
Hester Scheffer (Amsterdam, The Netherlands) advocates for the use of combined irreversible electroporation (IRE) and other immune stimulatory therapies to achieve greater overall survival in patients with pancreatic cancer. At the 2019 European Meeting on Interventional Oncology (ECIO), Scheffer presented the preliminary results of the first clinical proof of evidence study for an IRE-induced T cell specific immune response in pancreatic cancer in humans.
The presented work was a small side study of the recently completed PANFIRE trial, with the investigators conducting immune monitoring on 10 patients. Scheffer told the ECIO audience that this meant this “pilot study was therefore not powered for statistical significance”, and that they had carried it out for “exploratory purposes”. However, she said that the results were “interesting” nonetheless, and illuminating for the direction of future research.
The problem: Pancreatic cancer can “escape the immune system”
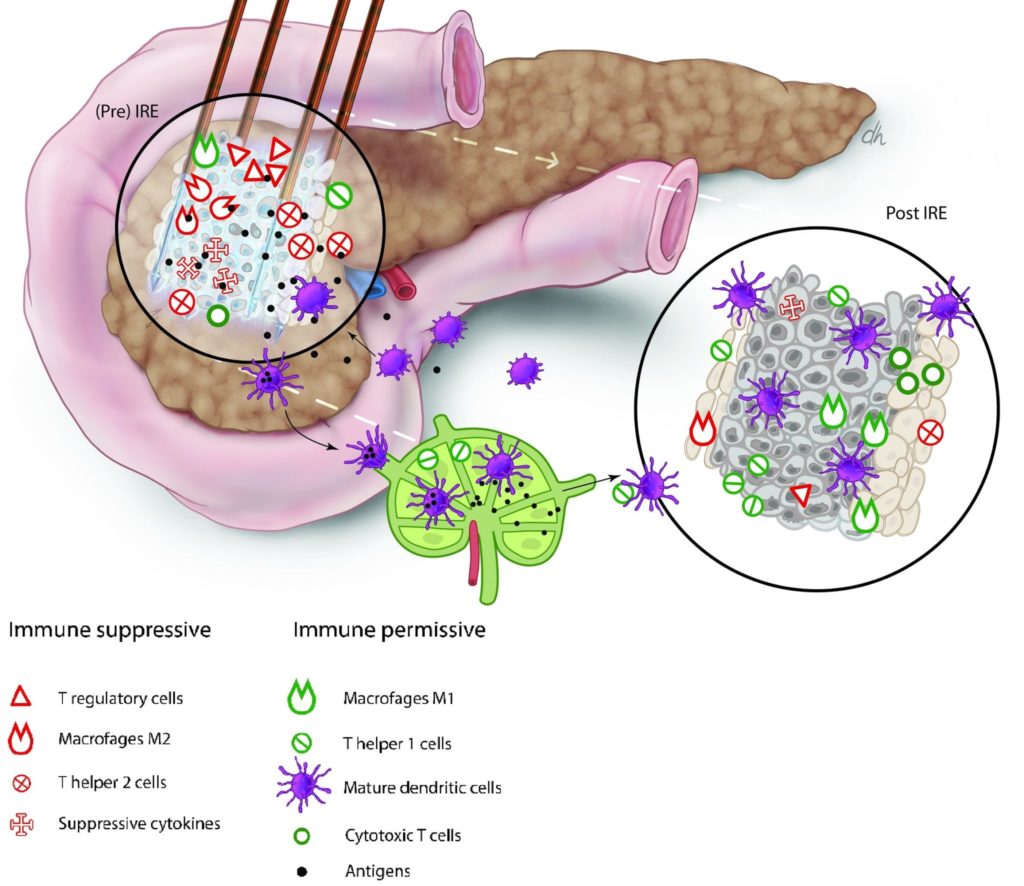
Pancreatic cancer is particularly aggressive, Scheffer explained, due to its ability to “escape the immune system”. The cancerous tumour is capable of this evasion through two mechanisms: its suppression of the tumour microenvironment, and the rarity of spontaneous apoptosis in pancreatic cancer cells.
Pancreatic cancer suppresses its microenvironment by releasing suppressive cytokines into the surrounding tissue, which upregulate immunosuppressive T cells (regulatory T cells and myeloid-derived suppressor cells [MDSCs]). These, in turn, downregulate effector T cells, which directly effectuate the immune response. The tumour is therefore not recognised by the immune system, and “T cell tolerance against the tumour develops”, Scheffer said.
The second way in which a pancreatic tumour limits the immunogenic potential is due to the low spontaneous apoptosis rate amongst pancreatic cancer cells: when a cell undergoes apoptosis, it breaks up into immunogenic epitopes that are taken up by antigen-presenting cells and transported to the lymph nodes, where a systemic, adaptive anti-tumour immune response can be elicited. This does not occur in pancreatic cancer.
The potential solution: shifting the balance “from immunosuppressive to immunostimulative”
Understanding these molecular machinations, Scheffer stated: “To improve the survival of pancreatic cancer patients, the cytokine balance needs to change from immunosuppressive to immunostimulative”. She and her colleagues hypothesised that IRE may be capable of altering this balance. As IRE reduces the tumour mass, it also leads to a reduction in the secretion of suppressive cytokines, which ultimately results in reduced T cell tolerance. Additionally, the apoptosis induced by the IRE treatment triggers the sequence of events that stimulates the systemic, adaptive, anti-tumour immune response not otherwise witnessed in pancreatic cancer patients. Scheffer added that “hopefully, memory T cells will then induce anti-tumour immunity and delay or maybe even prevent the development of metastases. Through this way, IRE could in fact be a type of in situ tumour immunisation.”
To test this hypothesis, Scheffer and colleagues sampled the venous blood of their patients three times: directly before IRE treatment, again two weeks after IRE treatment to investigate the immediate immune response, and then lastly three months post-IRE treatment, to investigate the durable immune response. White blood cells were isolated immediately after blood sampling and cryopreserved for later analysis. None of the patients in the pilot study had received pre- or post-IRE chemotherapy.
Speaking at the conference, Scheffer explained: “When we had collected the blood of all 10 patients, we broadly performed two different tests. In the first test, we determined the type, frequency and activation status of the circulating immune cells using flowcytometry. We investigated the MDSC and the T-cell subsets, and also activated PD-1 T-cells. But this only told us the number and the activation status of the circulating immune cells; it does not say anything about whether they were acting against pancreatic tumour specifically.”
To test the targeted immune response to the cancerous cells, the team performed tumour specific T-cell monitoring. They took the Wilms’ tumour 1 (WT1) epitope, which is expressed exclusively on the cell membrane of the pancreatic tumour, and coated it with an interferon-gamma (IFN-у) antibody so it could be detected. The investigators then combined the white blood cells collected from the patients with the Wilms’ tumour 1 epitope, and counted how many interferon-positive white blood cells—and thus Wilms’ tumour 1 positive white blood cells—there were. These represented tumour-specific T-cells, so tumour cells that were aggressive towards the pancreatic tumour.
The Dutch researchers reported a significant and a near-significant decrease in the immunosuppressive cells (the regulatory T cells [p=0.03] and the MDSCs [p=0.09]) two weeks after IRE. Scheffer said: “We also found a near-significant increase in the immune-effector cells [p=0.08]. So, the observed reduced immune suppression did seem to allow for the effector T cells to develop, just as we hypothesised.
“We also saw a significant de novo activation of PD-1 cytotoxic [p=0.04] and helper T-cells [p=0.01] two weeks after IRE, whereas the expression of the other immune checkpoints remained low and unchanged.”
Turning their attention next to the tumour-specific T cell monitoring, the investigators found an immune response against the Wilms’ tumour antigen, and thus against the pancreatic tumour, in five out of the 10 patients. Scheffer elaborated: “This Wilms’ tumour 1 response correlated with the reduced immune suppression. Most interestingly, the patients who had a positive, tumour-specific T-cell response had a higher median overall survival than patients who did not have this Wilms’ tumour 1 response [p=0.055].”
Scheffer summarised: “We found a temporary alleviation of the tumour-induced immune suppression, which created a window for anti-tumour T cell activation that was in turn associated with better overall median survival. These results advocate for the combination of IRE with other immune stimulatory therapies to further enhance this effect and achieve an even better overall survival.”
Future work, Scheffer said, will look at the possibilities of further stimulating the immune response through a combination of IRE and immune modulatory therapies: this is the remit of the PANFIRE III trial. Ideas included performing a PD-1 blockade to additionally suppress regulatory T cells (as the investigators reported an upregulation of the PD-1 antigen), and the intratumoural delivery of Toll-like receptor ligands.
According to Scheffer, the PANFIRE III trial will treat patients with oligometastatic pancreatic carcinoma—patients with between one and five liver metastases that are stable on four regimens of folforinox. “The patients will be randomised in three groups of six patients, and they will all receive PD-1 blockade, because we found upregulation of PD-1, so we think that is a very good thing to add,” Scheffer outlined. One arm will receive PD-1 blockade and IRE; one arm will receive PD-1 blockade and an intratumoural injection of Toll-like receptor ligand, and one arm will receive all three—PD-1 blockade, IRE, and the Toll-like receptor ligand. The PANFIRE III trial has just received full funding, and will begin recruiting patients in the coming months.
Hugo Rio Tinto (Lisbon, Portugal), one of the panel moderators, said that this was “an interesting result”, commenting: “Maybe in the future we can regulate this immune response to a greater degree. Though I think the most important thing is patient selection”, something Scheffer agreed with.

Rio Tinto also asked about the plausibility of predicting which patients would most benefit from this combined treatment, querying if Scheffer and colleagues will study factors that will predict patient outcomes, such as immune markers: “There are some immune types that are responding better to this therapy than others,” he said, “How will you identify these [possible] predictive factors?”. As half the patients showed the Wilms’ tumour 1 response, and half did not, Scheffer said at ECIO that this was something to consider. Speaking to Interventional News after the conference, Scheffer and Martijn Meijerink (Amsterdam, The Netherlands), panel moderator and senior author of the PANFIRE trial results, disclosed: “In our future study, we aim to perform NanoString sequencing and proteome analysis on pancreatic tissue pre IRE treatment. This will hopefully provide us with information about more than 700 oncogenes and just as many proteins and could possibly bridge the gap between cancer genome information, the observed cancer phenotype and the patient response to combined treatment with IRE and immunotherapy.”
Fielding a question from the audience regarding whether or not the investigators were targeting the primary pancreatic tumour itself or the metastases, “which are more easy to puncture”, Scheffer said: “We are lowering the pulse protocol because we want to induce apoptosis as we want the antigen release, but we do not need to destroy the tumour completely, because obviously there are also metastases, so we will never achieve complete elimination. Hopefully we will not find any complications with this less invasive protocol. We chose the primary tumour because of the lymph drainage directly around it; the antigens have to be taken to the lymph nodes. For now, we think that will give the highest chance of a response, and if we only treat one metastasis, there might be fewer lymph nodes that can pick up the antigens. It is just a hypothesis, but we had to make a choice.”








