
Despite being “perfectly placed” to help meet the increasing demand for stroke thrombectomy, there is not an established training structure for interventional radiologists wishing to perform the procedure in Europe. The findings of a recent online survey conducted by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) on stroke thrombectomy provide, according to the society, a “mandate [for] further European-wide initiatives” to establish such training programmes.
Writing to the Editor of CardioVascular and Interventional Radiology, CIRSE past president Robert Morgan (St George’s University Hospitals NHS Foundation Trust, London, UK) et al state that current barriers to interventional radiologists becoming key players in European stroke management, identified by CIRSE leadership, include “the absence of an established training structure for interventional radiologists performing stroke thrombectomy, a strong dependence on local conditions, limited 24/7 coverage, as well as varying opinions on the desired involvement of interventional radiology [IR] in stroke thrombectomy”. Therefore, to assess the level of interest and involvement by interventional radiologists in the procedure across Europe, CIRSE conducted an anonymous online survey on the current situation of stroke thrombectomy practice among European interventional radiologists.
Stroke thrombectomy was performed in 74.5% of the respondent’s centres, with an expected predominance in university hospitals, tertiary care hospitals and private hospitals, although the procedure was also performed in 52.5% of general hospitals. There was also an increasing tendency for the procedure to be performed in larger hospitals.
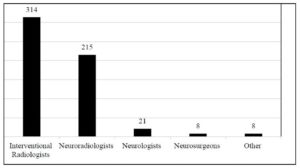
In centres where stroke thrombectomy is performed, it was most frequently delivered by interventional radiologists in 70.1% and by neuroradiologists in 48%. Stroke thrombectomy was provided by both interventional radiologists and neuroradiologists in 21% of centres. “Collaboration with other specialties appeared to be good throughout the obtained sample,” the letter says, “as interventional radiologists perform stroke thrombectomies in collaboration with other medical specialties in almost 90% of centres.”

It continues: “Training for stroke thrombectomy by interventional radiologists was either provided by a neuroradiologist at the same centre (47.7%) or was obtained by interventional radiologists independently (46.2%). However, opportunities for training in stroke thrombectomy are relatively limited for interventional radiologists, especially where there was reluctance by neuroradiologists to involve interventional radiologists in the stroke thrombectomy service, and almost a quarter of respondents who perform stroke thrombectomies indicated that they were ‘trained in another way’, indicating a large variety in training modes and options and reconfirming the need for more standardised training pathways and dedicated courses for IR.”
The survey also reported a broad consensus among respondents that “a significant growth in the demand for stroke thrombectomy was expected, due to factors such as improved infrastructure and service availability, increased awareness of this treatment option among referrers, better clinical evidence, and broader inclusion criteria”.
Speaking to Interventional News about the results of this survey, Morgan says: “This survey confirms that in many countries, interventional radiologists already have a significant role in the delivery of intraarterial stroke therapy. This was already known by CIRSE but had not been confirmed previously by a formal survey of CIRSE members.
“We all know that there are not enough interventional neuroradiologists to provide intraarterial stroke therapy in Europe in the volumes that are required by patient demand for this procedure. I would like the future of stroke thrombectomy to be a comprehensive service satisfying the widespread demand by patients and delivered by doctors who have been adequately trained to perform the procedure. Interventional radiologists would be key players in the stroke thrombectomy service, working alongside our colleagues in interventional neuroradiology.
“To bring this about, we need to form even better collaborative working relationships with our interventional neuroradiological colleagues. These improved relationships should be encouraged by our colleagues and not hampered by any counterproductive issues such as turf. Another important requirement is the recognition by leaders of national health systems that interventional radiologists can provide stroke thrombectomy and should be encouraged to do so in their country’s hospitals.”
CIRSE received a total of 601 valid responses, which the society claims is “a very high response rate (11.5%) for a CIRSE member survey”. Of these, 109 came from Germany, 87 from Italy, 68 from the UK, 38 from The Netherlands, 36 from Turkey, 32 from Spain, 28 from Belgium, 26 from Austria, 25 from Greece, and the remaining quarter from other European countries—“the sample was considered to be representative of CIRSE’s European membership in terms of geographical spread, centre type, and level of experience”. However, the letter writers acknowledge a potential bias that interventional radiologists involved in stroke thrombectomy may have been more likely to respond.










