

Within the context of liquid biopsy’s rising clinical application, Bruno Damascelli and Vladimira Tichà propose a means of improving this analytical technique through selective venous sampling. They argue that by drawing blood from a site nearer to the area affected by the malignancy, the sensitivity and specificity of the diagnosis would be enhanced. They present two illustrative cases that, according to the authors, “reinforce the interest for liquid biopsy”, a procedure they describe as “an important tool for the molecular definition of cancer and for its precise treatment”.
Incidence rates for malignant melanoma are currently rising more than those of any other malignancy. Predisposing factors are not fully known, except for the phenotype with fair complexion and light hair and eyes. A family history of melanoma accounts for 10% of all cases. Diagnosis is difficult because melanoma presents as a pigmented lesion, usually in a person with several cutaneous nevi. Electronic dermatoscopy has improved melanoma diagnosis, but excision of the skin lesion is normally conservative because staging is post-surgical unless there are distant lymph node metastases. Clinical-pathological staging is based on excisional biopsy, wide local excision, and sentinel lymph node biopsy. The American Joint Committee on Cancer (AJCC) melanoma committee strongly recommends sentinel lymph node biopsy because of the great difference in five-year survival rates in patients with negative lymph nodes. The sentinel lymph node must be removed for lesions with a Breslow thickness of 0 or >1mm, and those with spontaneous ulceration or with a mitotic rate of 1/mm2. This means planning at least three separate procedures: (1) excisional biopsy, (2) wide excision, and (3) selective lymphadenectomy (SLN).
It is now known that the DNA released by tumour cells (ctDNA) can be detected in blood even in an early stage of disease. This analytical technique, known as liquid biopsy, is increasingly finding clinical application. The limitation of liquid biopsy lies in the minimal amount of tumour DNA, which is masked by the prevalent amount of cell-free DNA (cfDNA) produced by the body’s normal tissue turnover. One or more mutations related to a certain tumour confirms the diagnosis with some certainty, as is the case when circulating tumour cells (CTCs) are found in blood samples. If blood is sampled in proximity to the venous drainage of the area affected by the malignancy, it is possible that a larger amount of tumour DNA will be obtained, with an increase in the sensitivity and therefore of the specificity of the liquid biopsy. Two cases presented here by way of example suggest that selective venous sampling should be considered in early-stage melanoma.
Case one
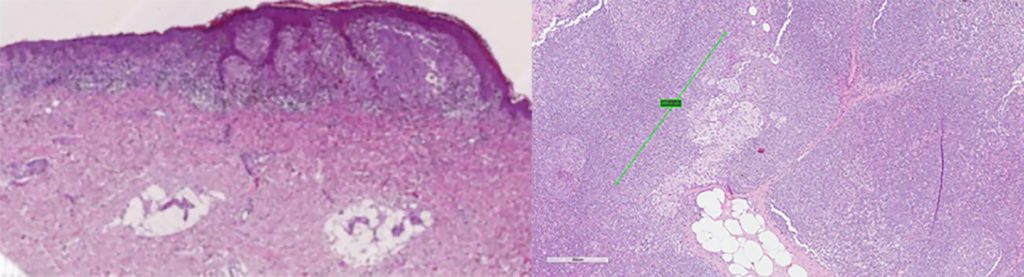
Figure 2 (Right): Intraparenchymal metastasis, diameter 1mm, in sentinel lymph node.
Fifty-three-year-old man with nevus on left arm and a diagnosis on excision of superficial melanoma, with a Breslow thickness of 0.7mm, Clark level 3, non-brisk tumour-infiltrating lymphocytes (TILs), no ulceration or regression, mitotic rate of 2/mm2, no vascular and perineural invasion, and negative lateral and deep margins. The indication for SLN was marginal. Peripheral liquid biopsy was negative. Selective liquid biopsy via transfemoral catheterisation of the left subclavian vein showed fragmented circulating DNA with a p.Y1021S mutation in codon 1021 of the PiK3CA gene. No mutations were found in the KRAS, BRAF and NRAS genes. On SLN, melanoma metastases were found in one of two sentinel lymph nodes in the left axilla, as well as two intraparenchymal micrometastases, the larger measuring 1mm (Figures 1 and 2). Radical lymphadenectomy with 27 lymph nodes was negative, as was two-year follow-up of the patient.
Case 2

Figure 4 (Right): Right transbrachial catheterisation of left subclavian vein for selective liquid biopsy blood sampling.
Seventy-nine-year-old man with nevus on left arm, suspected to be melanoma (Figure 3). Selective liquid biopsy with sampling from the left subclavian vein (Figure 4) at the same time as peripheral sampling was suggested. Mutation p.Q61R of the NRAS gene in exone 3 was found, leading to a diagnosis of melanoma and wide excision (Figure 5) with sentinel lymph node lymphoscintigraphy and biopsy (Figure 6). Histological diagnosis confirmed melanoma with horizontal growth, no vertical growth, Breslow thickness of 0.9mm, Clark level 3, non-brisk TIL, no ulceration or regression, pigmentation present, mitotic rate 0, no perineural invasion, associated nevus present, and negative lateral and deep margins. Molecular tissue analysis confirmed the NRAS gene mutation. SLN biopsy was negative, as was liquid biopsy molecular analysis six months after surgery.
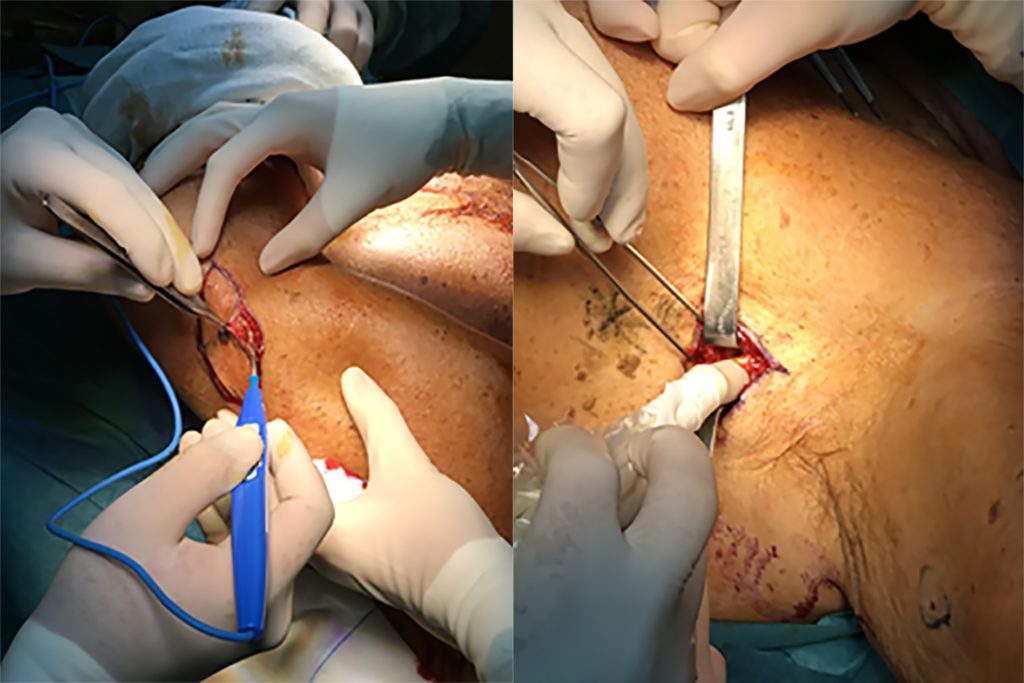
Figure 6 (Right): Sentinel lymph node identification at time of wide local excision.
Bruno Damascelli and Vladimira Tichà are interventionalists at the Department of Interventional Oncology EMO GVM Centrocuore Columbus in Milan, Italy. Their work is sponsored by the Falciani Foundation. The authors report no disclosures pertaining to this article.











