouraging results from a study of a similar procedure for the treatment of knee arthritis. Together, the knee, shoulder, and hip articulations account for approximately 95% of all arthritis cases.
The procedure could have numerous applications outside of treating arthritic pain, Gonzalez explains. Potential uses include treating pain related to diseases like cancer and sickle cell anaemia-related pain syndrome, for example.
“We are just scratching the surface here,” Gonzalez says. “We would like to explore efficacy of the treatment on patients in other settings like trauma, amputations, and especially in cancer patients with metastatic disease.”
The VIVA panel discuss Peter Schneider’s presentation on learnings from the paclitaxel “debacle”
This year’s Vascular Interventional Advances annual meeting (VIVA 2020; 6–8 November, online) opened with a session on controversial hot topics and advanced multidisciplinary approaches to vascular disease. Looking back on the paclitaxel “debacle”, Peter Schneider (University of California San Francisco, San Francisco, USA) detailed key learnings from the last year and a half, pointed to forthcoming data that will help add further clarity, and praised the combined and ongoing efforts of researchers, societies, and regulatory bodies.
Schneider began by stressing the patency of paclitaxel in the femoropopliteal segment. At 12 months, the four randomised controlled trials (RCTs) of paclitaxel drug-coated balloons (DCBs) and drug-eluting stents (DESs) versus percutaneous transluminal angioplasty (PTA) that are currently approved in the USA—ILLUMENATE, IN.PACT SFA, Zilver PTX, and LEVANT—show a “significant improvement” in patency with DCB/DES use compared to PTA, he noted. Speaking to Interventional News, Schneider noted that, since then, the Eluvia DES and the Ranger DCB (both Boston Scientific), have also shown “excellent” results and been approved by the US Food and Drug Administration (FDA).
In December 2018, a meta-analysis of summary-level data was published, “which we all know about,” remarked Schneider, that suggested an increased risk of death with paclitaxel use in the femoropopliteal segment at two and five years. Here Schneider was referencing the 2018 Journal of the American Heart Association (JAHA) paper by Konstantinos Katsanos (University of Patras, Patras, Greece) and colleagues.
Highlighting the instant and enduring impact of this publication, Schneider commented: “Overnight, the use of paclitaxel-delivering devices diminished substantially, which means that overnight the value of our field diminished substantially, because now it takes so many more repeat revascularisations in order to keep our patients whole and to keep these arteries open.”
The meta-analysis relied upon three RCTs—Zilver PTX, THUNDER, and IN.PACT SFA—that were followed up to four or five years and encompassed “a little over 800 patients,” Schneider remarked. Delving into the characteristics of the trials included, he noted that they were all powered for one-year patency, not long-term mortality, and that small control groups were used, leading to “unstable estimates”.
Key learnings: No dose effect, no clustering of deaths as to cause, and “substantial geographic variation” in mortality signal
As the meta-analysis pointed to causality between paclitaxel and mortality, Schneider stressed that it was necessary to assess whether or not there was a dose response. In the meta-analysis, dose was calculated as dose multiplied by time. Supposing a continuous, linear, and increasing exposure to paclitaxel over time is “quite an assumption,” said Schneider, detailing that tissue paclitaxel in pre-clinical models decreased over six months to nearly non-detectable levels and that time is disproportionately available for studies with longer-term follow-up.
When the FDA looked at dose response on mortality, Schneider recalled that “they found none,” specifying that the FDA included the LEVANT II, Zilver PTX, ILLUMENATE, and IN.PACT IDE trials in their assessment. Similarly, there was no dose relationship found in either the IN.PACT investigational device exemption (IDE) and Japan trials, or in the VIVA/North American Science Associates (NAMSA) individual patient data project, Schneider added.
The presenter stated that, along with dose response, it was also crucial to assess whether there was a clustering of deaths, as this would suggest a biological mechanism.
In the FDA analysis, Schneider relayed, there was no clustering of deaths. He elaborated: “There was an increase in deaths in the patients that had paclitaxel, but these were spread across numerous causes, really questioning the availability of a biological mechanism”. This led the FDA to issue a letter on 7 August 2019, stating that there was “no clear evidence of a paclitaxel dose effect on mortality, and no identified pathophysiologic mechanism for the late deaths”.
“We know that these trials were powered for one-year patency, so what about the five-year mortality?” Schneider wondered, stressing that many of the paclitaxel RCTs had a considerable number of patients lost to follow-up or who had withdrawn by this time point.
Through a “Herculean effort” by both the clinical sites and by the study sponsors, “a dramatic number” of these patients were identified, located, and their vital status ascertainment found, Schneider detailed. He noted that a five-year point estimate by the FDA developed a risk of 1.72, which after vital status ascertainment was 1.57, showing a decrease of 21%. The same happened in the IN.PACT IDE and Japan trials, he added, where the hazard ratio decreased by 38%, from 1.63 to 1.39 after vital status follow-up.
The third key point that Schneider addressed was the inconsistency of the mortality signal. In the IN.PACT SFA and the LEVANT II trials that were performed in both the USA and the European Union (EU), there was a “significant difference” in how the patients in the USA versus how those in the EU fared, with no apparent difference in mortality outside the USA, Schneider explained. “Why would this agent be more dangerous in one geography than another?” he asked.
“DCB and PTA patients are treated differently,” Schneider observed, adding that the difference in treatment is greater in the USA than in other geographies. Furthermore, he noted that the IN.PACT IDE and Japan trials, which were performed across different geographies using the same device, not only reveal this difference, but also show that PTA patients were more likely to follow up, with the biggest difference observed in the USA. “This really suggests that there may have been a treatment bias involved,” Schneider opined.
“When you include studies conducted outside the USA—ILLUMENATE EU, IN.PACT Japan, LEVANT I, and Lutonix Japan, for example—along with studies conducted on the same devices inside the USA—ILLUMENATE RCT, IN.PACT SFA, LEVANT II, and Zilver PTX—what you see is a significant drop in the hazard ratio,” he revealed.
Looking ahead: More data, continued collaboration, and trial design improvements
Summarising, Schneider noted that while paclitaxel is consistently efficacious, the mortality signal is not consistent. “There is no dose response and no biological mechanism, and the signal is not apparent so far in real-world data,” he communicated.
In addition, he told the VIVA audience that the signal is not consistent in the RCTs. The signal diminished with vital status ascertainment, and also when patients from outside the USA—where the signal was primarily observed—were included, he précised. “There is a possibility of treatment bias associated with trial design or practice patterns, which may help explain inconsistency of signal,” Schneider speculated.
The paclitaxel debacle is “crystalising,” the presenter concluded, pointing to an increasing volume of new data, with more to follow. Over the next five years, he revealed that 29 studies will yield randomised data on over 11,000 patients, including ILLUMENATE, IMPERIAL, TRANSCEND, VOYAGER, BEST, and SWEDEPAD.
Looking forward, Schneider pointed out that trial design improvements will be made with regards to the size, quality of follow-up, veracity of medical management, and vital status ascertainment.
Indeed, Schneider detailed how the VOYAGER trial sets an example for paclitaxel trials of the future. He commented: “One of the key things about VOYAGER, although it was not paclitaxel versus non-paclitaxel, is that it was a prospective randomised controlled trial in which they had excellent ascertainment, where they followed up more than 99% of the patients.” In addition, he mentioned that VOYAGER had “excellent control of medications”, which is “something that we did not do in the prospective randomised trials”.
At the end of his presentation, Schneider commended the continued collaboration of researchers, societies, manufacturers, and regulatory agencies “across specialties and countries” in the interest of moving things forward.
In relation to the role of the FDA specifically, an audience member asked what the agency has learned from the ongoing paclitaxel debate and how they will change things. “The FDA are in a challenging situation,” Schneider acknowledged. “Obviously they are there to protect the public health, but also to facilitate the ability for us to use the tools we need.”
He continued: “It is not clear to me what and how the FDA will use all the new information that is coming out, but there has been a massive amount of information. I did not go into the extensive amount of real-world data that we have but there is a tremendous amount, so I am sure the FDA is continually reconsidering this, but really the question is not the amount of data, but what is the threshold for them to act, for them to change the guidance that they gave us in August of 2019. Nobody knows that, and I do not know that they have even decided what that would look like.”
Schneider noted that the FDA has approved two paclitaxel devices since the paclitaxel situation began—the Ranger DCB from Boston Scientific and the IN.PACT AV Access balloon from Medtronic—which is “really the key”. He ended with the comment that “if [the FDA] felt there was a strong danger at this point, I do not believe they would approve new devices”.
The Infinity Angioplasty Balloon Company announced today that its angioplasty balloon platform—the Infinity angioplasty balloon catheter—has successfully completed a first-in-human clinical trial.
The platform was recently cleared by the US Food and Drug Administration (FDA) for percutaneous transluminal angioplasty (PTA) treatment of peripheral arterial disease.
“The Infinity catheter represents a game changing innovation in percutaneous angioplasty balloon design and utility,” states founder and vascular surgeon, John Pigott.
John A Phillips, an interventional cardiologist at OhioHealth Riverside Methodist in Columbus, USA, performed the first-in-human Infinity procedure. “I am extremely pleased with the catheter delivery and to-the-mm sizing of the balloon length to the lesion, particularly in this very challenging case,” commented Phillips. “The patient was a 60-year-old woman with highly angulated aortic bifurcation and a 78mm chronic total occlusion in the distal superficial femoral artery.”
According to a press release, the Infinity platform is the first and only therapy to provide Precision Angioplasty, to-the-mm sizing of balloon length to the lesion. Adopting the platform significantly reduces inventory needs and costs from dozens of stock keeping units and it reduces shelf space requirements, inventory management time, and trunk stock; while delivering the assurance that the right balloon size will always be on the shelf.
“Infinity is a highly differentiated product,” reports CEO Gary Smith. “This is an ideal product for both office-based labs and hospitals.” While initially launching the Infinity angioplasty balloon catheter, the company intends to follow quickly with the Infinity Defender, a drug-coated balloon (DCB) platform of similar design that will assure precise delivery of drug to the lesion site and minimise downstream and systematic effects.
Sinomed has announced the presentation of data from its inter-continental PIONEER III study comparing the safety and efficacy of the Supreme HT (healing-targeted) drug-eluting stent (DES), to the Xience (Abbott) or Promus durable polymer stent (Boston Scientific). One-year results were presented during a late-breaking trial session at the American Heart Association 2020 scientific sessions (AHA 2020, 13–17 November, virtual). The data showed equivalent clinical performance of the Supreme HT to the market-leading DES and will be used to support US Food and Drug Administration (FDA) and Japanese regulatory approvals.
The PIONEER III study enrolled 1,629 patients (randomised 2:1 experimental to control) from North America, Europe and Japan and had a primary composite endpoint of target lesion failure (TLF) at one-year. The TLF outcomes showed that the Supreme HT met the non-inferiority endpoint at 5.4% compared to 5.1% from the durable polymer DES (p=0.002). A grouped analysis of secondary endpoints showed a numerically better result for Supreme HT in cardiac death or target-vessel myocardial infarction (TV MI) with 3.5% in the Supreme HT arm compared to 4.6% in the control arm (p=0.27). Lower late stent thrombosis data (Supreme HT 0.1% compared to DP DES 0.4%, p=0.22) also suggested exceptional safety for the HT DES. A powered, landmark TLF analysis evaluating the healing superiority of Supreme HT between one and five years is ongoing.
“I am very pleased that Japanese patients will benefit from the most advanced DES in the US, Europe and Japan,” said Shigeru Saito, Shonan Kamakura General, Kamakura, Japan and primary investigator of the Japanese cohort of the PIONEER III study . “The results combined with the safety measurement of cardiac death, target vessel MI and late stent thrombosis favour the Supreme HT, supporting the early endothelial healing concept.”
The Supreme HT development was based on the “wound-healing window” concept originally proposed in 2013 and represents a novel class of DES that highlight the importance of early, timely healing, Sinomed said in a press release.
“We are very grateful to the extraordinary group of medical professionals and all the patients who have endured through this difficult pandemic and completed this study milestone in such a timely and professional manor,” said Jianhua Sun, chairman & chief executive officer of Sinomed. “The results have been extremely encouraging and if we reach superiority in the landmark analysis, we could revolutionise the understanding of healing and the future of implantable devices.”
Sean Lyden (Cleveland, USA), current VIVA Board president, speaks to Vascular News about his two years at the helm, which began with the “controversy on paclitaxel” and has led right up to COVID-19 and the first virtual VIVA meeting. Ten “amazing” late-breaking trials, two of which “brought increased clarity to the paclitaxel controversy”, were among the highlights of VIVA 2020, notes Lyden.
He goes on discuss the findings of a four-year meta-analysis from two major randomised controlled trials–ILLUMENATE EU and ILLUMENATE Pivotal– and explains why these results are so important. There was no significant difference in survival among patients treated with the low-dose Stellarex paclitaxel-coated balloon (85.7%) compared to those treated with percutaneous angioplasty (85.6%), notes Lyden.
More generally, Lyden brings attention to some of the current hot topics in the field of vascular medicine, including the continued vetting of the use of paclitaxel, the advent of new devices for the tibial section and the treatment of pulmonary embolism, which he states has been an “amazing breakthrough area”.
Moderate-to-severe calcification in peripheral arteries is an “ongoing battle” in in the endovascular treatment of complex lesions, William Gray (Philadelphia, USA), tells Vascular News.
Gray explains that there are a number of tools deployed to win the acute battle, but notes frankly that they have never been tested meaningfully in a randomised setting. In the longer-term patency war, when drug-coated balloons are employed as treatment options, interventionalists could use some “reinforcements”. he says.
It is in this context that the acute 30-days results from the DISRUPT PAD III data, billed as the largest-ever randomised clinical trial of severely calcified peripheral lesions, demonstrate superior outcomes with the use of intravascular lithotripsy (Shockwave) over percutaneous transluminal angioplasty.
“2020 has changed so much. But the need for IO education remains the same.” Cued to music and set against a backdrop of footage from previous conferences, lone individuals on laptops, and graphics of the now instantly-recognisable SARS-CoV-19 virus, this is the text that appears on the promotional video for the Symposium on Clinical Interventional Oncology (CIO), which took place virtually for the first time ever this year, with sessions livestreamed on each Tuesday in October 2020. “Undeterred by setbacks,” it continues, “this is your year to learn differently. Meet differently. See IO… differently.” At the time of writing, CIO 2020 is the most recent conference in the interventional radiology (IR) space to deliver education and networking opportunities online. As interventional radiologists look ahead to 2021, Interventional News speaks with thought leaders from IR societies across the world to capture their reflections on how the COVID-19 pandemic is impacting medical education.
“I do not think the pandemic is the end of the in-person meeting, rather the beginning of offering meetings accessible to all,” Erica Holland, interim executive director of the Society of Interventional Radiology (SIR), says. “SIR’s meetings, especially the annual scientific meeting, always feel like a family reunion, and we are looking forward to reuniting with our IR family as soon as it is safe to do so.”
Originally slated to be an in-person meeting in Seattle, USA, on 28 March–2 April 2020, the SIR annual scientific meeting was amongst the first events to be cancelled due to the COVID-19 pandemic. Constantino Peña (Miami Cardiac & Vascular Institute, Miami, USA), SIR 2020 programme chair, tells this newspaper this was “a disappointment”: “The annual meeting committee had spent so many months planning the programme, the awards ceremonies, and the networking events, and was excited to share them with our peers. We knew many of the researchers were eager to share their science with their colleagues and hear the feedback that is so important to expanding their work.
“But we were confident at the time that we made the right decision and that has been proven by how the spring unfolded. As a medical society, we knew we needed to lead by example during this public health emergency and ensure we were protecting our patients, colleagues, families, and communities by not creating a potential to spread the virus further. Interventional radiologists are data-driven, and the data we were presented at the time was unmistakable. There was community spread in the Seattle area, then the epicentre of America’s outbreak. There was a call from local officials, the Centers for Disease Control and Prevention [CDC] and the World Health Organisation [WHO] to limit social interactions and avoid large groups to stop the spread. There was the information from our members telling us their institutions were limiting travel to flatten the curve and ready to respond to the inevitable outbreaks in their hometowns. The team came together, and absorbed and analysed data quickly to make a correct and timely decision.”
The emergence of a post-pandemic hybrid model
Delegates attending CCI 2020 in person
The annual meeting of the Chinese College of Interventionalists (CCI), initially scheduled for April 2020, was postponed due to the pandemic. Whilst SIR 2020 took place as a fully virtual event 13–14 June, CCI 2020 was rescheduled for 27–30 August as a hybrid virtual/ in-person meeting in Nanjing, China.
“Although this new meeting mode brings a unique attendee experience for CCI meetings, it also presents a big challenge in terms of planning, in order to ensure audience satisfaction,” Gao-Jun Teng, CCI president, says, thinking back to the months of preparation that went into the 2020 event. Seven host venues were used in total; a “main” venue in Nanjing, and six “branch venues” across the country, which CCI say “were to let more IR professionals easily get involved”. In total, there were over 16,000 registered participants, who were able to access 153 scientific and workshop sessions, 796 lectures, and 76 live demonstrations of IR procedures.
“I am proud to conclude CCI 2020 a big success,” Teng told virtual and in-person attendees of the meeting’s closing ceremony, “and [declare] it a ‘sweet marriage’ between the virtual and physical meeting settings. Except for the completely online English- speaking sessions, almost all lectures were delivered in physical meeting rooms in Nanjing and the other six cities, while most audiences could just stay at home. This has no doubt brought attendees great convenience to participate with minimum travel and cost. Most importantly, it also broke territorial boundaries to allow more attendees to engage in and more citizens to appreciate this fairly new but strongly developing, medical specialty.” Indeed, following the strength of the hybrid model’s success at CCI 2020, the college is continuing with this format in 2021.
These boons of increased attendance and accessibility facilitated by the virtual meeting have been echoed by other IR societies. President of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Afshin Gangi (University Hospital of Strasbourg, Strasbourg, France) weighs in: “While I do believe that the virtual model brought a lot to the table in terms of accessibility, I strongly believe that the major congresses will go back to an in-person format after the pandemic. This, however, will not mean in-person only. We at CIRSE plan to also further develop a strong virtual component of our physical congresses; a hybrid model if you will. Medical education in general will of course require both in-person courses and congresses, as well as online learning opportunities. I believe for IR in particular, it is vital for professionals to be able to physically come together to meet, discuss important data, and interact with the latest technology. Virtual-only will not be the future.”
Speaking on behalf of SIR, Holland muses: “One of the interesting benefits of being all virtual is the fact that it has allowed us to expand access to our offerings to our members. We often hear that attendance at the annual scientific meeting is staggered in practices to ensure coverage at the home institutions, meaning some interventional radiologists attending may not be able to stay for the whole meeting, if they are able to attend at all. That is not generally an issue for virtual meetings as you can log on when you are available and absorb the discussion and even watch it on demand later on, depending on the meeting.
“Post-pandemic, I think you will see a pent-up demand for meeting again in person. Networking and community are a huge part of SIR’s meetings and part of the value of an in-person meeting are the sidebar conversations that happen after a presentation or when you bump into colleagues on your way to plenary session or expo hall. Those are impossible to replicate in the virtual space.
“At the same time, not everyone will be ready or able to attend our events in person, so we may see a hybrid model emerge that live streams what is happening on site for those who cannot be there in person.
“In addition, some of the virtual networking opportunities SIR created to fill the gaps while meeting sizes are still restricted, like our new virtual angio club series, are specifically designed to stay in the long term. Many of our members work in areas that do not have local angio clubs where they can regularly meet with their peers, learn, and exchange ideas. While SIR’s virtual club was born out of the necessity presented by the pandemic, it uncovered an important, longstanding need in our community, and we are excited to have this series continue in the long term to support interventional radiologists in their practice no matter where they are.”
When asked if she believed the future of medical conferences would follow a virtual, live, or hybrid model, Jena Eberly Stack, executive director of Society of Interventional Oncology (SIO), commented: “This is the million-dollar question! While I do not have a crystal ball, I can say that there are wonderful, unexpected benefits of virtual learning experiences, and there are also cherished, deeply missed aspects of in-person learning experiences. I am sure we will see a mix of both once we are able to safely meet in person again, offering tailored opportunities based on the type of information and education being shared.”
Spring IR conferences confirm they will be online-only events
Unlike the annual scientific meetings originally scheduled in the springtime, CIRSE had several months to anticipate the possibility of hosting a virtual meeting, something Gangi says was “essential […] to ensure everything went smoothly online”. Commenting on the event, held 12–15 September 2020, he adds: “We received overwhelmingly positive feedback from our stakeholders regarding the high calibre of educational content, interactive learning, and networking opportunities, and first-rate organisation. While of course we missed the opportunity of physically meeting together as in previous years, the CIRSE 2020 Summit was able to ensure an equally high level of educational content with our top-notch faculty streaming in from around the world, giving over 1,000 presentations, and also provide ample networking opportunities through the interactive presentation formats and chat functions available at every level of the platform.”
In total, there were 18,000 active users on the CIRSE 2020 Summit platform, the society claim, with almost 5,000 attendees from 115 different countries logging in and creating more than 20,000 chat messages over the course of the four live event days. While Gangi says these figures paint a positive picture of intra-conference communication, he adds this caveat: “I think the quality of interaction and collective creativity that is achievable online is not the same as we usually have at a physical congress. I therefore strongly hope that we will be able to meet again in-person at the CIRSE annual congress in 2021 in Lisbon, Portugal.” At the time of writing, this meeting is scheduled for 25–29 September 2021.
When questioned on his event expectations for 2021, Gangi said: “We are in the same spot as everyone else at the moment: waiting for a vaccine and hoping the situation will improve. While we hope and plan for in-person meetings, we are prepared to host the meetings in any format we can, and that might be online or in a hybrid format. One thing is certain—all CIRSE events in 2021, including the European Congress on Interventional Oncology (ECIO), the European Conference on Embolotherapy (ET), and the CIRSE annual scientific meeting will take place.”
Gearing up for SIO 2021, which will be held virtually 5–8 February 2021, Stack reflect on the 12 months’ experience the society has had to prepare for a potential online meeting (the society’s annual scientific meeting was one of the few IR congresses able to take place in person this year, 31 January–3 February 2020, New Orleans, USA). “The world certainly looks different today than it did a year ago, and our preparations for SIO 2021 reflect this shift in our landscape,” she says.
“We have held and observed several virtual events over the last seven months, and the learnings from those activities have provided feedback we are incorporating into our planning process for SIO 2021. Providing timely programming, valuable avenues to skill-build, and quality networking opportunities remain our commitment to our attendees, and we are achieving this through thoughtful programme development. SIO 2021 will be an interactive experience—not just a series of webinars—designed to mimic the best parts of an in-person event and capitalise on the unique opportunities a virtual event has to offer.”
SIR 2021 will also be held online. Peña assures readers that this “will be a completely different experience from any previous SIR meeting, including the SIR 2020 virtual offering”. He elaborates: “Given the uncertainty of the landscape, the unique nature of our specialty, and the need for members to stay safe and healthy to deliver patient care, we decided to postpone the in-person portion of our programming now so that we have adequate time to plan for and deliver an all virtual format that provides the same cutting-edge, high-quality programming that our members expect from the annual scientific meeting.
“Unlike SIR 2020’s virtual offering, which was deployed as a standard webinar platform, for 2021 we will replicate the feel of an in-person event as closely as possible through an interactive platform complete with meeting rooms, plenary sessions, an interactive expo hall, and on-demand offerings. We are also exploring ways to deliver the important networking opportunities, committee meetings, and our awards ceremonies honouring those who have greatly contributed to the advance of the specialty. […] We are confident that SIR members will find this online learning experience a not-to-be-missed event.”
Indeed, Holland believes the switch to all virtual education this year, which she says “is spurring SIR to move forward with a total reimagining” of their educational offerings, was actually already a part of the society’s strategic plan. “The pandemic has been a catalyst for us to take things down to the brass tacks and rebuild it anew in a way that is as agile as IR,” she surmises. The consensus amongst the international IR community is that conferences with at least a virtual component are here to stay. hybrid hybrid hybrid hybrid hybrid hybrid hybrid
According to a press release, Transit Scientific’s XO Score system has been successfully used to dilate multiple challenging fibrotic and calcific lesions in haemodialysis patients with stenotic and occluded fistulas. Richard Saxon (Tri City Medical Center Medical Center, Oceanside, USA) performed the first procedures using the XO Score. Treatment of all the lesions proved successful.
“The XO device performed well and demonstrated effective lesion dilatation at low pressures with a variety of our standard angioplasty balloons,” said Saxon. “The rotating scoring struts appeared to be effective against a mix of fibrous and calcified lesions which tend to be highly resistant to plain old angioplasty.”
Specialty scoring and cutting angioplasty balloons are manufactured with integrated struts, wires, or blades to reduce vessel dissection, dilation pressure, and assist with vessel preparation for atherectomy and/or stenting. However, scoring and cutting balloons also add profile, bulk, expense, inventory, and complexity.
The XO Score is different, a press release states, detailing that XO Score technology allows users to convert basic angioplasty balloons in the hospital’s existing inventory into sophisticated scoring, cutting, and infusion/delivery devices.
“One of the procedures required five separate inflations at various points along the native fistula and outflow vein, all of which were accomplished using the same XO Score device,” continued Saxon. “The ability to achieve a more predictable result at a lower and potentially safer pressure in resistant lesions could prove important in achieving the best possible PTA outcomes and thereby help in fistula maintenance. The fact that you can take quick angiograms through the XO Score and around the PTA balloon was a nice additional feature.”
During an XO Score procedure, clinicians insert a basic angioplasty balloon into the ultra-thin XO Score sheath and advance the combined balloon and XO sheath to the stenosis. When the balloon is inflated, up to 22 evenly spaced XO Score struts expand with the balloon and rotate 900 to score and cut the narrowed vessel. When the balloon is deflated, the struts rotate 900 back to an atraumatic position to assist balloon rewrap and removal.
“We are thrilled to see the XO Score contribute to patient care,” said Greg Method, president and CEO of Transit Scientific. “These procedures demonstrate XO Score effectiveness against a variety of lesion types. We look forward to growing the platform to treat complex peripheral arterial disease (PAD), critical limb ischaemia (CLI), along with haemodialysis access patients.”
The XO Score system has been cleared by the US Food and Drug Administration (FDA) to dilate stenotic material in iliac, femoral, iliofemoral, popliteal, infrapopliteal, and renal arteries and for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistula.
AngioDynamics has announced the safety and efficacy results from the RAPID (Registry of AngioVac system procedures in detail) database. Results were shared by principal investigator John Moriarty (University of California Los Angeles [UCLA], Los Angeles, USA), at this year’s Vascular Interventional Advances meeting (VIVA 2020; 6–8 November, virtual).
The registry was designed to evaluate the patterns of use, safety, and efficacy of the AngioVac system in the bulk removal of undesirable intravascular material. The registry enrolled 234 patients across 21 sites, surpassing its 200-patient enrolment goal. Among enrolled patients, 48.3% had a mass in the right heart, 35.9% had caval thromboemboli, 8.5% had catheter related thrombi, 1.7% had a pulmonary embolism, and 5.6% had a combination of the above.
“RAPID represents the largest catheter-based thromboaspiration study completed to date, and we are pleased to share its positive findings,” said Scott Centea, AngioDynamics senior vice president and general manager, VIT/PAD. “A growing number of providers are recognising the AngioVac system as a critically important tool in the treatment and removal of thrombi and emboli. The overwhelmingly positive results from the RAPID registry demonstrate that the AngioVac system is appropriate for use by a wide range of providers treating thrombus, clot, and vegetations in both peripheral deep vein thrombosis (DVT) and the right heart.”
Findings from the RAPID registry have been accepted for publication in the Journal of Vascular and Interventional Radiology.
The primary objective of the registry was to capture data on the use of the AngioVac system for various anatomic locations. Greater than 70% of clot/mass removal was achieved in a majority of the patient population. Overall, the study confirmed the AngioVac system to be versatile, safe, and effective for the removal of vascular thrombi and cardiac masses across a broad range of patient populations.
“Our goal threshold was to remove over 70% of the clot, which we felt was clinically relevant, and each of the three main groups—the caval group, the right heart group, and the catheter associated clot group—were associated with very high rates of clot removal,” commented Moriarty. “In the first two years of the registry, there were more caval thrombectomies than right heart mass procedures, and that flipped in the latter two years. If we were to extrapolate our trajectory, we would say that close to 70% of all procedures are being performed in the right heart. Additionally, the AngioVac system was successfully tested by a number of different practitioners, including cardiologists, EP cardiologists, cardiac surgeons, vascular surgeons, and interventional radiologists. Ultimately, the diversity of providers, combined with the efficacy and safety results, demonstrates the unique and versatile nature of the AngioVac system.”
Efthymios Avgerinos (Pittsburgh, USA) speaks to Interventional News about the SUNSET sPE trial, the one-year results of which he presented at VIVA 2020 (Vascular International Advances; 6–8 November, virtual), and which compared ultrasound-assisted thrombolysis (USAT) to standard catheter-directed thrombolysis (SCDT) in patients with submassive pulmonary embolism.
The primary endpoint was thrombus reduction and secondary endpoints included RV/LV ratio improvement, intensive care unit (ICU) stay, bleeding, and other serious adverse events. Participants were randomised 1:1 to a USAT catheter (EKOS System) or a SCDT catheter (Unifuse, Cragg-McNamara).
In the context of “cost-conscious health systems”, Avgerinos, who was one of the principal investigators of the trial, explains the importance of studying the financial viability of these two interventions. He outlines the key aims of the trial, whose findings showed that although a USAT catheter is “10 times more expensive” than a SCDT catheter, there was no significant difference in mean thrombus score reduction between the two groups (p=0.76) despite a similar average tPA dose and average lysis time.
In the USAT group (n=39), the mean raw pulmonary thrombus score was reduced from 31±4 at baseline to 22±7 (p<0.001). In the SCDT group (n=41), the score was reduced from 33±4 to 23±7 (p<0.001).
Avgerinos states that thrombolytic techniques are, in general, “safe and effective” and are “here to stay”, before concluding that despite this “we need to learn more and that is what we are doing”.
Steven Kum takes questions from the panel at VIVA 2020
Steven Kum takes questions from the panel at VIVA 2020
The Absorb bioresorbable vascular scaffold (BVS; Abbott Vascular) can be used for the treatment of chronic limb-threatening ischaemia (CLTI) patients in infrapopliteal arteries with no safety concerns and favourable patency, rates of reinterventions, and amputations at a mid-term follow-up of two years. This was the conclusion presented by Steven Kum (Changi General Hospital, Singapore) during a late-breaking data session at this year’s Vascular Interventional Advances annual meeting (VIVA 2020; 6–8 November, virtual).
CLTI continues to plague many patients worldwide and is associated with complex comorbidities, poor vessel patency, and major lower extremity amputations. Plain balloon angioplasty is still the mainstay of treatment although metallic drug-eluting stents have shown promise. This multicentre pooled analysis investigates the mid-term outcomes of a drug-eluting BVS in the treatment of CLTI.
Consecutive patients with de novo infrapopliteal lesions were treated with Absorb BVS at three centres (in Singapore, Chicago, and Sydney) between August 2012 and May 2017. Restenosis was defined on colour-flow Doppler examination with a sensitive peak systolic velocity (PSV) ratio >2 or PSV >2m/s (equivalent to >50% stenosis).
A total of 121 patients with 161 lesions were treated with 189 Absorb BVS in 126 limbs.
The mean age of the patients was 73 years. Fifty-seven per cent of patients had diabetes and 75% had tissue loss. Of the 161 lesions treated, 63% were calcified and 22% were occlusions. Median lesion length was 21mm (4–88mm). Successful deployment was achieved with all scaffolds.
Kum reported that there was no mortality in 30 days. Primary patency was 90.3% and 86.6%, and freedom from clinically driven target lesion revascularisation (CD-TLR) was 97.2% and 96.6% at one and two years, respectively. Major amputation occurred in 1.6% of the limbs and overall survival was 85.8% at two years.
Looking forward, Kum announced that the current LIFE-BTK randomised multicentre trial with the novel Esprit BTK drug-eluting resorbable scaffold (DRS) will help further assess the significance of these findings.
The Royal College of Radiologists (RCR) has welcomed the Getting It Right First Time (GIRFT) report into imaging services in England, released 10 November. One of the key recommendations of the report is for radiology departments to have dedicated provision of interventional radiology (IR) facilities.
The GIRFT radiology team, led by consultant radiologist Katharine ‘Kath’ Halliday (Nottingham University Hospitals NHS Trust, Nottingham, UK), and supported by RCR past-president Giles Maskell (Royal Cornwall Hospitals NHS Trust, UK) and radiology service experts Elaine Quick (Salford Royal NHS Foundation Trust, UK) and Lucy Beeley (Mid Yorkshire Hospitals NHS Trust, UK), spent more than two years investigating variation across National Health Service (NHS) imaging services, analysing data and visiting hundreds of hospital radiology departments. The team also consulted with the RCR and the wider radiology community.
The primary stated aim of the GIRFT radiology national specialty report is to make radiology services more patient-centric and accessible. Major themes include the need for standardised, streamlined radiology pathways and systems, and efficiencies in workload and workforce management.
The report covers the impact of COVID-19 on services and builds on issues highlighted in previous radiology investigations, such as the Care Quality Commission’s 2018 Radiology Review and a recent entitled “Diagnostics: Recovery and Renewal”, as well as various RCR publications.
Key patient-focussed recommendations include the ongoing creation of community-based diagnostic hubs recently promised by NHS England/Improvement (NHSE/I), online booking and extended hours to suit outpatient appointments, and dedicated provision of IR facilities.
The GIRFT team’s remit was to identify how imaging services can reduce variation and look to free up capacity and maximise existing resources.
However, the report authors emphasise that NHS imaging cannot provide the best possible service for patients or clinicians without more staff and resources.
They state: “Unless there is investment in increasing staff numbers overall, it will not be possible to provide the quality of service that patients expect, that other departments require, and that radiology teams wish to deliver.”
Welcoming the report’s publication, RCR vice president for clinical radiology William Ramsden (Leeds Children’s Hospital, Leeds, UK) says: “The GIRFT report is truly comprehensive, clearly stating the pivotal role of imaging in patient care, alongside the complex and significant pressures facing departments, and making positive recommendations to improve diagnostic and IR provision across England.
“As well as backing the RCR’s calls for increased investment in departmental space, equipment, and staffing, and the ongoing creation of imaging networks, the authors detail insightful suggestions for optimising imaging pathways and the use of resources and data. All of this will make NHS radiology more patient-focussed, accessible, and efficient, and we strongly endorse the team’s recommendations.”
The report makes 20 headline recommendations, with more than 50 supporting actions to be undertaken by trusts, the GIRFT team, NHSE/I, the RCR, and imaging community stakeholders.
The GIRFT report
Short-term and ongoing GIRFT recommendations include:
The creation of imaging networks, in line with NHSE/I’s target of 18 nation-wide networks by 2035
Imaging community stakeholders to continue ongoing work to review NHS coding for diagnostic and interventional radiology and end multiple NHS data submissions
National targets for time from imaging test-to-report, to be progressed by trusts and NHSE/I over the next six months
All radiology services to work towards providing dedicated facilities for IR day-case patients, with further guidance from GIRFT due in the next 12 months
Medium- and long-term recommendations include:
National protocols for imaging common conditions, to be progressed by GIRFT, the RCR, and the Society of Radiographers (SoR) over the next 18 months
Standard definitions and expected productivity for radiologists, to be progressed by the RCR over the next 18 months
Reporting standards for radiographers and radiology trainees, to be progressed by the RCR and SoR over the next 18 months
NHSE/I to create real-time demand management tools for diagnostic and interventional workflows, over the next two years
Commenting further on the GIRFT recommendations, Ramsden adds: “Despite being under-resourced, we know IR expertise saves lives and saves the NHS money. We particularly applaud the GIRFT team’s moves to boost recognition of IR via calls to expand IR day-case capacity on a national scale and improve monitoring.
“We agree there is scope to maximise existing diagnostic and interventional capacity through improved oversight and understanding of radiologists’ workloads, as well as enabling appropriate role extension for allied health professionals. We have started project work on those recommendation areas, alongside the SoR and other stakeholders. Trusts must also take seriously the report’s recommendation to assess workforce needs, and the RCR can help services here by sharing our comprehensive radiologist census data.
“However, given the ongoing crisis in imaging department staffing, we must again stress that these efficiency solutions will still only take us so far without the substantial workforce increases that NHS radiology desperately needs.
“On reporting targets, we previously welcomed the premise of national standards for the reporting of imaging, stating targets could be phased in to help benchmarking, and we appreciate GIRFT supporting a soft approach to any implementation.
“We are pleased to see GIRFT recommend standardised radiology IT solutions and the use of referral software. These are ‘quick win’ systematic improvements for helping to manage demand and have long been championed by the RCR. The suggested creation of real-time workflow management dashboards for both diagnostic and IR activities also has exciting potential.
“There are already many inspirational examples of local service innovation, as demonstrated by the host of departmental case studies featured throughout the GIRFT report, and the community as a whole is engaging with national initiatives such as the creation of imaging networks and guiding artificial intelligence tools in development.
“It is now essential that NHS leaders and providers engage with the GIRFT radiology programme as it progresses, supporting radiology teams to upskill, adapt and adopt best practice.
“The recommendations are ambitious but achievable, and we look forward to working with the GIRFT team, trusts, and other national bodies to see them realised.”
Surmodics recently announced that six-month data from the AVESS first-in-human (FIH) study of the company’s Avess arteriovenous fistula (AVF) drug-coated balloon (DCB) was shared at this year’s Vascular Interventional Advances virtual conference (VIVA 2020; 6–8 November, virtual).
The AVESS study is a prospective, multicentre, single-arm study to assess the safety and performance of the Avess DCB when used in the treatment of subjects with obstructive lesions of AVFs for haemodialysis.
Six-month data from the study show that target lesion patency at 30 days and six months was 100% and 90.9%, respectively. A single reintervention was required within six months, with no AVFs thrombosed. The study’s primary safety endpoints reported no mortality and no device or procedure related adverse events at 30 days, and all patients maintained functional AVFs for haemodialysis.
“This first-in-human study demonstrates that the Avess DCB is a safe and promising treatment for AVF stenosis, which can lead to vascular access dysfunction, thrombosis and loss,” said Ramon L Varcoe, associate professor of vascular surgery at Prince of Wales Hospital (Sydney, Australia) and co-lead investigator for the AVESS FIH clinical study.
“Previous AVF studies have demonstrated that DCBs effectively reduce rates of restenosis after percutaneous angioplasty,” added Andrew Holden, associate professor, director of Interventional Radiology at Auckland City Hospital (Auckland, New Zealand) and co-lead investigator for the AVESS FIH clinical trial. “The Avess DCB is a next-generation DCB that may provide further clinical benefits while minimising systemic paclitaxel exposure.”
Data presented include six-month results from 12 patients treated with an Avess DCB between December 2018 and August 2019. The majority of AVFs were radiocephalic (10/12, 83.3%) with the stenosis located in the juxta-anastomosis (7/12, 58.3%), cannulation zone (2/12, 16.7%), and outflow (3/12, 25%). All patients completed follow-up at or beyond six months.
“Our goal with all of our DCB platforms has been to advance the technology to improve drug transfer and distribution effect on the arterial wall offering the opportunity to use a lower drug dose,” said Gary Maharaj, president and CEO of Surmodics. “We are quite pleased with the AVESS first-in-human study results, which provide vital safety data on the Avess DCB and directional data on its effectiveness. This FIH data strengthens our believe that the Avess DCB could be a safe and promising treatment that improves patient outcomes while reducing the number of interventions needed to maintain patency.”
The first person to perform a transjugular intrahepatic portosystemic shunt procedure (TIPS) in Greece, Adam Hatzidakis discusses his career-long love affair with the hepato-biliary-pancreatic system, and describes the delights and difficulties of being a trailblazer in the interventional radiology (IR) space. Speaking seven months after the SARS-CoV-2 virus first caused multiple governments to impose national lockdowns and resulted in widespread international travel bans, Hatzidakis also hopes that the shift to digital conferences is here to stay, at least in part, “so that more colleagues may benefitfrom the international educational opportunities on offer”.
What initially attracted you to interventional radiology (IR)?
I was initially attracted to radiology because I loved imaging and trying to find the “pathological hidden in the physiological”. Then I discovered interventional radiology, where I had the possibility to “clean” the physiological from the pathological.
Have you had important mentors for you throughout your career?
Yes, several. To start, my first professor, Nicholas Gourtsoyiannis, in Heraklion, Crete. He taught us the importance of becoming clinical radiologists, and how to have a presence on the international stage. Together with my tutor and friend Spyros Karampekios, we performed the first IR procedures in Heraklion, back in 1993.
Next, my IR teacher, Panos Galis, at the AirForce Hospital in Athens, Greece. He was a Greek pioneer in vascular IR, and I learned many tricks from his experience.
Another three titans of IR who have been personally important: Plinio Rossi from Rome, Italy; Rolf Guenther from Aachen, Germany; and Andreas “Andy” Adam from London, UK. Beside great IR teaching, in London I learned how to manage, in Aachen how to organise, and in Rome how to improvise. All experiences were of great value.
Why are you specifically drawn to the hepato-bilio-pancreatic system? What do we still have to learn about treatment in this system?
In the era of magnetic resonance cholangiopancreatography (MRCP), endoscopists have fewer possibilities to practice so many endoscopic retrograde cholangiopancreatographies (ERCPs), with the result that new doctors are less well trained. So, radiologists usually have more to do. Biliary IR is delicate work, offering you a lot of challenging cases. Performing malignant cases is good training for tough benign cases.
In 1996, you performed the first transjugular intrahepatic portosystemic shunt procedure (TIPS) in Greece. How did this come about?
That was my passport to the future. The case went well, although the patient was not able to survive for a long time. Performing this case helped to create a lot of respect for my work and IR more generally, but the expectations others have from you can become a very heavy burden. I learned that I had to constantly perform at a high level, and try to be involved in novel procedures, so that everybody could benefit from this. I think one can feel that they have to fulfil the obligation to continue working at a high scientific level in order to show the younger generation of interventional radiologists their way to the top.
In 1998, you were one of the first interventional radiologists in Greece to perform percutaneous liver tumour ablation. What are the most exciting and the most intimidating aspects of working at the vanguard?
This is the reason why I like working in University Hospitals. Patients and other medical specialties can trust you more easily when it comes to new methods and techniques. Of course, you have to perform the procedures well and safely, with nice results to keep a good and trustful name. Sometimes this is not enough, because other specialties do not want to move to new methods and lose control of their patients, or stop performing what is common practice to them in favour of IR methods. The same happened in the old days with oncologists who did not want to stop chemotherapy protocols and send patients to radiofrequency ablation (RFA) in order to calculate total survival rates. The same thing still happens now with other IR techniques such as vertebroplasty, varicocele and fibroid embolization, and I am afraid it will also happen with prostatic artery embolization.
Could you describe a particularly memorable case?
Yes, definitely the first TIPS procedure done in Greece. I was still a last year radiology resident and I was asked to try to performed it. There were five university professors outside the angiography suite, and I needed five hours to complete the case. I would of course never have managed it without their trust and the good help of two senior radiologists who were my teachers and the backbone of our department.
As deputy chair of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) programme committee 2019–2021, and upcoming chair of the same committee, what are your goals for scientific education over the next two years?
Providing medical education has become difficult due to travelling restrictions. But this problem has convinced international medical societies to transition to a digital education format. Our last CIRSE Summit (12–15 September, virtual) is such an example. The set-up we managed to create in such a short time and the transformation of the programme from a live event to a digital one was a big challenge.
I am confident that this shift to online learning has come to stay. The future will be full of hybrid congresses with both live and distant participation. I hope during the next two years that we will be able to go back to face-to-face events, as these are very important for communication between doctors and industry, but also maintain some remote-learning capabilities, so that more colleagues may benefit from the international educational opportunities on offer.
How has the COVID-19 pandemic impacted IR this year, and do you foresee a lasting change to the discipline?
It was a hard time for everybody. Our University Hospital in Thessaloniki closed for almost every other activity. We were asked to perform only emergency cases. But due to the fact that the surgical departments also decreased their activities, we managed to keep a decreased but adequate number of cases to continue our clinical work. I am confident that the role of IR departments will come out of this crisis more powerful than before, because we provide minimally invasive solutions without need for intensive care unit (ICU) beds.
On a personal level, what are the central preoccupations when treating patients during a global pandemic?
Be aware of COVID-positive patients, treat them carefully, and keep your staff safe.
In your opinion, what is the most interesting research coming out of Greece in the IR space right now?
Greek interventional radiologists try hard to maintain a high level of medical services, and to convince patients and other physicians about the possibilities our treatments can offer. Research has always been a tough task in our country, usually due to a lack of financial resources. Nevertheless, there are Centres of Excellence like in Patras, where a lot of research work is conducted in the peripheral vascular disease space and in arteriovenous fistula creation. Athens also has a couple of centres working on interventional oncology therapies in the thorax, abdomen, and musculoskeletal systems. We in Thessaloniki are trying to create a Centre of Excellence for primary and secondary liver tumours, in good cooperation with a local transplant centre. I am pretty confident that this cooperation will be fruitful in the future.
What are the main challenges when treating HCC patients via IR techniques? How and why is interdisciplinary collaboration important?
HCC patients are quite complex. Experienced hepatologists, together with surgical oncology and transplant colleagues, are needed to decide how to treat every case. The cooperation of hospital tumour boards demonstrates the importance of being a clinical radiologist; being treated as an equal is the best reward for your work.
What are your hobbies and interests outside of medicine?
I love traveling and learning about other cultures. I am a big fan of various sports, especially soccer, basketball, and tennis, which I also played myself. I enjoy good company with my beautiful family and many good friends, which I am blessed to have. Hatzidakis Hatzidakis Hatzidakis Hatzidakis Hatzidakis Hatzidakis Hatzidakis
José Hugo Luz presenting at the virtual ECIO 2020 meeting
In a comparison of the regenerative capacity of portal vein embolization (PVE) before major hepatectomies with two different embolic materials, N-butyl-cyanoacrylate (NBCA) with lipiodol was shown to be superior to polyvinyl-alcohol (PVA) particles plus coils. Speaking during the virtual European Conference of Interventional Oncology (ECIO; 4 November 2020, online), José Hugo Luz (Curry Cabral Hospital and Nova Medical School, Lisbon, Portugal) presented the results of the randomised, controlled BestFLR (Best future liver remnant) trial.
Liver regeneration strategies, such as PVE, are crucial in enabling patients to undergo major hepatectomies, Luz informed delegates. Contextualising the BestFLR trial, he went on to explain that PVE has gained acceptance as the standard of care for inducing liver growth in the last few decades. However, the optimal embolic material for PVE has not yet been established. “There are some suggestions in the literature that NBCA glue (Glubran, GEM) with Lipiodol (Guerbet) might generate more liver hypertrophy,” he said.
The BestFLR investigators therefore set out to determine which embolic material, NBCA-Lipiodol or PVA plus coils, produces the highest healthy liver growth during PVE. In order to be enrolled in the study, the future liver remnant (FLR)—the volume of healthy liver that will remain with the patient after surgery—had to be 25% or less of the total liver volume in healthy liver patients, 35% or less in colorectal patients, and 40 to 45% or less in patients with cirrhosis or cholestatic liver disease.
The 60 patients enrolled in the trial were randomly assigned to receive PVE with either NBCA-lipiodol or PVA plus coils (30 in each group). Baseline characteristics, such as age, sex, comorbidities, weight, height, and presence of cirrhosis, were equivalent amongst the two cohorts. The most common tumour types included in the study were colorectal metastases (45%) and cholangiocarcinoma (35%).
Detailing the embolization technique used by the triallists, Luz recounted: “We injected PVA particles of increasing size until [we reached] flow stasis, followed by proximal coils (6–12mm in diameter) to achieve complete venous occlusion”. For NBCA-Lipiodol, they injected a solution of different concentrations depending on the approach used: when injecting from the contralateral side, a 1:3 dilution was used, and when obtaining ipsilateral access to the liver, they used a 1:5 dilution through a microcatheter.
The primary outcome of the BestFLR trial was liver regeneration 14 and 28 days after PVE, assessed by computed tomography (CT) volumetry. The specific endpoints measured were FLR degree of hypertrophy, FLR absolute hypertrophy, and kinetic growth rate (KGR). Secondary outcomes included the occurrence of post-hepatectomy liver failure, intraoperative incidents, blood loss, transfusions, surgery duration and hospital stay, PVE contrast volume used, fluoroscopy and total procedure time, as well as the rate of minor and major complications after PVE. All patients gave voluntary informed consent to participate in the trial, which is registered in a World Health Organisation (WHO) registry network.
Triallists encourage earlier assessment of patients for hepatectomy in light of positive results at 14 days post-embolization with NBCA-lipiodol.
After 14 and 28 days, all volumetric parameters were superior for PVE with NBCA-Lipiodol compared to PVE with PVA plus coils, such as greater absolute liver hypertrophy of 46.4 versus 29.6, p<0.001 and 57.0 versus 36.7, p<0.001, respectively.
“An interesting finding that we had in this study is that patients were ready for surgery after just 14 days,” Luz said. In the NBCA-Lipiodol cohort, 87% of patients had a sufficient FLR ratio for liver surgery after 14 days. This was higher than amongst the PVA plus coils cohort, where 55% of patients were eligible for surgery after the same time period (p=0.008).
“These data encourage us to assess patients earlier,” Luz told the ECIO audience, “14 days after PVE if we are using NBCA-lipiodol, which we are now after the Trial. This shorter waiting period to enable patients to undergo curative hepatectomy might decrease tumour progression, which is the main cause of precluding liver surgery.”
Addressing patient outcomes, he shared that 24 patients (80%) in the NBCA-lipiodol group underwent a successful hepatectomy after PVE, compared to 23 (76%) in the PVA plus coils group (p=0.32). Three patients in the NBCA-lipiodol cohort (12%) and seven patients in the PVA plus coils cohort (27%) had clinically-relevant liver failure (p=0.27).
Fluoroscopy and total PVE time were also significantly lower for NBCA-lipiodol versus PVA plus coils (16 minutes vs. 25 minutes, p<0.001, and 60 minutes vs. 80 minutes, p=0.0023, respectively).
At the time of writing, the results of the BestFLR trial are under submission for publication.
Ehrin Armstrong presents two-year DETOUR I outcomes at VIVA 2020
Ehrin Armstrong presents two-year DETOUR I outcomes at VIVA 2020
During a late-breaking data session at this year’s Vascular Interventional Advances annual meeting (VIVA 2020; 6–8 November, virtual), Ehrin Armstrong (University of Colorado, Denver, USA) presented two-year outcomes from the DETOUR I trial for percutaneous femoropopliteal bypass. He reported a 96% clinical success rate, with 83% of patients at Rutherford class 0 at two years, which “shows excellent functional improvement in a patient population facing severely debilitating PAD [peripheral arterial disease]”.
The DETOUR I trial was designed to evaluate the safety and effectiveness of the Detour system for percutaneous femoropopliteal bypass, which recently received US Food and Drug Administration (FDA) breakthrough device designation.
Using the novel PQ crossing device and a series of specially designed Torus stent grafts, the Detour procedure was created to route blood flow around severe lesions caused by complex peripheral arterial disease found in the superficial femoral artery. The procedure uses the femoral vein as a pathway for a Torus stent graft conduit and travels from the artery to the vein and back into the artery.
Now reporting two-year data, the trial enrolled a complex patient cohort with an average lesion length of 371mm; 96% of lesions had a confirmed chronic total occlusion, and 80% had evidence of moderate to severe calcification. At one and two years’ post-procedure, the study is reporting an 81% and 79% primary patency rate, respectively, as well as a rate of freedom from major adverse events of 83.7% and 82.1% at one and two years, respectively.
Armstrong also announced that, with FDA breakthrough designation and recent enrolment completion, DETOUR II is “on track to provide results earlier than expected”.
Concept Medical has announced the enrolment of the first patient in the SirPAD (Sirolimus in peripheral arterial disease) trial. According to a press release, SirPAD is the first all-comer randomised controlled clinical trial (RCT) investigating major adverse limb events in PAD patients with lesions below the inguinal ligament.
SirPAD is an investigator-initiated, single-centre, randomised, non-inferiority, open-label clinical trial investigating whether the use of MagicTouch PTA sirolimus-coated balloon catheters in patients with peripheral arterial disease of the femoropopliteal or below-the-knee segment is not inferior to that of uncoated balloon catheters for major clinical outcomes (unplanned major amputation, target limb revascularisation).
A total of 1,132 patients (1,200 after factoring for a 5% drop-out rate) are to be randomised 1:1 (566 [600 after factoring drop-out rate] patients per treatment group).
The primary objective is to evaluate whether the use of sirolimus-coated balloon catheters (MagicTouch PTA) is non-inferior to uncoated balloon catheters in infra-inguinal angioplasty to prevent one-year major adverse limb events (MALE), including unplanned major amputation of the target limb and target lesion revascularisation for critical limb ischaemia, in a representative population of patients with PAD (‘all-comers’).
If the criterion for non-inferiority is confirmed, the study will test whether sirolimus-coated catheters (MagicTouch PTA) are superior to uncoated catheters for important secondary outcomes and for the primary outcome itself according to pre-specified criteria for hierarchical analysis.
The index patient was successfully enrolled on 3 November 2020 at University Hospital Zurich (Zurich, Switzerland). The study was initiated by Nils Kucher (also the principal investigator) in charge of the Clinic of Angiology at University Hospital Zurich.
Kucher was excited to initiate the study and said, “Over the past decade, a few RCTs have compared the efficacy and safety of drug-coated (mainly paclitaxel-coated) devices versus that of uncoated ones, and demonstrated a significant reduction in restenosis rates, late lumen loss, and incidence of target lesion revascularisation. However, the size of these trials was often too small to draw firm conclusions concerning major clinical outcomes. Moreover, substantial heterogeneity of the study populations and too restrictive eligibility criteria limited their external validity, leading to a difficult interpretation of the results of meta-analyses. Indeed, these trials adopted as the primary outcome surrogate (and rather subjective) outcomes, such as vessel patency and target limb revascularisation, which may be difficult to objectively adjudicate in the setting of an open-label trial, rather than ‘hard’ objective clinical endpoints, such as major amputation or urgent revascularisation due to critical limb ischaemia.
“The aim of the SirPAD trial is to compare the efficacy, as defined by a composite of clinically relevant non-subjective ‘hard’ outcomes (major amputation and target lesion revascularisation for critical limb ischaemia), of sirolimus-coated versus uncoated balloon angioplasty for peripheral arterial disease.”
Daniel Clair takes questions from the panel after presenting new PROMISE I data at VIVA 2020
Daniel Clair takes questions from the panel after presenting new PROMISE I data at VIVA 2020
LimFlow SA has announced the presentation of one-year data from the full patient cohort in its PROMISE I study of the LimFlow percutaneous deep vein arterialisation system, showing sustained positive outcomes for both amputation-free survival and complete wound healing. Results were presented in the a late-breaking data session at this year’s Vascular Interventional Advances meeting (VIVA 2020; 6–8 November, virtual) conference by Daniel Clair (University of South Carolina [USC] and Prisma Health-USC Medical Group, Columbia, USA).
The one-year results from the PROMISE I study show that 70% of patients achieved major amputation-free survival, similar to what was seen at six months, following treatment with the LimFlow system. The patients in the trial also had 75% of their wounds classified as healed or healing one year after treatment. Technical success was reported at 97%.
“One-year outcomes demonstrate that the benefits from treatment with the LimFlow system are durable,” said Clair. “One of the greatest challenges in the treatment of CLTI [chronic limb-threatening ischaemia] is to achieve long-lasting outcomes due to disease progression. In this study, the vast majority of patients who would otherwise be facing major amputation were able to avoid it and, at the same time, heal their previously non-healing wounds. This type of lasting result in such a challenging, no-option patient population offers tremendous hope to CLTI patients and the physicians who treat them.”
PROMISE I is a multicentre, prospective, single-arm study of the LimFlow system conducted at seven US centres encompassing 32 end-stage—or “no option”—CLTI patients, 100% of whom had non-healing wounds on the target foot, 69% of whom had diabetes and 34% of whom had renal insufficiency. The minimally-invasive LimFlow system is designed to bypass blocked arteries in the leg and deliver oxygenated blood back into the foot via the veins in CLTI patients who are facing major amputation and have exhausted all other therapeutic options.
The pivotal PROMISE II clinical trial of the LimFlow system is currently enrolling patients at centres across the USA.
Efthymios Avgerinos begins his presentation on new SUNSET sPE data at VIVA 2020
Efthymios Avgerinos presents new SUNSET sPE data at VIVA 2020
Efthymios Avgerinos (University of Pittsburgh, Pittsburgh, USA) presented results from the SUNSET sPE trial during a late-breaking data session at this year’s Vascular Interventional Advances conference (VIVA 2020; 6–8 November, virtual). His concluded that catheter thrombolysis is safe and effective in tertiary expert centres and can achieve quick thrombus and right to left ventricular (RV/LV) ratio reduction, and that ultrasound-assisted thrombolysis may not confer additional benefits to standard catheter thrombolytic techniques.
The SUNSET sPE trial is a multicentre randomised trial that investigated whether ultrasound-assisted (USAT) is superior to standard-catheter (SCDT) thrombolysis in pulmonary arterial thrombus reduction.
Adults with sPE were randomised 1:1 to a USAT catheter (EKOS system, BTG) or a SCDT catheter. Thrombolysis dose and duration were left to the operators’ discretion. The primary outcome was 48-hour clearance of pulmonary thrombus assessed by pre- and post-procedure computed tomography angiography (CTA) using a refined Miller score. Secondary outcomes included RV/LV ratio improvement, intensive care unit (ICU), bleeding, and other serious adverse events.
Eighty-one patients with acute sPE were randomised and were available for analysis. The mean total dose of alteplase for USAT was 19±7mg and 18±7mg in SCDT (p=0.53) infused over 14±6 hours and 14±5 hours, respectively (p=0.99).
Addressing the VIVA audience, Avgerinos reported that in the USAT group (n=39), the mean raw pulmonary thrombus score was reduced from 31±4 at baseline to 22±7 (p<0.001). In the SCDT group (n=41), the score was reduced from 33±4 to 23±7 (p<0.001). There was no significant difference in mean thrombus score reduction between the two groups (p=0.76), and the obstruction index reduction was also similar between groups: 21% and 22% for USAT and SCDT, respectively (p=0.77). The mean difference in RV/LV ratio from baseline (1.54±0.30 for USAT, 1.69±.44 for SCDT) to 48 hours was 0.37±0.34 in USAT vs. 0.59±0.42 in SCDT (p=0.01). In five USAT and three SCDT patients there was no RV/LV ratio improvement.
He added that major bleeding (one stroke with hemianopia and one vaginal bleed requiring transfusion) occurred in two patients both in the USAT group. The average ICU stay for the entire cohort was 3.2±6.3, similar between groups.
Avgerinos summarised that in the SUNSET sPE trial, patients undergoing USAT had similar pulmonary arterial thrombus reduction compared to SCDT, using comparable mean lytic dose and duration of lysis.
Thomas Zeller takes questions from the VIVA panel after presenting five-year IN.PACT Global results
Thomas Zeller takes questions from the VIVA panel after presenting five-year IN.PACT Global results
In a late-breaking data session at this year’s Vascular Interventional Advances conference (VIVA 2020; 6–8 November, virtual) Thomas Zeller (University Heart Center Freiburg, Bad Krozingen, Germany) presented new data from the IN.PACT Global study. Safety and efficacy of Medtronic’s IN.PACT Admiral drug-coated balloon (DCB) has been sustained out to five years, Zeller revealed, adding that these results support use of the device for the management of real-world patients, including those with complex femoropopliteal artery lesions.
The IN.PACT Global study was a large, prospective, multicentre, single-arm study conducted at 64 international sites. Subjects with bilateral disease, multiple lesions (de novo or restenotic), TASC A, B, C, and D, in-stent restenosis, long lesions (≥15 cm) and chronic total occlusions (≥5cm) were enrolled.
The 1,406 intention-to-treat subjects with 1,774 target lesions were treated with the IN.PACT Admiral DCB and analysed as a part of the consecutively enrolled clinical cohort with safety and revascularisation events reviewed by an independent Clinical Events Committee. Assessments through five years using the Kaplan-Meier (K-M) method included freedom from clinically-driven target lesion revascularisation (CD-TLR), a safety composite (freedom from device- and procedure-related mortality through 30 days, freedom from major target limb amputation through five years, and clinically-driven target vessel revascularisation through five years), and all-cause death.
The mean lesion length in this clinical cohort was 12.1±9.54cm, with 18% in-stent restenosis, 35.5% total occlusions, and 68.7% calcification. The K-M estimate of freedom from CD-TLR through five years was 69.4%, and the K-M estimated primary safety composite endpoint was 67.4% with a low major target limb amputation K-M cumulative incidence of 1.7%, through five years. The K-M estimate of freedom from all-cause death was 78.9%. This all-cause death rate was calculated after 96.4% vital status follow-up and was collected through five years.
Anthony Comerota presents 12-month VIVO results at VIVA 2020
Anthony Comerota presents 12-month VIVO results at VIVA 2020
Results of the VIVO clinical study support the safety and effectiveness of Cook Medical’s recently FDA-cleared Zilver Vena venous stent for the treatment of symptomatic iliofemoral venous outflow obstruction, Anthony Comerota (Inova Fairfax Hospital, Alexandria, USA) revealed in a late-breaking data session at this year’s Vascular Interventional Advances conference (VIVA 2020; 6–8 November, virtual).
In addition, Comerota reported that VIVO study patients were “consistent with those in previous literature reports and reflective of a real-world population, including acute and chronic disease, and thrombotic and non-thrombotic lesions”.
Patients with symptomatic obstruction (CEAP clinical classification ≥3 or VCSS pain score ≥2) of one iliofemoral venous segment were included. The primary safety endpoint was 30-day freedom from major adverse events (MAE): procedural bleeding requiring transfusion, procedure- or device-related death, clinically-driven reintervention (reintervention with recurrent symptoms of venous outflow obstruction of the target lesion and a minimum lumen diameter [MLD] ≤50% of the immediate post-procedure MLD by venography), clinical migration, new symptomatic pulmonary embolism, or procedure-related perforation requiring open surgical repair or flow limiting dissection of the target vessel.
The primary effectiveness endpoint was 12-month rate of primary quantitative patency (intervention-free, MLD >50% of the immediate post-procedure MLD by venography). The secondary endpoint was the change in VCSS from baseline to 1 month and 12 months.
Comerota reported that 243 patients were enrolled (53±15 years; 70% female). Iliac vein compression by the iliac artery (n=191; 78.6%) was the primary indication for stent placement. The mean lesion length at baseline was 98.6±69.8mm. Technical success (ability to deliver and place stent in intended location) was achieved for 97.3% of stents. The 30-day freedom from MAE rate was 96.7%, exceeding the performance goal of 87% (95% confidence interval [CI]: 93.5–98.6%, p<0.0001). The 12-month primary quantitative patency rate was 89.9%, exceeding the performance goal of 76% (95% CI: 85.1–93.4%, p<0.0001). Clinical improvement was demonstrated by the improvement in VCSS from baseline: -3.0 (95% CI: -3.5 to -2.6, p<0.0001) at one month and -4.2 (95% CI: -4.7 to -3.7, p<0.0001) at 12 months.
Following Comerota’s presentation, panel member Kenneth Cavanaugh (US Food and Drug Administration [FDA] Office for Cardiovascular Devices, Silver Spring, USA) was interested in the potential value of adding a comparator into these studies now that there are other stents on the market.
Comerota responded by highlighting that certain factors would need to be taken into account in any head-to-head comparison of venous stents, including the potential for lesion length to vary widely. “If you were to choose an ideal lesion it would be short, it would be limited to the iliac segment, and it would be a stenosis, not an occlusion” he said, noting that in the VIVO study one-third of the patients had their stents extended to below the inguinal ligament, representing a “real challenge”.
Krishna Rocha-Singh presents 12-month results from the REALITY study at VIVA 2020
Krishna Rocha-Singh presents 12-month REALITY results at VIVA 2020
A vessel preparation treatment strategy of directional atherectomy prior to drug-coated balloon angioplasty with Medtronic’s IN.PACT Admiral drug-coated balloon (DCB) in long, calcified femoropoliteal lesions is effective out to one year, with an acceptable safety profile. This was the conclusion of Krishna-Rocha Singh (Prairie Heart Institute, Springfield, USA) in a late-breaking data session at this year’s Vascular Interventional Advances conference (VIVA 2020; 6–8 November, virtual), presenting new data from the REALITY study.
REALITY (Directional atherectomy plus drug-coated balloon to treat long, calcifIed femoropopliteal artery lesions) prospectively enrolled subjects at 13 multinational centres with 8–36cm femoropopliteal stenoses or occlusions with bilateral vessel wall calcification treated with directional atherectomy prior to DCB angioplasty. The primary effectiveness endpoint was 12-month primary patency and the primary safety endpoint was freedom from major adverse events through 30 days. Independent angiographic and duplex core laboratories assessed outcomes and Clinical Events Committee (CEC)-adjudicated events.
The study enrolled 102 subjects; one lesion was treated per subject. The mean lesion length was 17.9±8.1cm; 39% were chronic total occlusions (mean lesion length 22.6±8.6cm); and, 86% of lesions exhibited moderate to severe bilateral calcification. Provisional stents were implanted in 9% (9/102) of patients. Twelve-month primary patency rate was 77% (66/86) and freedom from clinically-driven target lesion revascularisation (CD-TLR) rate was 93% (87/94). No device- or procedure-related deaths were reported; one index-limb major amputation was reported.
Rocha-Singh concluded that plaque excision with directional atherectomy in patients with symptomatic severely calcified femoropopliteal arterial disease prior to IN.PACT Admiral DCB angioplasty is a safe and effective treatment strategy with a low provisional stent rate.
Commenting on the importance of these results, Rocha-Singh told Vascular News: “VIVA REALITY I think sets a new benchmark for the assessment of claudicants with severe femoropopliteal disease characterised by excessive lesion lengths […] and significant bilateral calcification, and suggests that the use of directional atherocath is very efficient in removing atheroma and that that is reflected in the primary safety and effectiveness endpoints at 12 months with a very compelling from CD-TLR and primary patency.”
However, he cautioned against generalisation: “Until another company steps forward, with the type of data that was presented with REALITY, with three core labs, specifically an angiographic core lab, a duplex Doppler core lab, a histology core lab, with all clinical advance adjudicated by a CEC, we cannot and must not equate the results of REALITY with any other combinations of atherectomy devices and drug-eluting balloons.”
Connie Hess details the most recent findings from VOYAGER PAD at VIVA 2020
Connie Hess details the most recent findings from VOYAGER PAD at VIVA 2020
Given the absence of a safety signal in data from the VOYAGER PAD trial, a new analysis examined the potential benefit of drug-coated device versus non-drug-coated device treatment for reducing limb outcomes. Connie Hess (University of Colorado, Aurora, USA) presented the most recent findings in a late-breaking data session at this year’s Vascular Interventional Advances conference (VIVA 2020; 6–8 November, virtual), reporting no excess mortality and improved limb outcomes with drug-coated device use in peripheral arterial disease (PAD).
Hess noted that patency remains a challenge, and that drug-coated devices are associated with a reduction in clinically-driven unplanned index limb revascularisation. However, she relayed that rivaroxaban 2.5mg twice daily plus aspirin reduces this risk, in addition to reducing major adverse events of the heart, limb, and brain, irrespective of device type. “These observations suggest that a ‘pharmaco-invasive’ approach combining innovative devices with effective medical therapy may optimise outcomes in PAD,” she told the VIVA audience.
The co-primary outcomes for this analysis were unplanned index limb revascularisation and major adverse limb events (MALE), defined as acute limb ischemia or major amputation of vascular cause. As drug-coated use was not randomised, inverse probability treatment weighting was used to account for known confounders.
Hess detailed that use of a drug-coated device was associated with a significant 16% reduction in relative risk of clinically-driven unplanned index limb revascularisation (hazard ratio [HR] 0.84, 95% confidence interval [CI] 0.76–0.92) but was not associated with a reduction in MALE (HR 1.08, 95% CI 0.9–1.3).
William Gray presents 30-day outcomes of the DISRUPT PAD III RCT at VIVA 2020
William Gray presents DISRUPT PAD III data at VIVA 2020
The DISRUPT PAD III randomised controlled trial (RCT) provides the largest level one evidence for the treatment of heavily calcified femoropopliteal arteries, noted William Gray (Main Line Health, Philadelphia, USA) during the second and final late-breaking data session at this year’s Vascular Interventional Advances conference (VIVA 2020; 6–8 November, virtual). Gray reported that Shockwave’s intravascular lithotripsy (IVL) was superior to percutaneous transluminal angioplasty (PTA) in acute procedural success out to 30 days.
In addition, Gray informed the VIVA audience that IVL demonstrated atraumatic treatment, characterised by a reduction in percentage diameter stenosis prior to drug-coated balloon or stent placement, lower maximum inflation pressure, reduction in frequency and severity of dissections, and lower post-dilatation and stent implantation rate. He stressed that these RCT outcomes are similar to the PAD III registry in multiple vessel beds, highlighting the consistency of IVL treatment in complex anatomy.
Endovascular treatment of calcified peripheral artery lesions may be associated with suboptimal vessel expansion, increased complication risk, and reduced long-term patency. Single-arm studies have reported promising results with IVL in the presence of moderate and severe calcium, yet comparative evidence from randomised trials is lacking.
The purpose of this study is to compare acute outcomes in patients receiving vessel preparation with IVL or PTA prior to drug-coated balloon (DCB) treatment for peripheral arterial disease (PAD) in calcified femoropopliteal arteries. The DISRUPT PAD III RCT enrolled PAD patients with moderate and severe calcification in a femoropopliteal artery who underwent vessel preparation with IVL or PTA. The primary effectiveness endpoint was procedural success, defined as core-lab adjudicated residual stenosis ≤30% without flow-limiting dissection prior to DCB or stenting. Secondary endpoints evaluated at 30 days included major adverse events (MAE) and clinically-driven target lesion revascularisation (CD-TLR).
Gray detailed that in patients receiving IVL (n=153) or PTA (n=153), the primary effectiveness endpoint of procedural success was significantly greater in the IVL group (65.8% vs. 50.4%, p=0.007). Post-treatment balloon dilatation (measured prior to DCB) residual diameter stenosis (27.3±11.5% vs. 30.5±13.9%, p=0.04), freedom from any dissection (81.5% vs.67.7%, p=0.009), flow-limiting dissection (1.4% vs. 6.8%, p=0.03), and provisional stent placement (4.6% vs. 18.3%, p<0.001) were also significantly lower in the IVL group. Secondary outcomes, including rates of MAE and CD-TLR at 30 days, were comparable between groups.
Sean Lyden takes questions from the VIVA 2020 panel
Sean Lyden takes questions from the panel at VIVA 2020
Royal Philips today announced the results of a patient-level meta-analysis that confirms the safety profile of its Stellarex drug-coated balloon (DCB) at four years. Including data from two major randomised controlled trials (RCTs), the results show no difference in mortality between patients treated with the Stellarex DCB and those treated with percutaneous angioplasty (PTA), the current standard of care. The meta-analysis was presented at the 2020 Vascular Interventional Advances conference (VIVA 2020; 6–8 November, virtual).
The meta-analysis found that over four years, there was no significant difference in survival among patients treated with the Stellarex DCB (85.7%) compared to those treated with PTA (85.6%). The data includes two Stellarex RCTs: the ILLUMENATE EU RCT and the ILLUMENATE Pivotal RCT, comprised of 589 patients in the USA and Europe followed up to four years with a high compliance on vital status data.
“The meta-analysis reinforces previously presented results from the ILLUMENATE RCTs, demonstrating low mortality rates each year through four years, with no difference in rates between the two patient cohorts,” said Sean Lyden (Cleveland Clinic, Cleveland, USA), who presented the data. Lyden is also co-primary Investigator for the ILLUMENATE Pivotal trial, one of the two RCTs included in the meta-analysis, and a paid consultant to Philips. “This independent, patient-level meta-analysis continues to provide consistent, long-term data for a large group of patients.”
In addition to demonstrating no significant difference in all-cause mortality between patients treated with the Stellarex DCB and those treated with PTA (14.3% vs. 14.4%), the results of the meta-analysis also show no difference in cardiovascular mortality (3.6% vs. 4%) and non-cardiovascular mortality (10.8% vs. 10.9%).
“The results of this study confirm the safety and performance of our unique Stellarex low-dose drug-coated balloon,” said Chris Landon, senior vice president and general manager Image Guided Therapy Devices at Philips. “We are committed to providing healthcare providers with accurate and transparent data in order to help them make an informed decision on the optimal treatment for each patient with peripheral arterial disease. Stellarex, with its low drug dose and unique drug coating composition, is a logical choice for those who require this option.”
Boston Scientific announced it has received US Food and Drug Administration (FDA) approval of the Ranger drug-coated balloon (DCB), developed for the treatment of patients with peripheral arterial disease (PAD) in the superficial femoral artery (SFA) and proximal popliteal artery (PPA).
According to a press release, the Ranger DCB was designed with a low therapeutic drug dose and proprietary coating which efficiently transfers the drug into the tissue, resulting in high primary patency rates and low systemic drug exposure for patients.
“This approval allows us to bring more treatment options with exceptional outcomes and proven safety to US physicians and their patients who are facing this challenging disease,” said Jeff Mirviss, president, Peripheral Interventions, Boston Scientific. “Adding the Ranger DCB to our drug-eluting portfolio, which also includes our Eluvia drug-eluting vascular stent system, reinforces our commitment to providing differentiated technology with strong clinical evidence that supports data-driven treatment decisions for millions of patients suffering from PAD worldwide.”
The FDA approval is based on results from the RANGER II SFA pivotal trial, which evaluated the safety and effectiveness of the Ranger DCB versus standard percutaneous transluminal angioplasty (PTA) for the treatment of patients with PAD in the SFA and PPA. In the randomised controlled trial, both primary endpoints were met:
The primary safety endpoint of 12-month freedom from major adverse events (MAE) was 94.1% for those treated with the Ranger DCB vs. 83.5% for standard PTA (Pnon-inferiority <0.0001).
Additionally, patients who received therapy with the Ranger DCB had a significantly lower target lesion revascularisation rate—a component of MAE—of 5.5% in contrast to 16.5% observed with standard PTA (p=0.0011), substantially reducing a patient’s need for repeat procedures.
The primary efficacy endpoint of 12-month binary primary patency—a measure of the target vessel remaining unobstructed—was 82.9% for the Ranger DCB and 66.3% for standard PTA (p=0.0017). Primary patency by Kaplan-Meier estimate was 89.8% for the Ranger DCB and 74% for PTA at 12 months (p=0.0005).
“The Ranger DCB eases deliverability for a wide range of lesion complexities via a low profile platform that is compatible with smaller diameter guidewires and has shown consistent results in multiple randomised controlled trials,” said Ravish Sachar, physician-in-chief for Heart and Vascular services at UNC Rex Hospital (Raleigh, USA) and principal investigator of the RANGER II SFA trial. “For physicians seeking to limit systemic drug loss without compromising outcomes, data demonstrate the Ranger DCB is a safe and effective treatment option.”
The Ranger DCB also demonstrated nearly 90% primary patency in the investigator-sponsored COMPARE trial—the first head-to-head prospective, randomised controlled trial to compare two different DCBs. In the trial, the Ranger DCB demonstrated a similar primary patency rate of 88.4% to that of the 89.4% observed with IN.PACT Admiral drug-coated balloon (Medtronic) by Kaplan-Meier estimate (p=0.81), with a significantly lower drug dose density (2µg/mm2 paclitaxel vs. 3.5µg/mm2 paclitaxel, respectively).
Boston Scientific expects to initiate a registry of the Ranger DCB and the Eluvia stent in the coming months to gather additional real-world evidence, which will add to the breadth of clinical data collected on these devices to date. The registry is expected to include five years of patient follow-up with an emphasis on enrolling patient populations who have been historically underrepresented in clinical trials studying treatments for PAD.
The company announced CE Mark for the Ranger DCB in 2014 and plans to immediately launch the device in the USA.
A new case report published in the Journal of Vascular Surgery (JVS) provides one of the first known opportunities to directly visualise the anastomosis that is created with Avenu Medical’s Ellipsys vascular access system, a press release reveals.
“This is the first published report of direct visualisation of a matured pAVF [percutaneous arteriovenous fistula] created with the Ellipsys System,” said lead author Alexandros Mallios (Paris Saint-Joseph Hospital, Paris, France). “It was an amazing opportunity that provided first hand proof of the permanent, fused vessel anastomosis made possible by this revolutionary technology.”
The subject of the case report was an 80-year-old male diabetic end-stage renal disease (ESRD) patient who had a pAVF created with the Ellipsys system six months prior. He was evaluated for decreasing blood flow (unrelated to his fistula) and required surgical intervention, which provided the opportunity to visualise the matured Ellipsys pAVF up close. According to Mallios, the lack of sutures or other foreign bodies made the fusion look “remarkably natural.”
Mallios has published numerous studies showing the ability of the Ellipsys system to easily and safely create durable vascular access for ESRD patients. In July 2020, he reported one-year follow-up results of 234 Ellipsys patients. Published in JVS, the study reported no adverse events and 96 percent of patients still had fully functioning fistulas with strong blood flow after a year. That “patency rate” is higher than published rates for surgically created fistulas, which average about 60% after one year.
In April 2020, JVS published a case report by Mallios that featured a 3D rendering of the Ellipsys pAVF on the cover of the publication. Mallios also co-authored two recent papers in the Journal of Vascular Access that discussed patient eligibility for Ellipsys and the similarities between an Ellipsys pAVF and a surgical AVF, the current standard of care.
Recently published long-term Ellipsys data showed a functional patency rate of 92% at two years. The study also found high levels of patient satisfaction with the procedure.
Medtronic recently announced its plan to acquire Avenu Medical for the Ellipsys percutaneous fistula creation technology. Terms of the deal were not disclosed.
Preclinical and clinical studies show that local, intra-tumoural injection of immunomodulatory agents can result in the shrinking of tumours distant from the site of inoculation. Furthermore, when chemotherapy drugs are used as the immunomodulator, it may circumnavigate the need for systemic chemotherapy delivery. These are the conclusions presented by Thierry de Baere (Institut Gustave Roussy Université Paris-Saclay, Villejuif, France) at the 2020 Symposium on Clinical Interventional Oncology (CIO; every Tuesday of October 2020, online). “Because this is a new field, there are a lot of open questions,” he said. “What is the best target, how should I access the target, is it safe, is it the correct organ, how should I deliver [the drugs], what dose, which regimen, can I monitor the delivery of the drugs?”
“This is a very new, exciting field, and there is a space for interventional radiologists,” he told viewers. Showing a graph depicting the number of new intratumoural immunotherapy trials conducted each year since 1992, de Baere demonstrated the rapid growth of research in this space: from a low of one trial in 1992, to a high of 40 trials in 2016.
When injecting immunostimulatory agents into the tumour, interventionalists hope to achieve local priming, de Baere explained. “We want to trigger a tumour-specific immune response, but we also hope that this [local] response will result in distant effects,” he continued. The idea underpinning human intra-tumoural injections in cancer care is that these “distant effects”—known as abscopal effects—will confer systematic anti-tumour immunity at non-injected tumour sites.
Many different compounds can be used as immunostimulatory agents, and can be used at different stages of tumour immunity. De Baere expanded: “We use products that will release tumour antigens—could be peptides, could be viruses. We want to activate antigen presentation, we want to stimulate cytotoxic cells on site, and we want to deplete or block regulatory T cells [Tregs].”
Providing a more granular breakdown of the agents currently under investigation for drug delivery, de Baere detailed potential combinations for in situ priming of anti-tumour immunity. At every stage of the immune response to cancer, different products are available. For the recruitment of antigen presenting cells, the stimulation of phagocytosis, and the triggering of tumour antigen presentation, interventionalists could consider using toll-like receptor agonists, STING (stimulator of interferon genes) agonists, RIG-I agonists, or anti-C040 agonists. To activate local immunogenic cancer cell death, there are a variety of options, including: the injection of oncolytic viruses, radiotherapy, transarterial chemoembolization (TACE), radiofrequency ablation (RFA), and cryoablation. Anti-PD-I or Anti-PD-LI could be deployed to activate cytotoxic cells, and anti-CTLA-4 could be used to deplete Treg numbers.
Addressing CIO attendees, de Baere said: “Of note, in most of the studies, you are injecting the drug locally, but there is also some intravenous [IV] drugs. Most of the time, you have a PD-LI inhibitor as an IV-combo with drug delivery.”
After detailing the procedural details of intra-tumoural injection, which involve many technical decisions, de Baere stated: “Of course we should be part of this journey, because I think nobody can deliver better local treatment than interventional radiologists.”
A systemic response from a local treatment
De Baere and other interested interventionalists hoping for confirmation of abscopal effects from local intra-tumoural injection are eagerly awaiting the results of ILLUMINATE 301, a randomised, phase III study of tilsotolimod in combination with ipilimumab compared with ipilimumab alone in patients with advanced melanoma following progression on or after anti-PD-1 therapy. Tilsotolimod is a toll-like receptor agonist with potent immunostimulating activity, as described in the literature. In a presentation given by Adi Diab (The University of Texas MD Anderson Cancer Center, Houston, USA) at the European Society of Molecular Oncology (ESMO) annual meeting back in October 2018, the intra-tumoural injection of tilsotolimod combined with ipilimumab resulted in a decrease in the size of an off-target melanoma tumour—one that was not injected with any drugs. Committing this finding to the collective medical memory, Diab and colleagues describe in Annals of Oncology how, in the phase I/II ILLUMINATE 301 study, intratumoural tilsotolimod with ipilimumab was “well-tolerated, demonstrating durable responses (including complete response >21 months), dendritic cell activation, type I interferon response, CD8+ T-cell proliferation in responders, and an abscopal effect”. At the time of writing, phase III results from ILLUMINATE 301 are anticipated in the first fiscal quarter of 2021.
Offering a personal example, de Baere showed the CIO audience a case performed at his own institution. The patient had a single injection of ipilimumab into a liver metastasis, as well as systemic treatment with nivolumab. “You can see we had an overall response from all of the tumours, despite [the fact that] only one tumour was injected.
Intra-tumoural injection potentially most suitable in neoadjuvant disease
Looking at the full spectrum of cancer development, from neo-adjuvant to metastatic disease, de Baere related how he believed that localised, intra-tumoural injections of chemotherapy drugs may be most successful in neo-adjuvant tumours. The interventionalist would inject immunomodulatory agents into a specific tumour, wait a few days or a few weeks to allow for the patient’s immune system to fight the cancer, and then perform surgery. “The reason for that is to prevent distant, metastatic disease to improve the overall survival,” he explained, “and maybe to improve the rate of R0 resection”. R0 resection indicates a cure or complete remission.
Data exist that supports this treatment approach. Presented at ESMO 2019, results of a phase 2, multicentre, randomised, open-label trial of efficacy and safety for neoadjuvant treatment plus surgery versus surgery alone in patients with resectable melanoma found that the combined treatment had improved overall survival and resection-free survival at two years (88.9% vs. 77.4%, p=0.050 and 50.5% vs. 30.2%, p=0.038, respectively). Results from the same dataset presented at the American Society of Clinical Oncology (ASCO) 2019 meeting also report an increased rate of R0 surgical resections.
As this is a new field of study, de Baere stressed the importance of collecting data and following up patients treated via an intratumoural injection of immunotherapeutic agents. “It is important that we use a specific way of looking at the tumour response,” he said. “We need to create a waterfall plots both of the tumours that have been injected, and a waterfall plot of the tumours that have not been injected.” Referencing a Journal of Clinical Oncology (JCO) paper from May 2020, de Baere told viewers that they should follow the intratumoural immunotherapy Response Evaluation Criteria in Solid Tumours (itRECIST) protocol when capturing data from their patients in order to assess any local and systemic responses in a standardised fashion.
Raul Uppot (Massachusetts General Hospital, Boston, USA) speaks to Interventional News about the evolution of hepatic ablation, following his talk on the same topic at the recent Symposium on Clinical Interventional Oncology (CIO).
He says: “What I want people to know is that liver ablation started off as a small trial: can we kill a tumour with a small needle? Over the past 30 years, we have shown that that is possible. It is exciting that, using a small probe, you can insert it into the liver and impact care—completely treat large tumours, multiple tumours, and yet the patient goes home as an outpatient with just a band-aid. The ability to do great oncological care and work with a small needle is exciting about ablation.”
RaFeVA (Rapid Femoral Vein Assessment), a new protocol, is a rapid and effective tool for the systematic ultrasound evaluation of the veins in the inguinal area and at mid-thigh, conclude Fabrizio Brescia (Unit of Anesthesia and Intensive Care Medicine, Vascular Access Team, Centro di Riferimento Oncologico di Aviano, IRCCS, Aviano, Italy) et al in The Journal of Vascular Access (JVA). Describing this new protocol step-by-step, the study authors say it is designed to evaluate patency and calibre of the common and superficial femoral veins and to help interventionalists choose the best venipuncture site before insertion of a femorally-inserted central catheter (FICC).
“In recent years, many factors have contributed to improving the practice of central venous access,” write Brescia and colleagues, enumerating: “adoption of biocompatible and high-pressure resistant materials, institution of multi-professional, multi-disciplinary teams focused on vascular access, and so on.” They go on to say that, “probably, the most important novelty of the 21st century in the field of venous access has been the adoption of ultrasound technology for minimising the costs and the complications associated with placement of central venous devices.”
Systemic and standardised approaches for the preliminary ultrasound evaluation before centrally-inserted central catheter (CICC) and peripherally-inserted central catheter (PICC) insertion have previously been developed, the authors state. The rapid central vein assessment—the RaCeVA protocol—is a systematic protocol of ultrasound evaluation of the veins of the neck and of the supra/infra-clavicular area before CICC insertion. According to Brescia and his co-authors, this protocol is “useful for teaching the different ultrasound-guided approaches to the central veins, for helping the operator to consider systematically all possible venous options, and for guiding the operator in choosing the most appropriate vein to be accessed, on a rational and well-informed basis”. The rapid peripheral vein assessment—RaPeVA—is the protocol developed in order to collect relevant anatomical information before positioning a PICC.
Rapid femoral vein assessment: RaFeVA
Brescia et al describe RaFeVA as “a clinical tool to evaluate different approaches to the veins of the groin and mid-thigh region, to provide operators with a systematic sequence for ultrasound evaluation of all the veins in the region with the aim of choosing the most appropriate vein for a tunnelled or non-tunnelled FICC”. It consists of seven steps, corresponding to seven different positions of the probe, and is always performed bilaterally. The seven steps of the RaFeVA protocol take into account the different possible visualisations of the vessels (along the short, long, or oblique axes), and propose different venipuncture techniques (out-of-plane and in-plane).
Ultrasound-guided positioning of a catheter in a superficial femoral vein
In brief, the seven steps go thus:
Start at the inguinal groove with the probe in a transverse position, perpendicular to the skin. Identify the common femoral artery (CFA) and the common femoral vein (CFV), both in short axis. Assess by probe compression the CFV in terms of depth, size, and patency.
Switch to a visualisation of the transition between the CFV and the external iliac vein (EIV) in long axis. Assess the longitudinal axis of the veins and its course.
Rotate the probe by 90° to return to a short axis view. Move the probe caudally, to visualise the CFA, CFV, and saphenous vein (SV), in the short axis view.
Slide the probe downward, far from the groin, still in a transverse view, to visualise the superficial femoral artery (SFA), the deep femoral artery (DFA), and the CFV, all in the short axis.
Move the probe even more caudally to visualise simultaneously the SFA, the DFA, the superficial femoral vein (SFV), and the deep femoral vein (DFV), all in the short axis.
Slide the probe caudally, toward mid-thigh, to visualise the SFA and the SFV in the short axis.
Perform a 45° rotation of the probe to obtain an oblique axis view of the SFA and SFV.
Brescia and colleagues elaborate on why standardising the approach to preliminary ultrasound evaluation ahead of FICC insertion is beneficial: “As for the choice of the venous approach and the technique of venipuncture, the preference or the personal experience of the operator should not be regarded any longer as an appropriate criterion,” they opine. “The venous approach that is more ‘comfortable’ for the operator is not necessarily the venous approach associated with the maximal safety for the patient. A rational choice of the venous approach should be based on objective anatomical criteria, verified in the specific patient who is candidate to the procedure. This rational, objective evaluation of the anatomic characteristics of the vasculature of each patient is possible by adopting systematically a pre-procedural ultrasound scan of the anatomic area where the central venous access device will be inserted. The inappropriate, ‘automatic’ choice of a venous access based only on the habits of the operator is potentially associated with repeated punctures, waste of time, poor clinical outcomes and/or puncture-related complications, due to the lack of knowledge of the possible anatomical variations or pathologic abnormalities of the local veins or the lack of identification of the surrounding structures (arteries, nerve bundles, and organs).”
They conclude that, in all phases of venous cannulation procedures—from preliminary assessment to the early identification of puncture-related complications—a correct use of ultrasound improves performance, “making them safer, faster, and more effective”. As the RaFeVA protocol provides a detailed anatomical assessment in advance of the venous cannulation procedure, they claim, it enables optimisation of the manoeuvre through the reduction of cannulation time and of number of attempts, and the avoidance of surrounding structures that could be accidentally damaged during the venous catheterisation.
Raul Uppot speaks to Interventional News over video call
Speaking during a livestreamed session dedicated to state-of-the-art liver therapy hosted by the Symposium on Clinical Interventional Oncology (CIO) on Tuesday 6 October, Raul Uppot (Massachusetts General Hospital, Boston, USA) discussed the evolution of liver ablation, from the first procedure in November 1986—where the patient was injected with alcohol into liver tumours—to the potential of this treatment modality to offer systemic, curative cancer care, possibly even without inserting a single needle. Here, he shares his thoughts on the past, present, and future of ablation with Interventional News.
What are the benefits of ablation of the liver, and are there any downsides?
The beauty of ablation is that, in a very minimally invasive way, you can treat tumours. In the past, when we were just doing biopsies, it was amazing to us that you could put a needle directly into the target to sample it for diagnostic purposes. Since the late 1980s, we have moved towards being able to treat tumours in a similarly minimally invasive fashion. The ability to use CT or ultrasound to put a small needle into something, to completely treat a tumour that previously would have required surgery, pull the needle out, put a band aid on, and send the patient home—that is what is unique about ablation.
Ablation allows you to treat tumours in a minimally invasively fashion, and we now have the data to show that the ability to do that has long-term impacts on our patients. As with any procedure that we do, there are risks. There are the same risks that you would have with any procedure: bleeding, infection, injury to adjacent organs.
How has the use of hepatic ablation changed over time?
The first hepatic ablation involved the insertion of a small needle into a tumour that was then injected with alcohol. People realised that alcohol could destroy tissue, so thought ‘Why not kill tumours by injecting alcohol into them?’ Since then, we have developed more advanced equipment that can burn or freeze tumours.
The applications have evolved as well. We initially treated primary hepatocellular tumours, and, over many studies, we have shown that [ablation] is very successful at local control and improving overall survival in patients. But we have also evolved into other tumours, such as treating metastatic disease. I think an exciting part of interventional radiology (IR) now is the ability to treat metastatic disease: colorectal cancer, pancreatic cancer, breast cancer metastases to the liver. Management of all of these tumours are based on a background knowledge from the surgical literature. For example, if you were able to surgically debulk disease in the liver for certain cancers (such as colorectal cancer), then you could improve survival. The same data is now being applied to IR, where, if you can debulk as much of the tumour in the liver, then you can potentially improve overall survival.
What is the evidence for ablation in the treatment of liver metastases?
I think the biggest trial out there that we are excited about is the COLLISION trial—this is a trial that will compare the treatment of colorectal cancer metastases with ablation versus surgery. The trial started in 2017, is expected to recruit 600 or so patients, and has a planned end date of 2022. The strength of this trial is that it is a multicentre, randomised controlled trial that will try to answer the question: is ablation as good or better than surgical resection, the current gold standard?
Given our historical data on ablation, especially for the treatment of hepatocellular cancer, we know that we can treat tumours with a good margin, so the expectation is that, in much the same way as surgery has improved survival in terms of debulking metastases disease to the liver, ablation could probably do the same thing, but with lower costs, less hospitalisation time, and with an equivalent survival to surgically treated patients.
What does the future of ablation look like?
When ablation first started, our goals were really just to provide a good option for locally controlling liver tumours. I do not think that the first time an ablation was done, there was ever any belief that we would treat widespread, systemic disease with a single probe. So it is very exciting now to learn that certain tools we now have, such as irreversible electroporation (IRE) and cryoablation, can potentially incite systemic effects. There are now a lot of trials going on exploring the combination of immunotherapy drugs and ablation.
I think where ablation fits into this whole paradigm is that, by destroying the tumour, you are able to release antigens; the release of these antigens, combined with immunotherapy drugs, could potentially affect overall systemic disease. I personally have had a few patients where treating a single tumour in the adrenal glands or the kidneys has ultimately resulted in a decrease in size of metastatic tumours in other parts of the body. This was accidental—we call it an abscopal effect. I think this has happened enough times that people have realised there is a way to study this, there is a way to learn how this could potentially be occurring, and control it, and use immunotherapy drugs to help it, so it is exciting, because I think for the first time it is a whole new world for IR. The ability to put a needle into one lesion, treat that, yet somehow affect systemic tumour control everywhere else, and improve overall survival in the patient.
What is the key message you would like your IR colleagues to take home from your CIO presentation on liver ablation?
What I want people to know is that liver ablation started off as a small trial: can we kill a tumour with a small needle? Over the past 30 years, we have shown that that is possible. It is exciting that, using a small probe, you can insert it into the liver and impact care: completely treat large tumours, multiple tumours, and yet the patient goes home as an outpatient with just a band-aid. The ability to do great oncological care and work with a small needle is exciting about ablation.
The other thing I am very excited about is that, over time, there has been a constant evolution in the technology [for ablation]. We started off with alcohol, but we evolved to radiofrequency ablation (RFA), cryoablation, microwave ablation, and IRE. There is a constant evolution in these technologies: we are constantly moving towards smaller and lighter probes that are more efficient in what they can destroy. There are new technologies on the horizon, such as histotripsy, that allow one to treat a tumour without inserting a needle. The ability to use ultrasound waves to kill tumour [cells] is what is coming down the pipeline. It is very exciting, the notion that a person could come in with a large liver tumour and one could treat it in a very minimally invasive fashion and, ultimately, improve the patient’s survival.
Medtronic today announced it has received US Food and Drug Administration (FDA) approval for the Abre venous self-expanding stent system. This device is indicated for use in the iliofemoral veins in patients with symptomatic iliofemoral venous outflow obstruction.
The FDA approval is based on 12-month results from the ABRE clinical study, presented at the 2020 Charing Cross Symposium. The ABRE study assessed the safety and effectiveness of the investigational Abre stent in 200 patients with iliofemoral venous outflow obstruction across the spectrum of deep venous obstruction including those with post thrombotic syndrome, non-thrombotic iliac vein lesions (NIVL), and those who presented with an acute deep vein thrombosis (aDVT).
The study also included a challenging patient population, 44% (88/200) of whom required stents that extended below the inguinal ligament into the common femoral vein (CFV). The study met its primary safety endpoint with a 2% (4/200) rate of major adverse events (MAEs) within 30 days. The study also met its 12-month primary effectiveness endpoint with an overall primary patency rate of 88% (162/184). Despite the challenging patient population, no stent fractures and no stent migrations were reported in the study.
“Patients with deep venous obstruction are often younger, therefore it’s critical to have a venous stent that is not only safe and effective, but also strong and flexible,” said Erin Murphy, global principal investigator for the ABRE clinical study and director of Atrium Health Sanger Heart & Vascular Institute’s Venous and Lymphatic Program in Charlotte, USA. “With FDA approval, we now have this important tool in our arsenal to treat patients with even the most challenging of deep venous lesions.”
A self-expanding stent system, Abre is intended for permanent implant and utilises an open-cell design with three off-set connection points to enable flexibility and stability during deployment. Based on data presented at the Leipzig Interventional Course (LINC) 2020 annual meeting by Stephen Black, consultant and vascular surgeon, Guy’s, and St Thomas’ Hospital and Kings College in London, UK, the Abre stent system demonstrated a 0% fracture rate in bench testing simulated out to 50 years.
“With Abre, our goal was to create a dedicated venous stent that combined a balance of the key characteristics necessary to treat patients with a broad spectrum of deep venous obstruction,” said Carolyn Sleeth, vice president and general manager of the endoVenous business, which is part of the Cardiac and Vascular Group at Medtronic. “We are excited to bring Abre to the US market, which we believe will provide both physicians and patients with a new option backed by clinical evidence to treat this disease safely and effectively.”
Abre received CE mark approval in April of 2017 and is also intended for use in the iliofemoral veins for treatment of symptomatic venous outflow obstruction.
The Janssen Pharmaceutical Companies of Johnson & Johnson announced today it has submitted a supplemental New Drug Application (sNDA) to the US Food and Drug Administration (FDA) for a new indication to expand the use of Xarelto (rivaroxaban) in patients with peripheral arterial disease (PAD).
If approved, this new indication for the Xarelto vascular dose (2.5mg twice daily plus aspirin 75–100mg once daily) would include reducing the risk of major thrombotic vascular events such as heart attack, stroke, and amputation in patients after recent lower extremity revascularisation.
The application is based on data from the VOYAGER PAD study, which showed Xarelto (2.5mg twice daily) plus aspirin (100mg once daily) was superior to aspirin alone in reducing the risk of major cardiovascular and limb events, with similar rates of thrombolysis in myocardial infarction (TIMI) major bleeding.
“Various antithrombotic regimens have been evaluated for short- and long-term prevention of major vascular events in patients with PAD, but only rivaroxaban in combination with aspirin has demonstrated a significant benefit over aspirin alone,” said James List, global therapeutic area head, Cardiovascular & Metabolism, Janssen Research & Development.
“Data from the VOYAGER PAD trial were the first in 20 years to show clinical benefit with an antithrombotic therapy in the symptomatic PAD population after lower-extremity revascularisation, which speaks to the need for a new treatment in this space. We look forward to discussing these data with the FDA.”
Janssen and its development partner Bayer have conducted two major Phase 3 trials, VOYAGER PAD and COMPASS, that evaluated the use of dual antithrombotic pathway inhibition with Xarelto plus aspirin in patients with PAD. Xarelto, in combination with aspirin, was approved by the FDA in 2018 to reduce the risk of major cardiovascular events in patients with chronic PAD and coronary artery disease—the only direct oral anticoagulant (DOAC) approved for use in these populations.
As presented at the Global Embolization Oncology Symposium Technologies (GEST) 2020 meeting (4–6 September, virtual), Robert Lewandowski discusses the evolution of radioembolization with Yttrium-90 (Y-90) over the past decade. Initially a lobar therapy, Y-90 can today be performed via a segmental delivery of microspheres to hepatocellular carcinoma (HCC) patients at earlier stages in their disease, and multiple tumours can be targeted in a same-day session. Furthermore, Lewandowski recounts how threshold dosimetry is now allowing for curative-intent therapy, and explains that the most recent data suggest this personalised dosimetry approach can be applied to a more advanced HCC population.
The historical role of radioembolization with Y-90 for patients with HCC is in the salvage setting; radioembolization has been employed to treat patients considered poor candidates for trans-arterial chemoembolization (TACE) or those that failed TACE. In contradistinction to the selective approach of TACE, radioembolization has been performed in a lobar (or sequential lobar) fashion. Despite these differences in patient selection and technique, evidence has supported the application of radioembolization over TACE in intermediate staged HCC patients because of improved quality of life metrics and longer time to progression. The median overall survival (OS) for patients with intermediate-stage HCC treated with Y-90 is 25 months.
A serendipitous observation following uni-lobar radioembolization was the development of an atrophy-hypertrophy complex; the treated hepatic lobe and targeted tumour decrease in size, with resultant hypertrophy in the contralateral lobe. For patients who would be candidates for surgical resection but present with an inadequate future liver remnant (FLR), radiation lobectomy was developed as a new paradigm to facilitate hepatic resection. With standard dosimetry, FLR hypertrophy is a time-dependent process with approximately 10% hypertrophy from baseline at one-month post Y-90, and 45% by nine-months post Y-90. More recently, modified radiation lobectomy techniques have been developed to increase the rate of hypertrophy and to deliver more effective cancer therapy.
The application of radioembolization is evolving from its lobar therapy origins; radioembolization is increasingly utilised in a segmental fashion to treat earlier stage disease. The results of the PREMIERE trial, a prospective, randomised trial for patients with unresectable tumours not amendable to ablation, revealed significantly improved outcomes for segmental radioembolization versus segmental TACE (time-to-progression >26 months vs. 6.8 months, respectively). These results have been corroborated by other US sites, including the University of Washington in Seattle, Mt Sinai Hospital in New York City, and the Mayo Clinic in Jacksonville. The true potential of segmental radioembolization, however, is in its ablative potential. Radiology-pathology correlative studies have revealed that complete pathologic necrosis at explant is best obtained when the volumes of perfusion are targeted with glass microsphere dosimetry >190 Gray. A recent multi-centre analysis has reset this threshold dose for segmental radioembolization. In this analysis, all tumours treated with a segmental radiation dose >400 Gray achieved complete pathologic necrosis at explant.
High tumour response rates on imaging, long time to tumour progression, and meaningful complete pathologic response rates have made radiation segmentectomy a versatile therapy, allowing for down-staging to liver transplant, bridging to liver transplant, or as a potentially definitive curative-intent therapy for early stage HCC. Median overall survival outcomes for Child-Pugh A patients with solitary HCC <5cm appear consistent with those for other curative therapies (i.e., ablation, surgical resection, liver transplant): 6.7 years from date of Y-90.
The evolution of radioembolization from a lobar therapy to a segmental therapy includes technical modifications beyond threshold dosimetry to achieve complete pathologic necrosis. Many of these techniques have been developed for TACE over the past several decades. The first concept is that of same-day radioembolization: the planning angiogram, macro-aggregated albumin (MAA) administration to determine lung shunt fraction (LSF), and Y-90 administration can be performed in a single session. This is particularly appealing for patients with early stage disease amenable to radiation segmentectomy. Same-day radioembolization might further be streamlined by eliminating the requirement for the MAA administration in patients with limited disease burden. Recent data support this concept by confirming low LSF for those HCC patients within Milan criteria. The second concept is that of performing radioembolization to extra-hepatic tumour perfusing branches. There is no established optimal embolic device to treat tumours via parasitised extra-hepatic arteries; there are now published reports describing the delivery of Y-90 via the inferior phrenic arteries, the adrenal artery, and the cystic artery. The final concept is that of segmental administration of Y-90 to multi-focal disease. With segmental radioembolization, multi-focal disease can be targeted in a single session through separate selective arterial catheterisations and dose vial administrations.
In conclusion, radioembolization with Y-90 has evolved over the past 10 years, morphing from a lobar therapy for patients with HCC advanced beyond being amendable to TACE into a versatile treatment option for patients across the Barcelona Clinic Liver Cancer staging paradigm. This evolution has allowed for radioembolization to be performed in a similar fashion to TACE: segmental/selective delivery of Y-90 microspheres to HCC patients at earlier stages in their disease, targeting multiple tumours as well as extra-hepatic tumour-perfusing branches, often in a same-day session. Most importantly, threshold dosimetry is now allowing for curative-intent therapy, supported by explant data. This concept of threshold, or personalised, dosimetry has more recently been expanded and applied to the advanced HCC population (DOSISPHERE-01 TRIAL), accepted for publication in the Lancet Gastroenterology & Hepatology.
Robert J Lewandowski is a professor of Radiology, Medicine, and Surgery, and the director of Interventional Oncologyat the Northwestern University Feinberg School of Medicine, Chicago, USA
Canon Medical Systems has launched its Aquilion Exceed LB (pending 510(k) clearance), a CT scanner dedicated to radiation therapy planning, at this week’s American Society for Radiation Oncology (ASTRO) virtual meeting (23–29 October). At 90cm, the new scanner sports what Canon believes to be the largest bore in the industry, and features a 90cm edge-to-edge extended field-of-view reconstruction and a wide detector coverage of 4cm.
The system also uses Canon’s Advanced intelligent Clear-IQ Engine (AiCE) Deep Learning Reconstruction (DLR) technology, pioneered on the company’s diagnostic radiology CT line.
“Accurate simulation across even the most challenging treatment plans is imperative during radiation therapy planning,” comments Erin Angel, managing director, CT Business Unit, Canon Medical Systems USA. “At Canon Medical, we deliver solutions that meet providers’ needs but also push the boundaries of traditional simulation. With the Aquilion Exceed LB, we brought deep learning reconstruction to the CT simulation space. This will revolutionise care for cancer patients and give the radiation oncology team the confidence and precision they need for accurate planning across patients.”
While the Aquilion Exceed LB is pending 510(k) clearance, international shipments outside the USA are ready to start now, the company said.
The Royal College of Radiologists (RCR) and the British Society of Interventional Radiology (BSIR) have called for a UK-wide clinical registry for ureteric stents, following the release of a report investigating delayed removal of the devices.
The Healthcare Safety Investigation Branch (HSIB) released a report on 22 October titled, “Unplanned delayed removal of ureteric stents”, highlighting the need for better clinical communication and monitoring standards around ureteric stent use.
The new HSIB report was instigated following a reference case involving a patient who was fitted with a stent following surgery for kidney stones. Removal of the stent was delayed, and the device became encrusted, causing ongoing urinary infections before it was eventually removed.
England-wide themes considered by HSIB include the different processes used for stent logging and tracking, varying communications between hospital teams and GPs, and the need for standardised advice for patients.
HSIB recommends the creation of national standards to support paper and electronic logging systems, enhanced patient information and guidance for clinicians, and for stent status and further information to be included on all hospital discharge letters and other communications sent to GPs.
The RCR and BSIR welcome the report and agree with its findings, but also argue that stent monitoring could be further centralised and given clear clinical incentives.
Ian McCafferty, BSIR president and member of the RCR’s Interventional Radiology Committee, says: “Interventional radiology (IR) plays a significant role in stent insertion and removal across specialties, including ureteric stenting. Radiology workload is also only increasing here, particularly as ‘COVID-secure’ IR services have picked up more cases during the pandemic. As a result, IR consultants and their teams are implicated in ensuring these devices are flagged and tracked.
“The RCR and BSIR fully agree stents should be removed at replaced at appropriate timescales, with a robust tracing system for their use.
“HSIB recommends more professional standards to support ureteric stent monitoring. However, ideally we believe there needs to be an open-access, UK-wide stent registry. In addition, tariff reimbursement should be linked to registration, to ensure all devices are properly registered and therefore monitored.
“Providers would also need to appoint leads to support clinicians logging the devices and to ensure local data is kept up-to-date.”
In a recently-published study, Jeremy Crane (Imperial College Healthcare NHS Trust, Hammersmith Hospital, London, UK) and colleagues conclude that a 3mm-long arteriotomy may be routinely utilised for brachiocephalic fistula creation in an attempt to limit the incidence of steal syndrome, while maintaining clinical patency outcomes. According to the authors, this is the first ever series in the literature of a 3mm arteriotomy.
“The arteriovenous fistula [AVF] is the modality of choice for long-term haemodialysis access,” the Journal of Vascular Access (JVA) paper begins. The authors cite lower rates of access-related infection and improved patient and access survival when compared to other modalities such as arteriovenous grafts or longstanding tunnelled central venous catheters as the reasons behind why the AVF is the most popular modality for haemodialysis access.
However, AVF formation is “not to be taken lightly,” Crane and colleagues warn, noting that dialysis access-associated steal syndrome (DASS) as an “important” and “potentially limb threatening” complication. They explain that the hallmarks of steal syndrome are symptoms and signs of peripheral vascular insufficiency within the limb distal to the AVF, which are often detected through a thorough clinical history and examination.
They go on to describe the feasibility of routinely fashioning a brachiocephalic fistula utilising a 3mm-long arteriotomy in an attempt to reduce the incidence of symptomatic steal syndrome, while maintaining clinical patency outcomes.
Crane and colleagues describe the study as a retrospective analysis of prospectively collected clinical data from a single surgeon. They detail that they included all patients who underwent brachiocephalic fistula formation using a routine 3mm-long arteriotomy within Hammersmith Hospital between January 2017 and March 2018 in the study. They note that primary outcomes included primary failure, failure of maturation, secondary patency, and steal syndrome.
Writing in JVA, Crane et al relay that 68 brachiocephalic AVFs were fashioned utilising a 3mm arteriotomy during study period, adding that the mean age was 60.5 years with 59% having a history of diabetes mellitus. The mean follow-up was 368 days, the authors write.
The authors report that primary failure occured in 10 (14.7%) of patients, and that cannulation was achieved in 67.3% of remaining fistulae within three months, rising to 87.3% by six months.
In terms of primary patency, Crane and colleagues note that this was 76% and 69% at six and 12 months, respectively. Secondary patency at the same time points was 91% and 94%, respectively. Finally, the authors detail that dialysis access steal syndrome was clinically apparent in three (4.4%) patients, with all cases being managed conservatively.
The authors acknowledge that the present study has certain limitations. Firstly, they recognise that steal syndrome is multifactorial in origin and not purely related to anastomosis calibre. In addition, “follow-up among the patients included in the study is limited,” Crane and colleagues write, adding that late presentations of DASS due to ongoing arterial and venous remodelling and subsequent increase in fistula flow may subsequently occur. They suggest that a randomised trial with clear documentation of venous and arterial diameter along with postoperative duplex ultrasound and haemodialysis access flow assessment would be useful.
Crane et al posit that comparison alongside other techniques such as the proximal radial artery AVF, particularly among patients deemed at higher risk of steal syndrome would be of interest. Nevertheless, they emphasise that a shorter length arteriotomy of 3mm “appears sufficient” to maintain fistula patency, while potentially minimising the risk of steal phenomena.
Editorial use only
Haemodialysis, Patient undergoing haemodialysis treatment, Limoges hospital, France.
Different risk factors affect patency between vascular access construction and the first percutaneous transluminal angioplasty, Mahoko Yoshida (Hiroshima University Hospital, Hiroshima, Japan) and colleagues conclude in The Journal of Vascular Access. Their results indicate that a poor patency rate is commonly associated with advanced age and diabetes mellitus.
“These findings suggest that older patients and those with diabetes mellitus are more likely to experience vascular access problems after both vascular access construction and percutaneous transluminal angioplasty [PTA], and that different risk factors should be taken into account when managing patients undergoing haemodialysis after vascular access construction and PTA,” the study authors write. “Understanding the risk factors that contribute to vascular access problems may lead to better surveillance and focused care in high-risk patients, resulting in more effective management of vascular access.”
Dialysis: “A global health concern”
The number of patients undergoing dialysis worldwide has been increasing each year, the study authors write, and is considered a global health concern. The majority of dialysis patients receive haemodialysis, and are known to suffer from various complications, including cardiovascular disease and infections. The most frequent issue relates to problems with vascular access: stenosis, thrombosis, aneurysm, and infection. “In fact,” Yoshida et al say, “the medical expenses for vascular access-related complications is estimated at JPY 10,953,310,000/year”. The investigators therefore surmise that “recognition of risk factors for vascular access failure is needed not only to improve the quality of life of patients undergoing haemodialysis, but also to reduce medical expenditure”.
They conducted a multicentre, prospective, observational study of 611 patients who had started haemodialysis between 1 April 2012 and 31 March 2018, and investigated the primary and secondary patency rates after construction of a radiocephalic arteriovenous fistula (AVF) and arteriovenous graft (AVG). Primary patency was defined as the period from vascular access construction to percutaneous transluminal angioplasty or surgical revision within 24 months; secondary patency was defined as the period from vascular access construction to the date of vascular access abandonment. The study also examined the patency rate following percutaneous transluminal angioplasty (PTA)—defined as the period from the first PTA to the next PTA or surgical revision within 12 months—as well as the clinical factors that contributed to the development of restenosis. All patients were followed-up until December 2018.
Post-PTA patency unaffected by vascular access form in older patients
The study results reveal that radiocephalic AVF exhibited better 24-month primary and secondary patency rates than AVG in patients who started haemodialysis: 54.5% and 91.6% versus 25.1% and 70.3%. The authors note that these 24-month primary and secondary patency rates after vascular access construction are higher than those reported in the literature by researchers investigating patients outside of Japan. They postulate that the higher patency rates seen in Japanese patients could be due to the fact that they undergo haemodialysis with lower blood flow, which they suggest may enable the vascular access to be used for longer periods.
While the patency rates after vascular access construction between the two vascular access forms (radiocephalic AVF and AVG) was not significantly different in the multivariate analysis, they did show a significant difference in the log-rank test. “With respect to the post-PTA patency rate, although radiocephalic AVF appeared to result in a better patency rate than that of AVG, the difference was not statistically significant in either the log-rank test or Cox proportional hazard model,” Yoshida and colleagues discuss. “A previous study reported that AVF exhibited a better patency rate after both vascular access construction and PTA than AVG. Notably, another study showed that the patency rate of AVF did not differ from that of AVG in advanced-age patients undergoing haemodialysis, especially those aged >65 years. In the present study, the median age of the patients was 70 years, suggesting that rather than the vascular access form, the background of the patients may be more strongly associated with the patency rate.”
Risk factors for vascular access complications
A Cox proportional hazard model demonstrated that aging, female sex, diabetes mellitus, low serum albumin, and use of an erythropoietin-stimulating agent were associated with poor primary patency after vascular access construction in this study. Of these identified risk factors, aging, diabetes mellitus, and low serum albumin may be indicative of a patient’s poor general condition, the study authors muse, while female sex has reportedly been associated with smaller vascular diameter, which can increase the number of vascular access problems. “Taken together these results indicate that vascular access patency might be improved if modifiable risk factors identified in the present study are well controlled,” Yoshida et al write.
Furthermore, aging, diabetes mellitus, polycystic kidney disease, initiation of haemodialysis with the use of a temporary catheter, and a shorter period from vascular access construction to use were associated with poor patency after the first PTA. These results led the study investigators to conclude that patients need to start haemodialysis “urgently”.
“These findings suggest that with the exception of aging and diabetes mellitus, different risk factors contribute to the incidence of vascular access problems after surgical construction of vascular access and restenosis after PTA,” the authors conclude.
“Our data showed that stenosis accounted for 92% of vascular access problems. […] These findings suggest that the presence or absence of procedure-induced stimulation may cause differences in the risk factors that influence the patency rates after vascular access construction and that after PTA.”
The VOYAGER PAD panel. Clockwise from top left: Sahil A Parikh, Frank Veith, Marc Bonaca, Connie N Hess, and Robert A Lookstein
Clockwise from top left: Sahil A Parikh, Frank Veith, Marc Bonaca, Connie N Hess, and Robert A Lookstein
Findings from a series of late-breaking trials in the endovascular field were presented recently at TCT Connect (14–18 October, virtual), the 32nd annual scientific symposium of the Cardiovascular Research Foundation (CRF). Sahil A Parikh (Columbia University Medical Center, New York, USA) and Frank Veith (New York University Medical Center, New York, USA) moderated the session, with Marc Bonaca (University of Colorado, Aurora, USA) and Robert A Lookstein (Mount Sinai Health System, New York, USA) on the panel.
First on the virtual podium was Connie N Hess (University of Colorado, Aurora, USA), who presented results of a large subgroup analysis of the VOYAGER PAD randomised clinical trial. This showed neither a mortality risk nor benefit associated with the use of paclitaxel drug-coated devices in the treatment of peripheral arterial disease (PAD). The study also found that the benefit of rivaroxaban use on reducing ischaemic limb and cardiovascular outcomes was consistent regardless of whether a drug-coated device was used.
This analysis examined the long-term safety of drug-coated devices and evaluated whether rivaroxaban 2.5mg twice daily plus low dose aspirin versus low dose aspirin alone on the primary efficacy endpoint was consistent with versus without drug-coated device (DCD) use.
During the qualifying endovascular lower extremity revascularisation, DCD was used for 31% (n=1,358) of patients. Patients receiving DCD more frequently had prior endovascular lower extremity revascularisation, had higher baseline use of dual antiplatelet therapy and statins, and were more often treated for claudication than non-DCD patients.
In the unweighted analysis, lower associated mortality was observed among patients receiving DCD versus non-DCD (2.9 vs. 3.9 per 100 patient-years; 3.5-year Kaplan-Meier cumulative incidence of 10.2% vs.13.8%). After weighting, there was no association between DCD use and mortality (3.5-year cumulative incidence 12.1% vs. 12.6%, HR 0.95, 95% CI 0.83-1.09, p=0.49). The benefit of rivaroxaban 2.5mg twice daily with aspirin compared to aspirin alone on reducing ischaemic limb and cardiovascular outcomes was also consistent regardless of whether a DCD was used.
The VOYAGER PAD trial was funded by research grants to CPC Clinical Research from Bayer and Janssen.
IN.PACT 0.014 DCB may offer a clinical benefit in patients with CLI
Antonio Micari (University of Messina, Messina, Italy) presented first-ever results from Medtronic’s IN.PACT BTK study, a feasibility study assessing the safety and effectiveness of the company’s IN.PACT 0.014 drug-coated balloon (DCB) in critical limb ischaemia (CLI) subjects with chronic total occlusion (CTO) in the infrapopliteal arteries.
The IN.PACT BTK study is a prospective, multicentre, 1:1, randomised feasibility study assessing the safety and effectiveness of the IN.PACT 0.014 DCB, a 3.5 μg/mm2 dose paclitaxel-coated balloon, versus conventional percutaneous transluminal angioplasty (PTA) for the treatment of CTOs in the infrapopliteal arteries. The study enrolled 50 subjects at nine sites in Europe.
At nine months, subjects in the DCB group experienced a reduction in sub-segmental late lumen loss compared to those in the PTA control group (0.59±0.94mm versus 1.26±0.81mm, respectively, p=0.017), a 53% lower late lumen loss than the PTA control group. Using the classic late lumen loss method, subjects in the DCB group experienced lower late lumen loss compared to those in the PTA control group at nine months (0.89±0.77mm versus 1.31±0.72mm respectively, p=0.07 ), a 32% lower late lumen loss than the PTA control group.
Historically, there has not been a DCB technology that has demonstrated effectiveness in this vessel bed. According to a Medtronic press release, the data presented at TCT demonstrate that IN.PACT 0.014 may offer a clinical benefit in patients with CLI.
The IN.PACT 0.014 DCB is an investigational device that is being evaluated in Europe. This device is not currently being evaluated in the USA.
ILLUMENATE Global: Four-year results support durable long-term outcomes with the Stellarex DCB
Andrew Holden (Auckland City Hospital, Auckland, New Zealand) reported on late safety and efficacy outcomes for the low-dose Stellarex DCB (Philips) in de novo and restenotic femoropopliteal lesions from a large cohort.
He revealed that four-year data from the trial show favourable safety and efficacy outcomes consistent with the ILLUMENATE randomised controlled trials, and also demonstrate similar efficacy in prespecified cohorts including different gender groups and diabetics.
ILLUMENATE Global is a prospective, single-arm, multicentre study conducted in the EU. The patient population included those with Rutherford Clinical Classification (RCC) of 2–4 indicated for treatment of the superficial femoral artery (SFA) and/or popliteal artery for de novo or restenotic lesions. Follow-up office visits were at one, six, 12, 24, and 36-months post-procedure and included clinical, haemodynamic, and functional outcomes.
At four years, the rate of major target limb amputation was 0.8% and that of all-cause mortality was 8.1%. Clinically-driven target lesion revascularisation through four years was 75.6% at day 1,460 and the subgroup analysis revealed no difference in prespecified cohorts.
“The ILLUMENATE Global study supports durable long-term outcomes with the Stellarex DCB and is applicable to a complex population,” Holden told the TCT audience.
Bullfrog device shows promise in TANGO Registry
Ehrin J Armstrong (UCHealth Heart and Vascular Center, Aurora, USA) presented results of the TANGO Registry. This Phase 2 study aimed to assess the six-month efficacy and safety of the Bullfrog micro-infusion device (Mercator MedSystems) adventitial deposition of two escalating doses of temsirolimus in reducing angiographic neointimal hyperplasia and target lesion failure after revascularisation of below-the-knee (BTK) arteries.
This prospective, multicentre, dose-escalation, comparative, double-blinded study enrolled 61 patients undergoing endovascular revascularisation of ≥1 angiographically significant BTK lesions. Treatment was applied after completion of artery revascularisation, and divided into control (saline; 0.25–0.5mL/cm of lesion length), low-dose temsirolimus (0.1mg/mL; 0.025–0.05mg/cm of lesion length) or high-dose temsirolimus (0.4mg/mL; 0.1–0.2mg/cm of lesion length) groups in a dual-blinded, randomised fashion.
Primary and secondary efficacy endpoints were transverse-view vessel area loss percentage (TVAL%) of the target lesion and clinically relevant target lesion failure (CR-TLF) at six months, respectively. Primary safety endpoint was freedom from a major adverse limb event or perioperative death (MALE+POD) at 30 days.
Armstrong reported that superior primary efficacy of the treatment arm was apparent in the per protocol (PP) and PP-TASC B-D (excluding 15 subjects with TASC A lesions) subgroups, and that TVAL% reductions of 13.9% and 22.3% were seen in the PP and PP-TASC B-D subgroups at six months, respectively.
In addition, freedom from CR-TLF rates were substantially higher in those patients treated with temsirolimus, and differences between treatment and control for freedom from CR-TLF at six months were 27.1% and 39.2% in the PP and PP TASC B-D subgroups, respectively. Freedom from composite of 30-day MALE+POD was 100% in all groups.
“Findings suggest that adventitial deposition of temsirolimus using the Bullfrog micro-infusion device improves six-month vessel patency when applied to BTK arteries after successful endovascular revascularisation,” Armstrong concluded.
FLASH Registry: Acute haemodynamic improvement with percutaneous mechanical thrombectomy in a real-world pulmonary embolism population
Catalin Toma (University of Pittsburgh, Pittsburgh, USA) presented results from the FLASH Registry. FLASH is a 500-patient prospective, multicentre registry study to evaluate real-world outcomes after treatment of patients with intermediate and high risk PE with FlowTriever (Inari Medical).
Toma reported that mortality through 48 hours was 0% and that just three patients out of 320 (1.3%) experienced major adverse events—all of which were major bleeds.
Ablation of peri-arterial nerves in ARA should result in an additional blood pressure reduction
Yu Sato (CVPath Institute, Gaithersburg, USA) gave the final presentation of the session, on the anatomy of the human accessory renal artery peri-arterial renal sympathetic nerve for renal denervation.
Sato began by detailing that accessory renal arteries (ARAs) have been reported in about 30% of patients. Some renal denervation clinical trials excluded patients with ARAs, while others included such patients but excluded those with ARAs less than 3 or 4mm in diameter. Moreover, some studies have suggested that renal denervation for ARAs may have an additional advantage of blood pressure reduction. The aim of this study was to evaluate the anatomic distribution of peri-arterial nerves in human ARAs.
Sato concluded that ARAs have two-thirds the number of nerves as compared to dominant renal arteries, and that the number of nerves around the ARAs is dependent on the size of the renal arteries.
“Our results suggest that ablation of peri-arterial nerves in ARA should result in an additional blood pressure reduction,” he remarked, adding that future renal denervation clinical trials should consider including ablation of peri-arterial nerves in ARAs.
Cook Medical today announced that the Zilver Vena received US Food and Drug Administration (FDA) premarket approval (PMA) in the USA. The product is expected to be commercially available to physicians in the USA in Q4 2020.
Zilver Vena is a self-expanding stent approved to treat patients suffering from iliofemoral venous disease. When implanted in a patient with venous disease, Zilver Vena expands to keep blood flowing through narrow or blocked veins.
To receive this FDA premarket approval, Cook Medical had to provide scientific evidence that the device is safe and effective for its intended use in treating venous outflow obstruction.
According to a press release, the stent was designed to balance flexibility and strength: it is flexible so that it can conform to a patient’s unique anatomy while it provides sufficient lumen expansion to open blocked veins.
“We are only in the early stages of understanding this complex disease, but Cook is committed to driving venous therapy development,” said Mark Breedlove, vice president of Cook Medical’s Vascular division. “We are engaged and committed to working alongside physicians and investing in thorough internal training, physician education, building clinical evidence, and more.”
Ra Medical Systems has announced enrolment of the tenth subject in its pivotal clinical trial to evaluate the safety and effectiveness of the Dabra excimer laser system as an atherectomy device for the treatment of peripheral arterial disease (PAD).
“Patient screening and enrolment have recently increased with five clinical sites now cleared to enrol subjects as we pursue an atherectomy indication for Dabra,” said Will McGuire, Ra Medical Systems CEO. “Earlier this year enrolment in this trial had stalled due to the COVID-19 pandemic, which also impacted our ability to activate new clinical sites. We are pleased that nine subjects have been enrolled in the past two months at our clinical study sites, all of which are operating via applicable COVID-19 protocols.”
The open-label pivotal atherectomy clinical trial can enrol up to 100 patients with symptoms of PAD (Rutherford Class 2–5) at up to 10 sites. Outcome measures include safety, acute technical success, and clinical success. The trial’s primary efficacy endpoint is the mean reduction in percent diameter stenosis in each patient’s primary lesion as measured by angiography immediately following treatment with Dabra, before any adjunctive treatment.
The trial’s safety and clinical success endpoints are major adverse events at 30 days and incidence of primary target lesion revascularisation at six months. Dabra received US Food and Drug Administration (FDA) 510(k) clearance in May 2017 for use in ablating a channel in occlusive peripheral vascular disease.
Bridging the gap between the IOs: “We need to determine whether to freeze, fry, shake, shock, zap, or choke a tumour,” writes Brad Wood
Ushering in “the era of IO”, Brad Wood calls for interventional oncologists to learn the language of immuno-oncology—“the other IO”—in order to improve care for cancer patients. Discussing the “speculative but huge potential impact” of combining interventional radiology (IR) approaches with an understanding of immune-oncology, Wood warns readers that this is not merely an exciting opportunity to increase the scope of interventional oncologists’ work, but a necessary step in ensuring the discipline stays at the vanguard of oncologic treatment. immuno-oncology
It has been known for decades that local-regional therapies like ablation and embolization can stimulate a tumour-specific systemic immune response, or even, on some occasions, tumour regression remote from the treated area. What is not known is who, what, where, when, and how to make it happen more often. Enter the era of IO, which to most people means immuno-oncology (IO), and not interventional oncology (IO). Bridging the gap (between IO and the other IO) requires learning the language and themes of cancer immunology. Interventional radiology (IR) has several hammers to pull out of our big IO toolbox. However, we need to determine whether to freeze, fry, shake, shock, zap, or choke a tumour—that is, whether to use cryoablation, radiofrequency ablation (RFA), microwave ablation (MWA), irreversible electroporation (IRE), high-intensity focused ultrasound (HIFU), histotripsy, transarterial chemoembolization [TACE], or Yttrium-90 (Y-90) radioembolization. We also need to determine which histology to treat, at what stage, alongside what IO drug, and in what sequence. Where in the cancer immunity cycle do the IO tools immuno-modulate? How do we balance pro-immune versus pro-metastatic pathways? The window of opportunity remains open for answering the many questions in a rational way.
Checkpoint inhibition takes the brakes off our natural immune response to tumours. Although revolutionary and Nobel-prize worthy, checkpoint inhibitors usually fail as monotherapy, are costly, and are not without side effects. Enter IR/IO. Local IO therapies alongside of checkpoint inhibition can convert an “immune-cold” tumour into an “immune-hot” tumour, potentially turning local into systemic. Immunomodulatory mechanisms boil down to enhancement of: 1) antigen release and presentation, 2) antigen-presenting cell (APC) maturation, 3) T-cell priming proliferation and trafficking, and, 4) reduction of immune tolerance and immune resistance. The molecular tumour micro-environment and the dynamic immune compartments (blood vessels, lymph nodes, target tumour, and remote tumours) also merit consideration.
Initial clinical experience with checkpoint inhibition drugs plus ablation or embolization for advanced hepatocellular carcinoma (HCC) was first reported over five years ago in a National Institute of Health (NIH) study.1, 2 This showed disease stabilisation in the bulk of patients with advanced and heavily pre-treated HCC via this combination approach, often with intentional subtotal treatment of the target tumours. This study also has strong blood and tissue evidence for an immune mechanism when looking at responders versus non-responders. For cholangiocarcinoma, a similar approach with subtotal ablation can be taken.3 Human tissue and survival data convince more medical oncologists at a multidisciplinary tumour board meeting than curing mice in 1,000 lab studies. In this setting, the local or regional therapy is meant to boost the immune system, deposit antigens, promote APC and T-cell maturation, broaden the T-cell receptor response, and tip the balance of immune-regulation away from immune tolerance and towards tumour-specific T-cell activation. More recently, Bevacizumab plus Atezolizumab was approved by the US Food and Drug Administration (FDA) for locally-advanced HCC,4 and ongoing clinical trials will hopefully address whether and when local ablation or embolization add value. The therapeutic options are evolving fast, so IR needs to organise a clinical trial infrastructure, so we can ask hypothesis-driven questions in a standardised fashion. Team science wins.
Brad Wood
Emerging data support aggressive local-regional therapies when immunotherapy fails locally in established tumors (versus new widespread metastases). Specifically, when stratified by patterns of failure, local therapy has been shown to be particularly effective after failed checkpoint inhibition, supporting an aggressive re-treatment approach, when progression is confined to established tumours (rather than new breakthrough metastases).5 Like ablation, drug-eluting bead TACE (DEB-TACE) and Y-90 radioembolization reduce regulatory T-cells (good) and expand T-cell responses in HCC. Doxorubicin potentiates immunogenic cell death and enhances cross-priming, but ischaemia cascades turn on damage/pathogen-associated molecular patterns (DAMPS/PAMPS), HIF1a, and cell stress pathways. IRE may leave vessel highways intact for APC and T-cell trafficking, which may explain why IRE (shock) may be better for immunomodulation than RFA (heat) or cryoablation (freeze) for T-cell activation. Histotripsy may be better than heat when combined with checkpoint inhibition.6 Both IRE and cryoablation release more proteins than heat. Yet RFA heat may have a favourable impact upon immunosuppressive T-regs than cryoablation. Cryoablation may have the most inflammation and cell stress signals. Any ablation might recruit more good macrophages than bad, when the margin interacts with the tumour (thus leaves tumour behind). Yet colorectal metastases may explode when partially treated and exposed to the hypoxia of partial treatment.
Clearly, we need to biopsy more after IO therapies. We need to learn more about the tools to measure immune effects (such as immunohistochemistry, flow cytometry, and sequencing). It is a great time to have coffee with an expert from another discipline!
So when you freeze, fry, shake, shock, zap, or choke the tumor—treat the patient, not the picture. Do not be a technical robot and just treat geometric spots in the liver. Think before ablating. Create the proper tumour micro-environment via timing, sequence, and delivery of rational IO plus IO immunomodulation. This is a one-time opportunity, with speculative but huge potential impact. New immuno-oncology trials with checkpoint inhibitor drug combinations have exploded in the past two years.7 Where is IR? We need to be at the table and not on the menu.
Brad Wood is an interventional oncologist at the National Institutes of Health (NIH) Center for Interventional Oncology, Bethesda, USA.
References:
Presentation at the American Society of Clinical Oncology (ASCO) Annual Meeting, 2015
Duffy AG et al. Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma. Journal of Hepatology. 2017 Mar;66(3):545–551. Doi: 10.1016/j.jhep.2016.10.029
Changqing Xie et al. Tremelimumab in combination with microwave ablation in patients with refractory biliary tract cancer. Hepatology. 2019 May;69(5):2048–2060. Doi: 10.1002/hep.30482
Richard Finn et al. Atezolizumab plus Bevacizumab in unresectable hepatocellular carcinoma. New England Journal of Medicine. 2020 May; 382:1894–1905. Doi: 10.1056/NEJMoa1915745
Nicholas Klemen et al. Patterns of failure after immunotherapy with checkpoint inhibitors predict durable progression-free survival after local therapy for metastatic melanoma. Journal of Immunotherapy of Cancer. 2019 July;7:196. Doi: 10.1186/s40425-019-0672-3
Eranki A, et al: High-Intensity Focused Ultrasound (HIFU) Triggers Immune Sensitization of Refractory Murine Neuroblastoma to Checkpoint Inhibitor Therapy. Clinical Cancer Research 2020 Mar 1;26(5):1152-1161. doi: 10.1158/1078-0432.CCR-19-1604
Greten TF, et al: Combined locoregional-immunotherapy for liver cancer. Journal of Hepatology 2019 May;70(5):999-1007. doi: 10.1016/j.jhep.2019.01.027
A new survey among vascular access (VA) and emergency department (ED) clinicians has revealed significant levels of variation in ultrasound-guided peripheral IV (UGPIV) practices and supply use across hospitals and alternate care settings. Published in the September issue of the Journal of the Association for Vascular Access, the findings carry critical implications for patient safety.
A total of 1,475 VA and ED practitioners responded to the survey, which was designed to gain better insight into clinicians’ current practices regarding UGPIV insertion. The survey also identified inconsistencies in supply use across hospital departments. The survey was conducted by Nancy Moureau (Griffith University, Brisbane, Australia) an internationally recognised expert and consultant in vascular access and CEO of PICC Excellence.
“Identifying gaps and variations in clinical practice forms the basis of quality initiatives intended to improve patient safety. This survey revealed clinically meaningful differences in all variables for UGPIV procedures and supplies,” said Moureau. “Aseptic technique is essential for minimising contamination, but its effectiveness is diminished if it is not done in a consistent manner. Often inconsistencies in supply usage point to variation in policy application and the potential for substandard practices. The survey results suggest a need for clinical education on the application of UGPIV guidelines, and for greater scrutiny over supplies and techniques in order to promote standardisation.”
The lack of consistency revealed by the survey is apparent in respondents’ varied use of transducer protection and gel. To minimise contamination during UGPIV insertions, current guidelines—such as those from the American College of Emergency Physicians and the American Institute of Ultrasound in Medicine—recommend use of a transducer cover and single-use gel packets (sterile or non-sterile). According to the survey, however, just 59% of VA clinicians and 11% of ED clinicians always use a sterile probe cover during UGPIV procedures, and only 64% of VA personnel and 13% of ED personnel use sterile gel. In addition, more than 22% of respondents stated that they vary between multi-use gel bottles and single-use gel packets, both sterile and non-sterile.
The survey results also highlight issues resulting from the presence of gel in the area of the sterile insertion site. Among the respondents, 41% of VA clinicians and 51% of ED clinicians reported instances of inadequate gel removal, which results in securement and dressing adherence issues. Poor adherence of dressings can lead to catheter failure and accidental dislodgement. Over half of all VA personnel (52%) said they felt that aseptic technique is often compromised by post-procedure gel clean-up.
PIV insertion is the most commonly performed invasive medical procedure among hospitalised patients. Over 70% of acute care patients require IV access at some point during their stay. According to Moureau, up to 60% of those patients may be considered to have difficult vascular access (DiVA). These patients frequently require ultrasound guidance in order to successfully achieve peripheral access and receive necessary treatments.
“This study confirms that the lack of consistent, evidence-based guidelines regarding ultrasound-guidance for PIV insertions has led to a great deal of fragmentation, and shows that clinicians are confused over when and how to use this technology in a way that protects patient safety,” said emergency vascular access expert Jon Bell (St Joseph Hospital, Bangor, USA). “There needs to be an objective standard for identifying difficult access patients, as well as a multidisciplinary effort to conduct research to determine the best practices that will minimise harm to the patient.”
The use of ultrasound may increase the risk of contamination during PIV insertions if certain guidelines are not followed to maintain a sterile insertion site and use the appropriate supplies (gel and transducer protection). According to Moureau, a specialty gel-free insertion dressing that separates the transducer and gel from the insertion site (UltraDrape, Parker Labs) may address and even mitigate many of these issues while reducing the cost of performing UGPIV insertions. In this study, 9% of survey respondents reported use of this gel separation safety dressing.
The survey results align with recent concerns from the healthcare quality and safety organisation, ECRI (Plymouth Meeting, PA). The non-profit technology assessment group addressed the issue of standardisation in its list of top patient safety concerns for 2020, writing that “policies and education must align across care settings to ensure patient safety.”
ECRI also included the use of point-of-care ultrasound in its briefing on 2020 Top 10 Health Technology Hazards, and noted that the rapid adoption of this technology across various care settings has left many organisations struggling to keep up with appropriate safety measures.
MedAlliance has announced enrolment of the first two patients in the PRISTINE registry with Selution sustained limus release (SLR) 018 drug-eluting balloon (DEB) for the treatment of patients with below-the-knee disease. This is the first DEB accepted by the US Food and Drug Administration (FDA) for its breakthrough programme.
The PRISTINE registry is a follow up to the encouraging results seen in the PRESTIGE clinical trial (below the knee, chronic limb threatening ischaemia [CLTI]) at six months.
PRISTINE is a prospective registry to investigate the safety and efficacy of treatment with Selution SLR sirolimus drug-coated balloon in TASC C and D athero-occlusive infrainguinal disease in patients with CLTI from Singapore.
The objective of the registry is to evaluate over 12 months safety and performance outcomes in 75 patients, with Selution SLR DEB in the treatment of infrainguinal occlusive lesions (TASC C and D) in patients with CLTI at Singapore General Hospital.
The clinical primary safety endpoint of the registry is freedom from major adverse events through 30 days and the performance primary endpoint is freedom from cd-TLR within six months. The secondary endpoints are primary patency at six and 12 months follow-up, freedom from cd-TLR at 12 months, clinical success at follow-up in Rutherford score by one class or more, wound healing at six months, and freedom from major target limb amputation within six and 12 months post index procedure.
“We are excited about the commencement of this large single-centre prospective study focusing on patients with chronic limb threatening ischemia receiving the novel sirolimus drug-eluting balloon (Selution SLR DEB) from MedAlliance”, said associate professor Chong Tze Tec, head and senior consultant, Department of Vascular Surgery, Singapore General Hospital. “We believe this registry will give us detailed insight into the efficacy and safety of this new balloon technology which will benefit this challenging group of patients.”
“We are delighted to report enrolment of the first two patients in the exciting PRISTINE registry”, added associate professor Tjun Tang, lead Investigator and a senior consultant in the Department of Vascular Surgery, Singapore General Hospital. “CLTI represents the worse part of the spectrum of peripheral artery disease and patients are at an increased risk of limb loss and mortality. The incidence is likely to increase in Singapore because of the rising trend in diabetes and end stage renal disease in the country and these patients are a challenging and frail population of patients.
“We currently do far too many major lower limb amputations: in fact the rate in Singapore is two to three times higher than in western countries. We seriously need to address this issue. One of the cornerstones of treatment is to re-establish pulsatile blood flow to the foot to promote wound healing and although percutaneous lower limb angioplasty has become the favoured option of revascularization, its Achilles heel is vessel recoil and restenosis from neointimal hyperplasia”.
“Singapore General Hospital performs over 900 lower limb salvage revascularisation procedures per year and has established multi-disciplinary wound management protocols and we are highly encouraged by the pilot data we have found using this technology so far and PRISTINE will offer further insight, leveraging on our experience with PRESTIGE, whether this sirolimus coated balloon will become an established device in our angioplasty armamentarium in the future”, concluded Tang.
The Surfacer Inside-Out access catheter system device (Bluegrass Vascular) is safe and effective for patients with thoracic central venous obstruction requiring central venous access. That is conclusion of the prospective, multicentre SAVE (Surfacer system to facilitate access in venous occlusions) registry, published today in the Journal of Vascular and Interventional Radiology (JVIR).
Central venous catheters were successfully placed in 29 of 30 patients (96.7%) with no device-related adverse events or intra- or postprocedural complications reported.
“The SAVE registry achieved its desired objective of confirming the safety and effectiveness of the Surfacer system to gain central venous access in patients with central venous occlusions,” comments Vladimir Matoussevitch, head of Vascular Access Unit University of Cologne (Cologne, Germany) and co-lead author for the paper.
“The publication of the results of the SAVE registry expands and strengthens the clinical evidence confirming the role the Surfacer system has in helping to establish central venous access in patients with venous obstructions,” states Maurizio Gallieni, director of Nephrology and Dialysis at the University of Milan (Milan, Italy), who was the other co-lead author.
President-elect of the Society of Interventional Oncology (SIO), Matthew Callstrom discusses his journey into cancer care, and how advances in percutaneous ablation have shaped the procedure’s integration into first-line therapy. “If we [interventional oncologists around the world] can work together to achieve common standards, we will be able to develop evidence to support interventional oncology [IO] procedures in guidelines at an earlier point in a patient’s care,” he says.
What initially drew you to interventional radiology, and then more specifically interventional oncology?
The opportunity to improve the care of patients through interventional radiology and IO by offering minimally invasive treatments that reduce pain and morbidity and also improve survival continues to motivate me. I strongly believe that what we offer patients is often a significant improvement over surgery and other treatment options.
Who have been important mentors for you throughout your career?
I was fortunate to have mentors that were advancing the care of patients in the very earliest days of IO. Both Bill Charboneau and Luigi Solbiati were great role models for driving improved care of patients with new, innovative technology and supporting the advancement through scholarship. They were instrumental in promoting an international approach to sharing lessons learned and advancing the care of patients with cancer.
As president-elect of the SIO, what are your hopes for the society over the next year?
The primary goal over the next year will be to work with the SIO leadership and membership to help advance the clinical evidence that demonstrates the value of IO for patient care. The SIO is focused on advancing the care of patients through supporting both investigator-initiated feasibility studies but also through pivotal clinical trials, industry partnership, and advocacy for IO. We are also committed to improving the care of patients by advancing IO through guidelines and standards.
You were very involved in the World Congress of Interventional Oncology (WCIO) 2013–2017. Could you describe the transition of WCIO to SIO: Why was this necessary, and what has SIO been able to achieve that a congress alone could not?
The WCIO was a great format for communication of the advances of IO, but it was only a meeting. The transition to a society and SIO was to build the support of education, research, and advocacy that expands the impact of the physicians and industry partners committed to IO. A good example of what SIO has accomplished is the support of teams that update the National Comprehensive Cancer Network (NCCN) guidelines on a regular basis. Another benefit of a society is the support of research efforts that advance the science of IO. If you look back at the history of radiation oncology, the formation of the Radiation Therapy Oncology Group (RTOG) was instrumental in advancing the evidence that supports the use of radiation therapy for patients with cancer. SIO is working to support IO through a similar infrastructure.
As a Section Editor of Cardiovascular and Interventional Radiology, what makes a good research paper, in your opinion?
I think a good research paper is focused on advancing the care of patients with clear communication of the findings. While early experience of new applications or advances is important, we need to produce evidence that shows how IO is important for patient care. It is important to recognise that decisions at tumour boards are driven by high-quality data with an emphasis on phase II/III studies.
Could you describe a particularly memorable case of yours?
I have been fortunate to be involved in the care of patients that have had improved survival due to the care that we provide in our practice. I was part of the team treating a patient that had metastatic hepatocellular carcinoma (HCC) but survived more than 10 years due to the care we provided. He had more than 10 ablation treatments involving his liver, adrenal, lung, spine, and body wall. Throughout the time that we cared for him, he continued in his medical practice and his son became a teenager. We developed a great friendship and I attended his funeral with his passing, which was difficult, but the celebration of his life at the service was a profound experience for me.
With your particular expertise and interest in percutaneous ablation, what do you think is currently the most exciting research involving this procedure?
I think we are now at the point in the use of ablation procedures where integration in first-line therapy has an important role. We have established that local control with ablation is complementary and comparable with surgery and radiation therapy for some applications. I think that in the next few years we will demonstrate that ablation procedures offer the advantage of tissue preservation and less morbidity over the course of a patient’s life with cancer. There is also promising research that ablation in combination with immune therapy may provide abscopal response for patients with metastatic disease.
How do you think the COVID-19 pandemic has influenced IO, over the short- and long term?
We experienced a continued need for the treatment of patients with cancer throughout this pandemic. We initially reduced our access in order to implement safety measures such as measuring aerosol clearance in our procedural suites and improved standards for personal protection equipment. We learned that we can safely offer cancer treatments with appropriate testing. We learned the necessity of continuing to offer treatment for patients rather than attempting to prioritise only for more acute or semi-acute patients as delayed care is a risk to patients for progression and potentially survival.
Which innovations have most influenced your career, and how?
The introduction of improved ablation devices has allowed better outcomes for IO treatments. The first heat-based devices we used were underpowered, and getting a complete treatment was often difficult. Percutaneous cryoablation devices have allowed the expansion of treatments that we can offer. I was involved in the use of the intraoperative liquid nitrogen systems many years ago and, although innovative, treatment of renal masses, lung tumours, and musculoskeletal tumours would not be possible. We now treat more than 500 patients a year with this technology. Hybrid rooms are also putting the best imaging methods in the hands of the proceduralists, allowing both CT and fluoroscopy imaging, where they offer the best visualisation and guidance approach.
What are the biggest challenges facing IR today?
I believe we need to work together to improve the standard performance and delivery of IO treatments. Many of the procedures that have matured and are helpful for patients are done differently in centres across the world. We have been involved in multicentre clinical trials where we have struggled to gain a common approach in the use of devices and technical performance, and the outcomes have been impacted negatively. Performing procedures with standard approaches and objective outcomes will both advance patient care and elevate the standing of IR/IO in the world. If we can work together to achieve common standards, we will be able to develop evidence to support IO procedures in guidelines at an earlier point in a patient’s care.
What are your hobbies and interests outside of medicine?
Outside of medicine, I am blessed to have a wonderful family, including my wife Brenda and my two boys, Joseph (30) and Peter (27). We also have two golden doodles (Charlie and Lucy) that are our constant companions and treated like children now that we are empty nesters. We spend as much time as we can at our lake cabin that is on the lake that Brenda and I first met and honeymooned—our family and friends often join us, and although there are 10,000 lakes in Minnesota, there is only one as far as our family is concerned. I enjoy making furniture in my wood shop even though there is usually more dust than any final product generated. I also enjoy riding a road bike—on the less travelled roads near our house and cabin, and in the basement on a trainer during the too-long winters in Minnesota.
In a session of the 2020 Cardiovascular and Radiological Society of Europe (CIRSE) meeting (12–15 September, virtual) focused on the hottest news in the endovascular thrombectomy space, Antonin Krajina (University Hospital, Hradec Králové, Czech Republic) shared new devices available for the procedure, and enthused about their potential in stroke management.
First describing his, hypothetical, ideal device for endovascular thrombectomy, Krajina said that it should be “easy to use and have fast access to the clot”. Stent retrievers are assessed by their ability to integrate the clot and to keep hold of it during retrieval; radiopacity of the stent retriever therefore plays an important role, Krajina stated. Additionally, he explained how there is a significant association between first-pass complete reperfusion and favourable clinical outcome, with two to three times higher odds for a favourable clinical outcome compared with complete reperfusion after multiple passes.
Indeed, his key take-home message was that clot integration is a function of delivery technique, duration of device implantation, and clot mechanics. His talk therefore detailed how device design influences these aspects of performance. In addition, he urged his listeners to “use all tricks in the attempt to remove the clot at the first pass (including aspiration via balloon guide), and detailed how the COMPASS trial results provide Level 1 data that an aspiration thrombectomy as first-pass approach is non-inferior to a stent-retriever as a first-line approach for the treatment of selected patients with acute large vessel ischaemic stroke.
The importance of device design
Comparing the Solitaire X device (Medtronic), the CatchView stent retriever (Balt), and the Embotrap III device (Cerenovus), Krajina showcased how each had platinum markers on the proximal and distal ends, explaining that these acted as radiopacity markers.
Turning to the capacity to integrate the clot, he next discussed the relative benefits of using a short (20mm) or a long (30mm) stent retriever: “A longer [stent retriever] may increase the capacity to catch the clot,” he said. This was proven by Gaurav Girdhar (Medtronic, Irvine, USA) et al in their January 2020 publication in Interventional Neurology, which concluded that stent length had a significant effect on first pass success rate (p<0.05). The authors wrote: “Longer stent retrievers may be safe and effective in improving first pass success for fibrin-rich clots in vitro and in vivo models of large vessel occlusion”. However, Krajina added that a longer stent retriever means higher friction, which in turn increases the probability of the device getting stuck and then elongating, resulting in a loss of apposition to the arterial wall. The embolisation risk of the clot is also higher with longer devices, he explained, as longer dwell times affect the likelihood of distal embolization.
“Stent retrieval length should be adjusted to clot extent,” Krajina said, citing a June 2020 paper published in Cerebrovascular Diseases from Hanna Styczen (University Hospital Essen, Essen, Germany) and colleagues. Styczen et al hypothesised that increased stent retriever length may improve the rate of complete angiographic reperfusion and decrease the respective number of attempts, resulting in a better clinical outcome. They conducted a retrospective analysis of 394 patients with large vessel occlusion in the anterior and posterior circulation treated with stent retriever mechanical thrombectomy, sorting patients by propensity matching into two groups: those treated with a short (20mm) device, and those treated with a long (30mm) device. They found that, in the anterior circulation, short stent retrievers had a significantly higher rate of first-pass reperfusion in cases with low clot burden, and in middle cerebral artery occlusions. Higher rates of favourable outcome at discharge and 90 days were observed for the short stent retriever group (p<0.001). This led them to conclude, as Krajina related to the CIRSE audience, that stent retriever length “should be adjusted to clot burden score and vessel occlusion site.” Krajina clarified: “Stents for short occlusion are appropriate if they are 20mm long; for longer occlusions, we need longer stent retrievers.”
“What position of the stent-retriever in relation to the occlusion/ embolus is the most effective?” Krajina asked his listeners rhetorically. “If it [the stent-retriever] is too –proximal and/or only partially engaged into the clot, it is less probable that we can remove the whole clot,” he explained. “If the clot is more proximal to the stent-retriever, the probability that we remove it during first-pass is higher. To verify the relationship of the clot and the stent-retriever position, we perform an angiogram after stent-retriever deployment.”
Next, Krajina discussed how to decide what diameter stent-retriever device to use to increase the probability of successfully removing the clot at first pass, 4mm or 6mm. “If you look at a diameter of the M1 segment in males, it is about 2.5mm, and the diameter of the internal carotid artery is around 3mm,” he informed delegates.
Writing in the Journal of Neurointerventional Surgery in 2018, Mark Davison (Rush University Medical Center, Chicago, USA) and colleagues said: “Compared with males, females consistently fare worse following mechanical thrombectomy for large vessel ischaemic strokes. Understanding why this gender disparity occurs may guide improvements in future treatment strategies.” In their study, they aimed to determine whether gender differences in cerebral arterial diameter correlated with clinical outcomes following stroke thrombectomy. They therefore performed an observational study of 92 consecutive acute ischaemic stroke patients (42 women) undergoing mechanical thrombectomy between June 2013 and August 2016 at a single, urban tertiary care medical centre. Catheter angiographic images were used to manually measure proximal segment arterial diameters in a standardised fashion, and medical record review was used to obtain relevant independent and dependent variables. Internal carotid artery terminus diameters for men and women were 3.08mm and 2.81mm, respectively (p=0.01). M1 segment middle cerebral artery diameters for men and women were 2.47mm and 2.18mm, respectively (p<0.0001). Nearly half (48%) the patients in the upper middle cerebral artery calibre tercile attained a favourable mRS 90-day value compared with 35% in each of the lower and middle terciles (p=0.51). Larger middle cerebral artery diameters correlated with favourable discharge disposition (p=0.21).
This led Davison et al to conclude: “These results provide limited evidence that males have larger cerebral arterial diameters than females and that larger arterial diameters may improve the odds for favourable clinical outcomes. If future studies validate these findings, arterial diameter may become a relevant variable in the design of improved thrombectomy strategies.”
However, Krajina went on to say that “More and more studies are proving that stent-retrievers with larger diameters do not appear to provide clear benefits”. Detailing a 2017 paper published in the American Journal of Neuroradiology, he reported how, in their investigation of the effects of different diameters of Solitaire retrievers on clinical outcomes, Dong Yang (Jinling Hospital, Second Military Medical University, Nanjing, China) and colleagues found “no evidence of a differential effect of intra-arterial therapy based on the size of the stent-retrievers”. Though they also found that, in patients with atherosclerotic disease, favourable reperfusion was associated with deployment of a small stent.
Demonstrating new designs for stent retrievers that he believes are improving interventionalists’ ability to successfully perform endovascular thrombectomy, Krajina introduced the NeVa stent retriever from Vesalio, which has clot pockets oriented at 90 degrees to each other that increase the first-pass effect. The Embotrap III device (Cerenovus) has an inner channel to stabilise the clot during retrieval, and an outer cage to engage and integrate the clot. With this latest re-design, the distal mesh of the Embotrap III device is also denser than previous iterations.
Access and delivery catheters and guidewires
“Besides stent-retrievers, we also need delivery catheters and guidewires,” Krajina said. In his view, the most important aspects to consider for these devices are navigability, pushability, kink resistance, and whether or not they can be assembled as a coaxial set.
A survey of Society of Neurointerventional Surgery (SNIS) neurointerventionalists that received 78 responses (approximately 10% of SNIS membership), published in the Journal of Neurointerventional Surgery, indicated an increase in aggressiveness in pursuing thrombectomy based on selection criteria. Nearly 40% of respondents (39.7%) reported using catheter aspiration thrombectomy as a frontline therapy. A further 28.2% opted for stent-retriever mechanical thrombectomy, and another 28.2% said they adopted a combined approach, utilising stent-retrievers with aspiration.
“Interventional neuroradiologists love to combine access catheters to create coaxial double, triple systems,” Krajina told CIRSE registrants, “sometimes in difficult or tortuous anatomy, referred to as a ‘tower of power’, to have enough support for intracranial catheters.” To create such a set, the length and diameter of the catheter used is important, the CIRSE audience heard: “Ideally one should use the shortest length necessary to do the job.”
Finally, he stressed that interventionalists should use balloon-guiding catheters to stop arterial flow, and to facilitate aspiration via these catheters during clot removal.
Reflow Medical has announced that Japan’s Pharmaceuticals and Medical Devices Agency (PMDA) has approved the Wingman chronic total occlusion (CTO) catheter. Reflow Medical has partnered with Century Medical, a medical device distributor based in Tokyo, to introduce the Wingman CTO catheter in Japan.
The Wingman catheter crosses peripheral CTOs using an extendable bevelled tip. The physician controls the advancement and activation of the tip to create a channel to help penetrate, or cross, the occlusion with a guidewire, enabling further treatment of the lesion with therapeutic devices. The catheter is compatible with the physician’s preferred guidewire and procedural technique.
Approval by Japan’s PMDA follows the completion of the Wing-IT CTO clinical trial, a prospective, international, multicentre study that treated 85 patients and followed them for 30 days. The Wingman catheter was able to demonstrate a 90% crossing rate when up to two previous guidewires could not cross the CTOs, meeting its primary safety and efficacy endpoints.
“Reflow Medical focuses their efforts on developing technologies based on physicians’ needs,” said John R Laird (Adventist Heart and Vascular Institute, St Helena, USA). Laird was the principal investigator for the study. “We rely on Reflow for real clinical evidence when utilising the technology.”
Reflow’s Wingman crossing catheter received clearance from the US Food and Drug Administration for the expanded CTO indication for the Wingman crossing catheter in March 2020 after completing the Wing-IT clinical trial.
An illustration of a completed Detour procedure within the superficial femoral artery and the femoral vein
PQ Bypass has announced enrolment of the final subject in the company’s DETOUR II investigational device exemption (IDE) clinical trial. This milestone occurs only a month after the Detour system entered the US Food and Drug Administration (FDA)’s breakthrough device programme.
DETOUR II is led by national co-principal investigators Sean Lyden (Cleveland Clinic, Cleveland, USA) and Jihad Mustapha (Advanced Cardiac and Vascular Centers, Grand Rapids, USA). Both national co-PIs receive compensation for their duties in this role.
“The speed with which we were able to enroll DETOUR2 in 2020 speaks to the large patient population that exists with long-segment femoropopliteal disease that has sub-optimal endovascular options,” says Lyden.
“If percutaneous fem-pop bypass is shown to be safe and effective, similar to the outcomes demonstrated in DETOUR1 study, it could be a game changer for the way we treat complex, long-segment SFA [superficial femoral artery] disease today,” continues Mustapha.
DETOUR II is a prospective, multicentre trial evaluating the Detour system for percutaneous femoral-popliteal bypass in patients with extremely long, complex lesions in the SFA. The study enrolled 202 patients in 36 sites in the USA and Europe, and is assessing freedom from major adverse events (MAE) within 30 days of the index procedure as the primary safety endpoint. The primary effectiveness is primary patency at 12 months.
“After finishing enrolment in DETOUR II and achieving the breakthrough device designation, PQ Bypass is on track to deliver results from this study much earlier than what we originally expected,” says Heather Simonsen, president of PQ Bypass. “We would like to thank the DETOUR II investigational sites for their ongoing contribution to this important research.”
A coalition organised by the CLI Global Society has announced its proposal to distinctly recognise “critical limb ischaemia” (CLI) and “chronic limb-threatening ischaemia” (CLTI) in the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) was approved by the Centers for Disease Control and Prevention (CDC) and went into effect on 1 October 2020.
The ICD-10-CM is a worldwide standard reference set of disease codes used to report medical services provided to patients. The announcement marks a major step forward in tracking patient treatments and outcomes for CLI and CLTI, which affect millions of patients globally.
The CLI Global Society worked in close partnership with the vascular specialist community to develop the proposal. Coalition members include:
Robert Lookstein, CLI Global Society (CLIGS)
Barry T Katzen, (CLIGS)
Sean Roddy, Society for Vascular Surgery (SVS)
Mitchell Weinberg, Society for Vascular Medicine (SVM)
Bulent Arslan, Society of Interventional Radiology (SIR)
Mehdi Shishehbohr, Society for Cardiac Angiography and Intervention (SCAI)
The goal of this initiative is to support coding professionals, educators, compliance staff, and physicians to identify and accurately report CLI and CLTI in clinical documentation, electronic medical records, and medical billing in order to track and monitor patient treatments and outcomes in the future.
“This effort is a first step in building awareness of the complexity associated with caring for patients who suffer from CLI within public and commercial payers and the broader healthcare community,” says Barry Katzen, board chair of the CLI Global Society. “These dedicated codes, now newly identified for CLI, are critical in our goal to improve quality of life by preventing amputations and death due to CLI.”
Robert Lookstein, chair of the Vascular Societies Workgroup and CLI Global Society board member, acknowledges the collective effort of his colleagues, “who came together to prioritise the need for a well-defined and accessible method to identify, report, and track CLI for the benefit of patients who suffer from this disease.
“We also look forward to continued partnership as we launch initiatives to educate our membership, our hospitals, and healthcare provider staff regarding these changes,” Lookstein explains. “They have the potential to positively impact the care we provide to these extremely vulnerable patients across the United States and around the world.”
CLI and CLTI are advanced forms of peripheral arterial disease (PAD), a common circulation problem that occurs when arteries that carry blood throughout the body become narrowed or blocked, restricting blood flow to legs and feet. Those who smoke, have diabetes or chronic kidney disease, or suffer from high blood pressure or high cholesterol are susceptible to CLI and its complications. Left untreated, CLI can lead to tissue loss, gangrene, amputations, and eventually death.
“The statistics are grim,” says Jihad Mustapha, founding board member of the CLI Global Society. “We know 60% of patients who receive an amputation due to PAD or CLI die within two years—this is higher than the five-year mortality rate for patients with breast, colon, and prostate cancer.
“In order to fight this deadly disease, we need to have accurate data. This seemingly small change to medical coding will allow us to save countless limbs—and lives.”
Interventionalists are being encouraged to take consideration of a set of talking points about the risks and benefits of paclitaxel-equipped devices—which has developed by a multispecialty panel of medical societies—in discussions with their patients.
The document is the work of the Multi-Specialty and Multi-Society Coalition for Patient Safety With Paclitaxel Technologies, which includes the following societies: the American College of Cardiology (ACC), American College of Radiology (ACR), American Heart Association (AHA), Society for Cardiovascular Angiography and Interventions (SCAI), Society for Vascular Medicine (SVM), the Society of Interventional Radiology (SIR), the Society for Vascular Surgery (SVS), the Vascular and Endovascular Surgery Society (VESS), and the Society for Clinical Vascular Surgery (SCVS).
The US Food and Drug Administration (FDA) tasked the coalition with putting together bullet points that reflect the current evidence around the hot topic of paclitaxel devices.
“The coalition bullet points reflect the current evidence surrounding this complex topic and is designed to help institutions and members to use when discussing increased rate of long-term mortality in patients treated with paclitaxel-coated balloons and paclitaxel-eluting stents,” the coalition stated.
“The statements are intended to summarise the current state of the evidence and to serve as starting points for discussion. We recognise this is a complex issue and the talking points and are not intended to take the place of thoughtful, individualised discussions with patients.
“The ability to effectively communicate risk and benefit of revascularisation is key part of procedure selection. Please consider the following statement in your discussions and informed consent process.” The document follows in full.
Peripheral vascular intervention talking points for informing patients about the paclitaxel safety signal
To this end, a Multi-Specialty Paclitaxel Coalition (American College of Cardiology, American College of Radiology, American Heart Association, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine, Society of Interventional Radiology, Society for Vascular Surgery, Vascular and Endovascular Surgery Society, and the Society for Clinical Vascular Surgery), representing the majority of specialists who evaluate and treat patients with PAD, developed the following talking points, which have been reviewed by the FDA, that physicians/providers may consider when discussing PAD treatment options with their patients:
Some balloons and stents used to treat symptoms resulting from blocked blood vessels in leg(s) are coated with the drug paclitaxel.
Research studies show that paclitaxel-coated balloons and stents improve the chance that the treated blood vessel in your leg will remain open after your treatment and lower the likelihood that you will need a repeat procedure to re-open the vessel.
However, an analysis in 2019 that combined the results from multiple studies indicated that the use of paclitaxel-coated balloons and stents may increase your chance of dying starting about two years after treatment. Although this analysis has limitations and further research is still ongoing, the available information as of April 2020 suggests that paclitaxel-coated device use may increase your chance of dying over the next 2–5 years compared to treatment with uncoated balloons or bare metal stents.
There may be other options for the treatment of your symptoms, including medications, exercise, balloons, stents or other devices that do not contain paclitaxel, and surgery. You and your doctor should discuss the possible risks and benefits of all treatments to identify those options that are best for you.
The Multi-Specialty Paclitaxel Coalition is actively working with the FDA, medical device manufacturers, and clinical investigators to advance our understanding of the long-term safety and effectiveness of paclitaxel-coated devices.
On behalf of the Multi-Specialty and Multi-Society Coalition for Patient Safety With Paclitaxel Technologies.
Teleflex has announced it has received 510(k) clearance from the US Food and Drug Administration to expand the indications for use of the Arrow EZ-IO intraosseous vascular access system. This device can be used when intravenous access is difficult or impossible to obtain in emergent, urgent, or medically necessary cases.
The Arrow EZ-IO system is now available with the expanded indication stating use of the device may be extended for up to 48 hours when alternate intravenous access is not available or reliably established in adults, and in paediatric patients 12 years and older.
“Vascular access is one of the most basic, yet critical, components of patient care,” said Michelle Fox, corporate vice president and chief medical officer, Teleflex. “The ability to use the EZ-IO system for a longer dwell time provides clinicians the option to utilise intraosseous (IO) access for the entire duration of therapy in patients with difficult vascular access where therapy is required for up to 48 hours.”
In patients who require longer-term access, the expanded indication gives clinicians additional time to establish vascular access safely, choosing the appropriate device and optimal site of insertion to meet the patient’s clinical needs. “These benefits are of particular importance in a time of constrained resources and patient surge,” said Fox.
Medtronic today announced the planned acquisition of Avenu Medical, a medical device company focused on the endovascular creation of arteriovenous (AV) fistulae for patients with end-stage renal disease (ESRD) undergoing dialysis. Terms of the transaction were not disclosed.
A press release explains that Avenu Medical’s Ellipsys vascular access system is a single-catheter, ultrasound-guided device that inserts a catheter percutaneously into the arm to create a durable AV fistula. The procedure can be performed in the hospital outpatient department, ambulatory surgery center (ASC), or physician’s office.
“AV fistulae are like lifelines to patients undergoing dialysis. Until recently, the only option to create a fistula was through invasive surgery, which is associated with high failure rates,” said Jeffrey Hull (Richmond Vascular Center, Richmond, USA), co-founder of Avenu Medical. “The Ellipsys system has shown durable outcomes out to two-years and has the ability to shorten procedure times and potentially reduce costs. Unlike open surgery, sutures are not required after the procedure and the patient leaves with just an adhesive bandage.”
“Medtronic’s acquisition of Avenu aligns directly with our vision of bringing less invasive, endovascular solutions to patients requiring durable vascular access,” said Mark Ritchart, president and chief executive officer of Avenu Medical. “With Medtronic’s extensive market presence, clinical leadership, and market development expertise, coupled with Avenu’s customer-focused team and innovative technology, we are confident that together, we can drive awareness and adoption of this technology globally.”
“Within the last year, we have seen significant momentum with the launch of the IN.PACT AV drug-coated balloon (DCB) in the USA and primary endpoint results of the IN.PACT AV Access study being published in The New England Journal of Medicine,” said Mark Pacyna, vice president and general manager of the Peripheral Vascular business at Medtronic. “Now with the acquisition of Avenu Medical, we can support procedures across the vascular access care continuum, while continuing to provide innovative endovascular therapies that will ultimately reach even more patients with ESRD around the world.”
The acquisition is expected to close in October, subject to the satisfaction of certain customary closing conditions.
Royal Philips has announced the launch of the QuickClear mechanical thrombectomy system. The single-use system delivers an all-in-one aspiration pump and catheter to remove blood clots from the vessels of the peripheral arterial and venous systems and has received US Food and Drug Administration (FDA) 510(k) clearance.
The system’s design aims to simplify the use of the device and improve procedure times without the need for capital equipment or accessories.
Chris Landon, senior vice president and general manager of image guided therapy devices at Philips claims that “by taking away the high initial capital expenditure costs associated with traditional mechanical thrombectomy systems, QuickClear can help bring cost-effective solutions to both the hospital and outpatient care settings.”
The small footprint of the sterile device allows it to be placed easily on the table next to the patient. The company claims that the system can easily work at maximum aspiration power within seconds and that the consistency of the aspiration power during the procedure supports faster procedure times.
Furthermore, the system’s range of catheters includes a large 10F aspiration catheter which, according to the company’s own in-house data, provides 59% more aspiration volume than 8F aspiration catheters.
Bryan Fisher (Nashville, USA) says that the “QuickClear is a simple and easy to use mechanical thrombectomy system.” He adds that it “is significantly smaller than other systems without compromising aspiration power.
The QuickClear mechanical thrombectomy system is the latest expansion of the company’s portfolio after acquiring Intact Vascular. Philips’ peripheral vascular portfolio already includes advanced interventional imaging systems for precision guidance; intravascular ultrasound (IVUS) catheters to assess the location of the disease and lesion morphology and guide and confirm the treatment; peripheral atherectomy devices to remove blockages; and peripheral therapy devices, such as Philips’ Stellarex drug-coated balloon, to treat lesions.
LimFlow percutaneous deep vein arterialisation system
Midterm results from a study of the largest population of patients with no-option chronic limb-threatening ischaemia (CLTI) treated with percutaneous deep vein arterialisation (pDVA) using the LimFlow device show that, in this complex group of patients, this treatment method is feasible, with a high technical success rate and amputation-free survival at six through to 24 months, coupled with effective wound healing. In selected patients with no-option CLTI, percutaneous deep vein arterialisation could be a recommended treatment to prevent amputation and heal wounds, Costantino Del Giudice (Université de Paris, Paris, France) told delegates attending the online 2020 meeting of the Cardiovascular and Radiological Society of Europe (CIRSE; 12–15 September, virtual).
These results from the ALPS (midterm outcomes of percutaneous deep venous arterialization with a dedicated system for patients with no-option chronic limb-threatening ischemia) multicentre study were published in the Journal of Endovascular Therapy in May this year, and appeared in the August print issue, in addition to being presented at the CIRSE congress. The ALPS registry is the largest study to date of no-option CLTI patients treated with the LimFlow system reporting mid- and long-term results, and is a multicentre, retrospective study conducted at centres in Alkmaar, The Netherlands; Leipzig, Germany; Paris, France; and Singapore encompassing 32 end-stage—or “no-option”—CLTI patients.
The investigators set out to evaluate the midterm results of patients suffering from no-option CLTI treated with a dedicated system (the Limflow system) for percutaneous deep venous arterialisation. Thirty-two consecutive CLTI patients (mean age 67±14 years; 20 men) were treated with this method using the Limflow device at four centres between 11 July 2014 and 11 June 2018 and retrospectively analysed. Of all patients, 21 (66%) had diabetes, eight (25%) were on immunosuppression, four (16%) had dialysis-dependent renal failure, nine (28%) had Rutherford category six ischaemia, and 25 (78%) were deemed at high risk of amputation. The primary outcome was amputation-free survival (AFS) at six months. Secondary outcomes were wound healing, limb salvage, and survival at six, 12, and 24 months.
Technical success was achieved in 31 patients (96.9%). The median follow-up was 34 months (range 16-63). At six, 12, and 24 months, estimates were 83.9%, 71%, and 67.2% for AFS, 86.8%, 79.8%, and 79.8% for limb salvage, and 36.6%, 68.2%, and 72.7% for complete wound healing, respectively. Median time to complete wound healing was 4.9 months (range 0.5–15). The deep vein arterialisation circuit occluded during follow-up in 21 patients; the median time to occlusion was 2.6 months. Reintervention for occlusion was performed in 17 patients: 16 because of unhealed wounds and one for a newly developed ulcer.
Deep vein arterialisation a hope for “no option” patients
“No option” patients are those where no possible endovascular or surgical procedure will help, due to either the absence of a target vessel or thanks to unsuccessful prior interventions. These patients frequently have calcified vessels, diabetes mellitus, dialysis, and/or long-term corticoid therapy. The risk of amputation and persistent wound is 58% when these patients are treated with conservative therapy, and the risk of death at one-year follow-up is 20%.
Deep vein arterialisation aims to improve the blood flow to the foot. “We direct nutritional improvement by reversal of flow through venules,” Del Giudice told the CIRSE audience, describing how deep vein arterialisation works. “This stimulates arteriogenesis, and recruits hibernating collaterals.”
The most important step, he shared, is patient selection. “Patients have to have a good heart function, a good life expectancy, foot arteries not treatable by an endovascular or surgical approach, a Rutherford class 5–6, a Wound, Ischaemia, and Foot Infection (Wifi) score of 3, and no infection,” Del Giudice listed.
According to the speaker, the Limflow technique is the most commonly used method.
The Limflow technique: How it works
Del Giudice talked CIRSE registrants through a case demonstrating the use of the Limflow technique. This first involved performing arteriography and venography scans to aid target vessel selection. Next, the interventionalists advanced the venous and arterial catheters to the target vessel, where the artery and vein were closest, and created an arteriovenous fistula, bridging the two vessels. Then, they advanced the guidewire along the vessel, using it to push the balloon through the arteriovenous fistula to create a passage. Blood flow is diverted from the blocked artery into the vein to salvage the lower leg.
Del Giudice also shared an alternative technique whereby entry in the distal lateral or medial plantar vein from a subintimal channel in the plantar artery can be intentionally pursued as a bailout tactic; this involves pointing the tip of the guidewire opposite to the arterial wall calcifications.
Yet another method is the venous arterialisation simplified technique (VAST). This utilises a low-profile balloon catheter and a snare to facilitate arteriovenous fistula creation during venous arterialisation.
An arteriovenous fistula could also be created using a low-profile balloon catheter and an outback catheter. Del Giudice described a case where he and his team treated a patient using this method, explaining how the patient had occlusion of the popliteal artery. “Without any target vessel in the distal leg,” he said, “we performed subintimal ligation towards the posterior tibial artery, and then we used the outback [catheter] to advance the balloon into the posterior tibial vein, and create the [arteriovenous] fistula, advancing the guidewire. Finally, we performed a valvotomy with a low-profile balloon, and stented the vein from the ankle to the arteriovenous fistula.”
Showing a table comparing the outcomes at six months from these different techniques, Del Giudice was positive: “There is good primary patency, ranging from 40–90% at six months, and good wound healing outcomes, ranging from 40–100%. Major amputations ranged from 0–33.3% at six months follow-up.”
Earlier trials: The Promise I study
PROMISE I study was an early feasibility study launched in mid-2017 to establish the clinical safety of the Limflow technique. It aimed to provide enough data for the investigators to move on to a pivotal trial, to identify and address any operator challenges, and to determine patient characteristics and therapeutic parameters that impact performance. Enrollment was completed in 2019, and the triallists have since reported a 97% technical success rate in the 32 patients treated in the USA as part of this study. Overall survival was 96%, freedom from amputation was 77%, and amputation-free survival was 74%.
“The importance of this study was that it allowed us to understand that not all patients are candidates for this procedure. We need salvageable tissue to obtain some results,” Del Giudice told the CIRSE audience. “Moreover,” he continued, “the results [show that] this is quite different from an arterial canalisation. Deep vein arterialisation requires four to six weeks for tissue granulation to start. Oedema can occur in the treated limb after deep vein arterialisation, but typically resolves within three to four weeks. We need to preserve native arterial perfusion and mange pedal loop outflow during the maturation process. It is also important to monitor changes in foot tissue colour. In terms of wound care, multidisciplinary collaboration is required, and patients may need some minor amputation management, debridement.”
Surmodics has announced receipt of US Food and Drug Administration (FDA) 510(k) clearance for its Pounce thrombus retrieval system.
The company describes the Pounce system as a mechanical thrombectomy device intended for the nonsurgical removal of thrombi and emboli from the peripheral arterial vasculature without the added expense or commitment to additional external capital equipment. The device includes a 5Fr basket delivery catheter, a basket wire assembly, and a trumpet assembly. Its mechanism of action is described as follows: “After the basket wire assembly is delivered distal to the location of the thrombus, two nitinol self-expanding baskets are deployed to collect and entrain the clot into a trumpet-shaped nitinol wire mesh. With the clot entrained, the trumpet assembly is then collapsed into a 7Fr guide sheath through which the clot is withdrawn and removed from the body.”
“The Surmodics team has done an excellent job finalising the product design and advancing the Pounce thrombus retrieval system into a medical device that has the potential to change the treatment algorithm for arterial thrombectomy,” comments Gary Ansel (OhioHealth Heart & Vascular Physicians, Columbus, USA), founder and former chief medical officer of Embolitech, from which Surmodics acquired the technology and intellectual property behind the Pounce thrombus retrieval system. “By providing peripheral interventionalists with an innovative, nonsurgical tool for treating arterial thrombotic occlusions, the Pounce thrombus retrieval system will serve an important clinical need and is a great fit with the company’s focus on advancing therapies for peripheral artery disease.”
Surmodics president and CEO Gary Maharaj adds: “The FDA 510(k) clearance of our Pounce thrombus retrieval system brings us one step closer to providing a technology that offers significant advances over the current treatment of complex, peripheral artery disease.” Maharaj also noted the company’s development efforts in the areas of deep vein thrombosis, pulmonary embolism, and ischaemic stroke. The company recently announced CE Mark for its Surveil drug-coated balloon and FDA clearance of its Sublime radial access 0.014 RX PTA dilatation catheter.
The first patient has been recruited into a trial investigating the BeGraft peripheral plus stent graft system (Bentley InnoMed) as a dedicated bridging stent in branched endovascular aortic repair (BEVAR) for the treatment of complex aortic aneurysms. It is the first study of its kind worldwide.
Martin Austermann (St Franziskus Hospital, and University of Münster, Münster, Germany) is the coordinating investigator of the prospective, single arm, multi-centre clinical study.
“Until now, we have not had a dedicated indicated bridging stent to connect branched endografts with renal and visceral arteries,” says Austermann. “There are many devices that could be used for this, but all in an off-label setting.”
“It is great news that we could start a trial in collaboration with the Foundation for Cardiovascular Research and Education and Bentley for this indication, it has been an unmet need for such a long time,” he adds. “We are very pleased to run this study, which is approved by the German national competent authority BfArM, together with some other colleagues working in high volume centres in Germany. For us, as endovascular specialists, it is key to work as much as possible with medical devices that are indicated for certain procedures.”
Eligible patients are those seeking elective repair of thoracoabdominal aortic aneurysm (TAAA) with BEVAR. The trial aims to carry out 100 BEVAR procedures with an average of 2.5 bridging stents per procedure.
The primary efficacy endpoint is comprised of a measure of technical success defined as the successfully introduction and deployment of the BeGraft Plus implanted as a bridging stent in BEVAR, with bridging stent patency at 12 months (absence of restenosis (≥50% stenosis) or sole target vessel occlusion based on computed tomography (CT) angiography at 12 months. The primary safety endpoint at 12 months relates to the absence of procedure-related complications and bridging stent related endoleaks.
“In one or two years, the trial will provide us with valuable information on occlusions or stent fracture, for example. We will be able to let the patient know what to expect, and it will make the procedure more predictable,” Austermann comments.
The BeGraft Plus combines radial force with flexibility, a Bentley press release states. It consists of two layers of micro-porous expanded polytetrafluoroethylene (ePTFE) tubing based on two cobalt chromium stents and has a sandwich design. The outer ePTFE layer provides fixation of the outer stent and guarantees sealing properties. It also protects the inner ePTFE layer and prevents endoleaks. The inner PTFE layer provides a sealing of the aneurysm and the inner stent supplies fixation of the inner and outer ePTFE layer. Compared to other available bridging stent grafts, Bentley claims it has an up to 3.5 times higher radial force and is kink-resistant.
Gore has announced the US launch of the lower profile, large diameter Gore Viabahn endoprosthesis.
Gore previously received approval from the US Food and Drug Administration (FDA) for the enhanced Gore Viabahn endoprosthesis.
“With broad clinical indications for use and numerous product improvements, the Viabahn device continues to be a dependable choice that demonstrates positive results in patients with complex vascular disease,” comments Amit J Dwivedi, (University of Louisville, Louisville, USA), who has implanted the lower profile device in complex arterial anatomy. “Older patients with co-morbidities such as hypertension, diabetes, and obesity may benefit from a less invasive endoluminal approach versus surgical bypass. These latest enhancements, including a lower profile, provide physicians with additional options for treating these patients.”
This innovative Viabahn device design reduces the delivery profile for larger 9–13mm diameter stent grafts by up to 3Fr, enabling delivery through smaller sheaths. Smaller introducer sheaths have resulted in a lower risk of vascular access complications in select patient populations, a Gore press release states. Additionally, new radiopaque markers on the distal and proximal ends enhance visualisation under fluoroscopy, facilitating positioning and device delivery, as well as precise and predictable placement.
“In addition to the radiopaque markers that facilitate positioning and deployment, the new lower profile enables use of a smaller sheath, potentially reducing the risk of damage at the access site,” says Yevgeniy (Eugene) Rits (Wayne State University; Detroit Medical Center; Harper University Hospital, Detroit, USA). “Combined with the trackability and flexibility I have always trusted with Viabahn devices, this new lower profile offering will become very instrumental in my dialysis access practice.”
Currently, the Viabahn device is indicated for use in superficial femoral artery (SFA) lesions, iliac lesions, in-stent restenosis of SFA lesions, and in stenosis or thrombotic occlusion at the venous anastomosis of synthetic arteriovenous access grafts for haemodialysis.
Outcomes of the BIO4AMB trial demonstrated that ambulatory treatment with 4-French (4F) devices is a valid and safe option for endovascular treatment of lower extremity peripheral arterial disease (PAD), a Biotronik press release reports.
In addition, The 4F compatible products showed similar results to 6-French (6F) devices, with the added benefit of an eliminated need for a vascular closure device. These results were presented at the 2020 meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 12–15 September, virtual).
The BIO4AMB multicentre, controlled trial compared the rate of access site complications and major adverse events in 4F versus 6F femoral access endovascular interventions. The full-cohort analysis of 766 patients showed no significant differences in safety and efficacy between the patient group treated with 6F devices and those treated with Biotronik’s 4F product portfolio.
“Compared to the already well-established 6F devices, 4F compatible devices were shown to be a valid alternative,” summarised co-principal investigator Marianne Brodmann (Medical University of Graz, Graz, Austria). The rate of freedom from access site complications was 97.2% in the 4F arm and 96.8% in the 6F arm (p=0.734).
Brodmann, who presented the data, highlighted a key difference: “Use of 4F sheaths creates 45% smaller puncture holes, which resulted in low rates of access site complications despite not needing vascular closure devices. This may offer a better potential for ambulatory treatment.”
The health economic evaluation of the BIO4AMB study, also presented at CIRSE, investigated the implications on safety, resource use and cost of lower-extremity peripheral treatment using 4F and 6F access in an ambulatory setting. In this analysis, the rate of vascular closure device use was 0% in the 4F arm versus 87.4% in the 6F arm (p<0.05).
“Depending on the country specific reimbursement situation, ambulatory treatment may offer a cost saving option compared to a stationary setting,” concluded co-principal investigator and presenter Jos van den Berg (Regional Hospital of Lugano, Lugano, Switzerland).
Two devices for creating minimally invasive dialysis access—the Ellipsys vascular access system (Avenu Medical) and the WavelinQ 4F system (BD)—demonstrated high rates of technical success and low rates of complications, according to a new study published in the Journal of Vascular and Interventional Radiology. In addition, both technologies enabled patients to start dialysis sooner compared to surgery, offering significant quality-of-life benefits.
WavelinQ (BD)
For patients with end-stage renal disease (ESRD) who require haemodialysis, the preferred type of vascular access is an arteriovenous fistula (AVF)—a permanent connection between a vein and artery in the arm. Until recently, the only way to create an AVF was through a surgical procedure that subjects patients to discomfort, longer recovery times and delayed dialysis.
Both the Ellipsys and WavelinQ devices offer a nonsurgical alternative by using a minimally invasive approach to create a percutaneous arteriovenous fistula (pAVF). The new single-centre study, led by vascular surgeon Robert Shahverdyan (Vascular Access Center, Hamburg, Germany), compared the outcomes for 100 patients who underwent pAVF procedures (65 Ellipsys and 35 WavelinQ) from December 2017 to December 2019.
The Ellipsys system had a technical success rate of 100%, and only 27.7% of patients required secondary interventions following fistula creation. The WavelinQ system demonstrated similar outcomes, with a technical success rate of 97% and 26.5% of patients requiring secondary interventions. Overall, 79.5% of Ellipsys patients and 58% of WavelinQ patients were able to successfully begin dialysis with their fistula. At 12 months, 82% of Ellipsys fistulas were still functional, compared to 60% of WavelinQ fistulas.
“For every patient, my goal is to create the best possible dialysis access with the fewest possible interventions,” said Shahverdyan. “Our data show that with careful planning, both systems can safely and quickly create percutaneous fistulas with a high rate of success, though the Ellipsys system appears to create more durable access that is also easier to repair if that becomes necessary.”
Compared to surgical fistulas, both devices reduced the time to dialysis (cannulation). The mean time to cannulation for WavelinQ was 90 days, compared to 60 days with Ellipsys. In fact, 75% of Ellipsys fistulas were ready for cannulation at just four weeks, with a small number of patients ready for early cannulation within a few days of fistula creation, Shahverdyan notes.
“This study confirms other newly published data showing how much faster we can start using the Ellipsys percutaneous fistula for dialysis—a finding that has significant patient safety benefits,” said interventional radiologist Jeffrey Hull (Richmond Vascular Center, Richmond, USA). “The sooner a patient can start dialysis with their fistula, the sooner we can get them off such riskier dialysis access methods as central venous catheters, which are associated with much higher rates of infection and other complications.”
Hull is the lead author on a recent study of Ellipsys pAVF that reported an average time to dialysis of 66 days. Vascular surgeon Alexandros Mallios (Hôpital Paris Saint-Joseph, Paris, France), recently published data showing that patients were able to begin using their pAVF for dialysis an average of 4 weeks after creation, with six percent of fistulas becoming functional in as little as 2 weeks.
The studied technologies differ significantly in their design, pAVF creation technique and fistula location. The single-catheter Ellipsys system uses ultrasound guidance and thermal energy to create the fused and permanent connection between the perforating vein and the proximal radial artery; no radiation or contrast media are required. The WavelinQ device is a two-catheter system that uses radio-frequency energy and fluoroscopy to create an aligned slit fistula. Differences between the systems can affect patient eligibility for the procedures based on anatomic constraints.
“Based on our preoperative ultrasound evaluations, we found that 65% of patients were eligible for an Ellipsys pAVF, compared to just 27% with the WavelinQ system,” said Shahverdyan. “By knowing that more than twice as many patients will be able to undergo the procedure, Ellipsys makes it more feasible for a center to offer this endovascular approach to creating dialysis access.”
Cleared by the US Food and Drug Administration (FDA) in 2018 for patients with end-stage renal disease, Ellipsys is the first significant innovation in AVF creation in over 50 years. It transforms a complex surgery into a minimally invasive procedure that can be performed in a hospital outpatient setting, ambulatory surgery center or physician’s office. Since 2015, nearly 3,000 patients worldwide have undergone the Ellipsys procedure. Recently published long-term data show that 92% of Ellipsys fistulas are still functional after two years. The study also found high levels of patient satisfaction with the procedure.
Panagiotis M Kitrou and Nicholas Inston discuss the impact of the COVID-19 pandemic on vascular access services. Despite the disruption caused, they are optimistic that the pandemic should be viewed as a catalyst for change. It is time to “redesign and restructure” vascular access programmes, they tell Vascular News.
The COVID-19 pandemic has resulted in major disruption in the delivery of clinical services on a scale previously unseen. In many countries, rationing of facilities and severely restricted or zero access to operating theatres has been imposed. It has been estimated that 28.4 million surgical procedures have been cancelled globally, with the highest cancellation rates in benign disease.1 The crisis has affected different countries and even different regions of countries variably. In Asia, 47% of healthcare practices suspended elective vascular surgery completely and 23% scaled down activity.2 In the UK, it has been estimated that to clear the backlog of cancelled surgery at 20% extra activity will require 11 months, even if further surgeries are not factored in.
To manage constrained services, many societies issued prioritisation to allow rationing based on clinical risk, mainly based on estimated urgency and need for treatment. These have been classified as 1a. emergency <24 hours; 1b. urgent (up to 72 hours); 2. up to one month; 3. up to three months; and 4. over three months by the Royal Colleges in the UK,3 and by the Society for Vascular Surgery (SVS) as 1. postpone; 2a. consider postponing; 2b. postpone if possible; and 3. do not postpone.4
Provision of vascular access for dialysis “less than ideal” before pandemic
The impact of COVID-19 on dialysis access is not yet known, but it is predicted that the rates of definitive access have been severely affected. Prior to the pandemic, the provision of vascular access for dialysis was already identified as being less than ideal. In the USA, 80% of patients initiate dialyses on a central venous catheter (CVC)5 and international rates of definitive access are highly variable.6
Despite this, benefits of definitive vascular access and avoidance of CVCs are clearly demonstrated, particularly in the younger and less comorbid patients.7,8
The problems encountered during the first peak of the pandemic are likely to have resulted in many patients starting dialysis on a CVC. This is multifactorial. Patients with chronic kidney disease (CKD) stages 4 and 5 require access in preparation for dialysis. These patients who were classed as a vulnerable group have been advised to follow enforced shielding practices. As such, they neither fall into a high priority group for surgery or are advised to attend hospital appointments in person. Assessment for vascular access generally requires ultrasound mapping and this may have been avoided due to patient concerns and/or clinical policies to avoid virus exposure. For the same patients, pre-emptive living donor transplantation, which may have avoided the need for vascular access, may have been suspended.
In patients infected with COVID-19, the requirement for renal replacement therapy was high, particularly in those requiring intensive care. The impact of multiple vascular access attempts on these patients and long-term effects on renal function remain to be seen, but may add a further healthcare need.
For patients with existing access data, is not yet possible to assess whether COVID-19 infection had adverse outcomes. Anecdotally, claims have been made for prothrombotic tendencies, particularly in those severely affected, but data on fistula loss secondary to infection is not yet clear. Dysfunctional access may have been afforded higher priority and performing maintenance procedures may have avoided CVC insertions. It is unclear yet whether patients presented later during the pandemic due to shielding risks, or hospitals operated policies of inserting a CVC to reduce lengthy salvage procedures.
The consequences arising from increased CVC placement and reduced fistula creation and salvage will result in multiple issues. Repeated hospitalisation, bloodstream infections, catheter dysfunction, central venous stenosis, and occlusion are all a product of increased catheter use and as a consequence healthcare costs will increase.9 This significant economic and healthcare burden will not only start to show now, but as renal failure is a chronic disease will have significant effect on health economics in the long term. In addition, CVCs have a negative impact on the quality of life and longevity of haemodialysis patients and constitutes a major deviation from best practice guidelines and a serious setback in the standard of care previously delivered.10
“Robust plans” needed for predicted second wave
Whilst some countries are unfortunately currently dealing with the first wave, others are now preparing for a predicted second wave. The needs of CKD and dialysis patients require robust plans to optimise safe creation, maintenance, and salvage of definitive vascular access and avoidance of the use of CVCs.
These strategies may require local modifications. Ideally cold (green) sites should be used, although dialysis patients’ inability to isolate due to thrice weekly treatment may prohibit pure “clean” pathways. Risk assessments may need specific “renal pathways” to be developed rather than apply standard surgical risk stratification.
Where surgical services are overwhelmed or resources compromised, other strategies should be considered, particularly endovascular approaches to maintenance, salvage, and even creation using percutaneous devices. This may increase the availability of additional operators, (e.g. interventional nephrologists and interventional radiologists) where staff redeployment or sickness is a problem, and also allow procedures to be performed in alternative facilities, avoiding hot sites and potentially freeing up theatres.
In order to recover from the first wave of COVID-19 and prepare for further phases, the provision of the best dialysis access, including peritoneal dialysis, will require close working with the wider multidisciplinary team involved in assessment, creation, cannulation, surveillance, maintenance, and salvage of definitive access.
An opportunity for change in the interest of renal patients
To manage dialysis access appropriately during peaks of COVID-19 will require better identification of those at need with more timely assessment and creation of access.
Early identification of problematic access through skilled clinical examination, timely and appropriate referral for diagnostics, and treatment using optimal technologies and devices by those with expertise should be available. Follow-up and surveillance should be based around dialysis sessions and training of dialysis centre staff to cannulate, examine, and identify problems with liaison and accessibility to expertise made easily available.
The challenges of dialysis access may have been exacerbated by the pandemic, but all these requirements were present before. This is an opportunity for vascular access programmes to redesign and restructure, not only to deal with the pandemic, but to build better programmes suited to the needs of the large global population of renal patients.
Panagiotis M Kitrou is an interventional radiologist at Patras University Hospital, Patras, Greece.
Nicholas Inston is a consultant transplant and vascular access surgeon at the University Hospital Birmingham NHS Trust, Birmingham, UK.
References
CovidSurg C, Nepogodiev D, Bhangu A. Elective surgery cancellations due to the COVID-19 pandemic: global predictive modelling to inform surgical recovery plans. Br J Surg 2020.
Ng JJ, Ho P, Dharmaraj RB, et al. The global impact of COVID-19 on vascular surgical services. J Vasc Surg 2020; 71(6):2182–3 e1.
RCS. Clinical guide to surgical prioritisation during the coronoavirus pandemic.
SVS. Vascular conditions by category, with Teir Class 2020 [Available from: https://vascular. org/sites/default/files/Vascular%20surgery%20 triage%20by%20Tier%20Class%203.24.20.pdf].
Pisoni RL ZL, Port FK, Robinson BM. Trends in US vascular access use, patient preferences, and related practices: an update from the US DOPPS Practice Monitor with international comparisons. Am J Kidney Dis 2015; 65(6):905–915. Am J Kidney Dis 2015; 65:905–15.
Ravani P, Quinn R, Oliver M, et al. Examining the association between hemodialysis access type and mortality: the role of access complications. Clin J Am Soc Nephrol 2017; 12(6):955–64.
Quinn RR, Oliver MJ, Devoe D, et al. The effect of predialysis fistula attempt on risk of all-cause and access-related death. J Am Soc Nephrol 2017; 28(2):613–20.
Vassalotti JA, Jennings WC, Beathard GA, et al. Fistula first breakthrough initiative: targeting catheter last in fistula first. Semin Dial 2012; 25(3):303–10.
Lok CE HT, Lee T, et al. KDOQI vascular access guideline work group. KDOQI clinical practice guideline for vascular access: 2019 update. Am J Kidney Dis 2020; 75(4).
Fertility in patients who have had uterine artery embolization (UAE) is still a “hot topic,” Jean-Pierre Pelage (University Hospital and Medical Center, Caen, France) told delegates attending the online meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 12–15 September, virtual). “We have confusing data in the literature—we know fertility after UAE is possible, and that UAE is a valuable alternative to hysterectomy and multiple myomectomy in symptomatic patients, but the role of embolization in the specific subset of women trying to get pregnant remains controversial.”
While some studies have demonstrated a 100% pregnancy rate following UAE, Pelage warned his audience that every patient is different, as is every procedure; there may be technical differences in how an embolization is conducted at different centres, for example. There are some reports in the literature of complications specifically associated with fertility after UAE. In the EMMY trial, the level of follicle-stimulating hormone (FSH)—used as a measure of ovarian impact, with higher values typically seen in patients with a diminished ovarian reserve—was seen to increase after embolization. However, this trend was more strongly observed in women over 45 years of age, and in those with higher FSH levels at baseline.
Complications from UAE include non-target embolization, mainly due to uterine-to-ovarian artery anastomoses, and extensive myometrial and endometrial ischaemic damage, largely due to an aggressive embolization technique. The latter complication can result in hysterectomy, which Pelage said “is obviously a disaster for women trying to get pregnant.” There are also reports of chronic endometriosis, which can also negatively impact fertility.
“There are some studies reporting very low pregnancy rates, including our initial experience: in 66 women offered embolization as a last resort treatment, there is virtually 0% pregnancy,” Pelage commented. He went on to give several examples of studies from other centres that also reported low fertility rates post-embolization.
“All these studies are confusing,” he said, “including the only randomised controlled trial dedicated to fertility [from Michal Mara (General Faculty Hospital and First Medical Faculty of Charles University, Prague, Czech Republic) et al, published in Cardiovascular and Interventional Radiology in 2008]. The pregnancy rate was lower after embolization, and the final term pregnancy rate was also very low.”
However, he did give the CIRSE audience some good news as well, informing them that embolization is known to be effective in the long-term for the treatment of heavy menstrual bleeding and pressure symptoms, and that the procedure leads to fully infarcted fibroids. “We know that you can expect spectacular volume reduction both of fibroids and of the uterus, which is good news for pregnancy. Embolization is a good alternative to myomectomy, which is the reference treatment for pregnancy-seeking women.”
In addition, Pelage’s group reported encouraging hormonal function following UAE, with no side effects of embolization on the ovarian reserve. Some studies have reported high rates of pregnancy: 61% (14 of 23 women) in a paper from Kavous Firouznia (Tehran University of Medical Sciences, Tehran, Iran) and colleagues published in American Journal of Roentgenology in 2009, which also reported no significant complications post-procedurally; and 59.5% (44 of 74 women) in a paper from João Pisco (St Louis Hospital, Lisbon, Portugal) et al, published in Fertility and Sterility in 2011.
Detailing his own institution’s recent experience, Pelage told registrants: “[We had a] 56% pregnancy rate in better-selected women, so younger than in our first cohort.” The 16 women included in this more recent study had an average age of 35 years, and nine of the group were actively trying to conceive. One-year post-embolization, five of the women were pregnant. Most of these pregnancies were not associated with any complications by the time of delivery.
Citing the July 2020 New England Journal of Medicine (NEJM) paper from Isaac Manyonda (St George’s, University of London, London, UK) detailing the results of the FEMME trial, Pelage highlighted the team’s fertility results: “They reported a significant number of pregnancies after embolization, even higher than in the surgery [myomectomy] group. Since it was not the primary objective, I well understand that you cannot draw definitive conclusions based on this paper.”
Attempting to make sense of these myriad results for fertility outcomes following UAE, Pelage summarised: “Pregnancy results are very variable, ranging from 14–61% from one study to another. The same [is true] for the miscarriage rate, obviously with miscarriage being more common in older women.
“From the existing literature, there seems to be an interest on the hormonal function [elevated FSH levels is more frequent after UAE], there seems to be a higher rate of pregnancy after myomectomy compared to embolization, and the rate of miscarriage seems to be higher after embolization. But again, most cases are not treated in a randomised trial, and treated women are older or have more fertility-confounding factors when treated with embolization.”
These summations led him to the conclusion that, “Despite the encouraging results of recent publications, we should still consider embolization with caution in pregnancy-seeking women. In our centre, we always discuss as a group with the referring gynaecologist to decide whether we should offer embolization or myomectomy, and we know that prospective randomised trials are very difficult to conduct in this group of women, especially in 2020, where women are well-aware of the potential interest of embolization as an alternative to surgery.”
Irreversible electroporation (IRE) significantly induces a window of reduced immune suppression two weeks post treatment, allowing the activation of effector T cells that seem to be correlated with improved survival, according to preliminary flow cytometry results of the CROSSFIRE trial (NCT02791503 on clinicaltrials.gov). Speaking during the 2020 meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 12–15 September, virtual), Bart Geboers (Amsterdam UMC, Amsterdam, The Netherlands) described how his team investigated the immune modulatory effects of IRE and MR-guided stereotactic ablative body radiotherapy (SABR) in patients with locally advanced pancreatic cancer.
Pancreatic cancer is one of the most aggressive cancers, Geboers informed the CIRSE audience, with a five-year overall survival of less than 10%. Thirty percent of all patients present with locally advanced disease, and are not amenable for surgical resection. The median overall survival for patients with locally advanced pancreatic cancer is approximately 12–14 months. “The problem with pancreatic cancer is that it is barely immunogenic, and the tumour cells can escape the immune system,” Geboers explained. “This might explain the disease aggressiveness.”
Describing the pathophysiology of the cancer, he said the low immunogenicity is “probably two-fold”: the cancer suppresses the tumour microenvironment, and is associated with a lack of spontaneous apoptosis.
In terms of suppressing its microenvironment, the tumour releases suppressive cytokines that induce activation and proliferation of specific T cell subsets that are immunosuppressive—regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSC). In turn, these reduce the activation and proliferation of effector T cells, including Helper T cells (CD4) and cytotoxic T cells (CD8), thereby providing the tumour with a “T cell tolerance”.
The second problem is the rarity of spontaneous tumour cell apoptosis. This means no epitopes are released that can be taken up by dendritic cells and used by the immune system to develop an adaptive response in the lymph nodes.
Altering the immune balance of the tumour microenvironment
Overcoming tumour-induced immune suppression is therefore difficult. Geboers and colleagues hypothesised that ablation can alter the immune balance, changing the microenvironment from an immunosuppressive one to a more immunopermissive one. “We know that ablation results in a reduction in the tumour mass, and so a reduction in suppressive cytokines. This will lead to a reduction in T cell tolerance, and allow the development of effector T cells,” he explained. In addition, ablation induces apoptosis and necrosis, meaning there will be a release of immunogenic epitopes that can be taken up by antigen-presenting cells. Furthermore, “IRE has the advancement of being vessel sparing,” Geboers said, so antigen-presenting cells can transport epitopic antibodies to lymph nodes, where an adaptive immune response can occur.
To test this thinking, the investigators conducted an Immunological side study of the CROSSFIRE trial, where pancreatic cancer patients were prospectively enrolled between January 2016 and February 2020. Patients with locally advanced pancreatic cancer were pre-treated with FOLFIRINOX, before being randomised between IRE or SABR.
Tumour microenvironment shifts to become more immunopermissive two weeks after IRE, but this is lost by three months post-IRE
In order to assess the immune response, Geboers and colleagues took a venous blood sample from each patient before IRE or SABR, two weeks after treatment (to evaluate the immediate response), and three months post-treatment (to evaluate the durable immune response). Flow cytometry analysis was used to detect the type, frequency, and activation status of circulating immune cells.
A T cell analysis of 36 patients (19 treated with IRE, 17 with SABR) revealed that, two weeks after IRE, there was a significant downregulation of the regulatory T cells in the peripheral blood flow, as predicted by Geboers and colleagues. This downregulation returned to baseline three months after IRE. There was a trend for down regulation of the regulatory T cells three months after SABR, though this was not significant.
The investigators next looked at checkpoint expression of CD4 and CD8 T cells (the effector or helper T cells that were suppressed by the tumour’s activities). Two weeks after IRE, there was a significant upregulation of PD1 on the CD4 T cells. All the other checkpoints remained low. None of the checkpoints were significantly upregulated in the SABR group at any time point following ablation. “When looking at the activation status of the CD4 and CD8 T cells, we found that Ki67, which is a marker for T cell activation, was significantly upregulated at two weeks after SABR, in both CD4 and CD8 T cells, but was only significantly upregulated on the CD8 T cells two weeks after IRE ablation,” Geboers shared.
A linear regression model demonstrated that an increase in PD 1, on both CD 4 and CD8 T cells two weeks after IRE, was significantly associated with improved overall survival. No significant correlation was seen between PD 1 upregulation and overall survival in the SABR group.
“We found a significant downregulation of regulatory T cells two weeks after IRE that was simultaneous with a PD 1 upregulation on CD 4 T cells,” Geboers summarised. “The fact that the expression of the other checkpoints remained low argues against T cell exhaustion, but rather indicates that we are looking at a real effector T cell activation that might be amenable for PD 1 blockade with checkpoint inhibitory drugs.”
The CIRSE audience were left with this promising take-home message: transient PD 1 T cell upregulation combined with simultaneous regulatory T cell decrease after IRE is consistent with previously described systemic immune stimulatory effects of IRE, and supports combination with pharmacologic PD 1 checkpoint inhibition.
“These findings warrant further studies, for which we designed the PANFIRE III trial,” Geboers told delegates (NCT04612530 on clinicaltrials.gov). This will be a Phase I trial in which 18 patients with oligometastatic pancreatic cancer will be included. The study has three arms: the first six patients will be treated with Nivolumab (a PD 1 blockade; this is the control); the second six patients will be treated with IRE ablation of the primary tumour followed by Nivolumab; the final six patients will be treated with TLR-9 ligand intra-tumoural injection, followed by incomplete IRE ablation of the primary tumour and Nivolumab.
Concept Medical has announced the enrolment of the first patient in the FUTURE SFA (Randomised controlled trial of first sirolimus coated balloon versus standard balloon angioplasty in the Treatment of superficial femoral artery and popliteal artery disease) study.
The index patient was successfully enrolled on 12 September in Singapore.
FUTURE SFA is a randomised, double blind, placebo-controlled, multicentre trial to determine the effectiveness of the MagicTouch PTA sirolimus drug-coated balloon (DCB) versus standard percutaneous transluminal angioplasty for the treatment of superficial femoral and popliteal arterial disease.
Sirolimus-coated balloons are considered to be the next new generation of DCBs and the novel MagicTouch PTA sirolimus-coated balloon (SCB), has emerged as one of the most promising transcatheter technologies in preventing restenosis for diseased arteries.
The principal investigator of FUTURE SFA is Edward Choke (Sengkang General Hospital, Singapore), who comments: “I am inspired by the bold, imaginative, and futuristic concepts presented by the Nanolute technology of the MagicTouch PTA sirolimus-coated balloon. In contrast to other contemporary technologies, MagicTouch PTA offers a solution which optimises both the deliverability and the absorption of sirolimus into the vessel wall.”
He adds: “Initial experience with the XTOSI first in man study suggested that MagicTouch PTA can provide an effective way of revascularisation for PAD patients, by keeping the vessels open longer and reducing the need of repeated angioplasty procedures. I look forward to the FUTURE SFA randomised controlled trial, which will test whether the Magic Touch PTA sirolimus-coated balloon can improve the patencies of femoral and popliteal arteries in PAD patients. We hope to establish whether SCB will emerge as the new standard of care which will impact the way we treat PAD.”
The trial will enrol 153 patients with Rutherford class 3 to 6 PAD. These subjects will be randomised in 2:1 fashion to receive either Magic Touch PTA or standard balloon angioplasty.
Primary outcome will be primary patency at six months, defined as duplex peak systolic velocity ratio (PSVR) of 2.4 or less.
The trial is designed to follow a rigorous blinding protocol in order to minimise bias. Patients, care providers, investigators and outcome assessors, including vascular technologists performing the duplex ultrasound, will be blinded to the treatment allocations. The patients will be followed up for two years.
Paul Gagne explains how intravascular ultrasound (IVUS) can be used to guide the treatment of chronic venous disease, discussing the various pathologies and patients in which the benefits of IVUS imaging are “irrefutable”
Stephen Black speaks about his experience using IVUS in venous procedures
Considering the addition of intravascular imaging to angiography in peripheral arterial disease (PAD) procedures, Michael Lichtenberg and Konstantinos Stavroulakis write that IVUS “should be available in all major interventional centres”
Case study by Jihad Mustapha: The value of IVUS in CLTI revascularisation
Jörg Tessarek provides a step-by-step procedural guide to using IVUS in endovascular aneurysm repair (EVAR) and thoracic endovascular aortic repair (TEVAR) procedures
Based on evidence in the literature and their own clinical experience, Fabrizio Fanelli and Gianmarco Falcone detail how IVUS has come to be considered a “valid and safe tool” in the endovascular treatment of thoracic and abdominal aortic pathologies
Symptomatic peripheral arterial disease (PAD) patients undergoing recurrent lower extremity revascularisation have higher rates of ischaemic events, particularly acute limb ischaemia, than those patients who are undergoing their first peripheral revascularisation. This is the conclusion presented by Marc Bonaca (University of Colorado, Aurora, USA) at the 2020 meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 12–15 September, virtual). Bonaca and colleagues conducted a subgroup analysis from the VOYAGER PAD trial, which examined the efficacy and safety of Rivaroxaban in patients with PAD undergoing recurrent lower extremity revascularisation.
“We know from trials of patients with PAD that a history of a prior peripheral revascularisation is associated with a very high risk of acute limb ischaemia, even long-term years after the intervention was done,” Bonaca told online attendees. “More recent data from the landmark COMPASS trial shows that, in patients with chronic PAD, those who had a prior history of revascularisation are at major heightened risk of major adverse limb events.”
VOYAGER PAD is a trial of 6,564 patients with symptomatic lower extremity PAD undergoing peripheral revascularisation. Patients were randomised 1:1 in a double blind fashion to either the Rivaroxaban group, where they received 2.5mg of the drug twice daily, or a placebo group. The primary efficacy endpoint was a five-point composite of acute limb ischaemia, major amputation of vascular aetiology, myocardial infarction, ischaemic stroke, or cardiovascular death. The primary safety endpoint was thrombolysis in myocardial infarction (TIMI) major bleeding.
In an assessment of the primary efficacy endpoint, the rivaroxaban group performed better than the placebo group, with fewer incidences of the five major complications included in the composite measurement. “In spite of best medical therapy in this population [those patients treated with a placebo], the event rate was nearly 20%, which was extremely high—nearly one in five had an event,” Bonaca said. A Kaplan-Meier curve plotting cumulative incidence of the composite measurement of major adverse events against time since randomisation revealed that, at three-years post-treatment initiation, the event rate was 19.9% in the placebo group, and 17.3% in the rivaroxaban arm (hazard ratio [HR], 0.85; 95% confidence interval [CI], 0.76–0.96; p=0.009).
“Rivaroxaban risk-benefit was apparent early, and continued over time,” Bonaca commented, “with an absolute risk reduction of 2.6% at three years, and a number needed to treat of just 39.”
Subhead
Against this backdrop of successful rivaroxaban use in the main VOYAGER PAD trial, Bonaca and colleagues conducted a subanalysis investigating symptomatic PAD patients undergoing recurrent lower extremity revascularisation versus those undergoing their first revascularisation. They hypothesised that repeat revascularisation patients would have a higher rate of acute limb ischaemia, and would derive “even greater benefits with a rivaroxaban plus aspirin strategy versus aspirin alone”.
The presence of known prior revascularisation was reported by investigators at baseline, and was defined as any history of endovascular, hybrid, or surgical lower extremity revascularisation. The primary outcome was the same composite as in the VOYAGER PAD study, and a COX model with interaction terms was used to assess for heterogeneity of efficacy and safety of rivaroxaban by prior lower extremity revascularisation status.
From a comorbidity perspective, the prior revascularisation group had a higher risk profile, Bonaca shared, with more hypertension, diabetes, and hyperlipidaemia. PAD characteristics were similar between the two cohorts, with the prior revascularisation group having a slightly lower risk: “they were more likely to be treated with an endovascular revascularisation, they had less frequently presented with acute limb ischaemia versus claudication, and the [average] ankle-brachial index was a bit higher. […] It is worth noting that they were very well-treated.”
In the placebo cohort, the cumulative event rate for those with no prior lower extremity revascularisation was 17.7%—“very high,” Bonaca pointed out, “even in this very well-treated population.” Nevertheless, those patients who had had a prior revascularisation had a higher cumulative event rate of 23.8%, representing a 6.1% increase in risk.
“When we look at the efficacy of Rivaroxaban, stratified in these two groups [prior revascularisation and no prior revascularisation], we see the benefit is there for both groups,” Bonaca explained.
In the Rivaroxaban cohort, those with no prior revascularisation had a cumulative event rate of 16.9%, while those who had undergone an earlier revascularisation had a cumulative event rate of 18.1%. The impact of prior revascularisation was therefore less in the Rivaroxaban cohort than in the placebo cohort.
Figure 1; LER is lower extremity revascularisation
Comparing the placebo and rivaroxaban cohorts (Figure 1), Bonaca told delegates: “The benefit [of Rivaroxaban] appears even greater in those who had a prior history of revascularisation, with a HR of 0.73, and a trend towards heterogeneity, meaning there may be an even greater benefit in this high-risk group.”
Wondering what could be driving this difference, Bonaca and colleagues looked at the limb outcomes of acute limb ischaemia and vascular amputation in patients treated with Rivaroxaban with and without prior lower extremity revascularisation. In placebo patients with no prior revascularisation, rates of acute limb ischaemia and vascular amputation were lower at three-years post-randomisation than they were in the group of patients who had had previous revascularisation: 6% versus 10.8%, and 3.4% versus 4.5%, respectively.
As Bonaca put it: “Patients in the prior revascularisation group have a very high risk of acute limb ischaemia, almost 11%, and that is driving this risk-profile, and that benefit for acute limb ischaemia [with Rivaroxaban] is even greater in patients with a prior history of revascularisation. This does look like our hypothesis—that repeat revascularisation patients are at higher risk and would derive a greater benefit of Rivaroxaban—was met in this analysis.
“Rivaroxaban plus aspirin versus aspirin alone reduces irreversible harm events, so the heart, limb, and brain in patients that are undergoing revascularisation, but in this subgroup with prior revascularisation, there is a particularly robust benefit, and really notably in acute limb ischaemia. The current analysis demonstrates that within this population, those with multiple revascularisations are at higher risk than those who have undergone a first revascularisation only, and may derive particularly robust benefit from Rivaroxaban plus aspirin versus aspirin alone. These observations further demonstrate the heterogeneity of risk in the PAD population, and may assist in clinical risk stratification and therapeutic decision-making.”
“Through 24 months, there was a significantly lower clinically-driven target lesion revascularisation (CD-TLR) rate for the Eluvia DES than for the Zilver PTX [12.7% vs. 20.1%; p=0.0495],” Müller-Hülsbeck told registrants. An “excellent” primary patency rate was sustained with the Eluvia DES (83% from Kaplan-Meier estimates), and both study devices showed a low mortality rate at 24 months: 7.1% for Eluvia, and 8.3% for Zilver PTX.
In addition, Müller-Hülsbeck reported a significant improvement in mobility and pain/discomfort dimensions of health-related quality of life, sustained over 24 months in both treatment arms.
Cost-effectiveness analysis of the US Medicare system and the German health insurance system showed cost savings; on average, US$1,300 per patient was saved when patients were treated with the Eluvia device in the USA, Müller-Hülsbeck said. “This shows, once again, that when we chose Eluvia, we might achieve a high value when treating our patients with this kind of drug-eluting technology, due to the higher TLR rates we might achieve.”
Moderator Fabrizio Fanelli (Careggi University Hospital, Florence, Italy) stated: “I am very curious about how, still after two years, there is a pretty important gap between the ELUVIA DES and the Zilver PTX”. He queried if Müller-Hülsbeck thought this gap would grow larger in the future, or if he believed that outcomes from using these two devices would become more similar in time.
“That is an excellent question, and it is hard to answer!” Müller-Hülsbeck responded. “Probably the results from [using] both stents could differ, but I think there is also a high probability that the curves in terms of target lesion revascularisation might come closer, so we have to see what will happen in five years.
“The five-year data Michael [Dake] presented [during the same FIRST@CIRSE session] with the Zilver PTX are really outstanding. My personal hope for the patient is that, with Eluvia, we might achieve equal or even slightly better data, but this is just a hope. We will have to see what will happen. Once again, I think that with both technologies, the Eluvia stent and the Zilver PTX, we have options to treat our patients adequately, to provide them with drug-eluting technology.”
Fanelli was in agreement, adding: “This is something everyone is watching with a lot of interest.”
Turning tack to discuss the cost-effective analysis, Fanelli next asked if Müller-Hülsbeck thought this could “push the use of Eluvia, or more generally drug-eluting stents” in the future.
“I think yes,” Müller-Hülsbeck replied, “especially in the USA, because there are some major differences. In Germany, I do not know exactly, because the difference there is slightly lower, but it is my hope—as we want to avoid patients coming back for early target lesion revascularisation—that this kind of technology becomes more accepted by insurance companies for reimbursement. I am mentioning that because, at the moment, especially in Germany, we do not receive any reimbursement if we use drug-eluting technology, either the Zilver PTX or the Eluvia stent.”
An ad hoc, two-year analysis of the EffPac study found no signal of increased risk of long-term mortality, nor any adverse events, within two years of drug-coated balloon (DCB) angioplasty using a Luminor-35 device (iVascular). This was the conclusion presented by Ulf Teichgräber (University Hospital Jena, Jean, Germany) at the 2020 meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 12–15 September, virtual).
Teichgräber is the principal investigator of the EffPac trial, a prospective, randomised controlled trial initiated by the federal authorities in Germany, and conducted at eleven study sites, that compares the paclitaxel-coated Luminor balloon with plain balloon angioplasty in the femoropopliteal artery segment of patients with peripheral arterial disease (PAD).
The primary efficacy endpoint of this study was late lumen loss at six months; secondary endpoints included primary patency, freedom from target lesion revascularisation (TLR), Rutherford category, ankle-brachial index, and quality of life score. All-cause mortality and target limb amputation were assessed as the primary safety endpoints.
Just published in Radiology, Teichgräber described to the CIRSE audience how he and his team conducted an ad hoc, two-year review of mortality and morbidity following DCB angioplasty in EffPac patients. The two-year follow-up of the EffPac trial was in fact completed in February 2019, but another study cast its shadow over the results. Konstantinos Katsanos (Patras, Greece) et al published a meta-analysis in the Journal of the American Heart Association (JAHA) in December 2018 that found an increased association between late mortality risk and paclitaxel use in the femoropopliteal arteries. “Numerous public debates about the safety of paclitaxel-coated balloons were triggered”, Teichgräber recalled.
This led the Federal Institute for Drug and Medical Devices in Germany (in German: Bundesinstitut für Arzneimittel und Medizinprodukte; BfArM) to request a formal hearing on mortality of all ongoing studies concerning paclitaxel use in the peripheral arteries.
While the EffPac trial could not confirm a correlation between paclitaxel application and all-cause mortality—there was one death in the DCB arm, out of a total of 82 patients, and seven out of 85 in the plain angioplasty arm—a lot of patients were lost to follow-up.
In total, the EffPac trial randomised 171 patients into two arms: those treated with the Luminor DCB (85 patients), and those who received plain angioplasty (86 patients). At 24 months, 60 patients were left in the DCB group, and 56 in the plain angioplasty group, due to a lack of follow-up in nearly one third of randomised patients. This represented a discontinuation of 25 patients in the DCB arm, and 30 patients in the plain angioplasty arm.
Under entreaty from the BfArM, Teichgräber set out to find those EffPac participants lost to follow-up in order to gain further information on two-year mortality rates with paclitaxel devices.
“Paclitaxel showed a very low [mortality] risk ratio of only 0.15 compared to other trials, meaning there is no correlation of all-cause mortality associated with Luminor balloons,” Teichgräber inferred from their results. “Another interesting aspect [to look at] is cause of death,” he said. “The only case of death in the DCB group was due to multiple comorbidities, which were hardly associated with the application of paclitaxel.” Patients in the plain balloon angioplasty cohort died of heart failure, sepsis, cholangiocarcinoma, respiratory failure, and suicide. “A correlation between paclitaxel and cause of death is [therefore] quite unlikely,” Teichgräber concluded.
The total number of adverse events per patient was higher in the DCB group than in the plain balloon angioplasty group, though this difference was not statistically significant (3.2±2.8 vs. 2.9±2.6; p=0.59). The proportion of patients who experienced any adverse event was slightly higher in the plain angioplasty arm of the study, but again, this difference was not statistically significant (88.5% vs. 86.5%, respectively; p=0.81). “So there is no real difference in adverse events between both groups,” Teichgräber summarised. Except for serious malignancies, there were no significant between-group differences in the incidence of adverse event types.
Summing up, Teichgräber said: “I believe that such an ad hoc analysis on discontinued patients in randomised controlled trials gives us a full picture on all-cause mortality for our follow-up patients.
“As we do not have a class effect between different DCB products, with our ad hoc analysis we can only give information on Luminor balloons, and their coating technology. Therefore, it is important that other trials, with other DCB products, go the same way as we did with EffPac, and assess what happened to their lack-of-follow-up patients, and [see] if they could show equivalent results of all-cause mortality in their full cohort.”
Stefan Müller-Hülsbeck and Konstantinos Stavroulakis at CIRSE 2020
“The SAVER registry reinforces the safety and effectiveness profile for the Stellarex drug-coated balloon (DCB; Philips) in a real-world patient population,” Konstantinos Stavroulakis (St Franziskus Hospital–Vascular Surgery, Munich, Germany) told the live, online audience during the 2020 meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE; 12–15 September, virtual).
“These real-world registry data provide important outcome information for healthcare providers for the debate on the safety of drug-eluting technology,” he opined.
The Stellarex DCB is a low dose (2µg/mm2) paclitaxel device, with proven effective drug tissue transfer and residency. Compared to competitors, it has limited drug loss, “a very important feature”, in Stavroulakis words.
The SAVER registry
SAVER stands for the Stellarex Vascular e-Registry, a multicentre, European registry with external monitoring and clinical event committee adjudication. Patients are followed up through to three years, and experience a 12-month visit. The aim of the SAVER registry is to assess the safety and efficacy of Stellarex DCB use in the superficial femoral, popliteal, and/or infra-popliteal arteries in a broad, real-world patient population.
The registry is split into two patient cohorts: claudicants, and chronic limb-threatening ischaemia (CLTI) patients.
In the claudicant group—where patients are classified as Rutherford category 2–3—the primary safety endpoints are freedom from 30-day device- and procedure-related death, and freedom from 12-month target limb major amputation and clinically-driven target lesion revascularisation (CD-TLR). The efficacy endpoint for claudicants is freedom from 12-month CD-TLR.
In the CLTI group—where patients are classified as Rutherford category 4–5—the primary safety endpoints are freedom from composite major adverse limb events and perioperative death through 30 days. The efficacy endpoint for CLTI patients is freedom from six-month CD-TLR.
Registry results “robustly” demonstrate safety of the Stellarex DCB
An interim analysis of the first 1,000 claudicant patients revealed a procedural success of 97.9%, and lesion success in 98.5%. “Bailout stenting was required in 24% of the patients, showing that we can treat the majority of these PAD patients effectively, […] with no additional permanent scaffold,” Stavroulakis said.
Regarding complications, there was a 0% periprocedural mortality, and “just” 0.6% significant distal embolization. Target vessel thrombosis was seen in 0.2% of the patient cohort, and emergent surgical revascularisation in 0.1%.
The majority of patients (87.4%; 892 of 1,021) reached the primary safety endpoint, with freedom from device- and procedure-related death through 30 days post-procedure, and freedom from target limb major amputation and CD-TLR through 12 months post-procedure. Giving additional outcomes at one-year, Stavroulakis told the CIRSE audience that all-cause death was 3.2%, and amputation rate was 2.7%, with the major amputation rate 0.8%—“acceptable” outcomes in this real-world population.
Regarding the efficacy endpoint, 87.7% (895 of 1,021) patients had freedom from CD-TLR at 12-months post-procedure, a “robust” finding, according to Stavroulakis. Kaplan-Meier evaluation demonstrated 98.7% freedom from CD-TLR at 30 days, 95% at 180 days, and 88.6% at 365 days.
Recounting the additional secondary outcomes, Stavroulakis told registrants that the majority of patients (87.6%) improved by at least one Rutherford class; 8.9% had no change in Rutherford category, and 3.5% worsened from baseline. There was a significant improvement in walking capacity at 12 months, as measured via the six-minute walk test: at baseline, the mean distance a patient could walk during the test was 52±24.4m; by 12 months, this had risen to 169±123.7m. Quality of life scores and the ankle-brachial index also improved from baseline to 12 months.
These results led Stavroulakis to conclude that there was a low rate of procedural complications when the Stellarex DCB was used in claudicants, and the device had a high safety profile.
This is the first level one trial dedicated solely to assess the safety and efficacy of the Covera (BD) covered stent designed to treat stenosis in the arteriovenous fistula (AVF) access circuit. The two-year results showed statistically superior target lesion primary patency and AVF circuit primary patency with the use of the covered stent compared with angioplasty alone.
Renal replacement is expensive, online attendees of the FIRST@CIRSE session heard, and largely achieved with haemodialysis using an arteriovenous AVF. However, Dolmatch explained how AVF stenosis interferes with efficient haemodialysis, leading physicians to try and find a treatment modality that reduces its occurrence.
“Angioplasty has been our go to for many years,” he said, “but we know that the durability after angioplasty is OK, but the question is, can we improve upon angioplasty durability when treating fistula stenosis?”
Enter the AVeNEW study, a prospective, multicentre, multinational clinical trial of 280 patients with stenotic AVFs and clinical AVF dysfunction. Patients were randomised 1:1 to either the percutaneous transluminal angioplasty (PTA) group, or the angioplasty with Covera covered stent group.
The study met both its primary safety and efficacy endpoints: freedom from a primary safety event out to 30 days, and target lesion primary patency at six months, respectively. There was no significant difference in freedom from a primary safety event out to 30 days between the covered stent cohort and the angioplasty alone cohort (95% and 96.4%, respectively; p=0.002). Target lesion primary patency at six months was “superb” and “statistically superior” in the covered stent group compared to angioplasty (78.7% and 47.9%, respectively; p<0.001).
A 12-month exploratory subgroup analysis of target lesion primary patency revealed that, regardless of certain lesion characteristics, “a preferential, better outcome using the covered stent compared to angioplasty alone. A Kaplan-Meier plot showed that the freedom from loss of target lesion primary patency was superior shortly after implantation of the covered stent compared to angioplasty, and remained statistically better at all time points, with more than a 30% better patency at 24 months.
Secondary outcomes were also better for the covered stent cohort, Dolmatch related. The index of patency function and mean access circuit reinterventions were both superior in the covered stent group, while secondary patency was the same in both groups (91.4%). “Interestingly, all-cause death was lower in the covered stent group than the angioplasty group,” Dolmatch continued. “I am not sure if this is statistically significant, we have not done that analysis yet, but it is a curious finding.”
Looking specifically at freedom from loss of access circuit primary patency, he commented: “Access circuit patency for an AVF drops off regardless of which group you are in, and yet, at 24 months, there is a statistically superior outcome of circuit patency for the covered stent group compared to the angioplasty group [p=0.02].”
The AVeNEW trial is still ongoing, with one more year of data collection and analysis ahead, to bring its total duration to three years.
Stefan Müller-Hülsbeck and Michael Dake during CIRSE 2020 Summit
“Please feel free to utilise this in your practice,” Michael Dake (University of Arizona Health Sciences, Tucson, USA) urged on the first day of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2020 Symposium (12–15 September, virtual). Speaking during a FIRST@CIRSE session, he presented a new, interactive, web-based tool built to predict patients’ freedom from target lesion revascularisation (TLR) following treatment with the Zilver PTX (Cook Medical) drug-eluting stent (DES).
Dake and colleagues used patient and lesion factors from five global clinical studies from Cook Medical to develop a prediction model for freedom from target lesion revascularisation (TLR) following use of Zilver PTX. These clinical studies studied both pre-market and post-market outcomes with the Zilver PTX stent in patients with femoropopliteal disease. In total, they collated data came from 2,374 patients, and included 15 risk factors in their creation of the model.
“It is note-worthy that over 50% of the patients included in the model had over five-year follow-up. In fact, this is the first prediction model to estimate the impact of patient and lesion characteristics on freedom from TLR through five years for patients with PAD,” Dake enthused. “Based on unique patient profiles, the model provides expected patient outcomes following treatment with the Zilver PTX DES, and may assist in defining algorithms for patients as the value of population management is increasingly recognised.”
Turning to the freedom from TLR results, Dake informed the CIRSE audience that 94% of the complete dataset (2,227 cases, with a median follow-up time of two years) was used to generate the model. Freedom from TLR was 90.5% at one-year, and 75.2% at five years.
Describing the model more closely, Dake next related the 15 risk factors that were considered when the tool was under construction: sex, age, diabetes, hypertension, hypercholesterolemia, renal disease, smoking status, Rutherford classification, lesion length, dexamethasone, popliteal involvement, total occlusion, calcification, prior interventions, and the number of patient runoff vessels. “Most all of these have been in the past implicated as being high-risk for TLR in studies performed over the last two decades,” Dake disclosed.
He continued: “Risk factors common in PAD patients collectively contributed to overall prognosis. As expected, chronic limb-threatening ischaemia (CLTI), lesion length, and total occlusion have a significant impact on TLR. Other factors, such as diabetes and calcification, do not have a significant impact on TLR.”
He then talked through three example patient profiles to illustrate how listening physicians could use this predictive model in their own practices. The risk factors any given patient may have are fed into the model, which then churns out an estimation of the risk that patient has of maintaining freedom from TLR out to five years, with a standard error given, when treated with the Zilver PTX. These results also translate into a freedom from TLR Kaplan-Meier curve. The physician can then make an informed treatment decision based on individual risk factors.
The baseline data
Teasing apart the larger dataset to examine trends in baseline patient demographics, Dake said: “Looking a bit closer at some of these individual patient demographics, and how they are distributed within the various trials included in the analysis, you can see some differences. Of note, in the Japan post-market study, [there is] a very high frequency of renal disease, and a higher frequency of CLTI. In terms of diabetes, there was a high frequency in all studies, approaching 50%.”
Appraising the baseline lesion characteristics, Dake informed viewers that 42% of patients had total occlusions, and that there was an increased number of prior interventions in both the single-arm study and the Japan post-market study, as both these trials included in-stent restenosis. “Patients with in-stent restenosis were not allowed to enter the other trials,” he explained.
“This is the first step”
Praising Dake for these results, moderator Stefan Müller-Hülsbeck (Diako Hospital, Flensburg, Germany) commented: “I think you have shown once again that paclitaxel is probably safe, and we meet a new level of security when using these kinds of devices, especially when using this kind of predictability model.” He then asked Dake if the model is already in use, and if so, if he was using it for his patients during his daily practice.
“This is actually the first debut of this model and this website,” Dake responded. “The manuscript will be published in Cardiovascular and Interventional Radiology (CVIR).” He encouraged CIRSE attendees to visit the site themselves and “really get a sense of getting comfortable with how individual risk factors can affect TLR going out through five years”.
Referring to his presentation as the launch of this predictive model, Dake closed the discussion by postulating: “Maybe other device manufacturers will look at this as a model and adopt predictive models as a way to counsel patients and their families in the clinic regarding their individual risk factors, modification of those risk factors, how we can really just predict and have them anticipate what results might be with individual different devices. I think this is the first step. I think this is an outcropping of what we have seen as a result of the Katsanos paper [Konstantinos Katsanos (Patras, Greece) et al published a paper in late 2018 that suggested the existence of an increased mortality risk with paclitaxel devices used in the peripheral arteries]. The next level now is [to evaluate the] efficacy in terms of using paclitaxel in individual patients.”
Biotronik today announced European market release of the Passeo-35 Xeo percutaneous transluminal angioplasty (PTA) balloon catheter. A company press release states that, compared to other available PTA balloons, the device offers physicians improved crossability, excellent trackability, and pushability in a wide range of sizes.
“The new Passeo-35 Xeo balloon handled impressively well, crossing easily even in an occlusive lesion,” comments Gerd Grözinger (University Hospital Tübingen, Tübingen, Germany), after performing the first-in-human procedure with the balloon. “The deflation time was also very fast compared to other balloons, which can save valuable procedure time.”
To aid in challenging lesion crossing, the Passeo-35 Xeo catheter offers a low entry profile, smooth tip taper, and up to 19.5% more pushability compared to competitors, facilitating improved catheter navigation in the peripheral vasculature. Catering to a full range of lesion sizes, the device is available in balloon diameters from 3–12mm and lengths of up to 250mm, with usable catheter lengths of 90, 130 and 170cm. Additionally, the Passeo-35 Xeo catheter is fully 5F compatible for balloon sizes up to 7mm in diameter and 250mm in length.
The Passeo-35 Xeo balloon is indicated to dilate stenosis in the iliac, femoral, popliteal and infrapopliteal arteries and for the treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulae. It is also recommended for post-dilatation of balloon-expandable and self-expanding stents in the peripheral vasculature. Passeo-35 Xeo is the platform for Biotronik’s recently released Dynetic-35 balloon-expandable cobalt chromium stent system.
Panellists at GEST discuss the single centre study presented by Dmitry Akinfiev
Uterine artery embolization (UAE) preserved fertility in “at least 75% of patients with acquired uterine arteriovenous malformations,” according to a recent single centre study presented at the virtual 2020 Global Embolization and Cancer Symposium Technologies (GEST) meeting (4–6 September). Dmitry Akinfiev (National Medical Research Center for Obstetrics, Gynecology and Perinatology, Kulakov, Russia) presented the clinical and reproductive findings of his research group to the live, global audience.
“In our work, the clinical effectiveness of UAE in acquired uterine arteriovenous malformations is 86.2%,” he shared.
Akinfiev and his team conducted a retrospective, single centre study involving 29 patients, with a mean age of 29.1 years—“rather low”, in the presenter’s words, with the oldest patient included in the study being 43 years old. “All [patients included in the study] were fertile,” Akinfiev informed delegates. The study investigators performed 34 UAE procedures, and the mean patient follow-up was 2.5 years (range: one to six years).
Uterine arteriovenous malformations are rare, the GEST audience were told. “Speaking of risk factors for acquired uterine arteriovenous malformations,” Akinfiev said, “in 80% of cases, the malformation was associated with curettage [19 patients had curettage following a miscarriage; four patients had a normal pregnancy and underwent curettage; one patient had a diagnostic curettage and no pregnancy]. Also, we had one patient with arteriovenous malformation after vacuum aspiration [following a normal pregnancy].” A further two patients developed uterine arteriovenous malformations due to gestational trophoblastic disease, and two patients acquired malformations for unknown reasons.
The team from Russia used irregular uterine bleeding as the primary indication for embolization. Eight patients (27%) needed a blood transfusion prior to UAE, and 10 procedures of 34 (29%) were emergency UAEs.
All patients underwent ultrasound and computed tomography (CT)-angiography before and after the procedure. “Those were our main diagnostic instruments,” Akinfiev divulged. “Importantly, we performed CT-angio from the diaphragm to the bottom of [the] pelvis.”
Detailing the procedures themselves, Akinfiev told the GEST attendees that 10 of the 34 procedures were expanded by embolizing additional arteries: branches of the internal iliacs, ovarian arteries, and superior mesenteric artery branches. Twenty-seven (80%) of the procedures were performed via the radial approach, and embolizations were performed with gelfoam and non-spherical polyvinyl acetate (PVA) particles under 500µm. “I prefer to use gelfoam in cubes,” Akinfiev opined.
The evaluation parameters for the study were the elimination of abnormal uterine bleeding, and the absence or significant reduction of arteriovenous shunting on CT-angio.
Of the 29 patients, 25 (86%) experienced clinical success after one procedure. Of the four who underwent a second procedure, the clinical success rate was 75%, with one patient having to have a third embolization. This third UAE was a clinical success.
There was a significant correlation between the clinical findings and the diagnostic findings, as presented on CT-angio. Twenty-seven of the 34 procedures were both clinically successful, and diagnostic imaging revealed a reduction or absence of arteriovenous shunting following UAE. In two cases, the interventionalists reported a clinical success, but diagnostic imaging showed the presence of arteriovenous shunting post-procedurally. All five clinical failures showed arteriovenous shunting on CT-angio. “There were no patients with CT-angio success and clinical failure,” Akinfiev said.
Next, he turned to reproductive outcomes. Of the 29 patients included in the study, 12 (41%) desired pregnancy, and 17 (59%) did not. In the desiring pregnancy subgroup, nine (75%) women did become pregnant, and all nine have since given birth, “a rather encouraging result,” according to Akinfiev.
“We had only one patient with a comorbidity during pregnancy,” he continued, “a patient with placental presentation. Our obstetricians had to perform a caesarean section in the 35th week of gestation due to threatening bleeding.”
Fielding a question from the audience concerning pulmonary embolisms, Akinfiev answered: “In this group, we did not see any sign of pulmonary embolism in our patients, but when we performed our procedures, we always tried to use the gelfoam first prior to PVA, as the cubic gelfoam particles are larger, and this way we try to prevent pulmonary embolism. Generally, we did not see any significant complications in this group except for one strange point, I cannot call it a complication, but about half of them demonstrated a very high temperature, higher than 38°C, on the second or third day after the procedure. I think it is because of using gelfoam.”
Another questioner asked if any of the 29 patients were given hormonal drugs prior to UAE, but Akinfiev replied that they did not use any form of systemic therapy ahead of embolization, “so zero,” he replied.
Lymphatic fistulae and/or lymphoceles in the groin following radical lymphadenectomy are frequent, and therapeutic options are needed to avoid severe restrictions for oncologic patients waiting for adjuvant medical therapies. This is the key message Florian Offensperger (General and Interventional Radiology, Stuttgart Clinics, Stuttgart, Germany) wants audience members to take home from the 2020 virtual Global Embolization and Cancer Symposium Technologies (GEST) meeting (4–6 September).
“It is important to say that there are treatment options,” he told attendees of the live event on Friday 4 September, “because we often have excellent patients who have been told that there is no other option but to wait.”
Stuttgart Clinics, where Offensperger works, is one of the largest surgical centres in Germany. Discussing postoperative lymphatic complications following radical inguinal lymphadenectomy in patients with malignant melanoma, Offensperger says: “Where wood is chopped, splinters must fall”. However, his talk offers hope for how best to deal with these splinters—a complication need not spell disaster for a patient.
The basic lymphatic intervention performed at the Stuttgart Clinics for patients with postoperative complications from radical inguinal lymphadenectomy is pedal Lipiodol lymphangiography combined with second-line interventions. “In our opinion,” Offensperger says, this is “the best treatment for these patients”.
He informs the GEST audience that the technical success rate of conventional lymphangiography is 75–100%, and the cure rate of postoperative lymphatic leakage for pedal conventional lymphangiography is 51–70% (time to cure, 2–29 days). “Conventional lymphangiography is safe, feasible, and effective in the management of postoperative lymphatic leakage,” he concludes, showing a pre-recorded video of the procedure to illustrate how it works to his listeners. “Personally, I really like this intervention, because it is a delicate task requiring many interventional techniques,” he shared.
In the present study, Offensperger and colleagues conducted a prospective analysis of their institutional digital databases for melanoma patients. They compared patients who had been treated with lymphatic angiography alone with those who had been treated with lymphatic angiography combined with sclerotherapy.
Between October 2014 and June 2019, 13 patients met the inclusion criteria: nine in the lymphatic angiography alone group, and four in the combined lymphatic angiography and sclerotherapy group. Mean patient age was 66.4 years (range: 46.8–83.4 years), and the interval between radical inguinal lymphadenectomy and lymphatic angiography was 17.8 days (range: seven to 34). The technical success rate for lymphatic angiography was 93%. The amount of Lipiodol used to perform the procedure was 15.4ml (range: six to 22ml), and in the combined group sclerotherapy was applied after an interval of 10 days (range: zero to 23). Sclerotherapy was performed either with 3–5ml ethanol, or with a glue/ Lipiodol 1:5 mixture (6–8ml) under fluoroscopy or computed tomography (CT) guidance.
The clinical success rate was higher in patients treated with lymphatic angiography and sclerotherapy, 100% compared with 78%. However, the interval between intervention and cure was slightly shorter in the cohort treated with lymphatic angiography alone: 23 days (range: four to seven) versus 29 days (range: 24–33). While there were no minor procedure-related complications in the group of patients treated with lymphatic angiography alone, there was one in the combined cohort (representing 25% of the patients treated in this arm of the study), a local infection cured by antibiotic treatment. There were no major procedure-related complications in the study.
These results led Offensperger to conclude that “Lymphatic angiography, with or without sclerotherapy, is an essential tool to cure therapy-refractory lymphatic fistulae after radical inguinal lymphadenectomy in patients with malignant melanoma.
“Lymphatic angiography in combination with sclerotherapy seems to result in higher clinical success rates,” he continued, “but also in higher complication rates when compared with lymphatic angiography alone.” However, he stressed that he wanted to leave GEST attendees with the understanding that lymphatic angiography in combination with sclerotherapy is a safe and effective option.
Boston Scientific announced that the US Centers for Medicare and Medicaid Services (CMS) granted a new technology add-on payment (NTAP) for the Eluvia drug-eluting vascular stent system as part of the 2021 inpatient prospective payment system (IPPS).
The NTAP designation, awarded to new medical devices determined to substantially improve the diagnosis or treatment of Medicare beneficiaries, will be effective on 1 October 1 2020 and will provide eligible hospitals with incremental reimbursement for the Eluvia stent system for up to three years. The Medicare criteria for an NTAP designation is based on newness of the device, cost, and a substantial clinical improvement.
The Eluvia stent system was developed for the treatment of peripheral arterial disease (PAD). The Eluvia stent reopens the blocked artery and restores blood flow, while also utilising a drug-polymer combination to offer a sustained, low-dose release of drug to prevent tissue regrowth within the stented artery.
“The CMS determination is a very positive development for patients with PAD and supports what we have confirmed through our clinical trials—the Eluvia stent offers clinically superior outcomes compared to other peripheral drug-coated technology available to clinicians and their patients,” said Jeff Mirviss, executive vice president and president, Peripheral Interventions, Boston Scientific.
“The decision is particularly important given the level of consideration and evaluation related to the role of paclitaxel in the peripheral vasculature, and we believe this designation reflects the unique attributes of the Eluvia stent, which are clearly differentiated and improve the quality of life for the millions of people suffering from symptoms of PAD.”
The NTAP designation will support access to the Eluvia stent for Medicare beneficiaries in the hospital inpatient setting, making it possible for eligible hospitals to receive NTAP payment in addition to the standard Medicare severity diagnosis related group (MS-DRG) payment.
The US Food and Drug Administration (FDA) approval of the Eluvia stent system in September 2018 was based on findings from the IMPERIAL trial, which exhibited the highest 24-month primary patency reported to date for the treatment of femoropopliteal disease in a US pivotal trial with a drug-coated balloon or drug-eluting stent. Trial data confirmed a statistically significant lower clinically-driven target lesion revascularisation (TLR) rate of 12.7% for patients treated with the Eluvia stent, in contrast to 20.1% observed within the Zilver PTX drug-eluting peripheral stent cohort (p=0.0495), thus reducing the need for repeat procedures at 24 months.
The Ellipsys vascular access system reduces the time before patients with kidney failure can start lifesaving dialysis treatments, while requiring fewer secondary procedures, according to a new study led by interventional radiologist Jeffrey Hull (Richmond Vascular Center, Richmond, USA).
This could have a significant impact on patient safety and healthcare costs by reducing the need for other forms of dialysis access that are associated with higher rates of complications, a press release states.
For patients with end-stage renal disease (ESRD) who require haemodialysis, the preferred type of vascular access is an arteriovenous fistula (AVF), a permanent connection between a vein and artery in the arm.
Until recently, surgery was the only way to create an AVF, but that subjects patients to longer recovery times and, as a result, delayed dialysis. Hull helped develop the Ellipsys system as a non-surgical alternative; the technology uses just a small needle puncture and catheter to create an endovascular AVF (endoAVF).
The prospective study, involving 123 patients at Richmond Vascular Center, evaluated patient selection and best practices for preparing (“maturing”) Ellipsys fistulas for dialysis. The results show that use of the Ellipsys system along with early maturation procedures reduced the average time from fistula creation to dialysis to just 66 days, down from 100 days in the initial US pivotal trial. In the USA, literature reports the time to dialysis with surgical fistulas averages 135 days.
This “rapid maturation” is important because it can potentially reduce or even eliminate the length of time patients require a central venous catheter (CVC) for dialysis. Compared to fistulas, CVCs are associated with significantly higher rates of complications, like infection and even death. Despite these risks, 80% of patients in the USA still start their dialysis with a catheter.
“Catheters are a less than optimal choice for dialysis access and the goal is to always get them out as soon as possible to avoid serious complications,” said Hull. “With Ellipsys, we have the unique ability to create fistulas in the office during the patient’s initial visit, thus avoiding surgery at the hospital and reducing physician visits. This enables us to streamline the dialysis timeline and reduce patients’ total catheter contact by a significant amount—sometimes by as much as four months. This will have a tremendous impact on quality of life for patients.”
Published in a recent issue of the Journal of Vascular and Interventional Radiology (JVIR), Hull’s study demonstrates real-world outpatient use of the Ellipsys endoAVF system. It is also the first US-based study to evaluate the application of best practices for early maturation. These best practices include performing balloon angioplasty during fistula creation to improve blood flow, as well as completing maturation after just four weeks. In addition to shortening the dialysis timeline, this protocol decreased the overall number of secondary maturation procedures required to prepare the fistula for dialysis and reduced the rate of thrombosis, a common complication with fistula creation.
Decreasing the number of procedures a patient must undergo to prepare for dialysis, as well as moving fistula creation from hospitals to outpatient settings, is a particular advantage for both patients and healthcare providers as the USA deals with COVID-19, according to kidney patient advocate Terry Litchfield.
“The ability to create a fistula with a minimally invasive procedure in an outpatient setting preserves limited hospital resources and lowers the risk of exposure for kidney patients, who already have a higher risk of developing complications with the virus,” said Litchfield. “Ellipsys enables physicians to safely create dialysis access, even in the midst of a pandemic, which will make it easier for these vulnerable patients to get the lifesaving dialysis treatments they need.”
An illustration of a completed Detour procedure within the superficial femoral artery and the femoral vein
PQ Bypass has announced that they received breakthrough device designation from the US Food and Drug Administration (FDA) for the Detour system. The Detour system is the world’s first fully-percutaneous femoral-popliteal bypass device intended to treat extremely long, complex blockages in the superficial femoral artery (SFA).
Physician access to this device can now be expedited as a result of this designation by the FDA breakthrough device programme, which is intended to help patients receive more timely access to breakthrough technologies that have the potential to provide more effective treatment or diagnosis for life-threatening or irreversibly debilitating diseases or conditions. Under the programme, the FDA will provide PQ Bypass with priority review and interactive communication regarding device development and clinical trial protocols, during the premarket review process.
“As this is a first-of-its-kind device, we are pleased to have the FDA recognise the novelty and potential of our therapeutic approach in treating severe SFA,” said Heather Simonsen, general manager at PQ Bypass. “We appreciate their collaborative review of our breakthrough device designation request and look forward to a continued productive relationship as we continue towards PMA submission.”
The Detour system is designed to treat patients who are unable to carry out activities of daily living and are unable to enjoy the liberties of free mobility as a result of their advanced symptomology, severe lesion morphology, and multiple comorbidities.
Once peripheral arterial disease (PAD) progresses to debilitating claudication or tissue loss, revascularisation becomes imperative to mitigate the ongoing deterioration and to prevent amputation. Left untreated, these patients are at greater risk for further functional deterioration, major adverse limb events, and mortality.
“This designation is a major milestone for PQ Bypass, and we expect this technology to change the paradigm for complex SFA treatment in the way EVAR [endovascular aneurysm repair] and TAVR [transcatheter aortic valve replacement] changed the paradigm for aortic repair,” said Rich Ferrari, chairman and CEO of PQ Bypass.
“We are nearing enrolment completion in our DETOUR2 and TORUS2 IDE [investigational device exemption] studies, and had new positive data on our technology published in the Journal of Vascular Surgery, making 2020 a momentous year for the company. This is an exciting time for all of us at PQ, with this important designation a credit to such a talented group. We are honoured and proud to be part of this important journey to develop a first-line therapy in the treatment of advanced PAD.”
Sirtex Medical and its shareholders, China Grand Pharmaceutical and Healthcare Holdings Limited (CGP) have been issued a “Notice of Drug Clinical Trial Approval” by the National Medical Products Administration (NMPA) of the People’s Republic of China.
The notice confirms that SIR-Spheres Y-90 resin microspheres meet the relevant requirements for drug registration in China. With this confirmation, Sirtex is approved to file a New Drug Application (NDA) in the country.
“We are grateful to the members of CGP, Sirtex China, and our Global Regulatory, Quality Assurance, Operations, and Medical teams for their dedicated work in achieving this approval from the NMPA and navigating the complex regulatory process,” comments Kevin R Smith, chief executive officer of Sirtex. “This is a critical milestone toward allowing us to provide a valuable treatment option to people with liver cancer in China.”
The announcement marks a step in Sirtex’s journey to gain market entry into China, thanks to the company’s collaboration with its shareholder, CGP.
“We are proud of our team’s accomplishment and work to achieve this goal,” says Weikun Tang, general manager of Sirtex China. “We are excited for the opportunity to work together with CGP to bring SIR-Spheres Y-90 resin microspheres to our country’s patients.”
Philips has announced the next generation of its Azurion imaging platform
Philips has announced the next generation of its Azurion imaging platform
Royal Philips has announced the next-generation of its Azurion image-guided therapy platform, designed to improve the quality and efficiency of interventional procedures. The Azurion platform has been used in over two million procedures worldwide since its introduction three years ago, according to a company press release.
In the past few decades, clinical practices around the world have evolved to successfully treat more patients and perform more complex procedures in interventional labs, the Philips press release noted, adding that with more staff and technologies involved during these procedures, interventional lab environments can become crowded and cluttered. In order to enhance clinician focus and control during procedures, Philips has integrated all the essential lab systems and tools into the new version of the Azurion platform.
The Azurion image-guided therapy platform now integrates control of imaging, physiology, haemodynamic and informatics applications, as well as intuitive control of the gantry, at the tableside, allowing clinicians to control all compatible applications from a single touch screen while performing procedures. This can eliminate the need for clinicians to leave the sterile field and step into an adjacent control room, as well as supporting faster and better informed decision making, the company said.
Philips is also introducing a new 3D imaging solution called SmartCT, where users are guided through image acquisition and can review and interact with the acquired CT-like 3D images on the tableside touch screen module using 3D visualisation and measurement tools. These tools have been designed to support procedures in a range of clinical domains, including neurology, oncology, and cardiovascular procedures.
“Our aim as an innovation company and global market leader in image-guided therapy is to push the boundaries and set new industry standards for delivering an outstanding experience for clinicians, helping them to deliver superior care to every patient,” said Ronald Tabaksblat, general manager image guided therapy systems at Philips. “This next-generation Azurion makes routine cardiovascular procedures more efficient and supports the development of new minimally-invasive techniques to treat complex diseases such as stroke, lung cancer and spine disorders.”
“The integrated platform enables us to efficiently carry out complex interventions at any time using a wide range of functions such as IVUS and iFR co-registration,” said Alexander Becker, head of the cardiac catheter laboratory at the Robert Bosch Hospital, Stuttgart, Germany, and one of the first hospitals to experience the new platform. “The use of the control panel by the examiner is intuitive, combining different sources of information to make patient evaluation much easier and faster.”
Philips adds that the new Azurion platform allows clinicians to easily switch between imaging, physiology, haemodynamic and informatics applications, including SmartCT and IntraSight—a suite of clinically proven iFR, FFR, IVUS and co-registration modalities.
The new Azurion also includes cybersecurity features, high-definition image display capabilities, and advanced remote and proactive services. The platform is available in three versions: complementing the Azurion 3 and 7 variants, Philips now also offers the Azurion 5 to facilitate tailored solutions to address specific customer needs.
The largest European-wide observational study on the treatment of primary and metastatic liver tumours with SIR-Spheres microspheres (Sirtex) will present its data on safety and overall survival from its 1,027-patient cohort for the first time at the virtual 2020 meeting of the Cardiovascular and Interventional Radiological Society of Europe (12–15 September).
The study, initiated by CIRSE, collected data on the clinical application of selective internal radiation therapy (SIRT), also known as radioembolization. The data will be presented virtually during a live hot topic symposium: “Research in IR: First results from CIRSE’s observational studies (HTS 1801, Monday 14 September, 14:30–15:30 CEST).
Thomas Helmberger (München Klinik Bogenhausen, Munich, Germany), speaking on behalf of CIRSE as the chairperson of the CIRT Steering Committee, states: “I am extremely proud of all the hard work that my colleagues have put into this study over the last six years. Its success is due to their continuous efforts, and I am very excited to present this data during the upcoming CIRSE 2020 Summit.”
The Society of Interventional Oncology (SIO) National Comprehensive Cancer Network (NCCN) Task Force submitted recommendations to the NCCN for the latest revision of the Neuroendocrine Tumour treatment guidelines. These have been accepted by the national body. According to the society, this is the first time interventional radiology (IR) has been called out as a separate body contributing to the guidelines (see figure 1).
The inverted “U” is the mathematical symbol for intersection; SIO describe this symbol as “a fitting designation for interventional oncology operating at the intersection of cancer therapies”.
For lung neuroendocrine tumours (NETS), ablation was added for treatment of primary tumours, and liver-directed therapy added for liver-dominant metastases.
An entirely new section on “Principles of Liver-Directed Therapy” was added to the guidelines and referenced in the sections on treatment of metastatic gastrointestinal and pancreatic NETS. The principles cover the spectrum of embolotherapies and include thermal ablation as an option, while acknowledging the limited prospective data for ablation. Adding an entirely new section of this name was the first request made from SIO late last year.
Cautions about liver-directed therapies in the setting of a Whipple were modified to include any prior biliary instrumentation.
Ablation was added as an option for malignant adrenal tumours.
A new section on “Principles of Imaging” was created to codify recommendations for anatomical and nuclear imaging.
Rony Avritscher (MD Anderson Cancer Center, Houston, USA), Nick Fidelman (University of California San Francisco, San Francisco, USA), and Etay Ziv (Memorial Sloan Kettering Cancer Center, New York, USA) authored the SIO submission. Their letter, dated 15 October 2019, requested the NCCN Neuroendocrine and Adrenal Tumours guideline panel review data regarding six specific changes to update the role of liver-directed therapies in the clinical practice guidelines in oncology.
In response to the global outcry following the murder of an unarmed black American, George Floyd, by police in Minneapolis in late May of this year, and as a contribution to the continuing conversation on racism in the USA and globally, the Society of Interventional Radiology (SIR) released a statement of commitment in support of diversity within medicine. It promised to “commit to anti-racist efforts, policies, and programmes that aim to increase the numbers of underrepresented minorities and women within our specialty”. Interventional News spoke with Paul J Rochon, chair of the SIR Diversity and Inclusion Advisory Council and a vascular and interventional radiologist at the University of Colorado School of Medicine, Aurora, USA, about the society’s continued anti-racist activities and intentions.
How is the SIR supporting diversity and combating racial inequality in the USA?
As we outlined in our statement, SIR has a number of activities underway to combat racial inequality. In addition to establishing the Diversity and Inclusiveness (D&I) advisory group and the Women in IR (WIR) section—both of which bring a powerful diverse voice to SIR’s leadership—the society and SIR Foundation offer a variety of grant programmes for medical students from diverse backgrounds to participate in clerkships that fund research by women and underrepresented minorities, and that fund the establishment and validation of programmes that aim to diversify the workforce. We also established a Speakers Bureau to ensure meeting planners have access to IR experts from underrepresented groups.
What strategies have been identified as essential to recalibrate any systemic imbalances within medicine and IR?
The formation of active diversity, equity, and inclusion committees and boards in institutions, both academic and private, is the first strategy. All specialties should have these incorporated. As this happens, specialties should come together in their efforts and strategies to recalibrate these systemic imbalances.
Workplace diversity (particularly of gender and race) is distinctly underrepresented in IR. Why do you think this is, and what actions is SIR taking to engage with this issue?
One of the biggest challenges facing IR is awareness of the specialty. For years, it was a subspecialty of radiology, and did not have that much exposure outside of radiology rotations. IR’s status as a primary specialty in the USA and its associated residency programmes are fairly new, but it is raising the profile of IR, which will hopefully help us recruit more people of diverse backgrounds into the specialty. The MATCH results are encouraging in that we remain among the most competitive specialties. We have routinely filled more than 98% of slots each year.
To help with recruitment among medical students, SIR’s D&I advisory group’s recruitment committee, in collaboration with SIR’s Residents, Fellows, and Students (RFS), WIR, and Association of Program Directors in Interventional Radiology (APDIR) sections, have been working to plan strategies related to ensuring that female and underrepresented minority medical students and undergraduates are aware of IR as a specialty option.
Through SIR Foundation, and a generous endowment from Alan Matsumoto and his family, we have issued grants to help people from underrepresented backgrounds participate in IR clerkships. The funding is critical to ensuring that those in various underrepresented groups are able to access the networking opportunities clerkships provide and be exposed to IR as a career path.
It will be some years before we train enough new interventional radiologists to build a truly diverse workforce, but in the meantime, we are working hard to raise the voices of those underrepresented in our workforce.
SIR has been collecting member demographic information for over five years; these data include gender and ethnicity, and cover all career stages, from medical student through to attending. The D&I advisory group has been reviewing this data as it relates to overall SIR membership, committee engagement, and speakers at its educational meetings, and is working to ensure that these posts and opportunities are accessible to people of diverse backgrounds.
Additionally, it is part of SIR’s strategic plan to conduct a study on the IR workforce, which will entail an overall look of the workforce trends and include insight on practice types, gender, and underrepresented minorities. This will further help us to tailor programmes to ensure we are effectively including all voices and views in all SIR activities. All in all, it all stems from intentionality. Workplaces need to not check boxes; strategic plans should be in place to recruit diversity in gender and race and ensure inclusion.
Could you elaborate on the role of the Women in IR committee and the Diversity & Inclusion committee within SIR?
Together, the WIR section and D&I advisory group promote diversity of gender, race, and ethnicity within SIR. The two groups collaborate to increase the participation and visibility of women and underrepresented minorities (URM) in SIR, as well as fostering the growth and awareness of women and URM in IR. It is expected that these initiatives will enhance our specialty and strengthen our society.
How do you describe to others why a Diversity and Inclusiveness advisory group is needed?
The success of our mission as a society draws strength not just from the clinical expertise of our physicians, but from the diversity of their backgrounds and experiences as human beings in the world. An innovative, competitive IR workforce requires more than market competencies—it must also carry the power of innate, authentic human connection. As a specialised group of medical practitioners, the diversity of our members and the patients they treat every day is of utmost importance to the overall health of our specialty. SIR’s commitment to these principles must be active and consistent. Having a dedicated D&I advisory group comprised of members and committees that are working across the society helps to ensure that diversity and inclusiveness is an active, living part of SIR’s culture and its work.
SIR has a limited number of grants for women and physicians who are underrepresented in medicine. What has the impact of these schemes been to date?
SIR and SIR Foundation have launched several programmes to encourage students of diverse backgrounds to enter into IR as their specialty. One of the key programmes, which I alluded to above, is the Grants for Education of Medical Students (GEMS), which was launched in 2019 thanks to the support of Alan Matsumoto and his family, as well as corporate partners. This scholarship programme allows up to 10 applicants from a variety of disadvantaged backgrounds to participate in an away clerkship rotation in IR.
Since its establishment in mid-2019, the GEMS programme has awarded seven medical students with US$10,500 in funding to participate in clerkships, and another US$7,000 in funding for travel to the SIR annual meeting, where they will be able to network with interventional radiologists and learn about the specialty. By the end of this year, we hope to increase that funding to US$16,500 and US$11,000, respectively. Due to the impact of COVID-19, the GEMS programme will be going virtual for a six-week course with a heavy health equity and diversity component. Each scholarship and travel stipend will still be paid out to the students for this year. In addition, the GEMS programme will also be issuing IR textbooks to the recipients and GEMS instructors from its endowment.
By the end of this year, the 2020 GEMS recipients will submit a Journal of Vascular and Interventional Radiology (JVIR) white paper outlining their vision for IR’s role in achieving healthcare and education justice moving forward as part of a group project during their GEMS curriculum.
In addition to this programme, SIR has an SIR Speakers Bureau, which aims to increase the visibility of URM and women nationally. The Speakers Bureau list is used to identify potential speakers for national and regional meetings, as well as invited guest speakers. Grants are available through the diversity and inclusion grant programme to defray the travel costs associated with speaking engagements.
How can SIR members help promote diversity and inclusivity in their own institutions?
Development of and/or involvement in diversity, equity, and inclusion committees in their own institutions is how SIR members can help promote diversity and inclusivity. The old saying of “it starts at home” cannot be truer for this endeavour.
In your opinion, how should a national society balance supporting the grassroots activism of its members with a top-down approach of implementing specific schemes and recommendations?
A national society should balance grassroots activism with a top-down approach by bridging the gap between both. While the grassroots efforts may be involved in producing resources to educate members and increase awareness, leadership of a national society should embrace, advocate, and support, in addition to incorporating them into all aspects of the society, leadership and executive committees not excluded. There needs to be representation at all levels. Pipeline programmes for underrepresented minorities and women should be established to get more representation in leadership and executive committees.
A world map showing the “huge disparity” between the number of UAEs and the number of uterine surgeries performed annually in Spain, France, Australia, and at one institution in El Salvador
“Unnecessary hysterectomies” could be avoided by involving interventional radiologists at gynaecology multidisciplinary team meetings and in the patient counselling process, Gregory Markris, Saqib Butt, and Tarun Sabharwal (all Guy’s and St Thomas’ Hospital, London, UK) write in a Letter to the Editor in Cardiovascular and Interventional Radiology (CVIR) Endovascular. UAE
Citing a 2019 article by Annefleur de Bruijn (Vrije Universiteit Amsterdam, Amsterdam, The Netherlands) and colleagues that concluded that adding uterine artery embolization (UAE) as a treatment option to the national Dutch guidelines did not change the number of performed UAEs for symptomatic fibroids, Makris et al claim: “Such low UAE rates are not isolated to The Netherlands”. As previously reported in this newspaper, approximately 145 UAEs are performed annually in Spain, a country with a population of over 44 million, and in France, there is an average of 2,000 UAEs performed each year, compared to 40,000 hysterectomies per annum. “This is concerning,” Markris et al opine, “especially in light of trial evidence showing that two thirds of women treated with UAE remain hysterectomy free at 10 years”.
Makris, Butt, and Sabharwall believe that promoting awareness of UAE amongst patients, and closer collaboration between interventional radiologists and gynaecologists, will help to raise the number of UAE patients. They say: “The interventional radiology community must continue to address the injustice of chronic underutilisation of this minimally invasive, safe, clinically and cost-effective procedure. Engaging with relevant stakeholders and lobbying at social and political levels is crucial for the success of this endeavour.”
The results of a randomised controlled trial—the Shunt simulation study—show that a new patient-specific computation model accurately calculated postoperative access flow. As flow is related to maturation, the authors argue that this model may potentially improve arteriovenous fistula (AVF) maturation rates.
Authors Niek Zonnebeld (Maastricht University, Maastricht, The Netherlands) and colleagues— on behalf of the Shunt simulation study group— add that further investigation is needed to improve the predictive power of these simulations in order to render the computational model an adjunct to surgical planning.
Writing in the July edition of the European Journal of Vascular and Endovascular Surgery (EJVES), Zonnebeld et al detail that an AVF needs to mature before it becomes suitable to cannulate for haemodialysis treatment, and that maturation depends on postoperative flow increase.
The authors highlight that AVF maturation remains a permanent issue in vascular access surgery for haemodialysis treatment, with 20–40% of AVFs failing to mature. To address this, they developed a patient-specific computational model that predicts immediate postoperative flow, and hypothesised that providing information from this model for planning of fistula creation might reduce failure rates. Zonnebeld and colleagues conducted a multicentre, randomised controlled trial in nine Dutch hospitals, in which they recruited patients with renal failure who were referred for AVF creation. Using 1:1 randomisation, they assigned patients to the control or computer simulation group. Both groups underwent a work up, with physical and duplex ultrasonography (DUS) examination.
In the simulation group, the data from the DUS examination were used for model simulations, and—based on the immediate postoperative flow prediction—the ideal AVF configuration was recommended.
Zonnebeld et al detail that the primary endpoint was AVF maturation defined as an AVF flow ≥500ml/min and a vein diameter of ≥4mm six weeks postoperatively. The secondary endpoint was model performance (i.e. comparisons between measured and predicted flows, and (multivariable) regression analysis for maturation probability with accompanying area under the receiver operator characteristic curve.
A total of 236 patients were randomly assigned (116 in the control and 120 in the simulation group), of whom 205 (100 and 105, respectively) were analysed for the primary endpoint.
The authors report in EJVES that there was no difference in failure to mature rates between the groups (29% and 32%, respectively). Immediate postoperative flow prediction had an odds ratio [OR] of 1.15 (1.06– 1.26; p<0.001) per 100ml/ min for maturation, and the accompanying operator characteristic curve was 0.67 (0.59–0.75).
Zonnebeld and colleagues recognise that the study has several limitations, including the fact that the primary endpoint was not a clinical one; it does not give any information on the functionality/usability of the AVF. However, they stress that it is an objective measure, and when patients reach the criteria of ≥500ml/min and a vein diameter of 4mm, as defined in this study, there is a 95% likelihood that the AVF will become functional.
Furthermore, to assess the vascular access functionality, the included patients should have initiated dialysis treatment. However, it remains very difficult to predict which and when a predialysis patient will progress to dialysis dependency and start haemodialysis. In the latter group of patients clinical AVF functionality cannot be determined.
Despite these limitations, the authors highlight the generalisable nature of their results, due to the fact that most of the (pre-)haemodialysis patients in need of an AVF were eligible for inclusion, and that the study was designed in such a way that it could be implemented easily in daily practice. In addition, DUS protocols were standardised to comply with the model’s demands. Usually, Dutch hospitals have well-equipped vascular laboratories with trained technicians who routinely perform preoperative DUS examination for AVF surgery.
Zonnebeld et al write that the multicentre design of the present study is a “major strength”, as it shows that the model can be implemented in other clinics. In addition, they note that selection of dialysis facilities for the multicentre study ensured a representative sample of the Dutch dialysis population, comparable with other European populations and studies. Compared with North American studies, however, they recognise that there is a considerably lower percentage of blacks included.
The authors summarise that simulating patient-specific immediate postoperative flows is an “innovative approach” to improve AVF maturation. “Since AVF maturation does not depend on blood flow enhancement through the anastomosed vessels exclusively, the predictive power of a single model was found to be insufficient to support clinical decision-making,” they write.
Looking to the future, the Shunt simulation study group speculate that incorporating the flow predictions in a hybrid model, in which other relevant but non-physical parameters or factors can be incorporated, might be beneficial.
The inaugural CX Aortic Vienna meeting will be livestreamed 8–11 September 2020 to an international, online audience, and will include registrant participation, interaction, and polling.
The programme will focus on all matters aortic—from the aortic valve to the iliac arteries. All known pathologies will be included, and imaging, diagnosis, and therapeutic options—open, endovascular, hybrid, and no intervention—will be applied to the length of the entire aorta, all the while keeping the patient front and centre. On each of the four days, the programme will cover abdominal and thoracic topics.
CX Aortic Vienna 2020 is brought to you with the participation of the Austrian Society of Vascular Surgery (ÖGG), the Italian Society of Vascular and Endovascular Surgery (SICVE), the Swiss Society for Vascular Surgery (SGG), and Aortic Surgery “HOW TO DO IT” (HTDI).
In the abdominal aortic section, there is an enduring fascination with the importance of diagnostic imaging modalities, as well as how to maintain endovascular aneurysm repair (EVAR) results, or instead turn to open repair. There will be dedicated discussion around open and endovascular choices to treat abdominal aortic aneurysm, with a focus on sac size and EVAR follow-up, ultrasound versus CT surveillance after EVAR, and current research into the best imaging modalities for EVAR. There is also a separate session on pathologies of the iliac vessels within the pelvis. In the juxtarenal section, the programme will explore methods to overcome the challenging aortic neck, using all manner of open and endovascular means.
In the thoracic aorta, there will be sections dedicated entirely to the aortic arch, and every aspect of dissecting aortic aneurysm, especially with regard to the timing of intervention. All treatment approaches will be considered and comparisons of open and endovascular methods made in a stepwise, methodical manner.
In the thoracoabdominal section, there remains obvious interest in spinal cord ischaemia and how to reduce the risk of this, with or without cerebrospinal fluid drainage.
In an important collaboration, the ÖGG will be joined by the SGG in the creation of a combined livestreamed programme. The SICVE will also have a livestreamed programme and HDTI will show Aortic Techniques & Technologies.
All about the aorta
Roger Greenhalgh (London, UK), the founding chair, explains the evolution of aortic management, contextualising the need for an aortic-specific educational meeting: “What I would like to know is the pathology behind any problems with the aorta. This might be very different: for example, with the ascending aorta, with the arch of the aorta, the great vessels to the brain and risk of stroke, the descending aorta—four different pathologies there, atherosclerosis, dissection, transection, and ulceration. How do you diagnose those, how do you image those, how do you know which is the best way to treat them in the first place?
“We still live in an era where it is possible for patients to be referred to one hospital and have an open operation for the aorta, and to another hospital and have an endovascular approach. It should not be right for it to dependent upon which hospital or specialist you get sent to, whether a patient should have endovascular or open. The patient should have the right treatment [speakers’ emphasis]. There should be discussions in centres on whether an open or an endovascular approach is best, it should not be a territorial matter. Let us encourage every patient to be considered with all options, and have an open mind about open surgery and endovascular.
A focus on decision-making in the patient’s interest
Roberto Chiesa (Milan, Italy) will be specially filming open and endovascular technical procedures of how to best manage the diseases of the arch of the aorta, considering whether to intervene or not based on the underlying pathology.
He will outline the importance of a forward-thinking, non-biased approach and running daily multidisciplinary meetings in the patient interest to decide which, if any, is the best treatment.
A comprehensive meeting on aortic therapies
Afshin Assadian (Vienna, Austria), the current president of the ÖGG, describes CX Aortic Vienna as a “comprehensive meeting on aortic therapies” taking in contributions from speakers covering a wide range of specialties.
Alexander Zimmermann (Zürich, Switzerland) comments that the livestream format will enable widespread participation, enabling all colleagues interested in vascular medicine “to participate and actively contribute to this event” easily, wherever they are in the world.
In octogenarians with chronic limb-threatening ischaemia (CLTI), researchers found a one-year mortality rate of 32% after revascularisation, which was significantly higher than in non-octogenarians. Amputation rates were comparable between both age groups.
The authors—Lina F Wübbeke (Maastricht University Medical Centre, Maastricht, The Netherlands), Barend ME Mees (Maastricht University Medical Centre, European Vascular Centre, Aachen-Maastricht, Germany, and European Vascular Centre, Maastricht, the Netherlands) and colleagues—comment that this mortality rate is “substantial”.
Writing in the European Journal of Vascular and Endovascular Surgery (EJVES), they remark: “This [outcome] is of major importance to clinical practice to inform patients and colleagues adequately during the decision-making process of any intervention in this fragile patient group.”
The authors do acknowledge, however, that only low-quality evidence could be obtained supporting the results of this meta-analysis, because only observational studies were available for inclusion. Therefore, they stress that the results should be “interpreted with caution”.
Discussing their methods, Wübbeke, Mees, and colleagues detail that two independent researchers searched systematically Medline, Embase, and Cochrane Library databases. Meta-analyses were performed to analyse one-year mortality, one-year major amputation, and one-year amputation-free survival (AFS) after revascularisation.
They specify that pooled outcome estimates were reported as percentages and odds ratio (OR) with 95% confidence intervals (CI). In addition, sensitivity and subgroup analyses were performed and the quality of evidence was determined according to the GRADE system.
Wübbeke, Mees et al write that the review includes 21 observational studies with patients who were treated for CLTI, and that a meta-analysis of 12 studies with a total of 17,118 patients was performed.
Writing in EJVES, the authors report that a mortality rate of 32% was found in octogenarians (95% CI 27–37%), which was almost double the mortality rate in the non-octogenarians (17%, 95% CI 11–22%/OR 2.52, 95% CI 1.93–3.29; GRADE: “low”).
They also state that no significant difference in amputation rate was found (octogenarians 15%, 95% CI 11–18%; non-octogenarians 12%, 95% CI 7–14%; GRADE: “very low”), and that amputation-free survival (AFS) was significantly lower in the octogenarian group (OR 1.55, 95% CI 1.03–2.43; GRADE: “very low”).
In a subgroup analysis differentiating between endovascular and surgical revascularisation, amputation rates were comparable, Wübbeke and colleagues detail. For octogenarians, those treated conservatively had a mortality rate significantly higher than those treated by revascularisation (OR 1.76, 95% CI 1.19–2.6; GRADE: “very low”). No significant difference in mortality rate was found between primary amputation and revascularisation in octogenarians (OR 0.7, 95% CI 0.24–2.03; GRADE: “very low”).
In the discussion of their findings, Wübbeke, Mees et al recognise that their study is limited by the weakness of the available evidence.
“No randomised controlled trials were available for inclusion,” they write, adding that 19 of the 21 studies were retrospective cohort studies, “increasing the risk of information bias”. They add that the current Global Vascular Guidelines on the Management of CLTI also stressed that high-quality data on ‘evidence-based revascularisation’ is limited.
Considering future research, Wübbeke, Mees et al recognise that additional studies are needed “to provide more solid results and to determine the optimal management of octogenarians with CLTI”. Moreover, they write that outcomes after revascularisation have to be compared with outcomes after conservative treatment or primary amputation and standardised study designs and endpoints should be used as promoted by the current Global Vascular Guidelines on the Management of CLTI.
Finally, they state that these results should also be used to develop adequate risk scores, enabling appropriate patient selection, and that quality of life studies should be performed to decide whether revascularisation interventions are always indicated in this group of frail patients.
Concept Medical has announced the enrolment of the first patient in the FUTURE BTK (Randomised controlled trial of first sirolimus coated balloon versus standard balloon angioplasty in the treatment of below-the-knee artery disease) trial. The index patient was successfully enrolled on 26 August 2020 in Singapore.
FUTURE BTK is a randomised, double-blind, placebo-controlled, multicentere trial. It is aimed at determining the effectiveness of MagicTouch PTA sirolimus-coated balloon versus standard balloon angioplasty for the treatment of below the knee arterial disease in chronic limb-threatening ischaemia (CLTI) patients.
Sirolimus-coated balloons are considered to be the next new generation of drug-coated balloons (DCBs), and MagicTouch PTA sirolimus-coated balloon offers a solution which optimises both the deliverability and the absorption of sirolimus into the vessel wall.
Edward Choke (Sengkang General Hospital, Singapore, Singapore), principal investigator of FUTURE-BTK comments: “CLTI is a condition which puts patients at an increased risk of limb amputation and death. Its burden is likely to grow in the coming years given the rising trends in key risk factors such as age and diabetes. Effective revascularisation is the cornerstone of treatment, but this is often hampered by high rates of restenosis and reintervention after conventional balloon angioplasty”.
He adds: “The novel MagicTouch PTA sirolimus-coated balloon has emerged as one of the most promising transcatheter technologies in preventing restenosis for below-the-knee lesions. The earlier data on the efficacy of MagicTouch PTA from small studies are encouraging but these need to be confirmed or refuted. I look forward to the FUTURE BTK randomised controlled trial, which will test whether the MagicTouch PTA sirolimus-coated balloon can improve the patency of below-the-knee arteries in CLTI patients, and this will hopefully bring us closer to our goal of reducing leg amputations”.
The trial will enrol 210 patients with Rutherford class 4 to 6 CLTI. These subjects will be randomised in 2:1 fashion to receive either MagicTouch PTA or standard balloon angioplasty. Primary outcome will be primary patency at six months, defined as duplex peak systolic velocity ratio (PSVR) of 2.4 or less.
The trial is designed to follow a rigorous blinding protocol in order to minimise bias. Patients, care providers, investigators, and outcome assessors, including vascular technologists performing the duplex ultrasound, will be blinded to the treatment allocations. The patients will be followed up for two years.
Royal Philips today announced that it has signed an agreement to acquire Intact Vascular. According to a press release, Intact Vascular will enhance Philips’ image-guided therapy portfolio, combining Philips’ interventional imaging platform and diagnostic and therapeutic devices with Intact Vascular’s unique, specialised implantable device to optimise the treatment of patients with peripheral arterial disease (PAD).
“Acquiring Intact Vascular will expand our portfolio of minimally invasive therapy options for PAD with the Tack endovascular system, a much needed implant that effectively restores blood flow in small limb vessels, promotes healing and preserves limbs,” said Chris Landon, senior vice president and general manager Image Guided Therapy Devices at Philips. “Through the integration of our interventional imaging systems and diagnostic and therapeutic devices, we will be able to provide clinicians with a complete procedural solution to optimise the treatment of patients with this disease.”
Philips’ peripheral vascular portfolio already includes advanced interventional imaging systems for precision guidance; intravascular ultrasound (IVUS) catheters to assess the location of the disease and lesion morphology and guide and confirm the treatment; peripheral atherectomy devices to remove blockages; and peripheral therapy devices, such as Philips’ Stellarex drug-coated balloon, to treat lesions.
Intact Vascular will strengthen this portfolio with the Tack endovascular system, which reinforces standard and drug-coated balloon PAD treatment results. Intact Vascular’s Tack implant is a first-of-its-kind, minimal-metal, dissection repair device that provides precision treatment of peripheral arterial dissections following balloon angioplasty in above-the-knee (ATK) and below-the-knee (BTK) therapeutic interventions. The Tack implant leaves less metal behind compared to stents, preserving future treatment options and ultimately preserving limbs. Moreover, Intact Vascular’s Tack implant offers a solution for repairing dissections and optimising post-angioplasty outcomes in the challenging chronic limb-threatening ischaemia (CLTI) patient population.
“We are excited about the strategic fit between our team, expertise and unique therapeutic device, and Philips’ Image-Guided Therapy business,” said Bruce Shook, president and CEO of Intact Vascular. “We share the same vision of complete procedural solutions to improve existing procedures and expand treatment options. We look forward to completing the transaction and working closely with Philips on a seamless transition.”
The transaction, which is subject to customary closing conditions, is expected to be completed in the third quarter of 2020. Philips will acquire Intact Vascular for an upfront cash consideration of US$275 million, and deferred payments for which the company expects to recognise a provision of US$85 million upon completion of the transaction.
Sirtex Medical reports that enrollment in the US RESiN registry has reached a milestone of 1,650 patients and 12.8 months of follow-up, allowing for a satisfactory number of patients enrolled for meaningful data analysis.
Under the leadership and direction of Daniel Brown and the trial’s executive committee, the registry will close enrollment at the 45 centres and will move to a new phase of data review and evaluation, publication, and presentation. The US RESiN registry, a database of patients eligible for treatment with SIR-Spheres Y-90 resin microspheres (Sirtex), started enrollment in 2015 and represents one of the largest prospective, multicentre, observational studies conducted in interventional radiology and the field of interventional oncology.
The registry should provide robust real-world evidence to characterise the effectiveness, safety, and clinical impact of SIR-Spheres Y-90 resin microspheres, a Sirtex press release states. To date, the RESiN registry has yielded several publications, including oral and poster presentations at international medical oncology and interventional radiology congresses, as well as a recent submission of “Incidence and risk factors for sustained hepatic function toxicity six months after Y-90 radioembolization: Interim analysis of the radiation-emitting SIR-spheres in non-resectable liver tumour (RESIN) registry.”
“I am extremely grateful to Sirtex for their support. Their commitment to developing and maintaining this first-of-its-kind interventional oncology registry has been unwavering over the five years of the study,” comments Brown, vice-chair of Innovation and Clinical Research, and chief of Interventional Oncology at Vanderbilt University Medical Center, Nashville, USA. “As this phase of the project winds down, I am looking forward to future collaborations with Sirtex to advance the data, science, and knowledge around patients treated with SIR-Spheres Y-90 resin microspheres.”
With completed enrollment, Sirtex and Vanderbilt will focus efforts to expand the number of publications arising from this data base and topic areas of interest, such as an assessment of different pre-treatment planning dosimetry methods, orphan tumour outcomes, and specific cohorts of interest.
As of August 2020, corresponding authors from more than 750 German universities and research institutions are able to publish in Cardiovascular and Interventional Radiology (CVIR) Endovascular free of charge thanks to a deal Springer Nature has signed with these German research institutions.
An explanatory statement on the Springer Nature website reads: “If you are a corresponding author affiliated with a German university or research institution, you are entitled to publish open access in our journals with fees covered by the German DEAL agreement.
“More than 900 German institutions are eligible to participate in the agreement between Springer Nature and Projekt DEAL, meaning that corresponding authors affiliated with these institutions are eligible to publish their articles open access without being invoiced by Springer Nature. The agreement includes more than 2,000 hybrid journals across the Springer Nature portfolio (from January 2020) and more than 500 fully OA journals (from August 2020).” CVIR
Sirtex Medical has announced a collaboration with Magle Chemoswed, a Sweden-based contract development and manufacturing organisation.
The development and commercial agreement grants Sirtex global use of Magle Chemoswed’s technology to develop a novel imaging agent for use in interventional oncology. Sirtex will have the exclusive license and commercialisation rights in the defined field of use. Magle Chemoswed maintains rights to its technology platform and to exclusively manufacture the product for supply to Sirtex. The development programme will begin in the third financial quarter of 2020.
“Our partnership with Magle Chemoswed marks an important step in our company growth, portfolio expansion, and investment in patient-centered care worldwide,” says Kevin R Smith, Chief Executive Officer (CEO) of Sirtex. “We are honoured to utilise this technology platform to advance innovative therapies for patients.”
“This is an incredibly exciting collaboration with a recognised global leader in the industry. Sirtex will be able to nimbly move the project from development to regulatory approvals and commercialisation, and we look forward to working closely with their team for optimal success,” says Justin Pierce, Magle Chemoswed’s CEO.
“We are thrilled to begin the collaborative programme with Magle Chemoswed to combine our resources and expertise,” says Mark Turco, Global Chief Medical Officer and EVP, Research and Development of Sirtex. “This technology will open the door to new product development opportunities for optimal patient care.”
The European Conference on Interventional Oncology (ECIO), hosted by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) have announced that their November meeting will no longer take place as a physical event. CIRSE says that, in order to provide continuing education in interventional oncology, a series of webinars will be taking place between November 2020 and February 2021.
In full, the letter from ECIO scientific programme committee (SPC) chairperson Alban Denys (CHUV University Hospital, Lausanne, Switzerland) and ECIO SPC deputy chairperson Philippe Pereira (SLK-Kliniken GmbH, Heilbronn, Germany) reads:
“We would like to update you on ECIO and how we are planning to proceed in light of the ongoing COVID-19 pandemic. As you all know, in the spring we had to postpone ECIO 2020 to November. At that time, we were hopeful that we could meet again in the fall to discuss the latest data and share our experience with a community that we have all come to appreciate so much.
“Unfortunately, COVID-19 is still far from being contained and the uncertainty involved in planning a major in-person event at this point has given us no choice but to take the difficult decision that ECIO 2020 will not take place as a physical meeting. It is with heavy hearts that we have to make this announcement, not only as physicians keen to push our specialty, but also as colleagues and friends looking forward to meeting you again soon in person.
“However, we are hopeful that ECIO 2021 will take place as planned from April 11–14 in Stockholm.”
In an entirely new endeavour for Yttrium-90 (Y-90) radioembolization, investigators from Northwestern University, Chicago, USA, have used the technique for the treatment of prostate cancer. “This is a new use for radioembolization, and an entirely new, more targeted treatment for prostate cancer,” Sam Mouli, who is leading the research group, tells Interventional News.
Sandeep Bagla (Prostate Centers USA and Vascular Interventional Partners NOVA, Falls Church, USA), course director of the STREAM meeting, which focuses on research at the vanguard of prostatic artery embolization (PAE) and musculoskeletal embolization, says of this novel use of Y-90: “It is the most cutting edge application of embolization going on right now, with extensive future long-term potential.”
The research team, led by Sam Mouli, set out to examine the potential role of intra-arterial radiotherapy in the setting of a large prostate and prostate cancer. “Radiotherapy has been a cornerstone of treatment for locally advanced prostate cancer for the last 30 years,” Mouli explains. “Despite several advances in the understanding and treatment of prostate cancer over this time, current therapies continue to be limited by significant toxicities, including risks of urinary, bowel, and erectile dysfunction following treatment. Patients continue to seek novel therapies that not only provide oncologic benefit, but also maximise quality of life.
“We posited that we could use our experience with Y-90 radioembolization in the treatment of liver cancer, and adapt it to what we have learned from our PAE programme.”
Prostate gland shrunk in early animal testing
The research team utilised the same canine model that they had initially used to study PAE, this time investigating the potential role of Y-90 radioembolization for the treatment of prostate cancer in a dose escalation study. They specifically looked into radiation changes to the prostatic tissues, as well as the effects of radiation on surrounding organs, such as the bladder and rectum, in addition to the erectile nerves, vasculature, and soft tissues.
Mouli describes the thought processes underpinning this early study: “External beam radiotherapy and transperineal brachytherapy are limited by nontarget radiation delivered to tissues surrounding the prostate, which is the source of the adverse event profile seen with current therapies. We hypothesised that targeted intra-arterial delivery of Y-90 microspheres could mitigate these off-target effects, while still delivering high-dose radiotherapy to the prostatic tissues.”
Utilising the techniques learned from both PAE for benign prostatic hyperplasia (BPH), and Y-90 radioembolization for liver malignancies, half of the prostates of the 14 animals included in the pr-clinical feasibility study were treated with Y-90 radioembolization, while the untreated contralateral sides were used as the control.
In this cohort, imaging follow-up performed at specific time-intervals demonstrated prostate gland size reduction in a dose-dependent fashion starting at two weeks’ post-embolization, continuing to three months post therapy. There were no clinical adverse events throughout the follow-up period. In addition, the investigators report no evidence of nontarget embolization or of any radiation damage to the surrounding bladder, rectum, and erectile tissues on MRI and pathologic analysis.
Expounding on the perceived importance of these early data, Mouli enthuses: “By demonstrating feasibility and safety in this model, we have shown that Y-90 microspheres can be safely delivered to prostatic tissues delivering highly targeted radiation without the off-target damage seen with current approaches. Additionally, given the radio-isotope characteristics of Y-90, this potentially offers a single-stage treatment option for patients. Current radiotherapy often requires multiple treatments over several weeks to deliver radiation safely.
Radioembolization tailored to treat the radiosensitive prostate
Radiation is a standard of care therapy for prostate cancer. However, Mouli says, current radiotherapy approaches are challenged by technical considerations, such as limited dosing due to the proximity of surrounding structures, and difficulty of brachytherapy seed placement in larger glands. He believes that radioembolization can overcome these limitations, while also delivering higher therapeutic doses with minimal off-target effects.
“Our initial results have been incredibly promising,” he comments, “demonstrating both feasibility and safety in an animal model. Of note, explant analysis demonstrated no radiation injury or scarring to adjacent tissue, and validated the initial hypothesis of using radiotherapy delivered trans-arterially: it maximises delivery to the gland and minimises non-target radiation. Our next step would be preparing a clinical study in men with unresectable, locally advanced prostate cancer in 2021. Similar to the current paradigm for Y-90 radioembolization, treatment volume-based dosimetry would be utilised to determine radiation dosing.”
However, Mouli also cautions that investigating new therapeutic options can be challenging: “The bar is very high when comparing to the standard of care,” he says. “Once demonstrating safety and feasibility pre-clinically, clinical translation requires collaboration between various medical specialties as well as industry support. Northwestern University is a highly collaborative enterprise, and we have a strong relationship with Boston Scientific, the sponsors of our Y-90 study. We will work together to move this therapy forward through the next phases of clinical trial testing.”
The future of embolization: “The field is advanced”
Mouli and Bagla belong to a generation of interventional radiologists enthusiastic about the potential of embolization in several guises. Mouli expands: “As interventional radiologists interested in advancing the science, we are always looking for ways to expand areas of clinical success into other organs. What 20 years of radioembolization research has shown is that the traditional dogmatic thinking of radiation dose limits no longer holds when radiotherapy is performed trans-arterially. It turns out that with microcatheter technique, 3D imaging, and proper patient selection, in fact doses much higher than can be delivered externally can be delivered to organs safely, in a single-setting. This is now being demonstrated by our current canine model, has been used in the kidney, spleen and, soon, in the brain. The radioembolization platform is quite simple to use, and when combined with modern imaging and contemporary state-of-the-art techniques, the field is advanced. Ultimately, the patients benefit.”
Julius Chapiro and Lynn Savic claim there is “no need for scepticism” about the recent emergence and growth of immuno-oncology from an interventional oncologists’ perspective. Indeed, they write that interventional oncology (IO) will thrive in this new research environment, and say that combinations of loco-regional therapies and immunotherapies are just now being trialled that may yet transform cancer care whilst centring the skills and clinical expertise of interventional oncologists.
Interventional Oncology (IO) brands itself as the fourth pillar of cancer care alongside medical, surgical, and radiation oncology. Across the board, IO is now the fastest growing sub-specialty in interventional radiology (IR) and certainly understands itself as the flag bearer of our entire field. The vast majority of National Institute of Health (NIH) funding for IR research supports IO science. The presence of an interventional oncologist at interdisciplinary tumour boards in every tertiary care centre has become the new normal. In fact, the rapidly growing IO culture—enhanced by our own society, the Society of Interventional Oncology (SIO)—can be seen as an organising principle among interventional radiologists that strive to abide by Charles Dotter’s everlasting legacy calling upon us to “provide clinical care” rather than practicing as “high-priced plumbers”.
Our dedication to curing cancer minimally invasively—one tumour at a time—and our involvement in patient care as clinicians rather than service providers was reinforced and invigorated during the COVID-19 pandemic. Precisely because of this level of maturity of our profession, there is no need for skepticism or concerns in light of the recent emergence of the “other IO”, immuno-oncology.
Without a doubt, novel immunotherapies transformed the way we approach cancer care. As such, five novel molecular targeted agents and their combinations have become available and US Food and Drug Administration (FDA)-approved for the use in advanced stage primary liver cancer within just roughly three years. While some in our community are overwhelmed and anxious in light of this rapid development, fearing replacement by the “other IO” in our key domain of liver-directed cancer therapies, the overall message remains reassuring: “our IO” will thrive in this new environment.
As the clinical trial data on immunotherapies in liver cancer continues to trickle in, we begin to realise that therapeutic outcomes in immunotherapy have not yet delivered upon the initial promise to make a substantial difference or even provide a cure. In fact, many in our community began to explore combinations of loco-regional and immunotherapy, and, meanwhile, numerous trials have been initiated to study this exciting new option.
While we eagerly await the first results from such prospective clinical trials, we must continue to do our homework in science and education. Historically, basic and translational research has been the Achilles’ heel of IR and this is especially true for the ethos of our professional training. The fellowship training model in IR was naturally focused on rapidly building up procedural hands-on skill in just 12 months of training by means of volume, frequently leaving no room to learn the “language of oncology”. Aware of its shortcomings, the generation before us wisely paved the way for a dedicated IR residency as the new training model. As such, we are now able to recruit trainees from a pool of medical students that have six years to make IR their professional identity, and interventional oncology their sub-specialty.
Therefore, and in order to succeed in this increasingly complex environment of advanced cancer care, we must substantially expand upon interventional oncology education and expect engagement in basic, translational, and clinical research from day one of training. Our interdisciplinary partners in tumour boards should sit across specialised peers with knowledge and profound understanding of tumour biology, disease staging, and clinical trial design when requesting our advice. We must therefore step up in those disciplines and offer more than just technical expertise on whether or not a tumour can be safely reached and targeted under image guidance. Formal oncologic training, increased participation in non-procedural patient care, shared therapeutic decision making, advice on expected outcome, and key opinion leadership in cutting edge research and guidelines must be the new hallmarks of our identity.
Consequently, we must leave behind our anxious heritage as proceduralists and no longer engage in meaningless conversations about “takeover” of our procedures by “competing” specialties. The future of cancer care lies in teamwork and it is time for us to recognise our qualitative edge and expand upon our expertise beyond a set of hands-on skills that can be easily learned by anyone with interest and access to equipment. Thus, we should define new role models in this rapidly evolving field and shift away from reverence and idolisation of procedural prowess as the final endpoint of career development.
Ultimately, the central task of our generation will be to establish formal interventional oncology training as part of the IR residency curriculum, and possibly even offer a formal IO fellowship for sub-specialisation. With that in mind, we will continue to strengthen our role as the fourth pillar of cancer care with content and substance to ensure a bright future of our specialty for the next generation of interventional oncologists.
Julius Chapiro is an assistant professor of Radiology and Biomedical Imaging, co-director of the Yale Interventional Oncology Research Lab, Department of Radiology and Biomedical Imaging, Yale University School of Medicine, New Haven, USA. Chapiro declares grants and research support from the Society of Interventional Oncology, Philips Healthcare, Boston Scientific, Guerbet, and the National Institutes of Health.
Lynn Savic is a diagnostic and interventional radiology resident and co-director of the Minimally Invasive Tumor Therapy Research Laboratory at the Charité University Hospital, Berlin, Germany. Savic has no disclosures.
A recent systematic review showed that randomised trials comparing different types of peripheral endovascular arterial intervention have a high level of heterogeneity in their antithrombotic regimens. It also revealed an increasing trend for use of dual antiplatelet therapy post intervention with no clear justification.
Authors Mahim I Qureshi (North Bristol NHS Trust and University of Bristol, Bristol, UK) and colleagues comment that this finding demonstrates a lack of standardisation and poor reporting of antithrombotic therapy in randomised controlled trials of endovascular intervention.
Writing in the July issue of the European Journal of Vascular and Endovascular Surgery (EJVES), they remark that antiplatelet therapy needs to be standardised in trials comparing endovascular technologies in order to reduce potential confounding.
Exploring this potential for confounding, they remark that dual antiplatelet therapy increases the major bleeding risk, which may contribute to late mortality if regimens were continued long term. “This is especially relevant in the current climate,” they comment, highlighting that the trials included in this systematic review contributed to the late mortality results attributed to paclitaxel.
Qureshi and colleagues say that while randomised trials of new devices for peripheral arterial endovascular intervention are published regularly, the evidence for which antiplatelet and/or anticoagulant (antithrombotic) therapy to use after an intervention is lacking.
The aim of this systematic review, therefore, was to examine the antithrombotic regimens in randomised trials for peripheral arterial endovascular intervention to understand choices made and trends with time or type of device.
Qureshi et al sourced information from the Medline, Embase, and Cochrane Library databases. They included randomised trials involving participants with peripheral arterial disease (PAD) undergoing any endovascular arterial intervention.
The investigators assessed trial methods to determine whether an antithrombotic protocol had been specified, its completeness, and the agent(s) prescribed. They classed antithrombotic therapy protocols as periprocedural, immediate post-procedural (up to 30 days following intervention), and maintenance post-procedural (therapy continuing beyond 30 days).
Qureshi and colleagues included 94 trials in the narrative synthesis. They note that study quality was low and that none of the trials justified their therapy protocol. Only 29% had complete periprocedural antithrombotic protocols, and 34% had complete post-procedural protocols.
The authors report in EJVES that antiplatelet monotherapy and unfractionated heparin were the most common regimen choices in the periprocedural setting, and dual antiplatelet therapy (55%) was most commonly utilised post procedure.
They write that over time there has been an increasing tendency to use dual therapy (p<0.001), which corresponds with the introduction of newer technologies and trials focused on below-the-knee interventions.
Qureshi et al’s results show that periprocedurally, aspirin remains the most widely adopted antiplatelet monotherapy, despite randomised evidence favouring clopidogrel. They note that reasons for this were unclear, but speculate that cost may be a factor as clopidogrel has only relatively recently come off patent. “There is the potential to reduce cardiovascular events periprocedurally by using clopidogrel in future trials,” they add.
In the discussion of their findings, the authors comment on potential bias in the randomised trials included in their study. They note that even though a formal meta-analysis could not be not performed, a risk of bias assessment was included as a marker of study quality. This showed a concerning amount of “unclear” bias such as detection bias and attrition bias, which can be compensated for by good trial design and follow-up.
Qureshi et al acknowledge that that their review has some limitations. They detail, for example, that it was impossible to tell whether some trials used antiplatelet agents alone in the periprocedural phase or whether they simply made no statement on heparin/anticoagulant use. They remark: “Because of this lack of clarity, it was impossible to confidently separate antiplatelet and anticoagulant use in these trials, which means some of the periprocedural regimens may not reflect ‘real-life’ practice during procedures.”
They emphasise also the strengths of their review, specifically its “all-encompassing search protocol” and “robust reporting of results,” but stress the need for an independent randomised trial specifically examining antiplatelet therapy following peripheral arterial endovascular intervention.
AngioDynamics has announced the enrolment of the first patient in the PATHFINDER I postmarket registry.
The PATHFINDER I registry is a pilot study to evaluate the safety and efficacy of the Auryon atherectomy system in the real-world treatment of de novo, restenotic, and in-stent restenosis (ISR) lesions in infrainguinal arteries of patients with peripheral arterial disease (PAD).
“We believe that the solid-state laser technology utilised in the Auryon system is the future of atherectomy treatment,” said Jim Clemmer, president and chief executive officer of AngioDynamics. “Providers are showing an eagerness to enrol patients in the study and treat patients with our game-changing technology. Their strong support of the PATHFINDER I registry, along with the enrolment of our first patient, represents a meaningful step toward achieving our shared goal of advancing the standard of care for patients with PAD and related conditions.”
Jason Yoho (Heart and Vascular Institute of Texas, New Braunfels, USA) enrolled the first PATHFINDER I registry patient, a 61-year-old woman with a past medical history of atrial fibrillation, hypertension, hyperlipidaemia, and prior myocardial infarction. She was initially evaluated for severe claudication at rest and was classified as Rutherford 5 (ischaemic ulceration not exceeding ulcers of the digits of the foot). A diagnostic angiography of her right leg revealed severely calcified and diseased anterior and posterior tibial arteries. She was treated with the Auryon atherectomy system.
“Thanks to the successful Auryon laser atherectomy procedure, which was performed in conjunction with balloon angioplasty, there is now excellent, rapid flow restored into the pedal arch. In this case of severely calcified and tortuous anatomy, other devices likely would not have been as successful,” said Yoho.
“Having a passion for CLI [critical limb ischaemia] and limb salvage, my staff and I are eager to advance the body of knowledge around the Auryon atherectomy system through the PATHFINDER I registry. I am excited that AngioDynamics is dedicated to improving upon existing atherectomy technology and increasing the quality of care in the peripheral space. It is critical that we aggressively seek out and support promising new technologies, such as the Auryon system, so that we can provide patients with the best outcomes possible.”
The Auryon system is a proprietary solid state laser technology platform that is US Food and Drug Administration (FDA)-indicated for use in the treatment, including atherectomy, of infrainguinal stenoses and occlusions, including ISR, which is the gradual re-narrowing of the artery after a blockage has been previously treated with a stent. The Auryon system uses a 355nm wavelength laser platform which enables the use of longer wavelengths and shorter pulses to produce the groundbreaking delivery of short UV laser pulses. The Auryon system’s targeted biological reactions address the risk of perforation and preserve the ability to vaporise lesions without thermal damage.
Ten healthcare delivery sites in the USA are expected to participate in the PATHFINDER I registry, each of which is equipped with an Auryon system. Sites are located in Texas, Iowa, Arizona, New Jersey, and Florida. AngioDynamics expects a total of 100 eligible PAD patients to participate in the PATHFINDER I registry, which will track outcomes for patients for 24 months after treatment with the Auryon system.
The PATHFINDER I registry is structured as a prospective, non-randomised, single-arm, multicentre observational study that will evaluate the performance of the Auryon system during procedures and measure clinical outcomes, both intermediate and long-term. Initial findings from the pilot registry study will inform and help shape a subsequent larger registry that is expected to include approximately 1,000 patients.
Just-published six-month results of the IN.PACT AV Access study show that drug-coated balloon (DCB) angioplasty is superior to standard angioplasty for the treatment of stenotic lesions in dysfunctional haemodialysis arteriovenous fistulas (AVFs). Furthermore, it was found to be non-inferior with respect to access circuit-related serious adverse events within 30 days.
These results were published on 19 August in the New England Journal of Medicine (NEJM).
Robert Lookstein (Mount Sinai Health System, New York, USA) and colleagues note that long-term outcomes for standard percutaneous transluminal angioplasty (PTA)—the current recommended treatment for dysfunctional haemodialysis fistulas—are poor. DCBs delivering the antirestonotic agent paclitaxel may improve outcomes, they write.
In this prospective, single-blinded, 1:1 randomised trial, the investigators enrolled 330 participants across 29 sites in the USA, Japan, and New Zealand. Patients with new or restenotic lesions in native upper-extremity AVFs were eligible for participation.
After successful high-pressure PTA, participants were randomly assigned to receive treatment with either the IN.PACT AV drug-coated balloon (Medtronic) or a standard balloon.
Lookstein and colleagues detail that the primary effectiveness endpoint was target-lesion primary patency, defined as freedom from clinically-driven target revascularisation or access-circuit thrombosis during the six months after the index procedure.
They assessed the primary safety endpoint—serious adverse events involving the arteriovenous access circuit within 30 days—in a noninferiority analysis (margin of noninferiority 7.5 percentage points).
Lookstein et al write that a total of 330 participants underwent randomisation, with 170 assigned to receive treatment with a DCB and 160 assigned to receive treatment with a standard balloon.
Writing in NEJM, the authors report that, during the six months after the index procedure, target-lesion primary patency was maintained more often in participants who had been treated with a DCB than in those who had been treated with a standard balloon (82.2% [125/152] vs. 59.5% [88/148]; difference in risk, 22.8 percentage points; 95% confidence interval [CI] 12.8–32.8; p<0.001).
In addition, they found that DCBs were noninferior to standard balloons with respect to the primary safety endpoint (4.2% [7/166] and 4.4% [7/158], respectively; difference in risk, -0.2 percentage points, 95% CI -5.5–5; p=0.002 for noninferiority).
In the NEJM paper, Lookstein et al detail that there has been a wide adoption of continuous haemodialysis through autologous AVFs. However, this has been associated with a high incidence of dysfunction caused by vascular stenosis within the fistula circuit, leading to inadequate haemodialysis.
Lookstein and colleagues acknowledge some limitations of the present study. For example, they note that the DCB has a different appearance than a standard balloon, which made a double-blind trial design “unfeasible”. In addition, the investigators recognise that further studies will be required to evaluate the safety and effectiveness of DCBs for the treatment of central vein obstruction, in-stent restenosis, or arteriovenous graft stenosis, as they investigated only lesions in AVFs.
“Improvements in patency could potentially have significant benefits for patients, leading to longer periods of successful and uninterrupted dialysis, as well as reducing the use of catheter-based dialysis and the substantial incidence of adverse events associated with this type of dialysis.”
Speaking to Vascular News, Lookstein commented on the clinical implications of the study: “We now have Level 1 evidence of a simple technology that is proven to be safe and effective at improving outcomes for patients with end-stage renal disease [ESKD] on haemodialysis.”
He continued: “This is the first US Food and Drug Administration [FDA]-approved paclitaxel-based device since the controversy last year, which is a testament not only to the incredible results seen in this trial, but also the significant needs of this population.”
A new study has found several racial disparities after mechanical thrombectomy for stroke with respect to post-procedure management and outcomes. Vineeth Thirunavu of Northwestern University Feinberg School of Medicine, Chicago, USA, presented the data at the Society of NeuroInterventional Surgery’s (SNIS) 17th Annual Meeting (4–7 August), which detailed key findings from the NVQI-QOD registry.
Specifically, Thirunavu explained that minority groups, including Hispanics, Asians, and African Americans, exhibited worse immediate post-procedural outcomes and a greater length of in-hospital and intensive care unit (ICU) stays.
“Race seems to be implicated in the length of treatment for acute ischaemic stroke,” he told the online audience. However, he said that the registry yielded an “interesting finding” in that in-hospital mortality for African Americans appears to be lower compared to their Caucasian counterparts. “This finding does not necessarily correlate with the findings that you would expect with longer length of stay and more ICU days.”
Discussing this finding further, Thirunavu added that in terms of outcome variables—modified Rankin scale (mRS) score and 90-day mRS—no difference in the rate of favourable outcome between races was observed, when excluding mRS scores of six.
Speculating as to why in-hospital mortality for African Americans was significantly lower, he said: “It could be a cultural thing, or not staying on the support of care, but we really have to do more research to see at what level these disparities are occurring at; is a patient level, a genetic level, or are healthcare providers treating patients differently?”.
Discussing the led the team to initially investigate racial disparities, Thirunavu said that since endovascular therapy has become the standard of care for stroke, research has focused on the disproportionate burden of stroke and cerebrovascular disease on African Americans. “Some studies have also looked into other minority groups […] but that research has focused on differences in the utilisation and access to mechanical thrombectomy; not a lot of research carried out has been on outcomes after mechanical thrombectomy, in terms of mRS scores or National Institutes of Health Stroke Scale [NIHSS] scores,” he added.
Therefore, according to Thirunavu, the current study utilised real-world evidence from the NVQI-QOD registry, enabling the team to study racial disparities in a large group of patients throughout the USA. In total, he reported that 3,261 patients from 23 US centres across 17 states, over a five year time period (January 2015–March 2020), were included.
He pointed to a slide displaying the population breakdown by race. It showed that 2,484 patients were Caucasian, 563 African American, 109 Hispanic, and 105 Asian. He admitted that there might be a slight underrepresentation of Hispanics in the cohort.
“We used a robust set of outcome variables; we were able to look up days to follow-up, and in-hospital mortality. In addition to the initial statistical analysis, we looked at regression models which controlled for demographics, comorbidities, intravenous tPA [tissue plasminogen activator] thrombolysis and pre-stroke functional measures,” Thirunavu explained.
However, he pointed to a particular caveat with the outcome variables, acknowledging that the registry contains some limited data. “Only 33% of patients that are alive at 90 days had mRS scores reported; two-thirds of the data are still up for grabs, and we do not know how those individuals faired,” he told viewers, and further emphasised that mRS, especially at 90-days, is an important outcome variable after mechanical thrombectomy.
In terms of moving forward with these findings, Thirunavu told the SNIS audience that time-to-event analyses need to be carried out. He noted that the NVQI registry has some data on this. “We also need to look into the relationship between sex and race, and think about how we can improve mRS data collection for registries, and have better outcome variables,” he concluded.
More than 15,000 professional delegates from 130 countries attended the virtual meeting, an increase of 5% compared with attendance at the virtual portion of ECR 2019. In addition, more than 2,000 people tuned in to the Imaging Interpretation Quiz, which was broadcasted live this year from Australia.
Furthermore, 216 companies exhibited at the meeting’s virtual exhibition, the ESR noted. Through the interactive experience, vendors could hold product demonstrations, host webinars, and invite attendees to visit their digital booths.
The meeting featured online educational, scientific, interactive, and industry-specific content, including more than 50 live sessions, and attendees could earn up to 28 continuing education credits. In a 21 July statement, congress president Boris Brkljačić (University of Zagreb School of Medicine, Zagreb, Croatia) deemed the virtual meeting a success.
“When we decided to convert ECR 2020 into an online-only congress, there was a lot of uncertainty about how this would look and whether it would still be possible to capture the magic of ECR in a digital format,” he stated in a press release. “After an incredible congress week, I am extremely pleased to say, there are no longer any doubts.”
Responding to the results of the FEMME (Fibroids with embolization or myomectomy to measure the effect on quality of life) trial, James Spies suggests that uterine artery embolization (UAE) is a favourable treatment option over myomectomy in many patients, as they take into consideration the recovery times and weigh up the benefits of having a minimally invasive procedure versus undergoing an open, operative one. “The important takeaway from the study is that both these treatments are highly effective and they produce comparable outcomes in this population,” he writes.
With the recent publishing of the FEMME trial outcomes in the New England Journal of Medicine,1 we gained additional insight into the outcomes of UAE, this time in a head-to-head comparison with myomectomy. Myomectomy has had growing acceptance in recent years as a first choice among surgical options for fibroids. Where myomectomy used to be limited to those who wished to have children in the future, there is a growing body of data suggesting that outcomes are similar to hysterectomy in women beyond their primary childbearing years,2 and it has been promoted by some in the gynaecology community as a preferred uterine-sparing treatment. It is in this context that we evaluate the FEMME study.
At first glance, some might be disappointed that the primary outcome from this study, the change in the quality of life score from the UFS QOL, showed a modest advantage for myomectomy, about eight points on a scale of 0 to 100. Higher scores on this scale reflect better quality of life. This was the primary conclusion reported in the abstract. However, when one looks closer some important points become clear. First, an eight-point difference is a modest difference at best, not reflecting a clinically important difference. As the authors note, the confidence interval suggests a range from no difference to a moderate 15-point difference.
The second important point is that, despite randomisation, the myomectomy group had lower baseline quality of life scores. This is a statistical aberration but with a direct impact on the primary outcome, which was the change in quality of life score. The final quality of life score was 80 for UAE patients and 84 for myomectomy patients, a minimal difference, below the threshold of what constitutes a clinically-important difference for this questionnaire.
A final point is that the more important measure on this questionnaire is the symptom score, which also showed a small, not clinically-important difference at six months in favor of myomectomy and no statistically significant difference at 12 months and two years. These findings confirm an earlier study using the same questionnaire comparing the outcomes of UAE, myomectomy, and hysterectomy with normal controls,3 in which myomectomy and UAE had similar quality of life and symptom scores.
So, the final scores are comparable, as were the safety and the limited fertility outcomes. The important takeaway from the study is that both these treatments are highly effective and they produce comparable outcomes in this population. When women choose a treatment for fibroids, they take a range of factors into consideration, including the outcomes mentioned, but also the time for recovery and time away from normal activities. In most cases, they will be comparing open operative myomectomy to a minimally invasive procedure, and many women are likely to believe that UAE is a better choice for them.
Having said that, the FEMME trial was not powered to address reproductive outcomes and, despite comparability in the very limited data presented, we cannot conclude that the reproductive outcomes are the same. There has only been one randomised trial reporting on reproductive outcomes of UAE versus myomectomy,4 and it showed an advantage for myomectomy. However, the data were not strong, and this lead the most recent Cochrane Review in 2012 to conclude that there was weak evidence favoring myomectomy over UAE for those seeking to become pregnant—to quote: “There was some indication that UAE may be associated with less favourable fertility outcomes than myomectomy, but it was very low quality evidence from a subgroup of a single study and should be regarded with extreme caution (live birth: odds ratio [OR], 0.26; 95% confidence interval [CI], 0.08–0.84; pregnancy: OR, 0.29; 95% CI, 0.10–0.85, one study, 66 women”.5
The FEMME trial investigators are to be congratulated on completing a randomised trial comparing these two therapies. The study has contributed significantly to our knowledge of these two therapies, demonstrating that the two procedures provide very similar outcomes and, while each patient’s circumstances are different, UAE should be considered whenever myomectomy is proposed.
James B Spies is an interventional radiologist at MedStar Georgetown University Hospital, Washington, DC, USA.
References:
Manyonda I, Belli AM, Lumsden MA, Moss J, McKinnon W, Middleton LJ, et al. Uterine-Artery Embolization or Myomectomy for Uterine Fibroids. N Engl J Med. 2020;383(5):440-51.
Wallace K, Zhang S, Thomas L, Stewart EA, Nicholson WK, Wegienka GR, et al. Comparative effectiveness of hysterectomy versus myomectomy on one-year health-related quality of life in women with uterine fibroids. Fertil Steril. 2020;113(3):618-26.
Spies J, Bradley L, Guido R, Maxwell GL, Levine BA, Coyne K. Outcomes for leiomyoma therapies: Comparison with normal controls. Obstet Gynecol. 2010;116:641-52.
Mara M, Maskova J, Fucikova Z, Kuzel D, Belsan T, Sosna O. Midterm clinical and first reproductive results of a randomized controlled trial comparing uterine fibroid embolization and myomectomy. Cardiovasc Intervent Radiol. 2008;31(1):73-85.
Gupta JK, Sinha A, Lumsden MA, Hickey M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst Rev. 2012;5:CD005073.
The Australian Medicare Services Advisory Committee (MSAC) has recommended restoring Medicare funding for vertebroplasty in patients with severely painful thoracolumbar fractures of less than three-weeks duration.
The MSAC is an independent, non-statutory committee established by the Australian Government Minister for Health in 1998. The body appraises new medical services proposed for public funding, and provides advice to government on whether a new medical service should be publicly funded (and, if so, under what circumstances) on an assessment of its comparative safety, clinical effectiveness, cost-effectiveness, and total cost, using the best available evidence. Interventional News has been informed by an Australian interventional radiologist that, following the MSAC recommendation, “It is now a formality that parliament will approve a Medicare item number for vertebroplasty”.
The MSAC recommendation comes after the Interventional Radiology Society of Australasia (IRSA) submitted an application to the Department of Health requesting the reinstatement of Medicare Benefits Schedule listing for vertebroplasty for severely painful osteoporotic thoracolumbar vertebral fractures of three-weeks duration or less in Australia, which was discussed at the 78th MSAC Meeting, on 3 April 2020.
MSAC’s advice to the Minister reads: “After considering the strength of the available evidence in relation to its safety, clinical effectiveness and cost-effectiveness, MSAC supported public funding for vertebroplasty for severely painful thoracolumbar osteoporotic fracture of three-weeks duration or less, as suggested during the MSAC Stakeholder Meeting on Vertebroplasty held on 7 June 2019. MSAC also advised that a prospective registry be developed to monitor this listing.”
Lead author of the VAPOUR trial (Vertebroplasty for Acute Painful Osteoporotic fractURes) William Clark (St George Private Hospital, Sydney, Australia) explains how the VAPOUR trial identified a subset of patients who benefit from the minimally invasive procedure, expanding on these ideas in a commentary for this newspaper how the VAPOUR trial results ultimately led to the reinstatement of Medicare funding in Australia.
Vertebroplasty is defined in the MSAC recommendation document as “A procedure in which acrylic cement is injected into a bone of the spine to treat a break (fracture) where the bone was already weakened due to osteoporosis, and where the break has resulted in pain and limited mobility affecting quality of life.”
“MSAC accepted that vertebroplasty has a benefit in a small population of patients by helping them regain their mobility sooner and reducing pain in the short term,” states the consumer summary. “However, MSAC noted that the cost-effectiveness of vertebroplasty is uncertain. MSAC also considered that the procedure might be used in patients for whom there is no evidence of any benefit. Therefore, MSAC advised that the use of vertebroplasty be limited to those patients with recent and severely painful fractures of a certain type and location. The Committee also suggested that this use is monitored through a registry for at least two years, so that information can be collected about who is receiving the treatment and the costs associated with that treatment. This will provide data that MSAC can review in the future to ensure that the procedure is being used appropriately according to these specified criteria.”
Vertebroplasty previously stripped of eligibility for Medicare funding: A timeline of events
Vertebroplasty was previously listed on the Medicare Benefits Schedule from 2005 to 2011 based on recommendation in the 2005 MSAC report. The interim item number was to be reassessed by 2010.
MSAC completed its second review in April 2011 and did not recommend continued public funding based on two randomised controlled trials, published together in the New England Journal of Medicine in 2009, that did not appear to support vertebroplasty.
An application for relisting vertebroplasty for severely painful osteoporotic vertebral fractures of less than six-weeks duration on the Medicare Benefits Schedule was submitted to MSAC after the results of the VAPOUR randomised controlled trial were published in The Lancet in 2016. The six-week limit for facture duration was later modified by consensus between MSAC and IRSA to three-weeks.
MSAC considered this application for relisting vertebroplasty in a November 2018 meeting, but did not support pubic funding for vertebroplasty due to the committee being “uncertain of its clinical significance”. They did, however, acknowledge that there may be “a small clinical benefit” from vertebroplasty.
In March 2019, MSAC again considered the application, but deferred its advice until a stakeholder meeting could be held, as the body believed this would “provide a broader clinical perspective and patient input, [and] could inform the uncertainties in the application”.
The June 2019 stakeholder meeting represented a turning-point for vertebroplasty advocates. In the publicly-available minutes of this meeting, it is noted: “One clinician commented that there is respect among his colleagues for the MSAC process. They feel it is fair and rigorous and prevents adoption of low value practice and wastage of health funding. However, there is some concern that the process is quite arduous, and the difficulty of obtaining the evidence required may discourage people from submitting applications for services that may be beneficial.
“The clinician suggested that MSAC needs to have procedural consistency in dealing with differences of opinion between professional groups. They commented that vertebroplasty is an established technique, and related that clinicians were achieving good results with it when it was previously funded. Clinicians were surprised when the 2009 randomised trials showed no benefit. The clinician commented that the VAPOUR trial compensated for problems in the early trials, and showed that with strict patient selection criteria, results can be positive. They expressed their disappointment that so far results of the VAPOUR trial had been combined with, and effectively ‘drowned out’ by, the other trials. Other clinicians agreed that there is no rationale for combining data from the VAPOUR trial for patients in the acute phase with data from other trials in patients with chronic fractures.”
Following the discussion at the stakeholder meeting, MSAC gave their funding recommendation.
Lead author of the VAPOUR trial (Vertebroplasty for Acute Painful Osteoporotic fractURes) William Clark discusses the recent history of Australian Medicare funding for vertebroplasty, detailing how the 2009 results of two negative trials resulted in the Medicare Services Advisory Committee (MSAC) pulling their financial backing of the procedure. He outlines how the VAPOUR trial identified a subset of patients who benefit from the minimally invasive procedure, and ultimately led to the reinstatement of Medicare funding nationally.
Our application for public funding of vertebroplasty in Australia was based on the VAPOUR trial. Medicare funding for vertebroplasty had been removed after two negative trials were published together in 2009. We felt that these trials had largely excluded the group of patients that we had been treating in Sydney—patients with severe pain and early fractures, especially hospitalised patients. We conducted the VAPOUR trial to gather evidence in this patient group and the trial showed positive benefits from vertebroplasty.
Consistent with the recent history of vertebroplasty debate, the Medicare Services Advisory Committee (MSAC) assessment was shrouded in controversy. The MSAC was torn between the positive evidence of VAPOUR, which was specific for this application, and the negative findings of the Cochrane vertebroplasty review. The situation was complicated by the first author of the Cochrane review being a committee member of the MSAC. Timing of the Cochrane review appeared designed to influence the MSAC assessment.
MSAC initially advised against funding vertebroplasty, citing negative findings of the Cochrane review. The Interventional Radiology Society of Australasia (IRSA) complained to the Australian government that the application had not received an impartial hearing and that the Cochrane review should have been excluded due to conflict of interest. VAPOUR authors have published a criticism that the Cochrane review misrepresented evidence from our trial.1
The MSAC agreed to reconsider the application and summoned a stakeholder meeting for vertebroplasty in June 2019, inviting additional input from a broader range of clinical, epidemiologic, and biostatistical experts. The consensus from this meeting supported public funding of vertebroplasty for a subgroup of patients with uncontrolled pain from acute thoracolumbar vertebral fractures of not more than three-weeks duration. This patient subgroup derived most benefit from vertebroplasty in the VAPOUR trial. It includes most of the patients who are hospitalised with osteoporotic spinal fracture pain.
Early vertebroplasty can reduce pain and the reliance on opiate analgesia, with its attendant negative side-effects (delirium and constipation), which so often complicate management of these patients. It can change the natural history of the fracture by restoring height and preventing further collapse while the fracture is still soft and pliable.
Two randomised trials have assessed vertebroplasty for patients with fractures of three weeks or less. Diamond and colleagues2 published findings of a sub-group analysis from the VAPOUR trial, looking at 93 patients (46 vertebroplasty, 47 placebo) who underwent an intervention within three-weeks of fracture. Yang and colleagues3 published an open label randomised trial of 107 patients (56 vertebroplasty, 51 control) for vertebroplasty performed within three-weeks of fracture. Both trials showed significantly better pain reduction in the vertebroplasty group and worse complications in the control group.
The authors of the VAPOUR trial are proud that we have helped identify a patient group likely to benefit from vertebroplasty. We encourage interventional radiologists to consider offering early vertebroplasty for patients with severe pain or immobility caused by osteoporotic vertebral fractures. Delay can mean missing the window of opportunity to change the natural history of the fracture to benefit these suffering patients.
William Clark is an interventional radiologist at St George Private Hospital, Sydney, Australia.
References
Clark W, Bird P, Diamond T, et al. The Cochrane vertebroplasty review misrepresented evidence for vertebroplasty with early intervention in severely affected patients. BMJ Evid Based Med. 2019
Diamond, T et al. Early vertebroplasty within three weeks of fracture for acute painful vertebral osteoporotic fractures: subgroup analysis of the VAPOUR trial and review of the literature. Eur Spine J. 2020
Yang EZ, Xu JG, Huang GZ, et al. Percutaneous vertebroplasty versus conservative treatment in aged patients with acute osteoporotic vertebral compression fractures. Spine 2016
ID3 Medical Belgium has announced the first two enrolments in the SUPERSURG study to investigate the safety and efficacy of Abbott’s Supera peripheral stent system versus surgical endarterectomy in treating patients with common femoral artery disease, with and without femoral bifurcation involvement.
The physician initiated, prospective, multicentre, randomised study is set to enrol 286 patients at 13 centres in four European countries (Belgium, Poland, the Netherlands, and the UK).
Patients will be stratified first based on three criteria: obesity, calcification, and femoral bifurcation involvement. After this stratification, consented patients will be 1:1 randomised in an open surgical or endovascular arm.
In addition to superior safety and non-inferior efficacy of the Supera peripheral stent system arm as primary endpoints, the study will also assess core lab-based angiographical outcomes post common femoral endarterectomy in a subcohort of 40 patients.
The principal investigator of the SUPERSURG study is Koen Deloose, head of the Department of Vascular Surgery at AZ Sint Blasius hospital in Dendermonde, Belgium, who performed the first two procedures (one open and one endo) in the trial.
“My enthusiasm about the use of the Supera peripheral stent system in the common femoral area was initiated by some case experiences at high risk for surgery with great longer-term follow-up,” comments Deloose in ID3 Medical’s announcement.
“Based on these findings, we set up the physician-initiated single-arm VMI-CFA trial,” Deloose continues. “The 12- and 24-months outcomes of this 100-patient cohort, presented at VIVA 2019, confirmed our initial enthusiasm with core lab-based primary patencies of 95% and 93%, respectively, and freedom from target lesion revascularisation (TLR) of 98% at two years (in press). As these results were very close to our surgical data, but with lower complication rates, the idea for a head-to-head randomisation between both treatment strategies, with the same stringent assessment methods was born. With a support grant from Abbott Vascular, we were able to launch this exciting project”.
Looking to the future, Deloose concludes: “Based on the outcome of this trial, I hope to be able to define subgroups of patients who are better treated with surgery, others with a minimal invasive Supera peripheral stent system implantation. I am convinced that there will be a place for both complementary strategies in the vascular future.”
In the EffPac trial, designed to compare a drug-coated and an uncoated balloon in the treatment of vascular occlusion in the femoropopliteal region, the drug-coated device proved to be superior. Additionally, the complete review of the study cohort two years after the intervention showed no increased mortality with the drug-coated balloon.
In cooperation with the Center for Clinical Studies, radiologists at Jena University Hospital, Jena, Germany, initiated an investigation to evaluate the efficiency of the Luminor paclitaxel drug-coated balloon catheter (iVascular) versus an uncoated balloon.
The success of the treatment was measured by the patient’s ability to walk and by ultrasound examinations of the vascular permeability in two follow-up examinations. This prospective, multicentre, randomised controlled trial enrolled a total of 171 participants at 11 centres throughout Germany.
Principal investigator of the EffPac trial Ulf Teichgräber (Jena University Hospital) summarises the result: “Compared to the control group, in the group treated with drug-coated balloon catheters, there was better vascular permeability and less tissue formation at the former constriction two years after the procedure.”
On behalf of the Federal Institute for Drugs and Medical Devices (BfArM) in Germany, the study authors re-checked the complete cohort with respect to morbidity and mortality. The reason for this was a meta-analysis of angioplasty studies published last year that warned of long-term increased mortality associated with paclitaxel-coated devices. This warning triggered discussions amongst experts, since subsequent analyses of patient-level data could not confirm the increased long-term risk.
According to a Jena University Hospital press release, a possible source of error in determining mortality rates is not considering patients who have not completed the entire follow-up programme. “Within the trials considered in the meta-analysis, these patients counted up to a quarter of the subjects. Their data are not included in the study result as if they had not participated at all. However, for mortality assessment, they have to be included. This happened for the first time in the EffPac trial: in the subsequent review, 167 patients were recorded, which represents almost the entire study cohort, thus preventing a misjudgement in comparing the groups,” the press release reads.
The review yielded no difference in the survival after two years between the groups treated with an uncoated balloon or with a paclitaxel-coated balloon. Teichgräber comments: “The mortality risk by drug-coated balloons turned out to be even lower than that shown in the original two-year results recently published. We could confirm angioplasty with paclitaxel-coated balloons to be a long-term successful and safe treatment option for intermittent claudication.”
The authors of this retrospective cohort study—Michael R Hall (The University of North Carolina at Chapel Hill, Chapel Hill, USA) et al—detail that there was no difference in outcomes between regional or general anaesthesia techniques in patients undergoing LEAMP, but add that further studies are needed to establish best practices in LEAMP procedures.
Hall et al emphasise the fact that major limb amputations are psychologically stressful and subject patients to perioperative cardiovascular risk. They note that up to 90% of major LEAMP are being performed under general anaesthesia, despite the fact that regional anaesthesia is an acceptable option in most cases.
The authors state that obtaining a better understanding of who would benefit from regional versus general anaesthesia could reduce complications and help to establish best evidence-based practice, and their hypothesis was that patients undergoing LEAMP with regional anaesthesia would have better postoperative outcomes than patients receiving general anaesthesia.
Hall and colleagues used the Vascular Quality Initiative (VQI) lower extremity amputation module to identify patients aged 18 or over who underwent LEAMP from 2013 to 2018.
They note that outcomes included 30-day incidence of major adverse cardiac events (MACE) and all-cause mortality, and used multivariate logistic regression modules to compute odds ratios (ORs) and 95% confidence intervals (CI). They analysed time to death using standard survival analysis.
Writing in EJVES, Hall et al detail that the final sample included 5,567 patients (median age: 65 years; 67% white, 65% male). They report that only 719 patients, representing 13% of the cohort, received regional anaesthesia. In addition, compared with patients undergoing general anaesthesia, patients in the regional group were older (67 vs. 65 years; p<0.001) and more likely to have diabetes (78% vs. 69%; p<0.001), end stage renal disease (26% vs. 18%; p<0.001), congestive heart failure (33% vs. 27%; p<0.01), and coronary artery disease (35% vs. 30%; p<0.01).
Hall and colleagues add that the overall incidence of MACE, death, and MACE or death was 5%, 6%, and 9%, respectively. In addition, there was no statistically significant difference by anaesthesia groups for MACE (OR 0.98, 95% CI 0.69–1.39) or mortality (hazard ratio [HR] 1.03, 95% CI 0.9–1.17).
According to Hall et al, this is the largest retrospective study analysing the outcomes for LEAMP using either regional or general anaesthesia. They note that other research using the National Surgical Quality Improvement Program (NSQIP) database demonstrated similar results, namely no difference in 30-day mortality or cardiac events, but was limited to above-knee amputations only and the majority of the regional anaesthesia used was spinal anaesthesia. “The present results parallel these studies while including regional nerve block techniques as well as all major LEAMP in the analysis,” they comment, which they add suggests acceptable short-term outcomes for all types of regional anaesthesia.
The authors recognise that physiological stress during and immediately after the major LEAMP operation may drive the postoperative outcomes regardless of anaesthetic approach and state that further study is warranted to determine whether regional anaesthesia can attenuate that stress by reducing the pain response during and after surgery.
Hall et al also acknowledge that the study is observational in nature and so the results do not imply causality, but instead describe the association between anaesthesia type and outcomes.
Commenting further on the study design, they concede that it made controlling for residual confounding impossible. “A randomised trial would be required to address this issue,” they remark.
Hall and colleagues end by stressing the many strengths of the methods they used. “The VQI represents a ‘real-world’ data source that provides a view of current outcomes in a large population of patients undergoing elective limb amputation,” they comment, and the findings “offer a critical insight into this highly complex, highly comorbid, and understudied population”.
The authors conclude that many patients are candidates for regional anaesthesia and this study “has shown that his method of anaesthesia is a reasonable alternative to general anaesthesia”.
A randomised controlled trial has found that clinical and patient-reported outcomes following radiofrequency ablation (RFA) of varicose veins without compression are no worse than with compression. Madu Onwudike (Manchester University NHS Foundation Trust, Manchester, UK) and colleagues conducted the study, which appeared as an Editor’s Choice paper in the July edition of the European Journal of Vascular and Endovascular Surgery (EJVES).
The authors detail that the target vein occlusion rate was not influenced by whether post-procedure compression was worn or not following RFA of varicose veins, where phlebectomies had not been performed adjunctively. Similarly, there was no evidence that quality of life (QoL) scores, patient satisfaction, and complications were inferior in the group that had no post-procedure compression.
Onwudike and colleagues write that post-procedure limb compression, hitherto routine following open varicose vein surgery, has been extended to endovenous procedures. “However,” they comment, “no robust evidence exists to support this practice”. Therefore, the investigators designed the present study to evaluate the clinical and patient-reported outcomes with and without post-procedure leg compression following RFA.
They note a few studies that raise doubts about the necessity for post-procedure compression, including a 2017 Annals of Vascular Surgery study by Ayo et al, which compared seven-day compression versus no compression and reported no difference in clinical (vein obliteration) and patient-reported outcomes (pain, ecchymosis, and QoL) following endovenous ablation. However, Onwudike et al’s study is the first to investigate the role of post-procedure compression where all the veins were exclusively ablated using RFA.
In this single-centre, prospective, non-inferiority randomised controlled trial, the investigators recruited adult patients into two groups: A (RFA with compression stockings for two weeks) and B: (RFA alone). The primary outcome was ultrasound determined target vein obliteration at 12 weeks. Secondary outcome measures included a QoL score (Aberdeen Varicose Vein Severity Score [AVSS] and Revised Venous Clinical Severity Score [RVCSS]), patient satisfaction, pain score, and complications.
In total, the investigators recruited 100 consecutive patients—51 to group A and 49 to group B—classified as clinical class C2–C6 of the Clinical-Etiological-Anatomical-Pathophysiological (CEAP) classification.
Onwudike and colleagues write in EJVES that, at 12 weeks, the occlusion rate of the target vein was similar in both groups at 98% (n=47) and 98% (n=45), respectively (p=1).
They also report that here was no statistically significant different in mean AVSS 6 vs. 5 (mean difference -1, 95% confidence interval [CI] -2–3, p=0.57) and mean RVCSS 3 vs. 4 (mean difference 1, 95% CI -1–2, p=0.46) scores at 12 weeks.
Finally, they observed comparable patient satisfaction scores (p=0.72) and pain score 2 vs. 2 (p=0.92) were achieved in both groups. Two patients in each group developed deep vein thrombosis at two-week follow-up (p=1 for above the knee and p=1 for below the knee).
In the discussion of their findings, Onwudike et al remark that the method of randomisation and the fact that both the chief investigator and the statistician were blinded to the allocated group reduced the risk of bias. In addition, the low dropout rate reduced the risk of type 2 error.
However, they also note some limitations. Firstly, Onwudike and colleagues recognise that the study is from a single centre and it only reports short-term results. “Long-term follow-up analysis may give further insight into differences in success rates based on compression therapy use,” they write.
Overall, while the authors “accept that the place or duration of compression post-RFA is far from settled,” they expect that this study will “contribute to development of the body of knowledge on the subject”.
Onwudike et al elaborate that, while earlier studies concentrated on the duration of compression, the present study and that of Ayo et al have moved the discussion on to answering the question of whether compression is required at all following RFA in situations where phlebectomies have not been performed. “This is consistent with a publication by the UK National Institute for Health and Care Excellent (NICE), which highlighted the knowledge gap in the role of compression following endothermal ablation,” they remark.
Furthermore, they note that this study is also a partial response to the European Society for Vascular Surgery (ESVS) guidelines, which recommend the need for further studies in this area. Onwudike and colleagues state that, if the present findings are confirmed by larger studies, “it is likely that the current recommendation of post-procedural compression for all cases of open surgery and endovenous superficial vein procedures will be revised”.
The authors summarise: “This trial supports the conclusion that the widely practised use of compression after RFA adds no clinical benefit for the patients.” However, they add that a much larger study, “preferably a multicentre trial,” may be required to confirm their findings.
In response to the COVID-19 pandemic, IR has taken a more prominent role in the hospital
Interventional radiology is “an operational and financial hedge” for hospitals during COVID-19, Mikin Patel (University of Arizona College of Medicine, Tucson, USA) and co-authors claim in Journal of Vascular and Interventional Radiology (JVIR).
“Under normal circumstances, interventional radiology (IR) efficiently cares for both inpatients and outpatients,” the authors note. “In response to the COVID-19 pandemic, IR has taken a more prominent role in the hospital, accounting for an increased share of both procedural volumes and gross charges at two academic medical centres [in the USA], the first with a total of 894 beds in Tucson, Arizona, and the second with 811 beds in Chicago, Illinois. This trend countered the observed, and notably opposite, trend towards a relative decrease in contribution from other prominent procedural services (surgery, cardiac catheterisation lab, and endoscopy).”
The JVIR report used aggregated departmental data from the two institutions studied to investigate procedural volume. At the start of the COVID-19 pandemic, the Centers for Medicare and Medicaid Services gave the recommendation that all elective surgeries, as well as all non-essential medical, surgical, and dental procedures, should be cancelled or delayed during the pandemic. Therefore, at both medical centres evaluated in this study, procedural volumes across the hospital decreased year-over-year (35% and 69%, respectively) in April 2020.
However, IR procedural volumes decreased by a much smaller amount (22% and 35%, respectively). Over the same time-frame, procedural volumes in surgery, cardiac catheterisation lab, and endoscopy decreased by a much larger proportion: -45%, -30%, and -40%, respectively, in the Tucson centre, and -72%, -56%, and -81%, respectively, in the Chicago hospital.
At the medical centre in Tucson, total gross procedural charges for the hospital decreased 40% year-over-year in April 2020, but IR charges had only decreased 20%. For surgery, this decrease was more stark, at 44%. Gross procedural charges in the catheterisation lab declined by 35%, and endoscopy charges were reduced by 43% in the same month.
“The data above demonstrate that, while other procedural services such as surgery, cardiac catheterisation lab, and endoscopy have suffered decreased procedural volume and charges, IR has filled the void,” Patel and colleagues write in their brief research letter. “The resultant increased disparity in work performed and charges generated should be recognised by hospital administration as a source of procedural revenue that is relatively spared. Furthermore, the work performed by IR during the pandemic likely provides value by contributing to patient discharges and length of stay metrics, however the authors acknowledge this would be difficult to quantify.”
They note that the majority of IR procedures took place in the outpatient setting in 2019, while most surgery and catheterisation lab procedures were performed on inpatients (56% and 60%, respectively). As the COVID-19 pandemic led to suspension of non-essential procedures, Patel et al say that resources were diverted towards inpatient care. “Paradoxically, IR pivoted from a predominantly outpatient-based practice to a service focused on hospital in patients, while services that were predominantly treating inpatients in 2019 decreased their role,” they relate.
Mikin V Patel
Speaking to Interventional News, Patel comments: “I do think that interventional radiology’s role in treating hospitalised patients will continue to grow whether or not we are under pandemic conditions. In the short term, the COVID-19 pandemic has exaggerated this trend. In the long term, I am optimistic the ‘new generation’ of interventional radiologists we have been training will push the advantages of IR therapies for patients.
“Ideally, hospitals will recognise the value IR brings in terms of efficacy, quality, and efficiency for patients. From the administrative perspective, it sometimes feels as if IR gets lumped in with the rest of radiology and is treated as a service to be ‘ordered’ by other physicians. It may be time for hospitals to start treating IR more like a surgical subspecialty, recognising the need for things like clinic space, scheduling support, and dedicated coders.”
“IR’s adaptation to the operational shocks of the COVID-19 pandemic was largely the result of two factors: efficiency in reconfiguring workflows and availability to treat patients,” the JVIR authors continue. “At both medical centres included in this report, IR departments promptly prepared for handling of COVID-19 patients by adding negative pressure air handling for IR suites, clearly assigning duties and personal protective equipment for staff, and establishing clear protocols on potentially aerosolising procedures requiring extra precautions. Notably, these changes took effect in IR before they were implemented in the operating rooms.”
In addition, interventional radiologists working at both institutions included in this study noted an increased number of consult requests for procedures which are traditionally areas of considerable overlap in scope of practice (central venous access, gastrostomy, nephrostomies, biopsies, and venous thromboembolism intervention). In many cases, other procedural services had rejected these consultations for lack of medical urgency, and IR was available and ready to treat these patients during the COVID-19 pandemic.
“The flexibility and motivation to accommodate the needs of the hospital are arguably core principles of IR which appear to be common across multiple institutions. During times of stress, these strengths allow IR to serve as an operational and financial hedge for ensuring the continued health of critically ill patients and burdened health systems,” they conclude.
Repeat prostatic artery embolization (PAE) is safe and effective for recurrence of lower urinary tract symptoms (LUTS) or acute urinary retention caused by benign prostatic hyperplasia (BPH), and may be used as a first-line treatment option. However, it has limited impact in patients who did not show a response to the initial embolization procedure. This is the conclusion presented by Nuno Costa (Saint Louis Hospital, Lisbon, Portugal) et al in their recent publication in Journal of Vascular and Interventional Radiology (JVIR).
The study investigators set out to evaluate the safety and efficacy of repeat PAE for LUTS caused by BPH, to define revascularisation patterns, and to establish predictors of outcome in larger cohort of treated patients. Costa and colleagues conducted a single-centre, retrospective study investigating 108 patients with BPH and clinical failure after PAE who then underwent repeat PAE between June 2009 and October 2018. Of these 108, 39 did not show a response to their initial PAE, and 69 had an initially favourable response in the first six months following PAE, but then experienced relapsing symptoms.
Clinical failure after initial PAE, as seen in the 39 non-responders, was defined as improvement in International Prostate Symptom Score (IPSS) after PAE of less than 25%, an IPSS after PAE of more than 15 points, no improvement in quality of life related to LUTS or a quality of life score greater than three points, acute urinary retention after PAE, and need for any additional medical or invasive therapy for LUTS.
The cumulative probability of clinical success at 12 months following repeat PAE was higher for patients who initially responded positively to embolization and were subsequently treated for a recurrence of initial symptoms than for patients who did not show a response at all to initial PAE: 56.7% versus 28.2%.
Indeed, for patients with symptom relapse after initial PAE, the clinical outcomes were comparable to those reported for PAE: mean IPSS improvement of 9.5 points, mean quality of life improvement of 1.3 points, and clinical success rates of 84% at one month, and more than 50% at mid-term and long-term follow-up appointments. Costa et al suggest that “these results may justify repeat PAE”.
They continue: “Of note, the subjective parameters of LUTS (IPSS/ quality of life scores) were not the only improvements noted after repeat PAE. Objective parameters such as prostate volume, postvoid residual volume, peak urinary flow [Qmax], and prostate-specific antigen level also showed significant improvements after repeat PAE.” They point out that the difference between non-responders and relapsers after repeat PAE were only observed in the IPSS/ quality of life analyses.
Tiago Bilhim
Speaking to Interventional News, Tiago Bilhim (Saint Louis Hospital, Lisbon, Portugal), a co-author of the JVIR paper, says: “This study is important because it is not uncommon to follow-up patients after PAE that still have residual LUTS and that may need additional treatments. These treatment options include medical management, surgery, and repeat PAE. In order to advise patients that still have LUTS after PAE about the best treatment options, one should have a clear idea on the potential outcomes from repeat PAE. We have previously shown [in a 2016 Radiology paper by Bilhim et al] that patient selection is important to improve outcomes.”
Up to 20% of PAE patients undergo repeat intervention after one year, with a minority of clinical failures occurring in patients who experience symptom relapse after initial improvement (80% of clinical failures never show any improvement post-procedurally, and are in the non-responders category of this study). By demonstrating the safety and efficacy of repeat PAE, the investigators hope that this clinical study sheds some light on the treatment options available for patients who are deemed clinical failures following embolization.
“The present study […] expands on the concept that not all patients respond to PAE the same way, and that patient selection plays a pivotal role in improving clinical outcomes,” the authors note. “Even with a technical success rate of 100% and a unilateral repeat PAE rate lower than 6% (similar between relapsers and non-responders), clinical outcomes in non-responders were inferior to those reported for PAE. Even though as many as 17% of patients who never showed a response to PAE may still exhibit clinical success 24 months after repeat PAE, the vast majority of these patients do not show improvement. Therefore, repeat PAE should probably be avoided in patients who do not show a response to initial PAE.”
Expanding on this idea, Bilhim tells this newspaper: “In this study, we prove once more that patient selection rather than PAE technique has a profound impact on outcomes. PAE is not a ‘perfect fit’ in all patients with LUTS and BPH, with up to 25% of clinical failures despite optimal technique. Correlation of clinical outcomes after PAE with prostate volume reduction are not clear, with many patients improving LUTS with minimum prostate volume reduction and vice-versa. We now know that patient factors play a role. A lot of studies exist nowadays looking at predictors of clinical outcome for PAE.”
Some identified predictors of clinical outcome listed by Bilhim include:
Baseline prostate volume—patients with a prostate volume <40cc have worse clinical outcomes. However, outcomes are not significantly different for patients with a prostate volume >40cc (including large or very large prostates). This means that larger prostates do not necessarily mean better outcomes. It is rather the other way around. Smaller prostates do worse after PAE.
Avoid pedunculated median lobes—avoid all prostates with a median lobe morphology that is taller than wide.
Patients under acute retention and large CG adenomas are good candidates—patients with prostate morphology with a central gland that is responsible for more than 50% of the whole prostate volume, with large central gland adenomas and those under acute urinary retention have very good outcomes with PAE.
Old patients—possible to have worse outcomes and more challenging PAE procedures
Patients with very severe baseline IPSS scores (>23 points) have a higher risk of clinical failure—PAE induces a mean IPSS reduction of 12–15 points. If your baseline is 30 points, this means that the probability of ending up with residual LUTS (>15 points) after PAE is very high. Again, this is important when counselling patients.
The embolization procedure
Patients were treated in an outpatient setting by a team of experienced interventional radiologists: two with nine years of experience with PAE each, one with four years experience, and one with one years experience. PAE was performed under local anaesthesia by a unilateral or bilateral femoral approach “wherever feasible”, the authors describe, stating that this was “usually through the right femoral artery”. In total, a unilateral femoral approach was used in 101 patients, and a bilateral approach in seven patients.
Embolization was performed with different embolic agents, including: non-spherical polyvinyl alcohol (PVA) particles (100–300μm), spherical PVA particles (Bead Block 100–300μm and 300–500μm; BTG International, London, UK), tris-acryl gelatin microspheres (Embosphere 100–300μm and 300–500μm; Merit Medical), and Polyzene-coated hydrogel microspheres (Embozene 250μm and 400μm; CeloNova, San Antonio, Texas).
Repeat PAE was considered more technically challenging than the initial embolization procedure: at 75 minutes (range: 20–120 minutes), the median procedure time of the repeat embolization was significantly higher versus initial PAE. Microspheres were used more often in repeat PAE procedures than the initial embolization, but Costa et al acknowledge that this “reflects a temporal trend rather than an intended method”.
There were no major complications. Among the 108 patients, 104 (96.3%) were discharged three to six hours after PAE, and the other four (3.7%) spent the night in the hospital and were discharged the next morning (18 hours later) per personal preference.
The endpoint of embolization was occlusion of all vessels to the prostate and reflux toward the prostatic artery. Embolization of at least one prostatic artery was considered a technically successful repeat PAE—repeat PAE was technically successful in all patients.
Endologix recently announced that it has received a CE mark for the Alto abdominal stent graft system.
“We are very excited to receive a CE mark for the Alto system, that has been achieved through a strong partnership and collaboration with our European notified body, NSAI ” commented Matt Thompson, chief medical officer of Endologix. “Alto will provide our physician partners and patients in the EU with a differentiated low profile endovascular treatment option designed to improve durability over traditional EVAR. In addition, with Alto, we anticipate observing improved short-term outcomes relative to the Ovation iX abdominal stent graft system (Ovation iX) as a result of the design and manufacturing changes incorporated into Alto. Lastly, CE mark of the Alto system is yet another critical milestone for Endologix as we seek to introduce a portfolio of devices to address the current unmet needs of endovascular aneurysm repair (EVAR).”
“Alto offers a highly differentiated endovascular treatment option to AAA patients and includes design features that we believe will enhance ease-of-use, improve acute outcomes and preserve the long-term durability associated with patient-specific anatomically adaptive sealing,” commented John Onopchenko, chief executive Officer of Endologix.
“We believe Alto, with its ultra-low profile and 7mm aortic neck length indication, will provide patients and physicians with an endograft capable of treating the highest proportion of patients within the indications for use of the device. As we continue with the global roll-out of the Alto system, which has commenced in the USA, Endologix is committed to investing in the highest levels of clinical evidence by initiating a head-to-head randomised controlled trial versus traditional undifferentiated EVAR grafts, with the intent of proving the superiority of Alto. Finally, with our recent announcement regarding our proposed transition to a private company, we are poised to meet the needs of our customers and the patients we proudly serve and fulfil our company mission.”
Surmodics recently announced it has received US Food and Drug Administration (FDA) 510(k) clearance for its Sublime radial access 0.014 rapid exchange (RX) percutaneous transluminal angioplasty (PTA) dilatation catheter.
According to a press release, the Sublime radial access 0.014 RX PTA catheter allows below-the-knee access through a transradial approach by providing the longest working length (250cm) on the market. Outer balloon diameters range from 2–4mm with balloon lengths between 20mm and 220mm. The product joins the previously cleared Sublime radial guide sheath within the company’s Sublime radial access platform and is designed to facilitate radial access for the treatment of above- or below-the-knee arteries.
“FDA 510(k) approval of the Sublime radial access 0.014 RX PTA dilation catheter is another step forward in our strategy to become a provider of whole-product vascular solutions through the design, development and manufacturing of highly differentiated products,” said Gary Maharaj, Surmodics president and CEO. “The continued expansion of our Sublime radial access platform demonstrates our commitment to developing the transradial peripheral market space through the introduction of longer, lower-profile devices that fill unmet physician and patient needs.”
Radial access offers many benefits relative to femoral access including reduced puncture site bleeding complications, earlier ambulation, reduced length of hospital stay, and lower healthcare costs. Although transradial access has become a mainstream technique in percutaneous coronary interventions (PCI), it has been less widely adopted in peripheral interventions due to the limited availability of purpose-designed access and therapeutic devices.
The Sublime 0.014 RX PTA dilatation catheter is compatible with a 5Fr guide sheath and is designed to provide the performance of an over-the-wire PTA catheter in an RX platform. Its proprietary reinforced shaft technology with flexible, kink-resistant construction and a tapered RX port transition are designed for optimal trackability and push through distal tortuosity.
A new post-market study investigating the effectiveness of the Renzan peripheral stent system (Terumo) in patients with peripheral arterial disease (PAD) has been initiated. PRIZER
The PRIZER (Prospective, multicentre post-market, single-arm study, to confirm the performance of the Renzan peripheral stent system in treating subjects with superficial femoral and/or popliteal artery disease) study plans to enrol 135 patients, in approximately 10 European centres in five countries. Patients will be stratified into two groups: 90 patients with arterial disease in both the femoral and popliteal segments, and 45 patients with isolated popliteal artery disease.
The Renzan peripheral stent system consists of a self-expanding nitinol stent pre-mounted on the distal portion of a rapid exchange (RX) delivery catheter, constructed from two layers of tubular braided nitinol wire mesh.
As well as aiming to confirm the safety and efficacy of the Renzan peripheral stent system in treating patients with superficial femoral and/or popliteal artery disease, the PRIZER study aims to assess the primary patency of the artery evaluated at 12 months, compared to clinical results coming from other clinical trials using similar metallic scaffolds.
“My enthusiasm about the dual layer Roadsaver stent in the carotid field can be investigated in this way in the even more challenging infra-inguinal area”, comments Koen Deloose, head of Department of Vascular Surgery at AZ Sint Blasius Dendermonde hospital in Dendermonde, Belgium, and principal investigator of the PRIZER study. “In current times, where drug-eluting technology is only reserved for high risk patients and where the need for scaffolding post drug-coated balloon treatment is high, a lot of interventionalists are really looking for a ‘daily practice’ modern scaffold that is extremely flexible, well balanced in chronic outward force and radial resistive force, and easy to implant accurately. The new 018″-compatible nitinol braided Renzan stent with dual layer technology over the full length showed in some proof of concept cases to respond extremely well to all my expectations. The PRIZER study offers us the possibility to further investigate the safety and efficacy of the Renzan peripheral stent system for treatment of superficial femoral and/or popliteal artery disease in 135 patients”, Deloose continues.
“We are very proud to contribute to our commitment to physicians and their patients and drive innovation in the field of peripheral artery disease”, says Jim Rushworth, chief commercial officer, Terumo Global. “With this clinical trial, we explore initiatives to increase our footprint in peripheral interventions.”
“This new technology ensures a great flexibility, conformability to the vessel, and fracture resistance”, comments Christophe Giot, chief medical officer, Terumo Europe. “The PRIZER study aims to provide scientific evidence for RENZAN stent in patients suffering from peripheral arterial disease.”
Peripheral arterial disease affects more than 200 million people worldwide
PAD is a progressive disorder caused by atherosclerotic changes in the blood vessel wall, which result in stenosis or occlusion of the arteries outside the heart and brain. The pathology affects more than 200 million people worldwide. In the last decade, the number of PAD-affected individuals increased by 13% in high- and by 29% in low-income countries. The PAD prevalence increases with age, affecting over 20% of octogenarians. Lower extremity PAD is its most common subset. PAD is associated with high morbidity and both cardiovascular and all-cause mortality rates. The pathology causes major personal, medical, and socio-economic burden, increasingly becoming a global healthcare concern.
Cerus Endovascular and AB Medica, a subsidiary of Balt, has announced that they have entered into a strategic distribution agreement providing AB Medica with the exclusive rights to market and sell the newly CE marked Contour Neurovascular System and the Neqstent Coil Assisted Flow Diverter devices in Germany.
“Our partnership with Balt will provide significantly increased awareness and more rapid penetration of both the Contour Neurovascular System and the Neqstent device within Germany, the largest market within the European Union (EU),” stated Stephen Griffin, president of Cerus Endovascular.
“Physicians in Germany have indicated their desire for greater access to our products and have, therefore, been very supportive of our decision to partner locally with AB Medica. We are excited to begin working closely together and eventually, to extending the distribution agreement into other key EU countries.”
Thomas Liebig, professor at the Institute for Diagnostic and Interventional Neuroradiology at Ludwig-Maximillian’s Universität München (LMU) and principal investigator of the CERUS clinical trial of the Contour Neurovascular System, noted, “I am delighted with the progress that Cerus has made thus far in Germany. At LMU, we performed the first case with the system in Germany back in 2018 and have been using the device consistently since CE mark was granted.”
“Balt has a long history of delivering innovative devices to the hands of physicians. With this partnership with Cerus, we are happy to continue with this tradition and look forward to providing two new unique products to physicians in Germany,” said Pascal Girin, CEO of Balt.
A new system designed to deliver Yttrium-90 (Y-90) resin microspheres during targeted liver cancer therapies, SIROS (Sirtex) has launched commercially.
A company press release states: “SIROS offers a visual, intuitive and versatile option for interventional radiologists to deliver SIR-Spheres to patients with liver cancer. With the system’s visually-controlled administration, physicians can determine and adjust the precise quantity and speed of SIR-Spheres microspheres delivery. Additionally, the system is designed to be simple to use yet versatile enough to allow expanded options for patient-tailored delivery.”
SIROS’ design features a peel-and-place tubing set, a proprietary needleless D-Vial specifically designed to suspend SIR-Spheres into a vortex that may allow for a more even distribution, and a locking cover to safely secure the microspheres during delivery. A three-step setup provides quick and simple administration and disposal.
“SIROS brings world-class expertise and innovation together to provide interventional radiologists with the support and technology they need to treat patients with liver cancer,” says Kevin R Smith, chief executive officer of Sirtex.
Siemens Healthineers has announced it has reached an agreement to acquire Varian Medical Systems, a US company active in the area of cancer research and therapy, in an all-cash transaction valued at $16.4 billion.
The combined company will offer an integrated platform of end-to-end oncology solutions to address the entire continuum of cancer care, from screening and diagnosis to care delivery and post-treatment survivorship. By bringing together the diagnostic tools, imaging, radiotherapy and AI capabilities across both companies, Varian and Siemens Healthineers aim to lead the digital transformation of oncology healthcare, to enable more efficient diagnosis, increased treatment quality and access, personalised precision cancer care, the companies said in a press release.
Under the terms of the agreement, Siemens Healthineers will acquire all outstanding shares of Varian for $177.50 per share in cash, representing a premium of approximately 42% to the 30-day volume weighted average closing price of Varian’s common stock as of July 31, 2020, the last trading day prior to the announcement of the transaction, and a premium of approximately 24% to the closing price of Varian’s common stock on July 31, 2020.
“Today’s announcement represents an important milestone in our company’s history,” said Dow Wilson, president and chief executive officer of Varian. “The combination with Siemens Healthineers brings us even closer to realising our transformative vision of a world without fear of cancer.
Bernd Montag, CEO of Siemens Healthineers AG said: “With this combination of two leading companies we make two leaps in one step: A leap in the fight against cancer and a leap in our overall impact on healthcare.”
The transaction is expected to close in the first half of calendar year 2021, subject to approval by Varian shareholders, receipt of regulatory approvals and other customary closing conditions.
Varian expects to continue to operate under the Varian name as an independent company within Siemens Healthineers following the completion of the transaction.
“Decreases in caseload and widespread cancellation of conferences have had significant impact on diagnostic and interventional radiology (DR/IR) training during COVID-19 restrictions,” Ahmed M Gabr (Oregon Health and Science University, Portland, USA; Tanta University, Tanta, Egypt) and colleagues reflect in Academic Radiology. “Whether remote learning can mitigate lost opportunities from in-person interactions remains uncertain. Optimising these strategies will be important for potential future restricted learning paradigms and can also be extrapolated to augment trainee education during unrestricted times.”
The study investigators set out to assess the immediate impact of the COVID-19 pandemic on diagnostic and interventional radiology education, and to propose measures to preserve and augment trainee education during future crises. They reviewed DR and IR procedures at a single tertiary-care teaching institution between 2015 and 2020, dividing DR up by section (body, cardiothoracic, musculoskeletal, neuroradiology, nuclear medicine, paediatrics, women’s imaging) and IR by procedural types (arterial, venous, lymphatic, core, neuro, paediatrics, dialysis, cancer embolization or ablation, non-cancer embolization, portal hypertension, and miscellaneous).
In their review, they note that remote learning technologies with annotated case recording, boards-style case reviews, procedural simulation, and narrated live cases, as well as online lectures and virtual journal clubs, have increased over the last few months.
Highlight findings
DR and IR caseloads decreased significantly in April 2020 compared to the same month in the previous five years (both p<0.0001).
Case volumes were reduced in body (49.2%, p<0.01), musculoskeletal (54.2%, p<0.05), neuroradiology (39.3%, p<0.05), and women’s imaging (75.5%, p<0.05) in DR
Case volumes were down in arterial (62.6%, p<0.01), neuro IR (57.6%, p<0.01) and core IR (42.6%, p<0.05) in IR.
The average IR trainee caseload in April 2020 was 51.9% lower than the IR trainee caseload in April in any of the previous five years (p < 0.01).
Utilisation of online learning increased in April. Trainees saw significant increases in overall DR didactics (31.3%, p=0.02) and no reduction in IR didactics, all online.
Twelve major national and international DR and IR meetings were cancelled or postponed between March and July.
Results from a multicentre, randomised controlled trial—FEMME—published today in the New England Journal of Medicine (NEJM) indicate that myomectomy shows superior fibroid-related quality of life at two years compared to uterine artery embolization (UAE) in women with symptomatic uterine fibroids. Several prominent interventional radiologists suggest that while gynaecologists may use this headline finding to cease recommending UAE, the treatment is still a good therapeutic option in patients with symptomatic fibroids. They highlight that informed patient choice is at the heart of personalised fibroid therapy.
Isaac Manyonda (St George’s, University of London, London, UK) and colleagues’ publication coincides with fibroid awareness month. July 2020 has seen healthcare workers, hospitals, and other organisations promoting uterine health, shining a spotlight on an underexposed condition that one in three women will experience in their lifetime.
The triallists set out to compare the effect of UAE and myomectomy on quality of life in women with symptomatic fibroids wishing to avoid hysterectomy. The primary outcome measure of the FEMME trial (Fibroids with embolization or myomectomy to measure the effect on quality of life) was the condition-specific quality of life domain score from the Uterine Fibroid Symptom Quality of Life questionnaire (UFS-QOL). Scores could range from 0–100, with higher numbers indicating a better quality of life.
Average quality of life scores at two years were substantially improved in both groups, but were greater in those assigned to myomectomy (mean-adjusted difference using complete case analysis: eight points; 95% confidence interval [CI], 1.8–14.1; p=0.01; mean-adjusted difference with missing responses imputed: 6.5 points; 95% CI, 1.1–11.9). Mean quality of life score at two years from randomisation was 84.6±21.5 in the myomectomy cohort, versus 80±22 in the UAE group.
In total, 254 patients were recruited from 29 hospitals, and randomly assigned to undergo myomectomy or UAE as the primary procedure in a 1:1 ratio. Women were only eligible for enrolment if they were considered suitable for either procedure.
“The six- to eight-point benefit on average in health-related quality of life scores in the myomectomy group, as compared with the UAE group, is consistent with small to moderate standardised treatment benefit at two years,” the authors write. “However, the 95% confidence interval around these estimates indicates that plausible results range from almost no benefit of myomectomy over embolization to a moderate (15 point) difference.”
Despite the increased quality of life scores in the myomectomy cohort, several interventional radiologists, including two of the study co-authors, have expressed to Interventional News that UAE is still a good option for patients with symptomatic fibroids. Jonathan Moss (University of Glasgow, Glasgow, UK), a co-author of the NEJM study, comments: “Although the quality of life was higher in the myomectomy group and [this difference was] statistically significant, it was only a few points better. Therefore, provided women understand this, then they can choose either procedure.”
Fellow study author Anna-Maria Belli (St George’s University Hospital NHS Foundation Trust, London, UK) echoes this sentiment, telling this newspaper that “The results show a substantial benefit to treatment in both groups with regard to quality of life and symptom severity, even though the results for myomectomy were better than UAE.” However, she adds that she believes “The results do not mean UAE is an inferior treatment to myomectomy.
“With regard to menstrual blood loss, the results in both groups were comparable. This means that women should be offered either treatment and choose for themselves. For some women, avoiding a general anaesthetic, having a shorter hospital stay, and avoiding an open surgical procedure (the majority of myomectomies in FEMME were open abdominal as fibroid and uterine sizes were large) is of paramount importance, in which case UAE would be their preferred option.”
Gerard Goh (The Alfred Hospital, Melbourne, Australia) also enumerates the benefits of UAE: “Individualised medicine, i.e. tailoring treatment to the patient, is an important part of patient care and as interventional radiologists we are able to offer patients an alternative treatment to surgery. Even before the FEMME trial was published, we knew that there were some patients better-suited to myomectomy, and some better-suited to UAE. Some benefits of UAE are its ability to be performed under conscious sedation, as well as a shorter recovery time that may be better-suited to young women with busy family and work commitments.”
Contextualising the investigators’ decision to use UFS-QOL score as the primary outcome measure, Moss explains that quality of life measurements are “included in almost all randomised controlled trials [RCTs]”. Early UAE trials, such as REST and EMMY (from Scotland and The Netherlands, respectively) used the SF36 questionnaire, which Moss describes as a “generic quality of life instrument”.
Weighing in on the primary outcome measure of the FEMME trial, James Spies (MedStar Georgetown University Hospital, Washington, DC, USA) comments: “The primary outcome was the change in quality of life, and the quality of life scores of the myomectomy patients were worse at baseline than the UAE group, despite the randomisation. If one looks at final quality of life scores, they are very comparable within the sensitivity of the questionnaire used, but the study was designed to use the change in scores as the primary outcome [Spies’ emphasis]. Thus, somewhat artefactually, there was a greater improvement in quality of life scores for myomectomy. If one compares final quality of life scores or symptom scores, there would have been no difference.”
The authors acknowledge that the presence of some baseline differences in health-related quality of life and age between the two groups is a limitation of their analysis, but note that prespecified analyses were adjusted for the baseline health-related quality of life, and a post-hoc analysis adjusted for age showed similar findings.
Spies describes FEMME as “an important study, one of the very few randomised trials comparing myomectomy versus UAE. It shows very comparable outcomes of both procedures in terms of symptom control, quality of life, complications, and in the limited fertility outcomes. Overall, I congratulate the authors on completing an outstanding study, which validates UAE as an effective therapy that yields comparable outcomes in this population of patients.”
UAE and myomectomy result in comparable pregnancy rates, but numbers too small to call
In terms of fertility, there were no consistent differences between groups in the FEMME trial with regard to biomarkers of ovarian reserve. Nine women in the UAE group (8%) and five women in the myomectomy group (4%) reported pregnancies within two years of randomisation, resulting in six and four live births, respectively, the authors report. However, they note there are too few pregnancies amongst the trial cohort to inform the effects of the procedures on fertility.
Expounding on the clinical implications of the two-year results, Moss relates: “We found no evidence of ovarian damage using several markers after either procedure. The number of pregnancies was low in both groups. The pregnancy data is difficult to interpret, and the intention to treat (ITT) and per protocol analysis showed no difference [between the UAE and myomectomy groups]. Interestingly, if you look at the women who actually received UAE, there were slightly more pregnancies than in those who actually had myomectomy. However, the numbers are small, and one cannot draw any firm conclusions.”
Belli believes that an “important aspect” of the trial is that the results reveal “no adverse effect on ovarian reserve from UAE, which opens up the potential for further research in younger women wishing to become pregnant”. She notes that the average age was 40 in the trial, “so low pregnancy rates are not so surprising”.
Belli adds: “Also, this trial reflects the real population of women suffering from symptomatic fibroids, with a high proportion of black women and large fibroid uteruses (mean >1,000cc).”
“There is a surprising amount of resistance from the gynaecological community across the world about offering UAE to women who wish to maintain their fertility,” Moss opines. Prior to the FEMME trial, Moss outlines how “several smaller RCTs compared these two techniques, but the numbers were small and results conflicting. Some, such as FUME, had to exclude women wishing to become pregnant. FEMME overcomes most of these problems, even though the number of pregnancies is small, with limited data on that outcome.”
He further informs Interventional News that his research team are currently considering a large trial using pregnancy outcomes as the primary outcome measure, which they believe is needed. “It would have to be a trial of several thousand women, and probably an international effort,” he says.
Other secondary outcome measures similar in both groups
In addition to fertility, other secondary outcomes measures were similar for both myomectomy and UAE: menstrual bleeding scores, peri and postoperative complication rates, and the percentage of patients who would recommend their procedure to a friend.
Specifically, at two years, the percentage of women who would recommend myomectomy to a friend was 93%, versus 84% with UAE, while respective percentages of women who said they would have the procedure again were 78% and 74%.
Peri and postoperative complication rates for both procedures were low, Manyonda et al relate, with one conversion of a myomectomy to a hysterectomy, and one conversion from a laparoscopic to an open myomectomy. At six months post-procedure, 32 of 80 (40%) fibroids treated by embolization were completely infarcted. Peri and postoperative complications from all initial procedures occurred in 34 out of 118 patients (29%) in the myomectomy arm, and in 27 out of 113 patients (24%) in the UAE group (relative risk, 1.2; 95% CI, 0.8–1.9; p=0.4).
Furthermore, a “substantially” greater number of patients in the UAE group underwent additional procedures within two years of follow-up: 18 of the 110 patients with two-year data (16%), versus eight of the 111 women (7%) in the myomectomy cohort. “This observation may be explained in part by the lower quality of life reported in the UAE group,” Manyonda et al muse. “However, more hysterectomies were performed as the initial procedure in the myomectomy group, owing either to patient preference or clinical decision.”
Moss acknowledges that the higher re-intervention rate with UAE was “a little surprising, as both procedures preserve the uterus”.
However, UAE was associated with a shorter length of hospital stay: the median time spent in the hospital for an embolization patient was two days, compared with four days for a myomectomy patient.
Belli articulates her opinion of these findings: “We knew that UAE had a greater repeat treatment rate, but the complication rate is no different between the two treatments, even though the blood transfusion and haemorrhage rate was higher in the myomectomy group. I have always believed that getting rid of the large bulky fibroids [as with myomectomy] is ultimately more satisfying for women than simply returning menstrual function and other fibroid symptoms to normal. My happiest patients were the ones who had the largest reduction in bulk, despite counselling them that this was not the main aim of UAE.”
However, reflecting on the impact of these FEMME trial data, Belli adds: “I hope that the results of this trial will make gynaecologists more accepting of UAE as an alternative, and allow a larger trial to address pregnancy rates and outcomes to go ahead. Unfortunately, I am afraid some gynaecologists might simply read the headline result and use this to confirm their prejudices and not even offer UAE.”
Moss concurs, commenting that “trying to ‘open many closed minds’ was the largest barrier” to running this trial. “At times it felt like trying to persuade someone to change their religion,” he says, “so firmly held are some views. Triallists, however, must never give up, and having a strong team, like we did, is essential.
“My message on the results it that UAE has some advantages, such as avoiding an incision, a general anaesthetic, and more rapid recovery. In my view, it is for fully-informed patients to make their own choice.”
C-arm developer Ziehm Imaging has purchased imaging software developer Therenva.
The acquisition comes after two years of work together, Ziehm said. The purchase will allow Ziehm to market Therenva’s EndoSize and EndoNaut intraoperative 3D navigation software for catheterisation procedures via Ziehm’s C-arm distribution network, according to the firm.
Instrumental to the development of interventional oncology in the USA and globally, William (Bill) Rilling tracks how the discipline has grown over the course of his career from a niche area of medicine for the most challenging cases to a subspecialty with its own society dedicated to revolutionising cancer care.
What initially drew you to interventional radiology (IR), and then specifically to cancer care?
My father was an engineer at GE Medical systems working on MR imaging systems and I had a summer job at GE working on MR spectroscopy experiments. This translated into additional research in MRI at UW Madison in undergrad and medical school so I was exposed to the power of rapidly progressing diagnostic imaging at an early age. In medical school, however, I was drawn to the operating room and the intensity of those experiences. I was torn between diagnostic radiology and surgical subspecialty training such as urology, but then I watched John McDermott drain a paraspinal abscess under CT guidance and the decision was made.
The decision to focus on cancer interventions was much more pragmatic. As a junior faculty member at the Medical College of Wisconsin, we were developing a strong multidisciplinary vascular practice but the turf battles with vascular surgery and cardiology were exploding at academic medical centres across the country. Cancer interventions were a blue ocean, with huge potential. I was also drawn to the cancer patient population—to see people face terrible circumstances with courage and grace is truly inspirational.
Who have been important mentors for you throughout your career?
I was fortunate to have wonderful mentors early in my career. During my fellowship at Northwestern University, both Bob Vogelzang and Al Nemcek influenced me greatly. At that time, Bob was spending many hours per week in meetings helping the Society of Interventional Radiology (SIR) construct the component coding system. Al was also doing work in multiple SIR committees and was starting to build some early quality infrastructure in IR. They both taught me that it was not enough to do the work of patient care every day, but that we should be giving back to this wonderful specialty by volunteering our time and expertise to help IR continue to grow. In my clinical practice, we were developing the foundations of a strong multidisciplinary vascular practice that continues to this day. It was my honour to work for 10 years with Jonathan Towne, who was a national leader in vascular surgery, a superb surgeon, and a fantastic and caring physician.
What challenges did you face in the early years of your interventional oncology (IO) practice, and do these differ to those IO faces now?
Initially, the challenges were to introduce the concept of IO techniques to colleagues in medical and surgical oncology. As with much of IR, we started out by treating the “hopeless cases” that had no other options. Once introduced, the power of these interventions were self evident—to see a patient walk out the door the same day after ablation of liver cancer, now cancer free. The integration of transarterial chemoembolization (TACE), radioembolization, and percutaneous ablation into practice patterns then followed, and so did the higher levels of evidence supporting their use.
Currently, the challenges are different. The rapid development of new targeted cancer drugs, and in particular immunotherapy, is revolutionising cancer care. We now have to discuss how and when to integrate IO therapies and systemic regimens and build the data to support such integration. We still have a very powerful case to make from patient quality of life and cost effectiveness perspectives, but we need to prove these as well.
You were involved in running the first ever meetings dedicated to IO back in 2001. How did this come about?
I joined the education committee for SIR as a junior faculty member to start getting involved in SIR. In the early 2000’s, the role of IR/IO in management of hepatocellular carcinoma (HCC) was beginning to blossom. At this time, I met Jeff Geschwind, and we planned and executed the first three stand-alone meetings focusing on multidisciplinary HCC management, beginning in 2001. To my knowledge, these were the first dedicated IO meetings ever organised, but of course, the term “interventional oncology” did not exist at that time.
As education counsellor on the Executive Council for the SIR, you helped develop the APDIR. How did this help improve IR education?
At that time, the IR programme directors met only once per year, for a couple of hours at the SIR annual meeting. The issues being faced by training programmes were becoming more complex, such as turf battles with other specialties, and it was clear we needed a more organised structure. With the support of SIR, we formed the Association of Program Directors in Interventional Radiology (APDIR). The APDIR had a stand alone meeting once per year with staff support from SIR. We started to tackle some urgent issues such as consistent participation in the National Resident Matching Program process and development of a core IR curriculum. Through APDIR, the programme directors were able to coordinate efforts and best practices to deal with the erosion of vascular cases, attracting medical students and residents to IR, and improving non procedural patient care skills.
You were also instrumental to the implementation of the IR residency task force. How did the existence of an IR-specific residency programme come about, and how has it shaped IR as a specialty?
In the early to mid 2000s, it was clear that IR was evolving into a specialty caring for a complex array of patient populations and that direct patient care was necessary to foster the growth of these new areas of practice. Delegation of the patient care aspects and just “doing procedures” was not an option. The complexity and diversity of interventions performed was expanding rapidly and the one year fellowship training pathway was not sufficient to adequately prepare IR trainees for future practice. Knowing that changing the training pathway was a process that would take many years, we formed the Primary Certificate Task Force in 2006 with an initial goal of a obtaining a stand alone IR certificate. I asked John Kaufman to chair the task force and he graciously accepted. As we went to work, it soon became clear that Diagnostic Radiology chairs and the American Board of Radiology and American College of Radiology would not support a pure IR certificate but would support a combined IR/DR certificate.
The ensuing process of navigating the politics, obtaining American Board of Medical Specialties (ABMS) and Accreditation Council for Graduate Medical Education (ACGME) approval, and implementation into the match was exceedingly complex and took over a decade from start to finish. In addition to John Kaufman, there were so many leaders in IR who pushed this to a successful completion, including Jeanne LaBerge, Gary Becker, Anne Roberts, Matt Mauro, Alan Matsumoto, Vicki Marx, Dan Siragusa, and Jan Durham. There have been countless others including my partner, Parag Patel, who have led the complex process of integration of the IR/DR residency into existing training programmes.
The IR/DR certificate was the first new primary specialty approved by ABMS in over two decades. Now, medical students can match direcly into a six year IR/DR programme that will prepare them for modern IR practice, including all the patient care skills necessary to succeed. By some measures, it is the most competitive specialty in American medicine. We are attracting the best and brightest to IR.
Would you describe the thought processes behind the decision to create the Society of Interventional Oncology (SIO) in 2017, and the reaction of the IR community at the time?
The decision to form SIO was made after a very long and thoughtful dialogue that occurred over a few years. The World Conference of Interventional Oncology (WCIO) had been in existence since 2005. WCIO was evolving into much broader activities, including research grants, clinical trial development, and advocacy with various cancer organisations. It was becoming much more than a meeting or conference. We also realised that there would be political ramifications to forming a new society. The last thing we wanted to do was damage or undermine IR as a whole, but felt that a small society focused on IO would have a positive impact on the future of patient care and, ultimately, IO as a subspecialty.
The reactions to forming SIO were varied. Certainly, there were some who feared this would weaken IR and might set a precedent for other subspecialties to “break off.” In my view, the development of subspecialty groups and societies is part of the natural evolution of IR. This process has occurred in many other medical specialties over time and is predictable. IR practice development is significantly driven by those who focus on subspecialty areas of practice, such as prostate artery ebmolization (PAE), venous disease, or women’s health. We need to enable subspecialisation and not fear it.
What has been the highlight of your presidency of the SIO?
For me personally, the highlight is to see forward progress on multiple fronts. We have initiated some simple processes which have the potential to make signifianct impacts on IO practice. We have organised expert panels to provide regular comments to disease specific National Comprehensive Cancer Network (NCCN) guidelines with some early evidence that we have initiated positive changes. We have organised committees working with existing cooperative groups such as Eastern Cooperative Oncology Group (ECOG) and the American College of Radiology Imaging Network (ACRIN) to develop IO trials. SIO has also had success in more complex initiatives. Working with our industry partners, SIO has awarded US$1.5 million in translational research grants, some of which have served as a springboard to larger national grants. We are working with SIR to build IO-CORE, a large and disease specific registry platform for IO. We have multiple clinical trials in development which will help raise the level of evidence for IO in meaningful ways.
How do SIO, CIRSE, and SIR work together?
We are working diligently to coordinate efforts with both the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and SIR. At the end of the day, we all have the same goals: to improve patient care and to advance IR/IO with education and research. SIO leadership is in frequent communication with CIRSE and SIR leaders to try to coordinate our efforts on various fronts, and to hopefully avoid duplicative or competitive activities. As a small society compared to SIR and CIRSE, SIO does not have the resouces for government advocacy, coding and billing initiatives, and some other broad scale IR practice issues that the large societies handle very capably.
As stated above, SIO and SIR are cooperating in building IO-CORE, which will be a registry platform for prospective disease-focused IO data collection with research questions and data elements developed by international expert panels. I believe it is a win for everyone that we do not have parallel or competitive IO registry platforms in development. SIO has had a number of meetings with CIRSE leaders regarding the International Accreditation System for Interventional Oncology Services (IASIOS) initiative, led by Professor Andy Adam. We support the goals of IASIOS to help raise the quality and consistency of IO practice worldwide. We look forward many future cooperative projects with both CIRSE and SIR.
How has SIO adapted during the COVID-19 crisis, and what is the role of medical societies during a pandemic?
SIO has had to change and adapt, similar to all other societies and organisations during this crisis. We now have virtual board meetings, our last in person meeting was in January at the SIO annual meeting. We are planning next year’s annual meeting very aware of uncertainty of future in person meetings—trying to be nimble and have the ability to adjust as circumstances change.
Medical societies provide a very important source of information to members during times like this. I believe that SIO, SIR ,and CIRSE have all done a fantastic job helping to keep members informed of best practices during these rapidly changing circumstances. The webinars regarding patient care during the pandemic hosted by all three societies have been very informative and well attended across the board.
On a personal level, what are the central preoccupations when treating patients with cancer during a global pandemic?
It is a very challenging situation given that cancer patients are vulnerable and have poor outcomes when infected with COVID-19. However, we also know that their cancer needs treatment and that, in most patients, delaying treatment could result in poorer outcomes. So we must balance the risk and benefit and in the majority of cases, we have proceeded with IO treatments as usual. The exceptions have been renal cell cancer ablations and a small number of very small liver tumours that have demonstrated relative stability on imaging. We have worked diligently, as I am certain all IR practices have, to separate inpatient and outpatient flows as much as possible to minimise risk for patients coming in for outpatient treatment.
How do you think this coronavirus pandemic influenced IO, over the short- and long-term?
I think that IR as a specialty has stepped up and shown that we can respond to a public health crisis. Much of our efforts during the pandemic were to support our colleagues in the intensive care unit (ICU), forming teams to perform portable urgent procedures if necessary during the surge of COVID-19 patients in our hospitals.
As stated earlier, much of our IO practice has continued as usual during the pandemic. Globally, I think there has been a shift in some regions toward increased IO treatments, which use fewer hospital resources, PPE, and probably also cause less decrement in the immune system compared to surgery. Over the long term, some of these advantages may result in changes in practice patterns, but it is too early to tell. For example, there has been an increase in overall Y90 treatments in the US during the pandemic—we do not know if this trend will continue.
What are your hobbies and interests outside of medicine?
Outside of medicine, I am blessed to have a wonderful family, including my wife Kate and my three children, Nicholas (24), Gabrielle (20), and Nathaniel (19). Kate has put up with my long hours at the hospital and travel to meetings and my grumpiness at the end of a long day. My children keep me grounded and remind me that there is much to life outside of medicine. I love to spend time with them and to spend time doing just about anything outdoors. I enjoy hiking, skiing, fly fishing, boating, running, and still manage to get up and down the basketball court.
Artio Medical today announced it has acquired Flow Forward Medical, a medical device company developing methods for establishing and maintaining vascular access sites.
This stock-for-stock merger transaction in which Flow Forward merged with and into Artio was approved by the Board of Directors and stockholders of both companies. The transaction closed on 8 June 2020.
“Flow Forward’s venous dilation technology is highly complementary to Artio’s existing peripheral vascular portfolio, with significant overlap in physician call points and procedures,” commented F Nicholas Franano, president and CEO of Artio Medical. “This acquisition provides a unique opportunity to diversify Artio’s endovascular pipeline, which will now include next generation vascular access solutions for kidney failure patients.”
Studies suggest baseline vein diameter may play an important role in achieving and maintaining routine, reliable AVF use. Flow Forward’s Arteriovenous Fistula Eligibility System (AFE System) stimulates flow-mediated vein dilation to expand the initial vein diameter prior to the creation of an AVF. This aims to increase the number of haemodialysis patients eligible for AVF and to enhance the usability and lifespan of newly created AVFs.
“Creating and maintaining reliable access sites is a complex vascular challenge, often resulting in complications, repeat procedures, and increased cost to patients, yet is critical for lifesaving hemodialysis treatment,” commented Paul Muller, chief technology officer and general manager of Flow Forward. “We are very excited Artio recognises the significant potential of our technology and we look forward to leveraging their expertise as we prepare for our first clinical use in the coming months and then move toward commercialisation.”
Maria Antonella Ruffino, a vascular interventional radiologist at Azienda Ospedaliera Universitaria Città della Salute e della Scienza in Turin, Italy, tells Vascular News about her team’s growing clinical experience with covered stents as a platform that offer a minimally invasive solution for arterial emergencies. Ruffino gives an insight into the advantages of covered stents in such cases, their potential limitations, and which ones may be a favourable option for emergency treatment.
Arterial emergencies, such as bleeding, pseudoaneurysm, dissection, or fistula are potentially life-threatening conditions. Spontaneous or iatrogenic arterial emergencies require prompt diagnosis and treatment. During the last few decades, the treatment of these lesions has shifted from emergency open surgery to an endovascular approach, and the latter is rapidly becoming part of the treatment algorithm.
What are the advantages of using covered stents in such emergency cases?
The main endovascular approaches include use of covered stents and embolisation. A key advantage of using a covered stent in an emergency case, when compared to embolisation, is that a stent graft guarantees the immediate exclusion of the lesion without the sacrifice of the target vessel, avoiding the risk of non-target embolisation, which can result in ischaemic complications and rebleeding. Preservation of flow is crucial – particularly in districts with a terminal vascularisation, without collaterals, such as the limbs and kidneys. Additionally, this also applies to the liver, where it is uncertain whether extrahepatic arteries provide sufficient collateral circulation in case of hepatic artery occlusion.
What is your clinical experience with covered stents?
At our centre, we started using the BeGraft peripheral stent graft (Bentley, Hechingen, Germany) in June 2015. In the beginning, we used it for iliac procedures in elective cases of severe aortoiliac occlusive disease. Subsequently, we expanded this to include cases of rupture or dissection, and for severe complications that can present when long, calcified iliac occlusions are treated. The availability, wide sizing range, good trackability and conformability of these stent grafts and their low profile (6F compatible up to 8mm diameter) led us to extend their use to other vessels in case of arterial injuries. Since 2018, we have also used the BeGraft aortic stent graft, which has allowed us to treat vessels of larger diameters. Our cardiology colleagues already use the BeGraft coronary stent.
During the last few years, we have treated many emergency cases with the BeGraft stent graft family. These include iliac ruptures or renal pseudoaneurysms – which are quite common – but also more complex cases, like common carotid artery bleeding or penetrating aortic ulcer rupture*. In these last two scenarios, in particular, where we needed a large stent graft (Ø12mm), we have experienced first-hand how a larger diameter BeGraft stent can perform in tortuous anatomies, thanks to its good trackability and low profile, as it can be used with small vascular sheaths (9F in these cases).
Part of our experience, which focused on iatrogenic arterial injuries, has been recently published in Medicine, reporting a technical success of 100% and a clinical success of 88%. No device- or procedure-related deaths, nor major complications were reported. There was no patency loss at mid-term follow-up (average FU 390 +/- 168 days).1
Are there any limitations associated with the use of covered stents for emergency cases?
Almost all arterial lesions can be treated with covered stents, except for those without anatomic suitability, such as very distal lesions, or those without an adequate proximal and distal neck. Similarly, arterial lesions that are located in vessels of a calibre not suitable for stenting cannot be treated with covered stents. Finally, in case of tortuous anatomy or at a joint, when possible, a self-expandable covered stent is the preferred option.
What are your must-have sizes of covered stents for emergencies?
Arterial emergencies can present with a variety of lesions that can be very different in aetiology and characteristics, and located in vessels that can vary significantly in size. This is why we require a wide array of differently sized stent grafts in order to select the most suitable one. It is, therefore, difficult to say which sizes are a “must-have”.
Our experience shows that, in the case of arterial injuries, the proper sizing of the stent graft is essential to achieve technical and clinical success, without complications and recurrences, which further highlights the importance of having a wide range of stent grafts on shelf to treat arterial emergencies, and the BeGraft family has the broadest covered stent platform in the market.
Overall, endovascular treatment with BeGraft covered stents, with preservation of distal flow, is minimally invasive, safe, and effective in the management of arterial injuries and emergencies. Furthermore, all the aforementioned device characteristics allow for the rapid treatment of the lesion, even in case of tortuous anatomy.
*The usage of the BeGraft aortic foot the treatment in the carotid artery or PAU is off-label
References
Ruffino MA, Fronda M, Varello S, et al. Emergency management of iatrogenic arterial injuries with a low-profile balloon-expandable stent-graft: Preliminary results. Medicine. 2020 April; 99(15): p e19655
Case images
Figure 1. Right common iliac artery stenosis in an 81-year-old male patientFigure 2. The angiographic control after lesion stenting with a balloon-expandable bare metal stent shows arterial rupture with medium contrast leakageFigure 3. The completion angiography after deployment of the BeGraft peripheral stent graft shows the sealing of the bleeding
MedAlliance’s partner in Japan, MDK Medical, has enrolled the first patient in the clinical study of its novel sirolimus drug-eluting balloon (DEB), SELUTION SLR, for the treatment of peripheral arterial disease (PAD). This follows the acceptance of a Clinical Trial Notification (CTN) by Japan’s Pharmaceutical and Medical Device Agency (PMDA) earlier this month.
The study involves up to 132 patients across a number of centres in Japan. Its objective is to assess the safety and efficacy of SELUTION SLR for the treatment of lesions of superficial femoral arteries and/or popliteal arteries. The study is a prospective, controlled, multicentre, open, single-arm clinical investigation. Its primary endpoint will be the primary patency rate at twelve months. Secondary endpoints will include major adverse events/TLR, primary patency, and the change of Rutherford classification/ABI/WIQ.
“We are extremely pleased with the regulatory and quality expertise demonstrated by our partner MDK, and particularly proud that Japanese patients can now benefit from our unique technology. This is the first sirolimus drug-eluting balloon implanted in Japan, where the current paclitaxel-coated balloon market generates more than US$100M in revenue”, commented MedAlliance chairman and CEO Jeffrey B Jump.
In February 2019, MedAlliance became the first DEB company in the world to receive Breakthrough Device Designation status for a sirolimus DEB from the US Food and Drug Administration (FDA). SELUTION SLR has now achieved three separate FDA Breakthrough Device Designations: for the treatment of AV-Fistula; coronary in-stent restenosis and peripheral below-the-knee lesions. The company announced the enrolment of the first patient in its FDA IDE pivotal coronary trial earlier this month.
In February 2020, MedAlliance announced the award of its first CE mark approval: for SELUTION SLR in the treatment of PAD. In May 2020, the company announced the award of its second CE mark: SELUTION SLR 014 PTCA for the treatment of coronary arterial disease (CAD).
A new study shows significant benefits of the Ellipsys vascular access system (Avenu Medical) in easily and safely creating durable vascular access for end-stage renal disease (ESRD) patients who require haemodialysis.
According to an Avenu Medical press release, the system also offers a standardised process for using the minimally invasive technology that other physicians can follow to reproduce the results, which “will make it easier for more practitioners to adopt this patient-friendly approach to dialysis access,” explained lead author Alexandros Mallios, a vascular surgeon at Institut Mutualiste Montsouris of Paris, France.
Published in the Journal of Vascular Surgery(JVS), this marks the largest study of any percutaneous arteriovenous fistula (pAVF) technique to date. Of the 232 patients who had an Ellipsys pAVF created between May 2017 and July 2019, there were no adverse events and 96% still had fully functioning fistulas with strong blood flow after a year. That “patency rate” is higher than published rates for surgically created fistulas, which average about 60% after one year.
“Vascular access is quite literally the lifeline for dialysis patients,” said Mallios. “The advantages of the percutaneous Ellipsys fistula are that it is a very safe, simple, and reproducible way to create a fistula that will function for a long time with minimal interventions.”
In addition, the study reported that patients were able to begin using their pAVF for dialysis an average of four weeks after creation, with six per cent of fistulas becoming functional (or “mature”) in as little as two weeks. Such rapid maturation can have a significant impact on patient safety, as it avoids the use of a central venous catheter (CVC) if they need to begin dialysis quickly. Compared to fistulas, CVCs are associated with significantly higher rates of complications, including infection and even death.
One of the most important aspects of the study, Mallios added, is that it offers a protocol for fistula creation, maturation and maintenance—which should make it easier for other physicians to adopt the relatively new procedure. For example, the study shows the benefit of adding a new step to the procedure—performing balloon angioplasty immediately after a fistula is created. That improves blood flow and speeds maturation, and could improve patency rates without increasing the need for additional maintenance procedures.
“Dr. Mallios’ results are very exciting, particularly with such a large patient population, as it adds to the growing body of evidence that this approach offers a safe and effective way to quickly create a functional percutaneous fistula,” said Mark Ritchart, president and CEO of Avenu Medical. “He also uses his valuable experience as a guide to enable more widespread use of percutaneous fistulas, which may improve patient safety by reducing reliance on riskier vascular access options.”
In April, JVS published a case report by Mallios that featured a 3D rendering of the Ellipsys pAVF on the cover of the publication. Mallios also co-authored two recent papers in the Journal of Vascular Access that discussed patient eligibility for Ellipsys and the similarities between an Ellipsys pAVF and a surgical AVF, the current standard of care.
In addition, recently published long-term Ellipsys data showed a functional patency rate of 92 percent at two years. The study also found high levels of patient satisfaction with the procedure.
Cleared by the FDA in 2018 for patients with end-stage kidney disease, Ellipsys is the first significant innovation in AVF creation in over 50 years. It transforms a complex surgery into a minimally invasive procedure that can be performed in a hospital outpatient setting or ambulatory surgery center. Since 2015, more than 1,800 patients worldwide have had the Ellipsys procedure.
Jim Reekers (Amsterdam UMC, Amsterdam, The Netherlands), Editor-in-chief of Cardiovascular and Interventional Radiology (CVIR) Endovascular, was awarded the European Society of Radiology (ESR) Gold Medal at this year’s—virtual—European Congress of Radiology (ECR; 15–19 July).
Reekers is a former president of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), and a professor Emeritus of Radiology and Interventional Radiology at the University of Amsterdam.
He has received the ESR Gold Medal in recognition of his achievements in the field of interventional radiology (IR). In a statement on their website, CVIR Endovascular say: “We hope [this award] will increase the visibility of IR and the importance of endovascular procedures”.
“It means a lot,” Reekers tells this newspaper, when asked about the impact of a prominent interventional radiologist receiving the Gold Medal award at the largest European radiology congress. “I think that diagnostic radiology (DR) is the basis for any interventional radiologist. Up to date diagnostic skills—and that means understanding the whole spectrum of diagnostic radiology—is mandatory to be an IR expert. Any medical specialist performing endovascular or interventional oncology procedures without high level diagnostic skills will always stay a craftsman, sometimes useful, but will never be able to make the real difference. Performing IR without up to date diagnostic skills is like driving with your eyes closed, and hoping for the best.”
Writing on Twitter, Reekers’ colleague Rick van Rijn (also Amsterdam UMC, Amsterdam, The Netherlands) wrote: “Proud moment for Dutch Radiology and for a great and inspiring colleague. For several years I have had the pleasure to work with him at the same department at the Amsterdam UMC #welldeserved”.
“I see this as a great honour,” Reekers says, “the golden crown on my career as an interventional radiologist (and trained radiologist), an innovator, a researcher, a mentor, and a teacher. To be only the second Dutch radiologist to receive this honour feels very special to me. This award symbolises to me personally that diagnostic and interventional radiology should always stay one close family. On equal base, with full clinical responsibilities for IR, and permanent cross fertilisation.”
Radiologists Richard FitzGerald (Royal Wolverhampton Hospitals National Health Service [NHS] Trust, Wolverhampton, UK) and Katrine Riklund (Umeå University, Umeå, Sweden) also received Gold Medals at this year’s ECR.
It was recently announced that Veryan Medical will support Walk Vascular in the commercialisation of the Jeti peripheral thrombectomy system in Germany.
Walk Vascular’s Jeti thrombectomy system employs an internal jet, located safely just inside its catheter mouth, capable of engaging large thrombus volumes through a miniature lumen, rapidly clearing peripheral vessels that can often prove challenging for standard aspiration devices.
“By working with Veryan Medical we can hit the ground running” comments David Look, president and CEO of Walk Vascular. “Veryan provides an invaluable catalyst to our commercial efforts, providing access to key opinion leaders in Germany through an experienced sales team with clinical expertise.”
“We are pleased to be working with Walk Vascular and the Jeti technology, a proven solution that safely and effectively restores blood flow in peripheral thrombectomy procedures,” says Nick Yeo, Veryan Medical’s CEO. “We are proud to support innovators like Walk Vascular to provide insights, marketing strategy, and a top-tier salesforce to ensure commercial success and clinical adoption. JETi and Veryan’s novel BioMimics 3D stent are an exciting combination both for our sales team and our customers.”
As the leader of an investigator-initiated, Phase 2 study evaluating the safety and efficacy of the SeQure® microcatheter (Guerbet), Francisco Cesar Carnevale here outlines his experience using the device, drawing particular attention to the reduced risk of reflux and non-target embolization. Originally scheduled to be presented at the Society of Interventional Radiology (SIR) Annual Scientific Meeting, this early experience with the SeQure® microcatheter in prostate artery embolization (PAE) is promising, with Carnevale hopeful it will enable the delivery of more therapeutics to the target vessel, while reducing damage to healthy tissue.
PAE is a novel, minimally invasive treatment for lower urinary tract symptoms (LUTS) attributed to benign prostate hyperplasia (BPH). Embolization of the prostatic arteries leads to ischaemic shrinkage of the prostate gland and subsequent reduction of LUTS. PAE’s therapeutic effect was first described in a case report in 2000. The first intentional treatment of BPH in humans was reported in 2010, and early cohort studies from around the world soon followed.
As with any new treatment, there is a learning curve. The more cases we perform, the more apparent it becomes to us that making even minor changes to our technique can make a difference to the outcome. One of the main concerns regarding PAE is related to non-target embolization (NTE). This is often due to one of three main causes: (A) reflux of embolic agents around the microcatheter into the main artery that feeds the prostatic artery (types I–V from the University of São Paulo Classification); (B) reflux or flow-direct injection of embolic agents to proximal, non-target branches; and (C) distal injection of embolic agents through intraprostatic shunts. The most common regions to NTE are the bladder, seminal vesical, rectum, penis, and pubic bone. So, having a refined technique and using dedicated microcatheters are key to a good and safe embolization.
With the aim of identifying a microcatheter that reduces the risk of NTE and which could be used as an alternative option, we have initiated the first PAE clinical study using the SeQure® microcatheter at the University of São Paulo Medical School (Prostate Artery Embolization using the SeQure® Microcatheter: A Phase 2 Study Addressing Safety and Efficacy).
The main goals of this microcatheter are to reduce the risk of reflux and NTE, and deliver more therapeutics to the target vessel while reducing damage to healthy tissue. Observations from our early experience—we have performed three procedures—indicate that PAE can be safely and effectively performed with the SeQure® microcatheter, even when navigating distally using the PErFecTED technique.
Case 1
A 70-year-old man with IPSS: 33 (nocturia 4x, weak urinary stream, incomplete voiding, frequency and intermittence). QoL: 6; PSA: 1.40 ng/mL; Qmax: 4.10 mL/sec; prostate volume by MRI: 70 grams; post-void residual volume by US: 40 mL. The patient was refractory to LUTS medication (taken for decades already) and PAE was chosen over surgery to avoid the risk of complications, mainly because of his age. To avoid NTE into the rectal branches—shown by digital subtraction angiography (DSA; Figure 1A) and cone beam computed tomography (CBCT; Figure 1B)—the SeQure® microcatheter was placed distally at the capsular branch, closing the communication with a metallic microcoil (Figure 1C). After injecting the embolic agents from the proximal position (before the bifurcation into the central gland and peripheral zone branches), the SeQure® microcatheter was easily navigated deeply into the central gland branch (Figure 1D) to inject additional particles according to the PErFecTED technique.
Case 2
A 65-year-old man with IPSS: 25 (nocturia 3x, urgency, frequency and weak urinary stream). QoL: 5; PSA: 3.40 ng/mL; Qmax: 6.50 mL/sec; prostate volume by MRI: 46.5 grams; postvoid residual volume by US: 5 mL. Refractory to LUTS medication after taking it for several years; PAE was chosen to avoid the risk of complications, and upon the recommendation of a friend of the patient previously treated with PAE.
During DSA of the right prostatic artery, some bladder branches were identified before the origin of the central gland and the capsular branches (Figure 2A). The SeQure® microcatheter was advanced distally to the bladder branches and positioned before the bifurcation of the central gland and capsular branches for a safer embolization (Figure 2B). One of the risks and consequences when performing this embolization step is the occlusion (NTE) of bladder branches proximal to the prostate resulting in bladder ischaemia. The side slits on the 1 cm distal tip of the SeQure® microcatheter allow the outflow of contrast media without passage of the embolic agent, meaning the bladder branches were saved from NTE (Figure 2C).
We hope that the data obtained from this important study will help bring a new, exciting device to those in the medical community performing this technically challenging procedure. Interventional radiologists should adopt a strategic, multidisciplinary approach to develop pre-clinical and clinical research, and to ultimately transfer current evidence into clinical practice.
Francisco Cesar Carnevale is the director of Vascular Interventional Radiology at the University of São Paulo Medical School, Sao Paulo, Brazil. He has received consulting and speaker honoraria from Guerbet.
Results from case studies are not necessarily predictive of results in other cases. Results in other cases may vary.
Ten-year data published in Radiologyshow that prostate artery embolization (PAE) is a safe and effective treatment for men with benign prostatic hyperplasia (BPH), which can result in long-term improvements in lower urinary tract symptoms (LUTS) and quality of life. Francisco Carnevale (University of São Paulo Medical School, São Paulo, Brazil) and colleagues note that, prior to their study, long-term experience with PAE for BPH was “limited”. They state that this research is an “important contribution” towards the wider medical community’s understanding of PAE not as an experimental procedure, but “as another alternative for patients suffering from LUTS related to BPH”.
Carnevale and colleagues set out to evaluate the efficacy, safety, and long-term results of PAE for BPH through a retrospective, single-centre study. Between June 2008 and June 2018, a total of 317 men (mean age, 65±8 years) were treated with the minimally-invasive procedure for the alleviation of moderate to severe BPH-related symptoms. PAE was performed with 100–500μm embolic microspheres, and the investigators report a 94% technical success rate for the procedure.
Patient follow-up ranged from three months to 96 months (mean, 27 months). International Prostate Symptom Score (IPSS), quality-of-life score, maximum urinary flow rate, post-void residual volume, prostate-specific antigen (PSA), and prostate volume were all assessed at baseline and during follow-up. Mean maximum improvement was as follows: IPSS, 16±7 points; quality-of-life score, 4±1 points; prostatic volume reduction, 39±39cm3 (39%±29); maximum urinary flow rate, 6±10mL/sec (155%±293); and post-void residual volume, 70±121mL (48% 81) (p<0.05 for all). Early clinical failure occurred in six (1.9%) and symptom recurrence in 72 (23%) men at a median follow-up of 72 months.
Unilateral PAE was associated with higher LUTS recurrence (42% vs. 21%; p=0.04), but the study authors note that the unilateral PAE cohort were on average slightly older than those treated with bilateral PAE (71 years old vs. 65 years old). However, log-rank analysis comparing unilateral and bilateral PAE groups showed no statistically significant difference in the median time to recurrence (48 months and 72 months, respectively; p=0.19).
Embolic particle size did not relate to symptom recurrence, with no difference observed in the median time to recurrence among men treated with microspheres 100–300μm or 300–500μm in diameter.
Baseline PSA was inversely related with recurrence, and was found to be an independent predictor of recurrence outcomes after PAE (hazard ratio [HR], 0.9 per nanograms per millilitre of PSA; 95% confidence interval [CI], 0.8, 0.9; p<0.001).
None of the patients presented with urinary incontinence or erectile dysfunction, an “important finding”, according to Carnevale.
Speaking to Interventional News, Carnevale stresses the significance of this research, the first decade-long dataset to follow-up outcomes in over 300 PAE patients: “It was published in the most reviewed journal with the highest impact factor in the radiology field. Urological societies have been waiting for these long-term data to decide if [they trust that] PAE can be offered as another alternative treatment for patients suffering from LUTS related to BPH. These data consolidate the pioneering, multidisciplinary work done by the Radiology and Urology Departments at the University of São Paulo Medical School. Without this mutual collaboration, this important contribution would not be achieved.
“To bring a new, alternative treatment to the medical community is not an easy assignment,” he continued. “This 10-year experience of using PAE confirms that this minimally invasive procedure is not only an alternative for candidates suffering from LUTS due to BPH-enlarged prostates. Several publications from different centres all over the world have shown that PAE has been accepted with excellent results for patients with urinary retention, for BPH-related bleedings, for patients with contraindications to traditional surgical treatments, and for patients with different prostate sizes (small and huge prostates). Now, PAE can be looked at with different eyes. Over the last decade, we have followed every ethical committee approval (local and national) and have followed several lines of inquiry (including investigating different prostate sizes and symptoms, as well as various embolic agent types and sizes). In this Radiology publication, we have included all patients during our ‘learning curve on PAE’. This means that, among all published patients following different prospective trials, we have tested and learned with every single patient and procedure. We were trying to identify the best way to perform PAE. It was really new and challenging to us.”
PAE excluded from urology guidelines globally
In March 2016, the Conselho Federal de Medicina (CFM), the authority in charge of professional regulation and medical licensing in the country, stated that PAE can be used as a new, alternative treatment for symptomatic patients with BPH. However, the board noted that five-year results should be analysed before a final decision is made on the procedure’s inclusion in the national urology guidelines. “Now, after 12 years of PAE and with this 10-year follow-up data, it is time the CFM gives the final approval for PAE,” comments Carnevale. “With that obtained, we hope the Brazilian Urological Society will include PAE in its guidelines for the treatment of BPH.”
This is a global issue. In 2018, results of the UK ROPE study, which compared embolization to conventional prostate surgery, led the National Institute of Health and Care Excellence (NICE) to determine that the evidence on the safety and efficacy of PAE for BPH was adequate to support the use of this procedure on the National Health Service (NHS). They recommended the procedure “provided that standard arrangements are in place for clinical governance, consent and audit”. NICE added: “This technically demanding procedure should only be done by an interventional radiologist with specific training and expertise in PAE”.
Nevertheless, the European Association of Urology (EAU) guidelines for the diagnosis and treatment of men with LUTS/BPH have not been updated, and remain cautious when describing the potential clinical role of PAE. They state: “A multidisciplinary team approach of urologists and radiologists is mandatory as the basis for future randomised controlled trials of good quality with long-term follow-up in order to integrate this treatment option into the spectrum of efficient, minimally invasive treatment options.” Since then, a 2019 study published in European Urologyfrom Tiago Bilhim (Hôpital Saint-Louis, Lisbon, Portugal) et al has demonstrated that improvements in quality of life measurements and IPSS are “far superior” following PAE than due to any placebo effect.
A US Food and Drug Administration (FDA) review in 2017 concluded that “the probable benefits outweigh the probable risks for this indication”, and in June the same year, the indication of Embosphere microspheres (Merit Medical) was expanded through the FDA’s 513(f)(2) de novo classification to include PAE. In 2018, the product was approved for the same indication by a 510(k) pathway. Embozene microspheres (Boston Scientific) also gained an expanded indication in 2018, with the FDA granting approval for its on-label use in PAE treatment in the USA via the 510(k) pathway. However, PAE is not recommended outside of a clinical trial in the American Urological Association (AUA) guidelines, something many interventional radiologists refute.
Addressing doubters of PAE, Carnevale says: “According to the Hippocratic oath, physicians should ‘Apply dietetic measures for the benefit of the sick according to their ability and judgement’. Interventional radiologists have faced turf battles for decades when aiming to bring new alternative treatments for patients. This happened with peripheral angioplasty, fibroid embolization, and abdominal aortic aneurysm repair, among others, and it will not be any different with PAE. We are not saying that PAE is the only or the best treatment for LUTS related to BPH. We have simply brought another option for patients and physicians to discuss. Each treatment has its indications and contraindications, and it is necessary to understand the patient’s aims and wishes. The publication of these exciting results from our 10-year experience of PAE is a great achievement, and should be considered by the medical community. Its time is now.”
Ahead of the first ever virtual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Thomas Kröncke, chairperson of the CIRSE 2020 scientific programme committee, speaks to Interventional News about the programme highlights, and the logistics of how an online congress will function.He encourages readers to participate, and notes that, for those who register for the event before 30 July, there will be a chance to win free CIRSE registration for life.
Due to the COVID-19 pandemic, this year’s annual CIRSE meeting will take place online. How will the programme look? Which sessions will stay the same as they were, and which will change?
As the CIRSE 2020 congress will be online this year, some of the presentation formats will be adapted, but the content of the congress will remain almost completely as originally planned. All authors of accepted abstracts and all invited speakers will have the opportunity to present their posters and lectures to a worldwide audience.
Part of the on-demand programme will be available online from 1 September, in order to give the interventional community the opportunity to prepare for the large virtual get-together during the four days of the congress. During the CIRSE 2020 Summit from 12–15 September, ten hours of live programming will be offered throughout three channels—the Dotter, Rösche, and Grüntzig auditoriums. On 15 and 15 September, a fourth channel will be added: the IDEAS auditorium. The preliminary programme and registration are already online at www.cirse.org.
During the summit, just as at a physical congress, the focus will be on interactivity and the opportunity to exchange views and ideas. There will be a number of interactive formats for this, such as case-based discussions, expert round tables, workshops, and much more. The participants will always have the opportunity to ask the lecturers questions and to participate in the discussion.
What is the focus for the CIRSE 2020 programme?
A clear focus of this year’s meeting is on the presentation of the latest data and the push for evidence-based practice in interventional radiology. For example, the results of the FEMME study will be presented, in which the quality of life of women after embolization versus myomectomy was examined. The presentation of the first results from two registry studies on transarterial radio- and chemoembolization carried out by CIRSE will also be very exciting. Regarding peripheral endovascular interventions, peripheral arterial disease (PAD) Day and the First @ CIRSE session on Saturday 12 September will certainly be a highlight.
Another important programme focus of the CIRSE Summit is new therapeutic approaches, such as the radiofrequency-based creation of arteriovenous fistulas or fluoroscopy-free 3D imaging.
Are there other programme highlights?
As mentioned, on the first day of the congress we will have a strong focus on peripheral arterial disease in a special PAD track. There will be a session scrutinising the latest study results, as well as an innovation forum in which new therapeutic approaches will be presented and discussed.
On the last two days of the congress the Interdisciplinary Endovascular Aortic Symposium—IDEAS—will again take place. This important format extremely successfully aims at all specialists who deal with the endovascular care of aortic pathologies. In contrast to many other meetings, IDEAS offers a truly interdisciplinary platform through which the pros and cons of all therapeutic approaches are presented and discussed based on evidence.
Another session I would like to highlight is “Women in IR”. With this format, CIRSE deliberately tackles the necessary discussion about a stronger female representation in leadership roles in intervention radiology.
What are the biggest challenges in transforming a physical congress into a virtual one?
Of course, we were disappointed that the physical meeting in Munich, Germany, would not be possible this year. But we soon realised that a virtual congress also offers many opportunities. We can reach a much wider audience online. Many doctors who would not have had the opportunity to travel to Munich will now be able to take part in the CIRSE 2020 Summit.
We are currently working tirelessly to create a virtual format that will further increase interactivity in the sessions. In addition to the opportunities for interaction with the speakers, there will also be break-out rooms where discussions can be continued on a smaller scale.
Our team in Vienna, Austria, has evaluated the best providers and is currently creating a platform through which the meetings, industrial exhibition, and communication between conference participants will be ideally served.
When will the first content be available?
The scientific programme for the CIRSE 2020 Summit is already available at www.cirse.org. The first presentations are expected to be available on the congress portal in early September. In order to stay up-to-date, I invite all those interested to sign up for the CIRSE e-newsletter and to follow our channels on Facebook, Twitter and LinkedIn.
When is registration open for the CIRSE 2020 Summit?
Registration is already open, and a discounted early bird fee is available until 30 July. Registering for CIRSE 2020 will not only give you access to the world’s largest interventional congress, but also exclusive on-demand access to all its scientific content in the six months after the congress. No healthcare professional involved in interventional radiology should miss this opportunity! As a special incentive, everyone who registers before 30 July will be entered for a chance to win free CIRSE registration for life. I warmly invite everyone to sign up!
The imaging system interface is a joint hardware and software development from Bayer and Siemens Healthineers, and the first injector scanner interface for the MRI suite. It synchronises the MEDRAD MRXperion MR injection system from Bayer and the Siemens Healthineers MR scanner, thereby overcoming significant challenges posed by the complex process used in conventional contrast-enhanced dynamic MRI, which can result in suboptimal imaging, according to a joint company press release. By enabling synchronised injector triggering from the MRI scanner operator console and a more efficient workflow, the imaging system interface allows users to conduct high quality, consistent contrast-enhanced procedures and spend more time focusing on the patient. Bayer and Siemens claim.
In a conventional, manually-controlled setting, radiographers must constantly plan, monitor, and time the various steps on the injector and scanner workstations separately during contrast-enhanced MRI procedures. If the required steps are not optimally-timed and synchronised, poor image quality may be generated, which can delay diagnosis as contrast-enhanced scans then have to be repeated. This can result in additional costs to healthcare systems and may cause unnecessary stress and inconvenience for patients as well as healthcare providers.
“Together with Siemens Healthineers, we were able to design an interface that directly addresses the challenges of conventional contrast-enhanced dynamic MRI workflows and improves both the user and patient experience,” comments Olaf Weber, head of Radiology Research and Development at Bayer.
“This is a very exciting time as we introduce the new technology to our customers that will further improve their experience with our MRXperion injector. We believe that the new interface will assist in allowing the MRI radiographers more time to care for their patients,” says Lynne Collins, country head Radiology at Bayer UK/Ireland.
The imaging system interface recently gained CE mark certification.
Terumo Corporation has announced it has completed the acquisition of Quirem Medical, a Netherlands-based healthcare start-up specialising in the development of next-generation microspheres for selective internal radiation therapy (SIRT), a treatment for liver tumours. Under the terms of the agreement, Terumo acquired 80.1% of the shares of Quirem Medical. This is over and above its current share position of 19.9%, making Quirem Medical now a wholly owned subsidiary of Terumo.
Terumo will make a one-time, up-front payment of US$20 million, with up to US$25 million additional payments based on the achievement of future milestones by 2030. It will be funded through cash on hand and will not significantly impact the company’s financial projections for the current fiscal year ending 31 March 2021.
Quirem Medical has developed and manufactures QuiremSpheres, the only commercially available microspheres containing the radioactive isotope Holmium-166. Recent trials have shown the safety and efficacy of holmium microspheres for the treatment of unresectable liver cancer. To improve patient selection, therapy planning, and treatment verification, QuiremSpheres can be visualised and quantified even in low concentrations by means of single-photon emission computed tomography (SPECT) and magnetic resonance imaging (MRI). This is unique and cannot be done with currently available Yttrium-90 based microspheres.
Furthermore, Quirem Medical also produces QuiremScout, a low dose holmium microsphere that helps evaluate the biodistribution of microspheres prior to therapy, and a dosimetry software package, Q-Suite, which is used to plan QuiremSpheres treatments based on QuiremScout dose imaging. Q-Suite is also able to determine SIRT success immediately after the procedure by converting SPECT and MR imaging into absorbed dose distributions. Together, these three integrated products (QuiremSpheres, QuiremScout, and Q-Suite) make up the full Holmium SIRT Platform. The Holmium Platform equips physicians with the necessary tools to optimise SIRT outcomes through more personalised treatment, a Terumo press release asserts, addressing the individual needs of each patient.
QuiremSpheres, QuiremScout, and Q-Suite are CE-marked and currently available in Europe, the Middle East, and Africa. In the coming years, Terumo intends to launch the Holmium Platform globally as part of the ongoing expansion of its interventional oncology portfolio.
The global interventional oncology market value is more than US$1 billion, which is a rapidly growing field with a compound annual growth rate (CAGR) of 7%. Within this field, SIRT is one of the main treatments that is expected to help to drive this growth year on year.
Terumo has been building its presence in the interventional oncology field, with product offerings such as the micro catheter system (Progreat), compressible microspheres for embolization (HydroPearl), drug-eluting microspheres (LifePearl), and biodegradable drug-eluting microspheres (BioPearl). In 2015, Terumo invested in Quirem Medical and became the exclusive global distributor of their technology.
Avicenna intracranial haemorrage and large vessel occlusion identified
Medical imaging artificial intelligence (AI) specialist Avicenna.AI has announced it has received 510(k) clearance from the US Food and Drug Administration (FDA) for its CINA Head triage AI solution for neurovascular emergencies. The FDA’s decision covers CINA’s automatic detection capabilities for both intracranial haemorrhage and large vessel occlusion (LVO) from CT-scan imaging.
Stroke is a leading cause of death in the USA, with more than 795,000 strokes resulting in more than 100,000 deaths each year. It is estimated that up to a third of the most common type of stroke are caused by LVO, when a clot blocks the circulation of the blood in the brain. Around one in 10 strokes are thought to be caused by intracranial haemorrhage. Using a combination of deep learning and machine learning technologies, CINA Head automatically detects and prioritises acute intracranial haemorrhage and LVO cases within 20 seconds, seamlessly alerting the radiologist within their existing systems and workflow.
Peter Chang, radiologist and co-founder of Avicenna.AI, says: “When dealing with a stroke, time is of the essence and being able to prioritise effectively is critical to saving lives and improving outcomes. Not only does CINA Head help radiologists to identify pathologies quickly, but also to highlight those that require the most urgent care.”
CINA’s intracranial haemorrhage detection capability was validated using data from 814 cases conducted at more than 250 imaging centres across the USA, with 96% accuracy, 91.4% sensitivity, and 97.5% specificity. The product’s LVO detection capability was validated based on 476 cases, with 97.7% accuracy, 97.9% sensitivity, and 97.6% specificity.
Cyril Di Grandi, co-founder and CEO of Avicenna.AI, comments: “We are excited to have received FDA clearance for CINA Head and are looking forward to working with emergency departments and stroke centres across the USA to help improve detection, decision-making, and patient outcomes. As a triage AI tool that identifies multiple pathologies, we believe that CINA Head delivers more value than AI tools or algorithms that only target a single condition.”
CINA Head is the first in a family of AI tools for emergency radiology being developed by Avicenna.AI. Subsequent products spanning the trauma and vascular fields are expected to be unveiled in the next 12 months.
Dynetic-35, the balloon-expandable cobalt chromium iliac stent system from Biotronik, is now commercially available in Europe. Indicated for the treatment of de novo or restenotic lesions in the iliac arteries, the product is approved for use in Europe and other markets that recognise CE mark certification.
The Dynetic-35 stent size matrix is 6F compatible, including stent diameters of 5–10mm and lengths of 18–78mm, and comes in working lengths of 90, 130, and 170cm, the largest range of iliac stent sizes on the market, a company press release states. Biotronik claim that the thin-strut stent combined with the low crossing profile of the balloon catheter delivery system enhances deliverability.
“The new Dynetic-35 is a true improvement over the previous-generation stainless steel iliac stent. The flexibility, lower profile, and improved deliverability allow direct stenting even in more challenging lesions,” says Michael Lichtenberg (Arnsberg Vascular Center, Arnsberg, Germany). “In my clinical experience with the new stent system, I have been impressed by the smooth placement and deployment for a direct stenting approach, as well as the radial strength of the stent.”
With the 170cm catheter length option, the Dynetic-35 system also enables a radial access approach. “In my practice, I often have the need to use radial access to treat iliac artery disease, which provides more patient comfort and earlier ambulation,” explains Mercedes Guerra-Requena (Guadalajara Hospital, Guadalajara, Spain). “Until now, available options for a radial approach have been limited. Fortunately, the new Dynetic-35 stent’s 170cm length delivery system option and 6F sheath compatibility enables me to comfortably use a radial approach.”
“The next-generation Dynetic-35 is a testament to BIOTRONIK’s continued mission to develop innovative devices that improve the lives of patients,” says Alexander Uhl, president of Vascular Intervention at Biotronik. “We are proud to be able to offer our signature thin-strut stent design in the largest size range on the market while staying 6F compatible for the entire product line.”
The Indigo System Lightning 12 (Penumbra) is now commercially available in the USA, the company has revealed. In addition, Penumbra has announced the appointment of interventional radiologist Corey L Teigen (formerly Sanford Health, Fargo, USA) as chief scientific officer, and interventional radiologist James Benenati (formerly Miami Cardiac & Vascular Institute, Baptist Hospital, Miami, USA) as chief medical officer. Both positions have been newly created.
The Indigo System Lightning 12 is the company’s next generation aspiration system for peripheral thrombectomy. Lightning 12 combines the new Indigo System CAT12 aspiration catheter with Lightning intelligent aspiration, enabling physicians to focus on optimising thrombus removal using the system’s clot detection mechanism. CAT12 is a large-lumen aspiration catheter that incorporates novel laser-cut hypotube-based catheter engineering to provide advanced deliverability and torqueability within the body, a company press release describes. This combination of intelligent aspiration and large-lumen catheter engineering makes Lightning 12 Penumbra’s most advanced clot removal technology.
“Penumbra continues to lead the field of clot management by bringing highly innovative technology to address the challenges that we as physicians face while caring for our patients,” says Frank Arko (Sanger Heart and Vascular Institute, Charlotte, USA). “When dealing with thrombus, we have learned that it is the combination of the catheter along with powered aspiration that yields the most effective results. Lightning 12 with intelligent aspiration is a giant leap forward for the field of thrombectomy, and we have been very impressed with the early results at Sanger.”
“The simplicity of Lightning intelligent aspiration combined with the significant advancements in catheter engineering will enable us as physicians to get closer to our thrombus removal goal in a safe manner, as well as our goal of improving clinical outcomes for our patients,” says Patrick Muck, (Good Samaritan Hospital, Cincinnati, USA).
“Lightning 12 provides physicians with an integrated system that not only removes large amounts of thrombus but also detects and manages clot removal,” comments Jay Mathews (Manatee Memorial Hospital, Bradenton, USA). “This is a very important advancement for the field of thrombus management, and our initial experience at Manatee Memorial with this technology shows us that we are now closer to single-setting care for our patients.”
New leadership appointments
Penumbra also announced appointments for two newly created positions: Corey L Teigen, as chief scientific officer and James F Benenati, as chief medical officer.
Teigen joins immediately as CSO and will contribute his extensive scientific and clinical expertise to ongoing and future research and development efforts.
“In my radiology practice, I have seen first-hand the challenges medical practitioners face while treating difficult medical conditions,” Teigen states. “At Penumbra, I have a profound opportunity to change the course of healthcare delivery for people living with vascular disease. I feel privileged to join Penumbra’s unparalleled group of talented engineers and leaders, and I look forward to contributing my scientific knowledge to help solve challenging medical problems.”
Benenati will join Penumbra on 1 September 2020 as CMO, and will contribute to clinical and medical affairs strategies and advise upon global commercialisation and market development activities.
“I am excited to join Penumbra at this very important time for the company, where it is poised for growth, as it moves into the next generation of intelligent clot removal and expand into rehabilitation with the recent launch of the REAL system,” Benenati says. “Penumbra has changed the landscape of healthcare by providing truly innovative solutions for a wide realm of medical challenges. In this next phase, Penumbra is set to broaden its reach on a global scale, and I am thrilled to join this excellent team and help accelerate the impact of its products.”
“I am thrilled we are bringing Lightning 12, the most advanced technology for aspiration thrombectomy, to the peripheral interventional community,” adds Adam Elsesser, president and chief executive officer, Penumbra. “It is an ideal time for us to welcome Corey and Jim to Penumbra’s leadership team as we progress into our next phase of growth. Their career-long focus on patient care and their innovative mind-set are a perfect fit with our vision and culture, which is dedicated to making a fundamental difference in patients’ lives.”
Barts Health NHS Trust has performed a UK-first operation outside of trial setting that could reduce mortality and risks of infection in patients with dialysis.
Interventional radiologists at The Royal London Hospital (London, UK) have carried out the new minimally invasive arteriovenous fistula (AVF) procedure, WavelinQ EndoAVF (BD Bard).
An endovascular AVF involves fusing a connection between the artery and adjacent vein within the forearm using direct heat which patients can use for dialysis. This procedure is an alternative to the more invasive traditional option of open surgery.
The novel EndoAVF procedure results in a closed circuit that provides adequate blood flow to the superficial veins for dialysis and blood can be withdrawn, cleaned through a dialysis machine, and returned to the body.
With the EndoAVF system—conducted by interventional radiologists Ounali Jaffer, Rashid Akhtar and Rajesh Sivaprakasam at The Royal London Hospital—two thin catheters are inserted into the artery and the vein through small needle punctures.
Magnets help to align the devices and a connection is made between the vein and artery in the forearm without the need for open surgery, which allows clinicians to access the blood stream and gives patients a reliable long-term dialysis AV fistula.
The dual magnetic catheter system is removed from the body once the connection is created and the arm heals without stitches with little or no scarring.
Ounali Jaffer, interventional radiologist at The Royal London Hospital, said:
“This new treatment really enhances our techniques in treating those patients with end stage kidney disease. Avoiding a CVC is imperative and now we have another procedure available to enable timely AVF creation.
“There are only a finite number of options available in creating an AVF, which is the lifeline for the patient. By extending these options, we can maximise the use of these vessels.
“The obvious added benefits are that the procedure is relatively quick and leaves no sign of a procedure, with no visible scar. These are early days, but the innovation is exciting and will hopefully benefit a number of our local population with end-stage kidney disease.”
The Global Embolization and Oncology Symposium Technology (GEST) has announced that it will take place virtually this year. Previously planned to be hosted in New York, USA, on 2–5 September, the event will now be online from 4–6 September 2020.
In an email addressed to the “GEST Community”, the GEST course directors write: “After careful consideration, GEST 2020 will go Virtual to protect the health and safety of our global community.
“GEST Meets Virtual 2020 will include both live interactive virtual sessions and an on-demand e-library. The GEST committees and faculty have been working diligently finalizing the virtual program. Stay tuned over the next week for the updated program!
“Our commitment to global education, innovation, research and improving patient care is stronger than ever. Please join us and take advantage of all the virtual content GEST has to offer.
“Until we ‘meet’ again, we hope you will join us virtually in September.”
The Journal of Vascular and Interventional Radiology‘s (JVIR‘s) impact factor—one measure of a journal’s influence based on the number of article citations compared to the total number of citable articles published—has broken 3 for the first time.
According to the Journal Citation Reports, published by Clarivate Analytics, JVIR‘s Impact Factor jumped 7% to 3.037 in 2019, up from 2.828 in 2018.
“This spectacular leap to the 3 range places JVIR in a distinct new class of peer journals, outdistancing all interventional radiology [IR] specialty journals,” comments Ziv J Haskal, the editor-in-chief of JVIR and a professor of radiology and medical imaging at the University of Virginia School of Medicine in Charlottesville, USA. “This continuing growth trajectory makes JVIR the commanding voice of IR science and the home of the highest-level IR research on its pages. It is a credit to the worldwide IR and endovascular researchers who choose JVIR for their most impactful work. This year’s numbers of submissions are projected to, again, reach record levels.”
Speaking specifically to Interventional News, Haskal adds: “I am incredibly proud that the new JVIR impact factor entered the ‘threes’ at 3.037. I have personally nudged, encouraged, curated, and sometimes ruthlessly edited over 17,000 manuscript drafts at all stages in a decade of living JVIR. The quality of our science has methodically and consistently improved, in JVIR, reflecting the pole position of this specialty in modern medicine. I could not be happier.”
“More than ever, there is a clear need for sound science and strong data to deliver optimal care for patients,” says SIR president Michael D Dake, senior vice president of the University of Arizona Health Sciences in Tucson, USA. “The research published in JVIR provides the support for image-guided therapies that interventional radiologists need to improve the lives of their patients.”
The impact factor, which reflects citations in the previous two years, is often used as a measure of the quality and influence of medical journals within scientific, professional, and academic communities. JVIR citations appeared in radiology, nuclear medicine, medical imaging, and peripheral vascular disease journals.
Patients who crossed over from the sham control arm of the RADIANCE-HTN SOLO trial to the renal denervation arm after 12 months of elevated blood pressure had decreased daytime ambulatory systolic blood pressure at both two and six months following renal denervation. The analysis of the crossover cohort was presented by Ajay J Kirtane (Columbia University Medical Center/NewYork-Presbyterian Hospital, New York, USA) during a late-breaking trial session at the PCR e-Course 2020 (25–27 June).
RADIANCE-HTN SOLO was a multicentre randomised controlled trial that demonstrated the blood pressure lowering effect of endovascular ultrasound based renal denervation (Paradise, ReCor Medical) compared with a sham control. Patients randomised to sham treatment who had daytime systolic ambulatory blood pressure ≥135mmHg or daytime diastolic ambulatory blood pressure ≥85mmHg after 12 months of follow-up were permitted to crossover to receive endovascular ultrasound based renal denervation.
Kirtane explained: “This analysis represents data on the cohort of 31 patients that had crossed-over as of January 2020. Complete two-month ambulatory blood pressure data are available on 31 participants, with complete six-month data available on 25 patients.”
Average age in the crossover population was 54 years, and 39% were female. Average daytime ambulatory blood pressure was 145/90mmHg, with a 24-hour ABP of 138/85mmHg, and office blood pressure of 146/95mmHg. The average number of hypertensive medications at crossover was 1.2±0.7, and the mean time from randomisation to crossover was 23±5 months.
There was 100% procedural success with renal denervation and there were no deaths from any cause.
Kirtane said: “This cohort demonstrated a daytime ambulatory systolic blood pressure change of -11.2mmHg at two months and -12.2mmHg at six months [p<0.001 in comparison to 12-month baseline for both], without an increase in medication burden; through six months, there were no major adverse events following crossover.”
At two months, 71% of patients had a decrease of ≥5mmHg in daytime ambulatory systolic blood pressure; at six months, this was 68%. Among these patients with a response 5mmHg in daytime ambulatory systolic blood pressure, At two and six months, the average daily ambulatory systolic blood pressure reduction was 17.7 and 20.6mmHg, respectively.
Summing up, Kirtane told the online audience: “Control of hypertension represents an unmet need globally, and renal denervation is an ‘adherence-independent’ adjunctive therapy to medications. These results are consistent with the primary SOLO results; however, there was no drug titration protocol between two to six months for crossover patients, so this may provide some added insight into six-month durability after renal denervation.”
He additionally stressed that, because crossover subjects and physicians were unblinded, the data are subject to behavioural and/or medication-related effects and as such these results need to be interpreted first and foremost within the context of the blinded study results. Nonetheless, “these data are further supportive of an adjunctive role of ultrasound-based renal denervation in the treatment of hypertension, especially when considering how many patients with hypertension worldwide are currently uncontrolled”, Kirtane said.
Transcatheter bariatric embolotherapy (TBE) for obesity is safe and leads to clinically significant weight loss in comparison to a sham procedure, a hotline and innovation session at PCR e-Course 2020 (25–27 June) has been told. TBE also demonstrated a greater improvement in quality of life and hunger scores. Vivek Y Reddy (Homolka Hospital, Prague, Czech Republic, and Icahn School of Medicine at Mount Sinai, New York, USA) presented the findings from a pilot, single-blind, sham procedure randomised controlled trial.
Reddy told the online audience: “Bariatric surgery is a highly effective procedure, and improves cardiovascular outcomes as well as mortality, but this invasive surgical procedure has significant morbidity and mortality associated with it, and that limits its utility to those patients who are severely obese, with BMIs [body mass index] almost always over 40. TBE is a novel catheter-based approach. It involves embolisation of microspheres to the left gastric artery [LGA] to cause ischaemia to the gastric submucosa. A number of preclinical studies, as well as clinical case series, have indicated that bariatric embolotherapy promotes weight loss—thought to be due to a mechanism of reducing ghrelin, which is the only known appetite-stimulating hormone in the body, and is secreted largely from the gastric fundus.”
The current study compared TBE to a sham procedure in a first-in-human trial conducted at two centres in Prague, The Czech Republic (PIs: Petr Neuzil MD PhD & Martin Fried MD). The first was a bariatric surgery centre that conducted most aspects of the trial, including patient enrolment, consent, weight counselling, and all of the follow-up. The second centre performed the randomisation and treated patients, either with embolotherapy or the sham procedure.
Key inclusion criteria were a BMI of between 35 and 50, and age 21–60 years. Patients were excluded if they had had prior bariatric surgery, had a history of ulcers, had type 2 diabetes, an active H. Pylori infection, or if they were chronic users of aspirin or non-steroidal anti-inflammatory drugs (NSAIDs).
Randomisation of consenting patients was 1:1 to TBE or a sham procedure. In TBE, femoral arterial access was obtained and a coeliac angiogram using a 6Fr guide was performed. Using an occlusion balloon microcatheter, beads which ranged between 300 µm and 500µm were injected into the LGA to achieve stasis. Injection was performed using a custom robotic manifold designed to inject the beads at the correct pressure. The Sham procedure involved the infiltration of lidocaine into the skin in the femoral area, and propofol was infused for one hour.
The primary efficacy endpoint was total body weight loss compared between TBE and sham therapy. Age, weight, and BMI were similar across the two groups. Patients were analysed in both intention-to-treat (ITT) and per protocol (PP) populations. After six months’ follow-up, crossover was permitted. TBE patients were followed for one year and sham patients for six months. After exclusions and withdrawals, 40 patients were randomised, 20 to each group. Following treatment, analysis of efficacy and safety was performed on 19 patients in the ITT population in the TBE group and on 18 patients in the sham group. The PP analysis of efficacy was performed in 15 patients treated with TBE and 16 with sham procedure.
Mean procedure time for TBE was 82.3 minutes. In 16 patients one vessel was injected, two were injected in two patients, and three in the remaining patient of the original 20 randomised to the procedure (19 treated with TBE).
Reddy announced the outcomes: “On the safety side, there was only mild nausea or vomiting that was self-limited, and minor ulcerations in five patients. All of these ulcers were asymptomatic and were self-limiting, requiring no additional treatment.”
At six months, the primary endpoint of weight loss for the ITT population was 7.4kg in the embolotherapy group versus 3kg in the control group (p=0.034). In the PP population, it was 9.4kg in the TBE cohort compared with 1.9kg for the sham therapy (p=0.0002). A comparison of TBE from baseline to 12 months found a 7.8kg loss in the ITT population (p=0.0011), and a 9.3kg loss in the PP population (p=0.0005). In addition, at both six and 12 months from baseline, TBE treatment led to a greater improvement in quality of life measures than sham treatment for physical function, self-esteem, sexual life, public distress, and work, as well as overall quality of life. Hunger scores also decreased to a greater extent for TBE than sham treatment at both six and 12 months from baseline.
Reddy concluded: “In this randomised pilot trial we established the proof of principle that transcatheter bariatric embolotherapy of the left gastric artery is safe, and it promotes clinically significant weight loss. There was an improvement in the hunger scores, significant weight loss that was maintained out to one year, and this also translated to improvements in quality of life.”
Reddy told Interventional News: “We believe this is an important trial that convincingly demonstrates for the first time that TBE helps promote weight loss. However, there is much additional work that remains to be done—most importantly a large multicentre trial to assess efficacy in the hands of a large number of operators, rare safety events that can only be identified after treating a large number of patients, and corroborating data on hormones (for example, ghrelin). My understanding is that the company that sponsored this pilot study is planning to conduct a large US pivotal FDA trial using a second generation TBE system (micro-infusion catheter and robotic manifold).
Cook Medical recently announced that the Advance Serenity hydrophilic percutaneous transluminal angioplasty (PTA) balloon catheter is now available to physicians in the USA. The catheter is manufactured by Surmodics and distributed by Cook Medical.
According to a press release, Advance Serenity is a hydrophilic-coated angioplasty balloon catheter designed to meet the technical needs of clinicians for treatment of patients who suffer from peripheral artery disease (PAD) which includes below-the- knee disease. The catheter portfolio includes both a 0.014- and an 0.018-inch diameter wire guide platform and will be available in a wide variety of balloon lengths and diameters.
“Now that we have added Advance Serenity to our product portfolio of vascular solutions, physicians have one more tool in their toolbox to help treat patients who have PAD,” said Mark Breedlove, vice president of Cook Medical’s Vascular division.
Cook Medical is working to make Advance Serenity balloon catheters available to physicians in Europe in the coming months.
Royal Philips recently announced the four-year results from the ILLUMENATE European randomised controlled trial (EU RCT). The Stellarex drug-coated balloon (DCB) cohort demonstrated similar all-cause mortality compared with the control arm through four years. This analysis included missing data found post hoc to achieve a follow-up compliance of 93.9%, increasing the robustness of the statistical analysis.
Along with the recently-published data on the ILLUMENATE Pivotal trial, this is the second RCT which has indicated similar mortality rates, further validating the long-term safety profile of Philips’ Stellarex low-dose DCB. The data were presented in the evening of 25 June as part of Vascular Interventional Advances’ (VIVA) first-ever Late-Breaking Clinical Trials Livestream.
The four-year ILLUMENATE EU RCT data are the latest from a series of trials evaluating the safety and efficacy of the Philips Stellarex .035″ DCB in restoring and maintaining blood flow in the superficial femoral artery and popliteal arteries of patients with peripheral arterial disease. The results were evaluated compared to percutaneous transluminal angioplasty (PTA) treatment with uncoated balloons, the current standard of care.
The mortality rate at four years shows no statistical difference between two patient groups, at 17.7% for the Stellarex patient group and 14.1% for the control group. Secondary safety outcomes were also similar across the two groups.
“These latest data from the ILLUMENATE EU RCT study add to the ILLUMENATE Pivotal RCT results and continue to demonstrate no statistical difference in mortality when comparing the DCB and PTA arms of the trial,” said William Gray, president of the Lankenau Heart Institute (Wynnewood, USA), an investigator for the Stellarex clinical trials who presented the results during the livestream.
“The results from the ILLUMENATE EU RCT trial continue to demonstrate durable long-term results at a high rate of follow-up compliance,” said Marianne Brodmann, professor, vascular specialist at the Medical University of Graz (Graz, Austria) and a primary investigator for the trial.
“The ILLUMENATE EU RCT results now establish Stellarex as the only paclitaxel DCB that has shown a consistent lack of statistical difference in mortality compared with PTA at each annual follow-up through four years across two randomised controlled trials,” said Chris Landon, general manager, Image Guided Therapy Devices at Philips. “We continue to proactively communicate relevant clinical findings to ensure physicians can make the best-informed decision for each patient.”
David Prologo from Emory University with Tanzanian IR trainees during a Uterine Fibroid Embolization (UFE)
Kenedy Foryoung (Yale, USA), Azza Naif (MUHAS, Tanzania), Fabian Laage Gaupp (Yale, USA), Ivan Rukundo (MUHAS, Tanzania), Frank Minja (Yale, USA), and Erick Mbuguje (MUHAS, Tanzania), who is holding a self made CT biopsy grid
“There is a general misconception that you cannot do interventional radiology (IR) in a resource limited setting,” says Fabian Laage Gaupp, IR resident at Yale School of Medicine (New Haven, USA), and a member of the Yale Radiology Outreach Program. He is outlining his work alongside colleagues to establish a radiology service at the Muhimbili National Hospital campus in Dar es Salaam, Tanzania, East Africa. “From having done this for almost three years, I can say that this is simply not true,” he says, picking up on the earlier statement.
The initiative has seen more than 50 volunteers travel to Tanzania in teams of up to five for two-week placements to provide hands-on training to radiology residents, nurses and technologists. Funded initially through donations and institutional grants, the project has recently been awarded funding through the Radiological Society of North America (RSNA) Derek Harwood-Nash International Education Scholar Grant scheme, which Laage Gaupp says will help to continue the initiative into the immediate future.
The project has grown out of work begun by Yale’s director of neuroradiology MRI and assistant professor of neuroradiology, Frank Minja, who initially sought to implement a Picture Archiving and Communication System (PACS) at the Muhimbili Orthopaedic Institute in Dar Es Salaam in 2014. Since then, Minja has made regular trips to Tanzania—the country of his birth—to support physician training in the country. Minja crossed paths with Laage Gaupp, who joined Yale as a radiology resident in 2016, and, hungry for outreach opportunities within the IR field himself, joined Minja on a trip to Dar es Salaam in 2017.
“In Africa you have around 1.3 billion people currently, and there are really only two countries where IR is established—South Africa and Egypt,” says Laage Gaupp, discussing the demand for IR services across the continent. Tanzania has a population of over 50 million, including over four million in Dar es Salaam, the country’s most populous city and the focal point of the outreach programme. During his first trip to the country, Laage Gaupp armed himself with an Interventional Radiology Readiness Assessment tool to establish the scope for setting up an IR service within the country. In terms of the availability of imaging equipment to support IR work, he found that this could be feasible, but the disposable equipment needed was lacking. Undeterred, he set about designing a training scheme that could bring IR into the country.
David Prologo from Emory University discussing the plan for a procedure with IR trainees Ziad Abdul and Ivan Rukundo from MUHAS
“We have followed the same training model that we do in the USA, doing three years of diagnostic radiology, followed by two years of an IR residency. In Tanzania they already have the three years of diagnostic radiology residency, so we essentially just have to add two years of interventional radiology.”
To date, six residents have enrolled over two year groups, with the first group of three residents set to graduate in September 2021. They are undertaking a combination of on-the-job training and lectures delivered by the visiting groups from institutions across the USA and Europe. Visiting groups, who visit for two weeks at a time, comprise at least one physician, nurse, and technologist, reflecting the fact that IR is, in Laage Gaupp’s words, “a team sport”. Groups may also be augmented by medical students and radiology residents. The ultimate aim of the programme is the establishment of a self-sustaining IR residency programme at Muhimbili, with Tanzanian IR faculty training Tanzanian residents. “Our focus has always been on getting them to be able to work independently quickly and we are already starting to see the outcomes of that,” Laage Gaupp comments. “They are already doing a lot of procedures independently, so now on a daily basis they do CT and ultrasound guided core needle biopsies, they do nephrostomy placements, and they do biliary drain placements, which is really considered a technically challenging procedure in many cases. There is no trained IR attending in Tanzania, but they are able to provide these really life-saving procedures, and have great success.”
IR technologist Julie Albrecht from Yale reviewing procedural images with Tanzanian IR technologist Msemo
The course has been designed to begin with teaching residents more basic procedures: “those that are more necessary”, Laage Gaupp says, such as core needle biopsies. “That might not be considered a life-saving procedure, but it is extremely necessary, because until then people were only doing fine needle aspiration, which has a much lower diagnostic yield.
“We felt that is something that would have a really significant impact on patient care because it is going to help you diagnose and help to guide the treatment. At the same time, it is a simple procedure where you can learn [to use] image guidance and you have a lower chance for complications.” Other procedures, including abscess drainage and nephrostomy and biliary drainage, have been prioritised, due to the potential impact these could have on morbidity and mortality compared to surgery. “Just by making those procedures available, that is the highest return in terms of patient outcomes that you can have. Even with those really basic procedures, you are going from a patient dying, to that patient surviving,” he emphasises.
Discussing some of the differences in running an IR service in East Africa, compared to the USA, Laage Gaupp comments that there is a significant difference in the “disease spectrum” of patients using healthcare services in Tanzania, with a high prevalence of parasitic infections, for example, as well as in the stage at which patients present in-hospital for treatment. “People present a lot later in general [in Tanzania],” Laage Gaupp remarks. “In the USA in particular, when people have the slightest headache or stomach ache, they usually go and see a doctor. In Tanzania, the coverage is different. For someone from a rural area to actually present to the national hospital in Dar es Salam takes months or sometimes years. Until they get to the national hospital, those are really the sickest of the sick, people show up with huge tumours, with roaring infections, with anything under the sun.”
David Prologo from Emory University with Tanzanian IR trainees during a Uterine Fibroid Embolization (UFE)
Another aspect he notes as being specific to Africa is a higher percentage of paediatric patients. “While paediatric interventional radiology in the USA is considered a bit of a fringe subset of IR, in sub Saharan Africa, paediatric interventional radiology will play a pretty big role because there are so many paediatric patients,” he notes. He also points to a large prevalence of uterine fibroids, which is particularly notable in black women compared to in predominantly white or Asian populations, adding that the introduction of uterine fibroid embolization (UFE) has the potential to have a huge benefit in throughout the region.
“If you look at UFE in particular, and you compare it with hysterectomy, one of the most common procedures worldwide, complication rates in sub Saharan Africa are on average higher than in Europe or the USA,” Laage Gaupp comments. “Now with UFE, the procedural risk is much lower, and second of all you do not need general anaesthesia, so you are taking that risk out. It is such a common problem, even if you said IR was limited only to UFE, that alone would justify bringing IR to sub Saharan Africa.”
The outbreak of COVID-19 has meant that outreach trips have been cancelled until it is safe to travel again. Laage Gaupp hopes that this will be before the end of 2020, but faculty have been able to offer online education through video conferencing. “If there is a positive thing that has come from COVID-19, it is the access to online teaching,” he comments, but notes that there is “no substitute” for hands-on teaching, particularly within IR.
Six-month clinical outcomes of the MERLION trial were presented as part of the VIVA Late-Breaking Clinical Trials Livesteam (25 June), by Tjun Tang (Singapore General Hospital, Singapore).
MERLION is a physician initiated, prospective, non-randomised multicentre trial investigating the safety and efficacy of the treatment with the luminor drug-coated balloon (DCB) and angiolite below-the-knee (BTK) drug-eluting stent (DES) in TASC C and D tibial occlusive disease, in patients with chronic limb-threatening ischaemia (CLTI).
Tang reported a 100% technical success rate, with a 4.5% bailout stenting for severe flow limiting dissection using angiolite BTK, and a primary patency of 78.9%.
Freedom from clinically driven TLR was 91.7% while the amputation free survival (AFS) was 88%, both at six months.
Tang concluded that the “luminor DCB is safe and efficacious, in treating highly complex infra-popliteal atherosclerotic lesions in challenging CLTI patients” and he added that “luminor is associated with highly satisfactory acute technical success, six-month target lesion patency, and AFS.”
IR equipment wrapped in plastic sheeting to aid cleaning and to prevent the spread of COVID-19
The COVID-19 pandemic will have a deep impact on the future of healthcare according to Tan Bien Soo, Singapore General Hospital (Singapore). He tells Interventional News how his institution has prepared for and dealt with the pandemic, including a six step programme for preventing the spread of the SARS-Cov-2 virus, how this response was influenced by Singapore’s experience tackling SARS and how the pandemic will shape healthcare services into the future.
Singapore General Hospital was well-equipped to deal with the COVID-19 outbreak due to previous experience with SARS. Could you expand on this, detailing the similarities and differences between COVID-19 and earlier viral epidemics?
SARS was also a coronavirus spread by droplets, as is the SARS-Cov-2 virus which is the cause of COVID-19. Based on this, we can conclude that the SARS-Cov-2 virus also spreads by droplets. However, beyond this, as it is a novel coronavirus, there is much that we still do not know about. We are now, for example, finding out that patients who are infected can have a pre-symptomatic phase when they can be very infectious. This is unlike SARS. After our experience with SARS, infection control and prevention has become an integral focus for all staff in Singapore General Hospital and we are constantly training and auditing ourselves to prepare for the next big disease outbreak. We have also, over the years, designed our infrastructure to allow for segregation of patients with different infection risks. Thus in Singapore General Hospital, we have different interventional radiology facilities for inpatients and outpatients.
What are the most important steps for interventional radiologists to take when ensuring their departments are ready for COVID-19 patients?
This has been summarised in six steps that we shared in the peer-reviewed journal Cardiovascular and Interventional Radiology. The six steps are:
Screen and segregate patients with different infection risks
Segregate staff to prevent health care worker infection
Prioritise requests to allow for reduction of workload and focus on ramping up infection control measures
Minimise movement of isolated patients
Review and enhance the workflows for infected patients
Adhere strictly to individual infection prevention and control guidelines
Elective procedures have been postponed or cancelled to mitigate the chances of coronavirus overwhelming the healthcare service. What counts as an elective procedure for an interventional radiologist, and what procedures are essential? Are elective procedures still cancelled in Singapore, or are you phasing them back in?
At Singapore General Hospital, we prioritise all clinically urgent and all inpatient procedures so that hospital length of stay can be shortened. For outpatient elective procedures, priority is given to patients with cancer who need treatment. Non-cancer related procedures that can be safely deferred, like fibroid embolisation, fallopian tube recanalisation and arteriovenous malformation embolisation have been postponed.
Interventional radiologists have also raised concerns over disposable sterile supplies. What actions did Singapore General Hospital take to conserve these supplies, and was there pressure from regulators to use them? Did you have any issues with your supply?
We quickly reviewed our existing guidelines for personal protective equipment (PPE) to ensure alignment with our institutional practice, and commenced refresher training in infection control. We stressed the need for appropriate use of PPE, and discouraged wastage. We also tracked our PPE stocks daily. That way, we have been able to maintain adequate supply.
On reflection, how do you feel Singapore has handled the COVID-19 outbreak? What lessons can other countries learn from the response in your country? What will the next few months look like?
In my opinion, we have handled the pandemic well. Even though we are now seeing a surge in case numbers, our hospitals are not overwhelmed, and mortality rate remains low. The response is co-ordinated nationally among all stakeholders, and not limited to just the healthcare sector. I feel that this holistic response will be the key to eventually overcoming this pandemic.
In your opinion, how will the COVID-19 pandemic impact the future of healthcare?
This pandemic will have deep impact on the future practice of healthcare. Much like how we in Singapore have learned from SARS which changed our practice and infrastructure to cater for future disease outbreaks. We now have to start thinking about the ‘new clinical practice norm’ in the post COVID-19 era by learning from our current experience.
This pandemic has created a global crisis and brought significant suffering upon millions of people, but I am confident that we will find a way to overcome it and emerge stronger, better and more resilient.
Tan Bien Soo is chairman of the Division of Radiological Sciences, and senior consultant, Department of Vascular and Interventional Radiology at Singapore General Hospital.
iVascular recently announced the launch of its Sergeant peripheral support catheter. Sergeant is a CE marked over-the-wire catheter, indicated for patients with peripheral arterial disease in small vessels or challenging anatomy during diagnostic and interventional procedures.
According to a press release, Sergeant is intended to facilitate, guide, and support guidewires. It also allows guidewire exchanges and provides a conduit for the delivery of saline solutions and diagnostic contrast agents. Sergeant’s guidewire support is possible thanks to its braided catheter that allows “exceptional” pushability and torque.
iVascular’s Hydrax proprietary hydrophilic coating increases the catheter’s trackability, allowing Sergeant to pass through tortuous anatomy. In terms of visibility, Sergeant features four radiopaque markers that asses accurately the catheters position and lesion length.
The device is available with the tip, straight, and 30º angled, and in lengths between 65 and 150cm, while offering compatibility with 0.014”, 0.018” and 0.035” guidewires, all of them being 4F introducer compatible.
Marc Sirvent, angiologist and vascular surgeon specialist at the University Hospital Germans Trias i Pujol in Barcelona, Spain, carried out the first procedures with the product, and notes that the product easily crossed the occlusion in the tibial posterior and plantar arch.
A BIBA MedTech Insights survey (conducted May 2020) indicates a trend towards centres only performing emergency percutaneous peripheral procedures during the COVID-19 pandemic. However, this trend is not seen with stenting/angioplasty for critical limb ischaemia. With critical limb ischaemia, the trend is for at least some elective procedures to still be performed.
BIBA MedTech Insights polled physicians at 238 centres across the globe about how the pandemic has affected clinical practice at their centre. More than half (55.8%) of respondents were vascular surgeons, with the rest of the respondents ranging from interventional radiologists to angiololgists. Furthermore, 46% of respondents came from the top four European countries: Italy, Germany, the UK, and Spain. Therefore, this article reviews the key Western European findings from the survey.
The survey showed that, in Western Europe, for both peripheral embolization and stenting/angioplasty for claudication, the majority of centres were only performing emergency procedures. For example, 69% of respondents reported that they were only performing emergency peripheral embolization and 61% said that they were only performing emergency stenting/angioplasty procedures for claudication. However, this tendency was not seen with critical limb ischaemia procedures. For stenting/angioplasty procedures for critical limb ischaemia, the majority of centres were performing at least some elective procedures: 40% for some procedures and 19% for all procedures versus 41% only performing emergency procedures. See Figure 1.
Source: BIBA MedTech Insights
Furthermore, of those still performing elective procedures for critical limb ischaemia, the tendency was for them to report seeing a reduction of 50% or less in elective procedures rather than a reduction of more than 50%. See Figure 2.
Source: BIBA MedTech Insights
The split between emergency only versus some versus all elective percutaneous procedures, for critical limb ischaemia, did vary depending on the country. For most countries, the majority of the centres were still performing at least some elective procedures. However, in the UK, 52% of centres reported performing emergency only procedures. In Spain, by contrast, only 29% of centres report performing emergency procedures (with 42% performing all procedures). See Figure 3
Source: BIBA MedTech Insights
Given that the survey suggests that elective critical limb ischaemia procedures have continued (albeit at a reduced level) during COVID-19, one may expect centres to “return to normal” relatively quickly once COVID-related restrictions have been lifted. Indeed, the survey does find that the majority of respondents in Western Europe estimate that their centre will go back to performing their usual level of elective critical limb ischaemia procedures within three months. Interestingly, although there is some variation, this trend is seen for all countries including the UK.
In terms of the measures needed to “clear the backlog” of elective procedures, overall, increased operating days, adjusted working practices (such as more frequently using a minimally invasive approach), and increased operating hours were the most common answers. However, of note, 10% felt no extra measures would be necessary.
The cover of June’s edition of the Journal of Hepatology featured a paper on transarterial radioembolization for the treatment of hepatocellular carcinoma (HCC). Publication of the paper, authored by Riad Salem (Department of Radiology, Northwestern University, Chicago, USA) and colleagues, has been described as a “milestone” for interventional radiology (IR) as a specialty and has heralded a call for greater collaboration between interventional radiologists and their Hepatology colleagues.
In the paper, Salem and colleagues investigate lung shunt function (LSF) observed in early HCC, and provide the scientific rationale for eliminating this step from routine practice. Salem and colleagues found that early stage patients, where segmental injections are planned, exhibited low lung shunting, effectively eliminating the risk of radiation pneumonitis. The study team proposed that the lung shunt study be eliminated in this subgroup, leading to fewer procedures, a cost reduction, and improved convenience for patients.
Riad Salem
Commenting on the clinical implication of eliminating lung shunt function in early HCC patients from routine practice, Salem tells this newspaper that “this would streamline the Yttrium-90 [Y90] algorithm, decrease the time to treatment, lower costs and minimise unnecessary hospital visits.” He continues: “This is particularly important in the time of COVID-19. Basically, we could take a patient selected for segmental Y90 at tumour board, schedule the procedure, and treat. This model also gets us one step closer to our ultimate goal of the ‘one-hour Y90’ as the standard of care.”
Julius Chapiro, co-director of the Interventional Oncology Research Laboratory at Yale School of Medicine, New Haven, USA, speaks to Interventional News about the publication of the data, and why its publication in one of the preeminent journals for research into the field of hepatology represents a landmark moment in the continuing development of interventional radiology (IR). He argues that the paper could help to forge stronger ties between interventional radiologists and their colleagues in hepatology.
Julius Chapiro
“The importance of publishing such data in the Journal of Hepatology and being featured as the cover story cannot be overstated for all of interventional radiology,” Chapiro comments. He cites the words of IR pioneer Charles Dotter, calling upon the practice to “provide clinical care” and “own” diseases and patients. “If we fail to do so,” Chapiro says, paraphrasing Dotter, “[we] become nothing more than high-priced plumbers”.
According to Chapiro, the manuscript takes these words from Dotter directly to heart. “Those of us who advocate for interventional oncology as the fourth pillar of cancer care must be rooting for Riad Salem’s team and this achievement,” he says. “Such high profile publications are changing clinical paradigms and inform a broad variety of specialists involved in therapy of liver cancer. The Journal of Hepatology is the official outlet of the European Association for the Study of the Liver (EASL) and has the highest impact factor of all journals focusing on liver disease. The publication reaches tens of thousands of people across the globe, including medical and surgical oncologists, both academic and in private practice. Having an IR cover story highlight our entire profession with such prominence legitimises our efforts, advocates for our therapies, establishes unquestionable authority, and protects our specialty.”
Describing the publication process, Salem says: “Once we had selected the prestigious Journal of Hepatology as our target, the manuscript was formatted accordingly and submitted. After receiving generally positive comments, we were encouraged to submit a revision with specific queries addressed. Once it was accepted, their production team sprang into action and enhanced the presentation style and graphics. They are a world-class team that significantly improved the manuscript quality, with the end result of the journal cover.
“The field of Hepatology is supremely competitive. Research groups from all around the world compete for a place in their high impact journals, with the Journal of Hepatology as one of the leaders, with an impact factor of 19. If the research is novel, impactful, and advances the field, the editors are universally fair and provide opportunities for all disciplines to publish in their journal. I have been very fortunate that in my career advancing IR, 26 manuscripts have been published in the highest impact journals of Gastroenterology, Hepatology, Journal of Hepatology and Gut. The editors placing our study on the cover reflects an acknowledgment of our team dedicating years of hard work investigating new concepts and challenging dogma. Our research group is humbled and honoured by this prestigious recognition.”
Discussing the efforts being made to improve teamwork between hepatologists and interventional radiologists, Chapiro comments that interventional radiologists are an integral part of liver tumour boards across most academic institutions, and that there has been a growing appreciation of their role in treating cancers of the liver. “Hepatologists and medical oncologists, who mostly lead those tumour boards in their cancer centres, have come to appreciate interventional oncologists as valuable team members and the spirit of those interactions is usually collaborative, productive, and cordial,” Chapiro states.
However, he argues that one of the most prevalent issues for interventional radiologists during these interactions with hepatology colleagues is the lack of unequivocal data in support of the therapeutic options. “This is especially true for the relative paucity of prospectively collected data from randomised controlled trials (RCTs) that would support the use of Y90, for example, in lieu of chemoembolization or as an option for patients with advanced stage disease.” Although not a randomised controlled trial, the data from Northwestern published in J Hep on the use of Y90 in early stage disease in patients waitlisted for transplant is an extremely valuable piece of information and has huge practical value, Chapiro suggests. “The elimination of shunt studies will make it more likely for transplant hepatologists and medical oncologists to choose this therapy, now that it has the stamp of approval from J Hep. Such data represent an important bridge between IR and other members of the tumour board.”
Exploring this idea further, Chapiro’s abiding message is that “teamwork begins at home”. “Our own institution has a very productive liver centre and interventional radiologists participate as full and associate members in collaborative projects and National Institute of Health [NIH]-funded research,” he says, adding that other avenues to collaborate are certainly through participation in NCCN guidelines, and through active memberships in national and international societies such as the American Association for the Study of the Liver Disease (AASLD), EASL and several Asian societies. Looking ahead at the opportunity for further opportunities to collaborate, he called for interventional radiologists to continue to make their voices heard within hepatology practice. “It is key for us to be present at their annual meetings and invite them to our own platforms such as the Society of Interventional Oncology Annual Meeting. At the end of the day, all we care about are patient outcomes and there is no better glue for us than this shared responsibility.”
The UK Royal College of Radiologists (RCR) has collaborated with the Society of Radiographers to create a leaflet for patients coming to the hospital for imaging and interventional radiology procedures.
The leaflet, “Protecting people attending for imaging tests or interventional radiology procedures,” outlines the new arrangements hospital sites are putting in place to protect visiting patients from COVID-19 so they may feel at ease. For example, patients with COVID-19 are scanned and treated separately, plus all patients coming to hospitals must wear a face covering or mask, it explains.
The leaflet also covers additional safety precautions patients will see, such as being asked about COVID-19, checking their temperature, new access routes, spacing around the imaging department and waiting areas, and staff wearing personal protective equipment.
“We want to reassure anyone visiting a hospital that radiology teams are doing everything they can to keep you safe from the virus,” notes RCR vice president for Clinical Radiology Caroline Rubin. “New protection measures are likely to include assessing you as you arrive, minimising contact in waiting areas, and potentially asking you to wait to be called in, as well as altering entry and exit points within the imaging department to keep people appropriately distanced.”
Intact Vascular announced the positive one-year results from its Tack optimised balloon angioplasty (TOBA) II BTK clinical trial during the 2020 Vascular Interventional Advances (VIVA) Late-Breaking Clinical Trial livestream.
Co-principal investigator Patrick Geraghty, professor of Surgery and Radiology at the Washington University School of Medicine in St Louis, USA, presented the one-year results, which successfully demonstrated sustained improvement in Rutherford category, toe-brachial index (TBI) and quality-of-life metrics following management of patients with post-PTA dissection with the Tack Endovascular System(4F), in conjunction with excellent limb salvage and amputation free survival rates.
“Effective treatment of below-the-knee arterial disease is a critical component of amputation prevention. Now, with Tack implants, we have an on-label treatment for post-angioplasty dissection that provides excellent outcomes through the first year of follow-up,” commented Geraghty. “The Tack device is a valuable treatment option that augments an aggressive approach to endovascular limb salvage.”
Notably the first vascular implant to receive US Food and Drug (FDA) premarket approval for below-the-knee (BTK) interventions, Tack implants impressively demonstrated an 81.3% Kaplan-Meier tacked segment patency and a 78.6% Kaplan-Meier target lesion patency, with an 83.1% Kaplan-Meier freedom from clinically-driven reintervention at one-year. No fractures, embolisation, or migration of the Tack device were observed, confirming the durability of the minimal metal implants.
Additionally, in the critical limb ischaemia (CLI) cohort, a population associated with high rates of amputation and mortality, Tack implants demonstrated remarkable 96.1% Kaplan-Meier target limb salvage and 89% amputation-free survival.
“This unprecedented trial is the first to investigate the safety and efficacy of a permanent vascular implant for repairing dissections in arteries below-the-knee. It enrolled a complex, predominantly CLI patient population that included 100% dissected vessels,” commented Peter Schneider, co-founder and chief medical officer of Intact Vascular. “These excellent one-year data highlight the clinical importance of below-the-knee dissection repair and validate the sustained durability of Tack implants.”
Additional co-principal Investigators for the trial included George Adams, director of Cardiovascular and Peripheral Vascular Research, UNC Rex Hospital, in Raleigh, USA, and Andrej Schmidt, Division of Interventional Angiology, University Hospital Leipzig, Leipzig, Germany.
“We are extremely pleased with the results from TOBA II BTK,” commented Bruce Shook, president and CEO of Intact Vascular. “The data from this clinical study add to the expanding evidence that repairing dissections following angioplasty improves long term outcomes for patients suffering from peripheral arterial disease (PAD). With FDA approval in hand, we are moving forward to address the large unmet need that exists among patients suffering from the most serious form of this disease, critical limb ischaemia.”
In a real-world retrospective analysis, recently published in JACC: Cardiovascular Interventions, the long-term mortality rate was lower after drug-coated balloon (DCB) angioplasty than after plain balloon angioplasty of femoropopliteal lesions. First author Tanja Böhme, senior author Thomas Zeller (both Universitäts-Herzzentrum Freiburg-Bad Krozingen, Bad Krozingen, Germany), and colleagues note that known co-morbidities, risk factors, and disease severity were identified as mortality predictors, but not paclitaxel.
Böhme et al cite the continuing debate surrounding the association between paclitaxel and late mortality in femoropopliteal interventions as the principal motivation behind their study.
They note that the conversion was sparked by the December 2018 meta-analysis by Konstantinos Katsanos (University of Patras, Patras, Greece) et al, which suggested an increased long-term mortality risk following femoropopliteal angioplasty using paclitaxel-coated devices.
“It remains unclear whether treatment of femoropopliteal lesions with a paclitaxel-coated DCBs leads to an increase in all-cause mortality in a real-world setting,” Böhmeand colleagues note, adding that health insurance data-based analyses even suggest a survival benefit for patients with paclitaxel-coated DCBs, referring specifically to a presentation given by William Schuyler Jones (Duke Heart Center, Durham, USA) at the TransCatherTherapeutics 2018 conference (TCT; 21–25 September) and a paper by Eva Freisinger (University of Münster, Münster, Germany) et al published last year in the European Heart Journal.
The authors of the present study therefore set out to evaluate the long-term mortality after paclitaxel DCB use and plain balloon angioplasty of femoropopliteal lesions in real-world practice.
Böhme et al conducted a retrospective mortality analysis of patients with at least three-year follow-up who underwent balloon-based endovascular therapy of femoropopliteal lesions. Between January 2011 and June 2016, 7,357 patients with femoropopliteal lesions were treated with either a DCB or plain balloon angioplasty; 1,579 fulfilled the study criteria. They detail that 514 patients were treated with plain balloon angioplasty without crossover to a paclitaxel-coated device during follow-up, and 1,065 patients were treated with DCB angioplasty.
The primary endpoint of the study was the difference in all-cause mortality rate after plain balloon and DCB angioplasty. Secondary endpoints included three-year and five-year mortality rates, the relationship between DCB length as a measure of drug concentration and mortality, as well as search for mortality predictors including type of treatment, age, gender, hyperlipidaemia, diabetes mellitus, renal insufficiency, cerebral artery disease, coronary heart disease, and Rutherford-Becker class 1–3 versus 4.
The authors report that mortality incidence at mean follow-up of 52±20.5 months (median 51 months) was 27.8% after plain balloon angioplasty and 16.9% after DCB (p<0.001). Equally, for a cohort excluding patients over 80 years of age, the mortality rate after plain balloon angioplasty treatment was significantly higher (23.6% vs. 12.3%, p<0.001).
In addition, they note that DCB length was not correlated to mortality rate and, after propensity score matching, independent mortality predictors were plain balloon angioplasty treatment (p=0.035), age (p<0.001), stroke (p=0.025), and renal insufficiency (p=0.007).
In the discussion of their findings, the authors remark that, despite including a large number of patients with long-term follow-up in this single-centre study, they were not able to confirm the findings of the Katsanos et al meta-analysis. “In this real-world study, even after adjusting for confounding variables, we found a significant mortality benefit for patients treated with DCB,” they write.
On the subject of mortality, the authors note that death was most common due to cardiovascular events. However, in a significant number of cases, the cause of death remained unknown.
Comparing their results to those of the Katsanos et al meta-analysis, Böhme and colleagues write that the mortality rates of their study are higher, “as expected”. They cite a potential reason for this as being Katsanos et al’s focus on randomised controlled trials, which “usually exclude patients at higher mortality risk, such as patients with end-stage renal disease. In addition, only patients with a certain life expectancy are included—frequently excluding elderly and frail patients results in a selection bias”.
The authors note that the single-centre observational design of their study is a potential limitation but defend the retrospective data analysis, which they state “does not affect the primary study endpoint of all-cause mortality”. They also note that this study design represents strength in terms of excluding potential confounding variables due to a standardised prescription of secondary preventive drugs, such as statins and antiplatelet agents following the intervention. Another limitation they mention is that in almost half of the study population the cause of death could not be determined.
Böhme et al conclude that, in this real-world study, treatment of femoropopliteal lesions with DCB excluding patients with ischaemic wounds resulted in a survival advantage. However, they note that all-comers randomised clinical trials are necessary to prove this long-term survival benefit and to identify the potential cause, such as a mobility benefit resulting in a positive risk profile modification as a result of a patent vessel.
The European Trainee Forum (ETF) Subcommittee of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has published a report on the status of vascular and interventional radiology training in Europe.
Interviews based on a specially designed questionnaire created to assess the various aspects of interventional radiology (IR) training were conducted with the subcommittee members of the ETF, where recipients gave answers regarding their country of residence. The report includes responses from representatives of 24 European countries.
Contextualising the report, editor-in-chief Gregory Makris (London, UK) writes in the executive summary: “IR is transforming medicine through minimally invasive image-guided procedures. Despite the explosive growth of the specialty and the huge demand for more interventional radiologists, the training pathways across Europe have not all evolved in parallel with the clinical and academic needs of the discipline. Our objective was to map the training pathways across Europe in order to identify potential issues and identify ways for further improvement and development.”
The report reveals that IR has gained subspecialty status in nine of the 24 included countries, though adds that a structured IR training programme is available in 15 (62.5%). Makris and co-authors also note that there is “significant heterogeneity in terms of duration of IR training, with nine countries offering up to one year, 10 countries offering up to two years, and only five offering more than two years”.
An official IR certification examination is awarded following completion of the training programme in just under half of the 24 countries (11). Clinical training is included as part of the IR curriculum in seven countries, and ranges from two to six months of vascular surgery or intensive care.
In addition, the report finds that endovascular training opportunities “vary significantly” at an international level, “with inconsistent levels of exposure for the trainees”.
“Finally”, Makris et al write, “only three national IR societies have trainee subcommittees in their structure”.
There is slow progress in terms of obtaining subspecialty status for IR in European countries, while the duration, structure and certification of IR training remains heterogeneous. Consensus among the European IR leaders is needed in order to achieve a homogenous, well-structured, competitive and clinically orientated IR curriculum in Europe with clear guidelines regarding the required duration and structure of training to achieve competency, especially regarding peripheral arterial and aortic work. More active involvement of the trainees in national and international IR societies is also deemed essential for the future growth of the specialty.
NOTE: This video is ONLY available to watch in selected countries and geographies
Ripal Gandhi (Miami, USA) outlines his initial experiences with the Caterpillar™ Arterial Embolization Device (BD), a product, which he says is easy to utilize, shows good trackability in tortuous vessels and allows for “very accurate placement”.
Gandhi describes the novel device, which consists of both distal and proximal nitinol fiber segments that are designed to promote thrombus formation and limit migration.* There are three versions of the device currently available, which treat varying vessel sizes (1.5-4mm, 3-6mm and 5-7mm), he says.
Gandhi presents a case in which a 46-year-old male with colorectal cancer with metastatic disease to the lung and liver was scheduled for treatment with systemic chemotherapy and concomitant radioembolization. The patient’s right gastric artery measured 3mm in diameter so the decision was made to use the Caterpillar™ Micro Arterial Embolization Device which “tracked quite smoothly along the curvature of this vessel to the desired embolization site”. The subsequent angiogram showed “immediate occlusion” of the right gastric artery.
Concluding, Gandhi states that the device tracked “very nicely through this tortuous anatomy” and notes that the three radio-opaque markers “allow for good visualisation of the device under fluoroscopy.”
This video is sponsored by BD
Indication For Use: The Caterpillar™ and Caterpillar™ Micro Arterial Embolization Devices are indicated for arterial embolization in the peripheral vasculature. The devices are contraindicated for use in vessels subject to cyclic bending, such as locomotive joints or muscle beds.
*Pre-clinical data and bench testing may not be indicative of clinical performance. Different test methods may yield different results. Data on file, Bard Peripheral Vascular, Inc.
The Transluminal Biliary Biopsy Forceps Set (BBFS) and a new 40-centimetre delivery system line extension of the existing Zilver 635 Biliary stent (both from Cook Medical) are now commercially available in the USA.
“We are excited to make these products available to physicians to provide more treatment options for biliary duct procedures. This continues our efforts to bring products to physicians that fill the unmet clinical needs for patients,” comments Mike Williams, director of Cook Medical’s vascular programmes.
According to a company press release, the Transluminal Biliary Biopsy Forceps Set is designed to facilitate percutaneous acquisition of accurate tissue samples for biopsy. Cook Medical go on to state that biopsy samples obtained during biliary procedures “must be sufficient and precise to reflect accurate diagnosis”. BBFS was developed to include an introduction system coupled with a “cup and jaw” forceps design to retrieve biopsy specimens. Supporting the use of the BBFS design, a study published in Cardiovascular and Interventional Radiology reported a 94.2% diagnostic accuracy, with appropriate technique, when evaluating malignant biliary strictures using BBFS.
The Zilver 635 Biliary Stent is designed for cases of abnormal constrictions of the biliary tree (biliary neoplasms). The product helps to restore the natural flow of the biliary duct system, Cook Medical claims in a statement on the product launch. The flexible stent is also resistant to shortening, helping to provide precise placement. Having a 40-centimetre long delivery system permits ease of access for placement of the stent in biliary neoplasms.
Rexgenero, a regenerative medicine company developing advanced cell therapies to treat chronic limb-threatening ischaemia (CLTI), has announced the acquisition of all the key assets of aratinga.bio SAS Group, a preclinical-stage immunotherapy biotechnology company based in Paris, France.
The acquisition, which follows the recent approval by the French Commercial Court, includes all patent applications and related intellectual property, the exclusive license agreement for polymeric nanoparticle technology and the bioproduction facilities of aratinga.bio SAS Group, as well as the entire aratinga.bio team.
All assets of aratinga.bio SAS Group will be transferred to a newly created French subsidiary of Rexgenero.
David Horn Solomon, chair of Rexgenero, comments: “The acquisition of the aratinga.bio SAS Group’s assets and intellectual property will enable the creation of an integrated cell and gene therapy platform that combines our innovative late-stage Phase III REX-001 programme for chronic limb-threatening ischaemia with aratinga.bio SAS Group’s potentially transformative in vivo CAR-T platform. In addition, the operating synergies between the two businesses are considerable.”
Renaud Vaillant, chief executive officer of aratinga.bio SAS Group, says: “This unique combination provides the solution we have been looking for, enabling us to continue the development of our breakthrough CAR-T technology to proof of concept in 2020 in preparation for a Phase I/II clinical trial.”
Cécile Bauche, chief scientific officer of aratinga.bio SAS Group, adds: “This acquisition will provide funding for experiments needed to demonstrate proof of concept of our CAR-T therapeutics in vivo.”
The transaction enables aratinga.bio SAS Group to continue the development of its technology, and for the Paris-based team (15 people in Villejuif, close to the Institut Gustave Roussy) to pursue this programme.
The Infinity Angioplasty Balloon Company has announced that its balloon platform—the INFINITY Angioplasty Balloon Catheter—has been cleared by the US Food and Drug Administration (FDA) for percutaneous treatment of peripheral arterial disease.
“The INFINITY catheter represents a game changing innovation in percutaneous angioplasty balloon design and utility,” states founder and vascular surgeon, John Pigott. “A single SKU to treat lesions from 40–250mm in length, is adjustable, to the millimetre, in vivo assuring Precision Angioplasty, while addressing over 95% of real-life clinical cases.”
“Adopting the INFINITY platform reduces inventory needs and costs from dozens of SKU’s to two, it reduces space requirements, inventory management time, and trunk stock, while delivering the assurance that the right balloon size will always be on the shelf—INFINTY is a highly differentiated product,” reports CEO Gary Smith. “This is an ideal product for both office-based labs and hospitals.”
While initially launching an uncoated angioplasty balloon, the company intends to follow quickly with a drug-coated balloon platform of similar design.
Surmodics recently announced it has received CE mark certification in the European Union for its SurVeil drug-coated balloon (DCB).
“I am excited about the potential of the SurVeil DCB to improve the treatment of PAD,” said Professor Marianne Brodmann, interventional cardiologist at Medical University Graz (Graz, Austria) and a principal investigator in TRANSCEND, Surmodics’ pivotal clinical trial for the SurVeil DCB. “Drug-coated balloons have been widely utilised in Europe as a frontline treatment for PAD.”
The SurVeil DCB, a next-generation device that utilises best-in-class technology in the treatment of peripheral artery disease (PAD), includes a proprietary drug-excipient formulation for a durable balloon coating and is manufactured using an innovative process to improve coating uniformity. Preclinical data have shown a more evenly distributed and durable drug effect, and lower incidence of downstream drug particles compared to the control drug-coated balloon.
“This CE mark is a critical milestone and an exciting step forward for Surmodics as we continue to demonstrate industry leadership in the development of pioneering vascular medical devices,” said Gary Maharaj, president and chief executive officer of Surmodics. “The design of the SurVeil DCB reflects our dedication to providing innovative solutions that bring real clinical value—benefitting both clinicians and the patients that they treat. Congratulations go out to the entire Surmodics team on this well-deserved achievement.”
In February 2018, Surmodics entered into an agreement with Abbott that provided Abbott with exclusive worldwide commercialisation rights for the SurVeil DCB. Pursuant to the terms of the agreement, Surmodics received a US$25 million upfront payment and a US$10 million milestone payment for the completion of patient enrolment in the TRANSCEND clinical trial. As a result of CE mark attainment, Surmodics will receive an additional US$10.8 million milestone payment. The company will recognise approximately US$6.5 million as revenue in its fiscal third quarter and could earn up to an additional US$45 million for future product development milestones. Surmodics is not forecasting material revenue from the sale of its SurVeil DCB product over the remainder of its fiscal year ending 30 September 2020.
Under the agreement, Surmodics will be responsible for the manufacture and supply of clinical and commercial quantities of the product and will realise revenue based on initial product sales to Abbott as well as a share of profits resulting from third-party sales. The SurVeil DCB is not available for sale and is for investigational use only in the USA.
Radiofrequency ablation (RFA) is a successful treatment option for patients with painful osteolytic bone metastases, Jason Levy (Northside, Forsyth, and Cherokee Hospitals, Atlanta, USA) and Sandeep Bagla (Vascular Interventional Partners of northern Virginia, Springfield, USA) conclude, discussing the results of the first 100 patients treated in the OPuS One clinical study. In light of the Society of Interventional Radiology (SIR) annual scientific meeting’s cancellation due to the COVID-19 pandemic, Bagla also shared these positive data, which were featured in an abstract presentation for the SIR’s virtual event, on 14 June 2020.
“RFA for musculoskeletal metastases is really significantly underutilised,” Levy notes. This led the OPuS One triallists to embark on the largest-ever prospective RFA study, with the aim of collecting more data on this treatment option. In this post-market study, patients were monitored at baseline, and then followed-up three days, one week, one month, three months, and six months after RFA with the Food and Drug Administration (FDA) cleared OsteoCool device (Medtronic).
At each of these follow-up time points, patient-reported pain scores improved, Levy and Bagla relate: “These patients were seeing significant pain reductions, significant improvement in quality of life and functionality scores, at three days post RFA. In addition, it was seen at every single time point, and it continued to improve over time.”
On a scale of zero to 10, with 10 being the most painful, the mean score for worst pain in the last 24 hours at baseline was 8.2. This fell to 5.6 three days’ post-procedure, and then continue to fall, to 4.7 after one week, 3.9 after one month, 3.7 after three months, and to 3.5 at six months’ follow-up. Enthusing about these results, Bagla says: “That pain improvement, from 8.2 to 5.6, was very rapid in these patients, and that is what is important, and it was durable, even out to six months.”
Function and quality of life scores also showed improvements at each follow-up appointment. The investigators also observed a decrease in transdermal and/or oral narcotic use in 46% of the patients at three months, “which is even more impressive when you take into account that these patients were at end-stage,” Levy opines.
Medtronic sponsored this video and its distribution in association with Interventional News.
In a new field safety notice, the UK Medicines and Healthcare products Regulatory Agency (MHRA) states that a warning and clinical summary section will be added to the instructions for use (IFU) of 12 paclitaxel-coated balloons and paclitaxel-eluting stents used in the treatment of peripheral arterial disease (PAD) of the lower limbs.
The medical devices that will be affected by the changes are BioPath (Biosensors International), ELUVIA (Boston Scientific), IN.PACT Admiral (Medtronic), IN.PACT Pacific (Medtronic), Luminor (iVascular), Lutonix (BD), Passeo-18 Lux (Biotronik), Ranger (Boston Scientific), Ranger SL (Boston Scientific), SeQuent Please OTW (B Braun), Stellarex (Philips), and Zilver PTX (Cook Medical).
The notice states that updates will be made to the IFUs for these devices throughout Europe, including a warning and a summary of the December 2018 meta-analysis by Konstantinos Katsanos (University of Patras, Patras, Greence) et al, which found an increased risk of death at two and five years following the application of paclitaxel-coated balloons and stents in the femoropopliteal artery in the studies analysed.
The notice clarifies that no product batch/lot is being recalled in relation to this field safety notice, noting in its first appendix that “the benefits of paclitaxel-coated devices (e.g. reduced reinterventions) should be considered in individual patients along with potential risks (e.g. late mortality,” and urges physicians to discuss this late mortality signal and the benefits and risks of available treatment options with patients.
Guerbet has announced the approval of an additional indication for Lipiodol Ultra-Fluid by the China NMPA (National Medical Products Administration) for use in transarterial chemoembolization (cTACE) for hepatocellular carcinoma (HCC) at intermediate-stage in adult patients in the People’s Republic of China.
HCC is the most common primary liver cancer and the fourth biggest cause of death due to cancer worldwide. China alone represents more than 50% of all primary liver cancers globally since the country has the highest liver cancer prevalence in the world according to the WHO with about 330 000 cases.
“Guerbet is honoured to receive the NMPA approval for this indication for Lipiodol Ultra-Fluid in China. This registration reflects a strong positive endorsement from Chinese interventional oncologists and provides them with an additional NMPA endorsed therapy for managing patients with HCC in China. This is also evidence of our commitment to making cTACE available to as many HCC patients as possible.” commented David Hale, Guerbet’s CEO. “Development of image-guided procedures is a top priority for Guerbet’s Interventional Imaging Business Unit as we work to enhance liver cancer patients’ prognosis and quality of life in China and worldwide.”
Lipiodol Ultra-Fluid is used in interventional oncology for conventional transarterial chemoembolization, a minimally invasive procedure which consists of mixing Lipiodol Ultra-Fluid with an anticancer drug. The mixture is injected trans-arterially in the liver as a locoregional targeted chemotherapy for unresectable liver tumors (HCC). Lipiodol UltraFluid acts as a contrast agent, a drug vehicle, and a dual arterioportal transient embolic.
For interventional oncology procedures, Lipiodol Ultra-Fluid is approved for cTACE indication in EMEA (Austria, Belgium, Czech Republic, Denmark, France, Hungary, Iran, Ireland, Luxembourg, Portugal, Switzerland, the Netherlands, Tunisia, Turkey), in the Americas (Argentina, Colombia, Brazil, Chile, Mexico, Peru, Uruguay) and in Asia-Pacific (Australia, Brunei Darussalam, Cambodia, Hong Kong, India, Mongolia, New Zealand, Philippines, South Korea, Sri Lanka, Taiwan, Thailand, Vietnam).
Lipiodol Ultra-Fluid is approved for Imaging of patients with known HCC in the USA, in Canada and in Germany. Lipiodol Ultra-Fluid is approved for adjustment of Epirubicin hydrochloride for transarterial injection in Japan.
The first patients have been enrolled in the single centre DEPPER LIMUS clinical trial, Reflow Medical has announced. The non-randomised pilot study will evaluate the temporary spur stent system for the treatment of lesions in the infrapopliteal arteries using a limus-base drug-coated balloon.
According to the company, the DEEPER LIMUS study is expected to enrol up to 30 patients for approximately six months at a single centre outside the USA. It will follow primary and secondary endpoints for safety and efficacy.
“This gives us an opportunity to truly understand how differently antirestenotic drugs can treat infrapopliteal disease,” the trial’s principal investigator Marianne Brodmann (Medical University of Graz, Graz, Austria) comments. “The unique design of the spur device may enable the antiproliferative drug to reach the medial layers of the arterial wall, without leaving anything behind, and minimising the need for follow-up procedures.”
The retrievable temporary spur stent system is designed to treat long, diffuse, and severely calcified infrapopliteal disease. The device has a series of radially expandable spikes intended to create multiple pathways to allow the increased uptake of antiproliferative drugs into the vessel wall and facilitate acute luminal gain, without leaving anything behind, state Reflow Medical.
The Advance Serenity Hydrophilic percutaneous transluminal angioplasty (PTA) balloon catheter is now available to physicians in the USA. The catheter is manufactured by Surmodics and distributed by Cook Medical.
Advance Serenity is a hydrophilic-coated angioplasty balloon catheter designed to meet the technical needs of clinicians for treatment of patients who suffer from peripheral arterial disease (PAD) which includes below-the-knee disease. The catheter portfolio includes both a 0.014- and an 0.018-inch diameter wire guide platform and will be available in a wide variety of balloon lengths and diameters.
“Now that we have added Advance Serenity to our product portfolio of vascular solutions, physicians have one more tool in their toolbox to help treat patients who have PAD,” says Mark Breedlove, vice president of Cook Medical’s Vascular division.
Cook Medical has said it is working to make Advance Serenity balloon catheters available to physicians in Europe in the coming months.
Throwback tothe 2019 Society of Interventional Radiology annual scientific meetingwhen Interventional Newsinterviewed Bart Dolmatch(Mountain View, USA) on the early results of the AVeNEW trial – the first Level One trial dedicated solely to assess the safety and efficacy of the Covera (BD) covered stent designed to treat stenosis in the arteriovenous (AV) fistula access circuit.
The early results were “quite compelling” says Dolmatch, who notes that a 71% treatment lesion primary patency was seen atsixmonths, which he notes is a greater than 30% improvement compared to angioplasty alone. The data also shows that “not only are we doing better than angioplasty historically has done” but also “much better than the original stent graft approved for this indication,” he adds.
Dolmatch also discusses some of the interesting developments in regard to vascular access and says that there is currently “a great amount of enthusiasm and excitement” for the use of catheter-based endovascular fistula creation.
A novel treatment for advanced mesothelioma is safe and effective and may improve the quality of life for patients who have few treatment options, according to a research abstract presented during a virtual session of the Society of Interventional Radiology’s 2020 Annual Scientific Meeting (13–14 June). Transarterial chemoperfusion with cisplatin, methotrexate, and gemcitabine every four weeks is a feasible and safe treatment for patients with relapsed unresectable malignant pleural mesothelioma (MPM). It comes with minimal side effects and shows promise for extending the lives of patients who have limited or no remaining treatment options.
Interim results from a phase 2 prospective study were announced at the SIR Virtual Meeting during an Abstract of the Year session. Presenting on behalf of his fellow researchers, Bela Kis (Moffitt Cancer Center, Tampa, USA), principal investigator of the study, said that the treatment shows a promising disease control rate in heavily pre-treated patients with relapsed MPM.
“MPM is a devastating cancer of the pleura, the membranes surrounding the lungs, that is very difficult to treat,” Kis said. “The typical survival rate of patients with stage 3 and 4 MPM is around 12 months from diagnosis; but with this new treatment, we are hoping we might be able to extend patients’ lives beyond that—giving them more time with friends and family.”
He explained that advanced MPM carries a poor prognosis, and that transarterial chemoperfusion treatment selectively delivers a relatively high concentration of chemotherapy to the targeted tissue’s arterial bed, maximising antitumoural effect and minimising systemic side effects. The study is investigating the disease control rate, overall survival and adverse events of the treatment in patients with relapsed unresectable MPM.
In all, 27 patients with MPM —four females and 23 males, mean age 70.8±6.8 years—were enrolled between March 2016 and June 2019. Patients had transarterial chemoperfusion treatment in every four weeks with cisplatin (35mg/m2), methotrexate (100mg/m2), and gemcitabine (1000mg/m2) via the ipsilateral internal mammary artery and/or descending thoracic aorta. All patients had received and progressed on prior chemotherapy. Four patients had also had radiation therapy, and three patients had had pleurectomy. Response rate was evaluated by modified RECIST for mesothelioma.
Transarterial chemoperfusion delivers a relatively high concentration of drugs to diseased tissue in the lining of the lungs to maximise the treatment effect with limited side effects. Unlike other chemotherapy that is delivered intravenously and circulates through the entire body, interventional radiologists inject one-third of the chemotherapy cocktail of cisplatin, methotrexate, and gemcitabine directly into the internal mammary artery that supplies the pleura. The other two-thirds of the drugs are injected into the descending aorta, which reaches the intercostal vessels that also supply the pleura. The treatment is an outpatient procedure and typically lasts an hour, followed by a one-hour recovery.
The interim results of the study show 70.3% disease control rate and median overall survival rate of 8.5 months from the start of the chemoperfusion treatment. The treatment was well-tolerated by patients with a major complication rate of 1.4%. Most side effects were relatively minor, including mild nausea and chest pain.
“We were pleasantly surprised to find that this treatment doesn’t come with the same side effects of traditional intravenous chemotherapy,” said Kis. “To see these promising results with so few side effects means we are able to make a positive impact on quality of life for these patients.”
Currently, surgery is the only truly effective treatment for MPM, but the disease must be diagnosed early. Only 10–20% of patients are candidates for surgery and often experience surgical complications.
The researchers are looking to expand their study to other cancer centres with larger MPM patient populations, since the cancer is so rare. They also hope to add flexibility to the study to allow for increasing the dosage and changing the combination of medications for individual patients to determine whether either approach could further improve outcomes.
Additional information about the clinical trial is available at ClinicalTrials.gov, using the identifier NCT02611037.
The research was originally scheduled to be presented in person at SIR’s Annual Scientific Meeting, 28 March–2 April, in Seattle, USA, before the meeting was cancelled due to COVID-19 concerns. See all our coverage of the virtual event here.
A covered stent provides significantly better target lesion primary patency than percutaneous transluminal angioplasty (PTA) of stenotic lesions in the venous outflow of upper extremity haemodialysis arteriovenous (AV) fistulae, according to interim results from the AVeNEW study announced at the Society of Interventional Radiology (SIR) 2020 Virtual Sessions (13–14 June).
Other findings presented by lead author Bart Dolmatch (Mountain View, USA) in the Abstract of the Year session were that safety was non-inferior with the expanded polytetrafluoroethylene (ePTFE)-covered, self-expanding Covera vascular covered stent (BD) at six months and, at 12 months, target lesion primary patency was statistically better for the covered-stent group, as was access circuit primary patency. In addition, about half as many reinterventions were required to maintain secondary circuit patency in the Covera stent group.
AVeNEW is a prospective, randomised study in 35 centres in the USA, Europe, Australia, and New Zealand, and is the first level-one clinical trial dedicated to the use of a covered stent designed to treat stenoses in AV fistulae.
Researchers randomised 280 patients with stenotic lesions (≥50%) and clinical or haemodynamic evidence of AV fistula dysfunction to either PTA alone (n=138) or PTA followed by covered stent placement (n=142). Primary endpoints were six-month target lesion primary patency and 30-day safety. Secondary measures included target lesion primary patency, access circuit primary patency, index of patency function, and the number of reinterventions needed to maintain patency at 12 months, with ongoing data collection to three years.
It found that safety at 30 days was non-inferior between groups (p=0.002). Target lesion primary patency at 180 days (Kaplan-Meier analysis) was superior for the covered-stent group compared to the PTA group (78.7% vs. 47.9%, respectively, one-sided p<0.001).
Among the 280 participants, 34 died (10.6% covered-stent group, 14.5% PTA group), and 10 patients withdrew or were lost to follow up (4.2% covered-stent group, 2.9% PTA group) prior to 12-month evaluation, leaving 83.9% of patients for follow up. Target lesion primary patency (Kaplan-Meier analysis) was superior for the covered stent group compared to the PTA (57.5% vs. 21.2%, respectively, p<0.001) at one year. Access circuit primary patency was also significantly better for the covered-stent group at 12 months, 28.9% versus 17.7% respectively (p=0.02). The mean number of reinterventions in the access circuit to maintain patency was 0.8+1 for the covered-stent group compared to 1.7+1.3 for the PTA group.
The research was originally scheduled to be presented in person at SIR’s Annual Scientific Meeting, 28 March–2 April, in Seattle, USA, before the meeting was cancelled due to COVID-19 concerns. See all our coverage of the virtual event here.
A new, nonsurgical treatment decreases errant blood flow in the shoulder to quickly reduce pain and improve function in patients with adhesive capsulitis, also known as “frozen shoulder,” according to a research abstract presented during a virtual session of the Society of Interventional Radiology’s 2020 Annual Scientific Meeting on 13 June. Frozen shoulder gradually causes significant pain and stiffness of the shoulder joint in an estimated 200,000 people in the USA each year. The symptoms are often treated with physical therapy or pain medications, until they resolve within one to three years.
“Patients with frozen shoulder are essentially told to tough it out until their symptoms improve, but considering the significant pain and decreased function many experience, we looked to determine if this treatment model of embolization, already in use in other areas of the body, could provide immediate and durable relief,” comments Sandeep Bagla (Vascular Institute at Virginia, Woodbridge, USA), CEO of Vascular Interventional Partners, NOVA, and lead author of the study. “We were shocked at the profound and dramatic improvement patients experienced in pain and use of their shoulder.”
In this Phase II US Food and Drug Administration (FDA)-approved Investigational Device Exemption clinical trial on arterial embolization of the shoulder (AES), interventional radiologists inserted a catheter through a pinhole-sized incision in patients’ wrists that was used to feed microsphere particles into as many as six arteries in the shoulder to reduce inflammation. The treatment was conducted on an outpatient basis and took approximately one hour. Each patient’s pain, disability, and blood flow in the shoulder were measured before and after the treatment using three scales, in addition to MRI imaging to visualise the shoulder joint.
The treatment was successfully completed in 16 patients whose symptoms had not responded to conservative treatment over 30 days. Minor adverse events such as temporary skin discoloration were reported in nine patients. One month later, researchers followed the progress of 11 patients and found that pain significantly decreased after arterial embolization of the shoulder (-57mm on the Visual Analog Scale) and improved physical function in all patients (+28mm on the Single Assessment Numeric Evaluation and +30mm on the American Shoulder and Elbow Surgeons Shoulder Score). Additional progress was reported at the three-month follow up.
“We are early in the investigation of this treatment but are inspired by its effectiveness in reducing pain and range of motion in patients’ shoulders,” Bagla says.
The research was conducted as a collaboration between interventional radiology and orthopaedic surgery to build on international studies of the procedure by adapting the treatment design and embolic agent to be more durable. The team plans to expand the study to additional patients in 2020.
The authors note that this treatment is still investigational and that conservative therapies should still be considered first. Additionally, there are several important limitations of the research, including small sample size and lack of control arm.
Additional information about the clinical trial is available at ClinicalTrials.gov, using the identifier NCT03676829. The trial is funded through Terumo Medical.
The research was originally scheduled to be presented in person at SIR’s Annual Scientific Meeting, 28 March–2 April, in Seattle, USA, before the meeting was cancelled due to COVID-19 concerns. See all our coverage of the virtual event here.
Interventional radiologists participating in a collaborative house call model in rural Indiana, USA, helped reduce emergency department use by 77% and hospital re-admissions by 50% for nearly 1,000 elderly home-bound patients with chronic illnesses, according to a research abstract presented during a virtual session of the Society of Interventional Radiology’s 2020 Annual Scientific Meeting on 13 June.The novel care model brings interventional radiology treatments into patients’ homes to provide more value through in-home advanced specialty care, prevent common complications of chronic diseases, and avoid unnecessary emergency department visits and hospital admissions.
“Older home-bound patients, including those in nursing home settings, have few resources available to receive specialty care and often delay care until preventable issues become urgent and acute,” explains Nazar Golewale, lead author of the study and an interventional radiologist with Modern Vascular & Vein Center (Valparaiso, USA). “By providing image-guided treatments in a patient’s home, we are improving access to care that otherwise would need to be delivered in the hospital.”
Golewale sees more than 900 of the practice’s patients to diagnose and manage their conditions. Through varieties of portable technology, he brings interventional radiology care into patients’ homes that would normally be delivered in clinics, such as ultrasound-guided needle biopsy, paracentesis and thoracentesis, ultrasound-guided joint injections for pain, wound care, and drug infusions. Payments for care are covered by Medicare reimbursement for home-bound patients.
The care partnership was formed to overcome the difficulty of providing specialty care for chronically ill, home-bound patients in Golewale’s rural community. As a result of the programme, patient satisfaction scores increased from 17% to 84% from before and after implementation of the programme. Primary care providers, including internists and nurse practitioners, recruited specialists based on the needs of the patients they serve. In addition to interventional radiology, the house call practice includes providers in internal medicine, podiatry, laboratory services, and wound care.
“Some specialty services are available at our local hospitals, but cost-effective ways of coordinating patients’ transportation and visits remained a significant barrier to care,” says Golewale. “By bringing the hospital care to the patient, we are eliminating these hurdles and providing timely, personalised care.”
The research was originally scheduled to be presented in person at SIR’s Annual Scientific Meeting, 28 March–2 April, in Seattle, USA, before the meeting was cancelled due to COVID-19 concerns. See all our coverage of the virtual event here.
Data from one of the first clinical uses of augmented reality guidance with electromagnetically tracked tools shows that the technology may help doctors quickly, safely, and accurately deliver targeted liver cancer treatments, according to a research abstract presented during a virtual session of the Society of Interventional Radiology’s 2020 Annual Scientific Meeting on 14 June. The technology provides a three-dimensional holographic view inside a patient’s body, allowing interventional radiologists to accurately burn away tumours while navigating to avoid organs and other critical structures.
“Converting traditional two-dimensional imaging into three-dimensional holograms which we can then utilise for guidance using augmented reality helps us to better view a patient’s internal structures as we navigate our way to the point of treatment,” says Gaurav Gadodia, lead author of the study and radiology resident at Cleveland Clinic (Cleveland, USA). “While conventional imaging like ultrasound and CT is safe, effective, and remains the gold-standard of care, augmented reality potentially improves the visualisation of the tumour and surrounding structures, increasing the speed of localisation and improving the treating-physician’s confidence.”
In this initial in-human pilot study, the technology was used to deliver a treatment known as percutaneous thermal ablation of solid liver tumours. To apply this technology, the physicians use multi-phase CT to coordinate markers placed on a patient’s body. This imaging data is added to a software application that allows for segmentation of the tumour and nearby structures within the marked coordinate space. This information is fed into a proprietary augmented reality application, which utilises Microsoft’s HoloLens technology, a virtual reality headset with transparent lenses, to project a segmented hologram of the patient’s imaged anatomy directly onto the patient. The hologram is registered to the coordinate markers to ensure accurate location of the relevant anatomy.
Utilising electromagnetic tracking, instruments including the ablation probe can also be visualised in the augmented reality space during the procedure, thus allowing for true holographic intraprocedural guidance. Interventional radiologists can then use the combination of the holographic images of the patient’s anatomy and tracked tools to find the tumour in the patient’s liver quickly, check for optimal targeting of the tumour by the ablation probe, and avoid key structures.
The study included five patients who were selected for microwave ablation of their liver tumours. For safety during this Institutional Review Board (IRB)-approved study, the gold standard of ultrasound was used for primary clinical decision making and probe guidance, with direct comparison to holographic guidance. Following ablation, images and video from post-procedural sonography, cone beam and multi-detector row CT, and HoloLens recordings were evaluated. In all five cases, intra-procedural holographic guidance was in agreement with the standard ultrasound-based guidance. Post-procedural imaging showed adequate tumour ablation, and no patients experienced tumour recurrence at the three-month follow-up. In this early phase pilot study, the authors anecdotally observed that the speed of tumour localisation was faster with holographic guidance, and that their confidence in optimal ablation and critical structure avoidance was improved over standard imaging guidance. They are further attempting to quantify these findings as they continue to enroll patients in the study.
Beyond its use during treatments, interventional radiologists also see value in using this tool for clinicians’ planning purposes and for improving patient engagement and understanding of the condition and treatment.
“This technique can be used intra-procedurally to check the accuracy and quality of the treatment, as well as pre-procedurally to engage with the patient in their own care,” says Charles Martin, an interventional radiologist at Cleveland Clinic (Cleveland, USA) who is the principal investigator of the IRB and the senior author of the study. “We can change 2D images into holograms of a patient’s distinct anatomy so that both the physician and the patient get a better understanding of the tumour and treatment.”
Researchers continue to test this technology for ablations in the abdominal area with plans to expand to other types of procedures and in other areas of the body. The technology has only been tested for feasibility and therefore cannot yet be used as a standalone method for delivering a treatment.
Additional information about the clinical trial is available at ClinicalTrials.gov, using the identifier NCT03500757. This work was funded through internal enterprise grants from Cleveland Clinic, as well as the Ohio-based biotechnology start-up, MediView.
The research was originally scheduled to be presented in person at SIR’s Annual Scientific Meeting, 28 March–2 April, in Seattle, USA, before the meeting was cancelled due to COVID-19 concerns. See all our coverage of the virtual event here.
CX 2020 LIVE’s Vascular Access Consensus panel, including (clockwise from top left): Roger Greenhalgh, Nick Inston, Domenico Valenti, Robert Jones, Robert Shahverdyan and Jennifer Hanko. Click on the image to watch the session on demand.
The CX 2020 LIVE Vascular Access Consensus session sparked global interest, with chair Nick Inston (Birmingham, UK) and moderator Domenico Valenti (London, UK) taking questions from 17 countries, spanning South America to South East Asia. The session pinpointed the latest developments in this fast-moving field, including cutting-edge technologies such as endovascular arteriovenous fistula (endoAVF) creation, the use of covered stents in dialysis access, and the advantages of external support. Jennifer Hanko (Belfast, UK) opened with the benefits and drawbacks of peritoneal dialysis compared to haemodialysis, stressing the importance of choosing “the right access, for the right patient, at the right time”. Polling revealed that audience members were split on whether endovascular fistula creation is the future, with Inston concluding that the topic is “still up for debate”.
“All modalities must be considered” when planning access, Hanko began, including peritoneal access, haemodialysis, conservative care “as appropriate,” and the patient’s suitability for kidney transplantation.
She suggested that more patients could benefit from peritoneal dialysis if they had it first, but also stressed that this approach is only recommended for certain patients. Indeed, while haemodialysis requires frequent hospitalisation and peritoneal dialysis can be managed at home, the latter does carry with it a risk of infection.
Among the factors that preclude peritoneal dialysis are the presence of cardiovascular disease, low serum albumin, and age greater than 75 years. Furthermore, Hanko noted that there is “no consensus” on when a patient should proceed to both peritoneal dialysis catheter and back-up fistula creation.
Patients with no fistula options “should be encouraged to do peritoneal dialysis if possible,” Hanko advised the CX 2020 LIVE audience.
“Traditionally, we have advocated radiocephalic fistula first.” However, Hanko acknowledged that there are situations in which this may not be appropriate. She pointed out that patient choice is also an important factor, summarising that the approach at the Belfast City Hospital “is no longer fistula first. It is the right access, for the right patient, at the right time”.
Valenti opened the discussion after Hanko’s presentation, asking how patient choice influences her decision-making in fistula creation. “I think it is a partnership,” Hanko replied, adding that “it is about working with [patients] to get to a solution”.
Inston asked whether it is common practice to insert a peritoneal dialysis tube at the same time as creating a fistula, to which Hanko responded that it is not something she would advocate for most patients. But she acknowledged that a “small subset, probably less than 5%” would benefit. “I think we can all testify to the fact that when patients fail peritoneal dialysis, we are not always that great at having their vascular access ready”.
In response to a question from the UK, about what to do if fistula formation is not what the patient wishes, Hanko said she would still strongly recommend it, and get additional education for the patient on the risks versus benefits of a catheter over a fistula. However, she noted that “it is the patient’s choice in the end”.
New era of vascular access must move beyond “fistula first” approach
Clockwise from top left: Roger Greenhalgh, Nick Inston, Domenico Valenti, Matteo Tozzi, David Kingsmore, and Panagiotis Kitrou
David Kingsmore (Glasgow, United Kingdom) also advocated a patient-tailored outlook to vascular access, describing in his presentation the “old era” approach of “fistula provision for all”—typified, he said, by European Society for Vascular Surgery (ESVS) 2018 guidelines on vascular access—as being ripe for change, in particular through greater use of early cannulation arteriovenous grafts (ecAVGs).
Kingsmore made the point that while, for some patients, fistulas remain the ideal treatment option, “for half [of patients] they are not”. Likewise, catheters for some patients are ideal, he commented, but for most they are not. “You have to consider what the patient aim is, and how to incorporate transplant with our vascular access planning. Overall, early cannulation grafts are certainly under-utilised and they can be optimised. We have an opportunity for a new era, to integrate and tailor optimal practices to patients’ aims, choices, and needs.”
Following his presentation, Valenti asked Kingsmore whether the “fistula first” approach has contributed to the underutilisation of grafts, to which he replied: “We are victims of looking at procedures rather than patients, [and] not integrating with other services and patient outcomes. Nick [Inston] has talked before about the outcomes and the changing success rate. We have got to bear in mind that dialysis has evolved substantially over the years, and transplant has evolved even more.”
Support for the use of external reinforcement is still limited
External support is currently not widely used in aid of vascular access, polling at CX 2020 LIVE’s Vascular Access Consensus Session has indicated
Developments in the use of external support devices were outlined by Robert Shahverdyan (Hamburg, Germany), who put forward a mechanical solution for fistula failure.
And, although an online poll of participants found that only 17% are currently using these devices to improve fistula outcomes, Inston was confident that the numbers would grow following Shahverdyan’s presentation on VasQ (Laminate Medical).
“The VasQ device improves the likelihood of an AVF becoming functional by addressing both haemodynamic and mechanical factors of failure. It produces consistent clinical benefits to patients, and also improves outcomes for an individual clinic when adopted as the standard of care for AVF creation.
“Several studies have been performed and more are under way to validate the clinical benefits of VasQ. So far, we are observing consistently high AVF usability and patency outcomes across the studies: 80–90% usability, with roughly 80% primary patency at six months for VasQ. [This] compares favourably with most other published results for standard AVF creations.”
Experience with endoAVF “encouraging,” but more data needed
Robert Jones (Birmingham, UK) provided a technology update on endoAVF, looking at the performance of two catheter systems—Ellipsys (Avenu Medical) and WavelinQ (BD).
One of the major benefits with this approach is the lack of surgical trauma, “therefore potentially less intimal hyperplasia and stenosis formation”. Jones also highlighted: “Both of these catheter systems utilise the forearm vascular anatomy to create an endoAVF, an area that is not typically used for surgical fistula creation”.
He added: “Multiple specialty operators can use both devices to create successful fistulas and this potentially can lead to a decreased waiting time for definitive access. Of utmost importance is patient preference.”
Polling reveals audience split over whether endovascular fistula creation is the way forward
Polling results revealed that audience members were split on whether endovascular fistula creation is the future
Polling of the online audience revealed that only 46% agreed with the statement: “Endovascular creation of a fistula is the way forward.” However, if a role for durability of the fistula can be established, consensus may be reached. In the discussion that followed the presentation, a participant from Buenos Aires in Argentina raised the issue of the difference in cost between endoAVF formation and a standard surgical procedure. Jones conceded that “the upfront cost of an endoAVF device is higher in most countries than it is for surgical fistula”. But he pointed out: “The evidence to date has demonstrated that these endoAVFs require less reinterventions.” Jones pointed to the potential for longer-term savings, citing an American study published in the Journal of Vascular Access that compared collective WavelinQ data with retrospective Medicare data that “demonstrated that there was a saving to be made in each patient over a period of time. The upfront costs are certainly more expensive with these devices but, overall, in a long period of time, according to the evidence, it suggests there is a cost saving.”
Edited case illustrates endovascular fistula creation with WavelinQ
Panagiotis M Kitrou (Patras, Greece) demonstrated an edited case on the endovascular creation of an arteriovenous fistula using WavelinQ.
The device consists of two rapid change catheters, with the arterial catheter inserted first. Kitrou detailed the steps involved in preparing the patient, as well as the other devices required for the procedure.
The issue of costs associated with endoAVF was raised again in the discussion that followed, with a question from Johannesburg in South Africa. Other queries on time-to-fistula maturation in endoAVF, and whether it is necessary to coil deep veins, were submitted from as far afield as Argentina and Pakistan.
Covered endoprostheses are “the gold standard” for venous anastomosis with prosthetic vascular access
A second edited case was presented by Matteo Tozzi (Varese, Italy) on the use of a self-expanding covered endoprosthesis—Viabahn (Gore)—to treat AVF failure at the venous anastomosis. Tozzi reviewed the case of a 69-year-old male receiving haemodialysis for diabetic nephropathy, starting the dialysis with a tunnelled central venous catheter filter for a bloodstream infection.
Following the edited case, Tozzi then fielded questions from the global audience, including one from India to which Tozzi responded by outlining that “in the cephalic arch, the stent graft is the first option for the stenosis because all other techniques such as drug-coated balloon, plain balloon or high-pressure balloon fail very fast”. In this instance, a covered stent graft is “the gold standard”.
Tozzi added that he “chose this terrible case to demonstrate the ability to maintain patency in the functionality of the early cannulation graft” and following a question from a physician in Malaysia, about the use of cutting or scoring balloons before deploying the stent graft, Tozzi noted that “I prefer scoring balloons for predilatation of arch stenosis like the prosthetic venous anastomosis. I do not use cutting [balloons] because the blade damages the elasticity of the internal lamina of the vessel and therefore increases the intimal hyperplasia.”
Roger Greenhalgh (top left), Gunnar Tepe (top right), Jean-Paul de Vries (bottom left), Andrew Holden (bottom middle) and Amer Zanabili (bottom right)
Roger Greenhalgh (top left), Gunnar Tepe (top right), Jean-Paul de Vries (bottom left), Andrew Holden (bottom middle) and Amer Zanabili (bottom right)
In a series of Podium 1st presentations from world-class faculty, CX 2020 LIVE attendees heard the latest data on peripheral arterial disease management and an evaluation of different types of stents, including covered and helical options for challenging lesions. In total, nearly 5,000 people, from 125 countries, have registered for the inaugural, CME-accreditedseries of 10 sessions. The first CX 2020 LIVE session dedicated to peripheral interventions has been viewed by 3,222 people, tuning in from five continents.
An overwhelming majority of 81% answered “yes” in agreement with the comment “I like relining”. The poll followed three sessions that looked at the concept of “relining”, using covered stents for the management of complex aortoiliac occlusive disease. Livestream attendees heard that the surgical management of complex lesions, which may be heavily calcified, is difficult, and may lead to rupture. Meanwhile, the endovascular approach is gaining ground.AmerZanabili (Oviedo, Spain)presented an edited case demonstrating the relining of an occluded, long TASC D iliac lesion, showcasing the potential of this technique. The polling results that followed then revealed an enthusiasm for this endovascular approach.
Roger Greenhalgh (London, UK) chaired the discussion, and Gunnar Tepe (Rosenheim, Germany) joined him as moderator for the session.
Covered balloon-expandable stents are effective treatment options for aortoiliac occlusive disease
In the first talk, Jean-Paul de Vries, (Groningen, The Netherlands) reported the key findings from a systematic review (published in the Journal of Vascular Surgery) of covered balloon-expandable stents for the management of aortoiliac occlusive disease. De Vries said: “Covered balloon-expandable stents are effective treatment options for aortoiliac occlusive disease as evidenced by the high rates of technical success and patency in all the stent grafts at one-year follow-up. They are preferred over bare metal stents for complex aortoiliac lesions, based on the documented five-year patency results for Advanta V12 in the COBEST trial.”
Overall, the studies explored five different stents: Advanta V12 (Getinge), Viabahn VBX (Gore), Lifestream (BD), BeGraft (Bentley), andJostent (Jomed).
De Vries said the rates of technical success and primary patency were both high, adding that that primary patency, at one year, “was 96.6% for Viabahn VBX and that is comparable to the Advanta V12 [83.6–96.4% at one year] and 94.4% for BeGraft [one-year data were not available for Lifestream or Jostent].” He further noted that five-year data were available for Advanta V12, showing a primary patency rate of 74.7% and a freedom from target lesion revascularisation rate of 67.4%.
During the discussion that followed his presentation, de Vries noted that comparative trials were required because, at present, the data are insufficient to provide “any proof that the new-generation devices perform better than the former generation ones”. However, he observed that three-year data for Viabahn VBX had recently been published and these were comparable to three-year results for Advanta V12.
“Excellent” three-year results with Viabahn VBX relate to stent graft’s unique design
Andrew Holden (Auckland, New Zealand), in his talk, further expanded on the three-year data from the VBX FLEX investigational device exemption (IDE) trial. The objective of the study, he explained, was “to evaluate the safety and efficacy of the VBX stent graft [Gore] for the treatment of arterial occlusive disease in patients with de novo or restenotic lesions in the common and/or external iliac arteries”. The primary outcome was a composite of major adverse events at nine months.
Overall, in VBX FLEX, 234 devices were implanted into 213 lesions (134 patients) across 27 sites. Holden said: “The Viabahn VBX is made up of a double polytetrafluoroethylene (PTFE) layer with independent stainless steel rings that give it flexibility and conformability.”
He reported that with the three-year data, freedom from target lesion revascularisation “was a very impressive 91.2%, which improves to 98.1% when we evaluate the clinically-driven target lesion revascularisation.” Furthermore, according to Holden, “a number of clinical parameters remained improved at three years,” including the Rutherford category, resting ankle brachial index, and walking impairment questionnaire scores. “In fact, of the patients who were at Rutherford 0 by three years, 80% had started from a baseline of Rutherford 3 or 4. Overall, 92% of patients improved at least one Rutherford category at three years,” he explained.
“The VBX FLEX clinical study is truly a real-world study, including complex aortoiliac occlusive disease (TASC II C and D lesions, 32.1%), that has shown excellent results. […] These are no doubt due to the unique design of this device,” Holden concluded.
The ensuing discussion emphasised that covered stents have become the first-line treatment for complex aortoiliac disease. “What we have seen, particularly in complex disease, is a real practice shift towards covered stents. I think one could consider using uncovered stents for very simple lesions, but obviously, for more complex cases, I think the standard of care is covered stents. Rupture of iliac arties is potentially catastrophic, but this is really very well managed by covered stents.”
Greenhalgh observed that there was a risk of rupture when implanting a covered stent because calcification meant that there was no elasticity in the artery. “When you start to expand it, surely, occasionally, there are ruptures? [Is the understanding that] the lining is going to take care of the leak?” he questioned.
Holden commented: “That is precisely right. As long as we are trying to optimise lumen diameter, we are going to see significant incidence of rupture. […] With covered stents, you are certainly much more comfortable being aggressive.”
Roger Greenhalgh (top left), Gunnar Tepe (top right), Rupert Bauersachs (bottom left), Thomas Zeller (bottom middle) and Joakim Nordanstig (bottom right)
Rivaroxaban reduces risk of comorbidities in patients with peripheral arterial disease
Three-quarters of the CX 2020 LIVE audience agreed with the statement: “I will use rivaroxaban in peripheral arterial disease lower extremity revascularisation”. Polling took place following a talk from Rupert Bauersachs (Darmstadt, Germany) giving the results of the VOYAGER PAD trial.
“After revascularisation, one in five peripheral arterial disease patients will suffer from acute limb ischaemia, major amputation, acute myocardial infarction, ischaemic stroke, or cardiovascular death within three years,” Bauersachs told CX 2020 LIVE delegates. The VOYAGER PAD trial, he went on to relate, therefore set out to evaluate the safety and efficacy of 2.5mg bid rivaroxaban plus aspirin versus aspirin alone to reduce thrombotic vascular events after peripheral revascularisation.
Bauersachs reported: “Rivaroxaban 2.5mg bid on top of aspirin was associated with a significant 15% reduction in major adverse limb events and major adverse cardiac events, with no significant increase in TIMI [thrombolysis in myocardial infarction] major bleeding. Acute limb ischaemia was significantly reduced by 33% compared to current standard of care.”
The study therefore met both its primary efficacy endpoint—a novel outcome measure combining major adverse limb events and major adverse cardiac events—and its primary safety endpoint—TIMI bleeding.
“Dual pathway inhibition treatment is the only antithrombotic regimen proven for significant benefit of the peripheral revascularisation in a large, randomised controlled trial,” Bauersachs concluded.
As questions began to flood in from Europe and Asia, it became clear that many pertained to Bauersachs’ rationale for using such a low dose of rivaroxaban. “It is a very low dose, 2.5mg,” Bauersachs agreed, adding, “the actual dose for treating venous thromboembolism, for example, is 30mg. Because it is such as low dose, it has to be given twice a day.
“As we know, these are high-risk patients, so the objective was, with a low dose of anticoagulants on top of antiplatelets, to reduce those outcomes.”
Responding to a question asking why a low dose of warfarin was not used, Bauersachs said that previous trials had shown “unacceptably high rates of bleeding” and had lacked efficacy.
Lastly, a CX 2020 LIVE viewer from Malaysia queried the recommended length of time for patients to take rivaroxaban plus aspirin, after revascularisation. In agreement with Tepe, Bauersachs said that it would be a lifelong treatment.
“I think the point we are talking about here,” Greenhalgh said in summary, “is that patients with that sort of peripheral arterial disease will have all of these other issues and comorbidities. It is not a standalone condition, it is a marker of arterial disease throughout the body’s vascular system; the more peripheral, the higher the likelihood it will be severe elsewhere in the body.
“So, the use of rivaroxaban enables the complications that come with this complex disease to be reduced, and comorbidities can be handled better.”
MIMICS-2 study three-year results: Swirling flow “is the answer”
Thomas Zeller (Bad Krozingen, Germany) presented the three-year results of a US IDE study, MIMICS-2, for which he is the European principal investigator. The prospective, single-arm, multicentre clinical trial found comparable efficacy and safety results for the helical BioMimics 3D stent (Veryan Medical) and drug-coated balloons or drug-eluting stents available on the market.
The primary endpoint for this study consisted of a safety endpoint, composite of deaths, major amputation, clinically-driven target lesion revascularisation through 30 days, and an effectiveness endpoint defined as primary patency at 12 months. The proportion of chronic total occlusions was 30%, and moderate-to-severe calcification was seen in 46% of lesions.
Both device and technical success was 100%, and the primary safety and primary efficacy endpoints were reached. Zeller told the audience that these results represent “a clear achievement” for the BioMimics 3D stent.
Three-year freedom from clinically-driven target lesion revascularisation was 81% for the entire patient cohort, and there was “only” a decrease by 8% of freedom from reintervention between one and three years, Zeller related.
Describing the device, Zeller said: “The BioMimics 3D stent represents a new bare metal stent, designed with a helical centreline, which imparts a nonplanar curvature to the stented femoropopliteal segment, inducing swirling flow.”
This mimics the natural flow of certain anatomy, Zeller explained. The vessel curvature in the aortic arch and the iliac arteries induces a swirling flow in normal anatomy, known to protect endothelial cells against atherosclerosis and restenosis, he noted. This is based on the lifetime work of Colin Caro (London, UK). Greenhalgh elaborated: “From what you have just told us, we can say Colin [Caro] was right, all along. Swirling flow is the answer.”
Zeller assessed the results of the BioMimics 3D stent from the MIMICS 2 study against those for contemporary devices, including bare metal stents, drug-coated balloons, and drug-eluting stents. “If you compare the BioMimics 3D stent results from the MIMICS 2 study with Supera (Abbott), Zilver PTX (Cook Medical), Eluvia (Boston Scientific), and the IN.PACT Admiral (Medtronic), we can see that freedom from reintervention up to three years is almost comparable,” Zeller said.
Zeller responded to a question from Tepe about the lower event rate seen in the long term,commenting: “It underlines the theory of the basal-protective and endothelial-protective effect of swirling flow. We have the acute phase, where we see the patency failures, which are induced by acute inflammation, resulting in neointimal hyperproliferation and, over time, it evens out regarding the need for reintervention. For me, the most interesting question would be: ‘What is the outcome of combining this sort of long-term protective stent design with acute suppression of neointimal hyperproliferation means with an antiproliferative agent?’ That would be a very interesting study to be seen in the future.”
Following Zeller’s presentation, Greenhalgh commented: “[The BioMimics 3D stent represents] a completely new way. We are hearing about the future here. This is not just practical reconstruction—you have just heard how the future is going to go.
“Caro spent his life analysing normal flow of an artery, and he believed that if the blood swirled, then it would reduce the risk of arterial disease, and we have just heard that that it is possible, and he was right. We have also had a peek into the future, about how the treatment might be.”
Absence of long-term benefit of revascularisation in claudicants, according to five-year data
The session also heard how a liberal strategy of revascularisation in patients with intermittent claudication resulted in a substantial improvement in health-related quality of life for two years, but this benefit was lost at five years. This is the conclusion presented by Joakim Nordanstig (Mölndal, Sweden), after he shared the five-year results from the IRONIC randomised trial.
The IRONIC trial investigators aimed to study the clinical effectiveness and cost-effectiveness of the two most widely offered treatment strategies for patients with intermittent claudication: lower limb revascularisation in combination with best medical treatment and exercise advice, versus best medical treatment and exercise advice only.
Speaking to the fact that the IRONIC trial included femoropopliteal lesions and aortoiliac lesions alike, Greenhalgh commented, “Assessors would say that the expectation of success or reconstruction over five years with the aortoiliac is far better than with the femoropopliteal. Some would argue that you should keep them separate because the expectation is different. They may present with intermittent claudication, so it is one presentation, but a different expectation of natural history.”
“I agree with that comment,” Nordanstig replied, “but for the purpose of this design, it was a real-world design.”
Asked if this would impact his clinical practice of patients with intermittent claudication going forward, Nordanstig said: “In a way, yes,” before elaborating. “It is a staged process, actually, and I try to really carefully inform every patient about the pros and cons with revascularisation. It is not a first line treatment for me, but I will re-evaluate all patients within a few months.”
The session was followed by an Industry Symposium supported by Concept Medical to explore where the field stands in terms of sirolimus devices, with a session titled “Overcoming the limitations of paclitaxel: A new sirolimus-coated balloon for the treatment of peripheral vascular disease”.
Shockwave Medical announced today that the Centers for Medicare & Medicaid Services (CMS) has issued new codes for intravascular lithotripsy (IVL) procedures performed in peripheral arteries in both the hospital outpatient and inpatient settings.
The new Healthcare Common Procedure Coding System (HCPCS) outpatient and International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) inpatient codes will go into effect on 1 July 1 October 1 2020, respectively. Under these new codes, Medicare payment rates for IVL procedures performed in the hospital outpatient and inpatient settings, respectively, are consistent with current payment levels for other similar peripheral artery interventional procedures.
“The decision by CMS to assign codes for peripheral IVL procedures in both outpatient and inpatient settings is an important validation of Shockwave’s technology as a unique and distinct therapy for treating complex calcified disease in the peripheral arteries,” said Doug Godshall, president and chief executive officer of Shockwave Medical.
He continued: “We look forward to continued engagement with CMS as these new codes will now enable the collection of cost data specific to IVL procedures, which is the information the agency utilises when making future adjustments to procedure payment levels. The appreciation for IVL’s unique ability to safely and effectively treat these challenging patients is growing globally and we are grateful that CMS has taken this important first step on the path towards establishing a reimbursement level that appropriately reflects the clinical value delivered by IVL.”
Roger Greenhalgh (top left), Stéphan Haulon (top right), Ludovic Canaud (bottom left), and Gustavo Oderich (bottom right)
Roger Greenhalgh (top left), Stéphan Haulon (top right), Ludovic Canaud (bottom left), and Gustavo Oderich (bottom right)
Last week week, the CX 2020 LIVE agenda turned to the technically challenging topic of aortic arch interventions. Through presentations, discussion, and polling, the session—chaired by Roger Greenhalgh (London, UK) and moderated by Stéphan Haulon (Paris, France)—aimed to tackle some vital questions, including how to reduce the risk of stroke in thoracic aortic endovascular procedures, what the best options are for the left subclavian branch, and how best to approach aortic arch aneurysms. The session covered atherosclerosis, dissection, transection and ulcers, and their role in guiding treatment was clearly emphasised, with audience polling revealing that 85% would alter reconstruction in the arch according to the underlying pathology. The session also dealt with the wider debate of open versus endovascular surgery and considered the benefits of a multidisciplinary team. In a boost for the endovascular approach in this difficulty anatomy, 63% of audience members disagreed with the statement “Open is best”.
Gustavo Oderich (Rochester, USA) outlined preliminary experience with a range of device options that would enable the left subclavian artery [LSA] to stay patent. He began with the statistic that “30–60% of thoracic endovascular aortic repair [TEVAR] patients require Zone 2 incorporation with coverage of the LSA”. Considering the implications, he detailed: “We know LSA coverage without revascularisation is associated with more arm ischaemia, posterior circulation events, and spinal cord injury”.
He noted that patient-specific fenestrated stent grafts have been available for over two decades, and added that reports from the Cleveland Clinic and the Hamburg group demonstrate that mortality and stroke can be an issue, particularly if there is misalignment of the stent graft requiring arch manipulations.
Considering options for left subclavian branch incorporation, Oderich began with the Terumo Aortic Scallop stent graft, outlining a Dutch registry of 30 patients showing “excellent outcomes”, with only one Type Ia endoleak, one mortality, and one stroke.
Moving on to the Gore Thoracic Branch Endoprosthesis (TBE), he noted that this is currently under investigation in the USA. “This device has a single retrograde portal and one-side branch stent,” he said, adding that “this is a self-expandable stent, specially designed for the subclavian artery, with flared diameters”.
“It is recommended for these cases to obtain brachiofemoral through-and-through access for better support of the side branch,” he told the CX 2020 LIVE audience, going on to detail his clinical experience: “My preference is to use a small incision to expose the distal brachial artery, obtain retrograde access, and snare the wire in the distal thoracic aorta. The device has been loaded via the aortic wire and the through-and-through brachiofemoral wire”.
Oderich detailed that the feasibility trial results with the Gore TBE were reported in the Annals of Thoracic Surgery, with “excellent outcomes for Zone 2, no mortality, one minor stroke, one late asymptomatic subclavian artery branch occlusion, no Type Ia endoleak, and no late neurological events”.
Going on to discuss the Medtronic Valiant Mona LSA stent graft, Oderich outlined that this was investigated in an early feasibility study of nine patients. “Although technical success was obtained in all patients, there were three minor non-disabling strokes,” he detailed.
The Cook LSA single branch device, which Oderich noted was designed by Stéphan Haulon (Le Plessis-Robinson, France) and colleagues, has a triple-wide scallop that incorporates the left carotid artery and a preloaded catheter. “Following deployment of this stent graft, a sheath is advanced via the preloaded catheter, the subclavian artery is catheterised, and the repair is extended with a bridging stent,” he described.
He concluded: “Zone 2 extension is needed in up to 60% of TEVAR patients, and the preliminary experience with LSA branch devices indicates low morbidity and stroke rates, with high patency rates”.
Global audience seeks expert opinion on LSA branch devices
In the discussion following his presentation, Oderich first addressed a question from Haulon on treatment with an off-the-shelf device. He responded: “We can have an off-the-shelf device for the subclavian artery, because the location of the left subclavian artery in relation to the left carotid artery is quite predictable”.
He continued: “I do think that a lot of these patients currently being treated with coverage will actually have the option of revascularisation. That would include acute cases, like dissection or even transection. In the pivotal trial from Gore, the enrolment has been quite fast for the chronic dissection group. It is quite impressive. They were tentatively trying to enrol 10 patients and they have already included 93. So, I think that there will be a large subset of patients that will benefit from the left subclavian branch”.
An audience member watching from Moldova then asked Oderich, “In what subgroup of patients would either a bypass or transposition be used rather than a branch endograft?” to which Oderich responded that the “obvious” cases would be when the subclavian artery is not suitable for a branch.
Oderich noted that, given the investigational nature of some grafts, surgeons are still “shying away” from treating patients with certain indications, for example a very dominant vertebral artery. That being said, “with increased experience, as we showed, the patency rate is excellent”. He was positive looking forward: “I do think there will be a benefit of a branch over a bypass”.
One limitation of branches may be for the low origin of the left vertebral artery, Oderich revealed in a response to a question from Brighton, UK. In these cases, “we have to consider another device, like a scallop subclavian artery incorporation,” he suggested.
Finally, a question from Singapore asked when you would choose an LSA branch device over a fenestrated one for the LSA. “The issues with fenestration are several-fold,” Oderich responded. “First of all, from the standpoint of industry, it becomes [a] totally patient-specific device for the most part. The nice think about the branches is the ability to deploy the aortic stent graft and commit to that position. You do not have to keep twisting and you can just focus on the branch.
“I would say people are probably going to move away from fenestration towards a branch,” he concluded.
Roger Greenhalgh (top left), Stéphan Haulon (top right), Roberto Chiesa (bottom left), Philippe Charbonneau (bottom centre), and Luca Bertoglio (bottom right)
Collaboration needed to respond to aortic arch aneurysms
Roberto Chiesa (Milan, Italy) provided a comprehensive overview of total endovascular, hybrid, open and frozen elephant trunk repair techniques, looking at which is the best strategy to use in different scenarios, and the European Society for Vascular Surgery (ESVS) recommendations for each. He stressed: “The clever surgeon chooses the best option for the patient.”
Chiesa’s key message on aortic arch aneurysms was the need for multidisciplinary decision-making. He revealed that, at his centre, meetings take place every day between vascular and cardiac surgeons to decide on the choice of technique. Chiesa’s message also illustrated the potential that exists for using patient characteristics to choose between endovascular and open reconstruction. This view was reflected in the polling result on whether to alter reconstruction in the arch according to underlying pathology, with which 85% of respondents agreed. “It [the approach chosen] depends on the extent of the disease and the situation of the patient. In a fit patient, also in a young patient … open surgery can represent a good option. Endovascular repair offers possibilities that open surgery cannot offer,” he said.
“Acceptable results in fit patients” can also be achieved using the Frozen Elephant Trunk technique, said Chiesa, describing a hybrid strategy—a combination of both open and endovascular technique—as “a good option in high to moderate-risk patients”, and total endovascular branch repair as providing improving results in anatomically suitable patients. He closed his presentation with the prediction: “I think that will represent the future.”
Chiesa’s colleague, Luca Bertoglio (Milan, Italy), also presented an edited case of a carotid subclavian bypass. He explained that LSA revascularisation is recommended in aortic procedures to reduce the incidence of spinal cord ischaemia and stroke. Bertoglio noted this was the procedure that “we prefer to perform in our centre”.
He outlined how the carotid subclavian bypass is performed, and dealt with common difficulties encountered, including the impact of anatomy on the choice of implant.
A lively discussion followed his presentation, at the end of which Greenhalgh declared himself to have “been extremely entertained”.
Kevin Mani (Uppsala, Sweden) echoed Chiesa’s comments on the need for consultation with cardiothoracic colleagues when he discussed the feasibility of endovascular arch repair for type A dissection. He explained that more than two-thirds of post type A dissection repair patients are technically eligible for endovascular arch repair. He said: “It is not an easy procedure for the surgeon or the patient, so everybody is happy if it can be done endovascularly at the second stage.”
He concluded: “More than two-thirds of post type A dissection repair patients are technically eligible for endovascular arch repair. Future advancements that may increase this number include a greater awareness among cardiovascular surgeons of a sufficient ascending graft length.
“Considering the high rate of eligible patients, it can be expected that the use of endovascular arch repair for type A dissection patients will increase over time and increasingly replace redo sternotomy as the treatment of choice,” Mani speculated.
Silent cerebral lesions study: Clinical stroke incidence small but infarction rate “substantial” on magnetic resonance
Philippe Charbonneau (Paris, France) presented findings from a multicentre study which looked to quantify silent cerebral lesions, evaluate their clinical impact and to identify predictive factors following endovascular arch repair. He noted that TEVAR is the primary repair technique for aneurysms of the descending thoracic aorta but added that “neurological complications from this technique remain a significant concern” with the stroke rate at around 5%.
The study found that a total of 245 silent cerebral infarcts were detected in 45 patients, which represented almost 50% of the cohort. Lesions were multiple in 78% with a “predilection for both hemispheres” (58%) as opposed to isolated hemispheres (33% left and 9% right). When comparing baselines characteristics between patients with and without silent cerebral lesions, “no difference was found on univariate analysis”. An operative analysis of patients with and without new lesions showed that urgent procedure, deployment in Ishimaru zone 0–1, placement of a branch or fenestrated endograft, a proximal stent diameter of more than 40mm and the use of a haemodynamic strategy during the deployment were all “significantly associated with the presence of ischaemic lesions”.
Haulon said the results are “really interesting” and noted that there is “room for improvement” in aortic arch repair procedures. After Charbonneau fielded questions from physicians across the globe, Greenhalgh remarked that “The STEP study was set up for this very reason” and concluded that the “key is to see whether we can modify technique to reduce that [the infarction rate].”
Double fenestrated stent graft associated with low risks of mortality and persistent stroke
During the session, Ludovic Canaud (Paris, France) described the double branch technique as the “gold standard” for endovascular repair of the arch, while acknowledging that it does carry a high risk of mortality, failure, and stroke. An alternative approach is the chimney procedure, Canaud said, noting that while this is associated with high technical success, it has also been known to carry a risk of endoleak that is higher than 20%. Canaud also outlined the current status of in situ fenestration, detailing its high technical success rate on the one hand, but also issues with long-term follow-up on the other, including fabric tears and poor-quality fenestration.
Roger Greenhalgh (top left), Stephen Black (top right), Armando Mansilha (bottom left), Manj Gohel (bottom middle) and Lowell Kabnick (bottom right)
In a boost for vascular education, the CX 2020 LIVE sessions have been granted European Union (EU) and US reciprocal Continuing Medical Education (CME) points in recognition of its highly interactive nature. In awarding this, the European Accreditation Council on CME (EACCME) is taking into account that this is a livestream with speakers performing from a panel and receiving questions from a global audience. On Tuesday, 759 attendees from 79 different countries tuned in. Each audience member could submit their name, country, and a question or point to the speaker in real-time, enabling interaction, discussion, and polling.Roger Greenhalgh (London, UK) chaired the most recent session, with Stephen Black (London, UK) moderating, as participants from five continents learnt about the latest development in superficial venous disease. Panellists fielded questions from 29 different countries, including the USA, Brazil, Ukraine, Kenya, Mexico, Spain, Saudi Arabia, Egypt, Argentina, Moldova, and the Russian Federation.
The first three talks of the session teased forthcoming, as-yet-unpublished guidelines from the European Venous Forum (EVF), the European Society for Vascular Surgery (ESVS), and the American Venous Forum (AVF)/Society for Vascular Surgery (SVS). These presentations were given by Armando Mansilha (Porto, Portugal), Manj Gohel (Cambridge, UK), and Lowell Kabnick (New York, USA), respectively. Additionally, a clinical assessment and work-up of patients with possible pelvic vein incompetence was presented by Aleksandra Jaworucka-Kaczorowska (Gorzów Wielkopolski, Poland), followed by a network meta-analysis on the use of cyanoacrylate glue, from Raghu Kolluri (Columbus, USA), audience polling, and, finally, an edited case from Kathleen Gibson (Bellevue, USA).
Spontaneous superficial vein thrombosis “far from a benign pathology”
Traditionally, superficial vein thrombosis (SVT) was treated with surgical management due to the perceived increased risk of deep vein thrombosis (DVT), which in turn could cause pulmonary embolism (PE), associated with a higher risk of death. Interestingly, it emerged in the CX 2020 LIVE discussion that surgical intervention is no longer mandatory. Instead, venous experts are searching for factors that explain a possible underlying hypercoagulable state that can lead to spontaneous thrombosis. One possible therapeutic option that is emerging for the treatment of SVT is the administration of anticoagulants. SVT is therefore no longer seen as requiring emergency surgery, but is indicative of an underlying condition that can be treated medically.
Manj Gohel (Cambridge, UK) told the CX 2020 LIVE audience that SVT is “far from a benign pathology”, discussing how the latest set of recommendations from the ESVS are set to pave the way for new approaches to treating this specific type of blood clot.
Though acknowledging that venous thrombosis is an “enormously varied topic”, Gohel said the writing committee felt strongly that superficial vein thrombosis should be included in the new guidelines, as it is “largely neglected” in other recommendations worldwide. “It is important to realise,” he added, “that it is significantly more common than deep vein thrombosis [DVT]; at least five times more common [as suggested] in most studies.”
Gohel said: “Anticoagulation, rather than antibiotics, is going to be the mainstay of treatment for most patients”. While he stated that “there will be a role for ablation of superficial venous reflux”, he clarified that he thought that this will probably not play a part in the treatment of sudden spontaneous thrombosis in the superficial vein.
A question posed to Gohel from a CX audience member from Iraq asked: “After treating superficial vein thrombosis, how long do you suggest waiting before treating the varicose vein in absence of any other contraindications?”
In his reply, Gohel highlighted the importance of treating the underlying superficial reflux. “All too often these patients have been treated and seen in thrombosis clinics, they have been told there is no DVT, and almost forgotten about”.
Multidisciplinary team important for managing pelvic vein incompetence
Roger Greenhalgh (top left), Stephen Black (top right), Aleksandra Jaworucka-Kaczorowska (bottom left), Raghu Kolluri (bottom middle), Kathleen Gibson (bottom right)
In her talk, Jaworucka-Kaczorowska looked at the clinical assessment and work-up of patients with possible pelvic vein incompetence. She showcased some extreme examples that she has encountered in her work as a gynaecologist, all the while emphasising the importance of drawing upon multiple skillsets in the treatment of these patients.
In particular, Jaworucka-Kaczorowska—noting she was a gynaecological surgeon—stated that she referred patients to a relevant centre with the appropriate radiological experience if they required percutaneous embolisation. Responding to this, Greenhalgh observed: “I think we have learned that when a physician can see a problem, the answer is that it is a multidisciplinary team that they require.”
Cyanoacrylate: A “good technique”, but “not a panacea”
The discussion next turned to the use of cyanoacrylate glue. Delivering his Podium 1st presentation, Kolluri said the VenaSeal closure system (Medtronic), a type of cyanoacrylate glue, is “a promising therapeutic option” with high rates of anatomic success, improved pain scores, and a low occurrence of adverse events compared with alternative treatment modalities. He made this conclusion based on the six-month results of a network meta-analysis published in the May issue of the Journal of Vascular Surgery: Venous and Lymphatic Disorders, comparing different interventions for chronic venous insufficiency (CVI) management. Following his talk, Gibson provided a step-by-step guide to cyanoacrylate closure using VenaSeal.
The discussion following the two cyanoacrylate-focused talks highlighted that this new technique may be particularly useful in carefully selected patients, but was not suitable for all veins.
When asked: “Are you a fan of cyanoacrylate glue”, 61% of CX 2020 LIVE respondents answered “no”.
Gibson summarised her take-home message: “It is not going to replace endothermal ablation. I think it is an advance; I think there are some situations where it is extremely good. For example, in the elderly population, where they have a very low incidence of hypersensitivity.”
Kolluri concurred, stating that his patients, who benefit from the use of cyanoacrylate glue, have quite severe disease, with multiple comorbidities, and are at high risk of bleeding.
Turning to the other panellists, Greenhalgh invited each to provide their take on the technique. Gohel: “It is not a panacea; it is not going to replace everything”; Kabnick: “Thermal is still the gold standard”; Mansilha: “One more good technique. The strategy is the point”.
Moderator Black concluded the session: “I think like all new techniques, you learn the good and the bad, and this will find a good place in the long term”.
CME accreditation
The 10 livestreams that comprise CX 2020 LIVE are together worth 10 CME points, with one point awarded for each session. Participants can only claim CME points for the sessions that they have watched live.
Transit Scientific has received US Food and Drug Administration (FDA) clearance for the XO Score percutaneous transluminal angioplasty (PTA) scoring sheath platform for use in iliac, ilio-femoral, popliteal, infra-popliteal, and renal arterial plus synthetic and/or native arteriovenous hemodialysis fistula.
Angioplasty is performed with expandable polymer balloon catheters to dilate stenosed, or narrowed, vessels. Calcified, fibrous, and/or resilient stenosis may require special scoring or cutting angioplasty balloons with integrated wires or blades on the balloon. The added features focus and improve dilating force but result in large crossing profiles and limited deliverability while increasing cost and inventory, Transit Scientific said in a press release announcing the regulatory approval.
“XO Score transforms regular PTA balloons into scoring and cutting systems,” said Greg Method, president of Transit Scientific. “Clinicians insert an off-the-shelf PTA balloon into the XO Score tableside and then the system can be used over-the-wire to dilate calcified plaque and prep vessels.”
The XO Score is a patented, low-profile, flexible, metal-alloy exoskeleton with a balloon expandable scoring section. One XO Score sheath can be used with a number of 4–8mm diameter and 20–40mm balloons to save the hospital, outpatient lab, ambulatory surgery centre (ASC), or office-based lab (OBL) money on each scoring or cutting procedure.
“XO Score is a new way to prep the vessel,” said Jihad Mustapha, interventional cardiologist, Advanced Cardiac & Vascular Center, (Grand Rapids, USA). “The low-profile design is smooth for tracking to and from the treatment site. But, during balloon inflation, XO Score struts rotate 90 degrees on edge to score and cut. Upon deflation, the XO Score rewraps back-to-flat for smooth withdraw.”
Competitive scoring/cutting balloons feature 1–5 fixed-depth scoring wires/blades that add bulk, profile, and stiffness. XO Score has up to 22 scoring/cutting struts that lay flat while tracking but rotate 90 degrees during balloon inflation to score and cut 0.25mm (0.010″), 0.35mm (0.014″), or 0.50mm (0.020″) deep. Struts rotate 90 degrees back during deflation.
This FDA clearance covers the 6.3Fr (French) XO Score in 65cm and 125cm working lengths with 0.25mm (0.010″), 0.35mm (0.014″), or 0.50mm (0.020″) scoring or cutting depths to enable precise dilation across a range of lesion types. Future 3Fr, 4Fr, and 5Fr over-the-wire and rapid-exchange XO Score versions are under development for smaller vessel and coronary use.
In May 2020, Transit Scientific received FDA clearance for the XO Cross 2Fr, 2.6Fr, and 3.8Fr low-profile, high-torque, and high-push non-tapered microcatheter platform. Transit Scientific is a private company with more than 26 combined issued and pending patents to commercialise medical devices including the FDA-cleared XO Score and XO Cross platforms.
VasQ external support (Laminate Medical Technologies)
VasQ external support (Laminate Medical)
The US Food and Drug Administration (FDA) has designated Laminate Medical’s VasQ external support for the creation of arteriovenous fistulas (AVF) in haemodialysis patients as a breakthrough device.
According to a press release, the designation was based in part on the breadth of clinical evidence collected so far for VasQ that consistently demonstrates improvement over the standard of care for creating functional AVFs for haemodialysis treatment.
“I have been anxious to get my hands back on VasQ ever since I reached the maximum enrolment for a site in the US clinical study,” said Jason Burgess of the Surgical Specialists of Charlotte (Charlotte, USA). “I am excited that the FDA has recognised the urgency we have as surgeons to improve the woeful outcomes that plague fistula creation.”
VasQ is currently in a US investigational device exemption (IDE) pivotal clinical study that is expected to have completed follow-up for its primary endpoints by August 2020 and will be evaluated by the FDA through the de novo pathway.
As of 4 February 2020, the single-arm study has prospectively enrolled its entire 144 male and female patient cohort from 15 sites across the USA. Both current and pre-dialysis patients referred for fistula creation where included in the study for either a brachiocephalic or radiocephalic fistulas with VasQ.
The patients will be followed for two years with the primary efficacy endpoint of unassisted primary patency to be analysed at six months. The FDA will consider the results from the study as well as the breadth of clinical evidence collected from use of the device around the world in its decision to grant US market clearance.
“This is a significant milestone for VasQ that will enable a faster and smoother regulatory process for the US market as well as support the necessary reimbursement for the use of the device in clinical practice to benefit patients,” stated Orit Yarden, vice president of Clinical and Regulatory Affairs for Laminate.
BD has announced the launch of the Halo One thin-walled guiding sheath, designed to perform as both a guiding sheath and an introducer sheath, for use in peripheral arterial and venous procedures requiring percutaneous introduction of intravascular devices.
According to the company, the device consists of a thin-walled (1-F wall thickness) sheath made from braided single-lumen tubing, fitted with a female luer hub at the proximal end and a formed atraumatic distal tip. The thin-walled design reduces the size of the arteriotomy compared with standard sheaths of equivalent French size to help minimise access-site complications. A stainless-steel braid construction fortifies the design for extra support.
The Halo One thin-walled guiding sheath is available in a broad size range (4, 5, and 6F) with shaft lengths of 10 and 25 cm, as well as shaft lengths of 45, 70, and 90 cm for 4 and 5 F sizes. The device is suitable for distal peripheral intervention as well as for alternative approaches, such as tibiopedal or radial access sites.
“With Halo One thin-walled guiding sheath, we’re focusing on where those interventions begin, at the point of access. It effectively downsizes the access profile of peripheral procedures compared to standard sheaths, making it a valuable complement to our innovative portfolio of peripheral artery disease interventional devices,” said Steve Williamson, worldwide president of BD Peripheral Intervention.
“Access site complications occur in up to 11% of peripheral vascular interventions,” said JD Meler, vice president for medical and clinical affairs at BD. “A low profile guiding sheath that is available in lengths suitable for distal peripheral interventions and with a design that can help to reduce access site complications, which have been shown to increase hospital length of stay and costs, is a meaningful addition to our interventional suite of products.”
Transradial, as opposed to transfemoral access, may be a safer approach for flow diversion procedures to treat cerebral aneurysms at a wide range of locations. This conclusion was reached by Yangchun Li from the University of Miami Miller School of Medicine (Miami, USA) and colleagues, as their retrospective study, published online in the Journal of NeuroInterventional Surgery (JNIS), found that both access site complication rate and overall complication rate were lower for transradial access flow diversion.
The investigators used a large multicentre registry to retrospectively analyse flow diversion cases for cerebral aneurysms from 14 institutions from 2010 to 2019. Pooled analysis of proportions was calculated using weighted analysis with a 95% confidence interval (CI) to account for results from multiple centres. Access site complication rates and overall complication rates were compared between the two approaches.
Of the 2,285 patients included in the study who underwent flow diversion, 135 (5.85%) were treated with transradial access, and 2,151 (94.14%) via transfemoral access. Li and the team reported that the two groups shared similar patient and aneurysm characteristics.
“There were no access site complication in the transradial access group,” highlight the authors. However, they write that the rate of access site complications for the transfemoral approach was 2.48% (95% CI, 2.4–2.57%, vs. 0%; p=0.039). Of note, one death resulted from a femoral access site complication.
The overall complication rate was also higher in the transfemoral group (9.02%; 95% CI, 8.15–9.89%) compared with the transradial group (3.73%; 95% CI, 3.13–4.28%; p=0.035), reported the investigators.
Why the authors are advocating for transradial access
These findings, Li et al say, help alleviate the apparent lack of neurointerventional literature directly comparing complication rates between the two approaches. Whilst the field of cardiology has conducted large randomised trials that have shown lower morbidity and mortality, as well as higher patient preference and cost reduction associated with transradial access, the same depth of investigation has yet to be applied to neuroendovascular medicine.
Moreover, Li and colleagues write: “Reducing access site complications isrelevant to flow diversion for two reasons. First, flow diversion employs larger bore access systems, which may increase the likelihood of access arterial injury, bleeding or occlusion. Second, prolonged dual antiplatelet therapy is administered to patients undergoing endovascular flow diversion along with heparin, which increases the risk of access site bleeding. Additionally, the smaller diameter of the radial artery raises the question of whether a transradial access approach is uniformly feasible for flow diverting procedures.”
The investigators state that the current study is “the largest series to date comparing transradial and transfemoral access for this type of neuroendovascular procedure”. Additionally, they argue that the study demonstrates a significant safety benefit with transradial access flow diversion, alongside the feasibility of treating both ruptured and unruptured aneurysms via transradial access at a wide range of locations.
Lastly, the team surmise: “Combining both these findings with other benefits of transradial access, including high patient preferences, elimination of post-procedural bed rest and decreased cost, we continue to advocate for the transition to a radial-first approach for endovascular flow diversion.”
The Society of Interventional Radiology (SIR) president Michael D Dake (University of Arizona Health Sciences, Tucson, USA) and diversity and inclusiveness group chair Paul J Rochon (University of Colorado Hospital, Aurora, USA), have issued the following statement on supporting diversity and combating racial inequality in the USA.
“Humanity has been dealt many challenges this year. While COVID-19 has undoubtedly received much of our attention, we suffer from another pandemic that remains a structural and pernicious threat—racism. The Society of Interventional Radiology (SIR) will not be silent on this issue.
“We denounce any act of hatred and bigotry on the basis of race, ethnicity, religion, sexual orientation, or gender identity. We denounce the long history of hatred and violence against the Black community and support our Black patients, physicians, trainees, nurses, technologists, industry partners, staff and administrators. We need to stand together in strength and work with a common purpose to realise a more diverse, equitable and inclusive organisation.
“We commit to anti-racist efforts, policies, and programmes that aim to increase the numbers of underrepresented minorities and women within our specialty. Our GEMS programme supports diversity in interventional radiology by providing a travel grant for medical students from diverse backgrounds who desire to participate in a visiting clerkship in interventional radiology (IR) outside of their home institution.
“We value a culture of inclusion in which all members of the IR community are accepted, respected, and embraced. The society’s IAmIR campaign has both celebrated and drawn attention to diversity within the specialty. SIR has microgrants that support research performed by female and underrepresented minority scientists and a speakers’ bureau to ensure interventional radiologists of colour are tapped as experts in their field at scientific meetings.
“We strongly support the need to reduce and eliminate health disparities that affect our Black patients and other patients of colour. SIR’s Diversity and Inclusiveness Group Task Force has been working for several years to ensure that these issues are a vital part of our strategic plan.
“We call upon our membership and affiliates to take this time to remember the families and communities of George Floyd, Breonna Taylor, Ahmaud Arbery and many others who have been subject to unconscionable acts of discrimination and hate. We ask that everyone look into his or her heart to understand the overdue need for change in the nation. With our intentional efforts, SIR calls to action the continuing need to develop strategies to ensure justice, diversity, equity and inclusion.”
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Annual Scientific Meeting will be taking place online 12–15 September. Read the full press release from the society below.
“It has been several months since the beginning of the COVID-19 pandemic and although infection numbers in some countries have declined, others are currently in the middle of experiencing the devastating effects of the virus. The situation remains uncertain and as governments struggle to find ways to prevent a second wave of infections, we all have to accept the new situation. Governments have imposed travel bans and strict limits on in-person meetings, which often means that we—at least for the time being—have to change the way we interact with others.
“It is for these reasons that the CIRSE Executive Committee has decided to hold CIRSE 2020 as an online event from September 12–15 instead of the physical meeting originally planned to take place in Munich. By offering a virtual event, CIRSE will provide a safe and reliable platform for knowledge exchange to IRs [interventional radiologists] around the world, regardless of the situation in their country or their ability to travel.
“We look forward to offering the usual high-quality sessions featuring the field’s top experts and the latest research further enhancing the evidence-base of our specialty. We would particularly like to thank our many faculty members for their patience and their unwavering commitment, as well as our corporate partners, who have been very supportive during the pandemic and will of course also form an important part of the CIRSE 2020 Summit.
“We invite all interested parties to access the CIRSE website, sign up for the CIRSE e-newsletters and join the CIRSE social media channels to stay up-to-date as we continue to plan an outstanding CIRSE 2020 Summit.
“We look forward to a lively knowledge exchange at the CIRSE 2020 Summit and to talking to you via its interactive platforms!”
Delivery of stroke thrombectomy services by discipline
Despite being “perfectly placed” to help meet the increasing demand for stroke thrombectomy, there is not an established training structure for interventional radiologists wishing to perform the procedure in Europe. The findings of a recent online survey conducted by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) on stroke thrombectomy provide, according to the society, a “mandate [for] further European-wide initiatives” to establish such training programmes.
Writing to the Editor of CardioVascular and Interventional Radiology, CIRSE past president Robert Morgan (St George’s University Hospitals NHS Foundation Trust, London, UK) et al state that current barriers to interventional radiologists becoming key players in European stroke management, identified by CIRSE leadership, include “the absence of an established training structure for interventional radiologists performing stroke thrombectomy, a strong dependence on local conditions, limited 24/7 coverage, as well as varying opinions on the desired involvement of interventional radiology [IR] in stroke thrombectomy”. Therefore, to assess the level of interest and involvement by interventional radiologists in the procedure across Europe, CIRSE conducted an anonymous online survey on the current situation of stroke thrombectomy practice among European interventional radiologists.
Stroke thrombectomy was performed in 74.5% of the respondent’s centres, with an expected predominance in university hospitals, tertiary care hospitals and private hospitals, although the procedure was also performed in 52.5% of general hospitals. There was also an increasing tendency for the procedure to be performed in larger hospitals.
In centres where stroke thrombectomy is performed, it was most frequently delivered by interventional radiologists in 70.1% and by neuroradiologists in 48%. Stroke thrombectomy was provided by both interventional radiologists and neuroradiologists in 21% of centres. “Collaboration with other specialties appeared to be good throughout the obtained sample,” the letter says, “as interventional radiologists perform stroke thrombectomies in collaboration with other medical specialties in almost 90% of centres.”
CIRSE past president and lead author of the Letter to the Editor of CVIR, Robert Morgan
It continues: “Training for stroke thrombectomy by interventional radiologists was either provided by a neuroradiologist at the same centre (47.7%) or was obtained by interventional radiologists independently (46.2%). However, opportunities for training in stroke thrombectomy are relatively limited for interventional radiologists, especially where there was reluctance by neuroradiologists to involve interventional radiologists in the stroke thrombectomy service, and almost a quarter of respondents who perform stroke thrombectomies indicated that they were ‘trained in another way’, indicating a large variety in training modes and options and reconfirming the need for more standardised training pathways and dedicated courses for IR.”
The survey also reported a broad consensus among respondents that “a significant growth in the demand for stroke thrombectomy was expected, due to factors such as improved infrastructure and service availability, increased awareness of this treatment option among referrers, better clinical evidence, and broader inclusion criteria”.
Speaking to Interventional News about the results of this survey, Morgan says: “This survey confirms that in many countries, interventional radiologists already have a significant role in the delivery of intraarterial stroke therapy. This was already known by CIRSE but had not been confirmed previously by a formal survey of CIRSE members.
“We all know that there are not enough interventional neuroradiologists to provide intraarterial stroke therapy in Europe in the volumes that are required by patient demand for this procedure. I would like the future of stroke thrombectomy to be a comprehensive service satisfying the widespread demand by patients and delivered by doctors who have been adequately trained to perform the procedure. Interventional radiologists would be key players in the stroke thrombectomy service, working alongside our colleagues in interventional neuroradiology.
“To bring this about, we need to form even better collaborative working relationships with our interventional neuroradiological colleagues. These improved relationships should be encouraged by our colleagues and not hampered by any counterproductive issues such as turf. Another important requirement is the recognition by leaders of national health systems that interventional radiologists can provide stroke thrombectomy and should be encouraged to do so in their country’s hospitals.”
CIRSE received a total of 601 valid responses, which the society claims is “a very high response rate (11.5%) for a CIRSE member survey”. Of these, 109 came from Germany, 87 from Italy, 68 from the UK, 38 from The Netherlands, 36 from Turkey, 32 from Spain, 28 from Belgium, 26 from Austria, 25 from Greece, and the remaining quarter from other European countries—“the sample was considered to be representative of CIRSE’s European membership in terms of geographical spread, centre type, and level of experience”. However, the letter writers acknowledge a potential bias that interventional radiologists involved in stroke thrombectomy may have been more likely to respond.
Straub Medical has approved a full acquisition by Becton, Dickinson and Company (BD). The acquisition was completed on 20 April 2020. Straub Medical manufactures, develops, and sells medical devices for the treatment of arterial and venous diseases that are used worldwide by vascular surgeons and interventional specialists in radiology, angiology, and surgery.
Gido Karges, CEO of Straub Medical, comments: “BD is the ideal strategic addition to Straub Medical. With its complementary product portfolio and established global sales channels, BD offers treatment solutions for vascular specialists around the world to advance the world of health.”
“With our extensive expertise in endovascular technologies and our strong global infrastructure, BD is the right company to offer Straub Medical products worldwide as an important building block of our modern treatment solutions,” says Steve Williamson, president of BD’s Peripheral Intervention business. “We are committed to improving the quality of life for the more than 200 million people worldwide who are affected by occlusive diseases of the peripheral arteries. We are also committed to providing more instruments for treating venous diseases. The acquisition of Straub Medical makes it possible to help physicians worldwide treat even more affected patients.”
All employees in all branches are taken over by BD.
Data from an unselected, real-world cohort of 64,000 claimants of the German BARMER Health Insurance reveals no signal of increased long-term mortality when paclitaxel-based devices are used in the femoropopliteal arteries, Eva Freisinger (Münster, Germany) told BLearning Peripheral at LINC 2020.
She explained that as German law mandates the mortality of every insurance holder be reported directly to the healthcare insurance provider, the investigators knew the exact date of death for every patient included in the analysis. “This is why we have no loss of follow-up on this important end-point,” Freisinger imparted.
“In 2020, I would consider these devices to not harm patients in the long-term, as was suggested by the Katsanos work,” she concluded, referencing the 2018 meta-analysis by Konstantinos Katsanos (Patras, Greece) et al that reported an increased association with mortality with paclitaxel-based devices in the leg. Freisinger believes these findings should “reassure physicians [that] we do not see an increased long-term mortality signal for paclitaxel-based devices”.
Bolstering the evidence-base for proponents of paclitaxel-based devices, Thomas Zeller (Bad Krozingen, Germany) also reported positive results for drug-coated balloons (DCBs) at LINC.
In an analysis of approximately 1,600 patients at his own institution treated with either a paclitaxel-coated balloon or through a paclitaxel-naïve method (either bare metal stenting, atherectomy, or plain balloon angioplasty), and with a follow-up of at least three years, Zeller and colleagues “found a mortality benefit of around 10% over time favouring the treatment with DCB angioplasty”.
He added that, despite being a single-centre, retrospective study, he believes “this is very high-level scientific data, because we enrolled really all-comers, we did not exclude any patient”. Additionally, an advantage of the single-centre setting is to exclude any confounding variables that may arise if patients are treated at different hospitals.
Based on both large, real-world data sets from insurance companies and this single-centre data analysis, Zeller concluded that his team “could not confirm” the 2018 findings that treatment with paclitaxel-coated devices in the femoropopliteal segment poses a greater risk to long-term mortality.
Mentice AB has announced the global introduction of its seventh-generation Vascular Interventional System Trainer (VIST) simulation platform.
According to the company, the VIST G7 includes artificial intelligence guidance, integration to robotics, and big data analytics. The newly redesigned platform of the VIST G7 incorporates the company’s latest advances in sensor and haptic technologies and uses newly developed software solutions.
A premium version of this platform with a higher level of realism is offered as the VIST G7+, which allows doctors to simultaneously manipulate multiple devices while using a single access point for therapies such as bifurcation lesion interventions and branched devices.
In the Mentice announcement, Lars Lönn, from National University Hospital (Copenhagen, Denmark), commented, “In the past, endovascular simulators were challenged to match the haptic feedback a seasoned doctor will experience on a real patient while pinning and advancing microcatheters, making microadjustments, selecting small vessels, and applying certain tricks and techniques acquired over many years of practice. Performing an interventional procedure on the new G7 platform feels incredibly like the real thing, even in intricate cases.”
Khalid Barakat from Queen Mary University, London, UK, added, “This new G7+ platform increases the fidelity of scenarios and is a much-needed addition to our practice, allowing us to simulate challenging bifurcation percutaneous coronary intervention (PCI) cases. Our aspiration is to perform procedure rehearsals for the most complex PCI cases, testing novel bifurcation strategies and devices.”
Merit Medical has received CE mark approval for the Wrapsody endovascular stent graft system from the British Standards Institution. The Wrapsody system is a flexible self-expanding endoprosthesis indicated for use in haemodialysis patients for the treatment of stenosis or occlusion within central veins as well as the dialysis outflow circuit of an arteriovenous (AV) fistula or AV graft.
According to the company, it will introduce the Wrapsody system in Europe as procedures are resumed following the ongoing lockdown due to COVID-19. Additionally, Merit Medical plans to initiate registration activities associated with the system in Australia, Canada, and certain countries in Latin America. The company recently completed enrolment and primary follow-up of its WRAPSODY FIRST study that included 46 patients in Europe.
Moreover, Merit Medical submitted an application for an investigational device exemption (IDE) to the US Food and Drug Administration (FDA) for its review and consideration before the initiation of its WAVE pivotal study. After completion of the WAVE pivotal study, Merit Medical intends to submit a premarket approval application to the FDA, a press release states.
The company intends to offer additional products using this technology platform, subject to additional submissions and review by the US FDA and the European Union notified body. Merit Medical recently received three US FDA breakthrough device designations covering indications and cohorts of the IDE for the Wrapsody system, which have been filed with the US FDA.
Tokai Medical Products announced CE mark approval for its Rescue balloon occlusion catheter, a low-profile device designed for resuscitative endovascular balloon occlusion of the aorta (REBOA).
According to Tokai, REBOA uses a balloon catheter for temporary control of non-compressible torso haemorrhage, as an alternative to traditional thoracotomy. The Rescue balloon is compatible with a 7-F sheath and 0.025-inch guidewire. Its maximum balloon diameter is 40mm. The device also features a radiopaque tip and marker band to facilitate precise positioning under fluoroscopy.
“As REBOA [is] being used more as part of the endovascular resuscitation and trauma management (EVTM) concept worldwide, there is a great need for this excellent tool,” comments Tal Hörer (Örebro University Hospital, Örebro, Sweden) in the company’s press release. He chairs the EVTM society and is Editor-in-Chief of the Journal of Endovascular Resuscitation and Trauma Management.
Hörer continues, “The Rescue balloon has been in use for several years in Japan and other countries. It has been proven clinically to be effective, reliable, and easy to use. The Rescue balloon can be used in trauma and non-trauma cases, and as a vascular surgeon clinically-active on vascular, endovascular, trauma, and resuscitation, I am looking forward to [being] able to use this product for life-saving procedures.”
Chair Roger Greenhalgh (top left), moderator Andrew Holden (top right), Sapan Desai (bottom left), Sabine Steiner (bottom middle), and Misti Malone (bottom right)
CX 2020 LIVEcame to life online—despite COVID-19—using state-of-the art broadcast technology to bring together more than 1,000 vascular specialists, live, from 95 countries across the world. The first session of the highly interactive conference, designed to deliver global vascular education in the CX style, saw participants from Stockholm to Santiago asking questions and engaging with leading vascular figures on the ongoing investigation into the safety of paclitaxel devices in the treatment of peripheral arterial disease (PAD). The session can now be viewed on demand here.
Roger Greenhalgh (London, UK) chaired the event, with Andrew Holden (Auckland, New Zealand) moderating the panel discussion. Six speakers gave their five-minute presentations, with each talk interceded with five minutes of discussion time.
A historic occasion for vascular education, attendees can earn continuing medical education (CME) points through their presence at this virtual event, taking place every Tuesday and Thursday from 16:00–17:20 BST from 25 May through to 25 June.
Podium first: “Paclitaxel devices are associated with improved survival” in new propensity score-matched analysis of claudicants and CLTI patients
“The debate on the safety and efficacy of paclitaxel continues to rage,” Sapan Desai (Chicago, USA) stated, kicking off the first session of CX 2020 LIVE with his podium 1st presentation on paclitaxel survival results related to drug-coated balloons (DCB) and drug-eluting stents (DES) out to five years. Contrary to the findings of Konstantinos Katsanos (Patras, Greece) et al in late 2018, Desai concluded that “paclitaxel devices are associated with improved survival, starting at nine months”. However, he added the usual caveat that “additional analyses, such as a more detailed subgroup evaluation, and causal inference determination, are urgently needed”.
In this propensity score-matched analysis, Desai and his co-investigators utilised a global healthcare registry to identify patients with femoropopliteal artery disease who subsequently underwent an endovascular intervention between 2010 and 2015. These patients—11,710 of whom underwent drug-coated balloon (DCB) or drug-eluting stent (DES) treatment, and 76,007 of whom underwent routine angioplasty or bare metal stenting—were followed for up to five years. In total, 61.5% of the paclitaxel cohort and 62.7% of the control group had chronic limb-threatening ischaemia (CLTI), respectively.
There was no difference in the rate of periprocedural complications between the paclitaxel-treated group and the control group, the investigators reported. Desai related how patients treated using paclitaxel “have a lower rate of reintervention at one year, with a significant decrease in major amputation rate at five years”.
Additionally, the triallists found that mortality is significantly lower for claudicants, starting at nine months. At five years, 42.9% of paclitaxel-treated patients had died, compared to 59.2% in the control group.
COMPARE trial highlights efficacy of low-dose paclitaxel balloons
Sabine Steiner (Leipzig, Germany) told the CX 2020 LIVE audience that the COMPARE trial, the first head-to head comparison of two paclitaxel-coated DCBs, the COMPARE trial, showed “excellent efficacy” at one year in both arms. There was a similar patency at one year with the low-dose (2µg/mm2) Ranger DCB (Boston Scientific) compared with the higher dose (3.5µg/mm2) IN.PACT Admiral DCB (Medtronic).
While earlier meta-analyses have suggested an association between paclitaxel dose and late mortality risk, Steiner told the CX 2020 LIVE audience that the COMPARE trial results “cannot identify any signal for a relationship between paclitaxel dose and mortality, at one year or beyond”.
The COMPARE trial, published in the European Heart Journal, was a prospective, randomised, non-inferiority trial of high- versus low-dose paclitaxel DCBs for femoropopliteal interventions. All patients enrolled in the study had PAD categorised as Rutherford class 2–4.
The trial met both its primary efficacy (primary patency through 12 months) and primary safety (freedom from major adverse events through 12 months) endpoints. Steiner says that the investigators, led by Dierk Scheinert (Leipzig, Germany), “will follow the patients up to five years by telephone calls in order to gain safety information”.
Focusing on all-cause mortality, Steiner noted that the COMPARE trial data show “an overlapping of Kaplan-Meier curves through four years”, indicating “no signal for any relevant difference [between the two different paclitaxel dosages] with respect to mortality”. She continued: “Actually, death rates are rather low. After two years, where we do have quite a good follow-up, we observe a death rate which is around 3%”.
When looking at individual causes of death, Steiner shared that the research team did not see any “clear signal of an excess rate of a specific cardiovascular or non-cardiovascular death subtype.
“Importantly,” she expanded, “the same holds true, or we see a similar pattern of causes of death, for the six patients who died in the high-dose DCB group. Importantly, no death was considered procedure- or device-related by the clinical events committee.”
Speaking as co-moderator of the session alongside Roger Greenhalgh (London, UK), Andrew Holden (Auckland, New Zealand) praised Steiner for bringing “new information that we are seeing for the first time” to CX 2020 LIVE.
Prompted by a question from Greenhalgh, Steiner clarified that the COMPARE trial was never designed to compare mortality between the Ranger DCB and the IN.PACT Admiral DCB, but rather efficacy. “What I would really like to highlight,” she stressed, “is that we have these meta-analyses showing us a signal that even for efficacy there will be a difference with respect to dose, so a higher dose will be more efficient. This was really the background of the COMPARE trial, that we wanted to have a non-inferiority design with respect to efficacy and primary patency. Here, we did not see a difference, which is really in contrast to the results from the meta-analyses.”
Holden, who was one of the authors of a 2019 paper published in the Journal of Endovascular Therapy (JEVT) refuting the idea of there being a dose-dependent impact of paclitaxel devices, said he “entirely” agreed with Steiner’s conclusions, adding: “I think it [the dose model] is the weakest part of the original [2018, Katsanos et al] meta-analysis.” Addressing Steiner, he said, “You have really shown that a low-dose device is as efficacious [as a high-dose one], and that there is no safety advantage or disadvantage.”
Steiner acknowledged that although she and her colleagues did not observe a signal with respect to mortality, the numbers in the COMPARE trial “are clearly very small in general, so there is a low mortality rate—we are definitely not powered for this question [detecting an association between increased mortality risk and paclitaxel dose].”
Therefore, the COMPARE trial can make “no statement about dose and mortality”, Greenhalgh concluded.
CX 2020 LIVE audience split over importance of dose effect
Polling during the CX 2020 LIVE session asked the audience: “Do you consider paclitaxel dose level to be crucial?” This split the CX audience with 53% of respondents voting “yes” (see Figure 1), sharing their belief that paclitaxel dose levels are crucial.
Figure 1
US FDA assessing “totality of evidence”, calls out specific value of individual patient-level data sets
Providing an update on the paclitaxel late-mortality signal from the US Food and Drug Administration (FDA) perspective, Misti Malone (Centre for Devices and Radiological Health, US FDA) said that the agency is in the “signal discernment/refinement phase” of the ongoing investigation.
Following the FDA Advisory Committee Meeting last summer (19–20 June, Washington, DC, USA), approved paclitaxel devices have remained on the US market with labelling updates that discuss ongoing uncertainties regarding the signal, as well as the conclusions of June’s meeting. At the time, the agency agreed that the mortality signal existed, but that the signal magnitude was uncertain.
“Because patient comorbidities, extent of disease, and lesion characteristics play a role in clinical outcomes, [the] FDA believes it is important for physicians to determine what patients are considered [at] high risk of restenosis, and they have a favourable risk–benefit profile from treatment with paclitaxel-coated devices.”
Clinical trials are continuing with revised informed consent and increased patient follow-up. Additionally, the FDA has also promoted efforts to increase trial robustness, such as attempts to reduce “missingness”. “We continue to collaborate with investigators of observational datasets, and through groups such as RAPID, a multi-stakeholder collaboration made of clinicians, industry members, and regulators aiming to improve the real-world evidence ecosystem, from data collection to analysis,” Malone explained. “These collaborations may provide insights into remaining questions, such as the precise magnitude of the signal, the mechanism for late-term mortality, and the benefit–risk profile in real-world patient populations.”
Malone stressed the importance of collaboration, finishing by saying: “This is a global issue that requires global collaborations.”
Referencing Desai’s earlier presentation on what he described as “another large, population-based study that failed to show a [mortality disadvantage], but in fact showed a mortality advantage of paclitaxel”, moderator Holden said he has found large population-based studies “reassuring”, and asked for the FDA’s thoughts on these types of analyses.
“We value the totality of evidence,” Malone replied, “be it from randomised controlled trials, single-arm trials, or observational datasets. The devil is in the details for many of these trials, in which we identify how many patients have been followed-up to four or five years, which is when the signal was noticed in our data sets. Many of these data sets have up to 50% missingness at this point, and although we may assume missingness accepts some level of randomness, it may not, so we typically need very robust, high-quality data with long follow-up in order to discern this mortality signal. So, we do value these observational datasets, and as part of the RAPID group, we are compiling all of the datasets we are aware of, and looking at the level of evidence and our confidence in the data that has been evaluated.”
Specifically commenting on individual, patient-level analyses, such as the VIVA individual patient-level data (IPD), Malone said: “We find those very valuable because we can dive into the details, we can see how the individual patients are affected, rather than looking at summary data. The higher-level meta-analyses help to guide us to our next step to do a more in-depth analysis.”
“High impact” of VIVA individual patient data analysis
The IPD analysis of the safety of paclitaxel-containing devices conducted by VIVA Physicians, based on the most complete available data set of mortality events from randomised controlled trials, identified an absolute 4.6% increased mortality risk—corresponding to a 38% increased relative mortality risk—associated with their use. This is a weaker mortality signal than that initially reported in December 2018 by Katsanos.
The analysis, based on the most complete available data set of mortality events from randomised controlled trials involving paclitaxel devices, included 2,185 patients (including those whose data were previously lost to follow-up) across eight studies, with a median follow-up of four years.
Presenting these results at CX 2020 LIVE, first published in Circulation, Gary Ansel (Columbus, USA) remarked: “The VIVA IPD has, and will continue to have, [a] high impact due to the richness of the dataset”.
Nearly two-thirds of the CX 2020 LIVE audience believe the VIVA Physicians’ IPD analysis does not provide consensus on the ongoing paclitaxel debate “once and for all”. When asked “Does the VIVA IPD settle this once and for all?”, 63% answered “no” (see Figure 2).
Figure 2
Greenhalgh concluded: “What we have learnt today, from various pieces of data, is that this matter is not settled. What I personally like is that the FDA’s comments have left room for doctors to decide what they consider to be the right thing to do for the patient.”
Recent meta-analyses have contradictory findings in patients with CLTI
Two analyses investigating the alleged increased rate of mortality with the use of paclitaxel-containing devices in the chronic limb-threatening ischaemia (CLTI) population were presented back-to-back during the inaugural CX 2020 LIVE session.
Though Ramon Varcoe (Randwick, Australia) put forward that paclitaxel-coated devices were not associated with increased mortality in patients with CLTI, Katsanos told viewers that paclitaxel-coated balloons seemed to increase the risk of all-cause death, as well as the risk of amputation, in the infrapopliteal segment.
Expounding on the differences between the methodologies used by each research team, Varcoe said: “As I see it, there are four main differences. The first was [that] we had a different primary endpoint. We looked at all-cause mortality, and we did that because we were asking whether paclitaxel was associated with death; it makes sense to look at overall survival, rather than amputation-free survival, which is more of an efficacy endpoint.
“We also looked at paclitaxel use in stents and balloons above and below the knee, so we did not restrict it, and this was a way to replicate the original 2018 meta-analyses. But also, the rationale was if you are exposed to paclitaxel, it should not matter how it was used in the leg or what device.
“We also used only published data. As we know, data change between their presentation at symposium level and the subsequent peer review at publication, so we thought it was important to use locked and verified data in our analysis.
“Most importantly, we included the five-year data from the Medtronic IN.PACT DEEP study. This was the largest study in the meta-analysis, and the longest follow-up, and had the largest number of event rates in terms of mortality. It was the most influential in terms of a meta-analysis, and it really needed to be included, and that is what we did.”
The five-year findings of the IN.PACT DEEP study, which tested a 3.5μg/mm2 device, were not part of the Katsanos meta-analysis, a fact that garnered criticism from CX 2020 LIVE attendees. Justifying this choice to viewers, Katsanos said: “All the otherstudies have presented six-month to one-year data. It would not be very reasonable to combine that with the five-year data because then it becomes heavily skewed towards this study, as it a lot more events due to the five-year follow-up.”
Greenhalgh summarised: “I think we will accept that six-month data follow-up is limited.”
The discussion continues 28 May 2020
Session Two of CX 2020 LIVE will focus on the durability of EVAR, sac diameter, and the UK National Institute for Health and Care Excellence (NICE) guidelines. To take part in the global conversation and participate in live polling, register here and join us from 16:00 to 17:20 BST on 28 May 2020. Roger Greenhalgh is returning as chair and Ian Loftus (London, UK) will moderate the discussion.
Guerbet has announced the registration of Vectorio, a kit for imaging hepatocellular carcinoma (HCC), in Canada.
The kit consists of a set of Lipiodol-resistant medical devices that includes patented syringes, stopcock and sampling devices.
Vectorio is dedicated to Lipiodol Ultra Fluid Injection for imaging of liver tumours in adults with known HCC during interventional oncology procedures.
HCC is the most common primary liver cancer and is the fourth biggest cause of death due to cancer worldwide.
This medical device:
Is 24 hours Lipiodol Ultra Fluid resistant
Contains Patented three-way stopcock with four connections offering possibility of “On-table Refill and optimised injection control” (interventional radiologists have the possibility of refill without disconnection from the micro-catheter)
Includes all devices in one set
Is user-friendly and allows ergonomic and quick device set-up.
Designed and manufactured in France, the product was launched commercially in September 2017 in Europe. Today, Vectoriofor HCC imaging is registered in Canada and Germany. Vectorio is also registered in 25 countries where conventional transarterial chemoembolization (cTACE) procedures are approved for Lipiodol Ultra Fluid.
LimFlow percutaneous deep vein arterialisation (pDVA) system
LimFlow SA today announced publication of positive two-year data from the ALPS registry of the LimFlow percutaneous deep vein arterialisation (pDVA) system. Results were published online yesterday in the Journal of Endovascular Therapy and will also appear in the August print issue of the journal.
The ALPS Registry is the largest study to date of no-option chronic limb-threatening ischaemia (CLTI) patients treated with the LimFlow system reporting mid- and long-term results.
“In this complex group of patients, pDVA using the LimFlow device has shown to be feasible and safe with high technical success and good amputation-free survival at six months up to 24 months coupled with good wound healing,” said the paper’s lead author, Andrej Schmidt, head of the Angiology CathLab at Leipzig University Hospital, Leipzig, Germany. “In selected patients with no-option CLTI, pDVA is a safe and effective treatment to prevent amputation and heal wounds.”
“Patients with this disease suffer with chronic ulcers, often including gangrene, recurrent pain, and a very poor quality of life. CLTI is associated with poor mid- and long-term survival, and no-option patients often face the worst outcomes,” said Roberto Ferraresi, chief of the Peripheral Interventional Unit at the San Carlo Clinic, Milan, Italy, co-author of the paper, and a pioneer in the interventional treatment of CLTI. “These patients desperately need an option to avoid amputation and improve their life, and LimFlow offers a very promising alternative for them.”
The ALPS Registry is a multicentre, retrospective study conducted at centres in Alkmaar, the Netherlands; Leipzig, Germany; Paris, France; and Singapore encompassing 32 end-stage—or “no-option”—CLTI patients.
All patients had non-healing wounds on the target foot and no arterial target for surgical or endovascular revascularisation. Among them, 66% had diabetes, 53% had renal insufficiency, and 16% were dialysis dependent. The majority of patients had experienced failed prior attempts at revascularisation.
The registry reported major amputation-free survival of 84%, 71%, and 67%, respectively, at six months, one year and two years. Additionally, a positive trend of successful wound healing was demonstrated, with 73% of wounds completely healed at two years. Technical success was 97%.
When all other therapeutic options have been exhausted and a CLTI patient is facing major amputation, the minimally-invasive LimFlow system is designed to bypass blocked arteries in the leg and deliver oxygenated blood back into the foot via the veins. For many patients, restoring perfusion in the lower limbs resolves chronic pain, improves quality of life, enables wound healing and prevents major amputation.
“It is very gratifying to see these durable results being demonstrated by the LimFlow system in a real-world setting with consecutive patients,” said LimFlow CEO Dan Rose. “For these no-option patients, the next intervention for their leg was going to be major amputation, with the associated morbidity and high mortality risk that comes with amputation. Instead, two years later, the vast majority of patients are alive, with almost three-quarters of them experiencing completely healed wounds. This registry adds to the building clinical evidence that LimFlow therapy is an effective solution for no-option patients.”
Click here to view a video of how the LimFlow System works.
Bluegrass Vascular Technologies has announced that the first US commercial cases using the Surfacer Inside-Out access catheter system were completed at Santa Clara Valley Medical Center in San Jose, California.
The procedures were performed by Ehab Sorial and Ajit Nair. Sorial is a clinical associate professor of Surgery in the Division of Vascular Surgery at Stanford University School of Medicine and staff surgeon at Santa Clara Valley Medical Center. Nair is a staff interventional radiologist at Santa Clara Valley Medical Center.
The device was used to obtain venous access in two haemodialysis patients with central venous obstructions, one of which had limited access options. Bluegrass Vascular was granted de novo classification by the US Food and Drug Administration (FDA) for the Surfacer system in February of this year.
“We are excited to be the first programme in the USA to incorporate use of the Surfacer system into our day-to-day clinical practice,” said Nair and Sorial. “The Surfacer system provides us with a safe and effective option for obtaining right-sided central venous access in patients with venous obstructions, enabling us to preserve secondary central veins and avoid alternative access procedures, which are not as effective and have a higher risk of complications.”
“Dr Sorial, Dr Nair and their team at Santa Clara Valley Medical Center played an integral role as one of several clinical sites for the US investigational device exemption (IDE) study, which led to our recent FDA de novo clearance. We are honoured to have Drs Sorial and Nair perform our first US cases,” stated Gabriele Niederauer, CEO and president of Bluegrass Vascular. “We envision US clinical adoption of the Surfacer system mirroring our positive commercial experiences in Europe and look forward to providing this truly novel technology to physicians and their patients across America.”
Getinge recently announced the launch of its Advanta V12 large diameter stent.
According to a press release, Getinge’s Advanta V12 stent has been shown to consistently improve patient outcomes by restoring iliac patency, reducing restenosis and re-intervention rates, improving ankle brachial index (ABIs) and sustaining symptom relief. Strong benchmark data demonstrates superior patency over bare metal stents.
“A clear need from our customers has encouraged us to now introduce a larger diameter size of Advanta V12 which expands from 12 to 16mm,” says Jens Viebke, president Acute Care Therapies at Getinge.
The first in the world implantation of the Advanta V12 large diameter stent, was performed by Franklin Pond, a vascular surgeon at the Western Hospital in Melbourne, Australia. Following the procedure, he reported, “I am delighted to expand the treatment spectrum of patients receiving the new Advanta V12 large diameter stent, and pleased with the excellent angiographic outcome.”
“Backed by long-term clinical data and over 500 publications, the Advanta V12 stent continues to prove itself every day when it comes to treating patients with this severe condition. We are of course excited to introduce this new larger size to help our customers treat a wider range of clinical cases,” says Jens Viebke.
According to Getinge, a unique full polytetrafluoroethylene (PTFE) encapsulation of the Advanta V12 stent provides a smooth flow lumen and offers an effective barrier to neointimal hyperplasia. It expands uniformly and prevents tissue from prolapsing through the expanded stent. 9F compatibility offers versatility and efficient delivery in complex endovascular procedures.
“The trusted design of Advanta V12 is conformable, deliverable and flexible to track through tortuous arteries and flex to accommodate the iliac arteries. It has the ability to post dilate up to 16mm, providing customization to the patients anatomy,” explains Michel Reijnen, professor at the University of Twente in Enschede, the Netherlands.
The larger diameter Advanta V12 balloon expandable covered stent is CE marked and TGA approved for restoring and improving the patency of iliac arteries.
This information is intended for an international audience outside of the USA.
Older age, being male, deprivation, living in a densely populated area, ethnicity, obesity, and chronic kidney disease are associated with a positive test for COVID-19, according to results from 3,802 people tested for SARS-CoV-2 in the UK. The observational study was conducted between 28 January and 4 April using routine electronic health records data from GP practices across England (UK), and results are published in The Lancet Infectious Diseases.
Study author Simon de Lusignan from the University of Oxford (Oxford, UK) and Director of the Royal College of GPs Surveillance Centre, UK, says: “While clear trends have emerged from hospital data for the people with severe symptoms, the risk of infection among the general population remains a grey area. It’s important to know which groups in the wider community are most at risk of infection so that we can better understand SARS-CoV-2 transmission and how to prevent new cases.”
The authors note that other socio-economic factors, which were not measured in this study, may also be linked with SARS-CoV-2 infection, such as employment in high-risk jobs, education, income, and differences in access to healthcare and testing among ethnic groups. Further research is needed to understand these associations.
de Lusignan and colleagues analysed data from 587 people with positive results and 3,215 with negative results, collated by GP practices in England who are part of the Royal College of General Practitioners Research and Surveillance Centre primary care network.
Among adults, those aged 40 to 64 years were at the greatest risk of testing positive for SARS-CoV-2 (18.5% tested positive, 243 out of 1,316 people), compared with children aged up to 17 years (4.6%, 23 of 499). Among 1,612 men, 18.4% (296) tested positive, compared with 13.3% (291/2,190) of women.
The only clinical conditions significantly associated with a positive test were chronic kidney disease and obesity. Of 207 people with chronic kidney disease, 32.9% (68) tested positive, compared with 14.4% (519/3,595) without kidney disease. While 20.9% of people who were obese tested positive (142/680), compared with 13.2% (171/1,296) people of normal weight.
Compared with people of white ethnicity, of whom 15.5% (388 of 2,497) tested positive, the proportion of people of black ethnicity testing positive were much higher, at 62.1% (36 of 58 people). This finding remained significant after adjusting for comorbidities such as high blood pressure and diabetes, the prevalence of which is increased in black ethnic groups. The authors say that these results should be interpreted with caution, as there were small numbers of people from England’s minority ethnic groups in the study.
There was a large difference between people living in the most and least deprived areas. Of 668 people in the most deprived areas, 29.5% (197) tested positive, compared with 7.7% (143 of 1,855) in the least deprived areas. People in urban areas were more at risk than those in rural areas. Of 1,816 people tested in urban areas, 26.2% (476) tested positive, while in rural areas 5.6% tested positive (111 of 1,986).
Co-author Gayatri Amirthalingam, from Public Health England, says: “With each day that passes our knowledge of COVID- 19 improves. This analysis of primary care outcomes of individuals testing positive for virus is an important contribution to our wider understanding of how COVID-19 is affecting people of different demographic groups. This study, which uses data from the Oxford RCGP Research and Surveillance Centre, will also inform Public Heath England’s ongoing review into factors impacting health outcomes from COVID-19 that is to be completed by the end of May, 2020. This review will also analyse hospitalisations and mortality, including excess mortality, to provide further insight on how COVID-19 may be having a disproportionate impact on different groups. It will also determine the impact of occupation (including healthcare workers) where data is available.”
While more than 60% of medical students are female, the number of women in endovascular medicine is low, report Bella Huasen and Agnieszka Solberg. Here, for Interventional News, they discuss the reasons behind this under-representation and consider the importance of creating a global support network to redress the imbalance.
“What hubris it was, he said, that mankind should think to halve the powers of the human race by ignoring the minds and words of the female half of it”—The Clockmaker’s Daughter, Kate Morton.
Charles Dotter’s first superficial femoral artery recanalisation in 1964 began a new era of endovascular medicine, a fairly new and evolving specialty compared to traditional career paths such as surgery or primary care.
The profession is practiced by multiple sub-specialists including interventional radiologists, vascular surgeons, angiologists, and interventional cardiologists. Despite the variation and interests, female trainee and consultants/residents remain under-represented in all of these specialities.
In the USA, fewer than 8% of interventional radiologists are women; in Europe fewer than 10%. The percentages are even more grim for vascular surgery, in the USA <6% and in Europe <8% are women. Despite >50% of medical students identifying as women in the USA and Europe, there is never a line to the ladies’ bathroom at endovascular medicine conferences.
This beautiful lifesaving carer should attract talent irrespective of gender. It is everyone’s responsibility to recognise this issue and encourage female doctors and students into this field. This is not as easy at is seems given the culture of misogyny and sexism engrained in cultures throughout the globe.
Conscious bias still exists in 2020 and trainees are still being told that endovascular medicine is not for them, based solely on the fact that they are women. Most of the time, however, this behaviour is unconscious and, sadly, it is prevalent in both men and women.
Many females have contributed to this field starting with Marie Curie-Sklodowski for the use of X-rays, yet the gender disparity is rife across the globe. When searching congresses, conferences, proctors, panels, and faculty members; the site or inclusion of females is rare if not none-existent.
We have attended multidisciplinary endovascular conferences with hundreds of attendees, but limited women speakers, chairs or panellists. Surely, there are qualified women endovascular specialists who can provide some insight.
Given the benefits of a diverse workforce and the effectiveness of female physicians compared to their male colleagues in respect to mortality rates and other outcomes (Tsugawa et al 2017; Wallis et al 2017), all specialities should be recruiting female physicians to join their teams.
The benefits of a diverse workforce are well known inclusive companies outperform the S&P 500 index, attract top talent rich in creativity and innovation, and can better anticipate a broad range of customer needs (Spalluto 2018).
Since women make over 90% of their family’s healthcare decisions (Spalluto 2018), female doctors have an edge at understanding and meeting the needs and expectations of the female health care consumer. As the minimally invasive options for patients grow to include gynecologic, urologic, gastrointestinal and breast procedures, female patients are likely to more often request a female physician.
One of the ways to increase the number of women in endovascular medicine is to provide trainees with more role models. Representation matters but there is a striking disparity between the genders in leadership positions in medical schools despite more female medical students; women represent a small fraction of medical school deans and full professors.
This is not occurring because women are uninterested in leadership positions; it is occurring because women are not being considered and not being selected for these positions despite having equal or higher qualifications than their male colleagues.
Many organisations have begun women’s sections to help combat biases and improve the representation of women in their societies. The Society of Interventional Radiology, for example, has a very active women-in-IR (WIR) section which meets monthly. There is also dedicated WIR programming at the annual SIR conference.
Multidisciplinary organisations (ISET, OEIS, VIVA, GEST, etc) tend to be smaller and have few, if any, women physicians in planning and execution of the annual event as well as a smaller percentage of women speakers and even attendees.
Grassroots organisations have tried to raise awareness about these discrepancies; however, it is challenging to enact any change without having adequate representation on the boards.
We met through “RadChicks” in interventional radiology and shared a passion for motivating females into interventional radiology. We work hard from both sides of the Atlantic to support and encourage this change as well as offer medical students and junior doctors’ opportunities to discover this fields as well as support those already in training.
Our main focus is twofold: 1. coordinate in our advocacy efforts for women in radiology/endovascular medicine and 2. provide platforms where medical students and student doctors/residents feel supported, including mentorship/sponsorship programs, book clubs/workshops on a myriad of topics, networking events, even anonymous counselling.
When women trainees see strong women in their field, even in another state/county or across the globe, they feel empowered. They are not only empowered to continue in their path, but they feel empowered to help other women and under-represented minorities. This chain reaction becomes a powerful global support network which one day will improve the representation of women in endovascular medicine.
Bella Huasen is a consultant interventional radiologist at Lancashire Teaching Hospitals NHS Foundation Trust in Preston, UK.
Agnieszka Solberg is a vascular and interventional radiologist at CHI St Alexius Health in Bismark, USA.
Erik Schadde (L), one of the lead investigators of the Dragon trials, and Christoph Binkert, the Dragon trials’ international coordinating investigator for interventional radiology
This week, the first patient has been enrolled in the Dragon trials, investigating the safety and feasibility of a novel, double vein embolization procedure in the treatment of patients with colorectal liver metastases.
Resection of liver metastases from colorectal cancer improves survival compared to chemotherapy alone and may lead to cure in up to 40% of patients. If the volume of the future liver remnant post-resection is too low to carry out the surgery, and liver growth needs to be stimulated to reduce the risk of post-procedural liver failure. Portal vein embolization (PVE) is the current gold standard for inducing liver regeneration prior to resection of liver metastases in patients with colorectal cancer. However, the triallists propose that as embolization of both the portal vein and the hepatic vein on one side of the liver leads to “faster and more extensive” liver growth, it could be an improvement compared to PVE.
To test this hypothesis, the investigators are conducting an international, prospective, multi-centre pre-trial—Dragon 1—to explore the safety and feasibility of the double embolization approach, and to test enrolment capacity. All participating centres have to include three patients. Currently, four centres are fully initiated into the study, nine have ethical approval but are not yet initiated, and a further 27 are awaiting ethics approval. Dragon 1 will then form the basis of a randomised controlled trial comparing PVE with hepatic vein embolization (HVE) to PVE alone—Dragon 2. Dragon 2 is expected to start in 2021.
Describing the combined embolization option, the clinicaltrials.gov page for the two Dragon studies notes: “PVE/HVE combines simultaneous embolization of the portal main branches into the tumour-bearing liver and the hepatic vein draining them. The tissue in the part of the liver treated with PVE/HVE stays viable because the hepatic artery continues to supply the liver deprived of portal and hepatic veins.”
Final radiograph after double vein embolization
Speaking to Interventional News, Christoph Binkert (Kantonsspital Winterthur, Winterthur, Switzerland), the international coordinating investigator for interventional radiology in the Dragon trials, comments: “The first double vein embolization in the Dragon 1 trial went very well. From our clinical experience, we always treat the right portal vein first in order to have good antegrade flow within the portal vein. We used a mixture of Lipiodol [Guerbet] and Glubran [Gem] as an embolic agent. In the same session, the hepatic veins were embolized with Amplatzer plugs. There were two main right hepatic veins and a prominent vein draining segment six, which was also embolized. The patient tolerated the procedure well and left the hospital the same afternoon.”
Earlier preclinical studies in pigs have demonstrated the feasibility of this method, and human case series show accelerated and increased liver growth.
Binkert enthuses: “The Dragon trial is a true international and interdisciplinary trial researching the potential of double vein embolization. The idea is to reach a faster growth of the future liver remnant without additional risks to the patient. After several months of intensive preparation, it is good to finally get started. I am convinced that soon other centres will also start enrolling.”
Binkert spoke to Interventional News last September at the first Embolotherapy (ET) conference in Valencia, Spain (26–29 June, 2019). You can see the full video interview here.
The Society for Cardiovascular Angiography and Interventions (SCAI) has released guidelines that provide a comprehensive review of comparative effectiveness data for devices used in aortoiliac arterial interventions.
The recommendations aim to provide clinicians with guidance for device selection in patients for whom these devices are intended as definitive therapy.
The document has just been published in SCAI’s official journal, Catheterization and Cardiovascular Interventions and presented during the SCAI 2020 Scientific Sessions Virtual Conference.
“Endovascular device selection in peripheral arterial interventions remains challenging due to paucity of comparative data and a wide spectrum of available devices. In 2018, SCAI developed the first-of-its-kind guidance document to address device selection in femoral-popliteal arterial interventions,” said Dmitriy Feldman, chair of the writing group.
“The purpose of newly released 2020 SCAI guidelines is to provide a comprehensive review of comparative effectiveness data for aortoiliac devices and to arm clinicians with evidence-based recommendations and practical guidance for selection of devices in aortoiliac arterial interventions,” Feldman continued.
The writing group used a modified Delphi panel methodology to form recommendations based on data extracted through a systematic review of available evidence.
The writing group graded recommendations for eleven relevant anatomical scenarios according to strength of the recommendation (magnitude of benefit or harm, including cost of use) and certainty of the evidence (type, quality, and consistency of data).
Micro Medical Solutions has announced the first implantation of the MicroStent vascular stent in the US Food and Drug Administration (FDA) randomised, multicentre pivotal clinical study, STAND (A Clinical Evaluation of the MicroSTent PeripherAl Vascular SteNt in subjects with Arterial Disease Below the Knee). The 25 leading medical institutions and outpatient centres designated across the USA are now enrolling patients in STAND.
The first procedure was performed 25 March 2020 by the study’s lead investigator, Robert E Beasley of Mount Sinai Medical Center in Miami Beach, USA. “With a very successful MicroStent procedure and positive early results from the feasibility study showing a 90.9% patency rate at one year, I am delighted that the STAND study is now underway,” Beasley comments. “MicroStent offers hope for limb salvage, better health and quality of life to patients at risk for below-the-knee amputation, and the clinical trial will bring us closer to offering this new solution to thousands more candidates.”
MicroStent is a vascular stent, with both a 3Fr and 4Fr delivery system that allows for multiple access points, designed to achieve and maintain vessel patency and improve blood flow in order to reduce below-the-knee amputations for patients with critical limb-threatening ischaemia (CLTI) resulting from peripheral arterial disease (PAD). Micro Medical Solutions received Investigational Device Exemption (IDE) approval from the FDA after completing a three-centre, 15-patient feasibility study in which MicroStent met all primary endpoints for both safety and efficacy. When complete, the STAND study will include approximately 177 patients at up to 25 sites across the US. MicroStent has already obtained CE mark approval for use outside the USA.
Micro Medical Solutions CEO, Gregory Sullivan, adds, “Our leadership team and scientific advisory board have worked diligently to design and plan the STAND trial, with encouraging response from the FDA every step of the way. This first case is a source of great pride and inspiration as we continue to work toward FDA approval, which will help save many patients with CLTI from the devastation of below-the-knee amputation.”
Intact Vascular has announced the peer-reviewed publication of its Tack optimised balloon angioplasty (TOBA) III 12-month clinical trial results in the Journal of Vascular Surgery.
The multi-centre, single-arm, prospective study investigated the combination of the Tack endovascular system with Medtronic’s IN.PACTAdmiraldrug-coated balloon as a treatment in the superficial femoral artery (SFA) and/or proximal popliteal artery (PPA).
The trial results were previously presented as part of the high impact clinical research session during the 2019 Transcatheter Cardiovascular Therapeutics (TCT) conference.
“We are thrilled to have the TOBA III data published in the Journal of Vascular Surgery,” commented Peter Schneider, co-founder and chief medical officer of Intact Vascular. “This peer-reviewed article adds to the strong body of evidence supporting use of the Tack endovascular system for focal dissection repair when treating lesions both above- and below-the-knee.”
The study was conducted in multiple sites across Europe and enrolled 201 patients, including 169 patients with arterial lesions ≤150 mm in length and a subset of 32 patients with long arterial lesions (>150 and ≤250 mm).
All patients suffered from peripheral arterial disease (PAD) and underwent drug-coated balloon angioplasty, consequently experiencing at least one dissection requiring repair.
Results from the 169-patient standard lesion cohort (≤150mm) impressively demonstrated a 95% primary K-M patency with 97.5% K-M freedom from clinically-driven reintervention at 12-months and a 0.6% bailout stent rate.
The observational data from the long lesion subset (>150 and ≤250mm) was analysed separately. Results from these 32 patients notably demonstrated 98.8% complete dissection resolution and 89.3% K-M vessel patency, with 96.8% K-M freedom from clinically-driven reintervention at 12-months and a 0% bailout stent rate.
“The TOBA III trial met all primary endpoints and impressively demonstrated the highest reported rates of safety, patency and freedom from clinically driven reintervention when treating above-the-knee lesions,” commented Marianne Brodmann, head of the Clinical Division of Angiology, Medical University of Graz, Austria and principal investigator of the TOBA III trial.
She continued: “This study is unique in that we enrolled patients with 100% dissected vessels and included a long lesion subset, notoriously a complex cohort. These clinically compelling data further validate Tack implants as safe and effective for PAD interventions.”
Kevin Stadtlander and two radiology technologists during the procedure
Kevin Stadtlander outlines how his institution is benefitting from the “creativity” of interventional radiologists during the coronavirus pandemic, here providing a step-by-step account of a bedside inferior vena cava (IVC) filter placement for a COVID-19-positive patient in intensive care.
A 38-year-old male with past medical history of hypertension, admitted for complications of COVID-19, required mechanical ventilation and extracorporeal membrane oxygenation (ECMO). The patient developed an intracranial parenchymal haemorrhage felt to be related to ECMO, with fluctuating haemodynamics, while on intravenous (IV) heparin protocol. After removal of the ECMO venous cannula from the right groin, the patient was also found to have right iliac vein and femoral deep venous thrombosis (DVT), as well as below-knee DVT. The patient was referred to interventional radiology (IR) for inferior vena cava (IVC) filter placement, with a contraindication to systemic anticoagulation due to his intracranial bleed.
Given the ongoing COVID-19 pandemic, we had already implemented a plan that included having a designated IR procedure room in the department. Our IR plan included the directive to try to do as much as possible at beside in COVID-positive patients. For this IVC filter placement, we quickly mapped out both options, and decided to take the care directly to the patient room.
We located a portable C-arm with digital subtraction angiography (DSA) capability and did a trial in an empty intensive care unit (ICU) room to ensure that the C-arm would fit under the bed, and that images would be clearly visible through the ICU bed. These goals were both accomplished, but it did necessitate maximum ICU bed height to fit the C-arm. The COVID patient room was negative pressure and separated from the hallway (considered dirty) by sliding glass doors. Since no true anteroom was available, we used the empty ICU room as a staging room across the hall. The entire procedure plan was first reviewed in a huddle with all team members. We chose to have one IR physician and two radiology technologists in the room for the procedure. We were also accompanied by IR nurses (outside the COVID room), who helped with staging and acted as buddies for donning and doffing. The sterile procedure tray for the IVC filter was made up in a second empty ICU room and covered. Informed consent was obtained via telephone from a family member.
The IR physician and two technologists donned their personal protective equipment (PPE) and lead aprons in the staging room with the help of the nursing buddies. The C-arm, the C-arm monitor, and the ultrasound unit were covered with a plastic barrier, and then taken into the COVID-positive patient’s room by the “dirty” technologist (who was wearing full PPE, excluding sterile surgical gown and gloves). The second technologist (wearing full PPE and designated as procedure scrub technologist) then wheeled the procedure tray into the room, put on her surgical gown and gloves, and began prepping the patient’s left groin. We chose the left groin due to a thrombus in the right iliac vein, and in order to stay away from the head of the bed. The IR physician then entered the room, put on a sterile gown and gloves over full PPE, and helped to complete patient preparation. Importantly, a step stool (covered in plastic) was used by the physician during the procedure, as bed height necessary for C-arm made this a requirement. Sign in/time out was performed, IVC filter placement was completed in 10 minutes, and sign out was performed. Throughout the procedure, the patient’s ICU nurse monitored the patient and controlled his IV sedation via drips that were outside the room as per COVID protocol.
The surgical scrub gowns and top layer of gloves were removed in the normal fashion in the room and discarded. The procedure tray breakdown was quickly performed, and all items were disposed of in the room trash. Plastic wraps were removed from equipment and discarded in the room as each unit was moved from room to hallway. Each unit was terminally cleaned with X-ray machine bleach wipes. Each of the three caregivers then performed careful doffing of PPE (with our nurse buddies using a checklist) at the door threshold, ultimately leaving only N95 mask and bottom layer eye goggles on as they exited back to the staging room. Lead aprons were removed and wiped down with a lead X-ray apron cleaner disinfectant. N95 mask and goggles were then removed, and caregivers were free to head to the surgical locker room for scrub change and shower. A debrief huddle with all team members was then performed.
Kevin Stadtlander wearing personal protective equipment (PPE)
This case illustrates how IR creativity allows for procedures to be performed “portably” at the bedside in a manner safe for both caregivers and patients, while having the added benefit of preserving PPE. By way of follow-up, this patient ultimately came off the ventilator, became COVID-negative, and a CT brain has since demonstrated resolution of the intracranial bleed. The patient has been discharged from hospital.
Kevin Stadtlander, MD is an interventional radiologist at the Cleveland Clinic Florida, Weston, USA.
The Charing Cross (CX) Symposium, with its world-class faculty and unique focus on live audience participation, has announced the launch of a not-to-be missed and timely vascular and endovascular education virtual event: CX 2020 LIVE. Mark your calendars for this live digital experience, designed to deliver high-quality vascular education and featuring extensive audience participation, including polling and Techniques & Technologies edited cases, every Tuesday and Thursday over five weeks from 26 May–25 June 2020.
Roger Greenhalgh (London, UK), symposium chair, invites you to CX 2020 LIVE, and outlines the content of the first two sessions. World-leading vascular experts will give short presentations on some of the hottest topics in the field, including the paclitaxel controversy in peripheral arterial interventions, and the UK’s recently published NICE abdominal aortic aneurysm guidelines.
The 10 live sessions, which will feature audience participation, will run from 16:00 BST/11:00 EDT/17:00 CEST, every Tuesday and Thursday, from 26 May until 25 June.
This meeting is a vascular and endovascular calendar special. Register now and read more on the programme here.
An individual patient-level data (IPD) analysis of the safety of paclitaxel-containing devices (PTXD), conducted by VIVA Physicians, identified an absolute 4.6% increased mortality risk associated with PTXD use.
The analysis, based on the most complete available data set of mortality events from PTXD randomised controlled trials, was led by Krishna Rocha-Singh (Prairie Heart Institute, Springfield, USA) and has been published in Circulation.
VIVA’s analysis included 2,185 subjects across 8 studies with a median follow-up of 4 years; ultimately, VIVA’s analysis identifies a weaker mortality signal than was initially reported in December 2018 by Katsanos et al.
VIVA Physicians’ paper, “Mortality and paclitaxel-coated devices: An individual patient data meta-analysis”, also acknowledges no drug-dose relationship was established.
This is VIVA’s second published article on the risk of increased late mortality in the context of PTXD from their independent, patient-level data analysis. The current study includes subjects whose data were previously lost to follow-up.
Manufacturers of US Food and Drug Administration (FDA) approved and commercially available devices in the USA provided de-identified data for VIVA’s independent analysis.
Cox proportional hazards one-stage meta-analysis models using intention-to-treat (ITT) methods were used for the primary analysis. A secondary analysis of additionally recovered missing vital status data was performed.
The impact of control crossover to paclitaxel-coated devices, cause-specific mortality and drug dose-mortality were all assessed. This IPD analysis was completed in collaboration with FDA, leading clinicians, researchers, and statistical analysts.
The paper appears in the May 2020 online edition of Circulation and is available here.
Reviewing the available evidence for below-the-ankle interventions in the treatment of critical limb-threatening ischaemia (CLTI), Srini Tummala proposes that pedal artery intervention “should be an integral part of the armamentarium” when physicians are faced with patients with both below-the-knee and below-the-ankle disease. Although he calls for more data to consolidate this view, he highlights how the existing literature demonstrates a higher rate of wound healing and a shorter time to wound healing when additional pedal artery revascularisation is performed with below-the-knee interventions.
CLTI is the most severe form of peripheral arterial disease (PAD), and is classified by ischaemic rest pain, ulcers, or gangrene in the lower extremities attributed to objectively proven arterial steno-occlusive disease. Diabetes is a major risk factor, resulting in atherosclerosis occurring at a younger age and affecting mostly the infrapopliteal arteries.1 Revascularisation with bypass or endovascular therapy (EVT) is an important treatment to avoid or minimise amputation based on the latest guidelines.2–4 Surgical bypass, however, is not always an option, as many CLTI patients with infrapopliteal disease may not be surgical candidates due to frailty, co-morbidities, advanced age, or poor distal bypass targets. 2–4 EVT for infrapopliteal disease has become commonplace, and studies have shown a comparable limb salvage rate to surgery, but there is still an apparent discrepancy between limb salvage rate and the rate of wound healing.5–10 Delayed wound healing has increased morbidity, lowers quality of life, and also increases medical costs even if limb loss is successfully prevented.6,9,10 Clinical trials have reported that the presence of below-the-ankle disease results in worse wound healing, thus pedal artery revascularisation is of paramount importance to achieve complete wound healing.7,10
About a decade ago, the safety and effectiveness of below-the-ankle angioplasty was unclear, and it was uncertain whether additional below-the-ankle angioplasty after below-the-knee (BTK) angioplasty improved clinical outcomes.11 Since then, new tools have been introduced, and many advanced techniques have been described for pedal artery revascularisation, but the lack of randomised controlled trial data and long-term results, coupled with the potential risks (including dissection, spasm, rupture, and thrombosis), have limited widespread adoption of these interventions.12–18
In 2009, Manzi and colleagues showed that below-the-ankle interventions in CLTI patients were not only feasible, but safe, and that they appeared to provide positive clinical results at both short and mid-term follow-up. In their analysis, they consecutively treated a total of 1,331 patients with BTK disease of which 135 (10.1%) underwent below-the-ankle revascularisation with pedal-plantar loop technique in order to recanalise the pedal arteries. Technical success for the pedal-plantar loop technique was 85%. Clinical improvement and functional status was obtained and maintained after an average of 12 months, with a significant improvement of transcutaneous oxygen tension (TcPO2) after 15 days. TcPO2 was 59+/-16mmHg in the below-the-ankle intervention group when it was successful versus 42+/-12mmHg in patients where patency was achieved in two BTK vessels down to the ankle level with partial out-flow in the foot (p<0.001).18
Shortly thereafter, Kawarada et al described a pedal arch classification system and demonstrated that the status of the pedal arch was an independent predictor of wound healing. Based on data from the RENDEZVOUS registry, Nakama et al demonstrated that the speed and extent of wound healing was improved with below-the-ankle angioplasty.19,20 This registry was multicentre, and included 317 CLTI patients presenting with infrapopliteal arterial disease who underwent EVT at five experienced cardiovascular centers in Japan. Nakama et al retrospectively reviewed 257 of these CLTI patients who presented with de novo infrapopliteal and pedal artery disease. Patients were then divided into two groups according to whether pedal artery angioplasty (PAA) was performed (n=140) or not (n=117). The rate of wound healing was higher in the PAA group (57.5% vs. 37.3%, p=0.003), and the time to wound healing shorter (211 days vs. 365 days; p=0.008).
More recently, in 2019, Huizing et al published a systematic review and meta-analysis of below-the-ankle angioplasty in CLTI patients. Their review included ten articles which reported a total of 478 patients with below-the-ankle angioplasty performed in 524 legs. The pooled 12-month limb salvage rate was 92%, and there was no statistically significant difference found in limb salvage when additional below-the-ankle angioplasty was compared to BTK angioplasty only. The pooled 12-month amputation-free survival was 78% and no statistically significant difference was found in amputation-free survival when additional below-the-ankle angioplasty was compared to BTK angioplasty only. This systematic review and meta-analysis showed that additional below-the-ankle angioplasty is a safe and feasible procedure, with a 92% pooled proportion of limb salvage at 12 months. Although no significant difference was found in limb salvage rates or amputation-free survival rates when BTK angioplasty only was compared to BTK angioplasty plus additional below-the-ankle angioplasty, the wound healing rates were better in the additional below-the-ankle angioplasty group. Specifically, Nakama et al in 2016 and 2017 showed wound healing rates of 93% versus 60%, and 59% versus 38%, respectively, favouring additional below-the-ankle angioplasty. Finally, with more severe pedal artery disease, wound healing results were better in the additional below-the-ankle angioplasty group compared to the BTK angioplasty only group.11
In conclusion, the currently available evidence suggests that pedal artery revascularisation is a safe and feasible procedure. Data also suggest no significant difference in limb salvage rates or amputation-free survival when additional below-the-ankle angioplasty was compared to BTK angioplasty only. However, wound healing rates are higher and time to wound healing shorter when patients undergo additional pedal artery revascularisation. This begs the question—is pedal artery revascularisation ready for prime time? While high-quality research is most certainly needed to clarify the benefits, available evidence suggests pedal artery intervention should be an integral part of the armamentarium to treat CLTI patients when there is BTK and co-existing below-the-ankle disease in cases of wound healing and limb salvage.
Srini Tummala is the director of the Limb Preservation Program, Department of Interventional Radiology at the University of Miami Health System, UM Miller School of Medicine, Miami, USA.
References
Marco Manzi, Giacomo Cester, Luis M Palena, Josef Alek, Alessandro Candeo, Roberto Ferraresi. Vascular Imaging of the Foot: The First Step Toward Endovascular Recanalization. Radiographics. 2011 Oct; 31(6): 1,623–36.
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. TASC II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg 2007; 33(Suppl. 1): S1e75.
Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, et al. Management of patients with peripheral artery disease (Compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation 2013; 127: 1425e43.
Tendera M, Aboyans V, Bartelik ML, Baumgartner I, Clement D, Collet JP, et al. ESC guidelines on the diagnosis and treatment of peripheral artery diseases. Eur Heart J 2011; 32: 2851e906.
Romiti M, Albers M, Brochado-Neto FC, Durazzo AE, Pereira CA, De Luccia N. Meta-analysis of infrapopliteal angioplasty for chronic critical limb ischemia. J Vasc Surg 2008; 47: 975e81.
Iida O, Soga Y, Hirano K, et al. Midterm outcomes and risk stratification after endovascular therapy for patients with critical limb ischaemia due to isolated below-the-knee lesions. Eur J Vasc Endovasc Surg 2012; 43: 313–21.
Kawarada O, Fujihara M, Higashimori A, et al. Predictors of adverse clinical outcomes after successful infrapopliteal intervention. Catheter Cardiovasc Interv 2012; 80: 861–71.
Iida O, Soga Y, Yamauchi Y, et al. Clinical efficacy of endovascular therapy for patients with critical limb ischemia attributable to pure isolated infrapopliteal lesions. J Vasc Surg 2013; 57: 974–81.
Kobayashi N, Hirano K, Nakano M, et al. Predictors of non-healing in patients with critical limb ischemia and tissue loss following successful endovascular therapy. Catheter Cardiovasc Interv 2015; 85: 850–8.
Shiraki T, Iida O, Takahara M, et al. Predictors of delayed wound healing after endovascular therapy of isolated infrapopliteal lesions under- lying critical limb ischemia in patients with high prevalence of diabetes mellitus and hemodialysis. Eur J Vasc Endovasc Surg 2015; 49: 565–73.
Eline Huizing, Michiel A Schreve, Jean-Paul PM de Vries, Roberto Ferraresi, Steven Kum, Çagdas ̧ Ü Below-the-Ankle Angioplasty in Patients with Critical Limb Ischemia: A Systematic Review and Meta-Analysis. J Vasc Interv Radiol 2019; 30: 1,361–1,368.
Bolia A. Subintimal angioplasty in lower limb ischaemia. J Cardiovasc Surg (Torino) 2005; 46(4): 385–394.
Montero-Baker M, Schmidt A, Bräunlich S, et al. Retrograde approach for complex popliteal and tibioperoneal occlusions. J Endovasc Ther 2008; 15(5): 594–604.
Spinosa DJ, Harthun NL, Bissonette EA, et al. Subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) for subintimal recanalization to treat chronic critical limb ischemia. J Vasc Interv Radiol 2005; 16(1): 37–44.
Gandini R, Pipitone V, Stefanini M, et al. The “Safari” technique to perform difficult subintimal infragenicular vessels. Cardiovasc Intervent Radiol 2007; 30(3): 469–473.
Graziani L, Silvestro A, Monge L, et al. Transluminal angioplasty of peroneal artery branches in diabetics: initial technical experience. Cardiovasc Intervent Radiol 2008; 31(1): 49–55.
Fusaro M, Dalla Paola L, Brigato C, et al. Plantar to dorsalis pedis artery subintimal angioplasty in a patient with critical foot ischemia: a novel technique in the armamentarium of the peripheral interventionist. J Cardiovasc Med (Hagerstown) 2007; 8(11): 977–980.
Manzi M, Fusaro M, Ceccacci T, Erente G, Dalla Paola L, Brocco E. Clinical results of below-the knee intervention using pedal-plantar loop technique for the revascularization of foot arteries. J Cardiovasc Surg (Torino) 2009; 50(3): 331–337.
Osami Kawarada, Masahiko Fujihara, Akihiro Higashimori, Yoshiaki Yokoi, Yasuhiro Honda, Peter J Fitzgerald. Predictors of Adverse Clinical Outcomes After Successful Infrapopliteal Intervention. Catheterization and Cardiovascular Interventions 2012, 80: 861–871.
Tatsuya Nakama, Nozomi Watanabe, Takuya Haraguchi, Hiroshi Sakamoto, Daisuke Kamoi, Yoshinori Tsubakimoto, Kenji Ogata, Katsuhiko Satoh, Kazushi Urasawa, Hiroshi Andoh, Hiroshi Fujita, Yoshisato Shibata. Clinical Outcomes of Pedal Artery Angioplasty for Patients With Ischemic Wounds Results From the Multicenter RENDEZVOUS Registry JACC: Cardiovascular Interventions 2017, Vol. 10, N 1: 79-90.
Control Medical Technology has announced that the US Food and Drug Administration (FDA) has cleared its Aspire MAX 7 – 11F mechanical thrombectomy platform to remove blood clots from peripheral vessels.
“This FDA clearance quadruples our product offering and improves our ability to help patients,” said Shawn Fojtik, president of Control Medical Technology in Park City, USA. “The Aspire MAX 7 – 11F mechanical thrombectomy system includes (20) new large-lumen, flexible, and kink-resistant catheters w/dilators powered by the Aspire aspirator and/or an electromechanical pump.”
During a procedure, clinicians typically access the femoral artery or vein, track a catheter over a guidewire to the thrombus, and then apply low-performance suction with a basic syringe or pulsed continual high-performance vacuum with an Aspire mechanical aspirator or an electromechanical pump.
“Blood clots range from soft-fresh clots to hard-aged thrombus,” continued Fojtik. “Clinicians need more cost-effective tools to remove blood clots. We plan to introduce more catheter and electromechanical pump innovations for use in peripheral, coronary, and neurovascular procedures.”
The new Aspire MAX 7 – 11F mechanical thrombectomy system includes 7F (0.090″) outer diameter (OD) to 11F (0.140″) OD catheters with flexible dilators for improved tracking. Catheters may be connected to the Aspire aspirator and/or an electromechanical pump for increased speed, force, volume, and control.
Control Medical’s platform also includes the Aspire MAX 5 – 6F mechanical thrombectomy system with over-the-wire catheters for peripheral vasculature and the Aspire RX-LP mechanical thrombectomy system with rapid exchange catheters for peripheral and coronary vasculature.
Data was recently published using the Aspire RX-LP mechanical thrombectomy system’s to remove blood clots from total occlusions during heart attack [Adams G, Cavros N, Tai Z, “Novel mechanical thrombectomy device for treatment of acute myocardial infarction: A retrospective report,” Journal of Invasive Cardiology, 2020;32(4):142-146].
APERTO, Cardionovum’s paclitaxel-coated balloon for arterio-venous access, has received market approval for China, making it the first high pressure drug-coated balloon (DCB) available in China to treat obstructive lesions of native arterio-venous dialysis fistulae (AVF).
The approval was given based on the statistical superiority shown in a clinical study in Chinese populations: APERTO AVF RCT CHINA.
This is the first AVF randomised controlled study to archive statistical superiority of a high pressure DCB versus high-pressure plain balloon angioplasty. In a population of 161 patients, treatment with the device achieved superiority in freedom from restenosis at six months, and better intervention-free survival of both the target lesion and target shunt at 12 months with equivalent safety. Additionally, patients treated with APERTO maintained patency for another three months.
In a recent webinar hosted by GEST (Global Embolization Oncology Symposium Technologies), Kristen Alexa Lee (Singapore General Hospital, Singapore) shares her experience of navigating the COVID-19 pandemic as a pregnant healthcare worker.
Singapore is using the DORSCON risk assessment system, conceptualised following the 2003 SARS (Severe acute respiratory syndrome) epidemic to provide guidance to the public. Currently, the country is at DORSCON orange, which means the disease is severe, spreads easily, but not spread widely, and is being contained. “It has been almost three months since the first COVID-19 case was diagnosed in Singapore, and we have certainly gone through waves of calm and panic,” Lee says.
Detailing the pandemic experience in her country, she explains: “Thanks to aggressive contact tracing and testing, we have [had] a lot of initial success in the containment of the outbreak in the first two months. We actually had our second wave with [the] return of Singapore nationals and other visitors from overseas sometime in February/March, and with progressive quarantine measures and strict travel restrictions, the surge of imported cases has largely ceased.
“Unfortunately, we are actually now tackling a new surge of cases. There are new foreign clusters which are popping up from foreign worker dormitories.” While part of this is due to increased testing, Lee adds that healthcare workers across the country are bracing for a surge of inpatient and intensive care unit (ICU) admissions in the coming weeks.
However, she asserts that the SARS experience in 2003 has “truly created an urgency for early action”. As measures were put in place within hospitals and the community in a timely manner, she adds, “Personally, despite the situation, I have felt safe both at work and outside of work.”
Education on appropriate infection control measures and ensuring compliance to quarantine are among many of the public health initiatives in Singapore that, according to Lee, the government are advocating. “They have largely been focusing on social distancing and protecting the vulnerable, such as the elderly and pregnant women.”
Due to an array of measures taken within the hospital, Lee acknowledges that they are seeing minimal social transmissions and healthcare worker infections. “Compared to SARS in 2003, 41% of the cases were infected healthcare workers. Now, in 2020 for COVID-19, less than 1% of cases are infected healthcare workers, and those are believed to be acquired from the community.”
She explains that early on, protocols were set in place for perimeter control, and screening occurs for all patients on arrival. Guidelines are also in place to identify suspect cases for immediate isolation and evaluation, while compliance to all policies regarding segregation, social distancing, and travel restrictions are strictly enforced. There are clear directives for staff with any respiratory symptoms to seek medical attention at the staff clinic, Lee says, adding that all healthcare workers at her hospital are obliged to take their temperature twice a day to ensure there are no fevers.
Yet, regarding restrictions on work responsibilities for pregnant healthcare workers, Lee comments that there is only one, as the N95 mask has been deemed unsuitable. Therefore, she says all pregnant staff have been reassigned to areas where only surgical masks are needed, and must avoid participating in aerosol-generating procedures.
“As the situation continues to evolve, we have to revise my day-to-day role. My main concern was that I did not want to compromise our man power. But working together with my chief, we are able to find productive ways to scale back my patient-fronting duties.”
Given that the number of outpatient procedures have been reduced, Lee has taken on diagnostic duties, which are usually assigned to interventional radiologists. She also now helps with the management of outpatient requests, and developing systems to triage such patients. “During peacetimes, our list usually runs from anywhere of 40–50 cases per day. For essential outpatient services, it is important to have a detailed and systematic workflow, so patients can still receive the care that they need.”
Pregnant radiographers and nurses have largely continued their duties, Lee affirms, but are taken out of rotation whenever contact with a suspected COVID-positive patient is required.
“Even though we may be tackling different phases of the pandemic around the world, there is no question that this is a very trying time for many healthcare workers. For expecting mothers, the information on pregnancy and COVID-19 is still relatively scarce.”
Addressing staff that are currently pregnant, Lee urges them to “be familiar with your hospitals occupational health policy regarding pregnant healthcare worker, and continue to have open and honest discussions with your departmental leadership, to minimise your risk.
“Continue to protect yourself with strict infection control measures. For some of us, we need to revise as necessary to minimise our patient-fronting activities. Ultimately, it is important to remember that we are all contributing to this fight, and segregation does not mean isolation.”
Maureen Kohi (University of California San Francisco [UCSF], San Francisco, USA), who was co-moderating the webinar discussion with John Kauffman (Oregon Health and Science University, Portland, USA), praised Lee’s work, saying: “All we have done at UCSF [for pregnant woman during the COVID-19 pandemic], we have done because of her [Lee] and her experience, and what she brings to the table.”
Female doctor reads senior patient files in hospital corridor
Prism Schneider (Cumming School of Medicine, University of Calgary, Calgary, Canada) and others write in a commentary in the Canadian Medical Association Journal—because of an increase in domestic violence during the pandemic—healthcare providers should be aware of the signs of intimate partner violence and learn strategies to safely ask about injuries.
According to the press release announcing the commentary, China, Italy and Spain have reported increases in calls to emergency support lines. Also some areas of the UK and France have had police reports of violence increase by 20% and 30%, respectively; and crisis lines in Canada have seen large jumps in the number of calls. The press release notes that the frequency of domestic violence increased markedly during the economic downturn after Hurricane Katrina, suggesting that those affected will continue to be at risk long after the current phase of the pandemic ends.
In the commentary, the authors write: “Healthcare providers, although facing the need to learn many new skills related to COVID-19, must also maintain awareness of intimate partner violence, seek opportunities for self-education, develop strategies for discussing intimate partner violence and become familiar with currently available local resources for patient referral.”
They add that evidence supports direct questioning by a healthcare provider in a private environment if they suspect injuries from violence, as many women will not offer this information without prompting. Schneider et al note: “The onus is on health practitioners to begin the conversation with patients who may have experienced intimate partner violence.”
Lead author Schneider says: “Measures to minimise the spread of severe acute respiratory syndrome coronavirus 2 reinforce environments that facilitate behaviours that an intimate partner may use to exert power over another to inflict psychological, physical or sexual harm. The stress of confinement, financial uncertainty, attitudes about gender roles and a desire for control during disasters all contribute to an increased risk of intimate partner violence.”
As many physicians have moved to telemedicine consults to maintain physical distancing, Canada has launched a “Safe Word” campaign and a “Signal for Help” campaign for patients to send a silent request for help.
This article is sponsored by Guerbet. immunotherapy
Preliminary evidence suggests that combining conventional transarterial chemoembolization (cTACE) with immunotherapy could be beneficial to patients with unresectable liver cancer, writes Rafael Duran. He highlights the role of Vectorio (Guerbet) in standardising the cTACE technique, which he says “is needed for better reproducibility”, and explains how immunotherapy could be given systematically, through locoregional delivery within the Lipiodol-based emulsion, or injected intratumourally. He urges interventional oncologists to watch this space, as he predicts that combined cTACE and immunotherapy will become an increasingly common treatment approach for hepatocellular carcinoma (HCC) patients.
cTACE is the most widely used treatment for unresectable HCC, and has been increasingly utilised in patients with liver metastases. As opposed to surgery, which completely removes the tumour, cTACE achieves tumor cell death in situ. Thus, cTACE-induced necrosis may unmask to the immune system previously shielded tumour antigens and induce antigenspecific T cell responses. cTACE can trigger a cascade of inflammatory and immune responses, induce systemic changes in the levels of cytokines and chemokines, and, notably, has a profound influence on T cell repertoire.
Ayaru and colleagues demonstrated that cTACE could uncover tumour-associated antigens (TAAs), such as alpha-fetoprotein (AFP), and elicit AFP-specific CD4+ T cell responses. Flecken and colleagues showed that the detection of TAAs by CD8+ cytotoxic T cells was increased following cTACE when compared to treatment-naïve HCC patients. A seminal study was conducted by Mizukoshi et al on immune responses in HCC patients treated with several liver-directed locoregional therapies. All the patients demonstrated an increased frequency of TAA specific T cells post therapy, and, intriguingly, T cells from some patients also exhibited novel recognition of TAA peptides that were not recognised prior to treatment, underscoring the importance of these therapies in inducing and enhancing tumour specific T cell responses.
Upon the application of immune checkpoint inhibitors, not only did the number of TAA-specific T cells significantly increase, but also their production of cytokines, suggesting that a combination with immunotherapy is beneficial. In another study by Liao and colleagues, type 17 helper T cells (Th17) cells, which are known to play an important role in inflammation and autoimmunity, were significantly increased in HCC patients treated with cTACE. Interestingly, this increased frequency of circulating Th17 cells following cTACE was predictive of better patient outcomes (improved survival and longer time to progression). Importantly, cTACE is able to significantly decrease the percentage of regulatory T cells (Tregs), which are known to correlate with disease stage (the more advanced disease stage, the more Tregs) and progression, and worse survival outcomes, as they dampen the effector T cell responses against tumours and promote an immunosuppressive tumour microenvironment (Li et al; Liao et al).
Although preliminary, these data highlight the rationale of combining cTACE with immunotherapy. Many trials are ongoing that combine cTACE with systematically delivered immunotherapies to maximise the anticancer efficacy of both therapies. Immunotherapy could be delivered locoregionally within the Lipiodol-based emulsion (i.e. replacing the chemotherapeutic drug or in combination with it), or injected intratumorally. More studies employing combinatorial approaches of cTACE and immunotherapy are expected, and further standardisation of the cTACE technique is needed for better reproducibility. Vectorio will help in the standardisation of the technique by decreasing the current heterogeneity in practices among interventional radiologists. The preparation of the water-in-oil emulsion is improved, and, thus, should be more densely retained within the tumours than the alternative oil-in-water emulsion. For this, it is crucial to have a volume of Lipiodol that is double the volume of the cytotoxic drug, and to adequately mix the chemotherapy with Lipiodol with at least 20 back and forth pumping movements through the stopcock.
To date, interventional oncology (IO) approaches such as cTACE have been highly effective in treating tumours locoregionally, and the effectiveness of these approaches can be augmented to achieve systemic anti-tumour effects by combining with targeted immunotherapies. Although the convergence of IO and immunotherapy is still in its infancy, it presents multitudinous possibilities to be explored, which will be pivotal in improving the standard of patient care.
Rafael Duran is an interventional radiologist at Lausanne University Hospital, Lausanne, Switzerland.
Workforce shortages in clinical radiology are increasing year-on-year, resulting in delayed diagnoses and lower-quality patient care, according to the latest annual census from the UK Royal College of Radiologists (RCR). Shortages of interventional and breast radiologists are of particular concern, the “Clinical Radiology UK Workforce Census 2019 Report” states.
“The 2019 clinical radiology workforce census findings are grave,” Mark Callaway, lead author of the workforce report and the RCR’s medical director of professional practice for clinical radiology, writes in the forward. “Once again, they highlight the continued growth in demand for diagnostic and interventional radiology (IR) services, alongside further increases in workforce shortages. These are issues we have raised for many years and, worryingly, the continuing workforce shortages are impacting the cost and quality of patient care.
“The 2019 census report demonstrates unequivocally that our current imaging and interventional radiology services are unsustainable; governments and policy makers from across the sector and from all four nations must take action. Otherwise, patients are at risk.”
Costs have risen as radiology departments struggle to meet the demand for complex imaging, and consultant radiologists are feeling overworked and undervalued, noted the report, which was released on 14 April.
The key findings from the 61-page report were as follows:
National Health Service (NHS) hospitals spent £193 million last year on outsourcing, overtime, and locums to cover radiologist shortages. UK outsourcing costs rose 32% in 2019. In Scotland, expenditure on outsourcing shot up by 73%.
Only 1% of NHS trusts (hospital groups) and health boards are able to report all scans within radiologists’ contracted hours.
70% of clinical directors of radiology departments feel they do not have enough radiology consultants to deliver safe care. Additionally, 46% of trusts and boards do not have the staff or transfer arrangements required for safe 24/7 IR services.
Demand for CT and MRI scans is growing at 9% a year, which is three times the speed of the radiologist workforce.
In 2020, approximately 200 doctors will qualify as radiology consultants—not enough to fill even half of the estimated 466 vacancies. Also, in the 12 months to September 2019, 196 consultant clinical radiologists (equivalent to 161 whole-time equivalents) left the workforce, equal to 4% attrition.
The UK radiologist workforce is now 33% short-staffed; without more consultants in training and better staff retention and recruitment, the shortfall will hit 43% by 2024.
Importantly, the document was finalised before the escalation of novel coronavirus management, and it underlines the precarious state of many hospital imaging services and the unprecedented challenge that lies ahead, stated an accompanying RCR press release.
“The global coronavirus pandemic brings a sustained period of uncertainty and demand for the NHS,” Callaway comments. “Our most recent report underlines how our staffing crisis, which has been evident and escalating for the past five years, is having an undeniable, direct impact on the cost and quality of patient care.”
He hopes politicians and health leaders will seriously consider how the ongoing shortage of radiologists limits patient care and poses a threat to patient safety and commit to improving trainee numbers and focusing on specialty-specific retention measures.
“Due to our consistent 100% completion rate for the workforce census, these powerful but concerning data can be used by the RCR to lobby government, health education bodies, and policy-makers for increased training numbers and improved working practices for clinical radiologists,” Callaway adds.
Questions concerning the provision of IR services in the UK included for the first time
This year’s report is the first to include questions about the provision of IR services across the UK. Minimally invasive therapy is vital for the delivery of safe patient care and avoiding unnecessary surgery, says Callaway, before opining: “The results make disappointing reading from a patient’s perspective; only half of trusts and health boards can provide a comprehensive 24-hour service, and there is a severe shortage of experts to provide both vascular and non-vascular IR procedures.”
The report concludes that IR provision is “patchy and puts patients at unacceptable risk”, explaining that trusts and health boards need a minimum of six whole-time equivalent interventional radiologists to provide an effective and sustainable 24 hour IR service, or that formal transfer arrangements need to be in place 24/7. This was not the case for all trusts. Specifically pertaining to IR service provision, the key findings of the report were:
In 2019, almost half of the trusts/ health boards (46%, n=79) did not provide adequate IR services, with insufficient radiologists on their rotas or no rota at all and no formal transfer arrangements for patients needing IR procedures. This pits patients at unacceptable risk.
Census data indicate that 386 additional interventional radiologists are currently needed in the UK to meet IR guidelines; this equates to an IR workforce shortfall of 37%.
Generalists versus specialists
In 2019, 73% of consultant radiologists were classified as generalists. Variations were seen across the UK, with generalists being more common in Northern Ireland, Scotland, and Wales (84% to 85% of the consultant workforce) than in England (71% of the consultant workforce).
“The proportion of specialist radiologists in England has increased gradually over the past five years, from 25% of the consultant workforce in 2014 to 29% in 2019. In comparison, there has been no shift from generalists to specialist consultant radiologists in Northern Ireland, Scotland and Wales, where specialist radiologists account for 15% to 16% of the consultant workforce,” the report noted.
Most generalists across the UK have one main area of specialty interest (57%), a third have two (33%), and a small number (10%) have none. The majority of specialists across the UK have one main area of specialty interest (83%), though some (17%) have two or more areas of specialty interest.
The most common specialty areas of practice are musculoskeletal, gastrointestinal, breast, vascular IR, and chest/lung. Together, these account for 53% of all specialty interests.
Breast radiology has slipped from 13% of all specialty interests in 2014 to 11% in 2019. Similarly, vascular IR has dropped from 12% of all specialty interests in 2014 to 10% in 2019. Shortages of breast radiologists and vascular interventional radiologists are an area of concern, the report stated.
There is an “urgent need” to improve specific venous thromboembolism (VTE) diagnostic strategies and investigate the efficacy and safety of thromboprophylaxis in ambulatory COVID-19 patients. This is the conclusion of a recent study into venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy.
Behind this conclusion are the investigators’ main findings that a high number of arterial and, in particular, venous thromboembolic events were diagnosed within 24 hours of admission and there was a high rate of positive VTE imaging tests among the few COVID-19 patients tested.
The authors elaborate: “Hospitalised patients with COVID-19 were characterised by substantial in-hospital mortality and a high rate of thromboembolic complications. Rapidly increasing D-dimer levels were observed in non-survivors, reflecting the inflammatory and procoagulant state of COVID-19.”
The study, authored by Corrado Lodigiani (Humanitas Clinical and Research Hospital and Humanitas University, Milan, Italy) and colleagues—on behalf of the Humanitas COVID-19 Task Force—was recently published in Thrombosis Research.
Lodigiani and colleagues note that few data are available on the rate and characteristics of thromboembolic complications in hospitalised patients with COVID-19.
The Humanitas COVID-19 Task Force studied consecutive symptomatic patients with laboratory-proven COVID-19 admitted to a university hospital in Milan, Italy. They detail that the primary outcome was any thromboembolic complication, including VTE, ischaemic stroke, and acute coronary syndrome/myocardial infarction and that the secondary outcome was overt disseminated intravascular coagulation.
Lodigiani et al report that, of 388 patients (median age 66 years, 68% men, 16% requiring intensive care [ICU]), thromboprophylaxis was used in 100% of ICU patients and 75% of those on the general ward. Thromboembolic events occurred in 28 (7.7% of closed cases; 95% CI 5.4–11%), corresponding to a cumulative rate of 21% (27.6% ICU, 6.6% general ward). Half of the thromboembolic events were diagnosed within 24 hours of hospital admission.
Forty-four patients underwent VTE imaging tests and VTE was confirmed in 16 (36%). Computed tomography pulmonary angiography was performed in 30 patients, corresponding to 7.7% of total, and pulmonary embolism was confirmed at 10 (33% of computed tomography pulmonary angiography). The rate of ischaemic stroke and acute coronary syndrome/myocardial infarction was 2.5% and 1.1%, respectively. Overt disseminated intravascular coagulation was present in eight (2.2%) patients.
The authors acknowledge limitations to the present study. “This was a retrospective analysis conducted at a large university hospital, therefore possibly not reflecting the management strategies and diagnostic facilities at other non-academic institutions,” they note.
Furthermore, the authors address a geographical limitation: “Patients included in this analysis were diagnosed at one of the ‘red zones’ where the European outbreak started. This may have influenced not only patients’ outcome, as no global experience on the disease was available yet, but also the execution and frequency of imaging tests during hospitalisation. From this perspective, we could not confirm whether thromboembolic events contributed substantially to such a dramatic mortality and no autopsies were routinely performed in COVID-19 patients. Indeed, we showed that the D-dimer levels, a marker of inflammation and coagulation activation, rapidly increases in non-survivors during the course of hospitalisation; overt disseminated intravascular coagulation was present in 2% of COVID-19 patients and fatal in almost all cases.”
On 18 March, the Centers for Medicare & Medicaid Services (CMS) recommended “limiting non-essential care and expanding surge capacity into ambulatory surgical centres and other areas” to conserve resources and staff for managing COVID-19 patients. However, in a statement issued on 19 April, it now recognises “at this time, many areas [in the USA] have a low, or relatively low and stable incidence of COVID-19, and that it is important to be flexible and allow facilities to provide care for patients needing non-emergent, non-COVID-19 healthcare”.
The CMS adds that, as states and localities begin to stabilise, “it is important to restart care that is currently being postponed, such as certain procedural care (surgeries and procedures), chronic disease care, and, ultimately, preventive care”. The CMS advises, therefore, that if states or regions have passed the Gating Criteria, they may proceed to Phase I and directs them to the new US Government’s “opening up American again” guidelines.
According to the CMS, “maximum use” of telehealth modalities is “strongly encouraged”. However, for care that cannot be accomplished virtually, the CMS has issued recommendations (the first in a series) to guide “healthcare systems and facilities as they consider resuming in-person care of non-COVID-19 patients in regions with low incidence of COVID-19 disease”.
It says that non-COVID-19 care should be offered to patients “as clinically appropriate and within a state, locality, or facility that has the resources to provide such care and the ability to quickly respond to a surge in COVID-19 cases, if necessary”. The CMS also notes that decisions should “be consistent with public health information and in collaboration with state public health authorities”.
The recommendations review, among others, general considerations, personal protective equipment, workforce availability, facility considerations, and testing capacity. They include creating non-COVID Care (NCC) zones that “would screen all patients [and staff] for symptoms of COVID-19, including temperature checks”. Another recommendation is that such NCC zones should have “have in place steps to reduce risk of COVID-19 exposure and transmission; these areas should be separate from other facilities to the degrees possible (i.e., separate building, or designated rooms or floor with a separate entrance and minimal crossover with COVID-19 areas).”
Terumo Europe today announced that their BioPearl microspheres have received CE mark, providing a new option for patients eligible for locoregional embolization for the treatment of liver cancer. BioPearl microspheres are designed to preserve post-transarterial chemoembolization (TACE) target artery access, opening up the potential for cyclic treatment.
Currently, drug-eluting microsphere TACE (DEM-TACE) and conventional TACE are both used worldwide. According to Terumo, BioPearl microspheres have been designed based upon clinicians’ desire to have controlled drug elution while keeping future treatment options open. BioPearl microspheres could change treatment algorithms and may offer more choices for patients.
“Interventional oncology is not a standalone speciality, and by working with medical oncologists, we will be able to optimise current and future treatments, namely by delivering drugs directly into the tumour. Through such collaboration, we may be able to reduce the dosage and improve the toxicity profile of anticancer drugs, and ultimately improve the field,” says Thierry De Baere (Institute Gustave Roussy, Villejuif, France). “BioPearl drug-eluting microspheres and its degradation profile is a significant next step toward enhancing localised drug delivery and hopefully improving patient outcomes”.
Last week, the Charing Cross (CX) Symposium 2020 would have taken place in London, UK. To mark the occasion virtually, experts from across the globe took part in a wide-ranging informal chat to share the impacts of the COVID-19 pandemic on the vascular community. Chaired by Roger Greenhalgh (London, UK), Enrico Ascher (New York, USA), Michel Makaroun (Pittsburgh, USA), Roberto Chiesa (Milan, Italy), Jürg Schmidli (Bern, Switzerland), Gunnar Tepe (Rosenheim, Germany), and Rebeca Reachi (San Luis Potosí, Mexico) discussed the effect of the virus on their daily practice, compared the differing readiness with which the threat was met by governments across Europe and North America, and deliberated on what healthcare will look like in the aftermath of the deadliest pandemic in living memory.
A key take-home message is that not all healthcare systems have been impacted equally. Those hit first by the virus had the least time to prepare, and are consequently seeing a greater loss of life. Anecdotally, poorer neighbourhoods and countries (such as Brooklyn in the USA and Mexico City, Mexico) also seem to be the most overwhelmed. On a positive note, governments and local authorities exposed to the virus later, such as those in Switzerland and Pittsburgh, USA, seem to have been able to prepare for the pandemic, having learned from those hit first. Schmidli and Makaroun were able to recount how their regions were able to effectively mobilise against the virus early, closing borders to reduce footfall and slowing the spread. This was possible, they related, due to a delay in the virus reaching their communities, providing a window of opportunity to witness the response from medical communities already exposed.
As an additional consequence of the COVID-19 pandemic, the webinar participants reported that the necessary cancellation of elective procedures has resulted in a backlog of surgeries, meaning the current crisis will potentially have ramifications for healthcare for years to come. Indeed, when considering life after the pandemic, the discussants agree that while virtual meetings are no match for face-to-face interaction, they have been an essential part of healthcare provision during government-enforced lockdowns. Chiesa proposed that a return to normality is possible, providing healthcare professionals work together in unity.
The effects of COVID-19 on physician environment and practice
Later hit countries benefit from early preparation
A key takeaway from the webinar is that there is a large geographic disparity in the severity of the virus’ impact. Timing is also crucial. Those vascular specialists practicing in countries or regions with a “head start” on the virus repeatedly reported being able to mobilise earlier and to prepare their wards for the coming influx of coronavirus patients. For those first impacted by COVID-19, this was not the case. Speaking from Milan, Italy, Chiesa relates the difficulties with being amongst the first hit with the COVID-19 pandemic in Europe. “The problem in Italy is that we are the first country to be infected with COVID-19, so other countries have had a one, two, or three-week delay. It was easier for the other countries. For example, for Switzerland, it was easier, after observing what has happened in Italy, to stop everything immediately, to close down everything.”
Schmidli concurred. “We were quite lucky in Switzerland,” he told webinar listeners. “We knew what happened in Italy, and our authorities shut down the country quite fast. Most of the hospitals had about two weeks to prepare for COVID-19 patients,” he relayed.
Providing a US perspective, Ascher said: “Unfortunately, we were hit with this horrible pandemic, and in particular in New York state we have been hit very hard.” Providing some statistics, Ascher shared that, to date, there were more than 130,000 confirmed cases of COVID-19 in the state, with over 35,000 hospitalisations, and more than 9,000 deaths from the virus. “Just in Brooklyn, which is a very endemic area, we had close to 35,000 diagnosed patients. This is double what you have in Manhattan. We have been particularly hit; although we do not have as many institutions in Brooklyn as in Manhattan, we have double the number of cases. Not only have we been doing what we know how to do within our specialty, but [we have] also been expanding our services to particular needs within the hospital.”
Ascher claims that there is a “poverty factor” associated with the differing proliferation of COVID-19 within New York state; when asked directly about why he believes the discrepancy exists between case numbers in Brooklyn and Manhattan, he replied: “I think it is because the average person in Brooklyn is poorer than in Manhattan.”
In neighbouring Pittsburgh, a city in Pennsylvania, USA, Makaroun reported that there have been very few COVID-19 cases. “We have been lucky in Pittsburgh,” he disclosed. “We have had very few cases, and certainly the system has not been overwhelmed.
Relating her experience of COVID-19 in Mexico, Reachi told the other panellists: “The government are not testing everybody. The number of [confirmed] cases right now is only 8,000, but it is estimated that there are over 50,000. […] The main problem for me is there is not enough testing of patients.
“We do not have anything. We do not have N95 masks. I bought one for myself because some public institutions do not have enough equipment. I am in fear of going to work. We do not know if the patient [we are treating] is infected or not because they are not being tested. We have to take our own protection, not to get infected, so that is a problem here.”
Footfall favours viral spread
Chiesa noted that a football game at the San Siro stadium near Milan in February has been attributed to the initial spike in COVID-19 patients in the region. Similarly, although Tepe described Germany as not being too inundated with COVID-19 patients, he acceded that “Bavaria is quite different”, elaborating: “Rosenheim is the number one spot for COVID-19 within Germany. This is because we are close to Italy and Austria, and quite a lot of people have travelled through who had been in ski resorts in the Alps. About 10% of the population of Rosenheim are affected. Our hospital has 600 beds, and 200 of those are COVID-19. So, we are quite heavily affected.”
Closing borders helped to stop the spread
Makaroun noted: “Pennsylvania borders New York, and when the number of cases started increasing, they put a lockdown on all of Pennsylvania. We are a six-hour drive away, so our region was locked down before the big increase in cases.” Greenhalgh noted Makaroun was the first vascular surgeon he had heard report being ready for the COVID-19 crisis. Most healthcare centres around the world were overwhelmed by the virus.
Schmidli concurred: “Only cities close to the border (such as Geneva, Lausanne, or Lugano, which is quite close to Italy) had a lot of novel coronavirus patients from the beginning. But in the Swiss-German part [of the country], we had very few patients.”
Effect of COVID-19 on surgical practice and emergencies: Increase in number of endovascular procedures performed as physicians aim to keep patients out of hospital
Many elective procedures have been delayed or postponed around the world in response to the COVID-19 pandemic. What is elucidated in the CX COVID-19 webinar is that as well as impacting the number of surgeries taking place globally, the virus has also influenced the type of surgery being performed. Chiesa reported seeing more endovascular procedures than normal, citing the lack of beds in the intensive care unit of his hospital as one explanation: “It is very difficult to do open surgery without intensive care on our ward.”
Making incisions brings greater risk of infection. Several vascular surgeons speaking testified to seeing fewer transplants and fewer cancer referrals because of this increased risk. “In our hospital and throughout Germany, emergencies like patients who present with stroke or heart attack have gone down by 50%,” Tepe stated.
“We have got to assume that heart attacks and stroke are still taking place,” Greenhalgh replied. “So, are we making the assumption that this means patients are not coming into the hospital, but they are in trouble somewhere in the community?” Both Tepe and Schmidli agreed, with the latter adding: “We have seen the same thing—we did not have one ruptured aneurysm [in the last few weeks], which is completely unusual.”
Ascher noted that the same story was true in New York: “We have fewer emergencies, much fewer heart attacks coming to the hospital, and the reason I believe this is happening is because patients are afraid of coming to the hospital. They are saying they might as well take an aspirin at home and take a telemedicine. So, I think we have seen fewer of all these patients.” He declared his concern that several of these patients may need more intensive treatment in the future, once the pandemic-induced panic has passed.
Contrary to the other speakers’ experiences, Makaroun shared that his institution has treated six ruptured aneurysms in the last two weeks, and that, although the number of trauma cases were down (which he attributed to fewer cars being on the road meaning fewer traffic accidents), the number of cancer surgeries “has not really stopped”. He expanded: “Elective work, as you have mentioned, is down to almost none, but in general the emergencies have stayed to about the same as where they were before, but we may be privileged in a way in terms of where we were before, not being overwhelmed with COVID-19, and the hospital actually has around 20% empty beds.”
Backlog of elective cases: Catch-up will vary by geography
The necessary deferral of elective procedures has resulted in a backlog of cases across healthcare systems worldwide. During the webinar a geographical disparity in readiness to restart procedures became clear.
Makaroun predicted some logistical problems in starting the catch-up. “How many operating rooms can you reopen? How many nurses are sick and cannot show up?” he asked. Putting the scale of the situation at his centre in perspective, Makaroun detailed: “Normally on our system there are over 2,800 procedures a day, so you can imagine the backlog after about five weeks of doing very little elective work.”
In general, however, Makaroun noted that his hospital still has “a lot of capacity”, so they are now trying to work out how to prioritise patients and provide a framework for the cases to restart with minimal risk. Schmidli anticipated this to be the case in Switzerland as well: “restarting cases will not be a big issue,” he disclosed, as the number of infections has been lower than expected.
In contrast, Reachi outlined that in Mexico, they will not be starting elective cases again any time soon. “I know that we are very far from where we have to be. We are trying to flatten the curve and we are trying to stay at home. The government says this will be the case until the end of May.”
Medical education during the time of COVID-19: Virtual meetings no match for face-to-face interaction
The discussion then moved towards medical education during an era of unprecedented social distancing. Greenhalgh noted that the CX Symposium had been ready to showcase numerous first-to-podium presentations, covering “a lot of new data which is important to communicate”.
The panel agreed that while virtual meetings have enabled communication whilst face-to-face meetings are not an option, they are no match for a live conference.
Makaroun commented on both the necessity and ubiquity of the online meeting at the present time: “I think virtual is something that we have to do. Most of our meetings are now virtual and I am spending more time in front of my computer than I ever did in my entire life.”
Ascher then emphasised the benefits of interacting in person, stating that “nothing will ever replace the live presence of your colleagues at a meeting”. However, he acknowledged that “right now, we are in a situation where we have no other option but to go online.”
Return to status quo desirable, but timeline remains unclear
It was made clear during the conversation that a return to the status quo ante is desired, however the rate at which this can happen will vary by geography.
While Makaroun is hopeful that things will go back to normal, he stressed that it would take time. “Until the science catches up with this virus, I am not sure that we will ever know how we are going to return to normal. I think we have to learn to live with it for the foreseeable future and it may be a year or two, but I hope we will all go back to where we used to be.”
Schmidli believes that until there is a vaccine, things cannot go back to normal. “In the meantime,” he said, “we hope that the second wave does not hit us too hard.”
There was universal consensus about the need to return to normality as soon as responsibly and feasibly possible.
Profession faces specific COVID-19 danger
On the specific risks faced by the medical profession, Tepe pointed out the importance of testing and how his centre is addressing this: “We have to know who is positive and who is negative. Here at our institution we are doing a lot of CT scans. It is quite sensitive and is faster than a test.”
On a personal note, Ascher raised the point of responsibility towards the families of physicians. “I do not think we should overlook the influence on the family of the surgeon or the provider. It is a big deal because you go and spend 12 hours working and when you get home you have small children, you have a wife, you have grandparents. It is a big problem, and this is affecting a lot of us.”
Role of medical students varies widely across the globe
On the topic of responsibility, the conversation then considered whether medical students were prematurely functioning as doctors in order to meet the needs of the COVID-19 pandemic, with answers once again revealing geographical imbalance.
“In Mexico, all the medical students are at home,” Reachi began. “They are not allowed to go to the hospital because they are not prepared and there is not enough equipment to protect them.”
Ascher outlined a contrasting situation in New York: “At NYU [New York University], 50% of our senior class graduated already. Many of them were given jobs as residents and those who were not were hired to help in other ways and paid as residents.”
In Pittsburgh, however, medical students are not required in the hospitals and have instead been providing childcare for healthcare workers who cannot be at home, and volunteering at clinics in disadvantaged areas of the city. “They are stepping up and helping but not necessarily as physicians,” Makaroun commented.
“If only I knew…”: Vascular community reflects on what they would have done differently
Tepe cited testing as a “major issue” at the beginning of the crisis and something he would like to have been better prepared for.
The conversation then turned to equipment, with Ascher commenting: “I would have called the governor and asked him to expedite an order of ventilators”. One a similar note, Reachi stated that she would have bought more equipment for her college. “It is gone. There is no more.”
In Switzerland, “we would not shut down the whole system completely,” said Schmidli, noting that they had overestimated the impact of the virus in their country.
Chiesa ended this part of the discussion by commenting that in Italy the onset was so sudden that “it would have been impossible to do something differently”.
With more forewarning, Chiesa would have implemented a different organisation of the healthcare system in order to better prepare for the crisis. He outlined that he would have created a hub for every type of specialty “as soon as possible”, stressing that this was “very important, because it would allow you to do all emergency or other important cases in one major hospital in the region and use all other hospitals to cure COVID-19 patients”.
Difficult decisions during the COVID-19 crisis
As the conversation came to an end, the panel revealed the most difficult decision they have had to make so far during the COVID-19 crisis.
Chiesa, Schmidli, and Tepe agreed that choosing not to operate on certain patients was their most difficult decision. Chiesa noted, for example, that he was not able to operate on patients with thoracoabdominal aneurysms of up to 10cm.
One of the most difficult decisions for Makaroun related to his responsibility towards his employees. “I had to make sure that most of our employees and personnel are protected by sending them home and making sure their jobs are protected.”
Ascher addressed the decision between loyalties to family on the one hand and to patients on the other, questioning “whether at my age I should put myself in the situation of being on call 24 days a month.”
Reachi also felt that her loyalties were split between her hospital duties and family ties. She cited her most difficult decision as simply going to the hospital, likening it to gambling in its risk and recalled feeling “petrified” when entering her institution, due to the unknown prevalence of the virus and the lack of PPE.
COVID-19 has illuminated stark differences in healthcare systems across the world. Responses to the pandemic have been reflective of the extent and timing of exposure to the virus, and the resultant impact on the vascular community is markedly variable. At the same time, COVID-19 has brought the medical profession together. While the CX Symposium would have assembled vascular specialists from nearly 80 countries this week, this conversation has revealed commonalities within the community during a crisis. The degree of testing, PPE provision, and the timing and suddenness of onset have determined the severity of the impact on healthcare systems. Speaking from one of the hardest-hit countries in the world, Reachi expressed that her enduring dilemma was between her professional and personal duties, something at the forefront of every physician’s mind today.
The European Congress of Radiology (ECR) will not take place onsite in Vienna, Austria, this year. Instead it will be a digital-only event from 15–19 July, the European Society of Radiology (ESR) has announced.
“It is with a heavy heart and much regret that the board of directors of the ESR has decided not to hold an onsite ECR in 2020,” the ESR statement noted. ” As you can imagine,”, the board of directors continue in a letter addressed to ECR participants, “this serious decision was not taken easily. The choice not to hold ECR 2020 onsite presents a significant burden for the European Society of Radiology and will also influence future congresses and endeavours. However, we have a social responsibility to our members, partners, staff, and the general public. In the current crisis, the ESR must lead by example, and it is clear that your safety will always be our number one priority, and we sincerely hope for your understanding and support of our decision.”
The society also noted: “Public health authorities in Austria, as well as much of the rest of the world, have restricted large meetings and enforced travel bans, with no official indication as to when these restrictions will be lifted. As we are currently witnessing, almost all specialty and subspecialty societies and other congress organisers have already, or will shortly, cancel their meetings for 2020.”
The ESR said it made its decision because the COVID-19 outbreak had worsened since the original resolution was made to postpone the conference, with Europe becoming the epicentre of the global pandemic.
The letter closes with a note of gratitude: “We are not only a medical profession, but a family, and helping and protecting one another during moments like these is of the utmost importance. At no time have your services to radiology and healthcare been more important than now and the ESR board of directors would like to thank you, not only for your ongoing contribution to helping fight coronavirus, in whatever form it might take, but also for your support of our congress and society. We sincerely hope that we can rely on a continuation of this support in the future.”
Registration fees and expenses
Registration fees paid by delegates for ECR 2020 will be valid for ECR 2021, due to take place on 3–7 March in Vienna. Also, an ECR 2020 registration will automatically grant free access to the online congress in July 2020, including on-demand access until 31 December 2020.
Any registration queries should go to the ESR staff at [email protected], although the ESR urged registered attendees to be patient.
With respect to flight and accommodation bookings, the ESR suggested people check the provider’s cancellation policy.
“As there is not yet an official statement by the Austrian government regarding travel restrictions, border openings, or the allowance to hold major events in July, you should consider waiting with the cancellation of your booking if you are not eligible for free cancellation now,” the ESR stated.
The ECR 2020 Book of Abstracts has also been published online in the society’s journal, Insights into Imaging.
Intact Vascular hasannounced the first commercial use of its Tack Endovascular System (4F) in multiple sites across the USA. Notably the first FDA-approved vascular implant for below-the-knee (BTK) post-angioplasty dissection repair, Tack implants are designed to optimise balloon angioplasty outcomes in the challenging critical limb ischaemia (CLI) patient population.
“Effectively treating the small arteries affected in CLI has always been challenging. Over the years, various technologies have attempted to address this unique vasculature, but failed to provide an effective solution,” commented John Rundback, vascular and interventional radiologist and partner at the American Endovascular & Amputation Prevention Services in Clifton, USA, one of the initial implanting sites. “Finally, I have an option that safely and effectively delivers better results below the knee for my CLI patients, and I am thrilled to incorporate this novel peripheral vascular implant into my treatment algorithm going forward.”
Regulatory approval was based on data from Intact Vascular’s Tack optimised balloon angioplasty II BTK (TOBA II BTK) clinical trial, which met all primary endpoints with 100% acute dissection resolution. The TOBA II BTK results were presented at the 2019 VIVA conference and demonstrated 95.7% K-M amputation-free survival, 87.3% K-M target lesion patency with significant improvement in toe-brachial index (TBI) and 92.0% K-M freedom from clinically driven reintervention at six months.
“As a company, Intact Vascular has sponsored multiple large-scale, prospective studies that have generated a solid and robust body of clinical evidence to support post-angioplasty dissection repair with the Tack Endovascular System,” noted S Jay Mathews, interventional cardiologist and endovascular specialist at Bradenton Cardiology Center in Bradenton, USA, another initial implanting site. “I am confident this game-changing technology will elevate the standard of care when performing endovascular procedures.”
“I would like to acknowledge our TOBA II BTK trial investigators for their collaboration and efforts to reach this important milestone,” commented Howard Rosen, vice president of marketing and business development for Intact Vascular. “There has been a long-standing and significant unmet need for a technology that addresses BTK disease. We are thrilled to provide the first FDA-approved peripheral vascular implant offering endovascular operators a novel tool that safely and effectively addresses this challenging condition and improves outcomes for their patients.”
Micro-practices can be anchored to already existing activities, such as hand-washing
“With coronavirus disease 2019 (COVID-19), the demands and stresses on radiologists and physicians have increased dramatically. Even before this pandemic, the high prevalence of burnout, complex causes, and critical consequences had been widely reported,” write David Fessell and Cary Cherniss in the Journal of the American College of Radiology. “The need for effective strategies and tools [to manage radiologists’ mental health] is only increasing as both individuals and institutions navigate the current anxiety and uncertainty.” Here, Fessell outlines some “micro-practices” physicians can implement in their daily life to help cope with the additional stresses of working amidst a global pandemic.
With increased stress and anxiety comes an increased risk of decreased functioning and potential burnout. “Macro-practices”, including quality sleep, exercise, and nutrition, are essential for well-being. “Micro-practices” may also be helpful in preventing burnout and promoting emotional wellness. Such practices take just a few seconds to a few minutes. In a recent article, Cary Cherniss [Rutgers University, New Brunswick, USA] and I reviewed the evidence for four such practices: a self-wellness “check-in” during handwashing; the practice of “name it to tame it,” for our emotions; using a gratitude journal; and deep breathing for activating the parasympathetic nervous system to promote calmness and relaxation.1
“Micro-practices” can be anchored to already existing activities, such as hand-washing or logging into the PACS [picture archiving and communication system], to help us form healthy habits.2 Almost any recurring event can be a cue for a wellness check in: focusing on your breath and reflecting: am I well hydrated? Hungry? Emotionally or physically exhausted? Such quick and simple micro-practices are potentially possible even for the busiest radiologist. Activities outside our work lives can be cues as well—waiting in line or online, before answering the phone or a text, or even before brushing one’s teeth. Over time, such built-in wellness moments have the potential to shift one’s energy level and the tone of one’s day.
“Name it to tame it,” to paraphrase [neuropsychiatrist and author] Dan Siegel (University of California Los Angeles [UCLA] School of Medicine, Los Angeles, USA), has fMRI research to back it up. Such a practice can help us regulate our emotions, such as frustration and anger, to bring calm and ease.3 There are many helpful resources, including lists of the range of human feelings, which can help facilitate this process.4,5
An additional evidence-based practice that can aid well-being is the simple act of writing down three things one is grateful for several times a week.6,7 Sharing this practice with a “gratitude partner” can help expand the positive feelings and bring support and encouragement. Such practices can be extended to groups by starting meetings with “kudos” for recent achievements. Such group practices can help develop positive and dynamics relationships among team members.
David Fessell
Finally, a simple breathing technique known as diaphragmatic breathing has also shown promise for reducing stress and self-perceived anxiety.8 The practice is simple: inhale deeply by expanding the lungs downward rather than inhalation using the abdomen or ribcage alone. Inhale through the nose, pause and then slowly exhale through the mouth. Silent counting during inhalation and exhalation may be helpful to establish a respiratory rate of six to eight breaths per minute. This kind of slow, deep breathing is thought to increase para-sympathetic activation. Many other breathing techniques exist—explore them, and find one or more that resonates with you.9,10
Throughout one’s day there are likely many opportunities to take a deep breath or three: before the start of a read-out session, between cases, or on a bathroom break. These micro-practices may seem too small and inconsequential to do any good. Small changes are, however, doable and sustainable. Over time, building moments of mindfulness and gratitude, emotional regulation, and deep breathing into one’s day can increase the wellness in one’s life. Try one or more. If you are bringing more calm and peace to your world, it is highly likely your colleagues, family, and friends will benefit as well.
These micro-practices are not treatments for burnout. If you are experiencing burnout, please seek professional help. We need you happy, healthy, and thriving. These micro-practices are meant to complement other individual efforts such as mindfulness-based stress reduction (MBSR) and personal coaching. Having a robust tool box of practices that resonate with you can be an invaluable resource for navigating challenges including COVID-19, and beyond.
David Fessell is a radiologist at the University of Michigan Medical School, Ann Arbor, USA.
References
Fessell D, Cherniss C. Covid-19 and Beyond: Micro-practices for Burnout Prevention and Emotional Wellness. J Am Coll Radiol.2020 Mar 24. pii: S1546-1440(20)30290-8. doi: 10.1016/j.jacr.2020.03.013. [Epub ahead of print].
Lieberman, M. D., Eisenberger, N. I., Crockett, M. J., Tom, S., Pfeifer, J. H., Way, B. M. Putting feelings into words: Affect labeling disrupts amygdala activity to affective stimuli. Psychological Science. 2007; 18:421–428.
Emmons, R. A., & McCullough, M. E. Counting blessings versus burdens: Experimental studies of gratitude and subjective well-being in daily life. Journal of Personality and Social Psychology. 2003:84;377–389.
Sexton JB, Adair KC. Forty-five good things: a prospective pilot study of the Three Good Things well-being intervention in the USA for healthcare worker emotional exhaustion, depression, work-life balance, and happiness. BMJ Open, 2019; e022695.
Hopper SI, Murray SL, Ferrara LR, Singleton JK. Effectiveness of diaphragmatic breathing for reducing physiological and psychological stress in adults: a quantitative systemic review. JBI Database of Systemic Reviews and Implementation Reports, 2019;17:1855-1876
Inspired by his father, an interventional radiologist who used to shape catheters over the stove at home, Matthew Johnson switched from a residency in surgery to pursue a career in interventional oncology, and began a lifelong love affair with the liver. “There is always more to learn”, he says.
What first attracted you to interventional radiology (IR)?
My father. He was a radiologist, radiation oncologist, and interventional radiologist in private practice in Battle Creek, Michigan, USA. He loved his job, and often spoke about his patients, mostly about his cancer patients. I once suggested that it must be difficult treating cancer patients, but he said “No; it is incredibly satisfying. There are two things you can cure in medicine: infection and cancer.” That positivity has always stuck with me. He did the first arteriogram in Battle Creek, but I did not know that until I was in medical school. I remembered that he used to shape catheters over the stove at home, but did not know that was unusual. It is what Dad did. After medical school, I started residency in surgery, following my brother, Mike. My father thought I was crazy. He said that I should be a radiologist. He was right. I switched to Radiology after two years in surgery, always with the intention of becoming an interventional radiologist.
Have you had important mentors throughout your career? What have they taught you?
My father and my brother Mike both taught me the importance of doing the work. Both led by example. The adages that “99% of life is showing up” and “do what you say you are going to do” were family mantras. Mike, two years ahead of me in medical school, and still a practicing surgeon, told me that as a resident, no matter how difficult your day was, you should study for an hour. He did that, all the way through his residency. While I was not 100% successful in matching his effort (his drive is unparalleled), I did understand the concept, and tried to adhere to it. I still do, even if sometimes that study is of ancient history rather than of the latest anticoagulant: there is always more to learn.
I have had many, many other mentors, including Rogelio Moncada, Leon Love, Terry Demos, and Richard Cooper at Loyola in Chicago. All were brilliant and all worked hard. They stressed and accepted only excellence, and were the best teachers. Tony Venbrux, part of the faculty at Johns Hopkins during my fellowship, demonstrated not only knowledge and ability, but unequalled empathy and kindness. I continue to strive to be more like Tony. Scott Trerotola, IR section head at IU when I joined and my chief for eight years, taught me how to be a researcher. His refusal to sacrifice his integrity was inspiring. Finally, in an inexhaustive list, and although he would be surprised to hear it (as he was a radiology resident when I joined the faculty at IU), I consider Himanshu Shah, my current chair, as a mentor. His always-positive demeanour, openness to discussion, keen intellect, and indefatigable spirit have made IU Radiology a wonderful department in which to work, one that continues to flourish under his stewardship.
What has been the highlight of your term as secretary of the Society of Interventional Radiology (SIR) this year?
Unquestionably, that as we have matured as a society and embraced the fact that we are now a primary specialty, we have recognised the importance of demonstrating to the world the value of what we provide to patients. That recognition has led to us having a robust strategic plan that includes supporting interventional radiologists in practice, and creating and maintaining a residency that trains excellent clinical physicians, as well as improving understanding by external groups of what IR is. The fourth pillar of that strategic plan excites me most: it is directed toward improving the quality and impact of IR research. We have grown the research infrastructure within SIR by adding staff experience (for example, a new methodologist) and undertaking advanced clinical practice guideline initiatives. The first SIR-sponsored Clinical Practice Guideline on IVC filter use will be published in the next few months, and two others will begin this year. We have also directed ample resources to support the growth of our registries to be used for both quality improvement efforts and original research. I am very excited about the shared commitment by SIR and the SIR Foundation to research, as I think that support is essential to the continuing success of our specialty.
You are co-principal investigator of the PRESERVE trial, the largest prospective study investigating real-world outcomes with contemporary use of IVC filters. Why is this study important?
It is important because it will give us the best data we can obtain regarding IVC [inferior vena cava] filter use in the USA. A randomised controlled trial is not really feasible, because of the impossibility of an appropriate control group: if that group is anticoagulated, it does not represent patients for whom filters are indicated; if that group is not anticoagulated, those patients are subjected (we believe) to increased risk of pulmonary embolus (PE). PRESERVE is designed to follow patients with filters until filter removal or for two years. With over 1,400 subjects, we will be able to evaluate real complication risks and incidences of PE before and after filter removal. We will begin evaluation of the results in May 2020, after all patients have completed one-year follow up or have had their filters removed. I hope and believe that PRESERVE will contribute greatly to our understanding of how filters are used, and will help to demonstrate who will benefit most from their use. As follow-up of patients with IVC filters is so important, I am hopeful that the structured follow-up we employed in PRESERVE will serve as a paradigm for such followup in clinical practice. learn
The PRESERVE trial is the result of a multi-stakeholder collaboration. What have you learnt from this?
The PRESERVE trial is a collaboration between SIR, the Society for Vascular Surgery (SVS), the US Food and Drug Administration (FDA), and industry partners. I think that that collaboration is one of the major benefits of PRESERVE. The trial was made possible by a shared goal: wanting to do what is best for our patients. We all recognised that the data surrounding venous thromboembolic disease in general, and especially around IVC filters, are limited, that we do not know who will benefit most from filter placement, how long to leave that filter in place, and how to follow it while it is there. PRESERVE has demonstrated that each of the entities involved has unique strengths—including skills, infrastructure, networks, understanding—and that as we work toward our shared goal, the sum of those combined strengths is greater than their components. I hope PRESERVE can serve as a paradigm for other SIR collaborative efforts. learn
You hold a number of patents. What drives you to innovate, and why specifically in the field of drug delivery?
There is always something more to learn. History repeatedly demonstrates the need for continuing innovation. Indeed, innovations changed the world: the stirrup changed warfare, the printing press changed thought. Happily, IR has always been immersed in innovation. That that process continues apace demonstrates how much more there is to improve. My clinical focus in the treatment of people with liver tumours led me to investigate ways to improve delivery of bioactive agents to those tumours. Our understanding of locoregional delivery of those agents is in its infancy, which is very exciting. What is the next thing that will really make a difference? I would like to contribute to the creation of that change-maker, to hear of a person whose life was made better by it. learn
Which innovations have most influenced your career, and how?
Transarterial radioembolization (TARE). Prior to the advent of ARE, my involvement in the treatment of patients with cancer was without much focus. When I considered treating patients with TARE, I thought that in order to provide adequate care to my patients, I would need to devote myself to interventional oncology (IO). So, prior to adding TARE to my practice, I spent a considerable amount of time learning about the treatment of patients with liver tumours. Not just IR treatments, but all possible treatments. It took me a few years to be somewhat comfortable with those treatment algorithms, but it was well worth it. That study made me a much better interventional oncologist, not just when I choose to use TARE for a particular patient, but also when I choose transarterial chemoembolization (TACE) or another locoregional therapy, or when I choose instead to refer to another doctors in our multidisciplinary team. I thank my IR partners at IU, as they allowed me the time to focus on IO. I am very grateful for their unwavering support. learn
Matthew Johnson
What are your hobbies and interests outside of medicine?
Mainly spending time with my family: my wife, Cynthia, and I have four children, all now adults with their own partners, and one grandson, Wesley. My hobbies include cycling, running, and rowing (machine); ancient history, from the beginning of civilisation to the Reformation, focusing primarily on the Roman republic and empire; playing and listening to music: I played piano and cello growing up, still play piano, and I took up guitar when I was 50 (I am not very good), and Cynthia and I very much enjoy going to concerts; and travel, which I very much enjoy when my wife is with me. learn
“Europe, including the European Union (EU) and the leaders of its nation states, needs to prepare better for future pandemics. I think we must develop a Europe-wide contingency plan providing clear guidance on effective measures,” says Afshin Gangi, president of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE). Speaking with Interventional News, he outlines the society’s response to the coronavirus pandemic, as well as measures taken by his own institution.
What is CIRSE doing currently to support its membership amidst the coronavirus pandemic?
The health of our members, congress goers, and industry partners has always been our top priority. This is why CIRSE reacted quickly following the outbreak of COVID-19 in Europe, moving our spring meetings to later dates in the year. The European Conference on Interventional Oncology (ECIO) 2020, which was planned for 26–29 April, has been moved to 2–5 November, in Nice, France. The European Conference on Embolotherapy (ET) and the International Conference on Complications in Interventional Radiology (ICCIR) were both going to take place in Austria in June, but since the restrictions on travel and gatherings will still be in place then, they have also been postponed. ET 2020 will take place 16–19 December in Vienna, Austria, with ICCIR 2020 running in parallel at the same congress centre from 16–18 December. The courses of the European School of Interventional Radiology (ESIR) are also being moved to autumn and spring 2021, hopefully once again enabling participants from around the world to join us for the comprehensive two-day courses on specific procedures.
With regards to the CIRSE annual congress, we are moving ahead with CIRSE 2020 to take place as planned in Munich, Germany, from 12–16 September.
In addition to these event-related activities, and in order to ensure that the exchange of experiences and medical education does not stop, we have put into action a series of measures to support online information exchange between interventional radiology (IR) professionals. Within a very short timeframe, a CIRSE/Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) working group put together a joint CIRSE-APSCVIR checklist to prepare IR departments for COVID 19. My special thanks go to main authors Bien Soo Tan and Kiang-Hiong Tay, both from Singapore General Hospital, Singapore, for sharing the knowledge they gained from both the SARS and the COVID-19 pandemics.
As the coronavirus continues to spread, it is key to be prepared to carry out emergency procedures in this new environment and treat possibly infected patients. Our knowledge in this regard is increasing by the day, which is why CIRSE is also planning to offer a series of freely available webinars in which front-line doctors will share their experience. In the first of these webinars, taking place on Monday 20 April at 5pm (CEST), Lorenzo Monfardini and Vittorio Pedicini from Milan, Italy, will talk about bedside procedures IR provides to COVID-19 patients. I encourage everybody to participate and use this unique opportunity to submit questions for this first CIRSE webinar. For more information please visit the CIRSE website at www.cirse.org
In addition, seven fully CME accredited CIRSE Academy courses have been made freely available, as have almost 200 lectures from previous CIRSE congresses via the CIRSE Library. We are confident that by taking these steps, we will be able to continue providing excellent IR education and supporting information exchange by an increased internet offering for the time being, and again in person once the pandemic has subsided.
CIRSE had to pull together a comprehensive resource centre very quickly. How did this come about? What needed to be prioritised, and how did you identify key stakeholders to work with?
In an effort to offer a concise and useful information hub amidst the myriad of online content on the pandemic, the CIRSE publications department has put together a collection of the most relevant links. These include the main stakeholders on an international scale, such as the World Health Organisation and the European Centre for Disease Prevention and Control, as well as articles, webinars, and checklists of particular relevance to interventional radiologists. Many thanks go to the CIRSE team. They really did an excellent job in putting all this together in such a short period of time.
In general, I think the internet is one of the big advantages we have during this pandemic and compared to past outbreaks. Even in comparison to SARS in 2002/2003, today it is so much easier for medical professionals to quickly share information and their experiences with colleagues from around the globe.
Is there a COVID-19 learning you wish to share with the interventional community?
I can only report on my own experiences in Strasbourg. The first major impact of the COVID-19 crisis was the cancellation of many elective interventions. Unfortunately, among the procedures that were classified as “not urgent” were many oncologic interventions, as well as benign pain management interventions. The delay in receiving their scheduled therapies is very stressful for patients and it will be important to start the interventional service again as soon as possible. I really admire how patients have reacted when learning that their therapies have been postponed. At the moment there is a lot of understanding and strong support for the medical community. However, it is not good to put them off from week to week and I hope that this situation will not persist for too long.
I think another important learning was that we are able, in a very short period of time, to change our work flows and patient pathways. Levels of safety and hygiene needed careful scrutiny and refinement to protect non-infected patients and hospital staff. Sadly, even with our immediate measures, it was impossible to avoid that some colleagues got infected and to my deepest regret a few colleagues even lost their lives.
I want to say that the medical and paramedical staff have been remarkable in this crisis, and I have the feeling that we are now even more united than before. In Strasbourg it seems that the peak has been reached and the situation is slowly starting to ease. However, we all know that this pandemic is far from over. We need to be careful not to provoke a second wave until medication, and hopefully a vaccination, against COVID-19 has been developed. Until that time, we will have to get used to our “new normal”.
Another important learning is that we need more of a European focus, not less. Europe, including the European Union (EU) and the leaders of its nation states, needs to prepare better for future pandemics. I think we must develop a Europe-wide contingency plan providing clear guidance on effective measures. Maybe there were good intentions from the EU leadership to introduce such a system after SARS in 2002/2003, but it seems that far too little was put into action. Among the many things that need improvement, I think, is that Europe should rebuild its infrastructure critical to the production of pharmaceuticals and medical equipment. This is essential, and would allow us to be independent and more proactive in the future.
What procedures are interventional radiologists still undertaking in this period?
In my experience, apart from the conventional emergencies such as bleeding, thrombectomies, or abscess drainages, we have of course also noticed more complications in the intensive care units related to COVID-19 patients with epistaxis or vascular damages.
In Strasbourg we also have seen an increase in thrombosis, but not necessarily in thrombectomy cases.
How has your personal daily practice been impacted by the pandemic? What measures has your hospital implemented?
Our department in Strasbourg has six operating rooms; three of them have been put out of function, with the removal of all anaesthesiologic devices and tools. We are fortunately still able to work in two angiography suites and one CT-angiography suite. Unfortunately, we have reduced collaboration with our colleagues from anaesthesiology. Outside of emergencies we currently receive their support only once a week. Additionally, all of our nurses have been assigned to other departments dealing with COVID-19 patients. Also, our medical staff has been temporarily reduced.
We are now preparing for the comeback and will be ready to catch up on the many postponed interventions once a regular IR service will again be possible.
What message would you like to give to the wider medical community at this time?
I think that the exchange of information is crucial. This is the first time that we have been confronted with a pandemic of this scale. We are gathering experience and seeing what works in real time, while at the same time having little to no data available on how exactly the virus works, and how it affects the body. We must therefore share all newly gained knowledge as quickly as possible. Each of us adding a piece of the puzzle on how to respond to and defeat this dreadful disease. It is a great challenge, but I am confident that we will get through this together, emerging stronger as physicians and a community.
Afshin Gangi is an interventional radiologist at the University Hospital of Strasbourg, Strasbourg, France, and is the president of the Cardiovascular and Interventional Radiological Society of Europe.
Medical oncologists Filippo Pietrantonio and Marina Chiara (both Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy) have launched a social media campaign called #knowyourstatus to advocate for the “periodical and frequent testing” of SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), the virus that causes COVID-19, in healthcare workers treating patients with cancer.
“Our aim is to guarantee separate and ‘clean’ pathways for patients with cancer,” they write in the Journal of the American Medical Association (JAMA) Oncology. “Even if this objective is failing in front of our very eyes, we will not give up on maintaining the involvement of institutions, patients’ advocacy organisations, and oncologist associations.”
In an opinion piece chronicling the dawning realisation of the severity of the current pandemic in Italy, Pietrantonio and Chiara write: “At this moment, we feel unprotected. Although everyone in the newspapers is praising physicians as heroes, we feel alone, thrown into jeopardy, thrown into an abyss. Our region has left us to fight the cancer battle and the COVID-19 war without true protection, without knowing whether we are infected with the virus. We go to work every day because we love our jobs, and this is the life we have chosen. But we are people, too; we are afraid of getting infected, of going home in the evening, of infecting our children, our parents. […] We live with the absurdity of trying to cure patients of a disease like cancer at the same time potentially being the vehicles for a virus that might kill these very patients.”
They dwell on the lack of personal protective equipment (PPE) available to physicians, and the criticise the low level of testing of healthcare workers in northern Italy. “We were terrified after reading the recent reports on undocumented infections as a crucial source of contagion. We were terrified when we thought about models of transmission when applied to our daily lives here at the hospital. Unfortunately, during the past few days, we have been facing the terrific and very real effects of the lack of prevention of intra-hospital infections. In the Lombardy region, the epicentre of the outbreak in Italy, and in many other regions in Italy, asymptomatic or paucisymptomatic health care workers who had contact with patients confirmed to have COVID-19 are not routinely tested unless they develop severe symptoms. Individual protection devices are often lacking and cannot be used for intermediate-risk scenarios. Some of our colleagues have tested positive and are now at home or, even worse, hospitalised in intensive care units. Some of us have already infected entire families, children, grandparents.”
Describing the initial approach to cancer care at the onset of the pandemic in Italy, Pietrantonio and Chiara say that they had to determine the risk-benefit ratio of using intensified treatments and treatment combinations, maintenance strategies, and later-line treatments for each of their patients. These “hard-to-make decisions” were discussed in multidisciplinary team meetings held over video call, and then communicated with patients. “As physicians of a referral centre facing the lockdown of the whole country, we had to decide what to do for some patients with cancer already enrolled in clinical trials, and the patients who faced travel disruptions and the lack of flights from the south of Italy to our hospital in the north, and the fear these patients with cancer had of being infected with COVID-19 while traveling,” they say.
Their piece also captures the emotional toll the COVID-19 pandemic is taking on physicians in Italy. With frequent mention of the “terror”, “loneliness”, “fear”, and “anger”, Pietrantonio and Chiara recount: “We meet colleagues and patients and even laugh about funny stories, but it is clear to all of us that the level of stress and the risk of burnout that health care professionals are facing is alarming.”
They conclude, however, on a hopeful note, emphasising the importance of international unity in the face of a shared global crisis: “In this time of fear and anger, the most important thing is sharing. We have found ourselves united across borders. We have felt the love of so many people for us and for our country. How do we survive, then? With love for our patients, for our professions, and thanks to the sharing that has been created between us.”
Sung-Han Kim. N.B: This picture was taken prior to the pandemic
Sung-Han Kim. N.B: This picture was taken prior to the pandemic
In a brief report in Annals of Internal Medicine, Seongman Bae (Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea) and colleagues report that neither surgical nor cotton masks appear to be an effective approach for preventing the dissemination of SARS-CoV-2 from the coughs of patients with COVID-19. They add that further research is needed to determine the effectiveness of cotton and surgical masks in stopping the spread of the virus from asymptomatic or non-coughing patients.
Bae et al note that previous research has suggested that surgical masks may be equally as effective as N95 masks at preventing the dissemination of the influenza virus, so surgical masks could potentially be used as an alternative to N95 masks during the current pandemic. However, they add: “The SARS-CoV-2 pandemic has contributed to shortages of both N95 and surgical masks, and cotton masks have gained interest as a substitute.” Therefore, the aim of their study was to evaluate the effectiveness of both surgical and cotton masks in preventing the dissemination of virus particles.
The authors asked four COVID-19 patients, while in a negative pressure isolation room, to cough five times into a petri dish while not wearing a mask. They were then asked to repeat this process while wearing a surgical mask, and then again while wearing a cotton mask (each time coughing into a different petri dish). “Mask surfaces were swabbed with aseptic Dacron swabs in the following sequence: outer surface of surgical mask, inner surface of surgical mask, outer surface of cotton mask, and inner surface of cotton mask,” Bae et al explain.
They report that the median viral loads after coughs without a mask, with a surgical mask, and with a cotton mask were 2.56 log copies/mL, 2.42 log copies/mL, and 1.85 log copies/ml, respectively. Furthermore, regardless of the type of mask (surgical or cotton), all swabs on the outside of the mask tested positive for SARS-CoV-2, but most swabs on the inside did not. According to Bae et al, these findings suggest that surgical or cotton masks do not adequately filter SARS-CoV-2 during coughs by infected patients.
The authors comment that while the size and concentrations of SARS-CoV-2 in aerosols generated through coughing are unknown, SARS-CoV particles from the 2002–2004 epidemic were estimated to be 0.08 to 0.014μm in diameter. They explain that a previous study found that surgical masks did not provide adequate filter performance against aerosols measuring 0.9, 2, and 3.1μm. “Assuming that SARS-CoV-2 has a similar size [to the 2002–2004 outbreak], surgical masks are unlikely to effectively filter this virus,” Bae et al note.
As to why there was SARS-CoV-2 on the outer surface of the masks but not the inner surface, the authors speculate that this could relate to the “aerodynamic features” of the masks. “Alternatively, the small aerosols of SARS-CoV-2 generated through a high-velocity cough might penetrate the masks,” they say. Whatever the reason for the finding, Bae et al state: “These observations support the importance of hand hygiene after touching the outer surface of a mask.”
Looking to the future, the authors say that further studies are needed to review whether face masks “decrease transmission of virus from asymptomatic individuals or those with suspected COVID-19 who are not coughing”. Another unknown is whether masks shorten the distance of droplets during coughing.
Study author Sung-Han Kim (Department of Infectious Diseases, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea) told Cardiovascular News that their findings did not mean that surgical or cotton had “no role” to play in stopping the spread of the virus. He explained: “Based on empirical evidence, masks might shorten the distance of aerosol containing virus and redirect the turbulent jets in less harmful directions (outward protection)—although the targeted studies using SARS-CoV-2 are unavailable. Furthermore, the inhaled air might have different aerodynamics in terms of low velocity particles with adherence of masks to face by depressurising. So, the ineffectiveness of outward protection of surgical or cotton masks in coughing COVID-19 patients do not mean ineffective inward protection of these masks. We recommend wearing any kind of masks in public settings with hand hygiene.”
Intact Vascular has received US Food and Drug Administration (FDA) approval for the Tack Endovascular System (4F), a novel, minimal metal implant for precision dissection repair in the mid/distal popliteal, tibial and/or peroneal arteries.
Regulatory approval was based on data from Intact Vascular’s Tack Optimised Balloon Angioplasty II BTK (TOBA II BTK) clinical trial, the first study to enrol patients with advanced disease below-the-knee and with 100% dissected vessels. The TOBA II BTK study enrolled patients suffering from critical limb-threatening ischemia (CLTI), a condition associated with high rates of amputation and mortality. Data from the trial were presented in a late-breaking scientific session at the 2019 Vascular and Interventional Advances conference (VIVA; 4–7 November 2019, Las Vegas, USA).
“Patients who have progressed to a CLTI diagnosis frequently endure debilitating pain, even at rest, infected foot ulcers, and are at an increased risk for amputation,” comments George Adams (UNC Rex Hospital, Raleigh, USA), co-principal investigator of the TOBA II BTK trial. “This is a complex patient population that historically had limited treatment options. The Tack implants deliver a much-needed solution that effectively restores blood flow, promotes healing, and preserves limbs.”
The prospective, multicentre, single-arm TOBA II BTK study met all primary endpoints with 100% acute dissection resolution and 73.8% of wounds healed or improved at six months. Results demonstrated 95.7% Kaplan-Meier amputation-free survival, 87.3% Kaplan-Meier target lesion patency with significant improvement in toe-brachial index, and 92% Kaplan-Meier freedom from clinically-driven reintervention.
Low-dose chest computed tomography (CT) has been an effective screening tool for COVID-19, writes Amir Davarpanah, outlining a novel screening and triage strategy successfully used in Iran to diagnose patients. “This strategy was valuable at the peak of the outbreak in Iran,” he says, “and added a new angle to the important role of radiologists and teleconsultation during a global health crisis”.
Healthcare systems across the world are facing a sudden surge in COVID-19 cases and thoracic radiologists are on the front-line of diagnosis in countries with limited supply of polymerase chain reaction (PCR) testing kits for definitive diagnosis. Due to the nature of the emergency in Iran at the peak of the outbreak and the reported low sensitivity and short supply of PCR testing, we temporarily used chest CT criteria of COVID-19 pneumonia as a surrogate for PCR testing. In our case study, published in the Journal of the American College of Radiology, we described the implementation of a novel triage strategy using humanitarian teleradiology service for the screening of symptomatic patients. The patients with early clinical and laboratory findings suspicious for COVID-19 underwent low-dose chest CT and categorised into two groups according to presence or absence of imaging features of viral lung infection.
Aiming to address the shortage of subspecialty-trained thoracic radiologists in Iran, we created a smartphone-based solution using a social media platform, WhatsApp, to provide expert interpretation of CT scans. Our goal was the early identification and isolation of infected patients to minimise disease transmission. Patients with CT finings suggestive of viral pneumonia were followed by PCR testing for confirmation and were isolated. Patients testing positive were transferred to designated hospitals. Patients with findings inconsistent with viral pneumonia on chest CT were treated according to alternative diagnosis and followed clinically.
Since radiographic findings of COVID-19 infection on chest CT are nonspecific and largely overlap with other viral infections, implementation of screening chest CT will result in a higher number of false-positive cases compared to PCR testing. Nonetheless, CT could be a valuable screening tool due to higher sensitivity, specifically in epidemic areas where there is a high pretest probability for disease. In addition, our priority was to identify the majority of suspicious cases and to use PCR testing in a more selective fashion to minimise resource drain.
Other important issues to consider are the cost and availability of CT scanners, the availability of thoracic radiology expertise, and the fact that at the time of crisis, referrals to major hospitals should be limited to decrease risk of exposure in the healthcare setting. A potential solution is using outpatient imaging centers and teleradiology, which eliminates the need to send patients to overpopulated hospitals and provides near-real time consultation from experts located around the world.
There are other certain downsides for using chest CT for triage, one of which is radiation exposure. We used low dose chest CT, which uses about 25–30% of regular chest CT dose, to minimise radiation exposure. Another concern for imaging centres is the possibility of becoming the new COVID-19 hot spots. In order to address this concern and limit the exposure of healthcare workers, employees, and patients, deep cleaning and disinfection of the room and scanner was performed after each patient, and staff wore personal protective equipment when handling these patients. The downside is the delay generated by the prolonged closure of CT scanning equipment for deep cleaning.
In spite of these limitations, this strategy has been valuable at the time of the outbreak in Iran, and has added a new angle to the important role of radiologists and teleconsultation during a global health crisis. The decision to implement a similar CT screening programme depends on the prevalence of infection in any given country or region, the availability of PCR testing, and the availability of CT scanners. Performing a cost-effectiveness analysis by regional healthcare authority is crucial before making the decision to use chest CT as a screening tool for COVID-19.
Amir H Davarpanah is an abdominal and cardiothoracic radiologist working in the Department of Radiology and Imaging Sciences at the Emory University School of Medicine, Atlanta, USA.
MedAlliance has announced enrolment of the first patient in the SAVE (Use of the Selution sirolimus-eluting balloon for dysfunctional AV access treatment indications) study utilising their novel sirolimus-eluting balloon, for the treatment of failed arteriovenous (AV) fistulae in renal dialysis patients.
The objectives of this prospective, randomised, single-blind multicentre study are to demonstrate the safety and efficacy of SELUTION SLR in the treatment of failed AV fistulae in patients undergoing renal dialysis. This study will also qualify for EU MDR approval.
Eighty-four subjects are being randomised to either SELUTION SLR or plain balloon angioplasty. To qualify for inclusion they must be aged 18–90, have a dialysis access that has performed at least one successful dialysis session, and a stenosis of more than 50% at the outflow vein.
“We are excited to study this novel sustained release of sirolimus in our dialysis patients with a malfunctioning fistula”, said Konstantinos Katsanos, consultant in Interventional Radiology at the University of Patras in Patras, Greece. “We truly look forward to the outcomes”.
The primary efficacy endpoint of the study will be primary patency of the treated lesion and of the treated circuit at six months post-intervention. The primary safety endpoint will be freedom from any serious adverse events involving the AV access circuit or the patient at 30 days.
“MedAlliance is honoured to initiate this important study with Dr Katsanos”, added chairman and CEO Jeffrey B Jump. “It will hopefully demonstrate extended life for AV Fistula patients around the world”.
SELUTION SLR’s technology involves unique Microreservoirs made from biodegradable polymer intermixed with the anti-restenotic drug sirolimus. These microreservoirs provide controlled and sustained release of the drug. Extended release of sirolimus from stents has been demonstrated highly efficacious in both coronary and peripheral vasculatures. MedAlliance’s proprietary CAT (Cell Adherent Technology) enables the microreservoirs to be coated onto balloons and adhered to the vessel lumen when delivered via an angioplasty balloon.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has made seven of ts Academy courses free to access online.
On its website, the society states: “While much of our regular routines have come to a halt as a result of the current crisis, your IR [interventional radiology] education should not have to. In an effort to support our community during these challenging times, CIRSE has now made seven CIRSE Academy courses free to access. This offer is only available for a limited time, so do not wait up! Find the courses that interest you, add them to your cart and check out—you will be enrolled at no cost!
“In addition, CIRSE has made more than 190 lectures from CIRSE congresses of the past year, including ECIO, ET, and CIRSE 2019 available free of charge.”
The seven online current courses currently available are:
Hepatocellular carcinoma
Management of acute arterial gastro-intestinal haemorrhage
Metastatic bone disease
Primary lung cancer
Renal cancer
Superior vena cave (SVC) stenting for treatment of malignant obstruction
Vascular access and closure
Completing each course earns the participant CME (continuing medical education) credits.
In the midst of the COVID-19 pandemic, CIRSE and the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) have jointly published a checklist for interventional radiologists to use when preparing their department for COVID-19 patients.
The Radiological Society of North America (RSNA) has launched a web page to help radiology professionals amid the ongoing COVID-19 outbreak.
The COVID-19 Resources webpage includes guidance, research, and a collection of images to help radiologists and other professionals. At time of publication, the page was last updated the page on 1 April, and the organisation will continue to post regular updates and advice.
The society state: “RSNA is committed to connecting radiologists and the radiology community to the most timely and useful COVID-19 information and resources.
“Stay in the know. Get COVID-19 updates sent directly to your inbox. We will send you the most important announcements and useful resources to help you manage the COVID-19 public health crisis.”
RSNA COVID-19 imaging data sharing survey
RSNA is also planning an open data repository “for international COVID-19 imaging research and education efforts”. In order to do this, the society has posted a form in its online resource centre where physicians can express their willingness to share their institution’s COVID-19 data for research purposed.
The society write at the start of the form: “The Radiological Society of North America (RSNA) has received numerous inquiries seeking access to COVID-19 related imaging data, both from radiology sites interested in sharing such data for use in research and education and from researchers.
“RSNA is committed to accelerating open source collaborative research on the uses of medical imaging in addressing the COVID-19 pandemic, including the use of new tools like artificial intelligence (AI). This form will enable institutions with COVID-19 data to express interest in participating in a planned open data repository for international COVID-19 imaging research and education efforts. Please complete this form if your institution has COVID-19 data that you may be willing and able to share for research purposes.
“Completing this brief survey does not represent a final commitment to collaborate with us or to share your data. RSNA staff will communicate directly with respondents in the next several days with further information about the next steps for organizations willing to participate in the RSNA COVID related research and education efforts.”
Organisations interested in participating are requested to respond to the survey by 15 April 2020.
Royal Philips has announced that the US government and Philips agreed to team up to increase the production of hospital ventilators in its manufacturing sites in the USA.
Philips plans to double the production by May 2020 and achieve a four-fold increase by the third quarter of 2020 for supply to the US and global markets. Such ventilators are critical for the treatment of patients with the new coronavirus disease (COVID-19). Philips will invest several tens of millions in its ventilator manufacturing sites in the USA.
“We are actively collaborating with the US government to help save lives in the USA and across the globe,” said Frans van Houten, CEO of Royal Philips. “There is an unprecedented global demand for medical equipment to help diagnose and treat patients with COVID-19. We welcome the support of the US government in our efforts to aggressively increase the production of hospital ventilators.”
He continued: “We believe in fair allocation of scarce medical equipment to those who need it the most, and we are ramping up to deliver 43,000 units to the most critical regions in the U.S. in the coming weeks and months through December 2020.”
In line with the recent call to action by the International Chamber of Commerce (ICC) and World Health Organization (WHO), Philips and the US government have agreed to work together to accelerate access to critical materials and components, expedite logistics and regulatory approvals, in order to rapidly increase the production of ventilators.
In the first three months of this year, Philips already delivered several thousand ventilators to US hospitals. As a result of its production ramp up, Philips was able to deliver an additional batch of ventilators to one of New York’s hospitals, to help provide immediate relief to the surge of COVID-19 patients within the city.
Philips believes that critical medical equipment, such as hospital ventilators, should be made available across the world using a fair and ethical approach to allocate supply to acute patient demands based on data such as the COVID-19 statistics per country/region (e.g. provided by the WHO and Johns Hopkins Coronavirus Resource Center) and the available critical care capacity. Philips may divide orders into batches to be delivered in phases, so that the company can simultaneously serve multiple countries/regions in need.
VIVA Physicians recently hosted a virtual roundtable to address COVID-19. Tony Das (Connected Cardiovascular Care Associates, Dallas and BSW Heart Hospital, Plano, USA), one of the VIVA Board Directors, lead the discussion, addressing topics such as resource management, triage, and telemedicine.
Das was joined by four other specialists—Niten Singh (University of Washington, Seattle, USA), Saher Sabri (MedStar Washington Hospital Center, Washington, DC, USA), Raghu Kolluri (OhioHealth Riverside Methodist Hospital, Columbus, USA), and John Rundback (Holy Name Medical Center, Teaneck, USA).
Das opened the virtual roundtable, available to watch on the VIVA Physicians website, by noting that Singh would have been one of the first to encounter COVID-19 in the USA in his centre in Seattle.
Singh went on to describe the fast-changing situation in the east coast city, noting that what is required is a “mentality change”. He noted in particular the importance of conserving resources. “In big systems, we all have to contribute,” he commented, pointing to the fact that elective vascular surgeries would have to be suspended so that enough resources would be available to cope with an increasing number of COVID-19 patients.
Singh also pointed to the issue of vascular patients being exposed to the virus whilst in hospital. “Our patients are generally in that age group where they are the most vulnerable to exposure and having a bad outcome with the contraction of COVID-19,” he remarked.
“Nobody stays in the hospital,” Singh added, elaborating that “if consultations can be managed telephonically, we do that.”
Singh also pointed out that, aside from clinical obligations, “fellows and residents still need teaching”. In this case, remote medicine is playing an important role.
Next to speak was Sabri, who mentioned that vascular surgeons and interventionalists are facing difficult decisions about who to treat and who not to treat, adding that “the triage process gets tighter” the more serious the COVID-19 situation becomes.
With regards to PPE [personal protective equipment], Sabri noted that, in his centre, they have started rationing their supply.
“We have to be vigilant,” said Sabri, urging fellow physicians to “think ahead”.
Raghu Kolluri (OhioHealth Riverside Methodist Hospital, Columbus, USA) was next to speak. He began by pointing out that his centre has not yet experienced a large number of cases but that they are expecting a surge in the near future.
The vascular lab “needs to be prepared,” he commented. He pointed out that it is a priority for him to be supportive of sonographers at this time—both from a triaging perspective and emotionally.
Last to speak was John Rundback (Holy Name Medical Center, Teaneck, USA), who is recovering from COVID-19.
He details that he likely contracted the virus in early March from a patient during regular office hours. “We have to assume we are getting infected by every patient walking in,” he said, adding that healthcare professionals are being “exposed in ways we cannot possibly anticipate”.
In terms of his practice, Rundback outlines that he has been “busy at home calling every single patient and triaging them appropriately,” stressing the importance of communication during this time, especially with elderly patients—making up the majority of vascular cases—who may have difficulty accessing telemedicine.
Rundback ended by emphasising that “CLI is not an elective thing,” noting that there are 300 amputations every day in the USA. “This is a serious matter.”
“The practice can adapt”
Das concluded the roundtable discussion on a positive note. “There is always good that comes out of these tragedies,” he began, elaborating that “untethering patients from hospitals and from offices is the reality of where this system is going”.
“The practice can adapt,” he continued. “This pandemic is creating an environment where I think everyone will say ‘I am not just going to do telemedicine right now, I am going to actually start to understand the infrastructure and the tools that are out there to be able to implement those in the future.’”
Considering the long-term impact of telemedicine, he gave the example that “CLI patients deserve more of a check-in than every six months”.
Afshin Gangi discusses IASIOS at the Asia Pacific Congress of Interventional Oncology (APCIO; 2–5 October 2019, Kuala Lumpur, Malaysia)
The newly established International Accreditation System for Interventional Oncology Services (IASIOS) gives medical facilities the opportunity to receive credentials for their interventional oncology (IO) service line. Developed by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), IASIOS focuses on the entire patient pathway, and as such has been heralded as a way of recognising that interventional oncologists are “clinicians, not just technicians”. Andreas ‘Andy’ Adam (Guy’s and St Thomas’ NHS Foundation Trust, London, UK) tells Interventional News that the project “will help establish IO as a mainstream clinical discipline, so is very important to IO as a whole”.
IASIOS is built on the standards outlined in the Standards of quality assurance in interventional oncology document, published in 2018 by CIRSE’s oncology alliance subcommittee, which is chaired by Adam. The idea of a global quality assurance scheme for IO goes back even further, to 2012, when radiation oncologist Lizbeth ‘Liz’ Kenny (Royal Brisbane and Women’s Hospital, Brisbane, Australia) delivered a talk at CIRSE’s annual congress on the interventional oncologist’s place in a multidisciplinary cancer care team.
Kenny emphasised the importance of recognising interventional oncologists as “clinicians, not just technicians”. She recalls: “I thought I was being very provocative, but CIRSE was very supportive. Since then [2012], I have been involved with the oncology alliance subcommittee, and have pushed the importance of standards of practice. In the world of radiation oncology, the stakes are very high, so quality assurance is built into every single step of all we do. I could see that with IO, we either needed to bring it into the mainstream, or it would disappear. IASIOS brings IO into the mainstream—by having a really serious quality assurance and standards programme underpinning the discipline, IO is in a great place to offer high benefit care to patients, and to fully integrate interventional oncologists into the multidisciplinary cancer care team.”
Establishing quality assurance standards in interventional oncology
In 2015, the CIRSE oncology alliance subcommittee—Adam, Kenny, Afshin Gangi (University Hospital Strasbourg, Strasbourg, France), Thierry de Baère (Institut Gustave Roussy, Villejuif, France), José Ignacio Bilbao (Clinica Universidad de Navarra, Pamplona, Spain), Thomas Helmberger (Klinikum Bogenhausen, Munich, Germany), Riccardo Lencioni (Pisa University School of Medicine, Pisa, Italy), and Philippe Pereira (Minimally Invasive Therapies and Nuclear Medicine Heilbronn, Heilbronn, Germany)—worked with interventional oncologist Shahzad Ilyas and former chief medical physicist Keith Ison (both Guy’s and St Thomas’ Hospital, London, UK) to adapt the Standards for Radiation Oncology developed and published by the Royal Australian and New Zealand College of Radiologists (RANZCR), the Australian Institute of Radiography, and the Australasian College of Physicists, Scientists and Engineers in Medicine. The group had to make these standards fit for purpose in the IO environment.
“This was a monumental effort,” Kenny describes. The standards went through 30 iterations over three years prior to publication. “The real complexity was to make the standards simple, understandable, and truly relevant to patients and care providers. This is not a tick box exercise. The standards describe what great care looks like, which then facilitates discussion between interventional oncologists and hospital management over necessary infrastructure, equipment, and patient pathways.”
Following the structure of the Australian and New Zealand Standards for Radiation Oncology, CIRSE’s Standards of Quality Assurance in Interventional Oncology document is split into three sections. These are: staff and facilities, treatment planning and delivery, and safety and quality. The IASIOS accreditation system is based on these standards. Between the three sections, there is a total of 52 criteria, 27 of which are “core”. After paying the enrolment fee, an institution can achieve accreditation if it meets all 27 core criteria. The IASIOS process is interactive: once an IO facility has applied for accreditation, a dialogue begins between it and the IASIOS team in the CIRSE office, which offers advice and guidance on how to improve the service, and is independent from the oncology alliance subcommittee. This conversation continues until accreditation is achieved. In exceptional cases, an institution may be awarded a “centre of excellence” accreditation if it fulfils the remaining 25 criteria.
Guy’s and St Thomas’ NHS Foundation Trust, London, UK, is the first in the world to be accredited through IASIOS. The centre gained accredited status in September 2019.
IASIOS is currently in a pilot phase, with eight centres across Europe, Asia, and Australasia enrolled in the programme to date. Two US centres are poised for potential future participation. CIRSE is working in collaboration with the Society of Interventional Oncology (SIO) to create a version of the IO standards appropriate to the pattern of practice in the USA.
While in this pilot phase of the programme, the IASIOS committee at CIRSE, chaired by Jean Palussière (l’Institut de cancérologie Bergonié, Bordeaux, France), is listening to feedback on the scheme from the enrolled institutions, and making any necessary modifications. Maria Weren, head of the department for certification and accreditation at CIRSE, expands: “I do not expect there to be too many changes at this stage. What I do foresee is some fine-tuning of our assessment process, and possibly to our application forms—so largely modifications to technical details. Any obstacles centres are repeatedly running into our expert group will of course also review.” The official, global launch of IASIOS is planned for early 2021.
Building a global IO network
Kenny is enthusiastic about the potential of the IASIOS scheme to build an international network of interventional oncologists. She tells this newspaper: “In due course, we anticipate building a network of centres that have achieved accreditation. I see this as ultimately an interconnected system of institutions offering support, encouragement, and advice for the betterment of all. IASIOS will uplift the whole of IO.”
There is no precedent for this type of international interconnectivity, Kenny explains: “There is no other movement that does what IASIOS does. The standards define the infrastructure, staffing, and safety requirements to bring IO into mainstream cancer care. If IO is to survive and flourish, it cannot just be a technical specialty under the direction of surgeons or medical and radiation oncologists. Interventional oncologists need to be considered a genuine partner in cancer care, and that is what IASIOS does.”
In Weren’s eyes, too, the IASIOS programme will bring increased recognition to the discipline, through giving interventional oncologists greater control of the entire patient pathway and a louder voice at interdisciplinary meetings. “IASIOS benefits not just patients, but also interventional oncologists,” she opines.
“It is an initiative by interventional oncologists, for interventional oncologists, because the standards look at the whole patient pathway. The standards will introduce systemic preprocedural assessment and patient follow-up by interventional oncologists, which I anticipate will provide greater visibility to IO. Interventional oncologists are ready to assume the role and responsibilities of a specialty, but they need to have a voice and they need to have a fixed place in the multidisciplinary cancer care team. This will enrich the discussion and widen the perspective for the patient.”
The European Commission (EC) has adopted a proposal to postpone by one year the date of application of the new Medical Devices Regulation (MDR), which was due to come into force on 26 May this year. The postponement, a press release reports, is to allow Member States, health institutions and economic operators to prioritise “the fight against the coronavirus pandemic”. As previously reported, the announcement follows the EC college (video) meeting on 25 March in which EC spokesperson Stefan de Keersmaecker stated that the commission were looking to delay the “entry into force” of the new MDR because of the global coronavirus pandemic.
According to the press release, the decision to delay “takes into account the unprecedented challenges of the coronavirus pandemic and the need for an increased availability of vitally important medical devices across the EU while continuing to ensure patient health and safety until the new legislation becomes applicable”. The proposal, therefore, delays the application of the MDR by one year (until 26 May 2021).
Additionally, the proposal also ensures that Member States and the Commission can address potential shortages of vitally important medical devices in the EU in a more effective manner through EU wide derogations. However, the press release notes that the proposal would need the full support of the European Parliament and the Council through an accelerated co-decision procedure.
Vice-president for Promoting our European Way of Life, Margaritis Schinas, says: “Shortages or delays in getting key medical devices certified and on the market are not an option right now. The Commission is, therefore, taking a pragmatic approach and delaying the entry into application of new EU rules on medical devices, so we can have our medical industries pouring all their energy into what we need them to be doing: helping fight the pandemic.”
Stella Kyriakides, commissioner for Health and Food Safety, adds: “Our priority is to support Member States to address the coronavirus crisis and protect public health as powerfully as possible—by all means necessary. Any potential market disruptions regarding the availability of safe and essential medical devices must and will be avoided.”
The Society of Interventional Radiology (SIR) has created a free online COVID-19 resource centre for physicians to access via their website.
The site states: “SIR has created this COVID-19 page to keep members apprised of interventional radiology (IR)-specific resources and information to help you, your practice, and your patients.
“Members are also encouraged to participate in the SIR Connect Open Forum for real-time sharing of knowledge, information and ideas among the IR community.”
The page is being continuously updated, but at time of publication includes two clinicalnotifications, a toolkit, webinars, and federal guidance.
The first clinical notification, effective from 18 March and updated on 19 March, lists SIR recommendations in response to statements from the Surgeon General and the Centers for Medicare and Medicaid Services (CMS) on elective surgeries as well as interim guidance from the Centers for Disease Control and Prevention (CDC).
The second clinical notification in the SIR resource centre, dated 26 March, provides medical decision-making guidance on how to perform aerosol-generating procedures (AGP) safely in the IR suite, following emerging data that indicates SARS-CoV-2 (the virus that causes COVID-19) is primarily spread via respiratory droplets produced when an infected person coughs or sneezes and has a “significant association with AGPs.”
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
This advertorial is sponsored by TriSalus Life Sciences.
NOTE: This article is intended only for healthcare professionals in the USA.
The Medicare Transitional Pass-Through Payment (TPT) programme is designed to foster innovation and increase access to cutting-edge treatments that benefit patients. The Centers for Medicare and Medicaid Services (CMS) believes the programme is important for hospitals to receive TPT payment for products that offer substantial clinical improvement. One goal of the programme is to target TPT payments for those devices where cost considerations might be most likely to interfere with Medicare patient access.
Patient access is at the heart of the TPT programme. CMS understands that relentless innovation is a crucial driver in creating value across all industries. Seema Verna, CMS administrator, remarks: “Innovation is the fuel that powers the engine of progress and creativity. […] We are committed to removing government barriers and modernising regulations around new technologies to ensure safe and effective treatments are readily accessible to beneficiaries without delaying patient care.”1
To facilitate beneficiary access to innovative medical devices, drugs, and biologicals, Congress established the TPT payment programme to prevent inadequate payment when used in an appropriate outpatient setting. CMS provides the TPT payment so as not to prevent use of new technologies due to cost concerns. The programme allows Medicare to collect data, and impacts CMS’ ability to establish appropriate permanent rates that are not described by existing categories. By addressing financial risk for outpatient facilities and mitigating the financial deterrent to innovative product utilisation, Medicare patients are more likely to gain access to new products through this programme.2
Historically, very few devices have qualified for TPT. In the last four years, only six device applications (out of 26) have been approved for the TPT programme. While TPT status has been in place for 20 years, only a very limited number of products have been approved because the programme requirements are so narrow. CMS reviews eligible device applications based on a demonstration of the following criteria:
Recent US Food and Drug Administration (FDA) approval/clearance (generally within three years)
Not appropriately described by another existing category or one previously established for TPT
Substantial clinical improvement over currently available treatments
TriNav™ Infusion System—one of five device TPT approvals granted this year
The TriNav Infusion System, which CMS approved TPT status for in November 2019, is the only TPT-approved device specifically designed for interventional radiology (IR) procedures. TriNav is designed to help overcome the infusion barriers that limit therapeutic uptake. In the Medicare hospital outpatient prospective payment system (OPPS) and ambulatory surgical center (ASC) payment system 2020 final rule, CMS stated that TriNav meets the criteria for device pass-through payment including newness, cost, and substantial clinical improvement. For those devices granted TPT status effective 1 January 2020, pass-through payments will mostly likely remain available until 31 December 2022.
A novel drug-delivery mechanism
Fundamental to TriNav is the Pressure-Enabled Drug Delivery™ (PEDD™) approach with SmartValve™ technology. To overcome pressure barriers that limit flow, PEDD with SmartValve creates a high-pressure gradient that improves delivery and penetration of therapeutic agents.3–7 The porous expandable SmartValve is a first-of-kind proprietary technology shown to modulate pressure and flow for optimal therapy delivery and deeper penetration into the vasculature while protecting heathy tissue.3, 5, 7
New HCPCS code information
Medicare’s transitional pass-through payment programme is designed to benefit patients who receive treatment with certain products in hospital outpatient departments (HOPDs) and ASCs. Medicare makes the additional TPT payment for devices where cost considerations might be most likely to interfere with patient access. It allows for CMS to collect necessary data and assign appropriate permanent codes and rates, paving the way for routine Medicare reimbursement later.
CMS assigned the TriNav Infusion System to the Health Care Common Procedure Coding System (HCPCS) code C1982 (catheter, pressure-generating, one-way valve, intermittently occlusive). When the device is used, CMS has stated it should always be billed with 37243 (vascular embolization or occlusion, inclusive of all radiological supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the intervention; for tumours, organ ischaemia, or infarction).
While most payers usually follow suit with Medicare B coverage policy, the reimbursement methodologies and amounts may vary. Facilities are encouraged to contact payers prior to using a product on TPT status to confirm coverage and reimbursement policies. For more information on TriNav, visit www.trinavinfusion.com, or call +1-888-321-5212.
None of the above statements are intended to imply a CMS endorsement of TriNav or any other product. The coding information provided is gathered from various resources, is general in nature, and is subject to change without notice. The provider is responsible for determining the appropriate health care setting and submitting accurate claims for products and services rendered. Providers should contact third-party payers for specific information on their coding, coverage, and payment policies. The TriNav Infusion System is available for sale in the USA. This product has not been approved for sale outside the USA. Contraindications: TriNav™ is not intended for use in the vasculature of the central nervous system (including the neurovasculature) or central circulatory system (including the coronary vasculature). Intended Use: The TriNav™ Infusion System is intended for use in angiographic procedures. It delivers radiopaque media and therapeutic agents to selected sites in the peripheral vascular system.9
References 1. Remarks of Centers for Medicare & Medicaid Services (CMS) Administrator Seema Verma to the Medical Device Manufacturers Association (MDMA) Annual Meeting (5/2/2019). 2. Gustafson, TA. ASC Focus. 2015 Sept:8-9. 3. Titano JJ, et al. Cardiovasc Intervent Radiol. 2019;42:560-568. * Study design: A retrospective, single-centre study included 88 treatment-naive patients with solitary HCC tumours <6.5cm who underwent treatment utilising either PEDD™ (n=18) or standard EH microcatheters (n=70). Twenty-three patients (five PEDD™, 18 EH) received a liver transplant during the study, with one PEDD™ and six EH patients excluded from the tumour necrosis analysis for receiving subsequent therapies prior to transplant. A pathologist performed a blinded review of the liver explant specimens to assess tumour necrosis and treatment distribution. Percentage necrosis was defined as the volume of necrotic areas divided by the total tumour volume. 4. Pasciak AS, et al. J Vasc Interv Radiol. 2015;26:660-669. *Study design: Sequential lobar infusion of 99mTc MAA in nine patients prior to 90Y treatment with PEDD™ and conventional microcatheter. 5. Durham ED, et al. J Vasc Interv Radiol. 2015;26:e54 (Poster 18). 6. Kim AY, et al. PloS One. 2017;12(9):e0183861. DOI: 10.1371/ journal.pone.0183861. 7. O’Hara R. Poster presented at: European Conference on Interventional Oncology (ECIO); April 22-25, 2018; Vienna, Austria. 8. Data on file (510K). TriSalus Life Sciences, 2019. 9. TriSalus TriNav™ Infusion System, Instructions for Use. None
In a new statement published on 2 April 2020, all 45 societies represented by the US Council of Medical Specialty Societies (CMSS)—over 800,000 physicians—emphatically declare their belief that all frontline healthcare professionals must have access to personal protective equipment (PPE) and be able to speak publicly about the lack of PPE without retribution while pushing for adequate supply and distribution.
This statement comes days after reports emerged in mainstream media outlets of threats made to hospital staff who have spoken publicly about the difficulties they are confronting on the frontlines of the COVID-19 pandemic. Among other cases, the story emerged of a Washington state emergency room physician who is said to have been fired after giving an interview to a newspaper on claims he had made about inadequate equipment and testing on his Facebook page, according to a report carried by Bloomberg News.
Susan E Sedory, executive director of the Society of Interventional Radiology (SIR), one of the 45 CMSS societies, says: “All physicians and health care professionals on the frontlines of the COVID-19 battle must be adequately protected to ensure they stay healthy and can continue to provide the care so urgently needed. Yet, the inadequate supply and distribution of PPE is magnifying the crisis here.
“Through CMSS, we can instead magnify the voice of nearly all of America’s specialty societies to send a clear and urgent message to policymakers and ensure that all frontline physician fighters have the protection they need. We are proud to advocate for interventional radiologists so they can continue to stay safe and care for patients in their communities.”
In full, the new CMSS statement reads:
“With more than 800,000 physicians across 45 specialties, the Council of Medical Specialty Societies (CMSS) strongly urges action to ensure safer working conditions for physicians and other healthcare professionals on the frontline of direct patient care.
“CMSS and its member societies believe that adequate personal protective equipment (PPE) should be a fundamental expectation for all frontline healthcare professionals:
“CMSS and its member societies urge federal, state and local authorities to ensure an adequate supply and distribution of PPE for every frontline healthcare professional in the United States. Physicians and other healthcare professionals can and should expect their institutions to provide appropriate means to limit occupational exposure.
“Physicians and other healthcare professionals should be allowed to bring their own PPE to protect themselves, colleagues, and patients when these items are in short supply at their institutions. CMSS supports the Joint Commission statement allowing the use of private PPE, but this option does not obviate an institution’s responsibility to provide adequate PPE to all healthcare personnel.
“The United States needs a simple, uniform mechanism for all healthcare facilities to report their PPE needs and other medical supply needs to help guide optimal distribution of supplies across the country.
“Physicians and other healthcare professionals should not be at risk of having their employment terminated, or be otherwise disciplined, for speaking out, within their health care systems or publicly, on conditions and practices related to care of COVID-19 patients (including lack of PPE) that the physician and other healthcare professional has direct knowledge of and deems to be in conflict with the health and safety of patients, themselves, and others involved in providing care to patients.
“CMSS supports the American Medical Association (AMA) statement that “no employer should restrict physicians’ freedom to advocate for the best interest of their patients.” Physicians and other healthcare professionals may appropriately decide that going public (including to the news media and on social media) with their concerns is necessary to achieve needed change for the health and safety of patients and clinicians, both within the healthcare facility and more broadly.”
Full list of CMSS societies
American Academy of Allergy, Asthma & Immunology
American Academy of Dermatology
American Academy of Family Physicians
American Academy of Hospice and Palliative Medicine
American Academy of Neurology
American Academy of Ophthalmology
American Academy of Orthopaedic Surgeons
American Academy of Pediatrics
American Academy of Physical Medicine and Rehabilitation
American Association of Clinical Endocrinologists
American College of Cardiology
American College of Emergency Physicians
American College of Medical Genetics and Genomics
American College of Obstetricians and Gynecologists
American College of Occupational and Environmental Medicine
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
The European Society of Radiology (ESR) has created a playlist on their YouTube channel dedicated to events and news related to the COVID-19 pandemic.
Currently, the playlist offers three videos. The first is a special report about radiology’s role in fighting the virus. Nicola Sverzellati (University of Parma, Parma, Italy) shares his experiences of working with patients and image management in Europe’s most affected area. He also discusses the challenges Italian radiology departments face and the diagnostic flowchart his team has developed since the outbreak.
The second video showcases geneticist and immunologist Josef Penninger (Institute of Molecular Biotechnology of the Austrian Academy of Sciences, Vienna, Austria), who discusses angiotensin-converting enzyme 2 (ACE2) as a potential treatment for the disease, as well as its relationship to the renin-angiotensin system (RAS) in instances of lung injury.
The third video again features Sverzellati, as well as Francesco Sardanelli (University of Milan, Milan, Italy). The two discuss the ongoing Italian response to the pandemic, and, chaired by Adrian Brady (Mercy University Hospital, Cork, Ireland), answer questions posed by audience members from the previous two broadcasts on the myecr YouTube channel.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
The Society of NeuroInterventional Surgery (SNIS) has published a set of recommendations for the care of emergent neurointerventional patients during the COVID-19 pandemic.
“Acute ischaemic stroke patients are a high-risk patient cohort,” the authors write, adding that patients with a history of ischaemic stroke and/or its risk factors are “particularly at risk” for the severe form of the coronavirus. The recommendations also acknowledge evidence that the disease can cause neurological signs, which have been reported in the brains of humans and in animal models.
Pointing to a study documenting neurological manifestations of hospitalised patients with COVID-19 in Wuhan, China, the society writes: “36.4% of SARS-CoV-2 [severe-acute respiratory syndrome-coronavirus 2] respiratory distress patients demonstrated neurological symptoms, with 4.5% of severe patients suffering ischaemic stroke.”
Given this evidence, the SNIS recommendations state that in this setting, neurointerventionalists should expect to be involved in the care of COVID-19-positive patients, as well as those whose status is unknown.
The document specifically advises on the criteria for mechanical thrombectomy: “The presence of COVID-19 as a public health issue should not alter the inclusion and exclusion criteria for mechanical thrombectomy […] denial of this treatment likely creates a greater drain on healthcare resources.”
However, the authors urge that maximum safety precautions should be taken when a patient with COVID-19 positive documentation requires treatment. If a patient’s COVID status is unknown, SNIS recommends that patients be treated as high risk for COVID-positive, provided institutional resources are available.
The document also details guidance on post-thrombectomy principals during the pandemic. The society recommends transferring uncomplicated post-thrombectomy patient’s out of the intensive care unit (ICU) “as soon as possible”, to maximise availability of ICU beds. Further, it advocates for COVID-19 testing of all acute ischaemic stroke patients on admission, if available, to allow preservation of personal protective equipment (PPE), and to “separate true COVID-19 positive patients to prevent nosocomial transmission.”
Due to how the cleaning of angiography equipment and suites will impact on the readiness of additional cases, SNIS advises that elective and non-urgent cerebrovascular cases be postponed until the pandemic’s peak has been reduced. Lastly, the society encourages the shift-based allocation of staff and physicians, to separate individuals with overlapping skillsets.
Given the number of identified COVID-19 patients is expected to increase, the authors underline the importance of safe delivery of care for both patients and providers. “If we fail to protect physicians, nursing staff, and ancillary providers, we will fail to meet the needs of future patients.
“The successful care of future COVID-19 patients will depend on the effective safety and prevention strategies for healthcare workers.”
As the COVID-19 pandemic continues to unfold, SNIS will consider revisiting these recommendations to match up-to-date information. Any such revisions will be provided as updates on the SNIS web page, the society advised.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
Michael Dake (University of Arizona Health Sciences, Tucson, USA) has become the new president of the Society of Interventional Radiology (SIR).
He officially assumed his new responsibilities after the annual members’ business meeting of the society, which was held this year via a webinar. Other officers of SIR’s 2020-2021 executive council include:
President-elect: Matthew Johnson (Indiana University School of Medicine, Indianapolis, USA)
Secretary: Parag Patel (Medical College of Wisconsin, Milwaukee, USA)
Immediate past-president: Laura Findeiss (Emory University School of Medicine, Atlanta, USA)
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) have jointly published a checklist for interventional radiologists to use when preparing their department for COVID-19 patients.
The full checklist, as well as other COVID-19 resources collated by CIRSE, is available here.
First author Bien Soo Tan (Singapore General Hospital, Singapore) and colleagues from South Korea, France, Switzerland, the UK, Germany, and New Zealand write: “The primary consideration in preparing the IR [interventional radiology] service for COVID-19 is prevention of intra hospital transmission so as to protect patients and health care workers from being contaminated or infected, while providing safe IR care for patients.”
Addressing the international IR community, CIRSE president Afshin Gangi stressed the importance of a rapid and coordinated IR response to the current coronavirus outbreak. He said: “The spreading COVID-19 pandemic has forced all of us to adjust to a new reality. While IR departments are trying to delay most non-emergency procedures until after the crisis, some interventions cannot be postponed. It is therefore adamant for interventional radiologists to adapt their departments accordingly, from the set-up of a COVID-19 task force to implementing infection prevention protocols and dedicated workflows.
“I am convinced that weathering this storm can only be done together, and when it has finally subsided, we will be stronger for it, as physicians, individuals and as a community.”
Outline of checklist
Set up COVID-19 task force or crisis management team in radiology/IR to sort out all COVID-19 related issues.
Implement and refresh infection prevention and control practices.
Create COVID-19 suspect case definitions and expanded case definitions.
Ensure appropriate personal protective equipment (PPE) is used. PPE recommendation for performing IR procedures on known COVID-19 patients and patients suspected of COVID-19 is: surgical cap, N95/FFP2 mask, eye protection (face shield or goggles), full length long-sleeved gown and gloves. For all other categories of patients, the PPE recommendation is stratified according to COVID-19 infection risk.
Use of powered air-purifying respirator is recommended when performing aerosol-generating procedures on suspected or confirmed COVID-19 patients.
Introduce screening measures to the hospital—this includes temperature screening and the completion of health declaration forms upon entry to the institution.
Limit the number of visitors; there should be a strict visitor policy.
Have designated wards for COVID-19 management.
Segregate inpatients from outpatients. Procedures should be performed in the outpatient setting where possible.
Reduce workload and cancel or defer elective procedures.
All requests for IR procedures for suspected or confirmed COVID-19 patients must be carefully vetted and prioritised.
Dedicated workflows need to be written and rehearsed to prevent cross transmission.
Segregation of staff into smaller functional teams is a key strategy to prevent the entire service from being decimated due to healthcare worker infection or quarantine.
Implement social distancing measures—meetings, such as multidisciplinary tumour board discussion, should be held over video calls, staff should eat separately; patients should have consultations over the phone.
Staff leave and travel advisory.
Staff surveillance should be implemented. This includes twice daily measuring of temperature.
Contact tracing: the names and designation of all staff involved in every IR procedure should be recorded. Staff rosters should be updated daily and archived.
Rapid dissemination of accurate information is critical.
Staff morale, welfare, and psychological support systems should be put in place.
Keep track of logistics: PPE usage and available stocks need to be tracked. It is important to stress at the institutional level that IR is given priority for PPE.
A plan must be devised for the management of residents and fellows. If feasible, residency and fellowship teaching should continue using video conferencing platforms.
Research activities are likely to be curtailed and IR should align with the prevailing institutional policies and directives.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
The American College of Surgeons (ACS) today leapt to the defense of healthcare workers who are heading to work in the face of increasing concerns over personal protective equipment (PPE) shortages as the COVID-19 pandemic cuts trails across the country.
The association released a statement in support of stretched surgeons, nurses and other key medical personnel as reports emerged in mainstream media outlets of threats made to staff who speak publicly about the difficulties they are confronting on the frontlines.
Among other cases, the story emerged of a Washington state emergency room physician who is said to have been fired after giving an interview to a newspaper on claims he’d made about inadequate equipment and testing on his Facebook page, according to a report carried by Bloomberg News.
The ACS outlined the picture confronting the medical field at large: Many healthcare facilities, it said, face shortages in PPE, including face masks, gowns and respirators.
However, the College’s statement went on to say: “The ACS believes it is essential that surgeons, nurses, anesthesiologists, and other healthcare personnel be able to speak freely, without fear of retribution, as they seek to find a solution to accessing PPE.
“We advise surgeons to speak with their institutional leadership on these matters and to be able to direct any concerns to the ACS, with the goal of protecting themselves and their colleagues.”
The ACS pointed out that the Joint Commission—which accredits and certifies more than 22,000 healthcare organisations and programs in the United States, including hospitals—had released a statement supporting the use of face masks and respirators provided from home when facilities are not able to provide access to PPE that matches the risk surrounding healthcare workers amid the COVID-19 pandemic.
The Joint Commission stepped forward with its statement yesterday, saying: “The Joint Commission supports allowing staff to bring their own standard face masks or respirators to wear at work when their healthcare organisations cannot routinely provide access to protective equipment that is commensurate with the risk to which they are exposed.”
Meanwhile, the ACS continued: “Where masks or respirators are recommended, the ACS maintains that surgeons should have access to and latitude to wear these masks at their sole discretion. The Centers for Disease Control and Prevention (CDC) also has released a document that offers a series of strategies or options to optimise supplies of disposable N95 filtering facepiece respirators.
“The ACS strongly supports the ability of surgeons to use their own masks or PPE, but this option does not obviate the hospital’s responsibility to provide adequate PPE to all their health care workers. In these extraordinary times, the ACS encourages institutions to adapt and be flexible so that health care personnel continue to feel safe; the Joint Commission guidelines are a reasonable starting point.”
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
This piece is one in a series of articles covering the GEST webinar. For dispatches from the frontlines of the COVID-19 pandemic, and the pertinent takeaways for interventional radiologists, click here.
“What have we learnt in the last month? We have to try to reduce or stop our activity—in the beginning, we thought we could continue to work as in standard life, but we realised that there is a high risk of infection, as the patient or operator could be a virus carrier. You have to really reduce your activity to only emergency cases.” So said Roberto Iezzi (Catholic University A Gemelli Hospital, Rome, Italy), speaking during the GEST (Global Embolization Oncology Technologies Symposium)-hosted webinar on 25 March, where an international group of interventional radiologists discussed the global response to the COVID-19 pandemic.
The first cluster of coronavirus patients was reported in Lombardy, a region of northern Italy, on 21 February. “It is just one month ago, but it feels like a year”, Iezzi stated. Sharing the key takeaways from the last five weeks’ experience, Iezzi summarised:
Reduce or stop your usual interventional radiology (IR) activity
Organise your activity: have dedicated routes to the angiosuites, for example, to reduce contamination
Stratify your patients, based on symptoms and based on testing
In the absence of test results, consider any patient as COVID-19 positive
Speaking specifically of his institution, the Catholic University A Gemelli Hospital in Rome, Iezzi described the changes made to its usual running. “With COVID, everything changed,” he said.
On 9 March, all IR cases were stopped, except for emergency cases or a few oncological treatments for patients that could not wait until the present pandemic passes. This freed up beds for potential COVID-19 patients, and reduced the risk of infection. In total, the A Gemelli Hospital now has six dedicated COVID-19 wards, one dedicated resuscitation ward, and three wards specifically for suspected COVID-19 patients. A smaller hospital nearby was translated into a COVID-19 only hospital, with 59 beds in its intensive care unit, and a further 80 standard beds.
“We should be ready for COVID patients,” Iezzi said of interventional radiologists, “because we know that COVID patients are [generally] older patients with multiple comorbidities, and they may need interventional treatment, such as a drainage.”
Roberto Iezzi
In order to limit the risk of infection, the nine interventional radiologists based at the A Gemelli Hospital (five neuro specialists and four “body” specialists) significantly reduced their case load. Two of the three angiosuites remain open: one is dedicated solely for COVID-19 patients, and the other is open for just six hours a day, the remaining 18 hours of each day being on-call. Usually, Iezzi’s institution has three slots a week for CT-guided procedures and two slots a week for ultrasound (US)-guided procedures; this is now down to one slot a week for CT-guided activity, and no dedicated slot for US-guided activity.
In addition, visitors, students, and external colleagues and specialists have been denied access to the hospital, to limit the number of people present. Operators also have reduced access: at any moment, one operator is on-call, and one is taking up an “active slot” in the hospital scheduling. Residents are only granted access to the IR section of the hospital if needed, and patients are being offered video consultations to limit person-to-person contact.
“We tried to determine which transport routes [to use] in the hospital to minimise exposure for staff and other patients,” Iezzi shared. This measure was also taken by healthcare workers in Singapore.
Furthermore, Iezzi recommended implementing additional precautions. “All patients should wear a medical mask,” he advised, “and for COVID-positive or COVID-suspected patients, try to avoid moving and transporting them out of their room or area. Where possible, you should perform bedside US-guided procedures.
“If we have to use general anaesthesia, for example when performing a stroke thrombectomy, we try to perform induction outside the angiosuite in order to reduce the risk for airborne contamination,” he continued. “We try to avoid or reduce waiting time in preoperative holding areas. It is also very important that we use adequate personal protective equipment (PPE).”
However, he said “there is an issue”, in Italy and in other European countries, notably Spain, with access to adequate PPE. Therefore, Iezzi highlighted the importance of setting up robust guidelines for when PPE is necessary, so as not to waste any protective gear. He recommended stratifying patients based on risk when deciding on what qualifies as appropriate PPE. Low risk patients are defined as those with no fever or respiratory tract symptoms, no loose contact with confirmed or suspected cases of COVID-19, and no residence in or travel to areas or attendance at events where widespread community transmission has been reported. Intermediate risk patients are those with fever and/or respiratory symptoms, but with no close contact with a confirmed or suspected case of COVID-19, and with no residence in or travel to areas or attendance at events where widespread community transmission has been reported. High risk patients have a fever and/or respiratory tract symptoms, and in the past 14 days have either been in close contact with a confirmed COVID-19 sufferer, and/or have lived in, travelled to, or attended an event where widespread community transmission has been reported.
Regardless of risk, Iezzi strongly advised that all patients wear a disposable surgical mask. Physicians should wear PPE appropriate for “contact and droplet precaution” when dealing with low risk patients, and PPE appropriate for “airborne precaution” when treating intermediate or high risk patients (see table 1).
Table 1: Categorising appropriate personal protective equipment (PPE)
Additionally, Iezzi recommended keeping doors closed when treating suspected or positive COVID-19 patients to reduce the potential for cross-contamination. Similarly, he urged those listening to adjust the team organisation in their own institutions when working with coronavirus patients. “We as interventional radiologists, our problem is devices,” he explained. “We need different devices, and we cannot have everything in the room [at the same time]. So we have a nurse in the room with three pairs of gloves in order to remove one, give the device to the interventional radiologist without touching it, and another nurse is outside. If we need something that we do not have in, they can bring it near the door to the angiosuite. The nurse inside can put on a new pair of gloves and can pick up the device, not touching anything else. This is very important.”
At the end of a procedure, any equipment in the angiosuite must be cleaned and disinfected, Iezzi explained, adding that the doors should remain closed during cleaning. “The IR area should then remain closed for 30 minutes,” he said.
Globally, Italy has experienced the highest death toll due to the coronavirus pandemic. On 9 March, the Italian government implemented a nation-wide quarantine, and on 21 March, they imposed a “significant lockdown” on the country, forcing the shut-down of all businesses and industries deemed “not necessary”.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
This is the first in a series of articles covering the GEST webinar. For dispatches from the frontlines of the COVID-19 pandemic, and the pertinent takeaways for interventional radiologists, click here.
Interventional radiologists must play their part in protecting patients and healthcare workers during the coronavirus pandemic, urge physicians fighting the COVID-19 outbreak in Singapore. Speaking in a webinar hosted by GEST (Global Embolization Oncology Symposium Technologies) on 25 March, Kiang Hiong Tay (Singapore General Hospital, Singapore) told the over 500 virtual attendees: “COVID-19 has exploded around the world. It took 67 days to reach the first 100,000 patients, but the last 100,000 were diagnosed in just the last two days. Europe is now the epicentre. In Italy and Spain, the death toll has exceeded that of China, and I think very soon, the USA will be the next epicentre for the epidemic.”
Singapore is no stranger to viral outbreaks. The 2003 epidemic of severe acute respiratory syndrome (SARS) had a disproportionately high mortality rate in the country compared to the worldwide average, with 14% of the 238 cases proving fatal. Recalling this experience, Tay said he believe it has led to the healthcare service in Singapore being relatively well-prepared for the current eruption in coronavirus cases, commenting: “For many years after SARS, our country has been slowly building up capacity to address big outbreaks such as this.”
He said that “the key principle is to try and prevent hospital transmission: you want to prevent cross transmission between different groups of people, and the way to do this is strict adherence to infection prevention measures. Social distance is another important strategy, especially in preventing healthcare [worker] to healthcare [worker] transmission.”
The crucial takeaways from his experience preventing viral transmission in Singapore that Tay wishes to impress on the international physician community are summarised below:
Protect patients
Segregate inpatients and outpatients. Singapore General Hospital are able to do this physically, with an upstairs/ downstairs divide between the two groups, but Tay advised that if this is not possible due to space limitations, then a temporal segregation can be implemented. For example, the outpatient list could be seen to in the morning, and inpatients in the afternoon.
Reduce the number of inpatients in the hospital. Postpone non-urgent elective cases, or do them as day cases where possible. This will free up beds for the COVID-19 surge in patient numbers.
Implement hospital perimeter control. Anyone with a recent travel history to a country with a COVID-19 outbreak, and anyone showing any symptoms, should be banned from the hospital. Tay also recommended introducing temperature screening for the patients.
Protect staff
Ensure infection prevention and control knowledge and practices are up to date and consistently practiced. This includes conducting refresher training in hand hygiene and personal protective equipment (PPE) use—proper donning and doffing of PPE. “Do not neglect the non-medical staff,” Tay cautioned, “in SARS, we had many healthcare assistants infected because we did not practice this. Please do not neglect them.”
PPE should be available. A surgical mask must be worn in all patient areas. PPE type calibrated to risk level—for example, full PPE is essential in Singapore when in contact with confirmed or suspected COVID-19 patients, when performing an interventional radiology (IR) procedure on a patient with pneumonia or acute respiratory symptoms, or when performing an aerosol-generating procedure. When treating patients from the general ward and for seeing outpatients with no risk factors for COVID-19, a surgical mask is adequate. Aerosol-generating procedures pertinent to interventional radiologists include bronchial stenting, gastrointestinal stenting, and naso-gastric or naso-jejunal tube insertions.
Walkabout and audit. “We have teams who daily walk about the hospital and audit people, ensuring every complies with the infection-control measures.”
Adequate staffing is “very important”. Tay said all vacation and conference leave must be put on hold. It is necessary to reduce the workload, he commented, as infection prevention measures are time consuming and labour intensive. “Do not rush,” he warned. “That is how mistakes are made.”
Staff monitoring. In Singapore General Hospital, there is a twice daily temperature check of all staff, and every employee is issued with a personal thermometer. “There is an app that we can submit our temperature to,” he recounted, “and this is to allow the early detection of COVID clusters.”
Travel restrictions to countries affected by COVID-19.
Prevent cross-transmission
Minimise transfer of COVID-19.
Patients suspected of COVID-19 handled the same way as confirmed cases. “This is because, if you do not have appropriate PPE and you become exposed, potentially a large group of people will end up with the infection or in quarantine.”
Do not come to work if ill.
Contact tracing is “key”. Any staff at the Singapore General Hospital not wearing appropriate PPE who are exposed to a COVID-19 patient are quarantined for 14 days. The names of staff involved in all interventional radiology (IR) procedures is captured in RIS/PACS (radiology information system/ picture archiving and communication system). Additionally, staff rosters are updated and archived.
Staff segregation and social distancing. Singapore has prohibited the cross-institution movement of staff. Tay urged webinar attendees to have dedicated interventional radiologists based at satellite sites who can cover calls. This prevents the shutting down of the entire service is staff is infected or if quarantine is necessary, he explained. “We have zoom or Webex lunches, where we eat separately, but are still socially connected,” he said.
Detailed workflow for COVID-19 patients
Chow Wei Too (Singapore General Hospital, Singapore) next talked listeners through the workflow for COVID-19 patients. “The objective is to provide vascular IR care for COVID-19 patients, whether they are suspected or confirmed, while practicing the highest level of infection control.
“We want to be part of the solution, and really not part of the problem,” he said, referencing an article published in Bloomberg where surgeons operating on patients without proper protection or testing was in part responsible for the rising death toll amongst physicians in Italy. He directed listeners to the Singaporean Ministry of Health website, where a 2017 document outlines the national infection prevention and control guidelines for acute healthcare facilities. The World Health Organisation (WHO) also have a document outlining the five “moments” when physicians should wash their hands. “This is also very important,” Too stressed.
Like Tay, Too mentioned the importance of minimising the movement of patients. Physicians seeing their patients at the bedside “is best”, he said, and if this is not possible, “we go to a designated operating theatre, which we share with other procedures, where we are guided by a C-arm, and for procedures like stroke [thrombectomy] or other things that involve CT scanning, we go to the IR centre”.
Bedside procedure
“For all of our procedures, we put up charts of who is involved, and we label them [extensively], so every staff member knows what to do,” Tay informed his listeners. He showcased an example of a procedure sheet, which included columns for staff members’ initials, the staff needed (for example controller and scrub nurse), the role they would play (for example “maintains command and control of the entire event and to coordinate with various external parties” and “scrubs for procedure”), the attire necessary (such as “N95/ eye protection” or “Full PPE”), and any additional remarks (such as “Walkie Talkie in breast pocket” or “Stays at corridor”). Staff are also given a schematic diagram of the procedure, for clarity.
Between the corridor and the isolation room or intensive care unit, where the patient is, there is an anteroom or air-locked lobby, which provides a barrier against loss of pressurisation, and allows for the transfer of equipment and staff, as well as the removal of PPE.
The workflow is as follows:
Circulating nurse goes in first and checks and briefs the patient
Circulating nurse communicates with controller via walkie talkie
Scrub nurse enters and prepares the trolley
All equipment wrapped so it is easier to clean
Circulating nurse and radiographer position the patient
Scrub nurse cleans and drapes the patient
Interventional radiologist goes into the room and perform the procedure
Procedure team exits room
Waste is disposed on in the anteroom—unused items bought into the room are also disposed of
Remove N95 in corridor and every staff member involved has a shower
Contact tracing form filled out
Interventional radiology suite procedure
Tay talks through a stroke thrombectomy procedure at the Singapore General Hospital for a suspected COVID-19 patient.
“The staffing here is a lot more elaborate,” he recounted. “We want separation of the procedural and the support teams. Reduce multi-tasking and assign clear roles for individuals. Very important here is the role of the controller. We found that with the creation of this role, of a controller, everyone is much calmer and much happier.”
The second floor of Singapore General Hospital, which is the IR centre, has been divided into seven suites operating across two levels. The hospital has set up a specific PPE removal and donning area, and has a clear traffic control policy in its corridors. A traffic nurse is in charge of directing people between rooms.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
The Imperial College Network of Excellence in Vascular Science at Imperial College London (UK) is to run a COVID-19 Cardiovascular Conference as a live webinar on Thursday 2 April for all healthcare professionals battling COVID-19.
The webinar aims to share current knowledge and key experiences of managing COVID-19 related cardiovascular manifestations, as well as critical issues in team preparedness, prevention, and command and control. Among the topics to be covered are:
cumulative clinical experience of COVID-19
the science behind COVID-19 and cardiovascular disease and therapeutic possibilities
prevention, equipment, and information technology
team working and adaptation.
Included among the presentations are Ajay Kirtane (Columbia University Irving Medical Centre/NewYork-Presbyterian Hospital, New York, USA) discussing his experience from New York, and Richard Schilling (St Bartholomew’s and the Royal London NHS Trust, London UK) sharing details of the establishment of an emergency field hospital, the Nightingale Excel, in London’s docklands. Other highlights are Simon Ray from the British Cardiology Society, who will outline a UK perspective on safe working in cardiology, and Sukh Nijjer and Ahran Arnold looking at IT measures to reduce COVID-19 infections.
The webinar will run from 14.00–18.00 BST.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
The American Board of Radiology (ABR) has announced that its Core Exam for diagnostic radiology (DR) and interventional radiology (IR/DR) will be held in November.
The ABR originally had the Core Exam scheduled for May and June, but it was forced to postpone the tests due to the novel coronavirus outbreak. The new dates for the DR and IR/DR exams will be 5–6 November and 9–10 November, respectively, in Chicago and Tucson, USA. Eligible candidates for the exam will receive invitations no later than 24 August.
At the same time, the ABR said it is making progress toward scheduling the Medical Physics and Radiation Oncology oral exams in Tucson, USA. The organisation has identified new dates and is waiting for confirmation from the hotel where the exams will take place.
The American Board of Radiology also said the Medical Physics and Radiation Oncology initial qualifying exams are scheduled to take place as planned in July and August.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
“More bleeding with background clopidogrel, even if not severe by adjudication, may be associated with broad consequences, including discontinuation of therapies. In the absence of clear benefit, clopidogrel exposure along with aspirin and rivaroxaban should be minimised or avoided to reduce this risk,” concluded William R Hiatt (University of Colorado Anschutz School of Medicine, Aurora, USA), presenting a subgroup analysis of the VOYAGER-PAD trial during the American College of Cardiology/World Congress of Cardiology’s virtual scientific sessions (ACC.20/WCC Virtual)—originally scheduled to take place on 28–30 March in Chicago, USA.
Hiatt detailed that VOYAGER-PAD aimed to assess the benefit and risk of rivaroxaban plus aspirin in patients with peripheral arterial disease (PAD) after lower extremity revascularisation with and without concomitant clopidogrel.
This subgroup analysis evaluated further the efficacy and safety of concomitant clopidogrel use at baseline. More specifically, the investigators aimed to determine if, in symptomatic PAD patients undergoing lower extremity revascularisation randomised to rivaroxaban 2.5mg twice daily with aspirin versus aspirin alone, the efficacy and safety of rivaroxaban were consistent regardless of background clopidogrel use, and to explore temporal patterns of bleeding in relation to exposure and duration of clopidogrel.
Hiatt said: “In patients with symptomatic PAD undergoing revascularisation, the benefit of dual antiplatelet therapy (DAPT) is uncertain, with the only randomised controlled trial in surgical bypass showing no benefit and significantly increasing bleeding.”
He continued: “Rivaroxaban added to aspirin significantly reduces limb and cardiovascular risk with consistent benefits regardless of clopidogrel; the safety and risk/benefit of rivaroxaban plus aspirin are consistent regardless of background clopidogrel; and, in patients receiving rivaroxaban, the addition of clopidogrel as a third agent, is associated with higher rates of bleeding during exposure”.
Background
The VOYAGER-PAD trial found that treatment with aspirin plus rivaroxaban following lower extremity revascularisation in patients with peripheral arterial disease (PAD) leads to a 15% reduction in the risk of major adverse limb and cardiovascular events when compared with aspirin alone. This conclusion was presented yesterday at ACC.20/WCC Virtual by Marc Bonaca (University of Colorado Anschutz School of Medicine) and simultaneously published in the New England Journal of Medicine (NEJM).
The trial found that a twice daily dose of 2.5mg rivaroxaban plus low dose aspirin is associated with significantly lower incidence of the composite primary efficacy outcome of acute limb ischaemia, major vascular amputation, myocardial infarction, ischaemic stroke, or death from cardiovascular causes than aspirin alone.
On the principal safety outcome of Thrombolysis in Myocardial Infarction (TIMI) major bleeding there was no significant difference between the therapies. However, rivaroxaban plus aspirin was associated with a significantly higher incidence for the secondary safety outcome of International Society on Thrombosis and Haemostasis (ISTH) major bleeding.
A total of 6,564 patients were randomised into VOYAGER-PAD and followed for a median of approximately three years with complete accrual of primary events through September 2019.
Three months after undergoing renal denervation, patients with untreated high blood pressure had statistically significant reductions in average blood pressure over 24 hours compared with patients who underwent a sham procedure according to results from the SPYRAL-HTN OFF MED pivotal trial presented at the American College of Cardiology/World Congress of Cardiology’s virtual scientific sessions (ACC.20/WCC Virtual).
Further, these patients experienced no major device- or procedure-related safety events through three months, data from an international, prospective, single-blinded, sham-controlled trial that enrolled at 46 global study sites shows. The findings were also published online on 29 March in The Lancet.
The SPYRAL HTN-OFF MED pivotal trial builds upon a previous pilot study and is powered to evaluate the efficacy of catheter-based renal denervation in the absence of medications. “These results show that renal denervation offers an effective alternative approach to traditional medications that require patient adherence for reducing blood pressure,” comments Michael Böhm (Saarland University Medical Center, Hamburg, Germany) and lead author of the study, in a press release from the ACC.
“Furthermore, the findings show that renal denervation lowers blood pressure not just during the day but also through the night and [in the] early morning periods when risk is highest for [adverse] clinical events and the effect of some medications on blood pressure is reduced,” Bohm adds.
Böhm and colleagues report in The Lancet: “Catheter-based renal denervation has significantly reduced blood pressure in previous studies. Following a positive pilot trial, the SPYRAL HTN-OFF MED (SPYRAL Pivotal) trial was designed to assess the efficacy of renal denervation in the absence of antihypertensive medications.”
The study enrolled 331 patients whose average systolic blood pressure over 24 hours was between 140 and 170mmHg. Their average age was 53 years, and 67% were men. Most had obesity, with an average body mass index of 31. Around 5% also had type 2 diabetes. A condition of enrolment was that patients either had not been taking any blood pressure-reducing medications or had discontinued those medications at least three weeks before their blood pressure was measured at study entry.
Patients were randomly assigned to receive either renal denervation or a sham procedure in which a catheter was inserted and only an angiography was performed. A total of 166 patients were assigned to renal denervation and 165 to the sham procedure.
At the end of three months, the primary efficacy endpoint was the change in average 24-hour systolic blood pressure, adjusted for systolic blood pressure at study entry. The secondary efficacy endpoint was the change in average blood pressure measured in the doctor’s office at three months, adjusted for office blood pressure at study entry. Major adverse safety events were also assessed at three months, including rates of death, stroke, changes in kidney function or any injury to the arteries surrounding the kidney.
For the primary and secondary efficacy endpoints, the difference between groups was –3.9mmHg for 24-hour systolic blood pressure and –6.5mmHg for office systolic blood pressure, both favouring the renal denervation group, with a 99.9% probability that renal denervation was superior to the sham procedure.
No deaths, strokes or changes in kidney function occurred during the three-month follow-up period, Böhm says. He added that these results may not demonstrate the total decrease in blood pressure achieved with renal denervation given the short follow-up period due to ethical and safety concerns that patients needed to be restarted on antihypertensive medications. In other studies of renal denervation, however, patients’ blood pressure has continued to decline at six months or more after the procedure, he states.
“This study establishes renal denervation as an additional option beyond exercise or lifestyle modification for patients with high blood pressure who are unwilling to take or cannot tolerate medication,” Böhm says, adding that the study results will be included in an application for FDA approval of the renal denervation device used in the trial for the treatment of patients who are not taking blood pressure-reducing medication. Currently there are no renal denervation devices approved for use in the USA.
Results from a companion study, the SPYRAL-HTN ON MED trial, which is testing the safety and effectiveness of renal denervation in patients who are taking up to three blood pressure-reducing medications, are expected in about 18 months. The results of that study will also be included in the application for FDA approval of the renal denervation device, Böhm said.
In stable atherosclerosis, a combination of aspirin plus rivaroxaban provided a similar relative degree of benefit on coronary, cerebrovascular, and peripheral endpoints in patients with and without diabetes, a prespecified analysis of the COMPASS trial has shown. It also noted that, given their higher baseline risk, the absolute benefits appeared greater in those with diabetes, including a three-fold greater reduction in all-cause mortality.
The findings were outlined in a virtual presentation by Deepak L Bhatt (Brigham and Women’s Hospital Heart and Vascular Center, and Harvard Medical School, Boston, USA) at the American College of Cardiology/World Congress of Cardiology’s virtual scientific sessions (ACC.20/WCC Virtual) which was originally scheduled to take place 28–30 March in Chicago, USA. The data were also simultaneously published online in Circulation.
“Diabetes with atherosclerosis either with or without ischaemic events is associated with an extremely high rate of cardiovascular death, myocardial infarction or stroke over just four years. One potential way to address this cardiovascular risk, this residual risk, is with dual pathway inhibition—that is, combining antiplatelet therapy with anticoagulation,” Bhatt explained on a video link. “This concept was tested in the COMPASS trial.”
The main COMPASS (Cardiovascular outcomes for people using anticoagulation strategies) trial demonstrated that aspirin plus rivaroxaban 2.5mg twice daily was superior to aspirin plus rivaroxaban placebo in reducing ischaemic events in 27,395 patients with coronary artery disease (CAD) and/or peripheral arterial disease (PAD). The study found a significant reduction in cardiovascular death with dual pathway inhibition, as well as lower all-cause mortality.
In the present prespecified analysis of COMPASS, investigators analysed the results of rivaroxaban plus aspirin versus aspirin alone in the subgroups of patients with or without diabetes mellitus at baseline.
The primary efficacy endpoint was the composite of cardiovascular death, myocardial infarction , or stroke. Secondary endpoints included all-cause mortality and all major vascular events (cardiovascular death, myocardial infarction, stroke, or major adverse limb events including amputation). The primary safety endpoint was a modification of the International Society on Thrombosis and Haemostasis (ISTH) criteria for major bleeding. There was also a prespecified net clinical benefit of cardiovascular death, myocardial infarction, stroke, fatal bleeding, and symptomatic bleeding into a critical organ.
In the overall trial, there were 10,341 patients with diabetes and 17,054 without diabetes. The COMPASS diabetes subanalysis found a consistent and similar relative risk reduction for benefit of rivaroxaban plus aspirin (n=9,152) versus placebo plus aspirin (n=9,126) in patients both with (n=6,922) and without (n=11,356) diabetes for the primary efficacy endpoint (hazard ratio [HR] 0.74, p=0.002, and HR 0.77, p=0.005, respectively, pinteraction=0.77) and all-cause mortality (HR 0.81, p=0.05 and HR 0.84, p=0.09, respectively, pinteraction=0.82). Although the absolute risk reductions (ARR) appeared numerically larger in patients with versus without diabetes, both subgroups derived similar benefit (2.3% vs. 1.4% for the primary efficacy endpoint at three years, pinteraction<0.0001; 1.9% vs. 0.6% for all-cause mortality, pinteraction=0.02, 2.7% vs. 1.7% for major vascular events, pinteraction<0.0001). Because the bleeding hazards were similar among patients with and without diabetes, the prespecified net benefit for rivaroxaban appeared particularly favourable among patients with diabetes (2.7% vs. 1.0%, pinteraction=0.001).
Bhatt also outlined that the findings on the primary outcome of cardiovascular death death, myocardial infarction or stroke in those with and without diabetes, either with or without prior ischaemic events or with or without revascularisation “demonstrated a consistent benefit across all these subgroups of subgroups, with interaction p values that are not significant, suggesting that the benefits of dual pathway inhibition are not predicated on a history of prior ischaemic events or revascularisation, per se, but rather on the presence of atherosclerosis”.
He acknowledged that the diabetes subgroup was not specifically powered to efficacy or safety, but pointed out that the analysis was prespecified “with sufficient power to show a significant reduction in the primary endpoint in the overall trial in [those] with or without diabetes”.
He also pointed that because the trial was stopped early by the data safety monitoring board (DSMB), subgroup analyses were further limited; however, he said: “The independent DSMB felt that the trial needed to be stopped due to overwhelming efficacy, including a reduction in all-cause mortality in the overall trial.”
In conclusion, Bhatt told the online audience: “Low-dose rivaroxaban plus aspirin reduced major adverse cardiovascular events in stable atherosclerosis, irrespective of the presence or absence of diabetes, although the absolute risk reductions were numerically larger with diabetes, including a three-fold greater reduction in all-cause mortality. As in the overall [COMPASS] trial, there was a significant increase in major bleeding, but not in fatal or intracranial bleeding. The net clinical benefit when examining irreversible outcomes appeared numerically greater in those with diabetes. Use of dual pathway inhibition with low-dose rivaroxaban plus aspirin is particularly attractive in high-risk patients, such as those with diabetes.”
Treatment with aspirin plus rivaroxaban following lower extremity revascularisation in patients with peripheral arterial disease (PAD) leads to a 15% reduction in the risk of major adverse limb and cardiovascular events when compared with aspirin alone.
The VOYAGER PAD study was presented at the American College of Cardiology/World Congress of Cardiology’s virtual scientific sessions (ACC.20/WCC Virtual)—originally scheduled to take place 28–30 March in Chicago, USA—and simultaneously published in the New England Journal of Medicine (NEJM). It found that a twice daily dose of 2.5mg rivaroxaban plus low dose aspirin is associated with significantly lower incidence of the composite primary efficacy outcome of acute limb ischaemia, major vascular amputation, myocardial infarction, ischaemic stroke, or death from cardiovascular causes than aspirin alone. On the principal safety outcome of Thrombolysis in Myocardial Infarction (TIMI) major bleeding there was no significant difference between the therapies. However, rivaroxaban plus aspirin was associated with a significantly higher incidence for the secondary safety outcome of International Society on Thrombosis and Haemostasis (ISTH) major bleeding.
Marc P Bonaca (University of Colorado Anschutz School of Medicine, Aurora, USA) outlined the findings for the virtual conference as part of a late-breaking session. He explained that the risks of major adverse limb and cardiovascular events are high in patients with PAD who have lower extremity revascularisation, but there is uncertainty about how effective and safe rivaroxaban is in this context. “In spite of this risk,” he said, “there are no proven antithrombotic strategies to reduce the risk of limb and cardiovascular outcomes after revascularisation. VOYAGER PAD was designed to address this gap.”
The double blind trial randomised 6,564 patients with PAD who had undergone revascularisation to receive either rivaroxaban 2.5mg twice daily plus aspirin (n=3,286) or placebo plus aspirin (n=3,278).
Baseline characteristics were well balanced across the two groups, with median age 67 years, and 26% of patients were female. Risk factors were common: 40% of patients had diabetes mellitus, 20% had an estimated glomerular filtration rate less than 60ml per minute per 1.73 m2 of body-surface area, and 35% were active smokers at randomisation. Less than one third of patients (31%) had known coronary artery disease, and 11% had previous myocardial infarction. The majority of patients (96%) had a history of claudication, and the median ankle–brachial index was 0.56. Bonaca described participants as “a sick population”.
The primary efficacy outcome occurred in 508 patients in the rivaroxaban group and 584 patients in the placebo group. Three-year Kaplan-Meier estimates of the incidence were 17.3% in the rivaroxaban arm and 19.9% in the placebo arm (hazard ratio [HR] 0.85, 95% confidence interval [CI] 0.76–0.96, p=0.009).
The incidences of the first five secondary outcomes in the testing hierarchy were all significantly lower in the rivaroxaban group than in the placebo group, including the incidence of unplanned index limb revascularisation for recurrent ischaemia (HR 0.88, 95% CI 0.79–0.99, p=0.03). All-cause mortality was not lower in the rivaroxaban group than in the placebo group (HR 1.08, 95% CI 0.92–1.27, p=0.34). Therefore, the researchers write in the NEJM: “In accordance with the prespecified hierarchical testing procedure, the assessment of the last secondary outcome (venous thromboembolism) was considered exploratory.”
There was no heterogeneity in the efficacy of rivaroxaban plus aspirin as compared with aspirin alone for the primary outcome across major subgroups, including those based on age, sex, and cardiovascular risk factors. Similarly, there was no heterogeneity on the basis of qualifying symptoms, type of intervention, ankle–brachial index at screening, or the presence of critical limb ischaemia at index revascularisation.
TIMI major bleeding occurred in 62 (2.65%) patients in the rivaroxaban group and 44 (1.87%) patients in the placebo group (HR 1.43, 95% CI 0.97-2.1, p=0.07.). Intracranial haemorrhage occurred in 13 patients in the rivaroxaban group and in 17 patients in the placebo group (hazard ratio, 0.78; 95% CI, 0.38 to 1.61). Fatal bleeding occurred in 6 patients in each group.
The second safety outcome of ISTH major bleeding occurred in 140 patients on rivaroxaban versus 100 patients in the placebo group (5.94% and 4.06%, respectively, HR 1.42, 95% CI 1.1–1.84, p=0.007).
Bonaca told the online audience: “To put these results into context, in patients with PAD requiring revascularisation, for 10,000 patients treated for one year with rivaroxaban 2.5mg twice daily with aspirin versus aspirin alone there would be the prevention of 181 first ischaemic events with the components of [the primary efficacy outcome events]. The cost of this would be 29 TIMI major bleeds without any excess in intracranial haemorrhage or fatal bleeding.”
Summing up he said: “In symptomatic peripheral arterial disease after revascularisation … in this population and in this setting, rivaroxaban 2.5mg twice daily with aspirin compared to aspirin alone significantly reduces this risk. The benefits appear early and continued over time, with consistent benefit across subgroups including those with critical limb ischaemia and broad benefits included reductions in the need for unplanned index limb revascularisation. It does increase bleeding and with VOYAGER PAD there was a numerical increase in TIMI major bleeding and statistically significant increase in ISTH major bleeding with no excess in intracranial or fatal bleeding, and putting them together there is about a six-fold increase in the number of ischaemic events prevented relative to bleeds caused.”
During a Q&A section of a European Commission (EC) college meeting on 25 March, EC spokesperson Stefan de Keersmaecker stated that the commission were looking to delay the “entry into force” of the new European medical device regulations (MDR) because of the global coronavirus pandemic.
de Keersmaecker, who spoke via video, said: “The EC is working on a proposal to postpone the entry into force of the new MDR for one year. We are working hard to submit this proposal by early April.” He added that he and his colleagues were calling on the European council and parliament to adopt the proposal (once complete) “quickly” given that the new MDR is due to come into force on 26 May this year. The delay, de Keersmaecker noted, “will relieve pressure from national authorities and industry and it will allow them to focus fully on urgent priorities related to the coronavirus”.
However, even before pandemic, there were calls to delay or revise the new MDR. In a commentary written last year (October 2019), Jeffrey Jump (chairman and CEO of MedAlliance), said: “My belief—one that is shared with others in the industry—is that the MDR could become the most disruptive factor to hit the European healthcare market since the start of the Second World War. For a start, around a half of the estimated 500,000 products currently available in Europe simply will not be re-approved, due to the time, cost and administrative input required.”
He added: “I believe that—even at this relatively late stage—the MDR can still be changed to make it more workable, and some of these changes are very simple. The first and most fundamental is to extend the deadline for the implementation of MDR until at least 20 notified bodies have been accredited.”
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
Interventional radiologists from Singapore have shared their strategies for the preparation of IR services to cope with COVID-19 patients, emphasising the need for clear planning and cross-departmental working to tackle the spread of the virus.
Lessons from Singapore’s healthcare system were shared by Kiang Hiong Tay, head of the Department of Vascular and Interventional Radiology at Singapore General Hospital and Chow Wei Too, director of IR Ops at the hospital’s Division of Radiological Services, alongside Farah Irani, director for IR at Seng Kang Hospital, as part of a webinar organised by the Society of Interventional Radiologists (SIR), “Is your IR service ready for COVID-19?”.
The webinar is a part of a suite of resources available to the IR community aimed at assisting in the response to the COVID-19 outbreak. SIR has released a toolkit featuring best practice guidance and recommendations for approaching the virus while the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) is also working on a number of initiatives to share information, including a resource centre on the CIRSE website with useful articles, checklists and webinars.
Rajesh Shah, (Stanford Healthcare, Palo Alto, USA) urged IR teams to adopt the recommendations, warning that the USA is “just at the beginning” of its battle against COVID-19. “You don’t want to be implementing these [recommendations] when COVID-19 patients are coming through your door, you need to be implementing these much earlier. In some places that might be too late, but you have to start right away.”
Speaking during the webinar, Tay explained that Singapore’s response to the 2020 COVID-19 outbreak has largely been informed by lessons learned from the 2003 outbreak of Severe Acute Respiratory Syndrome (SARS), which resulted in around 33 deaths, including those of two healthcare workers. “Because of this incident in Singapore, we have undertaken a number of changes to our system, to prepare ourselves for the next outbreak,” Tay explained. Significant post-SARS developments have included an increase in the number of negative pressure isolation rooms throughout Singapore’s public health system, as well as the establishment of a purpose-built National Centre for Infectious Disease, which itself has 330 negative pressure rooms.
Additionally, Tay explained, all public hospitals now have segregated inpatient and outpatient facilities, including in radiology departments, while the country also began a national stockpiling programme for personal protective equipment (PPE), including N95 respirator and surgical masks, to ensure it has adequate supplies to tackle future outbreaks. Singapore has also developed strong contact tracing capabilities, Tay said, which includes involvement of the police and criminal investigation bodies. “We also have a National Health Staff Surveillance System (S3) where we could survey the temperatures of all healthcare workers nationally. This would help pick up early fever clusters, before they spread out,” he added. “Importantly, we also had a major investment in biomedical science, with a significant focus in building expertise in infectious diseases.”
The strategy for tackling COVID-19 in Singapore has been one of containment, Tay noted, in order to ensure that the healthcare system can prevent itself from being overwhelmed by the number of cases coming in. “The key is to break the chain of transmission, and in Singapore we try to leave no stone unturned and with every single case, isolate them, and have rigorous contact tracing, and quarantining of the contacts,” he explained. Social distancing policies have also been introduced, and the Singapore government has emphasised the social responsibility for residents to remain in their homes, particularly if they begin to show symptoms of COVID-19.
At an institutional level, Tay commented that formation of a taskforce across departments is an important step in coordinating the response to an outbreak. “We meet daily to sort out any COVID-19 related issues. We review our manpower status, the sick leave and the temperature surveillance. We have an app that can easily enter this and staff are required to do this two times a day and this can be easily monitored,” Tay said. Other areas to be overseen by the taskforce include logistical issues, include monitoring PPE stocks, and ensuring that infection control practices are maintained on the ground.
Establishing segregated teams, comprising members of different sub specialities should also be considered, Tay suggested, so that essential functions can continue even if specialist staff are required to be quarantined, while elective cases should also be reduced. “For IR, the lessons learned from SARS are still relevant,” Tay remarked. “The concept is actually quite simple: you need to protect your patients, protect your staff and prevent intra-hospital transmission. Underbuilding all of this is strict adherence to infection control measures. We need to have business continuity plans because the likelihood of getting quarantined from exposure is high.”
Following Tay, Too Chow Wei outlined Singapore General Hospital’s approach from an IR operations perspective, noting that the institution had instigated a six-point plan for dealing with the virus.
The first step is patient segregation, Wei explained, with in- and outpatients separated into different areas or by time slots, so that there is no cross contamination between patients. “Here at Singapore General Hospital we have seven rooms separated into two levels, so that we can do an upstairs/downstairs space segregation. If you can’t, do it by time, finish [the] outpatient list in the morning before you are getting your inpatients in.” Reducing the workload of the hospital is also important, he noted. “Arbitrarily at the start of the infection we said that we wanted to reduce workload by about 50%. In reality it is probably closer to about 30–40%. We want fewer patients in the hospital as it is less likely they can overwhelm the system.”
The second part of the chain is staff segregation. Wei said that within Singapore General Hospital, the IR team has been split into two functional teams of doctors, nurses and radiographers, to keep certain functions running in case specialists need to be quarantined. A policy of social distancing, and staggered meal times has also been employed, to reduce the amount of social contact between staff, and potentially reduce the likelihood of infection. The institution has adopted a further policy of vetting and prioritising cases that are handled. “Non-urgent procedures have been given long waiting times,” Wei explained.
In addition, the hospital has sought to minimise the movement of isolated patients. “If we can treat by the bedside, we should do it by the bedside,” he said. This has necessitated the introduction of enhanced workflows, described by Wei as one of the most important parts of the strategy. “We reached out to our colleagues in anaesthesia, security, infection controls and we developed workflows. This is really a juggling act,” Wei said. The process involves ensuring that as a COVID-19 positive, or suspected patient leaves a ward en route to the IR centre, the area is cordoned off by security, so that a path can be found that minimises contact with other staff and patients. As the patient is moved, environmental services will clean down surfaces. “We need to bring everybody together just for transfer of the patients. We have simulations, rehearsals and after action reviews and we constantly improve our workflows,” Wei commented.
Alongside this, the IR room is prepared for the receipt of the patients. All equipment that is unnecessary for the procedure is removed, and the remaining equipment is wrapped in plastic sheeting. At the end of the procedure there is a wipe down of the equipment, with a disinfectant wipe, after which the walls and floor and other areas are cleaned with sodium hypochlorite solution at 1,000ppm. After this the room is then disinfected, either with ultraviolet c treatment or hydrogen peroxide vapour.
Offering his advice on putting a strong strategy in place for tackling the COVID-19 outbreak from an IR perspective, Wei posited: “You need to talk to different stakeholders in the hospital. Change has become the new constant. New workflows will need to be established, documented, rehearsed, reviewed and improved. Everybody plays a role, we really need to talk about infection controls. This is a labour intensive process, but training will pay off.”
Speaking after Wei, Irani outlined the Seng Kang General Hospital experience in having dealt with COVID-19 cases. Similar to the processes described by Wei, she sketched out the procedure for the movement of patients at Seng Kang, which seeks to minimise the risk of the spread of infection. This involves a similar level of coordination between departments, and within the IR department itself. Each member of the team has a defined role in handling the patient, and prepping the facilities for use.
After the patient has been moved on, there is a strict procedure for the removal and sterilisation of clothing and equipment. Safe removal of equipment is one area highlighted by Irani as being particularly important part of the process to prevent the spread of infection. “Doffing is more important than donning,” she said. “We always are very careful when we put on the equipment, but the time we will get infected is when we take off the equipment, and that is when we need to be really careful.”
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
A viewpoint in the Journal of the American Medical Association(JAMA) has offered potential solutions to modifying ongoing randomised clinical trials during the COVID-19 pandemic. It aims to “minimise disruption and preserve integrity”, while still ensuring participant health and safety.
Authors Mary M McDermott (deputy editor of JAMA, and Jeremiah Stamler Professor of Northwestern University, Chicago, USA) and Anne B Newman (University of Pittsburgh Graduate School of Public Health, Pittsburgh, USA) advise “creativity and persistence”. They point out: “Mitigation efforts interfere with all aspects of a successful clinical trial: efficient accrual and randomisation, intervention adherence and delivery, and outcome collection. Those most susceptible to severe consequences of coronavirus, older individuals and those with chronic disease, are commonly included in randomised trials designed to improve health in these vulnerable populations.”
They observe that, although one approach is to discontinue randomised trials that do not provide an immediate clear benefit to enrolled participants, the benefits of ongoing trials are unknown until the trial is completed, and discontinuing ongoing trials wastes previously invested resources, as well as the time and effort of those who have already completed the trial.
“In contrast, sustaining ongoing trials could help millions of people realise substantial, durable health benefits that will be important once the coronavirus pandemic ends. Therefore, efforts and resources should be dedicated to support continuing randomised trials using creative and thoughtful methods and proactive planning. Adapting protocols to facilitate continued intervention adherence, outcome measurement, and some aspects of recruitment for trials already underway is likely to have the greatest benefit for the most people.”
Among the modifications they recommend are changes to how outcome data are collected, and how interventions are delivered and monitored.
McDermott and Newman suggest prioritising outcomes, with the primary outcome given highest priority: “Outcomes that are exploratory or not prespecified are more appropriate to eliminate temporarily. Alternative methods for measuring primary outcomes that cannot be collected in-person should be prepared and protocols modified to facilitate collection of alternative self-reported or medical record data that can be adjudicated as a surrogate for the primary outcome.”
Those that can be collected remotely, such as self-administered outcomes or those collected by telephone or online, should be continued.
Safety and feasibility must be emphasised when considering the delivery of interventions, they say. Interventions that can be safely adhered to without leaving home should be continued, and it may be appropriate to continue some interventions, such as medications, beyond the originally intended stop date. Others may need modification—for example, those that require participants to attend behavioural interventions requiring group visits or exercise sessions at a gym could be temporarily converted to a home-based session with remote monitoring.
The authors also urge consideration of how an intervention might interact with coronavirus infection, and whether a study drug should be continued if a participant becomes ill with symptoms of coronavirus. “Conceivably,” they point out, “some interventions could improve outcomes. For example, a trial testing efficacy of a therapy such as a statin might mitigate the cardiovascular consequences of an acute inflammatory state. If continuing the intervention becomes untenable, intention-to-treat methods are essential for understanding risks and protective factors for infection, illness, or recovery.”
However, McDermott and Newman conclude, investigators should consider scaling back or placing selected studies on hold, if doing so does not substantially harm the trials, allowing research personnel to switch to work on urgent trials of interventions to address the coronavirus pandemic.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
The 2020 Charing Cross (CX) Symposium that was due to take place next month in London, UK, has been cancelled due to COVID-19.
In full, the statement from the CX Symposium team, reads:
“The CX Symposium team has made the difficult but necessary decision to cancel the Charing Cross Symposium 2020 that was scheduled to take place from 21 to 24 April in London, UK. We will be refunding in full all the registration fees incurred by delegates and will work with our Faculty members to assist with their travel cancellations.
“With the unprecedented spread of COVID-19, it has become clear that the CX Symposium could not take place in its usual format. Some alternatives were considered, including a digital symposium to be made available during the dates of CX, but even this would not be possible in these challenging times. The medical profession has a frontline role in the fight against the virus and we are committed to supporting our friends and colleagues in the vascular community at this difficult time.
“The CX and BIBA Medical teams will continue to work hard on the media and digital front to bring you useful and key educational learnings on how medical teams from all over the world are responding to the growing number of COVID-19 patients.
“In addition, when the time seems right, we are planning for some of the carefully selected CX programme presentations to be transformed into a free online educational resource for the vascular community.
“Finally, a copy of the CX Book, containing the high-quality contribution by some of our Faculty, will be made available free of charge on the CX website.”
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
The US Food and Drug Administration’s (FDA) Center for Devices and Radiological Health (CDRH) has written to the medical device industry to outline its response to the COVID-19 public health emergency in its day-to-day operations with industry.
The letter from the agency details that it aims to “prioritise work that advances the nation’s response during this national emergency”. Among the steps it has taken are converting in-person meetings to teleconferences, and changes to its processing of incoming documents, as well as extending response due dates for marketing applications that are currently on hold.
Meetings with industry scheduled up to 30 April are being switched to a teleconference to be held at the same date and time. The agency says it will continue to assess whether any in-person meetings arranged beyond that date should be converted to teleconferences, and promises to provide periodic updates.
The CDRH also indicates that although the Document Control Center continues to receive and process incoming documents it is “generally unable to accept incoming submissions via email”, and it is looking into other electronic options.
Marketing applications that were on hold as of 16 March with a response due date on or before 30 April have had their response due dates extended by 60 days. The extension relates to Premarket Notifications (510[k]s), Premarket Approval (PMA) applications (original and supplements), Humanitarian Device Exemption (HDE) applications (original and supplements) and De Novo classification requests. The agency says this will occur automatically, without the need to submit a request. In cases of additional submission types where a response or report is due (for example, Post Approval or 522 Study reports, Investigational Device Exemption annual reports, PMA reports), the CDRH encourages that the response or report be submitted when possible.
The Postmarket and Compliance Activities at the CDRH will continue to process and work on mission critical post-market and compliance activities. “Medical devices play an essential role in advancing public health in the response to the COVID-19 national emergency. As such, our work in supporting the availability of critically-needed medical devices is our highest priority,” states the organisation.
Share your story
If you have been affected or have any information, we’d like to hear from you. You can get in touch by emailing the editor at [email protected] and one of our journalists may contact you to discuss further.
Straub Medical (United States), the US direct-sales subsidiary of Straub Medical AG (Switzerland), has announced the launch and first intervention performed with the Rotarex S atherectomy device designed for treating (OPVD).
Baljeet Uppal (Pinnacle Vein and Vascular Center, Suncity, USA), who was the first physician to treat a US patient with Rotarex S commented, “This 70-year-old patient had a 5cm long, calcified, chronic total occlusion (CTO) of the popliteal artery.”
Discussing the case, he stated “The Rotarex S device performed flawlessly in opening the occlusion and restoring flow. It was simple to operate with a relatively short procedure time and no complications. The patient was able to go home just a few hours after the intervention.
Summarising the experience, he stated “In a field crowded by atherectomy devices, Rotarex S provides revascularisation of the lower extremities in virtually all lesion types, be it thrombus, soft or calcified plaque. In the process it has minimised distal embolisation. I see it becoming our tool of choice in the coming times.”
Intended for use as an atherectomy device and to break up and remove thrombus from upper and lower extremity peripheral arteries, Rotarex S is available in both 6F and 8F configurations and compatible with 0.018” guidewire. The device is intended to treat vessels of diameter 3–8mm.
Rotarex S is a hybrid device that removes both atheroma and thrombus at the same time. Straub Medical uses the acronym MATHto describe this process, meaning Mechanical Atherectomy plus Thrombectomy. Many similar devices are only able to remove one or other component, or to only treat stenosis. Use of the device is not restricted by the nature of the occluding material, nor by the length of the occlusion.
Scientific literature published on the device supports the safety of its use and the clinical benefit provided to patients.
Gido Karges, Straub Medical Group CEO, commented, “I am proud we finally can bring this proven technology to the USA. It is safe, fast, and produces reliable and lasting results. While we do not have specific US data in that regard yet, we expect it to have a positive effect on overall treatment cost and thus US OPVD health economics, too.”
He went on to explain, “Clinically proven in terms of safety, efficacy and clinical success, this multifunctional tool from Switzerland is sure to be welcomed by US physicians to increase their versatility and efficiency when treating their patients.” With a wink, he added,“Do the MATH!”
Mike Napack, national director sales and marketing at Straub Medical (United States), emphasised:“This device has been used successfully outside the USA for many years, and we have been eagerly waiting for it to be commercialised here. With the introduction of Rotarex S in the USA,today marks a milestone in the treatment of US patients with occlusive peripheral vascular disease.”
The Straub Medical Group has been marketing Rotarex S outside of the USA for more than two decades, with patients in more than 50 countries benefiting from its uniquely designed and safe operating mechanism.
Larry Scher (New York, USA) interviews John Aruny (Orangeburg, USA) and Stephen Hohmann (Dallas, USA) for VEITHtv at the VEITHsymposium (19–23 November, New York, USA) about the role of percutaneous AV fistulas in contemporary haemodialysis practice.
Aruny says physicians are “on the brink of a whole new paradigm in technology” in regards to creating AV fistulas for haemodialysis patients – who will be the “most impacted” by these procedures. He and Hohmann also discuss patient selection and exclusion criteria for the procedure.
Scher, for his part, says he remains sceptical about the new technology that allows AV fistulas to be inserted percutaneously rather than with open surgical procedures. He is also sceptical about non-surgeons using this technology when surgery may be a better option and goes on to emphasise the importance of a multidisciplinary approach to adopting this new technology.
However, Hohmann addresses these concerns and says that he believes this new technology expands physicians’ capabilities, rather than limiting them; adding that in most cases, physicians are “not sacrificing” but rather “expanding” the options available.
Edward Choke (Singapore) talks to BLearning Peripheral at LINC 2020 (Leipzig Interventional Course; 28–31 January 2020, Leipzig, Germany) about the first-in-man clinical study—XTOSI—which looked at the safety and efficacy of a sirolimus drug-coated balloon (DCB) in the treatment of peripheral arterial disease. interim
The interim findings showed that primary patency at six months in the XTOSI below-the-knee (BTK) patients was 74%. This, notes Choke, is “highly promising”, particularly when compared to a recent study by separate investigators which looked at a paclitaxel DCB in BTK patients and showed patency of just 40% at six months. Choke outlines some of the challenges with the critical limb ischaemia (CLI) patient cohort, including the strong prevalence of diabetes (90% of patients) and the “complexity of the lesions themselves”.
He concludes by discussing the next steps, including the need to gather level one data from a larger population of patients and also highlights two upcoming randomised controlled trials, FUTURE-SFA and FUTURE-BTK.
The 2020 European Conference on Embolotherapy (ET), run by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), has been postponed until 16–19 December due to the coronavirus pandemic.
In full, the statement from CIRSE president Afshin Gangi (University Hospital Strasbourg, Strasbourg, France), ET chairperson Christoph Binkert (Institute of Radiology and Nuclear Medicine Kantonsspital, Winterthur, Switzerland), and ET deputy chairperson Patrick Haage (HELIOS Universitätsklinikum, Wuppetal, Germany) reads:
“After careful consideration of the conditions surrounding the continuing spread of the COVID-19 epidemic throughout Europe and the uncertainty regarding the severity and duration of restrictions on travel and gatherings in Austria and globally, the CIRSE leadership has had to take the difficult decision of postponing ET 2020 in Vienna, Austria, to December 16-19.
“We are very grateful for the understanding and support we have received from our community in these challenging times and look forward to welcoming you to another engaging ET in December!”
The American Journal of Kidney Diseases (AJKD) has published the National Kidney Foundation’s KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update, a completely revamped set of 26 individual guidelines for clinicians that focuses on dialysis access choices tailored to individual patients’ goals and preferences, as well as clinical outcomes.
It is the third time the Kidney Disease Outcomes Quality Initiative (KDOQI) team has developed a vascular access guideline and the first time the guideline has been updated since 2006. About 500,000 patients in the USA receive dialysis treatment and in 2016 alone, nearly 125,000 people started treatment for end-stage kidney disease (ESKD).
This comprehensive update was developed due to the significant growth in the evidentiary database for vascular access. Haemodialysis access issues are managed by a multidisciplinary team of medical professionals, thus the working group that developed this update includes members representing not only clinical and academic-based adult and pediatric nephrologists, but also interventional nephrologists, radiologists, surgeons, and vascular access nurses.
“It is gratifying to see how much progress has been made in understanding how to place and maintain the various types of vascular access to maximise the effectiveness and reduce complications,” said NKF chief scientific officer Kerry Willis. “One of KDOQI’s most important contributions to improving outcomes for dialysis patients has been the stimulation of new research such as the studies used in creating this groundbreaking update.”
An important new approach introduced in this guideline is an individualised and comprehensive map for dialysis modalities for the lifetime of the patient called the “ESKD Life-Plan,” achieved by creating a “P-L-A-N” for each patient that considers the Patient’s Life-Plan and corresponding Access Needs. For each access, the “Access Needs” part of the P-L-A-N includes designing and documenting the patient’s access creation plan, contingency plan, succession plan and underlying vessel preservation plan. The end-result is a comprehensive vascular access management plan that will best suit the patient throughout his or her time with end stage kidney disease.
The Evidence Review Team from the University of Minnesota reviewed more than 4,600 peer-reviewed publications, of which 286 were included in the evidence tables. These evidence tables were used by the workgroup, chaired by Charmaine Lok from the University of Toronto, to develop this fresh and more patient-focused approach to vascular access care that takes into consideration each patient’s needs and preferences.
“The new guideline will have many benefits for patients on dialysis, including to help preserve vessels needed for successful future access creation and to minimise unnecessary access-related procedures and complications,” said KDOQI chair Michael Rocco.
NKF has produced clinical practice guidelines through KDOQI on all stages of kidney disease and related complications since 1997. Recognised around the world for improving the diagnosis and treatment of kidney disease, the KDOQI guidelines have changed the practices of numerous specialties and disciplines and improved the lives of thousands of kidney patients. All KDOQI guidelines and commentaries are published in AJKD.
“These Guidelines emphasise an integrated, individualised approach to patient care that promotes optimal dialysis access management based on the best available evidence,” said Guideline Chair Charmaine Lok. “It recognises the need for further research, data, and timely revision that incorporates evolving practices, innovation, and new advances in vascular access. We are excited for clinicians to start using these Guidelines to help get the right access in the right patient at the right time for the right reasons.”
The guidelines will appear in the National Kidney Foundation’s AJKD today. AJKD is the leading kidney disease journal. It reaches thousands of healthcare professionals each month. To read more about the authors and to read the commentary, please visit: https://www.ajkd.org/issue/S0272-6386(20)X0004-7.
NOTE: This video is ONLY available to watch in selected countries and geographies
Geert Maleux (Leuven, Belgium), one of the first users of the SeQure® reflux control microcatheter (Guerbet) in Europe, shares his experience with the new device. He tells BLearning IR that the current challenges of embolotherapy include incomplete devascularisation, which can occur in some cases of liver chemoembolisation procedures, as well as non-target embolisation.
Maleux shares that he was drawn to using the SeQure® microcatheter because it is a novel device that is designed to help reduce the risk of non-target embolization. “[.] I have also the impression that we can deliver more microparticles into the targeted areas, for instance in cases of liver chemoembolization, into the tumour,” he adds.
Guerbet sponsored this video and its distribution in association with Interventional News.
A review of data from Veteran Health Administration shows that there was a temporal increase in the use of revascularisations for the management of critical limb-threatening ischaemia (CLTI) between 2005 and 2014. This increase correlated with a reduction in both mortality and major amputation during the same time period. However, contrary to data for non-veteran association patients, the new data did not indicate a shift towards endovascular revascularisation strategies.
Amgad Mentias (University of Iowa Carver College of Medicine, Iowa City, USA) and others write in Circulation: Cardiovascular Interventionsthat prior studies of non-veteran patients have already shown a temporal increase in both the use of revascularisation and the use of statin therapy for the management of critical limb ischaemia, and these trends have been linked to a reduction in mortality. “However, contemporary studies of critical limb ischaemia incidence, clinical management, and outcomes among veterans remain limited,” the authors report. The senior study author Saket Girotra (University of Iowa Carver College of Medicine, Iowa City, USA) told BIBA Briefings via email that there is a general lack of research on peripheral arterial disease among veterans. He noted that “we do not know with any degree of certainty how common peripheral arterial disease is among veterans”. “How does peripheral arterial disease affect veterans’ health status and quality of life both in the short-term and the long-term? And are veterans with this condition being appropriately managed? If not, what are the barriers and how can we improve care?” he adds.
Therefore, the team reviewed data from the Veterans Health Administration to provide further information in critical limb ischemia, which represents an advanced stage of peripheral arterial disease. They identified data for 20,938 patients (mean age 67.8 years; range 40–100 years) who were admitted to a Veterans Affairs (VA) facility with a diagnosis of critical limb ischaemia between 2005 and 2014 (fiscal years). Overall, the incidence of critical limb ischaemia was 0.25 per 1,000 enrolees. The authors report that across the study period, there was a “modest” decrease in the incidence of critical limb ischaemia: 0.3 per 1,000 enrolees to 0.24 per 1,000 enrolees (p<0.01).
The authors note: “There was a significant temporal increase in the overall use of revascularisation at 90 days (41.4% in 2005 vs. 57.9% in 2014; p<0.01 for trend) and this trend was consistent across all modalities [surgery, endovascular, and hybrid] as well as revascularisation during hospital stay.” Furthermore, between 2005 and 2014, risk-adjusted 90-day mortality decreased: 11.8% in 2005 and 9.4% in 2014 (p<0.01). Both revascularisation and statin use (which also increased) were strongly associated with a lower risk of 90-day mortality; revascularisation was also associated with reduced rates of major amputation at 90 days.
The authors found that surgery was the primary method of revascularisation: 25.4% vs. 14.9% for endovascular vs. 9.2% for the hybrid approach. They note that although the ongoing BEST-CLI trial is evaluating the optimal revascularisation approach, “endovascular techniques provide a lower risk option for revascularisation in patients with critical limb ischaemia”. Furthermore, they observe their findings are in “sharp contrast” to non-VA studies that have “demonstrated a general shift in revascularisation towards an endovascular approach”. Girotra comments: “The suitability of treatment depends on several factors such as the extent and complexity of vascular disease, the availability of conduits, potential for wound healing, patient preference as well as availability of appropriate expertise. Our study did not capture these data to inform us about the reasons for this divergent pattern of care. There is currently equipoise between endovascular therapy and surgical revascularisation as treatment options for critical limb ischaemia and, thus, the result of BEST-CLI are eagerly awaited.”
The study also found more than four-fold variation in the use of revascularisation across the sites and differences in patient factors could only account for less than 10% of this variation. The authors comment that they could not determine, with the current analysis, if these differences were because of differences in speciality expertise or in the number of available operators. Therefore, future studies are needed. “Given the strong association of revascularisation with patient outcomes, the findings highlight an urgent need to develop processes for ensuring that patients with critical limb ischaemia receive care from specialists with expertise in critical limb ischaemia management,” they say.
The authors conclude: “Further studies are needed to examine the reason of low use of endovascular revascularisation in VA hospitals compared with surgical revascularisation.”
An ahead-of-print article in the April issue of the American Journal of Roentgenology (AJR) reviewing various techniques and clinical management paradigms to treat severe frostbite injuries—relevant for interventional radiologists, especially—shows promising results using both intra-arterial (IA) and intravenous (IV) tissue plasminogen activator (tPA) to reduce amputation.
“Severe frostbite injuries can lead to devastating outcomes with loss of limbs and digits,” write radiologists Mikhail Higgins and John Lee (both Boston Medical Center, Boston, USA). Speaking specifically to this newspaper, they add: “In an era where the clinical paradigm for management of frostbite injuries has been primarily tissue rewarming, prolonged watchful waiting, and often delayed amputation, it is particularly exciting to have a meta-analysis that supports and validates a promising endovascular therapy performed by interventional radiologists that can significantly mitigate digit loss.”
Elaborating to Interventional News, Higgins and Lee comment: “The management of frostbite injury has been limited to conservative management and supportive care until now, mainly due to lack of studies on additional treatment options. Patients with severe frostbite injuries have often had bad outcomes—including amputations—due to the lack of reliable treatment options in the acute setting. Our meta-analysis shows promising results of intra-arterial and intravenous tPA therapy in the acute management of severe frostbite involving thrombosis of the digital arteries.”
A search of the literature by Lee and Higgins yielded 157 citations. After manually screening for inclusion criteria of case reports, case series, cohort studies, and randomised prospective studies that reported the use of tPA to treat severe frostbite injuries, 16 qualified for review.
Higgins and Lee analysed series included 209 patients with 1,109 digits at risk of amputation treated with IA or IV tPA—116 and 77 patients, respectively. A total 926 at-risk digits were treated with IA tPA and resulted in amputation of 222 digits, for a salvage rate of 76%. Twenty-four of 63 patients underwent amputation after IV tPA, resulting in a 62% salvage rate.
Both digital subtraction angiography (DSA) and triple-phase bone scan were utilised for initial imaging evaluation of patients with severe frostbite injuries.
Additional concurrent treatment included therapeutic heparin at 500U/h, warfarin with target international normalised ratio of 2:3, nonsteroidal anti-inflammatory drugs, pain management, and light dressings with topical antimicrobial agents.
Interventional radiologists are well-placed to be offering this digit-saving treatment, they add. “Not only are we interventional radiologists trained in catheter and guidewire manipulation skills to successfully navigate the arterial anatomy, but we are also clinically facile with managing patients’ unique endovascular needs with tPA therapy, given our deep experience with its use in catheter-directed thrombolytic therapy of other pathologies, such as pulmonary thromboembolism and thrombosed arteriovenous fistulas and grafts. In addition, the skill of diagnostic angiography, particularly of micro-arterial anatomy, that is needed to quickly and accurately diagnose frostbite-related thrombosis of the digital arteries as well as during post treatment evaluation is a long-held point of expertise by the clinically trained interventional radiologist.”
“For many years,” Higgins and Lee concluded, “the axiom ‘frostbite in January, amputate in July’ was an accurate description of the common outcome in frostbite injuries. Through a meta-analysis of thrombolytic therapy in the management of severe frostbite, this article provides a useful guideline for interventional radiologists, including a suggested protocol, inclusion and exclusion criteria, and potential complications.”
The author’s recommendation is based off the multidisciplinary care protocol that they co-implemented at their own institution, Boston Medical Center. Higgins and Lee say this “begins with an objective evaluation of the affected digits, including grading post-rapid rewarming in the emergency department.” This might then include collaborative clinical triaging of severe frostbite injury patients to intravenous or intra-arterial thrombolytic management with conservative management for low grade injuries, with contributions from emergency medicine, trauma surgery, podiatry, orthopaedics, internal medicine, diagnostic and interventional radiology.
“It is important to note,” they add, “that such multidisciplinary efforts reliably and reproducibly support early and accurate diagnosis and triaging of patients with frostbite injuries and are vital in providing appropriate management and oversight of these patients, particularly during thrombolytic therapy.”
When asked how this research will impact clinical practice, Higgins emphasises the importance of promoting these procedures: “Publicity on the use of thrombolytic therapy in treating acute severe frostbite is vital to ensure that frostbite patients are afforded the most efficacious management option to preserve their digits in the unfortunate event of an acute frostbite injury. With global warming as a real though daunting consideration, who knows which city or hospital might experience a rush of frostbite cases amenable to this important digit-salvaging therapy, and when? Knowing how to protect our patients from digit loss should such events occur is now a critical consideration for the forward-thinking, patient-centric interventional radiologists that we all aspire to be. In that vein, I would consider encouraging periodic efforts to inform healthcare providers about thrombolytic management of severe frostbite, especially during each winter season.”
Higgins and Lee hope to see the results of randomised trials in comparing the effectiveness and complications of intra-arterial and intravenous thrombolytic therapy. “With these results,” they determine, “we will be able to provide more effective and safe digit-saving care for patients with acute severe frostbite injuries.”
The Society of Interventional Radiology (SIR) has cancelled its upcoming conference due to the coronavirus outbreak. The conference was to be held in Seattle, USA, from 28 March–2 April.
“Based on these recommendations, US Centers for Disease Control and Prevention (CDC) and World Health Organization (WHO) information, and numerous travel restrictions issued by companies and medical institutions, SIR and SIR Foundation leadership have made the difficult, but necessary and responsible, decision to cancel the SIR 2020 Annual Scientific Meeting in Seattle,” the society said.
SIR plans to refund attendees’ and exhibitors’ registration fees and will cancel any hotel reservations made through its official hotel block, it said. It will not refund individual travel costs. Exhibitors’ space rental fees will be refunded upon written request.
The society plans to explore other meeting options.
“In the coming weeks, we will tap into the innovative and agile spirit of [our] specialty to explore virtual meeting options that deliver world-class education, spotlight interventional radiologists’ ingenuity, and celebrate the many achievements we had planned to recognize in Seattle,” SIR said.
In addition, the European Society of Radiology (ESR) announced last week that is has postponed its annual meeting, the European Congress of Radiology (ECR), originally scheduled for 11–15 March in Vienna, Austria. This will now be held on 15–19 July.
Boris Brkljačić, ESR president, comments on the society’s website: “After careful evaluation of the spreading coronavirus epidemic, and considering the recent statements issued by the World Health Organization (WHO) and the European Centre for Disease Prevention (ECDP), and the related evolving world-wide restrictions and crisis, the ESR was forced to make this decision. Above all, we have analysed the recommendations from the Austrian health authorities for large-scale events and came to the conclusion that we are not in a position to fulfil their requirements and guarantee a safe congress for our participants and industry partners at this time. The safety, health and well-being of our delegates and partners will always be the highest priority for the ESR.”
Okami Medical has announced the successful completion of the first cases with the Lobo vascular occlusion system. The first offering in the company’s product portfolio, Lobo-3, recently received 510(k) clearance from the US Food and Drug Administration (FDA) for the occlusion of peripheral arteries.
The Lobo (Low-profile braided occluder) system is uniquely designed to provide interventional physicians with a single-device, one-and-done solution for the occlusion of various arterial targets without the need for multiple embolic devices. The Lobo system combines a patented design with proprietary Hdbraid technology to create a highly occlusive pore structure that substantially reduces blood flow and accelerates vessel closure. The Lobo-3 occluder is intended for use in 1.5–3mm diameter vessels.
Ripal Gandhi, interventional radiologist, Miami Cardiac and Vascular Institute, performed the first Lobo-3 implant. “We have successfully utilised the Lobo-3 occluder to embolise several small vessels via a microcatheter. The device has resulted in immediate occlusion of the target vessels. The device tracks well and deploys precisely at the desired location. The Lobo-3 occluder is a great addition to the embolic armamentarium for the occlusion of small vessels,” said Gandhi.
“Guided by world-class physician collaborators, Okami is committed to addressing numerous challenging aspects of peripheral vascular occlusion,” said Bob Rosenbluth, president and CEO of Okami Medical. “We are very pleased with the clinical performance of the Lobo-3 occluder in the initial cases. The device is in clinical use at key centres and we look forward to expanding our launch in 2020.”
Medtronic has issued an urgent field safety notice to warn on specific production lots of its Pipeline Flex embolization devices due to the potential for device fracture.
The company initiated verbal communication about the issue last month after identifying the potential for device fracture at the distal section during use, due to a weakened bond in a subset of recently manufactured devices.
Use of the affected product could result in unintended separation, where the distal portion of the device delivery system remains in the patient, which could cause significant patient injury, including a prolonged procedure, ischaemic stroke, intracranial haemorrhage, neurological deficit and/or death.
Medtronic has not received complaints related to the issue within the affected population, but the company is recalling the affected products due to the increased potential for fracture, according to the field safety notice.
If a Pipeline Flex embolization device was already successfully implanted, there is no increased risk to patients due to the issue, and those patients can continue with their normal course of treatment. The affected lots include devices with a “use-before” date on or after 21 October 2022.
The company urged those affected by the issue to cease the use of any affected products and to remove and quarantine all unused devices in their inventory before returning them to Medtronic.
Pipeline Flex is designed for the endovascular treatment of adults with large or giant wide-necked intracranial aneurysms from the petrous to the superior hypophyseal segments. In February 2019, it won expanded US Food and Drug Administration (FDA) indication for patients with small or medium wide-necked brain aneurysms in the territory from the petrous to the terminus of the internal carotid artery.
NOTE: This video is ONLY available to watch in selected countries and geographies
[xyz-ihs snippet=”vid-01″]
Andrew Holden (Auckland, New Zealand), Alexandros Mallios (Paris, France), Robert Lookstein (New York, USA) and Tobias Steinke (Dusseldorf, Germany) talk to BLearning Peripheral about the 12-month results of the IN.PACT AV Access randomised controlled trial (RCT) which compared drug-coated balloon (DCB) angioplasty to plain balloon angioplasty.
Holden, who presented the 12-month primary patency data for the first time at LINC 2020 (Leipzig Interventional Course; 28–31 January, Leipzig, Germany), explains that the data showed a “highly significant difference in patency” in the paclitaxel DCB arm (63.8%) when compared with the plain balloon arm (43.6%). He also highlights other key data including a 35.4% reduction in the number of reinterventions in the DCB group, which he notes “really resonates with clinicians as well as patients”.
Mallios notes that the six-month data was not only sustainable but improved and claims that another important point is that, regarding the risk of mortality, “apparently there is no evidence supporting this risk for arteriovenous access”. He discusses the clinical importance of the data which he believes is “very reassuring” and provides a “better quality of life for the patient”.
Lookstein for his part discusses the Economic Impact Model of the German and American healthcare systems which he says provided “a very telling argument” that the technology should be used in the “broadest population possible”. He goes on to look at how these “impressive” datasets, including both the 12-month data and the Economic Impact Model—which showed a DCB cost benefit—have led him to think “even more about using DCBs in AV access patients”.
Finally, Steinke gives his view on the 12-month IN.PACT AV Access data which he says was “really impressive”, noting that this was the first time that “significant results” were seen over this length of observation.
Reflow Medical has announced that they have received US Food and Drug Administration (FDA) clearance for an expanded indication for the Wingman crossing catheter after completing the Wing-IT clinical trial. The Wingman catheter crosses peripheral chronic total occlusions (CTOs) using an extendable bevelled tip that creates a channel to help penetrate, or cross, the occlusion with a guidewire, enabling further treatment of the lesion with therapeutic devices.
The Wing-IT CTO clinical trial was a prospective, international, multicentre study that treated 85 patients and followed them for 30 days. The Wingman catheter was able to demonstrate a 90% crossing rate when up to two previous guidewires could not cross these challenging lesions, meeting its primary safety and efficacy endpoints. These clinical trial results have garnered positive feedback in the physician community.
“With this expanded indication, physicians gain the ability to cross [CTOs] in peripheral lesions with a simple and very effective device,” according to John R Laird (Adventist Heart and Vascular Institute, St Helena, USA). Laird was the principal investigator for the study.
S Jay Mathews (Bradenton Cardiology Center, Bradenton, USA), who performed initial patient enrolments, said, “Reflow goes the extra mile to provide physicians with real clinical evidence for utilising their technology, including this new indication for the Wingman.”
Company co-founder and CEO Isa Rizk noted, “We are extremely grateful to the physician investigators, patients, research staff and employees who helped us conduct this very important and compelling clinical study that supported this expanded treatment option for crossing peripheral CTOs.”
A world map showing the “huge disparity” between the number of UAEs and the number of uterine surgeries performed annually in Spain, France, Australia, and at one institution in El Salvador
On average in France, 2,000 uterine artery embolizations (UAEs) are performed each year. In contrast, 40,000 patients have hysterectomies annually. This has led French interventional radiologists to protest the high number of “unnecessary” surgeries, and spurred the development of a nation-wide public awareness campaign. However, this is not just a French issue.
James Spies (Georgetown University Hospital, Washington, DC, USA) reports that, “despite some progress in reducing the number of hysterectomies for benign conditions such as fibroids, with about a 10% reduction in the past decade, there are still eight to 10 times the number of hysterectomies as UAEs for fibroids in the USA.”
A 2017 report by the Society of Interventional Radiology (SIR), The Fibroid Fix: What women need to know, provided insights into the lack of awareness. SIR commissioned a Harris Poll in June 2017 that surveyed 1,176 US women ages 18 and over. The poll found 62% of respondents had never heard of UAE and that 20% believed hysterectomy was the only treatment option for fibroids. Even those who were diagnosed with fibroids reported a lack of awareness, with 44% saying they had not heard of UAE. Of those who had, 75% said they did not learn about it from a gynaecologist.
“Our numbers for UAE are ridiculous,” José Urbano (Ramon y Cajal University Hospital, Madrid, Spain) says of Spain. According to the Spanish Society of Vascular and Interventional Radiology (SERVEI), 120–150 UAE are performed each year in the country, which has a population of 44 million. These experiences are echoed in Central America. Speaking at SIR’s annual meeting last year (23–28 March, Austin, USA), the only interventional radiologist in El Salvador, Ethel Rivas Zuleta (Universidad Dr José Matías Delgado, San Salvador, El Salvador), told delegates: “We face the same problems in our region”. Fibroids are the leading indication for hysterectomy in El Salvador. In 2018, 746 hysterectomies were performed in Zuleta’s institution, mostly in women between 30 and 50 years of age. Six women were treated with UAE. Zuleta noted that none of these six patients were referred by an obstetrician or gynaecologist: four were either doctors themselves, or related to one, and two had found out about UAE themselves online.
On the other side of the world, Gerard Goh (The Alfred Hospital, Melbourne, Australia) and colleagues recently analysed Australian Medicare data, and found a “huge disparity” between the number of hysterectomies performed each year compared with the number of UAEs. The data showed that, on average over the last five years, 30,332 uterine surgeries are performed each year. According to Goh, you would expect four to five thousand of these (approximately 30%) to be treatment for fibroids. Fewer than 145 UAEs were performed on average per year. “Based on the suggestion that 20% of hysterectomies in Australia are for fibroid-related disease, this estimates 6,066 fibroid-related surgeries per year,” Goh comments.
He adds that he thinks it is “interesting” that a procedure which has been proven to be efficacious has such a poor take-up globally. A major reason for this, he posits, is the lack of “patient and referrer awareness”. To tackle this issue, he believes interventional radiologists from across the world need to “come together” and work with societies to help educate patients and referrers, because currently “a lot of women are really missing out on uterus-sparing surgery for fibroids”.
Why this discrepancy?
Speaking specifically of the US population, Spies expands on his thoughts for the causes of the discrepancy between hysterectomy patient numbers and UAE patient numbers: “I believe that there are a range of factors, which could include economic considerations, but also persisting scepticism among gynaecologists about UAE. Despite considerable evidence of excellent outcomes after UAE, UAE patients are more likely to need additional interventions than those that have hysterectomy and many gynaecologists seem convinced that a definitive treatment like hysterectomy is best. [However, we must take into account] women’s desire to avoid hysterectomy.
“In the USA, we have made efforts for years to raise the profile of UAE, with some success. Still, it is an effort of decades that will cause change. Currently, SIR is engaged in a multi-disciplinary creation of practice guidelines for the procedure.”
These guidelines, which are expected to be published in early 2021, are being developed by physicians from the specialties of gynaecology, body imaging, and IR. “The guidelines will amplify SIR’s past awareness and education efforts by providing physicians and patients with evidence-based recommendations for the optimum care of patients with symptomatic fibroids,” SIR president Laura Findeiss (Grady Memorial Hospital, Emory University School of Medicine, Atlanta, USA) comments.
In addition to SIR, the participating societies are Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Fédération Internationale de Gynécologie et d’Obstétrique (FIGO), the American Association of Gynaecologic Laparoscopists (AAGL), the American Society for Reproductive Medicine (ASRM), and the Society for Advanced Body Imaging (SABI).
To attract a Medicare rebate for UAE in Australia, the patient must be referred by an obstetrician/gynaecologist, which Goh says “brings up potential referral bias”. However, he notes that the low UAE rate in Australia is “likely multifactorial”, and that IR can only fulfil its potential in terms of treating the appropriate number of eligible patients when interventional radiologists “take greater clinical ownership of their patients”. To Goh, this looks like preprocedural consultations with patients, postprocedural care, and having an inpatient bed card. He also stresses that gynaecologists and interventional radiologists alike should have an understanding of the pros and cons of both embolization and surgical options, to allow patients to make an informed decision about their fibroid treatment.
Urbano concurs with Goh’s assessment that there are numerous reasons for the underutilisation of UAE globally, and particularly in Spain. “Of course, like in France, gynaecologists actively block this treatment because they fear losing patients,” he says. “Furthermore, when obtaining informed consent for hysterectomy, it is mandatory to notify the patient that UAE is offered as an alternative, but it is often not even mentioned. Gynaecology tends to be a speciality that does not participate in multidisciplinary work. They have countless patients, they do their own diagnostic tests, and their patient management is routine.
“Interventional radiologists have too much work in Spanish public hospitals, so UAE is not an important focus for them. In addition, while they are experts at doing the procedure, they are not always involved in the diagnosis, pain management, and patient follow-up. Interventional radiologists are only fully involved in the UAE process in private practice and some public hospitals. Less than 50% of IR services in Spain have a clinic and beds. In my experience, this is crucial for us to do all those type of procedures in which IR competes with other specialties.”
Zuleta argues the same in El Salvador. She says the underutilisation of UAE is due to “a lack of knowledge by other specialties, the usage of old protocols and guidelines, and highly unequal access to healthcare for women. We do have access to technology: we have angiosuites, CTs, ultrasounds, MRI, but what we lack is education. We at SIDI [Sociedad Iberoamericana De Intervencionismo] believe that supporting education in our countries is the best way to improve the management of patients, especially in IR.”
Public awareness initiatives
In the USA, SIR is running its own campaign—the Vision to Heal, Together, launched in September 2019—to bring IR procedures to the forefront of the public consciousness. According to an SIR press release, this aims to “build stronger partnerships with referring physicians and to empower patients to ask about IR as a treatment option.” The campaign is not specific to UAE, it is focused more broadly on vascular disease, cancer, and men’s health conditions, which includes uterine fibroids. SIR is using a combination of radio, digital, and social media advertising in four pilot US markets (Washington, DC; Rochester; Little Rock; Portland) to spread its messaging.
The campaign was inspired in part by SIR’s 2017 report finding the lack of awareness among patients and the lack of information from referring physicians. “By educating both groups, we hope to not just reduce the knowledge gap, but to build trust among the specialties so that patients are presented with all of their treatment options up front,” says Findeiss.
The Vision to Heal, Together campaign ran through to the end of March 2020. SIR reports positive engagement and social media posts. “We have seen friends sharing information with friends in need and others simply commenting to vouch for the life-saving and quality-of-life improving power of interventional radiology,” Findeiss comments. “There is a real desire and need for more information about minimally invasive treatments across the board.”
In Australia, the wording of the Medicare item for UAE is under review, which Goh hopes will change to improve patient access to the procedure. The Interventional Radiology Society of Australasia (IRSA), of which Goh is president, is “working on the UAE issue.” Goh says: “We are working with some other stakeholders to increase public awareness online, and via print and social media.” IRSA is updating its website to list practitioners who can perform UAE, and is leading a global position statement to help further increase awareness.
In Spain, Urbano stresses that the key lesson from the French action is that it is patient-focused. “SERVEI’s position is not to start turf battles,” he says. “We have lost too much time and energy in the past with no-way fights. Our policy is to show what IR work is, and to demonstrate he advantages of our treatments to patients.”
French interventional radiologists are protesting the high number of “unnecessary” surgeries taking place nationwide, stressing that there are minimally invasive alternatives with fewer complications available. The Federation de Radiologie Interventionnelle (FRI), has launched a public awareness campaign to educate potential patients about interventional radiology (IR) procedures, with a specific emphasis on uterine artery embolization (UAE), which it claims is an underutilised, safe, and effective option for patients who do not want a hysterectomy. To read about this issue on an international stage, read the full coverage here.
“I think gynaecologists have a real scepticism of the effectiveness of UAE,” FRI president Hélène Vernhet-Kovacsik (Arnaud de Villeneuve Hospital and Montpellier University, Montpellier, France) tells Interventional News. “They do not trust this technique, which they do not practice.”
The French guidelines for the therapeutic management of uterine fibroid tumours, published in the European Journal of Obstetrics and Gynecology and Reproductive Biology and last updated in 2012, state that “Because UAE is an effective treatment with low long-term morbidity, it is an option for symptomatic fibroids in women who do not want to become pregnant, and a validated alternative to myomectomy and hysterectomy that must be offered to patients.” However, Vernhet-Kovacsik says that though UAE is in the guidelines, and “should be offered as an alternative to hysterectomy for all patients”, it is not. On average 2,000 UAEs are performed a year in France. In contrast, 40,000 patients have hysterectomies annually.
Raising awareness
When first elected president of the FRI, Vernhet-Kovacsik set up specific working groups within the society. The communications working group, headed by Vincent Vidal (Hôpital de la Timone, Marseille, France), have launched a public awareness campaign in an effort to educate the public about UAE and other minimally-invasive options. With a focus on pelvic interventional radiology (IR) in 2020, the society’s edifying efforts are dedicated to UAE, haemorrhoids, and prostate artery embolization (PAE). As a world-leading advocate of the “emborrhoid” technique—the embolization of the superior rectal arteries—and the lead author of the 2015 study demonstrating the procedure’s efficacy, Vidal is a global specialist on haemorrhoids. PAE is the principle purview of Marc Sapoval (Georges Pompidou European Hospital, Paris, France, and founder of the GEST Symposium), who is a prominent member of FRI. UAE was chosen for more political reasons: in Vernhet-Kovacsik’s words, the lack of referrals and general awareness “seemed to us very stigmatising and unfair. How is it that a technique recognised as effective and less morbid than hysterectomy, cited in the gynaecology guidelines [and] with long established scientific evidence, remains as little used?”
The communications working group organised a press conference with French media on 23 January at the Georges Pompidou European Hospital in Paris. This resulted in a double page spread appearing in the non-specialist daily newspaper Le Parisien, featuring patient testimonials in favour of UAE, and interviews with Vernhet-Kovacsik, Sapoval, and other French interventional radiologists with private practices explaining technical details of the procedure, as well as describing how and why it is underutilised. The article cited a lack of information provided to the patient from interventional radiologists’ medical colleagues leading to a low referral rate.
Following this, Vernhet-Kovacsik recounts how Sapoval appeared on French radio to discuss embolization. “[He] brilliantly exposed the clinical and economic effectiveness of all the IR treatments, and presented emerging techniques,” she enthuses. Following the success of these media engagements, FRI produced a press kit summarising current scientific data on pelvic IR, which can be used to inform future media opportunities, in France or abroad.
“We also wanted to communicate [the impact on] quality of life,” Vernhet-Kovacsik says of the FRI media strategy, “because it has become a major concern for patients, and is an advantage of IR procedures, which have very low morbidity and require very short hospitalisations in comparison with alternative surgical techniques. This also made it possible for us to directly address patients by proposing solutions to symptoms that are not always recognised as pathological, but [are] handicapping in everyday life, such as pelvic pain or urinary discomfort.”
FRI has taken a multimodal approach to disseminating their message. The society made a short animated film about pelvic IR, which is freely available on their YouTube channel. This also hosts video coverage of radiology congresses and the preprocedural film shown to patients in waiting rooms. Additionally, Sapoval is working on a patient-facing website, to launch 13 June this year. “We are testing and finalising it now,” Sapoval tells Interventional News, “then we will be launching it nationwide. The website will inform patients of treatments for fibroids other than hysterectomy, so they can be aware that they may not need one.” FRI also plans to use Facebook to engage the online community through question and answer sessions, mediated by specialised health publications, designed to offer patients a chance to speak directly with an interventional radiologist.
This direct engagement is part of a trend Vernhet-Kovacsik has identified. “The patient-doctor relationship is changing—it is no longer directive, but participative. The dissemination of information on the web via social media and the creation of user groups should be [a step] in the right direction.” Following the increased interest in UAE that succeeded the Le Parisien article, FRI set up an online directory of pelvic IR centres in France, allowing patients to find these services more easily.
Sapoval believes this increasingly participative relationship is important because patients will have to lead the charge in advocating for UAE. “We have a very unethical situation in France where women get hysterectomies instead of embolizations because the obstetricians/ gynaecologists are operating on patients instead of referring them to interventional radiologists. This is one of the interventions where we have strong, level one evidence, and despite a lot of effort, we have not seen a lot of movement in the last few years. This is the case in many other countries as well, so we wanted to take the lead and raise the flag for UAE.”
“Some resistence” to uterine artery embolization from referrers
When questioned about why he thinks the discrepancy between hysterectomy and UAE numbers exists, Sapoval is categorical: “There is some resistance. Some [obstetricians/ gynaecologists] do not know about UAE, and some do know, but do not want to refer patients because they are paid to perform hysterectomies.”
Vernhet-Kovacsik proposes another reason for the low referral rate: “In my opinion, this goes beyond simple corporatist considerations. Women have a doctor who has looked after them for years, has helped them give birth to their children, knows their intimate problems. A recognition has been created and it is difficult for patients to dare to express desire for a treatment different to the one proposed by the gynaecologist! However, it is shocking to offer a firstline technique (hysterectomy) which has twice as many serious complications as embolization, sometimes requires transfusions, and always prolongs work stoppage. Gynaecologists’ main argument is the increased risk of embolization versus myomectomy regarding fertility, but the vast majority of patients are over 43 years old, are not keen on pregnancy, and are treated by hysterectomy and not myomectomy: so why not perform an embolization? I think our target must be this population precisely!”
UAE preserves sexual function and bodily integrity
The EFUZEN study, conducted in 2017 by Vernhet-Kovacsik, Sapoval, and others from the French Society of Interventional and Cardiovascular Imaging (SFICV) research group, evaluated sexual function before and one year after UAE. The authors concluded that at one-year post-embolization, UAE significantly improves all aspects of sexual function and quality of life. Vernhet-Kovacsik stresses the pertinence of this finding: patient’s quality of life and sexual function “are rarely addressed by gynaecologists”, she says, adding that “there is a close link between fibroids and their treatment, and these aspects of life.
“The uterus is not only used for reproduction; preserving bodily integrity is also a current demand,” she comments. “I think we should all take advantage of the ‘me too’ phenomenon and, as interventional radiologists, speak out and encourage women to dare to ask for fair treatment when it comes to preserving their femininity and their quality of life. We could certainly work together: interventional radiologists, gynaecologists, and patients. I am less concerned about the future of PAE, however technically more difficult, because the importance of preserving sexual function in men will never be questioned!”
The US Food and Drug Administration (FDA) is hosting a public workshop entitled “Medical Extended Reality: Toward Best Evaluation Practices for Virtual and Augmented Reality in Medicine”. According to the agency’s website, the purpose of the public workshop is “to discuss evaluation techniques for hardware, standards development, and assessment challenges for applications of Extended Reality (XR) in medicine. The goal is to identify critical gaps that may impede medical XR device development, innovation, and to advance the evaluation of medical XR devices and applications, thus accelerating the development of safe and effective medical XR devices benefiting patients and healthcare.” Follow for live updates from Interventional News here.
13:41 GMT
Edward Margerrison (director, Office of Science and Engineering Labs, Center for Devices and Radiological Health, FDA) welcomes attendees. “I want to set the scene a bit, and explain why the FDA is involved,” he says. “We have representatives here from industry, from academia, we have healthcare professionals, and we have members of government as well. So we really have the whole community here.
“Much of the technology has been developed outside of healthcare, outside of medical devices, and is beginning to come into FDA to be regulated. It is a very interesting area for us, because companies are developing products that haven’t previously been in a regulated environment. Now is the time to get everyone on the same page, to have real discussions about how we are going to develop these technologies, and stimulate innovation.
“We are looking in a pre-competitive space. […] The technologies and products of the future should compete on how good they are for the customer. […] Being the FDA, a lot of people look to us as leaders. I anticipate a lot of people asking today, is this the end of the beginning, or the beginning of the end? We think it really is the end of the beginning. Particularly the AR/ VR space (augmented reality/ virtual reality), we know it is coming, but what are the things that we do not know yet? We want you to explain so we do not become a barrier.”
13:49 GMT
Technical session begins.
“At the end of the day, at around 4pm [ET], we will need to come up with ideas for how to move forward, and we want those ideas to come from you,” Aldo Badano (deputy director, DIDSR, OSEL, CDRH, FDA) says, encouraging attendees to “be bold” and come up to the microphone to ask questions and air opinions.
“With the exception of our keynote speaker, we do not want to focus on the hype or what would be possible if we had infinite amount of time and resources, but rather what are the current challenges that are impeding the application of these technologies in the medical field.”
13:55 GMT
General trauma surgeon Rafael Grossmann (Maine, USA), the first surgeon to use Google Glass, starts his keynote lecture.
Talking of VR, Grossmann enthuses: “It blows my mind, what the technologies allows you [to do] today. What you can see through s VR headset is incredible, and this is just the beginning. The future of this technology is to become more ergonomic, more economically viable, and, ultimately, much more common.
“We are going to see a paradigm cost in the cost, weight, size of these devices that will transform the way we do health care.”
He shares BrainLab, a company he claims is “revolutionising how we educate patients and providers in regards to surgery and planning”. A representative from BrainLab will speak later. Grossman stresses the importance of haptic feedback when using VR or AR in surgery, and says that BrainLab is a “pioneer” in this field.
Grossman is currently not using VR headsets clinically, but for teaching purposes. “This is not a matter of sterility, there is no infectious concern, but we have not found the right combination of this technology and procedure in the operating room. We are still waiting on regulations.”
14:23 GMT
Bernard Kress, an optical engineer at Microsoft, takes to the podium to present on advances in mixed reality devices and new evaluation challenges.
He says HoloLens is not advertised for general consumers, but is specifically for healthcare providers. The legal team at Microsoft requested Kress read the following disclaimer ahead of his talk: “HoloLens is not intended to be a medical or surgical device, but our clients say it can be effectively used in medical imaging and image assistant surgical planning.”
Several companies, including Philips, are already using HoloLens in the medical space, Kress comments. Atul Gupta will speak on behalf of Philips later in the programme.
“Everything that we do is centred on the human,” Kress explains. “The first pillar of mixed reality is immersion. Immersion has to be matched with what the human can actually sense. This is very difficult. You do not want to over-design your system; it has to fit what the actual human can see. You have to match the optical resolution and the field of view with that of the human eye.”
The second “pillar” is comfort. “This is especially important if the surgeon has to wear the headset for multiple hours”. There are four types of comfort Microsoft take into account: wearable comfort (taking into account size, weight, temperature, centre of gravity), vestibular comfort (the device has to be physically untethered, and a large, transparent, unobtrusive peripheral see-through is required so wearers are aware of their surroundings), visual comfort (having non-conflicting 3D cues and the shortest “motion to photon” latency possible), and social comfort (need to be able to make eye contact with nurses and technicians in the room, and not put off the patient).
“So where are we today with MR hardware?” Kress asks. “There is still a long way to go to provide full comfort to surgeons and medical professionals to allow for a revolutionary imaging and augmentation tool which will change forever the medical imaging field. This is just the tip of the ice berg.”
When asked by an audience member when the cost of MR headsets will go down (“Like VR headsets, which can be very cheap”), Kress says “It will take a long time. There is no AR market today for consumers, so we are not even looking at a consumer price point. For industry, right now, I think the device is around US$3,500. This will go down, but we are not constrained by consumer requirements.
“However, this ecosystem of companies that are trying to reduce the cost of these very complicated optics are emerging, so in five to ten years I think you will see a price decline of a degree of magnitude.”
14:52 GMT
Hiroshi Mukawa, of Sony, speaks on “Emerging technologies for addressing performance limitations in extended reality devices, such as motion-to-photon latency compensation, and retinal scan displays”.
15:09 GMT
Vinay Narayan, from HTC, delivers his talk, “Advances in virtual reality devices and characterization methods”.
“We started off in VR,” he says, “but the ability to build products that can scale in a meaningful time frame really made us switch our priorities to the VR space.” Echoing Kress, Narayan stresses that one of the key differences between AR and VR when thinking about commercialisation is that VR products are available for general consumers.
17:05 GMT
John Penczek, from NIST, takes to the podium to discuss progress in standards for extended reality devices. Providing a review of the International Organization for Standardization (ISO), he outlines how the standard-setting body has robust, specific guidance for consumer requirements for finding eye point, but that there is still more work to be done, in particular in the realm of eye tracking and direct retinal tracking.
18:45 GMT
Atul Gupta, from Philips, outlines the opportunities and challenges for extended reality devices in medicine.
Andrea Kahlberg (Milan, Italy) talks to BLearning Peripheral at LINC 2020 (Leipzig Interventional Course; 28–31 January 2020, Leipzig, Germany) about a novel sirolimus-eluting self-expanding nitinol stent that Kahlberg claims “has the ability to improve the long-term results” of superficial femoral artery (SFA) endovascular treatment.
Kahlberg outlines some of the main features and unique properties of the stent. He notes that one of the “unmet needs” of SFA stenting is durability over time, explaining that the Sirolimus is combined with fatty acids helps to improve the dispersion of the drug inside the arterial wall which helps improve durability.
He finally goes on to discuss the first in-human trial with the device, which enrolled 100 patients across Europe, and notes that the two year results were “very satisfactory” compared to other major trials that involved drug-eluting stents.
The first prospective study on the combination of peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTATATE and Holmium-166 (166Ho) radioembolization has shown that significant tumour reduction can be achieved in patients with bulky liver disease, a significant advancement considering the liver is the most commonly affected organ in metastatic disease and is the most incriminating factor for patient survival. Just published in Lancet Oncology, Arthur Braat (University Medical Center Utrecht, The Netherlands) et al conclude that the additional radiation boost provided by 166Ho-radioembolization following PRRT leads to a high objective response rate with acceptable side effects and only temporary changes in quality of life.
The HEPAR PLuS study (Holmium Embolization Particles for Arterial Radiotherapy Plus 177Lu-DOTATATE in Salvage NET [neuroendocrine tumour] patients) was a phase 2, single centre, non-randomised, noncomparative, open label study. Patients received additional 166Ho-radioembolization within 20 weeks after the fourth cycle of 177Lu-DOTATATE. Senior author Marnix Lam speaks about the study’s implications, highlighting the investigators’ use of Quiremspheres (Quirem/ Terumo Europe), and how these particles are helping to usher in a new era of more individualised treatment planning when it comes to selective internal radiation therapy (SIRT):
How is this data breaking new ground?
In my opinion, the phase 3 NETTER-1 trial in patients with grade 1 and 2 gastrointestinal neuroendocrine neoplasms was a landmark study, showing that PRRT has a huge benefit for patients in terms of progression-free survival [PFS] and overall survival [OS]. However, objective response rate after PRRT was limited to only 18%. In addition, a subanalysis showed that 68% of patients in the NETTER-1 study had bulky disease, and of those patients, 70% had bulky disease in the liver. The outcomes in terms of progression-free survival are much worse: most patients with bulky disease did not reach the median PFS of >40 weeks of the NETTER-1 trial. In other words, for patients with bulky liver disease, there is definitely room for improvement.
I was discussing this with Dik Kwekkeboom (Rotterdam, The Netherlands), one of the founders of PRRT, and a friend and colleague of mine who sadly passed away in 2017. He told me he had a fantastic new treatment for neuroendocrine tumours, but that improvements were needed for patients with bulky liver disease. At the time, we were developing 166Ho-radioembolization for liver disease, so we joined forces and came up with the design of the HEPAR PLuS study, which combines the treatments: four cycles of PRRT followed by additional 166Ho-radioembolization, which provides a radiation boost. While PRRT is a systemic treatment, 166Ho-radioembolization is a local treatment, targeting the liver metastases.
With this method, we were able to improve that 18% response rate. Total hepatic objective response rate at six months was 47% in HEPAR PLuS—a huge increase. Of course, we always have to keep in mind that response rates do not necessarily translate into improved PFS or OS, and that is definitely the next step that we want to take: conduct a randomised controlled trial to evaluate whether the increased response rate translates into a better outcome for patients with bulky liver disease.
The timing of this publication is significant. PRRT is now the standard of care, as a lot of hospitals around the world have been performing this therapy for six to 12 months. They have gained experience with PRRT, which is great, but have also found that the response rate for patients with bulky liver disease is limited.
What do you think is the future of SIRT?
I think the future of SIRT is individualised treatment planning. The HEPAR PLuS study shows that it is safe to combine PRRT and 166Ho-radioembolization. However, when combining two treatment modalities that involve radiation doses, dosimetry is essential. You have to calculate the absorbed dose coming from PRRT and from radioembolization, so combining these modalities is a call for improved treatment planning.
This is where the benefit of the 166Ho-microspheres comes in: we can use the exact same particles (QuieremScout) in the test procedure as in the treatment (QuieremSpheres). During the test, we only administer a small fraction of the microspheres to the patients for diagnostic purposes—a scout dose. We evaluate the biodistribution of the microspheres, and then draw an individualised treatment plan. This is possible because, even at low activities, 166Ho-microspheres are fit for imaging, unlike Yttrium-90 (90Y)-microspheres, which can only be properly imaged at high activities. Therefore, when using 90Y-microspheres, you have to use a surrogate for the pre-treatment testing, and this is not always predictive enough for the final outcome.
Having an individual treatment plan in place is crucial when combining treatments. This is not only true for PRRT, but also if we start combining immunotherapy or chemotherapy with radioembolization. This is really where the benefit of 166Ho-microspheres lies in comparison to the 90Y-microspheres.
How can other centres benefit from this combined treatment approach?
As with all innovation, study results need to be translated into clinical guidelines for reimbursement. In Germany and Belgium, 166Ho-radioembolization is already reimbursed specifically in the treatment of neuroendocrine tumours and liver metastases.
In the most recent US guidelines for neuroendocrine neoplasm patients with liver disease, PRRT is the standard of care. Radioembolization is listed as an option following the failure of systemic treatment such as PRRT, but is also considered investigational. We want to change that. This is the first step: we have shown that the combination is safe and effective in a prospective study; now we have to conduct a randomised controlled trial. If the outcomes of this concord with those of our present study, then I am convinced we will be able to change the guidelines and offer this combined treatment approach to patients with bulky liver disease.
Preliminary experience with 166Ho-radioembolization
Irene Bargellini (University of Pisa, Pisa, Italy) shares her early experience using 166Ho-microspheres (Quirem/ Terumo): “The initial cases we have performed have confirmed that there is something really interesting going on here that deserves more attention.
What drew you to 166Ho-microspheres?
Several interesting features attracted us to 166Ho-microspheres. Our physicists and nuclear medicine physicians in particular were very interested in the dosimetry—the idea of the scout dose (QuiremScout) was intriguing to them. The concept of being able to evaluate the distribution of the microspheres with MRI was also interesting to us.
How was incorporating 166Horadioembolization into your practice?
Initially, we had to set up a specific acquisition protocol for MRI and SPECT [Single photon emission computed tomography].
What therapeutic feedback have you got from using 166Homicrospheres?
We have treated 15 patients so far. In our limited experience, we have seen the majority of our patients responding much quicker than what we are used to seeing with 90Y microspheres. The lesions were already shrinking just 45 days post-procedure. In fact, two of our patients originally deemed to be non-surgical candidates had a resection and a transplant, respectively, after radioembolization with QuiremSpheres. The response might be so quick because 166Ho has a shorter half-life than 90Y, so the dose is deposited much quicker. This is the reason why we are currently using 166Ho-microspheres for patients that could be resected or transplanted after an adequate and fast tumour downstaging. In five patients, the Holmium scout dose (QuiremScout) was performed after an initial 99mTc-MAA diagnostic work-up, whose findings would have excluded the patients from treatment, due to high lung shunting in one patient and to heterogeneous 99mTc-MAA distribution within the tumours in the remaining four cases. In all 99mTccases, the scout dose provided different information that allowed us to safely and effectively perform Holmium radioembolization. We also try to use 166Ho-microspheres in patients with colorectal metastases, because so far we have not had very good results with 90Y in this cohort.
Mohamad Hamady (L), Oliver Llewellyn, and Neeral Patel
“Current evidence shows uterine artery embolization (UAE) is a safe and effective option to treat giant fibroids,” Oliver Llewellyn (Royal Infirmary of Edinburgh, Edinburgh, UK), Neeral Patel, and Mohamad Hamady (Imperial College NHS Trust, London, UK) et al conclude in Cardiovascular and Interventional Radiology (CVIR). They recommend that “patients should be selected, counselled, and managed accordingly” in order to benefit from this minimally invasive therapy and limit the “relatively higher risk of complications and reinterventions when compared with non-giant fibroids.”
Evidence supporting UAE for giant fibroids—defined as having a diameter of at least 10cm, and/ or with a uterine volume equal to or greater than 700cc—is sparse, according to Llewellyn and co-authors. They therefore performed a systemic review and meta-analysis of UAE outcomes for symptomatic giant versus non-giant fibroids to try and consolidate existing knowledge.
“This systematic review and meta-analysis of the current available data on the treatment of giant fibroids with UAE indicates there are several key factors required for the successful management of this unique cohort of patients,” Llewellyn tells Interventional News. “This includes close collaboration between gynaecology and interventional radiology colleagues, as well as careful follow-up in the post-procedure period.”
Primary outcome measures of the study were fibroid size, uterine volume reduction, procedure time, length of hospital stay, patent symptom improvement, reintervention rate, and complication rate. Following a systematic literature review, the authors extracted data from four relevant retrospective cohort studies, including a sum of 843 patients in their analysis. Of these, 163 (19.34%) had giant fibroids, and 676 (80.19%) had non-giant fibroids.
The main findings were:
UAE resulted in uterine volume reduction in both groups: patients with giant fibroids, 38.6%±16.2; non-giant fibroids, 37.5%±18.7. The difference between the groups was not significant.
Two studies indicated a statistically significant, but not clinically significant longer operative time for giant fibroids than non-giant fibroids (49±13.3 minutes versus 44.9±12.7 minutes, respectively, in one study, and 55.3±15.8 minutes versus 46.6±14.3 minutes; MD: 5.58 minutes; CI: 2.58–8.57; p=0.0003).
There was a statistically significant but not clinically significant longer hospital stay for the giant fibroid group, as reported in two studies (p=0.01).
Individually, included studies showed good overall patient satisfaction with the procedure, as well as effective postoperative symptom improvement, but meta-analysis was not possible.
All studies reported a higher reintervention rate when embolizing giant fibroids (odds ratio [OR]: 3.57; 95% CI: 1.7–7.49; p=0.0008).
Pooling analysis of all four studies found no significant difference in total postoperative complication rate associated with embolization of giant versus non-giant fibroids (OR: 1.45; 95% CI: 0.94–2.24; p=0.09).
The rate of major complications was relatively higher in the giant fibroid cohort (OR: 4.71; 95% CI:1.51–14.64; p=0.007).
Commenting on the reported major complication rate following embolization of giant fibroids, Llewellyn et al write: “Broadly, of the seven major complications within the giant fibroid group, three related to fibroid expulsion requiring reintervention/ endocavitatory transformation, three related to uterine infection, and one patient suffered sexual dysfunction post-UAE.” Complications can be minimised with meticulous post-procedure follow-up for women undergoing UAE for giant fibroids and dedicated management pathways for patients who present with uterine infection may expedite treatment in this patient group, subsequently reducing the requirement for emergency surgery.
Elaborating on the clinical implications of this research, Llewellyn says to this newspaper: “The results from this meta-analysis will allow interventional radiology clinicians to fully discuss the risk profile with patients in the clinic setting, allowing a fully informed decision to be made. Further work in this patient population includes a comparison with current surgical techniques such as myomectomy and hysterectomy, as well as standardising patient outcome measures for UAE, which will allow patient centred data to be pooled and compared, as has been achieved with the International Prostate Symptom Score (IPSS) for prostate artery embolization.”
While the study investigators conclude that UAE is safe and effective in the treatment of uterine fibroids of various sizes, they highlight “the heterogeneous methods used by included studies in assessing symptom severity and quality of life pre- and post-UAE”. None of the included papers used a validated measure such as the uterine fibroid symptom and health-related quality of life (UFS-QoL) questionnaire. Instead, each publication utilised their own local questionnaires, which Llewellyn and co-authors say “prevented direct comparison between studies”, missing a valuable opportunity to pool patient related outcome measures for UAE.
Cerus Endovascular receives FDA approval for its first microcatheter. The 021 microcatheter will be offered with three different distal configurations, and commercial sales are expected to begin during the second quarter of 2020.
According to a press release, the company will be developing additional microcatheters of various dimensions to offer a comprehensive selection of instrumentation for the needs of interventional neuroradiologists.
Moreover, the company announced it has successfully completed its Series B financing that has raised a total of US$19 million from current and new institutional investors since the commencement of the round in July 2018.
Completion of the Series B financing will allow the company to execute on its go-to-market strategy and to complete the planned expansion of its product portfolio, including a smaller delivery platform for its recently CE marked Contour Neurovascular System, for the treatment of intracranial aneurysms.
The company’s second implant device, the Neqstent aneurysm bridging device, is advancing through the regulatory process, with a clinical trial currently enrolling, aimed at providing additional safety and efficacy data. The Neqstent is designed to be used in conjunction with conventional embolic coils for endovascular embolisation of bifurcated saccular intracranial aneurysms.
February 2020 brings another paclitaxel device meta-analysis of randomised controlled trials in chronic limb-threatening ischaemia (CLTI) patients. Krystal Dinh (Westmead Hospital, Sydney, Australia) et al report online ahead of print the risk of all-cause mortality after treatment with paclitaxel-coated devices vs. uncoated controls in patients with CLTI in the Journal of Vascular and Endovascular Therapy (JEVT) very differently than did Katsanos and colleagues earlier this year.
Dinh and colleagues, including Ramon Varcoe (Prince of Wales Hospital, Sydney, Australia), Andrew Holden (Auckland Hospita, Auckland, New Zealand) and Peter Schneider (University of California San Francisco, San Francisco, USA) performed a systematic review on 5 November 2019 to identify randomised controlled trials using intention-to-treat analysis to compare a paclitaxel-coated device to an uncoated device in peripheral arterial disease patients having clinical follow-up of at least six months. Half of the study population had to have CLTI, or extractable data on the CLTI subgroup, if this constituted less than 50%, write the authors.
The search revealed 11 trials with 1,450 patients who were randomised to treatment with a paclitaxel-coated device (n=866) or an uncoated control (n=584). The group included 94.3% (1,367) patients with CLTI. The single endpoint was all-cause mortality, which was analysed by pooling the mortality data in a random effects model. Summary statistics are expressed as relative risk ratios (RR) with a 95% confidence interval (CI).
Ramon Varcoe
Importantly, Varcoe clarified that this meta-analysis included the five-year IN.PACT DEEP results that were overlooked by Katsanos and colleagues. Further, they included only studies that were published, or those that authors were able to confirm had been accepted for publication and were in press.
As described in JEVT, the mean follow-up was 25.6 months (range 6–60) and 10 of 11 studies reported a minimum 12-month follow-up. There were 18.6% (161) deaths in the 866 patients in the paclitaxel device group and 19.9% (116) deaths in 584 patients who received treatment with a non-coated devices (RR 0.93, 95% CI 0.78 to 1.12, p=0.45).
This led the investigators to conclude that “there was no observed difference in short- to mid-term mortality among a pooled patient population of predominately CLTI patients treated with paclitaxel-coated balloons or stents compared with uncoated controls”.
Ablative Solutions has announced that positive six-month results from the Peregrine post-market study demonstrating the safety and efficacy of the company’s CE-marked Peregrine System infusion catheter were published in the Journal of the American College of Cardiology: Cardiovascular Interventions.
The Peregrine post-market Study is a European multicentre open-label trial that evaluated additional safety and performance of the Peregrine System infusion catheter using a neurolytic agent (dehydrated alcohol) delivered into the space outside of the renal (kidney) arteries in 45 patients with systemic hypertension. Patients included in the study were taking at least three anti-hypertensive medications.
At six months, mean 24-hour ambulatory SBP was reduced by 11mm Hg, and diastolic blood pressure was reduced by 7mm Hg. Medication adherence was monitored and remained stable throughout the study. The primary safety endpoint, defined as absence of periprocedural major vascular complications, major bleeding, acute kidney injury, or death within one month, was met in 96% of patients (95% CI: 85–99%).
“Publication of the Peregrine post-market study results in a respected peer-reviewed journal is a significant milestone for Ablative Solutions and shows the potential of the Peregrine System to become an important adjunctive therapy for managing uncontrolled blood pressure in this large patient population,” said Kate Rumrill, president and chief executive officer at Ablative Solutions. “We are committed to robust clinical research through our ongoing Target BP clinical trials program to further substantiate the procedural, clinical, and health-economic benefits of the Peregrine catheter for the treatment of hypertension.”
In an accompanying editorial, Deepak L Bhatt and Arjun Majithia (Harvard Medical School, Boston, USA) noted that “although the Peregrine system will clearly need to be tested in a randomised, blinded, sham-controlled clinical trial environment, the study investigators should be complimented for using rigorous, contemporary methods including objective adherence measurements (urine toxicology analysis) and appropriate, clinically relevant endpoints (ambulatory blood pressure).”
Twelve-month results from the study presented last fall at the 2019 European Society of Cardiology (ESC) Congress (31 August–4 September, Paris, France) showed that the statistically significant reduction of 24-hour mean systolic ambulatory blood pressure measurement (ABPM) at six months was sustained at 12 months, providing evidence of consistent blood pressure-lowering effect. Twelve-month results also showed a reduction of mean systolic 24-hour ambulatory blood pressure of 10mmHg (±17mmHg, p=0.001) and a reduction in systolic office blood pressure of 20mmHg (±23 mmHg, p=0.001). No patients had major adverse events.
“Results from this trial show that the renal denervation procedure using the Peregrine Catheter and alcohol as a neurolytic agent may be safe and effective for lowering blood pressure in patients with poorly controlled hypertension on medications,” said Prof. Felix Mahfoud, Saarland University Hospital, Homburg, Germany. “The publication of these data further proves the potential value of the system for both physicians and patients. We look forward to further studying the investigational product in the randomised, sham-controlled TARGET BP clinical programme.”
Worldwide, hypertension affects more than one billion people. Management of hypertension often requires multiple medications. More than half of those treated with antihypertensive medications do not achieve their target blood pressure. High blood pressure can eventually lead to serious health problems such as heart attack, stroke and loss of vision. Approximately half of people with uncontrolled hypertension die of heart disease related to poor blood flow, and another third die of stroke.
The investigational Peregrine Kit, which includes the Peregrine System Infusion Catheter (Peregrine Catheter) and Ablative Solutions dehydrated alcohol, is currently being investigated in the TARGET BP clinical program which comprises two clinical trials. Data from the TARGET BP I and TARGET BP OFF-MED trials will be used to continue to advance the understanding of renal denervation.
At CRT 2019, (2–5 March (Washington, DC, USA) Horst Sievert (Sankt Katharinen Hospital, Frankfurt, Germany) shared early results of alcohol-mediated renal denervation, which were presented as a late-breaking abstract at the conference. Watch the video here.







 Interventional News covered a whole range of the specialty’s news during 2022, but readers’ attention was most piqued by acquisitions (Boston Scientific’s of Obsidio and Bentley’s of the GoBack catheter); study results from meetings that highlighted the “potential” and “promise” of both renal denervation and prostatic artery embolization (PAE); and the launch of a first-in-human trial of a sirolimus drug-coated balloon (DCB) for peripheral indication.
Interventional News covered a whole range of the specialty’s news during 2022, but readers’ attention was most piqued by acquisitions (Boston Scientific’s of Obsidio and Bentley’s of the GoBack catheter); study results from meetings that highlighted the “potential” and “promise” of both renal denervation and prostatic artery embolization (PAE); and the launch of a first-in-human trial of a sirolimus drug-coated balloon (DCB) for peripheral indication.
 AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases and advance development and preclinical work on a PIVL device for coronary cases.
AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases and advance development and preclinical work on a PIVL device for coronary cases.










 Data have been presented for the first time at the
Data have been presented for the first time at the 


 clearance of BodyTom 64")


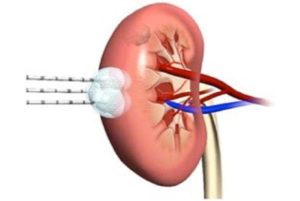

 The Swiss Federal Assembly has voted in favour of accepting medical devices with US Food and Drug Administration (FDA) marketing authorisation in Switzerland.
The Swiss Federal Assembly has voted in favour of accepting medical devices with US Food and Drug Administration (FDA) marketing authorisation in Switzerland.















 Hospices Civils de Lyon (HCL; Lyon, France) has acquired Epione, the
Hospices Civils de Lyon (HCL; Lyon, France) has acquired Epione, the 














 But, right now, in the immediate aftermath of lockdowns, Patel recounts witnessing “a chorus of excitement and eagerness to be completely in-person,” at SIR 2022. “Screen fatigue is real,” Patel adds, attributing the “[palpable] desire to continue to meet in person” to this fact. Jaworski has observed the same enthusiasm for the in-person RSNA annual meeting: “Currently, our in-person registration is up 54% from this time last year, while our virtual meeting is on a par with 2021,” he relays to Interventional News. This follows an RSNA 2021 meeting for which attendance was “in line with our expectations”—30,000 attendees, of whom 6,000 attended virtually.
But, right now, in the immediate aftermath of lockdowns, Patel recounts witnessing “a chorus of excitement and eagerness to be completely in-person,” at SIR 2022. “Screen fatigue is real,” Patel adds, attributing the “[palpable] desire to continue to meet in person” to this fact. Jaworski has observed the same enthusiasm for the in-person RSNA annual meeting: “Currently, our in-person registration is up 54% from this time last year, while our virtual meeting is on a par with 2021,” he relays to Interventional News. This follows an RSNA 2021 meeting for which attendance was “in line with our expectations”—30,000 attendees, of whom 6,000 attended virtually.


 BEST-CLI meets “astronomic” need for high-quality, practice-changing data
BEST-CLI meets “astronomic” need for high-quality, practice-changing data



















 In the USA,
In the USA, 





 XACT Robotics announced that its ACE Xtend remote control unit received US Food and Drug Administration (FDA) clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room. The first-of-its-kind feature for computed tomography (CT)-guided percutaneous procedures is designed to improve physician workflows while limiting physician and other users’ exposure to radiation, and to reduce physical strain.
XACT Robotics announced that its ACE Xtend remote control unit received US Food and Drug Administration (FDA) clearance, allowing users to robotically insert and steer the XACT ACE Robotic System remotely from the control room. The first-of-its-kind feature for computed tomography (CT)-guided percutaneous procedures is designed to improve physician workflows while limiting physician and other users’ exposure to radiation, and to reduce physical strain.




 Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.
Xeltis today announced what it describes as “very promising” preliminary efficacy and safety results from one of the centres participating in the AXESS study—a first-in-human (FIH) clinical trial of its restorative haemodialysis access graft, Axess.




 Paediatric interventional radiologist Alex Barnacle (Great Ormond Street Hospital, London, UK) gave the Josef Roesch Lecture at the
Paediatric interventional radiologist Alex Barnacle (Great Ormond Street Hospital, London, UK) gave the Josef Roesch Lecture at the 
















 Interventional News’ popular stories last month included acquisitions by Boston Scientific and Gore, studies of deep vein thrombosis and peripheral arterial disease treatments and, on the subject of the latter, research into the racial disparities affecting patients who receive peripheral vascular interventions. Stories covering data presented at two of the summer’s meetings—Society of Interventional Radiology (SIR) and the European Conference on Embolotherapy (ET)—also garnered ample views.
Interventional News’ popular stories last month included acquisitions by Boston Scientific and Gore, studies of deep vein thrombosis and peripheral arterial disease treatments and, on the subject of the latter, research into the racial disparities affecting patients who receive peripheral vascular interventions. Stories covering data presented at two of the summer’s meetings—Society of Interventional Radiology (SIR) and the European Conference on Embolotherapy (ET)—also garnered ample views.











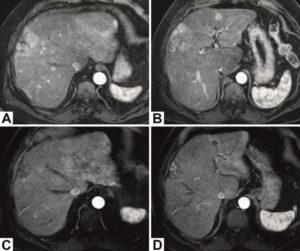


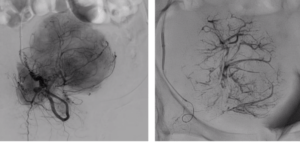


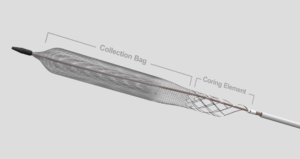




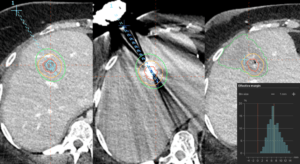









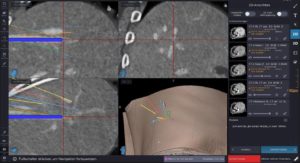


 Teleflex has announced a new agreement with FundamentalVR, a company providing virtual reality (VR) integration for medical simulation. The agreement will provide Teleflex with a VR training platform to accelerate the effective use of the company’s UroLift 2 system, a technology for treatment of benign prostatic hyperplasia (BPH), commonly known as enlarged prostate. The VR training platform integrates tactile feedback and a digital representation of the UroLift 2 system to provide urologists with a ‘hands-on’ VR experience that can accelerate their learning.
Teleflex has announced a new agreement with FundamentalVR, a company providing virtual reality (VR) integration for medical simulation. The agreement will provide Teleflex with a VR training platform to accelerate the effective use of the company’s UroLift 2 system, a technology for treatment of benign prostatic hyperplasia (BPH), commonly known as enlarged prostate. The VR training platform integrates tactile feedback and a digital representation of the UroLift 2 system to provide urologists with a ‘hands-on’ VR experience that can accelerate their learning.


 The first US patient has been enrolled in the US Food and Drug Administration (FDA) SELUTION4BTK (below-the-knee) clinical trial evaluating Selution SLR, MedAlliance’s novel sirolimus-eluting balloon. This follows investigational device exemption (IDE) approval in the USA in
The first US patient has been enrolled in the US Food and Drug Administration (FDA) SELUTION4BTK (below-the-knee) clinical trial evaluating Selution SLR, MedAlliance’s novel sirolimus-eluting balloon. This follows investigational device exemption (IDE) approval in the USA in 















 Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.
Gore has announced the acquisition of InnAVasc Medical, a privately held medical technology company focused on advancing care for patients with end-stage renal disease who utilise graft circuits for dialysis treatment.


 Fluidx Medical disclosed study results examining extent of vessel filling using the
Fluidx Medical disclosed study results examining extent of vessel filling using the 






 for Turbo-Elite laser atherectomy catheter reprocessing")
 Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US Food and Drug Administration (FDA) clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser
Northeast Scientific, a company that reprocesses single-use peripheral vascular catheters, announced recently in a press release that it has received US Food and Drug Administration (FDA) clearance for reprocessing the Philips Spectranetics 0.9mm over-the-wire Turbo-Elite laser 






 for new Soldier high-flow microcatheter")








 clearance for the Dabra 2.0 catheter")
 Ra Medical Systems has announced receipt of US Food and Drug Administration (FDA) 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. A company press release details that the catheter features enhancements including a braided overjacket design that is intended to improve deliverability and kink resistance when navigating tortuous anatomy, as well as a six-month shelf life.
Ra Medical Systems has announced receipt of US Food and Drug Administration (FDA) 510(k) clearance for the company’s Dabra 2.0 catheter as part of the Dabra excimer laser system. A company press release details that the catheter features enhancements including a braided overjacket design that is intended to improve deliverability and kink resistance when navigating tortuous anatomy, as well as a six-month shelf life.
 Konica Minolta Healthcare Americas has announced that the company’s Dynamic Digital Radiography (DDR) technology, enabling the visualisation of anatomy
Konica Minolta Healthcare Americas has announced that the company’s Dynamic Digital Radiography (DDR) technology, enabling the visualisation of anatomy 


 Among the most popular pieces from last month are reports on papers delivered at the
Among the most popular pieces from last month are reports on papers delivered at the 





 with Yttrium-90 in paediatric primary liver tumours")









 TriSalus’ clinical leadership team presented new preclinical data at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA). The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist,
TriSalus’ clinical leadership team presented new preclinical data at the Society of Interventional Radiology (SIR) 2022 Annual Scientific Meeting (11–16 June, Boston, USA). The data are the result of evaluations of the company’s immunotherapy platform, which integrates an investigational class C toll-like receptor 9 (TLR9) agonist, 







 SoniVie recently announced that on 5
SoniVie recently announced that on 5 


 Artio Medical today announced the closing of US$28 million in oversubscribed Series A2 and Series A3 financing, bringing the total amount raised by the company to date to US$74 million.
Artio Medical today announced the closing of US$28 million in oversubscribed Series A2 and Series A3 financing, bringing the total amount raised by the company to date to US$74 million.












 Arjo has announced the development of a new intraoperative Doppler system that includes a single-use, sterile intraoperative probe and Dopplex DMX Vascular Doppler.
Arjo has announced the development of a new intraoperative Doppler system that includes a single-use, sterile intraoperative probe and Dopplex DMX Vascular Doppler.



defining curative intent for HCC")










 The Royal Australian and New Zealand College of Radiologists (
The Royal Australian and New Zealand College of Radiologists (


 Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.
Germany-based endovascular simulator supplier CATHI has joined forces with UK-based Vascular Simulation Solutions (VSS) to offer the world’s first online training masterclass using endovascular simulation coupled to a structured curriculum, the company said in a press release.  A report from the American Venous Forum (AVF) 2022 meeting (23–26 February, Orlando, USA) on the comparative merits and demerits of dedicated and non-dedicated stents heads the list of Interventional News’ April
A report from the American Venous Forum (AVF) 2022 meeting (23–26 February, Orlando, USA) on the comparative merits and demerits of dedicated and non-dedicated stents heads the list of Interventional News’ April 



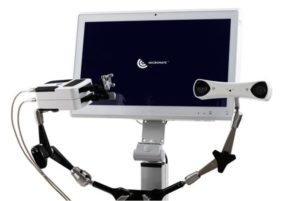

 Avail Medsystems, a healthcare technology company whose surgical telepresence platform facilitates real-time, interactive collaboration during live procedures among a network of physicians and medical device industry representatives, announced that it has entered into a partnership with the Stroke Thrombectomy and Aneurysm Registry (STAR).
Avail Medsystems, a healthcare technology company whose surgical telepresence platform facilitates real-time, interactive collaboration during live procedures among a network of physicians and medical device industry representatives, announced that it has entered into a partnership with the Stroke Thrombectomy and Aneurysm Registry (STAR).





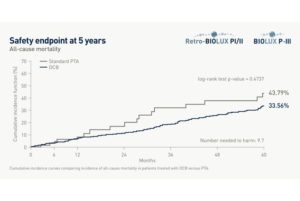 New long-term data presented at Charing Cross (CX) demonstrated the safety of BIOTRONIK’s
New long-term data presented at Charing Cross (CX) demonstrated the safety of BIOTRONIK’s 


 Suction thrombectomy has been studied many times over the years and decades. The challenge with suction is that the adherent clot material is still there and getting that stuff off the wall is still a problem, which is why wall contact thrombectomy devices are so popular. The bottom line is that there are lots of different ways to do this, as outlined in the literature. The one thing that I will reiterate is that using a US$10,000 device to do a thrombectomy is profligate. When I see it presented at meetings, it makes me cringe.
Suction thrombectomy has been studied many times over the years and decades. The challenge with suction is that the adherent clot material is still there and getting that stuff off the wall is still a problem, which is why wall contact thrombectomy devices are so popular. The bottom line is that there are lots of different ways to do this, as outlined in the literature. The one thing that I will reiterate is that using a US$10,000 device to do a thrombectomy is profligate. When I see it presented at meetings, it makes me cringe.
 EDDA Technology, a provider of advanced imaging-guided precision treatment solutions, announced it has entered into an agreement with the Society of Interventional Oncology (SIO) for its
EDDA Technology, a provider of advanced imaging-guided precision treatment solutions, announced it has entered into an agreement with the Society of Interventional Oncology (SIO) for its 



 The March
The March 



 clearance for Prodigy thrombectomy system")


 A study from Sweden published by
A study from Sweden published by 













 Tractus Vascular
Tractus Vascular






 Fist Assist Devices has announced a three-year affiliation with Regional Health Care Group to commercialise and launch sales of the
Fist Assist Devices has announced a three-year affiliation with Regional Health Care Group to commercialise and launch sales of the 


 A prospective multicentre study has evaluated the safety and efficacy of a polyethylene glycol (PEG)-based liquid embolic in treating hypervascular tumours, according to an Instylla press release.
A prospective multicentre study has evaluated the safety and efficacy of a polyethylene glycol (PEG)-based liquid embolic in treating hypervascular tumours, according to an Instylla press release.

















































 A new study reports that watching TV for four hours a day or more is associated with a 35% higher risk of venous thromboembolism (VTE) compared with less than 2.5 hours. The research is published today in the
A new study reports that watching TV for four hours a day or more is associated with a 35% higher risk of venous thromboembolism (VTE) compared with less than 2.5 hours. The research is published today in the 


















 Akura Medical has announced the closing of its $25M Series A1 financing, which will be used to support the development of its next-generation thrombectomy device.
Akura Medical has announced the closing of its $25M Series A1 financing, which will be used to support the development of its next-generation thrombectomy device.







 Fist Assist Devices has announced that it recently received Breakthrough Device designation from the US Food and Drug Administration (FDA) for its Fist Assist Model FA-1 device.
Fist Assist Devices has announced that it recently received Breakthrough Device designation from the US Food and Drug Administration (FDA) for its Fist Assist Model FA-1 device.









 Principal investigator of the
Principal investigator of the 














 Artio Medical has announced that full results from its first-in-human clinical study of the
Artio Medical has announced that full results from its first-in-human clinical study of the 





 Cardiovascular Systems has initiated a voluntary recall of unused Wirion embolic protection systems due to complaints of filter breakage during retrieval.
Cardiovascular Systems has initiated a voluntary recall of unused Wirion embolic protection systems due to complaints of filter breakage during retrieval.





























 Medtronic has announced its ambition to achieve net zero carbon emissions by fiscal year 2045 across its operations and value chain to accelerate efforts to combat climate change. The announcement comes amidst the 2021 United Nations Climate Change Conference (COP 26), where world leaders are focusing on collectively cutting greenhouse gas (GHG) emissions and limiting global warming to 1.5 degrees Celsius compared to pre-industrial levels.
Medtronic has announced its ambition to achieve net zero carbon emissions by fiscal year 2045 across its operations and value chain to accelerate efforts to combat climate change. The announcement comes amidst the 2021 United Nations Climate Change Conference (COP 26), where world leaders are focusing on collectively cutting greenhouse gas (GHG) emissions and limiting global warming to 1.5 degrees Celsius compared to pre-industrial levels.
 Randomised placebo-controlled trials show consistently that renal denervation provides significant reduction in ambulatory and office blood pressure, the findings of a systematic review and meta-analysis suggest.
Randomised placebo-controlled trials show consistently that renal denervation provides significant reduction in ambulatory and office blood pressure, the findings of a systematic review and meta-analysis suggest.
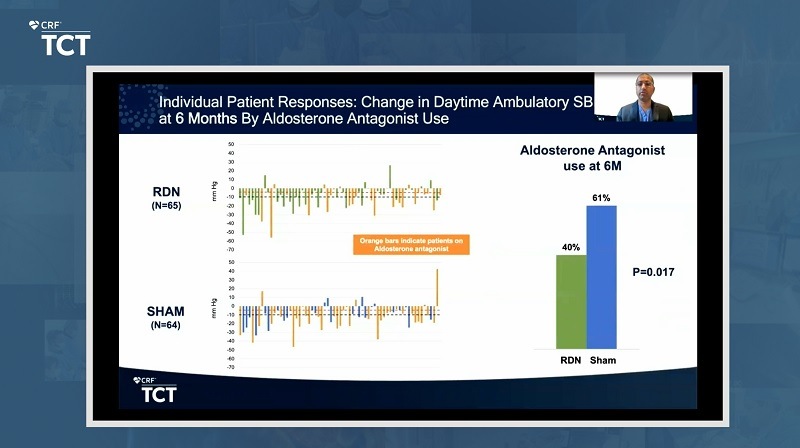 “Blood pressure reductions after renal denervation were achieved with a smaller increase in additional medications prescribed and less use of aldosterone antagonists compared with a sham procedure,” said Kirtane. “These results demonstrate the additional effects of pharmacologic intervention with maintenance of a blood pressure-lowering effect of endovascular ultrasound renal denervation at six months.”
“Blood pressure reductions after renal denervation were achieved with a smaller increase in additional medications prescribed and less use of aldosterone antagonists compared with a sham procedure,” said Kirtane. “These results demonstrate the additional effects of pharmacologic intervention with maintenance of a blood pressure-lowering effect of endovascular ultrasound renal denervation at six months.”











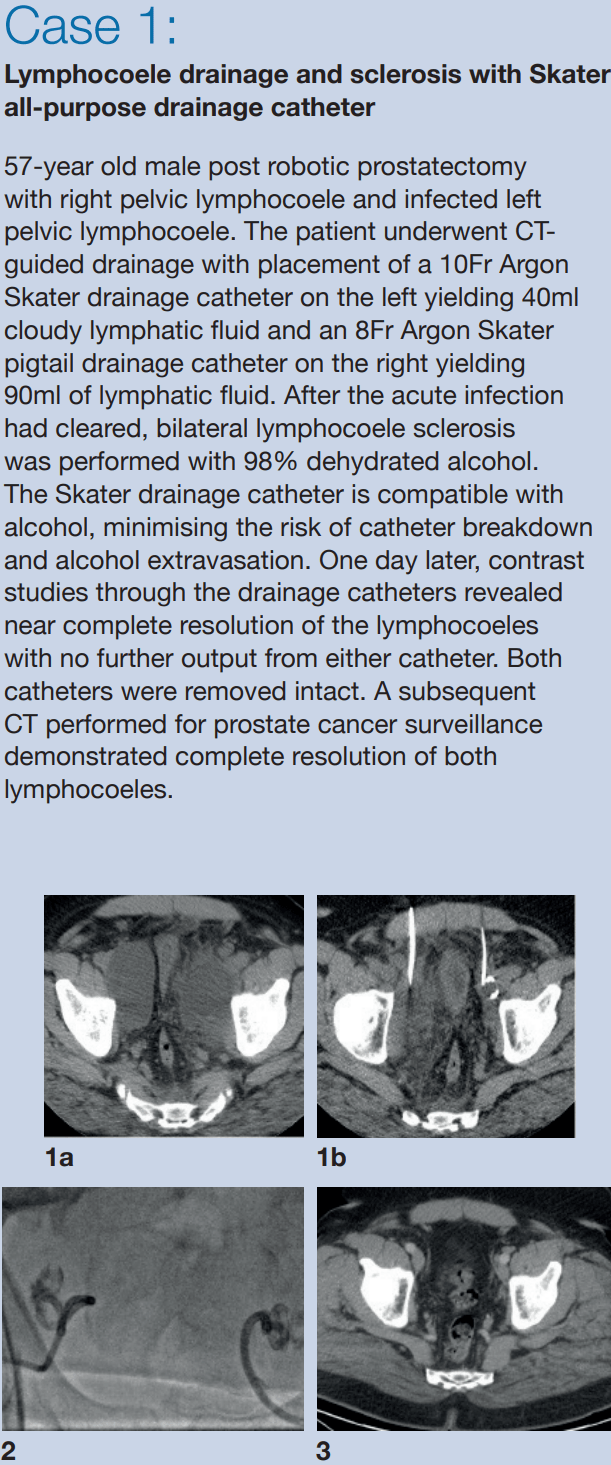
































 Preliminary clinical results from a first-in-human study assessing the
Preliminary clinical results from a first-in-human study assessing the 











 Sirtex Medical (Sirtex) has announced that the first procedure of selective internal radiation therapy (SIRT) using SIRSpheres Y-90 resin microspheres in China was successfully performed for a patient with hepatocellular carcinoma (HCC) on 28 September 2021. The milestone was reached with the support of Sirtex shareholder China Grand Pharmaceutical and Healthcare Holdings Limited.
Sirtex Medical (Sirtex) has announced that the first procedure of selective internal radiation therapy (SIRT) using SIRSpheres Y-90 resin microspheres in China was successfully performed for a patient with hepatocellular carcinoma (HCC) on 28 September 2021. The milestone was reached with the support of Sirtex shareholder China Grand Pharmaceutical and Healthcare Holdings Limited. clearance of expanded indications for the Rotarex atherectomy system")

















 Today,
Today, 









 Proposed cuts to physician reimbursements could shutter practices and leave thousands of medically vulnerable patients without access to care, the Society of Interventional Radiology (SIR) said in a comment letter submitted to Centers for Medicare and Medicaid Services (CMS) in September.
Proposed cuts to physician reimbursements could shutter practices and leave thousands of medically vulnerable patients without access to care, the Society of Interventional Radiology (SIR) said in a comment letter submitted to Centers for Medicare and Medicaid Services (CMS) in September. Johnson, an interventional radiologist and Gary J. Becker Professor of Radiology Research at Indiana University School of Medicine in Indianapolis, USA. “In many cases, practice costs have not been updated in 20 years. Due to purported budget neutrality, CMS made apparently arbitrary cuts rather than reimburse all practices and specialties at their true cost of care.” While CMS c onsiders such cuts “budget neutral” they disproportionately affect procedures performed by IRs in office-based settings, such as treatment of venous ulcers and dialysis access. More importantly, the services most affected treat diseases that disproportionately affect patients of colour, such as peripheral artery disease, venous disease, renal disease and cancer.
Johnson, an interventional radiologist and Gary J. Becker Professor of Radiology Research at Indiana University School of Medicine in Indianapolis, USA. “In many cases, practice costs have not been updated in 20 years. Due to purported budget neutrality, CMS made apparently arbitrary cuts rather than reimburse all practices and specialties at their true cost of care.” While CMS c onsiders such cuts “budget neutral” they disproportionately affect procedures performed by IRs in office-based settings, such as treatment of venous ulcers and dialysis access. More importantly, the services most affected treat diseases that disproportionately affect patients of colour, such as peripheral artery disease, venous disease, renal disease and cancer.













 The CardioVascular Coalition (CVC), a coalition of physicians, care providers, advocates, and manufacturers working to improve awareness and prevention of
The CardioVascular Coalition (CVC), a coalition of physicians, care providers, advocates, and manufacturers working to improve awareness and prevention of 















 Argon Medical Devices has announced the commercial launch of Skater mini-loop drainage catheters in the USA and the European Union.
Argon Medical Devices has announced the commercial launch of Skater mini-loop drainage catheters in the USA and the European Union.



 A research letter published in
A research letter published in 








 Artio Medical announced today it has completed enrolment in its first-in-human study evaluating the Amplifi vein dilation system. In the study, five patients were treated by Adrian Ebner, head of the Cardiovascular Department at Sanatorio Italiano Hospital in Asunción, Paraguay.
Artio Medical announced today it has completed enrolment in its first-in-human study evaluating the Amplifi vein dilation system. In the study, five patients were treated by Adrian Ebner, head of the Cardiovascular Department at Sanatorio Italiano Hospital in Asunción, Paraguay.

 “There appears to be heightened risk of major amputation after use of paclitaxel-coated balloons [PCBs] in the peripheral arteries,” findings from a systematic review and meta-analysis of randomised controlled trials (RCTs) published in the
“There appears to be heightened risk of major amputation after use of paclitaxel-coated balloons [PCBs] in the peripheral arteries,” findings from a systematic review and meta-analysis of randomised controlled trials (RCTs) published in the 



 A large, single-centre retrospective study has revealed the risk of
A large, single-centre retrospective study has revealed the risk of 




 Tara Graham (Trillium Health Partners, Toronto, Canada) has become the new president of the Canadian Association for Interventional Radiology (
Tara Graham (Trillium Health Partners, Toronto, Canada) has become the new president of the Canadian Association for Interventional Radiology (


 Royal
Royal 


 Scitech Medical, has announced that it has received CE mark approval for the Embosoft microspheres for use in vascular embolization of hypervascular tumours, symptomatic uterine fibroids and prostatic arteries to relieve symptoms related to benign prostatic hyperplasia, as well as for haemostatic embolization.
Scitech Medical, has announced that it has received CE mark approval for the Embosoft microspheres for use in vascular embolization of hypervascular tumours, symptomatic uterine fibroids and prostatic arteries to relieve symptoms related to benign prostatic hyperplasia, as well as for haemostatic embolization. A systematic review and meta-analysis has demonstrated that patients undergoing carotid interventions after thrombolysis have a higher risk of periprocedural hazards, compared with those patients who did not have prior thrombolysis. Authors Stavros K Kakkos (University Hospital of Patras, Patras, Greece) and colleagues report their findings in an article published online in the
A systematic review and meta-analysis has demonstrated that patients undergoing carotid interventions after thrombolysis have a higher risk of periprocedural hazards, compared with those patients who did not have prior thrombolysis. Authors Stavros K Kakkos (University Hospital of Patras, Patras, Greece) and colleagues report their findings in an article published online in the 









 Chair of the 2022 and 2023
Chair of the 2022 and 2023 
 Chair of the 2022 and 2023
Chair of the 2022 and 2023 



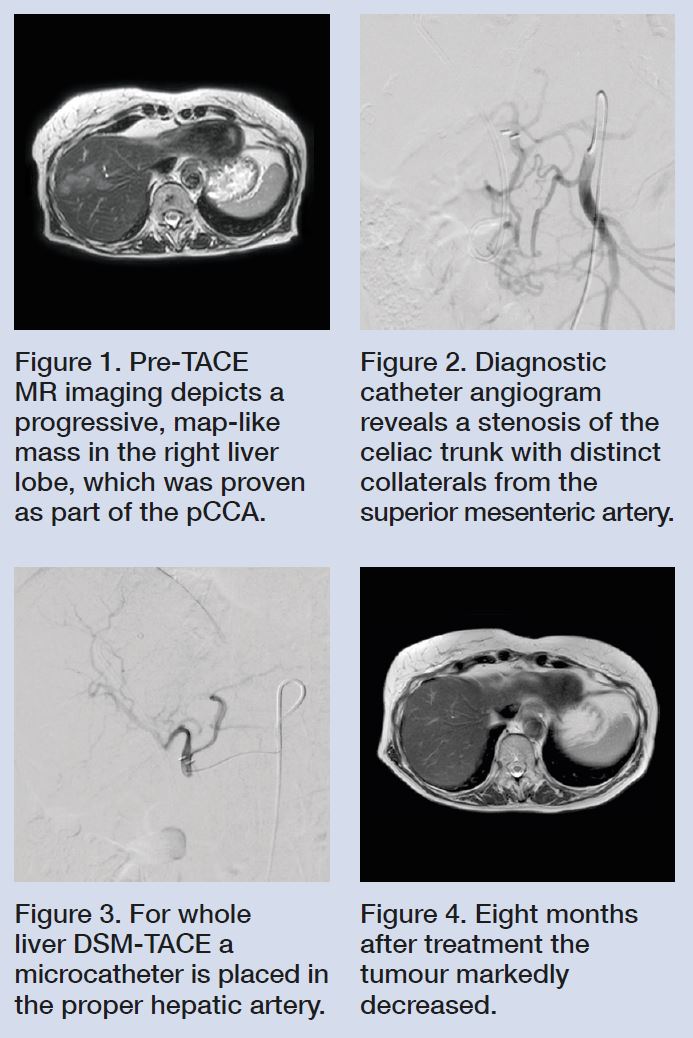 Cholangiocarcinoma is a highly lethal hepatic neoplasm with a median overall survival rate of about 16 months (Waseem 2017). Even after resection, the prognosis is poor, with reported three- and five-year survival rates after resection for perihilar cholangiocarcinoma (pCCA) of around 45% and 30% (Cillo 2019). In unresectable pCCA, common treatment options included chemotherapy with gemcitabine and cisplatinum, and transarterial chemoembolization (TACE).
Cholangiocarcinoma is a highly lethal hepatic neoplasm with a median overall survival rate of about 16 months (Waseem 2017). Even after resection, the prognosis is poor, with reported three- and five-year survival rates after resection for perihilar cholangiocarcinoma (pCCA) of around 45% and 30% (Cillo 2019). In unresectable pCCA, common treatment options included chemotherapy with gemcitabine and cisplatinum, and transarterial chemoembolization (TACE).
 This article is sponsored by
This article is sponsored by 







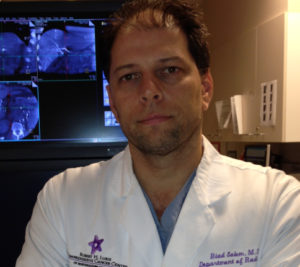

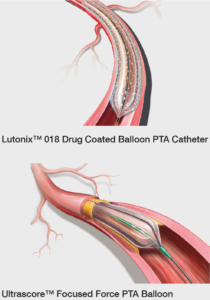 Subsequent diagnostic angiography confirmed the long SFA occlusion with diminished contrast flow below the knee and into the foot. For recanalisation of the long SFA occlusion, a crossover approach from the left groin was performed using the new Halo One™ Thin-Walled Guiding Sheath (BD) 70cm, 5 French. This sheath provides a 1 French wall thickness, which reduces the size of the arteriotomy compared to standard sheaths of the same French size without sacrificing inner diameter. The flush occlusion of the SFA (Figure 3) was penetrated with a 0.018” Glidewire Advantage (Terumo Interventional Systems). It was easy to achieve distal re-entry into the true lumen. Next, a two-minute lesion preparation was performed with an Ultrascore™ Focused Force PTA Balloon 5x150mm 5 French with repetitive inflation to 8atm over the whole length of the target lesion. This scoring balloon is designed to longitudinally fracture plaque at a lower inflation pressure. Compared to a standard balloon angioplasty, the Ultrascore™ Focused Force PTA Balloon provides approximately 24 times more force where the wire contracts the lesion. This lesion preparation was then followed by two-minute drug-coated balloon (DCB) angioplasty (Lutonix™ 018 Drug Coated Balloon PTA Catheter 5x220mm and 5x120mm; Figure 4). Subsequent angiographic analysis ruled out a persistent dissection or significant recoil.
Subsequent diagnostic angiography confirmed the long SFA occlusion with diminished contrast flow below the knee and into the foot. For recanalisation of the long SFA occlusion, a crossover approach from the left groin was performed using the new Halo One™ Thin-Walled Guiding Sheath (BD) 70cm, 5 French. This sheath provides a 1 French wall thickness, which reduces the size of the arteriotomy compared to standard sheaths of the same French size without sacrificing inner diameter. The flush occlusion of the SFA (Figure 3) was penetrated with a 0.018” Glidewire Advantage (Terumo Interventional Systems). It was easy to achieve distal re-entry into the true lumen. Next, a two-minute lesion preparation was performed with an Ultrascore™ Focused Force PTA Balloon 5x150mm 5 French with repetitive inflation to 8atm over the whole length of the target lesion. This scoring balloon is designed to longitudinally fracture plaque at a lower inflation pressure. Compared to a standard balloon angioplasty, the Ultrascore™ Focused Force PTA Balloon provides approximately 24 times more force where the wire contracts the lesion. This lesion preparation was then followed by two-minute drug-coated balloon (DCB) angioplasty (Lutonix™ 018 Drug Coated Balloon PTA Catheter 5x220mm and 5x120mm; Figure 4). Subsequent angiographic analysis ruled out a persistent dissection or significant recoil.
 © 2020 BD. BD, the BD logo, Bard, Halo One, Ultrascore and Lutonix are the property of Becton, Dickinson and Company. All other trademarks are property of their respective owners. Illustrations by Mike Austin. Copyright © 2020. All Rights Reserved.
© 2020 BD. BD, the BD logo, Bard, Halo One, Ultrascore and Lutonix are the property of Becton, Dickinson and Company. All other trademarks are property of their respective owners. Illustrations by Mike Austin. Copyright © 2020. All Rights Reserved.
 A new study, published online in
A new study, published online in 






 Researchers have found that the AMPREDICT decision support tool (DST) demonstrates “strong usability characteristics and clinical relevance” in amputation level decision making for patients with
Researchers have found that the AMPREDICT decision support tool (DST) demonstrates “strong usability characteristics and clinical relevance” in amputation level decision making for patients with 








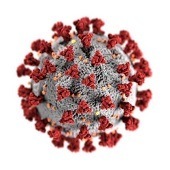 Many individuals with kidney failure have been unable to self-isolate during the COVID-19 pandemic because they require dialysis treatments in clinics several times a week. New research that will appear in an upcoming issue of the
Many individuals with kidney failure have been unable to self-isolate during the COVID-19 pandemic because they require dialysis treatments in clinics several times a week. New research that will appear in an upcoming issue of the 
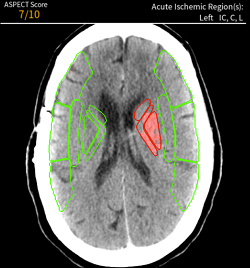









 The European Union (EU) Medical Devices Regulation (MDR) takes effect from today (26 May 2021).
The European Union (EU) Medical Devices Regulation (MDR) takes effect from today (26 May 2021).






 BoneView, an
BoneView, an 






 In a recent study, Victor Demaerel (University Hospitals Leuven, Leuven, Belgium) and colleagues found that tunnelled
In a recent study, Victor Demaerel (University Hospitals Leuven, Leuven, Belgium) and colleagues found that tunnelled 
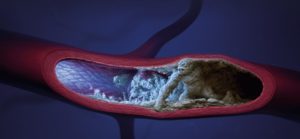 The Auryon atherectomy system (
The Auryon atherectomy system (








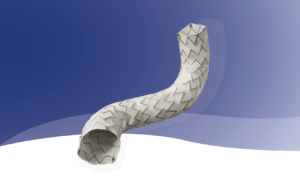






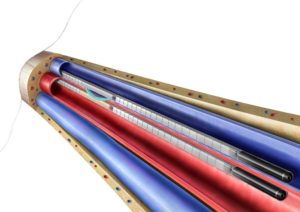






 The results of a recent investigation have revealed no association between infrainguinal bypass tunnelling technique and primary outcomes in patients with limb ischaemia. “Compared to subfascial tunnelling,” write Nallely Saldana-Ruiz (University of Southern California, Los Angeles, USA) and colleagues in the
The results of a recent investigation have revealed no association between infrainguinal bypass tunnelling technique and primary outcomes in patients with limb ischaemia. “Compared to subfascial tunnelling,” write Nallely Saldana-Ruiz (University of Southern California, Los Angeles, USA) and colleagues in the 
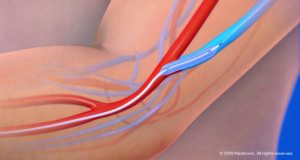






 Siemens Healthineers AG has completed the acquisition of Varian Medical Systems, Inc. The acquisition was
Siemens Healthineers AG has completed the acquisition of Varian Medical Systems, Inc. The acquisition was 









 clearance")





 Many of our top 10 stories of March 2021 highlight new data and ideas presented at the annual scientific meeting of the
Many of our top 10 stories of March 2021 highlight new data and ideas presented at the annual scientific meeting of the 


 From an early understanding in medical school that interventional radiology (IR) was “the future”, Parag Patel has dedicated his career to the discipline, notably as a primary investigator of the
From an early understanding in medical school that interventional radiology (IR) was “the future”, Parag Patel has dedicated his career to the discipline, notably as a primary investigator of the




















 Speaking more broadly of the hardships SIR members and attendees have experienced in the past year due to the ongoing COVID-19 pandemic, and in particular noting how this has affected the SIR meeting, Haskal commented: “On a professional level, 25 years of the Dotter Lecture means sitting in that giant hall, surrounded by thousands of our colleagues, the lights go down, an extraordinary speaker comes out, and something revealing, and visionary, pulls us all together. Instead, we are all separated, watching this on screens, alone.
Speaking more broadly of the hardships SIR members and attendees have experienced in the past year due to the ongoing COVID-19 pandemic, and in particular noting how this has affected the SIR meeting, Haskal commented: “On a professional level, 25 years of the Dotter Lecture means sitting in that giant hall, surrounded by thousands of our colleagues, the lights go down, an extraordinary speaker comes out, and something revealing, and visionary, pulls us all together. Instead, we are all separated, watching this on screens, alone.






 The US Food and Drug Administration (FDA) have granted approval of the TheraSphere Y-90 glass microspheres (
The US Food and Drug Administration (FDA) have granted approval of the TheraSphere Y-90 glass microspheres (




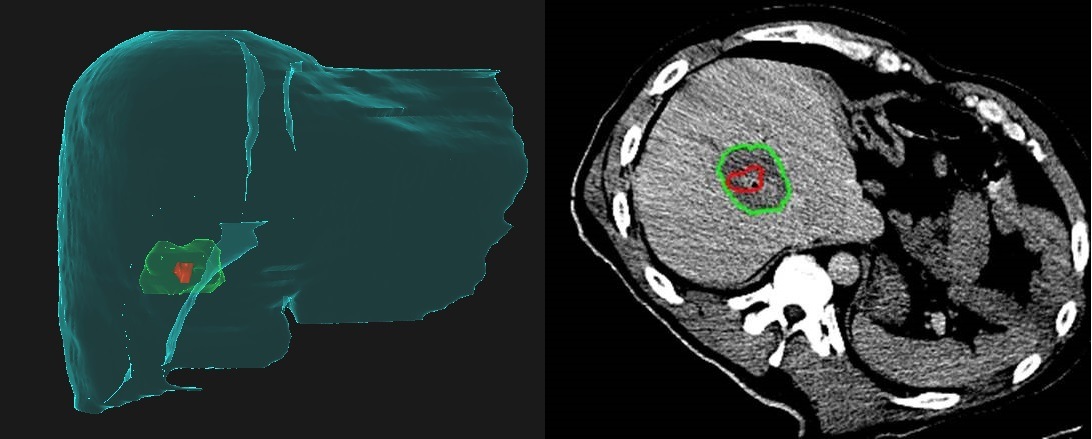
 Cardiovascular Systems has announced that the first patients in the USA have been treated with the Wirion embolic protection system. Wirion is a distal embolic protection filter used to capture thrombus and debris that can be associated with all types of peripheral vascular intervention procedures, including atherectomy.
Cardiovascular Systems has announced that the first patients in the USA have been treated with the Wirion embolic protection system. Wirion is a distal embolic protection filter used to capture thrombus and debris that can be associated with all types of peripheral vascular intervention procedures, including atherectomy.








 Renal artery involvement (RAI) in endovascular aneurysm repair (EVAR) is “highly predictive of the need for postoperative and permanent
Renal artery involvement (RAI) in endovascular aneurysm repair (EVAR) is “highly predictive of the need for postoperative and permanent 

 Former Editor of the Journal of Vascular and Interventional Radiology (JVIR)
Former Editor of the Journal of Vascular and Interventional Radiology (JVIR) 




 Our top 10 stories of February 2021: a success story for interventional oncology as intra-arterial delivery of chemotherapeutic agents is shown to improve survival, and a new trial investigating combined radioembolization and immunotherapy for hepatocellular carcinoma (HCC) treatment launches; the vascular community gears up for paclitaxel discussions at the
Our top 10 stories of February 2021: a success story for interventional oncology as intra-arterial delivery of chemotherapeutic agents is shown to improve survival, and a new trial investigating combined radioembolization and immunotherapy for hepatocellular carcinoma (HCC) treatment launches; the vascular community gears up for paclitaxel discussions at the 






 Contrast developer
Contrast developer 
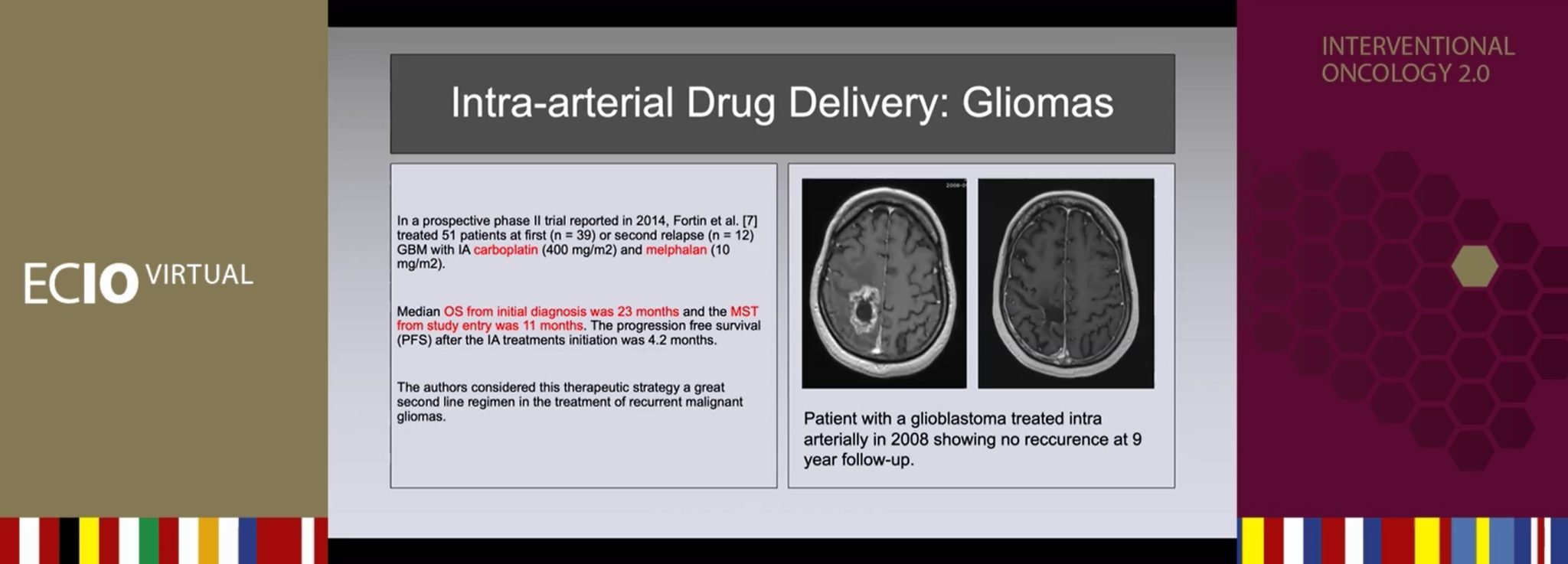






 In a recent meta-analysis, Yang Liu, Huan Lu (Henan Cancer Hospital, Zhengzhou, China), and colleagues found insufficient evidence to prove that
In a recent meta-analysis, Yang Liu, Huan Lu (Henan Cancer Hospital, Zhengzhou, China), and colleagues found insufficient evidence to prove that 



 Terumo Corporation has signed a definitive agreement to acquire all assets of Health Outcomes Sciences, a specialist in predictive analytics and clinical decision support for healthcare organisations.
Terumo Corporation has signed a definitive agreement to acquire all assets of Health Outcomes Sciences, a specialist in predictive analytics and clinical decision support for healthcare organisations.


 In response to the
In response to the 
 Acute kidney injury is a common complication after intervention for
Acute kidney injury is a common complication after intervention for 









")


 Endovascular stimulator company CATHI has launched a campaign promoting CATHIS Smart, its portable system, to medical technology and pharmaceutical companies. The system displays all types of endovascular intervention in any medical field, and is designed for neuroradiology, cardiology, radiology, angiology, and pneumology training.
Endovascular stimulator company CATHI has launched a campaign promoting CATHIS Smart, its portable system, to medical technology and pharmaceutical companies. The system displays all types of endovascular intervention in any medical field, and is designed for neuroradiology, cardiology, radiology, angiology, and pneumology training.







 Biomodex has announced its partnership with two of the top medical centres in France and a health system in the USA to develop Evias Plus, a training solution for treatment of ischaemic stroke.
Biomodex has announced its partnership with two of the top medical centres in France and a health system in the USA to develop Evias Plus, a training solution for treatment of ischaemic stroke.














 Forge Medical has announced the publication of results of an investigator-initiated randomised trial comparing its VasoStat haemostasis device to the TR Band (Terumo Medical) among patients undergoing radial artery coronary and peripheral procedures with planned same-day discharge.
Forge Medical has announced the publication of results of an investigator-initiated randomised trial comparing its VasoStat haemostasis device to the TR Band (Terumo Medical) among patients undergoing radial artery coronary and peripheral procedures with planned same-day discharge.


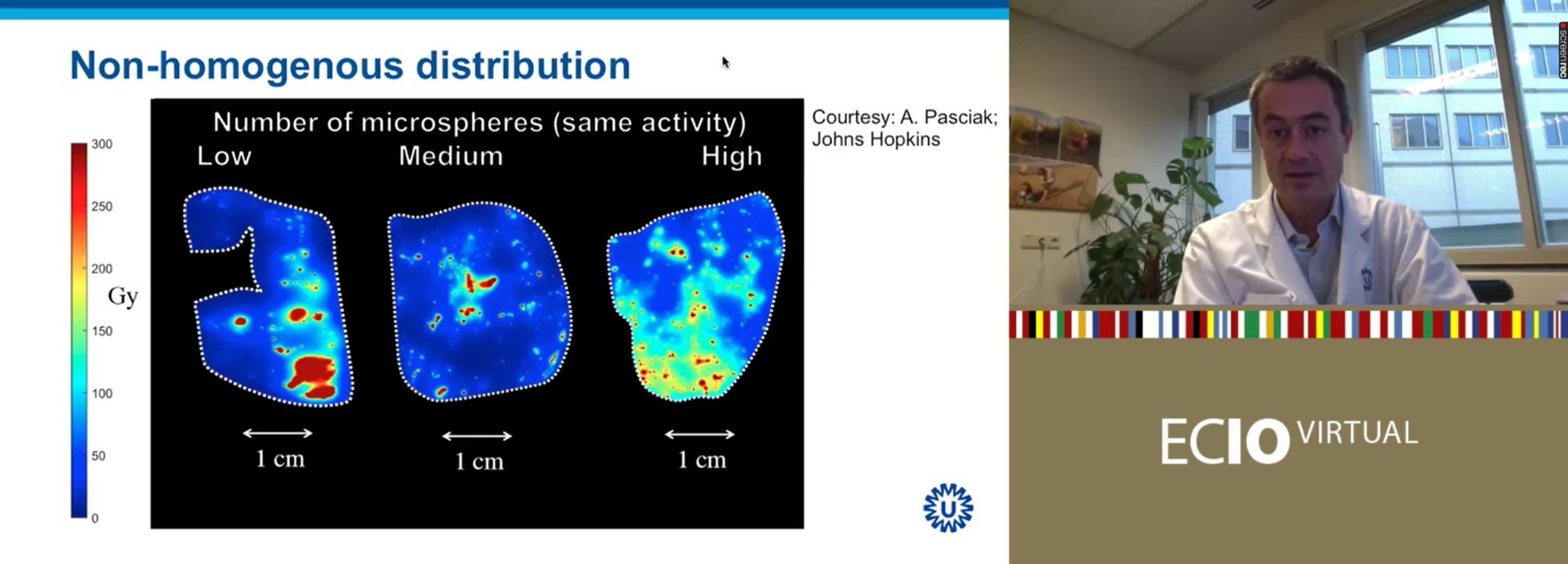


 A key theme among the late-breaking trial data presented at
A key theme among the late-breaking trial data presented at  New data presented for the first time at
New data presented for the first time at 















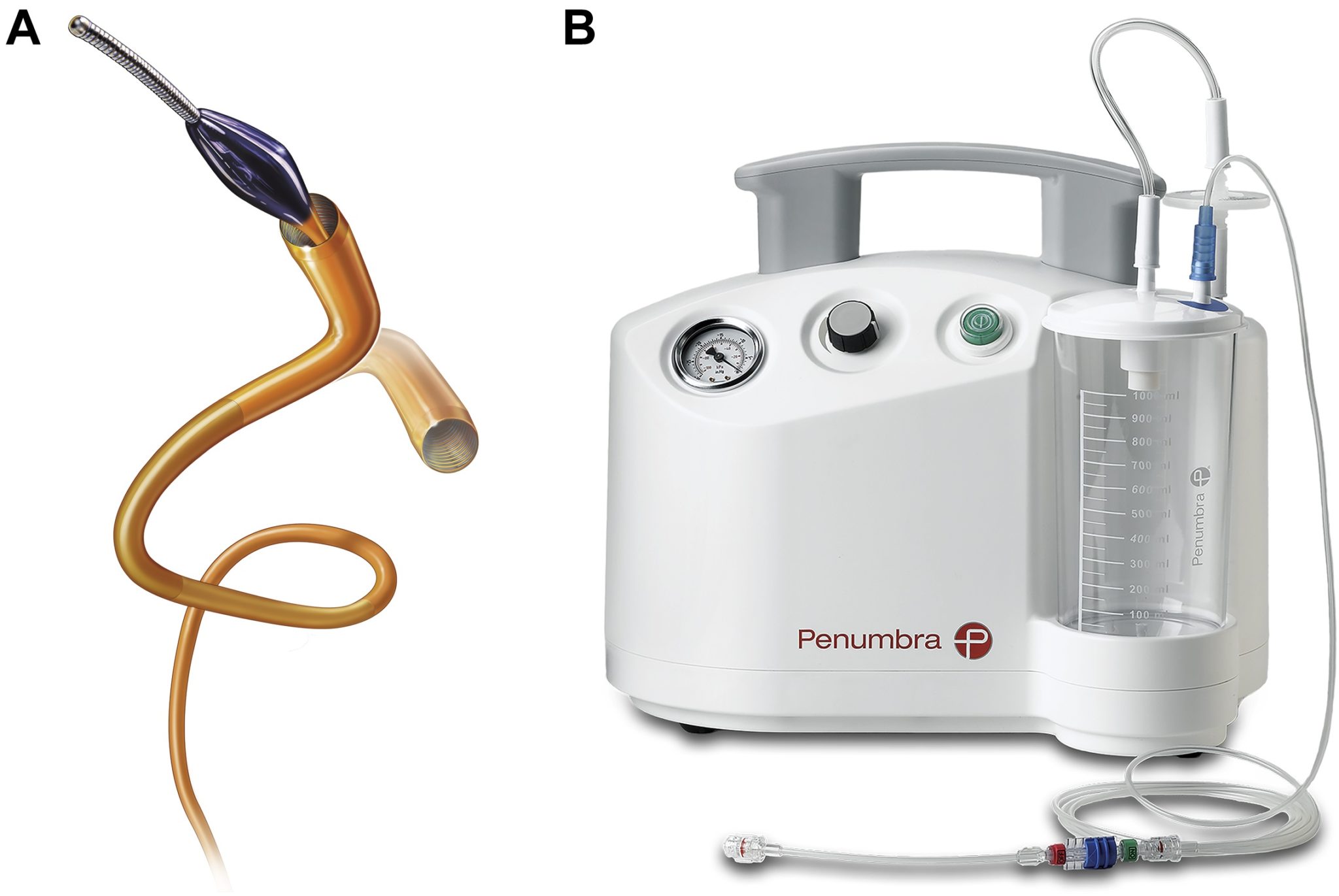

 New single-centre clinical study data published in the
New single-centre clinical study data published in the 





 The UK
The UK 

 There are several covered stents on the market that are used in an off-label setting as bridging stents for fenestrated and branched endovascular aneurysm repair (F/BEVAR). Currently, there is no consensus on when to use what—no gold standard, no proof, no evidence. According to three experts in the field, however, this is about to change. As trials take place and data begin to emerge, Vascular News speaks to Stéphan Haulon (Hôpital Marie Lannelongue, GHPSJ, Paris, France), Eric Verhoeven (Klinikum Nuremburg, Nuremberg Germany), and Tim Resch (Copenhagen Aortic Center, Rigshospitalet, Denmark), who express their views on the past, present, and future of bridging stents in FEVAR and BEVAR.
There are several covered stents on the market that are used in an off-label setting as bridging stents for fenestrated and branched endovascular aneurysm repair (F/BEVAR). Currently, there is no consensus on when to use what—no gold standard, no proof, no evidence. According to three experts in the field, however, this is about to change. As trials take place and data begin to emerge, Vascular News speaks to Stéphan Haulon (Hôpital Marie Lannelongue, GHPSJ, Paris, France), Eric Verhoeven (Klinikum Nuremburg, Nuremberg Germany), and Tim Resch (Copenhagen Aortic Center, Rigshospitalet, Denmark), who express their views on the past, present, and future of bridging stents in FEVAR and BEVAR.

 What is the significance of having the first CVIR Endovascular thematic series be dedicated to paediatric interventional radiology (PIR)?
What is the significance of having the first CVIR Endovascular thematic series be dedicated to paediatric interventional radiology (PIR)?












 The
The 

 Exercise can play an important role in treating
Exercise can play an important role in treating 





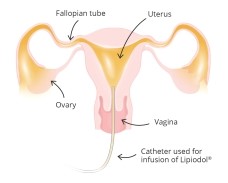















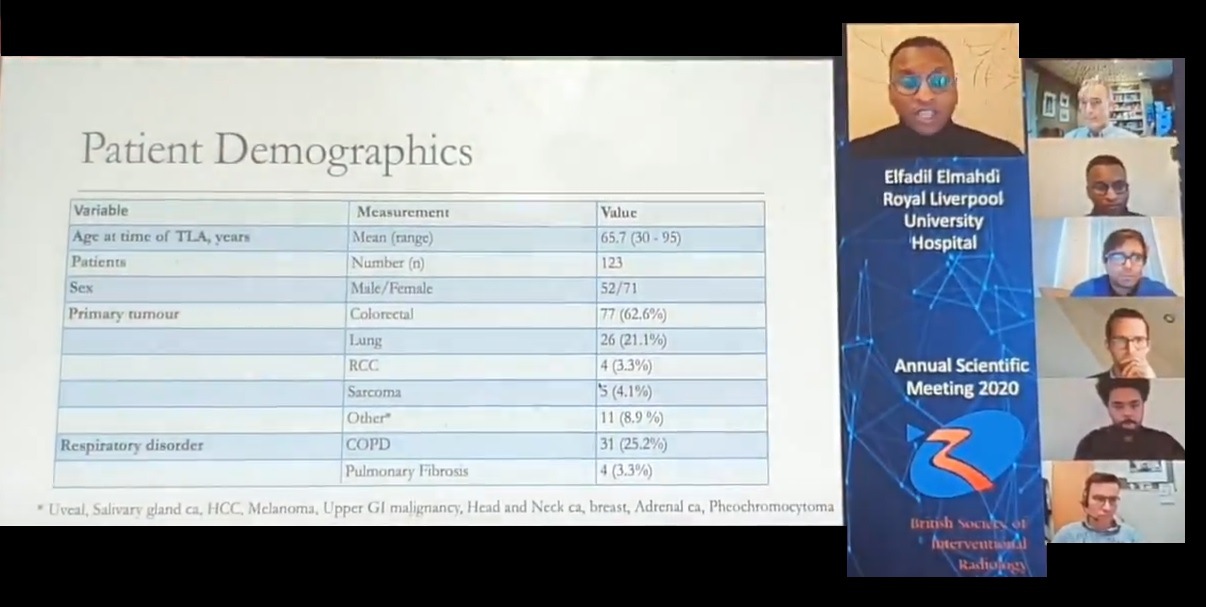




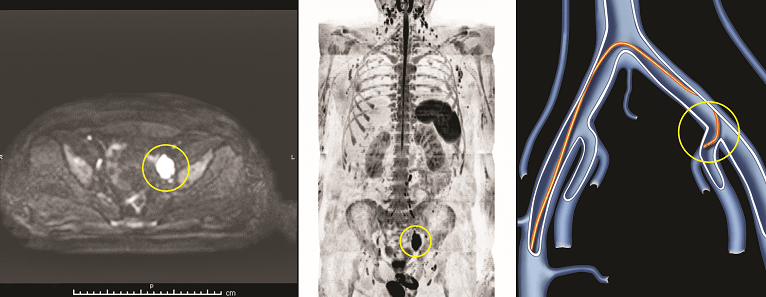 A 46-year-old male with no personal or family history of cancer underwent diffusion-weighted WB-MRI in the context of clinical screening, which revealed enlarged lymph nodes in the left iliac chain. The remaining lymph nodes, spleen, and bone marrow were unremarkable. Given the difficult access for instrumental biopsy, liquid biopsy with selective venous catheterisation was suggested. Only the sample from the left internal iliac vein was positive for the FGFR3 gene mutation, related to lymphoma. Subsequent percutaneous CT-guided biopsy and a video-laparoscopic procedure were both non-diagnostic. Blood tests were normal, while an 18F-FDG PET scan showed positive uptake coinciding with the MRI finding. No progression was seen at follow-up.
A 46-year-old male with no personal or family history of cancer underwent diffusion-weighted WB-MRI in the context of clinical screening, which revealed enlarged lymph nodes in the left iliac chain. The remaining lymph nodes, spleen, and bone marrow were unremarkable. Given the difficult access for instrumental biopsy, liquid biopsy with selective venous catheterisation was suggested. Only the sample from the left internal iliac vein was positive for the FGFR3 gene mutation, related to lymphoma. Subsequent percutaneous CT-guided biopsy and a video-laparoscopic procedure were both non-diagnostic. Blood tests were normal, while an 18F-FDG PET scan showed positive uptake coinciding with the MRI finding. No progression was seen at follow-up. A 50-year-old male presented with persistent thrombocytopenia. Liquid biopsy performed as a preliminary test showed BRAF gene mutation in selective venous samples as well as in peripheral blood. This mutation is related to lymphoma in 2.23% of cases. Low-grade lymphoma was confirmed by bone marrow biopsy. Chemotherapy led to the disappearance of the mutation in liquid biopsy samples, whereas a repeat bone marrow biopsy confirmed minimal disease. Diffusion-weighted WB-MRI revealed diffuse discrete lesions in the bone marrow, mainly in the spine and pelvis.
A 50-year-old male presented with persistent thrombocytopenia. Liquid biopsy performed as a preliminary test showed BRAF gene mutation in selective venous samples as well as in peripheral blood. This mutation is related to lymphoma in 2.23% of cases. Low-grade lymphoma was confirmed by bone marrow biopsy. Chemotherapy led to the disappearance of the mutation in liquid biopsy samples, whereas a repeat bone marrow biopsy confirmed minimal disease. Diffusion-weighted WB-MRI revealed diffuse discrete lesions in the bone marrow, mainly in the spine and pelvis. Liquid biopsy was performed in a 77-year-old asymptomatic female with a close family history of ovarian cancer. The peripheral sample was negative, whereas blood obtained from the inferior vena cava showed the PTEN gene mutation. This mutation is related to ovarian cancer in 3.5% of cases. On DWB-MRI, a right supraclavicular lymph node was enlarged with respect to a previous chest CT scan performed for other reasons. Lymph node biopsy was negative for epithelial cells or lymphoproliferative disease. Gynaecologic examination, transvaginal ultrasound, and abdominal CT scan were all negative. In this case, the liquid biopsy result may be the expression of a tumour clone not destined to develop into progressive ovarian cancer. The finding of the mutation in the sample collected from the blood draining the pelvis nonetheless reinforces the ovarian origin of pathological DNA. Follow-up over time is recommended.
Liquid biopsy was performed in a 77-year-old asymptomatic female with a close family history of ovarian cancer. The peripheral sample was negative, whereas blood obtained from the inferior vena cava showed the PTEN gene mutation. This mutation is related to ovarian cancer in 3.5% of cases. On DWB-MRI, a right supraclavicular lymph node was enlarged with respect to a previous chest CT scan performed for other reasons. Lymph node biopsy was negative for epithelial cells or lymphoproliferative disease. Gynaecologic examination, transvaginal ultrasound, and abdominal CT scan were all negative. In this case, the liquid biopsy result may be the expression of a tumour clone not destined to develop into progressive ovarian cancer. The finding of the mutation in the sample collected from the blood draining the pelvis nonetheless reinforces the ovarian origin of pathological DNA. Follow-up over time is recommended.
 The Royal College of Radiologists (RCR) and the British Society of Interventional Radiology (BSIR) have created a
The Royal College of Radiologists (RCR) and the British Society of Interventional Radiology (BSIR) have created a 


 BSIR vice president Phillip Haslam (Freeman Hospital Newcastle, Newcastle upon Tyne, UK) introduced Morgan to congress attendees, recounting his education background: Morgan trained at Bristol University Medical School (Bristol, UK), before heading to Plymouth, UK, for three years of radiology training, and then to St George’s Hospital in London, UK, for a further two years. He next completed a Fellowship at the University of Texas (Austin, USA) under Eric Van Sonneberg, specialising in hepatobiliary and vascular interventions. Returning to the UK, Morgan was a Fellow under Andreas ‘Andy’ Adams (Guys’ and St Thomas’ NHS Foundation Trust, London, UK) for 18 months, before becoming a consultant at St Mary’s Hospital, London, UK, between 1996 and 1999. He ultimately returned to St George’s Hospital, where he remains as a consultant interventional radiologist and the clinical director for Diagnostics.
BSIR vice president Phillip Haslam (Freeman Hospital Newcastle, Newcastle upon Tyne, UK) introduced Morgan to congress attendees, recounting his education background: Morgan trained at Bristol University Medical School (Bristol, UK), before heading to Plymouth, UK, for three years of radiology training, and then to St George’s Hospital in London, UK, for a further two years. He next completed a Fellowship at the University of Texas (Austin, USA) under Eric Van Sonneberg, specialising in hepatobiliary and vascular interventions. Returning to the UK, Morgan was a Fellow under Andreas ‘Andy’ Adams (Guys’ and St Thomas’ NHS Foundation Trust, London, UK) for 18 months, before becoming a consultant at St Mary’s Hospital, London, UK, between 1996 and 1999. He ultimately returned to St George’s Hospital, where he remains as a consultant interventional radiologist and the clinical director for Diagnostics.



 Boston Scientific has announced that it has entered into a definitive agreement with Stark International and SERB SAS, affiliates of the European specialty pharmaceutical group SERB, to sell its BTG Specialty Pharmaceuticals business for US$800 million in cash.
Boston Scientific has announced that it has entered into a definitive agreement with Stark International and SERB SAS, affiliates of the European specialty pharmaceutical group SERB, to sell its BTG Specialty Pharmaceuticals business for US$800 million in cash.
 The Society of Interventional Radiology (SIR) and the American Medical Association (AMA) have sent a letter to the Centers for Medicare and Medicaid Services (CMS) urging them to implement and pay for Current Procedural Terminology (CPT) code 99072 to compensate practices for the additional supplies and new staff activities required to provide safe patient care during the
The Society of Interventional Radiology (SIR) and the American Medical Association (AMA) have sent a letter to the Centers for Medicare and Medicaid Services (CMS) urging them to implement and pay for Current Procedural Terminology (CPT) code 99072 to compensate practices for the additional supplies and new staff activities required to provide safe patient care during the 

 In their recent systematic review and meta-analysis, Venkata Sai Jasty (University of Arizona, Tuscon, USA) and colleagues found that the risk of ischaemic steal syndrome, “one of the most feared complications in vascular access,” and patency rate are comparable for both tapered and non-tapered prosthetic arteriovenous grafts (AVGs) in dialysis access.
In their recent systematic review and meta-analysis, Venkata Sai Jasty (University of Arizona, Tuscon, USA) and colleagues found that the risk of ischaemic steal syndrome, “one of the most feared complications in vascular access,” and patency rate are comparable for both tapered and non-tapered prosthetic arteriovenous grafts (AVGs) in dialysis access.













 “2020 has changed so much. But the need for IO education remains the same.” Cued to music and set against a backdrop of footage from previous conferences, lone individuals on laptops, and graphics of the now instantly-recognisable SARS-CoV-19 virus, this is the text that appears on the promotional video for the
“2020 has changed so much. But the need for IO education remains the same.” Cued to music and set against a backdrop of footage from previous conferences, lone individuals on laptops, and graphics of the now instantly-recognisable SARS-CoV-19 virus, this is the text that appears on the promotional video for the 








 The first person to perform a
The first person to perform a 


















































 The Surfacer Inside-Out access catheter system device (
The Surfacer Inside-Out access catheter system device (



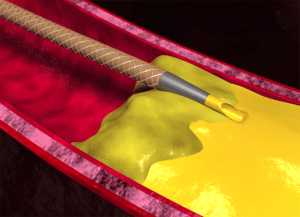





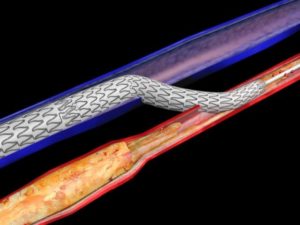












 Concept Medical has announced the enrolment of the first patient in the FUTURE SFA (Randomised controlled trial of first sirolimus coated balloon versus standard balloon angioplasty in the Treatment of superficial femoral artery and popliteal artery disease) study.
Concept Medical has announced the enrolment of the first patient in the FUTURE SFA (Randomised controlled trial of first sirolimus coated balloon versus standard balloon angioplasty in the Treatment of superficial femoral artery and popliteal artery disease) study.























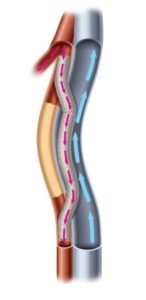





 The results of a randomised controlled trial—the Shunt simulation study—show that a new patient-specific computation model accurately calculated postoperative access flow. As flow is related to maturation, the authors argue that this model may potentially improve arteriovenous fistula (AVF) maturation rates.
The results of a randomised controlled trial—the Shunt simulation study—show that a new patient-specific computation model accurately calculated postoperative access flow. As flow is related to maturation, the authors argue that this model may potentially improve arteriovenous fistula (AVF) maturation rates.
 The inaugural
The inaugural 


 Concept Medical has announced the enrolment of the first patient in the FUTURE BTK (Randomised controlled trial of first sirolimus coated balloon versus standard balloon angioplasty in the treatment of below-the-knee artery disease) trial. The index patient was successfully enrolled on 26 August 2020 in Singapore.
Concept Medical has announced the enrolment of the first patient in the FUTURE BTK (Randomised controlled trial of first sirolimus coated balloon versus standard balloon angioplasty in the treatment of below-the-knee artery disease) trial. The index patient was successfully enrolled on 26 August 2020 in Singapore.
 Royal Philips today announced that it has signed an agreement to acquire Intact Vascular. According to a press release, Intact Vascular will enhance Philips’ image-guided therapy portfolio, combining Philips’ interventional imaging platform and diagnostic and therapeutic devices with Intact Vascular’s unique, specialised implantable device to optimise the treatment of patients with peripheral arterial disease (PAD).
Royal Philips today announced that it has signed an agreement to acquire Intact Vascular. According to a press release, Intact Vascular will enhance Philips’ image-guided therapy portfolio, combining Philips’ interventional imaging platform and diagnostic and therapeutic devices with Intact Vascular’s unique, specialised implantable device to optimise the treatment of patients with peripheral arterial disease (PAD).

 As of August 2020, corresponding authors from more than 750 German universities and research institutions are able to publish in
As of August 2020, corresponding authors from more than 750 German universities and research institutions are able to publish in 

 The
The 






 A new study has found several racial disparities after mechanical thrombectomy for stroke with respect to post-procedure management and outcomes. Vineeth Thirunavu of Northwestern University Feinberg School of Medicine, Chicago, USA, presented the data at the Society of NeuroInterventional Surgery’s (SNIS) 17th Annual Meeting (4–7 August), which detailed key findings from the NVQI-QOD registry.
A new study has found several racial disparities after mechanical thrombectomy for stroke with respect to post-procedure management and outcomes. Vineeth Thirunavu of Northwestern University Feinberg School of Medicine, Chicago, USA, presented the data at the Society of NeuroInterventional Surgery’s (SNIS) 17th Annual Meeting (4–7 August), which detailed key findings from the NVQI-QOD registry. 







 A recent study, published
A recent study, published 








 A new system designed to deliver Yttrium-90 (Y-90) resin microspheres during targeted liver cancer therapies, SIROS (
A new system designed to deliver Yttrium-90 (Y-90) resin microspheres during targeted liver cancer therapies, SIROS (
 “Decreases in caseload and widespread cancellation of conferences have had significant impact on diagnostic and interventional radiology (DR/IR) training during
“Decreases in caseload and widespread cancellation of conferences have had significant impact on diagnostic and interventional radiology (DR/IR) training during 
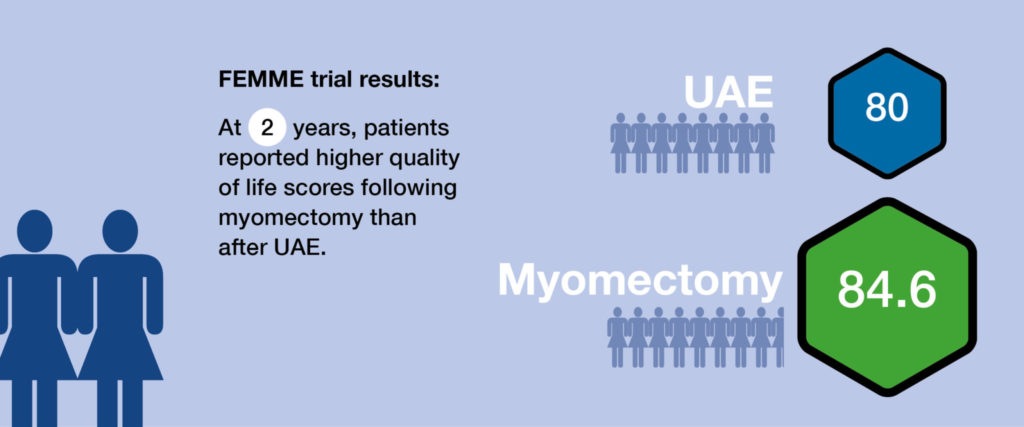 Results from a multicentre, randomised controlled trial—
Results from a multicentre, randomised controlled trial—
 Instrumental to the development of interventional oncology in the USA and globally, William (Bill) Rilling tracks how the discipline has grown over the course of his career from a niche area of medicine for the most challenging cases to a subspecialty with its own society dedicated to revolutionising cancer care.
Instrumental to the development of interventional oncology in the USA and globally, William (Bill) Rilling tracks how the discipline has grown over the course of his career from a niche area of medicine for the most challenging cases to a subspecialty with its own society dedicated to revolutionising cancer care.










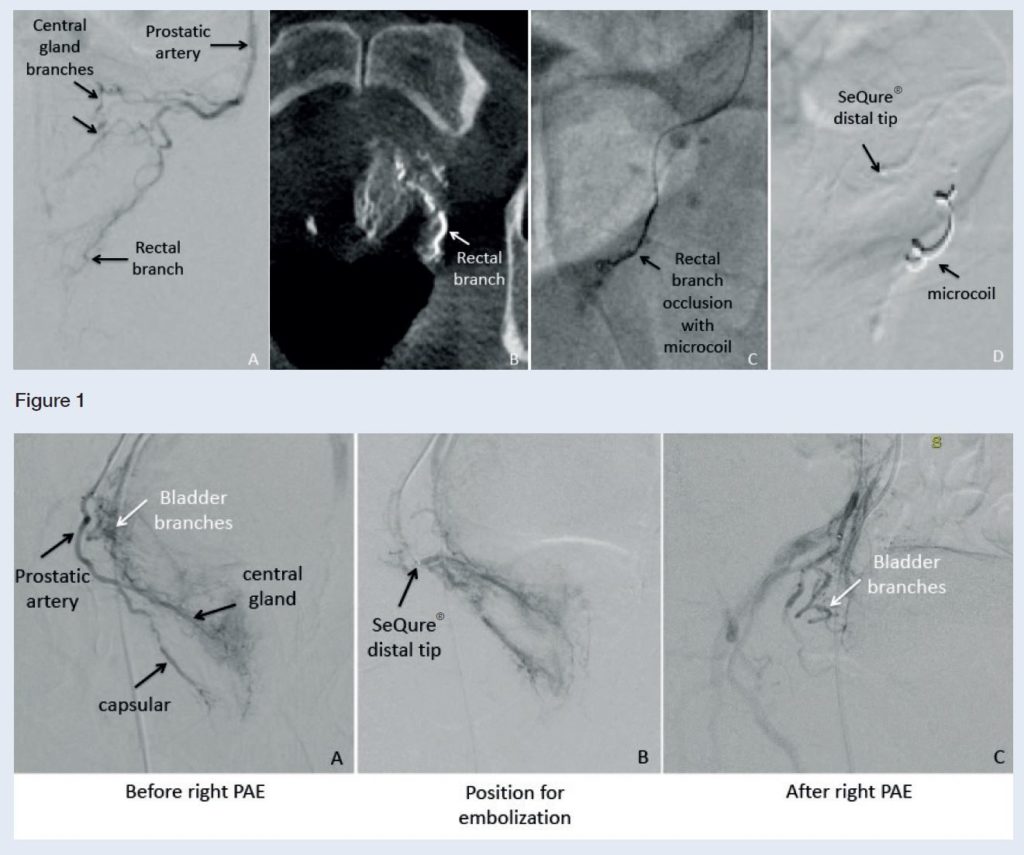 This advertorial is sponsored by Guerbet.
This advertorial is sponsored by Guerbet. 


 Ahead of the first ever virtual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Thomas Kröncke, chairperson of the CIRSE 2020 scientific programme committee, speaks to Interventional News about the programme highlights, and the logistics of how an online congress will function. He encourages readers to participate, and notes that, for those who
Ahead of the first ever virtual meeting of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), Thomas Kröncke, chairperson of the CIRSE 2020 scientific programme committee, speaks to Interventional News about the programme highlights, and the logistics of how an online congress will function. He encourages readers to participate, and notes that, for those who 




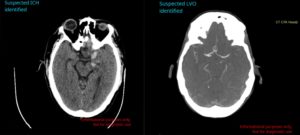





 Barts Health NHS Trust has performed a UK-first operation outside of trial setting that could reduce mortality and risks of infection in patients with dialysis.
Barts Health NHS Trust has performed a UK-first operation outside of trial setting that could reduce mortality and risks of infection in patients with dialysis. 
 The
The 
 The
The 





 Royal Philips recently announced the four-year results from the ILLUMENATE European randomised controlled trial (EU RCT). The Stellarex drug-coated balloon (DCB) cohort demonstrated similar all-cause mortality compared with the control arm through four years. This analysis included missing data found post hoc to achieve a follow-up compliance of 93.9%, increasing the robustness of the statistical analysis.
Royal Philips recently announced the four-year results from the ILLUMENATE European randomised controlled trial (EU RCT). The Stellarex drug-coated balloon (DCB) cohort demonstrated similar all-cause mortality compared with the control arm through four years. This analysis included missing data found post hoc to achieve a follow-up compliance of 93.9%, increasing the robustness of the statistical analysis.







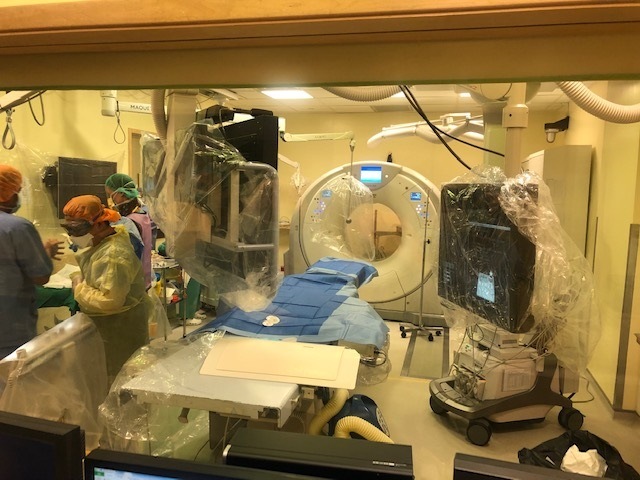
 In your opinion, how will the COVID-19 pandemic impact the future of healthcare?
In your opinion, how will the COVID-19 pandemic impact the future of healthcare?


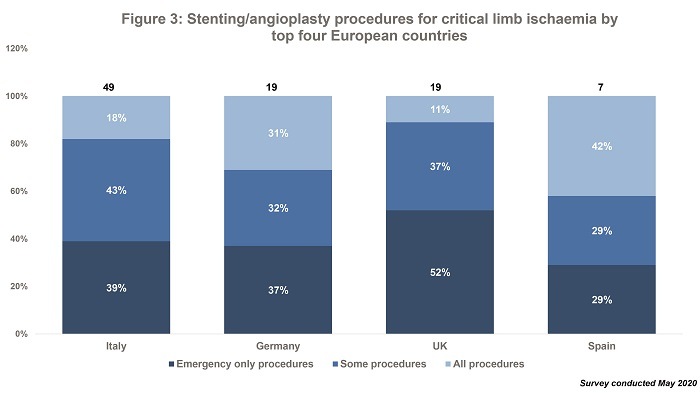








 The European Trainee Forum (ETF) Subcommittee of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has published a report on the status of vascular and interventional radiology training in Europe.
The European Trainee Forum (ETF) Subcommittee of the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has published a report on the status of vascular and interventional radiology training in Europe. 



 clearance")




















 In the first talk, Jean-Paul de Vries, (Groningen, The Netherlands) reported the key findings from a systematic review (published in the
In the first talk, Jean-Paul de Vries, (Groningen, The Netherlands) reported the key findings from a systematic review (published in the 








 The discussion next turned to the use of cyanoacrylate glue. Delivering his Podium 1
The discussion next turned to the use of cyanoacrylate glue. Delivering his Podium 1
 Transit Scientific has received US Food and Drug Administration (FDA) clearance for the XO Score percutaneous transluminal angioplasty (PTA) scoring sheath platform for use in iliac, ilio-femoral, popliteal, infra-popliteal, and renal arterial plus synthetic and/or native arteriovenous hemodialysis fistula.
Transit Scientific has received US Food and Drug Administration (FDA) clearance for the XO Score percutaneous transluminal angioplasty (PTA) scoring sheath platform for use in iliac, ilio-femoral, popliteal, infra-popliteal, and renal arterial plus synthetic and/or native arteriovenous hemodialysis fistula.


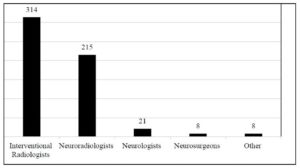










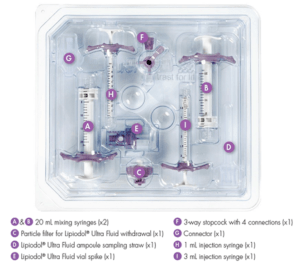 Guerbet has announced the registration of
Guerbet has announced the registration of 
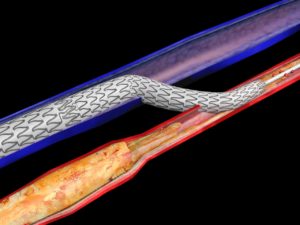

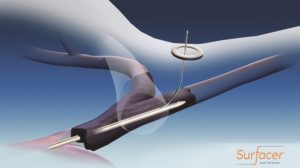

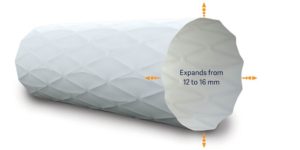



















 In a recent
In a recent 



 Workforce shortages in clinical radiology are increasing year-on-year, resulting in delayed diagnoses and lower-quality patient care, according to the latest
Workforce shortages in clinical radiology are increasing year-on-year, resulting in delayed diagnoses and lower-quality patient care, according to the latest 






 Inspired by his father, an interventional radiologist who used to shape catheters over the stove at home,
Inspired by his father, an interventional radiologist who used to shape catheters over the stove at home, 
 “Europe, including the European Union (EU) and the leaders of its nation states, needs to prepare better for future pandemics. I think we must develop a Europe-wide contingency plan providing clear guidance on effective measures,” says
“Europe, including the European Union (EU) and the leaders of its nation states, needs to prepare better for future pandemics. I think we must develop a Europe-wide contingency plan providing clear guidance on effective measures,” says 
 Medical oncologists Filippo Pietrantonio and Marina Chiara (both Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy) have launched a social media campaign called
Medical oncologists Filippo Pietrantonio and Marina Chiara (both Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy) have launched a social media campaign called 





 The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has made seven of ts Academy courses
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) has made seven of ts Academy courses 
 The Radiological Society of North America (
The Radiological Society of North America (




 This advertorial is sponsored by TriSalus Life Sciences.
This advertorial is sponsored by TriSalus Life Sciences.
 In a
In a 
 The European Society of Radiology (ESR) has created a playlist on their YouTube channel dedicated to events and news related to the
The European Society of Radiology (ESR) has created a playlist on their YouTube channel dedicated to events and news related to the 


 “Acute ischaemic stroke patients are a high-risk patient cohort,” the authors write, adding that patients with a history of ischaemic stroke and/or its risk factors are “particularly at risk” for the severe form of the coronavirus. The recommendations also acknowledge evidence that the disease can cause neurological signs, which have been reported in the brains of humans and in animal models.
“Acute ischaemic stroke patients are a high-risk patient cohort,” the authors write, adding that patients with a history of ischaemic stroke and/or its risk factors are “particularly at risk” for the severe form of the coronavirus. The recommendations also acknowledge evidence that the disease can cause neurological signs, which have been reported in the brains of humans and in animal models.


 The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) have jointly published a checklist for interventional radiologists to use when preparing their department for COVID-19 patients.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Asia Pacific Society of Cardiovascular and Interventional Radiology (APSCVIR) have jointly published a checklist for interventional radiologists to use when preparing their department for COVID-19 patients.


 This piece is one in a series of articles covering the
This piece is one in a series of articles covering the 


 This is the first in a series of articles covering the
This is the first in a series of articles covering the 
 The Imperial College Network of Excellence in Vascular Science at Imperial College London (UK) is to run a
The Imperial College Network of Excellence in Vascular Science at Imperial College London (UK) is to run a 



 Patients were randomly assigned to receive either renal denervation or a sham procedure in which a catheter was inserted and only an angiography was performed. A total of 166 patients were assigned to renal denervation and 165 to the sham procedure.
Patients were randomly assigned to receive either renal denervation or a sham procedure in which a catheter was inserted and only an angiography was performed. A total of 166 patients were assigned to renal denervation and 165 to the sham procedure.



 Interventional radiologists from Singapore have shared their strategies for the preparation of IR services to cope with COVID-19 patients, emphasising the need for clear planning and cross-departmental working to tackle the spread of the virus.
Interventional radiologists from Singapore have shared their strategies for the preparation of IR services to cope with COVID-19 patients, emphasising the need for clear planning and cross-departmental working to tackle the spread of the virus.


 The 2020 Charing Cross (CX) Symposium that was due to take place next month in London, UK, has been cancelled due to COVID-19.
The 2020 Charing Cross (CX) Symposium that was due to take place next month in London, UK, has been cancelled due to COVID-19. 












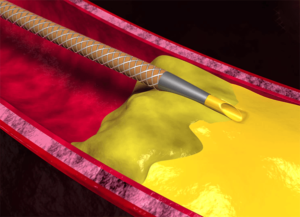



 The US
The US 




 Cerus Endovascular receives FDA approval for its first microcatheter. The 021 microcatheter will be offered with three different distal configurations, and commercial sales are expected to begin during the second quarter of 2020.
Cerus Endovascular receives FDA approval for its first microcatheter. The 021 microcatheter will be offered with three different distal configurations, and commercial sales are expected to begin during the second quarter of 2020.









